User login
Insulin Rules in the Hospital
Although new medications to manage and treat hyperglycemia and diabetes continuously appear on the market, national guidelines and position statements consistently refer to insulin as the treatment of choice in the inpatient hospital setting.
“When patients are admitted to the hospital, our standard is to switch from the outpatient regimen [wide variety of medications] to the inpatient regimen—insulin,” says Paul M. Szumita, PharmD, BCPS, clinical pharmacy practice manager director at Brigham and Women’s Hospital in Boston.
For critically ill patients in ICUs or during the peri-operative period, intravenous infusion of insulin is preferred. Most general medicine and surgery patients are managed with subcutaneous insulin.
“Using a basal bolus regimen starting at a total daily dose of 0.3-0.5 unit/kg is sufficient for most patients,” says Guillermo Umpierrez, MD, CDE, FCAE, FACP, professor of medicine at Emory University in Atlanta, Ga., and a member of the board of directors for the American Diabetes Association; however, for most general medicine and surgical patients who have low oral intake or are NPO, a recent trial reported that the administration of basal insulin alone plus correction doses with rapid-acting insulin analogs before meals is as good as a basal bolus regimen. A regimen should be tweaked throughout the inpatient’s stay with an aim to reach the goal of minimal or no hypoglycemia.1
Planning for a discharge regimen should start early in the hospital stay, Dr. Szumita says, and should be based on several factors:
- The patient’s Hb1c;
- The prior regimen and how it was performing;
- The patient’s wishes; and
- Collaboration with outpatient providers.
At discharge, it is critical that patients be clear about what medications they should be on post-discharge and that they follow-up with outpatient providers in a timely manner. TH
Karen Appold is a freelance writer in Pennsylvania.
Reference
- Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: basal plus trial. Diabetes Care. 2013;36(8):2169-2174.
Although new medications to manage and treat hyperglycemia and diabetes continuously appear on the market, national guidelines and position statements consistently refer to insulin as the treatment of choice in the inpatient hospital setting.
“When patients are admitted to the hospital, our standard is to switch from the outpatient regimen [wide variety of medications] to the inpatient regimen—insulin,” says Paul M. Szumita, PharmD, BCPS, clinical pharmacy practice manager director at Brigham and Women’s Hospital in Boston.
For critically ill patients in ICUs or during the peri-operative period, intravenous infusion of insulin is preferred. Most general medicine and surgery patients are managed with subcutaneous insulin.
“Using a basal bolus regimen starting at a total daily dose of 0.3-0.5 unit/kg is sufficient for most patients,” says Guillermo Umpierrez, MD, CDE, FCAE, FACP, professor of medicine at Emory University in Atlanta, Ga., and a member of the board of directors for the American Diabetes Association; however, for most general medicine and surgical patients who have low oral intake or are NPO, a recent trial reported that the administration of basal insulin alone plus correction doses with rapid-acting insulin analogs before meals is as good as a basal bolus regimen. A regimen should be tweaked throughout the inpatient’s stay with an aim to reach the goal of minimal or no hypoglycemia.1
Planning for a discharge regimen should start early in the hospital stay, Dr. Szumita says, and should be based on several factors:
- The patient’s Hb1c;
- The prior regimen and how it was performing;
- The patient’s wishes; and
- Collaboration with outpatient providers.
At discharge, it is critical that patients be clear about what medications they should be on post-discharge and that they follow-up with outpatient providers in a timely manner. TH
Karen Appold is a freelance writer in Pennsylvania.
Reference
- Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: basal plus trial. Diabetes Care. 2013;36(8):2169-2174.
Although new medications to manage and treat hyperglycemia and diabetes continuously appear on the market, national guidelines and position statements consistently refer to insulin as the treatment of choice in the inpatient hospital setting.
“When patients are admitted to the hospital, our standard is to switch from the outpatient regimen [wide variety of medications] to the inpatient regimen—insulin,” says Paul M. Szumita, PharmD, BCPS, clinical pharmacy practice manager director at Brigham and Women’s Hospital in Boston.
For critically ill patients in ICUs or during the peri-operative period, intravenous infusion of insulin is preferred. Most general medicine and surgery patients are managed with subcutaneous insulin.
“Using a basal bolus regimen starting at a total daily dose of 0.3-0.5 unit/kg is sufficient for most patients,” says Guillermo Umpierrez, MD, CDE, FCAE, FACP, professor of medicine at Emory University in Atlanta, Ga., and a member of the board of directors for the American Diabetes Association; however, for most general medicine and surgical patients who have low oral intake or are NPO, a recent trial reported that the administration of basal insulin alone plus correction doses with rapid-acting insulin analogs before meals is as good as a basal bolus regimen. A regimen should be tweaked throughout the inpatient’s stay with an aim to reach the goal of minimal or no hypoglycemia.1
Planning for a discharge regimen should start early in the hospital stay, Dr. Szumita says, and should be based on several factors:
- The patient’s Hb1c;
- The prior regimen and how it was performing;
- The patient’s wishes; and
- Collaboration with outpatient providers.
At discharge, it is critical that patients be clear about what medications they should be on post-discharge and that they follow-up with outpatient providers in a timely manner. TH
Karen Appold is a freelance writer in Pennsylvania.
Reference
- Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: basal plus trial. Diabetes Care. 2013;36(8):2169-2174.
The Increasing Presence of Pregnant Patients in Hospital Medicine
Twenty years ago, pregnant women rarely appeared in the hospital for reasons other than delivery. Two trends responsible for that shift are advanced maternal age and rising rates of obesity, defined as a body mass index of >30.
The birth rate for women ages 35-44 has continued to rise, and that has brought new challenges to treating pregnancy, many of which result in hospital visits.1
OB/GYN hospitalist Robert Olson, MD, SFHM, has witnessed the winds of change firsthand. “Older patients are more likely to have medical conditions such as hypertension and diabetes, as well as the unusual medical problems such as status post heart attack, status post heart transplant, status post chemotherapy for cancer, as well as being on medications for chronic disease,” says Dr. Olson, who practices in Bellingham, Wash., and is the founding president of the Society of OB/GYN Hospitalists.
According to the National Health and Nutrition Examination Survey, more than one third of U.S. women are obese and more than half of all pregnant women are overweight or obese and therefore prone to complications that send them to the hospital, including gestational diabetes, hypertension, and preeclampsia.3
As an inpatient, obese pregnant women present their own challenges, including increased risk of thromboembolism. When treating this type of patient, remember pneumatic compression devices are recommended if the patient will be immobile for any length of time.4
Click here to listen to Dr. Carolyn Zelop discuss cardiovascular emergencies in pregnant patients.
Clinicians might also have significant difficulty intubating the overweight mother-to-be. Whether for cesarean section, other surgical procedures, or an acute medical crisis, physicians must approach intubation with caution as a result of excessive adipose tissue, obscured landmarks, difficulty positioning, and edema, as well as progesterone-induced relaxation of the sphincter between the esophagus and stomach.5 It is vital to make use of your most experienced staff when intubating this special needs patient. TH
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Martin JA, Hamilton BE, Ventura SJ, et al. National Vital Statistics Reports: Volume 62, Number 1. June 28, 2013. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_01.pdf. Accessed October 6, 2014.
- Olson, Robert. Founding president, Society of OB/GYN Hospitalists; OB/GYN hospitalist, PeaceHealth St. Joseph Medical Center, Bellingham, Wash. E-mail interview. November 13, 2013.
- Leddy MA, Power ML, Schulkin J. The impact of maternal obesity on maternal and fetal health. Rev Obstet Gynecol. 2008;1(4):170-178.
- ACOG committee opinion number 549. Obstet Gynecol. 2013;121(1):213-217.
- Zelop, Carolyn M. Director, perinatal ultrasound and research, Valley Hospital, Ridgewood, N.J. Telephone interview. October 30, 2013.
Twenty years ago, pregnant women rarely appeared in the hospital for reasons other than delivery. Two trends responsible for that shift are advanced maternal age and rising rates of obesity, defined as a body mass index of >30.
The birth rate for women ages 35-44 has continued to rise, and that has brought new challenges to treating pregnancy, many of which result in hospital visits.1
OB/GYN hospitalist Robert Olson, MD, SFHM, has witnessed the winds of change firsthand. “Older patients are more likely to have medical conditions such as hypertension and diabetes, as well as the unusual medical problems such as status post heart attack, status post heart transplant, status post chemotherapy for cancer, as well as being on medications for chronic disease,” says Dr. Olson, who practices in Bellingham, Wash., and is the founding president of the Society of OB/GYN Hospitalists.
According to the National Health and Nutrition Examination Survey, more than one third of U.S. women are obese and more than half of all pregnant women are overweight or obese and therefore prone to complications that send them to the hospital, including gestational diabetes, hypertension, and preeclampsia.3
As an inpatient, obese pregnant women present their own challenges, including increased risk of thromboembolism. When treating this type of patient, remember pneumatic compression devices are recommended if the patient will be immobile for any length of time.4
Click here to listen to Dr. Carolyn Zelop discuss cardiovascular emergencies in pregnant patients.
Clinicians might also have significant difficulty intubating the overweight mother-to-be. Whether for cesarean section, other surgical procedures, or an acute medical crisis, physicians must approach intubation with caution as a result of excessive adipose tissue, obscured landmarks, difficulty positioning, and edema, as well as progesterone-induced relaxation of the sphincter between the esophagus and stomach.5 It is vital to make use of your most experienced staff when intubating this special needs patient. TH
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Martin JA, Hamilton BE, Ventura SJ, et al. National Vital Statistics Reports: Volume 62, Number 1. June 28, 2013. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_01.pdf. Accessed October 6, 2014.
- Olson, Robert. Founding president, Society of OB/GYN Hospitalists; OB/GYN hospitalist, PeaceHealth St. Joseph Medical Center, Bellingham, Wash. E-mail interview. November 13, 2013.
- Leddy MA, Power ML, Schulkin J. The impact of maternal obesity on maternal and fetal health. Rev Obstet Gynecol. 2008;1(4):170-178.
- ACOG committee opinion number 549. Obstet Gynecol. 2013;121(1):213-217.
- Zelop, Carolyn M. Director, perinatal ultrasound and research, Valley Hospital, Ridgewood, N.J. Telephone interview. October 30, 2013.
