User login
Accountable-Care Organizations on the Horizon for Hospitalists
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
Every HM group should look into transitioning from a fee-for-service model to an accountable-care organization (ACO), a leading hospitalist told conference attendees recently at the Third National Accountable Care Organization Congress.
"You need to be tackling it now, but that doesn't mean you need to be aggressively doing it now," Edward Murphy, MD, chairman of Sound Physicians, told eWire days before he spoke at the ACO Congress on Oct. 31 in Los Angeles. "By tackling it, you need to be doing a hard-nosed assessment of what's best for your group and your patients."
Question: Why is the ACO model so difficult in some instances?
Answer: The problem with the healthcare system today is we’ve spent 100 years building up a system that is designed around, and competent at, delivering services for fees. We're really not set up to manage care.
Q: What is the No. 1 thing you want hospitalists to know about ACOs today?
A: Figure out every single day how to improve the care of your patients at a lower cost. And then, how you can demonstrate it in a quantitative and clear way. ACO-style payments are really only a value proposition centered on providing superior outcomes for patients at higher satisfaction for lower cost. That’s a fundamental value that will always be noteworthy.
Q: Is a hospitalist's job to lead the charge toward ACOs, or support those who do?
A: That's the sort of thing that people on the ground don't have to be told. They just know. If I were the leader of a hospitalist group someplace and really thought the smart thing to do was to think about how to move to an accountable-care model … I would know from my discussions with my colleagues, my discussions with hospital executives where everybody was.
Visit our website for more information about ACOs.
End-of-Life Care Can Bring on Challenges for Hospitalists
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
How do you cope with a family that wants you to "do everything" for their seriously ill loved one? This dilemma was one of the topics explored at the Management of the Hospitalized Patient conference held last month at the University of California at San Francisco (UCSF).
"We don't actually know what 'everything' means to the family, not without probing into a range of possible meanings," said presenter Steve Pantilat, MD, FACP, SFHM, hospitalist and director of the palliative-care service at UCSF Medical Center. "The family may not have a clear understanding of what 'everything' entails, including mechanical ventilation or cardio-pulmonary resuscitation. I prefer to ask, 'How were you hoping we could help?' The answer can provide a great deal of insight."
In spite of various tools to aid decisions, prognosis is inherently uncertain, said co-presenter Matthew Gonzales, MD, assistant professor of hospital medicine and palliative care at UCSF Medical Center. "We use the Palliative Performance Scale [PDF]."
The family might not trust the hospitalist’s prognosis, especially when meeting the doctor for the first time in a stressful situation, and there might be disagreements within the family about the course of treatment, Dr. Gonzales said. Cultural differences also come into play.
"I have started to ask, 'How do you decide these questions in your family?' because of the differences within a cultural group," Dr. Pantilat said. "If they talk about hoping for a miracle, I probe the meaning of 'miracle' to them. Physicians can't work on the basis of miracles; they have to practice medicine. And you should resist getting drawn into a religious debate. That's a loser for the physician."
Visit our website for more information about palliative care.
Excessive Acetaminophen Dosing Seen Among Inpatients
Four percent of hospitalized adolescents and adults at two academic tertiary care medical centers received supratherapeutic doses of acetaminophen during their stays, according to a report published online Nov. 12 in Archives of Internal Medicine.
"These were not isolated events but often were successive and overlapping." Nearly half of the exposed patients received 5 g or more of acetaminophen per day, and 40% received excessive dosing for 3 or more days, said Dr. Li Zhou of Partners HealthCare System, Wellesley, Mass., and her associates.
Such overmedicating puts patients at unnecessary risk for hepatotoxicity, acute liver failure, and even death. In this study, even inpatients at specific risk for liver damage didn’t escape excessive dosing with acetaminophen: 22% of the elderly and 18% of patients with existing chronic liver disease were given acetaminophen in amounts exceeding their recommended limit of 3 g/day, said Dr. Zhou, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues.
The risk factors most strongly associated with supratherapeutic dosing were receiving recurring scheduled dosing (that is, standing orders) as opposed to as-needed or one-time-only administration, which carried a hazard ratio of 16.6; receiving multiple products containing acetaminophen, which carried a hazard ratio of 2.4 for each additional product; and receiving products containing 500 mg of acetaminophen, which carried an HR of 1.9.
The investigators used the hospitals’ electronic medication administration record systems to assess acetaminophen exposure in the inpatient setting – a topic that has received little attention from researchers before now, they wrote. The study population comprised the 14,411 inpatients aged 12 and older who received any acetaminophen during their stays in a 3-month period. That accounts for about 61% of the entire patient population hospitalized at the two centers during the study period.
The average age of the study subjects was 55 years (range, 12-110 years), and a little more than one-third were older than 65. Approximately 75 had chronic liver disease.
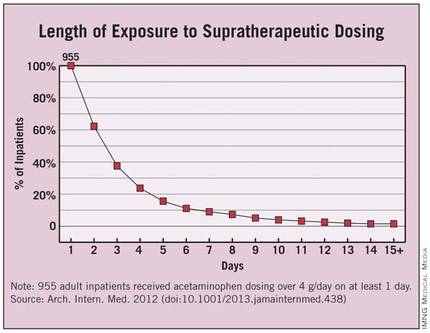
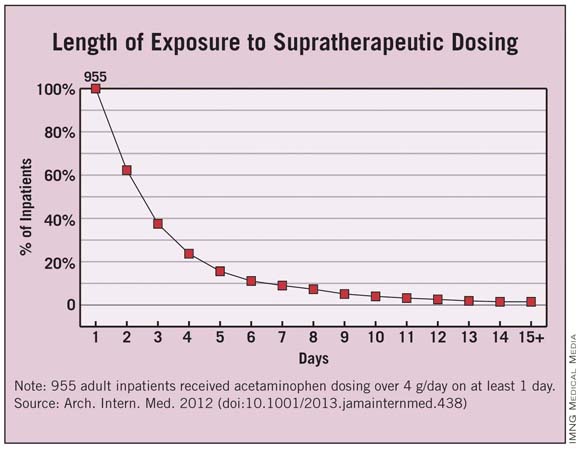
Overall, 955 patients were given acetaminophen in doses exceeding the 4-g/day limit. This represents 4% of the entire hospitalized population and 6.6% of the cohort of patients given any acetaminophen, the researchers said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.438]).
Each patient who received supratherapeutic dosing had a mean of five such incidents during the course of a mean of 3 days. Instances of such overmedicating ranged as high as 48 separate occasions over the course of 30 days.
Approximately 40% of the 955 patients received supratherapeutic dosing for 3 or more days, and 4% received it for 10 or more days.
"Our findings show that despite policies and procedures to monitor and control patients’ acetaminophen exposure, the incidence of supratherapeutic acetaminophen dosing in hospitalized patients remains high," Dr. Zhou and her associates said.
Previous studies have shown that many physicians and nurses aren’t aware of the maximal recommended daily dosing of acetaminophen, and that many have some difficulty identifying which products contain the agent. Therefore, increased training is warranted "to help clinicians identify acetaminophen-containing products and monitor closely the daily dose of acetaminophen," the investigators said.
A reassessment of long-accepted dosing regimens may also be warranted, "especially the scheduled use of products containing 500 mg of acetaminophen," they added.
The study was funded by the Partners-Siemens Research Council. The investigators reported no relevant financial conflicts.
Dr. Li Zhou and her colleagues have identified a serious threat to patient safety and a cause for great concern, said Dr. Walter H. Ettinger.
"On an annualized basis, more than 3,800 patients at these two hospitals alone were put at unnecessary risk. If the estimates in this manuscript are generalizable, hundreds of thousands of patients nationwide may be receiving toxic doses of acetaminophen while in the hospital," he noted.
The study is important, "but it is incomplete and illustrates the obstacles we must overcome in using [health information technology] to drive performance. The authors identified a major flaw in the way in which a common drug is used in the hospital setting, and in a rapid-learning, high-performance health system, the results would be rapidly disseminated, together with a definitive solution for preventing excessive dosing in the future. The authors suggested educating health care providers about the risks of acetaminophen use and changing hospital policies to reduce risk factors for excessive dosing as a means of prevention. But excessive dosing of acetaminophen should be a ‘never event.’ The best way to prevent excessive dosing is to engineer a process and imbed it in the [electronic health record] such that it creates a hard stop that prevents ordering and administering more than 4 g/day of acetaminophen."
Dr. Ettinger is at the University of Massachusetts, Worcester, and at Accretive Health, Chicago, a health care technology and services firm. He reported no other relevant financial conflicts. These remarks were taken from his invited commentary accompanying Dr. Zhou’s report (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.607]).
Dr. Li Zhou and her colleagues have identified a serious threat to patient safety and a cause for great concern, said Dr. Walter H. Ettinger.
"On an annualized basis, more than 3,800 patients at these two hospitals alone were put at unnecessary risk. If the estimates in this manuscript are generalizable, hundreds of thousands of patients nationwide may be receiving toxic doses of acetaminophen while in the hospital," he noted.
The study is important, "but it is incomplete and illustrates the obstacles we must overcome in using [health information technology] to drive performance. The authors identified a major flaw in the way in which a common drug is used in the hospital setting, and in a rapid-learning, high-performance health system, the results would be rapidly disseminated, together with a definitive solution for preventing excessive dosing in the future. The authors suggested educating health care providers about the risks of acetaminophen use and changing hospital policies to reduce risk factors for excessive dosing as a means of prevention. But excessive dosing of acetaminophen should be a ‘never event.’ The best way to prevent excessive dosing is to engineer a process and imbed it in the [electronic health record] such that it creates a hard stop that prevents ordering and administering more than 4 g/day of acetaminophen."
