User login
Biomechanical Evaluation of a Novel Suture Augment in Patella Fixation
Take-Home Points
- Suture augmentation improves construct strength for patella fixation.
- Krackow sutures may be placed in the quadriceps and patella tendons, then secured over the anterior patella (much like an anterior tension band).
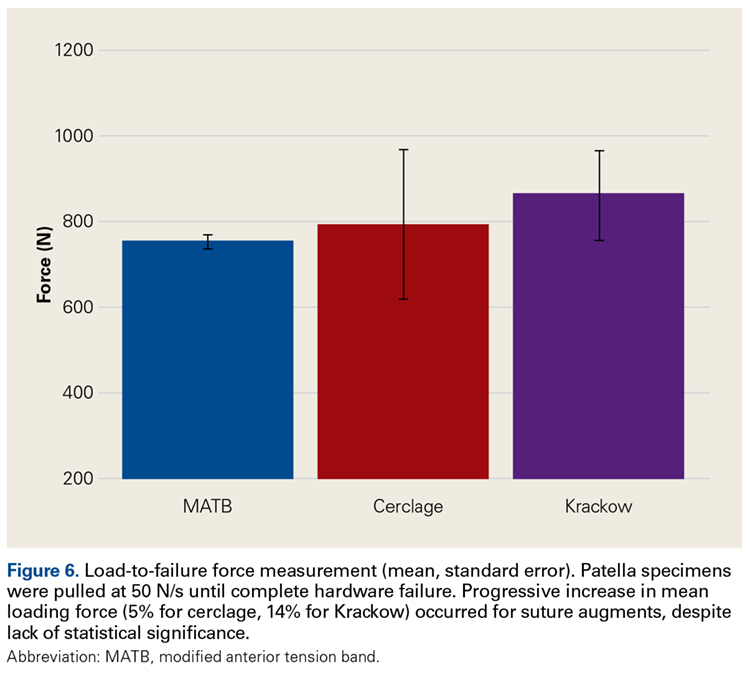
- The Krackow technique described was superior to the suture cerclage technique based on mean load values, but did not reach statistical significance.
- The Krackow suture technique is a viable and easily applied technique for suture augmentation of patella fixation constructs.
Patella fractures are relatively uncommon, accounting for only 1% of skeletal injuries.1 Restoration of the function of the patella and the extensor mechanism is vital for knee extension and gait. However, patella fractures have an inherently high rate of complications, making these injuries challenging to treat.2-4 In patients with intact extensor function, displacement of <4 mm, and articular step-off of <3 mm, nonoperative management is extremely effective, with 99% of patients reporting favorable results.5 However, for fractures in which the extensor mechanism is disrupted, surgical intervention typically is indicated.6
Authors have reported various surgical interventions, one of the most commonly used being the anterior tension band (ATB) technique, first described by the AO (Arbeitsgemeinschaft für Osteosynthesefragen) group in the 1950s.7 By converting distractive anterior force during knee flexion to compressive force at the fracture site, the ATB technique provides a repair stronger than the previously used cerclage repair.8 Although initially considered standard of care, the ATB technique was soon found to be associated with implant failure and subcutaneous irritation prompting implant removal.9
To address these issues, Berg10 and Carpenter and colleagues11 evaluated an ATB technique that used cannulated screws instead of Kirschner wires (K-wires). This variation on the ATB technique reduced the implant-related issues while maintaining the mechanical advantage of the tension band. The more rigid design also permitted earlier postoperative rehabilitation, which significantly reduced development of arthrofibrosis.6,7,10 This modified ATB (MATB) technique has since been investigated for additional augments, mainly focusing on use of different tension band materials, including polyester suture and braided composite suture.12-14
However, there is little research on augments that incorporate the surrounding soft tissue, specifically the quadriceps and patellar tendons. In a recent retrospective clinical study, Oh and colleagues15 found positive clinical results with use of Krackow sutures, though 2 or 3 vertically oriented stainless steel wires were used instead of cannulated screws.
We conducted a study to determine the biomechanical efficacy of using a cerclage suture augment and a Krackow suture augment coupled with and compared with conventional MATB repair. If effective, this technique may represent another strategy for increasing repair strength and thereby improve postoperative outcomes.
Materials and Methods
Specimen Preparation
Fresh-frozen cadaver extensor mechanisms (quadriceps tendon, patella, surrounding retinaculum, patellar tendon) were kept frozen at –4°C until preparation. Fifteen specimens were selected. Mean (SD) age at death was 68 (10) years (range, 51-85 years). One specimen was excluded for a short patella tendon, which precluded adequate attachment for testing. All specimens were free of overt osseous pathology.
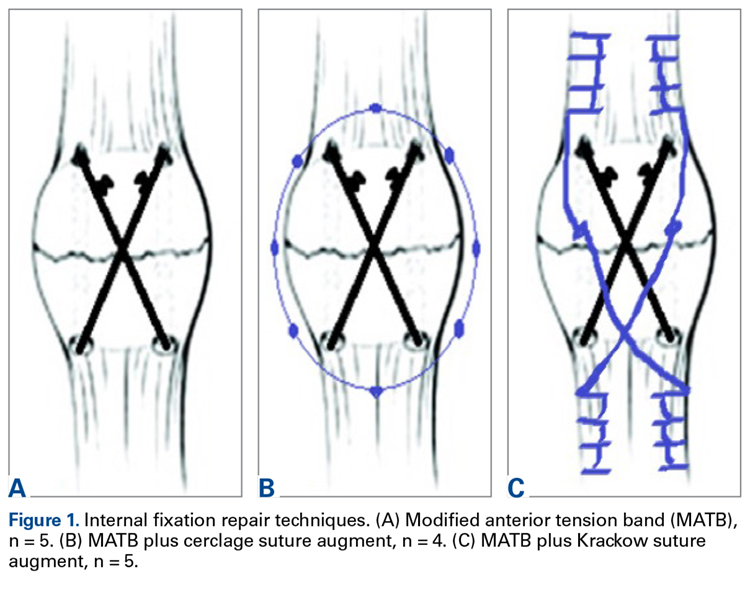
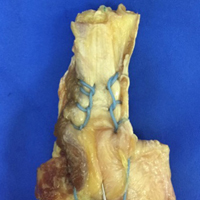
After specimens were thawed overnight, the patellae were transversely osteotomized with an osteotome at the junction of the middle and distal thirds of the patella. Sharp dissection was performed to carry the division through the medial and lateral retinaculum at the same level. All 14 specimens were then repaired using the MATB technique. First, the transverse fracture was reduced with a reduction clamp. Then, two 4-mm cannulated screws (DePuy Synthes) were inserted parallel to each other and perpendicular to the fracture. An 18-gauge stainless steel wire was then passed through each screw, crossed anteriorly, and tightened to create a figure-of-8 ATB. The specimens were then randomly divided into 3 groups—MATB; MATB with cerclage suture augment; MATB with Krackow suture augment—while ensuring specimens from a single cadaver were placed in different groups to avoid confounding based on bone density differences.
Experimental Setup
Repaired specimens were secured with tissue clamps at the quadriceps and patellar tendons on an MTS Bionix 858 (MTS Systems) hydraulic arm.

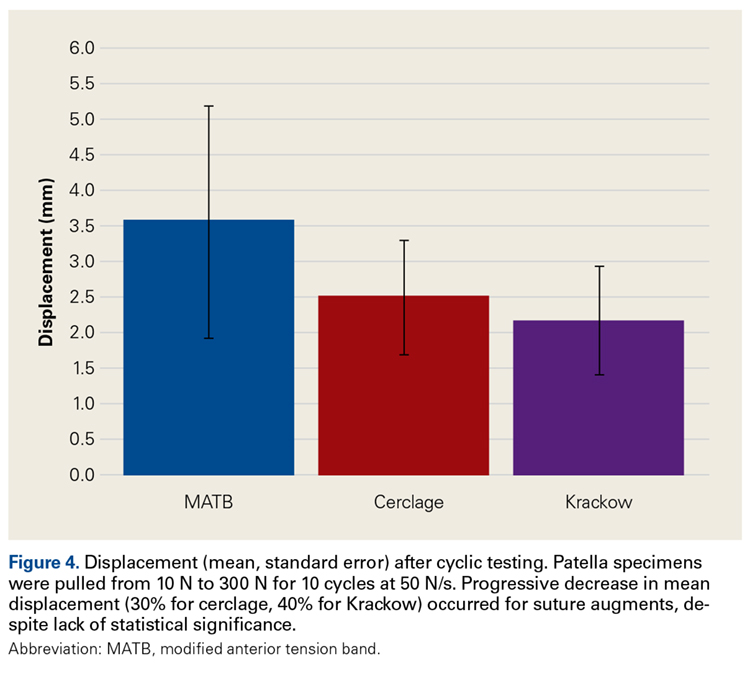
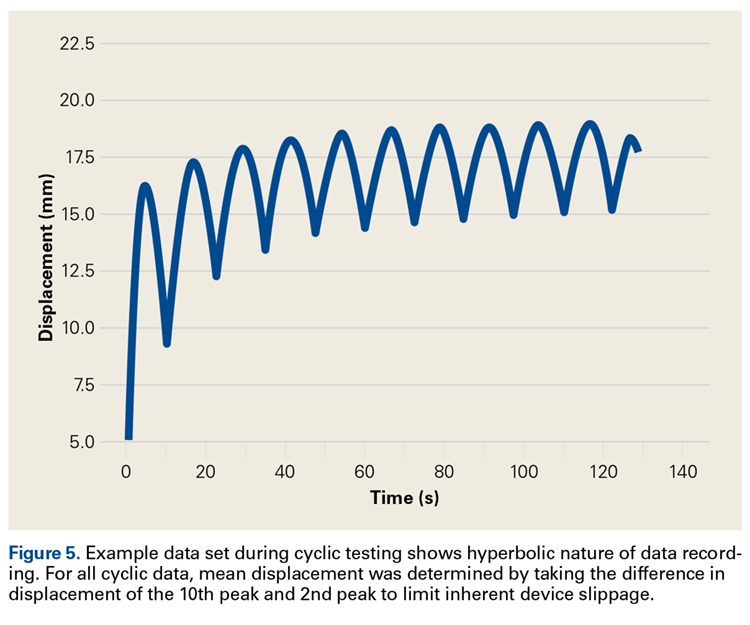
Each patella was secured for cyclic testing. Initially it was placed under 10 N of tension. Then it underwent tensile loading from 10 N to 300 N at 50 N/s for 10 cycles. These parameters were based on previous biomechanical patella studies.10,11 Load was measured with the MTS load cell and displacement with the displacement transducer. Fracture displacement associated with 300-N cyclic tension was recorded. Displacement was calculated as the difference between 10th cycle and 2nd cycle values, which accounted for any degree of initial tissue slippage. After cyclic testing, the patella was placed back in 10 N of tensile loading and subjected to maximum force loading to determine ultimate repair strength. For maximum loading, the patella was stretched progressively at 50 N/s until failure. Again, load and displacement were measured with MTS.
Statistical Analysis
After testing, fracture displacement and maximum load force data were compiled for analysis. One-way analysis of variance with Bonferroni correction was used to determine if there were significant differences between groups. Significance level was set at P < .05.
Results
For cyclic testing, mean total displacement was measured over 10 cycles for each group. Again, displacement was determined by taking the difference between 10th cycle and 2nd cycle values, allowing for system stabilization.
Discussion
Our main objective was to compare the efficacy of a novel suture augment technique with that of other patella fracture repair techniques. Our hypothesis—that adding a Krackow suture augment would increase strength in both cyclic and maximum loading—was supported. Although testing results were not statistically significant because of the small sample size, we think this novel technique has clinically relevant descriptive significance and warrants further investigation.
Proper anatomical reduction and postoperative stabilization are of utmost importance in clinical approaches to patella fractures. In addition, regardless of which technical procedure is used, open reduction should also allow for early range of motion to prevent joint arthrofibrosis. Ever since the ATB technique was first described by the AO group, postoperative outcomes have improved significantly. In a retrospective study by Levack and colleagues,17 30 of 64 patients with patella fractures underwent internal fixation. Mean follow-up was 6.2 years. By both objective and subjective measures, the best functional outcomes were associated with internal tension band fixation (vs cerclage repair). Lotke and Ecker18 also documented the efficacy of the tension band technique. Sixteen patients with patella fractures underwent anterior tension banding; those with a comminuted fracture also underwent cerclage repair for patella stabilization during tension banding. At 6-week follow-up, all patients had good range of motion (≥90° flexion), relatively few symptoms, and no implant failures. Results were similar to those of Levack and colleagues.17
Although it improves stability and functional outcomes over conventional patellectomy and cerclage wiring, the ATB technique has been associated with subcutaneous irritation caused by the K-wires used to secure the band. Hung and colleagues9 followed up 68 patients with patellar fractures. Five of these patients underwent tension banding. Although there was a high level of adequate functional outcomes, implant irritation was found to be “quite frequent.”
To address this issue, Carpenter and colleagues11 evaluated an ATB technique that uses K-wires instead of cannulated screws. Biomechanical testing in a cadaver model revealed less fracture displacement and overall more repair strength through cyclic and maximum load testing. Clinically, these results were supported by Berg,10 who followed up 10 patients with transverse patella fractures repaired with the MATB technique. At a mean follow-up of 24 months, 7 of the 10 patients had good to excellent outcomes, and there were no implant failures.
Further investigation into patella repairs has mainly focused on improving the MATB technique and experimenting with different tension band materials. Rabalais and colleagues13 biomechanically tested high-strength polyethylene suture as a replacement for standard 18-gauge wire, and Bryant and colleagues14 tested a braided composite suture (FiberWire; Arthrex) as a replacement for standard 18-gauge stainless steel wire. Both found no significant difference with use of augmented tension band material, but Rabalais and colleagues13 did find more advantages with a parallel tension band construct than with a standard figure-of-8 arrangement.
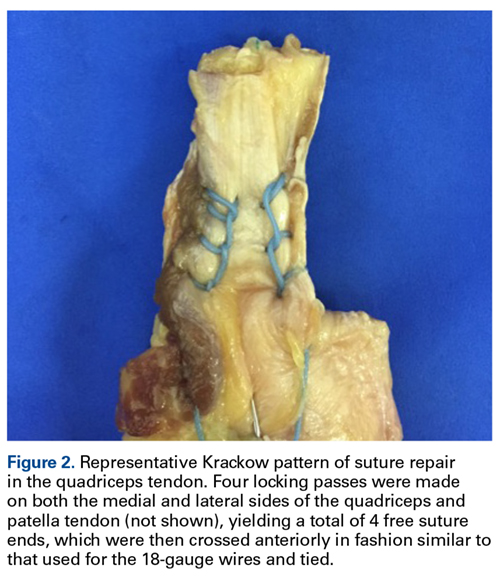
In developing our novel technique, we considered that Krackow sutures are routinely used in both quadriceps tendon repair and patellar tendon repair, including partial patellectomy for distal patella fracture. With a suture placed in both tendons, the augment could be expected to resist longitudinal gapping and augment the tension band across the anterior patella. First described by Krackow and colleagues,19 the Krackow suture is widely used for tendon reconstruction. In an interlocking system of sutures, the Krackow suture provides a repair that is more stable than repair with conventional suture techniques, specifically in the context of tendon repair.20 Given the sesamoidal nature of the patella, its repair shares the goal of gap prevention with other tendon repairs. In theory, anchoring the supporting structures that are above and below the patella provides support for the intervening patella and ultimately improves fracture fixation strength.
Oh and colleagues15 reported on the clinical efficacy of a Krackow augment in distal pole patella repairs. Similarly, we found a Krackow augment to be efficacious, supporting its potential in clinical approaches to patella repairs. Our results indicate this augment can be a useful clinical adjunct in biomechanical evaluation.
Limitations of this study include its use of dissected extensor mechanisms, which may have less biofidelity than whole-knee specimens. In our model, specimens were secured at the patellar tendon and the quadriceps tendons, as opposed to the quadriceps tendon and the tibia distally. Use of this model could have led to an increase in early displacement during cyclic testing as a result of tissue slippage. Furthermore, our small sample size could have affected our ability to demonstrate a difference between these techniques.
Given its increased strength as demonstrated by mean displacement during cyclic loading and mean load to failure, as well as the early clinical data recently published, the Krackow suture augment represents a feasible technique for patella fixation. It likely will be most useful in cases in which conventional techniques are prone to failure or cannot be applied, such as severe distal comminution or poor bone density. Further biomechanical testing with a larger number of specimens may be required for statistical significance.
Conclusion
In patella fracture repair strategies, the Krackow suture augment increased strength when used with a MATB technique. Failure to reach statistical significance likely resulted from our small sample size. Further biomechanical testing and clinical studies are needed for more complete evaluation of this technique. We think it will be most useful in the setting of poor bone quality or severe comminution, which can limit fixation options. As increased repair strength allows earlier postoperative rehabilitation and maintains fracture reduction, patient outcomes should improve. This novel technique represents another strategy for managing challenging patella fractures.
