User login
DNA vaccine + PD-1 blockade shows promise in mCRPC
NATIONAL HARBOR, MD. – Combining programmed death (PD)-1 blockade with tumor-targeted T-cell activation by a novel DNA vaccine safely enhanced antitumor immune responses in metastatic castration-resistant prostate cancer (mCRPC) patients in a randomized clinical study.

Of 26 patients with mCRPC who were evaluable for response, 13 received treatment with an investigational DNA vaccine (pTVG-HP) that encodes prostatic acid phosphatase (PAP) and concurrent PD-1 blockade, and 13 received sequential vaccination and PD-1 blockade. No difference was seen between the groups with respect to progression-free survival at 6 months, but of eight patients in the concurrent therapy arm who had measurable disease, one experienced a partial response and two experienced a reduction in tumor volume, Douglas G. McNeel, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We did not see objective responses in [six patients with measurable disease in the sequential treatment arm], said Dr. McNeel, a professor at the University of Wisconsin, Madison.
Prostate specific antigen (PSA) responses, which may be a more sensitive marker, were also more common in the concurrent treatment group; 8 of 13 patients in that group had a PSA decline from baseline, and 4 of those had a decline of greater than 25% from baseline, whereas only 1 of the 13 patients in the sequential treatment arm experienced any decline in PSA vs. baseline, Dr. McNeel said.
Responses to the vaccine’s target antigen, prostatic acid phosphatase, were seen in both arms, but only those who received the combined treatment and who had evidence of immune response experienced PSA decline, he added.
Pre- and postvaccination biopsies of metastatic sites showed that concurrent treatment, compared with sequential treatment, elicited tumor-infiltrating CD8+ T cells, PD-L1 expression in tumors, and changes associated with CD8+ T-cell activation, he said, adding that immunization with concurrent PD-1 blockade also elicits changes in proliferation detected by (18F) fluorothymidine PET/CT.
“We’ve been interested in vaccines for cancer, because we know that having the right kind of T cells in the tumor microenvironment is associated with better long-term outcomes,” Dr. McNeel said, noting that the ability of vaccines to activate T cells and augment cytolytic T cells, in particular, should have anticancer activity.
However, the clinical activity of single-agent tumor vaccines has been underwhelming, he noted.
PAP has been a focus in vaccine development, because it is essentially restricted to prostate tissue in humans. A nearly identical prostate-specific rat homologue was used in early studies, and PAP permits evaluation of serum PSA as an independent assessment of response in human trials, he explained.
“It’s the same target as the sipuleucel-T vaccine,” he said, referring to a Food and Drug Administration–approved vaccine for prostate cancer(Provenge).
Two prior phase 1/2 trials looking at DNA vaccine encoding PAP in patients with early biochemically recurrent prostate cancer showed that PAP-specific T-cell immune responses were elicited and that no significant adverse events occurred.
In both trials, the development of persistent PAP-specific, interferon-gamma–secreting T cells was associated with favorable change in PSA doubling time (suggesting a possible impact on the disease), and with PD-L1 expression in circulating tumor cells (suggesting a potential mechanism of resistance), he said.
Laboratory studies helped identify mechanisms of immune resistance following DNA immunization, he said, explaining that immunization elicits T cells secreting interferon-gamma, which leads to an increase in PD-L1 expression on tumor cells.
Encoding epitopes with increased major histocompatibility complex class 1 affinity elicited CD+ t cells with increased and persistent PD-1 expression, and blockade of PD-1 or PD-L1 with vaccination led to improved antitumor responses, he said.
The findings led to the new model focused on timing of PD-1 blockade with vaccine T-cell activation studied in the current trial.
It was hypothesized that PD-1 blockade at the time of T-cell activation with vaccination would be more effective than was blockade of PD-1-regulated T cells previously elicited with vaccination.
Study subjects had mCRPC and evidence of disease progression. Previous treatment with abiraterone(Zytiga), enzalutamide(Xtandi), or chemotherapy, was allowed, but patients with prior sipuleucel-T vaccine exposure were excluded.
Patients in the concurrent treatment arm received both the vaccine and PD-1 blockade with pembrolizumab (Keytruda)over 12 weeks, and those in the sequential therapy arm received vaccination first followed by PD-1 blockade, each for 12 weeks.
Both approaches were well tolerated.
“Essentially, we saw nothing that was unexpected,” Dr. McNeel said.
Adverse events greater than grade 2 included fatigue in one patient, diarrhea in one patient, and autoimmune hepatitis in one patient. No patients discontinued treatment from toxicity, he noted.
One death occurred during follow-up in a patient who had evidence of progression and refused further follow-up, therefore it could not be determined if the death was related to treatment.
The current findings, which are notable in part because PD-1 pathway inhibitors have demonstrated little clinical activity when used as single agents for prostate cancer and which expand upon data presented in a scientific poster at SITC 2016, demonstrate that combining this blockade with tumor-targeted T-cell activation by a DNA vaccine is safe and can augment tumor-specific T cells – as detectable within the peripheral blood and by imaging – and can result in objective antitumor changes.
“To summarize, plasmid DNA vaccines can elicit antigen-specific CD8+ T cells; immunization can increase PD-L1 expression on tumor cells – and we’ve demonstrated, in mice anyway, that this is mediated by the T cells elicited with immunization; PD-1 expression increases on CD8+ T cells following vaccination; and we think this is an opportunity to use checkpoint blockade at the point of vaccination to improve antitumor responses,” Dr. McNeel said.
“So we can look at this as PD-1 blockade to improve the effect of vaccination, but we can also look at it the other way around, and that is that anti-tumor vaccines can elicit the tumor-specific CD8+ T cells needed to enable PD-1 blockade to work,” he said. “ I think this has implications for the choice of vaccine approach, the antigen, and the timing of PD-1 blockade.”
Based on these results, an expansion arm has been opened to evaluate the safety and clinical efficacy of combination treatment beyond 12 weeks, and future studies will look at the combination of two different vaccines to improve antitumor response, he said.
Dr. McNeel disclosed financial relationships (intellectual property rights/patent holder, consultant, ownership interest) with Madison Vaccines Inc. The study is funded by a 2014 Movember PCF Challenge Award and Madison Vaccines.
SOURCE: McNeel D et al., J Immunother Cancer. 2017 5(Suppl 2):86 Abstract O11.
NATIONAL HARBOR, MD. – Combining programmed death (PD)-1 blockade with tumor-targeted T-cell activation by a novel DNA vaccine safely enhanced antitumor immune responses in metastatic castration-resistant prostate cancer (mCRPC) patients in a randomized clinical study.
Of 26 patients with mCRPC who were evaluable for response, 13 received treatment with an investigational DNA vaccine (pTVG-HP) that encodes prostatic acid phosphatase (PAP) and concurrent PD-1 blockade, and 13 received sequential vaccination and PD-1 blockade. No difference was seen between the groups with respect to progression-free survival at 6 months, but of eight patients in the concurrent therapy arm who had measurable disease, one experienced a partial response and two experienced a reduction in tumor volume, Douglas G. McNeel, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We did not see objective responses in [six patients with measurable disease in the sequential treatment arm], said Dr. McNeel, a professor at the University of Wisconsin, Madison.
Prostate specific antigen (PSA) responses, which may be a more sensitive marker, were also more common in the concurrent treatment group; 8 of 13 patients in that group had a PSA decline from baseline, and 4 of those had a decline of greater than 25% from baseline, whereas only 1 of the 13 patients in the sequential treatment arm experienced any decline in PSA vs. baseline, Dr. McNeel said.
Responses to the vaccine’s target antigen, prostatic acid phosphatase, were seen in both arms, but only those who received the combined treatment and who had evidence of immune response experienced PSA decline, he added.
Pre- and postvaccination biopsies of metastatic sites showed that concurrent treatment, compared with sequential treatment, elicited tumor-infiltrating CD8+ T cells, PD-L1 expression in tumors, and changes associated with CD8+ T-cell activation, he said, adding that immunization with concurrent PD-1 blockade also elicits changes in proliferation detected by (18F) fluorothymidine PET/CT.
“We’ve been interested in vaccines for cancer, because we know that having the right kind of T cells in the tumor microenvironment is associated with better long-term outcomes,” Dr. McNeel said, noting that the ability of vaccines to activate T cells and augment cytolytic T cells, in particular, should have anticancer activity.
However, the clinical activity of single-agent tumor vaccines has been underwhelming, he noted.
PAP has been a focus in vaccine development, because it is essentially restricted to prostate tissue in humans. A nearly identical prostate-specific rat homologue was used in early studies, and PAP permits evaluation of serum PSA as an independent assessment of response in human trials, he explained.
“It’s the same target as the sipuleucel-T vaccine,” he said, referring to a Food and Drug Administration–approved vaccine for prostate cancer(Provenge).
Two prior phase 1/2 trials looking at DNA vaccine encoding PAP in patients with early biochemically recurrent prostate cancer showed that PAP-specific T-cell immune responses were elicited and that no significant adverse events occurred.
In both trials, the development of persistent PAP-specific, interferon-gamma–secreting T cells was associated with favorable change in PSA doubling time (suggesting a possible impact on the disease), and with PD-L1 expression in circulating tumor cells (suggesting a potential mechanism of resistance), he said.
Laboratory studies helped identify mechanisms of immune resistance following DNA immunization, he said, explaining that immunization elicits T cells secreting interferon-gamma, which leads to an increase in PD-L1 expression on tumor cells.
Encoding epitopes with increased major histocompatibility complex class 1 affinity elicited CD+ t cells with increased and persistent PD-1 expression, and blockade of PD-1 or PD-L1 with vaccination led to improved antitumor responses, he said.
The findings led to the new model focused on timing of PD-1 blockade with vaccine T-cell activation studied in the current trial.
It was hypothesized that PD-1 blockade at the time of T-cell activation with vaccination would be more effective than was blockade of PD-1-regulated T cells previously elicited with vaccination.
Study subjects had mCRPC and evidence of disease progression. Previous treatment with abiraterone(Zytiga), enzalutamide(Xtandi), or chemotherapy, was allowed, but patients with prior sipuleucel-T vaccine exposure were excluded.
Patients in the concurrent treatment arm received both the vaccine and PD-1 blockade with pembrolizumab (Keytruda)over 12 weeks, and those in the sequential therapy arm received vaccination first followed by PD-1 blockade, each for 12 weeks.
Both approaches were well tolerated.
“Essentially, we saw nothing that was unexpected,” Dr. McNeel said.
Adverse events greater than grade 2 included fatigue in one patient, diarrhea in one patient, and autoimmune hepatitis in one patient. No patients discontinued treatment from toxicity, he noted.
One death occurred during follow-up in a patient who had evidence of progression and refused further follow-up, therefore it could not be determined if the death was related to treatment.
