User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'medstat-accordion-set article-series')]
Oral IL-23 receptor antagonist for psoriasis promising: Phase 2b study
SINGAPORE – across all doses, compared with placebo, according to results of the FRONTIER 1 trial.
In the 16-week phase 2b study, 255 adults with moderate to severe plaque psoriasis were randomly assigned into six treatment groups: placebo (n = 43), JNJ-2113 25 mg daily (n = 43), 25 mg twice daily (n = 41), 50 mg daily (n = 43), 100 mg daily (n = 43), or 100 mg twice daily (n = 42).
Of those who took the placebo, only 9.3% achieved the study’s primary endpoint of a 75% or greater improvement in the Psoriasis Area and Severity Index (PASI-75) by week 16. This was compared with 78.6% in the group that took the highest dose.

“Additionally, the onset of action was fairly fast: at week 4, more than 20% of patients had achieved PASI 75,” said Robert Bissonnette, MD, CEO of Innovaderm Research in Montreal, who presented the findings during a late-breaker session at the World Congress of Dermatology.
Patients in the remaining groups demonstrated a response that corresponded to dosing level: with 37.2%, 51.2%, 58.1%, and 65.1% achieving PASI-75 in the 25 mg daily, 25 mg twice-daily, 50 mg daily, and 100 mg daily groups, respectively.
“These results are very interesting because in terms of psoriasis treatment, if this is confirmed in phase 3, it would give us an oral alternative that would be selective for IL-23,” said Dr. Bissonnette, referring to the signaling pathway that plays a critical role in the pathogenesis of several immune-mediated inflammatory diseases, including plaque psoriasis.
Although rarely life-threatening, the skin disorder is often intractable to treatment. In recent years, therapies that block IL-23 signaling and downstream inflammatory cytokine production have proven useful. “We have on the market a number of biological agents targeting IL-23 that we use on a regular basis,” said Dr. Bissonnette. “However, there are currently no orally delivered therapies.”
If successful, JNJ-2113 – a first-in-class oral IL-23 antagonist peptide developed by Janssen – could change the treatment paradigm for patients with moderate to severe plaque psoriasis. “When I was first introduced to the concept, I thought it wouldn’t work as it’s a peptide, that it would be digested by the stomach,” he told the audience. “But because of its GI stability and its potency, when you administer it orally, you can detect pharmacological activity.”
A well-tolerated alternative
Participants in the FRONTIER 1 trial were on average about 44 years old and weighed 88.9 kg (195 lb). Most had been living with psoriasis for about 18 years, with a total PASI score of 19.05. In addition, 43.1% had been treated with phototherapy in the past, 22% with biologics, and 78.4% with systemics.
PASI 90 and 100 were among some of the secondary outcomes measured. Similar to the primary outcome of PASI 75, all treatment groups demonstrated a statistically significant dose-response in PASI 90, compared with placebo. For those on the highest dose of JNJ-2113, 59.5% and 40.5% achieved PASI 90 and PASI 100, respectively, by week 16. The corresponding figures for those receiving placebo were 2.3% and 0%.
The safety profile for JNJ-2113 across all doses was similar to that of placebo, with no evidence of a dose-dependent increase in the occurrence of adverse events (AEs). The most frequently reported AEs were COVID-19 and nasopharyngitis. There were three serious AEs (COVID-19, infected cyst, suicide attempt) among those on the active drug, but the investigators assessed that they were not related to the study intervention. No deaths, major adverse cardiac events, or malignancies were reported during the study.
Approached for an independent comment, Marius-Anton Ionescu, MD, PhD, from the University Hospital Saint Louis, Paris, who specializes in psoriasis, told this news organization that the new development with JNJ-2113 “is really promising.”
Treatment for plaque psoriasis has improved to the point where some biologics, such as risankizumab (Skyrizi), only require patients to have “four shots a year,” he says. “This is the future of psoriasis treatment; it might go down to two shots a year” – a regimen that will be easier than taking an oral medication once or twice a day.
“But it’s good to have an oral option because you will always have some patients who say: ‘Shots are not for me, I’m afraid,’ ” he says.
However, Dr. Ionescu noted that if JNJ-2113 were to pass phase 3 trials, it might face stiff competition from the selective tyrosine kinase 2 (TYK2) inhibitor deucravacitinib (Sotyktu), which the U.S. Food and Drug Administration approved for use in adults with moderate to severe plaque psoriasis last September. “It has very good results and is the first oral therapy that is comparable with biologics for plaque psoriasis,” he says.
But Dr. Bissonnette remains hopeful for the future. “I think JNJ-2113 goes way beyond psoriasis because this type of strategy using oral peptide–blocking receptors could be used in other immune-mediated diseases, including atopic dermatitis and other diseases outside of dermatology.” In addition to running a phase 3 study for moderate to severe plaque psoriasis, Janssen is planning to initiate a phase 2b clinical trial of JNJ-2113 in adults with ulcerative colitis.
The study was funded by Janssen. Dr. Bissonnette reports consulting and investigating for Janssen, and being on advisory panels and receiving research funding from multiple other pharmaceutical companies. Dr. Ionescu is an investigator for Psoriasis National Register France Psobioteq (no honoraria), and an investigator and speaker for Uriage cosmetics (honoraria).
A version of this article first appeared on Medscape.com.
SINGAPORE – across all doses, compared with placebo, according to results of the FRONTIER 1 trial.
In the 16-week phase 2b study, 255 adults with moderate to severe plaque psoriasis were randomly assigned into six treatment groups: placebo (n = 43), JNJ-2113 25 mg daily (n = 43), 25 mg twice daily (n = 41), 50 mg daily (n = 43), 100 mg daily (n = 43), or 100 mg twice daily (n = 42).
Of those who took the placebo, only 9.3% achieved the study’s primary endpoint of a 75% or greater improvement in the Psoriasis Area and Severity Index (PASI-75) by week 16. This was compared with 78.6% in the group that took the highest dose.
“Additionally, the onset of action was fairly fast: at week 4, more than 20% of patients had achieved PASI 75,” said Robert Bissonnette, MD, CEO of Innovaderm Research in Montreal, who presented the findings during a late-breaker session at the World Congress of Dermatology.
Patients in the remaining groups demonstrated a response that corresponded to dosing level: with 37.2%, 51.2%, 58.1%, and 65.1% achieving PASI-75 in the 25 mg daily, 25 mg twice-daily, 50 mg daily, and 100 mg daily groups, respectively.
“These results are very interesting because in terms of psoriasis treatment, if this is confirmed in phase 3, it would give us an oral alternative that would be selective for IL-23,” said Dr. Bissonnette, referring to the signaling pathway that plays a critical role in the pathogenesis of several immune-mediated inflammatory diseases, including plaque psoriasis.
Although rarely life-threatening, the skin disorder is often intractable to treatment. In recent years, therapies that block IL-23 signaling and downstream inflammatory cytokine production have proven useful. “We have on the market a number of biological agents targeting IL-23 that we use on a regular basis,” said Dr. Bissonnette. “However, there are currently no orally delivered therapies.”
If successful, JNJ-2113 – a first-in-class oral IL-23 antagonist peptide developed by Janssen – could change the treatment paradigm for patients with moderate to severe plaque psoriasis. “When I was first introduced to the concept, I thought it wouldn’t work as it’s a peptide, that it would be digested by the stomach,” he told the audience. “But because of its GI stability and its potency, when you administer it orally, you can detect pharmacological activity.”
A well-tolerated alternative
Participants in the FRONTIER 1 trial were on average about 44 years old and weighed 88.9 kg (195 lb). Most had been living with psoriasis for about 18 years, with a total PASI score of 19.05. In addition, 43.1% had been treated with phototherapy in the past, 22% with biologics, and 78.4% with systemics.
PASI 90 and 100 were among some of the secondary outcomes measured. Similar to the primary outcome of PASI 75, all treatment groups demonstrated a statistically significant dose-response in PASI 90, compared with placebo. For those on the highest dose of JNJ-2113, 59.5% and 40.5% achieved PASI 90 and PASI 100, respectively, by week 16. The corresponding figures for those receiving placebo were 2.3% and 0%.
The safety profile for JNJ-2113 across all doses was similar to that of placebo, with no evidence of a dose-dependent increase in the occurrence of adverse events (AEs). The most frequently reported AEs were COVID-19 and nasopharyngitis. There were three serious AEs (COVID-19, infected cyst, suicide attempt) among those on the active drug, but the investigators assessed that they were not related to the study intervention. No deaths, major adverse cardiac events, or malignancies were reported during the study.
Approached for an independent comment, Marius-Anton Ionescu, MD, PhD, from the University Hospital Saint Louis, Paris, who specializes in psoriasis, told this news organization that the new development with JNJ-2113 “is really promising.”
Treatment for plaque psoriasis has improved to the point where some biologics, such as risankizumab (Skyrizi), only require patients to have “four shots a year,” he says. “This is the future of psoriasis treatment; it might go down to two shots a year” – a regimen that will be easier than taking an oral medication once or twice a day.
“But it’s good to have an oral option because you will always have some patients who say: ‘Shots are not for me, I’m afraid,’ ” he says.
However, Dr. Ionescu noted that if JNJ-2113 were to pass phase 3 trials, it might face stiff competition from the selective tyrosine kinase 2 (TYK2) inhibitor deucravacitinib (Sotyktu), which the U.S. Food and Drug Administration approved for use in adults with moderate to severe plaque psoriasis last September. “It has very good results and is the first oral therapy that is comparable with biologics for plaque psoriasis,” he says.
But Dr. Bissonnette remains hopeful for the future. “I think JNJ-2113 goes way beyond psoriasis because this type of strategy using oral peptide–blocking receptors could be used in other immune-mediated diseases, including atopic dermatitis and other diseases outside of dermatology.” In addition to running a phase 3 study for moderate to severe plaque psoriasis, Janssen is planning to initiate a phase 2b clinical trial of JNJ-2113 in adults with ulcerative colitis.
The study was funded by Janssen. Dr. Bissonnette reports consulting and investigating for Janssen, and being on advisory panels and receiving research funding from multiple other pharmaceutical companies. Dr. Ionescu is an investigator for Psoriasis National Register France Psobioteq (no honoraria), and an investigator and speaker for Uriage cosmetics (honoraria).
A version of this article first appeared on Medscape.com.
SINGAPORE – across all doses, compared with placebo, according to results of the FRONTIER 1 trial.
In the 16-week phase 2b study, 255 adults with moderate to severe plaque psoriasis were randomly assigned into six treatment groups: placebo (n = 43), JNJ-2113 25 mg daily (n = 43), 25 mg twice daily (n = 41), 50 mg daily (n = 43), 100 mg daily (n = 43), or 100 mg twice daily (n = 42).
Of those who took the placebo, only 9.3% achieved the study’s primary endpoint of a 75% or greater improvement in the Psoriasis Area and Severity Index (PASI-75) by week 16. This was compared with 78.6% in the group that took the highest dose.
“Additionally, the onset of action was fairly fast: at week 4, more than 20% of patients had achieved PASI 75,” said Robert Bissonnette, MD, CEO of Innovaderm Research in Montreal, who presented the findings during a late-breaker session at the World Congress of Dermatology.
Patients in the remaining groups demonstrated a response that corresponded to dosing level: with 37.2%, 51.2%, 58.1%, and 65.1% achieving PASI-75 in the 25 mg daily, 25 mg twice-daily, 50 mg daily, and 100 mg daily groups, respectively.
“These results are very interesting because in terms of psoriasis treatment, if this is confirmed in phase 3, it would give us an oral alternative that would be selective for IL-23,” said Dr. Bissonnette, referring to the signaling pathway that plays a critical role in the pathogenesis of several immune-mediated inflammatory diseases, including plaque psoriasis.
Although rarely life-threatening, the skin disorder is often intractable to treatment. In recent years, therapies that block IL-23 signaling and downstream inflammatory cytokine production have proven useful. “We have on the market a number of biological agents targeting IL-23 that we use on a regular basis,” said Dr. Bissonnette. “However, there are currently no orally delivered therapies.”
If successful, JNJ-2113 – a first-in-class oral IL-23 antagonist peptide developed by Janssen – could change the treatment paradigm for patients with moderate to severe plaque psoriasis. “When I was first introduced to the concept, I thought it wouldn’t work as it’s a peptide, that it would be digested by the stomach,” he told the audience. “But because of its GI stability and its potency, when you administer it orally, you can detect pharmacological activity.”
A well-tolerated alternative
Participants in the FRONTIER 1 trial were on average about 44 years old and weighed 88.9 kg (195 lb). Most had been living with psoriasis for about 18 years, with a total PASI score of 19.05. In addition, 43.1% had been treated with phototherapy in the past, 22% with biologics, and 78.4% with systemics.
PASI 90 and 100 were among some of the secondary outcomes measured. Similar to the primary outcome of PASI 75, all treatment groups demonstrated a statistically significant dose-response in PASI 90, compared with placebo. For those on the highest dose of JNJ-2113, 59.5% and 40.5% achieved PASI 90 and PASI 100, respectively, by week 16. The corresponding figures for those receiving placebo were 2.3% and 0%.
The safety profile for JNJ-2113 across all doses was similar to that of placebo, with no evidence of a dose-dependent increase in the occurrence of adverse events (AEs). The most frequently reported AEs were COVID-19 and nasopharyngitis. There were three serious AEs (COVID-19, infected cyst, suicide attempt) among those on the active drug, but the investigators assessed that they were not related to the study intervention. No deaths, major adverse cardiac events, or malignancies were reported during the study.
Approached for an independent comment, Marius-Anton Ionescu, MD, PhD, from the University Hospital Saint Louis, Paris, who specializes in psoriasis, told this news organization that the new development with JNJ-2113 “is really promising.”
Treatment for plaque psoriasis has improved to the point where some biologics, such as risankizumab (Skyrizi), only require patients to have “four shots a year,” he says. “This is the future of psoriasis treatment; it might go down to two shots a year” – a regimen that will be easier than taking an oral medication once or twice a day.
“But it’s good to have an oral option because you will always have some patients who say: ‘Shots are not for me, I’m afraid,’ ” he says.
However, Dr. Ionescu noted that if JNJ-2113 were to pass phase 3 trials, it might face stiff competition from the selective tyrosine kinase 2 (TYK2) inhibitor deucravacitinib (Sotyktu), which the U.S. Food and Drug Administration approved for use in adults with moderate to severe plaque psoriasis last September. “It has very good results and is the first oral therapy that is comparable with biologics for plaque psoriasis,” he says.
But Dr. Bissonnette remains hopeful for the future. “I think JNJ-2113 goes way beyond psoriasis because this type of strategy using oral peptide–blocking receptors could be used in other immune-mediated diseases, including atopic dermatitis and other diseases outside of dermatology.” In addition to running a phase 3 study for moderate to severe plaque psoriasis, Janssen is planning to initiate a phase 2b clinical trial of JNJ-2113 in adults with ulcerative colitis.
The study was funded by Janssen. Dr. Bissonnette reports consulting and investigating for Janssen, and being on advisory panels and receiving research funding from multiple other pharmaceutical companies. Dr. Ionescu is an investigator for Psoriasis National Register France Psobioteq (no honoraria), and an investigator and speaker for Uriage cosmetics (honoraria).
A version of this article first appeared on Medscape.com.
