User login
Pembrolizumab showed ‘promising’ antitumor activity in small-cell lung cancer
One patient died of treatment-related mesenteric ischemia, reported Patrick A. Ott, MD, of Dana-Farber Cancer Institute in Boston, and his associates. Nonetheless, with an objective response rate of 33% and a median duration of response of 19 months, the checkpoint inhibitor “demonstrated a favorable safety profile and promising durable clinical activity,” they concluded.
Study participants received pembrolizumab (10 mg/kg) every 2 weeks for 24 months or until disease progression or intolerable toxicity occurred. After a median follow-up of 9.8 months (range, 0.5-24 months), one patient (4%) had a complete response, and seven (29%) had partial responses. The median onset of response was 2 months, and responses lasted from 3.6 to 20 months, Dr. Ott and his associates reported (J Clin Oncol. 2017 Aug 16. doi: 10.1200/JCO.2017.72.5069). Two-thirds of patients developed treatment-related adverse events, most often arthralgia, asthenia, rash, diarrhea, and fatigue. Two patients developed grade 3 or worse treatment-related adverse events, including a 65-year-old man with small cell lung cancer and liver metastasis who developed grade 3 bilirubin elevation, and a 58-year-old woman with a history of sleeve gastrectomy who developed grade 3 asthenia, grade 5 colitis, and intestinal ischemia.
The patient who died had received 10 cycles of pembrolizumab, was hospitalized with abdominal pain, nausea, and vomiting, and was discharged home with a diagnosis of food intolerance, the researchers reported. She received an 11th cycle of pembrolizumab and was readmitted with abdominal pain. A rectal biopsy showed chronic colitis. She received systemic corticosteroids and was discharged, was admitted to a different hospital several weeks later with diffuse abdominal pain and septic shock, and subsequently died. “Mesenteric ischemia resulted in death,” the researchers wrote. “The cause of the colitis and intestinal ischemia was reported as probably related to pembrolizumab.”
Pembrolizumab (Keytruda) is a programmed death receptor–1 blocking antibody approved for treating non–small cell lung cancer, head and neck squamous cell cancer, classical Hodgkin lymphoma, urothelial carcinoma, and microsatellite instability–high cancer or mismatch repair deficient solid tumors. Treatment with the checkpoint inhibitor led to grade 5 treatment-related adverse events in other trials. Most recently, in July 2017, the Food and Drug Administration placed clinical holds on phase 1 and phase 3 studies of pembrolizumab for treating multiple myeloma after more patients died in the pembrolizumab arms than did in the comparison arms. Pembrolizumab also recently came up short in a phase 3 trial of patients with head and neck cancer, although it has kept its FDA label for this indication. Multiple trials of pembrolizumab for small cell lung cancer are recruiting or ongoing.
Merck funded the study. Dr. Ott disclosed research funding from Merck and several other pharmaceutical companies, and advisory or consulting relationships with several companies, excluding Merck.
One patient died of treatment-related mesenteric ischemia, reported Patrick A. Ott, MD, of Dana-Farber Cancer Institute in Boston, and his associates. Nonetheless, with an objective response rate of 33% and a median duration of response of 19 months, the checkpoint inhibitor “demonstrated a favorable safety profile and promising durable clinical activity,” they concluded.
Study participants received pembrolizumab (10 mg/kg) every 2 weeks for 24 months or until disease progression or intolerable toxicity occurred. After a median follow-up of 9.8 months (range, 0.5-24 months), one patient (4%) had a complete response, and seven (29%) had partial responses. The median onset of response was 2 months, and responses lasted from 3.6 to 20 months, Dr. Ott and his associates reported (J Clin Oncol. 2017 Aug 16. doi: 10.1200/JCO.2017.72.5069). Two-thirds of patients developed treatment-related adverse events, most often arthralgia, asthenia, rash, diarrhea, and fatigue. Two patients developed grade 3 or worse treatment-related adverse events, including a 65-year-old man with small cell lung cancer and liver metastasis who developed grade 3 bilirubin elevation, and a 58-year-old woman with a history of sleeve gastrectomy who developed grade 3 asthenia, grade 5 colitis, and intestinal ischemia.
The patient who died had received 10 cycles of pembrolizumab, was hospitalized with abdominal pain, nausea, and vomiting, and was discharged home with a diagnosis of food intolerance, the researchers reported. She received an 11th cycle of pembrolizumab and was readmitted with abdominal pain. A rectal biopsy showed chronic colitis. She received systemic corticosteroids and was discharged, was admitted to a different hospital several weeks later with diffuse abdominal pain and septic shock, and subsequently died. “Mesenteric ischemia resulted in death,” the researchers wrote. “The cause of the colitis and intestinal ischemia was reported as probably related to pembrolizumab.”
Pembrolizumab (Keytruda) is a programmed death receptor–1 blocking antibody approved for treating non–small cell lung cancer, head and neck squamous cell cancer, classical Hodgkin lymphoma, urothelial carcinoma, and microsatellite instability–high cancer or mismatch repair deficient solid tumors. Treatment with the checkpoint inhibitor led to grade 5 treatment-related adverse events in other trials. Most recently, in July 2017, the Food and Drug Administration placed clinical holds on phase 1 and phase 3 studies of pembrolizumab for treating multiple myeloma after more patients died in the pembrolizumab arms than did in the comparison arms. Pembrolizumab also recently came up short in a phase 3 trial of patients with head and neck cancer, although it has kept its FDA label for this indication. Multiple trials of pembrolizumab for small cell lung cancer are recruiting or ongoing.
Merck funded the study. Dr. Ott disclosed research funding from Merck and several other pharmaceutical companies, and advisory or consulting relationships with several companies, excluding Merck.
One patient died of treatment-related mesenteric ischemia, reported Patrick A. Ott, MD, of Dana-Farber Cancer Institute in Boston, and his associates. Nonetheless, with an objective response rate of 33% and a median duration of response of 19 months, the checkpoint inhibitor “demonstrated a favorable safety profile and promising durable clinical activity,” they concluded.
Study participants received pembrolizumab (10 mg/kg) every 2 weeks for 24 months or until disease progression or intolerable toxicity occurred. After a median follow-up of 9.8 months (range, 0.5-24 months), one patient (4%) had a complete response, and seven (29%) had partial responses. The median onset of response was 2 months, and responses lasted from 3.6 to 20 months, Dr. Ott and his associates reported (J Clin Oncol. 2017 Aug 16. doi: 10.1200/JCO.2017.72.5069). Two-thirds of patients developed treatment-related adverse events, most often arthralgia, asthenia, rash, diarrhea, and fatigue. Two patients developed grade 3 or worse treatment-related adverse events, including a 65-year-old man with small cell lung cancer and liver metastasis who developed grade 3 bilirubin elevation, and a 58-year-old woman with a history of sleeve gastrectomy who developed grade 3 asthenia, grade 5 colitis, and intestinal ischemia.
The patient who died had received 10 cycles of pembrolizumab, was hospitalized with abdominal pain, nausea, and vomiting, and was discharged home with a diagnosis of food intolerance, the researchers reported. She received an 11th cycle of pembrolizumab and was readmitted with abdominal pain. A rectal biopsy showed chronic colitis. She received systemic corticosteroids and was discharged, was admitted to a different hospital several weeks later with diffuse abdominal pain and septic shock, and subsequently died. “Mesenteric ischemia resulted in death,” the researchers wrote. “The cause of the colitis and intestinal ischemia was reported as probably related to pembrolizumab.”
Pembrolizumab (Keytruda) is a programmed death receptor–1 blocking antibody approved for treating non–small cell lung cancer, head and neck squamous cell cancer, classical Hodgkin lymphoma, urothelial carcinoma, and microsatellite instability–high cancer or mismatch repair deficient solid tumors. Treatment with the checkpoint inhibitor led to grade 5 treatment-related adverse events in other trials. Most recently, in July 2017, the Food and Drug Administration placed clinical holds on phase 1 and phase 3 studies of pembrolizumab for treating multiple myeloma after more patients died in the pembrolizumab arms than did in the comparison arms. Pembrolizumab also recently came up short in a phase 3 trial of patients with head and neck cancer, although it has kept its FDA label for this indication. Multiple trials of pembrolizumab for small cell lung cancer are recruiting or ongoing.
Merck funded the study. Dr. Ott disclosed research funding from Merck and several other pharmaceutical companies, and advisory or consulting relationships with several companies, excluding Merck.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Pembrolizumab showed antitumor activity and was usually safe for treating extensive-stage small cell lung cancer.
Major finding: The objective response rate was 33%. Two patients developed grade 3 or worse treatment-related adverse events, which included fatal mesenteric ischemia and colitis.
Data source: A phase 1b open-label trial of 24 patients with PD-L1–positive extensive-stage small cell lung cancer.
Disclosures: Merck funded the study. Dr. Ott disclosed research funding from Merck and several other pharmaceutical companies, and advisory or consulting relationships with several companies, excluding Merck.
Comparison of Anterior and Posterior Corticosteroid Injections for Pain Relief and Functional Improvement in Shoulder Impingement Syndrome
Take-Home Points
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months
CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used.
Clinical response to CSI may not depend on injection accuracy.
Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
Shoulder pain, a common clinical problem, occurs in 7% to 34% of the general population and in 21% of people older than 70 years.1 Subacromial impingement refers to shoulder pain resulting from mechanical impingement of the rotator cuff underneath the coracoacromial arch between the acromion and the humeral head.2,3 Subacromial impingement syndrome (SIS) is the most common cause of shoulder pain, resulting in significant functional deficits and disability.3
Treatment options for SIS include conservative modalities such as use of nonsteroidal anti-inflammatory drugs, physical therapy (PT), and subacromial corticosteroid injections (CSIs). Studies have found short- and long-term improvement in pain, function, and range of motion after CSI.4-8 Subacromial CSI can be administered through an anterior or a posterior route.4,9 There have been several studies of the accuracy of anterior and posterior CSIs,10-12 with 2 studies finding similar accuracy for these routes.10,11 However, there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12
Although the accuracy of anterior and posterior routes has been studied, their effect on clinical outcomes has not. We conducted a study to understand the effects of anterior and posterior CSIs on SIS. As one of the accuracy studies suggested anterior CSI is more accurate—the anterior route was theorized to provide easier access to the subacromial space12—we hypothesized patients treated with anterior CSI would have superior clinical outcomes 6 months after injection.12,13
Materials and Methods
Study Participants and Randomization
After this study received Institutional Review Board approval, patients with shoulder pain of more than 3 months’ duration and consistent with SIS were screened for inclusion. Eligible patients had pain in the anterior biceps and over the top of the shoulder with overhead activities as well as one or more clinical findings on physical examination: Hawkins-Kennedy sign, Neer sign, painful arc, and infraspinatus pain (pain with external rotation).
Patients were excluded if their history included prior subacromial CSI, adhesive capsulitis (inability to passively abduct shoulder to 90° with scapular stabilization), calcific tendonitis, radiographic evidence of os acromiale, cervical radiculopathy, Spurling sign, neck pain, radiating arm pain or numbness, sensory deficits, or neck and upper extremity motor dysfunction. Also excluded were patients with full-thickness rotator cuff tear, weakness on arm elevation, positive "drop arm sign," or high-riding humerus on standing shoulder radiograph. Patients who had work-related injuries or who were involved in worker compensation were excluded as well.
Enrolled patients were randomly assigned (with use of a computer-based random number generator) to receive either anterior CSI or posterior CSI.
Injection Procedures
All patients were administered 5 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone by 2 board-certified orthopedic surgeons using a 22-gauge 1½-inch needle. For patients who received their subacromial CSI by the anterior route, the arm was held in 0° of abduction and 20° of external rotation. The needle was inserted medial to the humeral head, lateral to the coracoid process, beginning 1 cm inferior to the clavicle with the needle directed posteriorly and laterally toward the acromion.10 For patients who received their CSI by the posterior route, the arm was held in 0° of abduction, the posterolateral corner of the acromion was identified by palpation, and the needle was inserted 1 cm inferior and medial to this point with the needle directed anteriorly and laterally toward the acromion.10,12 In both groups, the subacromial space was identified when a drop in pressure was felt during needle insertion. Accuracy was assessed post hoc by asking patients to grade their response to the injection on a visual analog scale (VAS); VAS score was used as a surrogate for improvement. All patients had a positive Neer test: Pain decreased with impingement maneuvers immediately after injection.
All patients were referred for PT provided according to an evidence-based rehabilitation protocol.14 This program emphasized range of motion with shoulder shrugs, scapular retraction, and pendulum exercises; flexibility with stretching exercises targeting the anterior and posterior aspects of the shoulder and cane stretching for forward elevation and external rotation; and strength with strengthening exercises involving the rotator cuff and scapular stabilizers.
Outcome Measures
Pain was measured with VAS scores and function with Single Assessment Numeric Evaluation (SANE) scores. The VAS is a validated outcome measure of pain intensity. A numeric version of the VAS was used: Patients selected the whole number, from 0 (no pain) to 10 (worst possible pain), that best reflected their pain intensity. On SANE, another validated outcome measure, patients rated their shoulder function as a percentage of normal, from 0% (no function possible) to 100% (perfect).15 Before injection, all patients were administered the VAS and SANE questionnaires to establish their baseline pain level and opinion of shoulder function. These measures were repeated 1, 3, and 6 months after injection. Telephone interviews were conducted at 1 month and 6 months. Patients were asked to return to clinic 3 months after injection as part of the standard of care. At 3 months, 47 (86%) of the 55 patients returned for follow-up and were administered the VAS and SANE questionnaires; the other 8 completed the questionnaires by telephone. At each time point, patients were asked to report on their participation in PT and/or adherence to their home exercise program.
Statistical Analysis
Power analysis performed with Student t test and a 2-sided level of P = .05 compared VAS pain scores between the anterior and posterior injection routes and found a mean (SD) difference of 1.4 (1.7).16 Power calculations made with nQuery Advisor Version 7.0 (Statistical Solutions) indicated a total sample size of 60 patients (30/group) would provide 80% power for detecting a significant difference assuming a 20% dropout rate.
Two-way mixed-model analysis of variance (ANOVA) was used to compare the anterior and posterior routes for statistical differences in both VAS pain scores and SANE function scores at baseline and 1, 3, and 6 months after injection. Likewise, time at baseline (just before injection)was compared with follow-up (1, 3, 6 months) with 2-way mixed-model ANOVA adjusting for anterior or posterior route. Multivariate analysis was performed to evaluate differences between baseline and 6-month follow-up with respect to anterior and posterior injection routes, controlling for age, sex, and body mass index (BMI) for VAS and SANE scores. Parametric testing methods were used for statistical analysis, which was performed with IBM SPSS Statistics Version 21.0 (IBM Corp). Significance was set at P < .05.
Results
Patient Characteristics
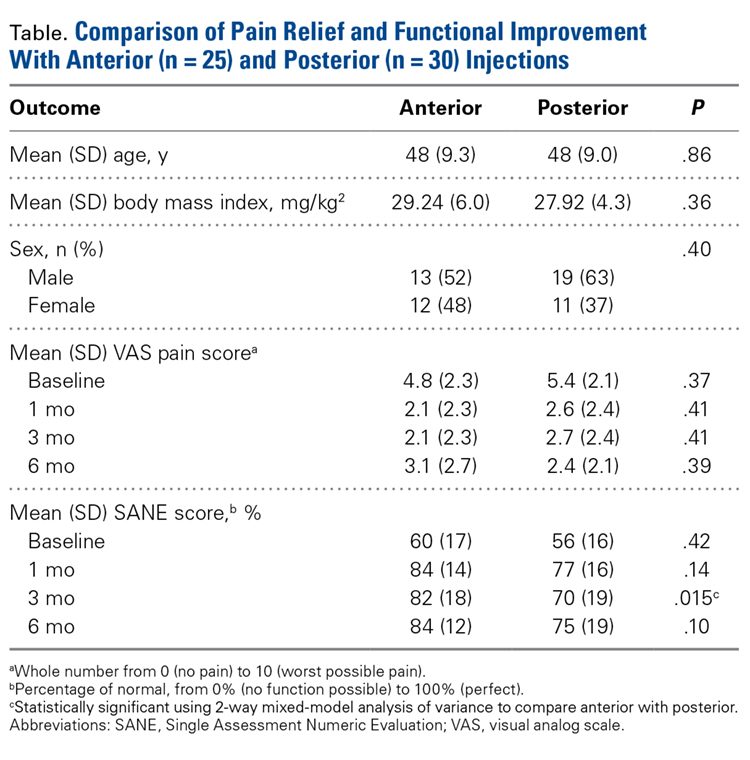
Of the 55 patients enrolled, 25 (46%) received anterior subacromial CSI and 30 (54%) received posterior CSI. All enrolled patients had a positive Neer impingement test immediately after injection. Mean (SD) age was 48 (9.3) years for anterior group patients and 48 (9.0) years for posterior group patients. There was no significant difference in age or BMI between the 2 groups (Table).
Five patients (9%) were excluded from the study after randomization and CSI: 2 for a full-thickness rotator cuff tear, 1 for a Bankart lesion, 1 for adhesive capsulitis, and 1 for a worker compensation claim.
One month after injection, 41 patients (75%) reported having engaged in PT as prescribed. Of the 47 patients (86%) who returned for the 3-month follow-up, 25 (46%) reported having engaged in PT between 1 month and 3 months after injection. Fourteen patients (26%) reported attending PT between 3 and 6 months post-injection.
Outcome Measures
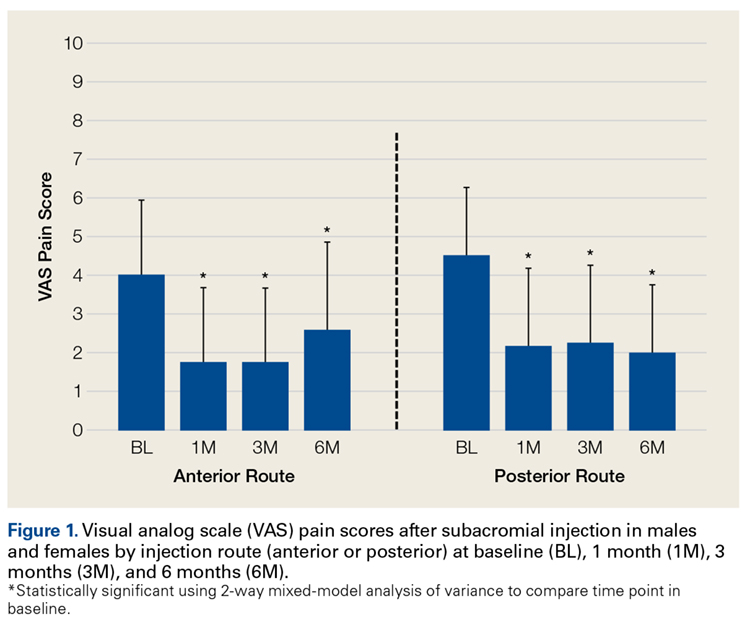
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in VAS scores between the anterior and posterior groups at any time point (P = .45). Both groups had highly significant pain reductions (anterior, F = 9.71, P < .001; posterior, F = 13.46, P < .001). Figure 1 shows mean VAS scores and significant reductions in pain 1, 3, and 6 months after injection (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of pain reduction over time, as indicated by a nonsignificant (P = .50) difference in slopes. These pain score reductions were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
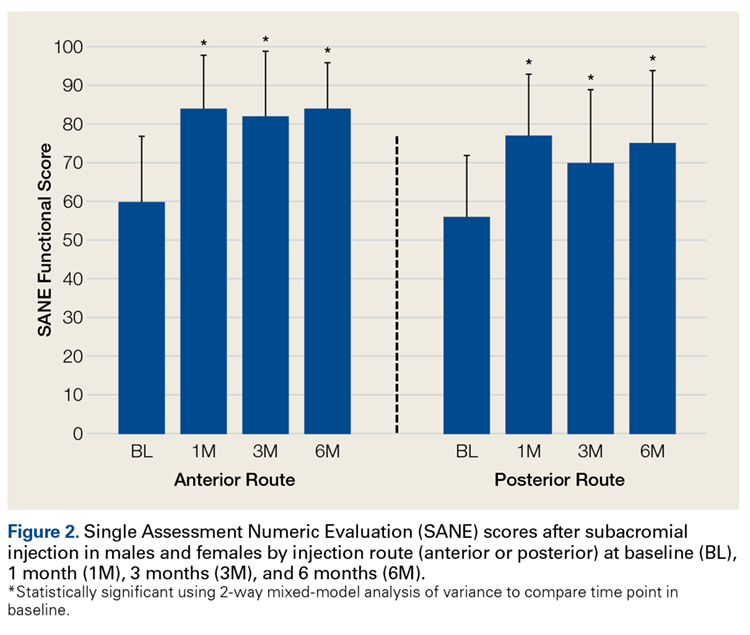
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in SANE scores between the anterior and posterior groups, except for a higher mean score in the anterior group at 3 months
(P = .02). There were no other group differences (P > .10 for all). Both groups had highly significant improvements in function (anterior, F = 17.34,
P < .001; posterior, F = 13.57, P < .001). Figure 2 shows mean SANE scores and significant improvement at 1, 3, and 6 months (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of improved function over time, as indicated by a nonsignificant (P = .51) difference in slopes. These function score improvements were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
From the results of this prospective randomized study, we concluded subacromial CSI significantly reduces pain and improves function regardless of route used. In addition, age, sex, and BMI do not significantly affect the efficacy of either anterior CSI or posterior CSI.
