User login
Elagolix safely offers long-term endometriosis pain relief
NATIONAL HARBOR, MD. – Elagolix, an oral gonadotropin-releasing hormone antagonist, improved dysmenorrhea and nonmenstrual pelvic pain for a year or more in women with surgically-diagnosed endometriosis in two extension studies.
Women who had participated in two pivotal, 6-month studies of elagolix were given the option to continue in an extension trial for another 6 months, Sukhbir S. Singh, MD, said at the AAGL Global Congress. He noted that “all my patients who completed the 6-month trial continued out to a year.”

Patients continued on one of two doses of elagolix – 150 mg daily or 200 mg twice a day – with the lower dose providing partial estradiol suppression and the higher dose providing nearly complete suppression.
Patients tracked their dysmenorrhea and nonmenstrual pelvic pain scores on a 4-point scale daily using an electronic pain impact diary. They were classified as being responders if they experienced reduced dysmenorrhea and nonmenstrual pelvic pain equal to or better than they had during the original trial (much or very much improved on the Patient Global Impression of Change scale).
For each dose of elagolix, rates of response seen at 6 months in the original trial were maintained at a year or longer of continuous treatment, demonstrating long-term efficacy, Dr. Singh said. The average number of analgesic pills taken per month decreased 46%-77% from baseline for all doses in the extension studies.
The most common adverse events were hot flushes, experienced by just over half (52%-55%) of women in the high-dose group and about 25%-30% of women in the lower-dose group. Severity was mild to moderate across the studies.
“The higher the dose you give, the more hot flushes you get,” said Dr. Singh, vice chair of gynecology at the University of Ottawa, Ontario. “But overall, patients often did not complain of this because they were getting pain relief as well.”
Other adverse events included headache in about 25%-30% of high-dose patients and 20% of low-dose patients, as well as nausea in about one-fifth of patients overall. Some decreases from baseline in bone mineral density were seen but there was progressive improvement upon discontinuation of elagolix, Dr. Singh noted.
Importantly, “these were patients who had endometriosis and pain, similar in makeup to groups studied by others. These studies did provide two dosing options to offer individualized approaches and pain results were controlled for use of rescue analgesia. But as extension trials, the studies are limited by having no placebo control and we did not know whether they had deep endometriosis or other pain issues,” Dr. Singh said.
Elagolix represents another treatment option for patients with endometriosis, Dr. Singh said. “One of the objections to taking currently approved [gonadotropin-releasing hormone] antagonists is that they are subcutaneous injections. Patients don’t like that – this is an oral option. It is quick to act and is rapidly reversible as well.”
Dr. Singh serves as a principal investigator and speaker for Allergan, AbbVie, and Bayer. The studies were sponsored by AbbVie.
[email protected]
On Twitter @denisefulton
NATIONAL HARBOR, MD. – Elagolix, an oral gonadotropin-releasing hormone antagonist, improved dysmenorrhea and nonmenstrual pelvic pain for a year or more in women with surgically-diagnosed endometriosis in two extension studies.
Women who had participated in two pivotal, 6-month studies of elagolix were given the option to continue in an extension trial for another 6 months, Sukhbir S. Singh, MD, said at the AAGL Global Congress. He noted that “all my patients who completed the 6-month trial continued out to a year.”
Patients continued on one of two doses of elagolix – 150 mg daily or 200 mg twice a day – with the lower dose providing partial estradiol suppression and the higher dose providing nearly complete suppression.
Patients tracked their dysmenorrhea and nonmenstrual pelvic pain scores on a 4-point scale daily using an electronic pain impact diary. They were classified as being responders if they experienced reduced dysmenorrhea and nonmenstrual pelvic pain equal to or better than they had during the original trial (much or very much improved on the Patient Global Impression of Change scale).
For each dose of elagolix, rates of response seen at 6 months in the original trial were maintained at a year or longer of continuous treatment, demonstrating long-term efficacy, Dr. Singh said. The average number of analgesic pills taken per month decreased 46%-77% from baseline for all doses in the extension studies.
The most common adverse events were hot flushes, experienced by just over half (52%-55%) of women in the high-dose group and about 25%-30% of women in the lower-dose group. Severity was mild to moderate across the studies.
“The higher the dose you give, the more hot flushes you get,” said Dr. Singh, vice chair of gynecology at the University of Ottawa, Ontario. “But overall, patients often did not complain of this because they were getting pain relief as well.”
Other adverse events included headache in about 25%-30% of high-dose patients and 20% of low-dose patients, as well as nausea in about one-fifth of patients overall. Some decreases from baseline in bone mineral density were seen but there was progressive improvement upon discontinuation of elagolix, Dr. Singh noted.
Importantly, “these were patients who had endometriosis and pain, similar in makeup to groups studied by others. These studies did provide two dosing options to offer individualized approaches and pain results were controlled for use of rescue analgesia. But as extension trials, the studies are limited by having no placebo control and we did not know whether they had deep endometriosis or other pain issues,” Dr. Singh said.
Elagolix represents another treatment option for patients with endometriosis, Dr. Singh said. “One of the objections to taking currently approved [gonadotropin-releasing hormone] antagonists is that they are subcutaneous injections. Patients don’t like that – this is an oral option. It is quick to act and is rapidly reversible as well.”
Dr. Singh serves as a principal investigator and speaker for Allergan, AbbVie, and Bayer. The studies were sponsored by AbbVie.
[email protected]
On Twitter @denisefulton
NATIONAL HARBOR, MD. – Elagolix, an oral gonadotropin-releasing hormone antagonist, improved dysmenorrhea and nonmenstrual pelvic pain for a year or more in women with surgically-diagnosed endometriosis in two extension studies.
Women who had participated in two pivotal, 6-month studies of elagolix were given the option to continue in an extension trial for another 6 months, Sukhbir S. Singh, MD, said at the AAGL Global Congress. He noted that “all my patients who completed the 6-month trial continued out to a year.”
Patients continued on one of two doses of elagolix – 150 mg daily or 200 mg twice a day – with the lower dose providing partial estradiol suppression and the higher dose providing nearly complete suppression.
Patients tracked their dysmenorrhea and nonmenstrual pelvic pain scores on a 4-point scale daily using an electronic pain impact diary. They were classified as being responders if they experienced reduced dysmenorrhea and nonmenstrual pelvic pain equal to or better than they had during the original trial (much or very much improved on the Patient Global Impression of Change scale).
For each dose of elagolix, rates of response seen at 6 months in the original trial were maintained at a year or longer of continuous treatment, demonstrating long-term efficacy, Dr. Singh said. The average number of analgesic pills taken per month decreased 46%-77% from baseline for all doses in the extension studies.
The most common adverse events were hot flushes, experienced by just over half (52%-55%) of women in the high-dose group and about 25%-30% of women in the lower-dose group. Severity was mild to moderate across the studies.
“The higher the dose you give, the more hot flushes you get,” said Dr. Singh, vice chair of gynecology at the University of Ottawa, Ontario. “But overall, patients often did not complain of this because they were getting pain relief as well.”
Other adverse events included headache in about 25%-30% of high-dose patients and 20% of low-dose patients, as well as nausea in about one-fifth of patients overall. Some decreases from baseline in bone mineral density were seen but there was progressive improvement upon discontinuation of elagolix, Dr. Singh noted.
Importantly, “these were patients who had endometriosis and pain, similar in makeup to groups studied by others. These studies did provide two dosing options to offer individualized approaches and pain results were controlled for use of rescue analgesia. But as extension trials, the studies are limited by having no placebo control and we did not know whether they had deep endometriosis or other pain issues,” Dr. Singh said.
Elagolix represents another treatment option for patients with endometriosis, Dr. Singh said. “One of the objections to taking currently approved [gonadotropin-releasing hormone] antagonists is that they are subcutaneous injections. Patients don’t like that – this is an oral option. It is quick to act and is rapidly reversible as well.”
Dr. Singh serves as a principal investigator and speaker for Allergan, AbbVie, and Bayer. The studies were sponsored by AbbVie.
[email protected]
On Twitter @denisefulton
AT AAGL 2107
Key clinical point:
Major finding: The most common adverse event was hot flushes seen in about half of women on the higher dose of elagolix.
Data source: Two randomized extension trials of 569 women.
Disclosures: Dr. Singh serves as a principal investigator and speaker for Allergan, AbbVie, and Bayer. The studies were sponsored by AbbVie.
Genetic testing may improve diagnosis of endometriosis
NATIONAL HARBOR, MD. –Genetic testing could provide a useful noninvasive diagnostic tool in identifying patients with endometriosis, according to a study conducted by Nick Fogelson, MD, of Pearl Women’s Center in Portland, Ore., and his colleagues.
Dr. Fogelson presented the findings from a blinded, randomized pilot study at the AAGL Global Congress. The study included two groups of 200 women each. The first group of women had previously been diagnosed with endometriosis. The second group comprised women with no evidence of endometriosis. In the group with endometriosis, the test correctly identified endometriosis in 189 of the 200 women (95%). The women with no evidence of endometriosis were accurately identified as having a low risk of developing endometriosis in 176 of 200 women (88%).
The samples were collected from around the United States as part of ongoing research by the Utah-based genetics company Juneau Biosciences.
Both groups were genotyped for 1,067 low-frequency DNA variants associated with endometriosis using a proprietary algorithm. The researchers then compared genotype results with a large dataset of 1,000 genotyped endometriosis patients and 33,000 published controls and assessed patient risk of developing endometriosis by weighting each genotype by the logarithm of the odds ratio.
“We’re getting toward a time when you will be able to tell if someone has endometriosis by looking at their genetics,” Dr. Fogelson said.
The genetic analysis hold potential in a disease state where misdiagnosis by nonexpert physicians can be high. Dr. Fogelson estimated that the misdiagnosis rate in endometriosis based on physical exam and patient history alone is about 50%. Compounding this issue, many insurers have reduced payment for diagnostic laparoscopy leading to surgeons’ placing patients on long-term medication treatments when they would benefit from surgery, Dr. Fogelson said.
“Noninvasive DNA testing may help to direct symptomatic patients to specialists who can effectively treat the disease state.” Dr. Fogelson and his colleagues wrote in the study abstract. “DNA markers might have better correlation to the subtypes and extent of disease than histology alone.”
Additional trials are currently underway using the genetic marker test; one is a prospective study and is expected to be completed in early 2018.
Dr. Fogelson reported having no conflicts of interest. Other researchers on the study work for Juneau Biosciences and receive stock options as part of their compensation.
NATIONAL HARBOR, MD. –Genetic testing could provide a useful noninvasive diagnostic tool in identifying patients with endometriosis, according to a study conducted by Nick Fogelson, MD, of Pearl Women’s Center in Portland, Ore., and his colleagues.
Dr. Fogelson presented the findings from a blinded, randomized pilot study at the AAGL Global Congress. The study included two groups of 200 women each. The first group of women had previously been diagnosed with endometriosis. The second group comprised women with no evidence of endometriosis. In the group with endometriosis, the test correctly identified endometriosis in 189 of the 200 women (95%). The women with no evidence of endometriosis were accurately identified as having a low risk of developing endometriosis in 176 of 200 women (88%).
The samples were collected from around the United States as part of ongoing research by the Utah-based genetics company Juneau Biosciences.
Both groups were genotyped for 1,067 low-frequency DNA variants associated with endometriosis using a proprietary algorithm. The researchers then compared genotype results with a large dataset of 1,000 genotyped endometriosis patients and 33,000 published controls and assessed patient risk of developing endometriosis by weighting each genotype by the logarithm of the odds ratio.
“We’re getting toward a time when you will be able to tell if someone has endometriosis by looking at their genetics,” Dr. Fogelson said.
The genetic analysis hold potential in a disease state where misdiagnosis by nonexpert physicians can be high. Dr. Fogelson estimated that the misdiagnosis rate in endometriosis based on physical exam and patient history alone is about 50%. Compounding this issue, many insurers have reduced payment for diagnostic laparoscopy leading to surgeons’ placing patients on long-term medication treatments when they would benefit from surgery, Dr. Fogelson said.
“Noninvasive DNA testing may help to direct symptomatic patients to specialists who can effectively treat the disease state.” Dr. Fogelson and his colleagues wrote in the study abstract. “DNA markers might have better correlation to the subtypes and extent of disease than histology alone.”
Additional trials are currently underway using the genetic marker test; one is a prospective study and is expected to be completed in early 2018.
Dr. Fogelson reported having no conflicts of interest. Other researchers on the study work for Juneau Biosciences and receive stock options as part of their compensation.
NATIONAL HARBOR, MD. –Genetic testing could provide a useful noninvasive diagnostic tool in identifying patients with endometriosis, according to a study conducted by Nick Fogelson, MD, of Pearl Women’s Center in Portland, Ore., and his colleagues.
Dr. Fogelson presented the findings from a blinded, randomized pilot study at the AAGL Global Congress. The study included two groups of 200 women each. The first group of women had previously been diagnosed with endometriosis. The second group comprised women with no evidence of endometriosis. In the group with endometriosis, the test correctly identified endometriosis in 189 of the 200 women (95%). The women with no evidence of endometriosis were accurately identified as having a low risk of developing endometriosis in 176 of 200 women (88%).
The samples were collected from around the United States as part of ongoing research by the Utah-based genetics company Juneau Biosciences.
Both groups were genotyped for 1,067 low-frequency DNA variants associated with endometriosis using a proprietary algorithm. The researchers then compared genotype results with a large dataset of 1,000 genotyped endometriosis patients and 33,000 published controls and assessed patient risk of developing endometriosis by weighting each genotype by the logarithm of the odds ratio.
“We’re getting toward a time when you will be able to tell if someone has endometriosis by looking at their genetics,” Dr. Fogelson said.
The genetic analysis hold potential in a disease state where misdiagnosis by nonexpert physicians can be high. Dr. Fogelson estimated that the misdiagnosis rate in endometriosis based on physical exam and patient history alone is about 50%. Compounding this issue, many insurers have reduced payment for diagnostic laparoscopy leading to surgeons’ placing patients on long-term medication treatments when they would benefit from surgery, Dr. Fogelson said.
“Noninvasive DNA testing may help to direct symptomatic patients to specialists who can effectively treat the disease state.” Dr. Fogelson and his colleagues wrote in the study abstract. “DNA markers might have better correlation to the subtypes and extent of disease than histology alone.”
Additional trials are currently underway using the genetic marker test; one is a prospective study and is expected to be completed in early 2018.
Dr. Fogelson reported having no conflicts of interest. Other researchers on the study work for Juneau Biosciences and receive stock options as part of their compensation.
AT AAGL 2017
Key clinical point:
Major finding: A total of 189 of 200 women (95%) with endometriosis were correctly classified with the disorder. Also, 176 of 200 women (88%) with no evidence of endometriosis were correctly classified as having a low risk of endometriosis.
Data source: Blinded, randomized pilot study of two groups composed of 200 women each. One group consisted of women with confirmed endometriosis and the other group consisted of women with no evidence of endometriosis.
Disclosures: Dr. Fogelson reported having no conflicts of interest. Other researchers on the study work for Juneau Biosciences and receive stock options as part of their compensation.
Primary Mucinous Carcinoma of the Eyelid Treated With Mohs Micrographic Surgery
To the Editor:
Primary mucinous carcinoma (PMC) is an exceedingly rare adnexal tumor with an incidence of 0.07 cases per million individuals.1,2 First described by Lennox et al3 in 1952, this entity often presents as slow-growing, solitary nodules that often are soft on palpation but may have an indurated quality and range in color from reddish blue to flesh colored to white.4 Primary mucinous carcinoma most commonly is found on the eyelid (38%) but may affect other sites on the face (20.3%), scalp (16%), and axilla (10%).5 Historically, it has been thought to be more common among men; however, a 2005 large case series by Kazakov et al5 found that women were twice as likely to be affected. Primary mucinous carcinoma most frequently is diagnosed in the fifth through seventh decades of life, with a median age at onset of 63 years.6,7 Because of its rarity, PMC is most frequently confused clinically with basal cell carcinoma, keratoacanthoma, apocrine hidrocystoma, epidermoid cyst, Kaposi sarcoma, neuroma, lacrimal sac tumor, squamous cell carcinoma, granulomatous tumors, and metastatic adenocarcinoma.1,8-10
Primary mucinous carcinoma is thought to be derived from sweat glands, and select features such as decapitation secretion are more suggestive of apocrine than eccrine differentiation.5,8 On histopathology, PMC classically is described as nests of epithelial cells floating in lakes of extracellular mucin, primarily in the dermis and subcutis. The nests are composed of basaloid cells in solid to cribriform arrangements, usually with a low mitotic count and little nuclear atypia. These nests are suspended within periodic acid–Schiff positive mucinous pools partitioned by delicate fibrous septa. The mucin produced by PMC is sialomucin, and as such it is hyaluronidase resistant and sialidase labile.6 At least 1 report has been made of the presence of psammoma bodies in PMC.11
The neoplasm is characterized by an indolent course with frequent recurrence but rare metastasis.5,12 Treatment is primarily surgical, with Mohs micrographic surgery (MMS) offering improved tissue conservation and reduced recurrence rates.12 The diagnostic challenge lies in distinguishing PMC from a variety of metastatic mucinous internal malignancies that portend a notably greater morbidity and mortality to the patient. We describe a case of PMC, discuss the differentiation of PMC from metastatic mucinous carcinoma, and review the literature regarding treatment of this rare neoplasm.
A 65-year-old white woman was referred to our tertiary-care dermatologic surgery clinic for treatment of an incompletely excised mucinous carcinoma of the right lateral canthus (Figure 1). The clinically evident scar measured 0.5×0.5 cm. Although difficult to appreciate in Figure 1, a slight textural change of the surrounding skin, including the upper and lower eyelid, was apparent. Prior to her arrival to our clinic, the referring physician had completed a thorough review of systems and physical examination, which did not suggest an underlying malignancy. Computed tomography of the head, neck, chest, abdomen, and pelvis revealed a mass in the thyroid that was removed and found to be benign. The patient’s cutaneous lesion was therefore considered to be a PMC of the skin.

Given the prior incomplete excision of the lesion and its periocular location, we treated the patient with MMS. After 6 surgical stages, we continued to see evidence of the neoplasm as it tracked medially along the orbicularis oculi muscle (Figure 2). Due to the patient’s physical and emotional exhaustion at this point, we discontinued MMS and referred her to a colleague in plastic surgery for further excision of the remaining focus of positivity as well as repair. The final Mohs defect measured 4.2×4.0 cm (Figure 3). Approximately 2.3×1.0 cm of tissue in the area of remaining tumor was excised by plastic surgery, and the defect was repaired with a cervicofacial advancement flap closure of the right cheek and lower eyelid and full-thickness skin graft of the left upper eyelid. Histopathologic investigation found the additional tissue resected to be free of residual tumor.

To diagnose a patient with PMC, one must first rule out cutaneous metastasis of various internal malignancies that may appear similar on histopathology. A full clinical investigation consisting of a thorough history, physical examination, and appropriate radiographic imaging is required. Cutaneous metastases most commonly arise from the breast or gastrointestinal tract (GIT) but also can originate from the prostate, lungs, ovaries, pancreas, and kidneys.5 Histologically, PMC may be identical to metastatic adenocarcinoma.13 Location on the body may be a clue to a lesion’s origin, as metastases from a mucinous adenocarcinoma of the breast typically occur on the chest, breast, or axilla,5 whereas PMC primarily is found on the head and neck.
Certain histopathologic features may be suggestive of either a primary or metastatic etiology. Lesions arising in the skin may reveal an in situ component representing ductal hyperplasia, atypical ductal hyperplasia, or ductal carcinoma in situ. Identification of an in situ component defines a cutaneous primary neoplasm, but its absence does not exclude PMC.5 Additionally, metastatic lesions from the GIT typically have greater pleomorphism and “dirty” necrosis defined as eosinophilic foci containing nuclear debris.5
The expression pattern of cytokeratins (CKs) also can be suggestive. Primary mucinous carcinoma and metastatic breast adenocarcinoma are both CK7+ and CK20−. By contrast, mucinous adenocarcinoma of the GIT stains CK20+ and CK7−.14 Another marker that stains PMC is CK5 and CK6, though infrequently present. Levy et al15 reported positive staining for CK5 and CK6 in only 1 of 5 PMC cases. Positive staining for CK5 and CK6 has not been reported in any metastatic mucinous carcinoma.