AT WCD 2023
The surprising occupations with higher-than-expected ovarian cancer rates
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.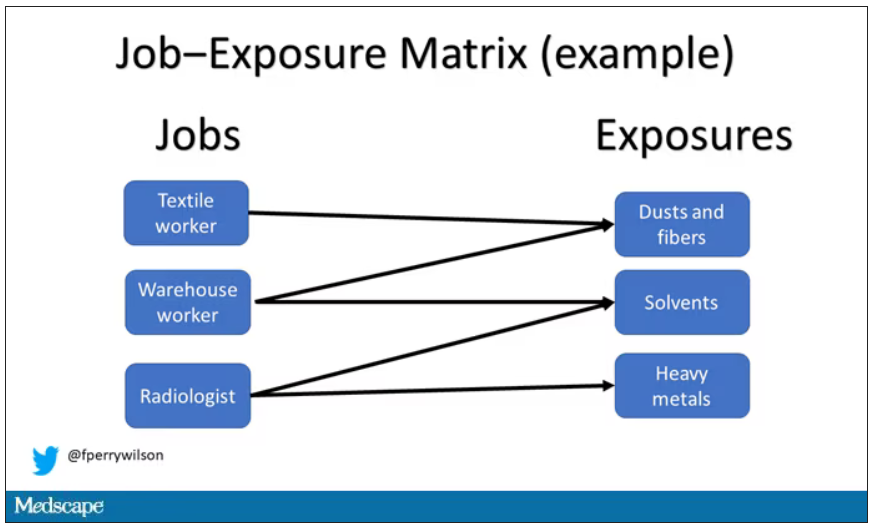
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.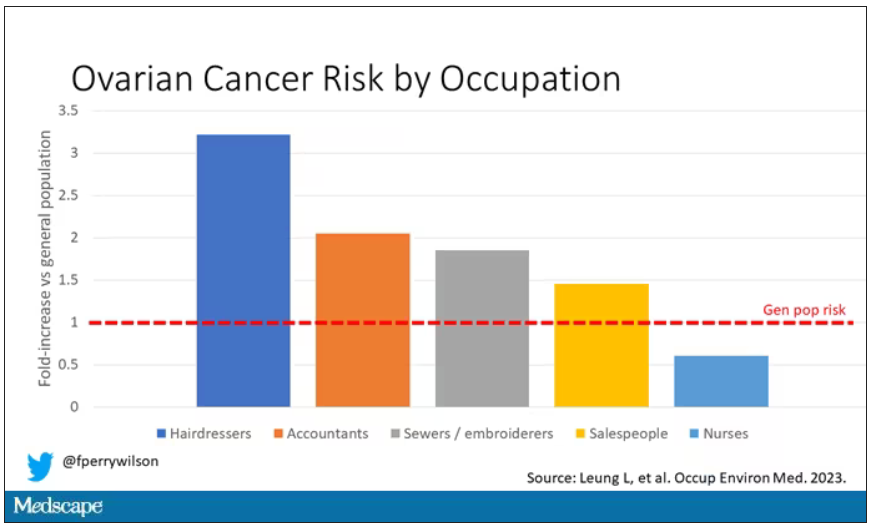
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study.
Basically, all cancers are caused by a mix of genetic and environmental factors, with some cancers driven more strongly by one or the other. When it comes to ovarian cancer, which kills more than 13,000 women per year in the United States, genetic factors like the BRCA gene mutations are well described.
Other risk factors, like early menarche and nulliparity, are difficult to modify. The only slam-dunk environmental toxin to be linked to ovarian cancer is asbestos. Still, the vast majority of women who develop ovarian cancer do not have a known high-risk gene or asbestos exposure, so other triggers may be out there. How do we find them? The answer may just be good old-fashioned epidemiology.
That’s just what researchers, led by Anita Koushik at the University of Montreal, did in a new study appearing in the journal Occupational and Environmental Medicine.
They identified 497 women in Montreal who had recently been diagnosed with ovarian cancer. They then matched those women to 897 women without ovarian cancer, based on age and address. (This approach would not work well in the United States, as diagnosis of ovarian cancer might depend on access to medical care, which is not universal here. In Canada, however, it’s safer to assume that anyone who could have gotten ovarian cancer in Montreal would have been detected.)
Cases and controls identified, the researchers took a detailed occupational history for each participant: every job they ever worked, and when, and for how long. Each occupation was mapped to a standardized set of industries and, interestingly, to a set of environmental exposures ranging from cosmetic talc to cooking fumes to cotton dust, in what is known as a job-exposure matrix. Of course, they also collected data on other ovarian cancer risk factors.
After that, it’s a simple matter of looking at the rate of ovarian cancer by occupation and occupation-associated exposures, accounting for differences in things like pregnancy rates.
A brief aside here. I was at dinner with my wife the other night and telling her about this study, and I asked, “What do you think the occupation with the highest rate of ovarian cancer is?” And without missing a beat, she said: “Hairdressers.” Which blew my mind because of how random that was, but she was also – as usual – 100% correct.
Hairdressers, at least those who had been in the industry for more than 10 years, had a threefold higher risk for ovarian cancer than matched controls who had never been hairdressers.
Of course, my wife is a cancer surgeon, so she has a bit of a leg up on me here. Many of you may also know that there is actually a decent body of literature showing higher rates of various cancers among hairdressers, presumably due to the variety of chemicals they are exposed to on a continuous basis.
The No. 2 highest-risk profession on the list? Accountants, with about a twofold higher risk. That one is more of a puzzler. It could be a false positive; after all, there were multiple occupations checked and random error might give a few hits that are meaningless. But there are certainly some occupational factors unique to accountants that might bear further investigation – maybe exposure to volatile organic compounds from office printers, or just a particularly sedentary office environment.
In terms of specific exposures, there were high risks seen with mononuclear aromatic hydrocarbons, bleaches, ethanol, and fluorocarbons, among others, but we have to be a bit more careful here. These exposures were not directly measured. Rather, based on the job category a woman described, the exposures were imputed based on the job-exposure matrix. As such, the correlations between the job and the particular exposure are really quite high, making it essentially impossible to tease out whether it is, for example, being a hairdresser, or being exposed to fluorocarbons as a hairdresser, or being exposed to something else as a hairdresser, that is the problem.
This is how these types of studies work; they tend to raise more questions than they answer. But in a world where a cancer diagnosis can seem to come completely out of the blue, they provide the starting point that someday may lead to a more definitive culprit agent or group of agents. Until then, it might be wise for hairdressers to make sure their workplace is well ventilated.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale University’s Clinical and Translational Research Accelerator in New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Mental health questions cut from MD licensing applications in 21 states
Since May, physicians in 21 states are no longer being asked broad mental health or substance abuse questions when they apply for a medical license. That’s a major shift that could ease doctors’ concerns about seeking treatment, according to the Dr. Lorna Breen Heroes› Foundation, a physician burnout prevention group that tracks such changes.
The foundation was named in honor of Lorna Breen, MD, an emergency medicine physician in New York City who died by suicide in April 2020 as the pandemic unfolded. The rate of suicide among physicians is twice that of the general population.
“The issue is not whether a physician may have had a serious or a mild mental illness ... but whether they have any disabilities that may affect their current work,” said Peter Yellowlees, MD, distinguished professor of psychiatry at the University of California, Davis. “Asking about any past mental illness episodes, which may have occurred years previously ... is simply discriminatory and is an example of the stigma associated with mental disorders.”
The Breen Foundation has been working with state medical boards and hospitals to remove stigmatizing mental health and substance abuse questions from licensing and credentialing applications.
Dr. Breen had told her sister and brother-in-law shortly before her suicide that she was afraid she could lose her license and the career she loved if the medical board found out that she had received inpatient mental health treatment, said J. Corey Feist, JD, MBA, her brother-in-law and cofounder and president of the foundation.
She wasn’t aware that New York was a state that didn’t ask physicians questions about their mental health, said Mr. Feist.
“That’s why we want to make it very clear to physicians which states continue to ask these questions and which ones don’t,” Mr. Feist said.
Many physicians share Dr. Breen’s concern about professional consequences.
Four in 10 physicians said that they did not seek help for burnout or depression because they worried that their employer or state medical board would find out, according to the Medscape ‘I Cry but No One Cares’: Physician Burnout & Depression Report 2023.
One Oregon emergency department physician said that informing her state medical board about an episode of mania resulted in public disclosures, a 4-month long investigation, lost income, and poorer work evaluations. Looking back on her decision to be transparent with the board, Susan Haney, MD, said that she was naive. “The board is not your friend.”
Fearing for her career, now-retired ob.gyn. Robyn Alley-Hay, MD, never disclosed on licensing applications that in the 1990s, she had been hospitalized and treated for depression. She stopped practicing medicine in 2014 and now works as a life coach.
“I hated those questions because I felt I could never tell the whole truth,” Dr. Alley-Hay said. “But I could always truthfully answer ‘no’ to questions about impairment. That was a line that I wouldn’t cross – if you’re impaired, you shouldn’t be practicing.”
Does the focus on current impairment protect the public?
New York, Texas, California, Montana, Illinois, and North Carolina are among the 21 states that either ask no health-related questions or ask only a single question to address physical and mental health, said Mr. Feist.
Most of these changes align with the 2018 Federation of State Medical Boards recommendations, said Joe Knickrehm, FSMB vice president of communications. “Application questions must focus only on current impairment and not on illness, diagnosis, or previous treatment in order to be compliant with the Americans With Disabilities Act,” states the FSMB.
Mental health questions were often added to licensing and credentialing applications out of a “misplaced desire to protect patients and families from clinicians who might not be fit to give care. Yet there is no evidence they serve that function,” said Mr. Feist.
Marian Hollingsworth, a patient safety advocate in California, says medical boards have a responsibility to ensure that doctors pose no risk or a negligible risk to the public. She questioned whether the medical boards can adequately protect the public if they only ask about medical conditions rather than mental illness or substance abuse.
“There’s a fine line between privacy and right to know for public protection. I would want to see the approving medical board have assurance from a treating professional that this physician is stable and is doing well with continued treatment,” said Ms. Hollingsworth.
Legislation requires that mental health questions be removed
In March, Virginia became the first state to enact a law that requires all health care profession regulatory boards, including medical boards, to remove or replace mental health questions on licensing, certification, and registration applications.
The law requires that boards use the following wording if they replace mental health questions: “Do you have any reason to believe you would pose a risk to the safety or well-being of patients?” “Are you able to perform the essential functions of your job with or without reasonable accommodations?”
The Illinois General Assembly passed a more limited bill in May that requires medical boards to remove or replace mental health questions on its licensing applications. Gov. J. B. Pritzker (D) is expected to sign the bill.
The Virginia Healthcare and Hospital Association, which represents more than 100 hospitals and health systems in the state, partnered with the Medical Society of Virginia and the Virginia Nurses Association to advocate for the new legislation.
“The reason that the Virginia coalition pushed for the law was because the state’s medical boards weren’t acting quickly enough. Although state laws vary about what medical boards can do, legislation isn’t necessary in most states to change licensing questions,” said Mr. Feist.
Virginia hospitals began working last year with the foundation to change their mental health questions on credentialing applications. About 20% of Virginia’s hospitals have completed the process, including four large health systems: Inova, UVA Health, Centerra, and Children’s Hospitals of King’s Daughters, said Mr. Feist.
The foundation also challenged Lisa MacLean, MD, a psychiatrist and chief clinical wellness officer at the Henry Ford Medical Group in Detroit, to review their credentialing application for any stigmatizing mental health questions.
Dr. MacLean told the American Medical Association that she had found one question that needed to be changed but that it took time to get through the hospital›s approval process. Ultimately, the wording was changed from “a diagnosis or treatment of a physical, mental, chemical dependency or emotional condition” to “a diagnosis or treatment of any condition which could impair your ability to practice medicine.”
National medical organizations back changes
The Joint Commission, which accredits hospitals, has emphasized since 2020 that it doesn’t require hospitals to ask about an applicant’s mental health history.
“We strongly encourage organizations to not ask about past history of mental health conditions or treatment,” the Commission said in a statement. “It is critical that we ensure health care workers can feel free to access mental health resources.”
The Joint Commission said it supports the FSMB recommendations and the AMA’s recommendation that questions about clinicians’ mental health be limited to “conditions that currently impair the clinicians’ ability to perform their job.”
More than 40 professional medical organizations, including the American Academy of Family Physicians and the American Psychiatric Association, signed a joint statement in 2020 calling for changes in disclosure rules about mental health.
“The backing of major organizations is helpful because it’s changing the conversation that occurs within and outside the house of medicine,” said Mr. Feist.
Should doctors answer mental health questions?
Many states continue to ask questions about hospitalization and mental health diagnoses or treatment on their licensing and credentialing applications.
Yellowlees advises doctors to “be honest and not lie or deny past mental health problems, as medical boards tend to take a very serious view of physicians who do not tell the truth.”
However, the questions asked by medical boards can vary by state. “If it’s possible, physicians can give accurate but minimal information while trying to focus mainly on their current work capacity,” said Dr. Yellowlees.
He also suggested that physicians who are uncertain about how to respond to mental health questions consider obtaining advice from lawyers accustomed to working with the relevant medical boards.
Physicians who want to get involved in removing licensing and credentialing barriers to mental health care can find resources here and here.
A version of this article first appeared on Medscape.com.
Since May, physicians in 21 states are no longer being asked broad mental health or substance abuse questions when they apply for a medical license. That’s a major shift that could ease doctors’ concerns about seeking treatment, according to the Dr. Lorna Breen Heroes› Foundation, a physician burnout prevention group that tracks such changes.
The foundation was named in honor of Lorna Breen, MD, an emergency medicine physician in New York City who died by suicide in April 2020 as the pandemic unfolded. The rate of suicide among physicians is twice that of the general population.
“The issue is not whether a physician may have had a serious or a mild mental illness ... but whether they have any disabilities that may affect their current work,” said Peter Yellowlees, MD, distinguished professor of psychiatry at the University of California, Davis. “Asking about any past mental illness episodes, which may have occurred years previously ... is simply discriminatory and is an example of the stigma associated with mental disorders.”
The Breen Foundation has been working with state medical boards and hospitals to remove stigmatizing mental health and substance abuse questions from licensing and credentialing applications.
Dr. Breen had told her sister and brother-in-law shortly before her suicide that she was afraid she could lose her license and the career she loved if the medical board found out that she had received inpatient mental health treatment, said J. Corey Feist, JD, MBA, her brother-in-law and cofounder and president of the foundation.
She wasn’t aware that New York was a state that didn’t ask physicians questions about their mental health, said Mr. Feist.
“That’s why we want to make it very clear to physicians which states continue to ask these questions and which ones don’t,” Mr. Feist said.
Many physicians share Dr. Breen’s concern about professional consequences.
Four in 10 physicians said that they did not seek help for burnout or depression because they worried that their employer or state medical board would find out, according to the Medscape ‘I Cry but No One Cares’: Physician Burnout & Depression Report 2023.
One Oregon emergency department physician said that informing her state medical board about an episode of mania resulted in public disclosures, a 4-month long investigation, lost income, and poorer work evaluations. Looking back on her decision to be transparent with the board, Susan Haney, MD, said that she was naive. “The board is not your friend.”
Fearing for her career, now-retired ob.gyn. Robyn Alley-Hay, MD, never disclosed on licensing applications that in the 1990s, she had been hospitalized and treated for depression. She stopped practicing medicine in 2014 and now works as a life coach.
“I hated those questions because I felt I could never tell the whole truth,” Dr. Alley-Hay said. “But I could always truthfully answer ‘no’ to questions about impairment. That was a line that I wouldn’t cross – if you’re impaired, you shouldn’t be practicing.”
Does the focus on current impairment protect the public?
New York, Texas, California, Montana, Illinois, and North Carolina are among the 21 states that either ask no health-related questions or ask only a single question to address physical and mental health, said Mr. Feist.
Most of these changes align with the 2018 Federation of State Medical Boards recommendations, said Joe Knickrehm, FSMB vice president of communications. “Application questions must focus only on current impairment and not on illness, diagnosis, or previous treatment in order to be compliant with the Americans With Disabilities Act,” states the FSMB.
Mental health questions were often added to licensing and credentialing applications out of a “misplaced desire to protect patients and families from clinicians who might not be fit to give care. Yet there is no evidence they serve that function,” said Mr. Feist.