Discussion
In patients with SIS, anterior CSI and posterior CSI provided significant improvements in pain and function 1, 3, and 6 months after injection. These effects were independent of age, sex, BMI, and PT participation. There were no significant differences in outcomes between injection routes.
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.4-8 Although clinical outcomes are inconsistent, CSI can be used to address SIS symptoms in appropriate patients. Specifically, Blair and colleagues6 found that, CSI consisting of 4 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone was effective in alleviating shoulder pain and improving shoulder range of motion. Other authors have similarly reported improved outcomes after subacromial injection and short-term follow-up with PT.4,7,8 Our findings are consistent with these reports: CSI coupled with a structured rehabilitation program is effective in alleviating symptoms associated with acute or subacute SIS.
Numerous studies have found improved clinical outcomes after anterior CSI and after posterior CSI,6-8 but no study has directly compared the clinical impact of anterior CSI with that of posterior CSI—which suggests injection route may not affect ultimate clinical outcomes.
CSI accuracy has been studied extensively.10-12,17-20 Although 2 studies found similar accuracy for anterior and posterior routes,10,11 there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12 Collectively, these studies expose the inherent difficulty in treating shoulder pain with localized subacromial injection. Therapy may fail because of errant needle positioning. Two prospective studies found improved clinical outcomes with successful delivery of medication into the subacromial space.17,18 Poor clinical outcomes may result from inaccurate CSI.
In contrast to other clinical studies, our study found that injection route was not associated with differences in clinical response. In a prospective randomized clinical trial in which 75 patients received a subacromial injection, Marder and colleagues12 found anterior routes 84% accurate and posterior routes 56% accurate; they concluded acromion anatomy and subacromial bursa anatomy make posterior injections more difficult. As theorized by Gruson and colleagues,13 with use of an anterior route, the needle enters inferior to the concavity of the acromion and provides easier access to the subacromial space. This idea is in line with Marder and colleagues’12 conclusion that subacromial bursa anatomy provides a favorable environment for accurate CSI.
If accuracy is positively correlated with clinical improvement and anterior routes are more accurate, there should be a difference in response to posterior injections. Our results provide evidence that clinical response to CSI may not depend on injection accuracy. Perhaps merely placing the corticosteroid near the bursa is adequate for improving symptoms or perhaps some of the clinical improvement is due to the systemic effect of corticosteroids. These possibilities require further analysis.
Establishing the efficacy of CSI in SIS is difficult. The literature includes various study designs, different CSI indications and medication formulations, and varying emphasis on the role of organized PT. Rehabilitation has been found to alleviate joint pain by reducing inflammation,14 but data do not universally support this finding.21,22 Nevertheless, use of PT might explain the divergence in clinical outcomes reported by Marder and colleagues,12 who found anterior CSI more accurate than posterior CSI. In our practice, PT is recommended for all SIS patients, not only those who have CSI. Thus, our findings are framed within the context of successful CSI but may include patients who improved with PT alone. This issue raises the question of whether subacromial CSI should be guided by ultrasound. Ultrasound guidance can improve CSI accuracy and clinical outcomes,23-25 though the value of this benefit is debated.26
This study had several limitations. First, pain relief was patient reported. Second, the treatment plan involved CSI with PT but did not control for CSI used alone. PT, which is part of the standard of care for patients with SIS, added another degree of complexity to the study. Third, there may have been some variability in SIS severity (stage 1, 2, or 3). Fourth, although the study design controlled for various shoulder pathologies, advanced imaging, which could have provided diagnosis confirmation, was not available for all patients. Therefore, concurrent conditions may have confounded results. However, randomization was used to try to minimize this effect. Fifth, although injection routes were randomly assigned, the trial was not blinded. Sixth, the study was underpowered by 1 patient, as there was an estimated 20% dropout rate over 3 and 6 months of follow-up. However, we do not think our results were significantly affected.
Although more research is needed to fully describe the role of subacromial CSI in SIS, our study findings suggested that CSI using either an anterior or a posterior route creates a window of symptomatic relief in which patients may be able to engage in PT.
Conclusion
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months. No differences were found between anterior and posterior CSIs. In the context of this study, CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used. Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
1. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev. 2003;(1):CD004016.
2. Bell AD, Conaway D. Corticosteroid injections for painful shoulders. Int J Clin Pract. 2005;59(10):1178-1186.
3. Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18(5):369-379.
4. Akgün K, Birtane M, Akarirmak U. Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome? Clin Rheumatol. 2004;23(6):496-500.
5. Bhagra A, Syed H, Reed DA, et al. Efficacy of musculoskeletal injections by primary care providers in the office: a retrospective cohort study. Int J Gen Med. 2013;6:237-243.
6. Blair B, Rokito AS, Cuomo F, Jarolem K, Zuckerman JD. Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am. 1996;78(11):1685-1689.
7. Cummins CA, Sasso LM, Nicholson D. Impingement syndrome: temporal outcomes of nonoperative treatment.
J Shoulder Elbow Surg. 2009;18(2):172-177.
8. Yu C, Chen CH, Liu HT, Dai MH, Wang IC, Wang KC. Subacromial injections of corticosteroids and Xylocaine for painful subacromial impingement syndrome. Chang Gung Med J. 2006;29(5):474-478.
9. Codsi MJ. The painful shoulder: when to inject and when to refer. Cleve Clin J Med. 2007;74(7):473-474, 477-478, 480-482 passim.
10. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
11. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(15):61S-66S.
12. Marder RA, Kim SH, Labson JD, Hunter JC. Injection of the subacromial bursa in patients with rotator cuff syndrome: a prospective, randomized study comparing the effectiveness of different routes. J Bone Joint Surg Am. 2012;94(16):
1442-1447.
13. Gruson, KI, Ruchelsman DE, Zuckerman JD. Subacromial corticosteroid injections. J Shoulder Elbow Surg. 2008;17(1 suppl):118S-130S.
14. Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009;18(1):138-160.
15. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
16. Tashjian RZ, Deloach J, Porucznik CA, Powell AP. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease.
J Shoulder Elbow Surg. 2009;88(6):927-932.
17. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
18. Esenyel CZ, Esenyel M, Yeiltepe R, et al. The correlation between the accuracy of steroid injections and subsequent shoulder pain and function in subacromial impingement
syndrome [in Turkish]. Acta Orthop Traumatol Turc. 2003;37(1):
41-45.
19. Powell SE, Davis SM, Lee EH, et al. Accuracy of palpation-directed intra-articular glenohumeral injection confirmed by magnetic resonance arthrography. Arthroscopy. 2015;31(2):205-208.
20. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
21. Desmeules F, Côté CH, Frémont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review. Clin J Sport Med. 2003;13(3):176-182.
22. Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study. BMJ. 1997;314(7090):1320-1325.
23. Chen MJ, Lew HL, Hsu TC, et al. Ultrasound-guided shoulder injections in the treatment of subacromial bursitis. Am J Phys Med Rehabil. 2006;85(1):31-35.
24. Hsieh LF, Hsu WC, Lin YJ, Wu SH, Chang KC, Chang HL. Is ultrasound-guided injection more effective in chronic subacromial bursitis? Med Sci Sports Exerc. 2013;45(12):
2205-2213.
25. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
26. Hall S, Buchbinder R. Do imaging methods that guide needle placement improve outcome? Ann Rheum Dis. 2004;63(9):1007-1008.
Take-Home Points
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months
CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used.
Clinical response to CSI may not depend on injection accuracy.
Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
Shoulder pain, a common clinical problem, occurs in 7% to 34% of the general population and in 21% of people older than 70 years.1 Subacromial impingement refers to shoulder pain resulting from mechanical impingement of the rotator cuff underneath the coracoacromial arch between the acromion and the humeral head.2,3 Subacromial impingement syndrome (SIS) is the most common cause of shoulder pain, resulting in significant functional deficits and disability.3
Treatment options for SIS include conservative modalities such as use of nonsteroidal anti-inflammatory drugs, physical therapy (PT), and subacromial corticosteroid injections (CSIs). Studies have found short- and long-term improvement in pain, function, and range of motion after CSI.4-8 Subacromial CSI can be administered through an anterior or a posterior route.4,9 There have been several studies of the accuracy of anterior and posterior CSIs,10-12 with 2 studies finding similar accuracy for these routes.10,11 However, there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12
Although the accuracy of anterior and posterior routes has been studied, their effect on clinical outcomes has not. We conducted a study to understand the effects of anterior and posterior CSIs on SIS. As one of the accuracy studies suggested anterior CSI is more accurate—the anterior route was theorized to provide easier access to the subacromial space12—we hypothesized patients treated with anterior CSI would have superior clinical outcomes 6 months after injection.12,13
Materials and Methods
Study Participants and Randomization
After this study received Institutional Review Board approval, patients with shoulder pain of more than 3 months’ duration and consistent with SIS were screened for inclusion. Eligible patients had pain in the anterior biceps and over the top of the shoulder with overhead activities as well as one or more clinical findings on physical examination: Hawkins-Kennedy sign, Neer sign, painful arc, and infraspinatus pain (pain with external rotation).
Patients were excluded if their history included prior subacromial CSI, adhesive capsulitis (inability to passively abduct shoulder to 90° with scapular stabilization), calcific tendonitis, radiographic evidence of os acromiale, cervical radiculopathy, Spurling sign, neck pain, radiating arm pain or numbness, sensory deficits, or neck and upper extremity motor dysfunction. Also excluded were patients with full-thickness rotator cuff tear, weakness on arm elevation, positive "drop arm sign," or high-riding humerus on standing shoulder radiograph. Patients who had work-related injuries or who were involved in worker compensation were excluded as well.
Enrolled patients were randomly assigned (with use of a computer-based random number generator) to receive either anterior CSI or posterior CSI.
Injection Procedures
All patients were administered 5 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone by 2 board-certified orthopedic surgeons using a 22-gauge 1½-inch needle. For patients who received their subacromial CSI by the anterior route, the arm was held in 0° of abduction and 20° of external rotation. The needle was inserted medial to the humeral head, lateral to the coracoid process, beginning 1 cm inferior to the clavicle with the needle directed posteriorly and laterally toward the acromion.10 For patients who received their CSI by the posterior route, the arm was held in 0° of abduction, the posterolateral corner of the acromion was identified by palpation, and the needle was inserted 1 cm inferior and medial to this point with the needle directed anteriorly and laterally toward the acromion.10,12 In both groups, the subacromial space was identified when a drop in pressure was felt during needle insertion. Accuracy was assessed post hoc by asking patients to grade their response to the injection on a visual analog scale (VAS); VAS score was used as a surrogate for improvement. All patients had a positive Neer test: Pain decreased with impingement maneuvers immediately after injection.
All patients were referred for PT provided according to an evidence-based rehabilitation protocol.14 This program emphasized range of motion with shoulder shrugs, scapular retraction, and pendulum exercises; flexibility with stretching exercises targeting the anterior and posterior aspects of the shoulder and cane stretching for forward elevation and external rotation; and strength with strengthening exercises involving the rotator cuff and scapular stabilizers.
Outcome Measures
Pain was measured with VAS scores and function with Single Assessment Numeric Evaluation (SANE) scores. The VAS is a validated outcome measure of pain intensity. A numeric version of the VAS was used: Patients selected the whole number, from 0 (no pain) to 10 (worst possible pain), that best reflected their pain intensity. On SANE, another validated outcome measure, patients rated their shoulder function as a percentage of normal, from 0% (no function possible) to 100% (perfect).15 Before injection, all patients were administered the VAS and SANE questionnaires to establish their baseline pain level and opinion of shoulder function. These measures were repeated 1, 3, and 6 months after injection. Telephone interviews were conducted at 1 month and 6 months. Patients were asked to return to clinic 3 months after injection as part of the standard of care. At 3 months, 47 (86%) of the 55 patients returned for follow-up and were administered the VAS and SANE questionnaires; the other 8 completed the questionnaires by telephone. At each time point, patients were asked to report on their participation in PT and/or adherence to their home exercise program.
Statistical Analysis
Power analysis performed with Student t test and a 2-sided level of P = .05 compared VAS pain scores between the anterior and posterior injection routes and found a mean (SD) difference of 1.4 (1.7).16 Power calculations made with nQuery Advisor Version 7.0 (Statistical Solutions) indicated a total sample size of 60 patients (30/group) would provide 80% power for detecting a significant difference assuming a 20% dropout rate.
Two-way mixed-model analysis of variance (ANOVA) was used to compare the anterior and posterior routes for statistical differences in both VAS pain scores and SANE function scores at baseline and 1, 3, and 6 months after injection. Likewise, time at baseline (just before injection)was compared with follow-up (1, 3, 6 months) with 2-way mixed-model ANOVA adjusting for anterior or posterior route. Multivariate analysis was performed to evaluate differences between baseline and 6-month follow-up with respect to anterior and posterior injection routes, controlling for age, sex, and body mass index (BMI) for VAS and SANE scores. Parametric testing methods were used for statistical analysis, which was performed with IBM SPSS Statistics Version 21.0 (IBM Corp). Significance was set at P < .05.
Results
Patient Characteristics
Of the 55 patients enrolled, 25 (46%) received anterior subacromial CSI and 30 (54%) received posterior CSI. All enrolled patients had a positive Neer impingement test immediately after injection. Mean (SD) age was 48 (9.3) years for anterior group patients and 48 (9.0) years for posterior group patients. There was no significant difference in age or BMI between the 2 groups (Table).
Five patients (9%) were excluded from the study after randomization and CSI: 2 for a full-thickness rotator cuff tear, 1 for a Bankart lesion, 1 for adhesive capsulitis, and 1 for a worker compensation claim.
One month after injection, 41 patients (75%) reported having engaged in PT as prescribed. Of the 47 patients (86%) who returned for the 3-month follow-up, 25 (46%) reported having engaged in PT between 1 month and 3 months after injection. Fourteen patients (26%) reported attending PT between 3 and 6 months post-injection.
Outcome Measures
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in VAS scores between the anterior and posterior groups at any time point (P = .45). Both groups had highly significant pain reductions (anterior, F = 9.71, P < .001; posterior, F = 13.46, P < .001). Figure 1 shows mean VAS scores and significant reductions in pain 1, 3, and 6 months after injection (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of pain reduction over time, as indicated by a nonsignificant (P = .50) difference in slopes. These pain score reductions were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in SANE scores between the anterior and posterior groups, except for a higher mean score in the anterior group at 3 months
(P = .02). There were no other group differences (P > .10 for all). Both groups had highly significant improvements in function (anterior, F = 17.34,
P < .001; posterior, F = 13.57, P < .001). Figure 2 shows mean SANE scores and significant improvement at 1, 3, and 6 months (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of improved function over time, as indicated by a nonsignificant (P = .51) difference in slopes. These function score improvements were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
From the results of this prospective randomized study, we concluded subacromial CSI significantly reduces pain and improves function regardless of route used. In addition, age, sex, and BMI do not significantly affect the efficacy of either anterior CSI or posterior CSI.
Discussion
In patients with SIS, anterior CSI and posterior CSI provided significant improvements in pain and function 1, 3, and 6 months after injection. These effects were independent of age, sex, BMI, and PT participation. There were no significant differences in outcomes between injection routes.
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.4-8 Although clinical outcomes are inconsistent, CSI can be used to address SIS symptoms in appropriate patients. Specifically, Blair and colleagues6 found that, CSI consisting of 4 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone was effective in alleviating shoulder pain and improving shoulder range of motion. Other authors have similarly reported improved outcomes after subacromial injection and short-term follow-up with PT.4,7,8 Our findings are consistent with these reports: CSI coupled with a structured rehabilitation program is effective in alleviating symptoms associated with acute or subacute SIS.
Numerous studies have found improved clinical outcomes after anterior CSI and after posterior CSI,6-8 but no study has directly compared the clinical impact of anterior CSI with that of posterior CSI—which suggests injection route may not affect ultimate clinical outcomes.
CSI accuracy has been studied extensively.10-12,17-20 Although 2 studies found similar accuracy for anterior and posterior routes,10,11 there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12 Collectively, these studies expose the inherent difficulty in treating shoulder pain with localized subacromial injection. Therapy may fail because of errant needle positioning. Two prospective studies found improved clinical outcomes with successful delivery of medication into the subacromial space.17,18 Poor clinical outcomes may result from inaccurate CSI.
In contrast to other clinical studies, our study found that injection route was not associated with differences in clinical response. In a prospective randomized clinical trial in which 75 patients received a subacromial injection, Marder and colleagues12 found anterior routes 84% accurate and posterior routes 56% accurate; they concluded acromion anatomy and subacromial bursa anatomy make posterior injections more difficult. As theorized by Gruson and colleagues,13 with use of an anterior route, the needle enters inferior to the concavity of the acromion and provides easier access to the subacromial space. This idea is in line with Marder and colleagues’12 conclusion that subacromial bursa anatomy provides a favorable environment for accurate CSI.
If accuracy is positively correlated with clinical improvement and anterior routes are more accurate, there should be a difference in response to posterior injections. Our results provide evidence that clinical response to CSI may not depend on injection accuracy. Perhaps merely placing the corticosteroid near the bursa is adequate for improving symptoms or perhaps some of the clinical improvement is due to the systemic effect of corticosteroids. These possibilities require further analysis.
Establishing the efficacy of CSI in SIS is difficult. The literature includes various study designs, different CSI indications and medication formulations, and varying emphasis on the role of organized PT. Rehabilitation has been found to alleviate joint pain by reducing inflammation,14 but data do not universally support this finding.21,22 Nevertheless, use of PT might explain the divergence in clinical outcomes reported by Marder and colleagues,12 who found anterior CSI more accurate than posterior CSI. In our practice, PT is recommended for all SIS patients, not only those who have CSI. Thus, our findings are framed within the context of successful CSI but may include patients who improved with PT alone. This issue raises the question of whether subacromial CSI should be guided by ultrasound. Ultrasound guidance can improve CSI accuracy and clinical outcomes,23-25 though the value of this benefit is debated.26
This study had several limitations. First, pain relief was patient reported. Second, the treatment plan involved CSI with PT but did not control for CSI used alone. PT, which is part of the standard of care for patients with SIS, added another degree of complexity to the study. Third, there may have been some variability in SIS severity (stage 1, 2, or 3). Fourth, although the study design controlled for various shoulder pathologies, advanced imaging, which could have provided diagnosis confirmation, was not available for all patients. Therefore, concurrent conditions may have confounded results. However, randomization was used to try to minimize this effect. Fifth, although injection routes were randomly assigned, the trial was not blinded. Sixth, the study was underpowered by 1 patient, as there was an estimated 20% dropout rate over 3 and 6 months of follow-up. However, we do not think our results were significantly affected.
Although more research is needed to fully describe the role of subacromial CSI in SIS, our study findings suggested that CSI using either an anterior or a posterior route creates a window of symptomatic relief in which patients may be able to engage in PT.
Conclusion
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months. No differences were found between anterior and posterior CSIs. In the context of this study, CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used. Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
Take-Home Points
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months
CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used.
Clinical response to CSI may not depend on injection accuracy.
Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
Shoulder pain, a common clinical problem, occurs in 7% to 34% of the general population and in 21% of people older than 70 years.1 Subacromial impingement refers to shoulder pain resulting from mechanical impingement of the rotator cuff underneath the coracoacromial arch between the acromion and the humeral head.2,3 Subacromial impingement syndrome (SIS) is the most common cause of shoulder pain, resulting in significant functional deficits and disability.3
Treatment options for SIS include conservative modalities such as use of nonsteroidal anti-inflammatory drugs, physical therapy (PT), and subacromial corticosteroid injections (CSIs). Studies have found short- and long-term improvement in pain, function, and range of motion after CSI.4-8 Subacromial CSI can be administered through an anterior or a posterior route.4,9 There have been several studies of the accuracy of anterior and posterior CSIs,10-12 with 2 studies finding similar accuracy for these routes.10,11 However, there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12
Although the accuracy of anterior and posterior routes has been studied, their effect on clinical outcomes has not. We conducted a study to understand the effects of anterior and posterior CSIs on SIS. As one of the accuracy studies suggested anterior CSI is more accurate—the anterior route was theorized to provide easier access to the subacromial space12—we hypothesized patients treated with anterior CSI would have superior clinical outcomes 6 months after injection.12,13
Materials and Methods
Study Participants and Randomization
After this study received Institutional Review Board approval, patients with shoulder pain of more than 3 months’ duration and consistent with SIS were screened for inclusion. Eligible patients had pain in the anterior biceps and over the top of the shoulder with overhead activities as well as one or more clinical findings on physical examination: Hawkins-Kennedy sign, Neer sign, painful arc, and infraspinatus pain (pain with external rotation).
