User login
Your age-based guide to comprehensive well-woman care
Preventive coding can be a snap
Billing for the well-woman exam, with Medicare Guide
Melanie Witt, RN, CPC, COBGC, MA
The American College of Obstetricians and Gynecologists (ACOG) has recommended dividing a woman's life cycle into four intervals—ages 13–18, 19–39, 40–64, and older than 65—in order to best organize the approach to primary and preventive health care.1 This paradigm provides a structure for organizing the clinical approach to physical examination, laboratory testing, counseling, and immunizations. In addition, it helps to highlight the diseases and health problems most prevalent among women at each life-stage.
Different professional organizations—US Preventive Services Task Force (USPSTF), American Medical Association, American College of Physicians, ACOG, American Academy of Family Physicians, American Academy of Pediatrics, and Advisory Committee on Immunization Practices—have used varying analytical methods to determine recommended health services by age group; consequently, these organizations have somewhat divergent recommendations. However, the recommendations of most organizations share many similarities. In this comprehensive guide, I point out those similarities. Keep in mind that recommendations change over time, and it is important to use your professional judgment when approaching each patient.
TABLE
Physical examination and laboratory testing services according to a patient's age, based on ACOG recommendations1
| Health service | 13–18 years | 19–39 years | 40–64 years | 65 years and older |
|---|---|---|---|---|
| Physical examination | ||||
| Height | X | X | X | X |
| Weight | X | X | X | X |
| BMI | X | X | X | X |
| Blood pressure | X | X | X | X |
| Tanner staging of secondary sexual characteristics | X | |||
| Neck exam (assess thyroid and presence of adenopathy) | X | X | X | |
| Breast exam | X | X (including axillae) | X (including axillae) | |
| Oral cavity | X | X | ||
| Abdominal exam | X | X | X | X |
| Pelvic exam | If indicated | Age 21 and older | X | X |
| Skin exam | X | X | X | |
| Laboratory testing | ||||
| Chlamydia | If sexually active | If age 25 or younger and sexually active | ||
| Gonorrhea | If sexually active | If age 25 or younger and sexually active | ||
| HIV | If sexually active | X | X | |
| Cervical cytology | Age 21-29: Every 2 years Age 30 and older, low risk: Every 3 years Age 30 and older, high risk (immunosuppressed or HIV infection): Annually | Low risk: Every 3 years High risk (immunosuppressed or HIV infection): Annually | Consider discontinuing in women with:
| |
| Colorectal cancer screening (colonoscopy preferred) | Age 50 and older, low risk: Every 10 years High risk: Consult colorectal screening guidelines* | Every 10 years | ||
| Fasting glucose | Age 45 and older: Every 5 years | Every 5 years | ||
| Lipid profile | Age 45 and older: Every 5 years | Every 5 years | ||
| Mammography | Age 40 to 49: Every 1-2 years Age 50 and older: Annually | Annually | ||
| BMD | Not more frequently than every 2 years | |||
| TSH | Every 5 years | |||
| Urinalysis | X | |||
| Abbreviations: BMD, bone mineral density; BMI, body mass index; HIV, human immunodeficiency virus; TSH, thyroid stimulating hormone. *Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130–160. | ||||
The adolescent: 13–18 years
Screen. Guide. Immunize. ACOG recommends that the first visit take place between 13 and 15 years of age, with annual visits thereafter. The purpose of the first, and subsequent, visits is to assess health status, including menstrual history and body mass index (BMI), and to provide health guidance, screening, and preventive health services. This initial visit generally does not include a pelvic examination. A physical examination is not required at every visit but is recommended to occur at least once during early, middle, and late adolescence.
Target your screening practices. Screen adolescents for the following conditions during clinical preventive services: hypertension; hyperlipidemia; obesity and eating disorders; physical, sexual, or emotional abuse; learning or school problems; substance use; depression and risk of suicide; sexual assault; sexual behavior that may lead to pregnancy or sexually transmitted disease (STD); and tuberculosis and HIV, unless the patient opts out (TABLE).
Anticipate. Then guide. Using anticipatory guidance, you can help adolescents understand their physical, psychosocial, and sexual development and motivate them to be involved in their health and health-care decisions. Issues relevant to adolescents include dietary habits; injury prevention, through the use of helmets and seatbelts; regular exercise; responsible sexual behaviors; avoidance of substances that can be abused; strategies for dealing with bullying; and avoidance of behaviors that might have negative consequences, such as vandalism, stealing, and sharing personal information with strangers.
Recommended immunizations. For this age group, immunizations, unless previously given, include:
- 1 or 2 doses of measles, mumps, and rubella
- 2 doses of varicella if not previously infected
- a booster dose of tetanus if ≥10 years have elapsed since the last dose
- human papillomavirus (HPV)
- annual influenza.
Other immunizations that may be warranted on the basis of medical condition, occupation, lifestyle, or other indications include: 3 doses of hepatitis B, 2 doses of hepatitis A, 1 or more doses of meningococcal, and 1 or 2 doses of pneumococcal.
Menses, an important "vital sign." Once menstruation begins, evaluating menstrual cycle characteristics is important. Patterns that may require evaluation include2:
- no menses within 3 years of thelarche
- no menses by age 13 with no sign of pubertal development
- no menses by age 14 with signs of hirsutism
- no menses by age 14 with indications of an eating disorder
- no menses by age 15
- history of regular menses that are now markedly irregular
- menses occur more frequently than 21 days or less frequently than every 45 days
- menses occur 90 days apart for one cycle
- menstrual bleeding that lasts more than 7 days
- frequent tampon/pad changes (more than 1 tampon/pad every 1 to 2 hours).
BMI predicts future disease. Overweight and obesity are important risk factors for diabetes mellitus, hyperlipidemia, hypertension, and various cancers. Eating disorders are common among adolescents and often occur in association with other mental health problems.
Non–sexually active teens and children
Gynecologic examination typically involves inspection of the genitalia and not instrumentation of the vagina. A careful explanation of the proposed examination is important. Ask young adolescents who they would like to have in the examination room with them. A hand mirror can be used to involve the patient in the genitalia inspection. If it's necessary to obtain magnification, use a hand lens, an otoscope without the speculum, or a colposcope. Record the configuration of the hymen, if present. If indicated, examination of the genitalia while the patient is in the knee-chest position often provides a good view of the vagina and sometimes the cervix, without instrumentation.
Sexually active teens
Effective contraception, including the use of emergency contraceptives, is an important health focus for sexually active teens. Vaginal speculum examination and bimanual gyn exam are not required prior to prescribing hormonal contraceptives to teens. Based on a review of the evidence and expert opinion,3 the current recommendation is that prior to prescribing a hormonal contraceptive, a medical history and blood pressure measurement are the only requirements; breast examination and a gyn exam (vaginal speculum and bimanual gyn exam) are not necessary. Testing for chlamydia and gonorrhea can be performed using a urine sample. A cervical cytology examination is not necessary until age 21 unless the patient is in a high-risk group, such as immunosuppressed or HIV-infected teens.
The young woman: 19–39 years
Focus on reproductive issues. Contraception, pregnancy, and cervical cancer screening are common reasons for visits among women in this age group. Gynecologic problems can include polycystic ovary syndrome (PCOS), endometriosis, fibroids, infertility, pelvic pain, vulvovaginal pain syndromes, vaginitis, adnexal masses, and STDs, including pelvic inflammatory diseases.
Offer effective contraception
Long-acting reversible contraceptives (LARCs) are the most clinically and cost-effective forms of reversible contraception. There are three LARC methods available in the United States: 1) the copper T380A intrauterine device (IUD; Paragard), 2) the levonorgestrel-releasing intrauterine system (Mirena), and 3) the single-rod etonogestrel implant (Implanon, Explanon).
The use of IUDs among American women has increased from about 2.4% of contracepting women of reproductive age in 2002 to 8.5% in 2009.4 In Norway and France, contracepting women of reproductive age use IUDs at a rate of 27% and 23%, respectively.5 Typical-use pregnancy rates for LARCs are lower and continuation rates are higher than observed with oral contraceptives (OCs).
In an economic analysis, the cost of LARCs was lower than almost all other forms of reversible contraception over a 5-year interval.6 When financial and access barriers are removed, most women starting a contraceptive will use a LARC, if offered.7
Be aware of STDs
STDs are common in this age group. In the United States, chlamydial genital infections reach a peak in women 18 to 25 years old, with a prevalence of about 4%.8
Counsel her about exercise and weight loss
Approximately 60% of women older than age 20 are overweight or obese.9 The rise in obesity is a key contributing factor to an increase in many diseases, including gestational diabetes, type 2 diabetes mellitus, and hypertension. Successful efforts to reduce the prevalence of obesity through diet and exercise could markedly improve population health.
Don't overlook autoimmune conditions
Many autoimmune diseases reach a peak incidence between ages 19 and 39, and, except for ankylosing spondylitis, are more of a concern for women than men. Systemic lupus erythematosus, lymphocytic thyroiditis, and rheumatoid arthritis occur much more frequently in women than in men, with ratios in the range of 7:1 observed during this age interval.
Keep her immunity up to date
Immunizations recommended in this age group include:
- one Tdap (tetanus toxoid, diphtheria, and pertussis)
- tetanus every 10 years
- influenza annually
- varicella if no evidence of immunity
- HPV for those aged 26 years or younger.
The mature woman: 40–64 years
Transition to postmenopause. The menstrual changes through perimenopause to postmenopause are often accompanied by changes in sleep patterns, vasomotor symptoms, and increasing vaginal dryness.
Open your eyes to a patient's insomnia
Perimenopausal and postmenopausal women report a much higher rate of insomnia than age-matched men.10 Women with moderate to severe vasomotor symptoms are more likely to report greater nighttime wakefulness and a greater number of nighttime long-awake episodes than women with mild vasomotor symptoms.11 Insomnia can be associated with poor work performance and mood changes.
Hormone therapy: Be conservative
In the past, hormone therapy, with various estrogen and progestin combinations, was recommended to help prevent a number of diseases, including cardiovascular disease (CD) and osteoporosis. Based on clinical trial results, the current recommendation is to limit the use of hormone therapy in postmenopausal women to the treatment of vasomotor symptoms and vaginal symptoms caused by hypoestrogenism. To treat these problems, the lowest doses of hormones that are effective should be used for the shortest periods of time that achieve symptom resolution.
The older woman: 65+ years
Successful aging. Based on observational studies, behavioral and health factors associated with successful aging include more than 12 years of education; high socioeconomic status; absence of diabetes, asthma, stroke, and lower respiratory tract disease; absence of depression; presence of at least five close personal contacts; frequent walking; moderate use of alcohol; and nonsmoking status.12
Know her risks, and watch for them
Cardiovascular disease. Among women, CDs cause more deaths than malignant neoplasms, chronic lower respiratory disease, Alzheimer's disease, and accidents combined. Black women have rates of CD approximately 40% greater than white women. Hypertension, hypertriglyceridemia, obesity, and sedentary lifestyle among black women account for a part of this increased risk.
Effective lifestyle interventions for primary CD prevention in women include smoking cessation, a diet such as DASH (Dietary Approaches to Stop Hypertension) rich in fruits and vegetables, regular physical activity, and weight management.13
There are important gender differences in aspirin efficacy for primary prevention of stroke and myocardial infarction (MI) in men and women. Among women, aspirin used for primary prevention appears to reduce the risk of stroke but not MI.14 Among men, aspirin used for primary prevention appears to reduce the risk of MI but not stroke.15,16 Based on these and other data, the USPSTF has recommended that aspirin not be used to prevent stroke in men but recommends aspirin to prevent stroke among women 55 to 79 years of age when benefits outweigh risks of gastrointestinal bleeding.17
Atrial fibrillation (AF), a risk factor for stroke, is more common in women than in men. In addition, women with AF who are not anticoagulated are at greater risk for stroke than men with AF who are not anticoagulated.18 The mechanisms that influence these gender differences are not well characterized.
Respiratory illness. Among women, the prevalence of chronic bronchitis and emphysema increased more than 2.8-fold from 1980 to 2000.19 These diseases are major contributors to physician office visits, hospitalizations, disability, and death. Tobacco use is the major risk factor that accounts for the marked increase in COPD among women during recent decades, although ambient pollutants in the environment, home, and workplace are also important contributors to COPD development.
Cognitive decline. Alzheimer's disease afflicts approximately twice as many women as men. Part of this difference is due to the greater longevity of women, but additional variables, such as gender differences in neurobiology, are also contributory. The role of estradiol in the development of Alzheimer's disease remains controversial.
Osteoporosis. This disease occurs about five times more frequently in women than in men. Among Medicare patients, the cost of caring for a hip fracture is more than $40,000 in the first year postfracture. Hip fracture is associated with a high risk of rapid health decline. Interventions that successfully prevent hip fracture are associated with a reduced mortality rate.20,21
Keep in mind the top causes of death for her age when you examine and counsel your patient. For a young teenager, for instance, accidents are the most common cause of death. Therefore, emphasize to her the importance of risk-reducing interventions, such as wearing helmets while biking and seatbelts while driving and practicing water sports safely.
| Age 13–18 years | Age 19–39 years |
|---|---|
|
|
| Age 40–64 years | Age 65 years and older |
|
|
| Source: Mortality Statistics Branch, National Center for Health Statistics; 2004. | |
Domestic violence
Domestic violence is common; approximately 5% of women report one episode during the past year and 25% report at least one lifetime episode.22 Domestic violence involves two people: a perpetrator and a victim. In some relationships, a recurrent cycle of violence and reconciliation is observed. Routine, confidential, and private screening is required to detect most cases of domestic violence.
Ask the right question(s). The single question, "At any time, has a partner hit, kicked, or otherwise hurt or threatened you?" can increase the rate of detection. Alternatively, a set of three questions can be used to screen for domestic violence:
- "Within the past year, have you been hit, slapped, kicked or otherwise physically hurt by someone?"
- "Within the past year, has anyone forced you to have sexual activity?"
- In pregnancy: "Since you have been pregnant, have you been hit, slapped, kicked, or otherwise physically hurt by someone?"
Follow-up and refer. If a woman reports that she has suffered or is at risk for domestic violence, document the finding in her medical record. Then try to assess her safety by asking: "Are there guns in the home?", "Have there been threats of suicide or homicide?", "Has there been violence toward children?" Choking, specifically, could be a sign of future escalated violence—as many perpetrators choke their victims prior to further, escalated violence occurring—and should be taken as a threat of homicide. Refer women who report domestic violence to a specialist; often, the best trained and most available experts are experienced social workers.
Sexual assault
About 25% of women report at least one lifetime sexual assault. Most women who report being raped initially receive care in a hospital-based emergency department from nurses who are credentialed in Sexual Assault Nurse Evaluation (SANE) skills.
The initial evaluation includes rapid access to treatment by a specialized clinical team, assessment and treatment of bodily injuries with a focus on genital trauma, psychological assessment and support, pregnancy assessment and prevention, preventive treatment of STDs, and collection of forensic data, including toxicology testing for the presence of date-rape drugs.
When sexual assault is reported, treat for an STD. The Centers for Disease Control and Prevention (CDC) recommends the following approach to prevent and treat STDs in victims of sexual assault23:
- ceftriaxone 125 mg IM to prevent gonorrhea
- azithromycin 1 g orally as a single dose or doxycycline 100 mg twice daily for 7 days to prevent chlamydia
- metronidazole 2 g orally as a single dose to prevent trichomoniasis
- hepatitis B vaccination, for women not previously vaccinated. (The CDC recommends against the use of hepatitis B immune globulin as the costs are believed to outweigh the benefits.)
- HIV postexposure prophylaxis for 3 to 7 days, with a follow-up visit to consider pros and cons of continued prophylaxis. (The risk of HIV infection following a sexual assault is low.)
- postcoital contraception (for example, levonorgestrel 1.5 mg orally as a single dose).
An antiemetic also should be offered to reduce the risk that the multiple prescribed medications will cause vomiting and nullify prophylaxis efforts. Approximately 2 weeks after the sexual assault the patient should have a pregnancy test and be assessed for ongoing mental health needs. If she did not adhere to the medications or if she shows relevant symptoms, perform follow-up STD testing. Follow-up HIV and syphilis testing can be performed at 12 and 24 weeks following the assault.
Sexual dysfunction
Sexuality is an important part of the human experience. Sexual dysfunction is the inability to participate as desired in a sexual relationship. Problems of sexual dysfunction are best approached from a biopsychosocial framework that recognizes the important contributions of biological, psychological, and social-cultural factors in sexual health. Masters and Johnson posited four stages of sexual response: excitement, plateau, orgasm, and resolution. Building on this linear model, investigators later divided the excitement phase into desire and arousal.
Recent models of sexual response have emphasized a circular model, in which sequential responses overlap and build on previous stimuli. These models also emphasize the importance of emotional intimacy and the quality of the relationship in achieving optimal sexual health.
Approximately 40% of women and 30% of men report sexual dysfunction.24 Common sexual problems reported by heterosexual women include:
- lack of interest in sex
- inability to achieve orgasm
- pain caused by sexual intercourse
- lack of pleasure with sex
- trouble lubricating.
The majority of men and women will not voluntarily report sexual dysfunction to their clinician. To elicit the presence of sexual concerns, you must initiate the conversation.25 You can begin the sexual history by asking, "Do you have any concerns about your sex life?" Additional helpful, open-ended questions include: "Are you having sexual relations currently? With men or women or both?", "If you are not having sex, when did you last have intercourse?", "Are you satisfied with the frequency and quality of your sexual experiences?", "What is the emotional quality and intimacy of your relationship with your sex partner?"
The common sexual disorders in women are categorized as desire, arousal, orgasm, and pain disorders. There are two desire disorders: hypoactive sexual desire disorder and sexual aversion disorder. There are two arousal disorders: female sexual arousal disorder and persistent genital arousal disorder. There are four pain disorders: dyspareunia, vulvodynia, vaginismus, and noncoital nonsexual pain.
Most experts recommend that treatment of female sexual dysfunction include multiple modalities that reflect the complex biopsychosocial factors that cause the problem. For example, a treatment plan might include cognitive behavioral therapy, sex therapy, and appropriate medications.
Mental health issues
Depression, anxiety, bulimia, and anorexia nervosa are more common in women than men. For instance, the lifetime risk of depression in women is approximately 20%, compared with about 10% in men. The gender difference is first observed in adolescence and becomes minimal after age 60. The gender differences are observed across racial and ethnic groups.26
It's on us
As leaders in women's health care, we are uniquely trained to guide, counsel, diagnose, and treat women across their entire lifetime, from adolescence to postmenopause. We are at the vanguard in the effort to continually improve the health of all women.
Melanie Witt, RN, CPC, COBGC, MA
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
"Guide to Billing the Medicare Annual Exam" is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
A special downloadable handout including all Medicare billing scenarios, at obgmanagement.com
Women's health under the Affordable Care Act: What is covered?
Lucia DiVenere, MA (September 2012)
Implementation of ICD-10 codes delayed 1 year
(Web NEWS, September 2012)
How state budget crises are putting the squeeze on Medicaid (and you)
Lucia DiVenere, MA (February 2012)
We want to hear from you! Tell us what you think.
1. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008-1015.
2. Diaz A, Laufer MR, Breech LL. American Academy of Pediatrics Committee on Adolescence, American College of Obstetricians and Gynecologists Committee on Adolescent Health Care. Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Pediatrics. 2006;118(5):2245-2250.
3. Stewart FH, Harper CC, Ellertson CE, Grimes DA, Sawaya GF, Trussell J. Clinical breast and pelvic examination requirements for hormonal contraception: current practice vs evidence. JAMA. 2001;285(17):2232-2239.
4. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States 2007-2009 [published online ahead of print July 13, 2012]. Fertil Steril. doi:10.1016/j.fertnstert.2012.06.027
5. Population Division, Department of Economic and Social Affairs, United Nations. World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf. Published April 2011. Accessed September 15, 2012.
6. Trussell J, Lalla AM, Doan QV, Reyes E, Pinto L, Gricar J. Cost effectiveness of contraceptives in the United States. Contraception. 2009;79(1):5-14.
7. Secura GM, Allsworth JE, Madden T, Mullersman JL, Peipert JF. The contraceptive CHOICE Project: reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010;203(2):115.e1-7.
8. Miller CW, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004;291(18):2229-2236.
9. Roger VL, Go AS, Lloyd-Jones, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18-e209.
10. Krystal AD. Insomnia in women. Clin Cornerstone. 2003;5(3):41-50.
11. Ensrud KE, Stone KL, Blackwell TL, et al. Frequency and severity of hot flashes and sleep disturbance in postmenopausal women with hot flashes. Menopause. 2009;16(2):286-292.
12. Strawbridge WJ, Cohen RD, Shema SJ, Kaplan GA. Successful aging: predictors and associated activities. Am J Epidemiol. 1996;144(2):135-141.
13. Mosca L, Benjamin EJ, Berra K, et al. American Heart Association. Effectiveness based guidelines for the prevention of cardiovascular disease in women—2011 update. J Amer Coll Cardiol. 2011;57(12):1404-1423.
14. Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352(13):1293-1304.
15. Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians’ Health Study. N Engl J Med. 1989;321(3):129-135.
16. Baigent C, Blackwell L, Collins R, et al. Antithrombotic Trialists’ Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomized trials. Lancet. 2009;373(9678):1849-1860.
17. U.S. Preventative Services Task Force. Aspirin for the prevention of cardiovascular disease. Ann Int Med. 2009;150(6):396-404.
18. Fang MC, Singer DE, Chang Y, et al. Gender differences in the risk of ischemic stroke and peripheral embolism in atrial fibrillation: the AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. Circulation. 2005;112(12):1687.-
19. Mannino Dm, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance—United States 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
20. Bolland MJ, Grey AB, Gamble GD, Reid IR. Effect of osteoporosis treatment on mortality: a meta-analysis. J Clin Endocrinol Metab. 2010;95(3):1174-1181.
21. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573-1579.
22. Centers for Disease Control and Prevention. Adverse health conditions and health risk behaviors associated with intimate partner violence—United States 2005. MMWR. 2008;57(9):113-117.
23. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. MMWR. 2006;55(RR-11):1-94.
24. Laumann EO, Nicolosi A, Glasser DB, et al. GSSAB Investigators’ Group. Sexual problems among women and men aged 40 to 80 years prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17(1):39-57.
25. Nusbaum MR, Helton MR, Ray N. The changing nature of women’s sexual health concerns through the midlife years. Maturitas. 2004;49(4):283-291.
26. Gutierrez-Lobos K, Scherer M, Anderer P, Katschnig H. The influence of age on the female/male ratio of treated incidence rates in depression. BMC Psychiatry. 2002;2:3.-

Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri is Chief, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri is Chief, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
Robert L. Barbieri, MD
Editor in Chief
Dr. Barbieri is Chief, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital, and Kate Macy Ladd Professor of Obstetrics, Gynecology, and Reproductive Biology, Harvard Medical School, Boston, Massachusetts
Dr. Barbieri reports no financial relationships relevant to this article.
Preventive coding can be a snap
Billing for the well-woman exam, with Medicare Guide
Melanie Witt, RN, CPC, COBGC, MA
The American College of Obstetricians and Gynecologists (ACOG) has recommended dividing a woman's life cycle into four intervals—ages 13–18, 19–39, 40–64, and older than 65—in order to best organize the approach to primary and preventive health care.1 This paradigm provides a structure for organizing the clinical approach to physical examination, laboratory testing, counseling, and immunizations. In addition, it helps to highlight the diseases and health problems most prevalent among women at each life-stage.
Different professional organizations—US Preventive Services Task Force (USPSTF), American Medical Association, American College of Physicians, ACOG, American Academy of Family Physicians, American Academy of Pediatrics, and Advisory Committee on Immunization Practices—have used varying analytical methods to determine recommended health services by age group; consequently, these organizations have somewhat divergent recommendations. However, the recommendations of most organizations share many similarities. In this comprehensive guide, I point out those similarities. Keep in mind that recommendations change over time, and it is important to use your professional judgment when approaching each patient.
TABLE
Physical examination and laboratory testing services according to a patient's age, based on ACOG recommendations1
| Health service | 13–18 years | 19–39 years | 40–64 years | 65 years and older |
|---|---|---|---|---|
| Physical examination | ||||
| Height | X | X | X | X |
| Weight | X | X | X | X |
| BMI | X | X | X | X |
| Blood pressure | X | X | X | X |
| Tanner staging of secondary sexual characteristics | X | |||
| Neck exam (assess thyroid and presence of adenopathy) | X | X | X | |
| Breast exam | X | X (including axillae) | X (including axillae) | |
| Oral cavity | X | X | ||
| Abdominal exam | X | X | X | X |
| Pelvic exam | If indicated | Age 21 and older | X | X |
| Skin exam | X | X | X | |
| Laboratory testing | ||||
| Chlamydia | If sexually active | If age 25 or younger and sexually active | ||
| Gonorrhea | If sexually active | If age 25 or younger and sexually active | ||
| HIV | If sexually active | X | X | |
| Cervical cytology | Age 21-29: Every 2 years Age 30 and older, low risk: Every 3 years Age 30 and older, high risk (immunosuppressed or HIV infection): Annually | Low risk: Every 3 years High risk (immunosuppressed or HIV infection): Annually | Consider discontinuing in women with:
| |
| Colorectal cancer screening (colonoscopy preferred) | Age 50 and older, low risk: Every 10 years High risk: Consult colorectal screening guidelines* | Every 10 years | ||
| Fasting glucose | Age 45 and older: Every 5 years | Every 5 years | ||
| Lipid profile | Age 45 and older: Every 5 years | Every 5 years | ||
| Mammography | Age 40 to 49: Every 1-2 years Age 50 and older: Annually | Annually | ||
| BMD | Not more frequently than every 2 years | |||
| TSH | Every 5 years | |||
| Urinalysis | X | |||
| Abbreviations: BMD, bone mineral density; BMI, body mass index; HIV, human immunodeficiency virus; TSH, thyroid stimulating hormone. *Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130–160. | ||||
The adolescent: 13–18 years
Screen. Guide. Immunize. ACOG recommends that the first visit take place between 13 and 15 years of age, with annual visits thereafter. The purpose of the first, and subsequent, visits is to assess health status, including menstrual history and body mass index (BMI), and to provide health guidance, screening, and preventive health services. This initial visit generally does not include a pelvic examination. A physical examination is not required at every visit but is recommended to occur at least once during early, middle, and late adolescence.
Target your screening practices. Screen adolescents for the following conditions during clinical preventive services: hypertension; hyperlipidemia; obesity and eating disorders; physical, sexual, or emotional abuse; learning or school problems; substance use; depression and risk of suicide; sexual assault; sexual behavior that may lead to pregnancy or sexually transmitted disease (STD); and tuberculosis and HIV, unless the patient opts out (TABLE).
Anticipate. Then guide. Using anticipatory guidance, you can help adolescents understand their physical, psychosocial, and sexual development and motivate them to be involved in their health and health-care decisions. Issues relevant to adolescents include dietary habits; injury prevention, through the use of helmets and seatbelts; regular exercise; responsible sexual behaviors; avoidance of substances that can be abused; strategies for dealing with bullying; and avoidance of behaviors that might have negative consequences, such as vandalism, stealing, and sharing personal information with strangers.
Recommended immunizations. For this age group, immunizations, unless previously given, include:
- 1 or 2 doses of measles, mumps, and rubella
- 2 doses of varicella if not previously infected
- a booster dose of tetanus if ≥10 years have elapsed since the last dose
- human papillomavirus (HPV)
- annual influenza.
Other immunizations that may be warranted on the basis of medical condition, occupation, lifestyle, or other indications include: 3 doses of hepatitis B, 2 doses of hepatitis A, 1 or more doses of meningococcal, and 1 or 2 doses of pneumococcal.
Menses, an important "vital sign." Once menstruation begins, evaluating menstrual cycle characteristics is important. Patterns that may require evaluation include2:
- no menses within 3 years of thelarche
- no menses by age 13 with no sign of pubertal development
- no menses by age 14 with signs of hirsutism
- no menses by age 14 with indications of an eating disorder
- no menses by age 15
- history of regular menses that are now markedly irregular
- menses occur more frequently than 21 days or less frequently than every 45 days
- menses occur 90 days apart for one cycle
- menstrual bleeding that lasts more than 7 days
- frequent tampon/pad changes (more than 1 tampon/pad every 1 to 2 hours).
BMI predicts future disease. Overweight and obesity are important risk factors for diabetes mellitus, hyperlipidemia, hypertension, and various cancers. Eating disorders are common among adolescents and often occur in association with other mental health problems.
Non–sexually active teens and children
Gynecologic examination typically involves inspection of the genitalia and not instrumentation of the vagina. A careful explanation of the proposed examination is important. Ask young adolescents who they would like to have in the examination room with them. A hand mirror can be used to involve the patient in the genitalia inspection. If it's necessary to obtain magnification, use a hand lens, an otoscope without the speculum, or a colposcope. Record the configuration of the hymen, if present. If indicated, examination of the genitalia while the patient is in the knee-chest position often provides a good view of the vagina and sometimes the cervix, without instrumentation.
Sexually active teens
Effective contraception, including the use of emergency contraceptives, is an important health focus for sexually active teens. Vaginal speculum examination and bimanual gyn exam are not required prior to prescribing hormonal contraceptives to teens. Based on a review of the evidence and expert opinion,3 the current recommendation is that prior to prescribing a hormonal contraceptive, a medical history and blood pressure measurement are the only requirements; breast examination and a gyn exam (vaginal speculum and bimanual gyn exam) are not necessary. Testing for chlamydia and gonorrhea can be performed using a urine sample. A cervical cytology examination is not necessary until age 21 unless the patient is in a high-risk group, such as immunosuppressed or HIV-infected teens.
The young woman: 19–39 years
Focus on reproductive issues. Contraception, pregnancy, and cervical cancer screening are common reasons for visits among women in this age group. Gynecologic problems can include polycystic ovary syndrome (PCOS), endometriosis, fibroids, infertility, pelvic pain, vulvovaginal pain syndromes, vaginitis, adnexal masses, and STDs, including pelvic inflammatory diseases.
Offer effective contraception
Long-acting reversible contraceptives (LARCs) are the most clinically and cost-effective forms of reversible contraception. There are three LARC methods available in the United States: 1) the copper T380A intrauterine device (IUD; Paragard), 2) the levonorgestrel-releasing intrauterine system (Mirena), and 3) the single-rod etonogestrel implant (Implanon, Explanon).
The use of IUDs among American women has increased from about 2.4% of contracepting women of reproductive age in 2002 to 8.5% in 2009.4 In Norway and France, contracepting women of reproductive age use IUDs at a rate of 27% and 23%, respectively.5 Typical-use pregnancy rates for LARCs are lower and continuation rates are higher than observed with oral contraceptives (OCs).
In an economic analysis, the cost of LARCs was lower than almost all other forms of reversible contraception over a 5-year interval.6 When financial and access barriers are removed, most women starting a contraceptive will use a LARC, if offered.7
Be aware of STDs
STDs are common in this age group. In the United States, chlamydial genital infections reach a peak in women 18 to 25 years old, with a prevalence of about 4%.8
Counsel her about exercise and weight loss
Approximately 60% of women older than age 20 are overweight or obese.9 The rise in obesity is a key contributing factor to an increase in many diseases, including gestational diabetes, type 2 diabetes mellitus, and hypertension. Successful efforts to reduce the prevalence of obesity through diet and exercise could markedly improve population health.
Don't overlook autoimmune conditions
Many autoimmune diseases reach a peak incidence between ages 19 and 39, and, except for ankylosing spondylitis, are more of a concern for women than men. Systemic lupus erythematosus, lymphocytic thyroiditis, and rheumatoid arthritis occur much more frequently in women than in men, with ratios in the range of 7:1 observed during this age interval.
Keep her immunity up to date
Immunizations recommended in this age group include:
- one Tdap (tetanus toxoid, diphtheria, and pertussis)
- tetanus every 10 years
- influenza annually
- varicella if no evidence of immunity
- HPV for those aged 26 years or younger.
The mature woman: 40–64 years
Transition to postmenopause. The menstrual changes through perimenopause to postmenopause are often accompanied by changes in sleep patterns, vasomotor symptoms, and increasing vaginal dryness.
Open your eyes to a patient's insomnia
Perimenopausal and postmenopausal women report a much higher rate of insomnia than age-matched men.10 Women with moderate to severe vasomotor symptoms are more likely to report greater nighttime wakefulness and a greater number of nighttime long-awake episodes than women with mild vasomotor symptoms.11 Insomnia can be associated with poor work performance and mood changes.
Hormone therapy: Be conservative
In the past, hormone therapy, with various estrogen and progestin combinations, was recommended to help prevent a number of diseases, including cardiovascular disease (CD) and osteoporosis. Based on clinical trial results, the current recommendation is to limit the use of hormone therapy in postmenopausal women to the treatment of vasomotor symptoms and vaginal symptoms caused by hypoestrogenism. To treat these problems, the lowest doses of hormones that are effective should be used for the shortest periods of time that achieve symptom resolution.
The older woman: 65+ years
Successful aging. Based on observational studies, behavioral and health factors associated with successful aging include more than 12 years of education; high socioeconomic status; absence of diabetes, asthma, stroke, and lower respiratory tract disease; absence of depression; presence of at least five close personal contacts; frequent walking; moderate use of alcohol; and nonsmoking status.12
Know her risks, and watch for them
Cardiovascular disease. Among women, CDs cause more deaths than malignant neoplasms, chronic lower respiratory disease, Alzheimer's disease, and accidents combined. Black women have rates of CD approximately 40% greater than white women. Hypertension, hypertriglyceridemia, obesity, and sedentary lifestyle among black women account for a part of this increased risk.
Effective lifestyle interventions for primary CD prevention in women include smoking cessation, a diet such as DASH (Dietary Approaches to Stop Hypertension) rich in fruits and vegetables, regular physical activity, and weight management.13
There are important gender differences in aspirin efficacy for primary prevention of stroke and myocardial infarction (MI) in men and women. Among women, aspirin used for primary prevention appears to reduce the risk of stroke but not MI.14 Among men, aspirin used for primary prevention appears to reduce the risk of MI but not stroke.15,16 Based on these and other data, the USPSTF has recommended that aspirin not be used to prevent stroke in men but recommends aspirin to prevent stroke among women 55 to 79 years of age when benefits outweigh risks of gastrointestinal bleeding.17
Atrial fibrillation (AF), a risk factor for stroke, is more common in women than in men. In addition, women with AF who are not anticoagulated are at greater risk for stroke than men with AF who are not anticoagulated.18 The mechanisms that influence these gender differences are not well characterized.
Respiratory illness. Among women, the prevalence of chronic bronchitis and emphysema increased more than 2.8-fold from 1980 to 2000.19 These diseases are major contributors to physician office visits, hospitalizations, disability, and death. Tobacco use is the major risk factor that accounts for the marked increase in COPD among women during recent decades, although ambient pollutants in the environment, home, and workplace are also important contributors to COPD development.
Cognitive decline. Alzheimer's disease afflicts approximately twice as many women as men. Part of this difference is due to the greater longevity of women, but additional variables, such as gender differences in neurobiology, are also contributory. The role of estradiol in the development of Alzheimer's disease remains controversial.
Osteoporosis. This disease occurs about five times more frequently in women than in men. Among Medicare patients, the cost of caring for a hip fracture is more than $40,000 in the first year postfracture. Hip fracture is associated with a high risk of rapid health decline. Interventions that successfully prevent hip fracture are associated with a reduced mortality rate.20,21
Keep in mind the top causes of death for her age when you examine and counsel your patient. For a young teenager, for instance, accidents are the most common cause of death. Therefore, emphasize to her the importance of risk-reducing interventions, such as wearing helmets while biking and seatbelts while driving and practicing water sports safely.
| Age 13–18 years | Age 19–39 years |
|---|---|
|
|
| Age 40–64 years | Age 65 years and older |
|
|
| Source: Mortality Statistics Branch, National Center for Health Statistics; 2004. | |
Domestic violence
Domestic violence is common; approximately 5% of women report one episode during the past year and 25% report at least one lifetime episode.22 Domestic violence involves two people: a perpetrator and a victim. In some relationships, a recurrent cycle of violence and reconciliation is observed. Routine, confidential, and private screening is required to detect most cases of domestic violence.
