User login
Now is the time to be heard: October is Advocacy Month!
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
The American College of Obstetricians and Gynecologists (ACOG) and specifically the Junior Fellow College Advisory Council (JFCAC) are rolling out steps to help you make your voice heard. Starting October 1, head to acog.org/advocacy to check out the ACOG Physician Advocacy video to get inspired. (Or watch it here!) Whether you are a seasoned advocate or just getting started, ACOG and women across the country are counting on you!
Week 1 (October 1–7): Why I advocate
The focus of this week is on delving into topics that interest you, learning why advocacy is critically important, and developing your own message to advocate for women’s health.
- View advocacy videos here to understand what advocacy is and why it is so important.
- See ACOG’s 2018 list of legislative priorities here to find topics that inspire you.
Week 2 (October 8–14): Use your voice
Explore the multitude of platforms available today for amplifying your message. Learn to use social media smartly, get advice for how to write op-eds for local outlets, add your name to support current legislative efforts, and find out who your representatives are to schedule sit-down meetings.
- For tips on communicating with elected officials, click here.
- Connect with ACOG and your district on social media, and remember to use social media responsibly to advocate effectively. See this link for more information!
- Don’t forget to include #JFadvoMonth in your posts while highlighting your advocacy work on social media!
Continued to: Week 3 (October 15–19): Empower your patients
Week 3 (October 15–21): Empower your patients
As a physician, advocating for your patient extends into the clinic itself. Access toolkits, patient websites, handouts, and resources available through ACOG.
- Familiarize yourself with the Patient Page for videos, infographics, and FAQs that are useful resources for your patients.
- Toolkits for providers are available here—use these to enhance your practice and empower your patients!
Week 4 (October 22–28): Take it forward
Advocacy happens year-round. Be sure you are actively involved in ACOG’s efforts. Participate in calls to action and remember on November 6 to GET OUT THE VOTE!
- Participate in the annual Congressional Leadership Conference (March 10–12, 2019) in Washington, DC. Descend on Washington with hundreds of fellow ObGyns to advocate to Congress on important issues. For more information, click here.
- Donate to the Ob-GynPAC, ACOG’s political action committee dedicated to electing officials who support our specialty.
- Run for office! ACOG has resources to support you. Be on the lookout for opportunities to attend candidate workshops sponsored by the Ob-GynPAC!
Get active now!
We are at a critical moment for women’s health and the future of our specialty. Key issues nationally include advocating to Congress to move forward with bills in the Senate (S 1112) and House (HR 1318) to support efforts to reduce maternal mortality. (See this article for background information on these bills.)
To find your elected officials and take action now, click here and tell Congress to help prevent maternal mortality, defend patient protections, and improve access and quality of maternity care.
You can be an advocate for your patients and your profession. Your voice matters. Now is the time to be heard.
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Family therapy and cultural conflicts
I recently had the privilege of treating a family who spoke my first language, Hindi. My patient, Ms. M, was 16 years old and struggling to adjust to her new life in the United States, having recently come from India. America’s schooling, culture, and “open society” was a contrast to her life in a semi-rural town, especially her close-knit family structure in which her parents and siblings are everything. Due to their cultural beliefs and religious faith in Islam, both Ms. M and her father were initially resistant to begin treatment for her depression and anxiety. “Let’s give it a trial” was the attitude I finally got from the father. But to me, there was a clear discordance in the communication among the family members in addition to the primary mental illness that led them to come for treatment. I was attracted to work with this family because I had a reasonable understanding of their faith, their culture, and their family system, and I have an inclination toward spirituality. Even though I recognized this family’s social isolation, I wondered why they were still in a state of unrest, given their deep commitment to their faith.
Ms. M was isolating herself at home, in an environment that wasn’t supportive of talking about her concerns. These included being bullied for being “different,” for how she dressed, and for having home-cooked traditional meals for lunch, and being unable to socialize with most of her male peers, except for those from her same community. This led her to dream of returning to India.
The family did not have a social life. Ms. M told me, “I wanted to socialize, but I cannot because of my faith and religion.” So she chose to wear attire to identify with her mother and her culture of origin. She also did this to hide her emotional pain from enduring trauma related to bullying at her school. It was a challenge to understand how faith, resilience, and trauma were intermingled in Ms. M and her family.
I saw Ms. M and her family for 12 one-hour family psychotherapy sessions. The initial session unfolded uneasily. It was a challenge to build rapport and help them understand how family therapy works. Circular inquiries to each family member, specifically to get the mother’s point of view, brought mourning, shame, and guilt to this family. The importance of marriage, education, and immigration were processed in reference to their culture and their incomplete acculturation to life in the United States.
I wondered if there were other families with different cultural backgrounds who struggled with similar conflicts. I also wondered if those families understood the value of family therapy or had ever experienced this therapeutic process.
The 3 key signs that made me believe that this family was making progress through our work together included:
- They complied with treatment; the family never missed a session.
- The parents acknowledged that their daughter was doing better.
- The mother brought me a dinner as a gesture of gratitude in our last session. This is a particularly meaningful gesture on the part of people with their cultural background.
I clearly remember our first meeting, when Ms. M asked
I recently had the privilege of treating a family who spoke my first language, Hindi. My patient, Ms. M, was 16 years old and struggling to adjust to her new life in the United States, having recently come from India. America’s schooling, culture, and “open society” was a contrast to her life in a semi-rural town, especially her close-knit family structure in which her parents and siblings are everything. Due to their cultural beliefs and religious faith in Islam, both Ms. M and her father were initially resistant to begin treatment for her depression and anxiety. “Let’s give it a trial” was the attitude I finally got from the father. But to me, there was a clear discordance in the communication among the family members in addition to the primary mental illness that led them to come for treatment. I was attracted to work with this family because I had a reasonable understanding of their faith, their culture, and their family system, and I have an inclination toward spirituality. Even though I recognized this family’s social isolation, I wondered why they were still in a state of unrest, given their deep commitment to their faith.
Ms. M was isolating herself at home, in an environment that wasn’t supportive of talking about her concerns. These included being bullied for being “different,” for how she dressed, and for having home-cooked traditional meals for lunch, and being unable to socialize with most of her male peers, except for those from her same community. This led her to dream of returning to India.
The family did not have a social life. Ms. M told me, “I wanted to socialize, but I cannot because of my faith and religion.” So she chose to wear attire to identify with her mother and her culture of origin. She also did this to hide her emotional pain from enduring trauma related to bullying at her school. It was a challenge to understand how faith, resilience, and trauma were intermingled in Ms. M and her family.
I saw Ms. M and her family for 12 one-hour family psychotherapy sessions. The initial session unfolded uneasily. It was a challenge to build rapport and help them understand how family therapy works. Circular inquiries to each family member, specifically to get the mother’s point of view, brought mourning, shame, and guilt to this family. The importance of marriage, education, and immigration were processed in reference to their culture and their incomplete acculturation to life in the United States.
I wondered if there were other families with different cultural backgrounds who struggled with similar conflicts. I also wondered if those families understood the value of family therapy or had ever experienced this therapeutic process.
The 3 key signs that made me believe that this family was making progress through our work together included:
- They complied with treatment; the family never missed a session.
- The parents acknowledged that their daughter was doing better.
- The mother brought me a dinner as a gesture of gratitude in our last session. This is a particularly meaningful gesture on the part of people with their cultural background.
I clearly remember our first meeting, when Ms. M asked
I recently had the privilege of treating a family who spoke my first language, Hindi. My patient, Ms. M, was 16 years old and struggling to adjust to her new life in the United States, having recently come from India. America’s schooling, culture, and “open society” was a contrast to her life in a semi-rural town, especially her close-knit family structure in which her parents and siblings are everything. Due to their cultural beliefs and religious faith in Islam, both Ms. M and her father were initially resistant to begin treatment for her depression and anxiety. “Let’s give it a trial” was the attitude I finally got from the father. But to me, there was a clear discordance in the communication among the family members in addition to the primary mental illness that led them to come for treatment. I was attracted to work with this family because I had a reasonable understanding of their faith, their culture, and their family system, and I have an inclination toward spirituality. Even though I recognized this family’s social isolation, I wondered why they were still in a state of unrest, given their deep commitment to their faith.
Ms. M was isolating herself at home, in an environment that wasn’t supportive of talking about her concerns. These included being bullied for being “different,” for how she dressed, and for having home-cooked traditional meals for lunch, and being unable to socialize with most of her male peers, except for those from her same community. This led her to dream of returning to India.
The family did not have a social life. Ms. M told me, “I wanted to socialize, but I cannot because of my faith and religion.” So she chose to wear attire to identify with her mother and her culture of origin. She also did this to hide her emotional pain from enduring trauma related to bullying at her school. It was a challenge to understand how faith, resilience, and trauma were intermingled in Ms. M and her family.
I saw Ms. M and her family for 12 one-hour family psychotherapy sessions. The initial session unfolded uneasily. It was a challenge to build rapport and help them understand how family therapy works. Circular inquiries to each family member, specifically to get the mother’s point of view, brought mourning, shame, and guilt to this family. The importance of marriage, education, and immigration were processed in reference to their culture and their incomplete acculturation to life in the United States.
I wondered if there were other families with different cultural backgrounds who struggled with similar conflicts. I also wondered if those families understood the value of family therapy or had ever experienced this therapeutic process.
The 3 key signs that made me believe that this family was making progress through our work together included:
- They complied with treatment; the family never missed a session.
- The parents acknowledged that their daughter was doing better.
- The mother brought me a dinner as a gesture of gratitude in our last session. This is a particularly meaningful gesture on the part of people with their cultural background.
I clearly remember our first meeting, when Ms. M asked

Proactive consultation: A new model of care in consultation-liaison psychiatry
During my residency training, I was trained in the standard “reactive” psychiatric consultation model. In this system, I would see consults placed by the primary team after they identified a behavioral issue in a patient. As a trainee, I experienced frequent frustrations working in this model: Consults that are discharge-dependent (“Can you see the patient before he is discharged this morning?”), consults for acute behavioral dysregulation (“The patient is near the elevator, can you come see him ASAP?”), or consults for consequences of poor management of alcohol/benzodiazepine withdrawal (“The patient is confused and trying to leave”).
As a fellow in consultation-liaison (C-L) psychiatry, I was introduced to the “proactive” consultation model, which avoids some of these issues. In this article, which is intended for residents who have not been exposed to this new approach, I explain how the proactive model changes our experience as C-L clinicians.
The Behavioral Intervention Team
At Yale New Haven Hospital, the Behavioral Intervention Team (BIT) is a proactive, multidisciplinary psychiatric consultation service that serves the internal medicine units at the hospital. The team consists of nurse practitioners, nurse liaison specialists, social workers, and psychiatrists. The team identifies and removes behavioral barriers in the care of hospitalized mentally ill patients.
The BIT collaborates closely with the medical team through formal and informal consultation; co-management of behavioral issues; education of medical, nursing, and social work staff; and direct care of complex patients with behavioral disorders. The BIT assists the medical team with transitions to appropriate outpatient and inpatient psychiatric care. The team also manages the relationship with the insurer when a patient requires a stay in a psychiatric unit.
