User login
Prognostic significance of HPV status in postoperative squamous-cell carcinoma of the head and neck
Background There are limited data on the prognostic significance of human papillomavirus (HPV) status in relation to traditional risk factors for head and neck squamous-cell carcinoma (HNSCC) in the postoperative setting.
Objective To clarify the impact of HPV status on the risk for HNSCC in the postoperative setting.
Methods We retrospectively evaluated an institutional cohort of 128 patients with HNSCC patients who had been treated with definitive surgery with or without adjuvant radiotherapy or chemoradiotherapy. Patient, disease, and treatment factors were analyzed as potential prognostic indicators.
Results Lymph node extracapsular extension (ECE), perineural invasion (PNI), and lymphovascular space invasion (LVSI) positivity predicted poorer locoregional control (LRC), disease-free survival (DFS), and overall survival (OS). Positive margins related to poorer DFS and OS. HPV status alone did not predict LRC, DFS, or OS. Compared with patients who were HPV-positive and ECE-negative, both HPV-positive and HPV-negative patients with ECE experienced significantly poorer OS (78.6%, 60%, and 43.7%, respectively; P = .010 and P = .018, respectively).
Limitations Retrospective, single-institution study; small patient cohort; short follow-up time
Conclusion The influence of HPV in postoperative HNSCC seems limited compared with traditional risk factors such as ECE, LVSI, and PNI. De-escalation of postoperative treatment based on HPV status alone should be approached with caution.
Click on the PDF icon at the top of this introduction to read the full article.
Background There are limited data on the prognostic significance of human papillomavirus (HPV) status in relation to traditional risk factors for head and neck squamous-cell carcinoma (HNSCC) in the postoperative setting.
Objective To clarify the impact of HPV status on the risk for HNSCC in the postoperative setting.
Methods We retrospectively evaluated an institutional cohort of 128 patients with HNSCC patients who had been treated with definitive surgery with or without adjuvant radiotherapy or chemoradiotherapy. Patient, disease, and treatment factors were analyzed as potential prognostic indicators.
Results Lymph node extracapsular extension (ECE), perineural invasion (PNI), and lymphovascular space invasion (LVSI) positivity predicted poorer locoregional control (LRC), disease-free survival (DFS), and overall survival (OS). Positive margins related to poorer DFS and OS. HPV status alone did not predict LRC, DFS, or OS. Compared with patients who were HPV-positive and ECE-negative, both HPV-positive and HPV-negative patients with ECE experienced significantly poorer OS (78.6%, 60%, and 43.7%, respectively; P = .010 and P = .018, respectively).
Limitations Retrospective, single-institution study; small patient cohort; short follow-up time
Conclusion The influence of HPV in postoperative HNSCC seems limited compared with traditional risk factors such as ECE, LVSI, and PNI. De-escalation of postoperative treatment based on HPV status alone should be approached with caution.
Click on the PDF icon at the top of this introduction to read the full article.
Background There are limited data on the prognostic significance of human papillomavirus (HPV) status in relation to traditional risk factors for head and neck squamous-cell carcinoma (HNSCC) in the postoperative setting.
Objective To clarify the impact of HPV status on the risk for HNSCC in the postoperative setting.
Methods We retrospectively evaluated an institutional cohort of 128 patients with HNSCC patients who had been treated with definitive surgery with or without adjuvant radiotherapy or chemoradiotherapy. Patient, disease, and treatment factors were analyzed as potential prognostic indicators.
Results Lymph node extracapsular extension (ECE), perineural invasion (PNI), and lymphovascular space invasion (LVSI) positivity predicted poorer locoregional control (LRC), disease-free survival (DFS), and overall survival (OS). Positive margins related to poorer DFS and OS. HPV status alone did not predict LRC, DFS, or OS. Compared with patients who were HPV-positive and ECE-negative, both HPV-positive and HPV-negative patients with ECE experienced significantly poorer OS (78.6%, 60%, and 43.7%, respectively; P = .010 and P = .018, respectively).
Limitations Retrospective, single-institution study; small patient cohort; short follow-up time
Conclusion The influence of HPV in postoperative HNSCC seems limited compared with traditional risk factors such as ECE, LVSI, and PNI. De-escalation of postoperative treatment based on HPV status alone should be approached with caution.
Click on the PDF icon at the top of this introduction to read the full article.
Painful Losses
A 58‐year‐old man presented to the emergency department with a 1‐month history of progressive, severe left hip pain that had become unbearable. The pain was constant and significantly worse with weight‐bearing, and the patient was now confined to bed. He denied back pain, falls, or trauma.
Although hip pain is a common complaint and a frequent manifestation of chronic degenerative joint disease, the debilitating and subacute nature of the pain suggests a potentially more serious underlying cause. Patients and even clinicians may refer to hip pain when the actual symptoms are periarticular, often presenting over the trochanter laterally, or muscular, presenting as posterior pain. The true hip joint is located in the anterior hip and groin area and often causes symptoms that radiate to the buttock. Pain can also be referred to the hip area from the spine, pelvis, or retroperitoneum, so it is crucial not to restrict the differential diagnosis to hip pathology.
Key diagnostic considerations include (1) inflammatory conditions such as trochanteric bursitis or gout; (2) bacterial infection of the hip joint, adjacent bone, or a nearby structure; (3) benign nerve compression (such as meralgia paresthetica); and (4) tumor (particularly myeloma or metastatic disease to the bone, but also potentially a pelvic or spinal mass with nerve compression). Polymyalgia rheumatica and other systemic rheumatologic complaints are a consideration, but because a single joint is involved, these conditions are less likely. The hip would be an unusual location for a first gout flare, and the duration of symptoms would be unusually long for gout. Avascular necrosis should be considered if the patient has received glucocorticoids for his previously diagnosed rheumatologic disease. If the patient is anticoagulated, consideration of spontaneous hematoma is reasonable, but usually this would present over a course of days, not weeks. The absence of trauma makes a fracture of the hip or pelvis less likely, and the insidious progression of symptoms makes a pathologic fracture less likely.
The patient reported 6 months of worsening proximal upper and lower extremity myalgia and weakness, with arthralgia of the hips and shoulders. The weakness was most notable in his proximal lower extremities, although he had remained ambulatory until the hip pain became limiting. He maintained normal use of his arms. The patient denied current rash but noted photosensitivity and a mild facial rash several months earlier. He described having transient mouth sores intermittently for several years. He denied fever, chills, night sweats, weight loss, dyspnea, recent travel, and outdoor exposures. Several months previously, he had been evaluated for these symptoms at another institution and given the diagnoses of rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE). At that time, he had initiated treatment with weekly dosing of methotrexate and etanercept.
The patient's medical history was also notable for hypertension, Graves' disease treated previously with radioiodine ablation, quiescent ulcerative colitis, and depression. Current medications included methotrexate, etanercept, levothyroxine, enalapril, hydrochlorothiazide, fluoxetine, ibuprofen, and oxycodone‐acetaminophen. He denied tobacco, alcohol, and recreational drug use.
Weakness occurring in the proximal lower extremities is the classic distribution for polymyositis and dermatomyositis. In contrast to polymyalgia rheumatica, dermatomyositis and polymyositis do not generally feature severe muscle pain, but they can be associated with a painful polyarthritis. Oral ulcers, photosensitivity, and facial rash are consistent with SLE, but dermatomyositis can also lead to a symmetrical erythema of the eyelids (commonly referred to as a heliotrope rash, named after the flower bearing that name) and sometimes can be associated with photosensitivity. Oral ulcers, particularly the painful ones known as canker sores, are extraordinarily common in the general population, and patients and providers may miss the mucosal lesions of SLE because they are usually painless. As methotrexate and etanercept are immunosuppressive, opportunistic pathogens such as typical or atypical mycobacteria and disseminated fungal infections should be considered, with special attention to the possibility of infection in or near the left hip. Given that SLE and RA rarely coexist, it would be helpful to seek outside medical records to know what the prior serologic evaluation entailed, but it is unlikely that this presentation is a manifestation of a diffuse connective tissue process.
Physical examination should focus on the features of dermatomyositis including heliotrope rash, truncal erythema, and papules over the knuckles (Gottron's papules); objective proximal muscle weakness in the shoulder and hip girdle; and findings that might suggest antisynthetase syndrome such as hyperkeratotic mechanic hand palmar and digital changes, and interstitial crackles on lung exam. If necrotic skin lesions are found, this would raise concern for a disseminated infection. The joints should be examined for inflammation and effusions.
His temperature was 36.6C, heart rate 74 beats per minute, blood pressure 134/76 mm Hg, respiratory rate 16 breaths per minute, and O2 saturation 97% on room air. He was obese but did not have moon facies or a buffalo hump. There were no rashes or mucosal lesions. Active and passive motion of his left hip joint elicited pain with both flexion/extension and internal/external rotation. Muscle strength was limited by pain in the left hip flexors and extenders, but was 5/5 in all other muscle groups. Palpation of the proximal muscles of his arms and legs did not elicit pain. His extremities were without edema, and examination of his shoulders, elbows, wrists, hands, knees, ankles, and feet did not reveal any erythema, synovial thickening, effusion, or deformity. Examination of the heart, chest, and abdomen was normal.
Given the reassuring strength examination, the absence of rashes or skin lesions, and the reassuring joint exam aside from the left hip, a focal infectious, inflammatory, or malignant process seems most likely. The pain with range of motion of the hip does not definitively localize the pathology to the hip joint, because pathology of the nearby structures can lead to pain when the hip is moved. Laboratory evaluation should include a complete blood count to screen for evidence of infection or marrow suppression, complete metabolic panel, and creatine kinase. The history of ulcerative colitis raises the possibility of an enthesitis (inflammation of tendons or ligaments) occurring near the hip. Enthesitis is sometimes a feature of the seronegative spondyloarthropathy‐associated conditions and can occur in the absence of sacroiliitis or spondyloarthropathy.
The patient's myalgias and arthralgias had recently been evaluated in the rheumatology clinic. Laboratory evaluation from that visit was remarkable only for an antinuclear antibody (ANA) test that was positive at a titer of 1:320 in a homogeneous pattern, creatine phosphokinase 366 IU/L (normal range [NR] 38240), and alkaline phosphatase 203 IU/L (NR 30130). All of the following labs from that visit were within normal ranges: cyclic citrullinated peptide, rheumatoid factor, antidouble stranded DNA, aldolase, complement levels, serum and urine protein electrophoresis, thyroglobulin antibody, thyroid microsomal antibody, thyroid‐stimulating hormone, erythrocyte sedimentation rate (10 mm/h), and C‐reactive protein (0.3 mg/dL).
The patient was admitted to the hospital. Initial blood test results on admission included sodium 139 mEq/L, potassium 3.9 mEq/L, chloride 105 mEq/L, bicarbonate 27 mEq/L, urea nitrogen 16 mg/dL, creatinine 0.6 mg/dL, glucose 85 mg/dL, calcium 9.2 mg/dL (NR 8.810.3), phosphate 1.3 mg/dL (NR 2.74.6), albumin 4.7 g/dL (NR 3.54.9), and alkaline phosphatase 195 IU/L (NR 30130). The remainder of a comprehensive metabolic profile, complete blood count with differential, and coagulation studies were all normal.
The homogeneous ANA titer of 1:320 is high enough to raise eyebrows, but is nonspecific for lupus and other ANA‐associated rheumatologic conditions, and may be a red herring, particularly given the low likelihood of a systemic inflammatory process explaining this new focal hip pain. The alkaline phosphatase is only mildly elevated and could be of bone or liver origin. The reassuringly low inflammatory markers are potentially helpful, because if checked now and substantially increased from the prior outpatient visit, they would be suggestive of a new inflammatory process. However, this would not point to a specific cause of inflammation.
Given the focality of the symptoms, imaging is warranted. As opposed to plain films, contrast‐enhanced computed tomography (CT) of the pelvis or magnetic resonance imaging (MRI) may be an efficient first step, because there is low suspicion for fracture and high suspicion for an inflammatory, neoplastic, or infectious process. MRI is more expensive and usually cannot be obtained as rapidly as CT. There is a chance that CT imaging alone will provide enough information to guide the next diagnostic steps, such as aspiration of an abscess or joint, or biopsy of a suspicious lesion. However, for soft tissue lesions and many bone lesions, including osteomyelitis, MRI offers better delineation of pathology.
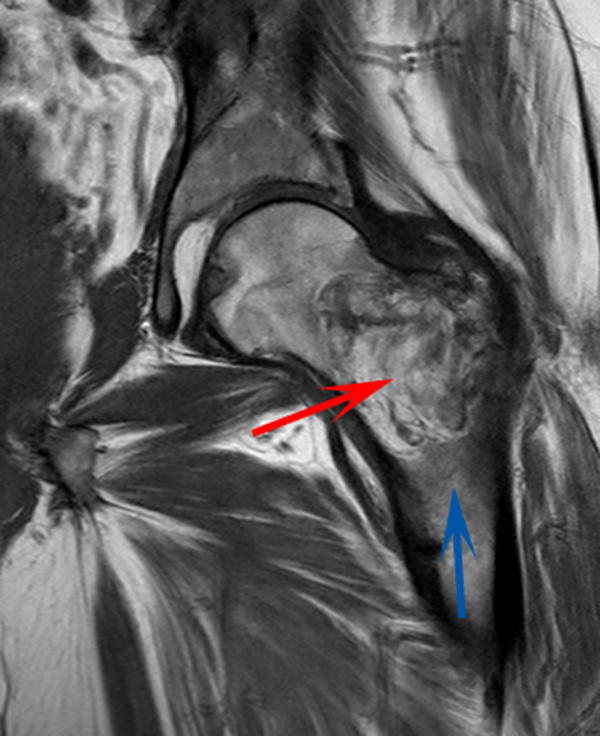
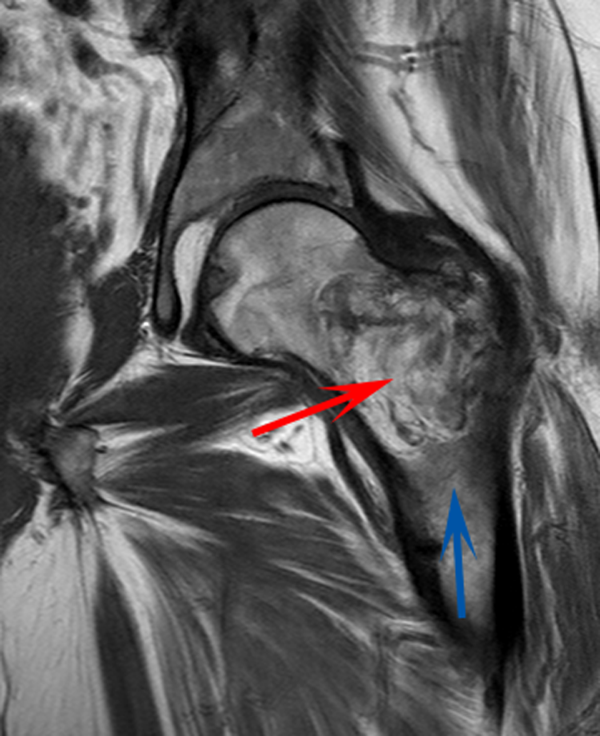
CT scan of the left femur demonstrated a large lytic lesion in the femoral neck that contained macroscopic fat and had an aggressive appearance with significant thinning of the cortex. MRI confirmed these findings and demonstrated a nondisplaced subtrochanteric femur fracture in the proximity of the lesion (Figure 1). Contrast‐enhanced CT scans of the thorax, abdomen, and pelvis revealed no other neoplastic lesions. Prostate‐specific antigen level was normal. The patient's significant hypophosphatemia persisted, with levels dropping to as low as 0.9 mg/dL despite aggressive oral phosphate replacement.
Although hypophosphatemia is often a nonspecific finding in hospitalized patients and is usually of little clinical importance, profound hypophosphatemia that is refractory to supplementation suggests an underlying metabolic disorder. Phosphate levels less than 1.0 mg/dL, particularly if prolonged, can lead to decreased adenosine triphosphate production and subsequent weakness of respiratory and cardiac muscles. Parathyroid hormone (PTH) excess and production of parathyroid hormone‐related protein (PTHrP) by a malignancy can cause profound hypophosphatemia, but are generally associated with hypercalcemia, a finding not seen in this case. Occasionally, tumors can lead to renal phosphate wasting via nonPTH‐related mechanisms. The best characterized example of this is the paraneoplastic syndrome oncogenic osteomalacia caused by tumor production of a fibroblast growth factor. Tumors that lead to this syndrome are usually benign mesenchymal tumors. This patient's tumor may be of this type, causing local destruction and metabolic disturbance. The next step would be consultation with orthopedic surgery for resection of the tumor and total hip arthroplasty with aggressive perioperative repletion of phosphate. Assessment of intact PTH, ionized calcium, 24‐hour urinary phosphate excretion, and even PTHrP levels may help to rule out other etiologies of hypophosphatemia, but given that surgery is needed regardless, it might be reasonable to proceed to the operating room without these diagnostics. If the phosphate levels return to normal postoperatively, then the diagnosis is clear and no further metabolic testing is needed.
PTH level was 47 pg/mL (NR 1065), 25‐hydroxyvitamin D level was 25 ng/mL (NR 2580), and 1,25‐dihydroxyvitamin D level was 18 pg/mL (NR 1872). Urinalysis was normal without proteinuria or glucosuria. A 24‐hour urine collection contained 1936 mg of phosphate (NR 4001200). The ratio of maximum rate of renal tubular reabsorption of phosphate to glomerular filtration rate (TmP/GFR) was 1.3 mg/dL (NR 2.44.2). Tissue obtained by CT‐guided needle biopsy of the femoral mass was consistent with a benign spindle cell neoplasm.
With normal calcium levels, the PTH level is appropriate, and hyperparathyroidism is excluded. The levels of 25‐hydroxyvitamin D and 1‐25‐dihydroxyvitamin D are not low enough to suggest that vitamin D deficiency is driving the impressive hypophosphatemia. What is impressive is the phosphate wasting demonstrated by the 24‐hour urine collection, consistent with paraneoplastic overproduction of fibroblast growth factor 23 (FGF23) by the benign bone tumor. Overproduction of this protein can be detected by blood tests or staining of the tumor specimen, but surgery should be performed as soon as possible independent of any further test results. Once the tumor is resected, phosphate metabolism should normalize.
FGF23 level was 266 RU/mL (NR 180). The patient was diagnosed with tumor‐induced osteomalacia (TIO). He underwent complete resection of the femoral tumor as well as open reduction and internal fixation of the fracture. After surgery, his symptoms of pain and subjective muscle weakness improved, his serum phosphate level normalized, his need for phosphate supplementation resolved, and his blood levels of FGF23 decreased into the normal range (111 RU/mL). The rapid improvement of his symptoms after surgery suggested that they were related to TIO, and not manifestations of SLE or RA. His immunosuppressant medications were discontinued. Surgical pathology demonstrated a heterogeneous tumor consisting of sheets of uniform spindle cells interspersed with mature adipose tissue. This was diagnosed descriptively as a benign spindle cell and lipomatous neoplasm without further classification. Two months later, the patient was ambulating without pain, and muscle strength was subjectively normal.
DISCUSSION
TIO is a rare paraneoplastic syndrome affecting phosphate and vitamin D metabolism, leading to hypophosphatemia and osteomalacia.[1] TIO is caused by the inappropriate tumor secretion of the phosphatonin hormone, FGF23.
