User login
VIDEO: The effect of removing pregnancy drug category labeling
AUSTIN, TEX. – In a randomized survey, the Food and Drug Administration’s previous letter-category labeling of drugs for pregnant women made prescribers more likely to prescribe appropriate medication than the new labeling standards without the letters.
The FDA removed the letter categories A, B, C, D, and X in 2014 in the belief “that a narrative structure for pregnancy labeling is best able to capture and convey the potential risks of drug exposure based on animal or human data, or both,” as stated in the FDA ruling.
“The [old] FDA categories are actually based upon the evidence related to clinical trials or animal trials and known risks to the fetus or the mother. The categorizations really reflect the evidence that we have or the absence of evidence as to whether medications can be safely used during pregnancy,” Dr. Robinson explained in a video interview. But letters can be perceived as overall “grades,” even though they aren’t.
The researchers sought to evaluate the effect of the letters’ removal by surveying doctors at two centers in New York City and two annual specialty meetings from October 2015 to May 2016.
The survey “included demographic information, followed by four clinical vignettes. Each vignette described a pregnant woman and presented an indication for prescribing a particular drug which was FDA approved. Each vignette was followed by detailed drug information as found in the FDA-approved package insert with the new [Pregnancy and Lactation Labeling Rule] content and formatting,” Dr. Robinson said at the meeting.
The 162 survey respondents estimated their likelihood of prescribing given the information in the vignette. The respondents were randomized to see the letter category or not. Category X (positive evidence of risk that clearly outweighs potential benefits) was not included. For all four remaining categories, the respondents who were shown the letter category were more likely to prescribe. Category B was significantly affected in a mixed linear model, and both categories B and C were significantly affected in a multivariate model.
“The new system of revised labeling may be more ambiguous and present new challenges for clinical decision making that could result in decreased access to medications for pregnant women,” Dr. Robinson said.
Dr. Robinson and her coauthors reported no relevant disclosures.
SOURCE: Robinson A et al. ACOG 2018. Abstract OP5.
AUSTIN, TEX. – In a randomized survey, the Food and Drug Administration’s previous letter-category labeling of drugs for pregnant women made prescribers more likely to prescribe appropriate medication than the new labeling standards without the letters.
The FDA removed the letter categories A, B, C, D, and X in 2014 in the belief “that a narrative structure for pregnancy labeling is best able to capture and convey the potential risks of drug exposure based on animal or human data, or both,” as stated in the FDA ruling.
“The [old] FDA categories are actually based upon the evidence related to clinical trials or animal trials and known risks to the fetus or the mother. The categorizations really reflect the evidence that we have or the absence of evidence as to whether medications can be safely used during pregnancy,” Dr. Robinson explained in a video interview. But letters can be perceived as overall “grades,” even though they aren’t.
The researchers sought to evaluate the effect of the letters’ removal by surveying doctors at two centers in New York City and two annual specialty meetings from October 2015 to May 2016.
The survey “included demographic information, followed by four clinical vignettes. Each vignette described a pregnant woman and presented an indication for prescribing a particular drug which was FDA approved. Each vignette was followed by detailed drug information as found in the FDA-approved package insert with the new [Pregnancy and Lactation Labeling Rule] content and formatting,” Dr. Robinson said at the meeting.
The 162 survey respondents estimated their likelihood of prescribing given the information in the vignette. The respondents were randomized to see the letter category or not. Category X (positive evidence of risk that clearly outweighs potential benefits) was not included. For all four remaining categories, the respondents who were shown the letter category were more likely to prescribe. Category B was significantly affected in a mixed linear model, and both categories B and C were significantly affected in a multivariate model.
“The new system of revised labeling may be more ambiguous and present new challenges for clinical decision making that could result in decreased access to medications for pregnant women,” Dr. Robinson said.
Dr. Robinson and her coauthors reported no relevant disclosures.
SOURCE: Robinson A et al. ACOG 2018. Abstract OP5.
AUSTIN, TEX. – In a randomized survey, the Food and Drug Administration’s previous letter-category labeling of drugs for pregnant women made prescribers more likely to prescribe appropriate medication than the new labeling standards without the letters.
The FDA removed the letter categories A, B, C, D, and X in 2014 in the belief “that a narrative structure for pregnancy labeling is best able to capture and convey the potential risks of drug exposure based on animal or human data, or both,” as stated in the FDA ruling.
“The [old] FDA categories are actually based upon the evidence related to clinical trials or animal trials and known risks to the fetus or the mother. The categorizations really reflect the evidence that we have or the absence of evidence as to whether medications can be safely used during pregnancy,” Dr. Robinson explained in a video interview. But letters can be perceived as overall “grades,” even though they aren’t.
The researchers sought to evaluate the effect of the letters’ removal by surveying doctors at two centers in New York City and two annual specialty meetings from October 2015 to May 2016.
The survey “included demographic information, followed by four clinical vignettes. Each vignette described a pregnant woman and presented an indication for prescribing a particular drug which was FDA approved. Each vignette was followed by detailed drug information as found in the FDA-approved package insert with the new [Pregnancy and Lactation Labeling Rule] content and formatting,” Dr. Robinson said at the meeting.
The 162 survey respondents estimated their likelihood of prescribing given the information in the vignette. The respondents were randomized to see the letter category or not. Category X (positive evidence of risk that clearly outweighs potential benefits) was not included. For all four remaining categories, the respondents who were shown the letter category were more likely to prescribe. Category B was significantly affected in a mixed linear model, and both categories B and C were significantly affected in a multivariate model.
“The new system of revised labeling may be more ambiguous and present new challenges for clinical decision making that could result in decreased access to medications for pregnant women,” Dr. Robinson said.
Dr. Robinson and her coauthors reported no relevant disclosures.
SOURCE: Robinson A et al. ACOG 2018. Abstract OP5.
REPORTING FROM ACOG 2018

VIDEO: Promoting upright and mobile labor could save over $700 million yearly
AUSTIN, TEX. – Encouraging an upright position and allowing mobility during labor is a cost-effective intervention that could save hundreds of millions of dollars while preventing cesarean deliveries, uterine rupture, and maternal deaths, according to a recent cost-effectiveness study.
Alyssa Hersh, a medical student at Oregon Health & Sciences University, Portland, developed the analysis using an innovative model that examines the costs associated not just with the first delivery, but also the probable next delivery.
“Our model was dependent on the ability to reduce cesareans and also reduce labor times,” said Ms. Hersh in a video interview. “So this reduction in cesareans allowed women to avoid having an increased risk of uterine rupture, of emergent hysterectomy, and other downstream consequences.”
The “two-delivery model” takes into account the average number of births per woman in the United States, “such that the risks, benefits, and costs are framed within the public health perspective of the average U.S. childrearing woman’s entire reproductive course,” she and her coauthors wrote in the poster accompanying the presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
This model captures the downstream effects of a first cesarean delivery on the next delivery, for example, providing a more realistic picture of the true costs of cesarean delivery for a nulliparous female.
Some of the known benefits of being upright and mobile during labor, Ms. Hersh said, include shortened labor and reduced risk for cesarean delivery. Cost-effectiveness of this approach for low-risk women, she said, had not been fully explored.
For the analysis, Ms. Hersh and her colleagues used a theoretical cohort of 1.8 million women, approximating the number of nulliparous term deliveries in the United States each year. They used rates of cesarean delivery for women laboring in upright and recumbent positions that were drawn from the literature, but lower than national averages: 7.8% of recumbent women and 5.4% of upright women went on to cesarean delivery in the model used by the investigators.
The outcomes tracked in the analysis included cesarean delivery, uterine rupture, hysterectomy attributed to uterine rupture, costs, and quality-adjusted life years (QALYs). All of the outcomes were tracked for the index pregnancy and the second pregnancy.
Ms. Hersh and her coinvestigators found that in the theoretical cohort, “laboring upright led to 64,890 fewer cesarean deliveries, 15 fewer maternal deaths, 113 fewer uterine ruptures, and 30 fewer hysterectomies.”
These reductions were associated with a savings for this cohort of $785 million, and an increase in QALYs of 2,142.
Using Monte Carlo simulation techniques to ascertain the effect of varying cesarean rates and other components of the model, Ms. Hersh and her colleagues found that the model remained cost-effective even with variation in all of the inputs.
“Laboring upright is a no-cost intervention that leads to improved outcomes, decreased costs, and increased QALYs during a woman’s first and second deliveries,” wrote Ms. Hersh and her associates. “This model argues for increasing systems factors that support women to be upright and mobile during labor, and in doing so, promoting improved health for our patients.”
Said Ms. Hersh, “This is an easy way for hospitals to adopt policies that can enable women to have improved outcomes.”
Ms. Hersh and her colleagues had no relevant financial disclosures.
SOURCE: Hersh A et al. ACOG 2018. Abstract 34C.
AUSTIN, TEX. – Encouraging an upright position and allowing mobility during labor is a cost-effective intervention that could save hundreds of millions of dollars while preventing cesarean deliveries, uterine rupture, and maternal deaths, according to a recent cost-effectiveness study.
Alyssa Hersh, a medical student at Oregon Health & Sciences University, Portland, developed the analysis using an innovative model that examines the costs associated not just with the first delivery, but also the probable next delivery.
“Our model was dependent on the ability to reduce cesareans and also reduce labor times,” said Ms. Hersh in a video interview. “So this reduction in cesareans allowed women to avoid having an increased risk of uterine rupture, of emergent hysterectomy, and other downstream consequences.”
The “two-delivery model” takes into account the average number of births per woman in the United States, “such that the risks, benefits, and costs are framed within the public health perspective of the average U.S. childrearing woman’s entire reproductive course,” she and her coauthors wrote in the poster accompanying the presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
This model captures the downstream effects of a first cesarean delivery on the next delivery, for example, providing a more realistic picture of the true costs of cesarean delivery for a nulliparous female.
Some of the known benefits of being upright and mobile during labor, Ms. Hersh said, include shortened labor and reduced risk for cesarean delivery. Cost-effectiveness of this approach for low-risk women, she said, had not been fully explored.
For the analysis, Ms. Hersh and her colleagues used a theoretical cohort of 1.8 million women, approximating the number of nulliparous term deliveries in the United States each year. They used rates of cesarean delivery for women laboring in upright and recumbent positions that were drawn from the literature, but lower than national averages: 7.8% of recumbent women and 5.4% of upright women went on to cesarean delivery in the model used by the investigators.
The outcomes tracked in the analysis included cesarean delivery, uterine rupture, hysterectomy attributed to uterine rupture, costs, and quality-adjusted life years (QALYs). All of the outcomes were tracked for the index pregnancy and the second pregnancy.
Ms. Hersh and her coinvestigators found that in the theoretical cohort, “laboring upright led to 64,890 fewer cesarean deliveries, 15 fewer maternal deaths, 113 fewer uterine ruptures, and 30 fewer hysterectomies.”
These reductions were associated with a savings for this cohort of $785 million, and an increase in QALYs of 2,142.
Using Monte Carlo simulation techniques to ascertain the effect of varying cesarean rates and other components of the model, Ms. Hersh and her colleagues found that the model remained cost-effective even with variation in all of the inputs.
“Laboring upright is a no-cost intervention that leads to improved outcomes, decreased costs, and increased QALYs during a woman’s first and second deliveries,” wrote Ms. Hersh and her associates. “This model argues for increasing systems factors that support women to be upright and mobile during labor, and in doing so, promoting improved health for our patients.”
Said Ms. Hersh, “This is an easy way for hospitals to adopt policies that can enable women to have improved outcomes.”
Ms. Hersh and her colleagues had no relevant financial disclosures.
SOURCE: Hersh A et al. ACOG 2018. Abstract 34C.
AUSTIN, TEX. – Encouraging an upright position and allowing mobility during labor is a cost-effective intervention that could save hundreds of millions of dollars while preventing cesarean deliveries, uterine rupture, and maternal deaths, according to a recent cost-effectiveness study.
Alyssa Hersh, a medical student at Oregon Health & Sciences University, Portland, developed the analysis using an innovative model that examines the costs associated not just with the first delivery, but also the probable next delivery.
“Our model was dependent on the ability to reduce cesareans and also reduce labor times,” said Ms. Hersh in a video interview. “So this reduction in cesareans allowed women to avoid having an increased risk of uterine rupture, of emergent hysterectomy, and other downstream consequences.”
The “two-delivery model” takes into account the average number of births per woman in the United States, “such that the risks, benefits, and costs are framed within the public health perspective of the average U.S. childrearing woman’s entire reproductive course,” she and her coauthors wrote in the poster accompanying the presentation at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists.
This model captures the downstream effects of a first cesarean delivery on the next delivery, for example, providing a more realistic picture of the true costs of cesarean delivery for a nulliparous female.
Some of the known benefits of being upright and mobile during labor, Ms. Hersh said, include shortened labor and reduced risk for cesarean delivery. Cost-effectiveness of this approach for low-risk women, she said, had not been fully explored.
For the analysis, Ms. Hersh and her colleagues used a theoretical cohort of 1.8 million women, approximating the number of nulliparous term deliveries in the United States each year. They used rates of cesarean delivery for women laboring in upright and recumbent positions that were drawn from the literature, but lower than national averages: 7.8% of recumbent women and 5.4% of upright women went on to cesarean delivery in the model used by the investigators.
The outcomes tracked in the analysis included cesarean delivery, uterine rupture, hysterectomy attributed to uterine rupture, costs, and quality-adjusted life years (QALYs). All of the outcomes were tracked for the index pregnancy and the second pregnancy.
