User login
FDA clears first-ever neurostimulation device for opioid withdrawal symptoms
The Food and Drug Administration has cleared a medical device that applies electrical stimulation to cranial nerves in order to reduce opioid withdrawal symptoms.
The clearance was granted amid the opioid crisis, which is killing 175 Americans each day, according to the recent report by The President’s Commission on Combating Drug Addiction and the Opioid Crisis. Currently, opioid addiction is treatable by three approved medications, said FDA Commissioner Scott Gottlieb, MD, in a press statement announcing the agency’s decision to permit marketing of the NSS-2 Bridge device.
“While we continue to pursue better medicines for the treatment of opioid use disorder, we also need to look to devices that can assist in this therapy,” Dr. Gottlieb said.
The NSS-2 Bridge device was cleared as an acupuncture aid in 2014. The new use of the device to reduce the symptoms of opioid withdrawal required a new clearance, which was granted based on a single, one-arm clinical study. In the study, 73 patients who were experiencing physical withdrawal from opioids used the neurostimulation device. They reported an initial mean score of 20.1 on the Clinical Opiate Withdrawal Score (COWS). All patients using the device had a reduction of at least 31% on the COWS within 30 minutes of beginning use of the NSS-2 Bridge. A total of 88% of participating patients transitioned to medication-assisted treatment after 5 days of using the device. Additional medications used to treat specific symptoms, such as nausea and vomiting, were permitted during the trial.
The physician-placed battery-powered device sits behind the ear and uses three percutaneous electrode arrays and one single-point needle to provide neurostimulation. The electrode placement is assisted with a transillumination technique, and also is based on known neuroanatomic landmarks for branches of cranial nerves V, VII, and IX, along with branches of the occipital nerve (Clin Med Diagnostics. 2015;5[4]:70-9).
The single-use device is designed to be used for up to 5 days during acute opioid withdrawal and is contraindicated for patients with hemophilia, patients with cardiac pacemakers, or those diagnosed with psoriasis vulgaris. The NSS-2 Bridge device requires a prescription and was cleared through the de novo premarket review pathway. This, said the FDA in the press statement, is “a regulatory pathway for some low- to moderate-risk devices that are novel and for which there is no legally marketed predicate device to which the device can claim substantial equivalence.”
The NSS-2 Bridge device will be marketed by Innovative Health Solutions.
[email protected]
On Twitter @karioakes
The Food and Drug Administration has cleared a medical device that applies electrical stimulation to cranial nerves in order to reduce opioid withdrawal symptoms.
The clearance was granted amid the opioid crisis, which is killing 175 Americans each day, according to the recent report by The President’s Commission on Combating Drug Addiction and the Opioid Crisis. Currently, opioid addiction is treatable by three approved medications, said FDA Commissioner Scott Gottlieb, MD, in a press statement announcing the agency’s decision to permit marketing of the NSS-2 Bridge device.
“While we continue to pursue better medicines for the treatment of opioid use disorder, we also need to look to devices that can assist in this therapy,” Dr. Gottlieb said.
The NSS-2 Bridge device was cleared as an acupuncture aid in 2014. The new use of the device to reduce the symptoms of opioid withdrawal required a new clearance, which was granted based on a single, one-arm clinical study. In the study, 73 patients who were experiencing physical withdrawal from opioids used the neurostimulation device. They reported an initial mean score of 20.1 on the Clinical Opiate Withdrawal Score (COWS). All patients using the device had a reduction of at least 31% on the COWS within 30 minutes of beginning use of the NSS-2 Bridge. A total of 88% of participating patients transitioned to medication-assisted treatment after 5 days of using the device. Additional medications used to treat specific symptoms, such as nausea and vomiting, were permitted during the trial.
The physician-placed battery-powered device sits behind the ear and uses three percutaneous electrode arrays and one single-point needle to provide neurostimulation. The electrode placement is assisted with a transillumination technique, and also is based on known neuroanatomic landmarks for branches of cranial nerves V, VII, and IX, along with branches of the occipital nerve (Clin Med Diagnostics. 2015;5[4]:70-9).
The single-use device is designed to be used for up to 5 days during acute opioid withdrawal and is contraindicated for patients with hemophilia, patients with cardiac pacemakers, or those diagnosed with psoriasis vulgaris. The NSS-2 Bridge device requires a prescription and was cleared through the de novo premarket review pathway. This, said the FDA in the press statement, is “a regulatory pathway for some low- to moderate-risk devices that are novel and for which there is no legally marketed predicate device to which the device can claim substantial equivalence.”
The NSS-2 Bridge device will be marketed by Innovative Health Solutions.
[email protected]
On Twitter @karioakes
The Food and Drug Administration has cleared a medical device that applies electrical stimulation to cranial nerves in order to reduce opioid withdrawal symptoms.
The clearance was granted amid the opioid crisis, which is killing 175 Americans each day, according to the recent report by The President’s Commission on Combating Drug Addiction and the Opioid Crisis. Currently, opioid addiction is treatable by three approved medications, said FDA Commissioner Scott Gottlieb, MD, in a press statement announcing the agency’s decision to permit marketing of the NSS-2 Bridge device.
“While we continue to pursue better medicines for the treatment of opioid use disorder, we also need to look to devices that can assist in this therapy,” Dr. Gottlieb said.
The NSS-2 Bridge device was cleared as an acupuncture aid in 2014. The new use of the device to reduce the symptoms of opioid withdrawal required a new clearance, which was granted based on a single, one-arm clinical study. In the study, 73 patients who were experiencing physical withdrawal from opioids used the neurostimulation device. They reported an initial mean score of 20.1 on the Clinical Opiate Withdrawal Score (COWS). All patients using the device had a reduction of at least 31% on the COWS within 30 minutes of beginning use of the NSS-2 Bridge. A total of 88% of participating patients transitioned to medication-assisted treatment after 5 days of using the device. Additional medications used to treat specific symptoms, such as nausea and vomiting, were permitted during the trial.
The physician-placed battery-powered device sits behind the ear and uses three percutaneous electrode arrays and one single-point needle to provide neurostimulation. The electrode placement is assisted with a transillumination technique, and also is based on known neuroanatomic landmarks for branches of cranial nerves V, VII, and IX, along with branches of the occipital nerve (Clin Med Diagnostics. 2015;5[4]:70-9).
