User login
Cariprazine for schizophrenia and bipolar I disorder
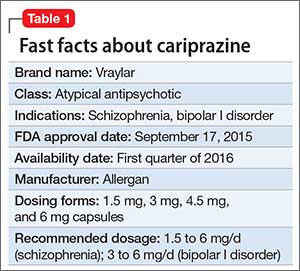
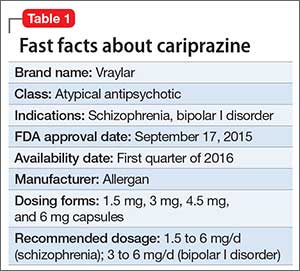
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
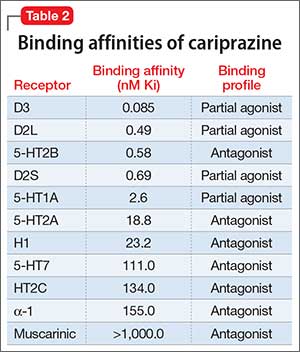
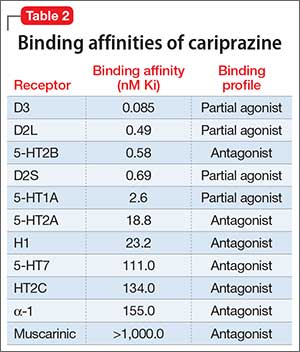
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
Cariprazine for schizophrenia and bipolar I disorder
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
Cariprazine is a newly approved (September 2015) dopamine D3/D2 receptor partial agonist with higher affinity for the D3 receptor than for D2. The drug is FDA-indicated for treating schizophrenia and bipolar I disorder (BD I)1,2 (Table 1). In clinical trials, cariprazine alleviated symptoms of schizophrenia and mixed and manic symptoms of BD I, with minimal effect on metabolic parameters, the prolactin level, and cardiac conduction.
Clinical implications
Despite numerous developments in pharmacotherapeutics, people with schizophrenia or bipolar disorder continue to struggle with residual symptoms or endure treatments that produce adverse effects (AEs). In particular, metabolic issues, sedation, and cognitive impairment plague many current treatment options for these disorders.
Receptor blocking. As a dopamine D3-preferring D3/D2 partial agonist, cariprazine offers an alternative to antipsychotics that preferentially modulate D2 receptors. First-generation (typical) antipsychotics block D2 receptors; atypical antipsychotics block D2 receptors and 5-HT2A receptors. Dopamine partial agonists aripiprazole and brexpiprazole are D2-preferring, with minimal D3 effects. In contrast, cariprazine has a 6-fold to 8-fold higher affinity for D3 receptors than for D2 receptors, and has specificity for the D3 receptor that is 3 to 10 times higher than what aripiprazole has for the D3 receptor3-5 (Table 2).
Use in schizophrenia. Recommended dosage range is 1.5 to 6 mg/d. In Phase-III clinical trials, dosages of 3 to 9 mg/d produced significant improvement on the Positive and Negative Symptom Scale (PANSS) and on the Clinical Global Impression scale. Higher dosages (6 to 9 mg/d) showed early separation from placebo—by the end of Week 1—but carried a dosage-related risk of AEs, leading the FDA to recommend 6 mg/d as the maximum dosage.1,6-8
Use in manic or mixed episodes of BD I. Recommended dosage range is 3 to 6 mg/d. In clinical trials, dosages in the range of 3 to 12 mg/d were effective for acute manic or mixed symptoms; significant improvement in the Young Mania Rating Scale (YMRS) score was seen as early as Day 4. Dosages >6 mg/d yielded no additional benefit and were associated with increased risk of AEs.9-12
Pharmacologic profile, adverse effects. Cariprazine has a pharmacologic profile consistent with the generally favorable metabolic profile and lack of anticholinergic effects seen in clinical trials. In short- and long-term trials, the drug had minimal effects on prolactin, blood pressure, and cardiac conduction.13
Across clinical trials for both disorders, akathisia and parkinsonism were among more common AEs of cariprazine. Both AEs were usually mild, resulting in relatively few premature discontinuations from trials. Parkinsonism appeared somewhat dosage-related; akathisia had no clear relationship to dosage.
How it works
The theory behind the use of partial agonists, including cariprazine, is that these agents restore homeostatic balance to neurochemical circuits by:
- decreasing the effects of endogenous neurotransmitters (dopamine tone) in regions of the brain where their transmission is excessive, such as mesolimbic regions in schizophrenia or mania
- simultaneously increasing neurotransmission in regions where transmission of endogenous neurotransmitters is low, such as the prefrontal cortex in schizophrenia
- exerting little effect in regions where neurotransmitter activity is normal, such as the pituitary gland.
- simultaneously
Cariprazine has higher binding affinity for dopamine D3 receptors (Ki 0.085 nM) than for D2L receptors (Ki 0.49 nM) and D2S receptors (Ki 0.69 nM). The drug also has strong affinity for serotonin receptor 5-HT2B; moderate affinity for 5-HT1A; and lower affinity for 5-HT2A, histamine H1, and 5-HT7 receptors. Cariprazine has little or no affinity for adrenergic or cholinergic receptors.14In patients with schizophrenia, as measured on PET scanning, a dosage of 1.5 mg/d yielded 69% to 75% D2/D3 receptor occupancy. A dosage of 3 mg/d yielded >90% occupancy.
Search for an understanding of action continues. The relative contribution of D3 partial agonism, compared with D2 partial agonism, is a subject of ongoing basic scientific and clinical research. D3 is an autoreceptor that (1) controls phasic, but not tonic, activity of dopamine nerve cells and (2) mediates behavioral abnormalities induced by glutamate and N-methyl-D-aspartate receptor antagonists.5,12 In animal studies, D3-preferring agents have been shown to exert pro-cognitive effects and improve anhedonic symptoms.
Pharmacokinetics
Cariprazine is a once-daily medication with a relatively long half-life that can be taken with or without food. Dosages of 3 to 12 mg/d yield a fairly linear, dose-proportional increase in plasma concentration. The peak serum concentration for cariprazine is 3 to 4 hours under fasting conditions; taking the drug with food causes a slight delay in absorption but does not have a significant effect on the area under the curve. Mean half-life for cariprazine is 2 to 5 days over a dosage range of 1.5 to 12.5 mg/d in otherwise healthy adults with schizophrenia.1
Cariprazine is metabolized primarily by cytochrome P450 (CYP) 3A4. It is a weak inhibitor of CYP2D6 and CYP3A4.1 Hepatic metabolism of cariprazine produces 2 active metabolites: desmethyl-cariprazine (DCAR) and didesmethyl-cariprazine (DDCAR), both of which are equipotent to cariprazine. After multiple dose administration, mean cariprazine and DCAR levels reach steady state in 1 to 2 weeks; DDCAR, in 4 to 8 weeks. The systemic exposure and serum levels of DDCAR are roughly 3-fold greater than cariprazine because of the longer elimination half-life of DDCAR.1
Efficacy in schizophrenia
The efficacy of cariprazine in schizophrenia was established by 3 six-week, randomized, placebo-controlled trials. Two trials were fixed-dosage; a third used 2 flexible dosage ranges. The primary efficacy measure was change from baseline in the total score of the PANSS at the end of Week 6, compared with placebo. In all trials, patients were adults (age 18 to 60) who met DSM-IV-TR criteria for schizophrenia and had a PANSS score between 80 and 120 at screening and baseline.
Study 1 (n = 711) compared dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d with placebo.7 All cariprazine dosages and an active control (risperdone) were superior to placebo in reducing symptoms of schizophrenia, as measured by the PANSS. The placebo-subtracted differences on PANSS score at 6 weeks for dosages of 1.5 mg/d, 3 mg/d, and 4.5 mg/d were –7.6, –8.8, –10.4, respectively (significant at 95% CI).
Study 2 (n = 151) compared 3 mg/d and 6 mg/d dosages of cariprazine with placebo.1 Both dosages and an active control (aripiprazole) were superior to placebo in reducing PANSS scores. Placebo-subtracted differences on PANSS score at 6 weeks for dosages of 3 mg/d and 6 mg/day were –6.0, –8.8, respectively (significant at 95% CI).
Study 3 (n = 147) was a fixed-flexible dosage trial comparing cariprazine, 3 to 6 mg/d and 6 to 9 mg/d dosage ranges, to placebo.8 Both ranges were superior to placebo in reducing symptoms on PANSS. Placebo-subtracted differences from placebo on PANSS at 6 weeks for cariprazine 3 to 6 or 6 to 9 mg/d were –6.8, –9.9, respectively (significant at 95% CI).
These trials established the efficacy of cariprazine for acute schizophrenia at dosages ranging from 1.5 to 9 mg/d. Although there was a modest trend toward higher efficacy at higher dosages, there was a dose-related increase in certain adverse reactions (extrapyramidal symptoms [EPS]) at dosages >6 mg/d.1
Efficacy in bipolar disorder
The efficacy of cariprazine for acute treatment of manic or mixed episodes of BD I was established in 3 randomized, placebo-controlled, flexibly dosed 3-week trials. In all trials, patients were adults (age 18 to 65) who met DSM-IV-TR criteria for BD I with manic or mixed episodes and with or without psychotic features (YMRS score, ≥20). The primary efficacy measure in the 3 trials was a change from baseline in the total YMRS score at the end of Week 3, compared with placebo.
Study 1 (n = 492) compared 2 flexibly dosed ranges of cariprazine (3 to 6 mg/d and 6 to 12 mg/d) with placebo.10 Both dosage ranges were superior to placebo in reducing mixed and manic symptoms, as measured by reduction in the total YMRS score. Placebo-subtracted differences in YMRS scores from placebo at Week 3 for cariprazine 3 to 6 mg/d and 6 to 12 mg/d were –6.1, –5.9, respectively (significant at 95% CI). The higher range offered no additional advantage over the lower range.
Study 2 (n = 235) compared flexibly dosed cariprazine, 3 to 12 mg/d, to placebo.11 Cariprazine was superior to placebo in reducing bipolar symptoms as measured by the YMRS. The difference between cariprazine 3 to 12 mg/d and placebo on the YMRS score at Week 3 was –6.1 (significant at 95% CI).
Study 3 (n = 310) compared flexibly dosed cariprazine, 3 to 12 mg/d, with placebo.15 Again, cariprazine was superior to placebo in reducing the YMRS score at Week 3: difference, –4.3 (significant at 95% CI).
These trials establish the efficacy of cariprazine in treating acute mania or mixed BD I episodes at dosages ranging from 3 to 12 mg/d. Dosages >6 mg/d did not offer additional benefit over lower dosages, and resulted in a dosage-related increase in EPS at dosages >6 mg/d.16
Tolerability
Cariprazine generally was well tolerated in short-term trials for schizophrenia and BD I. The only treatment-emergent adverse event reported for at least 1 treatment group in all trials at a rate of ≥10%, and at least twice the rate seen with placebo was akathisia. Adverse events reported at a lower rate than placebo included EPS (particularly parkinsonism), restlessness, headache, insomnia, fatigue, and gastrointestinal distress. The discontinuation rate due to AEs for treatment groups and placebo-treated patients generally was similar. In schizophrenia Study 3, for example, the discontinuation rate due to AEs was 13% for placebo; 14% for cariprazine, 3 to 6 mg/d; and 13% for cariprazine, 6 to 9 mg/d.1 48-Week open-label safety study. Patients with schizophrenia received open-label cariprazine for as long as 48 weeks.7 Serious adverse events were reported in 12.9%, including 1 death (suicide); exacerbation of symptoms of schizophrenia (4.3%); and psychosis (2.2%). Treatment-emergent adverse events reported in at least 10% of patients included akathisia (14.0%), insomnia (14.0%), and weight gain (11.8%). The mean change in laboratory values, blood pressure, pulse rate, and electrocardiographic parameters was clinically insignificant.
Other studies. In a 16-week, open-label extension study of patients with BD I, the major tolerability issue was akathisia. This AE developed in 37% of patients and led to a 5% withdrawal rate.12
In short- and long-term studies for either indication, the effect of the drug on metabolic parameters appears to be small. In studies with active controls, potentially significant weight gain (>7%) was greater for aripiprazole and risperidone than for cariprazine.6,7 The effect on the prolactin level was minimal. There do not appear to be clinically meaningful changes in laboratory values, vital signs, or QT interval.
Unique clinical issues
Preferential binding. Cariprazine is the third dopamine partial agonist approved for use in the United States; unlike the other 2—aripiprazole and brexpiprazole—cariprazine shows preference for D3 receptors over D2 receptors. The exact clinical impact of a preference for D3 and the drug’s partial agonism of 5-HT1A has not been fully elucidated.
EPS, including akathisia and parkinsonism, were among common adverse events. Both were usually mild, with 0.5% of schizophrenia patients and 2% of BD I patients dropping out of trials because of any type of EPS-related AEs.
Why Rx? On a practical medical level, reasons to prescribe cariprazine likely include:
- minimal effect on prolactin
- relative lack of effect on metabolic parameters, including weight (cariprazine showed less weight gain than risperidone or aripiprazole control arms in trials).
Dosing
The recommended dosage of cariprazine for schizophrenia ranges from 1.5 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
The recommended dosages of cariprazine for mixed and manic episodes of BD I range from 3 to 6 mg/d. The recommended starting dosage is 1.5 mg/d, which can be increased to 3 mg on Day 2, with further upward dosage adjustments of 1.5 to 3 mg/d, based on clinical response and tolerability.1
Other key aspects of dosing to keep in mind:
- Because of the long half-life and 2 equipotent active metabolites of cariprazine, any changes made to the dosage will not be reflected fully in the serum level for 2 weeks.
- Administering the drug with food slightly delays, but does not affect, the extent of absorption.
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 inhibitor; the recommended starting dosage of cariprazine is 1.5 mg every other day with a maximum dosage of 3 mg/d when it is administered concomitantly with a strong CYP3A4 inhibitor.
- Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4 inducer, this practice is not recommended.1
- Because the drug is metabolized primarily by CYP3A4, dosage adjustment is required in the presence of a CYP3A4 Because data are not available regarding concomitant use of cariprazine with a strong CYP3A4
Contraindications
Cariprazine carries a FDA black-box warning of increased mortality in older patients who have dementia-related psychosis, as other atypical antipsychotics do. Clinical trials produced few data about the use of cariprazine in geriatric patients; no data exist about use in the pediatric population.1
Metabolic, prolactin, and cardiac concerns about cariprazine appeared favorably minor in Phase-III and long-term safety trials. Concomitant use of cariprazine with any strong inducer of CYP3A4 has not been studied, and is not recommended. Dosage reduction is recommended when using cariprazine concomitantly with a CYP3A4 inhibitor.1
In conclusion
The puzzle in neuropsychiatry has always been to find ways to produce different effects in different brain regions—with a single drug. Cariprazine’s particular binding profile—higher affinity and higher selectivity for D3 receptors than for D2 receptors compared with either aripiprazole or brexpiprazole—may secure a role for it in managing psychosis and mood disorders.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
1. Vraylar [package insert]. Parsippany, NJ: Actavis Pharma, Inc.; 2015.
2. McCormack PL, Cariprazine: first global approval. Drugs. 2015;75(17):2035-2043.
3. Kiss B, Horváth A, Némethy Z, et al. Cariprazine (RGH-188), a dopamine D(3) receptor-preferring, D(3)/D(2) dopamine receptor antagonist-partial agonist antipsychotic candidate: in vitro and neurochemical profile. J Pharmacol Exp Ther. 2010;333(1):328-340.
4. Potkin, S, Keator, D, Mukherjee J, et al. P. 1. E 028 dopamine D3 and D2 receptor occupancy of cariprazine in schizophrenic patients. Eur Neuropsychopharmacology. 2009;19(suppl 3):S316.
5. Veselinovicˇ T, Paulzen M, Gründer G. Cariprazine, a new, orally active dopamine D2/3 receptor partial agonist for the treatment of schizophrenia, bipolar mania and depression. Expert Rev Neurother. 2013;13(11):1141-1159.
6. Cutler A, Mokliatchouk O, Laszlovszky I, et al. Cariprazine in acute schizophrenia: a fixed-dose phase III, randomized, double-blind, placebo- and active-controlled trial. Abstract presented at: 166th Annual Meeting of the American Psychiatric Association; May 18-22, 2013; San Francisco, CA.
7. Durgam S, Starace A, Li D, et al. An evaluation of the safety and efficacy of cariprazine in patients with acute exacerbation of schizophrenia: a phase II, randomized clinical trial. Schizophr Res. 2014;152(2-3):450-457.
8. Kane JM, Zukin S, Wang Y, et al. Efficacy and safety of cariprazine in acute exacerbation of schizophrenia: results from an international, phase III clinical trial. J Clin Psychopharmacol. 2015;35(4):367-373.
9. Bose A, Starace A, Lu, K, et al. Cariprazine in the treatment of acute mania in bipolar disorder: a double-blind, placebo-controlled, phase III trial. Poster presented at: 16th Annual Meeting of the College of Psychiatric and Neurologic Pharmacists; April 21-24, 2013; Colorado Springs, CO.
10. Calabrese JR, Keck PE Jr, Starace A, et al. Efficacy and safety of low- and high-dose cariprazine in acute and mixed mania associated with bipolar I disorder: a double-blind, placebo-controlled study. J Clin Psychiatry. 2015;76(3):284-292.
11. Durgam S, Starace A, Li D, et al. The efficacy and tolerability of cariprazine in acute mania associated with bipolar I disorder: a phase II trial. Bipolar Disord. 2015;17(1):63-75.
12. Ketter, T. A phase III, open-label, 16-week study of flexibly dosed cariprazine in 402 patients with bipolar I disorder. Presented at: 53rd Annual Meeting of the New Clinical Drug Evaluation Unit; May 28-31, 2013; Hollywood, FL.
13. Bose A, Li D, Migliore R. The efficacy and safety of the novel antipsychotic cariprazine in the acute exacerbation of schizophrenia. Poster presented at: 50th Annual Meeting of the New Clinical Drug Evaluation Unit; June 14-17, 2010; Boca Raton, FL.
14. Citrome L. Cariprazine: chemistry, pharmacodynamics, pharmacokinetics, and metabolism, clinical efficacy, safety, and tolerability. Expert Opin Drug Metab Toxicol. 2013;9(2):193-206.
15. Sachs GS, Greenberg WM, Starace A, et al. Cariprazine in the treatment of acute mania in bipolar I disorder: a double-blind, placebo-controlled, phase III trial. J Affect Disord. 2015;174:296-302.
16. Vieta E, Durgam S, Lu K, et al. Effect of cariprazine across the symptoms of mania in bipolar I disorder: analyses of pooled data from phase II/III trials. Eur Neuropsycholpharmacol. 2015;25(11):1882-1891.
The newest ‘rage’: disruptive mood dysregulation disorder
Outbursts by children when frustrated or when asked to “do something they don’t want to do” are among the most common behavioral complaints voiced by parents. But behavioral outbursts, beyond the typical tantrums of children up to age 4 years, can be signs of very severe mental health disorders and are the most common reason for psychiatric admission (50%-60%).
While behavioral dysregulation is undeniably a huge problem for families, there has been an unreasonable 40-fold rise in diagnosis of bipolar disorder from 1994 to 2003, and 48% were prescribed atypical neuroleptics – medications with serious side effects. In response to this overdiagnosis as bipolar disorder, in 2013 the DSM-5 created a new diagnosis called disruptive mood dysregulation disorder (DMDD) to differentiate children who experience explosive outbursts who have a different outcome. This new classification includes children aged 6-12 years with persistent irritability most of the time, nearly every day, lasting at least 12 months and starting before age 10 years. DMDD diagnosis is not used after age 18 years.
To be diagnosed, the child has to have frequent, severe temper outbursts “grossly out of proportion” to the situation, averaging at least three times per week. The outbursts can be verbal or physical aggression to people, things, or themselves. While tantrums can be severe in children with delayed development, for the DMDD diagnosis these behaviors must be inconsistent with developmental level and must occur in at least two settings, and in one setting it must be severe. While outbursts are common, only half of children in one study of severe tantrum behavior in 5- to 9-year-olds also had the required persistent irritability.

If this does sound a lot like bipolar disorder so far, you are right. So what is different? DMDD has a prevalence of 2%-5% and occurs mostly in boys, whereas bipolar disorder affects boys and girls equally and affects less than 1% prior to adolescence.
The key features distinguishing DMDD from bipolar disorder are lack of an episodic nature to the irritability and lack of mania. Irritability in DMDD has to be persistently present with breaks of no more than 3 consecutive months in the defining 12-month period. There also cannot be any more than 1 day of the elevated mood features of mania or hypomania. Identifying mania is the hardest part, even in diagnosing adult bipolar, where it occurs only 1% of the year, much less in children who are generally lively! Hypomania, while less intense than mania, is when the person is energetic, talkative, and confident to an extreme extent, often with a flight of creative ideas. Excitement over birthdays or Christmas specifically does not count! So getting this history has to be done carefully, generally by a mental health professional, to make the distinction.
Interestingly, DMDD is not diagnosed when outbursts and irritability are better explained by autism spectrum disorder, separation anxiety disorder, or PTSD. To me, these exclusions point out the importance of sorting out the “set conditions” for all problematic behaviors, not always an easy task. Symptoms of autism in high functioning individuals can be quite subtle. Was the upset from change in a rigid routine known only to the child? Were sensory stimuli such as loud noises intolerable to this child? Was a nonverbal signal of a peer mistaken as a threat? While violent outbursts precipitated by these factors would still be considered “grossly out of proportion to the situation” for a typical child, they are not uncommon in atypical children. Similarly, children with separation anxiety disorder experience a high level of threat from even thinking about being apart from their caregivers, setting them up for alarm by situations other children would not find difficult.
The American Academy of Pediatrics emphasizes the need to assess all children for a history of psychological trauma. Traumas are quite common, and their sequelae affect many aspects of the child’s life; in the case of outbursts, it is emotional resilience that is impaired. As for all DSM-5 diagnoses, DMDD is not diagnosed when the irritability is due to physiological effects of a substance (e.g. steroids) or another medical or neurological disorder. Children with chronic pain conditions such as rheumatoid arthritis or sickle cell usually cope remarkably well, but when they don’t, their irritability should not be considered a mental health disorder. More commonly, sleep debt can produce chronic irritability and always should be assessed.
When coaching families about outbursts, I work to help them recognize that the child is not just angry, but very distressed. While “typical” tantrums last 1-5 minutes and show a rise then decline in intensity of the anger and distress, anger outbursts are longer and have an initial short and rapid burst of anger that then declines over the duration of the outburst, and with a steady but lower level of distress throughout.
The option to hug and verbally console the child’s distress is sometimes effective and does not reinforce the behavior unless the parent also yields to demands. But once outbursts begin, I liken them to a bomb going off – there is no intervention possible then. Instead, the task of the family, and over time that of the child, is to recognize and better manage the triggers.
Dr. Ross Greene, in his book, “The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children,” asserts that the child’s anger and distress can be interpreted as frustration from a gap in skills. This has treatment implications for identifying, educating about, and ameliorating the child’s weaknesses (deficits in understanding, communication, emotion regulation, flexibility or performance; or excess jealousy or hypersensitivity), and coaching parents to recognize, acknowledge, and avoid stressing these areas, if possible. I coach families to give points to the child for progressive little steps toward being able to recognize, verbalize, and inhibit outbursts with a reward system for the points. This helps put the parents and child “on the same team” in working on improving these skills.
Research on children with DMDD indicates that they show less positive affect when winning a “fixed” video game and are less able to suppress negative affect when losing. (Don’t forget to examine the role of real video games as precipitants of tantrums and contingently remove them!) Threshold for upset is lower and the degree of the upsets less well handled by children with DMDD.
In another study, when presented with a series of ambiguous facial expressions, children with DMDD were more likely to see anger in the faces than were controls. One hopeful result was that they could be taught to shift their perceptions significantly away from seeing anger, also reducing irritability and resulting in functional MRI changes. Such hostile bias attribution (tending to see threat) is well known to predispose to aggression. Cognitive behavioral therapy, the most effective counseling intervention, similarly teaches children to rethink their own negative thoughts before acting.
If irritability and rages were not enough, most children with DMDD have other psychiatric disorders; 39% having two, and 51% three or more (J Child Adolesc Psychopharmacol. 2013 Nov;23[9]:588-96). If not for the DMDD diagnosis, 82% would meet criteria for oppositional defiant disorder (ODD). The other common comorbidities are attention-deficit/hyperactivity disorder (ADHD) (74.5%), anxiety disorders (49.0%), and depression that is not major depressive disorder (MDD)(33.3%). When MDD is present, that diagnosis takes precedence. One cannot diagnose ODD, intermittent explosive disorder, or bipolar disorder along with DMDD, conditions from which it is intended to differentiate. Each of these comorbid disorders can be difficult to manage alone much less in combination, making DMDD a disorder deserving diagnosis and treatment by a mental health professional.
One of the main reasons DMDD was created is that children with these features go on to depressive or anxiety disorder in adolescence, not bipolar disorder.
While there is no treatment specific to DMDD, the depression component and prognosis suggest use of SSRIs, in addition to psychosocial therapies, and stimulants for the comorbid ADHD. Unfortunately, these two classes of medication are relatively contraindicated in bipolar disorder because they can lead to treatment-induced episodic mania (TEM). TEM occurs twice as often with antidepressants compared with stimulants (44% vs. 18%) in children with bipolar disorder (J Affect Disord. 2004 Oct 1;82[1]:149-58). Getting the diagnosis correct is, therefore, of great importance when medication is considered.
Approaches such as behavior modification, family therapy, and inpatient treatment can be effective for chronic irritability and aggression. Stimulant treatment of comorbid ADHD can decrease aggression and irritability. Alpha agonists such as guanfacine or clonidine also can help. In cases of partial improvement, adding either risperidone or divalproex may further decrease aggression in ADHD. In refractory aggression, risperidone has the best evidence. The Affective Reactivity Index or Outburst Monitoring Scale can be helpful in assessing severity and monitoring outcomes.
While a prognosis for depression rather than bipolar disorder sounds like a plus, in a longitudinal study, adults who had DMDD as children had worse outcomes, including being more likely to have adverse health outcomes (smoking, sexually transmitted infection), police contact, and low educational attainment, and being more likely to live in poverty, compared with controls who had other psychiatric disorders. While DMDD is a new and different diagnosis, it is similar to bipolar in having a potential course of life disruption, dangerous behaviors, suicide risk, and hospitalization.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
Outbursts by children when frustrated or when asked to “do something they don’t want to do” are among the most common behavioral complaints voiced by parents. But behavioral outbursts, beyond the typical tantrums of children up to age 4 years, can be signs of very severe mental health disorders and are the most common reason for psychiatric admission (50%-60%).
While behavioral dysregulation is undeniably a huge problem for families, there has been an unreasonable 40-fold rise in diagnosis of bipolar disorder from 1994 to 2003, and 48% were prescribed atypical neuroleptics – medications with serious side effects. In response to this overdiagnosis as bipolar disorder, in 2013 the DSM-5 created a new diagnosis called disruptive mood dysregulation disorder (DMDD) to differentiate children who experience explosive outbursts who have a different outcome. This new classification includes children aged 6-12 years with persistent irritability most of the time, nearly every day, lasting at least 12 months and starting before age 10 years. DMDD diagnosis is not used after age 18 years.
To be diagnosed, the child has to have frequent, severe temper outbursts “grossly out of proportion” to the situation, averaging at least three times per week. The outbursts can be verbal or physical aggression to people, things, or themselves. While tantrums can be severe in children with delayed development, for the DMDD diagnosis these behaviors must be inconsistent with developmental level and must occur in at least two settings, and in one setting it must be severe. While outbursts are common, only half of children in one study of severe tantrum behavior in 5- to 9-year-olds also had the required persistent irritability.
If this does sound a lot like bipolar disorder so far, you are right. So what is different? DMDD has a prevalence of 2%-5% and occurs mostly in boys, whereas bipolar disorder affects boys and girls equally and affects less than 1% prior to adolescence.
The key features distinguishing DMDD from bipolar disorder are lack of an episodic nature to the irritability and lack of mania. Irritability in DMDD has to be persistently present with breaks of no more than 3 consecutive months in the defining 12-month period. There also cannot be any more than 1 day of the elevated mood features of mania or hypomania. Identifying mania is the hardest part, even in diagnosing adult bipolar, where it occurs only 1% of the year, much less in children who are generally lively! Hypomania, while less intense than mania, is when the person is energetic, talkative, and confident to an extreme extent, often with a flight of creative ideas. Excitement over birthdays or Christmas specifically does not count! So getting this history has to be done carefully, generally by a mental health professional, to make the distinction.
