User login
Enrollment Deadlines Coming Up for 2014 MOC Exams
The Hospital Medicine MOC secure exams are offered every spring and fall. Although the dates might seem far off now, hospitalists interested in taking the Hospital Medicine MOC exam must complete the entry process for the FPHM program at least two weeks before the exam registration deadline. For the spring MOC exam, this means hospitalists must complete the FPHM program entry process by Feb. 14, 2014, for the Spring 2014 exam, and Aug. 1, 2014, for the Fall 2014 exam.
To complete the entry process, hospitalists must:
- Be licensed and in good standing.
- Hold current or previous ABIM certification in Internal Medicine and current Advanced Cardiac Life Support (ACLS) certification.
- Complete at least three years of unsupervised hospital medicine practice experience prior to entry into the Focused Practice in Hospital Medicine MOC program. Formal fellowship training in a hospital medicine fellowship program can be counted toward the three-year practice experience criteria.
- Electronically submit a self-attestation and an attestation from a Senior Hospital Officer (SHO) that they meet the patient encounter thresholds for internal medicine practice in the hospital setting.
Once enrolled, hospitalists will be eligible to schedule a seat for the Hospital Medicine MOC exam during the registration period; however, the ABIM stipulates that hospitalists must be entered into the program at least two weeks prior to the exam date.
At the same time, hospitalists must have completed 100 points of self-evaluation within the last 10 years. Twenty of the points in Self-Evaluation of Medical Knowledge and 40 points in Self-Evaluation of Practice Performance must have been completed in the last three years.
The Hospital Medicine MOC secure exams are offered every spring and fall. Although the dates might seem far off now, hospitalists interested in taking the Hospital Medicine MOC exam must complete the entry process for the FPHM program at least two weeks before the exam registration deadline. For the spring MOC exam, this means hospitalists must complete the FPHM program entry process by Feb. 14, 2014, for the Spring 2014 exam, and Aug. 1, 2014, for the Fall 2014 exam.
To complete the entry process, hospitalists must:
- Be licensed and in good standing.
- Hold current or previous ABIM certification in Internal Medicine and current Advanced Cardiac Life Support (ACLS) certification.
- Complete at least three years of unsupervised hospital medicine practice experience prior to entry into the Focused Practice in Hospital Medicine MOC program. Formal fellowship training in a hospital medicine fellowship program can be counted toward the three-year practice experience criteria.
- Electronically submit a self-attestation and an attestation from a Senior Hospital Officer (SHO) that they meet the patient encounter thresholds for internal medicine practice in the hospital setting.
Once enrolled, hospitalists will be eligible to schedule a seat for the Hospital Medicine MOC exam during the registration period; however, the ABIM stipulates that hospitalists must be entered into the program at least two weeks prior to the exam date.
At the same time, hospitalists must have completed 100 points of self-evaluation within the last 10 years. Twenty of the points in Self-Evaluation of Medical Knowledge and 40 points in Self-Evaluation of Practice Performance must have been completed in the last three years.
The Hospital Medicine MOC secure exams are offered every spring and fall. Although the dates might seem far off now, hospitalists interested in taking the Hospital Medicine MOC exam must complete the entry process for the FPHM program at least two weeks before the exam registration deadline. For the spring MOC exam, this means hospitalists must complete the FPHM program entry process by Feb. 14, 2014, for the Spring 2014 exam, and Aug. 1, 2014, for the Fall 2014 exam.
To complete the entry process, hospitalists must:
- Be licensed and in good standing.
- Hold current or previous ABIM certification in Internal Medicine and current Advanced Cardiac Life Support (ACLS) certification.
- Complete at least three years of unsupervised hospital medicine practice experience prior to entry into the Focused Practice in Hospital Medicine MOC program. Formal fellowship training in a hospital medicine fellowship program can be counted toward the three-year practice experience criteria.
- Electronically submit a self-attestation and an attestation from a Senior Hospital Officer (SHO) that they meet the patient encounter thresholds for internal medicine practice in the hospital setting.
Once enrolled, hospitalists will be eligible to schedule a seat for the Hospital Medicine MOC exam during the registration period; however, the ABIM stipulates that hospitalists must be entered into the program at least two weeks prior to the exam date.
At the same time, hospitalists must have completed 100 points of self-evaluation within the last 10 years. Twenty of the points in Self-Evaluation of Medical Knowledge and 40 points in Self-Evaluation of Practice Performance must have been completed in the last three years.
ABIM Unveils New Process for Focused Practice in Hospital Medicine MOC
While the program is just a few years old, changes to the Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) from the American Board of Internal Medicine (ABIM) make it more attractive to hospitalists, bringing it in line with other MOC programs. And now is the time to act for 2014.
Not only do the changes to the FPHM MOC streamline the process, it remains the only ABIM certification designed exclusively for the growing ranks of hospitalists, according to hospitalists who have already earned the new certification. The hospitalist-centric program makes their board certification more applicable to their everyday practice and emphasizes their expertise in the specialty.
The alignment with the hospital medicine specialty has both practical and ideological benefits for hospitalists. On the practical side, the hospital medicine focused medical knowledge modules and preparation for the Hospital Medicine MOC exam are more focused, as the content better matches the day-to-day life of a hospitalist.
“From a content perspective, both for studying and the updates, it allows the hospitalist to focus on content that’s most relevant to their practice,” says hospitalist Jennifer Myers, MD, associate professor of clinical medicine and associate designated institutional official for graduate medical education at the Hospital of the University of Pennsylvania in Philadelphia.
Dr. Myers earned the FPHM certification in 2011. Compared to the internal medicine MOC, she says “the standard questions focused on ambulatory medicine do not always apply,” and the likelihood that hospitalists kept up on those topics was slim. Rather, “hospitalists will be better prepared to take the Focused Practice in Hospital Medicine. And as they’re updating and studying, they can focus on relevant topics for their practice,” she says.
For hospitalist and former SHM president Jeffrey Wiese, MD, MHM, the FPHM MOC program helps define his work in ways other than just the physical space of the hospital.
“If I am to have public accountability as a hospitalist, it has to be more than just geography. Intrinsic to a true hospitalist is systems architecture…improving the quality and patient safety delivered by the hospital system,” says Dr. Wiese, professor of medicine and senior associate dean of graduate medical education at Tulane University in New Orleans.
Dr. Wiese is intimately familiar with the process: He served on the ABIM’s Hospital Medicine MOC Exam Writing ABIM test writing committee for the FPHM pathway MOC program. He now serves on the new ABIM Council.
“This is a way to distinguish the ideals of the specialty,” he says. “What hospitalists do is more than just deliver inpatient care. … It’s about advancing the quality and safety of the system, and the FPHM MOC track ensures fidelity to that standard.”
FPHM’s ability to differentiate hospitalists resonates with Daniel Brotman, MD, director of the hospitalist program at Johns Hopkins Hospital in Baltimore and chair of SHM’s Annual Meeting Committee and Education Committee. And that differentiation extends from the individual hospitalist to the movement as a whole.
“If you’re a hospitalist and you’re invested in the field, this is an important statement to make on behalf of your specialty,” he says. “It can give you some added respect within your institution when people ask you about specialized training in hospital medicine.”
Even if hospitalists didn’t have specialized training, the FPHM MOC demonstrates that they “did have to pass a specialized certification process that gives different credentials,” Dr. Brotman says. “This is the best way to do that.”
He also sees it as an individual benefit for hospitalists—both for their career advancement and their peace of mind—knowing that they are more up to date with their clinical practice.
“You practice hospital medicine. If you want an exam that hits the ball to your forehand, this is it,” he says. “If you’re nervous about the board exam, I’d be more nervous about taking a generalized exam.”
Brendon Shank is SHM’s associate vice president of communications.
While the program is just a few years old, changes to the Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) from the American Board of Internal Medicine (ABIM) make it more attractive to hospitalists, bringing it in line with other MOC programs. And now is the time to act for 2014.
Not only do the changes to the FPHM MOC streamline the process, it remains the only ABIM certification designed exclusively for the growing ranks of hospitalists, according to hospitalists who have already earned the new certification. The hospitalist-centric program makes their board certification more applicable to their everyday practice and emphasizes their expertise in the specialty.
The alignment with the hospital medicine specialty has both practical and ideological benefits for hospitalists. On the practical side, the hospital medicine focused medical knowledge modules and preparation for the Hospital Medicine MOC exam are more focused, as the content better matches the day-to-day life of a hospitalist.
“From a content perspective, both for studying and the updates, it allows the hospitalist to focus on content that’s most relevant to their practice,” says hospitalist Jennifer Myers, MD, associate professor of clinical medicine and associate designated institutional official for graduate medical education at the Hospital of the University of Pennsylvania in Philadelphia.
Dr. Myers earned the FPHM certification in 2011. Compared to the internal medicine MOC, she says “the standard questions focused on ambulatory medicine do not always apply,” and the likelihood that hospitalists kept up on those topics was slim. Rather, “hospitalists will be better prepared to take the Focused Practice in Hospital Medicine. And as they’re updating and studying, they can focus on relevant topics for their practice,” she says.
For hospitalist and former SHM president Jeffrey Wiese, MD, MHM, the FPHM MOC program helps define his work in ways other than just the physical space of the hospital.
“If I am to have public accountability as a hospitalist, it has to be more than just geography. Intrinsic to a true hospitalist is systems architecture…improving the quality and patient safety delivered by the hospital system,” says Dr. Wiese, professor of medicine and senior associate dean of graduate medical education at Tulane University in New Orleans.
Dr. Wiese is intimately familiar with the process: He served on the ABIM’s Hospital Medicine MOC Exam Writing ABIM test writing committee for the FPHM pathway MOC program. He now serves on the new ABIM Council.
“This is a way to distinguish the ideals of the specialty,” he says. “What hospitalists do is more than just deliver inpatient care. … It’s about advancing the quality and safety of the system, and the FPHM MOC track ensures fidelity to that standard.”
FPHM’s ability to differentiate hospitalists resonates with Daniel Brotman, MD, director of the hospitalist program at Johns Hopkins Hospital in Baltimore and chair of SHM’s Annual Meeting Committee and Education Committee. And that differentiation extends from the individual hospitalist to the movement as a whole.
“If you’re a hospitalist and you’re invested in the field, this is an important statement to make on behalf of your specialty,” he says. “It can give you some added respect within your institution when people ask you about specialized training in hospital medicine.”
Even if hospitalists didn’t have specialized training, the FPHM MOC demonstrates that they “did have to pass a specialized certification process that gives different credentials,” Dr. Brotman says. “This is the best way to do that.”
He also sees it as an individual benefit for hospitalists—both for their career advancement and their peace of mind—knowing that they are more up to date with their clinical practice.
“You practice hospital medicine. If you want an exam that hits the ball to your forehand, this is it,” he says. “If you’re nervous about the board exam, I’d be more nervous about taking a generalized exam.”
Brendon Shank is SHM’s associate vice president of communications.
While the program is just a few years old, changes to the Focused Practice in Hospital Medicine (FPHM) Maintenance of Certification (MOC) from the American Board of Internal Medicine (ABIM) make it more attractive to hospitalists, bringing it in line with other MOC programs. And now is the time to act for 2014.
Not only do the changes to the FPHM MOC streamline the process, it remains the only ABIM certification designed exclusively for the growing ranks of hospitalists, according to hospitalists who have already earned the new certification. The hospitalist-centric program makes their board certification more applicable to their everyday practice and emphasizes their expertise in the specialty.
The alignment with the hospital medicine specialty has both practical and ideological benefits for hospitalists. On the practical side, the hospital medicine focused medical knowledge modules and preparation for the Hospital Medicine MOC exam are more focused, as the content better matches the day-to-day life of a hospitalist.
“From a content perspective, both for studying and the updates, it allows the hospitalist to focus on content that’s most relevant to their practice,” says hospitalist Jennifer Myers, MD, associate professor of clinical medicine and associate designated institutional official for graduate medical education at the Hospital of the University of Pennsylvania in Philadelphia.
Dr. Myers earned the FPHM certification in 2011. Compared to the internal medicine MOC, she says “the standard questions focused on ambulatory medicine do not always apply,” and the likelihood that hospitalists kept up on those topics was slim. Rather, “hospitalists will be better prepared to take the Focused Practice in Hospital Medicine. And as they’re updating and studying, they can focus on relevant topics for their practice,” she says.
For hospitalist and former SHM president Jeffrey Wiese, MD, MHM, the FPHM MOC program helps define his work in ways other than just the physical space of the hospital.
“If I am to have public accountability as a hospitalist, it has to be more than just geography. Intrinsic to a true hospitalist is systems architecture…improving the quality and patient safety delivered by the hospital system,” says Dr. Wiese, professor of medicine and senior associate dean of graduate medical education at Tulane University in New Orleans.
Dr. Wiese is intimately familiar with the process: He served on the ABIM’s Hospital Medicine MOC Exam Writing ABIM test writing committee for the FPHM pathway MOC program. He now serves on the new ABIM Council.
“This is a way to distinguish the ideals of the specialty,” he says. “What hospitalists do is more than just deliver inpatient care. … It’s about advancing the quality and safety of the system, and the FPHM MOC track ensures fidelity to that standard.”
FPHM’s ability to differentiate hospitalists resonates with Daniel Brotman, MD, director of the hospitalist program at Johns Hopkins Hospital in Baltimore and chair of SHM’s Annual Meeting Committee and Education Committee. And that differentiation extends from the individual hospitalist to the movement as a whole.
“If you’re a hospitalist and you’re invested in the field, this is an important statement to make on behalf of your specialty,” he says. “It can give you some added respect within your institution when people ask you about specialized training in hospital medicine.”
Even if hospitalists didn’t have specialized training, the FPHM MOC demonstrates that they “did have to pass a specialized certification process that gives different credentials,” Dr. Brotman says. “This is the best way to do that.”
He also sees it as an individual benefit for hospitalists—both for their career advancement and their peace of mind—knowing that they are more up to date with their clinical practice.
“You practice hospital medicine. If you want an exam that hits the ball to your forehand, this is it,” he says. “If you’re nervous about the board exam, I’d be more nervous about taking a generalized exam.”
Brendon Shank is SHM’s associate vice president of communications.
Affordable Care Act Latest in Half-Century of Healthcare Reform
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Initial Efforts
1965
• President Lyndon B. Johnson signs the Social Security Act, which authorizes both Medicare and Medicaid; the law is widely labeled the biggest healthcare reform of the past century.
1993
• President Bill Clinton attempts to craft universal healthcare legislation that includes both individual and employer mandates. He appoints his wife, Hillary Rodham Clinton, as chair of the White House Task Force on Health Reform. The President’s Health Security Act ultimately fails in Congress.
1997
• State Children’s Health Insurance Program (S-CHIP) authorized by Congress, covering low-income children in families above Medicaid eligibility levels.
2006
• Massachusetts (followed by Vermont in 2011) passes legislation that expands healthcare coverage to nearly all state residents; the Massachusetts law is later deemed a template for the Patient Protection and Affordable Care Act of 2010.
The Patient Protection and Affordable Care Act (ACA)
March 23, 2010
• President Obama signs the ACA into law. Among the law’s early provisions: Medicare beneficiaries who reach the Part D drug coverage gap begin receiving $250 rebates, and the IRS begins allowing tax credits to small employers that offer health insurance to their employees.
July 1, 2010
• Federal government begins enrolling patients with pre-existing conditions in a temporary Pre-Existing Condition Insurance Plan (PCIP).
• Healthcare.gov website debuts.
• IRS begins assessing 10% tax on indoor tanning.
Sep. 23, 2010
• Patient-Centered Outcomes Research Institute (PCORI) launches with 21-member board of directors.
• For new insurance plans or those renewed on or after this date, parents are allowed to keep adult children on their health policies until they turn 26 (many private plans voluntarily offered this option earlier).
• HHS bans insurers from imposing lifetime coverage limits and from denying health coverage to children with pre-existing conditions or excluding specific conditions from coverage.
• HHS requires new and renewing health plans to eliminate cost sharing for certain preventive services recommended by U.S. Preventive Services Task Force.
Sep. 30, 2010
• U.S. Comptroller General appoints 15 members to National Health Care Workforce Commission (commission does not secure funding).
December 30, 2010
• Medicare debuts first phase of Physician Compare website.
Jan. 1, 2011
• CMS begins closing Medicare Part D drug coverage gap.
• Medicare begins paying 10% bonus for primary care services (funded through 2015).
• Center for Medicare and Medicaid Innovation debuts, with a focus on testing new payment and care delivery systems.
March 23, 2011
• HHS begins providing grants to individual states to help set up health insurance exchanges.
July 1, 2011
• CMS stops paying for Medicaid services related to specific hospital-acquired infections.
Oct. 1, 2011
• Fifteen-member Independent Payment Advisory Board is formally established (but no members are nominated). The IPAB is charged with issuing legislative recommendations to lower Medicare spending growth, but only if projected costs exceed a certain threshold.
Jan. 1, 2012
• CMS launches Medicaid bundled-payment demonstration and Accountable Care Organization (ACO) incentive program.
• CMS reduces Medicare Advantage rebates but offers bonuses to high-quality plans.
Aug. 1, 2012
• HHS requires most new and renewing health plans to eliminate cost sharing for women’s preventive health services, including contraception.
Oct. 1, 2012
• CMS begins its Value-Based Purchasing (VBP) Program in Medicare, starting with a 1% withholding in FY2013.
• CMS begins reducing Medicare payments based on excess hospital readmissions, starting with a 1% penalty in FY2013.
Jan. 1, 2013
• CMS starts five-year bundled payment pilot program for Medicare, covering 10 conditions.
• CMS increases Medicaid payments for primary care services to 100% of Medicare’s rate (funded for two years).
• IRS increases Medicare tax rate to 2.35% on individuals earning more than $200,000 and on married couples earning more than $250,000; also imposes 3.8% tax on unearned income among high-income taxpayers.
• IRS begins assessing excise tax of 2.3% on sale of taxable medical devices.
Jan. 2, 2013
• Sequestration results in across-the-board cuts of 2% in Medicare reimbursements.
July 1, 2013
• DHS officially launches Consumer Operated and Oriented Plan (CO-OP) to encourage growth of nonprofit health insurers (roughly $2 billion in loans given to co-ops in 23 states by end of 2012).
Oct. 1, 2013
• Open enrollment begins for state- and federal government-run health insurance exchanges and expanded Medicaid; the rollout is marred by multiple computer glitches.
• CMS lowers Medicare Disproportionate Share Hospital (DSH) payments by 75%, starting in FY2014 but plans to supplement these payments based on each hospital’s share of uncompensated care.
• CMS lowers Medicaid DSH payments by $22 billion over 10 years, beginning with $500 million reduction in FY2014.
Jan. 1, 2014
• Coverage begins through health insurance exchanges. Individuals and families with incomes between 100% and 400% of the federal poverty level can receive subsidies to help pay for premiums.
• Voluntary Medicaid expansions expected to take place in roughly half of all states, for individuals up to 138% of the federal poverty level.
• Insurers banned from imposing annual limits on coverage, from restricting coverage due to pre-existing conditions, and from basing premiums on gender.
• Insurers required to cover 10 “essential health benefits,” including medication and maternity care.
March 31, 2014
• Open enrollment closes for health insurance exchanges; under the “individual mandate,” people who qualify but don’t buy insurance by this date will be penalized up to 1% of income (penalty increases in subsequent years).
Oct. 1, 2014
• CMS imposes 1% reduction in payments to hospitals with excess hospital-acquired conditions (FY2015).
• CMS imposes penalties on hospitals that haven’t met electronic health record (EHR) meaningful use requirements.
Jan. 1, 2015
• Employer Shared Responsibility Payment, or the “employer mandate,” begins (delayed from Jan. 1, 2014). With a few exceptions, employers with more than 50 employees must offer coverage or pay a fine.
• CMS begins imposing fines based on doctors who didn’t meet Physician Quality Reporting System requirements during 2013, with an initial 1.5% penalty that rises to 2% in 2016.
Jan. 1, 2018
• High-cost, or so-called “Cadillac,” insurance plans—those with premiums over $10,200 for individuals or $27,500 for family coverage—will be assessed an excise tax.
Sources: Healthcare.gov, Commonwealth Fund, Kaiser Family Foundation, American Medical Association, Greater New York Hospital Association.
Obamacare by the Numbers
Sometimes, numbers do tell a story. The Affordable Care Act has no shortage of them, and amid the densely packed provisions, regulations, pilots, demonstrations, fines, and other elements, a few numbers provide a glimpse of the intense wrangling that created both winners and losers in the healthcare reform effort.
One of the biggest numbers is also the mostly hotly contested: whether Obamacare will blow a hole in the nation’s deficit or lead to a trillion dollars or more in savings over the first two decades. In March 2010, the Congressional Budget Office predicted the latter, with savings of $143 billion through 2019 and a hazier guess of savings equivalent to 0.5% of gross domestic product—equal to $1 trillion or more—through the 2020s.
The problem? “That calculation reflects an assumption that the provisions of the legislation are enacted and remain unchanged throughout the next two decades, which is often not the case for major legislation,” the CBO wrote at the time. That prediction, at least, was spot on.
Amid the ongoing political back and forth, one point is often overlooked: Although still unsustainably high, per capita healthcare spending is now increasing at the lowest rate in decades. Robert Berenson, MD, an Institute Fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, notes that the trend (starting in 2006) predated the recession. Likewise, it is occurring in Medicare, where most beneficiaries have first-dollar coverage. Instead of being a side effect of the sluggish economy, Dr. Berenson believes fundamental change is occurring on the provider side, and that the additional focus on reform may be making a difference.
Some analysts, he says, believe that providers are responding to the anticipation of change in the system and are beginning to change their own behavior accordingly.
“That means we have more time to get it right, in terms of wholesale change in how healthcare is delivered, and, for me, that’s a good thing,” he says.
A few other numbers of note:
$1.075 trillion
The state- and federal-run healthcare exchanges are expected to cost $1.075 trillion through 2023, according to the CBO. That eye-popping number includes spending for “high-risk pools, premium review activities, loans to consumer-operated and -oriented plans, and grants to states for the establishment of exchanges.”
The big question, of course, is whether that investment will pay off, and a big part of the answer will rest with a well-balanced risk pool. In other words, long-term financial stability means getting as many young and healthy people into the exchanges as possible.
$2 billion
The ACA sought to increase competition by supporting the creation of consumer co-ops, despite opposition from the insurance industry. By the end of last year, HHS had doled out roughly $2 billion in loans to nonprofit co-ops in 23 states, as part of its Consumer Operated and Oriented Plan (CO-OP). Backers of these co-ops had initially sought $10 billion, however, based on estimates of what would be required to ensure a higher likelihood of success.
Although preliminary evidence suggests that these newcomers may be helping to drive down costs in some states, a lack of additional funding has prevented other potential co-ops from receiving startup loans. The co-ops also are barred from using any federal money for marketing, cannot jointly negotiate contracts with doctors, and have limited access to the large employer insurance market—casting doubt on their continued viability.
$0
On Sep. 30, 2010, the U.S. comptroller general appointed 15 members to the National Health Care Workforce Commission, an acknowledgment that the country needs more guidance in how to address existing shortages—expected to widen—in doctors and other healthcare providers. The commission, authorized by the ACA, has never met, however. The act didn’t appropriate any money for it, and Congress has yet to approve any funding either, meaning that the commission’s members are legally barred from conducting any work.
—Bryn Nelson, PhD
Sometimes, numbers do tell a story. The Affordable Care Act has no shortage of them, and amid the densely packed provisions, regulations, pilots, demonstrations, fines, and other elements, a few numbers provide a glimpse of the intense wrangling that created both winners and losers in the healthcare reform effort.
One of the biggest numbers is also the mostly hotly contested: whether Obamacare will blow a hole in the nation’s deficit or lead to a trillion dollars or more in savings over the first two decades. In March 2010, the Congressional Budget Office predicted the latter, with savings of $143 billion through 2019 and a hazier guess of savings equivalent to 0.5% of gross domestic product—equal to $1 trillion or more—through the 2020s.
The problem? “That calculation reflects an assumption that the provisions of the legislation are enacted and remain unchanged throughout the next two decades, which is often not the case for major legislation,” the CBO wrote at the time. That prediction, at least, was spot on.
Amid the ongoing political back and forth, one point is often overlooked: Although still unsustainably high, per capita healthcare spending is now increasing at the lowest rate in decades. Robert Berenson, MD, an Institute Fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, notes that the trend (starting in 2006) predated the recession. Likewise, it is occurring in Medicare, where most beneficiaries have first-dollar coverage. Instead of being a side effect of the sluggish economy, Dr. Berenson believes fundamental change is occurring on the provider side, and that the additional focus on reform may be making a difference.
Some analysts, he says, believe that providers are responding to the anticipation of change in the system and are beginning to change their own behavior accordingly.
“That means we have more time to get it right, in terms of wholesale change in how healthcare is delivered, and, for me, that’s a good thing,” he says.
A few other numbers of note:
$1.075 trillion
The state- and federal-run healthcare exchanges are expected to cost $1.075 trillion through 2023, according to the CBO. That eye-popping number includes spending for “high-risk pools, premium review activities, loans to consumer-operated and -oriented plans, and grants to states for the establishment of exchanges.”
The big question, of course, is whether that investment will pay off, and a big part of the answer will rest with a well-balanced risk pool. In other words, long-term financial stability means getting as many young and healthy people into the exchanges as possible.
$2 billion
The ACA sought to increase competition by supporting the creation of consumer co-ops, despite opposition from the insurance industry. By the end of last year, HHS had doled out roughly $2 billion in loans to nonprofit co-ops in 23 states, as part of its Consumer Operated and Oriented Plan (CO-OP). Backers of these co-ops had initially sought $10 billion, however, based on estimates of what would be required to ensure a higher likelihood of success.
Although preliminary evidence suggests that these newcomers may be helping to drive down costs in some states, a lack of additional funding has prevented other potential co-ops from receiving startup loans. The co-ops also are barred from using any federal money for marketing, cannot jointly negotiate contracts with doctors, and have limited access to the large employer insurance market—casting doubt on their continued viability.
$0
On Sep. 30, 2010, the U.S. comptroller general appointed 15 members to the National Health Care Workforce Commission, an acknowledgment that the country needs more guidance in how to address existing shortages—expected to widen—in doctors and other healthcare providers. The commission, authorized by the ACA, has never met, however. The act didn’t appropriate any money for it, and Congress has yet to approve any funding either, meaning that the commission’s members are legally barred from conducting any work.
—Bryn Nelson, PhD
Sometimes, numbers do tell a story. The Affordable Care Act has no shortage of them, and amid the densely packed provisions, regulations, pilots, demonstrations, fines, and other elements, a few numbers provide a glimpse of the intense wrangling that created both winners and losers in the healthcare reform effort.
One of the biggest numbers is also the mostly hotly contested: whether Obamacare will blow a hole in the nation’s deficit or lead to a trillion dollars or more in savings over the first two decades. In March 2010, the Congressional Budget Office predicted the latter, with savings of $143 billion through 2019 and a hazier guess of savings equivalent to 0.5% of gross domestic product—equal to $1 trillion or more—through the 2020s.
The problem? “That calculation reflects an assumption that the provisions of the legislation are enacted and remain unchanged throughout the next two decades, which is often not the case for major legislation,” the CBO wrote at the time. That prediction, at least, was spot on.
