User login
Noninvasive 1060-nm diode laser found effective for axillary hyperhidrosis
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.

The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”

The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”

SOURCE: Katz et. al. ASLMS 2018.
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.
The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”
The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”
SOURCE: Katz et. al. ASLMS 2018.
DALLAS – , a condition that affects an estimated 1.4% people in the United States.
“Newer treatments such as microwave technology, botulinum toxin injections, and lasers have emerged as effective methods,” lead study author Bruce E. Katz, MD, who directs the Juva Skin & Laser Center in New York, said at the annual conference of the American Society for Laser Medicine and Surgery Inc.
In a prospective pilot study, Dr. Katz and his associates examined the use of a noninvasive 1060-nm diode laser (SculpSure, Cynosure) in 10 subjects with moderate to severe hyperhidrosis of the axilla, which was defined as having Hyperhidrosis Disease Severity Scale (HDSS) scores of 3 or 4. The subjects, whose mean age was 42 years, received two laser treatments on the axillary area at 6-week intervals, and the researchers performed starch iodine tests and took two-dimensional photography of the axilla before and after treatment. Subjects were asked to rate their conditions on the HDSS and satisfaction with treatment. Two blinded dermatologist evaluators graded the reduction in sweat production on photos of starch iodine tests. The researchers also performed a retrospective analysis on all subjects to assess safety and efficacy of treatment.
The 1060-nm diode laser used for the study features four flat, nonsuction applicators. Dr. Katz and his associates positioned two applicators on the axilla simultaneously for 25 minutes. “The 1060-nm wavelength has minimal absorption in the melanin, so we can really treat any skin type,” he said. “It has a high affinity for adipose tissue, and we believe that its targeted effect at the level of the eccrine and apocrine glands should help improve hyperhidrosis. It works by elevating the tissue temperature to about 42 to 47 degrees Centigrade, without damaging surrounding tissue. The device has a sapphire cooling plate, so it’s comfortable for the patient.”
The retrospective analysis revealed minimal adverse events such as pain, mild erythema, and edema, which were transient and resolved without intervention in a day or two. To date, no cases have recurred, “which we were surprised by,” Dr. Katz said. “We were surprised that the effect lasted that long.”
SOURCE: Katz et. al. ASLMS 2018.
REPORTING FROM ASLMS 2018
Advanced training in hepatology
Unlike previous hepatologists, who were trained through gastroenterology programs, most new practitioners seek advanced training in a fellowship year focused exclusively on hepatology.
Like practitioners in many medical subspecialties, transplant hepatologists have varied career goals and responsibilities. Hepatologists who continue to specifically practice transplant hepatology are affiliated with a liver transplant center, which is generally a hospital-based practice. However, most hepatologists also treat nontransplant hepatology patients and some who have completed advanced hepatology training focus exclusively on these patients or provide community-based care for transplant recipients from other centers. Caring for patients with end-stage liver disease and liver transplant recipients can be clinically demanding but also very rewarding. There are also many opportunities for academic pursuits within a hepatology career including areas in urgent need of clinical and basic investigation, clinical trials for novel agents to treat common diseases, education (including leadership in advanced hepatology training), and involvement in professional societies such as the American Gastroenterological Association (AGA) and American Association for the Study of Liver Disease (AASLD).
What are the opportunities for advanced hepatology training?
In 1999, the AASLD determined that the practice of transplant hepatology required its own specialized knowledge and that most practicing gastroenterologists did not consider themselves adequately prepared to care for patients with advanced liver disease.1,2 The following year, the AASLD applied to the American Board of Internal Medicine (ABIM) to develop formalized liver transplant training. After several years of debate and development, the first ABIM certification exam in transplant hepatology was held in 2006 and is now offered every 2 years.2

There are currently three pathways to achieve advanced training in hepatology. The traditional pathway is a 1-year Accreditation Council for Graduate Medical Education (ACGME) transplant fellowship that is separate from, and must follow completion of, a gastroenterology fellowship. There are currently 51 ACGME-accredited 1-year transplant hepatology fellowships in the United States. These fellowships are only at institutions with ACGME-accredited training in internal medicine and gastroenterology as well. The full and updated list of programs can be found on the ACGME website.3 The second pathway is the relatively new ABIM “pilot” program during which the transplant hepatology fellowship year is combined with the third year of gastroenterology fellowship (discussed in detail below). Finally, there remain many 1-year training programs that are not ACGME-accredited, may not be associated with a gastroenterology fellowship program, and do have not regulated requirements for entry. Trainees who complete non-ACGME programs are not candidates for ABIM board certification.
How does one apply for transplant hepatology fellowship?
Transplant hepatology fellowships do not participate in a match system. Therefore, the interviews and offers for training spots may occur at different times depending on the program and the region of the country. In general, fellows apply by the fall of their second year of gastroenterology fellowship in order to begin training after graduating from the third year of fellowship. Each program has its individual approach to the application process and most have this information available on a website as to how to apply. A complete list of ACGME-accredited programs along with the program directors and contact information is available on the ABIM website.3
What is the gastroenterology/transplant hepatology pilot training program?
The AASLD and ABIM have developed a combined gastroenterology and transplant hepatology pilot fellowship training program that allows eligible gastroenterology fellows to spend their third year training in transplant hepatology. This approach has the potential to shorten the total training from 4 years to 3. In addition, if all gastroenterology and transplant hepatology competencies are achieved by the end of the third year, fellows approved to be in this program are eligible to take both gastroenterology and transplant hepatology ABIM certification exams.
Any ACGME-accredited gastroenterology fellowship program that has an accredited hepatology counterpart is eligible to participate in this pilot. Eligible programs and fellows must apply to AASLD during the fellow’s second year. The fellow applicant must complete all clinical gastroenterology requirements before the end of the second year of fellowship and be on a trajectory to meet competency milestones, as the majority of the third year will focus on hepatology.
Since 2012, 59 fellows from 31 programs have participated in this pilot program.4 If you are interested in participating in this pilot program at your institution, it is important to confer with program directors as early as possible to meet all training requirements. In addition, applications are submitted to the Pilot Steering Taskforce during the fellow’s second year for review. This is not meant to be a competitive process and all fellows who meet the criteria are approved.
This track may not be ideal for all fellows interested in advanced and transplant hepatology. In particular, there may be a trade-off between achieving clinical competency in a shortened training period and pursuing scholarly activity. This pilot program is designed to be an intensive clinical track, so fellows who wish to focus on research should discuss with their program directors whether this is the best approach.
What has been your career path after advanced training in hepatology?
I first became interested in hepatology during my inpatient rotations as a medical student. This interest led me to become involved in research in this area very early in my career. The current structure of the fellowship as well as the board certification exam were both developed while I was in training and I adjusted my plans to complete 3 years of gastroenterology fellowship followed by an ACGME-accredited liver transplant fellowship year. Since completing training, I have worked as an attending at an academic medical center in a large liver transplant program and continue to care for patients with all forms of liver disease. In addition, I continued to pursue research as a large component of my job and now have NIH funding and direct the Transplant Clinical Research Center at Columbia University. Finally, I have always been devoted to education and am the program director for the transplant hepatology fellowship at our institution.
What is the future of advanced hepatology training?
The current transplant hepatology training system has evolved significantly since its inception, including development of curricula, ongoing modification of training requirements, and the development of the innovative pilot program. However, there are issues that continue to be debated by the community. For example, it is not certain when or if the combined gastroenterology and transplant hepatology pilot program will become a permanent pathway for training or how best to select fellows for this approach.
Hepatology continues to be a very dynamic area of medicine. With diseases such as nonalcoholic fatty liver disease and hepatocellular carcinoma on the rise, the urgent need for training in HCV treatment to combat the global epidemic of viral hepatitis, and the growing number of patients on the liver transplant waiting list, there has never been a more exciting time to choose hepatology as a career.
References
1. Luxon BA. So you want to be a hepatologist? Gastroenterology. 2013;145(6):1182-5.
2. Bacon BR, Grosso LJ, Freedman N, Althouse LA. Subspecialty certification in transplant hepatology. Liver Transpl. 2007;13(11):1479-81.
3. https://apps.acgme.org/ads/public/reports/report/1.
4. https://www.aasld.org/events-professional-development/educational-learning-faq.
Dr. Verna is assistant professor of medicine, program director, transplant hepatology fellowship, director of clinical research, Transplant Clinical Research Center, Columbia University Medical Center, New York.
Unlike previous hepatologists, who were trained through gastroenterology programs, most new practitioners seek advanced training in a fellowship year focused exclusively on hepatology.
Like practitioners in many medical subspecialties, transplant hepatologists have varied career goals and responsibilities. Hepatologists who continue to specifically practice transplant hepatology are affiliated with a liver transplant center, which is generally a hospital-based practice. However, most hepatologists also treat nontransplant hepatology patients and some who have completed advanced hepatology training focus exclusively on these patients or provide community-based care for transplant recipients from other centers. Caring for patients with end-stage liver disease and liver transplant recipients can be clinically demanding but also very rewarding. There are also many opportunities for academic pursuits within a hepatology career including areas in urgent need of clinical and basic investigation, clinical trials for novel agents to treat common diseases, education (including leadership in advanced hepatology training), and involvement in professional societies such as the American Gastroenterological Association (AGA) and American Association for the Study of Liver Disease (AASLD).
What are the opportunities for advanced hepatology training?
In 1999, the AASLD determined that the practice of transplant hepatology required its own specialized knowledge and that most practicing gastroenterologists did not consider themselves adequately prepared to care for patients with advanced liver disease.1,2 The following year, the AASLD applied to the American Board of Internal Medicine (ABIM) to develop formalized liver transplant training. After several years of debate and development, the first ABIM certification exam in transplant hepatology was held in 2006 and is now offered every 2 years.2
There are currently three pathways to achieve advanced training in hepatology. The traditional pathway is a 1-year Accreditation Council for Graduate Medical Education (ACGME) transplant fellowship that is separate from, and must follow completion of, a gastroenterology fellowship. There are currently 51 ACGME-accredited 1-year transplant hepatology fellowships in the United States. These fellowships are only at institutions with ACGME-accredited training in internal medicine and gastroenterology as well. The full and updated list of programs can be found on the ACGME website.3 The second pathway is the relatively new ABIM “pilot” program during which the transplant hepatology fellowship year is combined with the third year of gastroenterology fellowship (discussed in detail below). Finally, there remain many 1-year training programs that are not ACGME-accredited, may not be associated with a gastroenterology fellowship program, and do have not regulated requirements for entry. Trainees who complete non-ACGME programs are not candidates for ABIM board certification.
How does one apply for transplant hepatology fellowship?
Transplant hepatology fellowships do not participate in a match system. Therefore, the interviews and offers for training spots may occur at different times depending on the program and the region of the country. In general, fellows apply by the fall of their second year of gastroenterology fellowship in order to begin training after graduating from the third year of fellowship. Each program has its individual approach to the application process and most have this information available on a website as to how to apply. A complete list of ACGME-accredited programs along with the program directors and contact information is available on the ABIM website.3
What is the gastroenterology/transplant hepatology pilot training program?
The AASLD and ABIM have developed a combined gastroenterology and transplant hepatology pilot fellowship training program that allows eligible gastroenterology fellows to spend their third year training in transplant hepatology. This approach has the potential to shorten the total training from 4 years to 3. In addition, if all gastroenterology and transplant hepatology competencies are achieved by the end of the third year, fellows approved to be in this program are eligible to take both gastroenterology and transplant hepatology ABIM certification exams.
Any ACGME-accredited gastroenterology fellowship program that has an accredited hepatology counterpart is eligible to participate in this pilot. Eligible programs and fellows must apply to AASLD during the fellow’s second year. The fellow applicant must complete all clinical gastroenterology requirements before the end of the second year of fellowship and be on a trajectory to meet competency milestones, as the majority of the third year will focus on hepatology.
Since 2012, 59 fellows from 31 programs have participated in this pilot program.4 If you are interested in participating in this pilot program at your institution, it is important to confer with program directors as early as possible to meet all training requirements. In addition, applications are submitted to the Pilot Steering Taskforce during the fellow’s second year for review. This is not meant to be a competitive process and all fellows who meet the criteria are approved.
This track may not be ideal for all fellows interested in advanced and transplant hepatology. In particular, there may be a trade-off between achieving clinical competency in a shortened training period and pursuing scholarly activity. This pilot program is designed to be an intensive clinical track, so fellows who wish to focus on research should discuss with their program directors whether this is the best approach.
What has been your career path after advanced training in hepatology?
I first became interested in hepatology during my inpatient rotations as a medical student. This interest led me to become involved in research in this area very early in my career. The current structure of the fellowship as well as the board certification exam were both developed while I was in training and I adjusted my plans to complete 3 years of gastroenterology fellowship followed by an ACGME-accredited liver transplant fellowship year. Since completing training, I have worked as an attending at an academic medical center in a large liver transplant program and continue to care for patients with all forms of liver disease. In addition, I continued to pursue research as a large component of my job and now have NIH funding and direct the Transplant Clinical Research Center at Columbia University. Finally, I have always been devoted to education and am the program director for the transplant hepatology fellowship at our institution.
