User login
Open thoracoabdominal aortic aneurysm repair in octogenarians: Special considerations
NEW YORK – Outcomes of thoracoabdominal aortic aneurysm (TAAA) repair in octogenarians vary considerably with the extent of repair. Those who undergo Extent II TAAA repair have significantly higher risks of morbidity and mortality, while Extent I, III, and IV repairs can be performed with relatively good outcomes, according to Dr. Muhammad Aftab, who presented the findings at the meeting sponsored by the American Association for Thoracic Surgery.
"Extensive TAAA repair should be performed with caution in octogenarians," says Dr. Aftab, a Fellow in cardiothoracic surgery at the Baylor College of Medicine–Texas Heart Institute, Houston. He recommends that a thorough preoperative discussion to assess the risks and benefits with the patient and his family is necessary before proceeding with surgery.
In this retrospective review of patients seen between January 2005 and September 2013, octogenarians with thoracoabdominal aortic aneurysms (TAAAs) (n = 88) were compared with a younger cohort (n = 1,179 patients, aged 70 years). Dr. Aftab found that octogenarians were threefold more likely to present with aneurysm rupture (13.6% vs. 4.6%; P less than .001) but less likely to present with aortic dissections (12.5% vs. 43.9%; P less than .001) than did the younger patients.
During surgery, the use of other types of adjunctive interventions, such as left heart bypass, cerebrospinal fluid drainage, cold renal perfusion, and visceral perfusion differed significantly among the octogenarians based on the extent of repair and clinical condition (all P less than .001). Because the octogenarians had a greater atherosclerotic burden and higher incidence of renal and mesenteric occlusive disease, they were also more likely to require renal/visceral endarterectomy, stenting, or both (57.9% vs. 33.6%; P less than.001).
Overall, octogenarians had higher rates of operative mortality (26.1% vs. 6.9%), in-hospital deaths (25% vs. 6.4%), 30-day deaths (13.6% vs. 4.8%), and adverse outcomes (36.4% vs. 15.7%; P less than .001) than did the younger group, all significant differences. The outcomes included significantly higher rates of permanent renal failure, cardiac complications, and pulmonary complications. The octogenarians had longer recovery times, as suggested by longer postoperative ICU and hospital stays. Spinal cord deficits and paraplegia were higher in the older group, but the difference was not significant.
Poor outcomes differed according to the extent of surgery, and seemed to be exacerbated for those who underwent repair of Extent II aneurysms (according to the Crawford Classification, these involve the subclavian artery and extend to the bifurcation of the aorta in the pelvis). For instance, the Extent II group had the highest risk of operative mortality (61.5%) vs. Extent I (31.6%), III (21.4%), and IV (10.7%), a significant difference. The Extent II group also had much higher rates of in-hospital and 30-day death rates. The most common causes of deaths for the Extent II octogenarians were multisystem organ failure and cardiac problems.
Adverse outcomes were also significantly much higher for the Extent II group (76.9%) than for the other groups (42.1%, 28.6%, and 21.4%). Similar patterns were found for permanent paraplegia, renal failure requiring permanent dialysis, stroke, and days spent in the ICU. Almost 85% of those who required Extent II repair needed renal/visceral endarterectomy, stenting, or both as a part of the surgical procedure.
Extent II TAAA repair was identified as an independent predictor of perioperative mortality by multivariate analysis, conferring an 11-fold increased risk of death. Aneurysm rupture and dissection were also identified as predictors of perioperative mortality while only Extent II TAAA and dissection were independent predictors of adverse outcomes.
While these problems were exacerbated in those with Extent II repairs, Extent I, III, and IV TAAA repairs may be performed with relatively low risk, according to Dr. Aftab. The results suggest that while octogenarians present more challenges than younger individuals, outcomes vary greatly according to the type of aneurysm repair.
Dr. Aftab had no relevant disclosures.
NEW YORK – Outcomes of thoracoabdominal aortic aneurysm (TAAA) repair in octogenarians vary considerably with the extent of repair. Those who undergo Extent II TAAA repair have significantly higher risks of morbidity and mortality, while Extent I, III, and IV repairs can be performed with relatively good outcomes, according to Dr. Muhammad Aftab, who presented the findings at the meeting sponsored by the American Association for Thoracic Surgery.
"Extensive TAAA repair should be performed with caution in octogenarians," says Dr. Aftab, a Fellow in cardiothoracic surgery at the Baylor College of Medicine–Texas Heart Institute, Houston. He recommends that a thorough preoperative discussion to assess the risks and benefits with the patient and his family is necessary before proceeding with surgery.
In this retrospective review of patients seen between January 2005 and September 2013, octogenarians with thoracoabdominal aortic aneurysms (TAAAs) (n = 88) were compared with a younger cohort (n = 1,179 patients, aged 70 years). Dr. Aftab found that octogenarians were threefold more likely to present with aneurysm rupture (13.6% vs. 4.6%; P less than .001) but less likely to present with aortic dissections (12.5% vs. 43.9%; P less than .001) than did the younger patients.
During surgery, the use of other types of adjunctive interventions, such as left heart bypass, cerebrospinal fluid drainage, cold renal perfusion, and visceral perfusion differed significantly among the octogenarians based on the extent of repair and clinical condition (all P less than .001). Because the octogenarians had a greater atherosclerotic burden and higher incidence of renal and mesenteric occlusive disease, they were also more likely to require renal/visceral endarterectomy, stenting, or both (57.9% vs. 33.6%; P less than.001).
Overall, octogenarians had higher rates of operative mortality (26.1% vs. 6.9%), in-hospital deaths (25% vs. 6.4%), 30-day deaths (13.6% vs. 4.8%), and adverse outcomes (36.4% vs. 15.7%; P less than .001) than did the younger group, all significant differences. The outcomes included significantly higher rates of permanent renal failure, cardiac complications, and pulmonary complications. The octogenarians had longer recovery times, as suggested by longer postoperative ICU and hospital stays. Spinal cord deficits and paraplegia were higher in the older group, but the difference was not significant.
Poor outcomes differed according to the extent of surgery, and seemed to be exacerbated for those who underwent repair of Extent II aneurysms (according to the Crawford Classification, these involve the subclavian artery and extend to the bifurcation of the aorta in the pelvis). For instance, the Extent II group had the highest risk of operative mortality (61.5%) vs. Extent I (31.6%), III (21.4%), and IV (10.7%), a significant difference. The Extent II group also had much higher rates of in-hospital and 30-day death rates. The most common causes of deaths for the Extent II octogenarians were multisystem organ failure and cardiac problems.
Adverse outcomes were also significantly much higher for the Extent II group (76.9%) than for the other groups (42.1%, 28.6%, and 21.4%). Similar patterns were found for permanent paraplegia, renal failure requiring permanent dialysis, stroke, and days spent in the ICU. Almost 85% of those who required Extent II repair needed renal/visceral endarterectomy, stenting, or both as a part of the surgical procedure.
Extent II TAAA repair was identified as an independent predictor of perioperative mortality by multivariate analysis, conferring an 11-fold increased risk of death. Aneurysm rupture and dissection were also identified as predictors of perioperative mortality while only Extent II TAAA and dissection were independent predictors of adverse outcomes.
While these problems were exacerbated in those with Extent II repairs, Extent I, III, and IV TAAA repairs may be performed with relatively low risk, according to Dr. Aftab. The results suggest that while octogenarians present more challenges than younger individuals, outcomes vary greatly according to the type of aneurysm repair.
Dr. Aftab had no relevant disclosures.
NEW YORK – Outcomes of thoracoabdominal aortic aneurysm (TAAA) repair in octogenarians vary considerably with the extent of repair. Those who undergo Extent II TAAA repair have significantly higher risks of morbidity and mortality, while Extent I, III, and IV repairs can be performed with relatively good outcomes, according to Dr. Muhammad Aftab, who presented the findings at the meeting sponsored by the American Association for Thoracic Surgery.
"Extensive TAAA repair should be performed with caution in octogenarians," says Dr. Aftab, a Fellow in cardiothoracic surgery at the Baylor College of Medicine–Texas Heart Institute, Houston. He recommends that a thorough preoperative discussion to assess the risks and benefits with the patient and his family is necessary before proceeding with surgery.
In this retrospective review of patients seen between January 2005 and September 2013, octogenarians with thoracoabdominal aortic aneurysms (TAAAs) (n = 88) were compared with a younger cohort (n = 1,179 patients, aged 70 years). Dr. Aftab found that octogenarians were threefold more likely to present with aneurysm rupture (13.6% vs. 4.6%; P less than .001) but less likely to present with aortic dissections (12.5% vs. 43.9%; P less than .001) than did the younger patients.
During surgery, the use of other types of adjunctive interventions, such as left heart bypass, cerebrospinal fluid drainage, cold renal perfusion, and visceral perfusion differed significantly among the octogenarians based on the extent of repair and clinical condition (all P less than .001). Because the octogenarians had a greater atherosclerotic burden and higher incidence of renal and mesenteric occlusive disease, they were also more likely to require renal/visceral endarterectomy, stenting, or both (57.9% vs. 33.6%; P less than.001).
Overall, octogenarians had higher rates of operative mortality (26.1% vs. 6.9%), in-hospital deaths (25% vs. 6.4%), 30-day deaths (13.6% vs. 4.8%), and adverse outcomes (36.4% vs. 15.7%; P less than .001) than did the younger group, all significant differences. The outcomes included significantly higher rates of permanent renal failure, cardiac complications, and pulmonary complications. The octogenarians had longer recovery times, as suggested by longer postoperative ICU and hospital stays. Spinal cord deficits and paraplegia were higher in the older group, but the difference was not significant.
Poor outcomes differed according to the extent of surgery, and seemed to be exacerbated for those who underwent repair of Extent II aneurysms (according to the Crawford Classification, these involve the subclavian artery and extend to the bifurcation of the aorta in the pelvis). For instance, the Extent II group had the highest risk of operative mortality (61.5%) vs. Extent I (31.6%), III (21.4%), and IV (10.7%), a significant difference. The Extent II group also had much higher rates of in-hospital and 30-day death rates. The most common causes of deaths for the Extent II octogenarians were multisystem organ failure and cardiac problems.
Adverse outcomes were also significantly much higher for the Extent II group (76.9%) than for the other groups (42.1%, 28.6%, and 21.4%). Similar patterns were found for permanent paraplegia, renal failure requiring permanent dialysis, stroke, and days spent in the ICU. Almost 85% of those who required Extent II repair needed renal/visceral endarterectomy, stenting, or both as a part of the surgical procedure.
