User login
Physicians as First Responders I
When I was an intern and junior resident there was a fellow house officer who seemed to be a magnet for out-of-hospital emergencies. There were a couple of car accidents, a baby to be delivered, an elderly neighbor with alarming chest pain, and a little old lady with syncope, plus a few playground incidents that required more than a little on-site tending and triage. It got to the point where he felt he needed to raid the hospital supply closets to build himself a proper emergency kit.
Envious of his excitement I, of course, followed suit. However, my well-appointed plastic tackle box remained unopened on the floor behind the driver’s seat in my car. Sure, there were Band-Aids to be dispensed from time to time but mostly I was the on-site reassurer and triage consultant at the playground. I almost never suggested a trip to the emergency room. No little old ladies crumpled to the floor in front of me in the checkout line at the grocery store. No distracted teenage drivers plowed into telephone poles anywhere within earshot.

When I began my practice here on the midcoast of Maine, my protective aura traveled with me. I went looking for excitement by signing on as the team physician for the local high school football team. But, other than a few minor concussions, which in those days we “treated” with a “sit on the bench for awhile and I’ll ask you a few questions,” my first responder experiences continued to be boringly undramatic. Not even any obvious dislocations or angulated fractures on the playground or athletic fields I frequented.
My professional adventures were confined to the hospital, where every physician regardless of specialty training was required to take a shift covering the emergency room. Talk about a situation looking for trouble. The concept of physicians with specialty training in emergency room medicine had not yet occurred to anyone in rural Maine. Although there were anxiety-provoking nights waiting for the disasters to arrive, somehow the shit never hit the fan while I was on duty.
Finally, after several more years of this bad (or good) fortune I was on a bike ride out in the country alone on a back road and came upon a fresh single-vehicle-single-occupant accident. Steam and smoke coming out of the engine compartment, the young driver slumped over the steering wheel. I was able to pry the door open but couldn’t find a pulse. I thumped him three times on the chest and eventually could detect a pulse and he began to stir. When the ambulance arrived I dragged my bike into the back of the ambulance with me and monitored him on the way to the hospital. He did fine, only to die in another accident a few years later.
A recent article in one of our local newspapers described a fledgling program in which three emergency room physicians are being equipped with supplies and communication links that will allow them to respond to emergent situations in the field. The program is currently seeking to extend its funding for another year. Its advocates argue that the need is twofold. There is currently a regional shortage of fully trained first responder EMTs. And having an extra pair of hands in the field could ease the burden of the already overutilized emergency rooms.
I am sure the physicians who have signed on to become first responders are passionate about the need and probably enjoy the excitement of in-the-field professional experiences, much as my fellow house officer did. However, were I sitting on the committee that controls the funding of programs like this I would want to take a step back and consider whether using primary care physicians, who are already in short supply, as first responders made sense. Some of the scenarios may be dramatic and the physician’s contribution may be life saving. But I suspect in the long run these headline-making stories will be few and far between.
The argument that putting physicians in the field will make a significant dent in the emergency room overutilization crisis we have in this country doesn’t hold water. Extending outpatient office hours, education, and improved phone triage to name just a few would have a bigger impact. I suspect there are other countries and even some counties in this country that may already use physicians as first responders. It just doesn’t seem to be a model that will work well given the realities in most semirural and suburban locales.
The real question that must wait for another Letters From Maine column is how well prepared should all of us who have graduated from medical school be to function as first responders. There are thousands of us out there who initially had the training and could, with some updating, become a valuable source of first-responders. Where do issues like continuing education requirements and Good Samaritan protection fit into the equation? The answers in a future Letter.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
When I was an intern and junior resident there was a fellow house officer who seemed to be a magnet for out-of-hospital emergencies. There were a couple of car accidents, a baby to be delivered, an elderly neighbor with alarming chest pain, and a little old lady with syncope, plus a few playground incidents that required more than a little on-site tending and triage. It got to the point where he felt he needed to raid the hospital supply closets to build himself a proper emergency kit.
Envious of his excitement I, of course, followed suit. However, my well-appointed plastic tackle box remained unopened on the floor behind the driver’s seat in my car. Sure, there were Band-Aids to be dispensed from time to time but mostly I was the on-site reassurer and triage consultant at the playground. I almost never suggested a trip to the emergency room. No little old ladies crumpled to the floor in front of me in the checkout line at the grocery store. No distracted teenage drivers plowed into telephone poles anywhere within earshot.
When I began my practice here on the midcoast of Maine, my protective aura traveled with me. I went looking for excitement by signing on as the team physician for the local high school football team. But, other than a few minor concussions, which in those days we “treated” with a “sit on the bench for awhile and I’ll ask you a few questions,” my first responder experiences continued to be boringly undramatic. Not even any obvious dislocations or angulated fractures on the playground or athletic fields I frequented.
My professional adventures were confined to the hospital, where every physician regardless of specialty training was required to take a shift covering the emergency room. Talk about a situation looking for trouble. The concept of physicians with specialty training in emergency room medicine had not yet occurred to anyone in rural Maine. Although there were anxiety-provoking nights waiting for the disasters to arrive, somehow the shit never hit the fan while I was on duty.
Finally, after several more years of this bad (or good) fortune I was on a bike ride out in the country alone on a back road and came upon a fresh single-vehicle-single-occupant accident. Steam and smoke coming out of the engine compartment, the young driver slumped over the steering wheel. I was able to pry the door open but couldn’t find a pulse. I thumped him three times on the chest and eventually could detect a pulse and he began to stir. When the ambulance arrived I dragged my bike into the back of the ambulance with me and monitored him on the way to the hospital. He did fine, only to die in another accident a few years later.
A recent article in one of our local newspapers described a fledgling program in which three emergency room physicians are being equipped with supplies and communication links that will allow them to respond to emergent situations in the field. The program is currently seeking to extend its funding for another year. Its advocates argue that the need is twofold. There is currently a regional shortage of fully trained first responder EMTs. And having an extra pair of hands in the field could ease the burden of the already overutilized emergency rooms.
I am sure the physicians who have signed on to become first responders are passionate about the need and probably enjoy the excitement of in-the-field professional experiences, much as my fellow house officer did. However, were I sitting on the committee that controls the funding of programs like this I would want to take a step back and consider whether using primary care physicians, who are already in short supply, as first responders made sense. Some of the scenarios may be dramatic and the physician’s contribution may be life saving. But I suspect in the long run these headline-making stories will be few and far between.
The argument that putting physicians in the field will make a significant dent in the emergency room overutilization crisis we have in this country doesn’t hold water. Extending outpatient office hours, education, and improved phone triage to name just a few would have a bigger impact. I suspect there are other countries and even some counties in this country that may already use physicians as first responders. It just doesn’t seem to be a model that will work well given the realities in most semirural and suburban locales.
The real question that must wait for another Letters From Maine column is how well prepared should all of us who have graduated from medical school be to function as first responders. There are thousands of us out there who initially had the training and could, with some updating, become a valuable source of first-responders. Where do issues like continuing education requirements and Good Samaritan protection fit into the equation? The answers in a future Letter.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
When I was an intern and junior resident there was a fellow house officer who seemed to be a magnet for out-of-hospital emergencies. There were a couple of car accidents, a baby to be delivered, an elderly neighbor with alarming chest pain, and a little old lady with syncope, plus a few playground incidents that required more than a little on-site tending and triage. It got to the point where he felt he needed to raid the hospital supply closets to build himself a proper emergency kit.
Envious of his excitement I, of course, followed suit. However, my well-appointed plastic tackle box remained unopened on the floor behind the driver’s seat in my car. Sure, there were Band-Aids to be dispensed from time to time but mostly I was the on-site reassurer and triage consultant at the playground. I almost never suggested a trip to the emergency room. No little old ladies crumpled to the floor in front of me in the checkout line at the grocery store. No distracted teenage drivers plowed into telephone poles anywhere within earshot.
When I began my practice here on the midcoast of Maine, my protective aura traveled with me. I went looking for excitement by signing on as the team physician for the local high school football team. But, other than a few minor concussions, which in those days we “treated” with a “sit on the bench for awhile and I’ll ask you a few questions,” my first responder experiences continued to be boringly undramatic. Not even any obvious dislocations or angulated fractures on the playground or athletic fields I frequented.
My professional adventures were confined to the hospital, where every physician regardless of specialty training was required to take a shift covering the emergency room. Talk about a situation looking for trouble. The concept of physicians with specialty training in emergency room medicine had not yet occurred to anyone in rural Maine. Although there were anxiety-provoking nights waiting for the disasters to arrive, somehow the shit never hit the fan while I was on duty.
Finally, after several more years of this bad (or good) fortune I was on a bike ride out in the country alone on a back road and came upon a fresh single-vehicle-single-occupant accident. Steam and smoke coming out of the engine compartment, the young driver slumped over the steering wheel. I was able to pry the door open but couldn’t find a pulse. I thumped him three times on the chest and eventually could detect a pulse and he began to stir. When the ambulance arrived I dragged my bike into the back of the ambulance with me and monitored him on the way to the hospital. He did fine, only to die in another accident a few years later.
A recent article in one of our local newspapers described a fledgling program in which three emergency room physicians are being equipped with supplies and communication links that will allow them to respond to emergent situations in the field. The program is currently seeking to extend its funding for another year. Its advocates argue that the need is twofold. There is currently a regional shortage of fully trained first responder EMTs. And having an extra pair of hands in the field could ease the burden of the already overutilized emergency rooms.
I am sure the physicians who have signed on to become first responders are passionate about the need and probably enjoy the excitement of in-the-field professional experiences, much as my fellow house officer did. However, were I sitting on the committee that controls the funding of programs like this I would want to take a step back and consider whether using primary care physicians, who are already in short supply, as first responders made sense. Some of the scenarios may be dramatic and the physician’s contribution may be life saving. But I suspect in the long run these headline-making stories will be few and far between.
The argument that putting physicians in the field will make a significant dent in the emergency room overutilization crisis we have in this country doesn’t hold water. Extending outpatient office hours, education, and improved phone triage to name just a few would have a bigger impact. I suspect there are other countries and even some counties in this country that may already use physicians as first responders. It just doesn’t seem to be a model that will work well given the realities in most semirural and suburban locales.
The real question that must wait for another Letters From Maine column is how well prepared should all of us who have graduated from medical school be to function as first responders. There are thousands of us out there who initially had the training and could, with some updating, become a valuable source of first-responders. Where do issues like continuing education requirements and Good Samaritan protection fit into the equation? The answers in a future Letter.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Doc Sues State Over ‘Antiquated’ Telehealth Rules
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Telemedicine visits skyrocketed during the pandemic, but
In the complaint filed on December 13 in New Jersey District Court, plaintiff Shannon MacDonald, MD, radiation oncologist at Massachusetts General Hospital, Boston, said that New Jersey’s telehealth rules make it illegal for her and other out-of-state specialists to consult with and treat residents who could benefit from their unique expertise, unless they first obtain licensure through the medical board.
While she currently maintains licenses in six states, New Jersey’s application process can take several months and requires an initial fee of $550, plus additional expenses for a background check and fingerprinting, court documents said.
Physicians providing telehealth services to New Jersey residents without a state-authorized medical license are subject to up to 5 years in prison and criminal and civil fines exceeding $10,000.
“Every day, my ethical obligations to my patients are in direct conflict with the legal framework,” said Dr. MacDonald.
She and coplaintiff Paul Gardner, MD, neurosurgical codirector of the Center for Cranial Base Surgery at the University of Pittsburgh Medical Center, are represented by the public interest law firm Pacific Legal Foundation, which recently sued Louisiana’s governor over its medical board diversity rules.
The lawsuit names Otto Sabando, DO, president of the New Jersey State Board of Medical Examiners. Representatives for Dr. Sabando and the medical board did not respond to a request for comment.
The complaint describes the care Dr. MacDonald provided several years before the pandemic for an out-of-state patient, J.A., also named as a plaintiff, who was diagnosed with pineoblastoma at 18 months old.
After initially undergoing treatment in New York, court documents indicate that J.A.’s medical team referred him to Dr. MacDonald “because of her nationally recognized expertise in proton therapy” targeting rare childhood cancers. Dr. MacDonald remotely reviewed J.A.’s scans and discussed options before his family pursued treatment with her in Boston.
Dr. MacDonald said that allowing more patients like J.A. to use telehealth to access services when specialists are unavailable in their state would go a long way toward achieving health equity. She says it could reduce the financial burden of travel and lodging expenses and provide timely consultations and follow-up care.
Many states, including New Jersey, waived or eased licensing regulations during the pandemic so physicians could temporarily practice in other states. Since those emergency orders have ended, physicians must again seek licensure in the states where their patients are located or potentially be subjected to fines or other penalties by state medical boards.
New Jersey Governor Phil Murphy signed a law in 2022 joining the Interstate Medical Licensure Compact, an agreement that offers a streamlined process for physicians already licensed in their home states to obtain licensure in 37 other member states as well as the District of Columbia and Territory of Guam. However, the lawsuit alleges that applications still take weeks and pose significant administrative and financial barriers for physicians.
Telehealth in a Post-COVID World
“Until COVID, we didn’t realize that a telephone call really was practicing medicine,” said Dr. MacDonald. “After being allowed to do telemedicine consultations across state lines for a year and 2 years for follow-ups, I thought it would last forever, but it’s placed a spotlight on what we cannot do.”
Dr. MacDonald, who recently penned a related editorial in the Wall Street Journal, said laws regarding interstate practice are outdated.
“They made sense in the preindustrial era when you had to be in the same location as your patient, but they make little sense in the modern era when distance disappears over the Internet or telephone,” she said.
The issue isn’t unique to New Jersey. Caleb Trotter, JD, attorney for the Pacific Legal Foundation, said that 30 states prohibit doctors from conducting telemedicine services in states where they are not licensed.
“Some hospitals instruct doctors and administrators to ask the patient where they are physically located at the beginning of a telehealth appointment, and if it isn’t a state where the physician is licensed, they are instructed to end the appointment immediately,” Mr. Trotter said. “A win in New Jersey would solve a very real problem for these [patients] of not having convenient legal access to specialists.”
Neither Dr. MacDonald nor Dr. Gardner have had any enforcement actions taken against them, said Mr. Trotter. Still, he said the New Jersey attorney general’s office reminded physicians last year that state licensure rules apply to out-of-state doctors using telemedicine to conduct follow-up appointments.
In November, the Center for Health Law and Policy Innovation at Harvard Law School, Cambridge, Massachusetts, proposed telemedicine reforms, including exceptions for the care of established patients and screening for specialty referrals.
