User login
Return of the Wild?
Last week I was on the last leg of my usual three-peninsula bicycle ride. Every now and then, I turned my gaze away from the spectacular ocean scenery and looked down at the road ahead. On one of those glances, I saw a small orange, noodlelike object that seemed to move. I braked and pedaled back, and I was surprised to find it was a salamander. I had not seen an orange salamander in nearly 60 years.
There are several reasons for that 6-decade gap. First, as I approached adolescence, I spent increasingly less time poking around in the woods and along the stream beds around my home, natural habitats for salamanders. However, after I finished my training and was a few years into practice, I returned to a woodsier lifestyle, and I spent hours on my hands and knees gardening in what should have been amphibian- and reptilian-friendly environs. I occasionally saw a toad, but never a salamander. While I had been metamorphing into an adult physician, the amphibians had been suffering a serious global decline, the causes of which are still largely unknown and hotly debated.
As I continued on my ride home, my mind drifted back to my childhood and my life with reptiles and amphibians. I spent hours on solitary forays along the streams and ponds in our neighborhood, collecting specimens. Most of my buddies were doing the same. There were tadpoles in Mason jars, toads in an old cracked aquarium I got from the neighbors, and turtles in cardboard boxes and discarded dishpans. Snakes were more of a challenge to catch and house, but every now and then I got lucky. None of the inhabitants of my menagerie ever made it into our house. My mother had a few, but sensible, rules.
These animals weren’t pets. Dog and cats were pets. Amphibians and reptiles were curiosities to be observed and studied, not stroked or petted. Those that survived their brief captivities were returned to the wild.
One could buy small turtles at the pet store. At the circus, there were racks of small perforated cellophane bags for sale, in which small lizards and chameleon were encased. Even as I child I knew those poor little captives were never going to survive for long after their car ride home. No, my friends and I were into wild specimens, caught for scientific study. Although there has been a surge of health warnings about the health risks from handling reptiles and amphibians, none of us ever got salmonella poisoning. Granted, our sample size was small, but our exposure was extensive.
When I arrived home from my ride, I decided to review the Centers for Disease Control and Prevention warnings, and to look a little bit more deeply into the real risks that we had survived from our amphibian and reptilian encounters. The CDC website list of cautions and recommendations are for the most part reasonable ... and not much different from my mother’s house rules and requirements for basic hygiene.
However, I was troubled by one warning that "children younger than 5 years old ... should not handle or touch reptiles, or anything in the area where they live and roam." If my parents had followed this recommendation, they would have set me down me in front of the television and never let me play outside. No more stream side exploring, no more turning over rocks and old logs, no more building fairy houses in the mossy woods.
No distinction is made in the CDC warnings between wild and captive animals. In the little research I could find on the subject, it turns out that wild reptiles are less likely to carry and shed salmonella. A study of red-sliders, a common pet store turtle with a long rap sheet of salmonella outbreaks, could find no salmonella in the wild specimens tested. Another study found that the tadpoles they cultured had no salmonella. One author postulated that the stress of captivity renders reptiles and amphibians more vulnerable to infection, as it has been found to do in other animals.
So it turns out that, as usual, my mother was correct. Go out and explore. Don’t buy at the pet store. Don’t bring ’em into the house. Sadly, even if we are successful in getting kids off the couch and into the woods, they will be less likely to find reptiles and amphibians when they go exploring. But, I am a hopeful guy. Maybe the little orange salamander I saw is the vanguard of an amphibian return.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
Last week I was on the last leg of my usual three-peninsula bicycle ride. Every now and then, I turned my gaze away from the spectacular ocean scenery and looked down at the road ahead. On one of those glances, I saw a small orange, noodlelike object that seemed to move. I braked and pedaled back, and I was surprised to find it was a salamander. I had not seen an orange salamander in nearly 60 years.
There are several reasons for that 6-decade gap. First, as I approached adolescence, I spent increasingly less time poking around in the woods and along the stream beds around my home, natural habitats for salamanders. However, after I finished my training and was a few years into practice, I returned to a woodsier lifestyle, and I spent hours on my hands and knees gardening in what should have been amphibian- and reptilian-friendly environs. I occasionally saw a toad, but never a salamander. While I had been metamorphing into an adult physician, the amphibians had been suffering a serious global decline, the causes of which are still largely unknown and hotly debated.
As I continued on my ride home, my mind drifted back to my childhood and my life with reptiles and amphibians. I spent hours on solitary forays along the streams and ponds in our neighborhood, collecting specimens. Most of my buddies were doing the same. There were tadpoles in Mason jars, toads in an old cracked aquarium I got from the neighbors, and turtles in cardboard boxes and discarded dishpans. Snakes were more of a challenge to catch and house, but every now and then I got lucky. None of the inhabitants of my menagerie ever made it into our house. My mother had a few, but sensible, rules.
These animals weren’t pets. Dog and cats were pets. Amphibians and reptiles were curiosities to be observed and studied, not stroked or petted. Those that survived their brief captivities were returned to the wild.
One could buy small turtles at the pet store. At the circus, there were racks of small perforated cellophane bags for sale, in which small lizards and chameleon were encased. Even as I child I knew those poor little captives were never going to survive for long after their car ride home. No, my friends and I were into wild specimens, caught for scientific study. Although there has been a surge of health warnings about the health risks from handling reptiles and amphibians, none of us ever got salmonella poisoning. Granted, our sample size was small, but our exposure was extensive.
When I arrived home from my ride, I decided to review the Centers for Disease Control and Prevention warnings, and to look a little bit more deeply into the real risks that we had survived from our amphibian and reptilian encounters. The CDC website list of cautions and recommendations are for the most part reasonable ... and not much different from my mother’s house rules and requirements for basic hygiene.
However, I was troubled by one warning that "children younger than 5 years old ... should not handle or touch reptiles, or anything in the area where they live and roam." If my parents had followed this recommendation, they would have set me down me in front of the television and never let me play outside. No more stream side exploring, no more turning over rocks and old logs, no more building fairy houses in the mossy woods.
No distinction is made in the CDC warnings between wild and captive animals. In the little research I could find on the subject, it turns out that wild reptiles are less likely to carry and shed salmonella. A study of red-sliders, a common pet store turtle with a long rap sheet of salmonella outbreaks, could find no salmonella in the wild specimens tested. Another study found that the tadpoles they cultured had no salmonella. One author postulated that the stress of captivity renders reptiles and amphibians more vulnerable to infection, as it has been found to do in other animals.
So it turns out that, as usual, my mother was correct. Go out and explore. Don’t buy at the pet store. Don’t bring ’em into the house. Sadly, even if we are successful in getting kids off the couch and into the woods, they will be less likely to find reptiles and amphibians when they go exploring. But, I am a hopeful guy. Maybe the little orange salamander I saw is the vanguard of an amphibian return.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
Last week I was on the last leg of my usual three-peninsula bicycle ride. Every now and then, I turned my gaze away from the spectacular ocean scenery and looked down at the road ahead. On one of those glances, I saw a small orange, noodlelike object that seemed to move. I braked and pedaled back, and I was surprised to find it was a salamander. I had not seen an orange salamander in nearly 60 years.
There are several reasons for that 6-decade gap. First, as I approached adolescence, I spent increasingly less time poking around in the woods and along the stream beds around my home, natural habitats for salamanders. However, after I finished my training and was a few years into practice, I returned to a woodsier lifestyle, and I spent hours on my hands and knees gardening in what should have been amphibian- and reptilian-friendly environs. I occasionally saw a toad, but never a salamander. While I had been metamorphing into an adult physician, the amphibians had been suffering a serious global decline, the causes of which are still largely unknown and hotly debated.
As I continued on my ride home, my mind drifted back to my childhood and my life with reptiles and amphibians. I spent hours on solitary forays along the streams and ponds in our neighborhood, collecting specimens. Most of my buddies were doing the same. There were tadpoles in Mason jars, toads in an old cracked aquarium I got from the neighbors, and turtles in cardboard boxes and discarded dishpans. Snakes were more of a challenge to catch and house, but every now and then I got lucky. None of the inhabitants of my menagerie ever made it into our house. My mother had a few, but sensible, rules.
These animals weren’t pets. Dog and cats were pets. Amphibians and reptiles were curiosities to be observed and studied, not stroked or petted. Those that survived their brief captivities were returned to the wild.
One could buy small turtles at the pet store. At the circus, there were racks of small perforated cellophane bags for sale, in which small lizards and chameleon were encased. Even as I child I knew those poor little captives were never going to survive for long after their car ride home. No, my friends and I were into wild specimens, caught for scientific study. Although there has been a surge of health warnings about the health risks from handling reptiles and amphibians, none of us ever got salmonella poisoning. Granted, our sample size was small, but our exposure was extensive.
When I arrived home from my ride, I decided to review the Centers for Disease Control and Prevention warnings, and to look a little bit more deeply into the real risks that we had survived from our amphibian and reptilian encounters. The CDC website list of cautions and recommendations are for the most part reasonable ... and not much different from my mother’s house rules and requirements for basic hygiene.
However, I was troubled by one warning that "children younger than 5 years old ... should not handle or touch reptiles, or anything in the area where they live and roam." If my parents had followed this recommendation, they would have set me down me in front of the television and never let me play outside. No more stream side exploring, no more turning over rocks and old logs, no more building fairy houses in the mossy woods.
No distinction is made in the CDC warnings between wild and captive animals. In the little research I could find on the subject, it turns out that wild reptiles are less likely to carry and shed salmonella. A study of red-sliders, a common pet store turtle with a long rap sheet of salmonella outbreaks, could find no salmonella in the wild specimens tested. Another study found that the tadpoles they cultured had no salmonella. One author postulated that the stress of captivity renders reptiles and amphibians more vulnerable to infection, as it has been found to do in other animals.
So it turns out that, as usual, my mother was correct. Go out and explore. Don’t buy at the pet store. Don’t bring ’em into the house. Sadly, even if we are successful in getting kids off the couch and into the woods, they will be less likely to find reptiles and amphibians when they go exploring. But, I am a hopeful guy. Maybe the little orange salamander I saw is the vanguard of an amphibian return.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including "How to Say No to Your Toddler." E-mail him at [email protected].
Mental health effects of concussions on adolescents and teens
A concussion or mild traumatic brain injury is defined as a transient neurologic change resulting from a biomechanical impact to the head. Given this broad definition, it is not surprising that concussion represents the most common type of traumatic brain injury (TBI). Concussions can be complicated and multifaceted, as patients usually present with various combinations of neurologic, cognitive, and psychiatric symptoms.
Fortunately, these injuries tend to have a more favorable outcome than do more severe brain injuries, with the vast majority of patients returning to usual functioning within days to weeks, with time and a guided return-to-activity plan. However, there is a subset of patients whose symptoms persist into what has been loosely defined as postconcussive syndrome. These individuals tend to be the greatest challenge for clinicians, and usually benefit from a multidisciplinary team approach, including neurologists, neuropsychologists, physical therapists, and speech pathologists.

Adolescents represent a commonly seen subgroup within the concussion population, most notably because of their frequent involvement in sports and higher-risk activities. Additionally, when injuries do occur at the high school and college level, the impact velocities tend to be at a higher rate than is seen in younger athletes, potentially resulting in more pronounced concussions. Further complicating the situation is that adolescents tend to have busy schedules and multiple responsibilities throughout the school year (when most concussions occur). Thus, when a concussion is sustained, the student athlete not only needs to deal with the immediate symptoms of the injury, but also the potential for academic and social derailment during the recovery process. Combine these issues with a strong body of literature suggesting adolescents tend to have slower resolution than do adults, and you have the recipe for a very bumpy recovery.
Neurologic symptoms usually present as headache, light and noise sensitivity, dizziness, and balance issues. Cognitive symptoms manifest as slower processing speed, feeling foggy, and occasional forgetting or transient confusion. Psychiatric symptoms often include irritability, lability, and sadness. A child may have one or many of these symptoms, although more often these symptoms overlap. The patient and their family may not recognize how persistent symptoms of headache and dizziness, for example, can contribute to memory problems and difficulty concentrating, irritability, and feelings of depression and hopelessness. Children with prolonged symptoms also can feel isolated from their peers while they are sitting out of play and school.
The treatment strategy for managing the emotional and mental health needs of the adolescent concussion patient is dictated by the underlying etiology. It is reasonable to suspect that irritability, a short fuse, and frequent crying during the first few days following injury are a direct result of neurologic disruption, which are not amenable to reason and behavioral interventions. In these cases, the best treatment is to educate the family that this is a transient neurologic state, while ensuring that the patient is protected from environmental stressors. One analogy that parents and patients find helpful is "weathering the storm," and with time, these symptoms tend to abate. The key here is to normalize the recovery process and provide parents with a realistic recovery trajectory.

The more challenging patient is the child whose symptoms persist for weeks or develop over time, or, even more complicated, the child who had preexisting known or unknown mental health issues. A common theme in working with TBI patients is that brain injuries tend to exacerbate preexisting conditions. In these cases, good history taking is the foundation for good mental health management.
Key questions include: Is there a preexisting history of learning disability and/or attention-deficit/hyperactivity disorder (ADHD)? Are there preexisting or current family stressors? Has the child ever been in therapy before? How much school has the child missed? How has the school responded to the child missing tests and assignments? Is the child being pressured by teachers or coaches to return to activity? The answer to these and other questions will dictate how mental health issues should be addressed.
As a pediatrician, a release to talk with the school can clear up many of the return-to-activity stressors or may help to better understand the contribution of preexisting learning struggles or ADHD. Again, it is particularly important to have an awareness of premorbid history, as head injuries tend to exacerbate or accentuate preexisting symptoms. The full utility of the multidisciplinary team is accentuated in these situations, and a referral to a psychologist familiar with concussion is often the next step. Short-term medication management also may be considered, with additional referral to a psychiatrist for long-term management as necessary.
Although fairly uncommon, the circumstances of a concussion can result in posttraumatic stress disorder (PTSD) or acute stress disorder, particularly when considering that concussions do not have to result in loss of consciousness during the event. It is important to at least screen for PTSD in situations in which there is the strong potential for this (in other words, an event that involved threatened death or serious injury to self or other, was the result of an assault, and resulted in intense fear or horror). Some symptoms to look for include intense psychological distress, recurrent distressing recollection, and frequent nightmares of the event, flashbacks, hypervigilance, and exaggerated startle response, and feelings of detachment from others. If these symptoms are present, a mental health evaluation and treatment would be the next logical step.
