User login
Children with Down syndrome and ALL have good outcomes today
PITTSBURGH – In the current era, children with Down syndrome who have standard risk B-cell precursor acute lymphoblastic leukemia have event-free and overall survival rates nearly as good as those of other children with standard-risk B–ALL, results of a Children’s Oncology Group study show.
Among 5,311 children enrolled in the COG AALL0331 trial, a study of combination chemotherapy for young patients with newly diagnosed ALL, the 5-year event-free survival (EFS) rate for children with Down syndrome was 86%, compared with 89% for children without Down syndrome (P = .025).

Although the differences in EFS and OS were significant, ”overall in this study, Down syndrome ALL had an excellent outcome that was similar to those patients without Down syndrome,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
The trial confirmed her group’s previous finding that there is a low rate of favorable cytogenetic features in patients with Down syndrome ALL; nonetheless, in the current study, 5-year continuous complete remission rates for standard-risk average, low, and high in patients with Down syndrome were similar to those for patients without Down syndrome, she said.
In the trial, patients were treated with a three-drug induction regimen, and following induction were assigned to standard-risk low, average, or high groups based on leukemia genetics and initial response to therapy.
Of the 5,311 children enrolled, 141 (2.7%) had Down syndrome, and these patients received risk-stratified therapy with additional supportive care guidelines, including leucovorin rescue after intrathecal methotrexate until maintenance. The care team strongly encouraged hospitalizations during high-risk blocks for this subgroup of patients until they experienced neutrophil recovery.
At the end of induction, patients who were judged to be standard-risk average were then randomized in a 2x2 design to either standard or intensified consolidation, and to standard interim maintenance with delayed intensification, or to intensified interim maintenance with delayed intensification.
The intensified interim maintenance with delayed intensification randomization was closed in 2008 because of superior results with escalating intravenous methotrexate during interim maintenance for standard-risk ALL patients treated in the CCG 1991 trial. Subsequently, all patients enrolled in AALL0331 received escalating intravenous methotrexate during interim maintenance.
Also in AALL0331, patients with Down syndrome who had standard-high ALL were given intensified consolidation and a single vs. double intensified interim maintenance with delayed intensification; patients without Down syndrome and standard risk high received the double intensified interim maintenance regimen.
Standard-risk low Down syndrome patients and non–Down syndrome patients participated in a randomization to additional pegaspargase doses during consolidation and interim maintenance.
There were no significant differences between patients with or without Down syndrome in the proportion of either rapid or slow early responses. Significantly fewer patients with Down syndrome had standard-risk low disease, and significantly more had average or high-risk disease.
Patients with Down syndrome initially had 11.5% excess risk for death during induction, but following additional treatment modifications, the excess risk decreased to 1.7%.
Among patients with Down syndrome, one died during intensive consolidation, and two died during delayed intensification. All three deaths were due to infections. No patients with Down syndrome died during maintenance.
Patients with Down syndrome also had a significantly increased risk for infection during induction (P less than .0001).
For patients with standard-risk low disease, 5-year EFS was 100% for those with Down syndrome, compared with 95.35% for patients without. Respective rates for standard risk average and high disease were 88.07% vs. 89.63%. and 82.35% vs. 86.18%.
Down syndrome was not an independent risk factor for survival in multivariate analyses accounting for risk group, Dr. Maloney said.
COG AALL0331 was supported by the National Cancer Institute. Dr. Maloney reported having no financial disclosures.
SOURCE: Maloney K et al. ASPHO 2018, Abstract PP 2001.
PITTSBURGH – In the current era, children with Down syndrome who have standard risk B-cell precursor acute lymphoblastic leukemia have event-free and overall survival rates nearly as good as those of other children with standard-risk B–ALL, results of a Children’s Oncology Group study show.
Among 5,311 children enrolled in the COG AALL0331 trial, a study of combination chemotherapy for young patients with newly diagnosed ALL, the 5-year event-free survival (EFS) rate for children with Down syndrome was 86%, compared with 89% for children without Down syndrome (P = .025).
Although the differences in EFS and OS were significant, ”overall in this study, Down syndrome ALL had an excellent outcome that was similar to those patients without Down syndrome,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
The trial confirmed her group’s previous finding that there is a low rate of favorable cytogenetic features in patients with Down syndrome ALL; nonetheless, in the current study, 5-year continuous complete remission rates for standard-risk average, low, and high in patients with Down syndrome were similar to those for patients without Down syndrome, she said.
In the trial, patients were treated with a three-drug induction regimen, and following induction were assigned to standard-risk low, average, or high groups based on leukemia genetics and initial response to therapy.
Of the 5,311 children enrolled, 141 (2.7%) had Down syndrome, and these patients received risk-stratified therapy with additional supportive care guidelines, including leucovorin rescue after intrathecal methotrexate until maintenance. The care team strongly encouraged hospitalizations during high-risk blocks for this subgroup of patients until they experienced neutrophil recovery.
At the end of induction, patients who were judged to be standard-risk average were then randomized in a 2x2 design to either standard or intensified consolidation, and to standard interim maintenance with delayed intensification, or to intensified interim maintenance with delayed intensification.
The intensified interim maintenance with delayed intensification randomization was closed in 2008 because of superior results with escalating intravenous methotrexate during interim maintenance for standard-risk ALL patients treated in the CCG 1991 trial. Subsequently, all patients enrolled in AALL0331 received escalating intravenous methotrexate during interim maintenance.
Also in AALL0331, patients with Down syndrome who had standard-high ALL were given intensified consolidation and a single vs. double intensified interim maintenance with delayed intensification; patients without Down syndrome and standard risk high received the double intensified interim maintenance regimen.
Standard-risk low Down syndrome patients and non–Down syndrome patients participated in a randomization to additional pegaspargase doses during consolidation and interim maintenance.
There were no significant differences between patients with or without Down syndrome in the proportion of either rapid or slow early responses. Significantly fewer patients with Down syndrome had standard-risk low disease, and significantly more had average or high-risk disease.
Patients with Down syndrome initially had 11.5% excess risk for death during induction, but following additional treatment modifications, the excess risk decreased to 1.7%.
Among patients with Down syndrome, one died during intensive consolidation, and two died during delayed intensification. All three deaths were due to infections. No patients with Down syndrome died during maintenance.
Patients with Down syndrome also had a significantly increased risk for infection during induction (P less than .0001).
For patients with standard-risk low disease, 5-year EFS was 100% for those with Down syndrome, compared with 95.35% for patients without. Respective rates for standard risk average and high disease were 88.07% vs. 89.63%. and 82.35% vs. 86.18%.
Down syndrome was not an independent risk factor for survival in multivariate analyses accounting for risk group, Dr. Maloney said.
COG AALL0331 was supported by the National Cancer Institute. Dr. Maloney reported having no financial disclosures.
SOURCE: Maloney K et al. ASPHO 2018, Abstract PP 2001.
PITTSBURGH – In the current era, children with Down syndrome who have standard risk B-cell precursor acute lymphoblastic leukemia have event-free and overall survival rates nearly as good as those of other children with standard-risk B–ALL, results of a Children’s Oncology Group study show.
Among 5,311 children enrolled in the COG AALL0331 trial, a study of combination chemotherapy for young patients with newly diagnosed ALL, the 5-year event-free survival (EFS) rate for children with Down syndrome was 86%, compared with 89% for children without Down syndrome (P = .025).
Although the differences in EFS and OS were significant, ”overall in this study, Down syndrome ALL had an excellent outcome that was similar to those patients without Down syndrome,” she said at the annual meeting of the American Society of Pediatric Hematology/Oncology.
The trial confirmed her group’s previous finding that there is a low rate of favorable cytogenetic features in patients with Down syndrome ALL; nonetheless, in the current study, 5-year continuous complete remission rates for standard-risk average, low, and high in patients with Down syndrome were similar to those for patients without Down syndrome, she said.
In the trial, patients were treated with a three-drug induction regimen, and following induction were assigned to standard-risk low, average, or high groups based on leukemia genetics and initial response to therapy.
Of the 5,311 children enrolled, 141 (2.7%) had Down syndrome, and these patients received risk-stratified therapy with additional supportive care guidelines, including leucovorin rescue after intrathecal methotrexate until maintenance. The care team strongly encouraged hospitalizations during high-risk blocks for this subgroup of patients until they experienced neutrophil recovery.
At the end of induction, patients who were judged to be standard-risk average were then randomized in a 2x2 design to either standard or intensified consolidation, and to standard interim maintenance with delayed intensification, or to intensified interim maintenance with delayed intensification.
The intensified interim maintenance with delayed intensification randomization was closed in 2008 because of superior results with escalating intravenous methotrexate during interim maintenance for standard-risk ALL patients treated in the CCG 1991 trial. Subsequently, all patients enrolled in AALL0331 received escalating intravenous methotrexate during interim maintenance.
Also in AALL0331, patients with Down syndrome who had standard-high ALL were given intensified consolidation and a single vs. double intensified interim maintenance with delayed intensification; patients without Down syndrome and standard risk high received the double intensified interim maintenance regimen.
Standard-risk low Down syndrome patients and non–Down syndrome patients participated in a randomization to additional pegaspargase doses during consolidation and interim maintenance.
There were no significant differences between patients with or without Down syndrome in the proportion of either rapid or slow early responses. Significantly fewer patients with Down syndrome had standard-risk low disease, and significantly more had average or high-risk disease.
Patients with Down syndrome initially had 11.5% excess risk for death during induction, but following additional treatment modifications, the excess risk decreased to 1.7%.
Among patients with Down syndrome, one died during intensive consolidation, and two died during delayed intensification. All three deaths were due to infections. No patients with Down syndrome died during maintenance.
Patients with Down syndrome also had a significantly increased risk for infection during induction (P less than .0001).
For patients with standard-risk low disease, 5-year EFS was 100% for those with Down syndrome, compared with 95.35% for patients without. Respective rates for standard risk average and high disease were 88.07% vs. 89.63%. and 82.35% vs. 86.18%.
Down syndrome was not an independent risk factor for survival in multivariate analyses accounting for risk group, Dr. Maloney said.
COG AALL0331 was supported by the National Cancer Institute. Dr. Maloney reported having no financial disclosures.
SOURCE: Maloney K et al. ASPHO 2018, Abstract PP 2001.
REPORTING FROM ASPHO 2018
Key clinical point:
Major finding: The 5-year event-free survival rate for children with Down syndrome was 86% vs. 89% for children without Down syndrome (P = .025).
Study details: Follow-up of 5,311 children with newly diagnosed ALL in the COG AALL0331 trial.
Disclosures: COG AALL0331 was supported by the National Cancer Institute. Dr. Maloney reported having no financial disclosures.
Source: Maloney K et al. ASPHO 2018, Abstract PP 2001.
How Does TBI Differ Among Older Patients?
LOS ANGELES—Most older adults recover well from traumatic brain injury (TBI), according to research presented at the 70th Annual Meeting of the American Academy of Neurology. Compared with younger patients, older adults endorse less independence after injury, but are less likely to report TBI-related neurobehavioral symptoms. A greater burden of preinjury disability among the elderly may explain these apparently conflicting results, according to the researchers.
Geriatric TBI is “a silent and growing epidemic,” said Raquel Gardner, MD, Assistant Professor of Neurology at the University of California, San Francisco. Older adults have the highest incidence of TBI-related emergency department visits, hospitalizations, and deaths, according to 2013 data from the CDC. Most research has indicated that this population has worse outcomes of TBI than younger populations do. Few studies, however, have examined age-related differences in neurobehavioral outcomes of TBI.
Injury Was More Severe Among Older Patients
To address this gap in the literature, Dr. Gardner and colleagues examined data from the TRACK-TBI pilot study. Eligible patients presented to participating trauma centers within 24 hours of sustaining a TBI that was severe enough to warrant head CT. The TRACK-TBI study excluded participants with a diagnosis of dementia or any pre-existing condition that would impair their ability to complete outcome assessments. Patients’ neurobehavioral outcomes were evaluated prospectively with measures such as the Glasgow Outcome Scale Extended (GOSE), Craig Handicap Assessment and Reporting Technique-Short Form (CHART-SF), Brief Symptom Inventory (BSI-18), Rivermead Post-Concussion Questionnaire (RPQ), Posttraumatic Stress Disorder Checklist-Civilian (PCL-C), and the Satisfaction With Life Scale (SWLS).

Dr. Gardner and colleagues categorized 586 patients as young (ie, younger than 40), middle-aged (ie, ages 40 to 59), or older (ie, age 60 or older). They compared baseline features and six-month neurobehavioral outcomes between the three groups using χ2, analysis of variance, and regression modeling.
Patients’ age ranged from 16 to 94. At baseline, the prevalence of female sex and white race increased with increasing age. Older adults were less likely to report a prior history of TBI than the other two age groups. TBI resulted from a fall for most older patients. At presentation, Glasgow Coma Scale scores did not differ significantly between the three patient groups, and older adults were less likely to report having experienced loss of consciousness or posttraumatic amnesia than the other groups.
Injury was more severe among older patients, however, as assessed by the Acute Injury Scale, the Injury Severity Scale, and CT pathology, compared with younger participants. Older patients also were more likely to be admitted to the intensive care unit.
Measures May Not Be Age-Appropriate
At six months, 415 of the participants completed the GOSE. The mortality rate was approximately 18% among older patients, compared with 7% among middle-aged patients and less than 1% among young patients. Among older patients who survived to six months, most achieved a good recovery, which was defined as a GOSE score of 7 to 8. After the researchers adjusted the data for baseline demographic differences, the rate of good recovery was not significantly different between the three age groups.
Older patients reported significantly less anxiety than other patients, as measured by the BSI-18. Older patients tended to report fewer symptoms overall on the BSI-18 and the RPQ, compared with the other groups. In addition, older patients reported fewer symptoms of PTSD and less dissatisfaction with life, compared with the other groups.
CHART-SF scores, however, were worse overall among older patients, said Dr. Gardner. Although they indicated better economic outcomes among older patients, compared with the other age groups, they also indicated less independence among older patients. Cognition and mobility in particular were worse among older patients than among the other groups.
Older patients were more likely to complete the GOSE than younger patients, but less likely to complete other assessments. The differences in response rates could create a misleadingly positive impression of six-month outcomes among older patients, said Dr. Gardner.
One interpretation of the results is that measures that are not age-appropriate are causing older patients to underreport TBI symptoms, she added. Survival bias also may partly explain the positive six-month outcomes. “We need studies that are truly representative of the entire geriatric TBI population and systematically measure, rather than exclude for, this huge heterogeneity in preinjury disability,” said Dr. Gardner. Investigators should take steps “to optimize enrollment, optimize retention, and optimize outcome completion in a frail and burdened population. We need to ultimately develop consensus NINDS geriatric TBI common data elements…. Only then can we unravel predictors of meaningful recovery in this vulnerable population, develop age-appropriate treatment guidelines, and improve outcomes.”
—Erik Greb
Suggested Reading
Yue JK, Winkler EA, Sharma S, et al. Temporal profile of care following mild traumatic brain injury: predictors of hospital admission, follow-up referral and six-month outcome. Brain Inj. 2017;31(13-14):1820-1829.
LOS ANGELES—Most older adults recover well from traumatic brain injury (TBI), according to research presented at the 70th Annual Meeting of the American Academy of Neurology. Compared with younger patients, older adults endorse less independence after injury, but are less likely to report TBI-related neurobehavioral symptoms. A greater burden of preinjury disability among the elderly may explain these apparently conflicting results, according to the researchers.
Geriatric TBI is “a silent and growing epidemic,” said Raquel Gardner, MD, Assistant Professor of Neurology at the University of California, San Francisco. Older adults have the highest incidence of TBI-related emergency department visits, hospitalizations, and deaths, according to 2013 data from the CDC. Most research has indicated that this population has worse outcomes of TBI than younger populations do. Few studies, however, have examined age-related differences in neurobehavioral outcomes of TBI.
Injury Was More Severe Among Older Patients
To address this gap in the literature, Dr. Gardner and colleagues examined data from the TRACK-TBI pilot study. Eligible patients presented to participating trauma centers within 24 hours of sustaining a TBI that was severe enough to warrant head CT. The TRACK-TBI study excluded participants with a diagnosis of dementia or any pre-existing condition that would impair their ability to complete outcome assessments. Patients’ neurobehavioral outcomes were evaluated prospectively with measures such as the Glasgow Outcome Scale Extended (GOSE), Craig Handicap Assessment and Reporting Technique-Short Form (CHART-SF), Brief Symptom Inventory (BSI-18), Rivermead Post-Concussion Questionnaire (RPQ), Posttraumatic Stress Disorder Checklist-Civilian (PCL-C), and the Satisfaction With Life Scale (SWLS).
Dr. Gardner and colleagues categorized 586 patients as young (ie, younger than 40), middle-aged (ie, ages 40 to 59), or older (ie, age 60 or older). They compared baseline features and six-month neurobehavioral outcomes between the three groups using χ2, analysis of variance, and regression modeling.
Patients’ age ranged from 16 to 94. At baseline, the prevalence of female sex and white race increased with increasing age. Older adults were less likely to report a prior history of TBI than the other two age groups. TBI resulted from a fall for most older patients. At presentation, Glasgow Coma Scale scores did not differ significantly between the three patient groups, and older adults were less likely to report having experienced loss of consciousness or posttraumatic amnesia than the other groups.
Injury was more severe among older patients, however, as assessed by the Acute Injury Scale, the Injury Severity Scale, and CT pathology, compared with younger participants. Older patients also were more likely to be admitted to the intensive care unit.
Measures May Not Be Age-Appropriate
At six months, 415 of the participants completed the GOSE. The mortality rate was approximately 18% among older patients, compared with 7% among middle-aged patients and less than 1% among young patients. Among older patients who survived to six months, most achieved a good recovery, which was defined as a GOSE score of 7 to 8. After the researchers adjusted the data for baseline demographic differences, the rate of good recovery was not significantly different between the three age groups.
Older patients reported significantly less anxiety than other patients, as measured by the BSI-18. Older patients tended to report fewer symptoms overall on the BSI-18 and the RPQ, compared with the other groups. In addition, older patients reported fewer symptoms of PTSD and less dissatisfaction with life, compared with the other groups.
CHART-SF scores, however, were worse overall among older patients, said Dr. Gardner. Although they indicated better economic outcomes among older patients, compared with the other age groups, they also indicated less independence among older patients. Cognition and mobility in particular were worse among older patients than among the other groups.
Older patients were more likely to complete the GOSE than younger patients, but less likely to complete other assessments. The differences in response rates could create a misleadingly positive impression of six-month outcomes among older patients, said Dr. Gardner.