Dr. MacDonald hopes the lawsuit will increase awareness of telehealth laws and spur changes.
A version of this article appeared on Medscape.com.
Mega Malpractice Verdicts Against Physicians on the Rise
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.
In December, in what’s known as the “Take Care of Maya” case, a Florida jury returned a record $261 million verdict against Johns Hopkins All Children’s Hospital, St. Petersburg, Florida, for its treatment of a young patient and her family after an emergency room visit.
A month earlier, in New York, a jury ordered Westchester Medical Center Health Network to pay $120 million to a patient and his family following delayed stroke care that resulted in brain damage.
Mega malpractice awards like these are rising against physicians and hospitals around the country, according to new data from TransRe, an international reinsurance company that tracks large verdicts.
“2023 blew away every record previously set among high medical malpractice verdicts,” said Richard Henderson, senior vice president for TransRe.
In 2023, there were 57 medical malpractice verdicts of $10 million or more in the United States, the data showed. Slightly more than half of those reached $25 million or more.
From 2012 to 2022, verdicts of $10 million or more ranged from 34 in 2013 to 52 in 2022, TransRe research found.
While New York, Illinois, and Florida typically saw the highest dollar verdicts in previous years, so-called “nuclear” verdicts now occur in states like Utah and Georgia where they once were uncommon, said Robert E. White Jr., president of TDC Group and The Doctors Company, a national medical liability insurer for physicians.
A rollback of tort reforms across the country is one contributor, he said. For example, Georgia’s cap on noneconomic damages is among those that have been ruled unconstitutional by courts. Utah’s cap on noneconomic damages still stands, but the limit was deemed unconstitutional in wrongful death cases. In 2019, a portion of Utah›s pre-litigation panel process was also struck down by the state’s Supreme Court.
“We used to be able to predict where these high verdicts would occur,” Mr. White said. “We can’t predict it anymore.”
Research shows a majority of malpractice cases are dropped or settled before trial, and claims that go before juries usually end in doctors’ favor. Plaintiffs’ attorneys cite large jury verdicts in similar cases to induce settlements and higher payouts, Mr. White said.
And while mega verdicts rarely stick, they can have lasting effects on future claims. The awards lead to larger settlement demands from plaintiffs and drive up the cost to resolve claims, according to Mr. Henderson and Mr. White.
“Verdicts are the yardstick by which all settlements are measured,” Mr. White said. “That’s where the damage is done.” The prospect of a mega verdict can make insurers leery of fighting some malpractice cases and motivate them to offer bigger settlements to stay out of the courtroom, he added.
Why Are Juries Awarding Higher Verdicts?
There’s no single reason for the rise in nuclear verdicts, Mr. Henderson said.
One theory is that plaintiffs’ attorneys held back on resolving high-dollar cases during the COVID pandemic and let loose with high-demand claims when courts returned to normal, he said.
Another theory is that people emerged from the pandemic angrier.
“Whether it was political dynamics, masking [mandates], or differences in opinions, people came out of it angry, and generally speaking, you don’t want an angry jury,” Mr. Henderson said. “For a while, there was the halo effect, where health professionals were seen as heroes. That went away, and all of a sudden [they] became ‘the bad guys.’ ”
“People are angry at the healthcare system, and this anger manifests itself in [liability] suits,” added Bill Burns, vice president of research for the Medical Professional Liability Association, an industry group for medical liability insurers.
Hospital and medical group consolidation also reduces the personal connection juries may have with healthcare providers, Mr. Burns said.
“Healthcare has become a big business, and the corporatization of medicine now puts companies on the stand and not your local community hospital or your family doctor that you have known since birth,” he said.
Plaintiffs’ attorneys also deploy tactics that can prompt higher verdicts, Mr. White said. They may tell a jury that the provider or hospital is a threat to the community and that awarding a large verdict will deter others in the healthcare community from repeating the same actions.
Juries may then want to punish the defendant in addition to assessing damages for economic harm or pain and suffering, Mr. White said.
“I am concerned that jurors are trying to right social wrongs rather than judging cases on the facts presented to them,” added Mike Stinson, vice president for policy and legal affairs for the Medical Professional Liability Association.
Third-party litigation financing also can lead to mega verdicts. That’s an emerging practice in which companies unrelated to a lawsuit provide capital to plaintiffs in return for a portion of any financial award. The firms essentially “invest” in the litigation.
“What this does is provide an additional financial backdrop for plaintiffs,” Mr. Henderson said. “It allows them to dig in harder on cases. They can hold out for higher numbers, and if nothing else, it can prolong litigation.”
Do High Awards Actually Stick?
Multimillion-dollar verdicts may grab headlines, but do plaintiffs actually receive them?
Rarely, said TransRe, which tracks the final outcomes of verdicts. In many cases, large verdicts are reduced on appeal.
In the Maya case, which involved child protection authorities, a judge later lowered the damages against Johns Hopkins All Children’s Hospital by $47.5 million.
A federal judge in October, for example, rejected a record $110 million medical malpractice award in Minnesota, reducing it to $10 million. The district judge ruled the award was “shockingly excessive” and that the plaintiff should either accept the $10 million award or retry the case.
After a verdict is awarded, the defendant typically challenges the award, and the case goes through the appellate pipeline, Mr. Henderson explained. A judge may reduce some elements of the verdict, he said, but more often, the plaintiff and defendant agree on a compromised figure.
Seattle medical liability defense attorney Jennifer Crisera has experienced this firsthand. She recalled a recent case where a plaintiff’s attorney demanded what she describes as an unreasonable amount to settle a claim. Ms. Crisera did not want to give exact numbers but said the plaintiff made an 8-figure demand and the defense offered a low 7-figure range.
“My impression was that plaintiff’s counsel believed that they could get a nuclear verdict from the jury, so they kept their settlement demand artificially high,” she said. “The division between the numbers was way too high. Ultimately, we had to let a jury decide the value.”
The plaintiff won the case, and the verdict was much less than the settlement demand, she said. Even so, the defense incurred trial costs, and the health provider was forced to endure the emotional stress of a trial that could have been avoided, Ms. Crisera said.
Higher medical malpractice premiums are another consequence of massive awards.
Premium rates are associated with how much insurers pay on average for cases and how frequently they are making payouts, Mr. White said.
Medical liability insurance premiums for physicians have steadily increased since 2019, according to data from the Medical Liability Monitor, a national publication that analyzes liability insurance premiums. The Monitor studies insurance premium data from insurers that cover internists, general surgeons, and obstetrician-gynecologists.
From 2019 to 2023, average premium rates for physicians increased between 1.1% and 3% each year in states without patient compensation funds, according to Monitor data.
“Nuclear verdicts are a real driver of the industry’s underwriting losses and remain top of mind for every malpractice insurance company,” said Michael Matray, editor for the Medical Liability Monitor. “Responses to this year’s rate survey questionnaire indicate that most responding companies have experienced an increase in claims greater than $1 million and claims greater than $5 million during the past 2 years.”
However, increases vary widely by region and among counties. In Montgomery County, Alabama, for instance, premiums for internists rose by 24% from 2022 to 2023, from $8,231 to $10,240. Premiums for Montgomery County general surgeons rose by 11.9% from 2022 to 2023, from $30,761 to $34,426, according to survey data.
In several counties in Illinois (Adams, Knox, Peoria, and Rock Island), premiums for some internists rose by 15% from $24,041 to $27,783, and premiums for some surgeons increased by 27% from $60,202 to $76,461, according to survey data. Some internists in Catoosa County, Georgia, meanwhile, paid $17,831 in 2023, up from $16,313 in 2022. Some surgeons in Catoosa County paid $65,616 in 2023, up from $60,032 in 2022. Inflation could be one factor behind higher liability premium rates. Claim severity is a key driver of higher premium rates, Mr. White added.
“We have not seen stability in claims severity,” he said. “It is continuing to go up and, in all likelihood, it will drive [premium] rates up further from this point.”
A version of this article appeared on Medscape.com.
US Board Discloses Cheating, Grads Say Problem Is Rampant
The United States Medical Licensing Examination (USMLE) program is invalidating scores attained by some examinees after an investigation revealed a pattern of anomalous exam performance associated with test-takers from Nepal.
In a January 31 announcement, the USMLE program said that officials are in the process of notifying examinees with results in question and that the examinees will be required to take validation exams. The program did not offer further details about its investigation or how the questionable performance was identified.
“The USMLE program regularly monitors and analyzes examinees’ test performances for unusual score patterns or variations, and other information that could raise questions about the validity of an examinee’s results,” the program said in a statement. “Highly irregular patterns can be indicative of prior unauthorized access to secure exam content.”
Some medical graduates say the action against students cheating on the USMLE is long overdue.
, particularly by groups within the international medical graduate (IMG) community, according to multiple IMGs who shared their concerns with this news organization. Sellers operate under pseudonyms across social media platforms and charge anywhere from $300 to $2000 for questions, Medscape research shows.
Facebook posts often advertise questions for sale, said Saqib Gul, MD, an IMG from Pakistan who has voiced concerns about the practice on social media.
“People make up fake profiles and tell others to [direct message] them for recalls,” he told this news organization. “There was a dedicated Facebook page that was doing this. In other cases, a couple of friends that took the exam remember a certain number of questions and write them down after the test.”
Ahmad Ozair, MD, an IMG from Lucknow, Uttar Pradesh, India, said that he has come across many groups online sharing or selling USMLE recalls. He first became suspicious when he saw several students, all from a few medical schools in Nepal, posting on social media about scoring in the 270 and 280-plus range.
“The statistical probability that you would have three or more candidates in the same year, scoring in the 99th percentile worldwide, belonging to a small geographical area is extremely low.”
Dr. Ozair, who now is studying public health at Johns Hopkins University in Baltimore, said that the issue is important for “all stakeholders” who care about patient safety: “Would you want a doctor who has cheated on the medical licensing exam to take care of you?”
In an interview, USMLE program spokesman Joe Knickrehm said that the program relies on multiple processes to detect and respond to claims that exam integrity is being compromised. The process includes monitoring performance data, an anonymous tip line for reporting suspicious behavior, and a thorough investigative process.
“The USMLE program regularly monitors social media channels for comments relating to exam security and irregular behavior and will initiate an investigation if warranted,” Mr. Knickrehm told this news organization. “ The covert nature of this activity does not lend itself to a definitive statement regarding whether the problem has increased or decreased in recent years.”
Mr. Knickrehm said that the program’s STOPit app allows people to report suspicious behavior electronically to the USMLE program. Since its launch in 2021, the program has received more than 80 tips per year through the app, according to Mr. Knickrehm. Security violations are investigated by USMLE staff and reviewed by the USMLE Committee for Individualized Review (CIR). Anyone found to have engaged in irregular behavior by the CIR for activities undermining exam integrity are typically barred from access to the USMLE for multiple years.
How Easy Is It to Buy Recalls?
Two years ago, Dr B was approached by a former study partner who had just completed Step 2 of the USMLE. She asked whether Dr B wanted to buy recalled questions to help her pass.
“She paid this guy almost $2000 for recalls and told me if I pay this money, he’ll give me the recalls,” said Dr B, who asked to remain anonymous for fear of being associated with students cheating on the USMLE. “I told her I was not interested, and she said the guy would lower the price. I broke contact with her.”
Dr B, an IMG from Pakistan, was appalled. But she said that the episode was not the first time she has come across groups selling USMLE recalls or heard peers brag about having access to exam content.
“I am baffled at how many [groups] post on social media and brazenly advertise their ‘services,’” she told this news organization. “No one arrests them, their customers go on to score abnormally high on the boards, making it unachievable for people who take the honest route, plus giving IMGs a bad rep.”
Groups offering recalls are easily findable on sites such as Telegram and Signal. Telegram is a cloud-based messaging app that focuses on security, and Signal is an encrypted messaging service.
The website recallmastery.com purports to offer a range of USMLE recall packages, from a free, unsorted version to Step 1 and Step 2 packages that include “fresh updates,” and sections with “mostly repeated topics. Prices range from the free version to the $799 VIP package.
Another site called MedPox.com boasts 2024 Step 2 recalls, advertising “ actual exam questions to get HIGH scores.” The website’s owner states that the recalls were collected “by my friends,” and to message the them to be added to the “recalls group.”
A reporter was able to easily download a free version of alleged USMLE questions and answers from recallmastery.com. The document was a combination of typed and handwritten notes about medical questions, with red circles around recalled answers.
J. Bryan Carmody, MD, who blogs about medical education, reviewed a copy of the document. He said that the content appeared “credible” and was in fact recalled USMLE questions. However, the extent of which the question stem was recalled was incomplete at best, and there was little production value to the document, said Dr. Carmody, a nephrologist and associate professor of pediatrics at the Eastern Virgina Medical School in Norfolk.
The person selling the recall packages states on the website that the free version is not organized or sorted, but it allows viewers to “see how this works before paying for premium recalls.”
Mr. Knickrehm said that the program could not comment on the document, but that “whenever the USMLE program receives or locates information about a potential security violation, we investigate and take necessary action.”
When asked about the specific websites noted above, Knickrehm said that the program routinely monitors a wide array of websites, message boards, and chat rooms for USMLE-related materials. Though many sites advertise having USMLE recalls for sale, it’s more likely they are selling non-USMLE content, he said.
Using past content to cheat on medical exams is an old problem. In 2010, for example, the American Board of Internal Medicine suspended 139 physicians after they were caught cheating on the board exams. The scandal involved a vast cheating ring that included physicians memorizing questions and reproducing them after the tests. The board later sued a gastroenterologist for her part in the scandal.
In 2012, a CNN investigation exposed doctors who were memorizing test questions and creating sophisticated recall banks to cheat on radiology boards. The Association of American Medical Colleges sued a medical student in 2017 for attempting to secretly record content on the MCAT using spyglasses.
In recent years, Dr. Carmody said that he has received multiple messages and screenshots from concerned students and residents who were offered or encountered recalls.
“One thing that’s unclear is how legitimate the claims are,” he said. “Many of these recalls may be faulty or outdated. It could be someone who took the exam yesterday and has a photographic memory or it could be some sparsely recalled or mis-recalled information. Unless you’re willing to pay these people, you can’t inspect the quality, or even if you did, you wouldn’t know if the information was current or not.”
‘As an IMG, There Is So Much at Stake’
Whether recall sellers — and those buying them — are more frequently IMGs has fostered heated debate on social media.