Twenty years ago, pregnant women rarely appeared in the hospital for reasons other than delivery. Two trends responsible for that shift are advanced maternal age and rising rates of obesity, defined as a body mass index of >30.
The birth rate for women ages 35-44 has continued to rise, and that has brought new challenges to treating pregnancy, many of which result in hospital visits.1
OB/GYN hospitalist Robert Olson, MD, SFHM, has witnessed the winds of change firsthand. “Older patients are more likely to have medical conditions such as hypertension and diabetes, as well as the unusual medical problems such as status post heart attack, status post heart transplant, status post chemotherapy for cancer, as well as being on medications for chronic disease,” says Dr. Olson, who practices in Bellingham, Wash., and is the founding president of the Society of OB/GYN Hospitalists.
According to the National Health and Nutrition Examination Survey, more than one third of U.S. women are obese and more than half of all pregnant women are overweight or obese and therefore prone to complications that send them to the hospital, including gestational diabetes, hypertension, and preeclampsia.3
As an inpatient, obese pregnant women present their own challenges, including increased risk of thromboembolism. When treating this type of patient, remember pneumatic compression devices are recommended if the patient will be immobile for any length of time.4
Click here to listen to Dr. Carolyn Zelop discuss cardiovascular emergencies in pregnant patients.
Clinicians might also have significant difficulty intubating the overweight mother-to-be. Whether for cesarean section, other surgical procedures, or an acute medical crisis, physicians must approach intubation with caution as a result of excessive adipose tissue, obscured landmarks, difficulty positioning, and edema, as well as progesterone-induced relaxation of the sphincter between the esophagus and stomach.5 It is vital to make use of your most experienced staff when intubating this special needs patient. TH
Maybelle Cowan-Lincoln is a freelance writer in New Jersey.
References
- Martin JA, Hamilton BE, Ventura SJ, et al. National Vital Statistics Reports: Volume 62, Number 1. June 28, 2013. Available at: http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_01.pdf. Accessed October 6, 2014.
- Olson, Robert. Founding president, Society of OB/GYN Hospitalists; OB/GYN hospitalist, PeaceHealth St. Joseph Medical Center, Bellingham, Wash. E-mail interview. November 13, 2013.
- Leddy MA, Power ML, Schulkin J. The impact of maternal obesity on maternal and fetal health. Rev Obstet Gynecol. 2008;1(4):170-178.
- ACOG committee opinion number 549. Obstet Gynecol. 2013;121(1):213-217.
- Zelop, Carolyn M. Director, perinatal ultrasound and research, Valley Hospital, Ridgewood, N.J. Telephone interview. October 30, 2013.
No survival benefit of RAI seen in early-stage thyroid cancer
CORONADO, CALIF. – In a large cohort of patients with differentiated thyroid cancer, the use of radioactive iodine was associated with improved disease-specific survival in those with advanced disease but not in those with papillary thyroid microcarcinoma.
“Everything in medicine is a risk-benefit balance,” lead author Dr. Ryan K. Orosco said in an interview in advance of the annual meeting of the American Thyroid Association, where the work was presented. “Any two patients that receive radioactive iodine (RAI) for differentiated thyroid cancer are likely to have different survival benefit from that therapy. This study provides a quantitative comparison of the impact of RAI in various patient subgroups.”

In one of the largest studies of its kind, Dr. Orosco of the division of head and neck surgery at the University of California, San Diego, and his associates identified 85,740 patients with differentiated thyroid carcinoma from the Surveillance, Epidemiology, and End Results database from 1973 through 2009. They used multivariate analyses to explore the association between RAI and cancer-specific survival in 149 population subgroups, controlling for age, decade of diagnosis, race, gender, tumor type, nodal involvement, metastasis stage, and RAI therapy.
More than three-quarters of the patients (78%) were female, 68% were white, their mean age at diagnosis was 46 years, and the median follow-up time was 85 months. The researchers found that nearly half of patients (43%) received RAI. By American Joint Committee on Cancer stage, RAI was used in 55% of stage I patients, 41% of stage II patients, 94% of stage III patients, and 85% of stage IV patients. In addition, 42% of patients with T1a disease and 88% of those with T4 disease received RAI.
Use of RAI was positively associated with survival in the overall cohort (hazard ratio 1.3; P = .002), while statistically significant HRs for RAI were observed in 49 population subgroups. In patients with metastatic disease, use of RAI was associated with a decreased risk for disease-specific mortality (HR range of 2.28-3.82). Protective effects of RAI were also observed in patients with regional metastases (HR 1.4-1.9), those with T3-positive tumors (HR 1.36-1.39), those with T4 tumors (HR 1.85), and in those with stage IV disease (HR 1.47-1.73).
Dr. Orosco and his associates observed a negative effect of RAI in patients with macropapillary carcinoma. Specifically, those with T1a disease had an increased likelihood of thyroid cancer–specific mortality (HR .13; P less than .001), while similar associations were seen in multiple subgroups of patients with T1a disease (HR 0.04-0.25). No statistically significant effects of RAI were observed in patients with T1b or T2 tumors.
“RAI appears to offer the best survival impact in patients with advanced differentiated thyroid carcinoma,” Dr. Orosco said. “Its use in early-stage patients should be carefully considered.”
In their abstract, the researchers noted that the findings “might help clinicians personalize RAI therapy to specific differentiated thyroid cancer populations – offering treatment in patients most likely to benefit, and sparing others unnecessary costs and potential side effects.”
Dr. Orosco acknowledged certain limitations of the study, including the fact that the SEER database does not contain details about each patient’s surgery, the dose of RAI used, other comorbidities, or data on cancer recurrence. “This study does not attempt to explore the reasons behind the apparent survival disadvantage seen in patients with T1a disease,” he said. “We don’t know exactly why early-stage patients have an increased risk of disease-specific mortality when RAI is used. Additional work is needed to explore this further.”
Dr. Orosco reported having no financial disclosures.
On Twitter @dougbrunk
CORONADO, CALIF. – In a large cohort of patients with differentiated thyroid cancer, the use of radioactive iodine was associated with improved disease-specific survival in those with advanced disease but not in those with papillary thyroid microcarcinoma.
“Everything in medicine is a risk-benefit balance,” lead author Dr. Ryan K. Orosco said in an interview in advance of the annual meeting of the American Thyroid Association, where the work was presented. “Any two patients that receive radioactive iodine (RAI) for differentiated thyroid cancer are likely to have different survival benefit from that therapy. This study provides a quantitative comparison of the impact of RAI in various patient subgroups.”
In one of the largest studies of its kind, Dr. Orosco of the division of head and neck surgery at the University of California, San Diego, and his associates identified 85,740 patients with differentiated thyroid carcinoma from the Surveillance, Epidemiology, and End Results database from 1973 through 2009. They used multivariate analyses to explore the association between RAI and cancer-specific survival in 149 population subgroups, controlling for age, decade of diagnosis, race, gender, tumor type, nodal involvement, metastasis stage, and RAI therapy.
More than three-quarters of the patients (78%) were female, 68% were white, their mean age at diagnosis was 46 years, and the median follow-up time was 85 months. The researchers found that nearly half of patients (43%) received RAI. By American Joint Committee on Cancer stage, RAI was used in 55% of stage I patients, 41% of stage II patients, 94% of stage III patients, and 85% of stage IV patients. In addition, 42% of patients with T1a disease and 88% of those with T4 disease received RAI.
Use of RAI was positively associated with survival in the overall cohort (hazard ratio 1.3; P = .002), while statistically significant HRs for RAI were observed in 49 population subgroups. In patients with metastatic disease, use of RAI was associated with a decreased risk for disease-specific mortality (HR range of 2.28-3.82). Protective effects of RAI were also observed in patients with regional metastases (HR 1.4-1.9), those with T3-positive tumors (HR 1.36-1.39), those with T4 tumors (HR 1.85), and in those with stage IV disease (HR 1.47-1.73).
Dr. Orosco and his associates observed a negative effect of RAI in patients with macropapillary carcinoma. Specifically, those with T1a disease had an increased likelihood of thyroid cancer–specific mortality (HR .13; P less than .001), while similar associations were seen in multiple subgroups of patients with T1a disease (HR 0.04-0.25). No statistically significant effects of RAI were observed in patients with T1b or T2 tumors.
“RAI appears to offer the best survival impact in patients with advanced differentiated thyroid carcinoma,” Dr. Orosco said. “Its use in early-stage patients should be carefully considered.”
In their abstract, the researchers noted that the findings “might help clinicians personalize RAI therapy to specific differentiated thyroid cancer populations – offering treatment in patients most likely to benefit, and sparing others unnecessary costs and potential side effects.”
Dr. Orosco acknowledged certain limitations of the study, including the fact that the SEER database does not contain details about each patient’s surgery, the dose of RAI used, other comorbidities, or data on cancer recurrence. “This study does not attempt to explore the reasons behind the apparent survival disadvantage seen in patients with T1a disease,” he said. “We don’t know exactly why early-stage patients have an increased risk of disease-specific mortality when RAI is used. Additional work is needed to explore this further.”
Dr. Orosco reported having no financial disclosures.
On Twitter @dougbrunk
CORONADO, CALIF. – In a large cohort of patients with differentiated thyroid cancer, the use of radioactive iodine was associated with improved disease-specific survival in those with advanced disease but not in those with papillary thyroid microcarcinoma.
“Everything in medicine is a risk-benefit balance,” lead author Dr. Ryan K. Orosco said in an interview in advance of the annual meeting of the American Thyroid Association, where the work was presented. “Any two patients that receive radioactive iodine (RAI) for differentiated thyroid cancer are likely to have different survival benefit from that therapy. This study provides a quantitative comparison of the impact of RAI in various patient subgroups.”
In one of the largest studies of its kind, Dr. Orosco of the division of head and neck surgery at the University of California, San Diego, and his associates identified 85,740 patients with differentiated thyroid carcinoma from the Surveillance, Epidemiology, and End Results database from 1973 through 2009. They used multivariate analyses to explore the association between RAI and cancer-specific survival in 149 population subgroups, controlling for age, decade of diagnosis, race, gender, tumor type, nodal involvement, metastasis stage, and RAI therapy.
More than three-quarters of the patients (78%) were female, 68% were white, their mean age at diagnosis was 46 years, and the median follow-up time was 85 months. The researchers found that nearly half of patients (43%) received RAI. By American Joint Committee on Cancer stage, RAI was used in 55% of stage I patients, 41% of stage II patients, 94% of stage III patients, and 85% of stage IV patients. In addition, 42% of patients with T1a disease and 88% of those with T4 disease received RAI.