This model has a critical financial benefit in reducing the length of stay, but it also has many other benefits. It focuses on early recognition and treatment, and helps mitigate the effects of mental or substance use disorders on patients’ recovery. BIT members educate their peers regarding management of a multitude of behavioral issues. This fosters extensive informal collaboration (“curbside consultation”), which helps patients who did not receive a formal consult. The model distributes work more rationally among different professional specialists. It yields a relationship with medical teams that is not only more effective, but also more enjoyable. In the BIT model, psychiatrists pick the cases where they feel they can have the most impact, and avoid the cases they feel they cannot have any.1-3
CASE A better approach to alcohol withdrawal
Mr. X, age 56, has a history of alcohol use disorder, hypertension, and coronary artery disease. He’s had multiple past admissions for complicated alcohol withdrawal. He is transferred from a local community hospital, where he had presented with chest pain. His last drink was 2 days prior to admission, and his blood alcohol level is <10 mg/dL.
During Mr. X’s previous hospitalizations, psychiatric consults were performed in the standard reactive model. The primary team initially prescribed an ineffective dosage of benzodiazepines for his alcohol withdrawal. This escalated his withdrawal into delirium tremens, after which psychiatry was involved. Due to this early ineffective management, the patient had a prolonged medical ICU stay and overall stay, experienced increased medical complications, and required increased staff resources because he was extremely agitated.
Continued to: During this hospitalization...
During this hospitalization, Mr. X arrives with similar medical complaints. The nurse practitioner on the BIT service, who screened all admissions each day, examines the prior notes (she finds the team sign-outs to be particularly useful). She suggests a psychiatric consult on Day 1 of the admission, which the primary medical team orders. The BIT nurse practitioner gives apt recommendations of evidence-based management, including a benzodiazepine taper, high-dose thiamine, and psychopharmacologic approaches to severe agitation. The nurse liaison specialist on the service makes behavioral plans for managing agitation, which she communicates to the nurses caring for Mr. X.
Because his withdrawal is managed more promptly, Mr. X’s length of stay is shorter and he does not experience any medical complications. The BIT social worker helps find appropriate aftercare options, including residential treatment and Alcoholics Anonymous meetings, to which the patient agrees.
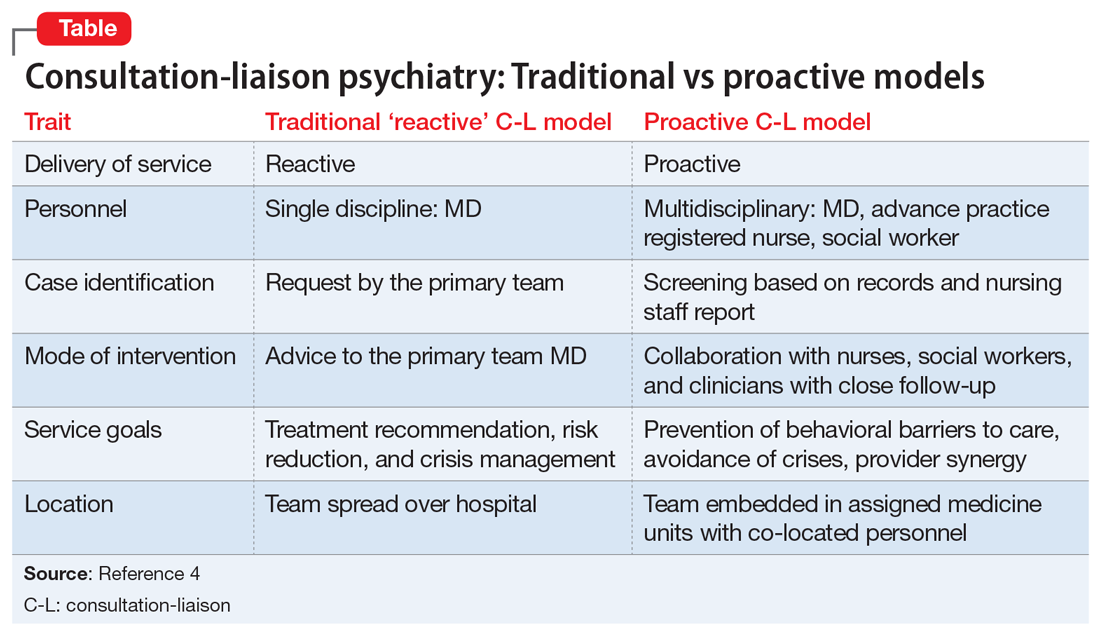
Participating in this case was highly educational for me as a trainee. This case is but one example among many where proactive consultation provided prompt care, lowered the rate of complications, reduced length of stay, and resulted in greater provider satisfaction. The Table4 contrasts the proactive and reactive consultation models. The following 5 factors are critical in the proactive consultation model4,5:
1. Standardized and reliable procedure screening of all admissions, involving a mental health professional, through record review and staff contact. This screening should identify patients with issues who will benefit specifically from in-hospital services, rather than just patients with any psychiatric issue. An electronic medical record is essential to efficient screening, team communication, and progress monitoring. Truly integrated consultation would be impossible with a paper chart.
Continued to: 2. Rapid intervention...
2. Rapid intervention that anticipates impending problems before a cascade of complications starts.
3. Collaborative engagement with the primary medical team, sharing the burden of caring for the complex inpatient, and transmitting critical behavioral management skills to all caregivers, including the skill of recognizing patients who can benefit from a psychiatric consultation.
4. Daily and close contact between behavioral and medical teams, ensuring that treatment recommendations are understood, enacted, and reinforced, ineffective treatments are discontinued, and new problems are addressed before complicating consequences arise. Dedicating specific personnel to specific hospital units and placing them in rounds simplifies communication and speeds intervention implementation.
5. A multidisciplinary consultation team, offering a range of responses, including informal curbside consultation, consultation with an advanced practice registered nurse, social work interventions, advice to discharge planning teams, psychological services, and access to specialized providers, such as addiction teams, as well as traditional consultation with an experienced psychiatrist.
Research has shown the effectiveness of proactive, embedded, multidisciplinary approaches.1-3,5 It was a gratifying experience to work in this model. I worked intimately with medical clinicians, and shared the burden of responsibilities leading to optimal patient outcomes. The proactive consultation model truly re-emphasizes the “liaison” component of C-L psychiatry, as it was originally envisioned.
1. Sledge WH, Gueorguieva R, Desan P, et al. Multidisciplinary proactive psychiatric consultation service: impact on length of stay for medical inpatients. Psychother Psychosom. 2015;84(4):208-216.
2. Desan PH, Zimbrean PC, Weinstein AJ, et al. Proactive psychiatric consultation services reduce length of stay for admissions to an inpatient medical team. Psychosomatics. 2011;52(6):513-520.
3. Sledge WH, Bozzo J, White-McCullum BA, et al. The cost-benefit from the perspective of the hospital of a proactive psychiatric consultation service on inpatient general medicine services. Health Econ Outcome Res Open Access. 2016;2(4):122.
4. Sledge WH, Lee HB. Proactive psychiatric consultation for hospitalized patients, a plan for the future. Health Affairs. www.healthaffairs.org/do/10.1377/hblog20150528.048026/full/. Published May 28, 2015. Accessed September 12, 2018.
5. Desan P, Lee H, Zimbrean P, et al. New models of psychiatric consultation in the general medical hospital: liaison psychiatry is back. Psychiatr Ann. 2017;47:355-361.
During my residency training, I was trained in the standard “reactive” psychiatric consultation model. In this system, I would see consults placed by the primary team after they identified a behavioral issue in a patient. As a trainee, I experienced frequent frustrations working in this model: Consults that are discharge-dependent (“Can you see the patient before he is discharged this morning?”), consults for acute behavioral dysregulation (“The patient is near the elevator, can you come see him ASAP?”), or consults for consequences of poor management of alcohol/benzodiazepine withdrawal (“The patient is confused and trying to leave”).
As a fellow in consultation-liaison (C-L) psychiatry, I was introduced to the “proactive” consultation model, which avoids some of these issues. In this article, which is intended for residents who have not been exposed to this new approach, I explain how the proactive model changes our experience as C-L clinicians.
The Behavioral Intervention Team
At Yale New Haven Hospital, the Behavioral Intervention Team (BIT) is a proactive, multidisciplinary psychiatric consultation service that serves the internal medicine units at the hospital. The team consists of nurse practitioners, nurse liaison specialists, social workers, and psychiatrists. The team identifies and removes behavioral barriers in the care of hospitalized mentally ill patients.
The BIT collaborates closely with the medical team through formal and informal consultation; co-management of behavioral issues; education of medical, nursing, and social work staff; and direct care of complex patients with behavioral disorders. The BIT assists the medical team with transitions to appropriate outpatient and inpatient psychiatric care. The team also manages the relationship with the insurer when a patient requires a stay in a psychiatric unit.
This model has a critical financial benefit in reducing the length of stay, but it also has many other benefits. It focuses on early recognition and treatment, and helps mitigate the effects of mental or substance use disorders on patients’ recovery. BIT members educate their peers regarding management of a multitude of behavioral issues. This fosters extensive informal collaboration (“curbside consultation”), which helps patients who did not receive a formal consult. The model distributes work more rationally among different professional specialists. It yields a relationship with medical teams that is not only more effective, but also more enjoyable. In the BIT model, psychiatrists pick the cases where they feel they can have the most impact, and avoid the cases they feel they cannot have any.1-3
CASE A better approach to alcohol withdrawal
Mr. X, age 56, has a history of alcohol use disorder, hypertension, and coronary artery disease. He’s had multiple past admissions for complicated alcohol withdrawal. He is transferred from a local community hospital, where he had presented with chest pain. His last drink was 2 days prior to admission, and his blood alcohol level is <10 mg/dL.
During Mr. X’s previous hospitalizations, psychiatric consults were performed in the standard reactive model. The primary team initially prescribed an ineffective dosage of benzodiazepines for his alcohol withdrawal. This escalated his withdrawal into delirium tremens, after which psychiatry was involved. Due to this early ineffective management, the patient had a prolonged medical ICU stay and overall stay, experienced increased medical complications, and required increased staff resources because he was extremely agitated.
Continued to: During this hospitalization...
During this hospitalization, Mr. X arrives with similar medical complaints. The nurse practitioner on the BIT service, who screened all admissions each day, examines the prior notes (she finds the team sign-outs to be particularly useful). She suggests a psychiatric consult on Day 1 of the admission, which the primary medical team orders. The BIT nurse practitioner gives apt recommendations of evidence-based management, including a benzodiazepine taper, high-dose thiamine, and psychopharmacologic approaches to severe agitation. The nurse liaison specialist on the service makes behavioral plans for managing agitation, which she communicates to the nurses caring for Mr. X.
Because his withdrawal is managed more promptly, Mr. X’s length of stay is shorter and he does not experience any medical complications. The BIT social worker helps find appropriate aftercare options, including residential treatment and Alcoholics Anonymous meetings, to which the patient agrees.
