User login
Acute Tender Papules on the Arms and Legs
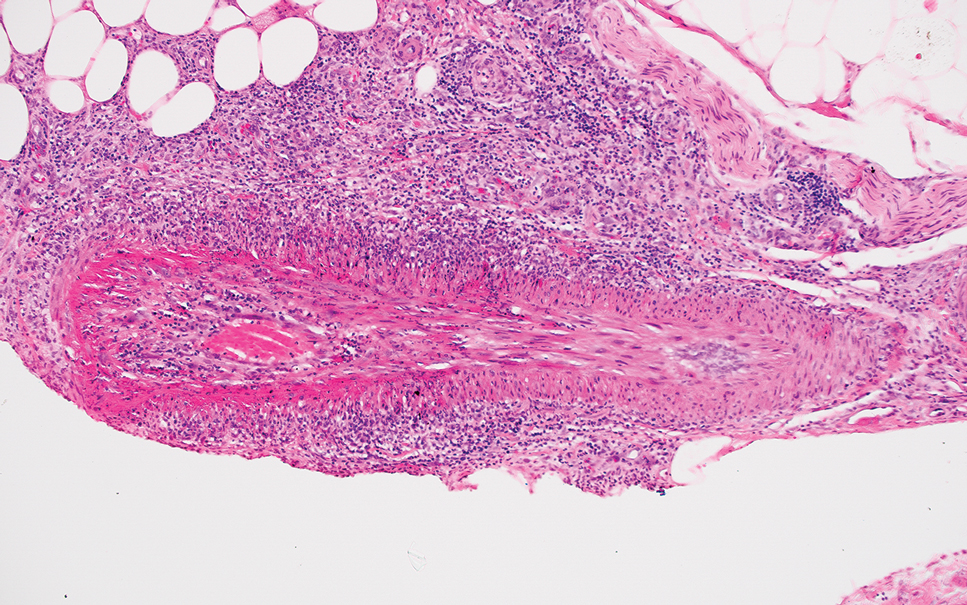
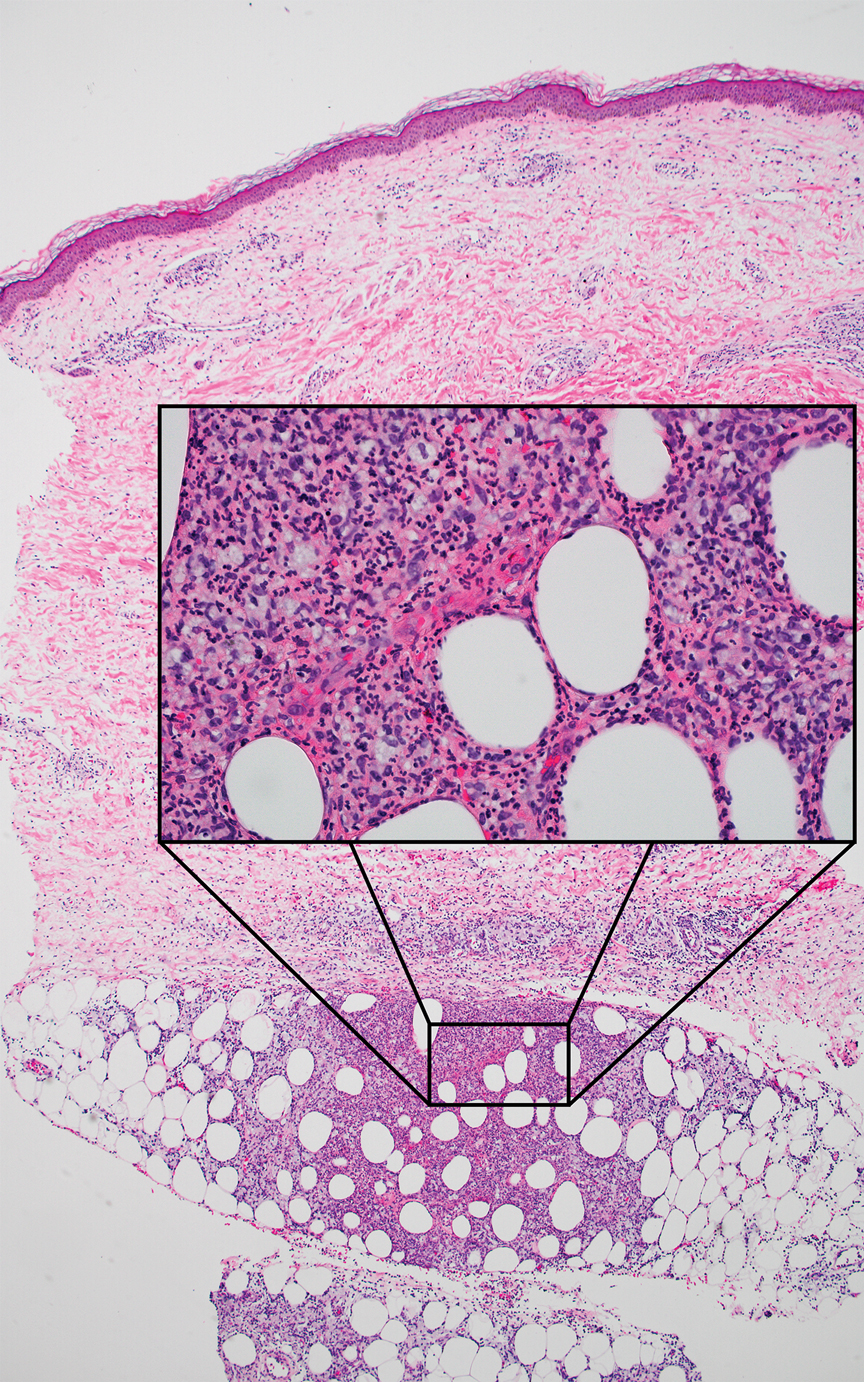
The Diagnosis: Erythema Nodosum Leprosum
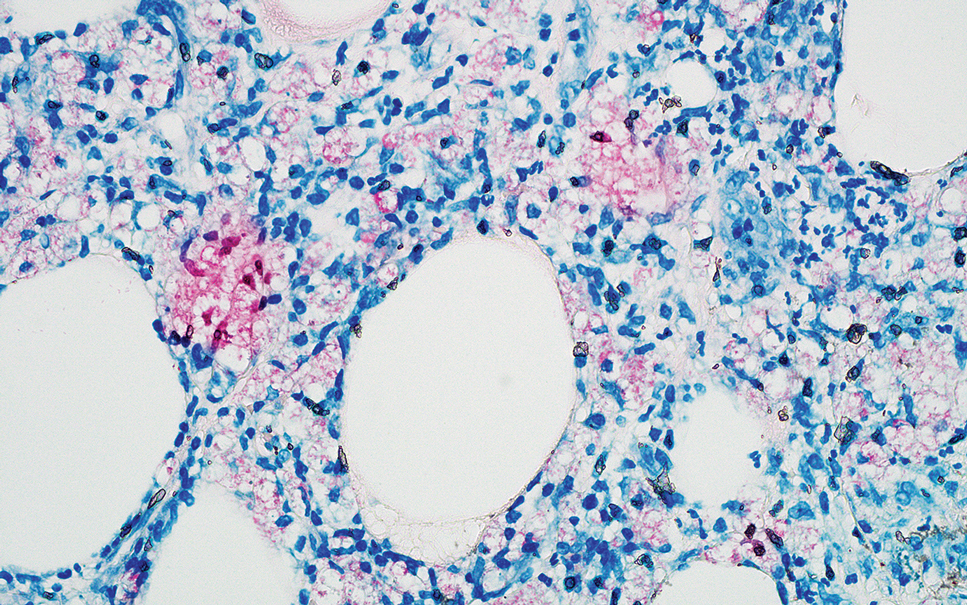
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
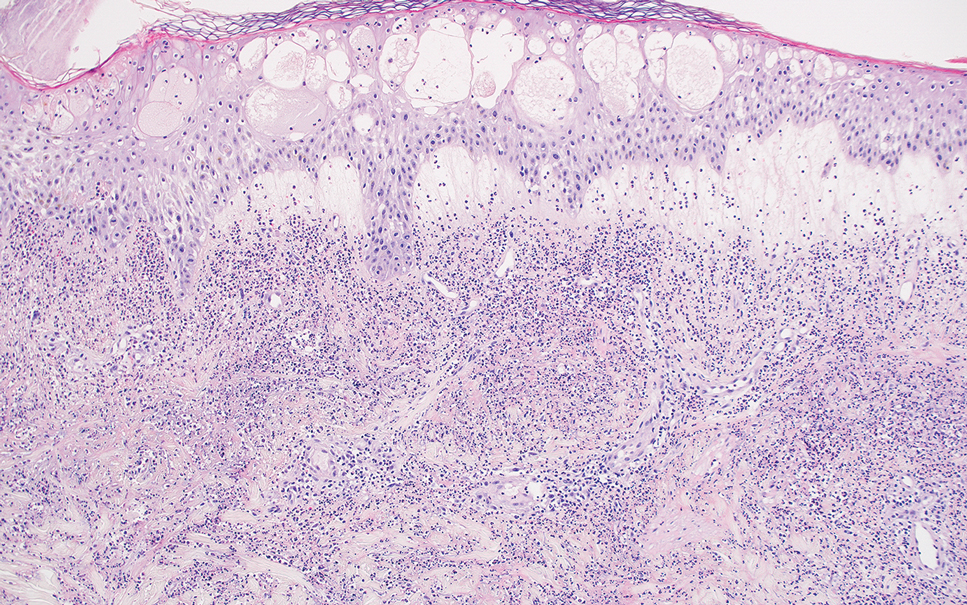
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
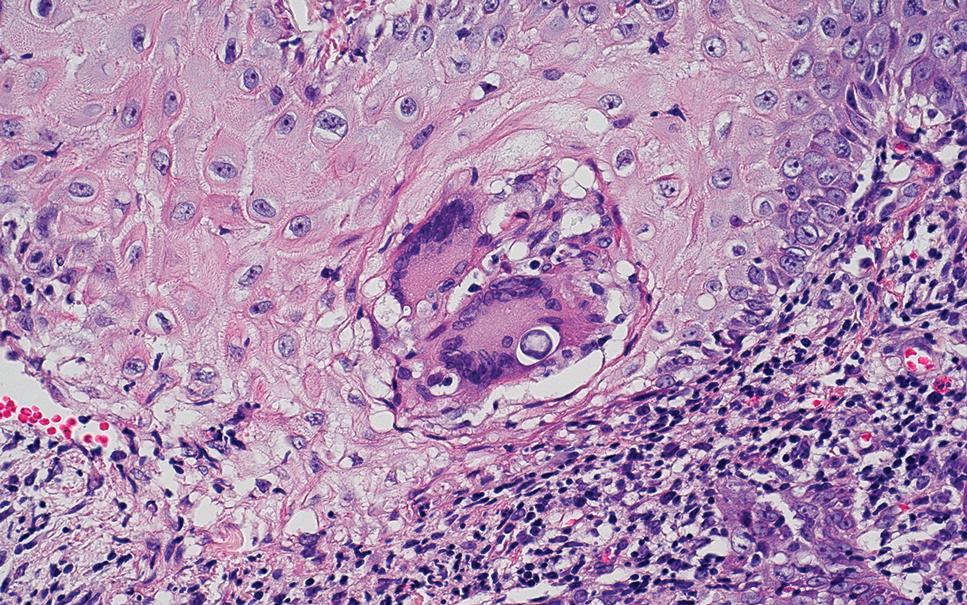
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
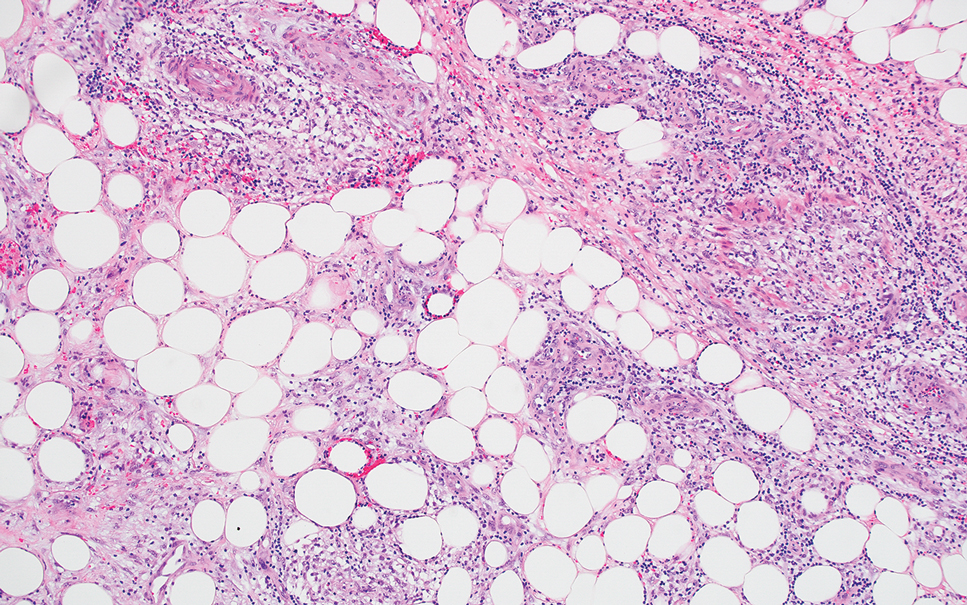
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
The Diagnosis: Erythema Nodosum Leprosum
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
The Diagnosis: Erythema Nodosum Leprosum
Erythema nodosum leprosum (ENL) is a type 2 reaction sometimes seen in patients infected with Mycobacterium leprae—primarily those with lepromatous or borderline lepromatous subtypes. Clinically, ENL manifests with abrupt onset of tender erythematous papules with associated fevers and general malaise. Studies have demonstrated a complex immune system reaction in ENL, but the detailed pathophysiology is not fully understood.1 Biopsies conducted within 24 hours of lesion formation are most elucidating. Foamy histiocytes admixed with neutrophils are seen in the subcutis, often causing a lobular panniculitis (quiz image).2 Neutrophils rarely are seen in other types of leprosy and thus are a useful diagnostic clue for ENL. Vasculitis of small- to medium-sized vessels can be seen but is not a necessary diagnostic criterion. Fite staining will highlight many acid-fast bacilli within the histiocytes (Figure 1).
Erythema nodosum leprosum is treated with a combination of immunosuppressants such as prednisone and thalidomide. Our patient was taking triple-antibiotic therapy—dapsone, rifampin, and clofazimine—for lepromatous leprosy when the erythematous papules developed on the arms and legs. After a skin biopsy confirmed the diagnosis of ENL, he was started on prednisone 20 mg daily with plans for close follow-up. Unfortunately, the patient was subsequently lost to follow-up.
Acute febrile neutrophilic dermatosis (also known as Sweet syndrome) is an acute inflammatory disease characterized by abrupt onset of painful erythematous papules, plaques, or nodules on the skin. It often is seen in association with preceding infections (especially those in the upper respiratory or gastrointestinal tracts), hematologic malignancies, inflammatory bowel disease, or exposure to certain classes of medications (eg, granulocyte colony-stimulating factor, tyrosine kinase inhibitors, various antibiotics).3 Histologically, acute febrile neutrophilic dermatosis is characterized by dense neutrophilic infiltrates, often with notable dermal edema (Figure 2).4 Many cases also show leukocytoclastic vasculitis; however, foamy histiocytes are not a notable component of the inflammatory infiltrate, though a histiocytoid form of acute febrile neutrophilic dermatosis has been described.5 Infections must be rigorously ruled out prior to diagnosing a patient with acute febrile neutrophilic dermatosis, making it a diagnosis of exclusion.
Cutaneous coccidioidomycosis is an infection caused by the dimorphic fungi Coccidioides immitis or Coccidioides posadasii. Cutaneous disease is rare but can occur from direct inoculation or dissemination from pulmonary disease in immunocompetent or immunocompromised patients. Papules, pustules, or plaques are seen clinically. Histologically, cutaneous coccidioidomycosis shows spherules that vary from 10 to 100 μm and are filled with multiple smaller endospores (Figure 3).6 Pseudoepitheliomatous hyperplasia with dense suppurative and granulomatous infiltrates also is seen.
