User login
Pasireotide decreases incidence of postoperative fistula
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
The somatostatin analogue pasireotide reduced postoperative pancreatic fistula leak or abscess by 56%, compared with placebo, a randomized study has determined.
Pasireotide (Signifor) was effective after both pancreaticoduodenectomy and distal pancreatectomy, whether or not the pancreatic duct was dilated, Dr. Peter J. Allen and his colleagues wrote in the May 21 issue of the New England Journal of Medicine (N. Engl. J. Med. 2014;370:2014-22).
In those patients who did develop fistulas or leaks, pasireotide was associated with fewer grade 3 occurrences.
"These results suggest that ... not only were many leaks and fistulas prevented, but when they did occur they were less clinically relevant," wrote Dr. Allen of the Memorial Sloan Kettering Cancer Center, New York, and his coauthors.
The study randomized 300 patients to subcutaneous injections of either placebo or pasireotide twice daily for 7 days after pancreatic surgery. The primary endpoint was the development of a pancreatic leak, fistula, or abscess of at least grade 3. Secondary endpoints included the overall rate of pancreatic complications (all grades) and the rate of grade B or grade C pancreatic fistula.
Patients were a mean of 64 years old. Most (73%) underwent a pancreaticoduodenectomy. The average length of stay for these patients was about 10 days. The active group received 900 mcg of pasireotide subcutaneously twice daily for 7 days, beginning on the morning of surgery.
Mean postoperative serum glucose levels were significantly higher in patients taking pasireotide (258 mg/dL vs. 215 mg/dL). Readmission occurred in significantly fewer pasireotide patients (17% vs. 29%).
Significantly fewer of those taking the active drug were able to finish the entire course of 14 doses (76% vs. 86% given placebo). The lower completion rate was mostly due to nausea and vomiting, which caused 26 patients in the active group and 3 in the placebo group to withdraw from the study.
A leak or fistula of grade 3 or higher developed in 45 patients. The outcome was significantly less common among those taking pasireotide than among those on placebo (9% vs. 21%; relative risk, 0.44). "This corresponded to an absolute risk reduction of 11.7 percentage points," with a number needed to treat of 8, the investigators said.
Pasireotide was significantly more effective than placebo in surgical subgroups, including pancreaticoduodenectomy (RR, 0.49) and distal pancreatectomy (RR, 0.32). The effect was also positive whether the pancreatic duct was dilated (RR, 0.11) or nondilated (RR, 0.55).
The secondary outcome (grade B or C postoperative fistula) occurred in 37 patients (12%). In the pasireotide group, there were 12 grade B fistulas and no grade C fistulas. In the placebo group, there were 20 grade B and 5 grade C fistulas.
Overall 60-day mortality was 0.7% (one death in each treatment group). Grade 3 and 4 complications were common, occurring in 92% of the pasireotide group and 90% of the placebo group. Most of these were expected postoperative serum abnormalities.
The investigators said that the other approved somatostatin analogue, octreotide, has not been clearly associated with pancreatic leak reduction. They suggested that pasireotide may be more effective because it has a longer half-life and binds to four of the five somatostatin-receptor subtypes, rather than just two, as octreotide does.
They added that the octreotide studies were conducted before 2005, when there was no consistent definition of postoperative pancreatic fistula. Therefore, they concluded, the extant data cannot be used to identify octreotide efficacy in this application.
Pasireotide, which is made by Novartis Pharmaceuticals, is currently approved as an injection for the treatment of Cushing’s disease patients who cannot be helped through surgery.
Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
FROM NEJM
Key clinical point: Pasireotide reduced the incidence of postoperative pancreatic fistula, leak, or abscess.
Major finding: Compared with placebo, pasireotide reduced the rate of fistula, leak, or abscess by 56%.
Data source: The randomized, placebo-controlled study included 300 patients.
Disclosures: Novartis Pharmaceuticals sponsored the trial. Dr. Allen received Novartis grant funding but had no other financial ties with the company.
MERS Cases Put Hospitalists on Alert for Infectious Disease
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
Patients diagnosed with Middle East Respiratory Syndrome (MERS) in Indiana and Florida have healthcare workers and hospitalists on the lookout for additional cases of the potentially fatal respiratory infection.
Hospitalists should pay attention to patients exhibiting fever and respiratory symptoms who traveled to the Arabian Peninsula in the 14 days prior to disease onset, and contact the hospital epidemiologist if MERS is suspected, says James Pile, MD, vice chair of the department of hospital medicine at the Cleveland Clinic.
The CDC has reported three cases of MERS this month. The first, reported on May 2, involved a healthcare worker from Saudi Arabia who traveled to Indiana to visit family. The second was reported on May 11, when another visiting healthcare worker from Saudi Arabia checked into the emergency department in Orlando, Fla., after he fell ill with fever, chills, and a slight cough. Both patients are considered to be fully recovered.
The third MERS case is in an Illinois man who had a business meeting with the patient from Indiana and represents the first case of the virus being contracted in the U.S. A blood test confirmed that the Illinois man had been infected with the virus, but he’s reported that he no longer feels sick.
Caused by a coronavirus called MERS-CoV, MERS was first reported in Saudi Arabia in 2012. So far, there have been more than 600 confirmed cases around the world and 181 people have died, according to the World Health Organization.
"The CDC suggests that the index U.S. case represents a very low threat to the general population in this country, and my sense is that that this will not turn out to be a major issue for the U.S. healthcare system, but there’s still a lot we don’t know about MERS," Dr. Pile says. “The scope of the issue should become much clearer over the next couple of months.”
For more information on MERS, check out this CDC fact sheet.
Read physician editor Danielle Scheurer's recent blog post on the MERS situation.
Visit our website for more information about hospitalists and infectious disease care.
New SHM Board Member Ron Greeno, MD, FCCP, MHM, Sets High Bar for Health System Improvements
Ron Greeno, MD, FCCP, MHM, says he plans to bring his passion for improving the U.S. healthcare system to his new role representing the interests of hospitalists as a member of the Society of Hospital Medicine's Board of Directors.

"SHM is a nontraditional professional society in that we do believe in advocacy for members, but we also believe we're advocating for patients and the integrity of the American healthcare system," he says.
On his to-do list as an SHM board member, Dr. Greeno plans to focus on overhauling the observation status admissions system, developing solutions to fix the flawed Medicare Sustainable Growth Rate formula, and improving how the quality of patient care provided by hospitalists is measured.
As executive vice president for strategy and innovation at Brentwood, Tenn.–based Cogent Healthcare, Dr. Greeno says his enthusiasm for system improvement has only increased over the years. In his concurrent role as Chairman of SHM's Public Policy Committee, Dr. Greeno and committee members will continue to provide input on hospital management practices to such federal agencies as the Centers for Medicare & Medicaid Services and offer feedback on improving the Affordable Care Act.
SHM Board Member Brian Harte, MD, SFHM, who is treasurer of SHM's Public Policy Committee, says Dr. Greeno's passion for policy is infectious.
"Ron brings an enthusiasm to the issues that really energize the committee," Dr. Harte says. "He does a really good job facilitating an equitable discussion and reaching consensus on a position to recommend to the SHM board."
Ron Greeno, MD, FCCP, MHM, says he plans to bring his passion for improving the U.S. healthcare system to his new role representing the interests of hospitalists as a member of the Society of Hospital Medicine's Board of Directors.
"SHM is a nontraditional professional society in that we do believe in advocacy for members, but we also believe we're advocating for patients and the integrity of the American healthcare system," he says.
On his to-do list as an SHM board member, Dr. Greeno plans to focus on overhauling the observation status admissions system, developing solutions to fix the flawed Medicare Sustainable Growth Rate formula, and improving how the quality of patient care provided by hospitalists is measured.
As executive vice president for strategy and innovation at Brentwood, Tenn.–based Cogent Healthcare, Dr. Greeno says his enthusiasm for system improvement has only increased over the years. In his concurrent role as Chairman of SHM's Public Policy Committee, Dr. Greeno and committee members will continue to provide input on hospital management practices to such federal agencies as the Centers for Medicare & Medicaid Services and offer feedback on improving the Affordable Care Act.
SHM Board Member Brian Harte, MD, SFHM, who is treasurer of SHM's Public Policy Committee, says Dr. Greeno's passion for policy is infectious.
"Ron brings an enthusiasm to the issues that really energize the committee," Dr. Harte says. "He does a really good job facilitating an equitable discussion and reaching consensus on a position to recommend to the SHM board."
Ron Greeno, MD, FCCP, MHM, says he plans to bring his passion for improving the U.S. healthcare system to his new role representing the interests of hospitalists as a member of the Society of Hospital Medicine's Board of Directors.
"SHM is a nontraditional professional society in that we do believe in advocacy for members, but we also believe we're advocating for patients and the integrity of the American healthcare system," he says.
On his to-do list as an SHM board member, Dr. Greeno plans to focus on overhauling the observation status admissions system, developing solutions to fix the flawed Medicare Sustainable Growth Rate formula, and improving how the quality of patient care provided by hospitalists is measured.
As executive vice president for strategy and innovation at Brentwood, Tenn.–based Cogent Healthcare, Dr. Greeno says his enthusiasm for system improvement has only increased over the years. In his concurrent role as Chairman of SHM's Public Policy Committee, Dr. Greeno and committee members will continue to provide input on hospital management practices to such federal agencies as the Centers for Medicare & Medicaid Services and offer feedback on improving the Affordable Care Act.
SHM Board Member Brian Harte, MD, SFHM, who is treasurer of SHM's Public Policy Committee, says Dr. Greeno's passion for policy is infectious.