Patients were excluded if their history included prior subacromial CSI, adhesive capsulitis (inability to passively abduct shoulder to 90° with scapular stabilization), calcific tendonitis, radiographic evidence of os acromiale, cervical radiculopathy, Spurling sign, neck pain, radiating arm pain or numbness, sensory deficits, or neck and upper extremity motor dysfunction. Also excluded were patients with full-thickness rotator cuff tear, weakness on arm elevation, positive "drop arm sign," or high-riding humerus on standing shoulder radiograph. Patients who had work-related injuries or who were involved in worker compensation were excluded as well.
Enrolled patients were randomly assigned (with use of a computer-based random number generator) to receive either anterior CSI or posterior CSI.
Injection Procedures
All patients were administered 5 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone by 2 board-certified orthopedic surgeons using a 22-gauge 1½-inch needle. For patients who received their subacromial CSI by the anterior route, the arm was held in 0° of abduction and 20° of external rotation. The needle was inserted medial to the humeral head, lateral to the coracoid process, beginning 1 cm inferior to the clavicle with the needle directed posteriorly and laterally toward the acromion.10 For patients who received their CSI by the posterior route, the arm was held in 0° of abduction, the posterolateral corner of the acromion was identified by palpation, and the needle was inserted 1 cm inferior and medial to this point with the needle directed anteriorly and laterally toward the acromion.10,12 In both groups, the subacromial space was identified when a drop in pressure was felt during needle insertion. Accuracy was assessed post hoc by asking patients to grade their response to the injection on a visual analog scale (VAS); VAS score was used as a surrogate for improvement. All patients had a positive Neer test: Pain decreased with impingement maneuvers immediately after injection.
All patients were referred for PT provided according to an evidence-based rehabilitation protocol.14 This program emphasized range of motion with shoulder shrugs, scapular retraction, and pendulum exercises; flexibility with stretching exercises targeting the anterior and posterior aspects of the shoulder and cane stretching for forward elevation and external rotation; and strength with strengthening exercises involving the rotator cuff and scapular stabilizers.
Outcome Measures
Pain was measured with VAS scores and function with Single Assessment Numeric Evaluation (SANE) scores. The VAS is a validated outcome measure of pain intensity. A numeric version of the VAS was used: Patients selected the whole number, from 0 (no pain) to 10 (worst possible pain), that best reflected their pain intensity. On SANE, another validated outcome measure, patients rated their shoulder function as a percentage of normal, from 0% (no function possible) to 100% (perfect).15 Before injection, all patients were administered the VAS and SANE questionnaires to establish their baseline pain level and opinion of shoulder function. These measures were repeated 1, 3, and 6 months after injection. Telephone interviews were conducted at 1 month and 6 months. Patients were asked to return to clinic 3 months after injection as part of the standard of care. At 3 months, 47 (86%) of the 55 patients returned for follow-up and were administered the VAS and SANE questionnaires; the other 8 completed the questionnaires by telephone. At each time point, patients were asked to report on their participation in PT and/or adherence to their home exercise program.
Statistical Analysis
Power analysis performed with Student t test and a 2-sided level of P = .05 compared VAS pain scores between the anterior and posterior injection routes and found a mean (SD) difference of 1.4 (1.7).16 Power calculations made with nQuery Advisor Version 7.0 (Statistical Solutions) indicated a total sample size of 60 patients (30/group) would provide 80% power for detecting a significant difference assuming a 20% dropout rate.
Two-way mixed-model analysis of variance (ANOVA) was used to compare the anterior and posterior routes for statistical differences in both VAS pain scores and SANE function scores at baseline and 1, 3, and 6 months after injection. Likewise, time at baseline (just before injection)was compared with follow-up (1, 3, 6 months) with 2-way mixed-model ANOVA adjusting for anterior or posterior route. Multivariate analysis was performed to evaluate differences between baseline and 6-month follow-up with respect to anterior and posterior injection routes, controlling for age, sex, and body mass index (BMI) for VAS and SANE scores. Parametric testing methods were used for statistical analysis, which was performed with IBM SPSS Statistics Version 21.0 (IBM Corp). Significance was set at P < .05.
Results
Patient Characteristics
Of the 55 patients enrolled, 25 (46%) received anterior subacromial CSI and 30 (54%) received posterior CSI. All enrolled patients had a positive Neer impingement test immediately after injection. Mean (SD) age was 48 (9.3) years for anterior group patients and 48 (9.0) years for posterior group patients. There was no significant difference in age or BMI between the 2 groups (Table).
Five patients (9%) were excluded from the study after randomization and CSI: 2 for a full-thickness rotator cuff tear, 1 for a Bankart lesion, 1 for adhesive capsulitis, and 1 for a worker compensation claim.
One month after injection, 41 patients (75%) reported having engaged in PT as prescribed. Of the 47 patients (86%) who returned for the 3-month follow-up, 25 (46%) reported having engaged in PT between 1 month and 3 months after injection. Fourteen patients (26%) reported attending PT between 3 and 6 months post-injection.
Outcome Measures
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in VAS scores between the anterior and posterior groups at any time point (P = .45). Both groups had highly significant pain reductions (anterior, F = 9.71, P < .001; posterior, F = 13.46, P < .001). Figure 1 shows mean VAS scores and significant reductions in pain 1, 3, and 6 months after injection (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of pain reduction over time, as indicated by a nonsignificant (P = .50) difference in slopes. These pain score reductions were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
Two-way repeated-measures ANOVA with age, sex, and BMI included as covariates revealed no significant differences in SANE scores between the anterior and posterior groups, except for a higher mean score in the anterior group at 3 months
(P = .02). There were no other group differences (P > .10 for all). Both groups had highly significant improvements in function (anterior, F = 17.34,
P < .001; posterior, F = 13.57, P < .001). Figure 2 shows mean SANE scores and significant improvement at 1, 3, and 6 months (see asterisks for anterior and posterior groups; P < .001 for all). The groups had parallel rates of improved function over time, as indicated by a nonsignificant (P = .51) difference in slopes. These function score improvements were significant for both injection routes and were independent of age, sex, and BMI (P > .05 for all).
From the results of this prospective randomized study, we concluded subacromial CSI significantly reduces pain and improves function regardless of route used. In addition, age, sex, and BMI do not significantly affect the efficacy of either anterior CSI or posterior CSI.
Discussion
In patients with SIS, anterior CSI and posterior CSI provided significant improvements in pain and function 1, 3, and 6 months after injection. These effects were independent of age, sex, BMI, and PT participation. There were no significant differences in outcomes between injection routes.
When conservative treatments for SIS do not resolve symptoms, inflammation and pain can be reduced with use of subacromial CSI.4-8 Although clinical outcomes are inconsistent, CSI can be used to address SIS symptoms in appropriate patients. Specifically, Blair and colleagues6 found that, CSI consisting of 4 mL of lidocaine 1% (without epinephrine) and 2 mL (80 mg) of triamcinolone was effective in alleviating shoulder pain and improving shoulder range of motion. Other authors have similarly reported improved outcomes after subacromial injection and short-term follow-up with PT.4,7,8 Our findings are consistent with these reports: CSI coupled with a structured rehabilitation program is effective in alleviating symptoms associated with acute or subacute SIS.
Numerous studies have found improved clinical outcomes after anterior CSI and after posterior CSI,6-8 but no study has directly compared the clinical impact of anterior CSI with that of posterior CSI—which suggests injection route may not affect ultimate clinical outcomes.
CSI accuracy has been studied extensively.10-12,17-20 Although 2 studies found similar accuracy for anterior and posterior routes,10,11 there may be a sex difference: In women, a posterior route may be less accurate than an anterior or a lateral route.12 Collectively, these studies expose the inherent difficulty in treating shoulder pain with localized subacromial injection. Therapy may fail because of errant needle positioning. Two prospective studies found improved clinical outcomes with successful delivery of medication into the subacromial space.17,18 Poor clinical outcomes may result from inaccurate CSI.
In contrast to other clinical studies, our study found that injection route was not associated with differences in clinical response. In a prospective randomized clinical trial in which 75 patients received a subacromial injection, Marder and colleagues12 found anterior routes 84% accurate and posterior routes 56% accurate; they concluded acromion anatomy and subacromial bursa anatomy make posterior injections more difficult. As theorized by Gruson and colleagues,13 with use of an anterior route, the needle enters inferior to the concavity of the acromion and provides easier access to the subacromial space. This idea is in line with Marder and colleagues’12 conclusion that subacromial bursa anatomy provides a favorable environment for accurate CSI.
If accuracy is positively correlated with clinical improvement and anterior routes are more accurate, there should be a difference in response to posterior injections. Our results provide evidence that clinical response to CSI may not depend on injection accuracy. Perhaps merely placing the corticosteroid near the bursa is adequate for improving symptoms or perhaps some of the clinical improvement is due to the systemic effect of corticosteroids. These possibilities require further analysis.
Establishing the efficacy of CSI in SIS is difficult. The literature includes various study designs, different CSI indications and medication formulations, and varying emphasis on the role of organized PT. Rehabilitation has been found to alleviate joint pain by reducing inflammation,14 but data do not universally support this finding.21,22 Nevertheless, use of PT might explain the divergence in clinical outcomes reported by Marder and colleagues,12 who found anterior CSI more accurate than posterior CSI. In our practice, PT is recommended for all SIS patients, not only those who have CSI. Thus, our findings are framed within the context of successful CSI but may include patients who improved with PT alone. This issue raises the question of whether subacromial CSI should be guided by ultrasound. Ultrasound guidance can improve CSI accuracy and clinical outcomes,23-25 though the value of this benefit is debated.26
This study had several limitations. First, pain relief was patient reported. Second, the treatment plan involved CSI with PT but did not control for CSI used alone. PT, which is part of the standard of care for patients with SIS, added another degree of complexity to the study. Third, there may have been some variability in SIS severity (stage 1, 2, or 3). Fourth, although the study design controlled for various shoulder pathologies, advanced imaging, which could have provided diagnosis confirmation, was not available for all patients. Therefore, concurrent conditions may have confounded results. However, randomization was used to try to minimize this effect. Fifth, although injection routes were randomly assigned, the trial was not blinded. Sixth, the study was underpowered by 1 patient, as there was an estimated 20% dropout rate over 3 and 6 months of follow-up. However, we do not think our results were significantly affected.
Although more research is needed to fully describe the role of subacromial CSI in SIS, our study findings suggested that CSI using either an anterior or a posterior route creates a window of symptomatic relief in which patients may be able to engage in PT.
Conclusion
Both anterior CSI and posterior CSI significantly improved pain and function for up to 6 months. No differences were found between anterior and posterior CSIs. In the context of this study, CSI combined with structured PT produced significant improvement in pain and function in patients with SIS, regardless of injection route used. Clinicians should rely on their clinical acumen when selecting injection routes, as anterior and posterior are both beneficial.
1. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev. 2003;(1):CD004016.
2. Bell AD, Conaway D. Corticosteroid injections for painful shoulders. Int J Clin Pract. 2005;59(10):1178-1186.
3. Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18(5):369-379.
4. Akgün K, Birtane M, Akarirmak U. Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome? Clin Rheumatol. 2004;23(6):496-500.
5. Bhagra A, Syed H, Reed DA, et al. Efficacy of musculoskeletal injections by primary care providers in the office: a retrospective cohort study. Int J Gen Med. 2013;6:237-243.
6. Blair B, Rokito AS, Cuomo F, Jarolem K, Zuckerman JD. Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am. 1996;78(11):1685-1689.
7. Cummins CA, Sasso LM, Nicholson D. Impingement syndrome: temporal outcomes of nonoperative treatment.
J Shoulder Elbow Surg. 2009;18(2):172-177.
8. Yu C, Chen CH, Liu HT, Dai MH, Wang IC, Wang KC. Subacromial injections of corticosteroids and Xylocaine for painful subacromial impingement syndrome. Chang Gung Med J. 2006;29(5):474-478.
9. Codsi MJ. The painful shoulder: when to inject and when to refer. Cleve Clin J Med. 2007;74(7):473-474, 477-478, 480-482 passim.
10. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
11. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(15):61S-66S.
12. Marder RA, Kim SH, Labson JD, Hunter JC. Injection of the subacromial bursa in patients with rotator cuff syndrome: a prospective, randomized study comparing the effectiveness of different routes. J Bone Joint Surg Am. 2012;94(16):
1442-1447.
13. Gruson, KI, Ruchelsman DE, Zuckerman JD. Subacromial corticosteroid injections. J Shoulder Elbow Surg. 2008;17(1 suppl):118S-130S.
14. Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009;18(1):138-160.
15. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
16. Tashjian RZ, Deloach J, Porucznik CA, Powell AP. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease.
J Shoulder Elbow Surg. 2009;88(6):927-932.
17. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
18. Esenyel CZ, Esenyel M, Yeiltepe R, et al. The correlation between the accuracy of steroid injections and subsequent shoulder pain and function in subacromial impingement
syndrome [in Turkish]. Acta Orthop Traumatol Turc. 2003;37(1):
41-45.
19. Powell SE, Davis SM, Lee EH, et al. Accuracy of palpation-directed intra-articular glenohumeral injection confirmed by magnetic resonance arthrography. Arthroscopy. 2015;31(2):205-208.
20. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
21. Desmeules F, Côté CH, Frémont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review. Clin J Sport Med. 2003;13(3):176-182.
22. Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study. BMJ. 1997;314(7090):1320-1325.
23. Chen MJ, Lew HL, Hsu TC, et al. Ultrasound-guided shoulder injections in the treatment of subacromial bursitis. Am J Phys Med Rehabil. 2006;85(1):31-35.
24. Hsieh LF, Hsu WC, Lin YJ, Wu SH, Chang KC, Chang HL. Is ultrasound-guided injection more effective in chronic subacromial bursitis? Med Sci Sports Exerc. 2013;45(12):
2205-2213.
25. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
26. Hall S, Buchbinder R. Do imaging methods that guide needle placement improve outcome? Ann Rheum Dis. 2004;63(9):1007-1008.
1. Buchbinder R, Green S, Youd JM. Corticosteroid injections for shoulder pain. Cochrane Database Syst Rev. 2003;(1):CD004016.
2. Bell AD, Conaway D. Corticosteroid injections for painful shoulders. Int J Clin Pract. 2005;59(10):1178-1186.
3. Michener LA, McClure PW, Karduna AR. Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clin Biomech. 2003;18(5):369-379.
4. Akgün K, Birtane M, Akarirmak U. Is local subacromial corticosteroid injection beneficial in subacromial impingement syndrome? Clin Rheumatol. 2004;23(6):496-500.
5. Bhagra A, Syed H, Reed DA, et al. Efficacy of musculoskeletal injections by primary care providers in the office: a retrospective cohort study. Int J Gen Med. 2013;6:237-243.
6. Blair B, Rokito AS, Cuomo F, Jarolem K, Zuckerman JD. Efficacy of injections of corticosteroids for subacromial impingement syndrome. J Bone Joint Surg Am. 1996;78(11):1685-1689.
7. Cummins CA, Sasso LM, Nicholson D. Impingement syndrome: temporal outcomes of nonoperative treatment.
J Shoulder Elbow Surg. 2009;18(2):172-177.
8. Yu C, Chen CH, Liu HT, Dai MH, Wang IC, Wang KC. Subacromial injections of corticosteroids and Xylocaine for painful subacromial impingement syndrome. Chang Gung Med J. 2006;29(5):474-478.
9. Codsi MJ. The painful shoulder: when to inject and when to refer. Cleve Clin J Med. 2007;74(7):473-474, 477-478, 480-482 passim.
10. Henkus HE, Cobben LP, Coerkamp EG, Nelissen RG, van Arkel ER. The accuracy of subacromial injections: a prospective randomized magnetic resonance imaging study. Arthroscopy. 2006;22(3):277-282.
11. Kang MN, Rizio L, Prybicien M, Middlemas DA, Blacksin MF. The accuracy of subacromial corticosteroid injections: a comparison of multiple methods. J Shoulder Elbow Surg. 2008;17(15):61S-66S.
12. Marder RA, Kim SH, Labson JD, Hunter JC. Injection of the subacromial bursa in patients with rotator cuff syndrome: a prospective, randomized study comparing the effectiveness of different routes. J Bone Joint Surg Am. 2012;94(16):
1442-1447.
13. Gruson, KI, Ruchelsman DE, Zuckerman JD. Subacromial corticosteroid injections. J Shoulder Elbow Surg. 2008;17(1 suppl):118S-130S.
14. Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009;18(1):138-160.
15. Williams GN, Gangel TJ, Arciero RA, Uhorchak JM, Taylor DC. Comparison of the Single Assessment Numeric Evaluation method and two shoulder rating scales. Outcomes measures after shoulder surgery. Am J Sports Med. 1999;27(2):214-221.
16. Tashjian RZ, Deloach J, Porucznik CA, Powell AP. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease.
J Shoulder Elbow Surg. 2009;88(6):927-932.
17. Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of the accuracy of steroid placement with clinical outcome in patients with shoulder symptoms. Ann Rheum Dis. 1997;56(1):59-63.
18. Esenyel CZ, Esenyel M, Yeiltepe R, et al. The correlation between the accuracy of steroid injections and subsequent shoulder pain and function in subacromial impingement
syndrome [in Turkish]. Acta Orthop Traumatol Turc. 2003;37(1):
41-45.
19. Powell SE, Davis SM, Lee EH, et al. Accuracy of palpation-directed intra-articular glenohumeral injection confirmed by magnetic resonance arthrography. Arthroscopy. 2015;31(2):205-208.
20. Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of the subacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop. 2007;78(2):254-257.
21. Desmeules F, Côté CH, Frémont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review. Clin J Sport Med. 2003;13(3):176-182.
22. Winters JC, Sobel JS, Groenier KH, Arendzen HJ, Meyboom-de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study. BMJ. 1997;314(7090):1320-1325.
23. Chen MJ, Lew HL, Hsu TC, et al. Ultrasound-guided shoulder injections in the treatment of subacromial bursitis. Am J Phys Med Rehabil. 2006;85(1):31-35.
24. Hsieh LF, Hsu WC, Lin YJ, Wu SH, Chang KC, Chang HL. Is ultrasound-guided injection more effective in chronic subacromial bursitis? Med Sci Sports Exerc. 2013;45(12):
2205-2213.
25. Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study of short term response to blind injection versus sonographic-guided injection of local corticosteroids in patients with painful shoulder. J Rheumatol. 2004;31(2):308-314.
26. Hall S, Buchbinder R. Do imaging methods that guide needle placement improve outcome? Ann Rheum Dis. 2004;63(9):1007-1008.
How to reduce NICU transfers for asymptomatic hypoglycemia
NASHVILLE, TENN. – At the University of North Carolina at Chapel Hill, many infants who would previously have been transferred to the NICU for asymptomatic hypoglycemia now are staying with their moms, thanks to a new protocol that holds off on blood glucose testing until infants are fed for the first time and glucose homeostasis can begin.
Not too long ago, the university realized it had a problem that’s probably familiar to other institutions: Its system to monitor newborns at risk for hypoglycemia – those born to diabetic mothers, or who are small or large for gestational age – put too many infants with asymptomatic hypoglycemia into the NICU when they didn’t really need to be there.
Nurse practitioners “were tired of transferring babies they felt were responsive to feeding and did not actually require NICU care,” and “a growing number of families were unhappy with being separated from infants that were well-appearing and feeding well at a time when moms were trying to establish breast feeding and bonding. There was frustration with our protocol,” which “seemed rigid and outdated,” said Ashley Sutton, MD, a pediatric hospitalist at the university.

To fix the problem, Dr. Sutton and others on a multidisciplinary team implemented the American Academy of Pediatrics’ 2011 guidelines for monitoring glucose homeostasis in late-preterm and term newborns at-risk for hypoglycemia, with an additional mandate to initiate immediate, continual skin-to-skin contact at delivery (Pediatrics. 2011 Mar;127[3]:575-9).
Under the new system, children are fed with either their mom’s or a donor’s breast milk within an hour of birth, and the initial glucose check comes at 90 minutes; infants are transferred if blood glucose remains below 25 mg/dL after the second feeding. After 4 hours of life, glucose levels below 35 mg/dL trigger an evaluation for symptoms, not necessarily an automatic NICU transfer.
Labor and delivery nurses also are empowered “to immediately feed the baby no matter what number [they are] seeing,” Dr. Sutton said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The efforts have made a difference. The transfer rate for at-risk infants has fallen from 17% to 3%, and skin-to-skin contact is initiated within the first hour of life in 64%, up from 45%. Feeding of at-risk infants within the first hour has increased from 43% to 61%, and the first glucose check comes at an average of 97 minutes. The number of unnecessary NICU transfers of at-risk infants has fallen sharply.
Meanwhile, there’s been no increase in sepsis evaluations, adverse events, readmissions, and the rates of symptomatic hypoglycemia.
