User login
Monoclonal antibody could improve treatment of ALL

Credit: Linda Bartlett
Preclinical research suggests the B-cell activating receptor (BAFF-R) may be a promising therapeutic target for treatment-resistant leukemia.
A monoclonal antibody (mAb) that targets BAFF-R overcame resistance to nilotinib and enhanced the efficacy of both nilotinib and vincristine in vitro.
The mAb, called B-1239, also demonstrated antileukemic effects in mouse models, when given alone. But it did not appear to improve upon the effects of nilotinib when given in combination.
Nora Heisterkamp, PhD, of Children’s Hospital Los Angeles in California, and her colleagues reported these findings in Molecular Cancer Therapeutics.
In a previous study, the researchers had shown that BAFF-R is expressed on pre-B ALL cells but not on their normal counterparts.
“We’ve now demonstrated that BAFF-R is a strong potential therapeutic target for treating chemotherapy-resistant leukemia cells, without damaging healthy cells,” Dr Heisterkamp said.
She and her colleagues began this research by generating pre-B ALL cells from the bone marrow of wild-type mice and BAFF-R-null mice with a retroviral vector carrying the BCR/ABL oncogene. They found that wild-type pre-B-ALL cells expressed high levels of BAFF-R.
The team then treated both wild-type and BAFF-R-deficient leukemic cells with nilotinib. The wild-type cells developed resistance to nilotinib in 9 to 10 days, but the BAFF-R-deficient cells were eradicated by treatment.
The researchers next tested the effects of B-1239, a human codon-optimized anti-BAFF-R mAb. B-1239 bound to BAFF-R on both Ph-positive and Ph-negative ALL cells in vitro, and the mAb inhibited BAFF-R in a dose-dependent manner.
In pre-B-ALL cells, B-1239 alone had little effect on cell viability or proliferation. However, when combined with vincristine or nilotinib, B-1239 reduced cell count and viability more than either agent alone.
The researchers also found that B-1239 stimulated natural killer cell-mediated cytotoxicity in patient-derived ALL cells. And the mAb stimulated phagocytosis by macrophages.
Finally, Dr Heisterkamp and her colleagues tested B-1239 in mice transplanted with TXL2 cells. Mice received human IgG, B-1239 alone, nilotinib alone, or nilotinib and B-1239.
At 12 days after the last treatment, leukemia cell numbers in the circulation of control mice and B-1239-treated mice were comparable.
However, B-1239-treated mice showed significant inhibition of ALL cell growth in the bone marrow and spleen, when compared to control mice. mAb-treated mice also had significantly lower spleen weights than controls.
Nilotinib alone also significantly reduced the ALL cell burden in the peripheral blood, spleen, and bone marrow, when compared to controls. But there was no significant difference in these measures between mice that received nilotinib alone or nilotinib plus B-1239.
Nevertheless, Dr Heisterkamp and her colleagues said they will continue to evaluate the use of B-1239 for the treatment of ALL. ![]()
Credit: Linda Bartlett
Preclinical research suggests the B-cell activating receptor (BAFF-R) may be a promising therapeutic target for treatment-resistant leukemia.
A monoclonal antibody (mAb) that targets BAFF-R overcame resistance to nilotinib and enhanced the efficacy of both nilotinib and vincristine in vitro.
The mAb, called B-1239, also demonstrated antileukemic effects in mouse models, when given alone. But it did not appear to improve upon the effects of nilotinib when given in combination.
Nora Heisterkamp, PhD, of Children’s Hospital Los Angeles in California, and her colleagues reported these findings in Molecular Cancer Therapeutics.
In a previous study, the researchers had shown that BAFF-R is expressed on pre-B ALL cells but not on their normal counterparts.
“We’ve now demonstrated that BAFF-R is a strong potential therapeutic target for treating chemotherapy-resistant leukemia cells, without damaging healthy cells,” Dr Heisterkamp said.
She and her colleagues began this research by generating pre-B ALL cells from the bone marrow of wild-type mice and BAFF-R-null mice with a retroviral vector carrying the BCR/ABL oncogene. They found that wild-type pre-B-ALL cells expressed high levels of BAFF-R.
The team then treated both wild-type and BAFF-R-deficient leukemic cells with nilotinib. The wild-type cells developed resistance to nilotinib in 9 to 10 days, but the BAFF-R-deficient cells were eradicated by treatment.
The researchers next tested the effects of B-1239, a human codon-optimized anti-BAFF-R mAb. B-1239 bound to BAFF-R on both Ph-positive and Ph-negative ALL cells in vitro, and the mAb inhibited BAFF-R in a dose-dependent manner.
In pre-B-ALL cells, B-1239 alone had little effect on cell viability or proliferation. However, when combined with vincristine or nilotinib, B-1239 reduced cell count and viability more than either agent alone.
The researchers also found that B-1239 stimulated natural killer cell-mediated cytotoxicity in patient-derived ALL cells. And the mAb stimulated phagocytosis by macrophages.
Finally, Dr Heisterkamp and her colleagues tested B-1239 in mice transplanted with TXL2 cells. Mice received human IgG, B-1239 alone, nilotinib alone, or nilotinib and B-1239.
At 12 days after the last treatment, leukemia cell numbers in the circulation of control mice and B-1239-treated mice were comparable.
However, B-1239-treated mice showed significant inhibition of ALL cell growth in the bone marrow and spleen, when compared to control mice. mAb-treated mice also had significantly lower spleen weights than controls.
Nilotinib alone also significantly reduced the ALL cell burden in the peripheral blood, spleen, and bone marrow, when compared to controls. But there was no significant difference in these measures between mice that received nilotinib alone or nilotinib plus B-1239.
Nevertheless, Dr Heisterkamp and her colleagues said they will continue to evaluate the use of B-1239 for the treatment of ALL. ![]()
Credit: Linda Bartlett
Preclinical research suggests the B-cell activating receptor (BAFF-R) may be a promising therapeutic target for treatment-resistant leukemia.
A monoclonal antibody (mAb) that targets BAFF-R overcame resistance to nilotinib and enhanced the efficacy of both nilotinib and vincristine in vitro.
The mAb, called B-1239, also demonstrated antileukemic effects in mouse models, when given alone. But it did not appear to improve upon the effects of nilotinib when given in combination.
Nora Heisterkamp, PhD, of Children’s Hospital Los Angeles in California, and her colleagues reported these findings in Molecular Cancer Therapeutics.
In a previous study, the researchers had shown that BAFF-R is expressed on pre-B ALL cells but not on their normal counterparts.
“We’ve now demonstrated that BAFF-R is a strong potential therapeutic target for treating chemotherapy-resistant leukemia cells, without damaging healthy cells,” Dr Heisterkamp said.
She and her colleagues began this research by generating pre-B ALL cells from the bone marrow of wild-type mice and BAFF-R-null mice with a retroviral vector carrying the BCR/ABL oncogene. They found that wild-type pre-B-ALL cells expressed high levels of BAFF-R.
The team then treated both wild-type and BAFF-R-deficient leukemic cells with nilotinib. The wild-type cells developed resistance to nilotinib in 9 to 10 days, but the BAFF-R-deficient cells were eradicated by treatment.
The researchers next tested the effects of B-1239, a human codon-optimized anti-BAFF-R mAb. B-1239 bound to BAFF-R on both Ph-positive and Ph-negative ALL cells in vitro, and the mAb inhibited BAFF-R in a dose-dependent manner.
In pre-B-ALL cells, B-1239 alone had little effect on cell viability or proliferation. However, when combined with vincristine or nilotinib, B-1239 reduced cell count and viability more than either agent alone.
The researchers also found that B-1239 stimulated natural killer cell-mediated cytotoxicity in patient-derived ALL cells. And the mAb stimulated phagocytosis by macrophages.
Finally, Dr Heisterkamp and her colleagues tested B-1239 in mice transplanted with TXL2 cells. Mice received human IgG, B-1239 alone, nilotinib alone, or nilotinib and B-1239.
At 12 days after the last treatment, leukemia cell numbers in the circulation of control mice and B-1239-treated mice were comparable.
However, B-1239-treated mice showed significant inhibition of ALL cell growth in the bone marrow and spleen, when compared to control mice. mAb-treated mice also had significantly lower spleen weights than controls.
Nilotinib alone also significantly reduced the ALL cell burden in the peripheral blood, spleen, and bone marrow, when compared to controls. But there was no significant difference in these measures between mice that received nilotinib alone or nilotinib plus B-1239.
Nevertheless, Dr Heisterkamp and her colleagues said they will continue to evaluate the use of B-1239 for the treatment of ALL. ![]()
Development and Evaluation of a Geriatric Mood Management Program
More older adults suffer from depression in a VHA setting (11%) than those in non-VHA settings (1%-5%).1 Depression and anxiety are evaluated less often in older adults and undertreated compared with younger adults.2-4 Unfortunately, older adults with depression and anxiety are vulnerable to suicide and disability; and they more frequently use medical services, such as the emergency department compared with older adults without these conditions.5-7
However, pharmacologic and behavioral treatments for late-life mood and anxiety disorders are available and are effective.8 These findings raise important questions about improving access to mental health care for older veterans with mood disorders. The VA Palo Alto Health Care System (VAPAHCS) Geriatric Research Education and Clinical Center (GRECC) fulfills one GRECC mission of carrying out transformative clinical demonstration projects by developing programs to address geriatric mood disorders.
The VHA has successfully implemented the nationwide integration of mental health management into primary care settings.9 To design and implement these programs locally, in 2007, all VHAs were invited to submit proposals related to mental health primary care integration. Local sites were given flexibility in their use of different evidence-based models for delivery of this integrated care.
Collaborative Models
Three models of mental health integration into primary care were adopted within VHA. All have resulted in improved patient outcomes.9 The co-located model places a behavioral health specialist within the same setting as primary care providers (PCPs), who shares in the evaluation, treatment planning, and monitoring of mental health outcomes. In the care management model, care managers facilitate evaluation and maintain communication with PCPs, but are not co-located with the PCPs. The third model is a blended model in which both a behavioral health specialist and a care manager may be involved in the management of mental health care. The care management model resulted in better participation in the evaluation and engagement in pharmacotherapy by older veterans in 2 VHA medical centers.10
Persistent Barriers for Older Veterans
The mental health-primary care integration initiative laid important foundations for improving access to mental health care. To provide a truly veteran-centered care option, however, programs require monitoring and analysis of the factors that impact care delivery and access. A recent evaluation of a local integration program, using a co-located model (ie, Primary Care Behavioral Health [PCBH]), demonstrated that there were several factors affecting older veterans’ access to mental health treatment.11 Older veterans with depression were less receptive to a mental health referral; 62% of older veterans refused mental health referrals compared with 32% of younger veterans who refused. Older veterans were less likely to complete at least 1 mental health clinic appointment, which was due in part to clinic location. All veterans were more likely to follow up with a mental health referral if first seen by the PCBH staff vs a referral by PCPs.
Geriatric-Specific Modifications to PCBH
The VAPAHCS GRECC, collaborating with the outpatient psychiatry service and the PCBH, sought to improve current mental health services for older veterans. Several barriers were identified: (1) limitations in types of interventions available to older veterans in the current PCBH and mental health programs; (2) the PCBH staff required geriatrics training, as recommended by the American Psychological Association12; and (3) resistance to receiving care in mental health clinics located several miles from the primary care setting. Therefore, a new pilot program was planned to address these barriers.
The Office of Geriatrics and Extended Care provided the funding for the initial program costs, and in September 2010, the Geriatric Primary Care Behavioral Health program (Geri-PCBH) was launched. The GRECC staff worked closely with the PCBH staff to offer a new service tailored to older veterans’ specific needs, which addressed the previously described program limitations.
Geri-PCBH Program
The Geri-PCBH program is a blended collaborative care model that provides outpatient-based mental health evaluation and treatment of mood disorders for older (aged ≥ 65 years) veterans. It is co-located with PCBH and PCPs within the primary care setting. The program extends PCBH services by providing psychotherapy that is contextually modified for older veterans. Older veterans may present with different therapy concerns than do younger veterans, such as caregiving, death of loved ones, and numerous and chronic medical illnesses. Illnesses may result in polypharmacy, giving rise to the need for understanding potential medication interactions in providing pharmacotherapy.
Within the program, geriatrics-trained psychologists and social workers offer psychotherapy. In addition, a geriatrician with expertise in polypharmacy offers pharmacotherapy. Psychotherapy, pharmacotherapy, or both are offered and initiated following evaluation and discussion with the veteran. Veterans are either referred by the PCBH staff because they screened positive for depression (Patient Health Questionnaire-2 [PHQ-2] ≥ 2) during a regularly scheduled primary care clinic appointment or they are directly referred by primary care physicians for suspected mood problems. Veterans are then contacted immediately by a staff member for a baseline assessment appointment with a geriatrician and one of the therapists. The type of treatment and goals of therapy are determined during the initial meeting. The program is a training site for psychology and social work interns, to increase their geriatric mental health training.
