User login
New and Noteworthy Information—January 2018
Sleep Improves After Retirement
Transition to statutory retirement is associated with a decrease in sleep difficulties, especially waking up too early in the morning and nonrestorative sleep, according to a study published online ahead of print November 16, 2017, in Sleep. The study included 5,807 public sector employees who retired between 2000 and 2011. Participants were administered the Jenkins Sleep Problem Scale Questionnaire before and after retirement in surveys conducted every four years. At the last study wave before retirement, 30% of the participants had sleep difficulties. The risk ratio for having sleep difficulties in the first study wave following retirement, compared with the last study wave preceding retirement, was 0.89. The decreases in sleep difficulties occurred primarily among people with psychologic distress, suboptimal self-rated health, short sleep duration, and job strain before retirement.
Myllyntausta S, Salo P, Kronholm E, et al. Changes in sleep difficulties during the transition to statutory retirement. Sleep. 2017 Nov 16 [Epub ahead of print].
Vigorous Exercise May Delay Parkinson’s Disease Progression
High-intensity treadmill exercise may be feasible and prescribed safely for patients with Parkinson’s disease, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. The randomized clinical trial included 128 participants between ages 40 and 80. Participants were at an early stage of the disease and not taking Parkinson’s disease medication. Investigators randomized the population to high-intensity exercise, moderate-intensity exercise, or a control condition. At baseline and six months, clinicians assessed the participants using the Unified Parkinson’s Disease Rating Scale (UPDRS). Participants in the study had a UPDRS score of about 20 at baseline. At six months, the high-intensity group’s score stayed at 20, and the moderate exercise group worsened by 1.5 points. The control group’s score worsened by three points.
Schenkman M, Moore CG, Kohrt WM, et al. Effect of high-intensity treadmill exercise on motor symptoms in patients with de novo Parkinson disease: a phase 2 randomized clinical trial. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Can Exposure to Terror Raise the Risk of Headache?
Exposure to terror increases the risk of persistent weekly and daily migraine and tension-type headache in adolescent survivors above expected levels, according to a study published online ahead of print December 13, 2017, in Neurology. Investigators interviewed 213 survivors of a terror attack in Norway. Half were male, the mean age was 17.7, and 13 survivors were severely injured. Participants provided information about their headache frequency four to five months after the attack. For each survivor, eight matched controls were drawn from the Young-HUNT3 Study. After exposure to terror, the odds ratio for migraine was 4.27, and that for tension-type headache was 3.39, as estimated in multivariable logistic regression models adjusted for injury, sex, age, family structure and economy, prior exposure to physical or sexual violence, and psychologic distress.
Stensland SØ, Zwart JA, Wentzel-Larsen T, Dyb G. The headache of terror: a matched cohort study of adolescents from the Utøya and the HUNT Study. Neurology. 2017 Dec 13 [Epub ahead of print].
Diet Reduces Disability and Symptoms of MS
A healthy diet and a composite healthy lifestyle are associated with less disability and symptom burden in multiple sclerosis (MS), according to a study published online ahead of print December 6, 2017, in Neurology. The study involved 6,989 people with MS who completed questionnaires about their diet as part of the North American Research Committee registry. The questionnaire estimated intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats. Researchers constructed an overall diet quality score for each individual based on the food groups. Participants with diet quality scores in the highest quintile had lower levels of disability and lower depression scores. Individuals reporting a composite healthy lifestyle had lower odds of reporting severe fatigue, depression, pain, or cognitive impairment.
Fitzgerald KC, Tyry T, Salter A, et al. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology. 2017 Dec 6 [Epub ahead of print].
What Are the Effects of Childhood Convulsive Status Epilepticus?
Childhood convulsive status epilepticus (CSE) is associated with substantial long-term neurologic morbidity, but primarily in people who have epilepsy, neurologic abnormalities, or both before the episode of CSE, according to a study published online ahead of print December 5, 2017, in Lancet Child & Adolescent Health. Researchers followed a population-based childhood CSE cohort. Of 203 survivors, 134 were assessed at a median follow-up of 8.9 years. Lasting neurologic conditions, including epilepsy, learning disabilities, and movement problems, were more common among participants than expected for children from the general population. Children who had existing neurologic or developmental issues at the time of CSE were more likely to have a neurologic problem at follow-up. Children without a neurologic or developmental issue tended to have better outcomes.
Pujar SS, Martinos MM, Cortina-Borja M, et al. Long-term prognosis after childhood convulsive status epilepticus: a prospective cohort study. Lancet Child Adolesc Health. 2017 Dec 5 [Epub ahead of print].
Protein Aggregation May Not Affect Cognition in Parkinson’s Disease
Patterns of cortical β-amyloid and tau do not differ between people with Parkinson’s disease who are cognitively normal (PD-CN), people with Parkinson’s disease with mild cognitive impairment (PD-MCI), and healthy older adults, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. This cross-sectional study included 29 patients with Parkinson’s disease from a tertiary care medical center and research institutions. Imaging measures were compared with those of 49 healthy control participants. Outcomes were tau PET measurements of groups of patients with PD-CN and PD-MCI. Of the participants, 47 were female, and the mean age was 71.1. Voxelwise contrasts of whole-brain tau PET uptake between patients with PD-CN and patients with PD-MCI, and between patients with Parkinson’s disease and β-amyloid-negative controls, did not reveal significant differences.
Winer JR, Maass A, Pressman P, et al. Associations between tau, β-amyloid, and cognition in Parkinson disease. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Hormone Therapy Not Linked to Increased Stroke Risk
Postmenopausal hormone therapy is not associated with increased risk of stroke, provided that it is started early, according to a study published November 17 in PLoS Medicine. Researchers analyzed data on postmenopausal hormone therapy from five cohort studies including 88,914 women, combined with data from national registries on diagnoses and causes of death during a follow-up period. During a median follow-up of 14.3 years, 6,371 first-time stroke events (1,080 hemorrhagic) were recorded. Hormone therapy was not linked to increased risk of stroke if the therapy was initiated within five years of menopausal onset, regardless of means of administration, type of therapy, active substance, and treatment duration. In subanalyses, researchers observed an increase in risk for hemorrhagic stroke if the therapy contained the active substance conjugated equine estrogens.
Carrasquilla GD, Frumento P, Berglund A, et al. Postmenopausal hormone therapy and risk of stroke: a pooled analysis of data from population-based cohort studies. PLoS Med. 2017;14(11):e1002445.
Restless Sleep May Be Linked to Parkinson’s Disease
In patients with idiopathic REM sleep behavior disorder (IRBD), PET shows increased microglial activation in the substantia nigra, along with reduced dopaminergic function in the putamen, according to a study published in the October 2017 issue of Lancet Neurology. This prospective, case–control PET study included 20 patients with IRBD and no clinical evidence of parkinsonism and cognitive impairment recruited from tertiary sleep centers and 19 healthy controls. 11C-PK11195 binding was increased on the left side of the substantia nigra in patients with IRBD, compared with controls, but not on the right side. 11C-PK11195 binding was not significantly increased in the putamen and caudate of patients with IRBD. 18F-DOPA uptake was reduced in IRBD in the left putamen and right putamen, but not in the caudate.
Stokholm MG, Iranzo A, Østergaard K, et al. Assessment of neuroinflammation in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a case-control study. Lancet Neurol. 2017;16(10):789-796.
Can Playing Video Games Benefit the Brains of Older Adults?
Playing 3D video games may prevent mild cognitive impairment and, perhaps, Alzheimer’s disease, according to a study published December 6, 2017, in PLoS One. In two separate studies, adults in their 20s played 3D video games on platforms such as Super Mario 64. The gray matter in their hippocampus increased after training. Researchers examined whether the results could be replicated in healthy seniors. Thirty-three people, ages 55 to 75, were randomly assigned to one of three groups. The video game experimental group engaged in 3D-platform video game training over six months. An active control group took a series of self-directed, computerized piano lessons, and a no-contact control group did not engage in any intervention. Participants in the video-game cohort had increases in gray matter volume in the hippocampus and cerebellum. Their short-term memory also improved.
West GL, Zendel BR, Konishi K, et al. Playing Super Mario 64 increases hippocampal grey matter in older adults. PLoS One. 2017;12(12):e0187779.
FDA Approves Vercise Deep Brain Stimulation System
The FDA has approved the Vercise Deep Brain Stimulation System (DBS) to treat symptoms of Parkinson’s disease. The approval is based on the INTREPID study, a multicenter, prospective, double-blind, randomized, sham-controlled trial of DBS for Parkinson’s disease in the US. The study evaluated the system’s safety and efficacy in 292 patients at 23 sites. The Vercise DBS System successfully met its primary end point of mean change in waking hours with good symptom control. The filing also was supported by safety data from the VANTAGE study, in which 40 patients treated with the system demonstrated a 63% improvement in motor function at 52 weeks from baseline, as measured by the Unified Parkinson’s Disease Rating Scale III. Boston Scientific markets Vercise.
Can Social Relationships Aid Cognitive Function?
Although superagers (ie, people older than 80 with episodic memory as good as that of a middle-aged adult) and their cognitively average-for-age peers report similarly high levels of psychological well-being, superagers demonstrate greater levels of positive social relationships, according to a study published October 23, 2017, in PLoS One. Thirty-one superagers and 19 cognitively average-for-age peers completed the Ryff 42-item Psychological Well-Being questionnaire, which includes subscales of autonomy, positive relations with others, environmental mastery, personal growth, purpose in life, and self-acceptance. The groups did not differ on demographic factors, including estimated premorbid intelligence. Compared with cognitively average-for-age peers, superagers endorsed greater levels of positive relations with others. Superagers had a median overall score of 40 in positive relations with others, compared with 36 in the control group.
Cook Maher A, Kielb S, Loyer E, et al. Psychological well-being in elderly adults with extraordinary episodic memory. PLoS One. 2017;12(10):e0186413.
—Kimberly Williams
Sleep Improves After Retirement
Transition to statutory retirement is associated with a decrease in sleep difficulties, especially waking up too early in the morning and nonrestorative sleep, according to a study published online ahead of print November 16, 2017, in Sleep. The study included 5,807 public sector employees who retired between 2000 and 2011. Participants were administered the Jenkins Sleep Problem Scale Questionnaire before and after retirement in surveys conducted every four years. At the last study wave before retirement, 30% of the participants had sleep difficulties. The risk ratio for having sleep difficulties in the first study wave following retirement, compared with the last study wave preceding retirement, was 0.89. The decreases in sleep difficulties occurred primarily among people with psychologic distress, suboptimal self-rated health, short sleep duration, and job strain before retirement.
Myllyntausta S, Salo P, Kronholm E, et al. Changes in sleep difficulties during the transition to statutory retirement. Sleep. 2017 Nov 16 [Epub ahead of print].
Vigorous Exercise May Delay Parkinson’s Disease Progression
High-intensity treadmill exercise may be feasible and prescribed safely for patients with Parkinson’s disease, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. The randomized clinical trial included 128 participants between ages 40 and 80. Participants were at an early stage of the disease and not taking Parkinson’s disease medication. Investigators randomized the population to high-intensity exercise, moderate-intensity exercise, or a control condition. At baseline and six months, clinicians assessed the participants using the Unified Parkinson’s Disease Rating Scale (UPDRS). Participants in the study had a UPDRS score of about 20 at baseline. At six months, the high-intensity group’s score stayed at 20, and the moderate exercise group worsened by 1.5 points. The control group’s score worsened by three points.
Schenkman M, Moore CG, Kohrt WM, et al. Effect of high-intensity treadmill exercise on motor symptoms in patients with de novo Parkinson disease: a phase 2 randomized clinical trial. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Can Exposure to Terror Raise the Risk of Headache?
Exposure to terror increases the risk of persistent weekly and daily migraine and tension-type headache in adolescent survivors above expected levels, according to a study published online ahead of print December 13, 2017, in Neurology. Investigators interviewed 213 survivors of a terror attack in Norway. Half were male, the mean age was 17.7, and 13 survivors were severely injured. Participants provided information about their headache frequency four to five months after the attack. For each survivor, eight matched controls were drawn from the Young-HUNT3 Study. After exposure to terror, the odds ratio for migraine was 4.27, and that for tension-type headache was 3.39, as estimated in multivariable logistic regression models adjusted for injury, sex, age, family structure and economy, prior exposure to physical or sexual violence, and psychologic distress.
Stensland SØ, Zwart JA, Wentzel-Larsen T, Dyb G. The headache of terror: a matched cohort study of adolescents from the Utøya and the HUNT Study. Neurology. 2017 Dec 13 [Epub ahead of print].