One interpretation of the results is that measures that are not age-appropriate are causing older patients to underreport TBI symptoms, she added. Survival bias also may partly explain the positive six-month outcomes. “We need studies that are truly representative of the entire geriatric TBI population and systematically measure, rather than exclude for, this huge heterogeneity in preinjury disability,” said Dr. Gardner. Investigators should take steps “to optimize enrollment, optimize retention, and optimize outcome completion in a frail and burdened population. We need to ultimately develop consensus NINDS geriatric TBI common data elements…. Only then can we unravel predictors of meaningful recovery in this vulnerable population, develop age-appropriate treatment guidelines, and improve outcomes.”
—Erik Greb
Suggested Reading
Yue JK, Winkler EA, Sharma S, et al. Temporal profile of care following mild traumatic brain injury: predictors of hospital admission, follow-up referral and six-month outcome. Brain Inj. 2017;31(13-14):1820-1829.
LOS ANGELES—Most older adults recover well from traumatic brain injury (TBI), according to research presented at the 70th Annual Meeting of the American Academy of Neurology. Compared with younger patients, older adults endorse less independence after injury, but are less likely to report TBI-related neurobehavioral symptoms. A greater burden of preinjury disability among the elderly may explain these apparently conflicting results, according to the researchers.
Geriatric TBI is “a silent and growing epidemic,” said Raquel Gardner, MD, Assistant Professor of Neurology at the University of California, San Francisco. Older adults have the highest incidence of TBI-related emergency department visits, hospitalizations, and deaths, according to 2013 data from the CDC. Most research has indicated that this population has worse outcomes of TBI than younger populations do. Few studies, however, have examined age-related differences in neurobehavioral outcomes of TBI.
Injury Was More Severe Among Older Patients
To address this gap in the literature, Dr. Gardner and colleagues examined data from the TRACK-TBI pilot study. Eligible patients presented to participating trauma centers within 24 hours of sustaining a TBI that was severe enough to warrant head CT. The TRACK-TBI study excluded participants with a diagnosis of dementia or any pre-existing condition that would impair their ability to complete outcome assessments. Patients’ neurobehavioral outcomes were evaluated prospectively with measures such as the Glasgow Outcome Scale Extended (GOSE), Craig Handicap Assessment and Reporting Technique-Short Form (CHART-SF), Brief Symptom Inventory (BSI-18), Rivermead Post-Concussion Questionnaire (RPQ), Posttraumatic Stress Disorder Checklist-Civilian (PCL-C), and the Satisfaction With Life Scale (SWLS).
Dr. Gardner and colleagues categorized 586 patients as young (ie, younger than 40), middle-aged (ie, ages 40 to 59), or older (ie, age 60 or older). They compared baseline features and six-month neurobehavioral outcomes between the three groups using χ2, analysis of variance, and regression modeling.
Patients’ age ranged from 16 to 94. At baseline, the prevalence of female sex and white race increased with increasing age. Older adults were less likely to report a prior history of TBI than the other two age groups. TBI resulted from a fall for most older patients. At presentation, Glasgow Coma Scale scores did not differ significantly between the three patient groups, and older adults were less likely to report having experienced loss of consciousness or posttraumatic amnesia than the other groups.
Injury was more severe among older patients, however, as assessed by the Acute Injury Scale, the Injury Severity Scale, and CT pathology, compared with younger participants. Older patients also were more likely to be admitted to the intensive care unit.
Measures May Not Be Age-Appropriate
At six months, 415 of the participants completed the GOSE. The mortality rate was approximately 18% among older patients, compared with 7% among middle-aged patients and less than 1% among young patients. Among older patients who survived to six months, most achieved a good recovery, which was defined as a GOSE score of 7 to 8. After the researchers adjusted the data for baseline demographic differences, the rate of good recovery was not significantly different between the three age groups.
Older patients reported significantly less anxiety than other patients, as measured by the BSI-18. Older patients tended to report fewer symptoms overall on the BSI-18 and the RPQ, compared with the other groups. In addition, older patients reported fewer symptoms of PTSD and less dissatisfaction with life, compared with the other groups.
CHART-SF scores, however, were worse overall among older patients, said Dr. Gardner. Although they indicated better economic outcomes among older patients, compared with the other age groups, they also indicated less independence among older patients. Cognition and mobility in particular were worse among older patients than among the other groups.
Older patients were more likely to complete the GOSE than younger patients, but less likely to complete other assessments. The differences in response rates could create a misleadingly positive impression of six-month outcomes among older patients, said Dr. Gardner.
One interpretation of the results is that measures that are not age-appropriate are causing older patients to underreport TBI symptoms, she added. Survival bias also may partly explain the positive six-month outcomes. “We need studies that are truly representative of the entire geriatric TBI population and systematically measure, rather than exclude for, this huge heterogeneity in preinjury disability,” said Dr. Gardner. Investigators should take steps “to optimize enrollment, optimize retention, and optimize outcome completion in a frail and burdened population. We need to ultimately develop consensus NINDS geriatric TBI common data elements…. Only then can we unravel predictors of meaningful recovery in this vulnerable population, develop age-appropriate treatment guidelines, and improve outcomes.”
—Erik Greb
Suggested Reading
Yue JK, Winkler EA, Sharma S, et al. Temporal profile of care following mild traumatic brain injury: predictors of hospital admission, follow-up referral and six-month outcome. Brain Inj. 2017;31(13-14):1820-1829.
New Medicare cards
By now, you are probably aware that . The new, completely random number-letter combinations – dubbed Medicare Beneficiary Identifiers (MBI) – replace the old Social Security number–based Health Insurance Claim Numbers (HICN). The idea is to make citizens’ private information less vulnerable to identity thieves and other nefarious parties.
The switch began on April 1, and is expected to take about a year as the CMS processes about half a dozen states at a time. As I write this (at the beginning of May), the CMS is mailing out the first group of new cards to patients in Pennsylvania, Virginia, West Virginia, Maryland, Delaware, and the District of Columbia. But regardless of where you practice, you can expect to start seeing MBIs in your office soon – if you haven’t already – because people enrolling in Medicare for the first time are also receiving the new cards, no matter where they live.
Unlike the abrupt switch in 2015 from ICD-9 coding to ICD-10, this changeover has a transition period: Both HICNs and MBIs can be used on all billing and Medicare transactions from now until the end of 2019; after that, only claims with MBIs will be accepted. The last day of 2019 may sound like a long way off, but the time to get up to speed on everything MBI is now. That way, you can begin processing MBIs as soon as you start receiving them, and you will have time to solve any processing glitches well before the deadline.
First, you’ll need to make sure that your electronic health records and claims processing software will accept the new format, and that your electronic clearinghouse, if you use one, is geared up to accept and transmit the data on the new cards. Not all of them are. Some have been seduced by the year-and-a-half buffer – during which time HICNs can still be used – into dragging their feet on the MBI issue. Now is the time to find out if a vendor’s software is hard-wired to accept a maximum of 10 digits (MBIs have 11), not when your claims start bouncing.
Second, you will need to educate your front desk staff, so they will be able to recognize the new cards at a glance. Unfortunately, it looks a lot like the current card, though it is slightly smaller. It has the traditional red and blue colors with black printing, but there is no birthday or gender designation – again, in the interest of protecting patients’ identities. Knowing the difference will become particularly important after your state has been processed, when all of your Medicare patients should have the new card. Those who don’t will need to be identified and urged to get one before the December 2019 deadline.
Finally, once your staff and vendors are up to speed, you can begin educating your patients. Inevitably, some will not receive a new card, especially if they have moved and have not notified the CMS of the change; and some who are not expecting a new card will believe it is a duplicate, and throw it away. The CMS will be airing public service announcements and mailing education pieces to Medicare recipients, but a substantial portion of the education burden will fall on doctors and hospitals.
Have your front office staff remind patients to be sure their addresses are updated online with Medicare (www.Medicare.gov) or the Social Security Administration (www.ssa.gov). Encourage them to take advantage of the free resources available at www.cms.gov. These include both downloadable options and printed materials that illustrate what the new card will look like, explain how to update a mailing address with the Social Security Administration, and remind seniors to keep an eye out for their cards in the mail.
For the many Medicare-age patients who are not particularly computer savvy, the CMS has free resources for physicians as well. You will need to open an account at the agency’s Product Ordering website (productordering.cms.hhs.gov), which in turn needs to be approved by an administrator. The posters and other free literature can be displayed in your waiting room, exam rooms, and other “patient flow” areas. There is also a 1-minute video, downloadable from YouTube (https://youtu.be/DusRmgzQnLY), which can be looped in your waiting area.

Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
By now, you are probably aware that . The new, completely random number-letter combinations – dubbed Medicare Beneficiary Identifiers (MBI) – replace the old Social Security number–based Health Insurance Claim Numbers (HICN). The idea is to make citizens’ private information less vulnerable to identity thieves and other nefarious parties.
The switch began on April 1, and is expected to take about a year as the CMS processes about half a dozen states at a time. As I write this (at the beginning of May), the CMS is mailing out the first group of new cards to patients in Pennsylvania, Virginia, West Virginia, Maryland, Delaware, and the District of Columbia. But regardless of where you practice, you can expect to start seeing MBIs in your office soon – if you haven’t already – because people enrolling in Medicare for the first time are also receiving the new cards, no matter where they live.
Unlike the abrupt switch in 2015 from ICD-9 coding to ICD-10, this changeover has a transition period: Both HICNs and MBIs can be used on all billing and Medicare transactions from now until the end of 2019; after that, only claims with MBIs will be accepted. The last day of 2019 may sound like a long way off, but the time to get up to speed on everything MBI is now. That way, you can begin processing MBIs as soon as you start receiving them, and you will have time to solve any processing glitches well before the deadline.
First, you’ll need to make sure that your electronic health records and claims processing software will accept the new format, and that your electronic clearinghouse, if you use one, is geared up to accept and transmit the data on the new cards. Not all of them are. Some have been seduced by the year-and-a-half buffer – during which time HICNs can still be used – into dragging their feet on the MBI issue. Now is the time to find out if a vendor’s software is hard-wired to accept a maximum of 10 digits (MBIs have 11), not when your claims start bouncing.
Second, you will need to educate your front desk staff, so they will be able to recognize the new cards at a glance. Unfortunately, it looks a lot like the current card, though it is slightly smaller. It has the traditional red and blue colors with black printing, but there is no birthday or gender designation – again, in the interest of protecting patients’ identities. Knowing the difference will become particularly important after your state has been processed, when all of your Medicare patients should have the new card. Those who don’t will need to be identified and urged to get one before the December 2019 deadline.
Finally, once your staff and vendors are up to speed, you can begin educating your patients. Inevitably, some will not receive a new card, especially if they have moved and have not notified the CMS of the change; and some who are not expecting a new card will believe it is a duplicate, and throw it away. The CMS will be airing public service announcements and mailing education pieces to Medicare recipients, but a substantial portion of the education burden will fall on doctors and hospitals.
Have your front office staff remind patients to be sure their addresses are updated online with Medicare (www.Medicare.gov) or the Social Security Administration (www.ssa.gov). Encourage them to take advantage of the free resources available at www.cms.gov. These include both downloadable options and printed materials that illustrate what the new card will look like, explain how to update a mailing address with the Social Security Administration, and remind seniors to keep an eye out for their cards in the mail.
For the many Medicare-age patients who are not particularly computer savvy, the CMS has free resources for physicians as well. You will need to open an account at the agency’s Product Ordering website (productordering.cms.hhs.gov), which in turn needs to be approved by an administrator. The posters and other free literature can be displayed in your waiting room, exam rooms, and other “patient flow” areas. There is also a 1-minute video, downloadable from YouTube (https://youtu.be/DusRmgzQnLY), which can be looped in your waiting area.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
By now, you are probably aware that . The new, completely random number-letter combinations – dubbed Medicare Beneficiary Identifiers (MBI) – replace the old Social Security number–based Health Insurance Claim Numbers (HICN). The idea is to make citizens’ private information less vulnerable to identity thieves and other nefarious parties.
The switch began on April 1, and is expected to take about a year as the CMS processes about half a dozen states at a time. As I write this (at the beginning of May), the CMS is mailing out the first group of new cards to patients in Pennsylvania, Virginia, West Virginia, Maryland, Delaware, and the District of Columbia. But regardless of where you practice, you can expect to start seeing MBIs in your office soon – if you haven’t already – because people enrolling in Medicare for the first time are also receiving the new cards, no matter where they live.
Unlike the abrupt switch in 2015 from ICD-9 coding to ICD-10, this changeover has a transition period: Both HICNs and MBIs can be used on all billing and Medicare transactions from now until the end of 2019; after that, only claims with MBIs will be accepted. The last day of 2019 may sound like a long way off, but the time to get up to speed on everything MBI is now. That way, you can begin processing MBIs as soon as you start receiving them, and you will have time to solve any processing glitches well before the deadline.
First, you’ll need to make sure that your electronic health records and claims processing software will accept the new format, and that your electronic clearinghouse, if you use one, is geared up to accept and transmit the data on the new cards. Not all of them are. Some have been seduced by the year-and-a-half buffer – during which time HICNs can still be used – into dragging their feet on the MBI issue. Now is the time to find out if a vendor’s software is hard-wired to accept a maximum of 10 digits (MBIs have 11), not when your claims start bouncing.
Second, you will need to educate your front desk staff, so they will be able to recognize the new cards at a glance. Unfortunately, it looks a lot like the current card, though it is slightly smaller. It has the traditional red and blue colors with black printing, but there is no birthday or gender designation – again, in the interest of protecting patients’ identities. Knowing the difference will become particularly important after your state has been processed, when all of your Medicare patients should have the new card. Those who don’t will need to be identified and urged to get one before the December 2019 deadline.
Finally, once your staff and vendors are up to speed, you can begin educating your patients. Inevitably, some will not receive a new card, especially if they have moved and have not notified the CMS of the change; and some who are not expecting a new card will believe it is a duplicate, and throw it away. The CMS will be airing public service announcements and mailing education pieces to Medicare recipients, but a substantial portion of the education burden will fall on doctors and hospitals.
Have your front office staff remind patients to be sure their addresses are updated online with Medicare (www.Medicare.gov) or the Social Security Administration (www.ssa.gov). Encourage them to take advantage of the free resources available at www.cms.gov. These include both downloadable options and printed materials that illustrate what the new card will look like, explain how to update a mailing address with the Social Security Administration, and remind seniors to keep an eye out for their cards in the mail.
For the many Medicare-age patients who are not particularly computer savvy, the CMS has free resources for physicians as well. You will need to open an account at the agency’s Product Ordering website (productordering.cms.hhs.gov), which in turn needs to be approved by an administrator. The posters and other free literature can be displayed in your waiting room, exam rooms, and other “patient flow” areas. There is also a 1-minute video, downloadable from YouTube (https://youtu.be/DusRmgzQnLY), which can be looped in your waiting area.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
CABANA: AF ablation ties drug management, with an asterisk for crossovers
BOSTON – Results from the CABANA trial, the long-awaited, head-to-head comparison of percutaneous catheter ablation with drug therapy for the treatment of atrial fibrillation by restoring sinus rhythm, failed to accomplish what it was designed to prove.
That is, that catheter ablation was superior to medical management for a combined endpoint of all-cause death, stroke, serious bleeding, or cardiac arrest.

The trial results also gave proponents of catheter ablation some tantalizing hints that this approach actually may have been superior to antiarrhythmic drugs, if only the randomization assignments had been more closely followed as the trial proceeded. But that didn’t happen, with about 30% of patients assigned to medical management crossing over to undergo catheter ablation, presumably because they had received inadequate symptom relief from their drug regimens. In addition, 10% of patients assigned to catheter ablation didn’t undergo it, primarily because they reconsidered after randomization and decided to not choose the invasive option. These crossovers produced a disparity in the outcomes between the standard, intention-to-treat analysis, which showed a neutral difference between the two study arms, and the per-protocol analysis that censored out crossover patients. The per-protocol analysis showed a statistically significant, 27% relative risk reduction in the primary endpoint among the patients randomized to and actually treated with catheter ablation, compared with those randomized to and exclusively treated medically.
“A patient can’t receive benefit from ablation if you don’t ablate,” noted the study’s lead investigation, Douglas L. Packer, MD, as he reported the results at the annual scientific sessions of the Heart Rhythm Society. “When you have this many crossovers and so many patients not getting their assigned treatments, then an on-treatment analysis is required, said Dr. Packer, a cardiac electrophysiologist and professor of medicine at the Mayo Clinic in Rochester, Minn.
The prespecified on-treatment analysis, which, instead of censoring crossover patients, analyzed outcomes based on the treatments that patients actually received, showed a statistically significant one-third reduction in the primary endpoint among the ablated patients and a statistically significant 40% relative reduction in all-cause mortality in the ablated arm, compared with those on medical management.
“For symptomatic treatment, and to restore and maintain sinus rhythm, there is no question that ablation is better. We knew that before this trial, and we know it even more convincingly now,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “To a large extent, we do ablations for symptomatic benefit; to get patients feeling better. And I think this trial will confirm that because this will likely follow the better reduction in atrial fibrillation burden, which was quite impressive in the study.” Dr. Packer said that the quality of life data collected in CABANA will come out in a report later in 2018.
The dilemma that Dr. Ruskin and other physicians who heard the results voiced was how best to interpret the study’s primary results.
“This trial was designed to address whether ablation has an impact [compared with medical management] on hard endpoints, like mortality, and the intention-to-treat analysis showed no difference. I feel bound to adhere to the intention-to-treat analysis, the primary result” the traditional default arbiter of a randomized trial’s outcome, Dr. Ruskin said in an interview, “But intention-to-treat analyses are built on a foundation where most patients are maintained on their assigned treatment.”

The results “tell us that there wasn’t harm from ablation,” Dr. Albert said during a press conference. “That is really important because, before this, we didn’t know for sure. These data make me a little more confident about offering patients ablation. I now have data to discuss with patients that’s useful for decision making.”
“There was certainly no signal whatsoever of harm by taking patients to ablation early” in their management, agreed Dr. Ruskin. “I find that very reassuring and encouraging.”
CABANA (Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial) started in 2009 and enrolled 2,204 patients with documented, new-onset paroxysmal or persistent atrial fibrillation (AF) at 110 centers in 10 countries. Patients averaged about 68 years of age, with about 15% at least 75 years old, and in general were what Dr. Packer characterized as a high-risk group, with a high prevalence of comorbidities: 23% with sleep apnea, 10% with cardiomyopathy, 15% with heart failure, 10% with a prior stroke or transient ischemic attack, and just over a third in a New York Heart Association functional class II or III. About 43% had paroxysmal AF, about 47% had persistent AF, and the remaining patients had long-standing persistent AF. The median duration of AF at the time of entry was just over 1 year.
The clinicians treating the patients assigned to medical management could decide on a case-by-case basis whether to use rate or rhythm control, and about 12% of patients received rate control. The trial design specified pulmonary-vein isolation as the method for left atrial ablation.