Ask the right question(s). The single question, "At any time, has a partner hit, kicked, or otherwise hurt or threatened you?" can increase the rate of detection. Alternatively, a set of three questions can be used to screen for domestic violence:
- "Within the past year, have you been hit, slapped, kicked or otherwise physically hurt by someone?"
- "Within the past year, has anyone forced you to have sexual activity?"
- In pregnancy: "Since you have been pregnant, have you been hit, slapped, kicked, or otherwise physically hurt by someone?"
Follow-up and refer. If a woman reports that she has suffered or is at risk for domestic violence, document the finding in her medical record. Then try to assess her safety by asking: "Are there guns in the home?", "Have there been threats of suicide or homicide?", "Has there been violence toward children?" Choking, specifically, could be a sign of future escalated violence—as many perpetrators choke their victims prior to further, escalated violence occurring—and should be taken as a threat of homicide. Refer women who report domestic violence to a specialist; often, the best trained and most available experts are experienced social workers.
Sexual assault
About 25% of women report at least one lifetime sexual assault. Most women who report being raped initially receive care in a hospital-based emergency department from nurses who are credentialed in Sexual Assault Nurse Evaluation (SANE) skills.
The initial evaluation includes rapid access to treatment by a specialized clinical team, assessment and treatment of bodily injuries with a focus on genital trauma, psychological assessment and support, pregnancy assessment and prevention, preventive treatment of STDs, and collection of forensic data, including toxicology testing for the presence of date-rape drugs.
When sexual assault is reported, treat for an STD. The Centers for Disease Control and Prevention (CDC) recommends the following approach to prevent and treat STDs in victims of sexual assault23:
- ceftriaxone 125 mg IM to prevent gonorrhea
- azithromycin 1 g orally as a single dose or doxycycline 100 mg twice daily for 7 days to prevent chlamydia
- metronidazole 2 g orally as a single dose to prevent trichomoniasis
- hepatitis B vaccination, for women not previously vaccinated. (The CDC recommends against the use of hepatitis B immune globulin as the costs are believed to outweigh the benefits.)
- HIV postexposure prophylaxis for 3 to 7 days, with a follow-up visit to consider pros and cons of continued prophylaxis. (The risk of HIV infection following a sexual assault is low.)
- postcoital contraception (for example, levonorgestrel 1.5 mg orally as a single dose).
An antiemetic also should be offered to reduce the risk that the multiple prescribed medications will cause vomiting and nullify prophylaxis efforts. Approximately 2 weeks after the sexual assault the patient should have a pregnancy test and be assessed for ongoing mental health needs. If she did not adhere to the medications or if she shows relevant symptoms, perform follow-up STD testing. Follow-up HIV and syphilis testing can be performed at 12 and 24 weeks following the assault.
Sexual dysfunction
Sexuality is an important part of the human experience. Sexual dysfunction is the inability to participate as desired in a sexual relationship. Problems of sexual dysfunction are best approached from a biopsychosocial framework that recognizes the important contributions of biological, psychological, and social-cultural factors in sexual health. Masters and Johnson posited four stages of sexual response: excitement, plateau, orgasm, and resolution. Building on this linear model, investigators later divided the excitement phase into desire and arousal.
Recent models of sexual response have emphasized a circular model, in which sequential responses overlap and build on previous stimuli. These models also emphasize the importance of emotional intimacy and the quality of the relationship in achieving optimal sexual health.
Approximately 40% of women and 30% of men report sexual dysfunction.24 Common sexual problems reported by heterosexual women include:
- lack of interest in sex
- inability to achieve orgasm
- pain caused by sexual intercourse
- lack of pleasure with sex
- trouble lubricating.
The majority of men and women will not voluntarily report sexual dysfunction to their clinician. To elicit the presence of sexual concerns, you must initiate the conversation.25 You can begin the sexual history by asking, "Do you have any concerns about your sex life?" Additional helpful, open-ended questions include: "Are you having sexual relations currently? With men or women or both?", "If you are not having sex, when did you last have intercourse?", "Are you satisfied with the frequency and quality of your sexual experiences?", "What is the emotional quality and intimacy of your relationship with your sex partner?"
The common sexual disorders in women are categorized as desire, arousal, orgasm, and pain disorders. There are two desire disorders: hypoactive sexual desire disorder and sexual aversion disorder. There are two arousal disorders: female sexual arousal disorder and persistent genital arousal disorder. There are four pain disorders: dyspareunia, vulvodynia, vaginismus, and noncoital nonsexual pain.
Most experts recommend that treatment of female sexual dysfunction include multiple modalities that reflect the complex biopsychosocial factors that cause the problem. For example, a treatment plan might include cognitive behavioral therapy, sex therapy, and appropriate medications.
Mental health issues
Depression, anxiety, bulimia, and anorexia nervosa are more common in women than men. For instance, the lifetime risk of depression in women is approximately 20%, compared with about 10% in men. The gender difference is first observed in adolescence and becomes minimal after age 60. The gender differences are observed across racial and ethnic groups.26
It's on us
As leaders in women's health care, we are uniquely trained to guide, counsel, diagnose, and treat women across their entire lifetime, from adolescence to postmenopause. We are at the vanguard in the effort to continually improve the health of all women.
Melanie Witt, RN, CPC, COBGC, MA
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
"Guide to Billing the Medicare Annual Exam" is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
A special downloadable handout including all Medicare billing scenarios, at obgmanagement.com
Women's health under the Affordable Care Act: What is covered?
Lucia DiVenere, MA (September 2012)
Implementation of ICD-10 codes delayed 1 year
(Web NEWS, September 2012)
How state budget crises are putting the squeeze on Medicaid (and you)
Lucia DiVenere, MA (February 2012)
We want to hear from you! Tell us what you think.
Preventive coding can be a snap
Billing for the well-woman exam, with Medicare Guide
Melanie Witt, RN, CPC, COBGC, MA
The American College of Obstetricians and Gynecologists (ACOG) has recommended dividing a woman's life cycle into four intervals—ages 13–18, 19–39, 40–64, and older than 65—in order to best organize the approach to primary and preventive health care.1 This paradigm provides a structure for organizing the clinical approach to physical examination, laboratory testing, counseling, and immunizations. In addition, it helps to highlight the diseases and health problems most prevalent among women at each life-stage.
Different professional organizations—US Preventive Services Task Force (USPSTF), American Medical Association, American College of Physicians, ACOG, American Academy of Family Physicians, American Academy of Pediatrics, and Advisory Committee on Immunization Practices—have used varying analytical methods to determine recommended health services by age group; consequently, these organizations have somewhat divergent recommendations. However, the recommendations of most organizations share many similarities. In this comprehensive guide, I point out those similarities. Keep in mind that recommendations change over time, and it is important to use your professional judgment when approaching each patient.
TABLE
Physical examination and laboratory testing services according to a patient's age, based on ACOG recommendations1
| Health service | 13–18 years | 19–39 years | 40–64 years | 65 years and older |
|---|---|---|---|---|
| Physical examination | ||||
| Height | X | X | X | X |
| Weight | X | X | X | X |
| BMI | X | X | X | X |
| Blood pressure | X | X | X | X |
| Tanner staging of secondary sexual characteristics | X | |||
| Neck exam (assess thyroid and presence of adenopathy) | X | X | X | |
| Breast exam | X | X (including axillae) | X (including axillae) | |
| Oral cavity | X | X | ||
| Abdominal exam | X | X | X | X |
| Pelvic exam | If indicated | Age 21 and older | X | X |
| Skin exam | X | X | X | |
| Laboratory testing | ||||
| Chlamydia | If sexually active | If age 25 or younger and sexually active | ||
| Gonorrhea | If sexually active | If age 25 or younger and sexually active | ||
| HIV | If sexually active | X | X | |
| Cervical cytology | Age 21-29: Every 2 years Age 30 and older, low risk: Every 3 years Age 30 and older, high risk (immunosuppressed or HIV infection): Annually | Low risk: Every 3 years High risk (immunosuppressed or HIV infection): Annually | Consider discontinuing in women with:
| |
| Colorectal cancer screening (colonoscopy preferred) | Age 50 and older, low risk: Every 10 years High risk: Consult colorectal screening guidelines* | Every 10 years | ||
| Fasting glucose | Age 45 and older: Every 5 years | Every 5 years | ||
| Lipid profile | Age 45 and older: Every 5 years | Every 5 years | ||
| Mammography | Age 40 to 49: Every 1-2 years Age 50 and older: Annually | Annually | ||
| BMD | Not more frequently than every 2 years | |||
| TSH | Every 5 years | |||
| Urinalysis | X | |||
| Abbreviations: BMD, bone mineral density; BMI, body mass index; HIV, human immunodeficiency virus; TSH, thyroid stimulating hormone. *Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. CA Cancer J Clin. 2008;58(3):130–160. | ||||
The adolescent: 13–18 years
Screen. Guide. Immunize. ACOG recommends that the first visit take place between 13 and 15 years of age, with annual visits thereafter. The purpose of the first, and subsequent, visits is to assess health status, including menstrual history and body mass index (BMI), and to provide health guidance, screening, and preventive health services. This initial visit generally does not include a pelvic examination. A physical examination is not required at every visit but is recommended to occur at least once during early, middle, and late adolescence.
Target your screening practices. Screen adolescents for the following conditions during clinical preventive services: hypertension; hyperlipidemia; obesity and eating disorders; physical, sexual, or emotional abuse; learning or school problems; substance use; depression and risk of suicide; sexual assault; sexual behavior that may lead to pregnancy or sexually transmitted disease (STD); and tuberculosis and HIV, unless the patient opts out (TABLE).
Anticipate. Then guide. Using anticipatory guidance, you can help adolescents understand their physical, psychosocial, and sexual development and motivate them to be involved in their health and health-care decisions. Issues relevant to adolescents include dietary habits; injury prevention, through the use of helmets and seatbelts; regular exercise; responsible sexual behaviors; avoidance of substances that can be abused; strategies for dealing with bullying; and avoidance of behaviors that might have negative consequences, such as vandalism, stealing, and sharing personal information with strangers.
Recommended immunizations. For this age group, immunizations, unless previously given, include:
- 1 or 2 doses of measles, mumps, and rubella
- 2 doses of varicella if not previously infected
- a booster dose of tetanus if ≥10 years have elapsed since the last dose
- human papillomavirus (HPV)
- annual influenza.
Other immunizations that may be warranted on the basis of medical condition, occupation, lifestyle, or other indications include: 3 doses of hepatitis B, 2 doses of hepatitis A, 1 or more doses of meningococcal, and 1 or 2 doses of pneumococcal.
Menses, an important "vital sign." Once menstruation begins, evaluating menstrual cycle characteristics is important. Patterns that may require evaluation include2:
- no menses within 3 years of thelarche
- no menses by age 13 with no sign of pubertal development
- no menses by age 14 with signs of hirsutism
- no menses by age 14 with indications of an eating disorder
- no menses by age 15
- history of regular menses that are now markedly irregular
- menses occur more frequently than 21 days or less frequently than every 45 days
- menses occur 90 days apart for one cycle
- menstrual bleeding that lasts more than 7 days
- frequent tampon/pad changes (more than 1 tampon/pad every 1 to 2 hours).
BMI predicts future disease. Overweight and obesity are important risk factors for diabetes mellitus, hyperlipidemia, hypertension, and various cancers. Eating disorders are common among adolescents and often occur in association with other mental health problems.
Non–sexually active teens and children
Gynecologic examination typically involves inspection of the genitalia and not instrumentation of the vagina. A careful explanation of the proposed examination is important. Ask young adolescents who they would like to have in the examination room with them. A hand mirror can be used to involve the patient in the genitalia inspection. If it's necessary to obtain magnification, use a hand lens, an otoscope without the speculum, or a colposcope. Record the configuration of the hymen, if present. If indicated, examination of the genitalia while the patient is in the knee-chest position often provides a good view of the vagina and sometimes the cervix, without instrumentation.
Sexually active teens
Effective contraception, including the use of emergency contraceptives, is an important health focus for sexually active teens. Vaginal speculum examination and bimanual gyn exam are not required prior to prescribing hormonal contraceptives to teens. Based on a review of the evidence and expert opinion,3 the current recommendation is that prior to prescribing a hormonal contraceptive, a medical history and blood pressure measurement are the only requirements; breast examination and a gyn exam (vaginal speculum and bimanual gyn exam) are not necessary. Testing for chlamydia and gonorrhea can be performed using a urine sample. A cervical cytology examination is not necessary until age 21 unless the patient is in a high-risk group, such as immunosuppressed or HIV-infected teens.
The young woman: 19–39 years
Focus on reproductive issues. Contraception, pregnancy, and cervical cancer screening are common reasons for visits among women in this age group. Gynecologic problems can include polycystic ovary syndrome (PCOS), endometriosis, fibroids, infertility, pelvic pain, vulvovaginal pain syndromes, vaginitis, adnexal masses, and STDs, including pelvic inflammatory diseases.
Offer effective contraception
Long-acting reversible contraceptives (LARCs) are the most clinically and cost-effective forms of reversible contraception. There are three LARC methods available in the United States: 1) the copper T380A intrauterine device (IUD; Paragard), 2) the levonorgestrel-releasing intrauterine system (Mirena), and 3) the single-rod etonogestrel implant (Implanon, Explanon).
The use of IUDs among American women has increased from about 2.4% of contracepting women of reproductive age in 2002 to 8.5% in 2009.4 In Norway and France, contracepting women of reproductive age use IUDs at a rate of 27% and 23%, respectively.5 Typical-use pregnancy rates for LARCs are lower and continuation rates are higher than observed with oral contraceptives (OCs).
In an economic analysis, the cost of LARCs was lower than almost all other forms of reversible contraception over a 5-year interval.6 When financial and access barriers are removed, most women starting a contraceptive will use a LARC, if offered.7
Be aware of STDs
STDs are common in this age group. In the United States, chlamydial genital infections reach a peak in women 18 to 25 years old, with a prevalence of about 4%.8
Counsel her about exercise and weight loss
Approximately 60% of women older than age 20 are overweight or obese.9 The rise in obesity is a key contributing factor to an increase in many diseases, including gestational diabetes, type 2 diabetes mellitus, and hypertension. Successful efforts to reduce the prevalence of obesity through diet and exercise could markedly improve population health.
Don't overlook autoimmune conditions
Many autoimmune diseases reach a peak incidence between ages 19 and 39, and, except for ankylosing spondylitis, are more of a concern for women than men. Systemic lupus erythematosus, lymphocytic thyroiditis, and rheumatoid arthritis occur much more frequently in women than in men, with ratios in the range of 7:1 observed during this age interval.
Keep her immunity up to date
Immunizations recommended in this age group include:
- one Tdap (tetanus toxoid, diphtheria, and pertussis)
- tetanus every 10 years
- influenza annually
- varicella if no evidence of immunity
- HPV for those aged 26 years or younger.
The mature woman: 40–64 years
Transition to postmenopause. The menstrual changes through perimenopause to postmenopause are often accompanied by changes in sleep patterns, vasomotor symptoms, and increasing vaginal dryness.
Open your eyes to a patient's insomnia
Perimenopausal and postmenopausal women report a much higher rate of insomnia than age-matched men.10 Women with moderate to severe vasomotor symptoms are more likely to report greater nighttime wakefulness and a greater number of nighttime long-awake episodes than women with mild vasomotor symptoms.11 Insomnia can be associated with poor work performance and mood changes.
Hormone therapy: Be conservative
In the past, hormone therapy, with various estrogen and progestin combinations, was recommended to help prevent a number of diseases, including cardiovascular disease (CD) and osteoporosis. Based on clinical trial results, the current recommendation is to limit the use of hormone therapy in postmenopausal women to the treatment of vasomotor symptoms and vaginal symptoms caused by hypoestrogenism. To treat these problems, the lowest doses of hormones that are effective should be used for the shortest periods of time that achieve symptom resolution.
The older woman: 65+ years
Successful aging. Based on observational studies, behavioral and health factors associated with successful aging include more than 12 years of education; high socioeconomic status; absence of diabetes, asthma, stroke, and lower respiratory tract disease; absence of depression; presence of at least five close personal contacts; frequent walking; moderate use of alcohol; and nonsmoking status.12
Know her risks, and watch for them
Cardiovascular disease. Among women, CDs cause more deaths than malignant neoplasms, chronic lower respiratory disease, Alzheimer's disease, and accidents combined. Black women have rates of CD approximately 40% greater than white women. Hypertension, hypertriglyceridemia, obesity, and sedentary lifestyle among black women account for a part of this increased risk.
Effective lifestyle interventions for primary CD prevention in women include smoking cessation, a diet such as DASH (Dietary Approaches to Stop Hypertension) rich in fruits and vegetables, regular physical activity, and weight management.13
There are important gender differences in aspirin efficacy for primary prevention of stroke and myocardial infarction (MI) in men and women. Among women, aspirin used for primary prevention appears to reduce the risk of stroke but not MI.14 Among men, aspirin used for primary prevention appears to reduce the risk of MI but not stroke.15,16 Based on these and other data, the USPSTF has recommended that aspirin not be used to prevent stroke in men but recommends aspirin to prevent stroke among women 55 to 79 years of age when benefits outweigh risks of gastrointestinal bleeding.17
Atrial fibrillation (AF), a risk factor for stroke, is more common in women than in men. In addition, women with AF who are not anticoagulated are at greater risk for stroke than men with AF who are not anticoagulated.18 The mechanisms that influence these gender differences are not well characterized.
Respiratory illness. Among women, the prevalence of chronic bronchitis and emphysema increased more than 2.8-fold from 1980 to 2000.19 These diseases are major contributors to physician office visits, hospitalizations, disability, and death. Tobacco use is the major risk factor that accounts for the marked increase in COPD among women during recent decades, although ambient pollutants in the environment, home, and workplace are also important contributors to COPD development.
Cognitive decline. Alzheimer's disease afflicts approximately twice as many women as men. Part of this difference is due to the greater longevity of women, but additional variables, such as gender differences in neurobiology, are also contributory. The role of estradiol in the development of Alzheimer's disease remains controversial.
Osteoporosis. This disease occurs about five times more frequently in women than in men. Among Medicare patients, the cost of caring for a hip fracture is more than $40,000 in the first year postfracture. Hip fracture is associated with a high risk of rapid health decline. Interventions that successfully prevent hip fracture are associated with a reduced mortality rate.20,21
Keep in mind the top causes of death for her age when you examine and counsel your patient. For a young teenager, for instance, accidents are the most common cause of death. Therefore, emphasize to her the importance of risk-reducing interventions, such as wearing helmets while biking and seatbelts while driving and practicing water sports safely.
| Age 13–18 years | Age 19–39 years |
|---|---|
|
|
| Age 40–64 years | Age 65 years and older |
|
|
| Source: Mortality Statistics Branch, National Center for Health Statistics; 2004. | |
Domestic violence
Domestic violence is common; approximately 5% of women report one episode during the past year and 25% report at least one lifetime episode.22 Domestic violence involves two people: a perpetrator and a victim. In some relationships, a recurrent cycle of violence and reconciliation is observed. Routine, confidential, and private screening is required to detect most cases of domestic violence.
Ask the right question(s). The single question, "At any time, has a partner hit, kicked, or otherwise hurt or threatened you?" can increase the rate of detection. Alternatively, a set of three questions can be used to screen for domestic violence:
- "Within the past year, have you been hit, slapped, kicked or otherwise physically hurt by someone?"
- "Within the past year, has anyone forced you to have sexual activity?"
- In pregnancy: "Since you have been pregnant, have you been hit, slapped, kicked, or otherwise physically hurt by someone?"
Follow-up and refer. If a woman reports that she has suffered or is at risk for domestic violence, document the finding in her medical record. Then try to assess her safety by asking: "Are there guns in the home?", "Have there been threats of suicide or homicide?", "Has there been violence toward children?" Choking, specifically, could be a sign of future escalated violence—as many perpetrators choke their victims prior to further, escalated violence occurring—and should be taken as a threat of homicide. Refer women who report domestic violence to a specialist; often, the best trained and most available experts are experienced social workers.
Sexual assault
About 25% of women report at least one lifetime sexual assault. Most women who report being raped initially receive care in a hospital-based emergency department from nurses who are credentialed in Sexual Assault Nurse Evaluation (SANE) skills.
The initial evaluation includes rapid access to treatment by a specialized clinical team, assessment and treatment of bodily injuries with a focus on genital trauma, psychological assessment and support, pregnancy assessment and prevention, preventive treatment of STDs, and collection of forensic data, including toxicology testing for the presence of date-rape drugs.
When sexual assault is reported, treat for an STD. The Centers for Disease Control and Prevention (CDC) recommends the following approach to prevent and treat STDs in victims of sexual assault23:
- ceftriaxone 125 mg IM to prevent gonorrhea
- azithromycin 1 g orally as a single dose or doxycycline 100 mg twice daily for 7 days to prevent chlamydia
- metronidazole 2 g orally as a single dose to prevent trichomoniasis
- hepatitis B vaccination, for women not previously vaccinated. (The CDC recommends against the use of hepatitis B immune globulin as the costs are believed to outweigh the benefits.)
- HIV postexposure prophylaxis for 3 to 7 days, with a follow-up visit to consider pros and cons of continued prophylaxis. (The risk of HIV infection following a sexual assault is low.)
- postcoital contraception (for example, levonorgestrel 1.5 mg orally as a single dose).
An antiemetic also should be offered to reduce the risk that the multiple prescribed medications will cause vomiting and nullify prophylaxis efforts. Approximately 2 weeks after the sexual assault the patient should have a pregnancy test and be assessed for ongoing mental health needs. If she did not adhere to the medications or if she shows relevant symptoms, perform follow-up STD testing. Follow-up HIV and syphilis testing can be performed at 12 and 24 weeks following the assault.
Sexual dysfunction
Sexuality is an important part of the human experience. Sexual dysfunction is the inability to participate as desired in a sexual relationship. Problems of sexual dysfunction are best approached from a biopsychosocial framework that recognizes the important contributions of biological, psychological, and social-cultural factors in sexual health. Masters and Johnson posited four stages of sexual response: excitement, plateau, orgasm, and resolution. Building on this linear model, investigators later divided the excitement phase into desire and arousal.
Recent models of sexual response have emphasized a circular model, in which sequential responses overlap and build on previous stimuli. These models also emphasize the importance of emotional intimacy and the quality of the relationship in achieving optimal sexual health.
Approximately 40% of women and 30% of men report sexual dysfunction.24 Common sexual problems reported by heterosexual women include:
- lack of interest in sex
- inability to achieve orgasm
- pain caused by sexual intercourse
- lack of pleasure with sex
- trouble lubricating.
The majority of men and women will not voluntarily report sexual dysfunction to their clinician. To elicit the presence of sexual concerns, you must initiate the conversation.25 You can begin the sexual history by asking, "Do you have any concerns about your sex life?" Additional helpful, open-ended questions include: "Are you having sexual relations currently? With men or women or both?", "If you are not having sex, when did you last have intercourse?", "Are you satisfied with the frequency and quality of your sexual experiences?", "What is the emotional quality and intimacy of your relationship with your sex partner?"
The common sexual disorders in women are categorized as desire, arousal, orgasm, and pain disorders. There are two desire disorders: hypoactive sexual desire disorder and sexual aversion disorder. There are two arousal disorders: female sexual arousal disorder and persistent genital arousal disorder. There are four pain disorders: dyspareunia, vulvodynia, vaginismus, and noncoital nonsexual pain.
Most experts recommend that treatment of female sexual dysfunction include multiple modalities that reflect the complex biopsychosocial factors that cause the problem. For example, a treatment plan might include cognitive behavioral therapy, sex therapy, and appropriate medications.
Mental health issues
Depression, anxiety, bulimia, and anorexia nervosa are more common in women than men. For instance, the lifetime risk of depression in women is approximately 20%, compared with about 10% in men. The gender difference is first observed in adolescence and becomes minimal after age 60. The gender differences are observed across racial and ethnic groups.26
It's on us
As leaders in women's health care, we are uniquely trained to guide, counsel, diagnose, and treat women across their entire lifetime, from adolescence to postmenopause. We are at the vanguard in the effort to continually improve the health of all women.
Melanie Witt, RN, CPC, COBGC, MA
Coding and billing for the care provided at a well-woman visit can be uncomplicated if you know the right codes for the right program. Here, I present information for straightforward preventive care. (I am assuming the patient has not also presented with a significant problem at the same visit.)
First, a patient who is not Medicare-eligible should have the annual well-woman exam billed using the CPT preventive medicine codes. There are some private insurers, however, that will only accept HCPCS codes for an annual gyn exam. These special codes are:
S0610 Annual gynecological examination, new patient
S0612 Annual gynecological examination, established patient
S0613 Annual gynecological examination; clinical breast examination without pelvic evaluation
Notably, Aetna Cigna, and United Healthcare require these codes for a gyn exam, but many BC/BS programs, for whom these codes were originally created, are now reverting to the CPT preventive medicine codes for all preventive care.
The CPT preventive codes are grouped by age and require an age- and gender-appropriate history, examination, and counseling/anticipatory guidance. The Medicare E/M documentation guidelines do not apply to preventive services, and a head-to-toe examination is also not required. CPT recognizes ACOG as an authoritative body to make recommendations for the expected preventive service for women, and if such a service is provided and documented, the preventive codes are to be reported.
The chart below summarizes the CPT preventive codes by patient status and age in comparison to ACOG age groupings.
| New Patient Preventive Medicine Code | |||
|---|---|---|---|
| New patient codes include an initial comprehensive preventive medicine evaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99384 (12–17 years) 99385 (18–39 years) | ACOG: 19–39 years 99385 (18–39 years) | ACOG: 40–64 years 99386 (40–64 years) | ACOG: 65 years and older 99387 (65 years and older) |
| Established Patient Preventive Medicine Codes | |||
| Established patient codes include periodic comprehensive preventive medicine reevaluation and management of an individual including an age- and gender-appropriate history, examination, counseling/anticipatory guidance/risk factor reduction interventions, and the ordering of laboratory/diagnostic procedures | |||
| ACOG: 13–18 years 99394 (12–17 years) 99395 (18–39 years) | ACOG: 19–39 years 99395 (18–39 years) | ACOG: 40–64 years 99396 (40–64 years) | ACOG: 65 years and older 99397 (65 years and older) |
The main code
The appropriate diagnostic link for the CPT preventive gyn annual well-woman exam is V72.31, whether or not a Pap specimen is collected. The collection of the Pap specimen is included in the preventive service, as is counseling regarding birth control, or general questions about preventing problems, including hormone replacement therapy.
If a pelvic examination is not performed, say because the patient is young and not sexually active, but an examination of other areas is carried out, the same preventive codes are reported, but the diagnosis code changes to V70.0, general health exam.
What about Medicare?
Coding. Medicare requirements are somewhat different. First, Medicare covers only a small portion of the preventive service; that is, they cover a physical examination of the genital organs and breasts and the collection and conveyance of a Pap specimen to the lab in the covered year only. Think of the complete preventive service as described in CPT as a pie—Medicare pays for 2 slices of that pie in a covered year. The two codes for these services are:
G0101 (Cervical or vaginal cancer screening; pelvic and clinical breast examination)
Q0091 (Screening Papanicolaou smear; obtaining, preparing, and conveyance of cervical or vaginal smear to laboratory)
If the patient is at low risk for developing cervical or vaginal cancer, the screening pelvic exam and Pap collection are paid every 2 years. If the woman is at high risk, Medicare will cover this portion of the encounter every year. The high-risk criteria must be re-documented every year and must include one of the following:
- Early onset of sexual activity (under age 16)
- Multiple sexual partners (five or more in a lifetime)
- History of a sexually transmitted disease (including HIV infection)
- Fewer than three negative Pap smears within the previous 7 years
- Diethylstilbestrol (DES)-exposed daughters of women who took DES during pregnancy.
If the Medicare-eligible patient is still of childbearing age, she is also considered high-risk if she has had an examination that indicated the presence of cervical or vaginal cancer or other genital abnormalities during any of the preceding 3 years. Note that these criteria do not include a history of breast cancer or a past history of cancer more than 3 years ago.
Billing. Because Medicare is paying only for a portion of the preventive service, you will need to subtract the Medicare allowable for codes G0101 and Q0091 from your normal fee for the preventive service.
- Example: If your usual fee for 99397 is $200, and the Medicare allowable for both the G and Q service is $82, you will charge the patient for the noncovered parts of the service at the rate of $118, and you will bill Medicare for their share of $82. You will collect from all sources the $200 for the preventive service. Remember, however, to get the patient to sign an ABN with regard to the Medicare part of the service. This will ensure that, if denied by Medicare, the patient will be held fully responsible for the denied amount.
The Medicare modifier is –GA (add it to codes G0101 and Q0091). Diagnostic coding is V72.31 (because a pelvic exam is performed). This code may also be linked to the collection code. For a high-risk patient, use code V15.89 (rather than V72.31). This code must be linked to the G and Q codes.
"Guide to Billing the Medicare Annual Exam" is a detailed Medicare checklist offered by the author that includes all billing scenarios for a Medicare patient. Click here to download a PDF.
Ms. Witt can be contacted directly at [email protected] should you have additional questions regarding coding and billing for preventive services.
Ms. Witt is an independent coding and documentation consultant and former program manager, department of coding and nomenclature, American Congress of Obstetricians and Gynecologists.
A special downloadable handout including all Medicare billing scenarios, at obgmanagement.com
Women's health under the Affordable Care Act: What is covered?
Lucia DiVenere, MA (September 2012)
Implementation of ICD-10 codes delayed 1 year
(Web NEWS, September 2012)
How state budget crises are putting the squeeze on Medicaid (and you)
Lucia DiVenere, MA (February 2012)
We want to hear from you! Tell us what you think.
1. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008-1015.
2. Diaz A, Laufer MR, Breech LL. American Academy of Pediatrics Committee on Adolescence, American College of Obstetricians and Gynecologists Committee on Adolescent Health Care. Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Pediatrics. 2006;118(5):2245-2250.
3. Stewart FH, Harper CC, Ellertson CE, Grimes DA, Sawaya GF, Trussell J. Clinical breast and pelvic examination requirements for hormonal contraception: current practice vs evidence. JAMA. 2001;285(17):2232-2239.
4. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States 2007-2009 [published online ahead of print July 13, 2012]. Fertil Steril. doi:10.1016/j.fertnstert.2012.06.027
5. Population Division, Department of Economic and Social Affairs, United Nations. World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf. Published April 2011. Accessed September 15, 2012.
6. Trussell J, Lalla AM, Doan QV, Reyes E, Pinto L, Gricar J. Cost effectiveness of contraceptives in the United States. Contraception. 2009;79(1):5-14.
7. Secura GM, Allsworth JE, Madden T, Mullersman JL, Peipert JF. The contraceptive CHOICE Project: reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010;203(2):115.e1-7.
8. Miller CW, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004;291(18):2229-2236.
9. Roger VL, Go AS, Lloyd-Jones, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18-e209.
10. Krystal AD. Insomnia in women. Clin Cornerstone. 2003;5(3):41-50.
11. Ensrud KE, Stone KL, Blackwell TL, et al. Frequency and severity of hot flashes and sleep disturbance in postmenopausal women with hot flashes. Menopause. 2009;16(2):286-292.
12. Strawbridge WJ, Cohen RD, Shema SJ, Kaplan GA. Successful aging: predictors and associated activities. Am J Epidemiol. 1996;144(2):135-141.
13. Mosca L, Benjamin EJ, Berra K, et al. American Heart Association. Effectiveness based guidelines for the prevention of cardiovascular disease in women—2011 update. J Amer Coll Cardiol. 2011;57(12):1404-1423.
14. Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352(13):1293-1304.
15. Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians’ Health Study. N Engl J Med. 1989;321(3):129-135.
16. Baigent C, Blackwell L, Collins R, et al. Antithrombotic Trialists’ Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomized trials. Lancet. 2009;373(9678):1849-1860.
17. U.S. Preventative Services Task Force. Aspirin for the prevention of cardiovascular disease. Ann Int Med. 2009;150(6):396-404.
18. Fang MC, Singer DE, Chang Y, et al. Gender differences in the risk of ischemic stroke and peripheral embolism in atrial fibrillation: the AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. Circulation. 2005;112(12):1687.-
19. Mannino Dm, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance—United States 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
20. Bolland MJ, Grey AB, Gamble GD, Reid IR. Effect of osteoporosis treatment on mortality: a meta-analysis. J Clin Endocrinol Metab. 2010;95(3):1174-1181.
21. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573-1579.
22. Centers for Disease Control and Prevention. Adverse health conditions and health risk behaviors associated with intimate partner violence—United States 2005. MMWR. 2008;57(9):113-117.
23. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. MMWR. 2006;55(RR-11):1-94.
24. Laumann EO, Nicolosi A, Glasser DB, et al. GSSAB Investigators’ Group. Sexual problems among women and men aged 40 to 80 years prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17(1):39-57.
25. Nusbaum MR, Helton MR, Ray N. The changing nature of women’s sexual health concerns through the midlife years. Maturitas. 2004;49(4):283-291.
26. Gutierrez-Lobos K, Scherer M, Anderer P, Katschnig H. The influence of age on the female/male ratio of treated incidence rates in depression. BMC Psychiatry. 2002;2:3.-
1. American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 483. Primary and preventive care: periodic assessments. Obstet Gynecol. 2011;117(4):1008-1015.
2. Diaz A, Laufer MR, Breech LL. American Academy of Pediatrics Committee on Adolescence, American College of Obstetricians and Gynecologists Committee on Adolescent Health Care. Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Pediatrics. 2006;118(5):2245-2250.
3. Stewart FH, Harper CC, Ellertson CE, Grimes DA, Sawaya GF, Trussell J. Clinical breast and pelvic examination requirements for hormonal contraception: current practice vs evidence. JAMA. 2001;285(17):2232-2239.
4. Finer LB, Jerman J, Kavanaugh ML. Changes in use of long-acting contraceptive methods in the United States 2007-2009 [published online ahead of print July 13, 2012]. Fertil Steril. doi:10.1016/j.fertnstert.2012.06.027
5. Population Division, Department of Economic and Social Affairs, United Nations. World Contraceptive Use 2011. http://www.un.org/esa/population/publications/contraceptive2011/wallchart_front.pdf. Published April 2011. Accessed September 15, 2012.
6. Trussell J, Lalla AM, Doan QV, Reyes E, Pinto L, Gricar J. Cost effectiveness of contraceptives in the United States. Contraception. 2009;79(1):5-14.
7. Secura GM, Allsworth JE, Madden T, Mullersman JL, Peipert JF. The contraceptive CHOICE Project: reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010;203(2):115.e1-7.
8. Miller CW, Ford CA, Morris M, et al. Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA. 2004;291(18):2229-2236.
9. Roger VL, Go AS, Lloyd-Jones, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123(4):e18-e209.
10. Krystal AD. Insomnia in women. Clin Cornerstone. 2003;5(3):41-50.
11. Ensrud KE, Stone KL, Blackwell TL, et al. Frequency and severity of hot flashes and sleep disturbance in postmenopausal women with hot flashes. Menopause. 2009;16(2):286-292.
12. Strawbridge WJ, Cohen RD, Shema SJ, Kaplan GA. Successful aging: predictors and associated activities. Am J Epidemiol. 1996;144(2):135-141.
13. Mosca L, Benjamin EJ, Berra K, et al. American Heart Association. Effectiveness based guidelines for the prevention of cardiovascular disease in women—2011 update. J Amer Coll Cardiol. 2011;57(12):1404-1423.
14. Ridker PM, Cook NR, Lee IM, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352(13):1293-1304.
15. Steering Committee of the Physicians’ Health Study Research Group. Final report on the aspirin component of the ongoing Physicians’ Health Study. N Engl J Med. 1989;321(3):129-135.