Erythema induratum is characterized by tender nodules on the lower extremities and has a substantial female predominance. Many cases are associated with Mycobacterium tuberculosis infection. The bacteria are not seen directly in the skin but are instead detectable through DNA polymerase chain reaction testing or investigation of other organ systems.7,8 Histologically, lesions show a lobular panniculitis with a mixed infiltrate. Vasculitis is seen in approximately 90% of erythema induratum cases vs approximately 25% of classic ENL cases (Figure 4),2,9 which has led some to use the term nodular vasculitis to describe this disease entity. Nodular vasculitis is considered by others to be a distinct disease entity in which there are clinical and histologic features similar to erythema induratum but no evidence of M tuberculosis infection.9
Polyarteritis nodosa is a vasculitis that affects medium- sized vessels of various organ systems. The presenting signs and symptoms vary based on the affected organ systems. Palpable to retiform purpura, livedo racemosa, subcutaneous nodules, or ulcers are seen when the skin is involved. The histologic hallmark is necrotizing vasculitis of medium-sized arterioles (Figure 5), although leukocytoclastic vasculitis of small-caliber vessels also can be seen in biopsies of affected skin.10 The vascular changes are said to be segmental, with uninvolved segments interspersed with involved segments. Antineutrophil cytoplasmic antibody (ANCA)– associated vasculitis also must be considered when one sees leukocytoclastic vasculitis of small-caliber vessels in the skin, as it can be distinguished most readily by detecting circulating antibodies specific for myeloperoxidase (MPO-ANCA) or proteinase 3 (PR3-ANCA).
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
- Polycarpou A, Walker SL, Lockwood DNJ. A systematic review of immunological studies of erythema nodosum leprosum. Front Immunol. 2017;8:233. doi:10.3389/fimmu.2017.00233
- Massone C, Belachew WA, Schettini A. Histopathology of the lepromatous skin biopsy. Clin Dermatol. 2015;33:38-45. doi:10.1016/j.clindermatol.2014.10.003
- Cohen PR. Sweet’s syndrome—a comprehensive review of an acute febrile neutrophilic dermatosis. Orphanet J Rare Dis. 2007;2:1-28. doi:10.1186/1750-1172-2-34
- Ratzinger G, Burgdorf W, Zelger BG, et al. Acute febrile neutrophilic dermatosis: a histopathologic study of 31 cases with review of literature. Am J Dermatopathol. 2007;29:125-133. doi:10.1097/01.dad.0000249887.59810.76
- Wilson TC, Stone MS, Swick BL. Histiocytoid Sweet syndrome with haloed myeloid cells masquerading as a cryptococcal infection. Am J Dermatopathology. 2014;36:264-269. doi:10.1097/DAD.0b013e31828b811b
- Guarner J, Brandt ME. Histopathologic diagnosis of fungal infections in the 21st century. Clin Microbiol Rev. 2011;24:247-280. doi:10.1128/CMR.00053-10
- Schneider JW, Jordaan HF, Geiger DH, et al. Erythema induratum of Bazin: a clinicopathological study of 20 cases of Mycobacterium tuberculosis DNA in skin lesions by polymerase chain reaction. Am J Dermatopathol. 1995;17:350-356. doi:10.1097/00000372-199508000-00008
- Boonchai W, Suthipinittharm P, Mahaisavariya P. Panniculitis in tuberculosis: a clinicopathologic study of nodular panniculitis associated with tuberculosis. Int J Dermatol. 1998;37:361-363. doi:10.1046/j.1365-4362.1998.00299.x
- Segura S, Pujol RM, Trindade F, et al. Vasculitis in erythema induratum of Bazin: a histopathologic study of 101 biopsy specimens from 86 patients. J Am Acad Dermatol. 2008;59:839-851. doi:10.1016/j.jaad.2008.07.030
- Ishiguro N, Kawashima M. Cutaneous polyarteritis nodosa: a report of 16 cases with clinical and histopathological analysis and a review of the published work. J Dermatol. 2010;37:85-93. doi:10.1111/j.1346-8138.2009.00752.x
A 66-year-old man presented with new tender erythematous papules scattered over the arms and legs. A biopsy of a lesion on the left thigh was performed.