The current findings, which are notable in part because PD-1 pathway inhibitors have demonstrated little clinical activity when used as single agents for prostate cancer and which expand upon data presented in a scientific poster at SITC 2016, demonstrate that combining this blockade with tumor-targeted T-cell activation by a DNA vaccine is safe and can augment tumor-specific T cells – as detectable within the peripheral blood and by imaging – and can result in objective antitumor changes.
“To summarize, plasmid DNA vaccines can elicit antigen-specific CD8+ T cells; immunization can increase PD-L1 expression on tumor cells – and we’ve demonstrated, in mice anyway, that this is mediated by the T cells elicited with immunization; PD-1 expression increases on CD8+ T cells following vaccination; and we think this is an opportunity to use checkpoint blockade at the point of vaccination to improve antitumor responses,” Dr. McNeel said.
“So we can look at this as PD-1 blockade to improve the effect of vaccination, but we can also look at it the other way around, and that is that anti-tumor vaccines can elicit the tumor-specific CD8+ T cells needed to enable PD-1 blockade to work,” he said. “ I think this has implications for the choice of vaccine approach, the antigen, and the timing of PD-1 blockade.”
Based on these results, an expansion arm has been opened to evaluate the safety and clinical efficacy of combination treatment beyond 12 weeks, and future studies will look at the combination of two different vaccines to improve antitumor response, he said.
Dr. McNeel disclosed financial relationships (intellectual property rights/patent holder, consultant, ownership interest) with Madison Vaccines Inc. The study is funded by a 2014 Movember PCF Challenge Award and Madison Vaccines.
SOURCE: McNeel D et al., J Immunother Cancer. 2017 5(Suppl 2):86 Abstract O11.
NATIONAL HARBOR, MD. – Combining programmed death (PD)-1 blockade with tumor-targeted T-cell activation by a novel DNA vaccine safely enhanced antitumor immune responses in metastatic castration-resistant prostate cancer (mCRPC) patients in a randomized clinical study.
Of 26 patients with mCRPC who were evaluable for response, 13 received treatment with an investigational DNA vaccine (pTVG-HP) that encodes prostatic acid phosphatase (PAP) and concurrent PD-1 blockade, and 13 received sequential vaccination and PD-1 blockade. No difference was seen between the groups with respect to progression-free survival at 6 months, but of eight patients in the concurrent therapy arm who had measurable disease, one experienced a partial response and two experienced a reduction in tumor volume, Douglas G. McNeel, MD, PhD, reported at the annual meeting of the Society for Immunotherapy of Cancer.
“We did not see objective responses in [six patients with measurable disease in the sequential treatment arm], said Dr. McNeel, a professor at the University of Wisconsin, Madison.
Prostate specific antigen (PSA) responses, which may be a more sensitive marker, were also more common in the concurrent treatment group; 8 of 13 patients in that group had a PSA decline from baseline, and 4 of those had a decline of greater than 25% from baseline, whereas only 1 of the 13 patients in the sequential treatment arm experienced any decline in PSA vs. baseline, Dr. McNeel said.
Responses to the vaccine’s target antigen, prostatic acid phosphatase, were seen in both arms, but only those who received the combined treatment and who had evidence of immune response experienced PSA decline, he added.
Pre- and postvaccination biopsies of metastatic sites showed that concurrent treatment, compared with sequential treatment, elicited tumor-infiltrating CD8+ T cells, PD-L1 expression in tumors, and changes associated with CD8+ T-cell activation, he said, adding that immunization with concurrent PD-1 blockade also elicits changes in proliferation detected by (18F) fluorothymidine PET/CT.
“We’ve been interested in vaccines for cancer, because we know that having the right kind of T cells in the tumor microenvironment is associated with better long-term outcomes,” Dr. McNeel said, noting that the ability of vaccines to activate T cells and augment cytolytic T cells, in particular, should have anticancer activity.
However, the clinical activity of single-agent tumor vaccines has been underwhelming, he noted.
PAP has been a focus in vaccine development, because it is essentially restricted to prostate tissue in humans. A nearly identical prostate-specific rat homologue was used in early studies, and PAP permits evaluation of serum PSA as an independent assessment of response in human trials, he explained.
“It’s the same target as the sipuleucel-T vaccine,” he said, referring to a Food and Drug Administration–approved vaccine for prostate cancer(Provenge).
Two prior phase 1/2 trials looking at DNA vaccine encoding PAP in patients with early biochemically recurrent prostate cancer showed that PAP-specific T-cell immune responses were elicited and that no significant adverse events occurred.
In both trials, the development of persistent PAP-specific, interferon-gamma–secreting T cells was associated with favorable change in PSA doubling time (suggesting a possible impact on the disease), and with PD-L1 expression in circulating tumor cells (suggesting a potential mechanism of resistance), he said.
Laboratory studies helped identify mechanisms of immune resistance following DNA immunization, he said, explaining that immunization elicits T cells secreting interferon-gamma, which leads to an increase in PD-L1 expression on tumor cells.
Encoding epitopes with increased major histocompatibility complex class 1 affinity elicited CD+ t cells with increased and persistent PD-1 expression, and blockade of PD-1 or PD-L1 with vaccination led to improved antitumor responses, he said.
The findings led to the new model focused on timing of PD-1 blockade with vaccine T-cell activation studied in the current trial.
It was hypothesized that PD-1 blockade at the time of T-cell activation with vaccination would be more effective than was blockade of PD-1-regulated T cells previously elicited with vaccination.
Study subjects had mCRPC and evidence of disease progression. Previous treatment with abiraterone(Zytiga), enzalutamide(Xtandi), or chemotherapy, was allowed, but patients with prior sipuleucel-T vaccine exposure were excluded.
Patients in the concurrent treatment arm received both the vaccine and PD-1 blockade with pembrolizumab (Keytruda)over 12 weeks, and those in the sequential therapy arm received vaccination first followed by PD-1 blockade, each for 12 weeks.
Both approaches were well tolerated.
“Essentially, we saw nothing that was unexpected,” Dr. McNeel said.
Adverse events greater than grade 2 included fatigue in one patient, diarrhea in one patient, and autoimmune hepatitis in one patient. No patients discontinued treatment from toxicity, he noted.
One death occurred during follow-up in a patient who had evidence of progression and refused further follow-up, therefore it could not be determined if the death was related to treatment.
The current findings, which are notable in part because PD-1 pathway inhibitors have demonstrated little clinical activity when used as single agents for prostate cancer and which expand upon data presented in a scientific poster at SITC 2016, demonstrate that combining this blockade with tumor-targeted T-cell activation by a DNA vaccine is safe and can augment tumor-specific T cells – as detectable within the peripheral blood and by imaging – and can result in objective antitumor changes.
“To summarize, plasmid DNA vaccines can elicit antigen-specific CD8+ T cells; immunization can increase PD-L1 expression on tumor cells – and we’ve demonstrated, in mice anyway, that this is mediated by the T cells elicited with immunization; PD-1 expression increases on CD8+ T cells following vaccination; and we think this is an opportunity to use checkpoint blockade at the point of vaccination to improve antitumor responses,” Dr. McNeel said.
“So we can look at this as PD-1 blockade to improve the effect of vaccination, but we can also look at it the other way around, and that is that anti-tumor vaccines can elicit the tumor-specific CD8+ T cells needed to enable PD-1 blockade to work,” he said. “ I think this has implications for the choice of vaccine approach, the antigen, and the timing of PD-1 blockade.”
Based on these results, an expansion arm has been opened to evaluate the safety and clinical efficacy of combination treatment beyond 12 weeks, and future studies will look at the combination of two different vaccines to improve antitumor response, he said.
Dr. McNeel disclosed financial relationships (intellectual property rights/patent holder, consultant, ownership interest) with Madison Vaccines Inc. The study is funded by a 2014 Movember PCF Challenge Award and Madison Vaccines.
SOURCE: McNeel D et al., J Immunother Cancer. 2017 5(Suppl 2):86 Abstract O11.
REPORTING FROM SITC 2017
Key clinical point: Concurrent PD-1 blockade enhanced DNA vaccine activity in mCRPC.
Major finding: A partial response and tumor volume reduction occurred in one and two patients, respectively.
Study details: A randomized clinical study of 26 patients.
Disclosures: Dr. McNeel disclosed financial relationships (intellectual property rights/patent holder, consultant, ownership interest) with Madison Vaccines. The study is funded by a 2014 Movember PCF Challenge Award and Madison Vaccines.
Source: Douglas McNeel D et al. J Immunother Cancer. 2017 Nov; 5(Suppl 2):86 Abstract O11.
Ovarian suppression during breast cancer chemo helps stave off early menopause, preserve fertility
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.

“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”

Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.
“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”
Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
SAN ANTONIO – Premenopausal women with early breast cancer should be offered temporary ovarian suppression during chemotherapy if they wish to remain fertile or avoid early menopause, suggests a meta-analysis of five randomized controlled trials among 873 women reported at the San Antonio Breast Cancer Symposium.
“Oocyte and embryo cryopreservation are standard strategies for fertility preservation in these patients, meaning increasing the chance of pregnancy after the end of treatment,” said lead author Matteo Lambertini, MD, medical oncologist and ESMO fellow at the Institut Jules Bordet in Brussels. “However, they do not prevent the risk of developing chemotherapy-induced premature ovarian insufficiency, and so patients are still at risk of developing early menopause.”
Data from individual trials of ovarian suppression have been mixed, and its use remains controversial, he further noted. As a result, guidelines from ASCO and ESMO for fertility preservation in cancer patients still consider ovarian suppression to be investigational.
Results of the new meta-analysis, reported in a press briefing and session, showed that, compared with control peers, premenopausal women given a gonadotropin-releasing hormone analog (GnRHa) to suppress ovarian function during breast cancer chemotherapy had a more than one-half reduction in odds of premature ovarian insufficiency and were almost twice as likely to become pregnant after completing their treatment.
“We believe that this strategy should now be considered a standard option to reduce the likelihood of chemotherapy-induced premature ovarian insufficiency and potentially improve future fertility in premenopausal early breast cancer patients who undergo adjuvant or neoadjuvant chemotherapy,” Dr. Lambertini maintained. The analysis and trial participants “remind us that there is a life after cancer and to cure the disease should not be considered enough any more.”
These new data are sufficient to put the controversy to rest, for several reasons, he contended. “First, this is an individual-patient meta-analysis of the five major randomized controlled trials in this setting, so it’s kind of the highest level of evidence that we can reach. Second, it’s very unlikely that we will have new randomized, controlled trials in this setting, and I would say also that, based on the results, it would probably be unethical to run randomized, controlled trials in this setting.”
Press briefing moderator Carlos L. Arteaga, MD, director of the Harold C. Simmons Comprehensive Cancer Center at UT Southwestern Medical Center, Dallas, wondered how trials were selected for inclusion in the meta-analysis.