Concussion is a relatively common occurrence in adolescence and has received increased interest in recent years. It is important for pediatricians to be aware of the neurologic, cognitive, and psychiatric/emotional symptoms of concussion and how these symptoms often overlap. The management of mental health issues in concussion depends on the stage of recovery, the impact of the concussion on academic and social functions, whether preexisting issues exist, and the circumstances of the injury. In certain situations, mental health symptoms can be headed off in the pediatrician’s office, while more complicated and protracted recoveries necessitate a multidisciplinary team that includes mental health professionals.
Dr. Romain is a neuropsychologist at the Children’s Hospital of Orange County, Calif., and was the primary author of this commentary. He provides neuropsychological evaluations at the CHOC multidisciplinary concussion clinic. Dr. Taraman is a pediatric neurologist at the hospital. Dr. Romain and Dr. Taraman said they have no relevant financial disclosures.
A concussion or mild traumatic brain injury is defined as a transient neurologic change resulting from a biomechanical impact to the head. Given this broad definition, it is not surprising that concussion represents the most common type of traumatic brain injury (TBI). Concussions can be complicated and multifaceted, as patients usually present with various combinations of neurologic, cognitive, and psychiatric symptoms.
Fortunately, these injuries tend to have a more favorable outcome than do more severe brain injuries, with the vast majority of patients returning to usual functioning within days to weeks, with time and a guided return-to-activity plan. However, there is a subset of patients whose symptoms persist into what has been loosely defined as postconcussive syndrome. These individuals tend to be the greatest challenge for clinicians, and usually benefit from a multidisciplinary team approach, including neurologists, neuropsychologists, physical therapists, and speech pathologists.
Adolescents represent a commonly seen subgroup within the concussion population, most notably because of their frequent involvement in sports and higher-risk activities. Additionally, when injuries do occur at the high school and college level, the impact velocities tend to be at a higher rate than is seen in younger athletes, potentially resulting in more pronounced concussions. Further complicating the situation is that adolescents tend to have busy schedules and multiple responsibilities throughout the school year (when most concussions occur). Thus, when a concussion is sustained, the student athlete not only needs to deal with the immediate symptoms of the injury, but also the potential for academic and social derailment during the recovery process. Combine these issues with a strong body of literature suggesting adolescents tend to have slower resolution than do adults, and you have the recipe for a very bumpy recovery.
Neurologic symptoms usually present as headache, light and noise sensitivity, dizziness, and balance issues. Cognitive symptoms manifest as slower processing speed, feeling foggy, and occasional forgetting or transient confusion. Psychiatric symptoms often include irritability, lability, and sadness. A child may have one or many of these symptoms, although more often these symptoms overlap. The patient and their family may not recognize how persistent symptoms of headache and dizziness, for example, can contribute to memory problems and difficulty concentrating, irritability, and feelings of depression and hopelessness. Children with prolonged symptoms also can feel isolated from their peers while they are sitting out of play and school.
The treatment strategy for managing the emotional and mental health needs of the adolescent concussion patient is dictated by the underlying etiology. It is reasonable to suspect that irritability, a short fuse, and frequent crying during the first few days following injury are a direct result of neurologic disruption, which are not amenable to reason and behavioral interventions. In these cases, the best treatment is to educate the family that this is a transient neurologic state, while ensuring that the patient is protected from environmental stressors. One analogy that parents and patients find helpful is "weathering the storm," and with time, these symptoms tend to abate. The key here is to normalize the recovery process and provide parents with a realistic recovery trajectory.
The more challenging patient is the child whose symptoms persist for weeks or develop over time, or, even more complicated, the child who had preexisting known or unknown mental health issues. A common theme in working with TBI patients is that brain injuries tend to exacerbate preexisting conditions. In these cases, good history taking is the foundation for good mental health management.
Key questions include: Is there a preexisting history of learning disability and/or attention-deficit/hyperactivity disorder (ADHD)? Are there preexisting or current family stressors? Has the child ever been in therapy before? How much school has the child missed? How has the school responded to the child missing tests and assignments? Is the child being pressured by teachers or coaches to return to activity? The answer to these and other questions will dictate how mental health issues should be addressed.
As a pediatrician, a release to talk with the school can clear up many of the return-to-activity stressors or may help to better understand the contribution of preexisting learning struggles or ADHD. Again, it is particularly important to have an awareness of premorbid history, as head injuries tend to exacerbate or accentuate preexisting symptoms. The full utility of the multidisciplinary team is accentuated in these situations, and a referral to a psychologist familiar with concussion is often the next step. Short-term medication management also may be considered, with additional referral to a psychiatrist for long-term management as necessary.
Although fairly uncommon, the circumstances of a concussion can result in posttraumatic stress disorder (PTSD) or acute stress disorder, particularly when considering that concussions do not have to result in loss of consciousness during the event. It is important to at least screen for PTSD in situations in which there is the strong potential for this (in other words, an event that involved threatened death or serious injury to self or other, was the result of an assault, and resulted in intense fear or horror). Some symptoms to look for include intense psychological distress, recurrent distressing recollection, and frequent nightmares of the event, flashbacks, hypervigilance, and exaggerated startle response, and feelings of detachment from others. If these symptoms are present, a mental health evaluation and treatment would be the next logical step.
Concussion is a relatively common occurrence in adolescence and has received increased interest in recent years. It is important for pediatricians to be aware of the neurologic, cognitive, and psychiatric/emotional symptoms of concussion and how these symptoms often overlap. The management of mental health issues in concussion depends on the stage of recovery, the impact of the concussion on academic and social functions, whether preexisting issues exist, and the circumstances of the injury. In certain situations, mental health symptoms can be headed off in the pediatrician’s office, while more complicated and protracted recoveries necessitate a multidisciplinary team that includes mental health professionals.
Dr. Romain is a neuropsychologist at the Children’s Hospital of Orange County, Calif., and was the primary author of this commentary. He provides neuropsychological evaluations at the CHOC multidisciplinary concussion clinic. Dr. Taraman is a pediatric neurologist at the hospital. Dr. Romain and Dr. Taraman said they have no relevant financial disclosures.
A concussion or mild traumatic brain injury is defined as a transient neurologic change resulting from a biomechanical impact to the head. Given this broad definition, it is not surprising that concussion represents the most common type of traumatic brain injury (TBI). Concussions can be complicated and multifaceted, as patients usually present with various combinations of neurologic, cognitive, and psychiatric symptoms.
Fortunately, these injuries tend to have a more favorable outcome than do more severe brain injuries, with the vast majority of patients returning to usual functioning within days to weeks, with time and a guided return-to-activity plan. However, there is a subset of patients whose symptoms persist into what has been loosely defined as postconcussive syndrome. These individuals tend to be the greatest challenge for clinicians, and usually benefit from a multidisciplinary team approach, including neurologists, neuropsychologists, physical therapists, and speech pathologists.
Adolescents represent a commonly seen subgroup within the concussion population, most notably because of their frequent involvement in sports and higher-risk activities. Additionally, when injuries do occur at the high school and college level, the impact velocities tend to be at a higher rate than is seen in younger athletes, potentially resulting in more pronounced concussions. Further complicating the situation is that adolescents tend to have busy schedules and multiple responsibilities throughout the school year (when most concussions occur). Thus, when a concussion is sustained, the student athlete not only needs to deal with the immediate symptoms of the injury, but also the potential for academic and social derailment during the recovery process. Combine these issues with a strong body of literature suggesting adolescents tend to have slower resolution than do adults, and you have the recipe for a very bumpy recovery.
Neurologic symptoms usually present as headache, light and noise sensitivity, dizziness, and balance issues. Cognitive symptoms manifest as slower processing speed, feeling foggy, and occasional forgetting or transient confusion. Psychiatric symptoms often include irritability, lability, and sadness. A child may have one or many of these symptoms, although more often these symptoms overlap. The patient and their family may not recognize how persistent symptoms of headache and dizziness, for example, can contribute to memory problems and difficulty concentrating, irritability, and feelings of depression and hopelessness. Children with prolonged symptoms also can feel isolated from their peers while they are sitting out of play and school.
The treatment strategy for managing the emotional and mental health needs of the adolescent concussion patient is dictated by the underlying etiology. It is reasonable to suspect that irritability, a short fuse, and frequent crying during the first few days following injury are a direct result of neurologic disruption, which are not amenable to reason and behavioral interventions. In these cases, the best treatment is to educate the family that this is a transient neurologic state, while ensuring that the patient is protected from environmental stressors. One analogy that parents and patients find helpful is "weathering the storm," and with time, these symptoms tend to abate. The key here is to normalize the recovery process and provide parents with a realistic recovery trajectory.
The more challenging patient is the child whose symptoms persist for weeks or develop over time, or, even more complicated, the child who had preexisting known or unknown mental health issues. A common theme in working with TBI patients is that brain injuries tend to exacerbate preexisting conditions. In these cases, good history taking is the foundation for good mental health management.
Key questions include: Is there a preexisting history of learning disability and/or attention-deficit/hyperactivity disorder (ADHD)? Are there preexisting or current family stressors? Has the child ever been in therapy before? How much school has the child missed? How has the school responded to the child missing tests and assignments? Is the child being pressured by teachers or coaches to return to activity? The answer to these and other questions will dictate how mental health issues should be addressed.
As a pediatrician, a release to talk with the school can clear up many of the return-to-activity stressors or may help to better understand the contribution of preexisting learning struggles or ADHD. Again, it is particularly important to have an awareness of premorbid history, as head injuries tend to exacerbate or accentuate preexisting symptoms. The full utility of the multidisciplinary team is accentuated in these situations, and a referral to a psychologist familiar with concussion is often the next step. Short-term medication management also may be considered, with additional referral to a psychiatrist for long-term management as necessary.
Although fairly uncommon, the circumstances of a concussion can result in posttraumatic stress disorder (PTSD) or acute stress disorder, particularly when considering that concussions do not have to result in loss of consciousness during the event. It is important to at least screen for PTSD in situations in which there is the strong potential for this (in other words, an event that involved threatened death or serious injury to self or other, was the result of an assault, and resulted in intense fear or horror). Some symptoms to look for include intense psychological distress, recurrent distressing recollection, and frequent nightmares of the event, flashbacks, hypervigilance, and exaggerated startle response, and feelings of detachment from others. If these symptoms are present, a mental health evaluation and treatment would be the next logical step.
Concussion is a relatively common occurrence in adolescence and has received increased interest in recent years. It is important for pediatricians to be aware of the neurologic, cognitive, and psychiatric/emotional symptoms of concussion and how these symptoms often overlap. The management of mental health issues in concussion depends on the stage of recovery, the impact of the concussion on academic and social functions, whether preexisting issues exist, and the circumstances of the injury. In certain situations, mental health symptoms can be headed off in the pediatrician’s office, while more complicated and protracted recoveries necessitate a multidisciplinary team that includes mental health professionals.
Dr. Romain is a neuropsychologist at the Children’s Hospital of Orange County, Calif., and was the primary author of this commentary. He provides neuropsychological evaluations at the CHOC multidisciplinary concussion clinic. Dr. Taraman is a pediatric neurologist at the hospital. Dr. Romain and Dr. Taraman said they have no relevant financial disclosures.

Calcium – Making deposits for a healthy adulthood
Likely, one of the most important roles of a pediatrician is to maximize health in childhood and positively impact health in adulthood. Bone density is one of the few things that can be maximized in adolescence. By maximizing bone density, we can directly slow and reduce the osteopenia that occurs later in life and the osteoporosis that 10 million Americans struggle with annually.
The physiology of calcium absorption changes throughout life. In early adolescence, the absorption is greater than the elimination. Between 30 and 50 years of age, absorption and elimination are about equal, but as we enter into the sixth decade of life, there is significant bone loss. Studies have shown that bone density is maximized by age 30 years, and little change is made later in life despite supplementation (Eur. J. Clin. Nutr. 1993;47:617-22). The greatest amount of bone loss occurs after the age of 65 years, and fractures after this age are predominantly at cortical sites.
Consumption of the appropriate amounts of calcium can be difficult given the inadequacies of most adolescents’ diet. The recommended daily intake is 1,200-1,500 mg of elemental calcium. But, absorption of calcium is quite variable and is dependent on other factors to be in place for it to be maximized.
The two most common form of calcium are calcium carbonate and calcium citrate malate. Calcium carbonate requires a higher pH of the stomach, and therefore needs to be taken with food. Calcium carbonate is more cost effective but is also associated with more side effects such as gas and bloating. Calcium citrate malate is found in many juices that are fortified with calcium, can be taken with or without food, is better absorbed with chronic conditions, and is thought to be protective against stone formation (J. Am. Coll. Nutr. 1996;15:313-6; Adv. Food. Nutr. Res. 2008;54:219-346).
Common sources of calcium include milk, yogurt, cheese, Chinese cabbage, kale, broccoli, and spinach. Appropriate levels of vitamin D are important to maximize the absorption of calcium, and recent studies have shown that 40% of adolescents are deficient in vitamin D (Arch. Pediatr. Adolesc. Med. 2004;158:531-7; Arch. Pediatr. Adolesc. Med. 2008;162:513-9). Many other adolescents are lactose intolerant or have a milk protein allergy, which also limit the calcium sources. Soymilk has similar levels of calcium, compared with whole milk. Almond-coconut milk has double the amount of calcium, compared with whole milk, so it is a great substitute for those who are lactose intolerant.
Oxalic acids are found in food such as spinach, collard greens, and sweet potatoes, all of which are rich in calcium, but the oxalic acid reduces the absorption of the calcium. Consumption of large amounts of tea and coffee also can reduce calcium absorption, so despite consuming appropriate amounts of calcium, limited amounts become bioavailable.
If using calcium supplements, ingesting less than or equal to 500 mg is better than taking 1,000 mg at once because it is better absorbed (Adv. Food Nutr. Res. 2008;54:219-346). Orange juice, apple juice, and cereals are fortified with calcium so these also are great sources that usually are accepted by adolescents.
Calcium is a critical dietary supplement that is needed for strong bones, metabolic functions, nerve transmission, and vascular contraction and vasodilation. Long-term deficiency will result in disease, and fragility of the bones. Early supplementation and calcium rich diets can ensure maximum bone development, but if parents are not educated on the appropriate delivery, this opportunity could be missed.
An excellent resource is the National Institutes of Health, Office of Dietary Supplements website. This site gives a wealth of information for sources and consumption of calcium. Another excellent resource for parents to use to guide them to make healthier choices is the U.S. Department of Agriculture site, www.choosemyplate.gov. Parents are looking for quick simple ways to maximize their children’s diet and ensure they are getting everything they need to be healthy adults. Becoming familiar with the basics will allow you to give informed advice that will significantly affect their children’s future.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
Likely, one of the most important roles of a pediatrician is to maximize health in childhood and positively impact health in adulthood. Bone density is one of the few things that can be maximized in adolescence. By maximizing bone density, we can directly slow and reduce the osteopenia that occurs later in life and the osteoporosis that 10 million Americans struggle with annually.