Use of RAI was positively associated with survival in the overall cohort (hazard ratio 1.3; P = .002), while statistically significant HRs for RAI were observed in 49 population subgroups. In patients with metastatic disease, use of RAI was associated with a decreased risk for disease-specific mortality (HR range of 2.28-3.82). Protective effects of RAI were also observed in patients with regional metastases (HR 1.4-1.9), those with T3-positive tumors (HR 1.36-1.39), those with T4 tumors (HR 1.85), and in those with stage IV disease (HR 1.47-1.73).
Dr. Orosco and his associates observed a negative effect of RAI in patients with macropapillary carcinoma. Specifically, those with T1a disease had an increased likelihood of thyroid cancer–specific mortality (HR .13; P less than .001), while similar associations were seen in multiple subgroups of patients with T1a disease (HR 0.04-0.25). No statistically significant effects of RAI were observed in patients with T1b or T2 tumors.
“RAI appears to offer the best survival impact in patients with advanced differentiated thyroid carcinoma,” Dr. Orosco said. “Its use in early-stage patients should be carefully considered.”
In their abstract, the researchers noted that the findings “might help clinicians personalize RAI therapy to specific differentiated thyroid cancer populations – offering treatment in patients most likely to benefit, and sparing others unnecessary costs and potential side effects.”
Dr. Orosco acknowledged certain limitations of the study, including the fact that the SEER database does not contain details about each patient’s surgery, the dose of RAI used, other comorbidities, or data on cancer recurrence. “This study does not attempt to explore the reasons behind the apparent survival disadvantage seen in patients with T1a disease,” he said. “We don’t know exactly why early-stage patients have an increased risk of disease-specific mortality when RAI is used. Additional work is needed to explore this further.”
Dr. Orosco reported having no financial disclosures.
On Twitter @dougbrunk
AT THE ATA ANNUAL MEETING
Key clinical point: Radioactive iodine appears to offer the best survival impact in patients with advanced differentiated thyroid carcinoma.
Major finding: In patients with metastatic disease, use of RAI was associated with a decreased risk for disease-specific mortality (HR range of 2.28-3.82). However, those with T1a disease had an increased likelihood of thyroid cancer-specific mortality (HR .13; P less than .001), while similar associations were seen in multiple subgroups of patients with T1a disease (HR .04-.25).
Data source: An analysis of 85,740 patients with differentiated thyroid carcinoma from the Surveillance, Epidemiology, and End Results database from 1973 through 2009.
Disclosures: Dr. Orosco reported having no financial disclosures.

Sulfur Spring Dermatitis
Sulfur spring dermatitis is characterized by multiple punched-out erosions and pits. In prior case reports, patients often presented with painful swollen lesions that developed within 24 hours of bathing in hot sulfur springs.1 Because spa therapy and thermal spring baths are common in modern society, dermatologists should be aware of sulfur spring dermatitis as a potential adverse effect.
Case Report
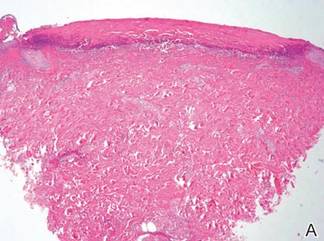
A healthy 65-year-old man presented with painful skin lesions on the legs that developed after bathing for 25 minutes in a hot sulfur spring 1 day prior. The patient had no history of dermatologic disease. He reported a 10-year history of bathing in a hot sulfur spring for 20 minutes every 3 days in the winter. This time, he bathed 5 minutes longer than usual. No skin condition was noted prior to bathing, but he reported feeling a tickling sensation and scratching the legs while he was immersed in the water. One hour after bathing, he noted confluent, punched-out, round ulcers with peripheral erythema on the thighs and shins (Figure 1).
|
|


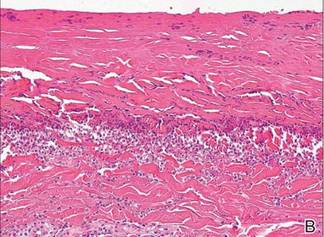
A skin biopsy revealed sharply demarcated, homogeneous coagulation necrosis of the epidermis. Many neutrophils were present under the necrosis (Figure 2). Periodic acid–Schiff and acid-fast stains were negative for infectious organisms, and a skin tissue culture yielded negative results. Intensive wound care was started with nitrofurazone ointment 0.2%. The ulcers healed gradually in the following months with scar formation and hyperpigmentation.
Comment
Thermal sulfur baths are a form of balneotherapy promoted in many cultures for improvement of skin conditions; however, certain uncommon skin problems may occur after bathing in hot sulfur springs.2 In particular, sulfur spring dermatitis is a potential adverse effect.
Thermal sulfur water is known to exert anti-inflammatory, keratoplastic, and antipruriginous effects. As a result, it often is used in many cultures as an alternative treatment of various skin conditions.2-4 Moreover, thermal sulfur baths are popular in northeastern Asian countries for their effects on mental health.5 Hot springs in northern Taiwan, which contain large amounts of hydrogen sulfide, sulfate, and sulfur differ from other thermal springs in that they are rather acidic in nature and release geothermal energy from volcanic activity.6 In addition to hot sulfur springs, there are neutral salt and CO2 springs in Taiwan.5 However, spring dermatitis has only been associated with bathing in hot sulfur springs due to high concentrations of hydrogen sulfide that break down keratin and cause dissolution of the stratum corneum.7
The incidence of sulfur spring dermatitis is unknown. Although the largest known case series reported 44 cases occurring within a decade in Taiwan,1 it is rarely seen in our daily practice. Previously reported cases of sulfur spring dermatitis noted clinical findings of swelling of the affected area followed by punched-out erosions with surrounding erythema. Most lesions gradually healed with dry brownish crusts. A patch test with sulfur spring water and sulfur compounds showed negative results; therefore, the mechanism is unlikely to be allergic reaction.1 The clinical differential diagnosis includes factitious ulcers as well as viral and fungal infections. A tissue culture should be performed to exclude infectious conditions.
This characteristic skin disease does not present in all individuals after bathing in hot sulfur springs. Lesions may present anywhere on the body with a predilection for skin folds, including the penis and scrotum. Preexisting skin conditions such as pruritus and xerosis are considered to be contributing factors. The possible etiology of sulfur spring dermatitis may be acid irritation from the unstable amount of soluble sulfur in the water, which is enhanced by the heat.1 In our patient, no prior skin disease was noted, but he scratched the skin on the thighs while bathing, which may have contributed to the development of lesions in this area rather than in the skin folds.
The skin biopsy specimen demonstrated epidermal coagulation necrosis, mild superficial dermal damage, and preservation of the pilosebaceous appendages. The ulcers were painful during healing and resolved with scarring and hyperpigmentation. The histopathologic findings and clinical course in our patient were similar to cases of superficial second-degree burns.8 It is possible that the keratoplastic effect of sulfur at high concentrations along with thermal water caused the skin condition.
Conclusion
Individuals who engage in thermal sulfur baths should be aware of potential adverse effects such as sulfur spring dermatitis, especially those with preexisting skin disorders.
1. Sun CC, Sue MS. Sulfur spring dermatitis. Contact Dermatitis. 1995;32:31-34.
2. Matz H, Orion E, Wolf R. Balneotherapy in dermatology. Dermatol Ther. 2003;16:132-140.
3. Leslie KS, Millington GW, Levell NJ. Sulphur and skin: from Satan to Saddam! J Cosmet Dermatol. 2004;3:94-98.
4. Millikan LE. Unapproved treatments or indications in dermatology: physical therapy including balneotherapy. Clin Dermatol. 2000;18:125-129.
5. Nirei H, Furuno K, Kusuda T. Medical geology in Japan. In: Selinus O, Finkelman RB, Centeno JA, eds. Medical Geology: A Regional Synthesis. New York, NY: Springer; 2010:329-354.
6. Liu CM, Song SR, Chen YL, et al. Characteristics and origins of hot springs in the Tatun Volcano Group in northern Taiwan. Terr Atmos Ocean Sci. 2011;22:475-489.
7. Lin AN, Reimer RJ, Carter DM. Sulfur revisited. J Am Acad Dermatol. 1988;18:553-558.
8. Weedon D. Reaction to physical agents. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. London, England: Churchill Livingstone, Elsevier Health; 2010:525-540.
Sulfur spring dermatitis is characterized by multiple punched-out erosions and pits. In prior case reports, patients often presented with painful swollen lesions that developed within 24 hours of bathing in hot sulfur springs.1 Because spa therapy and thermal spring baths are common in modern society, dermatologists should be aware of sulfur spring dermatitis as a potential adverse effect.
Case Report
A healthy 65-year-old man presented with painful skin lesions on the legs that developed after bathing for 25 minutes in a hot sulfur spring 1 day prior. The patient had no history of dermatologic disease. He reported a 10-year history of bathing in a hot sulfur spring for 20 minutes every 3 days in the winter. This time, he bathed 5 minutes longer than usual. No skin condition was noted prior to bathing, but he reported feeling a tickling sensation and scratching the legs while he was immersed in the water. One hour after bathing, he noted confluent, punched-out, round ulcers with peripheral erythema on the thighs and shins (Figure 1).
|
|
A skin biopsy revealed sharply demarcated, homogeneous coagulation necrosis of the epidermis. Many neutrophils were present under the necrosis (Figure 2). Periodic acid–Schiff and acid-fast stains were negative for infectious organisms, and a skin tissue culture yielded negative results. Intensive wound care was started with nitrofurazone ointment 0.2%. The ulcers healed gradually in the following months with scar formation and hyperpigmentation.
Comment
Thermal sulfur baths are a form of balneotherapy promoted in many cultures for improvement of skin conditions; however, certain uncommon skin problems may occur after bathing in hot sulfur springs.2 In particular, sulfur spring dermatitis is a potential adverse effect.