On a Reddit thread devoted to IMG issues, posters expressed frustration about being bombarded with recall advertisements and unwanted messages about buying USMLE questions while trying to find study materials. One poster called the practices a “huge slap to all those IMGs who are struggling day and night, just to get a good score.”
In an X thread about the same subject, however, some self-described IMGs took offense to claims that IMGs might score higher because they have access to recalls. The allegations are “incendiary” and “malign hardworking IMGs,” posters wrote.
When Dr. Gul spoke out online about the “biopsy” culture, he received multiple private messages from fellow IMGs telling him to remove his comments, he said.
“I received a lot of backlash on social media,” he told this news organization. “Some IMGs asked me to take down my posts because they thought I was making IMGs look bad, and it might prompt authorities to take action or shut down international examination centers for IMGs.”
Most of the IMGs who spoke to this news organization were afraid to be publicly identified. Several IMG advocates and IMG associations contacted for the story did not respond. One medical education expert said that his institution advised him to “steer clear” of commenting because the issue was “controversial.”
“As an IMG, there is so much at stake,” Dr B said. “Any association with shady operations like these is an absolute suicide. I’m personally afraid of any repercussions of the sort.”
USMLE officials declined to comment on whether the buying or selling of recalls appears to be more prevalent among the IMG community, saying it is “difficult to generalize this behavior as ‘prevalent’ simply due to the clandestine nature of this activity.”
Cheat-Proofing the USMLE
The USMLE program has taken several steps intended to prevent cheating, but more needs to be done, medical education advocates say.
For example, Dr. Carmody called the recent change in the attempt limit for taking USMLE exams from six to four times a good move.
“The reality is, if you’re taking a USMLE exam five-plus times, you’re far more likely to be memorizing questions and selling them for shady test prep operations than you are to be legitimately pursuing U.S. residency training or licensure,” he wrote on X.
The 2022 move to make USMLE Step 1 pass or fail is another positive change, said Dr. Gul, who added that US programs should also put less weight on test scores and focus more on clinical experience.
“Many programs in the US prioritize scores rather than clinical experiences in home countries,” he said. “If program directors would remove these criteria, probably the cheating practices would stop. Clinical practice matters. When a doctor gets matched, they have to be good at seeing and treating patients, not just good at sitting in front of a screen and taking an exam.”
Turning over questions more rapidly would help curb the practices, Dr. Carmody said. Another strategy is using math techniques to identify unusual deviations that suggest cheating, he said.
A blueprint for the strategy was created after a cheating scandal involving Canada’s Medical Council of Canada Qualifying Examination (MCCQE) in 2004. After learning which questions were circulated, MCCQE administrators evaluated exams by comparing answers of compromised questions with the answers of noncompromised questions.
“For a person who was not cheating, the error of performance should be pretty similar on those two groups of questions,” Dr. Carmody said. “But if you were given the questions in advance, you might have very poor performance on questions that had not been compromised, and very high performance on those that had been compromised. That disparity is very unlikely to occur just by chance alone.”
Based on his research, Dr. Ozair is working on an academic review paper about cheating on the USMLE and on the Medical Council of Canada Qualification Examination. He said that he hopes the paper will raise more awareness about the problem and drive more action.
He and others interviewed for this story shared that the websites they’ve reported to the USMLE program are still active and offering recalls to buyers.
“Even if they are not actually offering something tangible or true, appearance matters,” Dr. Ozair said. “I think it’s worth the USMLE sending cease and desist letters and getting these websites taken down. This would restore faith in the process and underscore that this issue is being taken seriously.”
A version of this article appeared on Medscape.com.
The United States Medical Licensing Examination (USMLE) program is invalidating scores attained by some examinees after an investigation revealed a pattern of anomalous exam performance associated with test-takers from Nepal.
In a January 31 announcement, the USMLE program said that officials are in the process of notifying examinees with results in question and that the examinees will be required to take validation exams. The program did not offer further details about its investigation or how the questionable performance was identified.
“The USMLE program regularly monitors and analyzes examinees’ test performances for unusual score patterns or variations, and other information that could raise questions about the validity of an examinee’s results,” the program said in a statement. “Highly irregular patterns can be indicative of prior unauthorized access to secure exam content.”
Some medical graduates say the action against students cheating on the USMLE is long overdue.
, particularly by groups within the international medical graduate (IMG) community, according to multiple IMGs who shared their concerns with this news organization. Sellers operate under pseudonyms across social media platforms and charge anywhere from $300 to $2000 for questions, Medscape research shows.
Facebook posts often advertise questions for sale, said Saqib Gul, MD, an IMG from Pakistan who has voiced concerns about the practice on social media.
“People make up fake profiles and tell others to [direct message] them for recalls,” he told this news organization. “There was a dedicated Facebook page that was doing this. In other cases, a couple of friends that took the exam remember a certain number of questions and write them down after the test.”
Ahmad Ozair, MD, an IMG from Lucknow, Uttar Pradesh, India, said that he has come across many groups online sharing or selling USMLE recalls. He first became suspicious when he saw several students, all from a few medical schools in Nepal, posting on social media about scoring in the 270 and 280-plus range.
“The statistical probability that you would have three or more candidates in the same year, scoring in the 99th percentile worldwide, belonging to a small geographical area is extremely low.”
Dr. Ozair, who now is studying public health at Johns Hopkins University in Baltimore, said that the issue is important for “all stakeholders” who care about patient safety: “Would you want a doctor who has cheated on the medical licensing exam to take care of you?”
In an interview, USMLE program spokesman Joe Knickrehm said that the program relies on multiple processes to detect and respond to claims that exam integrity is being compromised. The process includes monitoring performance data, an anonymous tip line for reporting suspicious behavior, and a thorough investigative process.
“The USMLE program regularly monitors social media channels for comments relating to exam security and irregular behavior and will initiate an investigation if warranted,” Mr. Knickrehm told this news organization. “ The covert nature of this activity does not lend itself to a definitive statement regarding whether the problem has increased or decreased in recent years.”
Mr. Knickrehm said that the program’s STOPit app allows people to report suspicious behavior electronically to the USMLE program. Since its launch in 2021, the program has received more than 80 tips per year through the app, according to Mr. Knickrehm. Security violations are investigated by USMLE staff and reviewed by the USMLE Committee for Individualized Review (CIR). Anyone found to have engaged in irregular behavior by the CIR for activities undermining exam integrity are typically barred from access to the USMLE for multiple years.
How Easy Is It to Buy Recalls?
Two years ago, Dr B was approached by a former study partner who had just completed Step 2 of the USMLE. She asked whether Dr B wanted to buy recalled questions to help her pass.
“She paid this guy almost $2000 for recalls and told me if I pay this money, he’ll give me the recalls,” said Dr B, who asked to remain anonymous for fear of being associated with students cheating on the USMLE. “I told her I was not interested, and she said the guy would lower the price. I broke contact with her.”
Dr B, an IMG from Pakistan, was appalled. But she said that the episode was not the first time she has come across groups selling USMLE recalls or heard peers brag about having access to exam content.
“I am baffled at how many [groups] post on social media and brazenly advertise their ‘services,’” she told this news organization. “No one arrests them, their customers go on to score abnormally high on the boards, making it unachievable for people who take the honest route, plus giving IMGs a bad rep.”
Groups offering recalls are easily findable on sites such as Telegram and Signal. Telegram is a cloud-based messaging app that focuses on security, and Signal is an encrypted messaging service.
The website recallmastery.com purports to offer a range of USMLE recall packages, from a free, unsorted version to Step 1 and Step 2 packages that include “fresh updates,” and sections with “mostly repeated topics. Prices range from the free version to the $799 VIP package.
Another site called MedPox.com boasts 2024 Step 2 recalls, advertising “ actual exam questions to get HIGH scores.” The website’s owner states that the recalls were collected “by my friends,” and to message the them to be added to the “recalls group.”
A reporter was able to easily download a free version of alleged USMLE questions and answers from recallmastery.com. The document was a combination of typed and handwritten notes about medical questions, with red circles around recalled answers.
J. Bryan Carmody, MD, who blogs about medical education, reviewed a copy of the document. He said that the content appeared “credible” and was in fact recalled USMLE questions. However, the extent of which the question stem was recalled was incomplete at best, and there was little production value to the document, said Dr. Carmody, a nephrologist and associate professor of pediatrics at the Eastern Virgina Medical School in Norfolk.
The person selling the recall packages states on the website that the free version is not organized or sorted, but it allows viewers to “see how this works before paying for premium recalls.”
Mr. Knickrehm said that the program could not comment on the document, but that “whenever the USMLE program receives or locates information about a potential security violation, we investigate and take necessary action.”
When asked about the specific websites noted above, Knickrehm said that the program routinely monitors a wide array of websites, message boards, and chat rooms for USMLE-related materials. Though many sites advertise having USMLE recalls for sale, it’s more likely they are selling non-USMLE content, he said.
Using past content to cheat on medical exams is an old problem. In 2010, for example, the American Board of Internal Medicine suspended 139 physicians after they were caught cheating on the board exams. The scandal involved a vast cheating ring that included physicians memorizing questions and reproducing them after the tests. The board later sued a gastroenterologist for her part in the scandal.
In 2012, a CNN investigation exposed doctors who were memorizing test questions and creating sophisticated recall banks to cheat on radiology boards. The Association of American Medical Colleges sued a medical student in 2017 for attempting to secretly record content on the MCAT using spyglasses.
In recent years, Dr. Carmody said that he has received multiple messages and screenshots from concerned students and residents who were offered or encountered recalls.
“One thing that’s unclear is how legitimate the claims are,” he said. “Many of these recalls may be faulty or outdated. It could be someone who took the exam yesterday and has a photographic memory or it could be some sparsely recalled or mis-recalled information. Unless you’re willing to pay these people, you can’t inspect the quality, or even if you did, you wouldn’t know if the information was current or not.”
‘As an IMG, There Is So Much at Stake’
Whether recall sellers — and those buying them — are more frequently IMGs has fostered heated debate on social media.
On a Reddit thread devoted to IMG issues, posters expressed frustration about being bombarded with recall advertisements and unwanted messages about buying USMLE questions while trying to find study materials. One poster called the practices a “huge slap to all those IMGs who are struggling day and night, just to get a good score.”
In an X thread about the same subject, however, some self-described IMGs took offense to claims that IMGs might score higher because they have access to recalls. The allegations are “incendiary” and “malign hardworking IMGs,” posters wrote.
When Dr. Gul spoke out online about the “biopsy” culture, he received multiple private messages from fellow IMGs telling him to remove his comments, he said.
“I received a lot of backlash on social media,” he told this news organization. “Some IMGs asked me to take down my posts because they thought I was making IMGs look bad, and it might prompt authorities to take action or shut down international examination centers for IMGs.”
Most of the IMGs who spoke to this news organization were afraid to be publicly identified. Several IMG advocates and IMG associations contacted for the story did not respond. One medical education expert said that his institution advised him to “steer clear” of commenting because the issue was “controversial.”
“As an IMG, there is so much at stake,” Dr B said. “Any association with shady operations like these is an absolute suicide. I’m personally afraid of any repercussions of the sort.”
USMLE officials declined to comment on whether the buying or selling of recalls appears to be more prevalent among the IMG community, saying it is “difficult to generalize this behavior as ‘prevalent’ simply due to the clandestine nature of this activity.”
Cheat-Proofing the USMLE
The USMLE program has taken several steps intended to prevent cheating, but more needs to be done, medical education advocates say.
For example, Dr. Carmody called the recent change in the attempt limit for taking USMLE exams from six to four times a good move.
“The reality is, if you’re taking a USMLE exam five-plus times, you’re far more likely to be memorizing questions and selling them for shady test prep operations than you are to be legitimately pursuing U.S. residency training or licensure,” he wrote on X.
The 2022 move to make USMLE Step 1 pass or fail is another positive change, said Dr. Gul, who added that US programs should also put less weight on test scores and focus more on clinical experience.
“Many programs in the US prioritize scores rather than clinical experiences in home countries,” he said. “If program directors would remove these criteria, probably the cheating practices would stop. Clinical practice matters. When a doctor gets matched, they have to be good at seeing and treating patients, not just good at sitting in front of a screen and taking an exam.”
Turning over questions more rapidly would help curb the practices, Dr. Carmody said. Another strategy is using math techniques to identify unusual deviations that suggest cheating, he said.
A blueprint for the strategy was created after a cheating scandal involving Canada’s Medical Council of Canada Qualifying Examination (MCCQE) in 2004. After learning which questions were circulated, MCCQE administrators evaluated exams by comparing answers of compromised questions with the answers of noncompromised questions.
“For a person who was not cheating, the error of performance should be pretty similar on those two groups of questions,” Dr. Carmody said. “But if you were given the questions in advance, you might have very poor performance on questions that had not been compromised, and very high performance on those that had been compromised. That disparity is very unlikely to occur just by chance alone.”
Based on his research, Dr. Ozair is working on an academic review paper about cheating on the USMLE and on the Medical Council of Canada Qualification Examination. He said that he hopes the paper will raise more awareness about the problem and drive more action.
He and others interviewed for this story shared that the websites they’ve reported to the USMLE program are still active and offering recalls to buyers.
“Even if they are not actually offering something tangible or true, appearance matters,” Dr. Ozair said. “I think it’s worth the USMLE sending cease and desist letters and getting these websites taken down. This would restore faith in the process and underscore that this issue is being taken seriously.”
A version of this article appeared on Medscape.com.
The United States Medical Licensing Examination (USMLE) program is invalidating scores attained by some examinees after an investigation revealed a pattern of anomalous exam performance associated with test-takers from Nepal.
In a January 31 announcement, the USMLE program said that officials are in the process of notifying examinees with results in question and that the examinees will be required to take validation exams. The program did not offer further details about its investigation or how the questionable performance was identified.
“The USMLE program regularly monitors and analyzes examinees’ test performances for unusual score patterns or variations, and other information that could raise questions about the validity of an examinee’s results,” the program said in a statement. “Highly irregular patterns can be indicative of prior unauthorized access to secure exam content.”
Some medical graduates say the action against students cheating on the USMLE is long overdue.
, particularly by groups within the international medical graduate (IMG) community, according to multiple IMGs who shared their concerns with this news organization. Sellers operate under pseudonyms across social media platforms and charge anywhere from $300 to $2000 for questions, Medscape research shows.
Facebook posts often advertise questions for sale, said Saqib Gul, MD, an IMG from Pakistan who has voiced concerns about the practice on social media.
“People make up fake profiles and tell others to [direct message] them for recalls,” he told this news organization. “There was a dedicated Facebook page that was doing this. In other cases, a couple of friends that took the exam remember a certain number of questions and write them down after the test.”
