User login
Coping with the influenza vaccine shortage
Help children and teens stop impulsive hair pulling
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
Trichotillomania (TTM) is distressing to pediatric patients who pull their hair and to their parents who feel helpless to stop the destructive behavior. Hair-pulling with psychiatric comorbidity requires comprehensive assessment and treatment, but we have found that cognitive-behavioral therapy (CBT) alone can help children and adolescents with uncomplicated TTM.
This article describes a typical patient with adolescent-onset mild-to-moderate TTM and the three-step CBT approach—awareness training, stimulus control, and habit reversal—that we find effective in reducing pediatric hair pulling.
Jane, age 12, was referred to our clinic by her primary doctor after an 8-week trial of fluoxetine, 80 mg/d, failed to stop her hair pulling. Jane, who is right-handed, has been pulling her hair for 2 years, mostly in the right front scalp. Her shame over the hair loss makes her reluctant to participate in social activities. A dermatologist found no medical cause for her behavior, such as alopecia or folliculitis.
Jane’s parents say she has no history of a major mood disorder or anxiety. Her hair pulling causes significant “tension and stress” for all family members.
WHY DO PATIENTS PULL HAIR?
Cognitive-behavioral theory suggests that chronic TTM originates as a normal response to stress that often escapes personal and social awareness but gradually increases in frequency and severity (Box).1-8 Thus, hair pulling becomes associated with internal and external cues through conditioning and is maintained primarily by positive reinforcement. Hair-pulling urges that are reinforced by pulling intensify the need to pull, perpetuating the behavioral cycle.
A genetic link? Familial research has associated TTM with increased rates of obsessive-compulsive disorder (OCD) or other excessive habits—such as nail biting or skin picking—among first-degree relatives.6,9,10 Neuroimaging of persons with TTM has shown hyperactivity in the left cerebellum and right superior parietal lobe11 as well as possible structural abnormalities in the left putamen,12 left inferior frontal gyrus, and right cluneal cortex.13
These findings do not necessarily indicate pre-existing brain pathology, however. Perhaps TTM leads to changes in brain structure or function, or both TTM and the brain abnormalities may be caused by another as-yet-unknown variable.
Decreased pain sensitivity. Patients with TTM often report that hair pulling is not painful,2 though we suspect that persons without TTM would disagree and derive no pleasure from it. Changes in pain sensitivity may influence the reinforcing quality of pulling behavior. One possible mechanism for such alterations is upregulation of the endogenous opioid system; some intriguing evidence suggests that opioid receptor antagonists such as naltrexone may reduce pulling.14
Trichotillomania (TTM) is an impulse control disorder characterized by repetitive hair pulling,1 which typically emerges during adolescence. In a large clinical sample of adult hair pullers, mean age of onset was 13.2 Very-early onset (before age 5) may be a more benign form of TTM that tends to abate spontaneously and requires little or no therapeutic intervention.3
Despite the absence of body hair in prepubertal children, their pulling patterns are consistent with those of adults. The scalp is the most common pulling site, followed by eyelashes and eyebrows.4
Psychiatric comorbidity. In two studies evaluating psychiatric comorbidity in pediatric clinical samples, 60% to 70% of children and teens with TTM had at least one comorbid axis I disorder.5,6 Disruptive behavior disorders were most common in one study,6 whereas overanxious disorder was most common in the other.5 In a large clinical sample of adults with TTM, 51% met criteria for comorbid depression.2
Early identification and treatment of TTM are recommended because of the disorder’s distressing nature and social stigma. Early interventions also may help prevent later adult psychiatric comorbidity and functional impairment, although no studies have been done to demonstrate this benefit.7,8
Pain tolerance at the preferred pulling site has not been studied, however. For patients who feel pain from hair pulling, the pain itself may reinforce the behavior by distracting the individual from negative emotional or physiologic states.15
CASE CONTINUED: COUNTING THE WAYS
Jane and her parents agree that she pulls her hair 5 to 8 times daily, one hair at a time with her right index finger and thumb while doing homework or watching TV. The trigger, she says, is “an itch” on her scalp; “sometimes pulling relieves the itch.” She fails to resist pulling her hair 9 out of 10 times.
Table 1
Defining hair pulling: What to ask the pediatric patient
| Response description | How many times do you pull your hair each day? |
| How many hairs do you pull each time? | |
| From what body areas do you pull hair? | |
| What are all the steps involved in pulling (Touching the head before pulling? Pulling one hair at a time with the thumb and index finger)? | |
| Response detection | Under what circumstances do you sense the urge to pull? |
| How strong is the urge on a scale of 1 to 10, with 10 being the greatest intensity you ever felt? | |
| How do you try to resist and overcome the urge to pull? | |
| Precursors | External cues (Do you pull when you look at yourself in a mirror?) |
| Internal cues (Do you pull when you are nervous?) | |
| High-risk situations | What are you usually doing when you get the urge to pull? (reading, talking on the telephone, watching TV, using a computer, etc.) |
| Consequences that reinforce the behavior | Do you pull to reduce physical sensations (such as itching) at the site of pulling? |
| Does pulling relieve sadness or worry about problems at home or in school? | |
| Do you pull to create a more even hairline? |
Psychiatric comorbidity is common—if not the norm—in adults with TTM. Although axis I comorbidity is also seen in children and adolescents, their hair pulling is frequently uncomplicated. Jane meets criteria for TTM, as determined by the Trichotillomania Diagnostic Interview,16 but her history does not support a comorbid disorder. After discussing the diagnosis with Jane and her parents, the psychiatrist begins treatment with CBT alone.
MEDICATION OR CBT?
SSRIs. Literature on TTM pharmacotherapy is very limited and equivocal. Medications that have helped adults with TTM have been described,17 but the lack of a single, randomized, controlled trial in pediatric TTM severely limits treatment recommendations for children.
Selective serotonin reuptake inhibitors (SSRIs) have shown efficacy for treating anger and other impulse control problems but not for TTM. Some practitioners use SSRIs for TTM because of the belief that TTM is a variant of OCD. However, TTM may be maintained by positive reinforcement rather than compulsive tendencies and thus may not respond to SSRIs.
CBT. Evidence on CBT justifies cautious recommendations for pediatric TTM. In randomized trials, CBT reduced hair pulling in adults and was more effective than SSRIs or placebo.18,19
REDUCING THE URGE
Obtain detailed information about a child or adolescent’s hair-pulling episodes (Table 1), as recognizing triggers and reactions is vital to effective CBT. Explain to the patient that:
- the pleasure or satisfaction she derives from pulling reinforces the urge to pull
- she can reduce the urge by learning and using awareness training, stimulus control, and habit reversal (Table 2).
Awareness training involves patient self-monitoring to gain awareness of urges to pull and of pulling behavior. The child must become alert to every hair pulled and to response precursors, such as placing her hand on her head. For a patient such as Jane, a useful technique is to post reminders on the TV and school notebook and in the bedroom and bathroom—wherever pulling typically occurs.
A “PULLING CALENDAR”
Jane begins a daily “pulling calendar” in which she records each time she pulls a hair while watching TV or doing homework. She is asked to include the total number of hairs pulled and the intensity of the “itch to pull” on a scale of 1 to 10.
Stimulus control. Most patients can identify high-risk situations, such as time in the bathroom, talking on the phone, watching TV, driving, reading, or while falling asleep. Boredom, frustration, anxiety, and sadness may serve as pulling cues.
With stimulus control, the patient tries to reduce her ability to freely engage in pulling behavior in high-risk situations. For instance, you might encourage a child who pulls hairs while doing homework to stick Band-Aid®-type adhesive strips on her thumb and index finger tips before she starts studying as an impediment to gripping hairs. Such “speed bumps” may allow her to delay pulling and reach for tools that assist in habit reversal.
TREATMENT THAT APPEALS
Jane agrees to apply adhesive strips to her fingers and understands why. Because she is a fan of Peter Pan, we place Peter Pan stickers on her books and notebooks and on the TV remote control as reminders not to pull.