Thirteen trials have been conducted on ovarian suppression in premenopausal patients with breast cancer, and the investigators included the five for which they were able to obtain patient-level data, a subset that contained both positive and negative trials, Dr. Lambertini replied. But findings would likely be the same had all trials been included, given that a 2015 analysis using trial-level data from the 12 trials completed at that time showed very similar results (Ann Oncol. 2015 Dec;26:2408-19).
“Societally, this is a hugely significant issue, but the difference you are showing I have to admit is rather modest,” commented Dr. Arteaga, who is also SABCS codirector and AACR past president. “So what kind of conversation do you have with the patient? Who are the ones who would be the best candidates for this approach?”
“The main message is that giving a GnRHa does not avoid the risk of early menopause in all patients, but still, it decreases significantly the number of patients who have this side effect,” Dr. Lambertini replied.
Two groups are optimal candidates for ovarian suppression, he proposed. “First, the patients who are concerned about developing early menopause and its related side effects, who are not interested per se in having a baby after the end of treatment, but may be preserving ovarian function. [Second], for patients interested in having a baby, so interested in fertility preservation, this strategy can be used after cryopreservation procedures or in patients who have no access, for different reasons, to cryopreservation strategies.”
Another point of view
In the session, attendee Kutluk Oktay, MD, PhD, professor of obstetrics & gynecology and reproductive sciences at Yale University, New Haven, and cochair of ASCO’s guideline committee on fertility preservation said, “I cannot agree with your conclusions based on what you presented to us.”
In particular, he took issue with the exclusion of additional trials in breast cancer as well as trials among patients with other types of cancers. “I’m wondering what the rationale is to limit this to breast cancer because chemotherapy is chemotherapy and ovary is ovary, so underlying disease should not matter. By limiting it to breast cancer, you are leaving out three important studies, all in hematological cancer, with better designs … three negative studies,” he commented.
From a clinical point of view, patients with lymphoma and patients with breast cancer differ greatly, Dr. Lambertini countered: The former are about 20 years younger, on average, and often receive less-granulotoxic chemotherapy. “For these reasons, I don’t believe that mixing these two populations would have been [appropriate] for analysis,” he said. “From a methodological point of view, the studies you have mentioned include overall [fewer] than 150 patients, so it’s a very small proportion in comparison to the data we have in breast cancer.”
Study details
For their meta-analysis, Dr. Lambertini and coinvestigators pooled individual patient data from five trials (PROMISE-GIM6, POEMS/SWOG S0230, Anglo-Celtic Group OPTION, GBG-37 ZORO, and a trial led by the Moffitt Cancer Center) that randomized premenopausal women with early breast cancer to adjuvant or neoadjuvant chemotherapy either with or without concurrent GnRHa therapy.
Two of the trials restricted enrollment to women with estrogen receptor (ER)-negative disease. The GnRHa agents used were triptorelin (Trelstar, Triptodur)and goserelin(Zoladex).
Main results showed that the rate of premature ovarian insufficiency, defined differently across trials, was 14.1% among women given a GnRHa and 30.9% among control women (adjusted odds ratio, 0.38; P less than .001), Dr. Lambertini reported. Findings were similar in subgroups stratified by age, ER status, and type and duration of chemotherapy.
The rate of amenorrhea, used as a standardized definition of premature ovarian insufficiency, was similar in the GnRHa and control groups at 1 year (36.8% and 40.4%) but sharply lower in the former at 2 years (18.2% vs. 30.0%; adjusted odds ratio, 0.51; P = .009).
Overall, 10.3% of women in the GnRHa group and 5.5% in the control group had at least one pregnancy after completing their breast cancer treatment (incidence rate ratio, 1.83; P = .030). “All of the randomized trials except for the POEMS study actually did not have fertility outcomes as a preplanned endpoint, and so the patients’ wish to have a pregnancy was not collected,” he noted; therefore, it was not possible to calculate pregnancy rates in the subset who actually wanted to conceive.
All pregnancies occurred among women aged 40 years or younger, and 86% occurred among women who had had ER-negative disease, likely reflecting use of adjuvant endocrine therapy in patients with ER-positive disease, he said. Of the 57 total pregnancies, 50 resulted in live births, and none of the infants had malformations; the other pregnancies ended in spontaneous or induced abortion.
With a median follow-up of 5 years, the groups did not differ significantly on rates of disease-free survival and overall survival, suggesting that ovarian suppression was safe, according to Dr. Lambertini. Findings were similar when patients were stratified by ER status.
“What I think researchers should do in the next year is to better understand how this strategy [of ovarian suppression] works because this is probably the main controversy right now, because it’s still not very clear how this strategy actually works,” he concluded.
SOURCE: Lambertini M et al., SABCS 2017 Abstract GS4-01.
REPORTING FROM SABCS 2017
Key clinical point:
Major finding: Compared with controls, women given a GnRHa during chemotherapy were less likely to develop premature ovarian insufficiency (adjusted OR, 0.38; P less than .001) and more likely to become pregnant after treatment (IRR, 1.83; P = .030).
Data source: A meta-analysis of individual patient data from five trials among 873 premenopausal women with early breast cancer.
Disclosures: Dr. Lambertini disclosed that he had no relevant conflicts of interest.
Source: Lambertini M et al., SABCS 2017 Abstract GS4-01.
Submit Research to VAM
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
Research done? Submit it as an abstract for the 2018 Vascular Annual Meeting, set for June 20-23, 2018, in Boston. Plenaries are June 21-23 and exhibits are June 21-22.
The submission site opened Monday. The deadline for submitting abstracts is Wednesday, Jan. 17, 2018.
Abstracts may be submitted in the following categories:
- Plenary
- Vascular and Endovascular Surgical Society
- International Forum
- International Fast Talk
- Poster Competition
- Interactive Poster
Guidelines, submission policies and general information on VAM are available online.
Obesity an independent risk factor for rosacea in cohort study of U.S. women
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
FROM JAAD
Key clinical point: independent of other risk factors such as smoking and alcohol intake.
Major finding: A BMI greater than 35 is associated with a 48% higher risk of rosacea, compared with a BMI of 21.
Data source: Information on rosacea diagnoses among 89,886 Nurses’ Health Study II participants.
Disclosures: The study was supported by the Warren Alpert Medical School of Brown University and a Nurses’ Health Study II grant. One author was supported by a research grant from the National Rosacea Society and the Dermatology Foundation; another author declared research funding, consultancies, and honoraria from the pharmaceutical industry.
Source: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
VIDEO: Weight loss cut risk of breast cancer
SAN ANTONIO – A new analysis from the Women’s Health Initiative Observational Study gives postmenopausal women yet another reason to mind their weight. Results showed that women losing at least 5% of their body weight had a significant 12% reduction in adjusted breast cancer risk relative to peers who maintained a stable weight, reported lead author Rowan Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. Findings were much the same regardless of whether women were of normal weight, overweight, or obese at baseline. Dr. Chlebowski discussed the implications for patient counseling and insurance coverage of weight loss interventions, as well as planned research that will assess the physiologic mechanisms at play in a video interview.
SAN ANTONIO – A new analysis from the Women’s Health Initiative Observational Study gives postmenopausal women yet another reason to mind their weight. Results showed that women losing at least 5% of their body weight had a significant 12% reduction in adjusted breast cancer risk relative to peers who maintained a stable weight, reported lead author Rowan Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. Findings were much the same regardless of whether women were of normal weight, overweight, or obese at baseline. Dr. Chlebowski discussed the implications for patient counseling and insurance coverage of weight loss interventions, as well as planned research that will assess the physiologic mechanisms at play in a video interview.
SAN ANTONIO – A new analysis from the Women’s Health Initiative Observational Study gives postmenopausal women yet another reason to mind their weight. Results showed that women losing at least 5% of their body weight had a significant 12% reduction in adjusted breast cancer risk relative to peers who maintained a stable weight, reported lead author Rowan Chlebowski, MD, PhD, research professor in the department of medical oncology and therapeutics research at City of Hope in Duarte, Calif. Findings were much the same regardless of whether women were of normal weight, overweight, or obese at baseline. Dr. Chlebowski discussed the implications for patient counseling and insurance coverage of weight loss interventions, as well as planned research that will assess the physiologic mechanisms at play in a video interview.
REPORTING FROM SABCS 2017

Inside the ‘mad rush’ for ketamine treatment
Ketamine, once best known as a pet anesthetic and party drug, is taking the United States by storm. Dozens of ketamine treatment centers are operating from coast to coast.
Big cities like Baltimore, Boston, and Phoenix have them. So do Charleston, S.C., and Boise, Idaho. Two such clinics are in sparsely populated New Mexico. And one national chain went from a pair of clinics to 10 in fewer than 2 years.

Never mind that these expensive treatments for conditions like depression are not covered by insurers or approved for this use by the Food and Drug Administration. Other questions also persist. “There is a considerable body of evidence that proves it really does work,” Dr. Lieberman said. “But we don’t know the extent of the range of conditions for which it might be effective, what the optimal frequency and concentration for dosing is, and what the long-term consequences are.”
To make matters more complicated, it’s anesthesiologists – not psychiatrists – who are leading the way toward a ketamine-infused future.

For now, however, hundreds and perhaps even thousands of patients are serving as ketamine test cases with psychiatrists only assisting remotely, if at all.
A stunningly rapid rise
Sara M. Markey, MD, is one of the rare psychiatrists in the United States who’s fully embraced ketamine treatment for mental illness.
She recalled first hearing about ketamine as an anesthetic in medical school. Best known as an anesthetic in animals, it’s also occasionally given to children and adults, although the drug’s dissociative properties have prevented widespread use.

In 2006, word spread about ketamine’s use as a painkiller. “I also began hearing and reading about its potential use/efficacy in treatment-resistant depression,” said Dr. Markey, who practices in Denver. “It was difficult to find information about ketamine, and many of my colleagues were hostile to the idea of using ketamine in clinical practice.”
She persisted, however, and prescribed intranasal and oral ketamine to depressed patients with “mild success.” She also saw patients whose psychiatrists refused to consider ketamine.
In early 2016, with Steven P. Levine, MD, a New Jersey psychiatrist who pioneered ketamine use for depression, Dr. Markey opened a ketamine infusion clinic in the Mile High City.
At at that time, it was only the second in a national chain called Ketamine Treatment Centers. Now, not even 2 years later, the chain has a new name – Actify Neurotherapies – and a total of 10 clinics from San Francisco and Beverly Hills, Calif., to Palm Beach, Fla.; Raleigh, N.C.; and New York City.
“It is wonderful,” she said, “to have an opportunity to provide a medication to people that does not cause weight gain, has very few medication interactions, and which is well tolerated and generic.”