The role of p63 immunostaining in the setting of mucinous carcinoma is controversial.16-18 Some practi-tioners have reported using p63 immunostaining to assist in establishing the diagnosis of PMC but only after performing a clinical workup to search for any primary sites of mucinous carcinoma in other organs.11 Other studies, however, have found select metastatic lesions from the breast17,18 and GIT18 to stain positively with p63. It is important to remember that these clinical and pathologic features are only suggestive of the primary etiology and are not replacement for a full clinical investigation.
Primary mucinous carcinoma is considered an indolent tumor with the majority of patient morbidity attributable to local recurrence and regional metastasis. Although uncommon, regional and distant metastasis rates have been reported to be 11% and 3%, respectively.19 Direct lymphatic invasion has been reported and indicates a more aggressive tumor with shorter recurrence-free intervals and predicts nodal metastases. Paradela et al20 recommended the use of D2-40, a monoclonal antibody and specific marker for lymphatic endothelium, to detect lymphatic invasion, particularly in node-negative primary tumors.
In one case of PMC on the jaw of a 39-year-old Japanese man, no recurrence or metastases were discovered until the 11th year of follow-up. At that time, he was found to have lung and bone metastases and died after 3 years.21 Other investigators report death occurring 4 to 24 months following diagnosis of distant metastases.7,22 Direct extension of the tumor into skeletal muscle, periosteum, bone, and dura also has been documented.7
Treatment principally is surgical, with PMC known to be resistant to both chemotherapy and radiation therapy.19,22 The recommended margins for simple excision range from 1 to 2 cm, but this method of treatment yields recurrence rates upward of 30% to 40%, especially for lesions located on the eyelid.12,13 First utilized in PMC of the eyelid to conserve tissue, MMS is rapidly becoming the treatment of choice because of its notably improved recurrence rate. A case series of 4 PMCs of the eyelid treated via MMS or frozen section control found the recurrence rate to be 7%.23 Another report of 2 cases of PMC treated by MMS reported no recurrence after 42 and 26 months.13 Ortiz et al7 reported an additional case of a patient treated by MMS that was recurrence free for 30 months at the time of publication. Further investigation is required to definitively recommend MMS on the basis of improved recurrence rate but should now be considered standard of care in recurrent, sizeable, or eyelid PMC.
Despite its ascension as treatment of choice in many cases of PMC, MMS is not without its risk of metastasis and recurrence. Tam et al24 reported a case of PMC with multiple recurrences and metastases following 3 simple excisions and 2 excisions via MMS. Although the lesion’s previously recurrent nature increased the likelihood of failure of MMS, this case demonstrates that all patients should be followed periodically after the treatment of PMC.
We presented a case of PMC in which standard surgical margins would have been insufficient to clear the lesion. Mohs micrographic surgery was used to remove the majority of the tumor. As is common in PMC, the lesion was indolent and periocular in location. It also was incompletely excised due to notable subclinical extension, which is common for PMC. The distinction of PMC from metastatic mucinous carcinoma is paramount but sometimes difficult. Randomized controlled trials are lacking with regards to preferred method of treatment, but MMS has shown benefit and should be considered for recurrent lesions and lesions in cosmetically sensitive areas.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Martinez SR, Young SE. Primary mucinous carcinoma of the skin: a review. Int J Oncol. 2005;2:432-437.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Marra DE, Schanbacher CF, Torres A. Mohs micrographic surgery of primary cutaneous mucinous carcinoma using immunohistochemistry for margin control. Dermatol Surg. 2004;30:799-802.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
- Mendoza S, Helwig EB. Mucinous (adenocystic) carcinoma of the skin. Arch Dermatol. 1971;103:68-78.
- Ortiz KJ, Gaughan MD, Bang RH, et al. A case of primary mucinous carcinoma of the scalp treated with Mohs surgery. Dermatol Surg. 2002;28:751-754.
- Bellezza G, Sidoni A, Bucciarelli E. Primary mucinous carcinoma of the skin. Am J Dermatopathol. 2000;22:166-170.
- Teng P, Muir J. Small primary cutaneous mucinous carcinoma mimicking an early basal cell carcinoma. Dermatol Online J. 2013;19:3.
- Terada T, Sato Y, Furukawa K, et al. Primary cutaneous mucinous carcinoma initially diagnosed as metastatic adenocarcinoma. Tohoku J Exp Med. 2004;203:345-348.
- Kalebi A, Hale M. Primary mucinous carcinoma of the skin: usefulness of p63 in excluding metastasis and first report of psammoma bodies. Am J Dermatopathol. 2008;30:510.
- Cabell CE, Helm KF, Sakol PJ, et al. Primary mucinous carcinoma in a 54-year-old man. J Am Acad Dermatol. 2003;49:941-943.
- Cecchi R, Rapicano V. Primary cutaneous mucinous carcinoma: report of two cases treated with Mohs’ micrographic surgery. Australas J Dermatol. 2006;47:192-194.
- Eckert F, Schmid U, Hardmeier T, et al. Cytokeratin expression in mucinous sweat gland carcinomas: an immunohistochemical analysis of four cases. Histopathology. 1992;21:161-165.
- Levy G, Finkelstein A, McNiff JM. Immunohistochemical techniques to compare primary vs. metastatic mucinous carcinoma of the skin. J Cutan Pathol. 2010;37:411-415.
- Ivan D, Hafeez Diwan A, Prieto VG. Expression of p63 in primary cutaneous adnexal neoplasms and adenocarcinoma metastatic to the skin. Mod Pathol. 2005;18:137-142.
- Kanitakis J, Chouvet B. Expression of p63 in cutaneous metastases. Am J Clin Pathol. 2007;128:753-758.
- Sariya D, Ruth K, Adams-McDonnell R, et al. Clinicopathologic correlation of cutaneous metastases: experience from a cancer center. Arch Dermatol. 2007;143:613-620.
- Snow SN, Reizner GT. Mucinous eccrine carcinoma of the eyelid. Cancer. 1992;70:2099-2104.
- Paradela S, Castiñeiras I, Cuevas J, et al. Mucinous carcinoma of the skin: evaluation of lymphatic invasion with D2-40. Am J Dermatopathol. 2008;30:504-508.
- Miyasaka M, Tanaka R, Hirabayashi K, et al. Primary mucinous carcinoma of the skin: a case of metastasis after 10 years of disease-free interval. Eur J Plast Surg. 2009;32:189-193.
- Yeung KY, Stinson JC. Mucinous (adenocystic) carcinoma of sweat glands with widespread metastasis. case report with ultrastructural study. Cancer. 1977;39:2556-2562.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathologic and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Tam CC, Dare DM, DiGiovanni JJ, et al. Recurrent and metastatic primary cutaneous mucinous carcinoma after excision and Mohs micrographic surgery. Cutis. 2011;87:245-248.
To the Editor:
Primary mucinous carcinoma (PMC) is an exceedingly rare adnexal tumor with an incidence of 0.07 cases per million individuals.1,2 First described by Lennox et al3 in 1952, this entity often presents as slow-growing, solitary nodules that often are soft on palpation but may have an indurated quality and range in color from reddish blue to flesh colored to white.4 Primary mucinous carcinoma most commonly is found on the eyelid (38%) but may affect other sites on the face (20.3%), scalp (16%), and axilla (10%).5 Historically, it has been thought to be more common among men; however, a 2005 large case series by Kazakov et al5 found that women were twice as likely to be affected. Primary mucinous carcinoma most frequently is diagnosed in the fifth through seventh decades of life, with a median age at onset of 63 years.6,7 Because of its rarity, PMC is most frequently confused clinically with basal cell carcinoma, keratoacanthoma, apocrine hidrocystoma, epidermoid cyst, Kaposi sarcoma, neuroma, lacrimal sac tumor, squamous cell carcinoma, granulomatous tumors, and metastatic adenocarcinoma.1,8-10
Primary mucinous carcinoma is thought to be derived from sweat glands, and select features such as decapitation secretion are more suggestive of apocrine than eccrine differentiation.5,8 On histopathology, PMC classically is described as nests of epithelial cells floating in lakes of extracellular mucin, primarily in the dermis and subcutis. The nests are composed of basaloid cells in solid to cribriform arrangements, usually with a low mitotic count and little nuclear atypia. These nests are suspended within periodic acid–Schiff positive mucinous pools partitioned by delicate fibrous septa. The mucin produced by PMC is sialomucin, and as such it is hyaluronidase resistant and sialidase labile.6 At least 1 report has been made of the presence of psammoma bodies in PMC.11
The neoplasm is characterized by an indolent course with frequent recurrence but rare metastasis.5,12 Treatment is primarily surgical, with Mohs micrographic surgery (MMS) offering improved tissue conservation and reduced recurrence rates.12 The diagnostic challenge lies in distinguishing PMC from a variety of metastatic mucinous internal malignancies that portend a notably greater morbidity and mortality to the patient. We describe a case of PMC, discuss the differentiation of PMC from metastatic mucinous carcinoma, and review the literature regarding treatment of this rare neoplasm.
A 65-year-old white woman was referred to our tertiary-care dermatologic surgery clinic for treatment of an incompletely excised mucinous carcinoma of the right lateral canthus (Figure 1). The clinically evident scar measured 0.5×0.5 cm. Although difficult to appreciate in Figure 1, a slight textural change of the surrounding skin, including the upper and lower eyelid, was apparent. Prior to her arrival to our clinic, the referring physician had completed a thorough review of systems and physical examination, which did not suggest an underlying malignancy. Computed tomography of the head, neck, chest, abdomen, and pelvis revealed a mass in the thyroid that was removed and found to be benign. The patient’s cutaneous lesion was therefore considered to be a PMC of the skin.
Given the prior incomplete excision of the lesion and its periocular location, we treated the patient with MMS. After 6 surgical stages, we continued to see evidence of the neoplasm as it tracked medially along the orbicularis oculi muscle (Figure 2). Due to the patient’s physical and emotional exhaustion at this point, we discontinued MMS and referred her to a colleague in plastic surgery for further excision of the remaining focus of positivity as well as repair. The final Mohs defect measured 4.2×4.0 cm (Figure 3). Approximately 2.3×1.0 cm of tissue in the area of remaining tumor was excised by plastic surgery, and the defect was repaired with a cervicofacial advancement flap closure of the right cheek and lower eyelid and full-thickness skin graft of the left upper eyelid. Histopathologic investigation found the additional tissue resected to be free of residual tumor.
To diagnose a patient with PMC, one must first rule out cutaneous metastasis of various internal malignancies that may appear similar on histopathology. A full clinical investigation consisting of a thorough history, physical examination, and appropriate radiographic imaging is required. Cutaneous metastases most commonly arise from the breast or gastrointestinal tract (GIT) but also can originate from the prostate, lungs, ovaries, pancreas, and kidneys.5 Histologically, PMC may be identical to metastatic adenocarcinoma.13 Location on the body may be a clue to a lesion’s origin, as metastases from a mucinous adenocarcinoma of the breast typically occur on the chest, breast, or axilla,5 whereas PMC primarily is found on the head and neck.
Certain histopathologic features may be suggestive of either a primary or metastatic etiology. Lesions arising in the skin may reveal an in situ component representing ductal hyperplasia, atypical ductal hyperplasia, or ductal carcinoma in situ. Identification of an in situ component defines a cutaneous primary neoplasm, but its absence does not exclude PMC.5 Additionally, metastatic lesions from the GIT typically have greater pleomorphism and “dirty” necrosis defined as eosinophilic foci containing nuclear debris.5
The expression pattern of cytokeratins (CKs) also can be suggestive. Primary mucinous carcinoma and metastatic breast adenocarcinoma are both CK7+ and CK20−. By contrast, mucinous adenocarcinoma of the GIT stains CK20+ and CK7−.14 Another marker that stains PMC is CK5 and CK6, though infrequently present. Levy et al15 reported positive staining for CK5 and CK6 in only 1 of 5 PMC cases. Positive staining for CK5 and CK6 has not been reported in any metastatic mucinous carcinoma.
The role of p63 immunostaining in the setting of mucinous carcinoma is controversial.16-18 Some practi-tioners have reported using p63 immunostaining to assist in establishing the diagnosis of PMC but only after performing a clinical workup to search for any primary sites of mucinous carcinoma in other organs.11 Other studies, however, have found select metastatic lesions from the breast17,18 and GIT18 to stain positively with p63. It is important to remember that these clinical and pathologic features are only suggestive of the primary etiology and are not replacement for a full clinical investigation.
Primary mucinous carcinoma is considered an indolent tumor with the majority of patient morbidity attributable to local recurrence and regional metastasis. Although uncommon, regional and distant metastasis rates have been reported to be 11% and 3%, respectively.19 Direct lymphatic invasion has been reported and indicates a more aggressive tumor with shorter recurrence-free intervals and predicts nodal metastases. Paradela et al20 recommended the use of D2-40, a monoclonal antibody and specific marker for lymphatic endothelium, to detect lymphatic invasion, particularly in node-negative primary tumors.
In one case of PMC on the jaw of a 39-year-old Japanese man, no recurrence or metastases were discovered until the 11th year of follow-up. At that time, he was found to have lung and bone metastases and died after 3 years.21 Other investigators report death occurring 4 to 24 months following diagnosis of distant metastases.7,22 Direct extension of the tumor into skeletal muscle, periosteum, bone, and dura also has been documented.7
Treatment principally is surgical, with PMC known to be resistant to both chemotherapy and radiation therapy.19,22 The recommended margins for simple excision range from 1 to 2 cm, but this method of treatment yields recurrence rates upward of 30% to 40%, especially for lesions located on the eyelid.12,13 First utilized in PMC of the eyelid to conserve tissue, MMS is rapidly becoming the treatment of choice because of its notably improved recurrence rate. A case series of 4 PMCs of the eyelid treated via MMS or frozen section control found the recurrence rate to be 7%.23 Another report of 2 cases of PMC treated by MMS reported no recurrence after 42 and 26 months.13 Ortiz et al7 reported an additional case of a patient treated by MMS that was recurrence free for 30 months at the time of publication. Further investigation is required to definitively recommend MMS on the basis of improved recurrence rate but should now be considered standard of care in recurrent, sizeable, or eyelid PMC.
Despite its ascension as treatment of choice in many cases of PMC, MMS is not without its risk of metastasis and recurrence. Tam et al24 reported a case of PMC with multiple recurrences and metastases following 3 simple excisions and 2 excisions via MMS. Although the lesion’s previously recurrent nature increased the likelihood of failure of MMS, this case demonstrates that all patients should be followed periodically after the treatment of PMC.
We presented a case of PMC in which standard surgical margins would have been insufficient to clear the lesion. Mohs micrographic surgery was used to remove the majority of the tumor. As is common in PMC, the lesion was indolent and periocular in location. It also was incompletely excised due to notable subclinical extension, which is common for PMC. The distinction of PMC from metastatic mucinous carcinoma is paramount but sometimes difficult. Randomized controlled trials are lacking with regards to preferred method of treatment, but MMS has shown benefit and should be considered for recurrent lesions and lesions in cosmetically sensitive areas.
To the Editor:
Primary mucinous carcinoma (PMC) is an exceedingly rare adnexal tumor with an incidence of 0.07 cases per million individuals.1,2 First described by Lennox et al3 in 1952, this entity often presents as slow-growing, solitary nodules that often are soft on palpation but may have an indurated quality and range in color from reddish blue to flesh colored to white.4 Primary mucinous carcinoma most commonly is found on the eyelid (38%) but may affect other sites on the face (20.3%), scalp (16%), and axilla (10%).5 Historically, it has been thought to be more common among men; however, a 2005 large case series by Kazakov et al5 found that women were twice as likely to be affected. Primary mucinous carcinoma most frequently is diagnosed in the fifth through seventh decades of life, with a median age at onset of 63 years.6,7 Because of its rarity, PMC is most frequently confused clinically with basal cell carcinoma, keratoacanthoma, apocrine hidrocystoma, epidermoid cyst, Kaposi sarcoma, neuroma, lacrimal sac tumor, squamous cell carcinoma, granulomatous tumors, and metastatic adenocarcinoma.1,8-10
Primary mucinous carcinoma is thought to be derived from sweat glands, and select features such as decapitation secretion are more suggestive of apocrine than eccrine differentiation.5,8 On histopathology, PMC classically is described as nests of epithelial cells floating in lakes of extracellular mucin, primarily in the dermis and subcutis. The nests are composed of basaloid cells in solid to cribriform arrangements, usually with a low mitotic count and little nuclear atypia. These nests are suspended within periodic acid–Schiff positive mucinous pools partitioned by delicate fibrous septa. The mucin produced by PMC is sialomucin, and as such it is hyaluronidase resistant and sialidase labile.6 At least 1 report has been made of the presence of psammoma bodies in PMC.11
The neoplasm is characterized by an indolent course with frequent recurrence but rare metastasis.5,12 Treatment is primarily surgical, with Mohs micrographic surgery (MMS) offering improved tissue conservation and reduced recurrence rates.12 The diagnostic challenge lies in distinguishing PMC from a variety of metastatic mucinous internal malignancies that portend a notably greater morbidity and mortality to the patient. We describe a case of PMC, discuss the differentiation of PMC from metastatic mucinous carcinoma, and review the literature regarding treatment of this rare neoplasm.
A 65-year-old white woman was referred to our tertiary-care dermatologic surgery clinic for treatment of an incompletely excised mucinous carcinoma of the right lateral canthus (Figure 1). The clinically evident scar measured 0.5×0.5 cm. Although difficult to appreciate in Figure 1, a slight textural change of the surrounding skin, including the upper and lower eyelid, was apparent. Prior to her arrival to our clinic, the referring physician had completed a thorough review of systems and physical examination, which did not suggest an underlying malignancy. Computed tomography of the head, neck, chest, abdomen, and pelvis revealed a mass in the thyroid that was removed and found to be benign. The patient’s cutaneous lesion was therefore considered to be a PMC of the skin.
Given the prior incomplete excision of the lesion and its periocular location, we treated the patient with MMS. After 6 surgical stages, we continued to see evidence of the neoplasm as it tracked medially along the orbicularis oculi muscle (Figure 2). Due to the patient’s physical and emotional exhaustion at this point, we discontinued MMS and referred her to a colleague in plastic surgery for further excision of the remaining focus of positivity as well as repair. The final Mohs defect measured 4.2×4.0 cm (Figure 3). Approximately 2.3×1.0 cm of tissue in the area of remaining tumor was excised by plastic surgery, and the defect was repaired with a cervicofacial advancement flap closure of the right cheek and lower eyelid and full-thickness skin graft of the left upper eyelid. Histopathologic investigation found the additional tissue resected to be free of residual tumor.
To diagnose a patient with PMC, one must first rule out cutaneous metastasis of various internal malignancies that may appear similar on histopathology. A full clinical investigation consisting of a thorough history, physical examination, and appropriate radiographic imaging is required. Cutaneous metastases most commonly arise from the breast or gastrointestinal tract (GIT) but also can originate from the prostate, lungs, ovaries, pancreas, and kidneys.5 Histologically, PMC may be identical to metastatic adenocarcinoma.13 Location on the body may be a clue to a lesion’s origin, as metastases from a mucinous adenocarcinoma of the breast typically occur on the chest, breast, or axilla,5 whereas PMC primarily is found on the head and neck.