"Ron brings an enthusiasm to the issues that really energize the committee," Dr. Harte says. "He does a really good job facilitating an equitable discussion and reaching consensus on a position to recommend to the SHM board."
Drugs approved in 2013
In 2013, the Food and Drug Administration approved 27 new molecular entities (i.e., drugs) for human use. Because of their indications, it is unlikely that four will be used in pregnancy or lactation, so they are not discussed here. The four agents are ospemifene (Osphena), an estrogen agonist/antagonist used for severe dyspareunia; [223Ra]radium dichloride (Xofigo), for late-stage metastatic prostate cancer; conjugated estrogens/bazedoxifene (Duavee) for hot flashes associated with menopause and to prevent osteoporosis; and flutemetamol F-18 injection (Vizamyl), a radioactive diagnostic agent to aid in the evaluation of Alzheimer’s disease and dementia.
There are two other drugs that are unlikely to be used in pregnancy: macitentan (Opsumit) and riociguat (Adempas). These drugs are oral vasodilators indicated for the treatment of pulmonary hypertension. Both are teratogenic in rats and rabbits, but there are no reports of their use in human pregnancy. For female patients of reproductive potential, they are only available through restricted programs. Pregnancy must be excluded before starting therapy, monthly during treatment, and for 1 month after treatment is stopped.
The remaining 21 agents can be classified into the following categories: anticonvulsant (1), antidepressant (1), antidiabetics (2), antineoplastics (7), antihyperlipidemic (1), anti-infectives (4), diagnostics (2), immunologic (1), and respiratory (2). It is important to note that, except for two drugs (fluticasone in a combination product and dimethyl fumarate), there is no reported human pregnancy experience for these agents. Moreover, all probably cross the placenta to the embryo and/or the fetus, at least in some part of pregnancy.
Eslicarbazepine (Aptiom) is indicated as adjunctive treatment of partial-onset seizures. Developmental toxicity was observed in three animals: teratogenicity (mice), embryolethality (rats), and fetal growth restriction (rabbits). The no-effect dose was not found in two species, and was less than the human dose based on body surface area in the third. If a pregnant woman is taking this drug, she should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry by calling 888-233-2334.
Vortioxetine (Brintellix) is indicated for the treatment of major depressive disorder. The drug was not teratogenic in animals but did cause developmental delays in one species. Although the antidepressant mechanism is not fully understood, it appears to be related to the inhibition of the reuptake of serotonin (5-hydroxytryptamine). If so, vortioxetine would be closely related to the drugs in the selective serotonin reuptake inhibitor (SSRI) class: citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), fluvoxamine (Luvox), paroxetine (Paxil), sertraline (Zoloft), and vilazodone (Viibryd). The relationship could be important because the use of SSRIs or serotonin norepinephrine reuptake inhibitors (SNRIs) close to birth is related to significant toxicity in the newborn.
There are two new antidiabetic agents for the treatment of type 2 diabetes. Alogliptin (Nesina), a dipeptidyl peptidase–4 inhibitor, is in the same pharmacologic class as linagliptin (Tradjenta), saxagliptin (Onglyza), and sitagliptin (Januvia). Canagliflozin (Invokana) is a sodium-glucose cotransporter 2 inhibitor, the first drug in this class to be approved. The animal data for alogliptin suggest low risk, whereas canagliflozin caused renal toxicity in rats at exposures corresponding to the late second and third trimester in humans. Insulin remains the treatment of choice for pregnant diabetics because tight control of glucose levels is beneficial for the mother, embryo-fetus, and newborn.
The seven new antineoplastic agents are ado-trastuzumab emtansine (Kadcyla) for HER2-positive breast cancer; afatinib (Gilotrif) for non–small cell lung cancer; dabrafenib (Tafinlar) for unresectable or metastatic melanoma; ibrutinib (Imbruvica) for mantle cell lymphoma or chronic lymphocytic leukemia; obinutuzumab (Gazyva) for chronic lymphocytic leukemia; pomalidomide (Pomalyst) for multiple myeloma; and trametinib (Mekinist) for unresectable or metastatic melanoma. Only pomalidomide is contraindicated in pregnancy. Although obinutuzumab did not cause teratogenicity in monkeys, its use in the latter portion of pregnancy resulted in newborn depletion of B cells that took up to 6 months after birth to restore. Moreover, it is used in combination with chlorambucil, a known teratogen. The animal data suggest risk in the other five agents. Nevertheless, the maternal condition should determine whether any of these antineoplastics are used in a pregnant woman.
Mipomersen sodium (Kynamro) is given subcutaneously once a week as an adjunct to lipid-lowering medications. The drug caused embryo toxicity in one of three animal species.
Among the four anti-infectives are two oral agents for the treatment of chronic hepatitis C virus infection: simeprevir (Olysio) and sofosbuvir (Sovaldi). Because both agents are recommended to be combined with peginterferon alfa and ribavirin, they are classified as contraindicated in pregnancy. However, when used alone, the animal data suggest that sofosbuvir was low risk, whereas simeprevir might have higher risk.
Luliconazole (Luzu), an azole antifungal, is a cream used for the treatment of tinea pedis, tinea cruris, and tinea corporis. Systemic absorption is minimal. The animal data suggest low risk, but there are no human pregnancy reports. Nevertheless, topical use is probably compatible in pregnancy, as are the other topical azole antifungals in this pharmacologic class: clotrimazole (Lotrimin), econazole (Spectazole), ketoconazole (Kuric), miconazole (Micatin), oxiconazole (Oxistat), sertaconazole (Ertaczo), and sulconazole (Exelderm).
Dolutegravir (Tivicay) is an HIV-1 integrase strand transfer inhibitor given in combination with other antiretroviral drugs. The animal data suggest low risk. If indicated, the drug should not be withheld because of pregnancy.
Gadoterate meglumine (Dotarem), a gadolinium-based contrast agent, is indicated to detect and visualize areas with disruption of the blood brain barrier and/or abnormal vascularity. No developmental toxicity was observed in pregnant animals. Closely related diagnostic agents are gadobenate dimeglumine (MultiHance), gadodiamide (Omniscan), gadofosveset (Ablavar), gadopentetate dimeglumine (Magnevist), gadoteridol (Prohance), and gadoversetamide (OptiMARK). Although the animal data for these agents show risk, no harm has been reported in human pregnancies. However, the available human data are very limited, and the risk magnitude for embryo-fetal harm remains unknown.
Technetium (99mTc) tilmanocept (Lymphoseek) is a radioactive diagnostic agent used in patients with breast cancer or melanoma. The active ingredient is technetium (99mTc). Animal reproduction studies have not been conducted. 99mTc is probably compatible in pregnancy (see Drugs in Pregnancy and Lactation, 10th ed.; Philadelphia: Lippincott, Williams and Wilkins, 2014:1317-8; to be released in August), but the risk of the tilmanocept moiety is unknown.
The immunologic agent dimethyl fumarate (Tecfidera) is indicated for the treatment of patients with relapsing forms of multiple sclerosis. The drug caused developmental toxicity (embryolethality, impaired growth, and birth defects) in animals during all portions of pregnancy. In clinical trials, there were 38 exposed pregnancies with the following outcomes: 22 live births, 3 spontaneous abortions, 9 elective abortions, 3 ongoing pregnancies, and 1 lost to follow-up (CNS Drugs 2014;28:89-94). A pregnancy registry has been established, and patients should be encouraged to enroll by calling 800-456-2255.
Two new respiratory combination products were approved in 2013, both for chronic obstructive pulmonary disease: fluticasone/vilanterol (Breo Ellipta) and umeclidinium/vilanterol (Anoro Ellipta). Inhaled fluticasone, a corticosteroid, is compatible in pregnancy (see Drugs in Pregnancy and Lactation, 9th ed.; Philadelphia: Lippincott, Williams and Wilkins; 2011:599-601). Vilanterol is a long-acting beta2-adrenergic agonist that is probably compatible in pregnancy. The absolute bioavailability of inhaled fluticasone and vilanterol in nonpregnant adults was about 15% and 27%, respectively. The animal data for the combination or when given individually suggest low risk in pregnancy. Umeclidinium is a long-acting anticholinergic. It also is absorbed from the lung, but the amount was not specified by the manufacturer. The animal data for umeclidinium suggest low risk.
There are no reports of the above drugs being used during breastfeeding, but excretion into breast milk should be expected. The effect of these exposures on a nursing infant is unknown. However, if a mother is taking one of these drugs and breastfeeding, her infant should be monitored for adverse effects, especially those that are the most common (typically listed on the first page of the package insert) in patients taking the drug. Close monitoring is particularly important during the first 2 postpartum months. A 2003 study found that most adverse reactions in nursing infants occurred within that time period (Clin. Pediatr. 2003;42:325-40).
Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; clinical professor of pharmacy at the University of California, San Francisco; and adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation," and coeditor of "Diseases, Complications, and Drug Therapy in Obstetrics." He had no other relevant financial disclosures. Contact him at [email protected].
In 2013, the Food and Drug Administration approved 27 new molecular entities (i.e., drugs) for human use. Because of their indications, it is unlikely that four will be used in pregnancy or lactation, so they are not discussed here. The four agents are ospemifene (Osphena), an estrogen agonist/antagonist used for severe dyspareunia; [223Ra]radium dichloride (Xofigo), for late-stage metastatic prostate cancer; conjugated estrogens/bazedoxifene (Duavee) for hot flashes associated with menopause and to prevent osteoporosis; and flutemetamol F-18 injection (Vizamyl), a radioactive diagnostic agent to aid in the evaluation of Alzheimer’s disease and dementia.