Amid the ongoing political back and forth, one point is often overlooked: Although still unsustainably high, per capita healthcare spending is now increasing at the lowest rate in decades. Robert Berenson, MD, an Institute Fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy, notes that the trend (starting in 2006) predated the recession. Likewise, it is occurring in Medicare, where most beneficiaries have first-dollar coverage. Instead of being a side effect of the sluggish economy, Dr. Berenson believes fundamental change is occurring on the provider side, and that the additional focus on reform may be making a difference.
Some analysts, he says, believe that providers are responding to the anticipation of change in the system and are beginning to change their own behavior accordingly.
“That means we have more time to get it right, in terms of wholesale change in how healthcare is delivered, and, for me, that’s a good thing,” he says.
A few other numbers of note:
$1.075 trillion
The state- and federal-run healthcare exchanges are expected to cost $1.075 trillion through 2023, according to the CBO. That eye-popping number includes spending for “high-risk pools, premium review activities, loans to consumer-operated and -oriented plans, and grants to states for the establishment of exchanges.”
The big question, of course, is whether that investment will pay off, and a big part of the answer will rest with a well-balanced risk pool. In other words, long-term financial stability means getting as many young and healthy people into the exchanges as possible.
$2 billion
The ACA sought to increase competition by supporting the creation of consumer co-ops, despite opposition from the insurance industry. By the end of last year, HHS had doled out roughly $2 billion in loans to nonprofit co-ops in 23 states, as part of its Consumer Operated and Oriented Plan (CO-OP). Backers of these co-ops had initially sought $10 billion, however, based on estimates of what would be required to ensure a higher likelihood of success.
Although preliminary evidence suggests that these newcomers may be helping to drive down costs in some states, a lack of additional funding has prevented other potential co-ops from receiving startup loans. The co-ops also are barred from using any federal money for marketing, cannot jointly negotiate contracts with doctors, and have limited access to the large employer insurance market—casting doubt on their continued viability.
$0
On Sep. 30, 2010, the U.S. comptroller general appointed 15 members to the National Health Care Workforce Commission, an acknowledgment that the country needs more guidance in how to address existing shortages—expected to widen—in doctors and other healthcare providers. The commission, authorized by the ACA, has never met, however. The act didn’t appropriate any money for it, and Congress has yet to approve any funding either, meaning that the commission’s members are legally barred from conducting any work.
—Bryn Nelson, PhD
Affordable Care Act Calls on Hospitalists to Hone Skills

Many of the buzzwords being bandied about in discussions of the Affordable Care Act, or ACA, already are familiar to hospitalists. HM providers regularly operate in an interdisciplinary environment and have been leading the charge in quality improvement initiatives over the past few years. But as the ACA kicks into high gear, hospitalists say it will ramp up the emphasis on tighter cost controls (especially identifying and eliminating waste), greater efficiency, and smoother transitions of care.
Supporters of the law have advanced the moral and ethical argument that everyone deserves at least basic healthcare.
“Money is not going to magically appear to pay for that,”
Dr. Hilger says. “So we’re all responsible for looking at what we do and where’s the waste in the system to help improve the care for the most at-risk patients.”
Some fundamentals of the work environment haven’t changed dramatically.
“Even before the ACA, there were core measures and coding and documentation requirements,” Dr. Hilger says. What’s different now, he says, is an added sense of urgency in scrutinizing quality and cost. That expectation may be especially acute for HM providers. “I think there’s a lot of pressure on hospitalists because organizations and hospitals are expecting us to be the primary care doctors in the hospital and to eliminate waste,” he says. That mandate dovetails with campaigns like Choosing Wisely that ask doctors to ponder the necessity of often overused or misused tests and procedures.

—Rick Hilger, MD, SFHM,medical director for care management, Regions Hospital, St. Paul, Minn., hospitalist, HealthPartners, member, SHM Public Policy Committee.
Another area of added emphasis is transitioning patients out of the hospital in a high-quality, low-cost way.
“That’s something we should have been doing 10 years ago,” Dr. Hilger says. “So that’s definitely a trend in the right direction that the ACA is helping to further.”
In effect, the heightened profile of ACOs, the rise of quality-based metrics, and the shift toward pay-for-performance models are extending the expectations around what happens to patients before, during, and after a hospital stay.
“We’re expected to not only provide excellent care to the patient while they’re in the hospital, but we’re expected to make sure that there is a good transition plan at discharge,” Dr. Hilger explains. “We’re expected to make sure that the patient has appropriate appointments lined up, that they’re getting appropriate services either at home or that we try to get them appropriately to a skilled nursing facility.”
Dr. Lenchus says a major objective of healthcare reform—at least in principle—is to devote more energy to preventive care to help ward off more expensive acute care.
“If we assume the hypothesis that the ACA really tries to keep people out of the hospital, that makes their time in the hospital that much more focused and concentrated, to the point where quality, cost control, and efficiency are really going to come into play,” he says.
And, at least initially, patients who have chronic conditions or were excluded from the healthcare system due to pre-existing illnesses or an inability to pay are likely to be clamoring for access the most. Consequently, those who do end up in the hospital will require more complex care.
“With respect to the workload, I believe we’ll see patients who are farther along in their disease process, in more acute, more dire need for healthcare,” Dr. Lenchus says.
Providers already accustomed to working in teams to improve quality and to communicating with a hospital’s chief medical officer and other C-suite executives over matters of cost will have a clear advantage.
“The ACA is not perfect, and it’s going to take time to figure out what works and what doesn’t, but what we have control over on a daily basis is to really focus on high-quality, low-cost, standardized best practices,” Dr. Hilger says.
What does that mean in practice? “Really work on perfecting or maximizing your transitions of care,” he says. “Really work with care management and social workers, and work with your hospital to try to develop relationships—if you haven’t already—with the primary care systems in your community.”
Bryn Nelson is a freelance medical writer in Seattle.
Many of the buzzwords being bandied about in discussions of the Affordable Care Act, or ACA, already are familiar to hospitalists. HM providers regularly operate in an interdisciplinary environment and have been leading the charge in quality improvement initiatives over the past few years. But as the ACA kicks into high gear, hospitalists say it will ramp up the emphasis on tighter cost controls (especially identifying and eliminating waste), greater efficiency, and smoother transitions of care.
Supporters of the law have advanced the moral and ethical argument that everyone deserves at least basic healthcare.
“Money is not going to magically appear to pay for that,”
Dr. Hilger says. “So we’re all responsible for looking at what we do and where’s the waste in the system to help improve the care for the most at-risk patients.”
Some fundamentals of the work environment haven’t changed dramatically.
“Even before the ACA, there were core measures and coding and documentation requirements,” Dr. Hilger says. What’s different now, he says, is an added sense of urgency in scrutinizing quality and cost. That expectation may be especially acute for HM providers. “I think there’s a lot of pressure on hospitalists because organizations and hospitals are expecting us to be the primary care doctors in the hospital and to eliminate waste,” he says. That mandate dovetails with campaigns like Choosing Wisely that ask doctors to ponder the necessity of often overused or misused tests and procedures.
—Rick Hilger, MD, SFHM,medical director for care management, Regions Hospital, St. Paul, Minn., hospitalist, HealthPartners, member, SHM Public Policy Committee.
Another area of added emphasis is transitioning patients out of the hospital in a high-quality, low-cost way.
“That’s something we should have been doing 10 years ago,” Dr. Hilger says. “So that’s definitely a trend in the right direction that the ACA is helping to further.”
In effect, the heightened profile of ACOs, the rise of quality-based metrics, and the shift toward pay-for-performance models are extending the expectations around what happens to patients before, during, and after a hospital stay.
“We’re expected to not only provide excellent care to the patient while they’re in the hospital, but we’re expected to make sure that there is a good transition plan at discharge,” Dr. Hilger explains. “We’re expected to make sure that the patient has appropriate appointments lined up, that they’re getting appropriate services either at home or that we try to get them appropriately to a skilled nursing facility.”
Dr. Lenchus says a major objective of healthcare reform—at least in principle—is to devote more energy to preventive care to help ward off more expensive acute care.
“If we assume the hypothesis that the ACA really tries to keep people out of the hospital, that makes their time in the hospital that much more focused and concentrated, to the point where quality, cost control, and efficiency are really going to come into play,” he says.
And, at least initially, patients who have chronic conditions or were excluded from the healthcare system due to pre-existing illnesses or an inability to pay are likely to be clamoring for access the most. Consequently, those who do end up in the hospital will require more complex care.
“With respect to the workload, I believe we’ll see patients who are farther along in their disease process, in more acute, more dire need for healthcare,” Dr. Lenchus says.
Providers already accustomed to working in teams to improve quality and to communicating with a hospital’s chief medical officer and other C-suite executives over matters of cost will have a clear advantage.
“The ACA is not perfect, and it’s going to take time to figure out what works and what doesn’t, but what we have control over on a daily basis is to really focus on high-quality, low-cost, standardized best practices,” Dr. Hilger says.
What does that mean in practice? “Really work on perfecting or maximizing your transitions of care,” he says. “Really work with care management and social workers, and work with your hospital to try to develop relationships—if you haven’t already—with the primary care systems in your community.”
Bryn Nelson is a freelance medical writer in Seattle.
Many of the buzzwords being bandied about in discussions of the Affordable Care Act, or ACA, already are familiar to hospitalists. HM providers regularly operate in an interdisciplinary environment and have been leading the charge in quality improvement initiatives over the past few years. But as the ACA kicks into high gear, hospitalists say it will ramp up the emphasis on tighter cost controls (especially identifying and eliminating waste), greater efficiency, and smoother transitions of care.
Supporters of the law have advanced the moral and ethical argument that everyone deserves at least basic healthcare.
“Money is not going to magically appear to pay for that,”
Dr. Hilger says. “So we’re all responsible for looking at what we do and where’s the waste in the system to help improve the care for the most at-risk patients.”
Some fundamentals of the work environment haven’t changed dramatically.
“Even before the ACA, there were core measures and coding and documentation requirements,” Dr. Hilger says. What’s different now, he says, is an added sense of urgency in scrutinizing quality and cost. That expectation may be especially acute for HM providers. “I think there’s a lot of pressure on hospitalists because organizations and hospitals are expecting us to be the primary care doctors in the hospital and to eliminate waste,” he says. That mandate dovetails with campaigns like Choosing Wisely that ask doctors to ponder the necessity of often overused or misused tests and procedures.
—Rick Hilger, MD, SFHM,medical director for care management, Regions Hospital, St. Paul, Minn., hospitalist, HealthPartners, member, SHM Public Policy Committee.
Another area of added emphasis is transitioning patients out of the hospital in a high-quality, low-cost way.
“That’s something we should have been doing 10 years ago,” Dr. Hilger says. “So that’s definitely a trend in the right direction that the ACA is helping to further.”
In effect, the heightened profile of ACOs, the rise of quality-based metrics, and the shift toward pay-for-performance models are extending the expectations around what happens to patients before, during, and after a hospital stay.
“We’re expected to not only provide excellent care to the patient while they’re in the hospital, but we’re expected to make sure that there is a good transition plan at discharge,” Dr. Hilger explains. “We’re expected to make sure that the patient has appropriate appointments lined up, that they’re getting appropriate services either at home or that we try to get them appropriately to a skilled nursing facility.”
Dr. Lenchus says a major objective of healthcare reform—at least in principle—is to devote more energy to preventive care to help ward off more expensive acute care.
“If we assume the hypothesis that the ACA really tries to keep people out of the hospital, that makes their time in the hospital that much more focused and concentrated, to the point where quality, cost control, and efficiency are really going to come into play,” he says.
And, at least initially, patients who have chronic conditions or were excluded from the healthcare system due to pre-existing illnesses or an inability to pay are likely to be clamoring for access the most. Consequently, those who do end up in the hospital will require more complex care.
“With respect to the workload, I believe we’ll see patients who are farther along in their disease process, in more acute, more dire need for healthcare,” Dr. Lenchus says.
Providers already accustomed to working in teams to improve quality and to communicating with a hospital’s chief medical officer and other C-suite executives over matters of cost will have a clear advantage.
“The ACA is not perfect, and it’s going to take time to figure out what works and what doesn’t, but what we have control over on a daily basis is to really focus on high-quality, low-cost, standardized best practices,” Dr. Hilger says.
What does that mean in practice? “Really work on perfecting or maximizing your transitions of care,” he says. “Really work with care management and social workers, and work with your hospital to try to develop relationships—if you haven’t already—with the primary care systems in your community.”
Bryn Nelson is a freelance medical writer in Seattle.
Hospitalists Will Be Critical to Obamacare Success
It has survived a bitterly divided Congress and a polarized public, a narrow Supreme Court ruling, and a 16-day government shutdown triggered by an effort to defund or repeal it. Hailed by some as the most significant healthcare reform in a half-century, it is also roundly scorned by others as an ill-advised debacle.
With some of its most hotly contested provisions now taking effect, the Affordable Care Act—or Obamacare, as both backers and detractors now call it—has been the object of admiration and animosity, of optimism and consternation. Its supporters have pointed to the promise of unprecedented access to healthcare for millions, while its critics have pointed to the trickle of consumers able to access the main web portal during an error-plagued rollout.
Beyond the heated rhetoric, however, what will the complicated and quickly evolving elements of Obamacare actually mean for hospitalists and for healthcare access, affordability, capacity, and delivery? In the short term, analysts say so much change is happening all at once that it’s nearly impossible to predict how it might turn out.
“Everyone’s kind of holding their breath to see what happens,” says Ann O’Malley, MD, MPH, a senior fellow at the Washington, D.C.-based Center for Studying Health System Change.
One thing is certain: more reliance on hospital-based providers.

“I think there are a lot of things on a hospitalist’s plate right now. And hospitals, because of the cost pressures, are definitely looking to us to lead the way through this uncertain time,” says Rick Hilger, MD, SFHM, medical director for care management at Regions Hospital in St. Paul, Minn., and a hospitalist for HealthPartners.
Amid the upheaval, experts are seeing the signs of a few major trends. In the short term, one emerging theme is considerable geographical variation in consumer access and costs, and in pressure on providers.
“How this is going to feel will depend, to a great extent, on where you live,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.

Analysts also have seen hints of more universal changes, including an accelerated trend toward the consolidation of provider groups, an added emphasis on team-based care, and significant momentum toward a pay-for-performance delivery model.
An Uneven Exchange
One of the law’s most visible and controversial elements, the health insurance exchange or marketplace, got off to a rocky start Oct. 1, 2013, when computer glitches hobbled the main healthcare.gov portal for 36 state exchanges and plagued many state-run sites as well.
While some state-run exchanges have generally earned high marks, others have struggled. Analysts are most worried about the balkiness of the main web-based portal, through which the majority of enrollees will have to pass. While older and sicker patients are generally more motivated to keep trying, the same isn’t necessarily true for younger and healthier people whose participation will be vital to help balance each state’s risk pool. Analysts sometimes call these people, “young invincibles.” Because they generally seek out care far less often than older consumers, their lower medical costs can help compensate for higher expenditures elsewhere.
If too few sign up, however, a state’s risk pool may be imbalanced toward costlier patients, causing insurance premiums to rise and creating a vicious cycle that destabilizes the market and makes more expensive insurance less attractive to younger people. Economists say the carrot-and-stick approach—offering subsidies to help lower-income people pay for premiums and gradually increasing financial penalties for those who choose not to buy any coverage—is likely to help. Nevertheless, supporters are nervous that malfunctioning exchange sites could cause would-be enrollees to delay or drop out, and, at the end of 2013, a worried Obama administration was scrambling to address the cascade of glitches.
Because the health insurance exchanges were highly controversial already, says Dr. Ku, who sits on the board of the Washington, D.C. Health Benefits Exchange Authority, every problem is likely to be magnified by critics. Although he doesn’t expect “huge changes” in physician payment rates from plans in the exchanges, he says varying degrees of competition could drive down insurers’ prices in some markets.
Doctors also are likely to encounter plenty of confusion among the newly insured, and Dr. Ku hopes educational sessions will help healthcare professionals take more of a leading role in helping patients navigate an often bewildering system.
“One of the most important things that a hospital can do to help in the beginning is to help on the enrollment end of things,” he says. “Help patients who don’t quite understand how to get in, how to use these systems.”
It’s too early to say whether the exchanges can still meet the Congressional Budget Office’s prediction of 7 million enrollees by the end of the 2014 enrollment period (and 13 million by 2015). But analysts say the composition of the risk pool—something that should be clearer this spring—may provide a glimpse into the ACA’s long-term financial viability.
Instead of a consistent pattern across the country, the exchanges will be shaped by local market forces, such as the number of competitors and the extent to which cheaper plans will try to limit access to providers. To minimize their costs, some exchange-based plans are promising in-network hospitals higher patient volumes in exchange for discounted reimbursements. Other hospitals now find themselves excluded from most private plans in favor of cheaper options.
In exchange for lower premiums, some of these insurers are offering “skinny networks” that give consumers more limited provider options.
“A primary objective in the marketplace is to offer the cheapest plan possible, and to do that the insurers are going to look at who are the least expensive providers,” says Christiane Mitchell, director of federal affairs for the Association of American Medical Colleges. Not surprisingly, some of the costliest providers tend to take care of sicker or higher-risk patients.
“It’s a very, very strong concern, and it’s one that we have been very vocal on since the enactment of the Affordable Care Act,” Mitchell says. The association also has expressed concern that lower-income patients buying into the cheapest plans may not have access to the specialty services they need the most. That possibility, she says, increases the importance of navigators helping the newly insured pick out the best plans.
A Question of Access
Another big question is how the healthcare system will accommodate the influx of newly insured. Because hospitals already have been the safety net for many patients lacking access to preventive and primary care, urgent and specialty care may go through a bigger adjustment period, says Dr. Hilger, who sits on SHM’s Public Policy Committee.
The growing provider shortage certainly won’t help. By 2015, the AAMC predicts a shortfall of 63,000 doctors, almost evenly split between primary and specialty care. By 2025, that number is expected to more than double.
Mitchell says the gap between supply and demand is worsening due to the sheer number of baby boomers entering Medicare. At the same time, she says, one in three doctors in the U.S. is now over the age of 60 and nearing retirement age. Whether through Medicaid or the marketplace, the ACA’s coverage expansion will exacerbate the shortages. “It’s not to the level of the boomers entering Medicare, but it certainly is having a major impact on access issues and exacerbating the shortage, again, across specialties,” she says.
Other analysts say the extent of the capacity problem will depend in large part on location.
“The truth is that the extent to which there are enough doctors or enough hospital beds is largely a function of geography,” Dr. Ku says. “So, if you’re in an urban area with lots of teaching hospitals, you probably have enough doctors and you probably have enough hospital beds. If, on the other hand, you’re in a poor, rural area, chances are you don’t.”
As both insurance and demand for healthcare expand, those areas that were having problems already “are going to be stretched even more,” Dr. Ku says.
Meeting demand also means training more doctors, and Mitchell worries about a pipeline that already is underfunded. Although medical school enrollment is at a record high, federal support for residency training has been frozen since 1997, meaning that the funded residency slots may not be sufficient to accommodate future graduates. Further declines in the clinical income that subsidizes training would place additional pressure on the educational mission of teaching hospitals, Mitchell says.
Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine in the division of hospital medicine at the University of Miami, says existing doctor deficits, the ACA’s new demands, and the growing medical training gap could swirl into a “perfect storm” of access problems. Longer delays in accessing primary and specialty care, in turn, could prevent timely interventions earlier during the course of a disease or condition.
“What it’s going to mean for hospitalists is that we’re going to see—over the short-term, maybe even the next three to five years—a real impact on when patients present, in terms of the acuity of their disease,” Dr. Lenchus says. That means sicker patients in the hospital.
Given the massive changes, observers like Mitchell and Dr. Hilger acknowledge that ironing out the rough spots will take time.
“There’s going to be two steps forward, one step back, but the simple question is: Was it ever OK to have tens of millions of patients who had no insurance or were underinsured and were using the emergency room as their primary care?” Dr. Hilger says. “I think, no matter what your political affiliation, that, in general, the answer is no.”

—Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine, division of hospital medicine, University of Miami, member, SHM Public Policy Committee.
Costs All Over the Map
One of the plan’s biggest goals and part of its name—affordability for those patients—also seems to vary considerably by geography. A recent analysis by The New York Times, for example, found that 58% of all counties served by the federal-run exchanges offer plans from only one or two insurance carriers. The relative lack of competition in many markets has created some huge cost disparities in premiums between neighboring states, and even neighboring counties.
With so many factors influencing costs, both proponents and opponents have found fodder to bolster their case that the law is either making insurance more affordable or sharply increasing premiums. One important consideration, Dr. Ku says, is that all plans must now include 10 “essential health benefits,” such as maternity care and medications, for example, and cannot allow gender to be a rating factor. As a result, he says, the cheapest plans for a relatively healthy young man may cost more now, while costs for a woman or an older person with a chronic condition like diabetes may go down.
Although the new mandates were designed to improve insurance standards, they sparked another firestorm when millions of Americans began receiving policy cancellation notices in 2013. Because many private insurance plans sold to individuals no longer met the ACA’s minimum requirements, insurers began dropping those plans or requiring enrollees to switch to other, often more expensive, ones. In November, in an effort to stem the mass cancellations, President Barack Obama bowed to mounting political pressure and announced a reprieve that allows insurance companies to renew existing policies for another year. That attempted fix has not been so straightforward, however. Many insurers were reluctant to reissue cancelled policies, and multiple states, which have the authority to regulate insurance sold within their borders, declined the administration’s request.

—Robert Berenson, MD, senior fellow, Urban Institute, Washington, D.C.
The Long View
Despite the intense focus on the first few months of health insurance enrollment, it may take several years before the markets begin to settle and other insurers waiting on the sidelines decide whether to participate. If they eventually succeed, the ACA exchanges could have several long-term consequences.
“If, in fact, the exchanges offer good insurance products that the public begins to accept and find that they have good information to make choices, it could affect the prevalence of employer-based insurance,” says Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy. Over many years, employers could begin moving their employees into exchanges rather than providing direct healthcare benefits.
If they prove viable, the exchanges also may help accelerate the trend toward more consolidation of physician practices or increase pressure to align with larger entities. Despite concerns over skinnier networks, for example, the more tightly controlled access to providers under certain plans dovetails with the ACA’s heightened emphasis on more integrated accountable care organizations (ACOs).
In fact, ACOs and other lower-profile provisions that enjoy more bipartisan support could ultimately play key roles in reshaping how healthcare is delivered in the U.S. Many of these reform efforts have been launched as pilots or demonstration projects. Salt Lake City-based healthcare consulting firm Leavitt Partners tallied nearly 500 ACOs through the end of July 2013, more than double the total in June 2012.
Other Obamacare provisions are levying fines based on excessive hospital-acquired conditions or readmissions and adjusting reimbursements based on e-prescribing, the Physician Quality Reporting System (PQRS), value-based purchasing, meaningful use of electronic health records, and other mandates.
“The overall theme is that the ACA is speeding up the move away from fee-for-service payment toward new payment methodologies that are going to be increasingly based on quality measures,” Dr. O’Malley says. “All of these are basically efforts to shift incentives away from rewarding volume of services toward value and quality of care for patients. And the crux of all of them is to try to get physicians to work together, not only with other specialists and their primary care colleagues, but also with other inter-professional members of their team.”
For hospitalists, it means relying more on nurses, physician assistants, and other support staff.
“In a collaborative agreement, where it’s a physician-led healthcare team, I think non-physician healthcare providers could help to support the physician hospitalists,” Dr. Lenchus says.
That extra help may be essential.
“I do think the workload will increase, and not just because we’ll have more people clamoring for healthcare and more patients who are sicker—remember, there are no more pre-existing conditions,” Dr. Lenchus says. “The other piece to this that goes outside the patient-physician interaction is that there’s a lot of additional regulations and administrative burdens, if you will, as individual hospitalists and as hospitals on the whole.”
The need to share resources to cut down on doctors’ workloads, Dr. O’Malley says, may be yet another factor in the accelerated rate of practice consolidation.
“There’s pressure among docs not just to function as teams but to consolidate among themselves either through physicians’ organizations like IPAs [independent practice associations] or becoming employees of hospitals,” she says. “That’s where you get economies of scale and shared infrastructure to do a lot of the things that the ACA is requiring of them.”
Consolidation or not, she sees plenty of potential for increased efficiency. Some medical groups may need to hire more support staff, whereas others may simply require more coordination and delegation among existing personnel to lighten the load and focus on priorities. The trick, Dr. Hilger says, is finding the right balance amid the dramatic change.
“Bottom line, it goes back to the triple aim that hospitalists should be aiming for: high quality, low-cost, patient-centered care,” he says. “I think the challenge over the next 10 years is how to find the sweet spot between all of those.”
Bryn Nelson is a freelance medical writer in Seattle.
It has survived a bitterly divided Congress and a polarized public, a narrow Supreme Court ruling, and a 16-day government shutdown triggered by an effort to defund or repeal it. Hailed by some as the most significant healthcare reform in a half-century, it is also roundly scorned by others as an ill-advised debacle.
With some of its most hotly contested provisions now taking effect, the Affordable Care Act—or Obamacare, as both backers and detractors now call it—has been the object of admiration and animosity, of optimism and consternation. Its supporters have pointed to the promise of unprecedented access to healthcare for millions, while its critics have pointed to the trickle of consumers able to access the main web portal during an error-plagued rollout.
Beyond the heated rhetoric, however, what will the complicated and quickly evolving elements of Obamacare actually mean for hospitalists and for healthcare access, affordability, capacity, and delivery? In the short term, analysts say so much change is happening all at once that it’s nearly impossible to predict how it might turn out.
“Everyone’s kind of holding their breath to see what happens,” says Ann O’Malley, MD, MPH, a senior fellow at the Washington, D.C.-based Center for Studying Health System Change.
One thing is certain: more reliance on hospital-based providers.
“I think there are a lot of things on a hospitalist’s plate right now. And hospitals, because of the cost pressures, are definitely looking to us to lead the way through this uncertain time,” says Rick Hilger, MD, SFHM, medical director for care management at Regions Hospital in St. Paul, Minn., and a hospitalist for HealthPartners.
Amid the upheaval, experts are seeing the signs of a few major trends. In the short term, one emerging theme is considerable geographical variation in consumer access and costs, and in pressure on providers.
“How this is going to feel will depend, to a great extent, on where you live,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.
Analysts also have seen hints of more universal changes, including an accelerated trend toward the consolidation of provider groups, an added emphasis on team-based care, and significant momentum toward a pay-for-performance delivery model.
An Uneven Exchange
One of the law’s most visible and controversial elements, the health insurance exchange or marketplace, got off to a rocky start Oct. 1, 2013, when computer glitches hobbled the main healthcare.gov portal for 36 state exchanges and plagued many state-run sites as well.
While some state-run exchanges have generally earned high marks, others have struggled. Analysts are most worried about the balkiness of the main web-based portal, through which the majority of enrollees will have to pass. While older and sicker patients are generally more motivated to keep trying, the same isn’t necessarily true for younger and healthier people whose participation will be vital to help balance each state’s risk pool. Analysts sometimes call these people, “young invincibles.” Because they generally seek out care far less often than older consumers, their lower medical costs can help compensate for higher expenditures elsewhere.