Ms. Hersh and her coinvestigators found that in the theoretical cohort, “laboring upright led to 64,890 fewer cesarean deliveries, 15 fewer maternal deaths, 113 fewer uterine ruptures, and 30 fewer hysterectomies.”
These reductions were associated with a savings for this cohort of $785 million, and an increase in QALYs of 2,142.
Using Monte Carlo simulation techniques to ascertain the effect of varying cesarean rates and other components of the model, Ms. Hersh and her colleagues found that the model remained cost-effective even with variation in all of the inputs.
“Laboring upright is a no-cost intervention that leads to improved outcomes, decreased costs, and increased QALYs during a woman’s first and second deliveries,” wrote Ms. Hersh and her associates. “This model argues for increasing systems factors that support women to be upright and mobile during labor, and in doing so, promoting improved health for our patients.”
Said Ms. Hersh, “This is an easy way for hospitals to adopt policies that can enable women to have improved outcomes.”
Ms. Hersh and her colleagues had no relevant financial disclosures.
SOURCE: Hersh A et al. ACOG 2018. Abstract 34C.
REPORTING FROM ACOG 2018

To detect subclinical AF, insertable monitor is unequaled
ORLANDO – with other intermittent ambulatory monitoring strategies, in a secondary analysis from the REVEAL AF study.
“If you really want to look for atrial fibrillation because your concern is that the patient has a high-risk profile, and if you saw it you would anticoagulate it and maybe prophylactically use rate control, nothing beats the implanted monitor,” James A. Reiffel, MD, said at the annual meeting of the American College of Cardiology.

As previously reported (JAMA Cardiol. 2017 Oct 1;2[10]:1120-7), the primary outcome – an AF episode lasting for at least 6 minutes – occurred during the first 18 months of the study in 29% of participants. By 30 months, it was 40%. At ACC 2018, Dr. Reiffel presented a new analysis looking at how the insertable cardiac monitor (ICM) would have stacked up against other device-based strategies aimed at detecting silent AF, including a 30-day implantable memory loop, daily transtelephonic ECG monitoring, and one-time or periodic 24- or 48-hour Holter monitoring.
To accomplish this, he and his coinvestigators conducted modeling studies harnessing the REVEAL AF continuous monitoring data. They looked at how many of the real-world patients found to have AF in the study would have been identified had they instead undergone a one-time recording period lasting 1, 2, 7, 14, or 30 days beginning at the time they would have received their ICM. They also looked at the yield of repeated monitoring strategies, including monthly or quarterly 24- or 48-hour Holter monitoring sessions. They repeated the various simulated monitoring strategies 10,000 times each in order to beef up the sample size and stability of the results.
It was no contest, according to Dr. Reiffel, professor of clinical medicine at Columbia University in New York.
That’s because the median time to AF detection in REVEAL AF was 123 days. Thus, any monitoring strategy of 30 days duration or less was doomed to be of comparatively low yield. Indeed, the 12-month AF incidence rate as detected by ICM in REVEAL AF was 27.1%, compared with 1.1%-13.5% for the various modeled monitoring strategies.
Among patients who met the primary endpoint in REVEAL AF, 10.2% had one or more AF episodes lasting 24 hours or more. So a significant proportion of the asymptomatic episodes of AF were not brief.
The take-home lesson of this analysis is straightforward, he said. “While the incidence of screen-detected atrial fibrillation is dependent upon the population screened, it is also strongly dependent upon the duration and intensity of monitoring.”
Session cochair Jeanne E. Poole, MD, observed that while the new REVEAL AF analysis is informative, it leaves unanswered the big questions regarding the clinical importance of these silent episodes of subclinical device-detected AF. That is, are these episodes associated with significantly increased stroke risk, and if so are they just another nonmodifiable risk marker, or are they a risk factor that can be dampened via oral anticoagulation, like symptomatic AF? said Dr. Poole, professor of medicine and director of the clinical cardiac electrophysiology program at the University of Washington, Seattle.
“My own belief is that they are both a risk marker and a risk factor that contributes to stroke,” Dr. Reiffel replied.
He noted that there are two major ongoing clinical trials evaluating the impact of oral anticoagulation in patients with ICM-detected AF. The 3,400-patient German multicenter Non–vitamin K Antagonist Oral Anticoagulants in Patients With Atrial High Rate Episodes (NOAH–AFNET 6 ) trial is testing whether oral anticoagulation with edoxaban (Savaysa) is superior to aspirin or no antithrombotic therapy for prevention of stroke or cardiovascular death. And the 4,000-patient Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation (ARTESIA) trial is randomizing patients to apixaban (Eliquis) or aspirin.
“We’ll know within the next 3-4 years whether patients with high-risk profiles for atrial fibrillation but no clinically manifest atrial fibrillation should in fact be detected and should in fact be anticoagulated if atrial fibrillation is detected. Putting on my ‘Carnac The Magnificent’ hat [made famous by Johnny Carson on the ‘Tonight Show’], I predict the answer to both of those questions is likely to be yes,” the cardiologist added.
He noted that the Medtronic ICM, which is one-third the size of a AAA battery, is implanted via a small incision, which is then covered by a adhesive bandage.
“There’s no major surgical technique involved in putting [int ICM] in,” he said.
The REVEAL AF study was sponsored by Medtronic. Dr. Reiffel reported serving as a consultant to the company.
SOURCE: Reiffel JA et al. ACC 2018, Abstract 900-08.
ORLANDO – with other intermittent ambulatory monitoring strategies, in a secondary analysis from the REVEAL AF study.
“If you really want to look for atrial fibrillation because your concern is that the patient has a high-risk profile, and if you saw it you would anticoagulate it and maybe prophylactically use rate control, nothing beats the implanted monitor,” James A. Reiffel, MD, said at the annual meeting of the American College of Cardiology.
As previously reported (JAMA Cardiol. 2017 Oct 1;2[10]:1120-7), the primary outcome – an AF episode lasting for at least 6 minutes – occurred during the first 18 months of the study in 29% of participants. By 30 months, it was 40%. At ACC 2018, Dr. Reiffel presented a new analysis looking at how the insertable cardiac monitor (ICM) would have stacked up against other device-based strategies aimed at detecting silent AF, including a 30-day implantable memory loop, daily transtelephonic ECG monitoring, and one-time or periodic 24- or 48-hour Holter monitoring.
To accomplish this, he and his coinvestigators conducted modeling studies harnessing the REVEAL AF continuous monitoring data. They looked at how many of the real-world patients found to have AF in the study would have been identified had they instead undergone a one-time recording period lasting 1, 2, 7, 14, or 30 days beginning at the time they would have received their ICM. They also looked at the yield of repeated monitoring strategies, including monthly or quarterly 24- or 48-hour Holter monitoring sessions. They repeated the various simulated monitoring strategies 10,000 times each in order to beef up the sample size and stability of the results.
It was no contest, according to Dr. Reiffel, professor of clinical medicine at Columbia University in New York.
That’s because the median time to AF detection in REVEAL AF was 123 days. Thus, any monitoring strategy of 30 days duration or less was doomed to be of comparatively low yield. Indeed, the 12-month AF incidence rate as detected by ICM in REVEAL AF was 27.1%, compared with 1.1%-13.5% for the various modeled monitoring strategies.
Among patients who met the primary endpoint in REVEAL AF, 10.2% had one or more AF episodes lasting 24 hours or more. So a significant proportion of the asymptomatic episodes of AF were not brief.
The take-home lesson of this analysis is straightforward, he said. “While the incidence of screen-detected atrial fibrillation is dependent upon the population screened, it is also strongly dependent upon the duration and intensity of monitoring.”
Session cochair Jeanne E. Poole, MD, observed that while the new REVEAL AF analysis is informative, it leaves unanswered the big questions regarding the clinical importance of these silent episodes of subclinical device-detected AF. That is, are these episodes associated with significantly increased stroke risk, and if so are they just another nonmodifiable risk marker, or are they a risk factor that can be dampened via oral anticoagulation, like symptomatic AF? said Dr. Poole, professor of medicine and director of the clinical cardiac electrophysiology program at the University of Washington, Seattle.
“My own belief is that they are both a risk marker and a risk factor that contributes to stroke,” Dr. Reiffel replied.
He noted that there are two major ongoing clinical trials evaluating the impact of oral anticoagulation in patients with ICM-detected AF. The 3,400-patient German multicenter Non–vitamin K Antagonist Oral Anticoagulants in Patients With Atrial High Rate Episodes (NOAH–AFNET 6 ) trial is testing whether oral anticoagulation with edoxaban (Savaysa) is superior to aspirin or no antithrombotic therapy for prevention of stroke or cardiovascular death. And the 4,000-patient Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation (ARTESIA) trial is randomizing patients to apixaban (Eliquis) or aspirin.
“We’ll know within the next 3-4 years whether patients with high-risk profiles for atrial fibrillation but no clinically manifest atrial fibrillation should in fact be detected and should in fact be anticoagulated if atrial fibrillation is detected. Putting on my ‘Carnac The Magnificent’ hat [made famous by Johnny Carson on the ‘Tonight Show’], I predict the answer to both of those questions is likely to be yes,” the cardiologist added.
He noted that the Medtronic ICM, which is one-third the size of a AAA battery, is implanted via a small incision, which is then covered by a adhesive bandage.
“There’s no major surgical technique involved in putting [int ICM] in,” he said.
The REVEAL AF study was sponsored by Medtronic. Dr. Reiffel reported serving as a consultant to the company.
SOURCE: Reiffel JA et al. ACC 2018, Abstract 900-08.
ORLANDO – with other intermittent ambulatory monitoring strategies, in a secondary analysis from the REVEAL AF study.
“If you really want to look for atrial fibrillation because your concern is that the patient has a high-risk profile, and if you saw it you would anticoagulate it and maybe prophylactically use rate control, nothing beats the implanted monitor,” James A. Reiffel, MD, said at the annual meeting of the American College of Cardiology.
As previously reported (JAMA Cardiol. 2017 Oct 1;2[10]:1120-7), the primary outcome – an AF episode lasting for at least 6 minutes – occurred during the first 18 months of the study in 29% of participants. By 30 months, it was 40%. At ACC 2018, Dr. Reiffel presented a new analysis looking at how the insertable cardiac monitor (ICM) would have stacked up against other device-based strategies aimed at detecting silent AF, including a 30-day implantable memory loop, daily transtelephonic ECG monitoring, and one-time or periodic 24- or 48-hour Holter monitoring.
To accomplish this, he and his coinvestigators conducted modeling studies harnessing the REVEAL AF continuous monitoring data. They looked at how many of the real-world patients found to have AF in the study would have been identified had they instead undergone a one-time recording period lasting 1, 2, 7, 14, or 30 days beginning at the time they would have received their ICM. They also looked at the yield of repeated monitoring strategies, including monthly or quarterly 24- or 48-hour Holter monitoring sessions. They repeated the various simulated monitoring strategies 10,000 times each in order to beef up the sample size and stability of the results.
It was no contest, according to Dr. Reiffel, professor of clinical medicine at Columbia University in New York.
That’s because the median time to AF detection in REVEAL AF was 123 days. Thus, any monitoring strategy of 30 days duration or less was doomed to be of comparatively low yield. Indeed, the 12-month AF incidence rate as detected by ICM in REVEAL AF was 27.1%, compared with 1.1%-13.5% for the various modeled monitoring strategies.
Among patients who met the primary endpoint in REVEAL AF, 10.2% had one or more AF episodes lasting 24 hours or more. So a significant proportion of the asymptomatic episodes of AF were not brief.
The take-home lesson of this analysis is straightforward, he said. “While the incidence of screen-detected atrial fibrillation is dependent upon the population screened, it is also strongly dependent upon the duration and intensity of monitoring.”
Session cochair Jeanne E. Poole, MD, observed that while the new REVEAL AF analysis is informative, it leaves unanswered the big questions regarding the clinical importance of these silent episodes of subclinical device-detected AF. That is, are these episodes associated with significantly increased stroke risk, and if so are they just another nonmodifiable risk marker, or are they a risk factor that can be dampened via oral anticoagulation, like symptomatic AF? said Dr. Poole, professor of medicine and director of the clinical cardiac electrophysiology program at the University of Washington, Seattle.
“My own belief is that they are both a risk marker and a risk factor that contributes to stroke,” Dr. Reiffel replied.
He noted that there are two major ongoing clinical trials evaluating the impact of oral anticoagulation in patients with ICM-detected AF. The 3,400-patient German multicenter Non–vitamin K Antagonist Oral Anticoagulants in Patients With Atrial High Rate Episodes (NOAH–AFNET 6 ) trial is testing whether oral anticoagulation with edoxaban (Savaysa) is superior to aspirin or no antithrombotic therapy for prevention of stroke or cardiovascular death. And the 4,000-patient Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation (ARTESIA) trial is randomizing patients to apixaban (Eliquis) or aspirin.
“We’ll know within the next 3-4 years whether patients with high-risk profiles for atrial fibrillation but no clinically manifest atrial fibrillation should in fact be detected and should in fact be anticoagulated if atrial fibrillation is detected. Putting on my ‘Carnac The Magnificent’ hat [made famous by Johnny Carson on the ‘Tonight Show’], I predict the answer to both of those questions is likely to be yes,” the cardiologist added.
He noted that the Medtronic ICM, which is one-third the size of a AAA battery, is implanted via a small incision, which is then covered by a adhesive bandage.
“There’s no major surgical technique involved in putting [int ICM] in,” he said.
The REVEAL AF study was sponsored by Medtronic. Dr. Reiffel reported serving as a consultant to the company.
SOURCE: Reiffel JA et al. ACC 2018, Abstract 900-08.