There are two other drugs that are unlikely to be used in pregnancy: macitentan (Opsumit) and riociguat (Adempas). These drugs are oral vasodilators indicated for the treatment of pulmonary hypertension. Both are teratogenic in rats and rabbits, but there are no reports of their use in human pregnancy. For female patients of reproductive potential, they are only available through restricted programs. Pregnancy must be excluded before starting therapy, monthly during treatment, and for 1 month after treatment is stopped.
The remaining 21 agents can be classified into the following categories: anticonvulsant (1), antidepressant (1), antidiabetics (2), antineoplastics (7), antihyperlipidemic (1), anti-infectives (4), diagnostics (2), immunologic (1), and respiratory (2). It is important to note that, except for two drugs (fluticasone in a combination product and dimethyl fumarate), there is no reported human pregnancy experience for these agents. Moreover, all probably cross the placenta to the embryo and/or the fetus, at least in some part of pregnancy.
Eslicarbazepine (Aptiom) is indicated as adjunctive treatment of partial-onset seizures. Developmental toxicity was observed in three animals: teratogenicity (mice), embryolethality (rats), and fetal growth restriction (rabbits). The no-effect dose was not found in two species, and was less than the human dose based on body surface area in the third. If a pregnant woman is taking this drug, she should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry by calling 888-233-2334.
Vortioxetine (Brintellix) is indicated for the treatment of major depressive disorder. The drug was not teratogenic in animals but did cause developmental delays in one species. Although the antidepressant mechanism is not fully understood, it appears to be related to the inhibition of the reuptake of serotonin (5-hydroxytryptamine). If so, vortioxetine would be closely related to the drugs in the selective serotonin reuptake inhibitor (SSRI) class: citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), fluvoxamine (Luvox), paroxetine (Paxil), sertraline (Zoloft), and vilazodone (Viibryd). The relationship could be important because the use of SSRIs or serotonin norepinephrine reuptake inhibitors (SNRIs) close to birth is related to significant toxicity in the newborn.
There are two new antidiabetic agents for the treatment of type 2 diabetes. Alogliptin (Nesina), a dipeptidyl peptidase–4 inhibitor, is in the same pharmacologic class as linagliptin (Tradjenta), saxagliptin (Onglyza), and sitagliptin (Januvia). Canagliflozin (Invokana) is a sodium-glucose cotransporter 2 inhibitor, the first drug in this class to be approved. The animal data for alogliptin suggest low risk, whereas canagliflozin caused renal toxicity in rats at exposures corresponding to the late second and third trimester in humans. Insulin remains the treatment of choice for pregnant diabetics because tight control of glucose levels is beneficial for the mother, embryo-fetus, and newborn.
The seven new antineoplastic agents are ado-trastuzumab emtansine (Kadcyla) for HER2-positive breast cancer; afatinib (Gilotrif) for non–small cell lung cancer; dabrafenib (Tafinlar) for unresectable or metastatic melanoma; ibrutinib (Imbruvica) for mantle cell lymphoma or chronic lymphocytic leukemia; obinutuzumab (Gazyva) for chronic lymphocytic leukemia; pomalidomide (Pomalyst) for multiple myeloma; and trametinib (Mekinist) for unresectable or metastatic melanoma. Only pomalidomide is contraindicated in pregnancy. Although obinutuzumab did not cause teratogenicity in monkeys, its use in the latter portion of pregnancy resulted in newborn depletion of B cells that took up to 6 months after birth to restore. Moreover, it is used in combination with chlorambucil, a known teratogen. The animal data suggest risk in the other five agents. Nevertheless, the maternal condition should determine whether any of these antineoplastics are used in a pregnant woman.
Mipomersen sodium (Kynamro) is given subcutaneously once a week as an adjunct to lipid-lowering medications. The drug caused embryo toxicity in one of three animal species.
Among the four anti-infectives are two oral agents for the treatment of chronic hepatitis C virus infection: simeprevir (Olysio) and sofosbuvir (Sovaldi). Because both agents are recommended to be combined with peginterferon alfa and ribavirin, they are classified as contraindicated in pregnancy. However, when used alone, the animal data suggest that sofosbuvir was low risk, whereas simeprevir might have higher risk.
Luliconazole (Luzu), an azole antifungal, is a cream used for the treatment of tinea pedis, tinea cruris, and tinea corporis. Systemic absorption is minimal. The animal data suggest low risk, but there are no human pregnancy reports. Nevertheless, topical use is probably compatible in pregnancy, as are the other topical azole antifungals in this pharmacologic class: clotrimazole (Lotrimin), econazole (Spectazole), ketoconazole (Kuric), miconazole (Micatin), oxiconazole (Oxistat), sertaconazole (Ertaczo), and sulconazole (Exelderm).
Dolutegravir (Tivicay) is an HIV-1 integrase strand transfer inhibitor given in combination with other antiretroviral drugs. The animal data suggest low risk. If indicated, the drug should not be withheld because of pregnancy.
Gadoterate meglumine (Dotarem), a gadolinium-based contrast agent, is indicated to detect and visualize areas with disruption of the blood brain barrier and/or abnormal vascularity. No developmental toxicity was observed in pregnant animals. Closely related diagnostic agents are gadobenate dimeglumine (MultiHance), gadodiamide (Omniscan), gadofosveset (Ablavar), gadopentetate dimeglumine (Magnevist), gadoteridol (Prohance), and gadoversetamide (OptiMARK). Although the animal data for these agents show risk, no harm has been reported in human pregnancies. However, the available human data are very limited, and the risk magnitude for embryo-fetal harm remains unknown.
Technetium (99mTc) tilmanocept (Lymphoseek) is a radioactive diagnostic agent used in patients with breast cancer or melanoma. The active ingredient is technetium (99mTc). Animal reproduction studies have not been conducted. 99mTc is probably compatible in pregnancy (see Drugs in Pregnancy and Lactation, 10th ed.; Philadelphia: Lippincott, Williams and Wilkins, 2014:1317-8; to be released in August), but the risk of the tilmanocept moiety is unknown.
The immunologic agent dimethyl fumarate (Tecfidera) is indicated for the treatment of patients with relapsing forms of multiple sclerosis. The drug caused developmental toxicity (embryolethality, impaired growth, and birth defects) in animals during all portions of pregnancy. In clinical trials, there were 38 exposed pregnancies with the following outcomes: 22 live births, 3 spontaneous abortions, 9 elective abortions, 3 ongoing pregnancies, and 1 lost to follow-up (CNS Drugs 2014;28:89-94). A pregnancy registry has been established, and patients should be encouraged to enroll by calling 800-456-2255.
Two new respiratory combination products were approved in 2013, both for chronic obstructive pulmonary disease: fluticasone/vilanterol (Breo Ellipta) and umeclidinium/vilanterol (Anoro Ellipta). Inhaled fluticasone, a corticosteroid, is compatible in pregnancy (see Drugs in Pregnancy and Lactation, 9th ed.; Philadelphia: Lippincott, Williams and Wilkins; 2011:599-601). Vilanterol is a long-acting beta2-adrenergic agonist that is probably compatible in pregnancy. The absolute bioavailability of inhaled fluticasone and vilanterol in nonpregnant adults was about 15% and 27%, respectively. The animal data for the combination or when given individually suggest low risk in pregnancy. Umeclidinium is a long-acting anticholinergic. It also is absorbed from the lung, but the amount was not specified by the manufacturer. The animal data for umeclidinium suggest low risk.
There are no reports of the above drugs being used during breastfeeding, but excretion into breast milk should be expected. The effect of these exposures on a nursing infant is unknown. However, if a mother is taking one of these drugs and breastfeeding, her infant should be monitored for adverse effects, especially those that are the most common (typically listed on the first page of the package insert) in patients taking the drug. Close monitoring is particularly important during the first 2 postpartum months. A 2003 study found that most adverse reactions in nursing infants occurred within that time period (Clin. Pediatr. 2003;42:325-40).
Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; clinical professor of pharmacy at the University of California, San Francisco; and adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation," and coeditor of "Diseases, Complications, and Drug Therapy in Obstetrics." He had no other relevant financial disclosures. Contact him at [email protected].
In 2013, the Food and Drug Administration approved 27 new molecular entities (i.e., drugs) for human use. Because of their indications, it is unlikely that four will be used in pregnancy or lactation, so they are not discussed here. The four agents are ospemifene (Osphena), an estrogen agonist/antagonist used for severe dyspareunia; [223Ra]radium dichloride (Xofigo), for late-stage metastatic prostate cancer; conjugated estrogens/bazedoxifene (Duavee) for hot flashes associated with menopause and to prevent osteoporosis; and flutemetamol F-18 injection (Vizamyl), a radioactive diagnostic agent to aid in the evaluation of Alzheimer’s disease and dementia.
There are two other drugs that are unlikely to be used in pregnancy: macitentan (Opsumit) and riociguat (Adempas). These drugs are oral vasodilators indicated for the treatment of pulmonary hypertension. Both are teratogenic in rats and rabbits, but there are no reports of their use in human pregnancy. For female patients of reproductive potential, they are only available through restricted programs. Pregnancy must be excluded before starting therapy, monthly during treatment, and for 1 month after treatment is stopped.
The remaining 21 agents can be classified into the following categories: anticonvulsant (1), antidepressant (1), antidiabetics (2), antineoplastics (7), antihyperlipidemic (1), anti-infectives (4), diagnostics (2), immunologic (1), and respiratory (2). It is important to note that, except for two drugs (fluticasone in a combination product and dimethyl fumarate), there is no reported human pregnancy experience for these agents. Moreover, all probably cross the placenta to the embryo and/or the fetus, at least in some part of pregnancy.