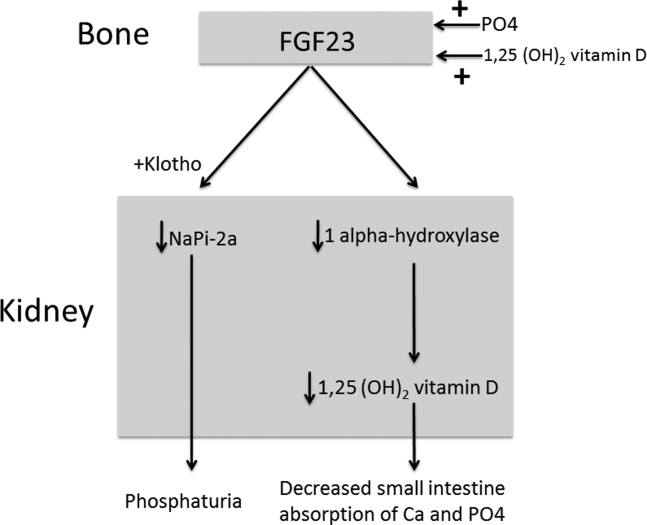
The normal physiology of FGF23 is illustrated in Figure 2. Osteocytes appear to be the primary source of FGF23, but the regulation of FGF23 production is not completely understood. FGF23 production may be influenced by several factors, including 1,25 dihydroxyvitamin D levels, and serum phosphate and PTH concentrations. This hormone binds to the FGF receptor and its coreceptor, Klotho,[2] causing 2 major physiological effects. First, it decreases the expression of the sodium‐phosphate cotransporters in the renal proximal tubular cells,[3, 4] resulting in increased tubular phosphate wasting. This effect appears to be partly PTH dependent.[5] Second, it has effects on vitamin D metabolism, decreasing renal production of activated vitamin D.[3, 4, 6]
In overproduction states, the elevated FGF23 leads to chronically low serum phosphate levels (with renal phosphate wasting) and the clinical syndrome of osteomalacia, manifested by bone pain, fractures, and deformities. Hypophosphatemia can also lead to painful proximal myopathy, cardiorespiratory dysfunction, and a spectrum of neuropsychiatric findings. The clinical findings in TIO are similar to those seen in genetic diseases in which hypophosphatemia results from the same mechanism.[3, 4]
In this case, measurement of the serum phosphate level was important in reaching the diagnosis. Although hypophosphatemia in the hospitalized patient is often easily explained, severe or persistent hypophosphatemia requires a focused evaluation. Causes of hypophosphatemia are categorized in Table 1.[7, 8, 9] In patients with hypophosphatemia that is not explained by the clinical situation (eg, osmotic diuresis, insulin treatment, refeeding syndrome, postparathyroidectomy, chronic diarrhea), measurement of serum calcium, PTH, and 25‐hydroxyvitamin D are used to investigate possible primary or secondary hyperparathyroidism. In addition, low‐normal or low serum 1,25‐dihydroxyvitamin D with normal PTH, normal 25‐hydroxyvitamin D stores, and normal renal function are clues to the presence of TIO. Urine phosphate wasting can be measured by collecting a 24‐hour urine sample. Calculation of the TmP/GFR (a measure of the maximum tubular resorption of phosphate relative to the glomerular filtration rate), as described by the nomogram of Walton and Bijvoet, may improve the accuracy of this assessment and confirm a renal source of the hypophosphatemia.[10]
|
| Internal redistribution |
| Insulin or catecholamine effect (including that related to refeeding syndrome, and infusion of glucose or TPN) |
| Acute respiratory alkalosis |
| Accelerated bone formation or rapid cell proliferation (eg, hungry bone syndrome, leukemic blast crisis, erythropoietin, or granulocyte colony stimulating factor administration) |
| Decreased absorption |
| Poor intake (including that seen in alcoholism*) |
| Vitamin D deficiency |
| Gastrointestinal losses (eg, chronic diarrhea) |
| Malabsorption (eg, phosphate‐binding antacids) |
| Urinary losses |
| Osmotic diuresis (eg, poorly controlled diabetes, acetazolamide) or volume expansion |
| Other diuretics: thiazides, indapamide |
| Hyperparathyroidism |
| Primary |
| Secondary (including vitamin D or calcium deficiency) |
| Parathyroid hormone‐related peptide |
| Renal tubular disease |
| Medications (eg, ethanol,* high‐dose glucocorticoids, cisplatin, bisphosphonates, estrogens, imatinib, acyclovir) |
| Fanconi syndrome |
| Medications inducing Fanconi syndrome: tenofovir, cidofovir, adefovir, aminoglycosides, ifosfamide, tetracyclines, valproic acid |
| Other (eg, postrenal transplant) |
| Excessive phosphatonin hormone activity (eg, hereditary syndromes [rickets], tumor‐induced osteomalacia) |
| Multifactorial causes |
| Alcoholism* |
| Acetaminophen toxicity |
| Parenteral iron administration |
The patient presented here had inappropriate urinary phosphate losses, and laboratory testing ruled out primary and secondary hyperparathyroidism and Fanconi syndrome. The patient was not taking medications known to cause tubular phosphate wasting. The patient's age and clinical history made hereditary syndromes unlikely. Therefore, the urinary phosphate wasting had to be related to an acquired defect in phosphate metabolism. The diagnostic characteristics of TIO are summarized in Table 2.
|
| Patients may present with symptoms of osteomalacia (eg, bone pain, fractures), hypophosphatemia (eg, proximal myopathy), and/or neoplasm. |
| Hypophosphatemia with urinary phosphate wasting. |
| Serum calcium level is usually normal. |
| Serum 1,25‐dihydroxyvitamin D level is usually low or low‐normal. |
| Parathyroid hormone is usually normal. |
| Plasma FGF23 level is elevated. |
| A neoplasm with the appropriate histology is identified, although the osteomalacia syndrome may precede identification of the tumor, which may be occult. |
| The syndrome resolves after complete resection of the tumor. |
The presence of a known neoplasm makes the diagnosis of TIO considerably easier. However, osteomalacia often precedes the tumor diagnosis. In these cases, the discovery of this clinical syndrome necessitates a search for the tumor. The tumors can be small, occult, and often located in the extremities. In addition to standard cross‐sectional imaging, specialized diagnostic modalities can be helpful in localizing culprit tumors. These include F‐18 flourodeoxyglucose positron emission tomography with computed tomography, 111‐Indium octreotide single photon emission CT/CT, 68‐Gallium‐DOTA‐octreotide positron emission tomography with computed tomography, and even selective venous sampling for FGF23 levels.[1, 11] The octreotide tests capitalize on the fact that culprit tumors often express somatostatin receptors.
TIO is most often associated with mesenchymal tumors of the bone or soft tissue. It has also been reported in association with several malignancies (small cell carcinoma, hematologic malignancies, prostate cancer), and with polyostotic fibrous dysplasia, neurofibromatosis, and the epidermal nevus syndrome. The mesenchymal tumors are heterogeneous in appearance and can be variably classified as hemangiopericytomas, hemangiomas, sarcomas, ossifying fibromas, granulomas, giant cell tumors, or osteoblastomas.[1] However, 1 review suggests that most of these tumors actually represent a distinct but heterogeneous, under‐recognized entity that is best classified as a phosphaturic mesenchymal tumor.[11]
TIO is only cured by complete resection of the tumor.[1] Local recurrences have been described, as have rare occurrences of metastatic disease.[1, 12] Medical treatment can be used to normalize serum phosphate levels in patients who are unable to be cured by surgery. The goal is to bring serum phosphate into the low‐normal range via phosphate supplementation (typically 13 g/day of elemental phosphorus is required) and treatment with either calcitriol or alfacalcidol. Due to the inhibition of 1,25‐dihydroxyvitamin D activation in TIO, relatively large doses of calcitriol are needed. A reasonable starting dose of calcitriol is 1.5 g/day, and most patients require 15 to 60 ng/kg per day. Because PTH action is involved in FGF23‐mediated hypophosphatemia, suppression of PTH may also be useful in these patients.[13]
This patient presented with a painful femoral tumor in the setting of muscle and joint pain that had been erroneously attributed to connective tissue disease. However, recognition and thorough evaluation of the patient's hypophosphatemia led to a unifying diagnosis of TIO. This diagnosis altered the surgical approach (emphasizing complete resection to eradicate the FGF23 production) and helped alleviate the patient's painful losses of phosphate.
TEACHING POINTS
- Hypophosphatemia, especially if severe or persistent, should not be dismissed as an unimportant laboratory finding. A focused evaluation should be performed to determine the etiology.
- In patients with unexplained hypophosphatemia, the measurement of serum calcium, parathyroid hormone, and vitamin D levels can identify primary or secondary hyperparathyroidism.
- The differential diagnosis of hypophosphatemia is narrowed if there is clinical evidence of inappropriate urinary phosphate wasting (ie, urinary phosphate levels remain high, despite low serum levels).
- TIO is a rare paraneoplastic syndrome caused by FGF23, a phosphatonin hormone that causes renal phosphate wasting, hypophosphatemia, and osteomalacia.
Disclosure: Nothing to report.
- , , , . Tumor‐induced osteomalacia. Endocr Relat Cancer. 2011;18:R53–R77.
- . The FGF23‐Klotho axis: endocrine regulation of phosphate homeostasis. Nat Rev Endocrinol. 2009;5:611–619.
- , . Genetic disorders of renal phosphate transport. N Engl J Med. 2010;362:2399–2409.
- . The expanding family of hypophosphatemic syndromes. J Bone Miner Metab. 2012;30:1–9.
- , , , , . FGF‐23 is elevated by chronic hyperphosphatemia. J Clin Endocrinol Metab. 2004;89:4489–4492.
- , , , et al. FGF‐23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004;19:429–435.
- , . Hypophosphatemia: an update on its etiology and treatment. Am J Med. 2005;118:1094–1101.
- , , . In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, eds. Williams Textbook of Endocrinology. 12th ed. Philadelphia, PA: Elsevier; 2011:1237–1304.
- , , . Medication‐induced hypophosphatemia: a review. QJM. 2010;103:449–459.
- , . Nomogram for derivation of renal threshold phosphate concentration. Lancet. 1975;2:309–310.
- , , , et al. Improving diagnosis of tumor‐induced osteomalacia with gallium‐68 DOTATATE PET/CT. J Clin Endocrinol Metab. 2013; 98:687–694.
- , , , et al. Most osteomalacia‐associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28:1–30.
- , , , , , . Cinacalcet in the management of tumor‐induced osteomalacia. J Bone Miner Res. 2007;22:931–937.
A 58‐year‐old man presented to the emergency department with a 1‐month history of progressive, severe left hip pain that had become unbearable. The pain was constant and significantly worse with weight‐bearing, and the patient was now confined to bed. He denied back pain, falls, or trauma.
Although hip pain is a common complaint and a frequent manifestation of chronic degenerative joint disease, the debilitating and subacute nature of the pain suggests a potentially more serious underlying cause. Patients and even clinicians may refer to hip pain when the actual symptoms are periarticular, often presenting over the trochanter laterally, or muscular, presenting as posterior pain. The true hip joint is located in the anterior hip and groin area and often causes symptoms that radiate to the buttock. Pain can also be referred to the hip area from the spine, pelvis, or retroperitoneum, so it is crucial not to restrict the differential diagnosis to hip pathology.
Key diagnostic considerations include (1) inflammatory conditions such as trochanteric bursitis or gout; (2) bacterial infection of the hip joint, adjacent bone, or a nearby structure; (3) benign nerve compression (such as meralgia paresthetica); and (4) tumor (particularly myeloma or metastatic disease to the bone, but also potentially a pelvic or spinal mass with nerve compression). Polymyalgia rheumatica and other systemic rheumatologic complaints are a consideration, but because a single joint is involved, these conditions are less likely. The hip would be an unusual location for a first gout flare, and the duration of symptoms would be unusually long for gout. Avascular necrosis should be considered if the patient has received glucocorticoids for his previously diagnosed rheumatologic disease. If the patient is anticoagulated, consideration of spontaneous hematoma is reasonable, but usually this would present over a course of days, not weeks. The absence of trauma makes a fracture of the hip or pelvis less likely, and the insidious progression of symptoms makes a pathologic fracture less likely.
The patient reported 6 months of worsening proximal upper and lower extremity myalgia and weakness, with arthralgia of the hips and shoulders. The weakness was most notable in his proximal lower extremities, although he had remained ambulatory until the hip pain became limiting. He maintained normal use of his arms. The patient denied current rash but noted photosensitivity and a mild facial rash several months earlier. He described having transient mouth sores intermittently for several years. He denied fever, chills, night sweats, weight loss, dyspnea, recent travel, and outdoor exposures. Several months previously, he had been evaluated for these symptoms at another institution and given the diagnoses of rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE). At that time, he had initiated treatment with weekly dosing of methotrexate and etanercept.
The patient's medical history was also notable for hypertension, Graves' disease treated previously with radioiodine ablation, quiescent ulcerative colitis, and depression. Current medications included methotrexate, etanercept, levothyroxine, enalapril, hydrochlorothiazide, fluoxetine, ibuprofen, and oxycodone‐acetaminophen. He denied tobacco, alcohol, and recreational drug use.
Weakness occurring in the proximal lower extremities is the classic distribution for polymyositis and dermatomyositis. In contrast to polymyalgia rheumatica, dermatomyositis and polymyositis do not generally feature severe muscle pain, but they can be associated with a painful polyarthritis. Oral ulcers, photosensitivity, and facial rash are consistent with SLE, but dermatomyositis can also lead to a symmetrical erythema of the eyelids (commonly referred to as a heliotrope rash, named after the flower bearing that name) and sometimes can be associated with photosensitivity. Oral ulcers, particularly the painful ones known as canker sores, are extraordinarily common in the general population, and patients and providers may miss the mucosal lesions of SLE because they are usually painless. As methotrexate and etanercept are immunosuppressive, opportunistic pathogens such as typical or atypical mycobacteria and disseminated fungal infections should be considered, with special attention to the possibility of infection in or near the left hip. Given that SLE and RA rarely coexist, it would be helpful to seek outside medical records to know what the prior serologic evaluation entailed, but it is unlikely that this presentation is a manifestation of a diffuse connective tissue process.
Physical examination should focus on the features of dermatomyositis including heliotrope rash, truncal erythema, and papules over the knuckles (Gottron's papules); objective proximal muscle weakness in the shoulder and hip girdle; and findings that might suggest antisynthetase syndrome such as hyperkeratotic mechanic hand palmar and digital changes, and interstitial crackles on lung exam. If necrotic skin lesions are found, this would raise concern for a disseminated infection. The joints should be examined for inflammation and effusions.
His temperature was 36.6C, heart rate 74 beats per minute, blood pressure 134/76 mm Hg, respiratory rate 16 breaths per minute, and O2 saturation 97% on room air. He was obese but did not have moon facies or a buffalo hump. There were no rashes or mucosal lesions. Active and passive motion of his left hip joint elicited pain with both flexion/extension and internal/external rotation. Muscle strength was limited by pain in the left hip flexors and extenders, but was 5/5 in all other muscle groups. Palpation of the proximal muscles of his arms and legs did not elicit pain. His extremities were without edema, and examination of his shoulders, elbows, wrists, hands, knees, ankles, and feet did not reveal any erythema, synovial thickening, effusion, or deformity. Examination of the heart, chest, and abdomen was normal.
Given the reassuring strength examination, the absence of rashes or skin lesions, and the reassuring joint exam aside from the left hip, a focal infectious, inflammatory, or malignant process seems most likely. The pain with range of motion of the hip does not definitively localize the pathology to the hip joint, because pathology of the nearby structures can lead to pain when the hip is moved. Laboratory evaluation should include a complete blood count to screen for evidence of infection or marrow suppression, complete metabolic panel, and creatine kinase. The history of ulcerative colitis raises the possibility of an enthesitis (inflammation of tendons or ligaments) occurring near the hip. Enthesitis is sometimes a feature of the seronegative spondyloarthropathy‐associated conditions and can occur in the absence of sacroiliitis or spondyloarthropathy.
The patient's myalgias and arthralgias had recently been evaluated in the rheumatology clinic. Laboratory evaluation from that visit was remarkable only for an antinuclear antibody (ANA) test that was positive at a titer of 1:320 in a homogeneous pattern, creatine phosphokinase 366 IU/L (normal range [NR] 38240), and alkaline phosphatase 203 IU/L (NR 30130). All of the following labs from that visit were within normal ranges: cyclic citrullinated peptide, rheumatoid factor, antidouble stranded DNA, aldolase, complement levels, serum and urine protein electrophoresis, thyroglobulin antibody, thyroid microsomal antibody, thyroid‐stimulating hormone, erythrocyte sedimentation rate (10 mm/h), and C‐reactive protein (0.3 mg/dL).
The patient was admitted to the hospital. Initial blood test results on admission included sodium 139 mEq/L, potassium 3.9 mEq/L, chloride 105 mEq/L, bicarbonate 27 mEq/L, urea nitrogen 16 mg/dL, creatinine 0.6 mg/dL, glucose 85 mg/dL, calcium 9.2 mg/dL (NR 8.810.3), phosphate 1.3 mg/dL (NR 2.74.6), albumin 4.7 g/dL (NR 3.54.9), and alkaline phosphatase 195 IU/L (NR 30130). The remainder of a comprehensive metabolic profile, complete blood count with differential, and coagulation studies were all normal.
The homogeneous ANA titer of 1:320 is high enough to raise eyebrows, but is nonspecific for lupus and other ANA‐associated rheumatologic conditions, and may be a red herring, particularly given the low likelihood of a systemic inflammatory process explaining this new focal hip pain. The alkaline phosphatase is only mildly elevated and could be of bone or liver origin. The reassuringly low inflammatory markers are potentially helpful, because if checked now and substantially increased from the prior outpatient visit, they would be suggestive of a new inflammatory process. However, this would not point to a specific cause of inflammation.
Given the focality of the symptoms, imaging is warranted. As opposed to plain films, contrast‐enhanced computed tomography (CT) of the pelvis or magnetic resonance imaging (MRI) may be an efficient first step, because there is low suspicion for fracture and high suspicion for an inflammatory, neoplastic, or infectious process. MRI is more expensive and usually cannot be obtained as rapidly as CT. There is a chance that CT imaging alone will provide enough information to guide the next diagnostic steps, such as aspiration of an abscess or joint, or biopsy of a suspicious lesion. However, for soft tissue lesions and many bone lesions, including osteomyelitis, MRI offers better delineation of pathology.
CT scan of the left femur demonstrated a large lytic lesion in the femoral neck that contained macroscopic fat and had an aggressive appearance with significant thinning of the cortex. MRI confirmed these findings and demonstrated a nondisplaced subtrochanteric femur fracture in the proximity of the lesion (Figure 1). Contrast‐enhanced CT scans of the thorax, abdomen, and pelvis revealed no other neoplastic lesions. Prostate‐specific antigen level was normal. The patient's significant hypophosphatemia persisted, with levels dropping to as low as 0.9 mg/dL despite aggressive oral phosphate replacement.
Although hypophosphatemia is often a nonspecific finding in hospitalized patients and is usually of little clinical importance, profound hypophosphatemia that is refractory to supplementation suggests an underlying metabolic disorder. Phosphate levels less than 1.0 mg/dL, particularly if prolonged, can lead to decreased adenosine triphosphate production and subsequent weakness of respiratory and cardiac muscles. Parathyroid hormone (PTH) excess and production of parathyroid hormone‐related protein (PTHrP) by a malignancy can cause profound hypophosphatemia, but are generally associated with hypercalcemia, a finding not seen in this case. Occasionally, tumors can lead to renal phosphate wasting via nonPTH‐related mechanisms. The best characterized example of this is the paraneoplastic syndrome oncogenic osteomalacia caused by tumor production of a fibroblast growth factor. Tumors that lead to this syndrome are usually benign mesenchymal tumors. This patient's tumor may be of this type, causing local destruction and metabolic disturbance. The next step would be consultation with orthopedic surgery for resection of the tumor and total hip arthroplasty with aggressive perioperative repletion of phosphate. Assessment of intact PTH, ionized calcium, 24‐hour urinary phosphate excretion, and even PTHrP levels may help to rule out other etiologies of hypophosphatemia, but given that surgery is needed regardless, it might be reasonable to proceed to the operating room without these diagnostics. If the phosphate levels return to normal postoperatively, then the diagnosis is clear and no further metabolic testing is needed.
PTH level was 47 pg/mL (NR 1065), 25‐hydroxyvitamin D level was 25 ng/mL (NR 2580), and 1,25‐dihydroxyvitamin D level was 18 pg/mL (NR 1872). Urinalysis was normal without proteinuria or glucosuria. A 24‐hour urine collection contained 1936 mg of phosphate (NR 4001200). The ratio of maximum rate of renal tubular reabsorption of phosphate to glomerular filtration rate (TmP/GFR) was 1.3 mg/dL (NR 2.44.2). Tissue obtained by CT‐guided needle biopsy of the femoral mass was consistent with a benign spindle cell neoplasm.
With normal calcium levels, the PTH level is appropriate, and hyperparathyroidism is excluded. The levels of 25‐hydroxyvitamin D and 1‐25‐dihydroxyvitamin D are not low enough to suggest that vitamin D deficiency is driving the impressive hypophosphatemia. What is impressive is the phosphate wasting demonstrated by the 24‐hour urine collection, consistent with paraneoplastic overproduction of fibroblast growth factor 23 (FGF23) by the benign bone tumor. Overproduction of this protein can be detected by blood tests or staining of the tumor specimen, but surgery should be performed as soon as possible independent of any further test results. Once the tumor is resected, phosphate metabolism should normalize.
FGF23 level was 266 RU/mL (NR 180). The patient was diagnosed with tumor‐induced osteomalacia (TIO). He underwent complete resection of the femoral tumor as well as open reduction and internal fixation of the fracture. After surgery, his symptoms of pain and subjective muscle weakness improved, his serum phosphate level normalized, his need for phosphate supplementation resolved, and his blood levels of FGF23 decreased into the normal range (111 RU/mL). The rapid improvement of his symptoms after surgery suggested that they were related to TIO, and not manifestations of SLE or RA. His immunosuppressant medications were discontinued. Surgical pathology demonstrated a heterogeneous tumor consisting of sheets of uniform spindle cells interspersed with mature adipose tissue. This was diagnosed descriptively as a benign spindle cell and lipomatous neoplasm without further classification. Two months later, the patient was ambulating without pain, and muscle strength was subjectively normal.