What is the future of advanced hepatology training?
The current transplant hepatology training system has evolved significantly since its inception, including development of curricula, ongoing modification of training requirements, and the development of the innovative pilot program. However, there are issues that continue to be debated by the community. For example, it is not certain when or if the combined gastroenterology and transplant hepatology pilot program will become a permanent pathway for training or how best to select fellows for this approach.
Hepatology continues to be a very dynamic area of medicine. With diseases such as nonalcoholic fatty liver disease and hepatocellular carcinoma on the rise, the urgent need for training in HCV treatment to combat the global epidemic of viral hepatitis, and the growing number of patients on the liver transplant waiting list, there has never been a more exciting time to choose hepatology as a career.
References
1. Luxon BA. So you want to be a hepatologist? Gastroenterology. 2013;145(6):1182-5.
2. Bacon BR, Grosso LJ, Freedman N, Althouse LA. Subspecialty certification in transplant hepatology. Liver Transpl. 2007;13(11):1479-81.
3. https://apps.acgme.org/ads/public/reports/report/1.
4. https://www.aasld.org/events-professional-development/educational-learning-faq.
Dr. Verna is assistant professor of medicine, program director, transplant hepatology fellowship, director of clinical research, Transplant Clinical Research Center, Columbia University Medical Center, New York.
Unlike previous hepatologists, who were trained through gastroenterology programs, most new practitioners seek advanced training in a fellowship year focused exclusively on hepatology.
Like practitioners in many medical subspecialties, transplant hepatologists have varied career goals and responsibilities. Hepatologists who continue to specifically practice transplant hepatology are affiliated with a liver transplant center, which is generally a hospital-based practice. However, most hepatologists also treat nontransplant hepatology patients and some who have completed advanced hepatology training focus exclusively on these patients or provide community-based care for transplant recipients from other centers. Caring for patients with end-stage liver disease and liver transplant recipients can be clinically demanding but also very rewarding. There are also many opportunities for academic pursuits within a hepatology career including areas in urgent need of clinical and basic investigation, clinical trials for novel agents to treat common diseases, education (including leadership in advanced hepatology training), and involvement in professional societies such as the American Gastroenterological Association (AGA) and American Association for the Study of Liver Disease (AASLD).
What are the opportunities for advanced hepatology training?
In 1999, the AASLD determined that the practice of transplant hepatology required its own specialized knowledge and that most practicing gastroenterologists did not consider themselves adequately prepared to care for patients with advanced liver disease.1,2 The following year, the AASLD applied to the American Board of Internal Medicine (ABIM) to develop formalized liver transplant training. After several years of debate and development, the first ABIM certification exam in transplant hepatology was held in 2006 and is now offered every 2 years.2
There are currently three pathways to achieve advanced training in hepatology. The traditional pathway is a 1-year Accreditation Council for Graduate Medical Education (ACGME) transplant fellowship that is separate from, and must follow completion of, a gastroenterology fellowship. There are currently 51 ACGME-accredited 1-year transplant hepatology fellowships in the United States. These fellowships are only at institutions with ACGME-accredited training in internal medicine and gastroenterology as well. The full and updated list of programs can be found on the ACGME website.3 The second pathway is the relatively new ABIM “pilot” program during which the transplant hepatology fellowship year is combined with the third year of gastroenterology fellowship (discussed in detail below). Finally, there remain many 1-year training programs that are not ACGME-accredited, may not be associated with a gastroenterology fellowship program, and do have not regulated requirements for entry. Trainees who complete non-ACGME programs are not candidates for ABIM board certification.
How does one apply for transplant hepatology fellowship?
Transplant hepatology fellowships do not participate in a match system. Therefore, the interviews and offers for training spots may occur at different times depending on the program and the region of the country. In general, fellows apply by the fall of their second year of gastroenterology fellowship in order to begin training after graduating from the third year of fellowship. Each program has its individual approach to the application process and most have this information available on a website as to how to apply. A complete list of ACGME-accredited programs along with the program directors and contact information is available on the ABIM website.3
What is the gastroenterology/transplant hepatology pilot training program?
The AASLD and ABIM have developed a combined gastroenterology and transplant hepatology pilot fellowship training program that allows eligible gastroenterology fellows to spend their third year training in transplant hepatology. This approach has the potential to shorten the total training from 4 years to 3. In addition, if all gastroenterology and transplant hepatology competencies are achieved by the end of the third year, fellows approved to be in this program are eligible to take both gastroenterology and transplant hepatology ABIM certification exams.
Any ACGME-accredited gastroenterology fellowship program that has an accredited hepatology counterpart is eligible to participate in this pilot. Eligible programs and fellows must apply to AASLD during the fellow’s second year. The fellow applicant must complete all clinical gastroenterology requirements before the end of the second year of fellowship and be on a trajectory to meet competency milestones, as the majority of the third year will focus on hepatology.
Since 2012, 59 fellows from 31 programs have participated in this pilot program.4 If you are interested in participating in this pilot program at your institution, it is important to confer with program directors as early as possible to meet all training requirements. In addition, applications are submitted to the Pilot Steering Taskforce during the fellow’s second year for review. This is not meant to be a competitive process and all fellows who meet the criteria are approved.
This track may not be ideal for all fellows interested in advanced and transplant hepatology. In particular, there may be a trade-off between achieving clinical competency in a shortened training period and pursuing scholarly activity. This pilot program is designed to be an intensive clinical track, so fellows who wish to focus on research should discuss with their program directors whether this is the best approach.
What has been your career path after advanced training in hepatology?
I first became interested in hepatology during my inpatient rotations as a medical student. This interest led me to become involved in research in this area very early in my career. The current structure of the fellowship as well as the board certification exam were both developed while I was in training and I adjusted my plans to complete 3 years of gastroenterology fellowship followed by an ACGME-accredited liver transplant fellowship year. Since completing training, I have worked as an attending at an academic medical center in a large liver transplant program and continue to care for patients with all forms of liver disease. In addition, I continued to pursue research as a large component of my job and now have NIH funding and direct the Transplant Clinical Research Center at Columbia University. Finally, I have always been devoted to education and am the program director for the transplant hepatology fellowship at our institution.
What is the future of advanced hepatology training?
The current transplant hepatology training system has evolved significantly since its inception, including development of curricula, ongoing modification of training requirements, and the development of the innovative pilot program. However, there are issues that continue to be debated by the community. For example, it is not certain when or if the combined gastroenterology and transplant hepatology pilot program will become a permanent pathway for training or how best to select fellows for this approach.
Hepatology continues to be a very dynamic area of medicine. With diseases such as nonalcoholic fatty liver disease and hepatocellular carcinoma on the rise, the urgent need for training in HCV treatment to combat the global epidemic of viral hepatitis, and the growing number of patients on the liver transplant waiting list, there has never been a more exciting time to choose hepatology as a career.
References
1. Luxon BA. So you want to be a hepatologist? Gastroenterology. 2013;145(6):1182-5.
2. Bacon BR, Grosso LJ, Freedman N, Althouse LA. Subspecialty certification in transplant hepatology. Liver Transpl. 2007;13(11):1479-81.
3. https://apps.acgme.org/ads/public/reports/report/1.
4. https://www.aasld.org/events-professional-development/educational-learning-faq.
Dr. Verna is assistant professor of medicine, program director, transplant hepatology fellowship, director of clinical research, Transplant Clinical Research Center, Columbia University Medical Center, New York.

Time for a facelift?
A few weeks ago I visited my primary care physician in her new office. As the first patient of the day I was immediately ushered into the examining room by a woman I assume was a medical assistant. She didn’t introduce herself, but her name tag read “Marcy” (not her real name). Her demeanor could best be described as cheerless. She efficiently took my vital signs, asked me my height, and weighed me. She ran through the usual list of screening questions without the slightest hint of a smile despite my efforts to gently inject a bit of levity into my answers.
With her work completed, she left me to wait for “the doctor” without a clue about who I was. She knew that I had one beer and one glass of wine each evening, and that I always wore a seatbelt and didn’t have gun. But she hadn’t provided any outward evidence that she cared about the person who had been providing the answers.
There was a welcome lifting of the chill when my former colleague and current physician entered the exam room. After we had done some catching up about our families and before we started talking about my blood pressure I said, “Marcy really needs to lighten up a bit.”
My observation came as no surprise to my doctor. The transition to a new hospital-owned group practice still had some rough edges including the struggle to instill a more customer-friendly culture among the support staff that she had inherited. She thanked me for my unsolicited feedback.
When Marcy returned to administer my “pneumonia shot” she was wearing a smile. And she was more than willing to engage in the kind of banter that may not have much substance, but is the currency that most of us use to ease the tension in potentially uncomfortable situations. Obviously, while I was waiting she had been given a quick course in customer service.
Marcy and the receptionists are the face of that office, and it certainly wasn’t a welcoming or friendly face. No one was rude. On the other hand, no one was trying to treat the patients as they would like to be treated themselves. You could accuse me of being a nit picky curmudgeon. You could ask if the addition of a smiling face or two would have made a difference in the quality of care coming out of that office. It may not have, but it wouldn’t have hurt, and it would be the nice thing to do.
But and take some of the edge off the anger of patients who are unhappy about the care they have been receiving. There is some evidence that hospitalized patients in customer-friendly situations do better. And I bet that patients seen in customer-friendly offices staff get better more quickly.

If you are aware of staff members whose behavior could be more customer friendly, have you said something to them? It can be touchy. You probably aren’t their supervisor. They may not being doing anything wrong. But their failure to make a pleasant and caring first impression may be making your job more difficult.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
A few weeks ago I visited my primary care physician in her new office. As the first patient of the day I was immediately ushered into the examining room by a woman I assume was a medical assistant. She didn’t introduce herself, but her name tag read “Marcy” (not her real name). Her demeanor could best be described as cheerless. She efficiently took my vital signs, asked me my height, and weighed me. She ran through the usual list of screening questions without the slightest hint of a smile despite my efforts to gently inject a bit of levity into my answers.
With her work completed, she left me to wait for “the doctor” without a clue about who I was. She knew that I had one beer and one glass of wine each evening, and that I always wore a seatbelt and didn’t have gun. But she hadn’t provided any outward evidence that she cared about the person who had been providing the answers.
There was a welcome lifting of the chill when my former colleague and current physician entered the exam room. After we had done some catching up about our families and before we started talking about my blood pressure I said, “Marcy really needs to lighten up a bit.”
My observation came as no surprise to my doctor. The transition to a new hospital-owned group practice still had some rough edges including the struggle to instill a more customer-friendly culture among the support staff that she had inherited. She thanked me for my unsolicited feedback.
When Marcy returned to administer my “pneumonia shot” she was wearing a smile. And she was more than willing to engage in the kind of banter that may not have much substance, but is the currency that most of us use to ease the tension in potentially uncomfortable situations. Obviously, while I was waiting she had been given a quick course in customer service.
Marcy and the receptionists are the face of that office, and it certainly wasn’t a welcoming or friendly face. No one was rude. On the other hand, no one was trying to treat the patients as they would like to be treated themselves. You could accuse me of being a nit picky curmudgeon. You could ask if the addition of a smiling face or two would have made a difference in the quality of care coming out of that office. It may not have, but it wouldn’t have hurt, and it would be the nice thing to do.
But and take some of the edge off the anger of patients who are unhappy about the care they have been receiving. There is some evidence that hospitalized patients in customer-friendly situations do better. And I bet that patients seen in customer-friendly offices staff get better more quickly.
If you are aware of staff members whose behavior could be more customer friendly, have you said something to them? It can be touchy. You probably aren’t their supervisor. They may not being doing anything wrong. But their failure to make a pleasant and caring first impression may be making your job more difficult.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
A few weeks ago I visited my primary care physician in her new office. As the first patient of the day I was immediately ushered into the examining room by a woman I assume was a medical assistant. She didn’t introduce herself, but her name tag read “Marcy” (not her real name). Her demeanor could best be described as cheerless. She efficiently took my vital signs, asked me my height, and weighed me. She ran through the usual list of screening questions without the slightest hint of a smile despite my efforts to gently inject a bit of levity into my answers.
With her work completed, she left me to wait for “the doctor” without a clue about who I was. She knew that I had one beer and one glass of wine each evening, and that I always wore a seatbelt and didn’t have gun. But she hadn’t provided any outward evidence that she cared about the person who had been providing the answers.
There was a welcome lifting of the chill when my former colleague and current physician entered the exam room. After we had done some catching up about our families and before we started talking about my blood pressure I said, “Marcy really needs to lighten up a bit.”