16. Baigent C, Blackwell L, Collins R, et al. Antithrombotic Trialists’ Collaboration. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomized trials. Lancet. 2009;373(9678):1849-1860.
17. U.S. Preventative Services Task Force. Aspirin for the prevention of cardiovascular disease. Ann Int Med. 2009;150(6):396-404.
18. Fang MC, Singer DE, Chang Y, et al. Gender differences in the risk of ischemic stroke and peripheral embolism in atrial fibrillation: the AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. Circulation. 2005;112(12):1687.-
19. Mannino Dm, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance—United States 1971-2000. MMWR Surveill Summ. 2002;51(6):1-16.
20. Bolland MJ, Grey AB, Gamble GD, Reid IR. Effect of osteoporosis treatment on mortality: a meta-analysis. J Clin Endocrinol Metab. 2010;95(3):1174-1181.
21. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence and mortality of hip fractures in the United States. JAMA. 2009;302(14):1573-1579.
22. Centers for Disease Control and Prevention. Adverse health conditions and health risk behaviors associated with intimate partner violence—United States 2005. MMWR. 2008;57(9):113-117.
23. Workowski KA, Berman SM. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2006. MMWR. 2006;55(RR-11):1-94.
24. Laumann EO, Nicolosi A, Glasser DB, et al. GSSAB Investigators’ Group. Sexual problems among women and men aged 40 to 80 years prevalence and correlates identified in the Global Study of Sexual Attitudes and Behaviors. Int J Impot Res. 2005;17(1):39-57.
25. Nusbaum MR, Helton MR, Ray N. The changing nature of women’s sexual health concerns through the midlife years. Maturitas. 2004;49(4):283-291.
26. Gutierrez-Lobos K, Scherer M, Anderer P, Katschnig H. The influence of age on the female/male ratio of treated incidence rates in depression. BMC Psychiatry. 2002;2:3.-
UPDATE: PELVIC FLOOR DYSFUNCTION
10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Megan O. Schimpf, MD (June 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Urinary tract infections (UTIs) are prevalent among women, afflicting as many as 60% of women during their lifetime.1 Symptoms include urgency, frequency, and dysuria. Although the diagnosis can be made on the basis of symptoms alone in many cases, urinalysis and urine cultures often are helpful in confirming it.2 The differential diagnosis includes infectious or atrophic vaginitis, urethritis from a sexually transmitted infection, urethral diverticulum, painful bladder syndrome, urinary tract calculi, and urinary tract neoplasms. Common risk factors for UTIs are listed in TABLE 1.3
TABLE 1
Risk factors for urinary tract infection in women
Premenopausal women •History of urinary tract infection (UTI) Postmenopausal women |
| SOURCE: Adapted from ACOG3 |
Recurrent UTIs are defined as three infections in 12 months or two infections in 6 months. In this Update, we explore strategies to prevent recurrent UTIs in three groups of women:
- sexually active premenopausal women
- postmenopausal women
- women undergoing pelvic surgery.
In the process, we summarize the results of five trials that explore treatment modalities such as prophylactic antibiotics, vaginal estrogen therapy, cranberry supplementation, and probiotics (TABLE 2).
TABLE 2
Summary of therapeutic strategies for prevention of recurrent urinary tract infections
| Strategy | Dose | Advantages | Disadvantages |
|---|---|---|---|
| Prophylactic antibiotics | Trimethoprim-sulfamethoxazole (Bactrim): 1 double-strength tablet* OR Nitrofurantoin: 50 or 100 mg Either drug can be given daily for 6 months or as one dose postcoitally | Highly effective Inexpensive | Potential for future microbial resistance Caution with nitrofurantoin, particularly in older patients or women who have renal insufficiency In pregnancy, nitrofurantoin is better studied |
| Vaginal estrogen** | Conjugated estrogens (0.625 mg conjugated estrogens/1 g cream [Premarin]). Give 0.5–2.0 g cream twice weekly. Estradiol (100 μg estradiol/1 g cream [Estrace]). Give 1–4 g cream | Highly effective in postmenopausal women, who can be difficult to treat Few true contraindications | Can be expensive Compliance may be an issue |
| Cranberry supplement | Dosing varies among products. Unsweetened natural cranberry juice or cranberry tablets, 1–3 times daily. | Generally well-tolerated Few side effects or contraindications | Can be expensive Compliance may be an issue May not be as effective in postmenopausal patients |
| Probiotics | Dosing varies among products and local availability | Few side effects or contraindications | Limited data Can be expensive |
| * Consider trimethoprim (100 mg) alone if the patient has an allergy to sulfa. ** Creams are preferred to the vaginal ring or tablets because they can be applied to periurethral tissues | |||
Postcoital antibiotic prophylaxis prevents some cases of recurrent UTI
Melekos MD, Asbach HW, Gerharz E, Zarakovitis IE, Weingaertner K, Naber KG. Post-intercourse versus daily ciprofloxacin prophylaxis for recurrent urinary tract infections in premenopausal women. J Urol. 1997;157(3):935–939.
UTIs typically involve fecal flora that colonize the vagina and perineum, most commonly Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis. These pathogens ascend to the bladder via the urethra. Sexual intercourse is thought to facilitate this process, and recurrent UTIs in premenopausal women are often postcoital in temporal pattern.
When fecal flora ascend via the urethra from the vagina and perineum to the bladder, the bladder mucosa and urethra may become inflamed, leading to urinary tract infection. The most commonly involved pathogens are Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis.Daily antibiotic prophylaxis for 6 to 12 months has proved to be effective in the prevention of recurrent UTIs, reducing the risk of recurrence by 95%, compared with placebo.4
In this trial by Melekos and colleagues, sexually active premenopausal women who had a history of three or more documented UTIs in the preceding 12 months were randomly assigned to:
- oral ciprofloxacin, one dose daily, or
- oral ciprofloxacin, one dose immediately after intercourse.
A total of 135 patients (65 in the daily group and 70 in the postcoital group) were followed for 12 months. The regimens were equally effective at preventing UTIs. The mean number of UTIs in 12 months decreased significantly in both groups—from 3.74 to 0.031 in the daily group and from 3.67 to 0.043 in the postcoital group.
The best antibiotic? Nitrofurantoin or trimethoprim-sulfamethoxazole
This randomized, controlled trial was rigorous and well-executed and included only healthy premenopausal women. However, given the emergence of antibiotic resistance since this trial was conducted, ciprofloxacin is not an ideal antibiotic for prophylaxis.
Both the American Urological Association and the Infectious Disease Society of America recommend that fluoroquinolones be avoided, if possible, in the treatment of uncomplicated UTIs.5 A better therapeutic choice would be nitrofurantoin or trimethoprim-sulfamethoxazole.
Postcoital antibiotic prophylaxis is an effective strategy for the prevention of UTIs associated with sexual intercourse in premenopausal women. Although the optimal duration of such a regimen was not addressed in this study, it would be appropriate to revisit the need for prophylaxis after 1 year.
Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175–178.
Urinary tract catheterization and urogynecologic surgery are associated with an increased risk for UTI. The risk of UTI following a midurethral sling procedure, in particular, ranges from 4.1% to 33.6% in the literature.6,7 To further explore the risk of UTI after placement of a midurethral sling, Dieter and colleagues followed 138 women who had undergone the procedure with and without concomitant pelvic surgery. The primary outcome was treatment of UTI within the first 3 weeks postoperatively.
Catheterization increased the risk of UTI
Fifty-eight percent of women required placement of a catheter postoperatively—either an indwelling Foley or intermittent self-catheterization. The duration of catheterization ranged from 1 to 14 days, with a mean of 4 days. The incidence of UTI was significantly higher in the group that was catheterized postoperatively, compared with the group that was not (30.0% vs 5.2%), and catheterization remained an independent risk factor for UTI after adjusting for other confounding factors.
Data may not be applicable to other types of surgery
This large retrospective cohort study of a well-characterized population was based on consistent postoperative data related to catheterization and UTI treatment. Because the study focused on patients who had undergone placement of a midurethral sling, its findings may not be applicable to women undergoing other types of pelvic surgery, including general gynecologic procedures. However, given the significant difference in the rate of UTI between the two groups, the increased risk of UTI may be at least partially attributable to short-term postoperative catheterization rather than urinary tract instrumentation during the procedure.
The risk of UTI is increased with short-term catheterization following placement of a midurethral sling. There may be a role for antibiotic prophylaxis in the setting of short-term postoperative catheterization; however, a prospective, randomized, placebo-controlled study is needed to determine whether the rate of UTI would be reduced.
Vaginal estrogen prevents recurrent UTIs among postmenopausal women
Raz R, Stamm WE. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753–756.
The tissues of the vagina, urethra, bladder, and pelvic floor musculature all express estrogen receptors.8 In postmenopausal women, the effects of decreased estrogen on the urinary tract include a rise in the vaginal pH level and decreased colonization with Lactobacillus. These effects predispose this population to an increased risk for UTI.3 The literature does not support the use of oral estrogen replacement as a therapy for recurrent UTI; however, data suggest that vaginal estrogen replacement may be helpful.9
Raz and Stamm conducted their randomized trial of 93 postmenopausal women with a history of recurrent UTIs to elucidate the effects of vaginal estrogen on the risk of UTI. Fifty women were randomly assigned to treatment with intravaginal estriol cream (0.5 mg nightly for 2 weeks, followed by 0.5 mg twice weekly for 8 months), and 43 women were randomly assigned to placebo (equivalent regimen). Compared with the placebo group, the women treated with estriol experienced a significantly reduced risk of UTI (0.5 vs 5.9 infections per patient-year), increased lactobacilli on vaginal cultures (61% vs 0%), decreased vaginal pH, and a lower rate of colonization with Enterobacteriaceae species.
Although this rigorous double-blind, randomized, placebo-controlled trial was published 20 years ago, its findings remain significant—and have been corroborated in other studies.9
Pros and cons of vaginal estrogen replacement
Raz and Stamm utilized vaginal estriol; the preparations used most commonly today are conjugated estrogens (Premarin) and estradiol (Estrace). Vaginal estrogen formulations can be expensive. Compliance also can wane over time. This study, in particular, showed a discontinuation rate of 28%; mild local reactions were the reason. Although the women who discontinued treatment in this study were included in the final analysis, no subanalysis of these patients was published.
Despite these challenges, local estrogen replacement is generally well-tolerated and, with infrequent dosing (twice weekly), has few contraindications. In fact, local estrogen replacement is one of the most highly effective regimens for UTI prevention among postmenopausal women, who can otherwise be difficult to treat for recurrent UTIs.
Vaginal estrogen is an effective therapy for the prevention of UTIs in postmenopausal women.
Cranberry supplementation may prevent UTIs,
but products vary widely
Stothers L. A randomized trial to evaluate effectiveness and cost-effectiveness of naturopathic cranberry products as prophylaxis against urinary tract infection in women. Can J Urol. 2002;9(3):1558–1562.
Cranberries have been used for many years in various formulations to prevent UTI, but no definitive mechanism has been established. In theory, cranberries keep bacteria from adhering to the urothelium.10 In vitro studies have revealed that Escherichia coli is prevented from adhering to uroepithelial cells by two components of cranberry—fructose and proanthocyanidins.10
In this trial of 150 sexually active women (ages 21–72 years) who had experienced at least two UTIs in the past calendar year, Stothers randomly assigned participants to one of three arms for 12 months:
- placebo tablets and cranberry juice (n = 50)
- cranberry tablets and placebo juice (n = 50)
- placebo tablets and placebo juice (n = 50).
Tablets were taken twice daily, and juice was consumed three times daily. All cranberry juice was organic, unsweetened, and unfiltered and taken in 250-mL servings; cranberry tablets were 1:30 parts concentrated cranberry juice.
The risk of UTI during treatment was reduced significantly in the groups taking a cranberry formulation, compared with placebo. Twenty percent of patients consuming cranberry juice experienced a UTI during treatment, compared with 18% of those taking a cranberry tablet and 32% of those in the placebo group (P<.05). In this study, the annual cost of prophylaxis with cranberry juice was $1,400 per woman, and it was $624 per woman for the cranberry tablets. Compliance was lowest among women consuming cranberry juice, decreasing at times to less than 80%.
Findings are difficult to extrapolate
This randomized, double-blind study demonstrated a significant reduction in the rate of UTI with cranberry supplementation, compared with placebo, among women with a mean age of 40 to 44 years. However, because cranberry preparations, juice, and tablets are not regulated as to the amount and bioavailability of the active ingredient, it is difficult to compare one to another and extrapolate to a particular type of preparation.
This study does highlight the higher rate of noncompliance and cost with cranberry juice, although it was as effective at reducing UTIs as cranberry tablets.
Cranberry supplementation reduced the risk of UTIs in sexually active women; placebo did not. Cranberry use may be an alternative to postcoital antibiotic prophylaxis; a randomized comparison of these therapies is needed.
Can nonhormonal therapy alter vaginal flora?
Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of a Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212–1217.
Probiotics have been used recently in attempts to prevent recurrent UTI, albeit with very little evidence in the literature. Their effectiveness is plausible due to promotion of healthy vaginal flora.
This study by Stapleton and colleagues enrolled premenopausal women (ages 18–40) with a history of one UTI within the past calendar year and a current, active, uncomplicated UTI. Ninety-nine percent of participants were sexually active. All women were treated with a standard antibiotic regimen for UTI. Seven to 10 days later, participants were randomly assigned to:
- Lactobacillus crispatus vaginal suppository [Lactin-V (Osel)], daily for 5 days and then weekly for 10 weeks (n = 50), or
- placebo (same regimen) (n = 50).
The risk of UTI was 15% among women in the probiotic group, compared with 27% in the placebo group—but this difference was only statistically significant for women who had a higher level of Lactobacillus crispatus vaginal colonization in the treatment group.
Vaginal probiotic formulations may be hard to obtain
The use of probiotics to prevent recurrent UTIs is new and innovative. However, vaginal probiotic formulations are not widely available, and most commercially available oral probiotic formulations are marketed for digestive health—an area where the effects have been studied widely.
In this study, the mean age was 21 years. Given that hypoestrogenization is associated with decreased vaginal colonization with Lactobacillus, an interesting area of future study would be the use of probiotics in postmenopausal women.
Continued investigation of probiotics is warranted, as this approach could help in the treatment of women who have intolerance to antibiotics and is generally considered safe and well-tolerated.
Intravaginal probiotic prophylaxis may reduce the risk of recurrent UTIs. However, further studies are needed to confirm early enthusiasm and delineate ideal populations.
We want to hear from you! Tell us what you think.
1. Foxman B, Barolow R, D’Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs. Ann Epidemiol. 2000;10(8):509-515.
2. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002;287(20):2701-2710.
3. ACOG Practice Bulletin #91: Treatment of urinary tract infections in nonpregnant women. Obstet Gynecol. 2008;111(3):785-794.
4. Hooton TM. Recurrent urinary tract infection in women. Int J Antimicrob Agents. 2001;17(4):259-268.
5. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Disease Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103-120.
6. Sutkin G, Alperin M, Meyn L, Wiesenfeld HC, Ellison R, Zyczynski HM. Symptomatic urinary tract infections after surgery for prolapse and/or incontinence. Int Urogynecol J. 2010;21(8):955-961.
7. Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175-178.
8. Robinson D, Cardozo L. Estrogens and the lower urinary tract. Neurourol Urodyn. 2011;30(5):754-757.
9. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;(2):CD005131.-
10. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;(1):CD001321.-
| Drs. Amundsen and Edenfield offer a novel strategy to prevent recurrent UTI in premenopausal women |

Autumn L. Edenfield, MD
Dr. Edenfield is a Fellow in Female Pelvic Medicine and Reconstructive Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University Medical Center in Durham, North Carolina.
Cindy L. Amundsen, MD
Dr. Amundsen is Professor and Fellowship Director in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, at Duke University Medical Center in Durham, North Carolina.
The authors report no financial relationships relevant to this article.
| Drs. Amundsen and Edenfield offer a novel strategy to prevent recurrent UTI in premenopausal women |
Autumn L. Edenfield, MD
Dr. Edenfield is a Fellow in Female Pelvic Medicine and Reconstructive Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University Medical Center in Durham, North Carolina.
Cindy L. Amundsen, MD
Dr. Amundsen is Professor and Fellowship Director in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, at Duke University Medical Center in Durham, North Carolina.
The authors report no financial relationships relevant to this article.
| Drs. Amundsen and Edenfield offer a novel strategy to prevent recurrent UTI in premenopausal women |
Autumn L. Edenfield, MD
Dr. Edenfield is a Fellow in Female Pelvic Medicine and Reconstructive Surgery and Clinical Instructor of Obstetrics and Gynecology at Duke University Medical Center in Durham, North Carolina.
Cindy L. Amundsen, MD
Dr. Amundsen is Professor and Fellowship Director in Female Pelvic Medicine and Reconstructive Surgery, Department of Obstetrics and Gynecology, at Duke University Medical Center in Durham, North Carolina.
The authors report no financial relationships relevant to this article.
10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Megan O. Schimpf, MD (June 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Urinary tract infections (UTIs) are prevalent among women, afflicting as many as 60% of women during their lifetime.1 Symptoms include urgency, frequency, and dysuria. Although the diagnosis can be made on the basis of symptoms alone in many cases, urinalysis and urine cultures often are helpful in confirming it.2 The differential diagnosis includes infectious or atrophic vaginitis, urethritis from a sexually transmitted infection, urethral diverticulum, painful bladder syndrome, urinary tract calculi, and urinary tract neoplasms. Common risk factors for UTIs are listed in TABLE 1.3
TABLE 1
Risk factors for urinary tract infection in women
Premenopausal women •History of urinary tract infection (UTI) Postmenopausal women |
| SOURCE: Adapted from ACOG3 |
Recurrent UTIs are defined as three infections in 12 months or two infections in 6 months. In this Update, we explore strategies to prevent recurrent UTIs in three groups of women:
- sexually active premenopausal women
- postmenopausal women
- women undergoing pelvic surgery.
In the process, we summarize the results of five trials that explore treatment modalities such as prophylactic antibiotics, vaginal estrogen therapy, cranberry supplementation, and probiotics (TABLE 2).
TABLE 2
Summary of therapeutic strategies for prevention of recurrent urinary tract infections
| Strategy | Dose | Advantages | Disadvantages |
|---|---|---|---|
| Prophylactic antibiotics | Trimethoprim-sulfamethoxazole (Bactrim): 1 double-strength tablet* OR Nitrofurantoin: 50 or 100 mg Either drug can be given daily for 6 months or as one dose postcoitally | Highly effective Inexpensive | Potential for future microbial resistance Caution with nitrofurantoin, particularly in older patients or women who have renal insufficiency In pregnancy, nitrofurantoin is better studied |
| Vaginal estrogen** | Conjugated estrogens (0.625 mg conjugated estrogens/1 g cream [Premarin]). Give 0.5–2.0 g cream twice weekly. Estradiol (100 μg estradiol/1 g cream [Estrace]). Give 1–4 g cream | Highly effective in postmenopausal women, who can be difficult to treat Few true contraindications | Can be expensive Compliance may be an issue |
| Cranberry supplement | Dosing varies among products. Unsweetened natural cranberry juice or cranberry tablets, 1–3 times daily. | Generally well-tolerated Few side effects or contraindications | Can be expensive Compliance may be an issue May not be as effective in postmenopausal patients |
| Probiotics | Dosing varies among products and local availability | Few side effects or contraindications | Limited data Can be expensive |
| * Consider trimethoprim (100 mg) alone if the patient has an allergy to sulfa. ** Creams are preferred to the vaginal ring or tablets because they can be applied to periurethral tissues | |||
Postcoital antibiotic prophylaxis prevents some cases of recurrent UTI
Melekos MD, Asbach HW, Gerharz E, Zarakovitis IE, Weingaertner K, Naber KG. Post-intercourse versus daily ciprofloxacin prophylaxis for recurrent urinary tract infections in premenopausal women. J Urol. 1997;157(3):935–939.
UTIs typically involve fecal flora that colonize the vagina and perineum, most commonly Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis. These pathogens ascend to the bladder via the urethra. Sexual intercourse is thought to facilitate this process, and recurrent UTIs in premenopausal women are often postcoital in temporal pattern.
When fecal flora ascend via the urethra from the vagina and perineum to the bladder, the bladder mucosa and urethra may become inflamed, leading to urinary tract infection. The most commonly involved pathogens are Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis.Daily antibiotic prophylaxis for 6 to 12 months has proved to be effective in the prevention of recurrent UTIs, reducing the risk of recurrence by 95%, compared with placebo.4
In this trial by Melekos and colleagues, sexually active premenopausal women who had a history of three or more documented UTIs in the preceding 12 months were randomly assigned to:
- oral ciprofloxacin, one dose daily, or
- oral ciprofloxacin, one dose immediately after intercourse.
A total of 135 patients (65 in the daily group and 70 in the postcoital group) were followed for 12 months. The regimens were equally effective at preventing UTIs. The mean number of UTIs in 12 months decreased significantly in both groups—from 3.74 to 0.031 in the daily group and from 3.67 to 0.043 in the postcoital group.
The best antibiotic? Nitrofurantoin or trimethoprim-sulfamethoxazole
This randomized, controlled trial was rigorous and well-executed and included only healthy premenopausal women. However, given the emergence of antibiotic resistance since this trial was conducted, ciprofloxacin is not an ideal antibiotic for prophylaxis.
Both the American Urological Association and the Infectious Disease Society of America recommend that fluoroquinolones be avoided, if possible, in the treatment of uncomplicated UTIs.5 A better therapeutic choice would be nitrofurantoin or trimethoprim-sulfamethoxazole.
Postcoital antibiotic prophylaxis is an effective strategy for the prevention of UTIs associated with sexual intercourse in premenopausal women. Although the optimal duration of such a regimen was not addressed in this study, it would be appropriate to revisit the need for prophylaxis after 1 year.
Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175–178.
Urinary tract catheterization and urogynecologic surgery are associated with an increased risk for UTI. The risk of UTI following a midurethral sling procedure, in particular, ranges from 4.1% to 33.6% in the literature.6,7 To further explore the risk of UTI after placement of a midurethral sling, Dieter and colleagues followed 138 women who had undergone the procedure with and without concomitant pelvic surgery. The primary outcome was treatment of UTI within the first 3 weeks postoperatively.
Catheterization increased the risk of UTI
Fifty-eight percent of women required placement of a catheter postoperatively—either an indwelling Foley or intermittent self-catheterization. The duration of catheterization ranged from 1 to 14 days, with a mean of 4 days. The incidence of UTI was significantly higher in the group that was catheterized postoperatively, compared with the group that was not (30.0% vs 5.2%), and catheterization remained an independent risk factor for UTI after adjusting for other confounding factors.
Data may not be applicable to other types of surgery
This large retrospective cohort study of a well-characterized population was based on consistent postoperative data related to catheterization and UTI treatment. Because the study focused on patients who had undergone placement of a midurethral sling, its findings may not be applicable to women undergoing other types of pelvic surgery, including general gynecologic procedures. However, given the significant difference in the rate of UTI between the two groups, the increased risk of UTI may be at least partially attributable to short-term postoperative catheterization rather than urinary tract instrumentation during the procedure.
The risk of UTI is increased with short-term catheterization following placement of a midurethral sling. There may be a role for antibiotic prophylaxis in the setting of short-term postoperative catheterization; however, a prospective, randomized, placebo-controlled study is needed to determine whether the rate of UTI would be reduced.
Vaginal estrogen prevents recurrent UTIs among postmenopausal women
Raz R, Stamm WE. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753–756.
The tissues of the vagina, urethra, bladder, and pelvic floor musculature all express estrogen receptors.8 In postmenopausal women, the effects of decreased estrogen on the urinary tract include a rise in the vaginal pH level and decreased colonization with Lactobacillus. These effects predispose this population to an increased risk for UTI.3 The literature does not support the use of oral estrogen replacement as a therapy for recurrent UTI; however, data suggest that vaginal estrogen replacement may be helpful.9
Raz and Stamm conducted their randomized trial of 93 postmenopausal women with a history of recurrent UTIs to elucidate the effects of vaginal estrogen on the risk of UTI. Fifty women were randomly assigned to treatment with intravaginal estriol cream (0.5 mg nightly for 2 weeks, followed by 0.5 mg twice weekly for 8 months), and 43 women were randomly assigned to placebo (equivalent regimen). Compared with the placebo group, the women treated with estriol experienced a significantly reduced risk of UTI (0.5 vs 5.9 infections per patient-year), increased lactobacilli on vaginal cultures (61% vs 0%), decreased vaginal pH, and a lower rate of colonization with Enterobacteriaceae species.
Although this rigorous double-blind, randomized, placebo-controlled trial was published 20 years ago, its findings remain significant—and have been corroborated in other studies.9
Pros and cons of vaginal estrogen replacement
Raz and Stamm utilized vaginal estriol; the preparations used most commonly today are conjugated estrogens (Premarin) and estradiol (Estrace). Vaginal estrogen formulations can be expensive. Compliance also can wane over time. This study, in particular, showed a discontinuation rate of 28%; mild local reactions were the reason. Although the women who discontinued treatment in this study were included in the final analysis, no subanalysis of these patients was published.
Despite these challenges, local estrogen replacement is generally well-tolerated and, with infrequent dosing (twice weekly), has few contraindications. In fact, local estrogen replacement is one of the most highly effective regimens for UTI prevention among postmenopausal women, who can otherwise be difficult to treat for recurrent UTIs.
Vaginal estrogen is an effective therapy for the prevention of UTIs in postmenopausal women.
Cranberry supplementation may prevent UTIs,
but products vary widely
Stothers L. A randomized trial to evaluate effectiveness and cost-effectiveness of naturopathic cranberry products as prophylaxis against urinary tract infection in women. Can J Urol. 2002;9(3):1558–1562.
Cranberries have been used for many years in various formulations to prevent UTI, but no definitive mechanism has been established. In theory, cranberries keep bacteria from adhering to the urothelium.10 In vitro studies have revealed that Escherichia coli is prevented from adhering to uroepithelial cells by two components of cranberry—fructose and proanthocyanidins.10
In this trial of 150 sexually active women (ages 21–72 years) who had experienced at least two UTIs in the past calendar year, Stothers randomly assigned participants to one of three arms for 12 months:
- placebo tablets and cranberry juice (n = 50)
- cranberry tablets and placebo juice (n = 50)
- placebo tablets and placebo juice (n = 50).
Tablets were taken twice daily, and juice was consumed three times daily. All cranberry juice was organic, unsweetened, and unfiltered and taken in 250-mL servings; cranberry tablets were 1:30 parts concentrated cranberry juice.
The risk of UTI during treatment was reduced significantly in the groups taking a cranberry formulation, compared with placebo. Twenty percent of patients consuming cranberry juice experienced a UTI during treatment, compared with 18% of those taking a cranberry tablet and 32% of those in the placebo group (P<.05). In this study, the annual cost of prophylaxis with cranberry juice was $1,400 per woman, and it was $624 per woman for the cranberry tablets. Compliance was lowest among women consuming cranberry juice, decreasing at times to less than 80%.
Findings are difficult to extrapolate
This randomized, double-blind study demonstrated a significant reduction in the rate of UTI with cranberry supplementation, compared with placebo, among women with a mean age of 40 to 44 years. However, because cranberry preparations, juice, and tablets are not regulated as to the amount and bioavailability of the active ingredient, it is difficult to compare one to another and extrapolate to a particular type of preparation.
This study does highlight the higher rate of noncompliance and cost with cranberry juice, although it was as effective at reducing UTIs as cranberry tablets.
Cranberry supplementation reduced the risk of UTIs in sexually active women; placebo did not. Cranberry use may be an alternative to postcoital antibiotic prophylaxis; a randomized comparison of these therapies is needed.
Can nonhormonal therapy alter vaginal flora?
Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of a Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212–1217.
Probiotics have been used recently in attempts to prevent recurrent UTI, albeit with very little evidence in the literature. Their effectiveness is plausible due to promotion of healthy vaginal flora.
This study by Stapleton and colleagues enrolled premenopausal women (ages 18–40) with a history of one UTI within the past calendar year and a current, active, uncomplicated UTI. Ninety-nine percent of participants were sexually active. All women were treated with a standard antibiotic regimen for UTI. Seven to 10 days later, participants were randomly assigned to:
- Lactobacillus crispatus vaginal suppository [Lactin-V (Osel)], daily for 5 days and then weekly for 10 weeks (n = 50), or
- placebo (same regimen) (n = 50).
The risk of UTI was 15% among women in the probiotic group, compared with 27% in the placebo group—but this difference was only statistically significant for women who had a higher level of Lactobacillus crispatus vaginal colonization in the treatment group.
Vaginal probiotic formulations may be hard to obtain
The use of probiotics to prevent recurrent UTIs is new and innovative. However, vaginal probiotic formulations are not widely available, and most commercially available oral probiotic formulations are marketed for digestive health—an area where the effects have been studied widely.
In this study, the mean age was 21 years. Given that hypoestrogenization is associated with decreased vaginal colonization with Lactobacillus, an interesting area of future study would be the use of probiotics in postmenopausal women.
Continued investigation of probiotics is warranted, as this approach could help in the treatment of women who have intolerance to antibiotics and is generally considered safe and well-tolerated.
Intravaginal probiotic prophylaxis may reduce the risk of recurrent UTIs. However, further studies are needed to confirm early enthusiasm and delineate ideal populations.
We want to hear from you! Tell us what you think.
10 practical, evidence-based recommendations for perioperative antibiotic prophylaxis
Megan O. Schimpf, MD (June 2012)
Update on Menopause
Andrew M. Kaunitz, MD (May 2012)
Urinary tract infections (UTIs) are prevalent among women, afflicting as many as 60% of women during their lifetime.1 Symptoms include urgency, frequency, and dysuria. Although the diagnosis can be made on the basis of symptoms alone in many cases, urinalysis and urine cultures often are helpful in confirming it.2 The differential diagnosis includes infectious or atrophic vaginitis, urethritis from a sexually transmitted infection, urethral diverticulum, painful bladder syndrome, urinary tract calculi, and urinary tract neoplasms. Common risk factors for UTIs are listed in TABLE 1.3
TABLE 1
Risk factors for urinary tract infection in women
Premenopausal women •History of urinary tract infection (UTI) Postmenopausal women |
| SOURCE: Adapted from ACOG3 |
Recurrent UTIs are defined as three infections in 12 months or two infections in 6 months. In this Update, we explore strategies to prevent recurrent UTIs in three groups of women:
- sexually active premenopausal women
- postmenopausal women
- women undergoing pelvic surgery.
In the process, we summarize the results of five trials that explore treatment modalities such as prophylactic antibiotics, vaginal estrogen therapy, cranberry supplementation, and probiotics (TABLE 2).
TABLE 2
Summary of therapeutic strategies for prevention of recurrent urinary tract infections
| Strategy | Dose | Advantages | Disadvantages |
|---|---|---|---|
| Prophylactic antibiotics | Trimethoprim-sulfamethoxazole (Bactrim): 1 double-strength tablet* OR Nitrofurantoin: 50 or 100 mg Either drug can be given daily for 6 months or as one dose postcoitally | Highly effective Inexpensive | Potential for future microbial resistance Caution with nitrofurantoin, particularly in older patients or women who have renal insufficiency In pregnancy, nitrofurantoin is better studied |
| Vaginal estrogen** | Conjugated estrogens (0.625 mg conjugated estrogens/1 g cream [Premarin]). Give 0.5–2.0 g cream twice weekly. Estradiol (100 μg estradiol/1 g cream [Estrace]). Give 1–4 g cream | Highly effective in postmenopausal women, who can be difficult to treat Few true contraindications | Can be expensive Compliance may be an issue |
| Cranberry supplement | Dosing varies among products. Unsweetened natural cranberry juice or cranberry tablets, 1–3 times daily. | Generally well-tolerated Few side effects or contraindications | Can be expensive Compliance may be an issue May not be as effective in postmenopausal patients |
| Probiotics | Dosing varies among products and local availability | Few side effects or contraindications | Limited data Can be expensive |
| * Consider trimethoprim (100 mg) alone if the patient has an allergy to sulfa. ** Creams are preferred to the vaginal ring or tablets because they can be applied to periurethral tissues | |||
Postcoital antibiotic prophylaxis prevents some cases of recurrent UTI
Melekos MD, Asbach HW, Gerharz E, Zarakovitis IE, Weingaertner K, Naber KG. Post-intercourse versus daily ciprofloxacin prophylaxis for recurrent urinary tract infections in premenopausal women. J Urol. 1997;157(3):935–939.
UTIs typically involve fecal flora that colonize the vagina and perineum, most commonly Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis. These pathogens ascend to the bladder via the urethra. Sexual intercourse is thought to facilitate this process, and recurrent UTIs in premenopausal women are often postcoital in temporal pattern.
When fecal flora ascend via the urethra from the vagina and perineum to the bladder, the bladder mucosa and urethra may become inflamed, leading to urinary tract infection. The most commonly involved pathogens are Escherichia coli, Staphylococcus saprophyticus, Klebsiella pneumonia, and Proteus mirabilis.Daily antibiotic prophylaxis for 6 to 12 months has proved to be effective in the prevention of recurrent UTIs, reducing the risk of recurrence by 95%, compared with placebo.4
In this trial by Melekos and colleagues, sexually active premenopausal women who had a history of three or more documented UTIs in the preceding 12 months were randomly assigned to:
- oral ciprofloxacin, one dose daily, or
- oral ciprofloxacin, one dose immediately after intercourse.
A total of 135 patients (65 in the daily group and 70 in the postcoital group) were followed for 12 months. The regimens were equally effective at preventing UTIs. The mean number of UTIs in 12 months decreased significantly in both groups—from 3.74 to 0.031 in the daily group and from 3.67 to 0.043 in the postcoital group.
The best antibiotic? Nitrofurantoin or trimethoprim-sulfamethoxazole
This randomized, controlled trial was rigorous and well-executed and included only healthy premenopausal women. However, given the emergence of antibiotic resistance since this trial was conducted, ciprofloxacin is not an ideal antibiotic for prophylaxis.
Both the American Urological Association and the Infectious Disease Society of America recommend that fluoroquinolones be avoided, if possible, in the treatment of uncomplicated UTIs.5 A better therapeutic choice would be nitrofurantoin or trimethoprim-sulfamethoxazole.
Postcoital antibiotic prophylaxis is an effective strategy for the prevention of UTIs associated with sexual intercourse in premenopausal women. Although the optimal duration of such a regimen was not addressed in this study, it would be appropriate to revisit the need for prophylaxis after 1 year.
Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175–178.
Urinary tract catheterization and urogynecologic surgery are associated with an increased risk for UTI. The risk of UTI following a midurethral sling procedure, in particular, ranges from 4.1% to 33.6% in the literature.6,7 To further explore the risk of UTI after placement of a midurethral sling, Dieter and colleagues followed 138 women who had undergone the procedure with and without concomitant pelvic surgery. The primary outcome was treatment of UTI within the first 3 weeks postoperatively.
Catheterization increased the risk of UTI
Fifty-eight percent of women required placement of a catheter postoperatively—either an indwelling Foley or intermittent self-catheterization. The duration of catheterization ranged from 1 to 14 days, with a mean of 4 days. The incidence of UTI was significantly higher in the group that was catheterized postoperatively, compared with the group that was not (30.0% vs 5.2%), and catheterization remained an independent risk factor for UTI after adjusting for other confounding factors.
Data may not be applicable to other types of surgery
This large retrospective cohort study of a well-characterized population was based on consistent postoperative data related to catheterization and UTI treatment. Because the study focused on patients who had undergone placement of a midurethral sling, its findings may not be applicable to women undergoing other types of pelvic surgery, including general gynecologic procedures. However, given the significant difference in the rate of UTI between the two groups, the increased risk of UTI may be at least partially attributable to short-term postoperative catheterization rather than urinary tract instrumentation during the procedure.
The risk of UTI is increased with short-term catheterization following placement of a midurethral sling. There may be a role for antibiotic prophylaxis in the setting of short-term postoperative catheterization; however, a prospective, randomized, placebo-controlled study is needed to determine whether the rate of UTI would be reduced.