DISCUSSION
TIO is a rare paraneoplastic syndrome affecting phosphate and vitamin D metabolism, leading to hypophosphatemia and osteomalacia.[1] TIO is caused by the inappropriate tumor secretion of the phosphatonin hormone, FGF23.
The normal physiology of FGF23 is illustrated in Figure 2. Osteocytes appear to be the primary source of FGF23, but the regulation of FGF23 production is not completely understood. FGF23 production may be influenced by several factors, including 1,25 dihydroxyvitamin D levels, and serum phosphate and PTH concentrations. This hormone binds to the FGF receptor and its coreceptor, Klotho,[2] causing 2 major physiological effects. First, it decreases the expression of the sodium‐phosphate cotransporters in the renal proximal tubular cells,[3, 4] resulting in increased tubular phosphate wasting. This effect appears to be partly PTH dependent.[5] Second, it has effects on vitamin D metabolism, decreasing renal production of activated vitamin D.[3, 4, 6]
In overproduction states, the elevated FGF23 leads to chronically low serum phosphate levels (with renal phosphate wasting) and the clinical syndrome of osteomalacia, manifested by bone pain, fractures, and deformities. Hypophosphatemia can also lead to painful proximal myopathy, cardiorespiratory dysfunction, and a spectrum of neuropsychiatric findings. The clinical findings in TIO are similar to those seen in genetic diseases in which hypophosphatemia results from the same mechanism.[3, 4]
In this case, measurement of the serum phosphate level was important in reaching the diagnosis. Although hypophosphatemia in the hospitalized patient is often easily explained, severe or persistent hypophosphatemia requires a focused evaluation. Causes of hypophosphatemia are categorized in Table 1.[7, 8, 9] In patients with hypophosphatemia that is not explained by the clinical situation (eg, osmotic diuresis, insulin treatment, refeeding syndrome, postparathyroidectomy, chronic diarrhea), measurement of serum calcium, PTH, and 25‐hydroxyvitamin D are used to investigate possible primary or secondary hyperparathyroidism. In addition, low‐normal or low serum 1,25‐dihydroxyvitamin D with normal PTH, normal 25‐hydroxyvitamin D stores, and normal renal function are clues to the presence of TIO. Urine phosphate wasting can be measured by collecting a 24‐hour urine sample. Calculation of the TmP/GFR (a measure of the maximum tubular resorption of phosphate relative to the glomerular filtration rate), as described by the nomogram of Walton and Bijvoet, may improve the accuracy of this assessment and confirm a renal source of the hypophosphatemia.[10]
|
| Internal redistribution |
| Insulin or catecholamine effect (including that related to refeeding syndrome, and infusion of glucose or TPN) |
| Acute respiratory alkalosis |
| Accelerated bone formation or rapid cell proliferation (eg, hungry bone syndrome, leukemic blast crisis, erythropoietin, or granulocyte colony stimulating factor administration) |
| Decreased absorption |
| Poor intake (including that seen in alcoholism*) |
| Vitamin D deficiency |
| Gastrointestinal losses (eg, chronic diarrhea) |
| Malabsorption (eg, phosphate‐binding antacids) |
| Urinary losses |
| Osmotic diuresis (eg, poorly controlled diabetes, acetazolamide) or volume expansion |
| Other diuretics: thiazides, indapamide |
| Hyperparathyroidism |
| Primary |
| Secondary (including vitamin D or calcium deficiency) |
| Parathyroid hormone‐related peptide |
| Renal tubular disease |
| Medications (eg, ethanol,* high‐dose glucocorticoids, cisplatin, bisphosphonates, estrogens, imatinib, acyclovir) |
| Fanconi syndrome |
| Medications inducing Fanconi syndrome: tenofovir, cidofovir, adefovir, aminoglycosides, ifosfamide, tetracyclines, valproic acid |
| Other (eg, postrenal transplant) |
| Excessive phosphatonin hormone activity (eg, hereditary syndromes [rickets], tumor‐induced osteomalacia) |
| Multifactorial causes |
| Alcoholism* |
| Acetaminophen toxicity |
| Parenteral iron administration |
The patient presented here had inappropriate urinary phosphate losses, and laboratory testing ruled out primary and secondary hyperparathyroidism and Fanconi syndrome. The patient was not taking medications known to cause tubular phosphate wasting. The patient's age and clinical history made hereditary syndromes unlikely. Therefore, the urinary phosphate wasting had to be related to an acquired defect in phosphate metabolism. The diagnostic characteristics of TIO are summarized in Table 2.
|
| Patients may present with symptoms of osteomalacia (eg, bone pain, fractures), hypophosphatemia (eg, proximal myopathy), and/or neoplasm. |
| Hypophosphatemia with urinary phosphate wasting. |
| Serum calcium level is usually normal. |
| Serum 1,25‐dihydroxyvitamin D level is usually low or low‐normal. |
| Parathyroid hormone is usually normal. |
| Plasma FGF23 level is elevated. |
| A neoplasm with the appropriate histology is identified, although the osteomalacia syndrome may precede identification of the tumor, which may be occult. |
| The syndrome resolves after complete resection of the tumor. |
The presence of a known neoplasm makes the diagnosis of TIO considerably easier. However, osteomalacia often precedes the tumor diagnosis. In these cases, the discovery of this clinical syndrome necessitates a search for the tumor. The tumors can be small, occult, and often located in the extremities. In addition to standard cross‐sectional imaging, specialized diagnostic modalities can be helpful in localizing culprit tumors. These include F‐18 flourodeoxyglucose positron emission tomography with computed tomography, 111‐Indium octreotide single photon emission CT/CT, 68‐Gallium‐DOTA‐octreotide positron emission tomography with computed tomography, and even selective venous sampling for FGF23 levels.[1, 11] The octreotide tests capitalize on the fact that culprit tumors often express somatostatin receptors.
TIO is most often associated with mesenchymal tumors of the bone or soft tissue. It has also been reported in association with several malignancies (small cell carcinoma, hematologic malignancies, prostate cancer), and with polyostotic fibrous dysplasia, neurofibromatosis, and the epidermal nevus syndrome. The mesenchymal tumors are heterogeneous in appearance and can be variably classified as hemangiopericytomas, hemangiomas, sarcomas, ossifying fibromas, granulomas, giant cell tumors, or osteoblastomas.[1] However, 1 review suggests that most of these tumors actually represent a distinct but heterogeneous, under‐recognized entity that is best classified as a phosphaturic mesenchymal tumor.[11]
TIO is only cured by complete resection of the tumor.[1] Local recurrences have been described, as have rare occurrences of metastatic disease.[1, 12] Medical treatment can be used to normalize serum phosphate levels in patients who are unable to be cured by surgery. The goal is to bring serum phosphate into the low‐normal range via phosphate supplementation (typically 13 g/day of elemental phosphorus is required) and treatment with either calcitriol or alfacalcidol. Due to the inhibition of 1,25‐dihydroxyvitamin D activation in TIO, relatively large doses of calcitriol are needed. A reasonable starting dose of calcitriol is 1.5 g/day, and most patients require 15 to 60 ng/kg per day. Because PTH action is involved in FGF23‐mediated hypophosphatemia, suppression of PTH may also be useful in these patients.[13]
This patient presented with a painful femoral tumor in the setting of muscle and joint pain that had been erroneously attributed to connective tissue disease. However, recognition and thorough evaluation of the patient's hypophosphatemia led to a unifying diagnosis of TIO. This diagnosis altered the surgical approach (emphasizing complete resection to eradicate the FGF23 production) and helped alleviate the patient's painful losses of phosphate.
TEACHING POINTS
- Hypophosphatemia, especially if severe or persistent, should not be dismissed as an unimportant laboratory finding. A focused evaluation should be performed to determine the etiology.
- In patients with unexplained hypophosphatemia, the measurement of serum calcium, parathyroid hormone, and vitamin D levels can identify primary or secondary hyperparathyroidism.
- The differential diagnosis of hypophosphatemia is narrowed if there is clinical evidence of inappropriate urinary phosphate wasting (ie, urinary phosphate levels remain high, despite low serum levels).
- TIO is a rare paraneoplastic syndrome caused by FGF23, a phosphatonin hormone that causes renal phosphate wasting, hypophosphatemia, and osteomalacia.
Disclosure: Nothing to report.
A 58‐year‐old man presented to the emergency department with a 1‐month history of progressive, severe left hip pain that had become unbearable. The pain was constant and significantly worse with weight‐bearing, and the patient was now confined to bed. He denied back pain, falls, or trauma.
Although hip pain is a common complaint and a frequent manifestation of chronic degenerative joint disease, the debilitating and subacute nature of the pain suggests a potentially more serious underlying cause. Patients and even clinicians may refer to hip pain when the actual symptoms are periarticular, often presenting over the trochanter laterally, or muscular, presenting as posterior pain. The true hip joint is located in the anterior hip and groin area and often causes symptoms that radiate to the buttock. Pain can also be referred to the hip area from the spine, pelvis, or retroperitoneum, so it is crucial not to restrict the differential diagnosis to hip pathology.
Key diagnostic considerations include (1) inflammatory conditions such as trochanteric bursitis or gout; (2) bacterial infection of the hip joint, adjacent bone, or a nearby structure; (3) benign nerve compression (such as meralgia paresthetica); and (4) tumor (particularly myeloma or metastatic disease to the bone, but also potentially a pelvic or spinal mass with nerve compression). Polymyalgia rheumatica and other systemic rheumatologic complaints are a consideration, but because a single joint is involved, these conditions are less likely. The hip would be an unusual location for a first gout flare, and the duration of symptoms would be unusually long for gout. Avascular necrosis should be considered if the patient has received glucocorticoids for his previously diagnosed rheumatologic disease. If the patient is anticoagulated, consideration of spontaneous hematoma is reasonable, but usually this would present over a course of days, not weeks. The absence of trauma makes a fracture of the hip or pelvis less likely, and the insidious progression of symptoms makes a pathologic fracture less likely.
The patient reported 6 months of worsening proximal upper and lower extremity myalgia and weakness, with arthralgia of the hips and shoulders. The weakness was most notable in his proximal lower extremities, although he had remained ambulatory until the hip pain became limiting. He maintained normal use of his arms. The patient denied current rash but noted photosensitivity and a mild facial rash several months earlier. He described having transient mouth sores intermittently for several years. He denied fever, chills, night sweats, weight loss, dyspnea, recent travel, and outdoor exposures. Several months previously, he had been evaluated for these symptoms at another institution and given the diagnoses of rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE). At that time, he had initiated treatment with weekly dosing of methotrexate and etanercept.
The patient's medical history was also notable for hypertension, Graves' disease treated previously with radioiodine ablation, quiescent ulcerative colitis, and depression. Current medications included methotrexate, etanercept, levothyroxine, enalapril, hydrochlorothiazide, fluoxetine, ibuprofen, and oxycodone‐acetaminophen. He denied tobacco, alcohol, and recreational drug use.
Weakness occurring in the proximal lower extremities is the classic distribution for polymyositis and dermatomyositis. In contrast to polymyalgia rheumatica, dermatomyositis and polymyositis do not generally feature severe muscle pain, but they can be associated with a painful polyarthritis. Oral ulcers, photosensitivity, and facial rash are consistent with SLE, but dermatomyositis can also lead to a symmetrical erythema of the eyelids (commonly referred to as a heliotrope rash, named after the flower bearing that name) and sometimes can be associated with photosensitivity. Oral ulcers, particularly the painful ones known as canker sores, are extraordinarily common in the general population, and patients and providers may miss the mucosal lesions of SLE because they are usually painless. As methotrexate and etanercept are immunosuppressive, opportunistic pathogens such as typical or atypical mycobacteria and disseminated fungal infections should be considered, with special attention to the possibility of infection in or near the left hip. Given that SLE and RA rarely coexist, it would be helpful to seek outside medical records to know what the prior serologic evaluation entailed, but it is unlikely that this presentation is a manifestation of a diffuse connective tissue process.
Physical examination should focus on the features of dermatomyositis including heliotrope rash, truncal erythema, and papules over the knuckles (Gottron's papules); objective proximal muscle weakness in the shoulder and hip girdle; and findings that might suggest antisynthetase syndrome such as hyperkeratotic mechanic hand palmar and digital changes, and interstitial crackles on lung exam. If necrotic skin lesions are found, this would raise concern for a disseminated infection. The joints should be examined for inflammation and effusions.
His temperature was 36.6C, heart rate 74 beats per minute, blood pressure 134/76 mm Hg, respiratory rate 16 breaths per minute, and O2 saturation 97% on room air. He was obese but did not have moon facies or a buffalo hump. There were no rashes or mucosal lesions. Active and passive motion of his left hip joint elicited pain with both flexion/extension and internal/external rotation. Muscle strength was limited by pain in the left hip flexors and extenders, but was 5/5 in all other muscle groups. Palpation of the proximal muscles of his arms and legs did not elicit pain. His extremities were without edema, and examination of his shoulders, elbows, wrists, hands, knees, ankles, and feet did not reveal any erythema, synovial thickening, effusion, or deformity. Examination of the heart, chest, and abdomen was normal.
Given the reassuring strength examination, the absence of rashes or skin lesions, and the reassuring joint exam aside from the left hip, a focal infectious, inflammatory, or malignant process seems most likely. The pain with range of motion of the hip does not definitively localize the pathology to the hip joint, because pathology of the nearby structures can lead to pain when the hip is moved. Laboratory evaluation should include a complete blood count to screen for evidence of infection or marrow suppression, complete metabolic panel, and creatine kinase. The history of ulcerative colitis raises the possibility of an enthesitis (inflammation of tendons or ligaments) occurring near the hip. Enthesitis is sometimes a feature of the seronegative spondyloarthropathy‐associated conditions and can occur in the absence of sacroiliitis or spondyloarthropathy.
The patient's myalgias and arthralgias had recently been evaluated in the rheumatology clinic. Laboratory evaluation from that visit was remarkable only for an antinuclear antibody (ANA) test that was positive at a titer of 1:320 in a homogeneous pattern, creatine phosphokinase 366 IU/L (normal range [NR] 38240), and alkaline phosphatase 203 IU/L (NR 30130). All of the following labs from that visit were within normal ranges: cyclic citrullinated peptide, rheumatoid factor, antidouble stranded DNA, aldolase, complement levels, serum and urine protein electrophoresis, thyroglobulin antibody, thyroid microsomal antibody, thyroid‐stimulating hormone, erythrocyte sedimentation rate (10 mm/h), and C‐reactive protein (0.3 mg/dL).
The patient was admitted to the hospital. Initial blood test results on admission included sodium 139 mEq/L, potassium 3.9 mEq/L, chloride 105 mEq/L, bicarbonate 27 mEq/L, urea nitrogen 16 mg/dL, creatinine 0.6 mg/dL, glucose 85 mg/dL, calcium 9.2 mg/dL (NR 8.810.3), phosphate 1.3 mg/dL (NR 2.74.6), albumin 4.7 g/dL (NR 3.54.9), and alkaline phosphatase 195 IU/L (NR 30130). The remainder of a comprehensive metabolic profile, complete blood count with differential, and coagulation studies were all normal.
The homogeneous ANA titer of 1:320 is high enough to raise eyebrows, but is nonspecific for lupus and other ANA‐associated rheumatologic conditions, and may be a red herring, particularly given the low likelihood of a systemic inflammatory process explaining this new focal hip pain. The alkaline phosphatase is only mildly elevated and could be of bone or liver origin. The reassuringly low inflammatory markers are potentially helpful, because if checked now and substantially increased from the prior outpatient visit, they would be suggestive of a new inflammatory process. However, this would not point to a specific cause of inflammation.
Given the focality of the symptoms, imaging is warranted. As opposed to plain films, contrast‐enhanced computed tomography (CT) of the pelvis or magnetic resonance imaging (MRI) may be an efficient first step, because there is low suspicion for fracture and high suspicion for an inflammatory, neoplastic, or infectious process. MRI is more expensive and usually cannot be obtained as rapidly as CT. There is a chance that CT imaging alone will provide enough information to guide the next diagnostic steps, such as aspiration of an abscess or joint, or biopsy of a suspicious lesion. However, for soft tissue lesions and many bone lesions, including osteomyelitis, MRI offers better delineation of pathology.
CT scan of the left femur demonstrated a large lytic lesion in the femoral neck that contained macroscopic fat and had an aggressive appearance with significant thinning of the cortex. MRI confirmed these findings and demonstrated a nondisplaced subtrochanteric femur fracture in the proximity of the lesion (Figure 1). Contrast‐enhanced CT scans of the thorax, abdomen, and pelvis revealed no other neoplastic lesions. Prostate‐specific antigen level was normal. The patient's significant hypophosphatemia persisted, with levels dropping to as low as 0.9 mg/dL despite aggressive oral phosphate replacement.
Although hypophosphatemia is often a nonspecific finding in hospitalized patients and is usually of little clinical importance, profound hypophosphatemia that is refractory to supplementation suggests an underlying metabolic disorder. Phosphate levels less than 1.0 mg/dL, particularly if prolonged, can lead to decreased adenosine triphosphate production and subsequent weakness of respiratory and cardiac muscles. Parathyroid hormone (PTH) excess and production of parathyroid hormone‐related protein (PTHrP) by a malignancy can cause profound hypophosphatemia, but are generally associated with hypercalcemia, a finding not seen in this case. Occasionally, tumors can lead to renal phosphate wasting via nonPTH‐related mechanisms. The best characterized example of this is the paraneoplastic syndrome oncogenic osteomalacia caused by tumor production of a fibroblast growth factor. Tumors that lead to this syndrome are usually benign mesenchymal tumors. This patient's tumor may be of this type, causing local destruction and metabolic disturbance. The next step would be consultation with orthopedic surgery for resection of the tumor and total hip arthroplasty with aggressive perioperative repletion of phosphate. Assessment of intact PTH, ionized calcium, 24‐hour urinary phosphate excretion, and even PTHrP levels may help to rule out other etiologies of hypophosphatemia, but given that surgery is needed regardless, it might be reasonable to proceed to the operating room without these diagnostics. If the phosphate levels return to normal postoperatively, then the diagnosis is clear and no further metabolic testing is needed.
PTH level was 47 pg/mL (NR 1065), 25‐hydroxyvitamin D level was 25 ng/mL (NR 2580), and 1,25‐dihydroxyvitamin D level was 18 pg/mL (NR 1872). Urinalysis was normal without proteinuria or glucosuria. A 24‐hour urine collection contained 1936 mg of phosphate (NR 4001200). The ratio of maximum rate of renal tubular reabsorption of phosphate to glomerular filtration rate (TmP/GFR) was 1.3 mg/dL (NR 2.44.2). Tissue obtained by CT‐guided needle biopsy of the femoral mass was consistent with a benign spindle cell neoplasm.
With normal calcium levels, the PTH level is appropriate, and hyperparathyroidism is excluded. The levels of 25‐hydroxyvitamin D and 1‐25‐dihydroxyvitamin D are not low enough to suggest that vitamin D deficiency is driving the impressive hypophosphatemia. What is impressive is the phosphate wasting demonstrated by the 24‐hour urine collection, consistent with paraneoplastic overproduction of fibroblast growth factor 23 (FGF23) by the benign bone tumor. Overproduction of this protein can be detected by blood tests or staining of the tumor specimen, but surgery should be performed as soon as possible independent of any further test results. Once the tumor is resected, phosphate metabolism should normalize.
FGF23 level was 266 RU/mL (NR 180). The patient was diagnosed with tumor‐induced osteomalacia (TIO). He underwent complete resection of the femoral tumor as well as open reduction and internal fixation of the fracture. After surgery, his symptoms of pain and subjective muscle weakness improved, his serum phosphate level normalized, his need for phosphate supplementation resolved, and his blood levels of FGF23 decreased into the normal range (111 RU/mL). The rapid improvement of his symptoms after surgery suggested that they were related to TIO, and not manifestations of SLE or RA. His immunosuppressant medications were discontinued. Surgical pathology demonstrated a heterogeneous tumor consisting of sheets of uniform spindle cells interspersed with mature adipose tissue. This was diagnosed descriptively as a benign spindle cell and lipomatous neoplasm without further classification. Two months later, the patient was ambulating without pain, and muscle strength was subjectively normal.
DISCUSSION
TIO is a rare paraneoplastic syndrome affecting phosphate and vitamin D metabolism, leading to hypophosphatemia and osteomalacia.[1] TIO is caused by the inappropriate tumor secretion of the phosphatonin hormone, FGF23.