Diet Reduces Disability and Symptoms of MS
A healthy diet and a composite healthy lifestyle are associated with less disability and symptom burden in multiple sclerosis (MS), according to a study published online ahead of print December 6, 2017, in Neurology. The study involved 6,989 people with MS who completed questionnaires about their diet as part of the North American Research Committee registry. The questionnaire estimated intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats. Researchers constructed an overall diet quality score for each individual based on the food groups. Participants with diet quality scores in the highest quintile had lower levels of disability and lower depression scores. Individuals reporting a composite healthy lifestyle had lower odds of reporting severe fatigue, depression, pain, or cognitive impairment.
Fitzgerald KC, Tyry T, Salter A, et al. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology. 2017 Dec 6 [Epub ahead of print].
What Are the Effects of Childhood Convulsive Status Epilepticus?
Childhood convulsive status epilepticus (CSE) is associated with substantial long-term neurologic morbidity, but primarily in people who have epilepsy, neurologic abnormalities, or both before the episode of CSE, according to a study published online ahead of print December 5, 2017, in Lancet Child & Adolescent Health. Researchers followed a population-based childhood CSE cohort. Of 203 survivors, 134 were assessed at a median follow-up of 8.9 years. Lasting neurologic conditions, including epilepsy, learning disabilities, and movement problems, were more common among participants than expected for children from the general population. Children who had existing neurologic or developmental issues at the time of CSE were more likely to have a neurologic problem at follow-up. Children without a neurologic or developmental issue tended to have better outcomes.
Pujar SS, Martinos MM, Cortina-Borja M, et al. Long-term prognosis after childhood convulsive status epilepticus: a prospective cohort study. Lancet Child Adolesc Health. 2017 Dec 5 [Epub ahead of print].
Protein Aggregation May Not Affect Cognition in Parkinson’s Disease
Patterns of cortical β-amyloid and tau do not differ between people with Parkinson’s disease who are cognitively normal (PD-CN), people with Parkinson’s disease with mild cognitive impairment (PD-MCI), and healthy older adults, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. This cross-sectional study included 29 patients with Parkinson’s disease from a tertiary care medical center and research institutions. Imaging measures were compared with those of 49 healthy control participants. Outcomes were tau PET measurements of groups of patients with PD-CN and PD-MCI. Of the participants, 47 were female, and the mean age was 71.1. Voxelwise contrasts of whole-brain tau PET uptake between patients with PD-CN and patients with PD-MCI, and between patients with Parkinson’s disease and β-amyloid-negative controls, did not reveal significant differences.
Winer JR, Maass A, Pressman P, et al. Associations between tau, β-amyloid, and cognition in Parkinson disease. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Hormone Therapy Not Linked to Increased Stroke Risk
Postmenopausal hormone therapy is not associated with increased risk of stroke, provided that it is started early, according to a study published November 17 in PLoS Medicine. Researchers analyzed data on postmenopausal hormone therapy from five cohort studies including 88,914 women, combined with data from national registries on diagnoses and causes of death during a follow-up period. During a median follow-up of 14.3 years, 6,371 first-time stroke events (1,080 hemorrhagic) were recorded. Hormone therapy was not linked to increased risk of stroke if the therapy was initiated within five years of menopausal onset, regardless of means of administration, type of therapy, active substance, and treatment duration. In subanalyses, researchers observed an increase in risk for hemorrhagic stroke if the therapy contained the active substance conjugated equine estrogens.
Carrasquilla GD, Frumento P, Berglund A, et al. Postmenopausal hormone therapy and risk of stroke: a pooled analysis of data from population-based cohort studies. PLoS Med. 2017;14(11):e1002445.
Restless Sleep May Be Linked to Parkinson’s Disease
In patients with idiopathic REM sleep behavior disorder (IRBD), PET shows increased microglial activation in the substantia nigra, along with reduced dopaminergic function in the putamen, according to a study published in the October 2017 issue of Lancet Neurology. This prospective, case–control PET study included 20 patients with IRBD and no clinical evidence of parkinsonism and cognitive impairment recruited from tertiary sleep centers and 19 healthy controls. 11C-PK11195 binding was increased on the left side of the substantia nigra in patients with IRBD, compared with controls, but not on the right side. 11C-PK11195 binding was not significantly increased in the putamen and caudate of patients with IRBD. 18F-DOPA uptake was reduced in IRBD in the left putamen and right putamen, but not in the caudate.
Stokholm MG, Iranzo A, Østergaard K, et al. Assessment of neuroinflammation in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a case-control study. Lancet Neurol. 2017;16(10):789-796.
Can Playing Video Games Benefit the Brains of Older Adults?
Playing 3D video games may prevent mild cognitive impairment and, perhaps, Alzheimer’s disease, according to a study published December 6, 2017, in PLoS One. In two separate studies, adults in their 20s played 3D video games on platforms such as Super Mario 64. The gray matter in their hippocampus increased after training. Researchers examined whether the results could be replicated in healthy seniors. Thirty-three people, ages 55 to 75, were randomly assigned to one of three groups. The video game experimental group engaged in 3D-platform video game training over six months. An active control group took a series of self-directed, computerized piano lessons, and a no-contact control group did not engage in any intervention. Participants in the video-game cohort had increases in gray matter volume in the hippocampus and cerebellum. Their short-term memory also improved.
West GL, Zendel BR, Konishi K, et al. Playing Super Mario 64 increases hippocampal grey matter in older adults. PLoS One. 2017;12(12):e0187779.
FDA Approves Vercise Deep Brain Stimulation System
The FDA has approved the Vercise Deep Brain Stimulation System (DBS) to treat symptoms of Parkinson’s disease. The approval is based on the INTREPID study, a multicenter, prospective, double-blind, randomized, sham-controlled trial of DBS for Parkinson’s disease in the US. The study evaluated the system’s safety and efficacy in 292 patients at 23 sites. The Vercise DBS System successfully met its primary end point of mean change in waking hours with good symptom control. The filing also was supported by safety data from the VANTAGE study, in which 40 patients treated with the system demonstrated a 63% improvement in motor function at 52 weeks from baseline, as measured by the Unified Parkinson’s Disease Rating Scale III. Boston Scientific markets Vercise.
Can Social Relationships Aid Cognitive Function?
Although superagers (ie, people older than 80 with episodic memory as good as that of a middle-aged adult) and their cognitively average-for-age peers report similarly high levels of psychological well-being, superagers demonstrate greater levels of positive social relationships, according to a study published October 23, 2017, in PLoS One. Thirty-one superagers and 19 cognitively average-for-age peers completed the Ryff 42-item Psychological Well-Being questionnaire, which includes subscales of autonomy, positive relations with others, environmental mastery, personal growth, purpose in life, and self-acceptance. The groups did not differ on demographic factors, including estimated premorbid intelligence. Compared with cognitively average-for-age peers, superagers endorsed greater levels of positive relations with others. Superagers had a median overall score of 40 in positive relations with others, compared with 36 in the control group.
Cook Maher A, Kielb S, Loyer E, et al. Psychological well-being in elderly adults with extraordinary episodic memory. PLoS One. 2017;12(10):e0186413.
—Kimberly Williams
Sleep Improves After Retirement
Transition to statutory retirement is associated with a decrease in sleep difficulties, especially waking up too early in the morning and nonrestorative sleep, according to a study published online ahead of print November 16, 2017, in Sleep. The study included 5,807 public sector employees who retired between 2000 and 2011. Participants were administered the Jenkins Sleep Problem Scale Questionnaire before and after retirement in surveys conducted every four years. At the last study wave before retirement, 30% of the participants had sleep difficulties. The risk ratio for having sleep difficulties in the first study wave following retirement, compared with the last study wave preceding retirement, was 0.89. The decreases in sleep difficulties occurred primarily among people with psychologic distress, suboptimal self-rated health, short sleep duration, and job strain before retirement.
Myllyntausta S, Salo P, Kronholm E, et al. Changes in sleep difficulties during the transition to statutory retirement. Sleep. 2017 Nov 16 [Epub ahead of print].
Vigorous Exercise May Delay Parkinson’s Disease Progression
High-intensity treadmill exercise may be feasible and prescribed safely for patients with Parkinson’s disease, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. The randomized clinical trial included 128 participants between ages 40 and 80. Participants were at an early stage of the disease and not taking Parkinson’s disease medication. Investigators randomized the population to high-intensity exercise, moderate-intensity exercise, or a control condition. At baseline and six months, clinicians assessed the participants using the Unified Parkinson’s Disease Rating Scale (UPDRS). Participants in the study had a UPDRS score of about 20 at baseline. At six months, the high-intensity group’s score stayed at 20, and the moderate exercise group worsened by 1.5 points. The control group’s score worsened by three points.
Schenkman M, Moore CG, Kohrt WM, et al. Effect of high-intensity treadmill exercise on motor symptoms in patients with de novo Parkinson disease: a phase 2 randomized clinical trial. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Can Exposure to Terror Raise the Risk of Headache?
Exposure to terror increases the risk of persistent weekly and daily migraine and tension-type headache in adolescent survivors above expected levels, according to a study published online ahead of print December 13, 2017, in Neurology. Investigators interviewed 213 survivors of a terror attack in Norway. Half were male, the mean age was 17.7, and 13 survivors were severely injured. Participants provided information about their headache frequency four to five months after the attack. For each survivor, eight matched controls were drawn from the Young-HUNT3 Study. After exposure to terror, the odds ratio for migraine was 4.27, and that for tension-type headache was 3.39, as estimated in multivariable logistic regression models adjusted for injury, sex, age, family structure and economy, prior exposure to physical or sexual violence, and psychologic distress.
Stensland SØ, Zwart JA, Wentzel-Larsen T, Dyb G. The headache of terror: a matched cohort study of adolescents from the Utøya and the HUNT Study. Neurology. 2017 Dec 13 [Epub ahead of print].
Diet Reduces Disability and Symptoms of MS
A healthy diet and a composite healthy lifestyle are associated with less disability and symptom burden in multiple sclerosis (MS), according to a study published online ahead of print December 6, 2017, in Neurology. The study involved 6,989 people with MS who completed questionnaires about their diet as part of the North American Research Committee registry. The questionnaire estimated intake of fruits, vegetables and legumes, whole grains, added sugars, and red and processed meats. Researchers constructed an overall diet quality score for each individual based on the food groups. Participants with diet quality scores in the highest quintile had lower levels of disability and lower depression scores. Individuals reporting a composite healthy lifestyle had lower odds of reporting severe fatigue, depression, pain, or cognitive impairment.
Fitzgerald KC, Tyry T, Salter A, et al. Diet quality is associated with disability and symptom severity in multiple sclerosis. Neurology. 2017 Dec 6 [Epub ahead of print].
What Are the Effects of Childhood Convulsive Status Epilepticus?
Childhood convulsive status epilepticus (CSE) is associated with substantial long-term neurologic morbidity, but primarily in people who have epilepsy, neurologic abnormalities, or both before the episode of CSE, according to a study published online ahead of print December 5, 2017, in Lancet Child & Adolescent Health. Researchers followed a population-based childhood CSE cohort. Of 203 survivors, 134 were assessed at a median follow-up of 8.9 years. Lasting neurologic conditions, including epilepsy, learning disabilities, and movement problems, were more common among participants than expected for children from the general population. Children who had existing neurologic or developmental issues at the time of CSE were more likely to have a neurologic problem at follow-up. Children without a neurologic or developmental issue tended to have better outcomes.
Pujar SS, Martinos MM, Cortina-Borja M, et al. Long-term prognosis after childhood convulsive status epilepticus: a prospective cohort study. Lancet Child Adolesc Health. 2017 Dec 5 [Epub ahead of print].
Protein Aggregation May Not Affect Cognition in Parkinson’s Disease
Patterns of cortical β-amyloid and tau do not differ between people with Parkinson’s disease who are cognitively normal (PD-CN), people with Parkinson’s disease with mild cognitive impairment (PD-MCI), and healthy older adults, according to a study published online ahead of print December 11, 2017, in JAMA Neurology. This cross-sectional study included 29 patients with Parkinson’s disease from a tertiary care medical center and research institutions. Imaging measures were compared with those of 49 healthy control participants. Outcomes were tau PET measurements of groups of patients with PD-CN and PD-MCI. Of the participants, 47 were female, and the mean age was 71.1. Voxelwise contrasts of whole-brain tau PET uptake between patients with PD-CN and patients with PD-MCI, and between patients with Parkinson’s disease and β-amyloid-negative controls, did not reveal significant differences.
Winer JR, Maass A, Pressman P, et al. Associations between tau, β-amyloid, and cognition in Parkinson disease. JAMA Neurol. 2017 Dec 11 [Epub ahead of print].
Hormone Therapy Not Linked to Increased Stroke Risk
Postmenopausal hormone therapy is not associated with increased risk of stroke, provided that it is started early, according to a study published November 17 in PLoS Medicine. Researchers analyzed data on postmenopausal hormone therapy from five cohort studies including 88,914 women, combined with data from national registries on diagnoses and causes of death during a follow-up period. During a median follow-up of 14.3 years, 6,371 first-time stroke events (1,080 hemorrhagic) were recorded. Hormone therapy was not linked to increased risk of stroke if the therapy was initiated within five years of menopausal onset, regardless of means of administration, type of therapy, active substance, and treatment duration. In subanalyses, researchers observed an increase in risk for hemorrhagic stroke if the therapy contained the active substance conjugated equine estrogens.