Vaginal estrogen prevents recurrent UTIs among postmenopausal women
Raz R, Stamm WE. A controlled trial of intravaginal estriol in postmenopausal women with recurrent urinary tract infections. N Engl J Med. 1993;329(11):753–756.
The tissues of the vagina, urethra, bladder, and pelvic floor musculature all express estrogen receptors.8 In postmenopausal women, the effects of decreased estrogen on the urinary tract include a rise in the vaginal pH level and decreased colonization with Lactobacillus. These effects predispose this population to an increased risk for UTI.3 The literature does not support the use of oral estrogen replacement as a therapy for recurrent UTI; however, data suggest that vaginal estrogen replacement may be helpful.9
Raz and Stamm conducted their randomized trial of 93 postmenopausal women with a history of recurrent UTIs to elucidate the effects of vaginal estrogen on the risk of UTI. Fifty women were randomly assigned to treatment with intravaginal estriol cream (0.5 mg nightly for 2 weeks, followed by 0.5 mg twice weekly for 8 months), and 43 women were randomly assigned to placebo (equivalent regimen). Compared with the placebo group, the women treated with estriol experienced a significantly reduced risk of UTI (0.5 vs 5.9 infections per patient-year), increased lactobacilli on vaginal cultures (61% vs 0%), decreased vaginal pH, and a lower rate of colonization with Enterobacteriaceae species.
Although this rigorous double-blind, randomized, placebo-controlled trial was published 20 years ago, its findings remain significant—and have been corroborated in other studies.9
Pros and cons of vaginal estrogen replacement
Raz and Stamm utilized vaginal estriol; the preparations used most commonly today are conjugated estrogens (Premarin) and estradiol (Estrace). Vaginal estrogen formulations can be expensive. Compliance also can wane over time. This study, in particular, showed a discontinuation rate of 28%; mild local reactions were the reason. Although the women who discontinued treatment in this study were included in the final analysis, no subanalysis of these patients was published.
Despite these challenges, local estrogen replacement is generally well-tolerated and, with infrequent dosing (twice weekly), has few contraindications. In fact, local estrogen replacement is one of the most highly effective regimens for UTI prevention among postmenopausal women, who can otherwise be difficult to treat for recurrent UTIs.
Vaginal estrogen is an effective therapy for the prevention of UTIs in postmenopausal women.
Cranberry supplementation may prevent UTIs,
but products vary widely
Stothers L. A randomized trial to evaluate effectiveness and cost-effectiveness of naturopathic cranberry products as prophylaxis against urinary tract infection in women. Can J Urol. 2002;9(3):1558–1562.
Cranberries have been used for many years in various formulations to prevent UTI, but no definitive mechanism has been established. In theory, cranberries keep bacteria from adhering to the urothelium.10 In vitro studies have revealed that Escherichia coli is prevented from adhering to uroepithelial cells by two components of cranberry—fructose and proanthocyanidins.10
In this trial of 150 sexually active women (ages 21–72 years) who had experienced at least two UTIs in the past calendar year, Stothers randomly assigned participants to one of three arms for 12 months:
- placebo tablets and cranberry juice (n = 50)
- cranberry tablets and placebo juice (n = 50)
- placebo tablets and placebo juice (n = 50).
Tablets were taken twice daily, and juice was consumed three times daily. All cranberry juice was organic, unsweetened, and unfiltered and taken in 250-mL servings; cranberry tablets were 1:30 parts concentrated cranberry juice.
The risk of UTI during treatment was reduced significantly in the groups taking a cranberry formulation, compared with placebo. Twenty percent of patients consuming cranberry juice experienced a UTI during treatment, compared with 18% of those taking a cranberry tablet and 32% of those in the placebo group (P<.05). In this study, the annual cost of prophylaxis with cranberry juice was $1,400 per woman, and it was $624 per woman for the cranberry tablets. Compliance was lowest among women consuming cranberry juice, decreasing at times to less than 80%.
Findings are difficult to extrapolate
This randomized, double-blind study demonstrated a significant reduction in the rate of UTI with cranberry supplementation, compared with placebo, among women with a mean age of 40 to 44 years. However, because cranberry preparations, juice, and tablets are not regulated as to the amount and bioavailability of the active ingredient, it is difficult to compare one to another and extrapolate to a particular type of preparation.
This study does highlight the higher rate of noncompliance and cost with cranberry juice, although it was as effective at reducing UTIs as cranberry tablets.
Cranberry supplementation reduced the risk of UTIs in sexually active women; placebo did not. Cranberry use may be an alternative to postcoital antibiotic prophylaxis; a randomized comparison of these therapies is needed.
Can nonhormonal therapy alter vaginal flora?
Stapleton AE, Au-Yeung M, Hooton TM, et al. Randomized, placebo-controlled phase 2 trial of a Lactobacillus crispatus probiotic given intravaginally for prevention of recurrent urinary tract infection. Clin Infect Dis. 2011;52(10):1212–1217.
Probiotics have been used recently in attempts to prevent recurrent UTI, albeit with very little evidence in the literature. Their effectiveness is plausible due to promotion of healthy vaginal flora.
This study by Stapleton and colleagues enrolled premenopausal women (ages 18–40) with a history of one UTI within the past calendar year and a current, active, uncomplicated UTI. Ninety-nine percent of participants were sexually active. All women were treated with a standard antibiotic regimen for UTI. Seven to 10 days later, participants were randomly assigned to:
- Lactobacillus crispatus vaginal suppository [Lactin-V (Osel)], daily for 5 days and then weekly for 10 weeks (n = 50), or
- placebo (same regimen) (n = 50).
The risk of UTI was 15% among women in the probiotic group, compared with 27% in the placebo group—but this difference was only statistically significant for women who had a higher level of Lactobacillus crispatus vaginal colonization in the treatment group.
Vaginal probiotic formulations may be hard to obtain
The use of probiotics to prevent recurrent UTIs is new and innovative. However, vaginal probiotic formulations are not widely available, and most commercially available oral probiotic formulations are marketed for digestive health—an area where the effects have been studied widely.
In this study, the mean age was 21 years. Given that hypoestrogenization is associated with decreased vaginal colonization with Lactobacillus, an interesting area of future study would be the use of probiotics in postmenopausal women.
Continued investigation of probiotics is warranted, as this approach could help in the treatment of women who have intolerance to antibiotics and is generally considered safe and well-tolerated.
Intravaginal probiotic prophylaxis may reduce the risk of recurrent UTIs. However, further studies are needed to confirm early enthusiasm and delineate ideal populations.
We want to hear from you! Tell us what you think.
1. Foxman B, Barolow R, D’Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs. Ann Epidemiol. 2000;10(8):509-515.
2. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002;287(20):2701-2710.
3. ACOG Practice Bulletin #91: Treatment of urinary tract infections in nonpregnant women. Obstet Gynecol. 2008;111(3):785-794.
4. Hooton TM. Recurrent urinary tract infection in women. Int J Antimicrob Agents. 2001;17(4):259-268.
5. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Disease Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103-120.
6. Sutkin G, Alperin M, Meyn L, Wiesenfeld HC, Ellison R, Zyczynski HM. Symptomatic urinary tract infections after surgery for prolapse and/or incontinence. Int Urogynecol J. 2010;21(8):955-961.
7. Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175-178.
8. Robinson D, Cardozo L. Estrogens and the lower urinary tract. Neurourol Urodyn. 2011;30(5):754-757.
9. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;(2):CD005131.-
10. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;(1):CD001321.-
1. Foxman B, Barolow R, D’Arcy H, Gillespie B, Sobel JD. Urinary tract infection: self-reported incidence and associated costs. Ann Epidemiol. 2000;10(8):509-515.
2. Bent S, Nallamothu BK, Simel DL, Fihn SD, Saint S. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002;287(20):2701-2710.
3. ACOG Practice Bulletin #91: Treatment of urinary tract infections in nonpregnant women. Obstet Gynecol. 2008;111(3):785-794.
4. Hooton TM. Recurrent urinary tract infection in women. Int J Antimicrob Agents. 2001;17(4):259-268.
5. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Disease Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis. 2011;52(5):e103-120.
6. Sutkin G, Alperin M, Meyn L, Wiesenfeld HC, Ellison R, Zyczynski HM. Symptomatic urinary tract infections after surgery for prolapse and/or incontinence. Int Urogynecol J. 2010;21(8):955-961.
7. Dieter AA, Amundsen CL, Visco AG, Siddiqui NY. Treatment for urinary tract infection after midurethral sling: a retrospective study comparing patients who receive short-term postoperative catheterization and patients who pass a void trial on the day of surgery. Female Pelvic Med Reconstr Surg. 2012;18(3):175-178.
8. Robinson D, Cardozo L. Estrogens and the lower urinary tract. Neurourol Urodyn. 2011;30(5):754-757.
9. Perrotta C, Aznar M, Mejia R, Albert X, Ng CW. Oestrogens for preventing recurrent urinary tract infection in postmenopausal women. Cochrane Database Syst Rev. 2008;(2):CD005131.-
10. Jepson RG, Craig JC. Cranberries for preventing urinary tract infections. Cochrane Database Syst Rev. 2008;(1):CD001321.-
Polycystic ovary syndrome: How are obesity and insulin resistance involved?
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Polycystic ovary syndrome, or PCOS, is an enigmatic condition. It presents with varying levels of severity of those symptoms and conditions associated with it—clinical hyperandrogenism (hirsutism, acne, alopecia), obesity, and menstrual disturbance. Although its exact cause is unknown, at least half of all women with PCOS are overweight or obese. What does obesity and, more specifically, insulin resistance, contribute to the pathogenesis of PCOS, and why is it important to screen your patient with PCOS for insulin resistance?
In part 2 of this 4-part series, which will continue to be posted here on the OBG Management Web site, we address these questions. [Editor’s note: As they are published, future installments of this series will continue to be collected on a single Web page for ease of access.]
The roles of obesity and insulin resistance
![]()
Overweight: BMI ≥ 25 kg/m2
Obesity: BMI ≥ 30 kg/m2
Morbid obesity: BMI ≥ 40 kg/m2
PCOS is associated with truncal fat distribution, manifesting as an increased waist-to-hip ratio. According to the Centers for Disease Control and Prevention (CDC), more than one-third of the population was obese in 2009 and 2010.1 Approximately 50% to 65% of women with PCOS are overweight or obese, and most of them have the truncal fat distribution phenotype. 2
Obesity is associated with an increase in insulin resistance (IR) and hyperinsulinemia. IR can be characterized as impaired action of insulin in the uptake and metabolism of glucose. Impaired insulin action leads to elevated insulin levels. Insulin synergizes with abnormally high secretion of luteinizing hormone (perhaps induced by hyperinsulinemia) to promote excess androgen production by intraovarian theca cells and an arrest of follicular development resulting in chronic anovulation.
In addition, hyperinsulinemia causes a decrease in hepatic sex hormone binding globulin, resulting in free circulating androgens and, thus, hirsutism and acne issues. While this picture tends to be more pronounced in women who have PCOS and are obese, it is important to realize that a nonobese patient with PCOS also may have IR, which suggests that insulin plays a major role in the pathogenesis of this disease.3,4
![]()
Most of the evidence suggests that hyperinsulinemia causes hyperandrogenism and not the reverse. Weight loss and insulin sensitizers are associated with a reduction in androgens, particularly testosterone and androstenedione. Gonadotropin-releasing hormone–analogs, which reduce androgen secretion from the ovaries, do not result in a reduction in insulin.3,4
Screening for insulin resistance: The rationale
![]()
The documented prevalence of IR and type 2 diabetes mellitus (DM) in women with PCOS suggests that impaired glucose tolerance (IGT) is present in 31% to 35% of women with PCOS5,6—and DM, classified according to World Health Organization (WHO) criteria, is present in 7.5% to 10% of women with PCOS.
The prevalence of IR and DM are considerably lower in women without PCOS. According to the Third National Health and Nutrition Examination Survey, in US women of similar age, the prevalence of IR is 1.6%, and the prevalence of DM is 2.2%.7
2003 consensus: Screen for IGT in obese PCOS patients. In view of the high prevalence of IR and IGT, a 2003 PCOS consensus8 established that obese women with PCOS should be screened for insulin sensitivity and undergo screening for the metabolic syndrome, including glucose intolerance. For nonobese women, the consensus recommended screening only if additional risk factors are present.
Unfortunately, IGT also occurs independent of obesity. In lean women with PCOS, 5% may have IGT, while 2% are frankly diabetic. Moreover, the conversion from normal glucose tolerance to IGT in patients with PCOS can be as high as 16% per year,9 while the conversion rate from IGT to DM among women with PCOS has been reported to be as high as 2% per year.
2007 position statement: Screen for IGT in all PCOS patients. A position statement by the Androgen Excess–PCOS Society on glucose intolerance and PCOS recommends screening for IGT in all PCOS women, regardless of BMI, at least once every 2 years.10
Screening for insulin resistance: The methods
There are two ways to determine insulin sensitivity:
- direct infusion of IV glucose and/or insulin
- indirect assessment using surrogate markers (such as fasting glucose and insulin, or C-peptide, and oral glucose tolerance test [OGTT]).
Direct infusion of IV glucose or insulin reveals how insulin disposes of glucose from the blood stream; however, this method is expensive, time consuming, and potentially dangerous due to possible hypoglycemia. Indirect assessments are less complex to perform and correlate reasonably well with the results of the more invasive direct measures.
![]()
Direct infusion of glucose and insulin
The hyperinsulinemic euglycemic clamp is the gold standard, but drawbacks relegate it to medical research only. This method measures the amount of glucose necessary to compensate for an increased insulin level without causing hypoglycemia. Numerous blood samplings (every 5 to 10 minutes) are taken to monitor serum glucose so that a steady “fasting” level can be maintained. The degree of insulin resistance is measured by the amount of glucose that is taken up by tissues during the procedure.11-14
The “clamp” technique is the most scientifically sound method for measuring insulin sensitivity, and it’s the standard against which all other tests are usually compared. Because the clamp technique is expensive, time consuming (about 2 hours), and labor intensive, however, it is not practical and is rarely performed in clinical care. It is primarily used in medical research.
Frequently sampled IV glucose tolerance tests: “minimal model.” The frequently sampled IV glucose tolerance test estimates insulin sensitivity through a computer-based mathematical analysis of the glucose-insulin dynamics. Though this test still requires 11 to 34 blood samples over a 3-hour period, it is less labor intensive than the clamp technique. However, in contrast to the clamp, it does not distinguish between peripheral and hepatic glucose utilization.15
Direct infusion of insulin
Insulin sensitivity test. This test involves IV infusion of a set glucose load and a fixed-rate infusion of insulin over approximately 3 hours. The mean plasma glucose concentration over the last 30 minutes of the test reflects insulin sensitivity. Although lengthy, the insulin sensitivity test is less labor intensive and requires fewer blood samples than the clamp technique.16
Insulin tolerance test. This test is a simplified version of the insulin sensitivity test, as it measures the decline in serum glucose after an IV bolus of insulin is administered. Several insulin and glucose levels are sampled over the following 15 minutes. In contrast to the clamp and the minimal model, the insulin tolerance test primarily measures insulin-stimulated uptake of glucose into skeletal muscle, and insulin sensitivity values reflect the rate of decline of log transformed glucose values.17
Direct infusion of glucose
Continuous infusion of glucose with model assessment. This method utilizes a constant IV glucose infusion; samples for glucose and insulin are drawn at 50, 55, and 60 minutes. A mathematical model is then used to calculate insulin sensitivity. The results are correlated with clamp techniques; however, few laboratories have used this continuous-infusion method for insulin sensitivity testing in women with PCOS.18
Unfortunately, all of these methods require IV access and multiple venipunctures, making them relatively impractical for office assessment. To overcome these obstacles, alternative tests have been developed including fasting methods and the OGTT, the latter of which does not require IV access and does correlate reasonably well with dynamic clamp techniques.
![]()
Fasting methods
Fasting insulin. The measurement of fasting serum insulin is simple and inexpensive. Generally, a fasting level of 30 μU/mL indicates greater insulin resistance in a diabetic individual than in a normoglycemic patient. However, fasting insulin levels may be in the “normal” range in up to 40% of PCOS patients who have impaired glucose tolerance diagnosed by the OGTT. It has been suggested by some investigators that a fasting insulin greater than 20 μU/mL in white women and greater than 23 μU/mL in Mexican-American women probably indicates insulin resistance in women with PCOS. Some have also advocated averaging two or three readings to account for day-to-day variability.19-21
Fasting plasma glucose. This is a simple blood test taken after 8 hours of fasting. Fasting plasma glucose (FPG) levels are considered normal up to 100 mg/dL (or 5.5 mmol/L). Levels between 100 and 125 mg/dL (5.5 to 7.0 mmol/L) are considered impaired fasting glucose or prediabetes. These levels are considered to be risk factors for DM and its complications. DM is diagnosed when FPG levels are 126 mg/dL (7.0 mmol/L) or higher. A “normal” result on the FPG test is not always reliable. Repeat testing with the OGTT is recommended if risk factors are suggestive for the presence of DM or a prediabetic condition.
Glucose/insulin ratio
The glucose/insulin (G/I) ratio has become very popular since its first description in 1998 as an accurate index of insulin sensitivity in women with PCOS. The ratio of glucose to insulin is easy to calculate, with lower values depicting higher degrees of insulin resistance. A G/I ratio of less than 4.5 has been shown to be sensitive (95%) and specific (84%) for insulin resistance in women with PCOS, compared with a control group. The normal range for G/I ratios may vary in different ethnic groups and have not been fully validated in nonobese patients.22-25
Homeostatic model assessment
First described in 1985, homeostatic model assessment (HOMA) has been used widely in clinical research to assess insulin sensitivity. Rather than using fasting insulin or a G/I ratio, the product of the fasting values of glucose (expressed as mg/dL) and insulin (expressed as μU/mL) is divided by a constant: I0 x G0 ÷ 405.
The constant 405 should be replaced by 22.5 if glucose is expressed in SI units (mmol/L). Unlike fasting insulin and the G/I ratio, the HOMA calculation compensates for fasting hyperglycemia. The HOMA value correlates well with clamp techniques and has been used frequently to assess changes in insulin sensitivity after treatment. HOMA also has been used to study insulin resistance among PCOS patients of differing ethnic origins.12,24-26
Quantitative insulin sensitivity check index
Like HOMA, quantitative insulin sensitivity check index (QUICKI) can be applied to normoglycemic and hyperglycemic patients. It is derived by calculating the inverse of the sum of logarithmically expressed values of fasting glucose and insulin: 1 ÷ [log(I0) + log(G0)].
Many investigators believe that QUICKI is superior to HOMA as a way of determining insulin sensitivity, although the two values correlate well. As the SI decreases, QUICKI values decrease.27
Oral glucose tolerance test
As OGTT does not require IV access, it is the current standard in practice for diagnosis of IGT and DM. It provides a better assessment of IGT and DM than fasting techniques because these patients may have normal fasting glucose values despite abnormal 2-hour fasting levels. The OGTT uses a 50-, 75-, or 100-g glucose load and measures glucose and insulin at various intervals over 1 to 3 hours. The WHO currently recommends a 75-g oral dose in all adults. A 50-g dose is used to screen for gestational diabetes over an hour, and the 100-g load over 3 hours if abnormal.28 See TABLE for normal and abnormal values. Insulin sensitivity has been assessed by calculating insulin area under the curve (AUC insulin), AUC glucose/AUC insulin, and by an insulin sensitivity index (ISI) that applies only the glucose and insulin values from 0 and 120 minutes into a complex mathematical formula.13,25,29-31
Criteria for diagnosis of diabetes
| Venous plasma glucose (mg/dL) | ||
|---|---|---|
| Fasting Level* | 2-hour postglucose load** | |
| Normal/Low risk | ≤99 | ≤139 |
| Prediabetes/Increased risk | 100–125 | 140–199 |
| Diabetes | ≥126 | ≥200 |
| *Fasting is defined as no caloric intake for at least 8 h **OGTT using a glucose load or 75 g as described by the World Health Organization SOURCE: American Diabetes Association. Standards of medical care in diabetes—2012. Diabetes Care. 2012;35 (suppl 1):s11–s63. doi:10.2337/dc12-s011. | ||
Test for glycosylated hemoglobin
Tests for blood levels of glycosylated hemoglobin, also known as hemoglobin A1c (HbA1c) are not currently used for an initial diagnosis because normal HbA1c levels do not necessarily rule out diabetes, but they are strongly associated with complications of diabetes. The test is not affected by food intake so it can be taken at any time. A normal HbA1c level is below 7%.
- “What is metabolic syndrome and what are the current diagnostic criteria?”
- “We know metformin is used to treat insulin resistance…but what about hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?”
We want to hear from you! Tell us what you think.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Polycystic ovary syndrome, or PCOS, is an enigmatic condition. It presents with varying levels of severity of those symptoms and conditions associated with it—clinical hyperandrogenism (hirsutism, acne, alopecia), obesity, and menstrual disturbance. Although its exact cause is unknown, at least half of all women with PCOS are overweight or obese. What does obesity and, more specifically, insulin resistance, contribute to the pathogenesis of PCOS, and why is it important to screen your patient with PCOS for insulin resistance?
In part 2 of this 4-part series, which will continue to be posted here on the OBG Management Web site, we address these questions. [Editor’s note: As they are published, future installments of this series will continue to be collected on a single Web page for ease of access.]
The roles of obesity and insulin resistance
![]()
Overweight: BMI ≥ 25 kg/m2
Obesity: BMI ≥ 30 kg/m2
Morbid obesity: BMI ≥ 40 kg/m2
PCOS is associated with truncal fat distribution, manifesting as an increased waist-to-hip ratio. According to the Centers for Disease Control and Prevention (CDC), more than one-third of the population was obese in 2009 and 2010.1 Approximately 50% to 65% of women with PCOS are overweight or obese, and most of them have the truncal fat distribution phenotype. 2
Obesity is associated with an increase in insulin resistance (IR) and hyperinsulinemia. IR can be characterized as impaired action of insulin in the uptake and metabolism of glucose. Impaired insulin action leads to elevated insulin levels. Insulin synergizes with abnormally high secretion of luteinizing hormone (perhaps induced by hyperinsulinemia) to promote excess androgen production by intraovarian theca cells and an arrest of follicular development resulting in chronic anovulation.
In addition, hyperinsulinemia causes a decrease in hepatic sex hormone binding globulin, resulting in free circulating androgens and, thus, hirsutism and acne issues. While this picture tends to be more pronounced in women who have PCOS and are obese, it is important to realize that a nonobese patient with PCOS also may have IR, which suggests that insulin plays a major role in the pathogenesis of this disease.3,4
![]()
Most of the evidence suggests that hyperinsulinemia causes hyperandrogenism and not the reverse. Weight loss and insulin sensitizers are associated with a reduction in androgens, particularly testosterone and androstenedione. Gonadotropin-releasing hormone–analogs, which reduce androgen secretion from the ovaries, do not result in a reduction in insulin.3,4
Screening for insulin resistance: The rationale
![]()
The documented prevalence of IR and type 2 diabetes mellitus (DM) in women with PCOS suggests that impaired glucose tolerance (IGT) is present in 31% to 35% of women with PCOS5,6—and DM, classified according to World Health Organization (WHO) criteria, is present in 7.5% to 10% of women with PCOS.
The prevalence of IR and DM are considerably lower in women without PCOS. According to the Third National Health and Nutrition Examination Survey, in US women of similar age, the prevalence of IR is 1.6%, and the prevalence of DM is 2.2%.7
2003 consensus: Screen for IGT in obese PCOS patients. In view of the high prevalence of IR and IGT, a 2003 PCOS consensus8 established that obese women with PCOS should be screened for insulin sensitivity and undergo screening for the metabolic syndrome, including glucose intolerance. For nonobese women, the consensus recommended screening only if additional risk factors are present.
Unfortunately, IGT also occurs independent of obesity. In lean women with PCOS, 5% may have IGT, while 2% are frankly diabetic. Moreover, the conversion from normal glucose tolerance to IGT in patients with PCOS can be as high as 16% per year,9 while the conversion rate from IGT to DM among women with PCOS has been reported to be as high as 2% per year.
2007 position statement: Screen for IGT in all PCOS patients. A position statement by the Androgen Excess–PCOS Society on glucose intolerance and PCOS recommends screening for IGT in all PCOS women, regardless of BMI, at least once every 2 years.10
Screening for insulin resistance: The methods
There are two ways to determine insulin sensitivity:
- direct infusion of IV glucose and/or insulin
- indirect assessment using surrogate markers (such as fasting glucose and insulin, or C-peptide, and oral glucose tolerance test [OGTT]).
Direct infusion of IV glucose or insulin reveals how insulin disposes of glucose from the blood stream; however, this method is expensive, time consuming, and potentially dangerous due to possible hypoglycemia. Indirect assessments are less complex to perform and correlate reasonably well with the results of the more invasive direct measures.
![]()
Direct infusion of glucose and insulin
The hyperinsulinemic euglycemic clamp is the gold standard, but drawbacks relegate it to medical research only. This method measures the amount of glucose necessary to compensate for an increased insulin level without causing hypoglycemia. Numerous blood samplings (every 5 to 10 minutes) are taken to monitor serum glucose so that a steady “fasting” level can be maintained. The degree of insulin resistance is measured by the amount of glucose that is taken up by tissues during the procedure.11-14
The “clamp” technique is the most scientifically sound method for measuring insulin sensitivity, and it’s the standard against which all other tests are usually compared. Because the clamp technique is expensive, time consuming (about 2 hours), and labor intensive, however, it is not practical and is rarely performed in clinical care. It is primarily used in medical research.
Frequently sampled IV glucose tolerance tests: “minimal model.” The frequently sampled IV glucose tolerance test estimates insulin sensitivity through a computer-based mathematical analysis of the glucose-insulin dynamics. Though this test still requires 11 to 34 blood samples over a 3-hour period, it is less labor intensive than the clamp technique. However, in contrast to the clamp, it does not distinguish between peripheral and hepatic glucose utilization.15
Direct infusion of insulin
Insulin sensitivity test. This test involves IV infusion of a set glucose load and a fixed-rate infusion of insulin over approximately 3 hours. The mean plasma glucose concentration over the last 30 minutes of the test reflects insulin sensitivity. Although lengthy, the insulin sensitivity test is less labor intensive and requires fewer blood samples than the clamp technique.16
Insulin tolerance test. This test is a simplified version of the insulin sensitivity test, as it measures the decline in serum glucose after an IV bolus of insulin is administered. Several insulin and glucose levels are sampled over the following 15 minutes. In contrast to the clamp and the minimal model, the insulin tolerance test primarily measures insulin-stimulated uptake of glucose into skeletal muscle, and insulin sensitivity values reflect the rate of decline of log transformed glucose values.17
Direct infusion of glucose
Continuous infusion of glucose with model assessment. This method utilizes a constant IV glucose infusion; samples for glucose and insulin are drawn at 50, 55, and 60 minutes. A mathematical model is then used to calculate insulin sensitivity. The results are correlated with clamp techniques; however, few laboratories have used this continuous-infusion method for insulin sensitivity testing in women with PCOS.18
Unfortunately, all of these methods require IV access and multiple venipunctures, making them relatively impractical for office assessment. To overcome these obstacles, alternative tests have been developed including fasting methods and the OGTT, the latter of which does not require IV access and does correlate reasonably well with dynamic clamp techniques.
![]()
Fasting methods
Fasting insulin. The measurement of fasting serum insulin is simple and inexpensive. Generally, a fasting level of 30 μU/mL indicates greater insulin resistance in a diabetic individual than in a normoglycemic patient. However, fasting insulin levels may be in the “normal” range in up to 40% of PCOS patients who have impaired glucose tolerance diagnosed by the OGTT. It has been suggested by some investigators that a fasting insulin greater than 20 μU/mL in white women and greater than 23 μU/mL in Mexican-American women probably indicates insulin resistance in women with PCOS. Some have also advocated averaging two or three readings to account for day-to-day variability.19-21
Fasting plasma glucose. This is a simple blood test taken after 8 hours of fasting. Fasting plasma glucose (FPG) levels are considered normal up to 100 mg/dL (or 5.5 mmol/L). Levels between 100 and 125 mg/dL (5.5 to 7.0 mmol/L) are considered impaired fasting glucose or prediabetes. These levels are considered to be risk factors for DM and its complications. DM is diagnosed when FPG levels are 126 mg/dL (7.0 mmol/L) or higher. A “normal” result on the FPG test is not always reliable. Repeat testing with the OGTT is recommended if risk factors are suggestive for the presence of DM or a prediabetic condition.
Glucose/insulin ratio
The glucose/insulin (G/I) ratio has become very popular since its first description in 1998 as an accurate index of insulin sensitivity in women with PCOS. The ratio of glucose to insulin is easy to calculate, with lower values depicting higher degrees of insulin resistance. A G/I ratio of less than 4.5 has been shown to be sensitive (95%) and specific (84%) for insulin resistance in women with PCOS, compared with a control group. The normal range for G/I ratios may vary in different ethnic groups and have not been fully validated in nonobese patients.22-25
Homeostatic model assessment
First described in 1985, homeostatic model assessment (HOMA) has been used widely in clinical research to assess insulin sensitivity. Rather than using fasting insulin or a G/I ratio, the product of the fasting values of glucose (expressed as mg/dL) and insulin (expressed as μU/mL) is divided by a constant: I0 x G0 ÷ 405.
The constant 405 should be replaced by 22.5 if glucose is expressed in SI units (mmol/L). Unlike fasting insulin and the G/I ratio, the HOMA calculation compensates for fasting hyperglycemia. The HOMA value correlates well with clamp techniques and has been used frequently to assess changes in insulin sensitivity after treatment. HOMA also has been used to study insulin resistance among PCOS patients of differing ethnic origins.12,24-26
Quantitative insulin sensitivity check index
Like HOMA, quantitative insulin sensitivity check index (QUICKI) can be applied to normoglycemic and hyperglycemic patients. It is derived by calculating the inverse of the sum of logarithmically expressed values of fasting glucose and insulin: 1 ÷ [log(I0) + log(G0)].
Many investigators believe that QUICKI is superior to HOMA as a way of determining insulin sensitivity, although the two values correlate well. As the SI decreases, QUICKI values decrease.27
Oral glucose tolerance test
As OGTT does not require IV access, it is the current standard in practice for diagnosis of IGT and DM. It provides a better assessment of IGT and DM than fasting techniques because these patients may have normal fasting glucose values despite abnormal 2-hour fasting levels. The OGTT uses a 50-, 75-, or 100-g glucose load and measures glucose and insulin at various intervals over 1 to 3 hours. The WHO currently recommends a 75-g oral dose in all adults. A 50-g dose is used to screen for gestational diabetes over an hour, and the 100-g load over 3 hours if abnormal.28 See TABLE for normal and abnormal values. Insulin sensitivity has been assessed by calculating insulin area under the curve (AUC insulin), AUC glucose/AUC insulin, and by an insulin sensitivity index (ISI) that applies only the glucose and insulin values from 0 and 120 minutes into a complex mathematical formula.13,25,29-31
Criteria for diagnosis of diabetes
| Venous plasma glucose (mg/dL) | ||
|---|---|---|
| Fasting Level* | 2-hour postglucose load** | |
| Normal/Low risk | ≤99 | ≤139 |
| Prediabetes/Increased risk | 100–125 | 140–199 |
| Diabetes | ≥126 | ≥200 |
| *Fasting is defined as no caloric intake for at least 8 h **OGTT using a glucose load or 75 g as described by the World Health Organization SOURCE: American Diabetes Association. Standards of medical care in diabetes—2012. Diabetes Care. 2012;35 (suppl 1):s11–s63. doi:10.2337/dc12-s011. | ||
Test for glycosylated hemoglobin
Tests for blood levels of glycosylated hemoglobin, also known as hemoglobin A1c (HbA1c) are not currently used for an initial diagnosis because normal HbA1c levels do not necessarily rule out diabetes, but they are strongly associated with complications of diabetes. The test is not affected by food intake so it can be taken at any time. A normal HbA1c level is below 7%.
- “What is metabolic syndrome and what are the current diagnostic criteria?”
- “We know metformin is used to treat insulin resistance…but what about hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?”
We want to hear from you! Tell us what you think.
Part 1. Where we stand with diagnosis and treatment—and
where we're going
Polycystic ovary syndrome, or PCOS, is an enigmatic condition. It presents with varying levels of severity of those symptoms and conditions associated with it—clinical hyperandrogenism (hirsutism, acne, alopecia), obesity, and menstrual disturbance. Although its exact cause is unknown, at least half of all women with PCOS are overweight or obese. What does obesity and, more specifically, insulin resistance, contribute to the pathogenesis of PCOS, and why is it important to screen your patient with PCOS for insulin resistance?
In part 2 of this 4-part series, which will continue to be posted here on the OBG Management Web site, we address these questions. [Editor’s note: As they are published, future installments of this series will continue to be collected on a single Web page for ease of access.]
The roles of obesity and insulin resistance
![]()
Overweight: BMI ≥ 25 kg/m2
Obesity: BMI ≥ 30 kg/m2
Morbid obesity: BMI ≥ 40 kg/m2
PCOS is associated with truncal fat distribution, manifesting as an increased waist-to-hip ratio. According to the Centers for Disease Control and Prevention (CDC), more than one-third of the population was obese in 2009 and 2010.1 Approximately 50% to 65% of women with PCOS are overweight or obese, and most of them have the truncal fat distribution phenotype. 2
Obesity is associated with an increase in insulin resistance (IR) and hyperinsulinemia. IR can be characterized as impaired action of insulin in the uptake and metabolism of glucose. Impaired insulin action leads to elevated insulin levels. Insulin synergizes with abnormally high secretion of luteinizing hormone (perhaps induced by hyperinsulinemia) to promote excess androgen production by intraovarian theca cells and an arrest of follicular development resulting in chronic anovulation.
In addition, hyperinsulinemia causes a decrease in hepatic sex hormone binding globulin, resulting in free circulating androgens and, thus, hirsutism and acne issues. While this picture tends to be more pronounced in women who have PCOS and are obese, it is important to realize that a nonobese patient with PCOS also may have IR, which suggests that insulin plays a major role in the pathogenesis of this disease.3,4
![]()
Most of the evidence suggests that hyperinsulinemia causes hyperandrogenism and not the reverse. Weight loss and insulin sensitizers are associated with a reduction in androgens, particularly testosterone and androstenedione. Gonadotropin-releasing hormone–analogs, which reduce androgen secretion from the ovaries, do not result in a reduction in insulin.3,4
Screening for insulin resistance: The rationale
![]()
The documented prevalence of IR and type 2 diabetes mellitus (DM) in women with PCOS suggests that impaired glucose tolerance (IGT) is present in 31% to 35% of women with PCOS5,6—and DM, classified according to World Health Organization (WHO) criteria, is present in 7.5% to 10% of women with PCOS.
The prevalence of IR and DM are considerably lower in women without PCOS. According to the Third National Health and Nutrition Examination Survey, in US women of similar age, the prevalence of IR is 1.6%, and the prevalence of DM is 2.2%.7
2003 consensus: Screen for IGT in obese PCOS patients. In view of the high prevalence of IR and IGT, a 2003 PCOS consensus8 established that obese women with PCOS should be screened for insulin sensitivity and undergo screening for the metabolic syndrome, including glucose intolerance. For nonobese women, the consensus recommended screening only if additional risk factors are present.
Unfortunately, IGT also occurs independent of obesity. In lean women with PCOS, 5% may have IGT, while 2% are frankly diabetic. Moreover, the conversion from normal glucose tolerance to IGT in patients with PCOS can be as high as 16% per year,9 while the conversion rate from IGT to DM among women with PCOS has been reported to be as high as 2% per year.
