User login
Hospitalist Perspective of Interactions with Medicine Subspecialty Consult Services
Hospitalist physicians care for an increasing proportion of general medicine inpatients and request a significant share of all subspecialty consultations.1 Subspecialty consultation in inpatient care is increasing,2,3 and effective hospitalist–consulting service interactions may affect team communication, patient care, and hospitalist learning. Therefore, enhancing hospitalist–consulting service interactions may have a broad-reaching, positive impact. Researchers in previous studies have explored resident–fellow consult interactions in the inpatient and emergency department settings as well as attending-to-attending consultation in the outpatient setting.4-7 However, to our knowledge, hospitalist–consulting team interactions have not been previously described. In academic medical centers, hospitalists are attending physicians who interact with both fellows (supervised by attending consultants) and directly with subspecialty attendings. Therefore, the exploration of the hospitalist–consultant interaction requires an evaluation of hospitalist–fellow and hospitalist–subspecialty attending interactions. The hospitalist–fellow interaction in particular is unique because it represents an unusual dynamic, in which an attending physician is primarily communicating with a trainee when requesting assistance with patient care.8 In order to explore hospitalist–consultant interactions (herein, the term “consultant” includes both fellow and attending consultants), we conducted a survey study in which we examine hospitalist practices and attitudes regarding consultation, with a specific focus on hospitalist consultation with internal medicine subspecialty consult services. In addition, we compared fellow–hospitalist and attending–hospitalist interactions and explored barriers to and facilitating factors of an effective hospitalist–consultant relationship.
METHODS
Survey Development
The survey instrument was developed by the authors based on findings of prior studies in which researchers examined consultation.2-6,9-16 The survey contained 31 questions (supplementary Appendix A) and evaluated 4 domains of the use of medical subspecialty consultation in direct patient care: (1) current consultation practices, (2) preferences regarding consultants, (3) barriers to and facilitating factors of effective consultation (both with respect to hospitalist learning and patient care), and (4) a comparison between hospitalist–fellow and hospitalist–subspecialty attending interactions. An evaluation of current consultation practices included a focus on communication methods (eg, in person, over the phone, through paging, or notes) because these have been found to be important during consultation.5,6,9,15,16 In order to explore hospitalist preferences regarding consult interactions and investigate perceptions of barriers to and facilitating factors of effective consultation, questions were developed based on previous literature, including our qualitative work examining resident–fellow interactions during consultation.4-6,9,12 We compared hospitalist consultation experiences among attending and fellow consultants because the interaction in which an attending hospitalist physician is primarily communicating with a trainee may differ from a consultation between a hospitalist attending and a subspecialty attending.8 Participants were asked to exclude their experiences when working on teaching services, during which students or housestaff often interact with consultants. The survey was cognitively tested with both hospitalist and non-hospitalist attending physicians not participating in the study and was revised by the authors using an iterative approach.
Study Participants
Hospitalist attending physicians at University of Texas Southwestern (UTSW) Medical Center, Emory University School of Medicine, Massachusetts General Hospital (MGH), and the Medical University of South Carolina (MUSC) were eligible to participate in the study. Consult team structures at each institution were composed of either a subspecialist-attending-only or a fellow-and-subspecialty-attending team. Fellows at all institutions are supervised by a subspecialty attending when performing consultations. Respondents who self-identified as nurse practitioners or physician assistants were excluded from the analysis. Hospitalists employed by the Veterans Affairs hospital system were also excluded. The study was approved by the institutional review boards of UTSW, Emory, MUSC, and MGH.
The survey was anonymous and administered to all hospitalists at participating institutions via a web-based survey tool (Qualtrics, Provo, UT). Participants were eligible to enter a raffle for a $500 gift card, and completion of the survey was not required for entry into the raffle.
Statistics
Results were summarized using the mean with standard deviation for continuous variables and the frequency with percentage for categorical variables after excluding missing values. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC). A 2-sided P value of ≤0.05 was considered statistically significant.
RESULTS
Current Consultation Practices
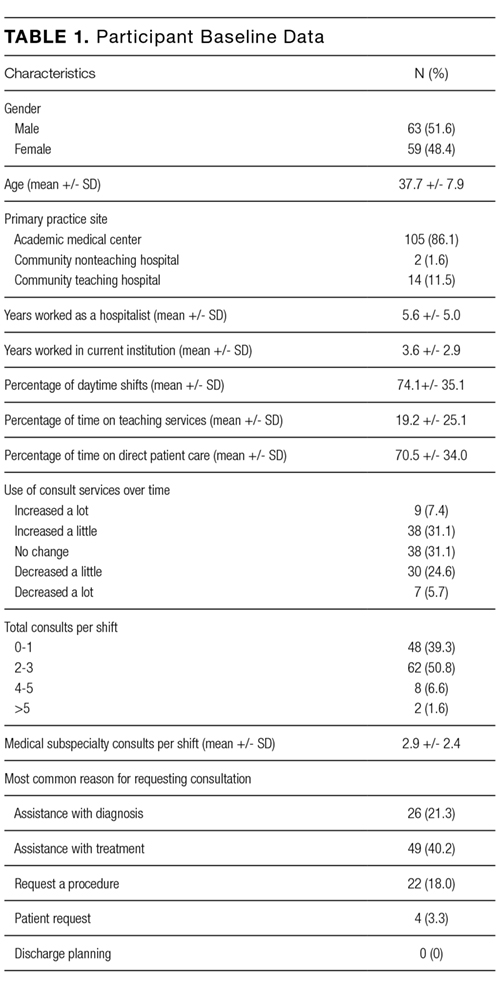
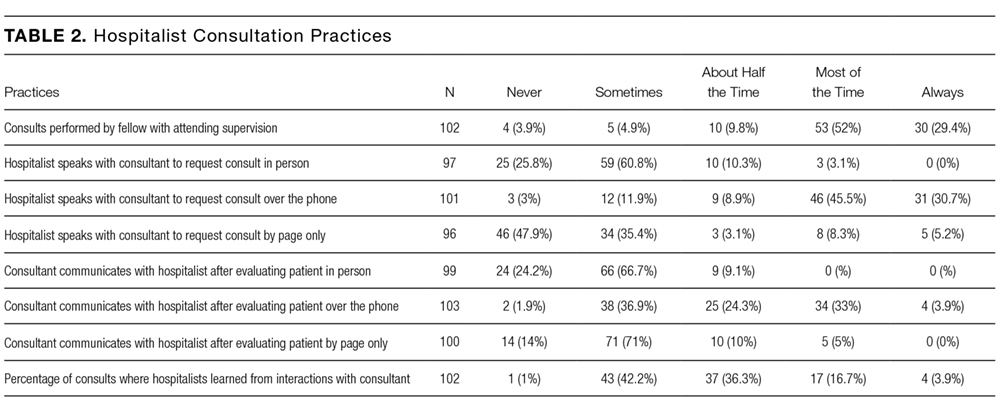
Current consultation practices and descriptions of hospitalist–consultant communication are shown in Table 2. Forty percent of respondents requested 0-1 consults per day, while 51.7% requested 2-3 per day. The most common reasons for requesting a consultation were assistance with treatment (48.5%), assistance with diagnosis (25.7%), and request for a procedure (21.8%). When asked whether the frequency of consultation is changing, slightly more hospitalists felt that their personal use of consultation was increasing as compared to those who felt that it was decreasing (38.5% vs 30.3%, respectively).
Hospitalist Preferences
Eighty-six percent of respondents agreed that consultants should be required to communicate their recommendations either in person or over the phone. Eighty-three percent of hospitalists agreed that they would like to receive more teaching from the consulting services, and 74.0% agreed that consultants should attempt to teach hospitalists during consult interactions regardless of whether the hospitalist initiates the teaching–learning interaction.
Barriers to and Facilitating Factors of Effective Consultation
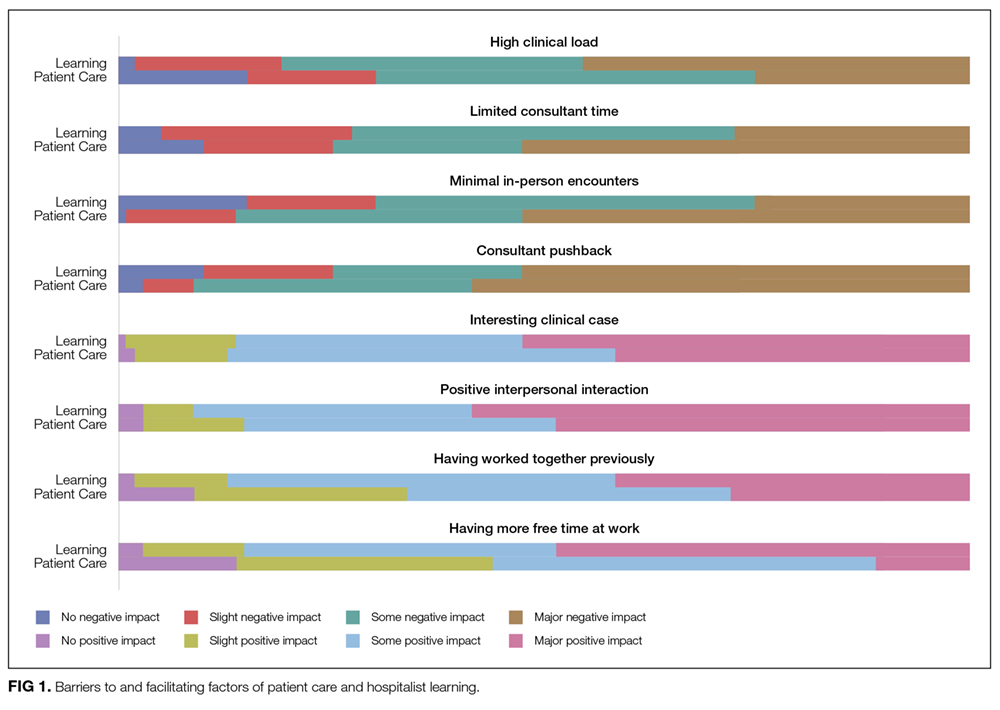
Participants reported that multiple factors affected patient care and their own learning during inpatient consultation (Figure 1). Consultant pushback, high hospitalist clinical workload, a perception that consultants had limited time, and minimal in-person interactions were all seen as factors that negatively affected the consult interaction. These generally affected both learning and patient care. Conversely, working on an interesting clinical case, more hospitalist free time, positive interaction with the consultant, and having previously worked with the consultant positively affected both learning and patient care (Figure 1).
Fellow Versus Attending Interactions
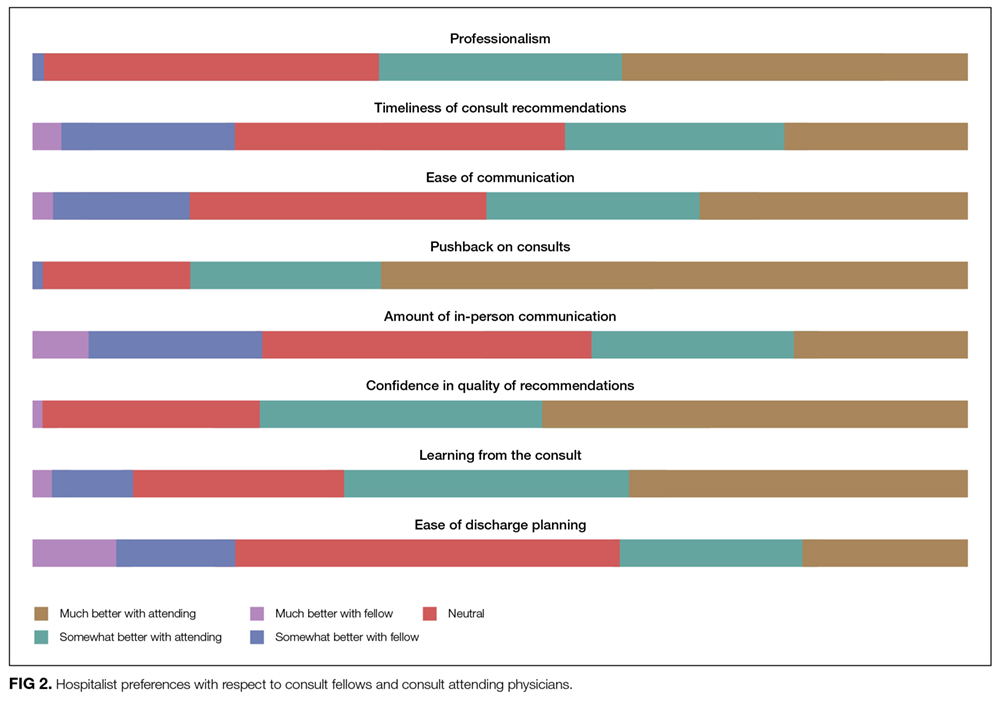
Respondents indicated that interacting directly with the consult attending was superior to hospitalist–fellow interactions in all aspects of care but particularly with respect to pushback, confidence in recommendations, professionalism, and hospitalist learning (Figure 2).
DISCUSSION
To our knowledge, this is the first study to describe hospitalist attending practices, attitudes, and perceptions of internal medicine subspecialty consultation. Our findings, which focus on the interaction between hospitalists and internal medicine subspecialty attendings and fellows, outline the hospitalist perspective on consultant interactions and identify a number of factors that are amenable to intervention. We found that hospitalists perceive the consult interaction to be important for patient care and a valuable opportunity for their own learning. In-person communication was seen as an important component of effective consultation but was reported to occur in a minority of consultations. We demonstrate that hospitalist–subspecialty attending consult interactions are perceived more positively than hospitalist–fellow interactions. Finally, we describe barriers and facilitating factors that may inform future interventions targeting this important interaction.
Effective communication between consultants and the primary team is critical for both patient care and teaching interactions.4-7 Pushback on consultation was reported to be the most significant barrier to hospitalist learning and had a major impact on patient care. Because hospitalists are attending physicians, we hypothesized that they may perceive pushback from fellows less frequently than residents.4 However, in our study, hospitalists reported pushback to be relatively frequent in their daily practice. Moreover, hospitalists reported a strong preference for in-person interactions with consultants, but our study demonstrated that such interactions are relatively infrequent. Researchers in studies of resident–fellow consult interactions have noted similar findings, suggesting that hospitalists and internal medicine residents face similar challenges during consultation.4-6 Hospitalists reported that positive interpersonal interactions and personal familiarity with the consultant positively affected the consult interaction. Most importantly, these effects were perceived to affect both hospitalist learning and patient care, suggesting the importance of interpersonal interactions in consultative medicine.
