User login
VIDEO: Loss of function in Rab10 gene cuts Alzheimer’s risk by up to 40%
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
TORONTO – A rare loss of function in a gene that influences gamma secretase trafficking has been found to reduce the risk of Alzheimer’s by up to 40%, even in people who are homozygous carriers of the apolipoprotein E (apo E) epsilon 4 allele.
The gene – Rab10 – is a member of a family of about 60 genes involved in intracellular protein transport, Keoni Kauwe, PhD, said at the Alzheimer’s Association International Conference 2016. In addition to influencing endocytosis, ciliary transport, phagosome maturation, and insulin transport, Rab10 appears to assist in the transport of gamma secretase to the cell membrane.
By studying a population of elders who appear resistant to developing Alzheimer’s, Dr. Kauwe of Brigham Young University, Provo, Utah, and his associates determined that many of them share a natural inhibition of Rab10 – a unique characteristic that strongly contributes to their resistance to Alzheimer’s, he said. This knocked-down function would decrease the amount of gamma secretase to reach the cell membrane, Dr. Kauwe reasoned. Therefore, the proteolytic pathway that creates amyloid beta (Abeta) should be attenuated, allowing much less amyloid beta to be created and, presumably, be around to initiate the amyloid cascade that sparks Alzheimer’s disease.
His study cohort was drawn from two large data sets of cognitively normal elders, including many who were apo E epsilon 4 homozygotes. About 5% of the sample showed the loss-of-function Rab10 variant, which Dr. Kauwe said conferred a 20%-40% risk reduction for developing Alzheimer’s disease.
To understand the gene’s effects on amyloid beta production, he both overexpressed it and silenced it in cell lines. Overexpression resulted in a significant increase in the Abeta42/Abeta40 ratio (a riskier Alzheimer’s profile), while silencing it resulted in a significant decrease in the Abeta42/Abeta40 ratio (a more favorable profile).
Rab10 could be a therapeutic target, similar to the PCSK9 gene that influences low-density lipoprotein creation, Dr. Kauwe said. Monoclonal antibodies that block PCSK9 have recently been developed after a similar observation that naturally occurring loss of functions in the gene was associated with lower LDL levels.
“We’re going to be looking at the same thing with Rab10,” he said. “We do think that Rab10 inhibition could be a big story. It’s a high-risk venture, certainly, but it could also be high reward.”
Dr. Kauwe discussed his findings in a video interview at the conference.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @alz_gal
AT AAIC 2016

ACOG: Offer immediate postpartum LARC as option
Use of long-acting reversible contraception immediately post partum can help reduce the risk of unintended and short-interval pregnancy, according to a new policy statement from the American College of Obstetricians and Gynecologists.
“Immediate postpartum LARC should be offered as an effective option for postpartum contraception; there are few contraindications to postpartum IUDs and implants,” according to the statement issued by ACOG’s Committee on Obstetric Practice (Obstet Gynecol. 2016;128:e32-37).

Unintended pregnancies account for approximately 45% of pregnancies in the United States overall, and at least 70% of pregnancies in the first year post partum, the committee noted.
The statement recommends prenatal counseling about the risks and benefits of LARCs, along with alternatives, to help patients make informed decisions. The committee emphasized that health care providers “should counsel women about the convenience and effectiveness of immediate postpartum LARC, as well as the benefits of reducing unintended pregnancy and lengthening pregnancy intervals.”
However, immediate postpartum use of IUDs is contraindicated in women with intrauterine infection at delivery, postpartum hemorrhage, and puerperal sepsis.
The committee called for systems to provide LARC at the comprehensive postpartum visit if necessary, and recommended stocking LARC devices in labor and delivery units for immediate postpartum placement. In addition, coding and reimbursement strategies are needed to support immediate postpartum LARC, according to the statement.
The policy statement was endorsed by the American College of Nurse-Midwives and the Society for Maternal-Fetal Medicine.
Use of long-acting reversible contraception immediately post partum can help reduce the risk of unintended and short-interval pregnancy, according to a new policy statement from the American College of Obstetricians and Gynecologists.
“Immediate postpartum LARC should be offered as an effective option for postpartum contraception; there are few contraindications to postpartum IUDs and implants,” according to the statement issued by ACOG’s Committee on Obstetric Practice (Obstet Gynecol. 2016;128:e32-37).
Unintended pregnancies account for approximately 45% of pregnancies in the United States overall, and at least 70% of pregnancies in the first year post partum, the committee noted.
The statement recommends prenatal counseling about the risks and benefits of LARCs, along with alternatives, to help patients make informed decisions. The committee emphasized that health care providers “should counsel women about the convenience and effectiveness of immediate postpartum LARC, as well as the benefits of reducing unintended pregnancy and lengthening pregnancy intervals.”
However, immediate postpartum use of IUDs is contraindicated in women with intrauterine infection at delivery, postpartum hemorrhage, and puerperal sepsis.
The committee called for systems to provide LARC at the comprehensive postpartum visit if necessary, and recommended stocking LARC devices in labor and delivery units for immediate postpartum placement. In addition, coding and reimbursement strategies are needed to support immediate postpartum LARC, according to the statement.
The policy statement was endorsed by the American College of Nurse-Midwives and the Society for Maternal-Fetal Medicine.
Use of long-acting reversible contraception immediately post partum can help reduce the risk of unintended and short-interval pregnancy, according to a new policy statement from the American College of Obstetricians and Gynecologists.
“Immediate postpartum LARC should be offered as an effective option for postpartum contraception; there are few contraindications to postpartum IUDs and implants,” according to the statement issued by ACOG’s Committee on Obstetric Practice (Obstet Gynecol. 2016;128:e32-37).
Unintended pregnancies account for approximately 45% of pregnancies in the United States overall, and at least 70% of pregnancies in the first year post partum, the committee noted.
The statement recommends prenatal counseling about the risks and benefits of LARCs, along with alternatives, to help patients make informed decisions. The committee emphasized that health care providers “should counsel women about the convenience and effectiveness of immediate postpartum LARC, as well as the benefits of reducing unintended pregnancy and lengthening pregnancy intervals.”
However, immediate postpartum use of IUDs is contraindicated in women with intrauterine infection at delivery, postpartum hemorrhage, and puerperal sepsis.
The committee called for systems to provide LARC at the comprehensive postpartum visit if necessary, and recommended stocking LARC devices in labor and delivery units for immediate postpartum placement. In addition, coding and reimbursement strategies are needed to support immediate postpartum LARC, according to the statement.
The policy statement was endorsed by the American College of Nurse-Midwives and the Society for Maternal-Fetal Medicine.
FROM OBSTETRICS & GYNECOLOGY

CDC Updates Zika Guidance for Managing Pregnant Women
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).

All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).
All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).
All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
FROM MMWR

CDC updates Zika guidance for managing pregnant women
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).

All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).
All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
Updated guidelines released by the Centers for Disease Control and Prevention outline how to diagnose suspected cases of Zika virus infection among pregnant women based on how quickly they present with symptoms.
The guidance was updated in light of “the emerging data indicating that Zika virus RNA can be detected for prolonged periods in some pregnant women,” the CDC wrote in the July 25 issue of the Morbidity and Mortality Weekly Report (doi: 10.15585/mmwr.mm6529e1).
All pregnant women should be assessed for Zika virus at each of their prenatal care visits, regardless of their recent travel history or exposure to mosquitoes, by being evaluated for signs and symptoms of infection, such as fever, rash, and arthralgia. From there, management can take one of two directions.
The first direction involves women who are tested within 2 weeks of either symptom onset, or their suspected exposure to the virus. Pregnant women who are asymptomatic and do not live in an area with an ongoing Zika virus outbreak, as well as women who are symptomatic, should have their serum and urine analyzed using a real-time reverse transcription–polymerase chain reaction (rRT-PCR) test. If the result of this test is positive, it should be considered as confirmation that the woman has a “recent Zika virus infection.”
However, if the test results are negative, symptomatic women should undergo immunoglobin M testing for both Zika virus and dengue virus, while asymptomatic women should undergo just Zika virus IgM testing within 2-12 weeks of the possible exposure. In either case, if the tests come back negative, then the patient can be definitively cleared of any recent Zika virus infection. However, if either the Zika virus or dengue virus tests are positive or equivocal, then there is a “presumptive recent Zika virus or dengue virus or Flavivirus infection” in the woman, at which point plaque reduction neutralization testing (PRNT) must be conducted.
