User login
Hepatitis C infection rates rising in women, young children
Rates of hepatitis C virus detection increased in U.S. women aged 15-44 years and in children less than 2 years old from 2011 to 2014, according to investigators from the Centers for Disease Control and Prevention.
A report published July 21 in Morbidity and Mortality Weekly Report revealed hepatitis C virus (HCV) detection rates (detection via antibody or RNA positivity) that were determined using data collected from Quest Diagnostics for Kentucky and for the United States. In Kentucky, the rate of HCV detection in women aged 15-44 increased 213% over the study period, from 275 to 862 cases per 100,000 people, and for the entire U.S., the rate of detection increased by 22% from 139 to 169 cases per 100,000 people (65[28]:705-10).
The rate of HCV testing for children under 2 years old in Kentucky increased 151% over the study period, rising from 403 to 1,011 per 100,000 people, and the rate of children born to HCV-positive mothers increased from 0.71% to 1.59%. Nationwide, the HCV testing rate for children under 2 years old increased 14% from 310 to 353 per 100,000, and the rate of children born to HCV-positive mothers increased from 0.19% to 0.32%.
“These findings underscore the importance of providing primary prevention services and following current recommendations to identify persons at risk for HCV infection and test accordingly; doing so among pregnant women would improve early identification of HCV-infected infants and linkage of the mother and infant to care and treatment,” the CDC investigators said.
Rates of hepatitis C virus detection increased in U.S. women aged 15-44 years and in children less than 2 years old from 2011 to 2014, according to investigators from the Centers for Disease Control and Prevention.
A report published July 21 in Morbidity and Mortality Weekly Report revealed hepatitis C virus (HCV) detection rates (detection via antibody or RNA positivity) that were determined using data collected from Quest Diagnostics for Kentucky and for the United States. In Kentucky, the rate of HCV detection in women aged 15-44 increased 213% over the study period, from 275 to 862 cases per 100,000 people, and for the entire U.S., the rate of detection increased by 22% from 139 to 169 cases per 100,000 people (65[28]:705-10).
The rate of HCV testing for children under 2 years old in Kentucky increased 151% over the study period, rising from 403 to 1,011 per 100,000 people, and the rate of children born to HCV-positive mothers increased from 0.71% to 1.59%. Nationwide, the HCV testing rate for children under 2 years old increased 14% from 310 to 353 per 100,000, and the rate of children born to HCV-positive mothers increased from 0.19% to 0.32%.
“These findings underscore the importance of providing primary prevention services and following current recommendations to identify persons at risk for HCV infection and test accordingly; doing so among pregnant women would improve early identification of HCV-infected infants and linkage of the mother and infant to care and treatment,” the CDC investigators said.
Rates of hepatitis C virus detection increased in U.S. women aged 15-44 years and in children less than 2 years old from 2011 to 2014, according to investigators from the Centers for Disease Control and Prevention.
A report published July 21 in Morbidity and Mortality Weekly Report revealed hepatitis C virus (HCV) detection rates (detection via antibody or RNA positivity) that were determined using data collected from Quest Diagnostics for Kentucky and for the United States. In Kentucky, the rate of HCV detection in women aged 15-44 increased 213% over the study period, from 275 to 862 cases per 100,000 people, and for the entire U.S., the rate of detection increased by 22% from 139 to 169 cases per 100,000 people (65[28]:705-10).
The rate of HCV testing for children under 2 years old in Kentucky increased 151% over the study period, rising from 403 to 1,011 per 100,000 people, and the rate of children born to HCV-positive mothers increased from 0.71% to 1.59%. Nationwide, the HCV testing rate for children under 2 years old increased 14% from 310 to 353 per 100,000, and the rate of children born to HCV-positive mothers increased from 0.19% to 0.32%.
“These findings underscore the importance of providing primary prevention services and following current recommendations to identify persons at risk for HCV infection and test accordingly; doing so among pregnant women would improve early identification of HCV-infected infants and linkage of the mother and infant to care and treatment,” the CDC investigators said.
FROM MMWR
Jury still out on value of r-HGH with IVF
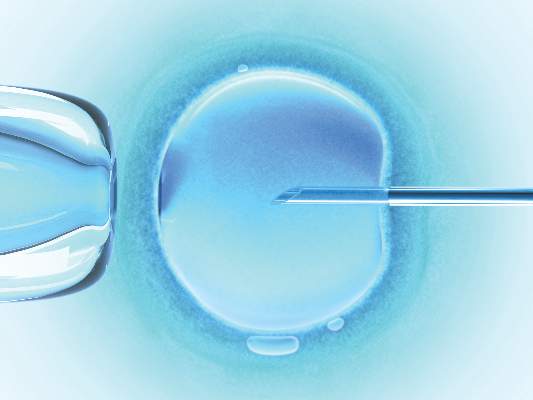
HELSINKI, FINLAND – Recombinant human growth hormone, or r-HGH, offered no advantage over placebo with respect to improving the live birth rate among poor-responding women undergoing in vitro fertilization in a randomized controlled study.
The current findings and those from previous studies leave questions about the value of r-HGH supplementation unanswered, Robert Norman, MD, said at the annual meeting of the European Society of Human Reproduction and Embryology.

An “extremely large” randomized trial would be needed to definitively show whether poor IVF responders benefit from r-HGH supplementation, he said.
The clinical pregnancy rate in 66 women randomized to receive r-HGH in the current study was 9.1%, compared with 9.2% in 65 patients in the placebo group. In the groups, respectively, the mean number of oocytes collected was 5.38 and 4.96, median embryo quality was 2.00 and 2.14, median days of a study drug were 8 and 9, and in both groups the median number of days of follicle stimulating hormone was 8, and the mean number of embryos transferred was 1.
The overall live birth rate per patient randomized was 12.3%; the groups did not differ significantly on any of these measures, said Dr. Norman of the University of Adelaide, and Fertility SA, Australia.
Human growth hormone is known to be important for ovarian steroidogenesis and follicular development, and prior research, including a recent Cochrane Review, has suggested it is associated with a trend toward improved live birth rates when used as an adjunct to IVF in poor responders (though not in routine IVF). The prior studies, however, have been underpowered, involved significant clinical heterogeneity between study groups, were not placebo controlled, and used pregnancy rather than live birth as the endpoint. Further, safety outcomes among patients treated with r-HGH were uncertain, Dr. Norman said.