The physiology of calcium absorption changes throughout life. In early adolescence, the absorption is greater than the elimination. Between 30 and 50 years of age, absorption and elimination are about equal, but as we enter into the sixth decade of life, there is significant bone loss. Studies have shown that bone density is maximized by age 30 years, and little change is made later in life despite supplementation (Eur. J. Clin. Nutr. 1993;47:617-22). The greatest amount of bone loss occurs after the age of 65 years, and fractures after this age are predominantly at cortical sites.
Consumption of the appropriate amounts of calcium can be difficult given the inadequacies of most adolescents’ diet. The recommended daily intake is 1,200-1,500 mg of elemental calcium. But, absorption of calcium is quite variable and is dependent on other factors to be in place for it to be maximized.
The two most common form of calcium are calcium carbonate and calcium citrate malate. Calcium carbonate requires a higher pH of the stomach, and therefore needs to be taken with food. Calcium carbonate is more cost effective but is also associated with more side effects such as gas and bloating. Calcium citrate malate is found in many juices that are fortified with calcium, can be taken with or without food, is better absorbed with chronic conditions, and is thought to be protective against stone formation (J. Am. Coll. Nutr. 1996;15:313-6; Adv. Food. Nutr. Res. 2008;54:219-346).
Common sources of calcium include milk, yogurt, cheese, Chinese cabbage, kale, broccoli, and spinach. Appropriate levels of vitamin D are important to maximize the absorption of calcium, and recent studies have shown that 40% of adolescents are deficient in vitamin D (Arch. Pediatr. Adolesc. Med. 2004;158:531-7; Arch. Pediatr. Adolesc. Med. 2008;162:513-9). Many other adolescents are lactose intolerant or have a milk protein allergy, which also limit the calcium sources. Soymilk has similar levels of calcium, compared with whole milk. Almond-coconut milk has double the amount of calcium, compared with whole milk, so it is a great substitute for those who are lactose intolerant.
Oxalic acids are found in food such as spinach, collard greens, and sweet potatoes, all of which are rich in calcium, but the oxalic acid reduces the absorption of the calcium. Consumption of large amounts of tea and coffee also can reduce calcium absorption, so despite consuming appropriate amounts of calcium, limited amounts become bioavailable.
If using calcium supplements, ingesting less than or equal to 500 mg is better than taking 1,000 mg at once because it is better absorbed (Adv. Food Nutr. Res. 2008;54:219-346). Orange juice, apple juice, and cereals are fortified with calcium so these also are great sources that usually are accepted by adolescents.
Calcium is a critical dietary supplement that is needed for strong bones, metabolic functions, nerve transmission, and vascular contraction and vasodilation. Long-term deficiency will result in disease, and fragility of the bones. Early supplementation and calcium rich diets can ensure maximum bone development, but if parents are not educated on the appropriate delivery, this opportunity could be missed.
An excellent resource is the National Institutes of Health, Office of Dietary Supplements website. This site gives a wealth of information for sources and consumption of calcium. Another excellent resource for parents to use to guide them to make healthier choices is the U.S. Department of Agriculture site, www.choosemyplate.gov. Parents are looking for quick simple ways to maximize their children’s diet and ensure they are getting everything they need to be healthy adults. Becoming familiar with the basics will allow you to give informed advice that will significantly affect their children’s future.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].
Likely, one of the most important roles of a pediatrician is to maximize health in childhood and positively impact health in adulthood. Bone density is one of the few things that can be maximized in adolescence. By maximizing bone density, we can directly slow and reduce the osteopenia that occurs later in life and the osteoporosis that 10 million Americans struggle with annually.
The physiology of calcium absorption changes throughout life. In early adolescence, the absorption is greater than the elimination. Between 30 and 50 years of age, absorption and elimination are about equal, but as we enter into the sixth decade of life, there is significant bone loss. Studies have shown that bone density is maximized by age 30 years, and little change is made later in life despite supplementation (Eur. J. Clin. Nutr. 1993;47:617-22). The greatest amount of bone loss occurs after the age of 65 years, and fractures after this age are predominantly at cortical sites.
Consumption of the appropriate amounts of calcium can be difficult given the inadequacies of most adolescents’ diet. The recommended daily intake is 1,200-1,500 mg of elemental calcium. But, absorption of calcium is quite variable and is dependent on other factors to be in place for it to be maximized.
The two most common form of calcium are calcium carbonate and calcium citrate malate. Calcium carbonate requires a higher pH of the stomach, and therefore needs to be taken with food. Calcium carbonate is more cost effective but is also associated with more side effects such as gas and bloating. Calcium citrate malate is found in many juices that are fortified with calcium, can be taken with or without food, is better absorbed with chronic conditions, and is thought to be protective against stone formation (J. Am. Coll. Nutr. 1996;15:313-6; Adv. Food. Nutr. Res. 2008;54:219-346).
Common sources of calcium include milk, yogurt, cheese, Chinese cabbage, kale, broccoli, and spinach. Appropriate levels of vitamin D are important to maximize the absorption of calcium, and recent studies have shown that 40% of adolescents are deficient in vitamin D (Arch. Pediatr. Adolesc. Med. 2004;158:531-7; Arch. Pediatr. Adolesc. Med. 2008;162:513-9). Many other adolescents are lactose intolerant or have a milk protein allergy, which also limit the calcium sources. Soymilk has similar levels of calcium, compared with whole milk. Almond-coconut milk has double the amount of calcium, compared with whole milk, so it is a great substitute for those who are lactose intolerant.
Oxalic acids are found in food such as spinach, collard greens, and sweet potatoes, all of which are rich in calcium, but the oxalic acid reduces the absorption of the calcium. Consumption of large amounts of tea and coffee also can reduce calcium absorption, so despite consuming appropriate amounts of calcium, limited amounts become bioavailable.
If using calcium supplements, ingesting less than or equal to 500 mg is better than taking 1,000 mg at once because it is better absorbed (Adv. Food Nutr. Res. 2008;54:219-346). Orange juice, apple juice, and cereals are fortified with calcium so these also are great sources that usually are accepted by adolescents.
Calcium is a critical dietary supplement that is needed for strong bones, metabolic functions, nerve transmission, and vascular contraction and vasodilation. Long-term deficiency will result in disease, and fragility of the bones. Early supplementation and calcium rich diets can ensure maximum bone development, but if parents are not educated on the appropriate delivery, this opportunity could be missed.
An excellent resource is the National Institutes of Health, Office of Dietary Supplements website. This site gives a wealth of information for sources and consumption of calcium. Another excellent resource for parents to use to guide them to make healthier choices is the U.S. Department of Agriculture site, www.choosemyplate.gov. Parents are looking for quick simple ways to maximize their children’s diet and ensure they are getting everything they need to be healthy adults. Becoming familiar with the basics will allow you to give informed advice that will significantly affect their children’s future.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at [email protected].

Catheter or bag?
It is such a common situation that you would think it would be a cut-and-dried decision. But in some ways it reflects at the core of medical professionalism. A 2-month-old infant presents to the emergency department with a 101.6° F fever. The history provides no hint at a specific diagnosis and the physical exam is unremarkable with a well-appearing baby. I’ve been using the Rochester criteria in this situation for nigh on 20 years. I need a CBC and urinalysis. Then I can decide on whether to do a lumbar puncture. The mother, however, resists the idea of doing a catheter for a urine sample. Now what?
The merits of bagged vs. catheter urine specimens have been debated for decades. In the United States, the experts have been in agreement for many years that catheter specimens are recommended.
My cause for skepticism has been that experts elsewhere have made contrary recommendations.
For many illnesses, I find the online resources of the Royal Children’s Hospital in Melbourne to be very helpful because they are so specific yet thorough, including those for urinary tract infections (UTIs).
Those guidelines were last updated in 2011. These are only two pages of bulleted items, so I strongly recommend reading them. You may find them eye opening. Those guidelines believe suprapubic aspiration remains the preferred method, at least in sick children. They also state that there is no indication for culture of urine from a bag specimen.
In Britain, the National Institute for Health and Care Excellence (NICE) guidelines have taken another approach. For them, "Noninvasive methods such as pads or bags should be used before trying to gain a sample by invasive methods," such as catheter or suprapubic aspiration. Those were 2007 NICE guidelines, referenced and reaffirmed in a 2013 guideline at the Royal Cornwall Hospitals Trust.
The British also have a protocol in which the baby is left undiapered and a parent waits to catch the urine in a sterile cup with the next void.
Furthermore, at least in the recent past, decisions in Britain about treating UTIs often were made based on dipstick alone if the child was well appearing. This made sterile collection less stringent. The costs of culture were thought excessive, compared with the improvement in accuracy of the diagnosis. This was analogous to the ongoing debate over whether to always test for strep throats before treating vs. treating empirically. The United States has moved strongly in the other direction. The 2011 American Academy of Pediatrics guidelines now require both a positive culture and a positive urinalysis to diagnose a UTI (Pediatrics 2011;128:595-610).
Why this difference? Because the diagnosis of a UTI in a young child in the United States under the now-discredited 1999 guidelines led to unnecessary admissions, intravenous therapy, renal ultrasounds, repeated voiding cystourethrograms, and long-term antibiotic prophylaxis. Invasive overtreatment certainly can be used to justify overly invasive diagnostic tests. The wiser course would be to stop the overtreatment.
All this knowledge and perspective didn’t help me in the ED with this mother. I suggested that to a control-freak toddler wearing a urine bag can be perceived as at least as invasive as the quick catheterization. I was not persuasive. Fortunately, the ED was empty at 3 a.m. So, if mom wanted to spend those extra 3 hours waiting for the child to pee into a bag, I could accommodate her autonomy.
My colleagues have differing opinions on what to do in this situation. One is a strong advocate for evidence-based medicine (EBM). Because the guidelines state that catheterization is the recommended method, he would argue that that is the only option that should be presented to the parent. That emphasis on EBM becomes his definition of professionalism. Other colleagues are less dogmatic. They will point out that at 10 p.m. with all the ED rooms full and the waiting room overflowing, accommodating this situation would be more problematic.
I think my experiences working in so many different parts of the country have shaped me to value flexibility and accommodation. I’ve seen many situations where differing locations are dogmatic in differing directions in how the local doctors believe care should be delivered. I’ve also anxiously received minor medical treatment while overseas when I didn’t speak the local language, so the phrase "delivering care" is a particularly meaningful concept.
I think I could have used my knowledge and status to bully this mother into permitting her infant to be catheterized. Perhaps that is the scientifically ideal approach. I worry, though, that it would not be the most compassionate approach. The risk to the infant in both scenarios is very small. So to me, it wasn’t a choice of catheter vs. bag. It was a choice of expressing compassion rather than expertise.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.
It is such a common situation that you would think it would be a cut-and-dried decision. But in some ways it reflects at the core of medical professionalism. A 2-month-old infant presents to the emergency department with a 101.6° F fever. The history provides no hint at a specific diagnosis and the physical exam is unremarkable with a well-appearing baby. I’ve been using the Rochester criteria in this situation for nigh on 20 years. I need a CBC and urinalysis. Then I can decide on whether to do a lumbar puncture. The mother, however, resists the idea of doing a catheter for a urine sample. Now what?
The merits of bagged vs. catheter urine specimens have been debated for decades. In the United States, the experts have been in agreement for many years that catheter specimens are recommended.
My cause for skepticism has been that experts elsewhere have made contrary recommendations.
For many illnesses, I find the online resources of the Royal Children’s Hospital in Melbourne to be very helpful because they are so specific yet thorough, including those for urinary tract infections (UTIs).
Those guidelines were last updated in 2011. These are only two pages of bulleted items, so I strongly recommend reading them. You may find them eye opening. Those guidelines believe suprapubic aspiration remains the preferred method, at least in sick children. They also state that there is no indication for culture of urine from a bag specimen.
In Britain, the National Institute for Health and Care Excellence (NICE) guidelines have taken another approach. For them, "Noninvasive methods such as pads or bags should be used before trying to gain a sample by invasive methods," such as catheter or suprapubic aspiration. Those were 2007 NICE guidelines, referenced and reaffirmed in a 2013 guideline at the Royal Cornwall Hospitals Trust.
The British also have a protocol in which the baby is left undiapered and a parent waits to catch the urine in a sterile cup with the next void.
Furthermore, at least in the recent past, decisions in Britain about treating UTIs often were made based on dipstick alone if the child was well appearing. This made sterile collection less stringent. The costs of culture were thought excessive, compared with the improvement in accuracy of the diagnosis. This was analogous to the ongoing debate over whether to always test for strep throats before treating vs. treating empirically. The United States has moved strongly in the other direction. The 2011 American Academy of Pediatrics guidelines now require both a positive culture and a positive urinalysis to diagnose a UTI (Pediatrics 2011;128:595-610).
Why this difference? Because the diagnosis of a UTI in a young child in the United States under the now-discredited 1999 guidelines led to unnecessary admissions, intravenous therapy, renal ultrasounds, repeated voiding cystourethrograms, and long-term antibiotic prophylaxis. Invasive overtreatment certainly can be used to justify overly invasive diagnostic tests. The wiser course would be to stop the overtreatment.
All this knowledge and perspective didn’t help me in the ED with this mother. I suggested that to a control-freak toddler wearing a urine bag can be perceived as at least as invasive as the quick catheterization. I was not persuasive. Fortunately, the ED was empty at 3 a.m. So, if mom wanted to spend those extra 3 hours waiting for the child to pee into a bag, I could accommodate her autonomy.
My colleagues have differing opinions on what to do in this situation. One is a strong advocate for evidence-based medicine (EBM). Because the guidelines state that catheterization is the recommended method, he would argue that that is the only option that should be presented to the parent. That emphasis on EBM becomes his definition of professionalism. Other colleagues are less dogmatic. They will point out that at 10 p.m. with all the ED rooms full and the waiting room overflowing, accommodating this situation would be more problematic.
I think my experiences working in so many different parts of the country have shaped me to value flexibility and accommodation. I’ve seen many situations where differing locations are dogmatic in differing directions in how the local doctors believe care should be delivered. I’ve also anxiously received minor medical treatment while overseas when I didn’t speak the local language, so the phrase "delivering care" is a particularly meaningful concept.
I think I could have used my knowledge and status to bully this mother into permitting her infant to be catheterized. Perhaps that is the scientifically ideal approach. I worry, though, that it would not be the most compassionate approach. The risk to the infant in both scenarios is very small. So to me, it wasn’t a choice of catheter vs. bag. It was a choice of expressing compassion rather than expertise.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.