The single-use device is designed to be used for up to 5 days during acute opioid withdrawal and is contraindicated for patients with hemophilia, patients with cardiac pacemakers, or those diagnosed with psoriasis vulgaris. The NSS-2 Bridge device requires a prescription and was cleared through the de novo premarket review pathway. This, said the FDA in the press statement, is “a regulatory pathway for some low- to moderate-risk devices that are novel and for which there is no legally marketed predicate device to which the device can claim substantial equivalence.”
The NSS-2 Bridge device will be marketed by Innovative Health Solutions.
[email protected]
On Twitter @karioakes
Heart transplantation: Preop LVAD erases adverse impact of pulmonary hypertension
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.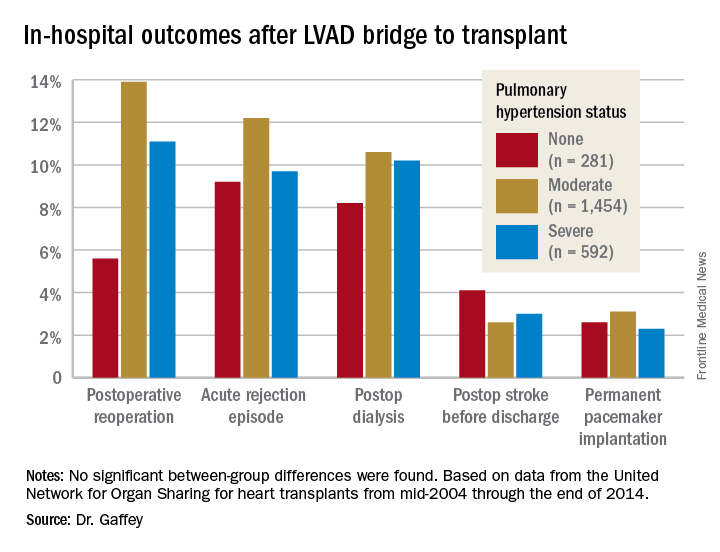
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
COLORADO SPRINGS – Reconsideration of the role of pulmonary hypertension in heart transplant outcomes is appropriate in the emerging era of the use of left ventricular assist devices (LVADs) as bridge to transplant, according to Ann C. Gaffey, MD, of the University of Pennsylvania, Philadelphia.
“Pulmonary hypertension secondary to congestive heart failure more than likely can be reversed to the values acceptable for heart transplant by the use of an LVAD. For bridge-to-transplant patients, pretransplant pulmonary hypertension does not affect recipient outcomes post transplantation,” she said at the annual meeting of the Western Thoracic Surgical Association.
Vasodilators are prescribed in an effort to reduce PH; however, 40% of patients with PH are unresponsive to the medications and have therefore been excluded from consideration as potential candidates for a donor heart.
But the growing use of LVADs as a bridge to transplant has changed all that, Dr. Gaffey said. As supporting evidence, she presented a retrospective analysis of the United Network for Organ Sharing database on adult heart transplants from mid-2004 through the end of 2014.
The review turned up 3,951 heart transplant recipients who had been bridged to transplant with an LVAD. Dr. Gaffey and her coinvestigators divided them into three groups: 281 patients without pretransplant PH; 1,454 with moderate PH as defined by 1-3 Wood units; and 592 with severe PH and more than 3 Wood units.
The three groups didn’t differ in terms of age, sex, wait-list time, or the prevalence of diabetes or renal, liver, or cerebrovascular disease. Nor did their donors differ in age, sex, left ventricular function, or allograft ischemic time.
Key in-hospital outcomes were similar between the groups with no, mild, and severe PH.
Moreover, there was no between-group difference in the rate of rejection at 1 year. Five-year survival rates were closely similar in the three groups, in the mid-70s.
Audience member Nahush A. Mokadam, MD, rose to praise Dr. Gaffey’s report.
“This is a great and important study. I think as a group we have been too conservative with pulmonary hypertension, so thank you for shining a good light on it,” said Dr. Mokadam of the University of Washington, Seattle.
Dr. Gaffey reported having no financial conflicts regarding the study, which was conducted free of commercial support.
AT THE WTSA ANNUAL MEETING
Key clinical point:
Major finding: It’s time to reconsider the practice of excluding patients with pulmonary hypertension from consideration for a donor heart.
Data source: A retrospective analysis of the United Network for Organ Sharing database including outcomes out to 5 years on 3,951 heart transplant recipients who had been bridged to transplant with an LVAD, most of whom had moderate or severe pulmonary hypertension before transplant.
Disclosures: This study was conducted free of commercial support. The presenter reported having no relevant financial conflicts of interest.
Incidence of adenomyosis in hysterectomy patients higher than previously reported
NATIONAL HARBOR, MD – Patients who experience chronic pelvic pain have higher rates of adenomyosis than previously thought, suggest new findings presented at the AAGL Global Congress.
Samantha P. Nadella, MD, and her associates conducted a retrospective cohort study analyzing 101 women with chronic pelvic pain who underwent hysterectomy between April 2014 and December 2016. In total, 51 patients (50.5%) were found to have adenomyosis. Previous studies of adenomyosis had suggested an overall incidence rate of 20%-35%. Dr. Nadella, currently of Kaiser Permanente South Bay Medical Center in Harbor City, Calif., conducted the study during her fellowship in minimally invasive gynecology surgery at St. Joseph’s Hospital and Medical Center in Phoenix.

“Anytime women have pelvic pain, or abdominal pain, they are always sent to their gynecologist,” Dr. Nadella said in an interview. However, there are many disorders that may present with pelvic pain but are not related to uterine pathology, including pelvic floor muscle dysfunction, interstitial cystitis, and irritable bowel syndrome. As suggested in this study, pelvic pain is frequently present in patients with IBS, both with and without adenomyosis.
“When we’re talking about hysterectomy and surgical management for pelvic pain, we need to do our due diligence to make sure we are not missing more treatable disorders, especially those with conservative treatments,” Dr. Nadella said. “It is important to counsel patients who are undergoing surgery for pelvic pain by explaining what will happen and what they can expect, including postsurgical pain and need for ongoing treatments. Additionally, cross-disciplinary communication is key in delivering more effective and personalized treatment of pelvic pain.”