Participating in this case was highly educational for me as a trainee. This case is but one example among many where proactive consultation provided prompt care, lowered the rate of complications, reduced length of stay, and resulted in greater provider satisfaction. The Table4 contrasts the proactive and reactive consultation models. The following 5 factors are critical in the proactive consultation model4,5:
1. Standardized and reliable procedure screening of all admissions, involving a mental health professional, through record review and staff contact. This screening should identify patients with issues who will benefit specifically from in-hospital services, rather than just patients with any psychiatric issue. An electronic medical record is essential to efficient screening, team communication, and progress monitoring. Truly integrated consultation would be impossible with a paper chart.
Continued to: 2. Rapid intervention...
2. Rapid intervention that anticipates impending problems before a cascade of complications starts.
3. Collaborative engagement with the primary medical team, sharing the burden of caring for the complex inpatient, and transmitting critical behavioral management skills to all caregivers, including the skill of recognizing patients who can benefit from a psychiatric consultation.
4. Daily and close contact between behavioral and medical teams, ensuring that treatment recommendations are understood, enacted, and reinforced, ineffective treatments are discontinued, and new problems are addressed before complicating consequences arise. Dedicating specific personnel to specific hospital units and placing them in rounds simplifies communication and speeds intervention implementation.
5. A multidisciplinary consultation team, offering a range of responses, including informal curbside consultation, consultation with an advanced practice registered nurse, social work interventions, advice to discharge planning teams, psychological services, and access to specialized providers, such as addiction teams, as well as traditional consultation with an experienced psychiatrist.
Research has shown the effectiveness of proactive, embedded, multidisciplinary approaches.1-3,5 It was a gratifying experience to work in this model. I worked intimately with medical clinicians, and shared the burden of responsibilities leading to optimal patient outcomes. The proactive consultation model truly re-emphasizes the “liaison” component of C-L psychiatry, as it was originally envisioned.
During my residency training, I was trained in the standard “reactive” psychiatric consultation model. In this system, I would see consults placed by the primary team after they identified a behavioral issue in a patient. As a trainee, I experienced frequent frustrations working in this model: Consults that are discharge-dependent (“Can you see the patient before he is discharged this morning?”), consults for acute behavioral dysregulation (“The patient is near the elevator, can you come see him ASAP?”), or consults for consequences of poor management of alcohol/benzodiazepine withdrawal (“The patient is confused and trying to leave”).
As a fellow in consultation-liaison (C-L) psychiatry, I was introduced to the “proactive” consultation model, which avoids some of these issues. In this article, which is intended for residents who have not been exposed to this new approach, I explain how the proactive model changes our experience as C-L clinicians.
The Behavioral Intervention Team
At Yale New Haven Hospital, the Behavioral Intervention Team (BIT) is a proactive, multidisciplinary psychiatric consultation service that serves the internal medicine units at the hospital. The team consists of nurse practitioners, nurse liaison specialists, social workers, and psychiatrists. The team identifies and removes behavioral barriers in the care of hospitalized mentally ill patients.
The BIT collaborates closely with the medical team through formal and informal consultation; co-management of behavioral issues; education of medical, nursing, and social work staff; and direct care of complex patients with behavioral disorders. The BIT assists the medical team with transitions to appropriate outpatient and inpatient psychiatric care. The team also manages the relationship with the insurer when a patient requires a stay in a psychiatric unit.
This model has a critical financial benefit in reducing the length of stay, but it also has many other benefits. It focuses on early recognition and treatment, and helps mitigate the effects of mental or substance use disorders on patients’ recovery. BIT members educate their peers regarding management of a multitude of behavioral issues. This fosters extensive informal collaboration (“curbside consultation”), which helps patients who did not receive a formal consult. The model distributes work more rationally among different professional specialists. It yields a relationship with medical teams that is not only more effective, but also more enjoyable. In the BIT model, psychiatrists pick the cases where they feel they can have the most impact, and avoid the cases they feel they cannot have any.1-3
CASE A better approach to alcohol withdrawal
Mr. X, age 56, has a history of alcohol use disorder, hypertension, and coronary artery disease. He’s had multiple past admissions for complicated alcohol withdrawal. He is transferred from a local community hospital, where he had presented with chest pain. His last drink was 2 days prior to admission, and his blood alcohol level is <10 mg/dL.
During Mr. X’s previous hospitalizations, psychiatric consults were performed in the standard reactive model. The primary team initially prescribed an ineffective dosage of benzodiazepines for his alcohol withdrawal. This escalated his withdrawal into delirium tremens, after which psychiatry was involved. Due to this early ineffective management, the patient had a prolonged medical ICU stay and overall stay, experienced increased medical complications, and required increased staff resources because he was extremely agitated.
Continued to: During this hospitalization...
During this hospitalization, Mr. X arrives with similar medical complaints. The nurse practitioner on the BIT service, who screened all admissions each day, examines the prior notes (she finds the team sign-outs to be particularly useful). She suggests a psychiatric consult on Day 1 of the admission, which the primary medical team orders. The BIT nurse practitioner gives apt recommendations of evidence-based management, including a benzodiazepine taper, high-dose thiamine, and psychopharmacologic approaches to severe agitation. The nurse liaison specialist on the service makes behavioral plans for managing agitation, which she communicates to the nurses caring for Mr. X.
Because his withdrawal is managed more promptly, Mr. X’s length of stay is shorter and he does not experience any medical complications. The BIT social worker helps find appropriate aftercare options, including residential treatment and Alcoholics Anonymous meetings, to which the patient agrees.
Participating in this case was highly educational for me as a trainee. This case is but one example among many where proactive consultation provided prompt care, lowered the rate of complications, reduced length of stay, and resulted in greater provider satisfaction. The Table4 contrasts the proactive and reactive consultation models. The following 5 factors are critical in the proactive consultation model4,5:
1. Standardized and reliable procedure screening of all admissions, involving a mental health professional, through record review and staff contact. This screening should identify patients with issues who will benefit specifically from in-hospital services, rather than just patients with any psychiatric issue. An electronic medical record is essential to efficient screening, team communication, and progress monitoring. Truly integrated consultation would be impossible with a paper chart.
Continued to: 2. Rapid intervention...
2. Rapid intervention that anticipates impending problems before a cascade of complications starts.
3. Collaborative engagement with the primary medical team, sharing the burden of caring for the complex inpatient, and transmitting critical behavioral management skills to all caregivers, including the skill of recognizing patients who can benefit from a psychiatric consultation.
4. Daily and close contact between behavioral and medical teams, ensuring that treatment recommendations are understood, enacted, and reinforced, ineffective treatments are discontinued, and new problems are addressed before complicating consequences arise. Dedicating specific personnel to specific hospital units and placing them in rounds simplifies communication and speeds intervention implementation.
5. A multidisciplinary consultation team, offering a range of responses, including informal curbside consultation, consultation with an advanced practice registered nurse, social work interventions, advice to discharge planning teams, psychological services, and access to specialized providers, such as addiction teams, as well as traditional consultation with an experienced psychiatrist.
Research has shown the effectiveness of proactive, embedded, multidisciplinary approaches.1-3,5 It was a gratifying experience to work in this model. I worked intimately with medical clinicians, and shared the burden of responsibilities leading to optimal patient outcomes. The proactive consultation model truly re-emphasizes the “liaison” component of C-L psychiatry, as it was originally envisioned.
1. Sledge WH, Gueorguieva R, Desan P, et al. Multidisciplinary proactive psychiatric consultation service: impact on length of stay for medical inpatients. Psychother Psychosom. 2015;84(4):208-216.
2. Desan PH, Zimbrean PC, Weinstein AJ, et al. Proactive psychiatric consultation services reduce length of stay for admissions to an inpatient medical team. Psychosomatics. 2011;52(6):513-520.
3. Sledge WH, Bozzo J, White-McCullum BA, et al. The cost-benefit from the perspective of the hospital of a proactive psychiatric consultation service on inpatient general medicine services. Health Econ Outcome Res Open Access. 2016;2(4):122.
4. Sledge WH, Lee HB. Proactive psychiatric consultation for hospitalized patients, a plan for the future. Health Affairs. www.healthaffairs.org/do/10.1377/hblog20150528.048026/full/. Published May 28, 2015. Accessed September 12, 2018.
5. Desan P, Lee H, Zimbrean P, et al. New models of psychiatric consultation in the general medical hospital: liaison psychiatry is back. Psychiatr Ann. 2017;47:355-361.
1. Sledge WH, Gueorguieva R, Desan P, et al. Multidisciplinary proactive psychiatric consultation service: impact on length of stay for medical inpatients. Psychother Psychosom. 2015;84(4):208-216.
2. Desan PH, Zimbrean PC, Weinstein AJ, et al. Proactive psychiatric consultation services reduce length of stay for admissions to an inpatient medical team. Psychosomatics. 2011;52(6):513-520.
3. Sledge WH, Bozzo J, White-McCullum BA, et al. The cost-benefit from the perspective of the hospital of a proactive psychiatric consultation service on inpatient general medicine services. Health Econ Outcome Res Open Access. 2016;2(4):122.
4. Sledge WH, Lee HB. Proactive psychiatric consultation for hospitalized patients, a plan for the future. Health Affairs. www.healthaffairs.org/do/10.1377/hblog20150528.048026/full/. Published May 28, 2015. Accessed September 12, 2018.
5. Desan P, Lee H, Zimbrean P, et al. New models of psychiatric consultation in the general medical hospital: liaison psychiatry is back. Psychiatr Ann. 2017;47:355-361.
Put the cash in the shoebox
Even when I was training back in the Pleistocene era, old Doc Greenberg was a throwback. During my pediatric residency, I accompanied him for a day to his office in the Parkchester neighborhood of the Bronx. With no secretary or office staff, Greenberg just processed patients himself. After he examined their kids, each mother handed him a $10 bill, which he stuffed into a box in his desk drawer. No records, no accountability, no payroll taxes ... Those were the days, bygone even then.

What prompted this reverie was recollecting a conversation I had quite some time ago with Stan, a retired drug rep of the old school: terrible combover, rumpled suit, beat-up briefcase. Stan regaled me with tales of derms he had called on many years before.
“Ed Gillooly down in Scituate used to charge $7 a visit,” Stan told me. “I asked him why so little – this was back in the ’60s – and he said, ‘Phil Gluckstern charges 20 bucks a visit in his fancy downtown office, but he has to spend half an hour with a patient. I just see ’em, diagnose ’em, prescribe for ’em, and they’re out the door.’
“Dermatology wasn’t the high-class deal it’s gotten to be,” said Stan. “It was sort of out there. Every doctor had his own special lotion or concoction, his calling card. The local pharmacist knew how to mix it up, but of course would never share the secret formula.
“Nobody referred anybody to another doctor if they could help it. They were terrified they’d never see the patient back.
“It was all cash. There was no Medicare, no third parties. The money would get put into a shoebox, which would go into the doctor’s closet. A lot of offices were in the doc’s house. Sometimes a babysitter would go through the closet, and wouldn’t you know, but the next time the doc’s wife looked, last week’s receipts were gone.