Carrasquilla GD, Frumento P, Berglund A, et al. Postmenopausal hormone therapy and risk of stroke: a pooled analysis of data from population-based cohort studies. PLoS Med. 2017;14(11):e1002445.
Restless Sleep May Be Linked to Parkinson’s Disease
In patients with idiopathic REM sleep behavior disorder (IRBD), PET shows increased microglial activation in the substantia nigra, along with reduced dopaminergic function in the putamen, according to a study published in the October 2017 issue of Lancet Neurology. This prospective, case–control PET study included 20 patients with IRBD and no clinical evidence of parkinsonism and cognitive impairment recruited from tertiary sleep centers and 19 healthy controls. 11C-PK11195 binding was increased on the left side of the substantia nigra in patients with IRBD, compared with controls, but not on the right side. 11C-PK11195 binding was not significantly increased in the putamen and caudate of patients with IRBD. 18F-DOPA uptake was reduced in IRBD in the left putamen and right putamen, but not in the caudate.
Stokholm MG, Iranzo A, Østergaard K, et al. Assessment of neuroinflammation in patients with idiopathic rapid-eye-movement sleep behaviour disorder: a case-control study. Lancet Neurol. 2017;16(10):789-796.
Can Playing Video Games Benefit the Brains of Older Adults?
Playing 3D video games may prevent mild cognitive impairment and, perhaps, Alzheimer’s disease, according to a study published December 6, 2017, in PLoS One. In two separate studies, adults in their 20s played 3D video games on platforms such as Super Mario 64. The gray matter in their hippocampus increased after training. Researchers examined whether the results could be replicated in healthy seniors. Thirty-three people, ages 55 to 75, were randomly assigned to one of three groups. The video game experimental group engaged in 3D-platform video game training over six months. An active control group took a series of self-directed, computerized piano lessons, and a no-contact control group did not engage in any intervention. Participants in the video-game cohort had increases in gray matter volume in the hippocampus and cerebellum. Their short-term memory also improved.
West GL, Zendel BR, Konishi K, et al. Playing Super Mario 64 increases hippocampal grey matter in older adults. PLoS One. 2017;12(12):e0187779.
FDA Approves Vercise Deep Brain Stimulation System
The FDA has approved the Vercise Deep Brain Stimulation System (DBS) to treat symptoms of Parkinson’s disease. The approval is based on the INTREPID study, a multicenter, prospective, double-blind, randomized, sham-controlled trial of DBS for Parkinson’s disease in the US. The study evaluated the system’s safety and efficacy in 292 patients at 23 sites. The Vercise DBS System successfully met its primary end point of mean change in waking hours with good symptom control. The filing also was supported by safety data from the VANTAGE study, in which 40 patients treated with the system demonstrated a 63% improvement in motor function at 52 weeks from baseline, as measured by the Unified Parkinson’s Disease Rating Scale III. Boston Scientific markets Vercise.
Can Social Relationships Aid Cognitive Function?
Although superagers (ie, people older than 80 with episodic memory as good as that of a middle-aged adult) and their cognitively average-for-age peers report similarly high levels of psychological well-being, superagers demonstrate greater levels of positive social relationships, according to a study published October 23, 2017, in PLoS One. Thirty-one superagers and 19 cognitively average-for-age peers completed the Ryff 42-item Psychological Well-Being questionnaire, which includes subscales of autonomy, positive relations with others, environmental mastery, personal growth, purpose in life, and self-acceptance. The groups did not differ on demographic factors, including estimated premorbid intelligence. Compared with cognitively average-for-age peers, superagers endorsed greater levels of positive relations with others. Superagers had a median overall score of 40 in positive relations with others, compared with 36 in the control group.
Cook Maher A, Kielb S, Loyer E, et al. Psychological well-being in elderly adults with extraordinary episodic memory. PLoS One. 2017;12(10):e0186413.
—Kimberly Williams

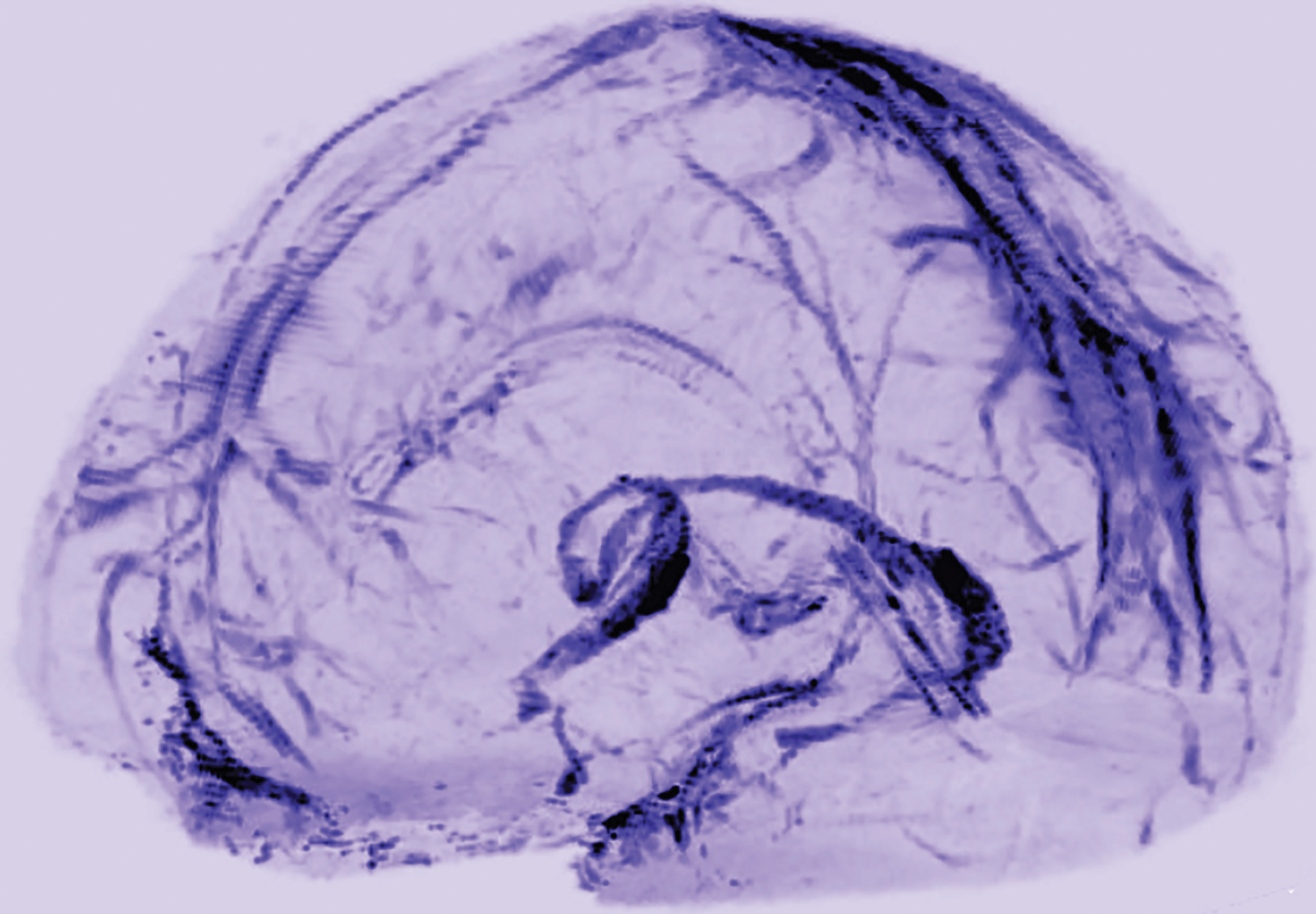
MRI Reveals Lymphatic Vessels in Dura
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.

A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.
A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Researchers have visualized lymphatic vessels in the dura mater of humans on MRI, according to a short report published October 3, 2017, in eLife. They also have identified lymphatic vessels in brain tissue samples using immunostaining. The results suggest that the vessels could act as a pipeline between the brain and the immune system.
“Overall, our data clearly and consistently demonstrate the existence of lymphatic vessels within the dura mater of human and nonhuman primates,” said Daniel S. Reich, MD, PhD, Senior Investigator at the NINDS, and colleagues. “The ability to image the meningeal lymphatics noninvasively immediately suggests the possibility of studying potential abnormalities” in neurologic disorders, they said.
A Fundamental Shift
In most of the body, lymphatic vessels transport immune cells and waste products from organs to the bloodstream, but the brain was thought not to have lymphatic vessels. In 2015, however, researchers found evidence of the brain’s lymphatic system in the dura of mice. Dr. Reich saw a presentation by an author of one the mouse studies, Jonathan Kipnis, PhD, Chair of the Department of Neuroscience at the University of Virginia in Charlottesville, and “was completely surprised.”
“In medical school, we were taught that the brain has no lymphatic system,” Dr. Reich said. “After Dr. Kipnis’s talk, I thought maybe we could find it in human brains.”
Dr. Reich and colleagues scanned the brains of five healthy volunteers who had been injected with gadobutrol, a dye used during MRI scans to visualize brain blood vessels. Gadobutrol that had leaked out of blood vessels in the dura as part of a normal process collected inside lymphatic vessels in the dura and showed up as bright white lines on MRI. “We watched people’s brains drain fluid into these vessels,” said Dr. Reich. When they repeated the experiment using a different dye that leaks much less out of blood vessels (ie, gadofosveset), the lymphatic vessels did not appear on imaging.
Similar findings were observed in monkeys.
The lymphatic vessels had been difficult to identify because they resemble blood vessels, which are far more numerous, the researchers said.
“These results could fundamentally change the way we think about how the brain and immune system interrelate,” said Walter J. Koroshetz, MD, NINDS director.
Meningeal Lymphatic Network
MRI showed collection of interstitial gadolinium within dural lymphatic vessels in all five of the healthy volunteers (ages 28 to 53, three women) and all three of the common marmoset monkeys studied. The vessels had a maximum apparent diameter of approximately 1 mm. “Our results suggest that in the dura, similar to many other organs throughout the body, small intravascular molecules extravasate into the interstitium and then, under a hydrostatic pressure gradient, collect into lymphatic capillaries through a loose lymphatic endothelium,” the researchers said. “On 3D rendering of subtraction MRI images, dural lymphatics are seen running parallel to the dural venous sinuses, especially the superior sagittal and straight sinuses, and alongside branches of the middle meningeal artery. The topography of the meningeal lymphatics fits with the previously described network in rodents.”
Although MRI shows large, slow-flow lymphatic ducts, “blind-ending and small lymphatic capillaries, clearly seen by histopathology, are unlikely to be revealed by MRI,” the researchers noted. In addition, they “could not prove whether dural lymphatic vessels drain immune cells, CSF, or other substances from the brain to deep cervical lymph nodes” or assess any link with the glymphatic system. “A comprehensive map of the meningeal lymphatic network would have implications for unraveling the ways in which the meningeal lymphatics participate in waste clearance and in immune cell trafficking within the CNS,” the researchers said.
Neuropathologic evaluation focused on dura samples from two formalin-fixed brains (from patients ages 60 and 77 with longstanding progressive multiple sclerosis) and from a 33-year-old patient with refractory epilepsy undergoing anterior temporal lobectomy.
Future studies may examine the role that dural lymphatics play in inflammatory pathologic conditions. The researchers have observed “clusters of extravascular CD3+ lymphocytes and CD68+ phagocytic meningeal macrophages … in the dura of several multiple sclerosis autopsies, confirming intense immune cell trafficking and communication.” Furthermore, “lymphatic dysfunction might impair waste clearance in neurodegenerative diseases and aging, in line with the recently captured deposition of β-amyloid in human dura in elderly people,” the researchers said.
—Jake Remaly
Suggested Reading
Absinta M, Ha SK, Nair G, et al. Human and nonhuman primate meninges harbor lymphatic vessels that can be visualized noninvasively by MRI. Elife. 2017 Oct 3;6:e29738.