It is such a common situation that you would think it would be a cut-and-dried decision. But in some ways it reflects at the core of medical professionalism. A 2-month-old infant presents to the emergency department with a 101.6° F fever. The history provides no hint at a specific diagnosis and the physical exam is unremarkable with a well-appearing baby. I’ve been using the Rochester criteria in this situation for nigh on 20 years. I need a CBC and urinalysis. Then I can decide on whether to do a lumbar puncture. The mother, however, resists the idea of doing a catheter for a urine sample. Now what?
The merits of bagged vs. catheter urine specimens have been debated for decades. In the United States, the experts have been in agreement for many years that catheter specimens are recommended.
My cause for skepticism has been that experts elsewhere have made contrary recommendations.
For many illnesses, I find the online resources of the Royal Children’s Hospital in Melbourne to be very helpful because they are so specific yet thorough, including those for urinary tract infections (UTIs).
Those guidelines were last updated in 2011. These are only two pages of bulleted items, so I strongly recommend reading them. You may find them eye opening. Those guidelines believe suprapubic aspiration remains the preferred method, at least in sick children. They also state that there is no indication for culture of urine from a bag specimen.
In Britain, the National Institute for Health and Care Excellence (NICE) guidelines have taken another approach. For them, "Noninvasive methods such as pads or bags should be used before trying to gain a sample by invasive methods," such as catheter or suprapubic aspiration. Those were 2007 NICE guidelines, referenced and reaffirmed in a 2013 guideline at the Royal Cornwall Hospitals Trust.
The British also have a protocol in which the baby is left undiapered and a parent waits to catch the urine in a sterile cup with the next void.
Furthermore, at least in the recent past, decisions in Britain about treating UTIs often were made based on dipstick alone if the child was well appearing. This made sterile collection less stringent. The costs of culture were thought excessive, compared with the improvement in accuracy of the diagnosis. This was analogous to the ongoing debate over whether to always test for strep throats before treating vs. treating empirically. The United States has moved strongly in the other direction. The 2011 American Academy of Pediatrics guidelines now require both a positive culture and a positive urinalysis to diagnose a UTI (Pediatrics 2011;128:595-610).
Why this difference? Because the diagnosis of a UTI in a young child in the United States under the now-discredited 1999 guidelines led to unnecessary admissions, intravenous therapy, renal ultrasounds, repeated voiding cystourethrograms, and long-term antibiotic prophylaxis. Invasive overtreatment certainly can be used to justify overly invasive diagnostic tests. The wiser course would be to stop the overtreatment.
All this knowledge and perspective didn’t help me in the ED with this mother. I suggested that to a control-freak toddler wearing a urine bag can be perceived as at least as invasive as the quick catheterization. I was not persuasive. Fortunately, the ED was empty at 3 a.m. So, if mom wanted to spend those extra 3 hours waiting for the child to pee into a bag, I could accommodate her autonomy.
My colleagues have differing opinions on what to do in this situation. One is a strong advocate for evidence-based medicine (EBM). Because the guidelines state that catheterization is the recommended method, he would argue that that is the only option that should be presented to the parent. That emphasis on EBM becomes his definition of professionalism. Other colleagues are less dogmatic. They will point out that at 10 p.m. with all the ED rooms full and the waiting room overflowing, accommodating this situation would be more problematic.
I think my experiences working in so many different parts of the country have shaped me to value flexibility and accommodation. I’ve seen many situations where differing locations are dogmatic in differing directions in how the local doctors believe care should be delivered. I’ve also anxiously received minor medical treatment while overseas when I didn’t speak the local language, so the phrase "delivering care" is a particularly meaningful concept.
I think I could have used my knowledge and status to bully this mother into permitting her infant to be catheterized. Perhaps that is the scientifically ideal approach. I worry, though, that it would not be the most compassionate approach. The risk to the infant in both scenarios is very small. So to me, it wasn’t a choice of catheter vs. bag. It was a choice of expressing compassion rather than expertise.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Dr. Powell said he had no relevant financial disclosures.

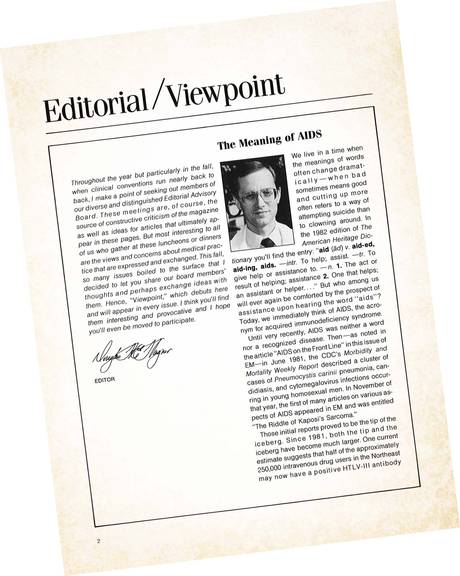
Editorial: The Meaning of AIDS—Then and Now
This month marks the 100th consecutive month of EM editorials. The accompanying editorial was written for EM way back in 1986, when, as a member of EM’s editorial board, I was asked to inaugurate a series of editorial/viewpoints by board members on the issues that “boiled to the surface” at the time. I chose to write about the relatively new and frightening epidemic of HIV infections and AIDS overwhelming EDs across the country. At that time, AIDS was a lethal illness accompanied by fears that it could accidentally spread to health care workers by needle sticks etc.
Predicting the future is a risky exercise but, young and undaunted, I wondered if we would have a vaccine in 3 to 5 years, a cure in 5 to 10 years, and by the latter, “cure cancer.” Though none of these possibilities actually occurred, by the beginning of the 21st century AIDS had been transformed into a chronic and mostly manageable illness—at least in the compliant patient. But in the years since 1986, we have indeed seen rapid scientific advances in identification of causative agents, followed by accurate tests for infection, and effective treatments or vaccines—all of which helped prevent the spread of SARS and other potentially lethal infections. In terms of outcome, not a bad forecast for 1986, though it would be more than 20 years before EM asked me to write another editorial!
Also next month, readers will be introduced to several new EM Advisory Board members who have achieved national recognition for their work in newer EM disciplines such as prehospital care, critical care, geriatric emergency medicine, wilderness medicine, and bedside ultrasonography.
Emergency Medicine, the first and oldest publication devoted to our specialty since 1969, continues to be the newest!
We live in a time when the meanings of words often change dramatically—when bad sometimes means good and “cutting up” more often refers to a way of attempting suicide rather than to clowning around. In the 1982 edition of The American Heritage Dictionary you’ll find the entry: “aid (ad) v. aid-ed, aid-ing, aids. –intr. To help: assist. –tr. To give help or assistance to. –n. 1. The act or result of helping; assistance 2. One that helps; an assistant or helper …” But who among us will ever again be comforted by the prospect of assistance upon hearing the word “aids”? Today, we immediately think of AIDS, the acronym for acquired immunodeficiency syndrome.
Until very recently, AIDS was neither a word nor a recognized disease. Then—as noted in the article “AIDS on the Frontline” [June 1981 issue of EM], the CDC’s Morbidity and mortality Weekly Report described a cluster of cases of Pneumocystis carinii pneumonia, candidiasis, and cytomegalovirus infections occurring in young homosexual men. In November of [1981], the first of many articles on various aspects of AIDS appeared in EM and was entitled “The Riddle of Kaposi’s Sarcoma.”
Those initial reports proved to be the tip of the iceberg. Since 1981, both the tip and the iceberg have become much larger. One current estimate suggests that half of the approximately 2,550,000 intravenous drug users in the Northeast may now have a positive HTLV-III (HIV) antibody blood test, indicating exposure to the virus. Another estimate suggests that 5% or more of those with positive blood tests will eventually be stricken with AIDS, while even more may be afflicted with AIDS-related complex, or ARC—another word that used to mean something else.
If one were asked to choose the half-dozen most significant events of [the 20th] century, along with the world at war, the theory of relativity and development of nuclear weapons, the use of antibiotics and vaccines, and the widespread employment of effective birth control methods, one would now have to include the phenomenon of AIDS—“phenomenon” because it remains to be seen whether by the end of the century it will be listed as “the AIDS epidemic and cure.” Whatever the outcome, AIDS is the scientific, clinical, and bioethical challenge to the medical profession in the last quarter of the 20th century.
The challenge is enormous. During our medical school training and clinical practice did we have any real understanding of what is was like to be physicians during an epidemic such as plague, the catastrophic influenza of 1918-19, or smallpox? We will probably learn. Did we consider how to negotiate the impossible demands by the public for the absolute truth—including our admission of vast areas of scientific ignorance—on the one hand, and their equally insistent demands for guarantees and reassurance beyond the limits of current scientific knowledge on the other? We do every day, now.
The ironies of AIDS are incredible. Until a few years ago, we were struggling along “just” trying to come up with a cure (cures) for cancer, when suddenly the struggle became a science-fiction nightmare no one would have believed possible: an infectious disease that causes cancer, spread both sexually and intravenously. And yet while the problem itself has grown, the scientific advances toward a solution have also been progressing in an incredibly short period of time—identification of an etiologic organism followed by a blood test indicating exposure in just a few years.
If we could consider the scientific advances alone, we could all stand around and justifiably congratulate ourselves. But of course, the advances are overshadowed by the disease itself. Will a vaccine be available in 3 to 5 years? A cure in 5 to 10? Will we ultimately cure cancer in curing AIDS? Or will we see a new “Darwinian selection” of the biologically fittest?
To get to the year 2000, we will have to continue to set aside nuclear weapons, effectively balance the world population with the world food supply, and cure or control AIDS and any similar new disease that may develop. To get to 1987, those of us who deal with medical emergencies daily will have to treat the complications of AIDS with the medications and antibiotics available, counsel our patients as best we can, reassure the public to the limits of current scientific knowledge, and neither panic ourselves nor become complacent in handling the needles and biological material that are part of everyday patient care.
It almost makes one long for the “good old days” of the 1970s, when aids were aids and the practice of medicine seemed so much simpler.
—Neal Flomenbaum, MD, New York
This month marks the 100th consecutive month of EM editorials. The accompanying editorial was written for EM way back in 1986, when, as a member of EM’s editorial board, I was asked to inaugurate a series of editorial/viewpoints by board members on the issues that “boiled to the surface” at the time. I chose to write about the relatively new and frightening epidemic of HIV infections and AIDS overwhelming EDs across the country. At that time, AIDS was a lethal illness accompanied by fears that it could accidentally spread to health care workers by needle sticks etc.
Predicting the future is a risky exercise but, young and undaunted, I wondered if we would have a vaccine in 3 to 5 years, a cure in 5 to 10 years, and by the latter, “cure cancer.” Though none of these possibilities actually occurred, by the beginning of the 21st century AIDS had been transformed into a chronic and mostly manageable illness—at least in the compliant patient. But in the years since 1986, we have indeed seen rapid scientific advances in identification of causative agents, followed by accurate tests for infection, and effective treatments or vaccines—all of which helped prevent the spread of SARS and other potentially lethal infections. In terms of outcome, not a bad forecast for 1986, though it would be more than 20 years before EM asked me to write another editorial!
Also next month, readers will be introduced to several new EM Advisory Board members who have achieved national recognition for their work in newer EM disciplines such as prehospital care, critical care, geriatric emergency medicine, wilderness medicine, and bedside ultrasonography.
Emergency Medicine, the first and oldest publication devoted to our specialty since 1969, continues to be the newest!
We live in a time when the meanings of words often change dramatically—when bad sometimes means good and “cutting up” more often refers to a way of attempting suicide rather than to clowning around. In the 1982 edition of The American Heritage Dictionary you’ll find the entry: “aid (ad) v. aid-ed, aid-ing, aids. –intr. To help: assist. –tr. To give help or assistance to. –n. 1. The act or result of helping; assistance 2. One that helps; an assistant or helper …” But who among us will ever again be comforted by the prospect of assistance upon hearing the word “aids”? Today, we immediately think of AIDS, the acronym for acquired immunodeficiency syndrome.
Until very recently, AIDS was neither a word nor a recognized disease. Then—as noted in the article “AIDS on the Frontline” [June 1981 issue of EM], the CDC’s Morbidity and mortality Weekly Report described a cluster of cases of Pneumocystis carinii pneumonia, candidiasis, and cytomegalovirus infections occurring in young homosexual men. In November of [1981], the first of many articles on various aspects of AIDS appeared in EM and was entitled “The Riddle of Kaposi’s Sarcoma.”
Those initial reports proved to be the tip of the iceberg. Since 1981, both the tip and the iceberg have become much larger. One current estimate suggests that half of the approximately 2,550,000 intravenous drug users in the Northeast may now have a positive HTLV-III (HIV) antibody blood test, indicating exposure to the virus. Another estimate suggests that 5% or more of those with positive blood tests will eventually be stricken with AIDS, while even more may be afflicted with AIDS-related complex, or ARC—another word that used to mean something else.
If one were asked to choose the half-dozen most significant events of [the 20th] century, along with the world at war, the theory of relativity and development of nuclear weapons, the use of antibiotics and vaccines, and the widespread employment of effective birth control methods, one would now have to include the phenomenon of AIDS—“phenomenon” because it remains to be seen whether by the end of the century it will be listed as “the AIDS epidemic and cure.” Whatever the outcome, AIDS is the scientific, clinical, and bioethical challenge to the medical profession in the last quarter of the 20th century.
The challenge is enormous. During our medical school training and clinical practice did we have any real understanding of what is was like to be physicians during an epidemic such as plague, the catastrophic influenza of 1918-19, or smallpox? We will probably learn. Did we consider how to negotiate the impossible demands by the public for the absolute truth—including our admission of vast areas of scientific ignorance—on the one hand, and their equally insistent demands for guarantees and reassurance beyond the limits of current scientific knowledge on the other? We do every day, now.
The ironies of AIDS are incredible. Until a few years ago, we were struggling along “just” trying to come up with a cure (cures) for cancer, when suddenly the struggle became a science-fiction nightmare no one would have believed possible: an infectious disease that causes cancer, spread both sexually and intravenously. And yet while the problem itself has grown, the scientific advances toward a solution have also been progressing in an incredibly short period of time—identification of an etiologic organism followed by a blood test indicating exposure in just a few years.
If we could consider the scientific advances alone, we could all stand around and justifiably congratulate ourselves. But of course, the advances are overshadowed by the disease itself. Will a vaccine be available in 3 to 5 years? A cure in 5 to 10? Will we ultimately cure cancer in curing AIDS? Or will we see a new “Darwinian selection” of the biologically fittest?