Table 2
CBT strategies to reduce the hair-pulling urge
| Awareness training | Increases patient’s awareness of pulling |
| Stimulus control | Establishes an environment less conducive to pulling |
| Habit reversal/ response | Patient develops alternate activities that provide competing positive reinforcement comparable to that gained from pulling |
Habit reversal and competing response procedures provide pleasurable physical stimulation as an alternative to pulling. The most effective methods engage the same motions as used in hair pulling. Examples include sculpting with clay, hulling sunflower seeds, and playing with Koosh® balls—small rubbery balls filled with a jellylike plasma and covered with hundreds of soft “tentacles.”
‘CALMER, HAPPIER’
We explain habit reversal to Jane and instruct her to use the Koosh ball a few times a day. She enjoys pulling its rubber strands, an action that uses the same muscles as hair pulling. Because she will need Koosh balls during all identified high-risk situations, we instruct her to buy one for her book bag and to leave one near the couch where she watches TV.
Over time, Jane reports a gradual decrease of hair pulling with the use of awareness training and stimulus control techniques. Using the Koosh ball (habit reversal) helps her improve. By the 10th week, Jane and her parents report a 70% decrease in hair pulling, based on the pulling calendar entries and other objective evidence of treatment response. All report feeling “calmer and happier.”
CONCLUSION
Cognitive and behavioral strategies are useful and safe for treating pediatric TTM. Enlisting the parents and patient in identifying problem situations and applying creative solutions may increase the chances of success.
Follow-up is important for maintaining new cognitive and behavioral patterns. We recommend that you see patients monthly for at least 3 months, depending on how the patient feels about additional sessions. We encourage families to call and report on progress or relapses. Booster CBT sessions can help deal with setbacks.
Related resources
- Trichotillomania Learning Center, Inc.; devoted to improving TTM understanding and providing access to treatments and support groups. www.trich.org. Accessed Sept. 17, 2004.
- Golomb RG, Vavrichek SM. The hair pulling “habit” and you: how to solve the trichotillomania puzzle (rev ed). Silver Spring, MD: Writer’s Cooperative of Greater Washington; 2000. Book for children and teenagers.
Drug brand names
- Fluoxetine • Prozac
- Naltrexone • Depade, ReVia
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Acknowledgment
Preparation of this article was supported in part by a grant from the National Institute of Mental Health (MH61457).
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev. Washington, DC: American Psychiatric Association Press; 2000;674-7.
2. Christenson GA, Mackenzie TB, Mitchell JE. Characteristics of 60 adult chronic hairpullers. Am J Psychiatry 1991;148:365-70.
3. Swedo SE, Leonard HL. Trichotillomania: an obsessive compulsive spectrum disorder? Psychiatr Clin North Am 1992;15:777-90.
4. Reeve E. Hair pulling in children and adolescents. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Association Press, 1999;201-24.
5. Reeve EA, Bernstein GA, Christenson GA. Clinical characteristics and psychiatric comorbidity in children with trichotillomania. J Am Acad Child Adolesc Psychiatry 1992;31:132-8.
6. King RA, Scahill L, Vitulano LA, et al. Childhood trichotillomania: clinical phenomenology, comorbidity, and family genetics. J Am Acad Child Adolesc Psychiatry 1995;34:1451-9.
7. Franklin ME, Bux DA, Foa EB. Pediatric trichotillomania: conceptualization and treatment implications. In: Orvashel H, Faust J, Hersen M, eds. Handbook of conceptualization and treatment of child psychopathology. Oxford, UK: Elsevier Science; 2001;379-98.
8. Keuthen NJ, Franklin ME. Trichotillomania: psychopathology and treatment development [presentation]. Reno, NV: Association for the Advancement of Behavior Therapy annual meeting, 2002.
9. Bienvenu OJ, Samuels JF, Riddle MA, et al. The relationship of obsessive-compulsive disorder to possible spectrum disorders: results from a family study. Biol Psychiatry 2000;48:287-93.
10. Lenane MC, Swedo SE, Rapoport JL, et al. Rates of obsessive compulsive disorder in first degree relatives of patients with trichotillomania: a research note. J Child Psychol Psychiatry 1992;33:925-33.
11. Swedo SE, Rapoport JL, Leonard HL, et al. Regional cerebral glucose metabolism of women in trichotillomania. Arch Gen Psychiatry 1991;48:828-33.
12. O’Sullivan RL, Rauch SL, Breiter HC, et al. Reduced basal ganglia volumes in trichotillomania measured via morphometric magnetic resonance imaging. Biol Psychiatry 1997;42:39-45.
13. Grachev ID. MRI-based morphometric topographic parcellation of human neocortex in trichotillomania. Psychiatry Clin Neurosci 1997;51:315-21.
14. Carrion VG. Naltrexone for the treatment of trichotillomania: a case report. J Clin Psychopharmacol 1995;15:444-5.
15. Christenson GA, Mansueto CS. Trichotillomania: descriptive characteristics and phenomenology. In: Stein DJ, Christenson GA, Hollander E, eds. Trichotillomania. Washington, DC: American Psychiatric Press, 1999;1-41.
16. Rothbaum BO, Ninan PT. The assessment of trichotillomania. Behav Res Ther 1994;32(6):651-62.
17. Lundt LP. Trichotillomania: a heads-up on severe cases. Current Psychiatry 2004;3(5):89-105.
18. Ninan PT, Rothbaum BO, Marsteller FA, et al. A placebo-controlled trial of cognitive-behavioral therapy and clomipramine in trichotillomania. J Clin Psychiatry. 2000;61:47-50.
19. Azrin NH, Nunn RG, Frantz SE. Treatment of hairpulling (trichotillomania): a comparative study of habit reversal and negative practice training. J Behav Ther Exp Psychiatry 1980;11:13-20.
Identify and manage 2 common non-Alzheimer’s dementias
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
Primary care doctors refer patients with dementia to psychiatrists when the diagnosis or disease course is unclear. Psychiatrists thus must often discern non-Alzheimer’s dementias— particularly the vascular and Lewy body types— from Alzheimer’s dementia. This article describes:
- features that distinguish vascular, Lewy body, and Alzheimer’s dementias
- cognitive and medical tests to help determine dementia type and facilitate treatment
- risk factors that promote cognitive and functional decline
- strategies for using medication while minimizing side-effect risks.
CASE REPORT: DISRUPTIVE IN DAY CARE
Ms. Z, age 82, is referred to a psychiatrist after numerous failed attempts by her primary care physician to stop her medical and psychiatric deterioration.
Table 1
Estimated dementia type prevalence among patients with dementia
| Dementia type | Prevalence |
|---|---|
| Alzheimer's | 65% |
| Lewy body | 0-15% |
| Vascular | 10-15% |
| Mixed | 10-15% |
| Source: reference 1 | |
The patient was functioning well at home until 6 months ago, when her husband’s death triggered a dramatic functional decline. She has Parkinson’s disease and has had dementia symptoms for 3 years, but family members do not recall a dementia diagnosis.
Ms. Z has become increasingly disruptive in day care; she yelled at and slapped a staff member during one episode. Her son is concerned that additional outbursts will prompt her dismissal. Her Mini-Mental State Examination (MMSE) score is 19, indicating moderate dementia.
Donepezil, 10 mg/d across 2 years, has not slowed Ms. Z’s memory decline. Carbidopa/levadopa, 25/250 mg tid over 1 year, has not improved her Parkinson’s symptoms. Risperidone, 0.5 mg bid, caused marked sedation and unsteady gait and was stopped after 4 weeks. She also is taking hydrocodone/acetaminophen, 5/500 mg/d for osteoarthritis, and lisinopril/hydrochlorothiazide, 10/12.5 mg/d for hypertension.
Discussion. As with Ms. Z, a significant other can mask a dementia patient’s cognitive deficits, but these deficits become apparent after the partner dies. Family members then discover that a parent or sibling cannot function independently.
Treatment should target Ms. Z’s aggression to allow her to stay in day care and her son to care for her at home. Determining the dementia type is crucial to planning treatment and preserving function.
WHICH DEMENTIA IS WHICH?
Non-Alzheimer’s dementias account for up to 35% of dementia cases (Table 1).1 The pathologic correlations separating Alzheimer’s, vascular, and Lewy body dementias are often confusing:
- Beta-amyloid plaques are common in Alzheimer’s and Lewy body dementias, although neurofibrillary tangles are much less common in the Lewy body type.