For the current study, women were recruited from nine fertility centers in Australia and from one center in New Zealand. All met the criteria for poor response, having had a previous IVF cycle with no more than five eggs collected following maximum stimulation. Of the 131 women randomized, all underwent ovarian stimulation with the same previous drug dose, and 116 had oocyte retrieval, 97 had embryo transfer, 25 reported a positive pregnancy test, and 16 had a live birth, which was the primary endpoint of the study. Three sets of twins were born – all to women in the r-HGH group. Four serious adverse events – all congenital abnormalities – were noted, including three in the r-HGH group and one in the placebo group. No serious adverse events occurred.
Of note, the study, which was expected to be completed in 2 years, was terminated after 4 years because of slow recruitment. Since the 390 patients required to demonstrate a difference between the groups were not enrolled, the study remained underpowered, Dr. Norman said.
Nonetheless, the findings, which highlight the challenges in answering the questions that could shed light on the best clinical treatment for a poor IVF responder, fail to provide any evidence either for benefit or for lack of benefit with the use of r-HGH in this group.
“If it were cheap, it might find a place in poor responders, but normal doses cost more than $1,000,” he said in a press statement regarding the findings.
Poor responders are a notoriously difficult group to treat, and although many strategies have been tried, there is no solid evidence that any of them improve the outcome of most concern to women undergoing IVF: the live birth rate, he added, noting that 30% of patients who are poor IVF responders and who have low pregnancy rates are over 40 years old.
Dr. Norman reported having no financial disclosures.
HELSINKI, FINLAND – Recombinant human growth hormone, or r-HGH, offered no advantage over placebo with respect to improving the live birth rate among poor-responding women undergoing in vitro fertilization in a randomized controlled study.
The current findings and those from previous studies leave questions about the value of r-HGH supplementation unanswered, Robert Norman, MD, said at the annual meeting of the European Society of Human Reproduction and Embryology.
An “extremely large” randomized trial would be needed to definitively show whether poor IVF responders benefit from r-HGH supplementation, he said.
The clinical pregnancy rate in 66 women randomized to receive r-HGH in the current study was 9.1%, compared with 9.2% in 65 patients in the placebo group. In the groups, respectively, the mean number of oocytes collected was 5.38 and 4.96, median embryo quality was 2.00 and 2.14, median days of a study drug were 8 and 9, and in both groups the median number of days of follicle stimulating hormone was 8, and the mean number of embryos transferred was 1.
The overall live birth rate per patient randomized was 12.3%; the groups did not differ significantly on any of these measures, said Dr. Norman of the University of Adelaide, and Fertility SA, Australia.
Human growth hormone is known to be important for ovarian steroidogenesis and follicular development, and prior research, including a recent Cochrane Review, has suggested it is associated with a trend toward improved live birth rates when used as an adjunct to IVF in poor responders (though not in routine IVF). The prior studies, however, have been underpowered, involved significant clinical heterogeneity between study groups, were not placebo controlled, and used pregnancy rather than live birth as the endpoint. Further, safety outcomes among patients treated with r-HGH were uncertain, Dr. Norman said.
For the current study, women were recruited from nine fertility centers in Australia and from one center in New Zealand. All met the criteria for poor response, having had a previous IVF cycle with no more than five eggs collected following maximum stimulation. Of the 131 women randomized, all underwent ovarian stimulation with the same previous drug dose, and 116 had oocyte retrieval, 97 had embryo transfer, 25 reported a positive pregnancy test, and 16 had a live birth, which was the primary endpoint of the study. Three sets of twins were born – all to women in the r-HGH group. Four serious adverse events – all congenital abnormalities – were noted, including three in the r-HGH group and one in the placebo group. No serious adverse events occurred.
Of note, the study, which was expected to be completed in 2 years, was terminated after 4 years because of slow recruitment. Since the 390 patients required to demonstrate a difference between the groups were not enrolled, the study remained underpowered, Dr. Norman said.
Nonetheless, the findings, which highlight the challenges in answering the questions that could shed light on the best clinical treatment for a poor IVF responder, fail to provide any evidence either for benefit or for lack of benefit with the use of r-HGH in this group.
“If it were cheap, it might find a place in poor responders, but normal doses cost more than $1,000,” he said in a press statement regarding the findings.
Poor responders are a notoriously difficult group to treat, and although many strategies have been tried, there is no solid evidence that any of them improve the outcome of most concern to women undergoing IVF: the live birth rate, he added, noting that 30% of patients who are poor IVF responders and who have low pregnancy rates are over 40 years old.
Dr. Norman reported having no financial disclosures.
HELSINKI, FINLAND – Recombinant human growth hormone, or r-HGH, offered no advantage over placebo with respect to improving the live birth rate among poor-responding women undergoing in vitro fertilization in a randomized controlled study.
The current findings and those from previous studies leave questions about the value of r-HGH supplementation unanswered, Robert Norman, MD, said at the annual meeting of the European Society of Human Reproduction and Embryology.
An “extremely large” randomized trial would be needed to definitively show whether poor IVF responders benefit from r-HGH supplementation, he said.
The clinical pregnancy rate in 66 women randomized to receive r-HGH in the current study was 9.1%, compared with 9.2% in 65 patients in the placebo group. In the groups, respectively, the mean number of oocytes collected was 5.38 and 4.96, median embryo quality was 2.00 and 2.14, median days of a study drug were 8 and 9, and in both groups the median number of days of follicle stimulating hormone was 8, and the mean number of embryos transferred was 1.
The overall live birth rate per patient randomized was 12.3%; the groups did not differ significantly on any of these measures, said Dr. Norman of the University of Adelaide, and Fertility SA, Australia.
Human growth hormone is known to be important for ovarian steroidogenesis and follicular development, and prior research, including a recent Cochrane Review, has suggested it is associated with a trend toward improved live birth rates when used as an adjunct to IVF in poor responders (though not in routine IVF). The prior studies, however, have been underpowered, involved significant clinical heterogeneity between study groups, were not placebo controlled, and used pregnancy rather than live birth as the endpoint. Further, safety outcomes among patients treated with r-HGH were uncertain, Dr. Norman said.