Dr. Nadella reported having no financial disclosures.
NATIONAL HARBOR, MD – Patients who experience chronic pelvic pain have higher rates of adenomyosis than previously thought, suggest new findings presented at the AAGL Global Congress.
Samantha P. Nadella, MD, and her associates conducted a retrospective cohort study analyzing 101 women with chronic pelvic pain who underwent hysterectomy between April 2014 and December 2016. In total, 51 patients (50.5%) were found to have adenomyosis. Previous studies of adenomyosis had suggested an overall incidence rate of 20%-35%. Dr. Nadella, currently of Kaiser Permanente South Bay Medical Center in Harbor City, Calif., conducted the study during her fellowship in minimally invasive gynecology surgery at St. Joseph’s Hospital and Medical Center in Phoenix.
“Anytime women have pelvic pain, or abdominal pain, they are always sent to their gynecologist,” Dr. Nadella said in an interview. However, there are many disorders that may present with pelvic pain but are not related to uterine pathology, including pelvic floor muscle dysfunction, interstitial cystitis, and irritable bowel syndrome. As suggested in this study, pelvic pain is frequently present in patients with IBS, both with and without adenomyosis.
“When we’re talking about hysterectomy and surgical management for pelvic pain, we need to do our due diligence to make sure we are not missing more treatable disorders, especially those with conservative treatments,” Dr. Nadella said. “It is important to counsel patients who are undergoing surgery for pelvic pain by explaining what will happen and what they can expect, including postsurgical pain and need for ongoing treatments. Additionally, cross-disciplinary communication is key in delivering more effective and personalized treatment of pelvic pain.”
Dr. Nadella reported having no financial disclosures.
NATIONAL HARBOR, MD – Patients who experience chronic pelvic pain have higher rates of adenomyosis than previously thought, suggest new findings presented at the AAGL Global Congress.
Samantha P. Nadella, MD, and her associates conducted a retrospective cohort study analyzing 101 women with chronic pelvic pain who underwent hysterectomy between April 2014 and December 2016. In total, 51 patients (50.5%) were found to have adenomyosis. Previous studies of adenomyosis had suggested an overall incidence rate of 20%-35%. Dr. Nadella, currently of Kaiser Permanente South Bay Medical Center in Harbor City, Calif., conducted the study during her fellowship in minimally invasive gynecology surgery at St. Joseph’s Hospital and Medical Center in Phoenix.
“Anytime women have pelvic pain, or abdominal pain, they are always sent to their gynecologist,” Dr. Nadella said in an interview. However, there are many disorders that may present with pelvic pain but are not related to uterine pathology, including pelvic floor muscle dysfunction, interstitial cystitis, and irritable bowel syndrome. As suggested in this study, pelvic pain is frequently present in patients with IBS, both with and without adenomyosis.
“When we’re talking about hysterectomy and surgical management for pelvic pain, we need to do our due diligence to make sure we are not missing more treatable disorders, especially those with conservative treatments,” Dr. Nadella said. “It is important to counsel patients who are undergoing surgery for pelvic pain by explaining what will happen and what they can expect, including postsurgical pain and need for ongoing treatments. Additionally, cross-disciplinary communication is key in delivering more effective and personalized treatment of pelvic pain.”
Dr. Nadella reported having no financial disclosures.
AT AAGL 2017
Key clinical point:
Major finding: In total, 51 of 101 (50.5%) patients undergoing hysterectomy had adenomyosis.
Data source: Retrospective cohort study of 101 patients with chronic pain undergoing hysterectomy between April 2014 and December 2016 at a community hospital.
Disclosures: Dr. Nadella reported having no financial disclosures.
Your online reputation
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.

Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].
Have you ever run across an unfair or even malicious comment about you or your practice on one of those “doctor-rating” web sites? Some curmudgeon, angry about something totally irrelevant to your clinical skills, decided to publicly trash you; and the site, of course, made no effort to authenticate the writer or fact-check the complaint.
What to do? You could hire one of the many companies in the rapidly burgeoning field of online reputation management; but that can cost hundreds to thousands of dollars per month for monitoring and intervention, and there are no guarantees of success.
Leave design and SEO to the pros, but don’t delegate the content itself; as captain of the ship you are responsible for all the facts and opinions on your site. And remember that, once it’s online, it’s online forever; consider the ramifications of anything you post on any site – yours or others – before hitting the “send” button. “The most damaging item about you,” one consultant told me, “could well be something you posted yourself.” Just ask any of several prominent politicians who have famously sabotaged their own careers online.
That said, don’t be shy about creating content. Patients appreciate factual information, but they value your opinions too. Add a blog to your web site and write about subjects – medical and otherwise – that interest you. If you have expertise in a particular field, be sure to write about that.
Incidentally, if the URL for your web site is not your own name, you should register your name as a separate domain name – even if you never use it – to be sure that a trickster or troll, or someone with the same name but a bad reputation, doesn’t get it.
A web site is a powerful resource, but not the only one. Take advantage of Google’s free profiling tool at https://profiles.google.com/me, where you can create a sterling bio, complete with links to URLs, photos, and anything else that shows you in the best possible light. Your Google profile will, of course, be at or near the top of any Google search.
Wikipedia articles also go to the top of most searches, so if you’re notable enough to merit mention in one – or to have one of your own – see that it is done and updated regularly. Remember that Wikipedia’s conflict of interest rules forbid adding or editing content about yourself, so someone with a theoretically “neutral point of view” will have to do it for you.
Other useful resources are the social networking sites. Whatever your opinion of online networks, the reality is that personal pages on Facebook, LinkedIn, and Twitter rank very high on major search engines. (Some consultants say a favorable LinkedIn profile is particularly helpful because of that site’s reputation as a “professional” network.) Make your (noncontroversial) opinions known on these portals. Your community activities, charitable work, interesting hobbies – anything that casts you in a favorable light – also need to be mentioned prominently.
Set up an RSS news feed for yourself (directions to follow in the next two columns), so you’ll know immediately if your name pops up in news or gossip sites, or on blogs. If something untrue is posted about you, take action. Reputable news sites and blogs have their own reputations to protect and can usually be persuaded to correct anything that is demonstrably false. Try to get the error removed entirely or corrected within the original article. An erratum on the last page of the next edition will be ignored and will leave the false information online, intact.