Massachusetts named healthiest state for 2017
A year of surprises ended with one more bit of unexpected news:
Massachusetts’ win may have knocked Hawaii out of the top spot for the first time since 2011, but the Aloha State was still second out of 50 in 2017. Two other New England states were in the top five: Vermont in third and Connecticut in fifth, with Utah sandwiched between them in fourth, the United Health Foundation said in its latest report.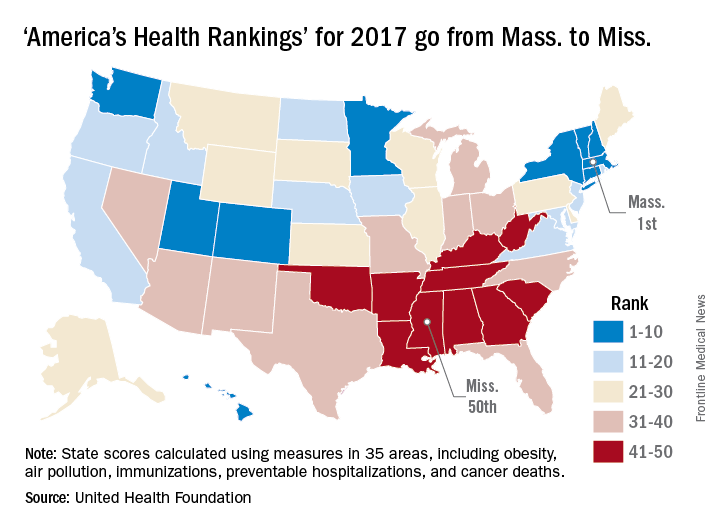
The report ranks states using 35 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. The measures include drug-related death rate, percentage of children in poverty, public health funding per person, mental health provider rate, and diabetes rate.
“America’s Health Rankings” is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
A year of surprises ended with one more bit of unexpected news:
Massachusetts’ win may have knocked Hawaii out of the top spot for the first time since 2011, but the Aloha State was still second out of 50 in 2017. Two other New England states were in the top five: Vermont in third and Connecticut in fifth, with Utah sandwiched between them in fourth, the United Health Foundation said in its latest report.
The report ranks states using 35 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. The measures include drug-related death rate, percentage of children in poverty, public health funding per person, mental health provider rate, and diabetes rate.
“America’s Health Rankings” is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
A year of surprises ended with one more bit of unexpected news:
Massachusetts’ win may have knocked Hawaii out of the top spot for the first time since 2011, but the Aloha State was still second out of 50 in 2017. Two other New England states were in the top five: Vermont in third and Connecticut in fifth, with Utah sandwiched between them in fourth, the United Health Foundation said in its latest report.
The report ranks states using 35 measures in five broad areas: behaviors, community and environment, policy, clinical care, and outcomes. The measures include drug-related death rate, percentage of children in poverty, public health funding per person, mental health provider rate, and diabetes rate.
“America’s Health Rankings” is funded entirely by the private, not-for-profit United Health Foundation, founded by UnitedHealth Group, which operates UnitedHealthcare.
Is mannitol a good alternative agent for evaluating ureteral patency after gynecologic surgery?
EXPERT COMMENTARY
Although the incidence of lower urinary tract and ureteral injury following gynecologic surgery is low, intraoperative identification of ureteral patency can prevent serious long-term sequelae. Since the indigo carmine shortage in 2014, US surgeons have searched for multiple alternative agents. Intravenous methylene blue is suboptimal due to its systemic adverse effects and the length of time for dye excretion in the urine.
Grimes and colleagues conducted a study to determine if there was any significant difference in surgeon satisfaction among 4 different alternatives to indigo carmine for intraoperative ureteral patency evaluation.
Related article:
Farewell to indigo carmine
Details of the study
The investigators conducted a randomized clinical trial of 130 women undergoing benign gynecologic or pelvic reconstructive surgery. Four different regimens were used for intraoperative ureteral evaluation: 1) oral phenazopyridine 200 mg, 2) intravenous sodium fluorescein 25 mg, 3) mannitol bladder distention, and 4) normal saline bladder distention.
Study outcomes. The primary outcome was surgeon satisfaction based on a 0 to 100 point visual analog scale rating (with 0 indicating strong agreement, 100 indicating disagreement). Secondary outcomes included ease of ureteral jet visualization, time to surgeon confidence of ureteral patency, and occurrence of adverse events over 6 weeks.
Surgeon satisfaction rating. The investigators found statistically significant physician satisfaction with the use of mannitol as a bladder distention medium over oral phenazopyridine, and slightly better satisfaction compared with the use of intravenous sodium fluorescein or normal saline distention. The median (range) visual analog scores for ureteral patency were phenazopyridine, 48 (0–83); sodium fluorescein 20 (0–82); mannitol, 0 (0–44); and normal saline, 23 (3–96) (P<.001).
There was no difference across the 4 groups in the timing to surgeon confidence of ureteral patency, length of cystoscopy (on average, 3 minutes), and development of postoperative urinary tract infections (UTIs).
Most dissatisfaction related to phenazopyridine is the fact that the resulting orange-stained urine can obscure the bladder mucosa.
One significant adverse event was a protocol deviation in which 1 patient received an incorrect dose of IV sodium fluorescein (500 mg) instead of the recommended 25-mg dose.
Related article:
Alternative options for visualizing ureteral patency during intraoperative cystoscopy
Study strengths and weaknesses
The strength of this study is in its randomized design and power. Its major weakness is surgeon bias, since the surgeons could not possibly be blinded to the method used.
The study confirms the problem that phenazopyridine makes the urine so orange that bladder mucosal lesions and de novo hematuria could be difficult to detect. Recommending mannitol as a hypertonic distending medium (as it is used in hysteroscopy procedures), however, may be premature. Prior studies have shown increased postoperative UTIs when 50% and 10% dextrose was used versus normal saline for cystoscopy.1,2 Since the Grimes study protocol did not include postoperative urine collection for cultures, more research on UTIs after mannitol use would be needed before surgeons confidently could use it routinely.
In our practice, surgeons prefer that intravenous sodium fluorescein be administered just prior to cystoscopy and oral phenazopyridine en route to the operating room. I agree that a major disadvantage to phenazopyridine is the heavy orange staining that obscures visualization.
Finally, this study did not account for cost of the various methods; standard normal saline would be cheapest, followed by phenazopyridine.
This study showed that surgeon satisfaction was greatest with the use of mannitol as a distending medium for intraoperative evaluation of ureteral patency compared with oral phenazopyridine, intravenous sodium fluorescein, and normal saline distention. However, time to surgeon confidence of ureteral patency was similar with all 4 methods. More data are needed related to UTIs and the cost of mannitol compared with the other 3 methods.
-- Cheryl B. Iglesia, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Narasimhulu DM, Prabakar C, Tang N, Bral P. 50% dextrose versus normal saline as distention media during cystoscopy for assessment of ureteric patency. Eur J Obstet Gynecol Reprod Biol. 2016;199:38–41.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM, Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–e6.
EXPERT COMMENTARY
Although the incidence of lower urinary tract and ureteral injury following gynecologic surgery is low, intraoperative identification of ureteral patency can prevent serious long-term sequelae. Since the indigo carmine shortage in 2014, US surgeons have searched for multiple alternative agents. Intravenous methylene blue is suboptimal due to its systemic adverse effects and the length of time for dye excretion in the urine.
Grimes and colleagues conducted a study to determine if there was any significant difference in surgeon satisfaction among 4 different alternatives to indigo carmine for intraoperative ureteral patency evaluation.
Related article:
Farewell to indigo carmine
Details of the study
The investigators conducted a randomized clinical trial of 130 women undergoing benign gynecologic or pelvic reconstructive surgery. Four different regimens were used for intraoperative ureteral evaluation: 1) oral phenazopyridine 200 mg, 2) intravenous sodium fluorescein 25 mg, 3) mannitol bladder distention, and 4) normal saline bladder distention.
Study outcomes. The primary outcome was surgeon satisfaction based on a 0 to 100 point visual analog scale rating (with 0 indicating strong agreement, 100 indicating disagreement). Secondary outcomes included ease of ureteral jet visualization, time to surgeon confidence of ureteral patency, and occurrence of adverse events over 6 weeks.
Surgeon satisfaction rating. The investigators found statistically significant physician satisfaction with the use of mannitol as a bladder distention medium over oral phenazopyridine, and slightly better satisfaction compared with the use of intravenous sodium fluorescein or normal saline distention. The median (range) visual analog scores for ureteral patency were phenazopyridine, 48 (0–83); sodium fluorescein 20 (0–82); mannitol, 0 (0–44); and normal saline, 23 (3–96) (P<.001).
There was no difference across the 4 groups in the timing to surgeon confidence of ureteral patency, length of cystoscopy (on average, 3 minutes), and development of postoperative urinary tract infections (UTIs).
Most dissatisfaction related to phenazopyridine is the fact that the resulting orange-stained urine can obscure the bladder mucosa.
One significant adverse event was a protocol deviation in which 1 patient received an incorrect dose of IV sodium fluorescein (500 mg) instead of the recommended 25-mg dose.
Related article:
Alternative options for visualizing ureteral patency during intraoperative cystoscopy
Study strengths and weaknesses
The strength of this study is in its randomized design and power. Its major weakness is surgeon bias, since the surgeons could not possibly be blinded to the method used.
The study confirms the problem that phenazopyridine makes the urine so orange that bladder mucosal lesions and de novo hematuria could be difficult to detect. Recommending mannitol as a hypertonic distending medium (as it is used in hysteroscopy procedures), however, may be premature. Prior studies have shown increased postoperative UTIs when 50% and 10% dextrose was used versus normal saline for cystoscopy.1,2 Since the Grimes study protocol did not include postoperative urine collection for cultures, more research on UTIs after mannitol use would be needed before surgeons confidently could use it routinely.
In our practice, surgeons prefer that intravenous sodium fluorescein be administered just prior to cystoscopy and oral phenazopyridine en route to the operating room. I agree that a major disadvantage to phenazopyridine is the heavy orange staining that obscures visualization.
Finally, this study did not account for cost of the various methods; standard normal saline would be cheapest, followed by phenazopyridine.
This study showed that surgeon satisfaction was greatest with the use of mannitol as a distending medium for intraoperative evaluation of ureteral patency compared with oral phenazopyridine, intravenous sodium fluorescein, and normal saline distention. However, time to surgeon confidence of ureteral patency was similar with all 4 methods. More data are needed related to UTIs and the cost of mannitol compared with the other 3 methods.
-- Cheryl B. Iglesia, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Although the incidence of lower urinary tract and ureteral injury following gynecologic surgery is low, intraoperative identification of ureteral patency can prevent serious long-term sequelae. Since the indigo carmine shortage in 2014, US surgeons have searched for multiple alternative agents. Intravenous methylene blue is suboptimal due to its systemic adverse effects and the length of time for dye excretion in the urine.
Grimes and colleagues conducted a study to determine if there was any significant difference in surgeon satisfaction among 4 different alternatives to indigo carmine for intraoperative ureteral patency evaluation.
Related article:
Farewell to indigo carmine
Details of the study
The investigators conducted a randomized clinical trial of 130 women undergoing benign gynecologic or pelvic reconstructive surgery. Four different regimens were used for intraoperative ureteral evaluation: 1) oral phenazopyridine 200 mg, 2) intravenous sodium fluorescein 25 mg, 3) mannitol bladder distention, and 4) normal saline bladder distention.
Study outcomes. The primary outcome was surgeon satisfaction based on a 0 to 100 point visual analog scale rating (with 0 indicating strong agreement, 100 indicating disagreement). Secondary outcomes included ease of ureteral jet visualization, time to surgeon confidence of ureteral patency, and occurrence of adverse events over 6 weeks.
Surgeon satisfaction rating. The investigators found statistically significant physician satisfaction with the use of mannitol as a bladder distention medium over oral phenazopyridine, and slightly better satisfaction compared with the use of intravenous sodium fluorescein or normal saline distention. The median (range) visual analog scores for ureteral patency were phenazopyridine, 48 (0–83); sodium fluorescein 20 (0–82); mannitol, 0 (0–44); and normal saline, 23 (3–96) (P<.001).
There was no difference across the 4 groups in the timing to surgeon confidence of ureteral patency, length of cystoscopy (on average, 3 minutes), and development of postoperative urinary tract infections (UTIs).
Most dissatisfaction related to phenazopyridine is the fact that the resulting orange-stained urine can obscure the bladder mucosa.
One significant adverse event was a protocol deviation in which 1 patient received an incorrect dose of IV sodium fluorescein (500 mg) instead of the recommended 25-mg dose.
Related article:
Alternative options for visualizing ureteral patency during intraoperative cystoscopy
Study strengths and weaknesses
The strength of this study is in its randomized design and power. Its major weakness is surgeon bias, since the surgeons could not possibly be blinded to the method used.
The study confirms the problem that phenazopyridine makes the urine so orange that bladder mucosal lesions and de novo hematuria could be difficult to detect. Recommending mannitol as a hypertonic distending medium (as it is used in hysteroscopy procedures), however, may be premature. Prior studies have shown increased postoperative UTIs when 50% and 10% dextrose was used versus normal saline for cystoscopy.1,2 Since the Grimes study protocol did not include postoperative urine collection for cultures, more research on UTIs after mannitol use would be needed before surgeons confidently could use it routinely.
In our practice, surgeons prefer that intravenous sodium fluorescein be administered just prior to cystoscopy and oral phenazopyridine en route to the operating room. I agree that a major disadvantage to phenazopyridine is the heavy orange staining that obscures visualization.