Interestingly, DMDD is not diagnosed when outbursts and irritability are better explained by autism spectrum disorder, separation anxiety disorder, or PTSD. To me, these exclusions point out the importance of sorting out the “set conditions” for all problematic behaviors, not always an easy task. Symptoms of autism in high functioning individuals can be quite subtle. Was the upset from change in a rigid routine known only to the child? Were sensory stimuli such as loud noises intolerable to this child? Was a nonverbal signal of a peer mistaken as a threat? While violent outbursts precipitated by these factors would still be considered “grossly out of proportion to the situation” for a typical child, they are not uncommon in atypical children. Similarly, children with separation anxiety disorder experience a high level of threat from even thinking about being apart from their caregivers, setting them up for alarm by situations other children would not find difficult.
The American Academy of Pediatrics emphasizes the need to assess all children for a history of psychological trauma. Traumas are quite common, and their sequelae affect many aspects of the child’s life; in the case of outbursts, it is emotional resilience that is impaired. As for all DSM-5 diagnoses, DMDD is not diagnosed when the irritability is due to physiological effects of a substance (e.g. steroids) or another medical or neurological disorder. Children with chronic pain conditions such as rheumatoid arthritis or sickle cell usually cope remarkably well, but when they don’t, their irritability should not be considered a mental health disorder. More commonly, sleep debt can produce chronic irritability and always should be assessed.
When coaching families about outbursts, I work to help them recognize that the child is not just angry, but very distressed. While “typical” tantrums last 1-5 minutes and show a rise then decline in intensity of the anger and distress, anger outbursts are longer and have an initial short and rapid burst of anger that then declines over the duration of the outburst, and with a steady but lower level of distress throughout.
The option to hug and verbally console the child’s distress is sometimes effective and does not reinforce the behavior unless the parent also yields to demands. But once outbursts begin, I liken them to a bomb going off – there is no intervention possible then. Instead, the task of the family, and over time that of the child, is to recognize and better manage the triggers.
Dr. Ross Greene, in his book, “The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children,” asserts that the child’s anger and distress can be interpreted as frustration from a gap in skills. This has treatment implications for identifying, educating about, and ameliorating the child’s weaknesses (deficits in understanding, communication, emotion regulation, flexibility or performance; or excess jealousy or hypersensitivity), and coaching parents to recognize, acknowledge, and avoid stressing these areas, if possible. I coach families to give points to the child for progressive little steps toward being able to recognize, verbalize, and inhibit outbursts with a reward system for the points. This helps put the parents and child “on the same team” in working on improving these skills.
Research on children with DMDD indicates that they show less positive affect when winning a “fixed” video game and are less able to suppress negative affect when losing. (Don’t forget to examine the role of real video games as precipitants of tantrums and contingently remove them!) Threshold for upset is lower and the degree of the upsets less well handled by children with DMDD.
In another study, when presented with a series of ambiguous facial expressions, children with DMDD were more likely to see anger in the faces than were controls. One hopeful result was that they could be taught to shift their perceptions significantly away from seeing anger, also reducing irritability and resulting in functional MRI changes. Such hostile bias attribution (tending to see threat) is well known to predispose to aggression. Cognitive behavioral therapy, the most effective counseling intervention, similarly teaches children to rethink their own negative thoughts before acting.
If irritability and rages were not enough, most children with DMDD have other psychiatric disorders; 39% having two, and 51% three or more (J Child Adolesc Psychopharmacol. 2013 Nov;23[9]:588-96). If not for the DMDD diagnosis, 82% would meet criteria for oppositional defiant disorder (ODD). The other common comorbidities are attention-deficit/hyperactivity disorder (ADHD) (74.5%), anxiety disorders (49.0%), and depression that is not major depressive disorder (MDD)(33.3%). When MDD is present, that diagnosis takes precedence. One cannot diagnose ODD, intermittent explosive disorder, or bipolar disorder along with DMDD, conditions from which it is intended to differentiate. Each of these comorbid disorders can be difficult to manage alone much less in combination, making DMDD a disorder deserving diagnosis and treatment by a mental health professional.
One of the main reasons DMDD was created is that children with these features go on to depressive or anxiety disorder in adolescence, not bipolar disorder.
While there is no treatment specific to DMDD, the depression component and prognosis suggest use of SSRIs, in addition to psychosocial therapies, and stimulants for the comorbid ADHD. Unfortunately, these two classes of medication are relatively contraindicated in bipolar disorder because they can lead to treatment-induced episodic mania (TEM). TEM occurs twice as often with antidepressants compared with stimulants (44% vs. 18%) in children with bipolar disorder (J Affect Disord. 2004 Oct 1;82[1]:149-58). Getting the diagnosis correct is, therefore, of great importance when medication is considered.
Approaches such as behavior modification, family therapy, and inpatient treatment can be effective for chronic irritability and aggression. Stimulant treatment of comorbid ADHD can decrease aggression and irritability. Alpha agonists such as guanfacine or clonidine also can help. In cases of partial improvement, adding either risperidone or divalproex may further decrease aggression in ADHD. In refractory aggression, risperidone has the best evidence. The Affective Reactivity Index or Outburst Monitoring Scale can be helpful in assessing severity and monitoring outcomes.
While a prognosis for depression rather than bipolar disorder sounds like a plus, in a longitudinal study, adults who had DMDD as children had worse outcomes, including being more likely to have adverse health outcomes (smoking, sexually transmitted infection), police contact, and low educational attainment, and being more likely to live in poverty, compared with controls who had other psychiatric disorders. While DMDD is a new and different diagnosis, it is similar to bipolar in having a potential course of life disruption, dangerous behaviors, suicide risk, and hospitalization.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].
Outbursts by children when frustrated or when asked to “do something they don’t want to do” are among the most common behavioral complaints voiced by parents. But behavioral outbursts, beyond the typical tantrums of children up to age 4 years, can be signs of very severe mental health disorders and are the most common reason for psychiatric admission (50%-60%).
While behavioral dysregulation is undeniably a huge problem for families, there has been an unreasonable 40-fold rise in diagnosis of bipolar disorder from 1994 to 2003, and 48% were prescribed atypical neuroleptics – medications with serious side effects. In response to this overdiagnosis as bipolar disorder, in 2013 the DSM-5 created a new diagnosis called disruptive mood dysregulation disorder (DMDD) to differentiate children who experience explosive outbursts who have a different outcome. This new classification includes children aged 6-12 years with persistent irritability most of the time, nearly every day, lasting at least 12 months and starting before age 10 years. DMDD diagnosis is not used after age 18 years.
To be diagnosed, the child has to have frequent, severe temper outbursts “grossly out of proportion” to the situation, averaging at least three times per week. The outbursts can be verbal or physical aggression to people, things, or themselves. While tantrums can be severe in children with delayed development, for the DMDD diagnosis these behaviors must be inconsistent with developmental level and must occur in at least two settings, and in one setting it must be severe. While outbursts are common, only half of children in one study of severe tantrum behavior in 5- to 9-year-olds also had the required persistent irritability.
If this does sound a lot like bipolar disorder so far, you are right. So what is different? DMDD has a prevalence of 2%-5% and occurs mostly in boys, whereas bipolar disorder affects boys and girls equally and affects less than 1% prior to adolescence.
The key features distinguishing DMDD from bipolar disorder are lack of an episodic nature to the irritability and lack of mania. Irritability in DMDD has to be persistently present with breaks of no more than 3 consecutive months in the defining 12-month period. There also cannot be any more than 1 day of the elevated mood features of mania or hypomania. Identifying mania is the hardest part, even in diagnosing adult bipolar, where it occurs only 1% of the year, much less in children who are generally lively! Hypomania, while less intense than mania, is when the person is energetic, talkative, and confident to an extreme extent, often with a flight of creative ideas. Excitement over birthdays or Christmas specifically does not count! So getting this history has to be done carefully, generally by a mental health professional, to make the distinction.
Interestingly, DMDD is not diagnosed when outbursts and irritability are better explained by autism spectrum disorder, separation anxiety disorder, or PTSD. To me, these exclusions point out the importance of sorting out the “set conditions” for all problematic behaviors, not always an easy task. Symptoms of autism in high functioning individuals can be quite subtle. Was the upset from change in a rigid routine known only to the child? Were sensory stimuli such as loud noises intolerable to this child? Was a nonverbal signal of a peer mistaken as a threat? While violent outbursts precipitated by these factors would still be considered “grossly out of proportion to the situation” for a typical child, they are not uncommon in atypical children. Similarly, children with separation anxiety disorder experience a high level of threat from even thinking about being apart from their caregivers, setting them up for alarm by situations other children would not find difficult.
The American Academy of Pediatrics emphasizes the need to assess all children for a history of psychological trauma. Traumas are quite common, and their sequelae affect many aspects of the child’s life; in the case of outbursts, it is emotional resilience that is impaired. As for all DSM-5 diagnoses, DMDD is not diagnosed when the irritability is due to physiological effects of a substance (e.g. steroids) or another medical or neurological disorder. Children with chronic pain conditions such as rheumatoid arthritis or sickle cell usually cope remarkably well, but when they don’t, their irritability should not be considered a mental health disorder. More commonly, sleep debt can produce chronic irritability and always should be assessed.
When coaching families about outbursts, I work to help them recognize that the child is not just angry, but very distressed. While “typical” tantrums last 1-5 minutes and show a rise then decline in intensity of the anger and distress, anger outbursts are longer and have an initial short and rapid burst of anger that then declines over the duration of the outburst, and with a steady but lower level of distress throughout.
The option to hug and verbally console the child’s distress is sometimes effective and does not reinforce the behavior unless the parent also yields to demands. But once outbursts begin, I liken them to a bomb going off – there is no intervention possible then. Instead, the task of the family, and over time that of the child, is to recognize and better manage the triggers.
Dr. Ross Greene, in his book, “The Explosive Child: A New Approach for Understanding and Parenting Easily Frustrated, Chronically Inflexible Children,” asserts that the child’s anger and distress can be interpreted as frustration from a gap in skills. This has treatment implications for identifying, educating about, and ameliorating the child’s weaknesses (deficits in understanding, communication, emotion regulation, flexibility or performance; or excess jealousy or hypersensitivity), and coaching parents to recognize, acknowledge, and avoid stressing these areas, if possible. I coach families to give points to the child for progressive little steps toward being able to recognize, verbalize, and inhibit outbursts with a reward system for the points. This helps put the parents and child “on the same team” in working on improving these skills.
Research on children with DMDD indicates that they show less positive affect when winning a “fixed” video game and are less able to suppress negative affect when losing. (Don’t forget to examine the role of real video games as precipitants of tantrums and contingently remove them!) Threshold for upset is lower and the degree of the upsets less well handled by children with DMDD.
In another study, when presented with a series of ambiguous facial expressions, children with DMDD were more likely to see anger in the faces than were controls. One hopeful result was that they could be taught to shift their perceptions significantly away from seeing anger, also reducing irritability and resulting in functional MRI changes. Such hostile bias attribution (tending to see threat) is well known to predispose to aggression. Cognitive behavioral therapy, the most effective counseling intervention, similarly teaches children to rethink their own negative thoughts before acting.
If irritability and rages were not enough, most children with DMDD have other psychiatric disorders; 39% having two, and 51% three or more (J Child Adolesc Psychopharmacol. 2013 Nov;23[9]:588-96). If not for the DMDD diagnosis, 82% would meet criteria for oppositional defiant disorder (ODD). The other common comorbidities are attention-deficit/hyperactivity disorder (ADHD) (74.5%), anxiety disorders (49.0%), and depression that is not major depressive disorder (MDD)(33.3%). When MDD is present, that diagnosis takes precedence. One cannot diagnose ODD, intermittent explosive disorder, or bipolar disorder along with DMDD, conditions from which it is intended to differentiate. Each of these comorbid disorders can be difficult to manage alone much less in combination, making DMDD a disorder deserving diagnosis and treatment by a mental health professional.
One of the main reasons DMDD was created is that children with these features go on to depressive or anxiety disorder in adolescence, not bipolar disorder.
While there is no treatment specific to DMDD, the depression component and prognosis suggest use of SSRIs, in addition to psychosocial therapies, and stimulants for the comorbid ADHD. Unfortunately, these two classes of medication are relatively contraindicated in bipolar disorder because they can lead to treatment-induced episodic mania (TEM). TEM occurs twice as often with antidepressants compared with stimulants (44% vs. 18%) in children with bipolar disorder (J Affect Disord. 2004 Oct 1;82[1]:149-58). Getting the diagnosis correct is, therefore, of great importance when medication is considered.
Approaches such as behavior modification, family therapy, and inpatient treatment can be effective for chronic irritability and aggression. Stimulant treatment of comorbid ADHD can decrease aggression and irritability. Alpha agonists such as guanfacine or clonidine also can help. In cases of partial improvement, adding either risperidone or divalproex may further decrease aggression in ADHD. In refractory aggression, risperidone has the best evidence. The Affective Reactivity Index or Outburst Monitoring Scale can be helpful in assessing severity and monitoring outcomes.
While a prognosis for depression rather than bipolar disorder sounds like a plus, in a longitudinal study, adults who had DMDD as children had worse outcomes, including being more likely to have adverse health outcomes (smoking, sexually transmitted infection), police contact, and low educational attainment, and being more likely to live in poverty, compared with controls who had other psychiatric disorders. While DMDD is a new and different diagnosis, it is similar to bipolar in having a potential course of life disruption, dangerous behaviors, suicide risk, and hospitalization.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline. E-mail her at [email protected].

The Starbucks generation
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.

But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.

The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.
But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.
The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.
Iced, Half-Caff, Ristretto, Venti, 4-Pump, Sugar Free, Cinnamon, Dolce Soy Skinny Latte. Or Non-Fat Frappuccino with Extra Whipped Cream and Chocolate Sauce. Sorry, let me simplify: Triple, Venti, Soy, No Foam Latte. If you’re thinking I am speaking a foreign language, just ask a teen and they likely will be able to translate for you. This is normal Starbucks lingo. If you’re not a coffee drinker, you’re likely completely lost, but for those of us who live by the bean, it’s the language of love, caffeine love.