Big short-term benefits
Treatment outcomes with ketamine – which is thought to act on glutamate and N-methyl-D-aspartate receptors – can be dramatic. “Some patients describe the ketamine treatments as life saving,” said Allison F. Wells, MD, an anesthesiologist who runs a clinic in Houston.

One depressed young man who tried ketamine at a Phoenix clinic in 2013 reportedly told the news site vice.com that he “felt good for a week” after his first treatment: “Not the kind of bipolar ‘good’ where I’d be manic. I just felt pleasant, and not crazy or compulsive. I felt normal for the first time in a long time.” Another depressed patient told National Public Radio that ketamine transformed his life: “I remember I was in my bathroom, and I literally fell to my knees crying because I had no anxiety; I had no depression.”
Enrique A. Abreu, DO, an anesthesiologist who offers ketamine therapy in Seattle and Portland, Ore., said he’s seen anxiety relief and a decrease in rumination in these patients. “They’re able to go back to work; a lot haven’t been able to work for a long time. And motivation is a big thing. They’re able to do things they haven’t been able to do.”
In addition, ketamine can reduce suicidal thinking, Dr. Markey said. “I am continually astounded to hear patients who come in with acute or chronic suicidal thinking report that those ideas and/or intrusive thoughts have disappeared. When they are absent, people need to be reminded of when they had them. They seem to have forgotten about them.”
‘Mystical experiences’
Dr. Markey said a retrospective analysis of about 740 patients at her chain’s clinics showed a response rate of about 75%. Other research has shown similarly high response levels.
“Multiple clinical trials suggest that a single low dose (0.5mg/kg) of IV ketamine results in a 50%-70% response rate in patients with treatment-resistant depression,” reported a 2016 clinical review. “Additional research has shown that depressed patients can experience symptom relief as early as 2 [hours], and lasting up to 2 weeks after a single administration of IV ketamine,” according to the review in Evidence Based Mental Health (2016 May;19[2]:35-8).

Adverse effects can include nausea and headache in patients with a history of migraine, he said. Over the long term, ketamine use can lead to incontinence and urinary urgency, he said.
As for ketamine addiction, Dr. Simelgor calls it unlikely at the lower doses that are used. However, he said, “I can’t say 100% that it won’t cause addiction.”
Who benefits? The jury’s still out
Considering its positive effects, why shouldn’t the mental health community embrace ketamine? Because, two prominent researchers say, best practices are still absent in a whole range of areas.
For example, there’s no agreement about who should undergo ketamine treatments beyond patients with treatment-resistant depression, especially those who have failed or cannot undergo electroconvulsive therapy. Ketamine therapy also is being touted by some as a treatment for a long list of other conditions from obsessive-compulsive disorder and anxiety to fibromyalgia and chronic pain disorders.
There are also limited data about dosing, making it “not possible to clarify the relative benefits and risks of doses other than 0.5 mg/kg delivered intravenously over 40 minutes,” cautioned Dr. Sanacora and Samuel T. Wilkinson, MD, also at Yale, in a 2017 commentary in JAMA (2017;318[9]:793-4).
In fact, they write, “Most published data supporting the use of ketamine as a treatment for mood disorders are based on trials that have followed up patients for just 1 week after a single administration of the drug.”
Unchartered waters
There’s also no accepted protocol beyond a typical six treatments over 2 or more weeks. This is relevant because the benefits of a series of treatments often fade away after a few weeks.
“Some patients describe the results lasting indefinitely, while most patients who respond to the treatments get to the point where they are going roughly 4-12 weeks with sustained results,” Dr. Wells said.
“When the effects start to wear off, they don’t crash,” said Dr. Abreu. Instead, he said, symptoms slowly reappear.
It’s typical for patients at Dr. Abreu’s clinic and others to return within a couple of months to go through another round of ketamine treatments. In some cases, “they continue to see us indefinitely to get them back up to where they need to be with a booster type of session,” he said.
Ketamine treatment costs vary widely, and insurers don’t cover this off-label treatment. The clinic operators quoted in this article reported a range of per-infusion costs from $350 (Dr. Markey’s clinic in Denver) to $675 (Dr. Abreu’s clinics in the Northwest).
“We have to have a talk with them: Can you afford this? This is going to take a significant amount of money every month to keep you well,” Dr. Abreu said. On the other hand, he said, the need for other medications goes away, eliminating that cost. (“They’re on [selective serotonin reputake inhibitors] usually,” he said, “but those drugs don’t work.”)
Nonpsychiatrists in forefront
At Dr. Markey’s clinic in Denver, all patients are required to see either her or a psychiatrist colleague. Some other ketamine clinics are run by psychiatrists, but that’s far from common.
Clinics often have no mental health professionals on staff and are run by anesthesiologists or other kinds of physicians.
Some clinic owners, Dr. Wells said, require patients to be under the care of a psychiatrist, neurologist, pain doctor, or other appropriate professional. “I do not intend, nor do I act, to displace psychiatrists, or the relationships our patients have with their psychiatrists, or the care they receive from their psychiatrists,” she said.
In the Northwest, Dr. Abreu said his patients take mood questionnaires, and he’s experimenting with a text-based mood monitoring system. In the Minneapolis area, anesthesiologist Dr. Simelgor is looking for a psychiatrist or psychiatrist partner for his ketamine clinic. “My thinking,” he said, “is that we need to work together.”
Still, there do not appear to be any requirements that ketamine clinic practitioners have connections to mental health professionals. Yet, as Dr. Sanacora put it: “Delivering the drug is the easiest part of the treatment. The hard part is managing the depression.”
Dr. Lieberman, Dr. Wells, Dr. Abreu, Dr. Simelgor, and Dr. Markey reported no relevant disclosures. Dr. Sanacora reported consulting fees and research contracts for multiple drug makers over the past 24 months. He holds shares in Biohaven Pharmaceuticals and is a coinventor on a U.S. patent (No. 8778979) on using glutamate agents to treat mental disorders held by Yale University.
Ketamine, once best known as a pet anesthetic and party drug, is taking the United States by storm. Dozens of ketamine treatment centers are operating from coast to coast.
Big cities like Baltimore, Boston, and Phoenix have them. So do Charleston, S.C., and Boise, Idaho. Two such clinics are in sparsely populated New Mexico. And one national chain went from a pair of clinics to 10 in fewer than 2 years.
Never mind that these expensive treatments for conditions like depression are not covered by insurers or approved for this use by the Food and Drug Administration. Other questions also persist. “There is a considerable body of evidence that proves it really does work,” Dr. Lieberman said. “But we don’t know the extent of the range of conditions for which it might be effective, what the optimal frequency and concentration for dosing is, and what the long-term consequences are.”
To make matters more complicated, it’s anesthesiologists – not psychiatrists – who are leading the way toward a ketamine-infused future.
For now, however, hundreds and perhaps even thousands of patients are serving as ketamine test cases with psychiatrists only assisting remotely, if at all.
A stunningly rapid rise
Sara M. Markey, MD, is one of the rare psychiatrists in the United States who’s fully embraced ketamine treatment for mental illness.
She recalled first hearing about ketamine as an anesthetic in medical school. Best known as an anesthetic in animals, it’s also occasionally given to children and adults, although the drug’s dissociative properties have prevented widespread use.
In 2006, word spread about ketamine’s use as a painkiller. “I also began hearing and reading about its potential use/efficacy in treatment-resistant depression,” said Dr. Markey, who practices in Denver. “It was difficult to find information about ketamine, and many of my colleagues were hostile to the idea of using ketamine in clinical practice.”
She persisted, however, and prescribed intranasal and oral ketamine to depressed patients with “mild success.” She also saw patients whose psychiatrists refused to consider ketamine.
In early 2016, with Steven P. Levine, MD, a New Jersey psychiatrist who pioneered ketamine use for depression, Dr. Markey opened a ketamine infusion clinic in the Mile High City.
At at that time, it was only the second in a national chain called Ketamine Treatment Centers. Now, not even 2 years later, the chain has a new name – Actify Neurotherapies – and a total of 10 clinics from San Francisco and Beverly Hills, Calif., to Palm Beach, Fla.; Raleigh, N.C.; and New York City.
“It is wonderful,” she said, “to have an opportunity to provide a medication to people that does not cause weight gain, has very few medication interactions, and which is well tolerated and generic.”
Big short-term benefits
Treatment outcomes with ketamine – which is thought to act on glutamate and N-methyl-D-aspartate receptors – can be dramatic. “Some patients describe the ketamine treatments as life saving,” said Allison F. Wells, MD, an anesthesiologist who runs a clinic in Houston.
One depressed young man who tried ketamine at a Phoenix clinic in 2013 reportedly told the news site vice.com that he “felt good for a week” after his first treatment: “Not the kind of bipolar ‘good’ where I’d be manic. I just felt pleasant, and not crazy or compulsive. I felt normal for the first time in a long time.” Another depressed patient told National Public Radio that ketamine transformed his life: “I remember I was in my bathroom, and I literally fell to my knees crying because I had no anxiety; I had no depression.”
Enrique A. Abreu, DO, an anesthesiologist who offers ketamine therapy in Seattle and Portland, Ore., said he’s seen anxiety relief and a decrease in rumination in these patients. “They’re able to go back to work; a lot haven’t been able to work for a long time. And motivation is a big thing. They’re able to do things they haven’t been able to do.”
In addition, ketamine can reduce suicidal thinking, Dr. Markey said. “I am continually astounded to hear patients who come in with acute or chronic suicidal thinking report that those ideas and/or intrusive thoughts have disappeared. When they are absent, people need to be reminded of when they had them. They seem to have forgotten about them.”
‘Mystical experiences’
Dr. Markey said a retrospective analysis of about 740 patients at her chain’s clinics showed a response rate of about 75%. Other research has shown similarly high response levels.
“Multiple clinical trials suggest that a single low dose (0.5mg/kg) of IV ketamine results in a 50%-70% response rate in patients with treatment-resistant depression,” reported a 2016 clinical review. “Additional research has shown that depressed patients can experience symptom relief as early as 2 [hours], and lasting up to 2 weeks after a single administration of IV ketamine,” according to the review in Evidence Based Mental Health (2016 May;19[2]:35-8).
Adverse effects can include nausea and headache in patients with a history of migraine, he said. Over the long term, ketamine use can lead to incontinence and urinary urgency, he said.
As for ketamine addiction, Dr. Simelgor calls it unlikely at the lower doses that are used. However, he said, “I can’t say 100% that it won’t cause addiction.”
Who benefits? The jury’s still out
Considering its positive effects, why shouldn’t the mental health community embrace ketamine? Because, two prominent researchers say, best practices are still absent in a whole range of areas.
For example, there’s no agreement about who should undergo ketamine treatments beyond patients with treatment-resistant depression, especially those who have failed or cannot undergo electroconvulsive therapy. Ketamine therapy also is being touted by some as a treatment for a long list of other conditions from obsessive-compulsive disorder and anxiety to fibromyalgia and chronic pain disorders.