If too few sign up, however, a state’s risk pool may be imbalanced toward costlier patients, causing insurance premiums to rise and creating a vicious cycle that destabilizes the market and makes more expensive insurance less attractive to younger people. Economists say the carrot-and-stick approach—offering subsidies to help lower-income people pay for premiums and gradually increasing financial penalties for those who choose not to buy any coverage—is likely to help. Nevertheless, supporters are nervous that malfunctioning exchange sites could cause would-be enrollees to delay or drop out, and, at the end of 2013, a worried Obama administration was scrambling to address the cascade of glitches.
Because the health insurance exchanges were highly controversial already, says Dr. Ku, who sits on the board of the Washington, D.C. Health Benefits Exchange Authority, every problem is likely to be magnified by critics. Although he doesn’t expect “huge changes” in physician payment rates from plans in the exchanges, he says varying degrees of competition could drive down insurers’ prices in some markets.
Doctors also are likely to encounter plenty of confusion among the newly insured, and Dr. Ku hopes educational sessions will help healthcare professionals take more of a leading role in helping patients navigate an often bewildering system.
“One of the most important things that a hospital can do to help in the beginning is to help on the enrollment end of things,” he says. “Help patients who don’t quite understand how to get in, how to use these systems.”
It’s too early to say whether the exchanges can still meet the Congressional Budget Office’s prediction of 7 million enrollees by the end of the 2014 enrollment period (and 13 million by 2015). But analysts say the composition of the risk pool—something that should be clearer this spring—may provide a glimpse into the ACA’s long-term financial viability.
Instead of a consistent pattern across the country, the exchanges will be shaped by local market forces, such as the number of competitors and the extent to which cheaper plans will try to limit access to providers. To minimize their costs, some exchange-based plans are promising in-network hospitals higher patient volumes in exchange for discounted reimbursements. Other hospitals now find themselves excluded from most private plans in favor of cheaper options.
In exchange for lower premiums, some of these insurers are offering “skinny networks” that give consumers more limited provider options.
“A primary objective in the marketplace is to offer the cheapest plan possible, and to do that the insurers are going to look at who are the least expensive providers,” says Christiane Mitchell, director of federal affairs for the Association of American Medical Colleges. Not surprisingly, some of the costliest providers tend to take care of sicker or higher-risk patients.
“It’s a very, very strong concern, and it’s one that we have been very vocal on since the enactment of the Affordable Care Act,” Mitchell says. The association also has expressed concern that lower-income patients buying into the cheapest plans may not have access to the specialty services they need the most. That possibility, she says, increases the importance of navigators helping the newly insured pick out the best plans.
A Question of Access
Another big question is how the healthcare system will accommodate the influx of newly insured. Because hospitals already have been the safety net for many patients lacking access to preventive and primary care, urgent and specialty care may go through a bigger adjustment period, says Dr. Hilger, who sits on SHM’s Public Policy Committee.
The growing provider shortage certainly won’t help. By 2015, the AAMC predicts a shortfall of 63,000 doctors, almost evenly split between primary and specialty care. By 2025, that number is expected to more than double.
Mitchell says the gap between supply and demand is worsening due to the sheer number of baby boomers entering Medicare. At the same time, she says, one in three doctors in the U.S. is now over the age of 60 and nearing retirement age. Whether through Medicaid or the marketplace, the ACA’s coverage expansion will exacerbate the shortages. “It’s not to the level of the boomers entering Medicare, but it certainly is having a major impact on access issues and exacerbating the shortage, again, across specialties,” she says.
Other analysts say the extent of the capacity problem will depend in large part on location.
“The truth is that the extent to which there are enough doctors or enough hospital beds is largely a function of geography,” Dr. Ku says. “So, if you’re in an urban area with lots of teaching hospitals, you probably have enough doctors and you probably have enough hospital beds. If, on the other hand, you’re in a poor, rural area, chances are you don’t.”
As both insurance and demand for healthcare expand, those areas that were having problems already “are going to be stretched even more,” Dr. Ku says.
Meeting demand also means training more doctors, and Mitchell worries about a pipeline that already is underfunded. Although medical school enrollment is at a record high, federal support for residency training has been frozen since 1997, meaning that the funded residency slots may not be sufficient to accommodate future graduates. Further declines in the clinical income that subsidizes training would place additional pressure on the educational mission of teaching hospitals, Mitchell says.
Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine in the division of hospital medicine at the University of Miami, says existing doctor deficits, the ACA’s new demands, and the growing medical training gap could swirl into a “perfect storm” of access problems. Longer delays in accessing primary and specialty care, in turn, could prevent timely interventions earlier during the course of a disease or condition.
“What it’s going to mean for hospitalists is that we’re going to see—over the short-term, maybe even the next three to five years—a real impact on when patients present, in terms of the acuity of their disease,” Dr. Lenchus says. That means sicker patients in the hospital.
Given the massive changes, observers like Mitchell and Dr. Hilger acknowledge that ironing out the rough spots will take time.
“There’s going to be two steps forward, one step back, but the simple question is: Was it ever OK to have tens of millions of patients who had no insurance or were underinsured and were using the emergency room as their primary care?” Dr. Hilger says. “I think, no matter what your political affiliation, that, in general, the answer is no.”
—Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine, division of hospital medicine, University of Miami, member, SHM Public Policy Committee.
Costs All Over the Map
One of the plan’s biggest goals and part of its name—affordability for those patients—also seems to vary considerably by geography. A recent analysis by The New York Times, for example, found that 58% of all counties served by the federal-run exchanges offer plans from only one or two insurance carriers. The relative lack of competition in many markets has created some huge cost disparities in premiums between neighboring states, and even neighboring counties.
With so many factors influencing costs, both proponents and opponents have found fodder to bolster their case that the law is either making insurance more affordable or sharply increasing premiums. One important consideration, Dr. Ku says, is that all plans must now include 10 “essential health benefits,” such as maternity care and medications, for example, and cannot allow gender to be a rating factor. As a result, he says, the cheapest plans for a relatively healthy young man may cost more now, while costs for a woman or an older person with a chronic condition like diabetes may go down.
Although the new mandates were designed to improve insurance standards, they sparked another firestorm when millions of Americans began receiving policy cancellation notices in 2013. Because many private insurance plans sold to individuals no longer met the ACA’s minimum requirements, insurers began dropping those plans or requiring enrollees to switch to other, often more expensive, ones. In November, in an effort to stem the mass cancellations, President Barack Obama bowed to mounting political pressure and announced a reprieve that allows insurance companies to renew existing policies for another year. That attempted fix has not been so straightforward, however. Many insurers were reluctant to reissue cancelled policies, and multiple states, which have the authority to regulate insurance sold within their borders, declined the administration’s request.
—Robert Berenson, MD, senior fellow, Urban Institute, Washington, D.C.
The Long View
Despite the intense focus on the first few months of health insurance enrollment, it may take several years before the markets begin to settle and other insurers waiting on the sidelines decide whether to participate. If they eventually succeed, the ACA exchanges could have several long-term consequences.
“If, in fact, the exchanges offer good insurance products that the public begins to accept and find that they have good information to make choices, it could affect the prevalence of employer-based insurance,” says Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy. Over many years, employers could begin moving their employees into exchanges rather than providing direct healthcare benefits.
If they prove viable, the exchanges also may help accelerate the trend toward more consolidation of physician practices or increase pressure to align with larger entities. Despite concerns over skinnier networks, for example, the more tightly controlled access to providers under certain plans dovetails with the ACA’s heightened emphasis on more integrated accountable care organizations (ACOs).
In fact, ACOs and other lower-profile provisions that enjoy more bipartisan support could ultimately play key roles in reshaping how healthcare is delivered in the U.S. Many of these reform efforts have been launched as pilots or demonstration projects. Salt Lake City-based healthcare consulting firm Leavitt Partners tallied nearly 500 ACOs through the end of July 2013, more than double the total in June 2012.
Other Obamacare provisions are levying fines based on excessive hospital-acquired conditions or readmissions and adjusting reimbursements based on e-prescribing, the Physician Quality Reporting System (PQRS), value-based purchasing, meaningful use of electronic health records, and other mandates.
“The overall theme is that the ACA is speeding up the move away from fee-for-service payment toward new payment methodologies that are going to be increasingly based on quality measures,” Dr. O’Malley says. “All of these are basically efforts to shift incentives away from rewarding volume of services toward value and quality of care for patients. And the crux of all of them is to try to get physicians to work together, not only with other specialists and their primary care colleagues, but also with other inter-professional members of their team.”
For hospitalists, it means relying more on nurses, physician assistants, and other support staff.
“In a collaborative agreement, where it’s a physician-led healthcare team, I think non-physician healthcare providers could help to support the physician hospitalists,” Dr. Lenchus says.
That extra help may be essential.
“I do think the workload will increase, and not just because we’ll have more people clamoring for healthcare and more patients who are sicker—remember, there are no more pre-existing conditions,” Dr. Lenchus says. “The other piece to this that goes outside the patient-physician interaction is that there’s a lot of additional regulations and administrative burdens, if you will, as individual hospitalists and as hospitals on the whole.”
The need to share resources to cut down on doctors’ workloads, Dr. O’Malley says, may be yet another factor in the accelerated rate of practice consolidation.
“There’s pressure among docs not just to function as teams but to consolidate among themselves either through physicians’ organizations like IPAs [independent practice associations] or becoming employees of hospitals,” she says. “That’s where you get economies of scale and shared infrastructure to do a lot of the things that the ACA is requiring of them.”
Consolidation or not, she sees plenty of potential for increased efficiency. Some medical groups may need to hire more support staff, whereas others may simply require more coordination and delegation among existing personnel to lighten the load and focus on priorities. The trick, Dr. Hilger says, is finding the right balance amid the dramatic change.
“Bottom line, it goes back to the triple aim that hospitalists should be aiming for: high quality, low-cost, patient-centered care,” he says. “I think the challenge over the next 10 years is how to find the sweet spot between all of those.”
Bryn Nelson is a freelance medical writer in Seattle.
It has survived a bitterly divided Congress and a polarized public, a narrow Supreme Court ruling, and a 16-day government shutdown triggered by an effort to defund or repeal it. Hailed by some as the most significant healthcare reform in a half-century, it is also roundly scorned by others as an ill-advised debacle.
With some of its most hotly contested provisions now taking effect, the Affordable Care Act—or Obamacare, as both backers and detractors now call it—has been the object of admiration and animosity, of optimism and consternation. Its supporters have pointed to the promise of unprecedented access to healthcare for millions, while its critics have pointed to the trickle of consumers able to access the main web portal during an error-plagued rollout.
Beyond the heated rhetoric, however, what will the complicated and quickly evolving elements of Obamacare actually mean for hospitalists and for healthcare access, affordability, capacity, and delivery? In the short term, analysts say so much change is happening all at once that it’s nearly impossible to predict how it might turn out.
“Everyone’s kind of holding their breath to see what happens,” says Ann O’Malley, MD, MPH, a senior fellow at the Washington, D.C.-based Center for Studying Health System Change.
One thing is certain: more reliance on hospital-based providers.
“I think there are a lot of things on a hospitalist’s plate right now. And hospitals, because of the cost pressures, are definitely looking to us to lead the way through this uncertain time,” says Rick Hilger, MD, SFHM, medical director for care management at Regions Hospital in St. Paul, Minn., and a hospitalist for HealthPartners.
Amid the upheaval, experts are seeing the signs of a few major trends. In the short term, one emerging theme is considerable geographical variation in consumer access and costs, and in pressure on providers.
“How this is going to feel will depend, to a great extent, on where you live,” says Leighton Ku, PhD, MPH, director of the Center for Health Policy Research at George Washington University School of Public Health and Health Services in Washington, D.C.
Analysts also have seen hints of more universal changes, including an accelerated trend toward the consolidation of provider groups, an added emphasis on team-based care, and significant momentum toward a pay-for-performance delivery model.
An Uneven Exchange
One of the law’s most visible and controversial elements, the health insurance exchange or marketplace, got off to a rocky start Oct. 1, 2013, when computer glitches hobbled the main healthcare.gov portal for 36 state exchanges and plagued many state-run sites as well.
While some state-run exchanges have generally earned high marks, others have struggled. Analysts are most worried about the balkiness of the main web-based portal, through which the majority of enrollees will have to pass. While older and sicker patients are generally more motivated to keep trying, the same isn’t necessarily true for younger and healthier people whose participation will be vital to help balance each state’s risk pool. Analysts sometimes call these people, “young invincibles.” Because they generally seek out care far less often than older consumers, their lower medical costs can help compensate for higher expenditures elsewhere.
If too few sign up, however, a state’s risk pool may be imbalanced toward costlier patients, causing insurance premiums to rise and creating a vicious cycle that destabilizes the market and makes more expensive insurance less attractive to younger people. Economists say the carrot-and-stick approach—offering subsidies to help lower-income people pay for premiums and gradually increasing financial penalties for those who choose not to buy any coverage—is likely to help. Nevertheless, supporters are nervous that malfunctioning exchange sites could cause would-be enrollees to delay or drop out, and, at the end of 2013, a worried Obama administration was scrambling to address the cascade of glitches.
Because the health insurance exchanges were highly controversial already, says Dr. Ku, who sits on the board of the Washington, D.C. Health Benefits Exchange Authority, every problem is likely to be magnified by critics. Although he doesn’t expect “huge changes” in physician payment rates from plans in the exchanges, he says varying degrees of competition could drive down insurers’ prices in some markets.
Doctors also are likely to encounter plenty of confusion among the newly insured, and Dr. Ku hopes educational sessions will help healthcare professionals take more of a leading role in helping patients navigate an often bewildering system.
“One of the most important things that a hospital can do to help in the beginning is to help on the enrollment end of things,” he says. “Help patients who don’t quite understand how to get in, how to use these systems.”
It’s too early to say whether the exchanges can still meet the Congressional Budget Office’s prediction of 7 million enrollees by the end of the 2014 enrollment period (and 13 million by 2015). But analysts say the composition of the risk pool—something that should be clearer this spring—may provide a glimpse into the ACA’s long-term financial viability.
Instead of a consistent pattern across the country, the exchanges will be shaped by local market forces, such as the number of competitors and the extent to which cheaper plans will try to limit access to providers. To minimize their costs, some exchange-based plans are promising in-network hospitals higher patient volumes in exchange for discounted reimbursements. Other hospitals now find themselves excluded from most private plans in favor of cheaper options.
In exchange for lower premiums, some of these insurers are offering “skinny networks” that give consumers more limited provider options.
“A primary objective in the marketplace is to offer the cheapest plan possible, and to do that the insurers are going to look at who are the least expensive providers,” says Christiane Mitchell, director of federal affairs for the Association of American Medical Colleges. Not surprisingly, some of the costliest providers tend to take care of sicker or higher-risk patients.
“It’s a very, very strong concern, and it’s one that we have been very vocal on since the enactment of the Affordable Care Act,” Mitchell says. The association also has expressed concern that lower-income patients buying into the cheapest plans may not have access to the specialty services they need the most. That possibility, she says, increases the importance of navigators helping the newly insured pick out the best plans.
A Question of Access
Another big question is how the healthcare system will accommodate the influx of newly insured. Because hospitals already have been the safety net for many patients lacking access to preventive and primary care, urgent and specialty care may go through a bigger adjustment period, says Dr. Hilger, who sits on SHM’s Public Policy Committee.
The growing provider shortage certainly won’t help. By 2015, the AAMC predicts a shortfall of 63,000 doctors, almost evenly split between primary and specialty care. By 2025, that number is expected to more than double.
Mitchell says the gap between supply and demand is worsening due to the sheer number of baby boomers entering Medicare. At the same time, she says, one in three doctors in the U.S. is now over the age of 60 and nearing retirement age. Whether through Medicaid or the marketplace, the ACA’s coverage expansion will exacerbate the shortages. “It’s not to the level of the boomers entering Medicare, but it certainly is having a major impact on access issues and exacerbating the shortage, again, across specialties,” she says.
Other analysts say the extent of the capacity problem will depend in large part on location.
“The truth is that the extent to which there are enough doctors or enough hospital beds is largely a function of geography,” Dr. Ku says. “So, if you’re in an urban area with lots of teaching hospitals, you probably have enough doctors and you probably have enough hospital beds. If, on the other hand, you’re in a poor, rural area, chances are you don’t.”
As both insurance and demand for healthcare expand, those areas that were having problems already “are going to be stretched even more,” Dr. Ku says.
Meeting demand also means training more doctors, and Mitchell worries about a pipeline that already is underfunded. Although medical school enrollment is at a record high, federal support for residency training has been frozen since 1997, meaning that the funded residency slots may not be sufficient to accommodate future graduates. Further declines in the clinical income that subsidizes training would place additional pressure on the educational mission of teaching hospitals, Mitchell says.
Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine in the division of hospital medicine at the University of Miami, says existing doctor deficits, the ACA’s new demands, and the growing medical training gap could swirl into a “perfect storm” of access problems. Longer delays in accessing primary and specialty care, in turn, could prevent timely interventions earlier during the course of a disease or condition.
“What it’s going to mean for hospitalists is that we’re going to see—over the short-term, maybe even the next three to five years—a real impact on when patients present, in terms of the acuity of their disease,” Dr. Lenchus says. That means sicker patients in the hospital.
Given the massive changes, observers like Mitchell and Dr. Hilger acknowledge that ironing out the rough spots will take time.
“There’s going to be two steps forward, one step back, but the simple question is: Was it ever OK to have tens of millions of patients who had no insurance or were underinsured and were using the emergency room as their primary care?” Dr. Hilger says. “I think, no matter what your political affiliation, that, in general, the answer is no.”
—Joshua Lenchus, DO, RPh, FACP, SFHM, associate professor of clinical medicine, division of hospital medicine, University of Miami, member, SHM Public Policy Committee.
Costs All Over the Map
One of the plan’s biggest goals and part of its name—affordability for those patients—also seems to vary considerably by geography. A recent analysis by The New York Times, for example, found that 58% of all counties served by the federal-run exchanges offer plans from only one or two insurance carriers. The relative lack of competition in many markets has created some huge cost disparities in premiums between neighboring states, and even neighboring counties.
With so many factors influencing costs, both proponents and opponents have found fodder to bolster their case that the law is either making insurance more affordable or sharply increasing premiums. One important consideration, Dr. Ku says, is that all plans must now include 10 “essential health benefits,” such as maternity care and medications, for example, and cannot allow gender to be a rating factor. As a result, he says, the cheapest plans for a relatively healthy young man may cost more now, while costs for a woman or an older person with a chronic condition like diabetes may go down.
Although the new mandates were designed to improve insurance standards, they sparked another firestorm when millions of Americans began receiving policy cancellation notices in 2013. Because many private insurance plans sold to individuals no longer met the ACA’s minimum requirements, insurers began dropping those plans or requiring enrollees to switch to other, often more expensive, ones. In November, in an effort to stem the mass cancellations, President Barack Obama bowed to mounting political pressure and announced a reprieve that allows insurance companies to renew existing policies for another year. That attempted fix has not been so straightforward, however. Many insurers were reluctant to reissue cancelled policies, and multiple states, which have the authority to regulate insurance sold within their borders, declined the administration’s request.
—Robert Berenson, MD, senior fellow, Urban Institute, Washington, D.C.
The Long View
Despite the intense focus on the first few months of health insurance enrollment, it may take several years before the markets begin to settle and other insurers waiting on the sidelines decide whether to participate. If they eventually succeed, the ACA exchanges could have several long-term consequences.
“If, in fact, the exchanges offer good insurance products that the public begins to accept and find that they have good information to make choices, it could affect the prevalence of employer-based insurance,” says Robert Berenson, MD, a senior fellow at the Washington, D.C.-based Urban Institute, a nonpartisan think tank focused on social and economic policy. Over many years, employers could begin moving their employees into exchanges rather than providing direct healthcare benefits.
If they prove viable, the exchanges also may help accelerate the trend toward more consolidation of physician practices or increase pressure to align with larger entities. Despite concerns over skinnier networks, for example, the more tightly controlled access to providers under certain plans dovetails with the ACA’s heightened emphasis on more integrated accountable care organizations (ACOs).
In fact, ACOs and other lower-profile provisions that enjoy more bipartisan support could ultimately play key roles in reshaping how healthcare is delivered in the U.S. Many of these reform efforts have been launched as pilots or demonstration projects. Salt Lake City-based healthcare consulting firm Leavitt Partners tallied nearly 500 ACOs through the end of July 2013, more than double the total in June 2012.
Other Obamacare provisions are levying fines based on excessive hospital-acquired conditions or readmissions and adjusting reimbursements based on e-prescribing, the Physician Quality Reporting System (PQRS), value-based purchasing, meaningful use of electronic health records, and other mandates.
“The overall theme is that the ACA is speeding up the move away from fee-for-service payment toward new payment methodologies that are going to be increasingly based on quality measures,” Dr. O’Malley says. “All of these are basically efforts to shift incentives away from rewarding volume of services toward value and quality of care for patients. And the crux of all of them is to try to get physicians to work together, not only with other specialists and their primary care colleagues, but also with other inter-professional members of their team.”
For hospitalists, it means relying more on nurses, physician assistants, and other support staff.
“In a collaborative agreement, where it’s a physician-led healthcare team, I think non-physician healthcare providers could help to support the physician hospitalists,” Dr. Lenchus says.
That extra help may be essential.
“I do think the workload will increase, and not just because we’ll have more people clamoring for healthcare and more patients who are sicker—remember, there are no more pre-existing conditions,” Dr. Lenchus says. “The other piece to this that goes outside the patient-physician interaction is that there’s a lot of additional regulations and administrative burdens, if you will, as individual hospitalists and as hospitals on the whole.”
The need to share resources to cut down on doctors’ workloads, Dr. O’Malley says, may be yet another factor in the accelerated rate of practice consolidation.
“There’s pressure among docs not just to function as teams but to consolidate among themselves either through physicians’ organizations like IPAs [independent practice associations] or becoming employees of hospitals,” she says. “That’s where you get economies of scale and shared infrastructure to do a lot of the things that the ACA is requiring of them.”
Consolidation or not, she sees plenty of potential for increased efficiency. Some medical groups may need to hire more support staff, whereas others may simply require more coordination and delegation among existing personnel to lighten the load and focus on priorities. The trick, Dr. Hilger says, is finding the right balance amid the dramatic change.
“Bottom line, it goes back to the triple aim that hospitalists should be aiming for: high quality, low-cost, patient-centered care,” he says. “I think the challenge over the next 10 years is how to find the sweet spot between all of those.”
Bryn Nelson is a freelance medical writer in Seattle.
Lung cancer found belatedly despite multiple chest radiographs
Lung cancer found belatedly despite multiple chest radiographs
DURING AN ANNUAL PHYSICAL EXAMINATION by her primary care physician, a 68-year-old woman with a history of smoking for more than 30 years had an in-house chest x-ray. The physician didn’t have a radiologist read the radiograph or order follow-up imaging. The chest film was repeated the following year. A year after that, the patient developed pulmonary symptoms. A chest x-ray showed an abnormality. The doctor prescribed antibiotics for presumed bronchitis or pneumonia. When the antibiotics didn’t relieve her symptoms, he referred her to a radiologist, who reported a large lesion suggestive of advanced lung cancer. Subsequent films confirmed stage IIIB lung cancer. After 16 rounds of chemotherapy, the patient died at age 73.
PLAINTIFF'S CLAIM The doctor missed an obvious lung lesion on the first radiograph; missed the lesion, which had grown and metastasized, on the second x-ray; and misinterpreted late-stage metastatic cancer on the third radiograph as bronchitis or pneumonia. The chest radiographs should have been over-read, especially when they showed an abnormality. A cancer diagnosis at the time of the first chest radiograph would have allowed a 75% possibility of cure with surgery alone. By the time of the diagnosis 2 years later, a surgical cure wasn’t possible.
THE DEFENSE The lesion could be seen only on retrospective review of the radiographs. The first and second radiographs were consistent with pulmonary hypertension and didn’t necessitate referral to a radiologist or additional imaging. The patient had many comorbid conditions, including obesity, hypertension, and stenosis of the carotid arteries. She also had a family history of heart disease and COPD.
VERDICT $2 million Virginia verdict.
COMMENT This case illustrates that a simple test, a chest x-ray in this instance, has the potential for litigation if it isn’t interpreted accurately and followed up. Failure to appropriately follow up on test results is one of the 2 major patient safety issues for family medicine; the other is medication errors/drug interactions.
Otitis media? Not likely
A 3-MONTH-OLD INFANT was taken to the emergency department with a fever of 103°F. The ED physician discharged her with a diagnosis of otitis media and a prescription for amoxicillin. He didn’t document which ear was infected or what he observed in the affected ear. The following day, the infant was pale, cool to the touch, and lethargic. She was brought to her pediatrician, then transferred immediately to a local medical center, where she was diagnosed with pneumococcal meningitis, hypoxic brain injury, and hydrocephalus and hospitalized for nearly a month. She was subsequently taken to the hospital 10 times and evaluated by several specialists. The child died of respiratory complications linked to the infection almost 2 years after her initial hospitalization.
PLAINTIFF'S CLAIM The ED physician should have ordered a blood count and urinalysis to rule out bacteremia and meningitis. He should have scheduled a follow-up within 24 to 48 hours of the ED visit.
THE DEFENSE The doctor wasn’t negligent; he couldn’t have anticipated the infant’s clinical course. The bacteremia and meningitis developed after the baby left the hospital, and the causative pneumococcal strain was resistant to amoxicillin.
VERDICT $1.72 million Pennsylvania verdict.
COMMENT Does otitis media ever cause a fever of 103°F in a 3-month-old? Although no definitive studies exist, I doubt it. Otitis media is a closed-space infection like an abscess, and abscesses rarely cause fever. Furthermore, the physical findings of otitis media, although not recorded in this case, are highly unreliable in a 3-month-old. Attributing a fever of 103°F in a 3-month-old to otitis media is always a bad idea.
Lung cancer found belatedly despite multiple chest radiographs
DURING AN ANNUAL PHYSICAL EXAMINATION by her primary care physician, a 68-year-old woman with a history of smoking for more than 30 years had an in-house chest x-ray. The physician didn’t have a radiologist read the radiograph or order follow-up imaging. The chest film was repeated the following year. A year after that, the patient developed pulmonary symptoms. A chest x-ray showed an abnormality. The doctor prescribed antibiotics for presumed bronchitis or pneumonia. When the antibiotics didn’t relieve her symptoms, he referred her to a radiologist, who reported a large lesion suggestive of advanced lung cancer. Subsequent films confirmed stage IIIB lung cancer. After 16 rounds of chemotherapy, the patient died at age 73.
PLAINTIFF'S CLAIM The doctor missed an obvious lung lesion on the first radiograph; missed the lesion, which had grown and metastasized, on the second x-ray; and misinterpreted late-stage metastatic cancer on the third radiograph as bronchitis or pneumonia. The chest radiographs should have been over-read, especially when they showed an abnormality. A cancer diagnosis at the time of the first chest radiograph would have allowed a 75% possibility of cure with surgery alone. By the time of the diagnosis 2 years later, a surgical cure wasn’t possible.
THE DEFENSE The lesion could be seen only on retrospective review of the radiographs. The first and second radiographs were consistent with pulmonary hypertension and didn’t necessitate referral to a radiologist or additional imaging. The patient had many comorbid conditions, including obesity, hypertension, and stenosis of the carotid arteries. She also had a family history of heart disease and COPD.