2007 position statement: Screen for IGT in all PCOS patients. A position statement by the Androgen Excess–PCOS Society on glucose intolerance and PCOS recommends screening for IGT in all PCOS women, regardless of BMI, at least once every 2 years.10
Screening for insulin resistance: The methods
There are two ways to determine insulin sensitivity:
- direct infusion of IV glucose and/or insulin
- indirect assessment using surrogate markers (such as fasting glucose and insulin, or C-peptide, and oral glucose tolerance test [OGTT]).
Direct infusion of IV glucose or insulin reveals how insulin disposes of glucose from the blood stream; however, this method is expensive, time consuming, and potentially dangerous due to possible hypoglycemia. Indirect assessments are less complex to perform and correlate reasonably well with the results of the more invasive direct measures.
![]()
Direct infusion of glucose and insulin
The hyperinsulinemic euglycemic clamp is the gold standard, but drawbacks relegate it to medical research only. This method measures the amount of glucose necessary to compensate for an increased insulin level without causing hypoglycemia. Numerous blood samplings (every 5 to 10 minutes) are taken to monitor serum glucose so that a steady “fasting” level can be maintained. The degree of insulin resistance is measured by the amount of glucose that is taken up by tissues during the procedure.11-14
The “clamp” technique is the most scientifically sound method for measuring insulin sensitivity, and it’s the standard against which all other tests are usually compared. Because the clamp technique is expensive, time consuming (about 2 hours), and labor intensive, however, it is not practical and is rarely performed in clinical care. It is primarily used in medical research.
Frequently sampled IV glucose tolerance tests: “minimal model.” The frequently sampled IV glucose tolerance test estimates insulin sensitivity through a computer-based mathematical analysis of the glucose-insulin dynamics. Though this test still requires 11 to 34 blood samples over a 3-hour period, it is less labor intensive than the clamp technique. However, in contrast to the clamp, it does not distinguish between peripheral and hepatic glucose utilization.15
Direct infusion of insulin
Insulin sensitivity test. This test involves IV infusion of a set glucose load and a fixed-rate infusion of insulin over approximately 3 hours. The mean plasma glucose concentration over the last 30 minutes of the test reflects insulin sensitivity. Although lengthy, the insulin sensitivity test is less labor intensive and requires fewer blood samples than the clamp technique.16
Insulin tolerance test. This test is a simplified version of the insulin sensitivity test, as it measures the decline in serum glucose after an IV bolus of insulin is administered. Several insulin and glucose levels are sampled over the following 15 minutes. In contrast to the clamp and the minimal model, the insulin tolerance test primarily measures insulin-stimulated uptake of glucose into skeletal muscle, and insulin sensitivity values reflect the rate of decline of log transformed glucose values.17
Direct infusion of glucose
Continuous infusion of glucose with model assessment. This method utilizes a constant IV glucose infusion; samples for glucose and insulin are drawn at 50, 55, and 60 minutes. A mathematical model is then used to calculate insulin sensitivity. The results are correlated with clamp techniques; however, few laboratories have used this continuous-infusion method for insulin sensitivity testing in women with PCOS.18
Unfortunately, all of these methods require IV access and multiple venipunctures, making them relatively impractical for office assessment. To overcome these obstacles, alternative tests have been developed including fasting methods and the OGTT, the latter of which does not require IV access and does correlate reasonably well with dynamic clamp techniques.
![]()
Fasting methods
Fasting insulin. The measurement of fasting serum insulin is simple and inexpensive. Generally, a fasting level of 30 μU/mL indicates greater insulin resistance in a diabetic individual than in a normoglycemic patient. However, fasting insulin levels may be in the “normal” range in up to 40% of PCOS patients who have impaired glucose tolerance diagnosed by the OGTT. It has been suggested by some investigators that a fasting insulin greater than 20 μU/mL in white women and greater than 23 μU/mL in Mexican-American women probably indicates insulin resistance in women with PCOS. Some have also advocated averaging two or three readings to account for day-to-day variability.19-21
Fasting plasma glucose. This is a simple blood test taken after 8 hours of fasting. Fasting plasma glucose (FPG) levels are considered normal up to 100 mg/dL (or 5.5 mmol/L). Levels between 100 and 125 mg/dL (5.5 to 7.0 mmol/L) are considered impaired fasting glucose or prediabetes. These levels are considered to be risk factors for DM and its complications. DM is diagnosed when FPG levels are 126 mg/dL (7.0 mmol/L) or higher. A “normal” result on the FPG test is not always reliable. Repeat testing with the OGTT is recommended if risk factors are suggestive for the presence of DM or a prediabetic condition.
Glucose/insulin ratio
The glucose/insulin (G/I) ratio has become very popular since its first description in 1998 as an accurate index of insulin sensitivity in women with PCOS. The ratio of glucose to insulin is easy to calculate, with lower values depicting higher degrees of insulin resistance. A G/I ratio of less than 4.5 has been shown to be sensitive (95%) and specific (84%) for insulin resistance in women with PCOS, compared with a control group. The normal range for G/I ratios may vary in different ethnic groups and have not been fully validated in nonobese patients.22-25
Homeostatic model assessment
First described in 1985, homeostatic model assessment (HOMA) has been used widely in clinical research to assess insulin sensitivity. Rather than using fasting insulin or a G/I ratio, the product of the fasting values of glucose (expressed as mg/dL) and insulin (expressed as μU/mL) is divided by a constant: I0 x G0 ÷ 405.
The constant 405 should be replaced by 22.5 if glucose is expressed in SI units (mmol/L). Unlike fasting insulin and the G/I ratio, the HOMA calculation compensates for fasting hyperglycemia. The HOMA value correlates well with clamp techniques and has been used frequently to assess changes in insulin sensitivity after treatment. HOMA also has been used to study insulin resistance among PCOS patients of differing ethnic origins.12,24-26
Quantitative insulin sensitivity check index
Like HOMA, quantitative insulin sensitivity check index (QUICKI) can be applied to normoglycemic and hyperglycemic patients. It is derived by calculating the inverse of the sum of logarithmically expressed values of fasting glucose and insulin: 1 ÷ [log(I0) + log(G0)].
Many investigators believe that QUICKI is superior to HOMA as a way of determining insulin sensitivity, although the two values correlate well. As the SI decreases, QUICKI values decrease.27
Oral glucose tolerance test
As OGTT does not require IV access, it is the current standard in practice for diagnosis of IGT and DM. It provides a better assessment of IGT and DM than fasting techniques because these patients may have normal fasting glucose values despite abnormal 2-hour fasting levels. The OGTT uses a 50-, 75-, or 100-g glucose load and measures glucose and insulin at various intervals over 1 to 3 hours. The WHO currently recommends a 75-g oral dose in all adults. A 50-g dose is used to screen for gestational diabetes over an hour, and the 100-g load over 3 hours if abnormal.28 See TABLE for normal and abnormal values. Insulin sensitivity has been assessed by calculating insulin area under the curve (AUC insulin), AUC glucose/AUC insulin, and by an insulin sensitivity index (ISI) that applies only the glucose and insulin values from 0 and 120 minutes into a complex mathematical formula.13,25,29-31
Criteria for diagnosis of diabetes
| Venous plasma glucose (mg/dL) | ||
|---|---|---|
| Fasting Level* | 2-hour postglucose load** | |
| Normal/Low risk | ≤99 | ≤139 |
| Prediabetes/Increased risk | 100–125 | 140–199 |
| Diabetes | ≥126 | ≥200 |
| *Fasting is defined as no caloric intake for at least 8 h **OGTT using a glucose load or 75 g as described by the World Health Organization SOURCE: American Diabetes Association. Standards of medical care in diabetes—2012. Diabetes Care. 2012;35 (suppl 1):s11–s63. doi:10.2337/dc12-s011. | ||
Test for glycosylated hemoglobin
Tests for blood levels of glycosylated hemoglobin, also known as hemoglobin A1c (HbA1c) are not currently used for an initial diagnosis because normal HbA1c levels do not necessarily rule out diabetes, but they are strongly associated with complications of diabetes. The test is not affected by food intake so it can be taken at any time. A normal HbA1c level is below 7%.
- “What is metabolic syndrome and what are the current diagnostic criteria?”
- “We know metformin is used to treat insulin resistance…but what about hyperandrogenism, anovulation, infertility, weight loss, and early pregnancy loss?”
We want to hear from you! Tell us what you think.
HCV Infection
The hepatitis C virus (HCV) is estimated to affect 180 million people worldwide, and the CDC estimates that approximately 3.2 million persons in the United States are chronically infected with HCV.1,2 In recent years, reported HCV-related deaths have outnumbered those attributed to HIV infection.3 Clinicians in almost any practice area are likely to encounter patients affected by HCV.
Infection with HCV is a major risk factor for cirrhosis, a disease associated with significant morbidity and mortality; HCV-associated cirrhosis is considered the leading cause of liver transplantation.4
Screening for HCV is important in patients with known risk factors for the disease1 (see Table 11,2,5). Of note, however, the CDC is in the process of expanding its recommendations to one-time screening for all Americans born between 1945 and 1965—an age-group that accounts for more than 75% of cases of HCV infection among US adults.6 (Clinicians interested in viewing the draft document for public comment can refer to www.regulations.gov, docket #CDC-2-12-0005.)
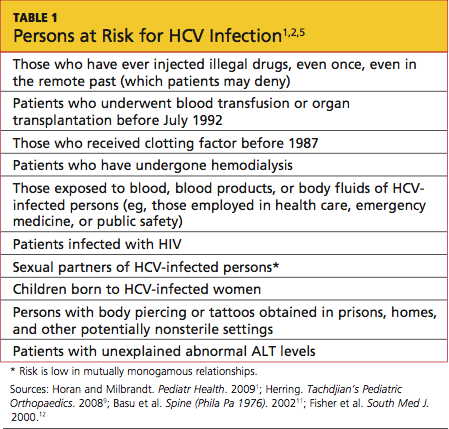
PATIENT PRESENTATION/ PATIENT HISTORY
Most patients with hepatitis C present without signs or symptoms of their illness. If symptoms are present, they may include fatigue, pruritus, abdominal pain/ discomfort, arthralgias, or anorexia; results on routine liver function tests may be abnormal.1,7-9 Liver function may appear normal in patients with HCV, although 30% of patients with a normal alanine aminotransferase (ALT) level may have significant fibrosis.10 Lichen planus is commonly associated with HCV infection,9-11 and patients with this condition should be screened for HCV.
HCV infection most commonly presents between the fourth and sixth decades of life. Many patients have had the disease for as long as 20 years by the time they present for treatment—often after abnormal laboratory findings are discovered7 (but see "Can Some Patients Defer Treatment?"7,10,12).
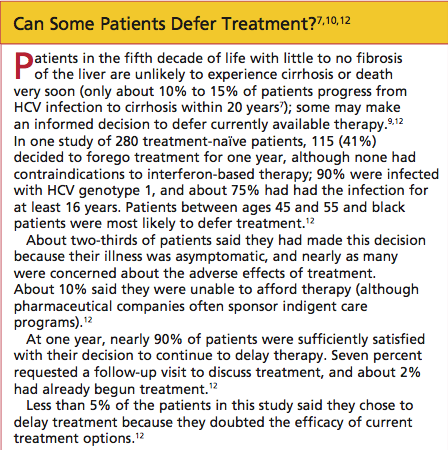
Patients with acute HCV infection usually do not appear jaundiced or exhibit other signs of acute hepatitis. Symptomatic illness occurs in only 20% to 40% of patients with acute hepatitis C.7 Patients who present with acute illness (15% to 25% of patients with HCV) typically have an improved prognosis and are less likely to convert to chronicity if they survive the initial symptoms (ie, malaise, weakness, anorexia, jaundice).2,7 In many such patients, the body appears to mount a full immune response, and patients are often virus-free within weeks.
For 75% to 85% of patients, however, it is believed that the immune system fails to overcome the virus, and chronic infection, with progressive damage to the liver tissue, ensues.7 In chronic HCV infection, the rate of progression varies, depending on the HCV genotype, the infected host's genetic factors and lifestyle (including level of alcohol consumption), the extent of liver injury, and possible coinfection (as with HIV or hepatitis B virus [HBV]).1,7
Cirrhosis and Hepatocellular Carcinoma
Complications of cirrhosis include portal hypertension, ascites, hepatic encephalopathy, esophageal varices, and hepatocellular carcinoma (HCC).13 In patients with HCV-related cirrhosis, HCC develops at a rate of 1% to 4% per year, with a twofold to fourfold increased risk among black patients and Asian patients, respectively, compared with whites.7 The risk for HCC appears to be reduced in patients who undergo treatment leading to a sustained virologic response (ie, a viral load that is no longer detectable); and the risk is increased in patients with diabetes mellitus and those with HCV genotypes 1b and 3.14-16
HCC is difficult to treat unless detected in its early stages. It often results in death.13
PHYSICAL EXAMINATION
An appropriate physical exam is critical in detecting sequelae of chronic liver disease, which may reflect complications of long-term HCV infection. The patient should be evaluated for the presence of spider angiomas, palmar erythema, scleral icterus, ascites, caput medusae, and evidence of umbilical hernias—all possible signs of advanced liver disease.8,9
The initial physical exam is also an appropriate time to screen and treat patients for hypertension and diabetes, and to identify disorders that may make them poor candidates for HCV treatment. These conditions include coronary heart disease, untreated cancers or thyroid disease, kidney or autoimmune diseases, and psychiatric illness.1,17
Evaluation of the skin for "track marks," tattoos or body piercings that may have been applied in prisons, homes, or other nonsterile settings, or nonhealing lesions that may indicate immune compromise or diabetes is important.5,8 Visual acuity testing and fundoscopic exams are critical to establish a baseline, because treatment with pegylated interferon has the potential to cause visual changes and retinopathy.18
Laboratory Work-up
Initial testing for HCV includes an HCV antibody test. This serum test is commonly performed as part of a hepatitis panel—testing for hepatitis A virus (HAV), HBV, and HCV. Testing for hepatitis D and E is not routinely recommended unless the patient routinely travels to the Mediterranean Basin, the Middle East, Central Asia, or West Africa (where hepatitis D is most prevalent19) or the patient is pregnant (because during the third trimester, hepatitis E infection carries a mortality rate of 20% and can be transmitted to the fetus20).
If immunity to HAV and HBV are not shown on laboratory findings, it is critical to vaccinate the HCV-positive patient against these diseases. Coinfection with HAV and HCV can progress to a fulminant form of hepatitis and poor hepatic function; coinfection with HBV and HCV is associated with severe liver disease and an increased risk for HCC.21,22
The patient with positive results on the HCV antibody screen should be tested next with a quantitative HCV RNA assay to confirm the presence of active infection (ie, viral load).1 Detection of virus is considered indicative of active disease.
It is possible for a patient with positive HCV antibody test results to have no circulating virus detected on HCV RNA testing. Perhaps 15% to 25% of patients are able to clear HCV infection spontaneously within weeks to months after infection.7
Testing Considerations Before Treatment
Several assays are available to identify the patient's HCV genotype. It is essential to obtain this information before agents, dosing, and duration are determined, as the regimen will be tailored to the patient's HCV genotype.1 There are six major known HCV genotypes (numbered 1 through 6) and at least 50 minor subtypes (eg, 1a, 2b, 3a).1,23
Also to be considered before initiating HCV treatment is screening for autoimmune hepatitis.17 Appropriate tests include the anti-actin antibody, anti-smooth muscle antibody, antinuclear antibody, and anti-liver kidney microsomal antibody tests.24,25 Additionally, ceruloplasmin testing should be ordered along with the iron studies and ferritin levels obtained at the patient's first visit, to screen for Wilson's disease, a disorder of copper metabolism, and hemochromatosis, a disorder of iron metabolism.
The risks associated with HAV or HBV coinfection have been described; patients with HCV and HAV, HBV, or HIV are at greater risk for disease progression to cirrhosis and/or HCC than are mono-infected patients.1,21,22,26 HIV testing is routinely recommended for patients with HCV, with repeat testing during treatment if the patient maintains any risk factors for HIV exposure. Patients with HCV who are found to be coinfected with HIV must be treated urgently, but therapeutic components must be selected with considerable care: Serious interactions are possible among the effective agents, and antiretroviral drugs are associated with hepatotoxicity.1,27
Before HCV treatment begins, it is essential to obtain baseline values: liver function testing (aspartate aminotransferase, ALT, alkaline phosphatase, bilirubin), coagulation testing (prothrombin time and partial thromboplastin time), and thyroid testing (thyroid-stimulating hormone, triiodothyronine, thyroxine),1 as changes may occur as a result of anti-HCV therapy. It is also important to establish a baseline complete blood count (CBC) and electrolyte levels in order to identify, and later monitor, the presence of anemia, thrombocytopenia, and renal or other abnormalities.
Finally, it is important to screen the patient early for HCC by testing for serum alphafetoprotein (AFP, ie, tumor marker).28 Serum AFP must then be monitored at six-month intervals (with a recommended threshold of 400 ng/mL, but even readings as modest as 6 to 20 ng/mL) for elevations that may indicate HCC.29,30
Liver Studies
In addition to the recommended AFP monitoring, the patient should undergo an imaging study of the liver twice yearly. Ultrasound is the most cost-effective screening tool for most patients (with high specificity but varying sensitivity); when combined with a serum AFP reading of 10 ng/mL or greater, ultrasound has a sensitivity of 100% for detection of HCC.29 However, if lesions are found, or if a patient has known cirrhosis, CT or MRI is more accurate in detecting small lesions of the liver (specificity, 100%).29
Liver biopsy is recommended for certain patients to stage liver fibrosis; biopsy may not be necessary, for example, in patients with genotypes 2 and 3, as 80% of these patients react to standard therapy with sustained virologic response.1 Detection of advanced fibrosis or cirrhosis increases the urgency for treatment to avert associated complications.31
Thanks to radiologic guidance, the risk for liver biopsy-related complications has been reduced; less than 1% of patients, according to 2008 study results, required hospitalization because of postprocedural pain or bleeding32; these are risks for which patients should be prepared,1 in addition to possible perforation of the bowel or lung, bile leak, or hematoma formation.33 Less than 10% of patients require analgesia two hours after the procedure,34 although prophylactic analgesia (as with sublingual tramadol and oral lorazepam) has been found helpful in reducing pain and anxiety.35
TREATMENT/MANAGEMENT
According to information from the CDC and practice guidelines from the American Association for the Study of Liver Diseases (AASLD),1,2 early diagnosis of HCV and treatment with currently available interventions can lead to cures in 75% of cases; otherwise, serious, life-threatening complications can be expected. In patients treated for HCV infection, cure (or sustained virologic response) is defined by an undetectable viral load, 24 weeks after completion of therapy.1 Patients with these test results are no longer able to transmit the virus to others.
For the past decade, pegylated interferon (or peginterferon) combined with ribavirin has been considered the standard of care for HCV; treatment response rates, depending on race and genotype, can range from 35% to 80%.36,37 Two forms of peginterferon, alfa-2a and alfa-2b, are FDA approved for treatment of chronic hepatitis C; both forms are administered subcutaneously in combination with oral ribavirin.1,38
The choice between peginterferon alfa-2a and alfa-2b and the recommended duration of treatment are dependent on the patient's HCV genotype (see Table 21,39-45) and prior exposure to treatment. These complex regimens are best managed by specialists in gastroenterology, hepatology, or infectious disease—clinicians who are familiar with the agents' associated adverse effects, the elements of attentive monitoring, and protocols for dosing adjustments.46

As noted in the AASLD guidelines,1 alcohol consumption constitutes a risk for worsening fibrosis and possibly for HCC. Additionally, drinking in excess may facilitate replication of HCV RNA, interfering with therapy.
Thus, patients should be urged to discontinue alcohol use during treatment for HCV—or at least restrict it to an occasional drink.
New Agents to Improve Cure Rates
HCV genotype 1 accounts for 70% to 75% of cases in the US, but with current standard treatment, a sustained virologic response is achieved in only 45% to 50% of these patients37 (including 30% of black patients and 50% of whites).1,36,38 However, adding one of two new protease inhibitors to the current peginterferon/ribavirin regimen has the potential to increase sustained virologic response rates to as high as 90% to 95% in early virologic responders with genotype 1 infection, both treatment-naïve and previously treated; and in some patients, to shorten treatment to 24 weeks.41,42,44,45 Both boceprevir and telaprevir were approved by the FDA in May 2011.
Both agents are given for 12 weeks during standard peginterferon/ribavirin therapy. Depending on the patient's viral response, the overall regimen may be shortened or extended. Neither telaprevir nor boceprevir is administered as monotherapy,47,48 nor are they ever administered together. As with any protease inhibitor, resuming treatment after the agent has been stopped incurs a risk for drug resistance.40
Both new agents are taken every 7 to 9 hours, with a meal or snack.47,48 The telaprevir dose should be taken with non-low-fat food.47
Drug interactions are common. Patients also being treated for HIV and those being treated for HCV genotype 1 infection with either of the two new protease inhibitors must very carefully communicate any prescription drug changes to their treating provider. Substances of greatest concern act via the cytochrome P450 3A (CYP3A) pathway. Examples include ritonavir, St. John's wort, statins, and daily-dosed sildenafil (as used to treat patients with pulmonary hypertension).
Package inserts accompanying all agents used should be reviewed for monitoring parameters and associated recommendations.
Monitoring for Treatment Effectiveness and Complications
Patients are closely monitored for treatment effectiveness by repeated measurements of HCV RNA (ie, weeks 4, 12, 24, then at four- to 12-week intervals; at end of treatment; and 24 weeks after treatment ends). A viral load not detectable at week 4 indicates a good chance for a cure.1 If at week 12 the viral load remains detectable, the patient with HCV genotype 1 is unlikely to respond to triple therapy; similarly, dual therapy is not likely to produce a cure in patients with HCV genotype 2 or 3. Without a 2-log drop in viral load by week 12, the patient has only an 8% chance of achieving a sustained virologic response.49-51 In these cases, treatment should be discontinued or modified.51
Regular visits and frequent blood testing make it possible to avoid potential disease- and treatment-related complications. At a minimum, it is recommended that a CBC, serum creatinine, and ALT level be measured at weeks 2, 4, 8, 12, 16, 20, and 24 of therapy.1 If significant abnormalities are detected (eg, anemia, thrombocytopenia, neutropenia), the clinician may decide to monitor the patient more closely. Measures of liver and kidney function, electrolytes, and coagulation times are part of the recommended monitoring parameters at regular intervals. In addition, interferon therapy is associated with thyroid dysfunction, so relevant monitoring is advised every 12 weeks.1
Anemia, neutropenia, thrombocytopenia, and other hematologic complications are known adverse effects of HCV therapy—particularly in cirrhotic patients.1,52 Ribavirin use (especially aggressive use, as for patients with recurrent infection or post-liver transplantation53) is associated with hemolytic anemia,54 as is protease inhibitor use.41,45 In cases of profound anemia, dosing reduction or treatment discontinuation may be necessary. Severe cases of hemolysis may require transfusion, but treatment with epoietin alfa has been found helpful in some patients.52,53 Conventional iron supplementation is not an effective treatment for hemolytic anemia resulting from ribavirin use.
For patients with low absolute neutrophil counts, treatment dosing reduction was once standard management.45,52 More recently, the use of epoietin alfa or a granulocyte colony-stimulating factor (eg, filgrastim) has been found helpful in raising neutrophil counts.52
Intervention for thrombocytopenia is not typically undertaken unless the total platelet count indicates a risk for spontaneous bleeding. In some patients, a new oral thrombopoietin mimetic called eltrombopag may reduce the need for dose reduction or early termination of therapy.52
Ribavirin is a major teratogen. This agent is listed in pregnancy category X, and its label carries a black box warning advising patients to avoid pregnancy while undergoing therapy and for six months following therapy. It has such a high potential for teratogenicity that male patients are even advised not to impregnate their female partners while on therapy or six months following therapy.54 Pregnant women should never handle ribavirin. It is important to educate medical professionals and office staff about this risk.
For management of other adverse reactions to one or more components of HCV treatment, see Table 3.1,41,43,45,55-57
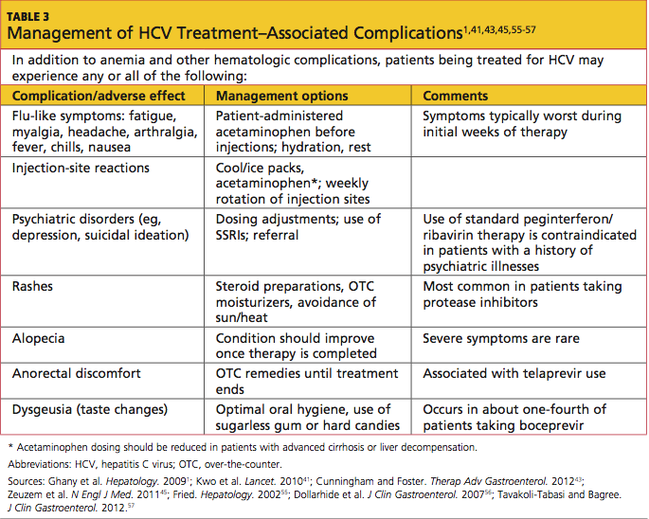
PATIENT EDUCATION/FOLLOW-UP DISCUSSION
Patient education is critical to successful treatment for HCV. Patients should be encouraged to avoid viral transmission to sexual partners by using condoms. They should also be advised to avoid sharing razors or toothbrushes with others in the home.1 Any patient with known HCV, HIV, or HBV should avoid undergoing body piercing or tattooing in any nonprofessional, nonsterile setting, where transmission may occur.5 Even successfully treated patients retain an HCV antibody and will test positive for HCV, making them ineligible to donate blood.
Six months after treatment, a viral load is drawn. If no active virus is found, patients will not need monitoring or follow-up labs unless they have known cirrhosis. Fibrosis is reversible in some patients following HCV treatment. However, if active disease is found at the six-month posttreatment follow-up visit, then the treatment was not effective, and the patient is considered a responder-relapser. Many such patients then consider enrolling in a drug trial or awaiting the potential approval of new treatments.
Herbal therapies, such as milk thistle and licorice root, have been widely tried by patients with HCV infection. The literature is mixed regarding the effectiveness of these substances or their potential for reducing liver function testing abnormalities. To date, no herbal compound has been proven to eradicate the virus. Most hepatologists encourage patients who take interferon, ribavirin, and/or protease inhibitors to avoid herbal or OTC substances with any potential for drug interactions or other complications.
ON THE HORIZON
Promising developments suggest a brightening future for patients with HCV infection. Researchers throughout the world are currently investigating new combinations of agents, effective against a wider range of genotypes and subtypes, that can control HCV infection without the emergence of drug-resistant strains. The near future may see more protease inhibitors added to current regimens and other direct-acting antivirals possibly replacing old treatment components. As is true of HIV, a vaccine for HCV will be difficult to develop; but in the meantime, new drug combinations will be created with a goal of sustained virologic response rates nearing 100% and ever-shorter treatment regimens.37,58
CONCLUSION
Since signs or symptoms are often not seen in patients infected with hepatitis C, it is important for primary care providers to question patients regarding known risk factors. At-risk patients should be screened using antibody testing, followed by confirmation of any positive results by HCV RNA testing. The patient's HCV genotype must be identified next, as it plays a key role in the therapeutic decisions to be made.
Because HCV therapy is complex, it is best managed by specialists who are experienced in all the aspects of each patient's regimen and who remain abreast of new therapeutic developments. Nevertheless, primary care providers can serve their patients well by acting as knowledgeable, supportive members of the health care team, accompanying their patients through the challenges of treatment and follow-up.
1. Ghany MG, Strader DB, Thomas DL, Seeff LB; American Association for the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49(4):1335-1374.
2. CDC. Hepatitis C FAQs for health professionals (2008). www.cdc.gov/hepatitis/HCV/HCVfaq. htm#section1. Accessed August 20, 2012.
3. Ly KN, Xing J, Klevens M, et al. The increasing burden of mortality from viral hepatitis in the United States between 1999 and 2007. Ann Intern Med. 2012;156(4):271-278.
4. Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR). OPTN/SRTR 2010 Annual Data Report (2011). Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. www.srtr.org/ annual_reports/2010/pdf/00_intro_pgs_11.pdf. Accessed August 20, 2012.
5. Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012;54(8):1167-1178.
6. CDC. Hepatitis C: proposed expansion of testing recommendations, 2012. www.cdc.gov/nchh-stp/newsroom/docs/HCV-TestingFactSheetNoEm-bargo508.pdf. Accessed August 20, 2012.
7. Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med Sci. 2006;3(2):47-52.
8. Al-Ali J, Al-Mutari N, Ahmed el-SF. Hepatitis C virus and the skin. Hepatogastroenterology. 2011;58(107-108):880-886.
9. Raslan HM, Ezzat WM, Abd El Hamid MF, et al. Skin manifestations of chronic hepatitis C virus infection in Cairo, Egypt. East Mediterr Health J. 2009;15(3):692-700.
10. Niederau C, Hüppe D, Zehnter E, et al. Chronic hepatitis C: treat or wait? Medical decision making in clinical practice. World J Gastroenterol. 2012;18(12):1339-1347.
11. Mahboobi N, Agha-Hosseini F, Lankarani K. Hepatitis C virus and lichen planus: the real association. Hepat Mon. 2010;10(3):161-164.
12. Khokhar OS, Lewis JH. Reasons why patients infected with chronic hepatitis C virus choose to defer treatment: do they alter their decision with time? Dig Dis Sci. 2007;52(5):1168-1176.
13. Bruno S, Zuin M, Crosignani A, et al. Predicting mortality risk in patients with compensated HCV-induced cirrhosis: a long-term prospective study. Am J Gastroenterol. 2009;104(5):1147-1158.
14. Cheinquer N, Cheinquer H, Wolff FH, Coelho-Borges S. Effect of sustained virologic response on the incidence of hepatocellular carcinoma in patients with HCV cirrhosis. Braz J Infect Dis. 2010;14(5):457-461.
15. Veldt BJ, Chen W, Heathcote EJ, et al. Increased risk of hepatocellular carcinoma among patients with hepatitis C cirrhosis and diabetes mellitus. Hepatology. 2008;47(6):1856-1862.
16. Nkontchou G, Ziol M, Aout M, et al. HCV genotype 3 is associated with a higher hepatocellular carcinoma incidence in patients with ongoing viral C cirrhosis. J Viral Hepat. 2011;18(10):e516-e522.
17. Czaja AJ, Freese DK. Diagnosis and treatment of autoimmune hepatitis. Hepatology. 2002;36:479-497.
18. Vujosevic S, Tempesta D, Noventa F, et al. Pegylated interferon-associated retinopathy is frequent in hepatitis C virus patients with hypertension and justifies ophthalmologic screening. Hepatology. 2012;56(2):455-463.
19. World Health Organization. Global alert and response: hepatitis D (2012). www.who.int/csr/ disease/hepatitis/whocdscsrncs20011/en/index3. html. Accessed August 20, 2012.
20. World Health Organization. Hepatitis E: fact sheet No 280 (July 2012). www.who.int/media centre/factsheets/fs280/en. Accessed August 20, 2012.
21. Bertino G, Ardiri AM, Bruno MC, et al. HAV infection in patients with chronic hepatitis C [in Italian]. Clin Ter. 2007;158(3):223-225.
22. Liu J, Hou J. Hepatitis B virus (HBV) and hepatitis C virus (HCV) dual infection. Int J Med Sci. 2006;3(2):57-62.
23. Schijman A, Colina R, Mukomolov S, et al. Comparison of hepatitis C viral loads in patients with or without coinfection with different genotypes. Clin Diagn Lab Immunol. 2004;11(2):433-435.
24. McClure JE, Shearer WT. Radioimmunoassay for anti-actin antibody: application in viral and autoimmune diseases. Mol Cell Probes. 1988;2(4):305-319.
25. Peakman M, Lobo-Yeo A, Mieli-Vergani, et al. Characterization of anti-liver kidney microsomal antibody in childhood autoimmune chronic active hepatitis: evidence for IgG1 subclass restriction, polyclonality and non cross-reactivity with hepatocyte surface antigens. Clin Exp Immunol. 1987;69(3):543-549.
26. Loko MA, Salmon D, Carrieri P, et al; ANRS CO 13 HEPAVIH Study Group. The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): early findings, 2006-2010. BMC Infect Dis. 2010 Oct 22;10:303.
27. Duclos-Vallée JC, Féray C, Sebagh M, et al; THEVIC Study Group. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2008;47(2):407-417.
28. Sato Y, Nakata K, Kato Y, et al. Early recognition of hepatocellular carcinoma based on altered profiles of alpha-fetoprotein. N Engl J Med. 1993;328(25):1802-1806.
29. Gebo KA, Chander G, Jenckes MW, et al. Screening tests for hepatocellular carcinoma in patients with chronic hepatitis C: a systematic review. Hepatology. 2002;36(5 suppl 1):S84-S92.
30. Tateyama M, Yatsuhashi H, Taura N, et al. Alpha-fetoprotein above normal levels as a risk factor for the development of hepatocellular carcinoma in patients infected with hepatitis C virus. J Gastroenterol. 2011;46(1):92-100.
31. Bruno S, Shiffman ML, Roberts SK, et al. Efficacy and safety of peginterferon alfa-2a (40KD) plus ribavirin in hepatitis C patients with advanced fibrosis and cirrhosis. Hepatology. 2010;51(2):388-397.
32. Myers RP, Fong A, Shaheen AA. Utilization rates, complications and costs of percutaneous liver biopsy: a population-based study including 4275 biopsies. Liver Int. 2008;28(5):705-712.
33. van der Poorten D, Kwok A, Lam T, et al. Twenty-year audit of percutaneous liver biopsy in a major Australian teaching hospital. Intern Med J. 2006;36(11):692-699.
34. Howard R, Karageorge G, van Harselaar K, et al. Post-procedure surveillance in liver biopsy: how long is long enough? N Z Med J. 2008;121(1280):8-14.
35. Kramskay R, Tansky A, Eisenberg, et al. Prophylactic analgesia before percutaneous liver biopsy: a clinical comparative study. Eur J Gastroenterol Hepatol. 2011;23(9):782-786.
36. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347(13):975-982.
37. Lemon SM, McKeating JA, Pietschmann T, et al. Development of novel therapies for hepatitis C. Antiviral Res. 2010;86(1):79-92.
38. Shepherd J, Brodin H, Cave C, et al. Pegylated interferon alpha-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation. Health Technol Assess. 2004;8(39):iii-iv, 1-125.
39. Kamal SM, El Kamary SS, Shardell MD, et al. Pegylated interferon alpha-2b plus ribavirin in patients with genotype 4 chronic hepatitis C: the role of rapid and early virologic response. Hepatology. 2007;46:1732-1740.
40. Hofmann WP, Sarrazin C, Zeuzem S. Current standards in the treatment of chronic hepatitis C. Dtsch Arztebl Int. 2012;109(19):352-358.
41. Kwo PY, Lawitz EJ, McCone J, et al; SPRINT-1 Investigators. Efficacy of boceprevir, an NS3 protease inhibitor, in combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): an open-label, randomised, multicentre phase 2 trial. Lancet. 2010;376(9742):705-716.
42. Klibanov OM, Vickery SB, Olin JL, et al. Boceprevir: a novel NS3/4 protease inhibitor for the treatment of hepatitis C. Pharmacotherapy. 2012;32(2):173-190.
43. Cunningham M, Foster GR. Efficacy and safety of telaprevir in patients with genotype 1 hepatitis C infection. Therap Adv Gastroenterol. 2012;5(2):139-151.
44. Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364(25):2405-2416.
45. Zeuzem S, Andreone P, Pol S, et al; REALIZE Study Team. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364(25):2417-2428.
46. Sagir A, Heintges T, Akyazi Z, et al. Therapy outcome in patients with chronic hepatitis C: role of therapy supervision by expert hepatologists. J Viral Hepat. 2007;14(9):633-638.
47. Highlights of prescribing information: INCIVEKTM (telaprevir) film coated tablets for oral use (2011). http://pi.vrtx.com/files/uspi_telaprevir. pdf. Accessed August 20, 2012.
48. Highlights of prescribing information: VICTRELISTM (boceprevir) capsules (2011). www .accessdata.fda.gov/drugsatfda_docs / label/2011/202258lbl.pdf. Accessed August 20, 2012.