Dr. Sutton and her colleagues had no industry disclosures. The work was funded by the National Institutes of Health.
NASHVILLE, TENN. – At the University of North Carolina at Chapel Hill, many infants who would previously have been transferred to the NICU for asymptomatic hypoglycemia now are staying with their moms, thanks to a new protocol that holds off on blood glucose testing until infants are fed for the first time and glucose homeostasis can begin.
Not too long ago, the university realized it had a problem that’s probably familiar to other institutions: Its system to monitor newborns at risk for hypoglycemia – those born to diabetic mothers, or who are small or large for gestational age – put too many infants with asymptomatic hypoglycemia into the NICU when they didn’t really need to be there.
Nurse practitioners “were tired of transferring babies they felt were responsive to feeding and did not actually require NICU care,” and “a growing number of families were unhappy with being separated from infants that were well-appearing and feeding well at a time when moms were trying to establish breast feeding and bonding. There was frustration with our protocol,” which “seemed rigid and outdated,” said Ashley Sutton, MD, a pediatric hospitalist at the university.
To fix the problem, Dr. Sutton and others on a multidisciplinary team implemented the American Academy of Pediatrics’ 2011 guidelines for monitoring glucose homeostasis in late-preterm and term newborns at-risk for hypoglycemia, with an additional mandate to initiate immediate, continual skin-to-skin contact at delivery (Pediatrics. 2011 Mar;127[3]:575-9).
Under the new system, children are fed with either their mom’s or a donor’s breast milk within an hour of birth, and the initial glucose check comes at 90 minutes; infants are transferred if blood glucose remains below 25 mg/dL after the second feeding. After 4 hours of life, glucose levels below 35 mg/dL trigger an evaluation for symptoms, not necessarily an automatic NICU transfer.
Labor and delivery nurses also are empowered “to immediately feed the baby no matter what number [they are] seeing,” Dr. Sutton said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The efforts have made a difference. The transfer rate for at-risk infants has fallen from 17% to 3%, and skin-to-skin contact is initiated within the first hour of life in 64%, up from 45%. Feeding of at-risk infants within the first hour has increased from 43% to 61%, and the first glucose check comes at an average of 97 minutes. The number of unnecessary NICU transfers of at-risk infants has fallen sharply.
Meanwhile, there’s been no increase in sepsis evaluations, adverse events, readmissions, and the rates of symptomatic hypoglycemia.
Dr. Sutton and her colleagues had no industry disclosures. The work was funded by the National Institutes of Health.
NASHVILLE, TENN. – At the University of North Carolina at Chapel Hill, many infants who would previously have been transferred to the NICU for asymptomatic hypoglycemia now are staying with their moms, thanks to a new protocol that holds off on blood glucose testing until infants are fed for the first time and glucose homeostasis can begin.
Not too long ago, the university realized it had a problem that’s probably familiar to other institutions: Its system to monitor newborns at risk for hypoglycemia – those born to diabetic mothers, or who are small or large for gestational age – put too many infants with asymptomatic hypoglycemia into the NICU when they didn’t really need to be there.
Nurse practitioners “were tired of transferring babies they felt were responsive to feeding and did not actually require NICU care,” and “a growing number of families were unhappy with being separated from infants that were well-appearing and feeding well at a time when moms were trying to establish breast feeding and bonding. There was frustration with our protocol,” which “seemed rigid and outdated,” said Ashley Sutton, MD, a pediatric hospitalist at the university.
To fix the problem, Dr. Sutton and others on a multidisciplinary team implemented the American Academy of Pediatrics’ 2011 guidelines for monitoring glucose homeostasis in late-preterm and term newborns at-risk for hypoglycemia, with an additional mandate to initiate immediate, continual skin-to-skin contact at delivery (Pediatrics. 2011 Mar;127[3]:575-9).
Under the new system, children are fed with either their mom’s or a donor’s breast milk within an hour of birth, and the initial glucose check comes at 90 minutes; infants are transferred if blood glucose remains below 25 mg/dL after the second feeding. After 4 hours of life, glucose levels below 35 mg/dL trigger an evaluation for symptoms, not necessarily an automatic NICU transfer.
Labor and delivery nurses also are empowered “to immediately feed the baby no matter what number [they are] seeing,” Dr. Sutton said at the meeting, sponsored by the Society of Hospital Medicine, the American Academy of Pediatrics, and the Academic Pediatric Association.
The efforts have made a difference. The transfer rate for at-risk infants has fallen from 17% to 3%, and skin-to-skin contact is initiated within the first hour of life in 64%, up from 45%. Feeding of at-risk infants within the first hour has increased from 43% to 61%, and the first glucose check comes at an average of 97 minutes. The number of unnecessary NICU transfers of at-risk infants has fallen sharply.
Meanwhile, there’s been no increase in sepsis evaluations, adverse events, readmissions, and the rates of symptomatic hypoglycemia.
Dr. Sutton and her colleagues had no industry disclosures. The work was funded by the National Institutes of Health.
AT PHM 2017
Key clinical point:
Major finding: After making that and other changes, the transfer rate for at-risk infants at a major academic center fell from 17% to 3%, without an increase in rates of symptomatic hypoglycemia and adverse events.
Data source: Quality improvement project at the University of North Carolina at Chapel Hill.
Disclosures: The investigators had no financial disclosures. The work was funded by the National Institutes of Health.

VESAP4 Mobile App Coming Soon
The mobile companion app (Apple products only) for VESAP4 is expected to be released by mid-September. The app permits users to access the program offline anywhere and sync up with the desktop app when later connected to the Internet.
It will be available on the iTunes store and is free to VESAP4 purchasers. Learn more about the fourth edition of the Vascular Education and Self-Assessment Program (VESAP4) here.
The mobile companion app (Apple products only) for VESAP4 is expected to be released by mid-September. The app permits users to access the program offline anywhere and sync up with the desktop app when later connected to the Internet.
It will be available on the iTunes store and is free to VESAP4 purchasers. Learn more about the fourth edition of the Vascular Education and Self-Assessment Program (VESAP4) here.
The mobile companion app (Apple products only) for VESAP4 is expected to be released by mid-September. The app permits users to access the program offline anywhere and sync up with the desktop app when later connected to the Internet.
It will be available on the iTunes store and is free to VESAP4 purchasers. Learn more about the fourth edition of the Vascular Education and Self-Assessment Program (VESAP4) here.
Submit VAM Session Topic Proposals
SVS is seeking proposals for invited sessions from internal committees and members alike for the 2018 Vascular Annual Meeting, June 20-23 (exhibits: June 21 to 22; plenaries: June 21 to 23) in Boston, Mass.
Invited sessions consist of postgraduate courses, breakfast sessions, concurrent sessions and workshops/small-group sessions. Submitters will be asked to address educational needs, provide objectives, indicate proposed formats and identify target audiences.
The deadline is 3 p.m. Central Daylight Time, Friday, Sept. 15. Submitters will be notified the week of Sept. 25 if their proposals have been selected for further development. Contact [email protected] or call 312-334-2327 with questions.
SVS is seeking proposals for invited sessions from internal committees and members alike for the 2018 Vascular Annual Meeting, June 20-23 (exhibits: June 21 to 22; plenaries: June 21 to 23) in Boston, Mass.
Invited sessions consist of postgraduate courses, breakfast sessions, concurrent sessions and workshops/small-group sessions. Submitters will be asked to address educational needs, provide objectives, indicate proposed formats and identify target audiences.
The deadline is 3 p.m. Central Daylight Time, Friday, Sept. 15. Submitters will be notified the week of Sept. 25 if their proposals have been selected for further development. Contact [email protected] or call 312-334-2327 with questions.
SVS is seeking proposals for invited sessions from internal committees and members alike for the 2018 Vascular Annual Meeting, June 20-23 (exhibits: June 21 to 22; plenaries: June 21 to 23) in Boston, Mass.
Invited sessions consist of postgraduate courses, breakfast sessions, concurrent sessions and workshops/small-group sessions. Submitters will be asked to address educational needs, provide objectives, indicate proposed formats and identify target audiences.
The deadline is 3 p.m. Central Daylight Time, Friday, Sept. 15. Submitters will be notified the week of Sept. 25 if their proposals have been selected for further development. Contact [email protected] or call 312-334-2327 with questions.
Adverse effects of PD-1/PD-L1 inhibitors varied by tumor type in systematic review
The immune-related adverse effects of inhibitors of programmed cell death protein 1 (PD-1) and its ligand varied by tumor type in a large systematic review and meta-analysis.
Patients with melanoma were significantly more likely to develop colitis (odds ratio, 4.2; 95% confidence interval, 1.3 to 14.0), diarrhea (OR, 1.9), pruritus (OR, 2.4), and rash (OR, 1.8) compared with patients with non–small cell lung cancer, who were significantly more likely to develop pneumonitis, reported Leila Khoja, MBChB, PhD, of AstraZeneca UK, Melbourn, England, and associates. Patients with melanoma also were significantly more likely to develop arthralgia, hypothyroidism, rash, pruritus, and diarrhea compared with patients with renal cell carcinoma, who were more likely to develop pneumonitis and dyspnea.
“In light of this study, we should be mindful that different tumor types may have different immune-related adverse effect patterns when treated with the same immune checkpoint inhibitor,” the reviewers noted (Ann Oncol. 2017 Aug 8. doi: 10.1093/annonc/mdx286).
The review included 48 trials of nearly 7,000 patients with solid tumors who received CTLA-4 inhibitors (26 studies), PD-1 inhibitors (17 studies), PD-1 ligand (PD-L1) inhibitors (two trials), or both CTLA-4 and PD-1 inhibitors (three trials). The reviewers identified the studies by searching the Medline, EMBASE, and COCHRANE databases for prospective trials published from 2003 through November 2015.
Severe or life-threatening immune-related adverse effects developed in 31% of patients who received CTLA-4 inhibitors and 10% of patients who received PD-1 inhibitors. Inhibitors of CTLA-4 were significantly more likely to cause all grades of colitis (OR, 8.7), hypophysitis (OR, 6.5), and rash (OR, 2.0), while PD-1 inhibitors were more strongly linked with pneumonitis (OR 6.4), hypothyroidism (OR 4.3), arthralgia (OR, 3.5), and vitiligo (OR, 3.5).
The reviewers also looked for significant predictors of immune-related colitis and pneumonitis, because these are potentially fatal. They found that pneumonitis was significantly linked to PD-1/PD-L1 inhibitor therapy (P less than .001) and colitis to CTLA-4 treatment (P = .04), even after accounting for therapeutic dose and tumor type. No other factors reached significance in this multivariable model.
“Clearly, a more thorough understanding of the mechanisms of immune-related adverse effects is needed, which may lead to the identification of biomarkers to predict the occurrence of toxicity in patients or predict those who have immune-related adverse effects that are unlikely to respond to corticosteroids,” the reviewers concluded. Researchers should also study whether clinical factors such as treatment history or comorbidities affect the risk of immune-related adverse effects from immune checkpoint inhibitors, they said.
The reviewers reported having no funding sources and no relevant conflicts of interest.
The immune-related adverse effects of inhibitors of programmed cell death protein 1 (PD-1) and its ligand varied by tumor type in a large systematic review and meta-analysis.
Patients with melanoma were significantly more likely to develop colitis (odds ratio, 4.2; 95% confidence interval, 1.3 to 14.0), diarrhea (OR, 1.9), pruritus (OR, 2.4), and rash (OR, 1.8) compared with patients with non–small cell lung cancer, who were significantly more likely to develop pneumonitis, reported Leila Khoja, MBChB, PhD, of AstraZeneca UK, Melbourn, England, and associates. Patients with melanoma also were significantly more likely to develop arthralgia, hypothyroidism, rash, pruritus, and diarrhea compared with patients with renal cell carcinoma, who were more likely to develop pneumonitis and dyspnea.
“In light of this study, we should be mindful that different tumor types may have different immune-related adverse effect patterns when treated with the same immune checkpoint inhibitor,” the reviewers noted (Ann Oncol. 2017 Aug 8. doi: 10.1093/annonc/mdx286).
The review included 48 trials of nearly 7,000 patients with solid tumors who received CTLA-4 inhibitors (26 studies), PD-1 inhibitors (17 studies), PD-1 ligand (PD-L1) inhibitors (two trials), or both CTLA-4 and PD-1 inhibitors (three trials). The reviewers identified the studies by searching the Medline, EMBASE, and COCHRANE databases for prospective trials published from 2003 through November 2015.
Severe or life-threatening immune-related adverse effects developed in 31% of patients who received CTLA-4 inhibitors and 10% of patients who received PD-1 inhibitors. Inhibitors of CTLA-4 were significantly more likely to cause all grades of colitis (OR, 8.7), hypophysitis (OR, 6.5), and rash (OR, 2.0), while PD-1 inhibitors were more strongly linked with pneumonitis (OR 6.4), hypothyroidism (OR 4.3), arthralgia (OR, 3.5), and vitiligo (OR, 3.5).
The reviewers also looked for significant predictors of immune-related colitis and pneumonitis, because these are potentially fatal. They found that pneumonitis was significantly linked to PD-1/PD-L1 inhibitor therapy (P less than .001) and colitis to CTLA-4 treatment (P = .04), even after accounting for therapeutic dose and tumor type. No other factors reached significance in this multivariable model.
“Clearly, a more thorough understanding of the mechanisms of immune-related adverse effects is needed, which may lead to the identification of biomarkers to predict the occurrence of toxicity in patients or predict those who have immune-related adverse effects that are unlikely to respond to corticosteroids,” the reviewers concluded. Researchers should also study whether clinical factors such as treatment history or comorbidities affect the risk of immune-related adverse effects from immune checkpoint inhibitors, they said.
The reviewers reported having no funding sources and no relevant conflicts of interest.
The immune-related adverse effects of inhibitors of programmed cell death protein 1 (PD-1) and its ligand varied by tumor type in a large systematic review and meta-analysis.
Patients with melanoma were significantly more likely to develop colitis (odds ratio, 4.2; 95% confidence interval, 1.3 to 14.0), diarrhea (OR, 1.9), pruritus (OR, 2.4), and rash (OR, 1.8) compared with patients with non–small cell lung cancer, who were significantly more likely to develop pneumonitis, reported Leila Khoja, MBChB, PhD, of AstraZeneca UK, Melbourn, England, and associates. Patients with melanoma also were significantly more likely to develop arthralgia, hypothyroidism, rash, pruritus, and diarrhea compared with patients with renal cell carcinoma, who were more likely to develop pneumonitis and dyspnea.
“In light of this study, we should be mindful that different tumor types may have different immune-related adverse effect patterns when treated with the same immune checkpoint inhibitor,” the reviewers noted (Ann Oncol. 2017 Aug 8. doi: 10.1093/annonc/mdx286).
The review included 48 trials of nearly 7,000 patients with solid tumors who received CTLA-4 inhibitors (26 studies), PD-1 inhibitors (17 studies), PD-1 ligand (PD-L1) inhibitors (two trials), or both CTLA-4 and PD-1 inhibitors (three trials). The reviewers identified the studies by searching the Medline, EMBASE, and COCHRANE databases for prospective trials published from 2003 through November 2015.
Severe or life-threatening immune-related adverse effects developed in 31% of patients who received CTLA-4 inhibitors and 10% of patients who received PD-1 inhibitors. Inhibitors of CTLA-4 were significantly more likely to cause all grades of colitis (OR, 8.7), hypophysitis (OR, 6.5), and rash (OR, 2.0), while PD-1 inhibitors were more strongly linked with pneumonitis (OR 6.4), hypothyroidism (OR 4.3), arthralgia (OR, 3.5), and vitiligo (OR, 3.5).
The reviewers also looked for significant predictors of immune-related colitis and pneumonitis, because these are potentially fatal. They found that pneumonitis was significantly linked to PD-1/PD-L1 inhibitor therapy (P less than .001) and colitis to CTLA-4 treatment (P = .04), even after accounting for therapeutic dose and tumor type. No other factors reached significance in this multivariable model.
“Clearly, a more thorough understanding of the mechanisms of immune-related adverse effects is needed, which may lead to the identification of biomarkers to predict the occurrence of toxicity in patients or predict those who have immune-related adverse effects that are unlikely to respond to corticosteroids,” the reviewers concluded. Researchers should also study whether clinical factors such as treatment history or comorbidities affect the risk of immune-related adverse effects from immune checkpoint inhibitors, they said.
The reviewers reported having no funding sources and no relevant conflicts of interest.
FROM ANNALS OF ONCOLOGY
Key clinical point: Immune-related adverse effects varied by tumor type in patients receiving programmed cell death protein 1 (PD-1) and PD-L1 inhibitors.
Major finding: Patients with melanoma who received PD-1/PD-L1 inhibitors were significantly more likely to develop colitis (odds ratio, 4.2; 95% confidence interval, 1.3 to 14.0), diarrhea (OR, 1.9), pruritus (OR, 2.4), and rash (OR, 1.8), compared with patients with non-small cell lung cancer, who were significantly more likely to develop pneumonitis.
Data source: A systematic review and meta-analysis of 48 prospective trials of immune checkpoint inhibitors in of 6,938 adults with solid tumors.
Disclosures: The reviewers reported having no funding sources and no relevant conflicts of interest.
Enasidenib data in IDH2-mutated AML are basis for combination therapy trials
Enasidenib was a well-tolerated, efficacious alternative to cytotoxic chemotherapy for patients with IDH2-mutated relapsed or refractory acute myeloid leukemia (AML), the results of a phase 1/2 study showed.
The Food and Drug Administration recently approved enasidenib (Idhifa, formerly AG-221; Celgene) for the treatment of adult patients with relapsed or refractory AML having an IDH2 mutation as detected by a companion diagnostic test (RealTime IDH2 Assay; Abbott Molecular Inc.). The drug was generally safe and well tolerated, according to reported trial results (Blood. 2017 Aug. 10;130[6]:722-31). The main grade 3-4 enasidenib-related adverse events were hyperbilirubinemia (12%) and IDH inhibitor–associated differentiation syndrome (6%).
The drug is an oral selective inhibitor of mutant isocitrate dehydrogenase 2 (IDH2) enzymes that is not myeloablative. Although enasidenib appears to work by inducing myeloblast differentiation, predictors of response to the drug generally remain elusive, according to Eytan M. Stein, MD, a hematologic oncologist at Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
About 12% of patients with AML have an IDH2 mutation. This genetic defect leads to accumulation of the metabolite 2-hydroxyglutarate (2-HG), causing DNA and histone hypermethylation. Hypermethylation, in turn, blocks hematopoietic cellular differentiation.
In a phase 1/2 trial sponsored by Celgene and Agios Pharmaceuticals, the investigators tested daily enasidenib monotherapy among 239 patients with IDH2-mutated advanced myeloid malignancies.
Among the 176 patients with relapsed or refractory AML (more than half of whom had already received at least two regimens directed against the disease), the overall response rate was 40.3%, and the complete response/remission rate was 19.3%. The median duration of response was 5.8 months.
Evaluation of serial bone marrow aspirates showed that responses were associated with myeloid cellular differentiation and maturation, generally without evidence of aplasia or hypoplasia.
With a median follow-up of 7.7 months, median overall survival was 9.3 months in the entire AML cohort and 19.7 months in the subset achieving complete response/remission. Ten percent of patients went on to allogeneic stem cell transplantation.
Although nearly all patients had a marked reduction in plasma levels of 2-HG, the extent of reduction did not predict response, suggesting that this metabolite is not a biomarker for benefit, and additional mechanisms are at play.
“Continuous daily enasidenib treatment was generally well tolerated and induced hematologic responses in patients for whom prior AML therapy had failed,” Dr. Stein and his coinvestigators wrote. “Inducing differentiation of myeloblasts, not cytotoxicity, seems to drive the clinical efficacy of enasidenib.”
They noted that an ongoing multicenter, randomized phase 3 trial, called IDHENTIFY (NCT02577406), is testing enasidenib against conventional regimens in older adults with late-stage AML harboring an IDH2 mutation.
In a companion translational study, investigators led by Michael D. Amatangelo, PhD, a scientist with Celgene in Summit, N.J., further explored mechanisms of enasidenib response and sought to identify alternative biomarkers for benefit in the AML cohort. They measured 2-HG levels, mutant IDH2 allele burden, and co-occurring somatic mutations in samples serially collected during the trial, and used flow cytometry to assess inhibition of mutant IDH2 on hematopoietic differentiation.
Enasidenib therapy induced 2-HG suppression regardless of whether patients’ IDH2 mutation affected the R140 or the R172 residue, according to reported results (Blood. 2017 Aug. 10;130[6]:732-41). However, analyses confirmed that 2-HG suppression alone did not predict response, as most nonresponders also had suppression.
In some patients with complete remission, mutant IDH2 persisted, but there was normalization of hematopoietic stem and progenitor compartments, and emergence of functional neutrophils having the IDH2 mutation. And some patients saw a reduction in mutant IDH2 allele burden, with levels remaining undetectable during response.