Certain histopathologic features may be suggestive of either a primary or metastatic etiology. Lesions arising in the skin may reveal an in situ component representing ductal hyperplasia, atypical ductal hyperplasia, or ductal carcinoma in situ. Identification of an in situ component defines a cutaneous primary neoplasm, but its absence does not exclude PMC.5 Additionally, metastatic lesions from the GIT typically have greater pleomorphism and “dirty” necrosis defined as eosinophilic foci containing nuclear debris.5
The expression pattern of cytokeratins (CKs) also can be suggestive. Primary mucinous carcinoma and metastatic breast adenocarcinoma are both CK7+ and CK20−. By contrast, mucinous adenocarcinoma of the GIT stains CK20+ and CK7−.14 Another marker that stains PMC is CK5 and CK6, though infrequently present. Levy et al15 reported positive staining for CK5 and CK6 in only 1 of 5 PMC cases. Positive staining for CK5 and CK6 has not been reported in any metastatic mucinous carcinoma.
The role of p63 immunostaining in the setting of mucinous carcinoma is controversial.16-18 Some practi-tioners have reported using p63 immunostaining to assist in establishing the diagnosis of PMC but only after performing a clinical workup to search for any primary sites of mucinous carcinoma in other organs.11 Other studies, however, have found select metastatic lesions from the breast17,18 and GIT18 to stain positively with p63. It is important to remember that these clinical and pathologic features are only suggestive of the primary etiology and are not replacement for a full clinical investigation.
Primary mucinous carcinoma is considered an indolent tumor with the majority of patient morbidity attributable to local recurrence and regional metastasis. Although uncommon, regional and distant metastasis rates have been reported to be 11% and 3%, respectively.19 Direct lymphatic invasion has been reported and indicates a more aggressive tumor with shorter recurrence-free intervals and predicts nodal metastases. Paradela et al20 recommended the use of D2-40, a monoclonal antibody and specific marker for lymphatic endothelium, to detect lymphatic invasion, particularly in node-negative primary tumors.
In one case of PMC on the jaw of a 39-year-old Japanese man, no recurrence or metastases were discovered until the 11th year of follow-up. At that time, he was found to have lung and bone metastases and died after 3 years.21 Other investigators report death occurring 4 to 24 months following diagnosis of distant metastases.7,22 Direct extension of the tumor into skeletal muscle, periosteum, bone, and dura also has been documented.7
Treatment principally is surgical, with PMC known to be resistant to both chemotherapy and radiation therapy.19,22 The recommended margins for simple excision range from 1 to 2 cm, but this method of treatment yields recurrence rates upward of 30% to 40%, especially for lesions located on the eyelid.12,13 First utilized in PMC of the eyelid to conserve tissue, MMS is rapidly becoming the treatment of choice because of its notably improved recurrence rate. A case series of 4 PMCs of the eyelid treated via MMS or frozen section control found the recurrence rate to be 7%.23 Another report of 2 cases of PMC treated by MMS reported no recurrence after 42 and 26 months.13 Ortiz et al7 reported an additional case of a patient treated by MMS that was recurrence free for 30 months at the time of publication. Further investigation is required to definitively recommend MMS on the basis of improved recurrence rate but should now be considered standard of care in recurrent, sizeable, or eyelid PMC.
Despite its ascension as treatment of choice in many cases of PMC, MMS is not without its risk of metastasis and recurrence. Tam et al24 reported a case of PMC with multiple recurrences and metastases following 3 simple excisions and 2 excisions via MMS. Although the lesion’s previously recurrent nature increased the likelihood of failure of MMS, this case demonstrates that all patients should be followed periodically after the treatment of PMC.
We presented a case of PMC in which standard surgical margins would have been insufficient to clear the lesion. Mohs micrographic surgery was used to remove the majority of the tumor. As is common in PMC, the lesion was indolent and periocular in location. It also was incompletely excised due to notable subclinical extension, which is common for PMC. The distinction of PMC from metastatic mucinous carcinoma is paramount but sometimes difficult. Randomized controlled trials are lacking with regards to preferred method of treatment, but MMS has shown benefit and should be considered for recurrent lesions and lesions in cosmetically sensitive areas.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Martinez SR, Young SE. Primary mucinous carcinoma of the skin: a review. Int J Oncol. 2005;2:432-437.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Marra DE, Schanbacher CF, Torres A. Mohs micrographic surgery of primary cutaneous mucinous carcinoma using immunohistochemistry for margin control. Dermatol Surg. 2004;30:799-802.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
- Mendoza S, Helwig EB. Mucinous (adenocystic) carcinoma of the skin. Arch Dermatol. 1971;103:68-78.
- Ortiz KJ, Gaughan MD, Bang RH, et al. A case of primary mucinous carcinoma of the scalp treated with Mohs surgery. Dermatol Surg. 2002;28:751-754.
- Bellezza G, Sidoni A, Bucciarelli E. Primary mucinous carcinoma of the skin. Am J Dermatopathol. 2000;22:166-170.
- Teng P, Muir J. Small primary cutaneous mucinous carcinoma mimicking an early basal cell carcinoma. Dermatol Online J. 2013;19:3.
- Terada T, Sato Y, Furukawa K, et al. Primary cutaneous mucinous carcinoma initially diagnosed as metastatic adenocarcinoma. Tohoku J Exp Med. 2004;203:345-348.
- Kalebi A, Hale M. Primary mucinous carcinoma of the skin: usefulness of p63 in excluding metastasis and first report of psammoma bodies. Am J Dermatopathol. 2008;30:510.
- Cabell CE, Helm KF, Sakol PJ, et al. Primary mucinous carcinoma in a 54-year-old man. J Am Acad Dermatol. 2003;49:941-943.
- Cecchi R, Rapicano V. Primary cutaneous mucinous carcinoma: report of two cases treated with Mohs’ micrographic surgery. Australas J Dermatol. 2006;47:192-194.
- Eckert F, Schmid U, Hardmeier T, et al. Cytokeratin expression in mucinous sweat gland carcinomas: an immunohistochemical analysis of four cases. Histopathology. 1992;21:161-165.
- Levy G, Finkelstein A, McNiff JM. Immunohistochemical techniques to compare primary vs. metastatic mucinous carcinoma of the skin. J Cutan Pathol. 2010;37:411-415.
- Ivan D, Hafeez Diwan A, Prieto VG. Expression of p63 in primary cutaneous adnexal neoplasms and adenocarcinoma metastatic to the skin. Mod Pathol. 2005;18:137-142.
- Kanitakis J, Chouvet B. Expression of p63 in cutaneous metastases. Am J Clin Pathol. 2007;128:753-758.
- Sariya D, Ruth K, Adams-McDonnell R, et al. Clinicopathologic correlation of cutaneous metastases: experience from a cancer center. Arch Dermatol. 2007;143:613-620.
- Snow SN, Reizner GT. Mucinous eccrine carcinoma of the eyelid. Cancer. 1992;70:2099-2104.
- Paradela S, Castiñeiras I, Cuevas J, et al. Mucinous carcinoma of the skin: evaluation of lymphatic invasion with D2-40. Am J Dermatopathol. 2008;30:504-508.
- Miyasaka M, Tanaka R, Hirabayashi K, et al. Primary mucinous carcinoma of the skin: a case of metastasis after 10 years of disease-free interval. Eur J Plast Surg. 2009;32:189-193.
- Yeung KY, Stinson JC. Mucinous (adenocystic) carcinoma of sweat glands with widespread metastasis. case report with ultrastructural study. Cancer. 1977;39:2556-2562.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathologic and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Tam CC, Dare DM, DiGiovanni JJ, et al. Recurrent and metastatic primary cutaneous mucinous carcinoma after excision and Mohs micrographic surgery. Cutis. 2011;87:245-248.
- Breiting L, Christensen L, Dahlstrom K, et al. Primary mucinous carcinoma of the skin: a population-based study. Int J Dermatol. 2008;47:242-245.
- Martinez SR, Young SE. Primary mucinous carcinoma of the skin: a review. Int J Oncol. 2005;2:432-437.
- Lennox B, Pearse AG, Richards HG. Mucin-secreting tumours of the skin with special reference to the so-called mixed-salivary tumour of the skin and its relation to hidradenoma. J Pathol Bacteriol. 1952;64:865-880.
- Marra DE, Schanbacher CF, Torres A. Mohs micrographic surgery of primary cutaneous mucinous carcinoma using immunohistochemistry for margin control. Dermatol Surg. 2004;30:799-802.
- Kazakov DV, Suster S, LeBoit PE, et al. Mucinous carcinoma of the skin, primary, and secondary: a clinicopathologic study of 63 cases with emphasis on the morphologic spectrum of primary cutaneous forms: homologies with mucinous lesions in the breast. Am J Surg Pathol. 2005;29:764-782.
- Mendoza S, Helwig EB. Mucinous (adenocystic) carcinoma of the skin. Arch Dermatol. 1971;103:68-78.
- Ortiz KJ, Gaughan MD, Bang RH, et al. A case of primary mucinous carcinoma of the scalp treated with Mohs surgery. Dermatol Surg. 2002;28:751-754.
- Bellezza G, Sidoni A, Bucciarelli E. Primary mucinous carcinoma of the skin. Am J Dermatopathol. 2000;22:166-170.
- Teng P, Muir J. Small primary cutaneous mucinous carcinoma mimicking an early basal cell carcinoma. Dermatol Online J. 2013;19:3.
- Terada T, Sato Y, Furukawa K, et al. Primary cutaneous mucinous carcinoma initially diagnosed as metastatic adenocarcinoma. Tohoku J Exp Med. 2004;203:345-348.
- Kalebi A, Hale M. Primary mucinous carcinoma of the skin: usefulness of p63 in excluding metastasis and first report of psammoma bodies. Am J Dermatopathol. 2008;30:510.
- Cabell CE, Helm KF, Sakol PJ, et al. Primary mucinous carcinoma in a 54-year-old man. J Am Acad Dermatol. 2003;49:941-943.
- Cecchi R, Rapicano V. Primary cutaneous mucinous carcinoma: report of two cases treated with Mohs’ micrographic surgery. Australas J Dermatol. 2006;47:192-194.
- Eckert F, Schmid U, Hardmeier T, et al. Cytokeratin expression in mucinous sweat gland carcinomas: an immunohistochemical analysis of four cases. Histopathology. 1992;21:161-165.
- Levy G, Finkelstein A, McNiff JM. Immunohistochemical techniques to compare primary vs. metastatic mucinous carcinoma of the skin. J Cutan Pathol. 2010;37:411-415.
- Ivan D, Hafeez Diwan A, Prieto VG. Expression of p63 in primary cutaneous adnexal neoplasms and adenocarcinoma metastatic to the skin. Mod Pathol. 2005;18:137-142.
- Kanitakis J, Chouvet B. Expression of p63 in cutaneous metastases. Am J Clin Pathol. 2007;128:753-758.
- Sariya D, Ruth K, Adams-McDonnell R, et al. Clinicopathologic correlation of cutaneous metastases: experience from a cancer center. Arch Dermatol. 2007;143:613-620.
- Snow SN, Reizner GT. Mucinous eccrine carcinoma of the eyelid. Cancer. 1992;70:2099-2104.
- Paradela S, Castiñeiras I, Cuevas J, et al. Mucinous carcinoma of the skin: evaluation of lymphatic invasion with D2-40. Am J Dermatopathol. 2008;30:504-508.
- Miyasaka M, Tanaka R, Hirabayashi K, et al. Primary mucinous carcinoma of the skin: a case of metastasis after 10 years of disease-free interval. Eur J Plast Surg. 2009;32:189-193.
- Yeung KY, Stinson JC. Mucinous (adenocystic) carcinoma of sweat glands with widespread metastasis. case report with ultrastructural study. Cancer. 1977;39:2556-2562.
- Papalas JA, Proia AD. Primary mucinous carcinoma of the eyelid: a clinicopathologic and immunohistochemical study of 4 cases and an update on recurrence rates. Arch Ophthalmol. 2010;128:1160-1165.
- Tam CC, Dare DM, DiGiovanni JJ, et al. Recurrent and metastatic primary cutaneous mucinous carcinoma after excision and Mohs micrographic surgery. Cutis. 2011;87:245-248.
Practice Points
- Primary mucinous carcinoma (PMC) of the skin is a rare adnexal tumor.
- Prior to treatment, the diagnostic importance lies in distinguishing PMC from metastatic mucinous malignancies, which portend a poorer prognosis.
- Treatment primarily is surgical, with Mohs micrographic surgery offering improved tissue conservation and reduced recurrence rates.

VIDEO: Innovative technology is opening doors for vaginal hysterectomy
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Innovative tools for vaginal hysterectomy were in the spotlight during a surgical demonstration at the AAGL Global Congress.
“I think it’s really compelling that we use the technologies that the AAGL is known for investigating and teaching each other,” said Charles Rardin, MD, director of the robotic surgery program at Women & Infants Hospital, Providence, R.I. “It’s nice to see a renewed interest in some newer technologies and applying them to vaginal hysterectomy.”
The presentation of new tools comes as the number of vaginal hysterectomies have decreased and laparoscopic procedures are on the rise. The rate of vaginal hysterectomy in the United States has fallen from 24.8% in 1998 to 16.7% in 2010, according to the Nationwide Inpatient Sample from the Agency for Healthcare Research and Quality.
Surgeons demonstrated new tools with the intent of showing physicians that the benefits some associate with laparoscopic procedures, such as having easier access or a better sense of the uterus, can be associated with vaginal hysterectomy as well.
Advanced tools, such as a self-retaining retractor and 3-D camera systems, could make it easier to teach students by allowing more mobility and easier visual access, Dr. Rardin said in a video interview.
The tutorial ended with a demonstration of the natural orifice transluminal endoscopic surgery tool that allows laparoscopic tools to be introduced through the vaginal pathway.
All the tools exhibited at AAGL are currently available.
Dr. Rardin reported having no relevant financial disclosures.
On Twitter @eaztweets
AT AAGL 2017

Acrodermatitis Enteropathica in a Patient With Short Bowel Syndrome
To the Editor:
Acrodermatitis enteropathica (AE) is an inherited defect in zinc absorption that leads to hypozincemia. Its clinical presentation can vary based on serum zinc level and ranges from periorificial erosive dermatitis to psoriasiform dermatitis.1 Recognition of the cutaneous manifestations of zinc deficiency can lead to early intervention with zinc supplementation and prevention of long-term morbidity and even mortality. In our case, the coexistence of a bullous acral dermatosis with the additional feature of extensor digital dermatitis with fissuring suggests a diagnosis of AE and can alert the astute clinician to the need for testing of serum zinc levels and/or treatment with zinc supplementation. Causes of acquired zinc deficiency that have been reported in the literature include eating disorders such as anorexia nervosa and bulimia nervosa, Crohn disease, food allergy, intestinal parasitic infestations, and an inborn error of metabolism known as nonketotic hyperglycemia (Table).2-4
RELATED ARTICLE: Acquired Acrodermatitis Enteropathica Secondary to Alcoholism
A 42-year-old woman with a medical history of rheumatoid arthritis and short bowel syndrome due to multiple small bowel obstructions with subsequent bowel resections who was on chronic total parenteral nutrition (TPN) presented with bullae on the hands, shins, and feet. The patient initially noticed small erythematous macules on the hands and feet months prior to presentation. Three weeks prior to presentation, bullae started to form on the hands, mostly between the web spaces; dorsal aspects of the feet; and anterior aspects of the shins. The patient denied any oral ulcers. One day prior to presentation the patient was seen at an outside hospital and was started on prednisone 5 mg daily, oral clindamycin, mupirocin ointment, and nystatin-triamcinolone cream. These medications failed to improve her condition. On review of systems, the patient denied any fever, chills, eye pain, or dysuria.
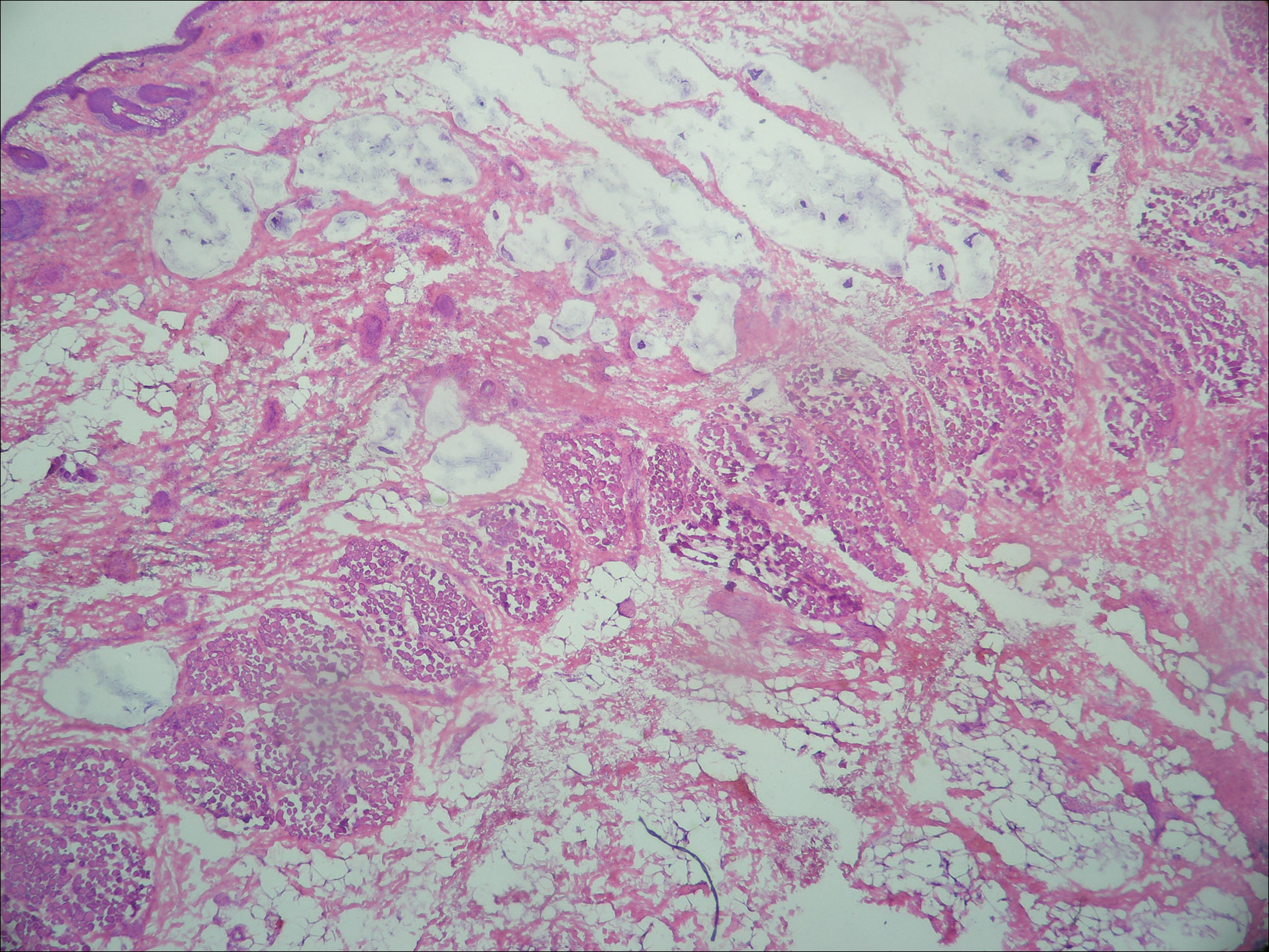
Upon initial presentation the patient appeared weak and fatigued, though vital signs were normal. Physical examination revealed multiple flaccid bullae in the web spaces of the hands and shallow erosions with hemorrhagic crusts on the bilateral wrists. She also had violaceous patches in the extensor creases of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints, which were strikingly symmetric (Figure 1). Prominent flaccid bullae and shallow erosions with hemorrhagic crusts also were present on the bilateral shins and dorsal aspects of the feet (Figure 2). No oral ulcers were present. A punch biopsy from the dorsal aspect of the left foot revealed psoriasiform hyperplasia of the epidermis with prominent ballooning degeneration and hyperkeratosis/parakeratosis (Figure 3); a periodic acid–Schiff stain was negative for fungal organisms.