Marian Hollingsworth, a patient safety advocate in California, says medical boards have a responsibility to ensure that doctors pose no risk or a negligible risk to the public. She questioned whether the medical boards can adequately protect the public if they only ask about medical conditions rather than mental illness or substance abuse.
“There’s a fine line between privacy and right to know for public protection. I would want to see the approving medical board have assurance from a treating professional that this physician is stable and is doing well with continued treatment,” said Ms. Hollingsworth.
Legislation requires that mental health questions be removed
In March, Virginia became the first state to enact a law that requires all health care profession regulatory boards, including medical boards, to remove or replace mental health questions on licensing, certification, and registration applications.
The law requires that boards use the following wording if they replace mental health questions: “Do you have any reason to believe you would pose a risk to the safety or well-being of patients?” “Are you able to perform the essential functions of your job with or without reasonable accommodations?”
The Illinois General Assembly passed a more limited bill in May that requires medical boards to remove or replace mental health questions on its licensing applications. Gov. J. B. Pritzker (D) is expected to sign the bill.
The Virginia Healthcare and Hospital Association, which represents more than 100 hospitals and health systems in the state, partnered with the Medical Society of Virginia and the Virginia Nurses Association to advocate for the new legislation.
“The reason that the Virginia coalition pushed for the law was because the state’s medical boards weren’t acting quickly enough. Although state laws vary about what medical boards can do, legislation isn’t necessary in most states to change licensing questions,” said Mr. Feist.
Virginia hospitals began working last year with the foundation to change their mental health questions on credentialing applications. About 20% of Virginia’s hospitals have completed the process, including four large health systems: Inova, UVA Health, Centerra, and Children’s Hospitals of King’s Daughters, said Mr. Feist.
The foundation also challenged Lisa MacLean, MD, a psychiatrist and chief clinical wellness officer at the Henry Ford Medical Group in Detroit, to review their credentialing application for any stigmatizing mental health questions.
Dr. MacLean told the American Medical Association that she had found one question that needed to be changed but that it took time to get through the hospital›s approval process. Ultimately, the wording was changed from “a diagnosis or treatment of a physical, mental, chemical dependency or emotional condition” to “a diagnosis or treatment of any condition which could impair your ability to practice medicine.”
National medical organizations back changes
The Joint Commission, which accredits hospitals, has emphasized since 2020 that it doesn’t require hospitals to ask about an applicant’s mental health history.
“We strongly encourage organizations to not ask about past history of mental health conditions or treatment,” the Commission said in a statement. “It is critical that we ensure health care workers can feel free to access mental health resources.”
The Joint Commission said it supports the FSMB recommendations and the AMA’s recommendation that questions about clinicians’ mental health be limited to “conditions that currently impair the clinicians’ ability to perform their job.”
More than 40 professional medical organizations, including the American Academy of Family Physicians and the American Psychiatric Association, signed a joint statement in 2020 calling for changes in disclosure rules about mental health.
“The backing of major organizations is helpful because it’s changing the conversation that occurs within and outside the house of medicine,” said Mr. Feist.
Should doctors answer mental health questions?
Many states continue to ask questions about hospitalization and mental health diagnoses or treatment on their licensing and credentialing applications.
Yellowlees advises doctors to “be honest and not lie or deny past mental health problems, as medical boards tend to take a very serious view of physicians who do not tell the truth.”
However, the questions asked by medical boards can vary by state. “If it’s possible, physicians can give accurate but minimal information while trying to focus mainly on their current work capacity,” said Dr. Yellowlees.
He also suggested that physicians who are uncertain about how to respond to mental health questions consider obtaining advice from lawyers accustomed to working with the relevant medical boards.
Physicians who want to get involved in removing licensing and credentialing barriers to mental health care can find resources here and here.
A version of this article first appeared on Medscape.com.
Since May, physicians in 21 states are no longer being asked broad mental health or substance abuse questions when they apply for a medical license. That’s a major shift that could ease doctors’ concerns about seeking treatment, according to the Dr. Lorna Breen Heroes› Foundation, a physician burnout prevention group that tracks such changes.
The foundation was named in honor of Lorna Breen, MD, an emergency medicine physician in New York City who died by suicide in April 2020 as the pandemic unfolded. The rate of suicide among physicians is twice that of the general population.
“The issue is not whether a physician may have had a serious or a mild mental illness ... but whether they have any disabilities that may affect their current work,” said Peter Yellowlees, MD, distinguished professor of psychiatry at the University of California, Davis. “Asking about any past mental illness episodes, which may have occurred years previously ... is simply discriminatory and is an example of the stigma associated with mental disorders.”
The Breen Foundation has been working with state medical boards and hospitals to remove stigmatizing mental health and substance abuse questions from licensing and credentialing applications.
Dr. Breen had told her sister and brother-in-law shortly before her suicide that she was afraid she could lose her license and the career she loved if the medical board found out that she had received inpatient mental health treatment, said J. Corey Feist, JD, MBA, her brother-in-law and cofounder and president of the foundation.
She wasn’t aware that New York was a state that didn’t ask physicians questions about their mental health, said Mr. Feist.
“That’s why we want to make it very clear to physicians which states continue to ask these questions and which ones don’t,” Mr. Feist said.
Many physicians share Dr. Breen’s concern about professional consequences.
Four in 10 physicians said that they did not seek help for burnout or depression because they worried that their employer or state medical board would find out, according to the Medscape ‘I Cry but No One Cares’: Physician Burnout & Depression Report 2023.
One Oregon emergency department physician said that informing her state medical board about an episode of mania resulted in public disclosures, a 4-month long investigation, lost income, and poorer work evaluations. Looking back on her decision to be transparent with the board, Susan Haney, MD, said that she was naive. “The board is not your friend.”
Fearing for her career, now-retired ob.gyn. Robyn Alley-Hay, MD, never disclosed on licensing applications that in the 1990s, she had been hospitalized and treated for depression. She stopped practicing medicine in 2014 and now works as a life coach.
“I hated those questions because I felt I could never tell the whole truth,” Dr. Alley-Hay said. “But I could always truthfully answer ‘no’ to questions about impairment. That was a line that I wouldn’t cross – if you’re impaired, you shouldn’t be practicing.”
Does the focus on current impairment protect the public?
New York, Texas, California, Montana, Illinois, and North Carolina are among the 21 states that either ask no health-related questions or ask only a single question to address physical and mental health, said Mr. Feist.
Most of these changes align with the 2018 Federation of State Medical Boards recommendations, said Joe Knickrehm, FSMB vice president of communications. “Application questions must focus only on current impairment and not on illness, diagnosis, or previous treatment in order to be compliant with the Americans With Disabilities Act,” states the FSMB.
Mental health questions were often added to licensing and credentialing applications out of a “misplaced desire to protect patients and families from clinicians who might not be fit to give care. Yet there is no evidence they serve that function,” said Mr. Feist.
Marian Hollingsworth, a patient safety advocate in California, says medical boards have a responsibility to ensure that doctors pose no risk or a negligible risk to the public. She questioned whether the medical boards can adequately protect the public if they only ask about medical conditions rather than mental illness or substance abuse.
“There’s a fine line between privacy and right to know for public protection. I would want to see the approving medical board have assurance from a treating professional that this physician is stable and is doing well with continued treatment,” said Ms. Hollingsworth.
Legislation requires that mental health questions be removed
In March, Virginia became the first state to enact a law that requires all health care profession regulatory boards, including medical boards, to remove or replace mental health questions on licensing, certification, and registration applications.
The law requires that boards use the following wording if they replace mental health questions: “Do you have any reason to believe you would pose a risk to the safety or well-being of patients?” “Are you able to perform the essential functions of your job with or without reasonable accommodations?”
The Illinois General Assembly passed a more limited bill in May that requires medical boards to remove or replace mental health questions on its licensing applications. Gov. J. B. Pritzker (D) is expected to sign the bill.
The Virginia Healthcare and Hospital Association, which represents more than 100 hospitals and health systems in the state, partnered with the Medical Society of Virginia and the Virginia Nurses Association to advocate for the new legislation.
“The reason that the Virginia coalition pushed for the law was because the state’s medical boards weren’t acting quickly enough. Although state laws vary about what medical boards can do, legislation isn’t necessary in most states to change licensing questions,” said Mr. Feist.
Virginia hospitals began working last year with the foundation to change their mental health questions on credentialing applications. About 20% of Virginia’s hospitals have completed the process, including four large health systems: Inova, UVA Health, Centerra, and Children’s Hospitals of King’s Daughters, said Mr. Feist.
The foundation also challenged Lisa MacLean, MD, a psychiatrist and chief clinical wellness officer at the Henry Ford Medical Group in Detroit, to review their credentialing application for any stigmatizing mental health questions.
Dr. MacLean told the American Medical Association that she had found one question that needed to be changed but that it took time to get through the hospital›s approval process. Ultimately, the wording was changed from “a diagnosis or treatment of a physical, mental, chemical dependency or emotional condition” to “a diagnosis or treatment of any condition which could impair your ability to practice medicine.”
National medical organizations back changes
The Joint Commission, which accredits hospitals, has emphasized since 2020 that it doesn’t require hospitals to ask about an applicant’s mental health history.
“We strongly encourage organizations to not ask about past history of mental health conditions or treatment,” the Commission said in a statement. “It is critical that we ensure health care workers can feel free to access mental health resources.”
The Joint Commission said it supports the FSMB recommendations and the AMA’s recommendation that questions about clinicians’ mental health be limited to “conditions that currently impair the clinicians’ ability to perform their job.”
More than 40 professional medical organizations, including the American Academy of Family Physicians and the American Psychiatric Association, signed a joint statement in 2020 calling for changes in disclosure rules about mental health.
“The backing of major organizations is helpful because it’s changing the conversation that occurs within and outside the house of medicine,” said Mr. Feist.
Should doctors answer mental health questions?
Many states continue to ask questions about hospitalization and mental health diagnoses or treatment on their licensing and credentialing applications.
Yellowlees advises doctors to “be honest and not lie or deny past mental health problems, as medical boards tend to take a very serious view of physicians who do not tell the truth.”
However, the questions asked by medical boards can vary by state. “If it’s possible, physicians can give accurate but minimal information while trying to focus mainly on their current work capacity,” said Dr. Yellowlees.
He also suggested that physicians who are uncertain about how to respond to mental health questions consider obtaining advice from lawyers accustomed to working with the relevant medical boards.
Physicians who want to get involved in removing licensing and credentialing barriers to mental health care can find resources here and here.
A version of this article first appeared on Medscape.com.
Lupus flares linked to gut bacteria overgrowth
Flares of systemic lupus erythematosus (SLE), particularly those involving severe kidney disease, were associated with growth spikes of the gut bacteria Ruminococcus blautia gnavus in a small, 4-year observational study that also demonstrated an underlying, inherent instability in the gut microbiome of patients with SLE.
Of 16 patients with SLE studied during the provision of routine care and monitoring, 5 had R. gnavus blooms that were “strikingly concordant with periods of raised disease activity,” Gregg J. Silverman, MD, of NYU Grossman School of Medicine, New York, and coinvestigators reported in Annals of the Rheumatic Diseases.

Four of the five patients with flare-associated R. gnavus blooms had lupus nephritis (LN); the other had a flare involving inflammation in multiple joints. The four patients with concurrent LN and spikes in R. gnavus also represented almost half of patients who had LN disease flares (four of nine) during the study period. The nine patients in the study with renal involvement, and the four with concurrent R. gnavus spikes and flares, represented different races and ethnicities.
The findings build upon research published by the NYU group several years ago showing that patients with SLE had more R. gnavus in the gut than similar patients without the disease, and that flares closely tracked major increases in R. gnavus growth. Evidence of R. gnavus expansions in patients with SLE now comes from several cohorts in the United States as well as cohorts in Europe and China, the researchers noted in their new paper.
An underlying, unstable microbiome
The new study at NYU took a “deeper dive” than previous research, looking at individuals over a longer period of time, Dr. Silverman, the study’s senior investigator and associate director of rheumatology at NYU Langone Health, said in an interview. Blood and a total of 44 stool samples from the 16 patients were analyzed, as were a total of 72 stool samples from 22 healthy control volunteers.
Importantly, he said, the gut microbiome in patients with SLE was found to be inherently unstable over time, compared with the microbiota communities of the controls. “There was an instability, a shifting dynamic composition of the microbiome [in patients with lupus]. ... Healthy individuals had more of a balance, with small changes over time” and a stable, low abundance of R. gnavus, Dr. Silverman said.
Transient expansions of several pathogenic species occurred in some of the patients with lupus (and not in controls), but blooms of R. gnavus were the most common. The researchers said in their paper that they “speculate that susceptibility for specific clinical features during R. gnavus blooms reflect in part differences in genetic susceptibility of the patient.”
Patients on cytotoxic agents or antibiotics were excluded from the study, but the study was not designed to disentangle the potential influence of diet or prior antibiotic exposure, they noted. Larger studies are needed that are better controlled and that include more frequent assessments, Dr. Silverman added.
A sure association and probable cause
“There seems to be a special connection [of R. gnavus] to lupus nephritis, which is an important, major subset of disease,” said Martin Kriegel, MD, PhD, chief or rheumatology and clinical immunology at the University of Munster (Germany). Dr. Kriegel also researches the gut microbiome in lupus and was asked to comment on the new findings from NYU.

The “difficult question is, is the bug driving the flare [as the NYU paper proposes], or is it the lupus nephritis that leads to overgrowth?” he said, noting that it “is well known that kidney disease, whether from lupus or other causes, creates disturbances in the microbiome.”
It’s “likely the case” that the pathobiome – with R. gnavus being an important pathobiont – helps to drive flares, he said. The new research shows only an association, but studies done in mice – including prior research by Dr. Silverman – support a mechanistic link, said Dr. Kriegel, also adjunct associate professor of immunobiology and of medicine at Yale University, New Haven, Conn.
Investigators in the microbiome space are moving toward more strain-level analysis – “not only measuring what organisms are there, but culturing them and sequencing them,” Dr. Kriegel noted, and the new study does just this.
The R. gnavus strains isolated during lupus flares were distinguishable from strains found in healthy people – and from strains found by other researchers in patients with inflammatory bowel disease – by their common expression of a novel type of cell membrane–associated lipoglycan. The lipoglycans were recognized by specific serum IgG2 antibodies that were detected concurrently with R. gnavus blooms and lupus flares, Dr. Silverman and his colleagues reported.
Dr. Silverman and Dr. Kriegel both study the paradigm of a gut-barrier breach, whereby pathogenic bacteria cause intestinal permeability, allowing bacterial leakages that trigger inflammation and immune responses. “We think that in lupus and other rheumatic diseases like rheumatoid arthritis, a leaky gut barrier is an important mechanism, even though these patients don’t have gastrointestinal symptoms,” said Dr. Kriegel, who has studied the role of another potentially pathogenic bacteria, Enterococcus gallinarum, in SLE.
Strengthening the gut barrier may be a plausible, general approach to reducing the severity of diseases like SLE and RA until more personalized approaches targeting individuals’ microbiome are developed, he noted.
Future treatments involving antibacterial agents, probiotics or dietary regimens that prevent imbalances in the gut microbiome would be “benign,” compared with currently utilized immunosuppressive medications, Dr. Silverman said.
The NYU study was funded in part by grants from the National Institutes of Health and the Lupus Research Alliance. Dr. Silverman disclosed that NYU has filed a patent application for an antibody test to detect serum antibodies to the lipoglycan made by some strains of R. gnavus. Dr. Kriegel disclosed that he holds a patent at Yale related to the Enterococcus bacteria he studies, and that he consults for Roche, Enterome, and Eligo Biosciences.
Flares of systemic lupus erythematosus (SLE), particularly those involving severe kidney disease, were associated with growth spikes of the gut bacteria Ruminococcus blautia gnavus in a small, 4-year observational study that also demonstrated an underlying, inherent instability in the gut microbiome of patients with SLE.