1. Boström Å. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl. 1972;143:1-80.
2. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979;(144):9-15.
3. LeBrun CT, Langford JR, Sagi HC. Functional outcomes after operatively treated patella fractures. J Orthop Trauma. 2012;26(7):422-426.
4. Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am. 1971;53(8):1551-1560.
5. Braun W, Wiedemann M, Rüter A, Kundel K, Kolbinger S. Indications and results of nonoperative treatment of patellar fractures. Clin Orthop Relat Res. 1993;(289):197-201.
6. Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg. 2011;19(4):198-207.
7. Müller M, Allgöwer M, Schneider R, Willeneger H. Manual of Internal Fixation: Techniques Recommended by the AO Group. Berlin, Germany: Springer; 1979.
8. Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Joint Surg Am. 1980;62(2):215-220.
9. Hung LK, Chan KM, Chow YN, Leung PC. Fractured patella: operative treatment using the tension band principle. Injury. 1985;16(5):343-347.
10. Berg EE. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws. J Orthop Trauma. 1997;11(8):573-576.
11. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma. 1997;11(5):351-356.
12. Hughes SC, Stott PM, Hearnden AJ, Ripley LG. A new and effective tension-band braided polyester suture technique for transverse patellar fracture fixation. Injury. 2007;38(2):212-222.
13. Rabalais RD, Burger E, Lu Y, Mansour A, Baratta RV. Comparison of two tension-band fixation materials and techniques in transverse patella fractures: a biomechanical study. Orthopedics. 2008;31(2):128.
14. Bryant TL, Anderson CL, Stevens CG, Conrad BP, Vincent HK, Sadasivan KK. Comparison of cannulated screws with FiberWire or stainless steel wire for patella fracture fixation: a pilot study. J Orthop. 2014;12(2):92-96.
15. Oh HK, Choo SK, Kim JW, Lee M. Internal fixation of displaced inferior pole of the patella fractures using vertical wiring augmented with Krachow suturing. Injury. 2015;46(12):2512-2515.
16. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. 1. Functional anatomy of the patello-femoral joint. J Bone Joint Surg Br. 1976;58(3):287-290.
17. Levack B, Flannagan JP, Hobbs S. Results of surgical treatment of patellar fractures. J Bone Joint Surg Br. 1985;67(3):416-419.
18. Lotke PA, Ecker ML. Transverse fractures of the patella. Clin Orthop Relat Res. 1981;(158):180-184.
19. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
20. Hahn JM, Inceoğlu S, Wongworawat MD. Biomechanical comparison of Krackow locking stitch versus nonlocking loop stitch with varying number of throws. Am J Sports Med. 2014;42(12):3003-3008.
Take-Home Points
- Suture augmentation improves construct strength for patella fixation.
- Krackow sutures may be placed in the quadriceps and patella tendons, then secured over the anterior patella (much like an anterior tension band).
- The Krackow technique described was superior to the suture cerclage technique based on mean load values, but did not reach statistical significance.
- The Krackow suture technique is a viable and easily applied technique for suture augmentation of patella fixation constructs.
Patella fractures are relatively uncommon, accounting for only 1% of skeletal injuries.1 Restoration of the function of the patella and the extensor mechanism is vital for knee extension and gait. However, patella fractures have an inherently high rate of complications, making these injuries challenging to treat.2-4 In patients with intact extensor function, displacement of <4 mm, and articular step-off of <3 mm, nonoperative management is extremely effective, with 99% of patients reporting favorable results.5 However, for fractures in which the extensor mechanism is disrupted, surgical intervention typically is indicated.6
Authors have reported various surgical interventions, one of the most commonly used being the anterior tension band (ATB) technique, first described by the AO (Arbeitsgemeinschaft für Osteosynthesefragen) group in the 1950s.7 By converting distractive anterior force during knee flexion to compressive force at the fracture site, the ATB technique provides a repair stronger than the previously used cerclage repair.8 Although initially considered standard of care, the ATB technique was soon found to be associated with implant failure and subcutaneous irritation prompting implant removal.9
To address these issues, Berg10 and Carpenter and colleagues11 evaluated an ATB technique that used cannulated screws instead of Kirschner wires (K-wires). This variation on the ATB technique reduced the implant-related issues while maintaining the mechanical advantage of the tension band. The more rigid design also permitted earlier postoperative rehabilitation, which significantly reduced development of arthrofibrosis.6,7,10 This modified ATB (MATB) technique has since been investigated for additional augments, mainly focusing on use of different tension band materials, including polyester suture and braided composite suture.12-14
However, there is little research on augments that incorporate the surrounding soft tissue, specifically the quadriceps and patellar tendons. In a recent retrospective clinical study, Oh and colleagues15 found positive clinical results with use of Krackow sutures, though 2 or 3 vertically oriented stainless steel wires were used instead of cannulated screws.
We conducted a study to determine the biomechanical efficacy of using a cerclage suture augment and a Krackow suture augment coupled with and compared with conventional MATB repair. If effective, this technique may represent another strategy for increasing repair strength and thereby improve postoperative outcomes.
Materials and Methods
Specimen Preparation
Fresh-frozen cadaver extensor mechanisms (quadriceps tendon, patella, surrounding retinaculum, patellar tendon) were kept frozen at –4°C until preparation. Fifteen specimens were selected. Mean (SD) age at death was 68 (10) years (range, 51-85 years). One specimen was excluded for a short patella tendon, which precluded adequate attachment for testing. All specimens were free of overt osseous pathology.
After specimens were thawed overnight, the patellae were transversely osteotomized with an osteotome at the junction of the middle and distal thirds of the patella. Sharp dissection was performed to carry the division through the medial and lateral retinaculum at the same level. All 14 specimens were then repaired using the MATB technique. First, the transverse fracture was reduced with a reduction clamp. Then, two 4-mm cannulated screws (DePuy Synthes) were inserted parallel to each other and perpendicular to the fracture. An 18-gauge stainless steel wire was then passed through each screw, crossed anteriorly, and tightened to create a figure-of-8 ATB. The specimens were then randomly divided into 3 groups—MATB; MATB with cerclage suture augment; MATB with Krackow suture augment—while ensuring specimens from a single cadaver were placed in different groups to avoid confounding based on bone density differences.
Experimental Setup
Repaired specimens were secured with tissue clamps at the quadriceps and patellar tendons on an MTS Bionix 858 (MTS Systems) hydraulic arm.
Each patella was secured for cyclic testing. Initially it was placed under 10 N of tension. Then it underwent tensile loading from 10 N to 300 N at 50 N/s for 10 cycles. These parameters were based on previous biomechanical patella studies.10,11 Load was measured with the MTS load cell and displacement with the displacement transducer. Fracture displacement associated with 300-N cyclic tension was recorded. Displacement was calculated as the difference between 10th cycle and 2nd cycle values, which accounted for any degree of initial tissue slippage. After cyclic testing, the patella was placed back in 10 N of tensile loading and subjected to maximum force loading to determine ultimate repair strength. For maximum loading, the patella was stretched progressively at 50 N/s until failure. Again, load and displacement were measured with MTS.
Statistical Analysis
After testing, fracture displacement and maximum load force data were compiled for analysis. One-way analysis of variance with Bonferroni correction was used to determine if there were significant differences between groups. Significance level was set at P < .05.
Results
For cyclic testing, mean total displacement was measured over 10 cycles for each group. Again, displacement was determined by taking the difference between 10th cycle and 2nd cycle values, allowing for system stabilization.
Discussion
Our main objective was to compare the efficacy of a novel suture augment technique with that of other patella fracture repair techniques. Our hypothesis—that adding a Krackow suture augment would increase strength in both cyclic and maximum loading—was supported. Although testing results were not statistically significant because of the small sample size, we think this novel technique has clinically relevant descriptive significance and warrants further investigation.
Proper anatomical reduction and postoperative stabilization are of utmost importance in clinical approaches to patella fractures. In addition, regardless of which technical procedure is used, open reduction should also allow for early range of motion to prevent joint arthrofibrosis. Ever since the ATB technique was first described by the AO group, postoperative outcomes have improved significantly. In a retrospective study by Levack and colleagues,17 30 of 64 patients with patella fractures underwent internal fixation. Mean follow-up was 6.2 years. By both objective and subjective measures, the best functional outcomes were associated with internal tension band fixation (vs cerclage repair). Lotke and Ecker18 also documented the efficacy of the tension band technique. Sixteen patients with patella fractures underwent anterior tension banding; those with a comminuted fracture also underwent cerclage repair for patella stabilization during tension banding. At 6-week follow-up, all patients had good range of motion (≥90° flexion), relatively few symptoms, and no implant failures. Results were similar to those of Levack and colleagues.17
Although it improves stability and functional outcomes over conventional patellectomy and cerclage wiring, the ATB technique has been associated with subcutaneous irritation caused by the K-wires used to secure the band. Hung and colleagues9 followed up 68 patients with patellar fractures. Five of these patients underwent tension banding. Although there was a high level of adequate functional outcomes, implant irritation was found to be “quite frequent.”
To address this issue, Carpenter and colleagues11 evaluated an ATB technique that uses K-wires instead of cannulated screws. Biomechanical testing in a cadaver model revealed less fracture displacement and overall more repair strength through cyclic and maximum load testing. Clinically, these results were supported by Berg,10 who followed up 10 patients with transverse patella fractures repaired with the MATB technique. At a mean follow-up of 24 months, 7 of the 10 patients had good to excellent outcomes, and there were no implant failures.
Further investigation into patella repairs has mainly focused on improving the MATB technique and experimenting with different tension band materials. Rabalais and colleagues13 biomechanically tested high-strength polyethylene suture as a replacement for standard 18-gauge wire, and Bryant and colleagues14 tested a braided composite suture (FiberWire; Arthrex) as a replacement for standard 18-gauge stainless steel wire. Both found no significant difference with use of augmented tension band material, but Rabalais and colleagues13 did find more advantages with a parallel tension band construct than with a standard figure-of-8 arrangement.
In developing our novel technique, we considered that Krackow sutures are routinely used in both quadriceps tendon repair and patellar tendon repair, including partial patellectomy for distal patella fracture. With a suture placed in both tendons, the augment could be expected to resist longitudinal gapping and augment the tension band across the anterior patella. First described by Krackow and colleagues,19 the Krackow suture is widely used for tendon reconstruction. In an interlocking system of sutures, the Krackow suture provides a repair that is more stable than repair with conventional suture techniques, specifically in the context of tendon repair.20 Given the sesamoidal nature of the patella, its repair shares the goal of gap prevention with other tendon repairs. In theory, anchoring the supporting structures that are above and below the patella provides support for the intervening patella and ultimately improves fracture fixation strength.
Oh and colleagues15 reported on the clinical efficacy of a Krackow augment in distal pole patella repairs. Similarly, we found a Krackow augment to be efficacious, supporting its potential in clinical approaches to patella repairs. Our results indicate this augment can be a useful clinical adjunct in biomechanical evaluation.
Limitations of this study include its use of dissected extensor mechanisms, which may have less biofidelity than whole-knee specimens. In our model, specimens were secured at the patellar tendon and the quadriceps tendons, as opposed to the quadriceps tendon and the tibia distally. Use of this model could have led to an increase in early displacement during cyclic testing as a result of tissue slippage. Furthermore, our small sample size could have affected our ability to demonstrate a difference between these techniques.
Given its increased strength as demonstrated by mean displacement during cyclic loading and mean load to failure, as well as the early clinical data recently published, the Krackow suture augment represents a feasible technique for patella fixation. It likely will be most useful in cases in which conventional techniques are prone to failure or cannot be applied, such as severe distal comminution or poor bone density. Further biomechanical testing with a larger number of specimens may be required for statistical significance.
Conclusion
In patella fracture repair strategies, the Krackow suture augment increased strength when used with a MATB technique. Failure to reach statistical significance likely resulted from our small sample size. Further biomechanical testing and clinical studies are needed for more complete evaluation of this technique. We think it will be most useful in the setting of poor bone quality or severe comminution, which can limit fixation options. As increased repair strength allows earlier postoperative rehabilitation and maintains fracture reduction, patient outcomes should improve. This novel technique represents another strategy for managing challenging patella fractures.
Take-Home Points
- Suture augmentation improves construct strength for patella fixation.
- Krackow sutures may be placed in the quadriceps and patella tendons, then secured over the anterior patella (much like an anterior tension band).
- The Krackow technique described was superior to the suture cerclage technique based on mean load values, but did not reach statistical significance.
- The Krackow suture technique is a viable and easily applied technique for suture augmentation of patella fixation constructs.
Patella fractures are relatively uncommon, accounting for only 1% of skeletal injuries.1 Restoration of the function of the patella and the extensor mechanism is vital for knee extension and gait. However, patella fractures have an inherently high rate of complications, making these injuries challenging to treat.2-4 In patients with intact extensor function, displacement of <4 mm, and articular step-off of <3 mm, nonoperative management is extremely effective, with 99% of patients reporting favorable results.5 However, for fractures in which the extensor mechanism is disrupted, surgical intervention typically is indicated.6
Authors have reported various surgical interventions, one of the most commonly used being the anterior tension band (ATB) technique, first described by the AO (Arbeitsgemeinschaft für Osteosynthesefragen) group in the 1950s.7 By converting distractive anterior force during knee flexion to compressive force at the fracture site, the ATB technique provides a repair stronger than the previously used cerclage repair.8 Although initially considered standard of care, the ATB technique was soon found to be associated with implant failure and subcutaneous irritation prompting implant removal.9
To address these issues, Berg10 and Carpenter and colleagues11 evaluated an ATB technique that used cannulated screws instead of Kirschner wires (K-wires). This variation on the ATB technique reduced the implant-related issues while maintaining the mechanical advantage of the tension band. The more rigid design also permitted earlier postoperative rehabilitation, which significantly reduced development of arthrofibrosis.6,7,10 This modified ATB (MATB) technique has since been investigated for additional augments, mainly focusing on use of different tension band materials, including polyester suture and braided composite suture.12-14
However, there is little research on augments that incorporate the surrounding soft tissue, specifically the quadriceps and patellar tendons. In a recent retrospective clinical study, Oh and colleagues15 found positive clinical results with use of Krackow sutures, though 2 or 3 vertically oriented stainless steel wires were used instead of cannulated screws.
We conducted a study to determine the biomechanical efficacy of using a cerclage suture augment and a Krackow suture augment coupled with and compared with conventional MATB repair. If effective, this technique may represent another strategy for increasing repair strength and thereby improve postoperative outcomes.
Materials and Methods
Specimen Preparation
Fresh-frozen cadaver extensor mechanisms (quadriceps tendon, patella, surrounding retinaculum, patellar tendon) were kept frozen at –4°C until preparation. Fifteen specimens were selected. Mean (SD) age at death was 68 (10) years (range, 51-85 years). One specimen was excluded for a short patella tendon, which precluded adequate attachment for testing. All specimens were free of overt osseous pathology.
After specimens were thawed overnight, the patellae were transversely osteotomized with an osteotome at the junction of the middle and distal thirds of the patella. Sharp dissection was performed to carry the division through the medial and lateral retinaculum at the same level. All 14 specimens were then repaired using the MATB technique. First, the transverse fracture was reduced with a reduction clamp. Then, two 4-mm cannulated screws (DePuy Synthes) were inserted parallel to each other and perpendicular to the fracture. An 18-gauge stainless steel wire was then passed through each screw, crossed anteriorly, and tightened to create a figure-of-8 ATB. The specimens were then randomly divided into 3 groups—MATB; MATB with cerclage suture augment; MATB with Krackow suture augment—while ensuring specimens from a single cadaver were placed in different groups to avoid confounding based on bone density differences.
Experimental Setup
Repaired specimens were secured with tissue clamps at the quadriceps and patellar tendons on an MTS Bionix 858 (MTS Systems) hydraulic arm.
Each patella was secured for cyclic testing. Initially it was placed under 10 N of tension. Then it underwent tensile loading from 10 N to 300 N at 50 N/s for 10 cycles. These parameters were based on previous biomechanical patella studies.10,11 Load was measured with the MTS load cell and displacement with the displacement transducer. Fracture displacement associated with 300-N cyclic tension was recorded. Displacement was calculated as the difference between 10th cycle and 2nd cycle values, which accounted for any degree of initial tissue slippage. After cyclic testing, the patella was placed back in 10 N of tensile loading and subjected to maximum force loading to determine ultimate repair strength. For maximum loading, the patella was stretched progressively at 50 N/s until failure. Again, load and displacement were measured with MTS.
Statistical Analysis
After testing, fracture displacement and maximum load force data were compiled for analysis. One-way analysis of variance with Bonferroni correction was used to determine if there were significant differences between groups. Significance level was set at P < .05.
Results
For cyclic testing, mean total displacement was measured over 10 cycles for each group. Again, displacement was determined by taking the difference between 10th cycle and 2nd cycle values, allowing for system stabilization.