Dr. Ettinger is at the University of Massachusetts, Worcester, and at Accretive Health, Chicago, a health care technology and services firm. He reported no other relevant financial conflicts. These remarks were taken from his invited commentary accompanying Dr. Zhou’s report (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.607]).
Dr. Li Zhou and her colleagues have identified a serious threat to patient safety and a cause for great concern, said Dr. Walter H. Ettinger.
"On an annualized basis, more than 3,800 patients at these two hospitals alone were put at unnecessary risk. If the estimates in this manuscript are generalizable, hundreds of thousands of patients nationwide may be receiving toxic doses of acetaminophen while in the hospital," he noted.
The study is important, "but it is incomplete and illustrates the obstacles we must overcome in using [health information technology] to drive performance. The authors identified a major flaw in the way in which a common drug is used in the hospital setting, and in a rapid-learning, high-performance health system, the results would be rapidly disseminated, together with a definitive solution for preventing excessive dosing in the future. The authors suggested educating health care providers about the risks of acetaminophen use and changing hospital policies to reduce risk factors for excessive dosing as a means of prevention. But excessive dosing of acetaminophen should be a ‘never event.’ The best way to prevent excessive dosing is to engineer a process and imbed it in the [electronic health record] such that it creates a hard stop that prevents ordering and administering more than 4 g/day of acetaminophen."
Dr. Ettinger is at the University of Massachusetts, Worcester, and at Accretive Health, Chicago, a health care technology and services firm. He reported no other relevant financial conflicts. These remarks were taken from his invited commentary accompanying Dr. Zhou’s report (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.607]).
Four percent of hospitalized adolescents and adults at two academic tertiary care medical centers received supratherapeutic doses of acetaminophen during their stays, according to a report published online Nov. 12 in Archives of Internal Medicine.
"These were not isolated events but often were successive and overlapping." Nearly half of the exposed patients received 5 g or more of acetaminophen per day, and 40% received excessive dosing for 3 or more days, said Dr. Li Zhou of Partners HealthCare System, Wellesley, Mass., and her associates.
Such overmedicating puts patients at unnecessary risk for hepatotoxicity, acute liver failure, and even death. In this study, even inpatients at specific risk for liver damage didn’t escape excessive dosing with acetaminophen: 22% of the elderly and 18% of patients with existing chronic liver disease were given acetaminophen in amounts exceeding their recommended limit of 3 g/day, said Dr. Zhou, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues.
The risk factors most strongly associated with supratherapeutic dosing were receiving recurring scheduled dosing (that is, standing orders) as opposed to as-needed or one-time-only administration, which carried a hazard ratio of 16.6; receiving multiple products containing acetaminophen, which carried a hazard ratio of 2.4 for each additional product; and receiving products containing 500 mg of acetaminophen, which carried an HR of 1.9.
The investigators used the hospitals’ electronic medication administration record systems to assess acetaminophen exposure in the inpatient setting – a topic that has received little attention from researchers before now, they wrote. The study population comprised the 14,411 inpatients aged 12 and older who received any acetaminophen during their stays in a 3-month period. That accounts for about 61% of the entire patient population hospitalized at the two centers during the study period.
The average age of the study subjects was 55 years (range, 12-110 years), and a little more than one-third were older than 65. Approximately 75 had chronic liver disease.
Overall, 955 patients were given acetaminophen in doses exceeding the 4-g/day limit. This represents 4% of the entire hospitalized population and 6.6% of the cohort of patients given any acetaminophen, the researchers said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.438]).
Each patient who received supratherapeutic dosing had a mean of five such incidents during the course of a mean of 3 days. Instances of such overmedicating ranged as high as 48 separate occasions over the course of 30 days.
Approximately 40% of the 955 patients received supratherapeutic dosing for 3 or more days, and 4% received it for 10 or more days.
"Our findings show that despite policies and procedures to monitor and control patients’ acetaminophen exposure, the incidence of supratherapeutic acetaminophen dosing in hospitalized patients remains high," Dr. Zhou and her associates said.
Previous studies have shown that many physicians and nurses aren’t aware of the maximal recommended daily dosing of acetaminophen, and that many have some difficulty identifying which products contain the agent. Therefore, increased training is warranted "to help clinicians identify acetaminophen-containing products and monitor closely the daily dose of acetaminophen," the investigators said.
A reassessment of long-accepted dosing regimens may also be warranted, "especially the scheduled use of products containing 500 mg of acetaminophen," they added.
The study was funded by the Partners-Siemens Research Council. The investigators reported no relevant financial conflicts.
Four percent of hospitalized adolescents and adults at two academic tertiary care medical centers received supratherapeutic doses of acetaminophen during their stays, according to a report published online Nov. 12 in Archives of Internal Medicine.
"These were not isolated events but often were successive and overlapping." Nearly half of the exposed patients received 5 g or more of acetaminophen per day, and 40% received excessive dosing for 3 or more days, said Dr. Li Zhou of Partners HealthCare System, Wellesley, Mass., and her associates.
Such overmedicating puts patients at unnecessary risk for hepatotoxicity, acute liver failure, and even death. In this study, even inpatients at specific risk for liver damage didn’t escape excessive dosing with acetaminophen: 22% of the elderly and 18% of patients with existing chronic liver disease were given acetaminophen in amounts exceeding their recommended limit of 3 g/day, said Dr. Zhou, who is also at Brigham and Women’s Hospital and Harvard Medical School, Boston, and her colleagues.
The risk factors most strongly associated with supratherapeutic dosing were receiving recurring scheduled dosing (that is, standing orders) as opposed to as-needed or one-time-only administration, which carried a hazard ratio of 16.6; receiving multiple products containing acetaminophen, which carried a hazard ratio of 2.4 for each additional product; and receiving products containing 500 mg of acetaminophen, which carried an HR of 1.9.
The investigators used the hospitals’ electronic medication administration record systems to assess acetaminophen exposure in the inpatient setting – a topic that has received little attention from researchers before now, they wrote. The study population comprised the 14,411 inpatients aged 12 and older who received any acetaminophen during their stays in a 3-month period. That accounts for about 61% of the entire patient population hospitalized at the two centers during the study period.
The average age of the study subjects was 55 years (range, 12-110 years), and a little more than one-third were older than 65. Approximately 75 had chronic liver disease.
Overall, 955 patients were given acetaminophen in doses exceeding the 4-g/day limit. This represents 4% of the entire hospitalized population and 6.6% of the cohort of patients given any acetaminophen, the researchers said (Arch. Intern. Med. 2012 [doi:10.1001/2013.jamainternmed.438]).
Each patient who received supratherapeutic dosing had a mean of five such incidents during the course of a mean of 3 days. Instances of such overmedicating ranged as high as 48 separate occasions over the course of 30 days.
Approximately 40% of the 955 patients received supratherapeutic dosing for 3 or more days, and 4% received it for 10 or more days.
"Our findings show that despite policies and procedures to monitor and control patients’ acetaminophen exposure, the incidence of supratherapeutic acetaminophen dosing in hospitalized patients remains high," Dr. Zhou and her associates said.
Previous studies have shown that many physicians and nurses aren’t aware of the maximal recommended daily dosing of acetaminophen, and that many have some difficulty identifying which products contain the agent. Therefore, increased training is warranted "to help clinicians identify acetaminophen-containing products and monitor closely the daily dose of acetaminophen," the investigators said.
A reassessment of long-accepted dosing regimens may also be warranted, "especially the scheduled use of products containing 500 mg of acetaminophen," they added.
The study was funded by the Partners-Siemens Research Council. The investigators reported no relevant financial conflicts.
FROM ARCHIVES OF INTERNAL MEDICINE
Major Finding: Four percent of all adolescent and adult inpatients at two hospitals received supratherapeutic doses of acetaminophen during their stays, including 22% of the elderly and 18% of patients with chronic liver disease.
Data Source: Data are based on acetaminophen exposure determined from electronic medication administration records for 14,411 inpatients aged 12 and older at two urban academic tertiary care hospitals during a 3-month period.
Disclosures: The study was funded by the Partners-Siemens Research Council. The authors reported no relevant financial conflicts.
Informed Consent: Information Transfer or Communication?
Obtaining informed consent for surgery is one of the most common tasks surgeons perform. Ensuring that a patient has the capacity to make a decision and then explaining the indications, risks, and alternatives to the surgery is something that surgeons do hundreds of times a year. Although the process is routine, it reflects the importance of respecting patients’ autonomy in making informed decisions about their health care. Informed consent has been an accepted practice in American surgery for decades, but questions about the process can arise and elicit varied responses among surgeons.
Recently, an experienced colleague (Dr. S) called me to discuss a case that had been troubling him. A 68-year-old man had been referred to him for a surgical opinion after experiencing recurrent episodes of diverticulitis. He was a former insurance executive, now retired. He was married, but came without his wife to the appointment with Dr. S.
After completing the history and physical examination and reviewing the imaging, Dr. S recommended an elective sigmoid colon resection. He explained to the patient what was involved in the surgery and the expected recovery. According to Dr. S, the patient then stated, "I understand. When can we schedule it?" At this point, Dr. S stated that a few more things needed to be reviewed and began to discuss the potential risks of the surgery. The patient stopped him abruptly, saying that he knew that there were risks, but he preferred not to hear about them.