In an era of increasing clinical workload, the consult interaction represents an important workplace-based learning opportunity.4 Centered on a consult question, the hospitalist–consultant interaction embodies a teachable moment and can be an efficient opportunity to learn because both parties are familiar with the patient. Indeed, survey respondents reported that they frequently learned from consultation, and there was a strong preference for more teaching from consultants in this setting. However, the hospitalist–fellow consult interaction is unique because attending hospitalists are frequently communicating with fellow trainees, which could limit fellows’ confidence in their role as teachers and hospitalists’ perception of their role as learners. Our study identifies a number of barriers and facilitating factors (including communication, pushback, familiarity, and clinical workload) that affect the hospitalist–consultant teaching interaction and may be amenable to intervention.
Hospitalists expressed a consistent preference for interacting with attending subspecialists compared to clinical fellows during consultation. Preference for interaction with attendings was strongest in the areas of pushback, confidence in recommendations, professionalism, and learning from consultation. Some of the factors that relate to consult service structure and fellow experience, such as timeliness of consultation and confidence in recommendations, may not be amenable to intervention. For instance, fellows must first see and then staff the consult with their attending prior to leaving formal recommendations, which makes their communication less timely than that of attending physicians, when they are the primary consultant. However, aspects of the hospitalist–consultant interaction (such as professionalism, ease of communication, and pushback) should not be affected by the difference in experience between fellows and attending physicians. The reasons for such perceptions deserve further exploration; however, differences in incentive structures, workload, and communication skills between fellows and attending consultants may be potential explanations.
Our findings suggest that interventions aimed at enhancing hospitalist–consultant interactions focus on enhancing direct communication and teaching while limiting the perception of pushback. A number of interventions that are primarily focused on instituting a systematic approach to requesting consultation have shown an improvement in resident and medical student consult communication17,18 as well as resident–fellow teaching interactions.9 However, it is not clear whether these interventions would be effective given that hospitalists have more experience communicating with consultants than trainees. Given the unique nature of the hospitalist–consultant interaction, multiple barriers may need to be addressed in order to have a significant impact. Efforts to increase direct communication, such as a mechanism for hospitalists to make and request in-person or direct verbal communication about a particular consultation during the consult request, can help consultants prioritize direct communication with hospitalists for specific patients. Familiarizing fellows with hospitalist workflow and the locations of hospitalist workrooms also may promote in-person communication. Fellowship training can focus on enhancing fellow teaching and communication skills,19-22 particularly as they relate to hospitalists. Fellows in particular may benefit because the hospitalist–fellow teaching interaction may be bidirectional, with hospitalists having expertise in systems practice and quality efforts that can inform fellows’ practice. Furthermore, interacting with hospitalists is an opportunity for fellows to practice professional interactions, which will be critical to their careers. Increasing familiarity between fellows and hospitalists through joint events may also serve to enhance the interaction. Finally, enabling hospitalists to provide feedback to fellows stands to benefit both parties because multisource feedback is an important tool in assessing trainee competence and improving performance.23 However, we should note that because our study focused on hospitalist perceptions, an exploration of subspecialty fellows’ and attendings’ perceptions of the hospitalist–consultant interaction would provide additional, important data for shaping interventions.
Strengths of our study include the inclusion of multiple study sites, which may increase generalizability; however, our study has several limitations. The incomplete response rate reduces both generalizability and statistical power and may have created selection or nonresponder bias. However, low response rates occur commonly when surveying medical professionals, and our results are consistent with many prior hospitalist survey studies.24-26 Further, we conducted our study at a single time point; therefore, we could not evaluate the effect of fellow experience on hospitalist perceptions. However, we conducted our study in the second half of the academic year, when fellows had already gained considerable experience in the consultation setting. We did not capture participants’ institutional affiliations; therefore, a subgroup analysis by institution could not be performed. Additionally, our study reflects hospitalist perception rather than objectively measured communication practices between hospitalists and consultants, and it does not include the perspective of subspecialists. The specific needs of nurse practitioners and physicians’ assistants, who were excluded from this study, should also be evaluated in future research. Lastly, this is a hypothesis-generating study and should be replicated in a national cohort.
CONCLUSION
The hospitalists represented in our sample population perceived the consult interaction to be important for patient care and a valuable opportunity for their own learning. Participants expressed that they would like to increase direct communication with consultants and enhance consultant–hospitalist teaching interactions. Multiple barriers to effective hospitalist–consultant interactions (including communication, pushback, and hospitalist–consultant familiarity) are amenable to intervention.
Disclosure
The authors have no financial disclosures or conflicts of interest.
1. Kravolec PD, Miller JA, Wellikson L, Huddleston JM. The status of hospital medicine groups in the United States. J Hosp Med.2006;1(2):75-80. PubMed
2. Cai Q, Bruno CJ, Hagedorn CH, Desbiens NA. Temporal trends over ten years in formal inpatient gastroenterology consultations at an inner-city hospital. J Clin Gastroenterol. 2003;36(1):34-38. PubMed
3. Ta K, Gardner GC. Evaluation of the activity of an academic rheumatology consult service over 10 years: using data to shape curriculum. J Rheumatol. 2007;34(3):563-566. PubMed
4. Miloslavsky EM, McSparron JI, Richards JB, Puig A, Sullivan AM. Teaching during consultation: factors affecting the resident-fellow teaching interaction. Med Educ. 2015;49(7):717-730. PubMed
5. Chan T, Sabir K, Sanhan S, Sherbino J. Understanding the impact of residents’ interpersonal relationships during emergency department referrals and consultations. J Grad Med Educ. 2013;5(4):576-581. PubMed
6. Chan T, Bakewell F, Orlich D, Sherbino J. Conflict prevention, conflict mitigation, and manifestations of conflict during emergency department consultations. Acad Emerg Med. 2014;21(3):308-313. PubMed
7. Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755. PubMed
8. Adams T. Barriers to hospitalist fellow interactions. Med Educ. 2016;50(3):370. PubMed
9. Gupta S, Alladina J, Heaton K, Miloslavsky E. A randomized trial of an intervention to improve resident-fellow teaching interaction on the wards. BMC Med Educ. 2016;16(1):276. PubMed
10. Day LW, Cello JP, Madden E, Segal M. Prospective assessment of inpatient gastrointestinal consultation requests in an academic teaching hospital. Am J Gastroenterol. 2010;105(3):484-489. PubMed
11. Kessler C, Kutka BM, Badillo C. Consultation in the emergency department: a qualitative analysis and review. J Emerg Med. 2012;42(6):704-711. PubMed
12. Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275. PubMed
13. Muzin LJ. Understanding the process of medical referral: part 1: critique of the literature. Can Fam Physician. 1991;37:2155-2161. PubMed
14. Muzin LJ. Understanding the process of medical referral: part 5: communication. Can Fam Physician. 1992;38:301-307. PubMed
15. Wadhwa A, Lingard L. A qualitative study examining tensions in interdoctor telephone consultations. Med Educ. 2006;40(8):759-767. PubMed
16. Grant IN, Dixon AS. “Thank you for seeing this patient”: studying the quality of communication between physicians. Can Fam Physician. 1987;33:605-611. PubMed
17. Kessler CS, Afshar Y, Sardar G, Yudkowsky R, Ankel F, Schwartz A. A prospective, randomized, controlled study demonstrating a novel, effective model of transfer of care between physicians: the 5 Cs of consultation. Acad Emerg Med. 2012;19(8):968-974. PubMed
18. Podolsky A, Stern DTP. The courteous consult: a CONSULT card and training to improve resident consults. J Grad Med Educ. 2015;7(1):113-117. PubMed
19. Tofil NM, Peterson DT, Harrington KF, et al. A novel iterative-learner simulation model: fellows as teachers. J. Grad. Med. Educ. 2014;6(1):127-132. PubMed
20. Kempainen RR, Hallstrand TS, Culver BH, Tonelli MR. Fellows as teachers: the teacher-assistant experience during pulmonary subspecialty training. Chest. 2005;128(1):401-406. PubMed
21. Backes CH, Reber KM, Trittmann JK, et al. Fellows as teachers: a model to enhance pediatric resident education. Med. Educ. Online. 2011;16:7205. PubMed
22. Miloslavsky EM, Degnan K, McNeill J, McSparron JI. Use of Fellow as Clinical Teacher (FACT) Curriculum for Teaching During Consultation: Effect on Subspecialty Fellow Teaching Skills. J Grad Med Educ. 2017;9(3):345-350 PubMed
23. Donnon T, Al Ansari A, Al Alawi S, Violato C. The reliability, validity, and feasibility of multisource feedback physician assessment: a systematic review. Acad. Med. 2014;89(3):511-516. PubMed
24. Monash B, Najafi N, Mourad M, et al. Standardized attending rounds to improve the patient experience: A pragmatic cluster randomized controlled trial. J Hosp Med. 2017;12(3):143-149. PubMed
25. Allen-Dicker J, Auerbach A, Herzig SJ. Perceived safety and value of inpatient “very important person” services. J Hosp Med. 2017;12(3):177-179. PubMed
26. Do D, Munchhof AM, Terry C, Emmett T, Kara A. Research and publication trends in hospital medicine. J Hosp Med. 2014;9(3):148-154. PubMed
Hospitalist physicians care for an increasing proportion of general medicine inpatients and request a significant share of all subspecialty consultations.1 Subspecialty consultation in inpatient care is increasing,2,3 and effective hospitalist–consulting service interactions may affect team communication, patient care, and hospitalist learning. Therefore, enhancing hospitalist–consulting service interactions may have a broad-reaching, positive impact. Researchers in previous studies have explored resident–fellow consult interactions in the inpatient and emergency department settings as well as attending-to-attending consultation in the outpatient setting.4-7 However, to our knowledge, hospitalist–consulting team interactions have not been previously described. In academic medical centers, hospitalists are attending physicians who interact with both fellows (supervised by attending consultants) and directly with subspecialty attendings. Therefore, the exploration of the hospitalist–consultant interaction requires an evaluation of hospitalist–fellow and hospitalist–subspecialty attending interactions. The hospitalist–fellow interaction in particular is unique because it represents an unusual dynamic, in which an attending physician is primarily communicating with a trainee when requesting assistance with patient care.8 In order to explore hospitalist–consultant interactions (herein, the term “consultant” includes both fellow and attending consultants), we conducted a survey study in which we examine hospitalist practices and attitudes regarding consultation, with a specific focus on hospitalist consultation with internal medicine subspecialty consult services. In addition, we compared fellow–hospitalist and attending–hospitalist interactions and explored barriers to and facilitating factors of an effective hospitalist–consultant relationship.
METHODS
Survey Development
The survey instrument was developed by the authors based on findings of prior studies in which researchers examined consultation.2-6,9-16 The survey contained 31 questions (supplementary Appendix A) and evaluated 4 domains of the use of medical subspecialty consultation in direct patient care: (1) current consultation practices, (2) preferences regarding consultants, (3) barriers to and facilitating factors of effective consultation (both with respect to hospitalist learning and patient care), and (4) a comparison between hospitalist–fellow and hospitalist–subspecialty attending interactions. An evaluation of current consultation practices included a focus on communication methods (eg, in person, over the phone, through paging, or notes) because these have been found to be important during consultation.5,6,9,15,16 In order to explore hospitalist preferences regarding consult interactions and investigate perceptions of barriers to and facilitating factors of effective consultation, questions were developed based on previous literature, including our qualitative work examining resident–fellow interactions during consultation.4-6,9,12 We compared hospitalist consultation experiences among attending and fellow consultants because the interaction in which an attending hospitalist physician is primarily communicating with a trainee may differ from a consultation between a hospitalist attending and a subspecialty attending.8 Participants were asked to exclude their experiences when working on teaching services, during which students or housestaff often interact with consultants. The survey was cognitively tested with both hospitalist and non-hospitalist attending physicians not participating in the study and was revised by the authors using an iterative approach.
Study Participants
Hospitalist attending physicians at University of Texas Southwestern (UTSW) Medical Center, Emory University School of Medicine, Massachusetts General Hospital (MGH), and the Medical University of South Carolina (MUSC) were eligible to participate in the study. Consult team structures at each institution were composed of either a subspecialist-attending-only or a fellow-and-subspecialty-attending team. Fellows at all institutions are supervised by a subspecialty attending when performing consultations. Respondents who self-identified as nurse practitioners or physician assistants were excluded from the analysis. Hospitalists employed by the Veterans Affairs hospital system were also excluded. The study was approved by the institutional review boards of UTSW, Emory, MUSC, and MGH.
The survey was anonymous and administered to all hospitalists at participating institutions via a web-based survey tool (Qualtrics, Provo, UT). Participants were eligible to enter a raffle for a $500 gift card, and completion of the survey was not required for entry into the raffle.
Statistics
Results were summarized using the mean with standard deviation for continuous variables and the frequency with percentage for categorical variables after excluding missing values. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC). A 2-sided P value of ≤0.05 was considered statistically significant.
RESULTS
Current Consultation Practices
Current consultation practices and descriptions of hospitalist–consultant communication are shown in Table 2. Forty percent of respondents requested 0-1 consults per day, while 51.7% requested 2-3 per day. The most common reasons for requesting a consultation were assistance with treatment (48.5%), assistance with diagnosis (25.7%), and request for a procedure (21.8%). When asked whether the frequency of consultation is changing, slightly more hospitalists felt that their personal use of consultation was increasing as compared to those who felt that it was decreasing (38.5% vs 30.3%, respectively).
Hospitalist Preferences
Eighty-six percent of respondents agreed that consultants should be required to communicate their recommendations either in person or over the phone. Eighty-three percent of hospitalists agreed that they would like to receive more teaching from the consulting services, and 74.0% agreed that consultants should attempt to teach hospitalists during consult interactions regardless of whether the hospitalist initiates the teaching–learning interaction.
Barriers to and Facilitating Factors of Effective Consultation
Participants reported that multiple factors affected patient care and their own learning during inpatient consultation (Figure 1). Consultant pushback, high hospitalist clinical workload, a perception that consultants had limited time, and minimal in-person interactions were all seen as factors that negatively affected the consult interaction. These generally affected both learning and patient care. Conversely, working on an interesting clinical case, more hospitalist free time, positive interaction with the consultant, and having previously worked with the consultant positively affected both learning and patient care (Figure 1).
