User login
Anidulafungin effectively treated invasive pediatric candidiasis in open-label trial
SAN DIEGO – The intravenous echinocandin anidulafungin effectively treated invasive candidiasis in a single-arm, multicenter, open-label trial of 47 children aged 2-17 years.
The overall global response rate of 72% resembled that from the prior adult registry study (76%), Emmanuel Roilides, MD, PhD, and his associates reported in a poster presented at an annual scientific meeting on infectious diseases.
At 6-week follow-up, two patients (4%) had relapsed, both with Candida parapsilosis, which was more resistant to treatment with anidulafungin (Eraxis) than other Candida species, the researchers reported. Treating the children with 3.0 mg/kg anidulafungin on day 1, followed by 1.5 mg/kg every 24 hours, yielded similar pharmacokinetics as the 200/100 mg regimen used in adults. The most common treatment-emergent adverse effects included diarrhea (23%), vomiting (23%), and fever (19%), which also reflected findings in adults, the investigators said. Five patients (10%) developed at least one severe treatment-emergent adverse event, including neutropenia, gastrointestinal hemorrhage, increased hepatic transaminases, hyponatremia, and myalgia. The study (NCT00761267) is ongoing and continues to recruit patients in 11 states in the United States and nine other countries, with final top-line results expected in 2019.
Although rates of invasive candidiasis appear to be decreasing in children overall, the population at risk is expanding, experts have noted. Relevant guidelines from the Infectious Disease Society of America and the European Society of Clinical Microbiology and Infectious Diseases list amphotericin B, echinocandins, and azoles as treatment options, but these recommendations are extrapolated mainly from adult studies, noted Dr. Roilides, who is a pediatric infectious disease specialist at Aristotle University School of Health Sciences and Hippokration General Hospital in Thessaloniki, Greece.
To better characterize the safety and efficacy of anidulafungin in children, the researchers enrolled patients up to 17 years of age who had signs and symptoms of invasive candidiasis and Candida cultured from a normally sterile site. Patients received intravenous anidulafungin (3 mg/kg on day 1, followed by 1.5 mg/kg every 24 hours) for at least 10 days, after which they could switch to oral fluconazole. Treatment continued for at least 14 days after blood cultures were negative and signs and symptoms resolved.
At interim data cutoff in October 2016, patients were exposed to anidulafungin for a median of 11.5 days (range, 1-28 days). Among 47 patients who received at least one dose of anidulafungin, about two-thirds were male, about 70% were white, and the average age was 8 years (standard deviation, 4.7 years). Rates of global success – a combination of clinical and microbiological response – were 82% in patients up to 5 years old and 67% in older children. Children whose baseline neutrophil count was at least 500 per mm3 had a 78% global response rate versus 50% among those with more severe neutropenia. C. parapsilosis had higher minimum inhibitory concentrations than other Candida species, and in vitro susceptibility rates of 85% for C. parapsilosis versus 100% for other species.
All patients experienced at least one treatment-emergent adverse effect. In addition to diarrhea, vomiting, and pyrexia, adverse events affecting more than 10% of patients included epistaxis (17%), headache (15%), and abdominal pain (13%). Half of patients switched to oral fluconazole. Four patients stopped treatment because of vomiting, generalized pruritus, or increased transaminases. A total of 15% of patients died, although no deaths were considered treatment related. The patient who stopped treatment because of pruritus later died of septic shock secondary to invasive candidiasis, despite having started treatment with fluconazole and micafungin, the investigators reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nearly all patients had bloodstream infections, and catheters also cultured positive in more than two-thirds of cases, the researchers said. Many patients had multiple risk factors for infection such as central venous catheters, broad-spectrum antibiotic therapy, total parenteral nutrition, and chemotherapy. Cultures were most often positive for Candida albicans (38%), followed by C. parapsilosis (26%) and C. tropicalis (13%).
Pfizer makes anidulafungin and sponsored the study. Dr. Roilides disclosed research grants and advisory relationships with Pfizer, Astellas, Gilead, and Merck.
SAN DIEGO – The intravenous echinocandin anidulafungin effectively treated invasive candidiasis in a single-arm, multicenter, open-label trial of 47 children aged 2-17 years.
The overall global response rate of 72% resembled that from the prior adult registry study (76%), Emmanuel Roilides, MD, PhD, and his associates reported in a poster presented at an annual scientific meeting on infectious diseases.
At 6-week follow-up, two patients (4%) had relapsed, both with Candida parapsilosis, which was more resistant to treatment with anidulafungin (Eraxis) than other Candida species, the researchers reported. Treating the children with 3.0 mg/kg anidulafungin on day 1, followed by 1.5 mg/kg every 24 hours, yielded similar pharmacokinetics as the 200/100 mg regimen used in adults. The most common treatment-emergent adverse effects included diarrhea (23%), vomiting (23%), and fever (19%), which also reflected findings in adults, the investigators said. Five patients (10%) developed at least one severe treatment-emergent adverse event, including neutropenia, gastrointestinal hemorrhage, increased hepatic transaminases, hyponatremia, and myalgia. The study (NCT00761267) is ongoing and continues to recruit patients in 11 states in the United States and nine other countries, with final top-line results expected in 2019.
Although rates of invasive candidiasis appear to be decreasing in children overall, the population at risk is expanding, experts have noted. Relevant guidelines from the Infectious Disease Society of America and the European Society of Clinical Microbiology and Infectious Diseases list amphotericin B, echinocandins, and azoles as treatment options, but these recommendations are extrapolated mainly from adult studies, noted Dr. Roilides, who is a pediatric infectious disease specialist at Aristotle University School of Health Sciences and Hippokration General Hospital in Thessaloniki, Greece.
To better characterize the safety and efficacy of anidulafungin in children, the researchers enrolled patients up to 17 years of age who had signs and symptoms of invasive candidiasis and Candida cultured from a normally sterile site. Patients received intravenous anidulafungin (3 mg/kg on day 1, followed by 1.5 mg/kg every 24 hours) for at least 10 days, after which they could switch to oral fluconazole. Treatment continued for at least 14 days after blood cultures were negative and signs and symptoms resolved.
At interim data cutoff in October 2016, patients were exposed to anidulafungin for a median of 11.5 days (range, 1-28 days). Among 47 patients who received at least one dose of anidulafungin, about two-thirds were male, about 70% were white, and the average age was 8 years (standard deviation, 4.7 years). Rates of global success – a combination of clinical and microbiological response – were 82% in patients up to 5 years old and 67% in older children. Children whose baseline neutrophil count was at least 500 per mm3 had a 78% global response rate versus 50% among those with more severe neutropenia. C. parapsilosis had higher minimum inhibitory concentrations than other Candida species, and in vitro susceptibility rates of 85% for C. parapsilosis versus 100% for other species.
All patients experienced at least one treatment-emergent adverse effect. In addition to diarrhea, vomiting, and pyrexia, adverse events affecting more than 10% of patients included epistaxis (17%), headache (15%), and abdominal pain (13%). Half of patients switched to oral fluconazole. Four patients stopped treatment because of vomiting, generalized pruritus, or increased transaminases. A total of 15% of patients died, although no deaths were considered treatment related. The patient who stopped treatment because of pruritus later died of septic shock secondary to invasive candidiasis, despite having started treatment with fluconazole and micafungin, the investigators reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nearly all patients had bloodstream infections, and catheters also cultured positive in more than two-thirds of cases, the researchers said. Many patients had multiple risk factors for infection such as central venous catheters, broad-spectrum antibiotic therapy, total parenteral nutrition, and chemotherapy. Cultures were most often positive for Candida albicans (38%), followed by C. parapsilosis (26%) and C. tropicalis (13%).
Pfizer makes anidulafungin and sponsored the study. Dr. Roilides disclosed research grants and advisory relationships with Pfizer, Astellas, Gilead, and Merck.
SAN DIEGO – The intravenous echinocandin anidulafungin effectively treated invasive candidiasis in a single-arm, multicenter, open-label trial of 47 children aged 2-17 years.
The overall global response rate of 72% resembled that from the prior adult registry study (76%), Emmanuel Roilides, MD, PhD, and his associates reported in a poster presented at an annual scientific meeting on infectious diseases.
At 6-week follow-up, two patients (4%) had relapsed, both with Candida parapsilosis, which was more resistant to treatment with anidulafungin (Eraxis) than other Candida species, the researchers reported. Treating the children with 3.0 mg/kg anidulafungin on day 1, followed by 1.5 mg/kg every 24 hours, yielded similar pharmacokinetics as the 200/100 mg regimen used in adults. The most common treatment-emergent adverse effects included diarrhea (23%), vomiting (23%), and fever (19%), which also reflected findings in adults, the investigators said. Five patients (10%) developed at least one severe treatment-emergent adverse event, including neutropenia, gastrointestinal hemorrhage, increased hepatic transaminases, hyponatremia, and myalgia. The study (NCT00761267) is ongoing and continues to recruit patients in 11 states in the United States and nine other countries, with final top-line results expected in 2019.
Although rates of invasive candidiasis appear to be decreasing in children overall, the population at risk is expanding, experts have noted. Relevant guidelines from the Infectious Disease Society of America and the European Society of Clinical Microbiology and Infectious Diseases list amphotericin B, echinocandins, and azoles as treatment options, but these recommendations are extrapolated mainly from adult studies, noted Dr. Roilides, who is a pediatric infectious disease specialist at Aristotle University School of Health Sciences and Hippokration General Hospital in Thessaloniki, Greece.
To better characterize the safety and efficacy of anidulafungin in children, the researchers enrolled patients up to 17 years of age who had signs and symptoms of invasive candidiasis and Candida cultured from a normally sterile site. Patients received intravenous anidulafungin (3 mg/kg on day 1, followed by 1.5 mg/kg every 24 hours) for at least 10 days, after which they could switch to oral fluconazole. Treatment continued for at least 14 days after blood cultures were negative and signs and symptoms resolved.