When Dr. S responded that it is always good to know the risks when deciding to have surgery, the patient stated, "Look, I trust my primary care doctor who sent me to see you. You seem like a good surgeon, and I have confidence in you. I don’t want to hear about the risks, because my hearing them won’t make them not happen and will only make me worry. I’ll sign anything that you want, but I don’t want you to tell me the risks."
Dr. S felt torn. He had always felt that the consent process was primarily about informing the patient of what could happen. Reviewing the potential risks would help the patient to become better informed in making the decision to have surgery. Dr. S felt that his patient’s desire not to be informed had short-circuited the process, and it now seemed incomplete.
Dr. S offered to call the patient’s wife to discuss the risks with her, but the patient said that would not be necessary since he was making his own decisions. Although there was no hostility in the patient’s remarks, Dr. S felt that he had pushed hard enough, so he obtained a signature on the consent form and documented in his note that he had offered to inform the patient of the risks but that the patient had refused to hear them.
In the 3 weeks between this office visit and the surgery, Dr. S related the case to a number of his surgical colleagues and received diametrically opposing views. One group of surgeons stated that as the surgeon, Dr. S had an ethical responsibility to ensure that his patient knew of the risks of the procedure. They felt strongly that unless Dr. S had reviewed these risks with the patient, the consent was not valid because "it was not truly informed." Another group of surgeons felt that the ethical responsibility was not to inform the patient, but rather to provide the opportunity for the patient to be informed. This second group felt that pushing the patient to hear information that he did not want to hear would actually be violating his autonomous choice not to be informed.
These opposing views of what to do in this case help to clarify what I believe is one of the central points of confusion about the informed consent process as it is currently used. Surgeons and patients alike often believe that the information transfer – that is, describing the risks of the surgery – is the central goal of the process. However, many studies have shown that patients do not actually remember much of what they are told by their surgeons. Specifically, few risks are remembered even on the same day that the surgeon has reviewed them and the consent form is signed. These data clearly suggest to me that the more important aspect of the informed consent process is the communication between the surgeon and the patient.
Communication suggests something more than providing a lecture to a patient. It suggests the importance of listening and responding to requests for more or less information. Given that the requirement for informed consent prior to surgery is grounded on the principle of respecting a patient’s autonomy, it seems clear that when a patient does not want to hear the information that a surgeon wants to convey, the surgeon must respect the patient’s choice not to be informed.
Although Dr. S had felt that something was missing in the consent process since it did not include "the usual discussion of risks," the patient’s choices had been respected and Dr. S had fully discharged his responsibilities in obtaining the patient’s informed consent.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Obtaining informed consent for surgery is one of the most common tasks surgeons perform. Ensuring that a patient has the capacity to make a decision and then explaining the indications, risks, and alternatives to the surgery is something that surgeons do hundreds of times a year. Although the process is routine, it reflects the importance of respecting patients’ autonomy in making informed decisions about their health care. Informed consent has been an accepted practice in American surgery for decades, but questions about the process can arise and elicit varied responses among surgeons.
Recently, an experienced colleague (Dr. S) called me to discuss a case that had been troubling him. A 68-year-old man had been referred to him for a surgical opinion after experiencing recurrent episodes of diverticulitis. He was a former insurance executive, now retired. He was married, but came without his wife to the appointment with Dr. S.
After completing the history and physical examination and reviewing the imaging, Dr. S recommended an elective sigmoid colon resection. He explained to the patient what was involved in the surgery and the expected recovery. According to Dr. S, the patient then stated, "I understand. When can we schedule it?" At this point, Dr. S stated that a few more things needed to be reviewed and began to discuss the potential risks of the surgery. The patient stopped him abruptly, saying that he knew that there were risks, but he preferred not to hear about them.
When Dr. S responded that it is always good to know the risks when deciding to have surgery, the patient stated, "Look, I trust my primary care doctor who sent me to see you. You seem like a good surgeon, and I have confidence in you. I don’t want to hear about the risks, because my hearing them won’t make them not happen and will only make me worry. I’ll sign anything that you want, but I don’t want you to tell me the risks."
Dr. S felt torn. He had always felt that the consent process was primarily about informing the patient of what could happen. Reviewing the potential risks would help the patient to become better informed in making the decision to have surgery. Dr. S felt that his patient’s desire not to be informed had short-circuited the process, and it now seemed incomplete.
Dr. S offered to call the patient’s wife to discuss the risks with her, but the patient said that would not be necessary since he was making his own decisions. Although there was no hostility in the patient’s remarks, Dr. S felt that he had pushed hard enough, so he obtained a signature on the consent form and documented in his note that he had offered to inform the patient of the risks but that the patient had refused to hear them.
In the 3 weeks between this office visit and the surgery, Dr. S related the case to a number of his surgical colleagues and received diametrically opposing views. One group of surgeons stated that as the surgeon, Dr. S had an ethical responsibility to ensure that his patient knew of the risks of the procedure. They felt strongly that unless Dr. S had reviewed these risks with the patient, the consent was not valid because "it was not truly informed." Another group of surgeons felt that the ethical responsibility was not to inform the patient, but rather to provide the opportunity for the patient to be informed. This second group felt that pushing the patient to hear information that he did not want to hear would actually be violating his autonomous choice not to be informed.
These opposing views of what to do in this case help to clarify what I believe is one of the central points of confusion about the informed consent process as it is currently used. Surgeons and patients alike often believe that the information transfer – that is, describing the risks of the surgery – is the central goal of the process. However, many studies have shown that patients do not actually remember much of what they are told by their surgeons. Specifically, few risks are remembered even on the same day that the surgeon has reviewed them and the consent form is signed. These data clearly suggest to me that the more important aspect of the informed consent process is the communication between the surgeon and the patient.
Communication suggests something more than providing a lecture to a patient. It suggests the importance of listening and responding to requests for more or less information. Given that the requirement for informed consent prior to surgery is grounded on the principle of respecting a patient’s autonomy, it seems clear that when a patient does not want to hear the information that a surgeon wants to convey, the surgeon must respect the patient’s choice not to be informed.
Although Dr. S had felt that something was missing in the consent process since it did not include "the usual discussion of risks," the patient’s choices had been respected and Dr. S had fully discharged his responsibilities in obtaining the patient’s informed consent.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Obtaining informed consent for surgery is one of the most common tasks surgeons perform. Ensuring that a patient has the capacity to make a decision and then explaining the indications, risks, and alternatives to the surgery is something that surgeons do hundreds of times a year. Although the process is routine, it reflects the importance of respecting patients’ autonomy in making informed decisions about their health care. Informed consent has been an accepted practice in American surgery for decades, but questions about the process can arise and elicit varied responses among surgeons.
Recently, an experienced colleague (Dr. S) called me to discuss a case that had been troubling him. A 68-year-old man had been referred to him for a surgical opinion after experiencing recurrent episodes of diverticulitis. He was a former insurance executive, now retired. He was married, but came without his wife to the appointment with Dr. S.
After completing the history and physical examination and reviewing the imaging, Dr. S recommended an elective sigmoid colon resection. He explained to the patient what was involved in the surgery and the expected recovery. According to Dr. S, the patient then stated, "I understand. When can we schedule it?" At this point, Dr. S stated that a few more things needed to be reviewed and began to discuss the potential risks of the surgery. The patient stopped him abruptly, saying that he knew that there were risks, but he preferred not to hear about them.
When Dr. S responded that it is always good to know the risks when deciding to have surgery, the patient stated, "Look, I trust my primary care doctor who sent me to see you. You seem like a good surgeon, and I have confidence in you. I don’t want to hear about the risks, because my hearing them won’t make them not happen and will only make me worry. I’ll sign anything that you want, but I don’t want you to tell me the risks."
Dr. S felt torn. He had always felt that the consent process was primarily about informing the patient of what could happen. Reviewing the potential risks would help the patient to become better informed in making the decision to have surgery. Dr. S felt that his patient’s desire not to be informed had short-circuited the process, and it now seemed incomplete.
Dr. S offered to call the patient’s wife to discuss the risks with her, but the patient said that would not be necessary since he was making his own decisions. Although there was no hostility in the patient’s remarks, Dr. S felt that he had pushed hard enough, so he obtained a signature on the consent form and documented in his note that he had offered to inform the patient of the risks but that the patient had refused to hear them.
In the 3 weeks between this office visit and the surgery, Dr. S related the case to a number of his surgical colleagues and received diametrically opposing views. One group of surgeons stated that as the surgeon, Dr. S had an ethical responsibility to ensure that his patient knew of the risks of the procedure. They felt strongly that unless Dr. S had reviewed these risks with the patient, the consent was not valid because "it was not truly informed." Another group of surgeons felt that the ethical responsibility was not to inform the patient, but rather to provide the opportunity for the patient to be informed. This second group felt that pushing the patient to hear information that he did not want to hear would actually be violating his autonomous choice not to be informed.
These opposing views of what to do in this case help to clarify what I believe is one of the central points of confusion about the informed consent process as it is currently used. Surgeons and patients alike often believe that the information transfer – that is, describing the risks of the surgery – is the central goal of the process. However, many studies have shown that patients do not actually remember much of what they are told by their surgeons. Specifically, few risks are remembered even on the same day that the surgeon has reviewed them and the consent form is signed. These data clearly suggest to me that the more important aspect of the informed consent process is the communication between the surgeon and the patient.
