User login
WPATH removes age limits from transgender treatment guidelines
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
Long-awaited global transgender care guidelines have dropped, with no recommendations regarding age limits for treatment and surgery in teenagers but acknowledging the complexity of dealing with such adolescents amid lack of longitudinal research on the impact of transitioning gender.
The World Professional Association of Transgender Health published its latest standards of care (SOC8) as it opens its annual meeting on Sept. 16 in Montreal.![]()
These are “the most comprehensive set of guidelines ever produced to assist health care professionals around the world in support of transgender and gender diverse adults, adolescents, and children who are taking steps to live their lives authentically,” wrote WPATH President Walter Bouman, MD, PhD, and WPATH President-Elect Marci Bowers, MD, in a news release.
The SOC8 is the first update to guidance on the treatment of transgender individuals in 10 years and appears online in the International Journal of Transgender Health.
For the first time, the association wrote a chapter dedicated to transgender and gender-diverse adolescents – distinct from the child chapter.
The complexity of treating adolescents
WPATH officials said that this was owed to exponential growth in adolescent referral rates, more research on adolescent gender diversity–related care, and the unique developmental and care issues of this age group.
Until recently, there was limited information regarding the prevalence of gender diversity among adolescents. Studies from high-school samples indicate much higher rates than was earlier thought, with reports of up to 1.2% of participants identifying as transgender and up to 2.7% or more (for example, 7%-9%) experiencing some level of self-reported gender diversity, WPATH said.
The new chapter “applies to adolescents from the start of puberty until the legal age of majority (in most cases 18 years),” it stated.
However, WPATH did not go as far as to recommend lowering the age at which youth can receive cross-sex hormone therapy or gender-affirming surgeries, as earlier decreed in a draft of the guidelines. That draft suggested that young people could receive hormone therapy at age 14 years and surgeries for double mastectomies at age 15 years and for genital reassignment at age 17 years.
The exception was phalloplasty – surgery to construct a penis in female-to-male individuals – which WPATH stressed should not be performed under the age of 18 years owing to its complexity.
Now, the final SOC8 emphasizes that each transgender adolescent is unique, and decisions must be made on an individual basis, with no recommendations on specific ages for any treatment. This could be interpreted in many ways.
The SOC8 also acknowledges the “very rare” regret of individuals who have transitioned to the opposite gender and then changed their minds.
“[Health care] providers may consider the possibility an adolescent may regret gender-affirming decisions made during adolescence, and a young person will want to stop treatment and return to living in the birth-assigned gender role in the future. Providers may discuss this topic in a collaborative and trusting manner with the adolescent and their parents/caregivers before gender-affirming medical treatments are started,” it states.
WPATH, in addition, stressed the importance of counseling and supporting regretting patients, many who “expressed difficulties finding help during their detransition process and reported their detransition was an isolating experience during which they did not receive either sufficient or appropriate support.”
Although it doesn’t put a firm figure on the rate of regret overall, in its chapter on surgery, WPATH estimates that 0.3%-3.8% of transgender individuals regret gender-affirming surgery.
SOC8 also acknowledges “A pattern of uneven ratios by assigned sex has been reported in gender clinics, with assigned female-at-birth patients initiating care 2.5-7.1 times more frequently” than patients who were assigned male at birth.
And WPATH states in SOC8 that another phenomenon is the growing number of adolescents seeking care who had not previously experienced or expressed gender diversity during their childhood years.
It goes on to cite the 2018 paper of Lisa Littman, MD, MPH, now president of the Institute for Comprehensive Gender Dysphoria Research. Dr. Littman coined the term, “rapid-onset gender dysphoria” to describe this phenomenon; SOC8 refrains from using this phrase, but does acknowledge: “For a select subgroup of young people, susceptibility to social influence impacting gender may be an important differential to consider.”
SOC8 recommends that before any medical or surgical treatment is considered, health care professionals “undertake a comprehensive biopsychosocial assessment of adolescents who present with gender identity-related concerns and seek medical/surgical transition-related care.”
And it specifically mentions that transgender adolescents “show high rates of autism spectrum disorder/characteristics,” and notes that “other neurodevelopmental presentations and/or mental health challenges may also be present, (e.g., ADHD, intellectual disability, and psychotic disorders).”
Who uses WPATH to guide care? This is ‘a big unknown’
WPATH is an umbrella organization with offshoots in most Western nations, such as USPATH in the United States, EPATH in Europe, and AUSPATH and NZPATH in Australia and New Zealand.
However, it is not the only organization to issue guidance on the care of transgender individuals; several specialties take care of this patient population, including, but not limited to: pediatricians, endocrinologists, psychiatrists, psychologists and plastic surgeons.
The extent to which any health care professional, or professional body, follows WPATH guidance is extremely varied.
“There is nothing binding clinicians to the SOC, and the SOC is so broad and vague that anyone can say they’re following it but according to their own biases and interpretation,” Aaron Kimberly, a trans man and mental health clinician from the Gender Dysphoria Alliance, said in an interview.
In North America, some clinics practice full “informed consent” with no assessment and prescriptions at the first visit, Mr. Kimberly said, whereas others do comprehensive assessments.
“I think SOC should be observed. It shouldn’t just be people going rogue,” Erica Anderson, a clinical psychologist in Berkeley, Calif., former president of USPATH, and former member of WPATH, who is herself transgender, said in an interview. “The reason there are standards of care is because hundreds of scientists have weighed in – is it perfect? No. We have a long way to go. But you can’t just ignore whatever it is that we know and let people make their own decisions.”
A version of this article first appeared on Medscape.com.
FROM THE INTERNATIONAL JOURNAL OF TRANSGENDER HEALTH
New ESC guidelines for cutting CV risk in noncardiac surgery
The European Society of Cardiology guidelines on cardiovascular assessment and management of patients undergoing noncardiac surgery have seen extensive revision since the 2014 version.
They still have the same aim – to prevent surgery-related bleeding complications, perioperative myocardial infarction/injury (PMI), stent thrombosis, acute heart failure, arrhythmias, pulmonary embolism, ischemic stroke, and cardiovascular (CV) death.
Cochairpersons Sigrun Halvorsen, MD, PhD, and Julinda Mehilli, MD, presented highlights from the guidelines at the annual congress of the European Society of Cardiology and the document was simultaneously published online in the European Heart Journal.
The document classifies noncardiac surgery into three levels of 30-day risk of CV death, MI, or stroke. Low (< 1%) risk includes eye or thyroid surgery; intermediate (1%-5%) risk includes knee or hip replacement or renal transplant; and high (> 5%) risk includes aortic aneurysm, lung transplant, or pancreatic or bladder cancer surgery (see more examples below).
It classifies patients as low risk if they are younger than 65 without CV disease or CV risk factors (smoking, hypertension, diabetes, dyslipidemia, family history); intermediate risk if they are 65 or older or have CV risk factors; and high risk if they have CVD.
In an interview, Dr. Halvorsen, professor in cardiology, University of Oslo, zeroed in on three important revisions:
First, recommendations for preoperative ECG and biomarkers are more specific, he noted.
The guidelines advise that before intermediate- or high-risk noncardiac surgery, in patients who have known CVD, CV risk factors (including age 65 or older), or symptoms suggestive of CVD:
- It is recommended to obtain a preoperative 12-lead ECG (class I).
- It is recommended to measure high-sensitivity cardiac troponin T (hs-cTn T) or high-sensitivity cardiac troponin I (hs-cTn I). It is also recommended to measure these biomarkers at 24 hours and 48 hours post surgery (class I).
- It should be considered to measure B-type natriuretic peptide or N-terminal of the prohormone BNP (NT-proBNP).
However, for low-risk patients undergoing low- and intermediate-risk noncardiac surgery, it is not recommended to routinely obtain preoperative ECG, hs-cTn T/I, or BNP/NT-proBNP concentrations (class III).
Troponins have a stronger class I recommendation, compared with the IIA recommendation for BNP, because they are useful for preoperative risk stratification and for diagnosis of PMI, Dr. Halvorsen explained. “Patients receive painkillers after surgery and may have no pain,” she noted, but they may have PMI, which has a bad prognosis.
Second, the guidelines recommend that “all patients should stop smoking 4 weeks before noncardiac surgery [class I],” she noted. Clinicians should also “measure hemoglobin, and if the patient is anemic, treat the anemia.”
Third, the sections on antithrombotic treatment have been significantly revised. “Bridging – stopping an oral antithrombotic drug and switching to a subcutaneous or IV drug – has been common,” Dr. Halvorsen said, “but recently we have new evidence that in most cases that increases the risk of bleeding.”
“We are [now] much more restrictive with respect to bridging” with unfractionated heparin or low-molecular-weight heparin, she said. “We recommend against bridging in patients with low to moderate thrombotic risk,” and bridging should only be considered in patients with mechanical prosthetic heart valves or with very high thrombotic risk.
More preoperative recommendations
In the guideline overview session at the congress, Dr. Halverson highlighted some of the new recommendations for preoperative risk assessment.
If time allows, it is recommended to optimize guideline-recommended treatment of CVD and control of CV risk factors including blood pressure, dyslipidemia, and diabetes, before noncardiac surgery (class I).
Patients commonly have “murmurs, chest pain, dyspnea, and edema that may suggest severe CVD, but may also be caused by noncardiac disease,” she noted. The guidelines state that “for patients with a newly detected murmur and symptoms or signs of CVD, transthoracic echocardiography is recommended before noncardiac surgery (class I).
“Many studies have been performed to try to find out if initiation of specific drugs before surgery could reduce the risk of complications,” Dr. Halvorsen noted. However, few have shown any benefit and “the question of presurgery initiation of beta-blockers has been greatly debated,” she said. “We have again reviewed the literature and concluded ‘Routine initiation of beta-blockers perioperatively is not recommended (class IIIA).’ “
“We adhere to the guidelines on acute and chronic coronary syndrome recommending 6-12 months of dual antiplatelet treatment as a standard before elective surgery,” she said. “However, in case of time-sensitive surgery, the duration of that treatment can be shortened down to a minimum of 1 month after elective PCI and a minimum of 3 months after PCI and ACS.”
Patients with specific types of CVD
Dr. Mehilli, a professor at Landshut-Achdorf (Germany) Hospital, highlighted some new guideline recommendations for patients who have specific types of cardiovascular disease.
Coronary artery disease (CAD). “For chronic coronary syndrome, a cardiac workup is recommended only for patients undergoing intermediate risk or high-risk noncardiac surgery.”
“Stress imaging should be considered before any high risk, noncardiac surgery in asymptomatic patients with poor functional capacity and prior PCI or coronary artery bypass graft (new recommendation, class IIa).”
Mitral valve regurgitation. For patients undergoing scheduled noncardiac surgery, who remain symptomatic despite guideline-directed medical treatment for mitral valve regurgitation (including resynchronization and myocardial revascularization), consider a valve intervention – either transcatheter or surgical – before noncardiac surgery in eligible patients with acceptable procedural risk (new recommendation).
Cardiac implantable electronic devices (CIED). For high-risk patients with CIEDs undergoing noncardiac surgery with high probability of electromagnetic interference, a CIED checkup and necessary reprogramming immediately before the procedure should be considered (new recommendation).
Arrhythmias. “I want only to stress,” Dr. Mehilli said, “in patients with atrial fibrillation with acute or worsening hemodynamic instability undergoing noncardiac surgery, an emergency electrical cardioversion is recommended (class I).”
Peripheral artery disease (PAD) and abdominal aortic aneurysm. For these patients “we do not recommend a routine referral for a cardiac workup. But we recommend it for patients with poor functional capacity or with significant risk factors or symptoms (new recommendations).”
Chronic arterial hypertension. “We have modified the recommendation, recommending avoidance of large perioperative fluctuations in blood pressure, and we do not recommend deferring noncardiac surgery in patients with stage 1 or 2 hypertension,” she said.
Postoperative cardiovascular complications
The most frequent postoperative cardiovascular complication is PMI, Dr. Mehilli noted.
“In the BASEL-PMI registry, the incidence of this complication around intermediate or high-risk noncardiac surgery was up to 15% among patients older than 65 years or with a history of CAD or PAD, which makes this kind of complication really important to prevent, to assess, and to know how to treat.”
“It is recommended to have a high awareness for perioperative cardiovascular complications, combined with surveillance for PMI in patients undergoing intermediate- or high-risk noncardiac surgery” based on serial measurements of high-sensitivity cardiac troponin.
The guidelines define PMI as “an increase in the delta of high-sensitivity troponin more than the upper level of normal,” Dr. Mehilli said. “It’s different from the one used in a rule-in algorithm for non-STEMI acute coronary syndrome.”
Postoperative atrial fibrillation (AFib) is observed in 2%-30% of noncardiac surgery patients in different registries, particularly in patients undergoing intermediate or high-risk noncardiac surgery, she noted.
“We propose an algorithm on how to prevent and treat this complication. I want to highlight that in patients with hemodynamic unstable postoperative AF[ib], an emergency cardioversion is indicated. For the others, a rate control with the target heart rate of less than 110 beats per minute is indicated.”
In patients with postoperative AFib, long-term oral anticoagulation therapy should be considered in all patients at risk for stroke, considering the anticipated net clinical benefit of oral anticoagulation therapy as well as informed patient preference (new recommendations).
Routine use of beta-blockers to prevent postoperative AFib in patients undergoing noncardiac surgery is not recommended.
The document also covers the management of patients with kidney disease, diabetes, cancer, obesity, and COVID-19. In general, elective noncardiac surgery should be postponed after a patient has COVID-19, until he or she recovers completely, and coexisting conditions are optimized.
The guidelines are available from the ESC website in several formats: pocket guidelines, pocket guidelines smartphone app, guidelines slide set, essential messages, and the European Heart Journal article.
Noncardiac surgery risk categories
The guideline includes a table that classifies noncardiac surgeries into three groups, based on the associated 30-day risk of death, MI, or stroke:
- Low (< 1%): breast, dental, eye, thyroid, and minor gynecologic, orthopedic, and urologic surgery.