Of 16 patients with SLE studied during the provision of routine care and monitoring, 5 had R. gnavus blooms that were “strikingly concordant with periods of raised disease activity,” Gregg J. Silverman, MD, of NYU Grossman School of Medicine, New York, and coinvestigators reported in Annals of the Rheumatic Diseases.
Four of the five patients with flare-associated R. gnavus blooms had lupus nephritis (LN); the other had a flare involving inflammation in multiple joints. The four patients with concurrent LN and spikes in R. gnavus also represented almost half of patients who had LN disease flares (four of nine) during the study period. The nine patients in the study with renal involvement, and the four with concurrent R. gnavus spikes and flares, represented different races and ethnicities.
The findings build upon research published by the NYU group several years ago showing that patients with SLE had more R. gnavus in the gut than similar patients without the disease, and that flares closely tracked major increases in R. gnavus growth. Evidence of R. gnavus expansions in patients with SLE now comes from several cohorts in the United States as well as cohorts in Europe and China, the researchers noted in their new paper.
An underlying, unstable microbiome
The new study at NYU took a “deeper dive” than previous research, looking at individuals over a longer period of time, Dr. Silverman, the study’s senior investigator and associate director of rheumatology at NYU Langone Health, said in an interview. Blood and a total of 44 stool samples from the 16 patients were analyzed, as were a total of 72 stool samples from 22 healthy control volunteers.
Importantly, he said, the gut microbiome in patients with SLE was found to be inherently unstable over time, compared with the microbiota communities of the controls. “There was an instability, a shifting dynamic composition of the microbiome [in patients with lupus]. ... Healthy individuals had more of a balance, with small changes over time” and a stable, low abundance of R. gnavus, Dr. Silverman said.
Transient expansions of several pathogenic species occurred in some of the patients with lupus (and not in controls), but blooms of R. gnavus were the most common. The researchers said in their paper that they “speculate that susceptibility for specific clinical features during R. gnavus blooms reflect in part differences in genetic susceptibility of the patient.”
Patients on cytotoxic agents or antibiotics were excluded from the study, but the study was not designed to disentangle the potential influence of diet or prior antibiotic exposure, they noted. Larger studies are needed that are better controlled and that include more frequent assessments, Dr. Silverman added.
A sure association and probable cause
“There seems to be a special connection [of R. gnavus] to lupus nephritis, which is an important, major subset of disease,” said Martin Kriegel, MD, PhD, chief or rheumatology and clinical immunology at the University of Munster (Germany). Dr. Kriegel also researches the gut microbiome in lupus and was asked to comment on the new findings from NYU.
The “difficult question is, is the bug driving the flare [as the NYU paper proposes], or is it the lupus nephritis that leads to overgrowth?” he said, noting that it “is well known that kidney disease, whether from lupus or other causes, creates disturbances in the microbiome.”
It’s “likely the case” that the pathobiome – with R. gnavus being an important pathobiont – helps to drive flares, he said. The new research shows only an association, but studies done in mice – including prior research by Dr. Silverman – support a mechanistic link, said Dr. Kriegel, also adjunct associate professor of immunobiology and of medicine at Yale University, New Haven, Conn.
Investigators in the microbiome space are moving toward more strain-level analysis – “not only measuring what organisms are there, but culturing them and sequencing them,” Dr. Kriegel noted, and the new study does just this.
The R. gnavus strains isolated during lupus flares were distinguishable from strains found in healthy people – and from strains found by other researchers in patients with inflammatory bowel disease – by their common expression of a novel type of cell membrane–associated lipoglycan. The lipoglycans were recognized by specific serum IgG2 antibodies that were detected concurrently with R. gnavus blooms and lupus flares, Dr. Silverman and his colleagues reported.
Dr. Silverman and Dr. Kriegel both study the paradigm of a gut-barrier breach, whereby pathogenic bacteria cause intestinal permeability, allowing bacterial leakages that trigger inflammation and immune responses. “We think that in lupus and other rheumatic diseases like rheumatoid arthritis, a leaky gut barrier is an important mechanism, even though these patients don’t have gastrointestinal symptoms,” said Dr. Kriegel, who has studied the role of another potentially pathogenic bacteria, Enterococcus gallinarum, in SLE.
Strengthening the gut barrier may be a plausible, general approach to reducing the severity of diseases like SLE and RA until more personalized approaches targeting individuals’ microbiome are developed, he noted.
Future treatments involving antibacterial agents, probiotics or dietary regimens that prevent imbalances in the gut microbiome would be “benign,” compared with currently utilized immunosuppressive medications, Dr. Silverman said.
The NYU study was funded in part by grants from the National Institutes of Health and the Lupus Research Alliance. Dr. Silverman disclosed that NYU has filed a patent application for an antibody test to detect serum antibodies to the lipoglycan made by some strains of R. gnavus. Dr. Kriegel disclosed that he holds a patent at Yale related to the Enterococcus bacteria he studies, and that he consults for Roche, Enterome, and Eligo Biosciences.
Flares of systemic lupus erythematosus (SLE), particularly those involving severe kidney disease, were associated with growth spikes of the gut bacteria Ruminococcus blautia gnavus in a small, 4-year observational study that also demonstrated an underlying, inherent instability in the gut microbiome of patients with SLE.
Of 16 patients with SLE studied during the provision of routine care and monitoring, 5 had R. gnavus blooms that were “strikingly concordant with periods of raised disease activity,” Gregg J. Silverman, MD, of NYU Grossman School of Medicine, New York, and coinvestigators reported in Annals of the Rheumatic Diseases.
Four of the five patients with flare-associated R. gnavus blooms had lupus nephritis (LN); the other had a flare involving inflammation in multiple joints. The four patients with concurrent LN and spikes in R. gnavus also represented almost half of patients who had LN disease flares (four of nine) during the study period. The nine patients in the study with renal involvement, and the four with concurrent R. gnavus spikes and flares, represented different races and ethnicities.
The findings build upon research published by the NYU group several years ago showing that patients with SLE had more R. gnavus in the gut than similar patients without the disease, and that flares closely tracked major increases in R. gnavus growth. Evidence of R. gnavus expansions in patients with SLE now comes from several cohorts in the United States as well as cohorts in Europe and China, the researchers noted in their new paper.
An underlying, unstable microbiome
The new study at NYU took a “deeper dive” than previous research, looking at individuals over a longer period of time, Dr. Silverman, the study’s senior investigator and associate director of rheumatology at NYU Langone Health, said in an interview. Blood and a total of 44 stool samples from the 16 patients were analyzed, as were a total of 72 stool samples from 22 healthy control volunteers.
Importantly, he said, the gut microbiome in patients with SLE was found to be inherently unstable over time, compared with the microbiota communities of the controls. “There was an instability, a shifting dynamic composition of the microbiome [in patients with lupus]. ... Healthy individuals had more of a balance, with small changes over time” and a stable, low abundance of R. gnavus, Dr. Silverman said.
Transient expansions of several pathogenic species occurred in some of the patients with lupus (and not in controls), but blooms of R. gnavus were the most common. The researchers said in their paper that they “speculate that susceptibility for specific clinical features during R. gnavus blooms reflect in part differences in genetic susceptibility of the patient.”
Patients on cytotoxic agents or antibiotics were excluded from the study, but the study was not designed to disentangle the potential influence of diet or prior antibiotic exposure, they noted. Larger studies are needed that are better controlled and that include more frequent assessments, Dr. Silverman added.
A sure association and probable cause
“There seems to be a special connection [of R. gnavus] to lupus nephritis, which is an important, major subset of disease,” said Martin Kriegel, MD, PhD, chief or rheumatology and clinical immunology at the University of Munster (Germany). Dr. Kriegel also researches the gut microbiome in lupus and was asked to comment on the new findings from NYU.
The “difficult question is, is the bug driving the flare [as the NYU paper proposes], or is it the lupus nephritis that leads to overgrowth?” he said, noting that it “is well known that kidney disease, whether from lupus or other causes, creates disturbances in the microbiome.”
It’s “likely the case” that the pathobiome – with R. gnavus being an important pathobiont – helps to drive flares, he said. The new research shows only an association, but studies done in mice – including prior research by Dr. Silverman – support a mechanistic link, said Dr. Kriegel, also adjunct associate professor of immunobiology and of medicine at Yale University, New Haven, Conn.
Investigators in the microbiome space are moving toward more strain-level analysis – “not only measuring what organisms are there, but culturing them and sequencing them,” Dr. Kriegel noted, and the new study does just this.
The R. gnavus strains isolated during lupus flares were distinguishable from strains found in healthy people – and from strains found by other researchers in patients with inflammatory bowel disease – by their common expression of a novel type of cell membrane–associated lipoglycan. The lipoglycans were recognized by specific serum IgG2 antibodies that were detected concurrently with R. gnavus blooms and lupus flares, Dr. Silverman and his colleagues reported.
Dr. Silverman and Dr. Kriegel both study the paradigm of a gut-barrier breach, whereby pathogenic bacteria cause intestinal permeability, allowing bacterial leakages that trigger inflammation and immune responses. “We think that in lupus and other rheumatic diseases like rheumatoid arthritis, a leaky gut barrier is an important mechanism, even though these patients don’t have gastrointestinal symptoms,” said Dr. Kriegel, who has studied the role of another potentially pathogenic bacteria, Enterococcus gallinarum, in SLE.
Strengthening the gut barrier may be a plausible, general approach to reducing the severity of diseases like SLE and RA until more personalized approaches targeting individuals’ microbiome are developed, he noted.
Future treatments involving antibacterial agents, probiotics or dietary regimens that prevent imbalances in the gut microbiome would be “benign,” compared with currently utilized immunosuppressive medications, Dr. Silverman said.
The NYU study was funded in part by grants from the National Institutes of Health and the Lupus Research Alliance. Dr. Silverman disclosed that NYU has filed a patent application for an antibody test to detect serum antibodies to the lipoglycan made by some strains of R. gnavus. Dr. Kriegel disclosed that he holds a patent at Yale related to the Enterococcus bacteria he studies, and that he consults for Roche, Enterome, and Eligo Biosciences.
FROM ANNALS OF THE RHEUMATIC DISEASES
Nearly one in five in U.S. still hadn’t gotten COVID by end of 2022
, according to a new estimate.
The findings came from an analysis of blood donations. The Centers for Disease Control and Prevention analyzed donor blood from 143,000 people every 3 months during 2022, looking for the presence of COVID antibodies that meant a person had previously been infected with the virus. The prevalence of antibodies from previous infections steadily rose throughout the year. Antibodies from prior infection were found in 49% of donors as of Feb. 15, 2022, 59% of donors as of May 15, 2022, 70% of donors as of Aug. 15, 2022, and 78% of donors as of Nov. 15, 2022.
Donor blood also was analyzed for the presence of antibodies known to come from COVID vaccination. When the vaccine-induced and infection-induced antibody data were combined, the CDC estimated that 97% of people had antibodies as of the end of the 2022.
In the report, CDC authors explained that while the presence of antibodies is related to protection from infection and to less severe disease, the level of antibodies that a person has can vary. The authors said that no standards have yet been set that show a minimum level of antibodies needed to provide protection.
As of July 3, more than 1.1 million people had died in the United States from COVID-19, according to CDC data. Deaths for the first half of 2023 are down dramatically, compared with the first 3 years of the pandemic, with just 41,538 death certificates this year listing the virus as an underlying or contributing cause. About two in three COVID deaths this year occurred in a hospital or nursing home, and 89% of people who died from the virus this year have been age 65 or older.
A version of this article first appeared on WebMD.com.
, according to a new estimate.
The findings came from an analysis of blood donations. The Centers for Disease Control and Prevention analyzed donor blood from 143,000 people every 3 months during 2022, looking for the presence of COVID antibodies that meant a person had previously been infected with the virus. The prevalence of antibodies from previous infections steadily rose throughout the year. Antibodies from prior infection were found in 49% of donors as of Feb. 15, 2022, 59% of donors as of May 15, 2022, 70% of donors as of Aug. 15, 2022, and 78% of donors as of Nov. 15, 2022.
Donor blood also was analyzed for the presence of antibodies known to come from COVID vaccination. When the vaccine-induced and infection-induced antibody data were combined, the CDC estimated that 97% of people had antibodies as of the end of the 2022.
In the report, CDC authors explained that while the presence of antibodies is related to protection from infection and to less severe disease, the level of antibodies that a person has can vary. The authors said that no standards have yet been set that show a minimum level of antibodies needed to provide protection.
As of July 3, more than 1.1 million people had died in the United States from COVID-19, according to CDC data. Deaths for the first half of 2023 are down dramatically, compared with the first 3 years of the pandemic, with just 41,538 death certificates this year listing the virus as an underlying or contributing cause. About two in three COVID deaths this year occurred in a hospital or nursing home, and 89% of people who died from the virus this year have been age 65 or older.
A version of this article first appeared on WebMD.com.
, according to a new estimate.
The findings came from an analysis of blood donations. The Centers for Disease Control and Prevention analyzed donor blood from 143,000 people every 3 months during 2022, looking for the presence of COVID antibodies that meant a person had previously been infected with the virus. The prevalence of antibodies from previous infections steadily rose throughout the year. Antibodies from prior infection were found in 49% of donors as of Feb. 15, 2022, 59% of donors as of May 15, 2022, 70% of donors as of Aug. 15, 2022, and 78% of donors as of Nov. 15, 2022.
Donor blood also was analyzed for the presence of antibodies known to come from COVID vaccination. When the vaccine-induced and infection-induced antibody data were combined, the CDC estimated that 97% of people had antibodies as of the end of the 2022.
In the report, CDC authors explained that while the presence of antibodies is related to protection from infection and to less severe disease, the level of antibodies that a person has can vary. The authors said that no standards have yet been set that show a minimum level of antibodies needed to provide protection.
As of July 3, more than 1.1 million people had died in the United States from COVID-19, according to CDC data. Deaths for the first half of 2023 are down dramatically, compared with the first 3 years of the pandemic, with just 41,538 death certificates this year listing the virus as an underlying or contributing cause. About two in three COVID deaths this year occurred in a hospital or nursing home, and 89% of people who died from the virus this year have been age 65 or older.
A version of this article first appeared on WebMD.com.
Higher alcohol consumption linked to early-onset CRC
TOPLINE:
Higher levels of alcohol consumption appear to increase an individual’s risk of early-onset colorectal cancer (CRC), particularly distal colon and rectal cancers, according to a population-based study from South Korea.
METHODOLOGY:
- The investigators retrospectively compared average daily alcohol consumption with early-onset CRC risk among nearly 5.7 million adults younger than 50 years, using data from the Korean National Health Insurance Service.
- Alcohol consumption levels were defined as nondrinker, light (< 10 g/day or < 0.7 U.S. drinks/day), moderate (10-30 g/day for men, 10-20 g/day for women), and heavy (≥ 30 g/day or ≥ 2.1 drinks/day for men, ≥ 20 g/day or ≥ 1.4 drinks/day for women).
- The primary outcome was incidence of early-onset CRC diagnosed before age 50. Models were adjusted for age, sex, smoking status, exercise, and income, as well as for comorbidities.
TAKEAWAY:
- Overall, 8,314 incident early-onset CRC cases occurred during the mean follow-up period of 7.4 years.
- Compared with light drinking, moderate and heavy drinking were associated with a significantly elevated risk of early-onset CRC (adjusted hazard ratio, 1.09 and 1.20, respectively); by sex, significant associations were found only among men.
- Among men, heavy drinking vs. light drinking was associated with a 26% increased risk of distal colon cancer, a 17% higher risk of rectal cancer, and a 29% higher risk of unspecified colon cancer (but not proximal colon cancer).