Extent II TAAA repair was identified as an independent predictor of perioperative mortality by multivariate analysis, conferring an 11-fold increased risk of death. Aneurysm rupture and dissection were also identified as predictors of perioperative mortality while only Extent II TAAA and dissection were independent predictors of adverse outcomes.
While these problems were exacerbated in those with Extent II repairs, Extent I, III, and IV TAAA repairs may be performed with relatively low risk, according to Dr. Aftab. The results suggest that while octogenarians present more challenges than younger individuals, outcomes vary greatly according to the type of aneurysm repair.
Dr. Aftab had no relevant disclosures.
AT AATS AORTIC SYMPOSIUM 2014
Key clinical point: Octogenarians with TAAAs present more challenges than younger individuals and their outcomes vary greatly according to the type of aneurysm repair.
Major finding: A study that compared octogenarians with thoracoabdominal aortic aneurysms (TAAAs) to a younger cohort found that octogenarians were more at risk for aneurysm rupture, were more likely to need visceral-branch endarterectomy/stenting, had more adverse postoperative outcomes, and higher rates of operative mortality and longer postoperative ICU and hospital stays. While these problems were exacerbated in those with Extent II repairs, Extent I, III, and IV TAAA repairs can be performed with relatively low risk. Younger patients were more likely than octogenarians to present with aortic dissections.
Data source: Retrospective review.
Disclosures: Dr. Aftab had no relevant disclosures.
C difficile vaccine generates immune response
on a blood agar plate
Credit: CDC
BOSTON—Results of a phase 2 study suggest an investigational vaccine may be able to prevent Clostridium difficile infection (CDI).
The vaccine generated an immune response against C difficile toxins A and B. And adverse reactions were generally mild and of short duration.
Researchers presented these results at the 114th General Meeting of the American Society for Microbiology. The study was sponsored by Sanofi, the company developing the vaccine.
“C diff infection threatens the many people who frequently use antibiotics, as well as older hospitalized patients and residents in long-term healthcare facilities,” said study investigator Jamshid Saleh, MD of the Northern California Clinical Research Center in Redding, California.
“It would be great if we could offer patients a way to help prevent this contagious and debilitating disease versus just treating it after it happens.”
To find out if Sanofi’s vaccine would do the job, Dr Saleh and his colleagues conducted a randomized, multicenter trial split into 2 stages.
The first stage, conducted with 455 volunteers, was placebo-controlled, double-blind, and designed for dose and formulation selection. The second stage, which included 206 additional volunteers, was designed to compare the dose and formulation chosen in the first stage against 2 alternate dosing schedules.
Volunteers ranged in age from 40 to 75 years and were at risk of CDI due to impending hospitalization or residence in a long-term healthcare facility.
In stage 1, volunteers were randomized into 1 of 5 study groups: high-dose or low-dose vaccine, either with or without adjuvant, or placebo. Each formulation was administered on days 0, 7, and 30.
Researchers measured immune responses using both enzyme linked immunosorbent assay (ELISA), which assesses antitoxin A and B immunoglobulin G (IgG) concentrations, and toxin neutralization activity (TNA), which measures antitoxin A and B neutralizing activity.
Composite ELISA ranking analysis determined that the high-dose plus adjuvant vaccine formulation (group 3) generated the greatest immune response over a 60-day period. ELISA results also showed a 4-fold increase in the development of detectable antibodies for both toxins A and B.
So the researchers selected the high-dose plus adjuvant vaccine formulation for further study in stage 2 of the trial. They compared its use across 3 schedules: days 0, 7, and 30 (group 3, n=101); days 0, 7, and 180 (group 6, n=103); and days 0, 30, and 180 (group 7, n=103). The team analyzed subjects on days 0, 7, 14, 30, 60, 180, and 210.
There were increased immune responses in all vaccine groups and with each dose, according to ELISA and TNA. Overall, group 3 demonstrated the most favorable immune profile over the 30-, 60- and 180-day periods, particularly in volunteers aged 65-75 years.
The safety profile of all vaccine doses was deemed acceptable throughout the study. Reactions were monitored until day 210 and were generally grade 1, of short duration, did not lead to study discontinuation, and were not considered clinically significant.
“Sanofi Pasteur’s investigational vaccine stimulates a person’s immune system to fight C diff toxins upon exposure and, ultimately, may help prevent a future CDI from occurring,” Dr Saleh said.
“Like other toxoid vaccines—such as tetanus, diphtheria, and whooping cough—this investigational vaccine targets the symptom-causing toxins generated by C diff bacteria and could be an important public health measure to help protect individuals from CDI.”
Based on the phase 2 results, researchers started a phase 3 trial in August 2013. ![]()
on a blood agar plate
Credit: CDC
BOSTON—Results of a phase 2 study suggest an investigational vaccine may be able to prevent Clostridium difficile infection (CDI).
The vaccine generated an immune response against C difficile toxins A and B. And adverse reactions were generally mild and of short duration.
Researchers presented these results at the 114th General Meeting of the American Society for Microbiology. The study was sponsored by Sanofi, the company developing the vaccine.
“C diff infection threatens the many people who frequently use antibiotics, as well as older hospitalized patients and residents in long-term healthcare facilities,” said study investigator Jamshid Saleh, MD of the Northern California Clinical Research Center in Redding, California.
“It would be great if we could offer patients a way to help prevent this contagious and debilitating disease versus just treating it after it happens.”
To find out if Sanofi’s vaccine would do the job, Dr Saleh and his colleagues conducted a randomized, multicenter trial split into 2 stages.
The first stage, conducted with 455 volunteers, was placebo-controlled, double-blind, and designed for dose and formulation selection. The second stage, which included 206 additional volunteers, was designed to compare the dose and formulation chosen in the first stage against 2 alternate dosing schedules.
Volunteers ranged in age from 40 to 75 years and were at risk of CDI due to impending hospitalization or residence in a long-term healthcare facility.
In stage 1, volunteers were randomized into 1 of 5 study groups: high-dose or low-dose vaccine, either with or without adjuvant, or placebo. Each formulation was administered on days 0, 7, and 30.
Researchers measured immune responses using both enzyme linked immunosorbent assay (ELISA), which assesses antitoxin A and B immunoglobulin G (IgG) concentrations, and toxin neutralization activity (TNA), which measures antitoxin A and B neutralizing activity.
Composite ELISA ranking analysis determined that the high-dose plus adjuvant vaccine formulation (group 3) generated the greatest immune response over a 60-day period. ELISA results also showed a 4-fold increase in the development of detectable antibodies for both toxins A and B.
So the researchers selected the high-dose plus adjuvant vaccine formulation for further study in stage 2 of the trial. They compared its use across 3 schedules: days 0, 7, and 30 (group 3, n=101); days 0, 7, and 180 (group 6, n=103); and days 0, 30, and 180 (group 7, n=103). The team analyzed subjects on days 0, 7, 14, 30, 60, 180, and 210.
There were increased immune responses in all vaccine groups and with each dose, according to ELISA and TNA. Overall, group 3 demonstrated the most favorable immune profile over the 30-, 60- and 180-day periods, particularly in volunteers aged 65-75 years.
The safety profile of all vaccine doses was deemed acceptable throughout the study. Reactions were monitored until day 210 and were generally grade 1, of short duration, did not lead to study discontinuation, and were not considered clinically significant.
“Sanofi Pasteur’s investigational vaccine stimulates a person’s immune system to fight C diff toxins upon exposure and, ultimately, may help prevent a future CDI from occurring,” Dr Saleh said.
“Like other toxoid vaccines—such as tetanus, diphtheria, and whooping cough—this investigational vaccine targets the symptom-causing toxins generated by C diff bacteria and could be an important public health measure to help protect individuals from CDI.”
Based on the phase 2 results, researchers started a phase 3 trial in August 2013. ![]()
on a blood agar plate
Credit: CDC
BOSTON—Results of a phase 2 study suggest an investigational vaccine may be able to prevent Clostridium difficile infection (CDI).
The vaccine generated an immune response against C difficile toxins A and B. And adverse reactions were generally mild and of short duration.
Researchers presented these results at the 114th General Meeting of the American Society for Microbiology. The study was sponsored by Sanofi, the company developing the vaccine.
“C diff infection threatens the many people who frequently use antibiotics, as well as older hospitalized patients and residents in long-term healthcare facilities,” said study investigator Jamshid Saleh, MD of the Northern California Clinical Research Center in Redding, California.
“It would be great if we could offer patients a way to help prevent this contagious and debilitating disease versus just treating it after it happens.”
To find out if Sanofi’s vaccine would do the job, Dr Saleh and his colleagues conducted a randomized, multicenter trial split into 2 stages.
The first stage, conducted with 455 volunteers, was placebo-controlled, double-blind, and designed for dose and formulation selection. The second stage, which included 206 additional volunteers, was designed to compare the dose and formulation chosen in the first stage against 2 alternate dosing schedules.
Volunteers ranged in age from 40 to 75 years and were at risk of CDI due to impending hospitalization or residence in a long-term healthcare facility.
In stage 1, volunteers were randomized into 1 of 5 study groups: high-dose or low-dose vaccine, either with or without adjuvant, or placebo. Each formulation was administered on days 0, 7, and 30.
Researchers measured immune responses using both enzyme linked immunosorbent assay (ELISA), which assesses antitoxin A and B immunoglobulin G (IgG) concentrations, and toxin neutralization activity (TNA), which measures antitoxin A and B neutralizing activity.
Composite ELISA ranking analysis determined that the high-dose plus adjuvant vaccine formulation (group 3) generated the greatest immune response over a 60-day period. ELISA results also showed a 4-fold increase in the development of detectable antibodies for both toxins A and B.
So the researchers selected the high-dose plus adjuvant vaccine formulation for further study in stage 2 of the trial. They compared its use across 3 schedules: days 0, 7, and 30 (group 3, n=101); days 0, 7, and 180 (group 6, n=103); and days 0, 30, and 180 (group 7, n=103). The team analyzed subjects on days 0, 7, 14, 30, 60, 180, and 210.
There were increased immune responses in all vaccine groups and with each dose, according to ELISA and TNA. Overall, group 3 demonstrated the most favorable immune profile over the 30-, 60- and 180-day periods, particularly in volunteers aged 65-75 years.
The safety profile of all vaccine doses was deemed acceptable throughout the study. Reactions were monitored until day 210 and were generally grade 1, of short duration, did not lead to study discontinuation, and were not considered clinically significant.