Fellow Versus Attending Interactions
Respondents indicated that interacting directly with the consult attending was superior to hospitalist–fellow interactions in all aspects of care but particularly with respect to pushback, confidence in recommendations, professionalism, and hospitalist learning (Figure 2).
DISCUSSION
To our knowledge, this is the first study to describe hospitalist attending practices, attitudes, and perceptions of internal medicine subspecialty consultation. Our findings, which focus on the interaction between hospitalists and internal medicine subspecialty attendings and fellows, outline the hospitalist perspective on consultant interactions and identify a number of factors that are amenable to intervention. We found that hospitalists perceive the consult interaction to be important for patient care and a valuable opportunity for their own learning. In-person communication was seen as an important component of effective consultation but was reported to occur in a minority of consultations. We demonstrate that hospitalist–subspecialty attending consult interactions are perceived more positively than hospitalist–fellow interactions. Finally, we describe barriers and facilitating factors that may inform future interventions targeting this important interaction.
Effective communication between consultants and the primary team is critical for both patient care and teaching interactions.4-7 Pushback on consultation was reported to be the most significant barrier to hospitalist learning and had a major impact on patient care. Because hospitalists are attending physicians, we hypothesized that they may perceive pushback from fellows less frequently than residents.4 However, in our study, hospitalists reported pushback to be relatively frequent in their daily practice. Moreover, hospitalists reported a strong preference for in-person interactions with consultants, but our study demonstrated that such interactions are relatively infrequent. Researchers in studies of resident–fellow consult interactions have noted similar findings, suggesting that hospitalists and internal medicine residents face similar challenges during consultation.4-6 Hospitalists reported that positive interpersonal interactions and personal familiarity with the consultant positively affected the consult interaction. Most importantly, these effects were perceived to affect both hospitalist learning and patient care, suggesting the importance of interpersonal interactions in consultative medicine.
In an era of increasing clinical workload, the consult interaction represents an important workplace-based learning opportunity.4 Centered on a consult question, the hospitalist–consultant interaction embodies a teachable moment and can be an efficient opportunity to learn because both parties are familiar with the patient. Indeed, survey respondents reported that they frequently learned from consultation, and there was a strong preference for more teaching from consultants in this setting. However, the hospitalist–fellow consult interaction is unique because attending hospitalists are frequently communicating with fellow trainees, which could limit fellows’ confidence in their role as teachers and hospitalists’ perception of their role as learners. Our study identifies a number of barriers and facilitating factors (including communication, pushback, familiarity, and clinical workload) that affect the hospitalist–consultant teaching interaction and may be amenable to intervention.
Hospitalists expressed a consistent preference for interacting with attending subspecialists compared to clinical fellows during consultation. Preference for interaction with attendings was strongest in the areas of pushback, confidence in recommendations, professionalism, and learning from consultation. Some of the factors that relate to consult service structure and fellow experience, such as timeliness of consultation and confidence in recommendations, may not be amenable to intervention. For instance, fellows must first see and then staff the consult with their attending prior to leaving formal recommendations, which makes their communication less timely than that of attending physicians, when they are the primary consultant. However, aspects of the hospitalist–consultant interaction (such as professionalism, ease of communication, and pushback) should not be affected by the difference in experience between fellows and attending physicians. The reasons for such perceptions deserve further exploration; however, differences in incentive structures, workload, and communication skills between fellows and attending consultants may be potential explanations.
Our findings suggest that interventions aimed at enhancing hospitalist–consultant interactions focus on enhancing direct communication and teaching while limiting the perception of pushback. A number of interventions that are primarily focused on instituting a systematic approach to requesting consultation have shown an improvement in resident and medical student consult communication17,18 as well as resident–fellow teaching interactions.9 However, it is not clear whether these interventions would be effective given that hospitalists have more experience communicating with consultants than trainees. Given the unique nature of the hospitalist–consultant interaction, multiple barriers may need to be addressed in order to have a significant impact. Efforts to increase direct communication, such as a mechanism for hospitalists to make and request in-person or direct verbal communication about a particular consultation during the consult request, can help consultants prioritize direct communication with hospitalists for specific patients. Familiarizing fellows with hospitalist workflow and the locations of hospitalist workrooms also may promote in-person communication. Fellowship training can focus on enhancing fellow teaching and communication skills,19-22 particularly as they relate to hospitalists. Fellows in particular may benefit because the hospitalist–fellow teaching interaction may be bidirectional, with hospitalists having expertise in systems practice and quality efforts that can inform fellows’ practice. Furthermore, interacting with hospitalists is an opportunity for fellows to practice professional interactions, which will be critical to their careers. Increasing familiarity between fellows and hospitalists through joint events may also serve to enhance the interaction. Finally, enabling hospitalists to provide feedback to fellows stands to benefit both parties because multisource feedback is an important tool in assessing trainee competence and improving performance.23 However, we should note that because our study focused on hospitalist perceptions, an exploration of subspecialty fellows’ and attendings’ perceptions of the hospitalist–consultant interaction would provide additional, important data for shaping interventions.
Strengths of our study include the inclusion of multiple study sites, which may increase generalizability; however, our study has several limitations. The incomplete response rate reduces both generalizability and statistical power and may have created selection or nonresponder bias. However, low response rates occur commonly when surveying medical professionals, and our results are consistent with many prior hospitalist survey studies.24-26 Further, we conducted our study at a single time point; therefore, we could not evaluate the effect of fellow experience on hospitalist perceptions. However, we conducted our study in the second half of the academic year, when fellows had already gained considerable experience in the consultation setting. We did not capture participants’ institutional affiliations; therefore, a subgroup analysis by institution could not be performed. Additionally, our study reflects hospitalist perception rather than objectively measured communication practices between hospitalists and consultants, and it does not include the perspective of subspecialists. The specific needs of nurse practitioners and physicians’ assistants, who were excluded from this study, should also be evaluated in future research. Lastly, this is a hypothesis-generating study and should be replicated in a national cohort.
CONCLUSION
The hospitalists represented in our sample population perceived the consult interaction to be important for patient care and a valuable opportunity for their own learning. Participants expressed that they would like to increase direct communication with consultants and enhance consultant–hospitalist teaching interactions. Multiple barriers to effective hospitalist–consultant interactions (including communication, pushback, and hospitalist–consultant familiarity) are amenable to intervention.
Disclosure
The authors have no financial disclosures or conflicts of interest.
Hospitalist physicians care for an increasing proportion of general medicine inpatients and request a significant share of all subspecialty consultations.1 Subspecialty consultation in inpatient care is increasing,2,3 and effective hospitalist–consulting service interactions may affect team communication, patient care, and hospitalist learning. Therefore, enhancing hospitalist–consulting service interactions may have a broad-reaching, positive impact. Researchers in previous studies have explored resident–fellow consult interactions in the inpatient and emergency department settings as well as attending-to-attending consultation in the outpatient setting.4-7 However, to our knowledge, hospitalist–consulting team interactions have not been previously described. In academic medical centers, hospitalists are attending physicians who interact with both fellows (supervised by attending consultants) and directly with subspecialty attendings. Therefore, the exploration of the hospitalist–consultant interaction requires an evaluation of hospitalist–fellow and hospitalist–subspecialty attending interactions. The hospitalist–fellow interaction in particular is unique because it represents an unusual dynamic, in which an attending physician is primarily communicating with a trainee when requesting assistance with patient care.8 In order to explore hospitalist–consultant interactions (herein, the term “consultant” includes both fellow and attending consultants), we conducted a survey study in which we examine hospitalist practices and attitudes regarding consultation, with a specific focus on hospitalist consultation with internal medicine subspecialty consult services. In addition, we compared fellow–hospitalist and attending–hospitalist interactions and explored barriers to and facilitating factors of an effective hospitalist–consultant relationship.
METHODS
Survey Development
The survey instrument was developed by the authors based on findings of prior studies in which researchers examined consultation.2-6,9-16 The survey contained 31 questions (supplementary Appendix A) and evaluated 4 domains of the use of medical subspecialty consultation in direct patient care: (1) current consultation practices, (2) preferences regarding consultants, (3) barriers to and facilitating factors of effective consultation (both with respect to hospitalist learning and patient care), and (4) a comparison between hospitalist–fellow and hospitalist–subspecialty attending interactions. An evaluation of current consultation practices included a focus on communication methods (eg, in person, over the phone, through paging, or notes) because these have been found to be important during consultation.5,6,9,15,16 In order to explore hospitalist preferences regarding consult interactions and investigate perceptions of barriers to and facilitating factors of effective consultation, questions were developed based on previous literature, including our qualitative work examining resident–fellow interactions during consultation.4-6,9,12 We compared hospitalist consultation experiences among attending and fellow consultants because the interaction in which an attending hospitalist physician is primarily communicating with a trainee may differ from a consultation between a hospitalist attending and a subspecialty attending.8 Participants were asked to exclude their experiences when working on teaching services, during which students or housestaff often interact with consultants. The survey was cognitively tested with both hospitalist and non-hospitalist attending physicians not participating in the study and was revised by the authors using an iterative approach.
Study Participants
Hospitalist attending physicians at University of Texas Southwestern (UTSW) Medical Center, Emory University School of Medicine, Massachusetts General Hospital (MGH), and the Medical University of South Carolina (MUSC) were eligible to participate in the study. Consult team structures at each institution were composed of either a subspecialist-attending-only or a fellow-and-subspecialty-attending team. Fellows at all institutions are supervised by a subspecialty attending when performing consultations. Respondents who self-identified as nurse practitioners or physician assistants were excluded from the analysis. Hospitalists employed by the Veterans Affairs hospital system were also excluded. The study was approved by the institutional review boards of UTSW, Emory, MUSC, and MGH.
The survey was anonymous and administered to all hospitalists at participating institutions via a web-based survey tool (Qualtrics, Provo, UT). Participants were eligible to enter a raffle for a $500 gift card, and completion of the survey was not required for entry into the raffle.
Statistics
Results were summarized using the mean with standard deviation for continuous variables and the frequency with percentage for categorical variables after excluding missing values. All analyses were conducted using SAS version 9.4 (SAS Institute, Cary, NC). A 2-sided P value of ≤0.05 was considered statistically significant.
RESULTS
Current Consultation Practices
Current consultation practices and descriptions of hospitalist–consultant communication are shown in Table 2. Forty percent of respondents requested 0-1 consults per day, while 51.7% requested 2-3 per day. The most common reasons for requesting a consultation were assistance with treatment (48.5%), assistance with diagnosis (25.7%), and request for a procedure (21.8%). When asked whether the frequency of consultation is changing, slightly more hospitalists felt that their personal use of consultation was increasing as compared to those who felt that it was decreasing (38.5% vs 30.3%, respectively).
Hospitalist Preferences
Eighty-six percent of respondents agreed that consultants should be required to communicate their recommendations either in person or over the phone. Eighty-three percent of hospitalists agreed that they would like to receive more teaching from the consulting services, and 74.0% agreed that consultants should attempt to teach hospitalists during consult interactions regardless of whether the hospitalist initiates the teaching–learning interaction.
Barriers to and Facilitating Factors of Effective Consultation
Participants reported that multiple factors affected patient care and their own learning during inpatient consultation (Figure 1). Consultant pushback, high hospitalist clinical workload, a perception that consultants had limited time, and minimal in-person interactions were all seen as factors that negatively affected the consult interaction. These generally affected both learning and patient care. Conversely, working on an interesting clinical case, more hospitalist free time, positive interaction with the consultant, and having previously worked with the consultant positively affected both learning and patient care (Figure 1).
Fellow Versus Attending Interactions
Respondents indicated that interacting directly with the consult attending was superior to hospitalist–fellow interactions in all aspects of care but particularly with respect to pushback, confidence in recommendations, professionalism, and hospitalist learning (Figure 2).
DISCUSSION
To our knowledge, this is the first study to describe hospitalist attending practices, attitudes, and perceptions of internal medicine subspecialty consultation. Our findings, which focus on the interaction between hospitalists and internal medicine subspecialty attendings and fellows, outline the hospitalist perspective on consultant interactions and identify a number of factors that are amenable to intervention. We found that hospitalists perceive the consult interaction to be important for patient care and a valuable opportunity for their own learning. In-person communication was seen as an important component of effective consultation but was reported to occur in a minority of consultations. We demonstrate that hospitalist–subspecialty attending consult interactions are perceived more positively than hospitalist–fellow interactions. Finally, we describe barriers and facilitating factors that may inform future interventions targeting this important interaction.
Effective communication between consultants and the primary team is critical for both patient care and teaching interactions.4-7 Pushback on consultation was reported to be the most significant barrier to hospitalist learning and had a major impact on patient care. Because hospitalists are attending physicians, we hypothesized that they may perceive pushback from fellows less frequently than residents.4 However, in our study, hospitalists reported pushback to be relatively frequent in their daily practice. Moreover, hospitalists reported a strong preference for in-person interactions with consultants, but our study demonstrated that such interactions are relatively infrequent. Researchers in studies of resident–fellow consult interactions have noted similar findings, suggesting that hospitalists and internal medicine residents face similar challenges during consultation.4-6 Hospitalists reported that positive interpersonal interactions and personal familiarity with the consultant positively affected the consult interaction. Most importantly, these effects were perceived to affect both hospitalist learning and patient care, suggesting the importance of interpersonal interactions in consultative medicine.
In an era of increasing clinical workload, the consult interaction represents an important workplace-based learning opportunity.4 Centered on a consult question, the hospitalist–consultant interaction embodies a teachable moment and can be an efficient opportunity to learn because both parties are familiar with the patient. Indeed, survey respondents reported that they frequently learned from consultation, and there was a strong preference for more teaching from consultants in this setting. However, the hospitalist–fellow consult interaction is unique because attending hospitalists are frequently communicating with fellow trainees, which could limit fellows’ confidence in their role as teachers and hospitalists’ perception of their role as learners. Our study identifies a number of barriers and facilitating factors (including communication, pushback, familiarity, and clinical workload) that affect the hospitalist–consultant teaching interaction and may be amenable to intervention.