At interim data cutoff in October 2016, patients were exposed to anidulafungin for a median of 11.5 days (range, 1-28 days). Among 47 patients who received at least one dose of anidulafungin, about two-thirds were male, about 70% were white, and the average age was 8 years (standard deviation, 4.7 years). Rates of global success – a combination of clinical and microbiological response – were 82% in patients up to 5 years old and 67% in older children. Children whose baseline neutrophil count was at least 500 per mm3 had a 78% global response rate versus 50% among those with more severe neutropenia. C. parapsilosis had higher minimum inhibitory concentrations than other Candida species, and in vitro susceptibility rates of 85% for C. parapsilosis versus 100% for other species.
All patients experienced at least one treatment-emergent adverse effect. In addition to diarrhea, vomiting, and pyrexia, adverse events affecting more than 10% of patients included epistaxis (17%), headache (15%), and abdominal pain (13%). Half of patients switched to oral fluconazole. Four patients stopped treatment because of vomiting, generalized pruritus, or increased transaminases. A total of 15% of patients died, although no deaths were considered treatment related. The patient who stopped treatment because of pruritus later died of septic shock secondary to invasive candidiasis, despite having started treatment with fluconazole and micafungin, the investigators reported at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Nearly all patients had bloodstream infections, and catheters also cultured positive in more than two-thirds of cases, the researchers said. Many patients had multiple risk factors for infection such as central venous catheters, broad-spectrum antibiotic therapy, total parenteral nutrition, and chemotherapy. Cultures were most often positive for Candida albicans (38%), followed by C. parapsilosis (26%) and C. tropicalis (13%).
Pfizer makes anidulafungin and sponsored the study. Dr. Roilides disclosed research grants and advisory relationships with Pfizer, Astellas, Gilead, and Merck.
AT IDWEEK 2017
Key clinical point: The intravenous echinocandin anidulafungin effectively treated invasive candidiasis in children, with a safety profile resembling what has been previously reported for adults.
Major finding: The overall global response rate was 72%. The most common treatment-emergent adverse effects included diarrhea (23%), vomiting (23%), and fever (19%). Five patients (10%) developed at least one severe treatment-emergent adverse event.
Data source: A multicenter, single-arm, open-label study of 47 patients aged 2-17 years.
Disclosures: Pfizer makes anidulafungin and sponsored the study. Dr. Roilides disclosed research grants and advisory relationships with Pfizer, Astellas, Gilead, and Merck.
Hitting a Rough Patch
Since they appeared in early childhood, the lesions on this 50-year-old woman’s arms have waxed and waned, becoming most noticeable in the winter. Although they are generally asymptomatic, the patient is bothered by their rough feel. She admits to picking at them, which causes further irritation. Moisturizers have provided some (temporary) relief.
The patient’s mother and sister have similar lesions, as well as very sensitive skin that overreacts to contactants. The entire family is markedly atopic, with seasonal allergies, asthma, and eczema.
EXAMINATION
The bumps can be seen on the deltoids, triceps, back, and anterior thighs but are particularly prominent on a small area of skin on the patient’s left triceps. The posterior third of both cheeks, which are faintly red, is mildly affected. Overall, glabrous (nonhairy) areas are completely spared.
The individual papules are hyperkeratotic, measure a millimeter or less, and are follicular. Many are faintly erythematous; when picked away, several reveal a coiled hair inside the papule.

What is the diagnosis?
DISCUSSION
One of the most common dermatologic conditions encountered in medical practice, keratosis pilaris (KP) affects 30% to 50% of the population. KP is an autosomal dominant disorder; the lesions are caused by an inherited overabundance of keratin around follicular orifices, which often precludes the ability of the hair to exit the follicle. The hairs keep growing, but curl up inside the keratotic papule. Fortunately, aside from mild irritation, KP is essentially asymptomatic.
It has a broad range of presentations, from mild to severe. Some children present with a few barely palpable keratotic papules limited to the bilateral triceps, while others have thousands of papules and large patches of prominent follicles that also involve extensor surfaces of hair-bearing skin. Another version of KP, rubra faceii, is distinguished by very red cheeks with keratotic follicular papules; the unwary provider may suspect acne, but that condition presents with comedones and/or a combination of papules, pustules, or cysts confined to sebaceous (oily) areas. The differential also includes Darier disease (keratosis follicularis), but this has a completely different distribution.
KP is often seen in conjunction with atopic stigmata such as eczema, seasonal allergies, xerosis, asthma, and urticaria. It is believed by some to be a marker for atopy.
Treatment is unsatisfactory in terms of a cure, though most patients see their disease lessen over time. Emollients (heavy moisturizers) containing salicylic acid, glycolic acid, ammonium lactate, or retinoic acid can minimize the height of the papules and smooth the skin, but they do not provide a long-term solution.
TAKE-HOME LEARNING POINTS
- Keratosis pilaris (KP) is an extremely common autosomal dominant condition that affects 30% to 50% of children.
- It manifests very early in life with tiny, hyperkeratotic, follicular papules in a characteristic distribution.
- The bilateral posterior triceps, deltoids, anterior thighs, buttocks, and face are typically affected, while glabrous skin is spared.
- Treatment is difficult; KP responds to emollients and keratolytics containing salicylic acid, glycolic acid, ammonium lactate, and retinoic acid—but any relief will be temporary.
Since they appeared in early childhood, the lesions on this 50-year-old woman’s arms have waxed and waned, becoming most noticeable in the winter. Although they are generally asymptomatic, the patient is bothered by their rough feel. She admits to picking at them, which causes further irritation. Moisturizers have provided some (temporary) relief.
The patient’s mother and sister have similar lesions, as well as very sensitive skin that overreacts to contactants. The entire family is markedly atopic, with seasonal allergies, asthma, and eczema.
EXAMINATION
The bumps can be seen on the deltoids, triceps, back, and anterior thighs but are particularly prominent on a small area of skin on the patient’s left triceps. The posterior third of both cheeks, which are faintly red, is mildly affected. Overall, glabrous (nonhairy) areas are completely spared.
The individual papules are hyperkeratotic, measure a millimeter or less, and are follicular. Many are faintly erythematous; when picked away, several reveal a coiled hair inside the papule.
What is the diagnosis?
DISCUSSION
One of the most common dermatologic conditions encountered in medical practice, keratosis pilaris (KP) affects 30% to 50% of the population. KP is an autosomal dominant disorder; the lesions are caused by an inherited overabundance of keratin around follicular orifices, which often precludes the ability of the hair to exit the follicle. The hairs keep growing, but curl up inside the keratotic papule. Fortunately, aside from mild irritation, KP is essentially asymptomatic.
It has a broad range of presentations, from mild to severe. Some children present with a few barely palpable keratotic papules limited to the bilateral triceps, while others have thousands of papules and large patches of prominent follicles that also involve extensor surfaces of hair-bearing skin. Another version of KP, rubra faceii, is distinguished by very red cheeks with keratotic follicular papules; the unwary provider may suspect acne, but that condition presents with comedones and/or a combination of papules, pustules, or cysts confined to sebaceous (oily) areas. The differential also includes Darier disease (keratosis follicularis), but this has a completely different distribution.
KP is often seen in conjunction with atopic stigmata such as eczema, seasonal allergies, xerosis, asthma, and urticaria. It is believed by some to be a marker for atopy.
Treatment is unsatisfactory in terms of a cure, though most patients see their disease lessen over time. Emollients (heavy moisturizers) containing salicylic acid, glycolic acid, ammonium lactate, or retinoic acid can minimize the height of the papules and smooth the skin, but they do not provide a long-term solution.
TAKE-HOME LEARNING POINTS
- Keratosis pilaris (KP) is an extremely common autosomal dominant condition that affects 30% to 50% of children.
- It manifests very early in life with tiny, hyperkeratotic, follicular papules in a characteristic distribution.
- The bilateral posterior triceps, deltoids, anterior thighs, buttocks, and face are typically affected, while glabrous skin is spared.
- Treatment is difficult; KP responds to emollients and keratolytics containing salicylic acid, glycolic acid, ammonium lactate, and retinoic acid—but any relief will be temporary.
Since they appeared in early childhood, the lesions on this 50-year-old woman’s arms have waxed and waned, becoming most noticeable in the winter. Although they are generally asymptomatic, the patient is bothered by their rough feel. She admits to picking at them, which causes further irritation. Moisturizers have provided some (temporary) relief.
The patient’s mother and sister have similar lesions, as well as very sensitive skin that overreacts to contactants. The entire family is markedly atopic, with seasonal allergies, asthma, and eczema.
EXAMINATION
The bumps can be seen on the deltoids, triceps, back, and anterior thighs but are particularly prominent on a small area of skin on the patient’s left triceps. The posterior third of both cheeks, which are faintly red, is mildly affected. Overall, glabrous (nonhairy) areas are completely spared.
The individual papules are hyperkeratotic, measure a millimeter or less, and are follicular. Many are faintly erythematous; when picked away, several reveal a coiled hair inside the papule.
What is the diagnosis?
DISCUSSION
One of the most common dermatologic conditions encountered in medical practice, keratosis pilaris (KP) affects 30% to 50% of the population. KP is an autosomal dominant disorder; the lesions are caused by an inherited overabundance of keratin around follicular orifices, which often precludes the ability of the hair to exit the follicle. The hairs keep growing, but curl up inside the keratotic papule. Fortunately, aside from mild irritation, KP is essentially asymptomatic.