Evaluation and Results
To determine improvements compared to PCBH program outcomes, the patients who attended the initial Geri-PCBH evaluation/intake appointment were tracked. A total of 79 older veterans were referred (average age, 82.7 years; range, aged 66-96 years); 14 veterans were ineligible due to significant cognitive impairment or lack of depressive symptoms. Compared with the 38% rate of attendance at intake for mental health referrals in the PCBH program, the Geri-PCBH program demonstrated a 90% attendance rate at the initial evaluation appointment. Fifty-five older veterans enrolled and received therapy: 39 received only psychotherapy, 14 received psychotherapy and antidepressant therapy, and 2 received only antidepressant therapy. Over the first 2 years of the program, 2 senior therapists and 5 trainees were able to see 53 patients for an average of 7 sessions per patient, which translated to about 14% of each therapist’s time.
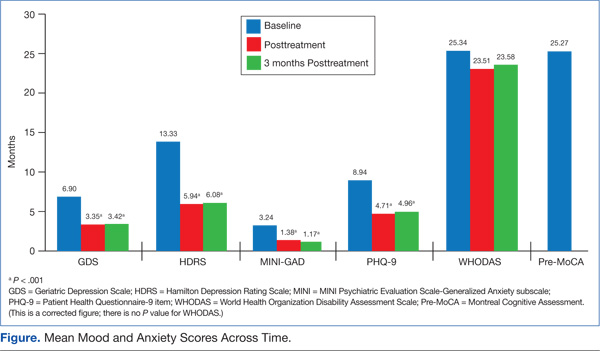
To determine the impact on patients, measures of depression (Hamilton Depression Rating Scale [HDRS]; Geriatric Depression Scale Short Form [GDS-SF]; and Patient Health Questionnaire 9 Item [PHQ-9]), anxiety (Mini Psychiatric Evaluation Scale-Generalized Anxiety subscale [MINI-GAD]), overall distress (clinical global inventory), and functional status (12-item World Health Organization Disability Assessment Scale [WHODAS]) were administered at baseline, posttreatment, and 3 months posttreatment. The veterans demonstrated a significant decrease (> 50% decline on mood symptoms) on the HDRS, GDS, PHQ-9, and MINI-GAD subscale, which were all sustained 3 months posttreatment (Figure).
Although the overall disability score did not improve, the percentage of older veterans reporting “bad” or “moderate” health decreased (pre = 42%; post = 31.1%; 3-month follow-up = 20.9%); while those reporting “good” or “very good” health increased (pre = 58%; post = 65.7%; 3-month follow-up = 79.2%) by the 3-month follow-up. Veterans also reported very high satisfaction rates with the program overall (Mean = 30, standard deviation = 2.03; anchors for measure: 0 = not satisfied; 32 = highly satisfied).
Patient Testimonials
“Not in my wildest dreams did I think I’d ever share, on this level, my personal, past and present life…You have been so helpful and allowed me to move forward with pride and self respect.”
“It makes you feel a lot better. I enjoy life more now than I used to. That first time that [my therapist and I] talked, she convinced me just a change in attitude was a big thing. And since I changed my attitude and started listening to people, it’s made a heck of a difference.”
Discussion and Conclusion
The results of the Geri-PCBH evaluation demonstrated improvements in acceptance by older veterans with depression of mental health referrals and in increased access to treatment. The program addressed several identified barriers, such as having a more accessible location, offering treatment by experienced geriatrics-trained providers, and providing a range of mental health services tailored to older veterans’ needs. These factors may have increased older veterans’ willingness to attend mental health referrals to the Geri-PCBH program. Having initial assessments done soon after initial referral (usually < 2 weeks) and calling patients personally to explain the program and make appointments likely improved referral acceptance.
There are some limits to implementing this program in other settings related to variability in staffing, infrastructure, and resources available. The project is currently sustained with the present staff, with the goal of expanding services by telehealth technology to disseminate the program to older veterans in rural settings.
The VHA has made impressive strides toward improving the lives of older veterans with depression and anxiety. The program described here provides an example of how quality improvement efforts, which take into account the specific needs of the older veteran, can lead to a dramatic impact on the services offered and more importantly on veterans’ mental health and functional abilities.
Acknowledgements
This material is the result of work supported with funding by the Office of Geriatrics and Extended Care T21T Fund-10/11 060B2 and resources and use of facilities at the VA Palo Alto Health Care System in Palo Alto, California.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Blow FC, Owen RE. Specialty care for veterans with depression in the VHA 2002 national registry report. Ann Arbor, MI: VHA Health Services Research and Development; 2003.
2. Fischer LR, Wei F, Solberg LI, Rush WA, Heinrich RL. Treatment of elderly and other adult patients for depression in primary care. J Am Geriatr Soc. 2003;51(11):1554-1562.
3. Stanley MA, Roberts RE, Bourland SL, Novy DM. Anxiety disorders among older primary care patients. J Clin Geropsychology. 2001;7(2):105-116.
4. Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelve-month use of mental health services in the United States: Results from the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):629-640.
5. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry. 2002;52(3):193-204.
6. Pérés K, Jagger C, Matthews FE; MRC CFAS. Impact of late-life self-reported emotional problems on disability-free life expectancy: Results from the MRC cognitive function and ageing study. Int J Geriatr Psychiatry. 2008;23(6):643-649.
7. Lee BW, Conwell Y, Shah MN, Barker WH, Delavan RL, Friedman B. Major depression and emergency medical services utilization in community-dwelling elderly persons with disabilities. Int J Geriatr Psychiatry. 2008;23(12):1276-1282.
8. Small GW. Treatment of geriatric depression. Depress Anxiety. 1998;8(suppl 1):32-42.
9. Post EP, Van Stone WW. Veterans health administration primary care-mental health integration initiative. N C Med J. 2008;69(1):49-52.
10. Mavandadi S, Klaus JR, Oslin DW. Age group differences among veterans enrolled in a clinical service for behavioral health issues in primary care. Am J Geriatr Psychiatry. 2012;20(3):205-214.
11. Lindley S, Cacciapaglia H, Noronha D, Carlson E, Schatzberg A. Monitoring mental health treatment acceptance and initial treatment adherence in veterans: Veterans of Operations Enduring Freedom and Iraqi Freedom versus other veterans of other eras. Ann N Y Acad Sci. 2010;1208:104-113.
12. American Psychological Association. Guidelines for psychological practice with older adults. American Psychologist. 2004;59(4):236-260.
More older adults suffer from depression in a VHA setting (11%) than those in non-VHA settings (1%-5%).1 Depression and anxiety are evaluated less often in older adults and undertreated compared with younger adults.2-4 Unfortunately, older adults with depression and anxiety are vulnerable to suicide and disability; and they more frequently use medical services, such as the emergency department compared with older adults without these conditions.5-7
However, pharmacologic and behavioral treatments for late-life mood and anxiety disorders are available and are effective.8 These findings raise important questions about improving access to mental health care for older veterans with mood disorders. The VA Palo Alto Health Care System (VAPAHCS) Geriatric Research Education and Clinical Center (GRECC) fulfills one GRECC mission of carrying out transformative clinical demonstration projects by developing programs to address geriatric mood disorders.
The VHA has successfully implemented the nationwide integration of mental health management into primary care settings.9 To design and implement these programs locally, in 2007, all VHAs were invited to submit proposals related to mental health primary care integration. Local sites were given flexibility in their use of different evidence-based models for delivery of this integrated care.
Collaborative Models
Three models of mental health integration into primary care were adopted within VHA. All have resulted in improved patient outcomes.9 The co-located model places a behavioral health specialist within the same setting as primary care providers (PCPs), who shares in the evaluation, treatment planning, and monitoring of mental health outcomes. In the care management model, care managers facilitate evaluation and maintain communication with PCPs, but are not co-located with the PCPs. The third model is a blended model in which both a behavioral health specialist and a care manager may be involved in the management of mental health care. The care management model resulted in better participation in the evaluation and engagement in pharmacotherapy by older veterans in 2 VHA medical centers.10
Persistent Barriers for Older Veterans
The mental health-primary care integration initiative laid important foundations for improving access to mental health care. To provide a truly veteran-centered care option, however, programs require monitoring and analysis of the factors that impact care delivery and access. A recent evaluation of a local integration program, using a co-located model (ie, Primary Care Behavioral Health [PCBH]), demonstrated that there were several factors affecting older veterans’ access to mental health treatment.11 Older veterans with depression were less receptive to a mental health referral; 62% of older veterans refused mental health referrals compared with 32% of younger veterans who refused. Older veterans were less likely to complete at least 1 mental health clinic appointment, which was due in part to clinic location. All veterans were more likely to follow up with a mental health referral if first seen by the PCBH staff vs a referral by PCPs.
Geriatric-Specific Modifications to PCBH
The VAPAHCS GRECC, collaborating with the outpatient psychiatry service and the PCBH, sought to improve current mental health services for older veterans. Several barriers were identified: (1) limitations in types of interventions available to older veterans in the current PCBH and mental health programs; (2) the PCBH staff required geriatrics training, as recommended by the American Psychological Association12; and (3) resistance to receiving care in mental health clinics located several miles from the primary care setting. Therefore, a new pilot program was planned to address these barriers.
The Office of Geriatrics and Extended Care provided the funding for the initial program costs, and in September 2010, the Geriatric Primary Care Behavioral Health program (Geri-PCBH) was launched. The GRECC staff worked closely with the PCBH staff to offer a new service tailored to older veterans’ specific needs, which addressed the previously described program limitations.
Geri-PCBH Program
The Geri-PCBH program is a blended collaborative care model that provides outpatient-based mental health evaluation and treatment of mood disorders for older (aged ≥ 65 years) veterans. It is co-located with PCBH and PCPs within the primary care setting. The program extends PCBH services by providing psychotherapy that is contextually modified for older veterans. Older veterans may present with different therapy concerns than do younger veterans, such as caregiving, death of loved ones, and numerous and chronic medical illnesses. Illnesses may result in polypharmacy, giving rise to the need for understanding potential medication interactions in providing pharmacotherapy.
Within the program, geriatrics-trained psychologists and social workers offer psychotherapy. In addition, a geriatrician with expertise in polypharmacy offers pharmacotherapy. Psychotherapy, pharmacotherapy, or both are offered and initiated following evaluation and discussion with the veteran. Veterans are either referred by the PCBH staff because they screened positive for depression (Patient Health Questionnaire-2 [PHQ-2] ≥ 2) during a regularly scheduled primary care clinic appointment or they are directly referred by primary care physicians for suspected mood problems. Veterans are then contacted immediately by a staff member for a baseline assessment appointment with a geriatrician and one of the therapists. The type of treatment and goals of therapy are determined during the initial meeting. The program is a training site for psychology and social work interns, to increase their geriatric mental health training.
Evaluation and Results
To determine improvements compared to PCBH program outcomes, the patients who attended the initial Geri-PCBH evaluation/intake appointment were tracked. A total of 79 older veterans were referred (average age, 82.7 years; range, aged 66-96 years); 14 veterans were ineligible due to significant cognitive impairment or lack of depressive symptoms. Compared with the 38% rate of attendance at intake for mental health referrals in the PCBH program, the Geri-PCBH program demonstrated a 90% attendance rate at the initial evaluation appointment. Fifty-five older veterans enrolled and received therapy: 39 received only psychotherapy, 14 received psychotherapy and antidepressant therapy, and 2 received only antidepressant therapy. Over the first 2 years of the program, 2 senior therapists and 5 trainees were able to see 53 patients for an average of 7 sessions per patient, which translated to about 14% of each therapist’s time.
To determine the impact on patients, measures of depression (Hamilton Depression Rating Scale [HDRS]; Geriatric Depression Scale Short Form [GDS-SF]; and Patient Health Questionnaire 9 Item [PHQ-9]), anxiety (Mini Psychiatric Evaluation Scale-Generalized Anxiety subscale [MINI-GAD]), overall distress (clinical global inventory), and functional status (12-item World Health Organization Disability Assessment Scale [WHODAS]) were administered at baseline, posttreatment, and 3 months posttreatment. The veterans demonstrated a significant decrease (> 50% decline on mood symptoms) on the HDRS, GDS, PHQ-9, and MINI-GAD subscale, which were all sustained 3 months posttreatment (Figure).
Although the overall disability score did not improve, the percentage of older veterans reporting “bad” or “moderate” health decreased (pre = 42%; post = 31.1%; 3-month follow-up = 20.9%); while those reporting “good” or “very good” health increased (pre = 58%; post = 65.7%; 3-month follow-up = 79.2%) by the 3-month follow-up. Veterans also reported very high satisfaction rates with the program overall (Mean = 30, standard deviation = 2.03; anchors for measure: 0 = not satisfied; 32 = highly satisfied).
Patient Testimonials
“Not in my wildest dreams did I think I’d ever share, on this level, my personal, past and present life…You have been so helpful and allowed me to move forward with pride and self respect.”
“It makes you feel a lot better. I enjoy life more now than I used to. That first time that [my therapist and I] talked, she convinced me just a change in attitude was a big thing. And since I changed my attitude and started listening to people, it’s made a heck of a difference.”
Discussion and Conclusion
The results of the Geri-PCBH evaluation demonstrated improvements in acceptance by older veterans with depression of mental health referrals and in increased access to treatment. The program addressed several identified barriers, such as having a more accessible location, offering treatment by experienced geriatrics-trained providers, and providing a range of mental health services tailored to older veterans’ needs. These factors may have increased older veterans’ willingness to attend mental health referrals to the Geri-PCBH program. Having initial assessments done soon after initial referral (usually < 2 weeks) and calling patients personally to explain the program and make appointments likely improved referral acceptance.