“Secretaries? Doctors wouldn’t bother with them. Sometimes their mothers or wives, who knew as little about office management as they did, would come in and mess things up.”
This observation resonated. Almost 40 years ago, I took over what was left of Al Shipman’s practice when the old-timer (as he seemed to me then) retired to Florida.
Al’s office was a converted garage. Rummaging through a closet, he offered me ancient samples of sulfur-resorcinol acne lotions. Then he pulled out a well-thumbed Merck Manual from the 1930s, with the front cover missing. “I always found this useful,” he said. “You can have it if you want.” I politely declined.
“You young fellas spend money like it’s going out of style,” said Al. “You all think you need secretaries. Never had one!”
My reverie done, I focused back on Stan, who was saying, “Doctors in those days did pretty much everything themselves.
“For instance, Jack Vallis had about thirty chairs in his waiting room. Whenever Jack came out to call the next patient, everybody got up and moved over one chair.
“Once – I swear this actually happened – a patient came in with a severe laceration on his wrist; his damned arm was dangling half-off. But he had to sit down in the last chair and take his turn, same as anybody else.
“I used to call on non-derms too. We carried cortisone creams and antifungal creams, and they used to stop and ask me, ‘Now Stan, I put this fungus cream on the fungus and the cortisone cream on the eczema, am I right?’”
Some things indeed don’t change.

I guess it’s just human nature to pine for When patients (or their biopsy specimens) could go to any lab you sent them to.
Ah, wasn’t that the life? When patients paid you 10 bucks in cash and you stuffed it in your shoebox? When if they didn’t have cash, they sent you a roast turkey on Thanksgiving, or a dozen eggs, or maybe nothing at all?
If you’re the sentimental sort, you can wax nostalgic about those good old days if you want. But you’ll forgive me if I don’t join you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
Even when I was training back in the Pleistocene era, old Doc Greenberg was a throwback. During my pediatric residency, I accompanied him for a day to his office in the Parkchester neighborhood of the Bronx. With no secretary or office staff, Greenberg just processed patients himself. After he examined their kids, each mother handed him a $10 bill, which he stuffed into a box in his desk drawer. No records, no accountability, no payroll taxes ... Those were the days, bygone even then.
What prompted this reverie was recollecting a conversation I had quite some time ago with Stan, a retired drug rep of the old school: terrible combover, rumpled suit, beat-up briefcase. Stan regaled me with tales of derms he had called on many years before.
“Ed Gillooly down in Scituate used to charge $7 a visit,” Stan told me. “I asked him why so little – this was back in the ’60s – and he said, ‘Phil Gluckstern charges 20 bucks a visit in his fancy downtown office, but he has to spend half an hour with a patient. I just see ’em, diagnose ’em, prescribe for ’em, and they’re out the door.’
“Dermatology wasn’t the high-class deal it’s gotten to be,” said Stan. “It was sort of out there. Every doctor had his own special lotion or concoction, his calling card. The local pharmacist knew how to mix it up, but of course would never share the secret formula.
“Nobody referred anybody to another doctor if they could help it. They were terrified they’d never see the patient back.
“It was all cash. There was no Medicare, no third parties. The money would get put into a shoebox, which would go into the doctor’s closet. A lot of offices were in the doc’s house. Sometimes a babysitter would go through the closet, and wouldn’t you know, but the next time the doc’s wife looked, last week’s receipts were gone.
“Secretaries? Doctors wouldn’t bother with them. Sometimes their mothers or wives, who knew as little about office management as they did, would come in and mess things up.”
This observation resonated. Almost 40 years ago, I took over what was left of Al Shipman’s practice when the old-timer (as he seemed to me then) retired to Florida.
Al’s office was a converted garage. Rummaging through a closet, he offered me ancient samples of sulfur-resorcinol acne lotions. Then he pulled out a well-thumbed Merck Manual from the 1930s, with the front cover missing. “I always found this useful,” he said. “You can have it if you want.” I politely declined.
“You young fellas spend money like it’s going out of style,” said Al. “You all think you need secretaries. Never had one!”
My reverie done, I focused back on Stan, who was saying, “Doctors in those days did pretty much everything themselves.
“For instance, Jack Vallis had about thirty chairs in his waiting room. Whenever Jack came out to call the next patient, everybody got up and moved over one chair.
“Once – I swear this actually happened – a patient came in with a severe laceration on his wrist; his damned arm was dangling half-off. But he had to sit down in the last chair and take his turn, same as anybody else.
“I used to call on non-derms too. We carried cortisone creams and antifungal creams, and they used to stop and ask me, ‘Now Stan, I put this fungus cream on the fungus and the cortisone cream on the eczema, am I right?’”
Some things indeed don’t change.
I guess it’s just human nature to pine for When patients (or their biopsy specimens) could go to any lab you sent them to.
Ah, wasn’t that the life? When patients paid you 10 bucks in cash and you stuffed it in your shoebox? When if they didn’t have cash, they sent you a roast turkey on Thanksgiving, or a dozen eggs, or maybe nothing at all?
If you’re the sentimental sort, you can wax nostalgic about those good old days if you want. But you’ll forgive me if I don’t join you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
Even when I was training back in the Pleistocene era, old Doc Greenberg was a throwback. During my pediatric residency, I accompanied him for a day to his office in the Parkchester neighborhood of the Bronx. With no secretary or office staff, Greenberg just processed patients himself. After he examined their kids, each mother handed him a $10 bill, which he stuffed into a box in his desk drawer. No records, no accountability, no payroll taxes ... Those were the days, bygone even then.
What prompted this reverie was recollecting a conversation I had quite some time ago with Stan, a retired drug rep of the old school: terrible combover, rumpled suit, beat-up briefcase. Stan regaled me with tales of derms he had called on many years before.
“Ed Gillooly down in Scituate used to charge $7 a visit,” Stan told me. “I asked him why so little – this was back in the ’60s – and he said, ‘Phil Gluckstern charges 20 bucks a visit in his fancy downtown office, but he has to spend half an hour with a patient. I just see ’em, diagnose ’em, prescribe for ’em, and they’re out the door.’
“Dermatology wasn’t the high-class deal it’s gotten to be,” said Stan. “It was sort of out there. Every doctor had his own special lotion or concoction, his calling card. The local pharmacist knew how to mix it up, but of course would never share the secret formula.
“Nobody referred anybody to another doctor if they could help it. They were terrified they’d never see the patient back.
“It was all cash. There was no Medicare, no third parties. The money would get put into a shoebox, which would go into the doctor’s closet. A lot of offices were in the doc’s house. Sometimes a babysitter would go through the closet, and wouldn’t you know, but the next time the doc’s wife looked, last week’s receipts were gone.
“Secretaries? Doctors wouldn’t bother with them. Sometimes their mothers or wives, who knew as little about office management as they did, would come in and mess things up.”
This observation resonated. Almost 40 years ago, I took over what was left of Al Shipman’s practice when the old-timer (as he seemed to me then) retired to Florida.
Al’s office was a converted garage. Rummaging through a closet, he offered me ancient samples of sulfur-resorcinol acne lotions. Then he pulled out a well-thumbed Merck Manual from the 1930s, with the front cover missing. “I always found this useful,” he said. “You can have it if you want.” I politely declined.
“You young fellas spend money like it’s going out of style,” said Al. “You all think you need secretaries. Never had one!”
My reverie done, I focused back on Stan, who was saying, “Doctors in those days did pretty much everything themselves.
“For instance, Jack Vallis had about thirty chairs in his waiting room. Whenever Jack came out to call the next patient, everybody got up and moved over one chair.
“Once – I swear this actually happened – a patient came in with a severe laceration on his wrist; his damned arm was dangling half-off. But he had to sit down in the last chair and take his turn, same as anybody else.
“I used to call on non-derms too. We carried cortisone creams and antifungal creams, and they used to stop and ask me, ‘Now Stan, I put this fungus cream on the fungus and the cortisone cream on the eczema, am I right?’”
Some things indeed don’t change.
I guess it’s just human nature to pine for When patients (or their biopsy specimens) could go to any lab you sent them to.
Ah, wasn’t that the life? When patients paid you 10 bucks in cash and you stuffed it in your shoebox? When if they didn’t have cash, they sent you a roast turkey on Thanksgiving, or a dozen eggs, or maybe nothing at all?
If you’re the sentimental sort, you can wax nostalgic about those good old days if you want. But you’ll forgive me if I don’t join you.
Dr. Rockoff practices dermatology in Brookline, Mass., and is a longtime contributor to Dermatology News. He serves on the clinical faculty at Tufts University, Boston, and has taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at amazon.com and barnesandnoble.com. Write to him at [email protected].
How to make psychiatry residency more rewarding
During my residency, I have taken advantage of several opportunities that helped me develop and become more confident as I assumed the role of Academic Chief Resident in my final year of residency. In this article, I describe some of these opportunities, including seeking extra supervision while providing psychotherapy, engaging in psychotherapy for oneself, becoming part of leadership, and participating in quality improvement (QI) projects.
Obtain extra supervision while providing psychotherapy. I feel it is important to become comfortable with different types of therapy during residency. There are various opportunities to receive additional education via 1- and 2-year courses. I attended the Prelude t
Consider seeking out psychotherapy. When I started providing therapy to my patients, I became aware of how important it is to invest in your own personal therapy to understand your mind. I researched the importance of personal therapy for psychiatric clinicians, and to my surprise there have been lengthy debates on both its positive and negative impacts. However, I have come to believe that personal therapy is an important part of training for mental health professionals because it helps us better understand ourselves, since it is impossible to take the therapist’s mind out of the session. Although personal psychotherapy is not required, residency is an opportune time to pursue it.
Get involved and become part of leadership. I always believed that when united, we are stronger. It is a great privilege that as residents, we can become an integral part of advocacy and leadership in different organizations at both the state and national level. Here are 2 examples of how I got involved:
- The American Psychiatric Association (APA). When I attended the APA to present my posters for the first time, I wanted to become more actively involved. So I contacted my district branch representatives for guidance. I attended meetings and became involved in the Brooklyn District Branch as a resident representative. I was elected APA Area 2 Resident Fellow Member Deputy representative (a 2-year position). In this position, I represent residents and fellows from New York in the APA assembly. This has been a gratifying experience, and I have come to appreciate the proceedings of the Assembly and the amount of work that goes into creating Action Papers and Policy Statements.
- The Committee of Interns and Residents (CIR). Representation in CIR is extremely important in this political climate. The resident CIR Delegates are selected via elections. Delegates have an excellent opportunity to attend the Delegate Conference to learn how CIR operates and represent the department in CIR meetings. CIR is extremely supportive of resident involvement in QI projects and provides opportunities to chair a quality council for residents.
Participate in QI projects. Involvement in QI projects provided me with the opportunity to learn unique skills, including how to think creatively, design a study, and work with statisticians to extract and analyze data. The main focus of my research has been resident well-being and burnout.
These are a few of the wonderful opportunities I have been able to experience during my residency. I would love to hear from other residents about their similar experiences.