Communication suggests something more than providing a lecture to a patient. It suggests the importance of listening and responding to requests for more or less information. Given that the requirement for informed consent prior to surgery is grounded on the principle of respecting a patient’s autonomy, it seems clear that when a patient does not want to hear the information that a surgeon wants to convey, the surgeon must respect the patient’s choice not to be informed.
Although Dr. S had felt that something was missing in the consent process since it did not include "the usual discussion of risks," the patient’s choices had been respected and Dr. S had fully discharged his responsibilities in obtaining the patient’s informed consent.
Dr. Angelos is an ACS Fellow, the Linda Kohler Anderson Professor of Surgery and Surgical Ethics, chief, endocrine surgery, and associate director of the MacLean Center for Clinical Medical Ethics at the University of Chicago.
Twelve Reasons for Considering Buprenorphine as a Frontline Analgesic in the Management of Pain
Mellar P. Davis, MD, FCCP, FAAHPM
ABSTRACT: Buprenorphine is an opioid that has a complex and unique pharmacology which provides some advantages over other potent mu agonists. We review 12 reasons for considering buprenorphine as a frontline analgesic for moderate to severe pain: (1) Buprenorphine is effective in cancer pain; (2) buprenorphine is effective in treating neuropathic pain; (3) buprenorphine treats a broader array of pain phenotypes than do certain potent mu agonists, is associated with less analgesic tolerance, and can be combined with other mu agonists; (4) buprenorphine produces less constipation than do certain other potent mu agonists, and does not adversely affect the sphincter of Oddi; (5) buprenorphine has a ceiling effect on respiratory depression but not analgesia; (6) buprenorphine causes less cognitive impairment than do certain other opioids; (7) buprenorphine is not immunosuppressive like morphine and fentanyl; (8) buprenorphine does not adversely affect the hypothalamic-pituitary-adrenal axis or cause hypogonadism; (9) buprenorphine does not significantly prolong the QTc interval, and is associated with less sudden death than is methadone; (10) buprenorphine is a safe and effective analgesic for the elderly; (11) buprenorphine is one of the safest opioids to use in patients in renal failure and those on dialysis; and (12) withdrawal symptoms are milder and drug dependence is less with buprenorphine. In light of evidence for efficacy, safety, versatility, and cost, buprenorphine should be considered as a first-line analgesic.
*For a PDF of the full article and a Commentary by Paul Sloan, MD, click on the links to the left of this introduction.
Mellar P. Davis, MD, FCCP, FAAHPM
ABSTRACT: Buprenorphine is an opioid that has a complex and unique pharmacology which provides some advantages over other potent mu agonists. We review 12 reasons for considering buprenorphine as a frontline analgesic for moderate to severe pain: (1) Buprenorphine is effective in cancer pain; (2) buprenorphine is effective in treating neuropathic pain; (3) buprenorphine treats a broader array of pain phenotypes than do certain potent mu agonists, is associated with less analgesic tolerance, and can be combined with other mu agonists; (4) buprenorphine produces less constipation than do certain other potent mu agonists, and does not adversely affect the sphincter of Oddi; (5) buprenorphine has a ceiling effect on respiratory depression but not analgesia; (6) buprenorphine causes less cognitive impairment than do certain other opioids; (7) buprenorphine is not immunosuppressive like morphine and fentanyl; (8) buprenorphine does not adversely affect the hypothalamic-pituitary-adrenal axis or cause hypogonadism; (9) buprenorphine does not significantly prolong the QTc interval, and is associated with less sudden death than is methadone; (10) buprenorphine is a safe and effective analgesic for the elderly; (11) buprenorphine is one of the safest opioids to use in patients in renal failure and those on dialysis; and (12) withdrawal symptoms are milder and drug dependence is less with buprenorphine. In light of evidence for efficacy, safety, versatility, and cost, buprenorphine should be considered as a first-line analgesic.
*For a PDF of the full article and a Commentary by Paul Sloan, MD, click on the links to the left of this introduction.
Mellar P. Davis, MD, FCCP, FAAHPM
ABSTRACT: Buprenorphine is an opioid that has a complex and unique pharmacology which provides some advantages over other potent mu agonists. We review 12 reasons for considering buprenorphine as a frontline analgesic for moderate to severe pain: (1) Buprenorphine is effective in cancer pain; (2) buprenorphine is effective in treating neuropathic pain; (3) buprenorphine treats a broader array of pain phenotypes than do certain potent mu agonists, is associated with less analgesic tolerance, and can be combined with other mu agonists; (4) buprenorphine produces less constipation than do certain other potent mu agonists, and does not adversely affect the sphincter of Oddi; (5) buprenorphine has a ceiling effect on respiratory depression but not analgesia; (6) buprenorphine causes less cognitive impairment than do certain other opioids; (7) buprenorphine is not immunosuppressive like morphine and fentanyl; (8) buprenorphine does not adversely affect the hypothalamic-pituitary-adrenal axis or cause hypogonadism; (9) buprenorphine does not significantly prolong the QTc interval, and is associated with less sudden death than is methadone; (10) buprenorphine is a safe and effective analgesic for the elderly; (11) buprenorphine is one of the safest opioids to use in patients in renal failure and those on dialysis; and (12) withdrawal symptoms are milder and drug dependence is less with buprenorphine. In light of evidence for efficacy, safety, versatility, and cost, buprenorphine should be considered as a first-line analgesic.
*For a PDF of the full article and a Commentary by Paul Sloan, MD, click on the links to the left of this introduction.
Highlights from the 2012 Annual Meeting of the American Society of Clinical Oncology
Highlights from the 2012 Annual Meeting of the American Society of Clinical Oncology 48th Annual Meeting
*For a PDF of the full article, click on the link to the left of this introduction.
Highlights from the 2012 Annual Meeting of the American Society of Clinical Oncology 48th Annual Meeting
*For a PDF of the full article, click on the link to the left of this introduction.
Highlights from the 2012 Annual Meeting of the American Society of Clinical Oncology 48th Annual Meeting
*For a PDF of the full article, click on the link to the left of this introduction.
Benefit of Young Liver Donors Scrutinized in Study
BOSTON – Younger age of deceased liver donors appeared to improve patient and graft survival when donors and recipients were both of younger age, but not when younger donor livers went to older recipients, according to a secondary analysis of the Organ Procurement and Transplantation Network national database from 2002 to 2011.
"Matching younger recipients with younger donors appears to be the best strategy in order to maximize life years after liver transplantation. However, before this can be considered for allocation policy, much more work needs to be done," including analyses specific to United Network for Organ Sharing regions, Model for End-Stage Liver Disease groups, and modeling of the potential life-years saved with a change in allocation policy, said lead investigator Dr. Neehar D. Parikh of the Comprehensive Transplant Center at Northwestern University, Chicago.
The risk of recipient death is known to increase with advancing donor age, beginning at ages older than 40 years and especially with donors older than 60 years. Also, advancing recipient age has been shown, with some controversy, to affect outcomes negatively, Dr. Parikh said at the annual meeting of the American Association for the Study of Liver Diseases.
Dr. Parikh and his colleagues’ study of the Organ Procurement and Transplantation Network database analyzed 26,849 cases of liver transplantation in which the donor was younger than the recipient, 782 cases in which they were the same age, and 12,107 cases in which the donor was older than the recipient. They also looked at outcomes of patients aged 18-40 years and those 60 years or older, based on the donor age.
As would be expected, recipients had progressively younger mean ages as the donor age increased: 56 years for recipients with younger donors, 52 years for same-age donors, and 48 years for older donors. Hepatitis C virus seropositivity was lowest in recipients who had an older donor (41%), followed by same-age recipient-donor pairs (51%), and recipients who had a younger donor (50%).
In Kaplan-Meier analyses, patient survival at 1 year was significantly worse for those who received a liver from a donor with an older age (86%) or the same age (86%) than from a younger donor (87.4%). Similar results were seen at 3 years between recipients of livers from older (74.5%), same age (73.5%), and younger donors (77.9%).
Older donor age increased the risk for patient death by 14% and graft failure by 13%, in comparison with younger donor age in an adjusted analysis.
For every 10-year increase in patient age for younger donors, the risk of patient mortality increased by 24% and graft failure by 17%. For every 10 years the donor was younger than the recipient, however, there was a 27% decline in the risk of patient mortality and 30% decrease in the risk of graft failure. A small but significance beneficial interaction was found between young donor age and young recipient age on both outcomes.
In contrast, for every 10 years the donor was older than the recipient, the risk of patient mortality increased 9% and the risk of graft failure increased by 22%, and there was no significant interaction between recipient and donor age.
When compared against donor and recipient pairs who were both aged 18-40 years, the risk of patient mortality and graft failure increased significantly for all other combinations of donor and recipient pairs: recipients aged 18-40 years and donors aged 60 years or older (hazard ratios of 1.76 and 1.49, respectively), recipients aged 60 years older and donors aged 18-40 years (HRs of 1.67 and 1.83), and recipients and donors both aged 60 years or older (HRs of 2.12 and 1.87). These results were consistent at both 1 and 3 years.
The overall results "suggest that there is something intrinsic about being older or having an older graft that cannot be remediated by graft or patient age factors," Dr. Parikh said.
The results might be explained in livers from older donors by impaired liver regeneration and increased susceptibility to ischemic reperfusion injury, while older recipients might have decreased circulating stem cells and more competing risks that are not adequately risk adjusted in the available data in older recipients, he said.
One audience member noted that there is still a "huge survival advantage" in all patient populations that receive younger donor livers and that allocating organs based on age is a slippery slope.