Analyses failed to identify any single mutation predictive of response to enasidenib. However, patients who did not achieve a response more commonly had mutations in NRAS and other MAPK pathway effectors, suggesting that RAS signaling plays a role in primary resistance to the drug.
“Although this is only a subgroup analysis of a large single-arm experience, taken together, the clinical response and translational data demonstrate that single-agent [mutant IDH2] inhibition by enasidenib in [relapsed or refractory AML] represents a critical and novel differentiation therapy,” Dr. Amatangelo and his coinvestigators wrote.
“Although enasidenib responses are clinically durable, the genetic heterogeneity observed in our patients suggests that combination with other therapies may be required to achieve long-term disease remission in more patients,” they added. “Current clinical studies combining enasidenib with combination chemotherapy or azacitidine (NCT02677922 and NCT02632708) and future orthogonal targeted therapies will address this question.”
Dr. Stein disclosed that he received grants and personal fees from Celgene and Agios Pharmaceuticals. Dr. Amatangelo disclosed that he is employed by and owns equity in Celgene.
Stein et al. provide for the first time answers to the questions of whether IDH inhibitors are tolerated in patients and whether these compounds induce clinical responses and, excitingly, both answers are positive.
Data from the phase 1/2 trial are encouraging, given that the population studied has a notoriously dismal prognosis when treated with conventional modalities.
Findings from the companion translational study suggest heterogeneity in the dynamics of response to enasidenib, with some responding patients retaining mutant alleles in mature cells, and a smaller group of responding patients clearing the mutation.
These findings raise the important question of whether enasidenib can target leukemic stem cells, the holy grail of AML therapy. Additional questions arising from the research pertain to the long-term effects of the drug, whether it will induce clonal selection, and how it affects leukemic cells that lack an IDH2 mutation.
Together, the results of these studies argue for the further clinical exploration of IDH inhibitors. It is expected that for more powerful responses, differentiation-based IDH2 inhibition will need to be combined with orthogonal treatment modalities, such as standard chemotherapy or other types of mechanism-based targeted therapy. Obviously, in the next phase, enasidenib-based regimens should be compared head to head to standard regimens in a randomized controlled fashion. Such studies, and studies with other IDH2 and IDH1 inhibitors, will address the full role of IDH inhibition in AML treatment.
Bas J. Wouters, MD, PhD, a hematologist at Erasmus University Medical Center, Rotterdam, the Netherlands, made his remarks in a related commentary ( Blood. 2017;130:693-4 ). Dr. Wouters reported no competing financial interests.
Stein et al. provide for the first time answers to the questions of whether IDH inhibitors are tolerated in patients and whether these compounds induce clinical responses and, excitingly, both answers are positive.
Data from the phase 1/2 trial are encouraging, given that the population studied has a notoriously dismal prognosis when treated with conventional modalities.
Findings from the companion translational study suggest heterogeneity in the dynamics of response to enasidenib, with some responding patients retaining mutant alleles in mature cells, and a smaller group of responding patients clearing the mutation.
These findings raise the important question of whether enasidenib can target leukemic stem cells, the holy grail of AML therapy. Additional questions arising from the research pertain to the long-term effects of the drug, whether it will induce clonal selection, and how it affects leukemic cells that lack an IDH2 mutation.
Together, the results of these studies argue for the further clinical exploration of IDH inhibitors. It is expected that for more powerful responses, differentiation-based IDH2 inhibition will need to be combined with orthogonal treatment modalities, such as standard chemotherapy or other types of mechanism-based targeted therapy. Obviously, in the next phase, enasidenib-based regimens should be compared head to head to standard regimens in a randomized controlled fashion. Such studies, and studies with other IDH2 and IDH1 inhibitors, will address the full role of IDH inhibition in AML treatment.
Bas J. Wouters, MD, PhD, a hematologist at Erasmus University Medical Center, Rotterdam, the Netherlands, made his remarks in a related commentary ( Blood. 2017;130:693-4 ). Dr. Wouters reported no competing financial interests.
Stein et al. provide for the first time answers to the questions of whether IDH inhibitors are tolerated in patients and whether these compounds induce clinical responses and, excitingly, both answers are positive.
Data from the phase 1/2 trial are encouraging, given that the population studied has a notoriously dismal prognosis when treated with conventional modalities.
Findings from the companion translational study suggest heterogeneity in the dynamics of response to enasidenib, with some responding patients retaining mutant alleles in mature cells, and a smaller group of responding patients clearing the mutation.
These findings raise the important question of whether enasidenib can target leukemic stem cells, the holy grail of AML therapy. Additional questions arising from the research pertain to the long-term effects of the drug, whether it will induce clonal selection, and how it affects leukemic cells that lack an IDH2 mutation.
Together, the results of these studies argue for the further clinical exploration of IDH inhibitors. It is expected that for more powerful responses, differentiation-based IDH2 inhibition will need to be combined with orthogonal treatment modalities, such as standard chemotherapy or other types of mechanism-based targeted therapy. Obviously, in the next phase, enasidenib-based regimens should be compared head to head to standard regimens in a randomized controlled fashion. Such studies, and studies with other IDH2 and IDH1 inhibitors, will address the full role of IDH inhibition in AML treatment.
Bas J. Wouters, MD, PhD, a hematologist at Erasmus University Medical Center, Rotterdam, the Netherlands, made his remarks in a related commentary ( Blood. 2017;130:693-4 ). Dr. Wouters reported no competing financial interests.
Enasidenib was a well-tolerated, efficacious alternative to cytotoxic chemotherapy for patients with IDH2-mutated relapsed or refractory acute myeloid leukemia (AML), the results of a phase 1/2 study showed.
The Food and Drug Administration recently approved enasidenib (Idhifa, formerly AG-221; Celgene) for the treatment of adult patients with relapsed or refractory AML having an IDH2 mutation as detected by a companion diagnostic test (RealTime IDH2 Assay; Abbott Molecular Inc.). The drug was generally safe and well tolerated, according to reported trial results (Blood. 2017 Aug. 10;130[6]:722-31). The main grade 3-4 enasidenib-related adverse events were hyperbilirubinemia (12%) and IDH inhibitor–associated differentiation syndrome (6%).
The drug is an oral selective inhibitor of mutant isocitrate dehydrogenase 2 (IDH2) enzymes that is not myeloablative. Although enasidenib appears to work by inducing myeloblast differentiation, predictors of response to the drug generally remain elusive, according to Eytan M. Stein, MD, a hematologic oncologist at Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
About 12% of patients with AML have an IDH2 mutation. This genetic defect leads to accumulation of the metabolite 2-hydroxyglutarate (2-HG), causing DNA and histone hypermethylation. Hypermethylation, in turn, blocks hematopoietic cellular differentiation.
In a phase 1/2 trial sponsored by Celgene and Agios Pharmaceuticals, the investigators tested daily enasidenib monotherapy among 239 patients with IDH2-mutated advanced myeloid malignancies.
Among the 176 patients with relapsed or refractory AML (more than half of whom had already received at least two regimens directed against the disease), the overall response rate was 40.3%, and the complete response/remission rate was 19.3%. The median duration of response was 5.8 months.
Evaluation of serial bone marrow aspirates showed that responses were associated with myeloid cellular differentiation and maturation, generally without evidence of aplasia or hypoplasia.
With a median follow-up of 7.7 months, median overall survival was 9.3 months in the entire AML cohort and 19.7 months in the subset achieving complete response/remission. Ten percent of patients went on to allogeneic stem cell transplantation.
Although nearly all patients had a marked reduction in plasma levels of 2-HG, the extent of reduction did not predict response, suggesting that this metabolite is not a biomarker for benefit, and additional mechanisms are at play.
“Continuous daily enasidenib treatment was generally well tolerated and induced hematologic responses in patients for whom prior AML therapy had failed,” Dr. Stein and his coinvestigators wrote. “Inducing differentiation of myeloblasts, not cytotoxicity, seems to drive the clinical efficacy of enasidenib.”
They noted that an ongoing multicenter, randomized phase 3 trial, called IDHENTIFY (NCT02577406), is testing enasidenib against conventional regimens in older adults with late-stage AML harboring an IDH2 mutation.
In a companion translational study, investigators led by Michael D. Amatangelo, PhD, a scientist with Celgene in Summit, N.J., further explored mechanisms of enasidenib response and sought to identify alternative biomarkers for benefit in the AML cohort. They measured 2-HG levels, mutant IDH2 allele burden, and co-occurring somatic mutations in samples serially collected during the trial, and used flow cytometry to assess inhibition of mutant IDH2 on hematopoietic differentiation.
Enasidenib therapy induced 2-HG suppression regardless of whether patients’ IDH2 mutation affected the R140 or the R172 residue, according to reported results (Blood. 2017 Aug. 10;130[6]:732-41). However, analyses confirmed that 2-HG suppression alone did not predict response, as most nonresponders also had suppression.
In some patients with complete remission, mutant IDH2 persisted, but there was normalization of hematopoietic stem and progenitor compartments, and emergence of functional neutrophils having the IDH2 mutation. And some patients saw a reduction in mutant IDH2 allele burden, with levels remaining undetectable during response.
Analyses failed to identify any single mutation predictive of response to enasidenib. However, patients who did not achieve a response more commonly had mutations in NRAS and other MAPK pathway effectors, suggesting that RAS signaling plays a role in primary resistance to the drug.
“Although this is only a subgroup analysis of a large single-arm experience, taken together, the clinical response and translational data demonstrate that single-agent [mutant IDH2] inhibition by enasidenib in [relapsed or refractory AML] represents a critical and novel differentiation therapy,” Dr. Amatangelo and his coinvestigators wrote.
“Although enasidenib responses are clinically durable, the genetic heterogeneity observed in our patients suggests that combination with other therapies may be required to achieve long-term disease remission in more patients,” they added. “Current clinical studies combining enasidenib with combination chemotherapy or azacitidine (NCT02677922 and NCT02632708) and future orthogonal targeted therapies will address this question.”
Dr. Stein disclosed that he received grants and personal fees from Celgene and Agios Pharmaceuticals. Dr. Amatangelo disclosed that he is employed by and owns equity in Celgene.
Enasidenib was a well-tolerated, efficacious alternative to cytotoxic chemotherapy for patients with IDH2-mutated relapsed or refractory acute myeloid leukemia (AML), the results of a phase 1/2 study showed.
The Food and Drug Administration recently approved enasidenib (Idhifa, formerly AG-221; Celgene) for the treatment of adult patients with relapsed or refractory AML having an IDH2 mutation as detected by a companion diagnostic test (RealTime IDH2 Assay; Abbott Molecular Inc.). The drug was generally safe and well tolerated, according to reported trial results (Blood. 2017 Aug. 10;130[6]:722-31). The main grade 3-4 enasidenib-related adverse events were hyperbilirubinemia (12%) and IDH inhibitor–associated differentiation syndrome (6%).
The drug is an oral selective inhibitor of mutant isocitrate dehydrogenase 2 (IDH2) enzymes that is not myeloablative. Although enasidenib appears to work by inducing myeloblast differentiation, predictors of response to the drug generally remain elusive, according to Eytan M. Stein, MD, a hematologic oncologist at Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
About 12% of patients with AML have an IDH2 mutation. This genetic defect leads to accumulation of the metabolite 2-hydroxyglutarate (2-HG), causing DNA and histone hypermethylation. Hypermethylation, in turn, blocks hematopoietic cellular differentiation.
In a phase 1/2 trial sponsored by Celgene and Agios Pharmaceuticals, the investigators tested daily enasidenib monotherapy among 239 patients with IDH2-mutated advanced myeloid malignancies.
Among the 176 patients with relapsed or refractory AML (more than half of whom had already received at least two regimens directed against the disease), the overall response rate was 40.3%, and the complete response/remission rate was 19.3%. The median duration of response was 5.8 months.
Evaluation of serial bone marrow aspirates showed that responses were associated with myeloid cellular differentiation and maturation, generally without evidence of aplasia or hypoplasia.
With a median follow-up of 7.7 months, median overall survival was 9.3 months in the entire AML cohort and 19.7 months in the subset achieving complete response/remission. Ten percent of patients went on to allogeneic stem cell transplantation.
Although nearly all patients had a marked reduction in plasma levels of 2-HG, the extent of reduction did not predict response, suggesting that this metabolite is not a biomarker for benefit, and additional mechanisms are at play.
“Continuous daily enasidenib treatment was generally well tolerated and induced hematologic responses in patients for whom prior AML therapy had failed,” Dr. Stein and his coinvestigators wrote. “Inducing differentiation of myeloblasts, not cytotoxicity, seems to drive the clinical efficacy of enasidenib.”
They noted that an ongoing multicenter, randomized phase 3 trial, called IDHENTIFY (NCT02577406), is testing enasidenib against conventional regimens in older adults with late-stage AML harboring an IDH2 mutation.
In a companion translational study, investigators led by Michael D. Amatangelo, PhD, a scientist with Celgene in Summit, N.J., further explored mechanisms of enasidenib response and sought to identify alternative biomarkers for benefit in the AML cohort. They measured 2-HG levels, mutant IDH2 allele burden, and co-occurring somatic mutations in samples serially collected during the trial, and used flow cytometry to assess inhibition of mutant IDH2 on hematopoietic differentiation.
Enasidenib therapy induced 2-HG suppression regardless of whether patients’ IDH2 mutation affected the R140 or the R172 residue, according to reported results (Blood. 2017 Aug. 10;130[6]:732-41). However, analyses confirmed that 2-HG suppression alone did not predict response, as most nonresponders also had suppression.
In some patients with complete remission, mutant IDH2 persisted, but there was normalization of hematopoietic stem and progenitor compartments, and emergence of functional neutrophils having the IDH2 mutation. And some patients saw a reduction in mutant IDH2 allele burden, with levels remaining undetectable during response.
Analyses failed to identify any single mutation predictive of response to enasidenib. However, patients who did not achieve a response more commonly had mutations in NRAS and other MAPK pathway effectors, suggesting that RAS signaling plays a role in primary resistance to the drug.
“Although this is only a subgroup analysis of a large single-arm experience, taken together, the clinical response and translational data demonstrate that single-agent [mutant IDH2] inhibition by enasidenib in [relapsed or refractory AML] represents a critical and novel differentiation therapy,” Dr. Amatangelo and his coinvestigators wrote.
“Although enasidenib responses are clinically durable, the genetic heterogeneity observed in our patients suggests that combination with other therapies may be required to achieve long-term disease remission in more patients,” they added. “Current clinical studies combining enasidenib with combination chemotherapy or azacitidine (NCT02677922 and NCT02632708) and future orthogonal targeted therapies will address this question.”
Dr. Stein disclosed that he received grants and personal fees from Celgene and Agios Pharmaceuticals. Dr. Amatangelo disclosed that he is employed by and owns equity in Celgene.
FROM BLOOD
Key clinical point:
Major finding: The overall response rate was 40.3%; 2-HG levels and co-occurring mutations were not reliable predictors of response.
Data source: A phase 1/2 trial of enasidenib monotherapy including 176 patients with relapsed or refractory IDH2-mutated AML, and a companion translational study of mechanisms and biomarkers of response in the same patients.
Disclosures: Dr. Stein disclosed that he received grants and personal fees from Celgene and Agios Pharmaceuticals, the trial sponsors. Dr. Amatangelo disclosed that he is employed by and owns equity in Celgene. The study was supported by the National Institutes of Health, National Cancer Institute.
New and Noteworthy Information—September 2017
Statin Prescription Varies in Stroke Belt
Less than half of patients with stroke discharged from the hospital receive a prescription for statins, and the likelihood of a prescription varies by patients’ location, sex, age, and race, according to a study published August 2 in the Journal of the American Heart Association. Researchers analyzed discharge medications for 323 participants hospitalized for an ischemic stroke during follow-up of the Reasons for Geographic and Racial Differences in Stroke study. In the Stroke Belt, participants ages 65 and older were 47% less likely to be discharged on a statin, compared with people younger than 65. Compared with women, men in the Stroke Belt were 31% less likely to be discharged on a statin, while men outside the Stroke Belt were more likely to be discharged on a statin.
Albright KC, Howard VJ, Howard G, et al. Age and sex disparities in discharge statin prescribing in the stroke belt: evidence from the Reasons for Geographic and Racial Differences in Stroke Study. J Am Heart Assoc. 2017;6(8).
Midlife Vascular Risk Factors Increase Risk of Dementia
Midlife vascular risk factors are associated with increased risk of dementia in blacks and whites, according to a study published online ahead of print August 7 in JAMA Neurology. In the Atherosclerosis Risk in Communities study, investigators measured demographic and vascular risk factors at baseline (ie, obesity, smoking, diabetes, prehypertension, hypertension, and hypercholesterolemia), along with the presence of the APOE ε4 genotype. After the baseline visit, participants had four additional in-person visits. In all, 1,516 cases of dementia (57.0% female and 34.9% black, with a mean age at visit 1 of 57.4) were identified among 15,744 participants. Black race, older age, lower educational attainment, and APOE ε4 genotype were associated with increased risk of dementia, as were midlife smoking, diabetes, prehypertension, and hypertension.
Gottesman RF, Albert MS, Alonso A, et al. Associations between midlife vascular risk factors and 25-year incident dementia in the Atherosclerosis Risk in Communities (ARIC) Cohort. JAMA Neurol. 2017 August 7 [Epub ahead of print].
Resistance Training May Slow the Progression of MS
Progressive resistance training may have a neuroprotective or neuroregenerative effect in relapsing-remitting multiple sclerosis (MS), according to a study published online ahead of print July 1 in Multiple Sclerosis Journal. This study was a 24-week randomized controlled crossover trial. Participants were assigned to training or to a wait list. Assessments included disability measures and MRI. The MS Functional Composite score improved in the training group, but disability, lesion load, and global brain volumes did not differ between groups. The researchers noted higher absolute cortical thickness values in 19 of 74 investigated cortical regions after progressive resistance training. Observed changes were confirmed and reproduced when comparing relative cortical thickness changes between groups in the anterior cingulate gyrus, temporal pole, orbital sulcus, and inferior temporal sulcus.
Kjølhede T, Siemonsen S, Wenzel D, et al. Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult Scler. 2017 Jul 1 [Epub ahead of print].
Noninvasive Device Measures Intracranial Pressure
A noninvasive device measures intracranial pressure (ICP) accurately, according to research published online ahead of print August 8 in the Journal of Neurosurgery. In patients with traumatic brain injury and subarachnoid hemorrhage who were undergoing treatment in a neurocritical intensive care unit, researchers recorded ICP using the gold-standard method of invasive external ventricular drainage or intraparenchymal monitoring. In addition, the authors simultaneously measured ICP noninvasively with a device that uses advanced signal-analysis algorithms for acoustic signals propagating through the cranium. Data were collected in 14 patients, yielding 2,543 data points of continuous parallel ICP values. For measurements at the ≥ 17-mm Hg cutoff, the sensitivity and specificity of the noninvasive device were 0.7541 and 0.8887, respectively. ICP values obtained using noninvasive and invasive monitoring methods correlated well.
Ganslandt O, Mourtzoukos S, Stadlbauer A, et al. Evaluation of a novel noninvasive ICP monitoring device in patients undergoing invasive ICP monitoring: preliminary results. J Neurosurg. 2017 Aug 8 [Epub ahead of print].
Strokes Decline Among Men, But Not Women
The rate of stroke in the US has declined among men, but not among women, according to a study published online ahead of print August 9 in Neurology. Researchers collected data on 1.3 million adults in Ohio and Kentucky between 1993 and 2010. They used medical records to identify first-ever strokes during four one-year periods. The researchers observed 7,710 incident strokes in the four periods, and 57% of them were among women. The incidence of all strokes decreased over time in men (263 to 192), but not in women (217 to 198). The researchers found a similar sex difference in the change in the rate of ischemic stroke (ie, a decline from 238 to 165 among men, and a change from 193 to 173 among women).
Madsen TE, Khoury J, Alwell K, et al. Sex-specific stroke incidence over time in the Greater Cincinnati/Northern Kentucky Stroke Study. Neurology. 2017 Aug 9 [Epub ahead of print].
Link Between Alcohol Intake and Cognitively Healthy Longevity
Older adults who consume alcohol moderately on a regular basis are more likely to live to age 85 without dementia or other cognitive impairments than nondrinkers, according to a study published in the August issue of the Journal of Alzheimer’s Disease. Researchers examined 1,344 older community-dwelling adults and assessed alcohol intake by questionnaire in 1984–1987. They evaluated cognitive function in approximately four-year intervals between 1988 and 2009. About 49% of participants reported moderate alcohol intake, and 48% reported drinking almost daily. Relative to nondrinkers, moderate and heavy drinkers had significantly higher adjusted odds of survival to age 85 without cognitive impairment. Near-daily drinkers had two- to threefold higher adjusted odds of cognitively healthy longevity versus living to at least age 85 with cognitive impairment or death before age 85.