During my residency, I have taken advantage of several opportunities that helped me develop and become more confident as I assumed the role of Academic Chief Resident in my final year of residency. In this article, I describe some of these opportunities, including seeking extra supervision while providing psychotherapy, engaging in psychotherapy for oneself, becoming part of leadership, and participating in quality improvement (QI) projects.
Obtain extra supervision while providing psychotherapy. I feel it is important to become comfortable with different types of therapy during residency. There are various opportunities to receive additional education via 1- and 2-year courses. I attended the Prelude t
Consider seeking out psychotherapy. When I started providing therapy to my patients, I became aware of how important it is to invest in your own personal therapy to understand your mind. I researched the importance of personal therapy for psychiatric clinicians, and to my surprise there have been lengthy debates on both its positive and negative impacts. However, I have come to believe that personal therapy is an important part of training for mental health professionals because it helps us better understand ourselves, since it is impossible to take the therapist’s mind out of the session. Although personal psychotherapy is not required, residency is an opportune time to pursue it.
Get involved and become part of leadership. I always believed that when united, we are stronger. It is a great privilege that as residents, we can become an integral part of advocacy and leadership in different organizations at both the state and national level. Here are 2 examples of how I got involved:
- The American Psychiatric Association (APA). When I attended the APA to present my posters for the first time, I wanted to become more actively involved. So I contacted my district branch representatives for guidance. I attended meetings and became involved in the Brooklyn District Branch as a resident representative. I was elected APA Area 2 Resident Fellow Member Deputy representative (a 2-year position). In this position, I represent residents and fellows from New York in the APA assembly. This has been a gratifying experience, and I have come to appreciate the proceedings of the Assembly and the amount of work that goes into creating Action Papers and Policy Statements.
- The Committee of Interns and Residents (CIR). Representation in CIR is extremely important in this political climate. The resident CIR Delegates are selected via elections. Delegates have an excellent opportunity to attend the Delegate Conference to learn how CIR operates and represent the department in CIR meetings. CIR is extremely supportive of resident involvement in QI projects and provides opportunities to chair a quality council for residents.
Participate in QI projects. Involvement in QI projects provided me with the opportunity to learn unique skills, including how to think creatively, design a study, and work with statisticians to extract and analyze data. The main focus of my research has been resident well-being and burnout.
These are a few of the wonderful opportunities I have been able to experience during my residency. I would love to hear from other residents about their similar experiences.
During my residency, I have taken advantage of several opportunities that helped me develop and become more confident as I assumed the role of Academic Chief Resident in my final year of residency. In this article, I describe some of these opportunities, including seeking extra supervision while providing psychotherapy, engaging in psychotherapy for oneself, becoming part of leadership, and participating in quality improvement (QI) projects.
Obtain extra supervision while providing psychotherapy. I feel it is important to become comfortable with different types of therapy during residency. There are various opportunities to receive additional education via 1- and 2-year courses. I attended the Prelude t
Consider seeking out psychotherapy. When I started providing therapy to my patients, I became aware of how important it is to invest in your own personal therapy to understand your mind. I researched the importance of personal therapy for psychiatric clinicians, and to my surprise there have been lengthy debates on both its positive and negative impacts. However, I have come to believe that personal therapy is an important part of training for mental health professionals because it helps us better understand ourselves, since it is impossible to take the therapist’s mind out of the session. Although personal psychotherapy is not required, residency is an opportune time to pursue it.
Get involved and become part of leadership. I always believed that when united, we are stronger. It is a great privilege that as residents, we can become an integral part of advocacy and leadership in different organizations at both the state and national level. Here are 2 examples of how I got involved:
- The American Psychiatric Association (APA). When I attended the APA to present my posters for the first time, I wanted to become more actively involved. So I contacted my district branch representatives for guidance. I attended meetings and became involved in the Brooklyn District Branch as a resident representative. I was elected APA Area 2 Resident Fellow Member Deputy representative (a 2-year position). In this position, I represent residents and fellows from New York in the APA assembly. This has been a gratifying experience, and I have come to appreciate the proceedings of the Assembly and the amount of work that goes into creating Action Papers and Policy Statements.
- The Committee of Interns and Residents (CIR). Representation in CIR is extremely important in this political climate. The resident CIR Delegates are selected via elections. Delegates have an excellent opportunity to attend the Delegate Conference to learn how CIR operates and represent the department in CIR meetings. CIR is extremely supportive of resident involvement in QI projects and provides opportunities to chair a quality council for residents.
Participate in QI projects. Involvement in QI projects provided me with the opportunity to learn unique skills, including how to think creatively, design a study, and work with statisticians to extract and analyze data. The main focus of my research has been resident well-being and burnout.
These are a few of the wonderful opportunities I have been able to experience during my residency. I would love to hear from other residents about their similar experiences.

CDC Publishes Guideline for Diagnosing and Treating Pediatric mTBI
The CDC has developed a guideline for the diagnosis and management of mild traumatic brain injury (mTBI) in children. The guideline was published online ahead of print September 4 in JAMA Pediatrics. To support the “multifaceted approach” that the authors recommend for implementing the guideline, the CDC has created materials such as a screening tool, online training, fact sheets, patient discharge instructions, and symptom-based recovery tips.
The number of emergency department visits for mTBI has increased significantly during the past decade, said the authors, yet no evidence-based clinical guidelines had been drafted in the United States to guide the diagnosis, prognosis, and management of this condition. To fill this gap, the CDC established the Pediatric mTBI Guideline Workgroup, which drafted recommendations based on a systematic review of research published from January 1990 through July 2015.
Diagnosis
The first section of the guideline offers recommendations for diagnosis. Health care professionals should not routinely obtain head CT in children with suspected mTBI, say the authors. They should, however, use validated clinical decision rules to identify children with mTBI at low risk for intracranial injury in whom CT is not indicated, as well as children at higher risk for intracranial injury for whom CT may be warranted. The authors cite the Pediatric Emergency Care Applied Research Network (PECARN) decision rules as an example.
Furthermore, health care professionals should not routinely use brain MRI to evaluate suspected or diagnosed mTBI in children, according to the guideline. No study examining whether this imaging technique is appropriate met the workgroup’s inclusion criteria.
An age-appropriate, validated symptom rating scale should be one component of the diagnostic evaluation, say the authors. The Standardized Assessment of Concussion, however, “should not be exclusively used to diagnose mTBI in children aged 6 to 18,” they add. Finally, the guideline discourages the use of biomarkers (ie, serum markers) for diagnosis outside of a research setting.
Prognosis
The second section of the document provides guidance on developing a prognosis. Clinicians should advise patients and their families that most children with mTBI do not have significant difficulties that last for more than one to three months after injury, say the authors. They also should state that even though certain factors predict a child’s risk for prolonged symptoms, “each child’s recovery from mTBI is unique and will follow its own trajectory.”
Health care professionals should evaluate a child’s premorbid history as soon as possible to help determine the prognosis, say the authors. Children and families should be advised that factors such as history of mTBI, lower cognitive ability, and neurologic disorder can delay recovery from mTBI. Clinicians should screen for known risk factors for persistent symptoms and use a combination of tools (eg, validated symptom scales, cognitive testing, and balance testing) to assess recovery, according to the guideline.
Children with mTBI at high risk for persistent symptoms should be monitored closely. “For children with mTBI whose symptoms do not resolve as expected with standard care (ie, within four to six weeks), health care professionals should provide or refer for appropriate assessments and interventions,” say the authors.
Management and Treatment
The guideline’s section devoted to management and treatment begins with recommendations for returning to normal activities. Clinicians should recommend restricting physical and cognitive activity during the first several days after pediatric mTBI, according to the authors. After that point, doctors should advise patients and families “to resume a gradual schedule of activity that does not exacerbate symptoms, with close monitoring of symptom expression.” If the patient completes this step successfully, the clinician should offer an active rehabilitation program that progressively reintroduces noncontact aerobic activity that does not worsen symptoms. The number and severity of symptoms should be monitored closely throughout the patient’s recovery. A patient should resume full activity when his or her performance returns to its premorbid level, provided that he or she has no symptoms at rest or with increasing levels of exertion, according to the guideline.
“To assist children returning to school after mTBI, medical and school-based teams should counsel the student and family regarding the process of gradually increasing the duration and intensity of academic activities as tolerated, with the goal of increasing participation without significantly exacerbating symptoms,” say the authors. Return-to-school protocols should be adapted to the severity of the child’s postconcussion symptoms. School personnel should assess the need for additional educational support in students with prolonged symptoms that harm their academic performance, according to the guideline.
If a child with mTBI develops severe headache, especially if the headache is associated with other risk factors or has worsened after mTBI, emergency department professionals should observe him or her and consider obtaining a head CT to evaluate for intracranial injury, say the authors. Health care professionals should explain proper sleep hygiene to all patients with mTBI and their families to facilitate recovery.
If a child with mTBI has cognitive dysfunction, clinicians should attempt to determine its etiology within the context of other mTBI symptoms, say the authors. Treatment for cognitive dysfunction should reflect its presumed etiology, they conclude.
—Erik Greb
Suggested Reading
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Diagnosis and management of mild traumatic brain injury in children: a systematic review. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
McCrea M, Manley G. State of the science on pediatric mild traumatic brain injury: progress toward clinical translation. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
The CDC has developed a guideline for the diagnosis and management of mild traumatic brain injury (mTBI) in children. The guideline was published online ahead of print September 4 in JAMA Pediatrics. To support the “multifaceted approach” that the authors recommend for implementing the guideline, the CDC has created materials such as a screening tool, online training, fact sheets, patient discharge instructions, and symptom-based recovery tips.
The number of emergency department visits for mTBI has increased significantly during the past decade, said the authors, yet no evidence-based clinical guidelines had been drafted in the United States to guide the diagnosis, prognosis, and management of this condition. To fill this gap, the CDC established the Pediatric mTBI Guideline Workgroup, which drafted recommendations based on a systematic review of research published from January 1990 through July 2015.
Diagnosis
The first section of the guideline offers recommendations for diagnosis. Health care professionals should not routinely obtain head CT in children with suspected mTBI, say the authors. They should, however, use validated clinical decision rules to identify children with mTBI at low risk for intracranial injury in whom CT is not indicated, as well as children at higher risk for intracranial injury for whom CT may be warranted. The authors cite the Pediatric Emergency Care Applied Research Network (PECARN) decision rules as an example.
Furthermore, health care professionals should not routinely use brain MRI to evaluate suspected or diagnosed mTBI in children, according to the guideline. No study examining whether this imaging technique is appropriate met the workgroup’s inclusion criteria.
An age-appropriate, validated symptom rating scale should be one component of the diagnostic evaluation, say the authors. The Standardized Assessment of Concussion, however, “should not be exclusively used to diagnose mTBI in children aged 6 to 18,” they add. Finally, the guideline discourages the use of biomarkers (ie, serum markers) for diagnosis outside of a research setting.