- Synaptic cholinergic deficiencies are seen in Alzheimer’s and vascular dementias.
- Hypertension and hyperlipidemia—both traditional vascular risk factors—also appear to contribute to Alzheimer’s dementia.
Vascular dementia. Large, single-vessel hemispheric infarcts cause substantial damage, whereas multiple small vascular lesions (such as lacunae or mini-infarcts) can have more-subtle effects when strategically located, such as in the basal ganglia, hippocampus, or thalamus. These smaller lesions can disrupt frontal cortical-subcortical neural pathways and contribute to difficulties with executive functions (judgment, insight), emotional control, and behavior.
Lesions from a cerebrovascular accident, however, do not necessarily cause dementia, and the mechanism by which lesions cause dementia is not fully understood. Post-stroke dementia sometimes is progressive, suggesting a degenerative rather than vascular cause.
Lewy body dementia is associated with Parkinson’s disease, as Lewy body inclusion deposits are common to both disorders. The deposits typically appear in the cerebral cortex in Lewy body dementia but not in Parkinson’s.
Amyloid protein deposits alter the clinical presentation. Patients with these lesions have fewer visual hallucinations and motor problems, making diagnosis more difficult.
Lewy body dementia, like all major dementias, usually surfaces after age 75. Its clinical course generally is considered worse than that of Alzheimer’s dementia, but these two dementia types do not differ substantially in age of onset, age of death, or survival rates.
Table 2
Clinical features that characterize Lewy body dementia
| Central | Progressive cognitive decline that interferes with normal social and occupational function; deficits on tests of attention, frontal-subcortical skills, and visuospatial ability can be especially prominent |
| Core | Two of three needed for probable diagnosis:
|
| Supportive | Repeated falls Syncope Transient loss of consciousness REM sleep behavior disorder Systematized delusions Hallucinations in other modalities Neuroleptic sensitivity Depression |
| Features less likely to be present | History of stroke Another physical illness or brain disorder that interferes with cognitive performance |
| Source: reference 6 | |
FEATURES OF VASCULAR DEMENTIA
Onset can be gradual but is more often sudden— usually occurring shortly after an ischemic stroke. Disease progression can be gradual or dramatic, depending on the vascular event type. Cognitive and physical decline in vascular dementia usually is stepwise over time, whereas decline in Alzheimer’s dementia is more gradual with progressive severity.
Patients with vascular dementia classically present with memory loss temporally associated with other typical stroke stigmata. Brain imaging often uncovers evidence of stroke that is otherwise not clinically evident.
CNS manifestations of vascular dementia often include memory loss, emotional lability (including depression), and executive-task dysfunction. Patients usually have atrial fibrillation or vascular risk factors, including diabetes mellitus, hypertension, hyperlipidemia, obesity, or tobacco use. Patients with previous stroke, coronary artery disease, or peripheral vascular disease are at increased risk.
Vascular dementia is categorized by stroke type:
Embolic infarct. Emboli, typically cardiac in origin, can occlude small or large cerebral arteries, resulting in correspondingly sized infarcts. Atrial fibrillation can promote areas in the atria with relatively low flow turbulence. Blood clots can form that eventually embolize via the carotid arteries. Multiple emboli can occur, causing progressive dementia.
Cerebral hemorrhage —small or large—can be devastating. Hypertension is the major risk factor for this form of stroke.
Multi-infarct dementia. Multiple cerebral blood vessel infarcts classically lead to stepwise functional decline after each event. Multiple small infarcts can occur in various brain regions, including the cortex and basal ganglia. Binswanger’s disease, a variant of vascular dementia in which incomplete ischemia is limited to the hemispheric white matter, tends to be fairly progressive.2
Small-vessel disease. Reduced blood flow and tissue perfusion can cause small-vessel disease. Often the ischemia is “silent,” detectable only on MRI or CT. The infarcts typically cause lacunar lesions, nerve demyelination, and gliosis.3 These can occur to some extent in nondemented patients but become significant with more-extensive disease.
FEATURES OF LEWY BODY DEMENTIA
As with all dementias, permanent memory loss must be present to diagnose this dementia sub-type. Overall cognitive deficits may be more prominent than memory loss, however. The patient may have trouble performing cognitive tasks that employ visuospatial abilities, executive functions, and attention. Neuropsychiatric symptoms that overlap with Alzheimer’s dementia include apathy, anxiety, agitation, depression, anhedonia, and paranoia.
The presence of visual hallucinations, fluctuating cognition, or extrapyramidal symptoms (EPS) distinguish Lewy body from Alzheimer’s dementia.
Visual hallucinations are prominent in Lewy body dementia and often prompt psychiatric referral (Table 2). They usually surface early in the disease course and tend to persist. Other sensory hallucinations also can occur.
The hallucinations often are detailed and vivid and the patient may be aware they are occurring, especially if the dementia is not advanced. Treatment might not be necessary for mild hallucinations, which can concern the caregiver more than the patient.
Antipsychotics paradoxically worsen hallucinations in Lewy body dementia, and many patients present to psychiatrists after failing an empiric trial. A failed antipsychotic course in a patient diagnosed with Alzheimer’s dementia could indicate that the diagnosis is incorrect.
Fluctuating cognition occurs in 50% to 75% of Lewy body cases. Alertness, attention, and concentration are variable and can cycle within hours to weeks. The patient often is fairly interactive and social for a time, then has periods of diminished function and being “out of it.” Some patients have recurrent delirium and undergo multiple workups in search of a cause.
EPS. As many as 75% of Lewy body patients have parkinsonian motor features.4 Because these features are not essential to the diagnosis, their absence is the most common reason Lewy body dementia goes unrecognized.1
Motor involvement varies and can be worsened by antipsychotics. Overuse of antipsychotics in Alzheimer’s or vascular dementia also can cause motor symptoms that mimic Lewy body features.
EPS orientation tends to be axial, showing less facial expressivity and more postural imbalance. Peripheral signs such as tremor and extremity rigidity tend to be less dominant.
MAKING THE DIAGNOSIS
Vascular and Lewy body dementia diagnoses are primarily based on clinical features and findings. Memory loss is necessary for either diagnosis.
Vascular dementia. Most consensus criteria require presence of dementia, physical or radiologic signs of a stroke, and a temporal relationship between the stroke and the dementia for a vascular dementia diagnosis.
Hachinski’s “ischemia scale” can help differentiate multi-infarct from Alzheimer’s dementia.5 Cases are scored on a 0-to-9 scale, with point values for abrupt onset; stepwise course; history of stroke; and presence of somatic complaints, emotional lability, hypertension, and focal neurologic signs. A score ≥4 suggests vascular dementia.
The scale, however, does not account for imaging studies, vascular risk factors other than hypertension, or repeated silent strokes that can cause symptoms. Also, some patients who score below the cutoff have strategic infarct dementias.
Lewy body dementia. Clinical consensus guidelines developed by McKeith et al6 can help clinicians recognize and categorize this dementia type (Table 2). Several studies of diagnostic criteria have shown very good specificity but variable sensitivity.7 Because no standard imaging modalities or serum markers exist, presence of progressive memory loss, fluctuating cognition, visual hallucinations, and EPS should drive the diagnosis.
Lewy body dementia is commonly misdiagnosed as Parkinson’s dementia. The two types are readily differentiated by onset of memory loss, which emerges late in Parkinson’s dementia but is early and prominent in Lewy body dementia.
CASE CONTINUED: HISTORY LEADS TO DIAGNOSIS
Ms. Z was diagnosed as having Lewy body dementia, as her cognitive decline clearly preceded her motor deficits. Further questioning revealed fluctuating attention levels and a history of visual hallucinations.
TESTING PATIENT FUNCTION
Neuropsychiatric tests. DSM-IV recommends testing memory, orientation, language, praxis, constructional ability, and executive control function in patients with dementia. Numerous tests can aid in diagnosis, but they generally are too lengthy to be practical. The MMSE takes 5 to 10 minutes, but it might miss mild memory loss or executive dysfunction.