Finally, this study did not account for cost of the various methods; standard normal saline would be cheapest, followed by phenazopyridine.
This study showed that surgeon satisfaction was greatest with the use of mannitol as a distending medium for intraoperative evaluation of ureteral patency compared with oral phenazopyridine, intravenous sodium fluorescein, and normal saline distention. However, time to surgeon confidence of ureteral patency was similar with all 4 methods. More data are needed related to UTIs and the cost of mannitol compared with the other 3 methods.
-- Cheryl B. Iglesia, MD
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Narasimhulu DM, Prabakar C, Tang N, Bral P. 50% dextrose versus normal saline as distention media during cystoscopy for assessment of ureteric patency. Eur J Obstet Gynecol Reprod Biol. 2016;199:38–41.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM, Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–e6.
- Narasimhulu DM, Prabakar C, Tang N, Bral P. 50% dextrose versus normal saline as distention media during cystoscopy for assessment of ureteric patency. Eur J Obstet Gynecol Reprod Biol. 2016;199:38–41.
- Siff LN, Unger CA, Jelovsek JE, Paraiso MF, Ridgeway BM, Barber MD. Assessing ureteral patency using 10% dextrose cystoscopy fluid: evaluation of urinary tract infection rates. Am J Obstet Gynecol. 2016;215(1):74.e1–e6.
Commentary—Study Heightens Awareness, But at What Cost?
The study conducted by Brookmeyer and colleagues is a logical and thoughtful attempt to size the potential impact of Alzheimer's disease now and in the future, updating old-technology estimates based on actual diagnoses with new technologically derived diagnoses of preclinical neurodegenerative states. They acknowledge that the uncertainty in the actual disease burden we will face is centered on the question of conversion rates, which vary between studies and are far less certain in the preclinical stages than the symptomatic ones.
Scientific interest aside, the main purpose of an article like this is to heighten awareness and concern by demonstrating that symptomatic Alzheimer's disease is the tip of a much larger iceberg and warrants more funding for research and clinical care. The worry that articles like this—or that the media attention they receive—create for me, however, is that they potentially contribute to a growing public panic at a time when we still lack truly meaningful therapy. As a doctor, I want to give my patients with MCI and dementia reason to believe they still have a meaningful life and that there is hope, rather than having them feel that I have just pronounced a death sentence.
The attention paid by the Alzheimer's Association is understandable, given its mission of increasing awareness and supporting more funding, but it omits to mention another important article showing that dementia rates are actually declining when data are adjusted for our aging population (observed vs expected).
We need to maintain public awareness without creating panic. There is no question that Alzheimer's disease is a major public health issue that warrants all the funding we can provide to researchers seeking a cure. How to balance that need with the need to give our population hope that all is not lost when they misplace their keys is the challenge this article raises.
—Richard J. Caselli, MD
Professor of Neurology
Mayo Clinic
Scottsdale, Arizona
The study conducted by Brookmeyer and colleagues is a logical and thoughtful attempt to size the potential impact of Alzheimer's disease now and in the future, updating old-technology estimates based on actual diagnoses with new technologically derived diagnoses of preclinical neurodegenerative states. They acknowledge that the uncertainty in the actual disease burden we will face is centered on the question of conversion rates, which vary between studies and are far less certain in the preclinical stages than the symptomatic ones.
Scientific interest aside, the main purpose of an article like this is to heighten awareness and concern by demonstrating that symptomatic Alzheimer's disease is the tip of a much larger iceberg and warrants more funding for research and clinical care. The worry that articles like this—or that the media attention they receive—create for me, however, is that they potentially contribute to a growing public panic at a time when we still lack truly meaningful therapy. As a doctor, I want to give my patients with MCI and dementia reason to believe they still have a meaningful life and that there is hope, rather than having them feel that I have just pronounced a death sentence.
The attention paid by the Alzheimer's Association is understandable, given its mission of increasing awareness and supporting more funding, but it omits to mention another important article showing that dementia rates are actually declining when data are adjusted for our aging population (observed vs expected).
We need to maintain public awareness without creating panic. There is no question that Alzheimer's disease is a major public health issue that warrants all the funding we can provide to researchers seeking a cure. How to balance that need with the need to give our population hope that all is not lost when they misplace their keys is the challenge this article raises.
—Richard J. Caselli, MD
Professor of Neurology
Mayo Clinic
Scottsdale, Arizona
The study conducted by Brookmeyer and colleagues is a logical and thoughtful attempt to size the potential impact of Alzheimer's disease now and in the future, updating old-technology estimates based on actual diagnoses with new technologically derived diagnoses of preclinical neurodegenerative states. They acknowledge that the uncertainty in the actual disease burden we will face is centered on the question of conversion rates, which vary between studies and are far less certain in the preclinical stages than the symptomatic ones.
Scientific interest aside, the main purpose of an article like this is to heighten awareness and concern by demonstrating that symptomatic Alzheimer's disease is the tip of a much larger iceberg and warrants more funding for research and clinical care. The worry that articles like this—or that the media attention they receive—create for me, however, is that they potentially contribute to a growing public panic at a time when we still lack truly meaningful therapy. As a doctor, I want to give my patients with MCI and dementia reason to believe they still have a meaningful life and that there is hope, rather than having them feel that I have just pronounced a death sentence.
The attention paid by the Alzheimer's Association is understandable, given its mission of increasing awareness and supporting more funding, but it omits to mention another important article showing that dementia rates are actually declining when data are adjusted for our aging population (observed vs expected).
We need to maintain public awareness without creating panic. There is no question that Alzheimer's disease is a major public health issue that warrants all the funding we can provide to researchers seeking a cure. How to balance that need with the need to give our population hope that all is not lost when they misplace their keys is the challenge this article raises.
—Richard J. Caselli, MD
Professor of Neurology
Mayo Clinic
Scottsdale, Arizona

Sodium Oxybate Reduces Daytime Sleepiness in Parkinson’s Disease
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.

The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.
The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Sodium oxybate effectively treats excessive daytime sleepiness and nocturnal sleep disturbance in patients with Parkinson’s disease, according to research published in the January issue of JAMA Neurology. Patients receiving this therapy should be monitored with follow-up polysomnography to rule out treatment-related complications, the investigators said.
Many patients with Parkinson’s disease have excessive daytime sleepiness and disturbed sleep, but few treatments are available for them. An open-label study found that sodium oxybate, a first-line therapy for narcolepsy type 1, improved sleep and reduced daytime sleepiness in Parkinson’s disease.
A Phase II Crossover Study
To investigate this treatment further, Christian Baumann, MD, Senior Physician at University Hospital Zürich, and colleagues enrolled 18 patients into a double-blind, placebo-controlled, crossover phase IIa study. Eligible participants had Parkinson’s disease and regularly took dopaminergic medication. People with sleep apnea, cognitive problems, or depression, and those who took hypnotics, were excluded from the study.
The researchers randomized participants in equal groups to sodium oxybate or placebo. Study medications were taken daily at bedtime and 2.5 to four hours later for six weeks. Doses were titrated between 3 g/night and 9 g/night according to efficacy and tolerability. After a two- to four-week washout period, participants crossed over to the opposite treatment arm for six weeks.
The trial’s primary efficacy end point was treatment effect on mean sleep latency (MSL), as measured by the Multiple Sleep Latency Test (MSLT). Secondary end points included change in subjective excessive daytime sleepiness (as measured by the Epworth Sleepiness Scale [ESS]), sleep quality, and objective sleep parameters. The investigators measured outcomes in the sleep laboratory at baseline and after six weeks of therapy.
Adverse Events Were Mild or Moderate
Five patients were excluded because of sleep apnea, and one patient withdrew consent. Of the 12 patients randomized, two were women. At baseline, participants’ mean age was 62, and mean disease duration was 8.4 years. Two patients developed de novo sleep apnea during sodium oxybate treatment, and one of them dropped out.
In the intention-to-treat analysis, sodium oxybate increased MSL by 2.9 minutes and reduced ESS score by 4.2 points. In the per-protocol analysis, sodium oxybate increased MSL by 3.5 minutes and reduced ESS score by 5.2 points. The responder rate for sodium oxybate (ie, the percentage of patients who had an improvement in MSL of more than 50%) was 67%. ESS score normalized for half of patients.
Every patient who received sodium oxybate had adverse events of mild or moderate intensity. The majority of these adverse events resolved after dose adjustment. Four patients continued to have adverse events until the end of the study, but none dropped out because of them.
Sodium oxybate had a treatment effect “that, to our knowledge, is unmatched by any other intervention reported so far,” said Dr. Baumann and colleagues. Although the sample size was large enough to provide class I evidence of efficacy, it was insufficient to support conclusions about safety, said the researchers. Larger follow-up trials thus are necessary, they concluded.
—Erik Greb
Suggested Reading
Büchele F, Hackius M, Schreglmann SR, et al. Sodium oxybate for excessive daytime sleepiness and sleep disturbance in Parkinson disease: a randomized clinical trial. JAMA Neurol. 2018;75(1):114-118.
Dementia: Past, Present, and Future
Jeffrey Cummings, MD, ScD
Director, Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas
Disclosure: Jeffrey Cummings has provided consultation to Axovant, biOasis Technologies, Biogen, Boehinger-Ingelheim, Bracket, Dart, Eisai, Genentech, Grifols, Intracellular Therapies, Kyowa, Eli Lilly, Lundbeck, Medavante, Merck, Neurotrope, Novartis, Nutricia, Orion, Otsuka, Pfizer, Probiodrug, QR, Resverlogix, Servier, Suven, Takeda, Toyoma, and United Neuroscience companies.

As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of dementia care and research. Most dementia research has focused on Alzheimer’s disease, although there have been important evolutions in the diagnosis, pathology, and potential interventions for frontotemporal dementia spectrum disorders, dementia with Lewy bodies, Parkinson’s disease dementia, and vascular dementia.
Alzheimer’s Disease
Twenty-five years ago—coinciding with the inauguration of Neurology Reviews—the first treatment for Alzheimer’s disease, the cholinesterase inhibitor tacrine, was approved by the FDA. Tacrine had many limitations, including a short half-life and a propensity to cause hepatotoxicity, but it represented an historical breakthrough in transforming an untreatable disease into a treatable one. The approval energized the field and gave hope to thousands of patients with Alzheimer’s disease dementia.
Tacrine was followed by other cholinesterase inhibitors and memantine in the next decade, with five drugs approved by the end of 2003. Unfortunately, no new agents have been approved for the treatment of Alzheimer’s disease since that fertile period.1 Tremendous efforts are now being devoted to developing disease-modifying treatments for Alzheimer’s disease and other dementias. There are promising preliminary observations for immunotherapies that remove amyloid-beta protein from the brain and stabilize cognitive decline.2 Progress in the development of disease-modifying treatments will transform the field, requiring much of the health care system and insurance companies, but offering an improved quality of life for millions of patients with Alzheimer’s disease.
Previous Advances
A major advance in understanding Alzheimer’s disease is the discovery that the disease begins with amyloid accumulation in mid-life, approximately 15 years before the onset of cognitive decline.3 The advent of amyloid imaging has allowed the visualization of fibrillar amyloid-comprising Alzheimer-type neuritic plaques in the brain of the living person. Scans become positive 15 years prior to the emergence of mild cognitive impairment (MCI) and progression to Alzheimer’s disease dementia. If one is destined to develop MCI at age 75, the scan would be positive by approximately age 60. CSF levels of amyloid beta decline simultaneously as the protein is trapped in the brain, thus resulting in positive amyloid imaging. More recently, findings from tau protein imaging have begun to remodel our understanding of the role of tau in Alzheimer’s disease. Tau imaging correlates with the emergence of symptoms in the MCI phase of Alzheimer’s disease.4 Tau correlates with cognitive decline; positive amyloid imaging does not.
Future Challenges
Looking to the future, it is likely that companion biomarkers such as amyloid and tau imaging will be approved for clinical use. They will enable neurologists to identify the patients whose brain changes match the mechanism of action of the intended treatment (eg, positive tau imaging for those to receive anti-tau therapy and positive amyloid imaging for individuals intended to receive anti-amyloid therapy).
Anticipated directions of therapy development include treatment of individuals before the onset of symptoms, phase-specific therapies that respond to the evolving state changes of Alzheimer’s disease, and combination therapies based on the observation that most patients with Alzheimer’s disease harbor multiple types of brain pathology.5 Alzheimer’s disease therapeutics will proceed in the direction of precision medicine with better matching of therapies to the features of the disorder for the individual patient.