My observation came as no surprise to my doctor. The transition to a new hospital-owned group practice still had some rough edges including the struggle to instill a more customer-friendly culture among the support staff that she had inherited. She thanked me for my unsolicited feedback.
When Marcy returned to administer my “pneumonia shot” she was wearing a smile. And she was more than willing to engage in the kind of banter that may not have much substance, but is the currency that most of us use to ease the tension in potentially uncomfortable situations. Obviously, while I was waiting she had been given a quick course in customer service.
Marcy and the receptionists are the face of that office, and it certainly wasn’t a welcoming or friendly face. No one was rude. On the other hand, no one was trying to treat the patients as they would like to be treated themselves. You could accuse me of being a nit picky curmudgeon. You could ask if the addition of a smiling face or two would have made a difference in the quality of care coming out of that office. It may not have, but it wouldn’t have hurt, and it would be the nice thing to do.
But and take some of the edge off the anger of patients who are unhappy about the care they have been receiving. There is some evidence that hospitalized patients in customer-friendly situations do better. And I bet that patients seen in customer-friendly offices staff get better more quickly.
If you are aware of staff members whose behavior could be more customer friendly, have you said something to them? It can be touchy. You probably aren’t their supervisor. They may not being doing anything wrong. But their failure to make a pleasant and caring first impression may be making your job more difficult.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
New rankings focus on child health care
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.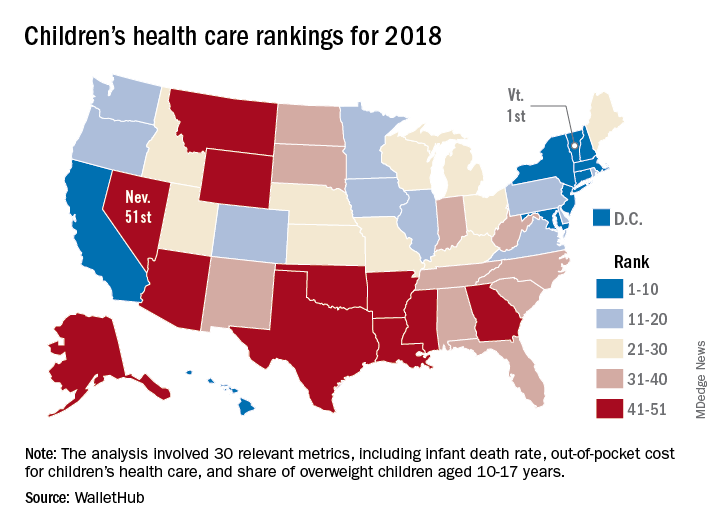
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
a personal finance website.
The District of Columbia joined the party and finished second to Vermont, which pushed Nevada down to 51st place, according to WalletHub’s “Best & Worst States for Children’s Health Care” for 2018.
Louisiana’s 50th-ranked health system was just ahead of Nevada’s, and those two were below Texas in 49th, Mississippi in 48th, Arkansas in 47th, and Montana in 46th. The top five had a strong New England flavor (think maple syrup and cranberries), with Vermont joined by Massachusetts in third and Connecticut in fourth, followed by New England’s neighbor New York in fifth, the report showed.
The analysis involved a 100-point system covering three broad areas of health care: health and access to health care (55 points); nutrition, physical activity, and obesity (40 points); and oral health (5 points). Those categories were divided into a total of 30 relevant metrics, including the share of children aged 0-17 years who were in excellent to very good health, pediatricians and family physicians per capita, share of obese children aged 10-17 years, and share of children aged 1-17 years with excellent or very good teeth.
Vermont’s strong showing in WalletHub’s metric system was driven by first-place finishes in lowest infant death rate, pediatricians and family physicians per capita, and percentage of children with recent medical and dental checkups, along with being in third place for percentage of uninsured children and for percentage of overweight children. D.C. had the lowest percentage of children with unaffordable medical bills, and Massachusetts had the lowest percentage of uninsured children, according to data collected by WalletHub from such sources as the U.S. Census Bureau, the Council for Community and Economic research, and the Trust for America’s Health.
“Parents should be supported to learn about and be active in [their] children’s development. … Since our safety net is anemic and our idea of health is about lack of symptoms, this answer challenges us to think more critically about our living conditions and those of our children,” Michael Montoya, PhD, associate professor emeritus in the departments of anthropology, public health, and the program in medical education for the Latino community at the University of California, Irvine, said in the report.
Another respondent to the report, Christina M. Dalton, PhD, of the department of economics at Wake Forest University, Winston-Salem, N.C., said, “Children’s health coverage has important potential to improve health and economic outcomes in the future since early good health enables children to learn better in school. However, any expansion of public options needs to take into account the idea that public insurance can end up taking enrollees away from the private market. … It’s always a trade-off of increasing coverage while not attracting too many of the enrollees that would have already bought insurance without government funding.”
Federal court puts chill on Maryland drug price-gouging law
The 2-to-1 ruling April 13 by the U.S. 4th Circuit Court of Appeals invalidated a Maryland law meant to limit “price-gouging” by makers of generic drugs. The measure was inspired by cases such as that of former Turing Pharmaceutical CEO Martin Shkreli, who raised one generic’s price 5,000% after buying the company.
If dissatisfied with the company’s justification, the attorney general could have filed suit in state court. Manufacturers would have faced a fine of up to $10,000 and potentially have to reverse the price hike. The generics industry was fiercely critical of the law.
“We are evaluating all options with regard to next steps,” said Maryland Attorney General Brian Frosh in a statement. His office would not elaborate further.
The state could appeal to have the case heard “en banc,” meaning by the full 4th Circuit, with jurisdiction over five states.
Such appeals aren’t commonly granted, but this law could be a strong candidate, suggested Aaron S. Kesselheim, MD, an associate professor at Harvard Medical School, Boston, who researches drug-price regulation.
The April 13 ruling looms large as other state legislatures grapple with ever-climbing drug prices.
Similar price-gouging legislation has been introduced in at least 13 states this year, though none of those measures became law, according to the National Conference of State Legislatures (NCSL). Three other bills failed to gain passage.
The NCSL also cited the law in a March advisory for states seeking new approaches to regulating drug prices.
The court’s finding could have a chilling effect on such efforts, especially as more state legislatures wrap up business for 2018.
“A negative court ruling will put a damper or a pause on state activities,” said Richard Cauchi, NCSL’s health program director. “Unless this topic is your No. 1 priority of the year, your legislators are juggling multiple bills, multiple strategies. When bill three gets in trouble, they move to bill four.”
The appeals court held that Maryland’s law overstepped limits on how states can regulate commerce – specifically, a constitutional ban on states controlling business that takes place outside their borders. The majority ruling argues that, since most generics manufacturers and drug wholesalers engage in trade outside Maryland, the state cannot control what prices they charge.
In a dissenting opinion, the panel’s third judge argued Maryland can regulate the drug prices charged within the state since the law is meant to affect only medications being sold to its own residents.
Dr. Kesselheim argued similarly in a JAMA viewpoint (2018;319[9]:865-866).
Regardless, striking down a law on constitutional grounds can be particularly discouraging, suggested Rachel Sachs, an associate law professor at Washington University in St. Louis who researches drug regulations.
“If it had been a rejection on vagueness grounds, that’s something you can cure with a more specific statute,” she said. “But the fact that they said this is unconstitutional poses real concern for other states.”
That’s important. While the federal government has talked a big game on bringing down drug prices, it has done little. Instead, states have taken the lead – spurred by the budget squeeze pricey prescriptions impose on their Medicaid programs and on state employee benefits packages.
But states have far fewer tools at their disposal than does Congress. Most state laws so far tackle only pieces of the problem – targeting a specific drug or particular practice, experts said.
“We’ll get more broad and better evolution on this issue if the federal government decides to take it seriously – which it hasn’t so far,” Dr. Kesselheim said.
To be fair, Maryland’s law is only one of a bevy of approaches.
Other states have focused on price transparency laws. In California, drug companies must disclose in advance if a price might increase by more than a set percent and that they justify the increase. Industry has sued to block the California law.
New York has limited what the state will pay for drugs, establishing a process to review if expensive drugs are priced out of step with their medical value.
A number of states have since 2017 passed laws regulating pharmacy benefit managers – the contractors who negotiate discounted drug coverage for insurance plans, but who rarely reveal what level of discount they actually pass on to consumers.
Experts expect that activity to continue, especially as escalating drug prices show little sign of letting up.
“The states are going to keep trying and experimenting,” Ms. Sachs added. “This is a problem that isn’t going away.”
Even efforts such as Maryland’s – which targeted price-gouging – will likely remain at the forefront.
“I don’t think this is the end of states trying to do something on price gouging,” said Ellen Albritton, a senior policy analyst at the left-leaning advocacy group Families USA who consults with states on drug-pricing policy. “It’s such an issue that offends people’s sensibilities. It’s crazy people can do this.”
KHN’s coverage of prescription drug development, costs, and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The 2-to-1 ruling April 13 by the U.S. 4th Circuit Court of Appeals invalidated a Maryland law meant to limit “price-gouging” by makers of generic drugs. The measure was inspired by cases such as that of former Turing Pharmaceutical CEO Martin Shkreli, who raised one generic’s price 5,000% after buying the company.
If dissatisfied with the company’s justification, the attorney general could have filed suit in state court. Manufacturers would have faced a fine of up to $10,000 and potentially have to reverse the price hike. The generics industry was fiercely critical of the law.
“We are evaluating all options with regard to next steps,” said Maryland Attorney General Brian Frosh in a statement. His office would not elaborate further.
The state could appeal to have the case heard “en banc,” meaning by the full 4th Circuit, with jurisdiction over five states.
Such appeals aren’t commonly granted, but this law could be a strong candidate, suggested Aaron S. Kesselheim, MD, an associate professor at Harvard Medical School, Boston, who researches drug-price regulation.
The April 13 ruling looms large as other state legislatures grapple with ever-climbing drug prices.
Similar price-gouging legislation has been introduced in at least 13 states this year, though none of those measures became law, according to the National Conference of State Legislatures (NCSL). Three other bills failed to gain passage.
The NCSL also cited the law in a March advisory for states seeking new approaches to regulating drug prices.
The court’s finding could have a chilling effect on such efforts, especially as more state legislatures wrap up business for 2018.
“A negative court ruling will put a damper or a pause on state activities,” said Richard Cauchi, NCSL’s health program director. “Unless this topic is your No. 1 priority of the year, your legislators are juggling multiple bills, multiple strategies. When bill three gets in trouble, they move to bill four.”
The appeals court held that Maryland’s law overstepped limits on how states can regulate commerce – specifically, a constitutional ban on states controlling business that takes place outside their borders. The majority ruling argues that, since most generics manufacturers and drug wholesalers engage in trade outside Maryland, the state cannot control what prices they charge.
In a dissenting opinion, the panel’s third judge argued Maryland can regulate the drug prices charged within the state since the law is meant to affect only medications being sold to its own residents.
Dr. Kesselheim argued similarly in a JAMA viewpoint (2018;319[9]:865-866).
Regardless, striking down a law on constitutional grounds can be particularly discouraging, suggested Rachel Sachs, an associate law professor at Washington University in St. Louis who researches drug regulations.
“If it had been a rejection on vagueness grounds, that’s something you can cure with a more specific statute,” she said. “But the fact that they said this is unconstitutional poses real concern for other states.”
That’s important. While the federal government has talked a big game on bringing down drug prices, it has done little. Instead, states have taken the lead – spurred by the budget squeeze pricey prescriptions impose on their Medicaid programs and on state employee benefits packages.
But states have far fewer tools at their disposal than does Congress. Most state laws so far tackle only pieces of the problem – targeting a specific drug or particular practice, experts said.
“We’ll get more broad and better evolution on this issue if the federal government decides to take it seriously – which it hasn’t so far,” Dr. Kesselheim said.
To be fair, Maryland’s law is only one of a bevy of approaches.
Other states have focused on price transparency laws. In California, drug companies must disclose in advance if a price might increase by more than a set percent and that they justify the increase. Industry has sued to block the California law.
New York has limited what the state will pay for drugs, establishing a process to review if expensive drugs are priced out of step with their medical value.
A number of states have since 2017 passed laws regulating pharmacy benefit managers – the contractors who negotiate discounted drug coverage for insurance plans, but who rarely reveal what level of discount they actually pass on to consumers.
Experts expect that activity to continue, especially as escalating drug prices show little sign of letting up.
“The states are going to keep trying and experimenting,” Ms. Sachs added. “This is a problem that isn’t going away.”
Even efforts such as Maryland’s – which targeted price-gouging – will likely remain at the forefront.
“I don’t think this is the end of states trying to do something on price gouging,” said Ellen Albritton, a senior policy analyst at the left-leaning advocacy group Families USA who consults with states on drug-pricing policy. “It’s such an issue that offends people’s sensibilities. It’s crazy people can do this.”
