User login
Landmark obesity legislation reintroduced in Congress
(TROA) (H.R. 4818/S. 2407). This legislation is a vital first step in expanding access to obesity treatment as it would expand Medicare coverage to include screening and treatment of obesity by a diverse range of health care providers who provide obesity care. The bill also includes coverage of behavioral counseling, prescription drugs for long-term weight management, and other prevention and treatment options.
The passage of TROA could lead to improved obesity care options because many private insurance companies model their covered health benefits to reflect Medicare.
You can help lawmakers understand the urgent need for expanded access to affordable, effective obesity treatments and how greater access to these tools will equip you to better care for your patients.
Use the new obesity advocacy toolkit to find the tools and resources you need, including an email template, sample phone script, op-ed template, and more, to assist you in reaching out to your elected officials and urging them to support the passage of TROA.
(TROA) (H.R. 4818/S. 2407). This legislation is a vital first step in expanding access to obesity treatment as it would expand Medicare coverage to include screening and treatment of obesity by a diverse range of health care providers who provide obesity care. The bill also includes coverage of behavioral counseling, prescription drugs for long-term weight management, and other prevention and treatment options.
The passage of TROA could lead to improved obesity care options because many private insurance companies model their covered health benefits to reflect Medicare.
You can help lawmakers understand the urgent need for expanded access to affordable, effective obesity treatments and how greater access to these tools will equip you to better care for your patients.
Use the new obesity advocacy toolkit to find the tools and resources you need, including an email template, sample phone script, op-ed template, and more, to assist you in reaching out to your elected officials and urging them to support the passage of TROA.
(TROA) (H.R. 4818/S. 2407). This legislation is a vital first step in expanding access to obesity treatment as it would expand Medicare coverage to include screening and treatment of obesity by a diverse range of health care providers who provide obesity care. The bill also includes coverage of behavioral counseling, prescription drugs for long-term weight management, and other prevention and treatment options.
The passage of TROA could lead to improved obesity care options because many private insurance companies model their covered health benefits to reflect Medicare.
You can help lawmakers understand the urgent need for expanded access to affordable, effective obesity treatments and how greater access to these tools will equip you to better care for your patients.
Use the new obesity advocacy toolkit to find the tools and resources you need, including an email template, sample phone script, op-ed template, and more, to assist you in reaching out to your elected officials and urging them to support the passage of TROA.
FDA panel deems phenylephrine ineffective
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.

The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.
The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
The Nonprescription Drug Advisory Committee discussed the efficacy and pharmacokinetic data for phenylephrine. The committee’s next move is to determine if the drug’s status as Generally Recognized as Safe and Effective should be revoked. This would mean manufacturers would have to come up with new formulations, or products containing the drug would be removed from store shelves. NDAC did not disclose a timeline for assessing GRASE status.
The vote that formally declared phenylephrine ineffective was in line with a review of pharmacology and clinical data presented by the FDA on Sept. 11, which found that the oral bioavailability of the drug is less than 1%, compared with 38%, a number often cited in the literature and based on outdated technology.
A mechanism potentially responsible for inefficacy may be the half-life of phenylephrine.
“The half-life of the parent phenylephrine is much shorter than that of total phenylephrine, suggesting that the duration of action for active parent phenylephrine is far shorter than the monographed dosing interval of every 4 hours and is therefore open to question,” the review states.
The side effects of phenylephrine include headaches, insomnia, and nervousness. At higher doses, it can increase blood pressure.
The review also found that original studies used to support the efficacy of phenylephrine were inconclusive at best and contained potential methodological, statistical, and data integrity issues.
Pseudoephedrine is the only other nonprescription oral nasal decongestant on the retail market but is only available behind the counter due to its use as a potential narcotic.
Manufacturers have used phenylephrine instead of pseudoephedrine in many products due to this limitation.
Revoking the GRASE status of phenylephrine would leave patients without an over-the-counter option.
According to the FDA review, 242 million packages or bottles of phenylephrine products were sold in 2022, resulting in $1.76 billion in sales. A little over 50 million packages of pseudoephedrine were sold that same year, resulting in $542 million in sales.
“I think there’s a huge potential for consumer concern,” Diane B. Ginsburg, PhD, MS, RPh, the pharmacy practice division associate dean for Healthcare Partnerships at The University of Texas at Austin, said during the panel.
She said patients may be confused and concerned about the panel vote, especially those who feel they have benefitted from phenylephrine products. In the event of GRASE removal, she advised reassuring patients that phenylephrine is being pulled from shelves due to inefficacy rather than immediate health risks.
“The real positive here to me is the opportunity from an educational perspective to show consumers the fact that there are a lot more ways to treat” conditions that present with the symptom of congestion, such as rhinitis.
According to the FDA review, “most consumers may simply need instruction on the alternatives, including how to obtain ‘behind-the-counter’ pseudoephedrine or to use alternative treatments, including intranasal decongestants (including intranasal phenylephrine), intranasal steroids, intranasal antihistamines, or intranasal saline products.”
Despite these complications, “there are a number of potential benefits that would be derived by changing the GRASE status of oral phenylephrine.”
These include avoiding unnecessary costs of taking an ineffective drug, potential allergic reactions and side effects, and the risks of patients taking a higher dosage.
A version of this article appeared on Medscape.com.
Bad blood: Could brain bleeds be contagious?
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.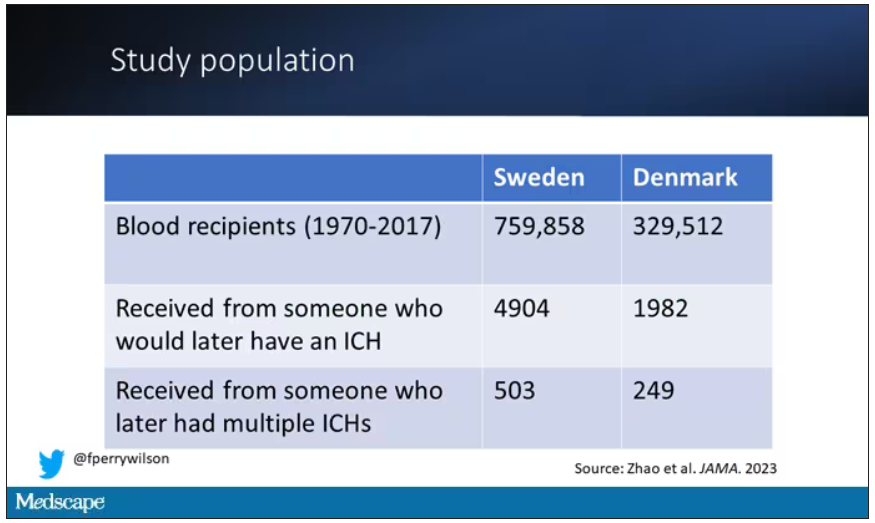
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.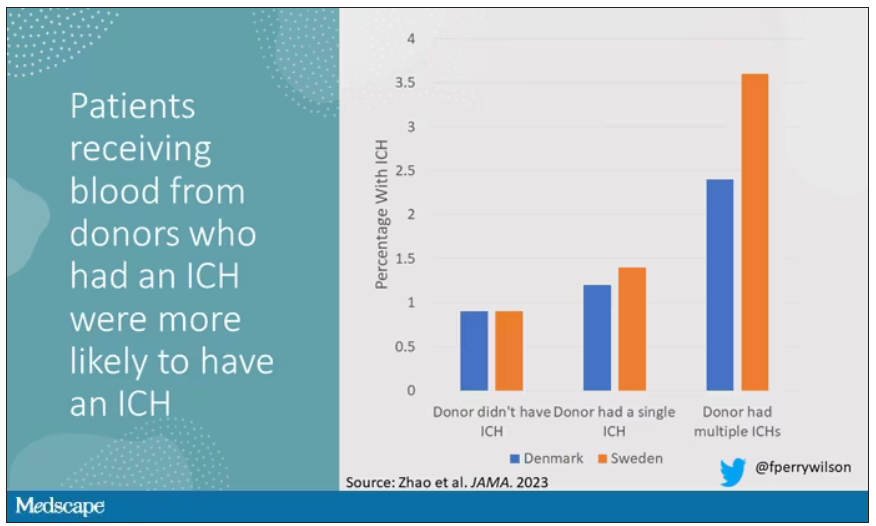
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.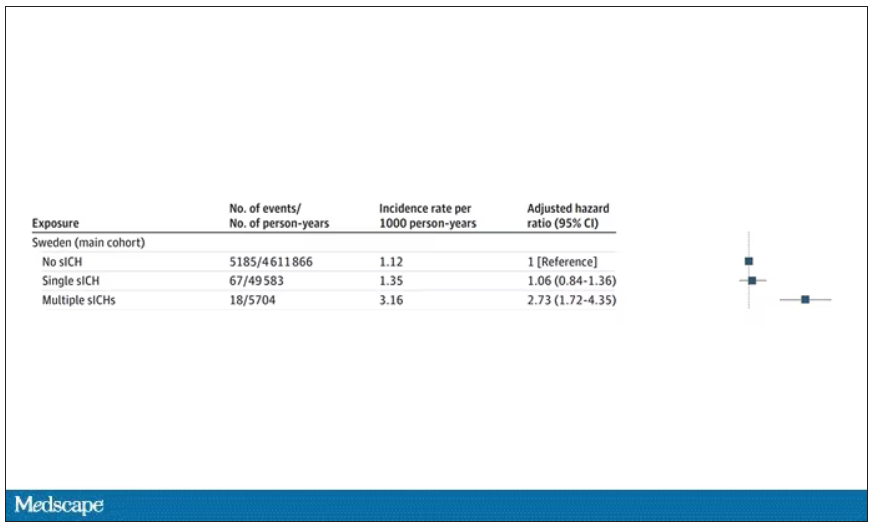
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
How do you tell if a condition is caused by an infection?