VERDICT $2 million Virginia verdict.
COMMENT This case illustrates that a simple test, a chest x-ray in this instance, has the potential for litigation if it isn’t interpreted accurately and followed up. Failure to appropriately follow up on test results is one of the 2 major patient safety issues for family medicine; the other is medication errors/drug interactions.
Otitis media? Not likely
A 3-MONTH-OLD INFANT was taken to the emergency department with a fever of 103°F. The ED physician discharged her with a diagnosis of otitis media and a prescription for amoxicillin. He didn’t document which ear was infected or what he observed in the affected ear. The following day, the infant was pale, cool to the touch, and lethargic. She was brought to her pediatrician, then transferred immediately to a local medical center, where she was diagnosed with pneumococcal meningitis, hypoxic brain injury, and hydrocephalus and hospitalized for nearly a month. She was subsequently taken to the hospital 10 times and evaluated by several specialists. The child died of respiratory complications linked to the infection almost 2 years after her initial hospitalization.
PLAINTIFF'S CLAIM The ED physician should have ordered a blood count and urinalysis to rule out bacteremia and meningitis. He should have scheduled a follow-up within 24 to 48 hours of the ED visit.
THE DEFENSE The doctor wasn’t negligent; he couldn’t have anticipated the infant’s clinical course. The bacteremia and meningitis developed after the baby left the hospital, and the causative pneumococcal strain was resistant to amoxicillin.
VERDICT $1.72 million Pennsylvania verdict.
COMMENT Does otitis media ever cause a fever of 103°F in a 3-month-old? Although no definitive studies exist, I doubt it. Otitis media is a closed-space infection like an abscess, and abscesses rarely cause fever. Furthermore, the physical findings of otitis media, although not recorded in this case, are highly unreliable in a 3-month-old. Attributing a fever of 103°F in a 3-month-old to otitis media is always a bad idea.
Lung cancer found belatedly despite multiple chest radiographs
DURING AN ANNUAL PHYSICAL EXAMINATION by her primary care physician, a 68-year-old woman with a history of smoking for more than 30 years had an in-house chest x-ray. The physician didn’t have a radiologist read the radiograph or order follow-up imaging. The chest film was repeated the following year. A year after that, the patient developed pulmonary symptoms. A chest x-ray showed an abnormality. The doctor prescribed antibiotics for presumed bronchitis or pneumonia. When the antibiotics didn’t relieve her symptoms, he referred her to a radiologist, who reported a large lesion suggestive of advanced lung cancer. Subsequent films confirmed stage IIIB lung cancer. After 16 rounds of chemotherapy, the patient died at age 73.
PLAINTIFF'S CLAIM The doctor missed an obvious lung lesion on the first radiograph; missed the lesion, which had grown and metastasized, on the second x-ray; and misinterpreted late-stage metastatic cancer on the third radiograph as bronchitis or pneumonia. The chest radiographs should have been over-read, especially when they showed an abnormality. A cancer diagnosis at the time of the first chest radiograph would have allowed a 75% possibility of cure with surgery alone. By the time of the diagnosis 2 years later, a surgical cure wasn’t possible.
THE DEFENSE The lesion could be seen only on retrospective review of the radiographs. The first and second radiographs were consistent with pulmonary hypertension and didn’t necessitate referral to a radiologist or additional imaging. The patient had many comorbid conditions, including obesity, hypertension, and stenosis of the carotid arteries. She also had a family history of heart disease and COPD.
VERDICT $2 million Virginia verdict.
COMMENT This case illustrates that a simple test, a chest x-ray in this instance, has the potential for litigation if it isn’t interpreted accurately and followed up. Failure to appropriately follow up on test results is one of the 2 major patient safety issues for family medicine; the other is medication errors/drug interactions.
Otitis media? Not likely
A 3-MONTH-OLD INFANT was taken to the emergency department with a fever of 103°F. The ED physician discharged her with a diagnosis of otitis media and a prescription for amoxicillin. He didn’t document which ear was infected or what he observed in the affected ear. The following day, the infant was pale, cool to the touch, and lethargic. She was brought to her pediatrician, then transferred immediately to a local medical center, where she was diagnosed with pneumococcal meningitis, hypoxic brain injury, and hydrocephalus and hospitalized for nearly a month. She was subsequently taken to the hospital 10 times and evaluated by several specialists. The child died of respiratory complications linked to the infection almost 2 years after her initial hospitalization.
PLAINTIFF'S CLAIM The ED physician should have ordered a blood count and urinalysis to rule out bacteremia and meningitis. He should have scheduled a follow-up within 24 to 48 hours of the ED visit.
THE DEFENSE The doctor wasn’t negligent; he couldn’t have anticipated the infant’s clinical course. The bacteremia and meningitis developed after the baby left the hospital, and the causative pneumococcal strain was resistant to amoxicillin.
VERDICT $1.72 million Pennsylvania verdict.
COMMENT Does otitis media ever cause a fever of 103°F in a 3-month-old? Although no definitive studies exist, I doubt it. Otitis media is a closed-space infection like an abscess, and abscesses rarely cause fever. Furthermore, the physical findings of otitis media, although not recorded in this case, are highly unreliable in a 3-month-old. Attributing a fever of 103°F in a 3-month-old to otitis media is always a bad idea.
Caring for Asian immigrants: Tips on culture that can enhance patient care
› Ask Asian immigrants open-ended questions and encourage them to share their use of alternative remedies. C
› Consider providing an interpretation service for patients not proficient in English, as opposed to asking family members to help. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Though often considered a “model minority,” Asian immigrants pose significant challenges for Western health care providers, including radically different ideas of disease causation, differing communication styles, and somatic presentations of mental illness. Asian diversity is tremendous, but several cultural trends are held in common: strong family structures, respect, adaptability, and, for first generation immigrants, widespread use of traditional therapies.1
While Asians and Pacific Islanders (APIs) represent only 5.6% of the US population, or 17.3 million people, that figure represents a 46% increase between 2000 and 2010, the most rapid for any ethnic group.2 A 79% increase is anticipated by 2050, bringing Asians to 9.3% of the US population. In order of population, API subpopulations include Chinese, Filipinos, Asian Indians, Vietnamese, Koreans, and Japanese.2 More than half of Asian Americans reside in the states of California, New York, and Hawaii, although enclaves exist in most major cities.3
Addressing the health needs of Asian immigrants in an increasingly diverse society mandates that US physicians develop the necessary skills to communicate, even when expectations for care may be very different. Fortunately, excellent resources are available (TABLE 1).
Barriers to good healthcare
The most formidable obstacle is limited English proficiency of patients, making them significantly less likely to seek care.4 They often struggle to arrange an appointment, although they arrive on time.5
Inadequate interpretation services. Frequently family members must interpret for patients, despite a federal mandate (Title VI of the 1964 Civil Rights Act) requiring professional services be provided at no charge if there is a federal payer (Medicare or Medicaid) involved.6 Unfortunately, these services are not currently reimbursable. Use of family or friends as interpreters, while convenient, results in far less accurate interpretation, frequent embarrassment, and loss of patient confidentiality. Trained medical interpreters or even telephone services are preferable, as they are much more accurate. Interviews involve a triad comprised of provider, patient, and interpreter, with the provider speaking directly to the patient using first-person address at all times. The interpreter should sit to the side or slightly behind the patient. All communication should be interpreted sentence by sentence so everyone is able to understand the entire conversation. It is well documented that proper interpretive services vastly improve the quality of care.7
Patient illiteracy. Health care illiteracy leads to medication errors due to the inability to understand instructions.8 Some immigrants have the added disadvantage of being illiterate both in English and in their native tongue.4 If not remedied, these situations easily lead to drug overdoses or missed allergies.9 Older immigrants neither understand the intricacies of the US health care system nor possess the language skills to master it.4
Stereotyping by caregivers must be surmounted if patients are to receive quality care. Many Asian patients report that physicians fail to understand them as unique individuals apart from their ethnic identity. Others feel excluded from the decision-making process or find culturally sensitive treatment options lacking.10
Subtleties of relational interaction. Asian culture has been defined as possessing a high Power Distance Index (PDI).11 The PDI refers to the distance or level of respect which an individual must afford to a superior, and this ideal is reflected in Asian conformance to a strict social hierarchy. Thus, physicians are viewed as authority figures and it is proper to nod or smile to indicate polite deference.12 However, showing respect and “buying in” to treatment recommendations are entirely different matters. Cultural factors make it difficult for patients to openly disagree with physician recommendations without feeling as though they have been disrespectful.12 Asian cultures are also “high context” cultures, having far more unwritten rules for conduct and communication that often prove baffling to westerners from “lower context” cultures.
Financial limitations. Socioeconomic influences also play a role. Although Asians have a higher income than other minority groups, 12.5% of Asians still live in poverty and 17.2% lack health insurance.2 Lack of coverage makes many Asians reluctant to seek regular medical care.13
Special medical concerns
Asian-Americans face a variety of challenging medical issues, including disproportionately high rates of tuberculosis (TB) and hepatitis B.
TB. Although rates of TB infection in the United States are low, rates in Asian immigrants are up to 100 times greater than that of the general population, more than any other immigrant group.14 Screening with interferon gamma release assays (IGRAs), such as T-SPOT TB, should be routine for Asian immigrants, since IGRAs do not cross-react with the bacillus Calmette-Guérin (BCG) vaccine. The Centers for Disease Control and Prevention now recommends IGRA blood testing in lieu of tuberculin skin testing (TST) for immigrants who received BCG in infancy, with the exception of children <5 years, for whom the TST is still preferable.15 Patients with positive IGRA tests are also more likely to be amenable to treatment.
Chronic hepatitis B infection in Asian immigrants is often due to perinatal transmission in their home countries. Rates of hepatitis B virus (HBV) infection in the United States have been steadily declining since vaccination began in 1981. However, chronic HBV infection in Asian immigrants approaches 10% of that population.16 An estimated 15% to 20% of patients with chronic HBV develop cirrhosis within 5 years and are at high risk for hepatocellular carcinoma (HCC).17,18
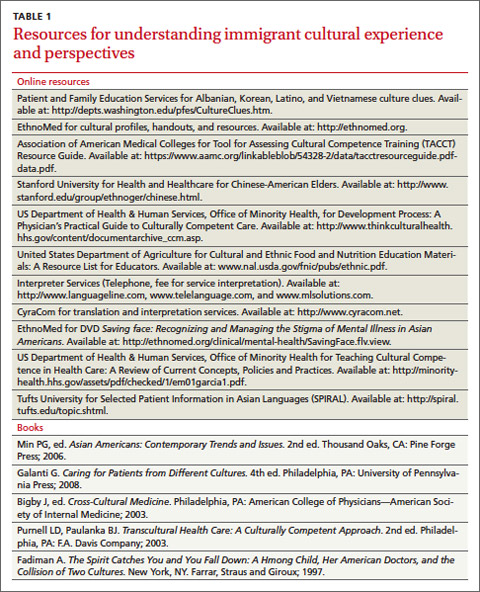
Evaluate HBV carriers annually with liver function testing (LFTs), hepatitis B surface Antigen (HBsAg), and hepatitis B e-Antigen (HBeAg). A positive HBsAg result indicates the virus is present; a positive HBeAg result indicates the virus is actively replicating. LFT elevation (AST >200 IU/L) or a positive HBeAg test should prompt referral to a gastroenterologist for liver biopsy and therapy. Screening for HCC with alpha-fetoprotein (AFP) levels and liver ultrasounds every 6 to 12 months has been recommended for all chronic HBV carriers,19 but this interval remains controversial. Screen men ≥40 years and women ≥50, or anyone who has had HBV infection >10 years, every 6 months.19,20 More recent recommendations favor ultrasound over AFP for screening, as the latter test lacks adequate sensitivity and specificity.20 Test partners and family members of HBV patients, and vaccinate them against HBV if not already immune.
Other medical issues. Asians from the Indian subcontinent have a significantly elevated risk of heart disease, in part due to low HDL-cholesterol levels.21 South Asian immigrant populations have a 3- to 5-fold increased risk of myocardial infarction and cardiovascular death compared with other ethnicities, and often exhibit coronary disease before the age of 40.22 The recent adoption of a Western diet and sedentary lifestyle has provoked an epidemic of diabetes throughout urban Asia and in Asians living abroad. This may be related to the “thrifty gene hypothesis,” which suggests that genes which evolved early in human history to facilitate storage of fat for periods of famine are detrimental in modern society where food is plentiful. A study of Asian Indian immigrants in Atlanta demonstrated an 18.3% prevalence rate for diabetes, higher than any other ethnic group.23 Tobacco and its causal relationship with lung cancer and heart disease only adds to this concern. Southeast Asians in particular demonstrate alarmingly high rates of tobacco consumption, and lung cancer is the leading cause of death among Asian Americans.12,24
Recently, a new acquired immune deficiency syndrome has been described in East Asia. In this syndrome, interferon–gamma (IFN–gamma) is blocked by an auto-antibody. Although not communicable like human immunodeficiency virus, this autoimmune syndrome may lead to similar opportunistic infections such as atypical mycobacterial infections.25
Mental health concerns
Perhaps no topic deserves more emphasis than that of mental health. In the aftermath of the war in Vietnam, Southeast Asian immigrants suffered a great deal from traumatic immigration experiences, with severe adjustment reactions.26 A high incidence of posttraumatic stress disorder (PTSD) among the Hmong in particular reflects their turbulent national history.27
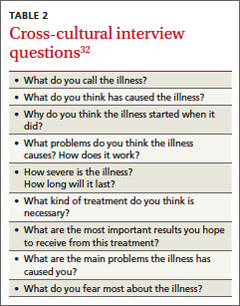
While the incidence of mental illness among Asians is comparable to that of the general population, Asian Americans are less likely to report such problems or to use mental health services26 due to the stigmatization of mental illness in Asian culture.28 Consequently, these symptoms may be subconsciously converted into the more socially acceptable medium of physical illness, which “saves face” and preserves family honor.29 In many ways, Asian culture still perceives mental illness as personal weakness.30 In Hmong culture, inability to speak about being depressed stems not just from cultural bias but from linguistic constraints—the language simply lacks a word for depression.31 Even Asian cultures recognizing mental illness deem depression to be more dependent on circumstances than on the psyche.31 A first-generation immigrant with mental illness is therefore more likely to present with somatic symptoms than a mood disturbance, and is likely to be resistant to counseling or medication for depression. (See “Cultural influence on self-perception: A case ”).
Asian health care beliefs and illnesses
Asian culture substantially influences the ways in which an individual perceives disease, experiences illness, and copes with the phenomenon of sickness. The interplay between illness, disease, and sickness was first elucidated by the pioneering work of Arthur Kleinman, MD, in 1978.32 The term disease denotes a pathological process, while illness describes the subjective impact of disease in a patient’s life. Sickness is the sum of both, as it relates to the total picture of biological and social disruption. The culturally competent physician must understand not only the patient’s disease but also his experience of illness. Asking Dr. Kleinman’s questions will help physicians understand their patient’s perception of illness (TABLE 2).32
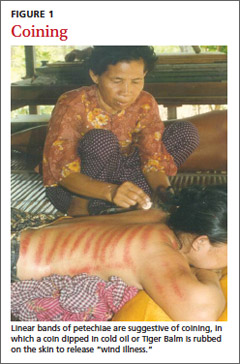
Traditional Chinese medicine
Many East Asians derive their conception of illness from traditional Chinese medicine (TCM), a broad range of therapies including herbs, acupuncture, massage (tuina), and diet that has been used for millennia. Similarly, South Asians are influenced by the Ayurvedic or Unani traditions. TCM views the body as an energy system, rather than a machine, through which the life force, or chi, flows. Health is not just the absence of disease, but a proper balance of the antithetic forces, yin and yang, maintained by herbs, diet, and acupuncture.33 TCM is often preferred for treating chronic conditions and viral syndromes, or as a substitute for Western medications with adverse effects.34 It is most popular among newly arrived immigrants, those with low literacy, and those with limited access to conventional medical treatment.34 Most Western physicians know little about TCM, feel uncomfortable when their patients use it, and fail to recognize its popularity.34,35 Likewise, most Asian patients are reluctant to discuss their use of TCM unless questioned about it in a nonjudgmental manner.

Many East Asian cultures practice a distinct form of folk healing known as “coining,” in which a coin dipped in cold oil or Tiger Balm is rubbed against the skin, enabling “wind illness” to escape the body (FIGURE 1). Linear bands of painless petechiae develop. The more extensive the bruising, the more illness is thought to be released. Failure to expel “wind-cold” from the body is believed to account for many ailments. Other traditions are moxibustion and cupping. In moxibustion, a smoldering plug of dried artemisia herb (moxi) is either impaled upon an acupuncture needle or placed directly on the skin to create a burn (FIGURE 2). In cupping, a flame is quickly passed through a glass bowl which is then placed against the skin. The resulting suction creates a circular bruise and draws blood to the area (FIGURE 3). Many folk remedies have been mistaken for child abuse by individuals unfamiliar with such practices.36 Occasionally TCM may result in harm from burns, unsterilized acupuncture needles, or (most commonly) adulterated herbal formulations.37
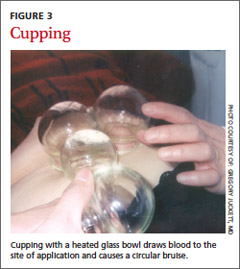
Culture-bound syndromes
Asian folk illnesses usually go unrecognized by western practitioners, and many of these are somatic presentations of mental illness or stress (TABLE 3). A classic example is the Korean folk condition Hwa-byung, which may include the sensation of an abdominal mass. US practitioners might pursue a fruitless abdominal workup before suspecting a psychiatric condition, even though a careful history would likely elicit other anxiety symptoms and loss of sleep and appetite.26
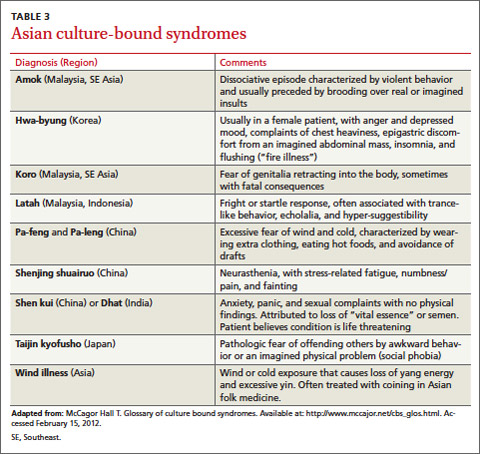
Asian social conventions
Asian cultural conventions often create considerable confusion. In India, head waggling (shaking the head back and forth) is equivalent to nodding in conversation, indicating an acknowledgement of communication. To western eyes, it appears that the patient is resisting advice rather than welcoming it. In East Asians, smiling expresses a variety of emotions, including polite disagreement. Acute embarrassment may provoke giggling. Eye contact is usually for social equals; avoiding it, especially between the sexes, is the norm. Only the right hand should be used when giving patients a prescription; the left hand is considered unclean. A patient’s head should only be touched with advance permission, as it is viewed as the seat of the soul and is therefore sacred. Under no circumstances should a patient ever see the bottom of the practitioner’s feet or be touched by them.38 Demonstrating respect (especially for older Asians) and preserving modesty are essential when examining patients.
Naming conventions can also be confusing. In China and much of Southeast Asia, it is customary for the surname to precede the given name, often with the 2 run together, rather than the other way round. It is best to ask how a patient would prefer to be addressed, regardless of how the name appears on the medical chart.38
Cultivating knowledge of Asian culture provides a framework from which practitioners can better understand and treat their patients. By asking respectful, open ended questions and encouraging patients to take an active role in their own treatment, physicians become therapeutic allies actively engaged in the healing process. Asking patients to share their use of alternative remedies allows the option of rationally integrating those most meaningful for the patient.
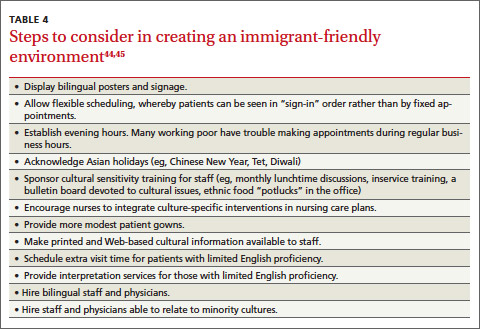
The cross-cultural interview
It is helpful to have a specific approach in mind when interviewing patients from other cultures. A number of mnemonic techniques exist.39-41 Perhaps the most useful of these is the LEARN model, which stands for Listen, Explain, Acknowledge, Recommend, and Negotiate.39 The physician first listens carefully to the patient’s perception of his illness before explaining any medical (disease) issues. This exchange is followed by acknowledging differences and similarities between the 2 viewpoints. Finally, the physician recommends a treatment plan and negotiates patient agreement.39 Negotiation implies flexibility and willingness to compromise with reasonable cultural demands, without compromising patient care. Use of the LEARN model aids in the identification and resolution of any cultural conflicts that might arise during the course of the clinical interview.
Teach back and patient activation
An extremely useful technique for all cultures is termed “teach back” or “show me,” which involves asking patients to repeat their care instructions at the end of the visit. This extra step provides an opportunity to correct errors that might have occurred during the transmission of instructions.42 Caregivers should also encourage or “activate” patients to become more involved in managing their own health care. Patient activation measures may be assessed on a one-to-4 point scale.43 Using both of these techniques combats passivity, promotes patient acceptance, and improves outcomes.
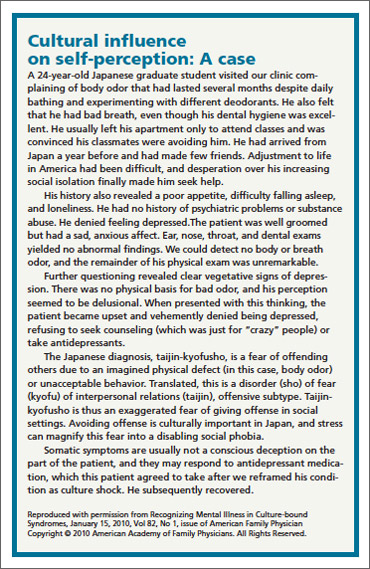
A caring environment
There are various strategies and approaches that can help make a medical practice more immigrant friendly (TABLE 4).44,45 Instructing office staff to assist patients in getting to the clinic is critical for those with limited mobility or who lack English proficiency. Adding evening hours that can also accommodate walk-ins helps working patients. For practices with larger immigrant populations, recognizing Asian holidays like Chinese New Year, Diwali, or Tet will be well received. These practices have been directly correlated with more positive health outcomes and better patient satisfaction.44
Conveying complex instructions to patients with little English takes effort for even the most unflappable providers. While written follow-up instructions in English could be interpreted by a more fluent family member, the ideal solution would be to have materials available in the native language. Fortunately, several Web sites, such as SPIRAL (Selective Patient Information in Asian Languages) provide downloadable Asian language instructions.46
Physicians should try to implement the Culturally & Linguistically Appropriate Services (CLAS) guidelines and mandates from the Office of Minority Health (http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15).6 They go far towards providing optimal care for patients of all cultures. Cultural competence does not imply being an expert in all cultures, let alone those of Asia. However, health care providers can develop the skills necessary for effective cross-cultural communication, which, to be most effective, must be accompanied by a caring attitude and respectful practice environment.
CORRESPONDENCE
Gregory Juckett, MD, MPH, West Virginia University School of Medicine, Box 9247, Robert C. Byrd Health Sciences Center, Morgantown, West Virginia, 26506; [email protected]
1. Min PG, ed. Asian Americans: Contemporary Trends and Issues. 2nd ed. Thousand Oaks, California: Pine Forge Press; 2006.
2. Ortman JM, Guarneri CE; National Census Bureau. United States population projections: 2000 to 2050. Available at: http://www.census.gov/population/projections/files/analytical-document09.pdf. Accessed February 20, 2012.
3. Barnes JS, Bennett CE; US Census Bureau Web site. The Asian population: 2000. Available at: http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed February 2, 2012.
4. Kim G, Worley CB, Allen RS, et al. Vulnerability of older Latino and Asian immigrants with limited English proficiency. J Am Geriatr Soc. 2011;59:1246-1252.
5. Silver D, Blustein J, Weitzman BC. Transportation to clinic: findings from a pilot clinic-based survey of low-income suburbanites. J Immigr Minor Health. 2012;14:350-355.
6. US Department of Health and Human Services Office of Minority Health Web site. The National CLAS Standards. Available at: http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15. Updated May 3, 2013. Accessed June 1, 2013.
7. Karliner LS, Jacobs EA, Chen AH, et al. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42:727-754.
8. Wilson E, Chen AH, Grumbach K, et al. Effects of limited English proficiency and physician language on health care comprehension. J Gen Intern Med. 2005;20:800-806.
9. Ku L, Flores G. Pay now or pay later: providing interpreter services in health care. Health Aff (Millwood). 2005;24:435-444.
10. Ngo-Metzger Q, Massagali MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med. 2003;18:44-52.
11. Basabe N, Ros M. Cultural dimensions and social behavior correlates: individualism-collectivism and power distance. Revue Internationale De Pscyhologie Sociale. 2005;17:189-225.
12. Ngo-Metzger Q, Legedza AT, Phillips RS. Asian Americans’ reports of their health care experiences. Results of a national survey. J Gen Intern Med. 2004;19:111-119.
13. Collins KS, Hughes DL, Doty MM, et al; The Commonwealth Fund. Diverse communities, common concerns: assessing health care quality for minority Americans. Available at: http://www.commonwealthfund.org/Publications/Fund-Reports/2002/Mar/Diverse-Communities--Common-Concerns--Assessing-Health-Care-Quality-for-Minority-Americans.aspx. Published March 2002. Accessed December 20, 2013.
14. Houston HR, Harada N, Makinodan T. Development of a culturally sensitive educational intervention program to reduce high incidence of tuberculosis among foreign-born Vietnamese. Ethn Health. 2002;7:255-265.
15. Mazurel GH, Jereb J, Vernon A, et al; Centers for Disease Control and Prevention (CDC). Updated guidelines for using interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection—United States, 2010. MMWR Recomm Rep. 2010;59(RR-5):1-25.
16. Hutton DW, Tan D, So SK, et al. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med. 2007;147:460-469.
17. Fattovich G, Brollo L, Giustina G, et al. Natural history and prognostic factors in chronic hepatitis B. Gut. 1991;32:294-298.
18. Beasley RP. Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer. 1988;61:1942-1956.
19. Smith C. Managing Adult Patients with Chronic HBV. Hepatitis B Foundation. Accessed February 15, 2012, at http://www.hepb.org/professionals/management_guidelines.htm.
20. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020-1022.
21. Hamaad A, Lip G. Assessing heart disease in your ethnic patients. Pulse. 2003;63:48-49.
22. Gupta M, Singh N, Verma S. South Asians and cardiovascular risk: what clinicians should know. Circulation. 2006;113:e924-e929.
23. Venkataraman R, Nanda NC, Beweja G, et al. Prevalence of diabetes mellitus and related conditions in Asian Indians living in the United States. Am J Cardiol. 2004;94:977-980.