- Among women, moderate drinking was associated with a 47% increased risk of distal colon cancer. Among nondrinkers, there was a 14% reduced risk of rectal cancer, compared with light drinkers.
IN PRACTICE:
“This population-based study provides evidence that higher levels of alcohol consumption may increase the risk of early-onset CRC,” the investigators concluded. “[E]ffective interventions are required to discourage alcohol consumption among young people and to tailor CRC screening approaches for high-risk individuals.”
SOURCE:
The study was led by researchers at Seoul National University, South Korea. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Study limitations include self-reported alcohol consumption. Data were missing for a higher number of male participants and younger participants, and there was a potential problem related to multiple comparisons and confounders. Only Korean individuals were included in the study, so larger studies involving various races are needed.
DISCLOSURES:
Funding was provided by grants from the Korea Health Technology R&D Project and the Ministry of Health and Welfare, Republic of Korea. No potential conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Higher levels of alcohol consumption appear to increase an individual’s risk of early-onset colorectal cancer (CRC), particularly distal colon and rectal cancers, according to a population-based study from South Korea.
METHODOLOGY:
- The investigators retrospectively compared average daily alcohol consumption with early-onset CRC risk among nearly 5.7 million adults younger than 50 years, using data from the Korean National Health Insurance Service.
- Alcohol consumption levels were defined as nondrinker, light (< 10 g/day or < 0.7 U.S. drinks/day), moderate (10-30 g/day for men, 10-20 g/day for women), and heavy (≥ 30 g/day or ≥ 2.1 drinks/day for men, ≥ 20 g/day or ≥ 1.4 drinks/day for women).
- The primary outcome was incidence of early-onset CRC diagnosed before age 50. Models were adjusted for age, sex, smoking status, exercise, and income, as well as for comorbidities.
TAKEAWAY:
- Overall, 8,314 incident early-onset CRC cases occurred during the mean follow-up period of 7.4 years.
- Compared with light drinking, moderate and heavy drinking were associated with a significantly elevated risk of early-onset CRC (adjusted hazard ratio, 1.09 and 1.20, respectively); by sex, significant associations were found only among men.
- Among men, heavy drinking vs. light drinking was associated with a 26% increased risk of distal colon cancer, a 17% higher risk of rectal cancer, and a 29% higher risk of unspecified colon cancer (but not proximal colon cancer).
- Among women, moderate drinking was associated with a 47% increased risk of distal colon cancer. Among nondrinkers, there was a 14% reduced risk of rectal cancer, compared with light drinkers.
IN PRACTICE:
“This population-based study provides evidence that higher levels of alcohol consumption may increase the risk of early-onset CRC,” the investigators concluded. “[E]ffective interventions are required to discourage alcohol consumption among young people and to tailor CRC screening approaches for high-risk individuals.”
SOURCE:
The study was led by researchers at Seoul National University, South Korea. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Study limitations include self-reported alcohol consumption. Data were missing for a higher number of male participants and younger participants, and there was a potential problem related to multiple comparisons and confounders. Only Korean individuals were included in the study, so larger studies involving various races are needed.
DISCLOSURES:
Funding was provided by grants from the Korea Health Technology R&D Project and the Ministry of Health and Welfare, Republic of Korea. No potential conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Higher levels of alcohol consumption appear to increase an individual’s risk of early-onset colorectal cancer (CRC), particularly distal colon and rectal cancers, according to a population-based study from South Korea.
METHODOLOGY:
- The investigators retrospectively compared average daily alcohol consumption with early-onset CRC risk among nearly 5.7 million adults younger than 50 years, using data from the Korean National Health Insurance Service.
- Alcohol consumption levels were defined as nondrinker, light (< 10 g/day or < 0.7 U.S. drinks/day), moderate (10-30 g/day for men, 10-20 g/day for women), and heavy (≥ 30 g/day or ≥ 2.1 drinks/day for men, ≥ 20 g/day or ≥ 1.4 drinks/day for women).
- The primary outcome was incidence of early-onset CRC diagnosed before age 50. Models were adjusted for age, sex, smoking status, exercise, and income, as well as for comorbidities.
TAKEAWAY:
- Overall, 8,314 incident early-onset CRC cases occurred during the mean follow-up period of 7.4 years.
- Compared with light drinking, moderate and heavy drinking were associated with a significantly elevated risk of early-onset CRC (adjusted hazard ratio, 1.09 and 1.20, respectively); by sex, significant associations were found only among men.
- Among men, heavy drinking vs. light drinking was associated with a 26% increased risk of distal colon cancer, a 17% higher risk of rectal cancer, and a 29% higher risk of unspecified colon cancer (but not proximal colon cancer).
- Among women, moderate drinking was associated with a 47% increased risk of distal colon cancer. Among nondrinkers, there was a 14% reduced risk of rectal cancer, compared with light drinkers.
IN PRACTICE:
“This population-based study provides evidence that higher levels of alcohol consumption may increase the risk of early-onset CRC,” the investigators concluded. “[E]ffective interventions are required to discourage alcohol consumption among young people and to tailor CRC screening approaches for high-risk individuals.”
SOURCE:
The study was led by researchers at Seoul National University, South Korea. It was published online in the Journal of Clinical Oncology.
LIMITATIONS:
Study limitations include self-reported alcohol consumption. Data were missing for a higher number of male participants and younger participants, and there was a potential problem related to multiple comparisons and confounders. Only Korean individuals were included in the study, so larger studies involving various races are needed.
DISCLOSURES:
Funding was provided by grants from the Korea Health Technology R&D Project and the Ministry of Health and Welfare, Republic of Korea. No potential conflicts of interest were reported.
A version of this article first appeared on Medscape.com.
Patient aggression against receptionists demands protocols
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
“I’ve been hit in the head by a walking stick,” a primary care receptionist reported.
“A mother came in and was screaming and swearing at me because she couldn’t get an appointment for her daughters,” another receptionist reported.
“I’ve had people throw a bag of syringes at me because we don’t accept syringes,” said another.
Reports such as these are part of the literature supporting a review that finds patient aggression against receptionists is a serious safety concern for primary care offices and affects delivery of health care.
The review was published online in the BMJ’s Family Medicine and Community Health journal.
“Receptionists in general practice deserve evidence-based measures to improve their working conditions and well-being,” say the authors, led by Fiona Willer, PhD, of the Centre for Community Health and Wellbeing at the University of Queensland, Brisbane, Australia.
Though the study looked primarily at European and Australian practices, physicians in the United States say the incidences are familiar.
Cause often lack of access
Dr. Willer and colleagues point out that the root cause of patient regression is typically related to operational factors, such as inefficient scheduling or lack of access to the medical providers.
“However, reception staff are placed in the unenviable position of having to deal with the aftermath of the poor function of these systems without having the status or autonomy to overhaul them,” the authors note.
Authors analyzed 20 studies on aggression against receptionists.
Among the findings:
- All studies reported that patient hostility and verbal abuse of receptionists “was a frequent, routine, and relatively unavoidable occurrence in general practice.”
- Nine studies reported acts of physical violence toward receptionists, with all reporting that physical abuse occurred much less frequently than verbal abuse.
- Some acts were very severe, including being hit, shaken, held at gunpoint, stalked, and threatened with a razorblade.
The studies also discussed ways to prevent potential aggression or react to it, including:
- Regular staff training for managing patient aggression.
- Designing clinics with “safe rooms” and “cool down” spaces.
- Providing clear acrylic shields between receptionists and patients.
- Developing formal policy/procedure/protocol/action guides relating to management of patients.
Behavior can interrupt health care delivery
Carrie Janiski, DO, regional medical director at Golden Valley Health Centers in California, who was not part of the review, said she has seen the aggressive behavior the authors document in her practice’s lobby, “including yelling, name-calling, and threatening language or physical behavior.”
The instances disrupt health care delivery to the patient, who is often in crisis, and all patients and staff in the clinic, she said.
“The patient needs help and the aggressive way they are seeking it could cause harm to others or prevent them from receiving all the help they need,” she said.
She says in practices she has worked in, some effective mitigation strategies have included open-access scheduling, increased walk-in availability for appointments, de-escalation training for front-line staff, and office and exam room layout designed for safety.
She added that incident review is important and should include a process for patient dismissal from the practice.
Dustin Arnold, DO, an internal medicine specialist and chief medical officer at UnityPoint Health-St. Luke’s Hospital, Cedar Rapids, IA, said he agrees with the authors on the urgency for action.
“This is an urgent concern for practices across the country. Your receptionist is the face of your practice, and you should invest in them,” said Dr. Arnold, who was not part of the review.
He said he has seen “verbal abuse and generalized incivility” from patients against receptionists in practices where he has worked.
He said the measure the authors list that he thinks is most effective is staff de-escalation training.
“However, the best preventative measure is for the physician to be on time and minimize cancellation of appointments,” he said. “These are the two primary triggers of a patient becoming disruptive.”
He said his practice has installed a panic button at the front desk and built an alert into the electronic health record indicating that a patient has shown disruptive behavior in the past.
The authors conclude: “Staff training and protocols to manage patient aggression and ongoing structured staff support should be considered essential in general practice. Evidence-based strategies to prevent, manage, and mitigate the harms of patient aggression towards general practice reception staff are urgently needed.”
The authors and Dr. Janiski and Dr. Arnold declared no relevant financial relationships.
FROM FAMILY MEDICINE AND COMMUNITY HEALTH
In-office infusions at risk with new Medicare Part B reimbursement recommendation
The Medicare Payment Advisory Commission (MedPAC) is an independent agency to advise Congress on Medicare (MC) policy, much of which pertains to payment issues. The 17 commissioners meet publicly and issue two reports a year with their recommendations to Congress, who then decides whether to enact these recommendations or not.
One MedPAC recommendation in 2023 was quickly introduced in the House of Representatives in May and passed the Energy and Commerce Committee 49-0. That recommendation relates to “site neutrality” payments to MC providers. If passed by Congress, it would result in some “site-neutral” cuts to hospitals. That MedPAC recommendation was acted upon very quickly by Congress. Consequently, it is important to discuss the potential negative ramifications of other MedPAC recommendations released in June regarding reimbursement of Medicare Part B drugs and proactively educate Congress accordingly on those ramifications.

Medicare Part B drugs
Medicare Part B drugs are those administered by providers, unlike the Part D medications which are generally obtained through pharmacies. Presently, MC reimburses providers for the administered Part B medication based on the average sales price (ASP) plus 6%. However, with sequestration, that add-on amount is reduced to ASP plus 4.3%. It has long been touted by MedPAC and other policy makers that physicians choose to infuse higher-priced drugs in order to increase reimbursements. That has not been borne out when it comes to rheumatologists, and, in fact, a retired MedPAC commissioner even stated that premise did not hold true for rheumatologists.
Regardless, it continues to be suggested that MC should reduce its costs for Part B medications by reducing reimbursement to physicians. It should be noted that often the margins on the drugs are already quite thin, and at times the reimbursement amount, compared with the acquisition cost of the drug even leaves the physician “underwater.”
A few years ago, there was a proposed Part B demonstration project that essentially removed the +6% add-on and replaced it with a very low fixed amount that would have left most physicians “underwater” in their Part B drug acquisitions. This was vigorously opposed by physicians around the country, who let Congress know exactly how they felt. We have been told that the Coalition of State Rheumatology Organizations was one of the most vociferous organizations that helped in fighting back this proposal and resulting in its withdrawal.
MedPAC recommendations
That brings us back to MedPAC. In June, MedPAC released recommendations to Congress in an attempt to address the “high price of drugs” covered under MC Part B. Unfortunately, the recommendations do nothing to address the root cause of high drug prices, but once again attempt to balance MC expenditures on the backs of physicians. In this case, it is physicians who infuse Part B drugs in their office to chronically ill patients. In-office infusions have been shown to be the most cost-effective site of care, as well as being safer when compared with home infusion for a number of rheumatologic medications.
One of the MedPAC recommendations gives the Secretary of Health & Human Services the authority to establish a single ASP for drugs with “similar health effects.” The ambiguity of the phrase “similar health effects” should put us all on alert as to the significant unintended consequences that may result. For example, HHS could assign one ASP to all drugs that treat rheumatoid arthritis based on the lowest ASP of the group. This certainly would lead to a number of drugs being out of reach for MC beneficiaries if the artificial ASP of the medication is much lower than the actual acquisition cost of the drug, leaving physicians unable to acquire it. Yet, MedPAC states this recommendation would not affect access to care for MC beneficiaries.
Another recommendation would require HHS to reduce or eliminate the add-on percentage to the ASP for higher-priced drugs and/or put in an added fixed amount. This recommendation is clearly reminiscent of the old ill-conceived Part B demonstration project.
A fixed “add-on amount” might work if it is sufficient to cover the overhead of maintaining a provider’s infusion suite. But if practices are left underwater in their purchases of certain Part B drugs, there may be no choice but to stop offering those infusions to MC beneficiaries or – worst-case scenario – shut the door completely. Yet again, MedPAC stated that this recommendation would not result in a loss of access to these treatments for MC beneficiaries.
Loss of access?
Rheumatologists have gone to great lengths to continue offering care to MC patients in spite of the yearly cuts and threats of more cuts in the future to physician reimbursements. In addition, physicians have no annual inflationary update to their reimbursements. I am not sure how MedPAC concludes that continued cuts to physician fee schedules, along with a decrease in reimbursement for administered drugs, will not affect access to care for MC beneficiaries.
Finally, the timing on these recommendations is confusing, considering that implementation of the Inflation Reduction Act (IRA) has just begun. Next quarter, a number of Part B drugs will be subject to inflationary penalties; there will also be additional Part B biosimilars coming to market, resulting in lower ASPs. And don’t forget, the IRA just instituted an ASP plus 8% reimbursement for biosimilars in an attempt to get physicians to do something that the Centers for Medicare & Medicaid Services has asked them not to do. That is, choose a drug based on its reimbursement, not necessarily the one which is right for the patient.
Overall, with so many variables up in the air, now is not the time to create even more uncertainty for physicians and the Medicare patients that they take care of.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
The Medicare Payment Advisory Commission (MedPAC) is an independent agency to advise Congress on Medicare (MC) policy, much of which pertains to payment issues. The 17 commissioners meet publicly and issue two reports a year with their recommendations to Congress, who then decides whether to enact these recommendations or not.
One MedPAC recommendation in 2023 was quickly introduced in the House of Representatives in May and passed the Energy and Commerce Committee 49-0. That recommendation relates to “site neutrality” payments to MC providers. If passed by Congress, it would result in some “site-neutral” cuts to hospitals. That MedPAC recommendation was acted upon very quickly by Congress. Consequently, it is important to discuss the potential negative ramifications of other MedPAC recommendations released in June regarding reimbursement of Medicare Part B drugs and proactively educate Congress accordingly on those ramifications.
Medicare Part B drugs
Medicare Part B drugs are those administered by providers, unlike the Part D medications which are generally obtained through pharmacies. Presently, MC reimburses providers for the administered Part B medication based on the average sales price (ASP) plus 6%. However, with sequestration, that add-on amount is reduced to ASP plus 4.3%. It has long been touted by MedPAC and other policy makers that physicians choose to infuse higher-priced drugs in order to increase reimbursements. That has not been borne out when it comes to rheumatologists, and, in fact, a retired MedPAC commissioner even stated that premise did not hold true for rheumatologists.
Regardless, it continues to be suggested that MC should reduce its costs for Part B medications by reducing reimbursement to physicians. It should be noted that often the margins on the drugs are already quite thin, and at times the reimbursement amount, compared with the acquisition cost of the drug even leaves the physician “underwater.”
A few years ago, there was a proposed Part B demonstration project that essentially removed the +6% add-on and replaced it with a very low fixed amount that would have left most physicians “underwater” in their Part B drug acquisitions. This was vigorously opposed by physicians around the country, who let Congress know exactly how they felt. We have been told that the Coalition of State Rheumatology Organizations was one of the most vociferous organizations that helped in fighting back this proposal and resulting in its withdrawal.