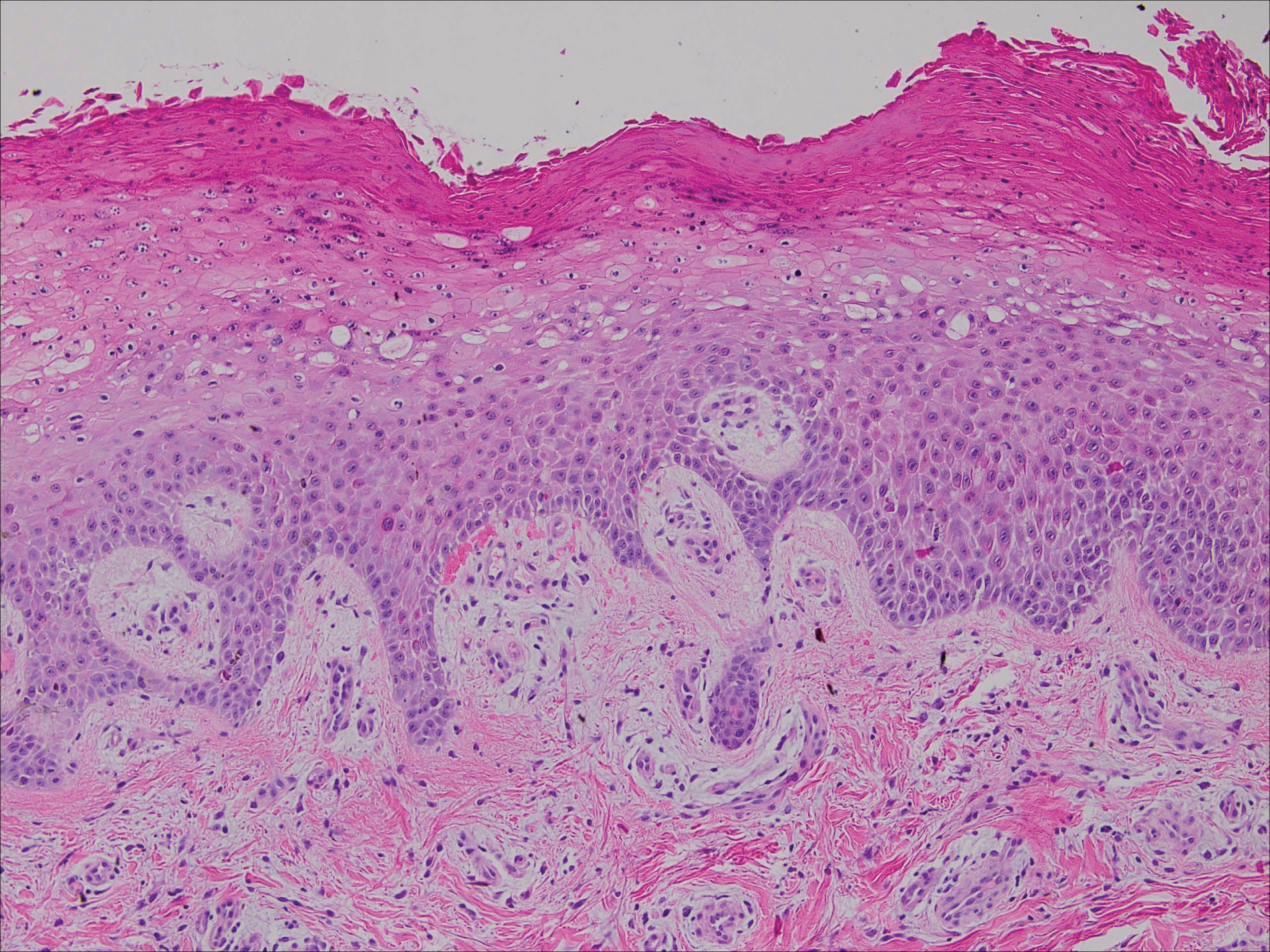
Given the biopsy results and clinical presentation, a nutritional deficiency was suspected and serum levels of zinc, vitamin B1, vitamin B2, and vitamin B3 were assessed. Vitamins B1, B2
Zinc is an essential trace element and can be found in high concentration in foods such as shellfish, green vegetables, legumes, nuts, and whole grains.6 The majority of zinc is absorbed in the jejunum; as such, many cases of acquired zinc deficiency leading to AE are dueto disorders that affect the small intestine.2 Conditions that may lead to poor gastrointestinal zinc absorption include alcoholism, eating disorders, TPN, burns, surgery, and malignancies.2,7
Diagnosis typically is made based on characteristic clinical features, biopsy results, and a measurement of the serum zinc concentration. Although a low serum zinc level supports the diagnosis, serum zinc concentration is not a reliable indicator of body zinc stores and a normal serum zinc concentration does not rule out AE. The gold standard for diagnosis is the resolution of lesions after zinc supplementation.1 Notably, because the production of alkaline phosphatase is dependent on zinc, levels of this enzyme also may be low in cases of AE,6 as in our patient.
The clinical manifestations of AE can vary greatly; patients may initially present with eczematous pink scaly plaques, which may subsequently become vesicular, bullous, pustular, or desquamative. The lesions may develop over the arms and legs as well as the anogenital and periorificial areas.5 Other notable manifestations that may present early in the course of AE include angular cheilitis followed by paronychia. In patients who are not promptly treated, long-term zinc deficiency may lead to growth delay, mental slowing, poor wound healing, anemia, and anorexia.5 Of note, deficiencies of branched-chain amino acids and essential fatty acids may appear clinically similar to AE.2
Zinc replacement is the treatment of choice for patients with AE due to dietary deficiency, and replacement therapy should begin with 0.5 to 1 mg/kg daily of elemental zinc.5 Response to acquired AE with zinc supplementation often is rapid. Lesions tend to resolve within days to weeks depending on the degree of deficiency.2
Although AE is an uncommon dermatosis in the United States, it is an important diagnosis to make because its clinical features are fairly specific and early zinc supplementation allows for full resolution of the disease without permanent sequelae. The diagnosis of AE should be strongly considered when features of an acral bullous dermatosis are combined with a fissured dermatitis of extensor joints of the hands or elbows. It is particularly important to recognize that alcoholics, burn victims, postsurgical patients, and those with malignancies and eating disorders are at an increased risk for developing this nutritional deficiency.
- Kumar P, Lal NR, Mondal AK, et al. Zinc and skin: a brief summary. Dermatol Online J. 2012;18:1.
- Suchithra N, Sreejith P, Pappachan JM, et al. Acrodermatitis enteropathica-like skin eruption in a case of short bowel syndrome following jejuno-transverse colon anastomosis. Dermatol Online J. 2007;13:20.
- Sundaram A, Koutkia P, Apovian CM. Nutritional management of short bowel syndrome in adults. J Clin Gastroenterol. 2002;34:207-220.
- Griffin IJ, Kim SC, Hicks PD, et al. Zinc metabolism in adolescents with Crohn’s disease. Pediatr Res. 2004;56:235-239.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism [published online October 30, 2006]. J Am Acad Dermatol. 2007;56:116-124.
- Cheshire H, Stather P, Vorster J. Acquired acrodermatitis enteropathica due to zinc deficiency in a patient with pre-existing Darier’s disease. J Dermatol Case Rep. 2009;3:41-43.
- Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol. 2005;6:165-173.
To the Editor:
Acrodermatitis enteropathica (AE) is an inherited defect in zinc absorption that leads to hypozincemia. Its clinical presentation can vary based on serum zinc level and ranges from periorificial erosive dermatitis to psoriasiform dermatitis.1 Recognition of the cutaneous manifestations of zinc deficiency can lead to early intervention with zinc supplementation and prevention of long-term morbidity and even mortality. In our case, the coexistence of a bullous acral dermatosis with the additional feature of extensor digital dermatitis with fissuring suggests a diagnosis of AE and can alert the astute clinician to the need for testing of serum zinc levels and/or treatment with zinc supplementation. Causes of acquired zinc deficiency that have been reported in the literature include eating disorders such as anorexia nervosa and bulimia nervosa, Crohn disease, food allergy, intestinal parasitic infestations, and an inborn error of metabolism known as nonketotic hyperglycemia (Table).2-4
RELATED ARTICLE: Acquired Acrodermatitis Enteropathica Secondary to Alcoholism
A 42-year-old woman with a medical history of rheumatoid arthritis and short bowel syndrome due to multiple small bowel obstructions with subsequent bowel resections who was on chronic total parenteral nutrition (TPN) presented with bullae on the hands, shins, and feet. The patient initially noticed small erythematous macules on the hands and feet months prior to presentation. Three weeks prior to presentation, bullae started to form on the hands, mostly between the web spaces; dorsal aspects of the feet; and anterior aspects of the shins. The patient denied any oral ulcers. One day prior to presentation the patient was seen at an outside hospital and was started on prednisone 5 mg daily, oral clindamycin, mupirocin ointment, and nystatin-triamcinolone cream. These medications failed to improve her condition. On review of systems, the patient denied any fever, chills, eye pain, or dysuria.
Upon initial presentation the patient appeared weak and fatigued, though vital signs were normal. Physical examination revealed multiple flaccid bullae in the web spaces of the hands and shallow erosions with hemorrhagic crusts on the bilateral wrists. She also had violaceous patches in the extensor creases of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints, which were strikingly symmetric (Figure 1). Prominent flaccid bullae and shallow erosions with hemorrhagic crusts also were present on the bilateral shins and dorsal aspects of the feet (Figure 2). No oral ulcers were present. A punch biopsy from the dorsal aspect of the left foot revealed psoriasiform hyperplasia of the epidermis with prominent ballooning degeneration and hyperkeratosis/parakeratosis (Figure 3); a periodic acid–Schiff stain was negative for fungal organisms.
Given the biopsy results and clinical presentation, a nutritional deficiency was suspected and serum levels of zinc, vitamin B1, vitamin B2, and vitamin B3 were assessed. Vitamins B1, B2
Zinc is an essential trace element and can be found in high concentration in foods such as shellfish, green vegetables, legumes, nuts, and whole grains.6 The majority of zinc is absorbed in the jejunum; as such, many cases of acquired zinc deficiency leading to AE are dueto disorders that affect the small intestine.2 Conditions that may lead to poor gastrointestinal zinc absorption include alcoholism, eating disorders, TPN, burns, surgery, and malignancies.2,7
Diagnosis typically is made based on characteristic clinical features, biopsy results, and a measurement of the serum zinc concentration. Although a low serum zinc level supports the diagnosis, serum zinc concentration is not a reliable indicator of body zinc stores and a normal serum zinc concentration does not rule out AE. The gold standard for diagnosis is the resolution of lesions after zinc supplementation.1 Notably, because the production of alkaline phosphatase is dependent on zinc, levels of this enzyme also may be low in cases of AE,6 as in our patient.
The clinical manifestations of AE can vary greatly; patients may initially present with eczematous pink scaly plaques, which may subsequently become vesicular, bullous, pustular, or desquamative. The lesions may develop over the arms and legs as well as the anogenital and periorificial areas.5 Other notable manifestations that may present early in the course of AE include angular cheilitis followed by paronychia. In patients who are not promptly treated, long-term zinc deficiency may lead to growth delay, mental slowing, poor wound healing, anemia, and anorexia.5 Of note, deficiencies of branched-chain amino acids and essential fatty acids may appear clinically similar to AE.2
Zinc replacement is the treatment of choice for patients with AE due to dietary deficiency, and replacement therapy should begin with 0.5 to 1 mg/kg daily of elemental zinc.5 Response to acquired AE with zinc supplementation often is rapid. Lesions tend to resolve within days to weeks depending on the degree of deficiency.2
Although AE is an uncommon dermatosis in the United States, it is an important diagnosis to make because its clinical features are fairly specific and early zinc supplementation allows for full resolution of the disease without permanent sequelae. The diagnosis of AE should be strongly considered when features of an acral bullous dermatosis are combined with a fissured dermatitis of extensor joints of the hands or elbows. It is particularly important to recognize that alcoholics, burn victims, postsurgical patients, and those with malignancies and eating disorders are at an increased risk for developing this nutritional deficiency.
To the Editor:
Acrodermatitis enteropathica (AE) is an inherited defect in zinc absorption that leads to hypozincemia. Its clinical presentation can vary based on serum zinc level and ranges from periorificial erosive dermatitis to psoriasiform dermatitis.1 Recognition of the cutaneous manifestations of zinc deficiency can lead to early intervention with zinc supplementation and prevention of long-term morbidity and even mortality. In our case, the coexistence of a bullous acral dermatosis with the additional feature of extensor digital dermatitis with fissuring suggests a diagnosis of AE and can alert the astute clinician to the need for testing of serum zinc levels and/or treatment with zinc supplementation. Causes of acquired zinc deficiency that have been reported in the literature include eating disorders such as anorexia nervosa and bulimia nervosa, Crohn disease, food allergy, intestinal parasitic infestations, and an inborn error of metabolism known as nonketotic hyperglycemia (Table).2-4
RELATED ARTICLE: Acquired Acrodermatitis Enteropathica Secondary to Alcoholism
A 42-year-old woman with a medical history of rheumatoid arthritis and short bowel syndrome due to multiple small bowel obstructions with subsequent bowel resections who was on chronic total parenteral nutrition (TPN) presented with bullae on the hands, shins, and feet. The patient initially noticed small erythematous macules on the hands and feet months prior to presentation. Three weeks prior to presentation, bullae started to form on the hands, mostly between the web spaces; dorsal aspects of the feet; and anterior aspects of the shins. The patient denied any oral ulcers. One day prior to presentation the patient was seen at an outside hospital and was started on prednisone 5 mg daily, oral clindamycin, mupirocin ointment, and nystatin-triamcinolone cream. These medications failed to improve her condition. On review of systems, the patient denied any fever, chills, eye pain, or dysuria.
Upon initial presentation the patient appeared weak and fatigued, though vital signs were normal. Physical examination revealed multiple flaccid bullae in the web spaces of the hands and shallow erosions with hemorrhagic crusts on the bilateral wrists. She also had violaceous patches in the extensor creases of the metacarpophalangeal, proximal interphalangeal, and distal interphalangeal joints, which were strikingly symmetric (Figure 1). Prominent flaccid bullae and shallow erosions with hemorrhagic crusts also were present on the bilateral shins and dorsal aspects of the feet (Figure 2). No oral ulcers were present. A punch biopsy from the dorsal aspect of the left foot revealed psoriasiform hyperplasia of the epidermis with prominent ballooning degeneration and hyperkeratosis/parakeratosis (Figure 3); a periodic acid–Schiff stain was negative for fungal organisms.
Given the biopsy results and clinical presentation, a nutritional deficiency was suspected and serum levels of zinc, vitamin B1, vitamin B2, and vitamin B3 were assessed. Vitamins B1, B2
Zinc is an essential trace element and can be found in high concentration in foods such as shellfish, green vegetables, legumes, nuts, and whole grains.6 The majority of zinc is absorbed in the jejunum; as such, many cases of acquired zinc deficiency leading to AE are dueto disorders that affect the small intestine.2 Conditions that may lead to poor gastrointestinal zinc absorption include alcoholism, eating disorders, TPN, burns, surgery, and malignancies.2,7
Diagnosis typically is made based on characteristic clinical features, biopsy results, and a measurement of the serum zinc concentration. Although a low serum zinc level supports the diagnosis, serum zinc concentration is not a reliable indicator of body zinc stores and a normal serum zinc concentration does not rule out AE. The gold standard for diagnosis is the resolution of lesions after zinc supplementation.1 Notably, because the production of alkaline phosphatase is dependent on zinc, levels of this enzyme also may be low in cases of AE,6 as in our patient.
The clinical manifestations of AE can vary greatly; patients may initially present with eczematous pink scaly plaques, which may subsequently become vesicular, bullous, pustular, or desquamative. The lesions may develop over the arms and legs as well as the anogenital and periorificial areas.5 Other notable manifestations that may present early in the course of AE include angular cheilitis followed by paronychia. In patients who are not promptly treated, long-term zinc deficiency may lead to growth delay, mental slowing, poor wound healing, anemia, and anorexia.5 Of note, deficiencies of branched-chain amino acids and essential fatty acids may appear clinically similar to AE.2
Zinc replacement is the treatment of choice for patients with AE due to dietary deficiency, and replacement therapy should begin with 0.5 to 1 mg/kg daily of elemental zinc.5 Response to acquired AE with zinc supplementation often is rapid. Lesions tend to resolve within days to weeks depending on the degree of deficiency.2
Although AE is an uncommon dermatosis in the United States, it is an important diagnosis to make because its clinical features are fairly specific and early zinc supplementation allows for full resolution of the disease without permanent sequelae. The diagnosis of AE should be strongly considered when features of an acral bullous dermatosis are combined with a fissured dermatitis of extensor joints of the hands or elbows. It is particularly important to recognize that alcoholics, burn victims, postsurgical patients, and those with malignancies and eating disorders are at an increased risk for developing this nutritional deficiency.
- Kumar P, Lal NR, Mondal AK, et al. Zinc and skin: a brief summary. Dermatol Online J. 2012;18:1.
- Suchithra N, Sreejith P, Pappachan JM, et al. Acrodermatitis enteropathica-like skin eruption in a case of short bowel syndrome following jejuno-transverse colon anastomosis. Dermatol Online J. 2007;13:20.
- Sundaram A, Koutkia P, Apovian CM. Nutritional management of short bowel syndrome in adults. J Clin Gastroenterol. 2002;34:207-220.
- Griffin IJ, Kim SC, Hicks PD, et al. Zinc metabolism in adolescents with Crohn’s disease. Pediatr Res. 2004;56:235-239.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism [published online October 30, 2006]. J Am Acad Dermatol. 2007;56:116-124.
- Cheshire H, Stather P, Vorster J. Acquired acrodermatitis enteropathica due to zinc deficiency in a patient with pre-existing Darier’s disease. J Dermatol Case Rep. 2009;3:41-43.
- Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol. 2005;6:165-173.
- Kumar P, Lal NR, Mondal AK, et al. Zinc and skin: a brief summary. Dermatol Online J. 2012;18:1.
- Suchithra N, Sreejith P, Pappachan JM, et al. Acrodermatitis enteropathica-like skin eruption in a case of short bowel syndrome following jejuno-transverse colon anastomosis. Dermatol Online J. 2007;13:20.
- Sundaram A, Koutkia P, Apovian CM. Nutritional management of short bowel syndrome in adults. J Clin Gastroenterol. 2002;34:207-220.
- Griffin IJ, Kim SC, Hicks PD, et al. Zinc metabolism in adolescents with Crohn’s disease. Pediatr Res. 2004;56:235-239.
- Maverakis E, Fung MA, Lynch PJ, et al. Acrodermatitis enteropathica and an overview of zinc metabolism [published online October 30, 2006]. J Am Acad Dermatol. 2007;56:116-124.
- Cheshire H, Stather P, Vorster J. Acquired acrodermatitis enteropathica due to zinc deficiency in a patient with pre-existing Darier’s disease. J Dermatol Case Rep. 2009;3:41-43.
- Strumia R. Dermatologic signs in patients with eating disorders. Am J Clin Dermatol. 2005;6:165-173.
Practice Points
- Acrodermatitis enteropathica can be a manifestation of zinc deficiency.
- Acrodermatitis enteropathica should be considered in patients with poor intestinal absorption of nutrients.

Patient handoffs and research methods
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform healthcare and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I wrap up my work for the summer, I am happy to reflect on my wonderful experiences. One of my greatest lessons from my mentors, Dr. Vineet Arora and Dr. Juan Rojas, is the development of a complete methods section and the careful necessity of approaching data and writing the abstract. I now realize the necessity of carefully maintaining a written account of how we approached the data, as it allows us to both communicate it to our audience and to look back on how to further organize it.

Furthermore, my approach towards research significantly shifted in the time I spent this summer. Previously, I would focus primarily on results; however, from having performed a comprehensive literature review, I now focus on the way the data was approached and presented, the way the team kept careful track of methods, and the way they use previous research to establish their project. My previous experience was around quantitative research; the way that research teams approach qualitative research often differs from one another, often requiring a special level of ingenuity in approach and analysis, often due to the highly variable data.
