User login
NICE recommends ofatumumab in CLL

Credit: Linda Bartlett
The UK’s National Institute for Health and Care Excellence (NICE) has issued a preliminary draft guidance recommending ofatumumab (Arzerra) for use in patients with chronic lymphocytic leukemia (CLL).
The agency is recommending the anti-CD20 monoclonal antibody in combination with chlorambucil for patients with untreated CLL who are ineligible for treatment with fludarabine combination therapy and for whom bendamustine is unsuitable.
NICE believes ofatumumab is a cost-effective use of National Health Service (NHS) resources for this patient population, as GlaxoSmithKline, the company developing ofatumumab, has agreed to provide the drug at a reduced price.
The company has agreed with the Department of Health that the size of the discount be confidential.
Clinical effectiveness
“The information provided by GlaxoSmithKline, who market the drug, showed that ofatumumab with chlorambucil is a clinically effective treatment option for those people unable to take fludarabine combination therapy or bendamustine,” said Sir Andrew Dillon, NICE chief executive.
In the phase 3 COMPLEMENT 1 trial, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
A NICE advisory committee also considered the use of ofatumumab in combination with bendamustine. But the committee said that, due to limited clinical evidence and the absence of cost-effectiveness estimates, it could not make a recommendation on this combination.
In a phase 2 trial known as OMB115991, ofatumumab plus bendamustine elicited an overall response rate of 95% and a complete response rate of 43%.
Cost-effectiveness
Ofatumumab’s list price is £182 for a 100 mg vial and £1820 for a 1000 mg vial. Assuming 6 cycles and no drug wastage, the mean cost of a treatment course for ofatumumab at its list price is £11,466 for 6300 mg.
GlaxoSmithKline has agreed to a patient access scheme with the Department of Health that makes ofatumumab available with a discount on the list price, though the exact amount is confidential.
The NICE advisory committee said the most plausible cost-effectiveness estimate for ofatumumab plus chlorambucil compared with chlorambucil alone using the
ofatumumab patient access scheme price was £26,000 per quality-adjusted life year gained.
Consultees, including GlaxoSmithKline, healthcare professionals, and members of the public, can now comment on NICE’s preliminary draft guidance. It will be available for public consultation until November 25, 2014.
Until the final guidance is issued, NHS bodies should make decisions locally on the funding of specific treatments. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
Credit: Linda Bartlett
The UK’s National Institute for Health and Care Excellence (NICE) has issued a preliminary draft guidance recommending ofatumumab (Arzerra) for use in patients with chronic lymphocytic leukemia (CLL).
The agency is recommending the anti-CD20 monoclonal antibody in combination with chlorambucil for patients with untreated CLL who are ineligible for treatment with fludarabine combination therapy and for whom bendamustine is unsuitable.
NICE believes ofatumumab is a cost-effective use of National Health Service (NHS) resources for this patient population, as GlaxoSmithKline, the company developing ofatumumab, has agreed to provide the drug at a reduced price.
The company has agreed with the Department of Health that the size of the discount be confidential.
Clinical effectiveness
“The information provided by GlaxoSmithKline, who market the drug, showed that ofatumumab with chlorambucil is a clinically effective treatment option for those people unable to take fludarabine combination therapy or bendamustine,” said Sir Andrew Dillon, NICE chief executive.
In the phase 3 COMPLEMENT 1 trial, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
A NICE advisory committee also considered the use of ofatumumab in combination with bendamustine. But the committee said that, due to limited clinical evidence and the absence of cost-effectiveness estimates, it could not make a recommendation on this combination.
In a phase 2 trial known as OMB115991, ofatumumab plus bendamustine elicited an overall response rate of 95% and a complete response rate of 43%.
Cost-effectiveness
Ofatumumab’s list price is £182 for a 100 mg vial and £1820 for a 1000 mg vial. Assuming 6 cycles and no drug wastage, the mean cost of a treatment course for ofatumumab at its list price is £11,466 for 6300 mg.
GlaxoSmithKline has agreed to a patient access scheme with the Department of Health that makes ofatumumab available with a discount on the list price, though the exact amount is confidential.
The NICE advisory committee said the most plausible cost-effectiveness estimate for ofatumumab plus chlorambucil compared with chlorambucil alone using the
ofatumumab patient access scheme price was £26,000 per quality-adjusted life year gained.
Consultees, including GlaxoSmithKline, healthcare professionals, and members of the public, can now comment on NICE’s preliminary draft guidance. It will be available for public consultation until November 25, 2014.
Until the final guidance is issued, NHS bodies should make decisions locally on the funding of specific treatments. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
Credit: Linda Bartlett
The UK’s National Institute for Health and Care Excellence (NICE) has issued a preliminary draft guidance recommending ofatumumab (Arzerra) for use in patients with chronic lymphocytic leukemia (CLL).
The agency is recommending the anti-CD20 monoclonal antibody in combination with chlorambucil for patients with untreated CLL who are ineligible for treatment with fludarabine combination therapy and for whom bendamustine is unsuitable.
NICE believes ofatumumab is a cost-effective use of National Health Service (NHS) resources for this patient population, as GlaxoSmithKline, the company developing ofatumumab, has agreed to provide the drug at a reduced price.
The company has agreed with the Department of Health that the size of the discount be confidential.
Clinical effectiveness
“The information provided by GlaxoSmithKline, who market the drug, showed that ofatumumab with chlorambucil is a clinically effective treatment option for those people unable to take fludarabine combination therapy or bendamustine,” said Sir Andrew Dillon, NICE chief executive.
In the phase 3 COMPLEMENT 1 trial, ofatumumab plus chlorambucil improved progression-free survival compared to chlorambucil alone. The median times were 22.4 months and 13.1 months, respectively, and the hazard ratio was 0.57 (P<0.001).
A NICE advisory committee also considered the use of ofatumumab in combination with bendamustine. But the committee said that, due to limited clinical evidence and the absence of cost-effectiveness estimates, it could not make a recommendation on this combination.
In a phase 2 trial known as OMB115991, ofatumumab plus bendamustine elicited an overall response rate of 95% and a complete response rate of 43%.
Cost-effectiveness
Ofatumumab’s list price is £182 for a 100 mg vial and £1820 for a 1000 mg vial. Assuming 6 cycles and no drug wastage, the mean cost of a treatment course for ofatumumab at its list price is £11,466 for 6300 mg.
GlaxoSmithKline has agreed to a patient access scheme with the Department of Health that makes ofatumumab available with a discount on the list price, though the exact amount is confidential.
The NICE advisory committee said the most plausible cost-effectiveness estimate for ofatumumab plus chlorambucil compared with chlorambucil alone using the
ofatumumab patient access scheme price was £26,000 per quality-adjusted life year gained.
Consultees, including GlaxoSmithKline, healthcare professionals, and members of the public, can now comment on NICE’s preliminary draft guidance. It will be available for public consultation until November 25, 2014.
Until the final guidance is issued, NHS bodies should make decisions locally on the funding of specific treatments. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
Point/Counterpoint: Dual antiplatelet therapy for vascular patients: Yes, no, or sometimes?
Introduction
As evidenced by this month’s Point/Counterpoint article by Dr. William Jordan and Dr. Joseph Mills, there is still debate as to the benefit of antiplatelet agents in patients with peripheral artery disease. Currently, dual antiplatelet agents refer to aspirin and clopidogrel, but over the last year or two, ticagrelor and vorapaxar are also being prescribed for patients with peripheral atherosclerosis. The addition of these medications will probably only add to our confusion! Why don’t you weigh in on this discussion by voting on our online poll at www.vascularspecialistonline.com?
Dr. Russell Samson is the medical editor of Vascular Specialist.
Definitely, maybe.
William D. Jordan, M.D.
First, primary prevention must be considered, as few patients with no prior intervention require dual antiplatelet therapy. It seems that we only have some scant data on the prevention of first-time events in at-risk patients when they are treated with aspirin alone.

While lipid management seems to be the most recent focus for primary prevention, single antiplatelet therapy seems appropriate for many patients who have higher risk due to atherosclerotic disease. A recent study from the University of Alabama at Birmingham found that asymptomatic carotid artery stenosis patients treated with dual antiplatelet therapy actually had higher bleed rates, higher mortality, and lower neurologic event rates, compared with those treated with aspirin alone.
While this study examined only a select group of patients treated for carotid artery disease, these vascular patients had worse outcomes when treated with aspirin and clopidogrel. Thus, caution should be considered before adding too many medical therapies.
Now, consider the short-term outlook for patients – specifically those who undergo some type of vascular intervention. The very nature of vascular intervention is disruptive to the arterial endothelium. Of course, most of the arteries that we enter have some underlying pathology; thus the intimal layer is not normal. The pathologic process is already, at least, partly underway. The concept of antiplatelet therapy is focused on limiting the platelet adhesions that might exaggerate the response to injury that creates a hyperplastic reaction within the vessels. We abhor the excessive response to injury due to the potential failure of the arterial reconstruction. Paradoxically, the same platelet inhibition can also cause excessive bleeding that may complicate the vascular repair. In the current medical climate, most of us tolerate the aggravation of diminished platelet function during open reconstruction in order to protect the target repair site and to avoid the dreaded “troponin leak” that may get classified as a myocardial infarction.
Some of our nonvascular colleagues avoid intervention (e.g., axial anesthesia, endoscopic biopsy) if stronger antiplatelet medication is present.
Now, to borrow some insight from other specialties, we should consider the extensive cardiology literature that shows the value of dual platelet inhibition after percutaneous coronary intervention or a recent cardiac event. While this strategy has shown improvement in PCI results, probably due to the great risk of thrombosis when disrupting the endothelial layer of a 2- to 3-mm coronary artery, the bleeding complications, including access-site hematomas, pseudoaneurysms, or retroperitoneal bleeding, are not analyzed as extensively. The preponderance of literature supports aggressive inhibition, but the long term needs to be considered – both expense and bleeding risk.
Currently, we use short-term dual treatment when the arterial endothelium is intentionally disrupted such as after an endarterectomy, angioplasty, with or without a stent, or atherectomy. Specifically, we add short-term IV dextran to oral agents for patients undergoing a carotid endarterectomy, but most are discharged on a single oral agent unless there is another indication for dual therapy.
Patients undergoing lower-extremity, catheter-based interventions are given dual therapy for the first 30 days, which is then adjusted according to the clinical response, duplex findings and other medical conditions. Bypass graft patients (yes, we still do some) are usually given a single agent unless the graft or patient has exhibited some concern for early failure.
In summary, I suspect that dual therapy is overused in our “pill-driven” population, but there still seem to be areas for its application. On each encounter with patients, I would encourage all vascular specialists to review the indications for antiplatelet therapy to consider removing a medication, improving compliance, and limiting bleeding risk.
Dr. Jordan is the director of the division of vascular surgery at the University of Alabama Birmingham School of Medicine. He has no relevant conflicts.
Dueling over dual antiplatelet therapy
Joseph L. Mills Sr., M.D.
Amidst a background of constant clamoring for data-driven and evidence-based medical decision-making, the practice of vascular medicine and surgery remains mired in the anecdotal. If a little is good, more must be better, seems the rationale for dual antiplatelet therapy. There may be small, as yet unclearly defined subsets of patients for whom dual therapy is actually beneficial, but an unbiased review of the current literature leads to the inescapable conclusion that more patients would be harmed by injudicious application of the more-is-better principle as concerns antiplatelet therapy for patients with carotid artery and peripheral artery disease (PAD).

The best evidence for antiplatelet therapy in patients with carotid disease suggests that aspirin as a single agent in doses ranging from 75 to 150 mg daily is preferred, and at least two meta-analyses and systematic reviews were unable to support the use of dual antiplatelet therapy.1 At least in symptomatic patients, combination or dual antiplatelet therapy may increase the short-term risk of hemorrhagic complications in patients with acute ischemic stroke caused by large-artery disease.2 Long-term dual therapy for secondary stroke prevention with aspirin and clopidogrel has been associated with four times the bleeding risk of monotherapy.3 These bleeds are often intracranial or gastrointestinal and are serious.