“Sanofi Pasteur’s investigational vaccine stimulates a person’s immune system to fight C diff toxins upon exposure and, ultimately, may help prevent a future CDI from occurring,” Dr Saleh said.
“Like other toxoid vaccines—such as tetanus, diphtheria, and whooping cough—this investigational vaccine targets the symptom-causing toxins generated by C diff bacteria and could be an important public health measure to help protect individuals from CDI.”
Based on the phase 2 results, researchers started a phase 3 trial in August 2013. ![]()
Olive oil may protect against adverse vascular effects

SAN DIEGO—Taking olive oil supplements may counteract some of the adverse cardiovascular effects of air pollution, according to a new study.
“Exposure to airborne particulate matter can lead to endothelial dysfunction, a condition in which the endothelium of blood vessels does not function normally, which is a risk factor for clinical cardiovascular events and progression of atherosclerosis,” said Haiyan Tong,
MD, PhD, of the US Environmental Protection Agency.
“As olive oil and fish oil are known to have beneficial effects on endothelial dysfunction, we examined whether use of these supplements would counteract the adverse cardiovascular effects of exposure to concentrated ambient particulate matter in a controlled setting.”
Dr Tong and his colleagues presented their findings at the American Thoracic Society’s 2014 International Conference (abstract 55100).
Their study involved 42 healthy adults who were randomized to receive 3 g/day of olive oil, fish oil, or no supplements for 4 weeks. Subjects then underwent controlled, 2-hour exposures to filtered air, followed on the next day by exposure to fine/ultrafine concentrated ambient particulate matter (CAP, mean mass concentration 253±16 µg/m3) in a controlled-exposure chamber.
The researchers assessed endothelial function by sonographic measurement of flow-mediated dilation of the brachial artery before, immediately after, and 20 hours after exposure to air and CAP. They also measured blood markers of vasoconstriction and fibrinolysis.
Immediately after exposure to CAP, there were significant particulate matter mass-dependent reductions in flow-mediated dilation in the control group (-19.4±8.4% per 100 µg/m3 increase in CAP concentration relative to pre-filtered air levels) and the fish oil group (-13.7±5.3%), but the decrease in the olive oil group was not significant (-7.6±6.8%).
Tissue plasminogen activator increased immediately after CAP exposure in the olive oil group (11.6±5%), and this effect persisted for up to 20 hours.
Olive oil supplementation also ameliorated changes in blood markers associated with vasoconstriction and fibrinolysis, while fish oil supplementation had no effect on endothelial function or fibrinolysis after CAP exposure.
“Our study suggests that use of olive oil supplements may protect against the adverse vascular effects of exposure to air pollution particles,” Dr Tong said. “If these results are replicated in further studies, use of these supplements might offer a safe, low-cost, and effective means of counteracting some of the health consequences of exposure to air pollution.” ![]()
SAN DIEGO—Taking olive oil supplements may counteract some of the adverse cardiovascular effects of air pollution, according to a new study.
“Exposure to airborne particulate matter can lead to endothelial dysfunction, a condition in which the endothelium of blood vessels does not function normally, which is a risk factor for clinical cardiovascular events and progression of atherosclerosis,” said Haiyan Tong,
MD, PhD, of the US Environmental Protection Agency.
“As olive oil and fish oil are known to have beneficial effects on endothelial dysfunction, we examined whether use of these supplements would counteract the adverse cardiovascular effects of exposure to concentrated ambient particulate matter in a controlled setting.”
Dr Tong and his colleagues presented their findings at the American Thoracic Society’s 2014 International Conference (abstract 55100).
Their study involved 42 healthy adults who were randomized to receive 3 g/day of olive oil, fish oil, or no supplements for 4 weeks. Subjects then underwent controlled, 2-hour exposures to filtered air, followed on the next day by exposure to fine/ultrafine concentrated ambient particulate matter (CAP, mean mass concentration 253±16 µg/m3) in a controlled-exposure chamber.
The researchers assessed endothelial function by sonographic measurement of flow-mediated dilation of the brachial artery before, immediately after, and 20 hours after exposure to air and CAP. They also measured blood markers of vasoconstriction and fibrinolysis.
Immediately after exposure to CAP, there were significant particulate matter mass-dependent reductions in flow-mediated dilation in the control group (-19.4±8.4% per 100 µg/m3 increase in CAP concentration relative to pre-filtered air levels) and the fish oil group (-13.7±5.3%), but the decrease in the olive oil group was not significant (-7.6±6.8%).
Tissue plasminogen activator increased immediately after CAP exposure in the olive oil group (11.6±5%), and this effect persisted for up to 20 hours.
Olive oil supplementation also ameliorated changes in blood markers associated with vasoconstriction and fibrinolysis, while fish oil supplementation had no effect on endothelial function or fibrinolysis after CAP exposure.
“Our study suggests that use of olive oil supplements may protect against the adverse vascular effects of exposure to air pollution particles,” Dr Tong said. “If these results are replicated in further studies, use of these supplements might offer a safe, low-cost, and effective means of counteracting some of the health consequences of exposure to air pollution.” ![]()
SAN DIEGO—Taking olive oil supplements may counteract some of the adverse cardiovascular effects of air pollution, according to a new study.
“Exposure to airborne particulate matter can lead to endothelial dysfunction, a condition in which the endothelium of blood vessels does not function normally, which is a risk factor for clinical cardiovascular events and progression of atherosclerosis,” said Haiyan Tong,
MD, PhD, of the US Environmental Protection Agency.
“As olive oil and fish oil are known to have beneficial effects on endothelial dysfunction, we examined whether use of these supplements would counteract the adverse cardiovascular effects of exposure to concentrated ambient particulate matter in a controlled setting.”
Dr Tong and his colleagues presented their findings at the American Thoracic Society’s 2014 International Conference (abstract 55100).
Their study involved 42 healthy adults who were randomized to receive 3 g/day of olive oil, fish oil, or no supplements for 4 weeks. Subjects then underwent controlled, 2-hour exposures to filtered air, followed on the next day by exposure to fine/ultrafine concentrated ambient particulate matter (CAP, mean mass concentration 253±16 µg/m3) in a controlled-exposure chamber.
The researchers assessed endothelial function by sonographic measurement of flow-mediated dilation of the brachial artery before, immediately after, and 20 hours after exposure to air and CAP. They also measured blood markers of vasoconstriction and fibrinolysis.
Immediately after exposure to CAP, there were significant particulate matter mass-dependent reductions in flow-mediated dilation in the control group (-19.4±8.4% per 100 µg/m3 increase in CAP concentration relative to pre-filtered air levels) and the fish oil group (-13.7±5.3%), but the decrease in the olive oil group was not significant (-7.6±6.8%).
Tissue plasminogen activator increased immediately after CAP exposure in the olive oil group (11.6±5%), and this effect persisted for up to 20 hours.
Olive oil supplementation also ameliorated changes in blood markers associated with vasoconstriction and fibrinolysis, while fish oil supplementation had no effect on endothelial function or fibrinolysis after CAP exposure.
“Our study suggests that use of olive oil supplements may protect against the adverse vascular effects of exposure to air pollution particles,” Dr Tong said. “If these results are replicated in further studies, use of these supplements might offer a safe, low-cost, and effective means of counteracting some of the health consequences of exposure to air pollution.” ![]()
Chip may allow for early cancer detection
Institute of Photonic Sciences
Scientists say they’ve developed a lab-on-a-chip device capable of detecting protein markers for cancer.
The device can detect very low concentrations of protein markers in the blood, enabling cancer diagnosis in its earliest stages, the team says.
Romain Quidant, PhD, of The Institute of Photonic Sciences in Barcelona, Spain, and his colleagues described the device in Nano Letters.
The lab on a chip hosts 32 sensing sites distributed across a network of 8 fluidic microchannels that enables it to conduct multiple analyses.
Gold nanoparticles lie on the surface of the chip and are chemically programed with an antibody receptor in such a way that they are capable of specifically attracting the protein markers circulating in blood.
When a drop of blood is injected into the chip, it circulates through the microchannels, and, if cancer markers are present in the blood, they will stick to the nanoparticles located on the microchannels as they pass by, setting off changes in what is known as the plasmonic resonance.
The device monitors these changes, the magnitude of which is directly related to the concentration/number of markers in the patient’s blood. In this way, it provides a direct assessment of the patient’s risk of developing cancer.
“The most fascinating finding is that we are capable of detecting extremely low concentrations of this protein in a matter of minutes, making this device an ultra-high-sensitivity, state-of-the-art, powerful instrument that will benefit early detection and treatment monitoring of cancer,” Dr Quidant said. ![]()
Institute of Photonic Sciences
Scientists say they’ve developed a lab-on-a-chip device capable of detecting protein markers for cancer.
The device can detect very low concentrations of protein markers in the blood, enabling cancer diagnosis in its earliest stages, the team says.
Romain Quidant, PhD, of The Institute of Photonic Sciences in Barcelona, Spain, and his colleagues described the device in Nano Letters.
The lab on a chip hosts 32 sensing sites distributed across a network of 8 fluidic microchannels that enables it to conduct multiple analyses.
Gold nanoparticles lie on the surface of the chip and are chemically programed with an antibody receptor in such a way that they are capable of specifically attracting the protein markers circulating in blood.
When a drop of blood is injected into the chip, it circulates through the microchannels, and, if cancer markers are present in the blood, they will stick to the nanoparticles located on the microchannels as they pass by, setting off changes in what is known as the plasmonic resonance.
The device monitors these changes, the magnitude of which is directly related to the concentration/number of markers in the patient’s blood. In this way, it provides a direct assessment of the patient’s risk of developing cancer.
“The most fascinating finding is that we are capable of detecting extremely low concentrations of this protein in a matter of minutes, making this device an ultra-high-sensitivity, state-of-the-art, powerful instrument that will benefit early detection and treatment monitoring of cancer,” Dr Quidant said. ![]()
Institute of Photonic Sciences
Scientists say they’ve developed a lab-on-a-chip device capable of detecting protein markers for cancer.
The device can detect very low concentrations of protein markers in the blood, enabling cancer diagnosis in its earliest stages, the team says.
Romain Quidant, PhD, of The Institute of Photonic Sciences in Barcelona, Spain, and his colleagues described the device in Nano Letters.
The lab on a chip hosts 32 sensing sites distributed across a network of 8 fluidic microchannels that enables it to conduct multiple analyses.