Prognosis
The second section of the document provides guidance on developing a prognosis. Clinicians should advise patients and their families that most children with mTBI do not have significant difficulties that last for more than one to three months after injury, say the authors. They also should state that even though certain factors predict a child’s risk for prolonged symptoms, “each child’s recovery from mTBI is unique and will follow its own trajectory.”
Health care professionals should evaluate a child’s premorbid history as soon as possible to help determine the prognosis, say the authors. Children and families should be advised that factors such as history of mTBI, lower cognitive ability, and neurologic disorder can delay recovery from mTBI. Clinicians should screen for known risk factors for persistent symptoms and use a combination of tools (eg, validated symptom scales, cognitive testing, and balance testing) to assess recovery, according to the guideline.
Children with mTBI at high risk for persistent symptoms should be monitored closely. “For children with mTBI whose symptoms do not resolve as expected with standard care (ie, within four to six weeks), health care professionals should provide or refer for appropriate assessments and interventions,” say the authors.
Management and Treatment
The guideline’s section devoted to management and treatment begins with recommendations for returning to normal activities. Clinicians should recommend restricting physical and cognitive activity during the first several days after pediatric mTBI, according to the authors. After that point, doctors should advise patients and families “to resume a gradual schedule of activity that does not exacerbate symptoms, with close monitoring of symptom expression.” If the patient completes this step successfully, the clinician should offer an active rehabilitation program that progressively reintroduces noncontact aerobic activity that does not worsen symptoms. The number and severity of symptoms should be monitored closely throughout the patient’s recovery. A patient should resume full activity when his or her performance returns to its premorbid level, provided that he or she has no symptoms at rest or with increasing levels of exertion, according to the guideline.
“To assist children returning to school after mTBI, medical and school-based teams should counsel the student and family regarding the process of gradually increasing the duration and intensity of academic activities as tolerated, with the goal of increasing participation without significantly exacerbating symptoms,” say the authors. Return-to-school protocols should be adapted to the severity of the child’s postconcussion symptoms. School personnel should assess the need for additional educational support in students with prolonged symptoms that harm their academic performance, according to the guideline.
If a child with mTBI develops severe headache, especially if the headache is associated with other risk factors or has worsened after mTBI, emergency department professionals should observe him or her and consider obtaining a head CT to evaluate for intracranial injury, say the authors. Health care professionals should explain proper sleep hygiene to all patients with mTBI and their families to facilitate recovery.
If a child with mTBI has cognitive dysfunction, clinicians should attempt to determine its etiology within the context of other mTBI symptoms, say the authors. Treatment for cognitive dysfunction should reflect its presumed etiology, they conclude.
—Erik Greb
Suggested Reading
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Diagnosis and management of mild traumatic brain injury in children: a systematic review. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
McCrea M, Manley G. State of the science on pediatric mild traumatic brain injury: progress toward clinical translation. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
The CDC has developed a guideline for the diagnosis and management of mild traumatic brain injury (mTBI) in children. The guideline was published online ahead of print September 4 in JAMA Pediatrics. To support the “multifaceted approach” that the authors recommend for implementing the guideline, the CDC has created materials such as a screening tool, online training, fact sheets, patient discharge instructions, and symptom-based recovery tips.
The number of emergency department visits for mTBI has increased significantly during the past decade, said the authors, yet no evidence-based clinical guidelines had been drafted in the United States to guide the diagnosis, prognosis, and management of this condition. To fill this gap, the CDC established the Pediatric mTBI Guideline Workgroup, which drafted recommendations based on a systematic review of research published from January 1990 through July 2015.
Diagnosis
The first section of the guideline offers recommendations for diagnosis. Health care professionals should not routinely obtain head CT in children with suspected mTBI, say the authors. They should, however, use validated clinical decision rules to identify children with mTBI at low risk for intracranial injury in whom CT is not indicated, as well as children at higher risk for intracranial injury for whom CT may be warranted. The authors cite the Pediatric Emergency Care Applied Research Network (PECARN) decision rules as an example.
Furthermore, health care professionals should not routinely use brain MRI to evaluate suspected or diagnosed mTBI in children, according to the guideline. No study examining whether this imaging technique is appropriate met the workgroup’s inclusion criteria.
An age-appropriate, validated symptom rating scale should be one component of the diagnostic evaluation, say the authors. The Standardized Assessment of Concussion, however, “should not be exclusively used to diagnose mTBI in children aged 6 to 18,” they add. Finally, the guideline discourages the use of biomarkers (ie, serum markers) for diagnosis outside of a research setting.
Prognosis
The second section of the document provides guidance on developing a prognosis. Clinicians should advise patients and their families that most children with mTBI do not have significant difficulties that last for more than one to three months after injury, say the authors. They also should state that even though certain factors predict a child’s risk for prolonged symptoms, “each child’s recovery from mTBI is unique and will follow its own trajectory.”
Health care professionals should evaluate a child’s premorbid history as soon as possible to help determine the prognosis, say the authors. Children and families should be advised that factors such as history of mTBI, lower cognitive ability, and neurologic disorder can delay recovery from mTBI. Clinicians should screen for known risk factors for persistent symptoms and use a combination of tools (eg, validated symptom scales, cognitive testing, and balance testing) to assess recovery, according to the guideline.
Children with mTBI at high risk for persistent symptoms should be monitored closely. “For children with mTBI whose symptoms do not resolve as expected with standard care (ie, within four to six weeks), health care professionals should provide or refer for appropriate assessments and interventions,” say the authors.
Management and Treatment
The guideline’s section devoted to management and treatment begins with recommendations for returning to normal activities. Clinicians should recommend restricting physical and cognitive activity during the first several days after pediatric mTBI, according to the authors. After that point, doctors should advise patients and families “to resume a gradual schedule of activity that does not exacerbate symptoms, with close monitoring of symptom expression.” If the patient completes this step successfully, the clinician should offer an active rehabilitation program that progressively reintroduces noncontact aerobic activity that does not worsen symptoms. The number and severity of symptoms should be monitored closely throughout the patient’s recovery. A patient should resume full activity when his or her performance returns to its premorbid level, provided that he or she has no symptoms at rest or with increasing levels of exertion, according to the guideline.
“To assist children returning to school after mTBI, medical and school-based teams should counsel the student and family regarding the process of gradually increasing the duration and intensity of academic activities as tolerated, with the goal of increasing participation without significantly exacerbating symptoms,” say the authors. Return-to-school protocols should be adapted to the severity of the child’s postconcussion symptoms. School personnel should assess the need for additional educational support in students with prolonged symptoms that harm their academic performance, according to the guideline.
If a child with mTBI develops severe headache, especially if the headache is associated with other risk factors or has worsened after mTBI, emergency department professionals should observe him or her and consider obtaining a head CT to evaluate for intracranial injury, say the authors. Health care professionals should explain proper sleep hygiene to all patients with mTBI and their families to facilitate recovery.
If a child with mTBI has cognitive dysfunction, clinicians should attempt to determine its etiology within the context of other mTBI symptoms, say the authors. Treatment for cognitive dysfunction should reflect its presumed etiology, they conclude.
—Erik Greb
Suggested Reading
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Centers for Disease Control and Prevention guideline on the diagnosis and management of mild traumatic brain injury among children. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
Lumba-Brown A, Yeates KO, Sarmiento K, et al. Diagnosis and management of mild traumatic brain injury in children: a systematic review. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
McCrea M, Manley G. State of the science on pediatric mild traumatic brain injury: progress toward clinical translation. JAMA Pediatr. 2018 Sep 4 [Epub ahead of print].
Embracing therapeutic silence: A resident’s perspective on learning psychotherapy
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
There is a tendency among young psychiatric residents, including me, to experience significant anxiety when providing outpatient psychotherapy for the first time. This anxiety often leads to rigid adherence to structured sessions aimed at a specific therapeutic target. Unfortunately, as patients begin to stray from the mold, this model breaks down and leaves the resident with little direction.
As a resident with an engineering background, I felt a strong affinity for this targeted approach, and have struggled for direction with patients whose symptoms or willingness to engage therapeutically did not match this method. I have slowly come to appreciate a more nimble approach that balances elements of both a structured method (such as cognitive-behavioral therapy [CBT]) with more free-flowing psychoanalytic techniques. This approach is based on several principles, including relinquishing a desire for a grand therapeutic arc, gaining comfort with silence, and, finally, allowing the patient to do the work.
Perhaps the most difficult part of this evolving realization is learning to resist the desire for an overarching path from session to session. As a novice therapist, I struggled with the apparent disconnect from session to session, and attempted to force this need for a therapeutic arc on each subsequent visit. This meant that rather than meeting the patient in his or her current state, I was forever reaching to the past, attempting to create a link between what was discussed previously to the topic of today’s session. While some patients readily identified with the concepts of CBT—where maladaptive cognitions are identified and challenged via reflection on past progress—there was another subset of patients who seemed unwilling to do so.
In his Notes On Memory and Desire,1 psychoanalyst Wilfred Bion proclaimed, “Do not remember past sessions.” As I discussed this concept in psychotherapy supervision, I began to understand the value of a less directed approach, and to try it with patients. I soon discovered interactions were more rewarding, and I gained a deeper understanding than I had before. Without a formulaic approach, patients were free to give voice to any issue, whether or not it conformed to their perceived “chief complaint.” It was refreshing to see the work progress over time as we began to slowly integrate the seemingly disparate themes of each session.
In addition to the naive idea of forcing a formulaic arc on the therapeutic process, I felt a strong desire for tangible results. Perhaps it was my engineering side yearning for the quantifiable, but nonetheless, I fell into the trap of trying to push patients to gain insights they may have not been ready to make. This led to dissatisfaction on both sides. I was reminded of another directive from Bion: “Desires for results, cure, or even understanding must not be allowed to proliferate.”1 It was interesting: the less I focused on results, the more patients began to open up and explore. By using their present experiences to examine patterns of behavior, we were able to slowly reach new levels of understanding.
The corollary to gaining comfort with relinquishing my desire for results was gaining comfort with silence and learning to meet patients where they are. The concept of using nonverbal cues to communicate is not a novel one. However, the idea that one might communicate by doing nothing at all is somewhat profound. I began to explore the use of silence with my patients, and have found an unknown richness that was previously hidden by my own tendency to interject. Psychotherapist Mark Epstein wrote, “When a therapist can sit with a patient without an agenda, without trying to force an experience, without thinking that she knows what is going to happen or who this person is…when he falls silent…the possibility of some real, spontaneous, unscripted communication exists.”2 Sitting in silence and allowing my patients to grow in their own insight has given them a sense of empowerment and mastery, and has greatly enriched our sessions.
Psychotherapy is not an easy thing for most embryonic psychiatrists or therapists, and many cling to formulaic methods because such methods are an easy approach. Initially, I, too, clung to this rigid approach, but it ultimately left me unfulfilled. I have learned to be more nimble, embrace silence, and relinquish my desire for results. I was initially uncomfortable with this unstructured model of psychotherapeutic interaction, preferring the more concrete thinking I had come to expect from engineering. It is likely that few residents will share this unique background, and thus may not struggle as I have, but I believe that the process of adaptation and change is relevant to all. As a young psychiatrist, I have gained much joy from being able to work with patients in psychotherapy. It is my hope that other young trainees, regardless of background, will learn to let go of their preconceived ideas and embrace change, for it is only through change that we grow.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.