Giving a quick clock-drawing test in tandem with the MMSE can help measure basic executive control and constructional ability. Also, patients with Lewy body or vascular dementia often are more proficient than patients with Alzheimer’s dementia on verbal memory tests but less proficient on visuospatial performance. Consider referring clinically challenging patients for more-extensive neuropsychiatric testing.
Lab tests. Blood tests including TSH and B12/folate screens are usually performed but rarely positive. Rapid plasma reagin testing for syphilis is no longer recommended unless syphilis is suspected.
Table 3
Potential cognitive side effects associated with psychotropic classes*
| Drug class | Potential cognitive side effects |
|---|---|
| Antidepressants Tricyclics, SSRIs, SNRIs | Confusion, sedation, falls |
| Antihistamines | Confusion, sedation, dizziness |
| Antipsychotics | Sedation, fatigue, anxiety |
| Antispasmodics | Confusion, sedation |
| Benzodiazepines | Sedation, confusion, ataxia, depression |
| Opioids | Sedation, confusion, dizziness |
| Sleep-promoting agents | Amnesia, confusion, ataxia |
| * Not all agents in each class are associated with listed side effects | |
| SSRIs: Selective serotonin reuptake inhibitors | |
| SNRIs: Serotonin-norepinephrine reuptake inhibitors | |
Radiologic imaging. Radiologic imaging (MRI or CT) can show infarcts in vascular dementia and can rule out:
- a brain tumor
- a subdural hemorrhage after recent head trauma
- or normal-pressure hydrocephalus in patients with dementia, gait instability, and/or urinary incontinence.
Brain imaging in Lewy body dementia can show hippocampal preservation8 but is not specific and does not significantly support the diagnosis. Specialized tests such as single-photon emission computed tomography or positron-emission tomography show occipital hypoperfusion9 but are expensive, not sufficiently specific, and do not add substantial value over clinical criteria.
MANAGING SYMPTOMS
Medication may be necessary if the patient is frequently and significantly agitated. Consider prescribing a selective serotonin reuptake inhibitor, an anticonvulsant such as divalproex or carbamazepine as a mood stabilizer, or a short-acting benzodiazepine. Start low and titrate slowly if needed.
Find out if the patient is taking medications that may be causing bothersome side effects. Avoid agents with potential cognitive or anticholinergic effects (Table 3); the latter can cause confusion, sedation, and falls in the elderly.
Cholinesterase inhibitors, FDA-approved for use in Alzheimer’s dementia, have been shown to reduce cognitive and global functioning decline in vascular dementia.10 A cholinergic deficit present in vascular dementia may explain the drugs’ effectiveness. Donepezil, galantamine, and rivastigmine have all shown positive effects on cognition.
Because patients with Lewy body hallucinations have greater synaptic acetylcholine deficits, cholinesterase inhibitors tend to be more effective in Lewy body dementia than in other dementia subtypes. In small open-label studies, patients taking cholinesterase inhibitors for Lewy body dementia have shown sustained improvements (up to 96 months) in cognition and behavior. Wild et al,11 however, concluded that the evidence supporting use of these agents—specifically rivastigmine—is weak.
Also, cholinesterase inhibitors offer fairly modest effectiveness, do not work for all patients, and do not prevent cognitive decline even when taken regularly. Because cholinesterase inhibitors are costly and most Medicare patients lack prescription medication coverage, an initial short (6-month) trial is recommended. Re-evaluate the patient periodically by using caregiver reports, caregiver assessment scales, and basic cognitive testing.
Cholinesterase inhibitor dosing is the same for vascular and Lewy body dementia as it is for Alzheimer’s disease. Tell patients to take the agents with food to minimize potential intestinal side effects.
Memantine. In European studies, memantine has shown positive effects on cognition and function in vascular dementia. Memantine, a N-methyl-D-aspartate receptor antagonist, is FDA-approved for moderate to severe Alzheimer’s dementia.12
DELAYING DECLINE
Controlling risk factors. Controlling vascular risk factors—especially high blood pressure—is the most effective way to prevent or treat vascular dementia. In primary prevention studies, patients with good hypertension and hyperlipidemia control developed dementia more slowly than did nontreated cohorts.
In patients with coronary artery disease, statins have been shown to lower cholesterol and stabilize pre-existing plaques in the arterial wall, reducing the risk of plaque rupture. Low-density lipoproteincholesterol goals vary according to vascular risk factors but should be <100 mg/dL for patients with vascular dementia, who are at highest risk. Blood pressure goals are ≤140 mm Hg (systolic) and ≤90 mm Hg (diastolic).
Glycemic control (fasting blood glucose <110 mg/dL) and smoking cessation can also reduce the risk of further vascular events. Most patients should be taking an antiplatelet medication, preferably aspirin, to reduce clotting risk.
Although Lewy body dementia has no known risk factors other than age, research will determine whether vascular or other factors contribute to its development.
CASE CONTINUED: TARGETING AGGRESSION
Ms. Z was given divalproex, 250 mg bid, to reduce her frequent aggression. Her visual hallucinations were considered mild and not problematic and therefore were not treated. She responded well to the medication, allowing her to remain in day care and avoid nursing home placement.
Related resources
- Alzheimer’s Association. http://www.alz.org
- American Geriatrics Society. http://www.americangeriatrics.org
Drug brand names
- Carbamazepine • Tegretol, others
- Carbidopa/Levodopa • Various
- Divalproex • Depakote
- Donepezil • Aricept
- Galantamine • Reminyl
- Hydrocodone/acetaminophen • Vicodin, others
- Lisinopril/hydrochlorothiazide • Prinzide, Zestoretic
- Memantine • Namenda
- Risperdone • Risperdal
- Rivastigmine • Exelon
Disclosure
Dr. Bartz is a speaker for Forest Pharmaceuticals and Novartis Pharmaceuticals Corp.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
1. McKeith JG, Ballard CG, Perry RH, et al. Prospective validation of consensus criteria for the diagnosis of dementia with Lewy bodies. Neurology 2000;54:1050-8.
2. Roman GC, Erkinjuntti T, Wallin A, et al. Subcortical ischemic vascular dementia. Lancet Neurol 2002;17:426-36.
3. Pohjasraara T, Mantyla R, Ylikoski MA, et al. Comparison of different clinical criteria (DSM-III, ADDTC, ICD-10, NINDS-AIREN, DSM-IV) for the diagnosis of vascular dementia. Stroke 2000;31:2952-7.
4. Del Ser T, McKeith I, Anand R, et al. Dementia with Lewy bodies: findings from an international multicenter study. Int J Geriatr Psychiatry 2000;15:1034-45.
5. Hachinski VC, Iliff LD, Zilhka E, et al. Cerebral blood flow in dementia. Arch Neurol 1975;32:632-7.
6. McKeith IG, Galasko D, Kosaka K, et al. Consensus guidelines for the clinical and pathologic diagnosis of dementia with Lewy bodies (DLB): report of the consortium on DLB international workshop. Neurology 1996;47:1113-24.
7. Luis CA, Barker WW, Gajaraj K, et al. Sensitivity and specificity of three clinical criteria for dementia with Lewy bodies in an autopsy-verified sample. Int J Geriatr Psychiatry 1999;14:526-33.
8. Barber R, Ballard C, McKeith IG, et al. MRI volumetric study of dementia with Lewy bodies: a comparison with AD and vascular dementia. Neurology 2000;54:1304-9.
9. Lobotesis K, Fenwick JD, Phipps A, et al. Occipital hypoperfusion on SPECT in dementia with Lewy bodies but not AD. Neurology 2001;56:643-9.
10. Pratt RD, Perdomo CA. Results of clinical studies with donepezil in vascular dementia. Am J Geriatr Psychiatry 2002;10(suppl 1):88-9.
11. Wild R, Pettit T, Burns A. Cholinesterase inhibitors for dementia with Lewy bodies. Cochrane Database Syst Rev 2003;3:CD003672.-
12. Tariot PN, Farlow MR, Grossberg GT, et al. Memantine treatment in patients with moderate to severe Alzheimer disease already receiving donepezil: a randomized controlled trial. JAMA 2004;291:317-24.