Hospitalists expressed a consistent preference for interacting with attending subspecialists compared to clinical fellows during consultation. Preference for interaction with attendings was strongest in the areas of pushback, confidence in recommendations, professionalism, and learning from consultation. Some of the factors that relate to consult service structure and fellow experience, such as timeliness of consultation and confidence in recommendations, may not be amenable to intervention. For instance, fellows must first see and then staff the consult with their attending prior to leaving formal recommendations, which makes their communication less timely than that of attending physicians, when they are the primary consultant. However, aspects of the hospitalist–consultant interaction (such as professionalism, ease of communication, and pushback) should not be affected by the difference in experience between fellows and attending physicians. The reasons for such perceptions deserve further exploration; however, differences in incentive structures, workload, and communication skills between fellows and attending consultants may be potential explanations.
Our findings suggest that interventions aimed at enhancing hospitalist–consultant interactions focus on enhancing direct communication and teaching while limiting the perception of pushback. A number of interventions that are primarily focused on instituting a systematic approach to requesting consultation have shown an improvement in resident and medical student consult communication17,18 as well as resident–fellow teaching interactions.9 However, it is not clear whether these interventions would be effective given that hospitalists have more experience communicating with consultants than trainees. Given the unique nature of the hospitalist–consultant interaction, multiple barriers may need to be addressed in order to have a significant impact. Efforts to increase direct communication, such as a mechanism for hospitalists to make and request in-person or direct verbal communication about a particular consultation during the consult request, can help consultants prioritize direct communication with hospitalists for specific patients. Familiarizing fellows with hospitalist workflow and the locations of hospitalist workrooms also may promote in-person communication. Fellowship training can focus on enhancing fellow teaching and communication skills,19-22 particularly as they relate to hospitalists. Fellows in particular may benefit because the hospitalist–fellow teaching interaction may be bidirectional, with hospitalists having expertise in systems practice and quality efforts that can inform fellows’ practice. Furthermore, interacting with hospitalists is an opportunity for fellows to practice professional interactions, which will be critical to their careers. Increasing familiarity between fellows and hospitalists through joint events may also serve to enhance the interaction. Finally, enabling hospitalists to provide feedback to fellows stands to benefit both parties because multisource feedback is an important tool in assessing trainee competence and improving performance.23 However, we should note that because our study focused on hospitalist perceptions, an exploration of subspecialty fellows’ and attendings’ perceptions of the hospitalist–consultant interaction would provide additional, important data for shaping interventions.
Strengths of our study include the inclusion of multiple study sites, which may increase generalizability; however, our study has several limitations. The incomplete response rate reduces both generalizability and statistical power and may have created selection or nonresponder bias. However, low response rates occur commonly when surveying medical professionals, and our results are consistent with many prior hospitalist survey studies.24-26 Further, we conducted our study at a single time point; therefore, we could not evaluate the effect of fellow experience on hospitalist perceptions. However, we conducted our study in the second half of the academic year, when fellows had already gained considerable experience in the consultation setting. We did not capture participants’ institutional affiliations; therefore, a subgroup analysis by institution could not be performed. Additionally, our study reflects hospitalist perception rather than objectively measured communication practices between hospitalists and consultants, and it does not include the perspective of subspecialists. The specific needs of nurse practitioners and physicians’ assistants, who were excluded from this study, should also be evaluated in future research. Lastly, this is a hypothesis-generating study and should be replicated in a national cohort.
CONCLUSION
The hospitalists represented in our sample population perceived the consult interaction to be important for patient care and a valuable opportunity for their own learning. Participants expressed that they would like to increase direct communication with consultants and enhance consultant–hospitalist teaching interactions. Multiple barriers to effective hospitalist–consultant interactions (including communication, pushback, and hospitalist–consultant familiarity) are amenable to intervention.
Disclosure
The authors have no financial disclosures or conflicts of interest.
1. Kravolec PD, Miller JA, Wellikson L, Huddleston JM. The status of hospital medicine groups in the United States. J Hosp Med.2006;1(2):75-80. PubMed
2. Cai Q, Bruno CJ, Hagedorn CH, Desbiens NA. Temporal trends over ten years in formal inpatient gastroenterology consultations at an inner-city hospital. J Clin Gastroenterol. 2003;36(1):34-38. PubMed
3. Ta K, Gardner GC. Evaluation of the activity of an academic rheumatology consult service over 10 years: using data to shape curriculum. J Rheumatol. 2007;34(3):563-566. PubMed
4. Miloslavsky EM, McSparron JI, Richards JB, Puig A, Sullivan AM. Teaching during consultation: factors affecting the resident-fellow teaching interaction. Med Educ. 2015;49(7):717-730. PubMed
5. Chan T, Sabir K, Sanhan S, Sherbino J. Understanding the impact of residents’ interpersonal relationships during emergency department referrals and consultations. J Grad Med Educ. 2013;5(4):576-581. PubMed
6. Chan T, Bakewell F, Orlich D, Sherbino J. Conflict prevention, conflict mitigation, and manifestations of conflict during emergency department consultations. Acad Emerg Med. 2014;21(3):308-313. PubMed
7. Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755. PubMed
8. Adams T. Barriers to hospitalist fellow interactions. Med Educ. 2016;50(3):370. PubMed
9. Gupta S, Alladina J, Heaton K, Miloslavsky E. A randomized trial of an intervention to improve resident-fellow teaching interaction on the wards. BMC Med Educ. 2016;16(1):276. PubMed
10. Day LW, Cello JP, Madden E, Segal M. Prospective assessment of inpatient gastrointestinal consultation requests in an academic teaching hospital. Am J Gastroenterol. 2010;105(3):484-489. PubMed
11. Kessler C, Kutka BM, Badillo C. Consultation in the emergency department: a qualitative analysis and review. J Emerg Med. 2012;42(6):704-711. PubMed
12. Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275. PubMed
13. Muzin LJ. Understanding the process of medical referral: part 1: critique of the literature. Can Fam Physician. 1991;37:2155-2161. PubMed
14. Muzin LJ. Understanding the process of medical referral: part 5: communication. Can Fam Physician. 1992;38:301-307. PubMed
15. Wadhwa A, Lingard L. A qualitative study examining tensions in interdoctor telephone consultations. Med Educ. 2006;40(8):759-767. PubMed
16. Grant IN, Dixon AS. “Thank you for seeing this patient”: studying the quality of communication between physicians. Can Fam Physician. 1987;33:605-611. PubMed
17. Kessler CS, Afshar Y, Sardar G, Yudkowsky R, Ankel F, Schwartz A. A prospective, randomized, controlled study demonstrating a novel, effective model of transfer of care between physicians: the 5 Cs of consultation. Acad Emerg Med. 2012;19(8):968-974. PubMed
18. Podolsky A, Stern DTP. The courteous consult: a CONSULT card and training to improve resident consults. J Grad Med Educ. 2015;7(1):113-117. PubMed
19. Tofil NM, Peterson DT, Harrington KF, et al. A novel iterative-learner simulation model: fellows as teachers. J. Grad. Med. Educ. 2014;6(1):127-132. PubMed
20. Kempainen RR, Hallstrand TS, Culver BH, Tonelli MR. Fellows as teachers: the teacher-assistant experience during pulmonary subspecialty training. Chest. 2005;128(1):401-406. PubMed
21. Backes CH, Reber KM, Trittmann JK, et al. Fellows as teachers: a model to enhance pediatric resident education. Med. Educ. Online. 2011;16:7205. PubMed
22. Miloslavsky EM, Degnan K, McNeill J, McSparron JI. Use of Fellow as Clinical Teacher (FACT) Curriculum for Teaching During Consultation: Effect on Subspecialty Fellow Teaching Skills. J Grad Med Educ. 2017;9(3):345-350 PubMed
23. Donnon T, Al Ansari A, Al Alawi S, Violato C. The reliability, validity, and feasibility of multisource feedback physician assessment: a systematic review. Acad. Med. 2014;89(3):511-516. PubMed
24. Monash B, Najafi N, Mourad M, et al. Standardized attending rounds to improve the patient experience: A pragmatic cluster randomized controlled trial. J Hosp Med. 2017;12(3):143-149. PubMed
25. Allen-Dicker J, Auerbach A, Herzig SJ. Perceived safety and value of inpatient “very important person” services. J Hosp Med. 2017;12(3):177-179. PubMed
26. Do D, Munchhof AM, Terry C, Emmett T, Kara A. Research and publication trends in hospital medicine. J Hosp Med. 2014;9(3):148-154. PubMed
1. Kravolec PD, Miller JA, Wellikson L, Huddleston JM. The status of hospital medicine groups in the United States. J Hosp Med.2006;1(2):75-80. PubMed
2. Cai Q, Bruno CJ, Hagedorn CH, Desbiens NA. Temporal trends over ten years in formal inpatient gastroenterology consultations at an inner-city hospital. J Clin Gastroenterol. 2003;36(1):34-38. PubMed
3. Ta K, Gardner GC. Evaluation of the activity of an academic rheumatology consult service over 10 years: using data to shape curriculum. J Rheumatol. 2007;34(3):563-566. PubMed
4. Miloslavsky EM, McSparron JI, Richards JB, Puig A, Sullivan AM. Teaching during consultation: factors affecting the resident-fellow teaching interaction. Med Educ. 2015;49(7):717-730. PubMed
5. Chan T, Sabir K, Sanhan S, Sherbino J. Understanding the impact of residents’ interpersonal relationships during emergency department referrals and consultations. J Grad Med Educ. 2013;5(4):576-581. PubMed
6. Chan T, Bakewell F, Orlich D, Sherbino J. Conflict prevention, conflict mitigation, and manifestations of conflict during emergency department consultations. Acad Emerg Med. 2014;21(3):308-313. PubMed
7. Goldman L, Lee T, Rudd P. Ten commandments for effective consultations. Arch Intern Med. 1983;143(9):1753-1755. PubMed
8. Adams T. Barriers to hospitalist fellow interactions. Med Educ. 2016;50(3):370. PubMed
9. Gupta S, Alladina J, Heaton K, Miloslavsky E. A randomized trial of an intervention to improve resident-fellow teaching interaction on the wards. BMC Med Educ. 2016;16(1):276. PubMed
10. Day LW, Cello JP, Madden E, Segal M. Prospective assessment of inpatient gastrointestinal consultation requests in an academic teaching hospital. Am J Gastroenterol. 2010;105(3):484-489. PubMed
11. Kessler C, Kutka BM, Badillo C. Consultation in the emergency department: a qualitative analysis and review. J Emerg Med. 2012;42(6):704-711. PubMed
12. Salerno SM, Hurst FP, Halvorson S, Mercado DL. Principles of effective consultation: an update for the 21st-century consultant. Arch Intern Med. 2007;167(3):271-275. PubMed
13. Muzin LJ. Understanding the process of medical referral: part 1: critique of the literature. Can Fam Physician. 1991;37:2155-2161. PubMed
14. Muzin LJ. Understanding the process of medical referral: part 5: communication. Can Fam Physician. 1992;38:301-307. PubMed
15. Wadhwa A, Lingard L. A qualitative study examining tensions in interdoctor telephone consultations. Med Educ. 2006;40(8):759-767. PubMed
16. Grant IN, Dixon AS. “Thank you for seeing this patient”: studying the quality of communication between physicians. Can Fam Physician. 1987;33:605-611. PubMed
17. Kessler CS, Afshar Y, Sardar G, Yudkowsky R, Ankel F, Schwartz A. A prospective, randomized, controlled study demonstrating a novel, effective model of transfer of care between physicians: the 5 Cs of consultation. Acad Emerg Med. 2012;19(8):968-974. PubMed
18. Podolsky A, Stern DTP. The courteous consult: a CONSULT card and training to improve resident consults. J Grad Med Educ. 2015;7(1):113-117. PubMed
19. Tofil NM, Peterson DT, Harrington KF, et al. A novel iterative-learner simulation model: fellows as teachers. J. Grad. Med. Educ. 2014;6(1):127-132. PubMed
20. Kempainen RR, Hallstrand TS, Culver BH, Tonelli MR. Fellows as teachers: the teacher-assistant experience during pulmonary subspecialty training. Chest. 2005;128(1):401-406. PubMed
21. Backes CH, Reber KM, Trittmann JK, et al. Fellows as teachers: a model to enhance pediatric resident education. Med. Educ. Online. 2011;16:7205. PubMed
22. Miloslavsky EM, Degnan K, McNeill J, McSparron JI. Use of Fellow as Clinical Teacher (FACT) Curriculum for Teaching During Consultation: Effect on Subspecialty Fellow Teaching Skills. J Grad Med Educ. 2017;9(3):345-350 PubMed
23. Donnon T, Al Ansari A, Al Alawi S, Violato C. The reliability, validity, and feasibility of multisource feedback physician assessment: a systematic review. Acad. Med. 2014;89(3):511-516. PubMed
24. Monash B, Najafi N, Mourad M, et al. Standardized attending rounds to improve the patient experience: A pragmatic cluster randomized controlled trial. J Hosp Med. 2017;12(3):143-149. PubMed
25. Allen-Dicker J, Auerbach A, Herzig SJ. Perceived safety and value of inpatient “very important person” services. J Hosp Med. 2017;12(3):177-179. PubMed
26. Do D, Munchhof AM, Terry C, Emmett T, Kara A. Research and publication trends in hospital medicine. J Hosp Med. 2014;9(3):148-154. PubMed
©2017 Society of Hospital Medicine
‘Untangling’ DNA Damage
“Imagine your DNA is a giant ball of yarn,” says Matthew Schellenberg, PhD. That is the metaphor he uses to help describe the findings of a study he conducted with other researchers from the NIH. They discovered how 2 proteins work together to “untangle” DNA damage known as a DNA-protein crosslink (DPC).
When DNA becomes tangled inside of cells, organisms use another protein called topoisomerase 2 (TOP2) to straighten things out, by cutting and “retying” individual threads. To do that, it first conceals the cut DNA ends within the core of the TOP2 protein, which allows it to then retie, or rejoin, the DNA ends. However, cancer drugs or environmental chemicals sometimes can block this retying ability, so the TOP2 remains stuck. That creates a stable environment for TOP2 and DPC, leading to an accumulation of severed DNA that kills cells.
Scott Williams, PhD, deputy chief of the Genome Integrity and Structural Biology Laboratory at the National Institute of Environmental Health Sciences, headed the team that identified ZATT as a new contributor to the process of removing DPCs. He uses another metaphor, likening the TOP2-DPCs to “ticking time bombs for cells.” The molecular charges are armed, Williams says, by TOP2’s interaction with environmental toxicants, chemical metabolites, tobacco exposures, or DNA damage caused by ultraviolet light.