Discussion
Our main objective was to compare the efficacy of a novel suture augment technique with that of other patella fracture repair techniques. Our hypothesis—that adding a Krackow suture augment would increase strength in both cyclic and maximum loading—was supported. Although testing results were not statistically significant because of the small sample size, we think this novel technique has clinically relevant descriptive significance and warrants further investigation.
Proper anatomical reduction and postoperative stabilization are of utmost importance in clinical approaches to patella fractures. In addition, regardless of which technical procedure is used, open reduction should also allow for early range of motion to prevent joint arthrofibrosis. Ever since the ATB technique was first described by the AO group, postoperative outcomes have improved significantly. In a retrospective study by Levack and colleagues,17 30 of 64 patients with patella fractures underwent internal fixation. Mean follow-up was 6.2 years. By both objective and subjective measures, the best functional outcomes were associated with internal tension band fixation (vs cerclage repair). Lotke and Ecker18 also documented the efficacy of the tension band technique. Sixteen patients with patella fractures underwent anterior tension banding; those with a comminuted fracture also underwent cerclage repair for patella stabilization during tension banding. At 6-week follow-up, all patients had good range of motion (≥90° flexion), relatively few symptoms, and no implant failures. Results were similar to those of Levack and colleagues.17
Although it improves stability and functional outcomes over conventional patellectomy and cerclage wiring, the ATB technique has been associated with subcutaneous irritation caused by the K-wires used to secure the band. Hung and colleagues9 followed up 68 patients with patellar fractures. Five of these patients underwent tension banding. Although there was a high level of adequate functional outcomes, implant irritation was found to be “quite frequent.”
To address this issue, Carpenter and colleagues11 evaluated an ATB technique that uses K-wires instead of cannulated screws. Biomechanical testing in a cadaver model revealed less fracture displacement and overall more repair strength through cyclic and maximum load testing. Clinically, these results were supported by Berg,10 who followed up 10 patients with transverse patella fractures repaired with the MATB technique. At a mean follow-up of 24 months, 7 of the 10 patients had good to excellent outcomes, and there were no implant failures.
Further investigation into patella repairs has mainly focused on improving the MATB technique and experimenting with different tension band materials. Rabalais and colleagues13 biomechanically tested high-strength polyethylene suture as a replacement for standard 18-gauge wire, and Bryant and colleagues14 tested a braided composite suture (FiberWire; Arthrex) as a replacement for standard 18-gauge stainless steel wire. Both found no significant difference with use of augmented tension band material, but Rabalais and colleagues13 did find more advantages with a parallel tension band construct than with a standard figure-of-8 arrangement.
In developing our novel technique, we considered that Krackow sutures are routinely used in both quadriceps tendon repair and patellar tendon repair, including partial patellectomy for distal patella fracture. With a suture placed in both tendons, the augment could be expected to resist longitudinal gapping and augment the tension band across the anterior patella. First described by Krackow and colleagues,19 the Krackow suture is widely used for tendon reconstruction. In an interlocking system of sutures, the Krackow suture provides a repair that is more stable than repair with conventional suture techniques, specifically in the context of tendon repair.20 Given the sesamoidal nature of the patella, its repair shares the goal of gap prevention with other tendon repairs. In theory, anchoring the supporting structures that are above and below the patella provides support for the intervening patella and ultimately improves fracture fixation strength.
Oh and colleagues15 reported on the clinical efficacy of a Krackow augment in distal pole patella repairs. Similarly, we found a Krackow augment to be efficacious, supporting its potential in clinical approaches to patella repairs. Our results indicate this augment can be a useful clinical adjunct in biomechanical evaluation.
Limitations of this study include its use of dissected extensor mechanisms, which may have less biofidelity than whole-knee specimens. In our model, specimens were secured at the patellar tendon and the quadriceps tendons, as opposed to the quadriceps tendon and the tibia distally. Use of this model could have led to an increase in early displacement during cyclic testing as a result of tissue slippage. Furthermore, our small sample size could have affected our ability to demonstrate a difference between these techniques.
Given its increased strength as demonstrated by mean displacement during cyclic loading and mean load to failure, as well as the early clinical data recently published, the Krackow suture augment represents a feasible technique for patella fixation. It likely will be most useful in cases in which conventional techniques are prone to failure or cannot be applied, such as severe distal comminution or poor bone density. Further biomechanical testing with a larger number of specimens may be required for statistical significance.
Conclusion
In patella fracture repair strategies, the Krackow suture augment increased strength when used with a MATB technique. Failure to reach statistical significance likely resulted from our small sample size. Further biomechanical testing and clinical studies are needed for more complete evaluation of this technique. We think it will be most useful in the setting of poor bone quality or severe comminution, which can limit fixation options. As increased repair strength allows earlier postoperative rehabilitation and maintains fracture reduction, patient outcomes should improve. This novel technique represents another strategy for managing challenging patella fractures.
1. Boström Å. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl. 1972;143:1-80.
2. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979;(144):9-15.
3. LeBrun CT, Langford JR, Sagi HC. Functional outcomes after operatively treated patella fractures. J Orthop Trauma. 2012;26(7):422-426.
4. Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am. 1971;53(8):1551-1560.
5. Braun W, Wiedemann M, Rüter A, Kundel K, Kolbinger S. Indications and results of nonoperative treatment of patellar fractures. Clin Orthop Relat Res. 1993;(289):197-201.
6. Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg. 2011;19(4):198-207.
7. Müller M, Allgöwer M, Schneider R, Willeneger H. Manual of Internal Fixation: Techniques Recommended by the AO Group. Berlin, Germany: Springer; 1979.
8. Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Joint Surg Am. 1980;62(2):215-220.
9. Hung LK, Chan KM, Chow YN, Leung PC. Fractured patella: operative treatment using the tension band principle. Injury. 1985;16(5):343-347.
10. Berg EE. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws. J Orthop Trauma. 1997;11(8):573-576.
11. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma. 1997;11(5):351-356.
12. Hughes SC, Stott PM, Hearnden AJ, Ripley LG. A new and effective tension-band braided polyester suture technique for transverse patellar fracture fixation. Injury. 2007;38(2):212-222.
13. Rabalais RD, Burger E, Lu Y, Mansour A, Baratta RV. Comparison of two tension-band fixation materials and techniques in transverse patella fractures: a biomechanical study. Orthopedics. 2008;31(2):128.
14. Bryant TL, Anderson CL, Stevens CG, Conrad BP, Vincent HK, Sadasivan KK. Comparison of cannulated screws with FiberWire or stainless steel wire for patella fracture fixation: a pilot study. J Orthop. 2014;12(2):92-96.
15. Oh HK, Choo SK, Kim JW, Lee M. Internal fixation of displaced inferior pole of the patella fractures using vertical wiring augmented with Krachow suturing. Injury. 2015;46(12):2512-2515.
16. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. 1. Functional anatomy of the patello-femoral joint. J Bone Joint Surg Br. 1976;58(3):287-290.
17. Levack B, Flannagan JP, Hobbs S. Results of surgical treatment of patellar fractures. J Bone Joint Surg Br. 1985;67(3):416-419.
18. Lotke PA, Ecker ML. Transverse fractures of the patella. Clin Orthop Relat Res. 1981;(158):180-184.
19. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
20. Hahn JM, Inceoğlu S, Wongworawat MD. Biomechanical comparison of Krackow locking stitch versus nonlocking loop stitch with varying number of throws. Am J Sports Med. 2014;42(12):3003-3008.
1. Boström Å. Fracture of the patella. A study of 422 patellar fractures. Acta Orthop Scand Suppl. 1972;143:1-80.
2. Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979;(144):9-15.
3. LeBrun CT, Langford JR, Sagi HC. Functional outcomes after operatively treated patella fractures. J Orthop Trauma. 2012;26(7):422-426.
4. Kaufer H. Mechanical function of the patella. J Bone Joint Surg Am. 1971;53(8):1551-1560.
5. Braun W, Wiedemann M, Rüter A, Kundel K, Kolbinger S. Indications and results of nonoperative treatment of patellar fractures. Clin Orthop Relat Res. 1993;(289):197-201.
6. Melvin JS, Mehta S. Patellar fractures in adults. J Am Acad Orthop Surg. 2011;19(4):198-207.
7. Müller M, Allgöwer M, Schneider R, Willeneger H. Manual of Internal Fixation: Techniques Recommended by the AO Group. Berlin, Germany: Springer; 1979.
8. Weber MJ, Janecki CJ, McLeod P, Nelson CL, Thompson JA. Efficacy of various forms of fixation of transverse fractures of the patella. J Bone Joint Surg Am. 1980;62(2):215-220.
9. Hung LK, Chan KM, Chow YN, Leung PC. Fractured patella: operative treatment using the tension band principle. Injury. 1985;16(5):343-347.
10. Berg EE. Open reduction internal fixation of displaced transverse patella fractures with figure-eight wiring through parallel cannulated compression screws. J Orthop Trauma. 1997;11(8):573-576.
11. Carpenter JE, Kasman RA, Patel N, Lee ML, Goldstein SA. Biomechanical evaluation of current patella fracture fixation techniques. J Orthop Trauma. 1997;11(5):351-356.
12. Hughes SC, Stott PM, Hearnden AJ, Ripley LG. A new and effective tension-band braided polyester suture technique for transverse patellar fracture fixation. Injury. 2007;38(2):212-222.
13. Rabalais RD, Burger E, Lu Y, Mansour A, Baratta RV. Comparison of two tension-band fixation materials and techniques in transverse patella fractures: a biomechanical study. Orthopedics. 2008;31(2):128.
14. Bryant TL, Anderson CL, Stevens CG, Conrad BP, Vincent HK, Sadasivan KK. Comparison of cannulated screws with FiberWire or stainless steel wire for patella fracture fixation: a pilot study. J Orthop. 2014;12(2):92-96.
15. Oh HK, Choo SK, Kim JW, Lee M. Internal fixation of displaced inferior pole of the patella fractures using vertical wiring augmented with Krachow suturing. Injury. 2015;46(12):2512-2515.
16. Goodfellow J, Hungerford DS, Zindel M. Patello-femoral joint mechanics and pathology. 1. Functional anatomy of the patello-femoral joint. J Bone Joint Surg Br. 1976;58(3):287-290.
17. Levack B, Flannagan JP, Hobbs S. Results of surgical treatment of patellar fractures. J Bone Joint Surg Br. 1985;67(3):416-419.
18. Lotke PA, Ecker ML. Transverse fractures of the patella. Clin Orthop Relat Res. 1981;(158):180-184.
19. Krackow KA, Thomas SC, Jones LC. Ligament-tendon fixation: analysis of a new stitch and comparison with standard techniques. Orthopedics. 1988;11(6):909-917.
20. Hahn JM, Inceoğlu S, Wongworawat MD. Biomechanical comparison of Krackow locking stitch versus nonlocking loop stitch with varying number of throws. Am J Sports Med. 2014;42(12):3003-3008.
FFR-guided PCI in stable CAD beats medical management
DENVER – Percutaneous coronary intervention plus optimal medical therapy in stable coronary artery disease (CAD) patients with at least one coronary lesion having an abnormal fractional flow reserve measurement resulted in superior clinical outcomes, better quality of life, and virtually identical cost, compared with optimal medical management alone over 3 years of follow-up in the FAME 2 trial.
“These results reinforce the point that the greater the burden of ischemia, the greater the benefit of revascularization with PCI [percutaneous coronary intervention],” William F. Fearon, MD, said while presenting the FAME 2 findings at the Transcatheter Cardiovascular Therapeutics annual meeting.

FAME 2 was a randomized, multicenter trial designed to help bring clarity regarding the optimal treatment strategy for patients with stable angina and CAD. This is an issue surrounded by considerable controversy. The fog descended a decade ago, when the COURAGE trial created a stir with its conclusion that optimal medical therapy (OMT) alone was as good as PCI plus OMT in terms of clinical outcome and quality of life – and was considerably less expensive as well. And the British ORBITA trial, presented earlier in the same session at TCT 2017 as Dr. Fearon’s report on FAME 2, caused an uproar with its finding that PCI plus OMT was no more effective than sham PCI plus OMT in the setting of stable CAD.
However, FAME 2 (Fractional Flow Reserve versus Angiography for Multivessel Evaluation) differed from those studies in a crucial aspect: randomization in FAME 2 was restricted to patients with physiologically significant cardiac ischemia as evidenced by a fractional flow reserve (FFR) measurement of 0.80 or less.
In contrast, COURAGE and ORBITA randomized patients without FFR guidance. As a result, in those trials PCI was performed in a substantial proportion of patients who actually should not have undergone the intervention because they didn’t have physiologic evidence of clinically important ischemia. The non–physiologically based approach to PCI utilized in COURAGE and ORBITA – disappointingly commonplace in daily clinical practice – diluted any true benefit of the procedure when applied appropriately, explained Dr. Fearon, professor of medicine and director of interventional cardiology at Stanford (Calif.) University.
FAME 2 randomized 888 patients with stable single- or multivessel CAD and an FFR of 0.80 or less to PCI plus OMT or an initial strategy of OMT alone at 28 European and North American sites. The primary outcome was the rate of major adverse cardiac events – death, MI, and urgent revascularization – at 3 years. The rate was 10.1% in the PCI group, compared with 22% in the medically managed cohort, Dr. Fearon reported at the meeting sponsored by the Cardiovascular Research Foundation.
Death or MI occurred in 8.3% of the PCI group versus 10.4% in the OMT group, a trend that didn’t reach significance. Of note, however, fully 44% of patients in the OMT group crossed over to PCI during the 3-year study. In the prespecified intent-to-treat analysis they were counted in the OMT group, whereas an as-treated analysis might well have shown statistically significant reductions in death and MI in the PCI group.
The proportion of patients with class II-IV angina was significantly lower in the PCI plus medical therapy group at every time point, including 5.9% versus 15.2% for OMT alone at 1 year, 5.9% versus 12% at 2 years, and 5.2% versus 9.7% at 3 years. This was the case even though the OMT group received significantly more antianginal therapy in an effort to control symptoms.
FAME 2 featured a first-of-its-kind comprehensive cost-effectiveness analysis of OMT vs. PCI over a 3-year period. It showed that, while mean initial costs were as expected higher in the PCI group ($9,944 versus $4,440), by 3 years the cumulative costs were near identical at $16,792 in the PCI group and $16,737 in the initial OMT group. The incremental cost-effectiveness ratio for PCI, compared with OMT at 3 years was attractive at $1,600 per quality-adjusted life-year gained.
The question on TCT attendees’ minds following presentation of the bombshell ORBITA findings was, what would have happened had FAME 2 featured a sham PCI arm? Could the advantageous outcomes for the initial PCI strategy seen in FAME 2 possibly have been due to a placebo effect?
Extremely unlikely, according to Dr. Fearon. For one thing, when he and his coinvestigators broke down the FFR values in the OMT group into quintiles, they saw a clear dose-response effect: The clinical event rate rose further with worsening quintile of FFR. Also, the study endpoints were death, MI, and urgent revascularization – triggered by ACS in half of cases – which are less susceptible to a placebo effect than, say, treadmill exercise time, the primary endpoint in ORBITA.
Moreover, as noted by Gary S. Mintz, MD, who moderated a press conference highlighting the ORBITA and FAME 2 results, placebo effects don’t last for years.
“Most people would say the placebo effect wanes over time. That’s why these 3-year data, analyzed by intent-to-treat, which allow for crossovers to still be analyzed in the medical therapy arm, are pretty compelling to me,” commented Dr. Mintz, chief medical officer for the Cardiovascular Research Foundation in New York.
FAME 2 was supported by St. Jude Medical. Dr. Fearon reported receiving institutional research support from Medtronic, Abbott Vascular, ACIST Medical, CathWorks, and Edwards LifeSciences.
DENVER – Percutaneous coronary intervention plus optimal medical therapy in stable coronary artery disease (CAD) patients with at least one coronary lesion having an abnormal fractional flow reserve measurement resulted in superior clinical outcomes, better quality of life, and virtually identical cost, compared with optimal medical management alone over 3 years of follow-up in the FAME 2 trial.
“These results reinforce the point that the greater the burden of ischemia, the greater the benefit of revascularization with PCI [percutaneous coronary intervention],” William F. Fearon, MD, said while presenting the FAME 2 findings at the Transcatheter Cardiovascular Therapeutics annual meeting.
FAME 2 was a randomized, multicenter trial designed to help bring clarity regarding the optimal treatment strategy for patients with stable angina and CAD. This is an issue surrounded by considerable controversy. The fog descended a decade ago, when the COURAGE trial created a stir with its conclusion that optimal medical therapy (OMT) alone was as good as PCI plus OMT in terms of clinical outcome and quality of life – and was considerably less expensive as well. And the British ORBITA trial, presented earlier in the same session at TCT 2017 as Dr. Fearon’s report on FAME 2, caused an uproar with its finding that PCI plus OMT was no more effective than sham PCI plus OMT in the setting of stable CAD.