- Intermediate (1%-5%): carotid surgery, endovascular aortic aneurysm repair, gallbladder surgery, head or neck surgery, hernia repair, peripheral arterial angioplasty, renal transplant, major gynecologic, orthopedic, or neurologic (hip or spine) surgery, or urologic surgery
- High (> 5%): aortic and major vascular surgery (including aortic aneurysm), bladder removal (usually as a result of cancer), limb amputation, lung or liver transplant, pancreatic surgery, or perforated bowel repair.
The guidelines were endorsed by the European Society of Anaesthesiology and Intensive Care. The guideline authors reported numerous disclosures.
A version of this article first appeared on Medscape.com.
The European Society of Cardiology guidelines on cardiovascular assessment and management of patients undergoing noncardiac surgery have seen extensive revision since the 2014 version.
They still have the same aim – to prevent surgery-related bleeding complications, perioperative myocardial infarction/injury (PMI), stent thrombosis, acute heart failure, arrhythmias, pulmonary embolism, ischemic stroke, and cardiovascular (CV) death.
Cochairpersons Sigrun Halvorsen, MD, PhD, and Julinda Mehilli, MD, presented highlights from the guidelines at the annual congress of the European Society of Cardiology and the document was simultaneously published online in the European Heart Journal.
The document classifies noncardiac surgery into three levels of 30-day risk of CV death, MI, or stroke. Low (< 1%) risk includes eye or thyroid surgery; intermediate (1%-5%) risk includes knee or hip replacement or renal transplant; and high (> 5%) risk includes aortic aneurysm, lung transplant, or pancreatic or bladder cancer surgery (see more examples below).
It classifies patients as low risk if they are younger than 65 without CV disease or CV risk factors (smoking, hypertension, diabetes, dyslipidemia, family history); intermediate risk if they are 65 or older or have CV risk factors; and high risk if they have CVD.
In an interview, Dr. Halvorsen, professor in cardiology, University of Oslo, zeroed in on three important revisions:
First, recommendations for preoperative ECG and biomarkers are more specific, he noted.
The guidelines advise that before intermediate- or high-risk noncardiac surgery, in patients who have known CVD, CV risk factors (including age 65 or older), or symptoms suggestive of CVD:
- It is recommended to obtain a preoperative 12-lead ECG (class I).
- It is recommended to measure high-sensitivity cardiac troponin T (hs-cTn T) or high-sensitivity cardiac troponin I (hs-cTn I). It is also recommended to measure these biomarkers at 24 hours and 48 hours post surgery (class I).
- It should be considered to measure B-type natriuretic peptide or N-terminal of the prohormone BNP (NT-proBNP).
However, for low-risk patients undergoing low- and intermediate-risk noncardiac surgery, it is not recommended to routinely obtain preoperative ECG, hs-cTn T/I, or BNP/NT-proBNP concentrations (class III).
Troponins have a stronger class I recommendation, compared with the IIA recommendation for BNP, because they are useful for preoperative risk stratification and for diagnosis of PMI, Dr. Halvorsen explained. “Patients receive painkillers after surgery and may have no pain,” she noted, but they may have PMI, which has a bad prognosis.
Second, the guidelines recommend that “all patients should stop smoking 4 weeks before noncardiac surgery [class I],” she noted. Clinicians should also “measure hemoglobin, and if the patient is anemic, treat the anemia.”
Third, the sections on antithrombotic treatment have been significantly revised. “Bridging – stopping an oral antithrombotic drug and switching to a subcutaneous or IV drug – has been common,” Dr. Halvorsen said, “but recently we have new evidence that in most cases that increases the risk of bleeding.”
“We are [now] much more restrictive with respect to bridging” with unfractionated heparin or low-molecular-weight heparin, she said. “We recommend against bridging in patients with low to moderate thrombotic risk,” and bridging should only be considered in patients with mechanical prosthetic heart valves or with very high thrombotic risk.
More preoperative recommendations
In the guideline overview session at the congress, Dr. Halverson highlighted some of the new recommendations for preoperative risk assessment.
If time allows, it is recommended to optimize guideline-recommended treatment of CVD and control of CV risk factors including blood pressure, dyslipidemia, and diabetes, before noncardiac surgery (class I).
Patients commonly have “murmurs, chest pain, dyspnea, and edema that may suggest severe CVD, but may also be caused by noncardiac disease,” she noted. The guidelines state that “for patients with a newly detected murmur and symptoms or signs of CVD, transthoracic echocardiography is recommended before noncardiac surgery (class I).
“Many studies have been performed to try to find out if initiation of specific drugs before surgery could reduce the risk of complications,” Dr. Halvorsen noted. However, few have shown any benefit and “the question of presurgery initiation of beta-blockers has been greatly debated,” she said. “We have again reviewed the literature and concluded ‘Routine initiation of beta-blockers perioperatively is not recommended (class IIIA).’ “
“We adhere to the guidelines on acute and chronic coronary syndrome recommending 6-12 months of dual antiplatelet treatment as a standard before elective surgery,” she said. “However, in case of time-sensitive surgery, the duration of that treatment can be shortened down to a minimum of 1 month after elective PCI and a minimum of 3 months after PCI and ACS.”
Patients with specific types of CVD
Dr. Mehilli, a professor at Landshut-Achdorf (Germany) Hospital, highlighted some new guideline recommendations for patients who have specific types of cardiovascular disease.
Coronary artery disease (CAD). “For chronic coronary syndrome, a cardiac workup is recommended only for patients undergoing intermediate risk or high-risk noncardiac surgery.”
“Stress imaging should be considered before any high risk, noncardiac surgery in asymptomatic patients with poor functional capacity and prior PCI or coronary artery bypass graft (new recommendation, class IIa).”
Mitral valve regurgitation. For patients undergoing scheduled noncardiac surgery, who remain symptomatic despite guideline-directed medical treatment for mitral valve regurgitation (including resynchronization and myocardial revascularization), consider a valve intervention – either transcatheter or surgical – before noncardiac surgery in eligible patients with acceptable procedural risk (new recommendation).
Cardiac implantable electronic devices (CIED). For high-risk patients with CIEDs undergoing noncardiac surgery with high probability of electromagnetic interference, a CIED checkup and necessary reprogramming immediately before the procedure should be considered (new recommendation).
Arrhythmias. “I want only to stress,” Dr. Mehilli said, “in patients with atrial fibrillation with acute or worsening hemodynamic instability undergoing noncardiac surgery, an emergency electrical cardioversion is recommended (class I).”
Peripheral artery disease (PAD) and abdominal aortic aneurysm. For these patients “we do not recommend a routine referral for a cardiac workup. But we recommend it for patients with poor functional capacity or with significant risk factors or symptoms (new recommendations).”
Chronic arterial hypertension. “We have modified the recommendation, recommending avoidance of large perioperative fluctuations in blood pressure, and we do not recommend deferring noncardiac surgery in patients with stage 1 or 2 hypertension,” she said.
Postoperative cardiovascular complications
The most frequent postoperative cardiovascular complication is PMI, Dr. Mehilli noted.
“In the BASEL-PMI registry, the incidence of this complication around intermediate or high-risk noncardiac surgery was up to 15% among patients older than 65 years or with a history of CAD or PAD, which makes this kind of complication really important to prevent, to assess, and to know how to treat.”
“It is recommended to have a high awareness for perioperative cardiovascular complications, combined with surveillance for PMI in patients undergoing intermediate- or high-risk noncardiac surgery” based on serial measurements of high-sensitivity cardiac troponin.
The guidelines define PMI as “an increase in the delta of high-sensitivity troponin more than the upper level of normal,” Dr. Mehilli said. “It’s different from the one used in a rule-in algorithm for non-STEMI acute coronary syndrome.”
Postoperative atrial fibrillation (AFib) is observed in 2%-30% of noncardiac surgery patients in different registries, particularly in patients undergoing intermediate or high-risk noncardiac surgery, she noted.
“We propose an algorithm on how to prevent and treat this complication. I want to highlight that in patients with hemodynamic unstable postoperative AF[ib], an emergency cardioversion is indicated. For the others, a rate control with the target heart rate of less than 110 beats per minute is indicated.”
In patients with postoperative AFib, long-term oral anticoagulation therapy should be considered in all patients at risk for stroke, considering the anticipated net clinical benefit of oral anticoagulation therapy as well as informed patient preference (new recommendations).
Routine use of beta-blockers to prevent postoperative AFib in patients undergoing noncardiac surgery is not recommended.
The document also covers the management of patients with kidney disease, diabetes, cancer, obesity, and COVID-19. In general, elective noncardiac surgery should be postponed after a patient has COVID-19, until he or she recovers completely, and coexisting conditions are optimized.
The guidelines are available from the ESC website in several formats: pocket guidelines, pocket guidelines smartphone app, guidelines slide set, essential messages, and the European Heart Journal article.
Noncardiac surgery risk categories
The guideline includes a table that classifies noncardiac surgeries into three groups, based on the associated 30-day risk of death, MI, or stroke:
- Low (< 1%): breast, dental, eye, thyroid, and minor gynecologic, orthopedic, and urologic surgery.
- Intermediate (1%-5%): carotid surgery, endovascular aortic aneurysm repair, gallbladder surgery, head or neck surgery, hernia repair, peripheral arterial angioplasty, renal transplant, major gynecologic, orthopedic, or neurologic (hip or spine) surgery, or urologic surgery
- High (> 5%): aortic and major vascular surgery (including aortic aneurysm), bladder removal (usually as a result of cancer), limb amputation, lung or liver transplant, pancreatic surgery, or perforated bowel repair.
The guidelines were endorsed by the European Society of Anaesthesiology and Intensive Care. The guideline authors reported numerous disclosures.
A version of this article first appeared on Medscape.com.
The European Society of Cardiology guidelines on cardiovascular assessment and management of patients undergoing noncardiac surgery have seen extensive revision since the 2014 version.
They still have the same aim – to prevent surgery-related bleeding complications, perioperative myocardial infarction/injury (PMI), stent thrombosis, acute heart failure, arrhythmias, pulmonary embolism, ischemic stroke, and cardiovascular (CV) death.
Cochairpersons Sigrun Halvorsen, MD, PhD, and Julinda Mehilli, MD, presented highlights from the guidelines at the annual congress of the European Society of Cardiology and the document was simultaneously published online in the European Heart Journal.
The document classifies noncardiac surgery into three levels of 30-day risk of CV death, MI, or stroke. Low (< 1%) risk includes eye or thyroid surgery; intermediate (1%-5%) risk includes knee or hip replacement or renal transplant; and high (> 5%) risk includes aortic aneurysm, lung transplant, or pancreatic or bladder cancer surgery (see more examples below).
It classifies patients as low risk if they are younger than 65 without CV disease or CV risk factors (smoking, hypertension, diabetes, dyslipidemia, family history); intermediate risk if they are 65 or older or have CV risk factors; and high risk if they have CVD.
In an interview, Dr. Halvorsen, professor in cardiology, University of Oslo, zeroed in on three important revisions:
First, recommendations for preoperative ECG and biomarkers are more specific, he noted.
The guidelines advise that before intermediate- or high-risk noncardiac surgery, in patients who have known CVD, CV risk factors (including age 65 or older), or symptoms suggestive of CVD:
- It is recommended to obtain a preoperative 12-lead ECG (class I).
- It is recommended to measure high-sensitivity cardiac troponin T (hs-cTn T) or high-sensitivity cardiac troponin I (hs-cTn I). It is also recommended to measure these biomarkers at 24 hours and 48 hours post surgery (class I).
- It should be considered to measure B-type natriuretic peptide or N-terminal of the prohormone BNP (NT-proBNP).
However, for low-risk patients undergoing low- and intermediate-risk noncardiac surgery, it is not recommended to routinely obtain preoperative ECG, hs-cTn T/I, or BNP/NT-proBNP concentrations (class III).
Troponins have a stronger class I recommendation, compared with the IIA recommendation for BNP, because they are useful for preoperative risk stratification and for diagnosis of PMI, Dr. Halvorsen explained. “Patients receive painkillers after surgery and may have no pain,” she noted, but they may have PMI, which has a bad prognosis.
Second, the guidelines recommend that “all patients should stop smoking 4 weeks before noncardiac surgery [class I],” she noted. Clinicians should also “measure hemoglobin, and if the patient is anemic, treat the anemia.”
Third, the sections on antithrombotic treatment have been significantly revised. “Bridging – stopping an oral antithrombotic drug and switching to a subcutaneous or IV drug – has been common,” Dr. Halvorsen said, “but recently we have new evidence that in most cases that increases the risk of bleeding.”
“We are [now] much more restrictive with respect to bridging” with unfractionated heparin or low-molecular-weight heparin, she said. “We recommend against bridging in patients with low to moderate thrombotic risk,” and bridging should only be considered in patients with mechanical prosthetic heart valves or with very high thrombotic risk.
More preoperative recommendations
In the guideline overview session at the congress, Dr. Halverson highlighted some of the new recommendations for preoperative risk assessment.
If time allows, it is recommended to optimize guideline-recommended treatment of CVD and control of CV risk factors including blood pressure, dyslipidemia, and diabetes, before noncardiac surgery (class I).
Patients commonly have “murmurs, chest pain, dyspnea, and edema that may suggest severe CVD, but may also be caused by noncardiac disease,” she noted. The guidelines state that “for patients with a newly detected murmur and symptoms or signs of CVD, transthoracic echocardiography is recommended before noncardiac surgery (class I).
“Many studies have been performed to try to find out if initiation of specific drugs before surgery could reduce the risk of complications,” Dr. Halvorsen noted. However, few have shown any benefit and “the question of presurgery initiation of beta-blockers has been greatly debated,” she said. “We have again reviewed the literature and concluded ‘Routine initiation of beta-blockers perioperatively is not recommended (class IIIA).’ “
“We adhere to the guidelines on acute and chronic coronary syndrome recommending 6-12 months of dual antiplatelet treatment as a standard before elective surgery,” she said. “However, in case of time-sensitive surgery, the duration of that treatment can be shortened down to a minimum of 1 month after elective PCI and a minimum of 3 months after PCI and ACS.”
Patients with specific types of CVD
Dr. Mehilli, a professor at Landshut-Achdorf (Germany) Hospital, highlighted some new guideline recommendations for patients who have specific types of cardiovascular disease.
Coronary artery disease (CAD). “For chronic coronary syndrome, a cardiac workup is recommended only for patients undergoing intermediate risk or high-risk noncardiac surgery.”