After my experience at University of Chicago, I feel significantly more comfortable approaching research. One of my greatest goals regarding my research was to gain a better understanding of the interaction between various departments and the general ward in order to better prepare myself to be an effective physician. By asking the question, “What do you think is the most important factor regarding the management of this patient?”, I fully realized my deep interest in medical management: any research I approach as a physician would be closely intertwined to clinical medicine.
I am very, very thankful for the opportunity to learn from highly experienced physicians and researchers, and I will use this experience going forward with any clinical and research experiences I encounter.
Anton Garazha is a medical student at Chicago Medical School at Rosalind Franklin University in North Chicago. He received his bachelor of science degree in biology from Loyola University in Chicago in 2015 and his master of biomedical science degree from Rosalind Franklin University in 2016. Anton is very interested in community outreach and quality improvement, and in his spare time tutors students in science-based subjects.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform healthcare and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I wrap up my work for the summer, I am happy to reflect on my wonderful experiences. One of my greatest lessons from my mentors, Dr. Vineet Arora and Dr. Juan Rojas, is the development of a complete methods section and the careful necessity of approaching data and writing the abstract. I now realize the necessity of carefully maintaining a written account of how we approached the data, as it allows us to both communicate it to our audience and to look back on how to further organize it.
Furthermore, my approach towards research significantly shifted in the time I spent this summer. Previously, I would focus primarily on results; however, from having performed a comprehensive literature review, I now focus on the way the data was approached and presented, the way the team kept careful track of methods, and the way they use previous research to establish their project. My previous experience was around quantitative research; the way that research teams approach qualitative research often differs from one another, often requiring a special level of ingenuity in approach and analysis, often due to the highly variable data.
After my experience at University of Chicago, I feel significantly more comfortable approaching research. One of my greatest goals regarding my research was to gain a better understanding of the interaction between various departments and the general ward in order to better prepare myself to be an effective physician. By asking the question, “What do you think is the most important factor regarding the management of this patient?”, I fully realized my deep interest in medical management: any research I approach as a physician would be closely intertwined to clinical medicine.
I am very, very thankful for the opportunity to learn from highly experienced physicians and researchers, and I will use this experience going forward with any clinical and research experiences I encounter.
Anton Garazha is a medical student at Chicago Medical School at Rosalind Franklin University in North Chicago. He received his bachelor of science degree in biology from Loyola University in Chicago in 2015 and his master of biomedical science degree from Rosalind Franklin University in 2016. Anton is very interested in community outreach and quality improvement, and in his spare time tutors students in science-based subjects.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform healthcare and revolutionize patient care. The program has been expanded for the 2017-18 year, offering two options for students to receive funding and engage in scholarly work during their first, second and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
As I wrap up my work for the summer, I am happy to reflect on my wonderful experiences. One of my greatest lessons from my mentors, Dr. Vineet Arora and Dr. Juan Rojas, is the development of a complete methods section and the careful necessity of approaching data and writing the abstract. I now realize the necessity of carefully maintaining a written account of how we approached the data, as it allows us to both communicate it to our audience and to look back on how to further organize it.
Furthermore, my approach towards research significantly shifted in the time I spent this summer. Previously, I would focus primarily on results; however, from having performed a comprehensive literature review, I now focus on the way the data was approached and presented, the way the team kept careful track of methods, and the way they use previous research to establish their project. My previous experience was around quantitative research; the way that research teams approach qualitative research often differs from one another, often requiring a special level of ingenuity in approach and analysis, often due to the highly variable data.
After my experience at University of Chicago, I feel significantly more comfortable approaching research. One of my greatest goals regarding my research was to gain a better understanding of the interaction between various departments and the general ward in order to better prepare myself to be an effective physician. By asking the question, “What do you think is the most important factor regarding the management of this patient?”, I fully realized my deep interest in medical management: any research I approach as a physician would be closely intertwined to clinical medicine.
I am very, very thankful for the opportunity to learn from highly experienced physicians and researchers, and I will use this experience going forward with any clinical and research experiences I encounter.
Anton Garazha is a medical student at Chicago Medical School at Rosalind Franklin University in North Chicago. He received his bachelor of science degree in biology from Loyola University in Chicago in 2015 and his master of biomedical science degree from Rosalind Franklin University in 2016. Anton is very interested in community outreach and quality improvement, and in his spare time tutors students in science-based subjects.
Providers’ Attitudes and Knowledge of Lesbian, Gay, Bisexual, and Transgender Health
Lesbian, gay, bisexual and transgender (LGBT) populations face significant social stigmatization, discrimination, and marginalization that contribute to negative patient outcomes. Consequently, the LGBT population experiences high rates of mental health issues, such as suicide and depression, as well as sexually transmitted diseases (STDs), drug abuse, poverty, and homelessness.1,2
Background
According to the CDC, gay men are at highest risk and have increased incidences of gonorrhea, chlamydia, herpes, human papilloma virus (HPV), and HIV.3 Lesbians and bisexual women are less likely to get preventive cancer screenings, such as Pap smears and mammograms, and have higher incidences of HIV, hepatitis C, self-reported gonorrhea, and are more likely to be overweight or obese.3-6 In addition, LGBT populations have high rates of use of tobacco, alcohol, and other drugs.
The National Transgender Discrimination Survey of 6,450 transgender and nonconforming participants also provides extensive data on the challenges faced by transgender individuals. Discrimination was frequently experienced in accessing health care. Due to their transgender status, 19% were denied care, and 28% postponed care due to perceived harassment and violence within a health care setting.1 The LGBT populations experience personal and structural barriers that interfere with their ability to access high-quality care. Sexual gender minority individuals also experience health care barriers due to isolation, insufficient social services, and a lack of culturally competent providers.4 At the same time, many health care providers (HCPs) experience various barriers to providing LGBT care and need to increase their cultural competence by improving awareness, receptivity, and knowledge.7,8 One personal barrier to quality care is stigmatization toward LGBT persons as expressed through HCP prejudices, beliefs, attitudes, and behaviors.2 Factors such as gender, race, and religious beliefs also influence attitudes to LGBT health care.
A study by Chapman and colleagues found significant differences in attitudes toward gay men by male and female medical and nursing students.9 Male students had a significantly more negative attitude toward gay men compared with the attitudes of female students. Cultural competence, defined in the study as gay affirmative action principles scores, were statistically significant and strongly correlated with negative attitudes. In this study there also was a statistically significant negative correlation between attitudes and knowledge scores indicating a considerable potential for personal values to influence the provision of health care.9
Various barriers inherent in the health care system restrict access to high-quality care. Institutional barriers that include a lack of legal recognition of same-sex partners, equality in visitation rights, and the ability of same-sex partners to access partner’s medical records hamper health care quality. The HCPs’ lack of knowledge of the health risks or health care needs of the LGBT population also present a structural barrier to quality of care and affects patient outcomes.2
Culturally competent interventions in health care delivery also have been studied to reduce LGBT health disparities. A systematic review of 56 studies by Butler and colleagues found that the term cultural competence was not well defined and often was denoted with the terms patient-centered or individualized care.10 A review on the impact of these interventions in LGBT populations also noted that the long-term effects of culturally competent interventions on health disparities in LGBT populations are still unknown.
The Joint Commission has identified the health and welfare of LGBT populations as a major priority. Beginning in 2012, The Joint Commission started assessing compliance with standards for cultural competence and patient-centered care for LGBT recipients as part of the accreditation criteria.11 The Joint Commission recommended that health care facilities begin to transform the health care environment to be a more welcoming, safe, and inclusive environment for LGBT patients and their families.11 Health care providers can play an important role in reducing the significant health disparities and unequal treatment.12
Problem Identification
Improving health outcomes and reducing health disparities are an important part of the HCP’s role. Yet, many HCPs lack the significant knowledge, skills, and cultural competencies needed to provide quality LGBT care.10 Evidence suggests that HCPs continue to receive little or no training to prepare them to manage this vulnerable population.10 Due to the growing evidence of health disparities and negative health outcomes affecting LGBT populations, the federal government has identified LGBT care and patient outcomes as a major health concern and priority under the Healthy 2020 goals.2,4
About 3.5% (9 million) of the U.S. adult population are identified as lesbian, gay, or bisexual and 0.3% or 700,000 as transgender.13,14 The VHA serves 9 million veterans at 1,245 facilities.15
Because the cooperation of HCPs can play a significant part in reducing health disparities and unequal treatment in the care LGBT patients receive, the VHA launched several initiatives to create a more welcoming, inclusive, and empowering environment for LGBT veterans and families. Among the initiatives, VHA established the Office of Health Equity to address health disparities and ensure that patient-centered care is provided in a positive environment.19,20 The VHA also issued a national directive mandating standardized services be provided for transgender veterans.20
Despite these initiatives, obstacles remain to the delivery of patient-centered LGBT care at the VA. A first step to identifying barriers to patient-centered, high-quality care to LGBT veterans is to evaluate personal and institutional barriers as expressed through HCPs’ preceptions and knowledge about the health of LGBT patients. The magnitude of barriers to providing patient-centered care must first be identified and understood before institutional recommendations can be made and implemented at the facility or national level.
This study examined attitudes and knowledge about LGBT patient health among 45 primary care providers (PCPs) in 4 VA community-based outpatient clinics (CBOCs). The first clinical question examined whether PCPs desired more education and training on LGBT health. The second clinical question asked whether there were gender differences in attitudes among providers about the need for LGBT health education.
The model presented in The Process of Cultural Competence in the Delivery of Healthcare Services by Campinha-Bacote provides an applicable conceptualization to guide HCPs’ actions toward delivering culturally responsive health care services to increasingly diverse health populations.21 The model defines cultural competence as an ongoing dynamic process of striving to effectively work within the cultural context of the client (person, family, or community). The model integrates 5 constructs that are fundamental to becoming culturally competent to provide appropriate culturally responsive care to diverse clients: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desires.21 The level of competence of the HCP is believed to have a direct relationship with their ability to provide culturally competent health care services. Table 1 provides the definitions of the 5 constructs and highlights the role of education and training in influencing competence in providing LGBT health services.21 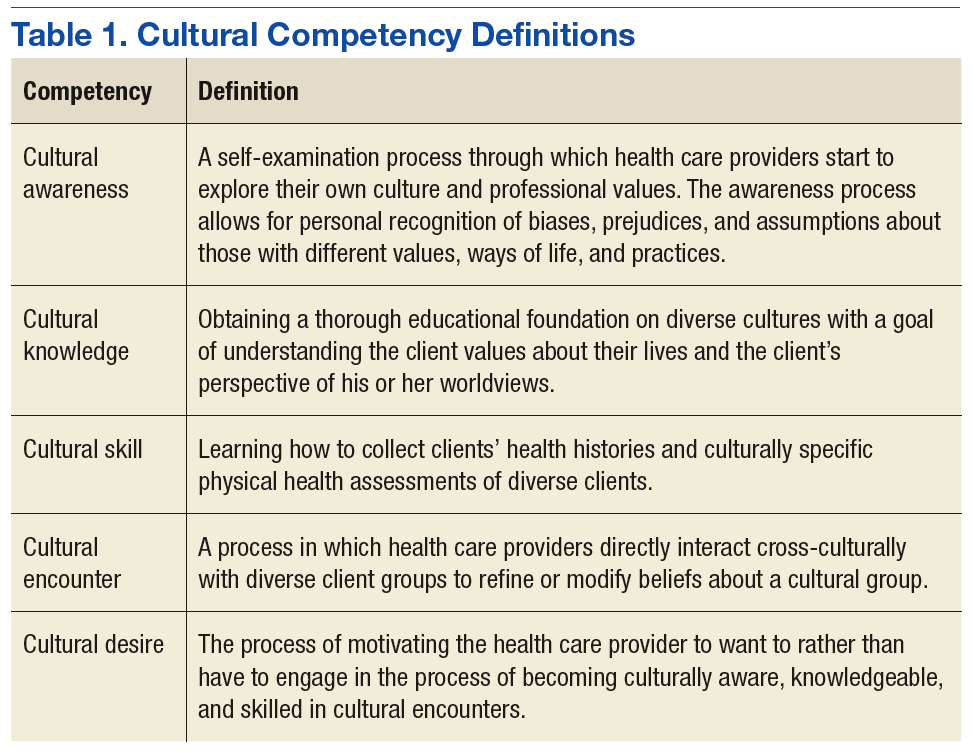
This project used a descriptive, cross-sectional one-group design to target physicians, nurse practitioners (NPs), and physician assistants (PAs) at VA Southern Nevada Healthcare System (VASNHS) CBOCs. Participation in the project was voluntary. The duration of project from data collection to completion of analysis and summation of the results was 4 months. The study was approved by the institutional review board (IRB) at the University of Alabama in Huntsville, and it was exempt from the VA IRB.
The survey consisted of 74 questions, including 8 demographic questions and 66 LGBT-related questions. The survey instrument, renamed the Perception and Knowledge of Sexual and Gender Minority Health (PKSGMH) survey was adapted with permission from an original study by Jabson and colleagues and used its format without revision or restructuring.22
Attitudinal questions asked personal opinions on LGBT orientation and gender identity (eAppendix:
Measures
The survey instrument integrated components of 4 different measures on attitudes and knowledge of LGBT health with questions about familiarity with organizational policies on discrimination, visitation, and staff training in LGBT care. The PKSGMH survey measured attitudes and knowledge levels on LGBT health by calculating the mean scores for each of 4 measures.
General Attitudes Toward LGBT Nonpatients.
Physician Attitudes Toward LGBT (ATLG) Patients. The attitudes toward LGBT scale assessed physicians’ feelings toward providing care to LGBT patients. This scale of 6 questions had modest reliability with a Cronbach α of .5. The measure used a 5-point Likert scale (5 = strongly agree). For this project, this scale was renamed the Provider subscale.
Knowledge of LGBT (KLGBT) Patients. The knowledge of LGBT patients’ scale included 13 true/false questions and had a Cronbach α of .74.
Gender and Sexual Minority Affirmative Practice (GSMAP). The GSMAP affirmative practice scale evaluated HCPs’ attitudes and beliefs about the treatment of LGBT patients. The 11-question measure with 2 subscales used a 5-point Likert scale with high reliability on the clinicians’ beliefs and behaviors subscales. Both subscales had a Cronbach α of .93 and .94, respectively.
Demographics and Data Analyses
Health care providers answered demographic questions about gender, sexual orientation, and marital status. They also were asked whether they had ever received any focused training in LGBT patient care. Descriptive and demographic data analyses were performed using SPSS version 24.0 (Armonk, New York). A significance level of P < .05 was used for all analyses. Analysis of variance (ANOVA) statistical analysis was conducted to evaluate the differences in mean scores between male and female PCP groups on the 4 attitudes toward LGBT subscales and the Provider subscale.
Results
Seventy-two PCPs participated in completing the PKSGMH survey. Fifty-seven surveys were returned; however, only 45 surveys were completely answered and included in the final analysis. Twelve surveys containing unanswered questions to the knowledge sections were excluded from the data analysis, and 14 distributed surveys were not returned. The overall response rate for completed surveys was 62.5% (Table 2). 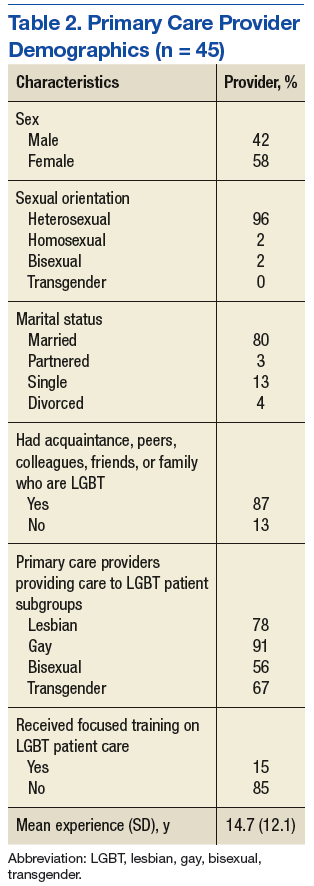
Attitudes Toward Care
Attitudes about competence in providing LGBT care was answered in question 23 of the PKSGMH survey. Overall, a total of 51.1% (n = 23) of PCPs agreed that they were competentto provide LGBT care, and 15.5% (n = 7) disagreed. By gender, 50% (n = 9) of males said they were competent in providing LGBT care compared with 51.8% (n = 14) of females.
Analysis of variance was used to test for differences between groups on the 5 ATLG subscales (gay, lesbian, bisexual, transgender, provider) of the PKSGMH survey (Table 3). A grouping variable was created by separating participants by gender and by their responses to a question that asked about their desire for more education about the health care needs of LGBT patients. The grouping resulted in 4 groups: (1) males who responded yes to need for additional education; (2) males who responded no to need for additional education; (3) females who responded yes to need for additional education; and (4) females who responded no to need for additional education. Results of the ANOVA demonstrated significant differences between groups for the bisexual subscale (F = 3.005, df = 3, 32; P = .045), transgender subscale (F = 4.545, df = 3, 32; P = .009), and the provider subscale (F = 12.602, df = 3, 32; P < .001).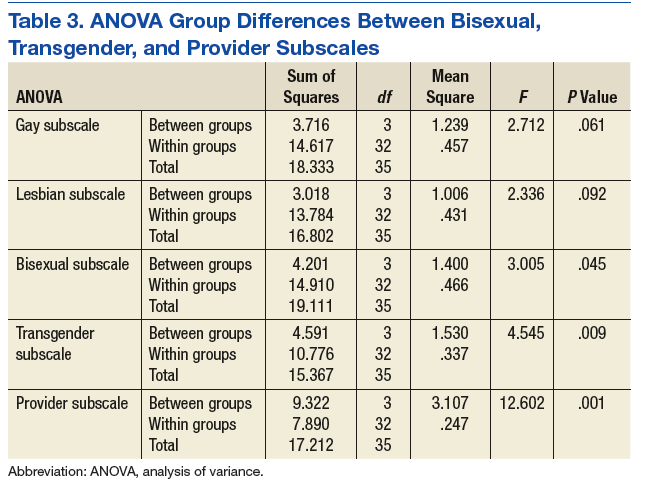
Attitudes toward adequacy of their medical training to address the health needs of the LGBT population were answered in question 26 of the PKSGMH survey. Overall a total of 29% (n = 13) of PCPs agreed that their training adequately prepared them to address the needs of the LGBT population while 51.1% (n = 23) disagreed (Figure).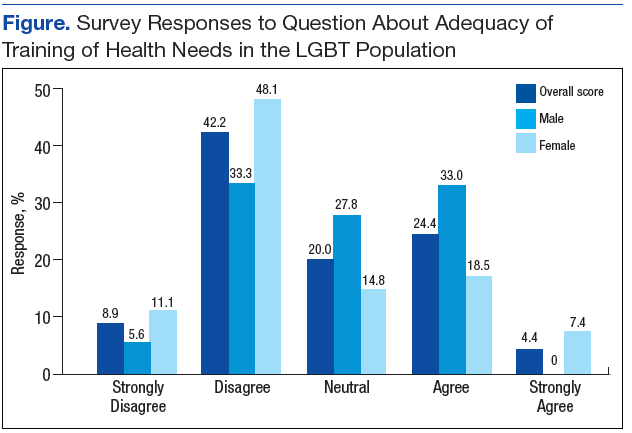
Knowledge of LGBT Care
Discussion
Federal health care agencies consider the health and welfare of LGBT persons to be a health priority despite the lack of available science-based knowledge about this population.2 In 2011, the National Academies of Medicine (NAM) noted that there are still research gaps concerning the well-being of LGBT individuals. The report stated that a significant contributor of health care inequities in LGBT patients is the lack of provider training and medical education.2 A major recommendation of the NAM is that additional training and education is needed to reduce barriers and improve patient outcomes in the LGBT population.