REPORTING FROM ACC 2018
Key clinical point: Most patients at high risk for previously unidentified atrial fibrillation whose arrhythmia is detected by means of an insertable continuous ECG monitor would go unidentified by any other detection strategy.
Major finding: The median time to insertable cardiac monitor–based detection of a first episode of silent AF of at least 6 minutes length was 123 days.
Study details: This was a multicenter, prospective, single-arm study of 385 patients at high risk for AF who received an insertable cardiac monitor and were followed for 30 months.
Disclosures: The REVEAL AF study was sponsored by Medtronic. The presenter reported serving as a consultant to the company.
Source: Reiffel JA et al. ACC 2018, Abstract 900-08.
VIDEO: Three questions with Aaron B. Caughey, MD
AUSTIN, TEX. – This interview was conducted at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. It has been edited for length and clarity.
OB.GYN. NEWS: Here at ACOG, there were two studies from your research group at Oregon Health & Sciences University, Portland, that examined the cost-effectiveness of pregnancy interventions using a “two-delivery” model. Could you explain a little more about what that is, and how you arrived at this model?
DR. CAUGHEY: We’ve been working on decision analytics and cost-effectiveness studies of a number of ways to approach pregnancy, whether it be complicated pregnancies or uncomplicated normal pregnancies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
One of the things that we think is really important to think about is the impact of management and outcomes in the current pregnancy, and how it might affect future pregnancies.
So, for example, if you have a vaginal delivery this time, that makes you multiparous with a prior vaginal delivery next time; that is kind of the goal in pregnancy. It just makes all future labor and delivery experiences so much easier. Whereas, if you have a prior C-section, we all know that now you’re high risk. Everybody gets nervous about you. Are you going to get a trial of labor? Can you find a hospital that will do a trial of labor? And there are all these downstream implications of the delivery in the first pregnancy.
If you think about it, there are a number of ways that we can manage the first pregnancy. There are a number of risk factors for increasing risk for cesarean delivery. And we can include those in models that are considered in downstream pregnancies. And so we’ve been doing that increasingly.
When we think about our vaginal birth after cesarean models, we had two presentations that considered that. One was how we manage the maternal position in labor, and the other was how we use doulas in labor. You think, well gosh, we’re spending money on this doula in this pregnancy – that’s a certain expenditure. Is it worth it?
Part of “Is it worth it?” is not just the current pregnancy, but the downstream pregnancy as well.
OB.GYN. NEWS: What has sparked your interest in looking at obstetric care delivery in this way?
DR. CAUGHEY: I did my PhD in health economics. I began it as a 3rd-year maternal fetal medicine fellow and during my early career as an assistant professor at the University of California, San Francisco.
A lot of people think that economics in general is kind of about finance. Actually, microeconomics in particular is about the allocation of scarce resources to optimize utility – utility as general wellbeing or happiness.
So people will say that this thing, or that intervention, is cost effective, and often what they think they mean is, “It saves money.” But most things don’t save money. Most things in health care cost money. There are a few things in health care that do save money – vaccinations, contraception. Contraception actually saves money – but most things cost money. We have to spend money to get something right.
And the way we do that in health economics is that we think we’re going to get some happiness, some utility, some better outcomes from the money we’re putting in. One of the things that we don’t do very well as a species is think about these downstream outcomes.
In our models, when we think about morbidity and mortality we’re incorporating two and three pregnancy models. Think about what happens in the future, and then think about if we do something – if we spend money on an induction of labor or having a doula or something like that, is it worth it for what we get?
Antenatal testing, for example. Or, is it worth it for you to be testing people with diabetes once a week? Twice a week? More? Less? Part of it is figuring out what you’ll get for it. The measurement of what you get for it is called quality-adjusted life years, and that’s the measure of happiness multiplied times life expectancy.
We incorporate that in standard ways to build these models, to help us make decisions around best practices. Now, the economics piece of it probably matters. We’re the richest country that’s probably ever going to be – not just ever has been but probably ever going to be – the way we’re using up scarce resources to beat the band.
Yet, we still have an issue of allocation. We have people that have less; we have enormous disparities, whether it be racial and ethnic disparities, or socioeconomic disparities. And so we need to figure out ways to be more efficient and allocate those scarce resources properly to the outcomes that will be the best.
I think that’s what we’re working on: creating models to think about how to allocate those scarce resources.
OB.GYN. NEWS: How can a busy obstetrician think about the work you’re doing and incorporate it into her practice on a day-to-day basis?
DR. CAUGHEY: As an economist, I want to step back from time to time and think about public health and allocation of scarce resources.
But as a busy practicing clinician, I don’t necessarily want you consciously to think about cost. There are people who will push back on this and say, “Oh no, we should always be cost conscious.” Actually, what I really want you to do is incorporate best practices into the care of the patient at that moment, and do the thing that improves her outcomes best at that moment.
What we want to do, instead, is design systems that will properly incentivize. Incentivize doesn’t mean you think, “Oh gosh, if I do this thing I’m going to get an extra dollar.” It means subconsciously that those incentives are there, and those incentives don’t have to just be about dollars. Often in our field, they’re about time – what takes less time and more time to do something. So if we provide little extra roadblocks, then you’re more likely to go the other way and do something else.
For example: the hard stop. We did all this research in the 2000s to show that you probably shouldn’t deliver babies just for fun before 39 weeks’ gestational age. There should be an indication. If we don’t allow any hard stop, if we don’t block the pathway, then patients are pushing us, they’re uncomfortable, they’re like, “Just deliver me.” So we said, “No, no, no, we’re going to block this. In fact, we’re actually going to provide a hard stop reimbursement-wise. And medical directors of hospitals are going to have to preapprove.” And so that provides a blockade, and makes it easier just not to do it.
So I think that’s what we want: At the bedside and in your office, we want clinicians to still just be really good doctors. But then, to get involved and help design systems to incentivize us to do the right things.
Aaron B. Caughey, MD, PhD, is professor and chair of the department of obstetrics and gynecology and associate dean for Women’s Health Research and Policy at Oregon Health & Science University, Portland, and is a member of the U.S. Preventive Services Task Force. He reported that he had no relevant financial disclosures.
AUSTIN, TEX. – This interview was conducted at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. It has been edited for length and clarity.
OB.GYN. NEWS: Here at ACOG, there were two studies from your research group at Oregon Health & Sciences University, Portland, that examined the cost-effectiveness of pregnancy interventions using a “two-delivery” model. Could you explain a little more about what that is, and how you arrived at this model?
DR. CAUGHEY: We’ve been working on decision analytics and cost-effectiveness studies of a number of ways to approach pregnancy, whether it be complicated pregnancies or uncomplicated normal pregnancies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
One of the things that we think is really important to think about is the impact of management and outcomes in the current pregnancy, and how it might affect future pregnancies.
So, for example, if you have a vaginal delivery this time, that makes you multiparous with a prior vaginal delivery next time; that is kind of the goal in pregnancy. It just makes all future labor and delivery experiences so much easier. Whereas, if you have a prior C-section, we all know that now you’re high risk. Everybody gets nervous about you. Are you going to get a trial of labor? Can you find a hospital that will do a trial of labor? And there are all these downstream implications of the delivery in the first pregnancy.
If you think about it, there are a number of ways that we can manage the first pregnancy. There are a number of risk factors for increasing risk for cesarean delivery. And we can include those in models that are considered in downstream pregnancies. And so we’ve been doing that increasingly.
When we think about our vaginal birth after cesarean models, we had two presentations that considered that. One was how we manage the maternal position in labor, and the other was how we use doulas in labor. You think, well gosh, we’re spending money on this doula in this pregnancy – that’s a certain expenditure. Is it worth it?
Part of “Is it worth it?” is not just the current pregnancy, but the downstream pregnancy as well.
OB.GYN. NEWS: What has sparked your interest in looking at obstetric care delivery in this way?
DR. CAUGHEY: I did my PhD in health economics. I began it as a 3rd-year maternal fetal medicine fellow and during my early career as an assistant professor at the University of California, San Francisco.
A lot of people think that economics in general is kind of about finance. Actually, microeconomics in particular is about the allocation of scarce resources to optimize utility – utility as general wellbeing or happiness.
So people will say that this thing, or that intervention, is cost effective, and often what they think they mean is, “It saves money.” But most things don’t save money. Most things in health care cost money. There are a few things in health care that do save money – vaccinations, contraception. Contraception actually saves money – but most things cost money. We have to spend money to get something right.
And the way we do that in health economics is that we think we’re going to get some happiness, some utility, some better outcomes from the money we’re putting in. One of the things that we don’t do very well as a species is think about these downstream outcomes.
In our models, when we think about morbidity and mortality we’re incorporating two and three pregnancy models. Think about what happens in the future, and then think about if we do something – if we spend money on an induction of labor or having a doula or something like that, is it worth it for what we get?
Antenatal testing, for example. Or, is it worth it for you to be testing people with diabetes once a week? Twice a week? More? Less? Part of it is figuring out what you’ll get for it. The measurement of what you get for it is called quality-adjusted life years, and that’s the measure of happiness multiplied times life expectancy.
We incorporate that in standard ways to build these models, to help us make decisions around best practices. Now, the economics piece of it probably matters. We’re the richest country that’s probably ever going to be – not just ever has been but probably ever going to be – the way we’re using up scarce resources to beat the band.
Yet, we still have an issue of allocation. We have people that have less; we have enormous disparities, whether it be racial and ethnic disparities, or socioeconomic disparities. And so we need to figure out ways to be more efficient and allocate those scarce resources properly to the outcomes that will be the best.
I think that’s what we’re working on: creating models to think about how to allocate those scarce resources.
OB.GYN. NEWS: How can a busy obstetrician think about the work you’re doing and incorporate it into her practice on a day-to-day basis?
DR. CAUGHEY: As an economist, I want to step back from time to time and think about public health and allocation of scarce resources.
But as a busy practicing clinician, I don’t necessarily want you consciously to think about cost. There are people who will push back on this and say, “Oh no, we should always be cost conscious.” Actually, what I really want you to do is incorporate best practices into the care of the patient at that moment, and do the thing that improves her outcomes best at that moment.
What we want to do, instead, is design systems that will properly incentivize. Incentivize doesn’t mean you think, “Oh gosh, if I do this thing I’m going to get an extra dollar.” It means subconsciously that those incentives are there, and those incentives don’t have to just be about dollars. Often in our field, they’re about time – what takes less time and more time to do something. So if we provide little extra roadblocks, then you’re more likely to go the other way and do something else.
For example: the hard stop. We did all this research in the 2000s to show that you probably shouldn’t deliver babies just for fun before 39 weeks’ gestational age. There should be an indication. If we don’t allow any hard stop, if we don’t block the pathway, then patients are pushing us, they’re uncomfortable, they’re like, “Just deliver me.” So we said, “No, no, no, we’re going to block this. In fact, we’re actually going to provide a hard stop reimbursement-wise. And medical directors of hospitals are going to have to preapprove.” And so that provides a blockade, and makes it easier just not to do it.
So I think that’s what we want: At the bedside and in your office, we want clinicians to still just be really good doctors. But then, to get involved and help design systems to incentivize us to do the right things.
Aaron B. Caughey, MD, PhD, is professor and chair of the department of obstetrics and gynecology and associate dean for Women’s Health Research and Policy at Oregon Health & Science University, Portland, and is a member of the U.S. Preventive Services Task Force. He reported that he had no relevant financial disclosures.
AUSTIN, TEX. – This interview was conducted at the annual clinical and scientific meeting of the American College of Obstetricians and Gynecologists. It has been edited for length and clarity.
OB.GYN. NEWS: Here at ACOG, there were two studies from your research group at Oregon Health & Sciences University, Portland, that examined the cost-effectiveness of pregnancy interventions using a “two-delivery” model. Could you explain a little more about what that is, and how you arrived at this model?
DR. CAUGHEY: We’ve been working on decision analytics and cost-effectiveness studies of a number of ways to approach pregnancy, whether it be complicated pregnancies or uncomplicated normal pregnancies.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
One of the things that we think is really important to think about is the impact of management and outcomes in the current pregnancy, and how it might affect future pregnancies.
So, for example, if you have a vaginal delivery this time, that makes you multiparous with a prior vaginal delivery next time; that is kind of the goal in pregnancy. It just makes all future labor and delivery experiences so much easier. Whereas, if you have a prior C-section, we all know that now you’re high risk. Everybody gets nervous about you. Are you going to get a trial of labor? Can you find a hospital that will do a trial of labor? And there are all these downstream implications of the delivery in the first pregnancy.
If you think about it, there are a number of ways that we can manage the first pregnancy. There are a number of risk factors for increasing risk for cesarean delivery. And we can include those in models that are considered in downstream pregnancies. And so we’ve been doing that increasingly.
When we think about our vaginal birth after cesarean models, we had two presentations that considered that. One was how we manage the maternal position in labor, and the other was how we use doulas in labor. You think, well gosh, we’re spending money on this doula in this pregnancy – that’s a certain expenditure. Is it worth it?
Part of “Is it worth it?” is not just the current pregnancy, but the downstream pregnancy as well.
OB.GYN. NEWS: What has sparked your interest in looking at obstetric care delivery in this way?
DR. CAUGHEY: I did my PhD in health economics. I began it as a 3rd-year maternal fetal medicine fellow and during my early career as an assistant professor at the University of California, San Francisco.
A lot of people think that economics in general is kind of about finance. Actually, microeconomics in particular is about the allocation of scarce resources to optimize utility – utility as general wellbeing or happiness.