For the current study, women were recruited from nine fertility centers in Australia and from one center in New Zealand. All met the criteria for poor response, having had a previous IVF cycle with no more than five eggs collected following maximum stimulation. Of the 131 women randomized, all underwent ovarian stimulation with the same previous drug dose, and 116 had oocyte retrieval, 97 had embryo transfer, 25 reported a positive pregnancy test, and 16 had a live birth, which was the primary endpoint of the study. Three sets of twins were born – all to women in the r-HGH group. Four serious adverse events – all congenital abnormalities – were noted, including three in the r-HGH group and one in the placebo group. No serious adverse events occurred.
Of note, the study, which was expected to be completed in 2 years, was terminated after 4 years because of slow recruitment. Since the 390 patients required to demonstrate a difference between the groups were not enrolled, the study remained underpowered, Dr. Norman said.
Nonetheless, the findings, which highlight the challenges in answering the questions that could shed light on the best clinical treatment for a poor IVF responder, fail to provide any evidence either for benefit or for lack of benefit with the use of r-HGH in this group.
“If it were cheap, it might find a place in poor responders, but normal doses cost more than $1,000,” he said in a press statement regarding the findings.
Poor responders are a notoriously difficult group to treat, and although many strategies have been tried, there is no solid evidence that any of them improve the outcome of most concern to women undergoing IVF: the live birth rate, he added, noting that 30% of patients who are poor IVF responders and who have low pregnancy rates are over 40 years old.
Dr. Norman reported having no financial disclosures.
AT ESHRE 2016
Key clinical point: Recombinant human growth hormone appears not to improve the live birth rate among poor-responding women undergoing in vitro fertilization.
Major finding: The overall live birth rate per patient randomized was 12.3% and did not differ between those who did and did not receive r-HGH.
Data source: A randomized controlled study involving 131 women.
Disclosures: Dr. Norman reported having no financial disclosures.
Teams boost confidence in IPF diagnoses
The accuracy of idiopathic pulmonary fibrosis (IPF) diagnoses is improving with the use of multidisciplinary team meetings and updated guidelines, based on the findings of a study that compared diagnostic agreement of individual clinicians and teams evaluating patients with interstitial lung disease.
Pulmonologists who participate in multidisciplinary team meetings said the findings validate the team approach.
“The [study’s] data confirm what we see in clinical practice ... it takes a multidisciplinary – and perhaps often multiple pulmonologists – to review these cases,” Marilyn K. Glassberg, MD,professor of medicine and surgery and director of the interstitial lung disease program at the University of Miami Health System, said in an interview.“This study demonstrates the importance of multiple perspectives when evaluating a patient and coming to a diagnosis at a time when reliable biomarkers are not available.”
The study, published in The Lancet Respiratory Medicine (2016;4[7]:557-65), is the first evaluation of multidisciplinary team agreement on diagnosis of interstitial lung disease since updated guidelines were published, according to Simon L. F. Walsh, MD, of Kings College Hospital NHS Foundation Trust, London, and his colleagues.
In 2015, the American Thoracic Society (ATS), European Respiratory Society (ERS), Japanese Respiratory Society (JRS), and Latin American Thoracic Association (ALTA) adopted joint guidelines for the treatment of IPF. In 2013, the ATS and ERS updated guidelines for the classification and terminology for idiopathic interstitial pneumonias.
“Our study shows ... in [IPF], MDTMs (multidisciplinary team meetings) have a higher level of agreement on diagnoses, assign diagnoses with higher confidence more frequently, and provide diagnoses that have non-significant greater prognostic separation than do clinicians or radiologists in most cases,” the researchers wrote.
Before MDTMs were initiated, the clinicians, radiologists, and pathologists who would be participating in them independently reviewed each patient’s case without consulting other specialists and provided up to five diagnoses with diagnostic likelihoods for each patient.
For the study, 70 patients were evaluated and the level of diagnostic agreement was assessed at seven international centers for the diagnosis of interstitial lung disease (diffuse parenchymal lung disease). Following independent reviews of the 70 cases, the clinician, radiologist, and pathologist from each center met as a multidisciplinary team to review the same cases together and give up to five diagnoses with diagnostic likelihoods.
All clinical information supplied in the first stage of the study, including pulmonary function test results, high-resolution CT at presentation, and digitalized surgical lung biopsy slides, were available to the multidisciplinary team. The patients’ outcomes were used to validate the diagnoses. The survival period for each patient was calculated based on the date of referral to the host institution to the minimum date of death, date patient was last known to be alive, or June 1, 2015 – the end of the study period.
The inter-MDTM agreement was better than interobserver agreement for all diagnoses (unweighted kappa value (K) = 0.50), and inter-MDTM agreement was highest for IPF (K = 0.60) and connective tissue disease-related interstitial lung disease (K = 0.64).
“We have shown an acceptable level [based on a K of greater than 0.40 being deemed clinically acceptable] of diagnostic agreement exists between multidisciplinary teams in the setting of diffuse parenchymal lung disease. Additionally, we showed that this agreement was validated by the nonsignificant increases toward greater prognostic separation of an IPF diagnosis made by multidisciplinary teams than by individual clinicians or radiologists,” the researchers wrote.
The weighted kappa (KW) values for estimation of diagnostic likelihood for diagnoses of IPF were 0.72 (0.67-0.76) for clinicians, 0.60 (0.46-0.66) for radiologists, 0.58 (0.45-0.66) for pathologists and 0.71 (0.64-0.77) for MDTMs.
For connective tissue disease–related interstitial lung diseases, the KW for estimation of diagnostic likelihood for diagnoses for MDTMs were 0.73 (0.68-0.78), compared with 0.76 (0.70-0.78) for clinicians, 0.17 (0.08-0.31) for radiologists, and 0.21 (0.06-0.36) for pathologists.
Krishna Thavarajah, MD,, who sees patients with interstitial lung disease within the Henry Ford Health System in Detroit, has been participating in MDTMs for nearly 6 years.
“The accuracies of diagnoses for patients with IPF are much better than even 10 years ago,” she said in an interview. “I think this is because of the improvement in consistency in diagnostic criteria based on the updated guidelines in IPF. Among the MDTMs that participated in the study, the agreement about diagnoses was highest for IPF. The interobserver agreement for clinicians was also pretty high for IPF.”
In her work within an academic center, Dr. Glassberg sees patients in an IPF clinic and in a separate autoimmune disorders clinic. For each clinic, there is a multidisciplinary team. In the IPF clinic, there are three pulmonologists and a radiologist, and when there is a biopsy, there are two pathologists. Dr. Glassberg’s IPF team also includes four pulmonary radiologists.