There are some limits to implementing this program in other settings related to variability in staffing, infrastructure, and resources available. The project is currently sustained with the present staff, with the goal of expanding services by telehealth technology to disseminate the program to older veterans in rural settings.
The VHA has made impressive strides toward improving the lives of older veterans with depression and anxiety. The program described here provides an example of how quality improvement efforts, which take into account the specific needs of the older veteran, can lead to a dramatic impact on the services offered and more importantly on veterans’ mental health and functional abilities.
Acknowledgements
This material is the result of work supported with funding by the Office of Geriatrics and Extended Care T21T Fund-10/11 060B2 and resources and use of facilities at the VA Palo Alto Health Care System in Palo Alto, California.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
More older adults suffer from depression in a VHA setting (11%) than those in non-VHA settings (1%-5%).1 Depression and anxiety are evaluated less often in older adults and undertreated compared with younger adults.2-4 Unfortunately, older adults with depression and anxiety are vulnerable to suicide and disability; and they more frequently use medical services, such as the emergency department compared with older adults without these conditions.5-7
However, pharmacologic and behavioral treatments for late-life mood and anxiety disorders are available and are effective.8 These findings raise important questions about improving access to mental health care for older veterans with mood disorders. The VA Palo Alto Health Care System (VAPAHCS) Geriatric Research Education and Clinical Center (GRECC) fulfills one GRECC mission of carrying out transformative clinical demonstration projects by developing programs to address geriatric mood disorders.
The VHA has successfully implemented the nationwide integration of mental health management into primary care settings.9 To design and implement these programs locally, in 2007, all VHAs were invited to submit proposals related to mental health primary care integration. Local sites were given flexibility in their use of different evidence-based models for delivery of this integrated care.
Collaborative Models
Three models of mental health integration into primary care were adopted within VHA. All have resulted in improved patient outcomes.9 The co-located model places a behavioral health specialist within the same setting as primary care providers (PCPs), who shares in the evaluation, treatment planning, and monitoring of mental health outcomes. In the care management model, care managers facilitate evaluation and maintain communication with PCPs, but are not co-located with the PCPs. The third model is a blended model in which both a behavioral health specialist and a care manager may be involved in the management of mental health care. The care management model resulted in better participation in the evaluation and engagement in pharmacotherapy by older veterans in 2 VHA medical centers.10
Persistent Barriers for Older Veterans
The mental health-primary care integration initiative laid important foundations for improving access to mental health care. To provide a truly veteran-centered care option, however, programs require monitoring and analysis of the factors that impact care delivery and access. A recent evaluation of a local integration program, using a co-located model (ie, Primary Care Behavioral Health [PCBH]), demonstrated that there were several factors affecting older veterans’ access to mental health treatment.11 Older veterans with depression were less receptive to a mental health referral; 62% of older veterans refused mental health referrals compared with 32% of younger veterans who refused. Older veterans were less likely to complete at least 1 mental health clinic appointment, which was due in part to clinic location. All veterans were more likely to follow up with a mental health referral if first seen by the PCBH staff vs a referral by PCPs.
Geriatric-Specific Modifications to PCBH
The VAPAHCS GRECC, collaborating with the outpatient psychiatry service and the PCBH, sought to improve current mental health services for older veterans. Several barriers were identified: (1) limitations in types of interventions available to older veterans in the current PCBH and mental health programs; (2) the PCBH staff required geriatrics training, as recommended by the American Psychological Association12; and (3) resistance to receiving care in mental health clinics located several miles from the primary care setting. Therefore, a new pilot program was planned to address these barriers.
The Office of Geriatrics and Extended Care provided the funding for the initial program costs, and in September 2010, the Geriatric Primary Care Behavioral Health program (Geri-PCBH) was launched. The GRECC staff worked closely with the PCBH staff to offer a new service tailored to older veterans’ specific needs, which addressed the previously described program limitations.
Geri-PCBH Program
The Geri-PCBH program is a blended collaborative care model that provides outpatient-based mental health evaluation and treatment of mood disorders for older (aged ≥ 65 years) veterans. It is co-located with PCBH and PCPs within the primary care setting. The program extends PCBH services by providing psychotherapy that is contextually modified for older veterans. Older veterans may present with different therapy concerns than do younger veterans, such as caregiving, death of loved ones, and numerous and chronic medical illnesses. Illnesses may result in polypharmacy, giving rise to the need for understanding potential medication interactions in providing pharmacotherapy.
Within the program, geriatrics-trained psychologists and social workers offer psychotherapy. In addition, a geriatrician with expertise in polypharmacy offers pharmacotherapy. Psychotherapy, pharmacotherapy, or both are offered and initiated following evaluation and discussion with the veteran. Veterans are either referred by the PCBH staff because they screened positive for depression (Patient Health Questionnaire-2 [PHQ-2] ≥ 2) during a regularly scheduled primary care clinic appointment or they are directly referred by primary care physicians for suspected mood problems. Veterans are then contacted immediately by a staff member for a baseline assessment appointment with a geriatrician and one of the therapists. The type of treatment and goals of therapy are determined during the initial meeting. The program is a training site for psychology and social work interns, to increase their geriatric mental health training.
Evaluation and Results
To determine improvements compared to PCBH program outcomes, the patients who attended the initial Geri-PCBH evaluation/intake appointment were tracked. A total of 79 older veterans were referred (average age, 82.7 years; range, aged 66-96 years); 14 veterans were ineligible due to significant cognitive impairment or lack of depressive symptoms. Compared with the 38% rate of attendance at intake for mental health referrals in the PCBH program, the Geri-PCBH program demonstrated a 90% attendance rate at the initial evaluation appointment. Fifty-five older veterans enrolled and received therapy: 39 received only psychotherapy, 14 received psychotherapy and antidepressant therapy, and 2 received only antidepressant therapy. Over the first 2 years of the program, 2 senior therapists and 5 trainees were able to see 53 patients for an average of 7 sessions per patient, which translated to about 14% of each therapist’s time.
To determine the impact on patients, measures of depression (Hamilton Depression Rating Scale [HDRS]; Geriatric Depression Scale Short Form [GDS-SF]; and Patient Health Questionnaire 9 Item [PHQ-9]), anxiety (Mini Psychiatric Evaluation Scale-Generalized Anxiety subscale [MINI-GAD]), overall distress (clinical global inventory), and functional status (12-item World Health Organization Disability Assessment Scale [WHODAS]) were administered at baseline, posttreatment, and 3 months posttreatment. The veterans demonstrated a significant decrease (> 50% decline on mood symptoms) on the HDRS, GDS, PHQ-9, and MINI-GAD subscale, which were all sustained 3 months posttreatment (Figure).
Although the overall disability score did not improve, the percentage of older veterans reporting “bad” or “moderate” health decreased (pre = 42%; post = 31.1%; 3-month follow-up = 20.9%); while those reporting “good” or “very good” health increased (pre = 58%; post = 65.7%; 3-month follow-up = 79.2%) by the 3-month follow-up. Veterans also reported very high satisfaction rates with the program overall (Mean = 30, standard deviation = 2.03; anchors for measure: 0 = not satisfied; 32 = highly satisfied).
Patient Testimonials
“Not in my wildest dreams did I think I’d ever share, on this level, my personal, past and present life…You have been so helpful and allowed me to move forward with pride and self respect.”
“It makes you feel a lot better. I enjoy life more now than I used to. That first time that [my therapist and I] talked, she convinced me just a change in attitude was a big thing. And since I changed my attitude and started listening to people, it’s made a heck of a difference.”
Discussion and Conclusion
The results of the Geri-PCBH evaluation demonstrated improvements in acceptance by older veterans with depression of mental health referrals and in increased access to treatment. The program addressed several identified barriers, such as having a more accessible location, offering treatment by experienced geriatrics-trained providers, and providing a range of mental health services tailored to older veterans’ needs. These factors may have increased older veterans’ willingness to attend mental health referrals to the Geri-PCBH program. Having initial assessments done soon after initial referral (usually < 2 weeks) and calling patients personally to explain the program and make appointments likely improved referral acceptance.
There are some limits to implementing this program in other settings related to variability in staffing, infrastructure, and resources available. The project is currently sustained with the present staff, with the goal of expanding services by telehealth technology to disseminate the program to older veterans in rural settings.
The VHA has made impressive strides toward improving the lives of older veterans with depression and anxiety. The program described here provides an example of how quality improvement efforts, which take into account the specific needs of the older veteran, can lead to a dramatic impact on the services offered and more importantly on veterans’ mental health and functional abilities.
Acknowledgements
This material is the result of work supported with funding by the Office of Geriatrics and Extended Care T21T Fund-10/11 060B2 and resources and use of facilities at the VA Palo Alto Health Care System in Palo Alto, California.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Blow FC, Owen RE. Specialty care for veterans with depression in the VHA 2002 national registry report. Ann Arbor, MI: VHA Health Services Research and Development; 2003.
2. Fischer LR, Wei F, Solberg LI, Rush WA, Heinrich RL. Treatment of elderly and other adult patients for depression in primary care. J Am Geriatr Soc. 2003;51(11):1554-1562.
3. Stanley MA, Roberts RE, Bourland SL, Novy DM. Anxiety disorders among older primary care patients. J Clin Geropsychology. 2001;7(2):105-116.
4. Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelve-month use of mental health services in the United States: Results from the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):629-640.
5. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry. 2002;52(3):193-204.
6. Pérés K, Jagger C, Matthews FE; MRC CFAS. Impact of late-life self-reported emotional problems on disability-free life expectancy: Results from the MRC cognitive function and ageing study. Int J Geriatr Psychiatry. 2008;23(6):643-649.
7. Lee BW, Conwell Y, Shah MN, Barker WH, Delavan RL, Friedman B. Major depression and emergency medical services utilization in community-dwelling elderly persons with disabilities. Int J Geriatr Psychiatry. 2008;23(12):1276-1282.
8. Small GW. Treatment of geriatric depression. Depress Anxiety. 1998;8(suppl 1):32-42.
9. Post EP, Van Stone WW. Veterans health administration primary care-mental health integration initiative. N C Med J. 2008;69(1):49-52.
10. Mavandadi S, Klaus JR, Oslin DW. Age group differences among veterans enrolled in a clinical service for behavioral health issues in primary care. Am J Geriatr Psychiatry. 2012;20(3):205-214.
11. Lindley S, Cacciapaglia H, Noronha D, Carlson E, Schatzberg A. Monitoring mental health treatment acceptance and initial treatment adherence in veterans: Veterans of Operations Enduring Freedom and Iraqi Freedom versus other veterans of other eras. Ann N Y Acad Sci. 2010;1208:104-113.
12. American Psychological Association. Guidelines for psychological practice with older adults. American Psychologist. 2004;59(4):236-260.
1. Blow FC, Owen RE. Specialty care for veterans with depression in the VHA 2002 national registry report. Ann Arbor, MI: VHA Health Services Research and Development; 2003.
2. Fischer LR, Wei F, Solberg LI, Rush WA, Heinrich RL. Treatment of elderly and other adult patients for depression in primary care. J Am Geriatr Soc. 2003;51(11):1554-1562.
3. Stanley MA, Roberts RE, Bourland SL, Novy DM. Anxiety disorders among older primary care patients. J Clin Geropsychology. 2001;7(2):105-116.
4. Wang PS, Lane M, Olfson M, Pincus HA, Wells KB, Kessler RC. Twelve-month use of mental health services in the United States: Results from the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):629-640.
5. Conwell Y, Duberstein PR, Caine ED. Risk factors for suicide in later life. Biol Psychiatry. 2002;52(3):193-204.
6. Pérés K, Jagger C, Matthews FE; MRC CFAS. Impact of late-life self-reported emotional problems on disability-free life expectancy: Results from the MRC cognitive function and ageing study. Int J Geriatr Psychiatry. 2008;23(6):643-649.
7. Lee BW, Conwell Y, Shah MN, Barker WH, Delavan RL, Friedman B. Major depression and emergency medical services utilization in community-dwelling elderly persons with disabilities. Int J Geriatr Psychiatry. 2008;23(12):1276-1282.
8. Small GW. Treatment of geriatric depression. Depress Anxiety. 1998;8(suppl 1):32-42.
9. Post EP, Van Stone WW. Veterans health administration primary care-mental health integration initiative. N C Med J. 2008;69(1):49-52.
10. Mavandadi S, Klaus JR, Oslin DW. Age group differences among veterans enrolled in a clinical service for behavioral health issues in primary care. Am J Geriatr Psychiatry. 2012;20(3):205-214.
11. Lindley S, Cacciapaglia H, Noronha D, Carlson E, Schatzberg A. Monitoring mental health treatment acceptance and initial treatment adherence in veterans: Veterans of Operations Enduring Freedom and Iraqi Freedom versus other veterans of other eras. Ann N Y Acad Sci. 2010;1208:104-113.
12. American Psychological Association. Guidelines for psychological practice with older adults. American Psychologist. 2004;59(4):236-260.
Team says antioxidant has no effect on cancer risk, overall health

Contrary to previous findings, a new study suggests the antioxidant resveratrol is not associated with improvements in health, including reducing the risk of cancer.
Researchers found that Italians who consumed a diet rich in resveratrol—a compound in red wine, dark chocolate, and berries—lived no longer than and were just as likely to develop cardiovascular disease or cancer as Italians who consumed smaller amounts of the antioxidant.