In the intention-to-treat analyses, ablation was linked to a 14% relative reduction in the composite primary endpoint, a nonsignificant difference. All-cause mortality was a relative 15% lower in the ablation arm, also not statistically significant. A third prespecified, secondary endpoint, all-cause mortality plus cardiovascular hospitalization, was 17% lower in the ablated patients than in those on drug treatment in the intention-to-treat analysis, a statistically significant difference (P = .002).
The adverse event rate in the ablation arm was “surprisingly” low, said Dr. Packer, with a 3.9% rate of complications from catheter insertion (more than half were hematomas), a 3.4% rate of complications from catheter manipulation within the heart (2.2% involved pericardial effusions that required no intervention), and a 1.8% rate of ablation-related events, most commonly severe pericardial chest pain. “The risks of ablation seem to be lower than we thought,” he said, but quickly added the caveat that all ablation operators in CABANA had to have performed at least 100 ablation cases prior to the trial. The observed safety applies to operators “who know what they’re doing,” he said. Adverse events in the medically treated patients were typical for patients treated with amiodarone, Dr. Packer said, with the most common events hyper- or hypothyroidism, in 1.6%, and an allergic reaction, in 0.6%. In the intention-to-treat analysis the incidence of recurrent AF following a 90-day blanking period after ablation was 47% lower in the ablated patients relative to the drug-treated patients (P less than .0001).
Dr. Packer also presented an intriguing subgroup analysis for the primary endpoint that showed ablation had the best performance relative to medical management in patients younger than 65 years, patients with a history of heart failure, minority patients, and those who entered the trial in NYHA functional class II or III. The subgroup analysis showed a signal for worse performance from ablation in patients who were at least 75 years old. “I’m concerned about these older patients; we need to look into this,” Dr. Packer said. He also expressed optimism that the good performance of ablation in heart failure patients, while an exploratory finding, suggested confirmation of the results reported recently from the CASTLE-AF trial, which also showed good outcomes from catheter ablation for treating patients with heart failure and AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
The main qualification Dr. Packer voiced about the CABANA results is that not every AF patient should get ablation. “All treatments are not right for all patients. Not everyone with AF needs ablation. You need to talk with patients about it.” But despite this caution, he declared that the results had already changed his practice.
“I much less often now say to patients ‘let’s go with a drug and see what happens.’ I’d still do that if I wasn’t sure that a patient’s symptoms were caused by their AF” as opposed to their underlying heart disease, but if I’m pretty certain that their symptoms are caused by their AF over the past few months, I’ve become more likely to say that front-line ablation is reasonable,” Dr. Packer said.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and has received research funding from all four of these companies and also from several other companies. Dr. Ruskin has been a consultant to Biosense Webster and Medtronic and several other companies, has an ownership interest in Amgen, Cameron Health, InfoBionic, Newpace, Portola, and Regeneron, and has a fiduciary role in Pharmaco-Kinesis. Dr. Albert has been a consultant to Myokardia and Sanofi Aventis and has received research funding from Roche Diagnostics and St. Jude.
SOURCE: Packer DL et al. HRS 2018, Abstract B-LBCT01-05.
The data from CABANA suggest that at the least, catheter ablation is the equivalent of drug therapy, and I think in many cases, it is probably superior. Patients with atrial fibrillation should be allowed to undergo ablation as their first treatment, performed by operators who know what they’re doing. These are excellent results, but they do not apply to every patient with atrial fibrillation; they apply to patients like those enrolled in the trial.

The results also speak very loudly about the importance of sinus rhythm in patients with heart failure. The results in the subgroup of patients with heart failure appear to support the findings from CASTLE-AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
Eric N. Prystowsky, MD , is a cardiac electrophysiologist with the St. Vincent Medical Group in Indianapolis. He has been a consultant to CardioNet and Medtronic, has an equity interest in Stereotaxis, and receives fellowship support from Medtronic and St. Jude. He made these comments as designated discussant for CABANA.
The data from CABANA suggest that at the least, catheter ablation is the equivalent of drug therapy, and I think in many cases, it is probably superior. Patients with atrial fibrillation should be allowed to undergo ablation as their first treatment, performed by operators who know what they’re doing. These are excellent results, but they do not apply to every patient with atrial fibrillation; they apply to patients like those enrolled in the trial.
The results also speak very loudly about the importance of sinus rhythm in patients with heart failure. The results in the subgroup of patients with heart failure appear to support the findings from CASTLE-AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
Eric N. Prystowsky, MD , is a cardiac electrophysiologist with the St. Vincent Medical Group in Indianapolis. He has been a consultant to CardioNet and Medtronic, has an equity interest in Stereotaxis, and receives fellowship support from Medtronic and St. Jude. He made these comments as designated discussant for CABANA.
The data from CABANA suggest that at the least, catheter ablation is the equivalent of drug therapy, and I think in many cases, it is probably superior. Patients with atrial fibrillation should be allowed to undergo ablation as their first treatment, performed by operators who know what they’re doing. These are excellent results, but they do not apply to every patient with atrial fibrillation; they apply to patients like those enrolled in the trial.
The results also speak very loudly about the importance of sinus rhythm in patients with heart failure. The results in the subgroup of patients with heart failure appear to support the findings from CASTLE-AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
Eric N. Prystowsky, MD , is a cardiac electrophysiologist with the St. Vincent Medical Group in Indianapolis. He has been a consultant to CardioNet and Medtronic, has an equity interest in Stereotaxis, and receives fellowship support from Medtronic and St. Jude. He made these comments as designated discussant for CABANA.
BOSTON – Results from the CABANA trial, the long-awaited, head-to-head comparison of percutaneous catheter ablation with drug therapy for the treatment of atrial fibrillation by restoring sinus rhythm, failed to accomplish what it was designed to prove.
That is, that catheter ablation was superior to medical management for a combined endpoint of all-cause death, stroke, serious bleeding, or cardiac arrest.
The trial results also gave proponents of catheter ablation some tantalizing hints that this approach actually may have been superior to antiarrhythmic drugs, if only the randomization assignments had been more closely followed as the trial proceeded. But that didn’t happen, with about 30% of patients assigned to medical management crossing over to undergo catheter ablation, presumably because they had received inadequate symptom relief from their drug regimens. In addition, 10% of patients assigned to catheter ablation didn’t undergo it, primarily because they reconsidered after randomization and decided to not choose the invasive option. These crossovers produced a disparity in the outcomes between the standard, intention-to-treat analysis, which showed a neutral difference between the two study arms, and the per-protocol analysis that censored out crossover patients. The per-protocol analysis showed a statistically significant, 27% relative risk reduction in the primary endpoint among the patients randomized to and actually treated with catheter ablation, compared with those randomized to and exclusively treated medically.
“A patient can’t receive benefit from ablation if you don’t ablate,” noted the study’s lead investigation, Douglas L. Packer, MD, as he reported the results at the annual scientific sessions of the Heart Rhythm Society. “When you have this many crossovers and so many patients not getting their assigned treatments, then an on-treatment analysis is required, said Dr. Packer, a cardiac electrophysiologist and professor of medicine at the Mayo Clinic in Rochester, Minn.
The prespecified on-treatment analysis, which, instead of censoring crossover patients, analyzed outcomes based on the treatments that patients actually received, showed a statistically significant one-third reduction in the primary endpoint among the ablated patients and a statistically significant 40% relative reduction in all-cause mortality in the ablated arm, compared with those on medical management.
“For symptomatic treatment, and to restore and maintain sinus rhythm, there is no question that ablation is better. We knew that before this trial, and we know it even more convincingly now,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “To a large extent, we do ablations for symptomatic benefit; to get patients feeling better. And I think this trial will confirm that because this will likely follow the better reduction in atrial fibrillation burden, which was quite impressive in the study.” Dr. Packer said that the quality of life data collected in CABANA will come out in a report later in 2018.
The dilemma that Dr. Ruskin and other physicians who heard the results voiced was how best to interpret the study’s primary results.
“This trial was designed to address whether ablation has an impact [compared with medical management] on hard endpoints, like mortality, and the intention-to-treat analysis showed no difference. I feel bound to adhere to the intention-to-treat analysis, the primary result” the traditional default arbiter of a randomized trial’s outcome, Dr. Ruskin said in an interview, “But intention-to-treat analyses are built on a foundation where most patients are maintained on their assigned treatment.”
The results “tell us that there wasn’t harm from ablation,” Dr. Albert said during a press conference. “That is really important because, before this, we didn’t know for sure. These data make me a little more confident about offering patients ablation. I now have data to discuss with patients that’s useful for decision making.”
“There was certainly no signal whatsoever of harm by taking patients to ablation early” in their management, agreed Dr. Ruskin. “I find that very reassuring and encouraging.”
CABANA (Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial) started in 2009 and enrolled 2,204 patients with documented, new-onset paroxysmal or persistent atrial fibrillation (AF) at 110 centers in 10 countries. Patients averaged about 68 years of age, with about 15% at least 75 years old, and in general were what Dr. Packer characterized as a high-risk group, with a high prevalence of comorbidities: 23% with sleep apnea, 10% with cardiomyopathy, 15% with heart failure, 10% with a prior stroke or transient ischemic attack, and just over a third in a New York Heart Association functional class II or III. About 43% had paroxysmal AF, about 47% had persistent AF, and the remaining patients had long-standing persistent AF. The median duration of AF at the time of entry was just over 1 year.
The clinicians treating the patients assigned to medical management could decide on a case-by-case basis whether to use rate or rhythm control, and about 12% of patients received rate control. The trial design specified pulmonary-vein isolation as the method for left atrial ablation.
In the intention-to-treat analyses, ablation was linked to a 14% relative reduction in the composite primary endpoint, a nonsignificant difference. All-cause mortality was a relative 15% lower in the ablation arm, also not statistically significant. A third prespecified, secondary endpoint, all-cause mortality plus cardiovascular hospitalization, was 17% lower in the ablated patients than in those on drug treatment in the intention-to-treat analysis, a statistically significant difference (P = .002).
The adverse event rate in the ablation arm was “surprisingly” low, said Dr. Packer, with a 3.9% rate of complications from catheter insertion (more than half were hematomas), a 3.4% rate of complications from catheter manipulation within the heart (2.2% involved pericardial effusions that required no intervention), and a 1.8% rate of ablation-related events, most commonly severe pericardial chest pain. “The risks of ablation seem to be lower than we thought,” he said, but quickly added the caveat that all ablation operators in CABANA had to have performed at least 100 ablation cases prior to the trial. The observed safety applies to operators “who know what they’re doing,” he said. Adverse events in the medically treated patients were typical for patients treated with amiodarone, Dr. Packer said, with the most common events hyper- or hypothyroidism, in 1.6%, and an allergic reaction, in 0.6%. In the intention-to-treat analysis the incidence of recurrent AF following a 90-day blanking period after ablation was 47% lower in the ablated patients relative to the drug-treated patients (P less than .0001).
Dr. Packer also presented an intriguing subgroup analysis for the primary endpoint that showed ablation had the best performance relative to medical management in patients younger than 65 years, patients with a history of heart failure, minority patients, and those who entered the trial in NYHA functional class II or III. The subgroup analysis showed a signal for worse performance from ablation in patients who were at least 75 years old. “I’m concerned about these older patients; we need to look into this,” Dr. Packer said. He also expressed optimism that the good performance of ablation in heart failure patients, while an exploratory finding, suggested confirmation of the results reported recently from the CASTLE-AF trial, which also showed good outcomes from catheter ablation for treating patients with heart failure and AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
The main qualification Dr. Packer voiced about the CABANA results is that not every AF patient should get ablation. “All treatments are not right for all patients. Not everyone with AF needs ablation. You need to talk with patients about it.” But despite this caution, he declared that the results had already changed his practice.
“I much less often now say to patients ‘let’s go with a drug and see what happens.’ I’d still do that if I wasn’t sure that a patient’s symptoms were caused by their AF” as opposed to their underlying heart disease, but if I’m pretty certain that their symptoms are caused by their AF over the past few months, I’ve become more likely to say that front-line ablation is reasonable,” Dr. Packer said.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and has received research funding from all four of these companies and also from several other companies. Dr. Ruskin has been a consultant to Biosense Webster and Medtronic and several other companies, has an ownership interest in Amgen, Cameron Health, InfoBionic, Newpace, Portola, and Regeneron, and has a fiduciary role in Pharmaco-Kinesis. Dr. Albert has been a consultant to Myokardia and Sanofi Aventis and has received research funding from Roche Diagnostics and St. Jude.
SOURCE: Packer DL et al. HRS 2018, Abstract B-LBCT01-05.
BOSTON – Results from the CABANA trial, the long-awaited, head-to-head comparison of percutaneous catheter ablation with drug therapy for the treatment of atrial fibrillation by restoring sinus rhythm, failed to accomplish what it was designed to prove.
That is, that catheter ablation was superior to medical management for a combined endpoint of all-cause death, stroke, serious bleeding, or cardiac arrest.
The trial results also gave proponents of catheter ablation some tantalizing hints that this approach actually may have been superior to antiarrhythmic drugs, if only the randomization assignments had been more closely followed as the trial proceeded. But that didn’t happen, with about 30% of patients assigned to medical management crossing over to undergo catheter ablation, presumably because they had received inadequate symptom relief from their drug regimens. In addition, 10% of patients assigned to catheter ablation didn’t undergo it, primarily because they reconsidered after randomization and decided to not choose the invasive option. These crossovers produced a disparity in the outcomes between the standard, intention-to-treat analysis, which showed a neutral difference between the two study arms, and the per-protocol analysis that censored out crossover patients. The per-protocol analysis showed a statistically significant, 27% relative risk reduction in the primary endpoint among the patients randomized to and actually treated with catheter ablation, compared with those randomized to and exclusively treated medically.
“A patient can’t receive benefit from ablation if you don’t ablate,” noted the study’s lead investigation, Douglas L. Packer, MD, as he reported the results at the annual scientific sessions of the Heart Rhythm Society. “When you have this many crossovers and so many patients not getting their assigned treatments, then an on-treatment analysis is required, said Dr. Packer, a cardiac electrophysiologist and professor of medicine at the Mayo Clinic in Rochester, Minn.
The prespecified on-treatment analysis, which, instead of censoring crossover patients, analyzed outcomes based on the treatments that patients actually received, showed a statistically significant one-third reduction in the primary endpoint among the ablated patients and a statistically significant 40% relative reduction in all-cause mortality in the ablated arm, compared with those on medical management.
“For symptomatic treatment, and to restore and maintain sinus rhythm, there is no question that ablation is better. We knew that before this trial, and we know it even more convincingly now,” commented Jeremy N. Ruskin, MD, professor of medicine at Harvard Medical School and director of the cardiac arrhythmia service at Massachusetts General Hospital, both in Boston. “To a large extent, we do ablations for symptomatic benefit; to get patients feeling better. And I think this trial will confirm that because this will likely follow the better reduction in atrial fibrillation burden, which was quite impressive in the study.” Dr. Packer said that the quality of life data collected in CABANA will come out in a report later in 2018.
The dilemma that Dr. Ruskin and other physicians who heard the results voiced was how best to interpret the study’s primary results.
“This trial was designed to address whether ablation has an impact [compared with medical management] on hard endpoints, like mortality, and the intention-to-treat analysis showed no difference. I feel bound to adhere to the intention-to-treat analysis, the primary result” the traditional default arbiter of a randomized trial’s outcome, Dr. Ruskin said in an interview, “But intention-to-treat analyses are built on a foundation where most patients are maintained on their assigned treatment.”
The results “tell us that there wasn’t harm from ablation,” Dr. Albert said during a press conference. “That is really important because, before this, we didn’t know for sure. These data make me a little more confident about offering patients ablation. I now have data to discuss with patients that’s useful for decision making.”
“There was certainly no signal whatsoever of harm by taking patients to ablation early” in their management, agreed Dr. Ruskin. “I find that very reassuring and encouraging.”
CABANA (Catheter Ablation vs. Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial) started in 2009 and enrolled 2,204 patients with documented, new-onset paroxysmal or persistent atrial fibrillation (AF) at 110 centers in 10 countries. Patients averaged about 68 years of age, with about 15% at least 75 years old, and in general were what Dr. Packer characterized as a high-risk group, with a high prevalence of comorbidities: 23% with sleep apnea, 10% with cardiomyopathy, 15% with heart failure, 10% with a prior stroke or transient ischemic attack, and just over a third in a New York Heart Association functional class II or III. About 43% had paroxysmal AF, about 47% had persistent AF, and the remaining patients had long-standing persistent AF. The median duration of AF at the time of entry was just over 1 year.
The clinicians treating the patients assigned to medical management could decide on a case-by-case basis whether to use rate or rhythm control, and about 12% of patients received rate control. The trial design specified pulmonary-vein isolation as the method for left atrial ablation.
In the intention-to-treat analyses, ablation was linked to a 14% relative reduction in the composite primary endpoint, a nonsignificant difference. All-cause mortality was a relative 15% lower in the ablation arm, also not statistically significant. A third prespecified, secondary endpoint, all-cause mortality plus cardiovascular hospitalization, was 17% lower in the ablated patients than in those on drug treatment in the intention-to-treat analysis, a statistically significant difference (P = .002).
The adverse event rate in the ablation arm was “surprisingly” low, said Dr. Packer, with a 3.9% rate of complications from catheter insertion (more than half were hematomas), a 3.4% rate of complications from catheter manipulation within the heart (2.2% involved pericardial effusions that required no intervention), and a 1.8% rate of ablation-related events, most commonly severe pericardial chest pain. “The risks of ablation seem to be lower than we thought,” he said, but quickly added the caveat that all ablation operators in CABANA had to have performed at least 100 ablation cases prior to the trial. The observed safety applies to operators “who know what they’re doing,” he said. Adverse events in the medically treated patients were typical for patients treated with amiodarone, Dr. Packer said, with the most common events hyper- or hypothyroidism, in 1.6%, and an allergic reaction, in 0.6%. In the intention-to-treat analysis the incidence of recurrent AF following a 90-day blanking period after ablation was 47% lower in the ablated patients relative to the drug-treated patients (P less than .0001).
Dr. Packer also presented an intriguing subgroup analysis for the primary endpoint that showed ablation had the best performance relative to medical management in patients younger than 65 years, patients with a history of heart failure, minority patients, and those who entered the trial in NYHA functional class II or III. The subgroup analysis showed a signal for worse performance from ablation in patients who were at least 75 years old. “I’m concerned about these older patients; we need to look into this,” Dr. Packer said. He also expressed optimism that the good performance of ablation in heart failure patients, while an exploratory finding, suggested confirmation of the results reported recently from the CASTLE-AF trial, which also showed good outcomes from catheter ablation for treating patients with heart failure and AF (N Engl J Med. 2018 Feb 1;378[5]:417-27).
The main qualification Dr. Packer voiced about the CABANA results is that not every AF patient should get ablation. “All treatments are not right for all patients. Not everyone with AF needs ablation. You need to talk with patients about it.” But despite this caution, he declared that the results had already changed his practice.