Ahmad Ozair, MD, an IMG from Lucknow, Uttar Pradesh, India, said that he has come across many groups online sharing or selling USMLE recalls. He first became suspicious when he saw several students, all from a few medical schools in Nepal, posting on social media about scoring in the 270 and 280-plus range.
“The statistical probability that you would have three or more candidates in the same year, scoring in the 99th percentile worldwide, belonging to a small geographical area is extremely low.”
Dr. Ozair, who now is studying public health at Johns Hopkins University in Baltimore, said that the issue is important for “all stakeholders” who care about patient safety: “Would you want a doctor who has cheated on the medical licensing exam to take care of you?”
In an interview, USMLE program spokesman Joe Knickrehm said that the program relies on multiple processes to detect and respond to claims that exam integrity is being compromised. The process includes monitoring performance data, an anonymous tip line for reporting suspicious behavior, and a thorough investigative process.
“The USMLE program regularly monitors social media channels for comments relating to exam security and irregular behavior and will initiate an investigation if warranted,” Mr. Knickrehm told this news organization. “ The covert nature of this activity does not lend itself to a definitive statement regarding whether the problem has increased or decreased in recent years.”
Mr. Knickrehm said that the program’s STOPit app allows people to report suspicious behavior electronically to the USMLE program. Since its launch in 2021, the program has received more than 80 tips per year through the app, according to Mr. Knickrehm. Security violations are investigated by USMLE staff and reviewed by the USMLE Committee for Individualized Review (CIR). Anyone found to have engaged in irregular behavior by the CIR for activities undermining exam integrity are typically barred from access to the USMLE for multiple years.
How Easy Is It to Buy Recalls?
Two years ago, Dr B was approached by a former study partner who had just completed Step 2 of the USMLE. She asked whether Dr B wanted to buy recalled questions to help her pass.
“She paid this guy almost $2000 for recalls and told me if I pay this money, he’ll give me the recalls,” said Dr B, who asked to remain anonymous for fear of being associated with students cheating on the USMLE. “I told her I was not interested, and she said the guy would lower the price. I broke contact with her.”
Dr B, an IMG from Pakistan, was appalled. But she said that the episode was not the first time she has come across groups selling USMLE recalls or heard peers brag about having access to exam content.
“I am baffled at how many [groups] post on social media and brazenly advertise their ‘services,’” she told this news organization. “No one arrests them, their customers go on to score abnormally high on the boards, making it unachievable for people who take the honest route, plus giving IMGs a bad rep.”
Groups offering recalls are easily findable on sites such as Telegram and Signal. Telegram is a cloud-based messaging app that focuses on security, and Signal is an encrypted messaging service.
The website recallmastery.com purports to offer a range of USMLE recall packages, from a free, unsorted version to Step 1 and Step 2 packages that include “fresh updates,” and sections with “mostly repeated topics. Prices range from the free version to the $799 VIP package.
Another site called MedPox.com boasts 2024 Step 2 recalls, advertising “ actual exam questions to get HIGH scores.” The website’s owner states that the recalls were collected “by my friends,” and to message the them to be added to the “recalls group.”
A reporter was able to easily download a free version of alleged USMLE questions and answers from recallmastery.com. The document was a combination of typed and handwritten notes about medical questions, with red circles around recalled answers.
J. Bryan Carmody, MD, who blogs about medical education, reviewed a copy of the document. He said that the content appeared “credible” and was in fact recalled USMLE questions. However, the extent of which the question stem was recalled was incomplete at best, and there was little production value to the document, said Dr. Carmody, a nephrologist and associate professor of pediatrics at the Eastern Virgina Medical School in Norfolk.
The person selling the recall packages states on the website that the free version is not organized or sorted, but it allows viewers to “see how this works before paying for premium recalls.”
Mr. Knickrehm said that the program could not comment on the document, but that “whenever the USMLE program receives or locates information about a potential security violation, we investigate and take necessary action.”
When asked about the specific websites noted above, Knickrehm said that the program routinely monitors a wide array of websites, message boards, and chat rooms for USMLE-related materials. Though many sites advertise having USMLE recalls for sale, it’s more likely they are selling non-USMLE content, he said.
Using past content to cheat on medical exams is an old problem. In 2010, for example, the American Board of Internal Medicine suspended 139 physicians after they were caught cheating on the board exams. The scandal involved a vast cheating ring that included physicians memorizing questions and reproducing them after the tests. The board later sued a gastroenterologist for her part in the scandal.
In 2012, a CNN investigation exposed doctors who were memorizing test questions and creating sophisticated recall banks to cheat on radiology boards. The Association of American Medical Colleges sued a medical student in 2017 for attempting to secretly record content on the MCAT using spyglasses.
In recent years, Dr. Carmody said that he has received multiple messages and screenshots from concerned students and residents who were offered or encountered recalls.
“One thing that’s unclear is how legitimate the claims are,” he said. “Many of these recalls may be faulty or outdated. It could be someone who took the exam yesterday and has a photographic memory or it could be some sparsely recalled or mis-recalled information. Unless you’re willing to pay these people, you can’t inspect the quality, or even if you did, you wouldn’t know if the information was current or not.”
‘As an IMG, There Is So Much at Stake’
Whether recall sellers — and those buying them — are more frequently IMGs has fostered heated debate on social media.
On a Reddit thread devoted to IMG issues, posters expressed frustration about being bombarded with recall advertisements and unwanted messages about buying USMLE questions while trying to find study materials. One poster called the practices a “huge slap to all those IMGs who are struggling day and night, just to get a good score.”
In an X thread about the same subject, however, some self-described IMGs took offense to claims that IMGs might score higher because they have access to recalls. The allegations are “incendiary” and “malign hardworking IMGs,” posters wrote.
When Dr. Gul spoke out online about the “biopsy” culture, he received multiple private messages from fellow IMGs telling him to remove his comments, he said.
“I received a lot of backlash on social media,” he told this news organization. “Some IMGs asked me to take down my posts because they thought I was making IMGs look bad, and it might prompt authorities to take action or shut down international examination centers for IMGs.”
Most of the IMGs who spoke to this news organization were afraid to be publicly identified. Several IMG advocates and IMG associations contacted for the story did not respond. One medical education expert said that his institution advised him to “steer clear” of commenting because the issue was “controversial.”
“As an IMG, there is so much at stake,” Dr B said. “Any association with shady operations like these is an absolute suicide. I’m personally afraid of any repercussions of the sort.”
USMLE officials declined to comment on whether the buying or selling of recalls appears to be more prevalent among the IMG community, saying it is “difficult to generalize this behavior as ‘prevalent’ simply due to the clandestine nature of this activity.”
Cheat-Proofing the USMLE
The USMLE program has taken several steps intended to prevent cheating, but more needs to be done, medical education advocates say.
For example, Dr. Carmody called the recent change in the attempt limit for taking USMLE exams from six to four times a good move.
“The reality is, if you’re taking a USMLE exam five-plus times, you’re far more likely to be memorizing questions and selling them for shady test prep operations than you are to be legitimately pursuing U.S. residency training or licensure,” he wrote on X.
The 2022 move to make USMLE Step 1 pass or fail is another positive change, said Dr. Gul, who added that US programs should also put less weight on test scores and focus more on clinical experience.
“Many programs in the US prioritize scores rather than clinical experiences in home countries,” he said. “If program directors would remove these criteria, probably the cheating practices would stop. Clinical practice matters. When a doctor gets matched, they have to be good at seeing and treating patients, not just good at sitting in front of a screen and taking an exam.”
Turning over questions more rapidly would help curb the practices, Dr. Carmody said. Another strategy is using math techniques to identify unusual deviations that suggest cheating, he said.
A blueprint for the strategy was created after a cheating scandal involving Canada’s Medical Council of Canada Qualifying Examination (MCCQE) in 2004. After learning which questions were circulated, MCCQE administrators evaluated exams by comparing answers of compromised questions with the answers of noncompromised questions.
“For a person who was not cheating, the error of performance should be pretty similar on those two groups of questions,” Dr. Carmody said. “But if you were given the questions in advance, you might have very poor performance on questions that had not been compromised, and very high performance on those that had been compromised. That disparity is very unlikely to occur just by chance alone.”
Based on his research, Dr. Ozair is working on an academic review paper about cheating on the USMLE and on the Medical Council of Canada Qualification Examination. He said that he hopes the paper will raise more awareness about the problem and drive more action.
He and others interviewed for this story shared that the websites they’ve reported to the USMLE program are still active and offering recalls to buyers.
“Even if they are not actually offering something tangible or true, appearance matters,” Dr. Ozair said. “I think it’s worth the USMLE sending cease and desist letters and getting these websites taken down. This would restore faith in the process and underscore that this issue is being taken seriously.”
A version of this article appeared on Medscape.com.
Federal Bill Seeks AI Tools to Stop Medicare Fraud
A new Senate bill would require Medicare to test two tools routinely used by credit card companies to prevent fraud: Artificial intelligence (AI)-trained algorithms to detect suspicious activity and a system to quickly alert Medicare patients on whose behalf payment is being sought.
Senator Mike Braun (R-IN) recently introduced the Medicare Transaction Fraud Prevention Act, which calls for a 2-year test of this approach.
The experiment, targeted to start in 2025, would focus on durable medical equipment and clinical diagnostic laboratory tests and cover Medicare beneficiaries who receive electronic notices about claims.
The legislation would direct the Center for Medicare and Medicaid Services (CMS) to test the use of predictive risk-scoring algorithms in finding fraud. The program would be modeled on the systems that credit card companies already use. Transactions could be scored from 1 (least risky) to 99 (most risky).
CMS would then check directly by email or phone call with selected Medicare enrollees about transactions considered to present a high risk for fraud.
Many consumers have benefited from this approach when used to check for fraud on their credit cards, Braun noted during a November hearing of the Senate Special Committee on Aging. Credit card companies often can intervene before a fraudulent transaction is cleared.
“There’s no reason we wouldn’t want to minimally at least mimic that,” Braun said at the hearing.
Asking Medicare enrollees to verify certain purchases could give CMS increased access to vital predictive data, test proof of concept, and save hundreds of millions of dollars, Braun said.
Concerns Raised
So far, Braun has only one cosponsor for the bill, Senator Bill Cassidy, MD (R-LA), and the bill has drawn some criticism.
Brett Meeks, executive director of the Health Innovation Alliance, a trade group representing technology companies, insurers, and consumer organizations, objected to requiring Medicare enrollees to verify flagged orders. CMS should internally root out fraud through technology, not burden seniors, Meeks told this news organization.
Meeks said he has been following the discussion about the use of AI in addressing Medicare fraud. Had a bill broadly targeted Medicare fraud through AI, his alliance might have backed it, he said. But the current proposed legislation has a narrower focus.
Focusing on durable medical equipment, for example, could have unintended consequences like denying power wheelchairs to people with debilitating conditions like multiple sclerosis, Meeks said.
But Braun’s bill won a quick nod of approval from a researcher who studies the use of AI to detect Medicare fraud. Taghi M. Khoshgoftaar, PhD, director of the Data Mining and Machine Learning Lab at Florida Atlantic University, Boca Raton, Florida, said he sees an advantage to Braun’s approach of involving Medicare enrollees in the protection of their benefits.
The bill does not authorize funding for the pilot project, and it’s unclear what it would cost.
Detecting Medicare Fraud
The federal government has stepped up Medicare fraud investigations in recent years, and more doctors are getting caught.
A study published in 2018 examined cases of physicians excluded from Medicare using data from the US Office of Inspector General (OIG) at the Department of Health and Human Services.
The OIG has the right to exclude clinicians from Medicare for fraud or other reasons. Chen and coauthors looked at Medicare physician exclusions from 2007 to 2017. They found that exclusions due to fraud increased an estimated 14% per year on average from a base level of 139 exclusions in 2007.
In 2019, CMS sought feedback on new ways to use AI to detect fraud. In a public request for information, the agency said Medicare scrutinizes fewer claims for payment than commercial insurers do.
About 99.7% of Medicare fee-for-service claims are processed and paid within 17 days without any medical review, CMS said at the time.
A version of this article appeared on Medscape.com .
A new Senate bill would require Medicare to test two tools routinely used by credit card companies to prevent fraud: Artificial intelligence (AI)-trained algorithms to detect suspicious activity and a system to quickly alert Medicare patients on whose behalf payment is being sought.
Senator Mike Braun (R-IN) recently introduced the Medicare Transaction Fraud Prevention Act, which calls for a 2-year test of this approach.
The experiment, targeted to start in 2025, would focus on durable medical equipment and clinical diagnostic laboratory tests and cover Medicare beneficiaries who receive electronic notices about claims.
The legislation would direct the Center for Medicare and Medicaid Services (CMS) to test the use of predictive risk-scoring algorithms in finding fraud. The program would be modeled on the systems that credit card companies already use. Transactions could be scored from 1 (least risky) to 99 (most risky).
CMS would then check directly by email or phone call with selected Medicare enrollees about transactions considered to present a high risk for fraud.
Many consumers have benefited from this approach when used to check for fraud on their credit cards, Braun noted during a November hearing of the Senate Special Committee on Aging. Credit card companies often can intervene before a fraudulent transaction is cleared.
“There’s no reason we wouldn’t want to minimally at least mimic that,” Braun said at the hearing.
Asking Medicare enrollees to verify certain purchases could give CMS increased access to vital predictive data, test proof of concept, and save hundreds of millions of dollars, Braun said.
Concerns Raised
So far, Braun has only one cosponsor for the bill, Senator Bill Cassidy, MD (R-LA), and the bill has drawn some criticism.
Brett Meeks, executive director of the Health Innovation Alliance, a trade group representing technology companies, insurers, and consumer organizations, objected to requiring Medicare enrollees to verify flagged orders. CMS should internally root out fraud through technology, not burden seniors, Meeks told this news organization.
Meeks said he has been following the discussion about the use of AI in addressing Medicare fraud. Had a bill broadly targeted Medicare fraud through AI, his alliance might have backed it, he said. But the current proposed legislation has a narrower focus.
Focusing on durable medical equipment, for example, could have unintended consequences like denying power wheelchairs to people with debilitating conditions like multiple sclerosis, Meeks said.
But Braun’s bill won a quick nod of approval from a researcher who studies the use of AI to detect Medicare fraud. Taghi M. Khoshgoftaar, PhD, director of the Data Mining and Machine Learning Lab at Florida Atlantic University, Boca Raton, Florida, said he sees an advantage to Braun’s approach of involving Medicare enrollees in the protection of their benefits.