With respect to asymptomatic patients, while the CHARISMA trial did demonstrate a modest reduction in subsequent thrombotic events in a subset analysis of patients with stable, preexisting vascular disease, the bottom line was that dual antiplatelet therapy was associated with a 4% risk of moderate to severe bleeding and that there were strong correlations between moderate bleeding and all cause mortality (hazard ratio, 2.55), myocardial infarction (HR, 2.92) and stroke (HR, 4.2).4 The bleeding risk of dual antiplatelet therapy thus seems to outweigh the benefits.
Other data muddy the situation, but only a little. While at least two small studies (one a randomized controlled trial – CARESS [Clopidogrel and Aspirin for Reduction of Emboli in Symptomatic Carotid Stenosis])5 have suggested that the combination of aspirin and clopidogrel may reduce the frequency of perioperative microembolic signals detected early after carotid endarterectomy compared with monotherapy, it is not established that this surrogate measure would translate into long-term clinical benefit and would outweigh the established bleeding risk of dual therapy.
At present, the vascular surgeon should urge his patients to stop smoking, prescribe a statin, control blood pressure (but not necessarily with a beta-blocker), control diabetes, and prescribe a single antiplatelet agent, most often baby aspirin, for most of his or her patients. More good than harm will result.
References
Dr. Mills is professor of surgery and chief, division of vascular and endovascular surgery, University of Arizona Health Sciences Center, Tucson, and an associate medical editor for Vascular Specialist. He has no relevant conflicts.
Introduction
As evidenced by this month’s Point/Counterpoint article by Dr. William Jordan and Dr. Joseph Mills, there is still debate as to the benefit of antiplatelet agents in patients with peripheral artery disease. Currently, dual antiplatelet agents refer to aspirin and clopidogrel, but over the last year or two, ticagrelor and vorapaxar are also being prescribed for patients with peripheral atherosclerosis. The addition of these medications will probably only add to our confusion! Why don’t you weigh in on this discussion by voting on our online poll at www.vascularspecialistonline.com?
Dr. Russell Samson is the medical editor of Vascular Specialist.
Definitely, maybe.
William D. Jordan, M.D.
First, primary prevention must be considered, as few patients with no prior intervention require dual antiplatelet therapy. It seems that we only have some scant data on the prevention of first-time events in at-risk patients when they are treated with aspirin alone.
While lipid management seems to be the most recent focus for primary prevention, single antiplatelet therapy seems appropriate for many patients who have higher risk due to atherosclerotic disease. A recent study from the University of Alabama at Birmingham found that asymptomatic carotid artery stenosis patients treated with dual antiplatelet therapy actually had higher bleed rates, higher mortality, and lower neurologic event rates, compared with those treated with aspirin alone.
While this study examined only a select group of patients treated for carotid artery disease, these vascular patients had worse outcomes when treated with aspirin and clopidogrel. Thus, caution should be considered before adding too many medical therapies.
Now, consider the short-term outlook for patients – specifically those who undergo some type of vascular intervention. The very nature of vascular intervention is disruptive to the arterial endothelium. Of course, most of the arteries that we enter have some underlying pathology; thus the intimal layer is not normal. The pathologic process is already, at least, partly underway. The concept of antiplatelet therapy is focused on limiting the platelet adhesions that might exaggerate the response to injury that creates a hyperplastic reaction within the vessels. We abhor the excessive response to injury due to the potential failure of the arterial reconstruction. Paradoxically, the same platelet inhibition can also cause excessive bleeding that may complicate the vascular repair. In the current medical climate, most of us tolerate the aggravation of diminished platelet function during open reconstruction in order to protect the target repair site and to avoid the dreaded “troponin leak” that may get classified as a myocardial infarction.
Some of our nonvascular colleagues avoid intervention (e.g., axial anesthesia, endoscopic biopsy) if stronger antiplatelet medication is present.
Now, to borrow some insight from other specialties, we should consider the extensive cardiology literature that shows the value of dual platelet inhibition after percutaneous coronary intervention or a recent cardiac event. While this strategy has shown improvement in PCI results, probably due to the great risk of thrombosis when disrupting the endothelial layer of a 2- to 3-mm coronary artery, the bleeding complications, including access-site hematomas, pseudoaneurysms, or retroperitoneal bleeding, are not analyzed as extensively. The preponderance of literature supports aggressive inhibition, but the long term needs to be considered – both expense and bleeding risk.
Currently, we use short-term dual treatment when the arterial endothelium is intentionally disrupted such as after an endarterectomy, angioplasty, with or without a stent, or atherectomy. Specifically, we add short-term IV dextran to oral agents for patients undergoing a carotid endarterectomy, but most are discharged on a single oral agent unless there is another indication for dual therapy.
Patients undergoing lower-extremity, catheter-based interventions are given dual therapy for the first 30 days, which is then adjusted according to the clinical response, duplex findings and other medical conditions. Bypass graft patients (yes, we still do some) are usually given a single agent unless the graft or patient has exhibited some concern for early failure.
In summary, I suspect that dual therapy is overused in our “pill-driven” population, but there still seem to be areas for its application. On each encounter with patients, I would encourage all vascular specialists to review the indications for antiplatelet therapy to consider removing a medication, improving compliance, and limiting bleeding risk.
Dr. Jordan is the director of the division of vascular surgery at the University of Alabama Birmingham School of Medicine. He has no relevant conflicts.
Dueling over dual antiplatelet therapy
Joseph L. Mills Sr., M.D.
Amidst a background of constant clamoring for data-driven and evidence-based medical decision-making, the practice of vascular medicine and surgery remains mired in the anecdotal. If a little is good, more must be better, seems the rationale for dual antiplatelet therapy. There may be small, as yet unclearly defined subsets of patients for whom dual therapy is actually beneficial, but an unbiased review of the current literature leads to the inescapable conclusion that more patients would be harmed by injudicious application of the more-is-better principle as concerns antiplatelet therapy for patients with carotid artery and peripheral artery disease (PAD).
The best evidence for antiplatelet therapy in patients with carotid disease suggests that aspirin as a single agent in doses ranging from 75 to 150 mg daily is preferred, and at least two meta-analyses and systematic reviews were unable to support the use of dual antiplatelet therapy.1 At least in symptomatic patients, combination or dual antiplatelet therapy may increase the short-term risk of hemorrhagic complications in patients with acute ischemic stroke caused by large-artery disease.2 Long-term dual therapy for secondary stroke prevention with aspirin and clopidogrel has been associated with four times the bleeding risk of monotherapy.3 These bleeds are often intracranial or gastrointestinal and are serious.
With respect to asymptomatic patients, while the CHARISMA trial did demonstrate a modest reduction in subsequent thrombotic events in a subset analysis of patients with stable, preexisting vascular disease, the bottom line was that dual antiplatelet therapy was associated with a 4% risk of moderate to severe bleeding and that there were strong correlations between moderate bleeding and all cause mortality (hazard ratio, 2.55), myocardial infarction (HR, 2.92) and stroke (HR, 4.2).4 The bleeding risk of dual antiplatelet therapy thus seems to outweigh the benefits.
Other data muddy the situation, but only a little. While at least two small studies (one a randomized controlled trial – CARESS [Clopidogrel and Aspirin for Reduction of Emboli in Symptomatic Carotid Stenosis])5 have suggested that the combination of aspirin and clopidogrel may reduce the frequency of perioperative microembolic signals detected early after carotid endarterectomy compared with monotherapy, it is not established that this surrogate measure would translate into long-term clinical benefit and would outweigh the established bleeding risk of dual therapy.
At present, the vascular surgeon should urge his patients to stop smoking, prescribe a statin, control blood pressure (but not necessarily with a beta-blocker), control diabetes, and prescribe a single antiplatelet agent, most often baby aspirin, for most of his or her patients. More good than harm will result.
References
Dr. Mills is professor of surgery and chief, division of vascular and endovascular surgery, University of Arizona Health Sciences Center, Tucson, and an associate medical editor for Vascular Specialist. He has no relevant conflicts.
Introduction
As evidenced by this month’s Point/Counterpoint article by Dr. William Jordan and Dr. Joseph Mills, there is still debate as to the benefit of antiplatelet agents in patients with peripheral artery disease. Currently, dual antiplatelet agents refer to aspirin and clopidogrel, but over the last year or two, ticagrelor and vorapaxar are also being prescribed for patients with peripheral atherosclerosis. The addition of these medications will probably only add to our confusion! Why don’t you weigh in on this discussion by voting on our online poll at www.vascularspecialistonline.com?
Dr. Russell Samson is the medical editor of Vascular Specialist.
Definitely, maybe.
William D. Jordan, M.D.
First, primary prevention must be considered, as few patients with no prior intervention require dual antiplatelet therapy. It seems that we only have some scant data on the prevention of first-time events in at-risk patients when they are treated with aspirin alone.
While lipid management seems to be the most recent focus for primary prevention, single antiplatelet therapy seems appropriate for many patients who have higher risk due to atherosclerotic disease. A recent study from the University of Alabama at Birmingham found that asymptomatic carotid artery stenosis patients treated with dual antiplatelet therapy actually had higher bleed rates, higher mortality, and lower neurologic event rates, compared with those treated with aspirin alone.
While this study examined only a select group of patients treated for carotid artery disease, these vascular patients had worse outcomes when treated with aspirin and clopidogrel. Thus, caution should be considered before adding too many medical therapies.
Now, consider the short-term outlook for patients – specifically those who undergo some type of vascular intervention. The very nature of vascular intervention is disruptive to the arterial endothelium. Of course, most of the arteries that we enter have some underlying pathology; thus the intimal layer is not normal. The pathologic process is already, at least, partly underway. The concept of antiplatelet therapy is focused on limiting the platelet adhesions that might exaggerate the response to injury that creates a hyperplastic reaction within the vessels. We abhor the excessive response to injury due to the potential failure of the arterial reconstruction. Paradoxically, the same platelet inhibition can also cause excessive bleeding that may complicate the vascular repair. In the current medical climate, most of us tolerate the aggravation of diminished platelet function during open reconstruction in order to protect the target repair site and to avoid the dreaded “troponin leak” that may get classified as a myocardial infarction.
Some of our nonvascular colleagues avoid intervention (e.g., axial anesthesia, endoscopic biopsy) if stronger antiplatelet medication is present.
Now, to borrow some insight from other specialties, we should consider the extensive cardiology literature that shows the value of dual platelet inhibition after percutaneous coronary intervention or a recent cardiac event. While this strategy has shown improvement in PCI results, probably due to the great risk of thrombosis when disrupting the endothelial layer of a 2- to 3-mm coronary artery, the bleeding complications, including access-site hematomas, pseudoaneurysms, or retroperitoneal bleeding, are not analyzed as extensively. The preponderance of literature supports aggressive inhibition, but the long term needs to be considered – both expense and bleeding risk.
Currently, we use short-term dual treatment when the arterial endothelium is intentionally disrupted such as after an endarterectomy, angioplasty, with or without a stent, or atherectomy. Specifically, we add short-term IV dextran to oral agents for patients undergoing a carotid endarterectomy, but most are discharged on a single oral agent unless there is another indication for dual therapy.
Patients undergoing lower-extremity, catheter-based interventions are given dual therapy for the first 30 days, which is then adjusted according to the clinical response, duplex findings and other medical conditions. Bypass graft patients (yes, we still do some) are usually given a single agent unless the graft or patient has exhibited some concern for early failure.
In summary, I suspect that dual therapy is overused in our “pill-driven” population, but there still seem to be areas for its application. On each encounter with patients, I would encourage all vascular specialists to review the indications for antiplatelet therapy to consider removing a medication, improving compliance, and limiting bleeding risk.
Dr. Jordan is the director of the division of vascular surgery at the University of Alabama Birmingham School of Medicine. He has no relevant conflicts.
Dueling over dual antiplatelet therapy
Joseph L. Mills Sr., M.D.
Amidst a background of constant clamoring for data-driven and evidence-based medical decision-making, the practice of vascular medicine and surgery remains mired in the anecdotal. If a little is good, more must be better, seems the rationale for dual antiplatelet therapy. There may be small, as yet unclearly defined subsets of patients for whom dual therapy is actually beneficial, but an unbiased review of the current literature leads to the inescapable conclusion that more patients would be harmed by injudicious application of the more-is-better principle as concerns antiplatelet therapy for patients with carotid artery and peripheral artery disease (PAD).
