User login
The Fountain of Youth
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion


This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
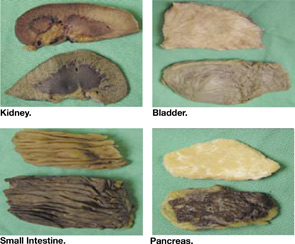
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
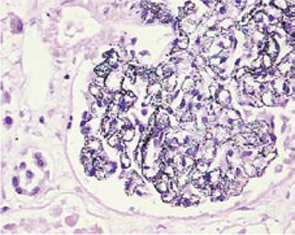
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Photo Quiz:
What is the etiology of the dermatologic and nail abnormalities in this 53‑year‑old man with cirrhosis due to chronic hepatitis B infection?
Diagnosis: Argyria
Discussion
This patient had progressive liver failure and was hospitalized for possible liver transplantation. During the initial history, he disclosed that he had noticed progressive discoloration of his skin, hair, and nails for the past several months. Our clinical suspicion of argyria was confirmed when the patient’s serum silver level returned at 54 ug/ml (normal range 0.0-14 ug/ml). Serum levels of arsenic, mercury, and lead were within normal limits.
Despite treatment of encephalopathy, esophageal varices, and peritonitis, this patient’s liver disease deteriorated and he underwent orthotopic liver transplantation. Unfortunately, he died 24 days post-transplantation from progressive multi-organ failure.
At autopsy, gross silver discoloration was noted in many organs, including the bowel, bladder, pancreas, and renal papillae.
Microscopically, fine black pigments were noted in almost all basement membranes, including the skin, glomeruli (see Figure), choroid plexus, and myocardial connective tissue.
Similar fine granules were seen in the basement membranes of the patient’s native liver but not within the newly transplanted liver.
The patient admitted to drinking one pint of colloid silver almost daily for 15 years. This homeopathic remedy has been purported to cure many illnesses, including the common cold, cancer, diabetes, and HIV. Equipment and recipes are readily available on the internet, and as a “food supplement” silver remedies bypass strict regulatory controls. Colloid silver can be made easily by connecting a 9-volt battery to two silver wires placed in a tub of water. The electric reaction draws silver off the wire and into the water, producing the liquid silver elixir.
After ingestion, silver deposits permanently in the skin, producing the characteristic color changes of argyria, especially pronounced in sun-exposed areas where sunlight reduces the metal to an inert salt, analogous to processes used in photography. Although ingested silver is known to alter skin color irreversibly and deposit widely in the body, permanent extracutaneous organ damage from silver ingestion has not been firmly established. Thus, argyria remains a cosmetically altering disease and is not a contraindication to liver transplant.
Like other homeopathic remedies, colloid silver recipes may be accessed by the public directly. Despite a lack of peer-reviewed scientific evidence to support its use, public testimonials touting silver as the new panacea nonetheless will remain prevalent. Physicians must educate themselves, and inform their patients, that colloid silver is not the “fountain of youth.”
Education: Hospitalists Add Value to Formal and Informal Learning Processes
Type a medical condition or term into a search engine and watch what happens. A search on the words “diabetes” yields more than 13 million Web pages, and “pneumonia” produces another 1.65 million. In 1998, the Internet hosted approximately 5000 health-related Web sites; two years later that number quadrupled (1). Between 30,000 and 45,000 medical articles on various drug therapies are published annually. The Patent and Trademark Office issued between 2000 and 4200 drug patents each year between 1979 and 1989 (2). The National Library of Medicine reports that it adds more than 2000 journal article citations to its MEDLINE database on a daily basis. In 2003, more than 460,000 citations were entered.
Deciphering and applying this myriad of changing information is a critical activity in the medical field. Without disseminating new knowledge through ongoing education, medical practices and procedures would become outdated, and uninformed medical professionals and patients would continue to operate under misinformation that might be detrimental to health or worse.
Hospitalists as Inpatient Experts
In an inpatient setting, hospitalists are uniquely qualified to play the role of educator. They analyze and interpret a wide range of medical information to treat their patients and provide updated information to patients and their families, residents, interns, nursing staff, other health care professionals, and hospital administrators. The hospitalist can be viewed as the “hub” of educational activities in the inpatient environment, absorbing, synthesizing, and disseminating information. They are “inpatient experts” in the following five spheres of knowledge:
- patient management
- clinical knowledge
- clinical skills
- health care industry issues
- research and management/leadership (3)
Hospitalists are uniquely qualified in the sphere of patient management, efficiently and effectively guiding the patient through the mazelike inpatient environment. Most hospitalists are quite familiar with critical hospital functions and activities, including treatment in the emergency department, the admissions process, bedside care on the medical floor, treatment in the intensive care unit, and the discharge process. Hospitalists, because they understand “how to get things done” by ancillary departments, including diagnostic and therapeutic services, often find themselves as conductors of inpatient care. Many hospitalists have developed unique proficiency in co-managing surgical cases due to expertise in peri-operative evaluation and care. Hospitalists are recognized as inpatient team leaders, facilitating and coordinating a range of support services needed to treat the patient, including nursing, case management, pharmacy, occupational/physical therapy, and social work. Hospitalists must also be effective in managing relationships with health care personnel external to the inpatient environment, including community physicians, homecare providers, extended care facilities, and visiting nurse services. Finally, hospitalists are oaen well informed about hospital processes, procedures, rules, regulations, and information systems.
As inpatient generalists, hospitalists continually treat the most common reasons for admission and have exceptional clinical knowledge of these conditions. These conditions include pneumonia, deep vein thrombosis (DVT), congestive heart failure (CHF), diabetes, end-of-life care, and other medical diagnoses. Since they treat many elderly patients, hospitalists are considered experts in managing patients with multiple co-morbidities. A related area of expertise is clinical guidelines/pathways, quality of care metrics, and practice standards. Since they spend nearly all of their time treating inpatients, hospitalists develop extraordinary familiarity with the clinical rules and tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have the experience and expertise to teach inpatient clinical skills. These skills include diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination, and oversight. Also, most hospitalists are familiar with a range of technical procedures, including insertion of central lines and arterial lines, lumbar puncture, arthrocentesis, paracentesis, and thoracentesis.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of health care industry issues. These include comprehension of the payer/insurance regulations regarding medication formularies, utilization review requirements, and other care policies. Their expertise may extend to knowledge of state and federal regulations, public health initiatives, and recently enacted or pending health care legislation. Finally, hospitalists also are often conversant in the field of health care economics, especially regarding the financial impact on hospitals of reimbursement policies, legislative initiatives, technology, etc.
The fifth sphere of hospitalist expertise combines several knowledge domains. Individual hospitalists have specialized expertise in particular fields related to hospital medicine. Some hospitalists, mostly affiliated with academic institutions, are researchers who may develop research protocols, gather data, perform statistical analyses, and write papers that may potentially become the basis of improved patient care. Other hospitalists are exceptionally experienced in management/leadership. A hospitalist may be highly qualified to manage projects (e.g., computer-based physician order entry systems, throughput initiatives, etc.),or a hospitalist could be a strategic thinker who is viewed as a key clinical member of the hospital’s management team.
As a growing specialty, hospitalists have established a proficiency in a range of disciplines and intellectual domains. They are well positioned to assume the role of educator in the hospital environment. Given the exceptional knowledge and skills needed to be a hospitalist, the Society of Hospital Medicine (SHM) is pursing an effort to standardize education and lend greater credibility to the hospitalist profession. The “core curriculum” project is currently formalizing training that will provide a solid foundation for effective clinical practice in the field of hospital medicine.
Dual Educational Tracks
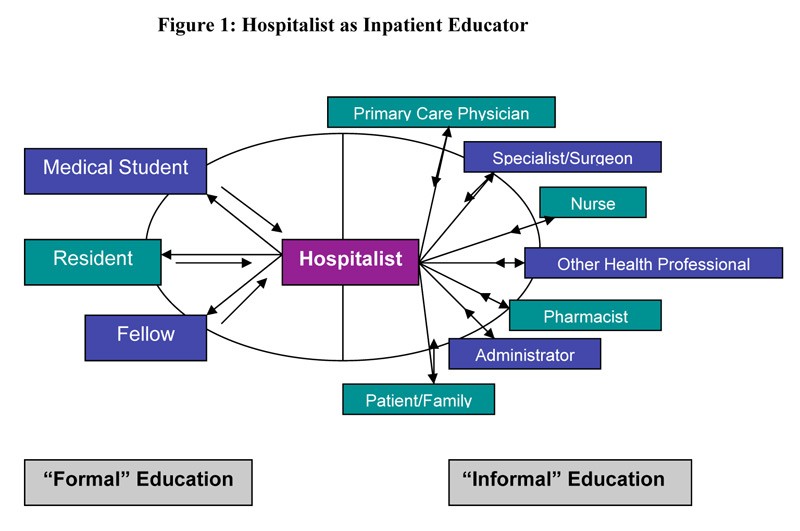
As depicted in Figure 1 below, medical education activity and the ways in which knowledge is imparted fall into two categories: formal and informal. Although some overlap may occur, there are distinct characteristics attributable to both classifications.
“Formal”
Formal education refers to the traditional “teacher-learner” roles in medicine. The learner can be a medical student, resident, or fellow. Education is typically transmitted from teacher to learner (as depicted in the diagram by a solid line), with some reciprocal feedback from the learner to the teacher (dotted line). It should be noted that as the importance and value of hospital medicine programs gain recognition, fellowship programs focusing on this specialty have been established. As of August 2004, eight active hospital medicine fellowship programs exist in the United States: three in California, two in Minnesota, and one each in Ohio, Illinois, and Texas. There are also pediatric hospital medicine fellowship programs in Boston, Washington DC, Houston, and San Diego. Each program enrolls one or two fellows annually (4).
Formal education can take place in both academic medical centers and community hospitals. By definition, academic medical centers provide supervised practical training for medical students, student nurses, and/or other health care professionals, as well as residents and fellows. In many academic medical centers throughout the country, hospitalists are emerging as core teachers of inpatient medicine. A prime example is the University of California, San Francisco. In 2002, 15 faculty hospitalists served as staff for approximately two-thirds of ward-attending months, as well as all medical consults (5).
By the same token, community hospitals that have residency programs also incorporate education to some degree into their daily operations. Today, medical education places a significant burden on residents and on the professionals charged with teaching students to absorb and understand vast amounts of science and medical information. On July 1, 2003, the Accreditation Council for Graduate Medical Education (ACGME) revised the regulations governing the number of resident duty hours. These changes have forced residency programs to find viable options for imparting the required knowledge and hands-on experience to residents in fewer hours. Many consider hospitalists, by virtue of their “superior clinical and educational skills,” as representative of “the solution to the residency work duty problem.” In addition to providing excellence in teaching, hospitalists, known for their “superior clinical and educational skills,” may lead the way in creating and leading a clinical research agenda, which presents as the ultimate pedagogical experience (6).
In 2002, ACGME required six general competencies to be incorporated into residency curriculum and evaluation: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice. Hospitalists, because their practice already incorporates many aspects of these competencies, may be more effective at teaching these concepts to residents.
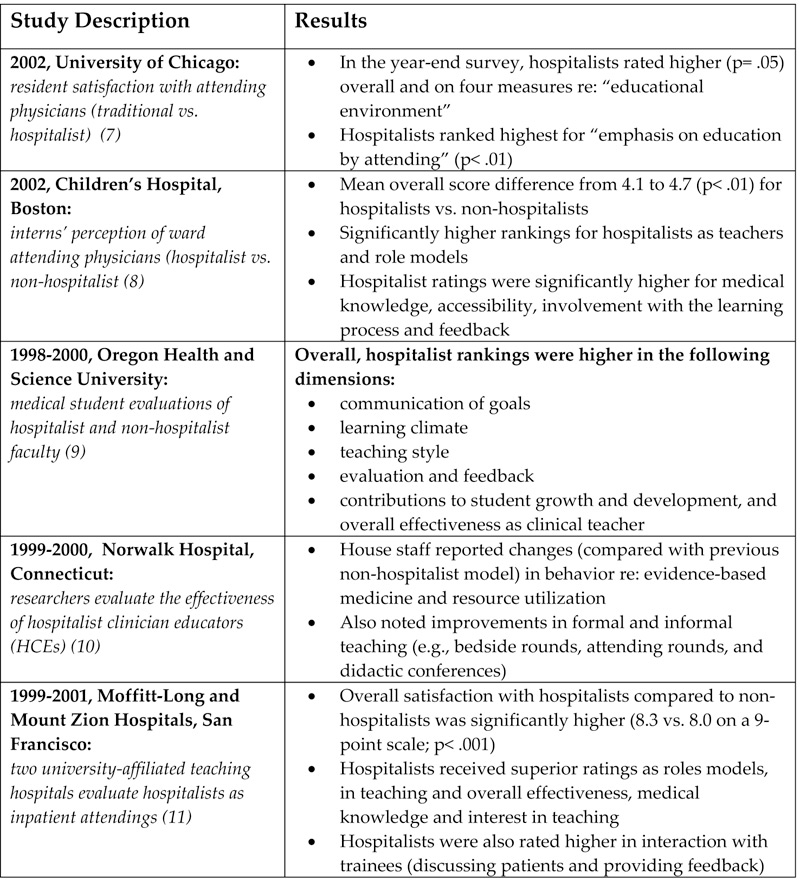
In the formal capacity of teacher, hospitalists can participate in attending/teaching rounds and in didactic patient-specific sessions presented in a case-based format, which provides residents with basic knowledge. As teaching supervisors, they can oversee the full range of clinical processes and procedures from the admission stage to post-discharge. Hospitalist teachers can also serve as mentors, providing a role model to residents who may be searching for direction regarding future plans. Through career counseling, hospitalists may steer learners into appropriate areas of study and training. Table 1 summarizes a series of research studies that document the positive impact hospitalists have achieved as educators in the academic environment.
Hospitalists may also have formal responsibility for developing curricula for learners in the academic environment. Whether the focus is on teaching medical students, residents, or hospitalist fellows, there is a need to determine the topics and material to be covered, incorporate them into a cogent curriculum, and update regularly to reflect the changing standards of care.
“Informal”
Informal education can be viewed as an exchange of information among stakeholders in the health care industry attempting to improve outcomes. Figure 1 depicts this as a two-way information exchange (solid arrows in both directions). As hospitalists impart knowledge to primary care physicians (PCPs), specialists/surgeons, other health care professionals (including nurses and pharmacists), patients, families, and hospital administrators, they reap benefits as well. These stakeholders stand to profit from the knowledge hospitalists can impart in daily interactions within the hospital and in less formal settings.
By working together with nurses, emergency room physicians, medical specialists, and PCPs, hospitalists can help achieve efficient and effective processes of care. The use of available software programs enables health care professionals to cooperatively exchange reliable information regarding patient management. Ongoing conversations regarding diagnoses, treatment, medications, and procedures serve to keep each member of the team educated and informed, thus ensuring more efficient delivery of care (12).
Alpesh Amin, MD, executive director of the hospitalist program at the University of California, Irvine, and chair of SHM’s Education Committee, points out that hospitalists frequently have opportunities to act as educators during case-by-case interactions with PCPs and other health care providers. “Every time you talk to a doctor about admitting or discharging a patient, it’s an opportunity to educate,” he says. In addition, “the hospitalist can apply and/or develop critical pathways and algorithms to educate others.” In the course of managing care, criteria can be developed for previously unaddressed medical issues.
This same opportunity for education extends to the hospital floor where team building serves to enlighten each member of the group providing patient care. In a reciprocal environment, both hospitalists and their medical professional “teammates” benefit from each other’s knowledge. Amin points out that specialists typically focus on one condition, while hospitalists consider the entire patient. By openly receiving the specialist’s input and advice, processing it, and then applying it to the patient, the hospitalist can develop a comprehensive approach to disease management. By considering co-morbidities and long-term care, the health care team should base decisions on “patient-centered education (13).”
Hospitalists can initiate informal in-house educational outreach, such as informational programs about medical breakthroughs, new medications, explanations of existing medical legislation, and other relevant topics. These programs can enlighten nurses, case managers, pharmacists, and other health care professionals about issues important to managing patients and/or achieving quality outcomes. The format for these programs may be one-on-one interactions (either in-person or by telephone) relating to one specific patient; formal in-service lectures; “Lunch and Learns”; pharmaceutically funded drug- or-disease-management seminars; committee or departmental meetings, and/or random written communications (sent electronically or by interoffice mail) that incorporate history and physical findings, consultations, discharge summaries, or hard-copy articles (12).
Conclusion
Because they spend so much time in the hospital, hospitalists are experts on all aspects of inpatient care: clinical, administrative, patient flow, and health care industry issues. Published research shows that academic institutions that employ hospitalists will have more satisfied and better-educated students. Common sense suggests that nurses and other stakeholders who work with hospitalists will be more informed and better-educated team members in the patient care process. Hospitalists can be the key ingredient and centerpiece in effective inpatient medical education.
References
- Yale New Haven Hospital Report, March 2004.
- Ward, Michael R. “Drug approval overregulation.” Regulation: the Review of Business and Government. Cato Institute, September 27, 2004.
- Pak, MH. Associate Professor of Medicine, Hospitalist, Director, General Medicine Consultation Service, University of Wisconsin School of Medicine, Madison, WI.
- Ranji S, Rosenman D. “Hospital medicine fellowship update.” The Hospitalist. 2004; 8 (5): 39.
- Wachter RM, Goldman L. “The hospitalist movement five years later.” JAMA.2002; 287(4): 487-94.
- Saint S, Flanders SA. “Hospitalists in teaching hospitals: opportunities but not without danger.” J Gen Intern Med. 2004; 19: 392-3.
- Chung P, Morrison J, Jin L, Levinson W, Humphrey H, Meltzer D. “Resident satisfaction on an academic hospitalist service: time to teach.” Am J Med. 2002; 112: 597-601.
- Landrigan CP, Muret-Wagstaff S, Chiang VW, Nigrin DJ, Goldmann DA, Finkelstein JA. “Effect of a pediatric hospitalist system on housestaff education and experience.” Arch Ped Adoles Med. 2002; 156 (9): 877-83.
- Hunter AJ, Desai SS, Harrison RA, Chan BK. “Medical student evaluation of the quality of hospitalist and non-hospitalist teaching faculty on inpatient medicine rotations.” Acad Med. 2004; 79:78-82.
- 10. Kulaga, ME. “The positive impact of initiation of hospitalist clinician educators.” J Gen Intern Med.2004; 19(4): 293-301.
- Hauer K, Wachter R, McCulloch C, Woo G, Auerbach A. Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations. Arch Intern Med. 2004; 164: 1866-71.
- Jones T, DO. Director of Medical Affairs, IPC, The Hospitalist Company, Mesa, AZ.
- Amin A, MD, MBA, FACP, executive director, Hospitalist Program, University of California, Irvine. Chair, Education Committee, Society of Hospital Medicine. Personal interview. October 7, 2004.
Type a medical condition or term into a search engine and watch what happens. A search on the words “diabetes” yields more than 13 million Web pages, and “pneumonia” produces another 1.65 million. In 1998, the Internet hosted approximately 5000 health-related Web sites; two years later that number quadrupled (1). Between 30,000 and 45,000 medical articles on various drug therapies are published annually. The Patent and Trademark Office issued between 2000 and 4200 drug patents each year between 1979 and 1989 (2). The National Library of Medicine reports that it adds more than 2000 journal article citations to its MEDLINE database on a daily basis. In 2003, more than 460,000 citations were entered.
Deciphering and applying this myriad of changing information is a critical activity in the medical field. Without disseminating new knowledge through ongoing education, medical practices and procedures would become outdated, and uninformed medical professionals and patients would continue to operate under misinformation that might be detrimental to health or worse.
Hospitalists as Inpatient Experts
In an inpatient setting, hospitalists are uniquely qualified to play the role of educator. They analyze and interpret a wide range of medical information to treat their patients and provide updated information to patients and their families, residents, interns, nursing staff, other health care professionals, and hospital administrators. The hospitalist can be viewed as the “hub” of educational activities in the inpatient environment, absorbing, synthesizing, and disseminating information. They are “inpatient experts” in the following five spheres of knowledge:
- patient management
- clinical knowledge
- clinical skills
- health care industry issues
- research and management/leadership (3)
Hospitalists are uniquely qualified in the sphere of patient management, efficiently and effectively guiding the patient through the mazelike inpatient environment. Most hospitalists are quite familiar with critical hospital functions and activities, including treatment in the emergency department, the admissions process, bedside care on the medical floor, treatment in the intensive care unit, and the discharge process. Hospitalists, because they understand “how to get things done” by ancillary departments, including diagnostic and therapeutic services, often find themselves as conductors of inpatient care. Many hospitalists have developed unique proficiency in co-managing surgical cases due to expertise in peri-operative evaluation and care. Hospitalists are recognized as inpatient team leaders, facilitating and coordinating a range of support services needed to treat the patient, including nursing, case management, pharmacy, occupational/physical therapy, and social work. Hospitalists must also be effective in managing relationships with health care personnel external to the inpatient environment, including community physicians, homecare providers, extended care facilities, and visiting nurse services. Finally, hospitalists are oaen well informed about hospital processes, procedures, rules, regulations, and information systems.
As inpatient generalists, hospitalists continually treat the most common reasons for admission and have exceptional clinical knowledge of these conditions. These conditions include pneumonia, deep vein thrombosis (DVT), congestive heart failure (CHF), diabetes, end-of-life care, and other medical diagnoses. Since they treat many elderly patients, hospitalists are considered experts in managing patients with multiple co-morbidities. A related area of expertise is clinical guidelines/pathways, quality of care metrics, and practice standards. Since they spend nearly all of their time treating inpatients, hospitalists develop extraordinary familiarity with the clinical rules and tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have the experience and expertise to teach inpatient clinical skills. These skills include diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination, and oversight. Also, most hospitalists are familiar with a range of technical procedures, including insertion of central lines and arterial lines, lumbar puncture, arthrocentesis, paracentesis, and thoracentesis.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of health care industry issues. These include comprehension of the payer/insurance regulations regarding medication formularies, utilization review requirements, and other care policies. Their expertise may extend to knowledge of state and federal regulations, public health initiatives, and recently enacted or pending health care legislation. Finally, hospitalists also are often conversant in the field of health care economics, especially regarding the financial impact on hospitals of reimbursement policies, legislative initiatives, technology, etc.
The fifth sphere of hospitalist expertise combines several knowledge domains. Individual hospitalists have specialized expertise in particular fields related to hospital medicine. Some hospitalists, mostly affiliated with academic institutions, are researchers who may develop research protocols, gather data, perform statistical analyses, and write papers that may potentially become the basis of improved patient care. Other hospitalists are exceptionally experienced in management/leadership. A hospitalist may be highly qualified to manage projects (e.g., computer-based physician order entry systems, throughput initiatives, etc.),or a hospitalist could be a strategic thinker who is viewed as a key clinical member of the hospital’s management team.
As a growing specialty, hospitalists have established a proficiency in a range of disciplines and intellectual domains. They are well positioned to assume the role of educator in the hospital environment. Given the exceptional knowledge and skills needed to be a hospitalist, the Society of Hospital Medicine (SHM) is pursing an effort to standardize education and lend greater credibility to the hospitalist profession. The “core curriculum” project is currently formalizing training that will provide a solid foundation for effective clinical practice in the field of hospital medicine.