Diet Rich in Processed Foods Linked to Elevated Risk for Colorectal Cancer
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- To date, no known studies have investigated how a dietary pattern (rather than just individual foods or nutrients) specifically directed at CRC-related microbes may contribute to an increased CRC risk.
- Using stool metagenomes and dietary information from 307 men and 212 women, researchers identified and then validated a dietary pattern specifically linked to an established CRC-related gut microbial signature, which they termed the CRC Microbial Dietary Score (CMDS).
- They then investigated the association between CMDS and the risk for CRC in 259,200 participants (50,637 men and 208,563 women) from three large US cohorts where health professionals provided detailed information on various lifestyle factors over long follow-up periods.
- Researchers also analyzed the risk for CRC on the basis of the presence of gut bacteria, such as F nucleatum, pks+ E coli, and ETBF, in the tumor tissues of the participants who underwent surgical resection for CRC.
TAKEAWAY:
- The CMDS was characterized by high intake of processed foods and low intake of fiber-rich foods.
- Over 6,467,378 person-years assessed in the three US cohorts, 3854 cases of incident CRC were documented, with 1172, 1096, and 1119 cases measured for F nucleatum, pks+ E coli, and ETBF, respectively.
- A higher CMDS was associated with an increased risk for CRC after adjusting for putative CRC risk factors (adjusted hazard ratio [HR], 1.25; Ptrend < .001).
- The association between CMDS and the risk for CRC was stronger for tumors with detectable levels of F nucleatum (HR, 2.51; Ptrend < .001), pks+ E coli (HR, 1.68; Ptrend = .005), and ETBF (HR, 2.06; Ptrend = .016).
IN PRACTICE:
“A dietary pattern with a low consumption of processed foods may help prevent colorectal cancer through modulation of the gut microbiome. The dietary pattern modulating the colorectal cancer–related gut microbial signature may particularly help prevent tumoral microbial positive colorectal cancer, which tends to have a worse prognosis,” the authors wrote.
SOURCE:
This study, led by Kai Wang and Chun-Han Lo, Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, was published online in Gastroenterology.
LIMITATIONS:
The study’s observational design may have limited the ability to establish causality between dietary patterns and the risk for CRC. The inclusion of participants who were all health professionals from a predominantly White US population may have limited the generalizability of the findings to other populations. The reliance on self-reported dietary data may have introduced recall bias and affected the accuracy of the dietary pattern assessed.
DISCLOSURES:
This work was supported by various sources, including the National Institutes of Health and the Cancer Research UK Grand Challenge Award. One author served as a consultant for some pharmaceutical companies, and another received funding from various sources, both unrelated to this study.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Systemic Sclerosis Without Scleroderma Has Unique Severity, Prognosis
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
Systemic sclerosis sine scleroderma (ssSSc) affects nearly 10% of patients with systemic sclerosis (SSc), with substantial internal organ involvement. Despite lacking skin fibrosis, patients with ssSSc are at a risk for interstitial lung disease, pulmonary arterial hypertension, and cardiac dysfunction.
METHODOLOGY:
- Driven by a fatal case of ssSSc with cardiac involvement, researchers aimed to evaluate its prevalence, severity, and prognosis.
- They conducted a systematic literature and qualitative synthesis of 35 studies on SSc cohorts from databases published between 1976 and 2023 that comprised data on the prevalence of SSc with or without organ involvement.
- A total of 25,455 patients with SSc were included, with 2437 identified as having ssSSc.
- Studies used various classification criteria for SSc, including the 1980 American Rheumatism Association criteria, 2001 LeRoy and Medsger criteria, and 2013 American College of Rheumatology/European League Against Rheumatism criteria, while ssSSc was classified on the basis of the definitions provided by Rodnan and Fennell and also Poormoghim.
- The analysis focused on ssSSc prevalence, reclassification rates, and internal organ involvement, including interstitial lung disease, pulmonary arterial hypertension, scleroderma renal crisis, and cardiac dysfunction.
TAKEAWAY:
- The overall mean prevalence of ssSSc was 9.6%, with a range of 0%-22.9% across different studies.
- Reclassification rates of ssSSc into limited cutaneous SSc (lcSSc) or diffuse cutaneous SSc (dcSSc) varied substantially, with some studies reporting rates as high as 27.8% over a 4-year follow-up period.
- The mean frequency of internal organ involvement in patients with ssSSc was 46% for interstitial lung disease, 15% for pulmonary arterial hypertension, 5% for scleroderma renal crisis, and 26.5% for cardiac dysfunction — mainly diastolic dysfunction.
- The survival rates in patients with ssSSc were similar to those with lcSSc and better than those with dcSSc.
IN PRACTICE:
“The results presented herein suggest a slightly more severe yet similar clinical picture of ssSSc compared to lcSSc [limited cutaneous SSc], while dcSSc [diffuse cutaneous SSc] remains the most severe disease form,” the authors wrote. “Although classification criteria should not impact appropriate management of patients, updated ssSSc subclassification criteria, which will take into account time from disease onset, should be considered,” they further added.
SOURCE:
The study was led by Anastasios Makris, MD, First Department of Propaedeutic & Internal Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece. It was published online on August 15, 2024, in The Journal of Rheumatology.
LIMITATIONS:
The variability in the classification criteria across different studies may affect the comparability of results. The included studies lacked data on cardiac MRI, restricting the identification of myocardial fibrosis patterns and characterization of cardiac disease activity.
DISCLOSURES:
The study did not receive any specific funding. Some authors disclosed having a consultancy relationship, serving as speakers, and receiving funding for research from multiple companies. One author reported having a patent and being a cofounder of CITUS AG.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
GIST Rates Rise, With Black Patients Facing Higher Mortality
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- A steep increase in GIST incidence was observed from 2000 to 2005, largely due to the reclassification of sarcomas as GISTs. The classification of GISTs has changed over time, with all GISTs now considered malignant instead of benign, likely further increasing the incidence. However, updated data on GIST trends are lacking.
- This study assessed recent trends in GIST incidence and survival outcomes across different racial and ethnic groups using data from the National Cancer Institute’s SEER database, including the SEER-22 and SEER-17 registries.
- Researchers evaluated annual percentage changes and incidences among 23,001 patients from SEER-22 (mean age, 64 years) and median overall and cancer-specific survival rates in 12,109 patients from SEER-17 (mean age, 64 years).
- More than half of the patients in both cohorts were White, 17.8%-19.6% were Black, 11.6%-12.3% were Hispanic, and 9.7%-13.2% were Asian or Pacific Islander.
TAKEAWAY:
- The rates of GISTs increased annually between 2000 and 2019 for all organ sites, except the colon, where it decreased by 0.2% per year. Esophageal GISTs increased by 7.3%, gastric by 5.1%, small intestine by 2.7%, and rectal by 1.9%.
- Black patients had significantly lower median overall survival than other racial groups. For example, the median survival for Black patients with esophageal GISTs was 3.6 years vs 15.3 years for White patients (hazard ratio [HR], 6.4; 95% CI, 2.0-20.3). Similar patterns were seen for gastric GISTs — 9.1 years for Black patients vs 11.8 years for White patients (HR, 1.4). GIST-specific mortality was also higher in Black patients for these two organ sites.
- Additionally, Asian or Pacific Islander patients with esophageal GISTs had lower survival rates, with a median of 8.8 years (HR, 5.6) vs 15.3 years for White patients. Similarly, American Indian or Alaska Native patients with gastric GIST had lower survival rates, with a median of 8.5 years (HR, 1.6) vs 11.8 years for White patients.
- Over the 20-year study period, 5-year relative survival rates improved for most patient groups but remained the lowest among American Indian or Alaska Native patients across various GIST sites.
IN PRACTICE:
“We observed a continued increase in the incidence of GISTs after 2005” with a “substantial increase in the last two decades,” the authors wrote. Therefore, “future research should explore lifestyle-related or environmental factors underlying the unfavorable trends” which “could not fully be explained by coding reclassification and advances in diagnostic technologies,” they further added.
SOURCE:
The study was led by Christian S. Alvarez, PhD, Division of Cancer Epidemiology and Genetics, National Cancer Institute, Rockville, Maryland. It was published online on August 19, 2024, in JAMA Network Open.
LIMITATIONS:
A lack of individual-level data on socioeconomic factors and healthcare access could have influenced the findings. Although the SEER registries used standardized codes and procedures for classifying the data on race and ethnicity, misclassification was possible. Additionally, data on prognostic factors were incomplete or missing, which limited the inferences of the analysis.
DISCLOSURES:
This work was supported by the National Institutes of Health Intramural Research Program of the National Cancer Institute. Two authors reported receiving grants or personal fees and having other ties with various sources.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Adjuvant Everolimus Offers No Survival Benefit in Non–Clear Cell RCC
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Non–clear cell RCC accounts for approximately 25% of RCC cases and includes various distinct tumor types such as papillary and chromophobe RCC. A common design flaw in clinical trials has been applying treatments effective in clear cell RCC to non–clear cell RCC subtypes without a strong biological rationale. The broad approval of drugs for RCC without considering subtype differences complicates treatment decisions.
- The EVEREST phase 3 randomized clinical trial evaluated everolimus in the adjuvant setting, enrolling patients with either clear cell (n = 1248) or non–clear cell (n = 208) RCC at high risk for recurrence after resection. The patients were randomly assigned to receive either everolimus or placebo.
- To assess the benefits of everolimus in patients with non–clear cell RCC, this analysis focused on the subgroup of 109 patients with papillary RCC (median age, 60 years) and 99 patients with chromophobe RCC (median age, 51 years).
- The primary outcome was recurrence-free survival, and the secondary outcome was overall survival. The median follow-up was 76 months.
TAKEAWAY:
- In the papillary RCC subgroup, the 5-year recurrence-free survival was lower among patients receiving everolimus vs placebo (62% vs 70%), but this difference was not significant (hazard ratio [HR], 1.19; 95% CI, 0.61-2.33; P = .61).
- In the chromophobe RCC subgroup, the 5-year recurrence-free survival was similar between the two groups — 79% for everolimus vs 77% for placebo (HR, 0.89; 95% CI, 0.37-2.13; P = .79).