Thermal sulfur water is known to exert anti-inflammatory, keratoplastic, and antipruriginous effects. As a result, it often is used in many cultures as an alternative treatment of various skin conditions.2-4 Moreover, thermal sulfur baths are popular in northeastern Asian countries for their effects on mental health.5 Hot springs in northern Taiwan, which contain large amounts of hydrogen sulfide, sulfate, and sulfur differ from other thermal springs in that they are rather acidic in nature and release geothermal energy from volcanic activity.6 In addition to hot sulfur springs, there are neutral salt and CO2 springs in Taiwan.5 However, spring dermatitis has only been associated with bathing in hot sulfur springs due to high concentrations of hydrogen sulfide that break down keratin and cause dissolution of the stratum corneum.7
The incidence of sulfur spring dermatitis is unknown. Although the largest known case series reported 44 cases occurring within a decade in Taiwan,1 it is rarely seen in our daily practice. Previously reported cases of sulfur spring dermatitis noted clinical findings of swelling of the affected area followed by punched-out erosions with surrounding erythema. Most lesions gradually healed with dry brownish crusts. A patch test with sulfur spring water and sulfur compounds showed negative results; therefore, the mechanism is unlikely to be allergic reaction.1 The clinical differential diagnosis includes factitious ulcers as well as viral and fungal infections. A tissue culture should be performed to exclude infectious conditions.
This characteristic skin disease does not present in all individuals after bathing in hot sulfur springs. Lesions may present anywhere on the body with a predilection for skin folds, including the penis and scrotum. Preexisting skin conditions such as pruritus and xerosis are considered to be contributing factors. The possible etiology of sulfur spring dermatitis may be acid irritation from the unstable amount of soluble sulfur in the water, which is enhanced by the heat.1 In our patient, no prior skin disease was noted, but he scratched the skin on the thighs while bathing, which may have contributed to the development of lesions in this area rather than in the skin folds.
The skin biopsy specimen demonstrated epidermal coagulation necrosis, mild superficial dermal damage, and preservation of the pilosebaceous appendages. The ulcers were painful during healing and resolved with scarring and hyperpigmentation. The histopathologic findings and clinical course in our patient were similar to cases of superficial second-degree burns.8 It is possible that the keratoplastic effect of sulfur at high concentrations along with thermal water caused the skin condition.
Conclusion
Individuals who engage in thermal sulfur baths should be aware of potential adverse effects such as sulfur spring dermatitis, especially those with preexisting skin disorders.
Sulfur spring dermatitis is characterized by multiple punched-out erosions and pits. In prior case reports, patients often presented with painful swollen lesions that developed within 24 hours of bathing in hot sulfur springs.1 Because spa therapy and thermal spring baths are common in modern society, dermatologists should be aware of sulfur spring dermatitis as a potential adverse effect.
Case Report
A healthy 65-year-old man presented with painful skin lesions on the legs that developed after bathing for 25 minutes in a hot sulfur spring 1 day prior. The patient had no history of dermatologic disease. He reported a 10-year history of bathing in a hot sulfur spring for 20 minutes every 3 days in the winter. This time, he bathed 5 minutes longer than usual. No skin condition was noted prior to bathing, but he reported feeling a tickling sensation and scratching the legs while he was immersed in the water. One hour after bathing, he noted confluent, punched-out, round ulcers with peripheral erythema on the thighs and shins (Figure 1).
|
|
A skin biopsy revealed sharply demarcated, homogeneous coagulation necrosis of the epidermis. Many neutrophils were present under the necrosis (Figure 2). Periodic acid–Schiff and acid-fast stains were negative for infectious organisms, and a skin tissue culture yielded negative results. Intensive wound care was started with nitrofurazone ointment 0.2%. The ulcers healed gradually in the following months with scar formation and hyperpigmentation.
Comment
Thermal sulfur baths are a form of balneotherapy promoted in many cultures for improvement of skin conditions; however, certain uncommon skin problems may occur after bathing in hot sulfur springs.2 In particular, sulfur spring dermatitis is a potential adverse effect.
Thermal sulfur water is known to exert anti-inflammatory, keratoplastic, and antipruriginous effects. As a result, it often is used in many cultures as an alternative treatment of various skin conditions.2-4 Moreover, thermal sulfur baths are popular in northeastern Asian countries for their effects on mental health.5 Hot springs in northern Taiwan, which contain large amounts of hydrogen sulfide, sulfate, and sulfur differ from other thermal springs in that they are rather acidic in nature and release geothermal energy from volcanic activity.6 In addition to hot sulfur springs, there are neutral salt and CO2 springs in Taiwan.5 However, spring dermatitis has only been associated with bathing in hot sulfur springs due to high concentrations of hydrogen sulfide that break down keratin and cause dissolution of the stratum corneum.7
The incidence of sulfur spring dermatitis is unknown. Although the largest known case series reported 44 cases occurring within a decade in Taiwan,1 it is rarely seen in our daily practice. Previously reported cases of sulfur spring dermatitis noted clinical findings of swelling of the affected area followed by punched-out erosions with surrounding erythema. Most lesions gradually healed with dry brownish crusts. A patch test with sulfur spring water and sulfur compounds showed negative results; therefore, the mechanism is unlikely to be allergic reaction.1 The clinical differential diagnosis includes factitious ulcers as well as viral and fungal infections. A tissue culture should be performed to exclude infectious conditions.
This characteristic skin disease does not present in all individuals after bathing in hot sulfur springs. Lesions may present anywhere on the body with a predilection for skin folds, including the penis and scrotum. Preexisting skin conditions such as pruritus and xerosis are considered to be contributing factors. The possible etiology of sulfur spring dermatitis may be acid irritation from the unstable amount of soluble sulfur in the water, which is enhanced by the heat.1 In our patient, no prior skin disease was noted, but he scratched the skin on the thighs while bathing, which may have contributed to the development of lesions in this area rather than in the skin folds.
The skin biopsy specimen demonstrated epidermal coagulation necrosis, mild superficial dermal damage, and preservation of the pilosebaceous appendages. The ulcers were painful during healing and resolved with scarring and hyperpigmentation. The histopathologic findings and clinical course in our patient were similar to cases of superficial second-degree burns.8 It is possible that the keratoplastic effect of sulfur at high concentrations along with thermal water caused the skin condition.
Conclusion
Individuals who engage in thermal sulfur baths should be aware of potential adverse effects such as sulfur spring dermatitis, especially those with preexisting skin disorders.
1. Sun CC, Sue MS. Sulfur spring dermatitis. Contact Dermatitis. 1995;32:31-34.
2. Matz H, Orion E, Wolf R. Balneotherapy in dermatology. Dermatol Ther. 2003;16:132-140.
3. Leslie KS, Millington GW, Levell NJ. Sulphur and skin: from Satan to Saddam! J Cosmet Dermatol. 2004;3:94-98.
4. Millikan LE. Unapproved treatments or indications in dermatology: physical therapy including balneotherapy. Clin Dermatol. 2000;18:125-129.
5. Nirei H, Furuno K, Kusuda T. Medical geology in Japan. In: Selinus O, Finkelman RB, Centeno JA, eds. Medical Geology: A Regional Synthesis. New York, NY: Springer; 2010:329-354.
6. Liu CM, Song SR, Chen YL, et al. Characteristics and origins of hot springs in the Tatun Volcano Group in northern Taiwan. Terr Atmos Ocean Sci. 2011;22:475-489.
7. Lin AN, Reimer RJ, Carter DM. Sulfur revisited. J Am Acad Dermatol. 1988;18:553-558.
8. Weedon D. Reaction to physical agents. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. London, England: Churchill Livingstone, Elsevier Health; 2010:525-540.
1. Sun CC, Sue MS. Sulfur spring dermatitis. Contact Dermatitis. 1995;32:31-34.
2. Matz H, Orion E, Wolf R. Balneotherapy in dermatology. Dermatol Ther. 2003;16:132-140.
3. Leslie KS, Millington GW, Levell NJ. Sulphur and skin: from Satan to Saddam! J Cosmet Dermatol. 2004;3:94-98.
4. Millikan LE. Unapproved treatments or indications in dermatology: physical therapy including balneotherapy. Clin Dermatol. 2000;18:125-129.
5. Nirei H, Furuno K, Kusuda T. Medical geology in Japan. In: Selinus O, Finkelman RB, Centeno JA, eds. Medical Geology: A Regional Synthesis. New York, NY: Springer; 2010:329-354.
6. Liu CM, Song SR, Chen YL, et al. Characteristics and origins of hot springs in the Tatun Volcano Group in northern Taiwan. Terr Atmos Ocean Sci. 2011;22:475-489.
7. Lin AN, Reimer RJ, Carter DM. Sulfur revisited. J Am Acad Dermatol. 1988;18:553-558.
8. Weedon D. Reaction to physical agents. In: Weedon D. Weedon’s Skin Pathology. 3rd ed. London, England: Churchill Livingstone, Elsevier Health; 2010:525-540.
Practice Points
- The clinical findings of sulfur spring dermatitis are similar to those of a superficial second-degree burn.
- Careful evaluation of the patient’s clinical history and recognition of characteristic findings are important for correct diagnosis.
- Patients with preexisting skin disorders who engage in thermal sulfur baths should be aware of the potential adverse effect of sulfur spring dermatitis.

Five Reasons You Should Attend Hospital Medicine 2013 in Washington, D.C.
Hospital Medicine 2013 offers expert speakers, 90 educational offerings, and networking with the best and brightest hospital medicine has to offer.
Hospital Medicine 2013 offers expert speakers, 90 educational offerings, and networking with the best and brightest hospital medicine has to offer.
Hospital Medicine 2013 offers expert speakers, 90 educational offerings, and networking with the best and brightest hospital medicine has to offer.
The Discount Dilemma
Health care reform has triggered considerable discussion both in print and online about the administrative problems it has created for private practitioners, including decreased cash flow, increased paperwork and business expenses, and an increasing number of high-deductible insurance exchanges with the infamous 90-day “grace periods.” Extending discounts to patients who pay at the time of service or out of pocket may mitigate damage caused by all 3 of these issues; however, caution is necessary, as discounts often can run afoul of federal and state laws, including anti-kickback statutes,1 the anti-inducement provision of the Health Insurance Portability and Accountability Act,2 the Medicare exclusion provision,3 and state insurance antidiscrimination provisions.4
Avoid Kickback Penalties From Patient Discounts
From a legal standpoint, any discount is technically a kickback of sorts because you are returning part of your fee to the patient, and many laws designed to thwart true kickbacks can apply to patient discounts. Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not normally covered by insurance. You would think that these transactions are strictly between you and your patients, but if these discounts appear to be marketing incentives to attract patients, you may face a penalty.5
Patient discounts also may impact third-party payers. Many provider agreements contain “most favored nation” clauses, which require you to automatically give that payer the lowest price you offer to anyone else, regardless of what would be paid otherwise. In other words, the payer could demand the same discount you offer any individual patient. A time-of-service discount is, of course, exactly that: it is offered only when payment is made immediately. Third parties never pay at the time of service and would not be entitled to it, but they may try to invoke their agreement.