Dual Educational Tracks
As depicted in Figure 1 below, medical education activity and the ways in which knowledge is imparted fall into two categories: formal and informal. Although some overlap may occur, there are distinct characteristics attributable to both classifications.
“Formal”
Formal education refers to the traditional “teacher-learner” roles in medicine. The learner can be a medical student, resident, or fellow. Education is typically transmitted from teacher to learner (as depicted in the diagram by a solid line), with some reciprocal feedback from the learner to the teacher (dotted line). It should be noted that as the importance and value of hospital medicine programs gain recognition, fellowship programs focusing on this specialty have been established. As of August 2004, eight active hospital medicine fellowship programs exist in the United States: three in California, two in Minnesota, and one each in Ohio, Illinois, and Texas. There are also pediatric hospital medicine fellowship programs in Boston, Washington DC, Houston, and San Diego. Each program enrolls one or two fellows annually (4).
Formal education can take place in both academic medical centers and community hospitals. By definition, academic medical centers provide supervised practical training for medical students, student nurses, and/or other health care professionals, as well as residents and fellows. In many academic medical centers throughout the country, hospitalists are emerging as core teachers of inpatient medicine. A prime example is the University of California, San Francisco. In 2002, 15 faculty hospitalists served as staff for approximately two-thirds of ward-attending months, as well as all medical consults (5).
By the same token, community hospitals that have residency programs also incorporate education to some degree into their daily operations. Today, medical education places a significant burden on residents and on the professionals charged with teaching students to absorb and understand vast amounts of science and medical information. On July 1, 2003, the Accreditation Council for Graduate Medical Education (ACGME) revised the regulations governing the number of resident duty hours. These changes have forced residency programs to find viable options for imparting the required knowledge and hands-on experience to residents in fewer hours. Many consider hospitalists, by virtue of their “superior clinical and educational skills,” as representative of “the solution to the residency work duty problem.” In addition to providing excellence in teaching, hospitalists, known for their “superior clinical and educational skills,” may lead the way in creating and leading a clinical research agenda, which presents as the ultimate pedagogical experience (6).
In 2002, ACGME required six general competencies to be incorporated into residency curriculum and evaluation: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice. Hospitalists, because their practice already incorporates many aspects of these competencies, may be more effective at teaching these concepts to residents.
In the formal capacity of teacher, hospitalists can participate in attending/teaching rounds and in didactic patient-specific sessions presented in a case-based format, which provides residents with basic knowledge. As teaching supervisors, they can oversee the full range of clinical processes and procedures from the admission stage to post-discharge. Hospitalist teachers can also serve as mentors, providing a role model to residents who may be searching for direction regarding future plans. Through career counseling, hospitalists may steer learners into appropriate areas of study and training. Table 1 summarizes a series of research studies that document the positive impact hospitalists have achieved as educators in the academic environment.
Hospitalists may also have formal responsibility for developing curricula for learners in the academic environment. Whether the focus is on teaching medical students, residents, or hospitalist fellows, there is a need to determine the topics and material to be covered, incorporate them into a cogent curriculum, and update regularly to reflect the changing standards of care.
“Informal”
Informal education can be viewed as an exchange of information among stakeholders in the health care industry attempting to improve outcomes. Figure 1 depicts this as a two-way information exchange (solid arrows in both directions). As hospitalists impart knowledge to primary care physicians (PCPs), specialists/surgeons, other health care professionals (including nurses and pharmacists), patients, families, and hospital administrators, they reap benefits as well. These stakeholders stand to profit from the knowledge hospitalists can impart in daily interactions within the hospital and in less formal settings.
By working together with nurses, emergency room physicians, medical specialists, and PCPs, hospitalists can help achieve efficient and effective processes of care. The use of available software programs enables health care professionals to cooperatively exchange reliable information regarding patient management. Ongoing conversations regarding diagnoses, treatment, medications, and procedures serve to keep each member of the team educated and informed, thus ensuring more efficient delivery of care (12).
Alpesh Amin, MD, executive director of the hospitalist program at the University of California, Irvine, and chair of SHM’s Education Committee, points out that hospitalists frequently have opportunities to act as educators during case-by-case interactions with PCPs and other health care providers. “Every time you talk to a doctor about admitting or discharging a patient, it’s an opportunity to educate,” he says. In addition, “the hospitalist can apply and/or develop critical pathways and algorithms to educate others.” In the course of managing care, criteria can be developed for previously unaddressed medical issues.
This same opportunity for education extends to the hospital floor where team building serves to enlighten each member of the group providing patient care. In a reciprocal environment, both hospitalists and their medical professional “teammates” benefit from each other’s knowledge. Amin points out that specialists typically focus on one condition, while hospitalists consider the entire patient. By openly receiving the specialist’s input and advice, processing it, and then applying it to the patient, the hospitalist can develop a comprehensive approach to disease management. By considering co-morbidities and long-term care, the health care team should base decisions on “patient-centered education (13).”
Hospitalists can initiate informal in-house educational outreach, such as informational programs about medical breakthroughs, new medications, explanations of existing medical legislation, and other relevant topics. These programs can enlighten nurses, case managers, pharmacists, and other health care professionals about issues important to managing patients and/or achieving quality outcomes. The format for these programs may be one-on-one interactions (either in-person or by telephone) relating to one specific patient; formal in-service lectures; “Lunch and Learns”; pharmaceutically funded drug- or-disease-management seminars; committee or departmental meetings, and/or random written communications (sent electronically or by interoffice mail) that incorporate history and physical findings, consultations, discharge summaries, or hard-copy articles (12).
Conclusion
Because they spend so much time in the hospital, hospitalists are experts on all aspects of inpatient care: clinical, administrative, patient flow, and health care industry issues. Published research shows that academic institutions that employ hospitalists will have more satisfied and better-educated students. Common sense suggests that nurses and other stakeholders who work with hospitalists will be more informed and better-educated team members in the patient care process. Hospitalists can be the key ingredient and centerpiece in effective inpatient medical education.
References
- Yale New Haven Hospital Report, March 2004.
- Ward, Michael R. “Drug approval overregulation.” Regulation: the Review of Business and Government. Cato Institute, September 27, 2004.
- Pak, MH. Associate Professor of Medicine, Hospitalist, Director, General Medicine Consultation Service, University of Wisconsin School of Medicine, Madison, WI.
- Ranji S, Rosenman D. “Hospital medicine fellowship update.” The Hospitalist. 2004; 8 (5): 39.
- Wachter RM, Goldman L. “The hospitalist movement five years later.” JAMA.2002; 287(4): 487-94.
- Saint S, Flanders SA. “Hospitalists in teaching hospitals: opportunities but not without danger.” J Gen Intern Med. 2004; 19: 392-3.
- Chung P, Morrison J, Jin L, Levinson W, Humphrey H, Meltzer D. “Resident satisfaction on an academic hospitalist service: time to teach.” Am J Med. 2002; 112: 597-601.
- Landrigan CP, Muret-Wagstaff S, Chiang VW, Nigrin DJ, Goldmann DA, Finkelstein JA. “Effect of a pediatric hospitalist system on housestaff education and experience.” Arch Ped Adoles Med. 2002; 156 (9): 877-83.
- Hunter AJ, Desai SS, Harrison RA, Chan BK. “Medical student evaluation of the quality of hospitalist and non-hospitalist teaching faculty on inpatient medicine rotations.” Acad Med. 2004; 79:78-82.
- 10. Kulaga, ME. “The positive impact of initiation of hospitalist clinician educators.” J Gen Intern Med.2004; 19(4): 293-301.
- Hauer K, Wachter R, McCulloch C, Woo G, Auerbach A. Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations. Arch Intern Med. 2004; 164: 1866-71.
- Jones T, DO. Director of Medical Affairs, IPC, The Hospitalist Company, Mesa, AZ.
- Amin A, MD, MBA, FACP, executive director, Hospitalist Program, University of California, Irvine. Chair, Education Committee, Society of Hospital Medicine. Personal interview. October 7, 2004.
Type a medical condition or term into a search engine and watch what happens. A search on the words “diabetes” yields more than 13 million Web pages, and “pneumonia” produces another 1.65 million. In 1998, the Internet hosted approximately 5000 health-related Web sites; two years later that number quadrupled (1). Between 30,000 and 45,000 medical articles on various drug therapies are published annually. The Patent and Trademark Office issued between 2000 and 4200 drug patents each year between 1979 and 1989 (2). The National Library of Medicine reports that it adds more than 2000 journal article citations to its MEDLINE database on a daily basis. In 2003, more than 460,000 citations were entered.
Deciphering and applying this myriad of changing information is a critical activity in the medical field. Without disseminating new knowledge through ongoing education, medical practices and procedures would become outdated, and uninformed medical professionals and patients would continue to operate under misinformation that might be detrimental to health or worse.
Hospitalists as Inpatient Experts
In an inpatient setting, hospitalists are uniquely qualified to play the role of educator. They analyze and interpret a wide range of medical information to treat their patients and provide updated information to patients and their families, residents, interns, nursing staff, other health care professionals, and hospital administrators. The hospitalist can be viewed as the “hub” of educational activities in the inpatient environment, absorbing, synthesizing, and disseminating information. They are “inpatient experts” in the following five spheres of knowledge:
- patient management
- clinical knowledge
- clinical skills
- health care industry issues
- research and management/leadership (3)
Hospitalists are uniquely qualified in the sphere of patient management, efficiently and effectively guiding the patient through the mazelike inpatient environment. Most hospitalists are quite familiar with critical hospital functions and activities, including treatment in the emergency department, the admissions process, bedside care on the medical floor, treatment in the intensive care unit, and the discharge process. Hospitalists, because they understand “how to get things done” by ancillary departments, including diagnostic and therapeutic services, often find themselves as conductors of inpatient care. Many hospitalists have developed unique proficiency in co-managing surgical cases due to expertise in peri-operative evaluation and care. Hospitalists are recognized as inpatient team leaders, facilitating and coordinating a range of support services needed to treat the patient, including nursing, case management, pharmacy, occupational/physical therapy, and social work. Hospitalists must also be effective in managing relationships with health care personnel external to the inpatient environment, including community physicians, homecare providers, extended care facilities, and visiting nurse services. Finally, hospitalists are oaen well informed about hospital processes, procedures, rules, regulations, and information systems.
As inpatient generalists, hospitalists continually treat the most common reasons for admission and have exceptional clinical knowledge of these conditions. These conditions include pneumonia, deep vein thrombosis (DVT), congestive heart failure (CHF), diabetes, end-of-life care, and other medical diagnoses. Since they treat many elderly patients, hospitalists are considered experts in managing patients with multiple co-morbidities. A related area of expertise is clinical guidelines/pathways, quality of care metrics, and practice standards. Since they spend nearly all of their time treating inpatients, hospitalists develop extraordinary familiarity with the clinical rules and tools supporting the patient care process.
In addition to clinical knowledge, hospitalists have the experience and expertise to teach inpatient clinical skills. These skills include diagnosis, physical examination, discharge planning, medical chart recording, family meeting coordination, and oversight. Also, most hospitalists are familiar with a range of technical procedures, including insertion of central lines and arterial lines, lumbar puncture, arthrocentesis, paracentesis, and thoracentesis.
Hospitalists often are the most knowledgeable inpatient clinicians with regard to a wide range of health care industry issues. These include comprehension of the payer/insurance regulations regarding medication formularies, utilization review requirements, and other care policies. Their expertise may extend to knowledge of state and federal regulations, public health initiatives, and recently enacted or pending health care legislation. Finally, hospitalists also are often conversant in the field of health care economics, especially regarding the financial impact on hospitals of reimbursement policies, legislative initiatives, technology, etc.
The fifth sphere of hospitalist expertise combines several knowledge domains. Individual hospitalists have specialized expertise in particular fields related to hospital medicine. Some hospitalists, mostly affiliated with academic institutions, are researchers who may develop research protocols, gather data, perform statistical analyses, and write papers that may potentially become the basis of improved patient care. Other hospitalists are exceptionally experienced in management/leadership. A hospitalist may be highly qualified to manage projects (e.g., computer-based physician order entry systems, throughput initiatives, etc.),or a hospitalist could be a strategic thinker who is viewed as a key clinical member of the hospital’s management team.
As a growing specialty, hospitalists have established a proficiency in a range of disciplines and intellectual domains. They are well positioned to assume the role of educator in the hospital environment. Given the exceptional knowledge and skills needed to be a hospitalist, the Society of Hospital Medicine (SHM) is pursing an effort to standardize education and lend greater credibility to the hospitalist profession. The “core curriculum” project is currently formalizing training that will provide a solid foundation for effective clinical practice in the field of hospital medicine.
Dual Educational Tracks
As depicted in Figure 1 below, medical education activity and the ways in which knowledge is imparted fall into two categories: formal and informal. Although some overlap may occur, there are distinct characteristics attributable to both classifications.
“Formal”
Formal education refers to the traditional “teacher-learner” roles in medicine. The learner can be a medical student, resident, or fellow. Education is typically transmitted from teacher to learner (as depicted in the diagram by a solid line), with some reciprocal feedback from the learner to the teacher (dotted line). It should be noted that as the importance and value of hospital medicine programs gain recognition, fellowship programs focusing on this specialty have been established. As of August 2004, eight active hospital medicine fellowship programs exist in the United States: three in California, two in Minnesota, and one each in Ohio, Illinois, and Texas. There are also pediatric hospital medicine fellowship programs in Boston, Washington DC, Houston, and San Diego. Each program enrolls one or two fellows annually (4).
Formal education can take place in both academic medical centers and community hospitals. By definition, academic medical centers provide supervised practical training for medical students, student nurses, and/or other health care professionals, as well as residents and fellows. In many academic medical centers throughout the country, hospitalists are emerging as core teachers of inpatient medicine. A prime example is the University of California, San Francisco. In 2002, 15 faculty hospitalists served as staff for approximately two-thirds of ward-attending months, as well as all medical consults (5).
By the same token, community hospitals that have residency programs also incorporate education to some degree into their daily operations. Today, medical education places a significant burden on residents and on the professionals charged with teaching students to absorb and understand vast amounts of science and medical information. On July 1, 2003, the Accreditation Council for Graduate Medical Education (ACGME) revised the regulations governing the number of resident duty hours. These changes have forced residency programs to find viable options for imparting the required knowledge and hands-on experience to residents in fewer hours. Many consider hospitalists, by virtue of their “superior clinical and educational skills,” as representative of “the solution to the residency work duty problem.” In addition to providing excellence in teaching, hospitalists, known for their “superior clinical and educational skills,” may lead the way in creating and leading a clinical research agenda, which presents as the ultimate pedagogical experience (6).
In 2002, ACGME required six general competencies to be incorporated into residency curriculum and evaluation: patient care, medical knowledge, practice-based learning and improvement, interpersonal and communication skills, professionalism, and systems-based practice. Hospitalists, because their practice already incorporates many aspects of these competencies, may be more effective at teaching these concepts to residents.
In the formal capacity of teacher, hospitalists can participate in attending/teaching rounds and in didactic patient-specific sessions presented in a case-based format, which provides residents with basic knowledge. As teaching supervisors, they can oversee the full range of clinical processes and procedures from the admission stage to post-discharge. Hospitalist teachers can also serve as mentors, providing a role model to residents who may be searching for direction regarding future plans. Through career counseling, hospitalists may steer learners into appropriate areas of study and training. Table 1 summarizes a series of research studies that document the positive impact hospitalists have achieved as educators in the academic environment.
Hospitalists may also have formal responsibility for developing curricula for learners in the academic environment. Whether the focus is on teaching medical students, residents, or hospitalist fellows, there is a need to determine the topics and material to be covered, incorporate them into a cogent curriculum, and update regularly to reflect the changing standards of care.
“Informal”
Informal education can be viewed as an exchange of information among stakeholders in the health care industry attempting to improve outcomes. Figure 1 depicts this as a two-way information exchange (solid arrows in both directions). As hospitalists impart knowledge to primary care physicians (PCPs), specialists/surgeons, other health care professionals (including nurses and pharmacists), patients, families, and hospital administrators, they reap benefits as well. These stakeholders stand to profit from the knowledge hospitalists can impart in daily interactions within the hospital and in less formal settings.
By working together with nurses, emergency room physicians, medical specialists, and PCPs, hospitalists can help achieve efficient and effective processes of care. The use of available software programs enables health care professionals to cooperatively exchange reliable information regarding patient management. Ongoing conversations regarding diagnoses, treatment, medications, and procedures serve to keep each member of the team educated and informed, thus ensuring more efficient delivery of care (12).
Alpesh Amin, MD, executive director of the hospitalist program at the University of California, Irvine, and chair of SHM’s Education Committee, points out that hospitalists frequently have opportunities to act as educators during case-by-case interactions with PCPs and other health care providers. “Every time you talk to a doctor about admitting or discharging a patient, it’s an opportunity to educate,” he says. In addition, “the hospitalist can apply and/or develop critical pathways and algorithms to educate others.” In the course of managing care, criteria can be developed for previously unaddressed medical issues.
This same opportunity for education extends to the hospital floor where team building serves to enlighten each member of the group providing patient care. In a reciprocal environment, both hospitalists and their medical professional “teammates” benefit from each other’s knowledge. Amin points out that specialists typically focus on one condition, while hospitalists consider the entire patient. By openly receiving the specialist’s input and advice, processing it, and then applying it to the patient, the hospitalist can develop a comprehensive approach to disease management. By considering co-morbidities and long-term care, the health care team should base decisions on “patient-centered education (13).”
Hospitalists can initiate informal in-house educational outreach, such as informational programs about medical breakthroughs, new medications, explanations of existing medical legislation, and other relevant topics. These programs can enlighten nurses, case managers, pharmacists, and other health care professionals about issues important to managing patients and/or achieving quality outcomes. The format for these programs may be one-on-one interactions (either in-person or by telephone) relating to one specific patient; formal in-service lectures; “Lunch and Learns”; pharmaceutically funded drug- or-disease-management seminars; committee or departmental meetings, and/or random written communications (sent electronically or by interoffice mail) that incorporate history and physical findings, consultations, discharge summaries, or hard-copy articles (12).
Conclusion
Because they spend so much time in the hospital, hospitalists are experts on all aspects of inpatient care: clinical, administrative, patient flow, and health care industry issues. Published research shows that academic institutions that employ hospitalists will have more satisfied and better-educated students. Common sense suggests that nurses and other stakeholders who work with hospitalists will be more informed and better-educated team members in the patient care process. Hospitalists can be the key ingredient and centerpiece in effective inpatient medical education.
References
- Yale New Haven Hospital Report, March 2004.
- Ward, Michael R. “Drug approval overregulation.” Regulation: the Review of Business and Government. Cato Institute, September 27, 2004.
- Pak, MH. Associate Professor of Medicine, Hospitalist, Director, General Medicine Consultation Service, University of Wisconsin School of Medicine, Madison, WI.
- Ranji S, Rosenman D. “Hospital medicine fellowship update.” The Hospitalist. 2004; 8 (5): 39.
- Wachter RM, Goldman L. “The hospitalist movement five years later.” JAMA.2002; 287(4): 487-94.
- Saint S, Flanders SA. “Hospitalists in teaching hospitals: opportunities but not without danger.” J Gen Intern Med. 2004; 19: 392-3.
- Chung P, Morrison J, Jin L, Levinson W, Humphrey H, Meltzer D. “Resident satisfaction on an academic hospitalist service: time to teach.” Am J Med. 2002; 112: 597-601.
- Landrigan CP, Muret-Wagstaff S, Chiang VW, Nigrin DJ, Goldmann DA, Finkelstein JA. “Effect of a pediatric hospitalist system on housestaff education and experience.” Arch Ped Adoles Med. 2002; 156 (9): 877-83.
- Hunter AJ, Desai SS, Harrison RA, Chan BK. “Medical student evaluation of the quality of hospitalist and non-hospitalist teaching faculty on inpatient medicine rotations.” Acad Med. 2004; 79:78-82.
- 10. Kulaga, ME. “The positive impact of initiation of hospitalist clinician educators.” J Gen Intern Med.2004; 19(4): 293-301.
- Hauer K, Wachter R, McCulloch C, Woo G, Auerbach A. Effects of hospitalist attending physicians on trainee satisfaction with teaching and with internal medicine rotations. Arch Intern Med. 2004; 164: 1866-71.
- Jones T, DO. Director of Medical Affairs, IPC, The Hospitalist Company, Mesa, AZ.
- Amin A, MD, MBA, FACP, executive director, Hospitalist Program, University of California, Irvine. Chair, Education Committee, Society of Hospital Medicine. Personal interview. October 7, 2004.
Disclosure: Who, What and Whether To
The concern for public safety has spawned both regulatory (1) and legislative (2) requirements for the reporting of medical errors. The evolution of this process has caused the discussion of issues related to the full disclosure of errors to patients. While the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has stated that patients are entitled to be informed about unanticipated outcomes (3), there is concern about what should be disclosed, who should disclose, and the possibility of resulting legal action. Concern is well placed as to the latter because there is little data from facilities with disclosure policies to show that the benefit of communicating errors to patients outweighs the risk of lawsuits.
Error has been defined by JCAHO as “…an unintended act, either of omission or commission, or an act that does not achieve its intended outcome”(4). It seems obvious that a major error which causes damage, e.g., sudden death related to a treatment or the wrong surgical procedure, will trigger disclosure of at least some information. However, a recent survey (5) surprisingly revealed that even death or serious harm related to an error is not always disclosed. To the author the harmless error creates a bigger dilemma. By extension it could be argued that based on the JCAHO entitlement (3) these errors have not affected outcome and therefore do not need to be communicated to the patient. On the other hand, if informed communication is a goal then even harmless errors should be disclosed. The bottom line is that required disclosure will be dictated by regulatory bodies, state requirements (2), and the policy of each health care facility or insurance carrier.
If events creating an unanticipated outcome are to be disclosed, a communicator must be identified. The designee should be carefully chosen based on communication skill, sensitivity, and awareness of the disclosure process. “Done incorrectly, disclosure may be an admission of liability (with possibly incorrect information) to a patient”(4). It is recommended that the attending physician at the time of the error be present at the time of disclosure if he is not the spokesperson (3). The rationale is that the attending physician has an established relationship with the patient and will be the most constant link in the communication chain to the patient. This should help to provide continuity of information and discourage inaccuracies. If the information conveyed is inconsistent, this could give rise to suspicion and may be the deciding factor to pursue legal action (4).
It is paramount that the spokesperson give thoughtful attention to what is conveyed to the patient. Consensus is that the information should be factual, accurate, yet broad (3). The emphasis should be on revealing the known facts and the immediate care to be given to the patient. Events take time for complete investigation and speculation is never beneficial (4). It is suggested that one should speak slowly, use simple language, be interactive, and not overwhelm the listener (3). There should never be the placement of blame. A study reported in JAMA showed that patients believed that the way an error was revealed to them affected their response to the experience (6). It has been suggested that expressing sincere regret, in effect an apology, may help to establish trust and even avoid litigation (7). In Healing Words by Michael Woods, MD practical hints are given about what to say and how to phrase information. The goal is for the patient/family to know that the provider genuinely cares for and respects them (3).