It has a broad range of presentations, from mild to severe. Some children present with a few barely palpable keratotic papules limited to the bilateral triceps, while others have thousands of papules and large patches of prominent follicles that also involve extensor surfaces of hair-bearing skin. Another version of KP, rubra faceii, is distinguished by very red cheeks with keratotic follicular papules; the unwary provider may suspect acne, but that condition presents with comedones and/or a combination of papules, pustules, or cysts confined to sebaceous (oily) areas. The differential also includes Darier disease (keratosis follicularis), but this has a completely different distribution.
KP is often seen in conjunction with atopic stigmata such as eczema, seasonal allergies, xerosis, asthma, and urticaria. It is believed by some to be a marker for atopy.
Treatment is unsatisfactory in terms of a cure, though most patients see their disease lessen over time. Emollients (heavy moisturizers) containing salicylic acid, glycolic acid, ammonium lactate, or retinoic acid can minimize the height of the papules and smooth the skin, but they do not provide a long-term solution.
TAKE-HOME LEARNING POINTS
- Keratosis pilaris (KP) is an extremely common autosomal dominant condition that affects 30% to 50% of children.
- It manifests very early in life with tiny, hyperkeratotic, follicular papules in a characteristic distribution.
- The bilateral posterior triceps, deltoids, anterior thighs, buttocks, and face are typically affected, while glabrous skin is spared.
- Treatment is difficult; KP responds to emollients and keratolytics containing salicylic acid, glycolic acid, ammonium lactate, and retinoic acid—but any relief will be temporary.
Healing Diabetic Foot Ulcers With Exercise
Foot ulcers are a common complication of diabetes, due to macro- and microvascular changes that lead to neuropathy. But despite treatment with standard interventions such as debridement and pressure relief, many diabetic foot ulcers persist as nonhealing wounds, say researchers from Nnamdi Azidiwe University and University of Nigeria.
Oxygenation is key to keep the tissues healthy, the researchers say. We already know that exercise enhances blood circulation and improves vascular blood perfusion and capillary oxygen tension. However, little research has associated increased vascular blood perfusion with wound healing in diabetic foot ulcers, the researchers say. They reanalyzed results from 1 of their earlier studies to find out whether aerobic exercise would lead to healing.
In a 12-week program, 61 patients with type 1 or 2 diabetes mellitus were randomly assigned to an intervention or control group. Each patient had had a persistent ulcer of at least 1 cm2. The intervention group rode a bicycle ergometer at 60% of their maximum heart rate and progressed to 85%. The researchers tested them for oxygen percentage saturation and ankle brachial index (ABI) at baseline every 2 weeks.
At the end of the program, the researchers found a “sharp contrast” between the 2 groups, including a significant difference in the oxygen percentage saturation (99.00 vs 97.20) and the ABI. The reduction in wound size was also significant for the exercise group.
There is evidence, the researchers say, that exercise enhances blood circulation by lowering plasma glucose concentration. Normally, endothelial cells metabolize the circulating blood glucose—unless they are overwhelmed by glucose molecules during hyperglycemia. Previously, the researchers also noted that plasma glucose dropped significantly, mostly at the end of the fourth week of the exercise program.
In this study, increases in ABIs, the researchers say, imply enhanced oxygen supply to the extremities. During the fourth week, they found greater wound size reductions and the ABI significantly correlated with oxygen percentage saturation. The ankle brachial index may be a useful tool, the researchers suggest, for predicting improvement in oxygen percentage saturation.
The researchers’ findings lead them to recommend that nonweight bearing exercise be made a “cornerstone” of management for people with diabetic foot ulcers.
Source:
Nwankwo MJ, Okoye GC, Victor EA, Obinna EA. Int J Diabetes Res. 2014;3(3):41-48.
doi:10.5923/j.diabetes.20140303.03
Foot ulcers are a common complication of diabetes, due to macro- and microvascular changes that lead to neuropathy. But despite treatment with standard interventions such as debridement and pressure relief, many diabetic foot ulcers persist as nonhealing wounds, say researchers from Nnamdi Azidiwe University and University of Nigeria.
Oxygenation is key to keep the tissues healthy, the researchers say. We already know that exercise enhances blood circulation and improves vascular blood perfusion and capillary oxygen tension. However, little research has associated increased vascular blood perfusion with wound healing in diabetic foot ulcers, the researchers say. They reanalyzed results from 1 of their earlier studies to find out whether aerobic exercise would lead to healing.
In a 12-week program, 61 patients with type 1 or 2 diabetes mellitus were randomly assigned to an intervention or control group. Each patient had had a persistent ulcer of at least 1 cm2. The intervention group rode a bicycle ergometer at 60% of their maximum heart rate and progressed to 85%. The researchers tested them for oxygen percentage saturation and ankle brachial index (ABI) at baseline every 2 weeks.
At the end of the program, the researchers found a “sharp contrast” between the 2 groups, including a significant difference in the oxygen percentage saturation (99.00 vs 97.20) and the ABI. The reduction in wound size was also significant for the exercise group.
There is evidence, the researchers say, that exercise enhances blood circulation by lowering plasma glucose concentration. Normally, endothelial cells metabolize the circulating blood glucose—unless they are overwhelmed by glucose molecules during hyperglycemia. Previously, the researchers also noted that plasma glucose dropped significantly, mostly at the end of the fourth week of the exercise program.
In this study, increases in ABIs, the researchers say, imply enhanced oxygen supply to the extremities. During the fourth week, they found greater wound size reductions and the ABI significantly correlated with oxygen percentage saturation. The ankle brachial index may be a useful tool, the researchers suggest, for predicting improvement in oxygen percentage saturation.
The researchers’ findings lead them to recommend that nonweight bearing exercise be made a “cornerstone” of management for people with diabetic foot ulcers.
Source:
Nwankwo MJ, Okoye GC, Victor EA, Obinna EA. Int J Diabetes Res. 2014;3(3):41-48.
doi:10.5923/j.diabetes.20140303.03
Foot ulcers are a common complication of diabetes, due to macro- and microvascular changes that lead to neuropathy. But despite treatment with standard interventions such as debridement and pressure relief, many diabetic foot ulcers persist as nonhealing wounds, say researchers from Nnamdi Azidiwe University and University of Nigeria.
Oxygenation is key to keep the tissues healthy, the researchers say. We already know that exercise enhances blood circulation and improves vascular blood perfusion and capillary oxygen tension. However, little research has associated increased vascular blood perfusion with wound healing in diabetic foot ulcers, the researchers say. They reanalyzed results from 1 of their earlier studies to find out whether aerobic exercise would lead to healing.
In a 12-week program, 61 patients with type 1 or 2 diabetes mellitus were randomly assigned to an intervention or control group. Each patient had had a persistent ulcer of at least 1 cm2. The intervention group rode a bicycle ergometer at 60% of their maximum heart rate and progressed to 85%. The researchers tested them for oxygen percentage saturation and ankle brachial index (ABI) at baseline every 2 weeks.
At the end of the program, the researchers found a “sharp contrast” between the 2 groups, including a significant difference in the oxygen percentage saturation (99.00 vs 97.20) and the ABI. The reduction in wound size was also significant for the exercise group.
There is evidence, the researchers say, that exercise enhances blood circulation by lowering plasma glucose concentration. Normally, endothelial cells metabolize the circulating blood glucose—unless they are overwhelmed by glucose molecules during hyperglycemia. Previously, the researchers also noted that plasma glucose dropped significantly, mostly at the end of the fourth week of the exercise program.
In this study, increases in ABIs, the researchers say, imply enhanced oxygen supply to the extremities. During the fourth week, they found greater wound size reductions and the ABI significantly correlated with oxygen percentage saturation. The ankle brachial index may be a useful tool, the researchers suggest, for predicting improvement in oxygen percentage saturation.
The researchers’ findings lead them to recommend that nonweight bearing exercise be made a “cornerstone” of management for people with diabetic foot ulcers.
Source:
Nwankwo MJ, Okoye GC, Victor EA, Obinna EA. Int J Diabetes Res. 2014;3(3):41-48.
doi:10.5923/j.diabetes.20140303.03
BRAIN Initiative update to whet appetite for main ANA meeting
Before the main American Neurological Association annual meeting begins in San Diego, plan on attending a special premeeting symposium, “Big Science and the BRAIN Initiative,” on the evening of Saturday, Oct. 14, to learn what a panel of experts has to say about the project, which is now entering its 4th year.
The Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative is aimed at supporting the development of an arsenal of new tools, multiscale maps, and new knowledge of neural circuits in both health and disease.
Walter Koroshetz, MD, director of the National Institute of Neurological Disorders and Stroke, Bethesda, Md., will chair the symposium and describe the structure of the initiative and its seven high-level research priorities.
Arnold Kriegstein, MD, PhD, of the University of California, San Francisco, will describe his research groups’ efforts at using single-cell approaches to establish an integrative definition of cell types in the developing human neocortex.
Viviana Gradinaru, PhD, of the California Institute of Technology, Pasadena, plans to provide insight on how her lab has developed safe, efficient, and specific vectors for targeting specific cells in the brain to learn about the circuits underlying locomotion, reward, and sleep, and to report on their activity history.
Sydney Cash, MD, PhD, of Massachusetts General Hospital, Boston, aims to survey the history and current landscape of available approaches toward obtaining single-neuron level information from patients, and to describe how this level of precision complements both meso- and macroscale information. He will describe how the huge amount of information being generated from these approaches is being examined with “big data” analytics.
Anna Devor, PhD, of the University of California, San Diego, intends to illustrate a “bottom-up” forward model for how to bridge the mechanistic insights we have gleaned from animal models and match them to noninvasive human neuroimaging data from functional MRI, functional near-infrared spectroscopy, magneto/electroencephalography, and positron emission tomography. This would involve identifying the noninvasive imaging signatures of specific neuronal cell types in order to derive better tools and techniques for estimating neuronal activity from multimodal noninvasive imaging data.