The US health care system is unprepared for the advent of disease-modifying treatments for Alzheimer’s disease. Recognition of patients with mild changes, availability of amyloid imaging to support diagnosis and identify therapeutic targets, and the number of infusion centers to administer monoclonal antibodies are all insufficient to respon
Advances in the understanding of frontotemporal dementia have not yet led to a breakthrough therapy. Frontotemporal dementia has been shown to be pathologically heterogeneous, with about half of the patients having an underlying tauopathy, and about half having TDP-43 as the associated aggregated protein.6 A few cases have rarer forms of pathology. Major phenotypes of frontotemporal dementia include behavioral variant frontotemporal dementia, progressive nonfluent aphasia, and semantic dementia. Trials of new candidate therapies are progressing for frontotemporal dementia spectrum disorders, and new treatments are anticipated.
Progress in understanding dementia with Lewy bodies has led to the publication of diagnostic criteria.7 The phenotype of parkinsonism, fluctuating cognition, and visual hallucinations is supported by decreased dopamine uptake on dopamine transporter (DaT) scanning and the presence of REM sleep behavior disorder. Lewy bodies are found in the limbic and neocortex at autopsy; many cases have concomitant amyloid plaques similar to those of Alzheimer’s disease. Parkinson’s disease dementia has many of the same features and is distinguished from dementia with Lewy bodies only by the order of appearance of major symptoms—dementia first in dementia with Lewy bodies, parkinsonism first in Parkinson’s disease dementia. Rivastigmine is approved for the symptomatic treatment of cognitive deficits in Parkinson’s disease dementia, and trials of new therapies are being conducted in Parkinson’s disease dementia and dementia with Lewy bodies. Alpha-synuclein is present in both disorders and is the target of new disease-modifying treatments currently in clinical trials.
Improved understanding of the basic biology of neurodegenerative disease is critically important and must be accelerated. This knowledge will provide the foundation for improved diagnostics and therapeutics essential for responding to the needs of the burgeoning number of patients with these late-life brain disorders.
References
1. Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37-43.
2. Sevigny J, Chiao P, Bussiere T, et al. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature. 2016;537(7618):50-56.
3. Villemagne VL, Burnham S, Bourgeat P, et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. 2013;12(4):357-367.
4. Johnson KA, Schultz A, Betensky RA, et al. Tau positron emission tomographic imaging in aging and early Alzheimer disease. Ann Neurol. 2016;79(1):110-119.
5. James BD, Wilson RS, Boyle PA, et al. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain. 2016;139(11):2983-2993.
6. Lashley T, Rohrer JD, Mead S, Revesz T. Review: an update on clinical, genetic and pathological aspects of frontotemporal lobar degenerations. Neuropathol Appl Neurobiol. 2015;41(7):858-881.
7. McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017;89(1):88-100.
Jeffrey Cummings, MD, ScD
Director, Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas
Disclosure: Jeffrey Cummings has provided consultation to Axovant, biOasis Technologies, Biogen, Boehinger-Ingelheim, Bracket, Dart, Eisai, Genentech, Grifols, Intracellular Therapies, Kyowa, Eli Lilly, Lundbeck, Medavante, Merck, Neurotrope, Novartis, Nutricia, Orion, Otsuka, Pfizer, Probiodrug, QR, Resverlogix, Servier, Suven, Takeda, Toyoma, and United Neuroscience companies.
As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of dementia care and research. Most dementia research has focused on Alzheimer’s disease, although there have been important evolutions in the diagnosis, pathology, and potential interventions for frontotemporal dementia spectrum disorders, dementia with Lewy bodies, Parkinson’s disease dementia, and vascular dementia.
Alzheimer’s Disease
Twenty-five years ago—coinciding with the inauguration of Neurology Reviews—the first treatment for Alzheimer’s disease, the cholinesterase inhibitor tacrine, was approved by the FDA. Tacrine had many limitations, including a short half-life and a propensity to cause hepatotoxicity, but it represented an historical breakthrough in transforming an untreatable disease into a treatable one. The approval energized the field and gave hope to thousands of patients with Alzheimer’s disease dementia.
Tacrine was followed by other cholinesterase inhibitors and memantine in the next decade, with five drugs approved by the end of 2003. Unfortunately, no new agents have been approved for the treatment of Alzheimer’s disease since that fertile period.1 Tremendous efforts are now being devoted to developing disease-modifying treatments for Alzheimer’s disease and other dementias. There are promising preliminary observations for immunotherapies that remove amyloid-beta protein from the brain and stabilize cognitive decline.2 Progress in the development of disease-modifying treatments will transform the field, requiring much of the health care system and insurance companies, but offering an improved quality of life for millions of patients with Alzheimer’s disease.
Previous Advances
A major advance in understanding Alzheimer’s disease is the discovery that the disease begins with amyloid accumulation in mid-life, approximately 15 years before the onset of cognitive decline.3 The advent of amyloid imaging has allowed the visualization of fibrillar amyloid-comprising Alzheimer-type neuritic plaques in the brain of the living person. Scans become positive 15 years prior to the emergence of mild cognitive impairment (MCI) and progression to Alzheimer’s disease dementia. If one is destined to develop MCI at age 75, the scan would be positive by approximately age 60. CSF levels of amyloid beta decline simultaneously as the protein is trapped in the brain, thus resulting in positive amyloid imaging. More recently, findings from tau protein imaging have begun to remodel our understanding of the role of tau in Alzheimer’s disease. Tau imaging correlates with the emergence of symptoms in the MCI phase of Alzheimer’s disease.4 Tau correlates with cognitive decline; positive amyloid imaging does not.
Future Challenges
Looking to the future, it is likely that companion biomarkers such as amyloid and tau imaging will be approved for clinical use. They will enable neurologists to identify the patients whose brain changes match the mechanism of action of the intended treatment (eg, positive tau imaging for those to receive anti-tau therapy and positive amyloid imaging for individuals intended to receive anti-amyloid therapy).
Anticipated directions of therapy development include treatment of individuals before the onset of symptoms, phase-specific therapies that respond to the evolving state changes of Alzheimer’s disease, and combination therapies based on the observation that most patients with Alzheimer’s disease harbor multiple types of brain pathology.5 Alzheimer’s disease therapeutics will proceed in the direction of precision medicine with better matching of therapies to the features of the disorder for the individual patient.
The US health care system is unprepared for the advent of disease-modifying treatments for Alzheimer’s disease. Recognition of patients with mild changes, availability of amyloid imaging to support diagnosis and identify therapeutic targets, and the number of infusion centers to administer monoclonal antibodies are all insufficient to respon
Advances in the understanding of frontotemporal dementia have not yet led to a breakthrough therapy. Frontotemporal dementia has been shown to be pathologically heterogeneous, with about half of the patients having an underlying tauopathy, and about half having TDP-43 as the associated aggregated protein.6 A few cases have rarer forms of pathology. Major phenotypes of frontotemporal dementia include behavioral variant frontotemporal dementia, progressive nonfluent aphasia, and semantic dementia. Trials of new candidate therapies are progressing for frontotemporal dementia spectrum disorders, and new treatments are anticipated.
Progress in understanding dementia with Lewy bodies has led to the publication of diagnostic criteria.7 The phenotype of parkinsonism, fluctuating cognition, and visual hallucinations is supported by decreased dopamine uptake on dopamine transporter (DaT) scanning and the presence of REM sleep behavior disorder. Lewy bodies are found in the limbic and neocortex at autopsy; many cases have concomitant amyloid plaques similar to those of Alzheimer’s disease. Parkinson’s disease dementia has many of the same features and is distinguished from dementia with Lewy bodies only by the order of appearance of major symptoms—dementia first in dementia with Lewy bodies, parkinsonism first in Parkinson’s disease dementia. Rivastigmine is approved for the symptomatic treatment of cognitive deficits in Parkinson’s disease dementia, and trials of new therapies are being conducted in Parkinson’s disease dementia and dementia with Lewy bodies. Alpha-synuclein is present in both disorders and is the target of new disease-modifying treatments currently in clinical trials.
Improved understanding of the basic biology of neurodegenerative disease is critically important and must be accelerated. This knowledge will provide the foundation for improved diagnostics and therapeutics essential for responding to the needs of the burgeoning number of patients with these late-life brain disorders.
References
1. Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37-43.
2. Sevigny J, Chiao P, Bussiere T, et al. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature. 2016;537(7618):50-56.
3. Villemagne VL, Burnham S, Bourgeat P, et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. 2013;12(4):357-367.
4. Johnson KA, Schultz A, Betensky RA, et al. Tau positron emission tomographic imaging in aging and early Alzheimer disease. Ann Neurol. 2016;79(1):110-119.
5. James BD, Wilson RS, Boyle PA, et al. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain. 2016;139(11):2983-2993.
6. Lashley T, Rohrer JD, Mead S, Revesz T. Review: an update on clinical, genetic and pathological aspects of frontotemporal lobar degenerations. Neuropathol Appl Neurobiol. 2015;41(7):858-881.
7. McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017;89(1):88-100.
Jeffrey Cummings, MD, ScD
Director, Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas
Disclosure: Jeffrey Cummings has provided consultation to Axovant, biOasis Technologies, Biogen, Boehinger-Ingelheim, Bracket, Dart, Eisai, Genentech, Grifols, Intracellular Therapies, Kyowa, Eli Lilly, Lundbeck, Medavante, Merck, Neurotrope, Novartis, Nutricia, Orion, Otsuka, Pfizer, Probiodrug, QR, Resverlogix, Servier, Suven, Takeda, Toyoma, and United Neuroscience companies.
As Neurology Reviews celebrates its 25th anniversary, we take this opportunity to look back and to look ahead in the area of dementia care and research. Most dementia research has focused on Alzheimer’s disease, although there have been important evolutions in the diagnosis, pathology, and potential interventions for frontotemporal dementia spectrum disorders, dementia with Lewy bodies, Parkinson’s disease dementia, and vascular dementia.
Alzheimer’s Disease
Twenty-five years ago—coinciding with the inauguration of Neurology Reviews—the first treatment for Alzheimer’s disease, the cholinesterase inhibitor tacrine, was approved by the FDA. Tacrine had many limitations, including a short half-life and a propensity to cause hepatotoxicity, but it represented an historical breakthrough in transforming an untreatable disease into a treatable one. The approval energized the field and gave hope to thousands of patients with Alzheimer’s disease dementia.
Tacrine was followed by other cholinesterase inhibitors and memantine in the next decade, with five drugs approved by the end of 2003. Unfortunately, no new agents have been approved for the treatment of Alzheimer’s disease since that fertile period.1 Tremendous efforts are now being devoted to developing disease-modifying treatments for Alzheimer’s disease and other dementias. There are promising preliminary observations for immunotherapies that remove amyloid-beta protein from the brain and stabilize cognitive decline.2 Progress in the development of disease-modifying treatments will transform the field, requiring much of the health care system and insurance companies, but offering an improved quality of life for millions of patients with Alzheimer’s disease.
Previous Advances
A major advance in understanding Alzheimer’s disease is the discovery that the disease begins with amyloid accumulation in mid-life, approximately 15 years before the onset of cognitive decline.3 The advent of amyloid imaging has allowed the visualization of fibrillar amyloid-comprising Alzheimer-type neuritic plaques in the brain of the living person. Scans become positive 15 years prior to the emergence of mild cognitive impairment (MCI) and progression to Alzheimer’s disease dementia. If one is destined to develop MCI at age 75, the scan would be positive by approximately age 60. CSF levels of amyloid beta decline simultaneously as the protein is trapped in the brain, thus resulting in positive amyloid imaging. More recently, findings from tau protein imaging have begun to remodel our understanding of the role of tau in Alzheimer’s disease. Tau imaging correlates with the emergence of symptoms in the MCI phase of Alzheimer’s disease.4 Tau correlates with cognitive decline; positive amyloid imaging does not.
Future Challenges
Looking to the future, it is likely that companion biomarkers such as amyloid and tau imaging will be approved for clinical use. They will enable neurologists to identify the patients whose brain changes match the mechanism of action of the intended treatment (eg, positive tau imaging for those to receive anti-tau therapy and positive amyloid imaging for individuals intended to receive anti-amyloid therapy).
Anticipated directions of therapy development include treatment of individuals before the onset of symptoms, phase-specific therapies that respond to the evolving state changes of Alzheimer’s disease, and combination therapies based on the observation that most patients with Alzheimer’s disease harbor multiple types of brain pathology.5 Alzheimer’s disease therapeutics will proceed in the direction of precision medicine with better matching of therapies to the features of the disorder for the individual patient.
The US health care system is unprepared for the advent of disease-modifying treatments for Alzheimer’s disease. Recognition of patients with mild changes, availability of amyloid imaging to support diagnosis and identify therapeutic targets, and the number of infusion centers to administer monoclonal antibodies are all insufficient to respon
Advances in the understanding of frontotemporal dementia have not yet led to a breakthrough therapy. Frontotemporal dementia has been shown to be pathologically heterogeneous, with about half of the patients having an underlying tauopathy, and about half having TDP-43 as the associated aggregated protein.6 A few cases have rarer forms of pathology. Major phenotypes of frontotemporal dementia include behavioral variant frontotemporal dementia, progressive nonfluent aphasia, and semantic dementia. Trials of new candidate therapies are progressing for frontotemporal dementia spectrum disorders, and new treatments are anticipated.