There are also limited data about dosing, making it “not possible to clarify the relative benefits and risks of doses other than 0.5 mg/kg delivered intravenously over 40 minutes,” cautioned Dr. Sanacora and Samuel T. Wilkinson, MD, also at Yale, in a 2017 commentary in JAMA (2017;318[9]:793-4).
In fact, they write, “Most published data supporting the use of ketamine as a treatment for mood disorders are based on trials that have followed up patients for just 1 week after a single administration of the drug.”
Unchartered waters
There’s also no accepted protocol beyond a typical six treatments over 2 or more weeks. This is relevant because the benefits of a series of treatments often fade away after a few weeks.
“Some patients describe the results lasting indefinitely, while most patients who respond to the treatments get to the point where they are going roughly 4-12 weeks with sustained results,” Dr. Wells said.
“When the effects start to wear off, they don’t crash,” said Dr. Abreu. Instead, he said, symptoms slowly reappear.
It’s typical for patients at Dr. Abreu’s clinic and others to return within a couple of months to go through another round of ketamine treatments. In some cases, “they continue to see us indefinitely to get them back up to where they need to be with a booster type of session,” he said.
Ketamine treatment costs vary widely, and insurers don’t cover this off-label treatment. The clinic operators quoted in this article reported a range of per-infusion costs from $350 (Dr. Markey’s clinic in Denver) to $675 (Dr. Abreu’s clinics in the Northwest).
“We have to have a talk with them: Can you afford this? This is going to take a significant amount of money every month to keep you well,” Dr. Abreu said. On the other hand, he said, the need for other medications goes away, eliminating that cost. (“They’re on [selective serotonin reputake inhibitors] usually,” he said, “but those drugs don’t work.”)
Nonpsychiatrists in forefront
At Dr. Markey’s clinic in Denver, all patients are required to see either her or a psychiatrist colleague. Some other ketamine clinics are run by psychiatrists, but that’s far from common.
Clinics often have no mental health professionals on staff and are run by anesthesiologists or other kinds of physicians.
Some clinic owners, Dr. Wells said, require patients to be under the care of a psychiatrist, neurologist, pain doctor, or other appropriate professional. “I do not intend, nor do I act, to displace psychiatrists, or the relationships our patients have with their psychiatrists, or the care they receive from their psychiatrists,” she said.
In the Northwest, Dr. Abreu said his patients take mood questionnaires, and he’s experimenting with a text-based mood monitoring system. In the Minneapolis area, anesthesiologist Dr. Simelgor is looking for a psychiatrist or psychiatrist partner for his ketamine clinic. “My thinking,” he said, “is that we need to work together.”
Still, there do not appear to be any requirements that ketamine clinic practitioners have connections to mental health professionals. Yet, as Dr. Sanacora put it: “Delivering the drug is the easiest part of the treatment. The hard part is managing the depression.”
Dr. Lieberman, Dr. Wells, Dr. Abreu, Dr. Simelgor, and Dr. Markey reported no relevant disclosures. Dr. Sanacora reported consulting fees and research contracts for multiple drug makers over the past 24 months. He holds shares in Biohaven Pharmaceuticals and is a coinventor on a U.S. patent (No. 8778979) on using glutamate agents to treat mental disorders held by Yale University.
Ketamine, once best known as a pet anesthetic and party drug, is taking the United States by storm. Dozens of ketamine treatment centers are operating from coast to coast.
Big cities like Baltimore, Boston, and Phoenix have them. So do Charleston, S.C., and Boise, Idaho. Two such clinics are in sparsely populated New Mexico. And one national chain went from a pair of clinics to 10 in fewer than 2 years.
Never mind that these expensive treatments for conditions like depression are not covered by insurers or approved for this use by the Food and Drug Administration. Other questions also persist. “There is a considerable body of evidence that proves it really does work,” Dr. Lieberman said. “But we don’t know the extent of the range of conditions for which it might be effective, what the optimal frequency and concentration for dosing is, and what the long-term consequences are.”
To make matters more complicated, it’s anesthesiologists – not psychiatrists – who are leading the way toward a ketamine-infused future.
For now, however, hundreds and perhaps even thousands of patients are serving as ketamine test cases with psychiatrists only assisting remotely, if at all.
A stunningly rapid rise
Sara M. Markey, MD, is one of the rare psychiatrists in the United States who’s fully embraced ketamine treatment for mental illness.
She recalled first hearing about ketamine as an anesthetic in medical school. Best known as an anesthetic in animals, it’s also occasionally given to children and adults, although the drug’s dissociative properties have prevented widespread use.
In 2006, word spread about ketamine’s use as a painkiller. “I also began hearing and reading about its potential use/efficacy in treatment-resistant depression,” said Dr. Markey, who practices in Denver. “It was difficult to find information about ketamine, and many of my colleagues were hostile to the idea of using ketamine in clinical practice.”
She persisted, however, and prescribed intranasal and oral ketamine to depressed patients with “mild success.” She also saw patients whose psychiatrists refused to consider ketamine.
In early 2016, with Steven P. Levine, MD, a New Jersey psychiatrist who pioneered ketamine use for depression, Dr. Markey opened a ketamine infusion clinic in the Mile High City.
At at that time, it was only the second in a national chain called Ketamine Treatment Centers. Now, not even 2 years later, the chain has a new name – Actify Neurotherapies – and a total of 10 clinics from San Francisco and Beverly Hills, Calif., to Palm Beach, Fla.; Raleigh, N.C.; and New York City.
“It is wonderful,” she said, “to have an opportunity to provide a medication to people that does not cause weight gain, has very few medication interactions, and which is well tolerated and generic.”
Big short-term benefits
Treatment outcomes with ketamine – which is thought to act on glutamate and N-methyl-D-aspartate receptors – can be dramatic. “Some patients describe the ketamine treatments as life saving,” said Allison F. Wells, MD, an anesthesiologist who runs a clinic in Houston.
One depressed young man who tried ketamine at a Phoenix clinic in 2013 reportedly told the news site vice.com that he “felt good for a week” after his first treatment: “Not the kind of bipolar ‘good’ where I’d be manic. I just felt pleasant, and not crazy or compulsive. I felt normal for the first time in a long time.” Another depressed patient told National Public Radio that ketamine transformed his life: “I remember I was in my bathroom, and I literally fell to my knees crying because I had no anxiety; I had no depression.”
Enrique A. Abreu, DO, an anesthesiologist who offers ketamine therapy in Seattle and Portland, Ore., said he’s seen anxiety relief and a decrease in rumination in these patients. “They’re able to go back to work; a lot haven’t been able to work for a long time. And motivation is a big thing. They’re able to do things they haven’t been able to do.”
In addition, ketamine can reduce suicidal thinking, Dr. Markey said. “I am continually astounded to hear patients who come in with acute or chronic suicidal thinking report that those ideas and/or intrusive thoughts have disappeared. When they are absent, people need to be reminded of when they had them. They seem to have forgotten about them.”
‘Mystical experiences’
Dr. Markey said a retrospective analysis of about 740 patients at her chain’s clinics showed a response rate of about 75%. Other research has shown similarly high response levels.
“Multiple clinical trials suggest that a single low dose (0.5mg/kg) of IV ketamine results in a 50%-70% response rate in patients with treatment-resistant depression,” reported a 2016 clinical review. “Additional research has shown that depressed patients can experience symptom relief as early as 2 [hours], and lasting up to 2 weeks after a single administration of IV ketamine,” according to the review in Evidence Based Mental Health (2016 May;19[2]:35-8).
Adverse effects can include nausea and headache in patients with a history of migraine, he said. Over the long term, ketamine use can lead to incontinence and urinary urgency, he said.
As for ketamine addiction, Dr. Simelgor calls it unlikely at the lower doses that are used. However, he said, “I can’t say 100% that it won’t cause addiction.”
Who benefits? The jury’s still out
Considering its positive effects, why shouldn’t the mental health community embrace ketamine? Because, two prominent researchers say, best practices are still absent in a whole range of areas.
For example, there’s no agreement about who should undergo ketamine treatments beyond patients with treatment-resistant depression, especially those who have failed or cannot undergo electroconvulsive therapy. Ketamine therapy also is being touted by some as a treatment for a long list of other conditions from obsessive-compulsive disorder and anxiety to fibromyalgia and chronic pain disorders.
There are also limited data about dosing, making it “not possible to clarify the relative benefits and risks of doses other than 0.5 mg/kg delivered intravenously over 40 minutes,” cautioned Dr. Sanacora and Samuel T. Wilkinson, MD, also at Yale, in a 2017 commentary in JAMA (2017;318[9]:793-4).
In fact, they write, “Most published data supporting the use of ketamine as a treatment for mood disorders are based on trials that have followed up patients for just 1 week after a single administration of the drug.”
Unchartered waters
There’s also no accepted protocol beyond a typical six treatments over 2 or more weeks. This is relevant because the benefits of a series of treatments often fade away after a few weeks.
“Some patients describe the results lasting indefinitely, while most patients who respond to the treatments get to the point where they are going roughly 4-12 weeks with sustained results,” Dr. Wells said.
“When the effects start to wear off, they don’t crash,” said Dr. Abreu. Instead, he said, symptoms slowly reappear.
It’s typical for patients at Dr. Abreu’s clinic and others to return within a couple of months to go through another round of ketamine treatments. In some cases, “they continue to see us indefinitely to get them back up to where they need to be with a booster type of session,” he said.
Ketamine treatment costs vary widely, and insurers don’t cover this off-label treatment. The clinic operators quoted in this article reported a range of per-infusion costs from $350 (Dr. Markey’s clinic in Denver) to $675 (Dr. Abreu’s clinics in the Northwest).
“We have to have a talk with them: Can you afford this? This is going to take a significant amount of money every month to keep you well,” Dr. Abreu said. On the other hand, he said, the need for other medications goes away, eliminating that cost. (“They’re on [selective serotonin reputake inhibitors] usually,” he said, “but those drugs don’t work.”)
Nonpsychiatrists in forefront
At Dr. Markey’s clinic in Denver, all patients are required to see either her or a psychiatrist colleague. Some other ketamine clinics are run by psychiatrists, but that’s far from common.
Clinics often have no mental health professionals on staff and are run by anesthesiologists or other kinds of physicians.
Some clinic owners, Dr. Wells said, require patients to be under the care of a psychiatrist, neurologist, pain doctor, or other appropriate professional. “I do not intend, nor do I act, to displace psychiatrists, or the relationships our patients have with their psychiatrists, or the care they receive from their psychiatrists,” she said.
In the Northwest, Dr. Abreu said his patients take mood questionnaires, and he’s experimenting with a text-based mood monitoring system. In the Minneapolis area, anesthesiologist Dr. Simelgor is looking for a psychiatrist or psychiatrist partner for his ketamine clinic. “My thinking,” he said, “is that we need to work together.”