Eslicarbazepine (Aptiom) is indicated as adjunctive treatment of partial-onset seizures. Developmental toxicity was observed in three animals: teratogenicity (mice), embryolethality (rats), and fetal growth restriction (rabbits). The no-effect dose was not found in two species, and was less than the human dose based on body surface area in the third. If a pregnant woman is taking this drug, she should be encouraged to enroll in the North American Antiepileptic Drug Pregnancy Registry by calling 888-233-2334.
Vortioxetine (Brintellix) is indicated for the treatment of major depressive disorder. The drug was not teratogenic in animals but did cause developmental delays in one species. Although the antidepressant mechanism is not fully understood, it appears to be related to the inhibition of the reuptake of serotonin (5-hydroxytryptamine). If so, vortioxetine would be closely related to the drugs in the selective serotonin reuptake inhibitor (SSRI) class: citalopram (Celexa), escitalopram (Lexapro), fluoxetine (Prozac), fluvoxamine (Luvox), paroxetine (Paxil), sertraline (Zoloft), and vilazodone (Viibryd). The relationship could be important because the use of SSRIs or serotonin norepinephrine reuptake inhibitors (SNRIs) close to birth is related to significant toxicity in the newborn.
There are two new antidiabetic agents for the treatment of type 2 diabetes. Alogliptin (Nesina), a dipeptidyl peptidase–4 inhibitor, is in the same pharmacologic class as linagliptin (Tradjenta), saxagliptin (Onglyza), and sitagliptin (Januvia). Canagliflozin (Invokana) is a sodium-glucose cotransporter 2 inhibitor, the first drug in this class to be approved. The animal data for alogliptin suggest low risk, whereas canagliflozin caused renal toxicity in rats at exposures corresponding to the late second and third trimester in humans. Insulin remains the treatment of choice for pregnant diabetics because tight control of glucose levels is beneficial for the mother, embryo-fetus, and newborn.
The seven new antineoplastic agents are ado-trastuzumab emtansine (Kadcyla) for HER2-positive breast cancer; afatinib (Gilotrif) for non–small cell lung cancer; dabrafenib (Tafinlar) for unresectable or metastatic melanoma; ibrutinib (Imbruvica) for mantle cell lymphoma or chronic lymphocytic leukemia; obinutuzumab (Gazyva) for chronic lymphocytic leukemia; pomalidomide (Pomalyst) for multiple myeloma; and trametinib (Mekinist) for unresectable or metastatic melanoma. Only pomalidomide is contraindicated in pregnancy. Although obinutuzumab did not cause teratogenicity in monkeys, its use in the latter portion of pregnancy resulted in newborn depletion of B cells that took up to 6 months after birth to restore. Moreover, it is used in combination with chlorambucil, a known teratogen. The animal data suggest risk in the other five agents. Nevertheless, the maternal condition should determine whether any of these antineoplastics are used in a pregnant woman.
Mipomersen sodium (Kynamro) is given subcutaneously once a week as an adjunct to lipid-lowering medications. The drug caused embryo toxicity in one of three animal species.
Among the four anti-infectives are two oral agents for the treatment of chronic hepatitis C virus infection: simeprevir (Olysio) and sofosbuvir (Sovaldi). Because both agents are recommended to be combined with peginterferon alfa and ribavirin, they are classified as contraindicated in pregnancy. However, when used alone, the animal data suggest that sofosbuvir was low risk, whereas simeprevir might have higher risk.
Luliconazole (Luzu), an azole antifungal, is a cream used for the treatment of tinea pedis, tinea cruris, and tinea corporis. Systemic absorption is minimal. The animal data suggest low risk, but there are no human pregnancy reports. Nevertheless, topical use is probably compatible in pregnancy, as are the other topical azole antifungals in this pharmacologic class: clotrimazole (Lotrimin), econazole (Spectazole), ketoconazole (Kuric), miconazole (Micatin), oxiconazole (Oxistat), sertaconazole (Ertaczo), and sulconazole (Exelderm).
Dolutegravir (Tivicay) is an HIV-1 integrase strand transfer inhibitor given in combination with other antiretroviral drugs. The animal data suggest low risk. If indicated, the drug should not be withheld because of pregnancy.
Gadoterate meglumine (Dotarem), a gadolinium-based contrast agent, is indicated to detect and visualize areas with disruption of the blood brain barrier and/or abnormal vascularity. No developmental toxicity was observed in pregnant animals. Closely related diagnostic agents are gadobenate dimeglumine (MultiHance), gadodiamide (Omniscan), gadofosveset (Ablavar), gadopentetate dimeglumine (Magnevist), gadoteridol (Prohance), and gadoversetamide (OptiMARK). Although the animal data for these agents show risk, no harm has been reported in human pregnancies. However, the available human data are very limited, and the risk magnitude for embryo-fetal harm remains unknown.
Technetium (99mTc) tilmanocept (Lymphoseek) is a radioactive diagnostic agent used in patients with breast cancer or melanoma. The active ingredient is technetium (99mTc). Animal reproduction studies have not been conducted. 99mTc is probably compatible in pregnancy (see Drugs in Pregnancy and Lactation, 10th ed.; Philadelphia: Lippincott, Williams and Wilkins, 2014:1317-8; to be released in August), but the risk of the tilmanocept moiety is unknown.
The immunologic agent dimethyl fumarate (Tecfidera) is indicated for the treatment of patients with relapsing forms of multiple sclerosis. The drug caused developmental toxicity (embryolethality, impaired growth, and birth defects) in animals during all portions of pregnancy. In clinical trials, there were 38 exposed pregnancies with the following outcomes: 22 live births, 3 spontaneous abortions, 9 elective abortions, 3 ongoing pregnancies, and 1 lost to follow-up (CNS Drugs 2014;28:89-94). A pregnancy registry has been established, and patients should be encouraged to enroll by calling 800-456-2255.
Two new respiratory combination products were approved in 2013, both for chronic obstructive pulmonary disease: fluticasone/vilanterol (Breo Ellipta) and umeclidinium/vilanterol (Anoro Ellipta). Inhaled fluticasone, a corticosteroid, is compatible in pregnancy (see Drugs in Pregnancy and Lactation, 9th ed.; Philadelphia: Lippincott, Williams and Wilkins; 2011:599-601). Vilanterol is a long-acting beta2-adrenergic agonist that is probably compatible in pregnancy. The absolute bioavailability of inhaled fluticasone and vilanterol in nonpregnant adults was about 15% and 27%, respectively. The animal data for the combination or when given individually suggest low risk in pregnancy. Umeclidinium is a long-acting anticholinergic. It also is absorbed from the lung, but the amount was not specified by the manufacturer. The animal data for umeclidinium suggest low risk.
There are no reports of the above drugs being used during breastfeeding, but excretion into breast milk should be expected. The effect of these exposures on a nursing infant is unknown. However, if a mother is taking one of these drugs and breastfeeding, her infant should be monitored for adverse effects, especially those that are the most common (typically listed on the first page of the package insert) in patients taking the drug. Close monitoring is particularly important during the first 2 postpartum months. A 2003 study found that most adverse reactions in nursing infants occurred within that time period (Clin. Pediatr. 2003;42:325-40).
Mr. Briggs is a pharmacist clinical specialist at the outpatient clinics of Memorial Care Center for Women at Miller Children’s Hospital in Long Beach, Calif.; clinical professor of pharmacy at the University of California, San Francisco; and adjunct professor of pharmacy at the University of Southern California, Los Angeles, and Washington State University, Spokane. He also is coauthor of "Drugs in Pregnancy and Lactation," and coeditor of "Diseases, Complications, and Drug Therapy in Obstetrics." He had no other relevant financial disclosures. Contact him at [email protected].

Team reports way to reduce sickling, SCD progression

Credit: Graham Colm
Through a series of preclinical experiments, scientists discovered they could reduce the sickling of red blood cells (RBCs) and slow the progression of sickle cell disease (SCD).
In a mouse model of SCD and blood samples from SCD patients, the researchers reduced sickling by manipulating sphingosine-1-phosphate (S1P) and sphingosine kinase 1 (SPHK1).
Yang Xia, MD, PhD, of The University of Texas Health Science Center at Houston, and colleagues described this work in The Journal of Clinical Investigation.
The scientists first discovered that S1P, a lipid enriched and stored in RBCs, is elevated in mice with SCD. Further investigation revealed that elevated SPHK1 activity underlies the increased levels of S1P and contributes to RBC sickling.
To confirm SPHK1’s role in SCD, the researchers tested 2 SPHK1 inhibitors, SK1-I and PF-543, in cells from mice with SCD. Both agents successfully inhibited SPHK1 activity and reduced S1P levels in a dose-dependent manner, but PF-543 demonstrated greater potency.
In subsequent experiments, PF-543 decreased intravascular hemolysis and reduced inflammation in mice with SCD. The treatment also decreased tissue injury and splenomegaly and increased survival in the mice.
When the scientists knocked down SPHK1 in hematopoietic stem cells (HSCs), they observed decreased sickling and reticulocytes in SCD chimeras, resulting from a reduction in S1P levels.
Knocking down SPHK1 in HSCs also decreased intravascular hemolysis, prolonged RBC life span, reduced inflammation, decreased splenomegaly and tissue injury, and increased survival in the mice.
Experiments in cells from patients with SCD showed that SPHK1 activity and S1P levels were elevated and directly contributed to sickling. So the researchers decided to evaluate how PF-543 would affect these cells.