Before the main American Neurological Association annual meeting begins in San Diego, plan on attending a special premeeting symposium, “Big Science and the BRAIN Initiative,” on the evening of Saturday, Oct. 14, to learn what a panel of experts has to say about the project, which is now entering its 4th year.
The Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative is aimed at supporting the development of an arsenal of new tools, multiscale maps, and new knowledge of neural circuits in both health and disease.
Walter Koroshetz, MD, director of the National Institute of Neurological Disorders and Stroke, Bethesda, Md., will chair the symposium and describe the structure of the initiative and its seven high-level research priorities.
Arnold Kriegstein, MD, PhD, of the University of California, San Francisco, will describe his research groups’ efforts at using single-cell approaches to establish an integrative definition of cell types in the developing human neocortex.
Viviana Gradinaru, PhD, of the California Institute of Technology, Pasadena, plans to provide insight on how her lab has developed safe, efficient, and specific vectors for targeting specific cells in the brain to learn about the circuits underlying locomotion, reward, and sleep, and to report on their activity history.
Sydney Cash, MD, PhD, of Massachusetts General Hospital, Boston, aims to survey the history and current landscape of available approaches toward obtaining single-neuron level information from patients, and to describe how this level of precision complements both meso- and macroscale information. He will describe how the huge amount of information being generated from these approaches is being examined with “big data” analytics.
Anna Devor, PhD, of the University of California, San Diego, intends to illustrate a “bottom-up” forward model for how to bridge the mechanistic insights we have gleaned from animal models and match them to noninvasive human neuroimaging data from functional MRI, functional near-infrared spectroscopy, magneto/electroencephalography, and positron emission tomography. This would involve identifying the noninvasive imaging signatures of specific neuronal cell types in order to derive better tools and techniques for estimating neuronal activity from multimodal noninvasive imaging data.
Before the main American Neurological Association annual meeting begins in San Diego, plan on attending a special premeeting symposium, “Big Science and the BRAIN Initiative,” on the evening of Saturday, Oct. 14, to learn what a panel of experts has to say about the project, which is now entering its 4th year.
The Brain Research through Advancing Innovative Neurotechnologies (BRAIN) Initiative is aimed at supporting the development of an arsenal of new tools, multiscale maps, and new knowledge of neural circuits in both health and disease.
Walter Koroshetz, MD, director of the National Institute of Neurological Disorders and Stroke, Bethesda, Md., will chair the symposium and describe the structure of the initiative and its seven high-level research priorities.
Arnold Kriegstein, MD, PhD, of the University of California, San Francisco, will describe his research groups’ efforts at using single-cell approaches to establish an integrative definition of cell types in the developing human neocortex.
Viviana Gradinaru, PhD, of the California Institute of Technology, Pasadena, plans to provide insight on how her lab has developed safe, efficient, and specific vectors for targeting specific cells in the brain to learn about the circuits underlying locomotion, reward, and sleep, and to report on their activity history.
Sydney Cash, MD, PhD, of Massachusetts General Hospital, Boston, aims to survey the history and current landscape of available approaches toward obtaining single-neuron level information from patients, and to describe how this level of precision complements both meso- and macroscale information. He will describe how the huge amount of information being generated from these approaches is being examined with “big data” analytics.
Anna Devor, PhD, of the University of California, San Diego, intends to illustrate a “bottom-up” forward model for how to bridge the mechanistic insights we have gleaned from animal models and match them to noninvasive human neuroimaging data from functional MRI, functional near-infrared spectroscopy, magneto/electroencephalography, and positron emission tomography. This would involve identifying the noninvasive imaging signatures of specific neuronal cell types in order to derive better tools and techniques for estimating neuronal activity from multimodal noninvasive imaging data.
Fever and bilateral ankle pain
A 35-year-old man presents with bilateral ankle pain and swelling. He has had fevers over the past 5 days. Physical examination: temperature, 38° C; pulse, 90; blood pressure, 140/70 mm Hg. Ext: Edema bilateral ankles, ankle joints tender. No other joints are involved. Lab: WBC, 6,000; polys, 4.8; mono, 0.5; lymph, 0.7.
What is the most useful diagnostic test?
A. CRP.
B. ESR.
C. Uric acid.
D. Chest x-ray.
E. Rheumatoid factor.
This patient has acute onset of fevers and bilateral ankle pain and swelling. The acute onset and presence of a fever makes rheumatoid arthritis unlikely. Bilateral ankle arthritis is a very unusual presentation for gout, and would be very unlikely in such a young patient unless there were other risk factors for gout. Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate) will not help make a specific diagnosis.
This patient has Lofgren’s syndrome (acute presentation of sarcoidosis). A chest x-ray would be diagnostic, as the presence of bilateral hilar adenopathy along with the other symptoms would be diagnostic of Lofgren’s syndrome. The patient also has a low peripheral lymphocyte count, which is common with active sarcoidosis.
The combination of bilateral ankle swelling and inflammation is a clue to think about sarcoidosis. Juan Mañá, MD, and his colleagues reviewed the charts of 330 sarcoid patients who presented over a 20-year period.1 A total of 33 patients presented with periarticular ankle inflammation. Interestingly, the majority of these patients presented in the spring (54%). The average age of the patients was 33 years, and about 80% had stage 1 sarcoid on chest radiography (bilateral hilar adenopathy). All 24 patients who were followed up were in remission a year later.
In another study, the same investigators reported on the clinical features and course of Lofgren’s syndrome in 186 patients. Almost all the patients (93%) had erythema nodosum or periarticular ankle inflammation at presentation.2 Half of the patients presented in the spring, and the vast majority (87%) had no respiratory symptoms at the time of presentation. Most of the 133 patients (86%) who were available for follow-up (mean follow-up, 5 years) were in complete remission from sarcoid.
Johan Grunewald, MD, and Anders Eklund, MD, reported on 150 patients with Lofgren’s syndrome.3 In that study, 87 patients had erythema nodosum, and 63 had no erythema nodosum but did have symmetric ankle inflammation. There was an increase in patients presenting in the spring, about 80% had stage 1 sarcoid on chest x-ray, and the majority of the patients who presented with bilateral ankle inflammation and no erythema nodosum were men. They also found that there was a strong association with the presence of HLA-DRB1*0301/DQB1*0201 in patients who developed Lofgren’s syndrome. Resolution of disease was very common (85%) without recurrences.
There are several pearls to emphasize. Think of Lofgren’s syndrome in patients with symmetrical ankle inflammation or erythema nodosum. Order a chest x-ray to make the diagnosis; these patients usually will have no pulmonary symptoms to lead you in that direction. The prognosis is very good for these patients, with the great majority of them having full clinical resolution without recurrences.
Key pearl: Think of Lofgren’s syndrome in patients presenting with bilateral ankle inflammation.

References
1. J Rheumatol. 1996 May;23(5):874-7.
2. Am J Med. 1999 Sep;107(3):240-5.
3. Am J Respir Crit Care Med. 2007 Jan 1;175(1):40-4.
A 35-year-old man presents with bilateral ankle pain and swelling. He has had fevers over the past 5 days. Physical examination: temperature, 38° C; pulse, 90; blood pressure, 140/70 mm Hg. Ext: Edema bilateral ankles, ankle joints tender. No other joints are involved. Lab: WBC, 6,000; polys, 4.8; mono, 0.5; lymph, 0.7.
What is the most useful diagnostic test?
A. CRP.
B. ESR.
C. Uric acid.
D. Chest x-ray.
E. Rheumatoid factor.
This patient has acute onset of fevers and bilateral ankle pain and swelling. The acute onset and presence of a fever makes rheumatoid arthritis unlikely. Bilateral ankle arthritis is a very unusual presentation for gout, and would be very unlikely in such a young patient unless there were other risk factors for gout. Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate) will not help make a specific diagnosis.
This patient has Lofgren’s syndrome (acute presentation of sarcoidosis). A chest x-ray would be diagnostic, as the presence of bilateral hilar adenopathy along with the other symptoms would be diagnostic of Lofgren’s syndrome. The patient also has a low peripheral lymphocyte count, which is common with active sarcoidosis.
The combination of bilateral ankle swelling and inflammation is a clue to think about sarcoidosis. Juan Mañá, MD, and his colleagues reviewed the charts of 330 sarcoid patients who presented over a 20-year period.1 A total of 33 patients presented with periarticular ankle inflammation. Interestingly, the majority of these patients presented in the spring (54%). The average age of the patients was 33 years, and about 80% had stage 1 sarcoid on chest radiography (bilateral hilar adenopathy). All 24 patients who were followed up were in remission a year later.
In another study, the same investigators reported on the clinical features and course of Lofgren’s syndrome in 186 patients. Almost all the patients (93%) had erythema nodosum or periarticular ankle inflammation at presentation.2 Half of the patients presented in the spring, and the vast majority (87%) had no respiratory symptoms at the time of presentation. Most of the 133 patients (86%) who were available for follow-up (mean follow-up, 5 years) were in complete remission from sarcoid.
Johan Grunewald, MD, and Anders Eklund, MD, reported on 150 patients with Lofgren’s syndrome.3 In that study, 87 patients had erythema nodosum, and 63 had no erythema nodosum but did have symmetric ankle inflammation. There was an increase in patients presenting in the spring, about 80% had stage 1 sarcoid on chest x-ray, and the majority of the patients who presented with bilateral ankle inflammation and no erythema nodosum were men. They also found that there was a strong association with the presence of HLA-DRB1*0301/DQB1*0201 in patients who developed Lofgren’s syndrome. Resolution of disease was very common (85%) without recurrences.