The best evidence for antiplatelet therapy in patients with carotid disease suggests that aspirin as a single agent in doses ranging from 75 to 150 mg daily is preferred, and at least two meta-analyses and systematic reviews were unable to support the use of dual antiplatelet therapy.1 At least in symptomatic patients, combination or dual antiplatelet therapy may increase the short-term risk of hemorrhagic complications in patients with acute ischemic stroke caused by large-artery disease.2 Long-term dual therapy for secondary stroke prevention with aspirin and clopidogrel has been associated with four times the bleeding risk of monotherapy.3 These bleeds are often intracranial or gastrointestinal and are serious.
With respect to asymptomatic patients, while the CHARISMA trial did demonstrate a modest reduction in subsequent thrombotic events in a subset analysis of patients with stable, preexisting vascular disease, the bottom line was that dual antiplatelet therapy was associated with a 4% risk of moderate to severe bleeding and that there were strong correlations between moderate bleeding and all cause mortality (hazard ratio, 2.55), myocardial infarction (HR, 2.92) and stroke (HR, 4.2).4 The bleeding risk of dual antiplatelet therapy thus seems to outweigh the benefits.
Other data muddy the situation, but only a little. While at least two small studies (one a randomized controlled trial – CARESS [Clopidogrel and Aspirin for Reduction of Emboli in Symptomatic Carotid Stenosis])5 have suggested that the combination of aspirin and clopidogrel may reduce the frequency of perioperative microembolic signals detected early after carotid endarterectomy compared with monotherapy, it is not established that this surrogate measure would translate into long-term clinical benefit and would outweigh the established bleeding risk of dual therapy.
At present, the vascular surgeon should urge his patients to stop smoking, prescribe a statin, control blood pressure (but not necessarily with a beta-blocker), control diabetes, and prescribe a single antiplatelet agent, most often baby aspirin, for most of his or her patients. More good than harm will result.
References
Dr. Mills is professor of surgery and chief, division of vascular and endovascular surgery, University of Arizona Health Sciences Center, Tucson, and an associate medical editor for Vascular Specialist. He has no relevant conflicts.
Guidelines: Urinate 2 liters daily to stop kidney stones’ return
Patients who have had kidney stones at least once should increase their fluid consumption to produce at least 2 L of urine per day to prevent the condition from recurring, according to new guidelines published by the American College of Physicians.
If increased fluid intake doesn’t prevent recurrent nephrolithiasis, the updated ACP guidelines recommend adding treatment with a thiazide diuretic, citrate, or allopurinol. “Increased fluid intake spread throughout the day can decrease stone recurrence by at least half with virtually no side effects,” said Dr. David A. Fleming, ACP president, in a statement. “However, people who already drink the recommended amount of liquids, or when increased fluid intake is contraindicated, should not increase their fluid intake.”

The guidelines are based on a review of nephrolithiasis studies, in which the ACP’s director of clinical policy, Dr. Amir Qaseem, and his associates examined baseline stone composition, blood and urine chemistries, and final health outcomes, among other factors. Only English-language trials were used, and research was collected through searches of MEDLINE, the Cochrane Database of Systematic Reviews, Google Scholar, ClinicalTrials.gov, and Web of Science (Ann. Intern. Med. 2014;161:659-67).
Thiazide diuretics, citrates, or allopurinol significantly reduced recurrence of calcium-based stones (the most common type of kidney stone) in patients who had nephrolithiasis at least twice before, according to the analysis.
The ACP guidelines also caution against consuming non-fruit–flavored sodas and carbonated beverages, because they are acidified by phosphoric acid, and dietary animal protein and purines.
However, the guidelines encourage consumption of dietary oxalate – commonly found in chocolate, beets, nuts, rhubarb, spinach, strawberries, tea, and wheat bran – and support maintaining normal dietary calcium. There was no evidence to suggest a risk reduction advantage in drinking tap water rather than mineral water.
The recommendations do not apply to “patients with suspected hyperparathyroidism or other rare cases,” the guidelines authors noted.
Financial support for the guidelines came from the ACP operating budget. The authors had no other relevant financial disclosures.
Patients who have had kidney stones at least once should increase their fluid consumption to produce at least 2 L of urine per day to prevent the condition from recurring, according to new guidelines published by the American College of Physicians.
If increased fluid intake doesn’t prevent recurrent nephrolithiasis, the updated ACP guidelines recommend adding treatment with a thiazide diuretic, citrate, or allopurinol. “Increased fluid intake spread throughout the day can decrease stone recurrence by at least half with virtually no side effects,” said Dr. David A. Fleming, ACP president, in a statement. “However, people who already drink the recommended amount of liquids, or when increased fluid intake is contraindicated, should not increase their fluid intake.”
The guidelines are based on a review of nephrolithiasis studies, in which the ACP’s director of clinical policy, Dr. Amir Qaseem, and his associates examined baseline stone composition, blood and urine chemistries, and final health outcomes, among other factors. Only English-language trials were used, and research was collected through searches of MEDLINE, the Cochrane Database of Systematic Reviews, Google Scholar, ClinicalTrials.gov, and Web of Science (Ann. Intern. Med. 2014;161:659-67).
Thiazide diuretics, citrates, or allopurinol significantly reduced recurrence of calcium-based stones (the most common type of kidney stone) in patients who had nephrolithiasis at least twice before, according to the analysis.
The ACP guidelines also caution against consuming non-fruit–flavored sodas and carbonated beverages, because they are acidified by phosphoric acid, and dietary animal protein and purines.
However, the guidelines encourage consumption of dietary oxalate – commonly found in chocolate, beets, nuts, rhubarb, spinach, strawberries, tea, and wheat bran – and support maintaining normal dietary calcium. There was no evidence to suggest a risk reduction advantage in drinking tap water rather than mineral water.
The recommendations do not apply to “patients with suspected hyperparathyroidism or other rare cases,” the guidelines authors noted.
Financial support for the guidelines came from the ACP operating budget. The authors had no other relevant financial disclosures.
Patients who have had kidney stones at least once should increase their fluid consumption to produce at least 2 L of urine per day to prevent the condition from recurring, according to new guidelines published by the American College of Physicians.
If increased fluid intake doesn’t prevent recurrent nephrolithiasis, the updated ACP guidelines recommend adding treatment with a thiazide diuretic, citrate, or allopurinol. “Increased fluid intake spread throughout the day can decrease stone recurrence by at least half with virtually no side effects,” said Dr. David A. Fleming, ACP president, in a statement. “However, people who already drink the recommended amount of liquids, or when increased fluid intake is contraindicated, should not increase their fluid intake.”
The guidelines are based on a review of nephrolithiasis studies, in which the ACP’s director of clinical policy, Dr. Amir Qaseem, and his associates examined baseline stone composition, blood and urine chemistries, and final health outcomes, among other factors. Only English-language trials were used, and research was collected through searches of MEDLINE, the Cochrane Database of Systematic Reviews, Google Scholar, ClinicalTrials.gov, and Web of Science (Ann. Intern. Med. 2014;161:659-67).
Thiazide diuretics, citrates, or allopurinol significantly reduced recurrence of calcium-based stones (the most common type of kidney stone) in patients who had nephrolithiasis at least twice before, according to the analysis.
The ACP guidelines also caution against consuming non-fruit–flavored sodas and carbonated beverages, because they are acidified by phosphoric acid, and dietary animal protein and purines.
However, the guidelines encourage consumption of dietary oxalate – commonly found in chocolate, beets, nuts, rhubarb, spinach, strawberries, tea, and wheat bran – and support maintaining normal dietary calcium. There was no evidence to suggest a risk reduction advantage in drinking tap water rather than mineral water.
The recommendations do not apply to “patients with suspected hyperparathyroidism or other rare cases,” the guidelines authors noted.
Financial support for the guidelines came from the ACP operating budget. The authors had no other relevant financial disclosures.
FROM THE ANNALS OF INTERNAL MEDICINE

Hospitalist Pioneer Bob Wachter Warns Waste Reduction Is New Quality Focus
Dr. Wachter closed SHM's 2013 annual meeting in National Harbor, MD, with a keynote address that identified cost and waste reduction as new planks of hospitalist's value proposition.
Dr. Wachter closed SHM's 2013 annual meeting in National Harbor, MD, with a keynote address that identified cost and waste reduction as new planks of hospitalist's value proposition.
Dr. Wachter closed SHM's 2013 annual meeting in National Harbor, MD, with a keynote address that identified cost and waste reduction as new planks of hospitalist's value proposition.
Evidence-Based Medicine Guru Implores Hospitalists to Join Cause
Gordon Guyatt, MD, who coined the term evidence-based medicine in a 1992 JAMA article, outlined EBM principles and challenged hospitalists to challenge the research.
Gordon Guyatt, MD, who coined the term evidence-based medicine in a 1992 JAMA article, outlined EBM principles and challenged hospitalists to challenge the research.
Gordon Guyatt, MD, who coined the term evidence-based medicine in a 1992 JAMA article, outlined EBM principles and challenged hospitalists to challenge the research.
Clomiphene better than letrozole to treat women with unexplained infertility
When the cause of infertility is unexplained, what is the best first-choice treatment option? Could letrozole, an oral nonsteroidal aromatase inhibitor, result in fewer multiple gestations than current standard therapy—gonadotropins or selective estrogen receptor modulators (clomiphene citrate)—without worsening the live birth rate?
Researchers from the Assessment of Multiple Intrauterine Gestations from Ovarian Stimulation (AMIGOS) trial investigated this question and presented data at the recent annual meeting of the American Society of Reproductive Medicine. The research was supported by the National Institutes of Health (NIH)/Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
Study details
This prospective, randomized, multicenter clinical trial involved 900 women aged 18 to 40 with at least one patent fallopian tube and regular menses. Patients underwent ovarian stimulation for up to four cycles with an injectable gonadotropin (Gn; n = 300), clomiphene citrate (n = 301), or letrozole (n = 299), followed by intrauterine insemination (IUI).
Birth rate. Conception occurred in 46.8%, 35.7%, and 28.4% of women receiving Gn, clomiphene, and letrozole, respectively, with a live birth occurring in 32.2%, 23.3%, and 18.7% of respective cases. Pregnancy rates with letrozole were significantly less than with Gn (P<.001) and less than with clomiphene (P<.015).
Multiple gestations. The rate of multiple gestations was highest among women treated with Gn (10.3%). But the multiple gestation rate for letrozole was higher than that for clomiphene (2.7% vs 1.3%, respectively). All multiples treated with letrozole and clomiphene were twins; in the Gn group, there were 24 twin and 10 triplet gestations.
No significant difference was found in the rates of infants with congenital anomalies or other fetal or neonatal complications.1
Clomiphene plus IUI remains first-line therapy for unexplained infertility
Although ovarian stimulation with letrozole was safe overall, the number of live births was reduced when treatment with letrozole was compared with clomiphene or Gn, and the multiple pregnancy rate for letrozole fell between clomiphene and Gn.
“CC [clomiphene citrate] /IUI remains first-line therapy for women with unexplained infertility,” concludes Michael P. Diamond, Chair and Professor of the Department of Obstetrics and Gynecology at Georgia Regents University in Augusta, Georgia.
Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Reference
Diamond MP. Outcomes of the NICHD’s comparative effectiveness assessment of multiple intrauterine gestations from ovarian stimulation (AMIGOS) trial. The NICHD cooperative reproductive medicine network. Fertil Steril. 2014;102(3):e39. http://www.fertstert.org/article/S0015-0282%2814%2900767-5/fulltext. Accessed October 31, 2014.
When the cause of infertility is unexplained, what is the best first-choice treatment option? Could letrozole, an oral nonsteroidal aromatase inhibitor, result in fewer multiple gestations than current standard therapy—gonadotropins or selective estrogen receptor modulators (clomiphene citrate)—without worsening the live birth rate?