- Everolimus was also not associated with a significant overall survival benefit in patients with papillary RCC (HR, 1.47; 95% CI, 0.67-3.24; P = .34) or chromophobe RCC (HR, 0.93; 95% CI, 0.33-2.65; P = .89). In the papillary RCC subgroup, 5-year overall survival rates were slightly lower in the everolimus group than in the placebo group (76% vs 82%); however, in the chromophobe RCC subgroup, the rates were the same for both arms (89%).
- Patients treated with everolimus reported an increased incidence of grade 3 or higher adverse events, compared with those treated with placebo (48% vs 9%). No treatment-related deaths were reported, but a significant number of patients — 54% with papillary RCC and 51% with chromophobe RCC — discontinued treatment early because of adverse events.
IN PRACTICE:
This secondary analysis “found that patients with papillary or chromophobe RCC did not benefit from treatment with everolimus in the adjuvant setting,” the authors wrote. “Our study highlights an area of unmet need in the kidney cancer field. It thus serves to provide a foundational background for future randomized clinical trials to address specific subgroups of RCC for risk mitigation strategies in the adjuvant setting.”
SOURCE:
The study was led by Shuchi Gulati, MD, MSc, University of California Davis Comprehensive Cancer Center, Sacramento, and was published online on August 6, 2024, in JAMA Network Open, along with an accompanying editorial.
LIMITATIONS:
The subgroup analyses were underpowered to detect a significant difference. Additionally, the study lacked a central pathology review to confirm non–clear cell histologies.
DISCLOSURES:
The study was supported by awards from the National Institutes of Health, National Cancer Institute, and National Clinical Trials Network. Several authors reported receiving grants or personal fees from various sources outside the submitted work.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
A New Era of Obesity Medicine
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Obesity has now reached epidemic proportions, with global prevalence of the condition increasing more than threefold between 1975 and 2022. In the United States alone, roughly two in five adults have obesity. As healthcare providers are intimately aware, obesity is linked to many serious health conditions, including type 2 diabetes, cardiovascular disease, and metabolic-associated steatotic liver disease, as well as some forms of cancer. As such, it presents a major challenge to chronic disease prevention and overall health.
For many years, management of obesity was considered within the purview of primary care as part of chronic disease management. However, as obesity has become more common, our understanding of the underlying causes of obesity has improved, and optimal strategies to manage and treat obesity have evolved. From glucagon-like peptide 1 agonists to an expanding armamentarium of bariatric procedures, emerging therapeutics have revolutionized treatment of patients with obesity and related health conditions.
In this month’s Member Spotlight, we introduce you to gastroenterologist Dr. Janese Laster, who has built a successful career with a primary focus on obesity medicine. She shares her passionate perspective on why gastroenterologists should play a more prominent role in management of this complex, chronic disease. We also include a summary of obesity-related content presented as part of this spring’s AGA Post-Graduate Course, with helpful clinical pearls from experts Dr. Andres Acosta, Dr. Violeta Popov, Dr. Sonali Paul, and Dr. Pooja Singhal.
Also in our September issue, we highlight a recent, practice-changing randomized controlled trial from Clinical Gastroenterology and Hepatology supporting use of snare tip soft coagulation as the preferred thermal margin treatment to reduce recurrence rates following colorectal endoscopic mucosal resection. In our quarterly Perspectives column, Dr. Maggie Ham and Dr. Petr Protiva offer their insights into a pressing question on many of our minds — whether to take the 10-year “high-stakes” exam or opt for the Longitudinal Knowledge Assessment to maintain American Board of Internal Medicine certification. As always, thanks for reading and please don’t hesitate to reach out with suggestions for future coverage.
Megan A. Adams, MD, JD, MSc
Editor in Chief
Alternative Paths to Recertification
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.

We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.

As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.

Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.
We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.
As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.
Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.
Dear colleagues,
When the American Board of Internal Medicine (ABIM) made changes to its recertification process, introducing its continuous Maintenance of Certification (MOC) in 2014, there was significant controversy across subspecialties. In response, the ABIM accreditation process has evolved. Currently, there remains the traditional 10-year MOC exam, and a newly introduced Longitudinal Knowledge Assessment (LKA) where questions are answered every quarter. But which is the better one for you?
In this issue of Perspectives, Dr. Petr Protiva and Dr. Maggie Ham discuss their experiences with these differing assessment methods. Dr. Ham touches on the flexibility and convenience of the LKA, while Dr. Protiva writes about the benefits of the focused preparation and clear endpoint that the 10-year exam offers.
We hope their experiences will help you decide on your approach to recertification. Good luck!
We look forward to hearing your thoughts on how endoscopy will continue to evolve@AGA_GIHN.
Gyanprakash A. Ketwaroo, MD, MSc, is associate professor of medicine, Yale University, New Haven, Conn., and chief of endoscopy at West Haven (Conn.) VA Medical Center. He is an associate editor for GI & Hepatology News.
Traditional 10-Year ABIM Exam: A Personal Perspective
BY PETR PROTIVA, MD, MPH, AGAF
The American Board of Internal Medicine (ABIM) offers board certification in gastroenterology, a mark of professional excellence. Physicians can maintain their certification through the traditional 10-year examination or the newer Longitudinal Knowledge Assessment (LKA).
I completed my initial certification exam in 2003 and currently practice gastroenterology full time at the West Haven (Conn.) VA, where I am associate chief of gastroenterology, and the Yale School of Medicine. I am a clinician educator, running clinical trials and performing general and some advanced endoscopy.
As an academic gastroenterologist, I recertified in November 2023 using the traditional 10-year examination. An informal survey among my colleagues revealed that most opted for the LKA route. The traditional exam offers consistency, a clear endpoint, and a comprehensive review but comes with high stakes, significant preparation requirements, and potential for outdated information. In contrast, the LKA promotes continuous learning, flexibility, and immediate feedback, though it requires ongoing commitment. The LKA is generally perceived as the preferable option for maintaining and enhancing a current knowledge base.
In a highly academic environment with ample opportunities for learning and staying current with clinical science, the traditional exam’s drawbacks can be mitigated. My decision to opt for the 10-year exam was based on prior experience and the ease of accessing and maintaining knowledge in an academic setting. I considered the LKA as well, but there’s no clear answer as to which exam is “better.” The choice ultimately depends on individual physician preferences, learning styles, and professional circumstances. This piece recounts my experience with the 10-year recertification exam in 2023.
Preparing for the 10-Year Exam
In the year my recertification was due, I logged into my ABIM account to verify requirements and deadlines. After signing up for the recertification exam on the ABIM website, I was directed to the Pearson Vue website to select my testing center and date. The process was straightforward and glitch-free.
To fulfill the Maintenance of Certification (MOC) point requirements, it is necessary to systematically accumulate points through accredited Continuing Medical Education (CME) activities. The ABIM web portal indicates how many MOC points you are missing for the recertification cycle. I converted my UpToDate CME credits into ABIM MOC points, a straightforward process if you follow the necessary steps and keep your accounts updated.
Numerous resources are available for assessing and testing your knowledge prior to the exam. My first assessment included an online GI Board question bank, followed by a virtual Board Review Course. Next, I used the GI society-based Self-Assessment Test, which was well-suited for honing testing skills as well as reviewing the questions and answers in detail. Both the online question bank and GI society tests offered additional MOC points upon successful completion of practice exams. I also found it useful to reread guidelines in areas outside my usual practice and use UpToDate on an ongoing basis, like in everyday clinical practice. Completing the MOC requirements well ahead of my exam date was relatively easy.
Exam Experience
The exam itself is a 10-hour, grueling experience, but I was familiar with the format and expectations. The exam day was divided into several sessions, each containing a maximum of 60 multiple-choice questions, usually totaling 220 questions with an average of 2 minutes per question. The use of UpToDate is permitted during the recertification exam. While UpToDate is an excellent clinical resource, it cannot substitute for comprehensive knowledge. It is useful for verifying specific facts but cannot fill knowledge gaps during the exam.
Pros and Cons of the 10-Year Exam
Pros:
- Focused Preparation: Preparing for a single, comprehensive exam leads to an in-depth review of the entire subspecialty, reinforcing foundational knowledge and ensuring breadth in less familiar areas.
- Clear Endpoint: The 10-year exam offers a clear endpoint. Once passed, the certification is valid for the next decade, allowing focus on practice or academic endeavors without a need for ongoing assessments.
- Consistency: The standardized nature of the exam ensures consistency in the assessment process, with all physicians tested under the same conditions.
- Benchmarking: A decade-long interval provides a significant time frame for measuring knowledge and expertise, allowing comparison with other test takers.
Cons:
- High Stakes: The exam is high stakes, creating significant stress. Failure can have serious professional consequences, potentially affecting credentials and career.
- Rigidity: The fixed schedule offers little flexibility, requiring careful planning and preparation, which may not align with personal or professional circumstances.
- Comprehensive Nature: Extensive preparation is challenging for busy physicians. Balancing study time with clinical responsibilities can be difficult.
- Outdated Information: Medical knowledge evolves rapidly, and the 10-year interval may not reflect the most current practices, leading to gaps in knowledge.
Conclusion
While I cannot directly compare my experience to the LKA, the traditional 10-year exam has both strengths and weaknesses. It requires extensive preparation and is high stakes, but it offers a clear endpoint and comprehensive review. The choice between the 10-year exam and the LKA depends on individual preferences, learning styles, and professional circumstances. In an academic environment, the traditional exam can be a good option, but continuous medical education remains essential regardless of the recertification method chosen.
Dr. Protiva is associate chief of gastroenterology at the West Haven (Conn.) VA Medical Center, and associate professor of medicine (digestive diseases) at Yale School of Medicine, New Haven, Conn. He has no disclosures related to this article.
The Longitudinal Knowledge Assessment: Flexible and Convenient
BY MAGGIE HAM, MD, AGAF
I completed my initial certification exam in 2013 when I completed gastroenterology fellowship training at the Beth Israel Deaconess Medical Center in Boston. I am currently in clinical practice at Southern California Permanente Medical Group in Ventura, California, where I see patients and perform endoscopy daily.