Twenty years ago, the thought of a teen drinking coffee was unheard of. Sure, soda has been there for decades, and in many cultures tea is a common drink, but today many kids are lining up at Starbucks for the caffeine jolt, and the new drinks such as 5-Hour Energy, Jolt, and Red Bull are making this generation the most sleep-deprived ever.
But how bad is caffeine for teens? The average adult consumes approximately 300 mg of caffeine per day,1 which is equivalent to 2-4 cups of coffee; this is considered to be a moderate intake. But the average teen intake of caffeine is not limited to just coffee. Many are consuming their favorite drink from Starbucks, then a few cans of soda, chocolate candy, and maybe even an energy drink – all before the school day is over. When we consider the content of caffeine in these products, the intake of caffeine is staggering.
For example, the average soda contains 35-55 mg of caffeine. Energy drinks such as Red Bull, Amp, and Monster contain approximately 150 mg of caffeine. A tall (small) Starbucks coffee also contains about 150 mg of caffeine, and when we increase the size to a grande, then we are looking at 320 mg.2,4 Simple math will show that the average teen likely has excessive intake of caffeine, resulting in adverse health effects.
The most concerning adverse effect is sleep deprivation.5 Physiologically, the circadian rhythm of adolescents changes and decreases the secretion of melatonin naturally, making it more difficult for them to fall asleep. With the addition of caffeine in high amounts, this is making falling asleep a greater challenge. Sleep deprivation leads to daytime sleepiness and inattention, resulting in learning issues.
Other ill effects found in some studies is that consumption of more than 220 mg of caffeine per day is associated with increased impulsivity, sensation seeking, and risk-taking behaviors.2 In people who are predisposed to arrhythmias, excessive intake can result in the onset of arrhythmias. Nervousness and jitteriness are other common effects.
Another consideration beyond the direct effects of caffeine is that it is usually coupled with sugary substances like those found in syrups used in Starbucks drinks, chocolate candy, and energy drinks. This has led to concerns of obesity as well as dental decay.
Now, when caffeine is taken in small to moderate amounts, less than 300 mg, there are health benefits. It certainly does improve concentration by attaching to the adenosine receptors that block the adenosine effect of sedation on the brain. This leads to improved concentration, memory retention, auditory vigilance, and reaction time.
Recent studies have shown that caffeine in moderate amounts can protect against Alzheimer’s, and is linked to a small decreased risk of cancer and liver disease. Coffee drinkers have also shown a moderate decrease in Parkinson’s disease and stroke.3,6
Regardless of the benefits of caffeine, the American Academy of Pediatrics has been very clear that it does not recommend caffeine in children. In its 2011 guideline,7 the extra calories, the risk of impulsive behavior, and sleep deprivation far outweighed any benefit that caffeine would have. It is critical that physicians educate their patients about foods that contain caffeine and the cumulative effect these foods have on their well-being, now and in the future.
References
1. “Trends in Caffeine Intake Among US Children and Adolescents” (Pediatrics 2014;133:386-93).
2. Caffeine Consumption Among Children and Adolescents. National Council on Strength and Fitness.
3. What is it about coffee? Harvard Health Letter (www.health.harvard.edu/staying-healthy/what-is-it-about-coffee).
4. Caffeine counts. American Physiological Association (Monitor on Psychology. 2001 June;32[6]).
5. J Pediatrics. 2011 March;158(3):508-9.
6. J Alzheimers Dis. 2010;20(suppl 1):s167-74.
7. Pediatrics 2011 June;127(6):1182-9
Dr. Pearce is a pediatrician in Frankfort, Ill.

Hernia repair: Studies don’t support use of higher-cost biological mesh
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
Balancing the need for innovation against the practicalities of demonstrating clinical benefit for novel ideas is a fundamental problem in surgery – a problem highlighted by Heurta et al., Dr. Benjamin K. Poulose and his colleagues said in an editorial.
“This issue is particularly timely given an unsustainable trajectory of health care spending in the United States,” they wrote (JAMA Surg 2016 Jan 27. doi: 10.1001/jamasurg2015.5236).
Like the authors of the literature review, the editorial authors stressed the importance of understanding the limitations of the 510(k) process, and noted that surgeons should consider that the FDA sees them as “the group responsible for understanding and evaluating the data before using expensive medical devices.
“Understanding who is in charge of making sure that the devices that we use during surgery are safe and effective is critical. Likely, it will require a collaborative effort of the FDA, medical device companies, and physicians,” they wrote. Establishing a more formal system of postmarketing surveillance for higher-risk medical devices will benefit patients, they added. Current efforts suffer from reliance on self-reporting and lack of standardized data collection.
Postmarketing surveillance can be greatly improved by directly linking medical device approval with the support of high-quality registries, and the end result should provide transparent data for monitoring effectiveness and safety to drive value-based care and maintain innovation, they said.
Dr. Poulose is with Vanderbilt University Medical Center, Nashville, Tenn. Dr. Poulose reported receiving personal fees from Ariste Medical for consulting work, and research grants from Bard-Davol outside the submitted work.
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, according to a systematic review of the literature.
Of 20 articles that met search criteria, only 3 were comparative studies and none was a randomized clinical trial. In fact, most were case series involving convenience samples of patients at single institutions, Dr. Sergio Huerta of the University of Texas Southwestern Medical Center, Dallas, and his colleagues reported online Jan. 27 in JAMA Surgery.
The authors used multiple electronic databases to identify articles published between 1948 and June 30, 2015, on the use of biological mesh materials for reinforcement of the abdominal wall for hernia repair. Included were 14 articles that described outcomes with human acellular dermal matrix, 2 that reported results for porcine collagen intestinal submucosa derivatives, 3 that reported on porcine acelluar collagen skin derivatives, and 1 that described results for bovine pericardium.
Several problems were noted with respect to the studies, including widely varying follow-up time, operative technique, types of mesh used, and patient selection criteria. Also, outcome measures were not reported consistently across studies.
In addition, 16 of the 20 studies that met search criteria did not report investigator conflicts of interest, the authors reported (JAMA Surg. 2016 Jan 27. doi: 10.10001/jamasurg.2015.5234).
Notably, all the meshes used in the studies were approved by the Food and Drug Administration and were considered to be comparable to a group of nonbiological predicate devices, which cost up to 25% less than the biological equivalents, they noted.
“We were unable to find any evidence that supported the use of expensive biological material relative to low-cost synthetic mesh. In fact, with one exception, the biological materials became commercially available by showing that these materials were equivalent to low-cost established synthetic mesh material in an FDA 510(k) approval process. This process does not require phase 0 through IV clinical trials as required for drugs or biological agents,” they wrote, noting that the one material that bypassed the 510(k) process (Alloderm) was not required to demonstrate equivalence because it was classified as human transplanted tissue.
Biological mesh materials were introduced in the 1990s to minimize the risk of complications commonly seen with the use of synthetic mesh for abdominal wall hernia repair – one of the most common procedures performed by general surgeons, the authors explained.
“Because the outcomes for biological mesh material are perceived to be better than those for polymer-based prosthetic mesh replacement materials, the use of biological grafts increased exponentially without clear clinical evidence of efficacy,” they wrote.
The current review suggests that the evidence remains insufficient to determine whether cost and clinical benefits exist.
“It is generally assumed that FDA-approved drug or biological agents have been rigorously evaluated and that there is demonstrable safety and efficacy. This is not the case for 510(k) medical devices. Before using a new medical device, physicians should know the approval basis for the device and recognize that if it is a 510(k) device neither safety nor efficacy is ensured,” they said, adding that physicians should assume such devices are no better than predicate devices to which they are equivalent, and that “there can be no justification for purchasing a more expensive device when a lower-cost predicate device, which is equivalent, is available.”
Though limited by certain factors such as lack of access to detailed FDA information such as the specific criteria used to determine equivalence, and a lack of published literature on the full market penetration of biological mesh materials vs. nonbiological counterparts, the authors maintained that until evidence demonstrates superiority of biological materials, the expense associated with their use cannot be justified.
This study was supported by the Hudson-Penn Endowment fund at the University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
FROM JAMA SURGERY
Key clinical point: The jury is still out on the costs and efficacy of biological mesh implants for abdominal wall hernia repair, and the expense associated with their use cannot be justified at this time, a systematic review of the literature suggested.
Major finding: Available evidence remains insufficient to determine whether cost and clinical benefits exist with the use of biological mesh for abdominal wall hernia repair.
Data source: A systematic review of the literature, yielding 20 eligible studies.
Disclosures: This study was supported by the Hudson-Penn Endowment fund at University of Texas Southwestern Medical Center. The authors reported having no relevant financial disclosures.
Level 1 activation reduces LOS, mortality in geriatric trauma
SAN ANTONIO – Automatically bumping elderly Level 2 trauma patients to Level 1 status reduced mortality and emergency department lengths of stay at Indiana University Health Methodist Hospital, Indianapolis.
Like trauma services elsewhere, the Methodist team is trying to figure out how best to handle the coming increase in elderly patients as the Baby Boom generation ages. It’s known that older trauma patients tend to be undertriaged. To improve the situation, “we need to respond quickly with a lot of resources up front so we don’t delay diagnosis” and treatment, said investigator Dr. Peter Hammer, assistant professor of surgery at Indiana University, Indianapolis.

The solution Methodist has tried since October 2013 is a Level 1 response to any patient aged 70 years or older who meets Level 2 criteria, regardless of vital sign stability or injury mechanism. With Level 1, trauma attendings, residents, respiratory therapists, clinical pharmacists, and others are at the bedside within 15 minutes and CT services and operating rooms are on standby, among other measures. Compared with the 1,271 patients aged 70 years or older treated in the almost 2 years before the change, the 998 treated in the year and a half afterwards were, after controlling for age, comorbidities, and injury severity scores (ISS), more likely to leave the ED in less than 2 hours (odds ratio, 1.614; 95% confidence interval, 1.088-2.394) and less likely to die (OR, 0.689, 95% CI, 0.484-0.979).
The before and after groups were similar, with a mean age of 81 years, a mean ISS of 12.2, a high comorbidity burden, and, for most, a blunt injury: 8.3% died in the before group, versus 7.6% in the after group. The shorter ED stays occurred despite a nursing staff reduction in 2014. Patients who went into cardiac arrest before arrival or died in the ED were excluded from the analysis.
“A simple, focused intervention of a higher level of trauma activation can decrease ED length of stay and in-hospital mortality in elderly trauma patients,” Dr. Hammer said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Among many initiatives as many trauma centers gear up for aging baby boomers, others are trying age as a criteria for higher activation, too, and recent guidelines from EAST recommend a lower threshold for trauma activation for patients 65 years or older, among other steps.
With more expertise and resources to brought to bear, it’s not surprising that Level 1 patients left the ED sooner, but it’s unclear what role that played in reducing mortality. “I wouldn’t hazard [to say] that shorter lengths of stay necessarily” saved lives, Dr. Hammer said.
Before the intervention, just 4.8% of geriatric patients left the ED within 2 hours, versus 6.5% afterwards. The numbers are low because, “as in most hospitals, there are more trauma patients than beds. [Reducing ED] length or stay [remains] an ongoing project” at Methodist, and not just for the elderly. “The ED is always overcrowded come afternoon and into the evening,” Dr. Hammer said.
That’s one of the reasons management supported the project. “They like the concept of getting patients moved through quickly. We have a lot of resources in the ED, so there doesn’t seem to be much of a slowdown” with increased Level 1 activation. It probably costs more up front, “but the hope is we’ll save money on the back end with lower mortality and shorter ED stays,” he said.
The investigators had no disclosures.
SAN ANTONIO – Automatically bumping elderly Level 2 trauma patients to Level 1 status reduced mortality and emergency department lengths of stay at Indiana University Health Methodist Hospital, Indianapolis.
Like trauma services elsewhere, the Methodist team is trying to figure out how best to handle the coming increase in elderly patients as the Baby Boom generation ages. It’s known that older trauma patients tend to be undertriaged. To improve the situation, “we need to respond quickly with a lot of resources up front so we don’t delay diagnosis” and treatment, said investigator Dr. Peter Hammer, assistant professor of surgery at Indiana University, Indianapolis.
The solution Methodist has tried since October 2013 is a Level 1 response to any patient aged 70 years or older who meets Level 2 criteria, regardless of vital sign stability or injury mechanism. With Level 1, trauma attendings, residents, respiratory therapists, clinical pharmacists, and others are at the bedside within 15 minutes and CT services and operating rooms are on standby, among other measures. Compared with the 1,271 patients aged 70 years or older treated in the almost 2 years before the change, the 998 treated in the year and a half afterwards were, after controlling for age, comorbidities, and injury severity scores (ISS), more likely to leave the ED in less than 2 hours (odds ratio, 1.614; 95% confidence interval, 1.088-2.394) and less likely to die (OR, 0.689, 95% CI, 0.484-0.979).
The before and after groups were similar, with a mean age of 81 years, a mean ISS of 12.2, a high comorbidity burden, and, for most, a blunt injury: 8.3% died in the before group, versus 7.6% in the after group. The shorter ED stays occurred despite a nursing staff reduction in 2014. Patients who went into cardiac arrest before arrival or died in the ED were excluded from the analysis.
“A simple, focused intervention of a higher level of trauma activation can decrease ED length of stay and in-hospital mortality in elderly trauma patients,” Dr. Hammer said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Among many initiatives as many trauma centers gear up for aging baby boomers, others are trying age as a criteria for higher activation, too, and recent guidelines from EAST recommend a lower threshold for trauma activation for patients 65 years or older, among other steps.
With more expertise and resources to brought to bear, it’s not surprising that Level 1 patients left the ED sooner, but it’s unclear what role that played in reducing mortality. “I wouldn’t hazard [to say] that shorter lengths of stay necessarily” saved lives, Dr. Hammer said.
Before the intervention, just 4.8% of geriatric patients left the ED within 2 hours, versus 6.5% afterwards. The numbers are low because, “as in most hospitals, there are more trauma patients than beds. [Reducing ED] length or stay [remains] an ongoing project” at Methodist, and not just for the elderly. “The ED is always overcrowded come afternoon and into the evening,” Dr. Hammer said.
That’s one of the reasons management supported the project. “They like the concept of getting patients moved through quickly. We have a lot of resources in the ED, so there doesn’t seem to be much of a slowdown” with increased Level 1 activation. It probably costs more up front, “but the hope is we’ll save money on the back end with lower mortality and shorter ED stays,” he said.
The investigators had no disclosures.