So people will say that this thing, or that intervention, is cost effective, and often what they think they mean is, “It saves money.” But most things don’t save money. Most things in health care cost money. There are a few things in health care that do save money – vaccinations, contraception. Contraception actually saves money – but most things cost money. We have to spend money to get something right.
And the way we do that in health economics is that we think we’re going to get some happiness, some utility, some better outcomes from the money we’re putting in. One of the things that we don’t do very well as a species is think about these downstream outcomes.
In our models, when we think about morbidity and mortality we’re incorporating two and three pregnancy models. Think about what happens in the future, and then think about if we do something – if we spend money on an induction of labor or having a doula or something like that, is it worth it for what we get?
Antenatal testing, for example. Or, is it worth it for you to be testing people with diabetes once a week? Twice a week? More? Less? Part of it is figuring out what you’ll get for it. The measurement of what you get for it is called quality-adjusted life years, and that’s the measure of happiness multiplied times life expectancy.
We incorporate that in standard ways to build these models, to help us make decisions around best practices. Now, the economics piece of it probably matters. We’re the richest country that’s probably ever going to be – not just ever has been but probably ever going to be – the way we’re using up scarce resources to beat the band.
Yet, we still have an issue of allocation. We have people that have less; we have enormous disparities, whether it be racial and ethnic disparities, or socioeconomic disparities. And so we need to figure out ways to be more efficient and allocate those scarce resources properly to the outcomes that will be the best.
I think that’s what we’re working on: creating models to think about how to allocate those scarce resources.
OB.GYN. NEWS: How can a busy obstetrician think about the work you’re doing and incorporate it into her practice on a day-to-day basis?
DR. CAUGHEY: As an economist, I want to step back from time to time and think about public health and allocation of scarce resources.
But as a busy practicing clinician, I don’t necessarily want you consciously to think about cost. There are people who will push back on this and say, “Oh no, we should always be cost conscious.” Actually, what I really want you to do is incorporate best practices into the care of the patient at that moment, and do the thing that improves her outcomes best at that moment.
What we want to do, instead, is design systems that will properly incentivize. Incentivize doesn’t mean you think, “Oh gosh, if I do this thing I’m going to get an extra dollar.” It means subconsciously that those incentives are there, and those incentives don’t have to just be about dollars. Often in our field, they’re about time – what takes less time and more time to do something. So if we provide little extra roadblocks, then you’re more likely to go the other way and do something else.
For example: the hard stop. We did all this research in the 2000s to show that you probably shouldn’t deliver babies just for fun before 39 weeks’ gestational age. There should be an indication. If we don’t allow any hard stop, if we don’t block the pathway, then patients are pushing us, they’re uncomfortable, they’re like, “Just deliver me.” So we said, “No, no, no, we’re going to block this. In fact, we’re actually going to provide a hard stop reimbursement-wise. And medical directors of hospitals are going to have to preapprove.” And so that provides a blockade, and makes it easier just not to do it.
So I think that’s what we want: At the bedside and in your office, we want clinicians to still just be really good doctors. But then, to get involved and help design systems to incentivize us to do the right things.
Aaron B. Caughey, MD, PhD, is professor and chair of the department of obstetrics and gynecology and associate dean for Women’s Health Research and Policy at Oregon Health & Science University, Portland, and is a member of the U.S. Preventive Services Task Force. He reported that he had no relevant financial disclosures.
REPORTING FROM ACOG 2018

White House pushes transparency in drug price plan
The Trump administration believes it is a “right that, when you are sitting there with your doctor, you ought to be able to know what your out-of-pocket [cost] is for drug you are going to be prescribed under your precise drug plan. And you ought to have information on what competing drugs are that your doctor is not prescribing and what you would pay out of pocket for that.”

Price transparency is a key theme to the broad package of proposals called American Patients First that the White House released May 11. The plan includes changes that can be made immediately as well as some upon which the administration will seek public comment, according to the plan.
Another tactic the administration is considering for quick action is requiring a drug’s list prices to be included in all direct-to-consumer advertising.
The plan also calls for the banning of gag rules that prevent pharmacists from alerting patients when it would be cheaper to buy a prescribed drug without going through their insurance coverage, as well as moving certain drugs from Medicare Part B to Medicare Part D to improve the government’s ability to negotiations for lower prices.
The overall strategy is laid out across four areas:
- Increasing competition though policy measures that prevent manufacturers from gaming the patent system and promoting innovation and competition among biologics.
- Improving negotiation abilities, including doing more with value-based purchasing; allowing for more substitution, especially in the case of single-source generics; and further examination of the competitive acquisition program for Part B.
- Providing incentives to manufacturers to lower their list prices.
- Lowering out-of-pocket costs.
Currently, there is no incentive to lower drug prices, Mr. Azar noted. He called out pharmacy benefit managers (PBMs) for financially benefiting from both manufacturers and the insurers they represent and said HHS is looking into banning financial compensation to PBMs from the manufacturers. He also said the agency will be releasing a request for information on the feasibility of doing away with rebates as a means of driving manufacturers to lower their prices.
PhRMA, the lobbying group representing pharmaceutical manufacturers, said in a statement that some of the changes related to Part D “could undermine the existing structure of the program that has successfully held down costs and provided seniors with access to comprehensive prescription drug coverage. We also must avoid changes to Medicare Part B that could raise costs for seniors and limit their access to lifesaving treatments.”
The Pharmaceutical Care Management Association, the lobbying group for pharmacy benefit managers, also spoke out against the idea of eliminating rebates, noting in a statement that getting rid of them “and other price concessions would leave patients and payers, including Medicaid and Medicare, at the mercy of drug manufacturer pricing strategies. PBMs have long encouraged manufacturers to offer payers alternative ways to reduce net costs. Simply put, the easiest way to lower costs would be for drug companies to lower their prices.”
The American Medical Association voiced support for the plan.
“The AMA is pleased the Trump administration is moving forward with its effort to address seemingly arbitrary pricing for prescription drugs,” President David Barbe, MD, said in a statement “Physicians see the impact of skyrocketing prices every day as patients are often unable to afford the most medically appropriate medications – even those that have effectively controlled their medical condition for years. No one can understand the logic behind the high and fluctuating prices. We hope the administration can bring some transparency – and relief – to patients.”
During a Rose Garden ceremony to introduce the initiative, President Trump said he is targeting foreign countries that require manufacturers to sell their products well below list prices as a condition of selling in their country, forcing Americans to absorb the research and development costs via higher prices for drugs.
“It’s time to end the global freeloading once and for all,” President Trump said. “I have directed U.S. Trade Representative Bob Lighthizer to make fixing this injustice a top priority with every trading partner.”
One proposal President Trump campaigned on – giving the federal government the power to directly negotiate for drug prices – was not included in the plan.
“I am very disappointed that he has apparently dropped his support for allowing Medicare to negotiate the price of prescription drugs,” Sen. Maggie Hassan (D-N.H.) said in a statement.
Also absent from the plan: a direct negotiation tactic for Part B drugs supported by Mr. Azar during his confirmation hearings.
The Trump administration believes it is a “right that, when you are sitting there with your doctor, you ought to be able to know what your out-of-pocket [cost] is for drug you are going to be prescribed under your precise drug plan. And you ought to have information on what competing drugs are that your doctor is not prescribing and what you would pay out of pocket for that.”
Price transparency is a key theme to the broad package of proposals called American Patients First that the White House released May 11. The plan includes changes that can be made immediately as well as some upon which the administration will seek public comment, according to the plan.
Another tactic the administration is considering for quick action is requiring a drug’s list prices to be included in all direct-to-consumer advertising.
The plan also calls for the banning of gag rules that prevent pharmacists from alerting patients when it would be cheaper to buy a prescribed drug without going through their insurance coverage, as well as moving certain drugs from Medicare Part B to Medicare Part D to improve the government’s ability to negotiations for lower prices.
The overall strategy is laid out across four areas:
- Increasing competition though policy measures that prevent manufacturers from gaming the patent system and promoting innovation and competition among biologics.
- Improving negotiation abilities, including doing more with value-based purchasing; allowing for more substitution, especially in the case of single-source generics; and further examination of the competitive acquisition program for Part B.
- Providing incentives to manufacturers to lower their list prices.
- Lowering out-of-pocket costs.
Currently, there is no incentive to lower drug prices, Mr. Azar noted. He called out pharmacy benefit managers (PBMs) for financially benefiting from both manufacturers and the insurers they represent and said HHS is looking into banning financial compensation to PBMs from the manufacturers. He also said the agency will be releasing a request for information on the feasibility of doing away with rebates as a means of driving manufacturers to lower their prices.
PhRMA, the lobbying group representing pharmaceutical manufacturers, said in a statement that some of the changes related to Part D “could undermine the existing structure of the program that has successfully held down costs and provided seniors with access to comprehensive prescription drug coverage. We also must avoid changes to Medicare Part B that could raise costs for seniors and limit their access to lifesaving treatments.”
The Pharmaceutical Care Management Association, the lobbying group for pharmacy benefit managers, also spoke out against the idea of eliminating rebates, noting in a statement that getting rid of them “and other price concessions would leave patients and payers, including Medicaid and Medicare, at the mercy of drug manufacturer pricing strategies. PBMs have long encouraged manufacturers to offer payers alternative ways to reduce net costs. Simply put, the easiest way to lower costs would be for drug companies to lower their prices.”
The American Medical Association voiced support for the plan.
“The AMA is pleased the Trump administration is moving forward with its effort to address seemingly arbitrary pricing for prescription drugs,” President David Barbe, MD, said in a statement “Physicians see the impact of skyrocketing prices every day as patients are often unable to afford the most medically appropriate medications – even those that have effectively controlled their medical condition for years. No one can understand the logic behind the high and fluctuating prices. We hope the administration can bring some transparency – and relief – to patients.”
During a Rose Garden ceremony to introduce the initiative, President Trump said he is targeting foreign countries that require manufacturers to sell their products well below list prices as a condition of selling in their country, forcing Americans to absorb the research and development costs via higher prices for drugs.
“It’s time to end the global freeloading once and for all,” President Trump said. “I have directed U.S. Trade Representative Bob Lighthizer to make fixing this injustice a top priority with every trading partner.”
One proposal President Trump campaigned on – giving the federal government the power to directly negotiate for drug prices – was not included in the plan.
“I am very disappointed that he has apparently dropped his support for allowing Medicare to negotiate the price of prescription drugs,” Sen. Maggie Hassan (D-N.H.) said in a statement.
Also absent from the plan: a direct negotiation tactic for Part B drugs supported by Mr. Azar during his confirmation hearings.
The Trump administration believes it is a “right that, when you are sitting there with your doctor, you ought to be able to know what your out-of-pocket [cost] is for drug you are going to be prescribed under your precise drug plan. And you ought to have information on what competing drugs are that your doctor is not prescribing and what you would pay out of pocket for that.”
Price transparency is a key theme to the broad package of proposals called American Patients First that the White House released May 11. The plan includes changes that can be made immediately as well as some upon which the administration will seek public comment, according to the plan.
Another tactic the administration is considering for quick action is requiring a drug’s list prices to be included in all direct-to-consumer advertising.
The plan also calls for the banning of gag rules that prevent pharmacists from alerting patients when it would be cheaper to buy a prescribed drug without going through their insurance coverage, as well as moving certain drugs from Medicare Part B to Medicare Part D to improve the government’s ability to negotiations for lower prices.
The overall strategy is laid out across four areas:
- Increasing competition though policy measures that prevent manufacturers from gaming the patent system and promoting innovation and competition among biologics.
- Improving negotiation abilities, including doing more with value-based purchasing; allowing for more substitution, especially in the case of single-source generics; and further examination of the competitive acquisition program for Part B.
- Providing incentives to manufacturers to lower their list prices.
- Lowering out-of-pocket costs.
Currently, there is no incentive to lower drug prices, Mr. Azar noted. He called out pharmacy benefit managers (PBMs) for financially benefiting from both manufacturers and the insurers they represent and said HHS is looking into banning financial compensation to PBMs from the manufacturers. He also said the agency will be releasing a request for information on the feasibility of doing away with rebates as a means of driving manufacturers to lower their prices.
PhRMA, the lobbying group representing pharmaceutical manufacturers, said in a statement that some of the changes related to Part D “could undermine the existing structure of the program that has successfully held down costs and provided seniors with access to comprehensive prescription drug coverage. We also must avoid changes to Medicare Part B that could raise costs for seniors and limit their access to lifesaving treatments.”
The Pharmaceutical Care Management Association, the lobbying group for pharmacy benefit managers, also spoke out against the idea of eliminating rebates, noting in a statement that getting rid of them “and other price concessions would leave patients and payers, including Medicaid and Medicare, at the mercy of drug manufacturer pricing strategies. PBMs have long encouraged manufacturers to offer payers alternative ways to reduce net costs. Simply put, the easiest way to lower costs would be for drug companies to lower their prices.”
The American Medical Association voiced support for the plan.
“The AMA is pleased the Trump administration is moving forward with its effort to address seemingly arbitrary pricing for prescription drugs,” President David Barbe, MD, said in a statement “Physicians see the impact of skyrocketing prices every day as patients are often unable to afford the most medically appropriate medications – even those that have effectively controlled their medical condition for years. No one can understand the logic behind the high and fluctuating prices. We hope the administration can bring some transparency – and relief – to patients.”
During a Rose Garden ceremony to introduce the initiative, President Trump said he is targeting foreign countries that require manufacturers to sell their products well below list prices as a condition of selling in their country, forcing Americans to absorb the research and development costs via higher prices for drugs.
“It’s time to end the global freeloading once and for all,” President Trump said. “I have directed U.S. Trade Representative Bob Lighthizer to make fixing this injustice a top priority with every trading partner.”