The second direction for management involves pregnant women who are initially tested within 2-12 weeks of either symptom onset or suspected exposure to the virus. Asymptomatic women who do not live in an area with active Zika virus transmission, or do live in an area with ongoing Zika virus cases but are already in the first or second trimester of their pregnancy – along with any women who are symptomatic – should have their serum analyzed through IgM testing for both Zika virus and dengue virus.
If both results are negative, then there is no Zika virus infection. If the Zika virus test is negative but the dengue virus test is either positive or equivocal, the woman has a “presumptive dengue virus infection” and should undergo PRNT. If the Zika virus test is either positive or equivocal, then the woman has a “presumptive recent Zika virus or Flavivirus infection,” regardless of the dengue virus IgM result. In the latter case, the next step is to conduct a reflex Zika virus rRT-PCR test on both serum and urine. A negative result on the serum test should be followed by PRNT; a positive result should be taken as proof of a “recent Zika virus infection.”
For any diagnostic chain that ends with a PRNT, the results of that test can be interpreted in one of three ways. If the Zika virus PRNT result is at least 10 and the dengue virus result is less than 10, then there is a recent Zika virus infection. If both the Zika virus and dengue virus PRNT results are 10 or greater, than there is a Flavivirus infection, but the specific one cannot be determined. Finally, if both results are less than 10, then there is no evidence of a recent Zika virus infection.
“For symptomatic and asymptomatic pregnant women with possible Zika virus exposure who seek care [more than] 12 weeks after symptom onset or possible exposure, IgM antibody testing might be considered,” the CDC wrote. “If fetal abnormalities are present, rRT-PCR testing should also be performed on maternal serum and urine [but] a negative IgM antibody test or rRT-PCR result [more than] 12 weeks after symptom onset or possible exposure does not rule out recent Zika virus infection.”
For pregnant women with a diagnosis of a confirmed or presumptive Flavivirus infection, regardless of whether it’s specifically Zika virus or not, the CDC recommends getting serial ultrasounds every 3-4 weeks during pregnancy in order to monitor the fetus’s development, while “decisions regarding amniocentesis should be individualized for each clinical circumstance.” After the child’s birth, rRT-PCR should be conducted on the child’s cord blood and serum; Zika virus and dengue virus IgM are also recommended.
Pregnant women without a diagnosis of either Zika virus or dengue virus should have a prenatal ultrasound; if abnormalities are found in the fetus, CDC recommends that they have a repeat Zika virus rRT-PCR and IgM test and that clinicians base management on corresponding laboratory results. If nothing is found, however, then standard care can resume with ongoing vigilance to avoid Zika virus infections. Women with dengue virus diagnoses should follow the guidance that is currently in place.
“Pregnant women with laboratory evidence of confirmed or possible Zika virus infection who experience a fetal loss or stillbirth should be offered pathology testing for Zika virus infection,” the CDC added. “This testing might provide insight into the etiology of the fetal loss, which could inform a woman’s future pregnancy planning.”
The CDC also issued updated guidance for preventing sexual transmission of Zika virus and that applies to all men and women who have traveled to or reside in areas with active Zika virus transmission and their sex partners (MMWR. ePub: 2016 25 Jul. doi: 10.15585/mmwr.mm6529e2). The CDC advises couples in which a woman is pregnant to use barriers methods or abstain from sex for the duration of the pregnancy. For couples not planning pregnancy and in which there is a male partner with confirmed Zika virus infection or symptoms of infection, the men should use barrier methods or abstain from sex for at least 6 months after the onset of illness. For women with Zika virus infection, they should use barrier protection or abstain from sex for at least 8 weeks after the onset of illness.
FROM MMWR

ASCO: Always Screen Cancer Survivors for Chronic Pain
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.

The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.
The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.
The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
FROM THE JOURNAL OF CLINICAL ONCOLOGY

New HER2-testing guidelines result in more women eligible for HER2-directed treatment
New guidelines for immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH) pathology testing categorize more breast cancers as “equivocal” regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive, investigators reported online in Journal of Clinical Oncology.
The American Society of Clinical Oncology and the College of American Pathologists released updated IHC and FISH guidelines in 2013, after the Food and Drug Administration approved the initial set of such guidelines in 1998 and ASCO/CAP issued their first such guidelines in 2007. “The intent of the 2013 guidelines was to decrease the number of equivocal [cancers],” said Mithun Vinod Shah, MD, PhD, of the Mayo Clinic, Rochester Minn., and his associates.
To assess the impact of implementing the new guidelines, the investigators analyzed 2,851 breast cancer samples sent to their cytogenetics laboratory by 139 medical centers for HER2 testing during a 1-year period. They compared the three sets of testing criteria – the FDA, the 2007, and the 2013 guidelines.
According to the 2013 guidelines, 69.7% of the tumors were classified as HER2 negative, 16.1% as HER2 positive, and 14.2% as equivocal. In contrast, the 2007 guidelines classified 85.1% as negative, 11.0% as positive, and 3.9% as equivocal, while the FDA guidelines classified 13.1% as positive and 86.9% as negative (there is no “equivocal” category in the FDA guidelines). Thus, “the final FISH interpretations indicate that by using 2013 guidelines, 358 additional patients were interpreted as positive, compared with the 2007 guidelines and that 298 additional patients were considered positive, compared with the FDA criteria,” Dr. Shah and his associates said.
The 2013 guidelines recommend additional chromosome 17 probe testing (among other strategies) to resolve equivocal results, so the investigators did so with the 405 samples classified as equivocal by the 2013 criteria. This resulted in 52.3% of the 405 equivocal tumors being reclassified as HER2 positive, 8.9% being reclassified as HER2 negative, and 38.8% remaining equivocal. Thus, HER2 positivity in the overall cohort rose significantly to 23.6% using the newest guidelines.
These findings demonstrate that using the 2013 guidelines for IHC and FISH pathology testing identifies more women who are eligible for HER2-directed therapy, the investigators said (J Clin Oncol. 2016 Jul 25. doi: 10.1200/JCO.2015.61.8983).
New guidelines for immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH) pathology testing categorize more breast cancers as “equivocal” regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive, investigators reported online in Journal of Clinical Oncology.
The American Society of Clinical Oncology and the College of American Pathologists released updated IHC and FISH guidelines in 2013, after the Food and Drug Administration approved the initial set of such guidelines in 1998 and ASCO/CAP issued their first such guidelines in 2007. “The intent of the 2013 guidelines was to decrease the number of equivocal [cancers],” said Mithun Vinod Shah, MD, PhD, of the Mayo Clinic, Rochester Minn., and his associates.
To assess the impact of implementing the new guidelines, the investigators analyzed 2,851 breast cancer samples sent to their cytogenetics laboratory by 139 medical centers for HER2 testing during a 1-year period. They compared the three sets of testing criteria – the FDA, the 2007, and the 2013 guidelines.
According to the 2013 guidelines, 69.7% of the tumors were classified as HER2 negative, 16.1% as HER2 positive, and 14.2% as equivocal. In contrast, the 2007 guidelines classified 85.1% as negative, 11.0% as positive, and 3.9% as equivocal, while the FDA guidelines classified 13.1% as positive and 86.9% as negative (there is no “equivocal” category in the FDA guidelines). Thus, “the final FISH interpretations indicate that by using 2013 guidelines, 358 additional patients were interpreted as positive, compared with the 2007 guidelines and that 298 additional patients were considered positive, compared with the FDA criteria,” Dr. Shah and his associates said.
The 2013 guidelines recommend additional chromosome 17 probe testing (among other strategies) to resolve equivocal results, so the investigators did so with the 405 samples classified as equivocal by the 2013 criteria. This resulted in 52.3% of the 405 equivocal tumors being reclassified as HER2 positive, 8.9% being reclassified as HER2 negative, and 38.8% remaining equivocal. Thus, HER2 positivity in the overall cohort rose significantly to 23.6% using the newest guidelines.
These findings demonstrate that using the 2013 guidelines for IHC and FISH pathology testing identifies more women who are eligible for HER2-directed therapy, the investigators said (J Clin Oncol. 2016 Jul 25. doi: 10.1200/JCO.2015.61.8983).
New guidelines for immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH) pathology testing categorize more breast cancers as “equivocal” regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive, investigators reported online in Journal of Clinical Oncology.
The American Society of Clinical Oncology and the College of American Pathologists released updated IHC and FISH guidelines in 2013, after the Food and Drug Administration approved the initial set of such guidelines in 1998 and ASCO/CAP issued their first such guidelines in 2007. “The intent of the 2013 guidelines was to decrease the number of equivocal [cancers],” said Mithun Vinod Shah, MD, PhD, of the Mayo Clinic, Rochester Minn., and his associates.