If you want to extend discounts for covered services, you must be sure that the discounted fee you charge the patient also is reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud.6 It is important to avoid discounting so regularly that the discounted fee becomes your usual and customary rate in the eyes of the insurer.
Waiving Costs and Kickbacks
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare & Medicaid Services (CMS) will see it as an inducement or kickback, especially if you do it routinely, and similar to private carriers, they will consider the discounted fee your new customary fee. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need,” according to the Office of Inspector General,7 but thorough documentation is necessary in such cases.
Waiving co-pays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable co-pays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and litigation may occur against providers who flout this requirement.8 As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but if there is a pattern of routine waivers and a paucity of documentation, you will have difficulty defending it.
Antidiscrimination Laws
In addition to kickback laws, some states also have antidiscrimination laws that forbid lower charges to any subset of insurance payers or to direct payers.4 Some states make specific exceptions for legitimate discounts, such as individual cases of financial hardship, or if you pass along your lower billing and collection expenditures to patients who pay immediately, but other states do not.
Determining Discount Amounts
The discount amount depends on the physician’s situation and deserves careful consideration. If the amount or percentage that you choose to offer as a discount is completely out of proportion with the administrative costs of submitting paperwork as well as the hassles associated with waiting for third-party payments, you could be accused of running a discount policy that is in effect a de facto increase to insurance carriers, which also could result in charges of fraud.2
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies as well as all hospitals have written policies for this system, often based on federal poverty guidelines. To avoid any potential issues, contact your local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence.
Final Thoughts
Consistency of administration, objectivity in policies, and documentation of individual eligibility will ensure that the discounts you offer patients are in line with legal and payer regulations. Before you establish a discount policy, be sure to check your state’s applicable laws, and as always, run everything by your attorney.
1. Guidance on the federal anti-kickback law. Health Resources and Services Administration Web site. http://bphc.hrsa.gov/policiesregulations/policies/pal199510.html. Accessed October 22, 2014.
2. US Department of Health & Human Services. A roadmap for new physicians: fraud & abuse laws. Office of Inspector General Web site.http://oig.hhs.gov/compliance/physician-education/01laws.asp. Accessed October 21, 2014.
3. Exclusion of certain individuals and entities from participation in Medicare and State health care programs, 42 USC §1320a–7 (2011).
4. Non-discrimination in health care, 42 USC §300gg–5 (2014).
5. US Department of Health and Human Services. Offering gifts and other inducements to beneficiaries. http://oig.hhs.gov/fraud/docs/alertsandbulletins/SABGiftsandInducements.pdf. Published August 2002. Accessed October 21, 2014.
6. The challenge of health care fraud. National Health Care Anti-Fraud Association Web site. http://www.nhcaa.org/resources/health-care-anti-fraud-resources/the-challenge-of-health-care-fraud.aspx. Accessed October 21, 2014.
7. US Department of Health & Human Services. Hospital discounts offered to patients who cannot afford to pay their hospital bills. Office of Inspector General Web site. http://oig.hhs.gov/fraud/docs/alertsandbulletins/2004/FA021904hospitaldiscounts.pdf. Published February 2, 2004. Accessed October 16, 2014.
8. Merritt M. Forgiving patient copays can lead to unforgiving consequences. Physicians Practice Web site. http://www.physicianspractice.com/blog/forgiving-patient-copays-can-lead-unforgiving-consequences. Published December 15, 2013. Accessed October 21, 2014.
Health care reform has triggered considerable discussion both in print and online about the administrative problems it has created for private practitioners, including decreased cash flow, increased paperwork and business expenses, and an increasing number of high-deductible insurance exchanges with the infamous 90-day “grace periods.” Extending discounts to patients who pay at the time of service or out of pocket may mitigate damage caused by all 3 of these issues; however, caution is necessary, as discounts often can run afoul of federal and state laws, including anti-kickback statutes,1 the anti-inducement provision of the Health Insurance Portability and Accountability Act,2 the Medicare exclusion provision,3 and state insurance antidiscrimination provisions.4
Avoid Kickback Penalties From Patient Discounts
From a legal standpoint, any discount is technically a kickback of sorts because you are returning part of your fee to the patient, and many laws designed to thwart true kickbacks can apply to patient discounts. Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not normally covered by insurance. You would think that these transactions are strictly between you and your patients, but if these discounts appear to be marketing incentives to attract patients, you may face a penalty.5
Patient discounts also may impact third-party payers. Many provider agreements contain “most favored nation” clauses, which require you to automatically give that payer the lowest price you offer to anyone else, regardless of what would be paid otherwise. In other words, the payer could demand the same discount you offer any individual patient. A time-of-service discount is, of course, exactly that: it is offered only when payment is made immediately. Third parties never pay at the time of service and would not be entitled to it, but they may try to invoke their agreement.
If you want to extend discounts for covered services, you must be sure that the discounted fee you charge the patient also is reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud.6 It is important to avoid discounting so regularly that the discounted fee becomes your usual and customary rate in the eyes of the insurer.
Waiving Costs and Kickbacks
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare & Medicaid Services (CMS) will see it as an inducement or kickback, especially if you do it routinely, and similar to private carriers, they will consider the discounted fee your new customary fee. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need,” according to the Office of Inspector General,7 but thorough documentation is necessary in such cases.
Waiving co-pays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable co-pays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and litigation may occur against providers who flout this requirement.8 As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but if there is a pattern of routine waivers and a paucity of documentation, you will have difficulty defending it.
Antidiscrimination Laws
In addition to kickback laws, some states also have antidiscrimination laws that forbid lower charges to any subset of insurance payers or to direct payers.4 Some states make specific exceptions for legitimate discounts, such as individual cases of financial hardship, or if you pass along your lower billing and collection expenditures to patients who pay immediately, but other states do not.
Determining Discount Amounts
The discount amount depends on the physician’s situation and deserves careful consideration. If the amount or percentage that you choose to offer as a discount is completely out of proportion with the administrative costs of submitting paperwork as well as the hassles associated with waiting for third-party payments, you could be accused of running a discount policy that is in effect a de facto increase to insurance carriers, which also could result in charges of fraud.2
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies as well as all hospitals have written policies for this system, often based on federal poverty guidelines. To avoid any potential issues, contact your local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence.
Final Thoughts
Consistency of administration, objectivity in policies, and documentation of individual eligibility will ensure that the discounts you offer patients are in line with legal and payer regulations. Before you establish a discount policy, be sure to check your state’s applicable laws, and as always, run everything by your attorney.
Health care reform has triggered considerable discussion both in print and online about the administrative problems it has created for private practitioners, including decreased cash flow, increased paperwork and business expenses, and an increasing number of high-deductible insurance exchanges with the infamous 90-day “grace periods.” Extending discounts to patients who pay at the time of service or out of pocket may mitigate damage caused by all 3 of these issues; however, caution is necessary, as discounts often can run afoul of federal and state laws, including anti-kickback statutes,1 the anti-inducement provision of the Health Insurance Portability and Accountability Act,2 the Medicare exclusion provision,3 and state insurance antidiscrimination provisions.4
Avoid Kickback Penalties From Patient Discounts
From a legal standpoint, any discount is technically a kickback of sorts because you are returning part of your fee to the patient, and many laws designed to thwart true kickbacks can apply to patient discounts. Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not normally covered by insurance. You would think that these transactions are strictly between you and your patients, but if these discounts appear to be marketing incentives to attract patients, you may face a penalty.5
Patient discounts also may impact third-party payers. Many provider agreements contain “most favored nation” clauses, which require you to automatically give that payer the lowest price you offer to anyone else, regardless of what would be paid otherwise. In other words, the payer could demand the same discount you offer any individual patient. A time-of-service discount is, of course, exactly that: it is offered only when payment is made immediately. Third parties never pay at the time of service and would not be entitled to it, but they may try to invoke their agreement.
If you want to extend discounts for covered services, you must be sure that the discounted fee you charge the patient also is reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud.6 It is important to avoid discounting so regularly that the discounted fee becomes your usual and customary rate in the eyes of the insurer.
Waiving Costs and Kickbacks
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare & Medicaid Services (CMS) will see it as an inducement or kickback, especially if you do it routinely, and similar to private carriers, they will consider the discounted fee your new customary fee. The CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need,” according to the Office of Inspector General,7 but thorough documentation is necessary in such cases.
Waiving co-pays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable co-pays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and litigation may occur against providers who flout this requirement.8 As with the CMS, accommodating patients with individually documented financial limitations is acceptable, but if there is a pattern of routine waivers and a paucity of documentation, you will have difficulty defending it.
Antidiscrimination Laws
In addition to kickback laws, some states also have antidiscrimination laws that forbid lower charges to any subset of insurance payers or to direct payers.4 Some states make specific exceptions for legitimate discounts, such as individual cases of financial hardship, or if you pass along your lower billing and collection expenditures to patients who pay immediately, but other states do not.
Determining Discount Amounts
The discount amount depends on the physician’s situation and deserves careful consideration. If the amount or percentage that you choose to offer as a discount is completely out of proportion with the administrative costs of submitting paperwork as well as the hassles associated with waiting for third-party payments, you could be accused of running a discount policy that is in effect a de facto increase to insurance carriers, which also could result in charges of fraud.2
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies as well as all hospitals have written policies for this system, often based on federal poverty guidelines. To avoid any potential issues, contact your local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence.
Final Thoughts
Consistency of administration, objectivity in policies, and documentation of individual eligibility will ensure that the discounts you offer patients are in line with legal and payer regulations. Before you establish a discount policy, be sure to check your state’s applicable laws, and as always, run everything by your attorney.
1. Guidance on the federal anti-kickback law. Health Resources and Services Administration Web site. http://bphc.hrsa.gov/policiesregulations/policies/pal199510.html. Accessed October 22, 2014.
2. US Department of Health & Human Services. A roadmap for new physicians: fraud & abuse laws. Office of Inspector General Web site.http://oig.hhs.gov/compliance/physician-education/01laws.asp. Accessed October 21, 2014.