However, the investigators said unknown compounds in these foods and drinks may still confer health benefits.
“The story of resveratrol turns out to be another case where you get a lot of hype about health benefits that doesn’t stand the test of time,” said study author Richard D. Semba, MD, MPH, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“The thinking was that certain foods are good for you because they contain resveratrol. We didn’t find that at all.”
Dr Semba and his colleagues recounted their findings in JAMA Internal Medicine.
Their study included 783 subjects, all of whom were older than 65 years of age. Participants were part of the Aging in the Chianti Region study, conducted from 1998 to 2009 in 2 Italian villages where supplement use is uncommon and the consumption of red wine is the norm. The subjects were not on any prescribed diet.
The researchers wanted to determine if diet-related resveratrol levels were associated with inflammation, cancer, cardiovascular disease, and death. So they collected urine samples from study participants and used advanced mass spectrometry to analyze the samples for metabolites of resveratrol.
After accounting for such factors as age and gender, the investigators found that subjects with the highest concentration of resveratrol metabolites were no less likely to have died of any cause than subjects with the lowest levels of resveratrol in their urine.
Likewise, the concentration of resveratrol was not associated with inflammatory markers (serum CRP, IL-6, IL-1β,TNF), cardiovascular disease, or cancer rates.
During 9 years of follow-up, 268 participants (34.3%) died. From the lowest to the highest quartile of baseline total urinary resveratrol metabolites, the proportion of subjects who died from all causes was 34.4%, 31.6%, 33.5%, and 37.4%, respectively (P=0.67).
Of the 734 participants who were free of cancer at enrollment, 34 (4.6%) developed cancer during follow-up. The proportions of subjects with incident cancer from the lowest to the highest quartiles of resveratrol were 4.4%, 4.9%, 5.0%, and 4.3%, respectively (P=0.98).
Of the 639 subjects who were free of cardiovascular disease at enrollment, 174 (27.2%) developed cardiovascular disease during follow-up. The proportions of participants with incident cardiovascular disease from the lowest to the highest quartiles of resveratrol were 22.3%, 29.6%, 28.4%, and 28.0%, respectively (P=0.44).
Despite these negative results, Dr Semba noted that studies have shown the consumption of red wine, dark chocolate, and berries does reduce inflammation in some people and still appears to protect the heart.
“It’s just that the benefits, if they are there, must come from other polyphenols or substances found in those foodstuffs,” he said. “These are complex foods, and all we really know from our study is that the benefits are probably not due to resveratrol.” ![]()
Contrary to previous findings, a new study suggests the antioxidant resveratrol is not associated with improvements in health, including reducing the risk of cancer.
Researchers found that Italians who consumed a diet rich in resveratrol—a compound in red wine, dark chocolate, and berries—lived no longer than and were just as likely to develop cardiovascular disease or cancer as Italians who consumed smaller amounts of the antioxidant.
However, the investigators said unknown compounds in these foods and drinks may still confer health benefits.
“The story of resveratrol turns out to be another case where you get a lot of hype about health benefits that doesn’t stand the test of time,” said study author Richard D. Semba, MD, MPH, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“The thinking was that certain foods are good for you because they contain resveratrol. We didn’t find that at all.”
Dr Semba and his colleagues recounted their findings in JAMA Internal Medicine.
Their study included 783 subjects, all of whom were older than 65 years of age. Participants were part of the Aging in the Chianti Region study, conducted from 1998 to 2009 in 2 Italian villages where supplement use is uncommon and the consumption of red wine is the norm. The subjects were not on any prescribed diet.
The researchers wanted to determine if diet-related resveratrol levels were associated with inflammation, cancer, cardiovascular disease, and death. So they collected urine samples from study participants and used advanced mass spectrometry to analyze the samples for metabolites of resveratrol.
After accounting for such factors as age and gender, the investigators found that subjects with the highest concentration of resveratrol metabolites were no less likely to have died of any cause than subjects with the lowest levels of resveratrol in their urine.
Likewise, the concentration of resveratrol was not associated with inflammatory markers (serum CRP, IL-6, IL-1β,TNF), cardiovascular disease, or cancer rates.
During 9 years of follow-up, 268 participants (34.3%) died. From the lowest to the highest quartile of baseline total urinary resveratrol metabolites, the proportion of subjects who died from all causes was 34.4%, 31.6%, 33.5%, and 37.4%, respectively (P=0.67).
Of the 734 participants who were free of cancer at enrollment, 34 (4.6%) developed cancer during follow-up. The proportions of subjects with incident cancer from the lowest to the highest quartiles of resveratrol were 4.4%, 4.9%, 5.0%, and 4.3%, respectively (P=0.98).
Of the 639 subjects who were free of cardiovascular disease at enrollment, 174 (27.2%) developed cardiovascular disease during follow-up. The proportions of participants with incident cardiovascular disease from the lowest to the highest quartiles of resveratrol were 22.3%, 29.6%, 28.4%, and 28.0%, respectively (P=0.44).
Despite these negative results, Dr Semba noted that studies have shown the consumption of red wine, dark chocolate, and berries does reduce inflammation in some people and still appears to protect the heart.
“It’s just that the benefits, if they are there, must come from other polyphenols or substances found in those foodstuffs,” he said. “These are complex foods, and all we really know from our study is that the benefits are probably not due to resveratrol.” ![]()
Contrary to previous findings, a new study suggests the antioxidant resveratrol is not associated with improvements in health, including reducing the risk of cancer.
Researchers found that Italians who consumed a diet rich in resveratrol—a compound in red wine, dark chocolate, and berries—lived no longer than and were just as likely to develop cardiovascular disease or cancer as Italians who consumed smaller amounts of the antioxidant.
However, the investigators said unknown compounds in these foods and drinks may still confer health benefits.
“The story of resveratrol turns out to be another case where you get a lot of hype about health benefits that doesn’t stand the test of time,” said study author Richard D. Semba, MD, MPH, of the Johns Hopkins University School of Medicine in Baltimore, Maryland.
“The thinking was that certain foods are good for you because they contain resveratrol. We didn’t find that at all.”
Dr Semba and his colleagues recounted their findings in JAMA Internal Medicine.
Their study included 783 subjects, all of whom were older than 65 years of age. Participants were part of the Aging in the Chianti Region study, conducted from 1998 to 2009 in 2 Italian villages where supplement use is uncommon and the consumption of red wine is the norm. The subjects were not on any prescribed diet.
The researchers wanted to determine if diet-related resveratrol levels were associated with inflammation, cancer, cardiovascular disease, and death. So they collected urine samples from study participants and used advanced mass spectrometry to analyze the samples for metabolites of resveratrol.
After accounting for such factors as age and gender, the investigators found that subjects with the highest concentration of resveratrol metabolites were no less likely to have died of any cause than subjects with the lowest levels of resveratrol in their urine.
Likewise, the concentration of resveratrol was not associated with inflammatory markers (serum CRP, IL-6, IL-1β,TNF), cardiovascular disease, or cancer rates.
During 9 years of follow-up, 268 participants (34.3%) died. From the lowest to the highest quartile of baseline total urinary resveratrol metabolites, the proportion of subjects who died from all causes was 34.4%, 31.6%, 33.5%, and 37.4%, respectively (P=0.67).
Of the 734 participants who were free of cancer at enrollment, 34 (4.6%) developed cancer during follow-up. The proportions of subjects with incident cancer from the lowest to the highest quartiles of resveratrol were 4.4%, 4.9%, 5.0%, and 4.3%, respectively (P=0.98).
Of the 639 subjects who were free of cardiovascular disease at enrollment, 174 (27.2%) developed cardiovascular disease during follow-up. The proportions of participants with incident cardiovascular disease from the lowest to the highest quartiles of resveratrol were 22.3%, 29.6%, 28.4%, and 28.0%, respectively (P=0.44).
Despite these negative results, Dr Semba noted that studies have shown the consumption of red wine, dark chocolate, and berries does reduce inflammation in some people and still appears to protect the heart.
“It’s just that the benefits, if they are there, must come from other polyphenols or substances found in those foodstuffs,” he said. “These are complex foods, and all we really know from our study is that the benefits are probably not due to resveratrol.” ![]()
90 US healthcare professionals charged with fraud

Credit: NIH
As a result of Medicare Fraud Strike Force operations in 6 US cities, 90 healthcare professionals have been charged with fraud.
These individuals—doctors, nurses, healthcare company owners, and others—are accused of participating in Medicare fraud schemes involving approximately $260 million in false billings.
They have been charged with various crimes, including conspiracy to commit healthcare fraud, violations of the anti-kickback statutes, and money laundering.
According to court documents, the defendants allegedly participated in schemes to submit claims to Medicare for treatments that were medically unnecessary and often never provided.
In many cases, court documents allege that patient recruiters, Medicare beneficiaries, and other co-conspirators were paid cash kickbacks in return for supplying beneficiary information to providers so the providers could then submit fraudulent bills to Medicare for services that were medically unnecessary or never performed.
“[T]he crimes charged represent the face of healthcare fraud today—doctors billing for services that were never rendered, supply companies providing motorized wheelchairs that were never needed, recruiters paying kickbacks to get Medicare billing numbers of patients,” said Acting Assistant Attorney General David O’Neil.
Case details
In Miami, Florida, 50 defendants were charged for their alleged participation in various fraud schemes involving approximately $65.5 million in false billings for home healthcare and mental health services, as well as pharmacy fraud.
Two of these defendants were charged in connection with a $23 million pharmacy kickback and laundering scheme. Court documents allege that the defendants solicited kickbacks from a pharmacy owner for Medicare beneficiary information, which was used to bill for drugs that were never dispensed.
The kickbacks were concealed as bi-weekly payments under a sham services contract and were laundered through shell entities owned by the defendants.
Eleven individuals were charged by the Medicare Strike Force in Houston, Texas. Five Houston-area physicians were charged with conspiring to bill Medicare for medically unnecessary home health services. According to court documents, the defendant doctors were paid by 2 co-conspirators to sign off on home healthcare services that were not necessary and often never provided.
Eight defendants were charged in Los Angeles, California, for their roles in schemes to defraud Medicare of approximately $32 million.
One doctor was charged for causing almost $24 million in losses to Medicare through his own fraudulent billing and referrals for durable medical equipment, including more than 1000 expensive power wheelchairs, and home health services that were not medically necessary and frequently not provided.
In Detroit, Michigan, 7 defendants were charged for their roles in fraud schemes involving approximately $30 million in false claims for medically unnecessary services, including home health services, psychotherapy, and infusion therapy.
Four of these individuals were charged in a $28 million fraud scheme, where a physician billed for expensive tests, physical therapy, and injections that were not necessary and not provided.
Court documents allege that when the physician’s billings raised red flags, he was put on payment review by Medicare. He was allegedly able to continue his scheme and evade detection by continuing to bill using the billing information of other Medicare providers, sometimes without their knowledge.
In Tampa, Florida, 7 individuals were charged in a variety of schemes, ranging from fraudulent physical therapy billings to a scheme involving millions of dollars in physician services and tests that never occurred.
Five of these individuals were charged for their alleged roles in a $12 million healthcare fraud and money laundering scheme that involved billing Medicare using names of beneficiaries from Miami-Dade County for services purportedly provided in Tampa-area clinics, 280 miles away. The defendants then allegedly laundered the proceeds through a number of transactions involving several shell entities.
In Brooklyn, New York, the Strike Force announced an indictment against Syed Imran Ahmed, MD, in connection with his alleged $85 million scheme involving billings for surgeries that never occurred. Dr Ahmed had been arrested last month and charged by complaint. He is now charged with healthcare fraud and making false statements.
The Brooklyn Strike Force also charged 6 other individuals, including a physician and 2 billers who allegedly concocted a $14.4 million scheme in which they recruited elderly Medicare beneficiaries and billed Medicare for medically unnecessary vitamin infusions, diagnostic tests, and physical and occupational therapy supposedly provided to these patients.
The cases are being prosecuted and investigated by Medicare Fraud Strike Force teams comprised of attorneys from the Fraud Section of the Justice Department’s Criminal Division and from the US Attorney’s Offices for the Southern District of Florida, the Eastern District of Michigan, the Eastern District of New York, the Southern District of Texas, the Central District of California, the Middle District of Louisiana, the Northern District of Illinois and the Middle District of Florida; and agents from the Federal Bureau of Investigation, Department of Health and Human Services (HHS)-Office of Inspector General (OIG), and state Medicaid Fraud Control Units.
About the Medicare Fraud Strike Force
This is the seventh national Medicare fraud takedown in Medicare Fraud Strike Force history. The Strike Force’s operations are part of the Health Care Fraud Prevention & Enforcement Action Team (HEAT), a joint initiative announced in May 2009 between the Department of Justice and the HHS to focus their efforts to prevent and deter fraud and enforce current anti-fraud laws around the country.
Since their inception in March 2007, Strike Force operations in 9 locations have charged almost 1900 defendants who collectively have falsely billed the Medicare program for almost $6 billion.
In addition, the Centers for Medicare & Medicaid Services, working in conjunction with HHS-OIG, has suspended enrollments of high-risk providers in 5 Strike Force locations and has removed more than 17,000 providers from the Medicare program since 2011.