Progress in understanding dementia with Lewy bodies has led to the publication of diagnostic criteria.7 The phenotype of parkinsonism, fluctuating cognition, and visual hallucinations is supported by decreased dopamine uptake on dopamine transporter (DaT) scanning and the presence of REM sleep behavior disorder. Lewy bodies are found in the limbic and neocortex at autopsy; many cases have concomitant amyloid plaques similar to those of Alzheimer’s disease. Parkinson’s disease dementia has many of the same features and is distinguished from dementia with Lewy bodies only by the order of appearance of major symptoms—dementia first in dementia with Lewy bodies, parkinsonism first in Parkinson’s disease dementia. Rivastigmine is approved for the symptomatic treatment of cognitive deficits in Parkinson’s disease dementia, and trials of new therapies are being conducted in Parkinson’s disease dementia and dementia with Lewy bodies. Alpha-synuclein is present in both disorders and is the target of new disease-modifying treatments currently in clinical trials.
Improved understanding of the basic biology of neurodegenerative disease is critically important and must be accelerated. This knowledge will provide the foundation for improved diagnostics and therapeutics essential for responding to the needs of the burgeoning number of patients with these late-life brain disorders.
References
1. Cummings JL, Morstorf T, Zhong K. Alzheimer’s disease drug-development pipeline: few candidates, frequent failures. Alzheimers Res Ther. 2014;6(4):37-43.
2. Sevigny J, Chiao P, Bussiere T, et al. The antibody aducanumab reduces Aβ plaques in Alzheimer’s disease. Nature. 2016;537(7618):50-56.
3. Villemagne VL, Burnham S, Bourgeat P, et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: a prospective cohort study. Lancet Neurol. 2013;12(4):357-367.
4. Johnson KA, Schultz A, Betensky RA, et al. Tau positron emission tomographic imaging in aging and early Alzheimer disease. Ann Neurol. 2016;79(1):110-119.
5. James BD, Wilson RS, Boyle PA, et al. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain. 2016;139(11):2983-2993.
6. Lashley T, Rohrer JD, Mead S, Revesz T. Review: an update on clinical, genetic and pathological aspects of frontotemporal lobar degenerations. Neuropathol Appl Neurobiol. 2015;41(7):858-881.
7. McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium. Neurology. 2017;89(1):88-100.
Forehead growth

Based on the doughnut shape of the growth, and other similar-looking lesions on the patient’s face, the FP diagnosed sebaceous hyperplasia (SH).
SH is a common, benign condition of the sebaceous glands. It becomes more common on the face starting in middle age. The cells that form the sebaceous gland (sebocytes) accumulate lipid material as they migrate from the basal layer of the gland to the central duct, where they release the lipid content as sebum. In younger individuals, turnover of sebocytes occurs approximately every month. With aging, the sebocyte turnover slows down. This results in crowding of primitive sebocytes within the sebaceous gland, causing the benign hamartomatous enlargement known as SH. Fortunately, there is no known potential for malignant transformation.
SH is located on the face, particularly the cheeks, forehead and nose. (There are other variations of sebaceous hyperplasia found on the lips, areolas, and genitalia.) Single—or groups—of lesions appear as yellowish, soft, small papules ranging in size from 2 to 9 mm. Aging and genetics are the most common risk factors. A small amount of sebum can sometimes be expressed with gentle pressure.
Dermoscopy aids in distinguishing between SH and nodular basal cell carcinoma (BCC). SH has a pattern of crown vessels that extend toward the center of the lesion and do not cross the midline, whereas BCC has branching vessels that can be found randomly distributed throughout the lesion. A biopsy isn’t usually necessary, unless there are features suspicious for BCC. Options for removal include electrodesiccation, cryotherapy, laser treatment, photodynamic therapy, and shave excision. Electrodessication can be performed without anesthesia using a very low setting of an electrosurgical instrument.
The patient in this case wanted the SH removed, so a shave biopsy was performed to make sure this was not a BCC. Pathology confirmed SH and the cosmetic result was excellent.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
Based on the doughnut shape of the growth, and other similar-looking lesions on the patient’s face, the FP diagnosed sebaceous hyperplasia (SH).
SH is a common, benign condition of the sebaceous glands. It becomes more common on the face starting in middle age. The cells that form the sebaceous gland (sebocytes) accumulate lipid material as they migrate from the basal layer of the gland to the central duct, where they release the lipid content as sebum. In younger individuals, turnover of sebocytes occurs approximately every month. With aging, the sebocyte turnover slows down. This results in crowding of primitive sebocytes within the sebaceous gland, causing the benign hamartomatous enlargement known as SH. Fortunately, there is no known potential for malignant transformation.
SH is located on the face, particularly the cheeks, forehead and nose. (There are other variations of sebaceous hyperplasia found on the lips, areolas, and genitalia.) Single—or groups—of lesions appear as yellowish, soft, small papules ranging in size from 2 to 9 mm. Aging and genetics are the most common risk factors. A small amount of sebum can sometimes be expressed with gentle pressure.
Dermoscopy aids in distinguishing between SH and nodular basal cell carcinoma (BCC). SH has a pattern of crown vessels that extend toward the center of the lesion and do not cross the midline, whereas BCC has branching vessels that can be found randomly distributed throughout the lesion. A biopsy isn’t usually necessary, unless there are features suspicious for BCC. Options for removal include electrodesiccation, cryotherapy, laser treatment, photodynamic therapy, and shave excision. Electrodessication can be performed without anesthesia using a very low setting of an electrosurgical instrument.
The patient in this case wanted the SH removed, so a shave biopsy was performed to make sure this was not a BCC. Pathology confirmed SH and the cosmetic result was excellent.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
Based on the doughnut shape of the growth, and other similar-looking lesions on the patient’s face, the FP diagnosed sebaceous hyperplasia (SH).
SH is a common, benign condition of the sebaceous glands. It becomes more common on the face starting in middle age. The cells that form the sebaceous gland (sebocytes) accumulate lipid material as they migrate from the basal layer of the gland to the central duct, where they release the lipid content as sebum. In younger individuals, turnover of sebocytes occurs approximately every month. With aging, the sebocyte turnover slows down. This results in crowding of primitive sebocytes within the sebaceous gland, causing the benign hamartomatous enlargement known as SH. Fortunately, there is no known potential for malignant transformation.
SH is located on the face, particularly the cheeks, forehead and nose. (There are other variations of sebaceous hyperplasia found on the lips, areolas, and genitalia.) Single—or groups—of lesions appear as yellowish, soft, small papules ranging in size from 2 to 9 mm. Aging and genetics are the most common risk factors. A small amount of sebum can sometimes be expressed with gentle pressure.
Dermoscopy aids in distinguishing between SH and nodular basal cell carcinoma (BCC). SH has a pattern of crown vessels that extend toward the center of the lesion and do not cross the midline, whereas BCC has branching vessels that can be found randomly distributed throughout the lesion. A biopsy isn’t usually necessary, unless there are features suspicious for BCC. Options for removal include electrodesiccation, cryotherapy, laser treatment, photodynamic therapy, and shave excision. Electrodessication can be performed without anesthesia using a very low setting of an electrosurgical instrument.
The patient in this case wanted the SH removed, so a shave biopsy was performed to make sure this was not a BCC. Pathology confirmed SH and the cosmetic result was excellent.
Photos and text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Smith M. Sebaceous hyperplasia. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 931-934.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

Gene Replacement Improves Survival in Spinal Muscular Atrophy
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
A single IV infusion to replace the gene encoding survival motor neuron 1 (SMN1) increases survival among infants with spinal muscular atrophy type 1 (SMA1), according to research published in the November 2, 2017, issue of the New England Journal of Medicine. The treatment also improves motor function, and its effects are maintained for two years, the researchers said.
The loss or dysfunction of SMN1 causes SMA, a progressive disease characterized by the degeneration and loss of lower motor neurons. Onset of SMA1 typically occurs at one month of age. Children with the disease usually are weak, fail to achieve motor milestones, and have declines in respiration and swallowing. At a median age of 10.5 months, patients die or need permanent ventilatory assistance.
In December 2016, the FDA approved nusinersen for the treatment of SMA. A phase III study found that patients treated with nusinersen were more likely than controls to have improved motor function and event-free survival. The trial was stopped early because of the treatment’s efficacy.
A Small, Open-Label Trial
A mouse study indicated that IV administration of an adenoassociated viral vector (ie, AAV9) containing SMN1 reduced the effects of SMA and extended survival. Jerry R. Mendell, MD, Principal Investigator at Nationwide Children’s Hospital’s Center for Gene Therapy in Columbus, Ohio, and colleagues studied this therapeutic technique in humans.
They enrolled 15 patients with a genetically confirmed diagnosis of SMA1 into two cohorts. The first cohort received a low dose (6.7×1013 vg/kg) of treatment, and the second cohort received a high dose (2.0×1014 vg/kg). Because the first patient in cohort one had serum aminotransferase elevations, the investigators gave 1 mg/kg/day of oral prednisolone to all subsequent patients for 30 days, starting 24 hours before gene therapy.
The study’s primary outcome was treatment-related adverse events of grade 3 or higher. The secondary outcome was time until death or the need for permanent ventilatory assistance, which was defined as at least 16 hours/day of continuous respiratory assistance for at least 14 days. The achievement of motor milestones and Children’s Hospital of Philadelphia Infant Test of Neuromuscular Disorders (CHOP INTEND) scores were exploratory outcomes.
Motor Scores Improved
Three patients entered the low-dose cohort, and 12 were enrolled in the high-dose cohort. Patients’ mean age at treatment was 6.3 months in cohort 1 and 3.4 months in cohort 2. At the last follow-up, all patients had reached age 20 months, and none required permanent mechanical ventilation. Approximately 8% of patients in a historical cohort met these criteria.
All patients had increases from baseline in CHOP INTEND score and maintained these increases throughout the study. Patients in cohort 2 had mean increases of 9.8 points at one month and 15.4 points at three months. Eleven patients achieved and sustained scores greater than 40 points, which is considered clinically meaningful in SMA.
Of the patients in cohort 2, 11 sat unassisted, nine rolled over, 11 fed orally and could speak, and two walked independently. No patients in the historical cohorts achieved any of these milestones, and they rarely became able to speak.
Dr. Mendell and colleagues observed two treatment-related grade 4 adverse events. Both were elevations in serum aminotransferase levels that were attenuated after treatment with prednisolone. The researchers also noted three treatment-related nonserious adverse events (ie, asymptomatic elevations in serum aminotransferase levels that were resolved without additional prednisolone treatment).
The study results were consistent with those of the preclinical mouse study. During a follow-up period of as long as two years, Dr. Mendell and colleagues did not observe any decrease in treatment effect or regression in motor function among the study participants. The presence of antibodies to AAV9 could be a potential limitation of the therapy, however. Further research to assess the treatment’s safety and the durability of its effect are needed, according to the authors.
Comparing Two Treatments
It is difficult to compare the results of Dr. Mendell and colleagues with those of the phase III nusinersen study, because of the two trials’ different designs, said Ans T. van der Ploeg, MD, PhD, Chair of the Center for Lysosomal and Metabolic Diseases at the Erasmus MC University in Rotterdam, the Netherlands, in an accompanying editorial. One potential advantage of AAV9 gene therapy is that it might require a single IV infusion. Nusinersen, on the other hand, may require lifelong intrathecal treatment.
“The durability of the effects is uncertain for both treatments,” said Dr. van der Ploeg. “If the expression of the scAAV9 gene therapy declines over time, the same treatment may not be able to be repeated, because antibodies against AAV capsid proteins are anticipated to form.”
In addition, neither of the two therapies cures SMA type 1. Earlier treatment could be beneficial, as could a combination of both treatments, said Dr. van der Ploeg. But the high expected cost of nusinersen is “an important constraint,” she concluded.
—Erik Greb
Suggested Reading
Mendell JR, Al-Zaidy S, Shell R, et al. Single-dose gene-replacement therapy for spinal muscular atrophy. N Engl J Med. 2017;377(18):1713-1722.
van der Ploeg AT. The dilemma of two innovative therapies for spinal muscular atrophy. N Engl J Med. 2017;377(18):1786-1787.
30 years in service to you, our community of women’s health clinicians
The mission of
OBG Management : Print and electronic portals for knowledge acquisition
Experienced clinicians acquire new knowledge and refresh established concepts through discussions with trusted colleagues and by reading journals and books that contain information relevant to their practice. A continuing trend in professional development is the accelerating transition from a reliance on print media (print journals and books) to electronic information delivery. Many clinicians continue to enjoy reading medical journals and magazines. ObGyns are no different; 96% report reading the print edition of medical journals.1 At
However, in the time-pressured setting of office- and hospital-based patient care, critical information is now frequently accessed through an electronic portal that is web based and focused on immediately answering a high priority question necessary for optimal patient care.