One proposal President Trump campaigned on – giving the federal government the power to directly negotiate for drug prices – was not included in the plan.
“I am very disappointed that he has apparently dropped his support for allowing Medicare to negotiate the price of prescription drugs,” Sen. Maggie Hassan (D-N.H.) said in a statement.
Also absent from the plan: a direct negotiation tactic for Part B drugs supported by Mr. Azar during his confirmation hearings.
Open Clinical Trials for Patients With Colorectal Cancer (FULL)
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors > 300 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of April 1, 2017; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Impact of Family History and Decision Support on High-Risk Cancer Screening
There is no standardized system for collecting and updating family health history, using this information to determine a patient’s disease risk level, and providing screening recommendations to patients and providers. Patients will enter their family health history into a program that will produce screening recommendations tailored to the patient’s family health history. The investigators will examine whether this process increases physician referrals for, and patient uptake of, guideline-recommended screening for colorectal cancer.
ID: NCT02247336
Sponsor: VA Office of Research and Development
Location (contact): Durham VAMC, North Carolina (Jamiyla Bolton, Susan B. Armstrong); William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin (Corrine Voils)
Colonoscopy Versus Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer
The investigators propose to perform a large, simple, multicenter, randomized, parallel-group trial directly comparing screening colonoscopy with annual fecal immunochemical test screening in average risk individuals. The hypothesis is that colonoscopy will be superior to fecal immunochemical testing in the prevention of colorectal cancer (CRC) mortality measured over 10 years. The primary study endpoint will be CRC mortality within 10 years of enrollment.
ID: NCT01239082
Sponsor: VA Office of Research and Development
Locations: 48 current locations
S0820, Adenoma and Second Primary Prevention Trial (PACES)
The investigators hypothesize that the combination of eflornithine and sulindac will be effective in reducing a 3-year event rate of adenomas and second primary colorectal cancers in patients previously treated for Stages 0 through III colon cancer.
ID: NCT01349881
Sponsor: Southwest Oncology Group
Location (contact): VA Connecticut Healthcare System-West Haven Campus (Michal Rose); Edward Hines Jr. VA Hospital, Hines, Illinois (Abdul Choudhury); Kansas City VAMC, Missouri (Joaquina Baranda); White River Junction VAMC, Vermont (Nancy Kuemmerle); Eisenhower Army Medical Center, Fort Gordon, Georgia (Andrew Delmas); Tripler Army Medical Center, Honolulu, Hawaii (Jeffrey Berenberg); Brooke Army Medical Center, Fort Sam Houston, Texas (John Renshaw)
Irinotecan Hydrochloride and Cetuximab With or Without Ramucirumab in Treating Patients With Advanced Colorectal Cancer With Progressive Disease After Treatment With Bevacizumab
This randomized phase II trial is studying the adverse effects and how well giving cetuximab and irinotecan hydrochloride with or without ramucirumab work in treating patients with advanced colorectal cancer with progressive disease after treatment with bevacizumab-containing chemotherapy.
ID: NCT01079780
Sponsor: Eastern Cooperative Oncology Group
Location (contact): Atlanta VAMC, Decatur, Georgia (Samuel Chan); VA New Jersey Health Care System East Orange Campus (Basil Kasimis)
Cancer Associated Thrombosis and Isoquercetin
This research study is evaluating a drug called isoquercetin to prevent venous thrombosis (blood clots) in participants who have pancreas, non-small cell lung cancer or colorectal cancer.
ID: NCT02195232
Sponsor: Dana-Farber Cancer Institute
Location (contact): Washington DC VAMC (Anita Aggarwal); Boston VA Healthcare System, Massachusetts (Kenneth Bauer); White River Junction VAMC, Vermont (Nancy Kuemmerle)
Studying Lymph Nodes in Patients With Stage II Colon Cancer
Diagnostic procedures that look for micrometastases in lymph nodes removed during surgery for colon cancer may help doctors learn the extent of disease. This phase I trial is studying lymph nodes in patients with stage II colon cancer.
ID: NCT00949312
Sponsor: John Wayne Cancer Institute
Location: Walter Reed Army Medical Center, Washington, DC
Click here to read the digital edition.
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors > 300 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of April 1, 2017; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Impact of Family History and Decision Support on High-Risk Cancer Screening
There is no standardized system for collecting and updating family health history, using this information to determine a patient’s disease risk level, and providing screening recommendations to patients and providers. Patients will enter their family health history into a program that will produce screening recommendations tailored to the patient’s family health history. The investigators will examine whether this process increases physician referrals for, and patient uptake of, guideline-recommended screening for colorectal cancer.
ID: NCT02247336
Sponsor: VA Office of Research and Development
Location (contact): Durham VAMC, North Carolina (Jamiyla Bolton, Susan B. Armstrong); William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin (Corrine Voils)
Colonoscopy Versus Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer
The investigators propose to perform a large, simple, multicenter, randomized, parallel-group trial directly comparing screening colonoscopy with annual fecal immunochemical test screening in average risk individuals. The hypothesis is that colonoscopy will be superior to fecal immunochemical testing in the prevention of colorectal cancer (CRC) mortality measured over 10 years. The primary study endpoint will be CRC mortality within 10 years of enrollment.
ID: NCT01239082
Sponsor: VA Office of Research and Development
Locations: 48 current locations
S0820, Adenoma and Second Primary Prevention Trial (PACES)
The investigators hypothesize that the combination of eflornithine and sulindac will be effective in reducing a 3-year event rate of adenomas and second primary colorectal cancers in patients previously treated for Stages 0 through III colon cancer.
ID: NCT01349881
Sponsor: Southwest Oncology Group
Location (contact): VA Connecticut Healthcare System-West Haven Campus (Michal Rose); Edward Hines Jr. VA Hospital, Hines, Illinois (Abdul Choudhury); Kansas City VAMC, Missouri (Joaquina Baranda); White River Junction VAMC, Vermont (Nancy Kuemmerle); Eisenhower Army Medical Center, Fort Gordon, Georgia (Andrew Delmas); Tripler Army Medical Center, Honolulu, Hawaii (Jeffrey Berenberg); Brooke Army Medical Center, Fort Sam Houston, Texas (John Renshaw)
Irinotecan Hydrochloride and Cetuximab With or Without Ramucirumab in Treating Patients With Advanced Colorectal Cancer With Progressive Disease After Treatment With Bevacizumab
This randomized phase II trial is studying the adverse effects and how well giving cetuximab and irinotecan hydrochloride with or without ramucirumab work in treating patients with advanced colorectal cancer with progressive disease after treatment with bevacizumab-containing chemotherapy.
ID: NCT01079780
Sponsor: Eastern Cooperative Oncology Group
Location (contact): Atlanta VAMC, Decatur, Georgia (Samuel Chan); VA New Jersey Health Care System East Orange Campus (Basil Kasimis)
Cancer Associated Thrombosis and Isoquercetin
This research study is evaluating a drug called isoquercetin to prevent venous thrombosis (blood clots) in participants who have pancreas, non-small cell lung cancer or colorectal cancer.
ID: NCT02195232
Sponsor: Dana-Farber Cancer Institute
Location (contact): Washington DC VAMC (Anita Aggarwal); Boston VA Healthcare System, Massachusetts (Kenneth Bauer); White River Junction VAMC, Vermont (Nancy Kuemmerle)
Studying Lymph Nodes in Patients With Stage II Colon Cancer
Diagnostic procedures that look for micrometastases in lymph nodes removed during surgery for colon cancer may help doctors learn the extent of disease. This phase I trial is studying lymph nodes in patients with stage II colon cancer.
ID: NCT00949312
Sponsor: John Wayne Cancer Institute
Location: Walter Reed Army Medical Center, Washington, DC
Click here to read the digital edition.
Providing access to clinical trials for veteran and active-duty military patients can be a challenge, but a significant number of trials are now recruiting patients from those patient populations. Many trials explicitly recruit patients from the VA, the military, and IHS. The VA Office of Research and Development alone sponsors > 300 research initiatives, and many more are sponsored by Walter Reed National Medical Center and other major defense and VA facilities. The clinical trials listed below are all open as of April 1, 2017; have at least 1 VA, DoD, or IHS location recruiting patients; and are focused on treatment for colorectal cancer. For additional information and full inclusion/exclusion criteria, please consult clinicaltrials.gov.
Impact of Family History and Decision Support on High-Risk Cancer Screening
There is no standardized system for collecting and updating family health history, using this information to determine a patient’s disease risk level, and providing screening recommendations to patients and providers. Patients will enter their family health history into a program that will produce screening recommendations tailored to the patient’s family health history. The investigators will examine whether this process increases physician referrals for, and patient uptake of, guideline-recommended screening for colorectal cancer.
ID: NCT02247336
Sponsor: VA Office of Research and Development
Location (contact): Durham VAMC, North Carolina (Jamiyla Bolton, Susan B. Armstrong); William S. Middleton Memorial Veterans Hospital, Madison, Wisconsin (Corrine Voils)
Colonoscopy Versus Fecal Immunochemical Test in Reducing Mortality From Colorectal Cancer
The investigators propose to perform a large, simple, multicenter, randomized, parallel-group trial directly comparing screening colonoscopy with annual fecal immunochemical test screening in average risk individuals. The hypothesis is that colonoscopy will be superior to fecal immunochemical testing in the prevention of colorectal cancer (CRC) mortality measured over 10 years. The primary study endpoint will be CRC mortality within 10 years of enrollment.
ID: NCT01239082
Sponsor: VA Office of Research and Development
Locations: 48 current locations
S0820, Adenoma and Second Primary Prevention Trial (PACES)
The investigators hypothesize that the combination of eflornithine and sulindac will be effective in reducing a 3-year event rate of adenomas and second primary colorectal cancers in patients previously treated for Stages 0 through III colon cancer.
ID: NCT01349881
Sponsor: Southwest Oncology Group
Location (contact): VA Connecticut Healthcare System-West Haven Campus (Michal Rose); Edward Hines Jr. VA Hospital, Hines, Illinois (Abdul Choudhury); Kansas City VAMC, Missouri (Joaquina Baranda); White River Junction VAMC, Vermont (Nancy Kuemmerle); Eisenhower Army Medical Center, Fort Gordon, Georgia (Andrew Delmas); Tripler Army Medical Center, Honolulu, Hawaii (Jeffrey Berenberg); Brooke Army Medical Center, Fort Sam Houston, Texas (John Renshaw)
Irinotecan Hydrochloride and Cetuximab With or Without Ramucirumab in Treating Patients With Advanced Colorectal Cancer With Progressive Disease After Treatment With Bevacizumab
This randomized phase II trial is studying the adverse effects and how well giving cetuximab and irinotecan hydrochloride with or without ramucirumab work in treating patients with advanced colorectal cancer with progressive disease after treatment with bevacizumab-containing chemotherapy.
ID: NCT01079780
Sponsor: Eastern Cooperative Oncology Group
Location (contact): Atlanta VAMC, Decatur, Georgia (Samuel Chan); VA New Jersey Health Care System East Orange Campus (Basil Kasimis)
Cancer Associated Thrombosis and Isoquercetin
This research study is evaluating a drug called isoquercetin to prevent venous thrombosis (blood clots) in participants who have pancreas, non-small cell lung cancer or colorectal cancer.
ID: NCT02195232
Sponsor: Dana-Farber Cancer Institute
Location (contact): Washington DC VAMC (Anita Aggarwal); Boston VA Healthcare System, Massachusetts (Kenneth Bauer); White River Junction VAMC, Vermont (Nancy Kuemmerle)
Studying Lymph Nodes in Patients With Stage II Colon Cancer
Diagnostic procedures that look for micrometastases in lymph nodes removed during surgery for colon cancer may help doctors learn the extent of disease. This phase I trial is studying lymph nodes in patients with stage II colon cancer.
ID: NCT00949312
Sponsor: John Wayne Cancer Institute
Location: Walter Reed Army Medical Center, Washington, DC
Click here to read the digital edition.
Group calls on WHO to help fight HTLV-1

A group of scientists and activists are calling on the World Health Organization (WHO) to fight the spread of human T-cell leukemia virus subtype 1 (HTLV-1).
The group has written a letter to the WHO highlighting the global prevalence of HTLV-1 infection and recommending strategies to prevent the transmission of HTLV-1.
An abbreviated version of the letter was published in The Lancet. The full letter is available on the Global Virus Network (GVN)* website.
“Since my colleagues and I discovered HTLV-1 . . ., we have learned that this destructive and lethal virus is causing much devastation in communities with high prevalence,” said Robert C. Gallo, MD, co-founder and director of GVN and a professor at the University of Maryland School of Medicine in Baltimore.
“During the GVN meeting last September, I was astounded to learn of the hyper-endemic numbers in the Aboriginal population of Australia. HTLV-1 is endemic in other regions, including several islands of the Caribbean, and in countries such as Brazil, Iran, Japan, and Peru. We hope that the WHO will agree with us and begin to take action in promoting prevention strategies against HTLV-1.”
HTLV-1 prevalence
In their letter, Dr Gallo and his colleagues cite statistics of HTLV-1 prevalence around the world.
The authors note that, in a hospital-based cohort study conducted in Central Australia, 33.6% of Indigenous people tested HTLV-1 positive, with the incidence rate reaching 48.5% in older men.
Research has suggested that, in Brazil, the HTLV-1 prevalence rate is 1.8% in the general population, 1.3% in blood donors in certain regions, and 1.05% in pregnant women.