Still, there do not appear to be any requirements that ketamine clinic practitioners have connections to mental health professionals. Yet, as Dr. Sanacora put it: “Delivering the drug is the easiest part of the treatment. The hard part is managing the depression.”
Dr. Lieberman, Dr. Wells, Dr. Abreu, Dr. Simelgor, and Dr. Markey reported no relevant disclosures. Dr. Sanacora reported consulting fees and research contracts for multiple drug makers over the past 24 months. He holds shares in Biohaven Pharmaceuticals and is a coinventor on a U.S. patent (No. 8778979) on using glutamate agents to treat mental disorders held by Yale University.
Tc-325 effective for immediate GI tumor bleeding
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
The powder Tc-325 is effective for immediate hemostasis in patients with malignant gastrointestinal bleeding, according to results published in Gastrointestinal Endoscopy.
The compound achieved immediate hemostasis in 97.7% of patients with GI tumor bleeding, reported Alan Barkun, MD, of the division of gastroenterology at McGill University Health Centre, Montreal, and his coauthors. Conventional endoscopic hemostatic methods, by contrast, have shown highly variable hemostasis rates in prior studies, ranging from 31% to 93%, the authors said.
“Tc-325 seems to be more predictably effective in providing initial hemostasis in upper GI tumor bleeding compared with conventional methods,” they added.
The study included 88 eligible patients who initially presented with bleeding either as a result of a primary GI tumor, or metastases to the upper or lower GI tract. Almost 60% had an upper GI cancer site. Twenty-five patients died before the end of the 30-day observation period.
The recurrent bleeding rate at 72 hours was 15%. Bleeding rates at 7, 14, and 30 days’ follow-up were 7%, 7.8%, and 1.9%, respectively.
Overall, 27.3% of patients experienced repeat bleeding within 30 days of Tc-325 treatment, all from upper GI sites. No recurrent bleeding occurred from lower GI lesions. Recurrent bleeding occurred in 38% patients who did not receive definite hemostasis within 30 days.
An international normalized ratio value greater than 1.3 was significantly associated with early recurrent bleeding in univariable analysis (P = .02; odds ratio, 5.08; 95% confidence interval, 1.33-19.33), as was an Eastern Cooperative Oncology Group (ECOG) score of at least 3 (P = .049; OR, 3.94; 95% CI, 1.01-15.38). Definite hemostatic treatment was associated with less recurrent bleeding (P = .009; OR, 0.15; 95% CI, 0.04-0.62).
Factors significantly associated with 6-month survival in multivariable analysis were an ECOG score of 0-2 (P = .001; hazard ratio, 0.14; 95% CI, 0.04-0.47); cancer stage 1-3 (P = .042; HR, 0.31; 95% CI, 0.10-0.96), and receiving definite hemostastic treatment (P = .002; HR, 0.24; 95% CI, 0.09-0.59), Dr. Barkun and his colleagues reported.
Although the results show promise for Tc-325 as an immediate treatment in the case of failed standard endoscopic hemostatic techniques or when definite hemostasis via radiation, surgery, and chemotherapy are unavailable, the long-term effects are comparable with conventional methods, at least in the upper GI tract, the authors said. Better results in the lower GI tract may be attributed to the presence of gastric juice in the upper GI tract, the investigators noted.
Limitations of the study include “its retrospective design with the possibility of missing information and selective data collection,” as well as the possibility of decreased generalizability of results, Dr. Barkun and coauthors wrote. Nevertheless, its immediate effectiveness at achieving hemostasis and prevention of early bleeding indicate that the results may still be “used with confidence as guidance for any physician managing such patients,” the authors said.
The investigators did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
SOURCE: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
FROM GASTROINTESTINAL ENDOSCOPY
Key clinical point: Tc-325 is promising for initial hemostasis in patients with gastrointestinal tumor bleeding.
Major finding: Tc-325 achieved immediate hemostasis in 97.7% of patients with bleeding from GI tumors.
Data source: A multicenter retrospective study of 88 eligible patients with GI tumor-related hemorrhage from 2011 to 2016.
Disclosures: The authors did not disclose any conflicts of interest. The study was funded by the Grant for International Research Integration: Chula Research Scholar, Ratchadaphiseksomphot Endowment Fund.
Source: Pittayanon R et al. Gastrointest Endosc. 2017 Nov 17. doi: 10.1016/j.gie.2017.11.013.
Hyperbaric oxygen may cut CO deaths
In patients with carbon monoxide poisoning, hyperbaric oxygen therapy was associated with a lower rate of mortality, according to results of a recent retrospective study.
The mortality reduction was particularly evident among patients under 20 years of age and in patients with acute respiratory failure, authors of the study said in a report published in Chest (2017 Nov. doi: 10.1016/j.chest.2017.03.049).
“The results provide important references for decision making in the treatment of carbon monoxide poisoning,” Chien-Cheng Huang, MD, department of emergency medicine, Chi-Mei Medical Center, Tainan, Taiwan, and colleagues said in their report.
While hyperbaric oxygen has been suggested for severe carbon monoxide poisoning, 100% normobaric oxygen is considered standard treatment, according to Dr. Huang and colleagues.
“There has been no consensus about whether hyperbaric oxygen therapy is better than 100% normobaric oxygen alone, or the number of sessions of hyperbaric oxygen therapy that are necessary regarding mortality and morbidity,” they wrote.
In a Taiwanese nationwide poisoning database, Dr. Huang and colleagues identified 25,737 patients diagnosed with carbon monoxide poisoning between 1999 and 2012. Of those patients, 7,278 had hyperbaric oxygen therapy.
After researchers adjusted for variables including age, sex, and underlying comorbidities, the mortality rate was lower in patients who underwent hyperbaric oxygen therapy, compared with those who did not (adjusted hazard ratio, 0.74; 95% confidence interval, 0.67-0.81), data show.
The reduction in mortality was especially notable in patients younger than age 20 years (adjusted HR, 0.45; 95% CI, 0.26-0.80), according to the researchers.
A similarly greater magnitude of mortality benefit also was found for patients who had acute respiratory failure, “which supports acute respiratory failure being an indication for hyperbaric oxygen therapy,” investigators wrote. “Further studies are warranted to clarify this issue.”
The number of hyperbaric oxygen therapy sessions appeared to make a difference in mortality. Patients who received two or more sessions had a lower rate of mortality than did those who had only one session, according to the report.
Predictors of mortality, described in more detail in the published report, included older age, diabetes, alcoholism, and suicide attempts, among other factors.
“In addition to considering hyperbaric oxygen therapy for reducing mortality, control of other concomitant mortality predictors is necessary,” the authors concluded based on their results.
Accidental deaths from carbon monoxide poisoning also are a major issue in the United States, where each year, there are an estimated 1,000-2,000 cases, according to the authors. Additionally, accidental carbon monoxide poisoning has “increased greatly in the past 10 years,” they said in the report.
Other studies have shown that, compared with normobaric oxygen, hyperbaric oxygen therapy did not reduce neurologic complications, the authors noted. Even so, that fact “does not suggest that hyperbaric oxygen therapy is not beneficial regarding mortality,” they wrote. “In fact, it is possible that reducing mortality may increase morbidities such as neurologic sequelae.”
Dr. Huang and coauthors reported no conflicts of interest related to the study, which was supported by Chi-Mei Medical Center in Taiwan.
Use of hyperbaric oxygen therapy to treat carbon monoxide poisioning has been “controversial since its inception” since early promoters “tended to place hyperbaric treatment ahead of strong supporting data,” wrote Clayton T. Cowl, MD, FCCP, in an editorial regarding the study by Dr. Huang and colleagues.

These data are compelling because they come from what is believed to be the first large-scale study that specifically examines mortality as an endpoint in an entire nation, as opposed to smaller cohorts in single centers or even multiple institutions, he said in his editorial.
“Have we reached the point of clearly establishing that delivery of pure oxygen in a high-pressure environment is more effective in treating patients who have carbon monoxide poisoning than is normobaric supplemental oxygen alone? Probably not,” Dr. Cowl wrote.
“The retrospective database study by Huang et al, despite its large size and interesting findings, remains distant from the ideal of a large blinded multicenter randomized controlled trial using a standardized protocol to compare normobaric supplemental oxygenation with hyperbaric oxygen therapy delivery for this cohort,” he explained. “However, its size, scale, and findings add credibility to the mounting data supporting HBOT for this indication.”
Clayton T. Cowl, MD, FCCP, is with the division of preventive, occupational, and aerospace medicine and the division of pulmonary and critical care medicine, Mayo Clinic. His comments came from an editorial in Chest (doi: 10.1016/j.chest.2017.07.022) He declared no financial or nonfinancial disclosures related to the editorial.
Use of hyperbaric oxygen therapy to treat carbon monoxide poisioning has been “controversial since its inception” since early promoters “tended to place hyperbaric treatment ahead of strong supporting data,” wrote Clayton T. Cowl, MD, FCCP, in an editorial regarding the study by Dr. Huang and colleagues.
These data are compelling because they come from what is believed to be the first large-scale study that specifically examines mortality as an endpoint in an entire nation, as opposed to smaller cohorts in single centers or even multiple institutions, he said in his editorial.
“Have we reached the point of clearly establishing that delivery of pure oxygen in a high-pressure environment is more effective in treating patients who have carbon monoxide poisoning than is normobaric supplemental oxygen alone? Probably not,” Dr. Cowl wrote.
“The retrospective database study by Huang et al, despite its large size and interesting findings, remains distant from the ideal of a large blinded multicenter randomized controlled trial using a standardized protocol to compare normobaric supplemental oxygenation with hyperbaric oxygen therapy delivery for this cohort,” he explained. “However, its size, scale, and findings add credibility to the mounting data supporting HBOT for this indication.”
Clayton T. Cowl, MD, FCCP, is with the division of preventive, occupational, and aerospace medicine and the division of pulmonary and critical care medicine, Mayo Clinic. His comments came from an editorial in Chest (doi: 10.1016/j.chest.2017.07.022) He declared no financial or nonfinancial disclosures related to the editorial.
Use of hyperbaric oxygen therapy to treat carbon monoxide poisioning has been “controversial since its inception” since early promoters “tended to place hyperbaric treatment ahead of strong supporting data,” wrote Clayton T. Cowl, MD, FCCP, in an editorial regarding the study by Dr. Huang and colleagues.
These data are compelling because they come from what is believed to be the first large-scale study that specifically examines mortality as an endpoint in an entire nation, as opposed to smaller cohorts in single centers or even multiple institutions, he said in his editorial.
“Have we reached the point of clearly establishing that delivery of pure oxygen in a high-pressure environment is more effective in treating patients who have carbon monoxide poisoning than is normobaric supplemental oxygen alone? Probably not,” Dr. Cowl wrote.