The normal physiology of FGF23 is illustrated in Figure 2. Osteocytes appear to be the primary source of FGF23, but the regulation of FGF23 production is not completely understood. FGF23 production may be influenced by several factors, including 1,25 dihydroxyvitamin D levels, and serum phosphate and PTH concentrations. This hormone binds to the FGF receptor and its coreceptor, Klotho,[2] causing 2 major physiological effects. First, it decreases the expression of the sodium‐phosphate cotransporters in the renal proximal tubular cells,[3, 4] resulting in increased tubular phosphate wasting. This effect appears to be partly PTH dependent.[5] Second, it has effects on vitamin D metabolism, decreasing renal production of activated vitamin D.[3, 4, 6]
In overproduction states, the elevated FGF23 leads to chronically low serum phosphate levels (with renal phosphate wasting) and the clinical syndrome of osteomalacia, manifested by bone pain, fractures, and deformities. Hypophosphatemia can also lead to painful proximal myopathy, cardiorespiratory dysfunction, and a spectrum of neuropsychiatric findings. The clinical findings in TIO are similar to those seen in genetic diseases in which hypophosphatemia results from the same mechanism.[3, 4]
In this case, measurement of the serum phosphate level was important in reaching the diagnosis. Although hypophosphatemia in the hospitalized patient is often easily explained, severe or persistent hypophosphatemia requires a focused evaluation. Causes of hypophosphatemia are categorized in Table 1.[7, 8, 9] In patients with hypophosphatemia that is not explained by the clinical situation (eg, osmotic diuresis, insulin treatment, refeeding syndrome, postparathyroidectomy, chronic diarrhea), measurement of serum calcium, PTH, and 25‐hydroxyvitamin D are used to investigate possible primary or secondary hyperparathyroidism. In addition, low‐normal or low serum 1,25‐dihydroxyvitamin D with normal PTH, normal 25‐hydroxyvitamin D stores, and normal renal function are clues to the presence of TIO. Urine phosphate wasting can be measured by collecting a 24‐hour urine sample. Calculation of the TmP/GFR (a measure of the maximum tubular resorption of phosphate relative to the glomerular filtration rate), as described by the nomogram of Walton and Bijvoet, may improve the accuracy of this assessment and confirm a renal source of the hypophosphatemia.[10]
|
| Internal redistribution |
| Insulin or catecholamine effect (including that related to refeeding syndrome, and infusion of glucose or TPN) |
| Acute respiratory alkalosis |
| Accelerated bone formation or rapid cell proliferation (eg, hungry bone syndrome, leukemic blast crisis, erythropoietin, or granulocyte colony stimulating factor administration) |
| Decreased absorption |
| Poor intake (including that seen in alcoholism*) |
| Vitamin D deficiency |
| Gastrointestinal losses (eg, chronic diarrhea) |
| Malabsorption (eg, phosphate‐binding antacids) |
| Urinary losses |
| Osmotic diuresis (eg, poorly controlled diabetes, acetazolamide) or volume expansion |
| Other diuretics: thiazides, indapamide |
| Hyperparathyroidism |
| Primary |
| Secondary (including vitamin D or calcium deficiency) |
| Parathyroid hormone‐related peptide |
| Renal tubular disease |
| Medications (eg, ethanol,* high‐dose glucocorticoids, cisplatin, bisphosphonates, estrogens, imatinib, acyclovir) |
| Fanconi syndrome |
| Medications inducing Fanconi syndrome: tenofovir, cidofovir, adefovir, aminoglycosides, ifosfamide, tetracyclines, valproic acid |
| Other (eg, postrenal transplant) |
| Excessive phosphatonin hormone activity (eg, hereditary syndromes [rickets], tumor‐induced osteomalacia) |
| Multifactorial causes |
| Alcoholism* |
| Acetaminophen toxicity |
| Parenteral iron administration |
The patient presented here had inappropriate urinary phosphate losses, and laboratory testing ruled out primary and secondary hyperparathyroidism and Fanconi syndrome. The patient was not taking medications known to cause tubular phosphate wasting. The patient's age and clinical history made hereditary syndromes unlikely. Therefore, the urinary phosphate wasting had to be related to an acquired defect in phosphate metabolism. The diagnostic characteristics of TIO are summarized in Table 2.
|
| Patients may present with symptoms of osteomalacia (eg, bone pain, fractures), hypophosphatemia (eg, proximal myopathy), and/or neoplasm. |
| Hypophosphatemia with urinary phosphate wasting. |
| Serum calcium level is usually normal. |
| Serum 1,25‐dihydroxyvitamin D level is usually low or low‐normal. |
| Parathyroid hormone is usually normal. |
| Plasma FGF23 level is elevated. |
| A neoplasm with the appropriate histology is identified, although the osteomalacia syndrome may precede identification of the tumor, which may be occult. |
| The syndrome resolves after complete resection of the tumor. |
The presence of a known neoplasm makes the diagnosis of TIO considerably easier. However, osteomalacia often precedes the tumor diagnosis. In these cases, the discovery of this clinical syndrome necessitates a search for the tumor. The tumors can be small, occult, and often located in the extremities. In addition to standard cross‐sectional imaging, specialized diagnostic modalities can be helpful in localizing culprit tumors. These include F‐18 flourodeoxyglucose positron emission tomography with computed tomography, 111‐Indium octreotide single photon emission CT/CT, 68‐Gallium‐DOTA‐octreotide positron emission tomography with computed tomography, and even selective venous sampling for FGF23 levels.[1, 11] The octreotide tests capitalize on the fact that culprit tumors often express somatostatin receptors.
TIO is most often associated with mesenchymal tumors of the bone or soft tissue. It has also been reported in association with several malignancies (small cell carcinoma, hematologic malignancies, prostate cancer), and with polyostotic fibrous dysplasia, neurofibromatosis, and the epidermal nevus syndrome. The mesenchymal tumors are heterogeneous in appearance and can be variably classified as hemangiopericytomas, hemangiomas, sarcomas, ossifying fibromas, granulomas, giant cell tumors, or osteoblastomas.[1] However, 1 review suggests that most of these tumors actually represent a distinct but heterogeneous, under‐recognized entity that is best classified as a phosphaturic mesenchymal tumor.[11]
TIO is only cured by complete resection of the tumor.[1] Local recurrences have been described, as have rare occurrences of metastatic disease.[1, 12] Medical treatment can be used to normalize serum phosphate levels in patients who are unable to be cured by surgery. The goal is to bring serum phosphate into the low‐normal range via phosphate supplementation (typically 13 g/day of elemental phosphorus is required) and treatment with either calcitriol or alfacalcidol. Due to the inhibition of 1,25‐dihydroxyvitamin D activation in TIO, relatively large doses of calcitriol are needed. A reasonable starting dose of calcitriol is 1.5 g/day, and most patients require 15 to 60 ng/kg per day. Because PTH action is involved in FGF23‐mediated hypophosphatemia, suppression of PTH may also be useful in these patients.[13]
This patient presented with a painful femoral tumor in the setting of muscle and joint pain that had been erroneously attributed to connective tissue disease. However, recognition and thorough evaluation of the patient's hypophosphatemia led to a unifying diagnosis of TIO. This diagnosis altered the surgical approach (emphasizing complete resection to eradicate the FGF23 production) and helped alleviate the patient's painful losses of phosphate.
TEACHING POINTS
- Hypophosphatemia, especially if severe or persistent, should not be dismissed as an unimportant laboratory finding. A focused evaluation should be performed to determine the etiology.
- In patients with unexplained hypophosphatemia, the measurement of serum calcium, parathyroid hormone, and vitamin D levels can identify primary or secondary hyperparathyroidism.
- The differential diagnosis of hypophosphatemia is narrowed if there is clinical evidence of inappropriate urinary phosphate wasting (ie, urinary phosphate levels remain high, despite low serum levels).
- TIO is a rare paraneoplastic syndrome caused by FGF23, a phosphatonin hormone that causes renal phosphate wasting, hypophosphatemia, and osteomalacia.
Disclosure: Nothing to report.
- , , , . Tumor‐induced osteomalacia. Endocr Relat Cancer. 2011;18:R53–R77.
- . The FGF23‐Klotho axis: endocrine regulation of phosphate homeostasis. Nat Rev Endocrinol. 2009;5:611–619.
- , . Genetic disorders of renal phosphate transport. N Engl J Med. 2010;362:2399–2409.
- . The expanding family of hypophosphatemic syndromes. J Bone Miner Metab. 2012;30:1–9.
- , , , , . FGF‐23 is elevated by chronic hyperphosphatemia. J Clin Endocrinol Metab. 2004;89:4489–4492.
- , , , et al. FGF‐23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004;19:429–435.
- , . Hypophosphatemia: an update on its etiology and treatment. Am J Med. 2005;118:1094–1101.
- , , . In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, eds. Williams Textbook of Endocrinology. 12th ed. Philadelphia, PA: Elsevier; 2011:1237–1304.
- , , . Medication‐induced hypophosphatemia: a review. QJM. 2010;103:449–459.
- , . Nomogram for derivation of renal threshold phosphate concentration. Lancet. 1975;2:309–310.
- , , , et al. Improving diagnosis of tumor‐induced osteomalacia with gallium‐68 DOTATATE PET/CT. J Clin Endocrinol Metab. 2013; 98:687–694.
- , , , et al. Most osteomalacia‐associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28:1–30.
- , , , , , . Cinacalcet in the management of tumor‐induced osteomalacia. J Bone Miner Res. 2007;22:931–937.
- , , , . Tumor‐induced osteomalacia. Endocr Relat Cancer. 2011;18:R53–R77.
- . The FGF23‐Klotho axis: endocrine regulation of phosphate homeostasis. Nat Rev Endocrinol. 2009;5:611–619.
- , . Genetic disorders of renal phosphate transport. N Engl J Med. 2010;362:2399–2409.
- . The expanding family of hypophosphatemic syndromes. J Bone Miner Metab. 2012;30:1–9.
- , , , , . FGF‐23 is elevated by chronic hyperphosphatemia. J Clin Endocrinol Metab. 2004;89:4489–4492.
- , , , et al. FGF‐23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004;19:429–435.
- , . Hypophosphatemia: an update on its etiology and treatment. Am J Med. 2005;118:1094–1101.
- , , . In: Melmed S, Polonsky KS, Larsen PR, Kronenberg HM, eds. Williams Textbook of Endocrinology. 12th ed. Philadelphia, PA: Elsevier; 2011:1237–1304.
- , , . Medication‐induced hypophosphatemia: a review. QJM. 2010;103:449–459.
- , . Nomogram for derivation of renal threshold phosphate concentration. Lancet. 1975;2:309–310.
- , , , et al. Improving diagnosis of tumor‐induced osteomalacia with gallium‐68 DOTATATE PET/CT. J Clin Endocrinol Metab. 2013; 98:687–694.
- , , , et al. Most osteomalacia‐associated mesenchymal tumors are a single histopathologic entity: an analysis of 32 cases and a comprehensive review of the literature. Am J Surg Pathol. 2004;28:1–30.
- , , , , , . Cinacalcet in the management of tumor‐induced osteomalacia. J Bone Miner Res. 2007;22:931–937.
Hospice Care Insurance and Readmissions
Palliative care and hospice specialists consult on a variety of patients in the acute care setting that span all diagnoses and specialties. These include patients in the intensive care units, oncology units, as well as patients with end‐stage pulmonary, cardiac, and renal diseases. Discharge of these patients is often complicated by social issues, intensive personal care needs, and decreased functional status, as well as by the patient's insurance. Options for discharge disposition for patients accepting enrollment in hospice are often limited by financial constraints. Medicare pays for a set package of hospice benefits that do not include payment for room and board for hospice residential care and have a limited number of hours for a personal care attendant.[1] Hospice inpatient units are typically covered only for patients with acute care needs. Patients with secondary commercial insurance similarly find that custodial care benefits are often lacking, as most private and managed care plans mimic the Medicare hospice benefit.[2]
Palliative care inpatient consultation and palliative or hospice home care are associated with decreased 30‐day readmission rates.[3, 4, 5, 6] None of these studies, however, evaluated the effect of insurance status on readmission rates. Patients with dual coverage of Medicare and Medicaid are eligible for coverage of room and board (covered by Medicaid) in addition to the standard hospice benefit (covered by Medicare), and therefore have more options for discharge planning, including admission to a hospice residence, nursing home care with hospice services, or increased personal care attendant hours at home. Dual eligible patients (those with both Medicare and Medicaid) represent 20% of the Medicare population. They are generally poorer and with worse health status that those with Medicare alone; they have on average 25% more medical conditions than Medicare‐only patients.[7] Previous studies of readmissions and healthcare costs in the general population have found that dual eligible patients have higher rates of readmissions and higher overall healthcare costs compared with other groups.[7, 8, 9] However, these studies did not specifically look at patients near the end of life receiving hospice services. We hypothesize that dual eligible patients may actually have a lower rate of readmission at end of life compared with other groups, and that this effect may be partially mediated by discharge location (facility or home).
Previous studies have identified risk factors for 30‐day readmission to hospital, including living alone, insurance status, and poor or fair satisfaction with their primary care provider (PCP).[10] This study aims to evaluate, in the cohort of patients who have received a palliative care consultation during their hospital stay and who were discharged with hospice services, whether type of insurance is associated with risk of early readmission.
METHODS
Data were extracted from a replicate of Montefiore's Clinical Information System using healthcare surveillance software (Clinical Looking Glass; Emerging Health Information Technology, Yonkers, NY). We queried this database to find patients who received palliative care consultation from August 2010 to January 2014 at Montefiore Medical Center, an academic medical center in Bronx, NY, consisting of 3 general hospitals with 1491 beds. The medical center provides care to many underserved and minority patients and serves as the University Hospital of the Albert Einstein College of Medicine.
Inclusion Criteria
Patients who received a palliative care consultation were included if they were 65 years of age, nonpregnant, and admitted to the medical intensive care unit, any surgical intensive care unit, cardiac care unit, general medicine, surgery or surgical subspecialty service, family medicine, cardiology or oncology service, and discharged with hospice services.
Exclusion Criteria
Patients 65 years old and patients who died during the index admission were excluded, as were admissions to pediatrics, obstetrics, and psychology services, and uninsured patients.
The admission with the first palliative care consultation resulting in hospice referral was considered the index admission for these patients. Sociodemographic variables related to readmission such as age, race, gender, primary language, and socioeconomic status (SES) were examined.[11, 12, 13, 14, 15, 16] Clinical variables shown to be related to 30‐day readmissions in the literature including lab‐based acute physiology score (LAPS), blood urea nitrogen level (BUN), serum sodium level, serum albumin level, documentation of weight loss, and Charlson Comorbidity Index as well as its specific components were also extracted.[11, 13, 16, 17, 18, 19] Other variables related to the index admission such as length of stay for index admission, admission source on index admission (eg, from home, nursing home, other), and whether the primary care physician was listed in the chart were also examined.[11, 13, 16, 17, 19, 20] All of the variables were examined because they were hypothesized to be related to both insurance status and readmission. Markers of clinical severity, such as LAPS, BUN, hyponatremia, hypoalbuminemia, weight loss, and comorbidity could lead to readmission for symptom management or acute deterioration, and have been found be related to readmission in previous literature.
The predictor variable was insurance status at the time of index admission (dual eligible or all other). The main outcome variable was readmission to Montefiore Medical Center for any reason within 30 days of the index admission. Discharge location (hospice services in a facility vs home hospice) was examined as a potential mediator.
Statistical Analysis
Based on quality metrics available from our department, we expected to find at least 1000 patients 65 years of age seen by the palliative care consultation service with a discharge disposition including hospice services. This would give our study 85% power to detect a 10% difference in readmission rates between the 2 groups.
Patients were categorized as dual eligible if they were covered by Medicare and Medicaid only or if they were covered by Medicare, Medicaid, and private insurance. Controls were patients who were covered by Medicare only, Medicaid only, private insurance only, or Medicare and private insurance or Medicaid and private insurance. For the primary analysis, patients with and without dual eligibility were compared with respect to sociodemographic characteristics, healthcare process variables, and measures of comorbidity and illness severity using t tests for continuous variables and 2 tests for categorical variables. We used a 2 test to assess the univariable association between dual eligibility and 30‐day readmission. To address the question as to whether dual eligibility reduces the likelihood of a 30 day readmission, logistic regression was used to model 30‐day readmission by selecting from the covariates associated with the 30‐day readmissions at the 0.15 significance level. The Hosmer‐Lemeshow goodness of fit test was used to evaluate overall model performance.
For the secondary analysis, we assessed whether type and location of hospice services mediate the effect of insurance status on 30‐day readmissions using a Sobel‐Goodman test for mediation. Statistical analysis was conducted using statistical software (Stata statistical software, release 12; StataCorp, College Station, TX).
This research protocol was reviewed by the Montefiore Medical Center/Albert Einstein College of Medicine Institutional Review Board.
RESULTS
A total of 2755 inpatients were seen by the palliative care consultation service across the Montefiore Medical Center sites and discharged with hospice services. Of those, 1688 were dual eligible for Medicare and Medicaid, and 1067 were not. Specifically, 695 patients had Medicare only, 148 had private insurance only, 126 had Medicaid only, 78 had Medicare and private insurance, and 19 had Medicaid and private insurance. Univariable relationships between patient characteristics, insurance status, and readmission are shown in Table 1.
| Characteristic | Dual Eligible, N = 1,688 |
Not Dual Eligible, N = 1,067 |
P Value | 30‐Day Readmission | P Value | |
|---|---|---|---|---|---|---|
| Yes, N = 296 | No, N = 2,459 | |||||
| ||||||
| Sociodemographic | ||||||
| Age, y, mean SD | 81.6 9.0 | 79.4 8.9 | 0.05 | 77.8 8.8 | 81.1 9.0 | 0.05 |
| Female, n (%) | 1,092 (64.7) | 622 (58.3) | 0.05 | 171 (57.8) | 1,543 (62.7) | 0.095 |
| Has PCP, n (%) | 1,451 (86.0) | 951 (89.1) | 0.05 | 263 (88.9) | 2,139 (87.0) | NS |
| Speaks English, n (%) | 1,064 (63.0) | 728 (68.2) | 0.05 | 181 (61.1) | 1,611 (65.5) | 0.137 |
| SES, mean SD | 2.76 2.81 | 2.51 2.67 | 0.05 | 3.11 2.72 | 2.61 2.77 | 0.05 |
| Race/ethnicity | 0.05 | 0.05 | ||||
| Hispanic, n (%) | 587 (34.8) | 267 (31.3) | 100 (33.8) | 754 (30.7) | ||
| White, n (%) | 532 (31.5) | 290 (27.2) | 58 (19.6) | 764 (31.1) | ||
| Black, n (%) | 449 (26.6) | 420 (39.4) | 121 (40.9) | 748 (30.4) | ||
| Comorbidities, n (%) | ||||||
| Congestive heart failure | 555 (32.9) | 264 (24.7) | 0.05 | 104 (35.1) | 751 (30.5) | 0.106 |
| Cardiac valvular disease | 179 (10.6) | 76 (7.1) | 0.05 | 19 (6.4) | 227 (9.2) | 0.109 |
| Myocardial infarction | 165 (9.8) | 85 (8.0) | 0.11 | 31 (10.5) | 219 (8.9) | NS |
| Pulmonary disease | 480 (28.4) | 292 (27.4) | NS | 98 (33.1) | 674 (27.4) | 0.039 |
| Liver disease | 60 (3.6) | 54 (5.1) | 0.053 | 22 (7.4) | 92 (3.7) | 0.05 |
| Dementia | 135 (8.0) | 52 (4.9) | 0.05 | 11 (3.7) | 176 (7.2) | 0.026 |
| Diabetes, complicated | 125 (7.4) | 52 (4.9) | 0.05 | 15 (5.1) | 163 (6.6) | NS |
| Malignancy | 589 (34.9) | 499 (46.8) | 0.05 | 124 (41.9) | 921 (37.5) | 0.137 |
| Renal disease | 394 (23.3) | 225 (21.1) | NS | 72 (24.3) | 547 (22.2) | NS |
| Depression | 174 (10.3) | 85 (8.0) | 0.05 | 25 (8.4) | 234 (9.5) | NS |
| Peripheral vascular disease | 166 (9.8) | 72 (6.7) | 0.05 | 16 (5.4) | 222 (9.0) | 0.036 |
| Cerebrovascular disease | 282 (16.7) | 125 (11.7) | 0.05 | 33 (11.1) | 374 (15.2) | 0.063 |
| Clinical characteristics | ||||||
| LOS, mean SD | 10.9 9.93 | 10.6 9.61 | 0.19 | 9.3 8.0 | 10.9 10.0 | 0.05 |
| LAPS, mean SD | 38.4 27.9 | 34.6 26.9 | 0.05 | 33.8 25.2 | 37.3 27.8 | 0.039 |
| BUN, mean SD | 34.4 32.3 | 30.9 28.3 | 0.05 | 29.5 24.4 | 33.4 31.6 | 0.036 |
| Charlson score, mean SD | 4.62 3.37 | 5.28 3.56 | 0.05 | 5.1 3.5 | 4.8 3.5 | 0.152 |
In this sample, 9.2% of patients in the dual eligible group were readmitted within 30 days compared with 13.1% of others (2 = 10.3, P = 0.001). Of the total cohort, 1500 patients, including 862 dual eligible patients, were discharged to a facility, and 1255 patients, including 826 dual eligible patients, were discharged home. Dual eligible patients had a lower readmission rate compared with others in both settings (Figure 1). In univariable analysis, gender, age, hospital length of stay, race/ethnicity, SES, English as a primary language, LAPS, BUN, Charlson score, and comorbid peripheral vascular disease, cerebrovascular disease, heart disease, dementia, cancer, and liver disease were found to be related both to the predictor and the outcome variables and were included in the logistic regression model. While controlling for these variables, dual eligible patients had a lower odds of readmission within 30 days compared with others (odds ratio [OR]: 0.77; P = 0.041; 95% confidence interval [CI]: 0.59‐0.98) (Table 2). The Hosmer‐Lemeshow test was not significant, indicating that the overall model fit was good.