Richard EL, Kritz-Silverstein D, Laughlin GA, et al. Alcohol intake and cognitively healthy longevity in community-dwelling adults: The Rancho Bernardo Study. J Alzheimers Dis. 2017;59(3):803-814.
MRI Shows Brain Differences in Genetic Autism
In two genetically related cohorts at high risk for autism, reciprocal neuroanatomic abnormalities were associated with cognitive and behavioral impairments, according to a study published online ahead of print August 8 in Radiology. Researchers performed MRI on 79 carriers of a deletion at 16p11.2, 79 carriers of a duplication at 16p11.2, 64 unaffected family members, and 109 controls. The participants completed cognitive and behavioral tests, and neuroradiologists reviewed the images for development-related abnormalities. The researchers found differences in the brain structures of deletion and duplication carriers, compared with noncarriers. Deletion carriers had brain overgrowth, and duplication carriers had brain undergrowth. When investigators compared cognitive assessments to imaging findings, they found that any imaging feature associated with the deletion carriers indicated worse daily living, communication, and social skills.
Owen JP, Bukshpun P, Pojman N, et al. Brain MR imaging findings and associated outcomes in carriers of the reciprocal copy number variation at 16p11.2. Radiology. 2017 Aug 8 [Epub ahead of print].
FDA Clears Stimpod NMS460 for Relief of Chronic Pain
The FDA has cleared Stimpod NMS460, a noninvasive neuromodulation device, for the symptomatic relief and management of chronic intractable pain. The unit also can be used for the adjunctive treatment of postsurgical pain, posttraumatic acute pain, and pain control due to rehabilitation. The device has a pulsed radio frequency waveform that creates electromagnetic effects similar to those of invasive pulsed radio frequency treatments. Treatment is applied transcutaneously. Case studies have shown quick and notable relief of chronic intractable pain. The treatment has no known side effects. The Stimpod NMS460 also incorporates nerve-locating technology that includes a nerve-mapping probe that enables practitioners to evaluate the treatment progress of damaged nerves. Xavant Technology, which markets Stimpod NMS460, is headquartered in Pretoria, South Africa.
Longer Sleep Is Associated With Lower BMI
Adults who have poor sleep patterns are more likely to be overweight or obese and have poorer metabolic health, according to a study published July 27 in PLoS One. Researchers analyzed associations between sleep duration and adiposity, selected metabolic health markers, and diet using National Diet and Nutrition Survey data. In all, 1,615 adults (57.1% female) between ages 19 and 65 completed questions about sleep duration and three to four days of food diaries. Investigators recorded blood pressure and waist circumference. Fasting blood lipids, glucose, glycated hemoglobin, thyroid hormones, and high-sensitivity C-reactive protein were measured in a subset of participants. After adjusting for age, ethnicity, sex, smoking, and socioeconomic status, sleep duration was negatively associated with BMI and waist circumference. Sleep duration was positively associated with high-density lipoprotein cholesterol.
Potter GDM, Cade JE, Hardie LJ. Longer sleep is associated with lower BMI and favorable metabolic profiles in UK adults: findings from the National Diet and Nutrition Survey. PLoS One. 2017; 12(7):e0182195.
Can Bleeding Risk After Stroke Be Predicted?
The S2TOP-BLEED score can estimate three-year major bleeding risk in patients with transient ischemic attack (TIA) or ischemic stroke who use antiplatelet agents, according to a study published online ahead of print August 2 in Neurology. To develop this prediction model, researchers combined data from six trials investigating antiplatelet therapy after TIA or ischemic stroke. They performed Cox regression analyses stratified by trial to study the association between predictors and major bleeding. Major bleeding occurred in 1,530 of the 43,112 patients during 94,833 person-years of follow-up. The observed three-year risk of major bleeding was 4.6%. The investigators identified male sex, smoking, type of antiplatelet agents, outcome on modified Rankin Scale ≥ 3, prior stroke, high blood pressure, lower BMI, elderly status, Asian ethnicity, and diabetes as predictors of major bleeding.
Hilkens NA, Algra A, Diener HC, et al. Predicting major bleeding in patients with noncardioembolic stroke on antiplatelets: S2TOP-BLEED. Neurology. 2017 Aug 2 [Epub ahead of print].
Questionnaires Predict Survival in MS
The way patients with multiple sclerosis (MS) answer questionnaires could help to predict their survival rate from the disease, according to a study published July 10 in PLoS Medicine. From July 15, 2004, onward, 2,126 people with MS completed MS Impact Scale-29 (MSIS-29) questionnaires. By 2014, 264 participants had died. Higher baseline MSIS-29 physical score and higher baseline MSIS-29 psychologic score were associated with reduced survival time. In participants with high baseline MSIS-29 scores, mortality risk was greater if the MSIS-29 score worsened over one year. MSIS-29 physical scores were associated with survival time, independent of age, sex, and patient-reported Expanded Disability Status Scale score in a Cox regression analysis.
Raffel J, Wallace A, Gveric D, et al. Patient-reported outcomes and survival in multiple sclerosis: a 10-year retrospective cohort study using the Multiple Sclerosis Impact Scale-29. PLoS Med. 2017;14(7):e1002346.
—Kimberly Williams
Statin Prescription Varies in Stroke Belt
Less than half of patients with stroke discharged from the hospital receive a prescription for statins, and the likelihood of a prescription varies by patients’ location, sex, age, and race, according to a study published August 2 in the Journal of the American Heart Association. Researchers analyzed discharge medications for 323 participants hospitalized for an ischemic stroke during follow-up of the Reasons for Geographic and Racial Differences in Stroke study. In the Stroke Belt, participants ages 65 and older were 47% less likely to be discharged on a statin, compared with people younger than 65. Compared with women, men in the Stroke Belt were 31% less likely to be discharged on a statin, while men outside the Stroke Belt were more likely to be discharged on a statin.
Albright KC, Howard VJ, Howard G, et al. Age and sex disparities in discharge statin prescribing in the stroke belt: evidence from the Reasons for Geographic and Racial Differences in Stroke Study. J Am Heart Assoc. 2017;6(8).
Midlife Vascular Risk Factors Increase Risk of Dementia
Midlife vascular risk factors are associated with increased risk of dementia in blacks and whites, according to a study published online ahead of print August 7 in JAMA Neurology. In the Atherosclerosis Risk in Communities study, investigators measured demographic and vascular risk factors at baseline (ie, obesity, smoking, diabetes, prehypertension, hypertension, and hypercholesterolemia), along with the presence of the APOE ε4 genotype. After the baseline visit, participants had four additional in-person visits. In all, 1,516 cases of dementia (57.0% female and 34.9% black, with a mean age at visit 1 of 57.4) were identified among 15,744 participants. Black race, older age, lower educational attainment, and APOE ε4 genotype were associated with increased risk of dementia, as were midlife smoking, diabetes, prehypertension, and hypertension.
Gottesman RF, Albert MS, Alonso A, et al. Associations between midlife vascular risk factors and 25-year incident dementia in the Atherosclerosis Risk in Communities (ARIC) Cohort. JAMA Neurol. 2017 August 7 [Epub ahead of print].
Resistance Training May Slow the Progression of MS
Progressive resistance training may have a neuroprotective or neuroregenerative effect in relapsing-remitting multiple sclerosis (MS), according to a study published online ahead of print July 1 in Multiple Sclerosis Journal. This study was a 24-week randomized controlled crossover trial. Participants were assigned to training or to a wait list. Assessments included disability measures and MRI. The MS Functional Composite score improved in the training group, but disability, lesion load, and global brain volumes did not differ between groups. The researchers noted higher absolute cortical thickness values in 19 of 74 investigated cortical regions after progressive resistance training. Observed changes were confirmed and reproduced when comparing relative cortical thickness changes between groups in the anterior cingulate gyrus, temporal pole, orbital sulcus, and inferior temporal sulcus.
Kjølhede T, Siemonsen S, Wenzel D, et al. Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult Scler. 2017 Jul 1 [Epub ahead of print].
Noninvasive Device Measures Intracranial Pressure
A noninvasive device measures intracranial pressure (ICP) accurately, according to research published online ahead of print August 8 in the Journal of Neurosurgery. In patients with traumatic brain injury and subarachnoid hemorrhage who were undergoing treatment in a neurocritical intensive care unit, researchers recorded ICP using the gold-standard method of invasive external ventricular drainage or intraparenchymal monitoring. In addition, the authors simultaneously measured ICP noninvasively with a device that uses advanced signal-analysis algorithms for acoustic signals propagating through the cranium. Data were collected in 14 patients, yielding 2,543 data points of continuous parallel ICP values. For measurements at the ≥ 17-mm Hg cutoff, the sensitivity and specificity of the noninvasive device were 0.7541 and 0.8887, respectively. ICP values obtained using noninvasive and invasive monitoring methods correlated well.
Ganslandt O, Mourtzoukos S, Stadlbauer A, et al. Evaluation of a novel noninvasive ICP monitoring device in patients undergoing invasive ICP monitoring: preliminary results. J Neurosurg. 2017 Aug 8 [Epub ahead of print].
Strokes Decline Among Men, But Not Women
The rate of stroke in the US has declined among men, but not among women, according to a study published online ahead of print August 9 in Neurology. Researchers collected data on 1.3 million adults in Ohio and Kentucky between 1993 and 2010. They used medical records to identify first-ever strokes during four one-year periods. The researchers observed 7,710 incident strokes in the four periods, and 57% of them were among women. The incidence of all strokes decreased over time in men (263 to 192), but not in women (217 to 198). The researchers found a similar sex difference in the change in the rate of ischemic stroke (ie, a decline from 238 to 165 among men, and a change from 193 to 173 among women).
Madsen TE, Khoury J, Alwell K, et al. Sex-specific stroke incidence over time in the Greater Cincinnati/Northern Kentucky Stroke Study. Neurology. 2017 Aug 9 [Epub ahead of print].
Link Between Alcohol Intake and Cognitively Healthy Longevity
Older adults who consume alcohol moderately on a regular basis are more likely to live to age 85 without dementia or other cognitive impairments than nondrinkers, according to a study published in the August issue of the Journal of Alzheimer’s Disease. Researchers examined 1,344 older community-dwelling adults and assessed alcohol intake by questionnaire in 1984–1987. They evaluated cognitive function in approximately four-year intervals between 1988 and 2009. About 49% of participants reported moderate alcohol intake, and 48% reported drinking almost daily. Relative to nondrinkers, moderate and heavy drinkers had significantly higher adjusted odds of survival to age 85 without cognitive impairment. Near-daily drinkers had two- to threefold higher adjusted odds of cognitively healthy longevity versus living to at least age 85 with cognitive impairment or death before age 85.
Richard EL, Kritz-Silverstein D, Laughlin GA, et al. Alcohol intake and cognitively healthy longevity in community-dwelling adults: The Rancho Bernardo Study. J Alzheimers Dis. 2017;59(3):803-814.
MRI Shows Brain Differences in Genetic Autism
In two genetically related cohorts at high risk for autism, reciprocal neuroanatomic abnormalities were associated with cognitive and behavioral impairments, according to a study published online ahead of print August 8 in Radiology. Researchers performed MRI on 79 carriers of a deletion at 16p11.2, 79 carriers of a duplication at 16p11.2, 64 unaffected family members, and 109 controls. The participants completed cognitive and behavioral tests, and neuroradiologists reviewed the images for development-related abnormalities. The researchers found differences in the brain structures of deletion and duplication carriers, compared with noncarriers. Deletion carriers had brain overgrowth, and duplication carriers had brain undergrowth. When investigators compared cognitive assessments to imaging findings, they found that any imaging feature associated with the deletion carriers indicated worse daily living, communication, and social skills.
Owen JP, Bukshpun P, Pojman N, et al. Brain MR imaging findings and associated outcomes in carriers of the reciprocal copy number variation at 16p11.2. Radiology. 2017 Aug 8 [Epub ahead of print].
FDA Clears Stimpod NMS460 for Relief of Chronic Pain
The FDA has cleared Stimpod NMS460, a noninvasive neuromodulation device, for the symptomatic relief and management of chronic intractable pain. The unit also can be used for the adjunctive treatment of postsurgical pain, posttraumatic acute pain, and pain control due to rehabilitation. The device has a pulsed radio frequency waveform that creates electromagnetic effects similar to those of invasive pulsed radio frequency treatments. Treatment is applied transcutaneously. Case studies have shown quick and notable relief of chronic intractable pain. The treatment has no known side effects. The Stimpod NMS460 also incorporates nerve-locating technology that includes a nerve-mapping probe that enables practitioners to evaluate the treatment progress of damaged nerves. Xavant Technology, which markets Stimpod NMS460, is headquartered in Pretoria, South Africa.
Longer Sleep Is Associated With Lower BMI
Adults who have poor sleep patterns are more likely to be overweight or obese and have poorer metabolic health, according to a study published July 27 in PLoS One. Researchers analyzed associations between sleep duration and adiposity, selected metabolic health markers, and diet using National Diet and Nutrition Survey data. In all, 1,615 adults (57.1% female) between ages 19 and 65 completed questions about sleep duration and three to four days of food diaries. Investigators recorded blood pressure and waist circumference. Fasting blood lipids, glucose, glycated hemoglobin, thyroid hormones, and high-sensitivity C-reactive protein were measured in a subset of participants. After adjusting for age, ethnicity, sex, smoking, and socioeconomic status, sleep duration was negatively associated with BMI and waist circumference. Sleep duration was positively associated with high-density lipoprotein cholesterol.
Potter GDM, Cade JE, Hardie LJ. Longer sleep is associated with lower BMI and favorable metabolic profiles in UK adults: findings from the National Diet and Nutrition Survey. PLoS One. 2017; 12(7):e0182195.
Can Bleeding Risk After Stroke Be Predicted?
The S2TOP-BLEED score can estimate three-year major bleeding risk in patients with transient ischemic attack (TIA) or ischemic stroke who use antiplatelet agents, according to a study published online ahead of print August 2 in Neurology. To develop this prediction model, researchers combined data from six trials investigating antiplatelet therapy after TIA or ischemic stroke. They performed Cox regression analyses stratified by trial to study the association between predictors and major bleeding. Major bleeding occurred in 1,530 of the 43,112 patients during 94,833 person-years of follow-up. The observed three-year risk of major bleeding was 4.6%. The investigators identified male sex, smoking, type of antiplatelet agents, outcome on modified Rankin Scale ≥ 3, prior stroke, high blood pressure, lower BMI, elderly status, Asian ethnicity, and diabetes as predictors of major bleeding.
Hilkens NA, Algra A, Diener HC, et al. Predicting major bleeding in patients with noncardioembolic stroke on antiplatelets: S2TOP-BLEED. Neurology. 2017 Aug 2 [Epub ahead of print].
Questionnaires Predict Survival in MS
The way patients with multiple sclerosis (MS) answer questionnaires could help to predict their survival rate from the disease, according to a study published July 10 in PLoS Medicine. From July 15, 2004, onward, 2,126 people with MS completed MS Impact Scale-29 (MSIS-29) questionnaires. By 2014, 264 participants had died. Higher baseline MSIS-29 physical score and higher baseline MSIS-29 psychologic score were associated with reduced survival time. In participants with high baseline MSIS-29 scores, mortality risk was greater if the MSIS-29 score worsened over one year. MSIS-29 physical scores were associated with survival time, independent of age, sex, and patient-reported Expanded Disability Status Scale score in a Cox regression analysis.
Raffel J, Wallace A, Gveric D, et al. Patient-reported outcomes and survival in multiple sclerosis: a 10-year retrospective cohort study using the Multiple Sclerosis Impact Scale-29. PLoS Med. 2017;14(7):e1002346.
—Kimberly Williams
Statin Prescription Varies in Stroke Belt
Less than half of patients with stroke discharged from the hospital receive a prescription for statins, and the likelihood of a prescription varies by patients’ location, sex, age, and race, according to a study published August 2 in the Journal of the American Heart Association. Researchers analyzed discharge medications for 323 participants hospitalized for an ischemic stroke during follow-up of the Reasons for Geographic and Racial Differences in Stroke study. In the Stroke Belt, participants ages 65 and older were 47% less likely to be discharged on a statin, compared with people younger than 65. Compared with women, men in the Stroke Belt were 31% less likely to be discharged on a statin, while men outside the Stroke Belt were more likely to be discharged on a statin.
Albright KC, Howard VJ, Howard G, et al. Age and sex disparities in discharge statin prescribing in the stroke belt: evidence from the Reasons for Geographic and Racial Differences in Stroke Study. J Am Heart Assoc. 2017;6(8).
Midlife Vascular Risk Factors Increase Risk of Dementia
Midlife vascular risk factors are associated with increased risk of dementia in blacks and whites, according to a study published online ahead of print August 7 in JAMA Neurology. In the Atherosclerosis Risk in Communities study, investigators measured demographic and vascular risk factors at baseline (ie, obesity, smoking, diabetes, prehypertension, hypertension, and hypercholesterolemia), along with the presence of the APOE ε4 genotype. After the baseline visit, participants had four additional in-person visits. In all, 1,516 cases of dementia (57.0% female and 34.9% black, with a mean age at visit 1 of 57.4) were identified among 15,744 participants. Black race, older age, lower educational attainment, and APOE ε4 genotype were associated with increased risk of dementia, as were midlife smoking, diabetes, prehypertension, and hypertension.
Gottesman RF, Albert MS, Alonso A, et al. Associations between midlife vascular risk factors and 25-year incident dementia in the Atherosclerosis Risk in Communities (ARIC) Cohort. JAMA Neurol. 2017 August 7 [Epub ahead of print].
Resistance Training May Slow the Progression of MS
Progressive resistance training may have a neuroprotective or neuroregenerative effect in relapsing-remitting multiple sclerosis (MS), according to a study published online ahead of print July 1 in Multiple Sclerosis Journal. This study was a 24-week randomized controlled crossover trial. Participants were assigned to training or to a wait list. Assessments included disability measures and MRI. The MS Functional Composite score improved in the training group, but disability, lesion load, and global brain volumes did not differ between groups. The researchers noted higher absolute cortical thickness values in 19 of 74 investigated cortical regions after progressive resistance training. Observed changes were confirmed and reproduced when comparing relative cortical thickness changes between groups in the anterior cingulate gyrus, temporal pole, orbital sulcus, and inferior temporal sulcus.
Kjølhede T, Siemonsen S, Wenzel D, et al. Can resistance training impact MRI outcomes in relapsing-remitting multiple sclerosis? Mult Scler. 2017 Jul 1 [Epub ahead of print].
Noninvasive Device Measures Intracranial Pressure
A noninvasive device measures intracranial pressure (ICP) accurately, according to research published online ahead of print August 8 in the Journal of Neurosurgery. In patients with traumatic brain injury and subarachnoid hemorrhage who were undergoing treatment in a neurocritical intensive care unit, researchers recorded ICP using the gold-standard method of invasive external ventricular drainage or intraparenchymal monitoring. In addition, the authors simultaneously measured ICP noninvasively with a device that uses advanced signal-analysis algorithms for acoustic signals propagating through the cranium. Data were collected in 14 patients, yielding 2,543 data points of continuous parallel ICP values. For measurements at the ≥ 17-mm Hg cutoff, the sensitivity and specificity of the noninvasive device were 0.7541 and 0.8887, respectively. ICP values obtained using noninvasive and invasive monitoring methods correlated well.
Ganslandt O, Mourtzoukos S, Stadlbauer A, et al. Evaluation of a novel noninvasive ICP monitoring device in patients undergoing invasive ICP monitoring: preliminary results. J Neurosurg. 2017 Aug 8 [Epub ahead of print].
Strokes Decline Among Men, But Not Women
The rate of stroke in the US has declined among men, but not among women, according to a study published online ahead of print August 9 in Neurology. Researchers collected data on 1.3 million adults in Ohio and Kentucky between 1993 and 2010. They used medical records to identify first-ever strokes during four one-year periods. The researchers observed 7,710 incident strokes in the four periods, and 57% of them were among women. The incidence of all strokes decreased over time in men (263 to 192), but not in women (217 to 198). The researchers found a similar sex difference in the change in the rate of ischemic stroke (ie, a decline from 238 to 165 among men, and a change from 193 to 173 among women).
Madsen TE, Khoury J, Alwell K, et al. Sex-specific stroke incidence over time in the Greater Cincinnati/Northern Kentucky Stroke Study. Neurology. 2017 Aug 9 [Epub ahead of print].
Link Between Alcohol Intake and Cognitively Healthy Longevity
Older adults who consume alcohol moderately on a regular basis are more likely to live to age 85 without dementia or other cognitive impairments than nondrinkers, according to a study published in the August issue of the Journal of Alzheimer’s Disease. Researchers examined 1,344 older community-dwelling adults and assessed alcohol intake by questionnaire in 1984–1987. They evaluated cognitive function in approximately four-year intervals between 1988 and 2009. About 49% of participants reported moderate alcohol intake, and 48% reported drinking almost daily. Relative to nondrinkers, moderate and heavy drinkers had significantly higher adjusted odds of survival to age 85 without cognitive impairment. Near-daily drinkers had two- to threefold higher adjusted odds of cognitively healthy longevity versus living to at least age 85 with cognitive impairment or death before age 85.