The information base needed to practice medicine is massive and continues to grow rapidly. No single print textbook or journal can cover this vast information base. Libraries of print material are cumbersome to use and ordinarily not accessible at the site of patient care. Electronic portals are the only means of providing immediate access to all medical knowledge. Electronic technology enables the aggregation of vast amounts of information in a database that is rapidly accessible from anywhere, and new search technology is making it easier to quickly locate the information you need.
The next frontier in medical information exchange is the application of artificial intelligence to cull “answers” from the vast aggregation of data. By combining all available medical information and artificial intelligence processes, in the near future, clinicians will be able to instantaneously get an answer to a question they have about how to care for a specific patient. A decade ago, when a question was entered into an Internet search engine, the response was typically a list of potential websites where the answer might be located. In the past few years, with the integration of huge databases and artificial intelligence, some advanced search engines now provide a specific answer to a question, followed by a list of relevant websites. For example, if you enter this question: “What countries have the greatest number of people?” into the Google search tool, in less than 1 second a direct answer is provided: “China has the world’s largest population (1.4 billion), followed by India (1.3 billion). The next most populous nations—the United States, Indonesia, Brazil and Pakistan—combined have less than 1 billion people.” The next step in medical information communication will be the deployment of artificial intelligence systems that can directly answer a query from a clinician about a specific patient.
Our distinguished Editorial Board and authors—the heart and mind of OBG Management
The editorial team at

Improving clinician wellness and resilience and reducing burnout
Clinicians throughout the world are reporting decreased levels of professional fulfillment and increased levels of burnout.2–4 This epidemic is likely caused by many factors, including the deployment of poorly designed electronic health systems, the administrative guidance for clinicians to work faster with fewer support staff, increasing administrative and secretarial burden on clinicians, and institutional constraints on clinician autonomy. Many of these problems only can be addressed at the level of the health system, but some are in the control of individual clinicians.
In the upcoming years,
The gratitude exercise
Showing more gratitude to those who have been most meaningful in your life may increase your wellness. Try the gratitude exercise outlined below.
To prepare for the exercise you will need about 15 minutes of uninterrupted time, a quiet room, and a method for recording your thoughts (pen/paper, electronic word processor, voice recorder).
Sit quietly and close your eyes. Spend 5 minutes thinking about the people in your life whose contributions have had the greatest positive impact on your development. Think deeply about the importance of their role in your life. Select one of those important people.
Open your eyes and spend 10 minutes expressing in writing your thoughts and feelings about that person. Once you have completed expressing yourself in writing, commit to reading your words, verbatim, to the person within the following 48 hours. This could be done by voice communication, video conferencing, or in-person.
The future of obstetrics and gynecology is bright
Medical students are electing to pursue a career in obstetrics and gynecology in record numbers. The students entering the field and the residents currently in training are superbly prepared and have demonstrated their commitment to advancing reproductive health by experiences in advocacy, research, and community service. We need to ensure that these super-star young physicians are able to have a 40-year career that is productive and fulfilling.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kantar Media. Sources and Interactions. Medical/Surgical Edition. Kantar Media; New York, New York; 2017.
- Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451.
- Vandenbroeck S, Van Gerven E, De Witte H, Vanhaecht K, Godderis L. Burnout in Belgian physicians and nurses. Occup Med (London). 2017;67(7):546-554.
- Siu C, Yuen SK, Cheung A. Burnout among public doctors in Hong Kong: cross-sectional survey. Hong Kong Med J. 2012;18(3):186-192.
- Cheng ST, Tsui PK, Lam JH. Improving mental health in health care practitioners: randomized controlled trial of a gratitude intervention. J Consult Clin Psychol. 2015;83(1):177-186.

Dr. Barbieri is Editor in Chief, OBG Management, and Chair, Department of Obstetrics and Gynecology, Brigham and Women's Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management, and Chair, Department of Obstetrics and Gynecology, Brigham and Women's Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
Dr. Barbieri reports no financial relationships relevant to this article.
Dr. Barbieri is Editor in Chief, OBG Management, and Chair, Department of Obstetrics and Gynecology, Brigham and Women's Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology and Reproductive Biology, Harvard Medical School.
Dr. Barbieri reports no financial relationships relevant to this article.
The mission of
OBG Management : Print and electronic portals for knowledge acquisition
Experienced clinicians acquire new knowledge and refresh established concepts through discussions with trusted colleagues and by reading journals and books that contain information relevant to their practice. A continuing trend in professional development is the accelerating transition from a reliance on print media (print journals and books) to electronic information delivery. Many clinicians continue to enjoy reading medical journals and magazines. ObGyns are no different; 96% report reading the print edition of medical journals.1 At
However, in the time-pressured setting of office- and hospital-based patient care, critical information is now frequently accessed through an electronic portal that is web based and focused on immediately answering a high priority question necessary for optimal patient care.
The information base needed to practice medicine is massive and continues to grow rapidly. No single print textbook or journal can cover this vast information base. Libraries of print material are cumbersome to use and ordinarily not accessible at the site of patient care. Electronic portals are the only means of providing immediate access to all medical knowledge. Electronic technology enables the aggregation of vast amounts of information in a database that is rapidly accessible from anywhere, and new search technology is making it easier to quickly locate the information you need.
The next frontier in medical information exchange is the application of artificial intelligence to cull “answers” from the vast aggregation of data. By combining all available medical information and artificial intelligence processes, in the near future, clinicians will be able to instantaneously get an answer to a question they have about how to care for a specific patient. A decade ago, when a question was entered into an Internet search engine, the response was typically a list of potential websites where the answer might be located. In the past few years, with the integration of huge databases and artificial intelligence, some advanced search engines now provide a specific answer to a question, followed by a list of relevant websites. For example, if you enter this question: “What countries have the greatest number of people?” into the Google search tool, in less than 1 second a direct answer is provided: “China has the world’s largest population (1.4 billion), followed by India (1.3 billion). The next most populous nations—the United States, Indonesia, Brazil and Pakistan—combined have less than 1 billion people.” The next step in medical information communication will be the deployment of artificial intelligence systems that can directly answer a query from a clinician about a specific patient.
Our distinguished Editorial Board and authors—the heart and mind of OBG Management
The editorial team at
Improving clinician wellness and resilience and reducing burnout
Clinicians throughout the world are reporting decreased levels of professional fulfillment and increased levels of burnout.2–4 This epidemic is likely caused by many factors, including the deployment of poorly designed electronic health systems, the administrative guidance for clinicians to work faster with fewer support staff, increasing administrative and secretarial burden on clinicians, and institutional constraints on clinician autonomy. Many of these problems only can be addressed at the level of the health system, but some are in the control of individual clinicians.
In the upcoming years,
The gratitude exercise
Showing more gratitude to those who have been most meaningful in your life may increase your wellness. Try the gratitude exercise outlined below.
To prepare for the exercise you will need about 15 minutes of uninterrupted time, a quiet room, and a method for recording your thoughts (pen/paper, electronic word processor, voice recorder).
Sit quietly and close your eyes. Spend 5 minutes thinking about the people in your life whose contributions have had the greatest positive impact on your development. Think deeply about the importance of their role in your life. Select one of those important people.
Open your eyes and spend 10 minutes expressing in writing your thoughts and feelings about that person. Once you have completed expressing yourself in writing, commit to reading your words, verbatim, to the person within the following 48 hours. This could be done by voice communication, video conferencing, or in-person.
The future of obstetrics and gynecology is bright
Medical students are electing to pursue a career in obstetrics and gynecology in record numbers. The students entering the field and the residents currently in training are superbly prepared and have demonstrated their commitment to advancing reproductive health by experiences in advocacy, research, and community service. We need to ensure that these super-star young physicians are able to have a 40-year career that is productive and fulfilling.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The mission of
OBG Management : Print and electronic portals for knowledge acquisition
Experienced clinicians acquire new knowledge and refresh established concepts through discussions with trusted colleagues and by reading journals and books that contain information relevant to their practice. A continuing trend in professional development is the accelerating transition from a reliance on print media (print journals and books) to electronic information delivery. Many clinicians continue to enjoy reading medical journals and magazines. ObGyns are no different; 96% report reading the print edition of medical journals.1 At
However, in the time-pressured setting of office- and hospital-based patient care, critical information is now frequently accessed through an electronic portal that is web based and focused on immediately answering a high priority question necessary for optimal patient care.
The information base needed to practice medicine is massive and continues to grow rapidly. No single print textbook or journal can cover this vast information base. Libraries of print material are cumbersome to use and ordinarily not accessible at the site of patient care. Electronic portals are the only means of providing immediate access to all medical knowledge. Electronic technology enables the aggregation of vast amounts of information in a database that is rapidly accessible from anywhere, and new search technology is making it easier to quickly locate the information you need.
The next frontier in medical information exchange is the application of artificial intelligence to cull “answers” from the vast aggregation of data. By combining all available medical information and artificial intelligence processes, in the near future, clinicians will be able to instantaneously get an answer to a question they have about how to care for a specific patient. A decade ago, when a question was entered into an Internet search engine, the response was typically a list of potential websites where the answer might be located. In the past few years, with the integration of huge databases and artificial intelligence, some advanced search engines now provide a specific answer to a question, followed by a list of relevant websites. For example, if you enter this question: “What countries have the greatest number of people?” into the Google search tool, in less than 1 second a direct answer is provided: “China has the world’s largest population (1.4 billion), followed by India (1.3 billion). The next most populous nations—the United States, Indonesia, Brazil and Pakistan—combined have less than 1 billion people.” The next step in medical information communication will be the deployment of artificial intelligence systems that can directly answer a query from a clinician about a specific patient.
Our distinguished Editorial Board and authors—the heart and mind of OBG Management
The editorial team at
Improving clinician wellness and resilience and reducing burnout
Clinicians throughout the world are reporting decreased levels of professional fulfillment and increased levels of burnout.2–4 This epidemic is likely caused by many factors, including the deployment of poorly designed electronic health systems, the administrative guidance for clinicians to work faster with fewer support staff, increasing administrative and secretarial burden on clinicians, and institutional constraints on clinician autonomy. Many of these problems only can be addressed at the level of the health system, but some are in the control of individual clinicians.
In the upcoming years,
The gratitude exercise
Showing more gratitude to those who have been most meaningful in your life may increase your wellness. Try the gratitude exercise outlined below.
To prepare for the exercise you will need about 15 minutes of uninterrupted time, a quiet room, and a method for recording your thoughts (pen/paper, electronic word processor, voice recorder).
Sit quietly and close your eyes. Spend 5 minutes thinking about the people in your life whose contributions have had the greatest positive impact on your development. Think deeply about the importance of their role in your life. Select one of those important people.
Open your eyes and spend 10 minutes expressing in writing your thoughts and feelings about that person. Once you have completed expressing yourself in writing, commit to reading your words, verbatim, to the person within the following 48 hours. This could be done by voice communication, video conferencing, or in-person.
The future of obstetrics and gynecology is bright
Medical students are electing to pursue a career in obstetrics and gynecology in record numbers. The students entering the field and the residents currently in training are superbly prepared and have demonstrated their commitment to advancing reproductive health by experiences in advocacy, research, and community service. We need to ensure that these super-star young physicians are able to have a 40-year career that is productive and fulfilling.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Kantar Media. Sources and Interactions. Medical/Surgical Edition. Kantar Media; New York, New York; 2017.
- Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451.
- Vandenbroeck S, Van Gerven E, De Witte H, Vanhaecht K, Godderis L. Burnout in Belgian physicians and nurses. Occup Med (London). 2017;67(7):546-554.
- Siu C, Yuen SK, Cheung A. Burnout among public doctors in Hong Kong: cross-sectional survey. Hong Kong Med J. 2012;18(3):186-192.
- Cheng ST, Tsui PK, Lam JH. Improving mental health in health care practitioners: randomized controlled trial of a gratitude intervention. J Consult Clin Psychol. 2015;83(1):177-186.
- Kantar Media. Sources and Interactions. Medical/Surgical Edition. Kantar Media; New York, New York; 2017.
- Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents and early career physicians relative to the general U.S. population. Acad Med. 2014;89(3):443-451.
- Vandenbroeck S, Van Gerven E, De Witte H, Vanhaecht K, Godderis L. Burnout in Belgian physicians and nurses. Occup Med (London). 2017;67(7):546-554.
- Siu C, Yuen SK, Cheung A. Burnout among public doctors in Hong Kong: cross-sectional survey. Hong Kong Med J. 2012;18(3):186-192.
- Cheng ST, Tsui PK, Lam JH. Improving mental health in health care practitioners: randomized controlled trial of a gratitude intervention. J Consult Clin Psychol. 2015;83(1):177-186.