Doctor-rating sites typically refuse to remove unfair comments unless they are blatantly libelous or a case of mistaken identity; but there is nothing wrong with encouraging happy patients to post favorable reviews on those sites. Sauce for the goose, and all that.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at [email protected].

Keep PCI patients on aspirin for noncardiac surgery
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.

The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.
The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
ANAHEIM, CALIF. – For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds, according to a substudy of the POISE-2 trial presented at the American Heart Association scientific sessions.
For patients with previous PCI undergoing noncardiac surgery, “I think aspirin will be more likely to benefit them than harm them,” so long as they are not having an operation where bleeding would be devastating.” These include “delicate neurosurgery in which, if you bleed into your spine, you end up paralyzed,” said lead investigator Michelle Graham, MD, an interventional cardiologist and professor of cardiology at the University of Alberta, Edmonton.
The original multisite POISE-2 trial (Perioperative Ischemic Evaluation 2) evaluated the effect of perioperative aspirin for noncardiac surgery. Patients were randomized to receive 200 mg aspirin or placebo within 4 hours of surgery and then 100 mg aspirin or placebo in the early postoperative period. There was no significant effect on the composite rate of death or myocardial infarction, but an increased risk of serious bleeding (N Engl J Med. 2014 Apr 17;370[16]:1494-503).
The new substudy focused on the 470 patients with previous PCIs, because such patients are known to have a higher risk for postop complications. More than half received bare-metal stents and a quarter got drug-eluting stents; in most of the rest, the stent type was not known. The median duration from PCI to noncardiac surgery was 64 months, ranging from 34 to 113 months. Patients with bare-metal stents placed within 6 weeks or drug-eluting stents within a year, were excluded.
Overall, 234 patients were randomized to the aspirin group, and 236 to placebo. Among those who came in on chronic, daily aspirin therapy – as almost all of the PCI subjects did – those who were randomized to perioperative aspirin stayed on daily 100 mg aspirin for a week postop, and then flipped back to whatever dose they were on at home. Likewise, placebo patients resumed their home aspirin after 1 week.
The results were very different from the main trial. At 30 days’ follow-up, just 6% of patients in the aspirin arm reached the primary endpoint of death or MI, versus 11.5% in the placebo group, a statistically significant 50% reduction.
This difference was driven almost entirely by a reduction in MIs. Whereas 5.1% of patients in the aspirin arm had MIs, 11% of the placebo group did, a significant 64% reduction. Meanwhile, the risk of major or life-threatening bleeding was not only similar between groups, but also to the overall trial, noted in 5.6% of aspirin and 4.2% of placebo subjects.
Over 75% of the participants were men, almost 60% were undergoing a major surgery, 30% had diabetes, and many had hypertension. Very few were on direct oral anticoagulants. The two arms were well matched, with a median age of about 68 years.
Simultaneously with Dr. Graham’s presentation, the results were published online (Ann Intern Med. 2017 Nov 14; doi: 10.7326/M17-2341)
The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. Dr. Graham has no industry disclosures.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: For every 1,000 patients with a history of percutaneous coronary intervention undergoing noncardiac surgery, perioperative aspirin would prevent 59 myocardial infarctions but cause 8 major/life-threatening bleeds.
Data source: POISE-2, a randomized trial of 470 PCI patients.
Disclosures: The work was funded mostly by the Canadian Institutes of Health Research. Bayer supplied the aspirin. The lead investigator has no industry disclosures.
DTaP vaccination rate highest in Maryland
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).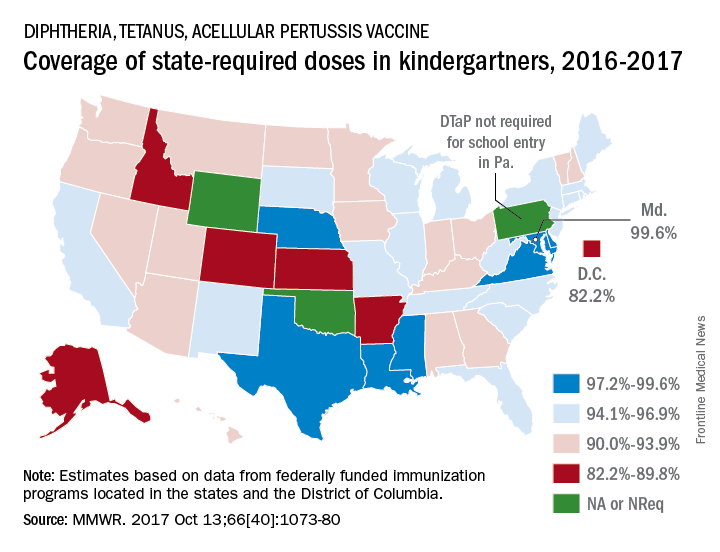
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
FROM MMWR
VIDEO: Regionalized STEMI care slashes in-hospital mortality
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.

Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.

Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.
Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.
Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
ANAHEIM, CALIF. – An American Heart Association program aimed at streamlining care of patients with ST-elevation MI resulted in a dramatic near-halving of in-hospital mortality, compared with STEMI patients treated in hospitals not participating in the project, James G. Jollis, MD, reported at the American Heart Association scientific sessions.
He presented the results of the STEMI ACCELERATOR 2 study, which involved 12 participating metropolitan regions across the United States, 132 percutaneous coronary intervention–capable hospitals, and 946 emergency medical services agencies. The ACCELERATOR 2 program entailed regional implementation of a structured STEMI care plan in which EMS personnel were trained to obtain prehospital ECGs and to activate cardiac catheterization labs prior to hospital arrival, bypassing the emergency department when appropriate.
Key elements of the project, which was part of the AHA’s Mission: Lifeline program, included having participating hospitals measure their performance of key processes and send that information as well as patient outcome data to the National Cardiovascular Data Registry’s ACTION–Get With The Guidelines registry. The hospitals in turn received quarterly feedback reports containing blinded hospital comparisons.
Dr. Jollis and his coinvestigators worked to obtain buy-in from local stakeholders, organize regional leadership, and help in drafting a central regional STEMI plan featuring prespecified treatment protocols.
The STEMI ACCELERATOR 2 study was carried out in 2015-2017, during which 10,730 patients with STEMI were transported directly to participating hospitals with PCI capability.