However, FAME 2 (Fractional Flow Reserve versus Angiography for Multivessel Evaluation) differed from those studies in a crucial aspect: randomization in FAME 2 was restricted to patients with physiologically significant cardiac ischemia as evidenced by a fractional flow reserve (FFR) measurement of 0.80 or less.
In contrast, COURAGE and ORBITA randomized patients without FFR guidance. As a result, in those trials PCI was performed in a substantial proportion of patients who actually should not have undergone the intervention because they didn’t have physiologic evidence of clinically important ischemia. The non–physiologically based approach to PCI utilized in COURAGE and ORBITA – disappointingly commonplace in daily clinical practice – diluted any true benefit of the procedure when applied appropriately, explained Dr. Fearon, professor of medicine and director of interventional cardiology at Stanford (Calif.) University.
FAME 2 randomized 888 patients with stable single- or multivessel CAD and an FFR of 0.80 or less to PCI plus OMT or an initial strategy of OMT alone at 28 European and North American sites. The primary outcome was the rate of major adverse cardiac events – death, MI, and urgent revascularization – at 3 years. The rate was 10.1% in the PCI group, compared with 22% in the medically managed cohort, Dr. Fearon reported at the meeting sponsored by the Cardiovascular Research Foundation.
Death or MI occurred in 8.3% of the PCI group versus 10.4% in the OMT group, a trend that didn’t reach significance. Of note, however, fully 44% of patients in the OMT group crossed over to PCI during the 3-year study. In the prespecified intent-to-treat analysis they were counted in the OMT group, whereas an as-treated analysis might well have shown statistically significant reductions in death and MI in the PCI group.
The proportion of patients with class II-IV angina was significantly lower in the PCI plus medical therapy group at every time point, including 5.9% versus 15.2% for OMT alone at 1 year, 5.9% versus 12% at 2 years, and 5.2% versus 9.7% at 3 years. This was the case even though the OMT group received significantly more antianginal therapy in an effort to control symptoms.
FAME 2 featured a first-of-its-kind comprehensive cost-effectiveness analysis of OMT vs. PCI over a 3-year period. It showed that, while mean initial costs were as expected higher in the PCI group ($9,944 versus $4,440), by 3 years the cumulative costs were near identical at $16,792 in the PCI group and $16,737 in the initial OMT group. The incremental cost-effectiveness ratio for PCI, compared with OMT at 3 years was attractive at $1,600 per quality-adjusted life-year gained.
The question on TCT attendees’ minds following presentation of the bombshell ORBITA findings was, what would have happened had FAME 2 featured a sham PCI arm? Could the advantageous outcomes for the initial PCI strategy seen in FAME 2 possibly have been due to a placebo effect?
Extremely unlikely, according to Dr. Fearon. For one thing, when he and his coinvestigators broke down the FFR values in the OMT group into quintiles, they saw a clear dose-response effect: The clinical event rate rose further with worsening quintile of FFR. Also, the study endpoints were death, MI, and urgent revascularization – triggered by ACS in half of cases – which are less susceptible to a placebo effect than, say, treadmill exercise time, the primary endpoint in ORBITA.
Moreover, as noted by Gary S. Mintz, MD, who moderated a press conference highlighting the ORBITA and FAME 2 results, placebo effects don’t last for years.
“Most people would say the placebo effect wanes over time. That’s why these 3-year data, analyzed by intent-to-treat, which allow for crossovers to still be analyzed in the medical therapy arm, are pretty compelling to me,” commented Dr. Mintz, chief medical officer for the Cardiovascular Research Foundation in New York.
FAME 2 was supported by St. Jude Medical. Dr. Fearon reported receiving institutional research support from Medtronic, Abbott Vascular, ACIST Medical, CathWorks, and Edwards LifeSciences.
DENVER – Percutaneous coronary intervention plus optimal medical therapy in stable coronary artery disease (CAD) patients with at least one coronary lesion having an abnormal fractional flow reserve measurement resulted in superior clinical outcomes, better quality of life, and virtually identical cost, compared with optimal medical management alone over 3 years of follow-up in the FAME 2 trial.
“These results reinforce the point that the greater the burden of ischemia, the greater the benefit of revascularization with PCI [percutaneous coronary intervention],” William F. Fearon, MD, said while presenting the FAME 2 findings at the Transcatheter Cardiovascular Therapeutics annual meeting.
FAME 2 was a randomized, multicenter trial designed to help bring clarity regarding the optimal treatment strategy for patients with stable angina and CAD. This is an issue surrounded by considerable controversy. The fog descended a decade ago, when the COURAGE trial created a stir with its conclusion that optimal medical therapy (OMT) alone was as good as PCI plus OMT in terms of clinical outcome and quality of life – and was considerably less expensive as well. And the British ORBITA trial, presented earlier in the same session at TCT 2017 as Dr. Fearon’s report on FAME 2, caused an uproar with its finding that PCI plus OMT was no more effective than sham PCI plus OMT in the setting of stable CAD.
However, FAME 2 (Fractional Flow Reserve versus Angiography for Multivessel Evaluation) differed from those studies in a crucial aspect: randomization in FAME 2 was restricted to patients with physiologically significant cardiac ischemia as evidenced by a fractional flow reserve (FFR) measurement of 0.80 or less.
In contrast, COURAGE and ORBITA randomized patients without FFR guidance. As a result, in those trials PCI was performed in a substantial proportion of patients who actually should not have undergone the intervention because they didn’t have physiologic evidence of clinically important ischemia. The non–physiologically based approach to PCI utilized in COURAGE and ORBITA – disappointingly commonplace in daily clinical practice – diluted any true benefit of the procedure when applied appropriately, explained Dr. Fearon, professor of medicine and director of interventional cardiology at Stanford (Calif.) University.
FAME 2 randomized 888 patients with stable single- or multivessel CAD and an FFR of 0.80 or less to PCI plus OMT or an initial strategy of OMT alone at 28 European and North American sites. The primary outcome was the rate of major adverse cardiac events – death, MI, and urgent revascularization – at 3 years. The rate was 10.1% in the PCI group, compared with 22% in the medically managed cohort, Dr. Fearon reported at the meeting sponsored by the Cardiovascular Research Foundation.
Death or MI occurred in 8.3% of the PCI group versus 10.4% in the OMT group, a trend that didn’t reach significance. Of note, however, fully 44% of patients in the OMT group crossed over to PCI during the 3-year study. In the prespecified intent-to-treat analysis they were counted in the OMT group, whereas an as-treated analysis might well have shown statistically significant reductions in death and MI in the PCI group.
The proportion of patients with class II-IV angina was significantly lower in the PCI plus medical therapy group at every time point, including 5.9% versus 15.2% for OMT alone at 1 year, 5.9% versus 12% at 2 years, and 5.2% versus 9.7% at 3 years. This was the case even though the OMT group received significantly more antianginal therapy in an effort to control symptoms.
FAME 2 featured a first-of-its-kind comprehensive cost-effectiveness analysis of OMT vs. PCI over a 3-year period. It showed that, while mean initial costs were as expected higher in the PCI group ($9,944 versus $4,440), by 3 years the cumulative costs were near identical at $16,792 in the PCI group and $16,737 in the initial OMT group. The incremental cost-effectiveness ratio for PCI, compared with OMT at 3 years was attractive at $1,600 per quality-adjusted life-year gained.
The question on TCT attendees’ minds following presentation of the bombshell ORBITA findings was, what would have happened had FAME 2 featured a sham PCI arm? Could the advantageous outcomes for the initial PCI strategy seen in FAME 2 possibly have been due to a placebo effect?
Extremely unlikely, according to Dr. Fearon. For one thing, when he and his coinvestigators broke down the FFR values in the OMT group into quintiles, they saw a clear dose-response effect: The clinical event rate rose further with worsening quintile of FFR. Also, the study endpoints were death, MI, and urgent revascularization – triggered by ACS in half of cases – which are less susceptible to a placebo effect than, say, treadmill exercise time, the primary endpoint in ORBITA.
Moreover, as noted by Gary S. Mintz, MD, who moderated a press conference highlighting the ORBITA and FAME 2 results, placebo effects don’t last for years.
“Most people would say the placebo effect wanes over time. That’s why these 3-year data, analyzed by intent-to-treat, which allow for crossovers to still be analyzed in the medical therapy arm, are pretty compelling to me,” commented Dr. Mintz, chief medical officer for the Cardiovascular Research Foundation in New York.
FAME 2 was supported by St. Jude Medical. Dr. Fearon reported receiving institutional research support from Medtronic, Abbott Vascular, ACIST Medical, CathWorks, and Edwards LifeSciences.
REPORTING FROM TCT 2017
Key clinical point:
Major finding: The rate of major adverse cardiac events at 3 years was 10.1% in the PCI group and 22% in the medically managed cohort.
Data source: The FAME 2 trial randomized 888 patients with stable single- or multivessel CAD and an FFR of 0.80 or less to PCI plus optimal medical therapy or an initial strategy of optimal medical management alone.
Disclosures: The trial was supported by St. Jude Medical. The presenter reported receiving institutional research support from Medtronic, Abbott Vascular, ACIST Medical, CathWorks, and Edwards LifeSciences.
EVAR, venous CPT coding revamped for 2018
CHICAGO – Current Procedural Terminology coding for endovascular aneurysm repair has been totally overhauled for 2018 with the introduction of a family of 20 new codes and codes for other vascular procedures have also been updated.
The new EVAR CPT codes attempt to capture the work involved in performing the procedures based upon the anatomy of the aneurysm and the treated vessels rather than being device-based, as previously, Matthew J. Sideman, MD, explained in presenting the coding and reimbursement for 2018 at a symposium on vascular surgery sponsored by Northwestern University.

“The new EVAR codes for 2018 have got a lot of gains. There are some losses as well, but overall, I think it’s going to be very positive moving forward,” according to Dr. Sideman, a vascular surgeon at the University of Texas, San Antonio, who serves as chair of the Society for Vascular Surgery Coding and Reimbursement Committee and an adviser to the American Medical Association Relative Value Scale Update Committee (RUC).
“What we gained was a new code for ruptured aneurysm repair, a new code for enhanced fixation, a new code for percutaneous access, new codes for alternative access options, and now all the access codes are add-on codes. But what we traded off was loss due to bundling. So catheterization is now bundled into the main procedure, radiographic supervision and interpretation is now bundled. The big thing that really hurt was we lost all proximal extensions to the renal arteries and all distal extensions to the iliac bifurcations – they’re also bundled into the main procedure,” he said.
Restructuring the EVAR codes was a multiyear collaborative project of the SVS, the American College of Surgeons, the Society of Interventional Radiology, the Society of Thoracic Surgery, the American College of Cardiology, and the Society for Cardiovascular Angiography and Interventions. The impetus was twofold: recognition that the existing codes seriously undervalued the work involved in EVAR because, for example, they didn’t distinguish between ruptured and elective aneurysm repair, nor did they recognize the unique challenges and advantages of percutaneous access.
Also, representatives of the professional societies involved with vascular medicine recognized that they had to develop a detailed proposal for coding restructuring or matters might be taken out of their hands. Bundling of codes has become the prevailing dogma at the RUC and the Centers for Medicare and Medicaid. Their current policy is that when analysis of coding patterns indicates two codes are billed together at least 51% of the time, that’s considered a ‘typical’ situation and a new code must be created combining them. The harsh reality for clinicians is that under what Dr. Sideman called “RUC math,” the new bundled codes invariably pay less than the two old ones.
“There was a little bit of smoke and mirrors – ‘Look at the pretty flashing lights and not what’s going on behind over here’ – as we tried to maintain value as we bundled these EVAR codes,” Dr. Sideman recalled. “I can stand here and tell you I did my very best to push for the best values possible. It can be a painful process, but I thought we came out ok.”
How the new EVAR codes work
Dr. Sideman explained that the impact of the new EVAR codes will depend upon a surgeon’s practice pattern.
He offered as a concrete example a patient undergoing elective EVAR of the aorta and both iliac arteries with percutaneous access and placement of a bifurcated device with one docking limb. In 2017, this might have been handled using CPT codes 34802, 36200-50, and 75952-26, for a total of 31.05 Relative Value Units (RVUs) of work.
In 2018, however, this same surgical strategy would be coded as 34705 (elective endovascular repair of infrarenal aorta and/or iliac artery or arteries) plus 34713 x 2 (percutaneous access and closure), for a total of 34.58 RVUs. Thus, the surgeon would come out 3.53 RVUs ahead in 2018, which at a conversion factor of $35.78/RVU translates to an extra $126.30.
On the other hand, if the surgeon chose to use a bifurcated device with one docking limb, a left iliac bell-bottom extension, a right iliac bell-bottom extension, and percutaneous access, in 2017, this would have been coded as 34802, 34825, 34826, 36200-50, 75952-26, and 75953-26 x 2, for a total of 44.29 RVUs of work. In 2018, this same treatment strategy would be coded as 34705 plus 34713 x 2, for a total of 34.58 RVUs, or a knockdown of 9.71 fewer RVUs compared with the year before, which translates to $347.42 less.
“The more extensions you use, the more you’re going to come out behind going forward,” according to Dr. Sideman.
Other coding changes in 2018
Sclerotherapy of single and multiple veins (codes 36470 and 36471) got down-valued from 1.10 and 2.49 to 0.75 and 1.5 RVUs, respectively.
Angiography of the extremities (75710 and 75716) will be better reimbursed in 2018. In what Dr. Sideman called “a good win,” unilateral angiography will be rated as 1.75 RVUs, up from 1.14 in 2017, while bilateral angiography increased from 1.31 to 1.97 RVUs.
“The other nice thing I can tell you is that through campaigning and lobbying and comments to CMS [Centers for Medicare & Medicaid Services], we got them to reverse their recommendations from 2017 to 2018 on the dialysis family of codes,” the surgeon continued.
Reimbursement for the dialysis codes took a big hit from 2016 to 2017, amounting to several hundred million dollars less in reimbursement, but CMS has reversed its policy on that score. The RVUs for the various dialysis codes have increased from 2017 to 2018 by 5%-21%, with central venous angioplasty (CPT 36907) garnering the biggest increase.
Existing RVUs were retained for 2018 in three of the four selective catheter placement codes. However, reimbursement for 36215 (first order catheterization of the thoracic or brachiocephalic branch) dropped from 4.67 to 4.17 RVUs because physician surveys showed the time involved was less than previously rated. Once the RUC and CMS saw that the time involved in a procedure has decreased, it became impossible to maintain the RVU, Dr. Sideman explained.
And speaking of time involved in procedures, Dr. Sideman offered a final plea to his vascular medicine colleagues:
“When you get surveys from the RUC asking for your input, please, please, please, fill them out because that’s how we get our direct physician input into the valuation of codes.”
He reported having no financial conflicts of interest regarding his presentation.
A detailed listing of many of the codes and changes can be found at the American College of Radiology website, and the Society for Vascular Surgery has coding resources available on their website, as well.
CHICAGO – Current Procedural Terminology coding for endovascular aneurysm repair has been totally overhauled for 2018 with the introduction of a family of 20 new codes and codes for other vascular procedures have also been updated.
The new EVAR CPT codes attempt to capture the work involved in performing the procedures based upon the anatomy of the aneurysm and the treated vessels rather than being device-based, as previously, Matthew J. Sideman, MD, explained in presenting the coding and reimbursement for 2018 at a symposium on vascular surgery sponsored by Northwestern University.
“The new EVAR codes for 2018 have got a lot of gains. There are some losses as well, but overall, I think it’s going to be very positive moving forward,” according to Dr. Sideman, a vascular surgeon at the University of Texas, San Antonio, who serves as chair of the Society for Vascular Surgery Coding and Reimbursement Committee and an adviser to the American Medical Association Relative Value Scale Update Committee (RUC).
“What we gained was a new code for ruptured aneurysm repair, a new code for enhanced fixation, a new code for percutaneous access, new codes for alternative access options, and now all the access codes are add-on codes. But what we traded off was loss due to bundling. So catheterization is now bundled into the main procedure, radiographic supervision and interpretation is now bundled. The big thing that really hurt was we lost all proximal extensions to the renal arteries and all distal extensions to the iliac bifurcations – they’re also bundled into the main procedure,” he said.
Restructuring the EVAR codes was a multiyear collaborative project of the SVS, the American College of Surgeons, the Society of Interventional Radiology, the Society of Thoracic Surgery, the American College of Cardiology, and the Society for Cardiovascular Angiography and Interventions. The impetus was twofold: recognition that the existing codes seriously undervalued the work involved in EVAR because, for example, they didn’t distinguish between ruptured and elective aneurysm repair, nor did they recognize the unique challenges and advantages of percutaneous access.
Also, representatives of the professional societies involved with vascular medicine recognized that they had to develop a detailed proposal for coding restructuring or matters might be taken out of their hands. Bundling of codes has become the prevailing dogma at the RUC and the Centers for Medicare and Medicaid. Their current policy is that when analysis of coding patterns indicates two codes are billed together at least 51% of the time, that’s considered a ‘typical’ situation and a new code must be created combining them. The harsh reality for clinicians is that under what Dr. Sideman called “RUC math,” the new bundled codes invariably pay less than the two old ones.