“Stress imaging should be considered before any high risk, noncardiac surgery in asymptomatic patients with poor functional capacity and prior PCI or coronary artery bypass graft (new recommendation, class IIa).”
Mitral valve regurgitation. For patients undergoing scheduled noncardiac surgery, who remain symptomatic despite guideline-directed medical treatment for mitral valve regurgitation (including resynchronization and myocardial revascularization), consider a valve intervention – either transcatheter or surgical – before noncardiac surgery in eligible patients with acceptable procedural risk (new recommendation).
Cardiac implantable electronic devices (CIED). For high-risk patients with CIEDs undergoing noncardiac surgery with high probability of electromagnetic interference, a CIED checkup and necessary reprogramming immediately before the procedure should be considered (new recommendation).
Arrhythmias. “I want only to stress,” Dr. Mehilli said, “in patients with atrial fibrillation with acute or worsening hemodynamic instability undergoing noncardiac surgery, an emergency electrical cardioversion is recommended (class I).”
Peripheral artery disease (PAD) and abdominal aortic aneurysm. For these patients “we do not recommend a routine referral for a cardiac workup. But we recommend it for patients with poor functional capacity or with significant risk factors or symptoms (new recommendations).”
Chronic arterial hypertension. “We have modified the recommendation, recommending avoidance of large perioperative fluctuations in blood pressure, and we do not recommend deferring noncardiac surgery in patients with stage 1 or 2 hypertension,” she said.
Postoperative cardiovascular complications
The most frequent postoperative cardiovascular complication is PMI, Dr. Mehilli noted.
“In the BASEL-PMI registry, the incidence of this complication around intermediate or high-risk noncardiac surgery was up to 15% among patients older than 65 years or with a history of CAD or PAD, which makes this kind of complication really important to prevent, to assess, and to know how to treat.”
“It is recommended to have a high awareness for perioperative cardiovascular complications, combined with surveillance for PMI in patients undergoing intermediate- or high-risk noncardiac surgery” based on serial measurements of high-sensitivity cardiac troponin.
The guidelines define PMI as “an increase in the delta of high-sensitivity troponin more than the upper level of normal,” Dr. Mehilli said. “It’s different from the one used in a rule-in algorithm for non-STEMI acute coronary syndrome.”
Postoperative atrial fibrillation (AFib) is observed in 2%-30% of noncardiac surgery patients in different registries, particularly in patients undergoing intermediate or high-risk noncardiac surgery, she noted.
“We propose an algorithm on how to prevent and treat this complication. I want to highlight that in patients with hemodynamic unstable postoperative AF[ib], an emergency cardioversion is indicated. For the others, a rate control with the target heart rate of less than 110 beats per minute is indicated.”
In patients with postoperative AFib, long-term oral anticoagulation therapy should be considered in all patients at risk for stroke, considering the anticipated net clinical benefit of oral anticoagulation therapy as well as informed patient preference (new recommendations).
Routine use of beta-blockers to prevent postoperative AFib in patients undergoing noncardiac surgery is not recommended.
The document also covers the management of patients with kidney disease, diabetes, cancer, obesity, and COVID-19. In general, elective noncardiac surgery should be postponed after a patient has COVID-19, until he or she recovers completely, and coexisting conditions are optimized.
The guidelines are available from the ESC website in several formats: pocket guidelines, pocket guidelines smartphone app, guidelines slide set, essential messages, and the European Heart Journal article.
Noncardiac surgery risk categories
The guideline includes a table that classifies noncardiac surgeries into three groups, based on the associated 30-day risk of death, MI, or stroke:
- Low (< 1%): breast, dental, eye, thyroid, and minor gynecologic, orthopedic, and urologic surgery.
- Intermediate (1%-5%): carotid surgery, endovascular aortic aneurysm repair, gallbladder surgery, head or neck surgery, hernia repair, peripheral arterial angioplasty, renal transplant, major gynecologic, orthopedic, or neurologic (hip or spine) surgery, or urologic surgery
- High (> 5%): aortic and major vascular surgery (including aortic aneurysm), bladder removal (usually as a result of cancer), limb amputation, lung or liver transplant, pancreatic surgery, or perforated bowel repair.
The guidelines were endorsed by the European Society of Anaesthesiology and Intensive Care. The guideline authors reported numerous disclosures.
A version of this article first appeared on Medscape.com.
FROM ESC CONGRESS 2022
ACC/AHA issue chest pain data standards update to 2021 guideline
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
The American College of Cardiology/American Heart Association have issued a set of data standards for chest pain and acute myocardial infarction to accompany the 2021 guidelines for evaluation and diagnosis of chest pain.
In October 2021, the AHA/ACC issued a joint clinical practice guideline encouraging clinicians to use standardized risk assessments, clinical pathways, and tools to evaluate and communicate with patients who present with chest pain, as reported by this news organization.
The writing group underscored the need to reach a consensus for the definitions of chest pain. The new document standardizes related data elements for consistent reporting on chest pain syndromes.
“This is an appendix to the guidelines and a planned effort to try to harmonize and bring uniformity to the language applied,” writing committee chair H.V. “Skip” Anderson, MD, with UT Health Science Center, Houston, told this news organization.
“You want heart attack to mean the same thing in Miami Beach as in Western Pennsylvania, as in Oregon and Washington and every place in between,” Dr. Anderson explained. “You want everybody to be using the same language, so that’s what these data standards are meant to do.”
In the document, data elements are grouped into three broad categories: chest pain, myocardial injury, and MI.
“We deliberately followed the plans contained in the new guideline and focused on potentially serious cardiovascular causes of chest pain as might be encountered in emergency departments,” the writing group notes in the document.
The terms “typical” and “atypical” as descriptors of chest pain or anginal syndromes are not used in the new document, in line with the 2021 guidance to abandon these terms.
Instead, the new document divides chest pain syndromes into three categories: “cardiac,” “possible cardiac,” and “noncardiac” – again, in keeping with the chest pain guideline.
The document also includes data elements for risk stratification scoring according to several common risk scoring algorithms and for procedure-related myocardial injury and procedure-related MI.
Each year, chest pain sends more than 7 million adults to the emergency department in the United States. Although noncardiac causes of chest pain make up a large majority of these cases, there are several life-threatening causes of chest pain that must be identified and treated promptly.
Distinguishing between serious and nonserious causes of chest pain is an urgent imperative, the writing group says.
Overall, they say this new clinical lexicon and set of data standards should be “broadly applicable” in various settings, including clinical trials and observational studies, patient care, electronic health records (EHRs), quality and performance improvement initiatives, registries, and public reporting programs.
The 2022 ACC/AHA Key Data Elements and Definitions for Chest Pain and Acute Myocardial Infarction was simultaneously published online in the Journal of the American College of Cardiology and Circulation: Cardiovascular Quality and Outcomes.
It was developed in collaboration with the American College of Emergency Physicians and the Society for Cardiac Angiography and Interventions and endorsed by the Society for Academic Emergency Medicine.
Dr. Anderson noted that “almost all of the guidelines that come out now, certainly in the last few years, have been followed after a certain interval by a set of data standards applicable to the guidelines.”
“It would be really great if it could actually be attached as an appendix, but the nature of the development of these things is such that there will always be a bit of a time lag between the writing group that develops the guidelines and the work group that develops the data standards; you can’t really have them working in parallel at the same time,” Dr. Anderson said in an interview.
This research had no commercial funding. The authors have no relevant disclosures.
A version of this article first appeared on Medscape.com.
AGA Clinical Practice Update: Expert review on endoscopic management for recurrent acute and chronic pancreatitis
Endoscopy plays an integral role in the evaluation and management of patients with recurrent acute pancreatitis and chronic pancreatitis, according to a new American Gastroenterological Association clinical practice update published in Gastroenterology.
Acute pancreatitis remains the leading cause of inpatient care among gastrointestinal conditions, with about 10%-30% of patients developing recurrent acute pancreatitis, wrote co–first authors Daniel Strand, MD, from the University of Virginia Health System, Charlottesville, and Ryan J. Law, MD, from the Mayo Clinic, Rochester, Minn., and colleagues. About 35% of patients with recurrent acute pancreatitis will progress to chronic pancreatitis. Both conditions are associated with significant morbidity and mortality.
“Interventions aimed to better evaluate, mitigate the progression of, and treat symptoms related to [acute pancreatitis] and [chronic pancreatitis] are critical to improve patients’ quality of life and other long-term outcomes,” the authors of the expert review wrote.
The authors reviewed randomized controlled trials, observational studies, systematic reviews and meta-analyses, and expert consensus in the field to develop eight clinical practice advice statements.
First, when the initial evaluation reveals no clear explanation for acute or recurrent pancreatitis, endoscopic ultrasound is the preferred diagnostic test. The authors noted that, although there isn’t a concretely defined optimal timing for EUS defined, most experts advise a short delay of 2-6 weeks after resolution of acute pancreatitis. MRI with contrast and cholangiopancreatography can be a reasonable complementary or alternative test, based on local expertise and availability.
Second, the role of ERCP remains controversial for reducing the frequency of acute pancreatitis episodes in patients with pancreas divisum, the most common congenital pancreatic anomaly, the authors wrote. However, minor papilla endotherapy may be useful, particularly for those with objective signs of outflow obstruction, such as a dilated dorsal pancreatic duct or santorinicele. However, there is no role for ERCP in treating pain alone in patients with pancreas divisum.
Third, ERCP remains even more controversial for reducing the frequency of pancreatitis episodes in patients with unexplained recurrent acute pancreatitis and standard pancreatic ductal anatomy, according to the authors. It should only be considered after a comprehensive discussion of the uncertain benefits and potentially severe procedure-related adverse events. When used, ERCP with biliary sphincterotomy alone may be preferable to dual sphincterotomy.
Fourth, for long-term treatment of patients with painful obstructive chronic pancreatitis, surgical intervention should be considered over endoscopic therapy, the study authors wrote. Pain is the most common symptom and important driver of impaired quality of life in patients with chronic pancreatitis, among whom a subset will be affected by intraductal hypertension from an obstructed pancreatic duct. The authors noted that endoscopic intervention remains a reasonable alternative to surgery for suboptimal operative candidates or patients who want a less-invasive approach, as long as they are clearly informed that the best practice advice primarily favors surgery.
Fifth, when using ERCP for pancreatic duct stones, small main pancreatic duct stones of 5 mm or less can be treated with pancreatography and conventional stone extraction maneuvers. For larger stones, however, extracorporeal shockwave lithotripsy or pancreatoscopy with intraductal lithotripsy can be considered, although the former is not widely available in the United States and the success rates for the latter vary.
Sixth, when using ERCP for pancreatic duct strictures, prolonged stent therapy for 6-12 months is effective for treating symptoms and remodeling main pancreatic duct strictures. The preferred approach is to place and sequentially add multiple plastic stents in parallel, or up-sizing. Emerging evidence suggests that fully covered self-expanding metal stents may be useful in this case, but additional research is needed. For example, one study suggested that patients treated with these self-expanding stents required fewer ERCPs, but their adverse event rate was significantly higher (39% vs. 14%).
Seventh, ERCP with stent insertion is the preferred treatment for benign biliary stricture caused by chronic pancreatitis. Fully covered self-expanding metal stents are favored over placing multiple plastic stents when feasible, given the similar efficacy but significantly lower need for stent exchange procedures during the treatment course.
Eighth, celiac plexus block shouldn’t be routinely performed for the management of pain caused by chronic pancreatitis. Celiac plexus block could be considered in certain patients on a case-by-case basis if they have debilitating pain that hasn’t responded to other therapeutic measures. However, this should only be considered after a discussion about the unclear outcomes and its procedural risks.
“Given the current lack of evidence, additional well-designed prospective comparative studies are needed to support a more unified diagnostic and therapeutic pathway for the treatment of these complex cases,” the authors concluded.
The authors reported no grant support or funding sources for this report. Several authors disclosed financial relationships with companies such as Olympus America, Medtronic, and Microtech.
Endoscopy plays an integral role in the evaluation and management of patients with recurrent acute pancreatitis and chronic pancreatitis, according to a new American Gastroenterological Association clinical practice update published in Gastroenterology.
Acute pancreatitis remains the leading cause of inpatient care among gastrointestinal conditions, with about 10%-30% of patients developing recurrent acute pancreatitis, wrote co–first authors Daniel Strand, MD, from the University of Virginia Health System, Charlottesville, and Ryan J. Law, MD, from the Mayo Clinic, Rochester, Minn., and colleagues. About 35% of patients with recurrent acute pancreatitis will progress to chronic pancreatitis. Both conditions are associated with significant morbidity and mortality.
“Interventions aimed to better evaluate, mitigate the progression of, and treat symptoms related to [acute pancreatitis] and [chronic pancreatitis] are critical to improve patients’ quality of life and other long-term outcomes,” the authors of the expert review wrote.
The authors reviewed randomized controlled trials, observational studies, systematic reviews and meta-analyses, and expert consensus in the field to develop eight clinical practice advice statements.
First, when the initial evaluation reveals no clear explanation for acute or recurrent pancreatitis, endoscopic ultrasound is the preferred diagnostic test. The authors noted that, although there isn’t a concretely defined optimal timing for EUS defined, most experts advise a short delay of 2-6 weeks after resolution of acute pancreatitis. MRI with contrast and cholangiopancreatography can be a reasonable complementary or alternative test, based on local expertise and availability.
Second, the role of ERCP remains controversial for reducing the frequency of acute pancreatitis episodes in patients with pancreas divisum, the most common congenital pancreatic anomaly, the authors wrote. However, minor papilla endotherapy may be useful, particularly for those with objective signs of outflow obstruction, such as a dilated dorsal pancreatic duct or santorinicele. However, there is no role for ERCP in treating pain alone in patients with pancreas divisum.
Third, ERCP remains even more controversial for reducing the frequency of pancreatitis episodes in patients with unexplained recurrent acute pancreatitis and standard pancreatic ductal anatomy, according to the authors. It should only be considered after a comprehensive discussion of the uncertain benefits and potentially severe procedure-related adverse events. When used, ERCP with biliary sphincterotomy alone may be preferable to dual sphincterotomy.