It is estimated that nearly 1 million people are HTLV-1-positive in Japan, and 850,000 to 1.7 million people in Nigeria are infected with the virus.
In Gabon, the HTLV-1 prevalence in adults is believed to be 5% to 10%. And in Central African Republic, 7% of older, female Pygmies in the southern region were found to be infected with HTLV-1.
Studies have indicated that 6.1% of the general population in Jamaica is positive for HTLV-1, and other Caribbean islands have similar prevalence rates.
The authors note that HTLV-1 and -2 have also been detected in non-endemic areas due to migration and sexual transmission.
It is estimated that 20,000 to 30,000 people are infected with HTLV-1 in the UK, and 10,000 to 25,000 people are infected in metropolitan France.
Other estimates suggest that 266,000 people are infected with HTLV-1 or -2 in the US, and 3600 people with HTLV-1 associated myelopathy/tropical spastic paraparesis (HAM/TSP) remain undiagnosed.
“The general neglect, globally, of the importance of HTLV-1 as a sexually transmitted infection that causes a range of debilitating inflammatory diseases does our patients, who request a sexual health screen, a disservice,” said Graham P. Taylor, MDMB, DSc, a professor at Imperial College London in the UK.
“It is also important to recognize the importance of mother-to-child transmission of HTLV-1 in the development of adult T-cell leukemia/lymphoma (ATLL) decades later. Despite the availability of highly sensitive and specific diagnostic tests for infection and a proven intervention, except for Japan, there are no antenatal screening programs. Evaluating the cost-effectiveness of such programs should now be a priority.”
“To prevent mother-to-child infection, the Japanese government has been offering HTLV-1 screening for all pregnant women without cost,” noted Yoshi Yamano, MD, PhD, a professor at St. Marianna University School of Medicine in Kawasaki, Japan.
“Taking a leadership role to promote research, it also provides grants for clinical trials and patient registries focused on ATLL and HAM/TSP.”
Preventing transmission
The letter outlines 5 strategies to prevent or reduce transmission of HTLV-1. The authors recommend:
- Protecting the sexually active population with routine HTLV-1 testing in sexual health clinics and through promotion of CMPC—Counsel & Monitor HTLV-1-positive patients, notify Partners, and promote Condom usage
- Protecting blood and organ donors and recipients by testing for HTLV, avoiding use of products that may be infected, and promoting CMPC
- Protecting mothers, babies, and fathers via routine antenatal care testing, advising HTLV-1-positive mothers against breastfeeding (when feasible), and promoting CMPC
- Protecting injectable drug users by promoting HTLV-1 testing, providing safe needles through needle exchange program, and promoting CMPC
- Supporting the general population and healthcare providers by providing access to an up-to-date WHO HTLV-1 Fact Sheet that can help healthcare providers diagnose HTLV-1 and related diseases and help patients protect themselves from HTLV-1.
“This virus has been underestimated since the time of its discovery perhaps because it is restricted to certain regions or because it is not terribly infectious,” said William Hall, MD, PhD, co-founder of GVN and a professor at the University College Dublin in Ireland.
“However, for decades, it has been known that HTLV-1 is highly carcinogenic and causes severe paralytic neurologic disease and immune disorders that can lead to bacterial infections. It is time that the WHO publicize prevention strategies against this devastating virus.”
*GVN is an international coalition of medical virologists dedicated to identifying, researching, fighting, and preventing current and emerging pandemic viruses that pose a threat to public health.
A group of scientists and activists are calling on the World Health Organization (WHO) to fight the spread of human T-cell leukemia virus subtype 1 (HTLV-1).
The group has written a letter to the WHO highlighting the global prevalence of HTLV-1 infection and recommending strategies to prevent the transmission of HTLV-1.
An abbreviated version of the letter was published in The Lancet. The full letter is available on the Global Virus Network (GVN)* website.
“Since my colleagues and I discovered HTLV-1 . . ., we have learned that this destructive and lethal virus is causing much devastation in communities with high prevalence,” said Robert C. Gallo, MD, co-founder and director of GVN and a professor at the University of Maryland School of Medicine in Baltimore.
“During the GVN meeting last September, I was astounded to learn of the hyper-endemic numbers in the Aboriginal population of Australia. HTLV-1 is endemic in other regions, including several islands of the Caribbean, and in countries such as Brazil, Iran, Japan, and Peru. We hope that the WHO will agree with us and begin to take action in promoting prevention strategies against HTLV-1.”
HTLV-1 prevalence
In their letter, Dr Gallo and his colleagues cite statistics of HTLV-1 prevalence around the world.
The authors note that, in a hospital-based cohort study conducted in Central Australia, 33.6% of Indigenous people tested HTLV-1 positive, with the incidence rate reaching 48.5% in older men.
Research has suggested that, in Brazil, the HTLV-1 prevalence rate is 1.8% in the general population, 1.3% in blood donors in certain regions, and 1.05% in pregnant women.
It is estimated that nearly 1 million people are HTLV-1-positive in Japan, and 850,000 to 1.7 million people in Nigeria are infected with the virus.
In Gabon, the HTLV-1 prevalence in adults is believed to be 5% to 10%. And in Central African Republic, 7% of older, female Pygmies in the southern region were found to be infected with HTLV-1.
Studies have indicated that 6.1% of the general population in Jamaica is positive for HTLV-1, and other Caribbean islands have similar prevalence rates.
The authors note that HTLV-1 and -2 have also been detected in non-endemic areas due to migration and sexual transmission.
It is estimated that 20,000 to 30,000 people are infected with HTLV-1 in the UK, and 10,000 to 25,000 people are infected in metropolitan France.
Other estimates suggest that 266,000 people are infected with HTLV-1 or -2 in the US, and 3600 people with HTLV-1 associated myelopathy/tropical spastic paraparesis (HAM/TSP) remain undiagnosed.
“The general neglect, globally, of the importance of HTLV-1 as a sexually transmitted infection that causes a range of debilitating inflammatory diseases does our patients, who request a sexual health screen, a disservice,” said Graham P. Taylor, MDMB, DSc, a professor at Imperial College London in the UK.
“It is also important to recognize the importance of mother-to-child transmission of HTLV-1 in the development of adult T-cell leukemia/lymphoma (ATLL) decades later. Despite the availability of highly sensitive and specific diagnostic tests for infection and a proven intervention, except for Japan, there are no antenatal screening programs. Evaluating the cost-effectiveness of such programs should now be a priority.”
“To prevent mother-to-child infection, the Japanese government has been offering HTLV-1 screening for all pregnant women without cost,” noted Yoshi Yamano, MD, PhD, a professor at St. Marianna University School of Medicine in Kawasaki, Japan.
“Taking a leadership role to promote research, it also provides grants for clinical trials and patient registries focused on ATLL and HAM/TSP.”
Preventing transmission
The letter outlines 5 strategies to prevent or reduce transmission of HTLV-1. The authors recommend:
- Protecting the sexually active population with routine HTLV-1 testing in sexual health clinics and through promotion of CMPC—Counsel & Monitor HTLV-1-positive patients, notify Partners, and promote Condom usage
- Protecting blood and organ donors and recipients by testing for HTLV, avoiding use of products that may be infected, and promoting CMPC
- Protecting mothers, babies, and fathers via routine antenatal care testing, advising HTLV-1-positive mothers against breastfeeding (when feasible), and promoting CMPC
- Protecting injectable drug users by promoting HTLV-1 testing, providing safe needles through needle exchange program, and promoting CMPC
- Supporting the general population and healthcare providers by providing access to an up-to-date WHO HTLV-1 Fact Sheet that can help healthcare providers diagnose HTLV-1 and related diseases and help patients protect themselves from HTLV-1.
“This virus has been underestimated since the time of its discovery perhaps because it is restricted to certain regions or because it is not terribly infectious,” said William Hall, MD, PhD, co-founder of GVN and a professor at the University College Dublin in Ireland.
“However, for decades, it has been known that HTLV-1 is highly carcinogenic and causes severe paralytic neurologic disease and immune disorders that can lead to bacterial infections. It is time that the WHO publicize prevention strategies against this devastating virus.”
*GVN is an international coalition of medical virologists dedicated to identifying, researching, fighting, and preventing current and emerging pandemic viruses that pose a threat to public health.
A group of scientists and activists are calling on the World Health Organization (WHO) to fight the spread of human T-cell leukemia virus subtype 1 (HTLV-1).
The group has written a letter to the WHO highlighting the global prevalence of HTLV-1 infection and recommending strategies to prevent the transmission of HTLV-1.
An abbreviated version of the letter was published in The Lancet. The full letter is available on the Global Virus Network (GVN)* website.
“Since my colleagues and I discovered HTLV-1 . . ., we have learned that this destructive and lethal virus is causing much devastation in communities with high prevalence,” said Robert C. Gallo, MD, co-founder and director of GVN and a professor at the University of Maryland School of Medicine in Baltimore.
“During the GVN meeting last September, I was astounded to learn of the hyper-endemic numbers in the Aboriginal population of Australia. HTLV-1 is endemic in other regions, including several islands of the Caribbean, and in countries such as Brazil, Iran, Japan, and Peru. We hope that the WHO will agree with us and begin to take action in promoting prevention strategies against HTLV-1.”
HTLV-1 prevalence
In their letter, Dr Gallo and his colleagues cite statistics of HTLV-1 prevalence around the world.
The authors note that, in a hospital-based cohort study conducted in Central Australia, 33.6% of Indigenous people tested HTLV-1 positive, with the incidence rate reaching 48.5% in older men.
Research has suggested that, in Brazil, the HTLV-1 prevalence rate is 1.8% in the general population, 1.3% in blood donors in certain regions, and 1.05% in pregnant women.
It is estimated that nearly 1 million people are HTLV-1-positive in Japan, and 850,000 to 1.7 million people in Nigeria are infected with the virus.
In Gabon, the HTLV-1 prevalence in adults is believed to be 5% to 10%. And in Central African Republic, 7% of older, female Pygmies in the southern region were found to be infected with HTLV-1.
Studies have indicated that 6.1% of the general population in Jamaica is positive for HTLV-1, and other Caribbean islands have similar prevalence rates.
The authors note that HTLV-1 and -2 have also been detected in non-endemic areas due to migration and sexual transmission.
It is estimated that 20,000 to 30,000 people are infected with HTLV-1 in the UK, and 10,000 to 25,000 people are infected in metropolitan France.
Other estimates suggest that 266,000 people are infected with HTLV-1 or -2 in the US, and 3600 people with HTLV-1 associated myelopathy/tropical spastic paraparesis (HAM/TSP) remain undiagnosed.
“The general neglect, globally, of the importance of HTLV-1 as a sexually transmitted infection that causes a range of debilitating inflammatory diseases does our patients, who request a sexual health screen, a disservice,” said Graham P. Taylor, MDMB, DSc, a professor at Imperial College London in the UK.
“It is also important to recognize the importance of mother-to-child transmission of HTLV-1 in the development of adult T-cell leukemia/lymphoma (ATLL) decades later. Despite the availability of highly sensitive and specific diagnostic tests for infection and a proven intervention, except for Japan, there are no antenatal screening programs. Evaluating the cost-effectiveness of such programs should now be a priority.”
“To prevent mother-to-child infection, the Japanese government has been offering HTLV-1 screening for all pregnant women without cost,” noted Yoshi Yamano, MD, PhD, a professor at St. Marianna University School of Medicine in Kawasaki, Japan.
“Taking a leadership role to promote research, it also provides grants for clinical trials and patient registries focused on ATLL and HAM/TSP.”
Preventing transmission
The letter outlines 5 strategies to prevent or reduce transmission of HTLV-1. The authors recommend:
- Protecting the sexually active population with routine HTLV-1 testing in sexual health clinics and through promotion of CMPC—Counsel & Monitor HTLV-1-positive patients, notify Partners, and promote Condom usage
- Protecting blood and organ donors and recipients by testing for HTLV, avoiding use of products that may be infected, and promoting CMPC
- Protecting mothers, babies, and fathers via routine antenatal care testing, advising HTLV-1-positive mothers against breastfeeding (when feasible), and promoting CMPC
- Protecting injectable drug users by promoting HTLV-1 testing, providing safe needles through needle exchange program, and promoting CMPC
- Supporting the general population and healthcare providers by providing access to an up-to-date WHO HTLV-1 Fact Sheet that can help healthcare providers diagnose HTLV-1 and related diseases and help patients protect themselves from HTLV-1.
“This virus has been underestimated since the time of its discovery perhaps because it is restricted to certain regions or because it is not terribly infectious,” said William Hall, MD, PhD, co-founder of GVN and a professor at the University College Dublin in Ireland.
“However, for decades, it has been known that HTLV-1 is highly carcinogenic and causes severe paralytic neurologic disease and immune disorders that can lead to bacterial infections. It is time that the WHO publicize prevention strategies against this devastating virus.”
*GVN is an international coalition of medical virologists dedicated to identifying, researching, fighting, and preventing current and emerging pandemic viruses that pose a threat to public health.
FDA expands fingolimod's indications to treat relapsing MS in pediatric patients
Pediatric patients with
The Food and Drug Administration approved on May 11 an expanded indication of the drug to allow it to be used to treat relapsing MS in children and adolescents age 10 and older. Gilenya was first approved by FDA to treat adults with relapsing MS in 2010.
“For the first time, we have an FDA-approved treatment specifically for children and adolescents with multiple sclerosis,” Billy Dunn, MD, director of the Division of Neurology Products in the FDA Center for Drug Evaluation and Research, said in a statement. “This represents an important and needed advance in the care of pediatric patients with multiple sclerosis.”