49. Alavian SM, Tabatabaei SV, Behnava B, Mahboobi N. Optimal duration of treatment for HCV genotype 1 infection in slow responders: a meta-analysis. Hepat Mon. 2011;11(8):612-619.
50. Fried MW, Hadziyannis SJ, Shiffman ML, et al. Rapid virological response is the most important predictor of sustained virological response across genotypes in patients with chronic hepatitis C virus infection. J Hepatol. 2011;55(1):69-75.
51. Reau N, Satoskar R, Te H, et al. Evaluation of early null response to pegylated interferon and ribavirin as a predictor of therapeutic nonresponse in patients undergoing treatment for chronic hepatitis C. Am J Gastroenterol. 2011;106(3):452-458.
52. Mac Nicholas R, Norris S. Optimizing SVR and management of the haematological side effects of peginterferon/ribavirin antiviral therapy for HCV: the role of epoietin, G-CSF and novel agents. Aliment Pharmacol Ther. 2010;31(9):929-937.
53. Singhal A, Jain AB, Burke M, Black M. Aggressive use of ribavirin and prolonged course of peginterferon to improve the rate of viral response in liver transplant patients with recurrent hepatitis C viral infection. Exp Clin Transplant. 2010;8(3):214-219.
54. Highlights of prescribing information: COPEGUSTM (ribavirin) tablets (2002). http://www.gene .com/gene/products/information/pegasys/pdf/ copegus_pi.pdf. Accessed August 20, 2012.
55. Fried MW. Side effects of therapy of hepatitis C and their management. Hepatology. 2002;36(5 suppl 1):S237-S244.
56. Dollarhide AW, Loh C, Leckband SG, et al. Psychiatric comorbidity does not predict interferon treatment completion rates in hepatitis C seropositive veterans. J Clin Gastroenterol. 2007;41(3):322-328.
57. Tavakoli-Tabasi S, Bagree A. A longitudinal cohort study of mucocutaneous drug eruptions during interferon and ribavirin treatment of hepatitis C. J Clin Gastroenterol. 2012;46(2):162-167.
58. Fox AN, Jacobson IM. Recent successes and noteworthy future prospects in the treatment of chronic hepatitis C. Clin Infect Dis. 2012;55 suppl 1:S16-S24.
The hepatitis C virus (HCV) is estimated to affect 180 million people worldwide, and the CDC estimates that approximately 3.2 million persons in the United States are chronically infected with HCV.1,2 In recent years, reported HCV-related deaths have outnumbered those attributed to HIV infection.3 Clinicians in almost any practice area are likely to encounter patients affected by HCV.
Infection with HCV is a major risk factor for cirrhosis, a disease associated with significant morbidity and mortality; HCV-associated cirrhosis is considered the leading cause of liver transplantation.4
Screening for HCV is important in patients with known risk factors for the disease1 (see Table 11,2,5). Of note, however, the CDC is in the process of expanding its recommendations to one-time screening for all Americans born between 1945 and 1965—an age-group that accounts for more than 75% of cases of HCV infection among US adults.6 (Clinicians interested in viewing the draft document for public comment can refer to www.regulations.gov, docket #CDC-2-12-0005.)
PATIENT PRESENTATION/ PATIENT HISTORY
Most patients with hepatitis C present without signs or symptoms of their illness. If symptoms are present, they may include fatigue, pruritus, abdominal pain/ discomfort, arthralgias, or anorexia; results on routine liver function tests may be abnormal.1,7-9 Liver function may appear normal in patients with HCV, although 30% of patients with a normal alanine aminotransferase (ALT) level may have significant fibrosis.10 Lichen planus is commonly associated with HCV infection,9-11 and patients with this condition should be screened for HCV.
HCV infection most commonly presents between the fourth and sixth decades of life. Many patients have had the disease for as long as 20 years by the time they present for treatment—often after abnormal laboratory findings are discovered7 (but see "Can Some Patients Defer Treatment?"7,10,12).
Patients with acute HCV infection usually do not appear jaundiced or exhibit other signs of acute hepatitis. Symptomatic illness occurs in only 20% to 40% of patients with acute hepatitis C.7 Patients who present with acute illness (15% to 25% of patients with HCV) typically have an improved prognosis and are less likely to convert to chronicity if they survive the initial symptoms (ie, malaise, weakness, anorexia, jaundice).2,7 In many such patients, the body appears to mount a full immune response, and patients are often virus-free within weeks.
For 75% to 85% of patients, however, it is believed that the immune system fails to overcome the virus, and chronic infection, with progressive damage to the liver tissue, ensues.7 In chronic HCV infection, the rate of progression varies, depending on the HCV genotype, the infected host's genetic factors and lifestyle (including level of alcohol consumption), the extent of liver injury, and possible coinfection (as with HIV or hepatitis B virus [HBV]).1,7
Cirrhosis and Hepatocellular Carcinoma
Complications of cirrhosis include portal hypertension, ascites, hepatic encephalopathy, esophageal varices, and hepatocellular carcinoma (HCC).13 In patients with HCV-related cirrhosis, HCC develops at a rate of 1% to 4% per year, with a twofold to fourfold increased risk among black patients and Asian patients, respectively, compared with whites.7 The risk for HCC appears to be reduced in patients who undergo treatment leading to a sustained virologic response (ie, a viral load that is no longer detectable); and the risk is increased in patients with diabetes mellitus and those with HCV genotypes 1b and 3.14-16
HCC is difficult to treat unless detected in its early stages. It often results in death.13
PHYSICAL EXAMINATION
An appropriate physical exam is critical in detecting sequelae of chronic liver disease, which may reflect complications of long-term HCV infection. The patient should be evaluated for the presence of spider angiomas, palmar erythema, scleral icterus, ascites, caput medusae, and evidence of umbilical hernias—all possible signs of advanced liver disease.8,9
The initial physical exam is also an appropriate time to screen and treat patients for hypertension and diabetes, and to identify disorders that may make them poor candidates for HCV treatment. These conditions include coronary heart disease, untreated cancers or thyroid disease, kidney or autoimmune diseases, and psychiatric illness.1,17
Evaluation of the skin for "track marks," tattoos or body piercings that may have been applied in prisons, homes, or other nonsterile settings, or nonhealing lesions that may indicate immune compromise or diabetes is important.5,8 Visual acuity testing and fundoscopic exams are critical to establish a baseline, because treatment with pegylated interferon has the potential to cause visual changes and retinopathy.18
Laboratory Work-up
Initial testing for HCV includes an HCV antibody test. This serum test is commonly performed as part of a hepatitis panel—testing for hepatitis A virus (HAV), HBV, and HCV. Testing for hepatitis D and E is not routinely recommended unless the patient routinely travels to the Mediterranean Basin, the Middle East, Central Asia, or West Africa (where hepatitis D is most prevalent19) or the patient is pregnant (because during the third trimester, hepatitis E infection carries a mortality rate of 20% and can be transmitted to the fetus20).
If immunity to HAV and HBV are not shown on laboratory findings, it is critical to vaccinate the HCV-positive patient against these diseases. Coinfection with HAV and HCV can progress to a fulminant form of hepatitis and poor hepatic function; coinfection with HBV and HCV is associated with severe liver disease and an increased risk for HCC.21,22
The patient with positive results on the HCV antibody screen should be tested next with a quantitative HCV RNA assay to confirm the presence of active infection (ie, viral load).1 Detection of virus is considered indicative of active disease.
It is possible for a patient with positive HCV antibody test results to have no circulating virus detected on HCV RNA testing. Perhaps 15% to 25% of patients are able to clear HCV infection spontaneously within weeks to months after infection.7
Testing Considerations Before Treatment
Several assays are available to identify the patient's HCV genotype. It is essential to obtain this information before agents, dosing, and duration are determined, as the regimen will be tailored to the patient's HCV genotype.1 There are six major known HCV genotypes (numbered 1 through 6) and at least 50 minor subtypes (eg, 1a, 2b, 3a).1,23
Also to be considered before initiating HCV treatment is screening for autoimmune hepatitis.17 Appropriate tests include the anti-actin antibody, anti-smooth muscle antibody, antinuclear antibody, and anti-liver kidney microsomal antibody tests.24,25 Additionally, ceruloplasmin testing should be ordered along with the iron studies and ferritin levels obtained at the patient's first visit, to screen for Wilson's disease, a disorder of copper metabolism, and hemochromatosis, a disorder of iron metabolism.
The risks associated with HAV or HBV coinfection have been described; patients with HCV and HAV, HBV, or HIV are at greater risk for disease progression to cirrhosis and/or HCC than are mono-infected patients.1,21,22,26 HIV testing is routinely recommended for patients with HCV, with repeat testing during treatment if the patient maintains any risk factors for HIV exposure. Patients with HCV who are found to be coinfected with HIV must be treated urgently, but therapeutic components must be selected with considerable care: Serious interactions are possible among the effective agents, and antiretroviral drugs are associated with hepatotoxicity.1,27
Before HCV treatment begins, it is essential to obtain baseline values: liver function testing (aspartate aminotransferase, ALT, alkaline phosphatase, bilirubin), coagulation testing (prothrombin time and partial thromboplastin time), and thyroid testing (thyroid-stimulating hormone, triiodothyronine, thyroxine),1 as changes may occur as a result of anti-HCV therapy. It is also important to establish a baseline complete blood count (CBC) and electrolyte levels in order to identify, and later monitor, the presence of anemia, thrombocytopenia, and renal or other abnormalities.
Finally, it is important to screen the patient early for HCC by testing for serum alphafetoprotein (AFP, ie, tumor marker).28 Serum AFP must then be monitored at six-month intervals (with a recommended threshold of 400 ng/mL, but even readings as modest as 6 to 20 ng/mL) for elevations that may indicate HCC.29,30
Liver Studies
In addition to the recommended AFP monitoring, the patient should undergo an imaging study of the liver twice yearly. Ultrasound is the most cost-effective screening tool for most patients (with high specificity but varying sensitivity); when combined with a serum AFP reading of 10 ng/mL or greater, ultrasound has a sensitivity of 100% for detection of HCC.29 However, if lesions are found, or if a patient has known cirrhosis, CT or MRI is more accurate in detecting small lesions of the liver (specificity, 100%).29
Liver biopsy is recommended for certain patients to stage liver fibrosis; biopsy may not be necessary, for example, in patients with genotypes 2 and 3, as 80% of these patients react to standard therapy with sustained virologic response.1 Detection of advanced fibrosis or cirrhosis increases the urgency for treatment to avert associated complications.31
Thanks to radiologic guidance, the risk for liver biopsy-related complications has been reduced; less than 1% of patients, according to 2008 study results, required hospitalization because of postprocedural pain or bleeding32; these are risks for which patients should be prepared,1 in addition to possible perforation of the bowel or lung, bile leak, or hematoma formation.33 Less than 10% of patients require analgesia two hours after the procedure,34 although prophylactic analgesia (as with sublingual tramadol and oral lorazepam) has been found helpful in reducing pain and anxiety.35
TREATMENT/MANAGEMENT
According to information from the CDC and practice guidelines from the American Association for the Study of Liver Diseases (AASLD),1,2 early diagnosis of HCV and treatment with currently available interventions can lead to cures in 75% of cases; otherwise, serious, life-threatening complications can be expected. In patients treated for HCV infection, cure (or sustained virologic response) is defined by an undetectable viral load, 24 weeks after completion of therapy.1 Patients with these test results are no longer able to transmit the virus to others.
For the past decade, pegylated interferon (or peginterferon) combined with ribavirin has been considered the standard of care for HCV; treatment response rates, depending on race and genotype, can range from 35% to 80%.36,37 Two forms of peginterferon, alfa-2a and alfa-2b, are FDA approved for treatment of chronic hepatitis C; both forms are administered subcutaneously in combination with oral ribavirin.1,38
The choice between peginterferon alfa-2a and alfa-2b and the recommended duration of treatment are dependent on the patient's HCV genotype (see Table 21,39-45) and prior exposure to treatment. These complex regimens are best managed by specialists in gastroenterology, hepatology, or infectious disease—clinicians who are familiar with the agents' associated adverse effects, the elements of attentive monitoring, and protocols for dosing adjustments.46
As noted in the AASLD guidelines,1 alcohol consumption constitutes a risk for worsening fibrosis and possibly for HCC. Additionally, drinking in excess may facilitate replication of HCV RNA, interfering with therapy.
Thus, patients should be urged to discontinue alcohol use during treatment for HCV—or at least restrict it to an occasional drink.
New Agents to Improve Cure Rates
HCV genotype 1 accounts for 70% to 75% of cases in the US, but with current standard treatment, a sustained virologic response is achieved in only 45% to 50% of these patients37 (including 30% of black patients and 50% of whites).1,36,38 However, adding one of two new protease inhibitors to the current peginterferon/ribavirin regimen has the potential to increase sustained virologic response rates to as high as 90% to 95% in early virologic responders with genotype 1 infection, both treatment-naïve and previously treated; and in some patients, to shorten treatment to 24 weeks.41,42,44,45 Both boceprevir and telaprevir were approved by the FDA in May 2011.
Both agents are given for 12 weeks during standard peginterferon/ribavirin therapy. Depending on the patient's viral response, the overall regimen may be shortened or extended. Neither telaprevir nor boceprevir is administered as monotherapy,47,48 nor are they ever administered together. As with any protease inhibitor, resuming treatment after the agent has been stopped incurs a risk for drug resistance.40
Both new agents are taken every 7 to 9 hours, with a meal or snack.47,48 The telaprevir dose should be taken with non-low-fat food.47
Drug interactions are common. Patients also being treated for HIV and those being treated for HCV genotype 1 infection with either of the two new protease inhibitors must very carefully communicate any prescription drug changes to their treating provider. Substances of greatest concern act via the cytochrome P450 3A (CYP3A) pathway. Examples include ritonavir, St. John's wort, statins, and daily-dosed sildenafil (as used to treat patients with pulmonary hypertension).
Package inserts accompanying all agents used should be reviewed for monitoring parameters and associated recommendations.
Monitoring for Treatment Effectiveness and Complications
Patients are closely monitored for treatment effectiveness by repeated measurements of HCV RNA (ie, weeks 4, 12, 24, then at four- to 12-week intervals; at end of treatment; and 24 weeks after treatment ends). A viral load not detectable at week 4 indicates a good chance for a cure.1 If at week 12 the viral load remains detectable, the patient with HCV genotype 1 is unlikely to respond to triple therapy; similarly, dual therapy is not likely to produce a cure in patients with HCV genotype 2 or 3. Without a 2-log drop in viral load by week 12, the patient has only an 8% chance of achieving a sustained virologic response.49-51 In these cases, treatment should be discontinued or modified.51
Regular visits and frequent blood testing make it possible to avoid potential disease- and treatment-related complications. At a minimum, it is recommended that a CBC, serum creatinine, and ALT level be measured at weeks 2, 4, 8, 12, 16, 20, and 24 of therapy.1 If significant abnormalities are detected (eg, anemia, thrombocytopenia, neutropenia), the clinician may decide to monitor the patient more closely. Measures of liver and kidney function, electrolytes, and coagulation times are part of the recommended monitoring parameters at regular intervals. In addition, interferon therapy is associated with thyroid dysfunction, so relevant monitoring is advised every 12 weeks.1
Anemia, neutropenia, thrombocytopenia, and other hematologic complications are known adverse effects of HCV therapy—particularly in cirrhotic patients.1,52 Ribavirin use (especially aggressive use, as for patients with recurrent infection or post-liver transplantation53) is associated with hemolytic anemia,54 as is protease inhibitor use.41,45 In cases of profound anemia, dosing reduction or treatment discontinuation may be necessary. Severe cases of hemolysis may require transfusion, but treatment with epoietin alfa has been found helpful in some patients.52,53 Conventional iron supplementation is not an effective treatment for hemolytic anemia resulting from ribavirin use.
For patients with low absolute neutrophil counts, treatment dosing reduction was once standard management.45,52 More recently, the use of epoietin alfa or a granulocyte colony-stimulating factor (eg, filgrastim) has been found helpful in raising neutrophil counts.52
Intervention for thrombocytopenia is not typically undertaken unless the total platelet count indicates a risk for spontaneous bleeding. In some patients, a new oral thrombopoietin mimetic called eltrombopag may reduce the need for dose reduction or early termination of therapy.52
Ribavirin is a major teratogen. This agent is listed in pregnancy category X, and its label carries a black box warning advising patients to avoid pregnancy while undergoing therapy and for six months following therapy. It has such a high potential for teratogenicity that male patients are even advised not to impregnate their female partners while on therapy or six months following therapy.54 Pregnant women should never handle ribavirin. It is important to educate medical professionals and office staff about this risk.
For management of other adverse reactions to one or more components of HCV treatment, see Table 3.1,41,43,45,55-57
PATIENT EDUCATION/FOLLOW-UP DISCUSSION
Patient education is critical to successful treatment for HCV. Patients should be encouraged to avoid viral transmission to sexual partners by using condoms. They should also be advised to avoid sharing razors or toothbrushes with others in the home.1 Any patient with known HCV, HIV, or HBV should avoid undergoing body piercing or tattooing in any nonprofessional, nonsterile setting, where transmission may occur.5 Even successfully treated patients retain an HCV antibody and will test positive for HCV, making them ineligible to donate blood.
Six months after treatment, a viral load is drawn. If no active virus is found, patients will not need monitoring or follow-up labs unless they have known cirrhosis. Fibrosis is reversible in some patients following HCV treatment. However, if active disease is found at the six-month posttreatment follow-up visit, then the treatment was not effective, and the patient is considered a responder-relapser. Many such patients then consider enrolling in a drug trial or awaiting the potential approval of new treatments.
Herbal therapies, such as milk thistle and licorice root, have been widely tried by patients with HCV infection. The literature is mixed regarding the effectiveness of these substances or their potential for reducing liver function testing abnormalities. To date, no herbal compound has been proven to eradicate the virus. Most hepatologists encourage patients who take interferon, ribavirin, and/or protease inhibitors to avoid herbal or OTC substances with any potential for drug interactions or other complications.
ON THE HORIZON
Promising developments suggest a brightening future for patients with HCV infection. Researchers throughout the world are currently investigating new combinations of agents, effective against a wider range of genotypes and subtypes, that can control HCV infection without the emergence of drug-resistant strains. The near future may see more protease inhibitors added to current regimens and other direct-acting antivirals possibly replacing old treatment components. As is true of HIV, a vaccine for HCV will be difficult to develop; but in the meantime, new drug combinations will be created with a goal of sustained virologic response rates nearing 100% and ever-shorter treatment regimens.37,58
CONCLUSION
Since signs or symptoms are often not seen in patients infected with hepatitis C, it is important for primary care providers to question patients regarding known risk factors. At-risk patients should be screened using antibody testing, followed by confirmation of any positive results by HCV RNA testing. The patient's HCV genotype must be identified next, as it plays a key role in the therapeutic decisions to be made.
Because HCV therapy is complex, it is best managed by specialists who are experienced in all the aspects of each patient's regimen and who remain abreast of new therapeutic developments. Nevertheless, primary care providers can serve their patients well by acting as knowledgeable, supportive members of the health care team, accompanying their patients through the challenges of treatment and follow-up.
The hepatitis C virus (HCV) is estimated to affect 180 million people worldwide, and the CDC estimates that approximately 3.2 million persons in the United States are chronically infected with HCV.1,2 In recent years, reported HCV-related deaths have outnumbered those attributed to HIV infection.3 Clinicians in almost any practice area are likely to encounter patients affected by HCV.
Infection with HCV is a major risk factor for cirrhosis, a disease associated with significant morbidity and mortality; HCV-associated cirrhosis is considered the leading cause of liver transplantation.4
Screening for HCV is important in patients with known risk factors for the disease1 (see Table 11,2,5). Of note, however, the CDC is in the process of expanding its recommendations to one-time screening for all Americans born between 1945 and 1965—an age-group that accounts for more than 75% of cases of HCV infection among US adults.6 (Clinicians interested in viewing the draft document for public comment can refer to www.regulations.gov, docket #CDC-2-12-0005.)
PATIENT PRESENTATION/ PATIENT HISTORY
Most patients with hepatitis C present without signs or symptoms of their illness. If symptoms are present, they may include fatigue, pruritus, abdominal pain/ discomfort, arthralgias, or anorexia; results on routine liver function tests may be abnormal.1,7-9 Liver function may appear normal in patients with HCV, although 30% of patients with a normal alanine aminotransferase (ALT) level may have significant fibrosis.10 Lichen planus is commonly associated with HCV infection,9-11 and patients with this condition should be screened for HCV.
HCV infection most commonly presents between the fourth and sixth decades of life. Many patients have had the disease for as long as 20 years by the time they present for treatment—often after abnormal laboratory findings are discovered7 (but see "Can Some Patients Defer Treatment?"7,10,12).
Patients with acute HCV infection usually do not appear jaundiced or exhibit other signs of acute hepatitis. Symptomatic illness occurs in only 20% to 40% of patients with acute hepatitis C.7 Patients who present with acute illness (15% to 25% of patients with HCV) typically have an improved prognosis and are less likely to convert to chronicity if they survive the initial symptoms (ie, malaise, weakness, anorexia, jaundice).2,7 In many such patients, the body appears to mount a full immune response, and patients are often virus-free within weeks.
For 75% to 85% of patients, however, it is believed that the immune system fails to overcome the virus, and chronic infection, with progressive damage to the liver tissue, ensues.7 In chronic HCV infection, the rate of progression varies, depending on the HCV genotype, the infected host's genetic factors and lifestyle (including level of alcohol consumption), the extent of liver injury, and possible coinfection (as with HIV or hepatitis B virus [HBV]).1,7
Cirrhosis and Hepatocellular Carcinoma
Complications of cirrhosis include portal hypertension, ascites, hepatic encephalopathy, esophageal varices, and hepatocellular carcinoma (HCC).13 In patients with HCV-related cirrhosis, HCC develops at a rate of 1% to 4% per year, with a twofold to fourfold increased risk among black patients and Asian patients, respectively, compared with whites.7 The risk for HCC appears to be reduced in patients who undergo treatment leading to a sustained virologic response (ie, a viral load that is no longer detectable); and the risk is increased in patients with diabetes mellitus and those with HCV genotypes 1b and 3.14-16
HCC is difficult to treat unless detected in its early stages. It often results in death.13
PHYSICAL EXAMINATION
An appropriate physical exam is critical in detecting sequelae of chronic liver disease, which may reflect complications of long-term HCV infection. The patient should be evaluated for the presence of spider angiomas, palmar erythema, scleral icterus, ascites, caput medusae, and evidence of umbilical hernias—all possible signs of advanced liver disease.8,9
The initial physical exam is also an appropriate time to screen and treat patients for hypertension and diabetes, and to identify disorders that may make them poor candidates for HCV treatment. These conditions include coronary heart disease, untreated cancers or thyroid disease, kidney or autoimmune diseases, and psychiatric illness.1,17
Evaluation of the skin for "track marks," tattoos or body piercings that may have been applied in prisons, homes, or other nonsterile settings, or nonhealing lesions that may indicate immune compromise or diabetes is important.5,8 Visual acuity testing and fundoscopic exams are critical to establish a baseline, because treatment with pegylated interferon has the potential to cause visual changes and retinopathy.18
Laboratory Work-up
Initial testing for HCV includes an HCV antibody test. This serum test is commonly performed as part of a hepatitis panel—testing for hepatitis A virus (HAV), HBV, and HCV. Testing for hepatitis D and E is not routinely recommended unless the patient routinely travels to the Mediterranean Basin, the Middle East, Central Asia, or West Africa (where hepatitis D is most prevalent19) or the patient is pregnant (because during the third trimester, hepatitis E infection carries a mortality rate of 20% and can be transmitted to the fetus20).
If immunity to HAV and HBV are not shown on laboratory findings, it is critical to vaccinate the HCV-positive patient against these diseases. Coinfection with HAV and HCV can progress to a fulminant form of hepatitis and poor hepatic function; coinfection with HBV and HCV is associated with severe liver disease and an increased risk for HCC.21,22
The patient with positive results on the HCV antibody screen should be tested next with a quantitative HCV RNA assay to confirm the presence of active infection (ie, viral load).1 Detection of virus is considered indicative of active disease.
It is possible for a patient with positive HCV antibody test results to have no circulating virus detected on HCV RNA testing. Perhaps 15% to 25% of patients are able to clear HCV infection spontaneously within weeks to months after infection.7
Testing Considerations Before Treatment
Several assays are available to identify the patient's HCV genotype. It is essential to obtain this information before agents, dosing, and duration are determined, as the regimen will be tailored to the patient's HCV genotype.1 There are six major known HCV genotypes (numbered 1 through 6) and at least 50 minor subtypes (eg, 1a, 2b, 3a).1,23
Also to be considered before initiating HCV treatment is screening for autoimmune hepatitis.17 Appropriate tests include the anti-actin antibody, anti-smooth muscle antibody, antinuclear antibody, and anti-liver kidney microsomal antibody tests.24,25 Additionally, ceruloplasmin testing should be ordered along with the iron studies and ferritin levels obtained at the patient's first visit, to screen for Wilson's disease, a disorder of copper metabolism, and hemochromatosis, a disorder of iron metabolism.
The risks associated with HAV or HBV coinfection have been described; patients with HCV and HAV, HBV, or HIV are at greater risk for disease progression to cirrhosis and/or HCC than are mono-infected patients.1,21,22,26 HIV testing is routinely recommended for patients with HCV, with repeat testing during treatment if the patient maintains any risk factors for HIV exposure. Patients with HCV who are found to be coinfected with HIV must be treated urgently, but therapeutic components must be selected with considerable care: Serious interactions are possible among the effective agents, and antiretroviral drugs are associated with hepatotoxicity.1,27
Before HCV treatment begins, it is essential to obtain baseline values: liver function testing (aspartate aminotransferase, ALT, alkaline phosphatase, bilirubin), coagulation testing (prothrombin time and partial thromboplastin time), and thyroid testing (thyroid-stimulating hormone, triiodothyronine, thyroxine),1 as changes may occur as a result of anti-HCV therapy. It is also important to establish a baseline complete blood count (CBC) and electrolyte levels in order to identify, and later monitor, the presence of anemia, thrombocytopenia, and renal or other abnormalities.
Finally, it is important to screen the patient early for HCC by testing for serum alphafetoprotein (AFP, ie, tumor marker).28 Serum AFP must then be monitored at six-month intervals (with a recommended threshold of 400 ng/mL, but even readings as modest as 6 to 20 ng/mL) for elevations that may indicate HCC.29,30
Liver Studies
In addition to the recommended AFP monitoring, the patient should undergo an imaging study of the liver twice yearly. Ultrasound is the most cost-effective screening tool for most patients (with high specificity but varying sensitivity); when combined with a serum AFP reading of 10 ng/mL or greater, ultrasound has a sensitivity of 100% for detection of HCC.29 However, if lesions are found, or if a patient has known cirrhosis, CT or MRI is more accurate in detecting small lesions of the liver (specificity, 100%).29
Liver biopsy is recommended for certain patients to stage liver fibrosis; biopsy may not be necessary, for example, in patients with genotypes 2 and 3, as 80% of these patients react to standard therapy with sustained virologic response.1 Detection of advanced fibrosis or cirrhosis increases the urgency for treatment to avert associated complications.31
Thanks to radiologic guidance, the risk for liver biopsy-related complications has been reduced; less than 1% of patients, according to 2008 study results, required hospitalization because of postprocedural pain or bleeding32; these are risks for which patients should be prepared,1 in addition to possible perforation of the bowel or lung, bile leak, or hematoma formation.33 Less than 10% of patients require analgesia two hours after the procedure,34 although prophylactic analgesia (as with sublingual tramadol and oral lorazepam) has been found helpful in reducing pain and anxiety.35
TREATMENT/MANAGEMENT
According to information from the CDC and practice guidelines from the American Association for the Study of Liver Diseases (AASLD),1,2 early diagnosis of HCV and treatment with currently available interventions can lead to cures in 75% of cases; otherwise, serious, life-threatening complications can be expected. In patients treated for HCV infection, cure (or sustained virologic response) is defined by an undetectable viral load, 24 weeks after completion of therapy.1 Patients with these test results are no longer able to transmit the virus to others.
For the past decade, pegylated interferon (or peginterferon) combined with ribavirin has been considered the standard of care for HCV; treatment response rates, depending on race and genotype, can range from 35% to 80%.36,37 Two forms of peginterferon, alfa-2a and alfa-2b, are FDA approved for treatment of chronic hepatitis C; both forms are administered subcutaneously in combination with oral ribavirin.1,38
The choice between peginterferon alfa-2a and alfa-2b and the recommended duration of treatment are dependent on the patient's HCV genotype (see Table 21,39-45) and prior exposure to treatment. These complex regimens are best managed by specialists in gastroenterology, hepatology, or infectious disease—clinicians who are familiar with the agents' associated adverse effects, the elements of attentive monitoring, and protocols for dosing adjustments.46
As noted in the AASLD guidelines,1 alcohol consumption constitutes a risk for worsening fibrosis and possibly for HCC. Additionally, drinking in excess may facilitate replication of HCV RNA, interfering with therapy.
Thus, patients should be urged to discontinue alcohol use during treatment for HCV—or at least restrict it to an occasional drink.
New Agents to Improve Cure Rates
HCV genotype 1 accounts for 70% to 75% of cases in the US, but with current standard treatment, a sustained virologic response is achieved in only 45% to 50% of these patients37 (including 30% of black patients and 50% of whites).1,36,38 However, adding one of two new protease inhibitors to the current peginterferon/ribavirin regimen has the potential to increase sustained virologic response rates to as high as 90% to 95% in early virologic responders with genotype 1 infection, both treatment-naïve and previously treated; and in some patients, to shorten treatment to 24 weeks.41,42,44,45 Both boceprevir and telaprevir were approved by the FDA in May 2011.
Both agents are given for 12 weeks during standard peginterferon/ribavirin therapy. Depending on the patient's viral response, the overall regimen may be shortened or extended. Neither telaprevir nor boceprevir is administered as monotherapy,47,48 nor are they ever administered together. As with any protease inhibitor, resuming treatment after the agent has been stopped incurs a risk for drug resistance.40
Both new agents are taken every 7 to 9 hours, with a meal or snack.47,48 The telaprevir dose should be taken with non-low-fat food.47
Drug interactions are common. Patients also being treated for HIV and those being treated for HCV genotype 1 infection with either of the two new protease inhibitors must very carefully communicate any prescription drug changes to their treating provider. Substances of greatest concern act via the cytochrome P450 3A (CYP3A) pathway. Examples include ritonavir, St. John's wort, statins, and daily-dosed sildenafil (as used to treat patients with pulmonary hypertension).
Package inserts accompanying all agents used should be reviewed for monitoring parameters and associated recommendations.
Monitoring for Treatment Effectiveness and Complications
Patients are closely monitored for treatment effectiveness by repeated measurements of HCV RNA (ie, weeks 4, 12, 24, then at four- to 12-week intervals; at end of treatment; and 24 weeks after treatment ends). A viral load not detectable at week 4 indicates a good chance for a cure.1 If at week 12 the viral load remains detectable, the patient with HCV genotype 1 is unlikely to respond to triple therapy; similarly, dual therapy is not likely to produce a cure in patients with HCV genotype 2 or 3. Without a 2-log drop in viral load by week 12, the patient has only an 8% chance of achieving a sustained virologic response.49-51 In these cases, treatment should be discontinued or modified.51
Regular visits and frequent blood testing make it possible to avoid potential disease- and treatment-related complications. At a minimum, it is recommended that a CBC, serum creatinine, and ALT level be measured at weeks 2, 4, 8, 12, 16, 20, and 24 of therapy.1 If significant abnormalities are detected (eg, anemia, thrombocytopenia, neutropenia), the clinician may decide to monitor the patient more closely. Measures of liver and kidney function, electrolytes, and coagulation times are part of the recommended monitoring parameters at regular intervals. In addition, interferon therapy is associated with thyroid dysfunction, so relevant monitoring is advised every 12 weeks.1
Anemia, neutropenia, thrombocytopenia, and other hematologic complications are known adverse effects of HCV therapy—particularly in cirrhotic patients.1,52 Ribavirin use (especially aggressive use, as for patients with recurrent infection or post-liver transplantation53) is associated with hemolytic anemia,54 as is protease inhibitor use.41,45 In cases of profound anemia, dosing reduction or treatment discontinuation may be necessary. Severe cases of hemolysis may require transfusion, but treatment with epoietin alfa has been found helpful in some patients.52,53 Conventional iron supplementation is not an effective treatment for hemolytic anemia resulting from ribavirin use.
For patients with low absolute neutrophil counts, treatment dosing reduction was once standard management.45,52 More recently, the use of epoietin alfa or a granulocyte colony-stimulating factor (eg, filgrastim) has been found helpful in raising neutrophil counts.52
Intervention for thrombocytopenia is not typically undertaken unless the total platelet count indicates a risk for spontaneous bleeding. In some patients, a new oral thrombopoietin mimetic called eltrombopag may reduce the need for dose reduction or early termination of therapy.52
Ribavirin is a major teratogen. This agent is listed in pregnancy category X, and its label carries a black box warning advising patients to avoid pregnancy while undergoing therapy and for six months following therapy. It has such a high potential for teratogenicity that male patients are even advised not to impregnate their female partners while on therapy or six months following therapy.54 Pregnant women should never handle ribavirin. It is important to educate medical professionals and office staff about this risk.
For management of other adverse reactions to one or more components of HCV treatment, see Table 3.1,41,43,45,55-57
PATIENT EDUCATION/FOLLOW-UP DISCUSSION
Patient education is critical to successful treatment for HCV. Patients should be encouraged to avoid viral transmission to sexual partners by using condoms. They should also be advised to avoid sharing razors or toothbrushes with others in the home.1 Any patient with known HCV, HIV, or HBV should avoid undergoing body piercing or tattooing in any nonprofessional, nonsterile setting, where transmission may occur.5 Even successfully treated patients retain an HCV antibody and will test positive for HCV, making them ineligible to donate blood.
Six months after treatment, a viral load is drawn. If no active virus is found, patients will not need monitoring or follow-up labs unless they have known cirrhosis. Fibrosis is reversible in some patients following HCV treatment. However, if active disease is found at the six-month posttreatment follow-up visit, then the treatment was not effective, and the patient is considered a responder-relapser. Many such patients then consider enrolling in a drug trial or awaiting the potential approval of new treatments.
Herbal therapies, such as milk thistle and licorice root, have been widely tried by patients with HCV infection. The literature is mixed regarding the effectiveness of these substances or their potential for reducing liver function testing abnormalities. To date, no herbal compound has been proven to eradicate the virus. Most hepatologists encourage patients who take interferon, ribavirin, and/or protease inhibitors to avoid herbal or OTC substances with any potential for drug interactions or other complications.
ON THE HORIZON
Promising developments suggest a brightening future for patients with HCV infection. Researchers throughout the world are currently investigating new combinations of agents, effective against a wider range of genotypes and subtypes, that can control HCV infection without the emergence of drug-resistant strains. The near future may see more protease inhibitors added to current regimens and other direct-acting antivirals possibly replacing old treatment components. As is true of HIV, a vaccine for HCV will be difficult to develop; but in the meantime, new drug combinations will be created with a goal of sustained virologic response rates nearing 100% and ever-shorter treatment regimens.37,58
CONCLUSION
Since signs or symptoms are often not seen in patients infected with hepatitis C, it is important for primary care providers to question patients regarding known risk factors. At-risk patients should be screened using antibody testing, followed by confirmation of any positive results by HCV RNA testing. The patient's HCV genotype must be identified next, as it plays a key role in the therapeutic decisions to be made.
Because HCV therapy is complex, it is best managed by specialists who are experienced in all the aspects of each patient's regimen and who remain abreast of new therapeutic developments. Nevertheless, primary care providers can serve their patients well by acting as knowledgeable, supportive members of the health care team, accompanying their patients through the challenges of treatment and follow-up.