Gold nanoparticles lie on the surface of the chip and are chemically programed with an antibody receptor in such a way that they are capable of specifically attracting the protein markers circulating in blood.
When a drop of blood is injected into the chip, it circulates through the microchannels, and, if cancer markers are present in the blood, they will stick to the nanoparticles located on the microchannels as they pass by, setting off changes in what is known as the plasmonic resonance.
The device monitors these changes, the magnitude of which is directly related to the concentration/number of markers in the patient’s blood. In this way, it provides a direct assessment of the patient’s risk of developing cancer.
“The most fascinating finding is that we are capable of detecting extremely low concentrations of this protein in a matter of minutes, making this device an ultra-high-sensitivity, state-of-the-art, powerful instrument that will benefit early detection and treatment monitoring of cancer,” Dr Quidant said. ![]()
CHF screening guidelines need another look, group says

patient and her father
Credit: Rhoda Baer
New research suggests a need to revisit cardiac screening guidelines for survivors of childhood cancers.
The study indicates that less frequent screening for early signs of impending congestive heart failure (CHF) may yield a similar clinical benefit as current screening recommendations.
Furthermore, some survivors might be better served by a different method of screening than the one currently used. And early treatment of patients at high risk of CHF may be beneficial.
The researchers reported these findings in the Annals of Internal Medicine.
Current CHF screening guidelines recommend that childhood cancer survivors treated with chemotherapeutic agents known to affect long-term heart health be screened as often as every year, with a schedule dependent on their level of CHF risk.
The Children’s Oncology Group (COG) recommends that survivors undergo screening by echocardiography for asymptomatic left ventricular dysfunction (ALVD). If left untreated, this clinically silent condition can progress to CHF, so clinicians typically prescribe beta blockers and ACE inhibitors to patients with signs of ALVD.
The COG recommends that patients at high risk of developing CHF be screened every year or 2 and those at low risk be screened every 2 or 5 years
“It is important to monitor survivors so we can reduce the late effects of treatment whenever possible, but we may be asking them to be tested too often, which burdens both individuals and the healthcare system,” said study author Lisa Diller, MD, of the Dana-Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts. “We think it is worthwhile to review the current CHF screening guidelines.”
To estimate the clinical benefits and cost-effectiveness of the current heart screening guidelines, Dr Diller and her colleagues constructed a computer model of a virtual cohort of 15-year-olds who had survived cancer at least 5 years.
Using data from the Childhood Cancer Survivors Study and the Framingham Heart Study, the researchers modeled the cohort’s CHF risk and clinical progression over the course of survivors’ lifetimes. Results suggested that routine screening may prevent as many as 1 in 12 cases of CHF.
The team then used Medicare data to estimate the costs and value (expressed in cost per quality-adjusted life-year [QALY]) of different screening schedules—every 1, 2, 5, or 10 years—and methods—echocardiography vs cardiac magnetic resonance imaging (cMRI)—for the different CHF risk groups.
At a cost-effectiveness threshold of $100,000/QALY, the model’s results indicated that echocardiographic screening might not be the best value for resources invested to reduce lifetime CHF risk among survivors at low risk of developing the disease.
On the other hand, the data suggested that biennial echocardiography screening may be a high-value strategy for high-risk survivors.
The simulation’s data also suggested that cMRI may be preferable to echocardiography as a screening method, with cMRI’s greater cost per test balanced by its greater sensitivity. According to the model, cMRI-based screening of low-risk survivors every 10 years and high-risk survivors every 5 years was more cost-effective than any echocardiography-based schedule.
Lastly, the data suggested it may be most beneficial to treat high-risk survivors before signs of ALVD even appear. For instance, proactively treating all high-risk patients in the virtual cohort with ACE inhibitors and beta blockers reduced their lifetime CHF risk more than if they received an echocardiograph every 2 years.
The researchers relied on simulation modeling using the best available clinical and epidemiologic data because of the logistical obstacles to conducting a prospective, randomized, clinical trial.
They said enrolling the number of survivors needed for such a study would be challenging, given how rare childhood cancers are. Yet guidance on the health benefits associated with current recommendations is needed.
“Our findings suggest that there is a long-term benefit in screening survivors at elevated risk for CHF,” said study author Jennifer Yeh, PhD, of the Harvard School of Public Health in Boston.
“Yet less frequent screening than currently recommended may be reasonable when other factors are considered. We hope these results can help inform the ongoing discussion about screening childhood cancer survivors.” ![]()
patient and her father
Credit: Rhoda Baer
New research suggests a need to revisit cardiac screening guidelines for survivors of childhood cancers.
The study indicates that less frequent screening for early signs of impending congestive heart failure (CHF) may yield a similar clinical benefit as current screening recommendations.
Furthermore, some survivors might be better served by a different method of screening than the one currently used. And early treatment of patients at high risk of CHF may be beneficial.
The researchers reported these findings in the Annals of Internal Medicine.
Current CHF screening guidelines recommend that childhood cancer survivors treated with chemotherapeutic agents known to affect long-term heart health be screened as often as every year, with a schedule dependent on their level of CHF risk.
The Children’s Oncology Group (COG) recommends that survivors undergo screening by echocardiography for asymptomatic left ventricular dysfunction (ALVD). If left untreated, this clinically silent condition can progress to CHF, so clinicians typically prescribe beta blockers and ACE inhibitors to patients with signs of ALVD.
The COG recommends that patients at high risk of developing CHF be screened every year or 2 and those at low risk be screened every 2 or 5 years
“It is important to monitor survivors so we can reduce the late effects of treatment whenever possible, but we may be asking them to be tested too often, which burdens both individuals and the healthcare system,” said study author Lisa Diller, MD, of the Dana-Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts. “We think it is worthwhile to review the current CHF screening guidelines.”
To estimate the clinical benefits and cost-effectiveness of the current heart screening guidelines, Dr Diller and her colleagues constructed a computer model of a virtual cohort of 15-year-olds who had survived cancer at least 5 years.
Using data from the Childhood Cancer Survivors Study and the Framingham Heart Study, the researchers modeled the cohort’s CHF risk and clinical progression over the course of survivors’ lifetimes. Results suggested that routine screening may prevent as many as 1 in 12 cases of CHF.
The team then used Medicare data to estimate the costs and value (expressed in cost per quality-adjusted life-year [QALY]) of different screening schedules—every 1, 2, 5, or 10 years—and methods—echocardiography vs cardiac magnetic resonance imaging (cMRI)—for the different CHF risk groups.
At a cost-effectiveness threshold of $100,000/QALY, the model’s results indicated that echocardiographic screening might not be the best value for resources invested to reduce lifetime CHF risk among survivors at low risk of developing the disease.
On the other hand, the data suggested that biennial echocardiography screening may be a high-value strategy for high-risk survivors.
The simulation’s data also suggested that cMRI may be preferable to echocardiography as a screening method, with cMRI’s greater cost per test balanced by its greater sensitivity. According to the model, cMRI-based screening of low-risk survivors every 10 years and high-risk survivors every 5 years was more cost-effective than any echocardiography-based schedule.
Lastly, the data suggested it may be most beneficial to treat high-risk survivors before signs of ALVD even appear. For instance, proactively treating all high-risk patients in the virtual cohort with ACE inhibitors and beta blockers reduced their lifetime CHF risk more than if they received an echocardiograph every 2 years.
The researchers relied on simulation modeling using the best available clinical and epidemiologic data because of the logistical obstacles to conducting a prospective, randomized, clinical trial.
They said enrolling the number of survivors needed for such a study would be challenging, given how rare childhood cancers are. Yet guidance on the health benefits associated with current recommendations is needed.
“Our findings suggest that there is a long-term benefit in screening survivors at elevated risk for CHF,” said study author Jennifer Yeh, PhD, of the Harvard School of Public Health in Boston.
“Yet less frequent screening than currently recommended may be reasonable when other factors are considered. We hope these results can help inform the ongoing discussion about screening childhood cancer survivors.” ![]()
patient and her father
Credit: Rhoda Baer
New research suggests a need to revisit cardiac screening guidelines for survivors of childhood cancers.
The study indicates that less frequent screening for early signs of impending congestive heart failure (CHF) may yield a similar clinical benefit as current screening recommendations.
Furthermore, some survivors might be better served by a different method of screening than the one currently used. And early treatment of patients at high risk of CHF may be beneficial.
The researchers reported these findings in the Annals of Internal Medicine.
Current CHF screening guidelines recommend that childhood cancer survivors treated with chemotherapeutic agents known to affect long-term heart health be screened as often as every year, with a schedule dependent on their level of CHF risk.
The Children’s Oncology Group (COG) recommends that survivors undergo screening by echocardiography for asymptomatic left ventricular dysfunction (ALVD). If left untreated, this clinically silent condition can progress to CHF, so clinicians typically prescribe beta blockers and ACE inhibitors to patients with signs of ALVD.
The COG recommends that patients at high risk of developing CHF be screened every year or 2 and those at low risk be screened every 2 or 5 years
“It is important to monitor survivors so we can reduce the late effects of treatment whenever possible, but we may be asking them to be tested too often, which burdens both individuals and the healthcare system,” said study author Lisa Diller, MD, of the Dana-Farber/Boston Children’s Cancer and Blood Disorders Center in Massachusetts. “We think it is worthwhile to review the current CHF screening guidelines.”
To estimate the clinical benefits and cost-effectiveness of the current heart screening guidelines, Dr Diller and her colleagues constructed a computer model of a virtual cohort of 15-year-olds who had survived cancer at least 5 years.
Using data from the Childhood Cancer Survivors Study and the Framingham Heart Study, the researchers modeled the cohort’s CHF risk and clinical progression over the course of survivors’ lifetimes. Results suggested that routine screening may prevent as many as 1 in 12 cases of CHF.
The team then used Medicare data to estimate the costs and value (expressed in cost per quality-adjusted life-year [QALY]) of different screening schedules—every 1, 2, 5, or 10 years—and methods—echocardiography vs cardiac magnetic resonance imaging (cMRI)—for the different CHF risk groups.
At a cost-effectiveness threshold of $100,000/QALY, the model’s results indicated that echocardiographic screening might not be the best value for resources invested to reduce lifetime CHF risk among survivors at low risk of developing the disease.
On the other hand, the data suggested that biennial echocardiography screening may be a high-value strategy for high-risk survivors.
The simulation’s data also suggested that cMRI may be preferable to echocardiography as a screening method, with cMRI’s greater cost per test balanced by its greater sensitivity. According to the model, cMRI-based screening of low-risk survivors every 10 years and high-risk survivors every 5 years was more cost-effective than any echocardiography-based schedule.