It seems like an obvious question, right? In the post–van Leeuwenhoek era we can look at whatever part of the body is diseased under a microscope and see microbes – you know, the usual suspects.
Except when we can’t. And there are plenty of cases where we can’t: where the microbe is too small to be seen without more advanced imaging techniques, like with viruses; or when the pathogen is sparsely populated or hard to culture, like Mycobacterium.
Finding out that a condition is the result of an infection is not only an exercise for 19th century physicians. After all, it was 2008 when Barry Marshall and Robin Warren won their Nobel Prize for proving that stomach ulcers, long thought to be due to “stress,” were actually caused by a tiny microbe called Helicobacter pylori.
And this week, we are looking at a study which, once again, begins to suggest that a condition thought to be more or less random – cerebral amyloid angiopathy – may actually be the result of an infectious disease.
We’re talking about this paper, appearing in JAMA, which is just a great example of old-fashioned shoe-leather epidemiology. But let’s get up to speed on cerebral amyloid angiopathy (CAA) first.
CAA is characterized by the deposition of amyloid protein in the brain. While there are some genetic causes, they are quite rare, and most cases are thought to be idiopathic. Recent analyses suggest that somewhere between 5% and 7% of cognitively normal older adults have CAA, but the rate is much higher among those with intracerebral hemorrhage – brain bleeds. In fact, CAA is the second-most common cause of bleeding in the brain, second only to severe hypertension.
An article in Nature highlights cases that seemed to develop after the administration of cadaveric pituitary hormone.
Other studies have shown potential transmission via dura mater grafts and neurosurgical instruments. But despite those clues, no infectious organism has been identified. Some have suggested that the long latent period and difficulty of finding a responsible microbe points to a prion-like disease not yet known. But these studies are more or less case series. The new JAMA paper gives us, if not a smoking gun, a pretty decent set of fingerprints.
Here’s the idea: If CAA is caused by some infectious agent, it may be transmitted in the blood. We know that a decent percentage of people who have spontaneous brain bleeds have CAA. If those people donated blood in the past, maybe the people who received that blood would be at risk for brain bleeds too.
Of course, to really test that hypothesis, you’d need to know who every blood donor in a country was and every person who received that blood and all their subsequent diagnoses for basically their entire lives. No one has that kind of data, right?
Well, if you’ve been watching this space, you’ll know that a few countries do. Enter Sweden and Denmark, with their national electronic health record that captures all of this information, and much more, on every single person who lives or has lived in those countries since before 1970. Unbelievable.
So that’s exactly what the researchers, led by Jingchen Zhao at Karolinska (Sweden) University, did. They identified roughly 760,000 individuals in Sweden and 330,000 people in Denmark who had received a blood transfusion between 1970 and 2017.
Of course, most of those blood donors – 99% of them, actually – never went on to have any bleeding in the brain. It is a rare thing, fortunately.
But some of the donors did, on average within about 5 years of the time they donated blood. The researchers characterized each donor as either never having a brain bleed, having a single bleed, or having multiple bleeds. The latter is most strongly associated with CAA.
The big question: Would recipients who got blood from individuals who later on had brain bleeds, have brain bleeds themselves?
The answer is yes, though with an asterisk. You can see the results here. The risk of recipients having a brain bleed was lowest if the blood they received was from people who never had a brain bleed, higher if the individual had a single brain bleed, and highest if they got blood from a donor who would go on to have multiple brain bleeds.
All in all, individuals who received blood from someone who would later have multiple hemorrhages were three times more likely to themselves develop bleeds themselves. It’s fairly compelling evidence of a transmissible agent.
Of course, there are some potential confounders to consider here. Whose blood you get is not totally random. If, for example, people with type O blood are just more likely to have brain bleeds, then you could get results like this, as type O tends to donate to type O and both groups would have higher risk after donation. But the authors adjusted for blood type. They also adjusted for number of transfusions, calendar year, age, sex, and indication for transfusion.
Perhaps most compelling, and most clever, is that they used ischemic stroke as a negative control. Would people who received blood from someone who later had an ischemic stroke themselves be more likely to go on to have an ischemic stroke? No signal at all. It does not appear that there is a transmissible agent associated with ischemic stroke – only the brain bleeds.
I know what you’re thinking. What’s the agent? What’s the microbe, or virus, or prion, or toxin? The study gives us no insight there. These nationwide databases are awesome but they can only do so much. Because of the vagaries of medical coding and the difficulty of making the CAA diagnosis, the authors are using brain bleeds as a proxy here; we don’t even know for sure whether these were CAA-associated brain bleeds.
It’s also worth noting that there’s little we can do about this. None of the blood donors in this study had a brain bleed prior to donation; it’s not like we could screen people out of donating in the future. We have no test for whatever this agent is, if it even exists, nor do we have a potential treatment. Fortunately, whatever it is, it is extremely rare.
Still, this paper feels like a shot across the bow. At this point, the probability has shifted strongly away from CAA being a purely random disease and toward it being an infectious one. It may be time to round up some of the unusual suspects.
Dr. F. Perry Wilson is an associate professor of medicine and public health and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Stress, insomnia tied to increased AFib risk for older women
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Eight psychosocial factors, grouped into two distinct clusters, are significantly associated with risk for atrial fibrillation in postmenopausal women, with insomnia and stressful life events (SLEs) being the most strongly associated with AFib, a large new study has found.
METHODOLOGY:
- In addition to traditional risk factors such as obesity, advanced age, ethnicity, smoking, alcohol, hypertension, diabetes, coronary artery disease, heart failure, and emotional and psychological distress may also affect AFib.
- The study included 83,736 postmenopausal women in the Women’s Health Initiative (mean age, 63.9 years; 88.1% White) who did not have AFib at baseline.
- From questionnaires, researchers collected information on psychosocial stressors and used hierarchical cluster analysis to identify patterns of psychosocial predictors.
- They separated these clusters into quartiles, identified associations between psychosocial exposure variables, and adjusted for traditional risk factors.
- Over an average follow-up of 10.5 years, 23,954 participants (28.6%) developed incident AFib.
TAKEAWAY:
- The analysis generated two clusters of distinct psychosocial variables that were significantly associated with AFib: the Stress Cluster, including SLEs, depressive symptoms, and insomnia; and the Strain Cluster, including three personality traits: optimism, cynical hostility, and emotional expressiveness; and two social measures: social support, and social strain.
- Those in the highest quartiles of both the Stress Cluster and the Strain Cluster had greater rates of AFib, compared with those in the lowest quartiles.
- In a final model, the association between SLEs (hazard ratio, 1.02; 95% confidence interval, 1.01-1.04) and insomnia (HR, 1.04; 95% CI, 1.03-1.06) were most strongly linked to increased incidence of AFib, and a sensitivity analysis using snoring as a surrogate marker for sleep apnea didn’t change this outcome, supporting the independent effect of insomnia on AFib.
- In subgroup analyses, the Stress Cluster had a stronger association with AFib incidence in younger (50-69 years) versus older women (70-79 years), and in non-Hispanic White and Asian women versus Hispanic and non-Hispanic Black women.
IN PRACTICE:
The results support the hypothesis that psychosocial predictors account for additional risk for AFib “above and beyond” traditional risk factors, the authors wrote. Identifying and addressing sex-specific, modifiable risk factors, including insomnia, “may help reduce the burden of AF[ib] in aging women.”
SOURCE:
The study was conducted by Susan X. Zhao, MD, division of cardiology, department of medicine, Santa Clara Valley Medical Center, San Jose, Calif., and colleagues. It was published online in the Journal of the American Heart Association.
LIMITATIONS:
The psychometric questionnaires were administered only at study entry, but psychosocial variables may change over time. Data on sleep apnea and other sleep disorders, which may confound the relationship between insomnia and AFib, were not available, and although the study included a sensitivity analysis controlling for snoring, this is an imperfect surrogate for sleep apnea. Generalizability to other demographic, racial, and ethnic groups is limited.
DISCLOSURES:
The Women’s Health Initiative program is funded by the National Heart, Lung, and Blood Institute; National Institutes of Health; and the Department of Health & Human Services. The authors have no relevant conflicts of interest.
A version of this article appeared on Medscape.com.
FROM JOURNAL OF THE AMERICAN HEART ASSOCIATION
Turmeric may be as effective as omeprazole for dyspepsia
TOPLINE:
METHODOLOGY:
- The researchers randomly assigned 206 patients to receive curcumin – the active ingredient in turmeric – alone; omeprazole alone; or curcumin plus omeprazole for 28 days. A total of 151 patients completed the study.
- Doses were two 250-mg curcumin pills four times daily, plus one placebo pill; one 20-mg omeprazole pill daily, plus two placebo pills four times daily; or two 250-mg curcumin pills four times daily, plus one 20-mg omeprazole pill once daily.
- Symptoms of functional dyspepsia were assessed on days 28 and 56 using the Severity of Dyspepsia Assessment (SODA) score.