1. Ghany MG, Strader DB, Thomas DL, Seeff LB; American Association for the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49(4):1335-1374.
2. CDC. Hepatitis C FAQs for health professionals (2008). www.cdc.gov/hepatitis/HCV/HCVfaq. htm#section1. Accessed August 20, 2012.
3. Ly KN, Xing J, Klevens M, et al. The increasing burden of mortality from viral hepatitis in the United States between 1999 and 2007. Ann Intern Med. 2012;156(4):271-278.
4. Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR). OPTN/SRTR 2010 Annual Data Report (2011). Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. www.srtr.org/ annual_reports/2010/pdf/00_intro_pgs_11.pdf. Accessed August 20, 2012.
5. Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012;54(8):1167-1178.
6. CDC. Hepatitis C: proposed expansion of testing recommendations, 2012. www.cdc.gov/nchh-stp/newsroom/docs/HCV-TestingFactSheetNoEm-bargo508.pdf. Accessed August 20, 2012.
7. Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med Sci. 2006;3(2):47-52.
8. Al-Ali J, Al-Mutari N, Ahmed el-SF. Hepatitis C virus and the skin. Hepatogastroenterology. 2011;58(107-108):880-886.
9. Raslan HM, Ezzat WM, Abd El Hamid MF, et al. Skin manifestations of chronic hepatitis C virus infection in Cairo, Egypt. East Mediterr Health J. 2009;15(3):692-700.
10. Niederau C, Hüppe D, Zehnter E, et al. Chronic hepatitis C: treat or wait? Medical decision making in clinical practice. World J Gastroenterol. 2012;18(12):1339-1347.
11. Mahboobi N, Agha-Hosseini F, Lankarani K. Hepatitis C virus and lichen planus: the real association. Hepat Mon. 2010;10(3):161-164.
12. Khokhar OS, Lewis JH. Reasons why patients infected with chronic hepatitis C virus choose to defer treatment: do they alter their decision with time? Dig Dis Sci. 2007;52(5):1168-1176.
13. Bruno S, Zuin M, Crosignani A, et al. Predicting mortality risk in patients with compensated HCV-induced cirrhosis: a long-term prospective study. Am J Gastroenterol. 2009;104(5):1147-1158.
14. Cheinquer N, Cheinquer H, Wolff FH, Coelho-Borges S. Effect of sustained virologic response on the incidence of hepatocellular carcinoma in patients with HCV cirrhosis. Braz J Infect Dis. 2010;14(5):457-461.
15. Veldt BJ, Chen W, Heathcote EJ, et al. Increased risk of hepatocellular carcinoma among patients with hepatitis C cirrhosis and diabetes mellitus. Hepatology. 2008;47(6):1856-1862.
16. Nkontchou G, Ziol M, Aout M, et al. HCV genotype 3 is associated with a higher hepatocellular carcinoma incidence in patients with ongoing viral C cirrhosis. J Viral Hepat. 2011;18(10):e516-e522.
17. Czaja AJ, Freese DK. Diagnosis and treatment of autoimmune hepatitis. Hepatology. 2002;36:479-497.
18. Vujosevic S, Tempesta D, Noventa F, et al. Pegylated interferon-associated retinopathy is frequent in hepatitis C virus patients with hypertension and justifies ophthalmologic screening. Hepatology. 2012;56(2):455-463.
19. World Health Organization. Global alert and response: hepatitis D (2012). www.who.int/csr/ disease/hepatitis/whocdscsrncs20011/en/index3. html. Accessed August 20, 2012.
20. World Health Organization. Hepatitis E: fact sheet No 280 (July 2012). www.who.int/media centre/factsheets/fs280/en. Accessed August 20, 2012.
21. Bertino G, Ardiri AM, Bruno MC, et al. HAV infection in patients with chronic hepatitis C [in Italian]. Clin Ter. 2007;158(3):223-225.
22. Liu J, Hou J. Hepatitis B virus (HBV) and hepatitis C virus (HCV) dual infection. Int J Med Sci. 2006;3(2):57-62.
23. Schijman A, Colina R, Mukomolov S, et al. Comparison of hepatitis C viral loads in patients with or without coinfection with different genotypes. Clin Diagn Lab Immunol. 2004;11(2):433-435.
24. McClure JE, Shearer WT. Radioimmunoassay for anti-actin antibody: application in viral and autoimmune diseases. Mol Cell Probes. 1988;2(4):305-319.
25. Peakman M, Lobo-Yeo A, Mieli-Vergani, et al. Characterization of anti-liver kidney microsomal antibody in childhood autoimmune chronic active hepatitis: evidence for IgG1 subclass restriction, polyclonality and non cross-reactivity with hepatocyte surface antigens. Clin Exp Immunol. 1987;69(3):543-549.
26. Loko MA, Salmon D, Carrieri P, et al; ANRS CO 13 HEPAVIH Study Group. The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): early findings, 2006-2010. BMC Infect Dis. 2010 Oct 22;10:303.
27. Duclos-Vallée JC, Féray C, Sebagh M, et al; THEVIC Study Group. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2008;47(2):407-417.
28. Sato Y, Nakata K, Kato Y, et al. Early recognition of hepatocellular carcinoma based on altered profiles of alpha-fetoprotein. N Engl J Med. 1993;328(25):1802-1806.
29. Gebo KA, Chander G, Jenckes MW, et al. Screening tests for hepatocellular carcinoma in patients with chronic hepatitis C: a systematic review. Hepatology. 2002;36(5 suppl 1):S84-S92.
30. Tateyama M, Yatsuhashi H, Taura N, et al. Alpha-fetoprotein above normal levels as a risk factor for the development of hepatocellular carcinoma in patients infected with hepatitis C virus. J Gastroenterol. 2011;46(1):92-100.
31. Bruno S, Shiffman ML, Roberts SK, et al. Efficacy and safety of peginterferon alfa-2a (40KD) plus ribavirin in hepatitis C patients with advanced fibrosis and cirrhosis. Hepatology. 2010;51(2):388-397.
32. Myers RP, Fong A, Shaheen AA. Utilization rates, complications and costs of percutaneous liver biopsy: a population-based study including 4275 biopsies. Liver Int. 2008;28(5):705-712.
33. van der Poorten D, Kwok A, Lam T, et al. Twenty-year audit of percutaneous liver biopsy in a major Australian teaching hospital. Intern Med J. 2006;36(11):692-699.
34. Howard R, Karageorge G, van Harselaar K, et al. Post-procedure surveillance in liver biopsy: how long is long enough? N Z Med J. 2008;121(1280):8-14.
35. Kramskay R, Tansky A, Eisenberg, et al. Prophylactic analgesia before percutaneous liver biopsy: a clinical comparative study. Eur J Gastroenterol Hepatol. 2011;23(9):782-786.
36. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347(13):975-982.
37. Lemon SM, McKeating JA, Pietschmann T, et al. Development of novel therapies for hepatitis C. Antiviral Res. 2010;86(1):79-92.
38. Shepherd J, Brodin H, Cave C, et al. Pegylated interferon alpha-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation. Health Technol Assess. 2004;8(39):iii-iv, 1-125.
39. Kamal SM, El Kamary SS, Shardell MD, et al. Pegylated interferon alpha-2b plus ribavirin in patients with genotype 4 chronic hepatitis C: the role of rapid and early virologic response. Hepatology. 2007;46:1732-1740.
40. Hofmann WP, Sarrazin C, Zeuzem S. Current standards in the treatment of chronic hepatitis C. Dtsch Arztebl Int. 2012;109(19):352-358.
41. Kwo PY, Lawitz EJ, McCone J, et al; SPRINT-1 Investigators. Efficacy of boceprevir, an NS3 protease inhibitor, in combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): an open-label, randomised, multicentre phase 2 trial. Lancet. 2010;376(9742):705-716.
42. Klibanov OM, Vickery SB, Olin JL, et al. Boceprevir: a novel NS3/4 protease inhibitor for the treatment of hepatitis C. Pharmacotherapy. 2012;32(2):173-190.
43. Cunningham M, Foster GR. Efficacy and safety of telaprevir in patients with genotype 1 hepatitis C infection. Therap Adv Gastroenterol. 2012;5(2):139-151.
44. Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364(25):2405-2416.
45. Zeuzem S, Andreone P, Pol S, et al; REALIZE Study Team. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364(25):2417-2428.
46. Sagir A, Heintges T, Akyazi Z, et al. Therapy outcome in patients with chronic hepatitis C: role of therapy supervision by expert hepatologists. J Viral Hepat. 2007;14(9):633-638.
47. Highlights of prescribing information: INCIVEKTM (telaprevir) film coated tablets for oral use (2011). http://pi.vrtx.com/files/uspi_telaprevir. pdf. Accessed August 20, 2012.
48. Highlights of prescribing information: VICTRELISTM (boceprevir) capsules (2011). www .accessdata.fda.gov/drugsatfda_docs / label/2011/202258lbl.pdf. Accessed August 20, 2012.
49. Alavian SM, Tabatabaei SV, Behnava B, Mahboobi N. Optimal duration of treatment for HCV genotype 1 infection in slow responders: a meta-analysis. Hepat Mon. 2011;11(8):612-619.
50. Fried MW, Hadziyannis SJ, Shiffman ML, et al. Rapid virological response is the most important predictor of sustained virological response across genotypes in patients with chronic hepatitis C virus infection. J Hepatol. 2011;55(1):69-75.
51. Reau N, Satoskar R, Te H, et al. Evaluation of early null response to pegylated interferon and ribavirin as a predictor of therapeutic nonresponse in patients undergoing treatment for chronic hepatitis C. Am J Gastroenterol. 2011;106(3):452-458.
52. Mac Nicholas R, Norris S. Optimizing SVR and management of the haematological side effects of peginterferon/ribavirin antiviral therapy for HCV: the role of epoietin, G-CSF and novel agents. Aliment Pharmacol Ther. 2010;31(9):929-937.
53. Singhal A, Jain AB, Burke M, Black M. Aggressive use of ribavirin and prolonged course of peginterferon to improve the rate of viral response in liver transplant patients with recurrent hepatitis C viral infection. Exp Clin Transplant. 2010;8(3):214-219.
54. Highlights of prescribing information: COPEGUSTM (ribavirin) tablets (2002). http://www.gene .com/gene/products/information/pegasys/pdf/ copegus_pi.pdf. Accessed August 20, 2012.
55. Fried MW. Side effects of therapy of hepatitis C and their management. Hepatology. 2002;36(5 suppl 1):S237-S244.
56. Dollarhide AW, Loh C, Leckband SG, et al. Psychiatric comorbidity does not predict interferon treatment completion rates in hepatitis C seropositive veterans. J Clin Gastroenterol. 2007;41(3):322-328.
57. Tavakoli-Tabasi S, Bagree A. A longitudinal cohort study of mucocutaneous drug eruptions during interferon and ribavirin treatment of hepatitis C. J Clin Gastroenterol. 2012;46(2):162-167.
58. Fox AN, Jacobson IM. Recent successes and noteworthy future prospects in the treatment of chronic hepatitis C. Clin Infect Dis. 2012;55 suppl 1:S16-S24.
1. Ghany MG, Strader DB, Thomas DL, Seeff LB; American Association for the Study of Liver Diseases. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology. 2009;49(4):1335-1374.
2. CDC. Hepatitis C FAQs for health professionals (2008). www.cdc.gov/hepatitis/HCV/HCVfaq. htm#section1. Accessed August 20, 2012.
3. Ly KN, Xing J, Klevens M, et al. The increasing burden of mortality from viral hepatitis in the United States between 1999 and 2007. Ann Intern Med. 2012;156(4):271-278.
4. Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR). OPTN/SRTR 2010 Annual Data Report (2011). Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation. www.srtr.org/ annual_reports/2010/pdf/00_intro_pgs_11.pdf. Accessed August 20, 2012.
5. Tohme RA, Holmberg SD. Transmission of hepatitis C virus infection through tattooing and piercing: a critical review. Clin Infect Dis. 2012;54(8):1167-1178.
6. CDC. Hepatitis C: proposed expansion of testing recommendations, 2012. www.cdc.gov/nchh-stp/newsroom/docs/HCV-TestingFactSheetNoEm-bargo508.pdf. Accessed August 20, 2012.
7. Chen SL, Morgan TR. The natural history of hepatitis C virus (HCV) infection. Int J Med Sci. 2006;3(2):47-52.
8. Al-Ali J, Al-Mutari N, Ahmed el-SF. Hepatitis C virus and the skin. Hepatogastroenterology. 2011;58(107-108):880-886.
9. Raslan HM, Ezzat WM, Abd El Hamid MF, et al. Skin manifestations of chronic hepatitis C virus infection in Cairo, Egypt. East Mediterr Health J. 2009;15(3):692-700.
10. Niederau C, Hüppe D, Zehnter E, et al. Chronic hepatitis C: treat or wait? Medical decision making in clinical practice. World J Gastroenterol. 2012;18(12):1339-1347.
11. Mahboobi N, Agha-Hosseini F, Lankarani K. Hepatitis C virus and lichen planus: the real association. Hepat Mon. 2010;10(3):161-164.
12. Khokhar OS, Lewis JH. Reasons why patients infected with chronic hepatitis C virus choose to defer treatment: do they alter their decision with time? Dig Dis Sci. 2007;52(5):1168-1176.
13. Bruno S, Zuin M, Crosignani A, et al. Predicting mortality risk in patients with compensated HCV-induced cirrhosis: a long-term prospective study. Am J Gastroenterol. 2009;104(5):1147-1158.
14. Cheinquer N, Cheinquer H, Wolff FH, Coelho-Borges S. Effect of sustained virologic response on the incidence of hepatocellular carcinoma in patients with HCV cirrhosis. Braz J Infect Dis. 2010;14(5):457-461.
15. Veldt BJ, Chen W, Heathcote EJ, et al. Increased risk of hepatocellular carcinoma among patients with hepatitis C cirrhosis and diabetes mellitus. Hepatology. 2008;47(6):1856-1862.
16. Nkontchou G, Ziol M, Aout M, et al. HCV genotype 3 is associated with a higher hepatocellular carcinoma incidence in patients with ongoing viral C cirrhosis. J Viral Hepat. 2011;18(10):e516-e522.
17. Czaja AJ, Freese DK. Diagnosis and treatment of autoimmune hepatitis. Hepatology. 2002;36:479-497.
18. Vujosevic S, Tempesta D, Noventa F, et al. Pegylated interferon-associated retinopathy is frequent in hepatitis C virus patients with hypertension and justifies ophthalmologic screening. Hepatology. 2012;56(2):455-463.
19. World Health Organization. Global alert and response: hepatitis D (2012). www.who.int/csr/ disease/hepatitis/whocdscsrncs20011/en/index3. html. Accessed August 20, 2012.
20. World Health Organization. Hepatitis E: fact sheet No 280 (July 2012). www.who.int/media centre/factsheets/fs280/en. Accessed August 20, 2012.
21. Bertino G, Ardiri AM, Bruno MC, et al. HAV infection in patients with chronic hepatitis C [in Italian]. Clin Ter. 2007;158(3):223-225.
22. Liu J, Hou J. Hepatitis B virus (HBV) and hepatitis C virus (HCV) dual infection. Int J Med Sci. 2006;3(2):57-62.
23. Schijman A, Colina R, Mukomolov S, et al. Comparison of hepatitis C viral loads in patients with or without coinfection with different genotypes. Clin Diagn Lab Immunol. 2004;11(2):433-435.
24. McClure JE, Shearer WT. Radioimmunoassay for anti-actin antibody: application in viral and autoimmune diseases. Mol Cell Probes. 1988;2(4):305-319.
25. Peakman M, Lobo-Yeo A, Mieli-Vergani, et al. Characterization of anti-liver kidney microsomal antibody in childhood autoimmune chronic active hepatitis: evidence for IgG1 subclass restriction, polyclonality and non cross-reactivity with hepatocyte surface antigens. Clin Exp Immunol. 1987;69(3):543-549.
26. Loko MA, Salmon D, Carrieri P, et al; ANRS CO 13 HEPAVIH Study Group. The French national prospective cohort of patients co-infected with HIV and HCV (ANRS CO13 HEPAVIH): early findings, 2006-2010. BMC Infect Dis. 2010 Oct 22;10:303.
27. Duclos-Vallée JC, Féray C, Sebagh M, et al; THEVIC Study Group. Survival and recurrence of hepatitis C after liver transplantation in patients coinfected with human immunodeficiency virus and hepatitis C virus. Hepatology. 2008;47(2):407-417.
28. Sato Y, Nakata K, Kato Y, et al. Early recognition of hepatocellular carcinoma based on altered profiles of alpha-fetoprotein. N Engl J Med. 1993;328(25):1802-1806.
29. Gebo KA, Chander G, Jenckes MW, et al. Screening tests for hepatocellular carcinoma in patients with chronic hepatitis C: a systematic review. Hepatology. 2002;36(5 suppl 1):S84-S92.
30. Tateyama M, Yatsuhashi H, Taura N, et al. Alpha-fetoprotein above normal levels as a risk factor for the development of hepatocellular carcinoma in patients infected with hepatitis C virus. J Gastroenterol. 2011;46(1):92-100.
31. Bruno S, Shiffman ML, Roberts SK, et al. Efficacy and safety of peginterferon alfa-2a (40KD) plus ribavirin in hepatitis C patients with advanced fibrosis and cirrhosis. Hepatology. 2010;51(2):388-397.
32. Myers RP, Fong A, Shaheen AA. Utilization rates, complications and costs of percutaneous liver biopsy: a population-based study including 4275 biopsies. Liver Int. 2008;28(5):705-712.
33. van der Poorten D, Kwok A, Lam T, et al. Twenty-year audit of percutaneous liver biopsy in a major Australian teaching hospital. Intern Med J. 2006;36(11):692-699.
34. Howard R, Karageorge G, van Harselaar K, et al. Post-procedure surveillance in liver biopsy: how long is long enough? N Z Med J. 2008;121(1280):8-14.
35. Kramskay R, Tansky A, Eisenberg, et al. Prophylactic analgesia before percutaneous liver biopsy: a clinical comparative study. Eur J Gastroenterol Hepatol. 2011;23(9):782-786.
36. Fried MW, Shiffman ML, Reddy KR, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347(13):975-982.
37. Lemon SM, McKeating JA, Pietschmann T, et al. Development of novel therapies for hepatitis C. Antiviral Res. 2010;86(1):79-92.
38. Shepherd J, Brodin H, Cave C, et al. Pegylated interferon alpha-2a and -2b in combination with ribavirin in the treatment of chronic hepatitis C: a systematic review and economic evaluation. Health Technol Assess. 2004;8(39):iii-iv, 1-125.
39. Kamal SM, El Kamary SS, Shardell MD, et al. Pegylated interferon alpha-2b plus ribavirin in patients with genotype 4 chronic hepatitis C: the role of rapid and early virologic response. Hepatology. 2007;46:1732-1740.
40. Hofmann WP, Sarrazin C, Zeuzem S. Current standards in the treatment of chronic hepatitis C. Dtsch Arztebl Int. 2012;109(19):352-358.
41. Kwo PY, Lawitz EJ, McCone J, et al; SPRINT-1 Investigators. Efficacy of boceprevir, an NS3 protease inhibitor, in combination with peginterferon alfa-2b and ribavirin in treatment-naive patients with genotype 1 hepatitis C infection (SPRINT-1): an open-label, randomised, multicentre phase 2 trial. Lancet. 2010;376(9742):705-716.
42. Klibanov OM, Vickery SB, Olin JL, et al. Boceprevir: a novel NS3/4 protease inhibitor for the treatment of hepatitis C. Pharmacotherapy. 2012;32(2):173-190.
43. Cunningham M, Foster GR. Efficacy and safety of telaprevir in patients with genotype 1 hepatitis C infection. Therap Adv Gastroenterol. 2012;5(2):139-151.
44. Jacobson IM, McHutchison JG, Dusheiko G, et al; ADVANCE Study Team. Telaprevir for previously untreated chronic hepatitis C virus infection. N Engl J Med. 2011;364(25):2405-2416.
45. Zeuzem S, Andreone P, Pol S, et al; REALIZE Study Team. Telaprevir for retreatment of HCV infection. N Engl J Med. 2011;364(25):2417-2428.
46. Sagir A, Heintges T, Akyazi Z, et al. Therapy outcome in patients with chronic hepatitis C: role of therapy supervision by expert hepatologists. J Viral Hepat. 2007;14(9):633-638.
47. Highlights of prescribing information: INCIVEKTM (telaprevir) film coated tablets for oral use (2011). http://pi.vrtx.com/files/uspi_telaprevir. pdf. Accessed August 20, 2012.
48. Highlights of prescribing information: VICTRELISTM (boceprevir) capsules (2011). www .accessdata.fda.gov/drugsatfda_docs / label/2011/202258lbl.pdf. Accessed August 20, 2012.
49. Alavian SM, Tabatabaei SV, Behnava B, Mahboobi N. Optimal duration of treatment for HCV genotype 1 infection in slow responders: a meta-analysis. Hepat Mon. 2011;11(8):612-619.
50. Fried MW, Hadziyannis SJ, Shiffman ML, et al. Rapid virological response is the most important predictor of sustained virological response across genotypes in patients with chronic hepatitis C virus infection. J Hepatol. 2011;55(1):69-75.
51. Reau N, Satoskar R, Te H, et al. Evaluation of early null response to pegylated interferon and ribavirin as a predictor of therapeutic nonresponse in patients undergoing treatment for chronic hepatitis C. Am J Gastroenterol. 2011;106(3):452-458.
52. Mac Nicholas R, Norris S. Optimizing SVR and management of the haematological side effects of peginterferon/ribavirin antiviral therapy for HCV: the role of epoietin, G-CSF and novel agents. Aliment Pharmacol Ther. 2010;31(9):929-937.
53. Singhal A, Jain AB, Burke M, Black M. Aggressive use of ribavirin and prolonged course of peginterferon to improve the rate of viral response in liver transplant patients with recurrent hepatitis C viral infection. Exp Clin Transplant. 2010;8(3):214-219.
54. Highlights of prescribing information: COPEGUSTM (ribavirin) tablets (2002). http://www.gene .com/gene/products/information/pegasys/pdf/ copegus_pi.pdf. Accessed August 20, 2012.
55. Fried MW. Side effects of therapy of hepatitis C and their management. Hepatology. 2002;36(5 suppl 1):S237-S244.
56. Dollarhide AW, Loh C, Leckband SG, et al. Psychiatric comorbidity does not predict interferon treatment completion rates in hepatitis C seropositive veterans. J Clin Gastroenterol. 2007;41(3):322-328.
57. Tavakoli-Tabasi S, Bagree A. A longitudinal cohort study of mucocutaneous drug eruptions during interferon and ribavirin treatment of hepatitis C. J Clin Gastroenterol. 2012;46(2):162-167.
58. Fox AN, Jacobson IM. Recent successes and noteworthy future prospects in the treatment of chronic hepatitis C. Clin Infect Dis. 2012;55 suppl 1:S16-S24.
Women, Weight, and Gout
Taking the Mystery Out of the Match: Histocompatibility Testing and Kidney Transplantation
Effect of Statins on Total Testosterone Levels in Male Veterans
Restless Legs Syndrome Complicating Iron Deficiency
Diagnosing Infantile Hypertrophic Pyloric Stenosis
Infantile hypertrophic pyloric stenosis (IHPS) is a common yet treatable condition in young infants, characterized by forceful vomiting after feeding as a result of hypertrophy of the pyloric muscle. Without proper diagnosis and surgical intervention, IHPS can eventually lead to dehydration, weight loss, and electrolyte disturbances, including the classic finding of hypochloremic alkalosis.1,2
IHPS occurs in two to four of every 1,000 births and is most common among white male infants.3,4 It develops between the first three to five weeks of life but rarely after age 12 weeks.1,2,5 IHPS is characterized by hypertrophy of the pyloric muscle (see figure), which eventually leads to gastric outlet obstruction.6,7
Because IHPS presents with symptoms that resemble those associated with other gastrointestinal disturbances, such as gastroesophageal reflux disease (GERD), it can be misdiagnosed in its early stages.1 Once it is identified, however, surgical correction by pyloromyotomy is considered curative, with a very low mortality rate (ie, 0.1%) and incidence recurrence in only 1% of patients. Typically, treated infants recover quickly and can begin feeding within hours after surgery.3,8
Although the etiology of IHPS remains unknown, providers can quickly recognize the signs and symptoms of IHPS in order for surgical treatment to be scheduled in a timely manner.
PATIENT PRESENTATION
Typically, an infant with IHPS will have a period of normal feeding for the first two to three weeks of life, followed by onset of nonbilious vomiting soon after feeding. Vomiting may become increasingly frequent and forceful—possibly described as “projectile.” Despite stomach distention, affected infants seem to have an insatiable appetite and may cry inconsolably. Depending on the duration of symptoms, patients may suffer significant weight loss, even falling below birth weight. In severe cases, a scaphoid abdomen and protruding ribcage may be present.1,2
Atypical Presentations
Premature infants with IHPS and those with certain medical or surgical conditions may present atypically. Vomiting may be less forceful, and the classic finding of visible gastric peristalsis may or may not be present.9 Researchers have documented cases in which hospitalized premature infants had nonprojectile vomiting, weight loss, and lethargy that were erroneously attributed to sepsis. IHPS should have been considered over sepsis when the infants’ clinical condition improved rapidly with rehydration, and when metabolic alkalosis (rather than acidosis) was identified.1,10,11
Projectile vomiting may not occur in infants with congenital anomalies that affect swallowing, such as cleft lip/palate or central nervous system disturbances. In infants who have recently undergone gastrointestinal (GI) surgery, IHPS may be misdiagnosed as adhesions or obstruction at an anastomotic site.1,10
RISK FACTORS
Despite the fact that IHPS is a relatively common condition, the etiology remains unknown. Research findings indicate that IHPS is not present at birth. Several hypotheses exist about potential risk factors, including genetics, use of macrolide antibiotics, and mechanical or environmental factors.6 IHPS has been associated with certain genetic conditions, including Cornelia de Lange syndrome and Smith-Lemli-Opitz syndrome, as well as chromosomal abnormalities, such as the translocation of chromosomes 8 and 17, and partial trisomy of chromosome 9.6,12
According to Chung,13 additional research has implicated the genetic loci IHPS1, also known as nitric oxide synthase 1 (NOS1), which encodes the gene for neuronal nitric oxide synthase (nNOS). This is the key enzyme for production of nitric oxide, which mediates relaxation of the pyloric smooth muscle.13
In a study by Mahon et al,12 an increased risk for IHPS was confirmed in young infants for whom systemic erythromycin had been prescribed as prophylactic treatment for pertussis. This may result from the agent’s motilin-like effects on antral smooth-muscle function.13
Mechanical defects, such as abnormal innervation of the pyloric muscle and neonatal hypergastrinemia and hyperacidity, have also been implicated.6 Infant sleeping position has been investigated as a possible environmental factor in the development of IHPS, correlating the decline in sudden infant death syndrome (attributed to decreased prone sleep position) with a decline in IHPS in recent years. However, no conclusive evidence has been shown to support this hypothesis.13
DIFFERENTIAL DIAGNOSIS
Typically, infants with nonbilious vomiting have either IHPS or GERD. Two factors to consider when evaluating the infant are its age and whether emesis is bilious or nonbilious. IHPS rarely causes bilious vomiting and most frequently occurs in infants between ages 3 and 6 weeks. Other GI disturbances that cause nonbilious emesis include adrenal crisis, gastroenteritis, pylorospasm, hiatal hernia, and preampullary duodenal stenosis.2 Malrotation or midgut volvulus may also be considered in the differential14 (see table1,2,14-16).
DIAGNOSIS
The diagnosis of IHPS is often made based on the history and physical exam. Imaging studies and labs can confirm the diagnosis, and surgery is usually deferred until dehydration has been addressed and any electrolyte disturbances corrected.1,17
Physical Examination
The infant may appear underweight and dehydrated, with visible peristaltic waves across the upper abdomen prior to emesis. Severe illness may be indicated in an underweight infant with the classic scaphoid abdomen.18
Palpation of an olive-shaped mass in the upper left quadrant of the epigastric region is pathognomonic for IHPS; the mass may be found more easily after emesis has occurred.19 To facilitate palpation, the hips can first be flexed to relax the abdominal wall. Next, the examiner should palpate gently for the “olive” in the space midway between the umbilicus and the xiphoid, between the two rectus muscles.3 All other findings in the physical exam should be within normal limits.
Imaging and Laboratory
Studies
An experienced provider can make a diagnosis of IHPS based on clinical examination alone in 60% to 80% of cases.20 However, most surgeons require the diagnosis to be confirmed with one of the following imaging studies before surgery.19
The diagnosis of IHPS can be confirmed by an upper GI series, but this is not commonly ordered as the primary diagnostic study. Ultrasound has become the modality of choice9; it can be used to quantify the size of an elongated, thickened pyloric muscle. The hypertrophied pylorus ranges in length from 14 to 16 mm, with thickness measuring more than 3.0 to 3.5 mm.1,19,21
An upper GI contrast study is rarely used for diagnosis of IHPS, but when this test is ordered to detect other gastrointestinal disease processes (eg, malrotation), IHPS may be identified incidentally.19 During an upper GI study, contrast material is propelled through the pyloric mucosa, and the string sign or the double-track sign may be visualized, revealing the mucosal filling defect.2
Abdominal x-ray may reveal a dilated stomach or a blockage, with a possible finding of gas in the gastric bubble but extending no further into the intestine.19
A study by Hernanz-Schulman2 was conducted to quantify the sensitivities and specificities associated with different diagnostic tools and the clinician’s experience and proficiency in using them. According to this study, palpation by a surgeon has a sensitivity of 31% to 99% and a specificity of 85% to 99% for detection of the pathognomonic olive-shaped mass. Ultrasound performed by an experienced technician has 97% to 100% sensitivity and 99% to 100% specificity for detecting IHPS. An upper GI series has 90% to 100% sensitivity and 99.5% specificity.
Venous blood gas and electrolyte levels are both helpful in making a diagnosis of IHPS.19,22 In a study by Oakley and Barnett,22 the following lab values were found useful in confirming the presence of pyloric stenosis: pH > 7.45; chloride 3 mEq/L. Sodium and potassium deficits may also be present.2,22
Before treatment is considered, the degree of dehydration must be determined by clinical examination and urinary output, as well as serum bicarbonate and chloride levels.3 Other laboratory tests to be ordered include urinalysis and a complete blood count (including platelets).
TREATMENT/MANAGEMENT
Initial management of vomiting in children should begin with fluid replacement if the patient appears dehydrated or if lab findings suggest an electrolyte imbalance. If surgery is later deemed necessary, this will reduce the risk for postoperative apnea.1,23
If IHPS is suspected, a pediatric surgery consult should be obtained. Before anesthesia is considered, serum bicarbonate should be measured with results no higher than 28 mEq/L, and the serum chloride level should be at least 100 mEq/L.3 Imaging, such as ultrasound or the upper GI series, may be ordered to confirm the diagnosis.
Surgical correction by a pyloromyotomy is curative. Presurgical gastric decompression via nasogastric tube placement will reduce the risk for postoperative vomiting and gastritis.20
Surgery
Although a variety of nonsurgical interventions, including oral and IV atropine and balloon dilation, have been described in the literature,3,24-26 the preferred treatment for IHPS is surgical intervention. Surgical correction has been so consistently successful (that is, provided the procedure is performed by a pediatric surgeon or other surgeon with appropriate experience3) that the treatment of choice for IHPS is the Ramstedt pyloromyotomy, which was first performed in 1912.6,27,28
Although the approach may differ based on the individual surgeon’s preference, the pyloric muscle is pulled through an incision in the abdominal wall. A longitudinal incision is made through the muscle with blunt dissection to the submucosa on the anterior surface of the pylorus. The pylorus is then returned to the abdominal cavity, and the abdominal incision is sutured.3,20
The laparoscopic approach, first described in the literature in the mid-1990s,29 is gaining popularity among surgeons, although recent studies have demonstrated that open and laparoscopic procedures are comparably safe and effective for the management of IHPS.30-33 Results from a recent study by Jia et al30 indicate that the laparoscopic approach results in reduced postoperative emesis, shorter length of hospital stay, and shorter recovery times; Hall et al31 emphasize the advantages of laparoscopic pyloromyotomy and recommend it over open surgery in facilities with experienced surgeons.
In follow-up ultrasound studies, hypertrophy of the pyloric muscle was reportedly resolved between two and 12 weeks after pyloromyotomy.34
Postoperative Care
The gastric tube can be removed and oral fluids reintroduced slowly at the surgeon’s discretion, between 8 and 12 hours after surgery. Postoperative vomiting is common (occurring in up to 80% of patients) but should resolve within 24 hours. Mild emesis should not delay the refeeding schedule.3
Patients should be evaluated by the surgeon one to two weeks following surgery unless the infant shows signs of infection (ie, fever, erythema, edema, bleeding, purulent drainage, excess pain, decreased fluid or nutritional intake). Follow-up imaging and laboratory studies are not indicated in an otherwise healthy infant.20
CONCLUSION
Early detection of IHPS, a condition characterized by hypertrophy of the pyloric muscle that results in gastric obstruction and projectile vomiting, can prevent complications of dehydration, malnutrition, and electrolyte disturbances. Surgery by open or laparoscopic pyloromyotomy is curative. Knowing the key physical exam findings, laboratory values, and typical patient history in IHPS enhances the clinician’s ability to make a timely diagnosis.
REFERENCES
1. Olivé AP, Endom EE. Infantile hypertrophic pyloric stenosis (2011). www.uptodate.com/contents/infan tile-hypertrophic-pyloric-stenosis. Accessed August 20, 2012.
2. Hernanz-Schulman M. Infantile hypertrophic pyloric stenosis. Radiology. 2003;227(2):319-331.
3. Aspelund G, Langer JC. Current management of hypertrophic pyloric stenosis. Semin Pediatr Surg. 2007;16(1):27-33.
4. To T, Wajja A, Wales PW, Langer JC. Population demographic indicators associated with incidence of pyloric stenosis. Arch Pediatr Adolesc Med. 2005;159(6):520-525.
5. MacMahon B. The continuing enigma of pyloric stenosis of infancy: a review. Epidemiology. 2006; 17(2):195-201.
6. Panteli C. New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 2009;25 (12):1043-1052.
7. Stone CK, Humphries RL, eds. Current Medical Diagnosis and Treatment: Emergency Medicine. 7th ed. Chapter 50. Pediatric emergencies (2008). http://accessmedicine.com/resourceTOC.aspx?resource ID=718. Accessed August 20, 2012.
8. Hulka F, Harrison MW, Campbell TJ, Campbell JR. Complications of pyloromyotomy for infantile hypertrophic pyloric stenosis. Am J Surg. 1997;173 (5):450-452.
9. Shaoul R, Enav B, Steiner Z, et al. Clinical presentation of pyloric stenosis: the change is in our hands. Isr Med Assoc J. 2004;6(3):134-137.
10. Weinstein MM, Seibert JJ, Ehrenberg A. Six atypical presentations of congenital hypertrophic pyloric stenosis. Clin Pediatr. 1979;18(2):120-122.
11. Eyal O, Asia A, Yorgenson U, et al. Atypical infantile hypertrophic pyloric stenosis [in Hebrew]. Harefuah. 1999;136(2):113-114, 175.
12. Mahon BE, Rosenman MB, Kleiman MB. Maternal and infant use of erythromycin and other macrolide antibiotics as risk factors for infantile hypertrophic pyloric stenosis. J Pediatr. 2001;139(3):380-384.
13. Chung E. Infantile hypertrophic pyloric stenosis: genes and environment. Arch Dis Child. 2008;93 (12):1003-1004.
14. Gilbertson-Dahdal DL, Dutta S, Varich LJ, Barth RA. Neonatal malrotation with midgut volvulus mimicking duodenal atresia. AJR Am J Roentgenol. 2009;192(5):1269-1271.