To assess the impact of implementing the new guidelines, the investigators analyzed 2,851 breast cancer samples sent to their cytogenetics laboratory by 139 medical centers for HER2 testing during a 1-year period. They compared the three sets of testing criteria – the FDA, the 2007, and the 2013 guidelines.
According to the 2013 guidelines, 69.7% of the tumors were classified as HER2 negative, 16.1% as HER2 positive, and 14.2% as equivocal. In contrast, the 2007 guidelines classified 85.1% as negative, 11.0% as positive, and 3.9% as equivocal, while the FDA guidelines classified 13.1% as positive and 86.9% as negative (there is no “equivocal” category in the FDA guidelines). Thus, “the final FISH interpretations indicate that by using 2013 guidelines, 358 additional patients were interpreted as positive, compared with the 2007 guidelines and that 298 additional patients were considered positive, compared with the FDA criteria,” Dr. Shah and his associates said.
The 2013 guidelines recommend additional chromosome 17 probe testing (among other strategies) to resolve equivocal results, so the investigators did so with the 405 samples classified as equivocal by the 2013 criteria. This resulted in 52.3% of the 405 equivocal tumors being reclassified as HER2 positive, 8.9% being reclassified as HER2 negative, and 38.8% remaining equivocal. Thus, HER2 positivity in the overall cohort rose significantly to 23.6% using the newest guidelines.
These findings demonstrate that using the 2013 guidelines for IHC and FISH pathology testing identifies more women who are eligible for HER2-directed therapy, the investigators said (J Clin Oncol. 2016 Jul 25. doi: 10.1200/JCO.2015.61.8983).
FROM JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: New IHC and FISH pathology guidelines categorize more breast cancers as “equivocal” regarding HER2 positivity and ultimately lead to identifying more of them as HER2 positive.
Major finding: By using 2013 guidelines, 358 additional tumors were interpreted as positive, compared with the 2007 guidelines and 298 additional tumors were considered positive, compared with the FDA criteria.
Data source: A cohort study involving 2,851 breast cancer samples analyzed according to three different pathology guidelines during a 1-year period.
Disclosures: This study was supported by the Mayo Clinic. Dr. Shah reported having no relevant financial disclosures; his associates reported ties to Merck, Hospira, Ariad Pharmaceuticals, Abbott Molecular, and Genome Diagnostics.
Study shows faster increase in obesity prevalence among cancer survivors
From 1997 to 2014, cancer survivors had a significantly faster increase in obesity prevalence compared with adults without a history of cancer, investigators found.
Furthermore, the elevated annual increase in rates of obesity was more pronounced in women, in breast and colorectal cancer survivors, and in non-Hispanic blacks.

Cancer patients may be at an increased risk for weight gain caused by specific cancer treatments such as chemotherapy, steroid modifications, and various hormone therapies, especially in “hormonally and metabolically driven cancers such as breast and colorectal cancer,” wrote Heather Greenlee, ND, PhD, of Columbia University, New York, and her associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.66.4391). “To better inform future research on obesity and cancer survival and to inform the planning and implementation of weight loss interventions in cancer survivors, we compared trends from 1997 to 2014 in obesity prevalence in U.S. adults with and without a history of cancer,” the researchers explained.
Obesity prevalence and trends were evaluated through the National Health Interview Survey, an ongoing cross-sectional survey of the health status, health care access, and behaviors of the U.S. civilian population conducted by the National Center for Health Statistics.
For the current study, surveys from a total of 538,969 adults aged 18-85 years with (n = 32,447) or without (n = 506,522) a history of cancer were analyzed. Participants provided self-reported height and weight measures from which body mass index was calculated. Obesity was defined as a BMI of 30 kg/m2 or higher for non-Asians and 27.5 kg/m2 or higher for Asians. Participants also self-reported sex, race, and cancer history.
Overall, the prevalence of obesity consistently increased from 1997 to 2014. Among cancer survivors, the prevalence of obesity increased from 22.4% to 31.7% while in adults without a history of cancer, prevalence increased from 20.9% to 29.5%.
The annual increase in the rate of obesity was significantly greater in both women and men with a history of cancer (2.9% and 2.8% respectively) compared with those without a history of cancer (2.3% and 2.4%, P less than .001 for all).
The elevated annual increase in rates of obesity was even higher in colorectal (3.1% in women and 3.7% in men) and breast (3.0%) cancer survivors compared with adults without a history of cancer, but was lower in prostate cancer survivors (2.1%; P = .001 for all).
“These findings call for public health planning of effective and scalable weight management and control programs for cancer survivors, especially for breast and colorectal cancer survivors and for non-Hispanic blacks,” the investigators concluded.
The National Cancer Institute funded the study. Dr. Greenlee and one other investigator reported serving in advisory roles for EHE International.
On Twitter @jessnicolecraig
From 1997 to 2014, cancer survivors had a significantly faster increase in obesity prevalence compared with adults without a history of cancer, investigators found.
Furthermore, the elevated annual increase in rates of obesity was more pronounced in women, in breast and colorectal cancer survivors, and in non-Hispanic blacks.
Cancer patients may be at an increased risk for weight gain caused by specific cancer treatments such as chemotherapy, steroid modifications, and various hormone therapies, especially in “hormonally and metabolically driven cancers such as breast and colorectal cancer,” wrote Heather Greenlee, ND, PhD, of Columbia University, New York, and her associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.66.4391). “To better inform future research on obesity and cancer survival and to inform the planning and implementation of weight loss interventions in cancer survivors, we compared trends from 1997 to 2014 in obesity prevalence in U.S. adults with and without a history of cancer,” the researchers explained.
Obesity prevalence and trends were evaluated through the National Health Interview Survey, an ongoing cross-sectional survey of the health status, health care access, and behaviors of the U.S. civilian population conducted by the National Center for Health Statistics.
For the current study, surveys from a total of 538,969 adults aged 18-85 years with (n = 32,447) or without (n = 506,522) a history of cancer were analyzed. Participants provided self-reported height and weight measures from which body mass index was calculated. Obesity was defined as a BMI of 30 kg/m2 or higher for non-Asians and 27.5 kg/m2 or higher for Asians. Participants also self-reported sex, race, and cancer history.
Overall, the prevalence of obesity consistently increased from 1997 to 2014. Among cancer survivors, the prevalence of obesity increased from 22.4% to 31.7% while in adults without a history of cancer, prevalence increased from 20.9% to 29.5%.
The annual increase in the rate of obesity was significantly greater in both women and men with a history of cancer (2.9% and 2.8% respectively) compared with those without a history of cancer (2.3% and 2.4%, P less than .001 for all).
The elevated annual increase in rates of obesity was even higher in colorectal (3.1% in women and 3.7% in men) and breast (3.0%) cancer survivors compared with adults without a history of cancer, but was lower in prostate cancer survivors (2.1%; P = .001 for all).
“These findings call for public health planning of effective and scalable weight management and control programs for cancer survivors, especially for breast and colorectal cancer survivors and for non-Hispanic blacks,” the investigators concluded.
The National Cancer Institute funded the study. Dr. Greenlee and one other investigator reported serving in advisory roles for EHE International.
On Twitter @jessnicolecraig
From 1997 to 2014, cancer survivors had a significantly faster increase in obesity prevalence compared with adults without a history of cancer, investigators found.
Furthermore, the elevated annual increase in rates of obesity was more pronounced in women, in breast and colorectal cancer survivors, and in non-Hispanic blacks.
Cancer patients may be at an increased risk for weight gain caused by specific cancer treatments such as chemotherapy, steroid modifications, and various hormone therapies, especially in “hormonally and metabolically driven cancers such as breast and colorectal cancer,” wrote Heather Greenlee, ND, PhD, of Columbia University, New York, and her associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.66.4391). “To better inform future research on obesity and cancer survival and to inform the planning and implementation of weight loss interventions in cancer survivors, we compared trends from 1997 to 2014 in obesity prevalence in U.S. adults with and without a history of cancer,” the researchers explained.
Obesity prevalence and trends were evaluated through the National Health Interview Survey, an ongoing cross-sectional survey of the health status, health care access, and behaviors of the U.S. civilian population conducted by the National Center for Health Statistics.
For the current study, surveys from a total of 538,969 adults aged 18-85 years with (n = 32,447) or without (n = 506,522) a history of cancer were analyzed. Participants provided self-reported height and weight measures from which body mass index was calculated. Obesity was defined as a BMI of 30 kg/m2 or higher for non-Asians and 27.5 kg/m2 or higher for Asians. Participants also self-reported sex, race, and cancer history.