The bill does not authorize funding for the pilot project, and it’s unclear what it would cost.
Detecting Medicare Fraud
The federal government has stepped up Medicare fraud investigations in recent years, and more doctors are getting caught.
A study published in 2018 examined cases of physicians excluded from Medicare using data from the US Office of Inspector General (OIG) at the Department of Health and Human Services.
The OIG has the right to exclude clinicians from Medicare for fraud or other reasons. Chen and coauthors looked at Medicare physician exclusions from 2007 to 2017. They found that exclusions due to fraud increased an estimated 14% per year on average from a base level of 139 exclusions in 2007.
In 2019, CMS sought feedback on new ways to use AI to detect fraud. In a public request for information, the agency said Medicare scrutinizes fewer claims for payment than commercial insurers do.
About 99.7% of Medicare fee-for-service claims are processed and paid within 17 days without any medical review, CMS said at the time.
A version of this article appeared on Medscape.com .
A new Senate bill would require Medicare to test two tools routinely used by credit card companies to prevent fraud: Artificial intelligence (AI)-trained algorithms to detect suspicious activity and a system to quickly alert Medicare patients on whose behalf payment is being sought.
Senator Mike Braun (R-IN) recently introduced the Medicare Transaction Fraud Prevention Act, which calls for a 2-year test of this approach.
The experiment, targeted to start in 2025, would focus on durable medical equipment and clinical diagnostic laboratory tests and cover Medicare beneficiaries who receive electronic notices about claims.
The legislation would direct the Center for Medicare and Medicaid Services (CMS) to test the use of predictive risk-scoring algorithms in finding fraud. The program would be modeled on the systems that credit card companies already use. Transactions could be scored from 1 (least risky) to 99 (most risky).
CMS would then check directly by email or phone call with selected Medicare enrollees about transactions considered to present a high risk for fraud.
Many consumers have benefited from this approach when used to check for fraud on their credit cards, Braun noted during a November hearing of the Senate Special Committee on Aging. Credit card companies often can intervene before a fraudulent transaction is cleared.
“There’s no reason we wouldn’t want to minimally at least mimic that,” Braun said at the hearing.
Asking Medicare enrollees to verify certain purchases could give CMS increased access to vital predictive data, test proof of concept, and save hundreds of millions of dollars, Braun said.
Concerns Raised
So far, Braun has only one cosponsor for the bill, Senator Bill Cassidy, MD (R-LA), and the bill has drawn some criticism.
Brett Meeks, executive director of the Health Innovation Alliance, a trade group representing technology companies, insurers, and consumer organizations, objected to requiring Medicare enrollees to verify flagged orders. CMS should internally root out fraud through technology, not burden seniors, Meeks told this news organization.
Meeks said he has been following the discussion about the use of AI in addressing Medicare fraud. Had a bill broadly targeted Medicare fraud through AI, his alliance might have backed it, he said. But the current proposed legislation has a narrower focus.
Focusing on durable medical equipment, for example, could have unintended consequences like denying power wheelchairs to people with debilitating conditions like multiple sclerosis, Meeks said.
But Braun’s bill won a quick nod of approval from a researcher who studies the use of AI to detect Medicare fraud. Taghi M. Khoshgoftaar, PhD, director of the Data Mining and Machine Learning Lab at Florida Atlantic University, Boca Raton, Florida, said he sees an advantage to Braun’s approach of involving Medicare enrollees in the protection of their benefits.
The bill does not authorize funding for the pilot project, and it’s unclear what it would cost.
Detecting Medicare Fraud
The federal government has stepped up Medicare fraud investigations in recent years, and more doctors are getting caught.
A study published in 2018 examined cases of physicians excluded from Medicare using data from the US Office of Inspector General (OIG) at the Department of Health and Human Services.
The OIG has the right to exclude clinicians from Medicare for fraud or other reasons. Chen and coauthors looked at Medicare physician exclusions from 2007 to 2017. They found that exclusions due to fraud increased an estimated 14% per year on average from a base level of 139 exclusions in 2007.
In 2019, CMS sought feedback on new ways to use AI to detect fraud. In a public request for information, the agency said Medicare scrutinizes fewer claims for payment than commercial insurers do.
About 99.7% of Medicare fee-for-service claims are processed and paid within 17 days without any medical review, CMS said at the time.
A version of this article appeared on Medscape.com .
Why Everyone Needs Their Own Emergency Medicine Doctor
How emerging models come close to making this reality
As emergency medicine doctors, we regularly give medical advice to family and close friends when they get sick or are injured and don’t know what to do. In a matter of moments, we triage, diagnose, and assemble a logical plan, whatever the issue may be. This skill comes from our training and years of experience in treating emergencies and also routine medical matters. The value proposition is clear.
Frankly, it’s a service everyone should have. Think about the potential time and money saved if this option for medical care and triage was broadly available. Overtriage would plummet. That’s when people run to the emergency department (ED) and wait endless hours, only to be reassured or receive limited treatment. Undertriage would also decline. That’s when people should go to the ED but, unwisely, wait. For example, this may occur when symptoms of dizziness end up being a stroke.
Why doesn’t everyone have an ED doctor they can call? The primary reason is that the current system mostly doesn’t support it. The most common scenario is that insurance companies pay us to see patients in an expensive box called the ED. Most EDs are situated within an even more expensive box, called a hospital.
Here’s the good news: Better access to emergency care and people who are formally trained in emergency medicine and routine matters of urgent care is increasing.
One example is telemedicine, where a remote doctor — either your own or a doctor through an app — conducts a visit. Telemedicine is more common since the pandemic, now that insurance pays for it. In emergency situations, it’s rare that your own doctor can see you immediately by telemedicine. By contrast, direct-to-consumer telemedicine (eg, Teladoc, Doctor On Demand, and others) connects you with a random doctor.
In many apps, it’s unclear not only who the doctor is, but more importantly, what their specific medical specialty or training is. It may be an ED doctor evaluating your child’s fever, or it may be a retired general surgeon or an adult rheumatology specialist in the midst of their fellowship, making an extra buck, who may have no pediatric training.
Training Matters
Clinical training and whether the doctor knows you matters. A recent JAMA study from Ontario, Canada, found that patients with virtual visits who saw outside family physicians (whom they had never met) compared with their own family physicians were 66% more likely to visit an ED within 7 days after the visit. This illustrates the importance of understanding your personal history in assessing acute symptoms.
Some healthcare systems do use ED physicians for on-demand telehealth services, such as Thomas Jefferson’s JeffConnect. Amazon Clinic recently entered this space, providing condition-specific acute or chronic care to adults aged 18-64 years for a fee that is, notably, not covered by insurance.
A second innovative approach, albeit not specifically in the realm of a personal emergency medicine doctor, is artificial intelligence (AI)–powered kiosks. A concierge medicine company known as Forward recently unveiled an innovative concept known as CarePods that are now available in Sacramento, California; Chandler, Arizona; and Chicago. For a membership fee, you swipe into what looks like an oversize, space-age porta-potty. You sit in a chair and run through a series of health apps, which includes a biometric body scan along with mental health screenings. It even takes your blood (without a needle) and sequences your DNA. Results are reviewed by a doctor (not yours) who talks to you by video. They advertise that AI helps make the diagnosis. Although diagnostic AI is emerging and exciting, its benefit is not clear in emergency conditions. Yet, one clear value in a kiosk over telemedicine is the ability to obtain vital signs and lab results, which are useful for diagnosis.
Another approach is the telehealth offerings used in integrated systems of care, such as Kaiser Permanente. Kaiser is both an insurance company and a deliverer of healthcare services. Kaiser maintains a nurse call center and can handle urgent e-visits. Integrated systems not only help triage patients’ acute issues but also have access to their personal health histories. They can also provide a definitive plan for in-person treatment or a specific referral. A downside of integrated care is that it often limits your choice of provider.
Insurance companies also maintain call-in lines such as HumanaFirst, which is also staffed by nurses. We have not seen data on the calls such services receive, but we doubt people that want to call their insurance company when sick or injured, knowing that the insurer benefits when you receive less care. Additionally, studies have found that nurse-only triage is not as effective as physician triage and results in higher ED referral rates.
The Concierge Option
Probably the closest thing to having your own personal emergency medicine doctor is concierge medicine, which combines personalized care and accessibility. Concierge doctors come in many forms, but they usually charge a fixed fee for 24/7 availability and same-day appointments. A downside of concierge medicine is its expense ($2000–$3500 per year), and that many don’t take insurance. Concierge medicine is also criticized because, as doctors gravitate toward it, people in the community often lose their physician if they can’t afford the fees.
Ultimately, remote medical advice for emergency care is clearly evolving in new ways. The inability of traditional care models to achieve this goal will lead to innovation to improve the available options that have led us to think outside of the proverbial “box” we refer to as the ED-in-the-case.
At this time, will any option come close to having a personal emergency medicine physician willing to answer your questions, real-time, as with family and close friends? We think not.
But the future certainly holds promise for alternatives that will hopefully make payers and the Centers for Medicare & Medicaid Services take notice. Innovations in personalized care that reduce costs will be critical in our current healthcare landscape.
Dr. Pines is clinical professor of emergency medicine at George Washington University in Washington, DC, and chief of clinical innovation at US Acute Care Solutions in Canton, Ohio. He disclosed ties with CSL Behring and Abbott Point-of-Care. Dr. Glatter is assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
How emerging models come close to making this reality
How emerging models come close to making this reality
As emergency medicine doctors, we regularly give medical advice to family and close friends when they get sick or are injured and don’t know what to do. In a matter of moments, we triage, diagnose, and assemble a logical plan, whatever the issue may be. This skill comes from our training and years of experience in treating emergencies and also routine medical matters. The value proposition is clear.
Frankly, it’s a service everyone should have. Think about the potential time and money saved if this option for medical care and triage was broadly available. Overtriage would plummet. That’s when people run to the emergency department (ED) and wait endless hours, only to be reassured or receive limited treatment. Undertriage would also decline. That’s when people should go to the ED but, unwisely, wait. For example, this may occur when symptoms of dizziness end up being a stroke.
Why doesn’t everyone have an ED doctor they can call? The primary reason is that the current system mostly doesn’t support it. The most common scenario is that insurance companies pay us to see patients in an expensive box called the ED. Most EDs are situated within an even more expensive box, called a hospital.
Here’s the good news: Better access to emergency care and people who are formally trained in emergency medicine and routine matters of urgent care is increasing.
One example is telemedicine, where a remote doctor — either your own or a doctor through an app — conducts a visit. Telemedicine is more common since the pandemic, now that insurance pays for it. In emergency situations, it’s rare that your own doctor can see you immediately by telemedicine. By contrast, direct-to-consumer telemedicine (eg, Teladoc, Doctor On Demand, and others) connects you with a random doctor.
In many apps, it’s unclear not only who the doctor is, but more importantly, what their specific medical specialty or training is. It may be an ED doctor evaluating your child’s fever, or it may be a retired general surgeon or an adult rheumatology specialist in the midst of their fellowship, making an extra buck, who may have no pediatric training.
Training Matters
Clinical training and whether the doctor knows you matters. A recent JAMA study from Ontario, Canada, found that patients with virtual visits who saw outside family physicians (whom they had never met) compared with their own family physicians were 66% more likely to visit an ED within 7 days after the visit. This illustrates the importance of understanding your personal history in assessing acute symptoms.
Some healthcare systems do use ED physicians for on-demand telehealth services, such as Thomas Jefferson’s JeffConnect. Amazon Clinic recently entered this space, providing condition-specific acute or chronic care to adults aged 18-64 years for a fee that is, notably, not covered by insurance.
A second innovative approach, albeit not specifically in the realm of a personal emergency medicine doctor, is artificial intelligence (AI)–powered kiosks. A concierge medicine company known as Forward recently unveiled an innovative concept known as CarePods that are now available in Sacramento, California; Chandler, Arizona; and Chicago. For a membership fee, you swipe into what looks like an oversize, space-age porta-potty. You sit in a chair and run through a series of health apps, which includes a biometric body scan along with mental health screenings. It even takes your blood (without a needle) and sequences your DNA. Results are reviewed by a doctor (not yours) who talks to you by video. They advertise that AI helps make the diagnosis. Although diagnostic AI is emerging and exciting, its benefit is not clear in emergency conditions. Yet, one clear value in a kiosk over telemedicine is the ability to obtain vital signs and lab results, which are useful for diagnosis.
Another approach is the telehealth offerings used in integrated systems of care, such as Kaiser Permanente. Kaiser is both an insurance company and a deliverer of healthcare services. Kaiser maintains a nurse call center and can handle urgent e-visits. Integrated systems not only help triage patients’ acute issues but also have access to their personal health histories. They can also provide a definitive plan for in-person treatment or a specific referral. A downside of integrated care is that it often limits your choice of provider.
Insurance companies also maintain call-in lines such as HumanaFirst, which is also staffed by nurses. We have not seen data on the calls such services receive, but we doubt people that want to call their insurance company when sick or injured, knowing that the insurer benefits when you receive less care. Additionally, studies have found that nurse-only triage is not as effective as physician triage and results in higher ED referral rates.
The Concierge Option
Probably the closest thing to having your own personal emergency medicine doctor is concierge medicine, which combines personalized care and accessibility. Concierge doctors come in many forms, but they usually charge a fixed fee for 24/7 availability and same-day appointments. A downside of concierge medicine is its expense ($2000–$3500 per year), and that many don’t take insurance. Concierge medicine is also criticized because, as doctors gravitate toward it, people in the community often lose their physician if they can’t afford the fees.
Ultimately, remote medical advice for emergency care is clearly evolving in new ways. The inability of traditional care models to achieve this goal will lead to innovation to improve the available options that have led us to think outside of the proverbial “box” we refer to as the ED-in-the-case.
At this time, will any option come close to having a personal emergency medicine physician willing to answer your questions, real-time, as with family and close friends? We think not.
But the future certainly holds promise for alternatives that will hopefully make payers and the Centers for Medicare & Medicaid Services take notice. Innovations in personalized care that reduce costs will be critical in our current healthcare landscape.
Dr. Pines is clinical professor of emergency medicine at George Washington University in Washington, DC, and chief of clinical innovation at US Acute Care Solutions in Canton, Ohio. He disclosed ties with CSL Behring and Abbott Point-of-Care. Dr. Glatter is assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
As emergency medicine doctors, we regularly give medical advice to family and close friends when they get sick or are injured and don’t know what to do. In a matter of moments, we triage, diagnose, and assemble a logical plan, whatever the issue may be. This skill comes from our training and years of experience in treating emergencies and also routine medical matters. The value proposition is clear.