Provider attitudes and education are among the gaps that contribute to inequities in the health care of LGBT populations as previously discussed. The findings from this survey suggest that PCPs in the VHA perceive that they have deficits in competencies and knowledge levels on LGBT care and that education influences attitudes toward LGBT care. The association between providers’ self-assessment of their competency and their knowledge and attitudes toward care for LGBT patients was not stated in the clinical question and was not investigated in this study.
An online search of 12,966 courses at the VA Talent Management System (TMS) was conducted to find web-based and/or instructor-led training courses focused on LGBT care. The search found 4 LGBT-focused courses that targeted physicians and nurses. Two 90-minute courses presented clinical and public health data on sexual health and addressed how providers can improve skills on taking sexual histories and incorporating these data into routine practice. Training and skills development in sexual history taking by clinicians is vital in reducing health disparities, such as STDs, and in helping LGBT patients feel more comfortable in accessing health care.4 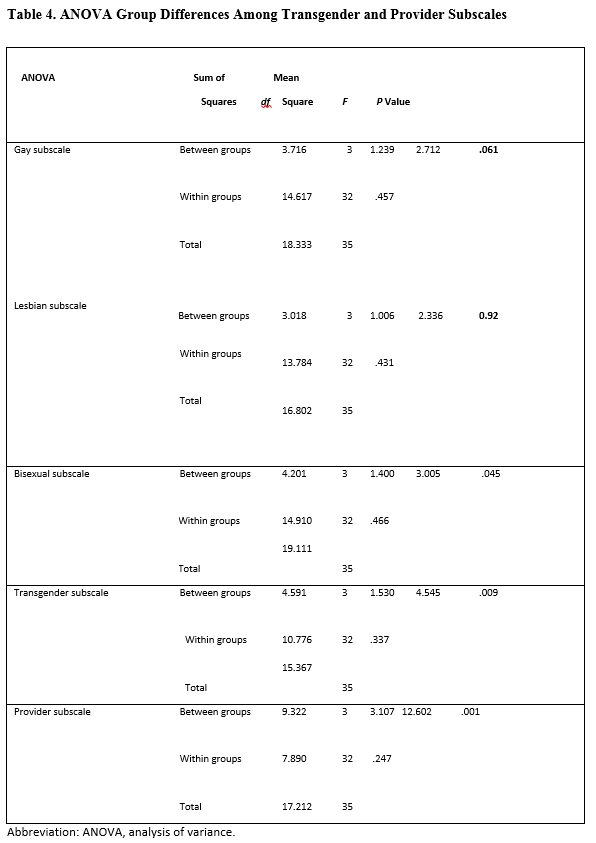
A 1-hour TMS course focused on training HCPs to develop as researchers, teachers, and leaders in improving the LGBT veteran experience by providing competent care. Information on LGBT-related subjects, such as sexual and physical trauma and STDs, were included in the content of some online courses. However, no other comprehensive courses specifically focused on LGBT care. The only exceptions were the Specialty Care Access Network Extension of Community Healthcare outcome video conferencing-based sequential training on transgender care and the VA Lesbian, Gay and Bisexual Education sharepoint and the transgender education sharepoint. At the VA, online LGBT health training is still limited.
Recommendations
Providing additional LGBT-focused TMS courses could help increase provider knowledge and cultural competencies. An online introductory LGBT health course could be offered at VA facilities for all new employees and HCPs as part of employee orientation. More specific courses with continuing education credits geared toward the HCP and focused on LGBT health could be included in the TMS learning portfolio for each HCP as annual learning refresher courses. This course could include specific knowledge questions on LGBT care and a posttest with a required passing score of 80%.
Training HCPs as designated LGBT educators in VA facilities should be considered. Classroom training could be offered annually or during times of increased LGBT patient focus, such as during LGBT Pride month when learning activities can be planned and/or coordinated with the VA Office of Diversity and Inclusion. Nurses, social workers, pharmacists, and medical assistants who provide supportive care to LGBT patients also should be included in the target audience for LGBT health education and training.
Limitations
The use of a cross-sectional project design with such a small convenience sample prevents generalizability of the findings to all PCPs. The lack of a survey design that included randomization and blinding in survey distribution could certainly deter participants from offering candid responses, particularly to some attitudinal questions that were emotional in context. The true-false responses wherein respondents had a 50% chance at guessing the correct response was not the most reliable method of measuring knowledge levels and thereby limited the ability to draw any strong conclusions about providers’ knowledge levels. Additionally, the project design did not allow for measures of other confounding factors, such as age, race/ethnicity, religion, and other social factors that could have influenced how participants responded. Additional randomized controlled studies with larger samples are needed to test specific interventions that evaluate the influence of gender on provider attitudes and knowledge as well as the effect of more HCP education and training on LGBT patient outcomes. Moreover, a literature review found no guidelines on how to specifically address provider gender differences in LGBT education and training or strategies for education and training interventions to address these differences.
Conclusion
Findings suggest that PCPs need additional education and training involving LGBT health issues. Although both male and female providers want more education, female PCPs as a group expressed a greater desire for more training compared with the responses of male PCPs. However, given the study’s small sample size, a strong conclusion regarding gender differences cannot be made. Research has shown that education is a factor that positively influences attitudes and feelings about providing LGBT care. The availability of education and training that is focused on LGBT health topics is still limited within the VHA. Within its stated mission to provide patient-centered care to all veterans, the
Better training on LGBT health topics is vital to improving health care delivery to LGBT populations. To meet this goal, ongoing HCP training to improve attitudes and knowledge and develop the skills necessary to effectively address LGBT health issues also must be a priority at VHA facilities. The VHA also should consider institutional changes that incorporate increased LGBT-focused health education into the learning activities of PCPs. This is essential to evaluating the quality of care given the impact on patient outcomes and health disparities in LGBT populations.
1. Grant JM, Mottet LA, Tanis J, Harrison J, Herman JL, Keisling M. Injustice at every turn: a report of the National Transgender Discrimination Survey. http://www.thetaskforce.org/static_html/downloads/reports/reports/ntds_full.pdf. Published 2011. Accessed October 5, 2017.
2. Institute of Medicine Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities.
3. Centers for Disease Control Prevention. Reported STDs in the United States. 2014 national data for chlamydia, gonorrhea, and syphilis. www.cdc.gov/std/stats14/std-trends-508.pdf. Published November 2015. Accessed October 5, 2017.
4. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Lesbian, gay, bisexual, and transgender health. http://www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health. Updated October 4, 2017. Accessed October 5, 2017.
5. Kerker BD, Mostashari F, Thorpe L. Health care access and utilization among women who have sex with women: sexual behavior and identity. J Urban Health. 2006;83(5):970-979.
6. Khan MA, Evans AT, Shah S. Caring for uninsured patients with diabetes: designing and evaluating a novel chronic care model for diabetes care. J Eval Clin Pract. 2010;16(4):700-706.
7. Herek GM. Sexual prejudice. In: Nelson TD, ed. Handbook of Prejudice, Stereotyping, and Discrimination. New York: Psychology Press; 2009:441-467.
8. McKay B. Lesbian, gay, bisexual, and transgender health issues, disparities, and information resources. Med Ref Serv Q. 2011;30(4):393-401.
9. Chapman R, Watkins R, Zappia T, Nicol P, Shields L. Nursing and medical students’ attitude, knowledge and beliefs regarding lesbian, gay, bisexual and transgender parents seeking health care for their children. J Clin Nurs. 2012;21(7‐8):938-945.
10. Butler M, McCreedy E, Schwer N, et al. Improving cultural competence to reduce health disparities. Review No. 170. https://ahrq-ehc-application.s3.amazonaws.com/media/pdf/cultural-competence_research.pdf. Published March 29, 2016. Accessed October 5, 2017.
11. The Joint Commission. Advancing effective communication, cultural competence, and patient-and family-centered care: a roadmap for hospitals. https://www.jointcommission.org/assets/1/6/ARoadmapforHospitalsfinalversion727.pdf. Published 2010. Accessed October 5, 2017.
12. Snelgrove JW, Jasudavisius AM, Rowe BW, Head EM, Bauer GR. “Completely out-at-sea” with “two-gender medicine”: a qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv Res. 2012;12:110.
13. Gates GJ. How many people are lesbian, gay, bisexual, and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Published April 2011. Accessed October 5, 2017.
14. Gates GJ, Herman J. Transgender military service in the United States. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Transgender-Military-Service-May-2014.pdf. Published May 2014. Accessed October 5, 2017.
15. U.S. Department of Veteran Affairs. Veterans Health Administration. http://www.va.gov/health. Updated October 2, 2017. Accessed October 5, 2017.
16. Gates GJ. Gay men and lesbians in the U.S. military: estimates from the 2000 census. http://www.lgbtdata.com/uploads/1/0/8/8/10884149/ds008_uscensus_gates.pdf. Published September 28, 2014. Accessed October 5, 2017.
17. Mattocks KM, Kauth MR, Sandfort T, Matza AR, Sullivan JC, Shipherd JC. Understanding health-care needs of sexual and gender minority veterans: how targeted research and policy can improve health. LGBT Health. 2014;1(1):50-57.
18. Kauth MR, Shipherd JC, Lindsay J, Blosnich JR, Brown GR, Jones KT. Access to care for transgender veterans in the Veterans Health Administration: 2006–2013. Am J Public Health. 2014;104(suppl 4):S532-S534.
19. Uchendu US. Veterans Health Administration Office of Health Equity: what is it a about? http://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/769-notes.pdf. Published November 4, 2013. Accessed October 5, 2017.
20. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2013-003: Providing Health Care for Transgender and Intersex Veterans. http://www.transequality.org/sites/default/files/docs/resources/VHAHealthcareDirective_2013.pdf. Published February 8, 2013. Accessed October 5, 2017.
21. Campinha-Bacote J. The process of cultural competence in the delivery of healthcare services: a model of care. J Transcult Nurs. 2002;13(3):181-184.
22. Jabson JM, Mitchell JW, Doty SB. Associations between non-discrimination and training policies and physicians’ attitudes and knowledge about sexual and gender minority patients: a comparison of physicians from two hospitals. BMC Public Health. 2016;16:256
Lesbian, gay, bisexual and transgender (LGBT) populations face significant social stigmatization, discrimination, and marginalization that contribute to negative patient outcomes. Consequently, the LGBT population experiences high rates of mental health issues, such as suicide and depression, as well as sexually transmitted diseases (STDs), drug abuse, poverty, and homelessness.1,2
Background
According to the CDC, gay men are at highest risk and have increased incidences of gonorrhea, chlamydia, herpes, human papilloma virus (HPV), and HIV.3 Lesbians and bisexual women are less likely to get preventive cancer screenings, such as Pap smears and mammograms, and have higher incidences of HIV, hepatitis C, self-reported gonorrhea, and are more likely to be overweight or obese.3-6 In addition, LGBT populations have high rates of use of tobacco, alcohol, and other drugs.
The National Transgender Discrimination Survey of 6,450 transgender and nonconforming participants also provides extensive data on the challenges faced by transgender individuals. Discrimination was frequently experienced in accessing health care. Due to their transgender status, 19% were denied care, and 28% postponed care due to perceived harassment and violence within a health care setting.1 The LGBT populations experience personal and structural barriers that interfere with their ability to access high-quality care. Sexual gender minority individuals also experience health care barriers due to isolation, insufficient social services, and a lack of culturally competent providers.4 At the same time, many health care providers (HCPs) experience various barriers to providing LGBT care and need to increase their cultural competence by improving awareness, receptivity, and knowledge.7,8 One personal barrier to quality care is stigmatization toward LGBT persons as expressed through HCP prejudices, beliefs, attitudes, and behaviors.2 Factors such as gender, race, and religious beliefs also influence attitudes to LGBT health care.
A study by Chapman and colleagues found significant differences in attitudes toward gay men by male and female medical and nursing students.9 Male students had a significantly more negative attitude toward gay men compared with the attitudes of female students. Cultural competence, defined in the study as gay affirmative action principles scores, were statistically significant and strongly correlated with negative attitudes. In this study there also was a statistically significant negative correlation between attitudes and knowledge scores indicating a considerable potential for personal values to influence the provision of health care.9
Various barriers inherent in the health care system restrict access to high-quality care. Institutional barriers that include a lack of legal recognition of same-sex partners, equality in visitation rights, and the ability of same-sex partners to access partner’s medical records hamper health care quality. The HCPs’ lack of knowledge of the health risks or health care needs of the LGBT population also present a structural barrier to quality of care and affects patient outcomes.2
Culturally competent interventions in health care delivery also have been studied to reduce LGBT health disparities. A systematic review of 56 studies by Butler and colleagues found that the term cultural competence was not well defined and often was denoted with the terms patient-centered or individualized care.10 A review on the impact of these interventions in LGBT populations also noted that the long-term effects of culturally competent interventions on health disparities in LGBT populations are still unknown.
The Joint Commission has identified the health and welfare of LGBT populations as a major priority. Beginning in 2012, The Joint Commission started assessing compliance with standards for cultural competence and patient-centered care for LGBT recipients as part of the accreditation criteria.11 The Joint Commission recommended that health care facilities begin to transform the health care environment to be a more welcoming, safe, and inclusive environment for LGBT patients and their families.11 Health care providers can play an important role in reducing the significant health disparities and unequal treatment.12
Problem Identification
Improving health outcomes and reducing health disparities are an important part of the HCP’s role. Yet, many HCPs lack the significant knowledge, skills, and cultural competencies needed to provide quality LGBT care.10 Evidence suggests that HCPs continue to receive little or no training to prepare them to manage this vulnerable population.10 Due to the growing evidence of health disparities and negative health outcomes affecting LGBT populations, the federal government has identified LGBT care and patient outcomes as a major health concern and priority under the Healthy 2020 goals.2,4
About 3.5% (9 million) of the U.S. adult population are identified as lesbian, gay, or bisexual and 0.3% or 700,000 as transgender.13,14 The VHA serves 9 million veterans at 1,245 facilities.15
Because the cooperation of HCPs can play a significant part in reducing health disparities and unequal treatment in the care LGBT patients receive, the VHA launched several initiatives to create a more welcoming, inclusive, and empowering environment for LGBT veterans and families. Among the initiatives, VHA established the Office of Health Equity to address health disparities and ensure that patient-centered care is provided in a positive environment.19,20 The VHA also issued a national directive mandating standardized services be provided for transgender veterans.20
Despite these initiatives, obstacles remain to the delivery of patient-centered LGBT care at the VA. A first step to identifying barriers to patient-centered, high-quality care to LGBT veterans is to evaluate personal and institutional barriers as expressed through HCPs’ preceptions and knowledge about the health of LGBT patients. The magnitude of barriers to providing patient-centered care must first be identified and understood before institutional recommendations can be made and implemented at the facility or national level.
This study examined attitudes and knowledge about LGBT patient health among 45 primary care providers (PCPs) in 4 VA community-based outpatient clinics (CBOCs). The first clinical question examined whether PCPs desired more education and training on LGBT health. The second clinical question asked whether there were gender differences in attitudes among providers about the need for LGBT health education.
The model presented in The Process of Cultural Competence in the Delivery of Healthcare Services by Campinha-Bacote provides an applicable conceptualization to guide HCPs’ actions toward delivering culturally responsive health care services to increasingly diverse health populations.21 The model defines cultural competence as an ongoing dynamic process of striving to effectively work within the cultural context of the client (person, family, or community). The model integrates 5 constructs that are fundamental to becoming culturally competent to provide appropriate culturally responsive care to diverse clients: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desires.21 The level of competence of the HCP is believed to have a direct relationship with their ability to provide culturally competent health care services. Table 1 provides the definitions of the 5 constructs and highlights the role of education and training in influencing competence in providing LGBT health services.21
This project used a descriptive, cross-sectional one-group design to target physicians, nurse practitioners (NPs), and physician assistants (PAs) at VA Southern Nevada Healthcare System (VASNHS) CBOCs. Participation in the project was voluntary. The duration of project from data collection to completion of analysis and summation of the results was 4 months. The study was approved by the institutional review board (IRB) at the University of Alabama in Huntsville, and it was exempt from the VA IRB.
The survey consisted of 74 questions, including 8 demographic questions and 66 LGBT-related questions. The survey instrument, renamed the Perception and Knowledge of Sexual and Gender Minority Health (PKSGMH) survey was adapted with permission from an original study by Jabson and colleagues and used its format without revision or restructuring.22
Attitudinal questions asked personal opinions on LGBT orientation and gender identity (eAppendix:
Measures
The survey instrument integrated components of 4 different measures on attitudes and knowledge of LGBT health with questions about familiarity with organizational policies on discrimination, visitation, and staff training in LGBT care. The PKSGMH survey measured attitudes and knowledge levels on LGBT health by calculating the mean scores for each of 4 measures.
General Attitudes Toward LGBT Nonpatients.
Physician Attitudes Toward LGBT (ATLG) Patients. The attitudes toward LGBT scale assessed physicians’ feelings toward providing care to LGBT patients. This scale of 6 questions had modest reliability with a Cronbach α of .5. The measure used a 5-point Likert scale (5 = strongly agree). For this project, this scale was renamed the Provider subscale.
Knowledge of LGBT (KLGBT) Patients. The knowledge of LGBT patients’ scale included 13 true/false questions and had a Cronbach α of .74.
Gender and Sexual Minority Affirmative Practice (GSMAP). The GSMAP affirmative practice scale evaluated HCPs’ attitudes and beliefs about the treatment of LGBT patients. The 11-question measure with 2 subscales used a 5-point Likert scale with high reliability on the clinicians’ beliefs and behaviors subscales. Both subscales had a Cronbach α of .93 and .94, respectively.
Demographics and Data Analyses
Health care providers answered demographic questions about gender, sexual orientation, and marital status. They also were asked whether they had ever received any focused training in LGBT patient care. Descriptive and demographic data analyses were performed using SPSS version 24.0 (Armonk, New York). A significance level of P < .05 was used for all analyses. Analysis of variance (ANOVA) statistical analysis was conducted to evaluate the differences in mean scores between male and female PCP groups on the 4 attitudes toward LGBT subscales and the Provider subscale.
Results
Seventy-two PCPs participated in completing the PKSGMH survey. Fifty-seven surveys were returned; however, only 45 surveys were completely answered and included in the final analysis. Twelve surveys containing unanswered questions to the knowledge sections were excluded from the data analysis, and 14 distributed surveys were not returned. The overall response rate for completed surveys was 62.5% (Table 2).
Attitudes Toward Care
Attitudes about competence in providing LGBT care was answered in question 23 of the PKSGMH survey. Overall, a total of 51.1% (n = 23) of PCPs agreed that they were competentto provide LGBT care, and 15.5% (n = 7) disagreed. By gender, 50% (n = 9) of males said they were competent in providing LGBT care compared with 51.8% (n = 14) of females.
Analysis of variance was used to test for differences between groups on the 5 ATLG subscales (gay, lesbian, bisexual, transgender, provider) of the PKSGMH survey (Table 3). A grouping variable was created by separating participants by gender and by their responses to a question that asked about their desire for more education about the health care needs of LGBT patients. The grouping resulted in 4 groups: (1) males who responded yes to need for additional education; (2) males who responded no to need for additional education; (3) females who responded yes to need for additional education; and (4) females who responded no to need for additional education. Results of the ANOVA demonstrated significant differences between groups for the bisexual subscale (F = 3.005, df = 3, 32; P = .045), transgender subscale (F = 4.545, df = 3, 32; P = .009), and the provider subscale (F = 12.602, df = 3, 32; P < .001).
Attitudes toward adequacy of their medical training to address the health needs of the LGBT population were answered in question 26 of the PKSGMH survey. Overall a total of 29% (n = 13) of PCPs agreed that their training adequately prepared them to address the needs of the LGBT population while 51.1% (n = 23) disagreed (Figure).
Knowledge of LGBT Care
Discussion
Federal health care agencies consider the health and welfare of LGBT persons to be a health priority despite the lack of available science-based knowledge about this population.2 In 2011, the National Academies of Medicine (NAM) noted that there are still research gaps concerning the well-being of LGBT individuals. The report stated that a significant contributor of health care inequities in LGBT patients is the lack of provider training and medical education.2 A major recommendation of the NAM is that additional training and education is needed to reduce barriers and improve patient outcomes in the LGBT population.