“I much less often now say to patients ‘let’s go with a drug and see what happens.’ I’d still do that if I wasn’t sure that a patient’s symptoms were caused by their AF” as opposed to their underlying heart disease, but if I’m pretty certain that their symptoms are caused by their AF over the past few months, I’ve become more likely to say that front-line ablation is reasonable,” Dr. Packer said.
CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and has received research funding from all four of these companies and also from several other companies. Dr. Ruskin has been a consultant to Biosense Webster and Medtronic and several other companies, has an ownership interest in Amgen, Cameron Health, InfoBionic, Newpace, Portola, and Regeneron, and has a fiduciary role in Pharmaco-Kinesis. Dr. Albert has been a consultant to Myokardia and Sanofi Aventis and has received research funding from Roche Diagnostics and St. Jude.
SOURCE: Packer DL et al. HRS 2018, Abstract B-LBCT01-05.
REPORTING FROM HEART RHYTHM 2018
Key clinical point: Catheter atrial fib ablation showed no significant benefit over medical management for the CABANA’s primary endpoint.
Major finding: The composite endpoint that included all-cause death was a nonsignificant 14% lower with ablation than with medical management in the intention-to-treat analysis.
Study details: CABANA, a multicenter, randomized trial with 2,204 patients.
Disclosures: CABANA received partial funding from Biosense Webster, Boston Scientific, Medtronic, and St. Jude. Dr. Packer has been a consultant to and has received research funding from all four of these companies and from several other companies. Dr. Ruskin has been a consultant to Biosense Webster and Medtronic and several other companies, has an ownership interest in Amgen, Cameron Health, InfoBionic, Newpace, Portola, and Regeneron, and has a fiduciary role in Pharmaco-Kinesis. Dr. Albert has been a consultant to Myokardia and Sanofi-Aventis and has received research funding from Roche Diagnostics and St. Jude.
Source: Packer D et al. HRS 2018, Abstract B-LBCT01-05.
Coverage of Hand Defects with Exposed Tendons: The Use of Dermal Regeneration Template
ABSTRACT
Soft tissue defects associated with exposed tendon pose difficult reconstructive problems because of tendon adhesions, poor range of motion, poor cosmetic appearance, and donor site morbidity. Dermal regeneration template is a skin substitute widely used in reconstructive surgery, including the occasional coverage of tendons. However, postoperative functionality of the tendons has not been well documented. We report a case of using dermal regeneration template for soft tissue reconstruction overlying tendons with loss of paratenon in a patient with Dupuytren’s contracture. Dermal regeneration template may offer an alternative option for immediate tendon coverage in the hand.
Soft tissue defects overlying exposed tendon with loss of paratenon often precipitate poor clinical outcomes because of the dichotomous demands of both closing the overlying soft-tissue defect and providing a gliding surface for the underlying tendons.1 Although avoidance of adhesions and restoration of function are the primary goals of the procedure, satisfactory appearance is also desirable. Likewise, any form of coverage should ideally provide good vasculature required for complete healing and an early form of closure following débridement.2 Simple skin grafts do not adequately meet these demands because they result in a high rate of tendon adhesions,3 and also are limited in patients with limited donor skin availability or questionable underlying wound bed viability, such as in scleroderma.
In order to reduce the frequency of tendon adhesions by creating a gliding surface, the use of interpositional materials, both artificial and biologic, has been employed with varying degrees of success, including cellophane, chitosan membrane, fibrin sealant, autogenous fascial flaps, and autogenous venous grafts.4-7 Many of the autogenous flaps and grafts have been employed with good success.8 However, complications and donor site morbidity encourage alternative procedures, including the use of artificial substances.2,8-10
We present our clinical experience with a patient who underwent successful placement of Integra (Integra LifeSciences) Dermal Regeneration Template (DRT) directly over exposed tendons with a subsequent full-thickness skin graft several weeks later. The procedures were performed per the manufacturer’s specifications, resulting in 2 stages of reconstruction. In our experience, DRT can offer immediate coverage unrestricted by wound size, and provides shorter operative time and decreased donor site and surgical morbidity compared with flap coverage, while demonstrating good cosmetic results. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 74-year-old right-handed man with Dupuytren’s contracture was evaluated for recurrent symptomatic contracture causing difficulty with daily activities. He reported palpable cords and contractures in the ring and small fingers of the right hand. He had 2 prior open surgical procedures, including palmar and digital fasciectomy of both hands. On the right hand, the ring and small fingers demonstrated 90° proximal interphalangeal (PIP) and 60° metacarpophalangeal (MCP) flexion contractures. Palpable central cords were present on the flexor surfaces of both the ring and small fingers. A well-healed surgical incision, performed 22 years earlier, was present over the palmar aspect of the ring finger.
Continue to: With consideration given...
With consideration given to the patient’s recurrent contracture after a prior surgical procedure, we discussed surgical excision of the diseased cords in order to eliminate the possibility of a second recurrence and maximize the gain of motion. Following discussion with the patient, we performed palmar and digital fasciectomy of the ring and small finger contractures. Postoperatively, the patient was followed closely for wound complications and vascular status. On his return to our clinic 11 days later, the patient was noted to have dehiscence of the digital wounds in the ring and small fingers (Figure 1). 
STAGE 1
During the first stage, completed 14 days following the index procedure, débridement of the wounds was performed, followed by provisional DRT coverage of the tendons, secured with 5-0 nylon sutures (Figure 2). 
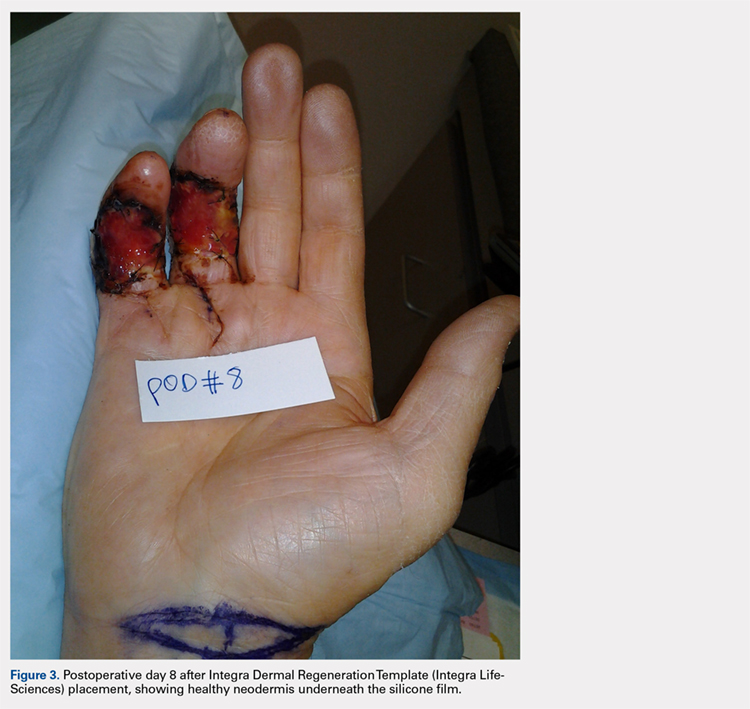
STAGE 2
At approximately 2 weeks after application of the DRT, a full-thickness skin graft was applied. The thickness of the graft was chosen to allow for durable coverage of the palmar skin defects. Upon successful completion of the second stage, the patient was followed and evaluated for complete wound healing. On performing an examination 14 days after surgery, the ring and small fingers demonstrated only partially healed skin graft but significantly improved range of motion (ROM), with 40° to 90° arc of motion in the PIP joint and 25° to 90° arc of motion in the MCP joint (Figure 4). Owing to their limited size, the wounds were treated with dressing changes until successful healing (Figure 5). 
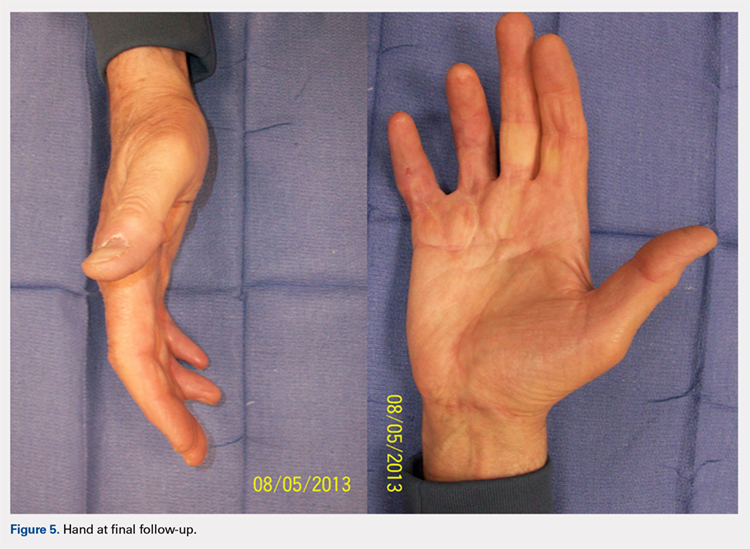
Hand therapy was instituted to achieve maximum mobility for covered soft tissue and tendons and to maximize tendon gliding. At 1-year follow-up, the skin was fully healed and the patient’s active PIP motion was 30° to 90°, active MCP motion was 0° to 90°, and grip strength was 90 lb on both sides. The tendons glided under a well-vascularized tissue at the DRT placement site, and no secondary tenolysis procedure was deemed necessary.
DISCUSSION
Soft tissue defects with exposed tendons may offer a number of challenges for coverage. The primary concern is the creation of a gliding surface and the restoration of a functional tendon without adhesions.2 However, surgeons must use their own clinical judgment when choosing the method of coverage so as to minimize the effects of donor site morbidity and maximize the overall functional and cosmetic outcomes. All options must be considered while selecting a material or flap that is likely to survive in the relatively avascular tendon plane.2,8,11 When considering the reconstructive ladder, skin grafts may not represent a viable option in the presence of a nonvascularized wound bed, such as exposed tendon or bone, where paratenon or periosteum have been damaged. That leaves the surgeon with local flaps, regional flaps, free flaps, and skin substitutes.
Continue to : Before planning closure...
Before planning closure, wound conditions should be optimized, including wound bed quality, vascularization, and bacterial loads. Experimental data suggest that the bacterial load should be brought down below a critical level of 105 bacteria per g of tissue to allow a skin graft to take. This may be problematic from a practical standpoint because quantitative bacterial cultures take about 48 hours to obtain the result, long after a decision to graft is made. As a result, the surgeon may take an aggressive approach to wound débridement, making sure that all necrotic material has been sharply débrided prior to coverage.
As Levin12 noted in 1993, decisions regarding repair of any soft tissue defect may follow a well-delineated ladder beginning with the primary choice of split-thickness skin grafts and ending with free flaps. When treating tissue defects in the hand complex, flaps are an excellent option as they replace like with like, allow minimal scarring and early rehabilitation. 13,14 Nevertheless, a few general disadvantages are inherent in flap procedure: increase in operating time, risk of flap loss, and in case of free flaps, knowledge, experience, and microsurgical ability.2 In reference to complications, the rate of flap loss found by Khouri and colleagues15 was 4.1% with a 12.1% chance of incurring some measured complication, including wound dehiscence, arterial insufficiency, and flap necrosis.
Likewise, some of the conventional local and free flaps, including cutaneous and muscular flaps, prove ineffective in preventing tendon adhesions, create unsightly postoperative contours, or increase the area of trauma on the wounded hand, encouraging the use of free fascial flaps.11 Among the wide array of potential free fascial flaps, the temporoparietal, scapular, lateral arm, radial forearm, and free serratus fascial flaps are some of the most popular for hand defects.8,9 However, these procedures require an additional surgical site, meticulous dissection, microsurgical technique at times, and increased operating cost and time.2,8-10 Furthermore, free fascial flaps have demonstrated occasional partial flap loss and a decreased survival of the overlying skin graft, leading some to advocate delayed skin graft placement.10,16,17
On the basis of these complications, Bray and colleagues11 noted that the utility of free flaps may be limited in smaller clinical settings. The primary disadvantage of using DRTs is the necessity for a second operative procedure to harvest and place the skin graft. Traditionally, this is performed 2 to 3 weeks after the initial DRT application. Nevertheless, a 1-stage procedure can be performed in an outpatient setup, minimizing the burden to the patient and the medical costs, followed by secondary intention healing.
In response to critics of the 2-stage technique, Sanger and colleagues18 described single-stage use of DRT with split-thickness skin grafts with placement of an overlying wound vacuum-assisted closure to help speed incorporation of the DRT and improve survival of the immediately grafted skin. Another viable alternative is the McCash open-palm technique.19 In the open-palm technique, a Brunner zigzag incision is made in the affected digit. A transverse incision is made in the palm. A partial fasciectomy is performed in the palm and digit. After release, the digital incision is closed, and the palmar incision is left open. Although this well-studied and well-reported technique is known to reduce the risk of flap necrosis due to tension and hematoma,20 its main application is in the palm, as the name implies. Because in our patient the defect was palmar-digital with exposed “white structures,” we elected to use DRT.
Continue to: Although there is still...
Although there is still no perfect answer for wound coverage and closure in the hand with exposed or damaged tendons, DRT certainly performs well as a primary choice by minimizing adhesions; allowing a good ROM; and providing a durable, satisfactory cosmetic outcome. Likewise, an initial treatment with DRT does not preclude later, more elaborate reconstructive efforts, such as local or free flaps, if they continue to be indicated. DRT also does not diminish the ability to revise a tendon reconstruction if a secondary procedure is necessary. In our patient, tendon revision has not been necessary. DRT gives the surgeon a minimally invasive, efficient initial alternative to more labor-intensive, potentially morbid reconstructive procedures, without sacrificing outcome. Therefore, DRT can offer an alternative procedure in the surgeon’s armamentarium for tendon coverage in complex hand defects.
1. Flügel A. Kehrer C. Heitmann C, German G, Sauerbier M. Coverage of soft tissue defects of the hand with free fascial flaps. Microsurgery.2005;25(1):47-53.
2. Chen H, Buchman MT, Wei FC. Free flaps for soft tissue coverage in the hand and fingers. Hand Clin. 1999;15(4):541-554.
3. Chia J, Lim A, Peng YP. Use of an arterialized venous flap for resurfacing a circumferential soft tissue defect of a digit. Microsurgery. 2001; 21(8):374-378.
4. Wheeldon T. The use of cellophane as a permanent tendon sheath. J Bone J Surg Am; 1939;21(2):393-396.
5. Frykman E, Jacobsson S, Widenfalk B. Fibrin sealant in prevention of flexor tendon adhesions: an experimental study in the rabbit. J Hand Surg Am. 1993;18(1):68-75.
6. Jones NF, Lister GD. Free skin and composite flaps. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green’s Operative hand surgery. 6th ed. New York, NY: Churchill Livingstone; 2011:1721-1756.
7. Yan D, Shi X, Lui Q. Reconstruction of tendon sheath by autogenous vein graft in preventing adhesion. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 1997;11(1):38-39.
8. Pederson WC. Upper extremity microsurgery. Plast Reconstr Surg. 2001;107(6):1524-1537; discussion 1538-15399, 1540-1543.
9. WintschK, Helaly P. Free flap of gliding tissue. J Reconstr Microsurg. 1986;2(3):143-151.
10. Meland NB, Weimar R. Microsurgical reconstruction: experience with free fascia flaps. Ann Plast Surg. 1991;27(1):1-8.
11. Bray PW, Boyer MI, Bowen CV. Complex injuries of the forearm. Coverage considerations. Hand Clin. 1997;13(2):263-278.
12. Levin LS. The reconstructive ladder: an orthoplastic approach. Ortho Clin North Am. 1993; 24(3):393-409.
13. Hallock GG. Utility of both muscle and fascia flaps in severe lower extremity trauma. J Trauma. 2000;48 (5):913-917. doi:10.1097/00005373-200005000-00016.
14. Hallock GG. The utility of both muscle and fascia flaps in severe upper extremity trauma. J Trauma. 2002;53(1):61-65. doi:10.1097/00005373-200207000-00013.
15. Khouri RK, Cooley BC, Kunselman AR, et al. A prospective study of microvascular free-flap surgery and outcome. Plast Reconstr Surg. 1998;102(3):711-721.
16. Woods JM 4th, Shack RB, Hagan KF. Free temporoparietal fascia flap in reconstruction of the lower extremity. Ann Plast Surg. 1995;34(5):501-506. doi:10.1097/00000637-199505000-00008.
17. Chung KC, Cederna PS. Endoscopic harvest of temporoparietal fascial free flaps for coverage of hand wounds. J Hand Surg Am. 2002;27(3):525-533.
18. Sanger C, Molnar JA, Newman CE, et al. Immediate skin grafting of an engineered dermal substitute: P37. Plast Reconstr Surg. 2005;116(3S):165.
19. McCash CR. The open palm technique in Dupuytren’s contracture. Br J Plast Surg. 1964;17:271-280.
20. Shaw DL, Wise DI, Holms W. Dupuytren's disease treated by palmar fasciectomy and an open palm technique. J Hand Surg Br. 1996;21(4):484-485.
ABSTRACT
Soft tissue defects associated with exposed tendon pose difficult reconstructive problems because of tendon adhesions, poor range of motion, poor cosmetic appearance, and donor site morbidity. Dermal regeneration template is a skin substitute widely used in reconstructive surgery, including the occasional coverage of tendons. However, postoperative functionality of the tendons has not been well documented. We report a case of using dermal regeneration template for soft tissue reconstruction overlying tendons with loss of paratenon in a patient with Dupuytren’s contracture. Dermal regeneration template may offer an alternative option for immediate tendon coverage in the hand.
Soft tissue defects overlying exposed tendon with loss of paratenon often precipitate poor clinical outcomes because of the dichotomous demands of both closing the overlying soft-tissue defect and providing a gliding surface for the underlying tendons.1 Although avoidance of adhesions and restoration of function are the primary goals of the procedure, satisfactory appearance is also desirable. Likewise, any form of coverage should ideally provide good vasculature required for complete healing and an early form of closure following débridement.2 Simple skin grafts do not adequately meet these demands because they result in a high rate of tendon adhesions,3 and also are limited in patients with limited donor skin availability or questionable underlying wound bed viability, such as in scleroderma.
In order to reduce the frequency of tendon adhesions by creating a gliding surface, the use of interpositional materials, both artificial and biologic, has been employed with varying degrees of success, including cellophane, chitosan membrane, fibrin sealant, autogenous fascial flaps, and autogenous venous grafts.4-7 Many of the autogenous flaps and grafts have been employed with good success.8 However, complications and donor site morbidity encourage alternative procedures, including the use of artificial substances.2,8-10
We present our clinical experience with a patient who underwent successful placement of Integra (Integra LifeSciences) Dermal Regeneration Template (DRT) directly over exposed tendons with a subsequent full-thickness skin graft several weeks later. The procedures were performed per the manufacturer’s specifications, resulting in 2 stages of reconstruction. In our experience, DRT can offer immediate coverage unrestricted by wound size, and provides shorter operative time and decreased donor site and surgical morbidity compared with flap coverage, while demonstrating good cosmetic results. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 74-year-old right-handed man with Dupuytren’s contracture was evaluated for recurrent symptomatic contracture causing difficulty with daily activities. He reported palpable cords and contractures in the ring and small fingers of the right hand. He had 2 prior open surgical procedures, including palmar and digital fasciectomy of both hands. On the right hand, the ring and small fingers demonstrated 90° proximal interphalangeal (PIP) and 60° metacarpophalangeal (MCP) flexion contractures. Palpable central cords were present on the flexor surfaces of both the ring and small fingers. A well-healed surgical incision, performed 22 years earlier, was present over the palmar aspect of the ring finger.