There are several pearls to emphasize. Think of Lofgren’s syndrome in patients with symmetrical ankle inflammation or erythema nodosum. Order a chest x-ray to make the diagnosis; these patients usually will have no pulmonary symptoms to lead you in that direction. The prognosis is very good for these patients, with the great majority of them having full clinical resolution without recurrences.
Key pearl: Think of Lofgren’s syndrome in patients presenting with bilateral ankle inflammation.
References
1. J Rheumatol. 1996 May;23(5):874-7.
2. Am J Med. 1999 Sep;107(3):240-5.
3. Am J Respir Crit Care Med. 2007 Jan 1;175(1):40-4.
A 35-year-old man presents with bilateral ankle pain and swelling. He has had fevers over the past 5 days. Physical examination: temperature, 38° C; pulse, 90; blood pressure, 140/70 mm Hg. Ext: Edema bilateral ankles, ankle joints tender. No other joints are involved. Lab: WBC, 6,000; polys, 4.8; mono, 0.5; lymph, 0.7.
What is the most useful diagnostic test?
A. CRP.
B. ESR.
C. Uric acid.
D. Chest x-ray.
E. Rheumatoid factor.
This patient has acute onset of fevers and bilateral ankle pain and swelling. The acute onset and presence of a fever makes rheumatoid arthritis unlikely. Bilateral ankle arthritis is a very unusual presentation for gout, and would be very unlikely in such a young patient unless there were other risk factors for gout. Inflammatory markers (C-reactive protein and erythrocyte sedimentation rate) will not help make a specific diagnosis.
This patient has Lofgren’s syndrome (acute presentation of sarcoidosis). A chest x-ray would be diagnostic, as the presence of bilateral hilar adenopathy along with the other symptoms would be diagnostic of Lofgren’s syndrome. The patient also has a low peripheral lymphocyte count, which is common with active sarcoidosis.
The combination of bilateral ankle swelling and inflammation is a clue to think about sarcoidosis. Juan Mañá, MD, and his colleagues reviewed the charts of 330 sarcoid patients who presented over a 20-year period.1 A total of 33 patients presented with periarticular ankle inflammation. Interestingly, the majority of these patients presented in the spring (54%). The average age of the patients was 33 years, and about 80% had stage 1 sarcoid on chest radiography (bilateral hilar adenopathy). All 24 patients who were followed up were in remission a year later.
In another study, the same investigators reported on the clinical features and course of Lofgren’s syndrome in 186 patients. Almost all the patients (93%) had erythema nodosum or periarticular ankle inflammation at presentation.2 Half of the patients presented in the spring, and the vast majority (87%) had no respiratory symptoms at the time of presentation. Most of the 133 patients (86%) who were available for follow-up (mean follow-up, 5 years) were in complete remission from sarcoid.
Johan Grunewald, MD, and Anders Eklund, MD, reported on 150 patients with Lofgren’s syndrome.3 In that study, 87 patients had erythema nodosum, and 63 had no erythema nodosum but did have symmetric ankle inflammation. There was an increase in patients presenting in the spring, about 80% had stage 1 sarcoid on chest x-ray, and the majority of the patients who presented with bilateral ankle inflammation and no erythema nodosum were men. They also found that there was a strong association with the presence of HLA-DRB1*0301/DQB1*0201 in patients who developed Lofgren’s syndrome. Resolution of disease was very common (85%) without recurrences.
There are several pearls to emphasize. Think of Lofgren’s syndrome in patients with symmetrical ankle inflammation or erythema nodosum. Order a chest x-ray to make the diagnosis; these patients usually will have no pulmonary symptoms to lead you in that direction. The prognosis is very good for these patients, with the great majority of them having full clinical resolution without recurrences.
Key pearl: Think of Lofgren’s syndrome in patients presenting with bilateral ankle inflammation.
References
1. J Rheumatol. 1996 May;23(5):874-7.
2. Am J Med. 1999 Sep;107(3):240-5.
3. Am J Respir Crit Care Med. 2007 Jan 1;175(1):40-4.
Rectal temps in the nursery
It seems to me that the closer one could get to the center of the child’s body, the more likely you would get a true reading – and the less likely you would fall victim to operator error. However, a study reported on the Pediatric News website suggests that our intuition is wrong again (“Axillary thermometry is the best choice for newborns,” by M. Alexander Otto, Aug. 24, 2017). In the study of 205 newborns at the University of North Carolina at Chapel Hill Medical Center, multiple temperatures were recorded using three methods over a 15-minute period. Rectal temperatures were accurate but less reliable than axillary readings, while temporal artery measurements tended to “overestimate temperatures by an average of about a quarter of a degree.”

However, before we jump on the no-rectal-temps in the nursery bandwagon, let’s look at the rectal probe not just as a way to assess a newborn’s temperature, but as a tool for examining the baby’s rectum. For a variety of reasons, the newborn perineum often seems to escape the careful examination it deserves, particularly if the initial exam is performed with the parents watching.
Of course, parents are interested in their baby’s hair and eye color, and whether it has the requisite number of fingers and toes. They will wait anxiously until you have lifted your stethoscope off the baby’s chest and given them a nod and smile. However, doing a thorough exam of the infant’s genitalia may appear a bit invasive and improper to some parents. Whether it is because we sense some unspoken parental discomfort or because we are trying to save time, the nether regions of little girls are inadequately examined.

But back to rectal temperatures. It seems to me that it would be prudent to adopt a guideline that says that a newborn’s first temperature be taken rectally. Not because it is any more accurate than an axillary temperature – which this study suggests that it is not. But because the process of taking the temperature would make it more likely (I hesitate to say guarantee) that someone will be taking a careful look at the newborn’s rectum. That initial rectal temperature is not going to detect every genital anomaly, but it may help find some in a more timely fashion. If nothing else, it will get that meconium moving.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
It seems to me that the closer one could get to the center of the child’s body, the more likely you would get a true reading – and the less likely you would fall victim to operator error. However, a study reported on the Pediatric News website suggests that our intuition is wrong again (“Axillary thermometry is the best choice for newborns,” by M. Alexander Otto, Aug. 24, 2017). In the study of 205 newborns at the University of North Carolina at Chapel Hill Medical Center, multiple temperatures were recorded using three methods over a 15-minute period. Rectal temperatures were accurate but less reliable than axillary readings, while temporal artery measurements tended to “overestimate temperatures by an average of about a quarter of a degree.”
However, before we jump on the no-rectal-temps in the nursery bandwagon, let’s look at the rectal probe not just as a way to assess a newborn’s temperature, but as a tool for examining the baby’s rectum. For a variety of reasons, the newborn perineum often seems to escape the careful examination it deserves, particularly if the initial exam is performed with the parents watching.
Of course, parents are interested in their baby’s hair and eye color, and whether it has the requisite number of fingers and toes. They will wait anxiously until you have lifted your stethoscope off the baby’s chest and given them a nod and smile. However, doing a thorough exam of the infant’s genitalia may appear a bit invasive and improper to some parents. Whether it is because we sense some unspoken parental discomfort or because we are trying to save time, the nether regions of little girls are inadequately examined.
But back to rectal temperatures. It seems to me that it would be prudent to adopt a guideline that says that a newborn’s first temperature be taken rectally. Not because it is any more accurate than an axillary temperature – which this study suggests that it is not. But because the process of taking the temperature would make it more likely (I hesitate to say guarantee) that someone will be taking a careful look at the newborn’s rectum. That initial rectal temperature is not going to detect every genital anomaly, but it may help find some in a more timely fashion. If nothing else, it will get that meconium moving.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
It seems to me that the closer one could get to the center of the child’s body, the more likely you would get a true reading – and the less likely you would fall victim to operator error. However, a study reported on the Pediatric News website suggests that our intuition is wrong again (“Axillary thermometry is the best choice for newborns,” by M. Alexander Otto, Aug. 24, 2017). In the study of 205 newborns at the University of North Carolina at Chapel Hill Medical Center, multiple temperatures were recorded using three methods over a 15-minute period. Rectal temperatures were accurate but less reliable than axillary readings, while temporal artery measurements tended to “overestimate temperatures by an average of about a quarter of a degree.”
However, before we jump on the no-rectal-temps in the nursery bandwagon, let’s look at the rectal probe not just as a way to assess a newborn’s temperature, but as a tool for examining the baby’s rectum. For a variety of reasons, the newborn perineum often seems to escape the careful examination it deserves, particularly if the initial exam is performed with the parents watching.
Of course, parents are interested in their baby’s hair and eye color, and whether it has the requisite number of fingers and toes. They will wait anxiously until you have lifted your stethoscope off the baby’s chest and given them a nod and smile. However, doing a thorough exam of the infant’s genitalia may appear a bit invasive and improper to some parents. Whether it is because we sense some unspoken parental discomfort or because we are trying to save time, the nether regions of little girls are inadequately examined.
But back to rectal temperatures. It seems to me that it would be prudent to adopt a guideline that says that a newborn’s first temperature be taken rectally. Not because it is any more accurate than an axillary temperature – which this study suggests that it is not. But because the process of taking the temperature would make it more likely (I hesitate to say guarantee) that someone will be taking a careful look at the newborn’s rectum. That initial rectal temperature is not going to detect every genital anomaly, but it may help find some in a more timely fashion. If nothing else, it will get that meconium moving.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
High percentage of nursing home residents found to harbor MDROs
SAN DIEGO – Nearly half of nursing home residents harbored multi-drug resistant organisms on their skin, results from a large multi-center surveillance study showed.
“Residents in skilled nursing homes are the most vulnerable patients in the health care system,” lead study author James A. McKinnell, MD, said in an interview in advance of an annual scientific meeting on infectious diseases. “Many residents depend on help from health care workers for routine needs like eating or bathing. Skilled nursing facilities have an obligation to optimize the personal hygiene and environmental cleanliness in skilled nursing facilities.”