Fourth, for long-term treatment of patients with painful obstructive chronic pancreatitis, surgical intervention should be considered over endoscopic therapy, the study authors wrote. Pain is the most common symptom and important driver of impaired quality of life in patients with chronic pancreatitis, among whom a subset will be affected by intraductal hypertension from an obstructed pancreatic duct. The authors noted that endoscopic intervention remains a reasonable alternative to surgery for suboptimal operative candidates or patients who want a less-invasive approach, as long as they are clearly informed that the best practice advice primarily favors surgery.
Fifth, when using ERCP for pancreatic duct stones, small main pancreatic duct stones of 5 mm or less can be treated with pancreatography and conventional stone extraction maneuvers. For larger stones, however, extracorporeal shockwave lithotripsy or pancreatoscopy with intraductal lithotripsy can be considered, although the former is not widely available in the United States and the success rates for the latter vary.
Sixth, when using ERCP for pancreatic duct strictures, prolonged stent therapy for 6-12 months is effective for treating symptoms and remodeling main pancreatic duct strictures. The preferred approach is to place and sequentially add multiple plastic stents in parallel, or up-sizing. Emerging evidence suggests that fully covered self-expanding metal stents may be useful in this case, but additional research is needed. For example, one study suggested that patients treated with these self-expanding stents required fewer ERCPs, but their adverse event rate was significantly higher (39% vs. 14%).
Seventh, ERCP with stent insertion is the preferred treatment for benign biliary stricture caused by chronic pancreatitis. Fully covered self-expanding metal stents are favored over placing multiple plastic stents when feasible, given the similar efficacy but significantly lower need for stent exchange procedures during the treatment course.
Eighth, celiac plexus block shouldn’t be routinely performed for the management of pain caused by chronic pancreatitis. Celiac plexus block could be considered in certain patients on a case-by-case basis if they have debilitating pain that hasn’t responded to other therapeutic measures. However, this should only be considered after a discussion about the unclear outcomes and its procedural risks.
“Given the current lack of evidence, additional well-designed prospective comparative studies are needed to support a more unified diagnostic and therapeutic pathway for the treatment of these complex cases,” the authors concluded.
The authors reported no grant support or funding sources for this report. Several authors disclosed financial relationships with companies such as Olympus America, Medtronic, and Microtech.
Endoscopy plays an integral role in the evaluation and management of patients with recurrent acute pancreatitis and chronic pancreatitis, according to a new American Gastroenterological Association clinical practice update published in Gastroenterology.
Acute pancreatitis remains the leading cause of inpatient care among gastrointestinal conditions, with about 10%-30% of patients developing recurrent acute pancreatitis, wrote co–first authors Daniel Strand, MD, from the University of Virginia Health System, Charlottesville, and Ryan J. Law, MD, from the Mayo Clinic, Rochester, Minn., and colleagues. About 35% of patients with recurrent acute pancreatitis will progress to chronic pancreatitis. Both conditions are associated with significant morbidity and mortality.
“Interventions aimed to better evaluate, mitigate the progression of, and treat symptoms related to [acute pancreatitis] and [chronic pancreatitis] are critical to improve patients’ quality of life and other long-term outcomes,” the authors of the expert review wrote.
The authors reviewed randomized controlled trials, observational studies, systematic reviews and meta-analyses, and expert consensus in the field to develop eight clinical practice advice statements.
First, when the initial evaluation reveals no clear explanation for acute or recurrent pancreatitis, endoscopic ultrasound is the preferred diagnostic test. The authors noted that, although there isn’t a concretely defined optimal timing for EUS defined, most experts advise a short delay of 2-6 weeks after resolution of acute pancreatitis. MRI with contrast and cholangiopancreatography can be a reasonable complementary or alternative test, based on local expertise and availability.
Second, the role of ERCP remains controversial for reducing the frequency of acute pancreatitis episodes in patients with pancreas divisum, the most common congenital pancreatic anomaly, the authors wrote. However, minor papilla endotherapy may be useful, particularly for those with objective signs of outflow obstruction, such as a dilated dorsal pancreatic duct or santorinicele. However, there is no role for ERCP in treating pain alone in patients with pancreas divisum.
Third, ERCP remains even more controversial for reducing the frequency of pancreatitis episodes in patients with unexplained recurrent acute pancreatitis and standard pancreatic ductal anatomy, according to the authors. It should only be considered after a comprehensive discussion of the uncertain benefits and potentially severe procedure-related adverse events. When used, ERCP with biliary sphincterotomy alone may be preferable to dual sphincterotomy.
Fourth, for long-term treatment of patients with painful obstructive chronic pancreatitis, surgical intervention should be considered over endoscopic therapy, the study authors wrote. Pain is the most common symptom and important driver of impaired quality of life in patients with chronic pancreatitis, among whom a subset will be affected by intraductal hypertension from an obstructed pancreatic duct. The authors noted that endoscopic intervention remains a reasonable alternative to surgery for suboptimal operative candidates or patients who want a less-invasive approach, as long as they are clearly informed that the best practice advice primarily favors surgery.
Fifth, when using ERCP for pancreatic duct stones, small main pancreatic duct stones of 5 mm or less can be treated with pancreatography and conventional stone extraction maneuvers. For larger stones, however, extracorporeal shockwave lithotripsy or pancreatoscopy with intraductal lithotripsy can be considered, although the former is not widely available in the United States and the success rates for the latter vary.
Sixth, when using ERCP for pancreatic duct strictures, prolonged stent therapy for 6-12 months is effective for treating symptoms and remodeling main pancreatic duct strictures. The preferred approach is to place and sequentially add multiple plastic stents in parallel, or up-sizing. Emerging evidence suggests that fully covered self-expanding metal stents may be useful in this case, but additional research is needed. For example, one study suggested that patients treated with these self-expanding stents required fewer ERCPs, but their adverse event rate was significantly higher (39% vs. 14%).
Seventh, ERCP with stent insertion is the preferred treatment for benign biliary stricture caused by chronic pancreatitis. Fully covered self-expanding metal stents are favored over placing multiple plastic stents when feasible, given the similar efficacy but significantly lower need for stent exchange procedures during the treatment course.
Eighth, celiac plexus block shouldn’t be routinely performed for the management of pain caused by chronic pancreatitis. Celiac plexus block could be considered in certain patients on a case-by-case basis if they have debilitating pain that hasn’t responded to other therapeutic measures. However, this should only be considered after a discussion about the unclear outcomes and its procedural risks.
“Given the current lack of evidence, additional well-designed prospective comparative studies are needed to support a more unified diagnostic and therapeutic pathway for the treatment of these complex cases,” the authors concluded.
The authors reported no grant support or funding sources for this report. Several authors disclosed financial relationships with companies such as Olympus America, Medtronic, and Microtech.
FROM GASTROENTEROLOGY
AGA clinical practice update: Expert review on managing short bowel syndrome
Caring for patients with short bowel syndrome (SBS) requires a multidisciplinary approach involving dietitians, nurses, surgeons, gastroenterologists or internists, and social workers experienced in SBS care, according to a clinical practice update expert review from the American Gastroenterological Association.
Kishore Iyer, MD, from Mount Sinai Hospital New York; John K. DiBaise, MD, from Mayo Clinic in Scottsdale, Ariz.; and Alberto Rubio-Tapia, MD, from the Cleveland Clinic, Ohio, developed 12 best practice advice statements based on available evidence. The items focus on adult patients with SBS; however, there was some overlap with the management of pediatric SBS. The review was published online in Clinical Gastroenterology and Hepatology.
Defining SBS
One update concerns defining SBS. The authors recommend that surgeons performing massive resections should report the residual bowel length, rather than the length of bowel resected.
“It is only the former that dictates outcome,” they wrote.
There is general agreement that a residual small intestinal length of 200 cm or less meets criteria for SBS. Measurement should be taken from “along the antimesenteric border of unstretched bowel, from the duodenojejunal flexure to the ileocecal junction, the site of any small bowel–colon anastomosis, or to the end-ostomy.”
Based on the residual bowel length, patients can be classified into three groups: end-jejunostomy, jejuno-colic, and jejuno-ileo-colic.
Assessing nutritional status
A dietitian experienced in SBS should perform a thorough nutritional assessment on all SBS patients. Long-term monitoring should include laboratory studies checking electrolytes and liver and kidney function, fluid balance, weight change, serum micronutrients, and bone density. Bone density should be repeated periodically, every 2-3 years.
Fluid and electrolyte problems may affect outcomes for SBS patients, particularly for those without a colon.
Adjusting diets
Most adult patients with SBS have significant malabsorption, so dietary intake “must be increased by at least 50% from their estimated needs,” the authors wrote. It’s best if the patient consumes the increased quantity throughout the day in 5-6 meals, they noted.
An experienced dietitian should counsel the patient based on the patient’s eating preferences. Incorporating preferences can help increase compliance with the adjustments that may become necessary based on symptoms, stool output, and weight.
Using pharmacologic therapy
Using antisecretory medications, including proton pump inhibitors or histamine-2 receptor antagonists, helps reduce gastric secretions, the damage of acid on the upper gut mucosa, and the function of pancreatic exocrine enzymes.
Antidiarrheals reduce intestinal motility but also cause a slight reduction in intestinal secretion. Common agents include loperamide, diphenoxylate with atropine, codeine, and tincture of opium. The review authors say loperamide should get preference over opiate drugs because it is not addictive or sedative.
Use of antidiarrheals should be guided by their effect on stool output.
“Loperamide and codeine may have a synergistic effect when used together,” the authors wrote.
Clonidine, which can be given transdermally, has also shown some benefit in treating high-output stool losses, presumably because of its effects on intestinal motility and secretion.
Weighing risks and benefits of teduglutide
The glucagonlike peptide–2 teduglutide is of particular interest for its ability to help improve intestinal absorption and hopefully wean patients off parenteral nutrition and some will achieve enteral autonomy, the authors wrote. “The very short half-life of native GLP-2 has been extended to allow daily subcutaneous injection in the recombinant molecule, teduglutide.”
However, because teduglutide is a growth factor and can boost the growth of polyps and cancer, it is contraindicated in patients with active gastrointestinal malignancies. Patients should undergo colonoscopy before treatment and periodically thereafter, the authors advised. The benefits of its use in patients with nongastrointestinal malignancy should be weighed carefully with these risks.
“The significant side effects of teduglutide and the cost mandate that teduglutide is employed only after optimizing diet and the more conventional SBS treatments described previously in carefully selected patients with [short bowel syndrome–intestinal failure],” the authors wrote.
Dosing drugs effectively
Medications in tablet form need to dissolve before being absorbed. Most oral medications are absorbed within the proximal jejunum, so they can be used in patients with SBS.
“However,” the authors noted, “sustained- and delayed-release medications should be avoided.”
They suggested that, when applicable, alternatives such as liquids and topical medications should be considered, as should the monitoring of medication levels in the blood.
If a patient does not respond, approaches to consider may include increasing a dose, changing dose frequency, or changing drug formulation or route of administration, such as intravenous, subcutaneous, or transdermal.
Including parenteral nutrition and oral rehydration
Almost all patients with SBS will need parenteral nutrition (PN) support following resection, and few will be able to stop it before discharge from the hospital.
“Although more than 50% of adults with SBS are able to be weaned completely from PN within 5 years of diagnosis, the probability of eliminating PN use is less than 6% if not successfully accomplished in the first 2 years following the individual’s last bowel resection,” the authors wrote.
For long-term PN, tunneled central venous catheters are preferred over peripherally inserted central venous catheters because of the higher risk of thrombosis and issues related to self-administration of PN with the central catheters. Also, tunneled catheters are preferred over totally implanted devices, or ports, for long-term patients because the main benefit of the port is not realized given that the device needs to be continually accessed and exchanged weekly.
“When calculating PN volume and content, changes in the patient’s weight, laboratory results, stool or ostomy output, urine output, and complaints of thirst should be monitored,” the authors noted.
The authors also discussed oral rehydration solution because patients lose more water and sodium from their stoma than they take in by mouth. Careful consideration of the glucose and sodium levels in oral fluids is important because inappropriate fluids will exacerbate fluid losses in SBS. For example, hypotonic (including water, tea, coffee, alcohol) and hypertonic (including fruit juices and sodas) solutions should be limited.
“A major misconception on the part of patients is that they should drink large quantities of water; however, this generally leads to an increase in ostomy output and creates a vicious cycle further exacerbating fluid and electrolyte disturbances,” they wrote, instead advising glucose–electrolyte rehydration solution to enhance absorption and reduce secretion.
Preventing complications
“A knowledge of these complications is critical for those caring for these patients to be able to not only identify and treat them when they occur but also to prevent their occurrence whenever possible,” the authors wrote. Although they considered it beyond the scope of the review to outline every complication, they indicated some complications and management strategies via an included table. These complications can include cirrhosis, osteoporosis, acute kidney disease, and central venous catheter–related infection or occlusion.
Considering further surgery or intestinal transplantation
The authors noted that any further surgery should be carefully considered, with the following three contexts having possible value: “(1) to recruit unused distal bowel, (2) to augment the function of residual bowel through specific lengthening and tapering operations, or (3) to slow intestinal transit.”
Surgeons involved in managing SBS may need to confront complex intra-abdominal problems such as massive desmoid tumors, mesenteric ischemia, or complex enterocutaneous fistulae; a multidisciplinary intestinal rehabilitation team may be better able to help these patients. The authors noted that care for patients starts even before the first operation, by taking every measure to avoid massive bowel resection and the resulting SBS.
The authors noted the importance of early referral for intestinal transplantation consideration for patients with refractory dependency on parenteral nutrition or even onset of parenteral nutrition failure, which refers to complications such as intestinal failure–associated liver disease.
“At present, nearly 50% of patients being considered for ITX are also requiring simultaneous liver replacement, indicating late referral for ITX,” they wrote, citing a data from a report by the Centers for Medicare and Medicaid.
They also noted that data have shown short- and medium-term outcomes are steadily improving; however, long-term outcomes have been challenged by opportunistic infections, long-term graft attrition, and other impediments that may be preventing early referral for intestinal transplantation.
Educating patients, caregivers
Long-term PN may restrict activity for patients, but patients and caregivers should know about some modifications.