Overall, the prevalence of obesity consistently increased from 1997 to 2014. Among cancer survivors, the prevalence of obesity increased from 22.4% to 31.7% while in adults without a history of cancer, prevalence increased from 20.9% to 29.5%.
The annual increase in the rate of obesity was significantly greater in both women and men with a history of cancer (2.9% and 2.8% respectively) compared with those without a history of cancer (2.3% and 2.4%, P less than .001 for all).
The elevated annual increase in rates of obesity was even higher in colorectal (3.1% in women and 3.7% in men) and breast (3.0%) cancer survivors compared with adults without a history of cancer, but was lower in prostate cancer survivors (2.1%; P = .001 for all).
“These findings call for public health planning of effective and scalable weight management and control programs for cancer survivors, especially for breast and colorectal cancer survivors and for non-Hispanic blacks,” the investigators concluded.
The National Cancer Institute funded the study. Dr. Greenlee and one other investigator reported serving in advisory roles for EHE International.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Cancer survivors had a significantly faster increase in obesity prevalence compared with adults without a history of cancer.
Major finding: The annual increase in the rate of obesity was significantly higher in both women and men with a history of cancer (2.9% and 2.8% respectively) compared with those without a history of cancer (2.3% and 2.4%, P less than .001 for all).
Data source: National Health Interview Survey responses from 538,969 adults aged 18-85 years with (n = 32,447) or without (n = 506,522) a history of cancer.
Disclosures: The National Cancer Institute funded the study. Dr. Greenlee and one other investigator reported serving in advisory roles for EHE International.

Overweight, obesity increase risk of cardiotoxicity from anthracyclines
Being overweight or obese was significantly associated with a greater risk of developing cardiotoxicity among breast cancer patients treated with anthracyclines and/or trastuzumab, investigators found.
Anthracyclines, a class of anticancer agents widely used to treat many cancer types, have a known association with cardiotoxicity. Furthermore, people who are overweight or obese have an increased risk for developing cardiovascular diseases. The purpose of this study was to “explore in greater depth the influence of overweight and obesity as aggravating factors in the development of cardiotoxicity” specifically among patients who received anthracycline and/or trastuzumab as part of their cancer treatment and were therefore at increased risk of experiencing cardiac-related adverse events, wrote Charles Guenancia, MD, PhD, of University Hospital, Dijon Cedex, France, and his associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.67.4846).
These results are from a meta-analysis of 15 published prospective or retrospective cohort studies that investigated or otherwise reported data on the association between overweight and/or obesity and cardiotoxicity resulting from anthracycline and/or trastuzumab use for treating localized or metastatic breast cancer. Together, the 15 studies represented a total of 8,745 breast cancer patients.
Overall, the mean rate of cardiotoxicity was 17% (95% confidence interval, 11%-25%). Patients treated with anthracyclines only (n = 3,898) had a mean rate of cardiotoxicity of 20% (95% CI, 5%-43%) while patients treated with trastuzumab with or without anthracyclines (n = 4,847) had a lower mean rate of cardiotoxicity at 16% (95% CI, 10%-24%).Paired meta-analysis revealed that overweight, defined as a body mass index score of 25 to 29.9, was associated with increased risk of cardiotoxicity with an odds ratio of 1.15 (95% CI, 0.83-1.58). Obesity, defined as a body mass index score of 30 or greater, was associated with a greater risk of cardiotoxicity with an odds ratio of 1.47 (95% CI, 0.95-2.28).
The association between body mass index and the risk of cardiotoxicity did not differ significantly by drug regimen (anthracyclines alone or sequential anthracyclines and trastuzumab).
This study’s funding source was not listed. Dr. Guenancia and one other investigator reported serving in advisory roles and/or receiving financial compensation from various companies.
On Twitter @jessnicolecraig
Being overweight or obese was significantly associated with a greater risk of developing cardiotoxicity among breast cancer patients treated with anthracyclines and/or trastuzumab, investigators found.
Anthracyclines, a class of anticancer agents widely used to treat many cancer types, have a known association with cardiotoxicity. Furthermore, people who are overweight or obese have an increased risk for developing cardiovascular diseases. The purpose of this study was to “explore in greater depth the influence of overweight and obesity as aggravating factors in the development of cardiotoxicity” specifically among patients who received anthracycline and/or trastuzumab as part of their cancer treatment and were therefore at increased risk of experiencing cardiac-related adverse events, wrote Charles Guenancia, MD, PhD, of University Hospital, Dijon Cedex, France, and his associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.67.4846).
These results are from a meta-analysis of 15 published prospective or retrospective cohort studies that investigated or otherwise reported data on the association between overweight and/or obesity and cardiotoxicity resulting from anthracycline and/or trastuzumab use for treating localized or metastatic breast cancer. Together, the 15 studies represented a total of 8,745 breast cancer patients.
Overall, the mean rate of cardiotoxicity was 17% (95% confidence interval, 11%-25%). Patients treated with anthracyclines only (n = 3,898) had a mean rate of cardiotoxicity of 20% (95% CI, 5%-43%) while patients treated with trastuzumab with or without anthracyclines (n = 4,847) had a lower mean rate of cardiotoxicity at 16% (95% CI, 10%-24%).Paired meta-analysis revealed that overweight, defined as a body mass index score of 25 to 29.9, was associated with increased risk of cardiotoxicity with an odds ratio of 1.15 (95% CI, 0.83-1.58). Obesity, defined as a body mass index score of 30 or greater, was associated with a greater risk of cardiotoxicity with an odds ratio of 1.47 (95% CI, 0.95-2.28).
The association between body mass index and the risk of cardiotoxicity did not differ significantly by drug regimen (anthracyclines alone or sequential anthracyclines and trastuzumab).
This study’s funding source was not listed. Dr. Guenancia and one other investigator reported serving in advisory roles and/or receiving financial compensation from various companies.
On Twitter @jessnicolecraig
Being overweight or obese was significantly associated with a greater risk of developing cardiotoxicity among breast cancer patients treated with anthracyclines and/or trastuzumab, investigators found.
Anthracyclines, a class of anticancer agents widely used to treat many cancer types, have a known association with cardiotoxicity. Furthermore, people who are overweight or obese have an increased risk for developing cardiovascular diseases. The purpose of this study was to “explore in greater depth the influence of overweight and obesity as aggravating factors in the development of cardiotoxicity” specifically among patients who received anthracycline and/or trastuzumab as part of their cancer treatment and were therefore at increased risk of experiencing cardiac-related adverse events, wrote Charles Guenancia, MD, PhD, of University Hospital, Dijon Cedex, France, and his associates (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.67.4846).
These results are from a meta-analysis of 15 published prospective or retrospective cohort studies that investigated or otherwise reported data on the association between overweight and/or obesity and cardiotoxicity resulting from anthracycline and/or trastuzumab use for treating localized or metastatic breast cancer. Together, the 15 studies represented a total of 8,745 breast cancer patients.
Overall, the mean rate of cardiotoxicity was 17% (95% confidence interval, 11%-25%). Patients treated with anthracyclines only (n = 3,898) had a mean rate of cardiotoxicity of 20% (95% CI, 5%-43%) while patients treated with trastuzumab with or without anthracyclines (n = 4,847) had a lower mean rate of cardiotoxicity at 16% (95% CI, 10%-24%).Paired meta-analysis revealed that overweight, defined as a body mass index score of 25 to 29.9, was associated with increased risk of cardiotoxicity with an odds ratio of 1.15 (95% CI, 0.83-1.58). Obesity, defined as a body mass index score of 30 or greater, was associated with a greater risk of cardiotoxicity with an odds ratio of 1.47 (95% CI, 0.95-2.28).
The association between body mass index and the risk of cardiotoxicity did not differ significantly by drug regimen (anthracyclines alone or sequential anthracyclines and trastuzumab).
This study’s funding source was not listed. Dr. Guenancia and one other investigator reported serving in advisory roles and/or receiving financial compensation from various companies.
On Twitter @jessnicolecraig
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Being overweight or obese was significantly associated with a greater risk of developing cardiotoxicity among breast cancer patients treated with anthracycline and/or trastuzumab.
Major finding: Being overweight was associated with increased risk of cardiotoxicity with an odds ratio of 1.15 (95% CI, 0.83-1.58). Obesity was associated with a greater risk of cardiotoxicity with an odds ratio of 1.47 (95% CI, 0.95-2.28).
Data source: A meta-analysis of 15 studies that investigated or otherwise reported data on the association between overweight and/or obesity and cardiotoxicity resulting from anthracyclines and/or trastuzumab use for treating breast cancer.
Disclosures: This study’s funding source was not identified. Dr. Guenancia and one other investigator reported serving in advisory roles and/or receiving financial compensation from various companies.