“There was a little bit of smoke and mirrors – ‘Look at the pretty flashing lights and not what’s going on behind over here’ – as we tried to maintain value as we bundled these EVAR codes,” Dr. Sideman recalled. “I can stand here and tell you I did my very best to push for the best values possible. It can be a painful process, but I thought we came out ok.”
How the new EVAR codes work
Dr. Sideman explained that the impact of the new EVAR codes will depend upon a surgeon’s practice pattern.
He offered as a concrete example a patient undergoing elective EVAR of the aorta and both iliac arteries with percutaneous access and placement of a bifurcated device with one docking limb. In 2017, this might have been handled using CPT codes 34802, 36200-50, and 75952-26, for a total of 31.05 Relative Value Units (RVUs) of work.
In 2018, however, this same surgical strategy would be coded as 34705 (elective endovascular repair of infrarenal aorta and/or iliac artery or arteries) plus 34713 x 2 (percutaneous access and closure), for a total of 34.58 RVUs. Thus, the surgeon would come out 3.53 RVUs ahead in 2018, which at a conversion factor of $35.78/RVU translates to an extra $126.30.
On the other hand, if the surgeon chose to use a bifurcated device with one docking limb, a left iliac bell-bottom extension, a right iliac bell-bottom extension, and percutaneous access, in 2017, this would have been coded as 34802, 34825, 34826, 36200-50, 75952-26, and 75953-26 x 2, for a total of 44.29 RVUs of work. In 2018, this same treatment strategy would be coded as 34705 plus 34713 x 2, for a total of 34.58 RVUs, or a knockdown of 9.71 fewer RVUs compared with the year before, which translates to $347.42 less.
“The more extensions you use, the more you’re going to come out behind going forward,” according to Dr. Sideman.
Other coding changes in 2018
Sclerotherapy of single and multiple veins (codes 36470 and 36471) got down-valued from 1.10 and 2.49 to 0.75 and 1.5 RVUs, respectively.
Angiography of the extremities (75710 and 75716) will be better reimbursed in 2018. In what Dr. Sideman called “a good win,” unilateral angiography will be rated as 1.75 RVUs, up from 1.14 in 2017, while bilateral angiography increased from 1.31 to 1.97 RVUs.
“The other nice thing I can tell you is that through campaigning and lobbying and comments to CMS [Centers for Medicare & Medicaid Services], we got them to reverse their recommendations from 2017 to 2018 on the dialysis family of codes,” the surgeon continued.
Reimbursement for the dialysis codes took a big hit from 2016 to 2017, amounting to several hundred million dollars less in reimbursement, but CMS has reversed its policy on that score. The RVUs for the various dialysis codes have increased from 2017 to 2018 by 5%-21%, with central venous angioplasty (CPT 36907) garnering the biggest increase.
Existing RVUs were retained for 2018 in three of the four selective catheter placement codes. However, reimbursement for 36215 (first order catheterization of the thoracic or brachiocephalic branch) dropped from 4.67 to 4.17 RVUs because physician surveys showed the time involved was less than previously rated. Once the RUC and CMS saw that the time involved in a procedure has decreased, it became impossible to maintain the RVU, Dr. Sideman explained.
And speaking of time involved in procedures, Dr. Sideman offered a final plea to his vascular medicine colleagues:
“When you get surveys from the RUC asking for your input, please, please, please, fill them out because that’s how we get our direct physician input into the valuation of codes.”
He reported having no financial conflicts of interest regarding his presentation.
A detailed listing of many of the codes and changes can be found at the American College of Radiology website, and the Society for Vascular Surgery has coding resources available on their website, as well.
CHICAGO – Current Procedural Terminology coding for endovascular aneurysm repair has been totally overhauled for 2018 with the introduction of a family of 20 new codes and codes for other vascular procedures have also been updated.
The new EVAR CPT codes attempt to capture the work involved in performing the procedures based upon the anatomy of the aneurysm and the treated vessels rather than being device-based, as previously, Matthew J. Sideman, MD, explained in presenting the coding and reimbursement for 2018 at a symposium on vascular surgery sponsored by Northwestern University.
“The new EVAR codes for 2018 have got a lot of gains. There are some losses as well, but overall, I think it’s going to be very positive moving forward,” according to Dr. Sideman, a vascular surgeon at the University of Texas, San Antonio, who serves as chair of the Society for Vascular Surgery Coding and Reimbursement Committee and an adviser to the American Medical Association Relative Value Scale Update Committee (RUC).
“What we gained was a new code for ruptured aneurysm repair, a new code for enhanced fixation, a new code for percutaneous access, new codes for alternative access options, and now all the access codes are add-on codes. But what we traded off was loss due to bundling. So catheterization is now bundled into the main procedure, radiographic supervision and interpretation is now bundled. The big thing that really hurt was we lost all proximal extensions to the renal arteries and all distal extensions to the iliac bifurcations – they’re also bundled into the main procedure,” he said.
Restructuring the EVAR codes was a multiyear collaborative project of the SVS, the American College of Surgeons, the Society of Interventional Radiology, the Society of Thoracic Surgery, the American College of Cardiology, and the Society for Cardiovascular Angiography and Interventions. The impetus was twofold: recognition that the existing codes seriously undervalued the work involved in EVAR because, for example, they didn’t distinguish between ruptured and elective aneurysm repair, nor did they recognize the unique challenges and advantages of percutaneous access.
Also, representatives of the professional societies involved with vascular medicine recognized that they had to develop a detailed proposal for coding restructuring or matters might be taken out of their hands. Bundling of codes has become the prevailing dogma at the RUC and the Centers for Medicare and Medicaid. Their current policy is that when analysis of coding patterns indicates two codes are billed together at least 51% of the time, that’s considered a ‘typical’ situation and a new code must be created combining them. The harsh reality for clinicians is that under what Dr. Sideman called “RUC math,” the new bundled codes invariably pay less than the two old ones.
“There was a little bit of smoke and mirrors – ‘Look at the pretty flashing lights and not what’s going on behind over here’ – as we tried to maintain value as we bundled these EVAR codes,” Dr. Sideman recalled. “I can stand here and tell you I did my very best to push for the best values possible. It can be a painful process, but I thought we came out ok.”
How the new EVAR codes work
Dr. Sideman explained that the impact of the new EVAR codes will depend upon a surgeon’s practice pattern.
He offered as a concrete example a patient undergoing elective EVAR of the aorta and both iliac arteries with percutaneous access and placement of a bifurcated device with one docking limb. In 2017, this might have been handled using CPT codes 34802, 36200-50, and 75952-26, for a total of 31.05 Relative Value Units (RVUs) of work.
In 2018, however, this same surgical strategy would be coded as 34705 (elective endovascular repair of infrarenal aorta and/or iliac artery or arteries) plus 34713 x 2 (percutaneous access and closure), for a total of 34.58 RVUs. Thus, the surgeon would come out 3.53 RVUs ahead in 2018, which at a conversion factor of $35.78/RVU translates to an extra $126.30.
On the other hand, if the surgeon chose to use a bifurcated device with one docking limb, a left iliac bell-bottom extension, a right iliac bell-bottom extension, and percutaneous access, in 2017, this would have been coded as 34802, 34825, 34826, 36200-50, 75952-26, and 75953-26 x 2, for a total of 44.29 RVUs of work. In 2018, this same treatment strategy would be coded as 34705 plus 34713 x 2, for a total of 34.58 RVUs, or a knockdown of 9.71 fewer RVUs compared with the year before, which translates to $347.42 less.
“The more extensions you use, the more you’re going to come out behind going forward,” according to Dr. Sideman.
Other coding changes in 2018
Sclerotherapy of single and multiple veins (codes 36470 and 36471) got down-valued from 1.10 and 2.49 to 0.75 and 1.5 RVUs, respectively.
Angiography of the extremities (75710 and 75716) will be better reimbursed in 2018. In what Dr. Sideman called “a good win,” unilateral angiography will be rated as 1.75 RVUs, up from 1.14 in 2017, while bilateral angiography increased from 1.31 to 1.97 RVUs.
“The other nice thing I can tell you is that through campaigning and lobbying and comments to CMS [Centers for Medicare & Medicaid Services], we got them to reverse their recommendations from 2017 to 2018 on the dialysis family of codes,” the surgeon continued.
Reimbursement for the dialysis codes took a big hit from 2016 to 2017, amounting to several hundred million dollars less in reimbursement, but CMS has reversed its policy on that score. The RVUs for the various dialysis codes have increased from 2017 to 2018 by 5%-21%, with central venous angioplasty (CPT 36907) garnering the biggest increase.
Existing RVUs were retained for 2018 in three of the four selective catheter placement codes. However, reimbursement for 36215 (first order catheterization of the thoracic or brachiocephalic branch) dropped from 4.67 to 4.17 RVUs because physician surveys showed the time involved was less than previously rated. Once the RUC and CMS saw that the time involved in a procedure has decreased, it became impossible to maintain the RVU, Dr. Sideman explained.
And speaking of time involved in procedures, Dr. Sideman offered a final plea to his vascular medicine colleagues:
“When you get surveys from the RUC asking for your input, please, please, please, fill them out because that’s how we get our direct physician input into the valuation of codes.”
He reported having no financial conflicts of interest regarding his presentation.
A detailed listing of many of the codes and changes can be found at the American College of Radiology website, and the Society for Vascular Surgery has coding resources available on their website, as well.
EXPERT ANALYSIS FROM THE NORTHWESTERN VASCULAR SYMPOSIUM
QI enthusiast to QI leader: Sheri Chernetsky Tejedor, MD
Armed with a background in engineering, Sheri Chernetsky Tejedor, MD, SFHM, had already adopted a mindset of system reliability and design improvement when she began her journey in hospital medicine at Johns Hopkins University in Baltimore.
After completing her studies there, Dr. Tejedor was quick to find a place at Emory Healthcare in Atlanta and began working toward a future in health care quality improvement (QI).
“I gravitated early on toward what was essentially quality improvement work,” Dr. Tejedor told The Hospitalist.
Dr. Tejedor worked with two mentors at a community hospital associated with Emory University who helped influence her success in QI: Mark V. Williams, MD, FACP, MHM, who is now the director of the Center for Health Services Research at the University of Kentucky in Lexington, and Jason Stein, MD, SFHM, who is currently a hospitalist at Emory University Hospital.
“They wanted to develop quality improvement expertise and get some of us trained,” she said. “These advocates, or mentors, were critical for me. They are people who went above and beyond to help with career planning and thinking through possibilities.”
Dr. Tejedor and Dr. Stein traveled to Intermountain Healthcare, a not-for-profit health system based in Salt Lake City that focuses on medical innovation, to participate in a rigorous quality training program.
“It was extremely intense,” said Dr. Tejedor. “You worked over several months to get a certificate from the Institute for Healthcare Delivery Research, and it’s all focused on quality improvement methodology.”
After completing this program, Dr. Tejedor continued on her quality improvement path by focusing on research while also simultaneously working part time and taking care of her three young children. During this phase of her career, Dr. Tejedor and her colleagues published a study on idle central venous catheters, which became a primary reference for part of the ABIM Foundation’s Choosing Wisely® campaign.
Dr. Tejedor said that, in addition to research, she explored different leadership roles, such as taking charge of central line teams and nurses working on device insertion practices. Her successful projects drew notice, and soon Dr. Tejedor and Dr. Stein helped to implement a stronger focus on quality improvement at their organization.
“Our health system was very entrenched in that QI culture,” Dr. Tejedor said. “After Jason and I went to Intermountain, many of the Emory Healthcare leadership also got trained in Utah, and we ultimately built a quality course at Emory that mirrored it.”
Dr. Tejedor’s research evolved to intersect with clinical informatics. She leveraged the organization’s electronic medical record to test her work.
“[The EMR] is ubiquitous, and that was a good way to reach staff, test interventions, and get data,” Dr. Tejedor said. “I built a lot of tools that were helpful for the health system.”
One of these tools was a device to monitor central line infections that was linked with clinical informatics as part of a large grant project. This led to another leadership opportunity: She assumed the role of chief research information officer and director for analytics at Emory Healthcare in 2013.

In 2014, Dr. Tejedor began working with the Centers for Disease Control and Prevention as the first hospitalist and informatics specialist on the Healthcare Infection Control Practices Advisory Committee, where she continues to hold a position. She is also a medical advisor for the CDC’s Division of Healthcare Quality Promotion, focusing on electronic quality measures.
For those hospitalists pursuing QI, exposure to formal training is essential, Dr. Tejedor said. That may not mean flying to Utah, she noted, but garnering a deeper understanding of informatics is crucial.
When it comes to leadership, Dr. Tejedor recommends that those looking to take charge develop social skills and embrace parts of medicine that may be unfamiliar yet essential.
“Learn a little bit about the business side, which you may not know much about as a doctor taking care of patients,” she said. “Learn just enough to understand what goes into people’s decision making when they are choosing what projects get approved.”
Dr. Tejedor encourages hospitalists to focus on developing relationships because that was one of the keys to her success as a quality improvement leader.
“It’s about gaining the trust of the staff, mutual respect, working with the nurses, and getting to know the leadership and the people who make the financial decisions,” she said. “Even if you have the money for a quality improvement project, it will fail if you don’t work with the various teams to understand their needs and how to make it work for them.”
[email protected]
On Twitter @eaztweets
Armed with a background in engineering, Sheri Chernetsky Tejedor, MD, SFHM, had already adopted a mindset of system reliability and design improvement when she began her journey in hospital medicine at Johns Hopkins University in Baltimore.
After completing her studies there, Dr. Tejedor was quick to find a place at Emory Healthcare in Atlanta and began working toward a future in health care quality improvement (QI).
“I gravitated early on toward what was essentially quality improvement work,” Dr. Tejedor told The Hospitalist.
Dr. Tejedor worked with two mentors at a community hospital associated with Emory University who helped influence her success in QI: Mark V. Williams, MD, FACP, MHM, who is now the director of the Center for Health Services Research at the University of Kentucky in Lexington, and Jason Stein, MD, SFHM, who is currently a hospitalist at Emory University Hospital.
“They wanted to develop quality improvement expertise and get some of us trained,” she said. “These advocates, or mentors, were critical for me. They are people who went above and beyond to help with career planning and thinking through possibilities.”
Dr. Tejedor and Dr. Stein traveled to Intermountain Healthcare, a not-for-profit health system based in Salt Lake City that focuses on medical innovation, to participate in a rigorous quality training program.
“It was extremely intense,” said Dr. Tejedor. “You worked over several months to get a certificate from the Institute for Healthcare Delivery Research, and it’s all focused on quality improvement methodology.”
After completing this program, Dr. Tejedor continued on her quality improvement path by focusing on research while also simultaneously working part time and taking care of her three young children. During this phase of her career, Dr. Tejedor and her colleagues published a study on idle central venous catheters, which became a primary reference for part of the ABIM Foundation’s Choosing Wisely® campaign.
Dr. Tejedor said that, in addition to research, she explored different leadership roles, such as taking charge of central line teams and nurses working on device insertion practices. Her successful projects drew notice, and soon Dr. Tejedor and Dr. Stein helped to implement a stronger focus on quality improvement at their organization.
“Our health system was very entrenched in that QI culture,” Dr. Tejedor said. “After Jason and I went to Intermountain, many of the Emory Healthcare leadership also got trained in Utah, and we ultimately built a quality course at Emory that mirrored it.”
Dr. Tejedor’s research evolved to intersect with clinical informatics. She leveraged the organization’s electronic medical record to test her work.
“[The EMR] is ubiquitous, and that was a good way to reach staff, test interventions, and get data,” Dr. Tejedor said. “I built a lot of tools that were helpful for the health system.”
One of these tools was a device to monitor central line infections that was linked with clinical informatics as part of a large grant project. This led to another leadership opportunity: She assumed the role of chief research information officer and director for analytics at Emory Healthcare in 2013.
In 2014, Dr. Tejedor began working with the Centers for Disease Control and Prevention as the first hospitalist and informatics specialist on the Healthcare Infection Control Practices Advisory Committee, where she continues to hold a position. She is also a medical advisor for the CDC’s Division of Healthcare Quality Promotion, focusing on electronic quality measures.
For those hospitalists pursuing QI, exposure to formal training is essential, Dr. Tejedor said. That may not mean flying to Utah, she noted, but garnering a deeper understanding of informatics is crucial.
When it comes to leadership, Dr. Tejedor recommends that those looking to take charge develop social skills and embrace parts of medicine that may be unfamiliar yet essential.
“Learn a little bit about the business side, which you may not know much about as a doctor taking care of patients,” she said. “Learn just enough to understand what goes into people’s decision making when they are choosing what projects get approved.”
Dr. Tejedor encourages hospitalists to focus on developing relationships because that was one of the keys to her success as a quality improvement leader.