Richard EL, Kritz-Silverstein D, Laughlin GA, et al. Alcohol intake and cognitively healthy longevity in community-dwelling adults: The Rancho Bernardo Study. J Alzheimers Dis. 2017;59(3):803-814.
MRI Shows Brain Differences in Genetic Autism
In two genetically related cohorts at high risk for autism, reciprocal neuroanatomic abnormalities were associated with cognitive and behavioral impairments, according to a study published online ahead of print August 8 in Radiology. Researchers performed MRI on 79 carriers of a deletion at 16p11.2, 79 carriers of a duplication at 16p11.2, 64 unaffected family members, and 109 controls. The participants completed cognitive and behavioral tests, and neuroradiologists reviewed the images for development-related abnormalities. The researchers found differences in the brain structures of deletion and duplication carriers, compared with noncarriers. Deletion carriers had brain overgrowth, and duplication carriers had brain undergrowth. When investigators compared cognitive assessments to imaging findings, they found that any imaging feature associated with the deletion carriers indicated worse daily living, communication, and social skills.
Owen JP, Bukshpun P, Pojman N, et al. Brain MR imaging findings and associated outcomes in carriers of the reciprocal copy number variation at 16p11.2. Radiology. 2017 Aug 8 [Epub ahead of print].
FDA Clears Stimpod NMS460 for Relief of Chronic Pain
The FDA has cleared Stimpod NMS460, a noninvasive neuromodulation device, for the symptomatic relief and management of chronic intractable pain. The unit also can be used for the adjunctive treatment of postsurgical pain, posttraumatic acute pain, and pain control due to rehabilitation. The device has a pulsed radio frequency waveform that creates electromagnetic effects similar to those of invasive pulsed radio frequency treatments. Treatment is applied transcutaneously. Case studies have shown quick and notable relief of chronic intractable pain. The treatment has no known side effects. The Stimpod NMS460 also incorporates nerve-locating technology that includes a nerve-mapping probe that enables practitioners to evaluate the treatment progress of damaged nerves. Xavant Technology, which markets Stimpod NMS460, is headquartered in Pretoria, South Africa.
Longer Sleep Is Associated With Lower BMI
Adults who have poor sleep patterns are more likely to be overweight or obese and have poorer metabolic health, according to a study published July 27 in PLoS One. Researchers analyzed associations between sleep duration and adiposity, selected metabolic health markers, and diet using National Diet and Nutrition Survey data. In all, 1,615 adults (57.1% female) between ages 19 and 65 completed questions about sleep duration and three to four days of food diaries. Investigators recorded blood pressure and waist circumference. Fasting blood lipids, glucose, glycated hemoglobin, thyroid hormones, and high-sensitivity C-reactive protein were measured in a subset of participants. After adjusting for age, ethnicity, sex, smoking, and socioeconomic status, sleep duration was negatively associated with BMI and waist circumference. Sleep duration was positively associated with high-density lipoprotein cholesterol.
Potter GDM, Cade JE, Hardie LJ. Longer sleep is associated with lower BMI and favorable metabolic profiles in UK adults: findings from the National Diet and Nutrition Survey. PLoS One. 2017; 12(7):e0182195.
Can Bleeding Risk After Stroke Be Predicted?
The S2TOP-BLEED score can estimate three-year major bleeding risk in patients with transient ischemic attack (TIA) or ischemic stroke who use antiplatelet agents, according to a study published online ahead of print August 2 in Neurology. To develop this prediction model, researchers combined data from six trials investigating antiplatelet therapy after TIA or ischemic stroke. They performed Cox regression analyses stratified by trial to study the association between predictors and major bleeding. Major bleeding occurred in 1,530 of the 43,112 patients during 94,833 person-years of follow-up. The observed three-year risk of major bleeding was 4.6%. The investigators identified male sex, smoking, type of antiplatelet agents, outcome on modified Rankin Scale ≥ 3, prior stroke, high blood pressure, lower BMI, elderly status, Asian ethnicity, and diabetes as predictors of major bleeding.
Hilkens NA, Algra A, Diener HC, et al. Predicting major bleeding in patients with noncardioembolic stroke on antiplatelets: S2TOP-BLEED. Neurology. 2017 Aug 2 [Epub ahead of print].
Questionnaires Predict Survival in MS
The way patients with multiple sclerosis (MS) answer questionnaires could help to predict their survival rate from the disease, according to a study published July 10 in PLoS Medicine. From July 15, 2004, onward, 2,126 people with MS completed MS Impact Scale-29 (MSIS-29) questionnaires. By 2014, 264 participants had died. Higher baseline MSIS-29 physical score and higher baseline MSIS-29 psychologic score were associated with reduced survival time. In participants with high baseline MSIS-29 scores, mortality risk was greater if the MSIS-29 score worsened over one year. MSIS-29 physical scores were associated with survival time, independent of age, sex, and patient-reported Expanded Disability Status Scale score in a Cox regression analysis.
Raffel J, Wallace A, Gveric D, et al. Patient-reported outcomes and survival in multiple sclerosis: a 10-year retrospective cohort study using the Multiple Sclerosis Impact Scale-29. PLoS Med. 2017;14(7):e1002346.
—Kimberly Williams

Annual mammograms from age 40 linked with greatest reductions in mortality
Annual mammograms starting at age 40 and continuing until age 84 will achieve the greatest reductions in breast cancer deaths, according to a modeling study published in Cancer.
Researchers used Cancer Intervention and Surveillance Modeling Network (CISNET) breast cancer models to compare three current mammography-based screening approaches for women at average risk of breast cancer. The first approach is for annual screening from ages 40-84 years, the second is a hybrid approach with annual screening from ages 45 to 54 then biennial screening from ages 55 to 79, and the third approach involves biennial mammograms from ages 50 to 74.
The modeling suggested that the largest mean reduction in mortality – 36.9% – was associated with annual screening starting at age 40. The second largest reduction of 30.8% occurred with the hybrid screening approach starting at age 45, while the smallest reduction in mortality – 23.2% – occurred with biennial screening starting at age 50 (Cancer 2017 Aug 21. doi: 10.1002/cncr.30842).
Annual screening also averted the most deaths from breast cancer – 11.9 per 1,000 women screened – and gained the most life-years (189 per 1,000 women screened, compared with 149 for the hybrid approach and 110 for biennial screening), reported Elizabeth K. Arleo, MD, of Weill Cornell Imaging at New York–Presbyterian, New York, and her coauthors.
However, the annual screening approach was also associated with the largest number of benign recalls and benign biopsies. The model suggested that a woman starting annual screening from age 40 could expect on average to be recalled for a benign diagnostic work-up every 13 years and undergo a benign biopsy every 187 years.
Overall, using a single-year cohort of women born in 1960 who were 100% compliant with screening, the model predicted that 44,671 would still die of breast cancer with annual screening, 51,211 would die under the hybrid screening model, and 56,887 would die under the biennial screening model.
“If the goal is to avert the most breast cancer deaths and gain the most life-years, CISNET modeling shows that the optimal age of initiation for screening mammography is 40 years, the optimal screening frequency is annual, and the optimal stopping age is when a woman’s life expectancy is less than 5-7 years,” the researchers wrote. “Individual women should continue to have the choice to reduce their risk of dying from breast cancer as much as possible, and as CISNET models show, annual mammography starting at age 40 years is the best way to do so.”
Two of the researchers reported consulting or institutional support from GE Healthcare. No other conflicts of interest were reported.
Annual mammograms starting at age 40 and continuing until age 84 will achieve the greatest reductions in breast cancer deaths, according to a modeling study published in Cancer.
Researchers used Cancer Intervention and Surveillance Modeling Network (CISNET) breast cancer models to compare three current mammography-based screening approaches for women at average risk of breast cancer. The first approach is for annual screening from ages 40-84 years, the second is a hybrid approach with annual screening from ages 45 to 54 then biennial screening from ages 55 to 79, and the third approach involves biennial mammograms from ages 50 to 74.
The modeling suggested that the largest mean reduction in mortality – 36.9% – was associated with annual screening starting at age 40. The second largest reduction of 30.8% occurred with the hybrid screening approach starting at age 45, while the smallest reduction in mortality – 23.2% – occurred with biennial screening starting at age 50 (Cancer 2017 Aug 21. doi: 10.1002/cncr.30842).
Annual screening also averted the most deaths from breast cancer – 11.9 per 1,000 women screened – and gained the most life-years (189 per 1,000 women screened, compared with 149 for the hybrid approach and 110 for biennial screening), reported Elizabeth K. Arleo, MD, of Weill Cornell Imaging at New York–Presbyterian, New York, and her coauthors.
However, the annual screening approach was also associated with the largest number of benign recalls and benign biopsies. The model suggested that a woman starting annual screening from age 40 could expect on average to be recalled for a benign diagnostic work-up every 13 years and undergo a benign biopsy every 187 years.
Overall, using a single-year cohort of women born in 1960 who were 100% compliant with screening, the model predicted that 44,671 would still die of breast cancer with annual screening, 51,211 would die under the hybrid screening model, and 56,887 would die under the biennial screening model.
“If the goal is to avert the most breast cancer deaths and gain the most life-years, CISNET modeling shows that the optimal age of initiation for screening mammography is 40 years, the optimal screening frequency is annual, and the optimal stopping age is when a woman’s life expectancy is less than 5-7 years,” the researchers wrote. “Individual women should continue to have the choice to reduce their risk of dying from breast cancer as much as possible, and as CISNET models show, annual mammography starting at age 40 years is the best way to do so.”
Two of the researchers reported consulting or institutional support from GE Healthcare. No other conflicts of interest were reported.
Annual mammograms starting at age 40 and continuing until age 84 will achieve the greatest reductions in breast cancer deaths, according to a modeling study published in Cancer.
Researchers used Cancer Intervention and Surveillance Modeling Network (CISNET) breast cancer models to compare three current mammography-based screening approaches for women at average risk of breast cancer. The first approach is for annual screening from ages 40-84 years, the second is a hybrid approach with annual screening from ages 45 to 54 then biennial screening from ages 55 to 79, and the third approach involves biennial mammograms from ages 50 to 74.
The modeling suggested that the largest mean reduction in mortality – 36.9% – was associated with annual screening starting at age 40. The second largest reduction of 30.8% occurred with the hybrid screening approach starting at age 45, while the smallest reduction in mortality – 23.2% – occurred with biennial screening starting at age 50 (Cancer 2017 Aug 21. doi: 10.1002/cncr.30842).
Annual screening also averted the most deaths from breast cancer – 11.9 per 1,000 women screened – and gained the most life-years (189 per 1,000 women screened, compared with 149 for the hybrid approach and 110 for biennial screening), reported Elizabeth K. Arleo, MD, of Weill Cornell Imaging at New York–Presbyterian, New York, and her coauthors.
However, the annual screening approach was also associated with the largest number of benign recalls and benign biopsies. The model suggested that a woman starting annual screening from age 40 could expect on average to be recalled for a benign diagnostic work-up every 13 years and undergo a benign biopsy every 187 years.
Overall, using a single-year cohort of women born in 1960 who were 100% compliant with screening, the model predicted that 44,671 would still die of breast cancer with annual screening, 51,211 would die under the hybrid screening model, and 56,887 would die under the biennial screening model.
“If the goal is to avert the most breast cancer deaths and gain the most life-years, CISNET modeling shows that the optimal age of initiation for screening mammography is 40 years, the optimal screening frequency is annual, and the optimal stopping age is when a woman’s life expectancy is less than 5-7 years,” the researchers wrote. “Individual women should continue to have the choice to reduce their risk of dying from breast cancer as much as possible, and as CISNET models show, annual mammography starting at age 40 years is the best way to do so.”
Two of the researchers reported consulting or institutional support from GE Healthcare. No other conflicts of interest were reported.
FROM CANCER
Key clinical point:
Major finding: Annual mammograms from age 40 are associated with a 36.9% mean reduction in mortality, compared with a 23.2% reduction with biennial screening from age 50.
Data source: A study using Cancer Intervention and Surveillance Modeling Network models.
Disclosures: Two of the researchers reported consulting or institutional support from GE Healthcare. No other conflicts of interest were reported.
The opioid crisis: Psychiatrists are well equipped to intervene
The U.S. opioid crisis and ongoing epidemic of chronic pain are inextricably intertwined, and psychiatrists are increasingly being called upon to intervene.
In a June 2016 blog post penned in the wake of new Centers for Disease Control and Prevention prescribing guidelines calling for a move away from opioids as the first-line treatment for many types of chronic noncancer pain, National Institute on Drug Abuse (NIDA) Director Nora D. Volkow, MD, decried the absence of psychiatrists on the front lines.
“Thus far, psychiatrists have not taken an active role in addressing the problem of chronic pain, but they have an important role to play here, for multiple reasons,” she wrote.
Chronic pain is closely linked to multiple psychiatric problems, she explained.

Furthermore, extensive evidence supports the use of some nonpharmacologic psychiatric therapies, she noted.
Indeed, there are numerous approaches, which have been shown to be effective or are showing promise in trials, that psychiatrists can take to intervene in the crisis and to help individual patients control pain and reduce the need for opioid medication. One that is underused and undervalued despite decades of research demonstrating its effectiveness, and which, according to David Spiegel, MD, has the potential to help at least two-thirds of affected adults, is hypnosis.
Power of hypnosis
“The brain has a whole lot to do with pain perception, and there’s a lot you can do to control it,” said Dr. Spiegel, the Jack, Samuel, and Lulu Willson Professor in Medicine in the department of psychiatry and behavioral sciences at Stanford (Calif.) University and a member of the Institute of Medicine.
And despite what many patients and physicians believe, it’s simply not true that if you’re not using a drug, you can’t actually control pain, he added.

For example, in a prospective randomized study of 241 patients undergoing percutaneous vascular and renal procedures, he and his colleagues found that self-hypnotic relaxation was superior to both intraoperative standard of care and structured attention (i.e., the “friendly nurse” group) for reducing pain and anxiety, and was better than standard of care for reducing drug use and reducing procedure time. It also improved hemodynamic stability compared with the other approaches (Lancet. 2000 Apr 29;355[9214]:1486-90).
“It works,” said Dr. Spiegel, also associate chair of the psychiatry department at Stanford.
Hypnotizability can be assessed using various validated scales; he said he can determine hypnotizability within 5 minutes, in part by giving a suggestion that the patient’s arm is getting lighter and is beginning to float. A component of involuntariness – if the patient’s arm feels like it is floating effortlessly and actually moves up in the air – indicates hypnotizability.
Most children, and about two of every three adults, can be hypnotized, he said.
Self-hypnosis, particularly in the chronic pain setting, can be life-changing, as patients can use it whenever needed once they learn how, he said, describing one young patient who had been suffering from intractable migraines and associated vomiting for years, and had failed to respond to numerous medications. Within minutes of being taught self-hypnosis, she said her pain had decreased from 7 to 3 on a 0-10 scale, and after coming out of the hypnotic state, she described feeling as rested as if she’d been sleeping for a decade.
Her mother broke down in tears of relief, Dr. Spiegel said.
Another patient who had suffered from immobilizing back pain had a similar experience: His back pain was immediately reduced by about 60% .
“Does it always work? No, but no treatment always works, and at worst it’s harmless,” Dr. Spiegel said, adding: “I don’t get people addicted to hypnosis. It just doesn’t happen.”
So why is hypnosis still considered outside the mainstream? In part that’s the case because of its “purple cape, dangling watch” image, but there also is a conception that hypnosis takes away control. In reality, it enhances control, he said.
“I think every psychiatrist – every physician – should know hypnosis,” he said.
Many, but not all medical schools teach hypnosis, and at least two U.S. societies – the American Society of Clinical Hypnosis and the Society for Clinical and Experimental Hypnosis – conduct workshops and annual scientific meetings where those interested can learn, he noted.
“It’s not that hard to learn ... and it’s a very useful skill for a professional,” he said.
Other approaches to pain management
For the one in three adults who are not hypnotizable, Dr. Spiegel teaches distraction techniques, and sometimes recommends acupuncture, which can be helpful for some patients. Exercise and physical therapy also can be of benefit for chronic pain.
“You can have very real pain that you can learn to deal with as people did throughout history. That doesn’t mean you should suffer unnecessarily; there is a time and place for opiates and other [pharmacologic] strategies, but they should be one among an array of choices,” he said, adding that for chronic pain, opioids can be more of a problem than a solution, and learning these techniques “can really help people safely deal with pain.”
Jeffrey Borckardt, PhD, professor and director of the division of biobehavioral medicine at the Medical University of South Carolina (MUSC), Charleston, agreed that hypnosis is a well-researched and effective treatment for pain, despite being better known for weight loss and smoking cessation. Another, lesser-known treatment that has been shown to have some effect for pain is acceptance and commitment therapy, or ACT, which incorporates the practice of mindfulness.

A 2014 study (J Pain. 2014 Jan;15[1]:101-13) demonstrated a beneficial effect of ACT in nearly 50% of patients studied, and in a 2017 study (J Pain. 2017 Jun;18[6]:664-72), ACT was associated with improved function in chronic pain patients.
However, there is another well-researched – and well-known – nonpharmacologic approach to the treatment of pain: cognitive-behavioral therapy, or CBT. CBT isn’t as new and exciting as some experimental approaches that Dr. Borckardt is working with and studying, such as transcranial magnetic stimulation and transcranial direct current stimulation. But CBT is readily available and typically covered by insurance (unlike those experimental therapies), and has been shown in numerous studies to be highly effective, he said.
CBT and ‘360’ programs
CBT also was mentioned by Dr. Volkow in her June 2016 blog post. She called it “one of the most effective pain treatments,” and said that “assisting patients in learning to change their pain-related thoughts, emotions, and behaviors is going to help with their condition, regardless of other pharmacological interventions.”
Dr. Borckardt said it is particularly effective in the context of programs that provide what he called “a 360 approach.” These multifaceted treatment programs aim to help chronic pain patients taper off of opioid medications and to find other approaches to managing pain.
Only a handful of such comprehensive, intensive outpatient programs exist across the United States, but the concept is taking hold, driven in part by the opioid crisis, and more centers are opening. In fact, Dr. Borckardt is helping to develop such a program at MUSC. The program will likely be housed in the MUSC Wellness Center, and much like the Mayo Clinic’s Pain Rehabilitation Center, which opened in 1974 and was one of the first such programs in the world, the MUSC program will involve an integrated team of health care professionals that provide CBT for pain, physical therapy, occupational therapy, and other programs designed to help patients living with pain.
This is widely accepted as being the best approach for pain rehabilitation, Dr. Borckardt said.
TMS and TDCS
Dr. Borckardt also has worked with some more cutting-edge approaches to pain management. Transcranial magnetic stimulation (TMS), which is approved for the treatment of depression, also has shown promise for treating pain. TMS can target areas in the brain involved with specific functioning, such as emotional regulation. The high-frequency stimulation is believed to enhance that particular area and produce a clinical effect.
“Pain is a subjective, largely psychological experience, and it involves an emotional component,” he said, explaining that the rationale for the use of TMS for pain is that the emotional component of the pain experience can be targeted along with the sensory and cognitive aspects of the pain experience.
TMS is being used in various studies, and has been used off label for pain management, but the out-of-pocket cost is high because it is not currently approved for pain and is therefore not covered by insurance, he said.
For depression, TMS typically is used 5 days per week for 3 weeks – at a cost ranging anywhere from $100 to $500 per session. It remains unclear how many sessions would be required for pain treatment to produce a sustained effect, but it would likely be similar to the requirements for depression treatment, and may also require follow-up treatments, Dr. Borckardt said.
“We do know with reasonable confidence that it impacts pain perception and can impact sensory or emotional components of pain, depending on the part of the brain treated. But we don’t know how long we have to treat, how often, or how durable the effects are,” he said, noting that several groups are studying TMS for pain.
Notably, there is also some very preliminary evidence that TMS may be useful for treating addiction by affecting cravings for substances such as opiates, nicotine, and alcohol. If that effect is confirmed, TMS could help chronic pain patients reduce their need for higher opioid doses, thereby lowering the risk of overdose, which is an important factor in the opioid crisis; most patients who use opioids don’t become addicted, but they can be at risk for overdose because of the need for high doses to control their pain, he explained.
In one study, the use of TMS postoperatively reduced the amount of in-hospital drug use by 40%, he said, noting that the reduction could convert to a reduction in the use of pain medication after discharge as well.
A related treatment, transcranial direct current stimulation, or tDCS, involves placement of electrodes directly on the scalp to run weak electrical currents through the brain, again trying to alter areas associated with pain perception. Ongoing studies are looking at combining tDCS and CBT with the hope that the two will have synergistic effects, including one in veterans with low back pain and opioid misuse. Another small pilot study in patients with fibromyalgia recently concluded and had some promising results.