The Joint Commission on Quality and Safety has enumerated some of the potential advantages and disadvantages of full disclosure of medical errors (1). Understandably it may be difficult for a physician to approach a person with the news that an injury or potential for injury has occurred. The JAMA study indicated that physicians would feel guilty about doing harm, disappointed about failing to practice to their own high standards, fearful about a possible lawsuit, and anxious about repercussions to their reputation (6). Of these, the most difficult hurdle may be the legal barriers to disclosure which are “entrenched in years of punitive attitudes and cultures of blame”(3).
Although there is the fear of increasing claims and lawsuits, increasing malpractice insurance, and increasing jury awards, there is no clear evidence of the impact on litigation. There has been no determination that lawsuits have increased. On the contrary it can be argued that failure to reveal medical errors “…could impair patient trust and satisfaction and increase the chances of a malpractice suit” (6). “Nearly 90 percent of jurors polled felt that there should be disclosure when there is a medical error or mistake” (4). So if disclosure is an expectation of jurors, this should give added credibility to an attending physician. There are anecdotal reports that verdict awards may be limited because of disclosure (4). In addition, the claim of concealment/“a cover up” and the request for punitive damages could be nullified by disclosure.
When disclosure is triggered by an outcome, prompt disclosure is encouraged but only after considering the following steps:
Steps:
- If your facility has a disclosure policy, become familiar with it. Be certain what is considered an “unexpected outcome.”
- Consult with risk management or your professional liability carrier.
- Carefully review the known facts and anticipate what care will be required by the patient.
- Decide who should do the disclosure.
- Decide who should be present.
- The content of the conversation should be prepared being careful not to place blame or admit liability.
- If the unexpected outcome is a recognized complication of treatment, this should be pointed out, including the fact that it was covered during the process of obtaining the patient’s consent.
- Disclosure should conclude with an offer to be available for further discussion. Do not avoid the patient or family.
- Documentation should conform to the policy of the facility or principles of risk management.
To make the theoretical more practical consider the following clinical scenarios.
- A 74 year old man weighing 63 Kg. with multiple co-morbidities (insulin dependent diabetes mellitus, congestive heart failure, coronary artery disease) underwent an anterior cervical laminectomy. His pain was difficult to control in the recovery room. Despite several doses of intravenous (IV) fentanyl, the pain level remained at 4. Over the next 6 ½ hours he received additional fentanyl, Percocet and Tylenol #3 without significant relief. The patient’s respiration rate and blood pressure remained stable. The nurse called the resident-physician and suggested Dilaudid because of the patient’s history of Demerol and morphine intolerance. An order was given for Dilaudid 2-4 mg. IV every 2‑3 hours as needed. Because of the uncontrolled pain the nurse gave 4 mg. Four hours later the patient was found pulseless and resuscitation was unsuccessful. After a discussion with the Risk Management staff, the surgeon disclosed to the family that the patient had received a large dose of narcotic but that he did not know if this contributed to the patient’s death. The family refused an autopsy initially but changed their decision with this added information.
- An infant with a congenital hypoplastic left heart syndrome underwent a modified Norwood procedure. The infant was doing well until a TPN programming error occurred. The baby received a 24 hour volume of TPN over a 2 hour period. There were symptoms of tamponade and the heart rate dropped from 140 to 43. The team opened the chest and resuscitated the infant. The TPN overload was not detected until the grossly abnormal laboratory values were reviewed. Because many hypoplastic-heart babies also have neurological problems, it will be impossible to determine the origin if any deficits become apparent. The mother was given the facts surrounding the event. The mother responded with support for the nurse in that she knew the nurse cared deeply about her child and then expressed that mistakes happen.
- A 55 year old man with a large pericardial effusion after a coronary artery bypass graft became hypotensive and was transferred to an intensive care unit. Dobutamine 7.5 mcg/kg/minute was ordered. However, dobutamine 18 mcg/kg/minute was administered. The patient did well and was discharged. The medication error was discovered on an audit. There was no indication of an associated injury. The Risk Management department recommended not disclosing to the patient. However, it was suggested that if the physician felt an obligation to inform the patient of the discrepancy, the physician should discuss the facts with a medical ethicist to work through his concerns which were separate from the legal ones.
Each of these scenarios presents a disclosure conundrum. Should there be disclosure when there is an unanticipated outcome without clear linkage to an error? How should you most appropriately disclose an obvious error with unknown damage? What is the correct action when there is a non-consequential mistake that is incidentally detected? Because each situation has unique facts and nuisances, there is no way to provide an exact roadmap.
Disclosure is a ripe topic for discussion but recognized to be in its practical and legal infancy. It is clear that education is the key to overcoming the pitfalls of this process. Outcomes should be measurable based on patient reaction. Because the lack of communication has generally been regarded as a source of patient dissatisfaction, it is reasonable to speculate that disclosure done properly should decrease litigation.
Agnes Yost can be contacted at [email protected].
References
- Kachalia A, Shojania K, Hofer T, et al. Does Full Disclosure of Medical Errors Affect Malpractice Liability? Joint Commission Journal on Quality and Safety. October 2003. Volume 29 Number 10:503-11.
- Rosental J, Booth M. Defining Reportable Adverse Events: A Guide for States Tracking Medical Errors. National Academy for State Health Policy. March 2003.
- Task Force of the American Society for Healthcare Risk Management. Monograph. Disclosure of unanticipated events: the next step in better communication with patients. May 2003. American Society for Healthcare Risk Management of the American Hospital Association.
- Popp P. How will disclosure affect future litigation? ASHRM J. Winter 2003:5-9.
- Safety Institute, Premier Inc. Survey on Disclosure Practices in Hospitals. 6th Annual NPSF Patient Safety Congress. Boston. May 3-7, 2004. (ECRI’s Healthcare Risk Control Weekly News. July 7, 2004).
- Gallagher T, Waterman A, Ebers A, et al. Patients’ and Physicians’ Attitudes Regarding the Disclosure of Medical Errors. JAMA. 2003;289:1001-1007.
- Apologies lead to trust, healing, help avoid litigation, new book says. Medical Liability Monitor. July, 2004. Vol 29, No. 7.
The concern for public safety has spawned both regulatory (1) and legislative (2) requirements for the reporting of medical errors. The evolution of this process has caused the discussion of issues related to the full disclosure of errors to patients. While the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has stated that patients are entitled to be informed about unanticipated outcomes (3), there is concern about what should be disclosed, who should disclose, and the possibility of resulting legal action. Concern is well placed as to the latter because there is little data from facilities with disclosure policies to show that the benefit of communicating errors to patients outweighs the risk of lawsuits.
Error has been defined by JCAHO as “…an unintended act, either of omission or commission, or an act that does not achieve its intended outcome”(4). It seems obvious that a major error which causes damage, e.g., sudden death related to a treatment or the wrong surgical procedure, will trigger disclosure of at least some information. However, a recent survey (5) surprisingly revealed that even death or serious harm related to an error is not always disclosed. To the author the harmless error creates a bigger dilemma. By extension it could be argued that based on the JCAHO entitlement (3) these errors have not affected outcome and therefore do not need to be communicated to the patient. On the other hand, if informed communication is a goal then even harmless errors should be disclosed. The bottom line is that required disclosure will be dictated by regulatory bodies, state requirements (2), and the policy of each health care facility or insurance carrier.
If events creating an unanticipated outcome are to be disclosed, a communicator must be identified. The designee should be carefully chosen based on communication skill, sensitivity, and awareness of the disclosure process. “Done incorrectly, disclosure may be an admission of liability (with possibly incorrect information) to a patient”(4). It is recommended that the attending physician at the time of the error be present at the time of disclosure if he is not the spokesperson (3). The rationale is that the attending physician has an established relationship with the patient and will be the most constant link in the communication chain to the patient. This should help to provide continuity of information and discourage inaccuracies. If the information conveyed is inconsistent, this could give rise to suspicion and may be the deciding factor to pursue legal action (4).
It is paramount that the spokesperson give thoughtful attention to what is conveyed to the patient. Consensus is that the information should be factual, accurate, yet broad (3). The emphasis should be on revealing the known facts and the immediate care to be given to the patient. Events take time for complete investigation and speculation is never beneficial (4). It is suggested that one should speak slowly, use simple language, be interactive, and not overwhelm the listener (3). There should never be the placement of blame. A study reported in JAMA showed that patients believed that the way an error was revealed to them affected their response to the experience (6). It has been suggested that expressing sincere regret, in effect an apology, may help to establish trust and even avoid litigation (7). In Healing Words by Michael Woods, MD practical hints are given about what to say and how to phrase information. The goal is for the patient/family to know that the provider genuinely cares for and respects them (3).
The Joint Commission on Quality and Safety has enumerated some of the potential advantages and disadvantages of full disclosure of medical errors (1). Understandably it may be difficult for a physician to approach a person with the news that an injury or potential for injury has occurred. The JAMA study indicated that physicians would feel guilty about doing harm, disappointed about failing to practice to their own high standards, fearful about a possible lawsuit, and anxious about repercussions to their reputation (6). Of these, the most difficult hurdle may be the legal barriers to disclosure which are “entrenched in years of punitive attitudes and cultures of blame”(3).
Although there is the fear of increasing claims and lawsuits, increasing malpractice insurance, and increasing jury awards, there is no clear evidence of the impact on litigation. There has been no determination that lawsuits have increased. On the contrary it can be argued that failure to reveal medical errors “…could impair patient trust and satisfaction and increase the chances of a malpractice suit” (6). “Nearly 90 percent of jurors polled felt that there should be disclosure when there is a medical error or mistake” (4). So if disclosure is an expectation of jurors, this should give added credibility to an attending physician. There are anecdotal reports that verdict awards may be limited because of disclosure (4). In addition, the claim of concealment/“a cover up” and the request for punitive damages could be nullified by disclosure.
When disclosure is triggered by an outcome, prompt disclosure is encouraged but only after considering the following steps:
Steps:
- If your facility has a disclosure policy, become familiar with it. Be certain what is considered an “unexpected outcome.”
- Consult with risk management or your professional liability carrier.
- Carefully review the known facts and anticipate what care will be required by the patient.
- Decide who should do the disclosure.
- Decide who should be present.
- The content of the conversation should be prepared being careful not to place blame or admit liability.
- If the unexpected outcome is a recognized complication of treatment, this should be pointed out, including the fact that it was covered during the process of obtaining the patient’s consent.
- Disclosure should conclude with an offer to be available for further discussion. Do not avoid the patient or family.
- Documentation should conform to the policy of the facility or principles of risk management.
To make the theoretical more practical consider the following clinical scenarios.
- A 74 year old man weighing 63 Kg. with multiple co-morbidities (insulin dependent diabetes mellitus, congestive heart failure, coronary artery disease) underwent an anterior cervical laminectomy. His pain was difficult to control in the recovery room. Despite several doses of intravenous (IV) fentanyl, the pain level remained at 4. Over the next 6 ½ hours he received additional fentanyl, Percocet and Tylenol #3 without significant relief. The patient’s respiration rate and blood pressure remained stable. The nurse called the resident-physician and suggested Dilaudid because of the patient’s history of Demerol and morphine intolerance. An order was given for Dilaudid 2-4 mg. IV every 2‑3 hours as needed. Because of the uncontrolled pain the nurse gave 4 mg. Four hours later the patient was found pulseless and resuscitation was unsuccessful. After a discussion with the Risk Management staff, the surgeon disclosed to the family that the patient had received a large dose of narcotic but that he did not know if this contributed to the patient’s death. The family refused an autopsy initially but changed their decision with this added information.
- An infant with a congenital hypoplastic left heart syndrome underwent a modified Norwood procedure. The infant was doing well until a TPN programming error occurred. The baby received a 24 hour volume of TPN over a 2 hour period. There were symptoms of tamponade and the heart rate dropped from 140 to 43. The team opened the chest and resuscitated the infant. The TPN overload was not detected until the grossly abnormal laboratory values were reviewed. Because many hypoplastic-heart babies also have neurological problems, it will be impossible to determine the origin if any deficits become apparent. The mother was given the facts surrounding the event. The mother responded with support for the nurse in that she knew the nurse cared deeply about her child and then expressed that mistakes happen.
- A 55 year old man with a large pericardial effusion after a coronary artery bypass graft became hypotensive and was transferred to an intensive care unit. Dobutamine 7.5 mcg/kg/minute was ordered. However, dobutamine 18 mcg/kg/minute was administered. The patient did well and was discharged. The medication error was discovered on an audit. There was no indication of an associated injury. The Risk Management department recommended not disclosing to the patient. However, it was suggested that if the physician felt an obligation to inform the patient of the discrepancy, the physician should discuss the facts with a medical ethicist to work through his concerns which were separate from the legal ones.
Each of these scenarios presents a disclosure conundrum. Should there be disclosure when there is an unanticipated outcome without clear linkage to an error? How should you most appropriately disclose an obvious error with unknown damage? What is the correct action when there is a non-consequential mistake that is incidentally detected? Because each situation has unique facts and nuisances, there is no way to provide an exact roadmap.
Disclosure is a ripe topic for discussion but recognized to be in its practical and legal infancy. It is clear that education is the key to overcoming the pitfalls of this process. Outcomes should be measurable based on patient reaction. Because the lack of communication has generally been regarded as a source of patient dissatisfaction, it is reasonable to speculate that disclosure done properly should decrease litigation.
Agnes Yost can be contacted at [email protected].
References
- Kachalia A, Shojania K, Hofer T, et al. Does Full Disclosure of Medical Errors Affect Malpractice Liability? Joint Commission Journal on Quality and Safety. October 2003. Volume 29 Number 10:503-11.
- Rosental J, Booth M. Defining Reportable Adverse Events: A Guide for States Tracking Medical Errors. National Academy for State Health Policy. March 2003.
- Task Force of the American Society for Healthcare Risk Management. Monograph. Disclosure of unanticipated events: the next step in better communication with patients. May 2003. American Society for Healthcare Risk Management of the American Hospital Association.
- Popp P. How will disclosure affect future litigation? ASHRM J. Winter 2003:5-9.
- Safety Institute, Premier Inc. Survey on Disclosure Practices in Hospitals. 6th Annual NPSF Patient Safety Congress. Boston. May 3-7, 2004. (ECRI’s Healthcare Risk Control Weekly News. July 7, 2004).
- Gallagher T, Waterman A, Ebers A, et al. Patients’ and Physicians’ Attitudes Regarding the Disclosure of Medical Errors. JAMA. 2003;289:1001-1007.
- Apologies lead to trust, healing, help avoid litigation, new book says. Medical Liability Monitor. July, 2004. Vol 29, No. 7.
The concern for public safety has spawned both regulatory (1) and legislative (2) requirements for the reporting of medical errors. The evolution of this process has caused the discussion of issues related to the full disclosure of errors to patients. While the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has stated that patients are entitled to be informed about unanticipated outcomes (3), there is concern about what should be disclosed, who should disclose, and the possibility of resulting legal action. Concern is well placed as to the latter because there is little data from facilities with disclosure policies to show that the benefit of communicating errors to patients outweighs the risk of lawsuits.
Error has been defined by JCAHO as “…an unintended act, either of omission or commission, or an act that does not achieve its intended outcome”(4). It seems obvious that a major error which causes damage, e.g., sudden death related to a treatment or the wrong surgical procedure, will trigger disclosure of at least some information. However, a recent survey (5) surprisingly revealed that even death or serious harm related to an error is not always disclosed. To the author the harmless error creates a bigger dilemma. By extension it could be argued that based on the JCAHO entitlement (3) these errors have not affected outcome and therefore do not need to be communicated to the patient. On the other hand, if informed communication is a goal then even harmless errors should be disclosed. The bottom line is that required disclosure will be dictated by regulatory bodies, state requirements (2), and the policy of each health care facility or insurance carrier.
If events creating an unanticipated outcome are to be disclosed, a communicator must be identified. The designee should be carefully chosen based on communication skill, sensitivity, and awareness of the disclosure process. “Done incorrectly, disclosure may be an admission of liability (with possibly incorrect information) to a patient”(4). It is recommended that the attending physician at the time of the error be present at the time of disclosure if he is not the spokesperson (3). The rationale is that the attending physician has an established relationship with the patient and will be the most constant link in the communication chain to the patient. This should help to provide continuity of information and discourage inaccuracies. If the information conveyed is inconsistent, this could give rise to suspicion and may be the deciding factor to pursue legal action (4).
It is paramount that the spokesperson give thoughtful attention to what is conveyed to the patient. Consensus is that the information should be factual, accurate, yet broad (3). The emphasis should be on revealing the known facts and the immediate care to be given to the patient. Events take time for complete investigation and speculation is never beneficial (4). It is suggested that one should speak slowly, use simple language, be interactive, and not overwhelm the listener (3). There should never be the placement of blame. A study reported in JAMA showed that patients believed that the way an error was revealed to them affected their response to the experience (6). It has been suggested that expressing sincere regret, in effect an apology, may help to establish trust and even avoid litigation (7). In Healing Words by Michael Woods, MD practical hints are given about what to say and how to phrase information. The goal is for the patient/family to know that the provider genuinely cares for and respects them (3).
The Joint Commission on Quality and Safety has enumerated some of the potential advantages and disadvantages of full disclosure of medical errors (1). Understandably it may be difficult for a physician to approach a person with the news that an injury or potential for injury has occurred. The JAMA study indicated that physicians would feel guilty about doing harm, disappointed about failing to practice to their own high standards, fearful about a possible lawsuit, and anxious about repercussions to their reputation (6). Of these, the most difficult hurdle may be the legal barriers to disclosure which are “entrenched in years of punitive attitudes and cultures of blame”(3).
Although there is the fear of increasing claims and lawsuits, increasing malpractice insurance, and increasing jury awards, there is no clear evidence of the impact on litigation. There has been no determination that lawsuits have increased. On the contrary it can be argued that failure to reveal medical errors “…could impair patient trust and satisfaction and increase the chances of a malpractice suit” (6). “Nearly 90 percent of jurors polled felt that there should be disclosure when there is a medical error or mistake” (4). So if disclosure is an expectation of jurors, this should give added credibility to an attending physician. There are anecdotal reports that verdict awards may be limited because of disclosure (4). In addition, the claim of concealment/“a cover up” and the request for punitive damages could be nullified by disclosure.
When disclosure is triggered by an outcome, prompt disclosure is encouraged but only after considering the following steps:
Steps:
- If your facility has a disclosure policy, become familiar with it. Be certain what is considered an “unexpected outcome.”
- Consult with risk management or your professional liability carrier.
- Carefully review the known facts and anticipate what care will be required by the patient.
- Decide who should do the disclosure.
- Decide who should be present.
- The content of the conversation should be prepared being careful not to place blame or admit liability.
- If the unexpected outcome is a recognized complication of treatment, this should be pointed out, including the fact that it was covered during the process of obtaining the patient’s consent.
- Disclosure should conclude with an offer to be available for further discussion. Do not avoid the patient or family.
- Documentation should conform to the policy of the facility or principles of risk management.
To make the theoretical more practical consider the following clinical scenarios.
- A 74 year old man weighing 63 Kg. with multiple co-morbidities (insulin dependent diabetes mellitus, congestive heart failure, coronary artery disease) underwent an anterior cervical laminectomy. His pain was difficult to control in the recovery room. Despite several doses of intravenous (IV) fentanyl, the pain level remained at 4. Over the next 6 ½ hours he received additional fentanyl, Percocet and Tylenol #3 without significant relief. The patient’s respiration rate and blood pressure remained stable. The nurse called the resident-physician and suggested Dilaudid because of the patient’s history of Demerol and morphine intolerance. An order was given for Dilaudid 2-4 mg. IV every 2‑3 hours as needed. Because of the uncontrolled pain the nurse gave 4 mg. Four hours later the patient was found pulseless and resuscitation was unsuccessful. After a discussion with the Risk Management staff, the surgeon disclosed to the family that the patient had received a large dose of narcotic but that he did not know if this contributed to the patient’s death. The family refused an autopsy initially but changed their decision with this added information.
- An infant with a congenital hypoplastic left heart syndrome underwent a modified Norwood procedure. The infant was doing well until a TPN programming error occurred. The baby received a 24 hour volume of TPN over a 2 hour period. There were symptoms of tamponade and the heart rate dropped from 140 to 43. The team opened the chest and resuscitated the infant. The TPN overload was not detected until the grossly abnormal laboratory values were reviewed. Because many hypoplastic-heart babies also have neurological problems, it will be impossible to determine the origin if any deficits become apparent. The mother was given the facts surrounding the event. The mother responded with support for the nurse in that she knew the nurse cared deeply about her child and then expressed that mistakes happen.
- A 55 year old man with a large pericardial effusion after a coronary artery bypass graft became hypotensive and was transferred to an intensive care unit. Dobutamine 7.5 mcg/kg/minute was ordered. However, dobutamine 18 mcg/kg/minute was administered. The patient did well and was discharged. The medication error was discovered on an audit. There was no indication of an associated injury. The Risk Management department recommended not disclosing to the patient. However, it was suggested that if the physician felt an obligation to inform the patient of the discrepancy, the physician should discuss the facts with a medical ethicist to work through his concerns which were separate from the legal ones.
Each of these scenarios presents a disclosure conundrum. Should there be disclosure when there is an unanticipated outcome without clear linkage to an error? How should you most appropriately disclose an obvious error with unknown damage? What is the correct action when there is a non-consequential mistake that is incidentally detected? Because each situation has unique facts and nuisances, there is no way to provide an exact roadmap.
Disclosure is a ripe topic for discussion but recognized to be in its practical and legal infancy. It is clear that education is the key to overcoming the pitfalls of this process. Outcomes should be measurable based on patient reaction. Because the lack of communication has generally been regarded as a source of patient dissatisfaction, it is reasonable to speculate that disclosure done properly should decrease litigation.
Agnes Yost can be contacted at [email protected].
References
- Kachalia A, Shojania K, Hofer T, et al. Does Full Disclosure of Medical Errors Affect Malpractice Liability? Joint Commission Journal on Quality and Safety. October 2003. Volume 29 Number 10:503-11.
- Rosental J, Booth M. Defining Reportable Adverse Events: A Guide for States Tracking Medical Errors. National Academy for State Health Policy. March 2003.
- Task Force of the American Society for Healthcare Risk Management. Monograph. Disclosure of unanticipated events: the next step in better communication with patients. May 2003. American Society for Healthcare Risk Management of the American Hospital Association.
- Popp P. How will disclosure affect future litigation? ASHRM J. Winter 2003:5-9.
- Safety Institute, Premier Inc. Survey on Disclosure Practices in Hospitals. 6th Annual NPSF Patient Safety Congress. Boston. May 3-7, 2004. (ECRI’s Healthcare Risk Control Weekly News. July 7, 2004).
- Gallagher T, Waterman A, Ebers A, et al. Patients’ and Physicians’ Attitudes Regarding the Disclosure of Medical Errors. JAMA. 2003;289:1001-1007.
- Apologies lead to trust, healing, help avoid litigation, new book says. Medical Liability Monitor. July, 2004. Vol 29, No. 7.
Sixth Annual Southern Regional Meeting Recap
Distinguished by the high quality that has become the trademark of the Society of Hospital Medicine’s meetings, the Sixth Annual Southern Regional Meeting began with a Practice Management pre-course directed by Joseph Miller. The course served as a template of SHM’s prospective educational efforts and generated immense enthusiasm from aTendees. Addressing the spectrum of hospital practices, pioneers of the specialty including Drs. Win Whitcomb and John Nelson presented topics ranging from recruitment to retention. Roger A. Heroux, PhD and Mr. Martin B. Buser emphasized practical means by which hospitalists can demonstrate value and how best to offer “proof” of return-on-investment in hospital practices.