3. Exclusion of certain individuals and entities from participation in Medicare and State health care programs, 42 USC §1320a–7 (2011).
4. Non-discrimination in health care, 42 USC §300gg–5 (2014).
5. US Department of Health and Human Services. Offering gifts and other inducements to beneficiaries. http://oig.hhs.gov/fraud/docs/alertsandbulletins/SABGiftsandInducements.pdf. Published August 2002. Accessed October 21, 2014.
6. The challenge of health care fraud. National Health Care Anti-Fraud Association Web site. http://www.nhcaa.org/resources/health-care-anti-fraud-resources/the-challenge-of-health-care-fraud.aspx. Accessed October 21, 2014.
7. US Department of Health & Human Services. Hospital discounts offered to patients who cannot afford to pay their hospital bills. Office of Inspector General Web site. http://oig.hhs.gov/fraud/docs/alertsandbulletins/2004/FA021904hospitaldiscounts.pdf. Published February 2, 2004. Accessed October 16, 2014.
8. Merritt M. Forgiving patient copays can lead to unforgiving consequences. Physicians Practice Web site. http://www.physicianspractice.com/blog/forgiving-patient-copays-can-lead-unforgiving-consequences. Published December 15, 2013. Accessed October 21, 2014.
1. Guidance on the federal anti-kickback law. Health Resources and Services Administration Web site. http://bphc.hrsa.gov/policiesregulations/policies/pal199510.html. Accessed October 22, 2014.
2. US Department of Health & Human Services. A roadmap for new physicians: fraud & abuse laws. Office of Inspector General Web site.http://oig.hhs.gov/compliance/physician-education/01laws.asp. Accessed October 21, 2014.
3. Exclusion of certain individuals and entities from participation in Medicare and State health care programs, 42 USC §1320a–7 (2011).
4. Non-discrimination in health care, 42 USC §300gg–5 (2014).
5. US Department of Health and Human Services. Offering gifts and other inducements to beneficiaries. http://oig.hhs.gov/fraud/docs/alertsandbulletins/SABGiftsandInducements.pdf. Published August 2002. Accessed October 21, 2014.
6. The challenge of health care fraud. National Health Care Anti-Fraud Association Web site. http://www.nhcaa.org/resources/health-care-anti-fraud-resources/the-challenge-of-health-care-fraud.aspx. Accessed October 21, 2014.
7. US Department of Health & Human Services. Hospital discounts offered to patients who cannot afford to pay their hospital bills. Office of Inspector General Web site. http://oig.hhs.gov/fraud/docs/alertsandbulletins/2004/FA021904hospitaldiscounts.pdf. Published February 2, 2004. Accessed October 16, 2014.
8. Merritt M. Forgiving patient copays can lead to unforgiving consequences. Physicians Practice Web site. http://www.physicianspractice.com/blog/forgiving-patient-copays-can-lead-unforgiving-consequences. Published December 15, 2013. Accessed October 21, 2014.
Practice Points
- Discounts to direct and immediate payers (patients) may run afoul of local and national statutes.
- Routine waiving of co-pays and deductibles can be problematic.
- Consistency of administration, objectivity in policies, and documentation of individual eligibility are essential in private practices.

CME, Procedures, and Advocacy Highlight Hospital Medicine 2013 Kickoff
Hospital Medicine 2013 starts off with a day of learning and advocacy on Capitol Hill.
Hospital Medicine 2013 starts off with a day of learning and advocacy on Capitol Hill.
Hospital Medicine 2013 starts off with a day of learning and advocacy on Capitol Hill.
Clear Cell Fibrous Papule
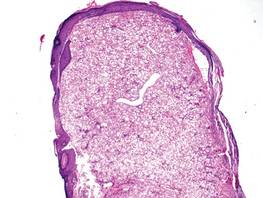
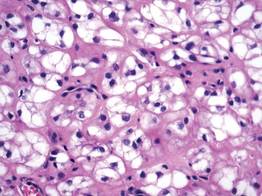
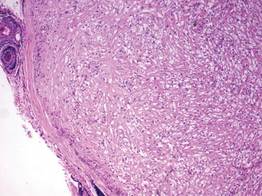
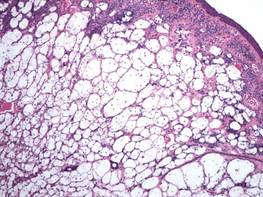
A fibrous papule is a common benign lesion that usually presents in adults on the face, especially on the lower portion of the nose. It typically presents as a small (2–5 mm), asymptomatic, flesh-colored, dome-shaped lesion that is firm and nontender. Several histopathologic variants of fibrous papules have been described, including clear cell, granular, epithelioid, hypercellular, pleomorphic, pigmented, and inflammatory.1 Clear cell fibrous papules are exceedingly rare. On microscopic examination the epidermis may be normal or show some degree of hyperkeratosis and parakeratosis, erosion, ulceration, or crust. The basal layer may show an increase of melanin. The dermis is expanded by a proliferation of clear cells arranged in sheets, clusters, or as single cells (Figure 1). The clear cells show variation in size and shape. The nuclei are small and round without pleomorphism, hyperchromasia, or mitoses. The nuclei may be centrally located or eccentrically displaced by a large intracytoplasmic vacuole (Figure 2). Some clear cells may exhibit finely vacuolated cytoplasm with nuclear scalloping. The surrounding stroma usually consists of sclerotic collagen and dilated blood vessels (Figure 3). Extravasated red blood cells may be present focally. Patchy lymphocytic infiltrates may be found in the stroma at the periphery of the lesion. Periodic acid–Schiff and mucicarmine staining of the clear cells is negative. On immunohistochemistry, the clear cells are diffusely positive for vimentin and negative for cytokeratin AE1/AE3, epithelial membrane antigen, carcinoembryonic antigen, and HMB-45 (human melanoma black 45).2,3 The clear cells often are positive for CD68, factor XIIIa, and NKI/C3 (anti-CD63) but also may be negative. The S-100 protein often is negative but may be focally positive.
The differential diagnosis for clear cell fibrous papules is broad but reasonably includes balloon cell nevus, clear cell hidradenoma, and cutaneous metastasis of clear cell (conventional) renal cell carcinoma (ccRCC). Balloon cell malignant melanoma is not considered strongly in the differential diagnosis because it usually exhibits invasive growth, cytologic atypia, and mitoses, all of which are not characteristic morphologic features of clear cell fibrous papules.
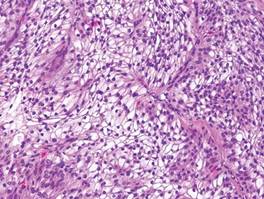
A balloon cell nevus may be difficult to distinguish from a clear cell fibrous papule on routine hematoxylin and eosin staining (Figure 4); however, the nuclei of a balloon cell nevus tend to be more rounded and centrally located. Any junctional nesting or nests of conventional nevus cells in the dermis also help differentiate a balloon cell nevus from a clear cell fibrous papule. Diffusely positive immunostaining for S-100 protein also is indicative of a balloon cell nevus.
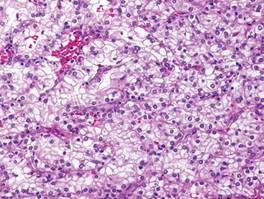
Clear cell hidradenoma consists predominantly of cells with clear cytoplasm and small dark nuclei that may closely mimic a clear cell fibrous papule (Figure 5) but often shows a second population of cells with more vesicular nuclei and dark eosinophilic cytoplasm. Cystic spaces containing hyaline material and foci of squamoid change are common, along with occasional tubular lumina that may be prominent or inconspicuous. Further, the tumor cells of clear cell hidradenoma show positive immunostaining for epithelial markers (eg, cytokeratin AE1/AE3, CAM5.2).
Cutaneous metastasis of ccRCC is rare and usually presents clinically as a larger lesion than a clear cell fibrous papule. The cells of ccRCC have moderate to abundant clear cytoplasm and nuclei with varying degrees of pleomorphism (Figure 6). Periodic acid–Schiff staining demonstrates intracytoplasmic glycogen. The stroma is abundantly vascular and extravasated blood cells are frequently observed. On immunohistochemistry, the tumor cells of ccRCC stain positively for cytokeratin AE1/AE3, CAM5.2, epithelial membrane antigen, CD10, and vimentin.
- Bansal C, Stewart D, Li A, et al. Histologic variants of fibrous papule. J Cutan Pathol. 2005;32:424-428.
- Chiang YY, Tsai HH, Lee WR, et al. Clear cell fibrous papule: report of a case mimicking a balloon cell nevus. J Cutan Pathol. 2009;36:381-384.
- Lee AN, Stein SL, Cohen LM. Clear cell fibrous papule with NKI/C3 expression: clinical and histologic features in six cases. Am J Dermatopathol. 2005;27:296-300.
A fibrous papule is a common benign lesion that usually presents in adults on the face, especially on the lower portion of the nose. It typically presents as a small (2–5 mm), asymptomatic, flesh-colored, dome-shaped lesion that is firm and nontender. Several histopathologic variants of fibrous papules have been described, including clear cell, granular, epithelioid, hypercellular, pleomorphic, pigmented, and inflammatory.1 Clear cell fibrous papules are exceedingly rare. On microscopic examination the epidermis may be normal or show some degree of hyperkeratosis and parakeratosis, erosion, ulceration, or crust. The basal layer may show an increase of melanin. The dermis is expanded by a proliferation of clear cells arranged in sheets, clusters, or as single cells (Figure 1). The clear cells show variation in size and shape. The nuclei are small and round without pleomorphism, hyperchromasia, or mitoses. The nuclei may be centrally located or eccentrically displaced by a large intracytoplasmic vacuole (Figure 2). Some clear cells may exhibit finely vacuolated cytoplasm with nuclear scalloping. The surrounding stroma usually consists of sclerotic collagen and dilated blood vessels (Figure 3). Extravasated red blood cells may be present focally. Patchy lymphocytic infiltrates may be found in the stroma at the periphery of the lesion. Periodic acid–Schiff and mucicarmine staining of the clear cells is negative. On immunohistochemistry, the clear cells are diffusely positive for vimentin and negative for cytokeratin AE1/AE3, epithelial membrane antigen, carcinoembryonic antigen, and HMB-45 (human melanoma black 45).2,3 The clear cells often are positive for CD68, factor XIIIa, and NKI/C3 (anti-CD63) but also may be negative. The S-100 protein often is negative but may be focally positive.