“It’s about gaining the trust of the staff, mutual respect, working with the nurses, and getting to know the leadership and the people who make the financial decisions,” she said. “Even if you have the money for a quality improvement project, it will fail if you don’t work with the various teams to understand their needs and how to make it work for them.”
[email protected]
On Twitter @eaztweets
Armed with a background in engineering, Sheri Chernetsky Tejedor, MD, SFHM, had already adopted a mindset of system reliability and design improvement when she began her journey in hospital medicine at Johns Hopkins University in Baltimore.
After completing her studies there, Dr. Tejedor was quick to find a place at Emory Healthcare in Atlanta and began working toward a future in health care quality improvement (QI).
“I gravitated early on toward what was essentially quality improvement work,” Dr. Tejedor told The Hospitalist.
Dr. Tejedor worked with two mentors at a community hospital associated with Emory University who helped influence her success in QI: Mark V. Williams, MD, FACP, MHM, who is now the director of the Center for Health Services Research at the University of Kentucky in Lexington, and Jason Stein, MD, SFHM, who is currently a hospitalist at Emory University Hospital.
“They wanted to develop quality improvement expertise and get some of us trained,” she said. “These advocates, or mentors, were critical for me. They are people who went above and beyond to help with career planning and thinking through possibilities.”
Dr. Tejedor and Dr. Stein traveled to Intermountain Healthcare, a not-for-profit health system based in Salt Lake City that focuses on medical innovation, to participate in a rigorous quality training program.
“It was extremely intense,” said Dr. Tejedor. “You worked over several months to get a certificate from the Institute for Healthcare Delivery Research, and it’s all focused on quality improvement methodology.”
After completing this program, Dr. Tejedor continued on her quality improvement path by focusing on research while also simultaneously working part time and taking care of her three young children. During this phase of her career, Dr. Tejedor and her colleagues published a study on idle central venous catheters, which became a primary reference for part of the ABIM Foundation’s Choosing Wisely® campaign.
Dr. Tejedor said that, in addition to research, she explored different leadership roles, such as taking charge of central line teams and nurses working on device insertion practices. Her successful projects drew notice, and soon Dr. Tejedor and Dr. Stein helped to implement a stronger focus on quality improvement at their organization.
“Our health system was very entrenched in that QI culture,” Dr. Tejedor said. “After Jason and I went to Intermountain, many of the Emory Healthcare leadership also got trained in Utah, and we ultimately built a quality course at Emory that mirrored it.”
Dr. Tejedor’s research evolved to intersect with clinical informatics. She leveraged the organization’s electronic medical record to test her work.
“[The EMR] is ubiquitous, and that was a good way to reach staff, test interventions, and get data,” Dr. Tejedor said. “I built a lot of tools that were helpful for the health system.”
One of these tools was a device to monitor central line infections that was linked with clinical informatics as part of a large grant project. This led to another leadership opportunity: She assumed the role of chief research information officer and director for analytics at Emory Healthcare in 2013.
In 2014, Dr. Tejedor began working with the Centers for Disease Control and Prevention as the first hospitalist and informatics specialist on the Healthcare Infection Control Practices Advisory Committee, where she continues to hold a position. She is also a medical advisor for the CDC’s Division of Healthcare Quality Promotion, focusing on electronic quality measures.
For those hospitalists pursuing QI, exposure to formal training is essential, Dr. Tejedor said. That may not mean flying to Utah, she noted, but garnering a deeper understanding of informatics is crucial.
When it comes to leadership, Dr. Tejedor recommends that those looking to take charge develop social skills and embrace parts of medicine that may be unfamiliar yet essential.
“Learn a little bit about the business side, which you may not know much about as a doctor taking care of patients,” she said. “Learn just enough to understand what goes into people’s decision making when they are choosing what projects get approved.”
Dr. Tejedor encourages hospitalists to focus on developing relationships because that was one of the keys to her success as a quality improvement leader.
“It’s about gaining the trust of the staff, mutual respect, working with the nurses, and getting to know the leadership and the people who make the financial decisions,” she said. “Even if you have the money for a quality improvement project, it will fail if you don’t work with the various teams to understand their needs and how to make it work for them.”
[email protected]
On Twitter @eaztweets
Burnout among surgical residents mitigated by traits of mindfulness
General surgery residents reported high levels of stress linked to burnout, but those who exhibited characteristics of mindfulness were less likely to experience this dynamic, a survey-based study has found.
Carter C. Lebares, MD, of the department of surgery at the University of California, San Francisco, and her colleagues wrote, “Stress is a double-edged sword, with a dose-response relationship between stress and performance described as an ‘inverted U-shaped curve.’ Although stress is initially stimulating, there is a tipping point when demands outstrip resources and stress becomes overwhelming,” the researchers wrote. Surgical trainees purposefully join a high-stress profession and presumably thrive on a demanding environment, but “that does not make individuals immune to the effects of overwhelming stress.”
The investigative team aimed to assess the prevalence and root causes of burnout among surgical trainees. They sent a survey questionnaire to 246 general surgery training program directors and asked them to distribute the survey to their residents (J Am Coll Surg. 2018 Jan;226[1]:80-90. doi: 10.1016/j.jamcollsurg.2017.10.010). The investigators focused on the components of burnout identified in the literature (emotional exhaustion, depersonalization, perceived stress, depression, anxiety, and alcohol misuse/abuse).
The survey, a voluntary and confidential exercise, was based on scales and tools to assess symptoms of burnout (Maslach Burnout Inventory), stress (Cohen’s Perceived Stress Scale), anxiety (Spielberger’s State Trait Anxiety Index), and depression/suicidal ideation (Patient Health Questionnaire).
The researchers also looked at personality traits that could make the difference between the usual stress of residency and burnout in individual trainees. Mindfulness was studied using the Cognitive Affective Mindfulness Scale–Revised. A personality characteristic “trait resilience” was captured in a 10-item Block Ego-Resiliency Scale, which measured ability to adapt to a demanding and changing environment. “Dispositional mindfulness, that is, the innate ability to pay attention to one’s thoughts, emotions, and experiences in a nonreactive way, has been shown to have a buffering effect against perceived stress and burnout among healthcare workers and trainees,” they wrote.
A total of 566 surgery residents responded to the survey; 51% were female and 76% were based in an academic training program. Overall, the survey found that burnout prevalence among general surgery residents was 69%, which confirms the findings of earlier studies of this population, and was significantly higher than rates seen in age-matched peers in the general population and among practicing surgeons. Burnout was equally prevalent among men and women, but men appeared more likely to experience depersonalization (62% vs. 51%). Emotional exhaustion was lower among lab trainees. Alcohol misuse and abuse was somewhat higher in women (58% vs. 41% and 40% vs. 26%, respectively). Although symptoms of burnout were not strongly associated with training level, PGY3 residents experienced the most (58% reported higher stress, 16% suicidal ideation, 50% high anxiety, and 61% alcohol abuse). A high level of stress was reported significantly less often by lab trainees, but alcohol misuse was significantly greater. A high level of stress and emotional exhaustion and depersonalization were strongly linked. And all of these elements were strongly associated with moderate to severe depressive symptoms, suicidal ideation, and high anxiety.
The study is limited by potential biases in the responses, inevitable in a voluntary, self-selected sample. The survey was sent to ACGME-accredited program directors who may or may not have distributed it to their trainees. The investigators suggested that whereas the findings of this study in general confirm earlier research on trainee burnout, the perception of lack personal accomplishment in this sample was less dominant in this sample. “Although this might be because we included residents in lab/research years (widely thought to be a time of very high productivity), it is more likely due to our use of an abbreviated (9-item) form of the Maslach Burnout Inventory-Human Services Survey” and therefore underreported the personal accomplishment factor.
The impact that personality traits (mindfulness and trait resilience) on burnout risk was notable in this sample. “Greater dispositional mindfulness was associated with an 85% decrease in the risk of high stress, and a greater trait resilience was associated with a 65% decrease in the risk of high stress.” Some individuals have traits to help them cope better with stress but the investigators stated that mindfulness and resilience can be taught and fostered in trainees.
The current research on burnout has identified both institutional factors and personal factors. This study suggests that strategies to address both, simultaneously, are needed to truly change the current burnout risk prevalence among surgical trainees. They concluded: “Our findings demonstrate that inherent mindfulness is already in use to combat stress and burnout in surgical trainees and, more importantly, it appears to work. Based on this evidence, mindfulness training can be a critical component of any intervention aimed at enhancing stress resilience and preventing or treating burnout in surgical trainees.”
The researchers reported no relevant financial conflicts.
SOURCE: J Am Coll Surg. 2018 Jan;226(1):80-90. doi: 10.1016/j.jamcollsurg.2017.10.010)
General surgery residents reported high levels of stress linked to burnout, but those who exhibited characteristics of mindfulness were less likely to experience this dynamic, a survey-based study has found.
Carter C. Lebares, MD, of the department of surgery at the University of California, San Francisco, and her colleagues wrote, “Stress is a double-edged sword, with a dose-response relationship between stress and performance described as an ‘inverted U-shaped curve.’ Although stress is initially stimulating, there is a tipping point when demands outstrip resources and stress becomes overwhelming,” the researchers wrote. Surgical trainees purposefully join a high-stress profession and presumably thrive on a demanding environment, but “that does not make individuals immune to the effects of overwhelming stress.”
The investigative team aimed to assess the prevalence and root causes of burnout among surgical trainees. They sent a survey questionnaire to 246 general surgery training program directors and asked them to distribute the survey to their residents (J Am Coll Surg. 2018 Jan;226[1]:80-90. doi: 10.1016/j.jamcollsurg.2017.10.010). The investigators focused on the components of burnout identified in the literature (emotional exhaustion, depersonalization, perceived stress, depression, anxiety, and alcohol misuse/abuse).
The survey, a voluntary and confidential exercise, was based on scales and tools to assess symptoms of burnout (Maslach Burnout Inventory), stress (Cohen’s Perceived Stress Scale), anxiety (Spielberger’s State Trait Anxiety Index), and depression/suicidal ideation (Patient Health Questionnaire).
The researchers also looked at personality traits that could make the difference between the usual stress of residency and burnout in individual trainees. Mindfulness was studied using the Cognitive Affective Mindfulness Scale–Revised. A personality characteristic “trait resilience” was captured in a 10-item Block Ego-Resiliency Scale, which measured ability to adapt to a demanding and changing environment. “Dispositional mindfulness, that is, the innate ability to pay attention to one’s thoughts, emotions, and experiences in a nonreactive way, has been shown to have a buffering effect against perceived stress and burnout among healthcare workers and trainees,” they wrote.
A total of 566 surgery residents responded to the survey; 51% were female and 76% were based in an academic training program. Overall, the survey found that burnout prevalence among general surgery residents was 69%, which confirms the findings of earlier studies of this population, and was significantly higher than rates seen in age-matched peers in the general population and among practicing surgeons. Burnout was equally prevalent among men and women, but men appeared more likely to experience depersonalization (62% vs. 51%). Emotional exhaustion was lower among lab trainees. Alcohol misuse and abuse was somewhat higher in women (58% vs. 41% and 40% vs. 26%, respectively). Although symptoms of burnout were not strongly associated with training level, PGY3 residents experienced the most (58% reported higher stress, 16% suicidal ideation, 50% high anxiety, and 61% alcohol abuse). A high level of stress was reported significantly less often by lab trainees, but alcohol misuse was significantly greater. A high level of stress and emotional exhaustion and depersonalization were strongly linked. And all of these elements were strongly associated with moderate to severe depressive symptoms, suicidal ideation, and high anxiety.
The study is limited by potential biases in the responses, inevitable in a voluntary, self-selected sample. The survey was sent to ACGME-accredited program directors who may or may not have distributed it to their trainees. The investigators suggested that whereas the findings of this study in general confirm earlier research on trainee burnout, the perception of lack personal accomplishment in this sample was less dominant in this sample. “Although this might be because we included residents in lab/research years (widely thought to be a time of very high productivity), it is more likely due to our use of an abbreviated (9-item) form of the Maslach Burnout Inventory-Human Services Survey” and therefore underreported the personal accomplishment factor.
The impact that personality traits (mindfulness and trait resilience) on burnout risk was notable in this sample. “Greater dispositional mindfulness was associated with an 85% decrease in the risk of high stress, and a greater trait resilience was associated with a 65% decrease in the risk of high stress.” Some individuals have traits to help them cope better with stress but the investigators stated that mindfulness and resilience can be taught and fostered in trainees.
The current research on burnout has identified both institutional factors and personal factors. This study suggests that strategies to address both, simultaneously, are needed to truly change the current burnout risk prevalence among surgical trainees. They concluded: “Our findings demonstrate that inherent mindfulness is already in use to combat stress and burnout in surgical trainees and, more importantly, it appears to work. Based on this evidence, mindfulness training can be a critical component of any intervention aimed at enhancing stress resilience and preventing or treating burnout in surgical trainees.”
The researchers reported no relevant financial conflicts.
SOURCE: J Am Coll Surg. 2018 Jan;226(1):80-90. doi: 10.1016/j.jamcollsurg.2017.10.010)
General surgery residents reported high levels of stress linked to burnout, but those who exhibited characteristics of mindfulness were less likely to experience this dynamic, a survey-based study has found.
Carter C. Lebares, MD, of the department of surgery at the University of California, San Francisco, and her colleagues wrote, “Stress is a double-edged sword, with a dose-response relationship between stress and performance described as an ‘inverted U-shaped curve.’ Although stress is initially stimulating, there is a tipping point when demands outstrip resources and stress becomes overwhelming,” the researchers wrote. Surgical trainees purposefully join a high-stress profession and presumably thrive on a demanding environment, but “that does not make individuals immune to the effects of overwhelming stress.”
The investigative team aimed to assess the prevalence and root causes of burnout among surgical trainees. They sent a survey questionnaire to 246 general surgery training program directors and asked them to distribute the survey to their residents (J Am Coll Surg. 2018 Jan;226[1]:80-90. doi: 10.1016/j.jamcollsurg.2017.10.010). The investigators focused on the components of burnout identified in the literature (emotional exhaustion, depersonalization, perceived stress, depression, anxiety, and alcohol misuse/abuse).
The survey, a voluntary and confidential exercise, was based on scales and tools to assess symptoms of burnout (Maslach Burnout Inventory), stress (Cohen’s Perceived Stress Scale), anxiety (Spielberger’s State Trait Anxiety Index), and depression/suicidal ideation (Patient Health Questionnaire).
The researchers also looked at personality traits that could make the difference between the usual stress of residency and burnout in individual trainees. Mindfulness was studied using the Cognitive Affective Mindfulness Scale–Revised. A personality characteristic “trait resilience” was captured in a 10-item Block Ego-Resiliency Scale, which measured ability to adapt to a demanding and changing environment. “Dispositional mindfulness, that is, the innate ability to pay attention to one’s thoughts, emotions, and experiences in a nonreactive way, has been shown to have a buffering effect against perceived stress and burnout among healthcare workers and trainees,” they wrote.
A total of 566 surgery residents responded to the survey; 51% were female and 76% were based in an academic training program. Overall, the survey found that burnout prevalence among general surgery residents was 69%, which confirms the findings of earlier studies of this population, and was significantly higher than rates seen in age-matched peers in the general population and among practicing surgeons. Burnout was equally prevalent among men and women, but men appeared more likely to experience depersonalization (62% vs. 51%). Emotional exhaustion was lower among lab trainees. Alcohol misuse and abuse was somewhat higher in women (58% vs. 41% and 40% vs. 26%, respectively). Although symptoms of burnout were not strongly associated with training level, PGY3 residents experienced the most (58% reported higher stress, 16% suicidal ideation, 50% high anxiety, and 61% alcohol abuse). A high level of stress was reported significantly less often by lab trainees, but alcohol misuse was significantly greater. A high level of stress and emotional exhaustion and depersonalization were strongly linked. And all of these elements were strongly associated with moderate to severe depressive symptoms, suicidal ideation, and high anxiety.
The study is limited by potential biases in the responses, inevitable in a voluntary, self-selected sample. The survey was sent to ACGME-accredited program directors who may or may not have distributed it to their trainees. The investigators suggested that whereas the findings of this study in general confirm earlier research on trainee burnout, the perception of lack personal accomplishment in this sample was less dominant in this sample. “Although this might be because we included residents in lab/research years (widely thought to be a time of very high productivity), it is more likely due to our use of an abbreviated (9-item) form of the Maslach Burnout Inventory-Human Services Survey” and therefore underreported the personal accomplishment factor.
The impact that personality traits (mindfulness and trait resilience) on burnout risk was notable in this sample. “Greater dispositional mindfulness was associated with an 85% decrease in the risk of high stress, and a greater trait resilience was associated with a 65% decrease in the risk of high stress.” Some individuals have traits to help them cope better with stress but the investigators stated that mindfulness and resilience can be taught and fostered in trainees.