Treating cells with PF-543 significantly inhibited hypoxia-induced SPHK1 activity and prevented the elevation of S1P in a dose-dependent manner. The treatment also significantly reduced the percentage of sickled cells in a dose-dependent manner.
Finally, the scientists found that S1P-induced sickling was independent of S1P receptor activation. S1P receptor antagonists did not inhibit hypoxia-induced sickling in cells from SCD patients. And treatment with S1P did not enhance sickling under hypoxic conditions.
“This work could lead to novel treatments for sickle cell disease,” said study author Harinder Juneja, MD, of The University of Texas Health Science Center. “The study provides a better understanding of the pathogenesis of the disease and reveals a new therapeutic target.”
Coauthor Rod Kellems, PhD, also of The University of Texas Health Science Center, added, “This research provides insight into how red blood cells work, revealing that SPHK1-mediated elevation of S1P contributes to sickling and promotes disease progression and highlights potential therapeutic opportunities for sickle cell disease.” ![]()
Credit: Graham Colm
Through a series of preclinical experiments, scientists discovered they could reduce the sickling of red blood cells (RBCs) and slow the progression of sickle cell disease (SCD).
In a mouse model of SCD and blood samples from SCD patients, the researchers reduced sickling by manipulating sphingosine-1-phosphate (S1P) and sphingosine kinase 1 (SPHK1).
Yang Xia, MD, PhD, of The University of Texas Health Science Center at Houston, and colleagues described this work in The Journal of Clinical Investigation.
The scientists first discovered that S1P, a lipid enriched and stored in RBCs, is elevated in mice with SCD. Further investigation revealed that elevated SPHK1 activity underlies the increased levels of S1P and contributes to RBC sickling.
To confirm SPHK1’s role in SCD, the researchers tested 2 SPHK1 inhibitors, SK1-I and PF-543, in cells from mice with SCD. Both agents successfully inhibited SPHK1 activity and reduced S1P levels in a dose-dependent manner, but PF-543 demonstrated greater potency.
In subsequent experiments, PF-543 decreased intravascular hemolysis and reduced inflammation in mice with SCD. The treatment also decreased tissue injury and splenomegaly and increased survival in the mice.
When the scientists knocked down SPHK1 in hematopoietic stem cells (HSCs), they observed decreased sickling and reticulocytes in SCD chimeras, resulting from a reduction in S1P levels.
Knocking down SPHK1 in HSCs also decreased intravascular hemolysis, prolonged RBC life span, reduced inflammation, decreased splenomegaly and tissue injury, and increased survival in the mice.
Experiments in cells from patients with SCD showed that SPHK1 activity and S1P levels were elevated and directly contributed to sickling. So the researchers decided to evaluate how PF-543 would affect these cells.
Treating cells with PF-543 significantly inhibited hypoxia-induced SPHK1 activity and prevented the elevation of S1P in a dose-dependent manner. The treatment also significantly reduced the percentage of sickled cells in a dose-dependent manner.
Finally, the scientists found that S1P-induced sickling was independent of S1P receptor activation. S1P receptor antagonists did not inhibit hypoxia-induced sickling in cells from SCD patients. And treatment with S1P did not enhance sickling under hypoxic conditions.
“This work could lead to novel treatments for sickle cell disease,” said study author Harinder Juneja, MD, of The University of Texas Health Science Center. “The study provides a better understanding of the pathogenesis of the disease and reveals a new therapeutic target.”
Coauthor Rod Kellems, PhD, also of The University of Texas Health Science Center, added, “This research provides insight into how red blood cells work, revealing that SPHK1-mediated elevation of S1P contributes to sickling and promotes disease progression and highlights potential therapeutic opportunities for sickle cell disease.” ![]()
Credit: Graham Colm
Through a series of preclinical experiments, scientists discovered they could reduce the sickling of red blood cells (RBCs) and slow the progression of sickle cell disease (SCD).
In a mouse model of SCD and blood samples from SCD patients, the researchers reduced sickling by manipulating sphingosine-1-phosphate (S1P) and sphingosine kinase 1 (SPHK1).
Yang Xia, MD, PhD, of The University of Texas Health Science Center at Houston, and colleagues described this work in The Journal of Clinical Investigation.
The scientists first discovered that S1P, a lipid enriched and stored in RBCs, is elevated in mice with SCD. Further investigation revealed that elevated SPHK1 activity underlies the increased levels of S1P and contributes to RBC sickling.
To confirm SPHK1’s role in SCD, the researchers tested 2 SPHK1 inhibitors, SK1-I and PF-543, in cells from mice with SCD. Both agents successfully inhibited SPHK1 activity and reduced S1P levels in a dose-dependent manner, but PF-543 demonstrated greater potency.
In subsequent experiments, PF-543 decreased intravascular hemolysis and reduced inflammation in mice with SCD. The treatment also decreased tissue injury and splenomegaly and increased survival in the mice.
When the scientists knocked down SPHK1 in hematopoietic stem cells (HSCs), they observed decreased sickling and reticulocytes in SCD chimeras, resulting from a reduction in S1P levels.
Knocking down SPHK1 in HSCs also decreased intravascular hemolysis, prolonged RBC life span, reduced inflammation, decreased splenomegaly and tissue injury, and increased survival in the mice.
Experiments in cells from patients with SCD showed that SPHK1 activity and S1P levels were elevated and directly contributed to sickling. So the researchers decided to evaluate how PF-543 would affect these cells.
Treating cells with PF-543 significantly inhibited hypoxia-induced SPHK1 activity and prevented the elevation of S1P in a dose-dependent manner. The treatment also significantly reduced the percentage of sickled cells in a dose-dependent manner.
Finally, the scientists found that S1P-induced sickling was independent of S1P receptor activation. S1P receptor antagonists did not inhibit hypoxia-induced sickling in cells from SCD patients. And treatment with S1P did not enhance sickling under hypoxic conditions.
“This work could lead to novel treatments for sickle cell disease,” said study author Harinder Juneja, MD, of The University of Texas Health Science Center. “The study provides a better understanding of the pathogenesis of the disease and reveals a new therapeutic target.”
Coauthor Rod Kellems, PhD, also of The University of Texas Health Science Center, added, “This research provides insight into how red blood cells work, revealing that SPHK1-mediated elevation of S1P contributes to sickling and promotes disease progression and highlights potential therapeutic opportunities for sickle cell disease.” ![]()
Inhibitor gets breakthrough designation for HL
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational PD-1 immune checkpoint inhibitor nivolumab to treat Hodgkin lymphoma (HL) in patients who have failed autologous stem cell transplant and treatment with brentuximab vedotin.
The FDA’s decision is based on data from a cohort of HL patients in an ongoing phase 1b study of patients with relapsed or refractory hematologic malignancies.
According to the FDA, breakthrough designation is intended to expedite the development and review of drugs for serious or life-threatening conditions.
For a treatment to receive this designation, there must be preliminary clinical evidence that demonstrates the drug may offer substantial improvement over currently available therapy on at least 1 clinically significant endpoint.
Nivolumab is an investigational agent that binds to the checkpoint receptor PD-1 expressed on activated T cells. Researchers are investigating whether, by blocking this pathway, nivolumab would enable the immune system to resume its ability to recognize, attack, and destroy cancer cells.
Nivolumab is under investigation in multiple tumor types as monotherapy or in combination with other therapies. There are 35 trials of the agent underway, in which more than 7000 patients have been enrolled.
The breakthrough designation for nivolumab in HL is based on results of a 2-part phase 1 study, which have not been made public.
The researchers planned to enroll 100 patients with relapsed or refractory hematologic malignancies on this study. For the dose-escalation portion, the team planned to treat successive cohorts of patients using a 6+3 escalation design.
Patients would receive 1 mg/kg or 3 mg/kg of intravenous nivolumab every 2 weeks (although the first dose would be followed by a 3-week evaluation period) for 2 years, with the potential for an additional year of therapy for patients who progress.
Then, the researchers would enroll 5 cohorts of 16 patients representing the following tumor sites: HL/primary mediastinal B-cell lymphoma, multiple myeloma, B-cell lymphoma, T-cell lymphoma, and chronic myelogenous leukemia.
These patients would receive nivolumab at the maximum-tolerated dose identified in the first part of the study.
A poster describing the study plan was presented at the 2013 ASCO Annual Meeting (abstract TPS3113). The study is funded by Bristol-Myers Squibb, the company developing nivolumab. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational PD-1 immune checkpoint inhibitor nivolumab to treat Hodgkin lymphoma (HL) in patients who have failed autologous stem cell transplant and treatment with brentuximab vedotin.
The FDA’s decision is based on data from a cohort of HL patients in an ongoing phase 1b study of patients with relapsed or refractory hematologic malignancies.
According to the FDA, breakthrough designation is intended to expedite the development and review of drugs for serious or life-threatening conditions.
For a treatment to receive this designation, there must be preliminary clinical evidence that demonstrates the drug may offer substantial improvement over currently available therapy on at least 1 clinically significant endpoint.
Nivolumab is an investigational agent that binds to the checkpoint receptor PD-1 expressed on activated T cells. Researchers are investigating whether, by blocking this pathway, nivolumab would enable the immune system to resume its ability to recognize, attack, and destroy cancer cells.
Nivolumab is under investigation in multiple tumor types as monotherapy or in combination with other therapies. There are 35 trials of the agent underway, in which more than 7000 patients have been enrolled.
The breakthrough designation for nivolumab in HL is based on results of a 2-part phase 1 study, which have not been made public.