For the first time the Southern Regional Meeting took place outside of Atlanta and with a new co-sponsor, Mayo Clinic. Orlando played host to the near‑record attendance conference that occurred on Walt Disney World property at the Wyndham Palace. The conference also included a new emphasis on families, offering a new spouse/family program that gave attendees and their families discounted tickets to parks and ideas for outings. The overwhelming success of the program suggested this may be a productive addition to other SHM meetings.
Day one of the main conference stressed the latest evidence in hospital medicine. The first plenary sessions focused on the most common cardiac hospital admissions: acute coronary syndromes (Dr. Keith Oken), atrial fibrillation (Dr. Joseph Blackshear), and diastolic heart failure (Dr. Eugene Page).
Given the increasing importance of the hospitalist in management of patients in the perioperative period, the conference then focused on unique aspects of pre-operative and intra-operative care. Perennial favorite Dr. Geno Merli presented data on the (lack of) evidence supporting most preoperative testing, while newcomers Drs. Neil Feinglass and Bruce Leone presented anesthesiologists’ perspectives on the impact of hospitalists on the surgical patient.

Hospitalists are increasingly on the frontlines of trying to minimize error and improve outcomes. Accordingly, early aaernoon topics looked at two issues in this regard: Heparin-Induced Thrombocytopenia (Dr. Jay Herman) and Improving Outcomes in Cardiac Arrest (Dr. Jason Persoff). Then attendees were able to choose from a spectrum of breakout sessions and workshops that ranged from the integration of nurse practitioners/PAs (Dr. Mitchell Wilson) to performing clinical research (Dr. Mike Picco). Dr. Merli held his popular discussion on anticoagulation in the perioperative period. Dr. Bruce Mitchell and Dr. Jared Morton spearheaded two sessions focusing on minorities in hospital medicine and on the unique aspects of hospitalists on physicians in training, respectively. Finally, Dr. Larry Wellikson provided practical information on how to get a job in hospital medicine as one of the closing sessions of the day.
Dr. Beril Cakir chaired the abstract competition at the end of the first day. Thirteen abstracts from over 6 institutions were presented. Dr. Greg Pendell, from Mayo Clinic Jacksonville, was awarded first place and the opportunity to present in April at the Annual Session in Chicago.
Day two built on the theme of hospital medicine’s diversity, with topics ranged from Emerging Infectious Threats (Dr. Walter Hellinger) and the CDC’s Mandate to Reduce Antimicrobial Resistance (Dr. Dan Dressler) to Status Epilepticus (Dr. David Chabolla). Dr. Amir Jaffer spoke about the Cleveland Clinic’s successful preoperative care clinic, while Dr. Archana Roy reviewed the most infl uential research articles to impact the specialty over the past year.
As a leader in advocating tighter glucose control in inpatients, Dr. Guillermo Umpierrez spoke about the paradigm change regarding what is truly considered “good” control of blood sugar in inpatients with diabetes, emphasizing how glucose control can impact mortality. The plenary session closed with an exciting update on the emergence of the specialty of Hospital Medicine by Dr. Larry Wellikson, SHM’s CEO.
Emphasizing the humanity of hospitalists, afternoon workshops included a special workshop by pediatrician Dr. Susie Gerik about the Spiritual Review of Systems, followed by Dr. James Lyman’s workshop on End-of-Life Opportunities for Hospitalists. Both spoke about the emotional aspects of caring for adult patients with severe illness and in those for whom hospice care is the mainstay of therapy.
Dr. Jeff Garland led a standing room only group through various approaches to oxygenation and ventilation in acutely ill patients. Dr. Solomon Tafari presented an evidence-based approach to the unconscious patient, and Dr. Mellena Bridges went over several CT scan case studies. Dr. Mike Picco reviewed the complexity of medical statistics, while Dr. Guillermo Umpierrez gave his perennially popular workshop on endocrine emergencies.
The success of any conference lies not only in the contribution of those who stand before podium, but in the countless movements and machinations that occur behind the scenes to allow a conference to operate so flawlessly. To that end, I would like to commend the herculean job performed by the SHM staff, particularly Angela Musial, Erica Pearson, and Jane Mihelic, whose savvy and dedication gave conference goers a highly organized, orchestrated CME event. The sheer breadth and scope of the speakers and topics presented stem from the creativity and enthusiasm of the conference’s committee members, with special mention to Drs. Donna Dean (the highly under recognized but not under appreciated assistant course director), Ryan McNamara, Mitchell Wilson, Patrick Cawley, Beril Cakir, and Ron Angus.
I would like to close with special acknowledgement of those whose great vision and leadership have guided this annual event and served as a focal point for SHM’s emergence: Dr. Mark Williams and Dr. Larry Wellikson. I thank you both.
Dr. Williams and Emory University plan to continue the annual autumn meeting, which will return to Atlanta in November, 2005.
Distinguished by the high quality that has become the trademark of the Society of Hospital Medicine’s meetings, the Sixth Annual Southern Regional Meeting began with a Practice Management pre-course directed by Joseph Miller. The course served as a template of SHM’s prospective educational efforts and generated immense enthusiasm from aTendees. Addressing the spectrum of hospital practices, pioneers of the specialty including Drs. Win Whitcomb and John Nelson presented topics ranging from recruitment to retention. Roger A. Heroux, PhD and Mr. Martin B. Buser emphasized practical means by which hospitalists can demonstrate value and how best to offer “proof” of return-on-investment in hospital practices.
For the first time the Southern Regional Meeting took place outside of Atlanta and with a new co-sponsor, Mayo Clinic. Orlando played host to the near‑record attendance conference that occurred on Walt Disney World property at the Wyndham Palace. The conference also included a new emphasis on families, offering a new spouse/family program that gave attendees and their families discounted tickets to parks and ideas for outings. The overwhelming success of the program suggested this may be a productive addition to other SHM meetings.
Day one of the main conference stressed the latest evidence in hospital medicine. The first plenary sessions focused on the most common cardiac hospital admissions: acute coronary syndromes (Dr. Keith Oken), atrial fibrillation (Dr. Joseph Blackshear), and diastolic heart failure (Dr. Eugene Page).
Given the increasing importance of the hospitalist in management of patients in the perioperative period, the conference then focused on unique aspects of pre-operative and intra-operative care. Perennial favorite Dr. Geno Merli presented data on the (lack of) evidence supporting most preoperative testing, while newcomers Drs. Neil Feinglass and Bruce Leone presented anesthesiologists’ perspectives on the impact of hospitalists on the surgical patient.
Hospitalists are increasingly on the frontlines of trying to minimize error and improve outcomes. Accordingly, early aaernoon topics looked at two issues in this regard: Heparin-Induced Thrombocytopenia (Dr. Jay Herman) and Improving Outcomes in Cardiac Arrest (Dr. Jason Persoff). Then attendees were able to choose from a spectrum of breakout sessions and workshops that ranged from the integration of nurse practitioners/PAs (Dr. Mitchell Wilson) to performing clinical research (Dr. Mike Picco). Dr. Merli held his popular discussion on anticoagulation in the perioperative period. Dr. Bruce Mitchell and Dr. Jared Morton spearheaded two sessions focusing on minorities in hospital medicine and on the unique aspects of hospitalists on physicians in training, respectively. Finally, Dr. Larry Wellikson provided practical information on how to get a job in hospital medicine as one of the closing sessions of the day.
Dr. Beril Cakir chaired the abstract competition at the end of the first day. Thirteen abstracts from over 6 institutions were presented. Dr. Greg Pendell, from Mayo Clinic Jacksonville, was awarded first place and the opportunity to present in April at the Annual Session in Chicago.
Day two built on the theme of hospital medicine’s diversity, with topics ranged from Emerging Infectious Threats (Dr. Walter Hellinger) and the CDC’s Mandate to Reduce Antimicrobial Resistance (Dr. Dan Dressler) to Status Epilepticus (Dr. David Chabolla). Dr. Amir Jaffer spoke about the Cleveland Clinic’s successful preoperative care clinic, while Dr. Archana Roy reviewed the most infl uential research articles to impact the specialty over the past year.
As a leader in advocating tighter glucose control in inpatients, Dr. Guillermo Umpierrez spoke about the paradigm change regarding what is truly considered “good” control of blood sugar in inpatients with diabetes, emphasizing how glucose control can impact mortality. The plenary session closed with an exciting update on the emergence of the specialty of Hospital Medicine by Dr. Larry Wellikson, SHM’s CEO.
Emphasizing the humanity of hospitalists, afternoon workshops included a special workshop by pediatrician Dr. Susie Gerik about the Spiritual Review of Systems, followed by Dr. James Lyman’s workshop on End-of-Life Opportunities for Hospitalists. Both spoke about the emotional aspects of caring for adult patients with severe illness and in those for whom hospice care is the mainstay of therapy.
Dr. Jeff Garland led a standing room only group through various approaches to oxygenation and ventilation in acutely ill patients. Dr. Solomon Tafari presented an evidence-based approach to the unconscious patient, and Dr. Mellena Bridges went over several CT scan case studies. Dr. Mike Picco reviewed the complexity of medical statistics, while Dr. Guillermo Umpierrez gave his perennially popular workshop on endocrine emergencies.
The success of any conference lies not only in the contribution of those who stand before podium, but in the countless movements and machinations that occur behind the scenes to allow a conference to operate so flawlessly. To that end, I would like to commend the herculean job performed by the SHM staff, particularly Angela Musial, Erica Pearson, and Jane Mihelic, whose savvy and dedication gave conference goers a highly organized, orchestrated CME event. The sheer breadth and scope of the speakers and topics presented stem from the creativity and enthusiasm of the conference’s committee members, with special mention to Drs. Donna Dean (the highly under recognized but not under appreciated assistant course director), Ryan McNamara, Mitchell Wilson, Patrick Cawley, Beril Cakir, and Ron Angus.
I would like to close with special acknowledgement of those whose great vision and leadership have guided this annual event and served as a focal point for SHM’s emergence: Dr. Mark Williams and Dr. Larry Wellikson. I thank you both.
Dr. Williams and Emory University plan to continue the annual autumn meeting, which will return to Atlanta in November, 2005.
Distinguished by the high quality that has become the trademark of the Society of Hospital Medicine’s meetings, the Sixth Annual Southern Regional Meeting began with a Practice Management pre-course directed by Joseph Miller. The course served as a template of SHM’s prospective educational efforts and generated immense enthusiasm from aTendees. Addressing the spectrum of hospital practices, pioneers of the specialty including Drs. Win Whitcomb and John Nelson presented topics ranging from recruitment to retention. Roger A. Heroux, PhD and Mr. Martin B. Buser emphasized practical means by which hospitalists can demonstrate value and how best to offer “proof” of return-on-investment in hospital practices.
For the first time the Southern Regional Meeting took place outside of Atlanta and with a new co-sponsor, Mayo Clinic. Orlando played host to the near‑record attendance conference that occurred on Walt Disney World property at the Wyndham Palace. The conference also included a new emphasis on families, offering a new spouse/family program that gave attendees and their families discounted tickets to parks and ideas for outings. The overwhelming success of the program suggested this may be a productive addition to other SHM meetings.
Day one of the main conference stressed the latest evidence in hospital medicine. The first plenary sessions focused on the most common cardiac hospital admissions: acute coronary syndromes (Dr. Keith Oken), atrial fibrillation (Dr. Joseph Blackshear), and diastolic heart failure (Dr. Eugene Page).
Given the increasing importance of the hospitalist in management of patients in the perioperative period, the conference then focused on unique aspects of pre-operative and intra-operative care. Perennial favorite Dr. Geno Merli presented data on the (lack of) evidence supporting most preoperative testing, while newcomers Drs. Neil Feinglass and Bruce Leone presented anesthesiologists’ perspectives on the impact of hospitalists on the surgical patient.
Hospitalists are increasingly on the frontlines of trying to minimize error and improve outcomes. Accordingly, early aaernoon topics looked at two issues in this regard: Heparin-Induced Thrombocytopenia (Dr. Jay Herman) and Improving Outcomes in Cardiac Arrest (Dr. Jason Persoff). Then attendees were able to choose from a spectrum of breakout sessions and workshops that ranged from the integration of nurse practitioners/PAs (Dr. Mitchell Wilson) to performing clinical research (Dr. Mike Picco). Dr. Merli held his popular discussion on anticoagulation in the perioperative period. Dr. Bruce Mitchell and Dr. Jared Morton spearheaded two sessions focusing on minorities in hospital medicine and on the unique aspects of hospitalists on physicians in training, respectively. Finally, Dr. Larry Wellikson provided practical information on how to get a job in hospital medicine as one of the closing sessions of the day.
Dr. Beril Cakir chaired the abstract competition at the end of the first day. Thirteen abstracts from over 6 institutions were presented. Dr. Greg Pendell, from Mayo Clinic Jacksonville, was awarded first place and the opportunity to present in April at the Annual Session in Chicago.
Day two built on the theme of hospital medicine’s diversity, with topics ranged from Emerging Infectious Threats (Dr. Walter Hellinger) and the CDC’s Mandate to Reduce Antimicrobial Resistance (Dr. Dan Dressler) to Status Epilepticus (Dr. David Chabolla). Dr. Amir Jaffer spoke about the Cleveland Clinic’s successful preoperative care clinic, while Dr. Archana Roy reviewed the most infl uential research articles to impact the specialty over the past year.
As a leader in advocating tighter glucose control in inpatients, Dr. Guillermo Umpierrez spoke about the paradigm change regarding what is truly considered “good” control of blood sugar in inpatients with diabetes, emphasizing how glucose control can impact mortality. The plenary session closed with an exciting update on the emergence of the specialty of Hospital Medicine by Dr. Larry Wellikson, SHM’s CEO.
Emphasizing the humanity of hospitalists, afternoon workshops included a special workshop by pediatrician Dr. Susie Gerik about the Spiritual Review of Systems, followed by Dr. James Lyman’s workshop on End-of-Life Opportunities for Hospitalists. Both spoke about the emotional aspects of caring for adult patients with severe illness and in those for whom hospice care is the mainstay of therapy.
Dr. Jeff Garland led a standing room only group through various approaches to oxygenation and ventilation in acutely ill patients. Dr. Solomon Tafari presented an evidence-based approach to the unconscious patient, and Dr. Mellena Bridges went over several CT scan case studies. Dr. Mike Picco reviewed the complexity of medical statistics, while Dr. Guillermo Umpierrez gave his perennially popular workshop on endocrine emergencies.
The success of any conference lies not only in the contribution of those who stand before podium, but in the countless movements and machinations that occur behind the scenes to allow a conference to operate so flawlessly. To that end, I would like to commend the herculean job performed by the SHM staff, particularly Angela Musial, Erica Pearson, and Jane Mihelic, whose savvy and dedication gave conference goers a highly organized, orchestrated CME event. The sheer breadth and scope of the speakers and topics presented stem from the creativity and enthusiasm of the conference’s committee members, with special mention to Drs. Donna Dean (the highly under recognized but not under appreciated assistant course director), Ryan McNamara, Mitchell Wilson, Patrick Cawley, Beril Cakir, and Ron Angus.
I would like to close with special acknowledgement of those whose great vision and leadership have guided this annual event and served as a focal point for SHM’s emergence: Dr. Mark Williams and Dr. Larry Wellikson. I thank you both.
Dr. Williams and Emory University plan to continue the annual autumn meeting, which will return to Atlanta in November, 2005.
Hospital Medicine: Growing Toward Specialty Status

When the Society of Hospital Medicine was very young and headquartered in the home computers of myself and Win Whitcomb (and known then as the National Association of Inpatient Physicians), I spent a lot of time thinking about the future of our field. Whether we would, or should, become a recognized specialty was one of the things I particularly enjoyed thinking about. Believing the history of Emergency Medicine might provide some insights for Hospital Medicine, I tracked down Dr. John Wiegenstein, who played a major role in the founding of the American College of Emergency Physicians (ACEP) in 1968, served as the group’s first president, and helped mold Emergency Medicine into a distinct specialty recognized by the American Board of Medical Specialties.
The parallels between the first few years of Emergency Medicine and Hospital Medicine are striking (see Table 1, milestones in Emergency Medicine). Dr. Wiegenstien told me that there was tremendous enthusiasm among early ACEP members for the opportunity to create a new specialty and invent the systems of care in the emergency room (now department) that would best serve patients and the overall enterprise of health care. At the time of ACEP’s founding, there was no group that was primarily devoted to ensuring that emergency rooms were held to high standards of care and operated efficiently. In the late 1960’s, when ACEP sought to fill this void, Dr. Wiegenstein said that the medical leaders of the day in the AMA and other organizations, tended to smile patronizingly, pat him on the shoulder figuratively, and suggest that it would be fine to busy himself with such a project since it would keep him and his colleagues out of the way of those who were doing the important things in medicine. After all, the leaders of the day reasoned, there were already existing specialties with more expertise at any kind of care that an ER doctor might provide, so creating a new breed of doctor or specialty seemed like it would be an unnecessary duplication of existing specialties. Yet Dr. Wiegenstein and his colleagues did exactly what they set out to do, and today there is probably no one who questions the importance of the contribution of Emergency Medicine to our healthcare system, and its status as a distinct specialty.
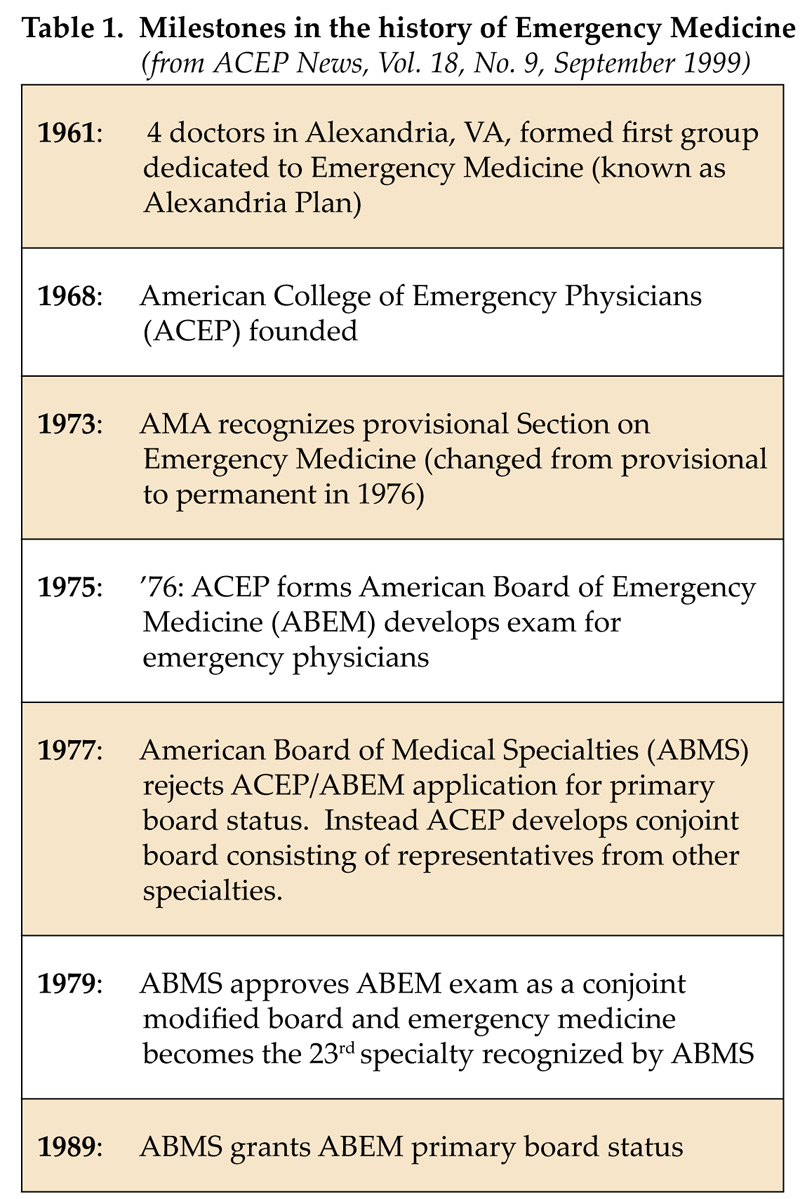
The case for Hospital Medicine becoming a recognized specialty or subspecialty.
The question for those of us in Hospital Medicine is should we, and can we, be about doing the same thing in our field that has happened, and is ongoing, in Emergency Medicine? I suspect nearly all hospitalists believe the answer is yes, and I sense growing support for this goal from those in nearly all other fields in medicine. And I think an important factor in ensuring success is to think of ourselves as a distinct specialty or subspecialty.
In fact, Hospital Medicine functions as a distinct specialty in many respects already. There is a growing body of distinct literature about clinical and operational aspects of hospitalist practice, distinct educational materials and CME courses, and an active and growing professional society. Hospitalists are taking leadership positions in developing optimal systems of inpatient care in many institutions. And SHM is now working to launch its own journal of Hospital Medicine.
What existing specialties have that Hospital Medicine does not (yet) is certification criteria, including an exam, and separate credentialing categories in hospitals and payer organizations such as Medicare. While I’m not eager to take or pay for another certifying exam myself, it would help to maintain high standards among hospitalists and encourage focus on the core competencies in Hospital Medicine. It would shape residency training and CME courses as well. At the outset, and maybe permanently, I envision a Hospital Medicine exam (with versions for pediatric and adult medicine hospitalists) as a certificate of added qualification to the existing board exams in Internal
Medicine, Family Practice, and Pediatrics. The American Board of Internal Medicine (ABIM) has developed criteria regarding when to develop a certificate (exam) in a new field (Table 2), and if/when Hospital Medicine passes that step, it will be time to think about whether Hospital Medicine should move up the hierarchy of specialization to become a recognized subspecialty of Internal Medicine. But the process of “sanctioning” a new certificate (exam) or subspecialty is a complex one, and many fields initiate it on their own; which for Hospital Medicine might mean doing so without the distinct approval or input of the ABIM or American Board of Medical Specialties (ABMS) at the outset. Once a field’s own efforts gain legitimacy, then the ABIM and ABMS often recognize it as a distinct specialty or subspecialty. Such was the path taken by Emergency Medicine and many other fields.
I see a process of becoming eligible for the exam by completing residency training in IM, FP, or Pediatrics, and working as a hospitalist for a specified period of time (e.g., 3 years). Those who meet these (and other?) criteria, and pass the exam, could benefit from increased prestige and stature, and better differentiate themselves from doctors who might call themselves hospitalists but not have the delivery of inpatient care as their primary professional focus. Research studies of hospitalist systems of care could benefit from a more rigorous definition of who is really a hospitalist based on certification. And a practical consequence of a growing number of certified hospitalists might be an improved ability to lobby for adjustments and improvements in the professional fee reimbursement for inpatient care.
Patients indicate that board certification is very important when choosing a doctor (1), so being able to show them that I am a certified practitioner in a recognized specialty will have value. Of course, all hospitalists have the opportunity to show patients (e.g., on a business card or stationary) board certification in the specialty of their residency training, but the ability to demonstrate additional competence and dedication to Hospital Medicine will be valuable in the same way it is valuable for other fields with certificates of added qualification such as Sports Medicine, and Geriatrics.