Dr. Parikh and his colleagues had no relevant financial disclosures.
BOSTON – Younger age of deceased liver donors appeared to improve patient and graft survival when donors and recipients were both of younger age, but not when younger donor livers went to older recipients, according to a secondary analysis of the Organ Procurement and Transplantation Network national database from 2002 to 2011.
"Matching younger recipients with younger donors appears to be the best strategy in order to maximize life years after liver transplantation. However, before this can be considered for allocation policy, much more work needs to be done," including analyses specific to United Network for Organ Sharing regions, Model for End-Stage Liver Disease groups, and modeling of the potential life-years saved with a change in allocation policy, said lead investigator Dr. Neehar D. Parikh of the Comprehensive Transplant Center at Northwestern University, Chicago.
The risk of recipient death is known to increase with advancing donor age, beginning at ages older than 40 years and especially with donors older than 60 years. Also, advancing recipient age has been shown, with some controversy, to affect outcomes negatively, Dr. Parikh said at the annual meeting of the American Association for the Study of Liver Diseases.
Dr. Parikh and his colleagues’ study of the Organ Procurement and Transplantation Network database analyzed 26,849 cases of liver transplantation in which the donor was younger than the recipient, 782 cases in which they were the same age, and 12,107 cases in which the donor was older than the recipient. They also looked at outcomes of patients aged 18-40 years and those 60 years or older, based on the donor age.
As would be expected, recipients had progressively younger mean ages as the donor age increased: 56 years for recipients with younger donors, 52 years for same-age donors, and 48 years for older donors. Hepatitis C virus seropositivity was lowest in recipients who had an older donor (41%), followed by same-age recipient-donor pairs (51%), and recipients who had a younger donor (50%).
In Kaplan-Meier analyses, patient survival at 1 year was significantly worse for those who received a liver from a donor with an older age (86%) or the same age (86%) than from a younger donor (87.4%). Similar results were seen at 3 years between recipients of livers from older (74.5%), same age (73.5%), and younger donors (77.9%).
Older donor age increased the risk for patient death by 14% and graft failure by 13%, in comparison with younger donor age in an adjusted analysis.
For every 10-year increase in patient age for younger donors, the risk of patient mortality increased by 24% and graft failure by 17%. For every 10 years the donor was younger than the recipient, however, there was a 27% decline in the risk of patient mortality and 30% decrease in the risk of graft failure. A small but significance beneficial interaction was found between young donor age and young recipient age on both outcomes.
In contrast, for every 10 years the donor was older than the recipient, the risk of patient mortality increased 9% and the risk of graft failure increased by 22%, and there was no significant interaction between recipient and donor age.
When compared against donor and recipient pairs who were both aged 18-40 years, the risk of patient mortality and graft failure increased significantly for all other combinations of donor and recipient pairs: recipients aged 18-40 years and donors aged 60 years or older (hazard ratios of 1.76 and 1.49, respectively), recipients aged 60 years older and donors aged 18-40 years (HRs of 1.67 and 1.83), and recipients and donors both aged 60 years or older (HRs of 2.12 and 1.87). These results were consistent at both 1 and 3 years.
The overall results "suggest that there is something intrinsic about being older or having an older graft that cannot be remediated by graft or patient age factors," Dr. Parikh said.
The results might be explained in livers from older donors by impaired liver regeneration and increased susceptibility to ischemic reperfusion injury, while older recipients might have decreased circulating stem cells and more competing risks that are not adequately risk adjusted in the available data in older recipients, he said.
One audience member noted that there is still a "huge survival advantage" in all patient populations that receive younger donor livers and that allocating organs based on age is a slippery slope.
Dr. Parikh and his colleagues had no relevant financial disclosures.
BOSTON – Younger age of deceased liver donors appeared to improve patient and graft survival when donors and recipients were both of younger age, but not when younger donor livers went to older recipients, according to a secondary analysis of the Organ Procurement and Transplantation Network national database from 2002 to 2011.
"Matching younger recipients with younger donors appears to be the best strategy in order to maximize life years after liver transplantation. However, before this can be considered for allocation policy, much more work needs to be done," including analyses specific to United Network for Organ Sharing regions, Model for End-Stage Liver Disease groups, and modeling of the potential life-years saved with a change in allocation policy, said lead investigator Dr. Neehar D. Parikh of the Comprehensive Transplant Center at Northwestern University, Chicago.
The risk of recipient death is known to increase with advancing donor age, beginning at ages older than 40 years and especially with donors older than 60 years. Also, advancing recipient age has been shown, with some controversy, to affect outcomes negatively, Dr. Parikh said at the annual meeting of the American Association for the Study of Liver Diseases.
Dr. Parikh and his colleagues’ study of the Organ Procurement and Transplantation Network database analyzed 26,849 cases of liver transplantation in which the donor was younger than the recipient, 782 cases in which they were the same age, and 12,107 cases in which the donor was older than the recipient. They also looked at outcomes of patients aged 18-40 years and those 60 years or older, based on the donor age.
As would be expected, recipients had progressively younger mean ages as the donor age increased: 56 years for recipients with younger donors, 52 years for same-age donors, and 48 years for older donors. Hepatitis C virus seropositivity was lowest in recipients who had an older donor (41%), followed by same-age recipient-donor pairs (51%), and recipients who had a younger donor (50%).
In Kaplan-Meier analyses, patient survival at 1 year was significantly worse for those who received a liver from a donor with an older age (86%) or the same age (86%) than from a younger donor (87.4%). Similar results were seen at 3 years between recipients of livers from older (74.5%), same age (73.5%), and younger donors (77.9%).
Older donor age increased the risk for patient death by 14% and graft failure by 13%, in comparison with younger donor age in an adjusted analysis.
For every 10-year increase in patient age for younger donors, the risk of patient mortality increased by 24% and graft failure by 17%. For every 10 years the donor was younger than the recipient, however, there was a 27% decline in the risk of patient mortality and 30% decrease in the risk of graft failure. A small but significance beneficial interaction was found between young donor age and young recipient age on both outcomes.
In contrast, for every 10 years the donor was older than the recipient, the risk of patient mortality increased 9% and the risk of graft failure increased by 22%, and there was no significant interaction between recipient and donor age.
When compared against donor and recipient pairs who were both aged 18-40 years, the risk of patient mortality and graft failure increased significantly for all other combinations of donor and recipient pairs: recipients aged 18-40 years and donors aged 60 years or older (hazard ratios of 1.76 and 1.49, respectively), recipients aged 60 years older and donors aged 18-40 years (HRs of 1.67 and 1.83), and recipients and donors both aged 60 years or older (HRs of 2.12 and 1.87). These results were consistent at both 1 and 3 years.
The overall results "suggest that there is something intrinsic about being older or having an older graft that cannot be remediated by graft or patient age factors," Dr. Parikh said.
The results might be explained in livers from older donors by impaired liver regeneration and increased susceptibility to ischemic reperfusion injury, while older recipients might have decreased circulating stem cells and more competing risks that are not adequately risk adjusted in the available data in older recipients, he said.
One audience member noted that there is still a "huge survival advantage" in all patient populations that receive younger donor livers and that allocating organs based on age is a slippery slope.
Dr. Parikh and his colleagues had no relevant financial disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
Major Finding: For every 10-year increase in patient age for younger donors, the risk of patient mortality increased by 24% and graft failure by 17%; for every 10 years the donor was younger than the recipient, there was a 27% decline in the risk of patient mortality and a 30% decrease in the risk of graft failure.
Data Source: This was a secondary analysis of the Organ Procurement and Transplantation Network national database from 2002 to 2011 for adult cadaveric liver transplantation.
Disclosures: Dr. Parikh and his colleagues had no relevant financial disclosures.
Acetaminophen Liver Failure Least Likely to Get Transplant
BOSTON – Acetaminophen toxicity is the most frequent cause of acute liver failure in the United States and its usually milder presentation, along with comorbid psychosocial issues, explain why fewer patients with the etiology undergo liver transplantation, compared with other causes, according to a 10-year retrospective study of the National Institute of Diabetes and Digestive and Kidney Diseases Acute Liver Failure database.
Dr. K. Rajender Reddy and his colleagues in the National Institutes of Health Acute Liver Failure Study Group set out to determine factors that could help clinicians to improve their selection of acute liver failure patients for liver transplantation listing and their decision to proceed with transplantation.

At the annual meeting of the American Association for the Study of Liver Diseases, Dr. Reddy reported that of 1,144 patients who had at least 1 year of follow-up in the database, 491 (43%) had an acetaminophen etiology for acute liver failure, but only 26% of all patients listed for transplantation had an acetaminophen etiology and just 14% of all transplants occurred in patients with acetaminophen toxicity as the underlying cause.
In comparison, patients with other etiologies had higher listing and transplantation rates, with the highest being for autoimmune hepatitis (62% of all patients listed and 50% of all transplanted).
Overall during 2000-2010, 697 patients were not listed and not transplanted (group A), 177 were listed and not transplanted (group B), and 270 were listed and transplanted (group C). After 2 years of follow-up, patient survival was highest in group C (82%), followed by group A (47%) and group B (41%). Survival at 21 days followed the same pattern (C, 89%; A, 58%; B, 45%). Patients in groups A and B with acetaminophen etiology had greater 21-day survival than did those without an acetaminophen etiology.
Patients in group A had significantly higher rates of positive toxicology screens than did groups B and C (43% vs. 35% and 19%, respectively) and history of illicit drug use (10% vs. 4% and 2%).