The primary study outcome was the change from the first to the final quarter of the study in the proportion of EMS-transported patients with a time from first medical contact to treatment in the cath lab of 90 minutes or less. This improved significantly, from 67% at baseline to 74% in the final quarter. Nine of the 12 participating regions reduced their time from first medical contact to treatment in the cath lab, and eight reached the national of goal of having 75% of STEMI patients treated within 90 minutes.
The other key time-to-care measures improved, too: At baseline, only 38% of patients had a time from first medical contact to cath lab activation of 20 minutes or less; by the final quarter, this figure had climbed to 56%. That’s an important metric, as evidenced by the study finding that in-hospital mortality occurred in 4.5% of patients with a time from first medical contact to cath lab activation of more than 20 minutes, compared with 2.2% in those with a time of 20 minutes or less.
Also, the proportion of patients who spent 20 minutes or less in the emergency department improved from 33% to 43%.
In-hospital mortality improved from 4.4% in the baseline quarter to 2.3% in the final quarter. No similar improvement in in-hospital mortality occurred in a comparison group of 22,651 STEMI patients treated at hospitals not involved in ACCELERATOR 2.
A significant reduction in the rate of in-hospital congestive heart failure occurred in the ACCELERATOR 2 centers, from 7.4% at baseline to 5.0%. In contrast, stroke, cardiogenic shock, and major bleeding rates were unchanged over time.
The ACCELERATOR 2 model of emergency cardiovascular care is designed to be highly generalizable, according to Dr. Jollis.
“This study supports the implementation of regionally coordinated systems across the United States to abort heart attacks, save lives, and enable heart attack victims to return to their families and productive lives,” he said.
The ACCELERATOR 2 operations manual – essentially a blueprint for organizing a regional STEMI system of care – is available gratis.
Dr. Allen, a cardiologist at the University of Colorado, Denver, said the ACCELERATOR 2 model has been successful because it is consistent with a fundamental principle of implementation science as described by Carolyn Clancy, MD, Executive in Charge at the Veterans Health Affairs Administration, who has said it’s a matter of making the right thing to do the easy thing to do.
Gregg C. Fonarow, MD, founder of the Get With the Guidelines program, predicted that the success of this program will lead to a ramping up of efforts to regionalize and coordinate STEMI care across the country. “I hope and anticipate that the AHA will take and run with the ACCELERATOR 2 model and adopt this into Mission: Lifeline, hoping to make this the standard approach to further improving care and outcomes in these patients,” said Dr. Fonarow, professor and cochief of cardiology at the University of California, Los Angeles, in a video interview.
Simultaneous with his presentation at the AHA conference, the results of STEMI ACCELERATOR 2 were published online in Circulation (2017 Nov 14; doi: 0.1161/CIRCULATIONAHA.117.032446).
The trial was sponsored by research and educational grants from AstraZeneca and The Medicines Company. Dr. Jollis reported having no financial conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point:
Major finding: The in-hospital mortality rate of STEMI patients dropped from 4.4% in the baseline quarter to 2.3% in the final quarter of a study that examined the impact of introducing regionalized STEMI care.
Data source: This was a prospective study of an intervention that involved implementation of regionalized STEMI care in a dozen U.S. metropolitan areas.
Disclosures: The study was sponsored by research and educational grants from AstraZeneca and The Medicines Company. The presenter reported having no financial conflicts of interest.
Long-term cholinesterase inhibition may slow cognitive decline – and more
BOSTON – Long-term use of cholinesterase inhibitors appears to confer a number of benefits, including protection from heart attack, stroke, diabetes-related mortality, and – according to a large new observational study – an annual 30% slowing of the cognitive decline associated with Alzheimer’s disease.
Long-term follow-up of thousands of patients in the Swedish Dementia Registry (SveDem) finds consistent, dose-dependent benefits associated with the drugs, Maria Eriksdotter, MD, said at the Clinical Trials on Alzheimer’s Disease conference. Most recently, her 3-year analysis of 29,000 patients showed that each year, those taking the drugs lost almost a point less on the Mini Mental State Exam (MMSE) than did nontreated patients.

“These drugs do reduce mortality and cardiovascular events, and improve cognitive decline,” she said in an interview. “It can be a difficult discussion to have with families, because yes, the patient is still declining, although more slowly. But combined with these other benefits that we are showing, I would say there is no reason not to get patients on a cholinesterase inhibitor as soon as possible. You want to get those benefits online as early as possible.”
The findings also strongly argue for cholinesterase inhibition to stay part of the standard treatment picture, even after disease-modifying medications do come on board.
“One could say you gain 30% of the decline back, and that 30% is something we could start from when we eventually begin talking about these therapies,” Dr. Eriksdotter said.
SveDem, launched in 2007, is a national project to improve the quality of diagnostics, treatment, and care of Swedish patients with dementia disorders. Patients newly diagnosed with a dementia disorder are registered and followed up yearly. Currently, it contains information on close to 70,000 patients.
The cognition study comprised almost 29,000 of those (CTAD abstract OC15). Dr. Eriksdotter and her colleagues categorized them as using or not using cholinesterase inhibitors (ChEI), and then examined the 3-year curves of cognitive decline, adjusting for age, sex, and a propensity score of whether or not they got a ChEI at baseline. The primary endpoint was MMSE decline by 3 years
At baseline, patients were a median of 80 years old. Alzheimer’s dementia was the most common diagnosis (63%), and 63% were taking a ChEI. Prescribing increased during each year of follow-up; by year 3, 91% were taking a ChEI. The median baseline MMSE was 22; this declined over time, to a median of 18. Patients taking the drugs were significantly younger than those not taking them (79 vs. 83 years), and less cognitively impaired (MMSE of 22 vs. 20). Most patients taking them had a diagnosis of Alzheimer’s dementia (70%), while others had a mix of vascular, frontotemporal, and Parkinson’s disease dementia.
Patients in both groups declined cognitively over the 3-year period, but the curves of decline were significantly different. The median MMSE decline regardless of treatment was 2.89 points. But in the fully adjusted model, those taking the drugs declined by about 0.85-point less each year than did those not taking them. This translated into an annual 30% reduction in cognitive decline, compared with untreated patients, Dr. Eriksdotter said.
She briefly discussed additional SveDem data supporting the drugs’ benefits in cardiovascular disorders and diabetes.