The researchers planned to enroll 100 patients with relapsed or refractory hematologic malignancies on this study. For the dose-escalation portion, the team planned to treat successive cohorts of patients using a 6+3 escalation design.
Patients would receive 1 mg/kg or 3 mg/kg of intravenous nivolumab every 2 weeks (although the first dose would be followed by a 3-week evaluation period) for 2 years, with the potential for an additional year of therapy for patients who progress.
Then, the researchers would enroll 5 cohorts of 16 patients representing the following tumor sites: HL/primary mediastinal B-cell lymphoma, multiple myeloma, B-cell lymphoma, T-cell lymphoma, and chronic myelogenous leukemia.
These patients would receive nivolumab at the maximum-tolerated dose identified in the first part of the study.
A poster describing the study plan was presented at the 2013 ASCO Annual Meeting (abstract TPS3113). The study is funded by Bristol-Myers Squibb, the company developing nivolumab. ![]()
The US Food and Drug Administration (FDA) has granted breakthrough therapy designation for the investigational PD-1 immune checkpoint inhibitor nivolumab to treat Hodgkin lymphoma (HL) in patients who have failed autologous stem cell transplant and treatment with brentuximab vedotin.
The FDA’s decision is based on data from a cohort of HL patients in an ongoing phase 1b study of patients with relapsed or refractory hematologic malignancies.
According to the FDA, breakthrough designation is intended to expedite the development and review of drugs for serious or life-threatening conditions.
For a treatment to receive this designation, there must be preliminary clinical evidence that demonstrates the drug may offer substantial improvement over currently available therapy on at least 1 clinically significant endpoint.
Nivolumab is an investigational agent that binds to the checkpoint receptor PD-1 expressed on activated T cells. Researchers are investigating whether, by blocking this pathway, nivolumab would enable the immune system to resume its ability to recognize, attack, and destroy cancer cells.
Nivolumab is under investigation in multiple tumor types as monotherapy or in combination with other therapies. There are 35 trials of the agent underway, in which more than 7000 patients have been enrolled.
The breakthrough designation for nivolumab in HL is based on results of a 2-part phase 1 study, which have not been made public.
The researchers planned to enroll 100 patients with relapsed or refractory hematologic malignancies on this study. For the dose-escalation portion, the team planned to treat successive cohorts of patients using a 6+3 escalation design.
Patients would receive 1 mg/kg or 3 mg/kg of intravenous nivolumab every 2 weeks (although the first dose would be followed by a 3-week evaluation period) for 2 years, with the potential for an additional year of therapy for patients who progress.
Then, the researchers would enroll 5 cohorts of 16 patients representing the following tumor sites: HL/primary mediastinal B-cell lymphoma, multiple myeloma, B-cell lymphoma, T-cell lymphoma, and chronic myelogenous leukemia.
These patients would receive nivolumab at the maximum-tolerated dose identified in the first part of the study.
A poster describing the study plan was presented at the 2013 ASCO Annual Meeting (abstract TPS3113). The study is funded by Bristol-Myers Squibb, the company developing nivolumab. ![]()
Method can help predict utility of tPA
Credit: Lucien Monfils
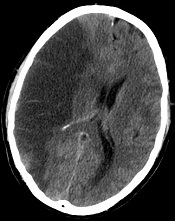
Researchers say they’ve developed a technique that can predict—with 95% accuracy—which stroke patients will benefit from tissue-type plasminogen activator (tPA) and which will suffer from intracranial hemorrhage if treated.
The team devised a method that uses standard MRI scans to measure damage to the blood-brain barrier.
If further tests confirm the method’s accuracy, the researchers say it could allow for more precise use of intravenous tPA.
“If we are able to replicate our findings in more patients, it will indicate we are able to identify which people are likely to have bad outcomes, improving the drug’s safety and also potentially allowing us to give the drug to patients who currently go untreated,” said study author Richard Leigh, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Leigh and his colleagues described their technique in Stroke.
The group’s method is a computer program that lets physicians see how much gadolinium, the contrast material injected into a patient’s vein during an MRI scan, has leaked into the brain tissue from surrounding blood vessels.
By quantifying this damage in 75 stroke patients, the researchers identified a threshold for determining how much leakage was dangerous.
Then, they applied this threshold to those 75 records to determine how well it would predict who had suffered a brain hemorrhage and who had not. The test correctly predicted the outcome with 95% accuracy.
The researchers noted that, until now, physicians haven’t been able to predict with any precision which patients are likely to suffer a drug-related bleed and which are not. In these situations, if physicians knew the extent of the damage to the blood-brain barrier, they would be able to more safely administer treatment.
Typically, physicians do a CT scan of a stroke victim to see if he or she has visible bleeding before administering tPA. Dr Leigh said his computer program, which works with an MRI scan instead, can detect subtle changes to the blood-brain barrier that are otherwise impossible to see.
If his findings hold up, Dr Leigh said, “We should probably be doing MRI scans in every stroke patient before we give tPA.”
He conceded that an MRI scan does take longer to conduct in most institutions than a CT scan. But if the benefits of getting tPA into the right patients outweigh the harms of waiting a little longer to get MRI results, physicians should consider changing their practice, according to Dr Leigh.
“If we could eliminate all intracranial hemorrhages, it would be worth it,” he said.
Dr Leigh is now analyzing data from patients who received other treatments for stroke outside the typical time window, in some cases many hours after the FDA-approved cutoff for tPA. It’s possible, he said, that some patients who come to the hospital many hours after a stroke can still benefit from tPA, the only FDA-approved treatment for ischemic stroke. ![]()
Credit: Lucien Monfils
Researchers say they’ve developed a technique that can predict—with 95% accuracy—which stroke patients will benefit from tissue-type plasminogen activator (tPA) and which will suffer from intracranial hemorrhage if treated.
The team devised a method that uses standard MRI scans to measure damage to the blood-brain barrier.
If further tests confirm the method’s accuracy, the researchers say it could allow for more precise use of intravenous tPA.
“If we are able to replicate our findings in more patients, it will indicate we are able to identify which people are likely to have bad outcomes, improving the drug’s safety and also potentially allowing us to give the drug to patients who currently go untreated,” said study author Richard Leigh, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Leigh and his colleagues described their technique in Stroke.
The group’s method is a computer program that lets physicians see how much gadolinium, the contrast material injected into a patient’s vein during an MRI scan, has leaked into the brain tissue from surrounding blood vessels.
By quantifying this damage in 75 stroke patients, the researchers identified a threshold for determining how much leakage was dangerous.
Then, they applied this threshold to those 75 records to determine how well it would predict who had suffered a brain hemorrhage and who had not. The test correctly predicted the outcome with 95% accuracy.
The researchers noted that, until now, physicians haven’t been able to predict with any precision which patients are likely to suffer a drug-related bleed and which are not. In these situations, if physicians knew the extent of the damage to the blood-brain barrier, they would be able to more safely administer treatment.
Typically, physicians do a CT scan of a stroke victim to see if he or she has visible bleeding before administering tPA. Dr Leigh said his computer program, which works with an MRI scan instead, can detect subtle changes to the blood-brain barrier that are otherwise impossible to see.
If his findings hold up, Dr Leigh said, “We should probably be doing MRI scans in every stroke patient before we give tPA.”
He conceded that an MRI scan does take longer to conduct in most institutions than a CT scan. But if the benefits of getting tPA into the right patients outweigh the harms of waiting a little longer to get MRI results, physicians should consider changing their practice, according to Dr Leigh.
“If we could eliminate all intracranial hemorrhages, it would be worth it,” he said.
Dr Leigh is now analyzing data from patients who received other treatments for stroke outside the typical time window, in some cases many hours after the FDA-approved cutoff for tPA. It’s possible, he said, that some patients who come to the hospital many hours after a stroke can still benefit from tPA, the only FDA-approved treatment for ischemic stroke. ![]()
Credit: Lucien Monfils
Researchers say they’ve developed a technique that can predict—with 95% accuracy—which stroke patients will benefit from tissue-type plasminogen activator (tPA) and which will suffer from intracranial hemorrhage if treated.
The team devised a method that uses standard MRI scans to measure damage to the blood-brain barrier.
If further tests confirm the method’s accuracy, the researchers say it could allow for more precise use of intravenous tPA.
“If we are able to replicate our findings in more patients, it will indicate we are able to identify which people are likely to have bad outcomes, improving the drug’s safety and also potentially allowing us to give the drug to patients who currently go untreated,” said study author Richard Leigh, MD, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
Dr Leigh and his colleagues described their technique in Stroke.
The group’s method is a computer program that lets physicians see how much gadolinium, the contrast material injected into a patient’s vein during an MRI scan, has leaked into the brain tissue from surrounding blood vessels.
By quantifying this damage in 75 stroke patients, the researchers identified a threshold for determining how much leakage was dangerous.
Then, they applied this threshold to those 75 records to determine how well it would predict who had suffered a brain hemorrhage and who had not. The test correctly predicted the outcome with 95% accuracy.
The researchers noted that, until now, physicians haven’t been able to predict with any precision which patients are likely to suffer a drug-related bleed and which are not. In these situations, if physicians knew the extent of the damage to the blood-brain barrier, they would be able to more safely administer treatment.
Typically, physicians do a CT scan of a stroke victim to see if he or she has visible bleeding before administering tPA. Dr Leigh said his computer program, which works with an MRI scan instead, can detect subtle changes to the blood-brain barrier that are otherwise impossible to see.
If his findings hold up, Dr Leigh said, “We should probably be doing MRI scans in every stroke patient before we give tPA.”