During her MDTMs, Dr. Thavarajah, a radiologist, and a pathologist will examine a patient’s chest imaging and pathology slides. They sit together until they become confident of their diagnosis in the absence of a biopsy.
There are times when the team tells a patient the probable diagnosis and acknowledges the small chance of an alternative diagnosis. “It was comforting to me that, in the Lancet study, there was a good level of agreement in diagnosis of IPF among multidisciplinary teams, whether the patients had undergone a biopsy or not,” said Dr. Thavarajah. “The mortality of patients given a diagnosis of IPF was worse than those given a diagnosis of non-IPF to validate the IPF diagnosis.”
Establishing and implementing MDTMs is challenging, though, said Dr. Glassberg.
“[We] need to address how multidisciplinary teams could work for doctors who are in smaller cities or who are not in academic centers. We need to utilize existing channels to create new avenues for these colleagues to present their cases – particularly challenging ones or patients who need to be referred – to be evaluated by an interdisciplinary team. The Internet may offer these opportunities for networking and decision making, said Dr. Glassberg.
The study was funded by the National Institute of Health Research, Imperial College London. Several of the study’s authors declared receiving personal fees, grants, or research support from a variety of sources, but had no financial disclosures relevant to this study.
Daniel R. Ouellette, MD, FCCP, comments: “Recommendations have been that multidisciplinary teams add to the accuracy of the diagnosis of IPF. The value of this study is that it provides objective data that this is so.”
Daniel R. Ouellette, MD, FCCP, comments: “Recommendations have been that multidisciplinary teams add to the accuracy of the diagnosis of IPF. The value of this study is that it provides objective data that this is so.”
Daniel R. Ouellette, MD, FCCP, comments: “Recommendations have been that multidisciplinary teams add to the accuracy of the diagnosis of IPF. The value of this study is that it provides objective data that this is so.”
The accuracy of idiopathic pulmonary fibrosis (IPF) diagnoses is improving with the use of multidisciplinary team meetings and updated guidelines, based on the findings of a study that compared diagnostic agreement of individual clinicians and teams evaluating patients with interstitial lung disease.
Pulmonologists who participate in multidisciplinary team meetings said the findings validate the team approach.
“The [study’s] data confirm what we see in clinical practice ... it takes a multidisciplinary – and perhaps often multiple pulmonologists – to review these cases,” Marilyn K. Glassberg, MD,professor of medicine and surgery and director of the interstitial lung disease program at the University of Miami Health System, said in an interview.“This study demonstrates the importance of multiple perspectives when evaluating a patient and coming to a diagnosis at a time when reliable biomarkers are not available.”
The study, published in The Lancet Respiratory Medicine (2016;4[7]:557-65), is the first evaluation of multidisciplinary team agreement on diagnosis of interstitial lung disease since updated guidelines were published, according to Simon L. F. Walsh, MD, of Kings College Hospital NHS Foundation Trust, London, and his colleagues.
In 2015, the American Thoracic Society (ATS), European Respiratory Society (ERS), Japanese Respiratory Society (JRS), and Latin American Thoracic Association (ALTA) adopted joint guidelines for the treatment of IPF. In 2013, the ATS and ERS updated guidelines for the classification and terminology for idiopathic interstitial pneumonias.
“Our study shows ... in [IPF], MDTMs (multidisciplinary team meetings) have a higher level of agreement on diagnoses, assign diagnoses with higher confidence more frequently, and provide diagnoses that have non-significant greater prognostic separation than do clinicians or radiologists in most cases,” the researchers wrote.
Before MDTMs were initiated, the clinicians, radiologists, and pathologists who would be participating in them independently reviewed each patient’s case without consulting other specialists and provided up to five diagnoses with diagnostic likelihoods for each patient.
For the study, 70 patients were evaluated and the level of diagnostic agreement was assessed at seven international centers for the diagnosis of interstitial lung disease (diffuse parenchymal lung disease). Following independent reviews of the 70 cases, the clinician, radiologist, and pathologist from each center met as a multidisciplinary team to review the same cases together and give up to five diagnoses with diagnostic likelihoods.
All clinical information supplied in the first stage of the study, including pulmonary function test results, high-resolution CT at presentation, and digitalized surgical lung biopsy slides, were available to the multidisciplinary team. The patients’ outcomes were used to validate the diagnoses. The survival period for each patient was calculated based on the date of referral to the host institution to the minimum date of death, date patient was last known to be alive, or June 1, 2015 – the end of the study period.
The inter-MDTM agreement was better than interobserver agreement for all diagnoses (unweighted kappa value (K) = 0.50), and inter-MDTM agreement was highest for IPF (K = 0.60) and connective tissue disease-related interstitial lung disease (K = 0.64).
“We have shown an acceptable level [based on a K of greater than 0.40 being deemed clinically acceptable] of diagnostic agreement exists between multidisciplinary teams in the setting of diffuse parenchymal lung disease. Additionally, we showed that this agreement was validated by the nonsignificant increases toward greater prognostic separation of an IPF diagnosis made by multidisciplinary teams than by individual clinicians or radiologists,” the researchers wrote.
The weighted kappa (KW) values for estimation of diagnostic likelihood for diagnoses of IPF were 0.72 (0.67-0.76) for clinicians, 0.60 (0.46-0.66) for radiologists, 0.58 (0.45-0.66) for pathologists and 0.71 (0.64-0.77) for MDTMs.
For connective tissue disease–related interstitial lung diseases, the KW for estimation of diagnostic likelihood for diagnoses for MDTMs were 0.73 (0.68-0.78), compared with 0.76 (0.70-0.78) for clinicians, 0.17 (0.08-0.31) for radiologists, and 0.21 (0.06-0.36) for pathologists.
Krishna Thavarajah, MD,, who sees patients with interstitial lung disease within the Henry Ford Health System in Detroit, has been participating in MDTMs for nearly 6 years.
“The accuracies of diagnoses for patients with IPF are much better than even 10 years ago,” she said in an interview. “I think this is because of the improvement in consistency in diagnostic criteria based on the updated guidelines in IPF. Among the MDTMs that participated in the study, the agreement about diagnoses was highest for IPF. The interobserver agreement for clinicians was also pretty high for IPF.”