KHN’s coverage of prescription drug development, costs, and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The 2-to-1 ruling April 13 by the U.S. 4th Circuit Court of Appeals invalidated a Maryland law meant to limit “price-gouging” by makers of generic drugs. The measure was inspired by cases such as that of former Turing Pharmaceutical CEO Martin Shkreli, who raised one generic’s price 5,000% after buying the company.
If dissatisfied with the company’s justification, the attorney general could have filed suit in state court. Manufacturers would have faced a fine of up to $10,000 and potentially have to reverse the price hike. The generics industry was fiercely critical of the law.
“We are evaluating all options with regard to next steps,” said Maryland Attorney General Brian Frosh in a statement. His office would not elaborate further.
The state could appeal to have the case heard “en banc,” meaning by the full 4th Circuit, with jurisdiction over five states.
Such appeals aren’t commonly granted, but this law could be a strong candidate, suggested Aaron S. Kesselheim, MD, an associate professor at Harvard Medical School, Boston, who researches drug-price regulation.
The April 13 ruling looms large as other state legislatures grapple with ever-climbing drug prices.
Similar price-gouging legislation has been introduced in at least 13 states this year, though none of those measures became law, according to the National Conference of State Legislatures (NCSL). Three other bills failed to gain passage.
The NCSL also cited the law in a March advisory for states seeking new approaches to regulating drug prices.
The court’s finding could have a chilling effect on such efforts, especially as more state legislatures wrap up business for 2018.
“A negative court ruling will put a damper or a pause on state activities,” said Richard Cauchi, NCSL’s health program director. “Unless this topic is your No. 1 priority of the year, your legislators are juggling multiple bills, multiple strategies. When bill three gets in trouble, they move to bill four.”
The appeals court held that Maryland’s law overstepped limits on how states can regulate commerce – specifically, a constitutional ban on states controlling business that takes place outside their borders. The majority ruling argues that, since most generics manufacturers and drug wholesalers engage in trade outside Maryland, the state cannot control what prices they charge.
In a dissenting opinion, the panel’s third judge argued Maryland can regulate the drug prices charged within the state since the law is meant to affect only medications being sold to its own residents.
Dr. Kesselheim argued similarly in a JAMA viewpoint (2018;319[9]:865-866).
Regardless, striking down a law on constitutional grounds can be particularly discouraging, suggested Rachel Sachs, an associate law professor at Washington University in St. Louis who researches drug regulations.
“If it had been a rejection on vagueness grounds, that’s something you can cure with a more specific statute,” she said. “But the fact that they said this is unconstitutional poses real concern for other states.”
That’s important. While the federal government has talked a big game on bringing down drug prices, it has done little. Instead, states have taken the lead – spurred by the budget squeeze pricey prescriptions impose on their Medicaid programs and on state employee benefits packages.
But states have far fewer tools at their disposal than does Congress. Most state laws so far tackle only pieces of the problem – targeting a specific drug or particular practice, experts said.
“We’ll get more broad and better evolution on this issue if the federal government decides to take it seriously – which it hasn’t so far,” Dr. Kesselheim said.
To be fair, Maryland’s law is only one of a bevy of approaches.
Other states have focused on price transparency laws. In California, drug companies must disclose in advance if a price might increase by more than a set percent and that they justify the increase. Industry has sued to block the California law.
New York has limited what the state will pay for drugs, establishing a process to review if expensive drugs are priced out of step with their medical value.
A number of states have since 2017 passed laws regulating pharmacy benefit managers – the contractors who negotiate discounted drug coverage for insurance plans, but who rarely reveal what level of discount they actually pass on to consumers.
Experts expect that activity to continue, especially as escalating drug prices show little sign of letting up.
“The states are going to keep trying and experimenting,” Ms. Sachs added. “This is a problem that isn’t going away.”
Even efforts such as Maryland’s – which targeted price-gouging – will likely remain at the forefront.
“I don’t think this is the end of states trying to do something on price gouging,” said Ellen Albritton, a senior policy analyst at the left-leaning advocacy group Families USA who consults with states on drug-pricing policy. “It’s such an issue that offends people’s sensibilities. It’s crazy people can do this.”
KHN’s coverage of prescription drug development, costs, and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a national health policy news service. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Will patients get on board with CMS’s new health data approach?
CMS is turning to patients to help drive health information technology toward greater interoperability, accessibility, and usability – elusive goals that have not been reached by working with health care professionals and IT vendors alone.
“MyHealthEData makes it clear that patients should have access and control to share their data with whomever they want, making the patient the center of our health system,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said at the annual HIMSS conference. “Patients need to be able to control their information and know that it is secure and private. Having access to their medical information will help them make decisions about their care and have a better understanding of their health.”

She added that “once information is freely flowing from the patient to the provider, the advances in coordinated, value-based care and patient-centric care will be even greater than anything we can imagine today.”
Patients could share their data with applications designed to help them make more informed health care decisions of with their providers and caregivers to help better manage their care,” Ms. Verma said in an interview.
For example, the initiative could lead to the development of products such as the following:
- Mobile apps to help patients manage medications and medical appointments.
- Simple processes that carry patients’ data when they switch providers or health insurance plans.
- Wearables, such as step trackers or glucose monitors, that are linked to patients’ clinical record.
To get to this future health IT nirvana, CMS will need to address the ongoing interoperability issues that continue to plague EHRs. And that’s where CMS is turning its efforts back to helping clinicians.
The agency “will be announcing a complete overhaul of the meaningful use program for hospitals and the advancing care information performance category of the Quality Payment Program,” Ms. Verma announced at HIMSS.
A complete overhaul is “the appropriate approach,” and one that doctors could support, according to a spokesman for the American Medical Association. “We are not talking about painting the walls. We are talking about stripping things down to the bare studs and coming back to this and looking at it from a fresh start.
“We have a perfect storm of opportunity here to really rethink the program,” the spokesman said. “It’s not just rethinking the program from the standpoint of burden; it’s rethinking CMS programs from the standpoint of collapsing some of the reporting into to one holistic picture where the doctor is participating with their patients in chronic care or different care teams or the patient-centered medical home.”
And fixing those regulations is going to go a long way in helping patients to actually interact with their data and to really put them in the center of their care; this is especially important since EHRs are currently built to comply with reporting requirements and not necessarily to help improve care, the AMA spokesman noted. And while current patient portal requirements promote engagement, the information is not necessarily useful for patients.
“What we see as the next step is an opportunity here to reduce some of the prescriptive nature of the regulation on the design and use of EHRs,” the spokesman said. “It is an interesting way to look at it because, while we want to encourage patients to access their complete record set, the front-to-back side of their entire medical record is not always available due to EHR design.”
Indeed, at HIMSS Ms. Verma said that “for those of you that still subscribe to the outdated idea that you can deny patients’ access to their health records, I encourage you, in the strongest way, to change course and accept that those practices will come to an end.”
CMS currently does not have a specific timeline for all the aspects of the MyHealthEData initiative, but Ms. Verma did note that the agency already is working with vendors on one aspect: Blue Button 2.0, a developer-friendly, standards-based developer tool that will allow the creation of apps to connect Medicare claims data to programs that can help create context and make informed medical decisions easier.
In 2019, new EHR requirements will follow that will require data to be shareable in a more standardized manner.
“Through the MyHealthEData initiative, this administration is focused on putting patients first, truly first, by empowering them to make cost and quality decisions, and giving them the information they need to prevent disease and improve their health,” Ms. Verma said.
CMS is turning to patients to help drive health information technology toward greater interoperability, accessibility, and usability – elusive goals that have not been reached by working with health care professionals and IT vendors alone.
“MyHealthEData makes it clear that patients should have access and control to share their data with whomever they want, making the patient the center of our health system,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said at the annual HIMSS conference. “Patients need to be able to control their information and know that it is secure and private. Having access to their medical information will help them make decisions about their care and have a better understanding of their health.”
She added that “once information is freely flowing from the patient to the provider, the advances in coordinated, value-based care and patient-centric care will be even greater than anything we can imagine today.”
Patients could share their data with applications designed to help them make more informed health care decisions of with their providers and caregivers to help better manage their care,” Ms. Verma said in an interview.
For example, the initiative could lead to the development of products such as the following:
- Mobile apps to help patients manage medications and medical appointments.
- Simple processes that carry patients’ data when they switch providers or health insurance plans.
- Wearables, such as step trackers or glucose monitors, that are linked to patients’ clinical record.
To get to this future health IT nirvana, CMS will need to address the ongoing interoperability issues that continue to plague EHRs. And that’s where CMS is turning its efforts back to helping clinicians.
The agency “will be announcing a complete overhaul of the meaningful use program for hospitals and the advancing care information performance category of the Quality Payment Program,” Ms. Verma announced at HIMSS.
A complete overhaul is “the appropriate approach,” and one that doctors could support, according to a spokesman for the American Medical Association. “We are not talking about painting the walls. We are talking about stripping things down to the bare studs and coming back to this and looking at it from a fresh start.
“We have a perfect storm of opportunity here to really rethink the program,” the spokesman said. “It’s not just rethinking the program from the standpoint of burden; it’s rethinking CMS programs from the standpoint of collapsing some of the reporting into to one holistic picture where the doctor is participating with their patients in chronic care or different care teams or the patient-centered medical home.”
And fixing those regulations is going to go a long way in helping patients to actually interact with their data and to really put them in the center of their care; this is especially important since EHRs are currently built to comply with reporting requirements and not necessarily to help improve care, the AMA spokesman noted. And while current patient portal requirements promote engagement, the information is not necessarily useful for patients.
“What we see as the next step is an opportunity here to reduce some of the prescriptive nature of the regulation on the design and use of EHRs,” the spokesman said. “It is an interesting way to look at it because, while we want to encourage patients to access their complete record set, the front-to-back side of their entire medical record is not always available due to EHR design.”
Indeed, at HIMSS Ms. Verma said that “for those of you that still subscribe to the outdated idea that you can deny patients’ access to their health records, I encourage you, in the strongest way, to change course and accept that those practices will come to an end.”
CMS currently does not have a specific timeline for all the aspects of the MyHealthEData initiative, but Ms. Verma did note that the agency already is working with vendors on one aspect: Blue Button 2.0, a developer-friendly, standards-based developer tool that will allow the creation of apps to connect Medicare claims data to programs that can help create context and make informed medical decisions easier.
In 2019, new EHR requirements will follow that will require data to be shareable in a more standardized manner.
“Through the MyHealthEData initiative, this administration is focused on putting patients first, truly first, by empowering them to make cost and quality decisions, and giving them the information they need to prevent disease and improve their health,” Ms. Verma said.
CMS is turning to patients to help drive health information technology toward greater interoperability, accessibility, and usability – elusive goals that have not been reached by working with health care professionals and IT vendors alone.
“MyHealthEData makes it clear that patients should have access and control to share their data with whomever they want, making the patient the center of our health system,” Seema Verma, administrator of the Centers for Medicare & Medicaid Services, said at the annual HIMSS conference. “Patients need to be able to control their information and know that it is secure and private. Having access to their medical information will help them make decisions about their care and have a better understanding of their health.”
She added that “once information is freely flowing from the patient to the provider, the advances in coordinated, value-based care and patient-centric care will be even greater than anything we can imagine today.”
Patients could share their data with applications designed to help them make more informed health care decisions of with their providers and caregivers to help better manage their care,” Ms. Verma said in an interview.
For example, the initiative could lead to the development of products such as the following:
- Mobile apps to help patients manage medications and medical appointments.
- Simple processes that carry patients’ data when they switch providers or health insurance plans.
- Wearables, such as step trackers or glucose monitors, that are linked to patients’ clinical record.
To get to this future health IT nirvana, CMS will need to address the ongoing interoperability issues that continue to plague EHRs. And that’s where CMS is turning its efforts back to helping clinicians.
The agency “will be announcing a complete overhaul of the meaningful use program for hospitals and the advancing care information performance category of the Quality Payment Program,” Ms. Verma announced at HIMSS.
A complete overhaul is “the appropriate approach,” and one that doctors could support, according to a spokesman for the American Medical Association. “We are not talking about painting the walls. We are talking about stripping things down to the bare studs and coming back to this and looking at it from a fresh start.
“We have a perfect storm of opportunity here to really rethink the program,” the spokesman said. “It’s not just rethinking the program from the standpoint of burden; it’s rethinking CMS programs from the standpoint of collapsing some of the reporting into to one holistic picture where the doctor is participating with their patients in chronic care or different care teams or the patient-centered medical home.”
And fixing those regulations is going to go a long way in helping patients to actually interact with their data and to really put them in the center of their care; this is especially important since EHRs are currently built to comply with reporting requirements and not necessarily to help improve care, the AMA spokesman noted. And while current patient portal requirements promote engagement, the information is not necessarily useful for patients.