The current research on burnout has identified both institutional factors and personal factors. This study suggests that strategies to address both, simultaneously, are needed to truly change the current burnout risk prevalence among surgical trainees. They concluded: “Our findings demonstrate that inherent mindfulness is already in use to combat stress and burnout in surgical trainees and, more importantly, it appears to work. Based on this evidence, mindfulness training can be a critical component of any intervention aimed at enhancing stress resilience and preventing or treating burnout in surgical trainees.”
The researchers reported no relevant financial conflicts.
SOURCE: J Am Coll Surg. 2018 Jan;226(1):80-90. doi: 10.1016/j.jamcollsurg.2017.10.010)
FROM JOURNAL OF THE AMERICAN COLLEGE OF SURGERY
Key clinical point: Burnout prevalence is high among surgical trainees, but individual traits such as mindfulness are linked to a lower risk of burnout.
Major finding: Among surgery residents, the total prevalence of burnout was 69%.
Study details: 566 responses to a voluntary and confidential survey of general surgery residents.
Disclosures: Investigators had no relevant financial disclosures.
Source: J Am Coll Surg. 2018 Jan;226(1):80-90. doi: 10.1016/j.jamcollsurg.2017.10.010.
Sneak Peek: The Hospital Leader blog – Dec. 2017
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.

Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.
Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Cultivating women leaders in health care #WIMmonth #ThisIsWhatADoctorLooksLike
On my flight home from Scotland, I had a moment to watch a movie while my daughter was caught up in the encore adventures of Moana. I stumbled upon “Hidden Figures,” the story of the African American women at NASA who helped launch John Glenn into space, reviving the nation’s space program.
Turns out I wasn’t the only one who stumbled upon this. Harvard researcher Julie Silver, MD, raised the question about invisible women leaders when reviewing quotes in magazines like Modern Healthcare or Forbes. Moreover, her research demonstrates that, for many professional society awards, 0% are given to women! This is happening in specialties that had nearly even proportions of women and men in practice, such as dermatology and rehab medicine. Last month, I was dumbfounded when I saw a full-page New York Times ad of Top Surgeons by Castle Connolly featuring 16 surgeons, all male.
While Castle Connolly does name female top doctors and market ad opportunities to women and men, I learned that only men sign up for the ads. While this raises more questions, the optics remain problematic – women doctors are hidden. Regardless of the venue, we must do a better job profiling our female leaders. In addition, it is important to recognize that female leaders face well-documented and somewhat controversial challenges that require careful thought:
- Stereotype threat: Some of the original research on stereotype threat done in college students showed that, if women who are about to take a math test are told that the test will expose gender differences, such as men do better at math, women will perform worse AND men will do better. The threat of stereotypes is that women can internalize them and this may hamper their progress. The good news is that education on stereotype threat apparently helps.
- Impostor syndrome: Even highly successful people apparently suffer from impostor syndrome, the fear that they do not deserve their success, but it is much worse in women than in men. You are always trying to conquer the little voice in your head that tells you that you are not good enough.
Read the full post at hospitalleader.org.
Also on The Hospital Leader …
- If I were you, I would not be bullish on long-term care by Brad Flansbaum, DO, MPH, MHM
- Da Vinci wuz here by Jordan Messler, MD, SFHM
- Making the implicit explicit by Leslie Flores, MHA, SFHM
- Should we really focus on “patient-centered care”? by Tracy Cardin, ACNP-BC, SFHM
Massachusetts and the opioid crisis: Can involuntary holds work?
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.

As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.
As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
My son played on a neighborhood little league team for several years. I have such sweet memories of little boys in baseball uniforms lined up on the bench singing cheers while they waited their turns to go to bat. The two devoted dads who worked together coaching the team were a gentle presence in the background of my family’s life every spring for years. One might hope that the love and attention those fathers invested in their sons and their teammates might confer some special protection from life’s tragedies, but the opioid epidemic spares no hostages, and last year, one of those singing little boys from so many years ago – the son of one of the coaches – died of a drug overdose.
President Trump has punted on how to stop the epidemic, one he finally deemed a national public health emergency in October, with no clear addition of federal resources. States have varied in their responses, and Massachusetts, in particular, has been aggressive with new legislation and funding. The laws in Massachusetts allow for involuntary rehab for substance abusers if a family member petitions the court under the state’s decades-old section 35. The irony is that much of this “involuntary” treatment is voluntary: People will ask family members to apply for them as a way of getting into treatment and as a way of bypassing the cost. Section 35 admissions are funded by the state, not by the individual or by health insurance.
As a Boston Globe article (“Mass. governor aims to expand battle against opioid addiction,” Nov. 15, 2017) explains, “Two years ago, Baker stirred controversy with a proposal to hold addicted patients for 72 hours against their will in emergency departments. That idea was rejected by the Legislature. The new bill takes a different approach to the 72-hour hold, enabling doctors to transfer patients with addiction to a treatment facility, much as they would with a person deemed a danger because of mental illness.”
The issues with involuntary care are complicated and nuanced in psychiatric disorders, and perhaps even more so with substance abuse. The time frame of 72 hours for mental health conditions allows for assessment and sometimes for the start of treatment. In some states, a hearing must be held for continued involuntary detention; in other states, a decision must be made as to whether further inpatient care will be pursued, and the actual hearing takes place days to weeks later, depending on the state. For the purposes of allowing someone to clear from an opioid intoxication, then persuading them to engage in voluntary substance abuse treatment, it seems that 72 hours could be the exact wrong time period.
Ideally, a patient would be placed in a comfortable inpatient unit, begun on medication-assisted withdrawal, and offered a high quality of care for those 72 hours so that continuing with treatment might be a palatable option. But would that actually happen? Does Massachusetts have the means and facilities for all its overdose patients? Massachusetts has, in fact, been aggressive with funding. Since 2015, the state has added 1,100 new treatment beds. The efforts to fund and offer novel treatments are commendable. My concern remains that without adequate treatment or a positive experience – a difficult target in the best of circumstances for a patient who is 72 hours into opioid withdrawal – patients would leave only to resume their substance abuse. In a disastrous scenario, patients who have overdosed and fear being detained might not call for help, and the death rate could actually rise.
John A. Renner Jr., MD, is the past president of the American Academy of Addiction Psychiatry and coeditor of Office-Based Buprenorphine Treatment of Opioid Use Disorder (American Psychiatric Association Publishing, 2018). Dr. Renner, who is a professor at Boston University, said, “I would like to see some evidence and research to be sure there were not unintended harms before we go this route.”
Eric C. Strain, MD, director of the Johns Hopkins Center for Substance Abuse Treatment and Research, Baltimore, noted: “Simply holding someone for 3 days, especially against their will, doesn’t make a lot of sense. They are certainly not going to be all better either from a physiological or psychological standpoint. It might, however, be possible to get a person who was not interested in treatment engaged in treatment, and that would be a success.”
Despite the increased numbers of beds and aggressive, thoughtful interventions, Massachusetts still had 1,450 overdose deaths in the first 9 months of 2017, a decrease of only 10% from the year before, according to the Globe article. For the sake of the former Little League players in Maryland, and all the other victims of this lethal nationwide epidemic, it is imperative that any untested treatments be the source of new research. If these measures are implemented, it is essential that Massachusetts follow the people who are the beneficiaries of interventions and create the data that allow other states to either follow suit if these efforts are successful, or allocate resources to other treatments if they are not.
Dr. Miller is coauthor with Annette Hanson, MD, of Committed: The Battle Over Involuntary Psychiatry Care (Baltimore: Johns Hopkins University Press, 2016).
Laparoscopic nerve-sparing approach is effective in deep infiltrating endometriosis
NATIONAL HARBOR, MD. – Laparoscopic retroperitoneal nerve-sparing surgery is a safe approach that relieves pain in women with deep infiltrating endometriosis, according to findings presented by Giovanni Roviglione, MD, at the AAGL Global Congress.
The prospective case series study with a single gynecologic surgeon in Verona, Italy, involved 382 women who had deep infiltrating endometriosis with sciatica and anogenital pain. All of the women had some level of nervous compression of somatic structures and infiltration of their fascial envelope.
The surgery involved whole decompression and partial neurolysis of nervous structures for most patients, while nearly 20% of women required complete neurolysis based on their level of infiltration. Most women (64%) had severe enough infiltration that a concomitant bowel resection was also necessary.
The surgeon performed a medial approach for deep pelvic endometriosis with rectal and/or parametrial involvement extending to the pelvic wall and somatic nerve, or a lateral approach for isolated endometriosis of the pelvic wall and somatic nerves.
At 6 months after surgery, all patients reported complete relief from pain. However, 77 women (20%) experienced postoperative neuritis, which was successfully treated with corticosteroids, antiepileptics, and opioids.
Endometriosis that extends into somatic nerves and the sacral roots is a common cause of pelvic pain, Dr. Roviglione said.
“This kind of endometriosis is resistant to opioids and drugs,” he said. The difficulty in treating deep infiltrating endometriosis is compounded by the often long delay in diagnosis, he added.
Using laparoscopy for neurolysis and decompression of somatic nerves affected by endometriosis is a “more accurate and effective treatment” for providing pain relief, Dr. Roviglione said. But laparoscopic retroperitoneal nerve-sparing surgery should be performed only by skilled neuroanatomy surgeons at referral centers because of the complex nature of the procedure, he noted.
Dr. Roviglione reported having no relevant financial disclosures.
SOURCE: Ceccaroni M et al. AAGL 2017 Abstract 166.
NATIONAL HARBOR, MD. – Laparoscopic retroperitoneal nerve-sparing surgery is a safe approach that relieves pain in women with deep infiltrating endometriosis, according to findings presented by Giovanni Roviglione, MD, at the AAGL Global Congress.
The prospective case series study with a single gynecologic surgeon in Verona, Italy, involved 382 women who had deep infiltrating endometriosis with sciatica and anogenital pain. All of the women had some level of nervous compression of somatic structures and infiltration of their fascial envelope.
The surgery involved whole decompression and partial neurolysis of nervous structures for most patients, while nearly 20% of women required complete neurolysis based on their level of infiltration. Most women (64%) had severe enough infiltration that a concomitant bowel resection was also necessary.
The surgeon performed a medial approach for deep pelvic endometriosis with rectal and/or parametrial involvement extending to the pelvic wall and somatic nerve, or a lateral approach for isolated endometriosis of the pelvic wall and somatic nerves.
At 6 months after surgery, all patients reported complete relief from pain. However, 77 women (20%) experienced postoperative neuritis, which was successfully treated with corticosteroids, antiepileptics, and opioids.
Endometriosis that extends into somatic nerves and the sacral roots is a common cause of pelvic pain, Dr. Roviglione said.
“This kind of endometriosis is resistant to opioids and drugs,” he said. The difficulty in treating deep infiltrating endometriosis is compounded by the often long delay in diagnosis, he added.
Using laparoscopy for neurolysis and decompression of somatic nerves affected by endometriosis is a “more accurate and effective treatment” for providing pain relief, Dr. Roviglione said. But laparoscopic retroperitoneal nerve-sparing surgery should be performed only by skilled neuroanatomy surgeons at referral centers because of the complex nature of the procedure, he noted.
Dr. Roviglione reported having no relevant financial disclosures.
SOURCE: Ceccaroni M et al. AAGL 2017 Abstract 166.
NATIONAL HARBOR, MD. – Laparoscopic retroperitoneal nerve-sparing surgery is a safe approach that relieves pain in women with deep infiltrating endometriosis, according to findings presented by Giovanni Roviglione, MD, at the AAGL Global Congress.
The prospective case series study with a single gynecologic surgeon in Verona, Italy, involved 382 women who had deep infiltrating endometriosis with sciatica and anogenital pain. All of the women had some level of nervous compression of somatic structures and infiltration of their fascial envelope.
The surgery involved whole decompression and partial neurolysis of nervous structures for most patients, while nearly 20% of women required complete neurolysis based on their level of infiltration. Most women (64%) had severe enough infiltration that a concomitant bowel resection was also necessary.
The surgeon performed a medial approach for deep pelvic endometriosis with rectal and/or parametrial involvement extending to the pelvic wall and somatic nerve, or a lateral approach for isolated endometriosis of the pelvic wall and somatic nerves.
At 6 months after surgery, all patients reported complete relief from pain. However, 77 women (20%) experienced postoperative neuritis, which was successfully treated with corticosteroids, antiepileptics, and opioids.
Endometriosis that extends into somatic nerves and the sacral roots is a common cause of pelvic pain, Dr. Roviglione said.
“This kind of endometriosis is resistant to opioids and drugs,” he said. The difficulty in treating deep infiltrating endometriosis is compounded by the often long delay in diagnosis, he added.
Using laparoscopy for neurolysis and decompression of somatic nerves affected by endometriosis is a “more accurate and effective treatment” for providing pain relief, Dr. Roviglione said. But laparoscopic retroperitoneal nerve-sparing surgery should be performed only by skilled neuroanatomy surgeons at referral centers because of the complex nature of the procedure, he noted.
Dr. Roviglione reported having no relevant financial disclosures.
SOURCE: Ceccaroni M et al. AAGL 2017 Abstract 166.
REPORTING FROM AAGL 2017
Key clinical point:
Major finding: All patients reported complete relief of neurologic symptoms at 6 months after surgery.
Study details: Single center, prospective case series of 382 women who underwent laparoscopic retroperitoneal nerve-sparing surgery to treat pain associated with deep infiltrating endometriosis.
Disclosures: Dr. Roviglione reported having no relevant financial disclosures.
Source: Ceccaroni M et al. AAGL 2017 Abstract 166.
Enzalutamide plus exemestane improves PFS in HR+ breast cancer subset
SAN ANTONIO – Enzalutamide added to exemestane improved progression-free survival (PFS) in patients with hormone receptor (HR)-positive advanced breast cancer, investigators reported.
Specifically, it improved outcomes in patients who had not received any prior endocrine therapy and who were positive for a gene signature-based biomarker indicating androgen receptor (AR) signaling.
Patients in this subset who were treated with combination enzalutamide and exemestane achieved a median PFS of 16.5 months, which was significantly higher than the 4 months observed with placebo and exemestane.
However, the addition of enzalutamide had no effect on PFS in the overall cohort or among patients who were biomarker positive but who had received prior endocrine therapy.
“The study met its primary endpoint in improving PFS in the enzalutamide plus exemestane-treated patients who were biomarker positive and HR positive with no prior endocrine therapy for advanced disease as compared [with] exemestane alone,” Denise A. Yardley, MD, of Tennessee Oncology, Nashville, said at the San Antonio Breast Cancer Symposium.
“The role of the AR in HR-positive breast cancer and the predictive value of the identified biomarker are still unclear and will require further studies and validation,” said Dr. Yardley.

Targeting AR is an active area of breast cancer research, as a majority of HR-positive tumors express the AR, as do a moderate number of HER2-positive tumors and almost a third of triple-negative breast cancers. AR signaling has also been associated with resistance to endocrine therapy. Aromatase inhibitors divert estrogen precursors to androgens and data from preclinical models have shown that enzalutamide blocked both estrogen- and androgen-mediated growth of HR+ cells.
Enzalutamide is an inhibitor of AR signaling that is currently used to treat patients with castration-resistant prostate cancer, and has demonstrated clinical activity and was well tolerated in patients with AR-positive advanced triple negative breast cancer, explained Dr. Yardley.
In this study, Dr. Yardley and her colleagues conducted a placebo-controlled phase 2 randomized trial that included 247 patients with HR+/HER2-normal advanced/metastatic breast cancer who were assigned to either 25 mg exemestane plus placebo or 50 mg exemestane and 160 mg enzalutamide daily.
The patients were divided into two parallel cohorts: those with no prior endocrine therapy (C1; n = 127) or those who had received one prior endocrine therapy for metastatic disease (C2; n = 120).
The primary endpoint was PFS in the intent-to-treat population and in the biomarker subgroup of each cohort. Secondary endpoints included the clinical benefit rate at 24 weeks, best overall response, and safety.
The authors found that the PFS in the intent-to-treat population did not significantly differ between those randomized to enzalutamide or placebo in either cohort. In cohort 1, the median PFS was 11.8 months in the enzalutamide arm and 5.8 months in the placebo arm (hazard ratio, 0.82; P = .3631), and in cohort 2, 3.6 months and 3.9 months, respectively (HR, 1.02; P = .9212).
However, statistically significant improvements in median PFS and clinical benefit rate at 24 weeks were observed only in the group with a positive biomarker who had not received any prior endocrine therapy. In cohort 1, the median PFS was 16.5 months in the enzalutamide arm vs. 4.3 months in the placebo arm (HR, 0.44, P = .0335). In cohort 2, median PFS did not significantly differ between groups (6.0 vs. 5.3 months; HR, 0.55; P = .1936).
The clinical response rate in cohort 1 of the biomarker positive group was 83% in the enzalutamide arm versus 38% in the placebo arm (P = .0012).
Adverse events with enzalutamide was similar to those previously reported, and the most common were nausea (39%) in cohort 1 and fatigue (37%) in cohort 2. Dose interruptions due to adverse events occurred in 21.0% and 25.0% of patients randomized to enzalutamide in cohorts 1 and 2 vs. 20.6% and 15.0% in the placebo group.