How should we diagnose and treat obstructive sleep apnea?
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
- What are the risk factors for obstructive sleep apnea (OSA)?
- What is the standard for diagnostic testing?
- How does management of mild OSA differ from severe OSA?
- Can other illnesses complicate OSA?
Obstructive sleep apnea is underdiagnosed.1 These recommendations (from the Institute for Clinical Systems Improvement’s Respiratory Steering Committee) can help providers more accurately identify adults who have OSA through a sleep study evaluation, prescribe appropriate treatment, document cases for appropriate follow-up, and increase patient understanding of related health risks. The target audience is physicians, nurses, advanced practice nurses, and physician assistants. The target population is adults.
The evidence categories for this guideline are diagnosis, evaluation, management, risk assessment, and treatment. Outcomes considered are signs and symptoms of OSA; patient risk factors, including comorbidities; accuracy of diagnostic tests; effects of treatment on apneahypopnea index and other measures; patient compliance and satisfaction with treatment; and complications of treatment. Their rating scheme has been updated to comply with the SORT taxonomy.2
Relevance and limitations
OSA affects more than 12 million people in the US, 2% of women and 4% of men aged >35 years. The patient with OSA commonly consults a physician after a sleep partner reports loud snoring and irregular breathing. The methods used to collect and select evidence is not stated.
Development and review
This guideline was accessed through the National Guideline Clearinghouse (www.ngc.gov). The Institute for Clinical Systems Improvement is an independent, nonprofit organization sponsored by 6 Minnesota health plans.
The authors completed an electronic search of databases. Data were analyzed by systematic review with evidence table and were validated by clinical validation-pilot testing and internal peer review. The methods used to make the recommendations were not discussed. Quality and strength of evidence were weighted according to a rating scheme furnished in the guideline. Two excellent algorithms are attached to this guideline: diagnosis and treatment. There are 92 references.
Guideline source
Institute for Clinical Systems Improvement. Diagnosis and Treatment of Obstructive Sleep Apnea. Bloomington, Minn: Institute for Clinical Systems Improvement; 2003. 53 pages.
Other guidelines on osa
- Practice parameters for the use of autotitrating continuous positive airway pressure devices for titrating pressures and treating adult patients with obstructive sleep apnea syndrome. Standards of Practice Committee. Sleep 2002; 25:143–147 [29 references]. Web access at: www.aasmnet.org/PDF/autotitratingreview.pdf.
- Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Chesson AL Jr, Berry RB, Pack A. Practice parameters for the use of portable monitoring devices in the investigation of suspected obstructive sleep apnea in adults. Sleep2003; 26:907–913 [11 references]. Web access at: www.aasmnet.org/PDF/260719.pdf.
- Clinical practice guideline: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics 2002; 109:704–712 [63 references]. Web access at: www.aappolicy. aappublications.org/cgi/content/full/pediatrics; 109/4/704.
Grade A Recommendations
- Large neck circumference, obesity, and hypertension are risk factors for OSA.
- OSA occurs frequently in patients with cardiovascular disease, coronary artery disease, and hypertension.
- Additional signs and symptoms of OSA include reports of choking by sleep partner, awakening with choking, intense snoring, severe daytime sleepiness (with driving impairment), and male gender.
- Polysomography should be performed to determine the diagnosis and is the standard for diagnosis. Unattended portable monitoring is a reasonable alternative when the patient has severe symptoms requiring prompt evaluation/treatment or for follow-up studies.
- Lifestyle modification, including weight loss, reduced alcohol consumption, and lateral sleep positioning are recommended for treatment.
- Severity of OSA is based on magnitude of sleepiness, hypoxia, and the Apnea-Hypopnea Index (AHI).
- Mild OSA can be treated with oral appliances, positive airway pressure devices, or surgical procedures.
- Moderate to severe obstructive sleep apnea should always be treated with positive airway pressure devices, continuous positive airway pressure (CPAP) most commonly.
Grade B Recommendations
- Unattended portable monitoring may be acceptable for rural areas where polysomography is unavailable.
- Surgical procedures (septoplasty, nasal polypectomy, tonsillectomy, turbinoplasty, and uvulopalatopharyngoplasty) to correct anatomical obstructions might be necessary for treatment of mild OSA prior to a positive pressure device.
- After initiating treatment patients should be seen in follow-up in 1 month to assess snoring and sleepiness.
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
1. Strollo PJ, Jr, Rogers RM. Obstructive sleep apnea. N Engl J Med 1996;334:99-104.
2. Ebell M, Siwek J, Weiss BD, et al. Strength of recommendation taxonomy (SORT): A patient-centered approach to grading evidence in the medical literature. Am Fam Physician 2004;69:548-556.
Correspondence: Keith B. Holten, MD, Clinton Memorial Hospital/University of Cincinnati Family Practice Residency, 825 W. Locust St., Wilmington, OH, 45177. E-mail: [email protected].
Safe use of opioids in chronic noncancer pain
Understanding valvular heart disease in patients with systemic autoimmune diseases
Melanoma Screening Behavior Among Primary Care Physicians
Is nedocromil effective in preventing asthmatic attacks in patients with asthma?
Nedocromil (Tilade) is effective for the treatment of mild persistent asthma. It has not been shown to be effective in more severe forms of asthma for both children and adults. Although no studies looked specifically at exacerbation rates, multiple clinical and biologic outcomes (symptom scores, quality of life measures, bronchodilator use, forced expiratory flow in 1 second [FEV1], and peak expiratory flow rate [PEFR]) improved with nedocromil use compared with placebo.
The most effective dose for preventing exacerbations appears to be 4 mg (2 puffs) 4 times a day (SOR: A, multiple randomized controlled trials [RCTs] and meta-analyses). More severe forms of asthma respond better to inhaled steroids than to nedocromil (SOR: A, multiple RCTs). Nedocromil may allow some patients with severe asthma to use lower doses of inhaled steroids (SOR: C, conflicting RCTs). Nedocromil is also effective for the treatment of exercise-induced asthma (SOR: A, multiple RCTs and meta-analyses).
In general, about 50% to 70% of patients respond to nedocromil (SOR: A, multiple RCTs and meta-analyses). Unfortunately, which patients respond is not predictable from clinical parameters.1 Nedocromil is worth trying in mild persistent asthma, particularly for children where the parents are worried about the growth issues associated with inhaled steroids. Side effects (sore throat, nausea, and headache) are mild and infrequent. Maximal efficacy is usually seen after 6 to 8 weeks.
Evidence summary
A systematic review encompassing 127 trial centers and 4723 patients concluded that inhaled nedocromil was effective for a variety of patients with asthma. Significant improvements were noted in FEV1, PEFR, use of bronchodilators, symptom scores, and quality of life scores. The reviewers found nedocromil to be most effective for patients with moderate disease already taking bronchodilators,2 corresponding to the “mild persistent asthma” category ( Table ).
A contemporaneous European RCT, not included in the review, compared 4 mg of inhaled nedocromil 4 times daily with inhaled placebo among 209 asthmatic children for 12 weeks.3 After 8 weeks, they found a statistically significant reduction in total daily asthma symptom scores (50% nedocromil vs 9% placebo; P<.01). The proportion of parents and children rating treatment as moderately or very effective was 78% in the treatment group and 59% in the placebo group (number needed to treat [NNT]=5.2; P<.01); clinicians’ ratings were 73% for nedocromil and 50% for placebo (NNT=4.3; P<.01). The frequency of side effects—including nausea, headache, and sleepiness—did not reach statistical significance; however, the nedocromil group reported up to a 20% incidence of sore throat. Most of the studies reported no dropouts due to side effects.
When patients are already using inhaled steroids, the evidence is less clear whether nedocromil confers additional benefits, such as fewer exacerbations or lower inhaled steroid doses. Two small studies of patients either already on inhaled steroids4 or considered to be steroid-resistant5 found nonsignificant trends towards reductions in bronchodilator use, increased PEFR, increased FEV1, and improved quality of life. Although both studies were underpowered, the study on steroid-resistant asthma did find a statistically significant 20% improvement in PEFR and decreased bronchodilator use for 50% of patients at 8 and 12 weeks.