Continue to: With consideration given...
With consideration given to the patient’s recurrent contracture after a prior surgical procedure, we discussed surgical excision of the diseased cords in order to eliminate the possibility of a second recurrence and maximize the gain of motion. Following discussion with the patient, we performed palmar and digital fasciectomy of the ring and small finger contractures. Postoperatively, the patient was followed closely for wound complications and vascular status. On his return to our clinic 11 days later, the patient was noted to have dehiscence of the digital wounds in the ring and small fingers (Figure 1).
STAGE 1
During the first stage, completed 14 days following the index procedure, débridement of the wounds was performed, followed by provisional DRT coverage of the tendons, secured with 5-0 nylon sutures (Figure 2).
STAGE 2
At approximately 2 weeks after application of the DRT, a full-thickness skin graft was applied. The thickness of the graft was chosen to allow for durable coverage of the palmar skin defects. Upon successful completion of the second stage, the patient was followed and evaluated for complete wound healing. On performing an examination 14 days after surgery, the ring and small fingers demonstrated only partially healed skin graft but significantly improved range of motion (ROM), with 40° to 90° arc of motion in the PIP joint and 25° to 90° arc of motion in the MCP joint (Figure 4). Owing to their limited size, the wounds were treated with dressing changes until successful healing (Figure 5).
Hand therapy was instituted to achieve maximum mobility for covered soft tissue and tendons and to maximize tendon gliding. At 1-year follow-up, the skin was fully healed and the patient’s active PIP motion was 30° to 90°, active MCP motion was 0° to 90°, and grip strength was 90 lb on both sides. The tendons glided under a well-vascularized tissue at the DRT placement site, and no secondary tenolysis procedure was deemed necessary.
DISCUSSION
Soft tissue defects with exposed tendons may offer a number of challenges for coverage. The primary concern is the creation of a gliding surface and the restoration of a functional tendon without adhesions.2 However, surgeons must use their own clinical judgment when choosing the method of coverage so as to minimize the effects of donor site morbidity and maximize the overall functional and cosmetic outcomes. All options must be considered while selecting a material or flap that is likely to survive in the relatively avascular tendon plane.2,8,11 When considering the reconstructive ladder, skin grafts may not represent a viable option in the presence of a nonvascularized wound bed, such as exposed tendon or bone, where paratenon or periosteum have been damaged. That leaves the surgeon with local flaps, regional flaps, free flaps, and skin substitutes.
Continue to : Before planning closure...
Before planning closure, wound conditions should be optimized, including wound bed quality, vascularization, and bacterial loads. Experimental data suggest that the bacterial load should be brought down below a critical level of 105 bacteria per g of tissue to allow a skin graft to take. This may be problematic from a practical standpoint because quantitative bacterial cultures take about 48 hours to obtain the result, long after a decision to graft is made. As a result, the surgeon may take an aggressive approach to wound débridement, making sure that all necrotic material has been sharply débrided prior to coverage.
As Levin12 noted in 1993, decisions regarding repair of any soft tissue defect may follow a well-delineated ladder beginning with the primary choice of split-thickness skin grafts and ending with free flaps. When treating tissue defects in the hand complex, flaps are an excellent option as they replace like with like, allow minimal scarring and early rehabilitation. 13,14 Nevertheless, a few general disadvantages are inherent in flap procedure: increase in operating time, risk of flap loss, and in case of free flaps, knowledge, experience, and microsurgical ability.2 In reference to complications, the rate of flap loss found by Khouri and colleagues15 was 4.1% with a 12.1% chance of incurring some measured complication, including wound dehiscence, arterial insufficiency, and flap necrosis.
Likewise, some of the conventional local and free flaps, including cutaneous and muscular flaps, prove ineffective in preventing tendon adhesions, create unsightly postoperative contours, or increase the area of trauma on the wounded hand, encouraging the use of free fascial flaps.11 Among the wide array of potential free fascial flaps, the temporoparietal, scapular, lateral arm, radial forearm, and free serratus fascial flaps are some of the most popular for hand defects.8,9 However, these procedures require an additional surgical site, meticulous dissection, microsurgical technique at times, and increased operating cost and time.2,8-10 Furthermore, free fascial flaps have demonstrated occasional partial flap loss and a decreased survival of the overlying skin graft, leading some to advocate delayed skin graft placement.10,16,17
On the basis of these complications, Bray and colleagues11 noted that the utility of free flaps may be limited in smaller clinical settings. The primary disadvantage of using DRTs is the necessity for a second operative procedure to harvest and place the skin graft. Traditionally, this is performed 2 to 3 weeks after the initial DRT application. Nevertheless, a 1-stage procedure can be performed in an outpatient setup, minimizing the burden to the patient and the medical costs, followed by secondary intention healing.
In response to critics of the 2-stage technique, Sanger and colleagues18 described single-stage use of DRT with split-thickness skin grafts with placement of an overlying wound vacuum-assisted closure to help speed incorporation of the DRT and improve survival of the immediately grafted skin. Another viable alternative is the McCash open-palm technique.19 In the open-palm technique, a Brunner zigzag incision is made in the affected digit. A transverse incision is made in the palm. A partial fasciectomy is performed in the palm and digit. After release, the digital incision is closed, and the palmar incision is left open. Although this well-studied and well-reported technique is known to reduce the risk of flap necrosis due to tension and hematoma,20 its main application is in the palm, as the name implies. Because in our patient the defect was palmar-digital with exposed “white structures,” we elected to use DRT.
Continue to: Although there is still...
Although there is still no perfect answer for wound coverage and closure in the hand with exposed or damaged tendons, DRT certainly performs well as a primary choice by minimizing adhesions; allowing a good ROM; and providing a durable, satisfactory cosmetic outcome. Likewise, an initial treatment with DRT does not preclude later, more elaborate reconstructive efforts, such as local or free flaps, if they continue to be indicated. DRT also does not diminish the ability to revise a tendon reconstruction if a secondary procedure is necessary. In our patient, tendon revision has not been necessary. DRT gives the surgeon a minimally invasive, efficient initial alternative to more labor-intensive, potentially morbid reconstructive procedures, without sacrificing outcome. Therefore, DRT can offer an alternative procedure in the surgeon’s armamentarium for tendon coverage in complex hand defects.
ABSTRACT
Soft tissue defects associated with exposed tendon pose difficult reconstructive problems because of tendon adhesions, poor range of motion, poor cosmetic appearance, and donor site morbidity. Dermal regeneration template is a skin substitute widely used in reconstructive surgery, including the occasional coverage of tendons. However, postoperative functionality of the tendons has not been well documented. We report a case of using dermal regeneration template for soft tissue reconstruction overlying tendons with loss of paratenon in a patient with Dupuytren’s contracture. Dermal regeneration template may offer an alternative option for immediate tendon coverage in the hand.
Soft tissue defects overlying exposed tendon with loss of paratenon often precipitate poor clinical outcomes because of the dichotomous demands of both closing the overlying soft-tissue defect and providing a gliding surface for the underlying tendons.1 Although avoidance of adhesions and restoration of function are the primary goals of the procedure, satisfactory appearance is also desirable. Likewise, any form of coverage should ideally provide good vasculature required for complete healing and an early form of closure following débridement.2 Simple skin grafts do not adequately meet these demands because they result in a high rate of tendon adhesions,3 and also are limited in patients with limited donor skin availability or questionable underlying wound bed viability, such as in scleroderma.
In order to reduce the frequency of tendon adhesions by creating a gliding surface, the use of interpositional materials, both artificial and biologic, has been employed with varying degrees of success, including cellophane, chitosan membrane, fibrin sealant, autogenous fascial flaps, and autogenous venous grafts.4-7 Many of the autogenous flaps and grafts have been employed with good success.8 However, complications and donor site morbidity encourage alternative procedures, including the use of artificial substances.2,8-10
We present our clinical experience with a patient who underwent successful placement of Integra (Integra LifeSciences) Dermal Regeneration Template (DRT) directly over exposed tendons with a subsequent full-thickness skin graft several weeks later. The procedures were performed per the manufacturer’s specifications, resulting in 2 stages of reconstruction. In our experience, DRT can offer immediate coverage unrestricted by wound size, and provides shorter operative time and decreased donor site and surgical morbidity compared with flap coverage, while demonstrating good cosmetic results. The patient provided written informed consent for print and electronic publication of this case report.
CASE
A 74-year-old right-handed man with Dupuytren’s contracture was evaluated for recurrent symptomatic contracture causing difficulty with daily activities. He reported palpable cords and contractures in the ring and small fingers of the right hand. He had 2 prior open surgical procedures, including palmar and digital fasciectomy of both hands. On the right hand, the ring and small fingers demonstrated 90° proximal interphalangeal (PIP) and 60° metacarpophalangeal (MCP) flexion contractures. Palpable central cords were present on the flexor surfaces of both the ring and small fingers. A well-healed surgical incision, performed 22 years earlier, was present over the palmar aspect of the ring finger.
Continue to: With consideration given...
With consideration given to the patient’s recurrent contracture after a prior surgical procedure, we discussed surgical excision of the diseased cords in order to eliminate the possibility of a second recurrence and maximize the gain of motion. Following discussion with the patient, we performed palmar and digital fasciectomy of the ring and small finger contractures. Postoperatively, the patient was followed closely for wound complications and vascular status. On his return to our clinic 11 days later, the patient was noted to have dehiscence of the digital wounds in the ring and small fingers (Figure 1).
STAGE 1
During the first stage, completed 14 days following the index procedure, débridement of the wounds was performed, followed by provisional DRT coverage of the tendons, secured with 5-0 nylon sutures (Figure 2).
STAGE 2
At approximately 2 weeks after application of the DRT, a full-thickness skin graft was applied. The thickness of the graft was chosen to allow for durable coverage of the palmar skin defects. Upon successful completion of the second stage, the patient was followed and evaluated for complete wound healing. On performing an examination 14 days after surgery, the ring and small fingers demonstrated only partially healed skin graft but significantly improved range of motion (ROM), with 40° to 90° arc of motion in the PIP joint and 25° to 90° arc of motion in the MCP joint (Figure 4). Owing to their limited size, the wounds were treated with dressing changes until successful healing (Figure 5).
Hand therapy was instituted to achieve maximum mobility for covered soft tissue and tendons and to maximize tendon gliding. At 1-year follow-up, the skin was fully healed and the patient’s active PIP motion was 30° to 90°, active MCP motion was 0° to 90°, and grip strength was 90 lb on both sides. The tendons glided under a well-vascularized tissue at the DRT placement site, and no secondary tenolysis procedure was deemed necessary.
DISCUSSION
Soft tissue defects with exposed tendons may offer a number of challenges for coverage. The primary concern is the creation of a gliding surface and the restoration of a functional tendon without adhesions.2 However, surgeons must use their own clinical judgment when choosing the method of coverage so as to minimize the effects of donor site morbidity and maximize the overall functional and cosmetic outcomes. All options must be considered while selecting a material or flap that is likely to survive in the relatively avascular tendon plane.2,8,11 When considering the reconstructive ladder, skin grafts may not represent a viable option in the presence of a nonvascularized wound bed, such as exposed tendon or bone, where paratenon or periosteum have been damaged. That leaves the surgeon with local flaps, regional flaps, free flaps, and skin substitutes.
Continue to : Before planning closure...
Before planning closure, wound conditions should be optimized, including wound bed quality, vascularization, and bacterial loads. Experimental data suggest that the bacterial load should be brought down below a critical level of 105 bacteria per g of tissue to allow a skin graft to take. This may be problematic from a practical standpoint because quantitative bacterial cultures take about 48 hours to obtain the result, long after a decision to graft is made. As a result, the surgeon may take an aggressive approach to wound débridement, making sure that all necrotic material has been sharply débrided prior to coverage.
As Levin12 noted in 1993, decisions regarding repair of any soft tissue defect may follow a well-delineated ladder beginning with the primary choice of split-thickness skin grafts and ending with free flaps. When treating tissue defects in the hand complex, flaps are an excellent option as they replace like with like, allow minimal scarring and early rehabilitation. 13,14 Nevertheless, a few general disadvantages are inherent in flap procedure: increase in operating time, risk of flap loss, and in case of free flaps, knowledge, experience, and microsurgical ability.2 In reference to complications, the rate of flap loss found by Khouri and colleagues15 was 4.1% with a 12.1% chance of incurring some measured complication, including wound dehiscence, arterial insufficiency, and flap necrosis.
Likewise, some of the conventional local and free flaps, including cutaneous and muscular flaps, prove ineffective in preventing tendon adhesions, create unsightly postoperative contours, or increase the area of trauma on the wounded hand, encouraging the use of free fascial flaps.11 Among the wide array of potential free fascial flaps, the temporoparietal, scapular, lateral arm, radial forearm, and free serratus fascial flaps are some of the most popular for hand defects.8,9 However, these procedures require an additional surgical site, meticulous dissection, microsurgical technique at times, and increased operating cost and time.2,8-10 Furthermore, free fascial flaps have demonstrated occasional partial flap loss and a decreased survival of the overlying skin graft, leading some to advocate delayed skin graft placement.10,16,17
On the basis of these complications, Bray and colleagues11 noted that the utility of free flaps may be limited in smaller clinical settings. The primary disadvantage of using DRTs is the necessity for a second operative procedure to harvest and place the skin graft. Traditionally, this is performed 2 to 3 weeks after the initial DRT application. Nevertheless, a 1-stage procedure can be performed in an outpatient setup, minimizing the burden to the patient and the medical costs, followed by secondary intention healing.
In response to critics of the 2-stage technique, Sanger and colleagues18 described single-stage use of DRT with split-thickness skin grafts with placement of an overlying wound vacuum-assisted closure to help speed incorporation of the DRT and improve survival of the immediately grafted skin. Another viable alternative is the McCash open-palm technique.19 In the open-palm technique, a Brunner zigzag incision is made in the affected digit. A transverse incision is made in the palm. A partial fasciectomy is performed in the palm and digit. After release, the digital incision is closed, and the palmar incision is left open. Although this well-studied and well-reported technique is known to reduce the risk of flap necrosis due to tension and hematoma,20 its main application is in the palm, as the name implies. Because in our patient the defect was palmar-digital with exposed “white structures,” we elected to use DRT.
Continue to: Although there is still...
Although there is still no perfect answer for wound coverage and closure in the hand with exposed or damaged tendons, DRT certainly performs well as a primary choice by minimizing adhesions; allowing a good ROM; and providing a durable, satisfactory cosmetic outcome. Likewise, an initial treatment with DRT does not preclude later, more elaborate reconstructive efforts, such as local or free flaps, if they continue to be indicated. DRT also does not diminish the ability to revise a tendon reconstruction if a secondary procedure is necessary. In our patient, tendon revision has not been necessary. DRT gives the surgeon a minimally invasive, efficient initial alternative to more labor-intensive, potentially morbid reconstructive procedures, without sacrificing outcome. Therefore, DRT can offer an alternative procedure in the surgeon’s armamentarium for tendon coverage in complex hand defects.
1. Flügel A. Kehrer C. Heitmann C, German G, Sauerbier M. Coverage of soft tissue defects of the hand with free fascial flaps. Microsurgery.2005;25(1):47-53.
2. Chen H, Buchman MT, Wei FC. Free flaps for soft tissue coverage in the hand and fingers. Hand Clin. 1999;15(4):541-554.
3. Chia J, Lim A, Peng YP. Use of an arterialized venous flap for resurfacing a circumferential soft tissue defect of a digit. Microsurgery. 2001; 21(8):374-378.
4. Wheeldon T. The use of cellophane as a permanent tendon sheath. J Bone J Surg Am; 1939;21(2):393-396.
5. Frykman E, Jacobsson S, Widenfalk B. Fibrin sealant in prevention of flexor tendon adhesions: an experimental study in the rabbit. J Hand Surg Am. 1993;18(1):68-75.
6. Jones NF, Lister GD. Free skin and composite flaps. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green’s Operative hand surgery. 6th ed. New York, NY: Churchill Livingstone; 2011:1721-1756.
7. Yan D, Shi X, Lui Q. Reconstruction of tendon sheath by autogenous vein graft in preventing adhesion. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 1997;11(1):38-39.
8. Pederson WC. Upper extremity microsurgery. Plast Reconstr Surg. 2001;107(6):1524-1537; discussion 1538-15399, 1540-1543.
9. WintschK, Helaly P. Free flap of gliding tissue. J Reconstr Microsurg. 1986;2(3):143-151.
10. Meland NB, Weimar R. Microsurgical reconstruction: experience with free fascia flaps. Ann Plast Surg. 1991;27(1):1-8.
11. Bray PW, Boyer MI, Bowen CV. Complex injuries of the forearm. Coverage considerations. Hand Clin. 1997;13(2):263-278.
12. Levin LS. The reconstructive ladder: an orthoplastic approach. Ortho Clin North Am. 1993; 24(3):393-409.
13. Hallock GG. Utility of both muscle and fascia flaps in severe lower extremity trauma. J Trauma. 2000;48 (5):913-917. doi:10.1097/00005373-200005000-00016.
14. Hallock GG. The utility of both muscle and fascia flaps in severe upper extremity trauma. J Trauma. 2002;53(1):61-65. doi:10.1097/00005373-200207000-00013.
15. Khouri RK, Cooley BC, Kunselman AR, et al. A prospective study of microvascular free-flap surgery and outcome. Plast Reconstr Surg. 1998;102(3):711-721.
16. Woods JM 4th, Shack RB, Hagan KF. Free temporoparietal fascia flap in reconstruction of the lower extremity. Ann Plast Surg. 1995;34(5):501-506. doi:10.1097/00000637-199505000-00008.
17. Chung KC, Cederna PS. Endoscopic harvest of temporoparietal fascial free flaps for coverage of hand wounds. J Hand Surg Am. 2002;27(3):525-533.
18. Sanger C, Molnar JA, Newman CE, et al. Immediate skin grafting of an engineered dermal substitute: P37. Plast Reconstr Surg. 2005;116(3S):165.
19. McCash CR. The open palm technique in Dupuytren’s contracture. Br J Plast Surg. 1964;17:271-280.
20. Shaw DL, Wise DI, Holms W. Dupuytren's disease treated by palmar fasciectomy and an open palm technique. J Hand Surg Br. 1996;21(4):484-485.