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.77 | 0.10 | 2.05 | 0.041 |
| Gender | 1.16 | 0.15 | 1.17 | 0.244 |
| Age | 0.96 | 0.01 | 4.54 | 0.000 |
| Hospital length of stay | 0.97 | 0.01 | 3.33 | 0.001 |
| Black | 1.93 | 0.53 | 2.37 | 0.018 |
| White | 1.02 | 0.30 | 0.08 | 0.939 |
| Hispanic | 1.29 | 0.37 | 0.90 | 0.368 |
| Socioeconomic status | 0.96 | 0.02 | 1.63 | 0.103 |
| Primary language English | 0.81 | 0.12 | 1.43 | 0.154 |
| Peripheral vascular disease | 0.67 | 0.18 | 1.48 | 0.139 |
| Cerebrovascular disease | 0.86 | 0.17 | 0.73 | 0.465 |
| Dementia | 0.61 | 0.20 | 1.50 | 0.135 |
| Congestive heart failure | 1.75 | 0.26 | 3.83 | 0.000 |
| Cardiac valvular disease | 0.73 | 0.19 | 1.23 | 0.219 |
| Cancer | 0.92 | 0.15 | 0.51 | 0.608 |
| Liver disease | 1.80 | 0.47 | 2.25 | 0.024 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.66 | 0.510 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.29 | 0.197 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.57 | 0.567 |
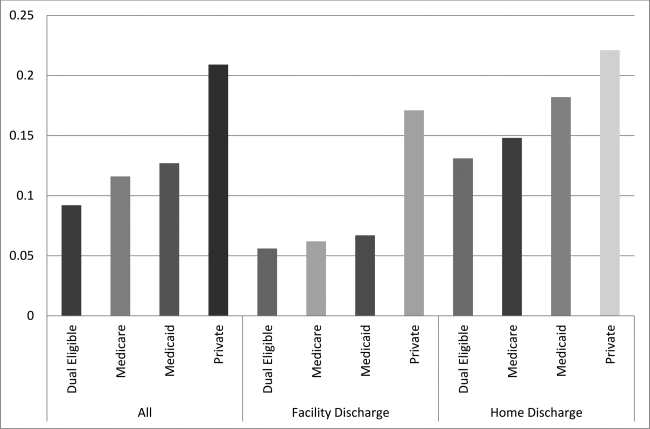
In the secondary analysis, we found that disposition (hospice services in a nursing home or hospice residence vs home hospice) partially mediates the relationship between insurance status and readmission, explaining 30% of the total effect (z = 5.06, P 0.001). When accounting for disposition as a mediator, dual eligible patients still had a lower odds of readmission within 30 days compared with others, although the difference was no longer statistically significant (OR: 0.86; P = 0.24; 95% CI: 0.66‐ 1.11). Patients discharged with hospice services in a nursing home or hospice residence were less likely to be readmitted within 30 days (OR: 0.41; P 0.001; 95% CI: 0.31‐0.54) (Table 3).
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.86 | 0.11 | 1.17 | 0.244 |
| Discharge location | 0.40 | 0.59 | 6.22 | 0.000 |
| Gender | 1.17 | 0.16 | 1.22 | 0.223 |
| Age | 0.96 | 0.01 | 4.69 | 0.000 |
| Hospital length of stay | 0.98 | 0.01 | 2.57 | 0.010 |
| Black | 1.95 | 0.54 | 2.39 | 0.017 |
| White | 1.02 | 0.30 | 0.10 | 0.924 |
| Hispanic | 1.20 | 0.35 | 0.63 | 0.526 |
| Socioeconomic status | 0.96 | 0.02 | 1.51 | 0.132 |
| Primary language English | 0.78 | 0.11 | 1.69 | 0.090 |
| Peripheral vascular disease | 0.70 | 0.19 | 1.31 | 0.190 |
| Cerebrovascular disease | 0.89 | 0.18 | 0.56 | 0.579 |
| Dementia | 0.64 | 0.21 | 1.36 | 0.174 |
| Congestive heart failure | 1.75 | 0.26 | 3.80 | 0.000 |
| Cardiac valvular disease | 0.70 | 0.18 | 1.35 | 0.176 |
| Cancer | 0.91 | 0.15 | 0.59 | 0.552 |
| Liver disease | 1.75 | 0.46 | 2.12 | 0.034 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.20 | 0.843 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.10 | 0.270 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.65 | 0.516 |
DISCUSSION
This study showed an association between dual coverage and lower odds of 30‐day readmission for patients discharged to hospice compared to all other insurance categories, excluding uninsured. This is the first study to date looking specifically at the association between insurance and readmission rates of patients discharged with hospice services. This association was attenuated, and no longer statistically significant, when accounting for discharge location.
These findings suggest that the added services available to patients enrolled in Medicare and Medicaid likely provide an enhanced level of postacute care. Patients with Medicaid have access to increased hours of personal care attendants as well as residential care, which often provides 24‐hour trained staff for rapid assessment of a change in clinical status and adjustment to therapeutic management. Combined with the Medicare hospice benefit, which provides better attention to symptom management, better supervision, and improved compliance with medications, as well as education of family and caregivers,[21, 22, 23] additional coverage with Medicaid is associated with a decrease in early readmission to the hospital.
It is often a financial hardship for family members or caregivers to take time off work to care for a dying patient. Without adequate postdischarge resources, the hospital to home transition will be ineffective, which has been shown to increase readmissions.[24] The option of increased attendant hours or residential care can have a positive impact on the financial and psychosocial stressors of caring for a family member at the end of life. Although we did not assess for this in our study, caregiver burnout often plays a role in emergency room visits and admissions of patients at the end of life.[25] The average age of the patients in our cohorts was 81 and 79 years; primary caregivers are often elderly with multiple medical conditions themselves and often struggle to provide the patient's care.[26, 27]
The main limitation of this study is that it is a retrospective observational study rather than a prospective randomized controlled trial. Many patients become dual eligible after requiring institutional custodial care, making the relationship between insurance status, discharge location, and readmissions complex and the causal relationship bidirectional. Patients discharged to hospice residence or to a nursing home with hospice services, who are more often dual eligible patients, are likely to receive more timely management of medical crises or changes in medical status, thus preventing readmission, whereas patients who receive home hospice with family providing the bulk of care may have a lower threshold for emergency room visits, possibly leading to greater incidence of readmission. Therefore, our results may be more a reflection of where the care is provided than what insurance the patient has. However, dual eligible patients discharged home also had a lower readmission rate compared with others, suggesting that insurance status has an independent association with readmission.
Unmeasured variables may explain the relationship between dual eligibility and 30‐day readmission rates. Some variables that we were not able to reliably measure in this study include functional status, number of hospitalizations in last year, patient educational level, patient self‐reported health status, quality of life, cognitive functioning, hearing or vision impairment, income, employment status, number of people in the home, and caregiver availability.[11, 12, 13, 19] However, omitting these variables from this study is more likely to bias our results toward the null, because these variables are likely related to dual eligibility and a higher, rather than lower, rate of readmission. We also did not measure whether participating decision makers were involved in the hospice admission or whether patients and families contacted their PCPs after discharge, variables found to be important in a previous pilot study.[5]
The generalizability of the results may be affected by the relative generosity of the New York State Medicaid benefits compared to many other states. New York State ranks third in the nation for eligibility and first for scope of services, including increased access to home‐ and community‐based services.[28] In addition, this study was a single‐center study in an urban, socioeconomically disadvantaged environment, explaining the higher rate of readmission compared to hospice patients nationally,[29] which is similar to other urban, academic medical centers.[5] For patients in our practice setting, the financial burden of paying privately for home care or residential custodial services is often prohibitive, which may not be the case in other settings.
Further research to identify whether discharge with hospice services mediates the relationship between insurance status and readmission could help confirm these findings. In addition, the relationship between caregiver burden and quality of life, and increased healthcare costs at the end of life should be explored. Overwhelming evidence suggests that being socioeconomically disadvantaged is a significant risk factor for early readmission, and enrolling these patients in Medicaid may modify this risk.[10, 30] Further research should explore whether policies that expand access to Medicaid or otherwise increase access to custodial care services can decrease burdensome hospital readmissions near the end of life.
Acknowledgements
The authors thank Galina Umanski for her technical support of this work.
Disclosure: This work was presented as a Power Point presentation on June 5, 2015 at the New York City Fellows' Palliative Care Research Day. The authors report no conflicts of interest.
- , . Hospice: comprehensive care at the end of life. Anest Clin N Am. 2006;24:181–204.
- . U.S. hospice benefits. J Pain Symptom Manage. 2009;38:105–109.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15:48–51.
- , , , . A hospice‐hospital partnership: reducing hospitalization costs and 30‐day readmissions among seriously ill adults. J Palliat Med. 2014;17:1005–1010.
- , , , , , . Rehospitalization of older adults discharged to home hospice care. J Palliat Med. 2014;17:841–844.
- , , , . Can palliative home care reduce 30‐day readmissions? Results of a propensity score matched cohort study. J Palliat Med. 2013;16:1290–1293.
- , , , , , . The Medicare Hospital Readmissions Reduction Program: potential unintended consequences for hospitals serving vulnerable populations. Health Serv Res. 2014;49:818–837.
- , , , . Understanding why patients with COPD get readmitted: a large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147:1219–1226.
- , , . Variations in 30‐day hospital readmission rates across primary care clinics within a tertiary referral center. J Hosp Med. 2014;9:688–694.
- , , , . Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62:489–494.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360:1418–1428.
- , , , , . Risk factors for 30‐day hospital readmission in patients >/=65 years of age. Proc (Bayl Univ Med Cent). 2008;21:363–372.
- , , , . Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6:54–60.
- , , , . Racial/ethnic disparities in potentially preventable readmissions: the case of diabetes. Am J Public Health. 2005;95:1561–1567.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681.
- , , , et al. Factors associated with 30‐day readmission rates after percutaneous coronary intervention. Arch Intern Med. 2012;172:112–117.
- , , , . Risk factors for 30‐day readmission in general medical patients admitted from the emergency department: a single centre study. Intern Med J. 2012;42:677–682.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688–1698.
- , , , , , . Thirty‐day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157:11–18.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25:211–219.
- , , , , , . An examination of adherence to pain medication plans in older cancer patients in hospice care. J Pain Symptom Manage. 2013;45:43–55.
- , , , et al. Hospice providers' key approaches to support informal caregivers in managing medications for patients in private residences. J Pain Symptom Manage. 2012;43:1060–1071.
- , . Hospice approach to palliative care, including Medicare hospice benefit. In: Yennurajalingam S, Bruera E, eds. Oxford American Handbook of Hospice and Palliative Medicine. New York, NY: Oxford University Press; 2011:229–239.
- , , . Predictors of thirty‐day readmission among hospitalized family medicine patients. J Am Board Fam Med. 2013;26:71–77.
- , , , , , . Emergency calls and need for emergency care in pateints looked after by a palliative care team: Retrospective interview study with bereaved relatives. BMC Palliat Care. 2008;7:11.
- , , , et al. Predictors of caregiver burden across the home‐based palliative care trajectory in Ontario, Canada [published online March 25, 2105]. Health Soc Care Community. doi: 10.1111/hsc.12219.
- , , , . Unique characteristics of informal hospice cancer caregiving. Support Care Cancer. 2015;23:2121–2128.
- , . Unsettling Scores: A Ranking of State Medicaid Programs. Washington, DC: Public Citizen Press; 2007.
- , , . 30‐day readmissions among seriously ill older adults. J Palliat Med. 2012;15:1–6.
- , . A path forward on Medicare readmissions. N Engl J Med. 2013;368:1175–1177.
Palliative care and hospice specialists consult on a variety of patients in the acute care setting that span all diagnoses and specialties. These include patients in the intensive care units, oncology units, as well as patients with end‐stage pulmonary, cardiac, and renal diseases. Discharge of these patients is often complicated by social issues, intensive personal care needs, and decreased functional status, as well as by the patient's insurance. Options for discharge disposition for patients accepting enrollment in hospice are often limited by financial constraints. Medicare pays for a set package of hospice benefits that do not include payment for room and board for hospice residential care and have a limited number of hours for a personal care attendant.[1] Hospice inpatient units are typically covered only for patients with acute care needs. Patients with secondary commercial insurance similarly find that custodial care benefits are often lacking, as most private and managed care plans mimic the Medicare hospice benefit.[2]
Palliative care inpatient consultation and palliative or hospice home care are associated with decreased 30‐day readmission rates.[3, 4, 5, 6] None of these studies, however, evaluated the effect of insurance status on readmission rates. Patients with dual coverage of Medicare and Medicaid are eligible for coverage of room and board (covered by Medicaid) in addition to the standard hospice benefit (covered by Medicare), and therefore have more options for discharge planning, including admission to a hospice residence, nursing home care with hospice services, or increased personal care attendant hours at home. Dual eligible patients (those with both Medicare and Medicaid) represent 20% of the Medicare population. They are generally poorer and with worse health status that those with Medicare alone; they have on average 25% more medical conditions than Medicare‐only patients.[7] Previous studies of readmissions and healthcare costs in the general population have found that dual eligible patients have higher rates of readmissions and higher overall healthcare costs compared with other groups.[7, 8, 9] However, these studies did not specifically look at patients near the end of life receiving hospice services. We hypothesize that dual eligible patients may actually have a lower rate of readmission at end of life compared with other groups, and that this effect may be partially mediated by discharge location (facility or home).
Previous studies have identified risk factors for 30‐day readmission to hospital, including living alone, insurance status, and poor or fair satisfaction with their primary care provider (PCP).[10] This study aims to evaluate, in the cohort of patients who have received a palliative care consultation during their hospital stay and who were discharged with hospice services, whether type of insurance is associated with risk of early readmission.
METHODS
Data were extracted from a replicate of Montefiore's Clinical Information System using healthcare surveillance software (Clinical Looking Glass; Emerging Health Information Technology, Yonkers, NY). We queried this database to find patients who received palliative care consultation from August 2010 to January 2014 at Montefiore Medical Center, an academic medical center in Bronx, NY, consisting of 3 general hospitals with 1491 beds. The medical center provides care to many underserved and minority patients and serves as the University Hospital of the Albert Einstein College of Medicine.
Inclusion Criteria
Patients who received a palliative care consultation were included if they were 65 years of age, nonpregnant, and admitted to the medical intensive care unit, any surgical intensive care unit, cardiac care unit, general medicine, surgery or surgical subspecialty service, family medicine, cardiology or oncology service, and discharged with hospice services.
Exclusion Criteria
Patients 65 years old and patients who died during the index admission were excluded, as were admissions to pediatrics, obstetrics, and psychology services, and uninsured patients.
The admission with the first palliative care consultation resulting in hospice referral was considered the index admission for these patients. Sociodemographic variables related to readmission such as age, race, gender, primary language, and socioeconomic status (SES) were examined.[11, 12, 13, 14, 15, 16] Clinical variables shown to be related to 30‐day readmissions in the literature including lab‐based acute physiology score (LAPS), blood urea nitrogen level (BUN), serum sodium level, serum albumin level, documentation of weight loss, and Charlson Comorbidity Index as well as its specific components were also extracted.[11, 13, 16, 17, 18, 19] Other variables related to the index admission such as length of stay for index admission, admission source on index admission (eg, from home, nursing home, other), and whether the primary care physician was listed in the chart were also examined.[11, 13, 16, 17, 19, 20] All of the variables were examined because they were hypothesized to be related to both insurance status and readmission. Markers of clinical severity, such as LAPS, BUN, hyponatremia, hypoalbuminemia, weight loss, and comorbidity could lead to readmission for symptom management or acute deterioration, and have been found be related to readmission in previous literature.
The predictor variable was insurance status at the time of index admission (dual eligible or all other). The main outcome variable was readmission to Montefiore Medical Center for any reason within 30 days of the index admission. Discharge location (hospice services in a facility vs home hospice) was examined as a potential mediator.
Statistical Analysis
Based on quality metrics available from our department, we expected to find at least 1000 patients 65 years of age seen by the palliative care consultation service with a discharge disposition including hospice services. This would give our study 85% power to detect a 10% difference in readmission rates between the 2 groups.
Patients were categorized as dual eligible if they were covered by Medicare and Medicaid only or if they were covered by Medicare, Medicaid, and private insurance. Controls were patients who were covered by Medicare only, Medicaid only, private insurance only, or Medicare and private insurance or Medicaid and private insurance. For the primary analysis, patients with and without dual eligibility were compared with respect to sociodemographic characteristics, healthcare process variables, and measures of comorbidity and illness severity using t tests for continuous variables and 2 tests for categorical variables. We used a 2 test to assess the univariable association between dual eligibility and 30‐day readmission. To address the question as to whether dual eligibility reduces the likelihood of a 30 day readmission, logistic regression was used to model 30‐day readmission by selecting from the covariates associated with the 30‐day readmissions at the 0.15 significance level. The Hosmer‐Lemeshow goodness of fit test was used to evaluate overall model performance.
For the secondary analysis, we assessed whether type and location of hospice services mediate the effect of insurance status on 30‐day readmissions using a Sobel‐Goodman test for mediation. Statistical analysis was conducted using statistical software (Stata statistical software, release 12; StataCorp, College Station, TX).
This research protocol was reviewed by the Montefiore Medical Center/Albert Einstein College of Medicine Institutional Review Board.