While cancer drugs induce formation of TOP2-DPCs to treat cancer, TOP2-DPC lesions also can cause rearrangement of an organism’s genome that leads to cancer. If they are not removed, they trigger cell death. That led Williams and the research team to find out how DPCs are located and broken down. In his metaphor, the protein ZATT “is like a bomb-sniffing dog.” When it locates the target, it sounds an alarm to mobilize the recruitment of TOP2, which “cuts the red wire to disarm these threats.”
Schellenberg says, “We’ve discovered how we defend against this potent means of killing.” The knowledge may help researchers make drugs that kill cancer cells more effective.
“Imagine your DNA is a giant ball of yarn,” says Matthew Schellenberg, PhD. That is the metaphor he uses to help describe the findings of a study he conducted with other researchers from the NIH. They discovered how 2 proteins work together to “untangle” DNA damage known as a DNA-protein crosslink (DPC).
When DNA becomes tangled inside of cells, organisms use another protein called topoisomerase 2 (TOP2) to straighten things out, by cutting and “retying” individual threads. To do that, it first conceals the cut DNA ends within the core of the TOP2 protein, which allows it to then retie, or rejoin, the DNA ends. However, cancer drugs or environmental chemicals sometimes can block this retying ability, so the TOP2 remains stuck. That creates a stable environment for TOP2 and DPC, leading to an accumulation of severed DNA that kills cells.
Scott Williams, PhD, deputy chief of the Genome Integrity and Structural Biology Laboratory at the National Institute of Environmental Health Sciences, headed the team that identified ZATT as a new contributor to the process of removing DPCs. He uses another metaphor, likening the TOP2-DPCs to “ticking time bombs for cells.” The molecular charges are armed, Williams says, by TOP2’s interaction with environmental toxicants, chemical metabolites, tobacco exposures, or DNA damage caused by ultraviolet light.
While cancer drugs induce formation of TOP2-DPCs to treat cancer, TOP2-DPC lesions also can cause rearrangement of an organism’s genome that leads to cancer. If they are not removed, they trigger cell death. That led Williams and the research team to find out how DPCs are located and broken down. In his metaphor, the protein ZATT “is like a bomb-sniffing dog.” When it locates the target, it sounds an alarm to mobilize the recruitment of TOP2, which “cuts the red wire to disarm these threats.”
Schellenberg says, “We’ve discovered how we defend against this potent means of killing.” The knowledge may help researchers make drugs that kill cancer cells more effective.
“Imagine your DNA is a giant ball of yarn,” says Matthew Schellenberg, PhD. That is the metaphor he uses to help describe the findings of a study he conducted with other researchers from the NIH. They discovered how 2 proteins work together to “untangle” DNA damage known as a DNA-protein crosslink (DPC).
When DNA becomes tangled inside of cells, organisms use another protein called topoisomerase 2 (TOP2) to straighten things out, by cutting and “retying” individual threads. To do that, it first conceals the cut DNA ends within the core of the TOP2 protein, which allows it to then retie, or rejoin, the DNA ends. However, cancer drugs or environmental chemicals sometimes can block this retying ability, so the TOP2 remains stuck. That creates a stable environment for TOP2 and DPC, leading to an accumulation of severed DNA that kills cells.
Scott Williams, PhD, deputy chief of the Genome Integrity and Structural Biology Laboratory at the National Institute of Environmental Health Sciences, headed the team that identified ZATT as a new contributor to the process of removing DPCs. He uses another metaphor, likening the TOP2-DPCs to “ticking time bombs for cells.” The molecular charges are armed, Williams says, by TOP2’s interaction with environmental toxicants, chemical metabolites, tobacco exposures, or DNA damage caused by ultraviolet light.
While cancer drugs induce formation of TOP2-DPCs to treat cancer, TOP2-DPC lesions also can cause rearrangement of an organism’s genome that leads to cancer. If they are not removed, they trigger cell death. That led Williams and the research team to find out how DPCs are located and broken down. In his metaphor, the protein ZATT “is like a bomb-sniffing dog.” When it locates the target, it sounds an alarm to mobilize the recruitment of TOP2, which “cuts the red wire to disarm these threats.”
Schellenberg says, “We’ve discovered how we defend against this potent means of killing.” The knowledge may help researchers make drugs that kill cancer cells more effective.
Method identifies effective treatments for leukemias, lymphomas

An ex vivo drug screening method can reveal optimal therapies for patients with hematologic malignancies, according to research published in The Lancet Haematology.
Researchers used a method called pharmacoscopy to measure single-cell responses to possible treatments in samples from patients with leukemias and lymphomas.
The team then used these results to guide treatment decisions and found that pharmacoscopy-guided treatment greatly improved response rates and progression-free survival (PFS).
“Having a robust, fast, and reliable predictive test at our disposal during the patient treatment process, especially at the time of relapse where a new intervention must be selected quickly, will change how medical doctors prioritize drugs to use for late-stage patients,” said study author Philipp Staber, MD, of Medical University of Vienna in Austria.
With pharmacoscopy, hundreds of drug options can be pre-tested ex vivo in small liquid biopsy samples collected from individual patients. The effects of each drug on the individual cells are quantified using high-throughput and high-content automated confocal microscopy.
In combination with specially developed analysis methods, machine learning, and other algorithms, pharmacoscopy allows quantification of never-before visualized phenotypes. The method was first described last April in Nature Chemical Biology.
Now, Dr Staber and his colleagues have reported, in The Lancet Haematology, an interim analysis of the first clinical trial testing pharmacoscopy-guided treatment.
There were 17 evaluable patients, all of whom had aggressive hematologic malignancies. This included diffuse large B-cell lymphoma (n=6), acute myeloid leukemia (n=3), B-cell acute lymphoblastic leukemia (n=2), precursor B-cell lymphoblastic lymphoma (n=1), peripheral T-cell lymphoma (n=1), primary mediastinal B-cell lymphoma (n=1), T-cell lymphoblastic lymphoma (n=1), follicular lymphoma (n=1), and T-cell prolymphocytic leukemia (n=1).
The researchers compared outcomes with pharmacoscopy-guided treatment to outcomes with the most recent regimen on which the patient had progressed.
The overall response rate was 88% with pharmacoscopy-guided treatment and 24% with the patients’ most recent previous treatment regimen (odds ratio=24.38; 95%, CI 3.99–125.4; P=0.0013).
None of the patients had progressive disease as their best overall response when they received pharmacoscopy-guided treatment. However, 7 patients had progressive disease in response to their most recent prior regimen.
At the time of analysis, 8 patients (47%) still had ongoing responses after pharmacoscopy-guided treatment.
In addition, pharmacoscopy-guided treatment significantly improved PFS. The median PFS was 22.6 weeks with pharmacoscopy-guided treatment and 5.7 weeks with the most recent prior regimen (hazard ratio=3.14; 95%, CI 1.37–7.22; P=0.0075).
“Evidence that the pharmacoscopy approach is helpful for clinical evaluation of therapy is wonderful,” said study author Giulio Superti-Furga, PhD, of CeMM Research Center for Molecular Medicine in Vienna, Austria.
“Single-cell functional analysis of primary material gives unprecedented resolution and precision that we are sure to further develop in the future to address yet more diseases.” ![]()
An ex vivo drug screening method can reveal optimal therapies for patients with hematologic malignancies, according to research published in The Lancet Haematology.
Researchers used a method called pharmacoscopy to measure single-cell responses to possible treatments in samples from patients with leukemias and lymphomas.
The team then used these results to guide treatment decisions and found that pharmacoscopy-guided treatment greatly improved response rates and progression-free survival (PFS).
“Having a robust, fast, and reliable predictive test at our disposal during the patient treatment process, especially at the time of relapse where a new intervention must be selected quickly, will change how medical doctors prioritize drugs to use for late-stage patients,” said study author Philipp Staber, MD, of Medical University of Vienna in Austria.
With pharmacoscopy, hundreds of drug options can be pre-tested ex vivo in small liquid biopsy samples collected from individual patients. The effects of each drug on the individual cells are quantified using high-throughput and high-content automated confocal microscopy.
In combination with specially developed analysis methods, machine learning, and other algorithms, pharmacoscopy allows quantification of never-before visualized phenotypes. The method was first described last April in Nature Chemical Biology.
Now, Dr Staber and his colleagues have reported, in The Lancet Haematology, an interim analysis of the first clinical trial testing pharmacoscopy-guided treatment.
There were 17 evaluable patients, all of whom had aggressive hematologic malignancies. This included diffuse large B-cell lymphoma (n=6), acute myeloid leukemia (n=3), B-cell acute lymphoblastic leukemia (n=2), precursor B-cell lymphoblastic lymphoma (n=1), peripheral T-cell lymphoma (n=1), primary mediastinal B-cell lymphoma (n=1), T-cell lymphoblastic lymphoma (n=1), follicular lymphoma (n=1), and T-cell prolymphocytic leukemia (n=1).
The researchers compared outcomes with pharmacoscopy-guided treatment to outcomes with the most recent regimen on which the patient had progressed.
The overall response rate was 88% with pharmacoscopy-guided treatment and 24% with the patients’ most recent previous treatment regimen (odds ratio=24.38; 95%, CI 3.99–125.4; P=0.0013).
None of the patients had progressive disease as their best overall response when they received pharmacoscopy-guided treatment. However, 7 patients had progressive disease in response to their most recent prior regimen.
At the time of analysis, 8 patients (47%) still had ongoing responses after pharmacoscopy-guided treatment.
In addition, pharmacoscopy-guided treatment significantly improved PFS. The median PFS was 22.6 weeks with pharmacoscopy-guided treatment and 5.7 weeks with the most recent prior regimen (hazard ratio=3.14; 95%, CI 1.37–7.22; P=0.0075).
“Evidence that the pharmacoscopy approach is helpful for clinical evaluation of therapy is wonderful,” said study author Giulio Superti-Furga, PhD, of CeMM Research Center for Molecular Medicine in Vienna, Austria.
“Single-cell functional analysis of primary material gives unprecedented resolution and precision that we are sure to further develop in the future to address yet more diseases.” ![]()
An ex vivo drug screening method can reveal optimal therapies for patients with hematologic malignancies, according to research published in The Lancet Haematology.
Researchers used a method called pharmacoscopy to measure single-cell responses to possible treatments in samples from patients with leukemias and lymphomas.
The team then used these results to guide treatment decisions and found that pharmacoscopy-guided treatment greatly improved response rates and progression-free survival (PFS).
“Having a robust, fast, and reliable predictive test at our disposal during the patient treatment process, especially at the time of relapse where a new intervention must be selected quickly, will change how medical doctors prioritize drugs to use for late-stage patients,” said study author Philipp Staber, MD, of Medical University of Vienna in Austria.
With pharmacoscopy, hundreds of drug options can be pre-tested ex vivo in small liquid biopsy samples collected from individual patients. The effects of each drug on the individual cells are quantified using high-throughput and high-content automated confocal microscopy.
In combination with specially developed analysis methods, machine learning, and other algorithms, pharmacoscopy allows quantification of never-before visualized phenotypes. The method was first described last April in Nature Chemical Biology.
Now, Dr Staber and his colleagues have reported, in The Lancet Haematology, an interim analysis of the first clinical trial testing pharmacoscopy-guided treatment.
There were 17 evaluable patients, all of whom had aggressive hematologic malignancies. This included diffuse large B-cell lymphoma (n=6), acute myeloid leukemia (n=3), B-cell acute lymphoblastic leukemia (n=2), precursor B-cell lymphoblastic lymphoma (n=1), peripheral T-cell lymphoma (n=1), primary mediastinal B-cell lymphoma (n=1), T-cell lymphoblastic lymphoma (n=1), follicular lymphoma (n=1), and T-cell prolymphocytic leukemia (n=1).
The researchers compared outcomes with pharmacoscopy-guided treatment to outcomes with the most recent regimen on which the patient had progressed.
The overall response rate was 88% with pharmacoscopy-guided treatment and 24% with the patients’ most recent previous treatment regimen (odds ratio=24.38; 95%, CI 3.99–125.4; P=0.0013).
None of the patients had progressive disease as their best overall response when they received pharmacoscopy-guided treatment. However, 7 patients had progressive disease in response to their most recent prior regimen.
At the time of analysis, 8 patients (47%) still had ongoing responses after pharmacoscopy-guided treatment.
In addition, pharmacoscopy-guided treatment significantly improved PFS. The median PFS was 22.6 weeks with pharmacoscopy-guided treatment and 5.7 weeks with the most recent prior regimen (hazard ratio=3.14; 95%, CI 1.37–7.22; P=0.0075).
“Evidence that the pharmacoscopy approach is helpful for clinical evaluation of therapy is wonderful,” said study author Giulio Superti-Furga, PhD, of CeMM Research Center for Molecular Medicine in Vienna, Austria.
“Single-cell functional analysis of primary material gives unprecedented resolution and precision that we are sure to further develop in the future to address yet more diseases.” ![]()
PTSD can persist in cancer survivors

Cancer patients may experience lasting post-traumatic stress disorder (PTSD), according to a study published in the journal Cancer.
Approximately one-fifth of patients involved in the study experienced PTSD several months after their cancer diagnosis, and roughly a third of these patients continued to live with PTSD 4 years later.
Researchers say these findings highlight the need for early identification, careful monitoring, and treatment of PTSD in cancer survivors.
Caryn Mei Hsien Chan, PhD, of the National University of Malaysia in Kuala Lumpur, and her colleagues conducted this research.
The study included 469 adults with various cancers who were within 1 month of cancer diagnosis at enrollment.
Patients who had significant psychological distress (defined as a Hospital Anxiety and Depression Scale total cutoff score of 16 or higher) underwent
testing for PTSD at 6 months of follow-up. All patients were tested for PTSD at 4 years of follow-up (regardless of their Hospital Anxiety and Depression Scale score).
The incidence of PTSD was 21.7% at 6 months and 6.1% at 4 years. Although overall rates of PTSD decreased with time, roughly one-third of patients initially diagnosed with PTSD were found to have persistent or worsening symptoms 4 years later.
“Many cancer patients believe they need to adopt a ‘warrior mentality’ and remain positive and optimistic from diagnosis through treatment to stand a better chance of beating their cancer,” Dr Chan said.
“To these patients, seeking help for the emotional issues they face is akin to admitting weakness. There needs to be greater awareness that there is nothing wrong with getting help to manage the emotional upheaval—particularly depression, anxiety, and PTSD—post-cancer.”