Dr. Yardley explained that the biomarker used in the study was identified on PAM50. “It was exploratory and proprietary,” she noted, adding that she is unable to share any further information about it at this time.
SOURCE: Yardley et al. SABCS Abstract GS4-07
SAN ANTONIO – Enzalutamide added to exemestane improved progression-free survival (PFS) in patients with hormone receptor (HR)-positive advanced breast cancer, investigators reported.
Specifically, it improved outcomes in patients who had not received any prior endocrine therapy and who were positive for a gene signature-based biomarker indicating androgen receptor (AR) signaling.
Patients in this subset who were treated with combination enzalutamide and exemestane achieved a median PFS of 16.5 months, which was significantly higher than the 4 months observed with placebo and exemestane.
However, the addition of enzalutamide had no effect on PFS in the overall cohort or among patients who were biomarker positive but who had received prior endocrine therapy.
“The study met its primary endpoint in improving PFS in the enzalutamide plus exemestane-treated patients who were biomarker positive and HR positive with no prior endocrine therapy for advanced disease as compared [with] exemestane alone,” Denise A. Yardley, MD, of Tennessee Oncology, Nashville, said at the San Antonio Breast Cancer Symposium.
“The role of the AR in HR-positive breast cancer and the predictive value of the identified biomarker are still unclear and will require further studies and validation,” said Dr. Yardley.
Targeting AR is an active area of breast cancer research, as a majority of HR-positive tumors express the AR, as do a moderate number of HER2-positive tumors and almost a third of triple-negative breast cancers. AR signaling has also been associated with resistance to endocrine therapy. Aromatase inhibitors divert estrogen precursors to androgens and data from preclinical models have shown that enzalutamide blocked both estrogen- and androgen-mediated growth of HR+ cells.
Enzalutamide is an inhibitor of AR signaling that is currently used to treat patients with castration-resistant prostate cancer, and has demonstrated clinical activity and was well tolerated in patients with AR-positive advanced triple negative breast cancer, explained Dr. Yardley.
In this study, Dr. Yardley and her colleagues conducted a placebo-controlled phase 2 randomized trial that included 247 patients with HR+/HER2-normal advanced/metastatic breast cancer who were assigned to either 25 mg exemestane plus placebo or 50 mg exemestane and 160 mg enzalutamide daily.
The patients were divided into two parallel cohorts: those with no prior endocrine therapy (C1; n = 127) or those who had received one prior endocrine therapy for metastatic disease (C2; n = 120).
The primary endpoint was PFS in the intent-to-treat population and in the biomarker subgroup of each cohort. Secondary endpoints included the clinical benefit rate at 24 weeks, best overall response, and safety.
The authors found that the PFS in the intent-to-treat population did not significantly differ between those randomized to enzalutamide or placebo in either cohort. In cohort 1, the median PFS was 11.8 months in the enzalutamide arm and 5.8 months in the placebo arm (hazard ratio, 0.82; P = .3631), and in cohort 2, 3.6 months and 3.9 months, respectively (HR, 1.02; P = .9212).
However, statistically significant improvements in median PFS and clinical benefit rate at 24 weeks were observed only in the group with a positive biomarker who had not received any prior endocrine therapy. In cohort 1, the median PFS was 16.5 months in the enzalutamide arm vs. 4.3 months in the placebo arm (HR, 0.44, P = .0335). In cohort 2, median PFS did not significantly differ between groups (6.0 vs. 5.3 months; HR, 0.55; P = .1936).
The clinical response rate in cohort 1 of the biomarker positive group was 83% in the enzalutamide arm versus 38% in the placebo arm (P = .0012).
Adverse events with enzalutamide was similar to those previously reported, and the most common were nausea (39%) in cohort 1 and fatigue (37%) in cohort 2. Dose interruptions due to adverse events occurred in 21.0% and 25.0% of patients randomized to enzalutamide in cohorts 1 and 2 vs. 20.6% and 15.0% in the placebo group.
Dr. Yardley explained that the biomarker used in the study was identified on PAM50. “It was exploratory and proprietary,” she noted, adding that she is unable to share any further information about it at this time.
SOURCE: Yardley et al. SABCS Abstract GS4-07
SAN ANTONIO – Enzalutamide added to exemestane improved progression-free survival (PFS) in patients with hormone receptor (HR)-positive advanced breast cancer, investigators reported.
Specifically, it improved outcomes in patients who had not received any prior endocrine therapy and who were positive for a gene signature-based biomarker indicating androgen receptor (AR) signaling.
Patients in this subset who were treated with combination enzalutamide and exemestane achieved a median PFS of 16.5 months, which was significantly higher than the 4 months observed with placebo and exemestane.
However, the addition of enzalutamide had no effect on PFS in the overall cohort or among patients who were biomarker positive but who had received prior endocrine therapy.
“The study met its primary endpoint in improving PFS in the enzalutamide plus exemestane-treated patients who were biomarker positive and HR positive with no prior endocrine therapy for advanced disease as compared [with] exemestane alone,” Denise A. Yardley, MD, of Tennessee Oncology, Nashville, said at the San Antonio Breast Cancer Symposium.
“The role of the AR in HR-positive breast cancer and the predictive value of the identified biomarker are still unclear and will require further studies and validation,” said Dr. Yardley.
Targeting AR is an active area of breast cancer research, as a majority of HR-positive tumors express the AR, as do a moderate number of HER2-positive tumors and almost a third of triple-negative breast cancers. AR signaling has also been associated with resistance to endocrine therapy. Aromatase inhibitors divert estrogen precursors to androgens and data from preclinical models have shown that enzalutamide blocked both estrogen- and androgen-mediated growth of HR+ cells.
Enzalutamide is an inhibitor of AR signaling that is currently used to treat patients with castration-resistant prostate cancer, and has demonstrated clinical activity and was well tolerated in patients with AR-positive advanced triple negative breast cancer, explained Dr. Yardley.
In this study, Dr. Yardley and her colleagues conducted a placebo-controlled phase 2 randomized trial that included 247 patients with HR+/HER2-normal advanced/metastatic breast cancer who were assigned to either 25 mg exemestane plus placebo or 50 mg exemestane and 160 mg enzalutamide daily.
The patients were divided into two parallel cohorts: those with no prior endocrine therapy (C1; n = 127) or those who had received one prior endocrine therapy for metastatic disease (C2; n = 120).
The primary endpoint was PFS in the intent-to-treat population and in the biomarker subgroup of each cohort. Secondary endpoints included the clinical benefit rate at 24 weeks, best overall response, and safety.
The authors found that the PFS in the intent-to-treat population did not significantly differ between those randomized to enzalutamide or placebo in either cohort. In cohort 1, the median PFS was 11.8 months in the enzalutamide arm and 5.8 months in the placebo arm (hazard ratio, 0.82; P = .3631), and in cohort 2, 3.6 months and 3.9 months, respectively (HR, 1.02; P = .9212).
However, statistically significant improvements in median PFS and clinical benefit rate at 24 weeks were observed only in the group with a positive biomarker who had not received any prior endocrine therapy. In cohort 1, the median PFS was 16.5 months in the enzalutamide arm vs. 4.3 months in the placebo arm (HR, 0.44, P = .0335). In cohort 2, median PFS did not significantly differ between groups (6.0 vs. 5.3 months; HR, 0.55; P = .1936).
The clinical response rate in cohort 1 of the biomarker positive group was 83% in the enzalutamide arm versus 38% in the placebo arm (P = .0012).
Adverse events with enzalutamide was similar to those previously reported, and the most common were nausea (39%) in cohort 1 and fatigue (37%) in cohort 2. Dose interruptions due to adverse events occurred in 21.0% and 25.0% of patients randomized to enzalutamide in cohorts 1 and 2 vs. 20.6% and 15.0% in the placebo group.
Dr. Yardley explained that the biomarker used in the study was identified on PAM50. “It was exploratory and proprietary,” she noted, adding that she is unable to share any further information about it at this time.
SOURCE: Yardley et al. SABCS Abstract GS4-07
REPORTING FROM SABCS 2017
Key clinical point: Enzalutamide added to exemestane improves progression-free survival in hormone receptor–positive advanced breast cancer patients with a biomarker indicating androgen receptor signaling.
Major finding: In this subset of patients, combination therapy improved PFS: 16.5 months vs. 4.3 months for the placebo arm (HR 0.44, P = .0335).
Data source: A placebo-controlled phase 2 randomized trial comprising 247 patients with HR+/HER2-normal advanced/metastatic breast cancer.
Disclosures: Study funding was not disclosed.
Source: Yardley et al. SABCS Abstract GS4-07.
FDA bans 24 ingredients from OTC health care antiseptic products
in hospital settings and other health care situations outside the hospital, the U.S. Food and Drug Administration announced in a final rule.
The affected products include health care personnel hand washes and hand rubs, surgical hand scrubs and hand rubs, and patient antiseptic skin preparations. The final rule was published Dec. 20 in the Federal Register and becomes effective in December 2018.
The agency determined that a deferral is warranted for six health care antiseptic active ingredients – benzalkonium chloride, benzethonium chloride, chloroxylenol, alcohol, isopropyl alcohol, and povidone-iodine – to allow more time for interested parties to complete the studies necessary to fill the safety and effectiveness data gaps identified for these ingredients.
“The FDA expects that this information may help better inform us on antiseptic resistance and antibiotic cross-resistance in the health care setting,” FDA Commissioner Scott Gottlieb, MD, said in a statement. “Importantly, this doesn’t mean that products containing these six ingredients are ineffective or unsafe. These antiseptic products remain an important resource in health care settings. Personnel should continue to use these products consistent with infection control guidelines while the additional data are gathered.”
No additional data was provided for another 24 products, which were deemed not generally recognized as safe and effective. The minimum data needed to demonstrate safety for all health care antiseptic active ingredients fall into four broad categories: human safety studies, nonclinical safety studies (developmental and reproductive toxicity studies and carcinogenicity studies), data to characterize potential hormonal effects, and data to evaluate the development of antimicrobial resistance, the final rule states.
The FDA noted that manufacturers started to remove nearly all of these 24 active ingredients from their products following a 2015 proposed rule. Triclosan is currently being used in available products.
The active ingredients affected are chlorhexidine gluconate; cloflucarban; fluorosalan; hexachlorophene; hexylresorcinol; iodophors (iodine-containing ingredients including iodine complex [ammonium ether sulfate and polyoxyethylene sorbitan monolaurate], iodine complex [phosphate ester of alkylaryloxy polyethylene glycol], iodine tincture USP, iodine topical solution USP, nonylphenoxypoly [ethyleneoxy] ethanoliodine, poloxamer–iodine complex, undecoylium chloride iodine complex); mercufenol chloride; methylbenzethonium chloride; phenol; secondary amyltricresols; sodium oxychlorosene; tribromsalan; triclocarban; triclosan; triple dye; combination of calomel, oxyquinoline benzoate, triethanolamine, and phenol derivative; and combination of mercufenol chloride and secondary amyltricresols in 50% alcohol.
If manufacturers want to use one or more of these 24 active ingredients in future OTC health care antiseptic drug products, those products will be considered new drugs for which a new drug application approval will be required, the agency said.
The rule does not affect health care antiseptics that are currently marketed under new drug applications and abbreviated new drug applications.
FDA’s action follows a similar final rule published Sept. 6, 2016, which removed triclosan and 18 other active ingredients from consumer antiseptic products.
in hospital settings and other health care situations outside the hospital, the U.S. Food and Drug Administration announced in a final rule.
The affected products include health care personnel hand washes and hand rubs, surgical hand scrubs and hand rubs, and patient antiseptic skin preparations. The final rule was published Dec. 20 in the Federal Register and becomes effective in December 2018.
The agency determined that a deferral is warranted for six health care antiseptic active ingredients – benzalkonium chloride, benzethonium chloride, chloroxylenol, alcohol, isopropyl alcohol, and povidone-iodine – to allow more time for interested parties to complete the studies necessary to fill the safety and effectiveness data gaps identified for these ingredients.
“The FDA expects that this information may help better inform us on antiseptic resistance and antibiotic cross-resistance in the health care setting,” FDA Commissioner Scott Gottlieb, MD, said in a statement. “Importantly, this doesn’t mean that products containing these six ingredients are ineffective or unsafe. These antiseptic products remain an important resource in health care settings. Personnel should continue to use these products consistent with infection control guidelines while the additional data are gathered.”
No additional data was provided for another 24 products, which were deemed not generally recognized as safe and effective. The minimum data needed to demonstrate safety for all health care antiseptic active ingredients fall into four broad categories: human safety studies, nonclinical safety studies (developmental and reproductive toxicity studies and carcinogenicity studies), data to characterize potential hormonal effects, and data to evaluate the development of antimicrobial resistance, the final rule states.
The FDA noted that manufacturers started to remove nearly all of these 24 active ingredients from their products following a 2015 proposed rule. Triclosan is currently being used in available products.
The active ingredients affected are chlorhexidine gluconate; cloflucarban; fluorosalan; hexachlorophene; hexylresorcinol; iodophors (iodine-containing ingredients including iodine complex [ammonium ether sulfate and polyoxyethylene sorbitan monolaurate], iodine complex [phosphate ester of alkylaryloxy polyethylene glycol], iodine tincture USP, iodine topical solution USP, nonylphenoxypoly [ethyleneoxy] ethanoliodine, poloxamer–iodine complex, undecoylium chloride iodine complex); mercufenol chloride; methylbenzethonium chloride; phenol; secondary amyltricresols; sodium oxychlorosene; tribromsalan; triclocarban; triclosan; triple dye; combination of calomel, oxyquinoline benzoate, triethanolamine, and phenol derivative; and combination of mercufenol chloride and secondary amyltricresols in 50% alcohol.
If manufacturers want to use one or more of these 24 active ingredients in future OTC health care antiseptic drug products, those products will be considered new drugs for which a new drug application approval will be required, the agency said.
The rule does not affect health care antiseptics that are currently marketed under new drug applications and abbreviated new drug applications.
FDA’s action follows a similar final rule published Sept. 6, 2016, which removed triclosan and 18 other active ingredients from consumer antiseptic products.
in hospital settings and other health care situations outside the hospital, the U.S. Food and Drug Administration announced in a final rule.
The affected products include health care personnel hand washes and hand rubs, surgical hand scrubs and hand rubs, and patient antiseptic skin preparations. The final rule was published Dec. 20 in the Federal Register and becomes effective in December 2018.
The agency determined that a deferral is warranted for six health care antiseptic active ingredients – benzalkonium chloride, benzethonium chloride, chloroxylenol, alcohol, isopropyl alcohol, and povidone-iodine – to allow more time for interested parties to complete the studies necessary to fill the safety and effectiveness data gaps identified for these ingredients.
“The FDA expects that this information may help better inform us on antiseptic resistance and antibiotic cross-resistance in the health care setting,” FDA Commissioner Scott Gottlieb, MD, said in a statement. “Importantly, this doesn’t mean that products containing these six ingredients are ineffective or unsafe. These antiseptic products remain an important resource in health care settings. Personnel should continue to use these products consistent with infection control guidelines while the additional data are gathered.”
No additional data was provided for another 24 products, which were deemed not generally recognized as safe and effective. The minimum data needed to demonstrate safety for all health care antiseptic active ingredients fall into four broad categories: human safety studies, nonclinical safety studies (developmental and reproductive toxicity studies and carcinogenicity studies), data to characterize potential hormonal effects, and data to evaluate the development of antimicrobial resistance, the final rule states.
The FDA noted that manufacturers started to remove nearly all of these 24 active ingredients from their products following a 2015 proposed rule. Triclosan is currently being used in available products.
The active ingredients affected are chlorhexidine gluconate; cloflucarban; fluorosalan; hexachlorophene; hexylresorcinol; iodophors (iodine-containing ingredients including iodine complex [ammonium ether sulfate and polyoxyethylene sorbitan monolaurate], iodine complex [phosphate ester of alkylaryloxy polyethylene glycol], iodine tincture USP, iodine topical solution USP, nonylphenoxypoly [ethyleneoxy] ethanoliodine, poloxamer–iodine complex, undecoylium chloride iodine complex); mercufenol chloride; methylbenzethonium chloride; phenol; secondary amyltricresols; sodium oxychlorosene; tribromsalan; triclocarban; triclosan; triple dye; combination of calomel, oxyquinoline benzoate, triethanolamine, and phenol derivative; and combination of mercufenol chloride and secondary amyltricresols in 50% alcohol.
If manufacturers want to use one or more of these 24 active ingredients in future OTC health care antiseptic drug products, those products will be considered new drugs for which a new drug application approval will be required, the agency said.
The rule does not affect health care antiseptics that are currently marketed under new drug applications and abbreviated new drug applications.
FDA’s action follows a similar final rule published Sept. 6, 2016, which removed triclosan and 18 other active ingredients from consumer antiseptic products.