Other features of a distinct specialty usually include things such as recognition in the AMA as a section; in the case of hospitalists a Section on Hospital Medicine. Such recognition would add legitimacy to the field and provide a stronger platform from which to lobby for the needs of our patients and our discipline. And with these credentials Hospital Medicine can relate to other specialties or subspecialties as peers rather than as a fledgling upstart.
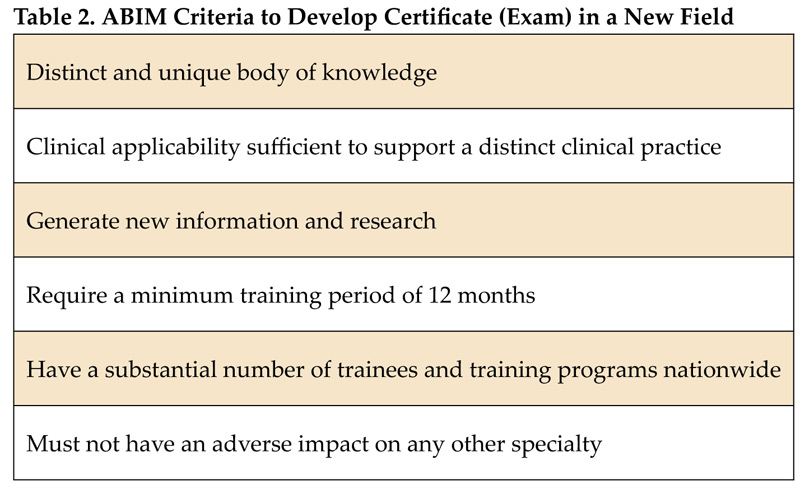
Costs of specialty recognition.
Some fear that developing an exam in Hospital Medicine will lead payers, which are usually enthusiastic supporters of the hospitalist movement, to discriminate between those who are and are not exam certified. In other words, if a payer has access to a group of certified (passed the exam) hospitalists, it might refuse to contract with non-certified PCPs to provide inpatient care. In this way the exam could be used as a way to restrict the practice of those who have not taken it, rather than simply enhancing the competence and stature of those who have passed it. I think there are many forces in medicine that would prevent this from happening to any significant degree. The history of many other specialties shows that an effort to restrict practice to certified doctors takes many years to gather steam (e.g., Emergency Medicine). And payers would only hurt themselves by restricting themselves to certified hospitalists early on, since it will likely be many years before the supply would be adequate to ensure enough doctors are available to do the work.
Something I hear often, and sometimes think myself, is “doesn’t medicine have enough specialties already?” After all, at the hospital where I practice the orthopedic doctors are segregated into those that focus on sports medicine, or the upper vs. lower extremity. Even though I know all of these orthopedists fairly well, I have a great deal of trouble remembering who is the knee person, and who to call for shoulders. If every traditional field in medicine continues to divide and subspecialize there is an increasing risk that we will grow further apart and have a harder time relating to each other professionally, and even more difficulty presenting a unified voice of all physicians before legislators or the public? I am very concerned about this problem, and do not see a simple solution. But concern about a potential “Tower of Babel” in medicine with many specialties which don’t speak the same language is not a good reason to inhibit specialization and increased expertise of any one group. The way to address this problem is through things such as improved mechanisms of communication.
Most patients believe our medical system clearly benefits from the existence of many different specialties. Few would want to go back to the system of limited physician specialization of 50 years ago. It seems likely that a person living in the middle of the last century would have all of their medical needs addressed by one or two doctors throughout their life (e.g., an internist or general practitioner, and possibly a surgeon at some point). That led to terrific patient-physician continuity for much of the population. And that continuity has been dissolving over the last 30 years, in large part due to the explosion of new specialties in medicine as well as economic forces and other factors. But I’m reminded regularly that patients want to see a number of different specialists at different times during their life, even if that means they see less of their primary care doctor (PCP) and have less overall continuity of care. After all, if a patient learns from her PCP that she needs to have her gallbladder removed, she isn’t likely to lean toward the PCP and say “You’re the doctor I know best, and I want you to take our my gallbladder instead of having it done by a stranger I’ve never met.” Instead patients say the opposite: “Send me to a doctor I’ve never met, but one who is an expert (experienced and board certified) in taking out gallbladders.”
So I think that we simply need to accept that increasing subspecialization is going to be part of our health care system for the foreseeable future. Rather than trying to resist or reverse it, we should simply be careful not to grant new subspecialty status too quickly. And all doctors should make sure that they spend time and energy focused on ensuring that doctors of all specialties maintain effective methods of communication about patients they care for together. Hospitalists will play an important role in this since ours is a specialty based on a site of practice rather than a particular disease or organ system. Like other generalists, such as PCPs and Emergency Physicians, we will be part of the glue that connects physicians by regular interaction with doctors from a wide variety of specialties.
We should also think about the effect a specialty of Hospital Medicine would have on the broader primary care community. For example, the American College of Physicians (ACP) has watched the birth of a number of medical subspecialties in the last 40 years, and most practitioners in each specialty have moved away from the ACP as their professional society and to their own subspecialty organization. This has led to a fracturing of internal medicine into many subgroups such that it might not be unusual to find one internal medicine subspecialty group arguing with another, rather than all speaking with one voice through the ACP. Each group has lost some clout and effectiveness as a result. But Hospital Medicine is still a generalist specialty (based on the site of care), unlike subspecialties such as cardiology and infectious disease, and should maintain a close connection with the ACP. If the formal recognition of Hospital Medicine as a specialty significantly dissolves the connection between ACP and SHM then both groups stand to lose a great deal. The leaders of these groups will need to work diligently to prevent this.
In my friend Mark Aronson’s accompanying article, “Be Careful What You Ask For,” he makes very reasonable proposals for what I see as intermediate steps toward specialty status. And he makes good points about some risks of becoming a specialty. I think we should move somewhat slowly toward specialty status so that the concerns he identifies can be addressed. But rather than identifying issues that are unique for Hospital Medicine, he has listed questions that probably arose in the formative years of every specialty and were subsequently addressed as the field “grew up.” He uses the example of electrophysiology as a field that requires additional training beyond the standard cardiology fellowship, and he suggests that it is the additional training that justifies the field’s exam and subspecialty status. But at some point in the early evolution of electrophysiology and any other field, there was no unique training program and practitioners learned the discipline through things such as self study, CME courses, and concentrating their practice on that clinical area. Isn’t that where we find ourselves in Hospital Medicine today?
Summary
The benefits of continued movement toward recognizing Hospital Medicine as a distinct specialty outweigh the costs. Indeed, without ever having an organized effort or agenda for this, our field has made many significant steps in that direction. What will require ongoing careful consideration is the pace at which the next steps in maturation of the field should proceed. While there are sure to be many differences in the path Hospital Medicine takes to specialty status, there are numerous lessons to be learned from the history of other specialties, such as Emergency Medicine. In 1969, Dr. John Wiegenstein wrote in the first Newsletter of the American College of Emergency Physicians that “We are, in a sense, a new breed of doctors dedicated to a new concept of medicine.” Most hospitalists feel the same way about Hospital Medicine, and I think we will mark very similar milestones toward specialty status in the coming years.
Reference
- Brennan TA, Horwitz RI, Duffy FD, Cassel CK, Goode LD, Lipner RS. The Role of Physician Specialty Board Certification Status in the Quality Movement. JAMA.2004;292:1038-43.
When the Society of Hospital Medicine was very young and headquartered in the home computers of myself and Win Whitcomb (and known then as the National Association of Inpatient Physicians), I spent a lot of time thinking about the future of our field. Whether we would, or should, become a recognized specialty was one of the things I particularly enjoyed thinking about. Believing the history of Emergency Medicine might provide some insights for Hospital Medicine, I tracked down Dr. John Wiegenstein, who played a major role in the founding of the American College of Emergency Physicians (ACEP) in 1968, served as the group’s first president, and helped mold Emergency Medicine into a distinct specialty recognized by the American Board of Medical Specialties.
The parallels between the first few years of Emergency Medicine and Hospital Medicine are striking (see Table 1, milestones in Emergency Medicine). Dr. Wiegenstien told me that there was tremendous enthusiasm among early ACEP members for the opportunity to create a new specialty and invent the systems of care in the emergency room (now department) that would best serve patients and the overall enterprise of health care. At the time of ACEP’s founding, there was no group that was primarily devoted to ensuring that emergency rooms were held to high standards of care and operated efficiently. In the late 1960’s, when ACEP sought to fill this void, Dr. Wiegenstein said that the medical leaders of the day in the AMA and other organizations, tended to smile patronizingly, pat him on the shoulder figuratively, and suggest that it would be fine to busy himself with such a project since it would keep him and his colleagues out of the way of those who were doing the important things in medicine. After all, the leaders of the day reasoned, there were already existing specialties with more expertise at any kind of care that an ER doctor might provide, so creating a new breed of doctor or specialty seemed like it would be an unnecessary duplication of existing specialties. Yet Dr. Wiegenstein and his colleagues did exactly what they set out to do, and today there is probably no one who questions the importance of the contribution of Emergency Medicine to our healthcare system, and its status as a distinct specialty.
The case for Hospital Medicine becoming a recognized specialty or subspecialty.
The question for those of us in Hospital Medicine is should we, and can we, be about doing the same thing in our field that has happened, and is ongoing, in Emergency Medicine? I suspect nearly all hospitalists believe the answer is yes, and I sense growing support for this goal from those in nearly all other fields in medicine. And I think an important factor in ensuring success is to think of ourselves as a distinct specialty or subspecialty.
In fact, Hospital Medicine functions as a distinct specialty in many respects already. There is a growing body of distinct literature about clinical and operational aspects of hospitalist practice, distinct educational materials and CME courses, and an active and growing professional society. Hospitalists are taking leadership positions in developing optimal systems of inpatient care in many institutions. And SHM is now working to launch its own journal of Hospital Medicine.
What existing specialties have that Hospital Medicine does not (yet) is certification criteria, including an exam, and separate credentialing categories in hospitals and payer organizations such as Medicare. While I’m not eager to take or pay for another certifying exam myself, it would help to maintain high standards among hospitalists and encourage focus on the core competencies in Hospital Medicine. It would shape residency training and CME courses as well. At the outset, and maybe permanently, I envision a Hospital Medicine exam (with versions for pediatric and adult medicine hospitalists) as a certificate of added qualification to the existing board exams in Internal
Medicine, Family Practice, and Pediatrics. The American Board of Internal Medicine (ABIM) has developed criteria regarding when to develop a certificate (exam) in a new field (Table 2), and if/when Hospital Medicine passes that step, it will be time to think about whether Hospital Medicine should move up the hierarchy of specialization to become a recognized subspecialty of Internal Medicine. But the process of “sanctioning” a new certificate (exam) or subspecialty is a complex one, and many fields initiate it on their own; which for Hospital Medicine might mean doing so without the distinct approval or input of the ABIM or American Board of Medical Specialties (ABMS) at the outset. Once a field’s own efforts gain legitimacy, then the ABIM and ABMS often recognize it as a distinct specialty or subspecialty. Such was the path taken by Emergency Medicine and many other fields.
I see a process of becoming eligible for the exam by completing residency training in IM, FP, or Pediatrics, and working as a hospitalist for a specified period of time (e.g., 3 years). Those who meet these (and other?) criteria, and pass the exam, could benefit from increased prestige and stature, and better differentiate themselves from doctors who might call themselves hospitalists but not have the delivery of inpatient care as their primary professional focus. Research studies of hospitalist systems of care could benefit from a more rigorous definition of who is really a hospitalist based on certification. And a practical consequence of a growing number of certified hospitalists might be an improved ability to lobby for adjustments and improvements in the professional fee reimbursement for inpatient care.
Patients indicate that board certification is very important when choosing a doctor (1), so being able to show them that I am a certified practitioner in a recognized specialty will have value. Of course, all hospitalists have the opportunity to show patients (e.g., on a business card or stationary) board certification in the specialty of their residency training, but the ability to demonstrate additional competence and dedication to Hospital Medicine will be valuable in the same way it is valuable for other fields with certificates of added qualification such as Sports Medicine, and Geriatrics.
Other features of a distinct specialty usually include things such as recognition in the AMA as a section; in the case of hospitalists a Section on Hospital Medicine. Such recognition would add legitimacy to the field and provide a stronger platform from which to lobby for the needs of our patients and our discipline. And with these credentials Hospital Medicine can relate to other specialties or subspecialties as peers rather than as a fledgling upstart.
Costs of specialty recognition.
Some fear that developing an exam in Hospital Medicine will lead payers, which are usually enthusiastic supporters of the hospitalist movement, to discriminate between those who are and are not exam certified. In other words, if a payer has access to a group of certified (passed the exam) hospitalists, it might refuse to contract with non-certified PCPs to provide inpatient care. In this way the exam could be used as a way to restrict the practice of those who have not taken it, rather than simply enhancing the competence and stature of those who have passed it. I think there are many forces in medicine that would prevent this from happening to any significant degree. The history of many other specialties shows that an effort to restrict practice to certified doctors takes many years to gather steam (e.g., Emergency Medicine). And payers would only hurt themselves by restricting themselves to certified hospitalists early on, since it will likely be many years before the supply would be adequate to ensure enough doctors are available to do the work.
Something I hear often, and sometimes think myself, is “doesn’t medicine have enough specialties already?” After all, at the hospital where I practice the orthopedic doctors are segregated into those that focus on sports medicine, or the upper vs. lower extremity. Even though I know all of these orthopedists fairly well, I have a great deal of trouble remembering who is the knee person, and who to call for shoulders. If every traditional field in medicine continues to divide and subspecialize there is an increasing risk that we will grow further apart and have a harder time relating to each other professionally, and even more difficulty presenting a unified voice of all physicians before legislators or the public? I am very concerned about this problem, and do not see a simple solution. But concern about a potential “Tower of Babel” in medicine with many specialties which don’t speak the same language is not a good reason to inhibit specialization and increased expertise of any one group. The way to address this problem is through things such as improved mechanisms of communication.
Most patients believe our medical system clearly benefits from the existence of many different specialties. Few would want to go back to the system of limited physician specialization of 50 years ago. It seems likely that a person living in the middle of the last century would have all of their medical needs addressed by one or two doctors throughout their life (e.g., an internist or general practitioner, and possibly a surgeon at some point). That led to terrific patient-physician continuity for much of the population. And that continuity has been dissolving over the last 30 years, in large part due to the explosion of new specialties in medicine as well as economic forces and other factors. But I’m reminded regularly that patients want to see a number of different specialists at different times during their life, even if that means they see less of their primary care doctor (PCP) and have less overall continuity of care. After all, if a patient learns from her PCP that she needs to have her gallbladder removed, she isn’t likely to lean toward the PCP and say “You’re the doctor I know best, and I want you to take our my gallbladder instead of having it done by a stranger I’ve never met.” Instead patients say the opposite: “Send me to a doctor I’ve never met, but one who is an expert (experienced and board certified) in taking out gallbladders.”
So I think that we simply need to accept that increasing subspecialization is going to be part of our health care system for the foreseeable future. Rather than trying to resist or reverse it, we should simply be careful not to grant new subspecialty status too quickly. And all doctors should make sure that they spend time and energy focused on ensuring that doctors of all specialties maintain effective methods of communication about patients they care for together. Hospitalists will play an important role in this since ours is a specialty based on a site of practice rather than a particular disease or organ system. Like other generalists, such as PCPs and Emergency Physicians, we will be part of the glue that connects physicians by regular interaction with doctors from a wide variety of specialties.
We should also think about the effect a specialty of Hospital Medicine would have on the broader primary care community. For example, the American College of Physicians (ACP) has watched the birth of a number of medical subspecialties in the last 40 years, and most practitioners in each specialty have moved away from the ACP as their professional society and to their own subspecialty organization. This has led to a fracturing of internal medicine into many subgroups such that it might not be unusual to find one internal medicine subspecialty group arguing with another, rather than all speaking with one voice through the ACP. Each group has lost some clout and effectiveness as a result. But Hospital Medicine is still a generalist specialty (based on the site of care), unlike subspecialties such as cardiology and infectious disease, and should maintain a close connection with the ACP. If the formal recognition of Hospital Medicine as a specialty significantly dissolves the connection between ACP and SHM then both groups stand to lose a great deal. The leaders of these groups will need to work diligently to prevent this.
In my friend Mark Aronson’s accompanying article, “Be Careful What You Ask For,” he makes very reasonable proposals for what I see as intermediate steps toward specialty status. And he makes good points about some risks of becoming a specialty. I think we should move somewhat slowly toward specialty status so that the concerns he identifies can be addressed. But rather than identifying issues that are unique for Hospital Medicine, he has listed questions that probably arose in the formative years of every specialty and were subsequently addressed as the field “grew up.” He uses the example of electrophysiology as a field that requires additional training beyond the standard cardiology fellowship, and he suggests that it is the additional training that justifies the field’s exam and subspecialty status. But at some point in the early evolution of electrophysiology and any other field, there was no unique training program and practitioners learned the discipline through things such as self study, CME courses, and concentrating their practice on that clinical area. Isn’t that where we find ourselves in Hospital Medicine today?
Summary
The benefits of continued movement toward recognizing Hospital Medicine as a distinct specialty outweigh the costs. Indeed, without ever having an organized effort or agenda for this, our field has made many significant steps in that direction. What will require ongoing careful consideration is the pace at which the next steps in maturation of the field should proceed. While there are sure to be many differences in the path Hospital Medicine takes to specialty status, there are numerous lessons to be learned from the history of other specialties, such as Emergency Medicine. In 1969, Dr. John Wiegenstein wrote in the first Newsletter of the American College of Emergency Physicians that “We are, in a sense, a new breed of doctors dedicated to a new concept of medicine.” Most hospitalists feel the same way about Hospital Medicine, and I think we will mark very similar milestones toward specialty status in the coming years.
Reference
- Brennan TA, Horwitz RI, Duffy FD, Cassel CK, Goode LD, Lipner RS. The Role of Physician Specialty Board Certification Status in the Quality Movement. JAMA.2004;292:1038-43.
When the Society of Hospital Medicine was very young and headquartered in the home computers of myself and Win Whitcomb (and known then as the National Association of Inpatient Physicians), I spent a lot of time thinking about the future of our field. Whether we would, or should, become a recognized specialty was one of the things I particularly enjoyed thinking about. Believing the history of Emergency Medicine might provide some insights for Hospital Medicine, I tracked down Dr. John Wiegenstein, who played a major role in the founding of the American College of Emergency Physicians (ACEP) in 1968, served as the group’s first president, and helped mold Emergency Medicine into a distinct specialty recognized by the American Board of Medical Specialties.
The parallels between the first few years of Emergency Medicine and Hospital Medicine are striking (see Table 1, milestones in Emergency Medicine). Dr. Wiegenstien told me that there was tremendous enthusiasm among early ACEP members for the opportunity to create a new specialty and invent the systems of care in the emergency room (now department) that would best serve patients and the overall enterprise of health care. At the time of ACEP’s founding, there was no group that was primarily devoted to ensuring that emergency rooms were held to high standards of care and operated efficiently. In the late 1960’s, when ACEP sought to fill this void, Dr. Wiegenstein said that the medical leaders of the day in the AMA and other organizations, tended to smile patronizingly, pat him on the shoulder figuratively, and suggest that it would be fine to busy himself with such a project since it would keep him and his colleagues out of the way of those who were doing the important things in medicine. After all, the leaders of the day reasoned, there were already existing specialties with more expertise at any kind of care that an ER doctor might provide, so creating a new breed of doctor or specialty seemed like it would be an unnecessary duplication of existing specialties. Yet Dr. Wiegenstein and his colleagues did exactly what they set out to do, and today there is probably no one who questions the importance of the contribution of Emergency Medicine to our healthcare system, and its status as a distinct specialty.
The case for Hospital Medicine becoming a recognized specialty or subspecialty.
The question for those of us in Hospital Medicine is should we, and can we, be about doing the same thing in our field that has happened, and is ongoing, in Emergency Medicine? I suspect nearly all hospitalists believe the answer is yes, and I sense growing support for this goal from those in nearly all other fields in medicine. And I think an important factor in ensuring success is to think of ourselves as a distinct specialty or subspecialty.
In fact, Hospital Medicine functions as a distinct specialty in many respects already. There is a growing body of distinct literature about clinical and operational aspects of hospitalist practice, distinct educational materials and CME courses, and an active and growing professional society. Hospitalists are taking leadership positions in developing optimal systems of inpatient care in many institutions. And SHM is now working to launch its own journal of Hospital Medicine.
What existing specialties have that Hospital Medicine does not (yet) is certification criteria, including an exam, and separate credentialing categories in hospitals and payer organizations such as Medicare. While I’m not eager to take or pay for another certifying exam myself, it would help to maintain high standards among hospitalists and encourage focus on the core competencies in Hospital Medicine. It would shape residency training and CME courses as well. At the outset, and maybe permanently, I envision a Hospital Medicine exam (with versions for pediatric and adult medicine hospitalists) as a certificate of added qualification to the existing board exams in Internal
Medicine, Family Practice, and Pediatrics. The American Board of Internal Medicine (ABIM) has developed criteria regarding when to develop a certificate (exam) in a new field (Table 2), and if/when Hospital Medicine passes that step, it will be time to think about whether Hospital Medicine should move up the hierarchy of specialization to become a recognized subspecialty of Internal Medicine. But the process of “sanctioning” a new certificate (exam) or subspecialty is a complex one, and many fields initiate it on their own; which for Hospital Medicine might mean doing so without the distinct approval or input of the ABIM or American Board of Medical Specialties (ABMS) at the outset. Once a field’s own efforts gain legitimacy, then the ABIM and ABMS often recognize it as a distinct specialty or subspecialty. Such was the path taken by Emergency Medicine and many other fields.
I see a process of becoming eligible for the exam by completing residency training in IM, FP, or Pediatrics, and working as a hospitalist for a specified period of time (e.g., 3 years). Those who meet these (and other?) criteria, and pass the exam, could benefit from increased prestige and stature, and better differentiate themselves from doctors who might call themselves hospitalists but not have the delivery of inpatient care as their primary professional focus. Research studies of hospitalist systems of care could benefit from a more rigorous definition of who is really a hospitalist based on certification. And a practical consequence of a growing number of certified hospitalists might be an improved ability to lobby for adjustments and improvements in the professional fee reimbursement for inpatient care.
Patients indicate that board certification is very important when choosing a doctor (1), so being able to show them that I am a certified practitioner in a recognized specialty will have value. Of course, all hospitalists have the opportunity to show patients (e.g., on a business card or stationary) board certification in the specialty of their residency training, but the ability to demonstrate additional competence and dedication to Hospital Medicine will be valuable in the same way it is valuable for other fields with certificates of added qualification such as Sports Medicine, and Geriatrics.
Other features of a distinct specialty usually include things such as recognition in the AMA as a section; in the case of hospitalists a Section on Hospital Medicine. Such recognition would add legitimacy to the field and provide a stronger platform from which to lobby for the needs of our patients and our discipline. And with these credentials Hospital Medicine can relate to other specialties or subspecialties as peers rather than as a fledgling upstart.
Costs of specialty recognition.