SAN ANTONIO – Automatically bumping elderly Level 2 trauma patients to Level 1 status reduced mortality and emergency department lengths of stay at Indiana University Health Methodist Hospital, Indianapolis.
Like trauma services elsewhere, the Methodist team is trying to figure out how best to handle the coming increase in elderly patients as the Baby Boom generation ages. It’s known that older trauma patients tend to be undertriaged. To improve the situation, “we need to respond quickly with a lot of resources up front so we don’t delay diagnosis” and treatment, said investigator Dr. Peter Hammer, assistant professor of surgery at Indiana University, Indianapolis.
The solution Methodist has tried since October 2013 is a Level 1 response to any patient aged 70 years or older who meets Level 2 criteria, regardless of vital sign stability or injury mechanism. With Level 1, trauma attendings, residents, respiratory therapists, clinical pharmacists, and others are at the bedside within 15 minutes and CT services and operating rooms are on standby, among other measures. Compared with the 1,271 patients aged 70 years or older treated in the almost 2 years before the change, the 998 treated in the year and a half afterwards were, after controlling for age, comorbidities, and injury severity scores (ISS), more likely to leave the ED in less than 2 hours (odds ratio, 1.614; 95% confidence interval, 1.088-2.394) and less likely to die (OR, 0.689, 95% CI, 0.484-0.979).
The before and after groups were similar, with a mean age of 81 years, a mean ISS of 12.2, a high comorbidity burden, and, for most, a blunt injury: 8.3% died in the before group, versus 7.6% in the after group. The shorter ED stays occurred despite a nursing staff reduction in 2014. Patients who went into cardiac arrest before arrival or died in the ED were excluded from the analysis.
“A simple, focused intervention of a higher level of trauma activation can decrease ED length of stay and in-hospital mortality in elderly trauma patients,” Dr. Hammer said at the annual scientific assembly of the Eastern Association for the Surgery of Trauma.
Among many initiatives as many trauma centers gear up for aging baby boomers, others are trying age as a criteria for higher activation, too, and recent guidelines from EAST recommend a lower threshold for trauma activation for patients 65 years or older, among other steps.
With more expertise and resources to brought to bear, it’s not surprising that Level 1 patients left the ED sooner, but it’s unclear what role that played in reducing mortality. “I wouldn’t hazard [to say] that shorter lengths of stay necessarily” saved lives, Dr. Hammer said.
Before the intervention, just 4.8% of geriatric patients left the ED within 2 hours, versus 6.5% afterwards. The numbers are low because, “as in most hospitals, there are more trauma patients than beds. [Reducing ED] length or stay [remains] an ongoing project” at Methodist, and not just for the elderly. “The ED is always overcrowded come afternoon and into the evening,” Dr. Hammer said.
That’s one of the reasons management supported the project. “They like the concept of getting patients moved through quickly. We have a lot of resources in the ED, so there doesn’t seem to be much of a slowdown” with increased Level 1 activation. It probably costs more up front, “but the hope is we’ll save money on the back end with lower mortality and shorter ED stays,” he said.
The investigators had no disclosures.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Consider treating Level 2 elderly trauma patients at Level 1 status.
Major finding: The 998 Level 2 elderly trauma patients treated as Level 1, after controlling for age, comorbidities, and injury severity scores, were more likely to leave the ED in less than 2 hours and were less likely to die, compared with patients treated in the previous 2 years.
Data source: More than 2,000 trauma patients aged 70 years or older.
Disclosures: The investigators had no disclosures.

Behavior problems in youth: Are things worse today than in the past?
Every generation of adults seems to worry that the next generation of youth is in trouble. The perception of kids today is no different, with theories abounding as to why the mental health of the newest generation is slipping, compared with previous standards. From mobile phones to helicopter parents, it might seem like a foregone conclusion that our current crop of young people is destined to be insecure, inattentive, and unable to cope with challenges and stress. Many news headlines on the latest mass shooting or standardized test results often seem to confirm these widespread concerns.
Pediatricians often hear parents lamenting the “good old days” when such things as corporal punishment were more easily accepted to help keep kids in line. But taking a step back, it may be worth a more objective look to examine the assumption that child behavioral problems are worse than ever. Measuring overall mental health is not an easy task, but looking at several important metrics indicate that things may not be nearly as bad as many people think.
Substance use

From the latest data from the Monitoring the Future Study, one of the nation’s most reliable sources on teen substance use, the use of both alcohol and tobacco among youth is at the lowest level since the study began in 1975. Use of drugs like heroin and ecstasy also are declining. The only major exception to this trend seems to be cannabis use, which has generally shown stable rates during this climate of marijuana decriminalization and, for some states, legalization.
Teen pregnancy rates
One area where there continues to be sustained progress is in teen pregnancy. According to the government’s Centers for Disease Control and Prevention, the overall pregnancy rate among adolescent females has been cut in half from 1991 to 2011, across many different ethnic groups. The rate fell from 61.8/1,000 teenagers aged 15-19 years to 31.3/1,000 teenagers.
Delinquency
Far fewer adolescents are being held against their will in juvenile detention centers. The number of youth who are incarcerated have dropped from a high of 381/100,000 in 1995 to 225/100,000 in 2010, according to a report by the Annie E. Casey Foundation.
Bullying
Bullying has been increasingly recognized as the public health problem that it is. The use of online technology also has created many new settings in which bullying can take place. Nevertheless, there is reason to be optimistic. From the National Center for Education Statistics and the National Crime Victimization Survey, the number of students who report being bullied at school has dropped from 32% in 2007 to an all-time low of 22% in 2013. Another recent study reached similar conclusions for bullying and many other forms of child victimization between 2003 and 2011 (JAMA Pediatr. 2014 Jun;168[6]:540-6).
Suicide
According to the CDC, the rate of completed suicide in youth peaked in the early1990s and then dropped and stabilized before starting to creep up again over the past 5 or so years. The trends are somewhat different, based on gender and the specific age group that is examined. The majority of completed youth suicides occur in males, with current rates still well below those historical highs.
Psychiatric disorders
This one is particularly tricky. While the rates of many specific psychiatric disorders such as ADHD and bipolar disorder have been rising in youth, as well as the use of psychiatric medications, it is much less clear whether this represents a true rise in these disorders versus other factors such as improved detection and a lower diagnostic threshold. One study by Achenbach et al. that measured quantitative levels of child behavior problems from the same rating scale over a 23-year time span found some increases in overall levels from the 1970s to the early 1990s, but then levels began to fall by the end of the millennium (J Abnorm Child Psychol. 2003 Feb;31[1]:1-11).
Of course, these hopeful trends in many significant areas do not mean that these problems have been overcome. While much work remains to be done on many fronts, it is still worth keeping in mind that the overall condition of youth mental health may not be as dire as we might be led to believe and that there is evidence that our efforts, perhaps, are leading to some progress.
Dr. Rettew is associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. He said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].
Every generation of adults seems to worry that the next generation of youth is in trouble. The perception of kids today is no different, with theories abounding as to why the mental health of the newest generation is slipping, compared with previous standards. From mobile phones to helicopter parents, it might seem like a foregone conclusion that our current crop of young people is destined to be insecure, inattentive, and unable to cope with challenges and stress. Many news headlines on the latest mass shooting or standardized test results often seem to confirm these widespread concerns.
Pediatricians often hear parents lamenting the “good old days” when such things as corporal punishment were more easily accepted to help keep kids in line. But taking a step back, it may be worth a more objective look to examine the assumption that child behavioral problems are worse than ever. Measuring overall mental health is not an easy task, but looking at several important metrics indicate that things may not be nearly as bad as many people think.
Substance use
From the latest data from the Monitoring the Future Study, one of the nation’s most reliable sources on teen substance use, the use of both alcohol and tobacco among youth is at the lowest level since the study began in 1975. Use of drugs like heroin and ecstasy also are declining. The only major exception to this trend seems to be cannabis use, which has generally shown stable rates during this climate of marijuana decriminalization and, for some states, legalization.
Teen pregnancy rates
One area where there continues to be sustained progress is in teen pregnancy. According to the government’s Centers for Disease Control and Prevention, the overall pregnancy rate among adolescent females has been cut in half from 1991 to 2011, across many different ethnic groups. The rate fell from 61.8/1,000 teenagers aged 15-19 years to 31.3/1,000 teenagers.
Delinquency
Far fewer adolescents are being held against their will in juvenile detention centers. The number of youth who are incarcerated have dropped from a high of 381/100,000 in 1995 to 225/100,000 in 2010, according to a report by the Annie E. Casey Foundation.
Bullying
Bullying has been increasingly recognized as the public health problem that it is. The use of online technology also has created many new settings in which bullying can take place. Nevertheless, there is reason to be optimistic. From the National Center for Education Statistics and the National Crime Victimization Survey, the number of students who report being bullied at school has dropped from 32% in 2007 to an all-time low of 22% in 2013. Another recent study reached similar conclusions for bullying and many other forms of child victimization between 2003 and 2011 (JAMA Pediatr. 2014 Jun;168[6]:540-6).
Suicide
According to the CDC, the rate of completed suicide in youth peaked in the early1990s and then dropped and stabilized before starting to creep up again over the past 5 or so years. The trends are somewhat different, based on gender and the specific age group that is examined. The majority of completed youth suicides occur in males, with current rates still well below those historical highs.
Psychiatric disorders
This one is particularly tricky. While the rates of many specific psychiatric disorders such as ADHD and bipolar disorder have been rising in youth, as well as the use of psychiatric medications, it is much less clear whether this represents a true rise in these disorders versus other factors such as improved detection and a lower diagnostic threshold. One study by Achenbach et al. that measured quantitative levels of child behavior problems from the same rating scale over a 23-year time span found some increases in overall levels from the 1970s to the early 1990s, but then levels began to fall by the end of the millennium (J Abnorm Child Psychol. 2003 Feb;31[1]:1-11).
Of course, these hopeful trends in many significant areas do not mean that these problems have been overcome. While much work remains to be done on many fronts, it is still worth keeping in mind that the overall condition of youth mental health may not be as dire as we might be led to believe and that there is evidence that our efforts, perhaps, are leading to some progress.
Dr. Rettew is associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. He said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].
Every generation of adults seems to worry that the next generation of youth is in trouble. The perception of kids today is no different, with theories abounding as to why the mental health of the newest generation is slipping, compared with previous standards. From mobile phones to helicopter parents, it might seem like a foregone conclusion that our current crop of young people is destined to be insecure, inattentive, and unable to cope with challenges and stress. Many news headlines on the latest mass shooting or standardized test results often seem to confirm these widespread concerns.
Pediatricians often hear parents lamenting the “good old days” when such things as corporal punishment were more easily accepted to help keep kids in line. But taking a step back, it may be worth a more objective look to examine the assumption that child behavioral problems are worse than ever. Measuring overall mental health is not an easy task, but looking at several important metrics indicate that things may not be nearly as bad as many people think.
Substance use
From the latest data from the Monitoring the Future Study, one of the nation’s most reliable sources on teen substance use, the use of both alcohol and tobacco among youth is at the lowest level since the study began in 1975. Use of drugs like heroin and ecstasy also are declining. The only major exception to this trend seems to be cannabis use, which has generally shown stable rates during this climate of marijuana decriminalization and, for some states, legalization.
Teen pregnancy rates
One area where there continues to be sustained progress is in teen pregnancy. According to the government’s Centers for Disease Control and Prevention, the overall pregnancy rate among adolescent females has been cut in half from 1991 to 2011, across many different ethnic groups. The rate fell from 61.8/1,000 teenagers aged 15-19 years to 31.3/1,000 teenagers.
Delinquency
Far fewer adolescents are being held against their will in juvenile detention centers. The number of youth who are incarcerated have dropped from a high of 381/100,000 in 1995 to 225/100,000 in 2010, according to a report by the Annie E. Casey Foundation.
Bullying
Bullying has been increasingly recognized as the public health problem that it is. The use of online technology also has created many new settings in which bullying can take place. Nevertheless, there is reason to be optimistic. From the National Center for Education Statistics and the National Crime Victimization Survey, the number of students who report being bullied at school has dropped from 32% in 2007 to an all-time low of 22% in 2013. Another recent study reached similar conclusions for bullying and many other forms of child victimization between 2003 and 2011 (JAMA Pediatr. 2014 Jun;168[6]:540-6).
Suicide
According to the CDC, the rate of completed suicide in youth peaked in the early1990s and then dropped and stabilized before starting to creep up again over the past 5 or so years. The trends are somewhat different, based on gender and the specific age group that is examined. The majority of completed youth suicides occur in males, with current rates still well below those historical highs.
Psychiatric disorders
This one is particularly tricky. While the rates of many specific psychiatric disorders such as ADHD and bipolar disorder have been rising in youth, as well as the use of psychiatric medications, it is much less clear whether this represents a true rise in these disorders versus other factors such as improved detection and a lower diagnostic threshold. One study by Achenbach et al. that measured quantitative levels of child behavior problems from the same rating scale over a 23-year time span found some increases in overall levels from the 1970s to the early 1990s, but then levels began to fall by the end of the millennium (J Abnorm Child Psychol. 2003 Feb;31[1]:1-11).
Of course, these hopeful trends in many significant areas do not mean that these problems have been overcome. While much work remains to be done on many fronts, it is still worth keeping in mind that the overall condition of youth mental health may not be as dire as we might be led to believe and that there is evidence that our efforts, perhaps, are leading to some progress.
Dr. Rettew is associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. He said he has no relevant financial disclosures. Follow him on Twitter @pedipsych. E-mail him at [email protected].

Study reveals how Tregs protect themselves

Image by Kathryn Iacono
Researchers say they have discovered how regulatory T cells (Tregs) remain intact and functional during activation.
The team found that once Tregs are activated, they are protected by autophagy, which maintains metabolic balance.
Hongbo Chi, PhD, of St. Jude Children’s Hospital in Memphis, Tennessee, and his colleagues described this discovery in Nature Immunology.
Until this study, no one knew how Tregs maintained themselves when activated.
“Regulatory T cells are very specialized cells that require activation to perform their function in curtailing undesirable immune responses,” Dr Chi explained. “But this activation is a double-edged sword, in that this very activation can destabilize them. They need to modulate this activation, or they will lose their stability and many of them will die. That could damage immune function.”
Dr Chi and his colleagues performed imaging studies in activated Tregs and found that autophagy was functional in the cells.