Lastly, the data suggested it may be most beneficial to treat high-risk survivors before signs of ALVD even appear. For instance, proactively treating all high-risk patients in the virtual cohort with ACE inhibitors and beta blockers reduced their lifetime CHF risk more than if they received an echocardiograph every 2 years.
The researchers relied on simulation modeling using the best available clinical and epidemiologic data because of the logistical obstacles to conducting a prospective, randomized, clinical trial.
They said enrolling the number of survivors needed for such a study would be challenging, given how rare childhood cancers are. Yet guidance on the health benefits associated with current recommendations is needed.
“Our findings suggest that there is a long-term benefit in screening survivors at elevated risk for CHF,” said study author Jennifer Yeh, PhD, of the Harvard School of Public Health in Boston.
“Yet less frequent screening than currently recommended may be reasonable when other factors are considered. We hope these results can help inform the ongoing discussion about screening childhood cancer survivors.” ![]()
Accessing Online Medical Information
Online publication of medical research continues to grow at a rapid pace, with approximately 2,000 to 4,000 new citations indexed daily by the National Library of Medicine.[1] Prior studies suggest use of web‐based applications such as Google and electronic databases may improve accuracy and efficiency in clinical decision‐making compared to accessing primary sources of medical information.[2, 3, 4] To date, however, no analyses have examined longitudinal patterns of utilization associated with these online resources. Accordingly, we sought to describe temporal trends in the online use of select sources of primary medical literature and drug information compared to UpToDate (
METHODS
We obtained data from Google Trends (Google Inc., Menlo Park, CA;
Ordinary least‐squares linear regression was used to calculate coefficients of trend for each source of online medical information, and postestimation differences across all pair‐wise combinations of coefficients were assessed using the generalized Hausman specification test. We performed locally weighted least squares regression to produce smoothed curves of each search query for graphical visualization. All analyses were performed using Stata SE 13.1 (StataCorp, College Station, TX), and all statistical tests were 2‐tailed with equal to 0.05.
RESULTS
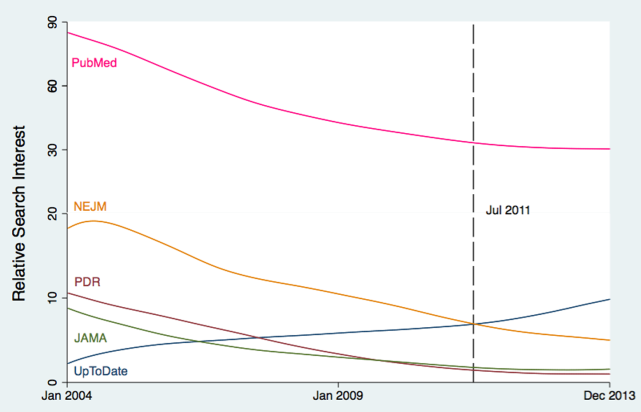
Since January 2004, relative search interest associated with UpToDate has increased steadily, whereas web‐based queries for other sources of online medical information have declined (Figure 1). Relative search interest in UpToDate has, on average, exceeded that of JAMA, NEJM, and PDR since approximately July 2011 (Figure 1), whereas PubMed has been associated with the greatest, albeit diminishing, relative search interest. Linear regression yielded the following significant (P0.001) coefficients of trend for UpToDate (coefficient=0.010), JAMA (coefficient=0.012), NEJM (coefficient=0.030), PDR (coefficient=0.020), and PubMed (coefficient=0.011). Every coefficient differed significantly from each other (P0.001).

DISCUSSION
Proliferation of medical researchin concert with expanding access to the Internethas dramatically magnified the amount and availability of medical information.[1] Our results support prior research indicating that medical information may be increasingly accessed by providers via interaction with online summary databases, rather than through electronic sources of primary medical literature or digital textbooks.[3, 6, 7]
Our study has implications for the practice of hospital‐based medicine. Our findings may reflect evolving provider preferences for synthesized medical information that can be translated efficiently to clinical practice.[8, 9] Use of summary databases may potentially lead to improved inpatient outcomes[10] by enhancing knowledge of current medical evidence, adherence to clinical guidelines, and subsequent consistency of care across providers. However, increased reliance on these resources necessitates that such databases are subject to ongoing evaluation and integration of novel research according to standardized criteria, such as those employed by the Cochrane Collaboration or the United States Preventive Services Task Force, to ensure the quality of the medical information they purport to deliver.
These results are also relevant to inpatient medical education. As summary databases are used more frequently, trainees may elect to memorize fewer medical facts and algorithms. Ideally, this transition would foster more opportunities to hone clinical reasoning skills and concentrate on delivering patient‐centered care. However, it may also create unwanted dependency on externalized expertise, which could impede the ability to critically evaluate primary medical literature, appropriately contextualize care options, and engage in real‐time problem solving.
Our study has several limitations. It is ecologic by design and cannot account for unknown secular trends. This analysis does not capture actual use or direct access of online medical resources, although we believe our observed results most likely mirror in‐person patterns of use. Additionally, because UpToDate is frequently incorporated into existing health information technology platforms (unlike journals), our results are biased conservatively. Finally, this study compares online medical information resources only, and we cannot account for concomitant use of printed/nondigital publications.
Our results signal an emergentand perhaps permanentshift in the utilization of online medical information in the United States. These trends may inform future efforts to optimize medical education and evidence‐based patient care as knowledge‐seeking behaviors continue to adapt to changes in technology and clinical demands.
- National Library of Medicine. MEDLINE factsheet. Available at: http://www.nlm.nih.gov/pubs/factsheets/medline.html. Accessed January 25, 2014.
- , , , . Speed, accuracy, and confidence in Google, Ovid, PubMed, and UpToDate: results of a randomised trial. Postgrad Med J. 2010;86:459–465.
- , , , . Should we Google it? Resource use by internal medicine residents for point‐of‐care clinical decision making. Acad Med. 2013;88:788–794.
- , , , , . A comparison of world wide web resources for identifying medical information. Acad Radiol. 2008;15:1165–1172.
- , . Predicting the present with Google Trends. Econ Rec. 2012;88:2–9.
- , , , , . Access of primary and secondary literature by health personnel in an academic health center: implications for open access. J Med Libr Assoc. 2013;101:205–212.
- , , . Public access and use health research: an exploratory study of the National Institutes of Health (NIH) public access policy using interviews and surveys of health personnel. J Med Internet Res. 2011;13:e97.
- , . Resource utilisation patterns of third‐year medical students. Clin Teach. 2011;8:43–47.
- , , , et al. A multi‐institutional survey of internal medicine residents' learning habits. Med Teach. 2010;32:773–775.
- , , . Use of UpToDate and outcomes in US hospitals. J Hosp Med. 2012;7:85–90.
Online publication of medical research continues to grow at a rapid pace, with approximately 2,000 to 4,000 new citations indexed daily by the National Library of Medicine.[1] Prior studies suggest use of web‐based applications such as Google and electronic databases may improve accuracy and efficiency in clinical decision‐making compared to accessing primary sources of medical information.[2, 3, 4] To date, however, no analyses have examined longitudinal patterns of utilization associated with these online resources. Accordingly, we sought to describe temporal trends in the online use of select sources of primary medical literature and drug information compared to UpToDate (
METHODS
We obtained data from Google Trends (Google Inc., Menlo Park, CA;
Ordinary least‐squares linear regression was used to calculate coefficients of trend for each source of online medical information, and postestimation differences across all pair‐wise combinations of coefficients were assessed using the generalized Hausman specification test. We performed locally weighted least squares regression to produce smoothed curves of each search query for graphical visualization. All analyses were performed using Stata SE 13.1 (StataCorp, College Station, TX), and all statistical tests were 2‐tailed with equal to 0.05.
RESULTS
Since January 2004, relative search interest associated with UpToDate has increased steadily, whereas web‐based queries for other sources of online medical information have declined (Figure 1). Relative search interest in UpToDate has, on average, exceeded that of JAMA, NEJM, and PDR since approximately July 2011 (Figure 1), whereas PubMed has been associated with the greatest, albeit diminishing, relative search interest. Linear regression yielded the following significant (P0.001) coefficients of trend for UpToDate (coefficient=0.010), JAMA (coefficient=0.012), NEJM (coefficient=0.030), PDR (coefficient=0.020), and PubMed (coefficient=0.011). Every coefficient differed significantly from each other (P0.001).
DISCUSSION
Proliferation of medical researchin concert with expanding access to the Internethas dramatically magnified the amount and availability of medical information.[1] Our results support prior research indicating that medical information may be increasingly accessed by providers via interaction with online summary databases, rather than through electronic sources of primary medical literature or digital textbooks.[3, 6, 7]
Our study has implications for the practice of hospital‐based medicine. Our findings may reflect evolving provider preferences for synthesized medical information that can be translated efficiently to clinical practice.[8, 9] Use of summary databases may potentially lead to improved inpatient outcomes[10] by enhancing knowledge of current medical evidence, adherence to clinical guidelines, and subsequent consistency of care across providers. However, increased reliance on these resources necessitates that such databases are subject to ongoing evaluation and integration of novel research according to standardized criteria, such as those employed by the Cochrane Collaboration or the United States Preventive Services Task Force, to ensure the quality of the medical information they purport to deliver.
These results are also relevant to inpatient medical education. As summary databases are used more frequently, trainees may elect to memorize fewer medical facts and algorithms. Ideally, this transition would foster more opportunities to hone clinical reasoning skills and concentrate on delivering patient‐centered care. However, it may also create unwanted dependency on externalized expertise, which could impede the ability to critically evaluate primary medical literature, appropriately contextualize care options, and engage in real‐time problem solving.
Our study has several limitations. It is ecologic by design and cannot account for unknown secular trends. This analysis does not capture actual use or direct access of online medical resources, although we believe our observed results most likely mirror in‐person patterns of use. Additionally, because UpToDate is frequently incorporated into existing health information technology platforms (unlike journals), our results are biased conservatively. Finally, this study compares online medical information resources only, and we cannot account for concomitant use of printed/nondigital publications.
Our results signal an emergentand perhaps permanentshift in the utilization of online medical information in the United States. These trends may inform future efforts to optimize medical education and evidence‐based patient care as knowledge‐seeking behaviors continue to adapt to changes in technology and clinical demands.