MedPAC recommendations
That brings us back to MedPAC. In June, MedPAC released recommendations to Congress in an attempt to address the “high price of drugs” covered under MC Part B. Unfortunately, the recommendations do nothing to address the root cause of high drug prices, but once again attempt to balance MC expenditures on the backs of physicians. In this case, it is physicians who infuse Part B drugs in their office to chronically ill patients. In-office infusions have been shown to be the most cost-effective site of care, as well as being safer when compared with home infusion for a number of rheumatologic medications.
One of the MedPAC recommendations gives the Secretary of Health & Human Services the authority to establish a single ASP for drugs with “similar health effects.” The ambiguity of the phrase “similar health effects” should put us all on alert as to the significant unintended consequences that may result. For example, HHS could assign one ASP to all drugs that treat rheumatoid arthritis based on the lowest ASP of the group. This certainly would lead to a number of drugs being out of reach for MC beneficiaries if the artificial ASP of the medication is much lower than the actual acquisition cost of the drug, leaving physicians unable to acquire it. Yet, MedPAC states this recommendation would not affect access to care for MC beneficiaries.
Another recommendation would require HHS to reduce or eliminate the add-on percentage to the ASP for higher-priced drugs and/or put in an added fixed amount. This recommendation is clearly reminiscent of the old ill-conceived Part B demonstration project.
A fixed “add-on amount” might work if it is sufficient to cover the overhead of maintaining a provider’s infusion suite. But if practices are left underwater in their purchases of certain Part B drugs, there may be no choice but to stop offering those infusions to MC beneficiaries or – worst-case scenario – shut the door completely. Yet again, MedPAC stated that this recommendation would not result in a loss of access to these treatments for MC beneficiaries.
Loss of access?
Rheumatologists have gone to great lengths to continue offering care to MC patients in spite of the yearly cuts and threats of more cuts in the future to physician reimbursements. In addition, physicians have no annual inflationary update to their reimbursements. I am not sure how MedPAC concludes that continued cuts to physician fee schedules, along with a decrease in reimbursement for administered drugs, will not affect access to care for MC beneficiaries.
Finally, the timing on these recommendations is confusing, considering that implementation of the Inflation Reduction Act (IRA) has just begun. Next quarter, a number of Part B drugs will be subject to inflationary penalties; there will also be additional Part B biosimilars coming to market, resulting in lower ASPs. And don’t forget, the IRA just instituted an ASP plus 8% reimbursement for biosimilars in an attempt to get physicians to do something that the Centers for Medicare & Medicaid Services has asked them not to do. That is, choose a drug based on its reimbursement, not necessarily the one which is right for the patient.
Overall, with so many variables up in the air, now is not the time to create even more uncertainty for physicians and the Medicare patients that they take care of.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
The Medicare Payment Advisory Commission (MedPAC) is an independent agency to advise Congress on Medicare (MC) policy, much of which pertains to payment issues. The 17 commissioners meet publicly and issue two reports a year with their recommendations to Congress, who then decides whether to enact these recommendations or not.
One MedPAC recommendation in 2023 was quickly introduced in the House of Representatives in May and passed the Energy and Commerce Committee 49-0. That recommendation relates to “site neutrality” payments to MC providers. If passed by Congress, it would result in some “site-neutral” cuts to hospitals. That MedPAC recommendation was acted upon very quickly by Congress. Consequently, it is important to discuss the potential negative ramifications of other MedPAC recommendations released in June regarding reimbursement of Medicare Part B drugs and proactively educate Congress accordingly on those ramifications.
Medicare Part B drugs
Medicare Part B drugs are those administered by providers, unlike the Part D medications which are generally obtained through pharmacies. Presently, MC reimburses providers for the administered Part B medication based on the average sales price (ASP) plus 6%. However, with sequestration, that add-on amount is reduced to ASP plus 4.3%. It has long been touted by MedPAC and other policy makers that physicians choose to infuse higher-priced drugs in order to increase reimbursements. That has not been borne out when it comes to rheumatologists, and, in fact, a retired MedPAC commissioner even stated that premise did not hold true for rheumatologists.
Regardless, it continues to be suggested that MC should reduce its costs for Part B medications by reducing reimbursement to physicians. It should be noted that often the margins on the drugs are already quite thin, and at times the reimbursement amount, compared with the acquisition cost of the drug even leaves the physician “underwater.”
A few years ago, there was a proposed Part B demonstration project that essentially removed the +6% add-on and replaced it with a very low fixed amount that would have left most physicians “underwater” in their Part B drug acquisitions. This was vigorously opposed by physicians around the country, who let Congress know exactly how they felt. We have been told that the Coalition of State Rheumatology Organizations was one of the most vociferous organizations that helped in fighting back this proposal and resulting in its withdrawal.
MedPAC recommendations
That brings us back to MedPAC. In June, MedPAC released recommendations to Congress in an attempt to address the “high price of drugs” covered under MC Part B. Unfortunately, the recommendations do nothing to address the root cause of high drug prices, but once again attempt to balance MC expenditures on the backs of physicians. In this case, it is physicians who infuse Part B drugs in their office to chronically ill patients. In-office infusions have been shown to be the most cost-effective site of care, as well as being safer when compared with home infusion for a number of rheumatologic medications.
One of the MedPAC recommendations gives the Secretary of Health & Human Services the authority to establish a single ASP for drugs with “similar health effects.” The ambiguity of the phrase “similar health effects” should put us all on alert as to the significant unintended consequences that may result. For example, HHS could assign one ASP to all drugs that treat rheumatoid arthritis based on the lowest ASP of the group. This certainly would lead to a number of drugs being out of reach for MC beneficiaries if the artificial ASP of the medication is much lower than the actual acquisition cost of the drug, leaving physicians unable to acquire it. Yet, MedPAC states this recommendation would not affect access to care for MC beneficiaries.
Another recommendation would require HHS to reduce or eliminate the add-on percentage to the ASP for higher-priced drugs and/or put in an added fixed amount. This recommendation is clearly reminiscent of the old ill-conceived Part B demonstration project.
A fixed “add-on amount” might work if it is sufficient to cover the overhead of maintaining a provider’s infusion suite. But if practices are left underwater in their purchases of certain Part B drugs, there may be no choice but to stop offering those infusions to MC beneficiaries or – worst-case scenario – shut the door completely. Yet again, MedPAC stated that this recommendation would not result in a loss of access to these treatments for MC beneficiaries.
Loss of access?
Rheumatologists have gone to great lengths to continue offering care to MC patients in spite of the yearly cuts and threats of more cuts in the future to physician reimbursements. In addition, physicians have no annual inflationary update to their reimbursements. I am not sure how MedPAC concludes that continued cuts to physician fee schedules, along with a decrease in reimbursement for administered drugs, will not affect access to care for MC beneficiaries.
Finally, the timing on these recommendations is confusing, considering that implementation of the Inflation Reduction Act (IRA) has just begun. Next quarter, a number of Part B drugs will be subject to inflationary penalties; there will also be additional Part B biosimilars coming to market, resulting in lower ASPs. And don’t forget, the IRA just instituted an ASP plus 8% reimbursement for biosimilars in an attempt to get physicians to do something that the Centers for Medicare & Medicaid Services has asked them not to do. That is, choose a drug based on its reimbursement, not necessarily the one which is right for the patient.
Overall, with so many variables up in the air, now is not the time to create even more uncertainty for physicians and the Medicare patients that they take care of.
Dr. Feldman is a rheumatologist in private practice with The Rheumatology Group in New Orleans. She is the CSRO’s Vice President of Advocacy and Government Affairs and its immediate Past President, as well as past chair of the Alliance for Safe Biologic Medicines and a past member of the American College of Rheumatology insurance subcommittee. You can reach her at [email protected].
New guidelines for MTX use in pediatric inflammatory skin disease unveiled
While the typical dose of methotrexate (MTX) for inflammatory disease in pediatric patients varies in published studies, the maximum dose is considered to be 1 mg/kg and not to exceed 25 mg/week. In addition, test doses are not necessary for pediatric patients starting low dose (1 mg/kg or less) MTX for inflammatory skin disease, and the onset of efficacy with MTX may take 8-16 weeks.
and published online in Pediatric Dermatology.
“Methotrexate is a cost-effective, readily accessible, well-tolerated, useful, and time-honored option for children with a spectrum of inflammatory skin diseases,” project cochair Elaine C. Siegfried, MD, professor of pediatrics and dermatology at Saint Louis University, told this news organization. “Although considered an ‘immune suppressant’ by some, it is more accurately classified as an immune modulator and has been widely used for more than 50 years, and remains the standard of care when administered at very high doses and intrathecally in children with acute lymphoblastic leukemia – a practice that supports safety. But many details that support optimized treatment are not widely appreciated.”

In their guidelines document, Dr. Siegfried and her 22 coauthors noted that Food and Drug Administration labeling does not include approved indications for the use of MTX for many inflammatory skin diseases in pediatric patients, including morphea, psoriasis, atopic dermatitis, and alopecia areata. “Furthermore, some clinicians may be unfamiliar or uncomfortable prescribing medications off label for pediatric patients, causing delayed initiation, premature drug discontinuation, or use of less advantageous alternatives,” they wrote.
To address this unmet need, Dr. Siegfried and the other committee members used a modified Delphi process to reach agreement on recommendations related to five key topic areas: indications and contraindications, dosing, interactions with immunizations and medications, potential for and management of adverse effects, and monitoring needs. Consensus was predefined as at least 70% of participants rating a statement as 7-9 on the Likert scale. The effort to develop 46 recommendations has been a work in progress for almost 5 years, “somewhat delayed by the pandemic,” Dr. Siegfried, past president and director of the American Board of Dermatology, said in an interview. “But it remains relevant, despite the emergence of biologics and JAK inhibitors for treating inflammatory skin conditions in children. Although the mechanism-of-action of low-dose MTX is not clear, it may overlap with the newer small molecules.”
The guidelines contain several pearls to guide optimal dosing, including the following key points:
- MTX can be discontinued abruptly without adverse effects, other than the risk of disease worsening.
- Folic acid supplementation (starting at 1 mg/day, regardless of weight) is an effective approach to minimizing associated gastrointestinal adverse effects.
- Concomitant use of MTX and antibiotics (including trimethoprim-sulfamethoxazole) and NSAIDS are not contraindicated for most pediatric patients treated for inflammatory skin disease.
- Live virus vaccine boosters such as varicella-zoster virus (VZV) and measles, mumps, and rubella (MMR) are not contraindicated in patients taking MTX; there are insufficient data to make recommendations for or against primary immunization with MMR vaccine in patients taking MTX; inactivated vaccines should be given to patients taking MTX.
- Routine surveillance laboratory monitoring (i.e., CBC with differential, alanine transaminase, aspartate aminotransferase, creatinine) is recommended at baseline, after 1 month of treatment, and every 3-4 months thereafter.
- Transient transaminase elevation (≤ 3 upper limit normal for < 3 months) is not uncommon with low-dose MTX and does not usually require interruption of MTX. The most likely causes are concomitant viral infection, MTX dosing within 24 hours prior to phlebotomy, recent administration of other medications (such as acetaminophen), and/or recent alcohol consumption.
- Liver biopsy is not indicated for routine monitoring of pediatric patients taking low-dose MTX.
According to Dr. Siegfried, consensus of the committee members was lowest on the need for a test dose of MTX.
Overall, she said in the interview, helping to craft the guidelines caused her to reflect on how her approach to using MTX has evolved over the past 35 years, after treating “many hundreds” of patients. “I was gratified to confirm similar practice patterns among my colleagues,” she added.
The project’s other cochair was Heather Brandling-Bennett, MD, a dermatologist at Seattle Children’s Hospital. This work was supported by a grant from the Pediatric Dermatology Research Alliance (PeDRA), with additional funding from the National Eczema Association and the National Psoriasis Foundation. Dr. Siegfried disclosed ties with AbbVie, Boehringer Ingelheim, Incyte, LEO Pharma, Novan, Novartis, Pierre Fabre, Pfizer, Regeneron, Sanofi Genzyme, UCB, and Verrica. She has participated in contracted research for AI Therapeutics, and has served as principal investigator for Janssen. Many of the guideline coauthors disclosed having received grant support and other funding from pharmaceutical companies.
While the typical dose of methotrexate (MTX) for inflammatory disease in pediatric patients varies in published studies, the maximum dose is considered to be 1 mg/kg and not to exceed 25 mg/week. In addition, test doses are not necessary for pediatric patients starting low dose (1 mg/kg or less) MTX for inflammatory skin disease, and the onset of efficacy with MTX may take 8-16 weeks.
and published online in Pediatric Dermatology.
“Methotrexate is a cost-effective, readily accessible, well-tolerated, useful, and time-honored option for children with a spectrum of inflammatory skin diseases,” project cochair Elaine C. Siegfried, MD, professor of pediatrics and dermatology at Saint Louis University, told this news organization. “Although considered an ‘immune suppressant’ by some, it is more accurately classified as an immune modulator and has been widely used for more than 50 years, and remains the standard of care when administered at very high doses and intrathecally in children with acute lymphoblastic leukemia – a practice that supports safety. But many details that support optimized treatment are not widely appreciated.”
In their guidelines document, Dr. Siegfried and her 22 coauthors noted that Food and Drug Administration labeling does not include approved indications for the use of MTX for many inflammatory skin diseases in pediatric patients, including morphea, psoriasis, atopic dermatitis, and alopecia areata. “Furthermore, some clinicians may be unfamiliar or uncomfortable prescribing medications off label for pediatric patients, causing delayed initiation, premature drug discontinuation, or use of less advantageous alternatives,” they wrote.
To address this unmet need, Dr. Siegfried and the other committee members used a modified Delphi process to reach agreement on recommendations related to five key topic areas: indications and contraindications, dosing, interactions with immunizations and medications, potential for and management of adverse effects, and monitoring needs. Consensus was predefined as at least 70% of participants rating a statement as 7-9 on the Likert scale. The effort to develop 46 recommendations has been a work in progress for almost 5 years, “somewhat delayed by the pandemic,” Dr. Siegfried, past president and director of the American Board of Dermatology, said in an interview. “But it remains relevant, despite the emergence of biologics and JAK inhibitors for treating inflammatory skin conditions in children. Although the mechanism-of-action of low-dose MTX is not clear, it may overlap with the newer small molecules.”
The guidelines contain several pearls to guide optimal dosing, including the following key points:
- MTX can be discontinued abruptly without adverse effects, other than the risk of disease worsening.
- Folic acid supplementation (starting at 1 mg/day, regardless of weight) is an effective approach to minimizing associated gastrointestinal adverse effects.
- Concomitant use of MTX and antibiotics (including trimethoprim-sulfamethoxazole) and NSAIDS are not contraindicated for most pediatric patients treated for inflammatory skin disease.
- Live virus vaccine boosters such as varicella-zoster virus (VZV) and measles, mumps, and rubella (MMR) are not contraindicated in patients taking MTX; there are insufficient data to make recommendations for or against primary immunization with MMR vaccine in patients taking MTX; inactivated vaccines should be given to patients taking MTX.
- Routine surveillance laboratory monitoring (i.e., CBC with differential, alanine transaminase, aspartate aminotransferase, creatinine) is recommended at baseline, after 1 month of treatment, and every 3-4 months thereafter.
- Transient transaminase elevation (≤ 3 upper limit normal for < 3 months) is not uncommon with low-dose MTX and does not usually require interruption of MTX. The most likely causes are concomitant viral infection, MTX dosing within 24 hours prior to phlebotomy, recent administration of other medications (such as acetaminophen), and/or recent alcohol consumption.
- Liver biopsy is not indicated for routine monitoring of pediatric patients taking low-dose MTX.