In 2013, she and her colleagues examined the link between ChEIs and heart attack in more than 7,000 SveDem registrants over a period of up to 5 years (Eur Heart J. 2013 Sep;34[33]:2585-91). After adjustment for confounding factors, the team found that ChEIs conferred a 34% risk reduction for a composite endpoint of myocardial infarction or death, compared with nonusers. The differences in the individual endpoints were also significant: a 36% lower risk of heart attack and 38% lower risk of death. She also found a dose-dependent response, with patients taking the highest recommended doses having the lowest risk of heart attack (hazard ratio, 0.35) and death (HR, 0.54).
Data from a similar study on stroke risk have been submitted for publication, Dr. Eriksdotter noted. This observational study comprised 22,300 patients followed for up to 5 years. Those who had ever taken a ChEI had a 33% decreased risk of ischemic stroke and 38% decreased risk of all-cause mortality. While the benefit was seen with the use of donepezil, rivastigmine, and galantamine, it was most pronounced with galantamine (30% decreased stroke risk, 32% decreased mortality risk). The study further determined that only patients taking high-dose ChEIs experienced the significant stroke benefit (HR, 0.59). The decreased risk of death was significant for all doses, but showed a dose-dependent benefit (low: HR, 0.85; medium: HR, 0.73; high: HR, 0.57).
Finally, Dr. Eriksdotter discussed a study in preparation comprising about 7,000 Alzheimer’s disease patients who also had diabetes. Of these, about 1,600 were taking a ChEI. In a fully adjusted model, the drugs were associated with a 16% decreased risk of death – exactly the same mortality benefit conferred by metformin. As an interesting side note, insulin use in this population was associated with a significant 15% increase in the risk of death, after full adjustment for confounding factors. None of the other antidiabetes medications (thiazolidinediones, dipeptidyl peptidase-4 inhibitors, or any newer drugs) showed any significant mortality benefit.
The protective mechanisms at work in these studies aren’t fully elucidated, Dr. Eriksdotter said. “But we do know that cholinesterase inhibitors exert an anti-inflammatory effect, and inflammation is definitely part of the cardiovascular disease and diabetes pictures. They also tend to slow heart rate, which has been found to have survival benefit in animal models.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
The cholinesterase inhibitors are widely used for patients with Alzheimer’s disease, and to some extent other forms of cognitive impairment (rightly or wrongly). Their observed symptomatic benefits are modest and families frequently question whether the drugs are having any beneficial effect. So the idea that they may have long-term benefits is an extremely encouraging thought.

We do not have all the information that may be available at this time, and all or many of these issues undoubtedly occurred to the investigators who may have controlled for them, or been able to at least partially control for them, so that for now, I want to believe and am hoping the investigators are able to justify that belief with further data.
Richard J. Caselli, MD, is professor of neurology and medical director for service at the Mayo Clinic, Scottsdale, Ariz., and is associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
The cholinesterase inhibitors are widely used for patients with Alzheimer’s disease, and to some extent other forms of cognitive impairment (rightly or wrongly). Their observed symptomatic benefits are modest and families frequently question whether the drugs are having any beneficial effect. So the idea that they may have long-term benefits is an extremely encouraging thought.
We do not have all the information that may be available at this time, and all or many of these issues undoubtedly occurred to the investigators who may have controlled for them, or been able to at least partially control for them, so that for now, I want to believe and am hoping the investigators are able to justify that belief with further data.
Richard J. Caselli, MD, is professor of neurology and medical director for service at the Mayo Clinic, Scottsdale, Ariz., and is associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
The cholinesterase inhibitors are widely used for patients with Alzheimer’s disease, and to some extent other forms of cognitive impairment (rightly or wrongly). Their observed symptomatic benefits are modest and families frequently question whether the drugs are having any beneficial effect. So the idea that they may have long-term benefits is an extremely encouraging thought.
We do not have all the information that may be available at this time, and all or many of these issues undoubtedly occurred to the investigators who may have controlled for them, or been able to at least partially control for them, so that for now, I want to believe and am hoping the investigators are able to justify that belief with further data.
Richard J. Caselli, MD, is professor of neurology and medical director for service at the Mayo Clinic, Scottsdale, Ariz., and is associate director and clinical core director of the Arizona Alzheimer’s Disease Center. He has no relevant disclosures.
BOSTON – Long-term use of cholinesterase inhibitors appears to confer a number of benefits, including protection from heart attack, stroke, diabetes-related mortality, and – according to a large new observational study – an annual 30% slowing of the cognitive decline associated with Alzheimer’s disease.
Long-term follow-up of thousands of patients in the Swedish Dementia Registry (SveDem) finds consistent, dose-dependent benefits associated with the drugs, Maria Eriksdotter, MD, said at the Clinical Trials on Alzheimer’s Disease conference. Most recently, her 3-year analysis of 29,000 patients showed that each year, those taking the drugs lost almost a point less on the Mini Mental State Exam (MMSE) than did nontreated patients.
“These drugs do reduce mortality and cardiovascular events, and improve cognitive decline,” she said in an interview. “It can be a difficult discussion to have with families, because yes, the patient is still declining, although more slowly. But combined with these other benefits that we are showing, I would say there is no reason not to get patients on a cholinesterase inhibitor as soon as possible. You want to get those benefits online as early as possible.”
The findings also strongly argue for cholinesterase inhibition to stay part of the standard treatment picture, even after disease-modifying medications do come on board.
“One could say you gain 30% of the decline back, and that 30% is something we could start from when we eventually begin talking about these therapies,” Dr. Eriksdotter said.
SveDem, launched in 2007, is a national project to improve the quality of diagnostics, treatment, and care of Swedish patients with dementia disorders. Patients newly diagnosed with a dementia disorder are registered and followed up yearly. Currently, it contains information on close to 70,000 patients.