Frankly, it’s a service everyone should have. Think about the potential time and money saved if this option for medical care and triage was broadly available. Overtriage would plummet. That’s when people run to the emergency department (ED) and wait endless hours, only to be reassured or receive limited treatment. Undertriage would also decline. That’s when people should go to the ED but, unwisely, wait. For example, this may occur when symptoms of dizziness end up being a stroke.
Why doesn’t everyone have an ED doctor they can call? The primary reason is that the current system mostly doesn’t support it. The most common scenario is that insurance companies pay us to see patients in an expensive box called the ED. Most EDs are situated within an even more expensive box, called a hospital.
Here’s the good news: Better access to emergency care and people who are formally trained in emergency medicine and routine matters of urgent care is increasing.
One example is telemedicine, where a remote doctor — either your own or a doctor through an app — conducts a visit. Telemedicine is more common since the pandemic, now that insurance pays for it. In emergency situations, it’s rare that your own doctor can see you immediately by telemedicine. By contrast, direct-to-consumer telemedicine (eg, Teladoc, Doctor On Demand, and others) connects you with a random doctor.
In many apps, it’s unclear not only who the doctor is, but more importantly, what their specific medical specialty or training is. It may be an ED doctor evaluating your child’s fever, or it may be a retired general surgeon or an adult rheumatology specialist in the midst of their fellowship, making an extra buck, who may have no pediatric training.
Training Matters
Clinical training and whether the doctor knows you matters. A recent JAMA study from Ontario, Canada, found that patients with virtual visits who saw outside family physicians (whom they had never met) compared with their own family physicians were 66% more likely to visit an ED within 7 days after the visit. This illustrates the importance of understanding your personal history in assessing acute symptoms.
Some healthcare systems do use ED physicians for on-demand telehealth services, such as Thomas Jefferson’s JeffConnect. Amazon Clinic recently entered this space, providing condition-specific acute or chronic care to adults aged 18-64 years for a fee that is, notably, not covered by insurance.
A second innovative approach, albeit not specifically in the realm of a personal emergency medicine doctor, is artificial intelligence (AI)–powered kiosks. A concierge medicine company known as Forward recently unveiled an innovative concept known as CarePods that are now available in Sacramento, California; Chandler, Arizona; and Chicago. For a membership fee, you swipe into what looks like an oversize, space-age porta-potty. You sit in a chair and run through a series of health apps, which includes a biometric body scan along with mental health screenings. It even takes your blood (without a needle) and sequences your DNA. Results are reviewed by a doctor (not yours) who talks to you by video. They advertise that AI helps make the diagnosis. Although diagnostic AI is emerging and exciting, its benefit is not clear in emergency conditions. Yet, one clear value in a kiosk over telemedicine is the ability to obtain vital signs and lab results, which are useful for diagnosis.
Another approach is the telehealth offerings used in integrated systems of care, such as Kaiser Permanente. Kaiser is both an insurance company and a deliverer of healthcare services. Kaiser maintains a nurse call center and can handle urgent e-visits. Integrated systems not only help triage patients’ acute issues but also have access to their personal health histories. They can also provide a definitive plan for in-person treatment or a specific referral. A downside of integrated care is that it often limits your choice of provider.
Insurance companies also maintain call-in lines such as HumanaFirst, which is also staffed by nurses. We have not seen data on the calls such services receive, but we doubt people that want to call their insurance company when sick or injured, knowing that the insurer benefits when you receive less care. Additionally, studies have found that nurse-only triage is not as effective as physician triage and results in higher ED referral rates.
The Concierge Option
Probably the closest thing to having your own personal emergency medicine doctor is concierge medicine, which combines personalized care and accessibility. Concierge doctors come in many forms, but they usually charge a fixed fee for 24/7 availability and same-day appointments. A downside of concierge medicine is its expense ($2000–$3500 per year), and that many don’t take insurance. Concierge medicine is also criticized because, as doctors gravitate toward it, people in the community often lose their physician if they can’t afford the fees.
Ultimately, remote medical advice for emergency care is clearly evolving in new ways. The inability of traditional care models to achieve this goal will lead to innovation to improve the available options that have led us to think outside of the proverbial “box” we refer to as the ED-in-the-case.
At this time, will any option come close to having a personal emergency medicine physician willing to answer your questions, real-time, as with family and close friends? We think not.
But the future certainly holds promise for alternatives that will hopefully make payers and the Centers for Medicare & Medicaid Services take notice. Innovations in personalized care that reduce costs will be critical in our current healthcare landscape.
Dr. Pines is clinical professor of emergency medicine at George Washington University in Washington, DC, and chief of clinical innovation at US Acute Care Solutions in Canton, Ohio. He disclosed ties with CSL Behring and Abbott Point-of-Care. Dr. Glatter is assistant professor of emergency medicine at Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. He is a medical advisor for Medscape and hosts the Hot Topics in EM series. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
In Search of the Nation’s Primary Care Providers
Clinicians at Valley-Wide Health Systems never know who will appear at their clinic in San Luis, a town of about 600 people in southern Colorado.
“If someone’s in labor, they’ll show up. If someone has a laceration, they’ll show up,” said nurse practitioner Emelin Martinez, the chief medical officer for the healthcare system serving 13 rural Colorado counties.
But she struggled to find a full-time medical provider for that clinic, the only one in Costilla County. Born and raised in the area, Martinez filled some of the gap by driving about 45 minutes from Alamosa, the nearest city, once a week for months. A physician assistant from another town chipped in, too.
As one of the nation’s more than 1000 federally designated primary care shortage areas, Costilla County has many carrots to dangle in front of medical providers willing to practice there, including federal student loan repayments, bonus Medicare payments, and expedited visas for foreign clinicians. Still, Ms. Martinez said, its latest opening remained unfilled for more than a year. Not a single physician applied.
Policymakers have long tried to lure more primary care providers to the areas of the nation that have fewer than one physician for every 3500 residents. Recent examples include the Biden administration boosting funding in 2022 to address shortages and Sen. Bernie Sanders (I-Vt.) pushing sweeping primary care legislation in 2023.
But researchers steeped in the issue have a persistent frustration: It’s hard to know if any policy is working given that the data the federal government collects on primary care shortage areas has been flawed for a long time. One of the biggest gaps is that the system counts only physicians, not the myriad other healthcare professionals who now provide much of our nation›s primary care.
Additionally, a Health Affairs study shows the federal designations, which help allocate an estimated $1 billion in annual funding through at least 20 federal programs aimed at boosting primary care capacity, haven›t helped much.
In fact, Costilla County is among more than 180 federally designated areas that have remained stuck on the primary care shortage list for at least 40 years, according to a KFF Health News analysis. That›s even as the overall number of licensed US physicians more than doubled from 1990 to 2022 to over 1 million, according to the Federation of State Medical Boards, outpacing overall population growth.
No one disputes that much of the nation is starved for primary care clinicians, with patients having to wait weeks to get appointments or travel long distances for basic preventive care. Many doctors decide against primary care career paths, let alone practicing in isolated communities, because those jobs entail heavy workloads and earn less money and respect than specialists. But how does the nation solve the problem without knowing exactly where it is? And what tools must be used? Does a physician need to be the one providing the care?
Whitney Zahnd, president of the board of the Iowa Rural Health Association, said the fact that some rural areas have had such federal shortage designations for decades doesn’t prove they are ineffective. “Had the program not been there, would it have been even worse?” she said.
Federal funding supports 18,000 primary care doctors, nurse practitioners, and physician assistants to provide care to more than 18 million patients in the highest-need urban and rural communities across the country, said David Bowman, a spokesperson for the Health Resources and Services Administration, which manages the shortage designations. He said more than 80% of clinicians who get such scholarships or loan repayments continue to practice in shortage areas beyond their obligation of several years.
But that doesn’t mean they stick around forever.
Justin Markowski, a Yale School of Public Health doctoral student, coauthored the Health Affairs study that found the federal shortage designation makes no difference in upping physician density long-term. He is skeptical of policy ideas that promise big primary care fixes. That includes the Biden administration’s investment in more scholarships and loan repayments through the National Health Service Corps.
“You’re just throwing more money at a set of programs that don’t really seem to work,” he said. “We’ll see in a few years, but I’ll be shocked if it actually moved any physicians or any other advanced practice providers.”
One possible explanation for the persistence of shortage areas is that such incentives are too small or too fleeting.
But another issue is how shortages are measured. The government considers geographic shortage areas, now numbering just over 1000, but also population groups such as migrant farmworkers and individual facilities such as prisons that lack enough providers. Yet it’s up to state offices to identify populations and locations that might qualify as shortage areas and submit them to HRSA, which then scores the extent of any shortages. The funding and staffing for those state offices vary, creating an uneven foundation from which to map actual shortages.
“Some states became very adept at the equivalent of gerrymandering, where they were piecing together census blocks or census tracts in odd shapes in order to maximize the areas that are eligible,” said Stephen Petterson, a senior scholar at the Robert Graham Center, a policy think tank in Washington, DC, that focuses on primary care.
The federal Government Accountability Office has highlighted such issues since at least 1995, when it released a report identifying widespread data problems with the shortage area system and concluding it had “little assurance that federal funds are used where most needed.” The report noted one of the persistent shortcomings is that the system counts only physicians, not other key primary care providers.
Since 1998, federal officials have made three attempts to update the 1970s-era rules that define what counts as a shortage area. The authors of the Affordable Care Act tried most recently, tasking a committee of experts to decide on an update.
Among other things, the committee concluded in its 2011 report that nurse practitioners, physician assistants, and certified nurse midwives should be counted as primary care providers. But the recommendations fell short by just a handful of votes.
“We failed and the committee as a whole failed and HRSA failed by not moving the process forward,” said Petterson, who presented to the committee on how to comprehensively measure primary care needs.
Steve Holloway, who directs the Colorado health department’s Primary Care Office, served on the committee. Without action at the federal level, he then led a team to create Colorado’s own health professional shortage area designations that factor in nurse practitioners and physician assistants, not just doctors.
He said it’s taken about 6 years to create a tool and map of Colorado to answer a deceptively simple question: “How many actual flesh-and-blood, live clinicians are seeing patients?”
Ed Salsberg, who was the lead federal government representative on that committee and who headed HRSA’s National Center for Health Workforce Analysis, said the rest of the nation needs more precise data, too.
“It’s so important for the nation to target its resources to the highest-need communities,” he said. “It’s time again to try one more time to develop an improved methodology.”
In the past few years, more readily available data from insurance claims has allowed researchers to distinguish the medical providers who are practicing primary care from those who have specialized or retired.
Candice Chen, an associate professor of health policy and management at George Washington University’s Fitzhugh Mullan Institute for Health Workforce Equity, used claims data that reflects one large slice of the American population — about 66 million Medicaid beneficiaries — to map the primary care workforce.
Meanwhile, Monica O’Reilly-Jacob, a nurse-scientist who recently moved from Boston College to Columbia University’s School of Nursing, studied Medicare claims to conclude that fewer than 70% of physicians typically considered primary care providers were actually providing primary care. The rest, she said, often find more lucrative positions, such as subspecializing or working in hospitals. By contrast, nurse practitioners are likely undercounted. Her study found that close to half are providing primary care.
But such publicly available data leaves out much of the country, given that fewer than 40% of Americans are insured through Medicaid or Medicare.
“There’s no government organization that’s tracking: Who trained in what, where, and where are they now, and what are they practicing,” said Alison Huffstetler, medical director of the Robert Graham Center. “And if we don’t know who is doing what kind of care — and where — then there is no way for us to equitably manage the patient-to-clinician ratio across every state.”
In Costilla County, Ms. Martinez finally found someone to provide primary care: An experienced physician assistant who moved from Texas in December.
The physician assistant’s presence should bump the county out of its dire shortage, according to Colorado’s measure. But since he isn’t a physician, he’ll remain invisible in the national data and Costilla County will likely remain on the books as a federal shortage area.
Data reporter Hannah Recht, data editor Holly K. Hacker, and rural editor/correspondent Tony Leys contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — an independent source of health policy research, polling, and journalism.
Clinicians at Valley-Wide Health Systems never know who will appear at their clinic in San Luis, a town of about 600 people in southern Colorado.
“If someone’s in labor, they’ll show up. If someone has a laceration, they’ll show up,” said nurse practitioner Emelin Martinez, the chief medical officer for the healthcare system serving 13 rural Colorado counties.
But she struggled to find a full-time medical provider for that clinic, the only one in Costilla County. Born and raised in the area, Martinez filled some of the gap by driving about 45 minutes from Alamosa, the nearest city, once a week for months. A physician assistant from another town chipped in, too.
As one of the nation’s more than 1000 federally designated primary care shortage areas, Costilla County has many carrots to dangle in front of medical providers willing to practice there, including federal student loan repayments, bonus Medicare payments, and expedited visas for foreign clinicians. Still, Ms. Martinez said, its latest opening remained unfilled for more than a year. Not a single physician applied.
Policymakers have long tried to lure more primary care providers to the areas of the nation that have fewer than one physician for every 3500 residents. Recent examples include the Biden administration boosting funding in 2022 to address shortages and Sen. Bernie Sanders (I-Vt.) pushing sweeping primary care legislation in 2023.
But researchers steeped in the issue have a persistent frustration: It’s hard to know if any policy is working given that the data the federal government collects on primary care shortage areas has been flawed for a long time. One of the biggest gaps is that the system counts only physicians, not the myriad other healthcare professionals who now provide much of our nation›s primary care.
Additionally, a Health Affairs study shows the federal designations, which help allocate an estimated $1 billion in annual funding through at least 20 federal programs aimed at boosting primary care capacity, haven›t helped much.
In fact, Costilla County is among more than 180 federally designated areas that have remained stuck on the primary care shortage list for at least 40 years, according to a KFF Health News analysis. That›s even as the overall number of licensed US physicians more than doubled from 1990 to 2022 to over 1 million, according to the Federation of State Medical Boards, outpacing overall population growth.
No one disputes that much of the nation is starved for primary care clinicians, with patients having to wait weeks to get appointments or travel long distances for basic preventive care. Many doctors decide against primary care career paths, let alone practicing in isolated communities, because those jobs entail heavy workloads and earn less money and respect than specialists. But how does the nation solve the problem without knowing exactly where it is? And what tools must be used? Does a physician need to be the one providing the care?