“What we see as the next step is an opportunity here to reduce some of the prescriptive nature of the regulation on the design and use of EHRs,” the spokesman said. “It is an interesting way to look at it because, while we want to encourage patients to access their complete record set, the front-to-back side of their entire medical record is not always available due to EHR design.”
Indeed, at HIMSS Ms. Verma said that “for those of you that still subscribe to the outdated idea that you can deny patients’ access to their health records, I encourage you, in the strongest way, to change course and accept that those practices will come to an end.”
CMS currently does not have a specific timeline for all the aspects of the MyHealthEData initiative, but Ms. Verma did note that the agency already is working with vendors on one aspect: Blue Button 2.0, a developer-friendly, standards-based developer tool that will allow the creation of apps to connect Medicare claims data to programs that can help create context and make informed medical decisions easier.
In 2019, new EHR requirements will follow that will require data to be shareable in a more standardized manner.
“Through the MyHealthEData initiative, this administration is focused on putting patients first, truly first, by empowering them to make cost and quality decisions, and giving them the information they need to prevent disease and improve their health,” Ms. Verma said.
Surgeon General wants naloxone widely on hand. Is that feasible?
This is an “unequivocally positive” step forward, said Leo Beletsky, an associate professor of law and health sciences at Northeastern University.
And not necessarily a surprise. Dr. Adams, who previously was Indiana’s health commissioner, was recruited to be the nation’s top doctor in part because of his work with then-Gov. Mike Pence, now the vice president. In Indiana, Dr. Adams pushed for harm-reduction approaches, which included expanded access to naloxone and the implementation of a needle exchange to combat the state’s much-publicized HIV outbreak, which began in 2015 and was linked to injection drug use.
Others cautioned, though, that his have-naloxone-will-carry recommendation is at best limited in what it can achieve, in part because the drug is relatively expensive.
Kaiser Health News breaks down what the advisory means, experts’ concerns, and what policy approaches may be in the pipeline.
Many public health advocates applaud the surgeon general’s position
Naloxone, which is a drug that can keep drug users alive by reversing opioid overdoses, is viewed by many as the cornerstone of the harm-reduction approach to the epidemic. Experts say people with addiction problems should carry it, and so should their family, friends and acquaintances.
“We want to put it more in reach,” said Traci Green, PhD, an associate professor of emergency medicine and community health sciences at Boston University, who has extensively researched the opioid abuse crisis. “It could not have been a better endorsement.”
Others, including Diane Goodman, who penned a recent Medscape commentary reflecting on the advisory, wonder whether this is a “rational” response to the scourge, since opioid addiction is one of many health problems people might encounter in everyday life and for which treatment options are still limited.
“I’m not sure it makes much more sense than any of us carrying a bottle of nitroglycerin to treat patients with end-stage angina,” wrote Ms. Goodman, an acute-care nurse practitioner.
“What, exactly, are we offering to addicts once their condition has been reversed?” she asked, noting that, without treatment and therapy programs that help wean people from addiction, “the odds of survival for any length of time remain low, no matter how much reversal medication is kept nearby.”
Results would likely be limited by naloxone’s price tag
Take Baltimore, which has been hit particularly hard by the opioid epidemic. Its health department already has pushed for more people to carry naloxone.
But the drug’s price is an issue, said Leana Wen, MD, the city’s health commissioner, and an emergency physician. She suggested that the federal government negotiate directly for a lower price, or give more money to organizations and agencies like hers so they can afford to maintain an adequate supply.
“Every day, people are calling us at the Baltimore City Health Department and requesting naloxone, and I have to tell them I can’t afford for them to have it,” Dr. Wen said.
The drug is available in generic form, which can be stored in a vial and injected via a needle, as well as in patented products, such as the nasal spray Narcan, sold by ADAPT Pharmaceuticals, and Kaleo’s Evzio, a talking auto-injector.
Generic naloxone costs $20-$40 per dose. Narcan, the nasal spray, costs $125 for a two-dose carton, according to ADAPT’s website. A two-pack of Evzio costs close to $4,000, according to GoodRx.
Health departments and first responders qualify for a discounted rate of $75 per carton of Narcan. Kaleo has made Evzio coupons available to consumers, so that some will not have a copay, and it advertises a discount for federal and state agencies.
Skeptics point out that similar methods have been used to build brand loyalty and potentially make a particular product a household name. That’s how Epi-Pen became synonymous with epinephrine for the treatment of anaphylactic shock.
“There’s clearly some overlap” here between the pricing strategies used by naloxone manufacturers and Epi-Pen distributor Mylan, said Richard Evans, cofounder of SSR Health, which tracks the pharmaceutical industry.
But it’s not a perfect comparison. The presence of low-cost generics changes the calculus, he said, as does the different level of demand.
Nonprofit organizations and health care providers keenly feel the pressures of increasing demand and cost
Experts say price breaks on naloxone are not sufficient to cover the costs on the ground.
“Sixty-four thousand people lost their lives [nationally in 2016] — that’s someone every 12 minutes,” said Justin Phillips, executive director of Overdose Lifeline, an Indianapolis-based nonprofit. “Ten free kits is not going to be enough.”
Ms. Phillips said her organization relies on generic naloxone, which is the least expensive formulation. It’s the only feasible option, using dedicated grant money the group received from the state attorney general’s office as part of a program funded by a settlement with pharmaceutical companies.
But that money is almost dried up. “We need to be able to access naloxone – which I’m told is pennies to make – for the pennies it cost to make it,” she said.
Ms. Phillips, who worked with Dr. Adams when he ran Indiana’s health department, said she has discussed the need for naloxone funding with the surgeon general, but never its price.
Pharmacies assess the hurdles of distribution
Local pharmacies are key in this chain, but the overdose antidote is new territory for many pharmacists, said Randy Hitchens, the executive vice president of the Indiana Pharmacists Alliance. He said in 2015, when Adams began his push to get naloxone into the hands of drug users and their families, only one or two retail pharmacies carried it.
“This has always been an emergency room drug. Retail pharmacists typically were not used to dealing with [it],” Mr. Hitchens said. “A lot were probably saying, ‘What in the devil is naloxone?’”
Today, he estimates 60%-70% of Indiana’s more than 1,100 retail pharmacies carry the drug. Walgreens has committed to stocking Narcan.
Access, though, is always subject to retail pressures.
“If pharmacies are not seeing a steady stream coming in asking for it, they won’t be incentivized to carry it on their shelves,” said Daniel Raymond, the deputy director of policy and planning for the Harm Reduction Coalition.
A patchwork of other decentralized sources for naloxone exist: syringe-exchange vans, county and state health departments, churches and community centers, all trying to find ways to get overdose medication into the hands of people who need it.
That supply stream “meets people where they are,” Mr. Raymond said, but those little programs don’t have the muscle to negotiate discounted prices.
“Individual health programs are trying to navigate the crisis on their own, but when you see … growing demand and limited supply, it’s a role for federal intervention,” Mr. Raymond said.
He’d like to see the federal government step in to negotiate prices where smaller programs can’t.
Even as Congress crafts an opioid epidemic response package, it’s not clear it will tackle these concerns
In the House Energy and Commerce Committee, one bill being discussed would require all state Medicaid programs to cover at least one form of naloxone. Currently, not all state Medicaid programs do so.
A Senate bill would authorize $300 million annually to equip first responders with naloxone.
But critics say those approaches still don’t address the underlying problems: cost and funding.
“You can either make naloxone available, at a much discounted price, or we need to have a lot more resources in order to purchase it,” Dr. Wen said. “I don’t care which one. My only concern is the health and well-being of our residents.”
KHN’s coverage of prescription drug development, costs and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
This is an “unequivocally positive” step forward, said Leo Beletsky, an associate professor of law and health sciences at Northeastern University.
And not necessarily a surprise. Dr. Adams, who previously was Indiana’s health commissioner, was recruited to be the nation’s top doctor in part because of his work with then-Gov. Mike Pence, now the vice president. In Indiana, Dr. Adams pushed for harm-reduction approaches, which included expanded access to naloxone and the implementation of a needle exchange to combat the state’s much-publicized HIV outbreak, which began in 2015 and was linked to injection drug use.
Others cautioned, though, that his have-naloxone-will-carry recommendation is at best limited in what it can achieve, in part because the drug is relatively expensive.
Kaiser Health News breaks down what the advisory means, experts’ concerns, and what policy approaches may be in the pipeline.
Many public health advocates applaud the surgeon general’s position
Naloxone, which is a drug that can keep drug users alive by reversing opioid overdoses, is viewed by many as the cornerstone of the harm-reduction approach to the epidemic. Experts say people with addiction problems should carry it, and so should their family, friends and acquaintances.
“We want to put it more in reach,” said Traci Green, PhD, an associate professor of emergency medicine and community health sciences at Boston University, who has extensively researched the opioid abuse crisis. “It could not have been a better endorsement.”
Others, including Diane Goodman, who penned a recent Medscape commentary reflecting on the advisory, wonder whether this is a “rational” response to the scourge, since opioid addiction is one of many health problems people might encounter in everyday life and for which treatment options are still limited.
“I’m not sure it makes much more sense than any of us carrying a bottle of nitroglycerin to treat patients with end-stage angina,” wrote Ms. Goodman, an acute-care nurse practitioner.
“What, exactly, are we offering to addicts once their condition has been reversed?” she asked, noting that, without treatment and therapy programs that help wean people from addiction, “the odds of survival for any length of time remain low, no matter how much reversal medication is kept nearby.”
Results would likely be limited by naloxone’s price tag
Take Baltimore, which has been hit particularly hard by the opioid epidemic. Its health department already has pushed for more people to carry naloxone.
But the drug’s price is an issue, said Leana Wen, MD, the city’s health commissioner, and an emergency physician. She suggested that the federal government negotiate directly for a lower price, or give more money to organizations and agencies like hers so they can afford to maintain an adequate supply.
“Every day, people are calling us at the Baltimore City Health Department and requesting naloxone, and I have to tell them I can’t afford for them to have it,” Dr. Wen said.
The drug is available in generic form, which can be stored in a vial and injected via a needle, as well as in patented products, such as the nasal spray Narcan, sold by ADAPT Pharmaceuticals, and Kaleo’s Evzio, a talking auto-injector.
Generic naloxone costs $20-$40 per dose. Narcan, the nasal spray, costs $125 for a two-dose carton, according to ADAPT’s website. A two-pack of Evzio costs close to $4,000, according to GoodRx.
Health departments and first responders qualify for a discounted rate of $75 per carton of Narcan. Kaleo has made Evzio coupons available to consumers, so that some will not have a copay, and it advertises a discount for federal and state agencies.
Skeptics point out that similar methods have been used to build brand loyalty and potentially make a particular product a household name. That’s how Epi-Pen became synonymous with epinephrine for the treatment of anaphylactic shock.
“There’s clearly some overlap” here between the pricing strategies used by naloxone manufacturers and Epi-Pen distributor Mylan, said Richard Evans, cofounder of SSR Health, which tracks the pharmaceutical industry.
But it’s not a perfect comparison. The presence of low-cost generics changes the calculus, he said, as does the different level of demand.
Nonprofit organizations and health care providers keenly feel the pressures of increasing demand and cost
Experts say price breaks on naloxone are not sufficient to cover the costs on the ground.
“Sixty-four thousand people lost their lives [nationally in 2016] — that’s someone every 12 minutes,” said Justin Phillips, executive director of Overdose Lifeline, an Indianapolis-based nonprofit. “Ten free kits is not going to be enough.”
Ms. Phillips said her organization relies on generic naloxone, which is the least expensive formulation. It’s the only feasible option, using dedicated grant money the group received from the state attorney general’s office as part of a program funded by a settlement with pharmaceutical companies.
But that money is almost dried up. “We need to be able to access naloxone – which I’m told is pennies to make – for the pennies it cost to make it,” she said.
Ms. Phillips, who worked with Dr. Adams when he ran Indiana’s health department, said she has discussed the need for naloxone funding with the surgeon general, but never its price.
Pharmacies assess the hurdles of distribution
Local pharmacies are key in this chain, but the overdose antidote is new territory for many pharmacists, said Randy Hitchens, the executive vice president of the Indiana Pharmacists Alliance. He said in 2015, when Adams began his push to get naloxone into the hands of drug users and their families, only one or two retail pharmacies carried it.
“This has always been an emergency room drug. Retail pharmacists typically were not used to dealing with [it],” Mr. Hitchens said. “A lot were probably saying, ‘What in the devil is naloxone?’”
Today, he estimates 60%-70% of Indiana’s more than 1,100 retail pharmacies carry the drug. Walgreens has committed to stocking Narcan.
Access, though, is always subject to retail pressures.
“If pharmacies are not seeing a steady stream coming in asking for it, they won’t be incentivized to carry it on their shelves,” said Daniel Raymond, the deputy director of policy and planning for the Harm Reduction Coalition.
A patchwork of other decentralized sources for naloxone exist: syringe-exchange vans, county and state health departments, churches and community centers, all trying to find ways to get overdose medication into the hands of people who need it.