ASCO: Always screen cancer survivors for chronic pain
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.

The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.
The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
All adult cancer survivors should be screened for chronic pain at every visit, according to the American Society of Clinical Oncology’s first clinical practice guideline for managing this patient population, published July 25 in the Journal of Clinical Oncology.
An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%. Yet most health care providers “haven’t been trained to recognize or treat long-term pain associated with cancer,” Judith A. Paice, PhD, RN, said in a press statement accompanying the release of the new guideline.
Existing guidelines focus on the acute pain of cancer and its treatment, or on acute pain related to advanced cancer, said Dr. Paice, cochair of the expert panel that developed the guideline and research professor of hematology/oncology at Northwestern University, Chicago.
The chronic pain addressed in the new guideline document can be related to the malignancy itself or to its treatment. Surgery, chemotherapy, hormone therapy, radiation treatment, and stem-cell transplantation can induce dozens of pain-producing complications, including osteonecrosis, bone fractures, peripheral or central nerve damage, fistulas, lymphedema, arthralgias, and myelopathy. The pain can develop months or years after diagnosis, significantly impacting patients’ quality of life well after treatment is completed.
“This guideline will help clinicians identify pain early and develop comprehensive treatment plans using a broad range of approaches,” Dr. Paice said in the statement.
The panel that developed the guideline comprised experts in medical oncology, hematology, pain medicine, palliative care, hospice, radiation oncology, social work, rehabilitation, psychology, and anesthesiology. They performed a systematic review of the literature and based their recommendations on 35 meta-analyses, 9 randomized controlled trials, 19 comparative studies, and expert consensus.
Some key recommendations include the following:
• Screen all survivors of adult cancers for chronic pain using both a physical exam and an in-depth interview that covers physical, functional, psychological, social, and spiritual aspects of pain, as well as the patient’s treatment history and comorbid conditions. The guideline includes a list of 36 common pain syndromes resulting from cancer treatments.
• Monitor patients at every visit for late-onset treatment effects that can produce pain, just as they are monitored for recurrent disease and secondary malignancy. Some cancer survivors may not recognize that their current pain is related to past disease or its treatments, or may consider it an untreatable complication that they have to endure.
• Consider the entire range of pain medicines – not just opioid analgesics – including NSAIDs, acetaminophen, and selected antidepressants and anticonvulsants with analgesic efficacy. The panel noted that some cancer survivors with chronic pain may benefit from other drugs, including muscle relaxants, benzodiazepines, N-methyl-D-aspartate receptor blockers, alpha-2 agonists, and neutraceuticals and botanicals. But they urged caution since the efficacy of these agents has not been fully established.
Consider nonmedical treatments such as physical, occupational, and recreation therapy; exercise; orthotics; ultrasound; massage; acupuncture; cognitive behavioral therapy; relaxation therapy; and TENS or other types of nerve stimulation.
Consider medical cannabis or cannabinoids as an adjuvant but not a first-line pain treatment, being sure to follow specific state regulations.
Consider a trial of opioids only for carefully selected patients who don’t respond to more conservative management. Weigh potential risks against benefits and employ universal precautions to minimize abuse and addiction, and be cautious in coprescribing other centrally-acting agents (J Clin Oncol. 2016 July 25. doi: 10.1200/JCO.2016.68.5206).
The full clinical practice guideline and other clinical tools and resources are available at www.asco.org/chronic-pai-guideline.
The guideline development process was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry sources.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point: Screen all survivors of adult cancers for chronic pain at every visit.
Major finding: An estimated 14 million adults with a history of cancer are living in the United States alone, and the prevalence of chronic pain related to their malignancy is reported to be as high as 40%.
Data source: The first ASCO clinical practice guideline for managing chronic pain in survivors of adult cancers.
Disclosures: This work was supported by ASCO. Dr. Paice reported having no relevant financial disclosures; some of her associates reported financial ties to industry.

Cervical cancer screening: How our approach may change
› Screen for cervical cancer in women ages 21 to 29 using cytology alone every 3 years. For women ages 30 to 65, screening with a combination of cytology and human papillomavirus (HPV) testing every 5 years is the preferred option. A
› Be aware of the alternative guideline proposed by several specialty organizations: All women ages 25 to 64 should receive primary HPV screening every 3 years with the FDA-approved HPV test. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
If the cervical cytology report you receive for a woman in her mid-20s is negative, how soon would you plan to repeat testing? Recommendations from the United States Preventive Services Task Force (USPSTF) and other leading organizations advise a combination of cytology and human papillomavirus (HPV) testing at specified intervals depending on a patient’s age. However, a study published in 2015 analyzed data from a statewide registry on provider behavior and found a wide array of screening intervals in practice and infrequent use of HPV testing.1 Clearly, adherence to published guidelines has been inconsistent.
Now, recommendations by several specialty groups are evolving based on newer evidence regarding HPV testing. These alternative guidelines recommend primary high-risk HPV testing for all women. This change is the topic of much national debate and is being researched for the USPSTF’s 2018 update on cervical cancer screening.
In this article, I review the USPSTF’s present recommendations and look ahead to how “best practices” for cervical cancer screening may be changing.
Current cervical cancer screening guidelines
Many subspecialty organizations and government agencies publish cervical cancer screening guidelines. The USPSTF guidelines, reviewed here, are evidence based, frequently updated, and widely used by primary care providers (TABLE).2,3 These guidelines recommend initiating cytology testing at age 21 and, if results are normal, repeating every 3 years. Reflex HPV testing is recommended if cytology results reveal atypical squamous cells of undetermined significance (ASCUS). For women ages 30 to 65, the preferred option is to undergo a combination of cytology and HPV testing every 5 years.2 Women older than 65 may discontinue screening.2 HPV immunization status does not affect USPSTF recommendations. Nationwide rates of HPV vaccination among females ages 13 to 17 vary among states, from ≤49% to ≥70%.4
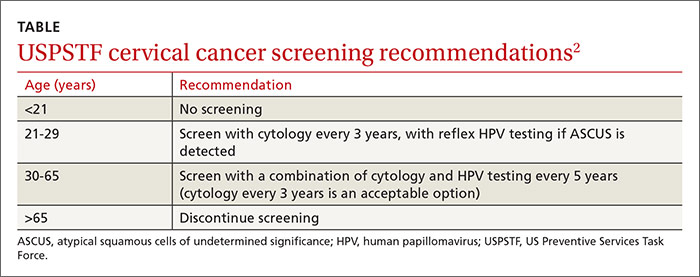
What the guidelines do, and do not, cover. The USPSTF screening intervals apply as long as testing results are normal.2 These guidelines apply to all women regardless of the age at which they began sexual activity. These guidelines do not apply to women who have had abnormal cytology or HPV results and have not undergone adequate follow-up to ensure their lesion has cleared.5 These guidelines also do not apply to women who are immunosuppressed, who were exposed to diethylstilbestrol (DES) in utero, who have had a hysterectomy for non-oncologic reasons, or who have had cervical cancer.5 A woman may stop routine screening after age 65 if she has had adequate follow-up including either 3 negative cytology samples or 2 negative co-tests (cytology and HPV test) in the last 10 years.6 A woman may also discontinue screening if she has had a total hysterectomy and has no history of cervical dysplasia.7
Evidence behind the guidelines. The USPSTF guidelines were updated to their current state in 2012 reflecting a growing body of evidence that, for women 30 years and older, detection of cervical intraepithelial neoplasia (CIN) 3+ lesions improves with HPV co-testing. The supporting studies also found that the risk of a high-grade lesion appearing 5 years following co-testing was equivalent to the risk seen with cytology samples alone taken at 3-year intervals.8 The sensitivity of a single cytology test is only about 50%.9 A patient’s risk of cervical cancer 18 months after 3 negative cytology tests is about 1.5/100,000.10 The risk at 36 months following 3 negative cytology results is about 4.5/100,000. Annual screening would require almost 100,000 women to be screened to detect 3 additional cases of cervical cancer.10
Additional benefits of the updated USPSTF guidelines. The updated strategy decreases the number of visits for patients and the number of colposcopies, minimizing harm and patient anxiety. The current management algorithms also recommend more conservative management of women in their early 20s who have reported abnormal cytology, as the likelihood of their lesion clearing within 12 to 24 months is high.5 The recommendation does not call for high-risk HPV testing of women ages 21 to 29 because the infection is highly prevalent in this age group and is also likely to clear before any significant pathology arises. This avoids unnecessary and potentially harmful treatment of younger women.11
What about the alternative screening guideline?