In her work within an academic center, Dr. Glassberg sees patients in an IPF clinic and in a separate autoimmune disorders clinic. For each clinic, there is a multidisciplinary team. In the IPF clinic, there are three pulmonologists and a radiologist, and when there is a biopsy, there are two pathologists. Dr. Glassberg’s IPF team also includes four pulmonary radiologists.
During her MDTMs, Dr. Thavarajah, a radiologist, and a pathologist will examine a patient’s chest imaging and pathology slides. They sit together until they become confident of their diagnosis in the absence of a biopsy.
There are times when the team tells a patient the probable diagnosis and acknowledges the small chance of an alternative diagnosis. “It was comforting to me that, in the Lancet study, there was a good level of agreement in diagnosis of IPF among multidisciplinary teams, whether the patients had undergone a biopsy or not,” said Dr. Thavarajah. “The mortality of patients given a diagnosis of IPF was worse than those given a diagnosis of non-IPF to validate the IPF diagnosis.”
Establishing and implementing MDTMs is challenging, though, said Dr. Glassberg.
“[We] need to address how multidisciplinary teams could work for doctors who are in smaller cities or who are not in academic centers. We need to utilize existing channels to create new avenues for these colleagues to present their cases – particularly challenging ones or patients who need to be referred – to be evaluated by an interdisciplinary team. The Internet may offer these opportunities for networking and decision making, said Dr. Glassberg.
The study was funded by the National Institute of Health Research, Imperial College London. Several of the study’s authors declared receiving personal fees, grants, or research support from a variety of sources, but had no financial disclosures relevant to this study.
The accuracy of idiopathic pulmonary fibrosis (IPF) diagnoses is improving with the use of multidisciplinary team meetings and updated guidelines, based on the findings of a study that compared diagnostic agreement of individual clinicians and teams evaluating patients with interstitial lung disease.
Pulmonologists who participate in multidisciplinary team meetings said the findings validate the team approach.
“The [study’s] data confirm what we see in clinical practice ... it takes a multidisciplinary – and perhaps often multiple pulmonologists – to review these cases,” Marilyn K. Glassberg, MD,professor of medicine and surgery and director of the interstitial lung disease program at the University of Miami Health System, said in an interview.“This study demonstrates the importance of multiple perspectives when evaluating a patient and coming to a diagnosis at a time when reliable biomarkers are not available.”
The study, published in The Lancet Respiratory Medicine (2016;4[7]:557-65), is the first evaluation of multidisciplinary team agreement on diagnosis of interstitial lung disease since updated guidelines were published, according to Simon L. F. Walsh, MD, of Kings College Hospital NHS Foundation Trust, London, and his colleagues.
In 2015, the American Thoracic Society (ATS), European Respiratory Society (ERS), Japanese Respiratory Society (JRS), and Latin American Thoracic Association (ALTA) adopted joint guidelines for the treatment of IPF. In 2013, the ATS and ERS updated guidelines for the classification and terminology for idiopathic interstitial pneumonias.
“Our study shows ... in [IPF], MDTMs (multidisciplinary team meetings) have a higher level of agreement on diagnoses, assign diagnoses with higher confidence more frequently, and provide diagnoses that have non-significant greater prognostic separation than do clinicians or radiologists in most cases,” the researchers wrote.
Before MDTMs were initiated, the clinicians, radiologists, and pathologists who would be participating in them independently reviewed each patient’s case without consulting other specialists and provided up to five diagnoses with diagnostic likelihoods for each patient.
For the study, 70 patients were evaluated and the level of diagnostic agreement was assessed at seven international centers for the diagnosis of interstitial lung disease (diffuse parenchymal lung disease). Following independent reviews of the 70 cases, the clinician, radiologist, and pathologist from each center met as a multidisciplinary team to review the same cases together and give up to five diagnoses with diagnostic likelihoods.
All clinical information supplied in the first stage of the study, including pulmonary function test results, high-resolution CT at presentation, and digitalized surgical lung biopsy slides, were available to the multidisciplinary team. The patients’ outcomes were used to validate the diagnoses. The survival period for each patient was calculated based on the date of referral to the host institution to the minimum date of death, date patient was last known to be alive, or June 1, 2015 – the end of the study period.
The inter-MDTM agreement was better than interobserver agreement for all diagnoses (unweighted kappa value (K) = 0.50), and inter-MDTM agreement was highest for IPF (K = 0.60) and connective tissue disease-related interstitial lung disease (K = 0.64).
“We have shown an acceptable level [based on a K of greater than 0.40 being deemed clinically acceptable] of diagnostic agreement exists between multidisciplinary teams in the setting of diffuse parenchymal lung disease. Additionally, we showed that this agreement was validated by the nonsignificant increases toward greater prognostic separation of an IPF diagnosis made by multidisciplinary teams than by individual clinicians or radiologists,” the researchers wrote.
The weighted kappa (KW) values for estimation of diagnostic likelihood for diagnoses of IPF were 0.72 (0.67-0.76) for clinicians, 0.60 (0.46-0.66) for radiologists, 0.58 (0.45-0.66) for pathologists and 0.71 (0.64-0.77) for MDTMs.
For connective tissue disease–related interstitial lung diseases, the KW for estimation of diagnostic likelihood for diagnoses for MDTMs were 0.73 (0.68-0.78), compared with 0.76 (0.70-0.78) for clinicians, 0.17 (0.08-0.31) for radiologists, and 0.21 (0.06-0.36) for pathologists.
Krishna Thavarajah, MD,, who sees patients with interstitial lung disease within the Henry Ford Health System in Detroit, has been participating in MDTMs for nearly 6 years.
“The accuracies of diagnoses for patients with IPF are much better than even 10 years ago,” she said in an interview. “I think this is because of the improvement in consistency in diagnostic criteria based on the updated guidelines in IPF. Among the MDTMs that participated in the study, the agreement about diagnoses was highest for IPF. The interobserver agreement for clinicians was also pretty high for IPF.”
In her work within an academic center, Dr. Glassberg sees patients in an IPF clinic and in a separate autoimmune disorders clinic. For each clinic, there is a multidisciplinary team. In the IPF clinic, there are three pulmonologists and a radiologist, and when there is a biopsy, there are two pathologists. Dr. Glassberg’s IPF team also includes four pulmonary radiologists.