1. Bion WR. Wilfred R. Bion: notes on memory and desire. In: Aguayo J, Malin B, eds. Wilfred Bion: Los Angeles seminars and supervision. London, UK: Karnac; 2013:136-138.
2. Epstein M. Remembering. In: Thoughts without a thinker. New York, NY: Basic Books; 1995:187-189.

Slowing down
This past Labor Day weekend, I did something radical. I slowed down. Way down. My wife slowed down with me, which helped. We spent the weekend close to home walking, talking, reading, contemplating, planning, assessing, doing puzzles and crosswords, and imbibing a craft beer or two, slowly, of course. Why? Because of Adam Grant, PhD, the organizational psychologist at the University of Pennsylvania’s Wharton School of Business, Philadelphia. I had recently reread his 2016 book I’m a big fan; he’s one of those professors who makes you fervently wish you were a student again, someone who will provoke you and challenge your way of thinking.
Dr. Grant’s basic premise, which he has proved through research, is that procrastination boosts productivity. Here’s how: Let’s say you’re facing a challenge or difficult task. He says to start working on it immediately, then take some time away for reflection. This “quick to start and slow to finish” method allows your brain to continually percolate on the problem. An incomplete task stays partially active in your brain. When you come back to it you often see it with fresh eyes. You will experience your highest productivity when you are toggling between these two modes.
This makes sense, and Dr. Grant cites numerous examples from Leonardo da Vinci to the founders of Warby-Parker, as examples of success. But how can it benefit physicians? Many of us are “precrastinators,” people who tend to complete or at least begin tasks as soon as possible, even when it’s unnecessary or not urgent. Unlike some jobs in which it’s easier to take a break from a project and return to it with more creative solutions, we often are racing against a clock to see more patients, read more slides, answer more emails, and make more phone calls. We are perpetually frenetic, which is not conducive to original thinking.
If this sounds like you, then you are likely to benefit from deliberate procrastination. Here are a few ways to slow down:
- Put it on your calendar. Yes, I see the irony, but it works. Start by scheduling one hour a week where you are to accomplish nothing. You can fill this time with whatever your mind wants to do at that moment.
- When faced with a diagnostic dilemma or treatment failure, resist the urge to solve that problem in that moment. Save that note for later, tell the patient you will call him back or bring him back for a visit later. Even if you’re not actively working on it, it will incubate somewhere in your brain, allowing more divergent thought processes to take over. It’s a little like trying to solve a crossword that seems impossible in the moment and then answers suddenly appear without effort.
- Take up a hobby: Play the guitar, learn to make pasta, climb a big rock. When you are fully engaged in such pursuits it requires complete mental focus. When you revisit the difficult problem you’re working on, you will likely see it from different perspectives.
- Meditate: Meditation requires our brains and bodies to slow down. It can help reduce self-doubt and criticism which stifle problem solving.
- Watch Slow TV. Slow TV is a Scandinavian phenomenon where you sit and watch meditative video such as a 7-hour train cam from Bergen, Norway, to Oslo. There’s no dialogue, no plot, no commercials. It’s just 7 hours of track and train and is weirdly comforting.

If you want to learn more, then when you get a chance, Google “slow living” and explore. Of course, some of you precrastinators probably have already started before finishing this column.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
This past Labor Day weekend, I did something radical. I slowed down. Way down. My wife slowed down with me, which helped. We spent the weekend close to home walking, talking, reading, contemplating, planning, assessing, doing puzzles and crosswords, and imbibing a craft beer or two, slowly, of course. Why? Because of Adam Grant, PhD, the organizational psychologist at the University of Pennsylvania’s Wharton School of Business, Philadelphia. I had recently reread his 2016 book I’m a big fan; he’s one of those professors who makes you fervently wish you were a student again, someone who will provoke you and challenge your way of thinking.
Dr. Grant’s basic premise, which he has proved through research, is that procrastination boosts productivity. Here’s how: Let’s say you’re facing a challenge or difficult task. He says to start working on it immediately, then take some time away for reflection. This “quick to start and slow to finish” method allows your brain to continually percolate on the problem. An incomplete task stays partially active in your brain. When you come back to it you often see it with fresh eyes. You will experience your highest productivity when you are toggling between these two modes.
This makes sense, and Dr. Grant cites numerous examples from Leonardo da Vinci to the founders of Warby-Parker, as examples of success. But how can it benefit physicians? Many of us are “precrastinators,” people who tend to complete or at least begin tasks as soon as possible, even when it’s unnecessary or not urgent. Unlike some jobs in which it’s easier to take a break from a project and return to it with more creative solutions, we often are racing against a clock to see more patients, read more slides, answer more emails, and make more phone calls. We are perpetually frenetic, which is not conducive to original thinking.
If this sounds like you, then you are likely to benefit from deliberate procrastination. Here are a few ways to slow down:
- Put it on your calendar. Yes, I see the irony, but it works. Start by scheduling one hour a week where you are to accomplish nothing. You can fill this time with whatever your mind wants to do at that moment.
- When faced with a diagnostic dilemma or treatment failure, resist the urge to solve that problem in that moment. Save that note for later, tell the patient you will call him back or bring him back for a visit later. Even if you’re not actively working on it, it will incubate somewhere in your brain, allowing more divergent thought processes to take over. It’s a little like trying to solve a crossword that seems impossible in the moment and then answers suddenly appear without effort.
- Take up a hobby: Play the guitar, learn to make pasta, climb a big rock. When you are fully engaged in such pursuits it requires complete mental focus. When you revisit the difficult problem you’re working on, you will likely see it from different perspectives.
- Meditate: Meditation requires our brains and bodies to slow down. It can help reduce self-doubt and criticism which stifle problem solving.
- Watch Slow TV. Slow TV is a Scandinavian phenomenon where you sit and watch meditative video such as a 7-hour train cam from Bergen, Norway, to Oslo. There’s no dialogue, no plot, no commercials. It’s just 7 hours of track and train and is weirdly comforting.
If you want to learn more, then when you get a chance, Google “slow living” and explore. Of course, some of you precrastinators probably have already started before finishing this column.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
This past Labor Day weekend, I did something radical. I slowed down. Way down. My wife slowed down with me, which helped. We spent the weekend close to home walking, talking, reading, contemplating, planning, assessing, doing puzzles and crosswords, and imbibing a craft beer or two, slowly, of course. Why? Because of Adam Grant, PhD, the organizational psychologist at the University of Pennsylvania’s Wharton School of Business, Philadelphia. I had recently reread his 2016 book I’m a big fan; he’s one of those professors who makes you fervently wish you were a student again, someone who will provoke you and challenge your way of thinking.
Dr. Grant’s basic premise, which he has proved through research, is that procrastination boosts productivity. Here’s how: Let’s say you’re facing a challenge or difficult task. He says to start working on it immediately, then take some time away for reflection. This “quick to start and slow to finish” method allows your brain to continually percolate on the problem. An incomplete task stays partially active in your brain. When you come back to it you often see it with fresh eyes. You will experience your highest productivity when you are toggling between these two modes.
This makes sense, and Dr. Grant cites numerous examples from Leonardo da Vinci to the founders of Warby-Parker, as examples of success. But how can it benefit physicians? Many of us are “precrastinators,” people who tend to complete or at least begin tasks as soon as possible, even when it’s unnecessary or not urgent. Unlike some jobs in which it’s easier to take a break from a project and return to it with more creative solutions, we often are racing against a clock to see more patients, read more slides, answer more emails, and make more phone calls. We are perpetually frenetic, which is not conducive to original thinking.
If this sounds like you, then you are likely to benefit from deliberate procrastination. Here are a few ways to slow down:
- Put it on your calendar. Yes, I see the irony, but it works. Start by scheduling one hour a week where you are to accomplish nothing. You can fill this time with whatever your mind wants to do at that moment.
- When faced with a diagnostic dilemma or treatment failure, resist the urge to solve that problem in that moment. Save that note for later, tell the patient you will call him back or bring him back for a visit later. Even if you’re not actively working on it, it will incubate somewhere in your brain, allowing more divergent thought processes to take over. It’s a little like trying to solve a crossword that seems impossible in the moment and then answers suddenly appear without effort.
- Take up a hobby: Play the guitar, learn to make pasta, climb a big rock. When you are fully engaged in such pursuits it requires complete mental focus. When you revisit the difficult problem you’re working on, you will likely see it from different perspectives.
- Meditate: Meditation requires our brains and bodies to slow down. It can help reduce self-doubt and criticism which stifle problem solving.
- Watch Slow TV. Slow TV is a Scandinavian phenomenon where you sit and watch meditative video such as a 7-hour train cam from Bergen, Norway, to Oslo. There’s no dialogue, no plot, no commercials. It’s just 7 hours of track and train and is weirdly comforting.
If you want to learn more, then when you get a chance, Google “slow living” and explore. Of course, some of you precrastinators probably have already started before finishing this column.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at [email protected].
Burnout may jeopardize patient care
because of depersonalization of care, according to recent research published in JAMA Internal Medicine.

“The primary conclusion of this review is that physician burnout might jeopardize patient care,” Maria Panagioti, PhD, from the National Institute for Health Research (NIHR) School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre at the University of Manchester (United Kingdom) and her colleagues wrote in their study. “Physician wellness and quality of patient care are critical [as are] complementary dimensions of health care organization efficiency.”
Dr. Panagioti and her colleagues performed a search of the MEDLINE, EMBASE, CINAHL, and PsycInfo databases and found 47 eligible studies on the topics of physician burnout and patient care, which altogether included data from a pooled cohort of 42,473 physicians. The physicians were median 38 years old, with 44.7% of studies looking at physicians in residency or early career (up to 5 years post residency) and 55.3% of studies examining experienced physicians. The meta-analysis also evaluated physicians in a hospital setting (63.8%), primary care (13.8%), and across various different health care settings (8.5%).
The researchers found physicians with burnout were significantly associated with higher rates of patient safety issues (odds ratio, 1.96; 95% confidence interval, 1.59-2.40), reduced patient satisfaction (OR, 2.28; 95% CI, 1.42-3.68), and lower quality of care (OR, 2.31; 95% CI, 1.87-2.85). System-reported instances of patient safety issues and low professionalism were not statistically significant, but the subgroup differences did reach statistical significance (Cohen Q, 8.14; P = .007). Among residents and physicians in their early career, there was a greater association between burnout and low professionalism (OR, 3.39; 95% CI, 2.38-4.40), compared with physicians in the middle or later in their career (OR, 1.73; 95% CI, 1.46-2.01; Cohen Q, 7.27; P = .003).
“Investments in organizational strategies to jointly monitor and improve physician wellness and patient care outcomes are needed,” Dr. Panagioti and her colleagues wrote in the study. “Interventions aimed at improving the culture of health care organizations, as well as interventions focused on individual physicians but supported and funded by health care organizations, are beneficial.”