The joint Department of Justice and HHS Medicare Fraud Strike Force is a multi-agency team of federal, state, and local investigators designed to combat Medicare fraud through the use of Medicare data analysis techniques and an increased focus on community policing.
To learn more, visit www.stopmedicarefraud.gov. ![]()
Credit: NIH
As a result of Medicare Fraud Strike Force operations in 6 US cities, 90 healthcare professionals have been charged with fraud.
These individuals—doctors, nurses, healthcare company owners, and others—are accused of participating in Medicare fraud schemes involving approximately $260 million in false billings.
They have been charged with various crimes, including conspiracy to commit healthcare fraud, violations of the anti-kickback statutes, and money laundering.
According to court documents, the defendants allegedly participated in schemes to submit claims to Medicare for treatments that were medically unnecessary and often never provided.
In many cases, court documents allege that patient recruiters, Medicare beneficiaries, and other co-conspirators were paid cash kickbacks in return for supplying beneficiary information to providers so the providers could then submit fraudulent bills to Medicare for services that were medically unnecessary or never performed.
“[T]he crimes charged represent the face of healthcare fraud today—doctors billing for services that were never rendered, supply companies providing motorized wheelchairs that were never needed, recruiters paying kickbacks to get Medicare billing numbers of patients,” said Acting Assistant Attorney General David O’Neil.
Case details
In Miami, Florida, 50 defendants were charged for their alleged participation in various fraud schemes involving approximately $65.5 million in false billings for home healthcare and mental health services, as well as pharmacy fraud.
Two of these defendants were charged in connection with a $23 million pharmacy kickback and laundering scheme. Court documents allege that the defendants solicited kickbacks from a pharmacy owner for Medicare beneficiary information, which was used to bill for drugs that were never dispensed.
The kickbacks were concealed as bi-weekly payments under a sham services contract and were laundered through shell entities owned by the defendants.
Eleven individuals were charged by the Medicare Strike Force in Houston, Texas. Five Houston-area physicians were charged with conspiring to bill Medicare for medically unnecessary home health services. According to court documents, the defendant doctors were paid by 2 co-conspirators to sign off on home healthcare services that were not necessary and often never provided.
Eight defendants were charged in Los Angeles, California, for their roles in schemes to defraud Medicare of approximately $32 million.
One doctor was charged for causing almost $24 million in losses to Medicare through his own fraudulent billing and referrals for durable medical equipment, including more than 1000 expensive power wheelchairs, and home health services that were not medically necessary and frequently not provided.
In Detroit, Michigan, 7 defendants were charged for their roles in fraud schemes involving approximately $30 million in false claims for medically unnecessary services, including home health services, psychotherapy, and infusion therapy.
Four of these individuals were charged in a $28 million fraud scheme, where a physician billed for expensive tests, physical therapy, and injections that were not necessary and not provided.
Court documents allege that when the physician’s billings raised red flags, he was put on payment review by Medicare. He was allegedly able to continue his scheme and evade detection by continuing to bill using the billing information of other Medicare providers, sometimes without their knowledge.
In Tampa, Florida, 7 individuals were charged in a variety of schemes, ranging from fraudulent physical therapy billings to a scheme involving millions of dollars in physician services and tests that never occurred.
Five of these individuals were charged for their alleged roles in a $12 million healthcare fraud and money laundering scheme that involved billing Medicare using names of beneficiaries from Miami-Dade County for services purportedly provided in Tampa-area clinics, 280 miles away. The defendants then allegedly laundered the proceeds through a number of transactions involving several shell entities.
In Brooklyn, New York, the Strike Force announced an indictment against Syed Imran Ahmed, MD, in connection with his alleged $85 million scheme involving billings for surgeries that never occurred. Dr Ahmed had been arrested last month and charged by complaint. He is now charged with healthcare fraud and making false statements.
The Brooklyn Strike Force also charged 6 other individuals, including a physician and 2 billers who allegedly concocted a $14.4 million scheme in which they recruited elderly Medicare beneficiaries and billed Medicare for medically unnecessary vitamin infusions, diagnostic tests, and physical and occupational therapy supposedly provided to these patients.
The cases are being prosecuted and investigated by Medicare Fraud Strike Force teams comprised of attorneys from the Fraud Section of the Justice Department’s Criminal Division and from the US Attorney’s Offices for the Southern District of Florida, the Eastern District of Michigan, the Eastern District of New York, the Southern District of Texas, the Central District of California, the Middle District of Louisiana, the Northern District of Illinois and the Middle District of Florida; and agents from the Federal Bureau of Investigation, Department of Health and Human Services (HHS)-Office of Inspector General (OIG), and state Medicaid Fraud Control Units.
About the Medicare Fraud Strike Force
This is the seventh national Medicare fraud takedown in Medicare Fraud Strike Force history. The Strike Force’s operations are part of the Health Care Fraud Prevention & Enforcement Action Team (HEAT), a joint initiative announced in May 2009 between the Department of Justice and the HHS to focus their efforts to prevent and deter fraud and enforce current anti-fraud laws around the country.
Since their inception in March 2007, Strike Force operations in 9 locations have charged almost 1900 defendants who collectively have falsely billed the Medicare program for almost $6 billion.
In addition, the Centers for Medicare & Medicaid Services, working in conjunction with HHS-OIG, has suspended enrollments of high-risk providers in 5 Strike Force locations and has removed more than 17,000 providers from the Medicare program since 2011.
The joint Department of Justice and HHS Medicare Fraud Strike Force is a multi-agency team of federal, state, and local investigators designed to combat Medicare fraud through the use of Medicare data analysis techniques and an increased focus on community policing.
To learn more, visit www.stopmedicarefraud.gov. ![]()
Credit: NIH
As a result of Medicare Fraud Strike Force operations in 6 US cities, 90 healthcare professionals have been charged with fraud.
These individuals—doctors, nurses, healthcare company owners, and others—are accused of participating in Medicare fraud schemes involving approximately $260 million in false billings.
They have been charged with various crimes, including conspiracy to commit healthcare fraud, violations of the anti-kickback statutes, and money laundering.
According to court documents, the defendants allegedly participated in schemes to submit claims to Medicare for treatments that were medically unnecessary and often never provided.
In many cases, court documents allege that patient recruiters, Medicare beneficiaries, and other co-conspirators were paid cash kickbacks in return for supplying beneficiary information to providers so the providers could then submit fraudulent bills to Medicare for services that were medically unnecessary or never performed.
“[T]he crimes charged represent the face of healthcare fraud today—doctors billing for services that were never rendered, supply companies providing motorized wheelchairs that were never needed, recruiters paying kickbacks to get Medicare billing numbers of patients,” said Acting Assistant Attorney General David O’Neil.
Case details
In Miami, Florida, 50 defendants were charged for their alleged participation in various fraud schemes involving approximately $65.5 million in false billings for home healthcare and mental health services, as well as pharmacy fraud.
Two of these defendants were charged in connection with a $23 million pharmacy kickback and laundering scheme. Court documents allege that the defendants solicited kickbacks from a pharmacy owner for Medicare beneficiary information, which was used to bill for drugs that were never dispensed.
The kickbacks were concealed as bi-weekly payments under a sham services contract and were laundered through shell entities owned by the defendants.
Eleven individuals were charged by the Medicare Strike Force in Houston, Texas. Five Houston-area physicians were charged with conspiring to bill Medicare for medically unnecessary home health services. According to court documents, the defendant doctors were paid by 2 co-conspirators to sign off on home healthcare services that were not necessary and often never provided.
Eight defendants were charged in Los Angeles, California, for their roles in schemes to defraud Medicare of approximately $32 million.
One doctor was charged for causing almost $24 million in losses to Medicare through his own fraudulent billing and referrals for durable medical equipment, including more than 1000 expensive power wheelchairs, and home health services that were not medically necessary and frequently not provided.
In Detroit, Michigan, 7 defendants were charged for their roles in fraud schemes involving approximately $30 million in false claims for medically unnecessary services, including home health services, psychotherapy, and infusion therapy.
Four of these individuals were charged in a $28 million fraud scheme, where a physician billed for expensive tests, physical therapy, and injections that were not necessary and not provided.
Court documents allege that when the physician’s billings raised red flags, he was put on payment review by Medicare. He was allegedly able to continue his scheme and evade detection by continuing to bill using the billing information of other Medicare providers, sometimes without their knowledge.
In Tampa, Florida, 7 individuals were charged in a variety of schemes, ranging from fraudulent physical therapy billings to a scheme involving millions of dollars in physician services and tests that never occurred.
Five of these individuals were charged for their alleged roles in a $12 million healthcare fraud and money laundering scheme that involved billing Medicare using names of beneficiaries from Miami-Dade County for services purportedly provided in Tampa-area clinics, 280 miles away. The defendants then allegedly laundered the proceeds through a number of transactions involving several shell entities.
In Brooklyn, New York, the Strike Force announced an indictment against Syed Imran Ahmed, MD, in connection with his alleged $85 million scheme involving billings for surgeries that never occurred. Dr Ahmed had been arrested last month and charged by complaint. He is now charged with healthcare fraud and making false statements.
The Brooklyn Strike Force also charged 6 other individuals, including a physician and 2 billers who allegedly concocted a $14.4 million scheme in which they recruited elderly Medicare beneficiaries and billed Medicare for medically unnecessary vitamin infusions, diagnostic tests, and physical and occupational therapy supposedly provided to these patients.
The cases are being prosecuted and investigated by Medicare Fraud Strike Force teams comprised of attorneys from the Fraud Section of the Justice Department’s Criminal Division and from the US Attorney’s Offices for the Southern District of Florida, the Eastern District of Michigan, the Eastern District of New York, the Southern District of Texas, the Central District of California, the Middle District of Louisiana, the Northern District of Illinois and the Middle District of Florida; and agents from the Federal Bureau of Investigation, Department of Health and Human Services (HHS)-Office of Inspector General (OIG), and state Medicaid Fraud Control Units.
About the Medicare Fraud Strike Force
This is the seventh national Medicare fraud takedown in Medicare Fraud Strike Force history. The Strike Force’s operations are part of the Health Care Fraud Prevention & Enforcement Action Team (HEAT), a joint initiative announced in May 2009 between the Department of Justice and the HHS to focus their efforts to prevent and deter fraud and enforce current anti-fraud laws around the country.
Since their inception in March 2007, Strike Force operations in 9 locations have charged almost 1900 defendants who collectively have falsely billed the Medicare program for almost $6 billion.
In addition, the Centers for Medicare & Medicaid Services, working in conjunction with HHS-OIG, has suspended enrollments of high-risk providers in 5 Strike Force locations and has removed more than 17,000 providers from the Medicare program since 2011.
The joint Department of Justice and HHS Medicare Fraud Strike Force is a multi-agency team of federal, state, and local investigators designed to combat Medicare fraud through the use of Medicare data analysis techniques and an increased focus on community policing.
To learn more, visit www.stopmedicarefraud.gov. ![]()
Cell phone records aid fight against malaria

Credit: James Gathany
Data that tracks cell phone activity can help us more accurately target antimalaria interventions, according to a paper published in Malaria Journal.
Researchers used anonymized cell phone records to measure population movements within Namibia, Africa, over a year.
By combining this data with information about malaria cases, topography, and climate, the group was able to identify geographical “hotspots” of the disease and design targeted plans for its elimination.
“If we are to eliminate this disease, we need to deploy the right measures in the right place, but figures on human movement patterns in endemic regions are hard to come by and often restricted to local travel surveys and census-based migration data,” said study author Andrew Tatem, PhD, of the University of Southampton in the UK.
“Our study demonstrates that the rapid global proliferation of mobile phones now provides us with an opportunity to study the movement of people, using sample sizes running in to millions. This data, combined with disease-case-based mapping, can help us plan where and how to intervene.”
Dr Tatem and his colleagues looked at anonymized Call Data Records from 2010 to 2011, provided by Mobile Telecommunications Limited. The data represented 9 billion communications from 1.19 million unique subscribers, around 52% of the population of Namibia.
The researchers analyzed aggregated movements of phone users between urban areas and urban and rural areas, in conjunction with data based on rapid diagnostic testing of malaria and information on the climate, environment, and topography of the country.
In this way, the team identified communities that were strongly connected by relatively higher levels of population movement. They quantified the net export and import of travelers and mapped malaria infection risks by region.
The researchers said these malaria risk maps can aid the design of targeted interventions to reduce the number of malaria cases exported to other regions and help manage the risk of infection in places that import the disease.
In fact, the maps have already helped the Namibia National Vector-borne Diseases Control Programme improve their targeting of malaria interventions to communities most at risk.
Specifically, the maps prompted the organization to target insecticide-treated bed net distribution in the Omusati, Kavango, and Zambezi regions in 2013.
“The importation of malaria from outside a country will always be a crucial focus of disease control programs, but movement of the disease within countries is also of huge significance,” Dr Tatem said. “Understanding the human element of this movement should be a critical component when designing elimination strategies—to help target resources most efficiently.”
“The use of mobile phone data is one example of how new technologies are overcoming past problems of quantifying and gaining a better understanding of human movement patterns in relation to disease control.” ![]()
Credit: James Gathany
Data that tracks cell phone activity can help us more accurately target antimalaria interventions, according to a paper published in Malaria Journal.
Researchers used anonymized cell phone records to measure population movements within Namibia, Africa, over a year.