The researchers obtained 2,797 body swabs from 1,400 residents in all. Swabs were processed for methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus spp. (VRE), extended spectrum beta-lactamase producers (ESBLs), and carbapenem-resistant Enterobacteriaceae (CRE). “MRSA is a relatively well known bacteria, but CRE is the new pathogen that the CDC has defined as an urgent public health threat,” Dr. McKinnell said.
The researchers also conducted environmental surveillance of commonly touched items in skilled nursing facilities. The five surfaces tested in resident rooms were the bedside table, TV remote, door knobs, light switch, and bathrooms. The five surfaces tested in common areas were the nursing station counter, tables, chairs, hallway hand rails, and drinking fountains.
Overall, 49% of residents harbored MDROs. MRSA was found in 37% of residents, followed by ESBL in 16%, VRE in 7%, and CRE in 1%. Resident MDRO status was known for 11% of MRSA carriers, compared with 18% of ESBL, 4% of VRE, and none of the CRE carriers. Rates of colonization did not differ whether residents had long stays at the facility or postacute stays (49% vs. 48%, respectively), but bed-bound residents were more likely to be MDRO colonized, compared with ambulatory residents (59% vs. 46%; P less than .001). In the analysis of environmental swabs, 93% of common areas and 74% of resident rooms had an MDRO-positive object, with an average of 2.5 and 1.9 objects, respectively, found to be contaminated.
“The fact that about half of patients were carrying a bacteria that could cause infection on their skin was very high,” said Dr. McKinnell, who is a member of the Infectious Disease Clinical Outcome Research Unit at the Los Angeles Biomedical Research Institute at Harbor-UCLA. “Studies conducted in other care settings, we would typically see less than a quarter of patients carry these types of bacteria. I was also surprised to see that 1% of patients were carrying the CRE bacteria on their skin.”
He acknowledged certain limitations of the study, including the fact that the data were taken from a select group of nursing homes that are participating in an interventional study to improve personal hygiene for skilled nursing facility residents. “They may not be representative of all skilled nursing facilities,” he said.
The Agency for Healthcare Research and Quality funded the study. Dr. McKinnell disclosed that he is conducting studies in health care facilities with products supplied from 3M, Clorox, Sage, and Xttrium Laboratories. Many of his coauthors disclosed numerous financial ties to the pharmaceutical industry. The event was the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
SAN DIEGO – Nearly half of nursing home residents harbored multi-drug resistant organisms on their skin, results from a large multi-center surveillance study showed.
“Residents in skilled nursing homes are the most vulnerable patients in the health care system,” lead study author James A. McKinnell, MD, said in an interview in advance of an annual scientific meeting on infectious diseases. “Many residents depend on help from health care workers for routine needs like eating or bathing. Skilled nursing facilities have an obligation to optimize the personal hygiene and environmental cleanliness in skilled nursing facilities.”
The researchers obtained 2,797 body swabs from 1,400 residents in all. Swabs were processed for methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus spp. (VRE), extended spectrum beta-lactamase producers (ESBLs), and carbapenem-resistant Enterobacteriaceae (CRE). “MRSA is a relatively well known bacteria, but CRE is the new pathogen that the CDC has defined as an urgent public health threat,” Dr. McKinnell said.
The researchers also conducted environmental surveillance of commonly touched items in skilled nursing facilities. The five surfaces tested in resident rooms were the bedside table, TV remote, door knobs, light switch, and bathrooms. The five surfaces tested in common areas were the nursing station counter, tables, chairs, hallway hand rails, and drinking fountains.
Overall, 49% of residents harbored MDROs. MRSA was found in 37% of residents, followed by ESBL in 16%, VRE in 7%, and CRE in 1%. Resident MDRO status was known for 11% of MRSA carriers, compared with 18% of ESBL, 4% of VRE, and none of the CRE carriers. Rates of colonization did not differ whether residents had long stays at the facility or postacute stays (49% vs. 48%, respectively), but bed-bound residents were more likely to be MDRO colonized, compared with ambulatory residents (59% vs. 46%; P less than .001). In the analysis of environmental swabs, 93% of common areas and 74% of resident rooms had an MDRO-positive object, with an average of 2.5 and 1.9 objects, respectively, found to be contaminated.
“The fact that about half of patients were carrying a bacteria that could cause infection on their skin was very high,” said Dr. McKinnell, who is a member of the Infectious Disease Clinical Outcome Research Unit at the Los Angeles Biomedical Research Institute at Harbor-UCLA. “Studies conducted in other care settings, we would typically see less than a quarter of patients carry these types of bacteria. I was also surprised to see that 1% of patients were carrying the CRE bacteria on their skin.”
He acknowledged certain limitations of the study, including the fact that the data were taken from a select group of nursing homes that are participating in an interventional study to improve personal hygiene for skilled nursing facility residents. “They may not be representative of all skilled nursing facilities,” he said.
The Agency for Healthcare Research and Quality funded the study. Dr. McKinnell disclosed that he is conducting studies in health care facilities with products supplied from 3M, Clorox, Sage, and Xttrium Laboratories. Many of his coauthors disclosed numerous financial ties to the pharmaceutical industry. The event was the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
SAN DIEGO – Nearly half of nursing home residents harbored multi-drug resistant organisms on their skin, results from a large multi-center surveillance study showed.
“Residents in skilled nursing homes are the most vulnerable patients in the health care system,” lead study author James A. McKinnell, MD, said in an interview in advance of an annual scientific meeting on infectious diseases. “Many residents depend on help from health care workers for routine needs like eating or bathing. Skilled nursing facilities have an obligation to optimize the personal hygiene and environmental cleanliness in skilled nursing facilities.”
The researchers obtained 2,797 body swabs from 1,400 residents in all. Swabs were processed for methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus spp. (VRE), extended spectrum beta-lactamase producers (ESBLs), and carbapenem-resistant Enterobacteriaceae (CRE). “MRSA is a relatively well known bacteria, but CRE is the new pathogen that the CDC has defined as an urgent public health threat,” Dr. McKinnell said.
The researchers also conducted environmental surveillance of commonly touched items in skilled nursing facilities. The five surfaces tested in resident rooms were the bedside table, TV remote, door knobs, light switch, and bathrooms. The five surfaces tested in common areas were the nursing station counter, tables, chairs, hallway hand rails, and drinking fountains.
Overall, 49% of residents harbored MDROs. MRSA was found in 37% of residents, followed by ESBL in 16%, VRE in 7%, and CRE in 1%. Resident MDRO status was known for 11% of MRSA carriers, compared with 18% of ESBL, 4% of VRE, and none of the CRE carriers. Rates of colonization did not differ whether residents had long stays at the facility or postacute stays (49% vs. 48%, respectively), but bed-bound residents were more likely to be MDRO colonized, compared with ambulatory residents (59% vs. 46%; P less than .001). In the analysis of environmental swabs, 93% of common areas and 74% of resident rooms had an MDRO-positive object, with an average of 2.5 and 1.9 objects, respectively, found to be contaminated.
“The fact that about half of patients were carrying a bacteria that could cause infection on their skin was very high,” said Dr. McKinnell, who is a member of the Infectious Disease Clinical Outcome Research Unit at the Los Angeles Biomedical Research Institute at Harbor-UCLA. “Studies conducted in other care settings, we would typically see less than a quarter of patients carry these types of bacteria. I was also surprised to see that 1% of patients were carrying the CRE bacteria on their skin.”
He acknowledged certain limitations of the study, including the fact that the data were taken from a select group of nursing homes that are participating in an interventional study to improve personal hygiene for skilled nursing facility residents. “They may not be representative of all skilled nursing facilities,” he said.
The Agency for Healthcare Research and Quality funded the study. Dr. McKinnell disclosed that he is conducting studies in health care facilities with products supplied from 3M, Clorox, Sage, and Xttrium Laboratories. Many of his coauthors disclosed numerous financial ties to the pharmaceutical industry. The event was the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
AT ID WEEK 2017
Key clinical point: About one of every two nursing home residents is colonized with multidrug resistant organisms.
Major finding:
Study details: A surveillance study of 1,400 residents at 28 skilled nursing facilities in Southern California.
Disclosures: The Agency for Healthcare Research and Quality funded the study. Dr. McKinnell disclosed that he is conducting studies in health care facilities with products supplied from 3M, Clorox, Sage, and Xttrium Laboratories. Many of his coauthors disclosed numerous financial ties to the pharmaceutical industry.
House, Senate committees clear CHIP reauthorization
Committees in the House and Senate passed bills to reauthorize funding for the Children’s Health Insurance Program for 5 years, but their efforts took very different paths.
Funding for CHIP expired on Sept. 30, adding a level of urgency for Congress to act.
The Senate Finance Committee needed only a voice vote during an Oct. 4 executive session, with support from both Republicans and Democrats, to move the Keeping Kids Insurance Dependable and Secure (KIDS) Act (S. 1827) to the Senate floor. The Senate version is a straight-forward bill that also extended a few childhood health demonstration projects.
Offsets in the Helping Ensure Access for Little Ones, Toddlers, and Hopeful Young by Keeping Insurance Delivery Stable (HEALTHY KIDS) Act (H.R. 3921) include means testing for Medicare Part B and D premiums by having those earning $500,000 or more on the hook for their entire Medicare Parts B and D premiums, inclusion of lottery and other lump sum awards in making Medicaid determinations, and help for states seeking to get payments from insurers.