To get to the year 2000, we will have to continue to set aside nuclear weapons, effectively balance the world population with the world food supply, and cure or control AIDS and any similar new disease that may develop. To get to 1987, those of us who deal with medical emergencies daily will have to treat the complications of AIDS with the medications and antibiotics available, counsel our patients as best we can, reassure the public to the limits of current scientific knowledge, and neither panic ourselves nor become complacent in handling the needles and biological material that are part of everyday patient care.
It almost makes one long for the “good old days” of the 1970s, when aids were aids and the practice of medicine seemed so much simpler.
—Neal Flomenbaum, MD, New York
This month marks the 100th consecutive month of EM editorials. The accompanying editorial was written for EM way back in 1986, when, as a member of EM’s editorial board, I was asked to inaugurate a series of editorial/viewpoints by board members on the issues that “boiled to the surface” at the time. I chose to write about the relatively new and frightening epidemic of HIV infections and AIDS overwhelming EDs across the country. At that time, AIDS was a lethal illness accompanied by fears that it could accidentally spread to health care workers by needle sticks etc.
Predicting the future is a risky exercise but, young and undaunted, I wondered if we would have a vaccine in 3 to 5 years, a cure in 5 to 10 years, and by the latter, “cure cancer.” Though none of these possibilities actually occurred, by the beginning of the 21st century AIDS had been transformed into a chronic and mostly manageable illness—at least in the compliant patient. But in the years since 1986, we have indeed seen rapid scientific advances in identification of causative agents, followed by accurate tests for infection, and effective treatments or vaccines—all of which helped prevent the spread of SARS and other potentially lethal infections. In terms of outcome, not a bad forecast for 1986, though it would be more than 20 years before EM asked me to write another editorial!
Also next month, readers will be introduced to several new EM Advisory Board members who have achieved national recognition for their work in newer EM disciplines such as prehospital care, critical care, geriatric emergency medicine, wilderness medicine, and bedside ultrasonography.
Emergency Medicine, the first and oldest publication devoted to our specialty since 1969, continues to be the newest!
We live in a time when the meanings of words often change dramatically—when bad sometimes means good and “cutting up” more often refers to a way of attempting suicide rather than to clowning around. In the 1982 edition of The American Heritage Dictionary you’ll find the entry: “aid (ad) v. aid-ed, aid-ing, aids. –intr. To help: assist. –tr. To give help or assistance to. –n. 1. The act or result of helping; assistance 2. One that helps; an assistant or helper …” But who among us will ever again be comforted by the prospect of assistance upon hearing the word “aids”? Today, we immediately think of AIDS, the acronym for acquired immunodeficiency syndrome.
Until very recently, AIDS was neither a word nor a recognized disease. Then—as noted in the article “AIDS on the Frontline” [June 1981 issue of EM], the CDC’s Morbidity and mortality Weekly Report described a cluster of cases of Pneumocystis carinii pneumonia, candidiasis, and cytomegalovirus infections occurring in young homosexual men. In November of [1981], the first of many articles on various aspects of AIDS appeared in EM and was entitled “The Riddle of Kaposi’s Sarcoma.”
Those initial reports proved to be the tip of the iceberg. Since 1981, both the tip and the iceberg have become much larger. One current estimate suggests that half of the approximately 2,550,000 intravenous drug users in the Northeast may now have a positive HTLV-III (HIV) antibody blood test, indicating exposure to the virus. Another estimate suggests that 5% or more of those with positive blood tests will eventually be stricken with AIDS, while even more may be afflicted with AIDS-related complex, or ARC—another word that used to mean something else.
If one were asked to choose the half-dozen most significant events of [the 20th] century, along with the world at war, the theory of relativity and development of nuclear weapons, the use of antibiotics and vaccines, and the widespread employment of effective birth control methods, one would now have to include the phenomenon of AIDS—“phenomenon” because it remains to be seen whether by the end of the century it will be listed as “the AIDS epidemic and cure.” Whatever the outcome, AIDS is the scientific, clinical, and bioethical challenge to the medical profession in the last quarter of the 20th century.
The challenge is enormous. During our medical school training and clinical practice did we have any real understanding of what is was like to be physicians during an epidemic such as plague, the catastrophic influenza of 1918-19, or smallpox? We will probably learn. Did we consider how to negotiate the impossible demands by the public for the absolute truth—including our admission of vast areas of scientific ignorance—on the one hand, and their equally insistent demands for guarantees and reassurance beyond the limits of current scientific knowledge on the other? We do every day, now.
The ironies of AIDS are incredible. Until a few years ago, we were struggling along “just” trying to come up with a cure (cures) for cancer, when suddenly the struggle became a science-fiction nightmare no one would have believed possible: an infectious disease that causes cancer, spread both sexually and intravenously. And yet while the problem itself has grown, the scientific advances toward a solution have also been progressing in an incredibly short period of time—identification of an etiologic organism followed by a blood test indicating exposure in just a few years.
If we could consider the scientific advances alone, we could all stand around and justifiably congratulate ourselves. But of course, the advances are overshadowed by the disease itself. Will a vaccine be available in 3 to 5 years? A cure in 5 to 10? Will we ultimately cure cancer in curing AIDS? Or will we see a new “Darwinian selection” of the biologically fittest?
To get to the year 2000, we will have to continue to set aside nuclear weapons, effectively balance the world population with the world food supply, and cure or control AIDS and any similar new disease that may develop. To get to 1987, those of us who deal with medical emergencies daily will have to treat the complications of AIDS with the medications and antibiotics available, counsel our patients as best we can, reassure the public to the limits of current scientific knowledge, and neither panic ourselves nor become complacent in handling the needles and biological material that are part of everyday patient care.
It almost makes one long for the “good old days” of the 1970s, when aids were aids and the practice of medicine seemed so much simpler.
—Neal Flomenbaum, MD, New York
Can a plant-based diet really reverse CAD?

We can all agree that this study is not the definitive study of this highly restrictive vegetarian diet. It is a case series of highly motivated patients, and we do not know how these findings would apply to others. Dr. Esselstyn and his colleagues admit that “(w)ithout a control group, it is challenging to establish causality and assess how much of the observed changes are specifically due to the diet.”
I think we can agree, too, that case series can lead us astray. A good example is the randomized trials of knee arthroscopy for relief of knee pain from meniscal tears that found lack of benefit compared to earlier case series that showed significant improvement (see “Surgery for persistent knee pain? Not so fast”). In a case series, it is not possible to answer the important question: compared to what? Without a control group and randomization, we cannot know if outcomes are due to the treatment, another factor, or the natural course of the disease.
On the other hand, case series can be the first step in medical breakthroughs. The first known successful trial of penicillin was a case series of 5 patients with eye infections performed in 1930,2 and the first published description of acquired immunodeficiency syndrome involved case reports of 5 patients with pneumocystis carinii pneumonia.3
In the present case, I was intrigued by Dr. Esselstyn’s findings and believe the methods and biological plausibility were good enough to get the word out, mostly to stimulate others’ thinking and actions. That is why, after the manuscript underwent peer review, we decided to publish it.
In a separate letter to me, Dr. Silverstein wrote, “Sometimes if something seems too good to be true, it isn’t [true].” I could not agree more. But the flip side of that statement is that sometimes something that seems too good to be true, actually is true.
We do not yet know which of these statements applies to Dr. Esselstyn’s work. I do, however, agree with Dr. Esselstyn and his colleagues that “...the time is right for a controlled trial.”
1. Esselstyn CB, Gendy G, Doyle J, et al. A way to reverse CAD? J Fam Pract. 2014;63:356-364,364a,364b.
2. Wainwright M, Swan HT. C.G. Paine and the earliest surviving clinical records of penicillin therapy. Med Hist. 1986;30:42-56.
3. Centers for Disease Control (CDC). Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep. 1981;30:250-252.
We can all agree that this study is not the definitive study of this highly restrictive vegetarian diet. It is a case series of highly motivated patients, and we do not know how these findings would apply to others. Dr. Esselstyn and his colleagues admit that “(w)ithout a control group, it is challenging to establish causality and assess how much of the observed changes are specifically due to the diet.”
I think we can agree, too, that case series can lead us astray. A good example is the randomized trials of knee arthroscopy for relief of knee pain from meniscal tears that found lack of benefit compared to earlier case series that showed significant improvement (see “Surgery for persistent knee pain? Not so fast”). In a case series, it is not possible to answer the important question: compared to what? Without a control group and randomization, we cannot know if outcomes are due to the treatment, another factor, or the natural course of the disease.
On the other hand, case series can be the first step in medical breakthroughs. The first known successful trial of penicillin was a case series of 5 patients with eye infections performed in 1930,2 and the first published description of acquired immunodeficiency syndrome involved case reports of 5 patients with pneumocystis carinii pneumonia.3
In the present case, I was intrigued by Dr. Esselstyn’s findings and believe the methods and biological plausibility were good enough to get the word out, mostly to stimulate others’ thinking and actions. That is why, after the manuscript underwent peer review, we decided to publish it.
In a separate letter to me, Dr. Silverstein wrote, “Sometimes if something seems too good to be true, it isn’t [true].” I could not agree more. But the flip side of that statement is that sometimes something that seems too good to be true, actually is true.
We do not yet know which of these statements applies to Dr. Esselstyn’s work. I do, however, agree with Dr. Esselstyn and his colleagues that “...the time is right for a controlled trial.”
We can all agree that this study is not the definitive study of this highly restrictive vegetarian diet. It is a case series of highly motivated patients, and we do not know how these findings would apply to others. Dr. Esselstyn and his colleagues admit that “(w)ithout a control group, it is challenging to establish causality and assess how much of the observed changes are specifically due to the diet.”
I think we can agree, too, that case series can lead us astray. A good example is the randomized trials of knee arthroscopy for relief of knee pain from meniscal tears that found lack of benefit compared to earlier case series that showed significant improvement (see “Surgery for persistent knee pain? Not so fast”). In a case series, it is not possible to answer the important question: compared to what? Without a control group and randomization, we cannot know if outcomes are due to the treatment, another factor, or the natural course of the disease.
On the other hand, case series can be the first step in medical breakthroughs. The first known successful trial of penicillin was a case series of 5 patients with eye infections performed in 1930,2 and the first published description of acquired immunodeficiency syndrome involved case reports of 5 patients with pneumocystis carinii pneumonia.3
In the present case, I was intrigued by Dr. Esselstyn’s findings and believe the methods and biological plausibility were good enough to get the word out, mostly to stimulate others’ thinking and actions. That is why, after the manuscript underwent peer review, we decided to publish it.
In a separate letter to me, Dr. Silverstein wrote, “Sometimes if something seems too good to be true, it isn’t [true].” I could not agree more. But the flip side of that statement is that sometimes something that seems too good to be true, actually is true.
We do not yet know which of these statements applies to Dr. Esselstyn’s work. I do, however, agree with Dr. Esselstyn and his colleagues that “...the time is right for a controlled trial.”
1. Esselstyn CB, Gendy G, Doyle J, et al. A way to reverse CAD? J Fam Pract. 2014;63:356-364,364a,364b.
2. Wainwright M, Swan HT. C.G. Paine and the earliest surviving clinical records of penicillin therapy. Med Hist. 1986;30:42-56.
3. Centers for Disease Control (CDC). Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep. 1981;30:250-252.
1. Esselstyn CB, Gendy G, Doyle J, et al. A way to reverse CAD? J Fam Pract. 2014;63:356-364,364a,364b.
2. Wainwright M, Swan HT. C.G. Paine and the earliest surviving clinical records of penicillin therapy. Med Hist. 1986;30:42-56.
3. Centers for Disease Control (CDC). Pneumocystis pneumonia—Los Angeles. MMWR Morb Mortal Wkly Rep. 1981;30:250-252.
Nursing home litigation: A vicious cycle
Nursing home neglect/abuse is growing fast, and so is related litigation. Cases typically involve wrongful death, decubitus ulcers, dehydration, malnutrition, sepsis, and falls.1 The financial burden nursing homes face in defending numerous lawsuits diverts funds that could be used to improve the quality of care.2
The families of victims of nursing home abuse/neglect often pursue lawsuits to get nursing homes to provide better quality of care to their residents. This can be difficult for nursing homes to achieve when they have to pour their financial resources into defending lawsuits. Historically, nursing home abuse/ neglect has been addressed by governmental regulation.3 Although victims and their families should not be deprived of their Seventh Amendment right, perhaps stricter government regulation is a more efficient means of addressing this problem.4
Mohammed Muqeet Adnan, MD
Huma Adnan, JD
Syed Amer, MD
Usman Bhutta, MD
Oklahoma City, Okla
1. Wunderlich GS, Kohler PO, eds. Improving the Quality of Long-Term Care. Washington, DC: National Academies Press; 2001.
2. Bourdon T, Doubin S. Long Term Care: General Liability and Professional Liability, Actuarial Analysis. New York, NY: Aon Risk Solutions; 2002.
3. Kapp MB. Quality of care and quality of life in nursing facilities: What’s regulation got to do with it? McGeorge Law Rev. 2000;31: 707-731.
4. Hemp SH. The right to a remedy: When should an abused nursing home resident sue? Elder Law J. 1994;2:195-224.
Nursing home neglect/abuse is growing fast, and so is related litigation. Cases typically involve wrongful death, decubitus ulcers, dehydration, malnutrition, sepsis, and falls.1 The financial burden nursing homes face in defending numerous lawsuits diverts funds that could be used to improve the quality of care.2
The families of victims of nursing home abuse/neglect often pursue lawsuits to get nursing homes to provide better quality of care to their residents. This can be difficult for nursing homes to achieve when they have to pour their financial resources into defending lawsuits. Historically, nursing home abuse/ neglect has been addressed by governmental regulation.3 Although victims and their families should not be deprived of their Seventh Amendment right, perhaps stricter government regulation is a more efficient means of addressing this problem.4
Mohammed Muqeet Adnan, MD
Huma Adnan, JD
Syed Amer, MD
Usman Bhutta, MD
Oklahoma City, Okla
Nursing home neglect/abuse is growing fast, and so is related litigation. Cases typically involve wrongful death, decubitus ulcers, dehydration, malnutrition, sepsis, and falls.1 The financial burden nursing homes face in defending numerous lawsuits diverts funds that could be used to improve the quality of care.2
The families of victims of nursing home abuse/neglect often pursue lawsuits to get nursing homes to provide better quality of care to their residents. This can be difficult for nursing homes to achieve when they have to pour their financial resources into defending lawsuits. Historically, nursing home abuse/ neglect has been addressed by governmental regulation.3 Although victims and their families should not be deprived of their Seventh Amendment right, perhaps stricter government regulation is a more efficient means of addressing this problem.4
Mohammed Muqeet Adnan, MD
Huma Adnan, JD
Syed Amer, MD
Usman Bhutta, MD
Oklahoma City, Okla
1. Wunderlich GS, Kohler PO, eds. Improving the Quality of Long-Term Care. Washington, DC: National Academies Press; 2001.