Dr Chan also stressed that many patients live in fear that their cancer may come back, and they may think the cancer has returned with every lump or bump, pain or ache, fatigue or fever.
In addition, cancer survivors might skip visits to their oncologists or other physicians to avoid triggering memories of their past cancer experience. This can lead to delays in seeking help for new symptoms or even refusal of treatment for unrelated conditions.
“We need psychological evaluation and support services for patients with cancer at an initial stage and at continued follows-up because psychological well-being and mental health—and by extension, quality of life—are just as important as physical health,” Dr Chan noted. ![]()
Cancer patients may experience lasting post-traumatic stress disorder (PTSD), according to a study published in the journal Cancer.
Approximately one-fifth of patients involved in the study experienced PTSD several months after their cancer diagnosis, and roughly a third of these patients continued to live with PTSD 4 years later.
Researchers say these findings highlight the need for early identification, careful monitoring, and treatment of PTSD in cancer survivors.
Caryn Mei Hsien Chan, PhD, of the National University of Malaysia in Kuala Lumpur, and her colleagues conducted this research.
The study included 469 adults with various cancers who were within 1 month of cancer diagnosis at enrollment.
Patients who had significant psychological distress (defined as a Hospital Anxiety and Depression Scale total cutoff score of 16 or higher) underwent
testing for PTSD at 6 months of follow-up. All patients were tested for PTSD at 4 years of follow-up (regardless of their Hospital Anxiety and Depression Scale score).
The incidence of PTSD was 21.7% at 6 months and 6.1% at 4 years. Although overall rates of PTSD decreased with time, roughly one-third of patients initially diagnosed with PTSD were found to have persistent or worsening symptoms 4 years later.
“Many cancer patients believe they need to adopt a ‘warrior mentality’ and remain positive and optimistic from diagnosis through treatment to stand a better chance of beating their cancer,” Dr Chan said.
“To these patients, seeking help for the emotional issues they face is akin to admitting weakness. There needs to be greater awareness that there is nothing wrong with getting help to manage the emotional upheaval—particularly depression, anxiety, and PTSD—post-cancer.”
Dr Chan also stressed that many patients live in fear that their cancer may come back, and they may think the cancer has returned with every lump or bump, pain or ache, fatigue or fever.
In addition, cancer survivors might skip visits to their oncologists or other physicians to avoid triggering memories of their past cancer experience. This can lead to delays in seeking help for new symptoms or even refusal of treatment for unrelated conditions.
“We need psychological evaluation and support services for patients with cancer at an initial stage and at continued follows-up because psychological well-being and mental health—and by extension, quality of life—are just as important as physical health,” Dr Chan noted. ![]()
Cancer patients may experience lasting post-traumatic stress disorder (PTSD), according to a study published in the journal Cancer.
Approximately one-fifth of patients involved in the study experienced PTSD several months after their cancer diagnosis, and roughly a third of these patients continued to live with PTSD 4 years later.
Researchers say these findings highlight the need for early identification, careful monitoring, and treatment of PTSD in cancer survivors.
Caryn Mei Hsien Chan, PhD, of the National University of Malaysia in Kuala Lumpur, and her colleagues conducted this research.
The study included 469 adults with various cancers who were within 1 month of cancer diagnosis at enrollment.
Patients who had significant psychological distress (defined as a Hospital Anxiety and Depression Scale total cutoff score of 16 or higher) underwent
testing for PTSD at 6 months of follow-up. All patients were tested for PTSD at 4 years of follow-up (regardless of their Hospital Anxiety and Depression Scale score).
The incidence of PTSD was 21.7% at 6 months and 6.1% at 4 years. Although overall rates of PTSD decreased with time, roughly one-third of patients initially diagnosed with PTSD were found to have persistent or worsening symptoms 4 years later.
“Many cancer patients believe they need to adopt a ‘warrior mentality’ and remain positive and optimistic from diagnosis through treatment to stand a better chance of beating their cancer,” Dr Chan said.
“To these patients, seeking help for the emotional issues they face is akin to admitting weakness. There needs to be greater awareness that there is nothing wrong with getting help to manage the emotional upheaval—particularly depression, anxiety, and PTSD—post-cancer.”
Dr Chan also stressed that many patients live in fear that their cancer may come back, and they may think the cancer has returned with every lump or bump, pain or ache, fatigue or fever.
In addition, cancer survivors might skip visits to their oncologists or other physicians to avoid triggering memories of their past cancer experience. This can lead to delays in seeking help for new symptoms or even refusal of treatment for unrelated conditions.
“We need psychological evaluation and support services for patients with cancer at an initial stage and at continued follows-up because psychological well-being and mental health—and by extension, quality of life—are just as important as physical health,” Dr Chan noted. ![]()
Withdrawn drug receives orphan designation for HA

The US Food and Drug Administration (FDA) has granted orphan drug designation to rofecoxib (TRM-201) as a potential treatment for degenerative joint disease in hemophilia, also known as hemophilic arthropathy (HA).
Rofecoxib is a COX-2 selective non-steroidal anti-inflammatory drug (NSAID) that was previously sold in the US under the name Vioxx.
Vioxx was FDA-approved to relieve the signs and symptoms of osteoarthritis, manage acute pain in adults, and treat primary dysmenorrhea.
Merck & Co. pulled Vioxx from the US market in 2004 due to safety concerns. The drug was shown to increase a person’s risk of cardiovascular events, including heart attack and stroke.
Now, Tremeau Pharmaceuticals, Inc., is working to bring rofecoxib back to market to treat patients with HA.
HA patients should not receive traditional NSAIDs due to their effects on platelet aggregation and the risk of gastrointestinal ulcers associated with these drugs. Therefore, high potency opioids are the current standard of care in HA.
“Being granted an orphan drug designation for rofecoxib by FDA is an important regulatory milestone for Tremeau and affirms our strategy of providing non-opioid pain treatments for rare diseases like hemophilic arthropathy,” said Bradford C. Sippy, chief executive officer of Tremeau.
Sippy is a former Merck employee who helped with the recall of Vioxx and knew the final patent protecting the drug’s monopoly was expiring this fall.
When it stopped making Vioxx, Merck was facing thousands of lawsuits from people claiming the drug caused their heart attacks or strokes.
Merck’s own research showed the drug doubled those risks, but lawyers for patients claimed the company downplayed or concealed that. Merck initially fought the lawsuits but, in 2007, agreed to a $4.85 billion settlement.
If approved to treat HA, rofecoxib would carry a warning about the increased risk of heart attack and stroke associated with the drug.
Although the orphan designation for rofecoxib is a step toward FDA approval, Sippy said Tremeau must still raise $25 million or more to fund trials of the drug in hemophilia patients.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to rofecoxib (TRM-201) as a potential treatment for degenerative joint disease in hemophilia, also known as hemophilic arthropathy (HA).
Rofecoxib is a COX-2 selective non-steroidal anti-inflammatory drug (NSAID) that was previously sold in the US under the name Vioxx.
Vioxx was FDA-approved to relieve the signs and symptoms of osteoarthritis, manage acute pain in adults, and treat primary dysmenorrhea.
Merck & Co. pulled Vioxx from the US market in 2004 due to safety concerns. The drug was shown to increase a person’s risk of cardiovascular events, including heart attack and stroke.
Now, Tremeau Pharmaceuticals, Inc., is working to bring rofecoxib back to market to treat patients with HA.
HA patients should not receive traditional NSAIDs due to their effects on platelet aggregation and the risk of gastrointestinal ulcers associated with these drugs. Therefore, high potency opioids are the current standard of care in HA.
“Being granted an orphan drug designation for rofecoxib by FDA is an important regulatory milestone for Tremeau and affirms our strategy of providing non-opioid pain treatments for rare diseases like hemophilic arthropathy,” said Bradford C. Sippy, chief executive officer of Tremeau.
Sippy is a former Merck employee who helped with the recall of Vioxx and knew the final patent protecting the drug’s monopoly was expiring this fall.
When it stopped making Vioxx, Merck was facing thousands of lawsuits from people claiming the drug caused their heart attacks or strokes.
Merck’s own research showed the drug doubled those risks, but lawyers for patients claimed the company downplayed or concealed that. Merck initially fought the lawsuits but, in 2007, agreed to a $4.85 billion settlement.
If approved to treat HA, rofecoxib would carry a warning about the increased risk of heart attack and stroke associated with the drug.
Although the orphan designation for rofecoxib is a step toward FDA approval, Sippy said Tremeau must still raise $25 million or more to fund trials of the drug in hemophilia patients.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
The US Food and Drug Administration (FDA) has granted orphan drug designation to rofecoxib (TRM-201) as a potential treatment for degenerative joint disease in hemophilia, also known as hemophilic arthropathy (HA).
Rofecoxib is a COX-2 selective non-steroidal anti-inflammatory drug (NSAID) that was previously sold in the US under the name Vioxx.
Vioxx was FDA-approved to relieve the signs and symptoms of osteoarthritis, manage acute pain in adults, and treat primary dysmenorrhea.
Merck & Co. pulled Vioxx from the US market in 2004 due to safety concerns. The drug was shown to increase a person’s risk of cardiovascular events, including heart attack and stroke.
Now, Tremeau Pharmaceuticals, Inc., is working to bring rofecoxib back to market to treat patients with HA.
HA patients should not receive traditional NSAIDs due to their effects on platelet aggregation and the risk of gastrointestinal ulcers associated with these drugs. Therefore, high potency opioids are the current standard of care in HA.
“Being granted an orphan drug designation for rofecoxib by FDA is an important regulatory milestone for Tremeau and affirms our strategy of providing non-opioid pain treatments for rare diseases like hemophilic arthropathy,” said Bradford C. Sippy, chief executive officer of Tremeau.
Sippy is a former Merck employee who helped with the recall of Vioxx and knew the final patent protecting the drug’s monopoly was expiring this fall.
When it stopped making Vioxx, Merck was facing thousands of lawsuits from people claiming the drug caused their heart attacks or strokes.
Merck’s own research showed the drug doubled those risks, but lawyers for patients claimed the company downplayed or concealed that. Merck initially fought the lawsuits but, in 2007, agreed to a $4.85 billion settlement.
If approved to treat HA, rofecoxib would carry a warning about the increased risk of heart attack and stroke associated with the drug.
Although the orphan designation for rofecoxib is a step toward FDA approval, Sippy said Tremeau must still raise $25 million or more to fund trials of the drug in hemophilia patients.
About orphan designation
The FDA grants orphan designation to products intended to treat, diagnose, or prevent diseases/disorders that affect fewer than 200,000 people in the US.
The designation provides incentives for sponsors to develop products for rare diseases. This may include tax credits toward the cost of clinical trials, prescription drug user fee waivers, and 7 years of market exclusivity if the product is approved. ![]()
Conjunctivitis and oral inflammation

This patient was diagnosed with reactive arthritis, based on her clinical syndrome of conjunctivitis, arthralgias, mucositis, and cervicitis. The widespread distribution of symptoms in this syndrome may be due to activation of the immune system by a viral or bacterial agent. In this case, a complete blood count revealed a white blood cell count of 17,000/mcL (with a left shift of 6% bands). An endocervical DNA probe was positive for Chlamydia trachomatis.
Interestingly, a test for the human leukocyte antigen HLA-B27 came back negative. This did not, however, change the diagnosis. Only 85% of patients with reactive arthritis are positive for HLA-B27, and the test results are frequently negative in African Americans.
Because many sexually transmitted diseases occur concurrently—or are transmitted together—the patient was also tested for human immunodeficiency virus, syphilis, and hepatitis B and C. All of these tests were negative.
The patient was hospitalized and given an injection of ceftriaxone 250 mg, as well as oral azithromycin 1 g for chlamydia (and possible gonorrhea). She also received nonsteroidal anti-inflammatory drugs for pain control. She responded rapidly to therapy as evidenced by decreased arthralgias, normalization of temperature and white blood cell count, and decreased abdominal pain. The patient was discharged after her third day in the hospital with instructions to take doxycycline twice daily, and to finish the 14-day course.
Historical note: “Reiter’s syndrome” is no longer the preferred term for reactive arthritis, as Dr. Reiter was affiliated with the Nazi Party and performed unethical experimentation on human subjects.
Photo courtesy of Joseph Mazziotta, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chumley H, Shedd A, Reddy S, et al. Reactive arthritis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 910-914; Mazziotta JM, Ahmed N. Conjunctivitis and cervicitis. J Fam Pract. 2004;53:121-123.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
This patient was diagnosed with reactive arthritis, based on her clinical syndrome of conjunctivitis, arthralgias, mucositis, and cervicitis. The widespread distribution of symptoms in this syndrome may be due to activation of the immune system by a viral or bacterial agent. In this case, a complete blood count revealed a white blood cell count of 17,000/mcL (with a left shift of 6% bands). An endocervical DNA probe was positive for Chlamydia trachomatis.
Interestingly, a test for the human leukocyte antigen HLA-B27 came back negative. This did not, however, change the diagnosis. Only 85% of patients with reactive arthritis are positive for HLA-B27, and the test results are frequently negative in African Americans.
Because many sexually transmitted diseases occur concurrently—or are transmitted together—the patient was also tested for human immunodeficiency virus, syphilis, and hepatitis B and C. All of these tests were negative.
The patient was hospitalized and given an injection of ceftriaxone 250 mg, as well as oral azithromycin 1 g for chlamydia (and possible gonorrhea). She also received nonsteroidal anti-inflammatory drugs for pain control. She responded rapidly to therapy as evidenced by decreased arthralgias, normalization of temperature and white blood cell count, and decreased abdominal pain. The patient was discharged after her third day in the hospital with instructions to take doxycycline twice daily, and to finish the 14-day course.
Historical note: “Reiter’s syndrome” is no longer the preferred term for reactive arthritis, as Dr. Reiter was affiliated with the Nazi Party and performed unethical experimentation on human subjects.
Photo courtesy of Joseph Mazziotta, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chumley H, Shedd A, Reddy S, et al. Reactive arthritis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 910-914; Mazziotta JM, Ahmed N. Conjunctivitis and cervicitis. J Fam Pract. 2004;53:121-123.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com
This patient was diagnosed with reactive arthritis, based on her clinical syndrome of conjunctivitis, arthralgias, mucositis, and cervicitis. The widespread distribution of symptoms in this syndrome may be due to activation of the immune system by a viral or bacterial agent. In this case, a complete blood count revealed a white blood cell count of 17,000/mcL (with a left shift of 6% bands). An endocervical DNA probe was positive for Chlamydia trachomatis.