I practice general gastroenterology and hepatology with an emphasis on inflammatory bowel disease, colon cancer prevention, and women’s health. I am also the medical director of the gastroenterology lab at Community Memorial Hospital in Ventura, physician in charge of a building at Kaiser, and assistant chief of gastroenterology. My husband and I are both gastroenterologists with a child in elementary school.
Two years ago, I decided to embark upon the Longitudinal Knowledge Assessment (LKA) for gastroenterology. This is offered by the American Board of Internal Medicine (ABIM) in lieu of the 10-year recertification examination. As a full-time working mother, I could not fathom the time it would take to study and sit down for the high-stakes 10-year exam.
The LKA consists of 30 questions per quarter, which equates to 600 questions over 5 years. One hundred questions may be skipped over the 5-year period. The questions can be answered from anywhere with an internet-connected device without any camera monitoring. I would often answer questions from the comfort of my own home using my laptop, but could also do so using my phone while waiting in line at the store or on a long plane ride. The 30 questions do not need to be answered in the same sitting, so within the quarter I can save my progress and answer the remaining questions at my convenience. This has worked well for me alongside my personal and professional obligations.
I can download my progress report which informs me of my score, and what the passing score is. I can see what the average score is, how I am performing relative to that, and how I am faring in each category (ie, esophagus, stomach and duodenum, liver, etc.). I also receive Maintenance of Certification points with each LKA question I answer correctly. With the 10-year ABIM recertification exam, I would still need to complete MOC.
While there is a 4-minute time limit for each question, it really has not been an issue. If needed, I can request to extend the time, to read or to look things up. It is an open book exam, so I have learned and kept abreast of GI knowledge. Any references other than another human may be used. I typically use UpToDate and the GI society guidelines, which have been sufficient. Occasionally there are experimental questions sprinkled throughout the exam, so I may never know the answer. Otherwise, the solution to each question will be presented to me immediately upon answering, with an explanation accompanied by references. I appreciate that this keeps me updated with the latest guidelines and recommendations, which was my primary reason for selecting the LKA.
At the end of the 5 years, you may choose to continue the LKA cycle, or take the 10-year exam. If you do not pass the LKA, they do give you a 1-year grace period to pass the exam if you want to continue to participate in MOC.
The quarter does seem to come around fairly quickly, but they do send frequent reminders by email or text as the deadline approaches. And if you forget to answer all the questions in a quarter, the LKA allows for 100 questions that may be skipped over the 5-year period.
Being able to answer questions from anywhere at any time is incredibly flexible and convenient. The immediate feedback is also great and helps me identify my strengths and weaknesses. While I will not know until the end of the 5-year period whether I have passed or not, I can check my progress report which gives me an idea of where I stand. Overall, I would say I am satisfied with the LKA, as it has been easy to maintain certification while effectively contributing to my continuing medical education.
Dr. Ham is a gastroenterologist at Southern California Permanente Medical Group in Ventura, California. She is also medical director of the gastroenterology lab at Southern Community Memorial Hospital in Ventura. She has no disclosures related to this article.
Obesity Is Not a Moral Failing, GI Physician Says
It takes a long time for some patients with obesity to acknowledge that they need help, said Dr. Laster, a bariatric endoscopist who specializes in gastroenterology, nutrition, and obesity medicine at Gut Theory Total Digestive Care, and Georgetown University Hospital in Washington. “If somebody has high blood pressure or has a cut or has chest pain, you don’t wait for things. You would go seek help immediately. I wish more patients reached out sooner and didn’t struggle.”

Another big challenge is making sure patients have insurance coverage for things like medications, surgery, and bariatric endoscopy, she added.
Her response: education and advocacy. “I’m giving as many talks as I can to fellows, creating courses for residents and fellows and medical students” to change the way physicians talk about obesity and excess weight, she said. Patients need to understand that physicians care about them, that “we’re not judging and we’re changing that perspective.”
Dr. Laster is also working with members of Congress to get bills passed for coverage of obesity medication and procedures. In an interview with GI & Hepatology News, she spoke more about the intersection between nutrition, medicine and bariatric procedures and the importance of offering patients multiple solutions.
Q: Why did you choose GI?
It allowed me a little bit of everything. You have clinic, where you can really interact with patients and get to the root of their problem. You have preventative care with routine colonoscopies and upper endoscopies to prevent for cancer. But then you also have fun stuff — which my mom told me to stop saying out loud — ‘bleeders’ and acute things that you get to fix immediately. So, you get the adrenaline rush too. I like it because you get the best of all worlds and it’s really hard to get bored.
Q: How did you become interested in nutrition and bariatric endoscopy?
My parents had a garden and never let us eat processed foods. In residency, I kept seeing the same medical problems over and over again. Everybody had high blood pressure, high cholesterol, and diabetes. Then in GI clinic, everybody had abdominal pain, bloating, constipation, heartburn, and a million GI appointments for these same things. Everyone’s upper endoscopy or colonoscopy was negative. Something else had to be going on.
And that’s sort of where it came from; figuring out the common denominator. It had to be what people were eating. There’s also the prevalence of patients with obesity going up every single year. Correlating all these other medical problems with people’s diets led me down the rabbit hole of: What else can we be doing?
Most people don’t want to undergo surgery. Only 2% of people eligible for surgery actually do it, even though it works. The reasons are because it’s invasive or there’s shame behind it. Bariatric endoscopy is another option that’s out here, that’s less invasive. I’m an endoscopist and gastroenterologist. I should be able to offer all those things and I should know more about nutrition. We don’t talk about it enough.
Q: Do you think more GI doctors should become better educated about nutrition?
100%. Every patient I see has seen a GI doctor before and says, ‘No one has ever told me that if I have carbonated beverages and cheese every day, I’m going to be bloated and constipated.’ And that shouldn’t be the case.
Q: Why do you think that more GI doctors don’t get the education on nutrition during their medical training?
I think it’s our healthcare system. It’s very much focused on secondary treatment rather than preventative care. There’s no emphasis on preventing things from happening.
We’re really good at reactionary medicine. People who have an ulcer, big polyps and colon cancer, esophageal cancer — we do those things really well. But I think because there’s no ICD-10 codes for preventive care via nutrition education, and no good reimbursement, then there’s no incentive for hospital systems to pay for these things. It’s a system based on RVUs (relative value units) and numbers. That’s been our trajectory. We’ve been so focused on reactionary medicine rather than saying, ‘Okay, let’s stop this from happening.’
We just didn’t talk about nutrition in medical school, in residency, or in fellowship. It was looked at as a soft science. When I was in school, people would also say, ‘No one’s going to change. So it’s a waste of your time essentially to talk to people about making dietary changes.’ I feel like if you give people the opportunity, you have to give them the chance. You can’t just write everybody off. Some people won’t change, but that’s okay. They should at least have the opportunity to do so.
Q: How do you determine whether a patient is a good candidate for bariatric surgery?
It’s based on the guidelines: If they meet the BMI requirements, if they have obesity-associated comorbidities, their risk for surgery is low. But it’s also whether they want to do it or not. A patient has to be in the mindset and be ready for it. They need to want to have surgery or bariatric endoscopy, or to use medications, or start to make a change. Some people aren’t there yet — that preemptive stage of making a change. They want the solution, but they’re not ready to do that legwork yet.
And all of it is work. I tell patients, ‘Whether it’s medication or bariatric endoscopy or bariatric surgery, you still have work to do. None of it is going to just magically happen where you could just continue to do the same thing you’re doing now and you’re going to lose weight and keep it off.’
Q: What advances in obesity prevention are you excited about?
I’m excited that bariatric endoscopy came about in the first place, because in every other field there are less invasive approaches that have become available. I’m also excited about the emergence of weight loss medication, like GLP-1s. I think they are a tool that we need.
Q: Do you think the weight loss medications may negate the need for surgery?
I don’t think they necessarily reduce the need for surgery. There’s still a lot we don’t know about why they work in some patients and why they don’t work in others.
Some of our colleagues have come up with phenotypes and blood tests so we can better understand which things will work in different patients. Surgery doesn’t work for some patients. People may need a combination of both after they reach a plateau. I’m excited that people see this as something that we should be researching and putting more effort into — that obesity isn’t a disease of moral failure, that people with excess weight just need to ‘move more’ or ‘eat less’ and it’s their fault. I’m glad people are starting to understand that.
Q: What teacher or mentor had the greatest impact on you?
Probably two. One of them is Andrea E Reid, MD, MPH, a dean of medicine at Harvard. She gives you such motivation to achieve things, no matter how big your idea is or how crazy it may seem. If you have something that you think is important, you go after it. Another person is Christopher C. Thompson, MD, at Brigham and Women’s Hospital, the father of bariatric endoscopy in a sense. He embodies what Dr. Reid talks about: crazy big ideas. And he goes after them and he succeeds. Having him push me and giving me that type of encouragement was invaluable.
Q: Describe how you would spend a free Saturday afternoon.
Every Saturday is yoga or some type of movement. Spending some time outside doing something, whether it’s messing around with plants that I’m not very good at, or going for a walk.
Lightning Round
Texting or talking?
Text
Favorite city in U.S. besides the one you live in?
New York
Favorite breakfast?
Avocado toast
Place you most want to travel to?
Istanbul
Favorite season?
Fall
Favorite ice cream flavor?
Raspberry sorbet
How many cups of coffee do you drink per day?
One
Best place you ever went on vacation?
Greece
If you weren’t a gastroenterologist, what would you be?
Own a clothing store
Favorite type of music?
Old school R&B
Favorite movie genre?
Romantic comedy or drama
Cat person or dog person?
Dog
Favorite sport?
Football
Favorite holiday?
Christmas
Optimist or pessimist?
Optimist
It takes a long time for some patients with obesity to acknowledge that they need help, said Dr. Laster, a bariatric endoscopist who specializes in gastroenterology, nutrition, and obesity medicine at Gut Theory Total Digestive Care, and Georgetown University Hospital in Washington. “If somebody has high blood pressure or has a cut or has chest pain, you don’t wait for things. You would go seek help immediately. I wish more patients reached out sooner and didn’t struggle.”
Another big challenge is making sure patients have insurance coverage for things like medications, surgery, and bariatric endoscopy, she added.