The inherent waxing and waning nature of asthma makes demonstrating benefits difficult. Furthermore, nedocromil tends to have an all-ornothing effect rather than a dose-response gradient. Unfortunately, none of these trials found useful predictors to help clinicians determine which patients respond.1,5
In a Cochrane Review, 20 RCTs involving 280 participants showed that 4 mg (2 puffs) of nedocromil inhaled 15 to 60 minutes prior to exercise significantly reduced the severity and duration of exercise-induced asthma for both adults and children. The maximum percentage fall in FEV1 improved significantly compared with placebo, with a weighted mean difference of 15.5% (95% confidence interval, 13.2–18.1). In addition, the time to complete recovery was shortened from 30 minutes with placebo to 10 minutes with nedocromil.6
TABLE
Classification of asthma
| Classification | Symptom frequency | Spirometry findings |
|---|---|---|
| Severe persistent | Continual symptoms | PEFR <60% Variability >30% |
| Moderate persistent | Daily symptoms, more than 1 night per week | PEFR >60% but <80% Variability >30% |
| Mild persistent | More than twice per week but less than daily; more than 2 nights per month | PEFR >80% Variability 20%–30% |
| Mild intermittent | Less than once per week; less than or equal to 2 nights per month | PEFR >80% Variability <20% |
| Source: Global Initiative for Asthma, National Heart, Lung and Blood Institute 2003.7 | ||
Recommendations from others
The Global Initiative for Asthma and the National Heart, Lung and Blood Institute Expert Panel Report list nedocromil as an option for the treatment of exercise-induced asthma and mild persistent asthma for adults and children. However, it is listed as a second choice to the use of inhaled steroids in the case of mild persistent asthma. It is not recommended for moderate or severe persistent asthma, or for mild intermittent asthma.7
Nedocromil and cromolyn sodium are safe but many patients do not respond
Ron Baldwin, MD
University of Wyoming Family Practice Residency at Casper
Inhaled nedocromil and cromolyn sodium have long been recognized as agents with an excellent safety profile. Unfortunately, as pointed about above, many patients do not respond to these agents. In addition, 4-times-daily dosing makes compliance difficult. Clinicians and parents must weigh the theoretical risk of inhaled corticosteroid-induced growth retardation with this potential differential in effectiveness.
1. Parish RC, Miller LJ. Nedocromil sodium. Ann Pharmacother 1993;27:599-606.
2. Edwards AM, Stevens MT. The clinical efficacy of inhaled nedocromil sodium (Tilade) in the treatment of asthma. Eur Respir J 1993;6:35-41.
3. Armenio L, Baldini G, Baldare M, et al. Double blind, placebo controlled study of nedocromil sodium in asthma. Arch Dis Child 1993;68:193-197.
4. O’Hickey SP, Rees PJ. High dose nedocromil sodium as an addition to inhaled corticosteroids in the treatment of asthma. Respir Med 1994;88:499-502.
5. Marin JM, Carrizo SJ, Garcia R, Ejea MV. Effects of nedocromil sodium in steroid-resistant asthma: a randomized controlled trial. J Allergy Clin Immunol 1996;97:602-610.
6. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction (Cochrane Review). The Cochrane Library, Issue 4, 2003. Chichester, UK: John Wiley & Sons, Ltd.
7. Global Strategy for Asthma Management and Prevention. Bethesda, Md: Global Initiative for Asthma, National Heart, Lung and Blood Institute; 2003.
Nedocromil (Tilade) is effective for the treatment of mild persistent asthma. It has not been shown to be effective in more severe forms of asthma for both children and adults. Although no studies looked specifically at exacerbation rates, multiple clinical and biologic outcomes (symptom scores, quality of life measures, bronchodilator use, forced expiratory flow in 1 second [FEV1], and peak expiratory flow rate [PEFR]) improved with nedocromil use compared with placebo.
The most effective dose for preventing exacerbations appears to be 4 mg (2 puffs) 4 times a day (SOR: A, multiple randomized controlled trials [RCTs] and meta-analyses). More severe forms of asthma respond better to inhaled steroids than to nedocromil (SOR: A, multiple RCTs). Nedocromil may allow some patients with severe asthma to use lower doses of inhaled steroids (SOR: C, conflicting RCTs). Nedocromil is also effective for the treatment of exercise-induced asthma (SOR: A, multiple RCTs and meta-analyses).
In general, about 50% to 70% of patients respond to nedocromil (SOR: A, multiple RCTs and meta-analyses). Unfortunately, which patients respond is not predictable from clinical parameters.1 Nedocromil is worth trying in mild persistent asthma, particularly for children where the parents are worried about the growth issues associated with inhaled steroids. Side effects (sore throat, nausea, and headache) are mild and infrequent. Maximal efficacy is usually seen after 6 to 8 weeks.
Evidence summary
A systematic review encompassing 127 trial centers and 4723 patients concluded that inhaled nedocromil was effective for a variety of patients with asthma. Significant improvements were noted in FEV1, PEFR, use of bronchodilators, symptom scores, and quality of life scores. The reviewers found nedocromil to be most effective for patients with moderate disease already taking bronchodilators,2 corresponding to the “mild persistent asthma” category ( Table ).
A contemporaneous European RCT, not included in the review, compared 4 mg of inhaled nedocromil 4 times daily with inhaled placebo among 209 asthmatic children for 12 weeks.3 After 8 weeks, they found a statistically significant reduction in total daily asthma symptom scores (50% nedocromil vs 9% placebo; P<.01). The proportion of parents and children rating treatment as moderately or very effective was 78% in the treatment group and 59% in the placebo group (number needed to treat [NNT]=5.2; P<.01); clinicians’ ratings were 73% for nedocromil and 50% for placebo (NNT=4.3; P<.01). The frequency of side effects—including nausea, headache, and sleepiness—did not reach statistical significance; however, the nedocromil group reported up to a 20% incidence of sore throat. Most of the studies reported no dropouts due to side effects.
When patients are already using inhaled steroids, the evidence is less clear whether nedocromil confers additional benefits, such as fewer exacerbations or lower inhaled steroid doses. Two small studies of patients either already on inhaled steroids4 or considered to be steroid-resistant5 found nonsignificant trends towards reductions in bronchodilator use, increased PEFR, increased FEV1, and improved quality of life. Although both studies were underpowered, the study on steroid-resistant asthma did find a statistically significant 20% improvement in PEFR and decreased bronchodilator use for 50% of patients at 8 and 12 weeks.
The inherent waxing and waning nature of asthma makes demonstrating benefits difficult. Furthermore, nedocromil tends to have an all-ornothing effect rather than a dose-response gradient. Unfortunately, none of these trials found useful predictors to help clinicians determine which patients respond.1,5
In a Cochrane Review, 20 RCTs involving 280 participants showed that 4 mg (2 puffs) of nedocromil inhaled 15 to 60 minutes prior to exercise significantly reduced the severity and duration of exercise-induced asthma for both adults and children. The maximum percentage fall in FEV1 improved significantly compared with placebo, with a weighted mean difference of 15.5% (95% confidence interval, 13.2–18.1). In addition, the time to complete recovery was shortened from 30 minutes with placebo to 10 minutes with nedocromil.6
TABLE
Classification of asthma
| Classification | Symptom frequency | Spirometry findings |
|---|---|---|
| Severe persistent | Continual symptoms | PEFR <60% Variability >30% |
| Moderate persistent | Daily symptoms, more than 1 night per week | PEFR >60% but <80% Variability >30% |
| Mild persistent | More than twice per week but less than daily; more than 2 nights per month | PEFR >80% Variability 20%–30% |
| Mild intermittent | Less than once per week; less than or equal to 2 nights per month | PEFR >80% Variability <20% |
| Source: Global Initiative for Asthma, National Heart, Lung and Blood Institute 2003.7 | ||
Recommendations from others
The Global Initiative for Asthma and the National Heart, Lung and Blood Institute Expert Panel Report list nedocromil as an option for the treatment of exercise-induced asthma and mild persistent asthma for adults and children. However, it is listed as a second choice to the use of inhaled steroids in the case of mild persistent asthma. It is not recommended for moderate or severe persistent asthma, or for mild intermittent asthma.7
Nedocromil and cromolyn sodium are safe but many patients do not respond
Ron Baldwin, MD
University of Wyoming Family Practice Residency at Casper
Inhaled nedocromil and cromolyn sodium have long been recognized as agents with an excellent safety profile. Unfortunately, as pointed about above, many patients do not respond to these agents. In addition, 4-times-daily dosing makes compliance difficult. Clinicians and parents must weigh the theoretical risk of inhaled corticosteroid-induced growth retardation with this potential differential in effectiveness.