By combining this data with information about malaria cases, topography, and climate, the group was able to identify geographical “hotspots” of the disease and design targeted plans for its elimination.
“If we are to eliminate this disease, we need to deploy the right measures in the right place, but figures on human movement patterns in endemic regions are hard to come by and often restricted to local travel surveys and census-based migration data,” said study author Andrew Tatem, PhD, of the University of Southampton in the UK.
“Our study demonstrates that the rapid global proliferation of mobile phones now provides us with an opportunity to study the movement of people, using sample sizes running in to millions. This data, combined with disease-case-based mapping, can help us plan where and how to intervene.”
Dr Tatem and his colleagues looked at anonymized Call Data Records from 2010 to 2011, provided by Mobile Telecommunications Limited. The data represented 9 billion communications from 1.19 million unique subscribers, around 52% of the population of Namibia.
The researchers analyzed aggregated movements of phone users between urban areas and urban and rural areas, in conjunction with data based on rapid diagnostic testing of malaria and information on the climate, environment, and topography of the country.
In this way, the team identified communities that were strongly connected by relatively higher levels of population movement. They quantified the net export and import of travelers and mapped malaria infection risks by region.
The researchers said these malaria risk maps can aid the design of targeted interventions to reduce the number of malaria cases exported to other regions and help manage the risk of infection in places that import the disease.
In fact, the maps have already helped the Namibia National Vector-borne Diseases Control Programme improve their targeting of malaria interventions to communities most at risk.
Specifically, the maps prompted the organization to target insecticide-treated bed net distribution in the Omusati, Kavango, and Zambezi regions in 2013.
“The importation of malaria from outside a country will always be a crucial focus of disease control programs, but movement of the disease within countries is also of huge significance,” Dr Tatem said. “Understanding the human element of this movement should be a critical component when designing elimination strategies—to help target resources most efficiently.”
“The use of mobile phone data is one example of how new technologies are overcoming past problems of quantifying and gaining a better understanding of human movement patterns in relation to disease control.” ![]()
Credit: James Gathany
Data that tracks cell phone activity can help us more accurately target antimalaria interventions, according to a paper published in Malaria Journal.
Researchers used anonymized cell phone records to measure population movements within Namibia, Africa, over a year.
By combining this data with information about malaria cases, topography, and climate, the group was able to identify geographical “hotspots” of the disease and design targeted plans for its elimination.
“If we are to eliminate this disease, we need to deploy the right measures in the right place, but figures on human movement patterns in endemic regions are hard to come by and often restricted to local travel surveys and census-based migration data,” said study author Andrew Tatem, PhD, of the University of Southampton in the UK.
“Our study demonstrates that the rapid global proliferation of mobile phones now provides us with an opportunity to study the movement of people, using sample sizes running in to millions. This data, combined with disease-case-based mapping, can help us plan where and how to intervene.”
Dr Tatem and his colleagues looked at anonymized Call Data Records from 2010 to 2011, provided by Mobile Telecommunications Limited. The data represented 9 billion communications from 1.19 million unique subscribers, around 52% of the population of Namibia.
The researchers analyzed aggregated movements of phone users between urban areas and urban and rural areas, in conjunction with data based on rapid diagnostic testing of malaria and information on the climate, environment, and topography of the country.
In this way, the team identified communities that were strongly connected by relatively higher levels of population movement. They quantified the net export and import of travelers and mapped malaria infection risks by region.
The researchers said these malaria risk maps can aid the design of targeted interventions to reduce the number of malaria cases exported to other regions and help manage the risk of infection in places that import the disease.
In fact, the maps have already helped the Namibia National Vector-borne Diseases Control Programme improve their targeting of malaria interventions to communities most at risk.
Specifically, the maps prompted the organization to target insecticide-treated bed net distribution in the Omusati, Kavango, and Zambezi regions in 2013.
“The importation of malaria from outside a country will always be a crucial focus of disease control programs, but movement of the disease within countries is also of huge significance,” Dr Tatem said. “Understanding the human element of this movement should be a critical component when designing elimination strategies—to help target resources most efficiently.”
“The use of mobile phone data is one example of how new technologies are overcoming past problems of quantifying and gaining a better understanding of human movement patterns in relation to disease control.” ![]()
COMMENTARY: How and why to perform research as a trainee
"Why do I need to do research if I'm going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature.
This is a skill that will serve you well throughout your career, guiding your clinical decision making, regardless if you choose private practice or academic surgery.
Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies.
Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings.
Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat.
There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor; a topic; a clear, novel question; and the appropriate study design.
Chances are that at some point, a mentor helped guide you toward a career in cardiovascular surgery. A research mentor is just as important as a clinical mentor for a young surgeon. The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time.
The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor that is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals.
Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
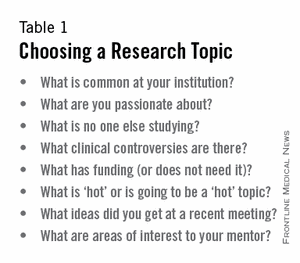
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is: "Do patients with a given disease treated with operation X live longer than those treated with operation Y?"
Stay away from the lure of "Let's review our experience of operation X…" or "Why don't I see how many of operation Y we've done over the past 10 years…" These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee.
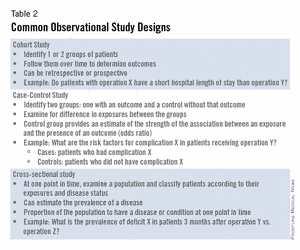
The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2).
Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
In the design of a study, one of the most important principles is defining a priori end points.
Every study will have one primary end point that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you do it only once.
The next step is to create a research proposal. To do this, you will need to go to the literature and see what published data relate to your study. Perhaps, there are previous studies examining your question with conflicting results?
Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval. This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed-upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
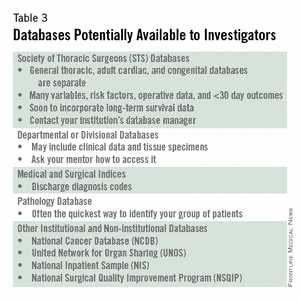
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project. Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity).
Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data exists regardless if the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward. Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct.
Next using your proposal as an outline, put together a rough draft of a manuscript. Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study.
Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product. Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing.
Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you.
Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don't know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions. Then spend as much time as possible after the session speaking with audience members about you and your study.
You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgment: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center, Chicago.
"Why do I need to do research if I'm going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature.
This is a skill that will serve you well throughout your career, guiding your clinical decision making, regardless if you choose private practice or academic surgery.
Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies.
Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings.
Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat.
There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor; a topic; a clear, novel question; and the appropriate study design.
Chances are that at some point, a mentor helped guide you toward a career in cardiovascular surgery. A research mentor is just as important as a clinical mentor for a young surgeon. The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time.
The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor that is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals.
Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is: "Do patients with a given disease treated with operation X live longer than those treated with operation Y?"
Stay away from the lure of "Let's review our experience of operation X…" or "Why don't I see how many of operation Y we've done over the past 10 years…" These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee.
The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2).
Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
In the design of a study, one of the most important principles is defining a priori end points.
Every study will have one primary end point that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you do it only once.
The next step is to create a research proposal. To do this, you will need to go to the literature and see what published data relate to your study. Perhaps, there are previous studies examining your question with conflicting results?
Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval. This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed-upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project. Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity).
Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data exists regardless if the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward. Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct.
Next using your proposal as an outline, put together a rough draft of a manuscript. Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study.
Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product. Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing.
Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you.
Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don't know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions. Then spend as much time as possible after the session speaking with audience members about you and your study.
You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgment: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center, Chicago.
"Why do I need to do research if I'm going into private practice anyway?"
I have heard this question multiple times throughout my career as a resident, fellow, and attending thoracic surgeon. The truth is, there are multiple reasons, any of which is sufficient to justify your participation in clinical research during training. First, and perhaps most importantly, it teaches you to critically appraise the literature.
This is a skill that will serve you well throughout your career, guiding your clinical decision making, regardless if you choose private practice or academic surgery.
Another reason is that performing clinical research allows you to become a content expert on a specific topic early in your career. This knowledge base is something that will serve as a foundation for ongoing learning and may help in designing future studies.
Once your project is complete, it will be your ticket to attend and present at regional, national, or international meetings. There is no better forum to gain public recognition for your investigative efforts and network with potential future partners than societal meetings.
Formal and informal interviews routinely occur at these gatherings and you do not want to be left out because you chose not to participate in research as a trainee. Finally, it is your responsibility to the patients that you have sworn to treat.
There are many ways to care for patients, and pushing back the frontiers of medical knowledge is as important as the day-to-day tasks that you perform on the ward or in the operating room.
So, now that you have decided that you want to participate in a research project as a trainee, how do you make it happen? Before you begin a project, you will have to choose a mentor; a topic; a clear, novel question; and the appropriate study design.
Chances are that at some point, a mentor helped guide you toward a career in cardiovascular surgery. A research mentor is just as important as a clinical mentor for a young surgeon. The most important trait that you should seek out in a research mentor is the ability to delineate important questions. All too often, residents and fellows are approached by attending surgeons with good intentions, but bad research ideas. Trainees then feel obligated to take them up on the project (in order to not appear like a slacker) and for various reasons, it does not result in an abstract, presentation, or publication. In fact, all it results in is frustration, a distaste for investigation, and wasted time.
The bottom line is that only you can protect your time, and as a surgical trainee, you must guard it ferociously. Look for a mentor that is an expert in your field of interest and who has a track record of publications.
He or she must be a logical thinker who can help you delineate a clear, novel question, choose the appropriate study design, guide your writing of the manuscript, and direct your submission to the appropriate meetings and journals.
Finally, your mentor must be dedicated to your success. We are all busy, but if your mentor cannot find the time to routinely meet with you at every step of your project, you need to find a new mentor.
Choosing a clear, novel clinical question starts with choosing an appropriate topic (Table 1). With the right topic and question, the hypothesis is obvious, it is easy to define your endpoints, and your study design will fall into place. But with the wrong question, your study will lack focus, it will be difficult to explain the relevance of your study, and you will not want to present your data on the podium. An example of a good question is: "Do patients with a given disease treated with operation X live longer than those treated with operation Y?"
Stay away from the lure of "Let's review our experience of operation X…" or "Why don't I see how many of operation Y we've done over the past 10 years…" These topics are vague and do not ask a specific question. There must be a clear hypothesis for any study that is expected to produce meaningful results.
Once you have chosen an appropriate question, you must decide on a study design. Although case reports are marginally publishable, they will not answer your clinical questions. For many reasons, randomized, controlled trials, the gold standard of research, are difficult to design, carry out, and complete in your short time as a trainee.
The good news is that well-designed and sufficiently powered observational studies often give similar results as randomized, controlled studies. Examples of common observational study designs include cohort studies, case control studies, and cross-sectional studies (Table 2).
Each study design is different and your mentor should be able to help you decide which is the best to answer the question you want to ask.
In the design of a study, one of the most important principles is defining a priori end points.
Every study will have one primary end point that reflects the hypothesis. Secondary endpoints are interesting and potentially helpful, but are not the main message. It will be important to meet with a statistician before you start data collection. Understanding the statistics to be used will allow you to collect your data in the correct way (categorical vs. continuous, etc.). Reviewing charts is very time consuming and you have to do everything in your power to ensure you do it only once.
The next step is to create a research proposal. To do this, you will need to go to the literature and see what published data relate to your study. Perhaps, there are previous studies examining your question with conflicting results?
Or if your question has not been previously investigated, what supporting literature suggests that yours is the next logical study? Your proposal should include a background section (1-2 paragraphs), hypothesis (1 sentence), the specific aims of the study (1-3 sentences), methods (2-4 paragraphs), anticipated results (1 paragraph), proposed timeline, and anticipated meeting to which it will be submitted. Your mentor will revise and critique the proposal and eventually give you a signature of approval. This proposal serves many purposes. It will allow you to fully understand the study before you begin, some form of it is usually required for the Institutional Review Board application, it will serve as the outline for your eventual manuscript, and it sets a timeline for completion of the project. Without an agreed-upon deadline, too many good studies are left in various states of completion when the trainee moves on, and are never finished. The deadline should be based on the meeting that you and your mentor agree is appropriate for reporting your results.
Most would agree that data collection is the most painful part of doing clinical research. However, there are a few tricks to ease your pain. First, there are many databases available that you may be able to harvest data from to minimize your chart work (Table 3). Before you hit the charts, it is essential to think through every step of the project. Anticipate problems (where in the chart will you locate each data point), do not collect unnecessary data points (postoperative data #3 serum [Na+] when looking at survival of thoracoscopic vs. open lobectomy), meet with your statistician beforehand to collect data for the correct analysis, collect the raw data (creatinine and weight, not presence of renal failure and obesity).
Finally, be sure that your data are backed up in multiple places. Some prefer to collect data on paper then enter it later into a spreadsheet. This ensures a hard copy of the data exists regardless if the electronic version is lost.
After the data are collected and the statistics are done, you will be faced with interpreting your results and composing an abstract and manuscript. If your study is focused and hypothesis driven, this step should be fairly straightforward. Schedule time with your mentor and discuss the results to ensure your interpretation of the data is correct.
Next using your proposal as an outline, put together a rough draft of a manuscript. Remember that manuscripts are the currency of academia. If you do not present and publish your work, you have not fully capitalized on the hard work you have put in to your study.