Online publication of medical research continues to grow at a rapid pace, with approximately 2,000 to 4,000 new citations indexed daily by the National Library of Medicine.[1] Prior studies suggest use of web‐based applications such as Google and electronic databases may improve accuracy and efficiency in clinical decision‐making compared to accessing primary sources of medical information.[2, 3, 4] To date, however, no analyses have examined longitudinal patterns of utilization associated with these online resources. Accordingly, we sought to describe temporal trends in the online use of select sources of primary medical literature and drug information compared to UpToDate (
METHODS
We obtained data from Google Trends (Google Inc., Menlo Park, CA;
Ordinary least‐squares linear regression was used to calculate coefficients of trend for each source of online medical information, and postestimation differences across all pair‐wise combinations of coefficients were assessed using the generalized Hausman specification test. We performed locally weighted least squares regression to produce smoothed curves of each search query for graphical visualization. All analyses were performed using Stata SE 13.1 (StataCorp, College Station, TX), and all statistical tests were 2‐tailed with equal to 0.05.
RESULTS
Since January 2004, relative search interest associated with UpToDate has increased steadily, whereas web‐based queries for other sources of online medical information have declined (Figure 1). Relative search interest in UpToDate has, on average, exceeded that of JAMA, NEJM, and PDR since approximately July 2011 (Figure 1), whereas PubMed has been associated with the greatest, albeit diminishing, relative search interest. Linear regression yielded the following significant (P0.001) coefficients of trend for UpToDate (coefficient=0.010), JAMA (coefficient=0.012), NEJM (coefficient=0.030), PDR (coefficient=0.020), and PubMed (coefficient=0.011). Every coefficient differed significantly from each other (P0.001).
DISCUSSION
Proliferation of medical researchin concert with expanding access to the Internethas dramatically magnified the amount and availability of medical information.[1] Our results support prior research indicating that medical information may be increasingly accessed by providers via interaction with online summary databases, rather than through electronic sources of primary medical literature or digital textbooks.[3, 6, 7]
Our study has implications for the practice of hospital‐based medicine. Our findings may reflect evolving provider preferences for synthesized medical information that can be translated efficiently to clinical practice.[8, 9] Use of summary databases may potentially lead to improved inpatient outcomes[10] by enhancing knowledge of current medical evidence, adherence to clinical guidelines, and subsequent consistency of care across providers. However, increased reliance on these resources necessitates that such databases are subject to ongoing evaluation and integration of novel research according to standardized criteria, such as those employed by the Cochrane Collaboration or the United States Preventive Services Task Force, to ensure the quality of the medical information they purport to deliver.
These results are also relevant to inpatient medical education. As summary databases are used more frequently, trainees may elect to memorize fewer medical facts and algorithms. Ideally, this transition would foster more opportunities to hone clinical reasoning skills and concentrate on delivering patient‐centered care. However, it may also create unwanted dependency on externalized expertise, which could impede the ability to critically evaluate primary medical literature, appropriately contextualize care options, and engage in real‐time problem solving.
Our study has several limitations. It is ecologic by design and cannot account for unknown secular trends. This analysis does not capture actual use or direct access of online medical resources, although we believe our observed results most likely mirror in‐person patterns of use. Additionally, because UpToDate is frequently incorporated into existing health information technology platforms (unlike journals), our results are biased conservatively. Finally, this study compares online medical information resources only, and we cannot account for concomitant use of printed/nondigital publications.
Our results signal an emergentand perhaps permanentshift in the utilization of online medical information in the United States. These trends may inform future efforts to optimize medical education and evidence‐based patient care as knowledge‐seeking behaviors continue to adapt to changes in technology and clinical demands.
- National Library of Medicine. MEDLINE factsheet. Available at: http://www.nlm.nih.gov/pubs/factsheets/medline.html. Accessed January 25, 2014.
- , , , . Speed, accuracy, and confidence in Google, Ovid, PubMed, and UpToDate: results of a randomised trial. Postgrad Med J. 2010;86:459–465.
- , , , . Should we Google it? Resource use by internal medicine residents for point‐of‐care clinical decision making. Acad Med. 2013;88:788–794.
- , , , , . A comparison of world wide web resources for identifying medical information. Acad Radiol. 2008;15:1165–1172.
- , . Predicting the present with Google Trends. Econ Rec. 2012;88:2–9.
- , , , , . Access of primary and secondary literature by health personnel in an academic health center: implications for open access. J Med Libr Assoc. 2013;101:205–212.
- , , . Public access and use health research: an exploratory study of the National Institutes of Health (NIH) public access policy using interviews and surveys of health personnel. J Med Internet Res. 2011;13:e97.
- , . Resource utilisation patterns of third‐year medical students. Clin Teach. 2011;8:43–47.
- , , , et al. A multi‐institutional survey of internal medicine residents' learning habits. Med Teach. 2010;32:773–775.
- , , . Use of UpToDate and outcomes in US hospitals. J Hosp Med. 2012;7:85–90.
- National Library of Medicine. MEDLINE factsheet. Available at: http://www.nlm.nih.gov/pubs/factsheets/medline.html. Accessed January 25, 2014.
- , , , . Speed, accuracy, and confidence in Google, Ovid, PubMed, and UpToDate: results of a randomised trial. Postgrad Med J. 2010;86:459–465.
- , , , . Should we Google it? Resource use by internal medicine residents for point‐of‐care clinical decision making. Acad Med. 2013;88:788–794.
- , , , , . A comparison of world wide web resources for identifying medical information. Acad Radiol. 2008;15:1165–1172.
- , . Predicting the present with Google Trends. Econ Rec. 2012;88:2–9.
- , , , , . Access of primary and secondary literature by health personnel in an academic health center: implications for open access. J Med Libr Assoc. 2013;101:205–212.
- , , . Public access and use health research: an exploratory study of the National Institutes of Health (NIH) public access policy using interviews and surveys of health personnel. J Med Internet Res. 2011;13:e97.
- , . Resource utilisation patterns of third‐year medical students. Clin Teach. 2011;8:43–47.
- , , , et al. A multi‐institutional survey of internal medicine residents' learning habits. Med Teach. 2010;32:773–775.
- , , . Use of UpToDate and outcomes in US hospitals. J Hosp Med. 2012;7:85–90.
Lobectomy suffices for surgery of small papillary thyroid cancers
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.

"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
This excellent study by Adam et al. contributes to a growing body of literature supporting thyroid lobectomy for low risk, small, differentiated thyroid tumors. I should say this represents a shift back toward lobectomy. Total thyroidectomy became the procedure of choice for nearly all differentiated thyroid tumors over the last 2-3 decades in part because of the landmark study by Bilimoria et al. (Surgery 2007;142:906-14).
Now the tide is shifting back the other direction.
I do not mean to imply that passing trends drive how we treat thyroid cancer. Mortality rates from differentiated thyroid cancer remain extremely low. This makes measuring any differences in mortality challenging. The outcome can differ depending on the cohort and the other variables included in the modeling. Recurrence is the real driver of morbidity in thyroid cancer, with anywhere from 10%-30% of patients experiencing a recurrence. Unfortunately, large national cancer registries do not capture recurrence very well.
This study controlled for many tumor features that will also impact disease specific survival apart from just the treatment received. The follow-up time is also impressive. So, if we are to undertake a more nuanced and stratified approach to determining the extent of surgery, there are a few things to consider. The first is patient selection.
In this study and in a growing body of retrospective, single institution studies looking at lobectomy for low-risk cancers, one must remember that these patients are selected based on other tumor features (multifocality, extrathyroidal extension, etc.) and not just size alone. Remember that 30%-40% of patients with papillary thyroid cancer will have multifocal disease.
The second is that successfully treating thyroid cancer patients with lobectomy requires buy-in from all parties involved - surgeons, endocrinologists, and, most importantly, the patient. Everyone must be comfortable with omitting radioactive iodine, detectable thyroglobulin levels, and following the remaining lobe with ultrasound. Some patients will not be comfortable with this and may choose to undergo total thyroidectomy. Even if we surgeons agree to shift back toward less aggressive surgery, we cannot do so in isolation.
Dr. David F. Schneider is an associate professor and the director of endocrine surgery research in the department of surgery, University of Wisconsin, Madison. He has no conflicts to disclose.
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.
"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
BOSTON – Extensive surgery beyond lobectomy offers no survival advantage for small papillary thyroid cancers, according to a large database analysis.
Total thyroidectomy was not associated with an overall survival benefit over lobectomy for papillary thyroid cancers sized 1-2 cm (hazard ratio, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21), even after adjusting for multiple patient and pathologic factors.
"Despite guidelines, our results call into question whether tumor size 1-4 cm should be an absolute determinant for extent of surgery," Dr. Mohamed Abdelgadir Adam said at the annual meeting of the American Surgical Association.
Current American Thyroid Association guidelines recommend lobectomy for tumors less than 1 cm in size and total thyroidectomy for those exceeding 1 cm.
"Using total thyroidectomy based on tumor size alone may unnecessarily subject patients to increased risks of complications without a survival benefit," he said. "In addition to tumor size up to 4 cm, other factors are important for determining extent of surgery such as nodal and distant metastases and patient preference."
The extent of surgery for papillary thyroid cancer, however, remains controversial. Recent analyses (Arch. Otolaryngol. Head Neck Surg. 2010;136:1055-61) have shown no survival difference between lobectomy and total thyroidectomy, while an earlier landmark study found improved overall survival with total thyroidectomy for tumors 1 cm or more (Ann. Surg. 2007;246;375-81). The latter study, however, has been criticized because it did not take into account patient comorbidities, multifocality, extrathyroidal extension, or completeness of resection, said Dr. Adam of Duke University School of Medicine, Durham, N.C.
The current analysis adjusted for age, gender, race, annual income, insurance status, hospital volume, patient comorbidities, tumor multifocality, extrathyroidal extension, lymph node involvement, metastases, surgical margins, and radioactive iodine ablation.
Discussant Dr. Blake Cady, professor emeritus of surgery at Harvard Medical School and Massachusetts General Hospital in Boston, said the current report is an important contribution to the controversy. It also supports his own bias against overtreatment of these mostly young patients with total thyroidectomy, which necessitates long-term medication and is accompanied by almost routine use of radioactive iodine, despite no evidence it improves outcomes in low-risk patients.
"In no other human cancer with a 99% 20-year survival is a policy of routine total primary organ removal practiced and routine systemic therapy used," he said. "Therefore, this report may help to scale back toward a more measured balance between treatment and morbidity."