During her MDTMs, Dr. Thavarajah, a radiologist, and a pathologist will examine a patient’s chest imaging and pathology slides. They sit together until they become confident of their diagnosis in the absence of a biopsy.
There are times when the team tells a patient the probable diagnosis and acknowledges the small chance of an alternative diagnosis. “It was comforting to me that, in the Lancet study, there was a good level of agreement in diagnosis of IPF among multidisciplinary teams, whether the patients had undergone a biopsy or not,” said Dr. Thavarajah. “The mortality of patients given a diagnosis of IPF was worse than those given a diagnosis of non-IPF to validate the IPF diagnosis.”
Establishing and implementing MDTMs is challenging, though, said Dr. Glassberg.
“[We] need to address how multidisciplinary teams could work for doctors who are in smaller cities or who are not in academic centers. We need to utilize existing channels to create new avenues for these colleagues to present their cases – particularly challenging ones or patients who need to be referred – to be evaluated by an interdisciplinary team. The Internet may offer these opportunities for networking and decision making, said Dr. Glassberg.
The study was funded by the National Institute of Health Research, Imperial College London. Several of the study’s authors declared receiving personal fees, grants, or research support from a variety of sources, but had no financial disclosures relevant to this study.
Australia Declares AIDS No Longer a Public Health Issue
SYDNEY - Australia declared on Monday the AIDS epidemic is no longer a public health issue there, a month after the United Nations adopted an ambitious target to eliminate the threat globally by 2030.
The government-backed Australian Federation of AIDS Organisations (AFAO) and top scientists said the number of people being diagnosed with AIDS in Australia was now so small it was no longer reported.
AIDS cases in Australia peaked in 1994, at 953 cases, according to the Kirby Institute for infection and immunity in society.
Since then, following the introduction of antiretroviral treatment, that prevent AIDS developing in people who are infected with the HIV virus, and awareness campaigns, AIDS diagnoses have declined sharply.
"Australia is incredibly fortunate to be in the position and its because of farsighted government policy," said Darryl O'Donnell, chief executive AFAO.
"We had community organizations of gay men, sex workers and drug users doing outreach campaigns that were extraordinarily effective," O'Donnell said.
A spokeswoman for the Federal Department of Health said while it was tremendous that AIDS was "not the automatic death sentence that it once was," approximately 1,100 cases of HIV are detected each year.
"We must not let down our guard."
Worldwide there are 36.7 million people living with HIV, according to the World Health Organisation, with 180,000 people dying from AIDS-related illness in the Asia-Pacific region last year.
The United Nations agreed a new declaration on ending the AIDS epidemic at a meeting in New York last month.
The UNAIDS Fast-Track approach to ending the AIDS epidemic has a set of time-bound targets, including reducing the number of people newly infected with HIV from 2.1 million in 2015 to fewer than 500,000 in 2020, reducing the number of people dying from AIDS-related illnesses from 1.1 million in 2015 to fewer than 500,000 in 2020 and eliminating HIV-related discrimination.
Andrew Grulich, head of the HIV Epidemiology and Prevention Program at the Kirby Institute, said other countries could learn from Australia.
"The thing that has characterized Australia is a partnership between all sectors involved," he said. "Community, research and the government - and having bipartisan political support."
SYDNEY - Australia declared on Monday the AIDS epidemic is no longer a public health issue there, a month after the United Nations adopted an ambitious target to eliminate the threat globally by 2030.
The government-backed Australian Federation of AIDS Organisations (AFAO) and top scientists said the number of people being diagnosed with AIDS in Australia was now so small it was no longer reported.
AIDS cases in Australia peaked in 1994, at 953 cases, according to the Kirby Institute for infection and immunity in society.
Since then, following the introduction of antiretroviral treatment, that prevent AIDS developing in people who are infected with the HIV virus, and awareness campaigns, AIDS diagnoses have declined sharply.
"Australia is incredibly fortunate to be in the position and its because of farsighted government policy," said Darryl O'Donnell, chief executive AFAO.
"We had community organizations of gay men, sex workers and drug users doing outreach campaigns that were extraordinarily effective," O'Donnell said.
A spokeswoman for the Federal Department of Health said while it was tremendous that AIDS was "not the automatic death sentence that it once was," approximately 1,100 cases of HIV are detected each year.
"We must not let down our guard."
Worldwide there are 36.7 million people living with HIV, according to the World Health Organisation, with 180,000 people dying from AIDS-related illness in the Asia-Pacific region last year.
The United Nations agreed a new declaration on ending the AIDS epidemic at a meeting in New York last month.
The UNAIDS Fast-Track approach to ending the AIDS epidemic has a set of time-bound targets, including reducing the number of people newly infected with HIV from 2.1 million in 2015 to fewer than 500,000 in 2020, reducing the number of people dying from AIDS-related illnesses from 1.1 million in 2015 to fewer than 500,000 in 2020 and eliminating HIV-related discrimination.
Andrew Grulich, head of the HIV Epidemiology and Prevention Program at the Kirby Institute, said other countries could learn from Australia.
"The thing that has characterized Australia is a partnership between all sectors involved," he said. "Community, research and the government - and having bipartisan political support."
SYDNEY - Australia declared on Monday the AIDS epidemic is no longer a public health issue there, a month after the United Nations adopted an ambitious target to eliminate the threat globally by 2030.
The government-backed Australian Federation of AIDS Organisations (AFAO) and top scientists said the number of people being diagnosed with AIDS in Australia was now so small it was no longer reported.
AIDS cases in Australia peaked in 1994, at 953 cases, according to the Kirby Institute for infection and immunity in society.
Since then, following the introduction of antiretroviral treatment, that prevent AIDS developing in people who are infected with the HIV virus, and awareness campaigns, AIDS diagnoses have declined sharply.
"Australia is incredibly fortunate to be in the position and its because of farsighted government policy," said Darryl O'Donnell, chief executive AFAO.
"We had community organizations of gay men, sex workers and drug users doing outreach campaigns that were extraordinarily effective," O'Donnell said.
A spokeswoman for the Federal Department of Health said while it was tremendous that AIDS was "not the automatic death sentence that it once was," approximately 1,100 cases of HIV are detected each year.
"We must not let down our guard."
Worldwide there are 36.7 million people living with HIV, according to the World Health Organisation, with 180,000 people dying from AIDS-related illness in the Asia-Pacific region last year.