2. Bourdon T, Doubin S. Long Term Care: General Liability and Professional Liability, Actuarial Analysis. New York, NY: Aon Risk Solutions; 2002.
3. Kapp MB. Quality of care and quality of life in nursing facilities: What’s regulation got to do with it? McGeorge Law Rev. 2000;31: 707-731.
4. Hemp SH. The right to a remedy: When should an abused nursing home resident sue? Elder Law J. 1994;2:195-224.
1. Wunderlich GS, Kohler PO, eds. Improving the Quality of Long-Term Care. Washington, DC: National Academies Press; 2001.
2. Bourdon T, Doubin S. Long Term Care: General Liability and Professional Liability, Actuarial Analysis. New York, NY: Aon Risk Solutions; 2002.
3. Kapp MB. Quality of care and quality of life in nursing facilities: What’s regulation got to do with it? McGeorge Law Rev. 2000;31: 707-731.
4. Hemp SH. The right to a remedy: When should an abused nursing home resident sue? Elder Law J. 1994;2:195-224.
Are these CAD study findings too good to be true?
I read with interest “A way to reverse CAD?” by Esselstyn et al (J Fam Pract. 2014;63:356-364,364a,364b) on the effects of a plant-based nutrition program on the incidence of cardiac events in patients with cardiovascular disease (CVD). If found to be effective in subsequent studies, this intervention could have tremendous clinical implications for patients. However, the article left me with many questions and concerns.
One of my concerns is that the article was written in a promotional, not scientific, tone. Although no potential conflicts of interest were reported, the lead author has published books on the topic from which he could profit. Even if one were to disregard these concerns, several methodological issues remain.
Specifically, Esselstyn et al report that over a mean 3.7 years of follow-up, 89% of patients were compliant to the program, defined as avoidance of all meat, fish, dairy, and added oils. Frankly, this statistic isn’t believable because the “compliant” patients undoubtedly consumed these products on occasion during this period. More likely, compliance was assessed by a simple Yes or No response over the phone; expectation bias would strongly influence patient reporting in this situation.
In addition, there’s no comparison of disease severity, prior interventions, weight loss, assessment of optimized medical management, or follow-up duration between the 2 groups. The differences in events reported in this study may be explained by unreported confounders.
The authors should be congratulated for presenting this work, but overall, the reporting is inadequate to form any scientific conclusions. The data lead to more questions than answers.
Larry E. Miller, PhD
Asheville, NC
Esselstyn et al report an extraordinary recurrent event rate of 0.6% among 177 patients with established cardiovascular disease who adhered to a plant-based diet for approximately 44 months. These results are so remarkable that several questions come to mind. Why didn’t the editors of The Journal of Family Practice offer any commentary on a revolutionary intervention that appears to cure cardiovascular disease? Why aren’t these results being reported and commented upon in the lay media? Why didn’t the journal note Dr. Esselstyn’s potential conflict of interest as an author who profits from the sale of books that advocate a plant-based diet?
I am glad to see studies that look at nutritional interventions getting equal billing with those funded by pharmaceutical companies, but publishing this report without comment certainly leads a reader to believe that the editors and peer reviewers accept this study at face value, and that physicians might practice accordingly.
David A. Silverstein, MD
Buffalo, NY
Authors' response:
We agree with the major point of Dr. Miller’s comments—this safe, inexpensive, and effective diet works so well at reducing coronary and other vascular disease that it raises more questions than answers, and deserves study by other groups. There was no intent to obscure the senior author’s 2007 book, Prevent and Reverse Heart Disease1; as it is mentioned in the article, a copy of the book was provided to each study participant, and it was listed among the references.
We agree that using standardized, validated instruments to evaluate dietary intake, such as food frequency questionnaires or 3- to 7-day food records, would provide more scientifically sound methodology, but we were able to assess several key features of the diet, including the 2 key ones, abstinence from animal food intake and avoidance of all oils, without such tools. Most patients transitioned to the whole foods plant-based diet from the meat and processed foods dietary pattern, with only a few eating ovo-lacto or lacto-vegetarian diets before participating in the study.
Regarding disease severity, 44 participants had a prior myocardial infarction and 119 had a prior percutaneous coronary intervention or coronary artery bypass graft surgery. Twenty-seven were scheduled for intervention that was unnecessary after they adopted the program. The frustration of current cardiovascular therapy and the potential of plant-based nutrition are succinctly expressed in our recent series of case reports.2
Caldwell B. Esselstyn Jr, MD
Mladen Golubic, MD, PhD
Michael F. Roizen, MD
Lyndhurst, Ohio
1. Esselstyn CB Jr. Prevent and Reverse Heart Disease. New York, New York: Penguin Group; 2007.
2. Esselstyn CB, Golubic M. The nutritional reversal of cardiovascular disease—fact or fiction? Three case reports. Exp Clin Cardiol. 2014;20:1901-1908.
I read with interest “A way to reverse CAD?” by Esselstyn et al (J Fam Pract. 2014;63:356-364,364a,364b) on the effects of a plant-based nutrition program on the incidence of cardiac events in patients with cardiovascular disease (CVD). If found to be effective in subsequent studies, this intervention could have tremendous clinical implications for patients. However, the article left me with many questions and concerns.
One of my concerns is that the article was written in a promotional, not scientific, tone. Although no potential conflicts of interest were reported, the lead author has published books on the topic from which he could profit. Even if one were to disregard these concerns, several methodological issues remain.
Specifically, Esselstyn et al report that over a mean 3.7 years of follow-up, 89% of patients were compliant to the program, defined as avoidance of all meat, fish, dairy, and added oils. Frankly, this statistic isn’t believable because the “compliant” patients undoubtedly consumed these products on occasion during this period. More likely, compliance was assessed by a simple Yes or No response over the phone; expectation bias would strongly influence patient reporting in this situation.
In addition, there’s no comparison of disease severity, prior interventions, weight loss, assessment of optimized medical management, or follow-up duration between the 2 groups. The differences in events reported in this study may be explained by unreported confounders.
The authors should be congratulated for presenting this work, but overall, the reporting is inadequate to form any scientific conclusions. The data lead to more questions than answers.
Larry E. Miller, PhD
Asheville, NC
Esselstyn et al report an extraordinary recurrent event rate of 0.6% among 177 patients with established cardiovascular disease who adhered to a plant-based diet for approximately 44 months. These results are so remarkable that several questions come to mind. Why didn’t the editors of The Journal of Family Practice offer any commentary on a revolutionary intervention that appears to cure cardiovascular disease? Why aren’t these results being reported and commented upon in the lay media? Why didn’t the journal note Dr. Esselstyn’s potential conflict of interest as an author who profits from the sale of books that advocate a plant-based diet?
I am glad to see studies that look at nutritional interventions getting equal billing with those funded by pharmaceutical companies, but publishing this report without comment certainly leads a reader to believe that the editors and peer reviewers accept this study at face value, and that physicians might practice accordingly.
David A. Silverstein, MD
Buffalo, NY
Authors' response:
We agree with the major point of Dr. Miller’s comments—this safe, inexpensive, and effective diet works so well at reducing coronary and other vascular disease that it raises more questions than answers, and deserves study by other groups. There was no intent to obscure the senior author’s 2007 book, Prevent and Reverse Heart Disease1; as it is mentioned in the article, a copy of the book was provided to each study participant, and it was listed among the references.
We agree that using standardized, validated instruments to evaluate dietary intake, such as food frequency questionnaires or 3- to 7-day food records, would provide more scientifically sound methodology, but we were able to assess several key features of the diet, including the 2 key ones, abstinence from animal food intake and avoidance of all oils, without such tools. Most patients transitioned to the whole foods plant-based diet from the meat and processed foods dietary pattern, with only a few eating ovo-lacto or lacto-vegetarian diets before participating in the study.
Regarding disease severity, 44 participants had a prior myocardial infarction and 119 had a prior percutaneous coronary intervention or coronary artery bypass graft surgery. Twenty-seven were scheduled for intervention that was unnecessary after they adopted the program. The frustration of current cardiovascular therapy and the potential of plant-based nutrition are succinctly expressed in our recent series of case reports.2
Caldwell B. Esselstyn Jr, MD
Mladen Golubic, MD, PhD
Michael F. Roizen, MD
Lyndhurst, Ohio
I read with interest “A way to reverse CAD?” by Esselstyn et al (J Fam Pract. 2014;63:356-364,364a,364b) on the effects of a plant-based nutrition program on the incidence of cardiac events in patients with cardiovascular disease (CVD). If found to be effective in subsequent studies, this intervention could have tremendous clinical implications for patients. However, the article left me with many questions and concerns.
One of my concerns is that the article was written in a promotional, not scientific, tone. Although no potential conflicts of interest were reported, the lead author has published books on the topic from which he could profit. Even if one were to disregard these concerns, several methodological issues remain.
Specifically, Esselstyn et al report that over a mean 3.7 years of follow-up, 89% of patients were compliant to the program, defined as avoidance of all meat, fish, dairy, and added oils. Frankly, this statistic isn’t believable because the “compliant” patients undoubtedly consumed these products on occasion during this period. More likely, compliance was assessed by a simple Yes or No response over the phone; expectation bias would strongly influence patient reporting in this situation.
In addition, there’s no comparison of disease severity, prior interventions, weight loss, assessment of optimized medical management, or follow-up duration between the 2 groups. The differences in events reported in this study may be explained by unreported confounders.
The authors should be congratulated for presenting this work, but overall, the reporting is inadequate to form any scientific conclusions. The data lead to more questions than answers.
Larry E. Miller, PhD
Asheville, NC
Esselstyn et al report an extraordinary recurrent event rate of 0.6% among 177 patients with established cardiovascular disease who adhered to a plant-based diet for approximately 44 months. These results are so remarkable that several questions come to mind. Why didn’t the editors of The Journal of Family Practice offer any commentary on a revolutionary intervention that appears to cure cardiovascular disease? Why aren’t these results being reported and commented upon in the lay media? Why didn’t the journal note Dr. Esselstyn’s potential conflict of interest as an author who profits from the sale of books that advocate a plant-based diet?
I am glad to see studies that look at nutritional interventions getting equal billing with those funded by pharmaceutical companies, but publishing this report without comment certainly leads a reader to believe that the editors and peer reviewers accept this study at face value, and that physicians might practice accordingly.
David A. Silverstein, MD
Buffalo, NY
Authors' response:
We agree with the major point of Dr. Miller’s comments—this safe, inexpensive, and effective diet works so well at reducing coronary and other vascular disease that it raises more questions than answers, and deserves study by other groups. There was no intent to obscure the senior author’s 2007 book, Prevent and Reverse Heart Disease1; as it is mentioned in the article, a copy of the book was provided to each study participant, and it was listed among the references.
We agree that using standardized, validated instruments to evaluate dietary intake, such as food frequency questionnaires or 3- to 7-day food records, would provide more scientifically sound methodology, but we were able to assess several key features of the diet, including the 2 key ones, abstinence from animal food intake and avoidance of all oils, without such tools. Most patients transitioned to the whole foods plant-based diet from the meat and processed foods dietary pattern, with only a few eating ovo-lacto or lacto-vegetarian diets before participating in the study.
Regarding disease severity, 44 participants had a prior myocardial infarction and 119 had a prior percutaneous coronary intervention or coronary artery bypass graft surgery. Twenty-seven were scheduled for intervention that was unnecessary after they adopted the program. The frustration of current cardiovascular therapy and the potential of plant-based nutrition are succinctly expressed in our recent series of case reports.2
Caldwell B. Esselstyn Jr, MD
Mladen Golubic, MD, PhD
Michael F. Roizen, MD
Lyndhurst, Ohio
1. Esselstyn CB Jr. Prevent and Reverse Heart Disease. New York, New York: Penguin Group; 2007.
2. Esselstyn CB, Golubic M. The nutritional reversal of cardiovascular disease—fact or fiction? Three case reports. Exp Clin Cardiol. 2014;20:1901-1908.
1. Esselstyn CB Jr. Prevent and Reverse Heart Disease. New York, New York: Penguin Group; 2007.
2. Esselstyn CB, Golubic M. The nutritional reversal of cardiovascular disease—fact or fiction? Three case reports. Exp Clin Cardiol. 2014;20:1901-1908.
Errata
The author listing for the Clinical Inquiry, “What is the best imaging method for patients with a presumed acute stroke?” (J Fam Pract. 2014;63:36-37) incorrectly listed Leilani St. Anna, MLIS, AHIP as one of the authors. It should have read: Roya Sadeghi, MD, and Jon Neher, MD (Valley Family Medicine Residency, Renton, Wash), and Sarah Safranek, MLIS (University of Washington Health Sciences Library, Seattle).
The article “4 EKG abnormalities: What are the lifesaving diagnoses?” (J Fam Pract. 2014;63:368-375) incorrectly stated that ventricular fibrillation was one of 4 arrhythmias associated with Wolff-Parkinson-White syndrome that should be treated with synchronized cardioversion. In fact, an unstable patient with ventricular fibrillation should receive defibrillation—not synchronized cardioversion. The passage, which appeared on page 373, has been corrected in the online edition of the article.
The author listing for the Clinical Inquiry, “What is the best imaging method for patients with a presumed acute stroke?” (J Fam Pract. 2014;63:36-37) incorrectly listed Leilani St. Anna, MLIS, AHIP as one of the authors. It should have read: Roya Sadeghi, MD, and Jon Neher, MD (Valley Family Medicine Residency, Renton, Wash), and Sarah Safranek, MLIS (University of Washington Health Sciences Library, Seattle).
The article “4 EKG abnormalities: What are the lifesaving diagnoses?” (J Fam Pract. 2014;63:368-375) incorrectly stated that ventricular fibrillation was one of 4 arrhythmias associated with Wolff-Parkinson-White syndrome that should be treated with synchronized cardioversion. In fact, an unstable patient with ventricular fibrillation should receive defibrillation—not synchronized cardioversion. The passage, which appeared on page 373, has been corrected in the online edition of the article.
The author listing for the Clinical Inquiry, “What is the best imaging method for patients with a presumed acute stroke?” (J Fam Pract. 2014;63:36-37) incorrectly listed Leilani St. Anna, MLIS, AHIP as one of the authors. It should have read: Roya Sadeghi, MD, and Jon Neher, MD (Valley Family Medicine Residency, Renton, Wash), and Sarah Safranek, MLIS (University of Washington Health Sciences Library, Seattle).