Researchers noted the study quality was low to moderate. Variation in outcomes across studies, heterogeneity among studies, potential selection bias by excluding gray literature, and the inability to establish causal links from findings because of the cross-sectional nature of the studies analyzed were potential limitations in the study, they reported.
The study was funded by the United Kingdom NIHR School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre. The authors report no relevant conflicts of interest.
SOURCE: Panagioti M et al. JAMA Intern Med. 2018 Sept 4. doi: 10.1001/jamainternmed.2018.3713.
Because of a lack of funding for research into burnout and the immediate need for change based on the effect it has on patient care seen in Pangioti et al., the question of how to address physician burnout should be answered with quality improvement programs aimed at making immediate changes in health care settings, Mark Linzer, MD, wrote in a related editorial.
“Resonating with these concepts, I propose that, for the burnout prevention and wellness field, we encourage quality improvement projects of high standards: multiple sites, concurrent control groups, longitudinal design, and blinding when feasible, with assessment of outcomes and costs,” he wrote. “These studies can point us toward what we will evaluate in larger trials and allow a place for the rapidly developing information base to be viewed and thus become part of the developing science of work conditions, burnout reduction, and the anticipated result on quality and safety.”
There are research questions that have yet to be answered on this topic, he added, such as to what extent do factors like workflow redesign, use and upkeep of electronic medical records, and chaotic workplaces affect burnout. Further, regulatory environments may play a role, and it is still not known whether reducing burnout among physicians will also reduce burnout among staff. Future studies should also look at how burnout affects trainees and female physicians, he suggested.
“The link between burnout and adverse patient outcomes is stronger, thanks to the work of Panagioti and colleagues,” Dr. Linzer said. “With close to half of U.S. physicians experiencing symptoms of burnout, more work is needed to understand how to reduce it and what we can expect from doing so.”
Dr. Linzer is from the Hennepin Healthcare Systems in Minneapolis. These comments summarize his editorial regarding the findings of Pangioti et al. He reported support for Wellness Champion training by the American College of Physicians and the Association of Chiefs and Leaders in General Internal Medicine and that he has received support for American Medical Association research projects.
Because of a lack of funding for research into burnout and the immediate need for change based on the effect it has on patient care seen in Pangioti et al., the question of how to address physician burnout should be answered with quality improvement programs aimed at making immediate changes in health care settings, Mark Linzer, MD, wrote in a related editorial.
“Resonating with these concepts, I propose that, for the burnout prevention and wellness field, we encourage quality improvement projects of high standards: multiple sites, concurrent control groups, longitudinal design, and blinding when feasible, with assessment of outcomes and costs,” he wrote. “These studies can point us toward what we will evaluate in larger trials and allow a place for the rapidly developing information base to be viewed and thus become part of the developing science of work conditions, burnout reduction, and the anticipated result on quality and safety.”
There are research questions that have yet to be answered on this topic, he added, such as to what extent do factors like workflow redesign, use and upkeep of electronic medical records, and chaotic workplaces affect burnout. Further, regulatory environments may play a role, and it is still not known whether reducing burnout among physicians will also reduce burnout among staff. Future studies should also look at how burnout affects trainees and female physicians, he suggested.
“The link between burnout and adverse patient outcomes is stronger, thanks to the work of Panagioti and colleagues,” Dr. Linzer said. “With close to half of U.S. physicians experiencing symptoms of burnout, more work is needed to understand how to reduce it and what we can expect from doing so.”
Dr. Linzer is from the Hennepin Healthcare Systems in Minneapolis. These comments summarize his editorial regarding the findings of Pangioti et al. He reported support for Wellness Champion training by the American College of Physicians and the Association of Chiefs and Leaders in General Internal Medicine and that he has received support for American Medical Association research projects.
Because of a lack of funding for research into burnout and the immediate need for change based on the effect it has on patient care seen in Pangioti et al., the question of how to address physician burnout should be answered with quality improvement programs aimed at making immediate changes in health care settings, Mark Linzer, MD, wrote in a related editorial.
“Resonating with these concepts, I propose that, for the burnout prevention and wellness field, we encourage quality improvement projects of high standards: multiple sites, concurrent control groups, longitudinal design, and blinding when feasible, with assessment of outcomes and costs,” he wrote. “These studies can point us toward what we will evaluate in larger trials and allow a place for the rapidly developing information base to be viewed and thus become part of the developing science of work conditions, burnout reduction, and the anticipated result on quality and safety.”
There are research questions that have yet to be answered on this topic, he added, such as to what extent do factors like workflow redesign, use and upkeep of electronic medical records, and chaotic workplaces affect burnout. Further, regulatory environments may play a role, and it is still not known whether reducing burnout among physicians will also reduce burnout among staff. Future studies should also look at how burnout affects trainees and female physicians, he suggested.
“The link between burnout and adverse patient outcomes is stronger, thanks to the work of Panagioti and colleagues,” Dr. Linzer said. “With close to half of U.S. physicians experiencing symptoms of burnout, more work is needed to understand how to reduce it and what we can expect from doing so.”
Dr. Linzer is from the Hennepin Healthcare Systems in Minneapolis. These comments summarize his editorial regarding the findings of Pangioti et al. He reported support for Wellness Champion training by the American College of Physicians and the Association of Chiefs and Leaders in General Internal Medicine and that he has received support for American Medical Association research projects.
because of depersonalization of care, according to recent research published in JAMA Internal Medicine.
“The primary conclusion of this review is that physician burnout might jeopardize patient care,” Maria Panagioti, PhD, from the National Institute for Health Research (NIHR) School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre at the University of Manchester (United Kingdom) and her colleagues wrote in their study. “Physician wellness and quality of patient care are critical [as are] complementary dimensions of health care organization efficiency.”
Dr. Panagioti and her colleagues performed a search of the MEDLINE, EMBASE, CINAHL, and PsycInfo databases and found 47 eligible studies on the topics of physician burnout and patient care, which altogether included data from a pooled cohort of 42,473 physicians. The physicians were median 38 years old, with 44.7% of studies looking at physicians in residency or early career (up to 5 years post residency) and 55.3% of studies examining experienced physicians. The meta-analysis also evaluated physicians in a hospital setting (63.8%), primary care (13.8%), and across various different health care settings (8.5%).
The researchers found physicians with burnout were significantly associated with higher rates of patient safety issues (odds ratio, 1.96; 95% confidence interval, 1.59-2.40), reduced patient satisfaction (OR, 2.28; 95% CI, 1.42-3.68), and lower quality of care (OR, 2.31; 95% CI, 1.87-2.85). System-reported instances of patient safety issues and low professionalism were not statistically significant, but the subgroup differences did reach statistical significance (Cohen Q, 8.14; P = .007). Among residents and physicians in their early career, there was a greater association between burnout and low professionalism (OR, 3.39; 95% CI, 2.38-4.40), compared with physicians in the middle or later in their career (OR, 1.73; 95% CI, 1.46-2.01; Cohen Q, 7.27; P = .003).
“Investments in organizational strategies to jointly monitor and improve physician wellness and patient care outcomes are needed,” Dr. Panagioti and her colleagues wrote in the study. “Interventions aimed at improving the culture of health care organizations, as well as interventions focused on individual physicians but supported and funded by health care organizations, are beneficial.”
Researchers noted the study quality was low to moderate. Variation in outcomes across studies, heterogeneity among studies, potential selection bias by excluding gray literature, and the inability to establish causal links from findings because of the cross-sectional nature of the studies analyzed were potential limitations in the study, they reported.
The study was funded by the United Kingdom NIHR School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre. The authors report no relevant conflicts of interest.
SOURCE: Panagioti M et al. JAMA Intern Med. 2018 Sept 4. doi: 10.1001/jamainternmed.2018.3713.
because of depersonalization of care, according to recent research published in JAMA Internal Medicine.
“The primary conclusion of this review is that physician burnout might jeopardize patient care,” Maria Panagioti, PhD, from the National Institute for Health Research (NIHR) School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre at the University of Manchester (United Kingdom) and her colleagues wrote in their study. “Physician wellness and quality of patient care are critical [as are] complementary dimensions of health care organization efficiency.”
Dr. Panagioti and her colleagues performed a search of the MEDLINE, EMBASE, CINAHL, and PsycInfo databases and found 47 eligible studies on the topics of physician burnout and patient care, which altogether included data from a pooled cohort of 42,473 physicians. The physicians were median 38 years old, with 44.7% of studies looking at physicians in residency or early career (up to 5 years post residency) and 55.3% of studies examining experienced physicians. The meta-analysis also evaluated physicians in a hospital setting (63.8%), primary care (13.8%), and across various different health care settings (8.5%).
The researchers found physicians with burnout were significantly associated with higher rates of patient safety issues (odds ratio, 1.96; 95% confidence interval, 1.59-2.40), reduced patient satisfaction (OR, 2.28; 95% CI, 1.42-3.68), and lower quality of care (OR, 2.31; 95% CI, 1.87-2.85). System-reported instances of patient safety issues and low professionalism were not statistically significant, but the subgroup differences did reach statistical significance (Cohen Q, 8.14; P = .007). Among residents and physicians in their early career, there was a greater association between burnout and low professionalism (OR, 3.39; 95% CI, 2.38-4.40), compared with physicians in the middle or later in their career (OR, 1.73; 95% CI, 1.46-2.01; Cohen Q, 7.27; P = .003).
“Investments in organizational strategies to jointly monitor and improve physician wellness and patient care outcomes are needed,” Dr. Panagioti and her colleagues wrote in the study. “Interventions aimed at improving the culture of health care organizations, as well as interventions focused on individual physicians but supported and funded by health care organizations, are beneficial.”
Researchers noted the study quality was low to moderate. Variation in outcomes across studies, heterogeneity among studies, potential selection bias by excluding gray literature, and the inability to establish causal links from findings because of the cross-sectional nature of the studies analyzed were potential limitations in the study, they reported.
The study was funded by the United Kingdom NIHR School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre. The authors report no relevant conflicts of interest.
SOURCE: Panagioti M et al. JAMA Intern Med. 2018 Sept 4. doi: 10.1001/jamainternmed.2018.3713.
FROM JAMA INTERNAL MEDICINE
Key clinical point: Burnout among physicians was associated with lower quality of care because of unprofessionalism, reduced patient satisfaction, and an increased risk of patient safety issues.
Major finding: Physicians with burnout were significantly associated with higher rates of patient safety issues (odds ratio, 1.96; 95% confidence interval, 1.59-2.40), reduced patient satisfaction (OR, 2.28; 95% CI, 1.42-3.68), and lower quality of care (OR, 2.31; 95% CI, 1.87-2.85).
Study details: A systematic review and meta-analysis of 42,473 physicians from 47 different studies.
Disclosures: The study was funded by the United Kingdom National Institute of Health Research (NIHR) School for Primary Care Research and the NIHR Greater Manchester Patient Safety Translational Research Centre. The authors reported no relevant conflicts of interest.
Source: Panagioti M et al. JAMA Intern Med. 2018 Sept 4. doi: 10.1001/jamainternmed.2018.3713.