1. Flügel A. Kehrer C. Heitmann C, German G, Sauerbier M. Coverage of soft tissue defects of the hand with free fascial flaps. Microsurgery.2005;25(1):47-53.
2. Chen H, Buchman MT, Wei FC. Free flaps for soft tissue coverage in the hand and fingers. Hand Clin. 1999;15(4):541-554.
3. Chia J, Lim A, Peng YP. Use of an arterialized venous flap for resurfacing a circumferential soft tissue defect of a digit. Microsurgery. 2001; 21(8):374-378.
4. Wheeldon T. The use of cellophane as a permanent tendon sheath. J Bone J Surg Am; 1939;21(2):393-396.
5. Frykman E, Jacobsson S, Widenfalk B. Fibrin sealant in prevention of flexor tendon adhesions: an experimental study in the rabbit. J Hand Surg Am. 1993;18(1):68-75.
6. Jones NF, Lister GD. Free skin and composite flaps. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, eds. Green’s Operative hand surgery. 6th ed. New York, NY: Churchill Livingstone; 2011:1721-1756.
7. Yan D, Shi X, Lui Q. Reconstruction of tendon sheath by autogenous vein graft in preventing adhesion. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 1997;11(1):38-39.
8. Pederson WC. Upper extremity microsurgery. Plast Reconstr Surg. 2001;107(6):1524-1537; discussion 1538-15399, 1540-1543.
9. WintschK, Helaly P. Free flap of gliding tissue. J Reconstr Microsurg. 1986;2(3):143-151.
10. Meland NB, Weimar R. Microsurgical reconstruction: experience with free fascia flaps. Ann Plast Surg. 1991;27(1):1-8.
11. Bray PW, Boyer MI, Bowen CV. Complex injuries of the forearm. Coverage considerations. Hand Clin. 1997;13(2):263-278.
12. Levin LS. The reconstructive ladder: an orthoplastic approach. Ortho Clin North Am. 1993; 24(3):393-409.
13. Hallock GG. Utility of both muscle and fascia flaps in severe lower extremity trauma. J Trauma. 2000;48 (5):913-917. doi:10.1097/00005373-200005000-00016.
14. Hallock GG. The utility of both muscle and fascia flaps in severe upper extremity trauma. J Trauma. 2002;53(1):61-65. doi:10.1097/00005373-200207000-00013.
15. Khouri RK, Cooley BC, Kunselman AR, et al. A prospective study of microvascular free-flap surgery and outcome. Plast Reconstr Surg. 1998;102(3):711-721.
16. Woods JM 4th, Shack RB, Hagan KF. Free temporoparietal fascia flap in reconstruction of the lower extremity. Ann Plast Surg. 1995;34(5):501-506. doi:10.1097/00000637-199505000-00008.
17. Chung KC, Cederna PS. Endoscopic harvest of temporoparietal fascial free flaps for coverage of hand wounds. J Hand Surg Am. 2002;27(3):525-533.
18. Sanger C, Molnar JA, Newman CE, et al. Immediate skin grafting of an engineered dermal substitute: P37. Plast Reconstr Surg. 2005;116(3S):165.
19. McCash CR. The open palm technique in Dupuytren’s contracture. Br J Plast Surg. 1964;17:271-280.
20. Shaw DL, Wise DI, Holms W. Dupuytren's disease treated by palmar fasciectomy and an open palm technique. J Hand Surg Br. 1996;21(4):484-485.
TAKE-HOME POINTS
- Full thickness skin grafts are generally considered unreliable for coverage of 3-dimensional defects of the hand with tendon exposure.
- Integra (Integra LifeSciences) is a bilayer skin substitute. The “dermal” (lower) layer is a bovine collagen base with glycosaminoglycan chondroitin-6-sulfate while the upper layer is a silicone sheet that acts as a temporary epidermis.
- Despite its popularity of Integra in burn reconstruction, little has been published regarding its utility in complex hand wounds with exposed tendons.
- Small areas of exposed tendons without remaining paratenon can be successfully grafted with Integra.
- In the presence of a healthy wound bed and no necrotic tissue or infection, Integra offers a reconstructive option that allows immediate coverage of complex hand wounds.

5-year data show deepening response with ibrutinib in CLL
Single-agent ibrutinib has had sustained efficacy and a rate of complete response that has increased over time, according to a 5-year follow-up report including 132 patients with chronic lymphocytic leukemia (CLL).
Efficacy has been maintained in both treatment-naive and relapsed/refractory CLL, despite the presence of high-risk genomic features in many patients, investigators reported in Blood.
Treatment has been well tolerated, and the occurrence of severe adverse events has diminished over time, according to Susan M. O’Brien, MD, of the Chao Family Comprehensive Cancer Center, University of California, Irvine, and her colleagues.
“The safety profile of ibrutinib over time remains acceptable and manageable, allowing almost one-half of the patients (48%) to be treated for more than 4 years and thus maximize response,” the investigators wrote.
The report was based on 5-year follow-up of patients with CLL who had been enrolled in a phase 1b/2 study (PCYC-1102) and an extension study (PCYC-1103). A total of 132 patients were evaluated, including 101 with relapsed/refractory disease and 31 who were treatment naive.
The overall response rate remained high, at 89% in this 5-year follow-up. Complete response rates increased over time, reaching 29% in treatment-naive patients and 10% in relapsed/refractory patients. In a previous report on 3-year follow-up for these patients, investigators reported complete response rates of 23% in the previously untreated group and 7% in the relapsed/refractory group. The new findings demonstrate “deepening of responses” with continued ibrutinib therapy, Dr. O’Brien and her coauthors wrote.
The 5-year rate of progression-free survival was 44% for relapsed/refractory patients and 92% for treatment-naive patients in this study. Median progression-free survival was 51 months for the relapsed/refractory cohort. “[Progression-free survival] with single-agent ibrutinib in [treatment-naive] patients appears particularly favorable, because the median has not been reached,” investigators wrote.
Adverse events that limited treatment were more frequent during the first year of treatment than in subsequent years, data show, while new onset of neutropenia and thrombocytopenia decreased over time.
The overall response rate was high even in patients with high-risk genetic features. Rates of overall response ranged from 79% to 97%, depending on genomic subgroup. That held true for relapsed/refractory CLL patients with del(17p), a significant negative prognostic factor for survival. In that group, the overall response rate was 79% and the duration of response was 31 months, representing “promising single-agent efficacy” in that group, investigators said.
Pharmacyclics, an AbbVie Company, provided funding for the study and writing support. The study was also supported by grants from the National Institutes of Health and a private foundation. Dr. O’Brien reported ties to AbbVie, Janssen, and Pharmacyclics. Other investigators reported financial relationships with various pharmaceutical companies.
SOURCE: O’Brien S et al. Blood. 2018;131(17):1910-9.
This report on the 5-year experience with single-agent ibrutinib in chronic lymphocytic leukemia (CLL) is a step forward in knowledge of the drug’s natural history, according to Jennifer R. Brown, MD, PhD.
“Ibrutinib data are starting to mature, but much opportunity for growth remains,” Dr. Brown said in an editorial.
One notable update in the report is that a median, progression-free survival has been reached in patients with relapsed/refractory CLL. The reported 51-month median progression-free survival is “strikingly good” in this cohort of patients with high-risk disease, and compares favorably to older regimens in similar patient populations, she said.
Regarding previously untreated CLL patients, it is notable that 45% of this cohort discontinued treatment, many apparently after year 4, Dr. Brown said. The finding that median duration on therapy was just about 5.5 years in the cohort could be “potentially quite useful” in counseling patients, if confirmed in a larger cohort, she added.
Given the discontinuation data, one unanswered question is the durability of remission after stopping ibrutinib in a “deep but probably not complete remission” versus continuing therapy.
“Further follow-up of patients who discontinue without disease progression, as well as systematic investigation of time-limited therapy, including novel likely combination approaches, is clearly warranted,” Dr. Brown said in her editorial.
Dr. Jennifer R. Brown is with the Dana-Farber Cancer Institute in Boston. These comments are adapted an accompanying editorial ( Blood. 2018;131:1880-2 ). Dr. Brown reported ties to Janssen, Pharmacyclics, AstraZeneca, Sun, Redx, Sunesis, Loxo, Gilead, TG Therapeutics, Verastem, and AbbVie.
This report on the 5-year experience with single-agent ibrutinib in chronic lymphocytic leukemia (CLL) is a step forward in knowledge of the drug’s natural history, according to Jennifer R. Brown, MD, PhD.
“Ibrutinib data are starting to mature, but much opportunity for growth remains,” Dr. Brown said in an editorial.
One notable update in the report is that a median, progression-free survival has been reached in patients with relapsed/refractory CLL. The reported 51-month median progression-free survival is “strikingly good” in this cohort of patients with high-risk disease, and compares favorably to older regimens in similar patient populations, she said.
Regarding previously untreated CLL patients, it is notable that 45% of this cohort discontinued treatment, many apparently after year 4, Dr. Brown said. The finding that median duration on therapy was just about 5.5 years in the cohort could be “potentially quite useful” in counseling patients, if confirmed in a larger cohort, she added.
Given the discontinuation data, one unanswered question is the durability of remission after stopping ibrutinib in a “deep but probably not complete remission” versus continuing therapy.
“Further follow-up of patients who discontinue without disease progression, as well as systematic investigation of time-limited therapy, including novel likely combination approaches, is clearly warranted,” Dr. Brown said in her editorial.
Dr. Jennifer R. Brown is with the Dana-Farber Cancer Institute in Boston. These comments are adapted an accompanying editorial ( Blood. 2018;131:1880-2 ). Dr. Brown reported ties to Janssen, Pharmacyclics, AstraZeneca, Sun, Redx, Sunesis, Loxo, Gilead, TG Therapeutics, Verastem, and AbbVie.
This report on the 5-year experience with single-agent ibrutinib in chronic lymphocytic leukemia (CLL) is a step forward in knowledge of the drug’s natural history, according to Jennifer R. Brown, MD, PhD.
“Ibrutinib data are starting to mature, but much opportunity for growth remains,” Dr. Brown said in an editorial.
One notable update in the report is that a median, progression-free survival has been reached in patients with relapsed/refractory CLL. The reported 51-month median progression-free survival is “strikingly good” in this cohort of patients with high-risk disease, and compares favorably to older regimens in similar patient populations, she said.
Regarding previously untreated CLL patients, it is notable that 45% of this cohort discontinued treatment, many apparently after year 4, Dr. Brown said. The finding that median duration on therapy was just about 5.5 years in the cohort could be “potentially quite useful” in counseling patients, if confirmed in a larger cohort, she added.
Given the discontinuation data, one unanswered question is the durability of remission after stopping ibrutinib in a “deep but probably not complete remission” versus continuing therapy.
“Further follow-up of patients who discontinue without disease progression, as well as systematic investigation of time-limited therapy, including novel likely combination approaches, is clearly warranted,” Dr. Brown said in her editorial.
Dr. Jennifer R. Brown is with the Dana-Farber Cancer Institute in Boston. These comments are adapted an accompanying editorial ( Blood. 2018;131:1880-2 ). Dr. Brown reported ties to Janssen, Pharmacyclics, AstraZeneca, Sun, Redx, Sunesis, Loxo, Gilead, TG Therapeutics, Verastem, and AbbVie.
Single-agent ibrutinib has had sustained efficacy and a rate of complete response that has increased over time, according to a 5-year follow-up report including 132 patients with chronic lymphocytic leukemia (CLL).
Efficacy has been maintained in both treatment-naive and relapsed/refractory CLL, despite the presence of high-risk genomic features in many patients, investigators reported in Blood.
Treatment has been well tolerated, and the occurrence of severe adverse events has diminished over time, according to Susan M. O’Brien, MD, of the Chao Family Comprehensive Cancer Center, University of California, Irvine, and her colleagues.
“The safety profile of ibrutinib over time remains acceptable and manageable, allowing almost one-half of the patients (48%) to be treated for more than 4 years and thus maximize response,” the investigators wrote.
The report was based on 5-year follow-up of patients with CLL who had been enrolled in a phase 1b/2 study (PCYC-1102) and an extension study (PCYC-1103). A total of 132 patients were evaluated, including 101 with relapsed/refractory disease and 31 who were treatment naive.
The overall response rate remained high, at 89% in this 5-year follow-up. Complete response rates increased over time, reaching 29% in treatment-naive patients and 10% in relapsed/refractory patients. In a previous report on 3-year follow-up for these patients, investigators reported complete response rates of 23% in the previously untreated group and 7% in the relapsed/refractory group. The new findings demonstrate “deepening of responses” with continued ibrutinib therapy, Dr. O’Brien and her coauthors wrote.
The 5-year rate of progression-free survival was 44% for relapsed/refractory patients and 92% for treatment-naive patients in this study. Median progression-free survival was 51 months for the relapsed/refractory cohort. “[Progression-free survival] with single-agent ibrutinib in [treatment-naive] patients appears particularly favorable, because the median has not been reached,” investigators wrote.
Adverse events that limited treatment were more frequent during the first year of treatment than in subsequent years, data show, while new onset of neutropenia and thrombocytopenia decreased over time.
The overall response rate was high even in patients with high-risk genetic features. Rates of overall response ranged from 79% to 97%, depending on genomic subgroup. That held true for relapsed/refractory CLL patients with del(17p), a significant negative prognostic factor for survival. In that group, the overall response rate was 79% and the duration of response was 31 months, representing “promising single-agent efficacy” in that group, investigators said.
Pharmacyclics, an AbbVie Company, provided funding for the study and writing support. The study was also supported by grants from the National Institutes of Health and a private foundation. Dr. O’Brien reported ties to AbbVie, Janssen, and Pharmacyclics. Other investigators reported financial relationships with various pharmaceutical companies.
SOURCE: O’Brien S et al. Blood. 2018;131(17):1910-9.
Single-agent ibrutinib has had sustained efficacy and a rate of complete response that has increased over time, according to a 5-year follow-up report including 132 patients with chronic lymphocytic leukemia (CLL).
Efficacy has been maintained in both treatment-naive and relapsed/refractory CLL, despite the presence of high-risk genomic features in many patients, investigators reported in Blood.
Treatment has been well tolerated, and the occurrence of severe adverse events has diminished over time, according to Susan M. O’Brien, MD, of the Chao Family Comprehensive Cancer Center, University of California, Irvine, and her colleagues.
“The safety profile of ibrutinib over time remains acceptable and manageable, allowing almost one-half of the patients (48%) to be treated for more than 4 years and thus maximize response,” the investigators wrote.
The report was based on 5-year follow-up of patients with CLL who had been enrolled in a phase 1b/2 study (PCYC-1102) and an extension study (PCYC-1103). A total of 132 patients were evaluated, including 101 with relapsed/refractory disease and 31 who were treatment naive.
The overall response rate remained high, at 89% in this 5-year follow-up. Complete response rates increased over time, reaching 29% in treatment-naive patients and 10% in relapsed/refractory patients. In a previous report on 3-year follow-up for these patients, investigators reported complete response rates of 23% in the previously untreated group and 7% in the relapsed/refractory group. The new findings demonstrate “deepening of responses” with continued ibrutinib therapy, Dr. O’Brien and her coauthors wrote.
The 5-year rate of progression-free survival was 44% for relapsed/refractory patients and 92% for treatment-naive patients in this study. Median progression-free survival was 51 months for the relapsed/refractory cohort. “[Progression-free survival] with single-agent ibrutinib in [treatment-naive] patients appears particularly favorable, because the median has not been reached,” investigators wrote.
Adverse events that limited treatment were more frequent during the first year of treatment than in subsequent years, data show, while new onset of neutropenia and thrombocytopenia decreased over time.
The overall response rate was high even in patients with high-risk genetic features. Rates of overall response ranged from 79% to 97%, depending on genomic subgroup. That held true for relapsed/refractory CLL patients with del(17p), a significant negative prognostic factor for survival. In that group, the overall response rate was 79% and the duration of response was 31 months, representing “promising single-agent efficacy” in that group, investigators said.
Pharmacyclics, an AbbVie Company, provided funding for the study and writing support. The study was also supported by grants from the National Institutes of Health and a private foundation. Dr. O’Brien reported ties to AbbVie, Janssen, and Pharmacyclics. Other investigators reported financial relationships with various pharmaceutical companies.
SOURCE: O’Brien S et al. Blood. 2018;131(17):1910-9.
FROM BLOOD
Key clinical point:
Major finding: The 5-year rate of progression-free survival was 44% for relapsed/refractory patients and 92% for treatment-naive patients.
Study details: Report on 5-year follow-up of 132 patients with CLL enrolled in a phase 1b/2 study (PCYC-1102) and an extension study (PCYC-1103).
Disclosures: Pharmacyclics, an AbbVie Company, provided funding for the study and writing support. The study was also supported by grants from the National Institutes of Health and a private foundation. The authors reported ties to Pharmacyclics and other companies.
Source: O’Brien S et al. Blood. 2018;131(17):1910-9.
Interferon treatment does not increase stroke risk in MS
LOS ANGELES – Patients with multiple sclerosis who are treated with subcutaneous interferon beta-1a have no increase in stroke risk, compared with those treated with placebo, according to pooled data from clinical trials and a safety database analysis.
Studies have shown that MS patients have a greater risk of stroke, compared with the general population, but the data with respect to the risk of stroke following interferon treatment are limited, Alan Gillett, PhD, explained in his presentation at the annual meeting of the American Academy of Neurology. He noted that a 2017 report on a series of nested case-control studies showed a 1.8-fold increased risk of stroke in relapsing-remitting MS patients who received interferon.
In the new analysis presented at the meeting, there was a trend toward decreased stroke incidence among patients treated with subcutaneous interferon beta-1a. Stroke incidence was 0.025 per 100 patient-years (25 events) in patients treated with subcutaneous interferon beta-1a vs. 0.051 per 100 patient-years (11 events) in patients who received placebo across 17 phase 2-4 clinical trials. The incidence rate ratio (IRR) and hazard ratio for stroke in interferon- vs. placebo-treated patients were 0.486 and 0.496, respectively, reported Dr. Gillett of EMD Serono, Mississauga, Ont.
Further, no significant difference in stroke incidence was seen between the treatment and placebo groups based on treatment duration, Dr. Gillett said. The IRR in patients treated for less than 2 years was 0.602 vs. 0.469 in those treated for 2 or more years.
“The incidence rate ratio [in both groups] was very comparable to that overall, so this indicates that treatment duration had little impact on the incidence rate of stroke,” he said.
The same was true in an analysis based on dose; the IRRs were similar in those exposed to 44 mcg vs. placebo, and in those receiving any dose vs. placebo, he noted.
The analysis is based on reports of 569 cerebrovascular events occurring over 19 years (2.7 per 10,000 patient-years) in 1,594,414 patient-years of follow-up through May 22, 2017, in the Global Patient Safety Database.