The article “4 EKG abnormalities: What are the lifesaving diagnoses?” (J Fam Pract. 2014;63:368-375) incorrectly stated that ventricular fibrillation was one of 4 arrhythmias associated with Wolff-Parkinson-White syndrome that should be treated with synchronized cardioversion. In fact, an unstable patient with ventricular fibrillation should receive defibrillation—not synchronized cardioversion. The passage, which appeared on page 373, has been corrected in the online edition of the article.
To improve our patients’ health, look beyond reducing readmissions
In this issue of the Cleveland Clinic Journal of Medicine, Drs. Ayache, Boyaji, and Pile share evidence-based strategies for reducing the risk of readmission for patients with acute exacerbations of chronic obstructive pulmonary disease (COPD).1 They emphasize standardizing practice by combining effective clinical management with appropriate patient education, communication, and postdischarge follow-up.
Reducing the rate of preventable hospital readmissions (as well as avoiding admissions in the first place) is the right thing to do for the patient. Moreover, broader adoption of the strategies that they outline in their article will be critical to the success of health care organizations in improving patient outcomes and navigating a rapidly evolving landscape of reimbursement and reporting changes associated with the Centers for Medicare and Medicaid Services (CMS) Readmissions Reduction Program. Hospital readmission rates, while imperfect measures of the quality of care, demonstrate opportunities to optimize transitions of care. Success in our efforts to improve the health of our patients will likely be aligned with reductions in preventable admissions and improved attention to care coordination.
HOSPITALS ARE PENALIZED FOR EXCESSIVE READMISSION RATES
With nearly 20% of Medicare beneficiaries being rehospitalized within 30 days of discharge, at a cost of $17 billion annually,2 Congress enacted the Hospital Readmissions Reduction Program3 as part of the Affordable Care Act (ACA) in 2012. The Centers for Medicare and Medicaid Services (CMS) had already been reporting the readmission rates for heart failure, acute myocardial infarction, and pneumonia since 2009 (www.medicare.gov/hospitalcompare). Building on this work, the Affordable Care Act implemented financial penalties against hospitals that had excessive rates of readmissions for these conditions.
The Affordable Care Act put 1% of a hospital’s Medicare base payment at risk for all inpatient diagnoses in 2013—not just the three listed here. The risk is 2% in 2014 and will rise to 3% in 2015. In its first year, more than 2,200 United States hospitals were penalized a total of approximately $280 million because of readmission rates above the national mean. Nearly 10% of hospitals incurred the maximum 1% penalty, and about 30% paid no penalty.
The Secretary of the Department of Health and Human Services has the authority to extend the Readmissions Reduction Program to additional high-volume or high-expenditure conditions, and the department has announced it will expand the program in October 2014 (fiscal year 2015) to include two additional conditions: elective hip or knee replacement and COPD.4 In both cases, CMS began by publicly reporting these rates before including them in the program. Additional readmission measures, including those for stroke and hospital-wide all-cause readmissions, are also publicly reported and receive increased attention but are not yet included in the Readmissions Reduction Program.
UNFAIRLY PENALIZING THOSE THAT SERVE THE POOR
Avoidable causes of readmissions include hospital-acquired infections and complications, inadequate medication reconciliation and management, poor communication and coordination of care among the members of the health care team, and suboptimal care transitions.5 But other important drivers of readmissions are outside of a hospital’s direct control. These include mental illness, lack of social support, and poverty.6
A criticism of the Readmissions Reduction Program is that it disproportionately penalizes hospitals that serve the poorest patients.7 Currently, CMS readmission risk models do not adjust for socioeconomic factors. Further, CMS responds to these concerns by noting that it does not want different outcome standards for poor patients, and that adjusting for these factors may conceal potential health care disparities in disadvantaged populations.
NEW MISSION FOR HOSPITALS: MITIGATE SOCIOECONOMIC BARRIERS
Effective programs to reduce hospital readmissions must address the clinical interventions and patient education needs in the COPD discharge checklist discussed by Ayache et al, but must also attempt to mitigate social disadvantages that drive up readmissions for patients at highest risk.
Are hospitals in a position to do this? Too often, it is assumed that patients have access to medications, transportation to follow-up appointments, and social support. Early identification of patients at highest risk of being affected by lack of these factors and innovative solutions for mitigating these risks are important considerations in our efforts to reduce hospital readmissions.
HOW MANY READMISSIONS ARE TRULY PREVENTABLE?
Experts disagree on how many readmissions are truly preventable. Readmission rates for the sickest patients treated at tertiary or academic medical centers may reflect high-quality care in well-managed patients who otherwise would have died during the index admission.8
In early studies, the Medicare Payment Advisory Commission estimated that up to three-quarters of readmissions are preventable.9 In contrast, studies that used clinical instead of administrative data suggest preventable readmissions make up as little as 12% of total readmissions.10
Regardless of the actual percentage, Medicare’s risk-adjustment model relies exclusively on administrative data that do not fully account for nonpreventable factors and do not completely address unrelated or planned rehospitalizations. CMS is attempting to address these issues with an expanded readmission algorithm that excludes more planned and unrelated readmissions from the penalty calculation.
Ironically, the current structure of the Readmissions Reduction Program does little to address its intended goal of eliminating the perverse financial incentives for hospitals and physicians to readmit patients. Payments are still episode-based and reward readmissions. The $280 million that CMS expects to receive from the program this year covers less than 5% of the nearly $12 billion attributed to preventable rehospitalizations.11
WHAT PATIENTS NEED, NOT WHAT SUITS PROVIDERS
Hospital readmission rates are publicly reported, but it is shortsighted to think about readmissions outside of the broader context of the “medical home.” One must consider the role of primary care providers before and after an index admission in addition to the role of postacute care providers for some patients after discharge. Neither is directly affected by the current penalty program, but both are critical to effective solutions and optimizing value-oriented care.
Readmission rates are suboptimal measures, as they address presumed failures of hospital transitions rather than measuring care coordination and providing meaningful incentives to coordinate care. Yes, there is much to do to ensure effective transitions from the hospital to home or postacute settings. But to truly transform health care and deliver value, shouldn’t we strive to redesign the work flow around what patients need rather than what suits providers?
This effort should focus on managing the conditions that bring patients to the hospital. Medical homes and optimizing chronic disease care can play pivotal roles in improving quality and reducing costs. Coordination of care and disease-management programs have led to cost reductions of 30% or more12 and have reduced admission rates by more than 10%.13 While the nation waits for health care reimbursement models to better reward patient quality outcomes and population health while reducing costs, we can use measures such as the Agency for Healthcare Research and Quality’s Prevention Quality Indicators to identify early interventions in the ambulatory care setting that can prevent admissions, complications, and exacerbation of disease.
Payers should also experiment with and promote innovative bundled-payment models such as Geisinger Health System’s ProvenCare program, which sets a fixed price for surgical procedures and up to 90 days of posthospital care, including readmission. These warranty-like programs overcome financial incentives to readmit patients in Medicare’s volume-based diagnosis-related group payment system.5
Re-engineering the delivery of care requires realigning resources to improve efficiency and effectiveness. In the short term, hospitals that successfully reduce readmission rates can expect reduced net reimbursements, as the penalties currently do not exceed the lost revenue of readmissions.
Reducing preventable readmissions is the right thing to do, but not all hospitalizations and rehospitalizations are avoidable. Many readmissions reflect appropriate and necessary care. The relentless focus on the readmission rate diverts attention and resources from more proactive solutions and innovative approaches for increasing health care safety, quality outcomes, and value.
Hospitals are caught between the volume and value paradigms. Payment programs that reward proactive disease management and care coordination will do the most to reduce health care costs and improve the quality of care. Hospitals have a responsibility to efficiently and effectively manage acute care and optimize handoffs to the next provider. Medicare’s payment policies do not do enough today to align the financial and quality-of-care incentives.
- Ayache MB, Boyaji S, Pile J. Can we reduce the risk of readmission for a patient with an exacerbation of COPD? Cleve Clin J Med 2014; 81:525–527.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360:1418–1428.
- Department of Health and Human Services. Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and FY 2012 Rates; Hospitals’ FTE Resident Caps for Graduate Medical Education Payment; Final Rule. Federal Register 2011; 76:51475–51846. www.gpo.gov/fdsys/pkg/FR-2011-08-18/pdf/2011-19719.pdf. Accessed August 5, 2014.
- Department of Health and Human Services. Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long term care; hospital prospective payment system and fiscal year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status; final rule. Federal Register 2013; 78:50495–51040. www.gpo.gov/fdsys/pkg/FR-2013-08-19/pdf/2013-18956.pdf. Accessed August 5, 2014.
- Berenson RA, Paulus RA, Kalman NS. Medicare’s readmissions-reduction program—a positive alternative. N Engl J Med 2012; 366:1364–1366.
- Joynt KE, Jha AK. Thirty-day readmissions—truth and consequences. N Engl J Med 2012; 366:1366–1369.
- Rau J. Medicare to penalize 2,217 hospitals for excess readmissions. Kaiser Health News 2012. www.kaiserhealthnews.org/stories/2012/august/13/medicare-hospitals-readmissions-penalties.aspx. Accessed August 5, 2014.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med 2010; 363:297–298.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare, June 2007. www.medpac.gov/documents/jun07_entirereport.pdf. Accessed August 5, 2014.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 2011; 183:E391–E402.
- CMS Fee For Service IPPS Payment File, Fiscal Year 2014. cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/FY_14_FR_Impact_File.zip. Accessed August 5, 2014.
- Dartmouth Medical School Center for the Evaluative Clinical Sciences. The Dartmouth Atlas of Health Care, 2006. www.dartmouthat-las.org/downloads/atlases/2006_Chronic_Care_Atlas.pdf. Accessed August 5, 2014.
- Gold W, Kongstvedt P. How broadening DM’s focus helped shrink one plan’s costs. Managed Care 2003. www.managedcaremag.com/archives/0311/0311.minnesota.html. Accessed August 5, 2014.
In this issue of the Cleveland Clinic Journal of Medicine, Drs. Ayache, Boyaji, and Pile share evidence-based strategies for reducing the risk of readmission for patients with acute exacerbations of chronic obstructive pulmonary disease (COPD).1 They emphasize standardizing practice by combining effective clinical management with appropriate patient education, communication, and postdischarge follow-up.
Reducing the rate of preventable hospital readmissions (as well as avoiding admissions in the first place) is the right thing to do for the patient. Moreover, broader adoption of the strategies that they outline in their article will be critical to the success of health care organizations in improving patient outcomes and navigating a rapidly evolving landscape of reimbursement and reporting changes associated with the Centers for Medicare and Medicaid Services (CMS) Readmissions Reduction Program. Hospital readmission rates, while imperfect measures of the quality of care, demonstrate opportunities to optimize transitions of care. Success in our efforts to improve the health of our patients will likely be aligned with reductions in preventable admissions and improved attention to care coordination.
HOSPITALS ARE PENALIZED FOR EXCESSIVE READMISSION RATES
With nearly 20% of Medicare beneficiaries being rehospitalized within 30 days of discharge, at a cost of $17 billion annually,2 Congress enacted the Hospital Readmissions Reduction Program3 as part of the Affordable Care Act (ACA) in 2012. The Centers for Medicare and Medicaid Services (CMS) had already been reporting the readmission rates for heart failure, acute myocardial infarction, and pneumonia since 2009 (www.medicare.gov/hospitalcompare). Building on this work, the Affordable Care Act implemented financial penalties against hospitals that had excessive rates of readmissions for these conditions.
The Affordable Care Act put 1% of a hospital’s Medicare base payment at risk for all inpatient diagnoses in 2013—not just the three listed here. The risk is 2% in 2014 and will rise to 3% in 2015. In its first year, more than 2,200 United States hospitals were penalized a total of approximately $280 million because of readmission rates above the national mean. Nearly 10% of hospitals incurred the maximum 1% penalty, and about 30% paid no penalty.
The Secretary of the Department of Health and Human Services has the authority to extend the Readmissions Reduction Program to additional high-volume or high-expenditure conditions, and the department has announced it will expand the program in October 2014 (fiscal year 2015) to include two additional conditions: elective hip or knee replacement and COPD.4 In both cases, CMS began by publicly reporting these rates before including them in the program. Additional readmission measures, including those for stroke and hospital-wide all-cause readmissions, are also publicly reported and receive increased attention but are not yet included in the Readmissions Reduction Program.
UNFAIRLY PENALIZING THOSE THAT SERVE THE POOR
Avoidable causes of readmissions include hospital-acquired infections and complications, inadequate medication reconciliation and management, poor communication and coordination of care among the members of the health care team, and suboptimal care transitions.5 But other important drivers of readmissions are outside of a hospital’s direct control. These include mental illness, lack of social support, and poverty.6
A criticism of the Readmissions Reduction Program is that it disproportionately penalizes hospitals that serve the poorest patients.7 Currently, CMS readmission risk models do not adjust for socioeconomic factors. Further, CMS responds to these concerns by noting that it does not want different outcome standards for poor patients, and that adjusting for these factors may conceal potential health care disparities in disadvantaged populations.
NEW MISSION FOR HOSPITALS: MITIGATE SOCIOECONOMIC BARRIERS
Effective programs to reduce hospital readmissions must address the clinical interventions and patient education needs in the COPD discharge checklist discussed by Ayache et al, but must also attempt to mitigate social disadvantages that drive up readmissions for patients at highest risk.
Are hospitals in a position to do this? Too often, it is assumed that patients have access to medications, transportation to follow-up appointments, and social support. Early identification of patients at highest risk of being affected by lack of these factors and innovative solutions for mitigating these risks are important considerations in our efforts to reduce hospital readmissions.
HOW MANY READMISSIONS ARE TRULY PREVENTABLE?
Experts disagree on how many readmissions are truly preventable. Readmission rates for the sickest patients treated at tertiary or academic medical centers may reflect high-quality care in well-managed patients who otherwise would have died during the index admission.8
In early studies, the Medicare Payment Advisory Commission estimated that up to three-quarters of readmissions are preventable.9 In contrast, studies that used clinical instead of administrative data suggest preventable readmissions make up as little as 12% of total readmissions.10
Regardless of the actual percentage, Medicare’s risk-adjustment model relies exclusively on administrative data that do not fully account for nonpreventable factors and do not completely address unrelated or planned rehospitalizations. CMS is attempting to address these issues with an expanded readmission algorithm that excludes more planned and unrelated readmissions from the penalty calculation.