Her response: education and advocacy. “I’m giving as many talks as I can to fellows, creating courses for residents and fellows and medical students” to change the way physicians talk about obesity and excess weight, she said. Patients need to understand that physicians care about them, that “we’re not judging and we’re changing that perspective.”
Dr. Laster is also working with members of Congress to get bills passed for coverage of obesity medication and procedures. In an interview with GI & Hepatology News, she spoke more about the intersection between nutrition, medicine and bariatric procedures and the importance of offering patients multiple solutions.
Q: Why did you choose GI?
It allowed me a little bit of everything. You have clinic, where you can really interact with patients and get to the root of their problem. You have preventative care with routine colonoscopies and upper endoscopies to prevent for cancer. But then you also have fun stuff — which my mom told me to stop saying out loud — ‘bleeders’ and acute things that you get to fix immediately. So, you get the adrenaline rush too. I like it because you get the best of all worlds and it’s really hard to get bored.
Q: How did you become interested in nutrition and bariatric endoscopy?
My parents had a garden and never let us eat processed foods. In residency, I kept seeing the same medical problems over and over again. Everybody had high blood pressure, high cholesterol, and diabetes. Then in GI clinic, everybody had abdominal pain, bloating, constipation, heartburn, and a million GI appointments for these same things. Everyone’s upper endoscopy or colonoscopy was negative. Something else had to be going on.
And that’s sort of where it came from; figuring out the common denominator. It had to be what people were eating. There’s also the prevalence of patients with obesity going up every single year. Correlating all these other medical problems with people’s diets led me down the rabbit hole of: What else can we be doing?
Most people don’t want to undergo surgery. Only 2% of people eligible for surgery actually do it, even though it works. The reasons are because it’s invasive or there’s shame behind it. Bariatric endoscopy is another option that’s out here, that’s less invasive. I’m an endoscopist and gastroenterologist. I should be able to offer all those things and I should know more about nutrition. We don’t talk about it enough.
Q: Do you think more GI doctors should become better educated about nutrition?
100%. Every patient I see has seen a GI doctor before and says, ‘No one has ever told me that if I have carbonated beverages and cheese every day, I’m going to be bloated and constipated.’ And that shouldn’t be the case.
Q: Why do you think that more GI doctors don’t get the education on nutrition during their medical training?
I think it’s our healthcare system. It’s very much focused on secondary treatment rather than preventative care. There’s no emphasis on preventing things from happening.
We’re really good at reactionary medicine. People who have an ulcer, big polyps and colon cancer, esophageal cancer — we do those things really well. But I think because there’s no ICD-10 codes for preventive care via nutrition education, and no good reimbursement, then there’s no incentive for hospital systems to pay for these things. It’s a system based on RVUs (relative value units) and numbers. That’s been our trajectory. We’ve been so focused on reactionary medicine rather than saying, ‘Okay, let’s stop this from happening.’
We just didn’t talk about nutrition in medical school, in residency, or in fellowship. It was looked at as a soft science. When I was in school, people would also say, ‘No one’s going to change. So it’s a waste of your time essentially to talk to people about making dietary changes.’ I feel like if you give people the opportunity, you have to give them the chance. You can’t just write everybody off. Some people won’t change, but that’s okay. They should at least have the opportunity to do so.
Q: How do you determine whether a patient is a good candidate for bariatric surgery?
It’s based on the guidelines: If they meet the BMI requirements, if they have obesity-associated comorbidities, their risk for surgery is low. But it’s also whether they want to do it or not. A patient has to be in the mindset and be ready for it. They need to want to have surgery or bariatric endoscopy, or to use medications, or start to make a change. Some people aren’t there yet — that preemptive stage of making a change. They want the solution, but they’re not ready to do that legwork yet.
And all of it is work. I tell patients, ‘Whether it’s medication or bariatric endoscopy or bariatric surgery, you still have work to do. None of it is going to just magically happen where you could just continue to do the same thing you’re doing now and you’re going to lose weight and keep it off.’
Q: What advances in obesity prevention are you excited about?
I’m excited that bariatric endoscopy came about in the first place, because in every other field there are less invasive approaches that have become available. I’m also excited about the emergence of weight loss medication, like GLP-1s. I think they are a tool that we need.
Q: Do you think the weight loss medications may negate the need for surgery?
I don’t think they necessarily reduce the need for surgery. There’s still a lot we don’t know about why they work in some patients and why they don’t work in others.
Some of our colleagues have come up with phenotypes and blood tests so we can better understand which things will work in different patients. Surgery doesn’t work for some patients. People may need a combination of both after they reach a plateau. I’m excited that people see this as something that we should be researching and putting more effort into — that obesity isn’t a disease of moral failure, that people with excess weight just need to ‘move more’ or ‘eat less’ and it’s their fault. I’m glad people are starting to understand that.
Q: What teacher or mentor had the greatest impact on you?
Probably two. One of them is Andrea E Reid, MD, MPH, a dean of medicine at Harvard. She gives you such motivation to achieve things, no matter how big your idea is or how crazy it may seem. If you have something that you think is important, you go after it. Another person is Christopher C. Thompson, MD, at Brigham and Women’s Hospital, the father of bariatric endoscopy in a sense. He embodies what Dr. Reid talks about: crazy big ideas. And he goes after them and he succeeds. Having him push me and giving me that type of encouragement was invaluable.
Q: Describe how you would spend a free Saturday afternoon.
Every Saturday is yoga or some type of movement. Spending some time outside doing something, whether it’s messing around with plants that I’m not very good at, or going for a walk.
Lightning Round
Texting or talking?
Text
Favorite city in U.S. besides the one you live in?
New York
Favorite breakfast?
Avocado toast
Place you most want to travel to?
Istanbul
Favorite season?
Fall
Favorite ice cream flavor?
Raspberry sorbet
How many cups of coffee do you drink per day?
One
Best place you ever went on vacation?
Greece
If you weren’t a gastroenterologist, what would you be?
Own a clothing store
Favorite type of music?
Old school R&B
Favorite movie genre?
Romantic comedy or drama
Cat person or dog person?
Dog
Favorite sport?
Football
Favorite holiday?
Christmas
Optimist or pessimist?
Optimist
It takes a long time for some patients with obesity to acknowledge that they need help, said Dr. Laster, a bariatric endoscopist who specializes in gastroenterology, nutrition, and obesity medicine at Gut Theory Total Digestive Care, and Georgetown University Hospital in Washington. “If somebody has high blood pressure or has a cut or has chest pain, you don’t wait for things. You would go seek help immediately. I wish more patients reached out sooner and didn’t struggle.”
Another big challenge is making sure patients have insurance coverage for things like medications, surgery, and bariatric endoscopy, she added.
Her response: education and advocacy. “I’m giving as many talks as I can to fellows, creating courses for residents and fellows and medical students” to change the way physicians talk about obesity and excess weight, she said. Patients need to understand that physicians care about them, that “we’re not judging and we’re changing that perspective.”
Dr. Laster is also working with members of Congress to get bills passed for coverage of obesity medication and procedures. In an interview with GI & Hepatology News, she spoke more about the intersection between nutrition, medicine and bariatric procedures and the importance of offering patients multiple solutions.
Q: Why did you choose GI?
It allowed me a little bit of everything. You have clinic, where you can really interact with patients and get to the root of their problem. You have preventative care with routine colonoscopies and upper endoscopies to prevent for cancer. But then you also have fun stuff — which my mom told me to stop saying out loud — ‘bleeders’ and acute things that you get to fix immediately. So, you get the adrenaline rush too. I like it because you get the best of all worlds and it’s really hard to get bored.
Q: How did you become interested in nutrition and bariatric endoscopy?
My parents had a garden and never let us eat processed foods. In residency, I kept seeing the same medical problems over and over again. Everybody had high blood pressure, high cholesterol, and diabetes. Then in GI clinic, everybody had abdominal pain, bloating, constipation, heartburn, and a million GI appointments for these same things. Everyone’s upper endoscopy or colonoscopy was negative. Something else had to be going on.
And that’s sort of where it came from; figuring out the common denominator. It had to be what people were eating. There’s also the prevalence of patients with obesity going up every single year. Correlating all these other medical problems with people’s diets led me down the rabbit hole of: What else can we be doing?
Most people don’t want to undergo surgery. Only 2% of people eligible for surgery actually do it, even though it works. The reasons are because it’s invasive or there’s shame behind it. Bariatric endoscopy is another option that’s out here, that’s less invasive. I’m an endoscopist and gastroenterologist. I should be able to offer all those things and I should know more about nutrition. We don’t talk about it enough.
Q: Do you think more GI doctors should become better educated about nutrition?
100%. Every patient I see has seen a GI doctor before and says, ‘No one has ever told me that if I have carbonated beverages and cheese every day, I’m going to be bloated and constipated.’ And that shouldn’t be the case.
Q: Why do you think that more GI doctors don’t get the education on nutrition during their medical training?
I think it’s our healthcare system. It’s very much focused on secondary treatment rather than preventative care. There’s no emphasis on preventing things from happening.
We’re really good at reactionary medicine. People who have an ulcer, big polyps and colon cancer, esophageal cancer — we do those things really well. But I think because there’s no ICD-10 codes for preventive care via nutrition education, and no good reimbursement, then there’s no incentive for hospital systems to pay for these things. It’s a system based on RVUs (relative value units) and numbers. That’s been our trajectory. We’ve been so focused on reactionary medicine rather than saying, ‘Okay, let’s stop this from happening.’
We just didn’t talk about nutrition in medical school, in residency, or in fellowship. It was looked at as a soft science. When I was in school, people would also say, ‘No one’s going to change. So it’s a waste of your time essentially to talk to people about making dietary changes.’ I feel like if you give people the opportunity, you have to give them the chance. You can’t just write everybody off. Some people won’t change, but that’s okay. They should at least have the opportunity to do so.
Q: How do you determine whether a patient is a good candidate for bariatric surgery?
It’s based on the guidelines: If they meet the BMI requirements, if they have obesity-associated comorbidities, their risk for surgery is low. But it’s also whether they want to do it or not. A patient has to be in the mindset and be ready for it. They need to want to have surgery or bariatric endoscopy, or to use medications, or start to make a change. Some people aren’t there yet — that preemptive stage of making a change. They want the solution, but they’re not ready to do that legwork yet.