Some fear that developing an exam in Hospital Medicine will lead payers, which are usually enthusiastic supporters of the hospitalist movement, to discriminate between those who are and are not exam certified. In other words, if a payer has access to a group of certified (passed the exam) hospitalists, it might refuse to contract with non-certified PCPs to provide inpatient care. In this way the exam could be used as a way to restrict the practice of those who have not taken it, rather than simply enhancing the competence and stature of those who have passed it. I think there are many forces in medicine that would prevent this from happening to any significant degree. The history of many other specialties shows that an effort to restrict practice to certified doctors takes many years to gather steam (e.g., Emergency Medicine). And payers would only hurt themselves by restricting themselves to certified hospitalists early on, since it will likely be many years before the supply would be adequate to ensure enough doctors are available to do the work.
Something I hear often, and sometimes think myself, is “doesn’t medicine have enough specialties already?” After all, at the hospital where I practice the orthopedic doctors are segregated into those that focus on sports medicine, or the upper vs. lower extremity. Even though I know all of these orthopedists fairly well, I have a great deal of trouble remembering who is the knee person, and who to call for shoulders. If every traditional field in medicine continues to divide and subspecialize there is an increasing risk that we will grow further apart and have a harder time relating to each other professionally, and even more difficulty presenting a unified voice of all physicians before legislators or the public? I am very concerned about this problem, and do not see a simple solution. But concern about a potential “Tower of Babel” in medicine with many specialties which don’t speak the same language is not a good reason to inhibit specialization and increased expertise of any one group. The way to address this problem is through things such as improved mechanisms of communication.
Most patients believe our medical system clearly benefits from the existence of many different specialties. Few would want to go back to the system of limited physician specialization of 50 years ago. It seems likely that a person living in the middle of the last century would have all of their medical needs addressed by one or two doctors throughout their life (e.g., an internist or general practitioner, and possibly a surgeon at some point). That led to terrific patient-physician continuity for much of the population. And that continuity has been dissolving over the last 30 years, in large part due to the explosion of new specialties in medicine as well as economic forces and other factors. But I’m reminded regularly that patients want to see a number of different specialists at different times during their life, even if that means they see less of their primary care doctor (PCP) and have less overall continuity of care. After all, if a patient learns from her PCP that she needs to have her gallbladder removed, she isn’t likely to lean toward the PCP and say “You’re the doctor I know best, and I want you to take our my gallbladder instead of having it done by a stranger I’ve never met.” Instead patients say the opposite: “Send me to a doctor I’ve never met, but one who is an expert (experienced and board certified) in taking out gallbladders.”
So I think that we simply need to accept that increasing subspecialization is going to be part of our health care system for the foreseeable future. Rather than trying to resist or reverse it, we should simply be careful not to grant new subspecialty status too quickly. And all doctors should make sure that they spend time and energy focused on ensuring that doctors of all specialties maintain effective methods of communication about patients they care for together. Hospitalists will play an important role in this since ours is a specialty based on a site of practice rather than a particular disease or organ system. Like other generalists, such as PCPs and Emergency Physicians, we will be part of the glue that connects physicians by regular interaction with doctors from a wide variety of specialties.
We should also think about the effect a specialty of Hospital Medicine would have on the broader primary care community. For example, the American College of Physicians (ACP) has watched the birth of a number of medical subspecialties in the last 40 years, and most practitioners in each specialty have moved away from the ACP as their professional society and to their own subspecialty organization. This has led to a fracturing of internal medicine into many subgroups such that it might not be unusual to find one internal medicine subspecialty group arguing with another, rather than all speaking with one voice through the ACP. Each group has lost some clout and effectiveness as a result. But Hospital Medicine is still a generalist specialty (based on the site of care), unlike subspecialties such as cardiology and infectious disease, and should maintain a close connection with the ACP. If the formal recognition of Hospital Medicine as a specialty significantly dissolves the connection between ACP and SHM then both groups stand to lose a great deal. The leaders of these groups will need to work diligently to prevent this.
In my friend Mark Aronson’s accompanying article, “Be Careful What You Ask For,” he makes very reasonable proposals for what I see as intermediate steps toward specialty status. And he makes good points about some risks of becoming a specialty. I think we should move somewhat slowly toward specialty status so that the concerns he identifies can be addressed. But rather than identifying issues that are unique for Hospital Medicine, he has listed questions that probably arose in the formative years of every specialty and were subsequently addressed as the field “grew up.” He uses the example of electrophysiology as a field that requires additional training beyond the standard cardiology fellowship, and he suggests that it is the additional training that justifies the field’s exam and subspecialty status. But at some point in the early evolution of electrophysiology and any other field, there was no unique training program and practitioners learned the discipline through things such as self study, CME courses, and concentrating their practice on that clinical area. Isn’t that where we find ourselves in Hospital Medicine today?
Summary
The benefits of continued movement toward recognizing Hospital Medicine as a distinct specialty outweigh the costs. Indeed, without ever having an organized effort or agenda for this, our field has made many significant steps in that direction. What will require ongoing careful consideration is the pace at which the next steps in maturation of the field should proceed. While there are sure to be many differences in the path Hospital Medicine takes to specialty status, there are numerous lessons to be learned from the history of other specialties, such as Emergency Medicine. In 1969, Dr. John Wiegenstein wrote in the first Newsletter of the American College of Emergency Physicians that “We are, in a sense, a new breed of doctors dedicated to a new concept of medicine.” Most hospitalists feel the same way about Hospital Medicine, and I think we will mark very similar milestones toward specialty status in the coming years.
Reference
- Brennan TA, Horwitz RI, Duffy FD, Cassel CK, Goode LD, Lipner RS. The Role of Physician Specialty Board Certification Status in the Quality Movement. JAMA.2004;292:1038-43.
Be Careful What You Ask For

I pose here a list of questions to consider before embarking on the creation of a new specialty in hospital medicine
1) What distinguishes the body of knowledge of hospital medicine from internal medicine (or pediatrics, for our colleagues in that field)?
While there is a body of literature supporting operational aspects of hospital care, as far as I can tell there is no difference in the way a hospitalist or office-based internist should treat pneumonia. Hospitalists develop areas of expertise in case management, understanding of hospital-based quality-improvement systems, communication skills, etc, but these fall short of a body of knowledge for a medical specialty. Books on hospital medicine do not differ from standard medicine texts in terms of disease pathophysiology, clinical presentation, diagnosis, or management. What then is the new body of knowledge?
2) Does hospital medicine really want to exclude office-based primary care doctors from managing their own cases in the hospital if they so choose?
Creating a new specialty of hospital medicine certainly would tend to do that. Let’s look at emergency medicine, for example. It used to be common for internists and surgeons to work in emergency rooms. That no longer is the case in many parts of this country because of the emergence of a new specialty. Do we want the same to be true for office-based doctors who care for their own patients?
3) Creating a new specialty requires special training. What is that going to be? Who teaches it and who will do it?
New subspecialties require additional training. For instance, electrophysiology is now a subspecialty of cardiology and requires an additional one or two years of training after a three-year cardiology fellowship. Working for 2-3 years as Dr. Nelson has proposed in the field of hospital medicine is not additional training, it is just additional practice. What is the formal training that the Society of Hospital Medicine proposes to qualify someone as a Board-certified hospitalist? Is it likely that young doctors are going to want to add on an additional 2 or 3 years of training beyond their internal medicine residency before they can start paying off their medical school loans? What will this training actually entail, and how will it merge with the internal medicine training programs that already exist?
I would point out that residents in fact are hospitalists in training. Certainly the vast majority of their clinical experience occurs in the hospital. Except for primary care residencies, I would estimate that 2/3 of the clinical care that internal medicine residents experience is in the hospital.
4) What about the primary care doctor or hospitalist who wants to switch careers?
Is the Society of Hospital Medicine going to require that a physician who has been in practice for 5 or 10 years and decides to switch to hospital medicine go through further training? Is that likely to occur? Alternatively, what about the hospitalist who gets tired of that field and wishes to become a primary care doctor? Might not office-based internists move to create their own specialty and thereby exclude hospitalists from work in that setting?
5) What about the malpractice risks that a new specialty will create?
Let’s imagine a world in which there are internists certified as hospitalists or as primary care physicians. Imagine this malpractice scenario. An office-based doctor caring for his/her own patients in the hospital is sued for some issue or another. The plaintiff attorney standing near the jury faces the doctor and asks “Doctor [he sighs, looking gravely serious], I understand there is a subspecialty in hospital medicine. Are you [now facing the jury] certified in that specialty? The doctor responds “No.” The attorney [turning abruptly back towards the nervous doctor] asks “No? Why not?” Let’s imagine another scenario. A hospitalist working part-time in an office-based practice 1 or 2 days a week faces a similar malpractice situation where he or she is sued. Attorney: “Doctor, I understand there is a subspecialty in primary care medicine? Are you certified in that specialty? Doctor: “No.” Attorney: “No? Why not?”
6) Why create more tests and expenses?
Enough said!
7) Do you want to bite the hand that feeds you?
In our hospital the vast majority of hospitalist admissions are from primary care doctors. Try to eliminate their admitting privileges and see what happens. It will be like the Flu vaccine fiasco this year. There is little vaccine available, but now everyone who has never gotten it in the past is asking for it. My guess is that most primary care doctors will protect their privileges and start admitting and caring for their own patients.
Why don’t we consider a more modest proposal? Here are three ideas.
First, identify areas of expertise that hospitalists actually develop. For instance, can they become procedural experts? Certainly the performance of lumbar punctures, thoracenteses, paracenteses, and central lines is something that most office-based doctors are not comfortable in carrying out any longer. Can we help create credentialing for these important procedures? That would go a long way towards initiating a set of skills that differentiates a hospitalist from an office-based doctor. Why not become a credentialing society for performance of these and other procedures? Monitoring numbers of procedures might constitute one measure, for example, of how to initiate credentialing. For instance, most centers no longer allow a cardiologist who has not performed a certain number of cardiac catheterizations a year to maintain privileges for that procedure. This does not seem discriminatory. It seems wise. I do not think office-based doctors would view credentialing for procedures as discriminatory.
Secondly, what about working to modify existing internal medicine training to perhaps provide added qualifications within hospital medicine for residents committed to the field? The board exams might actually differ then for primary care residents and for those interested in hospital medicine.
Thirdly, what about concentrating efforts on recertification? My guess is that very few residents coming out of practice would not feel qualified to take the hospital medicine or the ambulatory portion of an internal medicine exam. On the other hand, 10 years later during recertification many office-based doctors will not feel qualified to take an exam that emphasizes the treatment of vancomycin-resistant enterococci or management of cardiac arrests. Perhaps the recertification exam is the time to ask doctors to differentiate themselves. Some may wish to maintain certification in both hospital-based and ambulatory care, while others may choose one path or the other.
SHM has become the great organization it is in part because it reached out to hospitalists working in both community and teaching hospitals. Can we not bridge the gap with our office-based colleagues as well? In the field of internal medicine are we going to set ourselves up to become blue and red states? How about a nice shade of violet?
I pose here a list of questions to consider before embarking on the creation of a new specialty in hospital medicine
1) What distinguishes the body of knowledge of hospital medicine from internal medicine (or pediatrics, for our colleagues in that field)?
While there is a body of literature supporting operational aspects of hospital care, as far as I can tell there is no difference in the way a hospitalist or office-based internist should treat pneumonia. Hospitalists develop areas of expertise in case management, understanding of hospital-based quality-improvement systems, communication skills, etc, but these fall short of a body of knowledge for a medical specialty. Books on hospital medicine do not differ from standard medicine texts in terms of disease pathophysiology, clinical presentation, diagnosis, or management. What then is the new body of knowledge?
2) Does hospital medicine really want to exclude office-based primary care doctors from managing their own cases in the hospital if they so choose?
Creating a new specialty of hospital medicine certainly would tend to do that. Let’s look at emergency medicine, for example. It used to be common for internists and surgeons to work in emergency rooms. That no longer is the case in many parts of this country because of the emergence of a new specialty. Do we want the same to be true for office-based doctors who care for their own patients?
3) Creating a new specialty requires special training. What is that going to be? Who teaches it and who will do it?
New subspecialties require additional training. For instance, electrophysiology is now a subspecialty of cardiology and requires an additional one or two years of training after a three-year cardiology fellowship. Working for 2-3 years as Dr. Nelson has proposed in the field of hospital medicine is not additional training, it is just additional practice. What is the formal training that the Society of Hospital Medicine proposes to qualify someone as a Board-certified hospitalist? Is it likely that young doctors are going to want to add on an additional 2 or 3 years of training beyond their internal medicine residency before they can start paying off their medical school loans? What will this training actually entail, and how will it merge with the internal medicine training programs that already exist?
I would point out that residents in fact are hospitalists in training. Certainly the vast majority of their clinical experience occurs in the hospital. Except for primary care residencies, I would estimate that 2/3 of the clinical care that internal medicine residents experience is in the hospital.
4) What about the primary care doctor or hospitalist who wants to switch careers?
Is the Society of Hospital Medicine going to require that a physician who has been in practice for 5 or 10 years and decides to switch to hospital medicine go through further training? Is that likely to occur? Alternatively, what about the hospitalist who gets tired of that field and wishes to become a primary care doctor? Might not office-based internists move to create their own specialty and thereby exclude hospitalists from work in that setting?
5) What about the malpractice risks that a new specialty will create?
Let’s imagine a world in which there are internists certified as hospitalists or as primary care physicians. Imagine this malpractice scenario. An office-based doctor caring for his/her own patients in the hospital is sued for some issue or another. The plaintiff attorney standing near the jury faces the doctor and asks “Doctor [he sighs, looking gravely serious], I understand there is a subspecialty in hospital medicine. Are you [now facing the jury] certified in that specialty? The doctor responds “No.” The attorney [turning abruptly back towards the nervous doctor] asks “No? Why not?” Let’s imagine another scenario. A hospitalist working part-time in an office-based practice 1 or 2 days a week faces a similar malpractice situation where he or she is sued. Attorney: “Doctor, I understand there is a subspecialty in primary care medicine? Are you certified in that specialty? Doctor: “No.” Attorney: “No? Why not?”
6) Why create more tests and expenses?
Enough said!
7) Do you want to bite the hand that feeds you?
In our hospital the vast majority of hospitalist admissions are from primary care doctors. Try to eliminate their admitting privileges and see what happens. It will be like the Flu vaccine fiasco this year. There is little vaccine available, but now everyone who has never gotten it in the past is asking for it. My guess is that most primary care doctors will protect their privileges and start admitting and caring for their own patients.
Why don’t we consider a more modest proposal? Here are three ideas.
First, identify areas of expertise that hospitalists actually develop. For instance, can they become procedural experts? Certainly the performance of lumbar punctures, thoracenteses, paracenteses, and central lines is something that most office-based doctors are not comfortable in carrying out any longer. Can we help create credentialing for these important procedures? That would go a long way towards initiating a set of skills that differentiates a hospitalist from an office-based doctor. Why not become a credentialing society for performance of these and other procedures? Monitoring numbers of procedures might constitute one measure, for example, of how to initiate credentialing. For instance, most centers no longer allow a cardiologist who has not performed a certain number of cardiac catheterizations a year to maintain privileges for that procedure. This does not seem discriminatory. It seems wise. I do not think office-based doctors would view credentialing for procedures as discriminatory.
Secondly, what about working to modify existing internal medicine training to perhaps provide added qualifications within hospital medicine for residents committed to the field? The board exams might actually differ then for primary care residents and for those interested in hospital medicine.
Thirdly, what about concentrating efforts on recertification? My guess is that very few residents coming out of practice would not feel qualified to take the hospital medicine or the ambulatory portion of an internal medicine exam. On the other hand, 10 years later during recertification many office-based doctors will not feel qualified to take an exam that emphasizes the treatment of vancomycin-resistant enterococci or management of cardiac arrests. Perhaps the recertification exam is the time to ask doctors to differentiate themselves. Some may wish to maintain certification in both hospital-based and ambulatory care, while others may choose one path or the other.
SHM has become the great organization it is in part because it reached out to hospitalists working in both community and teaching hospitals. Can we not bridge the gap with our office-based colleagues as well? In the field of internal medicine are we going to set ourselves up to become blue and red states? How about a nice shade of violet?
I pose here a list of questions to consider before embarking on the creation of a new specialty in hospital medicine
1) What distinguishes the body of knowledge of hospital medicine from internal medicine (or pediatrics, for our colleagues in that field)?
While there is a body of literature supporting operational aspects of hospital care, as far as I can tell there is no difference in the way a hospitalist or office-based internist should treat pneumonia. Hospitalists develop areas of expertise in case management, understanding of hospital-based quality-improvement systems, communication skills, etc, but these fall short of a body of knowledge for a medical specialty. Books on hospital medicine do not differ from standard medicine texts in terms of disease pathophysiology, clinical presentation, diagnosis, or management. What then is the new body of knowledge?
2) Does hospital medicine really want to exclude office-based primary care doctors from managing their own cases in the hospital if they so choose?
Creating a new specialty of hospital medicine certainly would tend to do that. Let’s look at emergency medicine, for example. It used to be common for internists and surgeons to work in emergency rooms. That no longer is the case in many parts of this country because of the emergence of a new specialty. Do we want the same to be true for office-based doctors who care for their own patients?
3) Creating a new specialty requires special training. What is that going to be? Who teaches it and who will do it?
New subspecialties require additional training. For instance, electrophysiology is now a subspecialty of cardiology and requires an additional one or two years of training after a three-year cardiology fellowship. Working for 2-3 years as Dr. Nelson has proposed in the field of hospital medicine is not additional training, it is just additional practice. What is the formal training that the Society of Hospital Medicine proposes to qualify someone as a Board-certified hospitalist? Is it likely that young doctors are going to want to add on an additional 2 or 3 years of training beyond their internal medicine residency before they can start paying off their medical school loans? What will this training actually entail, and how will it merge with the internal medicine training programs that already exist?
I would point out that residents in fact are hospitalists in training. Certainly the vast majority of their clinical experience occurs in the hospital. Except for primary care residencies, I would estimate that 2/3 of the clinical care that internal medicine residents experience is in the hospital.
4) What about the primary care doctor or hospitalist who wants to switch careers?
Is the Society of Hospital Medicine going to require that a physician who has been in practice for 5 or 10 years and decides to switch to hospital medicine go through further training? Is that likely to occur? Alternatively, what about the hospitalist who gets tired of that field and wishes to become a primary care doctor? Might not office-based internists move to create their own specialty and thereby exclude hospitalists from work in that setting?
5) What about the malpractice risks that a new specialty will create?
Let’s imagine a world in which there are internists certified as hospitalists or as primary care physicians. Imagine this malpractice scenario. An office-based doctor caring for his/her own patients in the hospital is sued for some issue or another. The plaintiff attorney standing near the jury faces the doctor and asks “Doctor [he sighs, looking gravely serious], I understand there is a subspecialty in hospital medicine. Are you [now facing the jury] certified in that specialty? The doctor responds “No.” The attorney [turning abruptly back towards the nervous doctor] asks “No? Why not?” Let’s imagine another scenario. A hospitalist working part-time in an office-based practice 1 or 2 days a week faces a similar malpractice situation where he or she is sued. Attorney: “Doctor, I understand there is a subspecialty in primary care medicine? Are you certified in that specialty? Doctor: “No.” Attorney: “No? Why not?”
6) Why create more tests and expenses?
Enough said!
7) Do you want to bite the hand that feeds you?
In our hospital the vast majority of hospitalist admissions are from primary care doctors. Try to eliminate their admitting privileges and see what happens. It will be like the Flu vaccine fiasco this year. There is little vaccine available, but now everyone who has never gotten it in the past is asking for it. My guess is that most primary care doctors will protect their privileges and start admitting and caring for their own patients.
Why don’t we consider a more modest proposal? Here are three ideas.
First, identify areas of expertise that hospitalists actually develop. For instance, can they become procedural experts? Certainly the performance of lumbar punctures, thoracenteses, paracenteses, and central lines is something that most office-based doctors are not comfortable in carrying out any longer. Can we help create credentialing for these important procedures? That would go a long way towards initiating a set of skills that differentiates a hospitalist from an office-based doctor. Why not become a credentialing society for performance of these and other procedures? Monitoring numbers of procedures might constitute one measure, for example, of how to initiate credentialing. For instance, most centers no longer allow a cardiologist who has not performed a certain number of cardiac catheterizations a year to maintain privileges for that procedure. This does not seem discriminatory. It seems wise. I do not think office-based doctors would view credentialing for procedures as discriminatory.
Secondly, what about working to modify existing internal medicine training to perhaps provide added qualifications within hospital medicine for residents committed to the field? The board exams might actually differ then for primary care residents and for those interested in hospital medicine.
Thirdly, what about concentrating efforts on recertification? My guess is that very few residents coming out of practice would not feel qualified to take the hospital medicine or the ambulatory portion of an internal medicine exam. On the other hand, 10 years later during recertification many office-based doctors will not feel qualified to take an exam that emphasizes the treatment of vancomycin-resistant enterococci or management of cardiac arrests. Perhaps the recertification exam is the time to ask doctors to differentiate themselves. Some may wish to maintain certification in both hospital-based and ambulatory care, while others may choose one path or the other.
SHM has become the great organization it is in part because it reached out to hospitalists working in both community and teaching hospitals. Can we not bridge the gap with our office-based colleagues as well? In the field of internal medicine are we going to set ourselves up to become blue and red states? How about a nice shade of violet?
An Ongoing Analysis of the 2003-04 SHM Productivity and Compensation Survey
The survey analysis of productivity breaks this performance measure into two categories:
- Inputs: The hours worked by hospitalists. Three categories of hours worked are analyzed in this chapter: inpatient hours worked, non-patient hours worked, and on-call hours worked. Please note, the analysis excludes outpatient hours worked because only 15% of the survey respondents reported any outpatient hours.
- Outputs: The work completed by hospitalists. This includes charges generated, collections generated, patient encounters, patient admissions and consults, and relative value units (RVUs) of work completed. These measures are analyzed in chapter 5 (to be published in the March/April Hospitalist issue.