One is to cycle the PN over 10-14 hours overnight to allow freedom from the infusion pump during the day. Infusion pumps can be programmable, and some can be carried in a backpack for infusing during the day.
Authors recommend patient support groups, such as the Oley Foundation, which can help with issues surrounding body image and travel.
Because of the relative rarity of SBS, nonspecialist physicians may care for patients without a dedicated multidisciplinary team and may need education support in managing patients with complex care needs. One source the authors recommend is the Learn Intestinal Failure Tele-ECHO (Expanding Community Healthcare Outcomes) (LIFT-ECHO) project. The LIFT-ECHO project has become an online educational community with case-based learning in SBS, intestinal failure, and PN.
The authors disclose relationships with Takeda, Zealand, VectivBio, Napo, and Hanmi.
Caring for patients with short bowel syndrome (SBS) requires a multidisciplinary approach involving dietitians, nurses, surgeons, gastroenterologists or internists, and social workers experienced in SBS care, according to a clinical practice update expert review from the American Gastroenterological Association.
Kishore Iyer, MD, from Mount Sinai Hospital New York; John K. DiBaise, MD, from Mayo Clinic in Scottsdale, Ariz.; and Alberto Rubio-Tapia, MD, from the Cleveland Clinic, Ohio, developed 12 best practice advice statements based on available evidence. The items focus on adult patients with SBS; however, there was some overlap with the management of pediatric SBS. The review was published online in Clinical Gastroenterology and Hepatology.
Defining SBS
One update concerns defining SBS. The authors recommend that surgeons performing massive resections should report the residual bowel length, rather than the length of bowel resected.
“It is only the former that dictates outcome,” they wrote.
There is general agreement that a residual small intestinal length of 200 cm or less meets criteria for SBS. Measurement should be taken from “along the antimesenteric border of unstretched bowel, from the duodenojejunal flexure to the ileocecal junction, the site of any small bowel–colon anastomosis, or to the end-ostomy.”
Based on the residual bowel length, patients can be classified into three groups: end-jejunostomy, jejuno-colic, and jejuno-ileo-colic.
Assessing nutritional status
A dietitian experienced in SBS should perform a thorough nutritional assessment on all SBS patients. Long-term monitoring should include laboratory studies checking electrolytes and liver and kidney function, fluid balance, weight change, serum micronutrients, and bone density. Bone density should be repeated periodically, every 2-3 years.
Fluid and electrolyte problems may affect outcomes for SBS patients, particularly for those without a colon.
Adjusting diets
Most adult patients with SBS have significant malabsorption, so dietary intake “must be increased by at least 50% from their estimated needs,” the authors wrote. It’s best if the patient consumes the increased quantity throughout the day in 5-6 meals, they noted.
An experienced dietitian should counsel the patient based on the patient’s eating preferences. Incorporating preferences can help increase compliance with the adjustments that may become necessary based on symptoms, stool output, and weight.
Using pharmacologic therapy
Using antisecretory medications, including proton pump inhibitors or histamine-2 receptor antagonists, helps reduce gastric secretions, the damage of acid on the upper gut mucosa, and the function of pancreatic exocrine enzymes.
Antidiarrheals reduce intestinal motility but also cause a slight reduction in intestinal secretion. Common agents include loperamide, diphenoxylate with atropine, codeine, and tincture of opium. The review authors say loperamide should get preference over opiate drugs because it is not addictive or sedative.
Use of antidiarrheals should be guided by their effect on stool output.
“Loperamide and codeine may have a synergistic effect when used together,” the authors wrote.
Clonidine, which can be given transdermally, has also shown some benefit in treating high-output stool losses, presumably because of its effects on intestinal motility and secretion.
Weighing risks and benefits of teduglutide
The glucagonlike peptide–2 teduglutide is of particular interest for its ability to help improve intestinal absorption and hopefully wean patients off parenteral nutrition and some will achieve enteral autonomy, the authors wrote. “The very short half-life of native GLP-2 has been extended to allow daily subcutaneous injection in the recombinant molecule, teduglutide.”
However, because teduglutide is a growth factor and can boost the growth of polyps and cancer, it is contraindicated in patients with active gastrointestinal malignancies. Patients should undergo colonoscopy before treatment and periodically thereafter, the authors advised. The benefits of its use in patients with nongastrointestinal malignancy should be weighed carefully with these risks.
“The significant side effects of teduglutide and the cost mandate that teduglutide is employed only after optimizing diet and the more conventional SBS treatments described previously in carefully selected patients with [short bowel syndrome–intestinal failure],” the authors wrote.
Dosing drugs effectively
Medications in tablet form need to dissolve before being absorbed. Most oral medications are absorbed within the proximal jejunum, so they can be used in patients with SBS.
“However,” the authors noted, “sustained- and delayed-release medications should be avoided.”
They suggested that, when applicable, alternatives such as liquids and topical medications should be considered, as should the monitoring of medication levels in the blood.
If a patient does not respond, approaches to consider may include increasing a dose, changing dose frequency, or changing drug formulation or route of administration, such as intravenous, subcutaneous, or transdermal.
Including parenteral nutrition and oral rehydration
Almost all patients with SBS will need parenteral nutrition (PN) support following resection, and few will be able to stop it before discharge from the hospital.
“Although more than 50% of adults with SBS are able to be weaned completely from PN within 5 years of diagnosis, the probability of eliminating PN use is less than 6% if not successfully accomplished in the first 2 years following the individual’s last bowel resection,” the authors wrote.
For long-term PN, tunneled central venous catheters are preferred over peripherally inserted central venous catheters because of the higher risk of thrombosis and issues related to self-administration of PN with the central catheters. Also, tunneled catheters are preferred over totally implanted devices, or ports, for long-term patients because the main benefit of the port is not realized given that the device needs to be continually accessed and exchanged weekly.
“When calculating PN volume and content, changes in the patient’s weight, laboratory results, stool or ostomy output, urine output, and complaints of thirst should be monitored,” the authors noted.
The authors also discussed oral rehydration solution because patients lose more water and sodium from their stoma than they take in by mouth. Careful consideration of the glucose and sodium levels in oral fluids is important because inappropriate fluids will exacerbate fluid losses in SBS. For example, hypotonic (including water, tea, coffee, alcohol) and hypertonic (including fruit juices and sodas) solutions should be limited.
“A major misconception on the part of patients is that they should drink large quantities of water; however, this generally leads to an increase in ostomy output and creates a vicious cycle further exacerbating fluid and electrolyte disturbances,” they wrote, instead advising glucose–electrolyte rehydration solution to enhance absorption and reduce secretion.
Preventing complications
“A knowledge of these complications is critical for those caring for these patients to be able to not only identify and treat them when they occur but also to prevent their occurrence whenever possible,” the authors wrote. Although they considered it beyond the scope of the review to outline every complication, they indicated some complications and management strategies via an included table. These complications can include cirrhosis, osteoporosis, acute kidney disease, and central venous catheter–related infection or occlusion.
Considering further surgery or intestinal transplantation
The authors noted that any further surgery should be carefully considered, with the following three contexts having possible value: “(1) to recruit unused distal bowel, (2) to augment the function of residual bowel through specific lengthening and tapering operations, or (3) to slow intestinal transit.”
Surgeons involved in managing SBS may need to confront complex intra-abdominal problems such as massive desmoid tumors, mesenteric ischemia, or complex enterocutaneous fistulae; a multidisciplinary intestinal rehabilitation team may be better able to help these patients. The authors noted that care for patients starts even before the first operation, by taking every measure to avoid massive bowel resection and the resulting SBS.
The authors noted the importance of early referral for intestinal transplantation consideration for patients with refractory dependency on parenteral nutrition or even onset of parenteral nutrition failure, which refers to complications such as intestinal failure–associated liver disease.
“At present, nearly 50% of patients being considered for ITX are also requiring simultaneous liver replacement, indicating late referral for ITX,” they wrote, citing a data from a report by the Centers for Medicare and Medicaid.
They also noted that data have shown short- and medium-term outcomes are steadily improving; however, long-term outcomes have been challenged by opportunistic infections, long-term graft attrition, and other impediments that may be preventing early referral for intestinal transplantation.
Educating patients, caregivers
Long-term PN may restrict activity for patients, but patients and caregivers should know about some modifications.
One is to cycle the PN over 10-14 hours overnight to allow freedom from the infusion pump during the day. Infusion pumps can be programmable, and some can be carried in a backpack for infusing during the day.
Authors recommend patient support groups, such as the Oley Foundation, which can help with issues surrounding body image and travel.
Because of the relative rarity of SBS, nonspecialist physicians may care for patients without a dedicated multidisciplinary team and may need education support in managing patients with complex care needs. One source the authors recommend is the Learn Intestinal Failure Tele-ECHO (Expanding Community Healthcare Outcomes) (LIFT-ECHO) project. The LIFT-ECHO project has become an online educational community with case-based learning in SBS, intestinal failure, and PN.
The authors disclose relationships with Takeda, Zealand, VectivBio, Napo, and Hanmi.
Caring for patients with short bowel syndrome (SBS) requires a multidisciplinary approach involving dietitians, nurses, surgeons, gastroenterologists or internists, and social workers experienced in SBS care, according to a clinical practice update expert review from the American Gastroenterological Association.
Kishore Iyer, MD, from Mount Sinai Hospital New York; John K. DiBaise, MD, from Mayo Clinic in Scottsdale, Ariz.; and Alberto Rubio-Tapia, MD, from the Cleveland Clinic, Ohio, developed 12 best practice advice statements based on available evidence. The items focus on adult patients with SBS; however, there was some overlap with the management of pediatric SBS. The review was published online in Clinical Gastroenterology and Hepatology.
Defining SBS
One update concerns defining SBS. The authors recommend that surgeons performing massive resections should report the residual bowel length, rather than the length of bowel resected.
“It is only the former that dictates outcome,” they wrote.
There is general agreement that a residual small intestinal length of 200 cm or less meets criteria for SBS. Measurement should be taken from “along the antimesenteric border of unstretched bowel, from the duodenojejunal flexure to the ileocecal junction, the site of any small bowel–colon anastomosis, or to the end-ostomy.”
Based on the residual bowel length, patients can be classified into three groups: end-jejunostomy, jejuno-colic, and jejuno-ileo-colic.
Assessing nutritional status
A dietitian experienced in SBS should perform a thorough nutritional assessment on all SBS patients. Long-term monitoring should include laboratory studies checking electrolytes and liver and kidney function, fluid balance, weight change, serum micronutrients, and bone density. Bone density should be repeated periodically, every 2-3 years.
Fluid and electrolyte problems may affect outcomes for SBS patients, particularly for those without a colon.
Adjusting diets
Most adult patients with SBS have significant malabsorption, so dietary intake “must be increased by at least 50% from their estimated needs,” the authors wrote. It’s best if the patient consumes the increased quantity throughout the day in 5-6 meals, they noted.
An experienced dietitian should counsel the patient based on the patient’s eating preferences. Incorporating preferences can help increase compliance with the adjustments that may become necessary based on symptoms, stool output, and weight.
Using pharmacologic therapy
Using antisecretory medications, including proton pump inhibitors or histamine-2 receptor antagonists, helps reduce gastric secretions, the damage of acid on the upper gut mucosa, and the function of pancreatic exocrine enzymes.
Antidiarrheals reduce intestinal motility but also cause a slight reduction in intestinal secretion. Common agents include loperamide, diphenoxylate with atropine, codeine, and tincture of opium. The review authors say loperamide should get preference over opiate drugs because it is not addictive or sedative.
Use of antidiarrheals should be guided by their effect on stool output.
“Loperamide and codeine may have a synergistic effect when used together,” the authors wrote.
Clonidine, which can be given transdermally, has also shown some benefit in treating high-output stool losses, presumably because of its effects on intestinal motility and secretion.
Weighing risks and benefits of teduglutide
The glucagonlike peptide–2 teduglutide is of particular interest for its ability to help improve intestinal absorption and hopefully wean patients off parenteral nutrition and some will achieve enteral autonomy, the authors wrote. “The very short half-life of native GLP-2 has been extended to allow daily subcutaneous injection in the recombinant molecule, teduglutide.”
However, because teduglutide is a growth factor and can boost the growth of polyps and cancer, it is contraindicated in patients with active gastrointestinal malignancies. Patients should undergo colonoscopy before treatment and periodically thereafter, the authors advised. The benefits of its use in patients with nongastrointestinal malignancy should be weighed carefully with these risks.
“The significant side effects of teduglutide and the cost mandate that teduglutide is employed only after optimizing diet and the more conventional SBS treatments described previously in carefully selected patients with [short bowel syndrome–intestinal failure],” the authors wrote.
Dosing drugs effectively
Medications in tablet form need to dissolve before being absorbed. Most oral medications are absorbed within the proximal jejunum, so they can be used in patients with SBS.
“However,” the authors noted, “sustained- and delayed-release medications should be avoided.”
They suggested that, when applicable, alternatives such as liquids and topical medications should be considered, as should the monitoring of medication levels in the blood.
If a patient does not respond, approaches to consider may include increasing a dose, changing dose frequency, or changing drug formulation or route of administration, such as intravenous, subcutaneous, or transdermal.
Including parenteral nutrition and oral rehydration
Almost all patients with SBS will need parenteral nutrition (PN) support following resection, and few will be able to stop it before discharge from the hospital.
“Although more than 50% of adults with SBS are able to be weaned completely from PN within 5 years of diagnosis, the probability of eliminating PN use is less than 6% if not successfully accomplished in the first 2 years following the individual’s last bowel resection,” the authors wrote.
For long-term PN, tunneled central venous catheters are preferred over peripherally inserted central venous catheters because of the higher risk of thrombosis and issues related to self-administration of PN with the central catheters. Also, tunneled catheters are preferred over totally implanted devices, or ports, for long-term patients because the main benefit of the port is not realized given that the device needs to be continually accessed and exchanged weekly.
“When calculating PN volume and content, changes in the patient’s weight, laboratory results, stool or ostomy output, urine output, and complaints of thirst should be monitored,” the authors noted.