And all of it is work. I tell patients, ‘Whether it’s medication or bariatric endoscopy or bariatric surgery, you still have work to do. None of it is going to just magically happen where you could just continue to do the same thing you’re doing now and you’re going to lose weight and keep it off.’
Q: What advances in obesity prevention are you excited about?
I’m excited that bariatric endoscopy came about in the first place, because in every other field there are less invasive approaches that have become available. I’m also excited about the emergence of weight loss medication, like GLP-1s. I think they are a tool that we need.
Q: Do you think the weight loss medications may negate the need for surgery?
I don’t think they necessarily reduce the need for surgery. There’s still a lot we don’t know about why they work in some patients and why they don’t work in others.
Some of our colleagues have come up with phenotypes and blood tests so we can better understand which things will work in different patients. Surgery doesn’t work for some patients. People may need a combination of both after they reach a plateau. I’m excited that people see this as something that we should be researching and putting more effort into — that obesity isn’t a disease of moral failure, that people with excess weight just need to ‘move more’ or ‘eat less’ and it’s their fault. I’m glad people are starting to understand that.
Q: What teacher or mentor had the greatest impact on you?
Probably two. One of them is Andrea E Reid, MD, MPH, a dean of medicine at Harvard. She gives you such motivation to achieve things, no matter how big your idea is or how crazy it may seem. If you have something that you think is important, you go after it. Another person is Christopher C. Thompson, MD, at Brigham and Women’s Hospital, the father of bariatric endoscopy in a sense. He embodies what Dr. Reid talks about: crazy big ideas. And he goes after them and he succeeds. Having him push me and giving me that type of encouragement was invaluable.
Q: Describe how you would spend a free Saturday afternoon.
Every Saturday is yoga or some type of movement. Spending some time outside doing something, whether it’s messing around with plants that I’m not very good at, or going for a walk.
Lightning Round
Texting or talking?
Text
Favorite city in U.S. besides the one you live in?
New York
Favorite breakfast?
Avocado toast
Place you most want to travel to?
Istanbul
Favorite season?
Fall
Favorite ice cream flavor?
Raspberry sorbet
How many cups of coffee do you drink per day?
One
Best place you ever went on vacation?
Greece
If you weren’t a gastroenterologist, what would you be?
Own a clothing store
Favorite type of music?
Old school R&B
Favorite movie genre?
Romantic comedy or drama
Cat person or dog person?
Dog
Favorite sport?
Football
Favorite holiday?
Christmas
Optimist or pessimist?
Optimist
Rheumatologist Volunteers Make a Difference to Those in Need at Home and Overseas
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.

“There’s a language barrier no matter where you are,” Dr. Albert said.
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.

Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.

The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.
“There’s a language barrier no matter where you are,” Dr. Albert said.
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.
Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.
The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
As a resident, rheumatologist Daniel Albert, MD, did his first volunteer mission to Afghanistan. The clinic had one portable chest x-ray machine, and physicians could order a complete blood count but no other laboratory studies.
“We could do sputum stains, but that was about it. You had to use your clinical acumen and make decisions based on examining the patient and taking a history,” said Dr. Albert, a professor of medicine and pediatrics at the Geisel School of Medicine at Dartmouth, Hanover, and The Dartmouth Institute in Lebanon, both in New Hampshire. Such tasks can be difficult in a non–English-speaking country.
“There’s a language barrier no matter where you are,” Dr. Albert said.
In Nashville, Tennessee, James Gore, MD, had an epiphany about opening a free rheumatology clinic during a church service. His priest was discussing St. Sampson the Hospitable’s story and closed with “you don’t have to change the world. All you have to do is your little part,” Dr. Gore said. He knew he didn’t need much: a computer, a stethoscope, and a printer for prescriptions.
When his church expanded its building space, Dr. Gore took the opportunity to achieve his goal.
“I didn’t feel responsible for the clinic to succeed, but I did feel responsible to try my best,” he said. That was 14 years ago. To date, the monthly clinic has served 1124 patients representing 55 counties in Tennessee and several other patients from Kentucky.
Volunteer work is a juggling act. Dr. Gore divides his time between the clinic and his work as associate professor of clinical medicine at Vanderbilt University Medical Center (VUMC), also in Nashville.
Dr. Albert often gave up his vacation time and had to balance commitments with his own medical practice and family to do his overseas missions. In his view, it’s worth the extra time and effort.
“It makes you a better physician because you make reasonable decisions and conclusions based on the resources available. Various places had various limitations, but none of them had the kind of resources that we routinely avail ourselves of in the US,” he said.
Tennessee Clients Get Access to Care, Medications
In some parts of the United States, good rheumatology care is hard to come by. One in four people in Tennessee have no health insurance. There’s a big need for rheumatology care in the state, Dr. Gore said.
On the second Saturday of each month, he volunteers his services at the St. Sampson Medical Clinic at Holy Trinity Greek Orthodox Church, Nashville, Tennessee, from 9 AM to 4 PM, providing care for uninsured adult rheumatology patients.
Patients come by referral from a charity clinic or health department and appointment only. The clinic asks for a $10 payment for their visits. “If they can’t pay, we still see them. But we only take care of patients who don’t have insurance,” Dr. Gore said. Allowing patients to pay gives them an opportunity to show they are vested in their own care. Often, patients will donate extra in gratitude.
Dr. Gore, along with VUMC colleague and rheumatologist Narender Annapureddy, MD, and nurse practitioner Julie Barnes, treats a variety of rheumatic diseases. For Ms. Barnes, volunteering has many rewarding aspects, “as the patients would be unable to have the treatments they need without insurance,” she said.
“We have had patients waiting for many months or sometimes years and have not had a diagnosis, and in a short time, we have been able to diagnose and get them on specific treatment,” Dr. Annapureddy said.
Most people come in for rheumatoid arthritis (RA) and lupus and also positive antinuclear antibody tests. They also see patients with psoriatic arthritis, Sjögren’s disease, gout, scleroderma, Behçet disease, and leukocytoclastic vasculitis. On a typical clinic day, the team can treat up to 30-plus patients. The clinic recently expanded its services to include cardiology care, seeing about 10 patients each month.
Prior to St. Sampson, there were no volunteer clinics in Tennessee specifically dedicated to helping patients with rheumatologic disease. Untreated, these diseases may cause chronic, severe pain, lead to irreversible joint damage, and increase the risk for death.
Many patients have received medications such as adalimumab, etanercept, or tofacitinib for free. The drug companies will provide free medications, provided that they’re prescribed by a board-certified rheumatologist and the patient is uninsured and qualifies for the medication, Dr. Gore said.
Drugs like these can cost about $50,000 a year. “We have pharmacists that donate their time to help these patients get approved for those medicines,” Dr. Gore said. To date, more than 100 patients have received a biologic or targeted synthetic disease-modifying antirheumatic drug through the clinic.
The clinic has received more than $100,000 in donated professional fees, including $48,706 for consultations. Dr. Gore and colleagues relied on other volunteers to bring the clinic to life. He worked with his sister to develop an electronic medical record system that the clinic still uses today. “We did not buy expensive laptops or printers. I had a very generous volunteer, Damon Miltner, our IT guy, who set everything up to make our intranet secure,” he said.
The volunteer nurses, IT, and front desk all work together to make the clinic run efficiently, said Ms. Barnes, who also works as a nurse practitioner with Vanderbilt Rheumatology Cool Springs in Franklin, Tennessee. “We share a lunch together, all in a beautiful and holy church. I do not think of this as work, but as spending time with people who are appreciative and kind,” she said.
“It is amazing to see patients who are able to walk in by themselves after having used a cane for years,” Dr. Annapureddy said. “While doing this on weekends with young kids is challenging, having a supportive spouse who shares the same value makes it much easier to be able to do volunteer work.”
Working Outside Your Comfort Zone
Dr. Albert has traveled to all parts of the world to volunteer his services as a rheumatologist and general practitioner. This includes missions to Uganda, Rwanda, Ecuador, Peru, Nepal, and Borneo. He’s participated with several volunteer organizations, among them the International Student & Scholar Services program at the University of Pennsylvania, CARE, Global Volunteers, Project Amazonas, Asha Nepal, Health in Harmony, and several others.
Rheumatologists who volunteer in underdeveloped countries should be prepared to work outside of their specialty — and their comfort zone. In some instances, Dr. Albert took care of AIDS-related infectious diseases. “It’s not something I am particularly knowledgeable about, and I actually spent a fair amount of time reading about it before I went on the plane in order to get some comfort level.”
Dr. Albert often found himself doing more primary care and general pediatrics than rheumatology care. “I would see rheumatic conditions. But there’s not a lot of RA in developing countries, which is something that people have noted before. And the same goes for other autoimmune conditions. They’re just not that common.”
He did see a lot of septic arthritis and tuberculosis in Uganda. “We had a rheum clinic and saw a mixture of the consequences of septic arthritis and also a few RA and lupus patients.”
Limited resources are another thing to prepare for.
Whenever he traveled to a place that didn’t have a lot of resources, Dr. Albert would collect as many supplies as he could from the nearest hospital, pack them away, and try to get the supplies to the mission location.
Sometimes it worked out, and sometimes it didn’t, he said. “I probably had $10,000 worth of medical supplies when I went to Armenia, and American Airlines lost it. It ended up back in my apartment 3 months later. That was unfortunate because there was lot of good stuff there.”
He thought about FedEx-ing some supplies to a mission in Uganda, but it was astronomically expensive, so that didn’t work.
Luggage weight restrictions are another obstacle that sometimes requires a waiver. Dr. Albert once had to get the Red Cross to work with an airline to get a luggage waiver. “Other airlines were very good and didn’t have those kinds of restrictions. But most of the time I got some supplies to go with me, and sometimes that was a very helpful addition,” especially if the mission site was lacking in resources, he said.
When Charity Work Produces Success Stories
During one of his missions in Uganda with the University of Pennsylvania, Dr. Albert helped the Makerere University Medical School, Kampala, to establish a rheumatology clinic, which was affiliated with Mulago National Specialised Hospital. The clinic operated once a week for half a day, mostly treating patients with RA and lupus.