Ironically, the current structure of the Readmissions Reduction Program does little to address its intended goal of eliminating the perverse financial incentives for hospitals and physicians to readmit patients. Payments are still episode-based and reward readmissions. The $280 million that CMS expects to receive from the program this year covers less than 5% of the nearly $12 billion attributed to preventable rehospitalizations.11
WHAT PATIENTS NEED, NOT WHAT SUITS PROVIDERS
Hospital readmission rates are publicly reported, but it is shortsighted to think about readmissions outside of the broader context of the “medical home.” One must consider the role of primary care providers before and after an index admission in addition to the role of postacute care providers for some patients after discharge. Neither is directly affected by the current penalty program, but both are critical to effective solutions and optimizing value-oriented care.
Readmission rates are suboptimal measures, as they address presumed failures of hospital transitions rather than measuring care coordination and providing meaningful incentives to coordinate care. Yes, there is much to do to ensure effective transitions from the hospital to home or postacute settings. But to truly transform health care and deliver value, shouldn’t we strive to redesign the work flow around what patients need rather than what suits providers?
This effort should focus on managing the conditions that bring patients to the hospital. Medical homes and optimizing chronic disease care can play pivotal roles in improving quality and reducing costs. Coordination of care and disease-management programs have led to cost reductions of 30% or more12 and have reduced admission rates by more than 10%.13 While the nation waits for health care reimbursement models to better reward patient quality outcomes and population health while reducing costs, we can use measures such as the Agency for Healthcare Research and Quality’s Prevention Quality Indicators to identify early interventions in the ambulatory care setting that can prevent admissions, complications, and exacerbation of disease.
Payers should also experiment with and promote innovative bundled-payment models such as Geisinger Health System’s ProvenCare program, which sets a fixed price for surgical procedures and up to 90 days of posthospital care, including readmission. These warranty-like programs overcome financial incentives to readmit patients in Medicare’s volume-based diagnosis-related group payment system.5
Re-engineering the delivery of care requires realigning resources to improve efficiency and effectiveness. In the short term, hospitals that successfully reduce readmission rates can expect reduced net reimbursements, as the penalties currently do not exceed the lost revenue of readmissions.
Reducing preventable readmissions is the right thing to do, but not all hospitalizations and rehospitalizations are avoidable. Many readmissions reflect appropriate and necessary care. The relentless focus on the readmission rate diverts attention and resources from more proactive solutions and innovative approaches for increasing health care safety, quality outcomes, and value.
Hospitals are caught between the volume and value paradigms. Payment programs that reward proactive disease management and care coordination will do the most to reduce health care costs and improve the quality of care. Hospitals have a responsibility to efficiently and effectively manage acute care and optimize handoffs to the next provider. Medicare’s payment policies do not do enough today to align the financial and quality-of-care incentives.
In this issue of the Cleveland Clinic Journal of Medicine, Drs. Ayache, Boyaji, and Pile share evidence-based strategies for reducing the risk of readmission for patients with acute exacerbations of chronic obstructive pulmonary disease (COPD).1 They emphasize standardizing practice by combining effective clinical management with appropriate patient education, communication, and postdischarge follow-up.
Reducing the rate of preventable hospital readmissions (as well as avoiding admissions in the first place) is the right thing to do for the patient. Moreover, broader adoption of the strategies that they outline in their article will be critical to the success of health care organizations in improving patient outcomes and navigating a rapidly evolving landscape of reimbursement and reporting changes associated with the Centers for Medicare and Medicaid Services (CMS) Readmissions Reduction Program. Hospital readmission rates, while imperfect measures of the quality of care, demonstrate opportunities to optimize transitions of care. Success in our efforts to improve the health of our patients will likely be aligned with reductions in preventable admissions and improved attention to care coordination.
HOSPITALS ARE PENALIZED FOR EXCESSIVE READMISSION RATES
With nearly 20% of Medicare beneficiaries being rehospitalized within 30 days of discharge, at a cost of $17 billion annually,2 Congress enacted the Hospital Readmissions Reduction Program3 as part of the Affordable Care Act (ACA) in 2012. The Centers for Medicare and Medicaid Services (CMS) had already been reporting the readmission rates for heart failure, acute myocardial infarction, and pneumonia since 2009 (www.medicare.gov/hospitalcompare). Building on this work, the Affordable Care Act implemented financial penalties against hospitals that had excessive rates of readmissions for these conditions.
The Affordable Care Act put 1% of a hospital’s Medicare base payment at risk for all inpatient diagnoses in 2013—not just the three listed here. The risk is 2% in 2014 and will rise to 3% in 2015. In its first year, more than 2,200 United States hospitals were penalized a total of approximately $280 million because of readmission rates above the national mean. Nearly 10% of hospitals incurred the maximum 1% penalty, and about 30% paid no penalty.
The Secretary of the Department of Health and Human Services has the authority to extend the Readmissions Reduction Program to additional high-volume or high-expenditure conditions, and the department has announced it will expand the program in October 2014 (fiscal year 2015) to include two additional conditions: elective hip or knee replacement and COPD.4 In both cases, CMS began by publicly reporting these rates before including them in the program. Additional readmission measures, including those for stroke and hospital-wide all-cause readmissions, are also publicly reported and receive increased attention but are not yet included in the Readmissions Reduction Program.
UNFAIRLY PENALIZING THOSE THAT SERVE THE POOR
Avoidable causes of readmissions include hospital-acquired infections and complications, inadequate medication reconciliation and management, poor communication and coordination of care among the members of the health care team, and suboptimal care transitions.5 But other important drivers of readmissions are outside of a hospital’s direct control. These include mental illness, lack of social support, and poverty.6
A criticism of the Readmissions Reduction Program is that it disproportionately penalizes hospitals that serve the poorest patients.7 Currently, CMS readmission risk models do not adjust for socioeconomic factors. Further, CMS responds to these concerns by noting that it does not want different outcome standards for poor patients, and that adjusting for these factors may conceal potential health care disparities in disadvantaged populations.
NEW MISSION FOR HOSPITALS: MITIGATE SOCIOECONOMIC BARRIERS
Effective programs to reduce hospital readmissions must address the clinical interventions and patient education needs in the COPD discharge checklist discussed by Ayache et al, but must also attempt to mitigate social disadvantages that drive up readmissions for patients at highest risk.
Are hospitals in a position to do this? Too often, it is assumed that patients have access to medications, transportation to follow-up appointments, and social support. Early identification of patients at highest risk of being affected by lack of these factors and innovative solutions for mitigating these risks are important considerations in our efforts to reduce hospital readmissions.
HOW MANY READMISSIONS ARE TRULY PREVENTABLE?
Experts disagree on how many readmissions are truly preventable. Readmission rates for the sickest patients treated at tertiary or academic medical centers may reflect high-quality care in well-managed patients who otherwise would have died during the index admission.8
In early studies, the Medicare Payment Advisory Commission estimated that up to three-quarters of readmissions are preventable.9 In contrast, studies that used clinical instead of administrative data suggest preventable readmissions make up as little as 12% of total readmissions.10
Regardless of the actual percentage, Medicare’s risk-adjustment model relies exclusively on administrative data that do not fully account for nonpreventable factors and do not completely address unrelated or planned rehospitalizations. CMS is attempting to address these issues with an expanded readmission algorithm that excludes more planned and unrelated readmissions from the penalty calculation.
Ironically, the current structure of the Readmissions Reduction Program does little to address its intended goal of eliminating the perverse financial incentives for hospitals and physicians to readmit patients. Payments are still episode-based and reward readmissions. The $280 million that CMS expects to receive from the program this year covers less than 5% of the nearly $12 billion attributed to preventable rehospitalizations.11
WHAT PATIENTS NEED, NOT WHAT SUITS PROVIDERS
Hospital readmission rates are publicly reported, but it is shortsighted to think about readmissions outside of the broader context of the “medical home.” One must consider the role of primary care providers before and after an index admission in addition to the role of postacute care providers for some patients after discharge. Neither is directly affected by the current penalty program, but both are critical to effective solutions and optimizing value-oriented care.
Readmission rates are suboptimal measures, as they address presumed failures of hospital transitions rather than measuring care coordination and providing meaningful incentives to coordinate care. Yes, there is much to do to ensure effective transitions from the hospital to home or postacute settings. But to truly transform health care and deliver value, shouldn’t we strive to redesign the work flow around what patients need rather than what suits providers?
This effort should focus on managing the conditions that bring patients to the hospital. Medical homes and optimizing chronic disease care can play pivotal roles in improving quality and reducing costs. Coordination of care and disease-management programs have led to cost reductions of 30% or more12 and have reduced admission rates by more than 10%.13 While the nation waits for health care reimbursement models to better reward patient quality outcomes and population health while reducing costs, we can use measures such as the Agency for Healthcare Research and Quality’s Prevention Quality Indicators to identify early interventions in the ambulatory care setting that can prevent admissions, complications, and exacerbation of disease.
Payers should also experiment with and promote innovative bundled-payment models such as Geisinger Health System’s ProvenCare program, which sets a fixed price for surgical procedures and up to 90 days of posthospital care, including readmission. These warranty-like programs overcome financial incentives to readmit patients in Medicare’s volume-based diagnosis-related group payment system.5
Re-engineering the delivery of care requires realigning resources to improve efficiency and effectiveness. In the short term, hospitals that successfully reduce readmission rates can expect reduced net reimbursements, as the penalties currently do not exceed the lost revenue of readmissions.
Reducing preventable readmissions is the right thing to do, but not all hospitalizations and rehospitalizations are avoidable. Many readmissions reflect appropriate and necessary care. The relentless focus on the readmission rate diverts attention and resources from more proactive solutions and innovative approaches for increasing health care safety, quality outcomes, and value.
Hospitals are caught between the volume and value paradigms. Payment programs that reward proactive disease management and care coordination will do the most to reduce health care costs and improve the quality of care. Hospitals have a responsibility to efficiently and effectively manage acute care and optimize handoffs to the next provider. Medicare’s payment policies do not do enough today to align the financial and quality-of-care incentives.
- Ayache MB, Boyaji S, Pile J. Can we reduce the risk of readmission for a patient with an exacerbation of COPD? Cleve Clin J Med 2014; 81:525–527.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360:1418–1428.
- Department of Health and Human Services. Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and FY 2012 Rates; Hospitals’ FTE Resident Caps for Graduate Medical Education Payment; Final Rule. Federal Register 2011; 76:51475–51846. www.gpo.gov/fdsys/pkg/FR-2011-08-18/pdf/2011-19719.pdf. Accessed August 5, 2014.
- Department of Health and Human Services. Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long term care; hospital prospective payment system and fiscal year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status; final rule. Federal Register 2013; 78:50495–51040. www.gpo.gov/fdsys/pkg/FR-2013-08-19/pdf/2013-18956.pdf. Accessed August 5, 2014.
- Berenson RA, Paulus RA, Kalman NS. Medicare’s readmissions-reduction program—a positive alternative. N Engl J Med 2012; 366:1364–1366.
- Joynt KE, Jha AK. Thirty-day readmissions—truth and consequences. N Engl J Med 2012; 366:1366–1369.
- Rau J. Medicare to penalize 2,217 hospitals for excess readmissions. Kaiser Health News 2012. www.kaiserhealthnews.org/stories/2012/august/13/medicare-hospitals-readmissions-penalties.aspx. Accessed August 5, 2014.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med 2010; 363:297–298.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare, June 2007. www.medpac.gov/documents/jun07_entirereport.pdf. Accessed August 5, 2014.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 2011; 183:E391–E402.
- CMS Fee For Service IPPS Payment File, Fiscal Year 2014. cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/FY_14_FR_Impact_File.zip. Accessed August 5, 2014.
- Dartmouth Medical School Center for the Evaluative Clinical Sciences. The Dartmouth Atlas of Health Care, 2006. www.dartmouthat-las.org/downloads/atlases/2006_Chronic_Care_Atlas.pdf. Accessed August 5, 2014.
- Gold W, Kongstvedt P. How broadening DM’s focus helped shrink one plan’s costs. Managed Care 2003. www.managedcaremag.com/archives/0311/0311.minnesota.html. Accessed August 5, 2014.
- Ayache MB, Boyaji S, Pile J. Can we reduce the risk of readmission for a patient with an exacerbation of COPD? Cleve Clin J Med 2014; 81:525–527.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360:1418–1428.
- Department of Health and Human Services. Medicare Program; Hospital Inpatient Prospective Payment Systems for Acute Care Hospitals and the Long-Term Care Hospital Prospective Payment System and FY 2012 Rates; Hospitals’ FTE Resident Caps for Graduate Medical Education Payment; Final Rule. Federal Register 2011; 76:51475–51846. www.gpo.gov/fdsys/pkg/FR-2011-08-18/pdf/2011-19719.pdf. Accessed August 5, 2014.
- Department of Health and Human Services. Medicare program; hospital inpatient prospective payment systems for acute care hospitals and the long term care; hospital prospective payment system and fiscal year 2014 rates; quality reporting requirements for specific providers; hospital conditions of participation; payment policies related to patient status; final rule. Federal Register 2013; 78:50495–51040. www.gpo.gov/fdsys/pkg/FR-2013-08-19/pdf/2013-18956.pdf. Accessed August 5, 2014.
- Berenson RA, Paulus RA, Kalman NS. Medicare’s readmissions-reduction program—a positive alternative. N Engl J Med 2012; 366:1364–1366.
- Joynt KE, Jha AK. Thirty-day readmissions—truth and consequences. N Engl J Med 2012; 366:1366–1369.
- Rau J. Medicare to penalize 2,217 hospitals for excess readmissions. Kaiser Health News 2012. www.kaiserhealthnews.org/stories/2012/august/13/medicare-hospitals-readmissions-penalties.aspx. Accessed August 5, 2014.
- Gorodeski EZ, Starling RC, Blackstone EH. Are all readmissions bad readmissions? N Engl J Med 2010; 363:297–298.
- Medicare Payment Advisory Commission. Report to the Congress: Promoting Greater Efficiency in Medicare, June 2007. www.medpac.gov/documents/jun07_entirereport.pdf. Accessed August 5, 2014.
- van Walraven C, Bennett C, Jennings A, Austin PC, Forster AJ. Proportion of hospital readmissions deemed avoidable: a systematic review. CMAJ 2011; 183:E391–E402.
- CMS Fee For Service IPPS Payment File, Fiscal Year 2014. cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Downloads/FY_14_FR_Impact_File.zip. Accessed August 5, 2014.
- Dartmouth Medical School Center for the Evaluative Clinical Sciences. The Dartmouth Atlas of Health Care, 2006. www.dartmouthat-las.org/downloads/atlases/2006_Chronic_Care_Atlas.pdf. Accessed August 5, 2014.
- Gold W, Kongstvedt P. How broadening DM’s focus helped shrink one plan’s costs. Managed Care 2003. www.managedcaremag.com/archives/0311/0311.minnesota.html. Accessed August 5, 2014.