RESULTS
A total of 2755 inpatients were seen by the palliative care consultation service across the Montefiore Medical Center sites and discharged with hospice services. Of those, 1688 were dual eligible for Medicare and Medicaid, and 1067 were not. Specifically, 695 patients had Medicare only, 148 had private insurance only, 126 had Medicaid only, 78 had Medicare and private insurance, and 19 had Medicaid and private insurance. Univariable relationships between patient characteristics, insurance status, and readmission are shown in Table 1.
| Characteristic | Dual Eligible, N = 1,688 |
Not Dual Eligible, N = 1,067 |
P Value | 30‐Day Readmission | P Value | |
|---|---|---|---|---|---|---|
| Yes, N = 296 | No, N = 2,459 | |||||
| ||||||
| Sociodemographic | ||||||
| Age, y, mean SD | 81.6 9.0 | 79.4 8.9 | 0.05 | 77.8 8.8 | 81.1 9.0 | 0.05 |
| Female, n (%) | 1,092 (64.7) | 622 (58.3) | 0.05 | 171 (57.8) | 1,543 (62.7) | 0.095 |
| Has PCP, n (%) | 1,451 (86.0) | 951 (89.1) | 0.05 | 263 (88.9) | 2,139 (87.0) | NS |
| Speaks English, n (%) | 1,064 (63.0) | 728 (68.2) | 0.05 | 181 (61.1) | 1,611 (65.5) | 0.137 |
| SES, mean SD | 2.76 2.81 | 2.51 2.67 | 0.05 | 3.11 2.72 | 2.61 2.77 | 0.05 |
| Race/ethnicity | 0.05 | 0.05 | ||||
| Hispanic, n (%) | 587 (34.8) | 267 (31.3) | 100 (33.8) | 754 (30.7) | ||
| White, n (%) | 532 (31.5) | 290 (27.2) | 58 (19.6) | 764 (31.1) | ||
| Black, n (%) | 449 (26.6) | 420 (39.4) | 121 (40.9) | 748 (30.4) | ||
| Comorbidities, n (%) | ||||||
| Congestive heart failure | 555 (32.9) | 264 (24.7) | 0.05 | 104 (35.1) | 751 (30.5) | 0.106 |
| Cardiac valvular disease | 179 (10.6) | 76 (7.1) | 0.05 | 19 (6.4) | 227 (9.2) | 0.109 |
| Myocardial infarction | 165 (9.8) | 85 (8.0) | 0.11 | 31 (10.5) | 219 (8.9) | NS |
| Pulmonary disease | 480 (28.4) | 292 (27.4) | NS | 98 (33.1) | 674 (27.4) | 0.039 |
| Liver disease | 60 (3.6) | 54 (5.1) | 0.053 | 22 (7.4) | 92 (3.7) | 0.05 |
| Dementia | 135 (8.0) | 52 (4.9) | 0.05 | 11 (3.7) | 176 (7.2) | 0.026 |
| Diabetes, complicated | 125 (7.4) | 52 (4.9) | 0.05 | 15 (5.1) | 163 (6.6) | NS |
| Malignancy | 589 (34.9) | 499 (46.8) | 0.05 | 124 (41.9) | 921 (37.5) | 0.137 |
| Renal disease | 394 (23.3) | 225 (21.1) | NS | 72 (24.3) | 547 (22.2) | NS |
| Depression | 174 (10.3) | 85 (8.0) | 0.05 | 25 (8.4) | 234 (9.5) | NS |
| Peripheral vascular disease | 166 (9.8) | 72 (6.7) | 0.05 | 16 (5.4) | 222 (9.0) | 0.036 |
| Cerebrovascular disease | 282 (16.7) | 125 (11.7) | 0.05 | 33 (11.1) | 374 (15.2) | 0.063 |
| Clinical characteristics | ||||||
| LOS, mean SD | 10.9 9.93 | 10.6 9.61 | 0.19 | 9.3 8.0 | 10.9 10.0 | 0.05 |
| LAPS, mean SD | 38.4 27.9 | 34.6 26.9 | 0.05 | 33.8 25.2 | 37.3 27.8 | 0.039 |
| BUN, mean SD | 34.4 32.3 | 30.9 28.3 | 0.05 | 29.5 24.4 | 33.4 31.6 | 0.036 |
| Charlson score, mean SD | 4.62 3.37 | 5.28 3.56 | 0.05 | 5.1 3.5 | 4.8 3.5 | 0.152 |
In this sample, 9.2% of patients in the dual eligible group were readmitted within 30 days compared with 13.1% of others (2 = 10.3, P = 0.001). Of the total cohort, 1500 patients, including 862 dual eligible patients, were discharged to a facility, and 1255 patients, including 826 dual eligible patients, were discharged home. Dual eligible patients had a lower readmission rate compared with others in both settings (Figure 1). In univariable analysis, gender, age, hospital length of stay, race/ethnicity, SES, English as a primary language, LAPS, BUN, Charlson score, and comorbid peripheral vascular disease, cerebrovascular disease, heart disease, dementia, cancer, and liver disease were found to be related both to the predictor and the outcome variables and were included in the logistic regression model. While controlling for these variables, dual eligible patients had a lower odds of readmission within 30 days compared with others (odds ratio [OR]: 0.77; P = 0.041; 95% confidence interval [CI]: 0.59‐0.98) (Table 2). The Hosmer‐Lemeshow test was not significant, indicating that the overall model fit was good.
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.77 | 0.10 | 2.05 | 0.041 |
| Gender | 1.16 | 0.15 | 1.17 | 0.244 |
| Age | 0.96 | 0.01 | 4.54 | 0.000 |
| Hospital length of stay | 0.97 | 0.01 | 3.33 | 0.001 |
| Black | 1.93 | 0.53 | 2.37 | 0.018 |
| White | 1.02 | 0.30 | 0.08 | 0.939 |
| Hispanic | 1.29 | 0.37 | 0.90 | 0.368 |
| Socioeconomic status | 0.96 | 0.02 | 1.63 | 0.103 |
| Primary language English | 0.81 | 0.12 | 1.43 | 0.154 |
| Peripheral vascular disease | 0.67 | 0.18 | 1.48 | 0.139 |
| Cerebrovascular disease | 0.86 | 0.17 | 0.73 | 0.465 |
| Dementia | 0.61 | 0.20 | 1.50 | 0.135 |
| Congestive heart failure | 1.75 | 0.26 | 3.83 | 0.000 |
| Cardiac valvular disease | 0.73 | 0.19 | 1.23 | 0.219 |
| Cancer | 0.92 | 0.15 | 0.51 | 0.608 |
| Liver disease | 1.80 | 0.47 | 2.25 | 0.024 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.66 | 0.510 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.29 | 0.197 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.57 | 0.567 |
In the secondary analysis, we found that disposition (hospice services in a nursing home or hospice residence vs home hospice) partially mediates the relationship between insurance status and readmission, explaining 30% of the total effect (z = 5.06, P 0.001). When accounting for disposition as a mediator, dual eligible patients still had a lower odds of readmission within 30 days compared with others, although the difference was no longer statistically significant (OR: 0.86; P = 0.24; 95% CI: 0.66‐ 1.11). Patients discharged with hospice services in a nursing home or hospice residence were less likely to be readmitted within 30 days (OR: 0.41; P 0.001; 95% CI: 0.31‐0.54) (Table 3).
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.86 | 0.11 | 1.17 | 0.244 |
| Discharge location | 0.40 | 0.59 | 6.22 | 0.000 |
| Gender | 1.17 | 0.16 | 1.22 | 0.223 |
| Age | 0.96 | 0.01 | 4.69 | 0.000 |
| Hospital length of stay | 0.98 | 0.01 | 2.57 | 0.010 |
| Black | 1.95 | 0.54 | 2.39 | 0.017 |
| White | 1.02 | 0.30 | 0.10 | 0.924 |
| Hispanic | 1.20 | 0.35 | 0.63 | 0.526 |
| Socioeconomic status | 0.96 | 0.02 | 1.51 | 0.132 |
| Primary language English | 0.78 | 0.11 | 1.69 | 0.090 |
| Peripheral vascular disease | 0.70 | 0.19 | 1.31 | 0.190 |
| Cerebrovascular disease | 0.89 | 0.18 | 0.56 | 0.579 |
| Dementia | 0.64 | 0.21 | 1.36 | 0.174 |
| Congestive heart failure | 1.75 | 0.26 | 3.80 | 0.000 |
| Cardiac valvular disease | 0.70 | 0.18 | 1.35 | 0.176 |
| Cancer | 0.91 | 0.15 | 0.59 | 0.552 |
| Liver disease | 1.75 | 0.46 | 2.12 | 0.034 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.20 | 0.843 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.10 | 0.270 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.65 | 0.516 |
DISCUSSION
This study showed an association between dual coverage and lower odds of 30‐day readmission for patients discharged to hospice compared to all other insurance categories, excluding uninsured. This is the first study to date looking specifically at the association between insurance and readmission rates of patients discharged with hospice services. This association was attenuated, and no longer statistically significant, when accounting for discharge location.
These findings suggest that the added services available to patients enrolled in Medicare and Medicaid likely provide an enhanced level of postacute care. Patients with Medicaid have access to increased hours of personal care attendants as well as residential care, which often provides 24‐hour trained staff for rapid assessment of a change in clinical status and adjustment to therapeutic management. Combined with the Medicare hospice benefit, which provides better attention to symptom management, better supervision, and improved compliance with medications, as well as education of family and caregivers,[21, 22, 23] additional coverage with Medicaid is associated with a decrease in early readmission to the hospital.
It is often a financial hardship for family members or caregivers to take time off work to care for a dying patient. Without adequate postdischarge resources, the hospital to home transition will be ineffective, which has been shown to increase readmissions.[24] The option of increased attendant hours or residential care can have a positive impact on the financial and psychosocial stressors of caring for a family member at the end of life. Although we did not assess for this in our study, caregiver burnout often plays a role in emergency room visits and admissions of patients at the end of life.[25] The average age of the patients in our cohorts was 81 and 79 years; primary caregivers are often elderly with multiple medical conditions themselves and often struggle to provide the patient's care.[26, 27]
The main limitation of this study is that it is a retrospective observational study rather than a prospective randomized controlled trial. Many patients become dual eligible after requiring institutional custodial care, making the relationship between insurance status, discharge location, and readmissions complex and the causal relationship bidirectional. Patients discharged to hospice residence or to a nursing home with hospice services, who are more often dual eligible patients, are likely to receive more timely management of medical crises or changes in medical status, thus preventing readmission, whereas patients who receive home hospice with family providing the bulk of care may have a lower threshold for emergency room visits, possibly leading to greater incidence of readmission. Therefore, our results may be more a reflection of where the care is provided than what insurance the patient has. However, dual eligible patients discharged home also had a lower readmission rate compared with others, suggesting that insurance status has an independent association with readmission.
Unmeasured variables may explain the relationship between dual eligibility and 30‐day readmission rates. Some variables that we were not able to reliably measure in this study include functional status, number of hospitalizations in last year, patient educational level, patient self‐reported health status, quality of life, cognitive functioning, hearing or vision impairment, income, employment status, number of people in the home, and caregiver availability.[11, 12, 13, 19] However, omitting these variables from this study is more likely to bias our results toward the null, because these variables are likely related to dual eligibility and a higher, rather than lower, rate of readmission. We also did not measure whether participating decision makers were involved in the hospice admission or whether patients and families contacted their PCPs after discharge, variables found to be important in a previous pilot study.[5]
The generalizability of the results may be affected by the relative generosity of the New York State Medicaid benefits compared to many other states. New York State ranks third in the nation for eligibility and first for scope of services, including increased access to home‐ and community‐based services.[28] In addition, this study was a single‐center study in an urban, socioeconomically disadvantaged environment, explaining the higher rate of readmission compared to hospice patients nationally,[29] which is similar to other urban, academic medical centers.[5] For patients in our practice setting, the financial burden of paying privately for home care or residential custodial services is often prohibitive, which may not be the case in other settings.
Further research to identify whether discharge with hospice services mediates the relationship between insurance status and readmission could help confirm these findings. In addition, the relationship between caregiver burden and quality of life, and increased healthcare costs at the end of life should be explored. Overwhelming evidence suggests that being socioeconomically disadvantaged is a significant risk factor for early readmission, and enrolling these patients in Medicaid may modify this risk.[10, 30] Further research should explore whether policies that expand access to Medicaid or otherwise increase access to custodial care services can decrease burdensome hospital readmissions near the end of life.
Acknowledgements
The authors thank Galina Umanski for her technical support of this work.
Disclosure: This work was presented as a Power Point presentation on June 5, 2015 at the New York City Fellows' Palliative Care Research Day. The authors report no conflicts of interest.
Palliative care and hospice specialists consult on a variety of patients in the acute care setting that span all diagnoses and specialties. These include patients in the intensive care units, oncology units, as well as patients with end‐stage pulmonary, cardiac, and renal diseases. Discharge of these patients is often complicated by social issues, intensive personal care needs, and decreased functional status, as well as by the patient's insurance. Options for discharge disposition for patients accepting enrollment in hospice are often limited by financial constraints. Medicare pays for a set package of hospice benefits that do not include payment for room and board for hospice residential care and have a limited number of hours for a personal care attendant.[1] Hospice inpatient units are typically covered only for patients with acute care needs. Patients with secondary commercial insurance similarly find that custodial care benefits are often lacking, as most private and managed care plans mimic the Medicare hospice benefit.[2]
Palliative care inpatient consultation and palliative or hospice home care are associated with decreased 30‐day readmission rates.[3, 4, 5, 6] None of these studies, however, evaluated the effect of insurance status on readmission rates. Patients with dual coverage of Medicare and Medicaid are eligible for coverage of room and board (covered by Medicaid) in addition to the standard hospice benefit (covered by Medicare), and therefore have more options for discharge planning, including admission to a hospice residence, nursing home care with hospice services, or increased personal care attendant hours at home. Dual eligible patients (those with both Medicare and Medicaid) represent 20% of the Medicare population. They are generally poorer and with worse health status that those with Medicare alone; they have on average 25% more medical conditions than Medicare‐only patients.[7] Previous studies of readmissions and healthcare costs in the general population have found that dual eligible patients have higher rates of readmissions and higher overall healthcare costs compared with other groups.[7, 8, 9] However, these studies did not specifically look at patients near the end of life receiving hospice services. We hypothesize that dual eligible patients may actually have a lower rate of readmission at end of life compared with other groups, and that this effect may be partially mediated by discharge location (facility or home).
Previous studies have identified risk factors for 30‐day readmission to hospital, including living alone, insurance status, and poor or fair satisfaction with their primary care provider (PCP).[10] This study aims to evaluate, in the cohort of patients who have received a palliative care consultation during their hospital stay and who were discharged with hospice services, whether type of insurance is associated with risk of early readmission.
METHODS
Data were extracted from a replicate of Montefiore's Clinical Information System using healthcare surveillance software (Clinical Looking Glass; Emerging Health Information Technology, Yonkers, NY). We queried this database to find patients who received palliative care consultation from August 2010 to January 2014 at Montefiore Medical Center, an academic medical center in Bronx, NY, consisting of 3 general hospitals with 1491 beds. The medical center provides care to many underserved and minority patients and serves as the University Hospital of the Albert Einstein College of Medicine.
Inclusion Criteria
Patients who received a palliative care consultation were included if they were 65 years of age, nonpregnant, and admitted to the medical intensive care unit, any surgical intensive care unit, cardiac care unit, general medicine, surgery or surgical subspecialty service, family medicine, cardiology or oncology service, and discharged with hospice services.
Exclusion Criteria
Patients 65 years old and patients who died during the index admission were excluded, as were admissions to pediatrics, obstetrics, and psychology services, and uninsured patients.
The admission with the first palliative care consultation resulting in hospice referral was considered the index admission for these patients. Sociodemographic variables related to readmission such as age, race, gender, primary language, and socioeconomic status (SES) were examined.[11, 12, 13, 14, 15, 16] Clinical variables shown to be related to 30‐day readmissions in the literature including lab‐based acute physiology score (LAPS), blood urea nitrogen level (BUN), serum sodium level, serum albumin level, documentation of weight loss, and Charlson Comorbidity Index as well as its specific components were also extracted.[11, 13, 16, 17, 18, 19] Other variables related to the index admission such as length of stay for index admission, admission source on index admission (eg, from home, nursing home, other), and whether the primary care physician was listed in the chart were also examined.[11, 13, 16, 17, 19, 20] All of the variables were examined because they were hypothesized to be related to both insurance status and readmission. Markers of clinical severity, such as LAPS, BUN, hyponatremia, hypoalbuminemia, weight loss, and comorbidity could lead to readmission for symptom management or acute deterioration, and have been found be related to readmission in previous literature.
The predictor variable was insurance status at the time of index admission (dual eligible or all other). The main outcome variable was readmission to Montefiore Medical Center for any reason within 30 days of the index admission. Discharge location (hospice services in a facility vs home hospice) was examined as a potential mediator.
Statistical Analysis
Based on quality metrics available from our department, we expected to find at least 1000 patients 65 years of age seen by the palliative care consultation service with a discharge disposition including hospice services. This would give our study 85% power to detect a 10% difference in readmission rates between the 2 groups.
Patients were categorized as dual eligible if they were covered by Medicare and Medicaid only or if they were covered by Medicare, Medicaid, and private insurance. Controls were patients who were covered by Medicare only, Medicaid only, private insurance only, or Medicare and private insurance or Medicaid and private insurance. For the primary analysis, patients with and without dual eligibility were compared with respect to sociodemographic characteristics, healthcare process variables, and measures of comorbidity and illness severity using t tests for continuous variables and 2 tests for categorical variables. We used a 2 test to assess the univariable association between dual eligibility and 30‐day readmission. To address the question as to whether dual eligibility reduces the likelihood of a 30 day readmission, logistic regression was used to model 30‐day readmission by selecting from the covariates associated with the 30‐day readmissions at the 0.15 significance level. The Hosmer‐Lemeshow goodness of fit test was used to evaluate overall model performance.
For the secondary analysis, we assessed whether type and location of hospice services mediate the effect of insurance status on 30‐day readmissions using a Sobel‐Goodman test for mediation. Statistical analysis was conducted using statistical software (Stata statistical software, release 12; StataCorp, College Station, TX).
This research protocol was reviewed by the Montefiore Medical Center/Albert Einstein College of Medicine Institutional Review Board.
RESULTS
A total of 2755 inpatients were seen by the palliative care consultation service across the Montefiore Medical Center sites and discharged with hospice services. Of those, 1688 were dual eligible for Medicare and Medicaid, and 1067 were not. Specifically, 695 patients had Medicare only, 148 had private insurance only, 126 had Medicaid only, 78 had Medicare and private insurance, and 19 had Medicaid and private insurance. Univariable relationships between patient characteristics, insurance status, and readmission are shown in Table 1.
| Characteristic | Dual Eligible, N = 1,688 |
Not Dual Eligible, N = 1,067 |
P Value | 30‐Day Readmission | P Value | |
|---|---|---|---|---|---|---|
| Yes, N = 296 | No, N = 2,459 | |||||
| ||||||
| Sociodemographic | ||||||
| Age, y, mean SD | 81.6 9.0 | 79.4 8.9 | 0.05 | 77.8 8.8 | 81.1 9.0 | 0.05 |
| Female, n (%) | 1,092 (64.7) | 622 (58.3) | 0.05 | 171 (57.8) | 1,543 (62.7) | 0.095 |
| Has PCP, n (%) | 1,451 (86.0) | 951 (89.1) | 0.05 | 263 (88.9) | 2,139 (87.0) | NS |
| Speaks English, n (%) | 1,064 (63.0) | 728 (68.2) | 0.05 | 181 (61.1) | 1,611 (65.5) | 0.137 |
| SES, mean SD | 2.76 2.81 | 2.51 2.67 | 0.05 | 3.11 2.72 | 2.61 2.77 | 0.05 |
| Race/ethnicity | 0.05 | 0.05 | ||||
| Hispanic, n (%) | 587 (34.8) | 267 (31.3) | 100 (33.8) | 754 (30.7) | ||
| White, n (%) | 532 (31.5) | 290 (27.2) | 58 (19.6) | 764 (31.1) | ||
| Black, n (%) | 449 (26.6) | 420 (39.4) | 121 (40.9) | 748 (30.4) | ||
| Comorbidities, n (%) | ||||||
| Congestive heart failure | 555 (32.9) | 264 (24.7) | 0.05 | 104 (35.1) | 751 (30.5) | 0.106 |
| Cardiac valvular disease | 179 (10.6) | 76 (7.1) | 0.05 | 19 (6.4) | 227 (9.2) | 0.109 |
| Myocardial infarction | 165 (9.8) | 85 (8.0) | 0.11 | 31 (10.5) | 219 (8.9) | NS |
| Pulmonary disease | 480 (28.4) | 292 (27.4) | NS | 98 (33.1) | 674 (27.4) | 0.039 |
| Liver disease | 60 (3.6) | 54 (5.1) | 0.053 | 22 (7.4) | 92 (3.7) | 0.05 |
| Dementia | 135 (8.0) | 52 (4.9) | 0.05 | 11 (3.7) | 176 (7.2) | 0.026 |
| Diabetes, complicated | 125 (7.4) | 52 (4.9) | 0.05 | 15 (5.1) | 163 (6.6) | NS |
| Malignancy | 589 (34.9) | 499 (46.8) | 0.05 | 124 (41.9) | 921 (37.5) | 0.137 |
| Renal disease | 394 (23.3) | 225 (21.1) | NS | 72 (24.3) | 547 (22.2) | NS |
| Depression | 174 (10.3) | 85 (8.0) | 0.05 | 25 (8.4) | 234 (9.5) | NS |
| Peripheral vascular disease | 166 (9.8) | 72 (6.7) | 0.05 | 16 (5.4) | 222 (9.0) | 0.036 |
| Cerebrovascular disease | 282 (16.7) | 125 (11.7) | 0.05 | 33 (11.1) | 374 (15.2) | 0.063 |
| Clinical characteristics | ||||||
| LOS, mean SD | 10.9 9.93 | 10.6 9.61 | 0.19 | 9.3 8.0 | 10.9 10.0 | 0.05 |
| LAPS, mean SD | 38.4 27.9 | 34.6 26.9 | 0.05 | 33.8 25.2 | 37.3 27.8 | 0.039 |
| BUN, mean SD | 34.4 32.3 | 30.9 28.3 | 0.05 | 29.5 24.4 | 33.4 31.6 | 0.036 |
| Charlson score, mean SD | 4.62 3.37 | 5.28 3.56 | 0.05 | 5.1 3.5 | 4.8 3.5 | 0.152 |
In this sample, 9.2% of patients in the dual eligible group were readmitted within 30 days compared with 13.1% of others (2 = 10.3, P = 0.001). Of the total cohort, 1500 patients, including 862 dual eligible patients, were discharged to a facility, and 1255 patients, including 826 dual eligible patients, were discharged home. Dual eligible patients had a lower readmission rate compared with others in both settings (Figure 1). In univariable analysis, gender, age, hospital length of stay, race/ethnicity, SES, English as a primary language, LAPS, BUN, Charlson score, and comorbid peripheral vascular disease, cerebrovascular disease, heart disease, dementia, cancer, and liver disease were found to be related both to the predictor and the outcome variables and were included in the logistic regression model. While controlling for these variables, dual eligible patients had a lower odds of readmission within 30 days compared with others (odds ratio [OR]: 0.77; P = 0.041; 95% confidence interval [CI]: 0.59‐0.98) (Table 2). The Hosmer‐Lemeshow test was not significant, indicating that the overall model fit was good.