Researchers from the Assessment of Multiple Intrauterine Gestations from Ovarian Stimulation (AMIGOS) trial investigated this question and presented data at the recent annual meeting of the American Society of Reproductive Medicine. The research was supported by the National Institutes of Health (NIH)/Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
Study details
This prospective, randomized, multicenter clinical trial involved 900 women aged 18 to 40 with at least one patent fallopian tube and regular menses. Patients underwent ovarian stimulation for up to four cycles with an injectable gonadotropin (Gn; n = 300), clomiphene citrate (n = 301), or letrozole (n = 299), followed by intrauterine insemination (IUI).
Birth rate. Conception occurred in 46.8%, 35.7%, and 28.4% of women receiving Gn, clomiphene, and letrozole, respectively, with a live birth occurring in 32.2%, 23.3%, and 18.7% of respective cases. Pregnancy rates with letrozole were significantly less than with Gn (P<.001) and less than with clomiphene (P<.015).
Multiple gestations. The rate of multiple gestations was highest among women treated with Gn (10.3%). But the multiple gestation rate for letrozole was higher than that for clomiphene (2.7% vs 1.3%, respectively). All multiples treated with letrozole and clomiphene were twins; in the Gn group, there were 24 twin and 10 triplet gestations.
No significant difference was found in the rates of infants with congenital anomalies or other fetal or neonatal complications.1
Clomiphene plus IUI remains first-line therapy for unexplained infertility
Although ovarian stimulation with letrozole was safe overall, the number of live births was reduced when treatment with letrozole was compared with clomiphene or Gn, and the multiple pregnancy rate for letrozole fell between clomiphene and Gn.
“CC [clomiphene citrate] /IUI remains first-line therapy for women with unexplained infertility,” concludes Michael P. Diamond, Chair and Professor of the Department of Obstetrics and Gynecology at Georgia Regents University in Augusta, Georgia.
Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
When the cause of infertility is unexplained, what is the best first-choice treatment option? Could letrozole, an oral nonsteroidal aromatase inhibitor, result in fewer multiple gestations than current standard therapy—gonadotropins or selective estrogen receptor modulators (clomiphene citrate)—without worsening the live birth rate?
Researchers from the Assessment of Multiple Intrauterine Gestations from Ovarian Stimulation (AMIGOS) trial investigated this question and presented data at the recent annual meeting of the American Society of Reproductive Medicine. The research was supported by the National Institutes of Health (NIH)/Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD).
Study details
This prospective, randomized, multicenter clinical trial involved 900 women aged 18 to 40 with at least one patent fallopian tube and regular menses. Patients underwent ovarian stimulation for up to four cycles with an injectable gonadotropin (Gn; n = 300), clomiphene citrate (n = 301), or letrozole (n = 299), followed by intrauterine insemination (IUI).
Birth rate. Conception occurred in 46.8%, 35.7%, and 28.4% of women receiving Gn, clomiphene, and letrozole, respectively, with a live birth occurring in 32.2%, 23.3%, and 18.7% of respective cases. Pregnancy rates with letrozole were significantly less than with Gn (P<.001) and less than with clomiphene (P<.015).
Multiple gestations. The rate of multiple gestations was highest among women treated with Gn (10.3%). But the multiple gestation rate for letrozole was higher than that for clomiphene (2.7% vs 1.3%, respectively). All multiples treated with letrozole and clomiphene were twins; in the Gn group, there were 24 twin and 10 triplet gestations.
No significant difference was found in the rates of infants with congenital anomalies or other fetal or neonatal complications.1
Clomiphene plus IUI remains first-line therapy for unexplained infertility
Although ovarian stimulation with letrozole was safe overall, the number of live births was reduced when treatment with letrozole was compared with clomiphene or Gn, and the multiple pregnancy rate for letrozole fell between clomiphene and Gn.
“CC [clomiphene citrate] /IUI remains first-line therapy for women with unexplained infertility,” concludes Michael P. Diamond, Chair and Professor of the Department of Obstetrics and Gynecology at Georgia Regents University in Augusta, Georgia.