TAKEAWAY:
- In the combined group, the curcumin-alone group, and the omeprazole-alone group, SODA scores for pain severity declined significantly by day 28 (–4.83, –5.46, and –6.22, respectively), as did scores for severity of other symptoms (–2.22, –2.32, and –2.31, respectively).
- Symptom improvements were even stronger by day 56 for pain (–7.19, –8.07, –8.85) and other symptoms (–4.09, –4.12, –3.71) in the same groups.
- Curcumin was safe and well tolerated, but satisfaction scores did not change significantly over time among those taking it, suggesting the possible need for improvement in its taste or smell.
- There was no synergistic effect between omeprazole and curcumin.
IN PRACTICE:
“The new findings from our study may justify considering curcumin in clinical practice. This multicenter, randomized, controlled trial provides highly reliable evidence for the treatment of functional dyspepsia,” the authors wrote.
SOURCE:
Pradermchai Kongkam, MD, of Chulalongkorn University, Bangkok, and Wichittra Khongkha of Chao Phraya Abhaibhubejhr Hospital, Prachin Buri, Thailand, are joint first authors. The study was published online in BMJ Evidence-Based Medicine.
LIMITATIONS:
A small number of participants in each group were lost to follow-up, and the follow-up period was short (less than 2 months) for all.
DISCLOSURES:
The study was funded by the Thai Traditional and Alternative Medicine Fund. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The researchers randomly assigned 206 patients to receive curcumin – the active ingredient in turmeric – alone; omeprazole alone; or curcumin plus omeprazole for 28 days. A total of 151 patients completed the study.
- Doses were two 250-mg curcumin pills four times daily, plus one placebo pill; one 20-mg omeprazole pill daily, plus two placebo pills four times daily; or two 250-mg curcumin pills four times daily, plus one 20-mg omeprazole pill once daily.
- Symptoms of functional dyspepsia were assessed on days 28 and 56 using the Severity of Dyspepsia Assessment (SODA) score.
TAKEAWAY:
- In the combined group, the curcumin-alone group, and the omeprazole-alone group, SODA scores for pain severity declined significantly by day 28 (–4.83, –5.46, and –6.22, respectively), as did scores for severity of other symptoms (–2.22, –2.32, and –2.31, respectively).
- Symptom improvements were even stronger by day 56 for pain (–7.19, –8.07, –8.85) and other symptoms (–4.09, –4.12, –3.71) in the same groups.
- Curcumin was safe and well tolerated, but satisfaction scores did not change significantly over time among those taking it, suggesting the possible need for improvement in its taste or smell.
- There was no synergistic effect between omeprazole and curcumin.
IN PRACTICE:
“The new findings from our study may justify considering curcumin in clinical practice. This multicenter, randomized, controlled trial provides highly reliable evidence for the treatment of functional dyspepsia,” the authors wrote.
SOURCE:
Pradermchai Kongkam, MD, of Chulalongkorn University, Bangkok, and Wichittra Khongkha of Chao Phraya Abhaibhubejhr Hospital, Prachin Buri, Thailand, are joint first authors. The study was published online in BMJ Evidence-Based Medicine.
LIMITATIONS:
A small number of participants in each group were lost to follow-up, and the follow-up period was short (less than 2 months) for all.
DISCLOSURES:
The study was funded by the Thai Traditional and Alternative Medicine Fund. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The researchers randomly assigned 206 patients to receive curcumin – the active ingredient in turmeric – alone; omeprazole alone; or curcumin plus omeprazole for 28 days. A total of 151 patients completed the study.
- Doses were two 250-mg curcumin pills four times daily, plus one placebo pill; one 20-mg omeprazole pill daily, plus two placebo pills four times daily; or two 250-mg curcumin pills four times daily, plus one 20-mg omeprazole pill once daily.
- Symptoms of functional dyspepsia were assessed on days 28 and 56 using the Severity of Dyspepsia Assessment (SODA) score.
TAKEAWAY:
- In the combined group, the curcumin-alone group, and the omeprazole-alone group, SODA scores for pain severity declined significantly by day 28 (–4.83, –5.46, and –6.22, respectively), as did scores for severity of other symptoms (–2.22, –2.32, and –2.31, respectively).
- Symptom improvements were even stronger by day 56 for pain (–7.19, –8.07, –8.85) and other symptoms (–4.09, –4.12, –3.71) in the same groups.
- Curcumin was safe and well tolerated, but satisfaction scores did not change significantly over time among those taking it, suggesting the possible need for improvement in its taste or smell.
- There was no synergistic effect between omeprazole and curcumin.
IN PRACTICE:
“The new findings from our study may justify considering curcumin in clinical practice. This multicenter, randomized, controlled trial provides highly reliable evidence for the treatment of functional dyspepsia,” the authors wrote.
SOURCE:
Pradermchai Kongkam, MD, of Chulalongkorn University, Bangkok, and Wichittra Khongkha of Chao Phraya Abhaibhubejhr Hospital, Prachin Buri, Thailand, are joint first authors. The study was published online in BMJ Evidence-Based Medicine.
LIMITATIONS:
A small number of participants in each group were lost to follow-up, and the follow-up period was short (less than 2 months) for all.
DISCLOSURES:
The study was funded by the Thai Traditional and Alternative Medicine Fund. The authors have disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM BMJ EVIDENCE-BASED MEDICINE
Benralizumab hits target for eosinophilic granulomatosis with polyangiitis
(EGPA), based on data from 140 individuals.
The unpublished topline results of the phase 3 MANDARA study were shared in a press release from benralizumab’s manufacturer, AstraZeneca. More detailed findings are scheduled to be presented at a future medical meeting, according to the company.
EGPA, although rare, can damage multiple organs including the heart, lungs, gastrointestinal tract, skin, and nerves, and can be fatal if left untreated, but treatment options are limited, and mepolizumab, an anti-interleukin (IL)-5 monoclonal antibody, is the only currently approved treatment.
In the study, adults with EGPA were randomized to a single 30-mg subcutaneous injection of benralizumab or three separate 100-mg subcutaneous injections of mepolizumab once every 4 weeks. The primary endpoint was remission rates after 36 and 48 weeks of treatment. Remission was defined as a Birmingham Vasculitis Activity Score of 0 and use of 4 mg/day or less of oral corticosteroids.
At 36 weeks and 48 weeks, remission rates for benralizumab were noninferior to mepolizumab. According to Clinicaltrials.gov, the study is scheduled to last for 52 weeks to compare the remission rates with the two treatments, and collect data from an extension that allows each patient at least 1 year of treatment in an open-label format.
Benralizumab, also a monoclonal antibody, differs in action from mepolizumab by binding directly to the IL-5 receptor alpha on eosinophils.
“This trial demonstrates that a biologic medicine given in a single monthly injection could help patients achieve remission rates comparable to the current standard of care, adding to the importance of benralizumab as a potential treatment option for eosinophilic granulomatosis with polyangiitis,” Michael Wechsler, MD, principal investigator on the MANDARA study, said in the press release.
The safety and tolerability of benralizumab in the MANDARA study were consistent with drug’s known profile, according to the company.
Benralizumab is currently approved as an add-on maintenance treatment for severe eosinophilic asthma in the United States, the European Union, and Japan, among other countries, and for self-administration in the United States, the European Union, and other countries, according to the company.
Benralizumab also is in development for other eosinophilic diseases, including chronic obstructive pulmonary disease, chronic rhinosinusitis with nasal polyps, and hypereosinophilic syndrome, and received an Orphan Drug Designation from the U.S. Food and Drug Administration in 2018, according to the company.
(EGPA), based on data from 140 individuals.
The unpublished topline results of the phase 3 MANDARA study were shared in a press release from benralizumab’s manufacturer, AstraZeneca. More detailed findings are scheduled to be presented at a future medical meeting, according to the company.
EGPA, although rare, can damage multiple organs including the heart, lungs, gastrointestinal tract, skin, and nerves, and can be fatal if left untreated, but treatment options are limited, and mepolizumab, an anti-interleukin (IL)-5 monoclonal antibody, is the only currently approved treatment.
In the study, adults with EGPA were randomized to a single 30-mg subcutaneous injection of benralizumab or three separate 100-mg subcutaneous injections of mepolizumab once every 4 weeks. The primary endpoint was remission rates after 36 and 48 weeks of treatment. Remission was defined as a Birmingham Vasculitis Activity Score of 0 and use of 4 mg/day or less of oral corticosteroids.
At 36 weeks and 48 weeks, remission rates for benralizumab were noninferior to mepolizumab. According to Clinicaltrials.gov, the study is scheduled to last for 52 weeks to compare the remission rates with the two treatments, and collect data from an extension that allows each patient at least 1 year of treatment in an open-label format.
Benralizumab, also a monoclonal antibody, differs in action from mepolizumab by binding directly to the IL-5 receptor alpha on eosinophils.
“This trial demonstrates that a biologic medicine given in a single monthly injection could help patients achieve remission rates comparable to the current standard of care, adding to the importance of benralizumab as a potential treatment option for eosinophilic granulomatosis with polyangiitis,” Michael Wechsler, MD, principal investigator on the MANDARA study, said in the press release.
The safety and tolerability of benralizumab in the MANDARA study were consistent with drug’s known profile, according to the company.
Benralizumab is currently approved as an add-on maintenance treatment for severe eosinophilic asthma in the United States, the European Union, and Japan, among other countries, and for self-administration in the United States, the European Union, and other countries, according to the company.