He conceded that an MRI scan does take longer to conduct in most institutions than a CT scan. But if the benefits of getting tPA into the right patients outweigh the harms of waiting a little longer to get MRI results, physicians should consider changing their practice, according to Dr Leigh.
“If we could eliminate all intracranial hemorrhages, it would be worth it,” he said.
Dr Leigh is now analyzing data from patients who received other treatments for stroke outside the typical time window, in some cases many hours after the FDA-approved cutoff for tPA. It’s possible, he said, that some patients who come to the hospital many hours after a stroke can still benefit from tPA, the only FDA-approved treatment for ischemic stroke. ![]()
Drug granted orphan designation for AML

The US Food and Drug Administration (FDA) has granted selinexor (KPT-330) orphan designation for the treatment of acute myeloid leukemia (AML).
Selinexor is a selective inhibitor of nuclear transport that functions by binding to the nuclear export protein XPO1 (also called CRM1).
This leads to the accumulation of tumor suppressor proteins in the cell nucleus, which is thought to cause apoptosis in cancer cells while largely sparing normal cells.
The FDA grants orphan designation to promote the development of drugs that target conditions affecting 200,000 or fewer US patients annually and are expected to provide significant therapeutic advantage over existing treatments.
Selinexor’s orphan designation qualifies the drug’s developer, Karyopharm Therapeutics, Inc., for benefits that apply across all stages of development, including an accelerated approval process, 7 years of market exclusivity following marketing approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Promising early results
Selinexor has shown promising results in a phase 1 trial of older patients with relapsed or refractory AML. The study, which was sponsored by Karyopharm, was published in Blood.
Researchers enrolled 16 patients with relapsed or refractory AML. The median age was 71 years, and the median number of prior therapeutic regimens was 2.
Patients received 8 to 10 doses of selinexor on a 4-week cycle across 2 dose levels, 16.8 mg/m2 to 23 mg/m2 (with additional cohorts ongoing).
The researchers reported no dose-limiting toxicity, no clinically significant cumulative toxicities, and no major organ dysfunction.
However, 4 patients experienced drug-related grade 3/4 adverse events, including hypotension (n=1), increased AST (n=1), hypokalemia (n=1), nausea (n=1), headache (n=1), and fatigue (n=1).
The most common grade 1/2 toxicities were nausea (9/17; 53%), anorexia (8/17; 47%), vomiting (6/17; 35%), fatigue (5/17; 29%), weight loss (5/17; 29%), and diarrhea (3/17; 18%). But these events were manageable.
Fourteen of the patients were evaluable for response. Two (14%) achieved a complete response with full hematologic recovery, and 2 (14%) achieved a complete response without hematologic recovery. Four patients (29%) had stable disease for more than 30 days, and 6 (43%) experienced progression.
Other trials of selinexor in AML
Karyopharm’s development plans for selinexor in AML include a number of additional studies.
In a phase 2 trial, researchers will evaluate selinexor monotherapy in older patients with AML. The study will enroll patients 60 years of age or older with relapsed or refractory AML who are ineligible for intensive chemotherapy and/or transplant.
In another study, researchers will evaluate selinexor in combination with decitabine for patients with relapsed, refractory, or newly diagnosed AML. The study will enroll up to 42 patients aged 60 or older who are ineligible for intensive chemotherapy.
Lastly, researchers are planning a study of selinexor in pediatric leukemia patients. The goal of this study is to determine the oral dosing, toxicity, and preliminary clinical activity of selinexor in pediatric patients. It will enroll up to 28 children with relapsed or refractory AML or acute lymphoblastic leukemia. ![]()
The US Food and Drug Administration (FDA) has granted selinexor (KPT-330) orphan designation for the treatment of acute myeloid leukemia (AML).
Selinexor is a selective inhibitor of nuclear transport that functions by binding to the nuclear export protein XPO1 (also called CRM1).
This leads to the accumulation of tumor suppressor proteins in the cell nucleus, which is thought to cause apoptosis in cancer cells while largely sparing normal cells.
The FDA grants orphan designation to promote the development of drugs that target conditions affecting 200,000 or fewer US patients annually and are expected to provide significant therapeutic advantage over existing treatments.
Selinexor’s orphan designation qualifies the drug’s developer, Karyopharm Therapeutics, Inc., for benefits that apply across all stages of development, including an accelerated approval process, 7 years of market exclusivity following marketing approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Promising early results
Selinexor has shown promising results in a phase 1 trial of older patients with relapsed or refractory AML. The study, which was sponsored by Karyopharm, was published in Blood.
Researchers enrolled 16 patients with relapsed or refractory AML. The median age was 71 years, and the median number of prior therapeutic regimens was 2.
Patients received 8 to 10 doses of selinexor on a 4-week cycle across 2 dose levels, 16.8 mg/m2 to 23 mg/m2 (with additional cohorts ongoing).
The researchers reported no dose-limiting toxicity, no clinically significant cumulative toxicities, and no major organ dysfunction.
However, 4 patients experienced drug-related grade 3/4 adverse events, including hypotension (n=1), increased AST (n=1), hypokalemia (n=1), nausea (n=1), headache (n=1), and fatigue (n=1).
The most common grade 1/2 toxicities were nausea (9/17; 53%), anorexia (8/17; 47%), vomiting (6/17; 35%), fatigue (5/17; 29%), weight loss (5/17; 29%), and diarrhea (3/17; 18%). But these events were manageable.
Fourteen of the patients were evaluable for response. Two (14%) achieved a complete response with full hematologic recovery, and 2 (14%) achieved a complete response without hematologic recovery. Four patients (29%) had stable disease for more than 30 days, and 6 (43%) experienced progression.
Other trials of selinexor in AML
Karyopharm’s development plans for selinexor in AML include a number of additional studies.
In a phase 2 trial, researchers will evaluate selinexor monotherapy in older patients with AML. The study will enroll patients 60 years of age or older with relapsed or refractory AML who are ineligible for intensive chemotherapy and/or transplant.
In another study, researchers will evaluate selinexor in combination with decitabine for patients with relapsed, refractory, or newly diagnosed AML. The study will enroll up to 42 patients aged 60 or older who are ineligible for intensive chemotherapy.
Lastly, researchers are planning a study of selinexor in pediatric leukemia patients. The goal of this study is to determine the oral dosing, toxicity, and preliminary clinical activity of selinexor in pediatric patients. It will enroll up to 28 children with relapsed or refractory AML or acute lymphoblastic leukemia. ![]()
The US Food and Drug Administration (FDA) has granted selinexor (KPT-330) orphan designation for the treatment of acute myeloid leukemia (AML).
Selinexor is a selective inhibitor of nuclear transport that functions by binding to the nuclear export protein XPO1 (also called CRM1).
This leads to the accumulation of tumor suppressor proteins in the cell nucleus, which is thought to cause apoptosis in cancer cells while largely sparing normal cells.
The FDA grants orphan designation to promote the development of drugs that target conditions affecting 200,000 or fewer US patients annually and are expected to provide significant therapeutic advantage over existing treatments.
Selinexor’s orphan designation qualifies the drug’s developer, Karyopharm Therapeutics, Inc., for benefits that apply across all stages of development, including an accelerated approval process, 7 years of market exclusivity following marketing approval, tax credits on US clinical trials, eligibility for orphan drug grants, and a waiver of certain administrative fees.
Promising early results
Selinexor has shown promising results in a phase 1 trial of older patients with relapsed or refractory AML. The study, which was sponsored by Karyopharm, was published in Blood.
Researchers enrolled 16 patients with relapsed or refractory AML. The median age was 71 years, and the median number of prior therapeutic regimens was 2.
Patients received 8 to 10 doses of selinexor on a 4-week cycle across 2 dose levels, 16.8 mg/m2 to 23 mg/m2 (with additional cohorts ongoing).
The researchers reported no dose-limiting toxicity, no clinically significant cumulative toxicities, and no major organ dysfunction.
However, 4 patients experienced drug-related grade 3/4 adverse events, including hypotension (n=1), increased AST (n=1), hypokalemia (n=1), nausea (n=1), headache (n=1), and fatigue (n=1).
The most common grade 1/2 toxicities were nausea (9/17; 53%), anorexia (8/17; 47%), vomiting (6/17; 35%), fatigue (5/17; 29%), weight loss (5/17; 29%), and diarrhea (3/17; 18%). But these events were manageable.
Fourteen of the patients were evaluable for response. Two (14%) achieved a complete response with full hematologic recovery, and 2 (14%) achieved a complete response without hematologic recovery. Four patients (29%) had stable disease for more than 30 days, and 6 (43%) experienced progression.
Other trials of selinexor in AML
Karyopharm’s development plans for selinexor in AML include a number of additional studies.
In a phase 2 trial, researchers will evaluate selinexor monotherapy in older patients with AML. The study will enroll patients 60 years of age or older with relapsed or refractory AML who are ineligible for intensive chemotherapy and/or transplant.
In another study, researchers will evaluate selinexor in combination with decitabine for patients with relapsed, refractory, or newly diagnosed AML. The study will enroll up to 42 patients aged 60 or older who are ineligible for intensive chemotherapy.