Whitney Zahnd, president of the board of the Iowa Rural Health Association, said the fact that some rural areas have had such federal shortage designations for decades doesn’t prove they are ineffective. “Had the program not been there, would it have been even worse?” she said.
Federal funding supports 18,000 primary care doctors, nurse practitioners, and physician assistants to provide care to more than 18 million patients in the highest-need urban and rural communities across the country, said David Bowman, a spokesperson for the Health Resources and Services Administration, which manages the shortage designations. He said more than 80% of clinicians who get such scholarships or loan repayments continue to practice in shortage areas beyond their obligation of several years.
But that doesn’t mean they stick around forever.
Justin Markowski, a Yale School of Public Health doctoral student, coauthored the Health Affairs study that found the federal shortage designation makes no difference in upping physician density long-term. He is skeptical of policy ideas that promise big primary care fixes. That includes the Biden administration’s investment in more scholarships and loan repayments through the National Health Service Corps.
“You’re just throwing more money at a set of programs that don’t really seem to work,” he said. “We’ll see in a few years, but I’ll be shocked if it actually moved any physicians or any other advanced practice providers.”
One possible explanation for the persistence of shortage areas is that such incentives are too small or too fleeting.
But another issue is how shortages are measured. The government considers geographic shortage areas, now numbering just over 1000, but also population groups such as migrant farmworkers and individual facilities such as prisons that lack enough providers. Yet it’s up to state offices to identify populations and locations that might qualify as shortage areas and submit them to HRSA, which then scores the extent of any shortages. The funding and staffing for those state offices vary, creating an uneven foundation from which to map actual shortages.
“Some states became very adept at the equivalent of gerrymandering, where they were piecing together census blocks or census tracts in odd shapes in order to maximize the areas that are eligible,” said Stephen Petterson, a senior scholar at the Robert Graham Center, a policy think tank in Washington, DC, that focuses on primary care.
The federal Government Accountability Office has highlighted such issues since at least 1995, when it released a report identifying widespread data problems with the shortage area system and concluding it had “little assurance that federal funds are used where most needed.” The report noted one of the persistent shortcomings is that the system counts only physicians, not other key primary care providers.
Since 1998, federal officials have made three attempts to update the 1970s-era rules that define what counts as a shortage area. The authors of the Affordable Care Act tried most recently, tasking a committee of experts to decide on an update.
Among other things, the committee concluded in its 2011 report that nurse practitioners, physician assistants, and certified nurse midwives should be counted as primary care providers. But the recommendations fell short by just a handful of votes.
“We failed and the committee as a whole failed and HRSA failed by not moving the process forward,” said Petterson, who presented to the committee on how to comprehensively measure primary care needs.
Steve Holloway, who directs the Colorado health department’s Primary Care Office, served on the committee. Without action at the federal level, he then led a team to create Colorado’s own health professional shortage area designations that factor in nurse practitioners and physician assistants, not just doctors.
He said it’s taken about 6 years to create a tool and map of Colorado to answer a deceptively simple question: “How many actual flesh-and-blood, live clinicians are seeing patients?”
Ed Salsberg, who was the lead federal government representative on that committee and who headed HRSA’s National Center for Health Workforce Analysis, said the rest of the nation needs more precise data, too.
“It’s so important for the nation to target its resources to the highest-need communities,” he said. “It’s time again to try one more time to develop an improved methodology.”
In the past few years, more readily available data from insurance claims has allowed researchers to distinguish the medical providers who are practicing primary care from those who have specialized or retired.
Candice Chen, an associate professor of health policy and management at George Washington University’s Fitzhugh Mullan Institute for Health Workforce Equity, used claims data that reflects one large slice of the American population — about 66 million Medicaid beneficiaries — to map the primary care workforce.
Meanwhile, Monica O’Reilly-Jacob, a nurse-scientist who recently moved from Boston College to Columbia University’s School of Nursing, studied Medicare claims to conclude that fewer than 70% of physicians typically considered primary care providers were actually providing primary care. The rest, she said, often find more lucrative positions, such as subspecializing or working in hospitals. By contrast, nurse practitioners are likely undercounted. Her study found that close to half are providing primary care.
But such publicly available data leaves out much of the country, given that fewer than 40% of Americans are insured through Medicaid or Medicare.
“There’s no government organization that’s tracking: Who trained in what, where, and where are they now, and what are they practicing,” said Alison Huffstetler, medical director of the Robert Graham Center. “And if we don’t know who is doing what kind of care — and where — then there is no way for us to equitably manage the patient-to-clinician ratio across every state.”
In Costilla County, Ms. Martinez finally found someone to provide primary care: An experienced physician assistant who moved from Texas in December.
The physician assistant’s presence should bump the county out of its dire shortage, according to Colorado’s measure. But since he isn’t a physician, he’ll remain invisible in the national data and Costilla County will likely remain on the books as a federal shortage area.
Data reporter Hannah Recht, data editor Holly K. Hacker, and rural editor/correspondent Tony Leys contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — an independent source of health policy research, polling, and journalism.
Clinicians at Valley-Wide Health Systems never know who will appear at their clinic in San Luis, a town of about 600 people in southern Colorado.
“If someone’s in labor, they’ll show up. If someone has a laceration, they’ll show up,” said nurse practitioner Emelin Martinez, the chief medical officer for the healthcare system serving 13 rural Colorado counties.
But she struggled to find a full-time medical provider for that clinic, the only one in Costilla County. Born and raised in the area, Martinez filled some of the gap by driving about 45 minutes from Alamosa, the nearest city, once a week for months. A physician assistant from another town chipped in, too.
As one of the nation’s more than 1000 federally designated primary care shortage areas, Costilla County has many carrots to dangle in front of medical providers willing to practice there, including federal student loan repayments, bonus Medicare payments, and expedited visas for foreign clinicians. Still, Ms. Martinez said, its latest opening remained unfilled for more than a year. Not a single physician applied.
Policymakers have long tried to lure more primary care providers to the areas of the nation that have fewer than one physician for every 3500 residents. Recent examples include the Biden administration boosting funding in 2022 to address shortages and Sen. Bernie Sanders (I-Vt.) pushing sweeping primary care legislation in 2023.
But researchers steeped in the issue have a persistent frustration: It’s hard to know if any policy is working given that the data the federal government collects on primary care shortage areas has been flawed for a long time. One of the biggest gaps is that the system counts only physicians, not the myriad other healthcare professionals who now provide much of our nation›s primary care.
Additionally, a Health Affairs study shows the federal designations, which help allocate an estimated $1 billion in annual funding through at least 20 federal programs aimed at boosting primary care capacity, haven›t helped much.
In fact, Costilla County is among more than 180 federally designated areas that have remained stuck on the primary care shortage list for at least 40 years, according to a KFF Health News analysis. That›s even as the overall number of licensed US physicians more than doubled from 1990 to 2022 to over 1 million, according to the Federation of State Medical Boards, outpacing overall population growth.
No one disputes that much of the nation is starved for primary care clinicians, with patients having to wait weeks to get appointments or travel long distances for basic preventive care. Many doctors decide against primary care career paths, let alone practicing in isolated communities, because those jobs entail heavy workloads and earn less money and respect than specialists. But how does the nation solve the problem without knowing exactly where it is? And what tools must be used? Does a physician need to be the one providing the care?
Whitney Zahnd, president of the board of the Iowa Rural Health Association, said the fact that some rural areas have had such federal shortage designations for decades doesn’t prove they are ineffective. “Had the program not been there, would it have been even worse?” she said.
Federal funding supports 18,000 primary care doctors, nurse practitioners, and physician assistants to provide care to more than 18 million patients in the highest-need urban and rural communities across the country, said David Bowman, a spokesperson for the Health Resources and Services Administration, which manages the shortage designations. He said more than 80% of clinicians who get such scholarships or loan repayments continue to practice in shortage areas beyond their obligation of several years.
But that doesn’t mean they stick around forever.
Justin Markowski, a Yale School of Public Health doctoral student, coauthored the Health Affairs study that found the federal shortage designation makes no difference in upping physician density long-term. He is skeptical of policy ideas that promise big primary care fixes. That includes the Biden administration’s investment in more scholarships and loan repayments through the National Health Service Corps.
“You’re just throwing more money at a set of programs that don’t really seem to work,” he said. “We’ll see in a few years, but I’ll be shocked if it actually moved any physicians or any other advanced practice providers.”
One possible explanation for the persistence of shortage areas is that such incentives are too small or too fleeting.
But another issue is how shortages are measured. The government considers geographic shortage areas, now numbering just over 1000, but also population groups such as migrant farmworkers and individual facilities such as prisons that lack enough providers. Yet it’s up to state offices to identify populations and locations that might qualify as shortage areas and submit them to HRSA, which then scores the extent of any shortages. The funding and staffing for those state offices vary, creating an uneven foundation from which to map actual shortages.
“Some states became very adept at the equivalent of gerrymandering, where they were piecing together census blocks or census tracts in odd shapes in order to maximize the areas that are eligible,” said Stephen Petterson, a senior scholar at the Robert Graham Center, a policy think tank in Washington, DC, that focuses on primary care.
The federal Government Accountability Office has highlighted such issues since at least 1995, when it released a report identifying widespread data problems with the shortage area system and concluding it had “little assurance that federal funds are used where most needed.” The report noted one of the persistent shortcomings is that the system counts only physicians, not other key primary care providers.
Since 1998, federal officials have made three attempts to update the 1970s-era rules that define what counts as a shortage area. The authors of the Affordable Care Act tried most recently, tasking a committee of experts to decide on an update.
Among other things, the committee concluded in its 2011 report that nurse practitioners, physician assistants, and certified nurse midwives should be counted as primary care providers. But the recommendations fell short by just a handful of votes.
“We failed and the committee as a whole failed and HRSA failed by not moving the process forward,” said Petterson, who presented to the committee on how to comprehensively measure primary care needs.
Steve Holloway, who directs the Colorado health department’s Primary Care Office, served on the committee. Without action at the federal level, he then led a team to create Colorado’s own health professional shortage area designations that factor in nurse practitioners and physician assistants, not just doctors.
He said it’s taken about 6 years to create a tool and map of Colorado to answer a deceptively simple question: “How many actual flesh-and-blood, live clinicians are seeing patients?”
Ed Salsberg, who was the lead federal government representative on that committee and who headed HRSA’s National Center for Health Workforce Analysis, said the rest of the nation needs more precise data, too.
“It’s so important for the nation to target its resources to the highest-need communities,” he said. “It’s time again to try one more time to develop an improved methodology.”
In the past few years, more readily available data from insurance claims has allowed researchers to distinguish the medical providers who are practicing primary care from those who have specialized or retired.
Candice Chen, an associate professor of health policy and management at George Washington University’s Fitzhugh Mullan Institute for Health Workforce Equity, used claims data that reflects one large slice of the American population — about 66 million Medicaid beneficiaries — to map the primary care workforce.
Meanwhile, Monica O’Reilly-Jacob, a nurse-scientist who recently moved from Boston College to Columbia University’s School of Nursing, studied Medicare claims to conclude that fewer than 70% of physicians typically considered primary care providers were actually providing primary care. The rest, she said, often find more lucrative positions, such as subspecializing or working in hospitals. By contrast, nurse practitioners are likely undercounted. Her study found that close to half are providing primary care.
But such publicly available data leaves out much of the country, given that fewer than 40% of Americans are insured through Medicaid or Medicare.
“There’s no government organization that’s tracking: Who trained in what, where, and where are they now, and what are they practicing,” said Alison Huffstetler, medical director of the Robert Graham Center. “And if we don’t know who is doing what kind of care — and where — then there is no way for us to equitably manage the patient-to-clinician ratio across every state.”
In Costilla County, Ms. Martinez finally found someone to provide primary care: An experienced physician assistant who moved from Texas in December.
The physician assistant’s presence should bump the county out of its dire shortage, according to Colorado’s measure. But since he isn’t a physician, he’ll remain invisible in the national data and Costilla County will likely remain on the books as a federal shortage area.
Data reporter Hannah Recht, data editor Holly K. Hacker, and rural editor/correspondent Tony Leys contributed to this report.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF — an independent source of health policy research, polling, and journalism.
Doctors With Limited Vacation Have Increased Burnout Risk
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
A recent study sheds light on the heightened risk for burnout among physicians who take infrequent vacations and engage in patient-related work during their time off.
Conducted by the American Medical Association (AMA), the study focuses on the United States, where labor regulations regarding vacation days and compensation differ from German norms. Despite this distinction, it provides valuable insights into the vacation behavior of doctors and its potential impact on burnout risk.
Christine A. Sinsky, MD, study author and senior physician advisor for physician satisfaction at the AMA, and her colleagues invited more than 90,000 physicians to participate in a survey that used postal and computer-based methods. In all, 3024 physicians, mainly those contacted by mail, filled out the questionnaire.
Limited Vacation Days
A significant proportion (59.6%) of respondents reported having taken fewer than 15 vacation days in the previous year, with nearly 20% taking fewer than 5 days off. Even when officially on vacation, most (70.4%) found themselves dealing with patient-related tasks. For one-third, these tasks consumed at least 30 minutes on a typical vacation day, often longer. This phenomenon was noted especially among female physicians.
Doctors who took less vacation and worked during their time off displayed higher emotional exhaustion and reported feeling less fulfilled in their profession.
Administrative Tasks
Administrative tasks, though no longer confined to paper, significantly influenced physicians’ vacation behavior. In the United States, handling messages from patients through the electronic health records (EHR) inbox demands a considerable amount of time.
Courses and tutorials on EHR inbox management are on the rise. A 2023 review linked electronic health records management to an increased burnout risk in the US medical community.
Lack of Coverage
Many physicians lack coverage for their EHR inbox during their absence. Less than half (49.1%) stated that someone else manages their inbox while they are on vacation.
Difficulty in finding coverage, whether for the EHR inbox or patient care, is a leading reason why many physicians seldom take more than 3 weeks of vacation per year. Financial considerations also contribute to this decision, as revealed in the survey.
Vacation Lowers Risk
Further analysis showed that doctors who took more than 3 weeks of vacation per year, which is not common, had a lower risk of developing burnout. Having coverage for vacation was also associated with reduced burnout risk and increased professional fulfillment.
However, these benefits applied only when physicians truly took a break during their vacation. Respondents who spent 30 minutes or more per day on patient-related work had a higher burnout risk. The risk was 1.58 times greater for 30-60 minutes, 1.97 times greater for 60-90 minutes, and 1.92 times greater for more than 90 minutes.