15. Schmedel W, Ashe L, Kuznicki K. A 24-day-old child with projectile vomiting. J Emerg Nurs. 2009; 35(2):163-164.
16. Iijima T, Okamatsu T, Matsumura M, Yatsuzuka M. Hypertrophic pyloric stenosis associated with hiatal hernia. J Pediatr Surg. 1996;31(2):277-279.
17. Nakayama DK, Taylor LA. Hypertrophic pyloric stenosis in infancy: an analysis of treatment outcome. N C Med J. 1998;59(5):310-313.
18. Irish MS, Pearl RH, Caty M, Glick PL. The approach to common abdominal diagnoses in infants and children. Pediatr Clin North Am. 1998; 45(4):729-772.
19. Askew N. An overview of infantile hypertrophic pyloric stenosis: literature review. Paediatric Nurs. 2010;22(8):27-30.
20. Rudolph CD. Infantile hypertrophic pyloric stenosis. In: Rudolph CD, Rudolph AM, eds. Rudolph’s Pediatrics. 21st ed. New York, NY: McGraw-Hill; 2002:1402-1403.
21. Hallam D, Hansen B, Bødker B, et al. Pyloric size in normal infants and in infants suspected of having hypertrophic pyloric stenosis. Acta Radiol. 2005;36(3):261.
22. Oakley EA, Barnett PL. Is acid base determination an accurate predictor of pyloric stenosis? J Paediatr Child Health. 2000;36(6):587-589.
23. Steven IM, Allen TH, Sweeney DB. Congenital hypertrophic pyloric stenosis: the anaesthetist’s view. Anaesth Intensive Care. 1973;1(6):544-546.
24. Singh UK, Kumar R, Prasad R. Oral atropine sulfate for infantile hypertrophic pyloric stenosis. Indian Pediatr. 2005;42(5):473-476.
25. Nagita A, Yamaguchi J, Amemoto K, et al. Management and ultrasonographic appearance of infantile hypertrophic pyloric stenosis with intravenous atropine sulfate. J Pediatr Gastroenterol Nutr. 1996;23(2):172-177.
26. Ogawa Y, Higashimoto U, Nishijima E, et al. Successful endoscopic balloon dilatation for hypertrophic pyloric stenosis. J Pediatr Surg. 1996;31(12):1712-1714.
27. Langer JC, To T. Does pediatric surgical specialty training affect outcome after Ramstedt pyloromyotomy? A population-based study. Pediatrics. 2004;113(5):1342-1347.
28. Pollock WF, Norris WJ. Dr. Conrad Ramstedt and pyloromyotomy. Surgery. 1957;42(5):966-970.
29. Najmaldin A, Tan HL. Early experience with laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis. J Pediatr Surg. 1995;30(1):37-38.
30. Jia WQ, Tian JH, Yang KH, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a meta-analysis of randomized controlled trials. Eur J Pediatr Surg. 2011;21(2):77-81.
31. Hall NJ, Pacilli M, Eaton S, et al. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Lancet. 2009;373(9661):390-398.
32. Adibe OO, Nichol PF, Flake AAW, Mattei P. Comparison of outcomes after laparoscopic and open pyloromyotomy at a high-volume pediatric teaching hospital. J Pediatr Surg. 2006;41(10):1676-1678.
33. St. Peter SD, Holcomb GW, Calkins CM, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial. Ann Surg. 2006;244(3):363-370.
34. Okorie NM, Dickson JA, Carver RA, Steiner GM. What happens to the pylorus after pyloromyotomy? Arch Dis Child. 1988;63(11):1339-1341.
Infantile hypertrophic pyloric stenosis (IHPS) is a common yet treatable condition in young infants, characterized by forceful vomiting after feeding as a result of hypertrophy of the pyloric muscle. Without proper diagnosis and surgical intervention, IHPS can eventually lead to dehydration, weight loss, and electrolyte disturbances, including the classic finding of hypochloremic alkalosis.1,2
IHPS occurs in two to four of every 1,000 births and is most common among white male infants.3,4 It develops between the first three to five weeks of life but rarely after age 12 weeks.1,2,5 IHPS is characterized by hypertrophy of the pyloric muscle (see figure), which eventually leads to gastric outlet obstruction.6,7
Because IHPS presents with symptoms that resemble those associated with other gastrointestinal disturbances, such as gastroesophageal reflux disease (GERD), it can be misdiagnosed in its early stages.1 Once it is identified, however, surgical correction by pyloromyotomy is considered curative, with a very low mortality rate (ie, 0.1%) and incidence recurrence in only 1% of patients. Typically, treated infants recover quickly and can begin feeding within hours after surgery.3,8
Although the etiology of IHPS remains unknown, providers can quickly recognize the signs and symptoms of IHPS in order for surgical treatment to be scheduled in a timely manner.
PATIENT PRESENTATION
Typically, an infant with IHPS will have a period of normal feeding for the first two to three weeks of life, followed by onset of nonbilious vomiting soon after feeding. Vomiting may become increasingly frequent and forceful—possibly described as “projectile.” Despite stomach distention, affected infants seem to have an insatiable appetite and may cry inconsolably. Depending on the duration of symptoms, patients may suffer significant weight loss, even falling below birth weight. In severe cases, a scaphoid abdomen and protruding ribcage may be present.1,2
Atypical Presentations
Premature infants with IHPS and those with certain medical or surgical conditions may present atypically. Vomiting may be less forceful, and the classic finding of visible gastric peristalsis may or may not be present.9 Researchers have documented cases in which hospitalized premature infants had nonprojectile vomiting, weight loss, and lethargy that were erroneously attributed to sepsis. IHPS should have been considered over sepsis when the infants’ clinical condition improved rapidly with rehydration, and when metabolic alkalosis (rather than acidosis) was identified.1,10,11
Projectile vomiting may not occur in infants with congenital anomalies that affect swallowing, such as cleft lip/palate or central nervous system disturbances. In infants who have recently undergone gastrointestinal (GI) surgery, IHPS may be misdiagnosed as adhesions or obstruction at an anastomotic site.1,10
RISK FACTORS
Despite the fact that IHPS is a relatively common condition, the etiology remains unknown. Research findings indicate that IHPS is not present at birth. Several hypotheses exist about potential risk factors, including genetics, use of macrolide antibiotics, and mechanical or environmental factors.6 IHPS has been associated with certain genetic conditions, including Cornelia de Lange syndrome and Smith-Lemli-Opitz syndrome, as well as chromosomal abnormalities, such as the translocation of chromosomes 8 and 17, and partial trisomy of chromosome 9.6,12
According to Chung,13 additional research has implicated the genetic loci IHPS1, also known as nitric oxide synthase 1 (NOS1), which encodes the gene for neuronal nitric oxide synthase (nNOS). This is the key enzyme for production of nitric oxide, which mediates relaxation of the pyloric smooth muscle.13
In a study by Mahon et al,12 an increased risk for IHPS was confirmed in young infants for whom systemic erythromycin had been prescribed as prophylactic treatment for pertussis. This may result from the agent’s motilin-like effects on antral smooth-muscle function.13
Mechanical defects, such as abnormal innervation of the pyloric muscle and neonatal hypergastrinemia and hyperacidity, have also been implicated.6 Infant sleeping position has been investigated as a possible environmental factor in the development of IHPS, correlating the decline in sudden infant death syndrome (attributed to decreased prone sleep position) with a decline in IHPS in recent years. However, no conclusive evidence has been shown to support this hypothesis.13
DIFFERENTIAL DIAGNOSIS
Typically, infants with nonbilious vomiting have either IHPS or GERD. Two factors to consider when evaluating the infant are its age and whether emesis is bilious or nonbilious. IHPS rarely causes bilious vomiting and most frequently occurs in infants between ages 3 and 6 weeks. Other GI disturbances that cause nonbilious emesis include adrenal crisis, gastroenteritis, pylorospasm, hiatal hernia, and preampullary duodenal stenosis.2 Malrotation or midgut volvulus may also be considered in the differential14 (see table1,2,14-16).
DIAGNOSIS
The diagnosis of IHPS is often made based on the history and physical exam. Imaging studies and labs can confirm the diagnosis, and surgery is usually deferred until dehydration has been addressed and any electrolyte disturbances corrected.1,17
Physical Examination
The infant may appear underweight and dehydrated, with visible peristaltic waves across the upper abdomen prior to emesis. Severe illness may be indicated in an underweight infant with the classic scaphoid abdomen.18
Palpation of an olive-shaped mass in the upper left quadrant of the epigastric region is pathognomonic for IHPS; the mass may be found more easily after emesis has occurred.19 To facilitate palpation, the hips can first be flexed to relax the abdominal wall. Next, the examiner should palpate gently for the “olive” in the space midway between the umbilicus and the xiphoid, between the two rectus muscles.3 All other findings in the physical exam should be within normal limits.
Imaging and Laboratory
Studies
An experienced provider can make a diagnosis of IHPS based on clinical examination alone in 60% to 80% of cases.20 However, most surgeons require the diagnosis to be confirmed with one of the following imaging studies before surgery.19
The diagnosis of IHPS can be confirmed by an upper GI series, but this is not commonly ordered as the primary diagnostic study. Ultrasound has become the modality of choice9; it can be used to quantify the size of an elongated, thickened pyloric muscle. The hypertrophied pylorus ranges in length from 14 to 16 mm, with thickness measuring more than 3.0 to 3.5 mm.1,19,21
An upper GI contrast study is rarely used for diagnosis of IHPS, but when this test is ordered to detect other gastrointestinal disease processes (eg, malrotation), IHPS may be identified incidentally.19 During an upper GI study, contrast material is propelled through the pyloric mucosa, and the string sign or the double-track sign may be visualized, revealing the mucosal filling defect.2
Abdominal x-ray may reveal a dilated stomach or a blockage, with a possible finding of gas in the gastric bubble but extending no further into the intestine.19
A study by Hernanz-Schulman2 was conducted to quantify the sensitivities and specificities associated with different diagnostic tools and the clinician’s experience and proficiency in using them. According to this study, palpation by a surgeon has a sensitivity of 31% to 99% and a specificity of 85% to 99% for detection of the pathognomonic olive-shaped mass. Ultrasound performed by an experienced technician has 97% to 100% sensitivity and 99% to 100% specificity for detecting IHPS. An upper GI series has 90% to 100% sensitivity and 99.5% specificity.
Venous blood gas and electrolyte levels are both helpful in making a diagnosis of IHPS.19,22 In a study by Oakley and Barnett,22 the following lab values were found useful in confirming the presence of pyloric stenosis: pH > 7.45; chloride 3 mEq/L. Sodium and potassium deficits may also be present.2,22
Before treatment is considered, the degree of dehydration must be determined by clinical examination and urinary output, as well as serum bicarbonate and chloride levels.3 Other laboratory tests to be ordered include urinalysis and a complete blood count (including platelets).
TREATMENT/MANAGEMENT
Initial management of vomiting in children should begin with fluid replacement if the patient appears dehydrated or if lab findings suggest an electrolyte imbalance. If surgery is later deemed necessary, this will reduce the risk for postoperative apnea.1,23
If IHPS is suspected, a pediatric surgery consult should be obtained. Before anesthesia is considered, serum bicarbonate should be measured with results no higher than 28 mEq/L, and the serum chloride level should be at least 100 mEq/L.3 Imaging, such as ultrasound or the upper GI series, may be ordered to confirm the diagnosis.
Surgical correction by a pyloromyotomy is curative. Presurgical gastric decompression via nasogastric tube placement will reduce the risk for postoperative vomiting and gastritis.20
Surgery
Although a variety of nonsurgical interventions, including oral and IV atropine and balloon dilation, have been described in the literature,3,24-26 the preferred treatment for IHPS is surgical intervention. Surgical correction has been so consistently successful (that is, provided the procedure is performed by a pediatric surgeon or other surgeon with appropriate experience3) that the treatment of choice for IHPS is the Ramstedt pyloromyotomy, which was first performed in 1912.6,27,28
Although the approach may differ based on the individual surgeon’s preference, the pyloric muscle is pulled through an incision in the abdominal wall. A longitudinal incision is made through the muscle with blunt dissection to the submucosa on the anterior surface of the pylorus. The pylorus is then returned to the abdominal cavity, and the abdominal incision is sutured.3,20
The laparoscopic approach, first described in the literature in the mid-1990s,29 is gaining popularity among surgeons, although recent studies have demonstrated that open and laparoscopic procedures are comparably safe and effective for the management of IHPS.30-33 Results from a recent study by Jia et al30 indicate that the laparoscopic approach results in reduced postoperative emesis, shorter length of hospital stay, and shorter recovery times; Hall et al31 emphasize the advantages of laparoscopic pyloromyotomy and recommend it over open surgery in facilities with experienced surgeons.
In follow-up ultrasound studies, hypertrophy of the pyloric muscle was reportedly resolved between two and 12 weeks after pyloromyotomy.34
Postoperative Care
The gastric tube can be removed and oral fluids reintroduced slowly at the surgeon’s discretion, between 8 and 12 hours after surgery. Postoperative vomiting is common (occurring in up to 80% of patients) but should resolve within 24 hours. Mild emesis should not delay the refeeding schedule.3
Patients should be evaluated by the surgeon one to two weeks following surgery unless the infant shows signs of infection (ie, fever, erythema, edema, bleeding, purulent drainage, excess pain, decreased fluid or nutritional intake). Follow-up imaging and laboratory studies are not indicated in an otherwise healthy infant.20
CONCLUSION
Early detection of IHPS, a condition characterized by hypertrophy of the pyloric muscle that results in gastric obstruction and projectile vomiting, can prevent complications of dehydration, malnutrition, and electrolyte disturbances. Surgery by open or laparoscopic pyloromyotomy is curative. Knowing the key physical exam findings, laboratory values, and typical patient history in IHPS enhances the clinician’s ability to make a timely diagnosis.
REFERENCES
1. Olivé AP, Endom EE. Infantile hypertrophic pyloric stenosis (2011). www.uptodate.com/contents/infan tile-hypertrophic-pyloric-stenosis. Accessed August 20, 2012.
2. Hernanz-Schulman M. Infantile hypertrophic pyloric stenosis. Radiology. 2003;227(2):319-331.
3. Aspelund G, Langer JC. Current management of hypertrophic pyloric stenosis. Semin Pediatr Surg. 2007;16(1):27-33.
4. To T, Wajja A, Wales PW, Langer JC. Population demographic indicators associated with incidence of pyloric stenosis. Arch Pediatr Adolesc Med. 2005;159(6):520-525.
5. MacMahon B. The continuing enigma of pyloric stenosis of infancy: a review. Epidemiology. 2006; 17(2):195-201.
6. Panteli C. New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 2009;25 (12):1043-1052.
7. Stone CK, Humphries RL, eds. Current Medical Diagnosis and Treatment: Emergency Medicine. 7th ed. Chapter 50. Pediatric emergencies (2008). http://accessmedicine.com/resourceTOC.aspx?resource ID=718. Accessed August 20, 2012.
8. Hulka F, Harrison MW, Campbell TJ, Campbell JR. Complications of pyloromyotomy for infantile hypertrophic pyloric stenosis. Am J Surg. 1997;173 (5):450-452.
9. Shaoul R, Enav B, Steiner Z, et al. Clinical presentation of pyloric stenosis: the change is in our hands. Isr Med Assoc J. 2004;6(3):134-137.
10. Weinstein MM, Seibert JJ, Ehrenberg A. Six atypical presentations of congenital hypertrophic pyloric stenosis. Clin Pediatr. 1979;18(2):120-122.
11. Eyal O, Asia A, Yorgenson U, et al. Atypical infantile hypertrophic pyloric stenosis [in Hebrew]. Harefuah. 1999;136(2):113-114, 175.
12. Mahon BE, Rosenman MB, Kleiman MB. Maternal and infant use of erythromycin and other macrolide antibiotics as risk factors for infantile hypertrophic pyloric stenosis. J Pediatr. 2001;139(3):380-384.
13. Chung E. Infantile hypertrophic pyloric stenosis: genes and environment. Arch Dis Child. 2008;93 (12):1003-1004.
14. Gilbertson-Dahdal DL, Dutta S, Varich LJ, Barth RA. Neonatal malrotation with midgut volvulus mimicking duodenal atresia. AJR Am J Roentgenol. 2009;192(5):1269-1271.
15. Schmedel W, Ashe L, Kuznicki K. A 24-day-old child with projectile vomiting. J Emerg Nurs. 2009; 35(2):163-164.
16. Iijima T, Okamatsu T, Matsumura M, Yatsuzuka M. Hypertrophic pyloric stenosis associated with hiatal hernia. J Pediatr Surg. 1996;31(2):277-279.
17. Nakayama DK, Taylor LA. Hypertrophic pyloric stenosis in infancy: an analysis of treatment outcome. N C Med J. 1998;59(5):310-313.
18. Irish MS, Pearl RH, Caty M, Glick PL. The approach to common abdominal diagnoses in infants and children. Pediatr Clin North Am. 1998; 45(4):729-772.
19. Askew N. An overview of infantile hypertrophic pyloric stenosis: literature review. Paediatric Nurs. 2010;22(8):27-30.
20. Rudolph CD. Infantile hypertrophic pyloric stenosis. In: Rudolph CD, Rudolph AM, eds. Rudolph’s Pediatrics. 21st ed. New York, NY: McGraw-Hill; 2002:1402-1403.
21. Hallam D, Hansen B, Bødker B, et al. Pyloric size in normal infants and in infants suspected of having hypertrophic pyloric stenosis. Acta Radiol. 2005;36(3):261.
22. Oakley EA, Barnett PL. Is acid base determination an accurate predictor of pyloric stenosis? J Paediatr Child Health. 2000;36(6):587-589.
23. Steven IM, Allen TH, Sweeney DB. Congenital hypertrophic pyloric stenosis: the anaesthetist’s view. Anaesth Intensive Care. 1973;1(6):544-546.
24. Singh UK, Kumar R, Prasad R. Oral atropine sulfate for infantile hypertrophic pyloric stenosis. Indian Pediatr. 2005;42(5):473-476.
25. Nagita A, Yamaguchi J, Amemoto K, et al. Management and ultrasonographic appearance of infantile hypertrophic pyloric stenosis with intravenous atropine sulfate. J Pediatr Gastroenterol Nutr. 1996;23(2):172-177.
26. Ogawa Y, Higashimoto U, Nishijima E, et al. Successful endoscopic balloon dilatation for hypertrophic pyloric stenosis. J Pediatr Surg. 1996;31(12):1712-1714.
27. Langer JC, To T. Does pediatric surgical specialty training affect outcome after Ramstedt pyloromyotomy? A population-based study. Pediatrics. 2004;113(5):1342-1347.
28. Pollock WF, Norris WJ. Dr. Conrad Ramstedt and pyloromyotomy. Surgery. 1957;42(5):966-970.
29. Najmaldin A, Tan HL. Early experience with laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis. J Pediatr Surg. 1995;30(1):37-38.
30. Jia WQ, Tian JH, Yang KH, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a meta-analysis of randomized controlled trials. Eur J Pediatr Surg. 2011;21(2):77-81.
31. Hall NJ, Pacilli M, Eaton S, et al. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Lancet. 2009;373(9661):390-398.
32. Adibe OO, Nichol PF, Flake AAW, Mattei P. Comparison of outcomes after laparoscopic and open pyloromyotomy at a high-volume pediatric teaching hospital. J Pediatr Surg. 2006;41(10):1676-1678.
33. St. Peter SD, Holcomb GW, Calkins CM, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial. Ann Surg. 2006;244(3):363-370.
34. Okorie NM, Dickson JA, Carver RA, Steiner GM. What happens to the pylorus after pyloromyotomy? Arch Dis Child. 1988;63(11):1339-1341.
Infantile hypertrophic pyloric stenosis (IHPS) is a common yet treatable condition in young infants, characterized by forceful vomiting after feeding as a result of hypertrophy of the pyloric muscle. Without proper diagnosis and surgical intervention, IHPS can eventually lead to dehydration, weight loss, and electrolyte disturbances, including the classic finding of hypochloremic alkalosis.1,2
IHPS occurs in two to four of every 1,000 births and is most common among white male infants.3,4 It develops between the first three to five weeks of life but rarely after age 12 weeks.1,2,5 IHPS is characterized by hypertrophy of the pyloric muscle (see figure), which eventually leads to gastric outlet obstruction.6,7
Because IHPS presents with symptoms that resemble those associated with other gastrointestinal disturbances, such as gastroesophageal reflux disease (GERD), it can be misdiagnosed in its early stages.1 Once it is identified, however, surgical correction by pyloromyotomy is considered curative, with a very low mortality rate (ie, 0.1%) and incidence recurrence in only 1% of patients. Typically, treated infants recover quickly and can begin feeding within hours after surgery.3,8
Although the etiology of IHPS remains unknown, providers can quickly recognize the signs and symptoms of IHPS in order for surgical treatment to be scheduled in a timely manner.
PATIENT PRESENTATION
Typically, an infant with IHPS will have a period of normal feeding for the first two to three weeks of life, followed by onset of nonbilious vomiting soon after feeding. Vomiting may become increasingly frequent and forceful—possibly described as “projectile.” Despite stomach distention, affected infants seem to have an insatiable appetite and may cry inconsolably. Depending on the duration of symptoms, patients may suffer significant weight loss, even falling below birth weight. In severe cases, a scaphoid abdomen and protruding ribcage may be present.1,2
Atypical Presentations
Premature infants with IHPS and those with certain medical or surgical conditions may present atypically. Vomiting may be less forceful, and the classic finding of visible gastric peristalsis may or may not be present.9 Researchers have documented cases in which hospitalized premature infants had nonprojectile vomiting, weight loss, and lethargy that were erroneously attributed to sepsis. IHPS should have been considered over sepsis when the infants’ clinical condition improved rapidly with rehydration, and when metabolic alkalosis (rather than acidosis) was identified.1,10,11
Projectile vomiting may not occur in infants with congenital anomalies that affect swallowing, such as cleft lip/palate or central nervous system disturbances. In infants who have recently undergone gastrointestinal (GI) surgery, IHPS may be misdiagnosed as adhesions or obstruction at an anastomotic site.1,10
RISK FACTORS
Despite the fact that IHPS is a relatively common condition, the etiology remains unknown. Research findings indicate that IHPS is not present at birth. Several hypotheses exist about potential risk factors, including genetics, use of macrolide antibiotics, and mechanical or environmental factors.6 IHPS has been associated with certain genetic conditions, including Cornelia de Lange syndrome and Smith-Lemli-Opitz syndrome, as well as chromosomal abnormalities, such as the translocation of chromosomes 8 and 17, and partial trisomy of chromosome 9.6,12
According to Chung,13 additional research has implicated the genetic loci IHPS1, also known as nitric oxide synthase 1 (NOS1), which encodes the gene for neuronal nitric oxide synthase (nNOS). This is the key enzyme for production of nitric oxide, which mediates relaxation of the pyloric smooth muscle.13
In a study by Mahon et al,12 an increased risk for IHPS was confirmed in young infants for whom systemic erythromycin had been prescribed as prophylactic treatment for pertussis. This may result from the agent’s motilin-like effects on antral smooth-muscle function.13
Mechanical defects, such as abnormal innervation of the pyloric muscle and neonatal hypergastrinemia and hyperacidity, have also been implicated.6 Infant sleeping position has been investigated as a possible environmental factor in the development of IHPS, correlating the decline in sudden infant death syndrome (attributed to decreased prone sleep position) with a decline in IHPS in recent years. However, no conclusive evidence has been shown to support this hypothesis.13
DIFFERENTIAL DIAGNOSIS
Typically, infants with nonbilious vomiting have either IHPS or GERD. Two factors to consider when evaluating the infant are its age and whether emesis is bilious or nonbilious. IHPS rarely causes bilious vomiting and most frequently occurs in infants between ages 3 and 6 weeks. Other GI disturbances that cause nonbilious emesis include adrenal crisis, gastroenteritis, pylorospasm, hiatal hernia, and preampullary duodenal stenosis.2 Malrotation or midgut volvulus may also be considered in the differential14 (see table1,2,14-16).
DIAGNOSIS
The diagnosis of IHPS is often made based on the history and physical exam. Imaging studies and labs can confirm the diagnosis, and surgery is usually deferred until dehydration has been addressed and any electrolyte disturbances corrected.1,17
Physical Examination
The infant may appear underweight and dehydrated, with visible peristaltic waves across the upper abdomen prior to emesis. Severe illness may be indicated in an underweight infant with the classic scaphoid abdomen.18
Palpation of an olive-shaped mass in the upper left quadrant of the epigastric region is pathognomonic for IHPS; the mass may be found more easily after emesis has occurred.19 To facilitate palpation, the hips can first be flexed to relax the abdominal wall. Next, the examiner should palpate gently for the “olive” in the space midway between the umbilicus and the xiphoid, between the two rectus muscles.3 All other findings in the physical exam should be within normal limits.
Imaging and Laboratory
Studies
An experienced provider can make a diagnosis of IHPS based on clinical examination alone in 60% to 80% of cases.20 However, most surgeons require the diagnosis to be confirmed with one of the following imaging studies before surgery.19
The diagnosis of IHPS can be confirmed by an upper GI series, but this is not commonly ordered as the primary diagnostic study. Ultrasound has become the modality of choice9; it can be used to quantify the size of an elongated, thickened pyloric muscle. The hypertrophied pylorus ranges in length from 14 to 16 mm, with thickness measuring more than 3.0 to 3.5 mm.1,19,21
An upper GI contrast study is rarely used for diagnosis of IHPS, but when this test is ordered to detect other gastrointestinal disease processes (eg, malrotation), IHPS may be identified incidentally.19 During an upper GI study, contrast material is propelled through the pyloric mucosa, and the string sign or the double-track sign may be visualized, revealing the mucosal filling defect.2
Abdominal x-ray may reveal a dilated stomach or a blockage, with a possible finding of gas in the gastric bubble but extending no further into the intestine.19
A study by Hernanz-Schulman2 was conducted to quantify the sensitivities and specificities associated with different diagnostic tools and the clinician’s experience and proficiency in using them. According to this study, palpation by a surgeon has a sensitivity of 31% to 99% and a specificity of 85% to 99% for detection of the pathognomonic olive-shaped mass. Ultrasound performed by an experienced technician has 97% to 100% sensitivity and 99% to 100% specificity for detecting IHPS. An upper GI series has 90% to 100% sensitivity and 99.5% specificity.
Venous blood gas and electrolyte levels are both helpful in making a diagnosis of IHPS.19,22 In a study by Oakley and Barnett,22 the following lab values were found useful in confirming the presence of pyloric stenosis: pH > 7.45; chloride 3 mEq/L. Sodium and potassium deficits may also be present.2,22
Before treatment is considered, the degree of dehydration must be determined by clinical examination and urinary output, as well as serum bicarbonate and chloride levels.3 Other laboratory tests to be ordered include urinalysis and a complete blood count (including platelets).
TREATMENT/MANAGEMENT
Initial management of vomiting in children should begin with fluid replacement if the patient appears dehydrated or if lab findings suggest an electrolyte imbalance. If surgery is later deemed necessary, this will reduce the risk for postoperative apnea.1,23
If IHPS is suspected, a pediatric surgery consult should be obtained. Before anesthesia is considered, serum bicarbonate should be measured with results no higher than 28 mEq/L, and the serum chloride level should be at least 100 mEq/L.3 Imaging, such as ultrasound or the upper GI series, may be ordered to confirm the diagnosis.
Surgical correction by a pyloromyotomy is curative. Presurgical gastric decompression via nasogastric tube placement will reduce the risk for postoperative vomiting and gastritis.20
Surgery
Although a variety of nonsurgical interventions, including oral and IV atropine and balloon dilation, have been described in the literature,3,24-26 the preferred treatment for IHPS is surgical intervention. Surgical correction has been so consistently successful (that is, provided the procedure is performed by a pediatric surgeon or other surgeon with appropriate experience3) that the treatment of choice for IHPS is the Ramstedt pyloromyotomy, which was first performed in 1912.6,27,28
Although the approach may differ based on the individual surgeon’s preference, the pyloric muscle is pulled through an incision in the abdominal wall. A longitudinal incision is made through the muscle with blunt dissection to the submucosa on the anterior surface of the pylorus. The pylorus is then returned to the abdominal cavity, and the abdominal incision is sutured.3,20
The laparoscopic approach, first described in the literature in the mid-1990s,29 is gaining popularity among surgeons, although recent studies have demonstrated that open and laparoscopic procedures are comparably safe and effective for the management of IHPS.30-33 Results from a recent study by Jia et al30 indicate that the laparoscopic approach results in reduced postoperative emesis, shorter length of hospital stay, and shorter recovery times; Hall et al31 emphasize the advantages of laparoscopic pyloromyotomy and recommend it over open surgery in facilities with experienced surgeons.
In follow-up ultrasound studies, hypertrophy of the pyloric muscle was reportedly resolved between two and 12 weeks after pyloromyotomy.34
Postoperative Care
The gastric tube can be removed and oral fluids reintroduced slowly at the surgeon’s discretion, between 8 and 12 hours after surgery. Postoperative vomiting is common (occurring in up to 80% of patients) but should resolve within 24 hours. Mild emesis should not delay the refeeding schedule.3
Patients should be evaluated by the surgeon one to two weeks following surgery unless the infant shows signs of infection (ie, fever, erythema, edema, bleeding, purulent drainage, excess pain, decreased fluid or nutritional intake). Follow-up imaging and laboratory studies are not indicated in an otherwise healthy infant.20
CONCLUSION
Early detection of IHPS, a condition characterized by hypertrophy of the pyloric muscle that results in gastric obstruction and projectile vomiting, can prevent complications of dehydration, malnutrition, and electrolyte disturbances. Surgery by open or laparoscopic pyloromyotomy is curative. Knowing the key physical exam findings, laboratory values, and typical patient history in IHPS enhances the clinician’s ability to make a timely diagnosis.
REFERENCES
1. Olivé AP, Endom EE. Infantile hypertrophic pyloric stenosis (2011). www.uptodate.com/contents/infan tile-hypertrophic-pyloric-stenosis. Accessed August 20, 2012.
2. Hernanz-Schulman M. Infantile hypertrophic pyloric stenosis. Radiology. 2003;227(2):319-331.
3. Aspelund G, Langer JC. Current management of hypertrophic pyloric stenosis. Semin Pediatr Surg. 2007;16(1):27-33.
4. To T, Wajja A, Wales PW, Langer JC. Population demographic indicators associated with incidence of pyloric stenosis. Arch Pediatr Adolesc Med. 2005;159(6):520-525.
5. MacMahon B. The continuing enigma of pyloric stenosis of infancy: a review. Epidemiology. 2006; 17(2):195-201.
6. Panteli C. New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 2009;25 (12):1043-1052.
7. Stone CK, Humphries RL, eds. Current Medical Diagnosis and Treatment: Emergency Medicine. 7th ed. Chapter 50. Pediatric emergencies (2008). http://accessmedicine.com/resourceTOC.aspx?resource ID=718. Accessed August 20, 2012.
8. Hulka F, Harrison MW, Campbell TJ, Campbell JR. Complications of pyloromyotomy for infantile hypertrophic pyloric stenosis. Am J Surg. 1997;173 (5):450-452.
9. Shaoul R, Enav B, Steiner Z, et al. Clinical presentation of pyloric stenosis: the change is in our hands. Isr Med Assoc J. 2004;6(3):134-137.
10. Weinstein MM, Seibert JJ, Ehrenberg A. Six atypical presentations of congenital hypertrophic pyloric stenosis. Clin Pediatr. 1979;18(2):120-122.
11. Eyal O, Asia A, Yorgenson U, et al. Atypical infantile hypertrophic pyloric stenosis [in Hebrew]. Harefuah. 1999;136(2):113-114, 175.
12. Mahon BE, Rosenman MB, Kleiman MB. Maternal and infant use of erythromycin and other macrolide antibiotics as risk factors for infantile hypertrophic pyloric stenosis. J Pediatr. 2001;139(3):380-384.
13. Chung E. Infantile hypertrophic pyloric stenosis: genes and environment. Arch Dis Child. 2008;93 (12):1003-1004.
14. Gilbertson-Dahdal DL, Dutta S, Varich LJ, Barth RA. Neonatal malrotation with midgut volvulus mimicking duodenal atresia. AJR Am J Roentgenol. 2009;192(5):1269-1271.
15. Schmedel W, Ashe L, Kuznicki K. A 24-day-old child with projectile vomiting. J Emerg Nurs. 2009; 35(2):163-164.
16. Iijima T, Okamatsu T, Matsumura M, Yatsuzuka M. Hypertrophic pyloric stenosis associated with hiatal hernia. J Pediatr Surg. 1996;31(2):277-279.
17. Nakayama DK, Taylor LA. Hypertrophic pyloric stenosis in infancy: an analysis of treatment outcome. N C Med J. 1998;59(5):310-313.
18. Irish MS, Pearl RH, Caty M, Glick PL. The approach to common abdominal diagnoses in infants and children. Pediatr Clin North Am. 1998; 45(4):729-772.
19. Askew N. An overview of infantile hypertrophic pyloric stenosis: literature review. Paediatric Nurs. 2010;22(8):27-30.
20. Rudolph CD. Infantile hypertrophic pyloric stenosis. In: Rudolph CD, Rudolph AM, eds. Rudolph’s Pediatrics. 21st ed. New York, NY: McGraw-Hill; 2002:1402-1403.
21. Hallam D, Hansen B, Bødker B, et al. Pyloric size in normal infants and in infants suspected of having hypertrophic pyloric stenosis. Acta Radiol. 2005;36(3):261.
22. Oakley EA, Barnett PL. Is acid base determination an accurate predictor of pyloric stenosis? J Paediatr Child Health. 2000;36(6):587-589.
23. Steven IM, Allen TH, Sweeney DB. Congenital hypertrophic pyloric stenosis: the anaesthetist’s view. Anaesth Intensive Care. 1973;1(6):544-546.
24. Singh UK, Kumar R, Prasad R. Oral atropine sulfate for infantile hypertrophic pyloric stenosis. Indian Pediatr. 2005;42(5):473-476.
25. Nagita A, Yamaguchi J, Amemoto K, et al. Management and ultrasonographic appearance of infantile hypertrophic pyloric stenosis with intravenous atropine sulfate. J Pediatr Gastroenterol Nutr. 1996;23(2):172-177.
26. Ogawa Y, Higashimoto U, Nishijima E, et al. Successful endoscopic balloon dilatation for hypertrophic pyloric stenosis. J Pediatr Surg. 1996;31(12):1712-1714.
27. Langer JC, To T. Does pediatric surgical specialty training affect outcome after Ramstedt pyloromyotomy? A population-based study. Pediatrics. 2004;113(5):1342-1347.
28. Pollock WF, Norris WJ. Dr. Conrad Ramstedt and pyloromyotomy. Surgery. 1957;42(5):966-970.
29. Najmaldin A, Tan HL. Early experience with laparoscopic pyloromyotomy for infantile hypertrophic pyloric stenosis. J Pediatr Surg. 1995;30(1):37-38.
30. Jia WQ, Tian JH, Yang KH, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a meta-analysis of randomized controlled trials. Eur J Pediatr Surg. 2011;21(2):77-81.
31. Hall NJ, Pacilli M, Eaton S, et al. Recovery after open versus laparoscopic pyloromyotomy for pyloric stenosis: a double-blind multicentre randomised controlled trial. Lancet. 2009;373(9661):390-398.
32. Adibe OO, Nichol PF, Flake AAW, Mattei P. Comparison of outcomes after laparoscopic and open pyloromyotomy at a high-volume pediatric teaching hospital. J Pediatr Surg. 2006;41(10):1676-1678.
33. St. Peter SD, Holcomb GW, Calkins CM, et al. Open versus laparoscopic pyloromyotomy for pyloric stenosis: a prospective, randomized trial. Ann Surg. 2006;244(3):363-370.
34. Okorie NM, Dickson JA, Carver RA, Steiner GM. What happens to the pylorus after pyloromyotomy? Arch Dis Child. 1988;63(11):1339-1341.