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.77 | 0.10 | 2.05 | 0.041 |
| Gender | 1.16 | 0.15 | 1.17 | 0.244 |
| Age | 0.96 | 0.01 | 4.54 | 0.000 |
| Hospital length of stay | 0.97 | 0.01 | 3.33 | 0.001 |
| Black | 1.93 | 0.53 | 2.37 | 0.018 |
| White | 1.02 | 0.30 | 0.08 | 0.939 |
| Hispanic | 1.29 | 0.37 | 0.90 | 0.368 |
| Socioeconomic status | 0.96 | 0.02 | 1.63 | 0.103 |
| Primary language English | 0.81 | 0.12 | 1.43 | 0.154 |
| Peripheral vascular disease | 0.67 | 0.18 | 1.48 | 0.139 |
| Cerebrovascular disease | 0.86 | 0.17 | 0.73 | 0.465 |
| Dementia | 0.61 | 0.20 | 1.50 | 0.135 |
| Congestive heart failure | 1.75 | 0.26 | 3.83 | 0.000 |
| Cardiac valvular disease | 0.73 | 0.19 | 1.23 | 0.219 |
| Cancer | 0.92 | 0.15 | 0.51 | 0.608 |
| Liver disease | 1.80 | 0.47 | 2.25 | 0.024 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.66 | 0.510 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.29 | 0.197 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.57 | 0.567 |
In the secondary analysis, we found that disposition (hospice services in a nursing home or hospice residence vs home hospice) partially mediates the relationship between insurance status and readmission, explaining 30% of the total effect (z = 5.06, P 0.001). When accounting for disposition as a mediator, dual eligible patients still had a lower odds of readmission within 30 days compared with others, although the difference was no longer statistically significant (OR: 0.86; P = 0.24; 95% CI: 0.66‐ 1.11). Patients discharged with hospice services in a nursing home or hospice residence were less likely to be readmitted within 30 days (OR: 0.41; P 0.001; 95% CI: 0.31‐0.54) (Table 3).
| Independent Variable | Odds Ratio | Standard Error | z Ratio | P Value |
|---|---|---|---|---|
| Dual eligibility | 0.86 | 0.11 | 1.17 | 0.244 |
| Discharge location | 0.40 | 0.59 | 6.22 | 0.000 |
| Gender | 1.17 | 0.16 | 1.22 | 0.223 |
| Age | 0.96 | 0.01 | 4.69 | 0.000 |
| Hospital length of stay | 0.98 | 0.01 | 2.57 | 0.010 |
| Black | 1.95 | 0.54 | 2.39 | 0.017 |
| White | 1.02 | 0.30 | 0.10 | 0.924 |
| Hispanic | 1.20 | 0.35 | 0.63 | 0.526 |
| Socioeconomic status | 0.96 | 0.02 | 1.51 | 0.132 |
| Primary language English | 0.78 | 0.11 | 1.69 | 0.090 |
| Peripheral vascular disease | 0.70 | 0.19 | 1.31 | 0.190 |
| Cerebrovascular disease | 0.89 | 0.18 | 0.56 | 0.579 |
| Dementia | 0.64 | 0.21 | 1.36 | 0.174 |
| Congestive heart failure | 1.75 | 0.26 | 3.80 | 0.000 |
| Cardiac valvular disease | 0.70 | 0.18 | 1.35 | 0.176 |
| Cancer | 0.91 | 0.15 | 0.59 | 0.552 |
| Liver disease | 1.75 | 0.46 | 2.12 | 0.034 |
| Lab‐based acute physiology score | 1.00 | 0.00 | 0.20 | 0.843 |
| Blood urea nitrogen | 1.00 | 0.00 | 1.10 | 0.270 |
| Charlson comorbidity score | 0.99 | 0.02 | 0.65 | 0.516 |
DISCUSSION
This study showed an association between dual coverage and lower odds of 30‐day readmission for patients discharged to hospice compared to all other insurance categories, excluding uninsured. This is the first study to date looking specifically at the association between insurance and readmission rates of patients discharged with hospice services. This association was attenuated, and no longer statistically significant, when accounting for discharge location.
These findings suggest that the added services available to patients enrolled in Medicare and Medicaid likely provide an enhanced level of postacute care. Patients with Medicaid have access to increased hours of personal care attendants as well as residential care, which often provides 24‐hour trained staff for rapid assessment of a change in clinical status and adjustment to therapeutic management. Combined with the Medicare hospice benefit, which provides better attention to symptom management, better supervision, and improved compliance with medications, as well as education of family and caregivers,[21, 22, 23] additional coverage with Medicaid is associated with a decrease in early readmission to the hospital.
It is often a financial hardship for family members or caregivers to take time off work to care for a dying patient. Without adequate postdischarge resources, the hospital to home transition will be ineffective, which has been shown to increase readmissions.[24] The option of increased attendant hours or residential care can have a positive impact on the financial and psychosocial stressors of caring for a family member at the end of life. Although we did not assess for this in our study, caregiver burnout often plays a role in emergency room visits and admissions of patients at the end of life.[25] The average age of the patients in our cohorts was 81 and 79 years; primary caregivers are often elderly with multiple medical conditions themselves and often struggle to provide the patient's care.[26, 27]
The main limitation of this study is that it is a retrospective observational study rather than a prospective randomized controlled trial. Many patients become dual eligible after requiring institutional custodial care, making the relationship between insurance status, discharge location, and readmissions complex and the causal relationship bidirectional. Patients discharged to hospice residence or to a nursing home with hospice services, who are more often dual eligible patients, are likely to receive more timely management of medical crises or changes in medical status, thus preventing readmission, whereas patients who receive home hospice with family providing the bulk of care may have a lower threshold for emergency room visits, possibly leading to greater incidence of readmission. Therefore, our results may be more a reflection of where the care is provided than what insurance the patient has. However, dual eligible patients discharged home also had a lower readmission rate compared with others, suggesting that insurance status has an independent association with readmission.
Unmeasured variables may explain the relationship between dual eligibility and 30‐day readmission rates. Some variables that we were not able to reliably measure in this study include functional status, number of hospitalizations in last year, patient educational level, patient self‐reported health status, quality of life, cognitive functioning, hearing or vision impairment, income, employment status, number of people in the home, and caregiver availability.[11, 12, 13, 19] However, omitting these variables from this study is more likely to bias our results toward the null, because these variables are likely related to dual eligibility and a higher, rather than lower, rate of readmission. We also did not measure whether participating decision makers were involved in the hospice admission or whether patients and families contacted their PCPs after discharge, variables found to be important in a previous pilot study.[5]
The generalizability of the results may be affected by the relative generosity of the New York State Medicaid benefits compared to many other states. New York State ranks third in the nation for eligibility and first for scope of services, including increased access to home‐ and community‐based services.[28] In addition, this study was a single‐center study in an urban, socioeconomically disadvantaged environment, explaining the higher rate of readmission compared to hospice patients nationally,[29] which is similar to other urban, academic medical centers.[5] For patients in our practice setting, the financial burden of paying privately for home care or residential custodial services is often prohibitive, which may not be the case in other settings.
Further research to identify whether discharge with hospice services mediates the relationship between insurance status and readmission could help confirm these findings. In addition, the relationship between caregiver burden and quality of life, and increased healthcare costs at the end of life should be explored. Overwhelming evidence suggests that being socioeconomically disadvantaged is a significant risk factor for early readmission, and enrolling these patients in Medicaid may modify this risk.[10, 30] Further research should explore whether policies that expand access to Medicaid or otherwise increase access to custodial care services can decrease burdensome hospital readmissions near the end of life.
Acknowledgements
The authors thank Galina Umanski for her technical support of this work.
Disclosure: This work was presented as a Power Point presentation on June 5, 2015 at the New York City Fellows' Palliative Care Research Day. The authors report no conflicts of interest.
- , . Hospice: comprehensive care at the end of life. Anest Clin N Am. 2006;24:181–204.
- . U.S. hospice benefits. J Pain Symptom Manage. 2009;38:105–109.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15:48–51.
- , , , . A hospice‐hospital partnership: reducing hospitalization costs and 30‐day readmissions among seriously ill adults. J Palliat Med. 2014;17:1005–1010.
- , , , , , . Rehospitalization of older adults discharged to home hospice care. J Palliat Med. 2014;17:841–844.
- , , , . Can palliative home care reduce 30‐day readmissions? Results of a propensity score matched cohort study. J Palliat Med. 2013;16:1290–1293.
- , , , , , . The Medicare Hospital Readmissions Reduction Program: potential unintended consequences for hospitals serving vulnerable populations. Health Serv Res. 2014;49:818–837.
- , , , . Understanding why patients with COPD get readmitted: a large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147:1219–1226.
- , , . Variations in 30‐day hospital readmission rates across primary care clinics within a tertiary referral center. J Hosp Med. 2014;9:688–694.
- , , , . Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62:489–494.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360:1418–1428.
- , , , , . Risk factors for 30‐day hospital readmission in patients >/=65 years of age. Proc (Bayl Univ Med Cent). 2008;21:363–372.
- , , , . Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6:54–60.
- , , , . Racial/ethnic disparities in potentially preventable readmissions: the case of diabetes. Am J Public Health. 2005;95:1561–1567.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681.
- , , , et al. Factors associated with 30‐day readmission rates after percutaneous coronary intervention. Arch Intern Med. 2012;172:112–117.
- , , , . Risk factors for 30‐day readmission in general medical patients admitted from the emergency department: a single centre study. Intern Med J. 2012;42:677–682.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688–1698.
- , , , , , . Thirty‐day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157:11–18.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25:211–219.
- , , , , , . An examination of adherence to pain medication plans in older cancer patients in hospice care. J Pain Symptom Manage. 2013;45:43–55.
- , , , et al. Hospice providers' key approaches to support informal caregivers in managing medications for patients in private residences. J Pain Symptom Manage. 2012;43:1060–1071.
- , . Hospice approach to palliative care, including Medicare hospice benefit. In: Yennurajalingam S, Bruera E, eds. Oxford American Handbook of Hospice and Palliative Medicine. New York, NY: Oxford University Press; 2011:229–239.
- , , . Predictors of thirty‐day readmission among hospitalized family medicine patients. J Am Board Fam Med. 2013;26:71–77.
- , , , , , . Emergency calls and need for emergency care in pateints looked after by a palliative care team: Retrospective interview study with bereaved relatives. BMC Palliat Care. 2008;7:11.
- , , , et al. Predictors of caregiver burden across the home‐based palliative care trajectory in Ontario, Canada [published online March 25, 2105]. Health Soc Care Community. doi: 10.1111/hsc.12219.
- , , , . Unique characteristics of informal hospice cancer caregiving. Support Care Cancer. 2015;23:2121–2128.
- , . Unsettling Scores: A Ranking of State Medicaid Programs. Washington, DC: Public Citizen Press; 2007.
- , , . 30‐day readmissions among seriously ill older adults. J Palliat Med. 2012;15:1–6.
- , . A path forward on Medicare readmissions. N Engl J Med. 2013;368:1175–1177.
- , . Hospice: comprehensive care at the end of life. Anest Clin N Am. 2006;24:181–204.
- . U.S. hospice benefits. J Pain Symptom Manage. 2009;38:105–109.
- , , , , . Inpatient palliative care consults and the probability of hospital readmission. Perm J. 2011;15:48–51.
- , , , . A hospice‐hospital partnership: reducing hospitalization costs and 30‐day readmissions among seriously ill adults. J Palliat Med. 2014;17:1005–1010.
- , , , , , . Rehospitalization of older adults discharged to home hospice care. J Palliat Med. 2014;17:841–844.
- , , , . Can palliative home care reduce 30‐day readmissions? Results of a propensity score matched cohort study. J Palliat Med. 2013;16:1290–1293.
- , , , , , . The Medicare Hospital Readmissions Reduction Program: potential unintended consequences for hospitals serving vulnerable populations. Health Serv Res. 2014;49:818–837.
- , , , . Understanding why patients with COPD get readmitted: a large national study to delineate the Medicare population for the readmissions penalty expansion. Chest. 2015;147:1219–1226.
- , , . Variations in 30‐day hospital readmission rates across primary care clinics within a tertiary referral center. J Hosp Med. 2014;9:688–694.
- , , , . Risk factors for early hospital readmission in low‐income elderly adults. J Am Geriatr Soc. 2014;62:489–494.
- , , . Rehospitalizations among patients in the Medicare fee‐for‐service program. N Engl J Med. 2009;360:1418–1428.
- , , , , . Risk factors for 30‐day hospital readmission in patients >/=65 years of age. Proc (Bayl Univ Med Cent). 2008;21:363–372.
- , , , . Redefining readmission risk factors for general medicine patients. J Hosp Med. 2011;6:54–60.
- , , , . Racial/ethnic disparities in potentially preventable readmissions: the case of diabetes. Am J Public Health. 2005;95:1561–1567.
- , , . Thirty‐day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681.
- , , , et al. Factors associated with 30‐day readmission rates after percutaneous coronary intervention. Arch Intern Med. 2012;172:112–117.
- , , , . Risk factors for 30‐day readmission in general medical patients admitted from the emergency department: a single centre study. Intern Med J. 2012;42:677–682.
- , , , et al. Risk prediction models for hospital readmission: a systematic review. JAMA. 2011;306:1688–1698.
- , , , , , . Thirty‐day rehospitalizations after acute myocardial infarction: a cohort study. Ann Intern Med. 2012;157:11–18.
- , , , et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. 2009;25:211–219.
- , , , , , . An examination of adherence to pain medication plans in older cancer patients in hospice care. J Pain Symptom Manage. 2013;45:43–55.
- , , , et al. Hospice providers' key approaches to support informal caregivers in managing medications for patients in private residences. J Pain Symptom Manage. 2012;43:1060–1071.
- , . Hospice approach to palliative care, including Medicare hospice benefit. In: Yennurajalingam S, Bruera E, eds. Oxford American Handbook of Hospice and Palliative Medicine. New York, NY: Oxford University Press; 2011:229–239.
- , , . Predictors of thirty‐day readmission among hospitalized family medicine patients. J Am Board Fam Med. 2013;26:71–77.
- , , , , , . Emergency calls and need for emergency care in pateints looked after by a palliative care team: Retrospective interview study with bereaved relatives. BMC Palliat Care. 2008;7:11.
- , , , et al. Predictors of caregiver burden across the home‐based palliative care trajectory in Ontario, Canada [published online March 25, 2105]. Health Soc Care Community. doi: 10.1111/hsc.12219.
- , , , . Unique characteristics of informal hospice cancer caregiving. Support Care Cancer. 2015;23:2121–2128.
- , . Unsettling Scores: A Ranking of State Medicaid Programs. Washington, DC: Public Citizen Press; 2007.
- , , . 30‐day readmissions among seriously ill older adults. J Palliat Med. 2012;15:1–6.
- , . A path forward on Medicare readmissions. N Engl J Med. 2013;368:1175–1177.
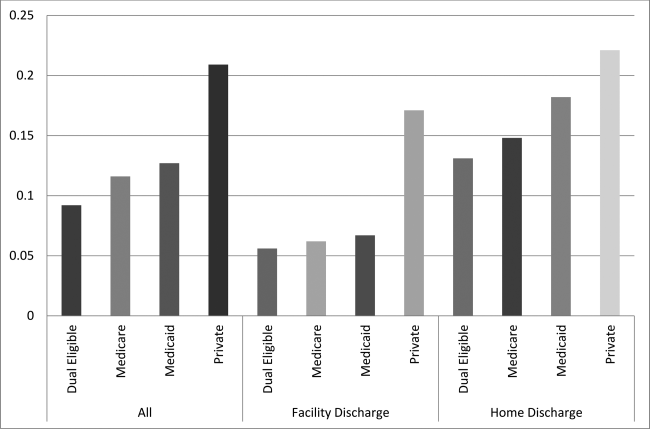
Omission of dexamethasone from antiemetic treatment for highly emetogenic chemotherapy in breast cancer patients with hepatitis B infection or diabetes mellitus
Patients and methods During August 2009 and September 2007, we reviewed the medical records of patients with breast cancer who were HBV carriers or had been diagnosed with DM. 97 patients were treated with anthracycline- and cyclophosphamide- containing regimens with omission of dexamethasone in antiemetic treatment because of their HBV or DM status.
Results The number of patients treated with Gra only, Apr and Gra, Apr and Pal, were 29, 29, and 39, respectively. Complete response (CR) in the acute phase (0-<24 hours after chemotherapy) or delayed phase (24-120 hours after chemotherapy) for Gra only, Apr-Gra, and Apr-Pal was 44.8% and 44.8%, 72.4% and 72.4%, and 76.9% and 74.4%, respectively. Complete control (CC) in the acute or delayed phase in each regimen for Gra only, Apr-Gra, and Apr-Pal was 31.0% and 27.6%, 48.2% and 51.7%, and 46.2% and 46.2%, respectively. Apr-Gra or Apr-Pal tended to be superior to Gra only in CR and CC in both the acute and delayed phases. HBV reactivation or aggravation of DM control was not observed in any of the 3 therapy options. CR and CC were about 20% higher for the dexamethasone-containing regimen than for the non-dexamethasone regimen in both the acute and delayed phases.
Conclusion Omission of dexamethasone in antiemetic treatment is tolerable when anthracycline- and cyclophosphamide-containing chemotherapy is administered to patients with breast cancer who have comorbidities of being HBV carriers or of DM.
Click on the PDF icon at the top of this introduction to read the full article.
Patients and methods During August 2009 and September 2007, we reviewed the medical records of patients with breast cancer who were HBV carriers or had been diagnosed with DM. 97 patients were treated with anthracycline- and cyclophosphamide- containing regimens with omission of dexamethasone in antiemetic treatment because of their HBV or DM status.
Results The number of patients treated with Gra only, Apr and Gra, Apr and Pal, were 29, 29, and 39, respectively. Complete response (CR) in the acute phase (0-<24 hours after chemotherapy) or delayed phase (24-120 hours after chemotherapy) for Gra only, Apr-Gra, and Apr-Pal was 44.8% and 44.8%, 72.4% and 72.4%, and 76.9% and 74.4%, respectively. Complete control (CC) in the acute or delayed phase in each regimen for Gra only, Apr-Gra, and Apr-Pal was 31.0% and 27.6%, 48.2% and 51.7%, and 46.2% and 46.2%, respectively. Apr-Gra or Apr-Pal tended to be superior to Gra only in CR and CC in both the acute and delayed phases. HBV reactivation or aggravation of DM control was not observed in any of the 3 therapy options. CR and CC were about 20% higher for the dexamethasone-containing regimen than for the non-dexamethasone regimen in both the acute and delayed phases.
Conclusion Omission of dexamethasone in antiemetic treatment is tolerable when anthracycline- and cyclophosphamide-containing chemotherapy is administered to patients with breast cancer who have comorbidities of being HBV carriers or of DM.
Click on the PDF icon at the top of this introduction to read the full article.
Patients and methods During August 2009 and September 2007, we reviewed the medical records of patients with breast cancer who were HBV carriers or had been diagnosed with DM. 97 patients were treated with anthracycline- and cyclophosphamide- containing regimens with omission of dexamethasone in antiemetic treatment because of their HBV or DM status.
Results The number of patients treated with Gra only, Apr and Gra, Apr and Pal, were 29, 29, and 39, respectively. Complete response (CR) in the acute phase (0-<24 hours after chemotherapy) or delayed phase (24-120 hours after chemotherapy) for Gra only, Apr-Gra, and Apr-Pal was 44.8% and 44.8%, 72.4% and 72.4%, and 76.9% and 74.4%, respectively. Complete control (CC) in the acute or delayed phase in each regimen for Gra only, Apr-Gra, and Apr-Pal was 31.0% and 27.6%, 48.2% and 51.7%, and 46.2% and 46.2%, respectively. Apr-Gra or Apr-Pal tended to be superior to Gra only in CR and CC in both the acute and delayed phases. HBV reactivation or aggravation of DM control was not observed in any of the 3 therapy options. CR and CC were about 20% higher for the dexamethasone-containing regimen than for the non-dexamethasone regimen in both the acute and delayed phases.
Conclusion Omission of dexamethasone in antiemetic treatment is tolerable when anthracycline- and cyclophosphamide-containing chemotherapy is administered to patients with breast cancer who have comorbidities of being HBV carriers or of DM.
Click on the PDF icon at the top of this introduction to read the full article.