Side effects for fingolimod in pediatric trial participants were similar to those experienced in adults, the most common of which include headache, liver enzyme elevation, diarrhea, cough, flu, sinusitis, back pain, abdominal pain, and pain in extremities. The drug must be dispensed with a medication guide that describes the product’s more serious risks.
The FDA, which granted the product a priority review and breakthrough designation for this indication, noted that 2%-5% of people with MS have symptoms onset before age 18 and suggested that 8,000-10,000 children and adolescents in the United States suffer from the disease.
The clinical trial evaluating the drug included 214 patients aged 10-17 years and compared fingolimod with interferon beta-1a. In that study, the FDA stated that 86% of patients receiving fingolimod remained relapse-free after 24 months of treatment, compared with 46% of those treated with interferon beta-1a.
Pediatric patients with
The Food and Drug Administration approved on May 11 an expanded indication of the drug to allow it to be used to treat relapsing MS in children and adolescents age 10 and older. Gilenya was first approved by FDA to treat adults with relapsing MS in 2010.
“For the first time, we have an FDA-approved treatment specifically for children and adolescents with multiple sclerosis,” Billy Dunn, MD, director of the Division of Neurology Products in the FDA Center for Drug Evaluation and Research, said in a statement. “This represents an important and needed advance in the care of pediatric patients with multiple sclerosis.”
Side effects for fingolimod in pediatric trial participants were similar to those experienced in adults, the most common of which include headache, liver enzyme elevation, diarrhea, cough, flu, sinusitis, back pain, abdominal pain, and pain in extremities. The drug must be dispensed with a medication guide that describes the product’s more serious risks.
The FDA, which granted the product a priority review and breakthrough designation for this indication, noted that 2%-5% of people with MS have symptoms onset before age 18 and suggested that 8,000-10,000 children and adolescents in the United States suffer from the disease.
The clinical trial evaluating the drug included 214 patients aged 10-17 years and compared fingolimod with interferon beta-1a. In that study, the FDA stated that 86% of patients receiving fingolimod remained relapse-free after 24 months of treatment, compared with 46% of those treated with interferon beta-1a.
Pediatric patients with
The Food and Drug Administration approved on May 11 an expanded indication of the drug to allow it to be used to treat relapsing MS in children and adolescents age 10 and older. Gilenya was first approved by FDA to treat adults with relapsing MS in 2010.
“For the first time, we have an FDA-approved treatment specifically for children and adolescents with multiple sclerosis,” Billy Dunn, MD, director of the Division of Neurology Products in the FDA Center for Drug Evaluation and Research, said in a statement. “This represents an important and needed advance in the care of pediatric patients with multiple sclerosis.”
Side effects for fingolimod in pediatric trial participants were similar to those experienced in adults, the most common of which include headache, liver enzyme elevation, diarrhea, cough, flu, sinusitis, back pain, abdominal pain, and pain in extremities. The drug must be dispensed with a medication guide that describes the product’s more serious risks.
The FDA, which granted the product a priority review and breakthrough designation for this indication, noted that 2%-5% of people with MS have symptoms onset before age 18 and suggested that 8,000-10,000 children and adolescents in the United States suffer from the disease.
The clinical trial evaluating the drug included 214 patients aged 10-17 years and compared fingolimod with interferon beta-1a. In that study, the FDA stated that 86% of patients receiving fingolimod remained relapse-free after 24 months of treatment, compared with 46% of those treated with interferon beta-1a.
Make the Diagnosis - May 2018
and through close skin contact, as well as contaminated clothes and bedding. Adult lice can live up to 36 hours away from its host. Pubic areas most commonly are affected, although other hair-bearing parts of the body often are affected, including eyelashes.
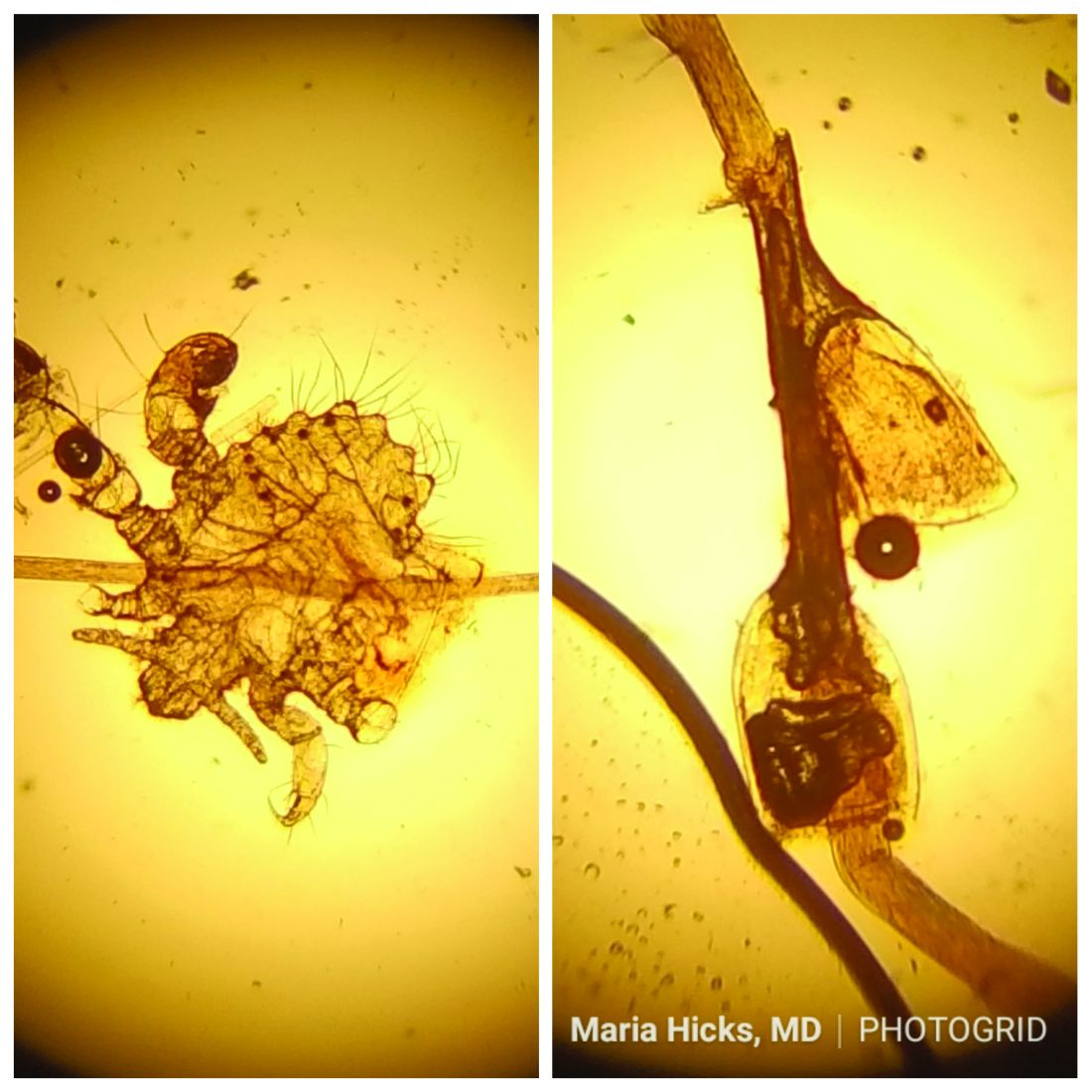
Pruritus can be severe. Secondary bacterial infections may occur as maculae ceruleae, or blue-colored macules, on the skin. The lice are visible to the naked eye and are approximately 1 mm in length. They have a crablike appearance, six legs, and a wide body. Nits may be present on the hair shaft. Unlike hair casts, which can be moved up and down along the hair shaft, nits firmly adhere to the hair. Diagnosis should prompt a workup for other sexually transmitted diseases, including HIV.
Treatment for patients and their sexual partners include permethrin topically; and laundering of clothing and bedding. Lice on the eyelashes can be treated with 8 days of twice-daily applications of petrolatum. Ivermectin can be used when topical therapy fails, although this is an off-label treatment (not approved by the Food and Drug Administration).
Pediculosis corporis – body lice or clothing lice – is also known as “vagabond’s disease” and is caused by Pediculus humanus var corporis. Body lice lay their eggs in clothing seams and can live in clothing for up to 1 month without feeding on human blood. Often homeless individuals and those living in overcrowded areas can be affected. The louse and nits also are visible to the naked eye. They have a longer, narrower body than Phthirus pubis and are more similar in appearance to head lice. They rarely are found on the skin.
Body lice may carry disease such as epidemic typhus, relapsing fever, and trench fever or endocarditis. Permethrin is the most widely used treatment to kill both lice and ova. Other treatments include Malathion, Lindane, and Crotamiton. Clothing and bedding should be laundered.
Scabies is a mite infestation caused by Sarcoptes scabiei. Unlike lice, scabies often affects the hands and feet. Characteristic linear burrows may be seen in the finger web spaces. The circle of Hebra describes the areas commonly infected by mites: axillae, antecubital fossa, wrists, hands, and the groin. Pruritus may be severe and worse at night. Patients may be afflicted with both lice and scabies at the same time. Mites are not visible to the naked eye but can be seen microscopically. Topical permethrin cream is used most often for treatment. All household contacts should be treated at the same time. As in louse infestations, clothing and bedding should be laundered. Ivermectin can be used for crusted scabies, although this is an off-label treatment.
This case and photo were submitted by Maria Hicks, MD, Advanced Dermatology and Cosmetic Surgery, Tampa, and Dr. Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
and through close skin contact, as well as contaminated clothes and bedding. Adult lice can live up to 36 hours away from its host. Pubic areas most commonly are affected, although other hair-bearing parts of the body often are affected, including eyelashes.
Pruritus can be severe. Secondary bacterial infections may occur as maculae ceruleae, or blue-colored macules, on the skin. The lice are visible to the naked eye and are approximately 1 mm in length. They have a crablike appearance, six legs, and a wide body. Nits may be present on the hair shaft. Unlike hair casts, which can be moved up and down along the hair shaft, nits firmly adhere to the hair. Diagnosis should prompt a workup for other sexually transmitted diseases, including HIV.
Treatment for patients and their sexual partners include permethrin topically; and laundering of clothing and bedding. Lice on the eyelashes can be treated with 8 days of twice-daily applications of petrolatum. Ivermectin can be used when topical therapy fails, although this is an off-label treatment (not approved by the Food and Drug Administration).
Pediculosis corporis – body lice or clothing lice – is also known as “vagabond’s disease” and is caused by Pediculus humanus var corporis. Body lice lay their eggs in clothing seams and can live in clothing for up to 1 month without feeding on human blood. Often homeless individuals and those living in overcrowded areas can be affected. The louse and nits also are visible to the naked eye. They have a longer, narrower body than Phthirus pubis and are more similar in appearance to head lice. They rarely are found on the skin.
Body lice may carry disease such as epidemic typhus, relapsing fever, and trench fever or endocarditis. Permethrin is the most widely used treatment to kill both lice and ova. Other treatments include Malathion, Lindane, and Crotamiton. Clothing and bedding should be laundered.
Scabies is a mite infestation caused by Sarcoptes scabiei. Unlike lice, scabies often affects the hands and feet. Characteristic linear burrows may be seen in the finger web spaces. The circle of Hebra describes the areas commonly infected by mites: axillae, antecubital fossa, wrists, hands, and the groin. Pruritus may be severe and worse at night. Patients may be afflicted with both lice and scabies at the same time. Mites are not visible to the naked eye but can be seen microscopically. Topical permethrin cream is used most often for treatment. All household contacts should be treated at the same time. As in louse infestations, clothing and bedding should be laundered. Ivermectin can be used for crusted scabies, although this is an off-label treatment.
This case and photo were submitted by Maria Hicks, MD, Advanced Dermatology and Cosmetic Surgery, Tampa, and Dr. Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
and through close skin contact, as well as contaminated clothes and bedding. Adult lice can live up to 36 hours away from its host. Pubic areas most commonly are affected, although other hair-bearing parts of the body often are affected, including eyelashes.
Pruritus can be severe. Secondary bacterial infections may occur as maculae ceruleae, or blue-colored macules, on the skin. The lice are visible to the naked eye and are approximately 1 mm in length. They have a crablike appearance, six legs, and a wide body. Nits may be present on the hair shaft. Unlike hair casts, which can be moved up and down along the hair shaft, nits firmly adhere to the hair. Diagnosis should prompt a workup for other sexually transmitted diseases, including HIV.
Treatment for patients and their sexual partners include permethrin topically; and laundering of clothing and bedding. Lice on the eyelashes can be treated with 8 days of twice-daily applications of petrolatum. Ivermectin can be used when topical therapy fails, although this is an off-label treatment (not approved by the Food and Drug Administration).
Pediculosis corporis – body lice or clothing lice – is also known as “vagabond’s disease” and is caused by Pediculus humanus var corporis. Body lice lay their eggs in clothing seams and can live in clothing for up to 1 month without feeding on human blood. Often homeless individuals and those living in overcrowded areas can be affected. The louse and nits also are visible to the naked eye. They have a longer, narrower body than Phthirus pubis and are more similar in appearance to head lice. They rarely are found on the skin.
Body lice may carry disease such as epidemic typhus, relapsing fever, and trench fever or endocarditis. Permethrin is the most widely used treatment to kill both lice and ova. Other treatments include Malathion, Lindane, and Crotamiton. Clothing and bedding should be laundered.