Your mentor will need to revise your manuscript repeatedly; use it as a learning experience for critiquing the literature and writing future manuscripts. He or she likely knows what editors and readers will be looking for in your finished product. Remember, you will need multiple revisions of the abstract and manuscript, so plan adequate time prior to your deadline for writing.
Most institutions have medical illustrators available for hire; consider including a drawing or photograph if it legitimately adds content to your manuscript.
The final step in the process is presenting your work in front of experts who likely know more about cardiothoracic surgery than you. Just remember, no one knows more about your data than you.
Prepare relentlessly for your talk, take a deep breath before you walk on stage, speak with confidence, and if you don't know the answer to a given question from the audience, admit it. Soon enough you will be the expert in the audience asking the tough questions. Then spend as much time as possible after the session speaking with audience members about you and your study.
You will meet lifelong colleagues, and maybe even your future partner. For many, research is a rewarding lifelong endeavor. For others, it is a means of learning to critically appraise the literature and landing a job. Either way, you cannot afford not to do research as a trainee.
Acknowledgment: I would like to thank my friend and colleague, Dr. Stephen H. McKellar (University of Utah), for his advice on performing research as a cardiothoracic trainee.
Dr. Seder is in the department of cardiovascular and thoracic surgery at Rush University Medical Center, Chicago.
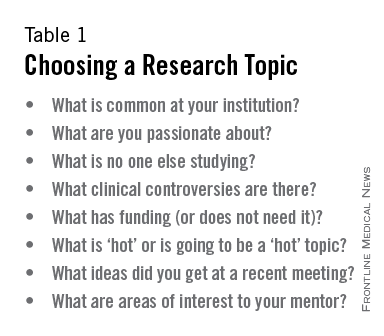
Is an MI following CEA or CAS just as clinically important as stroke?
The answer is yes!
I was not involved in the design of CREST, but I do have a responsibility to interpret the results and incorporate them into my clinical approach. When MI occurred after carotid endarterectomy (CEA) or carotid artery stenting (CAS) in CREST, the 1-year mortality was 14.2% versus 2.2% among those who did not have an MI (Blackshear et al. Circulation 2011;123:2571). This is consistent with the vascular literature, which is chock-full of strongly compelling data showing that we should take cardiac risk into account when planning our therapy.
It is not a mystery as to who is at risk for an MI. The significant independent risk factors for MI in CREST were known coronary artery disease or previous coronary revascularization. Since this is well known to us prior to treatment, shouldn’t this information be part of our therapeutic plan?
Suppose I said that perioperative MI is not important after abdominal aortic aneurysm repair, fem-pop bypass, or distal bypass?

A large part of the growth of endovascular approaches in recent years has been motivated by our best efforts to avoid MI. Think of the early days of endovascular aneurysm repair, prior to establishment of this as standard of care for most patients, and how many patients were treated with stent-grafts in an attempt to avoid cardiac risk. How could we now claim that it is unimportant?
There were two independent risk factors for mortality during CREST that increased the hazard ratio more than two times: stroke and MI (FDA panel presentation, Jan. 26, 2011).
The reason to revascularize the carotid is to prevent stroke, and this is a worthwhile endeavor. However, if the patient is harmed in some other way, especially in a manner associated with dramatically increased mortality, shouldn’t we understand that?
At some point, with further technological development, mesh-covered carotid stents, customized protection devices, and more informed patient selection, the stroke risk of CAS is likely to decrease. At that point, our relative concern about the risk of MI and the importance of MI as an endpoint is likely to increase, not decrease.
There is no doubt that we all fear stroke. Unfortunately, when something bad happens to a patient, they don’t get to select which complication they are going to have. We owe it to our patients to do what we can to diminish all the risks they face. I cannot envision an honest and useful future carotid trial design in which MI is not considered an endpoint.
Dr. Peter A. Schneider is chief of the division of vascular surgery, Hawaii Permanente Medical Group and Kaiser Foundation Hospital, Honolulu.
The answer is no!
Being given a choice between MI and stroke is like asking someone if they would rather be rich and healthy or poor and sick. The best option is to have neither an MI nor a stroke following carotid intervention. However, when given this unpleasant choice, the participants in CREST clearly stated that MI was preferable to either major or minor stroke. How often have we heard our patients state, "Doc, I’m not afraid to die, but I don’t want to live disabled from a stroke"?
A quality-of-life assessment was carried out in CREST patients using an SF-36.
This questionnaire looked at both the physical and the emotional effect of the complications of stroke and MI compared with those who were complication free.

One year after a complication, the patients stated that the worst thing that happened was a major stroke. The next worse thing was a minor stroke.
Myocardial infarction, 1 year later, from the patient’s perspective, was a nonevent. The argument that has been used regarding the importance of MI is that it has an adverse effect on life expectancy.
This is true, and it has been confirmed in several trials including CREST. The surprise finding is that stroke, including so-called minor strokes, also reduced life expectancy.
In CREST, 4 years following an adjudicated MI, the mortality rate was 19.1% versus 6.7% for those not suffering an MI.
However, the 4-year mortality rate among patients having suffered a stroke was 20%.
Therefore, compromised survival occurred equally among those patients following either stroke or MI.
However, not only did patients suffering a stroke have an equally high mortality, the group was further compromised by neurologic disability among the survivors, whereas the survivors following MI returned to their precomplication status.
Therefore, from the patients’ subjective status as well as objective clinical considerations, stroke is clearly more deleterious than MI.
Dr. Wesley S. Moore is a vascular and endovascular surgeon, and professor and chief, emeritus, of the division of vascular surgery, University of California, Los Angeles, Medical Center.
The answer is yes!
I was not involved in the design of CREST, but I do have a responsibility to interpret the results and incorporate them into my clinical approach. When MI occurred after carotid endarterectomy (CEA) or carotid artery stenting (CAS) in CREST, the 1-year mortality was 14.2% versus 2.2% among those who did not have an MI (Blackshear et al. Circulation 2011;123:2571). This is consistent with the vascular literature, which is chock-full of strongly compelling data showing that we should take cardiac risk into account when planning our therapy.
It is not a mystery as to who is at risk for an MI. The significant independent risk factors for MI in CREST were known coronary artery disease or previous coronary revascularization. Since this is well known to us prior to treatment, shouldn’t this information be part of our therapeutic plan?
Suppose I said that perioperative MI is not important after abdominal aortic aneurysm repair, fem-pop bypass, or distal bypass?
A large part of the growth of endovascular approaches in recent years has been motivated by our best efforts to avoid MI. Think of the early days of endovascular aneurysm repair, prior to establishment of this as standard of care for most patients, and how many patients were treated with stent-grafts in an attempt to avoid cardiac risk. How could we now claim that it is unimportant?
There were two independent risk factors for mortality during CREST that increased the hazard ratio more than two times: stroke and MI (FDA panel presentation, Jan. 26, 2011).
The reason to revascularize the carotid is to prevent stroke, and this is a worthwhile endeavor. However, if the patient is harmed in some other way, especially in a manner associated with dramatically increased mortality, shouldn’t we understand that?
At some point, with further technological development, mesh-covered carotid stents, customized protection devices, and more informed patient selection, the stroke risk of CAS is likely to decrease. At that point, our relative concern about the risk of MI and the importance of MI as an endpoint is likely to increase, not decrease.
There is no doubt that we all fear stroke. Unfortunately, when something bad happens to a patient, they don’t get to select which complication they are going to have. We owe it to our patients to do what we can to diminish all the risks they face. I cannot envision an honest and useful future carotid trial design in which MI is not considered an endpoint.
Dr. Peter A. Schneider is chief of the division of vascular surgery, Hawaii Permanente Medical Group and Kaiser Foundation Hospital, Honolulu.
The answer is no!
Being given a choice between MI and stroke is like asking someone if they would rather be rich and healthy or poor and sick. The best option is to have neither an MI nor a stroke following carotid intervention. However, when given this unpleasant choice, the participants in CREST clearly stated that MI was preferable to either major or minor stroke. How often have we heard our patients state, "Doc, I’m not afraid to die, but I don’t want to live disabled from a stroke"?
A quality-of-life assessment was carried out in CREST patients using an SF-36.
This questionnaire looked at both the physical and the emotional effect of the complications of stroke and MI compared with those who were complication free.
One year after a complication, the patients stated that the worst thing that happened was a major stroke. The next worse thing was a minor stroke.
Myocardial infarction, 1 year later, from the patient’s perspective, was a nonevent. The argument that has been used regarding the importance of MI is that it has an adverse effect on life expectancy.
This is true, and it has been confirmed in several trials including CREST. The surprise finding is that stroke, including so-called minor strokes, also reduced life expectancy.
In CREST, 4 years following an adjudicated MI, the mortality rate was 19.1% versus 6.7% for those not suffering an MI.
However, the 4-year mortality rate among patients having suffered a stroke was 20%.
Therefore, compromised survival occurred equally among those patients following either stroke or MI.
However, not only did patients suffering a stroke have an equally high mortality, the group was further compromised by neurologic disability among the survivors, whereas the survivors following MI returned to their precomplication status.
Therefore, from the patients’ subjective status as well as objective clinical considerations, stroke is clearly more deleterious than MI.
Dr. Wesley S. Moore is a vascular and endovascular surgeon, and professor and chief, emeritus, of the division of vascular surgery, University of California, Los Angeles, Medical Center.
The answer is yes!
I was not involved in the design of CREST, but I do have a responsibility to interpret the results and incorporate them into my clinical approach. When MI occurred after carotid endarterectomy (CEA) or carotid artery stenting (CAS) in CREST, the 1-year mortality was 14.2% versus 2.2% among those who did not have an MI (Blackshear et al. Circulation 2011;123:2571). This is consistent with the vascular literature, which is chock-full of strongly compelling data showing that we should take cardiac risk into account when planning our therapy.
It is not a mystery as to who is at risk for an MI. The significant independent risk factors for MI in CREST were known coronary artery disease or previous coronary revascularization. Since this is well known to us prior to treatment, shouldn’t this information be part of our therapeutic plan?
Suppose I said that perioperative MI is not important after abdominal aortic aneurysm repair, fem-pop bypass, or distal bypass?
A large part of the growth of endovascular approaches in recent years has been motivated by our best efforts to avoid MI. Think of the early days of endovascular aneurysm repair, prior to establishment of this as standard of care for most patients, and how many patients were treated with stent-grafts in an attempt to avoid cardiac risk. How could we now claim that it is unimportant?
There were two independent risk factors for mortality during CREST that increased the hazard ratio more than two times: stroke and MI (FDA panel presentation, Jan. 26, 2011).
The reason to revascularize the carotid is to prevent stroke, and this is a worthwhile endeavor. However, if the patient is harmed in some other way, especially in a manner associated with dramatically increased mortality, shouldn’t we understand that?
At some point, with further technological development, mesh-covered carotid stents, customized protection devices, and more informed patient selection, the stroke risk of CAS is likely to decrease. At that point, our relative concern about the risk of MI and the importance of MI as an endpoint is likely to increase, not decrease.
There is no doubt that we all fear stroke. Unfortunately, when something bad happens to a patient, they don’t get to select which complication they are going to have. We owe it to our patients to do what we can to diminish all the risks they face. I cannot envision an honest and useful future carotid trial design in which MI is not considered an endpoint.
Dr. Peter A. Schneider is chief of the division of vascular surgery, Hawaii Permanente Medical Group and Kaiser Foundation Hospital, Honolulu.
The answer is no!
Being given a choice between MI and stroke is like asking someone if they would rather be rich and healthy or poor and sick. The best option is to have neither an MI nor a stroke following carotid intervention. However, when given this unpleasant choice, the participants in CREST clearly stated that MI was preferable to either major or minor stroke. How often have we heard our patients state, "Doc, I’m not afraid to die, but I don’t want to live disabled from a stroke"?
A quality-of-life assessment was carried out in CREST patients using an SF-36.
This questionnaire looked at both the physical and the emotional effect of the complications of stroke and MI compared with those who were complication free.
One year after a complication, the patients stated that the worst thing that happened was a major stroke. The next worse thing was a minor stroke.
Myocardial infarction, 1 year later, from the patient’s perspective, was a nonevent. The argument that has been used regarding the importance of MI is that it has an adverse effect on life expectancy.
This is true, and it has been confirmed in several trials including CREST. The surprise finding is that stroke, including so-called minor strokes, also reduced life expectancy.
In CREST, 4 years following an adjudicated MI, the mortality rate was 19.1% versus 6.7% for those not suffering an MI.
However, the 4-year mortality rate among patients having suffered a stroke was 20%.
Therefore, compromised survival occurred equally among those patients following either stroke or MI.
However, not only did patients suffering a stroke have an equally high mortality, the group was further compromised by neurologic disability among the survivors, whereas the survivors following MI returned to their precomplication status.
Therefore, from the patients’ subjective status as well as objective clinical considerations, stroke is clearly more deleterious than MI.
Dr. Wesley S. Moore is a vascular and endovascular surgeon, and professor and chief, emeritus, of the division of vascular surgery, University of California, Los Angeles, Medical Center.

Be sure to keep mesenteric ischemia on your radar in your younger patients
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.

Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.

A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.
Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.
A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.
CHICAGO – Early recognition of mesenteric ischemia in young adults and children is essential to prevent bowel loss and other serious consequences associated with this rare condition, Dr. Michael Dalsing said at a vascular surgery symposium.