In experiments with mice, the researchers deleted Atg7 or Atg5, genes whose functions are necessary for autophagy in Tregs.
The mice showed key characteristics of Treg malfunction, including inflammatory and autoimmune disorders. The mice also more readily cleared tumors from their bodies, due to activated immune systems.
Dr Chi said that eliminating autophagy also affected the fate of Tregs.
“Once those T cells lack autophagy activity, they tend to undergo excessive cell death,” he said. “But even for the remaining surviving cells, they tend to be overly activated and lose their identity because they start to behave like non-regulatory T cells. That is why loss of autophagy in regulatory T cells produces a 2-fold effect on both survival and stability.”
Detailed analysis also revealed how the elimination of autophagy affected the basic energy-producing metabolic pathways of Tregs, compromising their function.
Dr Chi said this new understanding of autophagy’s role in Tregs could enable a 2-fold approach to immune therapy for cancers. Namely, by strengthening tumor-associated immune responses, targeting Treg autophagy could act in synergy with strategies that block autophagy in tumor cells.
In this study, the researchers used a transplanted colon cancer cell line. In further studies, they plan to explore the role of autophagy in immune reactions toward other tumor cell types to determine whether such therapies might be effective in a broad range of cancers.
The team also hopes to gain a better understanding of the detailed biochemical mechanisms regulating how autophagy connects to the cell’s metabolic pathways. ![]()
Image by Kathryn Iacono
Researchers say they have discovered how regulatory T cells (Tregs) remain intact and functional during activation.
The team found that once Tregs are activated, they are protected by autophagy, which maintains metabolic balance.
Hongbo Chi, PhD, of St. Jude Children’s Hospital in Memphis, Tennessee, and his colleagues described this discovery in Nature Immunology.
Until this study, no one knew how Tregs maintained themselves when activated.
“Regulatory T cells are very specialized cells that require activation to perform their function in curtailing undesirable immune responses,” Dr Chi explained. “But this activation is a double-edged sword, in that this very activation can destabilize them. They need to modulate this activation, or they will lose their stability and many of them will die. That could damage immune function.”
Dr Chi and his colleagues performed imaging studies in activated Tregs and found that autophagy was functional in the cells.
In experiments with mice, the researchers deleted Atg7 or Atg5, genes whose functions are necessary for autophagy in Tregs.
The mice showed key characteristics of Treg malfunction, including inflammatory and autoimmune disorders. The mice also more readily cleared tumors from their bodies, due to activated immune systems.
Dr Chi said that eliminating autophagy also affected the fate of Tregs.
“Once those T cells lack autophagy activity, they tend to undergo excessive cell death,” he said. “But even for the remaining surviving cells, they tend to be overly activated and lose their identity because they start to behave like non-regulatory T cells. That is why loss of autophagy in regulatory T cells produces a 2-fold effect on both survival and stability.”
Detailed analysis also revealed how the elimination of autophagy affected the basic energy-producing metabolic pathways of Tregs, compromising their function.
Dr Chi said this new understanding of autophagy’s role in Tregs could enable a 2-fold approach to immune therapy for cancers. Namely, by strengthening tumor-associated immune responses, targeting Treg autophagy could act in synergy with strategies that block autophagy in tumor cells.
In this study, the researchers used a transplanted colon cancer cell line. In further studies, they plan to explore the role of autophagy in immune reactions toward other tumor cell types to determine whether such therapies might be effective in a broad range of cancers.
The team also hopes to gain a better understanding of the detailed biochemical mechanisms regulating how autophagy connects to the cell’s metabolic pathways. ![]()
Image by Kathryn Iacono
Researchers say they have discovered how regulatory T cells (Tregs) remain intact and functional during activation.
The team found that once Tregs are activated, they are protected by autophagy, which maintains metabolic balance.
Hongbo Chi, PhD, of St. Jude Children’s Hospital in Memphis, Tennessee, and his colleagues described this discovery in Nature Immunology.
Until this study, no one knew how Tregs maintained themselves when activated.
“Regulatory T cells are very specialized cells that require activation to perform their function in curtailing undesirable immune responses,” Dr Chi explained. “But this activation is a double-edged sword, in that this very activation can destabilize them. They need to modulate this activation, or they will lose their stability and many of them will die. That could damage immune function.”
Dr Chi and his colleagues performed imaging studies in activated Tregs and found that autophagy was functional in the cells.
In experiments with mice, the researchers deleted Atg7 or Atg5, genes whose functions are necessary for autophagy in Tregs.
The mice showed key characteristics of Treg malfunction, including inflammatory and autoimmune disorders. The mice also more readily cleared tumors from their bodies, due to activated immune systems.
Dr Chi said that eliminating autophagy also affected the fate of Tregs.
“Once those T cells lack autophagy activity, they tend to undergo excessive cell death,” he said. “But even for the remaining surviving cells, they tend to be overly activated and lose their identity because they start to behave like non-regulatory T cells. That is why loss of autophagy in regulatory T cells produces a 2-fold effect on both survival and stability.”
Detailed analysis also revealed how the elimination of autophagy affected the basic energy-producing metabolic pathways of Tregs, compromising their function.
Dr Chi said this new understanding of autophagy’s role in Tregs could enable a 2-fold approach to immune therapy for cancers. Namely, by strengthening tumor-associated immune responses, targeting Treg autophagy could act in synergy with strategies that block autophagy in tumor cells.
In this study, the researchers used a transplanted colon cancer cell line. In further studies, they plan to explore the role of autophagy in immune reactions toward other tumor cell types to determine whether such therapies might be effective in a broad range of cancers.
The team also hopes to gain a better understanding of the detailed biochemical mechanisms regulating how autophagy connects to the cell’s metabolic pathways. ![]()
What Are Best Practices for Patients Discharged against Medical Advice?
Case No. 1
A 41-year-old woman with a history of asthma presents to the emergency department (ED) with shortness of breath and wheezing. She is diagnosed with a mild asthma exacerbation. After three albuterol nebulizer treatments, she still has wheezing on physical examination but appears comfortable and has no oxygen requirement. She has a primary medical doctor at the hospital and follows up with her regularly.

The hospitalist recommends that she stay in the hospital for further treatment, but the patient says she has a nebulizer machine at home and asks to be discharged. In addition, she is worried about her frail elderly mother, for whom she is the primary caretaker. The hospitalist acknowledges her concerns but continues to recommend that she remain in the hospital for additional care and monitoring. She becomes visibly upset and insists that she must return home. She asks for prescriptions for albuterol and prednisone and is discharged against medical advice (AMA).
Case No. 2
A 52-year-old man with a history of hypertension and diabetes presents to the ED with left foot pain. He frequently presents with this complaint but often leaves AMA before treatment is completed. He has no known physical address or telephone number and has no known outpatient healthcare providers. Physical examination reveals several ulcers on the dorsum of the foot, one with purulent drainage, and generalized lower extremity pallor. His left leg is cool to the touch, and vascular surgery is consulted for suspected limb-threatening ischemia; IV antibiotics are started for suspected osteomyelitis.
During the interview, he states that he wishes to leave the hospital because he has “things to take care of.” The hospitalist recommends that he remain in the hospital for limb-preserving surgery and antibiotics. He then explains that he is homeless and needs to return to his shelter to keep his bed. He is able to articulate the risks of premature discharge and the medical concerns, and it is determined that he has the capacity to participate in discharge planning. The hospitalist therefore discharges him AMA.
Background
AMA discharges represent 1%–2% of all inpatient discharges.¹,² Despite being a small percentage of total discharges, these patients have disproportionately high healthcare costs. One study reported that healthcare costs among these patients were 56% higher than expected.² Furthermore, AMA patients suffer higher than expected rates of morbidity, mortality, and hospital readmission.
For example, in one case-control study in an urban teaching hospital, patients discharged AMA from the general medicine service had a 21% 15-day readmission rate compared to a 3% readmission rate among age, gender, and diagnosis-matched controls.3,4,5
Additionally, history of AMA discharge appears to confer risk of increased future utilization of healthcare resources. In a cohort study of hospital admissions among HIV-infected patients with high rates of intravenous drug abuse, patients discharged AMA (13% of the cohort) were not only more likely to be readmitted within 30 days for a related diagnosis (odds ratio = 5.0) but also were more likely to have increased length of stay during the year following the index admission.6
These studies highlight the barriers to safe and effective transitions of care for this vulnerable population and demonstrate the increased burden that this population places on the health system.
Several retrospective studies have identified psychosocial and demographic risk factors associated with AMA discharge. These include younger age, male sex, substance abuse, lack of a primary care physician or health insurance, and history of previous AMA discharge.1,3,7,8 Insurance status is also associated with AMA discharge, with increased odds of AMA discharge among Medicare and Medicaid patients and patients without health insurance.9,10
Of note, one study found that race did not act as an independent predictor of AMA discharge when adjusted for age, gender, and socioeconomic factors.11
The AMA population is clinically heterogeneous. Among patients with pneumonia, for example, Saitz et al showed that a patient’s documented clinical severity did not independently predict AMA discharge, suggesting that there is great clinical heterogeneity even among AMA patients with similar admission diagnoses.12
These studies highlight the clinical and demographic heterogeneity within this population, suggesting that patients discharged AMA require individualized attention from hospitalists and other healthcare providers.
Patients describe numerous motivations for leaving the hospital prematurely, including needing to pick up public-assistance checks, personal financial issues, and familial obligations.13 Interestingly, in the cohort of HIV patients referenced above, discharge on the day welfare checks were distributed was an independent predictor of AMA discharge.6 In focus groups composed of patients discharged AMA and their treating nurses and physicians, several themes were identified as potential contributors to AMA discharge, including drug addiction, pain management issues, external obligations, wait time, the physician’s bedside manner, being in a teaching hospital, and communication issues.14
Clearly, patients have a diversity of reasons for requesting to be discharged AMA, and further research is necessary to define clear and potentially modifiable risk factors.
Discussion
The clinical scenarios outlined above present two patients with very different clinical presentations and outpatient support systems as well as demonstrate the great variability in clinical risk at the time of discharge AMA. These examples emphasize the importance of an individualized approach to care for each patient.
In Case No. 1, the patient is admitted with a mild asthma exacerbation with persistent bronchospasm, though she clinically appears well and has reliable follow-up. In contrast, in Case No. 2, the patient has life-threatening disease and no established primary care physician or mechanism for outpatient care. These examples demonstrate extremes on the clinical and psychosocial spectrum of patients requesting an “early” discharge and suggest that no two patients at risk of AMA discharge are the same. Patient 1 could likely be safely managed at home with close outpatient follow-up, while Patient 2 presents a high-risk scenario with very few safe outpatient treatment options.
We suggest that an individualized approach be taken for each patient, with attention to both clinical and psychosocial risk. In clinically low-risk cases (e.g., Case No. 1), an approach that prioritizes shared decision making and coordination with the outpatient care team may be preferable to an AMA discharge, particularly given the often adversarial nature of the later.2 In such cases, a collaborative approach may provide greater opportunity for harm reduction, provision of appropriate prescriptions, and follow-up appointments. In clinically high-risk patients such as Case No. 2, however, premature discharge is clearly inappropriate. Even in such clinically high-risk cases, however, we argue that a collaborative strategy aimed at identifying and addressing the patient’s psychosocial concerns is appropriate, as such an approach promotes shared decision making, builds trust between the patient and the care team, and therefore may facilitate improved follow-up at the time of discharge. Research is needed to formally assess the optimal approach for this patient population, including impact on rates of AMA discharge and the quality of post-discharge follow-up.
At present, the decision to classify a discharge as AMA falls solely on the treating provider, and we suspect that there is great variability in practice patterns, particularly as there are few established professional society practice guidelines regarding this difficult issue. As with all discharges from the hospital, the burden falls on the provider to engage the patient in shared decision making and ensure that the patient has the capacity to understand the risks and benefits of the proposed treatment plan. It is in this spirit that simply “filling out an AMA form” does not provide legal protection to a physician who does not adequately explain the full risks and benefits of refusal of inpatient treatment.2,15
We propose that a high-quality AMA discharge be defined as a discharge in which the patient is informed of the clinical team’s determination that further hospitalization is required but elects to leave the hospital, and it includes a clear discussion of the risks of outpatient treatment, a determination of capacity, and an exploration of safe alternative care plans that could satisfy both the patient’s medical and social needs. This definition places the burden on hospitalists and other providers to fully explore the motivations behind a patient’s request to leave the hospital and treats psychosocial motivators for premature discharge as variables in the complex risk-benefit analysis that underlies the informed consent discussion prior to AMA discharge.
Furthermore, AMA discharge does not obviate a physician’s responsibility to advocate for a patient’s well-being, and therefore an AMA discharge should be accompanied by reasonable efforts to coordinate a patient’s ongoing outpatient care. Of note, this approach is consistent with previous reviews and attempts to balance the physician’s duty to honor a patient’s autonomy with the responsibility to protect the patient from harm.2,16
Conclusion
Patients discharged AMA are a diverse population at markedly increased risk of morbidity, readmissions, and subsequent healthcare cost. We argue that in all cases of a potential premature discharge, a collaborative and patient-centered approach is crucial. Such an approach allows the provider to identify and address the patient’s concerns regarding further inpatient care, to explore possible safe outpatient treatment options, to document patient capacity, and to provide appropriate harm-reduction measures such as prescriptions.
Further research into the current practice patterns of hospitalists and other providers is necessary to allow for the formulation and adoption of best practices and implementation of appropriate harm-reduction strategies. TH
Dr. Tummalapalli is an internal medicine resident in the department of medicine at Icahn School of Medicine at Mount Sinai in New York City. Dr. Goodman is a hospitalist in the division of hospital medicine, department of medicine, at the Icahn School of Medicine at Mount Sinai.
References
- Aliyu ZY. Discharge against medical advice: sociodemographic, clinical and financial perspectives. Int J Clin Pract. 2002;56(5):325-327.
- Kahle CH, Rubio ML, Santos RA. Discharges against medical advice: considerations for the hospitalist and the patient. Hospital Medicine Clinics. 2015;4(3):421-429.
- Baptist AP, Warrier I, Arora R, Ager J, Massanari RM. Hospitalized patients with asthma who leave against medical advice: characteristics, reasons, and outcomes. J Allergy Clin Immunol. 2007;119(4):924-929.
- Hwang SW, Li J, Gupta R, Chien V, Martin RE. What happens to patients who leave hospital against medical advice? CMAJ. 2003;168(4):417-420.