Benralizumab also is in development for other eosinophilic diseases, including chronic obstructive pulmonary disease, chronic rhinosinusitis with nasal polyps, and hypereosinophilic syndrome, and received an Orphan Drug Designation from the U.S. Food and Drug Administration in 2018, according to the company.
(EGPA), based on data from 140 individuals.
The unpublished topline results of the phase 3 MANDARA study were shared in a press release from benralizumab’s manufacturer, AstraZeneca. More detailed findings are scheduled to be presented at a future medical meeting, according to the company.
EGPA, although rare, can damage multiple organs including the heart, lungs, gastrointestinal tract, skin, and nerves, and can be fatal if left untreated, but treatment options are limited, and mepolizumab, an anti-interleukin (IL)-5 monoclonal antibody, is the only currently approved treatment.
In the study, adults with EGPA were randomized to a single 30-mg subcutaneous injection of benralizumab or three separate 100-mg subcutaneous injections of mepolizumab once every 4 weeks. The primary endpoint was remission rates after 36 and 48 weeks of treatment. Remission was defined as a Birmingham Vasculitis Activity Score of 0 and use of 4 mg/day or less of oral corticosteroids.
At 36 weeks and 48 weeks, remission rates for benralizumab were noninferior to mepolizumab. According to Clinicaltrials.gov, the study is scheduled to last for 52 weeks to compare the remission rates with the two treatments, and collect data from an extension that allows each patient at least 1 year of treatment in an open-label format.
Benralizumab, also a monoclonal antibody, differs in action from mepolizumab by binding directly to the IL-5 receptor alpha on eosinophils.
“This trial demonstrates that a biologic medicine given in a single monthly injection could help patients achieve remission rates comparable to the current standard of care, adding to the importance of benralizumab as a potential treatment option for eosinophilic granulomatosis with polyangiitis,” Michael Wechsler, MD, principal investigator on the MANDARA study, said in the press release.
The safety and tolerability of benralizumab in the MANDARA study were consistent with drug’s known profile, according to the company.
Benralizumab is currently approved as an add-on maintenance treatment for severe eosinophilic asthma in the United States, the European Union, and Japan, among other countries, and for self-administration in the United States, the European Union, and other countries, according to the company.
Benralizumab also is in development for other eosinophilic diseases, including chronic obstructive pulmonary disease, chronic rhinosinusitis with nasal polyps, and hypereosinophilic syndrome, and received an Orphan Drug Designation from the U.S. Food and Drug Administration in 2018, according to the company.
Disenfranchised grief: What it looks like, where it goes
What happens to grief when those around you don’t understand it? Where does it go? How do you process it?
Disenfranchised grief, when someone or society more generally doesn’t see a loss as worthy of mourning, can deprive people of experiencing or processing their sadness. This grief, which may be triggered by the death of an ex-spouse, a pet, a failed adoption, can be painful and long-lasting.
Suzanne Cole, MD: ‘I didn’t feel the right to grieve’
During the COVID-19 pandemic, my little sister unexpectedly died. Though she was not one of the nearly 7 million people who died of the virus, in 2021 she became another type of statistic: one of the 109,699 people in the United State who died from a drug overdose. Hers was from fentanyl laced with methamphetamines.
Her death unraveled me. I felt deep guilt that I could not pull her from the sweeping current that had wrenched her from mainstream society into the underbelly of sex work and toward the solace of mind-altering drugs.
But I did not feel the right to grieve for her as I have grieved for other loved ones who were not blamed for their exit from this world. My sister was living a sordid life on the fringes of society. My grief felt invalid, undeserved. Yet, in the eyes of other “upstanding citizens,” her life was not as worth grieving – or so I thought. I tucked my sorrow into a small corner of my soul so no one would see, and I carried on.
To this day, the shame I feel robbed me of the ability to freely talk about her or share the searing pain I feel. Tears still prick my eyes when I think of her, but I have become adept at swallowing them, shaking off the waves of grief as though nothing happened. Even now, I cannot shake the pervasive feeling that my silent tears don’t deserve to be wept.
Don S. Dizon, MD: Working through tragedy
As a medical student, I worked with an outpatient physician as part of a third-year rotation. When we met, the first thing that struck me was how disheveled he looked. His clothes were wrinkled, and his pants were baggy. He took cigarette breaks, which I found disturbing.
But I quickly came to admire him. Despite my first impression, he was the type of doctor I aspired to be. He didn’t need to look at a patient’s chart to recall who they were. He just knew them. He greeted patients warmly, asked about their family. He even remembered the special occasions his patients had mentioned since their past visit. He epitomized empathy and connectedness.
Spending one day in clinic brought to light the challenges of forming such bonds with patients. A man came into the cancer clinic reporting chest pain and was triaged to an exam room. Soon after, the patient was found unresponsive on the floor. Nurses were yelling for help, and the doctor ran in and started CPR while minutes ticked by waiting for an ambulance that could take him to the ED.
By the time help arrived, the patient was blue.
He had died in the clinic in the middle of the day, as the waiting room filled. After the body was taken away, the doctor went into the bathroom. About 20 minutes later, he came out, eyes bloodshot, and continued with the rest of his day, ensuring each patient was seen and cared for.
As a medical student, it hit me how hard it must be to see something so tragic like the end of a life and then continue with your day as if nothing had happened. This is an experience of grief I later came to know well after nearly 30 years treating patients with advanced cancers: compartmentalizing it and carrying on.
A space for grieving: The Schwartz Center Rounds
Disenfranchised grief, the grief that is hard to share and often seems wrong to feel in the first place, can be triggered in many situations. Losing a person others don’t believe deserve to be grieved, such as an abusive partner or someone who committed a crime; losing someone you cared for in a professional role; a loss experienced in a breakup or same-sex partnership, if that relationship was not accepted by one’s family; loss from infertility, miscarriage, stillbirth, or failed adoption; loss that may be taboo or stigmatized, such as deaths via suicide or abortion; and loss of a job, home, or possession that you treasure.
Many of us have had similar situations or will, and the feeling that no one understands the need to mourn can be paralyzing and alienating. In the early days, intense, crushing feelings can cause intrusive, distracting thoughts, and over time, that grief can linger and find a permanent place in our minds.
More and more, though, we are being given opportunities to reflect on these sad moments.
The Schwartz Rounds are an example of such an opportunity. In these rounds, we gather to talk about the experience of caring for people, not the science of medicine.
During one particularly powerful rounds, I spoke to my colleagues about my initial meeting with a patient who was very sick. I detailed the experience of telling her children and her at that initial consult how I thought she was dying and that I did not recommend therapy. I remember how they cried. And I remembered how powerless I felt.
As I recalled that memory during Schwartz Rounds, I could not stop from crying. The unfairness of being a physician meeting someone for the first time and having to tell them such bad news overwhelmed me.
Even more poignant, I had the chance to reconnect with this woman’s children, who were present that day, not as audience members but as participants. Their presence may have brought my emotions to the surface more strongly. In that moment, I could show them the feelings I had bottled up for the sake of professionalism. Ultimately, I felt relieved, freer somehow, as if this burden my soul was carrying had been lifted.
Although we are both grateful for forums like this, these opportunities to share and express the grief we may have hidden away are not as common as they should be.
As physicians, we may express grief by shedding tears at the bedside of a patient nearing the end of life or through the anxiety we feel when our patient suffers a severe reaction to treatment. But we tend to put it away, to go on with our day, because there are others to be seen and cared for and more work to be done. Somehow, we move forward, shedding tears in one room and celebrating victories in another.
We need to create more spaces to express and feel grief, so we don’t get lost in it. Because understanding how grief impacts us, as people and as providers, is one of the most important realizations we can make as we go about our time-honored profession as healers.
Dr. Dizon is the director of women’s cancers at Lifespan Cancer Institute, director of medical oncology at Rhode Island Hospital, and a professor of medicine at Brown University, all in Providence. He reported conflicts of interest with Regeneron, AstraZeneca, Clovis, Bristol-Myers Squibb, and Kazia.
A version of this article first appeared on Medscape.com.
What happens to grief when those around you don’t understand it? Where does it go? How do you process it?
Disenfranchised grief, when someone or society more generally doesn’t see a loss as worthy of mourning, can deprive people of experiencing or processing their sadness. This grief, which may be triggered by the death of an ex-spouse, a pet, a failed adoption, can be painful and long-lasting.
Suzanne Cole, MD: ‘I didn’t feel the right to grieve’
During the COVID-19 pandemic, my little sister unexpectedly died. Though she was not one of the nearly 7 million people who died of the virus, in 2021 she became another type of statistic: one of the 109,699 people in the United State who died from a drug overdose. Hers was from fentanyl laced with methamphetamines.
Her death unraveled me. I felt deep guilt that I could not pull her from the sweeping current that had wrenched her from mainstream society into the underbelly of sex work and toward the solace of mind-altering drugs.
But I did not feel the right to grieve for her as I have grieved for other loved ones who were not blamed for their exit from this world. My sister was living a sordid life on the fringes of society. My grief felt invalid, undeserved. Yet, in the eyes of other “upstanding citizens,” her life was not as worth grieving – or so I thought. I tucked my sorrow into a small corner of my soul so no one would see, and I carried on.
To this day, the shame I feel robbed me of the ability to freely talk about her or share the searing pain I feel. Tears still prick my eyes when I think of her, but I have become adept at swallowing them, shaking off the waves of grief as though nothing happened. Even now, I cannot shake the pervasive feeling that my silent tears don’t deserve to be wept.