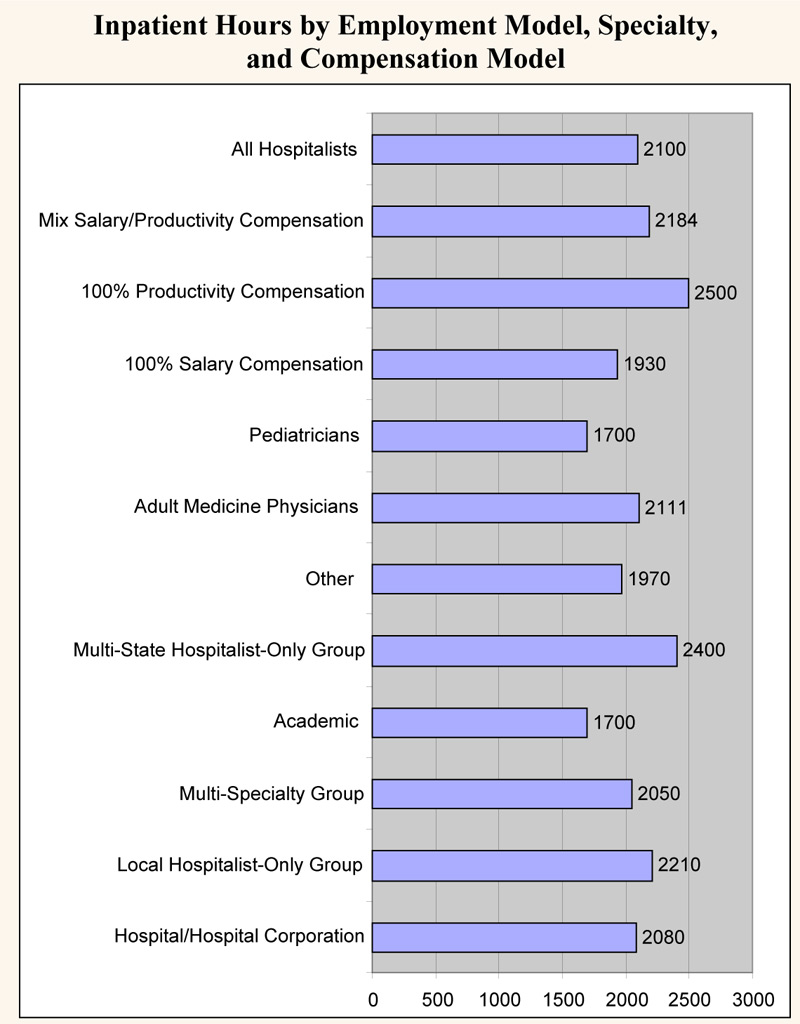
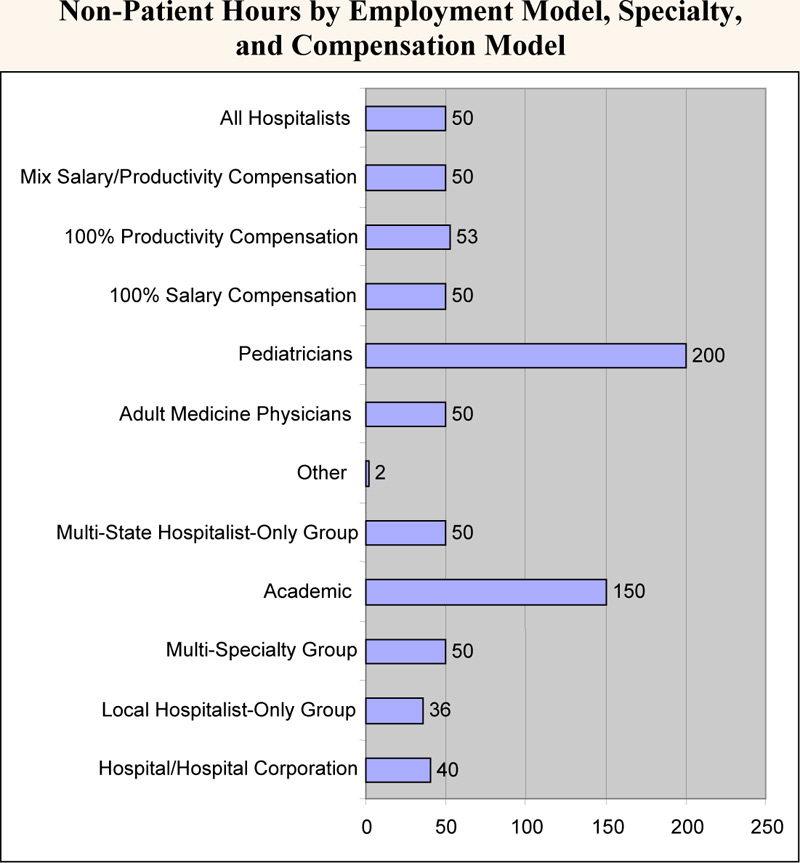
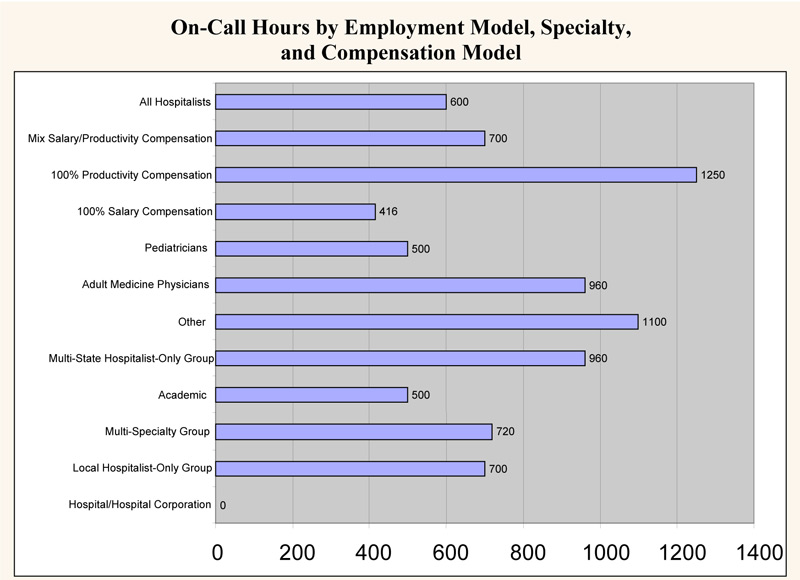
Overall, surveyed physician hospitalists worked a median of 2,100 inpatient hours per year. They had a median of 50 non-patient hours per year (about one per week) and worked a median of 600 on-call hours per year. The analyses below look at productivity inputs by region, employment model, specialty/provider type, and compensation model.
- Academic hospitalists work the least amount of inpatient hours (1,700 vs. an overall median of 2,100). However, they work significantly more non‑patient hours (150 vs. 50), probably because of their teaching responsibilities.
- Hospitalists that work for hospitalist-only groups work more inpatient hours than the overall median: multistate hospitalist only groups are 14% higher (2,400 vs. 2,100), while local hospitalist-only groups are 5% higher (2,210 vs. 2,100).
- Regarding on-call hours, hospitalists that work for hospital-based groups have a median of zero. This is probably because only 27% of hospital-based groups have call-based staffing, significantly less than other employment categories (see Chapter 1). This also is probably the explanation for the median of zero for eastern hospitalists, as that region has a high proportion of hospital-based groups.
- Adult medicine hospitalists work 24% more inpatient hours than pediatric hospitalists (2,111 vs. 1,700). Conversely, pediatric hospitalists have four times as many non-patient hours (200 vs. 50). This is likely explained by the fact that pediatricians are twice as likely to work in academia (see chapter 1).
- Non-physician hospitalists have a median of 1,900 inpatient hours and a median of only 10 non-patient hours
- There is a strong relationship between compensation model and hours worked. Hospitalists that work under a 100% productivity model have a median number of inpatient hours that is 30% more than those that work in a 100% salary model (2,500 vs. 1,930). Hospitalists that work in a mixed model fall in the middle (2,184).
- There is minimal difference in the non-patient hours worked among the three categories (approximately 50). However, 100% productivity-model hospitalists have a median number of on-call hours, which is almost 3 times greater than that of 100% salary-based hospitalists (1,250 vs. 416). Again, mixed-model hospitalists fall in the middle (700).
The survey analysis of productivity breaks this performance measure into two categories:
- Inputs: The hours worked by hospitalists. Three categories of hours worked are analyzed in this chapter: inpatient hours worked, non-patient hours worked, and on-call hours worked. Please note, the analysis excludes outpatient hours worked because only 15% of the survey respondents reported any outpatient hours.
- Outputs: The work completed by hospitalists. This includes charges generated, collections generated, patient encounters, patient admissions and consults, and relative value units (RVUs) of work completed. These measures are analyzed in chapter 5 (to be published in the March/April Hospitalist issue.
Overall, surveyed physician hospitalists worked a median of 2,100 inpatient hours per year. They had a median of 50 non-patient hours per year (about one per week) and worked a median of 600 on-call hours per year. The analyses below look at productivity inputs by region, employment model, specialty/provider type, and compensation model.
- Academic hospitalists work the least amount of inpatient hours (1,700 vs. an overall median of 2,100). However, they work significantly more non‑patient hours (150 vs. 50), probably because of their teaching responsibilities.
- Hospitalists that work for hospitalist-only groups work more inpatient hours than the overall median: multistate hospitalist only groups are 14% higher (2,400 vs. 2,100), while local hospitalist-only groups are 5% higher (2,210 vs. 2,100).
- Regarding on-call hours, hospitalists that work for hospital-based groups have a median of zero. This is probably because only 27% of hospital-based groups have call-based staffing, significantly less than other employment categories (see Chapter 1). This also is probably the explanation for the median of zero for eastern hospitalists, as that region has a high proportion of hospital-based groups.
- Adult medicine hospitalists work 24% more inpatient hours than pediatric hospitalists (2,111 vs. 1,700). Conversely, pediatric hospitalists have four times as many non-patient hours (200 vs. 50). This is likely explained by the fact that pediatricians are twice as likely to work in academia (see chapter 1).
- Non-physician hospitalists have a median of 1,900 inpatient hours and a median of only 10 non-patient hours
- There is a strong relationship between compensation model and hours worked. Hospitalists that work under a 100% productivity model have a median number of inpatient hours that is 30% more than those that work in a 100% salary model (2,500 vs. 1,930). Hospitalists that work in a mixed model fall in the middle (2,184).
- There is minimal difference in the non-patient hours worked among the three categories (approximately 50). However, 100% productivity-model hospitalists have a median number of on-call hours, which is almost 3 times greater than that of 100% salary-based hospitalists (1,250 vs. 416). Again, mixed-model hospitalists fall in the middle (700).
The survey analysis of productivity breaks this performance measure into two categories:
- Inputs: The hours worked by hospitalists. Three categories of hours worked are analyzed in this chapter: inpatient hours worked, non-patient hours worked, and on-call hours worked. Please note, the analysis excludes outpatient hours worked because only 15% of the survey respondents reported any outpatient hours.
- Outputs: The work completed by hospitalists. This includes charges generated, collections generated, patient encounters, patient admissions and consults, and relative value units (RVUs) of work completed. These measures are analyzed in chapter 5 (to be published in the March/April Hospitalist issue.
Overall, surveyed physician hospitalists worked a median of 2,100 inpatient hours per year. They had a median of 50 non-patient hours per year (about one per week) and worked a median of 600 on-call hours per year. The analyses below look at productivity inputs by region, employment model, specialty/provider type, and compensation model.
- Academic hospitalists work the least amount of inpatient hours (1,700 vs. an overall median of 2,100). However, they work significantly more non‑patient hours (150 vs. 50), probably because of their teaching responsibilities.
- Hospitalists that work for hospitalist-only groups work more inpatient hours than the overall median: multistate hospitalist only groups are 14% higher (2,400 vs. 2,100), while local hospitalist-only groups are 5% higher (2,210 vs. 2,100).
- Regarding on-call hours, hospitalists that work for hospital-based groups have a median of zero. This is probably because only 27% of hospital-based groups have call-based staffing, significantly less than other employment categories (see Chapter 1). This also is probably the explanation for the median of zero for eastern hospitalists, as that region has a high proportion of hospital-based groups.
- Adult medicine hospitalists work 24% more inpatient hours than pediatric hospitalists (2,111 vs. 1,700). Conversely, pediatric hospitalists have four times as many non-patient hours (200 vs. 50). This is likely explained by the fact that pediatricians are twice as likely to work in academia (see chapter 1).
- Non-physician hospitalists have a median of 1,900 inpatient hours and a median of only 10 non-patient hours
- There is a strong relationship between compensation model and hours worked. Hospitalists that work under a 100% productivity model have a median number of inpatient hours that is 30% more than those that work in a 100% salary model (2,500 vs. 1,930). Hospitalists that work in a mixed model fall in the middle (2,184).
- There is minimal difference in the non-patient hours worked among the three categories (approximately 50). However, 100% productivity-model hospitalists have a median number of on-call hours, which is almost 3 times greater than that of 100% salary-based hospitalists (1,250 vs. 416). Again, mixed-model hospitalists fall in the middle (700).
Thanks for the Memories
This issue of The Hospitalist marks the beginning of my sixth year as the chief executive officer at SHM. Much has happened at SHM and in our specialty in the last 5 years, and
I thought I would use this space to share with everyone what we have accomplished together and to recognize the many individuals who have made all of this possible.
Past
When I first came to SHM in January of 2000, SHM had two employees, three or four committees, and about 500members. There were estimated to be 1000-2000 hospitalists in the country. SHM did stage an Annual Meeting with 300 attendees and published a newsletter of 16 pages with minimal ad revenue and a circulation of about 1000. SHM had no external grants and limited relationships with industry.
SHM was a fledgling national organization with no local presence. SHM had minimal assets or infrastructure and was very reliant on ACP for support and direction. Most of the innovation and direction fell to a few hospitalists around the country, who, while devoted to SHM (then NAIP) and our specialty, still had a very full plate just doing their day jobs, growing their hospital medicine groups. It was amazing what they had accomplished with minimal staff support or infrastructure.
At the start of the new millennium, SHM didn’t know how many hospitals had hospitalists. There was no data on how hard hospitalists should be expected to work or how much they should be paid. There was limited data on the background or training of those doctors who were going into hospital medicine, and there was no understanding of what the knowledge base was for this new specialty. There was a vague sense that the importance of hospitalists was more than just seeing their own patients, but there was little understanding of what value hospitalists could add to their health communities.
Present
Over the last 5 years, together we have made enormous progress. We have changed our name from the National Association of Inpatient Physicians to the Society of Hospital Medicine to better reflect all the stakeholders in our growing specialty. We have grown our Philadelphia staff to 13 and employ another five staff in Boston, Atlanta, and California. The Hospitalist newsletter is now the recognized publication in hospital medicine with 65-80 pages per issue, 2-3 supplements each year, and a circulation well over 10,000. There are more than $75,000 in recruitment ads in each issue, as much a testament to the growth of the specialty as anything else.
SHM’s Annual Meeting now attracts almost 1000 attendees and is the primary networking opportunity for the fastest-growing medical specialty. SHM has almost 5000 members, and there are an estimated 10,000-12,000 hospitalists now practicing in over 1500 hospitals. SHM currently has more than 40 local chapters meeting at least once a year throughout the country.
SHM has developed unique expertise in the management aspects of hospital medicine and holds practice management courses at least three times each year. In addition, SHM has realized that hospitalists will need to be the leaders of the hospitals of the future and has created Leadership Academies to train these future leaders. SHM has worked with grants from the Hartford Foundation to establish the hospitalist as the physician for the acutely ill elderly. SHM is working with the Robert Wood Johnson Foundation and others in helping to create the physical design of the hospital of the future.
SHM is just completing the Core Curriculum for Hospital Medicine, which will define the knowledge base for our specialty and serve as the basis for SHM’s growing educational enterprise. SHM is defining the value that hospitalists add beyond just direct patient care. This phenomenon has been the basis for hospitals looking for innovative ways to grow and support their hospital medicine groups. SHM will publish these white papers for hospitalists and hospital executives to use in designing their hospital medicine programs.
SHM has defined the productivity and compensation data for our specialty in our biannual surveys that are the best source for hospitalist data. SHM has developed a Washington presence and is defining the advocacy issues for hospital medicine, including substantial reform of payment to de-emphasize compensation based solely on the unit of the visit or the procedure.
SHM is now an organization with almost $3 million in assets, completely autonomous, and functioning on its own. We have a strong and growing relationship with ACP, and SHM has reached out to partner with many other organizations, including the AHA, ACCP, JCAHO, RWJ, Hartford Foundation, CDC, AACN, ASHP, ABIM, AAP, SGIM, AAIM and many others.
Future
And there is much to look forward to in the next 5 years. In the coming months, SHM will launch the first journal in hospital medicine in January 2006. SHM’s Web site will come into the 21st century with the ability for each member to have their own Web page. The Web site will be the one location that hospitalists can come to for CME and other educational information. SHM will be working with AACP, AACN, ASHP, and others to establish an Acute Care Collaborative, reorganizing hospital workflow to deliver measurable higher-quality health care using interdisciplinary teams of health professionals. This will help to define the hospital of the future.
There will be a certification for hospitalists in the near future. This will define how hospitalists add value and how we are different from other internists, pediatricians, and family practitioners. SHM will also be using the Core Curriculum to not only drive SHM post-graduate education, but to help redefine residency training to produce more and better-trained individuals for a future that includes 30,000 to 40,000 hospitalists.
This has been quite a ride in the last 5 years. I have been fortunate enough to have had a front row seat. And I am not going anywhere soon. This is way too much fun. I just wanted to share with you a few others who have been instrumental in growing SHM.
A Special Thank You to Those Who Did the Work
SHM Presidents
John Nelson
Win Whitcomb
Bob Wachter
Ron Angus
Mark Williams
Jeff Dichter
Jeanne Huddleston
SHM Board Members (in addition to all Presidents)
Bill Atchley
Brad Flansbaum
David Zipes
Diane Craig
Herb Rogove
Jan Merin
Lisa Kettering
Mark Aronson
Mary Jo Gorman
Mike Ruhlen
Mitch Wilson
Pat Cawley
Peter Lindenauer
Richard Slataper
Russ Holman
Steve Pantilat
Editors, The Hospitalist
Scott Flanders
Jim Pile
Committee & Council Chairs (in addition to Board members)
Alpesh Amin
Andy Auerbach
Don Krause
Jack Percelay
Joe Li
Lakshmi Halasyamani
Mike Pistoria
Natalie Correia
Neil Kripalani
Preetha Basaviah
Sanjay Saint
Shaun Frost
Stacy Goldsholl
Sylvia McKean
Teresa Jones
Tim Cornell
Vineet Arora
SHM Staff
Angela Musial
Erica Pearson
Jane Mihelic
Kevin Stevens
Marie Francois
Marilyn Rivera
Michelle D’Agostino
Vera Bensch
Vernita Jackson
Veronica BeUs
Joe Miller
Tina Budnitz
This issue of The Hospitalist marks the beginning of my sixth year as the chief executive officer at SHM. Much has happened at SHM and in our specialty in the last 5 years, and
I thought I would use this space to share with everyone what we have accomplished together and to recognize the many individuals who have made all of this possible.
Past
When I first came to SHM in January of 2000, SHM had two employees, three or four committees, and about 500members. There were estimated to be 1000-2000 hospitalists in the country. SHM did stage an Annual Meeting with 300 attendees and published a newsletter of 16 pages with minimal ad revenue and a circulation of about 1000. SHM had no external grants and limited relationships with industry.
SHM was a fledgling national organization with no local presence. SHM had minimal assets or infrastructure and was very reliant on ACP for support and direction. Most of the innovation and direction fell to a few hospitalists around the country, who, while devoted to SHM (then NAIP) and our specialty, still had a very full plate just doing their day jobs, growing their hospital medicine groups. It was amazing what they had accomplished with minimal staff support or infrastructure.
At the start of the new millennium, SHM didn’t know how many hospitals had hospitalists. There was no data on how hard hospitalists should be expected to work or how much they should be paid. There was limited data on the background or training of those doctors who were going into hospital medicine, and there was no understanding of what the knowledge base was for this new specialty. There was a vague sense that the importance of hospitalists was more than just seeing their own patients, but there was little understanding of what value hospitalists could add to their health communities.
Present
Over the last 5 years, together we have made enormous progress. We have changed our name from the National Association of Inpatient Physicians to the Society of Hospital Medicine to better reflect all the stakeholders in our growing specialty. We have grown our Philadelphia staff to 13 and employ another five staff in Boston, Atlanta, and California. The Hospitalist newsletter is now the recognized publication in hospital medicine with 65-80 pages per issue, 2-3 supplements each year, and a circulation well over 10,000. There are more than $75,000 in recruitment ads in each issue, as much a testament to the growth of the specialty as anything else.
SHM’s Annual Meeting now attracts almost 1000 attendees and is the primary networking opportunity for the fastest-growing medical specialty. SHM has almost 5000 members, and there are an estimated 10,000-12,000 hospitalists now practicing in over 1500 hospitals. SHM currently has more than 40 local chapters meeting at least once a year throughout the country.
SHM has developed unique expertise in the management aspects of hospital medicine and holds practice management courses at least three times each year. In addition, SHM has realized that hospitalists will need to be the leaders of the hospitals of the future and has created Leadership Academies to train these future leaders. SHM has worked with grants from the Hartford Foundation to establish the hospitalist as the physician for the acutely ill elderly. SHM is working with the Robert Wood Johnson Foundation and others in helping to create the physical design of the hospital of the future.
SHM is just completing the Core Curriculum for Hospital Medicine, which will define the knowledge base for our specialty and serve as the basis for SHM’s growing educational enterprise. SHM is defining the value that hospitalists add beyond just direct patient care. This phenomenon has been the basis for hospitals looking for innovative ways to grow and support their hospital medicine groups. SHM will publish these white papers for hospitalists and hospital executives to use in designing their hospital medicine programs.
SHM has defined the productivity and compensation data for our specialty in our biannual surveys that are the best source for hospitalist data. SHM has developed a Washington presence and is defining the advocacy issues for hospital medicine, including substantial reform of payment to de-emphasize compensation based solely on the unit of the visit or the procedure.
SHM is now an organization with almost $3 million in assets, completely autonomous, and functioning on its own. We have a strong and growing relationship with ACP, and SHM has reached out to partner with many other organizations, including the AHA, ACCP, JCAHO, RWJ, Hartford Foundation, CDC, AACN, ASHP, ABIM, AAP, SGIM, AAIM and many others.
Future
And there is much to look forward to in the next 5 years. In the coming months, SHM will launch the first journal in hospital medicine in January 2006. SHM’s Web site will come into the 21st century with the ability for each member to have their own Web page. The Web site will be the one location that hospitalists can come to for CME and other educational information. SHM will be working with AACP, AACN, ASHP, and others to establish an Acute Care Collaborative, reorganizing hospital workflow to deliver measurable higher-quality health care using interdisciplinary teams of health professionals. This will help to define the hospital of the future.
There will be a certification for hospitalists in the near future. This will define how hospitalists add value and how we are different from other internists, pediatricians, and family practitioners. SHM will also be using the Core Curriculum to not only drive SHM post-graduate education, but to help redefine residency training to produce more and better-trained individuals for a future that includes 30,000 to 40,000 hospitalists.
This has been quite a ride in the last 5 years. I have been fortunate enough to have had a front row seat. And I am not going anywhere soon. This is way too much fun. I just wanted to share with you a few others who have been instrumental in growing SHM.
A Special Thank You to Those Who Did the Work
SHM Presidents
John Nelson
Win Whitcomb
Bob Wachter
Ron Angus
Mark Williams
Jeff Dichter
Jeanne Huddleston
SHM Board Members (in addition to all Presidents)
Bill Atchley
Brad Flansbaum
David Zipes
Diane Craig
Herb Rogove
Jan Merin
Lisa Kettering
Mark Aronson
Mary Jo Gorman
Mike Ruhlen
Mitch Wilson
Pat Cawley
Peter Lindenauer
Richard Slataper
Russ Holman
Steve Pantilat
Editors, The Hospitalist
Scott Flanders
Jim Pile
Committee & Council Chairs (in addition to Board members)
Alpesh Amin
Andy Auerbach
Don Krause
Jack Percelay
Joe Li
Lakshmi Halasyamani
Mike Pistoria
Natalie Correia
Neil Kripalani
Preetha Basaviah
Sanjay Saint
Shaun Frost
Stacy Goldsholl
Sylvia McKean
Teresa Jones
Tim Cornell
Vineet Arora
SHM Staff
Angela Musial
Erica Pearson
Jane Mihelic
Kevin Stevens
Marie Francois
Marilyn Rivera
Michelle D’Agostino
Vera Bensch
Vernita Jackson
Veronica BeUs
Joe Miller
Tina Budnitz
This issue of The Hospitalist marks the beginning of my sixth year as the chief executive officer at SHM. Much has happened at SHM and in our specialty in the last 5 years, and
I thought I would use this space to share with everyone what we have accomplished together and to recognize the many individuals who have made all of this possible.