24. Nishtar S. Prevention of coronary heart disease in south Asia. Lancet. 2002;360:1015-1018.
25. Browne SK, Burbelo PD, Chetchotisakd P, et al. Adult onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367:725-734.
26. Sorkin DH, Nguyen H, Ngo-Metzger Q. Assessing the mental health needs and barriers to care among a diverse sample of Asian American older adults. J Gen Intern Med. 2011;26:595-602.
27. PTSD, depression epidemic among Cambodian immigrants [press release]. Bethesda, MD: National Institutes of Health; August 2, 2005.
28. Sue S, Sue DW, Sue L, et al. Psychopathology among Asian Americans: a model minority? Cult Divers Ment Health. 1995;1:39-51.
29. Parker G, Cheah YC, Roy K. Do the Chinese somaticize depression? A cross-cultural study. Soc Psychiatry Psychiatr Epidemiol. 2001;36:287-293.
30. Sribney W, Elliot K, Aguilar-Gaxiola S, et al. The role of nonmedical human services and alternative medicine. In: Ruiz P, Primm A, eds. Disparities in Psychiatric Care. Baltimore, MD: Lippincott, Williams & Wilkins; 2010:274-289.
31. Lee HY, Lytle K, Yang PN, et al. Mental health literacy in Hmong and Cambodian elderly refugees: a barrier to understanding, recognizing, and responding to depression. Int J Aging Hum Dev. 2010;71:323-344.
32. Kleinman A, Eisenberg L, Good B. Culture, illness, and care: clinical lessons from anthroplologic and cross-cultural research. Ann Intern Med. 1978;88:251-258.
33. Patwardhan B, Warude D, Pushpangadan P, et al. Ayurveda and traditional Chinese medicine: a comparative overview. Evid Based Complement Alternat Med. 2005;2:465-473.
34. Wu AP, Burke A, LeBaron S. Use of traditional medicine by immigrant Chinese patients. Fam Med. 2007;39:195-200.
35. Nguyen G, Bowman M. Culture, language, and health literacy: communicating about health with Asians and Pacific Islanders. Fam Med. 2007;39:208-210.
36. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59:665-666.
37. Efferth T, Kaina B. Toxicities by herbal medicines with emphasis to traditional Chinese medicine. Curr Drug Metab. 2011;12:989-996.
38. Galanti G. Communication and time orientation. In: Caring for Patients from Different Cultures. 4th ed. Philadelphia, PA: University of Pennsylvania Press; 2008:27-51.
39. Berlin E, Fowkes WC Jr. A teaching framework for cross-cultural health care: application in family practice. West J Med. 1983;139:934-938.
40. Stuart MR, Lieberman JA III, eds. The Fifteen Minute Hour: Applied Psychotherapy for the Primary Care Physician. 2nd ed. Westport, CT: Praeger; 1993:101-183.
41. Kobylarz FA, Heath JM, Like RC. The ETHNIC(S) mnemonic: a clinical tool for ethnogeriatric education. J Am Geriat Soc. 2002;50:1582-1589.
42. Kountz DS. Strategies for improving low health literacy. Postgrad Med. 2009;121:171-177.
43. Patient Activation Measure Assessment. Insignia Health Web site. Available at: http://www.insigniahealth.com/solutions/patientactivation-measure. Accessed February 20, 2012.
44. Glenn-Vega A. Achieving a more minority-friendly practice. Fam Pract Manag. 2002;9:39-43.
45. Galanti G. Making a Difference. In: Caring for Patients from Different Cultures. 3rd ed. Philadelphia, PA: University of Pennsylvania Press; 2003:1222-1229.
46. SPIRAL: Selected Patient Information in Asian Languages. Tufts University Hirsh Health Sciences Web site. Available at: http://spiral.tufts.edu/topic.shtml. Accessed February 10, 2012.
› Ask Asian immigrants open-ended questions and encourage them to share their use of alternative remedies. C
› Consider providing an interpretation service for patients not proficient in English, as opposed to asking family members to help. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Though often considered a “model minority,” Asian immigrants pose significant challenges for Western health care providers, including radically different ideas of disease causation, differing communication styles, and somatic presentations of mental illness. Asian diversity is tremendous, but several cultural trends are held in common: strong family structures, respect, adaptability, and, for first generation immigrants, widespread use of traditional therapies.1
While Asians and Pacific Islanders (APIs) represent only 5.6% of the US population, or 17.3 million people, that figure represents a 46% increase between 2000 and 2010, the most rapid for any ethnic group.2 A 79% increase is anticipated by 2050, bringing Asians to 9.3% of the US population. In order of population, API subpopulations include Chinese, Filipinos, Asian Indians, Vietnamese, Koreans, and Japanese.2 More than half of Asian Americans reside in the states of California, New York, and Hawaii, although enclaves exist in most major cities.3
Addressing the health needs of Asian immigrants in an increasingly diverse society mandates that US physicians develop the necessary skills to communicate, even when expectations for care may be very different. Fortunately, excellent resources are available (TABLE 1).
Barriers to good healthcare
The most formidable obstacle is limited English proficiency of patients, making them significantly less likely to seek care.4 They often struggle to arrange an appointment, although they arrive on time.5
Inadequate interpretation services. Frequently family members must interpret for patients, despite a federal mandate (Title VI of the 1964 Civil Rights Act) requiring professional services be provided at no charge if there is a federal payer (Medicare or Medicaid) involved.6 Unfortunately, these services are not currently reimbursable. Use of family or friends as interpreters, while convenient, results in far less accurate interpretation, frequent embarrassment, and loss of patient confidentiality. Trained medical interpreters or even telephone services are preferable, as they are much more accurate. Interviews involve a triad comprised of provider, patient, and interpreter, with the provider speaking directly to the patient using first-person address at all times. The interpreter should sit to the side or slightly behind the patient. All communication should be interpreted sentence by sentence so everyone is able to understand the entire conversation. It is well documented that proper interpretive services vastly improve the quality of care.7
Patient illiteracy. Health care illiteracy leads to medication errors due to the inability to understand instructions.8 Some immigrants have the added disadvantage of being illiterate both in English and in their native tongue.4 If not remedied, these situations easily lead to drug overdoses or missed allergies.9 Older immigrants neither understand the intricacies of the US health care system nor possess the language skills to master it.4
Stereotyping by caregivers must be surmounted if patients are to receive quality care. Many Asian patients report that physicians fail to understand them as unique individuals apart from their ethnic identity. Others feel excluded from the decision-making process or find culturally sensitive treatment options lacking.10
Subtleties of relational interaction. Asian culture has been defined as possessing a high Power Distance Index (PDI).11 The PDI refers to the distance or level of respect which an individual must afford to a superior, and this ideal is reflected in Asian conformance to a strict social hierarchy. Thus, physicians are viewed as authority figures and it is proper to nod or smile to indicate polite deference.12 However, showing respect and “buying in” to treatment recommendations are entirely different matters. Cultural factors make it difficult for patients to openly disagree with physician recommendations without feeling as though they have been disrespectful.12 Asian cultures are also “high context” cultures, having far more unwritten rules for conduct and communication that often prove baffling to westerners from “lower context” cultures.
Financial limitations. Socioeconomic influences also play a role. Although Asians have a higher income than other minority groups, 12.5% of Asians still live in poverty and 17.2% lack health insurance.2 Lack of coverage makes many Asians reluctant to seek regular medical care.13
Special medical concerns
Asian-Americans face a variety of challenging medical issues, including disproportionately high rates of tuberculosis (TB) and hepatitis B.
TB. Although rates of TB infection in the United States are low, rates in Asian immigrants are up to 100 times greater than that of the general population, more than any other immigrant group.14 Screening with interferon gamma release assays (IGRAs), such as T-SPOT TB, should be routine for Asian immigrants, since IGRAs do not cross-react with the bacillus Calmette-Guérin (BCG) vaccine. The Centers for Disease Control and Prevention now recommends IGRA blood testing in lieu of tuberculin skin testing (TST) for immigrants who received BCG in infancy, with the exception of children <5 years, for whom the TST is still preferable.15 Patients with positive IGRA tests are also more likely to be amenable to treatment.
Chronic hepatitis B infection in Asian immigrants is often due to perinatal transmission in their home countries. Rates of hepatitis B virus (HBV) infection in the United States have been steadily declining since vaccination began in 1981. However, chronic HBV infection in Asian immigrants approaches 10% of that population.16 An estimated 15% to 20% of patients with chronic HBV develop cirrhosis within 5 years and are at high risk for hepatocellular carcinoma (HCC).17,18
Evaluate HBV carriers annually with liver function testing (LFTs), hepatitis B surface Antigen (HBsAg), and hepatitis B e-Antigen (HBeAg). A positive HBsAg result indicates the virus is present; a positive HBeAg result indicates the virus is actively replicating. LFT elevation (AST >200 IU/L) or a positive HBeAg test should prompt referral to a gastroenterologist for liver biopsy and therapy. Screening for HCC with alpha-fetoprotein (AFP) levels and liver ultrasounds every 6 to 12 months has been recommended for all chronic HBV carriers,19 but this interval remains controversial. Screen men ≥40 years and women ≥50, or anyone who has had HBV infection >10 years, every 6 months.19,20 More recent recommendations favor ultrasound over AFP for screening, as the latter test lacks adequate sensitivity and specificity.20 Test partners and family members of HBV patients, and vaccinate them against HBV if not already immune.
Other medical issues. Asians from the Indian subcontinent have a significantly elevated risk of heart disease, in part due to low HDL-cholesterol levels.21 South Asian immigrant populations have a 3- to 5-fold increased risk of myocardial infarction and cardiovascular death compared with other ethnicities, and often exhibit coronary disease before the age of 40.22 The recent adoption of a Western diet and sedentary lifestyle has provoked an epidemic of diabetes throughout urban Asia and in Asians living abroad. This may be related to the “thrifty gene hypothesis,” which suggests that genes which evolved early in human history to facilitate storage of fat for periods of famine are detrimental in modern society where food is plentiful. A study of Asian Indian immigrants in Atlanta demonstrated an 18.3% prevalence rate for diabetes, higher than any other ethnic group.23 Tobacco and its causal relationship with lung cancer and heart disease only adds to this concern. Southeast Asians in particular demonstrate alarmingly high rates of tobacco consumption, and lung cancer is the leading cause of death among Asian Americans.12,24
Recently, a new acquired immune deficiency syndrome has been described in East Asia. In this syndrome, interferon–gamma (IFN–gamma) is blocked by an auto-antibody. Although not communicable like human immunodeficiency virus, this autoimmune syndrome may lead to similar opportunistic infections such as atypical mycobacterial infections.25
Mental health concerns
Perhaps no topic deserves more emphasis than that of mental health. In the aftermath of the war in Vietnam, Southeast Asian immigrants suffered a great deal from traumatic immigration experiences, with severe adjustment reactions.26 A high incidence of posttraumatic stress disorder (PTSD) among the Hmong in particular reflects their turbulent national history.27
While the incidence of mental illness among Asians is comparable to that of the general population, Asian Americans are less likely to report such problems or to use mental health services26 due to the stigmatization of mental illness in Asian culture.28 Consequently, these symptoms may be subconsciously converted into the more socially acceptable medium of physical illness, which “saves face” and preserves family honor.29 In many ways, Asian culture still perceives mental illness as personal weakness.30 In Hmong culture, inability to speak about being depressed stems not just from cultural bias but from linguistic constraints—the language simply lacks a word for depression.31 Even Asian cultures recognizing mental illness deem depression to be more dependent on circumstances than on the psyche.31 A first-generation immigrant with mental illness is therefore more likely to present with somatic symptoms than a mood disturbance, and is likely to be resistant to counseling or medication for depression. (See “Cultural influence on self-perception: A case ”).
Asian health care beliefs and illnesses
Asian culture substantially influences the ways in which an individual perceives disease, experiences illness, and copes with the phenomenon of sickness. The interplay between illness, disease, and sickness was first elucidated by the pioneering work of Arthur Kleinman, MD, in 1978.32 The term disease denotes a pathological process, while illness describes the subjective impact of disease in a patient’s life. Sickness is the sum of both, as it relates to the total picture of biological and social disruption. The culturally competent physician must understand not only the patient’s disease but also his experience of illness. Asking Dr. Kleinman’s questions will help physicians understand their patient’s perception of illness (TABLE 2).32
Traditional Chinese medicine
Many East Asians derive their conception of illness from traditional Chinese medicine (TCM), a broad range of therapies including herbs, acupuncture, massage (tuina), and diet that has been used for millennia. Similarly, South Asians are influenced by the Ayurvedic or Unani traditions. TCM views the body as an energy system, rather than a machine, through which the life force, or chi, flows. Health is not just the absence of disease, but a proper balance of the antithetic forces, yin and yang, maintained by herbs, diet, and acupuncture.33 TCM is often preferred for treating chronic conditions and viral syndromes, or as a substitute for Western medications with adverse effects.34 It is most popular among newly arrived immigrants, those with low literacy, and those with limited access to conventional medical treatment.34 Most Western physicians know little about TCM, feel uncomfortable when their patients use it, and fail to recognize its popularity.34,35 Likewise, most Asian patients are reluctant to discuss their use of TCM unless questioned about it in a nonjudgmental manner.
Many East Asian cultures practice a distinct form of folk healing known as “coining,” in which a coin dipped in cold oil or Tiger Balm is rubbed against the skin, enabling “wind illness” to escape the body (FIGURE 1). Linear bands of painless petechiae develop. The more extensive the bruising, the more illness is thought to be released. Failure to expel “wind-cold” from the body is believed to account for many ailments. Other traditions are moxibustion and cupping. In moxibustion, a smoldering plug of dried artemisia herb (moxi) is either impaled upon an acupuncture needle or placed directly on the skin to create a burn (FIGURE 2). In cupping, a flame is quickly passed through a glass bowl which is then placed against the skin. The resulting suction creates a circular bruise and draws blood to the area (FIGURE 3). Many folk remedies have been mistaken for child abuse by individuals unfamiliar with such practices.36 Occasionally TCM may result in harm from burns, unsterilized acupuncture needles, or (most commonly) adulterated herbal formulations.37
Culture-bound syndromes
Asian folk illnesses usually go unrecognized by western practitioners, and many of these are somatic presentations of mental illness or stress (TABLE 3). A classic example is the Korean folk condition Hwa-byung, which may include the sensation of an abdominal mass. US practitioners might pursue a fruitless abdominal workup before suspecting a psychiatric condition, even though a careful history would likely elicit other anxiety symptoms and loss of sleep and appetite.26
Asian social conventions
Asian cultural conventions often create considerable confusion. In India, head waggling (shaking the head back and forth) is equivalent to nodding in conversation, indicating an acknowledgement of communication. To western eyes, it appears that the patient is resisting advice rather than welcoming it. In East Asians, smiling expresses a variety of emotions, including polite disagreement. Acute embarrassment may provoke giggling. Eye contact is usually for social equals; avoiding it, especially between the sexes, is the norm. Only the right hand should be used when giving patients a prescription; the left hand is considered unclean. A patient’s head should only be touched with advance permission, as it is viewed as the seat of the soul and is therefore sacred. Under no circumstances should a patient ever see the bottom of the practitioner’s feet or be touched by them.38 Demonstrating respect (especially for older Asians) and preserving modesty are essential when examining patients.
Naming conventions can also be confusing. In China and much of Southeast Asia, it is customary for the surname to precede the given name, often with the 2 run together, rather than the other way round. It is best to ask how a patient would prefer to be addressed, regardless of how the name appears on the medical chart.38
Cultivating knowledge of Asian culture provides a framework from which practitioners can better understand and treat their patients. By asking respectful, open ended questions and encouraging patients to take an active role in their own treatment, physicians become therapeutic allies actively engaged in the healing process. Asking patients to share their use of alternative remedies allows the option of rationally integrating those most meaningful for the patient.
The cross-cultural interview
It is helpful to have a specific approach in mind when interviewing patients from other cultures. A number of mnemonic techniques exist.39-41 Perhaps the most useful of these is the LEARN model, which stands for Listen, Explain, Acknowledge, Recommend, and Negotiate.39 The physician first listens carefully to the patient’s perception of his illness before explaining any medical (disease) issues. This exchange is followed by acknowledging differences and similarities between the 2 viewpoints. Finally, the physician recommends a treatment plan and negotiates patient agreement.39 Negotiation implies flexibility and willingness to compromise with reasonable cultural demands, without compromising patient care. Use of the LEARN model aids in the identification and resolution of any cultural conflicts that might arise during the course of the clinical interview.
Teach back and patient activation
An extremely useful technique for all cultures is termed “teach back” or “show me,” which involves asking patients to repeat their care instructions at the end of the visit. This extra step provides an opportunity to correct errors that might have occurred during the transmission of instructions.42 Caregivers should also encourage or “activate” patients to become more involved in managing their own health care. Patient activation measures may be assessed on a one-to-4 point scale.43 Using both of these techniques combats passivity, promotes patient acceptance, and improves outcomes.
A caring environment
There are various strategies and approaches that can help make a medical practice more immigrant friendly (TABLE 4).44,45 Instructing office staff to assist patients in getting to the clinic is critical for those with limited mobility or who lack English proficiency. Adding evening hours that can also accommodate walk-ins helps working patients. For practices with larger immigrant populations, recognizing Asian holidays like Chinese New Year, Diwali, or Tet will be well received. These practices have been directly correlated with more positive health outcomes and better patient satisfaction.44
Conveying complex instructions to patients with little English takes effort for even the most unflappable providers. While written follow-up instructions in English could be interpreted by a more fluent family member, the ideal solution would be to have materials available in the native language. Fortunately, several Web sites, such as SPIRAL (Selective Patient Information in Asian Languages) provide downloadable Asian language instructions.46
Physicians should try to implement the Culturally & Linguistically Appropriate Services (CLAS) guidelines and mandates from the Office of Minority Health (http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15).6 They go far towards providing optimal care for patients of all cultures. Cultural competence does not imply being an expert in all cultures, let alone those of Asia. However, health care providers can develop the skills necessary for effective cross-cultural communication, which, to be most effective, must be accompanied by a caring attitude and respectful practice environment.
CORRESPONDENCE
Gregory Juckett, MD, MPH, West Virginia University School of Medicine, Box 9247, Robert C. Byrd Health Sciences Center, Morgantown, West Virginia, 26506; [email protected]
› Ask Asian immigrants open-ended questions and encourage them to share their use of alternative remedies. C
› Consider providing an interpretation service for patients not proficient in English, as opposed to asking family members to help. C
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
Though often considered a “model minority,” Asian immigrants pose significant challenges for Western health care providers, including radically different ideas of disease causation, differing communication styles, and somatic presentations of mental illness. Asian diversity is tremendous, but several cultural trends are held in common: strong family structures, respect, adaptability, and, for first generation immigrants, widespread use of traditional therapies.1
While Asians and Pacific Islanders (APIs) represent only 5.6% of the US population, or 17.3 million people, that figure represents a 46% increase between 2000 and 2010, the most rapid for any ethnic group.2 A 79% increase is anticipated by 2050, bringing Asians to 9.3% of the US population. In order of population, API subpopulations include Chinese, Filipinos, Asian Indians, Vietnamese, Koreans, and Japanese.2 More than half of Asian Americans reside in the states of California, New York, and Hawaii, although enclaves exist in most major cities.3
Addressing the health needs of Asian immigrants in an increasingly diverse society mandates that US physicians develop the necessary skills to communicate, even when expectations for care may be very different. Fortunately, excellent resources are available (TABLE 1).
Barriers to good healthcare
The most formidable obstacle is limited English proficiency of patients, making them significantly less likely to seek care.4 They often struggle to arrange an appointment, although they arrive on time.5
Inadequate interpretation services. Frequently family members must interpret for patients, despite a federal mandate (Title VI of the 1964 Civil Rights Act) requiring professional services be provided at no charge if there is a federal payer (Medicare or Medicaid) involved.6 Unfortunately, these services are not currently reimbursable. Use of family or friends as interpreters, while convenient, results in far less accurate interpretation, frequent embarrassment, and loss of patient confidentiality. Trained medical interpreters or even telephone services are preferable, as they are much more accurate. Interviews involve a triad comprised of provider, patient, and interpreter, with the provider speaking directly to the patient using first-person address at all times. The interpreter should sit to the side or slightly behind the patient. All communication should be interpreted sentence by sentence so everyone is able to understand the entire conversation. It is well documented that proper interpretive services vastly improve the quality of care.7
Patient illiteracy. Health care illiteracy leads to medication errors due to the inability to understand instructions.8 Some immigrants have the added disadvantage of being illiterate both in English and in their native tongue.4 If not remedied, these situations easily lead to drug overdoses or missed allergies.9 Older immigrants neither understand the intricacies of the US health care system nor possess the language skills to master it.4
Stereotyping by caregivers must be surmounted if patients are to receive quality care. Many Asian patients report that physicians fail to understand them as unique individuals apart from their ethnic identity. Others feel excluded from the decision-making process or find culturally sensitive treatment options lacking.10
Subtleties of relational interaction. Asian culture has been defined as possessing a high Power Distance Index (PDI).11 The PDI refers to the distance or level of respect which an individual must afford to a superior, and this ideal is reflected in Asian conformance to a strict social hierarchy. Thus, physicians are viewed as authority figures and it is proper to nod or smile to indicate polite deference.12 However, showing respect and “buying in” to treatment recommendations are entirely different matters. Cultural factors make it difficult for patients to openly disagree with physician recommendations without feeling as though they have been disrespectful.12 Asian cultures are also “high context” cultures, having far more unwritten rules for conduct and communication that often prove baffling to westerners from “lower context” cultures.
Financial limitations. Socioeconomic influences also play a role. Although Asians have a higher income than other minority groups, 12.5% of Asians still live in poverty and 17.2% lack health insurance.2 Lack of coverage makes many Asians reluctant to seek regular medical care.13
Special medical concerns
Asian-Americans face a variety of challenging medical issues, including disproportionately high rates of tuberculosis (TB) and hepatitis B.
TB. Although rates of TB infection in the United States are low, rates in Asian immigrants are up to 100 times greater than that of the general population, more than any other immigrant group.14 Screening with interferon gamma release assays (IGRAs), such as T-SPOT TB, should be routine for Asian immigrants, since IGRAs do not cross-react with the bacillus Calmette-Guérin (BCG) vaccine. The Centers for Disease Control and Prevention now recommends IGRA blood testing in lieu of tuberculin skin testing (TST) for immigrants who received BCG in infancy, with the exception of children <5 years, for whom the TST is still preferable.15 Patients with positive IGRA tests are also more likely to be amenable to treatment.
Chronic hepatitis B infection in Asian immigrants is often due to perinatal transmission in their home countries. Rates of hepatitis B virus (HBV) infection in the United States have been steadily declining since vaccination began in 1981. However, chronic HBV infection in Asian immigrants approaches 10% of that population.16 An estimated 15% to 20% of patients with chronic HBV develop cirrhosis within 5 years and are at high risk for hepatocellular carcinoma (HCC).17,18
Evaluate HBV carriers annually with liver function testing (LFTs), hepatitis B surface Antigen (HBsAg), and hepatitis B e-Antigen (HBeAg). A positive HBsAg result indicates the virus is present; a positive HBeAg result indicates the virus is actively replicating. LFT elevation (AST >200 IU/L) or a positive HBeAg test should prompt referral to a gastroenterologist for liver biopsy and therapy. Screening for HCC with alpha-fetoprotein (AFP) levels and liver ultrasounds every 6 to 12 months has been recommended for all chronic HBV carriers,19 but this interval remains controversial. Screen men ≥40 years and women ≥50, or anyone who has had HBV infection >10 years, every 6 months.19,20 More recent recommendations favor ultrasound over AFP for screening, as the latter test lacks adequate sensitivity and specificity.20 Test partners and family members of HBV patients, and vaccinate them against HBV if not already immune.
Other medical issues. Asians from the Indian subcontinent have a significantly elevated risk of heart disease, in part due to low HDL-cholesterol levels.21 South Asian immigrant populations have a 3- to 5-fold increased risk of myocardial infarction and cardiovascular death compared with other ethnicities, and often exhibit coronary disease before the age of 40.22 The recent adoption of a Western diet and sedentary lifestyle has provoked an epidemic of diabetes throughout urban Asia and in Asians living abroad. This may be related to the “thrifty gene hypothesis,” which suggests that genes which evolved early in human history to facilitate storage of fat for periods of famine are detrimental in modern society where food is plentiful. A study of Asian Indian immigrants in Atlanta demonstrated an 18.3% prevalence rate for diabetes, higher than any other ethnic group.23 Tobacco and its causal relationship with lung cancer and heart disease only adds to this concern. Southeast Asians in particular demonstrate alarmingly high rates of tobacco consumption, and lung cancer is the leading cause of death among Asian Americans.12,24
Recently, a new acquired immune deficiency syndrome has been described in East Asia. In this syndrome, interferon–gamma (IFN–gamma) is blocked by an auto-antibody. Although not communicable like human immunodeficiency virus, this autoimmune syndrome may lead to similar opportunistic infections such as atypical mycobacterial infections.25
Mental health concerns
Perhaps no topic deserves more emphasis than that of mental health. In the aftermath of the war in Vietnam, Southeast Asian immigrants suffered a great deal from traumatic immigration experiences, with severe adjustment reactions.26 A high incidence of posttraumatic stress disorder (PTSD) among the Hmong in particular reflects their turbulent national history.27
While the incidence of mental illness among Asians is comparable to that of the general population, Asian Americans are less likely to report such problems or to use mental health services26 due to the stigmatization of mental illness in Asian culture.28 Consequently, these symptoms may be subconsciously converted into the more socially acceptable medium of physical illness, which “saves face” and preserves family honor.29 In many ways, Asian culture still perceives mental illness as personal weakness.30 In Hmong culture, inability to speak about being depressed stems not just from cultural bias but from linguistic constraints—the language simply lacks a word for depression.31 Even Asian cultures recognizing mental illness deem depression to be more dependent on circumstances than on the psyche.31 A first-generation immigrant with mental illness is therefore more likely to present with somatic symptoms than a mood disturbance, and is likely to be resistant to counseling or medication for depression. (See “Cultural influence on self-perception: A case ”).
Asian health care beliefs and illnesses
Asian culture substantially influences the ways in which an individual perceives disease, experiences illness, and copes with the phenomenon of sickness. The interplay between illness, disease, and sickness was first elucidated by the pioneering work of Arthur Kleinman, MD, in 1978.32 The term disease denotes a pathological process, while illness describes the subjective impact of disease in a patient’s life. Sickness is the sum of both, as it relates to the total picture of biological and social disruption. The culturally competent physician must understand not only the patient’s disease but also his experience of illness. Asking Dr. Kleinman’s questions will help physicians understand their patient’s perception of illness (TABLE 2).32
Traditional Chinese medicine
Many East Asians derive their conception of illness from traditional Chinese medicine (TCM), a broad range of therapies including herbs, acupuncture, massage (tuina), and diet that has been used for millennia. Similarly, South Asians are influenced by the Ayurvedic or Unani traditions. TCM views the body as an energy system, rather than a machine, through which the life force, or chi, flows. Health is not just the absence of disease, but a proper balance of the antithetic forces, yin and yang, maintained by herbs, diet, and acupuncture.33 TCM is often preferred for treating chronic conditions and viral syndromes, or as a substitute for Western medications with adverse effects.34 It is most popular among newly arrived immigrants, those with low literacy, and those with limited access to conventional medical treatment.34 Most Western physicians know little about TCM, feel uncomfortable when their patients use it, and fail to recognize its popularity.34,35 Likewise, most Asian patients are reluctant to discuss their use of TCM unless questioned about it in a nonjudgmental manner.