In early 2015, the American Society for Colposcopy and Cervical Pathology (ASCCP) and the Society of Gynecologic Oncology (SGO) co-sponsored an expert panel representing several specialty societies. The panel released interim guidelines for cervical cancer screening reflecting a growing body of evidence that favors HPV testing as the primary modality.12 Additionally, in January 2016, these guidelines received an evidence-level B rating from the American Congress of Obstetricians and Gynecologists.13 Primary HPV screening is also the topic of research and discussion for USPSTF’s pending 2018 update of cervical cancer screening strategies.14
The alternative algorithm from the ASCCP and SGO recommends cervical cancer screening with HPV testing alone starting at the age of 25 and, if results are negative, repeating at 3-year intervals.12 If a patient tests positive for any of the 14 identified high-risk HPV types, reflex cytology is indicated with a referral for colposcopy if an abnormality is identified.12 If the cytology result is normal, follow-up with another HPV test in 12 months is recommended.12
Over the last 12 years, multiple international studies have demonstrated the efficacy of high-risk HPV testing in primary screening for cervical cancer.15 The most recent study conducted in the United States from 2008 to 2011—Addressing THE Need for Advanced HPV Diagnostics (ATHENA)—enrolled 42,000 women older than 25 years to compare the screening modalities of cytology alone, cytology and HPV testing combined, and HPV testing alone.16 The purpose of the study was to determine the safety of the cobas HPV test as a co-test and as a primary screening modality in women older than 25 years. (Many HPV tests are commercially available, but only the cobas HPV test is FDA-approved for primary screening.12)
ATHENA researchers concluded that HPV testing was more sensitive than cytology, but less specific.16 The researchers also concluded that adding cytology to the HPV test increased the sensitivity by less than 5% and that HPV was better at detecting CIN 2+ lesions than cytology alone.12,16 Another recently published study conducted at a tertiary care hospital with a smaller sample (1000 patients) corroborated the ATHENA results.17
For patients in their late 20s, this alternative strategy may increase the number of subsequent colposcopies. However, during the clinical trials just described, the absolute number of colposcopies needed to detect high-grade disease was the same as seen with the current guidelines. This finding indicates that, with the current algorithm, clinically significant pathology due to high-risk HPV may be missed in the 25-to-29 age group.8
Looking ahead. The alternative screening strategy is already being adopted in Australia, the Netherlands, and the United Kingdom.15 For providers in the United States considering this alternative strategy, the recommendation is to initiate cervical cancer screening with cytology alone at age 21, manage results appropriately, and then transition the patient to primary HPV testing with the FDA-approved test at age 25.12 This recommendation may be modified in the future. However the guidelines might change, patients will benefit only if the guidelines are implemented consistently in practice.
CORRESPONDENCE
Sabrina Hofmeister, DO, 1121 E. North Ave, Milwaukee, WI 53212; [email protected].
1. Kim JJ, Campos NG, Sy S, et al. Inefficiencies and high-value improvements in U.S. cervical cancer screening practice: a cost-effective analysis. Ann Intern Med. 2015;163:589-597.
2. Moyer VA; U.S. Preventive Services Task Force. Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;156:880-891.
3. U.S. Preventive Services Task Force. Understanding How the USPSTF Works: USPSTF 101. Available at: http://www.uspreventiveservicestaskforce.org/Page/Name/understanding-how-the-uspstf-works. Accessed June 8, 2016.
4. Reagan-Steiner S, Yankey D, Jeyarajah J, et al; Centers for Disease Control and Prevention. National, regional, state, and selected local vaccination coverage among adolescents aged 13-17 years—United States, 2014. MMWR Morb Mortal Wkly Rep. 2015;64:784-792.
5. Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. J Low Genit Tract Dis. 2012;16:175-204.
6. Vesco KK, Whitlock EP, Eder M, et al. Risk factors and other epidemiologic considerations for cervical cancer screening: a narrative review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155:687-697.
7. Khan MJ, Massad LS, Kinney W, et al. A common clinical dilemma: management of abnormal vaginal cytology and human papilloma virus test results. J Low Genit Tract Dis. 2016;20:119-125.
8. Wright TC, Stoler MH, Behrens CM, et al. Primary cervical cancer screening with human papillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test. Gynecol Oncol. 2015;136:189-197.
9. Naucler P, Ryd W, Törnberg S, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med. 2007;357:1589-1597.
10. Sawaya GF, Sung HY, Kinney W, et al. Cervical cancer after multiple negative tests in long-term members of a prepaid health plan. Acta Cytol. 2005;49:391-397.
11. Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in the United States. JAMA. 2007;297:813-819.
12. Huh WK, Ault KA, Chelmow D, et al. Use of primary high-risk HPV testing for cervical cancer screening: interim clinical guidance. J Low Genit Tract Dis. 2015;19:91-96.
13. American Congress of Obstetricians and Gynecologists. Practice Bulletin No. 157: Cervical cancer screening and prevention. Obstet Gynecol. 2016;127:e1-e20.
14. U.S. Preventive Services Task Force. Final Research Plan: Cervical Cancer: Screening. October 2015. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/final-research-plan/cervical-cancer-screening2. Accessed June 22, 2016.
15. Ronco G, Dillner J, Elfström KM, et al; International HPV Working Group. Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet. 2014;383:524-532.
16. Stoler MH, Wright TC Jr, Sharma A, et al. High-risk human papilloma virus testing in women with ASC-US cytology: results from the ATHENA HPV study. Am J Clin Path. 2011;135:468-475.
17. Choi JW, Kim Y, Lee JH, et al. The clinical performance of primary HPV screening, primary HPV screening plus cytology cotesting, and cytology alone at a tertiary care hospital. Cancer Cytopathol. 2016;124:144-152.
› Screen for cervical cancer in women ages 21 to 29 using cytology alone every 3 years. For women ages 30 to 65, screening with a combination of cytology and human papillomavirus (HPV) testing every 5 years is the preferred option. A
› Be aware of the alternative guideline proposed by several specialty organizations: All women ages 25 to 64 should receive primary HPV screening every 3 years with the FDA-approved HPV test. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
If the cervical cytology report you receive for a woman in her mid-20s is negative, how soon would you plan to repeat testing? Recommendations from the United States Preventive Services Task Force (USPSTF) and other leading organizations advise a combination of cytology and human papillomavirus (HPV) testing at specified intervals depending on a patient’s age. However, a study published in 2015 analyzed data from a statewide registry on provider behavior and found a wide array of screening intervals in practice and infrequent use of HPV testing.1 Clearly, adherence to published guidelines has been inconsistent.
Now, recommendations by several specialty groups are evolving based on newer evidence regarding HPV testing. These alternative guidelines recommend primary high-risk HPV testing for all women. This change is the topic of much national debate and is being researched for the USPSTF’s 2018 update on cervical cancer screening.
In this article, I review the USPSTF’s present recommendations and look ahead to how “best practices” for cervical cancer screening may be changing.
Current cervical cancer screening guidelines
Many subspecialty organizations and government agencies publish cervical cancer screening guidelines. The USPSTF guidelines, reviewed here, are evidence based, frequently updated, and widely used by primary care providers (TABLE).2,3 These guidelines recommend initiating cytology testing at age 21 and, if results are normal, repeating every 3 years. Reflex HPV testing is recommended if cytology results reveal atypical squamous cells of undetermined significance (ASCUS). For women ages 30 to 65, the preferred option is to undergo a combination of cytology and HPV testing every 5 years.2 Women older than 65 may discontinue screening.2 HPV immunization status does not affect USPSTF recommendations. Nationwide rates of HPV vaccination among females ages 13 to 17 vary among states, from ≤49% to ≥70%.4
What the guidelines do, and do not, cover. The USPSTF screening intervals apply as long as testing results are normal.2 These guidelines apply to all women regardless of the age at which they began sexual activity. These guidelines do not apply to women who have had abnormal cytology or HPV results and have not undergone adequate follow-up to ensure their lesion has cleared.5 These guidelines also do not apply to women who are immunosuppressed, who were exposed to diethylstilbestrol (DES) in utero, who have had a hysterectomy for non-oncologic reasons, or who have had cervical cancer.5 A woman may stop routine screening after age 65 if she has had adequate follow-up including either 3 negative cytology samples or 2 negative co-tests (cytology and HPV test) in the last 10 years.6 A woman may also discontinue screening if she has had a total hysterectomy and has no history of cervical dysplasia.7
Evidence behind the guidelines. The USPSTF guidelines were updated to their current state in 2012 reflecting a growing body of evidence that, for women 30 years and older, detection of cervical intraepithelial neoplasia (CIN) 3+ lesions improves with HPV co-testing. The supporting studies also found that the risk of a high-grade lesion appearing 5 years following co-testing was equivalent to the risk seen with cytology samples alone taken at 3-year intervals.8 The sensitivity of a single cytology test is only about 50%.9 A patient’s risk of cervical cancer 18 months after 3 negative cytology tests is about 1.5/100,000.10 The risk at 36 months following 3 negative cytology results is about 4.5/100,000. Annual screening would require almost 100,000 women to be screened to detect 3 additional cases of cervical cancer.10
Additional benefits of the updated USPSTF guidelines. The updated strategy decreases the number of visits for patients and the number of colposcopies, minimizing harm and patient anxiety. The current management algorithms also recommend more conservative management of women in their early 20s who have reported abnormal cytology, as the likelihood of their lesion clearing within 12 to 24 months is high.5 The recommendation does not call for high-risk HPV testing of women ages 21 to 29 because the infection is highly prevalent in this age group and is also likely to clear before any significant pathology arises. This avoids unnecessary and potentially harmful treatment of younger women.11
What about the alternative screening guideline?