The authors also discussed oral rehydration solution because patients lose more water and sodium from their stoma than they take in by mouth. Careful consideration of the glucose and sodium levels in oral fluids is important because inappropriate fluids will exacerbate fluid losses in SBS. For example, hypotonic (including water, tea, coffee, alcohol) and hypertonic (including fruit juices and sodas) solutions should be limited.
“A major misconception on the part of patients is that they should drink large quantities of water; however, this generally leads to an increase in ostomy output and creates a vicious cycle further exacerbating fluid and electrolyte disturbances,” they wrote, instead advising glucose–electrolyte rehydration solution to enhance absorption and reduce secretion.
Preventing complications
“A knowledge of these complications is critical for those caring for these patients to be able to not only identify and treat them when they occur but also to prevent their occurrence whenever possible,” the authors wrote. Although they considered it beyond the scope of the review to outline every complication, they indicated some complications and management strategies via an included table. These complications can include cirrhosis, osteoporosis, acute kidney disease, and central venous catheter–related infection or occlusion.
Considering further surgery or intestinal transplantation
The authors noted that any further surgery should be carefully considered, with the following three contexts having possible value: “(1) to recruit unused distal bowel, (2) to augment the function of residual bowel through specific lengthening and tapering operations, or (3) to slow intestinal transit.”
Surgeons involved in managing SBS may need to confront complex intra-abdominal problems such as massive desmoid tumors, mesenteric ischemia, or complex enterocutaneous fistulae; a multidisciplinary intestinal rehabilitation team may be better able to help these patients. The authors noted that care for patients starts even before the first operation, by taking every measure to avoid massive bowel resection and the resulting SBS.
The authors noted the importance of early referral for intestinal transplantation consideration for patients with refractory dependency on parenteral nutrition or even onset of parenteral nutrition failure, which refers to complications such as intestinal failure–associated liver disease.
“At present, nearly 50% of patients being considered for ITX are also requiring simultaneous liver replacement, indicating late referral for ITX,” they wrote, citing a data from a report by the Centers for Medicare and Medicaid.
They also noted that data have shown short- and medium-term outcomes are steadily improving; however, long-term outcomes have been challenged by opportunistic infections, long-term graft attrition, and other impediments that may be preventing early referral for intestinal transplantation.
Educating patients, caregivers
Long-term PN may restrict activity for patients, but patients and caregivers should know about some modifications.
One is to cycle the PN over 10-14 hours overnight to allow freedom from the infusion pump during the day. Infusion pumps can be programmable, and some can be carried in a backpack for infusing during the day.
Authors recommend patient support groups, such as the Oley Foundation, which can help with issues surrounding body image and travel.
Because of the relative rarity of SBS, nonspecialist physicians may care for patients without a dedicated multidisciplinary team and may need education support in managing patients with complex care needs. One source the authors recommend is the Learn Intestinal Failure Tele-ECHO (Expanding Community Healthcare Outcomes) (LIFT-ECHO) project. The LIFT-ECHO project has become an online educational community with case-based learning in SBS, intestinal failure, and PN.
The authors disclose relationships with Takeda, Zealand, VectivBio, Napo, and Hanmi.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
New ovulatory disorder classifications from FIGO replace 50-year-old system
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.

The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.

The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.
The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.
The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
The first major revision in the systematic description of ovulatory disorders in nearly 50 years has been proposed by a consensus of experts organized by the International Federation of Gynecology and Obstetrics.
“The FIGO HyPO-P system for the classification of ovulatory disorders is submitted for consideration as a worldwide standard,” according to the writing committee, who published their methodology and their proposed applications in the International Journal of Gynecology and Obstetrics.
The classification system was created to replace the much-modified World Health Organization system first described in 1973. Since that time, many modifications have been proposed to accommodate advances in imaging and new information about underlying pathologies, but there has been no subsequent authoritative reference with these modifications or any other newer organizing system.
The new consensus was developed under the aegis of FIGO, but the development group consisted of representatives from national organizations and the major subspecialty societies. Recognized experts in ovulatory disorders and representatives from lay advocacy organizations also participated.
The HyPO-P system is based largely on anatomy. The acronym refers to ovulatory disorders related to the hypothalamus (type I), the pituitary (type II), and the ovary (type III).
Polycystic ovary syndrome (PCOS), one of the most common ovulatory disorders, was given a separate category (type IV) because of its complexity as well as the fact that PCOS is a heterogeneous systemic disorder with manifestations not limited to an impact on ovarian function.
As the first level of classification, three of the four primary categories (I-III) focus attention on the dominant anatomic source of the change in ovulatory function. The original WHO classification system identified as many as seven major groups, but they were based primarily on assays for gonadotropins and estradiol.
The new system “provides a different structure for determining the diagnosis. Blood tests are not a necessary first step,” explained Malcolm G. Munro, MD, clinical professor, department of obstetrics and gynecology, University of California, Los Angeles. Dr. Munro was the first author of the publication.
The classification system “is not as focused on the specific steps for investigation of ovulatory dysfunction as much as it explains how to structure an investigation of the girl or woman with an ovulatory disorder and then how to characterize the underlying cause,” Dr. Munro said in an interview. “It is designed to allow everyone, whether clinicians, researchers, or patients, to speak the same language.”
New system employs four categories
The four primary categories provide just the first level of classification. The next step is encapsulated in the GAIN-FIT-PIE acronym, which frames the presumed or documented categories of etiologies for the primary categories. GAIN stands for genetic, autoimmune, iatrogenic, or neoplasm etiologies. FIT stands for functional, infectious/inflammatory, or trauma and vascular etiologies. PIE stands for physiological, idiopathic, and endocrine etiologies.
By this methodology, a patient with irregular menses, galactorrhea, and elevated prolactin and an MRI showing a pituitary tumor would be identified a type 2-N, signifying pituitary (type 2) involvement with a neoplasm (N).
A third level of classification permits specific diagnostic entities to be named, allowing the patient in the example above to receive a diagnosis of a prolactin-secreting adenoma.
Not all etiologies can be identified with current diagnostic studies, even assuming clinicians have access to the resources, such as advanced imaging, that will increase diagnostic yield. As a result, the authors acknowledged that the classification system will be “aspirational” in at least some patients, but the structure of this system is expected to lead to greater precision in understanding the causes and defining features of ovulatory disorders, which, in turn, might facilitate new research initiatives.
In the published report, diagnostic protocols based on symptoms were described as being “beyond the spectrum” of this initial description. Rather, Dr. Munro explained that the most important contribution of this new classification system are standardization and communication. The system will be amenable for educating trainees and patients, for communicating between clinicians, and as a framework for research where investigators focus on more homogeneous populations of patients.
“There are many causes of ovulatory disorders that are not related to ovarian function. This is one message. Another is that ovulatory disorders are not binary. They occur on a spectrum. These range from transient instances of delayed or failed ovulation to chronic anovulation,” he said.
The new system is “ a welcome update,” according to Mark P. Trolice, MD, director of the IVF Center and professor of obstetrics and gynecology at the University of Central Florida, both in Orlando.
Dr. Trolice pointed to the clinical value of placing PCOS in a separate category. He noted that it affects 8%-13% of women, making it the most common single cause of ovulatory dysfunction.
“Another area that required clarification from prior WHO classifications was hyperprolactinemia, which is now placed in the type II category,” Dr. Trolice said in an interview.
Better terminology can help address a complex set of disorders with multiple causes and variable manifestations.
“In the evaluation of ovulation dysfunction, it is important to remember that regular menstrual intervals do not ensure ovulation,” Dr. Trolice pointed out. Even though a serum progesterone level of higher than 3 ng/mL is one of the simplest laboratory markers for ovulation, this level, he noted, “can vary through the luteal phase and even throughout the day.”
The proposed classification system, while providing a framework for describing ovulatory disorders, is designed to be adaptable, permitting advances in the understanding of the causes of ovulatory dysfunction, in the diagnosis of the causes, and in the treatments to be incorporated.
“No system should be considered permanent,” according to Dr. Munro and his coauthors. “Review and careful modification and revision should be carried out regularly.”
Dr. Munro reports financial relationships with AbbVie, American Regent, Daiichi Sankyo, Hologic, Myovant, and Pharmacosmos. Dr. Trolice reports no potential conflicts of interest.
FROM INTERNATIONAL JOURNAL OF GYNECOLOGY AND OBSTETRICS
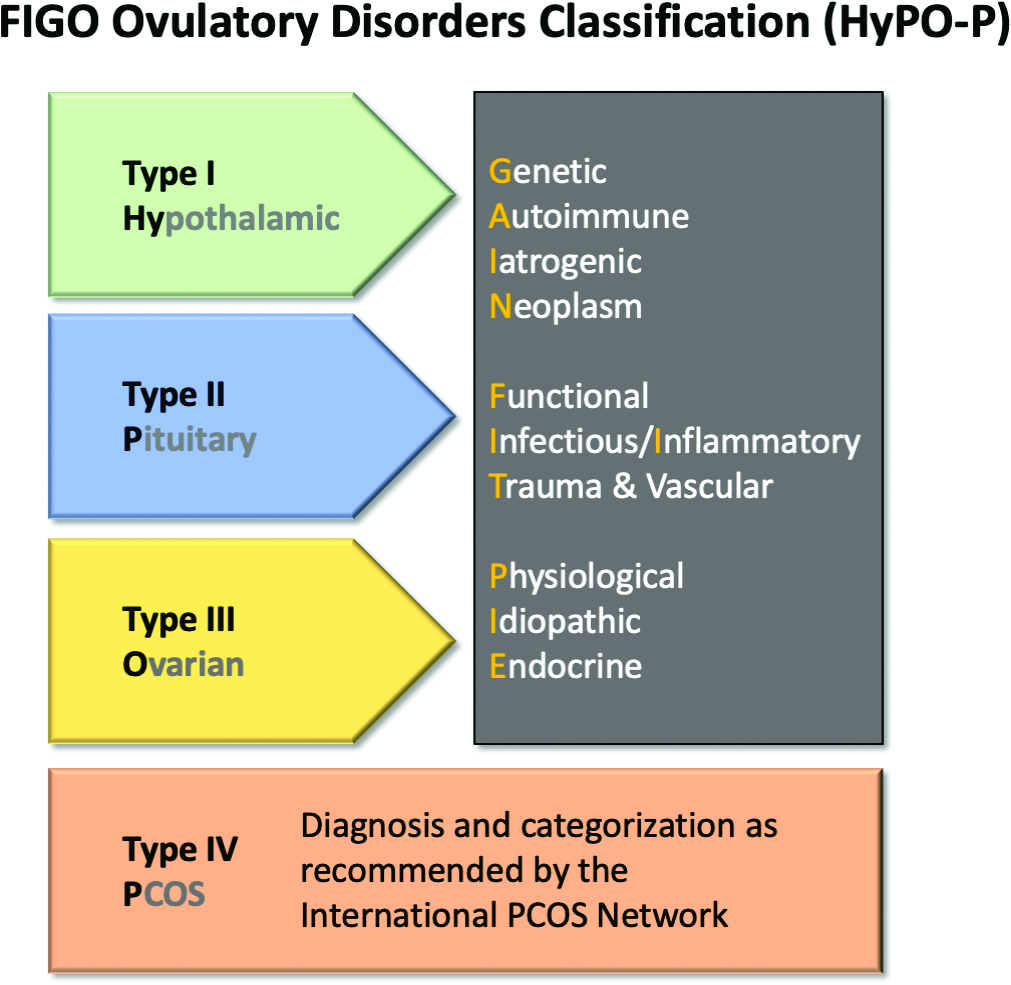
ACC fills gaps on guidance for nonstatin therapies for LDL-C lowering
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.

The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.
The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
To address current gaps in expert guidance on newer nonstatin agents, the American College of Cardiology has issued an expert consensus decision pathway on the role of nonstatin therapies in LDL cholesterol lowering for risk reduction in atherosclerotic cardiovascular disease (ASCVD).
Since the publication of the most recent AHA/ACC cholesterol guidelines in 2018, a number of newer nonstatin medications have become available for management of lipid-associated risk, including bempedoic acid, inclisiran, evinacumab, and icosapent ethyl.
These medications were not addressed in the 2018 AHA/ACC Guideline on the Management of Blood Cholesterol.
The 53-page document – 2022 ACC Expert Consensus Decision Pathway on the Role of Nonstatin Therapies for LDL-Cholesterol Lowering in the Management of Atherosclerotic Cardiovascular Disease Risk – was published online in the Journal of the American College of Cardiology.
The new expert consensus document provides guidance for clinicians until the next formal guidelines are produced, Donald Lloyd-Jones, MD, chair of the writing committee, told this news organization.
The writing group focused on three key areas regarding the use of nonstatin therapies where recent scientific evidence is still under review and clinical trials are still underway:
- In what patient populations should newer nonstatin therapies be considered?
- In what situations should newer nonstatin therapies be considered?
- If newer nonstatin therapies are to be added, which therapies should be considered and in what order to maximize patient benefit and preference?
The document provides algorithms that endorse the four evidence-based patient groups identified in the 2018 guidelines and assumes that the patient is currently taking or has attempted to take a statin, given that that is the most effective initial therapy, the writing group says.
“The algorithms have been streamlined for ease of use by clinicians to help them identify who may need adjunctive nonstatin medications, to provide thresholds for consideration of those medications, and to provide a prioritization of those medications based on the strength of available evidence of efficacy,” said Dr. Lloyd-Jones, chair of the department of preventive medicine at Northwestern University’s Feinberg School of Medicine, Chicago.
“We hope that these pathways will assist the decision-making process for clinicians and patients,” he added.
He also noted that statins remain the “most important first-line therapy for reducing ASCVD risk, because of their efficacy, safety, and low cost. However, for some patients, there are now options if statins do not fully achieve the goals for reducing ASCVD risk or if statins are not tolerated at effective doses.”
“The new expert consensus document highlights that higher-risk patients should be considered more often for adjunctive therapy and provides user-friendly decision pathways to assist in considering the reasonable choices available under different clinical scenarios,” Dr. Lloyd-Jones said.
The document has been endorsed by the National Lipid Association.
This research had no commercial funding. Dr. Lloyd-Jones has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
‘Conservative’ USPSTF primary prevention statin guidance finalized
Questions about how to prescribe statins for primary prevention abound more than 3 decades after the drugs swept into clinical practice to become a first-line medical approach to cutting cardiovascular (CV) risk. Statin usage recommendations from different bodies can vary in ways both limited and fundamental, spurring the kind of debate that accompanies such a document newly issued by the United States Preventive Services Task Force.