Many East Asian cultures practice a distinct form of folk healing known as “coining,” in which a coin dipped in cold oil or Tiger Balm is rubbed against the skin, enabling “wind illness” to escape the body (FIGURE 1). Linear bands of painless petechiae develop. The more extensive the bruising, the more illness is thought to be released. Failure to expel “wind-cold” from the body is believed to account for many ailments. Other traditions are moxibustion and cupping. In moxibustion, a smoldering plug of dried artemisia herb (moxi) is either impaled upon an acupuncture needle or placed directly on the skin to create a burn (FIGURE 2). In cupping, a flame is quickly passed through a glass bowl which is then placed against the skin. The resulting suction creates a circular bruise and draws blood to the area (FIGURE 3). Many folk remedies have been mistaken for child abuse by individuals unfamiliar with such practices.36 Occasionally TCM may result in harm from burns, unsterilized acupuncture needles, or (most commonly) adulterated herbal formulations.37
Culture-bound syndromes
Asian folk illnesses usually go unrecognized by western practitioners, and many of these are somatic presentations of mental illness or stress (TABLE 3). A classic example is the Korean folk condition Hwa-byung, which may include the sensation of an abdominal mass. US practitioners might pursue a fruitless abdominal workup before suspecting a psychiatric condition, even though a careful history would likely elicit other anxiety symptoms and loss of sleep and appetite.26
Asian social conventions
Asian cultural conventions often create considerable confusion. In India, head waggling (shaking the head back and forth) is equivalent to nodding in conversation, indicating an acknowledgement of communication. To western eyes, it appears that the patient is resisting advice rather than welcoming it. In East Asians, smiling expresses a variety of emotions, including polite disagreement. Acute embarrassment may provoke giggling. Eye contact is usually for social equals; avoiding it, especially between the sexes, is the norm. Only the right hand should be used when giving patients a prescription; the left hand is considered unclean. A patient’s head should only be touched with advance permission, as it is viewed as the seat of the soul and is therefore sacred. Under no circumstances should a patient ever see the bottom of the practitioner’s feet or be touched by them.38 Demonstrating respect (especially for older Asians) and preserving modesty are essential when examining patients.
Naming conventions can also be confusing. In China and much of Southeast Asia, it is customary for the surname to precede the given name, often with the 2 run together, rather than the other way round. It is best to ask how a patient would prefer to be addressed, regardless of how the name appears on the medical chart.38
Cultivating knowledge of Asian culture provides a framework from which practitioners can better understand and treat their patients. By asking respectful, open ended questions and encouraging patients to take an active role in their own treatment, physicians become therapeutic allies actively engaged in the healing process. Asking patients to share their use of alternative remedies allows the option of rationally integrating those most meaningful for the patient.
The cross-cultural interview
It is helpful to have a specific approach in mind when interviewing patients from other cultures. A number of mnemonic techniques exist.39-41 Perhaps the most useful of these is the LEARN model, which stands for Listen, Explain, Acknowledge, Recommend, and Negotiate.39 The physician first listens carefully to the patient’s perception of his illness before explaining any medical (disease) issues. This exchange is followed by acknowledging differences and similarities between the 2 viewpoints. Finally, the physician recommends a treatment plan and negotiates patient agreement.39 Negotiation implies flexibility and willingness to compromise with reasonable cultural demands, without compromising patient care. Use of the LEARN model aids in the identification and resolution of any cultural conflicts that might arise during the course of the clinical interview.
Teach back and patient activation
An extremely useful technique for all cultures is termed “teach back” or “show me,” which involves asking patients to repeat their care instructions at the end of the visit. This extra step provides an opportunity to correct errors that might have occurred during the transmission of instructions.42 Caregivers should also encourage or “activate” patients to become more involved in managing their own health care. Patient activation measures may be assessed on a one-to-4 point scale.43 Using both of these techniques combats passivity, promotes patient acceptance, and improves outcomes.
A caring environment
There are various strategies and approaches that can help make a medical practice more immigrant friendly (TABLE 4).44,45 Instructing office staff to assist patients in getting to the clinic is critical for those with limited mobility or who lack English proficiency. Adding evening hours that can also accommodate walk-ins helps working patients. For practices with larger immigrant populations, recognizing Asian holidays like Chinese New Year, Diwali, or Tet will be well received. These practices have been directly correlated with more positive health outcomes and better patient satisfaction.44
Conveying complex instructions to patients with little English takes effort for even the most unflappable providers. While written follow-up instructions in English could be interpreted by a more fluent family member, the ideal solution would be to have materials available in the native language. Fortunately, several Web sites, such as SPIRAL (Selective Patient Information in Asian Languages) provide downloadable Asian language instructions.46
Physicians should try to implement the Culturally & Linguistically Appropriate Services (CLAS) guidelines and mandates from the Office of Minority Health (http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15).6 They go far towards providing optimal care for patients of all cultures. Cultural competence does not imply being an expert in all cultures, let alone those of Asia. However, health care providers can develop the skills necessary for effective cross-cultural communication, which, to be most effective, must be accompanied by a caring attitude and respectful practice environment.
CORRESPONDENCE
Gregory Juckett, MD, MPH, West Virginia University School of Medicine, Box 9247, Robert C. Byrd Health Sciences Center, Morgantown, West Virginia, 26506; [email protected]
1. Min PG, ed. Asian Americans: Contemporary Trends and Issues. 2nd ed. Thousand Oaks, California: Pine Forge Press; 2006.
2. Ortman JM, Guarneri CE; National Census Bureau. United States population projections: 2000 to 2050. Available at: http://www.census.gov/population/projections/files/analytical-document09.pdf. Accessed February 20, 2012.
3. Barnes JS, Bennett CE; US Census Bureau Web site. The Asian population: 2000. Available at: http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed February 2, 2012.
4. Kim G, Worley CB, Allen RS, et al. Vulnerability of older Latino and Asian immigrants with limited English proficiency. J Am Geriatr Soc. 2011;59:1246-1252.
5. Silver D, Blustein J, Weitzman BC. Transportation to clinic: findings from a pilot clinic-based survey of low-income suburbanites. J Immigr Minor Health. 2012;14:350-355.
6. US Department of Health and Human Services Office of Minority Health Web site. The National CLAS Standards. Available at: http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15. Updated May 3, 2013. Accessed June 1, 2013.
7. Karliner LS, Jacobs EA, Chen AH, et al. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42:727-754.
8. Wilson E, Chen AH, Grumbach K, et al. Effects of limited English proficiency and physician language on health care comprehension. J Gen Intern Med. 2005;20:800-806.
9. Ku L, Flores G. Pay now or pay later: providing interpreter services in health care. Health Aff (Millwood). 2005;24:435-444.
10. Ngo-Metzger Q, Massagali MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med. 2003;18:44-52.
11. Basabe N, Ros M. Cultural dimensions and social behavior correlates: individualism-collectivism and power distance. Revue Internationale De Pscyhologie Sociale. 2005;17:189-225.
12. Ngo-Metzger Q, Legedza AT, Phillips RS. Asian Americans’ reports of their health care experiences. Results of a national survey. J Gen Intern Med. 2004;19:111-119.
13. Collins KS, Hughes DL, Doty MM, et al; The Commonwealth Fund. Diverse communities, common concerns: assessing health care quality for minority Americans. Available at: http://www.commonwealthfund.org/Publications/Fund-Reports/2002/Mar/Diverse-Communities--Common-Concerns--Assessing-Health-Care-Quality-for-Minority-Americans.aspx. Published March 2002. Accessed December 20, 2013.
14. Houston HR, Harada N, Makinodan T. Development of a culturally sensitive educational intervention program to reduce high incidence of tuberculosis among foreign-born Vietnamese. Ethn Health. 2002;7:255-265.
15. Mazurel GH, Jereb J, Vernon A, et al; Centers for Disease Control and Prevention (CDC). Updated guidelines for using interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection—United States, 2010. MMWR Recomm Rep. 2010;59(RR-5):1-25.
16. Hutton DW, Tan D, So SK, et al. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med. 2007;147:460-469.
17. Fattovich G, Brollo L, Giustina G, et al. Natural history and prognostic factors in chronic hepatitis B. Gut. 1991;32:294-298.
18. Beasley RP. Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer. 1988;61:1942-1956.
19. Smith C. Managing Adult Patients with Chronic HBV. Hepatitis B Foundation. Accessed February 15, 2012, at http://www.hepb.org/professionals/management_guidelines.htm.
20. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020-1022.
21. Hamaad A, Lip G. Assessing heart disease in your ethnic patients. Pulse. 2003;63:48-49.
22. Gupta M, Singh N, Verma S. South Asians and cardiovascular risk: what clinicians should know. Circulation. 2006;113:e924-e929.
23. Venkataraman R, Nanda NC, Beweja G, et al. Prevalence of diabetes mellitus and related conditions in Asian Indians living in the United States. Am J Cardiol. 2004;94:977-980.
24. Nishtar S. Prevention of coronary heart disease in south Asia. Lancet. 2002;360:1015-1018.
25. Browne SK, Burbelo PD, Chetchotisakd P, et al. Adult onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367:725-734.
26. Sorkin DH, Nguyen H, Ngo-Metzger Q. Assessing the mental health needs and barriers to care among a diverse sample of Asian American older adults. J Gen Intern Med. 2011;26:595-602.
27. PTSD, depression epidemic among Cambodian immigrants [press release]. Bethesda, MD: National Institutes of Health; August 2, 2005.
28. Sue S, Sue DW, Sue L, et al. Psychopathology among Asian Americans: a model minority? Cult Divers Ment Health. 1995;1:39-51.
29. Parker G, Cheah YC, Roy K. Do the Chinese somaticize depression? A cross-cultural study. Soc Psychiatry Psychiatr Epidemiol. 2001;36:287-293.
30. Sribney W, Elliot K, Aguilar-Gaxiola S, et al. The role of nonmedical human services and alternative medicine. In: Ruiz P, Primm A, eds. Disparities in Psychiatric Care. Baltimore, MD: Lippincott, Williams & Wilkins; 2010:274-289.
31. Lee HY, Lytle K, Yang PN, et al. Mental health literacy in Hmong and Cambodian elderly refugees: a barrier to understanding, recognizing, and responding to depression. Int J Aging Hum Dev. 2010;71:323-344.
32. Kleinman A, Eisenberg L, Good B. Culture, illness, and care: clinical lessons from anthroplologic and cross-cultural research. Ann Intern Med. 1978;88:251-258.
33. Patwardhan B, Warude D, Pushpangadan P, et al. Ayurveda and traditional Chinese medicine: a comparative overview. Evid Based Complement Alternat Med. 2005;2:465-473.
34. Wu AP, Burke A, LeBaron S. Use of traditional medicine by immigrant Chinese patients. Fam Med. 2007;39:195-200.
35. Nguyen G, Bowman M. Culture, language, and health literacy: communicating about health with Asians and Pacific Islanders. Fam Med. 2007;39:208-210.
36. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59:665-666.
37. Efferth T, Kaina B. Toxicities by herbal medicines with emphasis to traditional Chinese medicine. Curr Drug Metab. 2011;12:989-996.
38. Galanti G. Communication and time orientation. In: Caring for Patients from Different Cultures. 4th ed. Philadelphia, PA: University of Pennsylvania Press; 2008:27-51.
39. Berlin E, Fowkes WC Jr. A teaching framework for cross-cultural health care: application in family practice. West J Med. 1983;139:934-938.
40. Stuart MR, Lieberman JA III, eds. The Fifteen Minute Hour: Applied Psychotherapy for the Primary Care Physician. 2nd ed. Westport, CT: Praeger; 1993:101-183.
41. Kobylarz FA, Heath JM, Like RC. The ETHNIC(S) mnemonic: a clinical tool for ethnogeriatric education. J Am Geriat Soc. 2002;50:1582-1589.
42. Kountz DS. Strategies for improving low health literacy. Postgrad Med. 2009;121:171-177.
43. Patient Activation Measure Assessment. Insignia Health Web site. Available at: http://www.insigniahealth.com/solutions/patientactivation-measure. Accessed February 20, 2012.
44. Glenn-Vega A. Achieving a more minority-friendly practice. Fam Pract Manag. 2002;9:39-43.
45. Galanti G. Making a Difference. In: Caring for Patients from Different Cultures. 3rd ed. Philadelphia, PA: University of Pennsylvania Press; 2003:1222-1229.
46. SPIRAL: Selected Patient Information in Asian Languages. Tufts University Hirsh Health Sciences Web site. Available at: http://spiral.tufts.edu/topic.shtml. Accessed February 10, 2012.
1. Min PG, ed. Asian Americans: Contemporary Trends and Issues. 2nd ed. Thousand Oaks, California: Pine Forge Press; 2006.
2. Ortman JM, Guarneri CE; National Census Bureau. United States population projections: 2000 to 2050. Available at: http://www.census.gov/population/projections/files/analytical-document09.pdf. Accessed February 20, 2012.
3. Barnes JS, Bennett CE; US Census Bureau Web site. The Asian population: 2000. Available at: http://www.census.gov/prod/2002pubs/c2kbr01-16.pdf. Published February 2002. Accessed February 2, 2012.
4. Kim G, Worley CB, Allen RS, et al. Vulnerability of older Latino and Asian immigrants with limited English proficiency. J Am Geriatr Soc. 2011;59:1246-1252.
5. Silver D, Blustein J, Weitzman BC. Transportation to clinic: findings from a pilot clinic-based survey of low-income suburbanites. J Immigr Minor Health. 2012;14:350-355.
6. US Department of Health and Human Services Office of Minority Health Web site. The National CLAS Standards. Available at: http://minorityhealth.hhs.gov/templates/browse.aspx?lvl=2&lvlID=15. Updated May 3, 2013. Accessed June 1, 2013.
7. Karliner LS, Jacobs EA, Chen AH, et al. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv Res. 2007;42:727-754.
8. Wilson E, Chen AH, Grumbach K, et al. Effects of limited English proficiency and physician language on health care comprehension. J Gen Intern Med. 2005;20:800-806.
9. Ku L, Flores G. Pay now or pay later: providing interpreter services in health care. Health Aff (Millwood). 2005;24:435-444.
10. Ngo-Metzger Q, Massagali MP, Clarridge BR, et al. Linguistic and cultural barriers to care. J Gen Intern Med. 2003;18:44-52.
11. Basabe N, Ros M. Cultural dimensions and social behavior correlates: individualism-collectivism and power distance. Revue Internationale De Pscyhologie Sociale. 2005;17:189-225.
12. Ngo-Metzger Q, Legedza AT, Phillips RS. Asian Americans’ reports of their health care experiences. Results of a national survey. J Gen Intern Med. 2004;19:111-119.
13. Collins KS, Hughes DL, Doty MM, et al; The Commonwealth Fund. Diverse communities, common concerns: assessing health care quality for minority Americans. Available at: http://www.commonwealthfund.org/Publications/Fund-Reports/2002/Mar/Diverse-Communities--Common-Concerns--Assessing-Health-Care-Quality-for-Minority-Americans.aspx. Published March 2002. Accessed December 20, 2013.
14. Houston HR, Harada N, Makinodan T. Development of a culturally sensitive educational intervention program to reduce high incidence of tuberculosis among foreign-born Vietnamese. Ethn Health. 2002;7:255-265.
15. Mazurel GH, Jereb J, Vernon A, et al; Centers for Disease Control and Prevention (CDC). Updated guidelines for using interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection—United States, 2010. MMWR Recomm Rep. 2010;59(RR-5):1-25.
16. Hutton DW, Tan D, So SK, et al. Cost-effectiveness of screening and vaccinating Asian and Pacific Islander adults for hepatitis B. Ann Intern Med. 2007;147:460-469.
17. Fattovich G, Brollo L, Giustina G, et al. Natural history and prognostic factors in chronic hepatitis B. Gut. 1991;32:294-298.
18. Beasley RP. Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer. 1988;61:1942-1956.
19. Smith C. Managing Adult Patients with Chronic HBV. Hepatitis B Foundation. Accessed February 15, 2012, at http://www.hepb.org/professionals/management_guidelines.htm.
20. Bruix J, Sherman M. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53:1020-1022.
21. Hamaad A, Lip G. Assessing heart disease in your ethnic patients. Pulse. 2003;63:48-49.
22. Gupta M, Singh N, Verma S. South Asians and cardiovascular risk: what clinicians should know. Circulation. 2006;113:e924-e929.
23. Venkataraman R, Nanda NC, Beweja G, et al. Prevalence of diabetes mellitus and related conditions in Asian Indians living in the United States. Am J Cardiol. 2004;94:977-980.
24. Nishtar S. Prevention of coronary heart disease in south Asia. Lancet. 2002;360:1015-1018.
25. Browne SK, Burbelo PD, Chetchotisakd P, et al. Adult onset immunodeficiency in Thailand and Taiwan. N Engl J Med. 2012;367:725-734.
26. Sorkin DH, Nguyen H, Ngo-Metzger Q. Assessing the mental health needs and barriers to care among a diverse sample of Asian American older adults. J Gen Intern Med. 2011;26:595-602.
27. PTSD, depression epidemic among Cambodian immigrants [press release]. Bethesda, MD: National Institutes of Health; August 2, 2005.
28. Sue S, Sue DW, Sue L, et al. Psychopathology among Asian Americans: a model minority? Cult Divers Ment Health. 1995;1:39-51.
29. Parker G, Cheah YC, Roy K. Do the Chinese somaticize depression? A cross-cultural study. Soc Psychiatry Psychiatr Epidemiol. 2001;36:287-293.
30. Sribney W, Elliot K, Aguilar-Gaxiola S, et al. The role of nonmedical human services and alternative medicine. In: Ruiz P, Primm A, eds. Disparities in Psychiatric Care. Baltimore, MD: Lippincott, Williams & Wilkins; 2010:274-289.
31. Lee HY, Lytle K, Yang PN, et al. Mental health literacy in Hmong and Cambodian elderly refugees: a barrier to understanding, recognizing, and responding to depression. Int J Aging Hum Dev. 2010;71:323-344.
32. Kleinman A, Eisenberg L, Good B. Culture, illness, and care: clinical lessons from anthroplologic and cross-cultural research. Ann Intern Med. 1978;88:251-258.
33. Patwardhan B, Warude D, Pushpangadan P, et al. Ayurveda and traditional Chinese medicine: a comparative overview. Evid Based Complement Alternat Med. 2005;2:465-473.
34. Wu AP, Burke A, LeBaron S. Use of traditional medicine by immigrant Chinese patients. Fam Med. 2007;39:195-200.
35. Nguyen G, Bowman M. Culture, language, and health literacy: communicating about health with Asians and Pacific Islanders. Fam Med. 2007;39:208-210.
36. Oates RK. Overturning the diagnosis of child abuse. Arch Dis Child. 1984;59:665-666.
37. Efferth T, Kaina B. Toxicities by herbal medicines with emphasis to traditional Chinese medicine. Curr Drug Metab. 2011;12:989-996.
38. Galanti G. Communication and time orientation. In: Caring for Patients from Different Cultures. 4th ed. Philadelphia, PA: University of Pennsylvania Press; 2008:27-51.
39. Berlin E, Fowkes WC Jr. A teaching framework for cross-cultural health care: application in family practice. West J Med. 1983;139:934-938.
40. Stuart MR, Lieberman JA III, eds. The Fifteen Minute Hour: Applied Psychotherapy for the Primary Care Physician. 2nd ed. Westport, CT: Praeger; 1993:101-183.
41. Kobylarz FA, Heath JM, Like RC. The ETHNIC(S) mnemonic: a clinical tool for ethnogeriatric education. J Am Geriat Soc. 2002;50:1582-1589.
42. Kountz DS. Strategies for improving low health literacy. Postgrad Med. 2009;121:171-177.
43. Patient Activation Measure Assessment. Insignia Health Web site. Available at: http://www.insigniahealth.com/solutions/patientactivation-measure. Accessed February 20, 2012.
44. Glenn-Vega A. Achieving a more minority-friendly practice. Fam Pract Manag. 2002;9:39-43.
45. Galanti G. Making a Difference. In: Caring for Patients from Different Cultures. 3rd ed. Philadelphia, PA: University of Pennsylvania Press; 2003:1222-1229.
46. SPIRAL: Selected Patient Information in Asian Languages. Tufts University Hirsh Health Sciences Web site. Available at: http://spiral.tufts.edu/topic.shtml. Accessed February 10, 2012.

What is the best approach to goiter in euthyroid patients?
IN THE ABSENCE OF OUTCOME STUDIES, experts recommend ultrasound evaluation of nontoxic mulinodular goiters (MNG) followed by fine-needle aspiration (FNA) of suspicious nodules (strength of recommendation [SOR]: C, consensus-based guidelines).
Thyroid hormone suppression therapy reduces the size of MNG (SOR: A, systematic review of randomized controlled trials [RCTs]), but it risks inducing hyperthyroidism (SOR: C, expert opinion).
Experts recommend thyroidectomy for compressive symptoms, progressive growth, or ultrasound or FNA results indicating thyroid cancer (SOR: C, consensus based guidelines).
Expert guidelines recommend repeat ultrasound at 6 to 18 months to follow up benign nodules or nonendemic MNG in patients at low risk of malignancy and subsequent follow-up of stable nodules every 3 to 5 years (SOR: C, consensus-based guidelines).
EVIDENCE SUMMARY
This summary updates the 2007 Clinical Inquiry, “What is the best approach to goiter for euthyroid patients?”1
Initial evaluation of palpable goiter with a normal thyrotropin
In the United States, MNG is generally nonendemic and unrelated to iodine deficiency, as distinguished from endemic goiter caused by iodine deficiency in other parts of the world.
Our structured search of the literature found no randomized trials or prospective cohort studies comparing diagnostic approaches. The American Association of Clinical Endocrinologists’ (AACE) 2010 guidelines and American Thyroid Association (ATA) guidelines recommend ultrasound for all MNG.2,3 The AACE guidelines recommend thyroid scintigraphy when clinicians suspect retrosternal MNG.2
Ultrasound findings can change management, avoid biopsy
In a retrospective analysis of 223 patients with nodular thyroid disease, thyroid ultrasound altered clinical management of 63% of patients with abnormal thyroid exams.4 A single center retrospective cohort study of 650 FNA biopsies identified 4 morphologic patterns on ultrasound that predicted benign cytology with 100% specificity. The authors concluded that using ultrasound pattern to determine which patients require FNA could have obviated more than 60% of thyroid biopsies.5
Thyroid hormone suppression therapy risks hyperthyroidis
A systematic review of 9 RCTs of 18-month or shorter duration found that thyroid hormone suppression therapy reduced benign thyroid nodule volume (relative risk=1.88 compared with placebo or no treatment; 95% confidence interval [CI], 1.18-3.01; P=.008). The number needed to treat was 8 to reduce volume by >50% (risk difference=0.13; 95% CI, 0.06-0.19; P=.0003).6 However, thyroid hormone suppression therapy risks inducing hyperthyroidism and is not routinely recommended by the AACE or the ATA.2,3
Thyroidectomy: The treatment of choice
Thyroidectomy is the definitive therapy for MNG. A narrative review of 15 mostly retrospective cohort studies demonstrated MNG recurrence rates of 0% to 0.3% after total thyroidectomy, with follow-up intervals of 4.8 to 30 years.7
AACE consensus opinion recommends thyroidectomy for compressive symptoms, progressive growth, or when ultrasound or FNA results indicate thyroid cancer.2
A retrospective cohort study of 462 thyroidectomies for MNG found incidental thyroid carcinomas in 8.9% (41 patients). Risk factors included neck irradiation (odds ratio [OR]=21.64; 95% CI, 3.28-143), parenchymal calcifications on imaging (OR=2.30; 95% CI, 0.85-6.23), and family history of thyroid disease (OR=8.2; 95% CI, 2.15-29.87). Living in a goiter-endemic area was protective (OR=0.24; 95% CI, 0.07-0.83).8
Follow-up of patients with initial benign evaluation
Consensus opinion regarding follow-up of MNG is based on observational studies of the natural history of the condition. Benign MNG rarely progresses to malignancy. A review of 6 cohort studies, including 1265 patients with untreated nontoxic MNG who were followed for 60 to 130 months from 1990 to 2007, yielded an annual incidence range of 1.3 to 3.7 new cases of thyroid carcinoma per 1000 patients.9
Some goiters are more likely to enlarge. A retrospective cohort study of 488 patients treated surgically for MNG identified risk factors for enlargement: African American (OR=3.3; 95% CI, 2.0-5.4), age >40 years (OR=2.1; 95% CI, 1.2-3.8), and body mass index >30 (OR=2.5; 95% CI, 1.5-4.0).10
RECOMMENDATIONS
The AACE and the ATA recommend that patients with MNG with benign nodules have a repeat examination, TSH, and ultrasound in 6 to 18 months. Follow-up of stable nodules can then be done in 3 to 5 years.
An enlarging nodule requires repeat FNA.2 If palpation or ultrasound reveal evidence of nodule growth (more than a 50% change in volume or a 20% increase in at least 2 nodule dimensions, with a minimal increase of 2 mm in solid nodules or the solid portion of mixed cystic-solid nodules), the AACE and ATA recommend FNA, preferably with ultrasound guidance.3 Low TSH suggests autonomous nodules and the ATA recommends radionuclide scanning with FNA of hypofunctioning nodules with suspicious US features.3
1. Hoffman MR, Meadows SE, Langlois JP. Clinical inquiries. What is the best approach to goiter for euthyroid patients? J Fam Pract. 2007;56:479-480.
2. Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Pract. 2010;16(suppl 1):S1-S43.
3. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-1214.
4. Marqusee E, Benson CB, Frates MC, et al. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann Intern Med. 2000;133:696-700.
5. Bonavita JA, Mayo J, Babb J, et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol. 2009;193:207-213.
6. Sdano MT, Falciglia M, Welge JA, et al. Efficacy of thyroid hormone suppression for benign thyroid nodules: metaanalysis of randomized trials. Otolaryngol Head Neck Surg. 2005;133:391-396.
7. Moalem J, Suh I, Duh QY. Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J Surg. 2008;32:1301-1312.
8. Botrugno I, Lovisetto F, Cobianchi L, et al. Incidental carcinoma in multinodular goiter: risk factors. Am Surg. 2011;77:1553-1558.
9. Winbladh A, Järhult J. Fate of the non-operated, non-toxic goiter in a defined population. Brit J Surg. 2008;95:338-343.
10. Phitayakorn R, Super DM, McHenry CR. An investigation of epidemiologic factors associated with large nodular goiter. J Surg Res. 2006;133:16-21.
IN THE ABSENCE OF OUTCOME STUDIES, experts recommend ultrasound evaluation of nontoxic mulinodular goiters (MNG) followed by fine-needle aspiration (FNA) of suspicious nodules (strength of recommendation [SOR]: C, consensus-based guidelines).
Thyroid hormone suppression therapy reduces the size of MNG (SOR: A, systematic review of randomized controlled trials [RCTs]), but it risks inducing hyperthyroidism (SOR: C, expert opinion).