Don S. Dizon, MD: Working through tragedy
As a medical student, I worked with an outpatient physician as part of a third-year rotation. When we met, the first thing that struck me was how disheveled he looked. His clothes were wrinkled, and his pants were baggy. He took cigarette breaks, which I found disturbing.
But I quickly came to admire him. Despite my first impression, he was the type of doctor I aspired to be. He didn’t need to look at a patient’s chart to recall who they were. He just knew them. He greeted patients warmly, asked about their family. He even remembered the special occasions his patients had mentioned since their past visit. He epitomized empathy and connectedness.
Spending one day in clinic brought to light the challenges of forming such bonds with patients. A man came into the cancer clinic reporting chest pain and was triaged to an exam room. Soon after, the patient was found unresponsive on the floor. Nurses were yelling for help, and the doctor ran in and started CPR while minutes ticked by waiting for an ambulance that could take him to the ED.
By the time help arrived, the patient was blue.
He had died in the clinic in the middle of the day, as the waiting room filled. After the body was taken away, the doctor went into the bathroom. About 20 minutes later, he came out, eyes bloodshot, and continued with the rest of his day, ensuring each patient was seen and cared for.
As a medical student, it hit me how hard it must be to see something so tragic like the end of a life and then continue with your day as if nothing had happened. This is an experience of grief I later came to know well after nearly 30 years treating patients with advanced cancers: compartmentalizing it and carrying on.
A space for grieving: The Schwartz Center Rounds
Disenfranchised grief, the grief that is hard to share and often seems wrong to feel in the first place, can be triggered in many situations. Losing a person others don’t believe deserve to be grieved, such as an abusive partner or someone who committed a crime; losing someone you cared for in a professional role; a loss experienced in a breakup or same-sex partnership, if that relationship was not accepted by one’s family; loss from infertility, miscarriage, stillbirth, or failed adoption; loss that may be taboo or stigmatized, such as deaths via suicide or abortion; and loss of a job, home, or possession that you treasure.
Many of us have had similar situations or will, and the feeling that no one understands the need to mourn can be paralyzing and alienating. In the early days, intense, crushing feelings can cause intrusive, distracting thoughts, and over time, that grief can linger and find a permanent place in our minds.
More and more, though, we are being given opportunities to reflect on these sad moments.
The Schwartz Rounds are an example of such an opportunity. In these rounds, we gather to talk about the experience of caring for people, not the science of medicine.
During one particularly powerful rounds, I spoke to my colleagues about my initial meeting with a patient who was very sick. I detailed the experience of telling her children and her at that initial consult how I thought she was dying and that I did not recommend therapy. I remember how they cried. And I remembered how powerless I felt.
As I recalled that memory during Schwartz Rounds, I could not stop from crying. The unfairness of being a physician meeting someone for the first time and having to tell them such bad news overwhelmed me.
Even more poignant, I had the chance to reconnect with this woman’s children, who were present that day, not as audience members but as participants. Their presence may have brought my emotions to the surface more strongly. In that moment, I could show them the feelings I had bottled up for the sake of professionalism. Ultimately, I felt relieved, freer somehow, as if this burden my soul was carrying had been lifted.
Although we are both grateful for forums like this, these opportunities to share and express the grief we may have hidden away are not as common as they should be.
As physicians, we may express grief by shedding tears at the bedside of a patient nearing the end of life or through the anxiety we feel when our patient suffers a severe reaction to treatment. But we tend to put it away, to go on with our day, because there are others to be seen and cared for and more work to be done. Somehow, we move forward, shedding tears in one room and celebrating victories in another.
We need to create more spaces to express and feel grief, so we don’t get lost in it. Because understanding how grief impacts us, as people and as providers, is one of the most important realizations we can make as we go about our time-honored profession as healers.
Dr. Dizon is the director of women’s cancers at Lifespan Cancer Institute, director of medical oncology at Rhode Island Hospital, and a professor of medicine at Brown University, all in Providence. He reported conflicts of interest with Regeneron, AstraZeneca, Clovis, Bristol-Myers Squibb, and Kazia.
A version of this article first appeared on Medscape.com.
What happens to grief when those around you don’t understand it? Where does it go? How do you process it?
Disenfranchised grief, when someone or society more generally doesn’t see a loss as worthy of mourning, can deprive people of experiencing or processing their sadness. This grief, which may be triggered by the death of an ex-spouse, a pet, a failed adoption, can be painful and long-lasting.
Suzanne Cole, MD: ‘I didn’t feel the right to grieve’
During the COVID-19 pandemic, my little sister unexpectedly died. Though she was not one of the nearly 7 million people who died of the virus, in 2021 she became another type of statistic: one of the 109,699 people in the United State who died from a drug overdose. Hers was from fentanyl laced with methamphetamines.
Her death unraveled me. I felt deep guilt that I could not pull her from the sweeping current that had wrenched her from mainstream society into the underbelly of sex work and toward the solace of mind-altering drugs.
But I did not feel the right to grieve for her as I have grieved for other loved ones who were not blamed for their exit from this world. My sister was living a sordid life on the fringes of society. My grief felt invalid, undeserved. Yet, in the eyes of other “upstanding citizens,” her life was not as worth grieving – or so I thought. I tucked my sorrow into a small corner of my soul so no one would see, and I carried on.
To this day, the shame I feel robbed me of the ability to freely talk about her or share the searing pain I feel. Tears still prick my eyes when I think of her, but I have become adept at swallowing them, shaking off the waves of grief as though nothing happened. Even now, I cannot shake the pervasive feeling that my silent tears don’t deserve to be wept.
Don S. Dizon, MD: Working through tragedy
As a medical student, I worked with an outpatient physician as part of a third-year rotation. When we met, the first thing that struck me was how disheveled he looked. His clothes were wrinkled, and his pants were baggy. He took cigarette breaks, which I found disturbing.
But I quickly came to admire him. Despite my first impression, he was the type of doctor I aspired to be. He didn’t need to look at a patient’s chart to recall who they were. He just knew them. He greeted patients warmly, asked about their family. He even remembered the special occasions his patients had mentioned since their past visit. He epitomized empathy and connectedness.
Spending one day in clinic brought to light the challenges of forming such bonds with patients. A man came into the cancer clinic reporting chest pain and was triaged to an exam room. Soon after, the patient was found unresponsive on the floor. Nurses were yelling for help, and the doctor ran in and started CPR while minutes ticked by waiting for an ambulance that could take him to the ED.
By the time help arrived, the patient was blue.
He had died in the clinic in the middle of the day, as the waiting room filled. After the body was taken away, the doctor went into the bathroom. About 20 minutes later, he came out, eyes bloodshot, and continued with the rest of his day, ensuring each patient was seen and cared for.
As a medical student, it hit me how hard it must be to see something so tragic like the end of a life and then continue with your day as if nothing had happened. This is an experience of grief I later came to know well after nearly 30 years treating patients with advanced cancers: compartmentalizing it and carrying on.
A space for grieving: The Schwartz Center Rounds
Disenfranchised grief, the grief that is hard to share and often seems wrong to feel in the first place, can be triggered in many situations. Losing a person others don’t believe deserve to be grieved, such as an abusive partner or someone who committed a crime; losing someone you cared for in a professional role; a loss experienced in a breakup or same-sex partnership, if that relationship was not accepted by one’s family; loss from infertility, miscarriage, stillbirth, or failed adoption; loss that may be taboo or stigmatized, such as deaths via suicide or abortion; and loss of a job, home, or possession that you treasure.
Many of us have had similar situations or will, and the feeling that no one understands the need to mourn can be paralyzing and alienating. In the early days, intense, crushing feelings can cause intrusive, distracting thoughts, and over time, that grief can linger and find a permanent place in our minds.
More and more, though, we are being given opportunities to reflect on these sad moments.
The Schwartz Rounds are an example of such an opportunity. In these rounds, we gather to talk about the experience of caring for people, not the science of medicine.
During one particularly powerful rounds, I spoke to my colleagues about my initial meeting with a patient who was very sick. I detailed the experience of telling her children and her at that initial consult how I thought she was dying and that I did not recommend therapy. I remember how they cried. And I remembered how powerless I felt.
As I recalled that memory during Schwartz Rounds, I could not stop from crying. The unfairness of being a physician meeting someone for the first time and having to tell them such bad news overwhelmed me.
Even more poignant, I had the chance to reconnect with this woman’s children, who were present that day, not as audience members but as participants. Their presence may have brought my emotions to the surface more strongly. In that moment, I could show them the feelings I had bottled up for the sake of professionalism. Ultimately, I felt relieved, freer somehow, as if this burden my soul was carrying had been lifted.
Although we are both grateful for forums like this, these opportunities to share and express the grief we may have hidden away are not as common as they should be.
As physicians, we may express grief by shedding tears at the bedside of a patient nearing the end of life or through the anxiety we feel when our patient suffers a severe reaction to treatment. But we tend to put it away, to go on with our day, because there are others to be seen and cared for and more work to be done. Somehow, we move forward, shedding tears in one room and celebrating victories in another.
We need to create more spaces to express and feel grief, so we don’t get lost in it. Because understanding how grief impacts us, as people and as providers, is one of the most important realizations we can make as we go about our time-honored profession as healers.
Dr. Dizon is the director of women’s cancers at Lifespan Cancer Institute, director of medical oncology at Rhode Island Hospital, and a professor of medicine at Brown University, all in Providence. He reported conflicts of interest with Regeneron, AstraZeneca, Clovis, Bristol-Myers Squibb, and Kazia.