In early 2015, the American Society for Colposcopy and Cervical Pathology (ASCCP) and the Society of Gynecologic Oncology (SGO) co-sponsored an expert panel representing several specialty societies. The panel released interim guidelines for cervical cancer screening reflecting a growing body of evidence that favors HPV testing as the primary modality.12 Additionally, in January 2016, these guidelines received an evidence-level B rating from the American Congress of Obstetricians and Gynecologists.13 Primary HPV screening is also the topic of research and discussion for USPSTF’s pending 2018 update of cervical cancer screening strategies.14
The alternative algorithm from the ASCCP and SGO recommends cervical cancer screening with HPV testing alone starting at the age of 25 and, if results are negative, repeating at 3-year intervals.12 If a patient tests positive for any of the 14 identified high-risk HPV types, reflex cytology is indicated with a referral for colposcopy if an abnormality is identified.12 If the cytology result is normal, follow-up with another HPV test in 12 months is recommended.12
Over the last 12 years, multiple international studies have demonstrated the efficacy of high-risk HPV testing in primary screening for cervical cancer.15 The most recent study conducted in the United States from 2008 to 2011—Addressing THE Need for Advanced HPV Diagnostics (ATHENA)—enrolled 42,000 women older than 25 years to compare the screening modalities of cytology alone, cytology and HPV testing combined, and HPV testing alone.16 The purpose of the study was to determine the safety of the cobas HPV test as a co-test and as a primary screening modality in women older than 25 years. (Many HPV tests are commercially available, but only the cobas HPV test is FDA-approved for primary screening.12)
ATHENA researchers concluded that HPV testing was more sensitive than cytology, but less specific.16 The researchers also concluded that adding cytology to the HPV test increased the sensitivity by less than 5% and that HPV was better at detecting CIN 2+ lesions than cytology alone.12,16 Another recently published study conducted at a tertiary care hospital with a smaller sample (1000 patients) corroborated the ATHENA results.17
For patients in their late 20s, this alternative strategy may increase the number of subsequent colposcopies. However, during the clinical trials just described, the absolute number of colposcopies needed to detect high-grade disease was the same as seen with the current guidelines. This finding indicates that, with the current algorithm, clinically significant pathology due to high-risk HPV may be missed in the 25-to-29 age group.8
Looking ahead. The alternative screening strategy is already being adopted in Australia, the Netherlands, and the United Kingdom.15 For providers in the United States considering this alternative strategy, the recommendation is to initiate cervical cancer screening with cytology alone at age 21, manage results appropriately, and then transition the patient to primary HPV testing with the FDA-approved test at age 25.12 This recommendation may be modified in the future. However the guidelines might change, patients will benefit only if the guidelines are implemented consistently in practice.
CORRESPONDENCE
Sabrina Hofmeister, DO, 1121 E. North Ave, Milwaukee, WI 53212; [email protected].
› Screen for cervical cancer in women ages 21 to 29 using cytology alone every 3 years. For women ages 30 to 65, screening with a combination of cytology and human papillomavirus (HPV) testing every 5 years is the preferred option. A
› Be aware of the alternative guideline proposed by several specialty organizations: All women ages 25 to 64 should receive primary HPV screening every 3 years with the FDA-approved HPV test. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
If the cervical cytology report you receive for a woman in her mid-20s is negative, how soon would you plan to repeat testing? Recommendations from the United States Preventive Services Task Force (USPSTF) and other leading organizations advise a combination of cytology and human papillomavirus (HPV) testing at specified intervals depending on a patient’s age. However, a study published in 2015 analyzed data from a statewide registry on provider behavior and found a wide array of screening intervals in practice and infrequent use of HPV testing.1 Clearly, adherence to published guidelines has been inconsistent.
Now, recommendations by several specialty groups are evolving based on newer evidence regarding HPV testing. These alternative guidelines recommend primary high-risk HPV testing for all women. This change is the topic of much national debate and is being researched for the USPSTF’s 2018 update on cervical cancer screening.
In this article, I review the USPSTF’s present recommendations and look ahead to how “best practices” for cervical cancer screening may be changing.
Current cervical cancer screening guidelines
Many subspecialty organizations and government agencies publish cervical cancer screening guidelines. The USPSTF guidelines, reviewed here, are evidence based, frequently updated, and widely used by primary care providers (TABLE).2,3 These guidelines recommend initiating cytology testing at age 21 and, if results are normal, repeating every 3 years. Reflex HPV testing is recommended if cytology results reveal atypical squamous cells of undetermined significance (ASCUS). For women ages 30 to 65, the preferred option is to undergo a combination of cytology and HPV testing every 5 years.2 Women older than 65 may discontinue screening.2 HPV immunization status does not affect USPSTF recommendations. Nationwide rates of HPV vaccination among females ages 13 to 17 vary among states, from ≤49% to ≥70%.4
What the guidelines do, and do not, cover. The USPSTF screening intervals apply as long as testing results are normal.2 These guidelines apply to all women regardless of the age at which they began sexual activity. These guidelines do not apply to women who have had abnormal cytology or HPV results and have not undergone adequate follow-up to ensure their lesion has cleared.5 These guidelines also do not apply to women who are immunosuppressed, who were exposed to diethylstilbestrol (DES) in utero, who have had a hysterectomy for non-oncologic reasons, or who have had cervical cancer.5 A woman may stop routine screening after age 65 if she has had adequate follow-up including either 3 negative cytology samples or 2 negative co-tests (cytology and HPV test) in the last 10 years.6 A woman may also discontinue screening if she has had a total hysterectomy and has no history of cervical dysplasia.7
Evidence behind the guidelines. The USPSTF guidelines were updated to their current state in 2012 reflecting a growing body of evidence that, for women 30 years and older, detection of cervical intraepithelial neoplasia (CIN) 3+ lesions improves with HPV co-testing. The supporting studies also found that the risk of a high-grade lesion appearing 5 years following co-testing was equivalent to the risk seen with cytology samples alone taken at 3-year intervals.8 The sensitivity of a single cytology test is only about 50%.9 A patient’s risk of cervical cancer 18 months after 3 negative cytology tests is about 1.5/100,000.10 The risk at 36 months following 3 negative cytology results is about 4.5/100,000. Annual screening would require almost 100,000 women to be screened to detect 3 additional cases of cervical cancer.10
Additional benefits of the updated USPSTF guidelines. The updated strategy decreases the number of visits for patients and the number of colposcopies, minimizing harm and patient anxiety. The current management algorithms also recommend more conservative management of women in their early 20s who have reported abnormal cytology, as the likelihood of their lesion clearing within 12 to 24 months is high.5 The recommendation does not call for high-risk HPV testing of women ages 21 to 29 because the infection is highly prevalent in this age group and is also likely to clear before any significant pathology arises. This avoids unnecessary and potentially harmful treatment of younger women.11
What about the alternative screening guideline?