The differential diagnosis for clear cell fibrous papules is broad but reasonably includes balloon cell nevus, clear cell hidradenoma, and cutaneous metastasis of clear cell (conventional) renal cell carcinoma (ccRCC). Balloon cell malignant melanoma is not considered strongly in the differential diagnosis because it usually exhibits invasive growth, cytologic atypia, and mitoses, all of which are not characteristic morphologic features of clear cell fibrous papules.
A balloon cell nevus may be difficult to distinguish from a clear cell fibrous papule on routine hematoxylin and eosin staining (Figure 4); however, the nuclei of a balloon cell nevus tend to be more rounded and centrally located. Any junctional nesting or nests of conventional nevus cells in the dermis also help differentiate a balloon cell nevus from a clear cell fibrous papule. Diffusely positive immunostaining for S-100 protein also is indicative of a balloon cell nevus.
Clear cell hidradenoma consists predominantly of cells with clear cytoplasm and small dark nuclei that may closely mimic a clear cell fibrous papule (Figure 5) but often shows a second population of cells with more vesicular nuclei and dark eosinophilic cytoplasm. Cystic spaces containing hyaline material and foci of squamoid change are common, along with occasional tubular lumina that may be prominent or inconspicuous. Further, the tumor cells of clear cell hidradenoma show positive immunostaining for epithelial markers (eg, cytokeratin AE1/AE3, CAM5.2).
Cutaneous metastasis of ccRCC is rare and usually presents clinically as a larger lesion than a clear cell fibrous papule. The cells of ccRCC have moderate to abundant clear cytoplasm and nuclei with varying degrees of pleomorphism (Figure 6). Periodic acid–Schiff staining demonstrates intracytoplasmic glycogen. The stroma is abundantly vascular and extravasated blood cells are frequently observed. On immunohistochemistry, the tumor cells of ccRCC stain positively for cytokeratin AE1/AE3, CAM5.2, epithelial membrane antigen, CD10, and vimentin.
A fibrous papule is a common benign lesion that usually presents in adults on the face, especially on the lower portion of the nose. It typically presents as a small (2–5 mm), asymptomatic, flesh-colored, dome-shaped lesion that is firm and nontender. Several histopathologic variants of fibrous papules have been described, including clear cell, granular, epithelioid, hypercellular, pleomorphic, pigmented, and inflammatory.1 Clear cell fibrous papules are exceedingly rare. On microscopic examination the epidermis may be normal or show some degree of hyperkeratosis and parakeratosis, erosion, ulceration, or crust. The basal layer may show an increase of melanin. The dermis is expanded by a proliferation of clear cells arranged in sheets, clusters, or as single cells (Figure 1). The clear cells show variation in size and shape. The nuclei are small and round without pleomorphism, hyperchromasia, or mitoses. The nuclei may be centrally located or eccentrically displaced by a large intracytoplasmic vacuole (Figure 2). Some clear cells may exhibit finely vacuolated cytoplasm with nuclear scalloping. The surrounding stroma usually consists of sclerotic collagen and dilated blood vessels (Figure 3). Extravasated red blood cells may be present focally. Patchy lymphocytic infiltrates may be found in the stroma at the periphery of the lesion. Periodic acid–Schiff and mucicarmine staining of the clear cells is negative. On immunohistochemistry, the clear cells are diffusely positive for vimentin and negative for cytokeratin AE1/AE3, epithelial membrane antigen, carcinoembryonic antigen, and HMB-45 (human melanoma black 45).2,3 The clear cells often are positive for CD68, factor XIIIa, and NKI/C3 (anti-CD63) but also may be negative. The S-100 protein often is negative but may be focally positive.
The differential diagnosis for clear cell fibrous papules is broad but reasonably includes balloon cell nevus, clear cell hidradenoma, and cutaneous metastasis of clear cell (conventional) renal cell carcinoma (ccRCC). Balloon cell malignant melanoma is not considered strongly in the differential diagnosis because it usually exhibits invasive growth, cytologic atypia, and mitoses, all of which are not characteristic morphologic features of clear cell fibrous papules.
A balloon cell nevus may be difficult to distinguish from a clear cell fibrous papule on routine hematoxylin and eosin staining (Figure 4); however, the nuclei of a balloon cell nevus tend to be more rounded and centrally located. Any junctional nesting or nests of conventional nevus cells in the dermis also help differentiate a balloon cell nevus from a clear cell fibrous papule. Diffusely positive immunostaining for S-100 protein also is indicative of a balloon cell nevus.
Clear cell hidradenoma consists predominantly of cells with clear cytoplasm and small dark nuclei that may closely mimic a clear cell fibrous papule (Figure 5) but often shows a second population of cells with more vesicular nuclei and dark eosinophilic cytoplasm. Cystic spaces containing hyaline material and foci of squamoid change are common, along with occasional tubular lumina that may be prominent or inconspicuous. Further, the tumor cells of clear cell hidradenoma show positive immunostaining for epithelial markers (eg, cytokeratin AE1/AE3, CAM5.2).
Cutaneous metastasis of ccRCC is rare and usually presents clinically as a larger lesion than a clear cell fibrous papule. The cells of ccRCC have moderate to abundant clear cytoplasm and nuclei with varying degrees of pleomorphism (Figure 6). Periodic acid–Schiff staining demonstrates intracytoplasmic glycogen. The stroma is abundantly vascular and extravasated blood cells are frequently observed. On immunohistochemistry, the tumor cells of ccRCC stain positively for cytokeratin AE1/AE3, CAM5.2, epithelial membrane antigen, CD10, and vimentin.
- Bansal C, Stewart D, Li A, et al. Histologic variants of fibrous papule. J Cutan Pathol. 2005;32:424-428.
- Chiang YY, Tsai HH, Lee WR, et al. Clear cell fibrous papule: report of a case mimicking a balloon cell nevus. J Cutan Pathol. 2009;36:381-384.
- Lee AN, Stein SL, Cohen LM. Clear cell fibrous papule with NKI/C3 expression: clinical and histologic features in six cases. Am J Dermatopathol. 2005;27:296-300.
- Bansal C, Stewart D, Li A, et al. Histologic variants of fibrous papule. J Cutan Pathol. 2005;32:424-428.
- Chiang YY, Tsai HH, Lee WR, et al. Clear cell fibrous papule: report of a case mimicking a balloon cell nevus. J Cutan Pathol. 2009;36:381-384.
- Lee AN, Stein SL, Cohen LM. Clear cell fibrous papule with NKI/C3 expression: clinical and histologic features in six cases. Am J Dermatopathol. 2005;27:296-300.
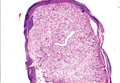
Probiotics for Radiation-Caused Diarrhea
Probiotics may help reduce the severity of one of the most common acute adverse effects of radiation—diarrhea. They just might not show results right away. According to a study by researchers from the Centre Hospitalier Universitaire de Québec in Canada, the effects of probiotics were positive and most effective in the weeks after radiation treatment.
No prophylactic agents are approved for preventing pelvic radiation enteritis, the researchers note, and evidence is weak for nutritional interventions that have been tried. But recently, more research is pointing to a powerful role for probiotics in a variety of gastrointestinal uses.
This study compared the efficacy of the probiotic Bifilact (Lactobacillus acidophilus LAC-361 and Bifidobacterium longum BB-536) with placebo. The main goal was to find whether probiotics would prevent or delay the incidence of moderate-to-severe radiation-induced diarrhea during a radiotherapy treatment. Secondary goals were to assess whether Bifilact reduced or delayed the need of antidiarrheal medication, reduced intestinal pain, reduced the need for hospitalization, minimized interruptions to radiotherapy treatments, and improved patient well-being.
In the study, 229 patients received either placebo or 1 of 2 Bifilact regimens: a standard dose twice a day or a high dose 3 times a day. Patients recorded their digestive symptoms every day and met with a registered dietitian and radiation oncologist every week during treatment.
Although the differences were not statistically significant, probiotics eventually halved the proportion of patients with moderate-to-severe diarrhea. The mean number of bowel movements per 24 hours was 2.3 in the placebo group, 2.3 in the standard-dose, and 2.1 in the high-dose patients (P = .84). During the treatment, those numbers changed to 2.9, 2.7, and 2.8 bowel movements per day (P = .80), respectively. For patients who underwent surgical procedures before radiation, probiotic intake tended to reduce all levels of diarrhea, especially the most severe grade 4 diarrhea. Median abdominal pain was initially 0 for all groups and < 1 during treatment for all groups (P = .23).
To their knowledge, the researchers say, only 6 human clinical studies have been published regarding using probiotics to prevent acute radiation-induced diarrhea, and only 1 for treating diarrhea after radiotherapy. The 6 studies showed positive results on diarrhea toxicity and/or frequency of bowel movement and/or stool consistency. Two of 3 systematic reviews also found a probable beneficial effect on prevention.
Their own study produced some interesting findings, the researchers say. For one, less diarrhea at 60 days meant the benefit began at the end of the treatment or after it. Patients with a standard dose of probiotic experienced less of the moderate-to-severe diarrhea at the end of treatment or during the 2 weeks following treatment. And after 60 days, 35% of patients in the standard-dose group did not have moderate-to-severe diarrhea, compared with 17% in the placebo group (P = .23). The researchers say the probiotic effect may be delayed because of the time required by bacteria to exert their influence on the inflammatory process.
Source
Demers M, Dagnault A, Desjardins J. Clin Nutr. 2014;33(5):761-767.
doi: 10.1016/j.clnu.2013.10.015.
Probiotics may help reduce the severity of one of the most common acute adverse effects of radiation—diarrhea. They just might not show results right away. According to a study by researchers from the Centre Hospitalier Universitaire de Québec in Canada, the effects of probiotics were positive and most effective in the weeks after radiation treatment.
No prophylactic agents are approved for preventing pelvic radiation enteritis, the researchers note, and evidence is weak for nutritional interventions that have been tried. But recently, more research is pointing to a powerful role for probiotics in a variety of gastrointestinal uses.