Experts recommend thyroidectomy for compressive symptoms, progressive growth, or ultrasound or FNA results indicating thyroid cancer (SOR: C, consensus based guidelines).
Expert guidelines recommend repeat ultrasound at 6 to 18 months to follow up benign nodules or nonendemic MNG in patients at low risk of malignancy and subsequent follow-up of stable nodules every 3 to 5 years (SOR: C, consensus-based guidelines).
EVIDENCE SUMMARY
This summary updates the 2007 Clinical Inquiry, “What is the best approach to goiter for euthyroid patients?”1
Initial evaluation of palpable goiter with a normal thyrotropin
In the United States, MNG is generally nonendemic and unrelated to iodine deficiency, as distinguished from endemic goiter caused by iodine deficiency in other parts of the world.
Our structured search of the literature found no randomized trials or prospective cohort studies comparing diagnostic approaches. The American Association of Clinical Endocrinologists’ (AACE) 2010 guidelines and American Thyroid Association (ATA) guidelines recommend ultrasound for all MNG.2,3 The AACE guidelines recommend thyroid scintigraphy when clinicians suspect retrosternal MNG.2
Ultrasound findings can change management, avoid biopsy
In a retrospective analysis of 223 patients with nodular thyroid disease, thyroid ultrasound altered clinical management of 63% of patients with abnormal thyroid exams.4 A single center retrospective cohort study of 650 FNA biopsies identified 4 morphologic patterns on ultrasound that predicted benign cytology with 100% specificity. The authors concluded that using ultrasound pattern to determine which patients require FNA could have obviated more than 60% of thyroid biopsies.5
Thyroid hormone suppression therapy risks hyperthyroidis
A systematic review of 9 RCTs of 18-month or shorter duration found that thyroid hormone suppression therapy reduced benign thyroid nodule volume (relative risk=1.88 compared with placebo or no treatment; 95% confidence interval [CI], 1.18-3.01; P=.008). The number needed to treat was 8 to reduce volume by >50% (risk difference=0.13; 95% CI, 0.06-0.19; P=.0003).6 However, thyroid hormone suppression therapy risks inducing hyperthyroidism and is not routinely recommended by the AACE or the ATA.2,3
Thyroidectomy: The treatment of choice
Thyroidectomy is the definitive therapy for MNG. A narrative review of 15 mostly retrospective cohort studies demonstrated MNG recurrence rates of 0% to 0.3% after total thyroidectomy, with follow-up intervals of 4.8 to 30 years.7
AACE consensus opinion recommends thyroidectomy for compressive symptoms, progressive growth, or when ultrasound or FNA results indicate thyroid cancer.2
A retrospective cohort study of 462 thyroidectomies for MNG found incidental thyroid carcinomas in 8.9% (41 patients). Risk factors included neck irradiation (odds ratio [OR]=21.64; 95% CI, 3.28-143), parenchymal calcifications on imaging (OR=2.30; 95% CI, 0.85-6.23), and family history of thyroid disease (OR=8.2; 95% CI, 2.15-29.87). Living in a goiter-endemic area was protective (OR=0.24; 95% CI, 0.07-0.83).8
Follow-up of patients with initial benign evaluation
Consensus opinion regarding follow-up of MNG is based on observational studies of the natural history of the condition. Benign MNG rarely progresses to malignancy. A review of 6 cohort studies, including 1265 patients with untreated nontoxic MNG who were followed for 60 to 130 months from 1990 to 2007, yielded an annual incidence range of 1.3 to 3.7 new cases of thyroid carcinoma per 1000 patients.9
Some goiters are more likely to enlarge. A retrospective cohort study of 488 patients treated surgically for MNG identified risk factors for enlargement: African American (OR=3.3; 95% CI, 2.0-5.4), age >40 years (OR=2.1; 95% CI, 1.2-3.8), and body mass index >30 (OR=2.5; 95% CI, 1.5-4.0).10
RECOMMENDATIONS
The AACE and the ATA recommend that patients with MNG with benign nodules have a repeat examination, TSH, and ultrasound in 6 to 18 months. Follow-up of stable nodules can then be done in 3 to 5 years.
An enlarging nodule requires repeat FNA.2 If palpation or ultrasound reveal evidence of nodule growth (more than a 50% change in volume or a 20% increase in at least 2 nodule dimensions, with a minimal increase of 2 mm in solid nodules or the solid portion of mixed cystic-solid nodules), the AACE and ATA recommend FNA, preferably with ultrasound guidance.3 Low TSH suggests autonomous nodules and the ATA recommends radionuclide scanning with FNA of hypofunctioning nodules with suspicious US features.3
IN THE ABSENCE OF OUTCOME STUDIES, experts recommend ultrasound evaluation of nontoxic mulinodular goiters (MNG) followed by fine-needle aspiration (FNA) of suspicious nodules (strength of recommendation [SOR]: C, consensus-based guidelines).
Thyroid hormone suppression therapy reduces the size of MNG (SOR: A, systematic review of randomized controlled trials [RCTs]), but it risks inducing hyperthyroidism (SOR: C, expert opinion).
Experts recommend thyroidectomy for compressive symptoms, progressive growth, or ultrasound or FNA results indicating thyroid cancer (SOR: C, consensus based guidelines).
Expert guidelines recommend repeat ultrasound at 6 to 18 months to follow up benign nodules or nonendemic MNG in patients at low risk of malignancy and subsequent follow-up of stable nodules every 3 to 5 years (SOR: C, consensus-based guidelines).
EVIDENCE SUMMARY
This summary updates the 2007 Clinical Inquiry, “What is the best approach to goiter for euthyroid patients?”1
Initial evaluation of palpable goiter with a normal thyrotropin
In the United States, MNG is generally nonendemic and unrelated to iodine deficiency, as distinguished from endemic goiter caused by iodine deficiency in other parts of the world.
Our structured search of the literature found no randomized trials or prospective cohort studies comparing diagnostic approaches. The American Association of Clinical Endocrinologists’ (AACE) 2010 guidelines and American Thyroid Association (ATA) guidelines recommend ultrasound for all MNG.2,3 The AACE guidelines recommend thyroid scintigraphy when clinicians suspect retrosternal MNG.2
Ultrasound findings can change management, avoid biopsy
In a retrospective analysis of 223 patients with nodular thyroid disease, thyroid ultrasound altered clinical management of 63% of patients with abnormal thyroid exams.4 A single center retrospective cohort study of 650 FNA biopsies identified 4 morphologic patterns on ultrasound that predicted benign cytology with 100% specificity. The authors concluded that using ultrasound pattern to determine which patients require FNA could have obviated more than 60% of thyroid biopsies.5
Thyroid hormone suppression therapy risks hyperthyroidis
A systematic review of 9 RCTs of 18-month or shorter duration found that thyroid hormone suppression therapy reduced benign thyroid nodule volume (relative risk=1.88 compared with placebo or no treatment; 95% confidence interval [CI], 1.18-3.01; P=.008). The number needed to treat was 8 to reduce volume by >50% (risk difference=0.13; 95% CI, 0.06-0.19; P=.0003).6 However, thyroid hormone suppression therapy risks inducing hyperthyroidism and is not routinely recommended by the AACE or the ATA.2,3
Thyroidectomy: The treatment of choice
Thyroidectomy is the definitive therapy for MNG. A narrative review of 15 mostly retrospective cohort studies demonstrated MNG recurrence rates of 0% to 0.3% after total thyroidectomy, with follow-up intervals of 4.8 to 30 years.7
AACE consensus opinion recommends thyroidectomy for compressive symptoms, progressive growth, or when ultrasound or FNA results indicate thyroid cancer.2
A retrospective cohort study of 462 thyroidectomies for MNG found incidental thyroid carcinomas in 8.9% (41 patients). Risk factors included neck irradiation (odds ratio [OR]=21.64; 95% CI, 3.28-143), parenchymal calcifications on imaging (OR=2.30; 95% CI, 0.85-6.23), and family history of thyroid disease (OR=8.2; 95% CI, 2.15-29.87). Living in a goiter-endemic area was protective (OR=0.24; 95% CI, 0.07-0.83).8
Follow-up of patients with initial benign evaluation
Consensus opinion regarding follow-up of MNG is based on observational studies of the natural history of the condition. Benign MNG rarely progresses to malignancy. A review of 6 cohort studies, including 1265 patients with untreated nontoxic MNG who were followed for 60 to 130 months from 1990 to 2007, yielded an annual incidence range of 1.3 to 3.7 new cases of thyroid carcinoma per 1000 patients.9
Some goiters are more likely to enlarge. A retrospective cohort study of 488 patients treated surgically for MNG identified risk factors for enlargement: African American (OR=3.3; 95% CI, 2.0-5.4), age >40 years (OR=2.1; 95% CI, 1.2-3.8), and body mass index >30 (OR=2.5; 95% CI, 1.5-4.0).10
RECOMMENDATIONS
The AACE and the ATA recommend that patients with MNG with benign nodules have a repeat examination, TSH, and ultrasound in 6 to 18 months. Follow-up of stable nodules can then be done in 3 to 5 years.
An enlarging nodule requires repeat FNA.2 If palpation or ultrasound reveal evidence of nodule growth (more than a 50% change in volume or a 20% increase in at least 2 nodule dimensions, with a minimal increase of 2 mm in solid nodules or the solid portion of mixed cystic-solid nodules), the AACE and ATA recommend FNA, preferably with ultrasound guidance.3 Low TSH suggests autonomous nodules and the ATA recommends radionuclide scanning with FNA of hypofunctioning nodules with suspicious US features.3
1. Hoffman MR, Meadows SE, Langlois JP. Clinical inquiries. What is the best approach to goiter for euthyroid patients? J Fam Pract. 2007;56:479-480.
2. Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Pract. 2010;16(suppl 1):S1-S43.
3. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-1214.
4. Marqusee E, Benson CB, Frates MC, et al. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann Intern Med. 2000;133:696-700.
5. Bonavita JA, Mayo J, Babb J, et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol. 2009;193:207-213.
6. Sdano MT, Falciglia M, Welge JA, et al. Efficacy of thyroid hormone suppression for benign thyroid nodules: metaanalysis of randomized trials. Otolaryngol Head Neck Surg. 2005;133:391-396.
7. Moalem J, Suh I, Duh QY. Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J Surg. 2008;32:1301-1312.
8. Botrugno I, Lovisetto F, Cobianchi L, et al. Incidental carcinoma in multinodular goiter: risk factors. Am Surg. 2011;77:1553-1558.
9. Winbladh A, Järhult J. Fate of the non-operated, non-toxic goiter in a defined population. Brit J Surg. 2008;95:338-343.
10. Phitayakorn R, Super DM, McHenry CR. An investigation of epidemiologic factors associated with large nodular goiter. J Surg Res. 2006;133:16-21.
1. Hoffman MR, Meadows SE, Langlois JP. Clinical inquiries. What is the best approach to goiter for euthyroid patients? J Fam Pract. 2007;56:479-480.
2. Gharib H, Papini E, Paschke R, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Pract. 2010;16(suppl 1):S1-S43.
3. American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167-1214.
4. Marqusee E, Benson CB, Frates MC, et al. Usefulness of ultrasonography in the management of nodular thyroid disease. Ann Intern Med. 2000;133:696-700.
5. Bonavita JA, Mayo J, Babb J, et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol. 2009;193:207-213.
6. Sdano MT, Falciglia M, Welge JA, et al. Efficacy of thyroid hormone suppression for benign thyroid nodules: metaanalysis of randomized trials. Otolaryngol Head Neck Surg. 2005;133:391-396.
7. Moalem J, Suh I, Duh QY. Treatment and prevention of recurrence of multinodular goiter: an evidence-based review of the literature. World J Surg. 2008;32:1301-1312.
8. Botrugno I, Lovisetto F, Cobianchi L, et al. Incidental carcinoma in multinodular goiter: risk factors. Am Surg. 2011;77:1553-1558.
9. Winbladh A, Järhult J. Fate of the non-operated, non-toxic goiter in a defined population. Brit J Surg. 2008;95:338-343.
10. Phitayakorn R, Super DM, McHenry CR. An investigation of epidemiologic factors associated with large nodular goiter. J Surg Res. 2006;133:16-21.
Evidence-based answers from the Family Physicians Inquiries Network
Neuroendocrine dysfunction following mild TBI: When to screen for it
› Consider neuroendocrine dysfunction (NED) following confirmed traumatic brain injury of any severity when symptoms suggestive of NED persist for >3 months after injury. A
› Order blood studies to detect deficiencies in pituitary and other key hormones when NED is suspected. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The Centers for Disease Control and Prevention (CDC) reports that >1.7 million cases of traumatic brain injury (TBI) occur annually in the United States.1 More than 266,000 military service members sustained at least one TBI from 2000 to 2012.2 Most TBIs (80%-85%), military and civilian, are classified as mild (mTBI), and most mTBI patients (80%-85%) experience a complete functional recovery within 3 months of injury.1,3 The remaining 15% to 20% of mTBI patients experience persistent symptoms and difficulty in rehabilitation, particularly if there are concomitant disorders, such as post-traumatic stress disorder (PTSD), sleep disorders, acute stress disorder, substance abuse disorder, and depression.4,5 Symptoms that mTBI and these other disorders have in common can make differential diagnosis difficult, requiring a high degree of clinical awareness by primary care providers. An additional concern following mTBI is neuroendocrine dysfunction (NED). This association has not been widely discussed and therefore may go largely undiagnosed.6 Consider NED in the setting of prolonged symptoms or in patients experiencing difficulty with rehabilitation following mTBI.7,8
NED following mTBI is more common than once thought
The term “neuroendocrine dysfunction,” as discussed in this article, refers to a variety of conditions caused by imbalances in the body’s hormone production directly related to the pituitary, hypothalamus, and their axes following TBI. Until the past decade, the incidence of TBI-associated pituitary dysfunction was thought to be an uncommon event, usually associated with catastrophic head injuries. Studies of NED in TBI patients focused primarily on moderate or severe TBI, usually from motor vehicle incidents, falls, and assaults.7 Other research has since shown that NED occurs more commonly than once believed.9 And while the risk of NED may be higher for patients who sustain more severe brain injuries, NED also occurs in mTBI.7,9,10,11 Interestingly, a recent literature review indicated that the incidence of NED in mTBI was 16.8%, while the incidence with moderate TBI was reported at 10.9%.7 Other research has noted that the incidence of NED in mTBI may be as high as 42%.9,12 No evidence suggests that the severity of NED is related to a specific hormonal dysfunction, nor is there evidence that NED may be associated with a specific mechanism of injury.
Pituitary anatomy is susceptible to injury and dysfunction
The anatomic and physiologic complexities of the hypothalamus and pituitary gland increase their susceptibility to injury from TBI. The pituitary gland is connected to the hypothalamus by a blood vessel-containing stalk, making the pituitary gland—particularly the anterior portion—susceptible to damage during a head injury.13 The hypothalamus secretes thyrotropin-releasing hormone (TRH) and luteinizing-releasing hormone (LRH) to stimulate or suppress the production of anterior pituitary gland hormones, which in turn stimulate the release of hormones and other substances from target organs. Anterior pituitary hormones are growth hormone (GH), luteinizing hormone (LH), follicle-stimulating hormone (FSH), adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), and prolactin (PRL). The posterior pituitary secretes oxytocin and vasopressin, also known as antidiuretic hormone (ADH).13
Impact from a direct blow with an object or from a concussive blast can cause focal trauma or rotational shearing of tissue internally. Resultant vascular injury, rupture, cerebral edema, vasospasm, pituitary swelling, or inflammation may then initiate an endocrine response that drives a cascade of complex hormonal processes.5,7,8 Anterior pituitary deficiencies account for the majority of chronic neuroendocrine disorders following mTBI. GH and gonadotropin deficiencies are the most common, but TSH deficiency (secondary hypothyroidism) and ACTH deficiency (adrenal insufficiency) may occur as well, although in <10% of cases with TBI associated NED.12
Clinical features of NED mimic those of other conditions
The symptoms of NED include fatigue, insomnia, impaired cognition, memory loss, difficulty concentrating, and emotional and mood disturbances (TABLE).7,12,14-17 Various combinations of these symptoms may occur and are similar to those of other post-mTBI conditions, such as sleep problems, postconcussive syndrome (PCS), and memory and attention difficulties.18 The onset of NED may be immediate (eg, in diabetes insipidus [DI] or syndrome of inappropriate antidiuretic hormone [SIADH], which are very rare in mTBI) and potentially life-threatening (eg, in sodium and potassium imbalances), or may be nonspecific and take years to manifest.6,10,15,19 Additionally, symptoms of NED may spontaneously resolve or persist. Studies have demonstrated pituitary dysfunction in the acute postinjury phase as well as its development as late as 2 to 3 years after injury.7,8,11,20
Due to the range of symptoms related to the combinations of possible hormonal derangements, NED can be an elusive diagnosis and may have a deleterious effect on individuals who sustain TBI.12 For example, an undiagnosed GH deficiency—which can result in increased abdominal fat mass and decreased lean muscle mass as well as impaired cardiac function, dyslipidemia, and insulin resistance—makes it more difficult for an affected individual either to recover from additional injuries or to maintain fitness. Considering NED may avoid a delay in diagnosis and improve prognosis.7,8,20
Findings leading to recommendations on diagnosis
Primary care providers, military and civilian alike, can benefit from the findings and recommendations of an expert panel assembled by the Defense Centers of Excellence (DCoE) for Psychological Health and Traumatic Brain Injury to address NED in mTBI. The panel that convened in December 2010 included experts representing the military services, the Department of Veterans Affairs, DCoE, and civilian sectors. Based on the group’s recommendations combined with literature review findings, the DCoE developed a clinical recommendation to encourage primary care providers to consider screening for NED in patients with persistent symptoms following mTBI.21 Key findings and issues identified by the group included the following:
• The most frequent mechanism of injury in the military deployed population is blast-induced TBI. Such injury could occur in the civilian population at construction blast sites or in factories producing or using highly flammable substances.
• The prevalence of any anterior pituitary hormone deficiency is as high as 30% to hormone deficiency is as high as 30% to 80% at 24 to 36 months post injury.
• The prevalence of posterior pituitary hormone deficiency is as high as 4% to 7% at 12 months post injury.
• The anterior pituitary hormones most frequently affected in survivors of TBI are ACTH, gonadotropin, prolactin, and GH.
• In 2004 Agha et al,22 reported >28% of survivors of TBI had at least one anterior pituitary hormone deficiency.
• According to research by Agha et al23 in 2005, >20% of survivors of TBI developed DI; those who developed DI, either acutely or permanently, were more likely to have sustained a severe TBI.
• The development of pituitary dysfunction is independent of the severity of TBI.
• In 2005, civilian guidelines4 recommended screening for pituitary dysfunction in all patients who sustained a moderate to severe TBI.
• In 2010, civilian guidelines7 recommended screening for pituitary dysfunction in patients who sustained a mild TBI.
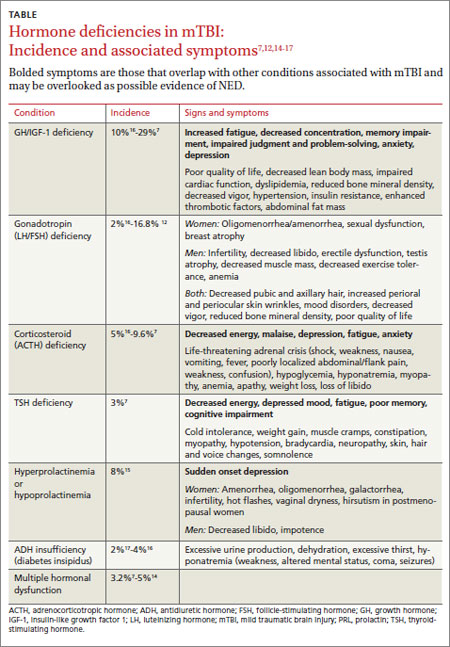
When to screen for NED after TBI
Given the complexities described—including the similarity of NED to other post-mTBI medical diagnoses and such concomitant disorders as a sleep disorder, memory difficulties, depression, PTSD, and PCS24—consider NED in the primary care setting following confirmed TBI of any severity level when symptoms suggestive of NED persist for >3 months following injury or appear up to 36 months later.7,8,12,20
Order a lab evaluation of blood levels for cortisol (drawn at 8 am), LH, FSH, PRL, insulin-like growth factor-1, TSH, free thyroxine-4, and testosterone for men (8 am) and estradiol for women (8 am). With frankly abnormal lab results or with borderline results and strong clinical suspicion for NED, refer for further endocrinology workup (FIGURE).21 Earlier diagnosis of NED results in more rapid improvement of symptoms and an improved prognosis.7,8,20 Postinjury screening for NED should be one component of a thorough clinical evaluation by a qualified provider, and not used in isolation for clinical decision making. NED screening should not be routinely ordered during the early stages of mTBI, defined as <3 months postinjury.
Provider awareness and willingness to include NED screening in a timely manner, and to refer to specialty services as indicated for symptoms that may be sleep related or psychiatric in nature, may increase the opportunities for early treatment, better rehabilitation outcomes, and better overall quality of life.
Looking ahead
While the DCoE expert group made recommendations on screening for NED in the military combat population, they also acknowledged that NED diagnosis and treatment would benefit from additional areas of research:
• the effect of GH replacement (for GH-deficient patients or as prophylaxis for all TBI patients) on rehabilitation response and quality of life
• the role of multiple TBIs on long-term cognition and possible premature aging
• the role of NED over time
• biomarkers for diagnosis
• factors affecting resiliency
• resiliency in the context of increased or decreased susceptibility to the development of an acute clinical syndrome, as well as susceptibility in developing the spectrum of consequences of TBI.
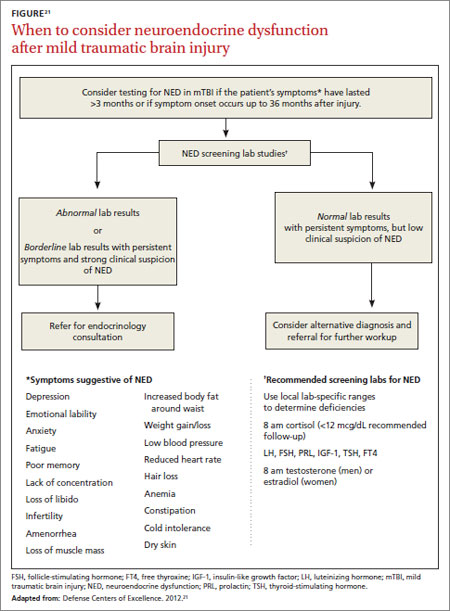
The research areas given the highest priority by the group were incidence and prevalence studies of pituitary dysfunction after TBI in the combat military population, including pre- and postdeployment rates of dysfunction and the incidence of comorbidities. Also of benefit would be a retrospective study of the consequences of pituitary dysfunction that additionally addresses the effects of comorbid conditions commonly associated with TBI. Considering the rapid expansion in the field of mTBI, additional research and provider awareness concerning early identification and treatments may improve the outcomes for those with persistent mTBI symptoms.
CORRESPONDENCE
Theres A. West, DNP, APN, BC, Defense and Veterans Brain Injury Center, 1335 East West Highway, 6th floor, Silver Spring, MD 20910; [email protected]
1. Injury prevention & control: Traumatic brain injury national TBI estimates. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/traumaticbraininjury/statistics.html. Accessed August 12, 2013.
2. Armed Forces Surveillance Center. DoD Worldwide Numbers for TBI. Defense and Veterans Brain Injury Centers Web site. Available at: www.dvbic.org/dod-worldwide-Numbers-tbi. Accessed August 12, 2013.
3. Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for management of concussion/mild traumatic brain injury (mTBI). Available at: http://www.healthquality.va.gov/management_of_concussion_mtbi.asp. Published April 2009. Accessed August 12, 2013.
4. Ghigo E, Masel B, Aimaretti G, et al. Consensus guidelines on screening for hypopituitarism following traumatic brain injury. Brain Inj. 2005;19:711-724.
5. Krahulik D, Zapletalova J, Frysak Z, et al. Dysfunction of hypothalamic-hyperphysical axis after traumatic brain injury in adults. J Neurosurg. 2010;113:581-584.
6. Behan LA, Phillips J, Thompson CJ, et al. Neuroendocrine disorders after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2008;79:753-759.
7. Tanriverdi F, Unluhizarci K, Kelestimur F. Pituitary function in subjects with mild traumatic brain injury: a review of literature and proposal of a screening strategy. Pituitary. 2010;13:146-153.
8. Bondanelli M, Ambrosio MR, Zatelli MC, et al. Hypopituitarism after traumatic brain injury. Eur J Endocrinol. 2005;152:679-691.
9. Wilkinson CW, Pagulayan KF, Petrie EC, et al. High prevalence of chronic pituitary and target-hormone abnormalities after blast related mild traumatic brain injury. Front Neurol. 2012;3:11.
10. Bondanelli M, Ambrosio MR, Cavazzini L, et al. Anterior pituitary function may predict functional and cognitive outcome in patients with traumatic brain injury undergoing rehabilitation. J Neurotrauma. 2007;24:1687-1697.
11. Benvenga S, Campenmi A, Ruggeri R, et al. Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab. 2000;85:1353-1361.
12. Schneider H, Kreitschman-Andermahr I, Ghigo E, et al. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA. 2007;298:1429-1438.
13. Amar AP, Weiss MH. Pituitary anatomy and physiology. Neurosurg Clin N Am. 2003;14:11-23.
14. Tanriverdi F, Unluhizarci K, Kocyigit I, et al. Brief communication: Pituitary volume and function in competing and retired male boxers. Ann Intern Med. 2008;148:827-831.
15. Bondanelli M, De Marinis L, Ambrosio MR, et al. Occurrence of pituitary dysfunction following traumatic brain injury. J Neurotrauma. 2004;21:685-696.
16. Klose M, Watt T, Brennum J, et al. Posttraumatic hypopituitarism is associated with an unfavorable body composition and lipid profile, and decreased quality of life in 12 months after injury. J Clin Endocrinol Metab. 2007;92:3861-3868.
17. Aimeretti G, Ambrosio MR, Di Somma C, et al. Residual pituitary function after brain injury-induced hypopituitaryism: a prospective 12-month study. J Clin Endocrinol Metab. 2005;90:6085-6092.
18. Agha A, Phillips J, Thompson CJ. Hypopituitarism following traumatic brain injury. Br J Neurosurg. 2007;21:210-216.
19. Cohan P, Wang C, McArthur DL, et al. Acute secondary adrenal insufficiency after traumatic brain injury: a prospective study. Crit Care Med. 2005;33:2358-2366.
20. Rothman MS, Arciniegas DS, Filley CM, et al. The neuroendocrine effects of traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2007;19:363-372.
21. Defense Centers of Excellence. Neuroendocrine screening post mild TBI clinical recommendation. Available at: http://www.dcoe.mil/Content/Navigation/Documents/DCoE_TBI_NED_Reference_Card.pdf. Published February 2012. Accessed August 12, 2013.
22. Agha A, Rogers B, Mylotte D, et al. Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin Endocrinol (Oxf). 2004;60:584-591.