These and other nonpharmacologic approaches to pain management could play an important role in the effort to reduce opioid prescribing. Currently, about 90 Americans die each day after overdosing on opioids, according to NIDA, and the CDC estimates that prescription opioid misuse alone in the United States costs $78.5 billion per year in health care, lost productivity, addiction treatment, and criminal justice involvement.
In her plea to psychiatrists to take action to intervene, Dr. Volkow underscored the value that they bring to the table.
“It is crucial that we not lose sight of the reality and complexity of chronic pain as management of chronic noncancer pain moves toward greater caution around opioid medication. This should not be solely an issue for primary care medicine or neurology, but also for specialties such as psychiatry that have much to offer people who are suffering from complex disorders in which physical symptoms merge with psychological distress,” she wrote.
Dr. Volkow has written hundreds of peer-reviewed articles, including analyses of the opioid crisis (N Engl J Med. 2017 Jul 27;377[4]:391-4) and (Neuron. 2016 Oct 19[2]:294-7). Dr. Spiegel is coauthor of Trance and Treatment: Clinical Uses of Hypnosis (Washington: American Psychiatric Association Publishing, 2004), a textbook written to help psychiatrists and other physicians learn to use hypnosis. Dr. Borckardt receives research funding from the National Institutes of Health.
The U.S. opioid crisis and ongoing epidemic of chronic pain are inextricably intertwined, and psychiatrists are increasingly being called upon to intervene.
In a June 2016 blog post penned in the wake of new Centers for Disease Control and Prevention prescribing guidelines calling for a move away from opioids as the first-line treatment for many types of chronic noncancer pain, National Institute on Drug Abuse (NIDA) Director Nora D. Volkow, MD, decried the absence of psychiatrists on the front lines.
“Thus far, psychiatrists have not taken an active role in addressing the problem of chronic pain, but they have an important role to play here, for multiple reasons,” she wrote.
Chronic pain is closely linked to multiple psychiatric problems, she explained.
Furthermore, extensive evidence supports the use of some nonpharmacologic psychiatric therapies, she noted.
Indeed, there are numerous approaches, which have been shown to be effective or are showing promise in trials, that psychiatrists can take to intervene in the crisis and to help individual patients control pain and reduce the need for opioid medication. One that is underused and undervalued despite decades of research demonstrating its effectiveness, and which, according to David Spiegel, MD, has the potential to help at least two-thirds of affected adults, is hypnosis.
Power of hypnosis
“The brain has a whole lot to do with pain perception, and there’s a lot you can do to control it,” said Dr. Spiegel, the Jack, Samuel, and Lulu Willson Professor in Medicine in the department of psychiatry and behavioral sciences at Stanford (Calif.) University and a member of the Institute of Medicine.
And despite what many patients and physicians believe, it’s simply not true that if you’re not using a drug, you can’t actually control pain, he added.
For example, in a prospective randomized study of 241 patients undergoing percutaneous vascular and renal procedures, he and his colleagues found that self-hypnotic relaxation was superior to both intraoperative standard of care and structured attention (i.e., the “friendly nurse” group) for reducing pain and anxiety, and was better than standard of care for reducing drug use and reducing procedure time. It also improved hemodynamic stability compared with the other approaches (Lancet. 2000 Apr 29;355[9214]:1486-90).
“It works,” said Dr. Spiegel, also associate chair of the psychiatry department at Stanford.
Hypnotizability can be assessed using various validated scales; he said he can determine hypnotizability within 5 minutes, in part by giving a suggestion that the patient’s arm is getting lighter and is beginning to float. A component of involuntariness – if the patient’s arm feels like it is floating effortlessly and actually moves up in the air – indicates hypnotizability.
Most children, and about two of every three adults, can be hypnotized, he said.
Self-hypnosis, particularly in the chronic pain setting, can be life-changing, as patients can use it whenever needed once they learn how, he said, describing one young patient who had been suffering from intractable migraines and associated vomiting for years, and had failed to respond to numerous medications. Within minutes of being taught self-hypnosis, she said her pain had decreased from 7 to 3 on a 0-10 scale, and after coming out of the hypnotic state, she described feeling as rested as if she’d been sleeping for a decade.
Her mother broke down in tears of relief, Dr. Spiegel said.
Another patient who had suffered from immobilizing back pain had a similar experience: His back pain was immediately reduced by about 60% .
“Does it always work? No, but no treatment always works, and at worst it’s harmless,” Dr. Spiegel said, adding: “I don’t get people addicted to hypnosis. It just doesn’t happen.”
So why is hypnosis still considered outside the mainstream? In part that’s the case because of its “purple cape, dangling watch” image, but there also is a conception that hypnosis takes away control. In reality, it enhances control, he said.
“I think every psychiatrist – every physician – should know hypnosis,” he said.
Many, but not all medical schools teach hypnosis, and at least two U.S. societies – the American Society of Clinical Hypnosis and the Society for Clinical and Experimental Hypnosis – conduct workshops and annual scientific meetings where those interested can learn, he noted.
“It’s not that hard to learn ... and it’s a very useful skill for a professional,” he said.
Other approaches to pain management
For the one in three adults who are not hypnotizable, Dr. Spiegel teaches distraction techniques, and sometimes recommends acupuncture, which can be helpful for some patients. Exercise and physical therapy also can be of benefit for chronic pain.
“You can have very real pain that you can learn to deal with as people did throughout history. That doesn’t mean you should suffer unnecessarily; there is a time and place for opiates and other [pharmacologic] strategies, but they should be one among an array of choices,” he said, adding that for chronic pain, opioids can be more of a problem than a solution, and learning these techniques “can really help people safely deal with pain.”
Jeffrey Borckardt, PhD, professor and director of the division of biobehavioral medicine at the Medical University of South Carolina (MUSC), Charleston, agreed that hypnosis is a well-researched and effective treatment for pain, despite being better known for weight loss and smoking cessation. Another, lesser-known treatment that has been shown to have some effect for pain is acceptance and commitment therapy, or ACT, which incorporates the practice of mindfulness.
A 2014 study (J Pain. 2014 Jan;15[1]:101-13) demonstrated a beneficial effect of ACT in nearly 50% of patients studied, and in a 2017 study (J Pain. 2017 Jun;18[6]:664-72), ACT was associated with improved function in chronic pain patients.
However, there is another well-researched – and well-known – nonpharmacologic approach to the treatment of pain: cognitive-behavioral therapy, or CBT. CBT isn’t as new and exciting as some experimental approaches that Dr. Borckardt is working with and studying, such as transcranial magnetic stimulation and transcranial direct current stimulation. But CBT is readily available and typically covered by insurance (unlike those experimental therapies), and has been shown in numerous studies to be highly effective, he said.
CBT and ‘360’ programs
CBT also was mentioned by Dr. Volkow in her June 2016 blog post. She called it “one of the most effective pain treatments,” and said that “assisting patients in learning to change their pain-related thoughts, emotions, and behaviors is going to help with their condition, regardless of other pharmacological interventions.”
Dr. Borckardt said it is particularly effective in the context of programs that provide what he called “a 360 approach.” These multifaceted treatment programs aim to help chronic pain patients taper off of opioid medications and to find other approaches to managing pain.
Only a handful of such comprehensive, intensive outpatient programs exist across the United States, but the concept is taking hold, driven in part by the opioid crisis, and more centers are opening. In fact, Dr. Borckardt is helping to develop such a program at MUSC. The program will likely be housed in the MUSC Wellness Center, and much like the Mayo Clinic’s Pain Rehabilitation Center, which opened in 1974 and was one of the first such programs in the world, the MUSC program will involve an integrated team of health care professionals that provide CBT for pain, physical therapy, occupational therapy, and other programs designed to help patients living with pain.
This is widely accepted as being the best approach for pain rehabilitation, Dr. Borckardt said.
TMS and TDCS
Dr. Borckardt also has worked with some more cutting-edge approaches to pain management. Transcranial magnetic stimulation (TMS), which is approved for the treatment of depression, also has shown promise for treating pain. TMS can target areas in the brain involved with specific functioning, such as emotional regulation. The high-frequency stimulation is believed to enhance that particular area and produce a clinical effect.
“Pain is a subjective, largely psychological experience, and it involves an emotional component,” he said, explaining that the rationale for the use of TMS for pain is that the emotional component of the pain experience can be targeted along with the sensory and cognitive aspects of the pain experience.
TMS is being used in various studies, and has been used off label for pain management, but the out-of-pocket cost is high because it is not currently approved for pain and is therefore not covered by insurance, he said.
For depression, TMS typically is used 5 days per week for 3 weeks – at a cost ranging anywhere from $100 to $500 per session. It remains unclear how many sessions would be required for pain treatment to produce a sustained effect, but it would likely be similar to the requirements for depression treatment, and may also require follow-up treatments, Dr. Borckardt said.
“We do know with reasonable confidence that it impacts pain perception and can impact sensory or emotional components of pain, depending on the part of the brain treated. But we don’t know how long we have to treat, how often, or how durable the effects are,” he said, noting that several groups are studying TMS for pain.
Notably, there is also some very preliminary evidence that TMS may be useful for treating addiction by affecting cravings for substances such as opiates, nicotine, and alcohol. If that effect is confirmed, TMS could help chronic pain patients reduce their need for higher opioid doses, thereby lowering the risk of overdose, which is an important factor in the opioid crisis; most patients who use opioids don’t become addicted, but they can be at risk for overdose because of the need for high doses to control their pain, he explained.
In one study, the use of TMS postoperatively reduced the amount of in-hospital drug use by 40%, he said, noting that the reduction could convert to a reduction in the use of pain medication after discharge as well.
A related treatment, transcranial direct current stimulation, or tDCS, involves placement of electrodes directly on the scalp to run weak electrical currents through the brain, again trying to alter areas associated with pain perception. Ongoing studies are looking at combining tDCS and CBT with the hope that the two will have synergistic effects, including one in veterans with low back pain and opioid misuse. Another small pilot study in patients with fibromyalgia recently concluded and had some promising results.
These and other nonpharmacologic approaches to pain management could play an important role in the effort to reduce opioid prescribing. Currently, about 90 Americans die each day after overdosing on opioids, according to NIDA, and the CDC estimates that prescription opioid misuse alone in the United States costs $78.5 billion per year in health care, lost productivity, addiction treatment, and criminal justice involvement.
In her plea to psychiatrists to take action to intervene, Dr. Volkow underscored the value that they bring to the table.
“It is crucial that we not lose sight of the reality and complexity of chronic pain as management of chronic noncancer pain moves toward greater caution around opioid medication. This should not be solely an issue for primary care medicine or neurology, but also for specialties such as psychiatry that have much to offer people who are suffering from complex disorders in which physical symptoms merge with psychological distress,” she wrote.
Dr. Volkow has written hundreds of peer-reviewed articles, including analyses of the opioid crisis (N Engl J Med. 2017 Jul 27;377[4]:391-4) and (Neuron. 2016 Oct 19[2]:294-7). Dr. Spiegel is coauthor of Trance and Treatment: Clinical Uses of Hypnosis (Washington: American Psychiatric Association Publishing, 2004), a textbook written to help psychiatrists and other physicians learn to use hypnosis. Dr. Borckardt receives research funding from the National Institutes of Health.
The U.S. opioid crisis and ongoing epidemic of chronic pain are inextricably intertwined, and psychiatrists are increasingly being called upon to intervene.
In a June 2016 blog post penned in the wake of new Centers for Disease Control and Prevention prescribing guidelines calling for a move away from opioids as the first-line treatment for many types of chronic noncancer pain, National Institute on Drug Abuse (NIDA) Director Nora D. Volkow, MD, decried the absence of psychiatrists on the front lines.
“Thus far, psychiatrists have not taken an active role in addressing the problem of chronic pain, but they have an important role to play here, for multiple reasons,” she wrote.
Chronic pain is closely linked to multiple psychiatric problems, she explained.
Furthermore, extensive evidence supports the use of some nonpharmacologic psychiatric therapies, she noted.
Indeed, there are numerous approaches, which have been shown to be effective or are showing promise in trials, that psychiatrists can take to intervene in the crisis and to help individual patients control pain and reduce the need for opioid medication. One that is underused and undervalued despite decades of research demonstrating its effectiveness, and which, according to David Spiegel, MD, has the potential to help at least two-thirds of affected adults, is hypnosis.
Power of hypnosis
“The brain has a whole lot to do with pain perception, and there’s a lot you can do to control it,” said Dr. Spiegel, the Jack, Samuel, and Lulu Willson Professor in Medicine in the department of psychiatry and behavioral sciences at Stanford (Calif.) University and a member of the Institute of Medicine.
And despite what many patients and physicians believe, it’s simply not true that if you’re not using a drug, you can’t actually control pain, he added.
For example, in a prospective randomized study of 241 patients undergoing percutaneous vascular and renal procedures, he and his colleagues found that self-hypnotic relaxation was superior to both intraoperative standard of care and structured attention (i.e., the “friendly nurse” group) for reducing pain and anxiety, and was better than standard of care for reducing drug use and reducing procedure time. It also improved hemodynamic stability compared with the other approaches (Lancet. 2000 Apr 29;355[9214]:1486-90).
“It works,” said Dr. Spiegel, also associate chair of the psychiatry department at Stanford.
Hypnotizability can be assessed using various validated scales; he said he can determine hypnotizability within 5 minutes, in part by giving a suggestion that the patient’s arm is getting lighter and is beginning to float. A component of involuntariness – if the patient’s arm feels like it is floating effortlessly and actually moves up in the air – indicates hypnotizability.
Most children, and about two of every three adults, can be hypnotized, he said.
Self-hypnosis, particularly in the chronic pain setting, can be life-changing, as patients can use it whenever needed once they learn how, he said, describing one young patient who had been suffering from intractable migraines and associated vomiting for years, and had failed to respond to numerous medications. Within minutes of being taught self-hypnosis, she said her pain had decreased from 7 to 3 on a 0-10 scale, and after coming out of the hypnotic state, she described feeling as rested as if she’d been sleeping for a decade.
Her mother broke down in tears of relief, Dr. Spiegel said.
Another patient who had suffered from immobilizing back pain had a similar experience: His back pain was immediately reduced by about 60% .
“Does it always work? No, but no treatment always works, and at worst it’s harmless,” Dr. Spiegel said, adding: “I don’t get people addicted to hypnosis. It just doesn’t happen.”
So why is hypnosis still considered outside the mainstream? In part that’s the case because of its “purple cape, dangling watch” image, but there also is a conception that hypnosis takes away control. In reality, it enhances control, he said.
“I think every psychiatrist – every physician – should know hypnosis,” he said.
Many, but not all medical schools teach hypnosis, and at least two U.S. societies – the American Society of Clinical Hypnosis and the Society for Clinical and Experimental Hypnosis – conduct workshops and annual scientific meetings where those interested can learn, he noted.
“It’s not that hard to learn ... and it’s a very useful skill for a professional,” he said.
Other approaches to pain management
For the one in three adults who are not hypnotizable, Dr. Spiegel teaches distraction techniques, and sometimes recommends acupuncture, which can be helpful for some patients. Exercise and physical therapy also can be of benefit for chronic pain.
“You can have very real pain that you can learn to deal with as people did throughout history. That doesn’t mean you should suffer unnecessarily; there is a time and place for opiates and other [pharmacologic] strategies, but they should be one among an array of choices,” he said, adding that for chronic pain, opioids can be more of a problem than a solution, and learning these techniques “can really help people safely deal with pain.”
Jeffrey Borckardt, PhD, professor and director of the division of biobehavioral medicine at the Medical University of South Carolina (MUSC), Charleston, agreed that hypnosis is a well-researched and effective treatment for pain, despite being better known for weight loss and smoking cessation. Another, lesser-known treatment that has been shown to have some effect for pain is acceptance and commitment therapy, or ACT, which incorporates the practice of mindfulness.
A 2014 study (J Pain. 2014 Jan;15[1]:101-13) demonstrated a beneficial effect of ACT in nearly 50% of patients studied, and in a 2017 study (J Pain. 2017 Jun;18[6]:664-72), ACT was associated with improved function in chronic pain patients.
However, there is another well-researched – and well-known – nonpharmacologic approach to the treatment of pain: cognitive-behavioral therapy, or CBT. CBT isn’t as new and exciting as some experimental approaches that Dr. Borckardt is working with and studying, such as transcranial magnetic stimulation and transcranial direct current stimulation. But CBT is readily available and typically covered by insurance (unlike those experimental therapies), and has been shown in numerous studies to be highly effective, he said.
CBT and ‘360’ programs
CBT also was mentioned by Dr. Volkow in her June 2016 blog post. She called it “one of the most effective pain treatments,” and said that “assisting patients in learning to change their pain-related thoughts, emotions, and behaviors is going to help with their condition, regardless of other pharmacological interventions.”
Dr. Borckardt said it is particularly effective in the context of programs that provide what he called “a 360 approach.” These multifaceted treatment programs aim to help chronic pain patients taper off of opioid medications and to find other approaches to managing pain.
Only a handful of such comprehensive, intensive outpatient programs exist across the United States, but the concept is taking hold, driven in part by the opioid crisis, and more centers are opening. In fact, Dr. Borckardt is helping to develop such a program at MUSC. The program will likely be housed in the MUSC Wellness Center, and much like the Mayo Clinic’s Pain Rehabilitation Center, which opened in 1974 and was one of the first such programs in the world, the MUSC program will involve an integrated team of health care professionals that provide CBT for pain, physical therapy, occupational therapy, and other programs designed to help patients living with pain.
This is widely accepted as being the best approach for pain rehabilitation, Dr. Borckardt said.
TMS and TDCS
Dr. Borckardt also has worked with some more cutting-edge approaches to pain management. Transcranial magnetic stimulation (TMS), which is approved for the treatment of depression, also has shown promise for treating pain. TMS can target areas in the brain involved with specific functioning, such as emotional regulation. The high-frequency stimulation is believed to enhance that particular area and produce a clinical effect.
“Pain is a subjective, largely psychological experience, and it involves an emotional component,” he said, explaining that the rationale for the use of TMS for pain is that the emotional component of the pain experience can be targeted along with the sensory and cognitive aspects of the pain experience.
TMS is being used in various studies, and has been used off label for pain management, but the out-of-pocket cost is high because it is not currently approved for pain and is therefore not covered by insurance, he said.
For depression, TMS typically is used 5 days per week for 3 weeks – at a cost ranging anywhere from $100 to $500 per session. It remains unclear how many sessions would be required for pain treatment to produce a sustained effect, but it would likely be similar to the requirements for depression treatment, and may also require follow-up treatments, Dr. Borckardt said.
“We do know with reasonable confidence that it impacts pain perception and can impact sensory or emotional components of pain, depending on the part of the brain treated. But we don’t know how long we have to treat, how often, or how durable the effects are,” he said, noting that several groups are studying TMS for pain.
Notably, there is also some very preliminary evidence that TMS may be useful for treating addiction by affecting cravings for substances such as opiates, nicotine, and alcohol. If that effect is confirmed, TMS could help chronic pain patients reduce their need for higher opioid doses, thereby lowering the risk of overdose, which is an important factor in the opioid crisis; most patients who use opioids don’t become addicted, but they can be at risk for overdose because of the need for high doses to control their pain, he explained.
In one study, the use of TMS postoperatively reduced the amount of in-hospital drug use by 40%, he said, noting that the reduction could convert to a reduction in the use of pain medication after discharge as well.
A related treatment, transcranial direct current stimulation, or tDCS, involves placement of electrodes directly on the scalp to run weak electrical currents through the brain, again trying to alter areas associated with pain perception. Ongoing studies are looking at combining tDCS and CBT with the hope that the two will have synergistic effects, including one in veterans with low back pain and opioid misuse. Another small pilot study in patients with fibromyalgia recently concluded and had some promising results.
These and other nonpharmacologic approaches to pain management could play an important role in the effort to reduce opioid prescribing. Currently, about 90 Americans die each day after overdosing on opioids, according to NIDA, and the CDC estimates that prescription opioid misuse alone in the United States costs $78.5 billion per year in health care, lost productivity, addiction treatment, and criminal justice involvement.
In her plea to psychiatrists to take action to intervene, Dr. Volkow underscored the value that they bring to the table.
“It is crucial that we not lose sight of the reality and complexity of chronic pain as management of chronic noncancer pain moves toward greater caution around opioid medication. This should not be solely an issue for primary care medicine or neurology, but also for specialties such as psychiatry that have much to offer people who are suffering from complex disorders in which physical symptoms merge with psychological distress,” she wrote.
Dr. Volkow has written hundreds of peer-reviewed articles, including analyses of the opioid crisis (N Engl J Med. 2017 Jul 27;377[4]:391-4) and (Neuron. 2016 Oct 19[2]:294-7). Dr. Spiegel is coauthor of Trance and Treatment: Clinical Uses of Hypnosis (Washington: American Psychiatric Association Publishing, 2004), a textbook written to help psychiatrists and other physicians learn to use hypnosis. Dr. Borckardt receives research funding from the National Institutes of Health.