Provider attitudes and education are among the gaps that contribute to inequities in the health care of LGBT populations as previously discussed. The findings from this survey suggest that PCPs in the VHA perceive that they have deficits in competencies and knowledge levels on LGBT care and that education influences attitudes toward LGBT care. The association between providers’ self-assessment of their competency and their knowledge and attitudes toward care for LGBT patients was not stated in the clinical question and was not investigated in this study.
An online search of 12,966 courses at the VA Talent Management System (TMS) was conducted to find web-based and/or instructor-led training courses focused on LGBT care. The search found 4 LGBT-focused courses that targeted physicians and nurses. Two 90-minute courses presented clinical and public health data on sexual health and addressed how providers can improve skills on taking sexual histories and incorporating these data into routine practice. Training and skills development in sexual history taking by clinicians is vital in reducing health disparities, such as STDs, and in helping LGBT patients feel more comfortable in accessing health care.4
A 1-hour TMS course focused on training HCPs to develop as researchers, teachers, and leaders in improving the LGBT veteran experience by providing competent care. Information on LGBT-related subjects, such as sexual and physical trauma and STDs, were included in the content of some online courses. However, no other comprehensive courses specifically focused on LGBT care. The only exceptions were the Specialty Care Access Network Extension of Community Healthcare outcome video conferencing-based sequential training on transgender care and the VA Lesbian, Gay and Bisexual Education sharepoint and the transgender education sharepoint. At the VA, online LGBT health training is still limited.
Recommendations
Providing additional LGBT-focused TMS courses could help increase provider knowledge and cultural competencies. An online introductory LGBT health course could be offered at VA facilities for all new employees and HCPs as part of employee orientation. More specific courses with continuing education credits geared toward the HCP and focused on LGBT health could be included in the TMS learning portfolio for each HCP as annual learning refresher courses. This course could include specific knowledge questions on LGBT care and a posttest with a required passing score of 80%.
Training HCPs as designated LGBT educators in VA facilities should be considered. Classroom training could be offered annually or during times of increased LGBT patient focus, such as during LGBT Pride month when learning activities can be planned and/or coordinated with the VA Office of Diversity and Inclusion. Nurses, social workers, pharmacists, and medical assistants who provide supportive care to LGBT patients also should be included in the target audience for LGBT health education and training.
Limitations
The use of a cross-sectional project design with such a small convenience sample prevents generalizability of the findings to all PCPs. The lack of a survey design that included randomization and blinding in survey distribution could certainly deter participants from offering candid responses, particularly to some attitudinal questions that were emotional in context. The true-false responses wherein respondents had a 50% chance at guessing the correct response was not the most reliable method of measuring knowledge levels and thereby limited the ability to draw any strong conclusions about providers’ knowledge levels. Additionally, the project design did not allow for measures of other confounding factors, such as age, race/ethnicity, religion, and other social factors that could have influenced how participants responded. Additional randomized controlled studies with larger samples are needed to test specific interventions that evaluate the influence of gender on provider attitudes and knowledge as well as the effect of more HCP education and training on LGBT patient outcomes. Moreover, a literature review found no guidelines on how to specifically address provider gender differences in LGBT education and training or strategies for education and training interventions to address these differences.
Conclusion
Findings suggest that PCPs need additional education and training involving LGBT health issues. Although both male and female providers want more education, female PCPs as a group expressed a greater desire for more training compared with the responses of male PCPs. However, given the study’s small sample size, a strong conclusion regarding gender differences cannot be made. Research has shown that education is a factor that positively influences attitudes and feelings about providing LGBT care. The availability of education and training that is focused on LGBT health topics is still limited within the VHA. Within its stated mission to provide patient-centered care to all veterans, the
Better training on LGBT health topics is vital to improving health care delivery to LGBT populations. To meet this goal, ongoing HCP training to improve attitudes and knowledge and develop the skills necessary to effectively address LGBT health issues also must be a priority at VHA facilities. The VHA also should consider institutional changes that incorporate increased LGBT-focused health education into the learning activities of PCPs. This is essential to evaluating the quality of care given the impact on patient outcomes and health disparities in LGBT populations.
Lesbian, gay, bisexual and transgender (LGBT) populations face significant social stigmatization, discrimination, and marginalization that contribute to negative patient outcomes. Consequently, the LGBT population experiences high rates of mental health issues, such as suicide and depression, as well as sexually transmitted diseases (STDs), drug abuse, poverty, and homelessness.1,2
Background
According to the CDC, gay men are at highest risk and have increased incidences of gonorrhea, chlamydia, herpes, human papilloma virus (HPV), and HIV.3 Lesbians and bisexual women are less likely to get preventive cancer screenings, such as Pap smears and mammograms, and have higher incidences of HIV, hepatitis C, self-reported gonorrhea, and are more likely to be overweight or obese.3-6 In addition, LGBT populations have high rates of use of tobacco, alcohol, and other drugs.
The National Transgender Discrimination Survey of 6,450 transgender and nonconforming participants also provides extensive data on the challenges faced by transgender individuals. Discrimination was frequently experienced in accessing health care. Due to their transgender status, 19% were denied care, and 28% postponed care due to perceived harassment and violence within a health care setting.1 The LGBT populations experience personal and structural barriers that interfere with their ability to access high-quality care. Sexual gender minority individuals also experience health care barriers due to isolation, insufficient social services, and a lack of culturally competent providers.4 At the same time, many health care providers (HCPs) experience various barriers to providing LGBT care and need to increase their cultural competence by improving awareness, receptivity, and knowledge.7,8 One personal barrier to quality care is stigmatization toward LGBT persons as expressed through HCP prejudices, beliefs, attitudes, and behaviors.2 Factors such as gender, race, and religious beliefs also influence attitudes to LGBT health care.
A study by Chapman and colleagues found significant differences in attitudes toward gay men by male and female medical and nursing students.9 Male students had a significantly more negative attitude toward gay men compared with the attitudes of female students. Cultural competence, defined in the study as gay affirmative action principles scores, were statistically significant and strongly correlated with negative attitudes. In this study there also was a statistically significant negative correlation between attitudes and knowledge scores indicating a considerable potential for personal values to influence the provision of health care.9
Various barriers inherent in the health care system restrict access to high-quality care. Institutional barriers that include a lack of legal recognition of same-sex partners, equality in visitation rights, and the ability of same-sex partners to access partner’s medical records hamper health care quality. The HCPs’ lack of knowledge of the health risks or health care needs of the LGBT population also present a structural barrier to quality of care and affects patient outcomes.2
Culturally competent interventions in health care delivery also have been studied to reduce LGBT health disparities. A systematic review of 56 studies by Butler and colleagues found that the term cultural competence was not well defined and often was denoted with the terms patient-centered or individualized care.10 A review on the impact of these interventions in LGBT populations also noted that the long-term effects of culturally competent interventions on health disparities in LGBT populations are still unknown.
The Joint Commission has identified the health and welfare of LGBT populations as a major priority. Beginning in 2012, The Joint Commission started assessing compliance with standards for cultural competence and patient-centered care for LGBT recipients as part of the accreditation criteria.11 The Joint Commission recommended that health care facilities begin to transform the health care environment to be a more welcoming, safe, and inclusive environment for LGBT patients and their families.11 Health care providers can play an important role in reducing the significant health disparities and unequal treatment.12
Problem Identification
Improving health outcomes and reducing health disparities are an important part of the HCP’s role. Yet, many HCPs lack the significant knowledge, skills, and cultural competencies needed to provide quality LGBT care.10 Evidence suggests that HCPs continue to receive little or no training to prepare them to manage this vulnerable population.10 Due to the growing evidence of health disparities and negative health outcomes affecting LGBT populations, the federal government has identified LGBT care and patient outcomes as a major health concern and priority under the Healthy 2020 goals.2,4
About 3.5% (9 million) of the U.S. adult population are identified as lesbian, gay, or bisexual and 0.3% or 700,000 as transgender.13,14 The VHA serves 9 million veterans at 1,245 facilities.15
Because the cooperation of HCPs can play a significant part in reducing health disparities and unequal treatment in the care LGBT patients receive, the VHA launched several initiatives to create a more welcoming, inclusive, and empowering environment for LGBT veterans and families. Among the initiatives, VHA established the Office of Health Equity to address health disparities and ensure that patient-centered care is provided in a positive environment.19,20 The VHA also issued a national directive mandating standardized services be provided for transgender veterans.20
Despite these initiatives, obstacles remain to the delivery of patient-centered LGBT care at the VA. A first step to identifying barriers to patient-centered, high-quality care to LGBT veterans is to evaluate personal and institutional barriers as expressed through HCPs’ preceptions and knowledge about the health of LGBT patients. The magnitude of barriers to providing patient-centered care must first be identified and understood before institutional recommendations can be made and implemented at the facility or national level.
This study examined attitudes and knowledge about LGBT patient health among 45 primary care providers (PCPs) in 4 VA community-based outpatient clinics (CBOCs). The first clinical question examined whether PCPs desired more education and training on LGBT health. The second clinical question asked whether there were gender differences in attitudes among providers about the need for LGBT health education.
The model presented in The Process of Cultural Competence in the Delivery of Healthcare Services by Campinha-Bacote provides an applicable conceptualization to guide HCPs’ actions toward delivering culturally responsive health care services to increasingly diverse health populations.21 The model defines cultural competence as an ongoing dynamic process of striving to effectively work within the cultural context of the client (person, family, or community). The model integrates 5 constructs that are fundamental to becoming culturally competent to provide appropriate culturally responsive care to diverse clients: cultural awareness, cultural knowledge, cultural skill, cultural encounters, and cultural desires.21 The level of competence of the HCP is believed to have a direct relationship with their ability to provide culturally competent health care services. Table 1 provides the definitions of the 5 constructs and highlights the role of education and training in influencing competence in providing LGBT health services.21
This project used a descriptive, cross-sectional one-group design to target physicians, nurse practitioners (NPs), and physician assistants (PAs) at VA Southern Nevada Healthcare System (VASNHS) CBOCs. Participation in the project was voluntary. The duration of project from data collection to completion of analysis and summation of the results was 4 months. The study was approved by the institutional review board (IRB) at the University of Alabama in Huntsville, and it was exempt from the VA IRB.
The survey consisted of 74 questions, including 8 demographic questions and 66 LGBT-related questions. The survey instrument, renamed the Perception and Knowledge of Sexual and Gender Minority Health (PKSGMH) survey was adapted with permission from an original study by Jabson and colleagues and used its format without revision or restructuring.22
Attitudinal questions asked personal opinions on LGBT orientation and gender identity (eAppendix:
Measures
The survey instrument integrated components of 4 different measures on attitudes and knowledge of LGBT health with questions about familiarity with organizational policies on discrimination, visitation, and staff training in LGBT care. The PKSGMH survey measured attitudes and knowledge levels on LGBT health by calculating the mean scores for each of 4 measures.
General Attitudes Toward LGBT Nonpatients.
Physician Attitudes Toward LGBT (ATLG) Patients. The attitudes toward LGBT scale assessed physicians’ feelings toward providing care to LGBT patients. This scale of 6 questions had modest reliability with a Cronbach α of .5. The measure used a 5-point Likert scale (5 = strongly agree). For this project, this scale was renamed the Provider subscale.
Knowledge of LGBT (KLGBT) Patients. The knowledge of LGBT patients’ scale included 13 true/false questions and had a Cronbach α of .74.
Gender and Sexual Minority Affirmative Practice (GSMAP). The GSMAP affirmative practice scale evaluated HCPs’ attitudes and beliefs about the treatment of LGBT patients. The 11-question measure with 2 subscales used a 5-point Likert scale with high reliability on the clinicians’ beliefs and behaviors subscales. Both subscales had a Cronbach α of .93 and .94, respectively.
Demographics and Data Analyses
Health care providers answered demographic questions about gender, sexual orientation, and marital status. They also were asked whether they had ever received any focused training in LGBT patient care. Descriptive and demographic data analyses were performed using SPSS version 24.0 (Armonk, New York). A significance level of P < .05 was used for all analyses. Analysis of variance (ANOVA) statistical analysis was conducted to evaluate the differences in mean scores between male and female PCP groups on the 4 attitudes toward LGBT subscales and the Provider subscale.
Results
Seventy-two PCPs participated in completing the PKSGMH survey. Fifty-seven surveys were returned; however, only 45 surveys were completely answered and included in the final analysis. Twelve surveys containing unanswered questions to the knowledge sections were excluded from the data analysis, and 14 distributed surveys were not returned. The overall response rate for completed surveys was 62.5% (Table 2).
Attitudes Toward Care
Attitudes about competence in providing LGBT care was answered in question 23 of the PKSGMH survey. Overall, a total of 51.1% (n = 23) of PCPs agreed that they were competentto provide LGBT care, and 15.5% (n = 7) disagreed. By gender, 50% (n = 9) of males said they were competent in providing LGBT care compared with 51.8% (n = 14) of females.
Analysis of variance was used to test for differences between groups on the 5 ATLG subscales (gay, lesbian, bisexual, transgender, provider) of the PKSGMH survey (Table 3). A grouping variable was created by separating participants by gender and by their responses to a question that asked about their desire for more education about the health care needs of LGBT patients. The grouping resulted in 4 groups: (1) males who responded yes to need for additional education; (2) males who responded no to need for additional education; (3) females who responded yes to need for additional education; and (4) females who responded no to need for additional education. Results of the ANOVA demonstrated significant differences between groups for the bisexual subscale (F = 3.005, df = 3, 32; P = .045), transgender subscale (F = 4.545, df = 3, 32; P = .009), and the provider subscale (F = 12.602, df = 3, 32; P < .001).
Attitudes toward adequacy of their medical training to address the health needs of the LGBT population were answered in question 26 of the PKSGMH survey. Overall a total of 29% (n = 13) of PCPs agreed that their training adequately prepared them to address the needs of the LGBT population while 51.1% (n = 23) disagreed (Figure).
Knowledge of LGBT Care
Discussion
Federal health care agencies consider the health and welfare of LGBT persons to be a health priority despite the lack of available science-based knowledge about this population.2 In 2011, the National Academies of Medicine (NAM) noted that there are still research gaps concerning the well-being of LGBT individuals. The report stated that a significant contributor of health care inequities in LGBT patients is the lack of provider training and medical education.2 A major recommendation of the NAM is that additional training and education is needed to reduce barriers and improve patient outcomes in the LGBT population.
Provider attitudes and education are among the gaps that contribute to inequities in the health care of LGBT populations as previously discussed. The findings from this survey suggest that PCPs in the VHA perceive that they have deficits in competencies and knowledge levels on LGBT care and that education influences attitudes toward LGBT care. The association between providers’ self-assessment of their competency and their knowledge and attitudes toward care for LGBT patients was not stated in the clinical question and was not investigated in this study.
An online search of 12,966 courses at the VA Talent Management System (TMS) was conducted to find web-based and/or instructor-led training courses focused on LGBT care. The search found 4 LGBT-focused courses that targeted physicians and nurses. Two 90-minute courses presented clinical and public health data on sexual health and addressed how providers can improve skills on taking sexual histories and incorporating these data into routine practice. Training and skills development in sexual history taking by clinicians is vital in reducing health disparities, such as STDs, and in helping LGBT patients feel more comfortable in accessing health care.4
A 1-hour TMS course focused on training HCPs to develop as researchers, teachers, and leaders in improving the LGBT veteran experience by providing competent care. Information on LGBT-related subjects, such as sexual and physical trauma and STDs, were included in the content of some online courses. However, no other comprehensive courses specifically focused on LGBT care. The only exceptions were the Specialty Care Access Network Extension of Community Healthcare outcome video conferencing-based sequential training on transgender care and the VA Lesbian, Gay and Bisexual Education sharepoint and the transgender education sharepoint. At the VA, online LGBT health training is still limited.
Recommendations
Providing additional LGBT-focused TMS courses could help increase provider knowledge and cultural competencies. An online introductory LGBT health course could be offered at VA facilities for all new employees and HCPs as part of employee orientation. More specific courses with continuing education credits geared toward the HCP and focused on LGBT health could be included in the TMS learning portfolio for each HCP as annual learning refresher courses. This course could include specific knowledge questions on LGBT care and a posttest with a required passing score of 80%.
Training HCPs as designated LGBT educators in VA facilities should be considered. Classroom training could be offered annually or during times of increased LGBT patient focus, such as during LGBT Pride month when learning activities can be planned and/or coordinated with the VA Office of Diversity and Inclusion. Nurses, social workers, pharmacists, and medical assistants who provide supportive care to LGBT patients also should be included in the target audience for LGBT health education and training.
Limitations
The use of a cross-sectional project design with such a small convenience sample prevents generalizability of the findings to all PCPs. The lack of a survey design that included randomization and blinding in survey distribution could certainly deter participants from offering candid responses, particularly to some attitudinal questions that were emotional in context. The true-false responses wherein respondents had a 50% chance at guessing the correct response was not the most reliable method of measuring knowledge levels and thereby limited the ability to draw any strong conclusions about providers’ knowledge levels. Additionally, the project design did not allow for measures of other confounding factors, such as age, race/ethnicity, religion, and other social factors that could have influenced how participants responded. Additional randomized controlled studies with larger samples are needed to test specific interventions that evaluate the influence of gender on provider attitudes and knowledge as well as the effect of more HCP education and training on LGBT patient outcomes. Moreover, a literature review found no guidelines on how to specifically address provider gender differences in LGBT education and training or strategies for education and training interventions to address these differences.
Conclusion
Findings suggest that PCPs need additional education and training involving LGBT health issues. Although both male and female providers want more education, female PCPs as a group expressed a greater desire for more training compared with the responses of male PCPs. However, given the study’s small sample size, a strong conclusion regarding gender differences cannot be made. Research has shown that education is a factor that positively influences attitudes and feelings about providing LGBT care. The availability of education and training that is focused on LGBT health topics is still limited within the VHA. Within its stated mission to provide patient-centered care to all veterans, the
Better training on LGBT health topics is vital to improving health care delivery to LGBT populations. To meet this goal, ongoing HCP training to improve attitudes and knowledge and develop the skills necessary to effectively address LGBT health issues also must be a priority at VHA facilities. The VHA also should consider institutional changes that incorporate increased LGBT-focused health education into the learning activities of PCPs. This is essential to evaluating the quality of care given the impact on patient outcomes and health disparities in LGBT populations.
1. Grant JM, Mottet LA, Tanis J, Harrison J, Herman JL, Keisling M. Injustice at every turn: a report of the National Transgender Discrimination Survey. http://www.thetaskforce.org/static_html/downloads/reports/reports/ntds_full.pdf. Published 2011. Accessed October 5, 2017.
2. Institute of Medicine Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities.
3. Centers for Disease Control Prevention. Reported STDs in the United States. 2014 national data for chlamydia, gonorrhea, and syphilis. www.cdc.gov/std/stats14/std-trends-508.pdf. Published November 2015. Accessed October 5, 2017.
4. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Lesbian, gay, bisexual, and transgender health. http://www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health. Updated October 4, 2017. Accessed October 5, 2017.
5. Kerker BD, Mostashari F, Thorpe L. Health care access and utilization among women who have sex with women: sexual behavior and identity. J Urban Health. 2006;83(5):970-979.
6. Khan MA, Evans AT, Shah S. Caring for uninsured patients with diabetes: designing and evaluating a novel chronic care model for diabetes care. J Eval Clin Pract. 2010;16(4):700-706.
7. Herek GM. Sexual prejudice. In: Nelson TD, ed. Handbook of Prejudice, Stereotyping, and Discrimination. New York: Psychology Press; 2009:441-467.
8. McKay B. Lesbian, gay, bisexual, and transgender health issues, disparities, and information resources. Med Ref Serv Q. 2011;30(4):393-401.
9. Chapman R, Watkins R, Zappia T, Nicol P, Shields L. Nursing and medical students’ attitude, knowledge and beliefs regarding lesbian, gay, bisexual and transgender parents seeking health care for their children. J Clin Nurs. 2012;21(7‐8):938-945.