The United Nations agreed a new declaration on ending the AIDS epidemic at a meeting in New York last month.
The UNAIDS Fast-Track approach to ending the AIDS epidemic has a set of time-bound targets, including reducing the number of people newly infected with HIV from 2.1 million in 2015 to fewer than 500,000 in 2020, reducing the number of people dying from AIDS-related illnesses from 1.1 million in 2015 to fewer than 500,000 in 2020 and eliminating HIV-related discrimination.
Andrew Grulich, head of the HIV Epidemiology and Prevention Program at the Kirby Institute, said other countries could learn from Australia.
"The thing that has characterized Australia is a partnership between all sectors involved," he said. "Community, research and the government - and having bipartisan political support."
Psoriasiform eruptions in Kawasaki disease reveal distinct phenotype
A comparison of psoriasis-like eruptions in Kawasaki disease (KD) with classic psoriasis shows a distinct phenotype with greater remission, report Ellen S. Haddock, AB, MBA and coauthors from the School of Medicine at the University of California, San Diego.
Investigators performed a retrospective study of 11 KD cases with a psoriasiform eruption matched by gender, age, and ethnicity with psoriasis-only and KD-only controls. Genotyping was performed in 10 cases for a deletion of two late cornified envelope genes associated with pediatric-onset psoriasis.
KD-associated eruptions were similar to classic psoriasis in presentation, but with less frequent diaper area involvement, more crust, more serious exudate, and significantly higher remission (91% vs. 23%; P less than .001), the authors noted.
The findings indicate that despite similarities to classic psoriasis, “this appears to be a distinct phenotype with significantly greater propensity for remission,” the authors concluded.
Read the full article in the Journal of the American Academy of Dermatology.
A comparison of psoriasis-like eruptions in Kawasaki disease (KD) with classic psoriasis shows a distinct phenotype with greater remission, report Ellen S. Haddock, AB, MBA and coauthors from the School of Medicine at the University of California, San Diego.
Investigators performed a retrospective study of 11 KD cases with a psoriasiform eruption matched by gender, age, and ethnicity with psoriasis-only and KD-only controls. Genotyping was performed in 10 cases for a deletion of two late cornified envelope genes associated with pediatric-onset psoriasis.
KD-associated eruptions were similar to classic psoriasis in presentation, but with less frequent diaper area involvement, more crust, more serious exudate, and significantly higher remission (91% vs. 23%; P less than .001), the authors noted.
The findings indicate that despite similarities to classic psoriasis, “this appears to be a distinct phenotype with significantly greater propensity for remission,” the authors concluded.
Read the full article in the Journal of the American Academy of Dermatology.
A comparison of psoriasis-like eruptions in Kawasaki disease (KD) with classic psoriasis shows a distinct phenotype with greater remission, report Ellen S. Haddock, AB, MBA and coauthors from the School of Medicine at the University of California, San Diego.
Investigators performed a retrospective study of 11 KD cases with a psoriasiform eruption matched by gender, age, and ethnicity with psoriasis-only and KD-only controls. Genotyping was performed in 10 cases for a deletion of two late cornified envelope genes associated with pediatric-onset psoriasis.
KD-associated eruptions were similar to classic psoriasis in presentation, but with less frequent diaper area involvement, more crust, more serious exudate, and significantly higher remission (91% vs. 23%; P less than .001), the authors noted.
The findings indicate that despite similarities to classic psoriasis, “this appears to be a distinct phenotype with significantly greater propensity for remission,” the authors concluded.
Read the full article in the Journal of the American Academy of Dermatology.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Intake of Vitamins and Minerals Is Inadequate for Most Americans: What Should We Advise Patients About Supplements?
This supplement examines the role of vitamin and mineral supplements in increasing nutrient intake and reducing nutrient deficiencies and inadequacies. Although research is needed to study the effects of dietary supplements on chronic disease outcomes, US health care providers need to know how to advise their patients about adding vitamins and minerals to their diets.
This supplement examines the role of vitamin and mineral supplements in increasing nutrient intake and reducing nutrient deficiencies and inadequacies. Although research is needed to study the effects of dietary supplements on chronic disease outcomes, US health care providers need to know how to advise their patients about adding vitamins and minerals to their diets.
This supplement examines the role of vitamin and mineral supplements in increasing nutrient intake and reducing nutrient deficiencies and inadequacies. Although research is needed to study the effects of dietary supplements on chronic disease outcomes, US health care providers need to know how to advise their patients about adding vitamins and minerals to their diets.
Clarifying a statement about efficacy of FGA, SGA
We appreciate Dr. Nasrallah referencing our work to assert that “most SGAs are similar to FGAs.” (Current Psychiatry, Comments & Controversies, October 2013, p. 39-40; http://bit.ly/177QOy6). What we actually found in our 20031 and 20112 meta-analyses was that “some antipsychotics are more efficacious than others,” and the first-generation antipsychotic vs second-generation antipsychotic distinction is not very useful clinically.3 These findings have repeatedly been replicated.3
John M. Davis, MD
Professor
Department of Psychiatry
University of Illinois at Chicago
Chicago, Illinois
Ira D. Glick, MD
Professor Emeritus of Psychiatry and Behavioral Sciences
Department of Psychiatry
Stanford University School of Medicine
Stanford, California
1. Davis JM, Chen N, Glick ID. A meta-analysis of the efficacy of second-generation antipsychotics. Arch Gen Psychiatry. 2003;60(6):553-564.
2. Glick ID, Correll CU, Altamura C, et al. Mid-term and long-term efficacy and effectiveness of antipsychotic medication for schizophrenia: a data-driven, personalized clinical approach. J Clin Psychiatry. 2011;72(12):1616-1627.
3. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)60733-3/abstract. Published June 27, 2013. Accessed November 15, 2013.