Comparisons between patients who died in group B and all patients in group C could not find significant risk factors to explain the higher mortality in group B, including longer wait list times and variations in survival and transplant rates by geographic location, although greater coma severity may have contributed to the higher mortality, said Dr. Reddy, professor of medicine in the division of gastroenterology at the Hospital of the University of Pennsylvania, Philadelphia.
Dr. Reddy said that he had no relevant financial disclosures. The study was funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases to the National Institutes of Health Acute Liver Failure Study Group.
BOSTON – Acetaminophen toxicity is the most frequent cause of acute liver failure in the United States and its usually milder presentation, along with comorbid psychosocial issues, explain why fewer patients with the etiology undergo liver transplantation, compared with other causes, according to a 10-year retrospective study of the National Institute of Diabetes and Digestive and Kidney Diseases Acute Liver Failure database.
Dr. K. Rajender Reddy and his colleagues in the National Institutes of Health Acute Liver Failure Study Group set out to determine factors that could help clinicians to improve their selection of acute liver failure patients for liver transplantation listing and their decision to proceed with transplantation.
At the annual meeting of the American Association for the Study of Liver Diseases, Dr. Reddy reported that of 1,144 patients who had at least 1 year of follow-up in the database, 491 (43%) had an acetaminophen etiology for acute liver failure, but only 26% of all patients listed for transplantation had an acetaminophen etiology and just 14% of all transplants occurred in patients with acetaminophen toxicity as the underlying cause.
In comparison, patients with other etiologies had higher listing and transplantation rates, with the highest being for autoimmune hepatitis (62% of all patients listed and 50% of all transplanted).
Overall during 2000-2010, 697 patients were not listed and not transplanted (group A), 177 were listed and not transplanted (group B), and 270 were listed and transplanted (group C). After 2 years of follow-up, patient survival was highest in group C (82%), followed by group A (47%) and group B (41%). Survival at 21 days followed the same pattern (C, 89%; A, 58%; B, 45%). Patients in groups A and B with acetaminophen etiology had greater 21-day survival than did those without an acetaminophen etiology.
Patients in group A had significantly higher rates of positive toxicology screens than did groups B and C (43% vs. 35% and 19%, respectively) and history of illicit drug use (10% vs. 4% and 2%).
Comparisons between patients who died in group B and all patients in group C could not find significant risk factors to explain the higher mortality in group B, including longer wait list times and variations in survival and transplant rates by geographic location, although greater coma severity may have contributed to the higher mortality, said Dr. Reddy, professor of medicine in the division of gastroenterology at the Hospital of the University of Pennsylvania, Philadelphia.
Dr. Reddy said that he had no relevant financial disclosures. The study was funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases to the National Institutes of Health Acute Liver Failure Study Group.
BOSTON – Acetaminophen toxicity is the most frequent cause of acute liver failure in the United States and its usually milder presentation, along with comorbid psychosocial issues, explain why fewer patients with the etiology undergo liver transplantation, compared with other causes, according to a 10-year retrospective study of the National Institute of Diabetes and Digestive and Kidney Diseases Acute Liver Failure database.
Dr. K. Rajender Reddy and his colleagues in the National Institutes of Health Acute Liver Failure Study Group set out to determine factors that could help clinicians to improve their selection of acute liver failure patients for liver transplantation listing and their decision to proceed with transplantation.
At the annual meeting of the American Association for the Study of Liver Diseases, Dr. Reddy reported that of 1,144 patients who had at least 1 year of follow-up in the database, 491 (43%) had an acetaminophen etiology for acute liver failure, but only 26% of all patients listed for transplantation had an acetaminophen etiology and just 14% of all transplants occurred in patients with acetaminophen toxicity as the underlying cause.
In comparison, patients with other etiologies had higher listing and transplantation rates, with the highest being for autoimmune hepatitis (62% of all patients listed and 50% of all transplanted).
Overall during 2000-2010, 697 patients were not listed and not transplanted (group A), 177 were listed and not transplanted (group B), and 270 were listed and transplanted (group C). After 2 years of follow-up, patient survival was highest in group C (82%), followed by group A (47%) and group B (41%). Survival at 21 days followed the same pattern (C, 89%; A, 58%; B, 45%). Patients in groups A and B with acetaminophen etiology had greater 21-day survival than did those without an acetaminophen etiology.
Patients in group A had significantly higher rates of positive toxicology screens than did groups B and C (43% vs. 35% and 19%, respectively) and history of illicit drug use (10% vs. 4% and 2%).
Comparisons between patients who died in group B and all patients in group C could not find significant risk factors to explain the higher mortality in group B, including longer wait list times and variations in survival and transplant rates by geographic location, although greater coma severity may have contributed to the higher mortality, said Dr. Reddy, professor of medicine in the division of gastroenterology at the Hospital of the University of Pennsylvania, Philadelphia.
Dr. Reddy said that he had no relevant financial disclosures. The study was funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases to the National Institutes of Health Acute Liver Failure Study Group.
AT THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
Major Finding: A total of 43% in the study had an acetaminophen etiology for acute liver failure, but only 26% of all patients listed for transplantation had an acetaminophen etiology and just 14% of all transplants occurred in patients with acetaminophen toxicity as the underlying cause.
Data Source: This was a 10-year retrospective study of the National Institute of Diabetes and Digestive and Kidney Diseases Acute Liver Failure database.
Disclosures: Dr. Reddy said he had no relevant financial disclosures. The study was funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases to the National Institutes of Health Acute Liver Failure Study Group.

Fatty Liver Disease Cited for Rise in Hepatocellular Carcinoma
BOSTON – Nonalcoholic fatty liver disease without cirrhosis appears to be a significant contributor to the rise in the incidence of hepatocellular carcinoma in the past two decades, according to a study linking population-based data from the National Cancer Institute with Medicare enrollment and claim files during 1993-2007.
"Our data suggest a unique underlying pathophysiology for development of HCC [hepatocellular carcinoma] in noncirrhotic NAFLD [nonalcoholic fatty liver disease]," Dr. Rubayat Rahman said at the annual meeting of the American Association for the Study of Liver Diseases.
The finding may help to explain the rise in the incidence of the malignancy, which has had no clear explanation, added Dr. Rahman of the division of gastroenterology and hepatology at the University of Missouri, Columbia.
Of 17,895 HCC cases in the linked Surveillance, Epidemiology and End Results (SEER)-Medicare database, 2,863 (16%) had only NAFLD without any other risk factors or etiologies for HCC. The linked database covers 30% of the U.S. Medicare population. SEER itself contains data from 18 cancer registries covering 28% of the U.S. population, and 93% of the individuals in the database who are at least 65 years are matched to a Medicare enrollment file.
At 16%, NAFLD was third most common risk factor for HCC after infection (44%) and alcoholic diseases (19%) – 21% were other causes – but it was the second most common risk factor after infection in Asians and Pacific islanders, said Dr. Rahman.
Cirrhosis was not present in 36% of the NAFLD-related HCC cases; of those, 18% had only steatosis and not nonalcoholic steatohepatitis (NASH) or other adverse changes in pathology. Patients without cirrhosis more often had early-stage disease (stage I or II) than did those with cirrhosis (62% vs. 44%), as well as favorable grades (I or II, 76% vs. 56%).
Although the annual percentage change of NAFLD-related HCC with cirrhosis has increased since 1993, 1999 marked a point when the annual growth of NAFLD-related cases of HCC without cirrhosis outpaced those with cirrhosis. The average number of cases per year of NAFLD-related HCC without cirrhosis grew significantly from 51 in 1993-2000 to 88 in 2001-2007, compared with no change in cases with cirrhosis.
Three components of the metabolic syndrome – body-mass index greater than 30 kg/m2, type 2 diabetes mellitus, and dyslipidemia – occurred in significantly greater proportions of patients with NAFLD-related HCC without cirrhosis than in those with cirrhosis. The odds of developing HCC for each of those three components among noncirrhotic NAFLD patients was higher than for those with cirrhotic NAFLD, although the overall odds of developing HCC were higher among patients with cirrhotic NAFLD (odds ratio, 16.5) than in those with noncirrhotic NAFLD (OR, 3.1).
One audience member expressed concern about determining the presence of cirrhosis or NASH in the data without a systematic assessment of histopathology performed in a centralized way, but Dr. Rahman noted that the Medicare-matched SEER data have CPT procedural codes and ICD-9 diagnostic codes for diagnoses made through liver biopsy. Another attendee also suggested caution in calling NAFLD a risk factor for cancer alone because the people in the database have a higher rate of cancer, and the database does not include the peak of NASH at age 55 years.
None of the study investigators had relevant financial disclosures.
BOSTON – Nonalcoholic fatty liver disease without cirrhosis appears to be a significant contributor to the rise in the incidence of hepatocellular carcinoma in the past two decades, according to a study linking population-based data from the National Cancer Institute with Medicare enrollment and claim files during 1993-2007.
"Our data suggest a unique underlying pathophysiology for development of HCC [hepatocellular carcinoma] in noncirrhotic NAFLD [nonalcoholic fatty liver disease]," Dr. Rubayat Rahman said at the annual meeting of the American Association for the Study of Liver Diseases.
The finding may help to explain the rise in the incidence of the malignancy, which has had no clear explanation, added Dr. Rahman of the division of gastroenterology and hepatology at the University of Missouri, Columbia.