- Glasgow JM, Vaughn-Sarrazin MV, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Int Med. 2010;25(9):926-929.
- Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637.
- Jeremiah J, O’Sullivan P, Stein MD. Who leaves against medical advice? J Gen Int Med. 1995; 10(7);403-405.
- O’Hara D, Hart W, McDonald I. Leaving hospital against medical advice. J Qual Clin Pract.1996;16(3):157-164.
- Ibrahim SA, Kwoh CK, Krishnan E. Factors associated with patients who leave acute-care hospitals against medical advice. Am J Public Health. 2007;97(12): 2204-2208.
- Weingart SN, Davis RB, Phillips RS. Patients discharged against medical advice from a general medicine service. J Gen Intern Med. 1998;13(8):568-571.
- Franks P, Meldrum S, Fiscella K. Discharges against medical advice: are race/ethnicity predictors? J Gen Intern Med. 2006;21(9):955-960.
- Saitz R, Ghali WA, Moskowitz MA. Characteristics of patients with pneumonia who are discharged from hospitals against medical advice. Am J Med. 1999;107(5):507-509.
- Alfandre, DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260.
- Onukwugha E, Saunders E, Mullins CD, Pradel FG, Zuckerman M, Weir MR. Reasons for discharges against medical advice: a qualitative study. Qual Saf Health Care. 2010;19(5):420-424. doi: 10.1136/qshc.2009.036269.
- Battenfeld v. Gregory, 589 A.2d 1059, 1061 (N.J. Super. Ct. App. Div. 1991).
- Berger J. Discharge against medical advice: ethical considerations and professional obligations. J Hosp Med. 2008;3(5):403-408.
Case No. 1
A 41-year-old woman with a history of asthma presents to the emergency department (ED) with shortness of breath and wheezing. She is diagnosed with a mild asthma exacerbation. After three albuterol nebulizer treatments, she still has wheezing on physical examination but appears comfortable and has no oxygen requirement. She has a primary medical doctor at the hospital and follows up with her regularly.
The hospitalist recommends that she stay in the hospital for further treatment, but the patient says she has a nebulizer machine at home and asks to be discharged. In addition, she is worried about her frail elderly mother, for whom she is the primary caretaker. The hospitalist acknowledges her concerns but continues to recommend that she remain in the hospital for additional care and monitoring. She becomes visibly upset and insists that she must return home. She asks for prescriptions for albuterol and prednisone and is discharged against medical advice (AMA).
Case No. 2
A 52-year-old man with a history of hypertension and diabetes presents to the ED with left foot pain. He frequently presents with this complaint but often leaves AMA before treatment is completed. He has no known physical address or telephone number and has no known outpatient healthcare providers. Physical examination reveals several ulcers on the dorsum of the foot, one with purulent drainage, and generalized lower extremity pallor. His left leg is cool to the touch, and vascular surgery is consulted for suspected limb-threatening ischemia; IV antibiotics are started for suspected osteomyelitis.
During the interview, he states that he wishes to leave the hospital because he has “things to take care of.” The hospitalist recommends that he remain in the hospital for limb-preserving surgery and antibiotics. He then explains that he is homeless and needs to return to his shelter to keep his bed. He is able to articulate the risks of premature discharge and the medical concerns, and it is determined that he has the capacity to participate in discharge planning. The hospitalist therefore discharges him AMA.
Background
AMA discharges represent 1%–2% of all inpatient discharges.¹,² Despite being a small percentage of total discharges, these patients have disproportionately high healthcare costs. One study reported that healthcare costs among these patients were 56% higher than expected.² Furthermore, AMA patients suffer higher than expected rates of morbidity, mortality, and hospital readmission.
For example, in one case-control study in an urban teaching hospital, patients discharged AMA from the general medicine service had a 21% 15-day readmission rate compared to a 3% readmission rate among age, gender, and diagnosis-matched controls.3,4,5
Additionally, history of AMA discharge appears to confer risk of increased future utilization of healthcare resources. In a cohort study of hospital admissions among HIV-infected patients with high rates of intravenous drug abuse, patients discharged AMA (13% of the cohort) were not only more likely to be readmitted within 30 days for a related diagnosis (odds ratio = 5.0) but also were more likely to have increased length of stay during the year following the index admission.6
These studies highlight the barriers to safe and effective transitions of care for this vulnerable population and demonstrate the increased burden that this population places on the health system.
Several retrospective studies have identified psychosocial and demographic risk factors associated with AMA discharge. These include younger age, male sex, substance abuse, lack of a primary care physician or health insurance, and history of previous AMA discharge.1,3,7,8 Insurance status is also associated with AMA discharge, with increased odds of AMA discharge among Medicare and Medicaid patients and patients without health insurance.9,10
Of note, one study found that race did not act as an independent predictor of AMA discharge when adjusted for age, gender, and socioeconomic factors.11
The AMA population is clinically heterogeneous. Among patients with pneumonia, for example, Saitz et al showed that a patient’s documented clinical severity did not independently predict AMA discharge, suggesting that there is great clinical heterogeneity even among AMA patients with similar admission diagnoses.12
These studies highlight the clinical and demographic heterogeneity within this population, suggesting that patients discharged AMA require individualized attention from hospitalists and other healthcare providers.
Patients describe numerous motivations for leaving the hospital prematurely, including needing to pick up public-assistance checks, personal financial issues, and familial obligations.13 Interestingly, in the cohort of HIV patients referenced above, discharge on the day welfare checks were distributed was an independent predictor of AMA discharge.6 In focus groups composed of patients discharged AMA and their treating nurses and physicians, several themes were identified as potential contributors to AMA discharge, including drug addiction, pain management issues, external obligations, wait time, the physician’s bedside manner, being in a teaching hospital, and communication issues.14
Clearly, patients have a diversity of reasons for requesting to be discharged AMA, and further research is necessary to define clear and potentially modifiable risk factors.
Discussion
The clinical scenarios outlined above present two patients with very different clinical presentations and outpatient support systems as well as demonstrate the great variability in clinical risk at the time of discharge AMA. These examples emphasize the importance of an individualized approach to care for each patient.
In Case No. 1, the patient is admitted with a mild asthma exacerbation with persistent bronchospasm, though she clinically appears well and has reliable follow-up. In contrast, in Case No. 2, the patient has life-threatening disease and no established primary care physician or mechanism for outpatient care. These examples demonstrate extremes on the clinical and psychosocial spectrum of patients requesting an “early” discharge and suggest that no two patients at risk of AMA discharge are the same. Patient 1 could likely be safely managed at home with close outpatient follow-up, while Patient 2 presents a high-risk scenario with very few safe outpatient treatment options.
We suggest that an individualized approach be taken for each patient, with attention to both clinical and psychosocial risk. In clinically low-risk cases (e.g., Case No. 1), an approach that prioritizes shared decision making and coordination with the outpatient care team may be preferable to an AMA discharge, particularly given the often adversarial nature of the later.2 In such cases, a collaborative approach may provide greater opportunity for harm reduction, provision of appropriate prescriptions, and follow-up appointments. In clinically high-risk patients such as Case No. 2, however, premature discharge is clearly inappropriate. Even in such clinically high-risk cases, however, we argue that a collaborative strategy aimed at identifying and addressing the patient’s psychosocial concerns is appropriate, as such an approach promotes shared decision making, builds trust between the patient and the care team, and therefore may facilitate improved follow-up at the time of discharge. Research is needed to formally assess the optimal approach for this patient population, including impact on rates of AMA discharge and the quality of post-discharge follow-up.
At present, the decision to classify a discharge as AMA falls solely on the treating provider, and we suspect that there is great variability in practice patterns, particularly as there are few established professional society practice guidelines regarding this difficult issue. As with all discharges from the hospital, the burden falls on the provider to engage the patient in shared decision making and ensure that the patient has the capacity to understand the risks and benefits of the proposed treatment plan. It is in this spirit that simply “filling out an AMA form” does not provide legal protection to a physician who does not adequately explain the full risks and benefits of refusal of inpatient treatment.2,15
We propose that a high-quality AMA discharge be defined as a discharge in which the patient is informed of the clinical team’s determination that further hospitalization is required but elects to leave the hospital, and it includes a clear discussion of the risks of outpatient treatment, a determination of capacity, and an exploration of safe alternative care plans that could satisfy both the patient’s medical and social needs. This definition places the burden on hospitalists and other providers to fully explore the motivations behind a patient’s request to leave the hospital and treats psychosocial motivators for premature discharge as variables in the complex risk-benefit analysis that underlies the informed consent discussion prior to AMA discharge.
Furthermore, AMA discharge does not obviate a physician’s responsibility to advocate for a patient’s well-being, and therefore an AMA discharge should be accompanied by reasonable efforts to coordinate a patient’s ongoing outpatient care. Of note, this approach is consistent with previous reviews and attempts to balance the physician’s duty to honor a patient’s autonomy with the responsibility to protect the patient from harm.2,16
Conclusion
Patients discharged AMA are a diverse population at markedly increased risk of morbidity, readmissions, and subsequent healthcare cost. We argue that in all cases of a potential premature discharge, a collaborative and patient-centered approach is crucial. Such an approach allows the provider to identify and address the patient’s concerns regarding further inpatient care, to explore possible safe outpatient treatment options, to document patient capacity, and to provide appropriate harm-reduction measures such as prescriptions.
Further research into the current practice patterns of hospitalists and other providers is necessary to allow for the formulation and adoption of best practices and implementation of appropriate harm-reduction strategies. TH
Dr. Tummalapalli is an internal medicine resident in the department of medicine at Icahn School of Medicine at Mount Sinai in New York City. Dr. Goodman is a hospitalist in the division of hospital medicine, department of medicine, at the Icahn School of Medicine at Mount Sinai.
References
- Aliyu ZY. Discharge against medical advice: sociodemographic, clinical and financial perspectives. Int J Clin Pract. 2002;56(5):325-327.
- Kahle CH, Rubio ML, Santos RA. Discharges against medical advice: considerations for the hospitalist and the patient. Hospital Medicine Clinics. 2015;4(3):421-429.
- Baptist AP, Warrier I, Arora R, Ager J, Massanari RM. Hospitalized patients with asthma who leave against medical advice: characteristics, reasons, and outcomes. J Allergy Clin Immunol. 2007;119(4):924-929.
- Hwang SW, Li J, Gupta R, Chien V, Martin RE. What happens to patients who leave hospital against medical advice? CMAJ. 2003;168(4):417-420.
- Glasgow JM, Vaughn-Sarrazin MV, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Int Med. 2010;25(9):926-929.
- Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637.
- Jeremiah J, O’Sullivan P, Stein MD. Who leaves against medical advice? J Gen Int Med. 1995; 10(7);403-405.
- O’Hara D, Hart W, McDonald I. Leaving hospital against medical advice. J Qual Clin Pract.1996;16(3):157-164.
- Ibrahim SA, Kwoh CK, Krishnan E. Factors associated with patients who leave acute-care hospitals against medical advice. Am J Public Health. 2007;97(12): 2204-2208.
- Weingart SN, Davis RB, Phillips RS. Patients discharged against medical advice from a general medicine service. J Gen Intern Med. 1998;13(8):568-571.
- Franks P, Meldrum S, Fiscella K. Discharges against medical advice: are race/ethnicity predictors? J Gen Intern Med. 2006;21(9):955-960.
- Saitz R, Ghali WA, Moskowitz MA. Characteristics of patients with pneumonia who are discharged from hospitals against medical advice. Am J Med. 1999;107(5):507-509.
- Alfandre, DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260.
- Onukwugha E, Saunders E, Mullins CD, Pradel FG, Zuckerman M, Weir MR. Reasons for discharges against medical advice: a qualitative study. Qual Saf Health Care. 2010;19(5):420-424. doi: 10.1136/qshc.2009.036269.
- Battenfeld v. Gregory, 589 A.2d 1059, 1061 (N.J. Super. Ct. App. Div. 1991).
- Berger J. Discharge against medical advice: ethical considerations and professional obligations. J Hosp Med. 2008;3(5):403-408.
Case No. 1
A 41-year-old woman with a history of asthma presents to the emergency department (ED) with shortness of breath and wheezing. She is diagnosed with a mild asthma exacerbation. After three albuterol nebulizer treatments, she still has wheezing on physical examination but appears comfortable and has no oxygen requirement. She has a primary medical doctor at the hospital and follows up with her regularly.
The hospitalist recommends that she stay in the hospital for further treatment, but the patient says she has a nebulizer machine at home and asks to be discharged. In addition, she is worried about her frail elderly mother, for whom she is the primary caretaker. The hospitalist acknowledges her concerns but continues to recommend that she remain in the hospital for additional care and monitoring. She becomes visibly upset and insists that she must return home. She asks for prescriptions for albuterol and prednisone and is discharged against medical advice (AMA).
Case No. 2
A 52-year-old man with a history of hypertension and diabetes presents to the ED with left foot pain. He frequently presents with this complaint but often leaves AMA before treatment is completed. He has no known physical address or telephone number and has no known outpatient healthcare providers. Physical examination reveals several ulcers on the dorsum of the foot, one with purulent drainage, and generalized lower extremity pallor. His left leg is cool to the touch, and vascular surgery is consulted for suspected limb-threatening ischemia; IV antibiotics are started for suspected osteomyelitis.
During the interview, he states that he wishes to leave the hospital because he has “things to take care of.” The hospitalist recommends that he remain in the hospital for limb-preserving surgery and antibiotics. He then explains that he is homeless and needs to return to his shelter to keep his bed. He is able to articulate the risks of premature discharge and the medical concerns, and it is determined that he has the capacity to participate in discharge planning. The hospitalist therefore discharges him AMA.
Background
AMA discharges represent 1%–2% of all inpatient discharges.¹,² Despite being a small percentage of total discharges, these patients have disproportionately high healthcare costs. One study reported that healthcare costs among these patients were 56% higher than expected.² Furthermore, AMA patients suffer higher than expected rates of morbidity, mortality, and hospital readmission.
For example, in one case-control study in an urban teaching hospital, patients discharged AMA from the general medicine service had a 21% 15-day readmission rate compared to a 3% readmission rate among age, gender, and diagnosis-matched controls.3,4,5
Additionally, history of AMA discharge appears to confer risk of increased future utilization of healthcare resources. In a cohort study of hospital admissions among HIV-infected patients with high rates of intravenous drug abuse, patients discharged AMA (13% of the cohort) were not only more likely to be readmitted within 30 days for a related diagnosis (odds ratio = 5.0) but also were more likely to have increased length of stay during the year following the index admission.6
These studies highlight the barriers to safe and effective transitions of care for this vulnerable population and demonstrate the increased burden that this population places on the health system.