That supply stream “meets people where they are,” Mr. Raymond said, but those little programs don’t have the muscle to negotiate discounted prices.
“Individual health programs are trying to navigate the crisis on their own, but when you see … growing demand and limited supply, it’s a role for federal intervention,” Mr. Raymond said.
He’d like to see the federal government step in to negotiate prices where smaller programs can’t.
Even as Congress crafts an opioid epidemic response package, it’s not clear it will tackle these concerns
In the House Energy and Commerce Committee, one bill being discussed would require all state Medicaid programs to cover at least one form of naloxone. Currently, not all state Medicaid programs do so.
A Senate bill would authorize $300 million annually to equip first responders with naloxone.
But critics say those approaches still don’t address the underlying problems: cost and funding.
“You can either make naloxone available, at a much discounted price, or we need to have a lot more resources in order to purchase it,” Dr. Wen said. “I don’t care which one. My only concern is the health and well-being of our residents.”
KHN’s coverage of prescription drug development, costs and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
This is an “unequivocally positive” step forward, said Leo Beletsky, an associate professor of law and health sciences at Northeastern University.
And not necessarily a surprise. Dr. Adams, who previously was Indiana’s health commissioner, was recruited to be the nation’s top doctor in part because of his work with then-Gov. Mike Pence, now the vice president. In Indiana, Dr. Adams pushed for harm-reduction approaches, which included expanded access to naloxone and the implementation of a needle exchange to combat the state’s much-publicized HIV outbreak, which began in 2015 and was linked to injection drug use.
Others cautioned, though, that his have-naloxone-will-carry recommendation is at best limited in what it can achieve, in part because the drug is relatively expensive.
Kaiser Health News breaks down what the advisory means, experts’ concerns, and what policy approaches may be in the pipeline.
Many public health advocates applaud the surgeon general’s position
Naloxone, which is a drug that can keep drug users alive by reversing opioid overdoses, is viewed by many as the cornerstone of the harm-reduction approach to the epidemic. Experts say people with addiction problems should carry it, and so should their family, friends and acquaintances.
“We want to put it more in reach,” said Traci Green, PhD, an associate professor of emergency medicine and community health sciences at Boston University, who has extensively researched the opioid abuse crisis. “It could not have been a better endorsement.”
Others, including Diane Goodman, who penned a recent Medscape commentary reflecting on the advisory, wonder whether this is a “rational” response to the scourge, since opioid addiction is one of many health problems people might encounter in everyday life and for which treatment options are still limited.
“I’m not sure it makes much more sense than any of us carrying a bottle of nitroglycerin to treat patients with end-stage angina,” wrote Ms. Goodman, an acute-care nurse practitioner.
“What, exactly, are we offering to addicts once their condition has been reversed?” she asked, noting that, without treatment and therapy programs that help wean people from addiction, “the odds of survival for any length of time remain low, no matter how much reversal medication is kept nearby.”
Results would likely be limited by naloxone’s price tag
Take Baltimore, which has been hit particularly hard by the opioid epidemic. Its health department already has pushed for more people to carry naloxone.
But the drug’s price is an issue, said Leana Wen, MD, the city’s health commissioner, and an emergency physician. She suggested that the federal government negotiate directly for a lower price, or give more money to organizations and agencies like hers so they can afford to maintain an adequate supply.
“Every day, people are calling us at the Baltimore City Health Department and requesting naloxone, and I have to tell them I can’t afford for them to have it,” Dr. Wen said.
The drug is available in generic form, which can be stored in a vial and injected via a needle, as well as in patented products, such as the nasal spray Narcan, sold by ADAPT Pharmaceuticals, and Kaleo’s Evzio, a talking auto-injector.
Generic naloxone costs $20-$40 per dose. Narcan, the nasal spray, costs $125 for a two-dose carton, according to ADAPT’s website. A two-pack of Evzio costs close to $4,000, according to GoodRx.
Health departments and first responders qualify for a discounted rate of $75 per carton of Narcan. Kaleo has made Evzio coupons available to consumers, so that some will not have a copay, and it advertises a discount for federal and state agencies.
Skeptics point out that similar methods have been used to build brand loyalty and potentially make a particular product a household name. That’s how Epi-Pen became synonymous with epinephrine for the treatment of anaphylactic shock.
“There’s clearly some overlap” here between the pricing strategies used by naloxone manufacturers and Epi-Pen distributor Mylan, said Richard Evans, cofounder of SSR Health, which tracks the pharmaceutical industry.
But it’s not a perfect comparison. The presence of low-cost generics changes the calculus, he said, as does the different level of demand.
Nonprofit organizations and health care providers keenly feel the pressures of increasing demand and cost
Experts say price breaks on naloxone are not sufficient to cover the costs on the ground.
“Sixty-four thousand people lost their lives [nationally in 2016] — that’s someone every 12 minutes,” said Justin Phillips, executive director of Overdose Lifeline, an Indianapolis-based nonprofit. “Ten free kits is not going to be enough.”
Ms. Phillips said her organization relies on generic naloxone, which is the least expensive formulation. It’s the only feasible option, using dedicated grant money the group received from the state attorney general’s office as part of a program funded by a settlement with pharmaceutical companies.
But that money is almost dried up. “We need to be able to access naloxone – which I’m told is pennies to make – for the pennies it cost to make it,” she said.
Ms. Phillips, who worked with Dr. Adams when he ran Indiana’s health department, said she has discussed the need for naloxone funding with the surgeon general, but never its price.
Pharmacies assess the hurdles of distribution
Local pharmacies are key in this chain, but the overdose antidote is new territory for many pharmacists, said Randy Hitchens, the executive vice president of the Indiana Pharmacists Alliance. He said in 2015, when Adams began his push to get naloxone into the hands of drug users and their families, only one or two retail pharmacies carried it.
“This has always been an emergency room drug. Retail pharmacists typically were not used to dealing with [it],” Mr. Hitchens said. “A lot were probably saying, ‘What in the devil is naloxone?’”
Today, he estimates 60%-70% of Indiana’s more than 1,100 retail pharmacies carry the drug. Walgreens has committed to stocking Narcan.
Access, though, is always subject to retail pressures.
“If pharmacies are not seeing a steady stream coming in asking for it, they won’t be incentivized to carry it on their shelves,” said Daniel Raymond, the deputy director of policy and planning for the Harm Reduction Coalition.
A patchwork of other decentralized sources for naloxone exist: syringe-exchange vans, county and state health departments, churches and community centers, all trying to find ways to get overdose medication into the hands of people who need it.
That supply stream “meets people where they are,” Mr. Raymond said, but those little programs don’t have the muscle to negotiate discounted prices.
“Individual health programs are trying to navigate the crisis on their own, but when you see … growing demand and limited supply, it’s a role for federal intervention,” Mr. Raymond said.
He’d like to see the federal government step in to negotiate prices where smaller programs can’t.
Even as Congress crafts an opioid epidemic response package, it’s not clear it will tackle these concerns
In the House Energy and Commerce Committee, one bill being discussed would require all state Medicaid programs to cover at least one form of naloxone. Currently, not all state Medicaid programs do so.
A Senate bill would authorize $300 million annually to equip first responders with naloxone.
But critics say those approaches still don’t address the underlying problems: cost and funding.
“You can either make naloxone available, at a much discounted price, or we need to have a lot more resources in order to purchase it,” Dr. Wen said. “I don’t care which one. My only concern is the health and well-being of our residents.”
KHN’s coverage of prescription drug development, costs and pricing is supported by the Laura and John Arnold Foundation. Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Henry J. Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
FDA panel recommends CBD for pediatric seizure disorders
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
Advisors to the Food and Drug Administration have found a generally favorable benefit-risk profile for cannabidiol oil solution in the treatment of two forms of severe pediatric seizure disorders. The drug is under expedited review by the agency.
If the FDA supports this recommendation, cannabidiol oral solution would be the first cannabis-based medication approved in the United States.
“At this point, this is a spectacular advance,” said committee member John Mendelson, MD, chief medical officer of Ria Health, San Francisco.
Fellow committee member Mark Green, MD, concurred. “It is clearly an honor to be making a decision based on science and public interest, rather than political discussion,” said Dr. Green, professor of neurology, anesthesiology, and rehabilitation medicine at Icahn School of Medicine, Mt Sinai, New York.
Patients with LGS taking cannabidiol oral solution at 20 mg/kg/day in two clinical trials saw a 42%-44% reduction in drop seizure frequency over a 14-week treatment period (P = .0047 and P = .0135, compared to placebo). A 50% reduction of drop seizure frequency was seen in 40% and 44% of LGS patients in the two clinical trials.![]()
For patients with DS, 20 mg/kg/day of cannabidiol oral solution resulted in a 39% decrease in convulsive seizure frequency during a 14-week treatment period (P less than .05). There was a numeric, but not statistically significant, increase in the number of DS patients who saw a 50% reduction in convulsive seizure frequency on this dose.
Sustained efficacy for both seizure disorders has been seen during an extended open-label follow-on study.
The potential for abuse of the non-psychoactive substance derived from cannabis plants was judged very low. Though animal studies didn’t yield a significant signal for abuse potential with cannabidiol oral solution, the fact that cannabis is currently a schedule I drug prompted the FDA to recommend a human abuse potential study.
From the totality of the studies, “We see little evidence that cannabidiol has meaningful abuse potential, even at supratherapeutic doses in adults,” said Katherine Bonson, PhD, a pharmacologist with the FDA’s Controlled Substance Staff, in the Office of the Center Director of the Center for Drug Evaluation and Research (CDER).
The committee also agreed with the FDA staff that the mild to moderate elevations in liver enzymes seen with cannabidiol oral solution administration can be managed with package labeling and patient monitoring.
Both the FDA and GW Pharmaceuticals, which seeks to market cannabidiol oral solution as Epidiolex, acknowledged that the cannabidiol oral solution was associated with a significant elevation in liver transaminases in some patients. In pooled data, 16.3% of patients taking the drug at the higher dose of 20 mg/kg/day experienced transaminase elevation greater than three times the upper limit of normal, compared with 0.9% of those taking placebo.
Concomitant use of valproic acid was associated with greater likelihood of transaminase elevation. In patients taking both valproic acid and cannabidiol oral solution at the higher dose, 13% experienced transaminase elevations over five times the upper limit of normal.
However, many patients had mild transaminase elevations at baseline, and most cases of transaminase elevation did not require discontinuation of cannabidiol oral solution. Both the sponsor and the FDA agreed that no cases of severe liver injury meeting Hy’s law criteria were seen during the clinical trials; the two cases of “hepatic failure” reported were not associated with elevated bilirubin or international normalized ratio (INR) levels.
The FDA staff clinical reviewer who presented the agency’s overview of liver safety did note one still-unknown factor.
“There are not enough patients exposed to this drug to know whether some might have a smoldering inflammatory response that might potentially – and I can only say potentially – cause a problem down the line,” said Lara Dimick-Santos, MD, of the Division of Gastroenterology and Inborn Errors Products of the Office of Drug Evaluation III, Office of New Drugs.
Advisory committee member Dr. Mendelson asked for long-term monitoring, noting that “we need to watch for long-term safety data because this is a novel drug.”
The FDA’s re-analysis of data from 3 randomized, double-blind, placebo-controlled trials agreed with the efficacy findings reported by GW Pharmaceuticals. Cannabidiol oral solution met its primary endpoint of a reduction in frequency of seizures in LGS and DS patients in all 3 pivotal clinical trials, showing a significant improvement in seizure control when added to standard of care antiepileptic drug therapy for patients with drug-resistant LGS and DS.
The safety evaluation was based on a total of 1,756 patients who were exposed to cannabidiol oral solution, “adequate exposure to allow for assessment of safety,” said Natalie Getzoff, MD, a clinical review in the CDER’s Division of Neurology Products. Though 20 deaths were seen in the study population, “overall, the causes of death were varied and not unexpected for the patient population, and not clearly linked to the drug,” she said. “At this point in our review, we have not identified any obstacles to approval.”
To be included in the clinical trials, LGS patients had to be 2-55 years old, using at least one antiepileptic drug and still having at least 8 drop seizures every 4 weeks and at least two drop seizures weekly. DS patients were aged 2-18 years old, also using at least one antiepileptic drug at baseline and having at least 4 convulsive seizures in a 4 week period.
A total of 235 patients with LGS and 88 patients with DS were enrolled in the clinical trials, and an additional 157 patients with LGS and 209 patients with DS were enrolled in the open-label extension study.
An expanded access program for individuals with refractory epilepsy is ongoing, and 684 patients have been enrolled to date, including 97 LGS patients and 64 DS patients.
The proposed indications for cannabidiol oral solution are for the adjunctive treatment of seizures associated with LGS and DS in patients 2 years of age and older. Initial dosing recommendations are to titrate to a dose of 10 mg/kg/day, with dose adjustments permissible up to 20 mg/kg/day depending on clinical response and tolerability. Cannabidiol received fast track designation in 2014, and rare pediatric designation for LGS and DS in 2017.