Of 17,895 HCC cases in the linked Surveillance, Epidemiology and End Results (SEER)-Medicare database, 2,863 (16%) had only NAFLD without any other risk factors or etiologies for HCC. The linked database covers 30% of the U.S. Medicare population. SEER itself contains data from 18 cancer registries covering 28% of the U.S. population, and 93% of the individuals in the database who are at least 65 years are matched to a Medicare enrollment file.
At 16%, NAFLD was third most common risk factor for HCC after infection (44%) and alcoholic diseases (19%) – 21% were other causes – but it was the second most common risk factor after infection in Asians and Pacific islanders, said Dr. Rahman.
Cirrhosis was not present in 36% of the NAFLD-related HCC cases; of those, 18% had only steatosis and not nonalcoholic steatohepatitis (NASH) or other adverse changes in pathology. Patients without cirrhosis more often had early-stage disease (stage I or II) than did those with cirrhosis (62% vs. 44%), as well as favorable grades (I or II, 76% vs. 56%).
Although the annual percentage change of NAFLD-related HCC with cirrhosis has increased since 1993, 1999 marked a point when the annual growth of NAFLD-related cases of HCC without cirrhosis outpaced those with cirrhosis. The average number of cases per year of NAFLD-related HCC without cirrhosis grew significantly from 51 in 1993-2000 to 88 in 2001-2007, compared with no change in cases with cirrhosis.
Three components of the metabolic syndrome – body-mass index greater than 30 kg/m2, type 2 diabetes mellitus, and dyslipidemia – occurred in significantly greater proportions of patients with NAFLD-related HCC without cirrhosis than in those with cirrhosis. The odds of developing HCC for each of those three components among noncirrhotic NAFLD patients was higher than for those with cirrhotic NAFLD, although the overall odds of developing HCC were higher among patients with cirrhotic NAFLD (odds ratio, 16.5) than in those with noncirrhotic NAFLD (OR, 3.1).
One audience member expressed concern about determining the presence of cirrhosis or NASH in the data without a systematic assessment of histopathology performed in a centralized way, but Dr. Rahman noted that the Medicare-matched SEER data have CPT procedural codes and ICD-9 diagnostic codes for diagnoses made through liver biopsy. Another attendee also suggested caution in calling NAFLD a risk factor for cancer alone because the people in the database have a higher rate of cancer, and the database does not include the peak of NASH at age 55 years.
None of the study investigators had relevant financial disclosures.
BOSTON – Nonalcoholic fatty liver disease without cirrhosis appears to be a significant contributor to the rise in the incidence of hepatocellular carcinoma in the past two decades, according to a study linking population-based data from the National Cancer Institute with Medicare enrollment and claim files during 1993-2007.
"Our data suggest a unique underlying pathophysiology for development of HCC [hepatocellular carcinoma] in noncirrhotic NAFLD [nonalcoholic fatty liver disease]," Dr. Rubayat Rahman said at the annual meeting of the American Association for the Study of Liver Diseases.
The finding may help to explain the rise in the incidence of the malignancy, which has had no clear explanation, added Dr. Rahman of the division of gastroenterology and hepatology at the University of Missouri, Columbia.
Of 17,895 HCC cases in the linked Surveillance, Epidemiology and End Results (SEER)-Medicare database, 2,863 (16%) had only NAFLD without any other risk factors or etiologies for HCC. The linked database covers 30% of the U.S. Medicare population. SEER itself contains data from 18 cancer registries covering 28% of the U.S. population, and 93% of the individuals in the database who are at least 65 years are matched to a Medicare enrollment file.
At 16%, NAFLD was third most common risk factor for HCC after infection (44%) and alcoholic diseases (19%) – 21% were other causes – but it was the second most common risk factor after infection in Asians and Pacific islanders, said Dr. Rahman.
Cirrhosis was not present in 36% of the NAFLD-related HCC cases; of those, 18% had only steatosis and not nonalcoholic steatohepatitis (NASH) or other adverse changes in pathology. Patients without cirrhosis more often had early-stage disease (stage I or II) than did those with cirrhosis (62% vs. 44%), as well as favorable grades (I or II, 76% vs. 56%).
Although the annual percentage change of NAFLD-related HCC with cirrhosis has increased since 1993, 1999 marked a point when the annual growth of NAFLD-related cases of HCC without cirrhosis outpaced those with cirrhosis. The average number of cases per year of NAFLD-related HCC without cirrhosis grew significantly from 51 in 1993-2000 to 88 in 2001-2007, compared with no change in cases with cirrhosis.
Three components of the metabolic syndrome – body-mass index greater than 30 kg/m2, type 2 diabetes mellitus, and dyslipidemia – occurred in significantly greater proportions of patients with NAFLD-related HCC without cirrhosis than in those with cirrhosis. The odds of developing HCC for each of those three components among noncirrhotic NAFLD patients was higher than for those with cirrhotic NAFLD, although the overall odds of developing HCC were higher among patients with cirrhotic NAFLD (odds ratio, 16.5) than in those with noncirrhotic NAFLD (OR, 3.1).
One audience member expressed concern about determining the presence of cirrhosis or NASH in the data without a systematic assessment of histopathology performed in a centralized way, but Dr. Rahman noted that the Medicare-matched SEER data have CPT procedural codes and ICD-9 diagnostic codes for diagnoses made through liver biopsy. Another attendee also suggested caution in calling NAFLD a risk factor for cancer alone because the people in the database have a higher rate of cancer, and the database does not include the peak of NASH at age 55 years.
None of the study investigators had relevant financial disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
Major Finding: The average number of cases per year of NAFLD-related hepatocellular carcinoma without cirrhosis grew significantly from 51 in 1993-2000 to 88 in 2001-2007, compared with no change in cases with cirrhosis.
Data Source: This population-based study used data from the SEER-Medicare database from 1993 to 2007.
Disclosures: None of the study investigators had relevant financial disclosures.
Doctors Need More Resources to Manage Pediatric Concussion
Pediatric primary care and emergency providers often feel ill prepared or lacking in resources, time, or training to effectively manage concussion in children and educate families about the condition and recovery, according to a survey published in the November 2012 issue of Pediatrics.
The findings come from a survey assessing what practicing physicians, nurse practitioners, and physician assistants know about concussion as well as their treatment practices and any perceived obstacles to managing the condition, reported by Dr. Mark R. Zonfrillo of the center for injury research and prevention at Children’s Hospital of Philadelphia and the University of Pennsylvania and his associates (Pediatrics 2012;130:1-6).
An online survey using multiple-choice, Likert scale, and open-ended questions was sent to 276 providers in the Children’s Hospital of Philadelphia Care Network and Emergency Department e-mail lists. The 53% response rate included 145 responding providers with a diverse range of experience. Sixty-one percent were pediatric primary care providers, and 39% were pediatric emergency care providers.

A total of 91% of respondents reported having cared for at least one patient with concussion in the past 3 months. Most of these providers (134, or 92%) referred at least one patient to a concussion specialist after the first exam, usually either because they were uncomfortable with managing the concussion (49%) or because they did not have the necessary resources to manage it (47%). In addition, 30% of primary care providers and 68% of emergency providers said their "setting is not always appropriate for management," the investigators said.
Both primary care providers and emergency providers were highly likely to refer concussion patients to sports medicine doctors or clinics (67% vs. 75%, respectively); primary care respondents were twice as likely as emergency providers to refer patients to neurologists (46% vs. 22%). Emergency providers also were likely to refer to a trauma surgeon or clinic (83%), while primary care providers rarely did (13%).
Past studies have found that approximately 100,000-140,000 U.S. children go to the emergency department each year for concussion, but parents and children may underreport concussion symptoms, and many youth sports coaches have misconceptions about them.
In the two scenarios presented in the survey – one of a patient with a subtle concussion and the other of a patient with more obvious symptoms – almost all respondents determined that both hypothetical patients had a concussion. However, some respondents did not recognize some of the symptoms of concussion, including abnormal eye tracking (17%), difficulty concentrating (11%), vestibular disturbance (9%), worsening school performance (6%), and sensitivity to light or noise (6%). "These more subtle signs of concussion may present in isolation and thus may be the only indication that a child has sustained the injury," the authors wrote.
A total of 104 providers reported they did not have access to a provider decision support tool relating to concussion, and 96% of these believed one would be helpful. All 57 respondents who said they didn’t have discharge instructions related to concussion said support tools would be helpful.
Doctors cited a lack of training most often when it came to obstacles to educating families about the diagnosis and recommending time off before returning to school or sports. Further, 69% of primary care providers and 77% of emergency providers said they don’t have enough time to complete formal neurocognitive testing for concussed patients.
The study was funded by the Children’s Hospital of Philadelphia Department of Pediatrics Chair’s Initiative. The authors said they had no relevant financial disclosures.
Concussion is an injury doctors will see in their practice regularly because it is happening more frequently. There is increased awareness about concussion, doctors are picking up previously unreported concussions, and more state laws require medical clearance after a concussion before a return to play. There also are more children participating in contact sports year-round and at younger ages, so there is more exposure for injury. Pediatricians need to feel confident that they can provide adequate frontline care, according to Dr. Kevin Walter.
Dr. Zonfrillo’s findings indicate there is still a lot of confusion about what a concussion is, most likely because medical education about concussion is lacking. Also, kids often lie to get back to playing. As with everything in medicine, providers are being asked to do more with less time. Although there are resources like the Centers for Disease Control and Prevention’s Heads-Up tool kit and the American Academy of Pediatrics 2010 clinical report (Pediatrics 2010;126:597-615), what would be most helpful is for health systems to have a protocol or best practice guideline for providers in that system.