A version of this article first appeared on Medscape.com.
Sedentary lifestyle tied to increased dementia risk
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The study of nearly 50,000 adults in the UK Biobank shows that dementia risk increased 8% with 10 hours of sedentary time and 63% with 12 hours. That’s particularly concerning because Americans spend an average of 9.5 hours a day sitting.
Sleep wasn’t factored into the sedentary time and how someone accumulated the 10 hours – either in one continuous block or broken up throughout the day – was irrelevant.
“Our analysis cannot determine whether there is a causal link, so prescriptive conclusions are not really possible; however. I think it is very reasonable to conclude that sitting less and moving more may help reduce risk of dementia,” lead investigator David Raichlen, PhD, professor of biological sciences and anthropology, University of Southern California, Los Angeles, said in an interview.
The findings were published online in JAMA.
A surprising find?
The study is a retrospective analysis of prospectively collected data from the UK Biobank of 49,841 adults aged 60 years or older who wore an accelerometer on their wrists 24 hours a day for a week. Participants had no history of dementia when they wore the movement monitoring device.
Investigators used machine-based learning to determine sedentary time based on readings from the accelerometers. Sleep was not included as sedentary behavior.
Over a mean follow-up of 6.72 years, 414 participants were diagnosed with dementia.
Investigators found that dementia risk rises by 8% at 10 hours a day (adjusted hazard ratio, 1.08; P < .001) and 63% at 12 hours a day (aHR, 1.63; P < .001), compared with 9.27 hours a day. Those who logged 15 hours of sedentary behavior a day had more than triple the dementia risk (aHR, 3.21; P < .001).
Although previous studies had found that breaking up sedentary periods with short bursts of activity help offset some negative health effects of sitting, that wasn’t the case here. Dementia risk was elevated whether participants were sedentary for 10 uninterrupted hours or multiple sedentary periods that totaled 10 hours over the whole day.
“This was surprising,” Dr. Raichlen said. “We expected to find that patterns of sedentary behavior would play a role in risk of dementia, but once you take into account the daily volume of time spent sedentary, how you get there doesn’t seem to matter as much.”
The study did not examine how participants spent sedentary time, but an earlier study by Dr. Raichlen found that watching TV was associated with a greater risk of dementia in older adults, compared with working on a computer.
More research welcome
Dr. Raichlen noted that the number of dementia cases in the study is low and that the view of sedentary behavior is based on 1 week of accelerometer readings. A longitudinal study is needed to determine if the findings last over a longer time period.
In a comment, Claire Sexton, DPhil, senior director of scientific programs and outreach for the Alzheimer’s Association, says that earlier studies reported an association between sedentary time and dementia, so these results aren’t “particularly surprising.”
“However, reports that did not find an association have also been published, so additional research on possible associations is welcome,” she said.
It’s also important to note that this observational study doesn’t establish a causal relationship between inactivity and cognitive function, which Dr. Sexton said means the influence of other dementia risk factors that are also exacerbated by sedentary behavior can’t be ruled out.
“Although results remained significant after adjusting for several of these factors, further research is required to better understand the various elements that may influence the observed relationship,” noted Dr. Sexton, who was not part of the study. “Reverse causality – that changes in the brain related to dementia are causing the sedentary behavior – cannot be ruled out.”
The study was funded by the National Institutes of Health, the state of Arizona, the Arizona Department of Health Services, and the McKnight Brain Research Foundation. Dr. Raichlen and Dr. Sexton report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA
Service dogs help veterans with PTSD lead better lives
When Ryan (not his real name), 37, returned home from two deployments with the 101st Airborne Division in Iraq from 2005 to 2008, he began withdrawing from social situations and experienced chronic anxiety. Nights brought no respite – his sleep was interrupted by punishing nightmares.
“I had every calling card of a veteran in distress,” he said in an interview. When his wife told him she thought he may have posttraumatic stress disorder (PTSD), he shrugged it off. “I wasn’t automatically going to accept [the diagnosis] because as an infantry veteran, we’re big tough guys. We don’t need help with anything.”
The dogs, mostly recruited from rescue organizations, receive 5-7 months of specialized training to assist the veterans.
Life-changing help
While Ryan was skeptical about the program and whether it would work for him, he agreed to try it. After working with Bullet, a cream-colored golden retriever, he realized his life was improving.
“I stopped self-medicating, started advocating for myself, and became more comfortable socializing in public.” In his 3 years with Bullet, Ryan was able to work on his marriage, advance his career, and become a homeowner.
“The dreams I never thought were attainable started coming to fruition, and I was happy and comfortable for the first time in as long as I could remember.”
Unfortunately, Bullet died from a rare heart condition after a few years, and when that happened, NWBB immediately began working with Ryan to find him a new dog to fill the void left by Bullet.
Soon, Ryan began working with Twitch, who, like Bullet, knew when Ryan was becoming anxious, angry, or depressed before he did, he said.
“These dogs pick up on PTSD symptoms and come over and press themselves against you, push their faces into yours, and give you those big puppy dog eyes as if to say, ‘I got you. Everything is going to be okay.’ ”
The same thing happened when Ryan had night terrors and nightmares. “These dogs wake you up, and again, you’re greeted with this sweet puppy dog face.”
NWBB founder and CEO Shannon Walker, who has been training dogs for 25 years and whose father served in the U.S. Air Force in the 1950s, leads a 5-week training course for the veterans and their “battle buddies” so that the veterans can learn how to bond with and benefit from their new service dogs.
Finding the perfect match
Veterans are paired with trained service dogs based on their lifestyle and personality. For instance, a Vietnam veteran who is having trouble walking may be paired with a calm dog while a younger veteran who runs each morning is paired with a more active dog.
NWBB operates on funds from private donors and nonprofit organizations that make it financially feasible for the veterans to travel to Washington State and stay for the time required to train with their service dogs.
“Our service dogs are there in the midnight hour when no one else is,” she said. “Our veterans are fighting internal battles that no one else sees but the dogs. The dogs alert on their adrenaline and bring them back to the moment of now, interrupting suicidal ideations, panic attacks, and night terrors.”
Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said in an interview that “PTSD can be devastating for service members and veterans and is often associated with comorbid mental health conditions, such as anxiety and substance use.”
He noted that for many people, dogs and other animals can be an important source of physical, emotional, and psychological comfort.
“Programs like the Northwest Battle Buddies are important for us to study and better understand the extent to which trained animals are able to help alleviate the symptoms of PTSD and associated disorders and, perhaps most importantly, enhance the ability of service members and veterans to function and live in ways that feel healthy and productive to them,” said Dr. Morganstein.
He added that the concept of a “battle buddy” is a term pioneered by the U.S. Army in 2002 and describes a “formal, rather than ad hoc, system of peer support in which service members are assigned buddies.
“Buddies look out for each other, encourage self-care and self-advocacy and, when needed, help their buddy to seek help. Buddies remind us that someone is looking out for us and there is someone we look out for as well, both of which are protective during difficult times,” he said.
A version of this article first appeared on Medscape.com.
When Ryan (not his real name), 37, returned home from two deployments with the 101st Airborne Division in Iraq from 2005 to 2008, he began withdrawing from social situations and experienced chronic anxiety. Nights brought no respite – his sleep was interrupted by punishing nightmares.
“I had every calling card of a veteran in distress,” he said in an interview. When his wife told him she thought he may have posttraumatic stress disorder (PTSD), he shrugged it off. “I wasn’t automatically going to accept [the diagnosis] because as an infantry veteran, we’re big tough guys. We don’t need help with anything.”
The dogs, mostly recruited from rescue organizations, receive 5-7 months of specialized training to assist the veterans.
Life-changing help
While Ryan was skeptical about the program and whether it would work for him, he agreed to try it. After working with Bullet, a cream-colored golden retriever, he realized his life was improving.
“I stopped self-medicating, started advocating for myself, and became more comfortable socializing in public.” In his 3 years with Bullet, Ryan was able to work on his marriage, advance his career, and become a homeowner.
“The dreams I never thought were attainable started coming to fruition, and I was happy and comfortable for the first time in as long as I could remember.”
Unfortunately, Bullet died from a rare heart condition after a few years, and when that happened, NWBB immediately began working with Ryan to find him a new dog to fill the void left by Bullet.
Soon, Ryan began working with Twitch, who, like Bullet, knew when Ryan was becoming anxious, angry, or depressed before he did, he said.
“These dogs pick up on PTSD symptoms and come over and press themselves against you, push their faces into yours, and give you those big puppy dog eyes as if to say, ‘I got you. Everything is going to be okay.’ ”
The same thing happened when Ryan had night terrors and nightmares. “These dogs wake you up, and again, you’re greeted with this sweet puppy dog face.”
NWBB founder and CEO Shannon Walker, who has been training dogs for 25 years and whose father served in the U.S. Air Force in the 1950s, leads a 5-week training course for the veterans and their “battle buddies” so that the veterans can learn how to bond with and benefit from their new service dogs.
Finding the perfect match
Veterans are paired with trained service dogs based on their lifestyle and personality. For instance, a Vietnam veteran who is having trouble walking may be paired with a calm dog while a younger veteran who runs each morning is paired with a more active dog.
NWBB operates on funds from private donors and nonprofit organizations that make it financially feasible for the veterans to travel to Washington State and stay for the time required to train with their service dogs.