Interestingly, a test for the human leukocyte antigen HLA-B27 came back negative. This did not, however, change the diagnosis. Only 85% of patients with reactive arthritis are positive for HLA-B27, and the test results are frequently negative in African Americans.
Because many sexually transmitted diseases occur concurrently—or are transmitted together—the patient was also tested for human immunodeficiency virus, syphilis, and hepatitis B and C. All of these tests were negative.
The patient was hospitalized and given an injection of ceftriaxone 250 mg, as well as oral azithromycin 1 g for chlamydia (and possible gonorrhea). She also received nonsteroidal anti-inflammatory drugs for pain control. She responded rapidly to therapy as evidenced by decreased arthralgias, normalization of temperature and white blood cell count, and decreased abdominal pain. The patient was discharged after her third day in the hospital with instructions to take doxycycline twice daily, and to finish the 14-day course.
Historical note: “Reiter’s syndrome” is no longer the preferred term for reactive arthritis, as Dr. Reiter was affiliated with the Nazi Party and performed unethical experimentation on human subjects.
Photo courtesy of Joseph Mazziotta, MD. Text for Photo Rounds Friday courtesy of Richard P. Usatine, MD. This case was adapted from: Chumley H, Shedd A, Reddy S, et al. Reactive arthritis. In: Usatine R, Smith M, Mayeaux EJ, et al, eds. Color Atlas of Family Medicine. 2nd ed. New York, NY: McGraw-Hill; 2013: 910-914; Mazziotta JM, Ahmed N. Conjunctivitis and cervicitis. J Fam Pract. 2004;53:121-123.
To learn more about the Color Atlas of Family Medicine, see: www.amazon.com/Color-Family-Medicine-Richard-Usatine/dp/0071769641/
You can now get the second edition of the Color Atlas of Family Medicine as an app by clicking on this link: usatinemedia.com

HTN in CKD: How Should I Be Treating It?
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

CMS to enlist Medicare Part D plans to combat opioid abuse
The Centers for Medicare & Medicaid Services aims to enlist the help of Medicare Part D plan sponsors in fighting opioid abuse, under a proposed rule scheduled for publication in the Federal Register on Nov. 28.
The agency is proposing to expand monitoring of patients taking opioids in its current Part D Opioid Drug Utilization Review (DUR) and Overutilization Monitoring System (OMS). To do so, officials would like to extend the use the criteria for overutilizers to identify at-risk beneficiaries. Part D plans then would be allowed to restrict at-risk beneficiaries’ access to opioids to a selected prescriber and/or network pharmacy, according to a fact sheet on proposal, which is part of the proposed 2018 update to regulations governing Medicare Advantage and Medicare Part D.
Under the proposal, plans would not be required to use these tools. However, CMS expects they will.
“While plan sponsors would have the option to implement a drug management program, our proposal codifies a framework that would place requirements upon such programs,” according to the proposal. “We foresee that all plan sponsors will implement such drug management programs based on our experience that all plan sponsors’ are complying with the current policy as laid out in guidance, the fact that our proposal largely incorporates the CARA [Comprehensive Addiction and Recovery Act of 2016] drug management provisions into existing CMS and sponsor operations, and especially, in light of the national opioid epidemic and the declaration that the opioid crisis is a nationwide Public Health Emergency.”
According to the proposal, potentially at-risk and at-risk beneficiaries would be identified based on the type and frequency of prescriptions. Those include the use of opioids with an average daily morphine milligram equivalent (MME) greater than or equal to 90 mg for any duration during the most recent 6 months and either four or more opioid prescribers plus four or more opioid-dispensing pharmacies or six or more opioid prescribers, regardless of pharmacies.
CMS notes in the regulation that, if the proposed 2019 criteria were used against those enrolled in Medicare Part D in 2015, it would have identified as at-risk about 33,000 Part D beneficiaries, or 0.08% of the 42 million people enrolled at that time. The agency said this population should be manageable for oversight by Part D plan sponsors, noting that, in Medicaid in 2015, 0.37% were included in some kind of pharmacy/prescriber lock-in program.
The proposed regulation includes an exemption for patients diagnosed with cancer, those in hospice, and those in a long-term care facility. CMS also plans to limit the availability of the special enrollment period for dual-eligible beneficiaries (those who qualify for both Medicare and Medicaid) and those who receive the low-income subsidy who are identified as at risk or potentially at risk.
Beneficiaries would be allowed to appeal their at-risk/potential at-risk determination under the proposal.
The Centers for Medicare & Medicaid Services aims to enlist the help of Medicare Part D plan sponsors in fighting opioid abuse, under a proposed rule scheduled for publication in the Federal Register on Nov. 28.
The agency is proposing to expand monitoring of patients taking opioids in its current Part D Opioid Drug Utilization Review (DUR) and Overutilization Monitoring System (OMS). To do so, officials would like to extend the use the criteria for overutilizers to identify at-risk beneficiaries. Part D plans then would be allowed to restrict at-risk beneficiaries’ access to opioids to a selected prescriber and/or network pharmacy, according to a fact sheet on proposal, which is part of the proposed 2018 update to regulations governing Medicare Advantage and Medicare Part D.
Under the proposal, plans would not be required to use these tools. However, CMS expects they will.
“While plan sponsors would have the option to implement a drug management program, our proposal codifies a framework that would place requirements upon such programs,” according to the proposal. “We foresee that all plan sponsors will implement such drug management programs based on our experience that all plan sponsors’ are complying with the current policy as laid out in guidance, the fact that our proposal largely incorporates the CARA [Comprehensive Addiction and Recovery Act of 2016] drug management provisions into existing CMS and sponsor operations, and especially, in light of the national opioid epidemic and the declaration that the opioid crisis is a nationwide Public Health Emergency.”
According to the proposal, potentially at-risk and at-risk beneficiaries would be identified based on the type and frequency of prescriptions. Those include the use of opioids with an average daily morphine milligram equivalent (MME) greater than or equal to 90 mg for any duration during the most recent 6 months and either four or more opioid prescribers plus four or more opioid-dispensing pharmacies or six or more opioid prescribers, regardless of pharmacies.
CMS notes in the regulation that, if the proposed 2019 criteria were used against those enrolled in Medicare Part D in 2015, it would have identified as at-risk about 33,000 Part D beneficiaries, or 0.08% of the 42 million people enrolled at that time. The agency said this population should be manageable for oversight by Part D plan sponsors, noting that, in Medicaid in 2015, 0.37% were included in some kind of pharmacy/prescriber lock-in program.
The proposed regulation includes an exemption for patients diagnosed with cancer, those in hospice, and those in a long-term care facility. CMS also plans to limit the availability of the special enrollment period for dual-eligible beneficiaries (those who qualify for both Medicare and Medicaid) and those who receive the low-income subsidy who are identified as at risk or potentially at risk.
Beneficiaries would be allowed to appeal their at-risk/potential at-risk determination under the proposal.
The Centers for Medicare & Medicaid Services aims to enlist the help of Medicare Part D plan sponsors in fighting opioid abuse, under a proposed rule scheduled for publication in the Federal Register on Nov. 28.
The agency is proposing to expand monitoring of patients taking opioids in its current Part D Opioid Drug Utilization Review (DUR) and Overutilization Monitoring System (OMS). To do so, officials would like to extend the use the criteria for overutilizers to identify at-risk beneficiaries. Part D plans then would be allowed to restrict at-risk beneficiaries’ access to opioids to a selected prescriber and/or network pharmacy, according to a fact sheet on proposal, which is part of the proposed 2018 update to regulations governing Medicare Advantage and Medicare Part D.
Under the proposal, plans would not be required to use these tools. However, CMS expects they will.
“While plan sponsors would have the option to implement a drug management program, our proposal codifies a framework that would place requirements upon such programs,” according to the proposal. “We foresee that all plan sponsors will implement such drug management programs based on our experience that all plan sponsors’ are complying with the current policy as laid out in guidance, the fact that our proposal largely incorporates the CARA [Comprehensive Addiction and Recovery Act of 2016] drug management provisions into existing CMS and sponsor operations, and especially, in light of the national opioid epidemic and the declaration that the opioid crisis is a nationwide Public Health Emergency.”
According to the proposal, potentially at-risk and at-risk beneficiaries would be identified based on the type and frequency of prescriptions. Those include the use of opioids with an average daily morphine milligram equivalent (MME) greater than or equal to 90 mg for any duration during the most recent 6 months and either four or more opioid prescribers plus four or more opioid-dispensing pharmacies or six or more opioid prescribers, regardless of pharmacies.
CMS notes in the regulation that, if the proposed 2019 criteria were used against those enrolled in Medicare Part D in 2015, it would have identified as at-risk about 33,000 Part D beneficiaries, or 0.08% of the 42 million people enrolled at that time. The agency said this population should be manageable for oversight by Part D plan sponsors, noting that, in Medicaid in 2015, 0.37% were included in some kind of pharmacy/prescriber lock-in program.
The proposed regulation includes an exemption for patients diagnosed with cancer, those in hospice, and those in a long-term care facility. CMS also plans to limit the availability of the special enrollment period for dual-eligible beneficiaries (those who qualify for both Medicare and Medicaid) and those who receive the low-income subsidy who are identified as at risk or potentially at risk.
Beneficiaries would be allowed to appeal their at-risk/potential at-risk determination under the proposal.
To predict macrosomia, focus on the abdomen
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
WASHINGTON – , John C. Hobbins, MD, said at the biennial meeting of the Diabetes in Pregnancy Study Group of North America.
“Everything that the estimated fetal weight [EFW] can do, the abdominal circumference can do better,” especially in diabetic mothers, said Dr. Hobbins, who is widely regarded as one of the early pioneers in the development and use of obstetric ultrasound as a diagnostic tool.
Because it reflects liver size and incorporates subcutaneous fat, the abdominal circumference (AC) “concentrates on where the action is,” he said. It also “roughly correlates” with the size of the fetal shoulders and is not affected by genetic factors.
Moreover, “it focuses on one task rather than putting into play four variables, each with its own standard error of the method,” said Dr. Hobbins, referring to the four fetal biometric parameters incorporated into the Hadlock formula for EFW that is provided “upon fire-up of virtually every ultrasound machine.”
These four parameters (biparietal diameter, head circumference, femur length, and AC) each contribute to fetal weight but the AC has been shown to correlate better with weight at birth than the other variables, and it is the only measure that reflects how corpulent the fetus is, he noted.
The “general rule of thumb is that the EFW [as calculated by ultrasound machine–based equations] has a standard error of the method of plus or minus 10%. … which means that an EFW of 4,000 g is associated with a splay of plus or minus 1.2 pounds,” said Dr. Hobbins, professor of obstetrics and gynecology at the University of Colorado at Denver, Aurora.
“But the problem for us is not the failure of the ultrasound – it’s the way we use it,” he said.
An assortment of customized formulas have been developed for macrosomia, including one designed for use in diabetes that incorporates AC, head circumference, femur length, and 3D volumes of the thigh and abdomen. “If one used this and set a cut-off at 4,300 g, you’d pick up 93%. … but at false positive rate of 38%,” he said.
While not perfect, the AC alone is as accurate as more complicated formulas to detect macrosomic fetuses, he emphasized. “It’s a tough [measurement] to get just before the baby is born, but you can do it a little bit earlier,” he said. Research has shown that screening at 30-34 weeks can capture a majority of the fetuses destined to be greater than 4,000 g at birth, with a lower false-positive rate.
He pointed to one “very interesting” recent study in which AC was measured with a handheld ultrasound device at 24-40 weeks’ gestation, prior to formal ultrasound estimation of EFW. Early AC was a better predictor of large-for-gestational age babies at birth than EFW or early fundal height measurement, with sensitivities of 67%, 25%, and 50%, respectively (Am J Obstet Gynecol. 2015 Jun;212[6]:820.e1-8).
“And AC had a false-positive rate of only 10%,” Dr. Hobbins said.
Macrosomia occurs in 20% of cases of gestational diabetes and 25% of pregestational diabetes, he said. “And even if there is adequate glucose control, 17% will be macrosomic.”
The condition correlates with childhood and adulthood metabolic dysfunction and is associated with significantly increased risk of birth injury to the infant and to the mother. The alternative – cesarean delivery – is “not innocuous,” and “[we have] a very low threshold for cesarean if macrosomia is suspected,” Dr. Hobbins said.
Dr. Hobbins reported having no financial disclosures.
EXPERT ANALYSIS FROM DPSG-NA 2017
Reducing harm: When doing less is enough
Launched in April 2012 – the same year an article in the Journal of the American Medical Association estimated the U.S. health care system was wasting between $600 billion and $1 trillion annually because of issues such as overtreatment – Choosing Wisely continues to change both conversations and practices across the medical field.1
In creating Choosing Wisely, the ABIM Foundation sought to establish a framework for physicians to think about managing resources and to talk to patients about which medical tests and procedures might be unnecessary – or even harmful.

Today, more than 75 medical specialties have their own “five things” lists: procedures that practitioners should question before ordering. Hospitalists have a total of 10 – 5 for adults and 5 for pediatrics – and hospitalists play a pivotal role in Choosing Wisely’s implementation, with crucial control over service lines. “Hospitalists are on the front line of patient care,” said Moises Auron, MD, FAAP, FACP, SFHM, a hospitalist at the Cleveland Clinic. “We are actually the frontline workers in the hospital.”
Choosing Wisely’s successes
In terms of its initial goal – starting a conversation and encouraging physicians to interrogate their habits – Choosing Wisely has been a success.
“It’s brought a lot of awareness about the problem of matching best evidence with the patient you have in front of you,” said John Bulger , DO, MACP, MBA, SFHM, chief medical officer of Geisinger Health Plan. “Some people call that evidence-based medicine, but the problem with calling it that is that you can have a study, but it may not match up with the patient you’re seeing right now. There are many things we do because we did them in the past or because we didn’t have all the information, and I think Choosing Wisely has made people think twice about some of the things they do.”