Mesenteric ischemia is generally seen in the elderly as the result of atherosclerotic and embolic occlusive diseases. Because young adults and children typically don’t have any of the telltale associated comorbidities such as cardiac arrhythmia or coronary artery disease to point physicians in this direction, the diagnosis of mesenteric ischemia is often delayed or misinterpreted as appendicitis, cholecystitis, or intra-abdominal abscess, he said.
Among 26 young adults under age 40 years who presented with acute mesenteric ischemia, only 6 were properly diagnosed preoperatively (Wien. Med. Wochenschr. 2012;162:349-53). The postoperative complication and mortality rates reached 61.5% and 27%, which is typical in this population, despite their otherwise good health, said Dr. Dalsing, director of vascular surgery at Indiana University, Indianapolis.
The hallmarks of acute mesenteric ischemia are standard in both young and old patients and include abdominal pain out of proportion to the physical exam, nausea, vomiting, and/or diarrhea. Acidosis, acute renal failure, and septic shock/sepsis can develop in roughly half of patients with more extensive liver or bowel ischemia or necrosis. The signs and symptoms of chronic ischemia are weight loss, food fear, and postprandial abdominal pain.
"For chronic mesenteric ischemia, what’s the important message? Consider the diagnosis," Dr. Dalsing said. "Do the imaging, find out what you have, and then you can worry about ancillary testing because, in general, these aren’t going to be your typical etiologies. In fact, they’re not standard fare at all."
The broad and atypical list of etiologies to consider in those under age 40 years include congenital aortic anomalies, hypercoagulable states, inflammatory conditions, collagen vascular disorders, and environmental agents such as cocaine use, smoking, or trauma. While MI is often suspected in those using cocaine, the vasoconstrictive effects of the drug can also cause vasospasm of the smaller branches of the mesenteric vessels, leading to nonocclusive mesenteric ischemia, he explained.
Once a diagnosis of chronic mesenteric ischemia is made in a young patient, management consists of fluid resuscitation, broad spectrum antibiotics, bowel rest, and imaging, often with a CT angiogram. The need for additional work-up, including hypercoagulable and inflammatory marker panels, varies based on initial clinical symptoms.
If vascular compromise is identified, the overall management goals should be to remove frankly necrotic bowel, reperfuse ischemic bowel, limit the resection length when possible to prevent short-gut syndrome, and treat the underlying etiology, Dr. Dalsing advised. Anticoagulation is also integral to prevent thrombus propagation.
Just six cases of mesenteric ischemia have been diagnosed at Indiana University in young adults over the last 16 years, with Takayasu’s arteritis the most common etiology, he noted. This includes a 20-year-old woman with a 5-year history of Takayasu’s, who presented with worsening abdominal pain despite remission of her Takayasu’s, as indicated by a normal sedimentation rate.
Repeat CT imaging revealed more than 70% celiac artery stenosis and more than 50% stenosis of the superior mesenteric artery (SMA). A median arcuate ligament division and celiac and SMA bypass graft, both with reverse saphenous vein originating from bilateral iliac arteries, was performed. "She’s had dramatic improvement" in her symptoms and remains on clopidogrel (Plavix) and low-dose steroids, Dr. Dalsing said.
A second patient with Takayasu’s presented with a 4-month history of abdominal pain, a 50-pound weight loss, stenosis of all major mesenteric arteries, and bowel pneumatosis. Despite this, her sedimentation rate was only slightly elevated at 33 mm/hour, and all other coagulation and inflammatory tests were normal. She remains symptom free at 2 years on daily aspirin after undergoing an emergent right common iliac-to-SMA bypass graft with reversed saphenous vein and bowel resection.
In cases in which bypass grafting is necessary, the internal iliac artery is the preferred conduit in children since the saphenous vein is very thin walled and thus, more prone to aneurysmal degeneration, Dr. Dalsing observed. In grown patients, the saphenous vein may be the best conduit in terms of ease of harvest and adequate length for even bifurcated grafts or C-loop alignment.
During postoperative follow-up, special effort should be taken because of the young age of these patients to reduce the detrimental effects of radiation from recurrent CT angiograms, he said. Patients with symptomatic improvement are followed at 1 month postoperatively with a physical exam that includes their weight and a mesenteric duplex to evaluate graft or stent patency. This is repeated every 6 months for 1-2 years, and decreased to yearly visits, if no disease progression is detected. More aggressive imaging with CT angiography is reserved for patients with recurrent symptoms or if duplex ultrasound is insufficient or shows progressive disease, he said at the meeting, sponsored by Northwestern University.
Dr. Dalsing reported having no financial disclosures.

'Walk out the snot'
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
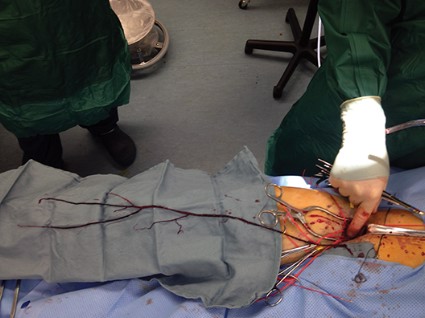
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
Balloon embolectomy revolutionized the treatment of acute thromboembolism involving peripheral arteries. However, an often overlooked method that actually may be more beneficial is to "walk out the snot."
This may sound somewhat disgusting but as can be seen from the accompanying photograph, the surgeon can often retrieve the entire clot from the main artery including extensions into collateral vessels.
In this picture of a patient undergoing femoral embolectomy with this technique, we retrieved a cast of the entire superficial femoral artery as well as the peroneal and posterior tibial arteries and two major collaterals.
The technique is simple. With proximal control of the inflow artery, the visible clot is gently pulled out of the arteriotomy in a slow but deliberate fashion, hand over hand. Often back bleeding will aid in pushing the specimen out of the arteriotomy. The maneuver is very similar to what children do when they feel the need to empty their nostrils! (No adult would do that – would they?)
Retrieval of a specimen like the one in the photo will usually reassure the surgeon that there will not be more thrombus left behind.
The technique also prevents possible arterial injury from a balloon catheter. For both reasons a postcompletion arteriogram may sometimes be avoided.
Dr. Showalter is clinical assistant professor of surgery at Florida State University Medical School and attending vascular surgeon, Sarasota Vascular Specialists.
Dr. Samson is clinical professor of surgery at Florida State University Medical School, attending vascular surgeon, Sarasota Vascular Specialists, and the medical editor of Vascular Specialist.
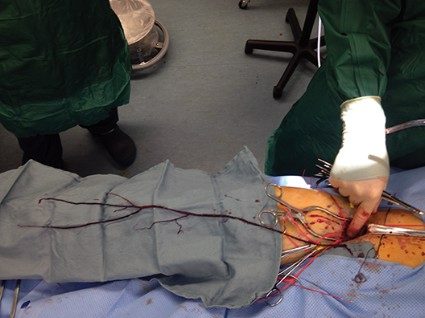
MRD test can predict HSCT outcomes in ALL patients

Credit: Graham Colm
A method of measuring minimal residual disease (MRD) can predict transplant outcomes in adults with acute lymphoblastic leukemia (ALL), according to a study published in Biology of Blood and Marrow Transplantation.
Researchers used the test, called LymphoSIGHT, to evaluate MRD in patient blood samples.
The test successfully predicted both relapse and survival and detected evidence of disease a median of 3 months prior to relapse.
This research was conducted by Aaron C. Logan, MD, PhD, of the University of California, San Francisco, and his colleagues. It was sponsored by Sequenta, Inc., makers of the LymphoSIGHT test.
The researchers used LymphoSIGHT to analyze 237 blood samples from 29 adults who underwent allogeneic hematopoietic stem cell transplant (HSCT) to treat ALL.
The LymphoSIGHT test consists of a 2-step process. First, cancer cell DNA sequences are identified in a diagnostic sample. Follow-up samples are then screened for these sequences to detect MRD.
The results, which are generated in 7 days using Sequenta’s CLIA-certified laboratory, are provided in a report that shows a patient’s MRD status and level, as well as MRD trends over time.
The researchers found the test could quantify MRD in 93% of patients. MRD positivity was defined as more than 1 leukemia cell per 1 million white blood cells.
Patients who were MRD-positive before HSCT conditioning were significantly more likely than MRD-negative patients to relapse after transplant (hazard ratio=7.7, P=0.003).
And patients who were MRD-positive in the first 90 days after transplant had a significantly higher risk of relapse than patients who were MRD-negative (hazard ratio=14; P<0.0001).
Patients who were MRD-positive at any point after HSCT (17 of 25 evaluable patients) all relapsed and died from their disease. Their median survival was 359 days (range, 85-1991 days). The median lead-time from MRD detection to clinical relapse was 89 days (range, 0-207 days).
Of the 8 patients who remained MRD-negative, 6 were still alive at a median of 1853 days post-HSCT (range, 1641-2732). Two patients died from complications of graft-vs-host disease, without evidence of leukemia recurrence.
The researchers said these results suggest the LymphoSIGHT test can help physicians understand treatment responses and patient prognoses, as well as guide treatment decisions. ![]()
Credit: Graham Colm
A method of measuring minimal residual disease (MRD) can predict transplant outcomes in adults with acute lymphoblastic leukemia (ALL), according to a study published in Biology of Blood and Marrow Transplantation.
Researchers used the test, called LymphoSIGHT, to evaluate MRD in patient blood samples.
The test successfully predicted both relapse and survival and detected evidence of disease a median of 3 months prior to relapse.
This research was conducted by Aaron C. Logan, MD, PhD, of the University of California, San Francisco, and his colleagues. It was sponsored by Sequenta, Inc., makers of the LymphoSIGHT test.
The researchers used LymphoSIGHT to analyze 237 blood samples from 29 adults who underwent allogeneic hematopoietic stem cell transplant (HSCT) to treat ALL.
The LymphoSIGHT test consists of a 2-step process. First, cancer cell DNA sequences are identified in a diagnostic sample. Follow-up samples are then screened for these sequences to detect MRD.
The results, which are generated in 7 days using Sequenta’s CLIA-certified laboratory, are provided in a report that shows a patient’s MRD status and level, as well as MRD trends over time.
The researchers found the test could quantify MRD in 93% of patients. MRD positivity was defined as more than 1 leukemia cell per 1 million white blood cells.
Patients who were MRD-positive before HSCT conditioning were significantly more likely than MRD-negative patients to relapse after transplant (hazard ratio=7.7, P=0.003).
And patients who were MRD-positive in the first 90 days after transplant had a significantly higher risk of relapse than patients who were MRD-negative (hazard ratio=14; P<0.0001).
Patients who were MRD-positive at any point after HSCT (17 of 25 evaluable patients) all relapsed and died from their disease. Their median survival was 359 days (range, 85-1991 days). The median lead-time from MRD detection to clinical relapse was 89 days (range, 0-207 days).
Of the 8 patients who remained MRD-negative, 6 were still alive at a median of 1853 days post-HSCT (range, 1641-2732). Two patients died from complications of graft-vs-host disease, without evidence of leukemia recurrence.
The researchers said these results suggest the LymphoSIGHT test can help physicians understand treatment responses and patient prognoses, as well as guide treatment decisions. ![]()
Credit: Graham Colm
A method of measuring minimal residual disease (MRD) can predict transplant outcomes in adults with acute lymphoblastic leukemia (ALL), according to a study published in Biology of Blood and Marrow Transplantation.
Researchers used the test, called LymphoSIGHT, to evaluate MRD in patient blood samples.
The test successfully predicted both relapse and survival and detected evidence of disease a median of 3 months prior to relapse.
This research was conducted by Aaron C. Logan, MD, PhD, of the University of California, San Francisco, and his colleagues. It was sponsored by Sequenta, Inc., makers of the LymphoSIGHT test.
The researchers used LymphoSIGHT to analyze 237 blood samples from 29 adults who underwent allogeneic hematopoietic stem cell transplant (HSCT) to treat ALL.
The LymphoSIGHT test consists of a 2-step process. First, cancer cell DNA sequences are identified in a diagnostic sample. Follow-up samples are then screened for these sequences to detect MRD.
The results, which are generated in 7 days using Sequenta’s CLIA-certified laboratory, are provided in a report that shows a patient’s MRD status and level, as well as MRD trends over time.
The researchers found the test could quantify MRD in 93% of patients. MRD positivity was defined as more than 1 leukemia cell per 1 million white blood cells.
Patients who were MRD-positive before HSCT conditioning were significantly more likely than MRD-negative patients to relapse after transplant (hazard ratio=7.7, P=0.003).
And patients who were MRD-positive in the first 90 days after transplant had a significantly higher risk of relapse than patients who were MRD-negative (hazard ratio=14; P<0.0001).
Patients who were MRD-positive at any point after HSCT (17 of 25 evaluable patients) all relapsed and died from their disease. Their median survival was 359 days (range, 85-1991 days). The median lead-time from MRD detection to clinical relapse was 89 days (range, 0-207 days).
Of the 8 patients who remained MRD-negative, 6 were still alive at a median of 1853 days post-HSCT (range, 1641-2732). Two patients died from complications of graft-vs-host disease, without evidence of leukemia recurrence.
The researchers said these results suggest the LymphoSIGHT test can help physicians understand treatment responses and patient prognoses, as well as guide treatment decisions. ![]()