We appreciate Dr. Nasrallah referencing our work to assert that “most SGAs are similar to FGAs.” (Current Psychiatry, Comments & Controversies, October 2013, p. 39-40; http://bit.ly/177QOy6). What we actually found in our 20031 and 20112 meta-analyses was that “some antipsychotics are more efficacious than others,” and the first-generation antipsychotic vs second-generation antipsychotic distinction is not very useful clinically.3 These findings have repeatedly been replicated.3
John M. Davis, MD
Professor
Department of Psychiatry
University of Illinois at Chicago
Chicago, Illinois
Ira D. Glick, MD
Professor Emeritus of Psychiatry and Behavioral Sciences
Department of Psychiatry
Stanford University School of Medicine
Stanford, California
We appreciate Dr. Nasrallah referencing our work to assert that “most SGAs are similar to FGAs.” (Current Psychiatry, Comments & Controversies, October 2013, p. 39-40; http://bit.ly/177QOy6). What we actually found in our 20031 and 20112 meta-analyses was that “some antipsychotics are more efficacious than others,” and the first-generation antipsychotic vs second-generation antipsychotic distinction is not very useful clinically.3 These findings have repeatedly been replicated.3
John M. Davis, MD
Professor
Department of Psychiatry
University of Illinois at Chicago
Chicago, Illinois
Ira D. Glick, MD
Professor Emeritus of Psychiatry and Behavioral Sciences
Department of Psychiatry
Stanford University School of Medicine
Stanford, California
1. Davis JM, Chen N, Glick ID. A meta-analysis of the efficacy of second-generation antipsychotics. Arch Gen Psychiatry. 2003;60(6):553-564.
2. Glick ID, Correll CU, Altamura C, et al. Mid-term and long-term efficacy and effectiveness of antipsychotic medication for schizophrenia: a data-driven, personalized clinical approach. J Clin Psychiatry. 2011;72(12):1616-1627.
3. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)60733-3/abstract. Published June 27, 2013. Accessed November 15, 2013.
1. Davis JM, Chen N, Glick ID. A meta-analysis of the efficacy of second-generation antipsychotics. Arch Gen Psychiatry. 2003;60(6):553-564.
2. Glick ID, Correll CU, Altamura C, et al. Mid-term and long-term efficacy and effectiveness of antipsychotic medication for schizophrenia: a data-driven, personalized clinical approach. J Clin Psychiatry. 2011;72(12):1616-1627.
3. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)60733-3/abstract. Published June 27, 2013. Accessed November 15, 2013.
Webcast: Hormonal contraception and risk of venous thromboembolism

Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:
Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:
Access Dr. Burkman's Webcasts on contraception:
- Factors that contribute to overall contraceptive efficacy and risks
- Obesity and contraceptive efficacy and risks
- How to use the CDC's online tools to manage complex cases in contraception
Helpful resource for your practice:

Places to connect online
Thinking of joining an online physician collaboration network but don't know where to start?
Here is a list of large physician online communities and listservs to help you connect, communicate, and network with your colleagues.
Sermo: This online community of physicians has over 200,000 members in 68 specialties. It is a place where physicians can securely post questions, insights, and observations for discussion.
Medscape Physician Connect: This is another online private community of physicians that has over 170,000 members.
Doximity: This online networking site is similar to LinkedIn, except that is is only for physicians. Users create a profile to connect with colleagues and to access the "nation’s most complete physician directory," according to their website.
DermRounds: This online networking site is the Facebook of dermatology. Users can pose questions, share videos and images, learn about upcoming CME conferences, and more.
RxDerm-L: This listserv group is open to dermatologists and dermatology residents only. To subscribe, send an email to [email protected], and in the body of the message write "subscribe rxderm-L" followed by your name.
ACADERM-L: This listserv group is open to teaching dermatolgists, or dermatologists serving in an administraction for a dermatology program. To subscribe, send an email to [email protected], and in the body of the message write "subscribe acaderm-L" followed by your name.
AMA Listservs: The AMA offers multiple listservs, including ones for residents and fellows and young physicians.
Thinking of joining an online physician collaboration network but don't know where to start?
Here is a list of large physician online communities and listservs to help you connect, communicate, and network with your colleagues.
Sermo: This online community of physicians has over 200,000 members in 68 specialties. It is a place where physicians can securely post questions, insights, and observations for discussion.
Medscape Physician Connect: This is another online private community of physicians that has over 170,000 members.
Doximity: This online networking site is similar to LinkedIn, except that is is only for physicians. Users create a profile to connect with colleagues and to access the "nation’s most complete physician directory," according to their website.
DermRounds: This online networking site is the Facebook of dermatology. Users can pose questions, share videos and images, learn about upcoming CME conferences, and more.
RxDerm-L: This listserv group is open to dermatologists and dermatology residents only. To subscribe, send an email to [email protected], and in the body of the message write "subscribe rxderm-L" followed by your name.
ACADERM-L: This listserv group is open to teaching dermatolgists, or dermatologists serving in an administraction for a dermatology program. To subscribe, send an email to [email protected], and in the body of the message write "subscribe acaderm-L" followed by your name.
AMA Listservs: The AMA offers multiple listservs, including ones for residents and fellows and young physicians.
Thinking of joining an online physician collaboration network but don't know where to start?
Here is a list of large physician online communities and listservs to help you connect, communicate, and network with your colleagues.
Sermo: This online community of physicians has over 200,000 members in 68 specialties. It is a place where physicians can securely post questions, insights, and observations for discussion.
Medscape Physician Connect: This is another online private community of physicians that has over 170,000 members.
Doximity: This online networking site is similar to LinkedIn, except that is is only for physicians. Users create a profile to connect with colleagues and to access the "nation’s most complete physician directory," according to their website.
DermRounds: This online networking site is the Facebook of dermatology. Users can pose questions, share videos and images, learn about upcoming CME conferences, and more.
RxDerm-L: This listserv group is open to dermatologists and dermatology residents only. To subscribe, send an email to [email protected], and in the body of the message write "subscribe rxderm-L" followed by your name.
ACADERM-L: This listserv group is open to teaching dermatolgists, or dermatologists serving in an administraction for a dermatology program. To subscribe, send an email to [email protected], and in the body of the message write "subscribe acaderm-L" followed by your name.
AMA Listservs: The AMA offers multiple listservs, including ones for residents and fellows and young physicians.
Where do you network?
According to a CDC study, 59% of physicians use social media networks.
Do you use social media networking? If so, share your favorite places to network in the poll below, or leave a note for your colleagues in the comments field.
According to a CDC study, 59% of physicians use social media networks.
Do you use social media networking? If so, share your favorite places to network in the poll below, or leave a note for your colleagues in the comments field.
According to a CDC study, 59% of physicians use social media networks.
Do you use social media networking? If so, share your favorite places to network in the poll below, or leave a note for your colleagues in the comments field.