The FDA is not obligated to support the recommendations of its advisory committees, though it often does. The agency is slated to take action on cannabidiol oral solution by June.
This article was updated 4/19/18.
REPORTING FROM AN FDA ADVISORY COMMITTEE MEETING
Providers’ prior imaging patterns and ownership of equipment are strong predictors of low-value imaging
Background: For many common conditions, expert guidelines such as Choosing Wisely recommend against ordering specific low-value tests, yet overuse of these tests remains widespread, and unnecessary care may account for up to a third of all medical expenditures. Studies have demonstrated that there is considerable geographic variation in health care usage and higher overall imaging among clinicians who own imaging equipment. No prior study has assessed whether prior ordering patterns of low-value care predict future ordering patterns or whether providers who order low-value imaging in one clinical scenario are more likely to do so in another scenario.
Study design: Retrospective analysis of insurance claims data.
Setting: Medical claims data from a large U.S. commercial health insurer, inclusive of 29 million commercially insured members across all 50 states from January 2010 to December 2014.
Synopsis: Using the claims database, researchers created three unique study samples to examine clinician predictors of low-value imaging. The study involved outpatient visits by patients aged 18-64 years without red-flag symptoms. The first included 1,007,392 visits across 878,720 patients with acute, uncomplicated low-back pain. Physicians who ordered imaging for the prior patient with back pain were 1.8 times more likely to do so again. Similarly, in 492,804 visits by 417,010 patients with headache, clinicians who ordered imaging on the prior patient demonstrated a twofold higher odds of imaging. Physicians who practiced low-value ordering for one condition were 1.8 times more likely to do so for the other. Across all studies, imaging ownership was an independent predictor (odds ratio, 1.8).
As this study analyzed only claims data, some patients may have warranted imaging based on red-flag symptoms that were not documented. Hospitalists designing initiatives to reduce low-value testing should consider targeting specific providers with a history of low-value test use.
Bottom line: Among commercially insured patients, a clinician’s prior imaging pattern and ownership of imaging equipment were strong independent predictors of low-value back pain and headache imaging.
Citation: Hong AS et al. Clinician-level predictors for ordering low-value imaging. JAMA Intern Med. 2017 Nov 1;177(11):1577-85.

Background: For many common conditions, expert guidelines such as Choosing Wisely recommend against ordering specific low-value tests, yet overuse of these tests remains widespread, and unnecessary care may account for up to a third of all medical expenditures. Studies have demonstrated that there is considerable geographic variation in health care usage and higher overall imaging among clinicians who own imaging equipment. No prior study has assessed whether prior ordering patterns of low-value care predict future ordering patterns or whether providers who order low-value imaging in one clinical scenario are more likely to do so in another scenario.
Study design: Retrospective analysis of insurance claims data.
Setting: Medical claims data from a large U.S. commercial health insurer, inclusive of 29 million commercially insured members across all 50 states from January 2010 to December 2014.
Synopsis: Using the claims database, researchers created three unique study samples to examine clinician predictors of low-value imaging. The study involved outpatient visits by patients aged 18-64 years without red-flag symptoms. The first included 1,007,392 visits across 878,720 patients with acute, uncomplicated low-back pain. Physicians who ordered imaging for the prior patient with back pain were 1.8 times more likely to do so again. Similarly, in 492,804 visits by 417,010 patients with headache, clinicians who ordered imaging on the prior patient demonstrated a twofold higher odds of imaging. Physicians who practiced low-value ordering for one condition were 1.8 times more likely to do so for the other. Across all studies, imaging ownership was an independent predictor (odds ratio, 1.8).
As this study analyzed only claims data, some patients may have warranted imaging based on red-flag symptoms that were not documented. Hospitalists designing initiatives to reduce low-value testing should consider targeting specific providers with a history of low-value test use.
Bottom line: Among commercially insured patients, a clinician’s prior imaging pattern and ownership of imaging equipment were strong independent predictors of low-value back pain and headache imaging.
Citation: Hong AS et al. Clinician-level predictors for ordering low-value imaging. JAMA Intern Med. 2017 Nov 1;177(11):1577-85.
Background: For many common conditions, expert guidelines such as Choosing Wisely recommend against ordering specific low-value tests, yet overuse of these tests remains widespread, and unnecessary care may account for up to a third of all medical expenditures. Studies have demonstrated that there is considerable geographic variation in health care usage and higher overall imaging among clinicians who own imaging equipment. No prior study has assessed whether prior ordering patterns of low-value care predict future ordering patterns or whether providers who order low-value imaging in one clinical scenario are more likely to do so in another scenario.
Study design: Retrospective analysis of insurance claims data.
Setting: Medical claims data from a large U.S. commercial health insurer, inclusive of 29 million commercially insured members across all 50 states from January 2010 to December 2014.
Synopsis: Using the claims database, researchers created three unique study samples to examine clinician predictors of low-value imaging. The study involved outpatient visits by patients aged 18-64 years without red-flag symptoms. The first included 1,007,392 visits across 878,720 patients with acute, uncomplicated low-back pain. Physicians who ordered imaging for the prior patient with back pain were 1.8 times more likely to do so again. Similarly, in 492,804 visits by 417,010 patients with headache, clinicians who ordered imaging on the prior patient demonstrated a twofold higher odds of imaging. Physicians who practiced low-value ordering for one condition were 1.8 times more likely to do so for the other. Across all studies, imaging ownership was an independent predictor (odds ratio, 1.8).
As this study analyzed only claims data, some patients may have warranted imaging based on red-flag symptoms that were not documented. Hospitalists designing initiatives to reduce low-value testing should consider targeting specific providers with a history of low-value test use.
Bottom line: Among commercially insured patients, a clinician’s prior imaging pattern and ownership of imaging equipment were strong independent predictors of low-value back pain and headache imaging.
Citation: Hong AS et al. Clinician-level predictors for ordering low-value imaging. JAMA Intern Med. 2017 Nov 1;177(11):1577-85.
What is HIPEC?
Ovarian cancer most commonly follows a pattern of intraperitoneal spread, and even in the setting of bulky extra-ovarian disease, it can be thought of as being largely localized to the peritoneal compartment. This forms some of the rationale for performing extensive cytoreductive surgery (CRS) on ovarian cancer metastatic within the peritoneal cavity, and also some of the rationale for delivery of cytotoxic therapy directly to this compartment (intraperitoneal or “IP” chemotherapy). To be most effective, IP chemotherapy should be able to contact all peritoneal surfaces and be exposed to very low volume tumors (ideally no thicker than 2-mm implants).

There is a large body of evidence demonstrating the benefits of conventional IP chemotherapy in women who have received complete or “optimal” CRS to disease measuring less than 1 cm3.1 However, IP chemotherapy is complicated by difficult administration and can be difficult for patients to tolerate. It is associated with significant toxicity, more so than what is seen from intravenous chemotherapy, and this toxicity is drawn out over the 18 (or more) weeks of therapy. It requires placement of an intraperitoneal port, and there are many problems associated with this foreign body including infection, malposition, and even erosions into underlying visceral structures. There are also concerns regarding the ability of the intraperitoneal infusions to reach all peritoneal surfaces when postoperative adhesions may have formed to pocket-off areas of the peritoneal cavity.
Hyperthermic intraperitoneal chemotherapy (HIPEC), at the time of CRS, is a strategy that has been explored to overcome some of these challenges.2 HIPEC has the most history as an adjunct to the surgical management of gastrointestinal cancers (particularly appendiceal and colorectal). The technique first described by Dr. Paul H. Sugarbaker for gastrointestinal tumors remains similar to that performed in ovarian cancer.3 Patients first undergo extensive CRS until there is no macroscopic residual disease. Immediately following cytoreduction, catheters are placed into the peritoneal cavity, the main incision is temporarily closed (to prevent spillage), and an infusion of cytotoxic agents (commonly cisplatin, often with a second agent such as mitomycin C or doxorubicin) is warmed and then distilled into the peritoneal cavity until it is “moderately distended.” The patient’s body is then rolled back and forth to “wash” down the entire peritoneal cavity. All peritoneal surfaces can be touched by the agent as this procedure is happening intraoperatively prior to adhesion formation.
The “H” in HIPEC stands for hyperthermic, which is a key differentiator from traditional intraperitoneal and intravenous chemotherapy administration. Some chemotherapy agents, such as cisplatin, have a synergistic effect with hyperthermia. Some of these effects include increased oxygen free radical formation, increased cellular uptake of drug, reversal of mechanisms of drug resistance, and increases in DNA damage. The ideal range of hyperthermia is between 41° C and 44° C. At higher temperatures, infusions rates can be faster; however, higher temperatures are associated with more toxicity, particularly of the small bowel.4
Toxicity is a concern with HIPEC.5 Cytoreductive surgery for ovarian cancer can be associated with substantial morbidity, and exposing patients to prolonged operative time, extended periods of hyperthermia, and high doses of cytotoxic agents is a concern. When performed by high volume, experienced practitioners, approximately 12% of patients experience serious (grade 3-5) toxicity after CRS with HIPEC, with a procedure-related mortality of 1.2%. The majority of major toxicities were bone marrow suppression and nephrotoxicity (which in some cases can result in patients requiring hemodialysis in the immediate postoperative period). It is for this reason that most HIPEC protocols include a routine ICU admission postoperatively to closely monitor patients for major renal toxicity and electrolyte disturbances. These complications are associated with higher doses of administered cisplatin. Febrile neutropenia and gastrointestinal complications (such as bowel perforation, fistula, or anastomotic leak) also comprise the most common major toxicities. Patient factors to consider as higher risk for morbidity and mortality include underlying cardiac or pulmonary disease, poor performance status, extreme obesity, and preexisting renal disease.
While the history of HIPEC was focused around the treatment of GI peritoneal malignancies, in more recent years, the technique has been applied and studied in women with ovarian cancer.
The indications for use can vary from the upfront setting (at the time of primary CRS), following neoadjuvant chemotherapy (at the time of interval CRS), or in the recurrent setting (at the time of secondary CRS).2 Possibly the most compelling study exploring HIPEC in ovarian cancer was published earlier this year in the New England Journal of Medicine.6 This study explored the use of HIPEC at the time of interval CRS following three cycles of neoadjuvant platinum and taxane intravenous chemotherapy. Two hundred and forty-five patients were randomly assigned at the time of optimal interval CRS to either CRS alone or CRS with HIPEC with cisplatin administered over 90 minutes. All patients received three additional cycles of intravenous platinum and taxane chemotherapy. Death was observed in a significantly higher proportion of patients in the non-HIPEC group (62% versus 50%). HIPEC was associated with a hazard ratio for death of 0.67 (P = .02). In this study, a similar number of severe adverse outcomes were observed in the two groups, though specific information was lacking, particularly with respect to renal toxicity.
These findings are intriguing and have energized interest in HIPEC by many gynecologic oncology providers; however, there are some concerns regarding the results. Patients in this study received not one intervention, but in fact three interventions (hyperthermia, an additional cycle of chemotherapy, and the peritoneal administration of chemotherapy). Any one of these three variables could explain the outcomes and it is difficult to know if all three (in the form of HIPEC) are necessary to see this observed benefit. Others have questioned the finding of no added toxicity when HIPEC is applied. This is inconsistent with what has been presented elsewhere. It is unclear from the data whether or not the nephrotoxicity was comparable between the two groups or more severe among those who received HIPEC.
An additional concern regarding HIPEC is the feasibility. Additional operative times (by up to 90 minutes), increased duration of hospitalization (including ICU admission), and additional equipment and specialized personnel are required for this technique. This may further hinder its uptake and routine practice. In the meantime, we continue to await further clinical trials that will better define the ovarian cancer patient population who might benefit from this technique and provide further data regarding its risk/benefit profile.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Armstrong DK et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354:34-43.
2. Helm CW et al. Hyperthermic intraperitoneal chemotherapy with and without cytoreductive surgery for epithelial ovarian cancer. J Surg Oncol. 2008;98(4):283-90.
3. Glehen O et al. Hyperthermic intraperitoneal chemotherapy: nomenclature and modalities of perfusion. J Surg Oncol. 2008;98(4):242-6.
4. Kusamura S et al. Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy. J Surg Oncol. 2008;98(4):247-52.
5. Kusamura S et al. Impact of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy on systemic toxicity. Ann Surg Oncol. 2007;14(9):2550-8.
6. van Driel WJ et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N Engl J Med. 2018 Jan;378(3):230-240.
Ovarian cancer most commonly follows a pattern of intraperitoneal spread, and even in the setting of bulky extra-ovarian disease, it can be thought of as being largely localized to the peritoneal compartment. This forms some of the rationale for performing extensive cytoreductive surgery (CRS) on ovarian cancer metastatic within the peritoneal cavity, and also some of the rationale for delivery of cytotoxic therapy directly to this compartment (intraperitoneal or “IP” chemotherapy). To be most effective, IP chemotherapy should be able to contact all peritoneal surfaces and be exposed to very low volume tumors (ideally no thicker than 2-mm implants).