In early 2015, the American Society for Colposcopy and Cervical Pathology (ASCCP) and the Society of Gynecologic Oncology (SGO) co-sponsored an expert panel representing several specialty societies. The panel released interim guidelines for cervical cancer screening reflecting a growing body of evidence that favors HPV testing as the primary modality.12 Additionally, in January 2016, these guidelines received an evidence-level B rating from the American Congress of Obstetricians and Gynecologists.13 Primary HPV screening is also the topic of research and discussion for USPSTF’s pending 2018 update of cervical cancer screening strategies.14
The alternative algorithm from the ASCCP and SGO recommends cervical cancer screening with HPV testing alone starting at the age of 25 and, if results are negative, repeating at 3-year intervals.12 If a patient tests positive for any of the 14 identified high-risk HPV types, reflex cytology is indicated with a referral for colposcopy if an abnormality is identified.12 If the cytology result is normal, follow-up with another HPV test in 12 months is recommended.12
Over the last 12 years, multiple international studies have demonstrated the efficacy of high-risk HPV testing in primary screening for cervical cancer.15 The most recent study conducted in the United States from 2008 to 2011—Addressing THE Need for Advanced HPV Diagnostics (ATHENA)—enrolled 42,000 women older than 25 years to compare the screening modalities of cytology alone, cytology and HPV testing combined, and HPV testing alone.16 The purpose of the study was to determine the safety of the cobas HPV test as a co-test and as a primary screening modality in women older than 25 years. (Many HPV tests are commercially available, but only the cobas HPV test is FDA-approved for primary screening.12)
ATHENA researchers concluded that HPV testing was more sensitive than cytology, but less specific.16 The researchers also concluded that adding cytology to the HPV test increased the sensitivity by less than 5% and that HPV was better at detecting CIN 2+ lesions than cytology alone.12,16 Another recently published study conducted at a tertiary care hospital with a smaller sample (1000 patients) corroborated the ATHENA results.17
For patients in their late 20s, this alternative strategy may increase the number of subsequent colposcopies. However, during the clinical trials just described, the absolute number of colposcopies needed to detect high-grade disease was the same as seen with the current guidelines. This finding indicates that, with the current algorithm, clinically significant pathology due to high-risk HPV may be missed in the 25-to-29 age group.8
Looking ahead. The alternative screening strategy is already being adopted in Australia, the Netherlands, and the United Kingdom.15 For providers in the United States considering this alternative strategy, the recommendation is to initiate cervical cancer screening with cytology alone at age 21, manage results appropriately, and then transition the patient to primary HPV testing with the FDA-approved test at age 25.12 This recommendation may be modified in the future. However the guidelines might change, patients will benefit only if the guidelines are implemented consistently in practice.
CORRESPONDENCE
Sabrina Hofmeister, DO, 1121 E. North Ave, Milwaukee, WI 53212; [email protected].
1. Kim JJ, Campos NG, Sy S, et al. Inefficiencies and high-value improvements in U.S. cervical cancer screening practice: a cost-effective analysis. Ann Intern Med. 2015;163:589-597.
2. Moyer VA; U.S. Preventive Services Task Force. Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;156:880-891.
3. U.S. Preventive Services Task Force. Understanding How the USPSTF Works: USPSTF 101. Available at: http://www.uspreventiveservicestaskforce.org/Page/Name/understanding-how-the-uspstf-works. Accessed June 8, 2016.
4. Reagan-Steiner S, Yankey D, Jeyarajah J, et al; Centers for Disease Control and Prevention. National, regional, state, and selected local vaccination coverage among adolescents aged 13-17 years—United States, 2014. MMWR Morb Mortal Wkly Rep. 2015;64:784-792.
5. Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. J Low Genit Tract Dis. 2012;16:175-204.
6. Vesco KK, Whitlock EP, Eder M, et al. Risk factors and other epidemiologic considerations for cervical cancer screening: a narrative review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155:687-697.
7. Khan MJ, Massad LS, Kinney W, et al. A common clinical dilemma: management of abnormal vaginal cytology and human papilloma virus test results. J Low Genit Tract Dis. 2016;20:119-125.
8. Wright TC, Stoler MH, Behrens CM, et al. Primary cervical cancer screening with human papillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test. Gynecol Oncol. 2015;136:189-197.
9. Naucler P, Ryd W, Törnberg S, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med. 2007;357:1589-1597.
10. Sawaya GF, Sung HY, Kinney W, et al. Cervical cancer after multiple negative tests in long-term members of a prepaid health plan. Acta Cytol. 2005;49:391-397.
11. Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in the United States. JAMA. 2007;297:813-819.
12. Huh WK, Ault KA, Chelmow D, et al. Use of primary high-risk HPV testing for cervical cancer screening: interim clinical guidance. J Low Genit Tract Dis. 2015;19:91-96.
13. American Congress of Obstetricians and Gynecologists. Practice Bulletin No. 157: Cervical cancer screening and prevention. Obstet Gynecol. 2016;127:e1-e20.
14. U.S. Preventive Services Task Force. Final Research Plan: Cervical Cancer: Screening. October 2015. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/final-research-plan/cervical-cancer-screening2. Accessed June 22, 2016.
15. Ronco G, Dillner J, Elfström KM, et al; International HPV Working Group. Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet. 2014;383:524-532.
16. Stoler MH, Wright TC Jr, Sharma A, et al. High-risk human papilloma virus testing in women with ASC-US cytology: results from the ATHENA HPV study. Am J Clin Path. 2011;135:468-475.
17. Choi JW, Kim Y, Lee JH, et al. The clinical performance of primary HPV screening, primary HPV screening plus cytology cotesting, and cytology alone at a tertiary care hospital. Cancer Cytopathol. 2016;124:144-152.
1. Kim JJ, Campos NG, Sy S, et al. Inefficiencies and high-value improvements in U.S. cervical cancer screening practice: a cost-effective analysis. Ann Intern Med. 2015;163:589-597.
2. Moyer VA; U.S. Preventive Services Task Force. Screening for cervical cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2012;156:880-891.
3. U.S. Preventive Services Task Force. Understanding How the USPSTF Works: USPSTF 101. Available at: http://www.uspreventiveservicestaskforce.org/Page/Name/understanding-how-the-uspstf-works. Accessed June 8, 2016.
4. Reagan-Steiner S, Yankey D, Jeyarajah J, et al; Centers for Disease Control and Prevention. National, regional, state, and selected local vaccination coverage among adolescents aged 13-17 years—United States, 2014. MMWR Morb Mortal Wkly Rep. 2015;64:784-792.
5. Saslow D, Solomon D, Lawson HW, et al. American Cancer Society, American Society for Colposcopy and Cervical Pathology, and American Society for Clinical Pathology screening guidelines for the prevention and early detection of cervical cancer. J Low Genit Tract Dis. 2012;16:175-204.
6. Vesco KK, Whitlock EP, Eder M, et al. Risk factors and other epidemiologic considerations for cervical cancer screening: a narrative review for the U.S. Preventive Services Task Force. Ann Intern Med. 2011;155:687-697.
7. Khan MJ, Massad LS, Kinney W, et al. A common clinical dilemma: management of abnormal vaginal cytology and human papilloma virus test results. J Low Genit Tract Dis. 2016;20:119-125.
8. Wright TC, Stoler MH, Behrens CM, et al. Primary cervical cancer screening with human papillomavirus: end of study results from the ATHENA study using HPV as the first-line screening test. Gynecol Oncol. 2015;136:189-197.
9. Naucler P, Ryd W, Törnberg S, et al. Human papillomavirus and Papanicolaou tests to screen for cervical cancer. N Engl J Med. 2007;357:1589-1597.
10. Sawaya GF, Sung HY, Kinney W, et al. Cervical cancer after multiple negative tests in long-term members of a prepaid health plan. Acta Cytol. 2005;49:391-397.
11. Dunne EF, Unger ER, Sternberg M, et al. Prevalence of HPV infection among females in the United States. JAMA. 2007;297:813-819.
12. Huh WK, Ault KA, Chelmow D, et al. Use of primary high-risk HPV testing for cervical cancer screening: interim clinical guidance. J Low Genit Tract Dis. 2015;19:91-96.
13. American Congress of Obstetricians and Gynecologists. Practice Bulletin No. 157: Cervical cancer screening and prevention. Obstet Gynecol. 2016;127:e1-e20.
14. U.S. Preventive Services Task Force. Final Research Plan: Cervical Cancer: Screening. October 2015. Available at: http://www.uspreventiveservicestaskforce.org/Page/Document/final-research-plan/cervical-cancer-screening2. Accessed June 22, 2016.
15. Ronco G, Dillner J, Elfström KM, et al; International HPV Working Group. Efficacy of HPV-based screening for prevention of invasive cervical cancer: follow-up of four European randomised controlled trials. Lancet. 2014;383:524-532.
16. Stoler MH, Wright TC Jr, Sharma A, et al. High-risk human papilloma virus testing in women with ASC-US cytology: results from the ATHENA HPV study. Am J Clin Path. 2011;135:468-475.
17. Choi JW, Kim Y, Lee JH, et al. The clinical performance of primary HPV screening, primary HPV screening plus cytology cotesting, and cytology alone at a tertiary care hospital. Cancer Cytopathol. 2016;124:144-152.