23. Agha A, Phillips J, O’Kelly P, et al. The natural history of post-traumatic hypopituitarism: implications for assessment and treatment. Am J Med. 2005;118:1416.
24. Guerrero AF, Alfonso A. Traumatic brain injury related hypopituitarism: a review and recommendations for screening combat veterans. Mil Med. 2010;175:574-580.
› Consider neuroendocrine dysfunction (NED) following confirmed traumatic brain injury of any severity when symptoms suggestive of NED persist for >3 months after injury. A
› Order blood studies to detect deficiencies in pituitary and other key hormones when NED is suspected. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The Centers for Disease Control and Prevention (CDC) reports that >1.7 million cases of traumatic brain injury (TBI) occur annually in the United States.1 More than 266,000 military service members sustained at least one TBI from 2000 to 2012.2 Most TBIs (80%-85%), military and civilian, are classified as mild (mTBI), and most mTBI patients (80%-85%) experience a complete functional recovery within 3 months of injury.1,3 The remaining 15% to 20% of mTBI patients experience persistent symptoms and difficulty in rehabilitation, particularly if there are concomitant disorders, such as post-traumatic stress disorder (PTSD), sleep disorders, acute stress disorder, substance abuse disorder, and depression.4,5 Symptoms that mTBI and these other disorders have in common can make differential diagnosis difficult, requiring a high degree of clinical awareness by primary care providers. An additional concern following mTBI is neuroendocrine dysfunction (NED). This association has not been widely discussed and therefore may go largely undiagnosed.6 Consider NED in the setting of prolonged symptoms or in patients experiencing difficulty with rehabilitation following mTBI.7,8
NED following mTBI is more common than once thought
The term “neuroendocrine dysfunction,” as discussed in this article, refers to a variety of conditions caused by imbalances in the body’s hormone production directly related to the pituitary, hypothalamus, and their axes following TBI. Until the past decade, the incidence of TBI-associated pituitary dysfunction was thought to be an uncommon event, usually associated with catastrophic head injuries. Studies of NED in TBI patients focused primarily on moderate or severe TBI, usually from motor vehicle incidents, falls, and assaults.7 Other research has since shown that NED occurs more commonly than once believed.9 And while the risk of NED may be higher for patients who sustain more severe brain injuries, NED also occurs in mTBI.7,9,10,11 Interestingly, a recent literature review indicated that the incidence of NED in mTBI was 16.8%, while the incidence with moderate TBI was reported at 10.9%.7 Other research has noted that the incidence of NED in mTBI may be as high as 42%.9,12 No evidence suggests that the severity of NED is related to a specific hormonal dysfunction, nor is there evidence that NED may be associated with a specific mechanism of injury.
Pituitary anatomy is susceptible to injury and dysfunction
The anatomic and physiologic complexities of the hypothalamus and pituitary gland increase their susceptibility to injury from TBI. The pituitary gland is connected to the hypothalamus by a blood vessel-containing stalk, making the pituitary gland—particularly the anterior portion—susceptible to damage during a head injury.13 The hypothalamus secretes thyrotropin-releasing hormone (TRH) and luteinizing-releasing hormone (LRH) to stimulate or suppress the production of anterior pituitary gland hormones, which in turn stimulate the release of hormones and other substances from target organs. Anterior pituitary hormones are growth hormone (GH), luteinizing hormone (LH), follicle-stimulating hormone (FSH), adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), and prolactin (PRL). The posterior pituitary secretes oxytocin and vasopressin, also known as antidiuretic hormone (ADH).13
Impact from a direct blow with an object or from a concussive blast can cause focal trauma or rotational shearing of tissue internally. Resultant vascular injury, rupture, cerebral edema, vasospasm, pituitary swelling, or inflammation may then initiate an endocrine response that drives a cascade of complex hormonal processes.5,7,8 Anterior pituitary deficiencies account for the majority of chronic neuroendocrine disorders following mTBI. GH and gonadotropin deficiencies are the most common, but TSH deficiency (secondary hypothyroidism) and ACTH deficiency (adrenal insufficiency) may occur as well, although in <10% of cases with TBI associated NED.12
Clinical features of NED mimic those of other conditions
The symptoms of NED include fatigue, insomnia, impaired cognition, memory loss, difficulty concentrating, and emotional and mood disturbances (TABLE).7,12,14-17 Various combinations of these symptoms may occur and are similar to those of other post-mTBI conditions, such as sleep problems, postconcussive syndrome (PCS), and memory and attention difficulties.18 The onset of NED may be immediate (eg, in diabetes insipidus [DI] or syndrome of inappropriate antidiuretic hormone [SIADH], which are very rare in mTBI) and potentially life-threatening (eg, in sodium and potassium imbalances), or may be nonspecific and take years to manifest.6,10,15,19 Additionally, symptoms of NED may spontaneously resolve or persist. Studies have demonstrated pituitary dysfunction in the acute postinjury phase as well as its development as late as 2 to 3 years after injury.7,8,11,20
Due to the range of symptoms related to the combinations of possible hormonal derangements, NED can be an elusive diagnosis and may have a deleterious effect on individuals who sustain TBI.12 For example, an undiagnosed GH deficiency—which can result in increased abdominal fat mass and decreased lean muscle mass as well as impaired cardiac function, dyslipidemia, and insulin resistance—makes it more difficult for an affected individual either to recover from additional injuries or to maintain fitness. Considering NED may avoid a delay in diagnosis and improve prognosis.7,8,20
Findings leading to recommendations on diagnosis
Primary care providers, military and civilian alike, can benefit from the findings and recommendations of an expert panel assembled by the Defense Centers of Excellence (DCoE) for Psychological Health and Traumatic Brain Injury to address NED in mTBI. The panel that convened in December 2010 included experts representing the military services, the Department of Veterans Affairs, DCoE, and civilian sectors. Based on the group’s recommendations combined with literature review findings, the DCoE developed a clinical recommendation to encourage primary care providers to consider screening for NED in patients with persistent symptoms following mTBI.21 Key findings and issues identified by the group included the following:
• The most frequent mechanism of injury in the military deployed population is blast-induced TBI. Such injury could occur in the civilian population at construction blast sites or in factories producing or using highly flammable substances.
• The prevalence of any anterior pituitary hormone deficiency is as high as 30% to hormone deficiency is as high as 30% to 80% at 24 to 36 months post injury.
• The prevalence of posterior pituitary hormone deficiency is as high as 4% to 7% at 12 months post injury.
• The anterior pituitary hormones most frequently affected in survivors of TBI are ACTH, gonadotropin, prolactin, and GH.
• In 2004 Agha et al,22 reported >28% of survivors of TBI had at least one anterior pituitary hormone deficiency.
• According to research by Agha et al23 in 2005, >20% of survivors of TBI developed DI; those who developed DI, either acutely or permanently, were more likely to have sustained a severe TBI.
• The development of pituitary dysfunction is independent of the severity of TBI.
• In 2005, civilian guidelines4 recommended screening for pituitary dysfunction in all patients who sustained a moderate to severe TBI.
• In 2010, civilian guidelines7 recommended screening for pituitary dysfunction in patients who sustained a mild TBI.
When to screen for NED after TBI
Given the complexities described—including the similarity of NED to other post-mTBI medical diagnoses and such concomitant disorders as a sleep disorder, memory difficulties, depression, PTSD, and PCS24—consider NED in the primary care setting following confirmed TBI of any severity level when symptoms suggestive of NED persist for >3 months following injury or appear up to 36 months later.7,8,12,20
Order a lab evaluation of blood levels for cortisol (drawn at 8 am), LH, FSH, PRL, insulin-like growth factor-1, TSH, free thyroxine-4, and testosterone for men (8 am) and estradiol for women (8 am). With frankly abnormal lab results or with borderline results and strong clinical suspicion for NED, refer for further endocrinology workup (FIGURE).21 Earlier diagnosis of NED results in more rapid improvement of symptoms and an improved prognosis.7,8,20 Postinjury screening for NED should be one component of a thorough clinical evaluation by a qualified provider, and not used in isolation for clinical decision making. NED screening should not be routinely ordered during the early stages of mTBI, defined as <3 months postinjury.
Provider awareness and willingness to include NED screening in a timely manner, and to refer to specialty services as indicated for symptoms that may be sleep related or psychiatric in nature, may increase the opportunities for early treatment, better rehabilitation outcomes, and better overall quality of life.
Looking ahead
While the DCoE expert group made recommendations on screening for NED in the military combat population, they also acknowledged that NED diagnosis and treatment would benefit from additional areas of research:
• the effect of GH replacement (for GH-deficient patients or as prophylaxis for all TBI patients) on rehabilitation response and quality of life
• the role of multiple TBIs on long-term cognition and possible premature aging
• the role of NED over time
• biomarkers for diagnosis
• factors affecting resiliency
• resiliency in the context of increased or decreased susceptibility to the development of an acute clinical syndrome, as well as susceptibility in developing the spectrum of consequences of TBI.
The research areas given the highest priority by the group were incidence and prevalence studies of pituitary dysfunction after TBI in the combat military population, including pre- and postdeployment rates of dysfunction and the incidence of comorbidities. Also of benefit would be a retrospective study of the consequences of pituitary dysfunction that additionally addresses the effects of comorbid conditions commonly associated with TBI. Considering the rapid expansion in the field of mTBI, additional research and provider awareness concerning early identification and treatments may improve the outcomes for those with persistent mTBI symptoms.
CORRESPONDENCE
Theres A. West, DNP, APN, BC, Defense and Veterans Brain Injury Center, 1335 East West Highway, 6th floor, Silver Spring, MD 20910; [email protected]
› Consider neuroendocrine dysfunction (NED) following confirmed traumatic brain injury of any severity when symptoms suggestive of NED persist for >3 months after injury. A
› Order blood studies to detect deficiencies in pituitary and other key hormones when NED is suspected. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
The Centers for Disease Control and Prevention (CDC) reports that >1.7 million cases of traumatic brain injury (TBI) occur annually in the United States.1 More than 266,000 military service members sustained at least one TBI from 2000 to 2012.2 Most TBIs (80%-85%), military and civilian, are classified as mild (mTBI), and most mTBI patients (80%-85%) experience a complete functional recovery within 3 months of injury.1,3 The remaining 15% to 20% of mTBI patients experience persistent symptoms and difficulty in rehabilitation, particularly if there are concomitant disorders, such as post-traumatic stress disorder (PTSD), sleep disorders, acute stress disorder, substance abuse disorder, and depression.4,5 Symptoms that mTBI and these other disorders have in common can make differential diagnosis difficult, requiring a high degree of clinical awareness by primary care providers. An additional concern following mTBI is neuroendocrine dysfunction (NED). This association has not been widely discussed and therefore may go largely undiagnosed.6 Consider NED in the setting of prolonged symptoms or in patients experiencing difficulty with rehabilitation following mTBI.7,8
NED following mTBI is more common than once thought
The term “neuroendocrine dysfunction,” as discussed in this article, refers to a variety of conditions caused by imbalances in the body’s hormone production directly related to the pituitary, hypothalamus, and their axes following TBI. Until the past decade, the incidence of TBI-associated pituitary dysfunction was thought to be an uncommon event, usually associated with catastrophic head injuries. Studies of NED in TBI patients focused primarily on moderate or severe TBI, usually from motor vehicle incidents, falls, and assaults.7 Other research has since shown that NED occurs more commonly than once believed.9 And while the risk of NED may be higher for patients who sustain more severe brain injuries, NED also occurs in mTBI.7,9,10,11 Interestingly, a recent literature review indicated that the incidence of NED in mTBI was 16.8%, while the incidence with moderate TBI was reported at 10.9%.7 Other research has noted that the incidence of NED in mTBI may be as high as 42%.9,12 No evidence suggests that the severity of NED is related to a specific hormonal dysfunction, nor is there evidence that NED may be associated with a specific mechanism of injury.
Pituitary anatomy is susceptible to injury and dysfunction
The anatomic and physiologic complexities of the hypothalamus and pituitary gland increase their susceptibility to injury from TBI. The pituitary gland is connected to the hypothalamus by a blood vessel-containing stalk, making the pituitary gland—particularly the anterior portion—susceptible to damage during a head injury.13 The hypothalamus secretes thyrotropin-releasing hormone (TRH) and luteinizing-releasing hormone (LRH) to stimulate or suppress the production of anterior pituitary gland hormones, which in turn stimulate the release of hormones and other substances from target organs. Anterior pituitary hormones are growth hormone (GH), luteinizing hormone (LH), follicle-stimulating hormone (FSH), adrenocorticotropic hormone (ACTH), thyroid-stimulating hormone (TSH), and prolactin (PRL). The posterior pituitary secretes oxytocin and vasopressin, also known as antidiuretic hormone (ADH).13
Impact from a direct blow with an object or from a concussive blast can cause focal trauma or rotational shearing of tissue internally. Resultant vascular injury, rupture, cerebral edema, vasospasm, pituitary swelling, or inflammation may then initiate an endocrine response that drives a cascade of complex hormonal processes.5,7,8 Anterior pituitary deficiencies account for the majority of chronic neuroendocrine disorders following mTBI. GH and gonadotropin deficiencies are the most common, but TSH deficiency (secondary hypothyroidism) and ACTH deficiency (adrenal insufficiency) may occur as well, although in <10% of cases with TBI associated NED.12
Clinical features of NED mimic those of other conditions
The symptoms of NED include fatigue, insomnia, impaired cognition, memory loss, difficulty concentrating, and emotional and mood disturbances (TABLE).7,12,14-17 Various combinations of these symptoms may occur and are similar to those of other post-mTBI conditions, such as sleep problems, postconcussive syndrome (PCS), and memory and attention difficulties.18 The onset of NED may be immediate (eg, in diabetes insipidus [DI] or syndrome of inappropriate antidiuretic hormone [SIADH], which are very rare in mTBI) and potentially life-threatening (eg, in sodium and potassium imbalances), or may be nonspecific and take years to manifest.6,10,15,19 Additionally, symptoms of NED may spontaneously resolve or persist. Studies have demonstrated pituitary dysfunction in the acute postinjury phase as well as its development as late as 2 to 3 years after injury.7,8,11,20
Due to the range of symptoms related to the combinations of possible hormonal derangements, NED can be an elusive diagnosis and may have a deleterious effect on individuals who sustain TBI.12 For example, an undiagnosed GH deficiency—which can result in increased abdominal fat mass and decreased lean muscle mass as well as impaired cardiac function, dyslipidemia, and insulin resistance—makes it more difficult for an affected individual either to recover from additional injuries or to maintain fitness. Considering NED may avoid a delay in diagnosis and improve prognosis.7,8,20
Findings leading to recommendations on diagnosis
Primary care providers, military and civilian alike, can benefit from the findings and recommendations of an expert panel assembled by the Defense Centers of Excellence (DCoE) for Psychological Health and Traumatic Brain Injury to address NED in mTBI. The panel that convened in December 2010 included experts representing the military services, the Department of Veterans Affairs, DCoE, and civilian sectors. Based on the group’s recommendations combined with literature review findings, the DCoE developed a clinical recommendation to encourage primary care providers to consider screening for NED in patients with persistent symptoms following mTBI.21 Key findings and issues identified by the group included the following:
• The most frequent mechanism of injury in the military deployed population is blast-induced TBI. Such injury could occur in the civilian population at construction blast sites or in factories producing or using highly flammable substances.
• The prevalence of any anterior pituitary hormone deficiency is as high as 30% to hormone deficiency is as high as 30% to 80% at 24 to 36 months post injury.
• The prevalence of posterior pituitary hormone deficiency is as high as 4% to 7% at 12 months post injury.
• The anterior pituitary hormones most frequently affected in survivors of TBI are ACTH, gonadotropin, prolactin, and GH.
• In 2004 Agha et al,22 reported >28% of survivors of TBI had at least one anterior pituitary hormone deficiency.
• According to research by Agha et al23 in 2005, >20% of survivors of TBI developed DI; those who developed DI, either acutely or permanently, were more likely to have sustained a severe TBI.
• The development of pituitary dysfunction is independent of the severity of TBI.
• In 2005, civilian guidelines4 recommended screening for pituitary dysfunction in all patients who sustained a moderate to severe TBI.
• In 2010, civilian guidelines7 recommended screening for pituitary dysfunction in patients who sustained a mild TBI.
When to screen for NED after TBI
Given the complexities described—including the similarity of NED to other post-mTBI medical diagnoses and such concomitant disorders as a sleep disorder, memory difficulties, depression, PTSD, and PCS24—consider NED in the primary care setting following confirmed TBI of any severity level when symptoms suggestive of NED persist for >3 months following injury or appear up to 36 months later.7,8,12,20
Order a lab evaluation of blood levels for cortisol (drawn at 8 am), LH, FSH, PRL, insulin-like growth factor-1, TSH, free thyroxine-4, and testosterone for men (8 am) and estradiol for women (8 am). With frankly abnormal lab results or with borderline results and strong clinical suspicion for NED, refer for further endocrinology workup (FIGURE).21 Earlier diagnosis of NED results in more rapid improvement of symptoms and an improved prognosis.7,8,20 Postinjury screening for NED should be one component of a thorough clinical evaluation by a qualified provider, and not used in isolation for clinical decision making. NED screening should not be routinely ordered during the early stages of mTBI, defined as <3 months postinjury.
Provider awareness and willingness to include NED screening in a timely manner, and to refer to specialty services as indicated for symptoms that may be sleep related or psychiatric in nature, may increase the opportunities for early treatment, better rehabilitation outcomes, and better overall quality of life.
Looking ahead
While the DCoE expert group made recommendations on screening for NED in the military combat population, they also acknowledged that NED diagnosis and treatment would benefit from additional areas of research:
• the effect of GH replacement (for GH-deficient patients or as prophylaxis for all TBI patients) on rehabilitation response and quality of life
• the role of multiple TBIs on long-term cognition and possible premature aging
• the role of NED over time
• biomarkers for diagnosis
• factors affecting resiliency
• resiliency in the context of increased or decreased susceptibility to the development of an acute clinical syndrome, as well as susceptibility in developing the spectrum of consequences of TBI.
The research areas given the highest priority by the group were incidence and prevalence studies of pituitary dysfunction after TBI in the combat military population, including pre- and postdeployment rates of dysfunction and the incidence of comorbidities. Also of benefit would be a retrospective study of the consequences of pituitary dysfunction that additionally addresses the effects of comorbid conditions commonly associated with TBI. Considering the rapid expansion in the field of mTBI, additional research and provider awareness concerning early identification and treatments may improve the outcomes for those with persistent mTBI symptoms.
CORRESPONDENCE
Theres A. West, DNP, APN, BC, Defense and Veterans Brain Injury Center, 1335 East West Highway, 6th floor, Silver Spring, MD 20910; [email protected]
1. Injury prevention & control: Traumatic brain injury national TBI estimates. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/traumaticbraininjury/statistics.html. Accessed August 12, 2013.
2. Armed Forces Surveillance Center. DoD Worldwide Numbers for TBI. Defense and Veterans Brain Injury Centers Web site. Available at: www.dvbic.org/dod-worldwide-Numbers-tbi. Accessed August 12, 2013.
3. Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for management of concussion/mild traumatic brain injury (mTBI). Available at: http://www.healthquality.va.gov/management_of_concussion_mtbi.asp. Published April 2009. Accessed August 12, 2013.
4. Ghigo E, Masel B, Aimaretti G, et al. Consensus guidelines on screening for hypopituitarism following traumatic brain injury. Brain Inj. 2005;19:711-724.
5. Krahulik D, Zapletalova J, Frysak Z, et al. Dysfunction of hypothalamic-hyperphysical axis after traumatic brain injury in adults. J Neurosurg. 2010;113:581-584.
6. Behan LA, Phillips J, Thompson CJ, et al. Neuroendocrine disorders after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2008;79:753-759.
7. Tanriverdi F, Unluhizarci K, Kelestimur F. Pituitary function in subjects with mild traumatic brain injury: a review of literature and proposal of a screening strategy. Pituitary. 2010;13:146-153.
8. Bondanelli M, Ambrosio MR, Zatelli MC, et al. Hypopituitarism after traumatic brain injury. Eur J Endocrinol. 2005;152:679-691.
9. Wilkinson CW, Pagulayan KF, Petrie EC, et al. High prevalence of chronic pituitary and target-hormone abnormalities after blast related mild traumatic brain injury. Front Neurol. 2012;3:11.
10. Bondanelli M, Ambrosio MR, Cavazzini L, et al. Anterior pituitary function may predict functional and cognitive outcome in patients with traumatic brain injury undergoing rehabilitation. J Neurotrauma. 2007;24:1687-1697.
11. Benvenga S, Campenmi A, Ruggeri R, et al. Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab. 2000;85:1353-1361.
12. Schneider H, Kreitschman-Andermahr I, Ghigo E, et al. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA. 2007;298:1429-1438.
13. Amar AP, Weiss MH. Pituitary anatomy and physiology. Neurosurg Clin N Am. 2003;14:11-23.
14. Tanriverdi F, Unluhizarci K, Kocyigit I, et al. Brief communication: Pituitary volume and function in competing and retired male boxers. Ann Intern Med. 2008;148:827-831.
15. Bondanelli M, De Marinis L, Ambrosio MR, et al. Occurrence of pituitary dysfunction following traumatic brain injury. J Neurotrauma. 2004;21:685-696.
16. Klose M, Watt T, Brennum J, et al. Posttraumatic hypopituitarism is associated with an unfavorable body composition and lipid profile, and decreased quality of life in 12 months after injury. J Clin Endocrinol Metab. 2007;92:3861-3868.
17. Aimeretti G, Ambrosio MR, Di Somma C, et al. Residual pituitary function after brain injury-induced hypopituitaryism: a prospective 12-month study. J Clin Endocrinol Metab. 2005;90:6085-6092.
18. Agha A, Phillips J, Thompson CJ. Hypopituitarism following traumatic brain injury. Br J Neurosurg. 2007;21:210-216.
19. Cohan P, Wang C, McArthur DL, et al. Acute secondary adrenal insufficiency after traumatic brain injury: a prospective study. Crit Care Med. 2005;33:2358-2366.
20. Rothman MS, Arciniegas DS, Filley CM, et al. The neuroendocrine effects of traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2007;19:363-372.
21. Defense Centers of Excellence. Neuroendocrine screening post mild TBI clinical recommendation. Available at: http://www.dcoe.mil/Content/Navigation/Documents/DCoE_TBI_NED_Reference_Card.pdf. Published February 2012. Accessed August 12, 2013.
22. Agha A, Rogers B, Mylotte D, et al. Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin Endocrinol (Oxf). 2004;60:584-591.
23. Agha A, Phillips J, O’Kelly P, et al. The natural history of post-traumatic hypopituitarism: implications for assessment and treatment. Am J Med. 2005;118:1416.
24. Guerrero AF, Alfonso A. Traumatic brain injury related hypopituitarism: a review and recommendations for screening combat veterans. Mil Med. 2010;175:574-580.
1. Injury prevention & control: Traumatic brain injury national TBI estimates. Centers for Disease Control and Prevention Web site. Available at: http://www.cdc.gov/traumaticbraininjury/statistics.html. Accessed August 12, 2013.
2. Armed Forces Surveillance Center. DoD Worldwide Numbers for TBI. Defense and Veterans Brain Injury Centers Web site. Available at: www.dvbic.org/dod-worldwide-Numbers-tbi. Accessed August 12, 2013.
3. Department of Veterans Affairs, Department of Defense. VA/DoD clinical practice guideline for management of concussion/mild traumatic brain injury (mTBI). Available at: http://www.healthquality.va.gov/management_of_concussion_mtbi.asp. Published April 2009. Accessed August 12, 2013.
4. Ghigo E, Masel B, Aimaretti G, et al. Consensus guidelines on screening for hypopituitarism following traumatic brain injury. Brain Inj. 2005;19:711-724.
5. Krahulik D, Zapletalova J, Frysak Z, et al. Dysfunction of hypothalamic-hyperphysical axis after traumatic brain injury in adults. J Neurosurg. 2010;113:581-584.
6. Behan LA, Phillips J, Thompson CJ, et al. Neuroendocrine disorders after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2008;79:753-759.
7. Tanriverdi F, Unluhizarci K, Kelestimur F. Pituitary function in subjects with mild traumatic brain injury: a review of literature and proposal of a screening strategy. Pituitary. 2010;13:146-153.
8. Bondanelli M, Ambrosio MR, Zatelli MC, et al. Hypopituitarism after traumatic brain injury. Eur J Endocrinol. 2005;152:679-691.
9. Wilkinson CW, Pagulayan KF, Petrie EC, et al. High prevalence of chronic pituitary and target-hormone abnormalities after blast related mild traumatic brain injury. Front Neurol. 2012;3:11.
10. Bondanelli M, Ambrosio MR, Cavazzini L, et al. Anterior pituitary function may predict functional and cognitive outcome in patients with traumatic brain injury undergoing rehabilitation. J Neurotrauma. 2007;24:1687-1697.
11. Benvenga S, Campenmi A, Ruggeri R, et al. Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab. 2000;85:1353-1361.
12. Schneider H, Kreitschman-Andermahr I, Ghigo E, et al. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage: a systematic review. JAMA. 2007;298:1429-1438.
13. Amar AP, Weiss MH. Pituitary anatomy and physiology. Neurosurg Clin N Am. 2003;14:11-23.
14. Tanriverdi F, Unluhizarci K, Kocyigit I, et al. Brief communication: Pituitary volume and function in competing and retired male boxers. Ann Intern Med. 2008;148:827-831.
15. Bondanelli M, De Marinis L, Ambrosio MR, et al. Occurrence of pituitary dysfunction following traumatic brain injury. J Neurotrauma. 2004;21:685-696.
16. Klose M, Watt T, Brennum J, et al. Posttraumatic hypopituitarism is associated with an unfavorable body composition and lipid profile, and decreased quality of life in 12 months after injury. J Clin Endocrinol Metab. 2007;92:3861-3868.
17. Aimeretti G, Ambrosio MR, Di Somma C, et al. Residual pituitary function after brain injury-induced hypopituitaryism: a prospective 12-month study. J Clin Endocrinol Metab. 2005;90:6085-6092.
18. Agha A, Phillips J, Thompson CJ. Hypopituitarism following traumatic brain injury. Br J Neurosurg. 2007;21:210-216.
19. Cohan P, Wang C, McArthur DL, et al. Acute secondary adrenal insufficiency after traumatic brain injury: a prospective study. Crit Care Med. 2005;33:2358-2366.
20. Rothman MS, Arciniegas DS, Filley CM, et al. The neuroendocrine effects of traumatic brain injury. J Neuropsychiatry Clin Neurosci. 2007;19:363-372.
21. Defense Centers of Excellence. Neuroendocrine screening post mild TBI clinical recommendation. Available at: http://www.dcoe.mil/Content/Navigation/Documents/DCoE_TBI_NED_Reference_Card.pdf. Published February 2012. Accessed August 12, 2013.
22. Agha A, Rogers B, Mylotte D, et al. Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin Endocrinol (Oxf). 2004;60:584-591.
23. Agha A, Phillips J, O’Kelly P, et al. The natural history of post-traumatic hypopituitarism: implications for assessment and treatment. Am J Med. 2005;118:1416.
24. Guerrero AF, Alfonso A. Traumatic brain injury related hypopituitarism: a review and recommendations for screening combat veterans. Mil Med. 2010;175:574-580.