Study coauthor Dr. Julie Ann Sosa, chief of endocrine surgery at Duke, challenged the audience to promote the growing body of evidence supporting equivalence in overall survival, such as a recent study described as coming the closest to a head-to-head comparison and having the longest follow-up at 18 years. It showed equivalence between lobectomy, without radioactive iodine, and total thyroidectomy for overall, progression-free, and disease-specific survival and risk of recurrence in tumors 40 mm or less (World J. Surg. 2014;38:68-79.
"In light of these data, I think it is probably high time for guidelines to potentially reconsider this issue," she said, noting that the American Thyroid Association will issue new guidelines later this spring or summer.
Dr. Sosa also advocated for "a more sophisticated approach" to preoperative evaluation and risk stratification for papillary thyroid cancer that distinguishes between low-, medium-, and high-risk tumors. The Duke study did not exclude most high-risk tumors, but rather adjusted for high-risk characteristics such as extrathyroidal extension, lymph node involvement, and distant metastases.
"When you adjust for these high-risk characteristics, the afforded overall survival benefit disappears," she said. "So what I think we would argue is that there is equivalence in outcome for the majority of patients for low- and medium-risk tumors. But for those patients who have high-risk tumors, as defined by some of these high-risk characteristics, then I think all of us would agree that total thyroidectomy, with or without radioactive iodine, would be indicated."
The study involved 61,775 patients in the National Cancer Database who underwent total thyroidectomy (n = 54,926) or lobectomy with or without isthmusectomy (n = 6,849) for papillary thyroid cancer from 1998 to 2006. Compared with the lobectomy group, the thyroidectomy group had more tumor multifocality (44% vs. 29%), positive surgical margins (27% vs. 7%), distant metastases (1% vs. 0.4%), and radioactive iodine (65% vs. 33%; P value less than .01 for all).
In multivariable analysis, nodal and distant metastases were associated with compromised survival, Dr. Adam said.
The complete manuscript of this study and its presentation at the American Surgical Association’s 134th Annual Meeting, April 2014 in Boston, is anticipated to be published in the Annals of Surgery, pending editorial review.
The authors reported no conflicting interests
AT THE ASA ANNUAL MEETING
Major finding: After adjustment, total thyroidectomy did not improve overall survival over lobectomy for tumors 1-2 cm (HR, 1.05; P = .61) or 2.1-4.0 cm (HR, 0.89; P = .21).
Data source: A retrospective database analysis of 61,775 papillary thyroid cancers.
Disclosures: The authors reported no conflicting interests.

Test detects PE with greater specificity than D-dimer

Credit: Andre E.X. Brown
SAN DIEGO—New research suggests a urine test can be used to detect a pulmonary embolism (PE), providing similar sensitivity and greater specificity than the D-dimer test.
The urine test measures levels of fibrinopeptide B (FPB), a peptide released when a thrombus forms.
“The urine FPB test offers advantages over other screening methods because it doesn’t require blood to be drawn, and it can provide more accurate results than the D-dimer test,” said Timothy Fernandes, MD, of the University of California, San Diego.
Dr Fernandes and his colleagues presented results observed with the FPB test at the American Thoracic Society’s 2014 International Conference (abstract 53841).
The researchers tested samples taken from 344 patients who participated in the Pulmonary Embolism Diagnosis Study (PEDS), a multicenter study of patients considered likely to have an acute PE. Sixty-one of these patients (18%) had a confirmed PE, and 283 (83%) did not.
For all urine samples, the researchers measured the FPB concentration and evaluated the sensitivity and specificity of the test at various cut-off points in relation to its ability to predict the presence of PE.
The team found that, at concentrations of 2.5 ng/mL, urine FPB demonstrated sensitivity comparable to previously published values for plasma latex and whole-blood D-dimer levels, but with greater specificity.
Specifically, at a threshold of 2.5 ng/mL, urine FPB could predict PE with sensitivity of 75.4%, specificity of 28.9%, and a negative likelihood ratio of 0.18. Sensitivity was lower at thresholds of 5 ng/mL and 7.5 ng/mL, at 55.7% and 42.6%, respectively.
The researchers noted that the FPB test has the potential for greater specificity than the D-dimer test because FPB can reflect ongoing clot activity, while D-dimer can only be measured once a thrombus has already become degraded.
“The results of our study indicate that urine FPB tests may be a useful complement to current biomarkers such as D-dimer to measure for the
presence and activity of venous thromboembolism,” Dr Fernandes said.
He and his colleagues are now planning to develop a urine dipstick test for FBP. The patent for the urine FPB test is held by the University of California Board of Regents.
The researchers are also planning studies to assess urine FPB in other settings where D-dimer is used, including the use of urine FPB after anticoagulation to determine the risk of recurrent venous thromboembolism. ![]()
Credit: Andre E.X. Brown
SAN DIEGO—New research suggests a urine test can be used to detect a pulmonary embolism (PE), providing similar sensitivity and greater specificity than the D-dimer test.
The urine test measures levels of fibrinopeptide B (FPB), a peptide released when a thrombus forms.
“The urine FPB test offers advantages over other screening methods because it doesn’t require blood to be drawn, and it can provide more accurate results than the D-dimer test,” said Timothy Fernandes, MD, of the University of California, San Diego.
Dr Fernandes and his colleagues presented results observed with the FPB test at the American Thoracic Society’s 2014 International Conference (abstract 53841).
The researchers tested samples taken from 344 patients who participated in the Pulmonary Embolism Diagnosis Study (PEDS), a multicenter study of patients considered likely to have an acute PE. Sixty-one of these patients (18%) had a confirmed PE, and 283 (83%) did not.
For all urine samples, the researchers measured the FPB concentration and evaluated the sensitivity and specificity of the test at various cut-off points in relation to its ability to predict the presence of PE.
The team found that, at concentrations of 2.5 ng/mL, urine FPB demonstrated sensitivity comparable to previously published values for plasma latex and whole-blood D-dimer levels, but with greater specificity.
Specifically, at a threshold of 2.5 ng/mL, urine FPB could predict PE with sensitivity of 75.4%, specificity of 28.9%, and a negative likelihood ratio of 0.18. Sensitivity was lower at thresholds of 5 ng/mL and 7.5 ng/mL, at 55.7% and 42.6%, respectively.
The researchers noted that the FPB test has the potential for greater specificity than the D-dimer test because FPB can reflect ongoing clot activity, while D-dimer can only be measured once a thrombus has already become degraded.
“The results of our study indicate that urine FPB tests may be a useful complement to current biomarkers such as D-dimer to measure for the
presence and activity of venous thromboembolism,” Dr Fernandes said.
He and his colleagues are now planning to develop a urine dipstick test for FBP. The patent for the urine FPB test is held by the University of California Board of Regents.
The researchers are also planning studies to assess urine FPB in other settings where D-dimer is used, including the use of urine FPB after anticoagulation to determine the risk of recurrent venous thromboembolism. ![]()
Credit: Andre E.X. Brown
SAN DIEGO—New research suggests a urine test can be used to detect a pulmonary embolism (PE), providing similar sensitivity and greater specificity than the D-dimer test.
The urine test measures levels of fibrinopeptide B (FPB), a peptide released when a thrombus forms.
“The urine FPB test offers advantages over other screening methods because it doesn’t require blood to be drawn, and it can provide more accurate results than the D-dimer test,” said Timothy Fernandes, MD, of the University of California, San Diego.
Dr Fernandes and his colleagues presented results observed with the FPB test at the American Thoracic Society’s 2014 International Conference (abstract 53841).
The researchers tested samples taken from 344 patients who participated in the Pulmonary Embolism Diagnosis Study (PEDS), a multicenter study of patients considered likely to have an acute PE. Sixty-one of these patients (18%) had a confirmed PE, and 283 (83%) did not.
For all urine samples, the researchers measured the FPB concentration and evaluated the sensitivity and specificity of the test at various cut-off points in relation to its ability to predict the presence of PE.
The team found that, at concentrations of 2.5 ng/mL, urine FPB demonstrated sensitivity comparable to previously published values for plasma latex and whole-blood D-dimer levels, but with greater specificity.
Specifically, at a threshold of 2.5 ng/mL, urine FPB could predict PE with sensitivity of 75.4%, specificity of 28.9%, and a negative likelihood ratio of 0.18. Sensitivity was lower at thresholds of 5 ng/mL and 7.5 ng/mL, at 55.7% and 42.6%, respectively.
The researchers noted that the FPB test has the potential for greater specificity than the D-dimer test because FPB can reflect ongoing clot activity, while D-dimer can only be measured once a thrombus has already become degraded.
“The results of our study indicate that urine FPB tests may be a useful complement to current biomarkers such as D-dimer to measure for the
presence and activity of venous thromboembolism,” Dr Fernandes said.
He and his colleagues are now planning to develop a urine dipstick test for FBP. The patent for the urine FPB test is held by the University of California Board of Regents.
The researchers are also planning studies to assess urine FPB in other settings where D-dimer is used, including the use of urine FPB after anticoagulation to determine the risk of recurrent venous thromboembolism. ![]()
Team unearths surprising sepsis finding

Credit: NHLBI
SAN DIEGO—Results of a retrospective study suggest sepsis may contribute to as many as half of all hospital deaths in the US.
Researchers analyzed information from 6.5 million hospital discharge records and found that, of all hospital deaths, as many as 52% occurred in patients with sepsis.
“We were surprised to find that as many as 1 in 2 patients dying in US hospitals had sepsis,” said Vincent Liu, MD, of the Kaiser Permanente Northern California Division of Research.
He and his colleagues presented this finding at the American Thoracic Society’s 2014 International Conference (abstract 50626). The results have also been published in JAMA.
The researchers analyzed data from 6.5 million hospital discharge records derived from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample (NIS) in 2010. The NIS is the largest publicly available, all-payer inpatient database in the US, containing data from 100% of hospital discharges from a stratified sample of 1051 community hospitals.
The team also evaluated records for 482,828 adult patients admitted to 21 Kaiser Permanente Northern California (KPNC) hospitals.
Using diagnosis and procedure codes, the researchers identified hospital admissions and deaths of patients with sepsis and estimated the percentage of total hospital charges associated with sepsis hospitalizations.
They used 2 approaches to identify patients with sepsis from International Statistical Classification of Diseases, Ninth Revision, Clinical Modification codes. The explicit approach identified patients with codes 038 (septicemia), 995.91 (sepsis), 995.92 (severe sepsis), or 785.52 (septic shock). The team also used an implicit approach, which included patients with evidence of both infection and acute organ failure.