This study compared the efficacy of the probiotic Bifilact (Lactobacillus acidophilus LAC-361 and Bifidobacterium longum BB-536) with placebo. The main goal was to find whether probiotics would prevent or delay the incidence of moderate-to-severe radiation-induced diarrhea during a radiotherapy treatment. Secondary goals were to assess whether Bifilact reduced or delayed the need of antidiarrheal medication, reduced intestinal pain, reduced the need for hospitalization, minimized interruptions to radiotherapy treatments, and improved patient well-being.
In the study, 229 patients received either placebo or 1 of 2 Bifilact regimens: a standard dose twice a day or a high dose 3 times a day. Patients recorded their digestive symptoms every day and met with a registered dietitian and radiation oncologist every week during treatment.
Although the differences were not statistically significant, probiotics eventually halved the proportion of patients with moderate-to-severe diarrhea. The mean number of bowel movements per 24 hours was 2.3 in the placebo group, 2.3 in the standard-dose, and 2.1 in the high-dose patients (P = .84). During the treatment, those numbers changed to 2.9, 2.7, and 2.8 bowel movements per day (P = .80), respectively. For patients who underwent surgical procedures before radiation, probiotic intake tended to reduce all levels of diarrhea, especially the most severe grade 4 diarrhea. Median abdominal pain was initially 0 for all groups and < 1 during treatment for all groups (P = .23).
To their knowledge, the researchers say, only 6 human clinical studies have been published regarding using probiotics to prevent acute radiation-induced diarrhea, and only 1 for treating diarrhea after radiotherapy. The 6 studies showed positive results on diarrhea toxicity and/or frequency of bowel movement and/or stool consistency. Two of 3 systematic reviews also found a probable beneficial effect on prevention.
Their own study produced some interesting findings, the researchers say. For one, less diarrhea at 60 days meant the benefit began at the end of the treatment or after it. Patients with a standard dose of probiotic experienced less of the moderate-to-severe diarrhea at the end of treatment or during the 2 weeks following treatment. And after 60 days, 35% of patients in the standard-dose group did not have moderate-to-severe diarrhea, compared with 17% in the placebo group (P = .23). The researchers say the probiotic effect may be delayed because of the time required by bacteria to exert their influence on the inflammatory process.
Source
Demers M, Dagnault A, Desjardins J. Clin Nutr. 2014;33(5):761-767.
doi: 10.1016/j.clnu.2013.10.015.
Probiotics may help reduce the severity of one of the most common acute adverse effects of radiation—diarrhea. They just might not show results right away. According to a study by researchers from the Centre Hospitalier Universitaire de Québec in Canada, the effects of probiotics were positive and most effective in the weeks after radiation treatment.
No prophylactic agents are approved for preventing pelvic radiation enteritis, the researchers note, and evidence is weak for nutritional interventions that have been tried. But recently, more research is pointing to a powerful role for probiotics in a variety of gastrointestinal uses.
This study compared the efficacy of the probiotic Bifilact (Lactobacillus acidophilus LAC-361 and Bifidobacterium longum BB-536) with placebo. The main goal was to find whether probiotics would prevent or delay the incidence of moderate-to-severe radiation-induced diarrhea during a radiotherapy treatment. Secondary goals were to assess whether Bifilact reduced or delayed the need of antidiarrheal medication, reduced intestinal pain, reduced the need for hospitalization, minimized interruptions to radiotherapy treatments, and improved patient well-being.
In the study, 229 patients received either placebo or 1 of 2 Bifilact regimens: a standard dose twice a day or a high dose 3 times a day. Patients recorded their digestive symptoms every day and met with a registered dietitian and radiation oncologist every week during treatment.
Although the differences were not statistically significant, probiotics eventually halved the proportion of patients with moderate-to-severe diarrhea. The mean number of bowel movements per 24 hours was 2.3 in the placebo group, 2.3 in the standard-dose, and 2.1 in the high-dose patients (P = .84). During the treatment, those numbers changed to 2.9, 2.7, and 2.8 bowel movements per day (P = .80), respectively. For patients who underwent surgical procedures before radiation, probiotic intake tended to reduce all levels of diarrhea, especially the most severe grade 4 diarrhea. Median abdominal pain was initially 0 for all groups and < 1 during treatment for all groups (P = .23).
To their knowledge, the researchers say, only 6 human clinical studies have been published regarding using probiotics to prevent acute radiation-induced diarrhea, and only 1 for treating diarrhea after radiotherapy. The 6 studies showed positive results on diarrhea toxicity and/or frequency of bowel movement and/or stool consistency. Two of 3 systematic reviews also found a probable beneficial effect on prevention.
Their own study produced some interesting findings, the researchers say. For one, less diarrhea at 60 days meant the benefit began at the end of the treatment or after it. Patients with a standard dose of probiotic experienced less of the moderate-to-severe diarrhea at the end of treatment or during the 2 weeks following treatment. And after 60 days, 35% of patients in the standard-dose group did not have moderate-to-severe diarrhea, compared with 17% in the placebo group (P = .23). The researchers say the probiotic effect may be delayed because of the time required by bacteria to exert their influence on the inflammatory process.
Source
Demers M, Dagnault A, Desjardins J. Clin Nutr. 2014;33(5):761-767.
doi: 10.1016/j.clnu.2013.10.015.
Sugar beets can be used to create hemoglobin

holding a sugar beet
Credit: Lund University
Biochemists have found evidence to suggest that sugar beets can be used to create a substitute for human hemoglobin.
While studying the genome of the sugar beet, the researchers identified 4 hemoglobin genes—3 non-symbiotic genes (BvHb1.1, BvHb1.2, and BvHb2) and 1 truncated gene (BvHb3).
The team then discovered they could extract hemoglobin from sugar beets using a process that’s about as simple as the one used to extract sugar.
The researchers cloned the hemoglobin genes and inserted them into bacteria, which facilitates their expression and purification.
The group described the gene discovery in Plant and Cell Physiology. Study author Nélida Leiva-Eriksson, a doctoral student at Lund University in Sweden, disclosed additional details in her dissertation. And a short video on the research is available on YouTube.
The researchers discovered that the hemoglobin extracted from sugar beets is almost identical to human hemoglobin, especially the form of hemoglobin in the brain.
“There is a difference in a small detail on the surface of the protein, but this simply appears to extend the lifespan of the hemoglobin from sugar beet, which is good news,” Leiva-Eriksson said.
On the other hand, sugar beet hemoglobin has a completely different function from human hemoglobin.
“We have found that the hemoglobin in the plant binds nitric oxide,” Leiva-Eriksson said. “It is probably needed to keep certain processes in check, for example, so that the nitric oxide doesn’t become toxic, and to ward off bacteria.”
The researchers are planning to start testing the sugar beet hemoglobin in animal experiments in just over a year.
The team said there is good reason to think hemoglobin derived from sugar beets and other crops could become a realistic alternative to human hemoglobin.
“From 1 hectare, we could produce 1 to 2 tons of hemoglobin,” said Leif Bülow, PhD, of Lund University, “which could save thousands of lives.” ![]()
holding a sugar beet
Credit: Lund University
Biochemists have found evidence to suggest that sugar beets can be used to create a substitute for human hemoglobin.
While studying the genome of the sugar beet, the researchers identified 4 hemoglobin genes—3 non-symbiotic genes (BvHb1.1, BvHb1.2, and BvHb2) and 1 truncated gene (BvHb3).
The team then discovered they could extract hemoglobin from sugar beets using a process that’s about as simple as the one used to extract sugar.
The researchers cloned the hemoglobin genes and inserted them into bacteria, which facilitates their expression and purification.
The group described the gene discovery in Plant and Cell Physiology. Study author Nélida Leiva-Eriksson, a doctoral student at Lund University in Sweden, disclosed additional details in her dissertation. And a short video on the research is available on YouTube.
The researchers discovered that the hemoglobin extracted from sugar beets is almost identical to human hemoglobin, especially the form of hemoglobin in the brain.
“There is a difference in a small detail on the surface of the protein, but this simply appears to extend the lifespan of the hemoglobin from sugar beet, which is good news,” Leiva-Eriksson said.
On the other hand, sugar beet hemoglobin has a completely different function from human hemoglobin.
“We have found that the hemoglobin in the plant binds nitric oxide,” Leiva-Eriksson said. “It is probably needed to keep certain processes in check, for example, so that the nitric oxide doesn’t become toxic, and to ward off bacteria.”
The researchers are planning to start testing the sugar beet hemoglobin in animal experiments in just over a year.
The team said there is good reason to think hemoglobin derived from sugar beets and other crops could become a realistic alternative to human hemoglobin.
“From 1 hectare, we could produce 1 to 2 tons of hemoglobin,” said Leif Bülow, PhD, of Lund University, “which could save thousands of lives.” ![]()
holding a sugar beet
Credit: Lund University
Biochemists have found evidence to suggest that sugar beets can be used to create a substitute for human hemoglobin.
While studying the genome of the sugar beet, the researchers identified 4 hemoglobin genes—3 non-symbiotic genes (BvHb1.1, BvHb1.2, and BvHb2) and 1 truncated gene (BvHb3).
The team then discovered they could extract hemoglobin from sugar beets using a process that’s about as simple as the one used to extract sugar.
The researchers cloned the hemoglobin genes and inserted them into bacteria, which facilitates their expression and purification.
The group described the gene discovery in Plant and Cell Physiology. Study author Nélida Leiva-Eriksson, a doctoral student at Lund University in Sweden, disclosed additional details in her dissertation. And a short video on the research is available on YouTube.
The researchers discovered that the hemoglobin extracted from sugar beets is almost identical to human hemoglobin, especially the form of hemoglobin in the brain.
“There is a difference in a small detail on the surface of the protein, but this simply appears to extend the lifespan of the hemoglobin from sugar beet, which is good news,” Leiva-Eriksson said.
On the other hand, sugar beet hemoglobin has a completely different function from human hemoglobin.
“We have found that the hemoglobin in the plant binds nitric oxide,” Leiva-Eriksson said. “It is probably needed to keep certain processes in check, for example, so that the nitric oxide doesn’t become toxic, and to ward off bacteria.”
The researchers are planning to start testing the sugar beet hemoglobin in animal experiments in just over a year.
The team said there is good reason to think hemoglobin derived from sugar beets and other crops could become a realistic alternative to human hemoglobin.
“From 1 hectare, we could produce 1 to 2 tons of hemoglobin,” said Leif Bülow, PhD, of Lund University, “which could save thousands of lives.” ![]()