According to Dr. Siegfried, consensus of the committee members was lowest on the need for a test dose of MTX.
Overall, she said in the interview, helping to craft the guidelines caused her to reflect on how her approach to using MTX has evolved over the past 35 years, after treating “many hundreds” of patients. “I was gratified to confirm similar practice patterns among my colleagues,” she added.
The project’s other cochair was Heather Brandling-Bennett, MD, a dermatologist at Seattle Children’s Hospital. This work was supported by a grant from the Pediatric Dermatology Research Alliance (PeDRA), with additional funding from the National Eczema Association and the National Psoriasis Foundation. Dr. Siegfried disclosed ties with AbbVie, Boehringer Ingelheim, Incyte, LEO Pharma, Novan, Novartis, Pierre Fabre, Pfizer, Regeneron, Sanofi Genzyme, UCB, and Verrica. She has participated in contracted research for AI Therapeutics, and has served as principal investigator for Janssen. Many of the guideline coauthors disclosed having received grant support and other funding from pharmaceutical companies.
While the typical dose of methotrexate (MTX) for inflammatory disease in pediatric patients varies in published studies, the maximum dose is considered to be 1 mg/kg and not to exceed 25 mg/week. In addition, test doses are not necessary for pediatric patients starting low dose (1 mg/kg or less) MTX for inflammatory skin disease, and the onset of efficacy with MTX may take 8-16 weeks.
and published online in Pediatric Dermatology.
“Methotrexate is a cost-effective, readily accessible, well-tolerated, useful, and time-honored option for children with a spectrum of inflammatory skin diseases,” project cochair Elaine C. Siegfried, MD, professor of pediatrics and dermatology at Saint Louis University, told this news organization. “Although considered an ‘immune suppressant’ by some, it is more accurately classified as an immune modulator and has been widely used for more than 50 years, and remains the standard of care when administered at very high doses and intrathecally in children with acute lymphoblastic leukemia – a practice that supports safety. But many details that support optimized treatment are not widely appreciated.”
In their guidelines document, Dr. Siegfried and her 22 coauthors noted that Food and Drug Administration labeling does not include approved indications for the use of MTX for many inflammatory skin diseases in pediatric patients, including morphea, psoriasis, atopic dermatitis, and alopecia areata. “Furthermore, some clinicians may be unfamiliar or uncomfortable prescribing medications off label for pediatric patients, causing delayed initiation, premature drug discontinuation, or use of less advantageous alternatives,” they wrote.
To address this unmet need, Dr. Siegfried and the other committee members used a modified Delphi process to reach agreement on recommendations related to five key topic areas: indications and contraindications, dosing, interactions with immunizations and medications, potential for and management of adverse effects, and monitoring needs. Consensus was predefined as at least 70% of participants rating a statement as 7-9 on the Likert scale. The effort to develop 46 recommendations has been a work in progress for almost 5 years, “somewhat delayed by the pandemic,” Dr. Siegfried, past president and director of the American Board of Dermatology, said in an interview. “But it remains relevant, despite the emergence of biologics and JAK inhibitors for treating inflammatory skin conditions in children. Although the mechanism-of-action of low-dose MTX is not clear, it may overlap with the newer small molecules.”
The guidelines contain several pearls to guide optimal dosing, including the following key points:
- MTX can be discontinued abruptly without adverse effects, other than the risk of disease worsening.
- Folic acid supplementation (starting at 1 mg/day, regardless of weight) is an effective approach to minimizing associated gastrointestinal adverse effects.
- Concomitant use of MTX and antibiotics (including trimethoprim-sulfamethoxazole) and NSAIDS are not contraindicated for most pediatric patients treated for inflammatory skin disease.
- Live virus vaccine boosters such as varicella-zoster virus (VZV) and measles, mumps, and rubella (MMR) are not contraindicated in patients taking MTX; there are insufficient data to make recommendations for or against primary immunization with MMR vaccine in patients taking MTX; inactivated vaccines should be given to patients taking MTX.
- Routine surveillance laboratory monitoring (i.e., CBC with differential, alanine transaminase, aspartate aminotransferase, creatinine) is recommended at baseline, after 1 month of treatment, and every 3-4 months thereafter.
- Transient transaminase elevation (≤ 3 upper limit normal for < 3 months) is not uncommon with low-dose MTX and does not usually require interruption of MTX. The most likely causes are concomitant viral infection, MTX dosing within 24 hours prior to phlebotomy, recent administration of other medications (such as acetaminophen), and/or recent alcohol consumption.
- Liver biopsy is not indicated for routine monitoring of pediatric patients taking low-dose MTX.
According to Dr. Siegfried, consensus of the committee members was lowest on the need for a test dose of MTX.
Overall, she said in the interview, helping to craft the guidelines caused her to reflect on how her approach to using MTX has evolved over the past 35 years, after treating “many hundreds” of patients. “I was gratified to confirm similar practice patterns among my colleagues,” she added.
The project’s other cochair was Heather Brandling-Bennett, MD, a dermatologist at Seattle Children’s Hospital. This work was supported by a grant from the Pediatric Dermatology Research Alliance (PeDRA), with additional funding from the National Eczema Association and the National Psoriasis Foundation. Dr. Siegfried disclosed ties with AbbVie, Boehringer Ingelheim, Incyte, LEO Pharma, Novan, Novartis, Pierre Fabre, Pfizer, Regeneron, Sanofi Genzyme, UCB, and Verrica. She has participated in contracted research for AI Therapeutics, and has served as principal investigator for Janssen. Many of the guideline coauthors disclosed having received grant support and other funding from pharmaceutical companies.
FROM PEDIATRIC DERMATOLOGY
The invisible effect medical notes could have on care
In the mid-1990s, when Somnath Saha was a medical resident at the University of California, San Francisco, School of Medicine, he came across a cluster of studies showing that Black people with cardiovascular disease were treated less aggressively, compared with White people. The findings were “appalling” to the young physician who describes himself as a “Brown kid from suburban St. Louis, Missouri.”
Dr. Saha had experienced racism growing up, but was surprised to see such clear signs of inequity within the field of medicine. “There was an injustice happening in my own backyard,” he said.
Indeed, bias towards Black patients can be challenging because many doctors either don’t realize their biases or won’t admit to them. Dr. Saha, now a professor of medicine at Johns Hopkins University, likens implicit bias – unconscious judgments that can affect behavior – to “an invisible force.”
While numerous studies have found evidence of racial discrimination in medicine through patient reports, less is known about how implicit bias shows up in medical records, and how stigmatizing language in patient notes can affect the care that Black patients receive.
That’s part of the reason why, about 7 years ago, Dr. Saha began poring through medical records. For him, they offered a window into doctors’ feelings about their patients.
As part of his latest research, Dr. Saha’s team examined the records of nearly 19,000 patients, paying particular attention to negative descriptions that may influence a clinician’s decision-making. The data, which were recently presented at the 2023 American Association for the Advancement of Science annual meeting, aren’t yet published, but it suggests what researchers have long speculated: The notes provide, at times, a surprisingly candid view of how patients are perceived by doctors, and how their race may affect treatment.
The study adds to a concerning body of literature that explores how racial bias manifests in health care. Researchers like Dr. Saha are interested in how such prejudice leaves a paper trail, which can then reinforce negative stereotypes. Because medical notes get passed between physicians, Dr. Saha’s research suggests they can affect the health of Black patients down the line.
“The medical record is like a rap sheet, it stays with you,” Dr. Saha said, adding that “these things that we say about patients get eternalized.”
Research has long shown that Black patients experience worse health outcomes, compared with White patients, in part because of biased medical care. Black women, for example, are three times more likely to die from pregnancy-related complications, compared with White women. And Black patients often report feeling like physicians don’t listen to their needs or don’t believe their concerns.
Studies appear to back that up. Last year, researchers at the University of Washington found that non-Hispanic White children who went to the emergency room for migraines were more likely to receive pain medications, compared with children of color – even though the two groups reported similar pain scores. Other studies echo similar results for adults as well.
While Michael Sun, a resident physician at the University of Chicago, knew about such health disparities, by his own admission, he was naive about the biases in medical records. At that time, Dr. Sun had “no experience in the medical record, in documentation, or in physician language and culture,” he said.
But in Dr. Sun’s first year of medical school, his professor shared the story of a longtime patient, whom she had referred to an outside specialist. In his recollection, the professor regarded her patient in kind terms, having worked with her for some time to treat a chronic illness. But when she got the specialist’s notes back, she was confused by the description of her patient: Terms like “really difficult,” “noncompliant,” and “uninterested in their health.” This was not the patient she remembered.
“This, as a first-year medical student, really shocked me because I had taken at face value that any words used in notes were true, were valid, or rightfully used,” said Dr. Sun. “I realized all the ways that bias, untold stories, and unknown context may change the way that we view our patients.”
Like Dr. Saha, Dr. Sun became interested in how bias influenced the relationship between doctor and patient, and how these interactions were memorialized in the medical record. In a study published last year, he and his colleagues looked at more than 40,000 medical notes from 18,459 patients. Researchers first manually combed through the notes, then used this information to teach a machine learning algorithm to interpret the connotations of words. Compared with White patients, Black patients were about 2.5 times more likely to be described negatively, with terms like “challenging,” “angry,” and “noncompliant.”
Dr. Saha has used similar methodology – and found similar results – in his own research. For the study presented at the AAAS meeting, his team first read through more than 100,000 medical notes to identify language their team considered to be disparaging – which they chose based on a list of words and phrases from prior research. They then used machine learning to find those terms in medical notes, taking care to ensure context was considered. For example, if the word “aggressive” was used to describe a treatment plan, it was excluded from their analysis. But if “aggressive” was used to describe the patient, it was included.
Dr. Saha pointed to three categories of stigmatizing language that were the most pronounced: expressing doubt or disbelief in what the patient said, such as reporting they “claimed” to experience pain; insinuating that the patient was confrontational, using words like “belligerent” or combative;” and suggesting a patient was not cooperating with a doctor’s orders by saying they “refused” medical advice.
“We’ve known for some time that in health care we sometimes use language that can be confusing or even insulting,” Matthew Wynia, director of the Center for Bioethics and Humanities at the University of Colorado at Denver, Aurora, wrote in an email to Undark. But he noted that research such as Dr. Saha’s has drawn attention to a previously overlooked issue. Describing a patient as “noncompliant” with medications, he said, “makes it sound like the patient is intentionally refusing to follow advice when, in fact, there are many reasons why people might not be able to follow our advice and intentional refusal isn’t even a very common one.”
Dr. Saha noted that, if a patient isn’t taking their medication, it’s important that doctors note that, so that the next physician doesn’t overprescribe them. But the concern, he said, is whether doctors are using these terms appropriately and for the right reasons because of the implications they have for patients.
If a doctor portrays their patient negatively, Dr. Saha said, it can “trigger the next clinician to read them and formulate a potentially negative opinion about that patient” before they’ve even had a chance to interact.
Still, stigmatizing language is only one small piece of the puzzle. What also matters, Dr. Saha said, is how those words can have an impact on care. In prior work, Dr. Saha has shown how implicit and, in some cases, explicit bias, affects a patient’s treatment recommendations.
In a 2018 study, Dr. Saha, along with his wife, Mary Catherine Beach – also a professor at Johns Hopkins University – combed through reports of patients with sickle cell anemia. Their team focused on that particular population since sickle cell patients are some of the most stigmatized in the health care system: Most patients are Black and many require regular doses of opioids for pain management.
In the notes, they found numerous examples of details that were irrelevant to patients’ health concerns: phrases like “girlfriend requests bus token,” “cursing at nurse,” “girlfriend on bed with shoes on,” and “narcotic dependent.”
Dr. Saha and Dr. Beach wanted to see how these remarks might influence a physician’s treatment recommendations, so they used vignettes they had found in the medical records of sickle cell patients. They showed either a vignette which had described patients negatively, or one that was edited with neutral language. Then they asked medical students and residents about the dose of pain medication they would hypothetically recommend. Dr. Beach said that the purpose was to see how what she called “dog whistles about social class or race or something that would make the person seem less educated” would impact treatment recommendations.
The study found that medical notes with stigmatizing language were associated with “less aggressive management of the patient’s pain.” Doctors who read the stigmatizing language chart notes prescribed less pain medication to patients even in cases when they commented that their pain was a 10 out of 10.
“The fact that we were able to show that this bias transmits to the next doctor has been the thing that I think motivates doctors to take it seriously,” said Dr. Beach.
Pain management has become a focal point for researchers because many of the most glaring racial tropes about patient care have revolved around pain. In 2016, a study conducted at the University of Virginia found that half of the 418 medical students and residents surveyed endorsed false beliefs about Black patients. For example, that “Blacks’ nerve endings are less sensitive than whites” and “Blacks’ skin is thicker than whites.” What’s more, those who endorsed these false beliefs also rated Black patients’ pain as lower than White patients’.
Antoinette M. Schoenthaler, a professor of population health and medicine at New York University and associate director of research at the school’s Institute for Excellence in Health Equity, said that disparities in pain management are pervasive and widespread across the medical profession. They seep into treatments for sickle cell anemia, but also prenatal care. As a result, she said, Black patients across the board are often fearful of attending appointments.
“Patients of color go into an appointment with feelings of heightened anxiety because they’re expecting mistreatment,” said Dr. Schoenthaler. “We’ve seen minoritized patients have higher blood pressure in the context of a clinical visit because of these expectations of anxiety and fear, and disappointment.”
Disparities in health care between Black and White patients is a complex issue – one which can’t be solved by addressing medical records alone. But, for researchers like Dr. Saha, Dr. Beach, and Dr. Sun, they can offer a road map that outlines where differences in care begin. The words a clinician uses sets the path for how a patient may be treated in the future.
One way to combat implicit bias, Dr. Saha suggested, is to use an algorithm that identifies stigmatizing language to “give hospital departments or clinicians report cards on how much of this language that they’re using.” By benchmarking averages against one another, clinicians could know if they’re using stigmatizing language at an above average rate. This is something he is considering for future research.
When clinicians are made aware of their biases – when the unconscious becomes conscious – Dr. Saha told Undark that he’s optimistic they’ll work to change them: “We’re using language that we’ve used forever without realizing the potential impact that it has on patient care.”
This article originated on Undark. A version of this article appeared on Medscape.com.
In the mid-1990s, when Somnath Saha was a medical resident at the University of California, San Francisco, School of Medicine, he came across a cluster of studies showing that Black people with cardiovascular disease were treated less aggressively, compared with White people. The findings were “appalling” to the young physician who describes himself as a “Brown kid from suburban St. Louis, Missouri.”
Dr. Saha had experienced racism growing up, but was surprised to see such clear signs of inequity within the field of medicine. “There was an injustice happening in my own backyard,” he said.
Indeed, bias towards Black patients can be challenging because many doctors either don’t realize their biases or won’t admit to them. Dr. Saha, now a professor of medicine at Johns Hopkins University, likens implicit bias – unconscious judgments that can affect behavior – to “an invisible force.”
While numerous studies have found evidence of racial discrimination in medicine through patient reports, less is known about how implicit bias shows up in medical records, and how stigmatizing language in patient notes can affect the care that Black patients receive.
That’s part of the reason why, about 7 years ago, Dr. Saha began poring through medical records. For him, they offered a window into doctors’ feelings about their patients.
As part of his latest research, Dr. Saha’s team examined the records of nearly 19,000 patients, paying particular attention to negative descriptions that may influence a clinician’s decision-making. The data, which were recently presented at the 2023 American Association for the Advancement of Science annual meeting, aren’t yet published, but it suggests what researchers have long speculated: The notes provide, at times, a surprisingly candid view of how patients are perceived by doctors, and how their race may affect treatment.
The study adds to a concerning body of literature that explores how racial bias manifests in health care. Researchers like Dr. Saha are interested in how such prejudice leaves a paper trail, which can then reinforce negative stereotypes. Because medical notes get passed between physicians, Dr. Saha’s research suggests they can affect the health of Black patients down the line.