The mission also established an AIDS clinic. Many of the patients with musculoskeletal complaints also had HIV and were able to get antiretroviral drugs through the clinic, he said.
For Dr. Gore, seeing patients from more than half the counties in Tennessee was one of the clinic’s biggest accomplishments. “That was all through word of mouth,” he said.
In rheumatology, many patients may feel their condition is hopeless, Ms. Barnes noted. “There have been many patients that, through months of proper treatment, have normal lives. A high percentage would be disabled without the needed medical therapies.”
Dr. Gore has seen patients who literally couldn’t walk or had severe, painful psoriasis all over their body. The clinic would put them on medicine that would give them new life. The psoriasis would clear up, or their joints would heal, and they could walk again.
One of Dr. Gore’s patients, a woman in her mid-50s, got on an expensive medication that brought her arthritis into remission. She’s now able to care for her grandchildren.
The fact that the clinic, with the help of volunteer pharmacologists, can provide medications to enable patients to have a less destructive disease and improved quality of life “is a major reward,” Ms. Barnes said.
Balancing Your Priorities
Overseas missions can last for a few weeks to several months, depending on the mission, the organization, and the type of care involved.
Rheumatologists who want to volunteer need to do so in a way that doesn’t generate a lot of angst with supervisors or colleagues. Dr. Albert balanced this by keeping his missions reasonably short. “I would have someone cover my service. And since there’s reciprocity in the places I worked for, if they covered me for a month, I would cover them for a month, so it wasn’t a burden on anybody.”
“By and large, I used my vacation time to do it, and it does cost some money, but it’s a lot less than the cost of a typical vacation,” Dr. Albert said.
Volunteer work can also compete with family time. Dr. Albert ended up taking his family along on several of his missions to Ecuador and Uganda. He would tell the organization: “My family wants to come. Is there anything they can do while I’m working in the program? And they usually found an occupation.”
At St. Sampson, volunteering is also a family affair. “My wife acts as the administrator, so she’s the one that helps schedule patients and deals with a lot of the faxes.” It’s a big commitment for Dr. Gore’s family and for the church, which gives up a significant chunk of the building one Saturday a month.
“However, for us, I think that it’s a real manifestation of giving back and trying to help those in need and doing what we can do,” he said.
Volunteer Work Involves Prep Work
Establishing the St. Sampson clinic took some planning. Dr. Gore and colleagues had to fill out a 501(c)(3) application; establish a charter, bylaws, articles of incorporation, policies, and procedures; and obtain medical malpractice and general liability insurance.
The clinic was able to get financing from the Mid-South Chapter of the Lupus Foundation of America as well as in-kind donations from the church. “We’ve had a lot of different companies who were very generous in donating money and excited to help the clinic continue,” Dr. Gore said.
All volunteers sign a Health Insurance Portability and Accountability Act consent form.
Although the clinic operates for about 7 hours a month, it’s still important to have malpractice insurance, Dr. Gore said. He and his colleagues also have tail insurance that covers medical malpractice insurance for up to 7 years if the clinic closes.
“If somebody were to slip and fall and then try to sue the church, we have a separate policy for the clinic for that. We also have a director’s and officer’s insurance policy,” he said.
Anyone who volunteers abroad should get a travel medicine clinic consultation. “Most of the time, it’s of very little consequence. You might have to get [a] yellow fever vaccine” when traveling to certain parts of the world, Dr. Albert said.
“If you’re going into an area that is all volatile politically or in some way a threat to your personal security, I think you have to think very carefully about that,” he said, suggesting that doctors consult with the US Department of State about potential dangers.
Talk to other physicians who have gone on missions and your sponsoring institution. “By and large, you want to go with a large organization that’s been doing ongoing work,” Dr. Albert said.
Volunteer work teaches you about the breadth of humanist endeavors across the world, he noted. “The people that you deal with are very grateful for your help. Whether you’re successful or not, they’re still very appreciative of the efforts that you’re making to help.”
Dr. Albert and Dr. Gore had no disclosures. Dr. Annapureddy has done consulting for GlaxoSmithKline. Ms. Barnes had no disclosures.
A version of this article first appeared on Medscape.com.
Ustekinumab’s ‘Egregious’ Medicare Part B and D Pricing Differences Led to Federal Intervention
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.
A US government report showed how a Medicare policy change made the drug ustekinumab (Stelara) for autoimmune diseases much more expensive, a finding that experts say illustrates the need for reforms created by the Inflation Reduction Act of 2022 (IRA).
The topline findings of an August report from the Department of Health and Human Services (HHS) about ustekinumab may seem somewhat surprising and a bit counterintuitive.
Ustekinumab costs spiked as Medicare pushed patients to get their supply through the Part D pharmacy program. The aim of Part D is to make medicines more affordable and accessible for patients. It runs on a model of insurers to negotiate deals for pharmaceuticals.
Earlier, many patients who needed ustekinumab had the drug covered by Medicare Part B. For many years, Medicare Part B has been largely a passive purchaser of medicines. Part B covers drugs administered by physicians. Its longtime model has been to add a premium of 6% to the reported average sales price to reimburse physicians who buy and administer the drug for patients.
But it was Part D, the Medicare program based on insurers’ negotiating clout, that saw a spike in ustekinumab costs after patients were shifted out of Part B coverage, where the cost of the medicine fell.
The average reported Part B cost for an ustekinumab injection slipped from $14,450 in 2016 to $12,912 by 2023, according to the report from HHS’ Office of Inspector General (OIG).
The Part D cost jumped in the same period. It rose by 84% from $17,717 in 2016 to $32,559 by 2023.
The IRA is intended to curb these kinds of increases in the future for drugs covered by Medicare, said Stacie B. Dusetzina, PhD, professor of health policy at Vanderbilt University School of Medicine, Nashville, Tennessee. The law demands companies pay rebates to Medicare if they increase drug prices faster than consumer inflation.
“That should at least help with some of this price growth that over time has seemed quite egregious,” Dr. Dusetzina told this news organization.
The IRA contains several provisions intended to curb rising drug costs for people enrolled in Medicare, including allowing the federal government to directly negotiate on some medicines.
Ustekinumab is one of the first 10 medicines that are subject to negotiations. Medicare will select as many as 15 additional drugs covered under Part D for negotiation in 2025, another 15 Part B and D drugs in 2026, and up to 20 drugs every year after that.
Earlier in August, the Centers for Medicare & Medicaid Services (CMS) announced the results of its first drug negotiations, with prices set to take effect in 2026. The Part D price for a 30-day supply of ustekinumab will be $4695 in 2026, a 66% reduction from the list price last year of $13,836.
Even at the negotiated price, ustekinumab’s cost will be high enough to trigger a new cap on out-of-pocket Part D spending, Dr. Dusetzina said.
Starting in 2025, Part D will have a cap of $2000 on individuals’ out-of-pocket costs, with annual adjustments in future years.
“It may not be better for someone who was filling this on Part B, who had a supplement [that covered their share of the ustekinumab cost], but it will be better for a lot of people that it’s covered under Part D,” Dr. Dusetzina said. “The good news is that at least from a beneficiary affordability standpoint, they’re going to have some price protection.”
OIG noted that the US Food and Drug Administration has approved three competing biosimilar versions of ustekinumab. These could also potentially work to lower costs.
‘A Complicated and Not Particularly Transparent Process’
OIG said it expects to release a report later this year with more detail about the decision that shifted ustekinumab coverage from Part B to Part D.
First cleared for US sales in 2009, ustekinumab is approved for psoriasis, psoriatic arthritis, Crohn’s disease, and ulcerative colitis. It can be given subcutaneously or intravenously.
Part B does not generally cover self-administered drugs. The infused version of ustekinumab has been covered under Medicare Part B since it reached the market.
“However, Part B coverage of the subcutaneous versions has been less straightforward,” OIG said in the report.
In 2020, Medicare administrative contractors — the units or affiliates of insurers that for decades have processed Part B claims for the traditional Medicare programs — determined that subcutaneous ustekinumab did not meet the criteria for coverage under Part B. Implementation of this change was delayed due to the COVID public health emergency but has since taken effect.
The shift in ustekinumab coverage to Part D eroded financial protections of many people on Medicare when Part B covered the drug.
Almost 9 in 10 people enrolled in Medicare Part B have supplemental insurance such as Medigap, employer coverage, or Medicaid to fully or partially cover their cost-sharing requirements, the OIG report said. That means Part B coverage shielded many patients from high ustekinumab costs.
In contrast, patients who self-administered the drug at home under Part D coverage paid an average of almost $6000 out of pocket if they did not receive any type of financial assistance, OIG said.
“From a financial standpoint, as long as you have Part B coinsurance, it would be much cheaper to get the drug in your doctor’s office than getting it through a pharmacy, unless you qualify for the low-income subsidy,” OIG Regional Inspector General David Tawes, who supervised the team that produced the report, told this news organization.
OIG has previously reported that post–point-of-sale rebates paid by manufacturers sometimes lower the costs incurred by Part D plans by a significant margin. But this was not the case with ustekinumab. Instead, OIG said the gap between initial and actual costs of ustekinumab was reduced by less than one third even with rebates. Rebate information is considered confidential.
“The whole negotiation structure is a complicated and not particularly transparent process,” Mr. Tawes said.
Backchannel Discounts, Top-Line Prices
The IRA is bringing some more transparency to the process through negotiations, said Mariana P. Socal, MD, associate professor at the Johns Hopkins Bloomberg School of Public Health in Baltimore. Patients who buy medicines that have been through the CMS negotiation process will be able to see if they are being charged correctly.
Dr. Socal noted that there’s something of a disconnect in discussions of Part D between how insurers and consumers view prices.
For Part D plans, the list prices represent the beginning of negotiations. They get rebates from drugmakers’ list prices for medicines, which insurers say work to lower premium costs.
“For plans, those prices are unrealistic. They are simply a sticker price. But for patients, for the Medicare beneficiaries, these prices are very real” because they are used to set copays, Dr. Socal said.
Dr. Dusetzina reported receiving funding from Arnold Ventures and the Commonwealth Fund for research related to drug pricing. Dr. Socal reported receiving funding from Arnold Ventures.
A version of this article first appeared on Medscape.com.