There is a large body of evidence demonstrating the benefits of conventional IP chemotherapy in women who have received complete or “optimal” CRS to disease measuring less than 1 cm3.1 However, IP chemotherapy is complicated by difficult administration and can be difficult for patients to tolerate. It is associated with significant toxicity, more so than what is seen from intravenous chemotherapy, and this toxicity is drawn out over the 18 (or more) weeks of therapy. It requires placement of an intraperitoneal port, and there are many problems associated with this foreign body including infection, malposition, and even erosions into underlying visceral structures. There are also concerns regarding the ability of the intraperitoneal infusions to reach all peritoneal surfaces when postoperative adhesions may have formed to pocket-off areas of the peritoneal cavity.
Hyperthermic intraperitoneal chemotherapy (HIPEC), at the time of CRS, is a strategy that has been explored to overcome some of these challenges.2 HIPEC has the most history as an adjunct to the surgical management of gastrointestinal cancers (particularly appendiceal and colorectal). The technique first described by Dr. Paul H. Sugarbaker for gastrointestinal tumors remains similar to that performed in ovarian cancer.3 Patients first undergo extensive CRS until there is no macroscopic residual disease. Immediately following cytoreduction, catheters are placed into the peritoneal cavity, the main incision is temporarily closed (to prevent spillage), and an infusion of cytotoxic agents (commonly cisplatin, often with a second agent such as mitomycin C or doxorubicin) is warmed and then distilled into the peritoneal cavity until it is “moderately distended.” The patient’s body is then rolled back and forth to “wash” down the entire peritoneal cavity. All peritoneal surfaces can be touched by the agent as this procedure is happening intraoperatively prior to adhesion formation.
The “H” in HIPEC stands for hyperthermic, which is a key differentiator from traditional intraperitoneal and intravenous chemotherapy administration. Some chemotherapy agents, such as cisplatin, have a synergistic effect with hyperthermia. Some of these effects include increased oxygen free radical formation, increased cellular uptake of drug, reversal of mechanisms of drug resistance, and increases in DNA damage. The ideal range of hyperthermia is between 41° C and 44° C. At higher temperatures, infusions rates can be faster; however, higher temperatures are associated with more toxicity, particularly of the small bowel.4
Toxicity is a concern with HIPEC.5 Cytoreductive surgery for ovarian cancer can be associated with substantial morbidity, and exposing patients to prolonged operative time, extended periods of hyperthermia, and high doses of cytotoxic agents is a concern. When performed by high volume, experienced practitioners, approximately 12% of patients experience serious (grade 3-5) toxicity after CRS with HIPEC, with a procedure-related mortality of 1.2%. The majority of major toxicities were bone marrow suppression and nephrotoxicity (which in some cases can result in patients requiring hemodialysis in the immediate postoperative period). It is for this reason that most HIPEC protocols include a routine ICU admission postoperatively to closely monitor patients for major renal toxicity and electrolyte disturbances. These complications are associated with higher doses of administered cisplatin. Febrile neutropenia and gastrointestinal complications (such as bowel perforation, fistula, or anastomotic leak) also comprise the most common major toxicities. Patient factors to consider as higher risk for morbidity and mortality include underlying cardiac or pulmonary disease, poor performance status, extreme obesity, and preexisting renal disease.
While the history of HIPEC was focused around the treatment of GI peritoneal malignancies, in more recent years, the technique has been applied and studied in women with ovarian cancer.
The indications for use can vary from the upfront setting (at the time of primary CRS), following neoadjuvant chemotherapy (at the time of interval CRS), or in the recurrent setting (at the time of secondary CRS).2 Possibly the most compelling study exploring HIPEC in ovarian cancer was published earlier this year in the New England Journal of Medicine.6 This study explored the use of HIPEC at the time of interval CRS following three cycles of neoadjuvant platinum and taxane intravenous chemotherapy. Two hundred and forty-five patients were randomly assigned at the time of optimal interval CRS to either CRS alone or CRS with HIPEC with cisplatin administered over 90 minutes. All patients received three additional cycles of intravenous platinum and taxane chemotherapy. Death was observed in a significantly higher proportion of patients in the non-HIPEC group (62% versus 50%). HIPEC was associated with a hazard ratio for death of 0.67 (P = .02). In this study, a similar number of severe adverse outcomes were observed in the two groups, though specific information was lacking, particularly with respect to renal toxicity.
These findings are intriguing and have energized interest in HIPEC by many gynecologic oncology providers; however, there are some concerns regarding the results. Patients in this study received not one intervention, but in fact three interventions (hyperthermia, an additional cycle of chemotherapy, and the peritoneal administration of chemotherapy). Any one of these three variables could explain the outcomes and it is difficult to know if all three (in the form of HIPEC) are necessary to see this observed benefit. Others have questioned the finding of no added toxicity when HIPEC is applied. This is inconsistent with what has been presented elsewhere. It is unclear from the data whether or not the nephrotoxicity was comparable between the two groups or more severe among those who received HIPEC.
An additional concern regarding HIPEC is the feasibility. Additional operative times (by up to 90 minutes), increased duration of hospitalization (including ICU admission), and additional equipment and specialized personnel are required for this technique. This may further hinder its uptake and routine practice. In the meantime, we continue to await further clinical trials that will better define the ovarian cancer patient population who might benefit from this technique and provide further data regarding its risk/benefit profile.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Armstrong DK et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354:34-43.
2. Helm CW et al. Hyperthermic intraperitoneal chemotherapy with and without cytoreductive surgery for epithelial ovarian cancer. J Surg Oncol. 2008;98(4):283-90.
3. Glehen O et al. Hyperthermic intraperitoneal chemotherapy: nomenclature and modalities of perfusion. J Surg Oncol. 2008;98(4):242-6.
4. Kusamura S et al. Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy. J Surg Oncol. 2008;98(4):247-52.
5. Kusamura S et al. Impact of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy on systemic toxicity. Ann Surg Oncol. 2007;14(9):2550-8.
6. van Driel WJ et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N Engl J Med. 2018 Jan;378(3):230-240.
Ovarian cancer most commonly follows a pattern of intraperitoneal spread, and even in the setting of bulky extra-ovarian disease, it can be thought of as being largely localized to the peritoneal compartment. This forms some of the rationale for performing extensive cytoreductive surgery (CRS) on ovarian cancer metastatic within the peritoneal cavity, and also some of the rationale for delivery of cytotoxic therapy directly to this compartment (intraperitoneal or “IP” chemotherapy). To be most effective, IP chemotherapy should be able to contact all peritoneal surfaces and be exposed to very low volume tumors (ideally no thicker than 2-mm implants).
There is a large body of evidence demonstrating the benefits of conventional IP chemotherapy in women who have received complete or “optimal” CRS to disease measuring less than 1 cm3.1 However, IP chemotherapy is complicated by difficult administration and can be difficult for patients to tolerate. It is associated with significant toxicity, more so than what is seen from intravenous chemotherapy, and this toxicity is drawn out over the 18 (or more) weeks of therapy. It requires placement of an intraperitoneal port, and there are many problems associated with this foreign body including infection, malposition, and even erosions into underlying visceral structures. There are also concerns regarding the ability of the intraperitoneal infusions to reach all peritoneal surfaces when postoperative adhesions may have formed to pocket-off areas of the peritoneal cavity.
Hyperthermic intraperitoneal chemotherapy (HIPEC), at the time of CRS, is a strategy that has been explored to overcome some of these challenges.2 HIPEC has the most history as an adjunct to the surgical management of gastrointestinal cancers (particularly appendiceal and colorectal). The technique first described by Dr. Paul H. Sugarbaker for gastrointestinal tumors remains similar to that performed in ovarian cancer.3 Patients first undergo extensive CRS until there is no macroscopic residual disease. Immediately following cytoreduction, catheters are placed into the peritoneal cavity, the main incision is temporarily closed (to prevent spillage), and an infusion of cytotoxic agents (commonly cisplatin, often with a second agent such as mitomycin C or doxorubicin) is warmed and then distilled into the peritoneal cavity until it is “moderately distended.” The patient’s body is then rolled back and forth to “wash” down the entire peritoneal cavity. All peritoneal surfaces can be touched by the agent as this procedure is happening intraoperatively prior to adhesion formation.
The “H” in HIPEC stands for hyperthermic, which is a key differentiator from traditional intraperitoneal and intravenous chemotherapy administration. Some chemotherapy agents, such as cisplatin, have a synergistic effect with hyperthermia. Some of these effects include increased oxygen free radical formation, increased cellular uptake of drug, reversal of mechanisms of drug resistance, and increases in DNA damage. The ideal range of hyperthermia is between 41° C and 44° C. At higher temperatures, infusions rates can be faster; however, higher temperatures are associated with more toxicity, particularly of the small bowel.4
Toxicity is a concern with HIPEC.5 Cytoreductive surgery for ovarian cancer can be associated with substantial morbidity, and exposing patients to prolonged operative time, extended periods of hyperthermia, and high doses of cytotoxic agents is a concern. When performed by high volume, experienced practitioners, approximately 12% of patients experience serious (grade 3-5) toxicity after CRS with HIPEC, with a procedure-related mortality of 1.2%. The majority of major toxicities were bone marrow suppression and nephrotoxicity (which in some cases can result in patients requiring hemodialysis in the immediate postoperative period). It is for this reason that most HIPEC protocols include a routine ICU admission postoperatively to closely monitor patients for major renal toxicity and electrolyte disturbances. These complications are associated with higher doses of administered cisplatin. Febrile neutropenia and gastrointestinal complications (such as bowel perforation, fistula, or anastomotic leak) also comprise the most common major toxicities. Patient factors to consider as higher risk for morbidity and mortality include underlying cardiac or pulmonary disease, poor performance status, extreme obesity, and preexisting renal disease.
While the history of HIPEC was focused around the treatment of GI peritoneal malignancies, in more recent years, the technique has been applied and studied in women with ovarian cancer.
The indications for use can vary from the upfront setting (at the time of primary CRS), following neoadjuvant chemotherapy (at the time of interval CRS), or in the recurrent setting (at the time of secondary CRS).2 Possibly the most compelling study exploring HIPEC in ovarian cancer was published earlier this year in the New England Journal of Medicine.6 This study explored the use of HIPEC at the time of interval CRS following three cycles of neoadjuvant platinum and taxane intravenous chemotherapy. Two hundred and forty-five patients were randomly assigned at the time of optimal interval CRS to either CRS alone or CRS with HIPEC with cisplatin administered over 90 minutes. All patients received three additional cycles of intravenous platinum and taxane chemotherapy. Death was observed in a significantly higher proportion of patients in the non-HIPEC group (62% versus 50%). HIPEC was associated with a hazard ratio for death of 0.67 (P = .02). In this study, a similar number of severe adverse outcomes were observed in the two groups, though specific information was lacking, particularly with respect to renal toxicity.
These findings are intriguing and have energized interest in HIPEC by many gynecologic oncology providers; however, there are some concerns regarding the results. Patients in this study received not one intervention, but in fact three interventions (hyperthermia, an additional cycle of chemotherapy, and the peritoneal administration of chemotherapy). Any one of these three variables could explain the outcomes and it is difficult to know if all three (in the form of HIPEC) are necessary to see this observed benefit. Others have questioned the finding of no added toxicity when HIPEC is applied. This is inconsistent with what has been presented elsewhere. It is unclear from the data whether or not the nephrotoxicity was comparable between the two groups or more severe among those who received HIPEC.
An additional concern regarding HIPEC is the feasibility. Additional operative times (by up to 90 minutes), increased duration of hospitalization (including ICU admission), and additional equipment and specialized personnel are required for this technique. This may further hinder its uptake and routine practice. In the meantime, we continue to await further clinical trials that will better define the ovarian cancer patient population who might benefit from this technique and provide further data regarding its risk/benefit profile.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Armstrong DK et al. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med. 2006;354:34-43.
2. Helm CW et al. Hyperthermic intraperitoneal chemotherapy with and without cytoreductive surgery for epithelial ovarian cancer. J Surg Oncol. 2008;98(4):283-90.
3. Glehen O et al. Hyperthermic intraperitoneal chemotherapy: nomenclature and modalities of perfusion. J Surg Oncol. 2008;98(4):242-6.
4. Kusamura S et al. Drugs, carrier solutions and temperature in hyperthermic intraperitoneal chemotherapy. J Surg Oncol. 2008;98(4):247-52.
5. Kusamura S et al. Impact of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy on systemic toxicity. Ann Surg Oncol. 2007;14(9):2550-8.
6. van Driel WJ et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. N Engl J Med. 2018 Jan;378(3):230-240.