10. Butler M, McCreedy E, Schwer N, et al. Improving cultural competence to reduce health disparities. Review No. 170. https://ahrq-ehc-application.s3.amazonaws.com/media/pdf/cultural-competence_research.pdf. Published March 29, 2016. Accessed October 5, 2017.
11. The Joint Commission. Advancing effective communication, cultural competence, and patient-and family-centered care: a roadmap for hospitals. https://www.jointcommission.org/assets/1/6/ARoadmapforHospitalsfinalversion727.pdf. Published 2010. Accessed October 5, 2017.
12. Snelgrove JW, Jasudavisius AM, Rowe BW, Head EM, Bauer GR. “Completely out-at-sea” with “two-gender medicine”: a qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv Res. 2012;12:110.
13. Gates GJ. How many people are lesbian, gay, bisexual, and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Published April 2011. Accessed October 5, 2017.
14. Gates GJ, Herman J. Transgender military service in the United States. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Transgender-Military-Service-May-2014.pdf. Published May 2014. Accessed October 5, 2017.
15. U.S. Department of Veteran Affairs. Veterans Health Administration. http://www.va.gov/health. Updated October 2, 2017. Accessed October 5, 2017.
16. Gates GJ. Gay men and lesbians in the U.S. military: estimates from the 2000 census. http://www.lgbtdata.com/uploads/1/0/8/8/10884149/ds008_uscensus_gates.pdf. Published September 28, 2014. Accessed October 5, 2017.
17. Mattocks KM, Kauth MR, Sandfort T, Matza AR, Sullivan JC, Shipherd JC. Understanding health-care needs of sexual and gender minority veterans: how targeted research and policy can improve health. LGBT Health. 2014;1(1):50-57.
18. Kauth MR, Shipherd JC, Lindsay J, Blosnich JR, Brown GR, Jones KT. Access to care for transgender veterans in the Veterans Health Administration: 2006–2013. Am J Public Health. 2014;104(suppl 4):S532-S534.
19. Uchendu US. Veterans Health Administration Office of Health Equity: what is it a about? http://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/769-notes.pdf. Published November 4, 2013. Accessed October 5, 2017.
20. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2013-003: Providing Health Care for Transgender and Intersex Veterans. http://www.transequality.org/sites/default/files/docs/resources/VHAHealthcareDirective_2013.pdf. Published February 8, 2013. Accessed October 5, 2017.
21. Campinha-Bacote J. The process of cultural competence in the delivery of healthcare services: a model of care. J Transcult Nurs. 2002;13(3):181-184.
22. Jabson JM, Mitchell JW, Doty SB. Associations between non-discrimination and training policies and physicians’ attitudes and knowledge about sexual and gender minority patients: a comparison of physicians from two hospitals. BMC Public Health. 2016;16:256
1. Grant JM, Mottet LA, Tanis J, Harrison J, Herman JL, Keisling M. Injustice at every turn: a report of the National Transgender Discrimination Survey. http://www.thetaskforce.org/static_html/downloads/reports/reports/ntds_full.pdf. Published 2011. Accessed October 5, 2017.
2. Institute of Medicine Committee on Lesbian, Gay, Bisexual, and Transgender Health Issues and Research Gaps and Opportunities.
3. Centers for Disease Control Prevention. Reported STDs in the United States. 2014 national data for chlamydia, gonorrhea, and syphilis. www.cdc.gov/std/stats14/std-trends-508.pdf. Published November 2015. Accessed October 5, 2017.
4. U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion. Lesbian, gay, bisexual, and transgender health. http://www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health. Updated October 4, 2017. Accessed October 5, 2017.
5. Kerker BD, Mostashari F, Thorpe L. Health care access and utilization among women who have sex with women: sexual behavior and identity. J Urban Health. 2006;83(5):970-979.
6. Khan MA, Evans AT, Shah S. Caring for uninsured patients with diabetes: designing and evaluating a novel chronic care model for diabetes care. J Eval Clin Pract. 2010;16(4):700-706.
7. Herek GM. Sexual prejudice. In: Nelson TD, ed. Handbook of Prejudice, Stereotyping, and Discrimination. New York: Psychology Press; 2009:441-467.
8. McKay B. Lesbian, gay, bisexual, and transgender health issues, disparities, and information resources. Med Ref Serv Q. 2011;30(4):393-401.
9. Chapman R, Watkins R, Zappia T, Nicol P, Shields L. Nursing and medical students’ attitude, knowledge and beliefs regarding lesbian, gay, bisexual and transgender parents seeking health care for their children. J Clin Nurs. 2012;21(7‐8):938-945.
10. Butler M, McCreedy E, Schwer N, et al. Improving cultural competence to reduce health disparities. Review No. 170. https://ahrq-ehc-application.s3.amazonaws.com/media/pdf/cultural-competence_research.pdf. Published March 29, 2016. Accessed October 5, 2017.
11. The Joint Commission. Advancing effective communication, cultural competence, and patient-and family-centered care: a roadmap for hospitals. https://www.jointcommission.org/assets/1/6/ARoadmapforHospitalsfinalversion727.pdf. Published 2010. Accessed October 5, 2017.
12. Snelgrove JW, Jasudavisius AM, Rowe BW, Head EM, Bauer GR. “Completely out-at-sea” with “two-gender medicine”: a qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv Res. 2012;12:110.
13. Gates GJ. How many people are lesbian, gay, bisexual, and transgender? http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Published April 2011. Accessed October 5, 2017.
14. Gates GJ, Herman J. Transgender military service in the United States. https://williamsinstitute.law.ucla.edu/wp-content/uploads/Transgender-Military-Service-May-2014.pdf. Published May 2014. Accessed October 5, 2017.
15. U.S. Department of Veteran Affairs. Veterans Health Administration. http://www.va.gov/health. Updated October 2, 2017. Accessed October 5, 2017.
16. Gates GJ. Gay men and lesbians in the U.S. military: estimates from the 2000 census. http://www.lgbtdata.com/uploads/1/0/8/8/10884149/ds008_uscensus_gates.pdf. Published September 28, 2014. Accessed October 5, 2017.
17. Mattocks KM, Kauth MR, Sandfort T, Matza AR, Sullivan JC, Shipherd JC. Understanding health-care needs of sexual and gender minority veterans: how targeted research and policy can improve health. LGBT Health. 2014;1(1):50-57.
18. Kauth MR, Shipherd JC, Lindsay J, Blosnich JR, Brown GR, Jones KT. Access to care for transgender veterans in the Veterans Health Administration: 2006–2013. Am J Public Health. 2014;104(suppl 4):S532-S534.
19. Uchendu US. Veterans Health Administration Office of Health Equity: what is it a about? http://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/769-notes.pdf. Published November 4, 2013. Accessed October 5, 2017.
20. U.S. Department of Veterans Affairs, Veterans Health Administration. VHA Directive 2013-003: Providing Health Care for Transgender and Intersex Veterans. http://www.transequality.org/sites/default/files/docs/resources/VHAHealthcareDirective_2013.pdf. Published February 8, 2013. Accessed October 5, 2017.
21. Campinha-Bacote J. The process of cultural competence in the delivery of healthcare services: a model of care. J Transcult Nurs. 2002;13(3):181-184.
22. Jabson JM, Mitchell JW, Doty SB. Associations between non-discrimination and training policies and physicians’ attitudes and knowledge about sexual and gender minority patients: a comparison of physicians from two hospitals. BMC Public Health. 2016;16:256
Are We Ready for the Next Global Health Crisis?
The outbreak of Ebola in West Africa in 2014 provided a wake-up call for global health care experts. Responding to the next global health care crisis will require a more coherent and strategic response, and U.S. leadership, to protect both U.S. and global health security. The Ebola crisis “raised consciousness generally that health and security have become more directly linked,” said CAPT Paul Reed, MD, USPHS, interim director of the Center for Global Health Engagement (CGHE) at the Uniformed Services University.
According to CAPT Reed, global health engagement is an essential part of force preparedness and a key part of U.S. dialogue with global partners. The CGHE will host a series of sessions at the upcoming AMSUS meeting on November 28, outside Washington, DC, that will focus on global health strategies, the importance of global health engagement to combat commands, and projects underway to expand global health engagement.

The CGHE mission is to lead, integrate, and bring together thought leadership, research, and advocacy from public health experts, Uniformed Services University faculty, combatant commands, and the Military Health System to national security objectives. The CGHE is focused on developing partnerships to build global capacity and increase resiliency for disaster preparation. In addition, the center is engaged in research studies, including the Measures Of Effectiveness in Defense Engagement and Learning (MODEL) and the Improving Processes and Coordination in Theater (IMPACT) studies.
As the Ebola outbreak made clear, global health threats can impact both military and domestic operations. “There is not distinction between global and domestic health issues,” Dr. Reed told Federal Practitioner. “Global health engagement is a unique aspects of public health. We need to develop a new doctrine. We have to do it collectively and we can't do that in silos. We can't even do it within a federal government silo.”
The outbreak of Ebola in West Africa in 2014 provided a wake-up call for global health care experts. Responding to the next global health care crisis will require a more coherent and strategic response, and U.S. leadership, to protect both U.S. and global health security. The Ebola crisis “raised consciousness generally that health and security have become more directly linked,” said CAPT Paul Reed, MD, USPHS, interim director of the Center for Global Health Engagement (CGHE) at the Uniformed Services University.
According to CAPT Reed, global health engagement is an essential part of force preparedness and a key part of U.S. dialogue with global partners. The CGHE will host a series of sessions at the upcoming AMSUS meeting on November 28, outside Washington, DC, that will focus on global health strategies, the importance of global health engagement to combat commands, and projects underway to expand global health engagement.
The CGHE mission is to lead, integrate, and bring together thought leadership, research, and advocacy from public health experts, Uniformed Services University faculty, combatant commands, and the Military Health System to national security objectives. The CGHE is focused on developing partnerships to build global capacity and increase resiliency for disaster preparation. In addition, the center is engaged in research studies, including the Measures Of Effectiveness in Defense Engagement and Learning (MODEL) and the Improving Processes and Coordination in Theater (IMPACT) studies.
As the Ebola outbreak made clear, global health threats can impact both military and domestic operations. “There is not distinction between global and domestic health issues,” Dr. Reed told Federal Practitioner. “Global health engagement is a unique aspects of public health. We need to develop a new doctrine. We have to do it collectively and we can't do that in silos. We can't even do it within a federal government silo.”
The outbreak of Ebola in West Africa in 2014 provided a wake-up call for global health care experts. Responding to the next global health care crisis will require a more coherent and strategic response, and U.S. leadership, to protect both U.S. and global health security. The Ebola crisis “raised consciousness generally that health and security have become more directly linked,” said CAPT Paul Reed, MD, USPHS, interim director of the Center for Global Health Engagement (CGHE) at the Uniformed Services University.
According to CAPT Reed, global health engagement is an essential part of force preparedness and a key part of U.S. dialogue with global partners. The CGHE will host a series of sessions at the upcoming AMSUS meeting on November 28, outside Washington, DC, that will focus on global health strategies, the importance of global health engagement to combat commands, and projects underway to expand global health engagement.
The CGHE mission is to lead, integrate, and bring together thought leadership, research, and advocacy from public health experts, Uniformed Services University faculty, combatant commands, and the Military Health System to national security objectives. The CGHE is focused on developing partnerships to build global capacity and increase resiliency for disaster preparation. In addition, the center is engaged in research studies, including the Measures Of Effectiveness in Defense Engagement and Learning (MODEL) and the Improving Processes and Coordination in Theater (IMPACT) studies.
As the Ebola outbreak made clear, global health threats can impact both military and domestic operations. “There is not distinction between global and domestic health issues,” Dr. Reed told Federal Practitioner. “Global health engagement is a unique aspects of public health. We need to develop a new doctrine. We have to do it collectively and we can't do that in silos. We can't even do it within a federal government silo.”

Study Will Compare Mammography Screening Methods
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
Which method is better for breast cancer screening: 3-D mammography or 2-D mammography? Researchers from the ECOG-ACRIN Cancer Research Group and the National Cancer Institute are hoping to find out, with the Tomosynthesis Mammographic Imaging Screening Trial (TMIST).
It has been decades since the last large-scale randomized trial of mammography, points out Worta McCaskill-Stevens, MD, director of the NCI Community Oncology Research Program. In the meantime, mammography technology has evolved, from “conventional” 2-D mammography to tomosynthesis, also known as 3-D mammography.
However, although 3-D mammography is more likely to detect more findings that require follow-up, it is also likely to lead to more procedures and treatments. “If a newer screening technology does not reduce the numbers of advanced, life-threatening cancers, then are we really improving screening for breast cancer?” said Etta Pisano, MD, ECOG-ACRIN study chair.
Researchers plan to enroll 165,000 participants aged between 45 and 74 years who already are scheduled for routine mammograms. They will follow all participants for breast cancer status, treatment, and outcomes until at least 2025. About 100 mammography clinics are expected to take part.
Restrictive transfusion method safe in cardiac surgery patients

ANAHEIM, CA—Results of a large study suggest a restrictive transfusion strategy is safe for moderate- to high-risk patients undergoing cardiac surgery.
Researchers found that patients had similar rates of various outcomes—death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis—whether they received red blood cell (RBC) transfusions according to a restrictive strategy or a liberal one.
C. David Mazer, MD, of St. Michael’s Hospital in Toronto, Ontario, Canada, presented these results at the American Heart Association’s Scientific Sessions 2017.
Results were simultaneously published in NEJM.
Dr Mazer and his colleagues studied 5243 adults undergoing cardiac surgery. They all had a European System for Cardiac Operative Risk Evaluation I score of 6 or more (on a scale from 0 to 47, with higher scores indicating a higher risk of death after cardiac surgery).
Patients were randomized to receive RBC transfusions according to a restrictive strategy or a liberal one.
With the restrictive strategy, patients received transfusions if their hemoglobin level was below 7.5 g/dL, starting from induction of anesthesia.
With the liberal strategy, patients were transfused if their hemoglobin level was less than 9.5 g/dL in the operating room or intensive care unit (ICU) or was less than 8.5 g/dL in the non-ICU ward.
Results
There were 4860 patients in the per-protocol analysis—2430 in each transfusion group. Baseline characteristics were similar between the groups.
The rate of RBC transfusion was 52.3% in the restrictive group and 72.6% in the liberal group. The odds ratio (OR) was 0.41 (95% confidence interval [CI], 0.37 to 0.47).
Transfused patients received a median of 2 RBC units (interquartile range [IQR], 1 to 4) in the restrictive group and 3 units (IQR, 2 to 5) in the liberal group.
The study’s primary composite outcome was death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis by hospital discharge or by day 28, whichever came first.
This outcome occurred in 11.4% of patients in the restrictive group and 12.5% of those in the liberal group. The absolute risk difference was −1.11 percentage points (95% CI, −2.93 to 0.72), and the odds ratio was 0.90 (95% CI, 0.76 to 1.07; P<0.001 for noninferiority).
There were no significant differences between the groups when it came to the individual components of the composite outcome.
“We have shown that this [restrictive] approach to transfusion is safe in moderate- to high-risk patients undergoing cardiac surgery,” Dr Mazer said.
“Such practices can also reduce the number of patients transfused, the amount of blood transfused, the impact on blood supply, and costs to the healthcare system.” ![]()
ANAHEIM, CA—Results of a large study suggest a restrictive transfusion strategy is safe for moderate- to high-risk patients undergoing cardiac surgery.
Researchers found that patients had similar rates of various outcomes—death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis—whether they received red blood cell (RBC) transfusions according to a restrictive strategy or a liberal one.
C. David Mazer, MD, of St. Michael’s Hospital in Toronto, Ontario, Canada, presented these results at the American Heart Association’s Scientific Sessions 2017.
Results were simultaneously published in NEJM.
Dr Mazer and his colleagues studied 5243 adults undergoing cardiac surgery. They all had a European System for Cardiac Operative Risk Evaluation I score of 6 or more (on a scale from 0 to 47, with higher scores indicating a higher risk of death after cardiac surgery).
Patients were randomized to receive RBC transfusions according to a restrictive strategy or a liberal one.
With the restrictive strategy, patients received transfusions if their hemoglobin level was below 7.5 g/dL, starting from induction of anesthesia.
With the liberal strategy, patients were transfused if their hemoglobin level was less than 9.5 g/dL in the operating room or intensive care unit (ICU) or was less than 8.5 g/dL in the non-ICU ward.
Results
There were 4860 patients in the per-protocol analysis—2430 in each transfusion group. Baseline characteristics were similar between the groups.
The rate of RBC transfusion was 52.3% in the restrictive group and 72.6% in the liberal group. The odds ratio (OR) was 0.41 (95% confidence interval [CI], 0.37 to 0.47).
Transfused patients received a median of 2 RBC units (interquartile range [IQR], 1 to 4) in the restrictive group and 3 units (IQR, 2 to 5) in the liberal group.
The study’s primary composite outcome was death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis by hospital discharge or by day 28, whichever came first.
This outcome occurred in 11.4% of patients in the restrictive group and 12.5% of those in the liberal group. The absolute risk difference was −1.11 percentage points (95% CI, −2.93 to 0.72), and the odds ratio was 0.90 (95% CI, 0.76 to 1.07; P<0.001 for noninferiority).
There were no significant differences between the groups when it came to the individual components of the composite outcome.
“We have shown that this [restrictive] approach to transfusion is safe in moderate- to high-risk patients undergoing cardiac surgery,” Dr Mazer said.
“Such practices can also reduce the number of patients transfused, the amount of blood transfused, the impact on blood supply, and costs to the healthcare system.” ![]()
ANAHEIM, CA—Results of a large study suggest a restrictive transfusion strategy is safe for moderate- to high-risk patients undergoing cardiac surgery.
Researchers found that patients had similar rates of various outcomes—death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis—whether they received red blood cell (RBC) transfusions according to a restrictive strategy or a liberal one.
C. David Mazer, MD, of St. Michael’s Hospital in Toronto, Ontario, Canada, presented these results at the American Heart Association’s Scientific Sessions 2017.
Results were simultaneously published in NEJM.
Dr Mazer and his colleagues studied 5243 adults undergoing cardiac surgery. They all had a European System for Cardiac Operative Risk Evaluation I score of 6 or more (on a scale from 0 to 47, with higher scores indicating a higher risk of death after cardiac surgery).
Patients were randomized to receive RBC transfusions according to a restrictive strategy or a liberal one.
With the restrictive strategy, patients received transfusions if their hemoglobin level was below 7.5 g/dL, starting from induction of anesthesia.
With the liberal strategy, patients were transfused if their hemoglobin level was less than 9.5 g/dL in the operating room or intensive care unit (ICU) or was less than 8.5 g/dL in the non-ICU ward.
Results
There were 4860 patients in the per-protocol analysis—2430 in each transfusion group. Baseline characteristics were similar between the groups.
The rate of RBC transfusion was 52.3% in the restrictive group and 72.6% in the liberal group. The odds ratio (OR) was 0.41 (95% confidence interval [CI], 0.37 to 0.47).
Transfused patients received a median of 2 RBC units (interquartile range [IQR], 1 to 4) in the restrictive group and 3 units (IQR, 2 to 5) in the liberal group.
The study’s primary composite outcome was death from any cause, myocardial infarction, stroke, or new-onset renal failure with dialysis by hospital discharge or by day 28, whichever came first.
This outcome occurred in 11.4% of patients in the restrictive group and 12.5% of those in the liberal group. The absolute risk difference was −1.11 percentage points (95% CI, −2.93 to 0.72), and the odds ratio was 0.90 (95% CI, 0.76 to 1.07; P<0.001 for noninferiority).
There were no significant differences between the groups when it came to the individual components of the composite outcome.
“We have shown that this [restrictive] approach to transfusion is safe in moderate- to high-risk patients undergoing cardiac surgery,” Dr Mazer said.
“Such practices can also reduce the number of patients transfused, the amount of blood transfused, the impact on blood supply, and costs to the healthcare system.” ![]()