Nedocromil (Tilade) is effective for the treatment of mild persistent asthma. It has not been shown to be effective in more severe forms of asthma for both children and adults. Although no studies looked specifically at exacerbation rates, multiple clinical and biologic outcomes (symptom scores, quality of life measures, bronchodilator use, forced expiratory flow in 1 second [FEV1], and peak expiratory flow rate [PEFR]) improved with nedocromil use compared with placebo.
The most effective dose for preventing exacerbations appears to be 4 mg (2 puffs) 4 times a day (SOR: A, multiple randomized controlled trials [RCTs] and meta-analyses). More severe forms of asthma respond better to inhaled steroids than to nedocromil (SOR: A, multiple RCTs). Nedocromil may allow some patients with severe asthma to use lower doses of inhaled steroids (SOR: C, conflicting RCTs). Nedocromil is also effective for the treatment of exercise-induced asthma (SOR: A, multiple RCTs and meta-analyses).
In general, about 50% to 70% of patients respond to nedocromil (SOR: A, multiple RCTs and meta-analyses). Unfortunately, which patients respond is not predictable from clinical parameters.1 Nedocromil is worth trying in mild persistent asthma, particularly for children where the parents are worried about the growth issues associated with inhaled steroids. Side effects (sore throat, nausea, and headache) are mild and infrequent. Maximal efficacy is usually seen after 6 to 8 weeks.
Evidence summary
A systematic review encompassing 127 trial centers and 4723 patients concluded that inhaled nedocromil was effective for a variety of patients with asthma. Significant improvements were noted in FEV1, PEFR, use of bronchodilators, symptom scores, and quality of life scores. The reviewers found nedocromil to be most effective for patients with moderate disease already taking bronchodilators,2 corresponding to the “mild persistent asthma” category ( Table ).
A contemporaneous European RCT, not included in the review, compared 4 mg of inhaled nedocromil 4 times daily with inhaled placebo among 209 asthmatic children for 12 weeks.3 After 8 weeks, they found a statistically significant reduction in total daily asthma symptom scores (50% nedocromil vs 9% placebo; P<.01). The proportion of parents and children rating treatment as moderately or very effective was 78% in the treatment group and 59% in the placebo group (number needed to treat [NNT]=5.2; P<.01); clinicians’ ratings were 73% for nedocromil and 50% for placebo (NNT=4.3; P<.01). The frequency of side effects—including nausea, headache, and sleepiness—did not reach statistical significance; however, the nedocromil group reported up to a 20% incidence of sore throat. Most of the studies reported no dropouts due to side effects.
When patients are already using inhaled steroids, the evidence is less clear whether nedocromil confers additional benefits, such as fewer exacerbations or lower inhaled steroid doses. Two small studies of patients either already on inhaled steroids4 or considered to be steroid-resistant5 found nonsignificant trends towards reductions in bronchodilator use, increased PEFR, increased FEV1, and improved quality of life. Although both studies were underpowered, the study on steroid-resistant asthma did find a statistically significant 20% improvement in PEFR and decreased bronchodilator use for 50% of patients at 8 and 12 weeks.
The inherent waxing and waning nature of asthma makes demonstrating benefits difficult. Furthermore, nedocromil tends to have an all-ornothing effect rather than a dose-response gradient. Unfortunately, none of these trials found useful predictors to help clinicians determine which patients respond.1,5
In a Cochrane Review, 20 RCTs involving 280 participants showed that 4 mg (2 puffs) of nedocromil inhaled 15 to 60 minutes prior to exercise significantly reduced the severity and duration of exercise-induced asthma for both adults and children. The maximum percentage fall in FEV1 improved significantly compared with placebo, with a weighted mean difference of 15.5% (95% confidence interval, 13.2–18.1). In addition, the time to complete recovery was shortened from 30 minutes with placebo to 10 minutes with nedocromil.6
TABLE
Classification of asthma
| Classification | Symptom frequency | Spirometry findings |
|---|---|---|
| Severe persistent | Continual symptoms | PEFR <60% Variability >30% |
| Moderate persistent | Daily symptoms, more than 1 night per week | PEFR >60% but <80% Variability >30% |
| Mild persistent | More than twice per week but less than daily; more than 2 nights per month | PEFR >80% Variability 20%–30% |
| Mild intermittent | Less than once per week; less than or equal to 2 nights per month | PEFR >80% Variability <20% |
| Source: Global Initiative for Asthma, National Heart, Lung and Blood Institute 2003.7 | ||
Recommendations from others
The Global Initiative for Asthma and the National Heart, Lung and Blood Institute Expert Panel Report list nedocromil as an option for the treatment of exercise-induced asthma and mild persistent asthma for adults and children. However, it is listed as a second choice to the use of inhaled steroids in the case of mild persistent asthma. It is not recommended for moderate or severe persistent asthma, or for mild intermittent asthma.7
Nedocromil and cromolyn sodium are safe but many patients do not respond
Ron Baldwin, MD
University of Wyoming Family Practice Residency at Casper
Inhaled nedocromil and cromolyn sodium have long been recognized as agents with an excellent safety profile. Unfortunately, as pointed about above, many patients do not respond to these agents. In addition, 4-times-daily dosing makes compliance difficult. Clinicians and parents must weigh the theoretical risk of inhaled corticosteroid-induced growth retardation with this potential differential in effectiveness.
1. Parish RC, Miller LJ. Nedocromil sodium. Ann Pharmacother 1993;27:599-606.
2. Edwards AM, Stevens MT. The clinical efficacy of inhaled nedocromil sodium (Tilade) in the treatment of asthma. Eur Respir J 1993;6:35-41.
3. Armenio L, Baldini G, Baldare M, et al. Double blind, placebo controlled study of nedocromil sodium in asthma. Arch Dis Child 1993;68:193-197.
4. O’Hickey SP, Rees PJ. High dose nedocromil sodium as an addition to inhaled corticosteroids in the treatment of asthma. Respir Med 1994;88:499-502.
5. Marin JM, Carrizo SJ, Garcia R, Ejea MV. Effects of nedocromil sodium in steroid-resistant asthma: a randomized controlled trial. J Allergy Clin Immunol 1996;97:602-610.
6. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction (Cochrane Review). The Cochrane Library, Issue 4, 2003. Chichester, UK: John Wiley & Sons, Ltd.
7. Global Strategy for Asthma Management and Prevention. Bethesda, Md: Global Initiative for Asthma, National Heart, Lung and Blood Institute; 2003.
1. Parish RC, Miller LJ. Nedocromil sodium. Ann Pharmacother 1993;27:599-606.
2. Edwards AM, Stevens MT. The clinical efficacy of inhaled nedocromil sodium (Tilade) in the treatment of asthma. Eur Respir J 1993;6:35-41.
3. Armenio L, Baldini G, Baldare M, et al. Double blind, placebo controlled study of nedocromil sodium in asthma. Arch Dis Child 1993;68:193-197.
4. O’Hickey SP, Rees PJ. High dose nedocromil sodium as an addition to inhaled corticosteroids in the treatment of asthma. Respir Med 1994;88:499-502.
5. Marin JM, Carrizo SJ, Garcia R, Ejea MV. Effects of nedocromil sodium in steroid-resistant asthma: a randomized controlled trial. J Allergy Clin Immunol 1996;97:602-610.
6. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exercise-induced bronchoconstriction (Cochrane Review). The Cochrane Library, Issue 4, 2003. Chichester, UK: John Wiley & Sons, Ltd.
7. Global Strategy for Asthma Management and Prevention. Bethesda, Md: Global Initiative for Asthma, National Heart, Lung and Blood Institute; 2003.