“And according to prescribing information ... this would be classified as rare, with less than 1 in 1,000,” Dr. Gillett said.
“So this led us to our objective to really assess the risk of stroke in patients treated with subcutaneous interferon beta-1a ... and the association with treatment duration and dose,” he said. “What we can conclude from [our] study is that a trend toward decreased risk of stroke for subcutaneous interferon beta-1a, compared to placebo, was observed in 17 clinical trials ... and the safety data from both clinical trials and postmarketing [surveillance] suggests that treatment with subcutaneous interferon beta-1a ... does not increase the risk of stroke in patients with MS.”
This study was supported by Merck KGaA of Darmstadt, Germany. Dr. Gillett is an employee of EMD Serono, the biopharmaceutical division of Merck KGaA.
SOURCE: Sabidó M et al. Neurology. 2018 Apr 90(15 Suppl.):S36.008.
LOS ANGELES – Patients with multiple sclerosis who are treated with subcutaneous interferon beta-1a have no increase in stroke risk, compared with those treated with placebo, according to pooled data from clinical trials and a safety database analysis.
Studies have shown that MS patients have a greater risk of stroke, compared with the general population, but the data with respect to the risk of stroke following interferon treatment are limited, Alan Gillett, PhD, explained in his presentation at the annual meeting of the American Academy of Neurology. He noted that a 2017 report on a series of nested case-control studies showed a 1.8-fold increased risk of stroke in relapsing-remitting MS patients who received interferon.
In the new analysis presented at the meeting, there was a trend toward decreased stroke incidence among patients treated with subcutaneous interferon beta-1a. Stroke incidence was 0.025 per 100 patient-years (25 events) in patients treated with subcutaneous interferon beta-1a vs. 0.051 per 100 patient-years (11 events) in patients who received placebo across 17 phase 2-4 clinical trials. The incidence rate ratio (IRR) and hazard ratio for stroke in interferon- vs. placebo-treated patients were 0.486 and 0.496, respectively, reported Dr. Gillett of EMD Serono, Mississauga, Ont.
Further, no significant difference in stroke incidence was seen between the treatment and placebo groups based on treatment duration, Dr. Gillett said. The IRR in patients treated for less than 2 years was 0.602 vs. 0.469 in those treated for 2 or more years.
“The incidence rate ratio [in both groups] was very comparable to that overall, so this indicates that treatment duration had little impact on the incidence rate of stroke,” he said.
The same was true in an analysis based on dose; the IRRs were similar in those exposed to 44 mcg vs. placebo, and in those receiving any dose vs. placebo, he noted.
The analysis is based on reports of 569 cerebrovascular events occurring over 19 years (2.7 per 10,000 patient-years) in 1,594,414 patient-years of follow-up through May 22, 2017, in the Global Patient Safety Database.
“And according to prescribing information ... this would be classified as rare, with less than 1 in 1,000,” Dr. Gillett said.
“So this led us to our objective to really assess the risk of stroke in patients treated with subcutaneous interferon beta-1a ... and the association with treatment duration and dose,” he said. “What we can conclude from [our] study is that a trend toward decreased risk of stroke for subcutaneous interferon beta-1a, compared to placebo, was observed in 17 clinical trials ... and the safety data from both clinical trials and postmarketing [surveillance] suggests that treatment with subcutaneous interferon beta-1a ... does not increase the risk of stroke in patients with MS.”
This study was supported by Merck KGaA of Darmstadt, Germany. Dr. Gillett is an employee of EMD Serono, the biopharmaceutical division of Merck KGaA.
SOURCE: Sabidó M et al. Neurology. 2018 Apr 90(15 Suppl.):S36.008.
LOS ANGELES – Patients with multiple sclerosis who are treated with subcutaneous interferon beta-1a have no increase in stroke risk, compared with those treated with placebo, according to pooled data from clinical trials and a safety database analysis.
Studies have shown that MS patients have a greater risk of stroke, compared with the general population, but the data with respect to the risk of stroke following interferon treatment are limited, Alan Gillett, PhD, explained in his presentation at the annual meeting of the American Academy of Neurology. He noted that a 2017 report on a series of nested case-control studies showed a 1.8-fold increased risk of stroke in relapsing-remitting MS patients who received interferon.
In the new analysis presented at the meeting, there was a trend toward decreased stroke incidence among patients treated with subcutaneous interferon beta-1a. Stroke incidence was 0.025 per 100 patient-years (25 events) in patients treated with subcutaneous interferon beta-1a vs. 0.051 per 100 patient-years (11 events) in patients who received placebo across 17 phase 2-4 clinical trials. The incidence rate ratio (IRR) and hazard ratio for stroke in interferon- vs. placebo-treated patients were 0.486 and 0.496, respectively, reported Dr. Gillett of EMD Serono, Mississauga, Ont.
Further, no significant difference in stroke incidence was seen between the treatment and placebo groups based on treatment duration, Dr. Gillett said. The IRR in patients treated for less than 2 years was 0.602 vs. 0.469 in those treated for 2 or more years.
“The incidence rate ratio [in both groups] was very comparable to that overall, so this indicates that treatment duration had little impact on the incidence rate of stroke,” he said.
The same was true in an analysis based on dose; the IRRs were similar in those exposed to 44 mcg vs. placebo, and in those receiving any dose vs. placebo, he noted.
The analysis is based on reports of 569 cerebrovascular events occurring over 19 years (2.7 per 10,000 patient-years) in 1,594,414 patient-years of follow-up through May 22, 2017, in the Global Patient Safety Database.
“And according to prescribing information ... this would be classified as rare, with less than 1 in 1,000,” Dr. Gillett said.
“So this led us to our objective to really assess the risk of stroke in patients treated with subcutaneous interferon beta-1a ... and the association with treatment duration and dose,” he said. “What we can conclude from [our] study is that a trend toward decreased risk of stroke for subcutaneous interferon beta-1a, compared to placebo, was observed in 17 clinical trials ... and the safety data from both clinical trials and postmarketing [surveillance] suggests that treatment with subcutaneous interferon beta-1a ... does not increase the risk of stroke in patients with MS.”
This study was supported by Merck KGaA of Darmstadt, Germany. Dr. Gillett is an employee of EMD Serono, the biopharmaceutical division of Merck KGaA.
SOURCE: Sabidó M et al. Neurology. 2018 Apr 90(15 Suppl.):S36.008.
REPORTING FROM AAN 2018
Key clinical point: Pooled data show no increase in stroke risk in MS patients treated with interferon.
Major finding: A trend toward decreased stroke incidence was seen with interferon treatment vs. placebo (IRR, 0.486).
Study details: A review of pooled data from 17 clinical trials and postmarketing surveillance.
Disclosures: This study was supported by Merck KGaA of Darmstadt, Germany. Dr. Gillett is an employee of EMD Serono, the biopharmaceutical division of Merck KGaA.
Source: Sabidó M et al. Neurology. 2018 Apr:90(15 Suppl.):S36.008.
U.S. public largely ignores firearm access and suicide completion link
WASHINGTON – The evidence linking firearm access and suicide completion is largely ignored in current U.S. discussions on guns, Michael D. Anestis, PhD, said at the annual conference of the American Association of Suicidology.
“Only a tiny fraction of media discussions on gun deaths involve suicide. We must make a concerted and sustained effort to change this conversation,” said Dr. Anestis, a clinical psychologist at the University of Southern Mississippi in Hattiesburg. When the relationship between firearms and suicide is discussed, it often is as a “footnote” and includes a lot of inaccurate information.

Dr. Anestis reviewed results from a survey he and his associates ran in 2017 that documented these inaccurate beliefs regarding firearms and suicide. The researchers had 300 American adults who owned at least one firearm complete a questionnaire on their practices for firearm storage and their beliefs on the connections between firearm storage and suicide risk. The results showed a clear link between unsafe firearm storage and reduced belief of a link between firearm access and suicide risk (J Affect Disord. 2018 Feb;227:530-5). They also showed that fearlessness about death moderated the relationship: People with a higher level of fearlessness showed a tighter link between storage practices and beliefs about suicide risk.
During the conference, Dr. Anestis and his associates reported additional, as-yet unpublished findings that further detailed risks for suicide among gun owners. A survey of 100 adults from the Hattiesburg area showed that greater experience firing a gun linked with “factors thought to facilitate the transition from suicidal desire to suicidal behavior. We need to consider an individual’s experience and comfort with firearms, not just ownership and storage,” Dr. Anestis said.
. But additional research from his group showed that another route to acquiring “capability” for suicide, such as fearlessness of death, can occur through exposure to violent video games.
Dr. Anestis had no disclosures.
;
WASHINGTON – The evidence linking firearm access and suicide completion is largely ignored in current U.S. discussions on guns, Michael D. Anestis, PhD, said at the annual conference of the American Association of Suicidology.
“Only a tiny fraction of media discussions on gun deaths involve suicide. We must make a concerted and sustained effort to change this conversation,” said Dr. Anestis, a clinical psychologist at the University of Southern Mississippi in Hattiesburg. When the relationship between firearms and suicide is discussed, it often is as a “footnote” and includes a lot of inaccurate information.
Dr. Anestis reviewed results from a survey he and his associates ran in 2017 that documented these inaccurate beliefs regarding firearms and suicide. The researchers had 300 American adults who owned at least one firearm complete a questionnaire on their practices for firearm storage and their beliefs on the connections between firearm storage and suicide risk. The results showed a clear link between unsafe firearm storage and reduced belief of a link between firearm access and suicide risk (J Affect Disord. 2018 Feb;227:530-5). They also showed that fearlessness about death moderated the relationship: People with a higher level of fearlessness showed a tighter link between storage practices and beliefs about suicide risk.
During the conference, Dr. Anestis and his associates reported additional, as-yet unpublished findings that further detailed risks for suicide among gun owners. A survey of 100 adults from the Hattiesburg area showed that greater experience firing a gun linked with “factors thought to facilitate the transition from suicidal desire to suicidal behavior. We need to consider an individual’s experience and comfort with firearms, not just ownership and storage,” Dr. Anestis said.
. But additional research from his group showed that another route to acquiring “capability” for suicide, such as fearlessness of death, can occur through exposure to violent video games.
Dr. Anestis had no disclosures.
;
WASHINGTON – The evidence linking firearm access and suicide completion is largely ignored in current U.S. discussions on guns, Michael D. Anestis, PhD, said at the annual conference of the American Association of Suicidology.
“Only a tiny fraction of media discussions on gun deaths involve suicide. We must make a concerted and sustained effort to change this conversation,” said Dr. Anestis, a clinical psychologist at the University of Southern Mississippi in Hattiesburg. When the relationship between firearms and suicide is discussed, it often is as a “footnote” and includes a lot of inaccurate information.
Dr. Anestis reviewed results from a survey he and his associates ran in 2017 that documented these inaccurate beliefs regarding firearms and suicide. The researchers had 300 American adults who owned at least one firearm complete a questionnaire on their practices for firearm storage and their beliefs on the connections between firearm storage and suicide risk. The results showed a clear link between unsafe firearm storage and reduced belief of a link between firearm access and suicide risk (J Affect Disord. 2018 Feb;227:530-5). They also showed that fearlessness about death moderated the relationship: People with a higher level of fearlessness showed a tighter link between storage practices and beliefs about suicide risk.
During the conference, Dr. Anestis and his associates reported additional, as-yet unpublished findings that further detailed risks for suicide among gun owners. A survey of 100 adults from the Hattiesburg area showed that greater experience firing a gun linked with “factors thought to facilitate the transition from suicidal desire to suicidal behavior. We need to consider an individual’s experience and comfort with firearms, not just ownership and storage,” Dr. Anestis said.
. But additional research from his group showed that another route to acquiring “capability” for suicide, such as fearlessness of death, can occur through exposure to violent video games.
Dr. Anestis had no disclosures.
;
REPORTING FROM THE AAS ANNUAL CONFERENCE
‘You are what kind of doctor?’
Editor’s note: The Hospitalist is pleased to introduce a new recurring column: “The Legacies of Hospital Medicine.” This will be a recurring feature submitted by some of the best and brightest hospitalists in the field who have helped shape our specialty into what it is today. It will be a series of articles that will reflect on hospital medicine and it’s evolution over time from a variety of unique and innovative perspectives. We hope you enjoy this series, and we welcome any feedback as it evolves!
Hearkening back to my early time as a hospital-based physician, I recall the pleasure of waking every day and feeling like I belonged to an exclusive club. I felt passion for my work, along with a tiny cohort of similarly situated docs. We lacked a kinship with other medical organizations, however. We had no union of our own and were invisible upstarts.

And the question always came: “Tell me again ... you are what kind of doctor?”
The response changed every week. Ditto for my job responsibilities and charges. The memories are wonderful, though, and I have great affection for the early years.
Initially, I recall networking and attending national meetings – SGIM and ACP in particular – spreading the faith and talking up our bona fides. In addition to the registration fees, there came an earful of guff from irate physicians about the new breed of doctors, yet unnamed, who were destroying medicine. Likewise, I recall opinion columns from newspapers and peer-reviewed journals from a spate of “simple country docs.” The writing had a pretense of politeness but with a hint of disdain, predicting nothing less than the destruction of health care as we knew it. And to be standing next to them in conversation: “How dare you hospital docs exhale CO2!” We might as well have had “KICK ME” signs on our backs.
Inpatient medicine was upending the status quo – or so we believed – while also overturning a generations’ worth of dogma on how hospitals should do their business. Fate also played a role, and we could not have anticipated the arrival of health care consolidation, “To Err Is Human,” managed care, and payment reform – all of which upset practice conditions that had been in existence for decades. We walked a line between old and new, down a path whose purpose we felt but toward a destination we could not entirely envision.
That transformed with time.
Like most hospitalists, my ticket in began after some sleuthing and calls to Win Whitcomb, MD, and John Nelson, MD – still trusted friends today. They will make their marks in future columns, but as I am the inaugural contributor, let me be the first to state they both had a sixth sense steering our group of disciples. They became the obvious chiefs, along with Bob Wachter, MD, and took the lead in articulating what we aspired to be. Sounds saccharine now, but it did not then.
But lucky for us, hospital medicine took off. Our wise choices laid the groundwork for what is now a discipline in repose. “Hospitalist” no longer sounds like a neologism, and the term entered Merriam-Webster to seal our fate.
Twenty years out, hospital medicine still feels like a figurative case of Moore’s law. I cannot keep up with the strange faces at annual meetings and membership size, the throng of published articles (I used to pride myself on knowing all the hospitalist studies – no longer), and the lengthy list of initiatives and Society of Hospital Medicine resources on hand.
Without question, SHM has been the most rewarding part of my professional life. Hospital medicine mates sustain and keep me in good stead and have done so since training. Their insights teach me more than journals or any day on the job could impart and have given me a learning windfall for the cost of a song.
I initiated my hospitalist path as a 20-something tenderfoot, but from my interactions with colleagues both liberal and conservative, urban and rural, corporate and academic, and specialist and generalist, I developed into a seasoned craftsman.
Countless times I strode into an SHM activity thinking one way, and through the intellect and conviction of my peers, I got smart. Working in the same setting for most of my career, unchallenged, I could have assimilated a sclerotic worldview, but my hospital medicine colleagues would have none of that – kudos and thanks to them for it.
I could cite endless anecdotes – and they are swirling as I write. Crucial positions discussed and adopted, roads taken and those not, specialties angered and appeased, wonderful meals had, and on and on. They are and were the building blocks of a journey – and a joyful one.
As truly notable memories go, however, for me, there is only one.
By far, watching and absorbing the lessons of how an organization develops – goes from zero to sixty – has been a master class in enterprise and execution.
A PGY4 sees a president, CEO, board, ad hoc committees, staff, big budgets, and capital outlays make things happen and assumes it just is. But an operational charter with an instruction manual in-tow didn’t just drop from on high; that’s not how things go down. The right personnel selections, value choices (“SHM is a big tent” was not an accident), affiliate alliances, assessment of risks, and strategies pursued occurred for a reason; keen minds had the vision to set the board right.
The privilege of participating in the SHM project has been an education no grant or scholarship could equal. To say I had a tiny role in all of that is just reward.
Through SHM I have made lifelong friends, advanced my perspective and development as a healer, acquired a nifty board certification (one of 1,400 with a Focused Practice in Hospital Medicine), gained a mastership, and yes, met President Obama.
As odysseys go, how many docs can make such lofty claims?
Dr. Flansbaum works for Geisinger Health System in Danville, Pa., in both the divisions of hospital medicine and population health. He began working as a hospitalist in 1996 and is a founding member of the Society of Hospital Medicine.
Editor’s note: The Hospitalist is pleased to introduce a new recurring column: “The Legacies of Hospital Medicine.” This will be a recurring feature submitted by some of the best and brightest hospitalists in the field who have helped shape our specialty into what it is today. It will be a series of articles that will reflect on hospital medicine and it’s evolution over time from a variety of unique and innovative perspectives. We hope you enjoy this series, and we welcome any feedback as it evolves!
Hearkening back to my early time as a hospital-based physician, I recall the pleasure of waking every day and feeling like I belonged to an exclusive club. I felt passion for my work, along with a tiny cohort of similarly situated docs. We lacked a kinship with other medical organizations, however. We had no union of our own and were invisible upstarts.
And the question always came: “Tell me again ... you are what kind of doctor?”
The response changed every week. Ditto for my job responsibilities and charges. The memories are wonderful, though, and I have great affection for the early years.
Initially, I recall networking and attending national meetings – SGIM and ACP in particular – spreading the faith and talking up our bona fides. In addition to the registration fees, there came an earful of guff from irate physicians about the new breed of doctors, yet unnamed, who were destroying medicine. Likewise, I recall opinion columns from newspapers and peer-reviewed journals from a spate of “simple country docs.” The writing had a pretense of politeness but with a hint of disdain, predicting nothing less than the destruction of health care as we knew it. And to be standing next to them in conversation: “How dare you hospital docs exhale CO2!” We might as well have had “KICK ME” signs on our backs.
Inpatient medicine was upending the status quo – or so we believed – while also overturning a generations’ worth of dogma on how hospitals should do their business. Fate also played a role, and we could not have anticipated the arrival of health care consolidation, “To Err Is Human,” managed care, and payment reform – all of which upset practice conditions that had been in existence for decades. We walked a line between old and new, down a path whose purpose we felt but toward a destination we could not entirely envision.
That transformed with time.
Like most hospitalists, my ticket in began after some sleuthing and calls to Win Whitcomb, MD, and John Nelson, MD – still trusted friends today. They will make their marks in future columns, but as I am the inaugural contributor, let me be the first to state they both had a sixth sense steering our group of disciples. They became the obvious chiefs, along with Bob Wachter, MD, and took the lead in articulating what we aspired to be. Sounds saccharine now, but it did not then.
But lucky for us, hospital medicine took off. Our wise choices laid the groundwork for what is now a discipline in repose. “Hospitalist” no longer sounds like a neologism, and the term entered Merriam-Webster to seal our fate.