The document, little changed from the draft guidance released for public comment in February, was published online Aug. 23 in JAMA and the USPSTF website. It replaces a similar document issued by the task force in 2016.
The guidance has much in common with, but also sharp differences from, the influential 2018 guidelines on blood cholesterol management developed by the American College of Cardiology, American Heart Association, and 10 other medical societies.
And it is provocative enough to elicit at least four editorials issued the same day across the JAMA family of journals. They highlight key differences between the two documents, among them the USPSTF guidance’s consistent, narrow reliance on 7.5% and 10% cut points for 10-year risk levels as estimated from the ACC/AHA pooled cohort equations (PCE).
The guidance pairs the 10-year risk metric with at least one of only four prescribed CV risk factors to arrive at a limited choice of statin therapy recommendations. But its decision process isn’t bolstered by coronary artery calcium (CAC) scores or the prespecified “risk enhancers” that allowed the ACC/AHA-multisociety guidelines to be applied broadly and still be closely personalized. Those guidelines provide more PCE-based risk tiers for greater discrimination of risk and allow statins to be considered across a broader age group.
The USPSTF guidance’s evidence base consists of 23 clinical trials and three observational studies that directly compared a statin to either placebo or no statin, task force member John B. Wong, MD, Tufts University School of Medicine, Boston, told this news organization.
“In either kind of study, we found that the vast majority of patients had one or more of four risk factors – dyslipidemia, hypertension, diabetes, or smoking. So, when we categorized high risk or increased risk, we included the presence of one or more of those risk factors,” said Dr. Wong, who is director of comparative effectiveness research at Tufts Clinical Translational Science Institute.
‘Sensible and practical’
The USPSTF guidance applies only to adults aged 40-75 without CV signs or symptoms and recommends a statin prescription for persons at “high risk,” that is with an estimated 10-year PCE-based risk for death or CV events of 10% or higher plus at least one of the four risk factors, a level B recommendation.
It recommends that “clinicians selectively offer a statin” to such persons at “increased risk,” who have at least one of the risk factors and an estimated 10-year risk for death or CV events of 7.5% to less than 10%, a level C recommendation. “The likelihood of benefit is smaller in this group” than in persons at high risk, the document states.

“These recommendations from the USPSTF are sensible and practical,” states Salim S. Virani, MD, PhD, DeBakey Veterans Affairs Medical Center, Houston, in a related editorial published the same day in JAMA Network Open. He calls the former B-level recommendation “a conservative approach” and the latter C-level recommendation a “nuanced approach.”
Both are “understandable” given that some studies suggest that the PCE may overestimate the CV risk, Dr. Virani observes. “On the other hand, statin therapy has been shown to be efficacious” at 10-year CV-risk levels down to about 5%.
The USPSTF document “I think is going to perpetuate a problem that we have in this country, which is vast undertreatment of lipids,” Eric D. Peterson, MD, MPH, University of Texas Southwestern Medical Center, Dallas, said in an interview.
“We have a ton of good drugs that can lower cholesterol like crazy. If you lower cholesterol a lot, you improve outcomes,” he said. Dyslipidemia needs to be more widely and consistently treated, but “right now we have a pool of people in primary prevention who undertreat lipids and wait until disease happens – and then cardiologists get engaged. That’s an avoidable miss,” Dr. Peterson adds. He and JAMA Cardiology associate editor Ann Marie Navar, MD, PhD, provided JAMA with an editorial that accompanies the USPSTF guidance.
“My own personal bias would be that the [ACC/AHA-multisociety guidelines] are closer to being right,” Dr. Peterson said. They – unlike the USPSTF guidance – cover people with risk levels below 7.5%, down to at least 5%. They allow risk enhancers like metabolic syndrome, inflammatory diseases, or family history into the decision process. “And they’re more aggressive in diabetes and more aggressive in older people,” he said.
Higher threshold for therapy
The USPSTF guidance also explicitly omits some high-risk groups and makes little accommodation for others who might especially benefit from statins, several of the editorials contend. For example, states a related JAMA Cardiology editorial published the same day, “The USPSTF does not comment on familial hypercholesterolemia or an LDL-C level of 190 mg/dL or higher,” yet they are covered by the ACC/AHA-multispecialty guidelines.
In addition, write the editorialists, led by Neil J. Stone, MD, Northwestern University, Chicago, “the USPSTF uses a slightly higher threshold for initiation of statin therapy” than was used in the ACC/AHA-multisociety guidelines. USPSTF, for example, calls for 10-year risk to reach 10% before recommending a statin prescription.
“One concern about the USPSTF setting the bar higher for statin initiation is that it reduces the number of young patients (age 40-50 years) at risk for premature myocardial infarction considered for treatment,” write Dr. Stone and colleagues.
That may be related to a weakness of the PCE-based decision process. “Because the PCE estimates of 10-year CV disease risk rely so heavily on age, sex, and race, use of these estimates to identify candidates for statins results in significant skewing of the population recommended for statins,” write Dr. Navar and Dr. Peterson in their JAMA editorial.
The risk enhancers in the ACC/AHA-multispecialty guidelines, about a dozen of them, compensate for that limitation to some extent. But the PCE-dominated USPSTF risk estimates will likely miss some groups that could potentially benefit from statin therapy, Dr. Peterson agreed in an interview.
For example, younger adults facing years of high LDL-cholesterol levels could easily have PCE-based 10-year risk below 10%. “Having a high LDL over a lifetime puts you at really high risk,” he said. “Young people are missed even though their longitudinal risk is high.” So, by waiting for the lofty 10% level of risk over 10 years, “we limit the use of medicine that’s pretty cheap and highly effective.”
Dose intensity, adverse events
Also at variance from the ACC/AHA-multispecialty guidelines, the USPSTF states that, “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CV disease in most persons.”
The task force specifically explored whether evidence supports some use of high-intensity vs. moderate-intensity statins, Tufts University’s Dr. Wong said. “We found only one study that looked at that particular question, and it didn’t give us a strong answer.” An elevated rosuvastatin-related diabetes risk was apparent in the JUPITER trial, “but for the other studies, we did not find that association.”
Most of the studies that explored statins for reducing risk for a first stroke or myocardial infarction used a moderate-dose statin, Dr. Wong said. “So that’s what we would usually recommend.”
But, Dr. Virani writes, consistent with the ACC/AHA-multispecialty guidelines, “clinicians should consider titrating the intensity of therapy to the risk of the individual.” Persons in certain high-risk primary prevention groups, such as those with end-organ injury from diabetes or LDL cholesterol at least 190 mg/dL, “may derive further benefit from the use of high-intensity statin therapy.”
Low-intensity statins are another potential option, but “in contrast with its 2016 recommendations, the USPSTF no longer recommends use of low-intensity statins in certain situations,” observes a fourth editorial published the same day in JAMA Internal Medicine, with lead author Anand R. Habib, MD, MPhil, and senior author Rita F. Redberg, MD, MSc, both of the University of California, San Francisco. Dr. Redberg is the journal’s editor and has long expressed cautions about statin safety.
“While it is understandable that the Task Force was limited by lack of data on dosing, this change is unfortunate for patients because the frequency of adverse effects increases as the statin dose increases,” the editorial states. Although USPSTF did not find statistically significant harm from the drugs, “in clinical practice, adverse events are commonly reported with use of statins.”
It continues: “At present, there are further reasons to curb our enthusiasm about the use of statins for primary prevention of CV disease.” To illustrate, the editorial questioned primary-prevention statins’ balance of risk vs. clinically meaningful benefit, not benefit that is merely statistically significant.
“The purported benefits of statins in terms of relative risk reduction are fairly constant across baseline lipid levels and cardiovascular risk score categories for primary prevention,” the editorial states.
“Therefore, the absolute benefit for those in lower-risk categories is likely small given that their baseline absolute risk is low, while the chance of adverse effects is constant across risk categories.”
However, USPSTF states, “In pooled analyses of trial data, statin therapy was not associated with increased risk of study withdrawal due to adverse events or serious adverse events.” Nor did it find significant associations with cancers, liver enzyme abnormalities, or diabetes, including new-onset diabetes.
And, the USPSTF adds, “Evidence on the association between statins and renal or cognitive harms is very limited but does not indicate increased risk.”
USPSTF is supported by the U.S. Agency for Healthcare Research and Quality. Dr. Virani discloses receiving grants from the Department of Veterans Affairs, National Institutes of Health, and the World Heart Federation; and personal fees from the American College of Cardiology. Dr. Peterson discloses serving on the JAMA editorial board and receiving research support to his institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and consulting fees from Novo Nordisk, Bayer, and Novartis. Dr. Navar discloses receiving research support to her institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and receiving honoraria and consulting fees from AstraZeneca, Boehringer Ingelheim, Bayer, Janssen, Lilly, Novo Nordisk, Novartis, New Amsterdam, and Pfizer. Dr. Stone discloses receiving an honorarium from Knowledge to Practice, an educational company not associated with the pharmaceutical industry; disclosures for the other authors are in the report. Dr. Redberg discloses receiving research funding from the Arnold Ventures Foundation and the Greenwall Foundation.
A version of this article first appeared on Medscape.com.
Questions about how to prescribe statins for primary prevention abound more than 3 decades after the drugs swept into clinical practice to become a first-line medical approach to cutting cardiovascular (CV) risk. Statin usage recommendations from different bodies can vary in ways both limited and fundamental, spurring the kind of debate that accompanies such a document newly issued by the United States Preventive Services Task Force.
The document, little changed from the draft guidance released for public comment in February, was published online Aug. 23 in JAMA and the USPSTF website. It replaces a similar document issued by the task force in 2016.
The guidance has much in common with, but also sharp differences from, the influential 2018 guidelines on blood cholesterol management developed by the American College of Cardiology, American Heart Association, and 10 other medical societies.
And it is provocative enough to elicit at least four editorials issued the same day across the JAMA family of journals. They highlight key differences between the two documents, among them the USPSTF guidance’s consistent, narrow reliance on 7.5% and 10% cut points for 10-year risk levels as estimated from the ACC/AHA pooled cohort equations (PCE).
The guidance pairs the 10-year risk metric with at least one of only four prescribed CV risk factors to arrive at a limited choice of statin therapy recommendations. But its decision process isn’t bolstered by coronary artery calcium (CAC) scores or the prespecified “risk enhancers” that allowed the ACC/AHA-multisociety guidelines to be applied broadly and still be closely personalized. Those guidelines provide more PCE-based risk tiers for greater discrimination of risk and allow statins to be considered across a broader age group.
The USPSTF guidance’s evidence base consists of 23 clinical trials and three observational studies that directly compared a statin to either placebo or no statin, task force member John B. Wong, MD, Tufts University School of Medicine, Boston, told this news organization.
“In either kind of study, we found that the vast majority of patients had one or more of four risk factors – dyslipidemia, hypertension, diabetes, or smoking. So, when we categorized high risk or increased risk, we included the presence of one or more of those risk factors,” said Dr. Wong, who is director of comparative effectiveness research at Tufts Clinical Translational Science Institute.
‘Sensible and practical’
The USPSTF guidance applies only to adults aged 40-75 without CV signs or symptoms and recommends a statin prescription for persons at “high risk,” that is with an estimated 10-year PCE-based risk for death or CV events of 10% or higher plus at least one of the four risk factors, a level B recommendation.
It recommends that “clinicians selectively offer a statin” to such persons at “increased risk,” who have at least one of the risk factors and an estimated 10-year risk for death or CV events of 7.5% to less than 10%, a level C recommendation. “The likelihood of benefit is smaller in this group” than in persons at high risk, the document states.
“These recommendations from the USPSTF are sensible and practical,” states Salim S. Virani, MD, PhD, DeBakey Veterans Affairs Medical Center, Houston, in a related editorial published the same day in JAMA Network Open. He calls the former B-level recommendation “a conservative approach” and the latter C-level recommendation a “nuanced approach.”
Both are “understandable” given that some studies suggest that the PCE may overestimate the CV risk, Dr. Virani observes. “On the other hand, statin therapy has been shown to be efficacious” at 10-year CV-risk levels down to about 5%.
The USPSTF document “I think is going to perpetuate a problem that we have in this country, which is vast undertreatment of lipids,” Eric D. Peterson, MD, MPH, University of Texas Southwestern Medical Center, Dallas, said in an interview.
“We have a ton of good drugs that can lower cholesterol like crazy. If you lower cholesterol a lot, you improve outcomes,” he said. Dyslipidemia needs to be more widely and consistently treated, but “right now we have a pool of people in primary prevention who undertreat lipids and wait until disease happens – and then cardiologists get engaged. That’s an avoidable miss,” Dr. Peterson adds. He and JAMA Cardiology associate editor Ann Marie Navar, MD, PhD, provided JAMA with an editorial that accompanies the USPSTF guidance.
“My own personal bias would be that the [ACC/AHA-multisociety guidelines] are closer to being right,” Dr. Peterson said. They – unlike the USPSTF guidance – cover people with risk levels below 7.5%, down to at least 5%. They allow risk enhancers like metabolic syndrome, inflammatory diseases, or family history into the decision process. “And they’re more aggressive in diabetes and more aggressive in older people,” he said.
Higher threshold for therapy
The USPSTF guidance also explicitly omits some high-risk groups and makes little accommodation for others who might especially benefit from statins, several of the editorials contend. For example, states a related JAMA Cardiology editorial published the same day, “The USPSTF does not comment on familial hypercholesterolemia or an LDL-C level of 190 mg/dL or higher,” yet they are covered by the ACC/AHA-multispecialty guidelines.
In addition, write the editorialists, led by Neil J. Stone, MD, Northwestern University, Chicago, “the USPSTF uses a slightly higher threshold for initiation of statin therapy” than was used in the ACC/AHA-multisociety guidelines. USPSTF, for example, calls for 10-year risk to reach 10% before recommending a statin prescription.
“One concern about the USPSTF setting the bar higher for statin initiation is that it reduces the number of young patients (age 40-50 years) at risk for premature myocardial infarction considered for treatment,” write Dr. Stone and colleagues.