The cognition study comprised almost 29,000 of those (CTAD abstract OC15). Dr. Eriksdotter and her colleagues categorized them as using or not using cholinesterase inhibitors (ChEI), and then examined the 3-year curves of cognitive decline, adjusting for age, sex, and a propensity score of whether or not they got a ChEI at baseline. The primary endpoint was MMSE decline by 3 years
At baseline, patients were a median of 80 years old. Alzheimer’s dementia was the most common diagnosis (63%), and 63% were taking a ChEI. Prescribing increased during each year of follow-up; by year 3, 91% were taking a ChEI. The median baseline MMSE was 22; this declined over time, to a median of 18. Patients taking the drugs were significantly younger than those not taking them (79 vs. 83 years), and less cognitively impaired (MMSE of 22 vs. 20). Most patients taking them had a diagnosis of Alzheimer’s dementia (70%), while others had a mix of vascular, frontotemporal, and Parkinson’s disease dementia.
Patients in both groups declined cognitively over the 3-year period, but the curves of decline were significantly different. The median MMSE decline regardless of treatment was 2.89 points. But in the fully adjusted model, those taking the drugs declined by about 0.85-point less each year than did those not taking them. This translated into an annual 30% reduction in cognitive decline, compared with untreated patients, Dr. Eriksdotter said.
She briefly discussed additional SveDem data supporting the drugs’ benefits in cardiovascular disorders and diabetes.
In 2013, she and her colleagues examined the link between ChEIs and heart attack in more than 7,000 SveDem registrants over a period of up to 5 years (Eur Heart J. 2013 Sep;34[33]:2585-91). After adjustment for confounding factors, the team found that ChEIs conferred a 34% risk reduction for a composite endpoint of myocardial infarction or death, compared with nonusers. The differences in the individual endpoints were also significant: a 36% lower risk of heart attack and 38% lower risk of death. She also found a dose-dependent response, with patients taking the highest recommended doses having the lowest risk of heart attack (hazard ratio, 0.35) and death (HR, 0.54).
Data from a similar study on stroke risk have been submitted for publication, Dr. Eriksdotter noted. This observational study comprised 22,300 patients followed for up to 5 years. Those who had ever taken a ChEI had a 33% decreased risk of ischemic stroke and 38% decreased risk of all-cause mortality. While the benefit was seen with the use of donepezil, rivastigmine, and galantamine, it was most pronounced with galantamine (30% decreased stroke risk, 32% decreased mortality risk). The study further determined that only patients taking high-dose ChEIs experienced the significant stroke benefit (HR, 0.59). The decreased risk of death was significant for all doses, but showed a dose-dependent benefit (low: HR, 0.85; medium: HR, 0.73; high: HR, 0.57).
Finally, Dr. Eriksdotter discussed a study in preparation comprising about 7,000 Alzheimer’s disease patients who also had diabetes. Of these, about 1,600 were taking a ChEI. In a fully adjusted model, the drugs were associated with a 16% decreased risk of death – exactly the same mortality benefit conferred by metformin. As an interesting side note, insulin use in this population was associated with a significant 15% increase in the risk of death, after full adjustment for confounding factors. None of the other antidiabetes medications (thiazolidinediones, dipeptidyl peptidase-4 inhibitors, or any newer drugs) showed any significant mortality benefit.
The protective mechanisms at work in these studies aren’t fully elucidated, Dr. Eriksdotter said. “But we do know that cholinesterase inhibitors exert an anti-inflammatory effect, and inflammation is definitely part of the cardiovascular disease and diabetes pictures. They also tend to slow heart rate, which has been found to have survival benefit in animal models.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
BOSTON – Long-term use of cholinesterase inhibitors appears to confer a number of benefits, including protection from heart attack, stroke, diabetes-related mortality, and – according to a large new observational study – an annual 30% slowing of the cognitive decline associated with Alzheimer’s disease.
Long-term follow-up of thousands of patients in the Swedish Dementia Registry (SveDem) finds consistent, dose-dependent benefits associated with the drugs, Maria Eriksdotter, MD, said at the Clinical Trials on Alzheimer’s Disease conference. Most recently, her 3-year analysis of 29,000 patients showed that each year, those taking the drugs lost almost a point less on the Mini Mental State Exam (MMSE) than did nontreated patients.
“These drugs do reduce mortality and cardiovascular events, and improve cognitive decline,” she said in an interview. “It can be a difficult discussion to have with families, because yes, the patient is still declining, although more slowly. But combined with these other benefits that we are showing, I would say there is no reason not to get patients on a cholinesterase inhibitor as soon as possible. You want to get those benefits online as early as possible.”
The findings also strongly argue for cholinesterase inhibition to stay part of the standard treatment picture, even after disease-modifying medications do come on board.
“One could say you gain 30% of the decline back, and that 30% is something we could start from when we eventually begin talking about these therapies,” Dr. Eriksdotter said.
SveDem, launched in 2007, is a national project to improve the quality of diagnostics, treatment, and care of Swedish patients with dementia disorders. Patients newly diagnosed with a dementia disorder are registered and followed up yearly. Currently, it contains information on close to 70,000 patients.
The cognition study comprised almost 29,000 of those (CTAD abstract OC15). Dr. Eriksdotter and her colleagues categorized them as using or not using cholinesterase inhibitors (ChEI), and then examined the 3-year curves of cognitive decline, adjusting for age, sex, and a propensity score of whether or not they got a ChEI at baseline. The primary endpoint was MMSE decline by 3 years
At baseline, patients were a median of 80 years old. Alzheimer’s dementia was the most common diagnosis (63%), and 63% were taking a ChEI. Prescribing increased during each year of follow-up; by year 3, 91% were taking a ChEI. The median baseline MMSE was 22; this declined over time, to a median of 18. Patients taking the drugs were significantly younger than those not taking them (79 vs. 83 years), and less cognitively impaired (MMSE of 22 vs. 20). Most patients taking them had a diagnosis of Alzheimer’s dementia (70%), while others had a mix of vascular, frontotemporal, and Parkinson’s disease dementia.
Patients in both groups declined cognitively over the 3-year period, but the curves of decline were significantly different. The median MMSE decline regardless of treatment was 2.89 points. But in the fully adjusted model, those taking the drugs declined by about 0.85-point less each year than did those not taking them. This translated into an annual 30% reduction in cognitive decline, compared with untreated patients, Dr. Eriksdotter said.
She briefly discussed additional SveDem data supporting the drugs’ benefits in cardiovascular disorders and diabetes.