Scabies is a mite infestation caused by Sarcoptes scabiei. Unlike lice, scabies often affects the hands and feet. Characteristic linear burrows may be seen in the finger web spaces. The circle of Hebra describes the areas commonly infected by mites: axillae, antecubital fossa, wrists, hands, and the groin. Pruritus may be severe and worse at night. Patients may be afflicted with both lice and scabies at the same time. Mites are not visible to the naked eye but can be seen microscopically. Topical permethrin cream is used most often for treatment. All household contacts should be treated at the same time. As in louse infestations, clothing and bedding should be laundered. Ivermectin can be used for crusted scabies, although this is an off-label treatment.
This case and photo were submitted by Maria Hicks, MD, Advanced Dermatology and Cosmetic Surgery, Tampa, and Dr. Martin.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Fla. More diagnostic cases are available at edermatologynews.com. To submit a case for possible publication, send an email to [email protected].
A 40-year-old HIV-positive male presented with a 1-month history of severely pruritic papules on his chest. The patient reported that he "removes bugs" from his skin. Microscopic examination of a hair clipping was performed.
Make the Diagnosis:
Structured PPH management cuts severe hemorrhage
AUSTIN, TEX. – Taking a page from critical care, an obstetrical team that implemented a checklist-based management protocol for postpartum hemorrhage saw a significant drop in severe obstetric hemorrhage, with numeric reductions in other maternal outcomes.
The protocol, piloted in a single hospital, is now being rolled out in all 28 hospitals of a large, multistate health care system.
“Our medical critical care colleagues long ago abandoned the notion that physician judgment should guide the provision of basic and advanced cardiac life support in favor of highly specific and uniform protocols,” wrote first author Rachael Smith, DO, and her coauthors in the poster accompanying the presentation at the annual clinical and scientific meeting of the American Society of Obstetricians and Gynecologists.
“While existing guidelines outlining a general approach to postpartum hemorrhage are useful, recent data suggest that greater specificity is necessary to significantly impact morbidity and mortality,” they wrote.
When comparing outcomes for 9 matched months before and after implementation of the protocol, Dr. Smith and her collaborators found that rates of severe postpartum hemorrhage (PPH), defined as estimated blood loss (EBL) of at least 2,500 cc, were halved, dropping from 18% to 9% (P = .035).

“Patients with life-threatening illnesses seem to do better when their providers are following very structured, regimented protocols, and [advanced cardiac life support protocols] is probably the best example of that,” said Ms. Hermann.
They then produced a training video to educate nursing and house staff and attending physicians about the new checklist-based protocol. In this way, each team member would understand the rationale behind the checklist, know the steps in the care pathway, and understand his or her specific role.
The protocol, which begins when uterine atony is suspected, first calls the physician to the patient room, along with a second nurse to be the recorder and timekeeper. Among other duties, this individual tracks blood loss during a maternal bleeding event, weighing linens and sponges, and alerting the team when EBL exceeds 500, 1,000, and 1,500 cc, or when pulse or blood pressure fall outside of designated parameters.
“Having a second nurse in the room who is keeping the team on track, saying ‘Hey, we’re at this much blood loss; these are the next steps,’ and who is recording everything” can avert the sense of chaos that sometimes occurs in critical scenarios, said Ms. Hermann.
When stage 1 PPH (EBL of at least 500 cc) has occurred, a team lead is called. At this point, a PPH cart containing necessary equipment and medication, including uterotonics, is brought to the room.
Having the uterotonic kit in the room, said Ms. Hermann, is a key component of the protocol. “Having a kit you can wheel into the room, and having everything you need to manage PPH” saves critical time, she said. “The nurses aren’t running back and forth to the Pyxis to get the next uterotonic that you need.”
If EBL of at least 1,500 cc is reached, a third nurse is called and the obstetric rapid-response team is activated, meaning that a code cart and additional supportive equipment are also brought to the patient.
The checklist paperwork lays out all interventions, including uterotonic dosing, timing, and contraindications. It also includes differential diagnoses for PPH, and provides directions for visual estimation of blood loss.
Finally, a structured debrief takes place after each PPH, said Ms. Hermann.
The study included women who experienced PPH during matched 9-month periods before and after the PPH protocol implementation. PPH was defined as EBL of at least 500 cc for vaginal delivery, and 1,000 cc for cesarean delivery. Women were excluded if they delivered before 22 weeks’ gestation, or if there was a diagnosis of or suspicion for placenta accreta, increta, or percreta.
A total of 147 women were in the preintervention group; of these, 98 (66%) had vaginal deliveries. In the postintervention group, 110 out of150 women (73%) had vaginal deliveries.
In addition to the significant reduction in severe PPH that followed implementation of the protocol, numeric reductions were also seen in other surrogate measures of maternal morbidity, including stage 1 hemorrhage, the need for transfusion, surgical interventions, intensive care admissions, and length of stay.
“Across all of these surrogates, we saw an improvement in our postprotocol patients,” said Ms. Hermann. “We think that the reason the rest of them weren’t statistically significant was due to lack of power” in the single-center study, she said. “The clinical trend speaks for itself.”
Once the protocol is rolled out in all 28 hospitals, she anticipates seeing statistics that confirm what the investigators are already seeing clinically.
SOURCE: Smith R et al. ACOG 2018, Abstract 26R.
AUSTIN, TEX. – Taking a page from critical care, an obstetrical team that implemented a checklist-based management protocol for postpartum hemorrhage saw a significant drop in severe obstetric hemorrhage, with numeric reductions in other maternal outcomes.
The protocol, piloted in a single hospital, is now being rolled out in all 28 hospitals of a large, multistate health care system.
“Our medical critical care colleagues long ago abandoned the notion that physician judgment should guide the provision of basic and advanced cardiac life support in favor of highly specific and uniform protocols,” wrote first author Rachael Smith, DO, and her coauthors in the poster accompanying the presentation at the annual clinical and scientific meeting of the American Society of Obstetricians and Gynecologists.
“While existing guidelines outlining a general approach to postpartum hemorrhage are useful, recent data suggest that greater specificity is necessary to significantly impact morbidity and mortality,” they wrote.
When comparing outcomes for 9 matched months before and after implementation of the protocol, Dr. Smith and her collaborators found that rates of severe postpartum hemorrhage (PPH), defined as estimated blood loss (EBL) of at least 2,500 cc, were halved, dropping from 18% to 9% (P = .035).
“Patients with life-threatening illnesses seem to do better when their providers are following very structured, regimented protocols, and [advanced cardiac life support protocols] is probably the best example of that,” said Ms. Hermann.
They then produced a training video to educate nursing and house staff and attending physicians about the new checklist-based protocol. In this way, each team member would understand the rationale behind the checklist, know the steps in the care pathway, and understand his or her specific role.
The protocol, which begins when uterine atony is suspected, first calls the physician to the patient room, along with a second nurse to be the recorder and timekeeper. Among other duties, this individual tracks blood loss during a maternal bleeding event, weighing linens and sponges, and alerting the team when EBL exceeds 500, 1,000, and 1,500 cc, or when pulse or blood pressure fall outside of designated parameters.
“Having a second nurse in the room who is keeping the team on track, saying ‘Hey, we’re at this much blood loss; these are the next steps,’ and who is recording everything” can avert the sense of chaos that sometimes occurs in critical scenarios, said Ms. Hermann.
When stage 1 PPH (EBL of at least 500 cc) has occurred, a team lead is called. At this point, a PPH cart containing necessary equipment and medication, including uterotonics, is brought to the room.
Having the uterotonic kit in the room, said Ms. Hermann, is a key component of the protocol. “Having a kit you can wheel into the room, and having everything you need to manage PPH” saves critical time, she said. “The nurses aren’t running back and forth to the Pyxis to get the next uterotonic that you need.”
If EBL of at least 1,500 cc is reached, a third nurse is called and the obstetric rapid-response team is activated, meaning that a code cart and additional supportive equipment are also brought to the patient.
The checklist paperwork lays out all interventions, including uterotonic dosing, timing, and contraindications. It also includes differential diagnoses for PPH, and provides directions for visual estimation of blood loss.
Finally, a structured debrief takes place after each PPH, said Ms. Hermann.
The study included women who experienced PPH during matched 9-month periods before and after the PPH protocol implementation. PPH was defined as EBL of at least 500 cc for vaginal delivery, and 1,000 cc for cesarean delivery. Women were excluded if they delivered before 22 weeks’ gestation, or if there was a diagnosis of or suspicion for placenta accreta, increta, or percreta.
A total of 147 women were in the preintervention group; of these, 98 (66%) had vaginal deliveries. In the postintervention group, 110 out of150 women (73%) had vaginal deliveries.
In addition to the significant reduction in severe PPH that followed implementation of the protocol, numeric reductions were also seen in other surrogate measures of maternal morbidity, including stage 1 hemorrhage, the need for transfusion, surgical interventions, intensive care admissions, and length of stay.
“Across all of these surrogates, we saw an improvement in our postprotocol patients,” said Ms. Hermann. “We think that the reason the rest of them weren’t statistically significant was due to lack of power” in the single-center study, she said. “The clinical trend speaks for itself.”
Once the protocol is rolled out in all 28 hospitals, she anticipates seeing statistics that confirm what the investigators are already seeing clinically.
SOURCE: Smith R et al. ACOG 2018, Abstract 26R.
AUSTIN, TEX. – Taking a page from critical care, an obstetrical team that implemented a checklist-based management protocol for postpartum hemorrhage saw a significant drop in severe obstetric hemorrhage, with numeric reductions in other maternal outcomes.
The protocol, piloted in a single hospital, is now being rolled out in all 28 hospitals of a large, multistate health care system.
“Our medical critical care colleagues long ago abandoned the notion that physician judgment should guide the provision of basic and advanced cardiac life support in favor of highly specific and uniform protocols,” wrote first author Rachael Smith, DO, and her coauthors in the poster accompanying the presentation at the annual clinical and scientific meeting of the American Society of Obstetricians and Gynecologists.
“While existing guidelines outlining a general approach to postpartum hemorrhage are useful, recent data suggest that greater specificity is necessary to significantly impact morbidity and mortality,” they wrote.
When comparing outcomes for 9 matched months before and after implementation of the protocol, Dr. Smith and her collaborators found that rates of severe postpartum hemorrhage (PPH), defined as estimated blood loss (EBL) of at least 2,500 cc, were halved, dropping from 18% to 9% (P = .035).
“Patients with life-threatening illnesses seem to do better when their providers are following very structured, regimented protocols, and [advanced cardiac life support protocols] is probably the best example of that,” said Ms. Hermann.
They then produced a training video to educate nursing and house staff and attending physicians about the new checklist-based protocol. In this way, each team member would understand the rationale behind the checklist, know the steps in the care pathway, and understand his or her specific role.
The protocol, which begins when uterine atony is suspected, first calls the physician to the patient room, along with a second nurse to be the recorder and timekeeper. Among other duties, this individual tracks blood loss during a maternal bleeding event, weighing linens and sponges, and alerting the team when EBL exceeds 500, 1,000, and 1,500 cc, or when pulse or blood pressure fall outside of designated parameters.
“Having a second nurse in the room who is keeping the team on track, saying ‘Hey, we’re at this much blood loss; these are the next steps,’ and who is recording everything” can avert the sense of chaos that sometimes occurs in critical scenarios, said Ms. Hermann.
When stage 1 PPH (EBL of at least 500 cc) has occurred, a team lead is called. At this point, a PPH cart containing necessary equipment and medication, including uterotonics, is brought to the room.
Having the uterotonic kit in the room, said Ms. Hermann, is a key component of the protocol. “Having a kit you can wheel into the room, and having everything you need to manage PPH” saves critical time, she said. “The nurses aren’t running back and forth to the Pyxis to get the next uterotonic that you need.”
If EBL of at least 1,500 cc is reached, a third nurse is called and the obstetric rapid-response team is activated, meaning that a code cart and additional supportive equipment are also brought to the patient.
The checklist paperwork lays out all interventions, including uterotonic dosing, timing, and contraindications. It also includes differential diagnoses for PPH, and provides directions for visual estimation of blood loss.
Finally, a structured debrief takes place after each PPH, said Ms. Hermann.
The study included women who experienced PPH during matched 9-month periods before and after the PPH protocol implementation. PPH was defined as EBL of at least 500 cc for vaginal delivery, and 1,000 cc for cesarean delivery. Women were excluded if they delivered before 22 weeks’ gestation, or if there was a diagnosis of or suspicion for placenta accreta, increta, or percreta.
A total of 147 women were in the preintervention group; of these, 98 (66%) had vaginal deliveries. In the postintervention group, 110 out of150 women (73%) had vaginal deliveries.
In addition to the significant reduction in severe PPH that followed implementation of the protocol, numeric reductions were also seen in other surrogate measures of maternal morbidity, including stage 1 hemorrhage, the need for transfusion, surgical interventions, intensive care admissions, and length of stay.
“Across all of these surrogates, we saw an improvement in our postprotocol patients,” said Ms. Hermann. “We think that the reason the rest of them weren’t statistically significant was due to lack of power” in the single-center study, she said. “The clinical trend speaks for itself.”
Once the protocol is rolled out in all 28 hospitals, she anticipates seeing statistics that confirm what the investigators are already seeing clinically.
SOURCE: Smith R et al. ACOG 2018, Abstract 26R.
REPORTING FROM ACOG 2018
Key clinical point: Indicators of maternal morbidity decreased after a postpartum hemorrhage checklist was implemented.
Major finding: Severe postpartum hemorrhage rates fell from 18% to 9% (P = .035).
Study details: A prospective pre/post implementation study of 297 women experiencing postpartum hemorrhage.
Disclosures: The study authors reported no relevant financial conflicts of interest.
Source: Smith R et al. ACOG 2018, Abstract 26R.