Evidence-based answers from the Family Physicians Inquiries Network
Blocking the ‘munchies’ receptor: A novel approach to obesity
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
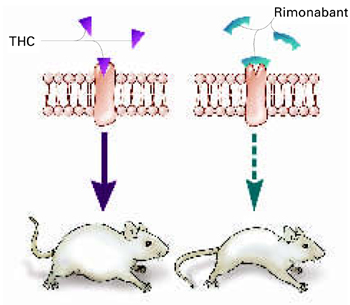
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
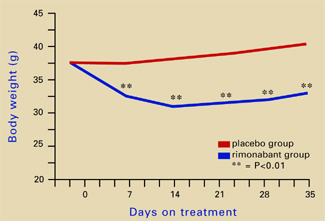
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
Marijuana has long been known to stimulate appetite, particularly for sweet foods.1 The naughty boys in my fraternity called it “the munchies;” the professionals call it hyperphagia. Cannabinoid receptor (CB1) stimulation by marijuana’s main active component—9-THC—is believed to induce this behavior. Clinicians have successfully used this effect to treat AIDS-related wasting syndrome and other anorexic conditions.2
CB1 is widely expressed throughout the brain and seems to inhibit release of various neurotransmitters.3 How this effect leads to increased appetite is unclear, but it may result from a decrease in the appetite-suppressing effects of hormones such as leptin. In other words, tweaking the CB1 receptor may take the “brakes” off appetite.
Some researchers have speculated that if stimulating CB1 triggers appetite, blocking the receptor might inhibit it (Figure 1).
THE ‘MUNCHIES’ IN MICE
Rimonabant (SR141716), an experimental agent, is a potent and selective CB1 antagonist.
Ravinet Trillou et al fed mice a high-fat diet known to induce obesity.4 The mice were randomized to receive rimonabant or placebo while maintained on the highly palatable diet. The authors asked: Would rimonabant help the mice lose weight even when they could eat as much delicious fatty food as they wanted?
Figure 1 Blocking CB1 may prevent weight gain
Δ9-THC activates the cannabinoid receptor (CB1), stimulating appetite and leading to weight gain in mice (left). When the same receptor is blocked, appetite is controlled (right).
Source: Illustration for CURRENT PSYCHIATRY by Marcia HartsockRimonabant induced a sustained body weight reduction of approximately 20% in the treatment group compared with the placebo group across 5 weeks (Figure 2). Estimated fat stores among the treatment group were depleted by slightly more than 50%.
The authors noted that the mice in the treatment group had decreased their food intake, but the decrease was not sufficient to explain the weight loss. They speculate that rimonabant could activate metabolic processes and decrease intake.
RIMONABANT’S ROLE IN PSYCHIATRY
Phase III human trials of rimonabant are under way for obesity as well as smoking cessation.5 In uncontrolled studies, rimonabant has been shown to help people avoid weight gain while quitting smoking.5
If rimonabant shows effectiveness in controlled trials and is safe in humans, it could be most valuable. Obesity in industrial countries is epidemic and causes serious secondary morbidity, including diabetes, arthritis, and hypertension. Rimonabant, if approved by the FDA, could reach the market by early 2006.6
It is unknown whether rimonabant’s metabolic effects could offset those of many psychotropics. As psychiatrists, we often must stop an effective antipsychotic or antidepressant because it is causing significant weight gain. A treatment that would prevent medication-induced weight gain could improve patient compliance and, ultimately, outcomes.
MANAGING SCHIZOPHRENIA
Some evidence also suggests that rimonabant may offer additional benefits for patients with schizophrenia beyond weight reduction or smoking cessation.
Figure 2 Rimonabant’s effects on weight in mice on a high-fat diet
Source: Adapted from reference 4.Leweke et al found increased endogenous cannabinoids in the CSF of patients with schizophrenia, suggesting that a cannabinoid signaling imbalance may contribute to the disorder’s pathogenesis.7 However, 72 patients with schizophrenia or schizoaffective disorder who took rimonabant for 6 weeks showed no improvement compared with a placebo group.8
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
1. Abel EL. Cannabis: effects on hunger and thirst. Behav Biol 1975;15:255-81.
2. Beal JE, Olson R, Laubenstein L, et al. Dronabinol as a treatment for anorexia associated with weight loss in patients with AIDS. J Pain Symptom Manage 1995;10:89-97.
3. Iversen L. Cannabis and the brain. Brain 2003;126:1252-70.
4. Ravinet Trillou C, Arnone M, Delgorge C, et al. Anti-obesity effect of SR141716, a CB1 receptor antagonist, in diet-induced obese mice. Am J Physiol Regul Integr Comp Physiol 2003;284:R345-53.
5. Fernandez JR, Allison DB. Rimonabant Sanofi-Synthelabo. Curr Opin Investig Drugs 2004;5:430-5.
6. The Website for the Drug Development Industry. Acomplia (rimonabant)—investigational agent for the management of obesity. London: SPGMedia. Available at: http://www. drugdevelopment-technology.com/projects/rimonabant/. Accessed Oct. 14, 2004.
7. Leweke FM, Giuffrida A, Wurster U, et al. Elevated endogenous cannabinoids in schizophrenia. Neuroreport 1999;10:1665-9.
8. Meltzer HY, Arvanitis L, Bauer D, et al. Placebo-controlled evaluation of four novel compounds for the treatment of schizophrenia and schizoaffective disorder. Am J Psychiatry 2004;161:975-84.
A ‘FRESH’ way to manage trauma
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
Ameliorating emotional trauma is key to avoiding long-term functional impairment. Consider a FRESH approach that involves families/friends, reassurance/retelling, education, addressing substance abuse, sleeplessness, and suicide risk, and taking a careful history.
Family and friends can be valuable to treatment but clinicians often overlook their importance. Overwhelmed or traumatized family members who are not counseled about the patient’s symptoms can undermine treatment by dismissing symptoms and withdrawing support. Involve them by emphasizing their supportive role. Alert them to normal and problematic trauma responses and stress disorder symptoms.
Reassurance/retelling. Explain that emotional pain is normal but usually fades with time. Consider effects of survivor guilt: Encourage the patient to retell the experience, but do not demand this. Help patients identify and correct thought distortions that foster avoidance. Though controversial,1 critical incident debriefing and cognitive-behavioral therapy can help the patient recount the trauma and ultimately restore a sense of self, enjoyment of life, and expectations of safety, control, and trust.2
Educate patients about normal variable stress responses. Warn traumatized patients against engaging in high-risk behaviors, through which they may try to deny their vulnerability, fear, and loss of control. Explain symptoms and risk factors for depression, posttraumatic stress disorder (PTSD), and other anxiety disorders.
Substance abuse, sleeplessness, and suicide are possible outcomes of trauma. Prescribe a non-narcotic sleep-promoting medication if insomnia is problematic. Alternately, consider a selective serotonin or serotonin-norepinephrine reuptake inhibitor3,4 at normal or low starting dosages if presenting symptoms suggest an emerging anxiety or mood disorder or PTSD. Watch for signs of survivor guilt—such as an unrealistic sense of responsibility for the trauma—that can lead to depression with suicide risk after a significant loss.
History. Watch for factors that predict PTSD and comorbid disorders (trauma severity and chronicity, involvement of interpersonal violence, fear of death). Previous trauma, PTSD, depression, anxiety, personality disorder, childhood victimization, substance abuse, and poor social support increase the risk. Avoidance, numbing, dissociation, high guilt, and low acknowledged anger correlate with increased PTSD risk. Follow up with patients who exhibit these risk factors every 1 to 2 weeks with medication and/or psychotherapy.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.
1. Cloak NL, Edwards P. Psychological first aid: Emergency care for terrorism and disaster survivors. Current Psychiatry 2004;3(5):12-23.
2. Bisson JI. Early interventions following traumatic events. Psychiatr Ann 2003;1:37-44.
3. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry 2001;58:485-92.
4. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry 2001;158:1982-8.
Dr. Sobel is a clinical instructor, University of California-San Diego School of Medicine, and consulting psychiatrist, University of San Diego Counseling Center.