“The retrospective database study by Huang et al, despite its large size and interesting findings, remains distant from the ideal of a large blinded multicenter randomized controlled trial using a standardized protocol to compare normobaric supplemental oxygenation with hyperbaric oxygen therapy delivery for this cohort,” he explained. “However, its size, scale, and findings add credibility to the mounting data supporting HBOT for this indication.”
Clayton T. Cowl, MD, FCCP, is with the division of preventive, occupational, and aerospace medicine and the division of pulmonary and critical care medicine, Mayo Clinic. His comments came from an editorial in Chest (doi: 10.1016/j.chest.2017.07.022) He declared no financial or nonfinancial disclosures related to the editorial.
In patients with carbon monoxide poisoning, hyperbaric oxygen therapy was associated with a lower rate of mortality, according to results of a recent retrospective study.
The mortality reduction was particularly evident among patients under 20 years of age and in patients with acute respiratory failure, authors of the study said in a report published in Chest (2017 Nov. doi: 10.1016/j.chest.2017.03.049).
“The results provide important references for decision making in the treatment of carbon monoxide poisoning,” Chien-Cheng Huang, MD, department of emergency medicine, Chi-Mei Medical Center, Tainan, Taiwan, and colleagues said in their report.
While hyperbaric oxygen has been suggested for severe carbon monoxide poisoning, 100% normobaric oxygen is considered standard treatment, according to Dr. Huang and colleagues.
“There has been no consensus about whether hyperbaric oxygen therapy is better than 100% normobaric oxygen alone, or the number of sessions of hyperbaric oxygen therapy that are necessary regarding mortality and morbidity,” they wrote.
In a Taiwanese nationwide poisoning database, Dr. Huang and colleagues identified 25,737 patients diagnosed with carbon monoxide poisoning between 1999 and 2012. Of those patients, 7,278 had hyperbaric oxygen therapy.
After researchers adjusted for variables including age, sex, and underlying comorbidities, the mortality rate was lower in patients who underwent hyperbaric oxygen therapy, compared with those who did not (adjusted hazard ratio, 0.74; 95% confidence interval, 0.67-0.81), data show.
The reduction in mortality was especially notable in patients younger than age 20 years (adjusted HR, 0.45; 95% CI, 0.26-0.80), according to the researchers.
A similarly greater magnitude of mortality benefit also was found for patients who had acute respiratory failure, “which supports acute respiratory failure being an indication for hyperbaric oxygen therapy,” investigators wrote. “Further studies are warranted to clarify this issue.”
The number of hyperbaric oxygen therapy sessions appeared to make a difference in mortality. Patients who received two or more sessions had a lower rate of mortality than did those who had only one session, according to the report.
Predictors of mortality, described in more detail in the published report, included older age, diabetes, alcoholism, and suicide attempts, among other factors.
“In addition to considering hyperbaric oxygen therapy for reducing mortality, control of other concomitant mortality predictors is necessary,” the authors concluded based on their results.
Accidental deaths from carbon monoxide poisoning also are a major issue in the United States, where each year, there are an estimated 1,000-2,000 cases, according to the authors. Additionally, accidental carbon monoxide poisoning has “increased greatly in the past 10 years,” they said in the report.
Other studies have shown that, compared with normobaric oxygen, hyperbaric oxygen therapy did not reduce neurologic complications, the authors noted. Even so, that fact “does not suggest that hyperbaric oxygen therapy is not beneficial regarding mortality,” they wrote. “In fact, it is possible that reducing mortality may increase morbidities such as neurologic sequelae.”
Dr. Huang and coauthors reported no conflicts of interest related to the study, which was supported by Chi-Mei Medical Center in Taiwan.
In patients with carbon monoxide poisoning, hyperbaric oxygen therapy was associated with a lower rate of mortality, according to results of a recent retrospective study.
The mortality reduction was particularly evident among patients under 20 years of age and in patients with acute respiratory failure, authors of the study said in a report published in Chest (2017 Nov. doi: 10.1016/j.chest.2017.03.049).
“The results provide important references for decision making in the treatment of carbon monoxide poisoning,” Chien-Cheng Huang, MD, department of emergency medicine, Chi-Mei Medical Center, Tainan, Taiwan, and colleagues said in their report.
While hyperbaric oxygen has been suggested for severe carbon monoxide poisoning, 100% normobaric oxygen is considered standard treatment, according to Dr. Huang and colleagues.
“There has been no consensus about whether hyperbaric oxygen therapy is better than 100% normobaric oxygen alone, or the number of sessions of hyperbaric oxygen therapy that are necessary regarding mortality and morbidity,” they wrote.
In a Taiwanese nationwide poisoning database, Dr. Huang and colleagues identified 25,737 patients diagnosed with carbon monoxide poisoning between 1999 and 2012. Of those patients, 7,278 had hyperbaric oxygen therapy.
After researchers adjusted for variables including age, sex, and underlying comorbidities, the mortality rate was lower in patients who underwent hyperbaric oxygen therapy, compared with those who did not (adjusted hazard ratio, 0.74; 95% confidence interval, 0.67-0.81), data show.
The reduction in mortality was especially notable in patients younger than age 20 years (adjusted HR, 0.45; 95% CI, 0.26-0.80), according to the researchers.
A similarly greater magnitude of mortality benefit also was found for patients who had acute respiratory failure, “which supports acute respiratory failure being an indication for hyperbaric oxygen therapy,” investigators wrote. “Further studies are warranted to clarify this issue.”
The number of hyperbaric oxygen therapy sessions appeared to make a difference in mortality. Patients who received two or more sessions had a lower rate of mortality than did those who had only one session, according to the report.
Predictors of mortality, described in more detail in the published report, included older age, diabetes, alcoholism, and suicide attempts, among other factors.
“In addition to considering hyperbaric oxygen therapy for reducing mortality, control of other concomitant mortality predictors is necessary,” the authors concluded based on their results.
Accidental deaths from carbon monoxide poisoning also are a major issue in the United States, where each year, there are an estimated 1,000-2,000 cases, according to the authors. Additionally, accidental carbon monoxide poisoning has “increased greatly in the past 10 years,” they said in the report.
Other studies have shown that, compared with normobaric oxygen, hyperbaric oxygen therapy did not reduce neurologic complications, the authors noted. Even so, that fact “does not suggest that hyperbaric oxygen therapy is not beneficial regarding mortality,” they wrote. “In fact, it is possible that reducing mortality may increase morbidities such as neurologic sequelae.”
Dr. Huang and coauthors reported no conflicts of interest related to the study, which was supported by Chi-Mei Medical Center in Taiwan.
FROM CHEST
Key clinical point: In patients with carbon monoxide poisoning, hyperbaric oxygen therapy was associated with a lower rate of mortality.
Major finding: The mortality rate was lower in patients who received hyperbaric oxygen therapy, compared with those who did not (adjusted HR, 0.74; 95% CI, 0.67-0.81).
Data source: A retrospective nationwide population-based study from Taiwan including 25,737 individuals diagnosed with carbon monoxide poisoning during 1999-2012.
Disclosures: Chi-Mei Medical Center in Taiwan supported the study. The authors reported no conflicts of interest.
Adherence to Psychotherapy May Improve Outcomes in Patients With Psychogenic Nonepileptic Seizures
WASHINGTON, DC—Adherence to psychotherapy is associated with a 50% or greater reduction in psychogenic nonepileptic seizures (PNES), improved quality of life, and decreased emergency department visits, according to research presented at the 71st Annual Meeting of the American Epilepsy Society.
Twenty-five percent to 40% of patients in epilepsy monitoring units are ultimately diagnosed with PNES. Research has indicated that psychotherapy reduces seizure frequency and improves quality of life in patients with PNES, but 20% to 30% of patients fail to attend their first appointment after diagnosis.
An Obstacle to Treatment
To determine whether nonadherence to psychotherapy may affect patient outcomes, Benjamin Tolchin, MD, Assistant Professor of Neurology at Yale School of Medicine in New Haven, Connecticut, and colleagues followed 105 consecutive patients with video-EEG confirmed PNES at Brigham and Women’s Hospital in Boston from March 2013 to August 2015. At baseline, researchers assessed patients’ psychiatric comorbidities and abuse history in a semistructured neuropsychiatric interview.

Following diagnosis, participants were referred for psychotherapy at Brigham and Women’s Hospital or with a local community therapist. Psychotherapy at Brigham and Women’s Hospital included a manualized regimen of 12 weekly one-hour sessions. In addition, a neuropsychiatrist called all local therapists to review the diagnosis and principles of treatment.
The researchers defined adherence to psychotherapy as attending at least eight sessions over the course of 16 weeks. The primary outcome was the proportion of participants with a 50% or greater reduction in PNES frequency at a 12- to 24-month telephone follow-up. Secondary outcomes included the rate of seizure freedom, change in quality of life, and change in number of monthly emergency department visits, which were assessed during the telephone follow-up and with medical chart review. Researchers used Fischer’s exact test and Student’s t-test to assess the correlation of outcomes with adherence to psychotherapy.
At follow-up, 84% of patients who were adherent with treatment achieved a significant reduction in seizure frequency, compared with 61% of patients who were nonadherent. Patients who were adherent had an average 7.2-point improvement on the Quality of Life in Epilepsy-10, whereas patients who were nonadherent had a mean 2.8-point improvement. Mean change in monthly emergency department visits was significantly reduced among patients who were adherent to treatment, compared with patients who were not adherent. After adjusting for potential confounders, treatment adherence remained a significant predictor of 50% reduction in seizure frequency (odds ratio, 3.81). Overall, 60% of participants were nonadherent. Risk factors for nonadherence included self-identified minority status and history of childhood abuse.
“New interventions, such as motivational interviewing, are needed to improve adherence with psychotherapy among patients with PNES,” Dr. Tolchin said.
Motivational Interviewing
In a separate study, Dr. Tolchin and colleagues evaluated whether motivational interviewing improved treatment adherence and outcomes among 60 patients with video-EEG confirmed PNES. Patients who were randomized to receive a 30-minute motivational interviewing session before psychotherapy were more adherent to psychotherapy and had greater improvements in PNES frequency and quality of life, compared with patients randomized to psychotherapy alone. “Motivational interviewing-based interventions can improve the common problem of nonadherence with psychotherapy among patients diagnosed with PNES,” the researchers said. They added that this technique potentially could be delivered remotely to improve outcomes.
—Erica Tricarico
WASHINGTON, DC—Adherence to psychotherapy is associated with a 50% or greater reduction in psychogenic nonepileptic seizures (PNES), improved quality of life, and decreased emergency department visits, according to research presented at the 71st Annual Meeting of the American Epilepsy Society.