Twenty years out, hospital medicine still feels like a figurative case of Moore’s law. I cannot keep up with the strange faces at annual meetings and membership size, the throng of published articles (I used to pride myself on knowing all the hospitalist studies – no longer), and the lengthy list of initiatives and Society of Hospital Medicine resources on hand.
Without question, SHM has been the most rewarding part of my professional life. Hospital medicine mates sustain and keep me in good stead and have done so since training. Their insights teach me more than journals or any day on the job could impart and have given me a learning windfall for the cost of a song.
I initiated my hospitalist path as a 20-something tenderfoot, but from my interactions with colleagues both liberal and conservative, urban and rural, corporate and academic, and specialist and generalist, I developed into a seasoned craftsman.
Countless times I strode into an SHM activity thinking one way, and through the intellect and conviction of my peers, I got smart. Working in the same setting for most of my career, unchallenged, I could have assimilated a sclerotic worldview, but my hospital medicine colleagues would have none of that – kudos and thanks to them for it.
I could cite endless anecdotes – and they are swirling as I write. Crucial positions discussed and adopted, roads taken and those not, specialties angered and appeased, wonderful meals had, and on and on. They are and were the building blocks of a journey – and a joyful one.
As truly notable memories go, however, for me, there is only one.
By far, watching and absorbing the lessons of how an organization develops – goes from zero to sixty – has been a master class in enterprise and execution.
A PGY4 sees a president, CEO, board, ad hoc committees, staff, big budgets, and capital outlays make things happen and assumes it just is. But an operational charter with an instruction manual in-tow didn’t just drop from on high; that’s not how things go down. The right personnel selections, value choices (“SHM is a big tent” was not an accident), affiliate alliances, assessment of risks, and strategies pursued occurred for a reason; keen minds had the vision to set the board right.
The privilege of participating in the SHM project has been an education no grant or scholarship could equal. To say I had a tiny role in all of that is just reward.
Through SHM I have made lifelong friends, advanced my perspective and development as a healer, acquired a nifty board certification (one of 1,400 with a Focused Practice in Hospital Medicine), gained a mastership, and yes, met President Obama.
As odysseys go, how many docs can make such lofty claims?
Dr. Flansbaum works for Geisinger Health System in Danville, Pa., in both the divisions of hospital medicine and population health. He began working as a hospitalist in 1996 and is a founding member of the Society of Hospital Medicine.
Editor’s note: The Hospitalist is pleased to introduce a new recurring column: “The Legacies of Hospital Medicine.” This will be a recurring feature submitted by some of the best and brightest hospitalists in the field who have helped shape our specialty into what it is today. It will be a series of articles that will reflect on hospital medicine and it’s evolution over time from a variety of unique and innovative perspectives. We hope you enjoy this series, and we welcome any feedback as it evolves!
Hearkening back to my early time as a hospital-based physician, I recall the pleasure of waking every day and feeling like I belonged to an exclusive club. I felt passion for my work, along with a tiny cohort of similarly situated docs. We lacked a kinship with other medical organizations, however. We had no union of our own and were invisible upstarts.
And the question always came: “Tell me again ... you are what kind of doctor?”
The response changed every week. Ditto for my job responsibilities and charges. The memories are wonderful, though, and I have great affection for the early years.
Initially, I recall networking and attending national meetings – SGIM and ACP in particular – spreading the faith and talking up our bona fides. In addition to the registration fees, there came an earful of guff from irate physicians about the new breed of doctors, yet unnamed, who were destroying medicine. Likewise, I recall opinion columns from newspapers and peer-reviewed journals from a spate of “simple country docs.” The writing had a pretense of politeness but with a hint of disdain, predicting nothing less than the destruction of health care as we knew it. And to be standing next to them in conversation: “How dare you hospital docs exhale CO2!” We might as well have had “KICK ME” signs on our backs.
Inpatient medicine was upending the status quo – or so we believed – while also overturning a generations’ worth of dogma on how hospitals should do their business. Fate also played a role, and we could not have anticipated the arrival of health care consolidation, “To Err Is Human,” managed care, and payment reform – all of which upset practice conditions that had been in existence for decades. We walked a line between old and new, down a path whose purpose we felt but toward a destination we could not entirely envision.
That transformed with time.
Like most hospitalists, my ticket in began after some sleuthing and calls to Win Whitcomb, MD, and John Nelson, MD – still trusted friends today. They will make their marks in future columns, but as I am the inaugural contributor, let me be the first to state they both had a sixth sense steering our group of disciples. They became the obvious chiefs, along with Bob Wachter, MD, and took the lead in articulating what we aspired to be. Sounds saccharine now, but it did not then.
But lucky for us, hospital medicine took off. Our wise choices laid the groundwork for what is now a discipline in repose. “Hospitalist” no longer sounds like a neologism, and the term entered Merriam-Webster to seal our fate.
Twenty years out, hospital medicine still feels like a figurative case of Moore’s law. I cannot keep up with the strange faces at annual meetings and membership size, the throng of published articles (I used to pride myself on knowing all the hospitalist studies – no longer), and the lengthy list of initiatives and Society of Hospital Medicine resources on hand.
Without question, SHM has been the most rewarding part of my professional life. Hospital medicine mates sustain and keep me in good stead and have done so since training. Their insights teach me more than journals or any day on the job could impart and have given me a learning windfall for the cost of a song.
I initiated my hospitalist path as a 20-something tenderfoot, but from my interactions with colleagues both liberal and conservative, urban and rural, corporate and academic, and specialist and generalist, I developed into a seasoned craftsman.
Countless times I strode into an SHM activity thinking one way, and through the intellect and conviction of my peers, I got smart. Working in the same setting for most of my career, unchallenged, I could have assimilated a sclerotic worldview, but my hospital medicine colleagues would have none of that – kudos and thanks to them for it.
I could cite endless anecdotes – and they are swirling as I write. Crucial positions discussed and adopted, roads taken and those not, specialties angered and appeased, wonderful meals had, and on and on. They are and were the building blocks of a journey – and a joyful one.
As truly notable memories go, however, for me, there is only one.
By far, watching and absorbing the lessons of how an organization develops – goes from zero to sixty – has been a master class in enterprise and execution.
A PGY4 sees a president, CEO, board, ad hoc committees, staff, big budgets, and capital outlays make things happen and assumes it just is. But an operational charter with an instruction manual in-tow didn’t just drop from on high; that’s not how things go down. The right personnel selections, value choices (“SHM is a big tent” was not an accident), affiliate alliances, assessment of risks, and strategies pursued occurred for a reason; keen minds had the vision to set the board right.
The privilege of participating in the SHM project has been an education no grant or scholarship could equal. To say I had a tiny role in all of that is just reward.
Through SHM I have made lifelong friends, advanced my perspective and development as a healer, acquired a nifty board certification (one of 1,400 with a Focused Practice in Hospital Medicine), gained a mastership, and yes, met President Obama.
As odysseys go, how many docs can make such lofty claims?
Dr. Flansbaum works for Geisinger Health System in Danville, Pa., in both the divisions of hospital medicine and population health. He began working as a hospitalist in 1996 and is a founding member of the Society of Hospital Medicine.
San Antonio hotels for CHEST 2018
Are you ready for CHEST Annual Meeting 2018? Get ready with exclusive hotel deals for your trip to San Antonio from onPeak, the official hotel provider for CHEST 2018. Through onPeak, we are able to bring you the lowest rates, best hotels, and great amenities for your trip all along the beautiful San Antonio River Walk. onPeak also provides flexible booking policies, great group tools, and a full team of wonderful customer service agents to ensure you have a smooth booking process.
Marriott Rivercenter – HQ Hotel
The San Antonio Marriott Rivercenter, a magnificent 38-story hotel, is just steps away from premier shopping, dining, and entertainment destinations. Guests will enjoy supreme comfort conveniently located near many hot attractions, including Six Flags Fiesta Texas and the San Antonio Zoo. The Alamo, one of the nation’s most storied and revered landmarks, is within easy walking distance from the hotel.
Grand Hyatt San Antonio
Discover the distinctly diverse personality of the Alamo City in grand style. Also along the spectacular River Walk, Grand Hyatt San Antonio is steps from trendy downtown bars, Zagat-rated restaurants, and all the sites and attractions that make San Antonio one of the most culturally rich cities in the country.
Hilton Palacio Del Rio
Located in beautiful downtown San Antonio, the Hilton Palacio del Rio hotel is surrounded by Texas culture and attractions, including the Alamo, just two blocks away. The Hilton Palacio del Rio offers superior service, extensive guest amenities, and is the only hotel in downtown San Antonio that features a private balcony in every room. Tex’s Riverwalk Sports Bar & Grill, Durty Nelley’s Irish Pub, Ibiza Riverwalk Patio Restaurant & Bar, and the Rincon Allegre Lobby Bar await to satisfy individual tastes.
Hotel Contessa
Step into the marble lobby accented with glass sconces and towering palm trees and you’ll know you’ve made the right choice on where to stay. The ambiance of this 265 all-suite property with heated rooftop pool, full-service spa, gourmet restaurant, and modern meeting space is unmatched by any other downtown hotel. Our dedicated service team is devoted to making any stay – leisure or business – a memorable experience. The Hotel Contessa extends to her guests a relaxing respite in an urban setting coupled with all the amenities of a large resort.
Hyatt Regency San Antonio
Experience the heart of the River Walk at Hyatt Regency San Antonio. This is the only hotel on the River Walk directly overlooking the historic Alamo, connecting two of San Antonio’s top destinations through the 16-story atrium lobby. This four-diamond hotel includes contemporary guest rooms, a rooftop pool, Stay-Fit gym, and a relaxing spa. The experienced staff adds a genuine touch to world-class amenities.
Marriott Riverwalk
The San Antonio Marriott Riverwalk hotel charmingly captures the vibrant culture and style of this romantic city, welcoming you and ensuring an enchanting stay. This hotel is located in the heart of downtown San Antonio, offering sweeping balcony views of the fabulous River Walk district. The 30-story hotel invites guests into a contemporary lobby with Texas flair: chili-red walls, dark-wood trim, and wrought-iron accents. Explore the history, culture, and culinary delights along the River Walk.
Westin Riverwalk Hotel
The Westin Riverwalk Hotel boasts 473 rooms and luxury suites with Texan hospitality and warm residential style. This riverfront hotel is the perfect location to relax and recharge. Expect a warm welcome when you visit the best of San Antonio River Walk hotels. Enjoy delicious dark chocolates imported from Venezuela when you check in and amenities such as The Westin Heavenly Bed® and Heavenly Bath® products that will leave you feeling refreshed and rejuvenated. The hotel rooms also include sparkling city or river views and elegant, oversized marble bathrooms with pampering bath amenities.
Don’t forget to book your hotel before they sell out! View the official hotel block at http://onpeak.com/CHEST-2018.
Note that onPeak is the only official hotel provider associated with our event. While other hotel resellers may contact you offering accommodations for your trip, they are not endorsed by or affiliated with the meeting. Beware that entering into financial agreements with unendorsed companies can have costly consequences.
Hotel information provided by onPeak.
Are you ready for CHEST Annual Meeting 2018? Get ready with exclusive hotel deals for your trip to San Antonio from onPeak, the official hotel provider for CHEST 2018. Through onPeak, we are able to bring you the lowest rates, best hotels, and great amenities for your trip all along the beautiful San Antonio River Walk. onPeak also provides flexible booking policies, great group tools, and a full team of wonderful customer service agents to ensure you have a smooth booking process.
Marriott Rivercenter – HQ Hotel
The San Antonio Marriott Rivercenter, a magnificent 38-story hotel, is just steps away from premier shopping, dining, and entertainment destinations. Guests will enjoy supreme comfort conveniently located near many hot attractions, including Six Flags Fiesta Texas and the San Antonio Zoo. The Alamo, one of the nation’s most storied and revered landmarks, is within easy walking distance from the hotel.
Grand Hyatt San Antonio
Discover the distinctly diverse personality of the Alamo City in grand style. Also along the spectacular River Walk, Grand Hyatt San Antonio is steps from trendy downtown bars, Zagat-rated restaurants, and all the sites and attractions that make San Antonio one of the most culturally rich cities in the country.
Hilton Palacio Del Rio
Located in beautiful downtown San Antonio, the Hilton Palacio del Rio hotel is surrounded by Texas culture and attractions, including the Alamo, just two blocks away. The Hilton Palacio del Rio offers superior service, extensive guest amenities, and is the only hotel in downtown San Antonio that features a private balcony in every room. Tex’s Riverwalk Sports Bar & Grill, Durty Nelley’s Irish Pub, Ibiza Riverwalk Patio Restaurant & Bar, and the Rincon Allegre Lobby Bar await to satisfy individual tastes.
Hotel Contessa
Step into the marble lobby accented with glass sconces and towering palm trees and you’ll know you’ve made the right choice on where to stay. The ambiance of this 265 all-suite property with heated rooftop pool, full-service spa, gourmet restaurant, and modern meeting space is unmatched by any other downtown hotel. Our dedicated service team is devoted to making any stay – leisure or business – a memorable experience. The Hotel Contessa extends to her guests a relaxing respite in an urban setting coupled with all the amenities of a large resort.
Hyatt Regency San Antonio
Experience the heart of the River Walk at Hyatt Regency San Antonio. This is the only hotel on the River Walk directly overlooking the historic Alamo, connecting two of San Antonio’s top destinations through the 16-story atrium lobby. This four-diamond hotel includes contemporary guest rooms, a rooftop pool, Stay-Fit gym, and a relaxing spa. The experienced staff adds a genuine touch to world-class amenities.
Marriott Riverwalk
The San Antonio Marriott Riverwalk hotel charmingly captures the vibrant culture and style of this romantic city, welcoming you and ensuring an enchanting stay. This hotel is located in the heart of downtown San Antonio, offering sweeping balcony views of the fabulous River Walk district. The 30-story hotel invites guests into a contemporary lobby with Texas flair: chili-red walls, dark-wood trim, and wrought-iron accents. Explore the history, culture, and culinary delights along the River Walk.
Westin Riverwalk Hotel
The Westin Riverwalk Hotel boasts 473 rooms and luxury suites with Texan hospitality and warm residential style. This riverfront hotel is the perfect location to relax and recharge. Expect a warm welcome when you visit the best of San Antonio River Walk hotels. Enjoy delicious dark chocolates imported from Venezuela when you check in and amenities such as The Westin Heavenly Bed® and Heavenly Bath® products that will leave you feeling refreshed and rejuvenated. The hotel rooms also include sparkling city or river views and elegant, oversized marble bathrooms with pampering bath amenities.
Don’t forget to book your hotel before they sell out! View the official hotel block at http://onpeak.com/CHEST-2018.
Note that onPeak is the only official hotel provider associated with our event. While other hotel resellers may contact you offering accommodations for your trip, they are not endorsed by or affiliated with the meeting. Beware that entering into financial agreements with unendorsed companies can have costly consequences.
Hotel information provided by onPeak.
Are you ready for CHEST Annual Meeting 2018? Get ready with exclusive hotel deals for your trip to San Antonio from onPeak, the official hotel provider for CHEST 2018. Through onPeak, we are able to bring you the lowest rates, best hotels, and great amenities for your trip all along the beautiful San Antonio River Walk. onPeak also provides flexible booking policies, great group tools, and a full team of wonderful customer service agents to ensure you have a smooth booking process.
Marriott Rivercenter – HQ Hotel
The San Antonio Marriott Rivercenter, a magnificent 38-story hotel, is just steps away from premier shopping, dining, and entertainment destinations. Guests will enjoy supreme comfort conveniently located near many hot attractions, including Six Flags Fiesta Texas and the San Antonio Zoo. The Alamo, one of the nation’s most storied and revered landmarks, is within easy walking distance from the hotel.
Grand Hyatt San Antonio
Discover the distinctly diverse personality of the Alamo City in grand style. Also along the spectacular River Walk, Grand Hyatt San Antonio is steps from trendy downtown bars, Zagat-rated restaurants, and all the sites and attractions that make San Antonio one of the most culturally rich cities in the country.
Hilton Palacio Del Rio
Located in beautiful downtown San Antonio, the Hilton Palacio del Rio hotel is surrounded by Texas culture and attractions, including the Alamo, just two blocks away. The Hilton Palacio del Rio offers superior service, extensive guest amenities, and is the only hotel in downtown San Antonio that features a private balcony in every room. Tex’s Riverwalk Sports Bar & Grill, Durty Nelley’s Irish Pub, Ibiza Riverwalk Patio Restaurant & Bar, and the Rincon Allegre Lobby Bar await to satisfy individual tastes.
Hotel Contessa
Step into the marble lobby accented with glass sconces and towering palm trees and you’ll know you’ve made the right choice on where to stay. The ambiance of this 265 all-suite property with heated rooftop pool, full-service spa, gourmet restaurant, and modern meeting space is unmatched by any other downtown hotel. Our dedicated service team is devoted to making any stay – leisure or business – a memorable experience. The Hotel Contessa extends to her guests a relaxing respite in an urban setting coupled with all the amenities of a large resort.
Hyatt Regency San Antonio
Experience the heart of the River Walk at Hyatt Regency San Antonio. This is the only hotel on the River Walk directly overlooking the historic Alamo, connecting two of San Antonio’s top destinations through the 16-story atrium lobby. This four-diamond hotel includes contemporary guest rooms, a rooftop pool, Stay-Fit gym, and a relaxing spa. The experienced staff adds a genuine touch to world-class amenities.
Marriott Riverwalk
The San Antonio Marriott Riverwalk hotel charmingly captures the vibrant culture and style of this romantic city, welcoming you and ensuring an enchanting stay. This hotel is located in the heart of downtown San Antonio, offering sweeping balcony views of the fabulous River Walk district. The 30-story hotel invites guests into a contemporary lobby with Texas flair: chili-red walls, dark-wood trim, and wrought-iron accents. Explore the history, culture, and culinary delights along the River Walk.
Westin Riverwalk Hotel
The Westin Riverwalk Hotel boasts 473 rooms and luxury suites with Texan hospitality and warm residential style. This riverfront hotel is the perfect location to relax and recharge. Expect a warm welcome when you visit the best of San Antonio River Walk hotels. Enjoy delicious dark chocolates imported from Venezuela when you check in and amenities such as The Westin Heavenly Bed® and Heavenly Bath® products that will leave you feeling refreshed and rejuvenated. The hotel rooms also include sparkling city or river views and elegant, oversized marble bathrooms with pampering bath amenities.
Don’t forget to book your hotel before they sell out! View the official hotel block at http://onpeak.com/CHEST-2018.
Note that onPeak is the only official hotel provider associated with our event. While other hotel resellers may contact you offering accommodations for your trip, they are not endorsed by or affiliated with the meeting. Beware that entering into financial agreements with unendorsed companies can have costly consequences.
Hotel information provided by onPeak.