Effects of exercise interventions during different treatments in breast cancer
Previous findings suggest that exercise is a safe and efficacious means of improving physiological and psychosocial outcomes in female breast cancer survivors. To date, most research has focused on post-treatment interventions. However, given that the type and severity of treatment-related adverse effects may be dependent on the type of treatment, and that the effects are substantially more pronounced during treatment, an assessment of the safety and efficacy of exercise during treatment is warranted. In this review, we present and evaluate the results of randomized controlled trials (RCTs) conducted during breast cancer treatment. We conducted literature searches to identify studies examining exercise interventions in breast cancer patients who were undergoing chemotherapy or radiation. Data were extracted on physiological and psychosocial outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Previous findings suggest that exercise is a safe and efficacious means of improving physiological and psychosocial outcomes in female breast cancer survivors. To date, most research has focused on post-treatment interventions. However, given that the type and severity of treatment-related adverse effects may be dependent on the type of treatment, and that the effects are substantially more pronounced during treatment, an assessment of the safety and efficacy of exercise during treatment is warranted. In this review, we present and evaluate the results of randomized controlled trials (RCTs) conducted during breast cancer treatment. We conducted literature searches to identify studies examining exercise interventions in breast cancer patients who were undergoing chemotherapy or radiation. Data were extracted on physiological and psychosocial outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Previous findings suggest that exercise is a safe and efficacious means of improving physiological and psychosocial outcomes in female breast cancer survivors. To date, most research has focused on post-treatment interventions. However, given that the type and severity of treatment-related adverse effects may be dependent on the type of treatment, and that the effects are substantially more pronounced during treatment, an assessment of the safety and efficacy of exercise during treatment is warranted. In this review, we present and evaluate the results of randomized controlled trials (RCTs) conducted during breast cancer treatment. We conducted literature searches to identify studies examining exercise interventions in breast cancer patients who were undergoing chemotherapy or radiation. Data were extracted on physiological and psychosocial outcomes.
Click on the PDF icon at the top of this introduction to read the full article.
Growing Subcutaneous Mass on the Thigh
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
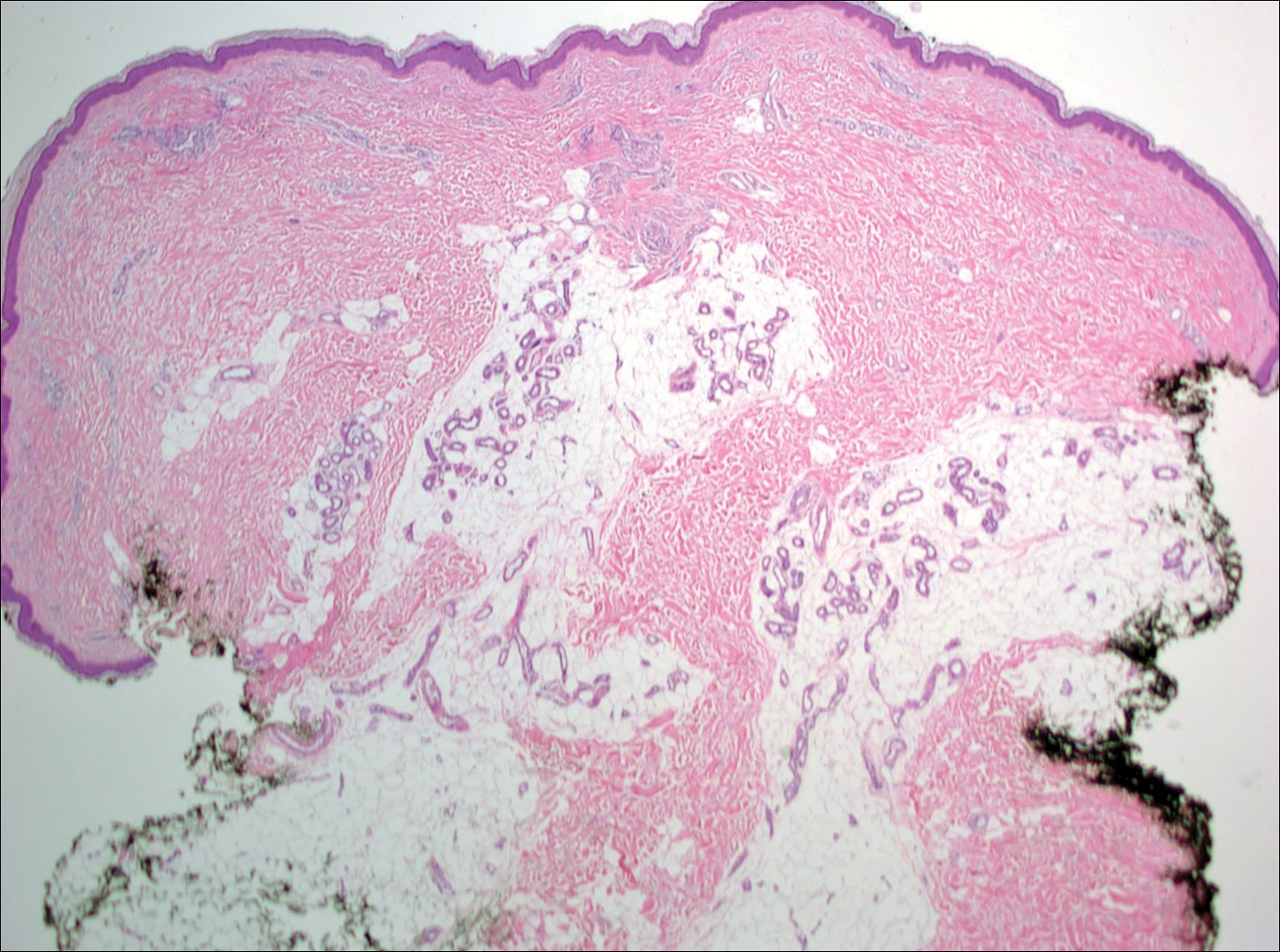
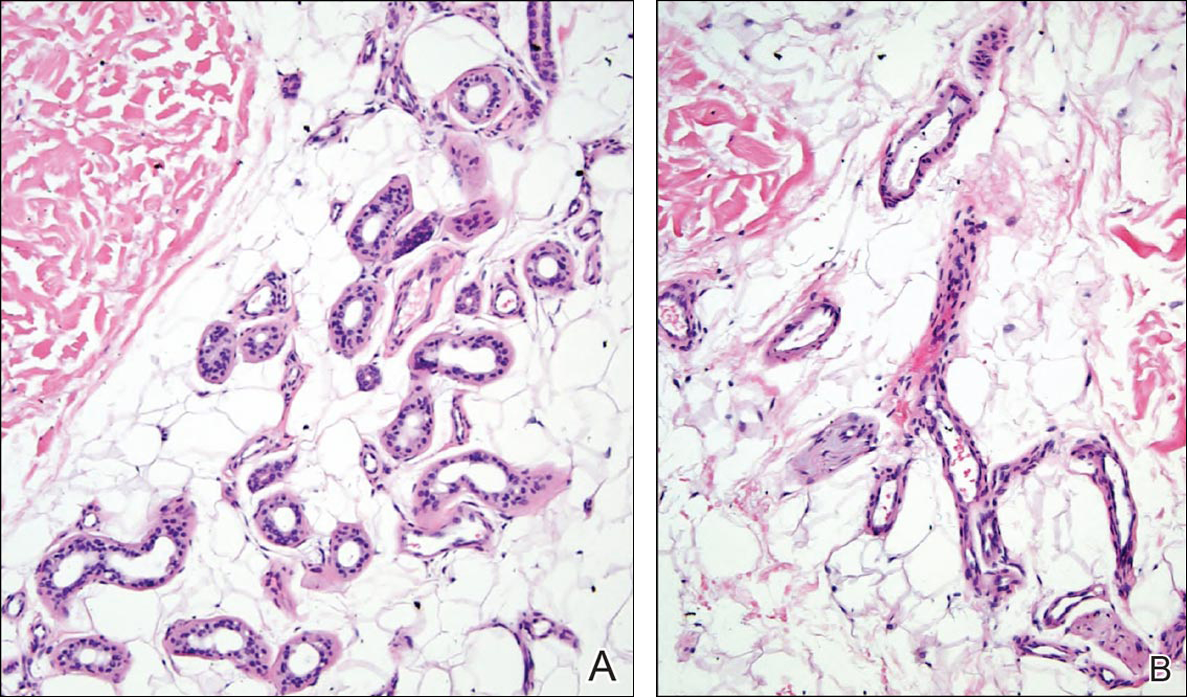
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
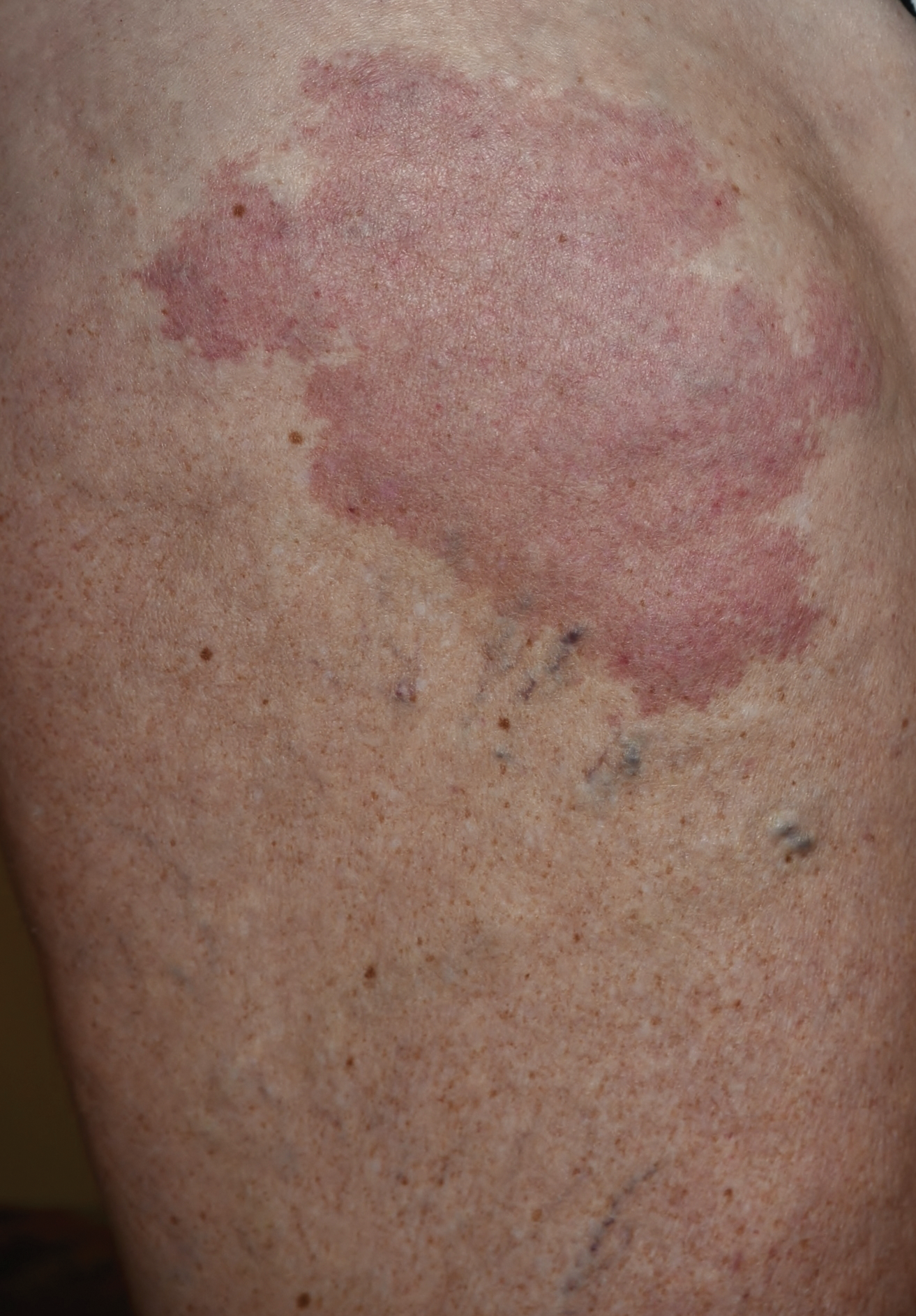
Histologic examination of anastomotic stapler doughnuts may not yield clinical benefit
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”

Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
LOS ANGELES – A multicenter of patients who had low anterior resection with stapled anastomosis for rectal cancer found no clinical or economic benefit in routinely sending anastomotic doughnuts for histopathological evaluation.
“Several small studies outside the United States have found no benefit in histologic examination of anastomotic stapler doughnuts,” lead study author Dr. Jeremy Sugrue said at the annual meeting of the American Society of Colon and Rectal Surgeons. “We wanted to see if this held true in our population.”
Dr. Sugrue, of the division of colon and rectal surgery in the department of surgery at the University of Illinois at Chicago, and his associates performed a retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions. The primary outcome was pathologic findings in the doughnuts and their impact on patient management. Secondary outcomes included tumor characteristics that may influence how often a surgeon may send a doughnut to pathology, along with approximate cost.
The mean age of the 486 patients was 60 years, 55% were male, and the mean gross distal margin of the primary tumor specimen was 2.9 cm. “The majority of tumors were located in the middle rectum, and the rest were evenly distributed between the lower rectum, upper rectum, and rectosigmoid regions,” said Dr. Sugrue, who is a general surgery resident. About half of the patients received neoadjuvant radiation or chemotherapy.
Benign findings were found in 33 patients. Among these, 16 had inflammatory changes, including 12 who had nonspecific changes, 3 who had changes from radiation, and 1 had inflammatory bowel disease changes. In addition, 13 patients with benign findings had polyps in their doughnuts (10 hyperplastic and 3 adenomatous), while 4 patients had miscellaneous changes including two cases of vessel micro calcification, one case of diverticuli, and one case of melanosis coli.
Among the 412 patients with malignant findings, 410 (99.5%) had no cancer in the doughnuts and no cancer at the distal resection margin in the primary tumor specimens. “In the two patients where we found cancer in the doughnuts, these patients also had a positive distal margin,” Dr. Sugrue said. “We did not find any patients with a positive distal margin and a negative doughnut. Likewise, we did not find any patients with a negative distal margin or an unexpectedly positive doughnut.”
The researchers also found that patients with low rectal tumors were significantly more likely to have their doughnut sent to pathology, compared with those with rectosigmoid tumors. “However, when we looked at distal margin comparing patients who had doughnuts reported on pathology with those who did not, there was no statistically significant difference,” Dr. Sugrue said. After averaging pathology professional fees and technical fees across all three institutions, he and his associates determined that doughnuts add $643 in cost when processed by pathology as a unique specimen.
Limitations of the study, he said, include its retrospective design, “which inherently introduces selection bias, and we did not perform a precise cost-benefit analysis.”
Dr. Sugrue reported having no financial disclosures.
AT THE ASCRS ANNUAL MEETING
Key clinical point: The routine histologic examination of anastomotic doughnuts at lower anterior resection for rectal cancer has no clinical benefit.
Major finding: Of the 412 patients with anastomotic doughnuts included in their pathology reports, only 2 had cancer cells in their doughnuts and both of these patients also had a positive distal margin in their primary tumor specimen.
Data source: A retrospective review of 486 patients who underwent a low anterior resection with stapled anastomosis for rectal cancer between 2002 and 2015 at three medical institutions.
Disclosures: Dr. Sugrue reported having no financial disclosures.

VIDEO: Experts discuss progress in schizophrenia treatment
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Over the last 20 years, there have been many signs of progress in treating schizophrenia, two experts said at the annual meeting of the American Psychiatric Association.
In this video, Dr. Henry A. Nasrallah and Dr. Michael Y. Hwang review the latest research in everything from genetic profiles predisposed to schizophrenia to their relationship with addiction, as well as the interplay between schizophrenia. They also discuss medical and psychiatric comorbidities – particularly obsessive-compulsive disorder. “We did a study where we looked at the onset of schizophrenia vs. the onset of OCD,” Dr. Nasrallah said. “We found that OCD symptoms precede the onset of psychosis by about a year.”
In addition, Dr. Nasrallah and Dr. Hwang discuss the impact of heterogeneity in schizophrenia not only when it comes to identifying appropriate interventions but also to conducting clinical trials.
Dr. Nasrallah is the Sydney W. Souers Professor and chair of the department of neurology and psychiatry at Saint Louis University. He has multiple disclosures, including Alkermes, Boehringer Ingelheim, Lundbeck, Otsuka, Sunovion, and others. Dr. Hwang, a staff physician at the East Orange (N.J.) Veterans Administration Medical Center, did not have any relevant disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE APA ANNUAL MEETING

VIDEO: Identifying patients who will benefit from pulmonary metastasectomy
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
BALTIMORE – New research from Memorial Sloan Kettering Cancer Center in New York could help surgeons better determine which patients with soft tissue sarcoma may benefit most from pulmonary metastasectomy.
The results of the research, presented at the annual meeting of the American Association for Thoracic Surgery, suggest that preoperative factors such as primary tumor histology and size, number of metastases, time from initial resection of the primary, absence of extrapulmonary disease, and thoracoscopic resection are associated with improved survival in STS patients.
Dr. Garrett L. Walsh, professor of surgery at the University of Texas MD Anderson Cancer Center, Houston, and a discussant on the paper at the meeting, said the study was important because it showed the power of a prospective surgical database, retrospectively viewed in this particular case. He said that the Sloan Kettering research was likely “as good as it’s going to get,” given that a randomized controlled trial is unlikely ever to occur with STS patients.
“Trying to select the patients we think are going to do well with surgery has always been one of the challenging aspects of thoracic surgery,” Dr. Walsh said in a video interview. “This paper may help with better selection of patients from that large cohort who are referred to us for pulmonary metastasectomy.”
Dr. Walsh reported no relevant financial disclosures.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @richpizzi
AT THE AATS ANNUAL MEETING

Novel drug shows preclinical success in pancreatic cancer
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”

Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”
Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
SAN DIEGO – The experimental drug Metavert was effective in a mouse model of aggressive pancreatic cancer, and phase I trials in humans are expected to begin in early 2017.
“Metavert significantly slows tumor growth with less toxicity in preclinical trials. The drug prevents metastasis and reduces resistance to chemotherapy. Hopefully the drug will be a good partner with other drugs,” said presenting author Mouad Edderkaoui, Ph.D., of Cedars-Sinai, Los Angeles. “We hope this drug will improve the outcome of treatment of pancreatic cancer, knowing that the drugs now available are not effective and outcome is dismal. The last drug approved for pancreatic cancer – nab-paclitaxel – extended survival by only 7 weeks.”
Dr. Edderkaoui and Dr. Stephen Pandol, director, basic and translational pancreas research, gastroenterology, at Cedars-Sinai, are cofounders of Avenzoar Pharmaceuticals, the developer of Metavert.
Metavert is a small molecular dual inhibitor that targets two procancer pathways. Preclinical results show strong prevention of pancreatic cancer growth and metastasis with no significant toxicity, according to Dr. Edderkaoui, who explained that the novel agent has two linked moieties that target the glycogen synthase kinase–3 (GSK-3) beta and histone deacetylase (HDAC).
GSK-3 beta, which is highly expressed in pancreatic cancer, stimulates proliferation and resistance to apoptosis in cancer cells. HDAC inhibits epithelial cells. In combination, the two should simultaneously affect proliferation and metastasis.
The investigators studied pancreatic cell lines and KPC mice – an animal model of aggressive pancreatic cancer that carries KRAS and p53 mutations. Metavert reduced the survival of cancer cell lines but not of normal cells.
“The [combination] drug was more potent in cell lines than the two inhibitors separately,” he said. In dose-dependent fashion, Metavert inhibited GSK-3 beta and HDAC, decreased markers of epithelial to mesenchymal transition, and decreased migration of pancreatic cancer cells.
Further, Metavert sensitized pancreatic cancer cells to chemotherapy with gemcitabine and to radiation.
In KPC mice with advanced pancreatic cancer, treatment with Metavert increased survival by about 50%. At 6 months, all control mice had died, while 42% of Metavert-treated mice were still alive.
Tumor shrinkage was observed in Metavert-treated mice. Micrometastasis was seen in 29% of controls and in none of the Metavert-treated mice.
Fibrosis was not significantly affected by treatment, and the level of M2 macrophages significantly declined in treated mice.
AT DDW® 2016
Key clinical point: A novel compound appears to have potential in the treatment of pancreatic cancer.
Major finding: In experimental animal models of pancreatic cancer, Metavert improved survival by 50% and prevented micrometastasis.
Data source: Cell lines and a mouse model of pancreatic cancer.
Disclosures: Metavert was developed with financial support from the Hirshberg Foundation, NIH/VA Awards, and the Cedars-Sinai Intellectual Property office.