In addition to general arguments against the use of offsets for this bill and not other measures that were also marked up during the Oct. 4 session and complaints about the inadequacy of funding for Puerto Rico’s Medicaid program in light of the recent hurricane, Energy and Commerce Committee Democrats also voiced strong objection to the use of means testing for Medicare.
“The way they are put together today will likely mean more delay and possibly no action in Congress until the end of the year as part of an omnibus appropriations bill,” Energy & Commerce Ranking Member Frank Pallone (D-N.J.) said.

Committees in the House and Senate passed bills to reauthorize funding for the Children’s Health Insurance Program for 5 years, but their efforts took very different paths.
Funding for CHIP expired on Sept. 30, adding a level of urgency for Congress to act.
The Senate Finance Committee needed only a voice vote during an Oct. 4 executive session, with support from both Republicans and Democrats, to move the Keeping Kids Insurance Dependable and Secure (KIDS) Act (S. 1827) to the Senate floor. The Senate version is a straight-forward bill that also extended a few childhood health demonstration projects.
Offsets in the Helping Ensure Access for Little Ones, Toddlers, and Hopeful Young by Keeping Insurance Delivery Stable (HEALTHY KIDS) Act (H.R. 3921) include means testing for Medicare Part B and D premiums by having those earning $500,000 or more on the hook for their entire Medicare Parts B and D premiums, inclusion of lottery and other lump sum awards in making Medicaid determinations, and help for states seeking to get payments from insurers.
In addition to general arguments against the use of offsets for this bill and not other measures that were also marked up during the Oct. 4 session and complaints about the inadequacy of funding for Puerto Rico’s Medicaid program in light of the recent hurricane, Energy and Commerce Committee Democrats also voiced strong objection to the use of means testing for Medicare.
“The way they are put together today will likely mean more delay and possibly no action in Congress until the end of the year as part of an omnibus appropriations bill,” Energy & Commerce Ranking Member Frank Pallone (D-N.J.) said.
Committees in the House and Senate passed bills to reauthorize funding for the Children’s Health Insurance Program for 5 years, but their efforts took very different paths.
Funding for CHIP expired on Sept. 30, adding a level of urgency for Congress to act.
The Senate Finance Committee needed only a voice vote during an Oct. 4 executive session, with support from both Republicans and Democrats, to move the Keeping Kids Insurance Dependable and Secure (KIDS) Act (S. 1827) to the Senate floor. The Senate version is a straight-forward bill that also extended a few childhood health demonstration projects.
Offsets in the Helping Ensure Access for Little Ones, Toddlers, and Hopeful Young by Keeping Insurance Delivery Stable (HEALTHY KIDS) Act (H.R. 3921) include means testing for Medicare Part B and D premiums by having those earning $500,000 or more on the hook for their entire Medicare Parts B and D premiums, inclusion of lottery and other lump sum awards in making Medicaid determinations, and help for states seeking to get payments from insurers.
In addition to general arguments against the use of offsets for this bill and not other measures that were also marked up during the Oct. 4 session and complaints about the inadequacy of funding for Puerto Rico’s Medicaid program in light of the recent hurricane, Energy and Commerce Committee Democrats also voiced strong objection to the use of means testing for Medicare.
“The way they are put together today will likely mean more delay and possibly no action in Congress until the end of the year as part of an omnibus appropriations bill,” Energy & Commerce Ranking Member Frank Pallone (D-N.J.) said.
SHM suggests tweaks to CMS QPP proposal
The Society of Hospital Medicine approves of the direction the Centers for Medicare & Medicaid Services is heading when it comes to measuring pay-for-performance for hospitalists in its Quality Payment Program (QPP) but is suggesting some tweaks to make it a better system.
The proposed CMS 2018 update to the QPP, the value-based payment scheme developed by the Medicare Access and CHIP Reauthorization Act (MACRA), included an option that would allow all physicians who primarily practice in a hospital setting to report as a unified group under the hospital umbrella – as an alternative to reporting as an individual in the Merit-Based Incentive Payment System (MIPS) track.

He said there is lot to like in that option, although there are things that need to be changed as well.
One key area SHM would like to see changed is how time spent in a hospital is measured. In the CMS proposal, codes related to site of service capture only those in the emergency room and those admitted for in-patient services. Doctors who are seeing patients on an observation basis before they are admitted are not captured and could not be included in the facility payment.
“Observation services are virtually indistinguishable from inpatient care and frequently occur on the same wards of the hospital,” SHM said in Aug. 21, 2017, comments to CMS on the proposed QPP update, noting that observational care is built around the two-midnight rule.
“We disagree with this interpretation,” the SHM letter continues. “While it is true observation is generally time limited for a given patient, practice structures and provider scheduling have a profound [impact] on the proportion of observation care an individual clinician provides.” The letter noted that hospitalists who are on observation service could have a high proportion of observation (outpatient) billing, which could in turn exclude them from qualifying for a facility-based reporting option “despite the fact they are truly hospital-based inpatient providers.”
Dr. Greeno noted that some hospitals have hospitalists that exclusively provide observational care.
The proposal designates physicians who meet a 75% threshold of providing care in an emergency room or in-patient setting as eligible to opt into facility-based reporting.
SHM suggests that if observation services cannot be included in the 75% threshold, those services should be included and “couple the calculation with a cross-check to ensure most other billing is also hospital-based. As a further check, CMS could look at specialty codes – is the provider also enrolled in Medicare as a hospitalist?” SHM also recommends lowering the threshold “to 70% or, ideally, 60%. Due to the wide variation in hospitalist practice, we are uncomfortable with the use of thresholds in general, but lowering this threshold would at least provide a kind of safety net for hospitalists who are caring for high numbers of patients on observation.”
Another key area that needs to be addressed is the quality metrics that are used for scoring, which Dr. Greeno acknowledged is “surprisingly hard to do.”
For the 2018 reporting year, CMS is proposing that the required number of measures for the MIPS program be six, that same is it currently is for 2017. While SHM agrees with this level, “we remind CMS that even six measures may be a challenge for some providers, including hospitalists, to meet. Concerted efforts should be made to ensure that those providers who have fewer than six measures available for reporting are not disadvantaged in any way.”

Two of the six hospitalist-specific quality metrics relate to heart attacks, Dr. Seymann noted.
“Most hospitalists do take care of these patients, but they can only be reported via registry or via an electronic health record, and I don’t know that all hospitalist groups have access to reporting those ways,” Dr. Seymann said. “Most folks are reporting when they submit their billing claims. That takes two measures away from them. That may significantly decrease your score, even if you are trying your best.”
While Dr. Seymann applauded CMS for the slow rollout of the MIPS program in general, “we haven’t seen great progress as far as the growth of available relevant measures for hospitalists, and I am not confident that 2 years down the line we are going to have 12 measures to choose from.”
He did suggest that hospitalists would like a greater variety of measures and want to be measured on the quality of care they provide.
“We truly believe that the majority of hospitalist groups are really heavily invested in improving the quality of care that is provided at their hospitals – that is a big part of the culture of hospital medicine in general,” Dr. Seymann said. “We want to make our ability to succeed and participate in this program as effective as we can. We want to try to minimize barriers to hospitalists hitting this one out of the park.”
SHM also noted that certain measures rarely meet the volume threshold, which could ultimately put hospitalists at a disadvantage when it comes to receiving bonus payments.
“This is not an acceptable outcome, and we strongly urge CMS to develop a solution for providers with low-volume measures, such as removing low-volume measures from the Quality category score,” SHM wrote.
Ultimately, Dr. Greeno believes the facility reporting opt-in will survive when the rule is finalized.
“We fully expect there to be a facility-based option for hospital-based doctors, including hospitalists,” he said. “So rather than reporting on physician metrics, especially metrics through MIPS, they can get rewarded or penalized based on the hospital value-based purchasing metrics for their hospital.”
The Society of Hospital Medicine approves of the direction the Centers for Medicare & Medicaid Services is heading when it comes to measuring pay-for-performance for hospitalists in its Quality Payment Program (QPP) but is suggesting some tweaks to make it a better system.
The proposed CMS 2018 update to the QPP, the value-based payment scheme developed by the Medicare Access and CHIP Reauthorization Act (MACRA), included an option that would allow all physicians who primarily practice in a hospital setting to report as a unified group under the hospital umbrella – as an alternative to reporting as an individual in the Merit-Based Incentive Payment System (MIPS) track.
He said there is lot to like in that option, although there are things that need to be changed as well.
One key area SHM would like to see changed is how time spent in a hospital is measured. In the CMS proposal, codes related to site of service capture only those in the emergency room and those admitted for in-patient services. Doctors who are seeing patients on an observation basis before they are admitted are not captured and could not be included in the facility payment.
“Observation services are virtually indistinguishable from inpatient care and frequently occur on the same wards of the hospital,” SHM said in Aug. 21, 2017, comments to CMS on the proposed QPP update, noting that observational care is built around the two-midnight rule.
“We disagree with this interpretation,” the SHM letter continues. “While it is true observation is generally time limited for a given patient, practice structures and provider scheduling have a profound [impact] on the proportion of observation care an individual clinician provides.” The letter noted that hospitalists who are on observation service could have a high proportion of observation (outpatient) billing, which could in turn exclude them from qualifying for a facility-based reporting option “despite the fact they are truly hospital-based inpatient providers.”
Dr. Greeno noted that some hospitals have hospitalists that exclusively provide observational care.
The proposal designates physicians who meet a 75% threshold of providing care in an emergency room or in-patient setting as eligible to opt into facility-based reporting.
SHM suggests that if observation services cannot be included in the 75% threshold, those services should be included and “couple the calculation with a cross-check to ensure most other billing is also hospital-based. As a further check, CMS could look at specialty codes – is the provider also enrolled in Medicare as a hospitalist?” SHM also recommends lowering the threshold “to 70% or, ideally, 60%. Due to the wide variation in hospitalist practice, we are uncomfortable with the use of thresholds in general, but lowering this threshold would at least provide a kind of safety net for hospitalists who are caring for high numbers of patients on observation.”