Lastly, researchers are planning a study of selinexor in pediatric leukemia patients. The goal of this study is to determine the oral dosing, toxicity, and preliminary clinical activity of selinexor in pediatric patients. It will enroll up to 28 children with relapsed or refractory AML or acute lymphoblastic leukemia. ![]()
How I am adapting my morcellation practice: Voices from across the country
Hear from:
Michael Baggish, MD (St. Helena, California)
Rupen Baxi, MD (Royal Oak, Michigan)
Jennifer Hollings, MD (Richmond, Virginia)
Gwinnett Ladson, MD (Nashville, Tennessee)
Rich Persino, MD (McHenry, Illinois)
Teresa Tam, MD (Chicago, Illinois)
Yvonne Wolny, MD (Chicago, Illinois)
Hear from:
Michael Baggish, MD (St. Helena, California)
Rupen Baxi, MD (Royal Oak, Michigan)
Jennifer Hollings, MD (Richmond, Virginia)
Gwinnett Ladson, MD (Nashville, Tennessee)
Rich Persino, MD (McHenry, Illinois)
Teresa Tam, MD (Chicago, Illinois)
Yvonne Wolny, MD (Chicago, Illinois)
Hear from:
Michael Baggish, MD (St. Helena, California)
Rupen Baxi, MD (Royal Oak, Michigan)
Jennifer Hollings, MD (Richmond, Virginia)
Gwinnett Ladson, MD (Nashville, Tennessee)
Rich Persino, MD (McHenry, Illinois)
Teresa Tam, MD (Chicago, Illinois)
Yvonne Wolny, MD (Chicago, Illinois)
The springtime eruptions
The spectrum of idiopathic ultraviolet-induced dermatoses includes the most severe variant, polymorphous light eruption (PMLE), in which erythematous papules, papulovesicles, and plaques form from a delayed type IV hypersensitivity reaction to the sun. Its milder cousins, benign summer light eruption and juvenile springtime eruption, are milder, more transient variants.
Patients may experience sudden-onset, pruritic, sometimes painful papules and papulovesicles or cheilitis within 30 minutes to several hours of exposure to UV light in areas normally covered in the winter months. The rash subsides over 1-7 days (or sooner with effective topical steroid administration and strict sun avoidance) and without scarring. Occasionally, patients experience systemic flulike symptoms after sun exposure. Triggers can be UVA, UVB, or UVC. However, because most cases appear in the spring, describing these variants as benign summer light eruption is something of a misnomer.
These seasonal rashes are often underrecognized in skin of color patients, particularly those with Fitzpatrick skin types III-VI, because many practitioners assume a protective role of melanin (Photochem. Photobiol. Sci. 2013;12:65-77). A study by Kerr and Lim identified 280 patients with photodermatoses; 135 (48%) were African American, 110 (40%) were white, and 35 (12%) were other ethnicities. They noted a significantly higher proportion of African Americans with PMLE, compared with whites (J. Am. Acad. Dermatol. 2007;57:638-43). Also, Native Americans have a hereditary form of PMLE with autosomal dominant inheritance that can involve the face and is most common in patients with Fitzpatrick skin types III-VI.
For sun-sensitive patients, and especially skin of color patients, diagnosis and treatment include ruling out other photosensitive diseases such as systemic lupus, and then counseling about the importance of sun avoidance and the use of sunscreens, which include both UVA and UVB protection. Prophylactic phototherapy or photochemotherapy at the beginning of spring for several weeks may prevent flare-ups throughout the summer. PUVA (psoralen and UVA) therapy, as well as UVB phototherapy, have been successful at preventing flares in several studies. Topical steroids, antihistamines, and oral prednisone are mainstays of treatment for severe flares, alone or in combination with phototherapy. For severe cases, or those recalcitrant to first-line treatment, antimalarials, azathioprine, and thalidomide have been used with variable efficacy.
Particularly at this time of year, I always ask patients with photo-distributed rashes about their ethnicities. One can never assume ethnicity, culture, skin type, background, or even photosensitivity based on skin color alone. I have been surprised by the many patients with dark skin who may have Native American origins who present with photosensitive rashes, or the many patients with hereditary photosensitive rashes with fair skin. Our beautiful, multicultural society makes it harder to define or categorize dermatoses by skin type alone, based on the definitions we have set for skin type in our literature today.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice at McLean (Va.) Dermatology Center. Dr. Wesley practices dermatology in Beverly Hills, Calif.
The spectrum of idiopathic ultraviolet-induced dermatoses includes the most severe variant, polymorphous light eruption (PMLE), in which erythematous papules, papulovesicles, and plaques form from a delayed type IV hypersensitivity reaction to the sun. Its milder cousins, benign summer light eruption and juvenile springtime eruption, are milder, more transient variants.
Patients may experience sudden-onset, pruritic, sometimes painful papules and papulovesicles or cheilitis within 30 minutes to several hours of exposure to UV light in areas normally covered in the winter months. The rash subsides over 1-7 days (or sooner with effective topical steroid administration and strict sun avoidance) and without scarring. Occasionally, patients experience systemic flulike symptoms after sun exposure. Triggers can be UVA, UVB, or UVC. However, because most cases appear in the spring, describing these variants as benign summer light eruption is something of a misnomer.
These seasonal rashes are often underrecognized in skin of color patients, particularly those with Fitzpatrick skin types III-VI, because many practitioners assume a protective role of melanin (Photochem. Photobiol. Sci. 2013;12:65-77). A study by Kerr and Lim identified 280 patients with photodermatoses; 135 (48%) were African American, 110 (40%) were white, and 35 (12%) were other ethnicities. They noted a significantly higher proportion of African Americans with PMLE, compared with whites (J. Am. Acad. Dermatol. 2007;57:638-43). Also, Native Americans have a hereditary form of PMLE with autosomal dominant inheritance that can involve the face and is most common in patients with Fitzpatrick skin types III-VI.
For sun-sensitive patients, and especially skin of color patients, diagnosis and treatment include ruling out other photosensitive diseases such as systemic lupus, and then counseling about the importance of sun avoidance and the use of sunscreens, which include both UVA and UVB protection. Prophylactic phototherapy or photochemotherapy at the beginning of spring for several weeks may prevent flare-ups throughout the summer. PUVA (psoralen and UVA) therapy, as well as UVB phototherapy, have been successful at preventing flares in several studies. Topical steroids, antihistamines, and oral prednisone are mainstays of treatment for severe flares, alone or in combination with phototherapy. For severe cases, or those recalcitrant to first-line treatment, antimalarials, azathioprine, and thalidomide have been used with variable efficacy.
Particularly at this time of year, I always ask patients with photo-distributed rashes about their ethnicities. One can never assume ethnicity, culture, skin type, background, or even photosensitivity based on skin color alone. I have been surprised by the many patients with dark skin who may have Native American origins who present with photosensitive rashes, or the many patients with hereditary photosensitive rashes with fair skin. Our beautiful, multicultural society makes it harder to define or categorize dermatoses by skin type alone, based on the definitions we have set for skin type in our literature today.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice at McLean (Va.) Dermatology Center. Dr. Wesley practices dermatology in Beverly Hills, Calif.
The spectrum of idiopathic ultraviolet-induced dermatoses includes the most severe variant, polymorphous light eruption (PMLE), in which erythematous papules, papulovesicles, and plaques form from a delayed type IV hypersensitivity reaction to the sun. Its milder cousins, benign summer light eruption and juvenile springtime eruption, are milder, more transient variants.
Patients may experience sudden-onset, pruritic, sometimes painful papules and papulovesicles or cheilitis within 30 minutes to several hours of exposure to UV light in areas normally covered in the winter months. The rash subsides over 1-7 days (or sooner with effective topical steroid administration and strict sun avoidance) and without scarring. Occasionally, patients experience systemic flulike symptoms after sun exposure. Triggers can be UVA, UVB, or UVC. However, because most cases appear in the spring, describing these variants as benign summer light eruption is something of a misnomer.
These seasonal rashes are often underrecognized in skin of color patients, particularly those with Fitzpatrick skin types III-VI, because many practitioners assume a protective role of melanin (Photochem. Photobiol. Sci. 2013;12:65-77). A study by Kerr and Lim identified 280 patients with photodermatoses; 135 (48%) were African American, 110 (40%) were white, and 35 (12%) were other ethnicities. They noted a significantly higher proportion of African Americans with PMLE, compared with whites (J. Am. Acad. Dermatol. 2007;57:638-43). Also, Native Americans have a hereditary form of PMLE with autosomal dominant inheritance that can involve the face and is most common in patients with Fitzpatrick skin types III-VI.
For sun-sensitive patients, and especially skin of color patients, diagnosis and treatment include ruling out other photosensitive diseases such as systemic lupus, and then counseling about the importance of sun avoidance and the use of sunscreens, which include both UVA and UVB protection. Prophylactic phototherapy or photochemotherapy at the beginning of spring for several weeks may prevent flare-ups throughout the summer. PUVA (psoralen and UVA) therapy, as well as UVB phototherapy, have been successful at preventing flares in several studies. Topical steroids, antihistamines, and oral prednisone are mainstays of treatment for severe flares, alone or in combination with phototherapy. For severe cases, or those recalcitrant to first-line treatment, antimalarials, azathioprine, and thalidomide have been used with variable efficacy.
Particularly at this time of year, I always ask patients with photo-distributed rashes about their ethnicities. One can never assume ethnicity, culture, skin type, background, or even photosensitivity based on skin color alone. I have been surprised by the many patients with dark skin who may have Native American origins who present with photosensitive rashes, or the many patients with hereditary photosensitive rashes with fair skin. Our beautiful, multicultural society makes it harder to define or categorize dermatoses by skin type alone, based on the definitions we have set for skin type in our literature today.
Dr. Talakoub and Dr. Wesley are co-contributors to a monthly Aesthetic Dermatology column in Skin & Allergy News. Dr. Talakoub is in private practice at McLean (Va.) Dermatology Center. Dr. Wesley practices dermatology in Beverly Hills, Calif.