Several retrospective studies have identified psychosocial and demographic risk factors associated with AMA discharge. These include younger age, male sex, substance abuse, lack of a primary care physician or health insurance, and history of previous AMA discharge.1,3,7,8 Insurance status is also associated with AMA discharge, with increased odds of AMA discharge among Medicare and Medicaid patients and patients without health insurance.9,10
Of note, one study found that race did not act as an independent predictor of AMA discharge when adjusted for age, gender, and socioeconomic factors.11
The AMA population is clinically heterogeneous. Among patients with pneumonia, for example, Saitz et al showed that a patient’s documented clinical severity did not independently predict AMA discharge, suggesting that there is great clinical heterogeneity even among AMA patients with similar admission diagnoses.12
These studies highlight the clinical and demographic heterogeneity within this population, suggesting that patients discharged AMA require individualized attention from hospitalists and other healthcare providers.
Patients describe numerous motivations for leaving the hospital prematurely, including needing to pick up public-assistance checks, personal financial issues, and familial obligations.13 Interestingly, in the cohort of HIV patients referenced above, discharge on the day welfare checks were distributed was an independent predictor of AMA discharge.6 In focus groups composed of patients discharged AMA and their treating nurses and physicians, several themes were identified as potential contributors to AMA discharge, including drug addiction, pain management issues, external obligations, wait time, the physician’s bedside manner, being in a teaching hospital, and communication issues.14
Clearly, patients have a diversity of reasons for requesting to be discharged AMA, and further research is necessary to define clear and potentially modifiable risk factors.
Discussion
The clinical scenarios outlined above present two patients with very different clinical presentations and outpatient support systems as well as demonstrate the great variability in clinical risk at the time of discharge AMA. These examples emphasize the importance of an individualized approach to care for each patient.
In Case No. 1, the patient is admitted with a mild asthma exacerbation with persistent bronchospasm, though she clinically appears well and has reliable follow-up. In contrast, in Case No. 2, the patient has life-threatening disease and no established primary care physician or mechanism for outpatient care. These examples demonstrate extremes on the clinical and psychosocial spectrum of patients requesting an “early” discharge and suggest that no two patients at risk of AMA discharge are the same. Patient 1 could likely be safely managed at home with close outpatient follow-up, while Patient 2 presents a high-risk scenario with very few safe outpatient treatment options.
We suggest that an individualized approach be taken for each patient, with attention to both clinical and psychosocial risk. In clinically low-risk cases (e.g., Case No. 1), an approach that prioritizes shared decision making and coordination with the outpatient care team may be preferable to an AMA discharge, particularly given the often adversarial nature of the later.2 In such cases, a collaborative approach may provide greater opportunity for harm reduction, provision of appropriate prescriptions, and follow-up appointments. In clinically high-risk patients such as Case No. 2, however, premature discharge is clearly inappropriate. Even in such clinically high-risk cases, however, we argue that a collaborative strategy aimed at identifying and addressing the patient’s psychosocial concerns is appropriate, as such an approach promotes shared decision making, builds trust between the patient and the care team, and therefore may facilitate improved follow-up at the time of discharge. Research is needed to formally assess the optimal approach for this patient population, including impact on rates of AMA discharge and the quality of post-discharge follow-up.
At present, the decision to classify a discharge as AMA falls solely on the treating provider, and we suspect that there is great variability in practice patterns, particularly as there are few established professional society practice guidelines regarding this difficult issue. As with all discharges from the hospital, the burden falls on the provider to engage the patient in shared decision making and ensure that the patient has the capacity to understand the risks and benefits of the proposed treatment plan. It is in this spirit that simply “filling out an AMA form” does not provide legal protection to a physician who does not adequately explain the full risks and benefits of refusal of inpatient treatment.2,15
We propose that a high-quality AMA discharge be defined as a discharge in which the patient is informed of the clinical team’s determination that further hospitalization is required but elects to leave the hospital, and it includes a clear discussion of the risks of outpatient treatment, a determination of capacity, and an exploration of safe alternative care plans that could satisfy both the patient’s medical and social needs. This definition places the burden on hospitalists and other providers to fully explore the motivations behind a patient’s request to leave the hospital and treats psychosocial motivators for premature discharge as variables in the complex risk-benefit analysis that underlies the informed consent discussion prior to AMA discharge.
Furthermore, AMA discharge does not obviate a physician’s responsibility to advocate for a patient’s well-being, and therefore an AMA discharge should be accompanied by reasonable efforts to coordinate a patient’s ongoing outpatient care. Of note, this approach is consistent with previous reviews and attempts to balance the physician’s duty to honor a patient’s autonomy with the responsibility to protect the patient from harm.2,16
Conclusion
Patients discharged AMA are a diverse population at markedly increased risk of morbidity, readmissions, and subsequent healthcare cost. We argue that in all cases of a potential premature discharge, a collaborative and patient-centered approach is crucial. Such an approach allows the provider to identify and address the patient’s concerns regarding further inpatient care, to explore possible safe outpatient treatment options, to document patient capacity, and to provide appropriate harm-reduction measures such as prescriptions.
Further research into the current practice patterns of hospitalists and other providers is necessary to allow for the formulation and adoption of best practices and implementation of appropriate harm-reduction strategies. TH
Dr. Tummalapalli is an internal medicine resident in the department of medicine at Icahn School of Medicine at Mount Sinai in New York City. Dr. Goodman is a hospitalist in the division of hospital medicine, department of medicine, at the Icahn School of Medicine at Mount Sinai.
References
- Aliyu ZY. Discharge against medical advice: sociodemographic, clinical and financial perspectives. Int J Clin Pract. 2002;56(5):325-327.
- Kahle CH, Rubio ML, Santos RA. Discharges against medical advice: considerations for the hospitalist and the patient. Hospital Medicine Clinics. 2015;4(3):421-429.
- Baptist AP, Warrier I, Arora R, Ager J, Massanari RM. Hospitalized patients with asthma who leave against medical advice: characteristics, reasons, and outcomes. J Allergy Clin Immunol. 2007;119(4):924-929.
- Hwang SW, Li J, Gupta R, Chien V, Martin RE. What happens to patients who leave hospital against medical advice? CMAJ. 2003;168(4):417-420.
- Glasgow JM, Vaughn-Sarrazin MV, Kaboli PJ. Leaving against medical advice (AMA): risk of 30-day mortality and hospital readmission. J Gen Int Med. 2010;25(9):926-929.
- Anis AH, Sun H, Guh DP, Palepu A, Schechter MT, O’Shaughnessy MV. Leaving hospital against medical advice among HIV-positive patients. CMAJ. 2002;167(6):633-637.
- Jeremiah J, O’Sullivan P, Stein MD. Who leaves against medical advice? J Gen Int Med. 1995; 10(7);403-405.
- O’Hara D, Hart W, McDonald I. Leaving hospital against medical advice. J Qual Clin Pract.1996;16(3):157-164.
- Ibrahim SA, Kwoh CK, Krishnan E. Factors associated with patients who leave acute-care hospitals against medical advice. Am J Public Health. 2007;97(12): 2204-2208.
- Weingart SN, Davis RB, Phillips RS. Patients discharged against medical advice from a general medicine service. J Gen Intern Med. 1998;13(8):568-571.
- Franks P, Meldrum S, Fiscella K. Discharges against medical advice: are race/ethnicity predictors? J Gen Intern Med. 2006;21(9):955-960.
- Saitz R, Ghali WA, Moskowitz MA. Characteristics of patients with pneumonia who are discharged from hospitals against medical advice. Am J Med. 1999;107(5):507-509.
- Alfandre, DJ. “I’m going home”: discharges against medical advice. Mayo Clin Proc. 2009;84(3):255-260.
- Onukwugha E, Saunders E, Mullins CD, Pradel FG, Zuckerman M, Weir MR. Reasons for discharges against medical advice: a qualitative study. Qual Saf Health Care. 2010;19(5):420-424. doi: 10.1136/qshc.2009.036269.
- Battenfeld v. Gregory, 589 A.2d 1059, 1061 (N.J. Super. Ct. App. Div. 1991).
- Berger J. Discharge against medical advice: ethical considerations and professional obligations. J Hosp Med. 2008;3(5):403-408.
Malaria test granted CE mark

Image by Peter H. Seeberger
A malaria test called illumigene® Malaria has received the CE mark, which suggests it meets European health and safety standards.
illumigene Malaria is a molecular test that involves the use of loop-mediated isothermal amplification (LAMP) technology.
According to the test’s developers, it provides results in under an hour, doesn’t require a high level technical expertise, and is up to 80,000 times more sensitive than conventional malaria tests.
illumigene Malaria was developed by Meridian Bioscience, Inc., with technical assistance from the US Centers for Disease Control and Prevention (CDC) and Cheikh Anta Diop University in Dakar, Senegal.
“illumigene Malaria has the potential to change current practices,” said Daouda NDIAYE, PharmD, PhD, of Cheikh Anta Diop University.
“Faster and more accurate diagnosis is vital in the fight against malaria. Earlier diagnosis enables the correct treatment to be prescribed, which leads to better clinical outcomes for the person with malaria and keeps malaria treatments for the right people.”
“Because of submicroscopic parasitemia carriage among the populations, a robust, sensitive, and field-community-deployable screening tool is needed to track the malaria reservoir in pre-elimination regions. illumigene Malaria shows this capacity.”
illumigene Malaria uses LAMP technology to amplify DNA and detect the presence of the malaria parasite.
LAMP technology is isothermal and can be used at room temperature without the need to heat reagents or the material being tested, unlike the rapid diagnostic tests currently used in malaria, which use polymerase chain reaction technology. illumigene Malaria does not require refrigeration.
Meridian Bioscience has worked with experts at the CDC and the Cheikh Anta Diop University of Dakar during the development of illumigene Malaria and collaborated with these organizations to design clinical trials.
According to Meridian, data from more than 200 patients in Senegal validated the performance of illumigene Malaria. The test demonstrated 100% sensitivity and detected infected patients that were missed by conventional testing methods.
Meridian said illumigene Malaria will be distributed in the European, Middle Eastern, and African regions by Meridian Bioscience Europe and in additional international markets by the company’s global distribution network. ![]()
Image by Peter H. Seeberger
A malaria test called illumigene® Malaria has received the CE mark, which suggests it meets European health and safety standards.
illumigene Malaria is a molecular test that involves the use of loop-mediated isothermal amplification (LAMP) technology.
According to the test’s developers, it provides results in under an hour, doesn’t require a high level technical expertise, and is up to 80,000 times more sensitive than conventional malaria tests.
illumigene Malaria was developed by Meridian Bioscience, Inc., with technical assistance from the US Centers for Disease Control and Prevention (CDC) and Cheikh Anta Diop University in Dakar, Senegal.
“illumigene Malaria has the potential to change current practices,” said Daouda NDIAYE, PharmD, PhD, of Cheikh Anta Diop University.
“Faster and more accurate diagnosis is vital in the fight against malaria. Earlier diagnosis enables the correct treatment to be prescribed, which leads to better clinical outcomes for the person with malaria and keeps malaria treatments for the right people.”
“Because of submicroscopic parasitemia carriage among the populations, a robust, sensitive, and field-community-deployable screening tool is needed to track the malaria reservoir in pre-elimination regions. illumigene Malaria shows this capacity.”
illumigene Malaria uses LAMP technology to amplify DNA and detect the presence of the malaria parasite.
LAMP technology is isothermal and can be used at room temperature without the need to heat reagents or the material being tested, unlike the rapid diagnostic tests currently used in malaria, which use polymerase chain reaction technology. illumigene Malaria does not require refrigeration.
Meridian Bioscience has worked with experts at the CDC and the Cheikh Anta Diop University of Dakar during the development of illumigene Malaria and collaborated with these organizations to design clinical trials.
According to Meridian, data from more than 200 patients in Senegal validated the performance of illumigene Malaria. The test demonstrated 100% sensitivity and detected infected patients that were missed by conventional testing methods.
Meridian said illumigene Malaria will be distributed in the European, Middle Eastern, and African regions by Meridian Bioscience Europe and in additional international markets by the company’s global distribution network. ![]()
Image by Peter H. Seeberger
A malaria test called illumigene® Malaria has received the CE mark, which suggests it meets European health and safety standards.
illumigene Malaria is a molecular test that involves the use of loop-mediated isothermal amplification (LAMP) technology.
According to the test’s developers, it provides results in under an hour, doesn’t require a high level technical expertise, and is up to 80,000 times more sensitive than conventional malaria tests.
illumigene Malaria was developed by Meridian Bioscience, Inc., with technical assistance from the US Centers for Disease Control and Prevention (CDC) and Cheikh Anta Diop University in Dakar, Senegal.
“illumigene Malaria has the potential to change current practices,” said Daouda NDIAYE, PharmD, PhD, of Cheikh Anta Diop University.
“Faster and more accurate diagnosis is vital in the fight against malaria. Earlier diagnosis enables the correct treatment to be prescribed, which leads to better clinical outcomes for the person with malaria and keeps malaria treatments for the right people.”
“Because of submicroscopic parasitemia carriage among the populations, a robust, sensitive, and field-community-deployable screening tool is needed to track the malaria reservoir in pre-elimination regions. illumigene Malaria shows this capacity.”
illumigene Malaria uses LAMP technology to amplify DNA and detect the presence of the malaria parasite.
LAMP technology is isothermal and can be used at room temperature without the need to heat reagents or the material being tested, unlike the rapid diagnostic tests currently used in malaria, which use polymerase chain reaction technology. illumigene Malaria does not require refrigeration.
Meridian Bioscience has worked with experts at the CDC and the Cheikh Anta Diop University of Dakar during the development of illumigene Malaria and collaborated with these organizations to design clinical trials.
According to Meridian, data from more than 200 patients in Senegal validated the performance of illumigene Malaria. The test demonstrated 100% sensitivity and detected infected patients that were missed by conventional testing methods.
Meridian said illumigene Malaria will be distributed in the European, Middle Eastern, and African regions by Meridian Bioscience Europe and in additional international markets by the company’s global distribution network. ![]()