Share your thoughts on this article. Send your Letter to the Editor to: [email protected]
Reference
Diamond MP. Outcomes of the NICHD’s comparative effectiveness assessment of multiple intrauterine gestations from ovarian stimulation (AMIGOS) trial. The NICHD cooperative reproductive medicine network. Fertil Steril. 2014;102(3):e39. http://www.fertstert.org/article/S0015-0282%2814%2900767-5/fulltext. Accessed October 31, 2014.
Reference
Diamond MP. Outcomes of the NICHD’s comparative effectiveness assessment of multiple intrauterine gestations from ovarian stimulation (AMIGOS) trial. The NICHD cooperative reproductive medicine network. Fertil Steril. 2014;102(3):e39. http://www.fertstert.org/article/S0015-0282%2814%2900767-5/fulltext. Accessed October 31, 2014.
Bob Wachter Says Cost Equation Is Shifting in Ever-Changing Healthcare Paradigm
HM pioneer says hospitalists who have flown under radar soon will be counted on to produce cost, waste reduction.
HM pioneer says hospitalists who have flown under radar soon will be counted on to produce cost, waste reduction.
HM pioneer says hospitalists who have flown under radar soon will be counted on to produce cost, waste reduction.
Hospitalists Flock to Annual Meeting's Bedside Procedures Pre-Courses
From early-career hospitalists looking to gain hands-on experience with intraosseous lines to family-medicine trained physicians brushing up on ultrasound usage, the procedures' pre-courses at SHM annual meetings receive rave reviews.
From early-career hospitalists looking to gain hands-on experience with intraosseous lines to family-medicine trained physicians brushing up on ultrasound usage, the procedures' pre-courses at SHM annual meetings receive rave reviews.
From early-career hospitalists looking to gain hands-on experience with intraosseous lines to family-medicine trained physicians brushing up on ultrasound usage, the procedures' pre-courses at SHM annual meetings receive rave reviews.
Congenital uterine anomalies: A resource of diagnostic images, Part 1
INTRODUCTION
Steven R. Goldstein, MD, CCD, NCMP
Professor, Department of Obstetrics and Gynecology, New York University School of Medicine; Director, Gynecologic Ultrasound; and Co-Director, Bone Densitometry, New York University Medical Center, New York
In this month’s Images in GYN Ultrasound, Drs. Stalnaker and Kaunitz have done an excellent job of discussing the various uterine malformations as well as characterizing their appearance on 3D transvaginal ultrasound.
Unfortunately, many women are still subjected to the cost, inconvenience, and time involvement of magnetic resonance imaging (MRI) in cases of suspected uterine malformations. The exquisite visualization of 3D transvaginal ultrasound, so nicely depicted in this installment of Images in GYN Ultrasound, allow the observer to see the endometrial contours in the same plane as the serosal surface. This view is not available in traditional 2D ultrasound images. Thus, it is akin to doing laparoscopy and hysteroscopy simultaneously in order to arrive at the proper diagnosis. Although not mandatory, when such 3D ultrasound is performed late in the cycle, the thickened endometrium acts as a nice sonic backdrop to better delineate these structures. Alternatively, 3D saline infusion sonohysterography can be performed.
As more and more ultrasound equipment becomes available with 3D capability as a standard feature, clinicians who do perform ultrasonography will find that obtaining this “z-plane” is relatively simple and extremely informative, and can and should be done in cases of suspected uterine malformations in lieu of ordering MRI.
Congenital uterine anomalies: A resource of diagnostic images, Part 1

Michelle L. Stalnaker Ozcan, MD
Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville

Andrew M. Kaunitz, MD
University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz is a member of the OBG Management Board of Editors.
Uterine malformations make up a diverse group of congenital anomalies that can result from various alterations in the normal development of the Müllerian ducts, including underdevelopment of one or both Müllerian ducts, disorders in Müllerian duct fusion, and alterations in septum reabsorption. How common are such anomalies, how are they classified, and what is the best approach for optimal visualization? Here, we explore these questions and offer an atlas of diagnostic images as an ongoing reference for your practice. Many of the images we offer will be found only online at obgmanagement.com.