In 2013, she and her colleagues examined the link between ChEIs and heart attack in more than 7,000 SveDem registrants over a period of up to 5 years (Eur Heart J. 2013 Sep;34[33]:2585-91). After adjustment for confounding factors, the team found that ChEIs conferred a 34% risk reduction for a composite endpoint of myocardial infarction or death, compared with nonusers. The differences in the individual endpoints were also significant: a 36% lower risk of heart attack and 38% lower risk of death. She also found a dose-dependent response, with patients taking the highest recommended doses having the lowest risk of heart attack (hazard ratio, 0.35) and death (HR, 0.54).
Data from a similar study on stroke risk have been submitted for publication, Dr. Eriksdotter noted. This observational study comprised 22,300 patients followed for up to 5 years. Those who had ever taken a ChEI had a 33% decreased risk of ischemic stroke and 38% decreased risk of all-cause mortality. While the benefit was seen with the use of donepezil, rivastigmine, and galantamine, it was most pronounced with galantamine (30% decreased stroke risk, 32% decreased mortality risk). The study further determined that only patients taking high-dose ChEIs experienced the significant stroke benefit (HR, 0.59). The decreased risk of death was significant for all doses, but showed a dose-dependent benefit (low: HR, 0.85; medium: HR, 0.73; high: HR, 0.57).
Finally, Dr. Eriksdotter discussed a study in preparation comprising about 7,000 Alzheimer’s disease patients who also had diabetes. Of these, about 1,600 were taking a ChEI. In a fully adjusted model, the drugs were associated with a 16% decreased risk of death – exactly the same mortality benefit conferred by metformin. As an interesting side note, insulin use in this population was associated with a significant 15% increase in the risk of death, after full adjustment for confounding factors. None of the other antidiabetes medications (thiazolidinediones, dipeptidyl peptidase-4 inhibitors, or any newer drugs) showed any significant mortality benefit.
The protective mechanisms at work in these studies aren’t fully elucidated, Dr. Eriksdotter said. “But we do know that cholinesterase inhibitors exert an anti-inflammatory effect, and inflammation is definitely part of the cardiovascular disease and diabetes pictures. They also tend to slow heart rate, which has been found to have survival benefit in animal models.”
She had no financial disclosures.
[email protected]
On Twitter @Alz_Gal
AT CTAD
Key clinical point:
Major finding: Patients taking the drugs lost almost 1 point less on the Mini Mental State Exam each year than did those who didn’t take them.
Data source: The 3-year observational study comprised almost 29,000 patients in the Swedish Dementia Registry.
Disclosures: Dr. Eriksdotter had no financial disclosures.
Cancer patients with TKI-induced hypothyroidism had better survival rates
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.

Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.

Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.
Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.
Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
VICTORIA, B.C. – When it comes to the adverse effects of tyrosine kinase inhibitors (TKIs), hypothyroidism appears to have a bright side, according to a retrospective cohort study among patients with nonthyroid cancers.
While taking one of these targeted agents, roughly a quarter of patients became overtly hypothyroid, an adverse effect that appears to be due in part to immune destruction. Risk was higher for women and earlier in therapy.
Relative to counterparts who remained euthyroid, overtly hypothyroid patients were 44% less likely to die after other factors were taken into account.
Hypothyroidism may reflect changes in immune activation, Dr. Angell proposed. “Additional studies may be helpful, both prospectively looking at the clinical importance of this finding [of survival benefit], and also potentially mechanistically, to understand the relationship between hypothyroidism and survival in these patients.”
“This is an innovative study that looked at an interesting clinical question,” observed session cochair Angela M. Leung, MD, of the University of California, Los Angeles, and an endocrinologist at both UCLA and the VA Greater Los Angeles Healthcare System.
Thyroid dysfunction is a well-known, common side effect of TKI therapy, Dr. Angell noted. “The possible mechanisms that have been suggested for this are direct toxicity on the thyroid gland, destructive thyroiditis, increased thyroid hormone clearance, and vascular endothelial growth factor (VEGF) inhibition, among others.”
Some previous research has suggested a possible survival benefit of TKI-induced hypothyroidism. But “there are limitations in our understanding of hypothyroidism in this setting, including the timing of onset, what risk factors there may be, and the effect of additional clinical variables on the survival effect seen,” Dr. Angell pointed out.
He and his coinvestigators studied 538 adult patients with nonthyroid cancers (mostly stage III or IV) who received a first TKI during 2000-2013 and were followed up through 2017. They excluded those who had preexisting thyroid disease or were on thyroid-related medications.
During TKI therapy, 26.7% of patients developed overt hypothyroidism, and another 13.2% developed subclinical hypothyroidism.
“For a given drug, patients were less likely to develop hypothyroidism when they were given it subsequent to another TKI, as opposed to it being the initial TKI,” Dr. Angell reported. But median time to onset of hypothyroidism was about 2.5 months, regardless.
Cumulative months of all TKI exposure during cancer treatment were not significantly associated with development of hypothyroidism.
In a multivariate analysis, patients were significantly more likely to develop hypothyroidism if they were female (odds ratio, 1.99) and significantly less likely if they had a longer total time on treatment (OR, 0.98) or received a non-TKI VEGF inhibitor (OR, 0.43). Age, race, and cumulative TKI exposure did not influence the outcome.
In a second multivariate analysis, patients’ risk of death was significantly lower if they developed overt hypothyroidism (hazard ratio, 0.56; P less than .0001), but not if they developed subclinical hypothyroidism (HR, 0.79; P = .1655).
Treatment of hypothyroidism did not appear to influence survival, according to Dr. Angell. However, “there wasn’t a specific decision on who was treated, how they were treated, [or] when they were treated,” he said. “So, it is difficult within this cohort to look specifically at which cutoff would be ideal” for initiating treatment.
Similarly, thyroid function testing was not standardized in this retrospectively identified cohort, so it was not possible to determine how long patients were hypothyroid and whether that had an impact, according to Dr. Angell.
Dr. Angell had no relevant conflicts of interest.
AT ATA 2017
Key clinical point:
Major finding: Relative to peers who remained euthyroid, patients who developed overt hypothyroidism had a reduced risk of death (HR, 0.56; P less than .0001).
Data source: A retrospective cohort study of 538 adult patients with mainly advanced nonthyroid cancers treated with a tyrosine kinase inhibitor.
Disclosures: Dr. Angell had no relevant conflicts of interest.
Higher hospital mortality in pediatric emergency transfer patients
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.

After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.
After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.
After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.