Twenty-five percent to 40% of patients in epilepsy monitoring units are ultimately diagnosed with PNES. Research has indicated that psychotherapy reduces seizure frequency and improves quality of life in patients with PNES, but 20% to 30% of patients fail to attend their first appointment after diagnosis.
An Obstacle to Treatment
To determine whether nonadherence to psychotherapy may affect patient outcomes, Benjamin Tolchin, MD, Assistant Professor of Neurology at Yale School of Medicine in New Haven, Connecticut, and colleagues followed 105 consecutive patients with video-EEG confirmed PNES at Brigham and Women’s Hospital in Boston from March 2013 to August 2015. At baseline, researchers assessed patients’ psychiatric comorbidities and abuse history in a semistructured neuropsychiatric interview.
Following diagnosis, participants were referred for psychotherapy at Brigham and Women’s Hospital or with a local community therapist. Psychotherapy at Brigham and Women’s Hospital included a manualized regimen of 12 weekly one-hour sessions. In addition, a neuropsychiatrist called all local therapists to review the diagnosis and principles of treatment.
The researchers defined adherence to psychotherapy as attending at least eight sessions over the course of 16 weeks. The primary outcome was the proportion of participants with a 50% or greater reduction in PNES frequency at a 12- to 24-month telephone follow-up. Secondary outcomes included the rate of seizure freedom, change in quality of life, and change in number of monthly emergency department visits, which were assessed during the telephone follow-up and with medical chart review. Researchers used Fischer’s exact test and Student’s t-test to assess the correlation of outcomes with adherence to psychotherapy.
At follow-up, 84% of patients who were adherent with treatment achieved a significant reduction in seizure frequency, compared with 61% of patients who were nonadherent. Patients who were adherent had an average 7.2-point improvement on the Quality of Life in Epilepsy-10, whereas patients who were nonadherent had a mean 2.8-point improvement. Mean change in monthly emergency department visits was significantly reduced among patients who were adherent to treatment, compared with patients who were not adherent. After adjusting for potential confounders, treatment adherence remained a significant predictor of 50% reduction in seizure frequency (odds ratio, 3.81). Overall, 60% of participants were nonadherent. Risk factors for nonadherence included self-identified minority status and history of childhood abuse.
“New interventions, such as motivational interviewing, are needed to improve adherence with psychotherapy among patients with PNES,” Dr. Tolchin said.
Motivational Interviewing
In a separate study, Dr. Tolchin and colleagues evaluated whether motivational interviewing improved treatment adherence and outcomes among 60 patients with video-EEG confirmed PNES. Patients who were randomized to receive a 30-minute motivational interviewing session before psychotherapy were more adherent to psychotherapy and had greater improvements in PNES frequency and quality of life, compared with patients randomized to psychotherapy alone. “Motivational interviewing-based interventions can improve the common problem of nonadherence with psychotherapy among patients diagnosed with PNES,” the researchers said. They added that this technique potentially could be delivered remotely to improve outcomes.
—Erica Tricarico
WASHINGTON, DC—Adherence to psychotherapy is associated with a 50% or greater reduction in psychogenic nonepileptic seizures (PNES), improved quality of life, and decreased emergency department visits, according to research presented at the 71st Annual Meeting of the American Epilepsy Society.
Twenty-five percent to 40% of patients in epilepsy monitoring units are ultimately diagnosed with PNES. Research has indicated that psychotherapy reduces seizure frequency and improves quality of life in patients with PNES, but 20% to 30% of patients fail to attend their first appointment after diagnosis.
An Obstacle to Treatment
To determine whether nonadherence to psychotherapy may affect patient outcomes, Benjamin Tolchin, MD, Assistant Professor of Neurology at Yale School of Medicine in New Haven, Connecticut, and colleagues followed 105 consecutive patients with video-EEG confirmed PNES at Brigham and Women’s Hospital in Boston from March 2013 to August 2015. At baseline, researchers assessed patients’ psychiatric comorbidities and abuse history in a semistructured neuropsychiatric interview.
Following diagnosis, participants were referred for psychotherapy at Brigham and Women’s Hospital or with a local community therapist. Psychotherapy at Brigham and Women’s Hospital included a manualized regimen of 12 weekly one-hour sessions. In addition, a neuropsychiatrist called all local therapists to review the diagnosis and principles of treatment.
The researchers defined adherence to psychotherapy as attending at least eight sessions over the course of 16 weeks. The primary outcome was the proportion of participants with a 50% or greater reduction in PNES frequency at a 12- to 24-month telephone follow-up. Secondary outcomes included the rate of seizure freedom, change in quality of life, and change in number of monthly emergency department visits, which were assessed during the telephone follow-up and with medical chart review. Researchers used Fischer’s exact test and Student’s t-test to assess the correlation of outcomes with adherence to psychotherapy.
At follow-up, 84% of patients who were adherent with treatment achieved a significant reduction in seizure frequency, compared with 61% of patients who were nonadherent. Patients who were adherent had an average 7.2-point improvement on the Quality of Life in Epilepsy-10, whereas patients who were nonadherent had a mean 2.8-point improvement. Mean change in monthly emergency department visits was significantly reduced among patients who were adherent to treatment, compared with patients who were not adherent. After adjusting for potential confounders, treatment adherence remained a significant predictor of 50% reduction in seizure frequency (odds ratio, 3.81). Overall, 60% of participants were nonadherent. Risk factors for nonadherence included self-identified minority status and history of childhood abuse.
“New interventions, such as motivational interviewing, are needed to improve adherence with psychotherapy among patients with PNES,” Dr. Tolchin said.
Motivational Interviewing
In a separate study, Dr. Tolchin and colleagues evaluated whether motivational interviewing improved treatment adherence and outcomes among 60 patients with video-EEG confirmed PNES. Patients who were randomized to receive a 30-minute motivational interviewing session before psychotherapy were more adherent to psychotherapy and had greater improvements in PNES frequency and quality of life, compared with patients randomized to psychotherapy alone. “Motivational interviewing-based interventions can improve the common problem of nonadherence with psychotherapy among patients diagnosed with PNES,” the researchers said. They added that this technique potentially could be delivered remotely to improve outcomes.
—Erica Tricarico
Dermatologists paying for errors during procedures
according to a review of over 90,000 lawsuits filed from 2006 to 2015.
Data from the Physician Insurers Association of America Data Sharing Project registry show that dermatologists paid 102 claims for errors that occurred during a procedure over that period. Misdiagnosis, with 62 payments, was the next most common reason, followed by medication errors (23 payments). Failure to supervise or monitor case, failure to instruct or communicate with patients, and failure to recognize a complication of treatment each had 15 payments, Heather Kornmehl and her associates reported (JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713).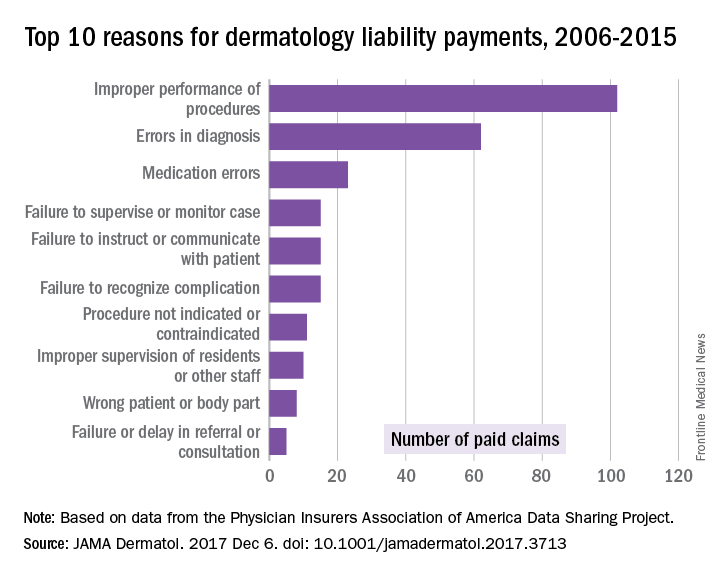
From 2006 to 2015, the total cost of the 281 claims paid by dermatologists was $71.8 million, and dermatologists were involved in 1,084 (1.2%) of the 90,743 closed claims against physicians in all specialties, said Ms. Kornwehl, who is a medical student at Drexel University, Philadelphia, and her associates.
Closed claims include any lawsuit that is subsequently abandoned, withdrawn, or dismissed; is settled; or goes to trial and results in a verdict.
One of Ms. Kornmehl’s coinvestigators has served as an investigator and/or advisor to a number of companies. No other disclosures were reported.
SOURCE: Kornmehl H et al. JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713
according to a review of over 90,000 lawsuits filed from 2006 to 2015.
Data from the Physician Insurers Association of America Data Sharing Project registry show that dermatologists paid 102 claims for errors that occurred during a procedure over that period. Misdiagnosis, with 62 payments, was the next most common reason, followed by medication errors (23 payments). Failure to supervise or monitor case, failure to instruct or communicate with patients, and failure to recognize a complication of treatment each had 15 payments, Heather Kornmehl and her associates reported (JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713).
From 2006 to 2015, the total cost of the 281 claims paid by dermatologists was $71.8 million, and dermatologists were involved in 1,084 (1.2%) of the 90,743 closed claims against physicians in all specialties, said Ms. Kornwehl, who is a medical student at Drexel University, Philadelphia, and her associates.
Closed claims include any lawsuit that is subsequently abandoned, withdrawn, or dismissed; is settled; or goes to trial and results in a verdict.
One of Ms. Kornmehl’s coinvestigators has served as an investigator and/or advisor to a number of companies. No other disclosures were reported.
SOURCE: Kornmehl H et al. JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713
according to a review of over 90,000 lawsuits filed from 2006 to 2015.
Data from the Physician Insurers Association of America Data Sharing Project registry show that dermatologists paid 102 claims for errors that occurred during a procedure over that period. Misdiagnosis, with 62 payments, was the next most common reason, followed by medication errors (23 payments). Failure to supervise or monitor case, failure to instruct or communicate with patients, and failure to recognize a complication of treatment each had 15 payments, Heather Kornmehl and her associates reported (JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713).
From 2006 to 2015, the total cost of the 281 claims paid by dermatologists was $71.8 million, and dermatologists were involved in 1,084 (1.2%) of the 90,743 closed claims against physicians in all specialties, said Ms. Kornwehl, who is a medical student at Drexel University, Philadelphia, and her associates.
Closed claims include any lawsuit that is subsequently abandoned, withdrawn, or dismissed; is settled; or goes to trial and results in a verdict.
One of Ms. Kornmehl’s coinvestigators has served as an investigator and/or advisor to a number of companies. No other disclosures were reported.
SOURCE: Kornmehl H et al. JAMA Dermatol. 2017 Dec 6. doi: 10.1001/jamadermatol.2017.3713
FROM JAMA DERMATOLOGY