How common are congenital uterine anomalies?
The reported prevalence of uterine malformations varies among publications due to heterogeneous population samples, differences in diagnostic techniques, and variations in nomenclature. In general, they are estimated to occur in 0.4% (0.1% to 3.0%) of the population at large, 4% of infertile women, and between 3% and 38% of women with repetitive spontaneous miscarriage.1
Classical classification
A classification of the Müllerian anomalies was introduced in 1980 and, with few modifications, was adopted by the American Fertility Society (currently, ASRM). The Society identified seven basic groups according to Müllerian development and their relationship to fertility: agenesis and hypoplasias, unicornuate uteri (unilateral hypoplasia), didelphys uteri (complete nonfusion), bicornuate uteri (incomplete fusion), septate uteri (nonreabsorption of septum), arcuate uteri (almost complete reabsorption of septum), and anomalies related to fetal DES exposure.2
Anomalies also can be categorized in terms of progression along the developmental continuum, taking into account that many cases result from partial failure of fusion and reabsorption: agenesis (Types I and II), lack of fusion (Types III and IV), lack of reabsorption(Types V and VI), and lack of posterior development (Type VII) (FIGURE 1).3
| FIGURE 1. Classification of müllerian anomalies |
|---|

|
| Source: The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988. 49(6):944-955. |
3D ultrasonography offers accurate, cost-efficient diagnosis
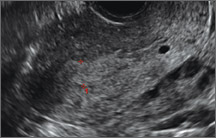
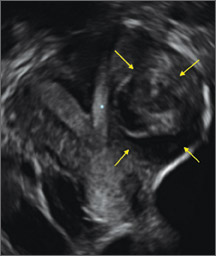
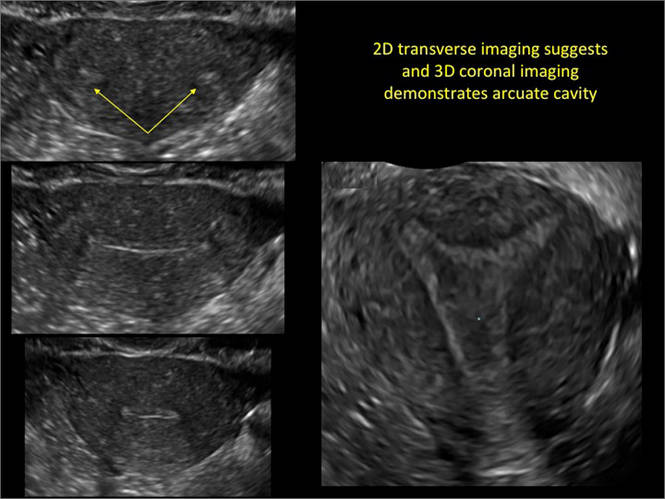
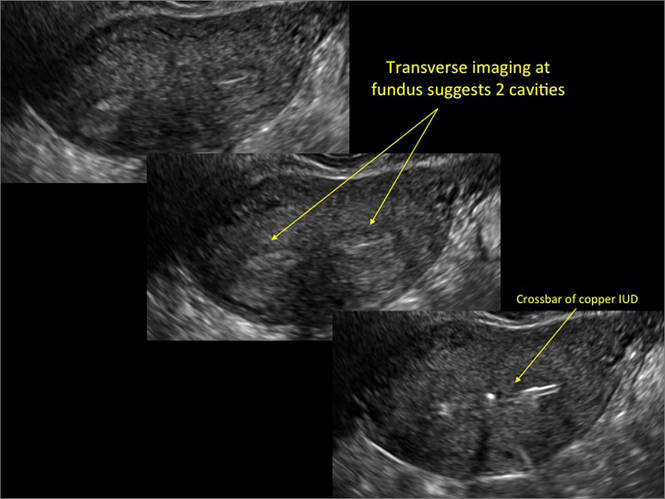
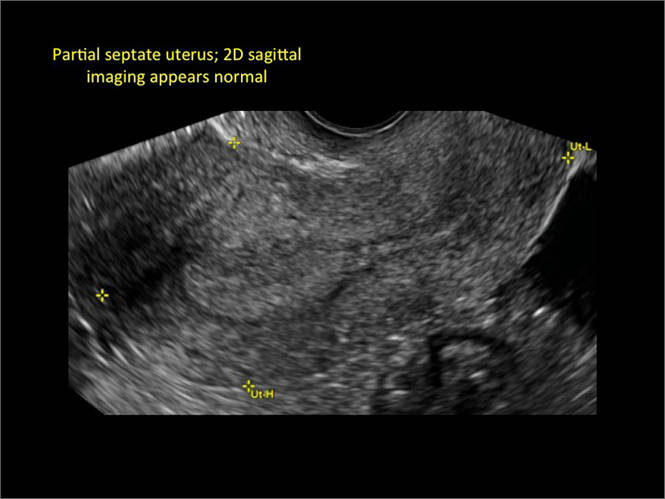
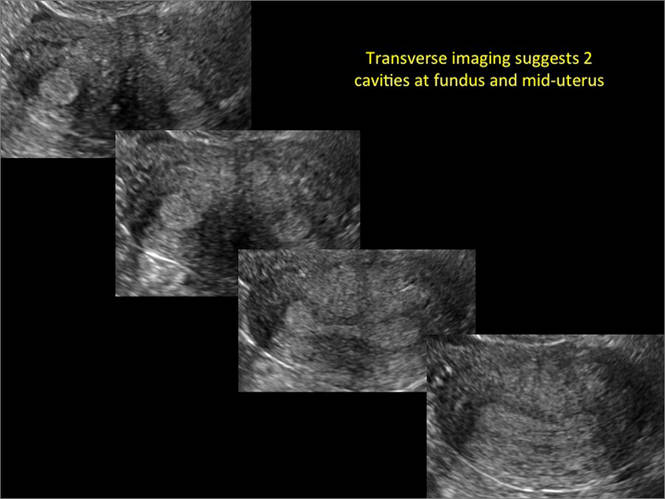
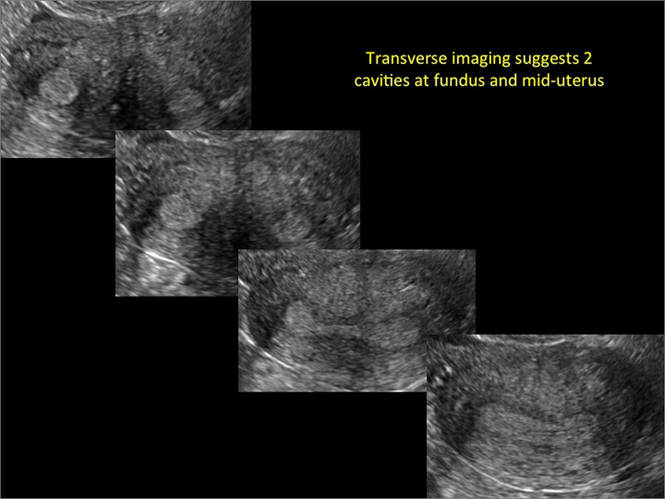
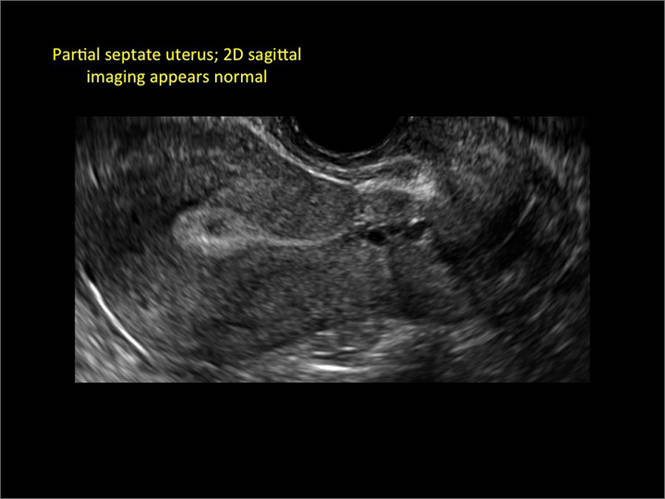
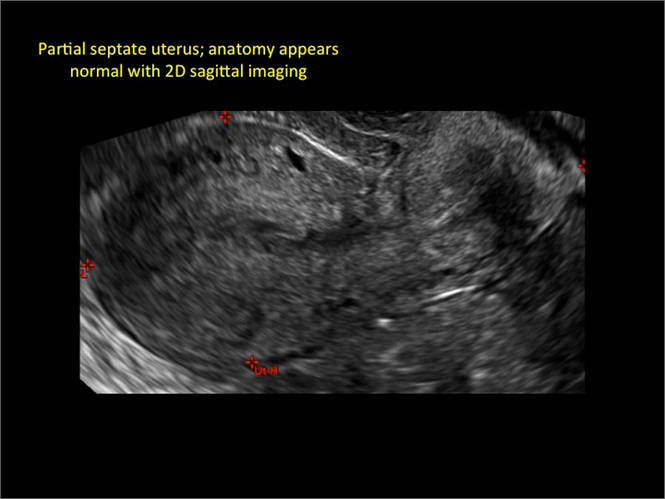
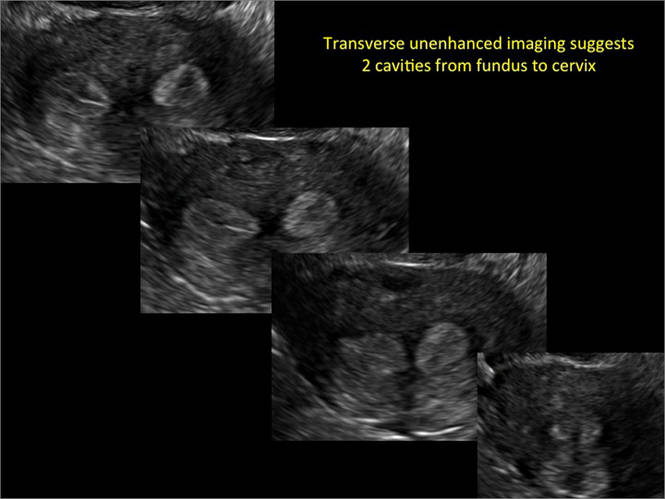
Using only 2D imaging, neither an unenhanced sonogram nor a sonohysterogram can provide definitive information regarding the possibility of a uterine anomaly. The fundal contour cannot be evaluated with 2D imaging; likewise, details regarding the configuration of the uterine cavity (or cavities) may not be appreciated with the use of 2D imaging (FIGURE 2).
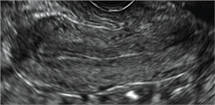
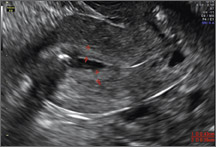
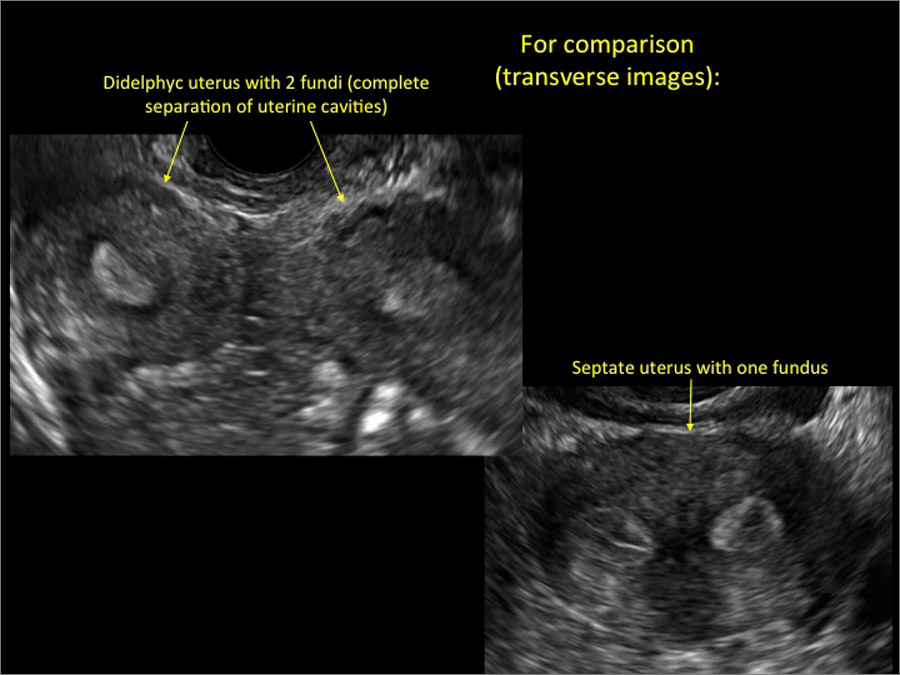
Figure 2: Normal appearance, but abnormal uteri
In sagittal view, a uterus with a congenital anomaly can appear normal. 2D sagittal views of a normal uterus (top), a didelphic uterus (middle), and a sonohysterogram of a septate uterus (bottom). |

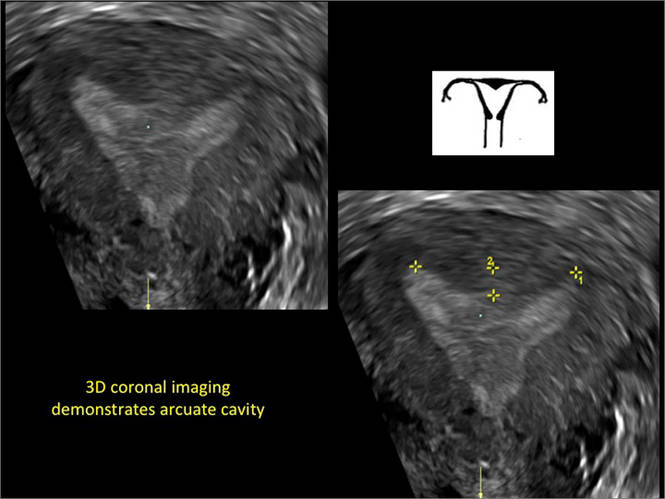
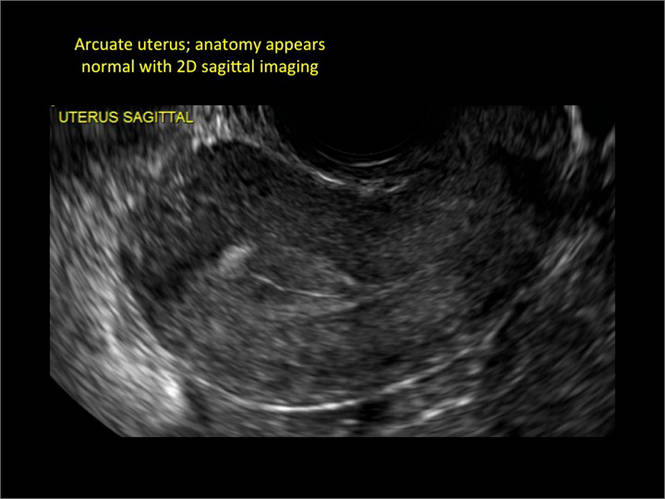
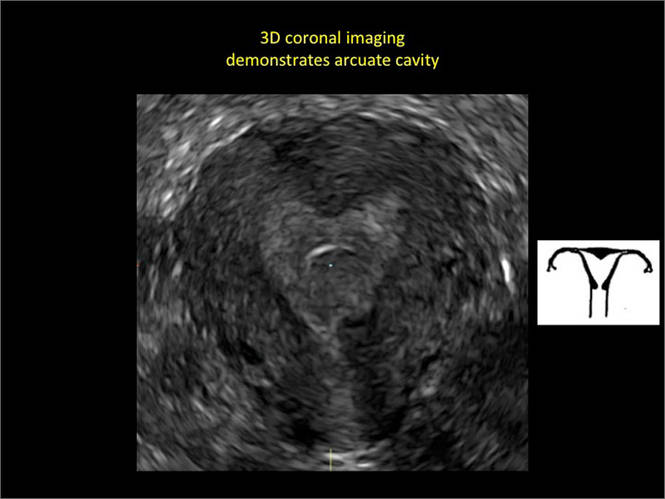
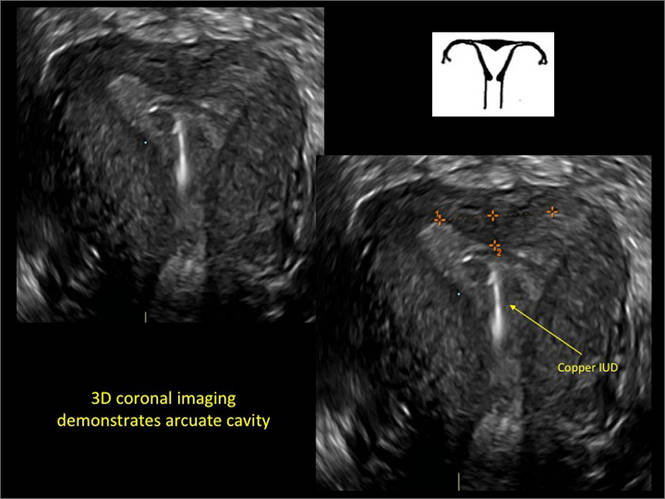
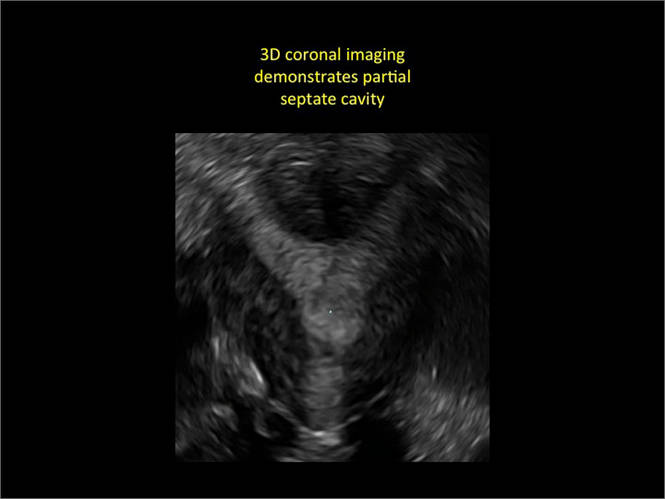
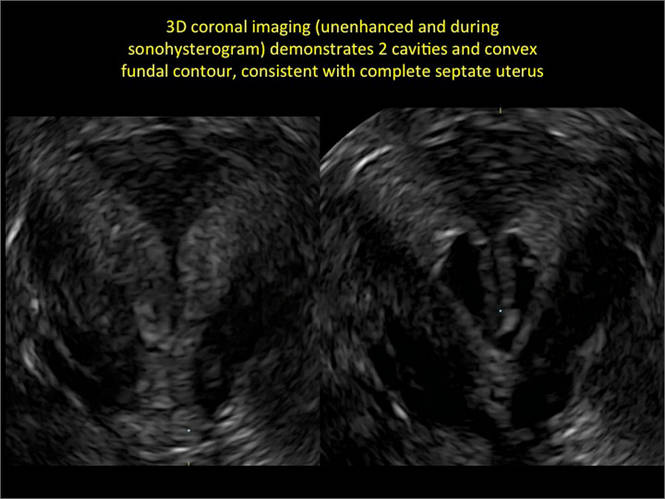
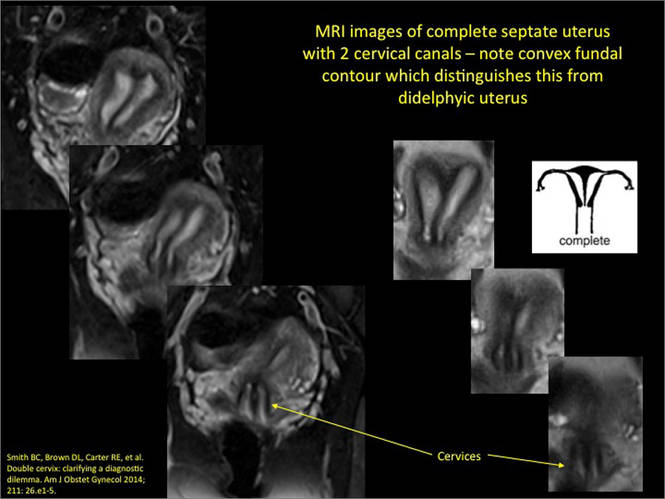
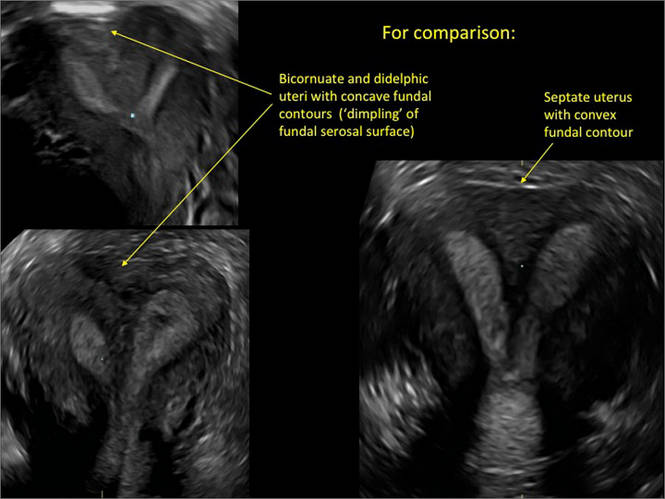
To fully evaluate the uterine fundal contour and determine the type of uterine anomaly, it previously was necessary to obtain magnetic resonance imaging (MRI) or perform laparoscopy. Today, however, 3D coronal ultrasonography (US) can allow for accurate evaluation of fundal contour and diagnosis of uterine anomalies with lower cost and greater patient convenience. Several studies have confirmed the high accuracy of 3D US compared with MRI and surgical findings in the diagnosis of uterine anomalies (with 3D US showing 98% to 100% sensitivity and specificity).4-6
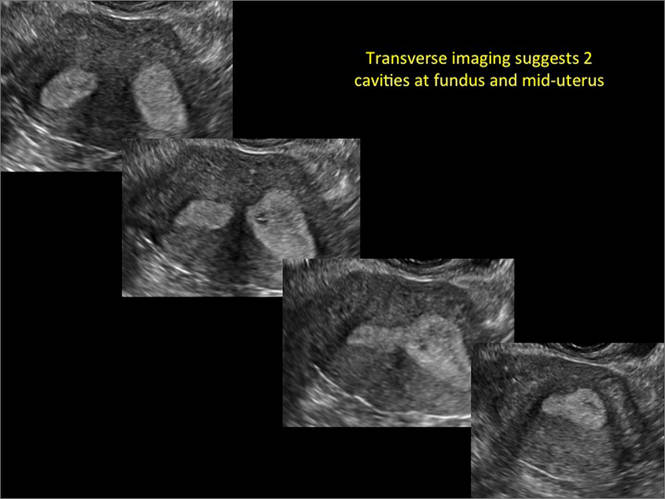
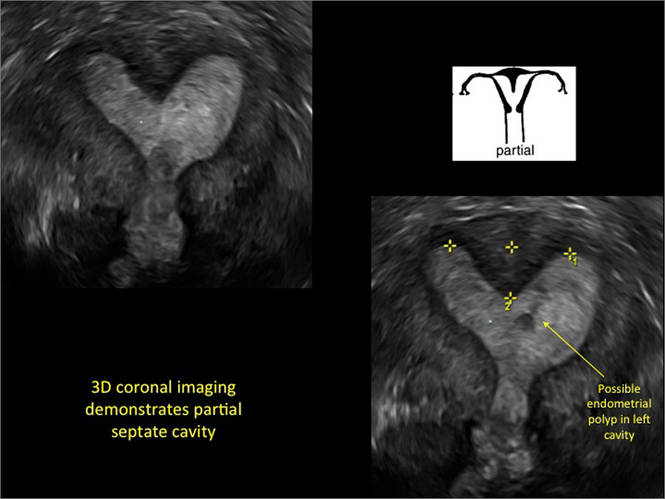
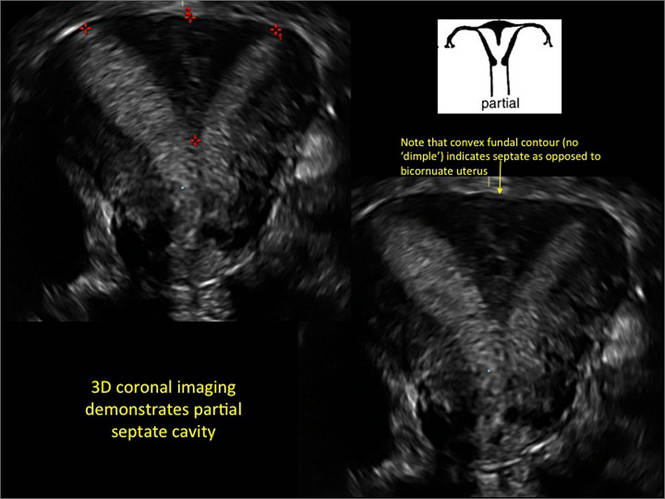
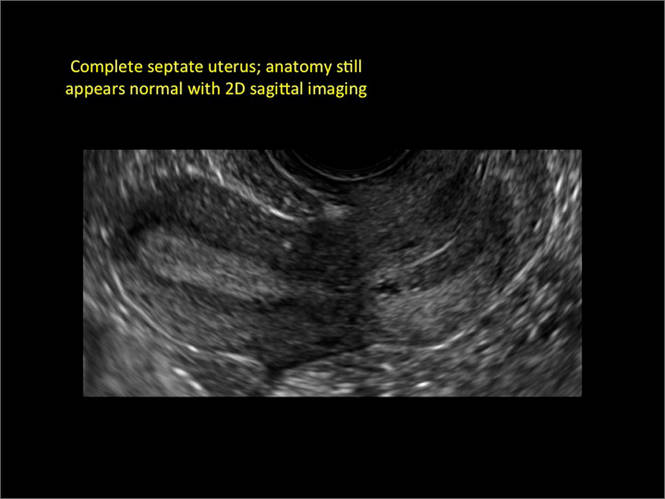
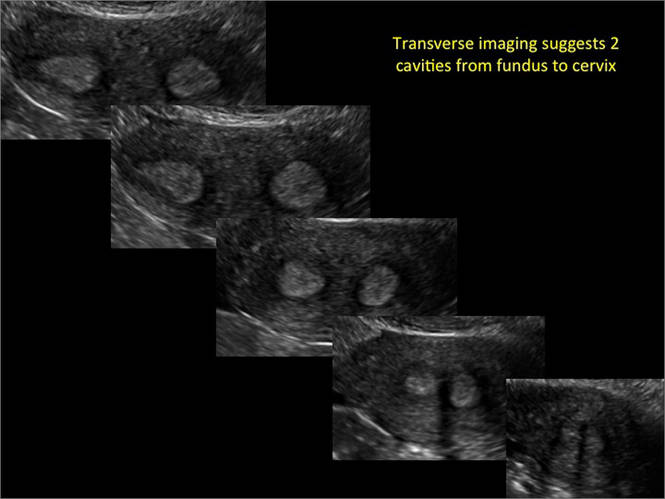
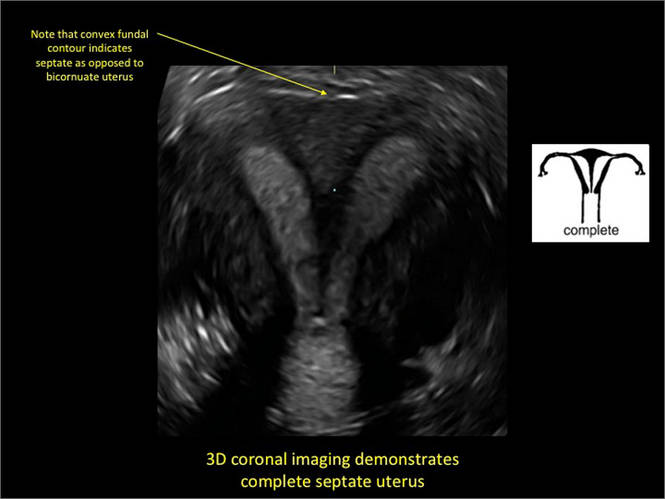
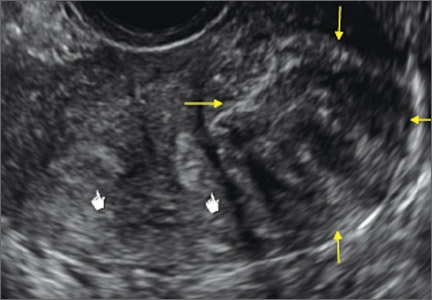
Case: Partial septate uterus
|

ADDITIONAL IMAGES


Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Bermejo C, Martinez Ten P, Cantarero R, et al. Three-dimensional ultrasound in the diagnosis of Müllerian duct anomalies and concordance with magnetic resonance imaging. Ultrasound Obstet Gynecol. 2010;35(5):593–601.