Past
When I first came to SHM in January of 2000, SHM had two employees, three or four committees, and about 500members. There were estimated to be 1000-2000 hospitalists in the country. SHM did stage an Annual Meeting with 300 attendees and published a newsletter of 16 pages with minimal ad revenue and a circulation of about 1000. SHM had no external grants and limited relationships with industry.
SHM was a fledgling national organization with no local presence. SHM had minimal assets or infrastructure and was very reliant on ACP for support and direction. Most of the innovation and direction fell to a few hospitalists around the country, who, while devoted to SHM (then NAIP) and our specialty, still had a very full plate just doing their day jobs, growing their hospital medicine groups. It was amazing what they had accomplished with minimal staff support or infrastructure.
At the start of the new millennium, SHM didn’t know how many hospitals had hospitalists. There was no data on how hard hospitalists should be expected to work or how much they should be paid. There was limited data on the background or training of those doctors who were going into hospital medicine, and there was no understanding of what the knowledge base was for this new specialty. There was a vague sense that the importance of hospitalists was more than just seeing their own patients, but there was little understanding of what value hospitalists could add to their health communities.
Present
Over the last 5 years, together we have made enormous progress. We have changed our name from the National Association of Inpatient Physicians to the Society of Hospital Medicine to better reflect all the stakeholders in our growing specialty. We have grown our Philadelphia staff to 13 and employ another five staff in Boston, Atlanta, and California. The Hospitalist newsletter is now the recognized publication in hospital medicine with 65-80 pages per issue, 2-3 supplements each year, and a circulation well over 10,000. There are more than $75,000 in recruitment ads in each issue, as much a testament to the growth of the specialty as anything else.
SHM’s Annual Meeting now attracts almost 1000 attendees and is the primary networking opportunity for the fastest-growing medical specialty. SHM has almost 5000 members, and there are an estimated 10,000-12,000 hospitalists now practicing in over 1500 hospitals. SHM currently has more than 40 local chapters meeting at least once a year throughout the country.
SHM has developed unique expertise in the management aspects of hospital medicine and holds practice management courses at least three times each year. In addition, SHM has realized that hospitalists will need to be the leaders of the hospitals of the future and has created Leadership Academies to train these future leaders. SHM has worked with grants from the Hartford Foundation to establish the hospitalist as the physician for the acutely ill elderly. SHM is working with the Robert Wood Johnson Foundation and others in helping to create the physical design of the hospital of the future.
SHM is just completing the Core Curriculum for Hospital Medicine, which will define the knowledge base for our specialty and serve as the basis for SHM’s growing educational enterprise. SHM is defining the value that hospitalists add beyond just direct patient care. This phenomenon has been the basis for hospitals looking for innovative ways to grow and support their hospital medicine groups. SHM will publish these white papers for hospitalists and hospital executives to use in designing their hospital medicine programs.
SHM has defined the productivity and compensation data for our specialty in our biannual surveys that are the best source for hospitalist data. SHM has developed a Washington presence and is defining the advocacy issues for hospital medicine, including substantial reform of payment to de-emphasize compensation based solely on the unit of the visit or the procedure.
SHM is now an organization with almost $3 million in assets, completely autonomous, and functioning on its own. We have a strong and growing relationship with ACP, and SHM has reached out to partner with many other organizations, including the AHA, ACCP, JCAHO, RWJ, Hartford Foundation, CDC, AACN, ASHP, ABIM, AAP, SGIM, AAIM and many others.
Future
And there is much to look forward to in the next 5 years. In the coming months, SHM will launch the first journal in hospital medicine in January 2006. SHM’s Web site will come into the 21st century with the ability for each member to have their own Web page. The Web site will be the one location that hospitalists can come to for CME and other educational information. SHM will be working with AACP, AACN, ASHP, and others to establish an Acute Care Collaborative, reorganizing hospital workflow to deliver measurable higher-quality health care using interdisciplinary teams of health professionals. This will help to define the hospital of the future.
There will be a certification for hospitalists in the near future. This will define how hospitalists add value and how we are different from other internists, pediatricians, and family practitioners. SHM will also be using the Core Curriculum to not only drive SHM post-graduate education, but to help redefine residency training to produce more and better-trained individuals for a future that includes 30,000 to 40,000 hospitalists.
This has been quite a ride in the last 5 years. I have been fortunate enough to have had a front row seat. And I am not going anywhere soon. This is way too much fun. I just wanted to share with you a few others who have been instrumental in growing SHM.
A Special Thank You to Those Who Did the Work
SHM Presidents
John Nelson
Win Whitcomb
Bob Wachter
Ron Angus
Mark Williams
Jeff Dichter
Jeanne Huddleston
SHM Board Members (in addition to all Presidents)
Bill Atchley
Brad Flansbaum
David Zipes
Diane Craig
Herb Rogove
Jan Merin
Lisa Kettering
Mark Aronson
Mary Jo Gorman
Mike Ruhlen
Mitch Wilson
Pat Cawley
Peter Lindenauer
Richard Slataper
Russ Holman
Steve Pantilat
Editors, The Hospitalist
Scott Flanders
Jim Pile
Committee & Council Chairs (in addition to Board members)
Alpesh Amin
Andy Auerbach
Don Krause
Jack Percelay
Joe Li
Lakshmi Halasyamani
Mike Pistoria
Natalie Correia
Neil Kripalani
Preetha Basaviah
Sanjay Saint
Shaun Frost
Stacy Goldsholl
Sylvia McKean
Teresa Jones
Tim Cornell
Vineet Arora
SHM Staff
Angela Musial
Erica Pearson
Jane Mihelic
Kevin Stevens
Marie Francois
Marilyn Rivera
Michelle D’Agostino
Vera Bensch
Vernita Jackson
Veronica BeUs
Joe Miller
Tina Budnitz
The Campaign to Save 100,000 Lives

I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
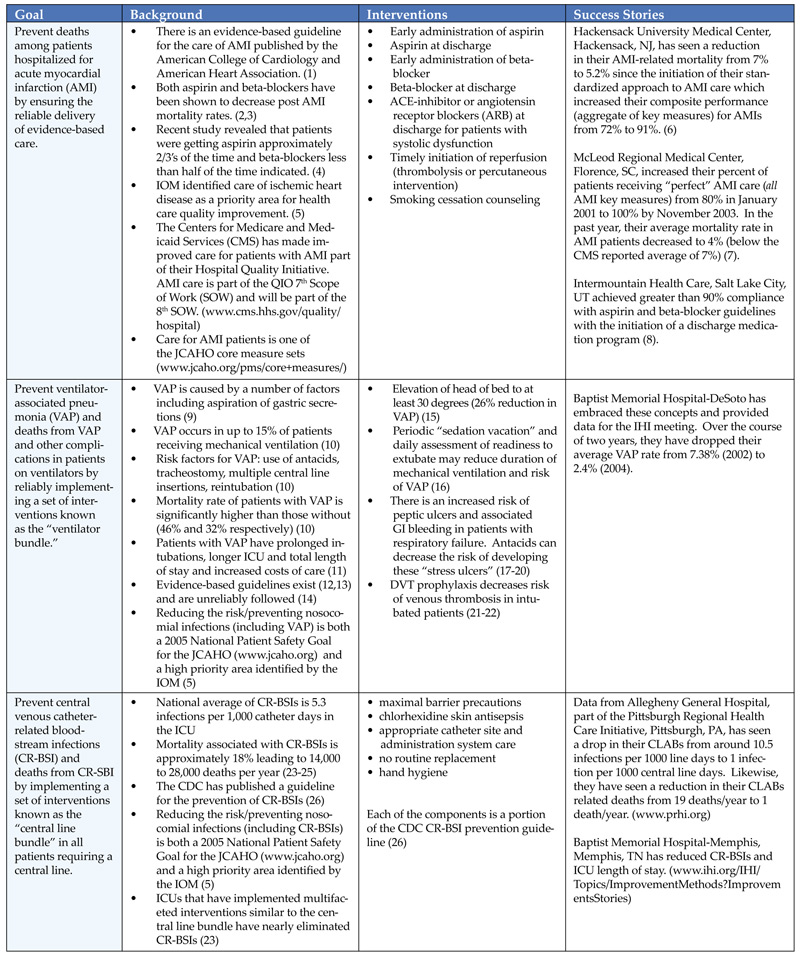
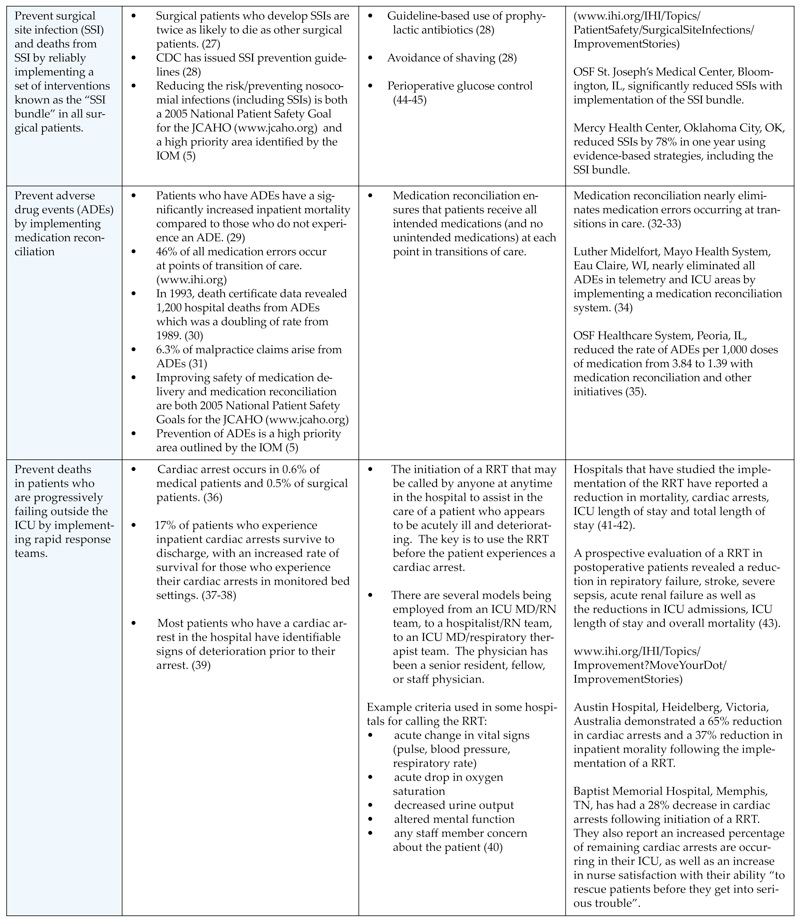
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.
I am on a plane on my way back to Minnesota after being professionally rejuvenated by the content of the Institute of Healthcare Improvement’s 16th Annual Forum, in Orlando, FL. The theme of the meeting called on all hospitals, and hence I believe all hospitalists, to save lives. Dr. Donald Berwick, President and CEO of the Institute of Healthcare Improvement (IHI) kicked off this years’ Annual Forum with his plenary speech “Some is not a number, Soon is not a time.” Saving some lives, some time in the future is not a clear goal. “Some is not a number and soon is not a time.” So, he put the challenge forth for hospitals to join IHI in a campaign to save 100K lives by June 14, 2006 at 9:00 a.m. EDT.
“Some is not a number. Soon is not a time.” We all get “why” this is important, at least in so much as what we have been told by the Institute of Medicine Reports “To Err is Human” and “Crossing the Quality Chasm”. But “how” can this be done? By doing things that we already know impact mortality in a hospital setting. By engaging in the reliable care delivery of six changes that save lives. These include recommendations in each of the following areas: rapid response or emergency medical teams, reliable care for acute myocardial infarctions, reliable use of the ventilator pneumonia and central venous line “bundles”, surgical site infection prophylaxis, and prevention of adverse drug events with reconciliation. Each is described in more detail below.
- Rapid Response Teams (also known as Medical Emergency or Pre-Code Teams): This is a team of healthcare providers that may be summoned at any time by anyone in the hospital to assist in the care of a patient who appears acutely ill, before the patient has respiratory failure, a cardiac arrest or other adverse event. The aim is to prevent situations of “failure to rescue”, to recognize the early signs and symptoms of clinical deterioration prior to requiring transfer to the intensive care unit.
- Reliable Care for Acute Myocardial Infarction (AMI): For appropriate AMI patients, reliable use of all of the following treatments: early administration of aspirin, aspirin at discharge, early administration of a beta-blocker, beta-blocker at discharge, ACE‑inhibitor or angiotensin receptor blocker (ARB) at discharge (if systolic dysfunction), timely reperfusion, and smoking cessation counseling.
- Reliable use of the Ventilator Bundle: A number of hospitals have initiated the use of the ventilator bundle to prevent ventilator associated pneumonia (VAP). VAP carries a high mortality rate. The “bundle” is a grouping of 5 treatments/preventions measured as a composite (% of patients that get all 5).
- Elevate head of bed to 30 degrees
- Peptic ulcer prophylaxis
- Deep venous thrombosis prophylaxis
- Daily “sedation vacation”
- Daily assessment of readiness to extubate
Not all of the items have a specific relationship to VAP (e.g., DVT prophylaxis), but when reliably performed in concert with the other items, leads to a decrease in VAP.
- Reliable use of Central Venous Line Bundles: This is a grouping of 5 preventative measures that when done in concert and measured as a composite have had maximal effectiveness for the reduction of central line associated blood stream infections (CLABs) in some hospitals.
- Hand hygiene
- Maximal barrier precautions
- Chlorhexidine skin antisepsis
- Appropriate catheter site and administration system care
- No routine line replacement
- Surgical site infection (SSI) prophylaxis with a “SSI bundle”: Hospitals participating with the IHI in a variety of different formats have found the most substantial reduction/prevention of SSIs when 3 preventative measures are done in concert with each other for every surgical patient. These preventative measures include:
- Guideline-based use of prophylactic perioperative antibiotics (including both choice and timing of administration of antibiotic)
- Appropriate hair removal (avoiding shaving)
- Perioperative glucose control
- Prevention of adverse drug events with medication reconciliation: This refers to the procedures that can be put in place at the time of any transition of care to mitigate the increased risk of wrong dose of medication or even wrong drug being administered immediately following that transition. Each time we have to transfer information from one sheet of paper to another or from a sheet of paper to a computer, there is chance for human error. Medication reconciliation can virtually eliminate errors occurring at transitions in care.
I have placed in Table 1, the information (goals, background, proposed interventions and success stories) handed out during Dr. Donald Berwick’s opening plenary session, the kick-off for the campaign to save 100,000 lives.
Two key components of the descriptions above deserve further explanation. One of the key components is the concept of reliability. Reliability is how often something in health care does what it is supposed to do, in the time frame it is supposed to do it in. The formula is the number of times that something (delivery of a medication or service) is done correctly divided by the number of times that same something is attempted. In work published by Karl Weick, one common principle within high reliability organizations is that of a preoccupation with failure. As such, the notation of reliability is a measure of defects. Currently much of healthcare (including use of beta-blockers after AMI) functions at a 10-1 level of performance (one defect in 10 tries) or less than a 90% success rate. Organizations that have actively embraced this concept of reliability in their quality improvement work have rejected the usual satisfaction with 10-1 performance. Shouldn’t 99 out of 100 (or 999 out of a 1,000) patients with an AMI get what they are supposed to get?
The other key component embedded within some of the six items that save lives is the concept of bundles. Rather than considering individual measures for each of the items within a bundle, a composite or aggregate measure is reported. Bottom line is that doing any one or two of the items in a bundle is not good enough. It will not achieve the same reduction in hospital acquired infection rates or mortality, as doing all of the items in concert for every appropriate patient.
How can hospitalists help achieve this national goal, to participate in this campaign with the IHI? As individuals, we can be a hospital “precinct captain” or champion, speak to our hospital boards, convene colleagues to standardize to science, start medication reconciliation, and seek composite reliability in our own individual practices.
The IHI will measure this campaign in four ways.
Level 1. Number of hospitals “signing up”
Level 2. Changes in process of care reported
Level 3. Actual changes in deaths and death rates (sample amongst volunteer hospitals)
Level 4. Hospital Standardized Mortality Rates (work of Brian Jarman)
More detailed and specific information about the campaign (and how to participate) can be found on IHI’s Web site (www.ihi.org/ihi/programs/campaign).
“Some is not a number. Soon is not a time.”
The number: 100,000 lives.
The time: June 14, 2006 – 9 a.m. EDT.
References
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction). J Am Coll Cardiol. 2004;44:671-719.
- Antman EM, Lau J, Kupelnick B, Mosteller F, Chalmers TC. A comparison of results of meta-analyses of randomized controlled trials and recommendations of clinical experts: treatments for myocardial infarction. JAMA. 1992;268:240-8.
- Hennekens CH, Albert CM, Godfried SL, Gaziano JM, Buring JE. Adjunctive drug therapy of acute myocardial infarction – evidence from clinical trials. N Engl J Med. 1996;335:1660-7.
- McGlynn EA, Asch SM, Adams J, et al. The quality of health care delivered to adults in the United States. N Engl J Med. 2003;348:2635-45.
- Adams K, Corrigan JM, eds. Priority areas for national action: transforming health care quality. Washington, DC: The National Academics Press, 2003.
- Lappe JM, Muhlstein JB, Lappe DL, et al. Improvements in 1-year cardiovascular clinical outcomes associated with a hospital-based discharge medication program. Ann Intern Med. 2004;141:446-53.
- Hackensack University Medical Center AMI Report, Sept 10, 2004.
- McLeod Regional Medical Center Storyboard for the 2004 IHI National Forum.
- Craven DE, Steger KA. Nosocomial pneumonia in mechanically ventilated adult patients: epidemiology and prevention in 1996. Semin Respir Infect. 1996;11:32-53.
- Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH. The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest. 2001;120:555-61.
- Rello J, Ollendorf DA, Oster G, et al. Epidemiology and outcomes of ventilator associated pneumonia in a large U.S. database. Chest. 2002;122:2115-21.
- Guidelines for Preventing Health-Care-Associated Pneumonia, 2003. Recommendations of CDC and the Healthcare Infection Control Practices Advisory Commi Tee. MMWR. 2004;53(No.RR‑3):1-36.
- Dodek P, Keenan S, Cook D, et al. Evidence-based clinical practice guideline for the prevention of ventilator-associated pneumonia. Ann Intern Med. 2004;141:305-13.
- Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia? A survey based on the opinions of an international panel of intensivists. Chest. 2002;122:656-61.
- Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomized trial. Lancet. 1999;354:1851-58.
- Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. N Engl J Med. 2000;342:1471-77.
- Cook DJ, Fuller HD, Guyatt GH, et al. Risk factors for gastrointestinal bleeding in critically ill patients. N Engl J Med. 1994;330:377-81.
- Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients: resolving discordant meta-analyses. JAMA. 1996;275:308-314.
- Cook D, Guyatt G, Marshall J, et al. A comparison of sucralfate and ranitidine for the prevention of upper gastrointestinal bleeding in patients requiring mechanical ventilation. N Engl J Med. 1998;338:791-97.
- Cook D, Heyland, Griffith L, Cook R, Marshall J, Pagliarello J. Risk factors for clinically important upper gastrointestinal bleeding in patients requiring mechanical ventilation. Canadian Critical Care Trials Group. Crit Care Med. 1999;27:2812-17.
- Attia J, Ray JG, Cook DJ, Douketis J, Ginsberg JS, Geerts WH. Deep vein thrombosis and its prevention in critically ill adults. Arch Intern Med. 2001;161:1268-79.
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism. The seventh ACCP conference on antithrombotic and thrombolytic therapy. Chest. 2004;126:338S-400S.
- Berenholtz SM, Pronovost PJ, Lipsett PA, et al. Eliminating catheter-related bloodstream infections in the intensive care unit. Crit Care Med. 2004;32:2014-20.
- Pittet D, Tarara D, Wenzel RP. Nosocomial bloodstream infection in critically ill patients. Excess length of stay, extra costs, and aTributable mortality. JAMA. 1994;271:1598-1601.
- Saint S. Chapter 16. Prevention of intravascular catheter-related infection. Making health care safer: a critical analysis of patient safety practices. AHRQ evidence report, number 43, July 20, 2001. www.ncbi.nlm.nih.gov/vooks.
- O’Grady NP; Alexander M, Dellinger EP, et al. Guidelines for the prevention of intravascular catheter-related infections. MMWR Morb Mort Wkly Rep. 2002;51(RR-10):1-29.
- Kirkland KB, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725-30.
- Mangram AJ, Horan TC, Pearson ML, et al. Guidelines for prevention of surgical site infection, 1999. Infect Control Hosp Epidemiol. 1999;20:247-78.
- Classen DC, Pestotnik SL, Evans RS, Lloyd JF, Burke JP. Adverse drug events in hospitalized patients. Excess length of stay, extra costs, and attributable mortality. JAMA. 1997;277:301-06.
- Phillips DP, Christenfeld N, Glynn LM. Increase in U.S. medication-error deaths between 1983 and 1993. Lancet. 1998;351:643-4.
- Rothschild JM, Federic FA, Gandhi TK, Kaushal R, Williams DH, Bates DW. Analysis of medication-related malpractice claims. Causes, preventability, and costs. Arch Intern Med. 2002;162:2414-20.
- Pronovost P, Weast B, Schwarz M, et al. Medication reconciliation: a practical tool to reduce the risk of medication errors. J Crit Care. 2003;18:201-205.
- Rozich JD, Resar RK. Medication safety: one organization’s approach to the challenge. JCOM. 2001;8(10):27-34.
- Rozich JD, Howard RJ, Justeson JM, Macken PD, Lindsay ME, Resar RK. Standardization as a mechanism to improve safety in healthcare. Jt Comm J Qual Saf. 2004;30:5-14.
- Whittington J, Cohen H. OSF Healthcare’s journey in patient safety. Qual Manag Health Care. 2004;13:53-59.
- Needleman J, Buerhaus P, Mattke S, et al. Nursing-staffing levels and the quality of care in hospitals. N Engl J Med. 2002;346:1715-22.
- Peberdy MA, Kaye W, Ornato JP, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14,270 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297-308.
- Sandroni C, Ferro G, Santangelo S, et al. In-hospital cardiac arrest: survival depends mainly on the emergency response. Resuscitation. 2004;62:291-7.
- Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388-92.
- Hillman K, Parr M, Flabouris A, Bishop G, Stewart A. Redefining in-hospital resuscitation: the concept of the medical emergency team. Resuscitation. 2001;48:105-10.
- Buist MD, Moore GE, Bernard SA, Waxman BP, Anderson JN, Nguyen TV. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. BMJ. 2002;324:387-90.
- Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. MJA. 2003;179:283-7.
- Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trail of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Car Med. 2004;32:916-21.
- Furnary AP, Zerr KJ, Grunkemeier GL, Starr AL. Continuous intravenous insulin infusion reduces the incidence of deep sternal wound infection in diabetic patients after cardiac surgical procedures. Ann Thorac Surg. 1999;67: 352-62.
- Van de Berghe G, Wouters P, Weekers F, et all. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359-67.