“The medical record is like a rap sheet, it stays with you,” Dr. Saha said, adding that “these things that we say about patients get eternalized.”
Research has long shown that Black patients experience worse health outcomes, compared with White patients, in part because of biased medical care. Black women, for example, are three times more likely to die from pregnancy-related complications, compared with White women. And Black patients often report feeling like physicians don’t listen to their needs or don’t believe their concerns.
Studies appear to back that up. Last year, researchers at the University of Washington found that non-Hispanic White children who went to the emergency room for migraines were more likely to receive pain medications, compared with children of color – even though the two groups reported similar pain scores. Other studies echo similar results for adults as well.
While Michael Sun, a resident physician at the University of Chicago, knew about such health disparities, by his own admission, he was naive about the biases in medical records. At that time, Dr. Sun had “no experience in the medical record, in documentation, or in physician language and culture,” he said.
But in Dr. Sun’s first year of medical school, his professor shared the story of a longtime patient, whom she had referred to an outside specialist. In his recollection, the professor regarded her patient in kind terms, having worked with her for some time to treat a chronic illness. But when she got the specialist’s notes back, she was confused by the description of her patient: Terms like “really difficult,” “noncompliant,” and “uninterested in their health.” This was not the patient she remembered.
“This, as a first-year medical student, really shocked me because I had taken at face value that any words used in notes were true, were valid, or rightfully used,” said Dr. Sun. “I realized all the ways that bias, untold stories, and unknown context may change the way that we view our patients.”
Like Dr. Saha, Dr. Sun became interested in how bias influenced the relationship between doctor and patient, and how these interactions were memorialized in the medical record. In a study published last year, he and his colleagues looked at more than 40,000 medical notes from 18,459 patients. Researchers first manually combed through the notes, then used this information to teach a machine learning algorithm to interpret the connotations of words. Compared with White patients, Black patients were about 2.5 times more likely to be described negatively, with terms like “challenging,” “angry,” and “noncompliant.”
Dr. Saha has used similar methodology – and found similar results – in his own research. For the study presented at the AAAS meeting, his team first read through more than 100,000 medical notes to identify language their team considered to be disparaging – which they chose based on a list of words and phrases from prior research. They then used machine learning to find those terms in medical notes, taking care to ensure context was considered. For example, if the word “aggressive” was used to describe a treatment plan, it was excluded from their analysis. But if “aggressive” was used to describe the patient, it was included.
Dr. Saha pointed to three categories of stigmatizing language that were the most pronounced: expressing doubt or disbelief in what the patient said, such as reporting they “claimed” to experience pain; insinuating that the patient was confrontational, using words like “belligerent” or combative;” and suggesting a patient was not cooperating with a doctor’s orders by saying they “refused” medical advice.
“We’ve known for some time that in health care we sometimes use language that can be confusing or even insulting,” Matthew Wynia, director of the Center for Bioethics and Humanities at the University of Colorado at Denver, Aurora, wrote in an email to Undark. But he noted that research such as Dr. Saha’s has drawn attention to a previously overlooked issue. Describing a patient as “noncompliant” with medications, he said, “makes it sound like the patient is intentionally refusing to follow advice when, in fact, there are many reasons why people might not be able to follow our advice and intentional refusal isn’t even a very common one.”
Dr. Saha noted that, if a patient isn’t taking their medication, it’s important that doctors note that, so that the next physician doesn’t overprescribe them. But the concern, he said, is whether doctors are using these terms appropriately and for the right reasons because of the implications they have for patients.
If a doctor portrays their patient negatively, Dr. Saha said, it can “trigger the next clinician to read them and formulate a potentially negative opinion about that patient” before they’ve even had a chance to interact.
Still, stigmatizing language is only one small piece of the puzzle. What also matters, Dr. Saha said, is how those words can have an impact on care. In prior work, Dr. Saha has shown how implicit and, in some cases, explicit bias, affects a patient’s treatment recommendations.
In a 2018 study, Dr. Saha, along with his wife, Mary Catherine Beach – also a professor at Johns Hopkins University – combed through reports of patients with sickle cell anemia. Their team focused on that particular population since sickle cell patients are some of the most stigmatized in the health care system: Most patients are Black and many require regular doses of opioids for pain management.
In the notes, they found numerous examples of details that were irrelevant to patients’ health concerns: phrases like “girlfriend requests bus token,” “cursing at nurse,” “girlfriend on bed with shoes on,” and “narcotic dependent.”
Dr. Saha and Dr. Beach wanted to see how these remarks might influence a physician’s treatment recommendations, so they used vignettes they had found in the medical records of sickle cell patients. They showed either a vignette which had described patients negatively, or one that was edited with neutral language. Then they asked medical students and residents about the dose of pain medication they would hypothetically recommend. Dr. Beach said that the purpose was to see how what she called “dog whistles about social class or race or something that would make the person seem less educated” would impact treatment recommendations.
The study found that medical notes with stigmatizing language were associated with “less aggressive management of the patient’s pain.” Doctors who read the stigmatizing language chart notes prescribed less pain medication to patients even in cases when they commented that their pain was a 10 out of 10.
“The fact that we were able to show that this bias transmits to the next doctor has been the thing that I think motivates doctors to take it seriously,” said Dr. Beach.
Pain management has become a focal point for researchers because many of the most glaring racial tropes about patient care have revolved around pain. In 2016, a study conducted at the University of Virginia found that half of the 418 medical students and residents surveyed endorsed false beliefs about Black patients. For example, that “Blacks’ nerve endings are less sensitive than whites” and “Blacks’ skin is thicker than whites.” What’s more, those who endorsed these false beliefs also rated Black patients’ pain as lower than White patients’.
Antoinette M. Schoenthaler, a professor of population health and medicine at New York University and associate director of research at the school’s Institute for Excellence in Health Equity, said that disparities in pain management are pervasive and widespread across the medical profession. They seep into treatments for sickle cell anemia, but also prenatal care. As a result, she said, Black patients across the board are often fearful of attending appointments.
“Patients of color go into an appointment with feelings of heightened anxiety because they’re expecting mistreatment,” said Dr. Schoenthaler. “We’ve seen minoritized patients have higher blood pressure in the context of a clinical visit because of these expectations of anxiety and fear, and disappointment.”
Disparities in health care between Black and White patients is a complex issue – one which can’t be solved by addressing medical records alone. But, for researchers like Dr. Saha, Dr. Beach, and Dr. Sun, they can offer a road map that outlines where differences in care begin. The words a clinician uses sets the path for how a patient may be treated in the future.
One way to combat implicit bias, Dr. Saha suggested, is to use an algorithm that identifies stigmatizing language to “give hospital departments or clinicians report cards on how much of this language that they’re using.” By benchmarking averages against one another, clinicians could know if they’re using stigmatizing language at an above average rate. This is something he is considering for future research.
When clinicians are made aware of their biases – when the unconscious becomes conscious – Dr. Saha told Undark that he’s optimistic they’ll work to change them: “We’re using language that we’ve used forever without realizing the potential impact that it has on patient care.”
This article originated on Undark. A version of this article appeared on Medscape.com.
In the mid-1990s, when Somnath Saha was a medical resident at the University of California, San Francisco, School of Medicine, he came across a cluster of studies showing that Black people with cardiovascular disease were treated less aggressively, compared with White people. The findings were “appalling” to the young physician who describes himself as a “Brown kid from suburban St. Louis, Missouri.”
Dr. Saha had experienced racism growing up, but was surprised to see such clear signs of inequity within the field of medicine. “There was an injustice happening in my own backyard,” he said.
Indeed, bias towards Black patients can be challenging because many doctors either don’t realize their biases or won’t admit to them. Dr. Saha, now a professor of medicine at Johns Hopkins University, likens implicit bias – unconscious judgments that can affect behavior – to “an invisible force.”
While numerous studies have found evidence of racial discrimination in medicine through patient reports, less is known about how implicit bias shows up in medical records, and how stigmatizing language in patient notes can affect the care that Black patients receive.
That’s part of the reason why, about 7 years ago, Dr. Saha began poring through medical records. For him, they offered a window into doctors’ feelings about their patients.
As part of his latest research, Dr. Saha’s team examined the records of nearly 19,000 patients, paying particular attention to negative descriptions that may influence a clinician’s decision-making. The data, which were recently presented at the 2023 American Association for the Advancement of Science annual meeting, aren’t yet published, but it suggests what researchers have long speculated: The notes provide, at times, a surprisingly candid view of how patients are perceived by doctors, and how their race may affect treatment.
The study adds to a concerning body of literature that explores how racial bias manifests in health care. Researchers like Dr. Saha are interested in how such prejudice leaves a paper trail, which can then reinforce negative stereotypes. Because medical notes get passed between physicians, Dr. Saha’s research suggests they can affect the health of Black patients down the line.
“The medical record is like a rap sheet, it stays with you,” Dr. Saha said, adding that “these things that we say about patients get eternalized.”
Research has long shown that Black patients experience worse health outcomes, compared with White patients, in part because of biased medical care. Black women, for example, are three times more likely to die from pregnancy-related complications, compared with White women. And Black patients often report feeling like physicians don’t listen to their needs or don’t believe their concerns.
Studies appear to back that up. Last year, researchers at the University of Washington found that non-Hispanic White children who went to the emergency room for migraines were more likely to receive pain medications, compared with children of color – even though the two groups reported similar pain scores. Other studies echo similar results for adults as well.
While Michael Sun, a resident physician at the University of Chicago, knew about such health disparities, by his own admission, he was naive about the biases in medical records. At that time, Dr. Sun had “no experience in the medical record, in documentation, or in physician language and culture,” he said.
But in Dr. Sun’s first year of medical school, his professor shared the story of a longtime patient, whom she had referred to an outside specialist. In his recollection, the professor regarded her patient in kind terms, having worked with her for some time to treat a chronic illness. But when she got the specialist’s notes back, she was confused by the description of her patient: Terms like “really difficult,” “noncompliant,” and “uninterested in their health.” This was not the patient she remembered.
“This, as a first-year medical student, really shocked me because I had taken at face value that any words used in notes were true, were valid, or rightfully used,” said Dr. Sun. “I realized all the ways that bias, untold stories, and unknown context may change the way that we view our patients.”
Like Dr. Saha, Dr. Sun became interested in how bias influenced the relationship between doctor and patient, and how these interactions were memorialized in the medical record. In a study published last year, he and his colleagues looked at more than 40,000 medical notes from 18,459 patients. Researchers first manually combed through the notes, then used this information to teach a machine learning algorithm to interpret the connotations of words. Compared with White patients, Black patients were about 2.5 times more likely to be described negatively, with terms like “challenging,” “angry,” and “noncompliant.”
Dr. Saha has used similar methodology – and found similar results – in his own research. For the study presented at the AAAS meeting, his team first read through more than 100,000 medical notes to identify language their team considered to be disparaging – which they chose based on a list of words and phrases from prior research. They then used machine learning to find those terms in medical notes, taking care to ensure context was considered. For example, if the word “aggressive” was used to describe a treatment plan, it was excluded from their analysis. But if “aggressive” was used to describe the patient, it was included.
Dr. Saha pointed to three categories of stigmatizing language that were the most pronounced: expressing doubt or disbelief in what the patient said, such as reporting they “claimed” to experience pain; insinuating that the patient was confrontational, using words like “belligerent” or combative;” and suggesting a patient was not cooperating with a doctor’s orders by saying they “refused” medical advice.
“We’ve known for some time that in health care we sometimes use language that can be confusing or even insulting,” Matthew Wynia, director of the Center for Bioethics and Humanities at the University of Colorado at Denver, Aurora, wrote in an email to Undark. But he noted that research such as Dr. Saha’s has drawn attention to a previously overlooked issue. Describing a patient as “noncompliant” with medications, he said, “makes it sound like the patient is intentionally refusing to follow advice when, in fact, there are many reasons why people might not be able to follow our advice and intentional refusal isn’t even a very common one.”
Dr. Saha noted that, if a patient isn’t taking their medication, it’s important that doctors note that, so that the next physician doesn’t overprescribe them. But the concern, he said, is whether doctors are using these terms appropriately and for the right reasons because of the implications they have for patients.
If a doctor portrays their patient negatively, Dr. Saha said, it can “trigger the next clinician to read them and formulate a potentially negative opinion about that patient” before they’ve even had a chance to interact.
Still, stigmatizing language is only one small piece of the puzzle. What also matters, Dr. Saha said, is how those words can have an impact on care. In prior work, Dr. Saha has shown how implicit and, in some cases, explicit bias, affects a patient’s treatment recommendations.
In a 2018 study, Dr. Saha, along with his wife, Mary Catherine Beach – also a professor at Johns Hopkins University – combed through reports of patients with sickle cell anemia. Their team focused on that particular population since sickle cell patients are some of the most stigmatized in the health care system: Most patients are Black and many require regular doses of opioids for pain management.
In the notes, they found numerous examples of details that were irrelevant to patients’ health concerns: phrases like “girlfriend requests bus token,” “cursing at nurse,” “girlfriend on bed with shoes on,” and “narcotic dependent.”
Dr. Saha and Dr. Beach wanted to see how these remarks might influence a physician’s treatment recommendations, so they used vignettes they had found in the medical records of sickle cell patients. They showed either a vignette which had described patients negatively, or one that was edited with neutral language. Then they asked medical students and residents about the dose of pain medication they would hypothetically recommend. Dr. Beach said that the purpose was to see how what she called “dog whistles about social class or race or something that would make the person seem less educated” would impact treatment recommendations.
The study found that medical notes with stigmatizing language were associated with “less aggressive management of the patient’s pain.” Doctors who read the stigmatizing language chart notes prescribed less pain medication to patients even in cases when they commented that their pain was a 10 out of 10.
“The fact that we were able to show that this bias transmits to the next doctor has been the thing that I think motivates doctors to take it seriously,” said Dr. Beach.
Pain management has become a focal point for researchers because many of the most glaring racial tropes about patient care have revolved around pain. In 2016, a study conducted at the University of Virginia found that half of the 418 medical students and residents surveyed endorsed false beliefs about Black patients. For example, that “Blacks’ nerve endings are less sensitive than whites” and “Blacks’ skin is thicker than whites.” What’s more, those who endorsed these false beliefs also rated Black patients’ pain as lower than White patients’.
Antoinette M. Schoenthaler, a professor of population health and medicine at New York University and associate director of research at the school’s Institute for Excellence in Health Equity, said that disparities in pain management are pervasive and widespread across the medical profession. They seep into treatments for sickle cell anemia, but also prenatal care. As a result, she said, Black patients across the board are often fearful of attending appointments.
“Patients of color go into an appointment with feelings of heightened anxiety because they’re expecting mistreatment,” said Dr. Schoenthaler. “We’ve seen minoritized patients have higher blood pressure in the context of a clinical visit because of these expectations of anxiety and fear, and disappointment.”
Disparities in health care between Black and White patients is a complex issue – one which can’t be solved by addressing medical records alone. But, for researchers like Dr. Saha, Dr. Beach, and Dr. Sun, they can offer a road map that outlines where differences in care begin. The words a clinician uses sets the path for how a patient may be treated in the future.
One way to combat implicit bias, Dr. Saha suggested, is to use an algorithm that identifies stigmatizing language to “give hospital departments or clinicians report cards on how much of this language that they’re using.” By benchmarking averages against one another, clinicians could know if they’re using stigmatizing language at an above average rate. This is something he is considering for future research.
When clinicians are made aware of their biases – when the unconscious becomes conscious – Dr. Saha told Undark that he’s optimistic they’ll work to change them: “We’re using language that we’ve used forever without realizing the potential impact that it has on patient care.”
This article originated on Undark. A version of this article appeared on Medscape.com.