That may be related to a weakness of the PCE-based decision process. “Because the PCE estimates of 10-year CV disease risk rely so heavily on age, sex, and race, use of these estimates to identify candidates for statins results in significant skewing of the population recommended for statins,” write Dr. Navar and Dr. Peterson in their JAMA editorial.
The risk enhancers in the ACC/AHA-multispecialty guidelines, about a dozen of them, compensate for that limitation to some extent. But the PCE-dominated USPSTF risk estimates will likely miss some groups that could potentially benefit from statin therapy, Dr. Peterson agreed in an interview.
For example, younger adults facing years of high LDL-cholesterol levels could easily have PCE-based 10-year risk below 10%. “Having a high LDL over a lifetime puts you at really high risk,” he said. “Young people are missed even though their longitudinal risk is high.” So, by waiting for the lofty 10% level of risk over 10 years, “we limit the use of medicine that’s pretty cheap and highly effective.”
Dose intensity, adverse events
Also at variance from the ACC/AHA-multispecialty guidelines, the USPSTF states that, “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CV disease in most persons.”
The task force specifically explored whether evidence supports some use of high-intensity vs. moderate-intensity statins, Tufts University’s Dr. Wong said. “We found only one study that looked at that particular question, and it didn’t give us a strong answer.” An elevated rosuvastatin-related diabetes risk was apparent in the JUPITER trial, “but for the other studies, we did not find that association.”
Most of the studies that explored statins for reducing risk for a first stroke or myocardial infarction used a moderate-dose statin, Dr. Wong said. “So that’s what we would usually recommend.”
But, Dr. Virani writes, consistent with the ACC/AHA-multispecialty guidelines, “clinicians should consider titrating the intensity of therapy to the risk of the individual.” Persons in certain high-risk primary prevention groups, such as those with end-organ injury from diabetes or LDL cholesterol at least 190 mg/dL, “may derive further benefit from the use of high-intensity statin therapy.”
Low-intensity statins are another potential option, but “in contrast with its 2016 recommendations, the USPSTF no longer recommends use of low-intensity statins in certain situations,” observes a fourth editorial published the same day in JAMA Internal Medicine, with lead author Anand R. Habib, MD, MPhil, and senior author Rita F. Redberg, MD, MSc, both of the University of California, San Francisco. Dr. Redberg is the journal’s editor and has long expressed cautions about statin safety.
“While it is understandable that the Task Force was limited by lack of data on dosing, this change is unfortunate for patients because the frequency of adverse effects increases as the statin dose increases,” the editorial states. Although USPSTF did not find statistically significant harm from the drugs, “in clinical practice, adverse events are commonly reported with use of statins.”
It continues: “At present, there are further reasons to curb our enthusiasm about the use of statins for primary prevention of CV disease.” To illustrate, the editorial questioned primary-prevention statins’ balance of risk vs. clinically meaningful benefit, not benefit that is merely statistically significant.
“The purported benefits of statins in terms of relative risk reduction are fairly constant across baseline lipid levels and cardiovascular risk score categories for primary prevention,” the editorial states.
“Therefore, the absolute benefit for those in lower-risk categories is likely small given that their baseline absolute risk is low, while the chance of adverse effects is constant across risk categories.”
However, USPSTF states, “In pooled analyses of trial data, statin therapy was not associated with increased risk of study withdrawal due to adverse events or serious adverse events.” Nor did it find significant associations with cancers, liver enzyme abnormalities, or diabetes, including new-onset diabetes.
And, the USPSTF adds, “Evidence on the association between statins and renal or cognitive harms is very limited but does not indicate increased risk.”
USPSTF is supported by the U.S. Agency for Healthcare Research and Quality. Dr. Virani discloses receiving grants from the Department of Veterans Affairs, National Institutes of Health, and the World Heart Federation; and personal fees from the American College of Cardiology. Dr. Peterson discloses serving on the JAMA editorial board and receiving research support to his institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and consulting fees from Novo Nordisk, Bayer, and Novartis. Dr. Navar discloses receiving research support to her institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and receiving honoraria and consulting fees from AstraZeneca, Boehringer Ingelheim, Bayer, Janssen, Lilly, Novo Nordisk, Novartis, New Amsterdam, and Pfizer. Dr. Stone discloses receiving an honorarium from Knowledge to Practice, an educational company not associated with the pharmaceutical industry; disclosures for the other authors are in the report. Dr. Redberg discloses receiving research funding from the Arnold Ventures Foundation and the Greenwall Foundation.
A version of this article first appeared on Medscape.com.
Questions about how to prescribe statins for primary prevention abound more than 3 decades after the drugs swept into clinical practice to become a first-line medical approach to cutting cardiovascular (CV) risk. Statin usage recommendations from different bodies can vary in ways both limited and fundamental, spurring the kind of debate that accompanies such a document newly issued by the United States Preventive Services Task Force.
The document, little changed from the draft guidance released for public comment in February, was published online Aug. 23 in JAMA and the USPSTF website. It replaces a similar document issued by the task force in 2016.
The guidance has much in common with, but also sharp differences from, the influential 2018 guidelines on blood cholesterol management developed by the American College of Cardiology, American Heart Association, and 10 other medical societies.
And it is provocative enough to elicit at least four editorials issued the same day across the JAMA family of journals. They highlight key differences between the two documents, among them the USPSTF guidance’s consistent, narrow reliance on 7.5% and 10% cut points for 10-year risk levels as estimated from the ACC/AHA pooled cohort equations (PCE).
The guidance pairs the 10-year risk metric with at least one of only four prescribed CV risk factors to arrive at a limited choice of statin therapy recommendations. But its decision process isn’t bolstered by coronary artery calcium (CAC) scores or the prespecified “risk enhancers” that allowed the ACC/AHA-multisociety guidelines to be applied broadly and still be closely personalized. Those guidelines provide more PCE-based risk tiers for greater discrimination of risk and allow statins to be considered across a broader age group.
The USPSTF guidance’s evidence base consists of 23 clinical trials and three observational studies that directly compared a statin to either placebo or no statin, task force member John B. Wong, MD, Tufts University School of Medicine, Boston, told this news organization.
“In either kind of study, we found that the vast majority of patients had one or more of four risk factors – dyslipidemia, hypertension, diabetes, or smoking. So, when we categorized high risk or increased risk, we included the presence of one or more of those risk factors,” said Dr. Wong, who is director of comparative effectiveness research at Tufts Clinical Translational Science Institute.
‘Sensible and practical’
The USPSTF guidance applies only to adults aged 40-75 without CV signs or symptoms and recommends a statin prescription for persons at “high risk,” that is with an estimated 10-year PCE-based risk for death or CV events of 10% or higher plus at least one of the four risk factors, a level B recommendation.
It recommends that “clinicians selectively offer a statin” to such persons at “increased risk,” who have at least one of the risk factors and an estimated 10-year risk for death or CV events of 7.5% to less than 10%, a level C recommendation. “The likelihood of benefit is smaller in this group” than in persons at high risk, the document states.
“These recommendations from the USPSTF are sensible and practical,” states Salim S. Virani, MD, PhD, DeBakey Veterans Affairs Medical Center, Houston, in a related editorial published the same day in JAMA Network Open. He calls the former B-level recommendation “a conservative approach” and the latter C-level recommendation a “nuanced approach.”
Both are “understandable” given that some studies suggest that the PCE may overestimate the CV risk, Dr. Virani observes. “On the other hand, statin therapy has been shown to be efficacious” at 10-year CV-risk levels down to about 5%.
The USPSTF document “I think is going to perpetuate a problem that we have in this country, which is vast undertreatment of lipids,” Eric D. Peterson, MD, MPH, University of Texas Southwestern Medical Center, Dallas, said in an interview.
“We have a ton of good drugs that can lower cholesterol like crazy. If you lower cholesterol a lot, you improve outcomes,” he said. Dyslipidemia needs to be more widely and consistently treated, but “right now we have a pool of people in primary prevention who undertreat lipids and wait until disease happens – and then cardiologists get engaged. That’s an avoidable miss,” Dr. Peterson adds. He and JAMA Cardiology associate editor Ann Marie Navar, MD, PhD, provided JAMA with an editorial that accompanies the USPSTF guidance.
“My own personal bias would be that the [ACC/AHA-multisociety guidelines] are closer to being right,” Dr. Peterson said. They – unlike the USPSTF guidance – cover people with risk levels below 7.5%, down to at least 5%. They allow risk enhancers like metabolic syndrome, inflammatory diseases, or family history into the decision process. “And they’re more aggressive in diabetes and more aggressive in older people,” he said.
Higher threshold for therapy
The USPSTF guidance also explicitly omits some high-risk groups and makes little accommodation for others who might especially benefit from statins, several of the editorials contend. For example, states a related JAMA Cardiology editorial published the same day, “The USPSTF does not comment on familial hypercholesterolemia or an LDL-C level of 190 mg/dL or higher,” yet they are covered by the ACC/AHA-multispecialty guidelines.
In addition, write the editorialists, led by Neil J. Stone, MD, Northwestern University, Chicago, “the USPSTF uses a slightly higher threshold for initiation of statin therapy” than was used in the ACC/AHA-multisociety guidelines. USPSTF, for example, calls for 10-year risk to reach 10% before recommending a statin prescription.
“One concern about the USPSTF setting the bar higher for statin initiation is that it reduces the number of young patients (age 40-50 years) at risk for premature myocardial infarction considered for treatment,” write Dr. Stone and colleagues.
That may be related to a weakness of the PCE-based decision process. “Because the PCE estimates of 10-year CV disease risk rely so heavily on age, sex, and race, use of these estimates to identify candidates for statins results in significant skewing of the population recommended for statins,” write Dr. Navar and Dr. Peterson in their JAMA editorial.
The risk enhancers in the ACC/AHA-multispecialty guidelines, about a dozen of them, compensate for that limitation to some extent. But the PCE-dominated USPSTF risk estimates will likely miss some groups that could potentially benefit from statin therapy, Dr. Peterson agreed in an interview.
For example, younger adults facing years of high LDL-cholesterol levels could easily have PCE-based 10-year risk below 10%. “Having a high LDL over a lifetime puts you at really high risk,” he said. “Young people are missed even though their longitudinal risk is high.” So, by waiting for the lofty 10% level of risk over 10 years, “we limit the use of medicine that’s pretty cheap and highly effective.”
Dose intensity, adverse events
Also at variance from the ACC/AHA-multispecialty guidelines, the USPSTF states that, “Based on available evidence, use of moderate-intensity statin therapy seems reasonable for the primary prevention of CV disease in most persons.”
The task force specifically explored whether evidence supports some use of high-intensity vs. moderate-intensity statins, Tufts University’s Dr. Wong said. “We found only one study that looked at that particular question, and it didn’t give us a strong answer.” An elevated rosuvastatin-related diabetes risk was apparent in the JUPITER trial, “but for the other studies, we did not find that association.”
Most of the studies that explored statins for reducing risk for a first stroke or myocardial infarction used a moderate-dose statin, Dr. Wong said. “So that’s what we would usually recommend.”
But, Dr. Virani writes, consistent with the ACC/AHA-multispecialty guidelines, “clinicians should consider titrating the intensity of therapy to the risk of the individual.” Persons in certain high-risk primary prevention groups, such as those with end-organ injury from diabetes or LDL cholesterol at least 190 mg/dL, “may derive further benefit from the use of high-intensity statin therapy.”
Low-intensity statins are another potential option, but “in contrast with its 2016 recommendations, the USPSTF no longer recommends use of low-intensity statins in certain situations,” observes a fourth editorial published the same day in JAMA Internal Medicine, with lead author Anand R. Habib, MD, MPhil, and senior author Rita F. Redberg, MD, MSc, both of the University of California, San Francisco. Dr. Redberg is the journal’s editor and has long expressed cautions about statin safety.
“While it is understandable that the Task Force was limited by lack of data on dosing, this change is unfortunate for patients because the frequency of adverse effects increases as the statin dose increases,” the editorial states. Although USPSTF did not find statistically significant harm from the drugs, “in clinical practice, adverse events are commonly reported with use of statins.”
It continues: “At present, there are further reasons to curb our enthusiasm about the use of statins for primary prevention of CV disease.” To illustrate, the editorial questioned primary-prevention statins’ balance of risk vs. clinically meaningful benefit, not benefit that is merely statistically significant.
“The purported benefits of statins in terms of relative risk reduction are fairly constant across baseline lipid levels and cardiovascular risk score categories for primary prevention,” the editorial states.
“Therefore, the absolute benefit for those in lower-risk categories is likely small given that their baseline absolute risk is low, while the chance of adverse effects is constant across risk categories.”
However, USPSTF states, “In pooled analyses of trial data, statin therapy was not associated with increased risk of study withdrawal due to adverse events or serious adverse events.” Nor did it find significant associations with cancers, liver enzyme abnormalities, or diabetes, including new-onset diabetes.
And, the USPSTF adds, “Evidence on the association between statins and renal or cognitive harms is very limited but does not indicate increased risk.”
USPSTF is supported by the U.S. Agency for Healthcare Research and Quality. Dr. Virani discloses receiving grants from the Department of Veterans Affairs, National Institutes of Health, and the World Heart Federation; and personal fees from the American College of Cardiology. Dr. Peterson discloses serving on the JAMA editorial board and receiving research support to his institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and consulting fees from Novo Nordisk, Bayer, and Novartis. Dr. Navar discloses receiving research support to her institution from Amgen, Bristol-Myers Squibb, Esperion, and Janssen; and receiving honoraria and consulting fees from AstraZeneca, Boehringer Ingelheim, Bayer, Janssen, Lilly, Novo Nordisk, Novartis, New Amsterdam, and Pfizer. Dr. Stone discloses receiving an honorarium from Knowledge to Practice, an educational company not associated with the pharmaceutical industry; disclosures for the other authors are in the report. Dr. Redberg discloses receiving research funding from the Arnold Ventures Foundation and the Greenwall Foundation.
A version of this article first appeared on Medscape.com.
FROM JAMA
Updates on treatment/prevention of VTE in cancer patients
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
ACR makes changes to adult, pediatric vaccinations guidance
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.

The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.
The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.
The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.