- The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49(6):944–955.
- Acien P, Acien M. Updated classification of malformations. Hum Reprod. 2010;25(suppl 1):i81–i82.
- Deutch T, Bocca S, Oehninger S, Stadtmauer L, Abuhamad AZ. Magnetic resonance imaging versus three-dimensional transvaginal ultrasound for the diagnosis of Müllerian anomalies [abstract P-465]. Fertil Steril. 2006;86(suppl):S308.
- Wu MH, Hsu CC, Huang KE. Detection of congenital Müllerian duct anomalies using three-dimensional ultrasound. J Clin Ultrasound. 1997;25(9):487–492.
- Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of Müllerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
INTRODUCTION
Steven R. Goldstein, MD, CCD, NCMP
Professor, Department of Obstetrics and Gynecology, New York University School of Medicine; Director, Gynecologic Ultrasound; and Co-Director, Bone Densitometry, New York University Medical Center, New York
In this month’s Images in GYN Ultrasound, Drs. Stalnaker and Kaunitz have done an excellent job of discussing the various uterine malformations as well as characterizing their appearance on 3D transvaginal ultrasound.
Unfortunately, many women are still subjected to the cost, inconvenience, and time involvement of magnetic resonance imaging (MRI) in cases of suspected uterine malformations. The exquisite visualization of 3D transvaginal ultrasound, so nicely depicted in this installment of Images in GYN Ultrasound, allow the observer to see the endometrial contours in the same plane as the serosal surface. This view is not available in traditional 2D ultrasound images. Thus, it is akin to doing laparoscopy and hysteroscopy simultaneously in order to arrive at the proper diagnosis. Although not mandatory, when such 3D ultrasound is performed late in the cycle, the thickened endometrium acts as a nice sonic backdrop to better delineate these structures. Alternatively, 3D saline infusion sonohysterography can be performed.
As more and more ultrasound equipment becomes available with 3D capability as a standard feature, clinicians who do perform ultrasonography will find that obtaining this “z-plane” is relatively simple and extremely informative, and can and should be done in cases of suspected uterine malformations in lieu of ordering MRI.
Congenital uterine anomalies: A resource of diagnostic images, Part 1
Michelle L. Stalnaker Ozcan, MD
Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville
Andrew M. Kaunitz, MD
University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz is a member of the OBG Management Board of Editors.
Uterine malformations make up a diverse group of congenital anomalies that can result from various alterations in the normal development of the Müllerian ducts, including underdevelopment of one or both Müllerian ducts, disorders in Müllerian duct fusion, and alterations in septum reabsorption. How common are such anomalies, how are they classified, and what is the best approach for optimal visualization? Here, we explore these questions and offer an atlas of diagnostic images as an ongoing reference for your practice. Many of the images we offer will be found only online at obgmanagement.com.
How common are congenital uterine anomalies?
The reported prevalence of uterine malformations varies among publications due to heterogeneous population samples, differences in diagnostic techniques, and variations in nomenclature. In general, they are estimated to occur in 0.4% (0.1% to 3.0%) of the population at large, 4% of infertile women, and between 3% and 38% of women with repetitive spontaneous miscarriage.1
Classical classification
A classification of the Müllerian anomalies was introduced in 1980 and, with few modifications, was adopted by the American Fertility Society (currently, ASRM). The Society identified seven basic groups according to Müllerian development and their relationship to fertility: agenesis and hypoplasias, unicornuate uteri (unilateral hypoplasia), didelphys uteri (complete nonfusion), bicornuate uteri (incomplete fusion), septate uteri (nonreabsorption of septum), arcuate uteri (almost complete reabsorption of septum), and anomalies related to fetal DES exposure.2
Anomalies also can be categorized in terms of progression along the developmental continuum, taking into account that many cases result from partial failure of fusion and reabsorption: agenesis (Types I and II), lack of fusion (Types III and IV), lack of reabsorption(Types V and VI), and lack of posterior development (Type VII) (FIGURE 1).3
| FIGURE 1. Classification of müllerian anomalies |
|---|
|
|
| Source: The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988. 49(6):944-955. |
3D ultrasonography offers accurate, cost-efficient diagnosis
Using only 2D imaging, neither an unenhanced sonogram nor a sonohysterogram can provide definitive information regarding the possibility of a uterine anomaly. The fundal contour cannot be evaluated with 2D imaging; likewise, details regarding the configuration of the uterine cavity (or cavities) may not be appreciated with the use of 2D imaging (FIGURE 2).
Figure 2: Normal appearance, but abnormal uteri
In sagittal view, a uterus with a congenital anomaly can appear normal. 2D sagittal views of a normal uterus (top), a didelphic uterus (middle), and a sonohysterogram of a septate uterus (bottom). |
To fully evaluate the uterine fundal contour and determine the type of uterine anomaly, it previously was necessary to obtain magnetic resonance imaging (MRI) or perform laparoscopy. Today, however, 3D coronal ultrasonography (US) can allow for accurate evaluation of fundal contour and diagnosis of uterine anomalies with lower cost and greater patient convenience. Several studies have confirmed the high accuracy of 3D US compared with MRI and surgical findings in the diagnosis of uterine anomalies (with 3D US showing 98% to 100% sensitivity and specificity).4-6
Case: Partial septate uterus
|
ADDITIONAL IMAGES
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
INTRODUCTION
Steven R. Goldstein, MD, CCD, NCMP
Professor, Department of Obstetrics and Gynecology, New York University School of Medicine; Director, Gynecologic Ultrasound; and Co-Director, Bone Densitometry, New York University Medical Center, New York
In this month’s Images in GYN Ultrasound, Drs. Stalnaker and Kaunitz have done an excellent job of discussing the various uterine malformations as well as characterizing their appearance on 3D transvaginal ultrasound.
Unfortunately, many women are still subjected to the cost, inconvenience, and time involvement of magnetic resonance imaging (MRI) in cases of suspected uterine malformations. The exquisite visualization of 3D transvaginal ultrasound, so nicely depicted in this installment of Images in GYN Ultrasound, allow the observer to see the endometrial contours in the same plane as the serosal surface. This view is not available in traditional 2D ultrasound images. Thus, it is akin to doing laparoscopy and hysteroscopy simultaneously in order to arrive at the proper diagnosis. Although not mandatory, when such 3D ultrasound is performed late in the cycle, the thickened endometrium acts as a nice sonic backdrop to better delineate these structures. Alternatively, 3D saline infusion sonohysterography can be performed.
As more and more ultrasound equipment becomes available with 3D capability as a standard feature, clinicians who do perform ultrasonography will find that obtaining this “z-plane” is relatively simple and extremely informative, and can and should be done in cases of suspected uterine malformations in lieu of ordering MRI.
Congenital uterine anomalies: A resource of diagnostic images, Part 1
Michelle L. Stalnaker Ozcan, MD
Assistant Professor and Associate Program Director, Obstetrics and Gynecology Residency, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville
Andrew M. Kaunitz, MD
University of Florida Research Foundation Professor and Associate Chairman, Department of Obstetrics and Gynecology at the University of Florida College of Medicine–Jacksonville. Dr. Kaunitz is a member of the OBG Management Board of Editors.
Uterine malformations make up a diverse group of congenital anomalies that can result from various alterations in the normal development of the Müllerian ducts, including underdevelopment of one or both Müllerian ducts, disorders in Müllerian duct fusion, and alterations in septum reabsorption. How common are such anomalies, how are they classified, and what is the best approach for optimal visualization? Here, we explore these questions and offer an atlas of diagnostic images as an ongoing reference for your practice. Many of the images we offer will be found only online at obgmanagement.com.
How common are congenital uterine anomalies?
The reported prevalence of uterine malformations varies among publications due to heterogeneous population samples, differences in diagnostic techniques, and variations in nomenclature. In general, they are estimated to occur in 0.4% (0.1% to 3.0%) of the population at large, 4% of infertile women, and between 3% and 38% of women with repetitive spontaneous miscarriage.1
Classical classification
A classification of the Müllerian anomalies was introduced in 1980 and, with few modifications, was adopted by the American Fertility Society (currently, ASRM). The Society identified seven basic groups according to Müllerian development and their relationship to fertility: agenesis and hypoplasias, unicornuate uteri (unilateral hypoplasia), didelphys uteri (complete nonfusion), bicornuate uteri (incomplete fusion), septate uteri (nonreabsorption of septum), arcuate uteri (almost complete reabsorption of septum), and anomalies related to fetal DES exposure.2
Anomalies also can be categorized in terms of progression along the developmental continuum, taking into account that many cases result from partial failure of fusion and reabsorption: agenesis (Types I and II), lack of fusion (Types III and IV), lack of reabsorption(Types V and VI), and lack of posterior development (Type VII) (FIGURE 1).3
| FIGURE 1. Classification of müllerian anomalies |
|---|
|
|
| Source: The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988. 49(6):944-955. |
3D ultrasonography offers accurate, cost-efficient diagnosis
Using only 2D imaging, neither an unenhanced sonogram nor a sonohysterogram can provide definitive information regarding the possibility of a uterine anomaly. The fundal contour cannot be evaluated with 2D imaging; likewise, details regarding the configuration of the uterine cavity (or cavities) may not be appreciated with the use of 2D imaging (FIGURE 2).
Figure 2: Normal appearance, but abnormal uteri
In sagittal view, a uterus with a congenital anomaly can appear normal. 2D sagittal views of a normal uterus (top), a didelphic uterus (middle), and a sonohysterogram of a septate uterus (bottom). |
To fully evaluate the uterine fundal contour and determine the type of uterine anomaly, it previously was necessary to obtain magnetic resonance imaging (MRI) or perform laparoscopy. Today, however, 3D coronal ultrasonography (US) can allow for accurate evaluation of fundal contour and diagnosis of uterine anomalies with lower cost and greater patient convenience. Several studies have confirmed the high accuracy of 3D US compared with MRI and surgical findings in the diagnosis of uterine anomalies (with 3D US showing 98% to 100% sensitivity and specificity).4-6
Case: Partial septate uterus
|
ADDITIONAL IMAGES
Share your thoughts on this article! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
- Bermejo C, Martinez Ten P, Cantarero R, et al. Three-dimensional ultrasound in the diagnosis of Müllerian duct anomalies and concordance with magnetic resonance imaging. Ultrasound Obstet Gynecol. 2010;35(5):593–601.
- The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49(6):944–955.
- Acien P, Acien M. Updated classification of malformations. Hum Reprod. 2010;25(suppl 1):i81–i82.
- Deutch T, Bocca S, Oehninger S, Stadtmauer L, Abuhamad AZ. Magnetic resonance imaging versus three-dimensional transvaginal ultrasound for the diagnosis of Müllerian anomalies [abstract P-465]. Fertil Steril. 2006;86(suppl):S308.
- Wu MH, Hsu CC, Huang KE. Detection of congenital Müllerian duct anomalies using three-dimensional ultrasound. J Clin Ultrasound. 1997;25(9):487–492.
- Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of Müllerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
- Bermejo C, Martinez Ten P, Cantarero R, et al. Three-dimensional ultrasound in the diagnosis of Müllerian duct anomalies and concordance with magnetic resonance imaging. Ultrasound Obstet Gynecol. 2010;35(5):593–601.
- The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49(6):944–955.
- Acien P, Acien M. Updated classification of malformations. Hum Reprod. 2010;25(suppl 1):i81–i82.
- Deutch T, Bocca S, Oehninger S, Stadtmauer L, Abuhamad AZ. Magnetic resonance imaging versus three-dimensional transvaginal ultrasound for the diagnosis of Müllerian anomalies [abstract P-465]. Fertil Steril. 2006;86(suppl):S308.