Another key area that needs to be addressed is the quality metrics that are used for scoring, which Dr. Greeno acknowledged is “surprisingly hard to do.”
For the 2018 reporting year, CMS is proposing that the required number of measures for the MIPS program be six, that same is it currently is for 2017. While SHM agrees with this level, “we remind CMS that even six measures may be a challenge for some providers, including hospitalists, to meet. Concerted efforts should be made to ensure that those providers who have fewer than six measures available for reporting are not disadvantaged in any way.”
Two of the six hospitalist-specific quality metrics relate to heart attacks, Dr. Seymann noted.
“Most hospitalists do take care of these patients, but they can only be reported via registry or via an electronic health record, and I don’t know that all hospitalist groups have access to reporting those ways,” Dr. Seymann said. “Most folks are reporting when they submit their billing claims. That takes two measures away from them. That may significantly decrease your score, even if you are trying your best.”
While Dr. Seymann applauded CMS for the slow rollout of the MIPS program in general, “we haven’t seen great progress as far as the growth of available relevant measures for hospitalists, and I am not confident that 2 years down the line we are going to have 12 measures to choose from.”
He did suggest that hospitalists would like a greater variety of measures and want to be measured on the quality of care they provide.
“We truly believe that the majority of hospitalist groups are really heavily invested in improving the quality of care that is provided at their hospitals – that is a big part of the culture of hospital medicine in general,” Dr. Seymann said. “We want to make our ability to succeed and participate in this program as effective as we can. We want to try to minimize barriers to hospitalists hitting this one out of the park.”
SHM also noted that certain measures rarely meet the volume threshold, which could ultimately put hospitalists at a disadvantage when it comes to receiving bonus payments.
“This is not an acceptable outcome, and we strongly urge CMS to develop a solution for providers with low-volume measures, such as removing low-volume measures from the Quality category score,” SHM wrote.
Ultimately, Dr. Greeno believes the facility reporting opt-in will survive when the rule is finalized.
“We fully expect there to be a facility-based option for hospital-based doctors, including hospitalists,” he said. “So rather than reporting on physician metrics, especially metrics through MIPS, they can get rewarded or penalized based on the hospital value-based purchasing metrics for their hospital.”
The Society of Hospital Medicine approves of the direction the Centers for Medicare & Medicaid Services is heading when it comes to measuring pay-for-performance for hospitalists in its Quality Payment Program (QPP) but is suggesting some tweaks to make it a better system.
The proposed CMS 2018 update to the QPP, the value-based payment scheme developed by the Medicare Access and CHIP Reauthorization Act (MACRA), included an option that would allow all physicians who primarily practice in a hospital setting to report as a unified group under the hospital umbrella – as an alternative to reporting as an individual in the Merit-Based Incentive Payment System (MIPS) track.
He said there is lot to like in that option, although there are things that need to be changed as well.
One key area SHM would like to see changed is how time spent in a hospital is measured. In the CMS proposal, codes related to site of service capture only those in the emergency room and those admitted for in-patient services. Doctors who are seeing patients on an observation basis before they are admitted are not captured and could not be included in the facility payment.
“Observation services are virtually indistinguishable from inpatient care and frequently occur on the same wards of the hospital,” SHM said in Aug. 21, 2017, comments to CMS on the proposed QPP update, noting that observational care is built around the two-midnight rule.
“We disagree with this interpretation,” the SHM letter continues. “While it is true observation is generally time limited for a given patient, practice structures and provider scheduling have a profound [impact] on the proportion of observation care an individual clinician provides.” The letter noted that hospitalists who are on observation service could have a high proportion of observation (outpatient) billing, which could in turn exclude them from qualifying for a facility-based reporting option “despite the fact they are truly hospital-based inpatient providers.”
Dr. Greeno noted that some hospitals have hospitalists that exclusively provide observational care.
The proposal designates physicians who meet a 75% threshold of providing care in an emergency room or in-patient setting as eligible to opt into facility-based reporting.
SHM suggests that if observation services cannot be included in the 75% threshold, those services should be included and “couple the calculation with a cross-check to ensure most other billing is also hospital-based. As a further check, CMS could look at specialty codes – is the provider also enrolled in Medicare as a hospitalist?” SHM also recommends lowering the threshold “to 70% or, ideally, 60%. Due to the wide variation in hospitalist practice, we are uncomfortable with the use of thresholds in general, but lowering this threshold would at least provide a kind of safety net for hospitalists who are caring for high numbers of patients on observation.”
Another key area that needs to be addressed is the quality metrics that are used for scoring, which Dr. Greeno acknowledged is “surprisingly hard to do.”
For the 2018 reporting year, CMS is proposing that the required number of measures for the MIPS program be six, that same is it currently is for 2017. While SHM agrees with this level, “we remind CMS that even six measures may be a challenge for some providers, including hospitalists, to meet. Concerted efforts should be made to ensure that those providers who have fewer than six measures available for reporting are not disadvantaged in any way.”
Two of the six hospitalist-specific quality metrics relate to heart attacks, Dr. Seymann noted.
“Most hospitalists do take care of these patients, but they can only be reported via registry or via an electronic health record, and I don’t know that all hospitalist groups have access to reporting those ways,” Dr. Seymann said. “Most folks are reporting when they submit their billing claims. That takes two measures away from them. That may significantly decrease your score, even if you are trying your best.”
While Dr. Seymann applauded CMS for the slow rollout of the MIPS program in general, “we haven’t seen great progress as far as the growth of available relevant measures for hospitalists, and I am not confident that 2 years down the line we are going to have 12 measures to choose from.”
He did suggest that hospitalists would like a greater variety of measures and want to be measured on the quality of care they provide.
“We truly believe that the majority of hospitalist groups are really heavily invested in improving the quality of care that is provided at their hospitals – that is a big part of the culture of hospital medicine in general,” Dr. Seymann said. “We want to make our ability to succeed and participate in this program as effective as we can. We want to try to minimize barriers to hospitalists hitting this one out of the park.”
SHM also noted that certain measures rarely meet the volume threshold, which could ultimately put hospitalists at a disadvantage when it comes to receiving bonus payments.
“This is not an acceptable outcome, and we strongly urge CMS to develop a solution for providers with low-volume measures, such as removing low-volume measures from the Quality category score,” SHM wrote.
Ultimately, Dr. Greeno believes the facility reporting opt-in will survive when the rule is finalized.
“We fully expect there to be a facility-based option for hospital-based doctors, including hospitalists,” he said. “So rather than reporting on physician metrics, especially metrics through MIPS, they can get rewarded or penalized based on the hospital value-based purchasing metrics for their hospital.”
Lifesaving future seen for electronic cigarettes
A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).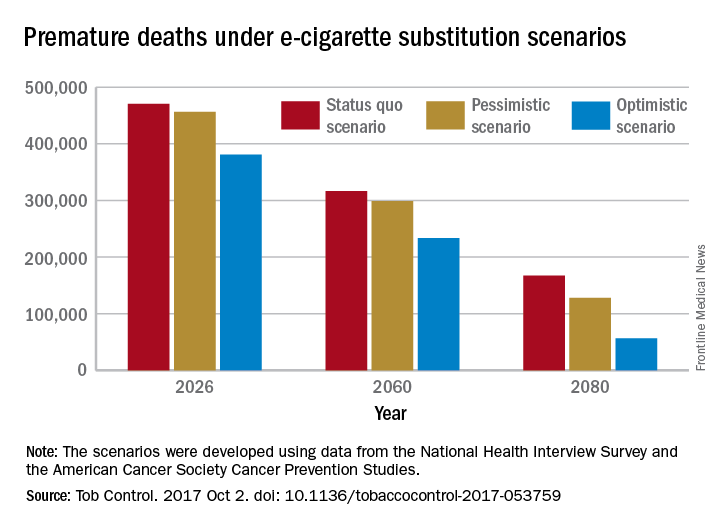
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.

A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.
A switch from cigarettes to e-cigarettes has the potential to prevent almost 90,000 premature deaths in the United States in the year 2026, according to a study examining e-cigarette substitution scenarios.
The investigators’ “optimistic scenario” – in which new smokers use e-cigarettes instead of cigarettes, smoking prevalence falls to 5% over a 10-year period, and e-cigarettes have a 5% excess risk over regular cigarettes – projects 380,832 premature deaths from smoking in the year 2026. Under a “status quo scenario,” which projected current cigarette initiation and cessation rates and did not include e-cigarettes or other tobacco products, there would be 470,743 deaths, reported David T. Levy, PhD, and his associates (Tob Control. 2017 Oct 2. doi: 10.1136/tobaccocontrol-2017-053759).
Further projections suggest that the optimistic scenario could result in almost 6.6 million fewer premature deaths and 86.7 million years of life gained by the year 2100, compared with the status quo scenario, while the pessimistic scenario would prevent 1.6 million deaths and add an extra 20.8 million years of life, they noted.
Since “a strategy of replacing cigarette by e-cigarette use can yield substantial gains, even with conservative assumptions about related risks … an endgame scenario for cigarettes might well be within reach, if new technologies for delivering nicotine with substantially less harm, but sufficient satisfaction, are harnessed with sufficient passion and political will to aggressively phase out tobacco cigarettes,” Dr. Levy and his associates wrote.
The study was funded by grants from the National Institute on Drug Abuse and the National Cancer Institute. One investigator received a research grant from Pfizer and served as an advisory board member to Johnson & Johnson, which manufactures smoking cessation medications. No other conflicts of interest were declared.
FROM TOBACCO CONTROL