“Our service dogs are there in the midnight hour when no one else is,” she said. “Our veterans are fighting internal battles that no one else sees but the dogs. The dogs alert on their adrenaline and bring them back to the moment of now, interrupting suicidal ideations, panic attacks, and night terrors.”
Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said in an interview that “PTSD can be devastating for service members and veterans and is often associated with comorbid mental health conditions, such as anxiety and substance use.”
He noted that for many people, dogs and other animals can be an important source of physical, emotional, and psychological comfort.
“Programs like the Northwest Battle Buddies are important for us to study and better understand the extent to which trained animals are able to help alleviate the symptoms of PTSD and associated disorders and, perhaps most importantly, enhance the ability of service members and veterans to function and live in ways that feel healthy and productive to them,” said Dr. Morganstein.
He added that the concept of a “battle buddy” is a term pioneered by the U.S. Army in 2002 and describes a “formal, rather than ad hoc, system of peer support in which service members are assigned buddies.
“Buddies look out for each other, encourage self-care and self-advocacy and, when needed, help their buddy to seek help. Buddies remind us that someone is looking out for us and there is someone we look out for as well, both of which are protective during difficult times,” he said.
A version of this article first appeared on Medscape.com.
When Ryan (not his real name), 37, returned home from two deployments with the 101st Airborne Division in Iraq from 2005 to 2008, he began withdrawing from social situations and experienced chronic anxiety. Nights brought no respite – his sleep was interrupted by punishing nightmares.
“I had every calling card of a veteran in distress,” he said in an interview. When his wife told him she thought he may have posttraumatic stress disorder (PTSD), he shrugged it off. “I wasn’t automatically going to accept [the diagnosis] because as an infantry veteran, we’re big tough guys. We don’t need help with anything.”
The dogs, mostly recruited from rescue organizations, receive 5-7 months of specialized training to assist the veterans.
Life-changing help
While Ryan was skeptical about the program and whether it would work for him, he agreed to try it. After working with Bullet, a cream-colored golden retriever, he realized his life was improving.
“I stopped self-medicating, started advocating for myself, and became more comfortable socializing in public.” In his 3 years with Bullet, Ryan was able to work on his marriage, advance his career, and become a homeowner.
“The dreams I never thought were attainable started coming to fruition, and I was happy and comfortable for the first time in as long as I could remember.”
Unfortunately, Bullet died from a rare heart condition after a few years, and when that happened, NWBB immediately began working with Ryan to find him a new dog to fill the void left by Bullet.
Soon, Ryan began working with Twitch, who, like Bullet, knew when Ryan was becoming anxious, angry, or depressed before he did, he said.
“These dogs pick up on PTSD symptoms and come over and press themselves against you, push their faces into yours, and give you those big puppy dog eyes as if to say, ‘I got you. Everything is going to be okay.’ ”
The same thing happened when Ryan had night terrors and nightmares. “These dogs wake you up, and again, you’re greeted with this sweet puppy dog face.”
NWBB founder and CEO Shannon Walker, who has been training dogs for 25 years and whose father served in the U.S. Air Force in the 1950s, leads a 5-week training course for the veterans and their “battle buddies” so that the veterans can learn how to bond with and benefit from their new service dogs.
Finding the perfect match
Veterans are paired with trained service dogs based on their lifestyle and personality. For instance, a Vietnam veteran who is having trouble walking may be paired with a calm dog while a younger veteran who runs each morning is paired with a more active dog.
NWBB operates on funds from private donors and nonprofit organizations that make it financially feasible for the veterans to travel to Washington State and stay for the time required to train with their service dogs.
“Our service dogs are there in the midnight hour when no one else is,” she said. “Our veterans are fighting internal battles that no one else sees but the dogs. The dogs alert on their adrenaline and bring them back to the moment of now, interrupting suicidal ideations, panic attacks, and night terrors.”
Joshua Morganstein, MD, chair of the American Psychiatric Association’s Committee on the Psychiatric Dimensions of Disaster, said in an interview that “PTSD can be devastating for service members and veterans and is often associated with comorbid mental health conditions, such as anxiety and substance use.”
He noted that for many people, dogs and other animals can be an important source of physical, emotional, and psychological comfort.
“Programs like the Northwest Battle Buddies are important for us to study and better understand the extent to which trained animals are able to help alleviate the symptoms of PTSD and associated disorders and, perhaps most importantly, enhance the ability of service members and veterans to function and live in ways that feel healthy and productive to them,” said Dr. Morganstein.
He added that the concept of a “battle buddy” is a term pioneered by the U.S. Army in 2002 and describes a “formal, rather than ad hoc, system of peer support in which service members are assigned buddies.
“Buddies look out for each other, encourage self-care and self-advocacy and, when needed, help their buddy to seek help. Buddies remind us that someone is looking out for us and there is someone we look out for as well, both of which are protective during difficult times,” he said.
A version of this article first appeared on Medscape.com.
Early glucocorticoid bridging in RA supported by meta-analysis, but concerns remain
In a new salvo in the dispute over the wisdom of early “bridging” treatment with glucocorticoids in rheumatoid arthritis, Dutch researchers suggested in a new meta-analysis that the American College of Rheumatology guideline is too cautious.
The report, published in Annals of the Rheumatic Diseases, examined three randomized trials of bridging versus nonbridging. The findings “emphasize the benefits of bridging therapy and shows that bridgers are not using more glucocorticoids after their intended bridging period, compared with nonbridgers, during a 2-year follow-up,” study coauthor Sytske Anne Bergstra, PhD, a postdoctoral researcher at Leiden (the Netherlands) University Medical Center, said in an interview.

However, an American researcher who helped create the 2021 ACR guideline is unmoved by the new report. “This publication didn’t do anything to assuage my concerns,” Joel Kremer, MD, founder and president of the Corrona Research Foundation and professor of medicine emeritus at Albany (N.Y.) Medical College, said in an interview.
At issue is whether patients with early RA should be temporarily treated with glucocorticoids in order to provide rapid relief. The ACR’s 2021 guideline on the treatment of RA says short-term glucocorticoids should not be “systematically prescribed” but notes that they are still “frequently necessary to alleviate symptoms” before disease-modifying therapies are given. The guideline adds that “these recommendations were made in recognition of the frequent difficulty tapering glucocorticoids, leading to undesirable prolonged use and the increasing evidence of the negative impact of glucocorticoids on long-term patient outcomes, including risk for infection, osteoporosis, and cardiovascular disease, in RA and other rheumatic diseases.”
For its part, the European Alliance of Associations for Rheumatology’s 2022 recommendations state that short-term glucocorticoids “should be considered when initiating or changing [disease-modifying antirheumatic drugs], in different dose regimens and routes of administration, but should be tapered and discontinued as rapidly as clinically feasible.”
Members of the Dutch team behind the new meta-analysis have been supporters of “bridging” therapy. For the new report, they analyzed three studies, including one led by a member of the team. Each study had at least one arm that randomized patients with RA to glucocorticoid bridging. Patients also took disease-modifying antirheumatic drugs (DMARDs).
There were 252 patients in study arms that started with bridging (mean age, 52 years; 68% female) and 373 other patients (mean age, 53 years; 67% female).
The researchers found that glucocorticoid use was higher in the bridgers at 12 months (odds ratio, 3.27; 95% confidence interval, 1.06-10.08), but the excess risk at 18 months (OR, 1.60; 95% CI, 0.46-5.60) and 24 months (OR, 1.70; 95% CI, 0.58-4.97) dipped below statistical significance. Also, they reported that “bridgers improved more rapidly (P < .001) in the first 6 months and the bridgers required significantly fewer changes in DMARDs (incidence rate ratio, 0.59; 95% CI, 0.38-0.94).”
“Based on our results, combined with two earlier publications [here and here], we show that most patients included in clinical trials with protocolized tapering schedules are able to stop glucocorticoids after bridging,” Dr. Bergstra said. “We also confirm the well-known short-term clinical effects and show that patients using glucocorticoid bridging require fewer DMARD changes. For a re-evaluation of the ACR guideline, this evidence should be combined with the extensive evidence showing short- as well as long-term clinical benefits of glucocorticoid bridging but also with evidence on potential side effects at different doses.”
She added that “implementing predefined tapering protocols may help clinicians and patients to stop glucocorticoids after bridging.” As for limitations, “patients included in these trials may differ from patients in clinical practice. We cannot be sure whether these results can be generalized to the full patient population.”
Dr. Kremer, a coauthor of the ACR guideline, pointed out that the patients who took glucocorticoids early were much more likely to be on them at 12 months.
By definition, “bridging” is temporary, he said, a brief period to help patients tolerate RA until DMARDs kick in. But in the studies, many of the patients clearly took the drugs for extended periods of time. In those cases, “it not a bridge,” and the risk is that “you’re treating people with a lifelong disease with doses of glucocorticoids that have been shown in multiple studies to be dangerous.”
He added that, while the excess likelihood of these patients staying on the drugs at 18 or 24 months wasn’t deemed to be statistically significant in the meta-analysis, the confidence intervals were unusually wide. That raises questions about whether some of the patients actually stay on the drugs.
Dr. Kremer said it can still be appropriate to give glucocorticoids to patients in distress, although it’s crucial in those cases to take the patients off them as soon as possible. It’s best, though, to not prescribe them at all. “If you can avoid it,” he said, “definitely avoid it.”