- Wu MH, Hsu CC, Huang KE. Detection of congenital Müllerian duct anomalies using three-dimensional ultrasound. J Clin Ultrasound. 1997;25(9):487–492.
- Deutch TD, Abuhamad AZ. The role of 3-dimensional ultrasonography and magnetic resonance imaging in the diagnosis of Müllerian duct anomalies. J Ultrasound Med. 2008;27(3):413–423.
Hair Loss in a 12-Year-Old
A mother brings her 12-year-old son to dermatology following a referral from the boy’s pediatrician. Several months ago, she noticed her son’s hair loss. The change had been preceded by a stressful period in which she and her husband divorced and one of the boy’s grandparents died unexpectedly.
Both the mother and other relatives and friends had observed the boy reaching for his scalp frequently and twirling his hair “absentmindedly.” When asked if the area in question bothers him, the boy always answers in the negative. Although he knows he should leave his scalp and hair alone, he says he finds it difficult to do so—even though he acknowledges the social liability of his hair loss. According to the mother, the more his family discourages his behavior, the more it persists.

EXAMINATION
Distinct but incomplete hair loss is noted in an 8 x 10–cm area of his scalp crown. There is neither redness nor any disturbance to the skin there. On palpation, there is no tenderness or increased warmth. No nodes are felt in the adjacent head or neck. Hair pull test is negative.
Closer examination shows hairs of varying lengths in the affected area: many quite short, others of normal length, and many of intermediate length.
Blood work done by the referring pediatrician—including complete blood count, chemistry panel, antinuclear antibody test, and thyroid testing—yielded no abnormal results.
What is the diagnosis?
DISCUSSION
Hair loss, collectively termed alopecia, is a disturbing development, especially in a child. In this case, we had localized hair loss most likely caused by behavior that was not only witnessed by the boy’s parents but also admitted to by the patient. (We’re not always so fortunate.) Thus, it was fairly straightforward to diagnosis trichotillomania, also known as trichotillosis or hair-pulling disorder. This condition can mimic alopecia areata and tinea capitis.
In this case, the lack of epidermal change (scaling, redness, edema) and palpable adenopathy spoke loudly against fungal infection. The hair loss in alopecia areata (AA) is usually sharply defined and complete, which our patient’s hair loss was not. And the blood work that was done effectively ruled out systemic disease (an unlikely cause of localized hair loss in any case).
The jury is still out as to how exactly to classify trichotillomania (TTM). The new DSM-V lists it as an anxiety disorder, in part because it often appears in that context. What we do know is that girls are twice as likely as boys to be affected. And children ages 4 to 13 are seven times more likely than adults to develop TTM.
TTM can involve hair anywhere on the body, though children almost always confine their behavior to their scalp. Actual hair-pulling is not necessarily seen. Manipulation, such as the twirling in this case, is enough to weaken hair follicles, causing hair to fall out. In cases involving hair-pulling, a small percentage of patients actually ingest the hairs they’ve plucked out (trichophagia). Being indigestible, the hairs can accumulate in hairballs (trichobezoars).
Even though TTM is most likely a psychiatric disorder lying somewhere in the obsessive-compulsive spectrum, it is seen more often in primary care and dermatology offices. Scalp biopsy would certainly settle the matter, but a better alternative is simply shaving a dime-sized area of scalp and watching it for normal hair growth.
Most cases eventually resolve with time and persistent but gentle reminders, but a few will require psychiatric intervention. This typically includes habit reversal therapy or cognitive behavioral therapy, plus or minus combinations of psychoactive medications. (The latter decision depends on whether there psychiatric comorbidities.) Despite all these efforts, severe cases of TTM can persist for years or even a lifetime.
It remains to be seen how this particular patient responds to his parents’ efforts. It was an immense relief for them to know the cause of their son’s hair loss and that the condition is likely self-limiting.
TAKE-HOME LEARNING POINTS
• Trichotillomania (TTM) is an unusual form of localized hair loss, usually involving children’s scalps.
• TTM affects children ages 4 to 13 and at least twice as many girls as boys.
• TTM does not always involve actual plucking of hairs. Repetitive manipulation, such as twirling, can weaken the hairs enough to cause hair loss.
• Unlike alopecia areata (the main item in the alopecia differential for children), TTM is more likely to cause incomplete, poorly defined hair loss in an area where hairs of varying length can be seen.
• Usually self-limiting, TTM can require psychiatric attention, for which a variety of habit training techniques can be used.
A mother brings her 12-year-old son to dermatology following a referral from the boy’s pediatrician. Several months ago, she noticed her son’s hair loss. The change had been preceded by a stressful period in which she and her husband divorced and one of the boy’s grandparents died unexpectedly.
Both the mother and other relatives and friends had observed the boy reaching for his scalp frequently and twirling his hair “absentmindedly.” When asked if the area in question bothers him, the boy always answers in the negative. Although he knows he should leave his scalp and hair alone, he says he finds it difficult to do so—even though he acknowledges the social liability of his hair loss. According to the mother, the more his family discourages his behavior, the more it persists.
EXAMINATION
Distinct but incomplete hair loss is noted in an 8 x 10–cm area of his scalp crown. There is neither redness nor any disturbance to the skin there. On palpation, there is no tenderness or increased warmth. No nodes are felt in the adjacent head or neck. Hair pull test is negative.
Closer examination shows hairs of varying lengths in the affected area: many quite short, others of normal length, and many of intermediate length.
Blood work done by the referring pediatrician—including complete blood count, chemistry panel, antinuclear antibody test, and thyroid testing—yielded no abnormal results.
What is the diagnosis?
DISCUSSION
Hair loss, collectively termed alopecia, is a disturbing development, especially in a child. In this case, we had localized hair loss most likely caused by behavior that was not only witnessed by the boy’s parents but also admitted to by the patient. (We’re not always so fortunate.) Thus, it was fairly straightforward to diagnosis trichotillomania, also known as trichotillosis or hair-pulling disorder. This condition can mimic alopecia areata and tinea capitis.
In this case, the lack of epidermal change (scaling, redness, edema) and palpable adenopathy spoke loudly against fungal infection. The hair loss in alopecia areata (AA) is usually sharply defined and complete, which our patient’s hair loss was not. And the blood work that was done effectively ruled out systemic disease (an unlikely cause of localized hair loss in any case).
The jury is still out as to how exactly to classify trichotillomania (TTM). The new DSM-V lists it as an anxiety disorder, in part because it often appears in that context. What we do know is that girls are twice as likely as boys to be affected. And children ages 4 to 13 are seven times more likely than adults to develop TTM.
TTM can involve hair anywhere on the body, though children almost always confine their behavior to their scalp. Actual hair-pulling is not necessarily seen. Manipulation, such as the twirling in this case, is enough to weaken hair follicles, causing hair to fall out. In cases involving hair-pulling, a small percentage of patients actually ingest the hairs they’ve plucked out (trichophagia). Being indigestible, the hairs can accumulate in hairballs (trichobezoars).
Even though TTM is most likely a psychiatric disorder lying somewhere in the obsessive-compulsive spectrum, it is seen more often in primary care and dermatology offices. Scalp biopsy would certainly settle the matter, but a better alternative is simply shaving a dime-sized area of scalp and watching it for normal hair growth.
Most cases eventually resolve with time and persistent but gentle reminders, but a few will require psychiatric intervention. This typically includes habit reversal therapy or cognitive behavioral therapy, plus or minus combinations of psychoactive medications. (The latter decision depends on whether there psychiatric comorbidities.) Despite all these efforts, severe cases of TTM can persist for years or even a lifetime.
It remains to be seen how this particular patient responds to his parents’ efforts. It was an immense relief for them to know the cause of their son’s hair loss and that the condition is likely self-limiting.
TAKE-HOME LEARNING POINTS
• Trichotillomania (TTM) is an unusual form of localized hair loss, usually involving children’s scalps.
• TTM affects children ages 4 to 13 and at least twice as many girls as boys.
• TTM does not always involve actual plucking of hairs. Repetitive manipulation, such as twirling, can weaken the hairs enough to cause hair loss.
• Unlike alopecia areata (the main item in the alopecia differential for children), TTM is more likely to cause incomplete, poorly defined hair loss in an area where hairs of varying length can be seen.
• Usually self-limiting, TTM can require psychiatric attention, for which a variety of habit training techniques can be used.
A mother brings her 12-year-old son to dermatology following a referral from the boy’s pediatrician. Several months ago, she noticed her son’s hair loss. The change had been preceded by a stressful period in which she and her husband divorced and one of the boy’s grandparents died unexpectedly.
Both the mother and other relatives and friends had observed the boy reaching for his scalp frequently and twirling his hair “absentmindedly.” When asked if the area in question bothers him, the boy always answers in the negative. Although he knows he should leave his scalp and hair alone, he says he finds it difficult to do so—even though he acknowledges the social liability of his hair loss. According to the mother, the more his family discourages his behavior, the more it persists.
EXAMINATION
Distinct but incomplete hair loss is noted in an 8 x 10–cm area of his scalp crown. There is neither redness nor any disturbance to the skin there. On palpation, there is no tenderness or increased warmth. No nodes are felt in the adjacent head or neck. Hair pull test is negative.
Closer examination shows hairs of varying lengths in the affected area: many quite short, others of normal length, and many of intermediate length.
Blood work done by the referring pediatrician—including complete blood count, chemistry panel, antinuclear antibody test, and thyroid testing—yielded no abnormal results.
What is the diagnosis?
DISCUSSION
Hair loss, collectively termed alopecia, is a disturbing development, especially in a child. In this case, we had localized hair loss most likely caused by behavior that was not only witnessed by the boy’s parents but also admitted to by the patient. (We’re not always so fortunate.) Thus, it was fairly straightforward to diagnosis trichotillomania, also known as trichotillosis or hair-pulling disorder. This condition can mimic alopecia areata and tinea capitis.
In this case, the lack of epidermal change (scaling, redness, edema) and palpable adenopathy spoke loudly against fungal infection. The hair loss in alopecia areata (AA) is usually sharply defined and complete, which our patient’s hair loss was not. And the blood work that was done effectively ruled out systemic disease (an unlikely cause of localized hair loss in any case).
The jury is still out as to how exactly to classify trichotillomania (TTM). The new DSM-V lists it as an anxiety disorder, in part because it often appears in that context. What we do know is that girls are twice as likely as boys to be affected. And children ages 4 to 13 are seven times more likely than adults to develop TTM.
TTM can involve hair anywhere on the body, though children almost always confine their behavior to their scalp. Actual hair-pulling is not necessarily seen. Manipulation, such as the twirling in this case, is enough to weaken hair follicles, causing hair to fall out. In cases involving hair-pulling, a small percentage of patients actually ingest the hairs they’ve plucked out (trichophagia). Being indigestible, the hairs can accumulate in hairballs (trichobezoars).
Even though TTM is most likely a psychiatric disorder lying somewhere in the obsessive-compulsive spectrum, it is seen more often in primary care and dermatology offices. Scalp biopsy would certainly settle the matter, but a better alternative is simply shaving a dime-sized area of scalp and watching it for normal hair growth.
Most cases eventually resolve with time and persistent but gentle reminders, but a few will require psychiatric intervention. This typically includes habit reversal therapy or cognitive behavioral therapy, plus or minus combinations of psychoactive medications. (The latter decision depends on whether there psychiatric comorbidities.) Despite all these efforts, severe cases of TTM can persist for years or even a lifetime.
It remains to be seen how this particular patient responds to his parents’ efforts. It was an immense relief for them to know the cause of their son’s hair loss and that the condition is likely self-limiting.
TAKE-HOME LEARNING POINTS
• Trichotillomania (TTM) is an unusual form of localized hair loss, usually involving children’s scalps.
• TTM affects children ages 4 to 13 and at least twice as many girls as boys.
• TTM does not always involve actual plucking of hairs. Repetitive manipulation, such as twirling, can weaken the hairs enough to cause hair loss.
• Unlike alopecia areata (the main item in the alopecia differential for children), TTM is more likely to cause incomplete, poorly defined hair loss in an area where hairs of varying length can be seen.
• Usually self-limiting, TTM can require psychiatric attention, for which a variety of habit training techniques can be used.