The message of Choosing Wisely continues to spread, even internationally. It’s now present in 18 countries, Mr. Wolfson said. “We’re also seeing on the horizon many state efforts, such as in Connecticut and Rhode Island; and Delaware is organizing a statewide effort. I see that as the next big thing: statewide efforts that pair delivery systems with multistakeholder groups, regional health collaboratives, and physician organizations, all working to reduce use.”As it spreads, Choosing Wisely is sparking a new generation of related initiatives, such as Costs of Care and Johns Hopkins’ High Value Practice Academic Alliance. There’s a new section in the Journal of Hospital Medicine called “Things We Do for No Reason” highlighting different practices each month, and a nationwide Student High Value Care Initiative introduces value concepts to medical students. “It’s not Choosing Wisely by itself; it’s provided the backbone for all these new efforts,” Dr. Auron said.
Challenges remain
While it has spread, Choosing Wisely also has met some obstacles. Among them is that even with the help of Consumer Reports’ tools, the physician-patient conversations can be difficult. A behavioral economics concept called loss aversion is part of the reason: It’s basic human nature to feel the pain of loss more acutely than the pleasure of gain.

“It’s tough because that conversation requires specific training,” he said. “It’s one thing to tell the clinician, or to have it pop up on an EHR, that provision of an antibiotic for this clinical presentation is not appropriate. However, it’s an entirely different thing to look a patient in the face who comes in expecting a course of antibiotics and tell them that they’re not going to get it.”
Another hurdle is the existing fee-for-service system, which obviously does not promote cost consciousness. Since there’s really no disincentive to a physician ordering an additional test, acceptance of Choosing Wisely can vary widely between institutions. “Choosing Wisely permeated very nicely here at the Cleveland Clinic,” Dr. Auron said. “But other hospitals – especially private hospitals that are not owned by doctors – what they want is just the service line.”
Physicians’ discomfort with uncertainty is another challenge, according to Mr. Mainor. “A lot of it can be by virtue of medical training and how particular residents were taught to always run this panel when you have this presentation,” he said. “Sometimes it’s hard to separate Choosing Wisely from the concept of defensive medicine, but this is more wanting to be able to tell the patient that you did everything that you could before proceeding to a particular next step or treatment.”
Getting patient input from the outset and making sure goals are aligned can help with some of these issues – but can itself be a hurdle.

The road ahead
The time it takes to have these conversations is more than a sticking point for Choosing Wisely, it’s an underlying challenge in our health care system.
“For example, it takes more time to have a discussion about what the alternatives are to alleviate pain – other than taking an opiate,” Dr. Bulger said. “The easiest thing to do is to write the script for the opiate – which is part of the reason why we got where we are with opioids – or to write the script for an antibiotic – which is part of the reason why we got here with drug resistance. We haven’t done a great deal to address those underlying drivers. Without doing that, you can only go so far with a campaign like Choosing Wisely.”
Issues around costs fall into a similar category: an underlying issue that demands a broader conversation. ”It’s just so elusive,” Dr. Cho said. “There are so many different versions of cost, and from a hospital medicine standpoint, that process is so prolonged. We may not touch base with that patient when they get their bill, so for us to have a conversation about exactly how much this would cost can be difficult. It’s so complex; I would love for that to be tackled so that it’s a little more straightforward.”
“There are people involved in career paths in education, quality and safety, research, and administration, but there are very few people actually focused on value – and then finding the resources and the mobilization to do that,” Dr. Cho said. “I think it would really be helpful moving forward to find more people doing this and getting more support from their organizations.”
In one step toward that goal, a value track has been added to the Society of Hospital Medicine annual meeting.
“I think you’re going to see more emphasis on this, especially with younger hospitalists that are really pushing the value theme,” Dr. Bulger said. “I think those are really the lessons learned in what we started with Choosing Wisely.”
References
1. Berwick DM et al. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
2. Colla CH et al. Physician perceptions of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016 May;22(5):337-43.
Launched in April 2012 – the same year an article in the Journal of the American Medical Association estimated the U.S. health care system was wasting between $600 billion and $1 trillion annually because of issues such as overtreatment – Choosing Wisely continues to change both conversations and practices across the medical field.1
In creating Choosing Wisely, the ABIM Foundation sought to establish a framework for physicians to think about managing resources and to talk to patients about which medical tests and procedures might be unnecessary – or even harmful.
Today, more than 75 medical specialties have their own “five things” lists: procedures that practitioners should question before ordering. Hospitalists have a total of 10 – 5 for adults and 5 for pediatrics – and hospitalists play a pivotal role in Choosing Wisely’s implementation, with crucial control over service lines. “Hospitalists are on the front line of patient care,” said Moises Auron, MD, FAAP, FACP, SFHM, a hospitalist at the Cleveland Clinic. “We are actually the frontline workers in the hospital.”
Choosing Wisely’s successes
In terms of its initial goal – starting a conversation and encouraging physicians to interrogate their habits – Choosing Wisely has been a success.
“It’s brought a lot of awareness about the problem of matching best evidence with the patient you have in front of you,” said John Bulger , DO, MACP, MBA, SFHM, chief medical officer of Geisinger Health Plan. “Some people call that evidence-based medicine, but the problem with calling it that is that you can have a study, but it may not match up with the patient you’re seeing right now. There are many things we do because we did them in the past or because we didn’t have all the information, and I think Choosing Wisely has made people think twice about some of the things they do.”
The message of Choosing Wisely continues to spread, even internationally. It’s now present in 18 countries, Mr. Wolfson said. “We’re also seeing on the horizon many state efforts, such as in Connecticut and Rhode Island; and Delaware is organizing a statewide effort. I see that as the next big thing: statewide efforts that pair delivery systems with multistakeholder groups, regional health collaboratives, and physician organizations, all working to reduce use.”As it spreads, Choosing Wisely is sparking a new generation of related initiatives, such as Costs of Care and Johns Hopkins’ High Value Practice Academic Alliance. There’s a new section in the Journal of Hospital Medicine called “Things We Do for No Reason” highlighting different practices each month, and a nationwide Student High Value Care Initiative introduces value concepts to medical students. “It’s not Choosing Wisely by itself; it’s provided the backbone for all these new efforts,” Dr. Auron said.
Challenges remain
While it has spread, Choosing Wisely also has met some obstacles. Among them is that even with the help of Consumer Reports’ tools, the physician-patient conversations can be difficult. A behavioral economics concept called loss aversion is part of the reason: It’s basic human nature to feel the pain of loss more acutely than the pleasure of gain.
“It’s tough because that conversation requires specific training,” he said. “It’s one thing to tell the clinician, or to have it pop up on an EHR, that provision of an antibiotic for this clinical presentation is not appropriate. However, it’s an entirely different thing to look a patient in the face who comes in expecting a course of antibiotics and tell them that they’re not going to get it.”
Another hurdle is the existing fee-for-service system, which obviously does not promote cost consciousness. Since there’s really no disincentive to a physician ordering an additional test, acceptance of Choosing Wisely can vary widely between institutions. “Choosing Wisely permeated very nicely here at the Cleveland Clinic,” Dr. Auron said. “But other hospitals – especially private hospitals that are not owned by doctors – what they want is just the service line.”
Physicians’ discomfort with uncertainty is another challenge, according to Mr. Mainor. “A lot of it can be by virtue of medical training and how particular residents were taught to always run this panel when you have this presentation,” he said. “Sometimes it’s hard to separate Choosing Wisely from the concept of defensive medicine, but this is more wanting to be able to tell the patient that you did everything that you could before proceeding to a particular next step or treatment.”
Getting patient input from the outset and making sure goals are aligned can help with some of these issues – but can itself be a hurdle.
The road ahead
The time it takes to have these conversations is more than a sticking point for Choosing Wisely, it’s an underlying challenge in our health care system.
“For example, it takes more time to have a discussion about what the alternatives are to alleviate pain – other than taking an opiate,” Dr. Bulger said. “The easiest thing to do is to write the script for the opiate – which is part of the reason why we got where we are with opioids – or to write the script for an antibiotic – which is part of the reason why we got here with drug resistance. We haven’t done a great deal to address those underlying drivers. Without doing that, you can only go so far with a campaign like Choosing Wisely.”
Issues around costs fall into a similar category: an underlying issue that demands a broader conversation. ”It’s just so elusive,” Dr. Cho said. “There are so many different versions of cost, and from a hospital medicine standpoint, that process is so prolonged. We may not touch base with that patient when they get their bill, so for us to have a conversation about exactly how much this would cost can be difficult. It’s so complex; I would love for that to be tackled so that it’s a little more straightforward.”
“There are people involved in career paths in education, quality and safety, research, and administration, but there are very few people actually focused on value – and then finding the resources and the mobilization to do that,” Dr. Cho said. “I think it would really be helpful moving forward to find more people doing this and getting more support from their organizations.”
In one step toward that goal, a value track has been added to the Society of Hospital Medicine annual meeting.
“I think you’re going to see more emphasis on this, especially with younger hospitalists that are really pushing the value theme,” Dr. Bulger said. “I think those are really the lessons learned in what we started with Choosing Wisely.”
References
1. Berwick DM et al. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
2. Colla CH et al. Physician perceptions of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016 May;22(5):337-43.
Launched in April 2012 – the same year an article in the Journal of the American Medical Association estimated the U.S. health care system was wasting between $600 billion and $1 trillion annually because of issues such as overtreatment – Choosing Wisely continues to change both conversations and practices across the medical field.1
In creating Choosing Wisely, the ABIM Foundation sought to establish a framework for physicians to think about managing resources and to talk to patients about which medical tests and procedures might be unnecessary – or even harmful.
Today, more than 75 medical specialties have their own “five things” lists: procedures that practitioners should question before ordering. Hospitalists have a total of 10 – 5 for adults and 5 for pediatrics – and hospitalists play a pivotal role in Choosing Wisely’s implementation, with crucial control over service lines. “Hospitalists are on the front line of patient care,” said Moises Auron, MD, FAAP, FACP, SFHM, a hospitalist at the Cleveland Clinic. “We are actually the frontline workers in the hospital.”
Choosing Wisely’s successes
In terms of its initial goal – starting a conversation and encouraging physicians to interrogate their habits – Choosing Wisely has been a success.
“It’s brought a lot of awareness about the problem of matching best evidence with the patient you have in front of you,” said John Bulger , DO, MACP, MBA, SFHM, chief medical officer of Geisinger Health Plan. “Some people call that evidence-based medicine, but the problem with calling it that is that you can have a study, but it may not match up with the patient you’re seeing right now. There are many things we do because we did them in the past or because we didn’t have all the information, and I think Choosing Wisely has made people think twice about some of the things they do.”
The message of Choosing Wisely continues to spread, even internationally. It’s now present in 18 countries, Mr. Wolfson said. “We’re also seeing on the horizon many state efforts, such as in Connecticut and Rhode Island; and Delaware is organizing a statewide effort. I see that as the next big thing: statewide efforts that pair delivery systems with multistakeholder groups, regional health collaboratives, and physician organizations, all working to reduce use.”As it spreads, Choosing Wisely is sparking a new generation of related initiatives, such as Costs of Care and Johns Hopkins’ High Value Practice Academic Alliance. There’s a new section in the Journal of Hospital Medicine called “Things We Do for No Reason” highlighting different practices each month, and a nationwide Student High Value Care Initiative introduces value concepts to medical students. “It’s not Choosing Wisely by itself; it’s provided the backbone for all these new efforts,” Dr. Auron said.
Challenges remain
While it has spread, Choosing Wisely also has met some obstacles. Among them is that even with the help of Consumer Reports’ tools, the physician-patient conversations can be difficult. A behavioral economics concept called loss aversion is part of the reason: It’s basic human nature to feel the pain of loss more acutely than the pleasure of gain.
“It’s tough because that conversation requires specific training,” he said. “It’s one thing to tell the clinician, or to have it pop up on an EHR, that provision of an antibiotic for this clinical presentation is not appropriate. However, it’s an entirely different thing to look a patient in the face who comes in expecting a course of antibiotics and tell them that they’re not going to get it.”
Another hurdle is the existing fee-for-service system, which obviously does not promote cost consciousness. Since there’s really no disincentive to a physician ordering an additional test, acceptance of Choosing Wisely can vary widely between institutions. “Choosing Wisely permeated very nicely here at the Cleveland Clinic,” Dr. Auron said. “But other hospitals – especially private hospitals that are not owned by doctors – what they want is just the service line.”
Physicians’ discomfort with uncertainty is another challenge, according to Mr. Mainor. “A lot of it can be by virtue of medical training and how particular residents were taught to always run this panel when you have this presentation,” he said. “Sometimes it’s hard to separate Choosing Wisely from the concept of defensive medicine, but this is more wanting to be able to tell the patient that you did everything that you could before proceeding to a particular next step or treatment.”
Getting patient input from the outset and making sure goals are aligned can help with some of these issues – but can itself be a hurdle.
The road ahead
The time it takes to have these conversations is more than a sticking point for Choosing Wisely, it’s an underlying challenge in our health care system.
“For example, it takes more time to have a discussion about what the alternatives are to alleviate pain – other than taking an opiate,” Dr. Bulger said. “The easiest thing to do is to write the script for the opiate – which is part of the reason why we got where we are with opioids – or to write the script for an antibiotic – which is part of the reason why we got here with drug resistance. We haven’t done a great deal to address those underlying drivers. Without doing that, you can only go so far with a campaign like Choosing Wisely.”
Issues around costs fall into a similar category: an underlying issue that demands a broader conversation. ”It’s just so elusive,” Dr. Cho said. “There are so many different versions of cost, and from a hospital medicine standpoint, that process is so prolonged. We may not touch base with that patient when they get their bill, so for us to have a conversation about exactly how much this would cost can be difficult. It’s so complex; I would love for that to be tackled so that it’s a little more straightforward.”
“There are people involved in career paths in education, quality and safety, research, and administration, but there are very few people actually focused on value – and then finding the resources and the mobilization to do that,” Dr. Cho said. “I think it would really be helpful moving forward to find more people doing this and getting more support from their organizations.”
In one step toward that goal, a value track has been added to the Society of Hospital Medicine annual meeting.
“I think you’re going to see more emphasis on this, especially with younger hospitalists that are really pushing the value theme,” Dr. Bulger said. “I think those are really the lessons learned in what we started with Choosing Wisely.”
References
1. Berwick DM et al. Eliminating waste in US health care. JAMA. 2012;307(14):1513-6.
2. Colla CH et al. Physician perceptions of Choosing Wisely and drivers of overuse. Am J Manag Care. 2016 May;22(5):337-43.