With concussions, everyone is different, and the cookie cutter approach used for other conditions doesn’t work with concussion. Concussion is broader and more general, so providers have to individualize care management to each patient according to the patient’s injury and situation.
Dr. Walter is with the department of orthopedic surgery and the department of pediatrics at the Medical College of Wisconsin, Milwaukee, and was lead author of the AAP’s clinical report "Sport-Related Concussion in Children and Adolescents." He made these comments during an interview.
Concussion is an injury doctors will see in their practice regularly because it is happening more frequently. There is increased awareness about concussion, doctors are picking up previously unreported concussions, and more state laws require medical clearance after a concussion before a return to play. There also are more children participating in contact sports year-round and at younger ages, so there is more exposure for injury. Pediatricians need to feel confident that they can provide adequate frontline care, according to Dr. Kevin Walter.
Dr. Zonfrillo’s findings indicate there is still a lot of confusion about what a concussion is, most likely because medical education about concussion is lacking. Also, kids often lie to get back to playing. As with everything in medicine, providers are being asked to do more with less time. Although there are resources like the Centers for Disease Control and Prevention’s Heads-Up tool kit and the American Academy of Pediatrics 2010 clinical report (Pediatrics 2010;126:597-615), what would be most helpful is for health systems to have a protocol or best practice guideline for providers in that system.
With concussions, everyone is different, and the cookie cutter approach used for other conditions doesn’t work with concussion. Concussion is broader and more general, so providers have to individualize care management to each patient according to the patient’s injury and situation.
Dr. Walter is with the department of orthopedic surgery and the department of pediatrics at the Medical College of Wisconsin, Milwaukee, and was lead author of the AAP’s clinical report "Sport-Related Concussion in Children and Adolescents." He made these comments during an interview.
Concussion is an injury doctors will see in their practice regularly because it is happening more frequently. There is increased awareness about concussion, doctors are picking up previously unreported concussions, and more state laws require medical clearance after a concussion before a return to play. There also are more children participating in contact sports year-round and at younger ages, so there is more exposure for injury. Pediatricians need to feel confident that they can provide adequate frontline care, according to Dr. Kevin Walter.
Dr. Zonfrillo’s findings indicate there is still a lot of confusion about what a concussion is, most likely because medical education about concussion is lacking. Also, kids often lie to get back to playing. As with everything in medicine, providers are being asked to do more with less time. Although there are resources like the Centers for Disease Control and Prevention’s Heads-Up tool kit and the American Academy of Pediatrics 2010 clinical report (Pediatrics 2010;126:597-615), what would be most helpful is for health systems to have a protocol or best practice guideline for providers in that system.
With concussions, everyone is different, and the cookie cutter approach used for other conditions doesn’t work with concussion. Concussion is broader and more general, so providers have to individualize care management to each patient according to the patient’s injury and situation.
Dr. Walter is with the department of orthopedic surgery and the department of pediatrics at the Medical College of Wisconsin, Milwaukee, and was lead author of the AAP’s clinical report "Sport-Related Concussion in Children and Adolescents." He made these comments during an interview.
Pediatric primary care and emergency providers often feel ill prepared or lacking in resources, time, or training to effectively manage concussion in children and educate families about the condition and recovery, according to a survey published in the November 2012 issue of Pediatrics.
The findings come from a survey assessing what practicing physicians, nurse practitioners, and physician assistants know about concussion as well as their treatment practices and any perceived obstacles to managing the condition, reported by Dr. Mark R. Zonfrillo of the center for injury research and prevention at Children’s Hospital of Philadelphia and the University of Pennsylvania and his associates (Pediatrics 2012;130:1-6).
An online survey using multiple-choice, Likert scale, and open-ended questions was sent to 276 providers in the Children’s Hospital of Philadelphia Care Network and Emergency Department e-mail lists. The 53% response rate included 145 responding providers with a diverse range of experience. Sixty-one percent were pediatric primary care providers, and 39% were pediatric emergency care providers.
A total of 91% of respondents reported having cared for at least one patient with concussion in the past 3 months. Most of these providers (134, or 92%) referred at least one patient to a concussion specialist after the first exam, usually either because they were uncomfortable with managing the concussion (49%) or because they did not have the necessary resources to manage it (47%). In addition, 30% of primary care providers and 68% of emergency providers said their "setting is not always appropriate for management," the investigators said.
Both primary care providers and emergency providers were highly likely to refer concussion patients to sports medicine doctors or clinics (67% vs. 75%, respectively); primary care respondents were twice as likely as emergency providers to refer patients to neurologists (46% vs. 22%). Emergency providers also were likely to refer to a trauma surgeon or clinic (83%), while primary care providers rarely did (13%).
Past studies have found that approximately 100,000-140,000 U.S. children go to the emergency department each year for concussion, but parents and children may underreport concussion symptoms, and many youth sports coaches have misconceptions about them.
In the two scenarios presented in the survey – one of a patient with a subtle concussion and the other of a patient with more obvious symptoms – almost all respondents determined that both hypothetical patients had a concussion. However, some respondents did not recognize some of the symptoms of concussion, including abnormal eye tracking (17%), difficulty concentrating (11%), vestibular disturbance (9%), worsening school performance (6%), and sensitivity to light or noise (6%). "These more subtle signs of concussion may present in isolation and thus may be the only indication that a child has sustained the injury," the authors wrote.
A total of 104 providers reported they did not have access to a provider decision support tool relating to concussion, and 96% of these believed one would be helpful. All 57 respondents who said they didn’t have discharge instructions related to concussion said support tools would be helpful.
Doctors cited a lack of training most often when it came to obstacles to educating families about the diagnosis and recommending time off before returning to school or sports. Further, 69% of primary care providers and 77% of emergency providers said they don’t have enough time to complete formal neurocognitive testing for concussed patients.
The study was funded by the Children’s Hospital of Philadelphia Department of Pediatrics Chair’s Initiative. The authors said they had no relevant financial disclosures.
Pediatric primary care and emergency providers often feel ill prepared or lacking in resources, time, or training to effectively manage concussion in children and educate families about the condition and recovery, according to a survey published in the November 2012 issue of Pediatrics.
The findings come from a survey assessing what practicing physicians, nurse practitioners, and physician assistants know about concussion as well as their treatment practices and any perceived obstacles to managing the condition, reported by Dr. Mark R. Zonfrillo of the center for injury research and prevention at Children’s Hospital of Philadelphia and the University of Pennsylvania and his associates (Pediatrics 2012;130:1-6).
An online survey using multiple-choice, Likert scale, and open-ended questions was sent to 276 providers in the Children’s Hospital of Philadelphia Care Network and Emergency Department e-mail lists. The 53% response rate included 145 responding providers with a diverse range of experience. Sixty-one percent were pediatric primary care providers, and 39% were pediatric emergency care providers.
A total of 91% of respondents reported having cared for at least one patient with concussion in the past 3 months. Most of these providers (134, or 92%) referred at least one patient to a concussion specialist after the first exam, usually either because they were uncomfortable with managing the concussion (49%) or because they did not have the necessary resources to manage it (47%). In addition, 30% of primary care providers and 68% of emergency providers said their "setting is not always appropriate for management," the investigators said.
Both primary care providers and emergency providers were highly likely to refer concussion patients to sports medicine doctors or clinics (67% vs. 75%, respectively); primary care respondents were twice as likely as emergency providers to refer patients to neurologists (46% vs. 22%). Emergency providers also were likely to refer to a trauma surgeon or clinic (83%), while primary care providers rarely did (13%).
Past studies have found that approximately 100,000-140,000 U.S. children go to the emergency department each year for concussion, but parents and children may underreport concussion symptoms, and many youth sports coaches have misconceptions about them.
In the two scenarios presented in the survey – one of a patient with a subtle concussion and the other of a patient with more obvious symptoms – almost all respondents determined that both hypothetical patients had a concussion. However, some respondents did not recognize some of the symptoms of concussion, including abnormal eye tracking (17%), difficulty concentrating (11%), vestibular disturbance (9%), worsening school performance (6%), and sensitivity to light or noise (6%). "These more subtle signs of concussion may present in isolation and thus may be the only indication that a child has sustained the injury," the authors wrote.
A total of 104 providers reported they did not have access to a provider decision support tool relating to concussion, and 96% of these believed one would be helpful. All 57 respondents who said they didn’t have discharge instructions related to concussion said support tools would be helpful.
Doctors cited a lack of training most often when it came to obstacles to educating families about the diagnosis and recommending time off before returning to school or sports. Further, 69% of primary care providers and 77% of emergency providers said they don’t have enough time to complete formal neurocognitive testing for concussed patients.
The study was funded by the Children’s Hospital of Philadelphia Department of Pediatrics Chair’s Initiative. The authors said they had no relevant financial disclosures.
FROM PEDIATRICS
Major Finding: Although 91% of pediatric and emergency providers reported caring for at least one concussed patient in the past 3 months, pediatric providers reported referring patients to specialists because they did not feel comfortable with management (49%) or lacked adequate resources for management (47%).
Data Source: Results are from a survey of 145 providers that included physicians, nurse practitioners, and physician assistants in the emergency department and primary care network of the Children’s Hospital of Philadelphia Care Network and Emergency Department.
Disclosures: The research was funded by the Children’s Hospital of Philadelphia Department of Pediatrics Chair’s Initiative. The authors said they had no relevant financial disclosures.