The study was conducted without outside funding. Dr. Bergstra reported receiving grant funding from Pfizer, and some of the other study authors reported various relationships with industry. Dr. Kremer had no relevant disclosures.
In a new salvo in the dispute over the wisdom of early “bridging” treatment with glucocorticoids in rheumatoid arthritis, Dutch researchers suggested in a new meta-analysis that the American College of Rheumatology guideline is too cautious.
The report, published in Annals of the Rheumatic Diseases, examined three randomized trials of bridging versus nonbridging. The findings “emphasize the benefits of bridging therapy and shows that bridgers are not using more glucocorticoids after their intended bridging period, compared with nonbridgers, during a 2-year follow-up,” study coauthor Sytske Anne Bergstra, PhD, a postdoctoral researcher at Leiden (the Netherlands) University Medical Center, said in an interview.
However, an American researcher who helped create the 2021 ACR guideline is unmoved by the new report. “This publication didn’t do anything to assuage my concerns,” Joel Kremer, MD, founder and president of the Corrona Research Foundation and professor of medicine emeritus at Albany (N.Y.) Medical College, said in an interview.
At issue is whether patients with early RA should be temporarily treated with glucocorticoids in order to provide rapid relief. The ACR’s 2021 guideline on the treatment of RA says short-term glucocorticoids should not be “systematically prescribed” but notes that they are still “frequently necessary to alleviate symptoms” before disease-modifying therapies are given. The guideline adds that “these recommendations were made in recognition of the frequent difficulty tapering glucocorticoids, leading to undesirable prolonged use and the increasing evidence of the negative impact of glucocorticoids on long-term patient outcomes, including risk for infection, osteoporosis, and cardiovascular disease, in RA and other rheumatic diseases.”
For its part, the European Alliance of Associations for Rheumatology’s 2022 recommendations state that short-term glucocorticoids “should be considered when initiating or changing [disease-modifying antirheumatic drugs], in different dose regimens and routes of administration, but should be tapered and discontinued as rapidly as clinically feasible.”
Members of the Dutch team behind the new meta-analysis have been supporters of “bridging” therapy. For the new report, they analyzed three studies, including one led by a member of the team. Each study had at least one arm that randomized patients with RA to glucocorticoid bridging. Patients also took disease-modifying antirheumatic drugs (DMARDs).
There were 252 patients in study arms that started with bridging (mean age, 52 years; 68% female) and 373 other patients (mean age, 53 years; 67% female).
The researchers found that glucocorticoid use was higher in the bridgers at 12 months (odds ratio, 3.27; 95% confidence interval, 1.06-10.08), but the excess risk at 18 months (OR, 1.60; 95% CI, 0.46-5.60) and 24 months (OR, 1.70; 95% CI, 0.58-4.97) dipped below statistical significance. Also, they reported that “bridgers improved more rapidly (P < .001) in the first 6 months and the bridgers required significantly fewer changes in DMARDs (incidence rate ratio, 0.59; 95% CI, 0.38-0.94).”
“Based on our results, combined with two earlier publications [here and here], we show that most patients included in clinical trials with protocolized tapering schedules are able to stop glucocorticoids after bridging,” Dr. Bergstra said. “We also confirm the well-known short-term clinical effects and show that patients using glucocorticoid bridging require fewer DMARD changes. For a re-evaluation of the ACR guideline, this evidence should be combined with the extensive evidence showing short- as well as long-term clinical benefits of glucocorticoid bridging but also with evidence on potential side effects at different doses.”
She added that “implementing predefined tapering protocols may help clinicians and patients to stop glucocorticoids after bridging.” As for limitations, “patients included in these trials may differ from patients in clinical practice. We cannot be sure whether these results can be generalized to the full patient population.”
Dr. Kremer, a coauthor of the ACR guideline, pointed out that the patients who took glucocorticoids early were much more likely to be on them at 12 months.
By definition, “bridging” is temporary, he said, a brief period to help patients tolerate RA until DMARDs kick in. But in the studies, many of the patients clearly took the drugs for extended periods of time. In those cases, “it not a bridge,” and the risk is that “you’re treating people with a lifelong disease with doses of glucocorticoids that have been shown in multiple studies to be dangerous.”
He added that, while the excess likelihood of these patients staying on the drugs at 18 or 24 months wasn’t deemed to be statistically significant in the meta-analysis, the confidence intervals were unusually wide. That raises questions about whether some of the patients actually stay on the drugs.
Dr. Kremer said it can still be appropriate to give glucocorticoids to patients in distress, although it’s crucial in those cases to take the patients off them as soon as possible. It’s best, though, to not prescribe them at all. “If you can avoid it,” he said, “definitely avoid it.”
The study was conducted without outside funding. Dr. Bergstra reported receiving grant funding from Pfizer, and some of the other study authors reported various relationships with industry. Dr. Kremer had no relevant disclosures.
In a new salvo in the dispute over the wisdom of early “bridging” treatment with glucocorticoids in rheumatoid arthritis, Dutch researchers suggested in a new meta-analysis that the American College of Rheumatology guideline is too cautious.
The report, published in Annals of the Rheumatic Diseases, examined three randomized trials of bridging versus nonbridging. The findings “emphasize the benefits of bridging therapy and shows that bridgers are not using more glucocorticoids after their intended bridging period, compared with nonbridgers, during a 2-year follow-up,” study coauthor Sytske Anne Bergstra, PhD, a postdoctoral researcher at Leiden (the Netherlands) University Medical Center, said in an interview.
However, an American researcher who helped create the 2021 ACR guideline is unmoved by the new report. “This publication didn’t do anything to assuage my concerns,” Joel Kremer, MD, founder and president of the Corrona Research Foundation and professor of medicine emeritus at Albany (N.Y.) Medical College, said in an interview.
At issue is whether patients with early RA should be temporarily treated with glucocorticoids in order to provide rapid relief. The ACR’s 2021 guideline on the treatment of RA says short-term glucocorticoids should not be “systematically prescribed” but notes that they are still “frequently necessary to alleviate symptoms” before disease-modifying therapies are given. The guideline adds that “these recommendations were made in recognition of the frequent difficulty tapering glucocorticoids, leading to undesirable prolonged use and the increasing evidence of the negative impact of glucocorticoids on long-term patient outcomes, including risk for infection, osteoporosis, and cardiovascular disease, in RA and other rheumatic diseases.”
For its part, the European Alliance of Associations for Rheumatology’s 2022 recommendations state that short-term glucocorticoids “should be considered when initiating or changing [disease-modifying antirheumatic drugs], in different dose regimens and routes of administration, but should be tapered and discontinued as rapidly as clinically feasible.”
Members of the Dutch team behind the new meta-analysis have been supporters of “bridging” therapy. For the new report, they analyzed three studies, including one led by a member of the team. Each study had at least one arm that randomized patients with RA to glucocorticoid bridging. Patients also took disease-modifying antirheumatic drugs (DMARDs).
There were 252 patients in study arms that started with bridging (mean age, 52 years; 68% female) and 373 other patients (mean age, 53 years; 67% female).
The researchers found that glucocorticoid use was higher in the bridgers at 12 months (odds ratio, 3.27; 95% confidence interval, 1.06-10.08), but the excess risk at 18 months (OR, 1.60; 95% CI, 0.46-5.60) and 24 months (OR, 1.70; 95% CI, 0.58-4.97) dipped below statistical significance. Also, they reported that “bridgers improved more rapidly (P < .001) in the first 6 months and the bridgers required significantly fewer changes in DMARDs (incidence rate ratio, 0.59; 95% CI, 0.38-0.94).”
“Based on our results, combined with two earlier publications [here and here], we show that most patients included in clinical trials with protocolized tapering schedules are able to stop glucocorticoids after bridging,” Dr. Bergstra said. “We also confirm the well-known short-term clinical effects and show that patients using glucocorticoid bridging require fewer DMARD changes. For a re-evaluation of the ACR guideline, this evidence should be combined with the extensive evidence showing short- as well as long-term clinical benefits of glucocorticoid bridging but also with evidence on potential side effects at different doses.”
She added that “implementing predefined tapering protocols may help clinicians and patients to stop glucocorticoids after bridging.” As for limitations, “patients included in these trials may differ from patients in clinical practice. We cannot be sure whether these results can be generalized to the full patient population.”
Dr. Kremer, a coauthor of the ACR guideline, pointed out that the patients who took glucocorticoids early were much more likely to be on them at 12 months.
By definition, “bridging” is temporary, he said, a brief period to help patients tolerate RA until DMARDs kick in. But in the studies, many of the patients clearly took the drugs for extended periods of time. In those cases, “it not a bridge,” and the risk is that “you’re treating people with a lifelong disease with doses of glucocorticoids that have been shown in multiple studies to be dangerous.”
He added that, while the excess likelihood of these patients staying on the drugs at 18 or 24 months wasn’t deemed to be statistically significant in the meta-analysis, the confidence intervals were unusually wide. That raises questions about whether some of the patients actually stay on the drugs.
Dr. Kremer said it can still be appropriate to give glucocorticoids to patients in distress, although it’s crucial in those cases to take the patients off them as soon as possible. It’s best, though, to not prescribe them at all. “If you can avoid it,” he said, “definitely avoid it.”
The study was conducted without outside funding. Dr. Bergstra reported receiving grant funding from Pfizer, and some of the other study authors reported various relationships with industry. Dr. Kremer had no relevant disclosures.
FROM ANNALS OF THE RHEUMATIC DISEASES