In the NIS cohort, there were 280,663 explicit and 717,718 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 4.3% (explicit) to 10.9% (implicit) of all hospitalizations.
There were 143,312 deaths in the NIS cohort, and 34.7% (explicit) to 52.0% (implicit) occurred among patients with sepsis.
In the KPNC cohort, there were 55,008 explicit and 80,678 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 11.4% (explicit) to 16.7% (implicit) of all hospitalizations.
There were 14,206 inpatient deaths in this cohort, and 36.9% (explicit) to 55.9% (implicit) occurred among patients with sepsis.
“[W]e found that most patients already had sepsis at the time of hospital admission,” Dr Liu said. “There was also a large number of patients with less severe sepsis, a group for whom treatment guidelines are less well-defined. The results of our study suggest that improved care for sepsis patients of all severity levels and in all hospital settings could result in many future lives saved.” ![]()
Credit: NHLBI
SAN DIEGO—Results of a retrospective study suggest sepsis may contribute to as many as half of all hospital deaths in the US.
Researchers analyzed information from 6.5 million hospital discharge records and found that, of all hospital deaths, as many as 52% occurred in patients with sepsis.
“We were surprised to find that as many as 1 in 2 patients dying in US hospitals had sepsis,” said Vincent Liu, MD, of the Kaiser Permanente Northern California Division of Research.
He and his colleagues presented this finding at the American Thoracic Society’s 2014 International Conference (abstract 50626). The results have also been published in JAMA.
The researchers analyzed data from 6.5 million hospital discharge records derived from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample (NIS) in 2010. The NIS is the largest publicly available, all-payer inpatient database in the US, containing data from 100% of hospital discharges from a stratified sample of 1051 community hospitals.
The team also evaluated records for 482,828 adult patients admitted to 21 Kaiser Permanente Northern California (KPNC) hospitals.
Using diagnosis and procedure codes, the researchers identified hospital admissions and deaths of patients with sepsis and estimated the percentage of total hospital charges associated with sepsis hospitalizations.
They used 2 approaches to identify patients with sepsis from International Statistical Classification of Diseases, Ninth Revision, Clinical Modification codes. The explicit approach identified patients with codes 038 (septicemia), 995.91 (sepsis), 995.92 (severe sepsis), or 785.52 (septic shock). The team also used an implicit approach, which included patients with evidence of both infection and acute organ failure.
In the NIS cohort, there were 280,663 explicit and 717,718 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 4.3% (explicit) to 10.9% (implicit) of all hospitalizations.
There were 143,312 deaths in the NIS cohort, and 34.7% (explicit) to 52.0% (implicit) occurred among patients with sepsis.
In the KPNC cohort, there were 55,008 explicit and 80,678 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 11.4% (explicit) to 16.7% (implicit) of all hospitalizations.
There were 14,206 inpatient deaths in this cohort, and 36.9% (explicit) to 55.9% (implicit) occurred among patients with sepsis.
“[W]e found that most patients already had sepsis at the time of hospital admission,” Dr Liu said. “There was also a large number of patients with less severe sepsis, a group for whom treatment guidelines are less well-defined. The results of our study suggest that improved care for sepsis patients of all severity levels and in all hospital settings could result in many future lives saved.” ![]()
Credit: NHLBI
SAN DIEGO—Results of a retrospective study suggest sepsis may contribute to as many as half of all hospital deaths in the US.
Researchers analyzed information from 6.5 million hospital discharge records and found that, of all hospital deaths, as many as 52% occurred in patients with sepsis.
“We were surprised to find that as many as 1 in 2 patients dying in US hospitals had sepsis,” said Vincent Liu, MD, of the Kaiser Permanente Northern California Division of Research.
He and his colleagues presented this finding at the American Thoracic Society’s 2014 International Conference (abstract 50626). The results have also been published in JAMA.
The researchers analyzed data from 6.5 million hospital discharge records derived from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample (NIS) in 2010. The NIS is the largest publicly available, all-payer inpatient database in the US, containing data from 100% of hospital discharges from a stratified sample of 1051 community hospitals.
The team also evaluated records for 482,828 adult patients admitted to 21 Kaiser Permanente Northern California (KPNC) hospitals.
Using diagnosis and procedure codes, the researchers identified hospital admissions and deaths of patients with sepsis and estimated the percentage of total hospital charges associated with sepsis hospitalizations.
They used 2 approaches to identify patients with sepsis from International Statistical Classification of Diseases, Ninth Revision, Clinical Modification codes. The explicit approach identified patients with codes 038 (septicemia), 995.91 (sepsis), 995.92 (severe sepsis), or 785.52 (septic shock). The team also used an implicit approach, which included patients with evidence of both infection and acute organ failure.
In the NIS cohort, there were 280,663 explicit and 717,718 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 4.3% (explicit) to 10.9% (implicit) of all hospitalizations.
There were 143,312 deaths in the NIS cohort, and 34.7% (explicit) to 52.0% (implicit) occurred among patients with sepsis.
In the KPNC cohort, there were 55,008 explicit and 80,678 implicit sepsis hospitalizations. Sepsis hospitalizations accounted for 11.4% (explicit) to 16.7% (implicit) of all hospitalizations.
There were 14,206 inpatient deaths in this cohort, and 36.9% (explicit) to 55.9% (implicit) occurred among patients with sepsis.
“[W]e found that most patients already had sepsis at the time of hospital admission,” Dr Liu said. “There was also a large number of patients with less severe sepsis, a group for whom treatment guidelines are less well-defined. The results of our study suggest that improved care for sepsis patients of all severity levels and in all hospital settings could result in many future lives saved.” ![]()
Protein may be therapeutic target for AML

Credit: Lance Liotta
Researchers have found evidence to suggest that the phosphoinositide (PI) modulator PIP4K2A plays a key role in acute myeloid leukemia (AML).
PIs appear to control the transformation of hematopoietic stem cells into leukemic cells.
Some of these PIs switch on specific cell-signaling pathways, resulting in rapid growth and enhanced survival. Regulation of the PIs is carried out by a variety of proteins known as PI modulators.
“Little is known about the role of PI modulators in leukemia,” said Tim Somervaille, PhD, of The University of Manchester in the UK.
“We wanted to find out which ones were responsible for cell growth or survival in acute myeloid leukemia.”
He and his colleagues described this research in Oncogene.
The researchers performed a targeted knockdown screen of PI modulator genes in human AML cells, looking for genes required to sustain proliferation or prevent apoptosis.
They found that one PI modulator, PIP4K2A, was essential for the growth of leukemia. PIP4K2A knockdown resulted in leukemic cell death. This occurred in both murine MLL-AF9 AML cells and primary human AML cells.
Additional investigation showed that PIP4K2A knockdown resulted in the accumulation of the cyclin-dependent kinase inhibitors CDKN1A and CDKN1B, as well as G1 cell-cycle arrest and apoptosis. CDKN1A accumulation and apoptosis were partially dependent on activation of the mTOR pathway.
Fortunately, PIP4K2A knockdown did not adversely affect normal hematopoietic stem and progenitor cells from mice or human subjects. Neither clonogenic nor multilineage differentiation potential was affected.
“This makes [PIP4K2A] an ideal target for future drug development in leukemia,” Dr Somervaille concluded. ![]()
Credit: Lance Liotta
Researchers have found evidence to suggest that the phosphoinositide (PI) modulator PIP4K2A plays a key role in acute myeloid leukemia (AML).
PIs appear to control the transformation of hematopoietic stem cells into leukemic cells.
Some of these PIs switch on specific cell-signaling pathways, resulting in rapid growth and enhanced survival. Regulation of the PIs is carried out by a variety of proteins known as PI modulators.
“Little is known about the role of PI modulators in leukemia,” said Tim Somervaille, PhD, of The University of Manchester in the UK.
“We wanted to find out which ones were responsible for cell growth or survival in acute myeloid leukemia.”
He and his colleagues described this research in Oncogene.
The researchers performed a targeted knockdown screen of PI modulator genes in human AML cells, looking for genes required to sustain proliferation or prevent apoptosis.
They found that one PI modulator, PIP4K2A, was essential for the growth of leukemia. PIP4K2A knockdown resulted in leukemic cell death. This occurred in both murine MLL-AF9 AML cells and primary human AML cells.
Additional investigation showed that PIP4K2A knockdown resulted in the accumulation of the cyclin-dependent kinase inhibitors CDKN1A and CDKN1B, as well as G1 cell-cycle arrest and apoptosis. CDKN1A accumulation and apoptosis were partially dependent on activation of the mTOR pathway.
Fortunately, PIP4K2A knockdown did not adversely affect normal hematopoietic stem and progenitor cells from mice or human subjects. Neither clonogenic nor multilineage differentiation potential was affected.
“This makes [PIP4K2A] an ideal target for future drug development in leukemia,” Dr Somervaille concluded. ![]()
Credit: Lance Liotta
Researchers have found evidence to suggest that the phosphoinositide (PI) modulator PIP4K2A plays a key role in acute myeloid leukemia (AML).
PIs appear to control the transformation of hematopoietic stem cells into leukemic cells.
Some of these PIs switch on specific cell-signaling pathways, resulting in rapid growth and enhanced survival. Regulation of the PIs is carried out by a variety of proteins known as PI modulators.
“Little is known about the role of PI modulators in leukemia,” said Tim Somervaille, PhD, of The University of Manchester in the UK.
“We wanted to find out which ones were responsible for cell growth or survival in acute myeloid leukemia.”
He and his colleagues described this research in Oncogene.
The researchers performed a targeted knockdown screen of PI modulator genes in human AML cells, looking for genes required to sustain proliferation or prevent apoptosis.
They found that one PI modulator, PIP4K2A, was essential for the growth of leukemia. PIP4K2A knockdown resulted in leukemic cell death. This occurred in both murine MLL-AF9 AML cells and primary human AML cells.
Additional investigation showed that PIP4K2A knockdown resulted in the accumulation of the cyclin-dependent kinase inhibitors CDKN1A and CDKN1B, as well as G1 cell-cycle arrest and apoptosis. CDKN1A accumulation and apoptosis were partially dependent on activation of the mTOR pathway.
Fortunately, PIP4K2A knockdown did not adversely affect normal hematopoietic stem and progenitor cells from mice or human subjects. Neither clonogenic nor multilineage differentiation potential was affected.
“This makes [PIP4K2A] an ideal target for future drug development in leukemia,” Dr Somervaille concluded.