System-Level Interventions
The vacation behavior observed in this study likely exacerbates the effects of chronic workplace overload that are associated with long working hours, thus increasing the risk for burnout, according to the researchers.
“System-level measures must be implemented to ensure physicians take an appropriate number of vacation days,” wrote the researchers. “This includes having coverage available to handle clinical activities and administrative tasks, such as managing the EHR inbox. This could potentially reduce the burnout rate among physicians.”
This article was translated from the Medscape German edition. A version of this article appeared on Medscape.com.
PCPs Increasingly Chained to EHRs
If you feel like the day doesn’t hold enough hours for you to get your work done, you’re right: (EHRs).
Investigators followed 141 academic PCPs between May 2019 and March 2023 and found they spent considerably more time engaging in EHR tasks during the final year of the study than in the prepandemic period. EHR time increased by over 8% on days with scheduled appointments and almost 20% on days without scheduled appointments.
“Physicians spend an unsustainable amount of time on EHR-based work, and that amount has increased steadily from 2019 to 2023,” Christine Sinsky, MD, vice president of professional satisfaction at the American Medical Association (AMA) and the senior author of the study, told this news organization. “It is imperative for healthcare systems to develop strategies to change the overall EHR workload trajectory to minimize PCPs’ occupational stress, including improved workflows, where the work is more appropriately distributed amongst the team.”
The study was published online on January 22, 2024, in the Annals of Family Medicine.
‘Pajama Time’
Dr. Sinsky said the motivation for conducting the current study was that PCPs have reported an increase in their workload, especially EHR tasks outside of work (“pajama time”) since the onset of the pandemic.
The research followed up on a 2017 analysis from the same group and other findings showing an increase in the time physicians spend in EHR tasks and the number of Inbox messages they receive from patients seeking medical advice increased during the months following the start of the pandemic.
“As a busy practicing PCP with a large panel of patients, my sense was that the workload was increasing even more, which is what our study confirmed,” said Brian G. Arndt, MD, of the Department of Family Medicine and Community Heath at the University of Wisconsin School of Medicine and Public Health, in Madison, Wisconsin, who led the new study.
The researchers analyzed EHR usage of 141 academic PCPs practicing family medicine, internal medicine, and general pediatrics, two thirds (66.7%) of whom were female. They compared the amount of time spent on EHR tasks during four timespans:
- May 2019 to February 2020
- June 2020 to March 2021
- May 2021 to March 2022
- April 2022 to March 2023
Each PCP’s time and Inbox message volume were calculated and then normalized over 8 hours of scheduled clinic appointments.
Increased Time, Increased Burnout
The study found evidence PCPs have reduced their clinical hours in response to their growing digital workload.
“We have a serious shortage of primary care physicians,” Dr. Sinsky said. “When PCPs cut back their clinical [work] as a coping mechanism for an unmanageable workload, this further exacerbates the primary care shortage, reducing access to care for patients.”
The researchers found increases from the first prepandemic period to the final period of their study in average time that PCPs spent at the EHR per 8 hours of scheduled clinic appointments (Table).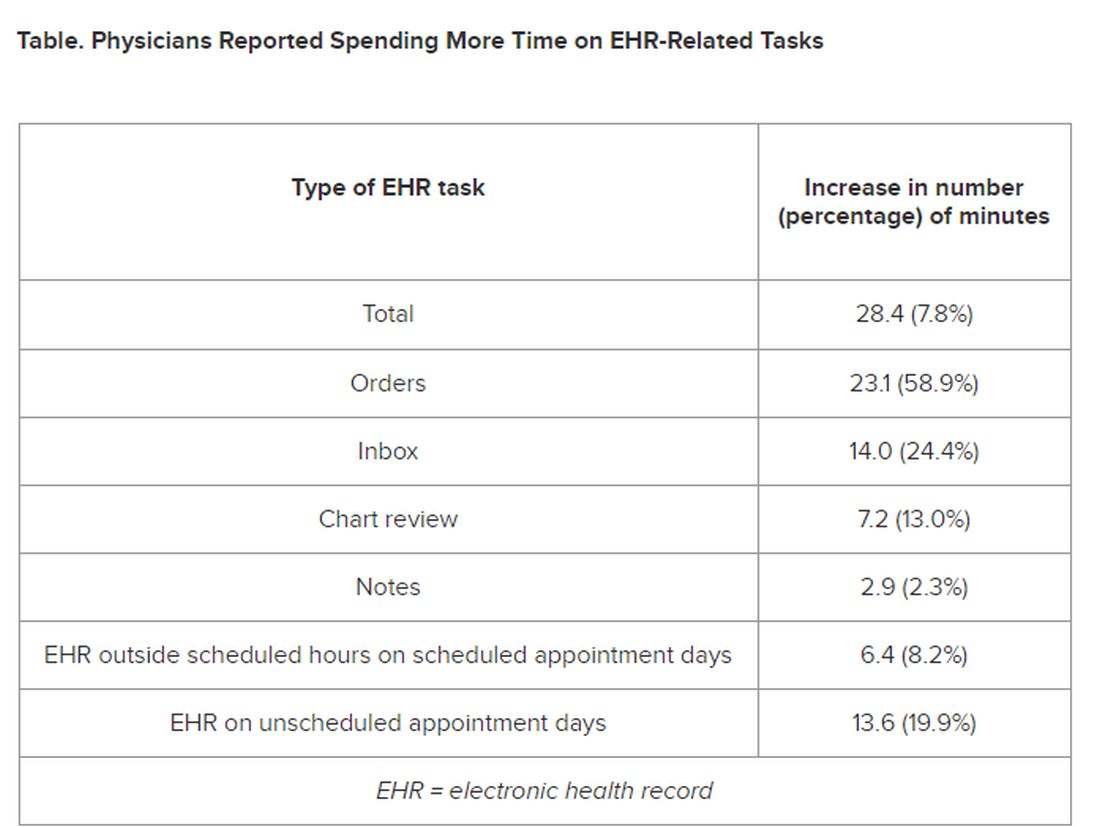
PCPs were inundated with several types of EHR-related responsibilities, including more medical advice requests (+55.5%) and more prescription messages (+19.5%) per 8 hours of scheduled clinic appointments. On the other hand, they had slightly fewer patient calls (−10.5%) and messages concerning test results (−2.7%).
A recent study of 307 PCPs across 31 primary care practices paralleled these findings. It found that physicians spent 36.2 minutes on the EHR per visit (interquartile range, 28.9-45.7 minutes). Included were 6.2 minutes of “pajama time” per visit and 7.8 minutes on the EHR per visit.
The amount of EHR time exceeded the amount of time allotted to a primary care visit (30 minutes). The authors commented that the EHR time burden “and the burnout associated with this burden represent a serious threat to the primary care physician workforce.”
“As more health systems across the country transition from fee-for-service to value-based payment arrangements, they need to balance the time PCPs and their care teams need for face-to-face care — in-person or video visits — with the increasing asynchronous care patients are seeking from us through the portal, for example, MyChart,” Dr. Arndt said.
Sinsky noted that when patients receive care from a PCP, quality is higher and costs are lower. “When access to primary care is further limited by virtue of physicians being overwhelmed by administrative work implemented via the EHR, so that they are reducing their hours, then we can expect negative consequences for patient care and costs of care.”
Tips for Reducing EHR Time
Arndt noted that some “brief investments” of time with patients “lead to high rates of return on decreased MyChart messaging.” For example, he has said to patients: “In the future, there’s no need to respond in MyChart with a ‘Thank you.’” Or “In the future, if you have questions from preappointment labs, no need to send me a separate message in MyChart prior to your visit since they’re typically just a few days out. I look closely at your labs and would always pick up the phone and call you if there was anything more urgent or pressing that needs more immediate action.”
Sinsky recommended two “high-yield opportunities” to reduce EHR-associated workload. The AMA offers a brief Inbox reduction checklist as well as a detailed toolkit to guide physicians and operational leaders in reducing the volume of unnecessary Inbox messages, she said.
Distribution of work among the team also can reduce the time physicians spent on order entry. “It doesn’t take a medical school education to enter orders for flu shots, lipid profiles, mammograms, and other tests, and yet we have primary care physicians around the country spending an hour or more per 8 hours of patient visits on this task,” she said.
‘Growing Mountain’
Sally Baxter, MD, assistant professor of ophthalmology and division chief for Ophthalmology Informatics and Data Sciences at University of California San Diego, said, “Studies like this ... are important for continuing to quantify the burden of EHR work and to evaluate potential interventions to reduce this burden and subsequent burnout.”
Baxter’s health system allows physicians to bill for asynchronous messaging when certain eligibility criteria are met. “This can deter frivolous messaging and also provide some compensation for the work involved,” she said.
“In addition, we’ve recently piloted using AI tools to help draft replies to patient messages in the EHR as another approach to tackling this important issue,” said Baxter, who wasn’t involved with the current study.
Eve Rittenberg, MD, an assistant professor at Harvard Medical School and a PCP at Brigham and Women’s Hospital Fish Center for Women’s Health, in Boston, recommended that healthcare systems “monitor EHR workload across gender, specialty, and other variables to develop equitable support and compensation models.”
Dr. Rittenberg, who wasn’t involved with the current study, said healthcare systems should consider supporting physicians by blocking out time during clinic sessions to manage their EHR work. “Cross-coverage systems are vital so that on their days off, physicians can unplug from the computer and know that their patients’ needs are being met,” she added.
This work was supported in part by the AMA Practice Transformation Initiative: EHR-Use Metrics Research which provided grant funding to several of the authors. Sinsky is employed by the AMA. Dr. Arndt and coauthors disclosed no relevant financial information. Dr. Baxter received nonfinancial support from Optonmed and Topcon for research studies and collaborated with some of the study authors on other research but not this particular study. Dr. Rittenberg received internal funding from the Brigham Care Redesign Incubator and Startup Program, Brigham and Women’s Hospital, for a previous pilot project of inbasket cross-coverage. She had no relevant current disclosures.
A version of this article appeared on Medscape.com.
If you feel like the day doesn’t hold enough hours for you to get your work done, you’re right: (EHRs).
Investigators followed 141 academic PCPs between May 2019 and March 2023 and found they spent considerably more time engaging in EHR tasks during the final year of the study than in the prepandemic period. EHR time increased by over 8% on days with scheduled appointments and almost 20% on days without scheduled appointments.
“Physicians spend an unsustainable amount of time on EHR-based work, and that amount has increased steadily from 2019 to 2023,” Christine Sinsky, MD, vice president of professional satisfaction at the American Medical Association (AMA) and the senior author of the study, told this news organization. “It is imperative for healthcare systems to develop strategies to change the overall EHR workload trajectory to minimize PCPs’ occupational stress, including improved workflows, where the work is more appropriately distributed amongst the team.”
The study was published online on January 22, 2024, in the Annals of Family Medicine.
‘Pajama Time’
Dr. Sinsky said the motivation for conducting the current study was that PCPs have reported an increase in their workload, especially EHR tasks outside of work (“pajama time”) since the onset of the pandemic.
The research followed up on a 2017 analysis from the same group and other findings showing an increase in the time physicians spend in EHR tasks and the number of Inbox messages they receive from patients seeking medical advice increased during the months following the start of the pandemic.
“As a busy practicing PCP with a large panel of patients, my sense was that the workload was increasing even more, which is what our study confirmed,” said Brian G. Arndt, MD, of the Department of Family Medicine and Community Heath at the University of Wisconsin School of Medicine and Public Health, in Madison, Wisconsin, who led the new study.
The researchers analyzed EHR usage of 141 academic PCPs practicing family medicine, internal medicine, and general pediatrics, two thirds (66.7%) of whom were female. They compared the amount of time spent on EHR tasks during four timespans:
- May 2019 to February 2020
- June 2020 to March 2021
- May 2021 to March 2022
- April 2022 to March 2023
Each PCP’s time and Inbox message volume were calculated and then normalized over 8 hours of scheduled clinic appointments.
Increased Time, Increased Burnout
The study found evidence PCPs have reduced their clinical hours in response to their growing digital workload.
“We have a serious shortage of primary care physicians,” Dr. Sinsky said. “When PCPs cut back their clinical [work] as a coping mechanism for an unmanageable workload, this further exacerbates the primary care shortage, reducing access to care for patients.”
The researchers found increases from the first prepandemic period to the final period of their study in average time that PCPs spent at the EHR per 8 hours of scheduled clinic appointments (Table).
PCPs were inundated with several types of EHR-related responsibilities, including more medical advice requests (+55.5%) and more prescription messages (+19.5%) per 8 hours of scheduled clinic appointments. On the other hand, they had slightly fewer patient calls (−10.5%) and messages concerning test results (−2.7%).
A recent study of 307 PCPs across 31 primary care practices paralleled these findings. It found that physicians spent 36.2 minutes on the EHR per visit (interquartile range, 28.9-45.7 minutes). Included were 6.2 minutes of “pajama time” per visit and 7.8 minutes on the EHR per visit.
The amount of EHR time exceeded the amount of time allotted to a primary care visit (30 minutes). The authors commented that the EHR time burden “and the burnout associated with this burden represent a serious threat to the primary care physician workforce.”
“As more health systems across the country transition from fee-for-service to value-based payment arrangements, they need to balance the time PCPs and their care teams need for face-to-face care — in-person or video visits — with the increasing asynchronous care patients are seeking from us through the portal, for example, MyChart,” Dr. Arndt said.
Sinsky noted that when patients receive care from a PCP, quality is higher and costs are lower. “When access to primary care is further limited by virtue of physicians being overwhelmed by administrative work implemented via the EHR, so that they are reducing their hours, then we can expect negative consequences for patient care and costs of care.”
Tips for Reducing EHR Time
Arndt noted that some “brief investments” of time with patients “lead to high rates of return on decreased MyChart messaging.” For example, he has said to patients: “In the future, there’s no need to respond in MyChart with a ‘Thank you.’” Or “In the future, if you have questions from preappointment labs, no need to send me a separate message in MyChart prior to your visit since they’re typically just a few days out. I look closely at your labs and would always pick up the phone and call you if there was anything more urgent or pressing that needs more immediate action.”
Sinsky recommended two “high-yield opportunities” to reduce EHR-associated workload. The AMA offers a brief Inbox reduction checklist as well as a detailed toolkit to guide physicians and operational leaders in reducing the volume of unnecessary Inbox messages, she said.
Distribution of work among the team also can reduce the time physicians spent on order entry. “It doesn’t take a medical school education to enter orders for flu shots, lipid profiles, mammograms, and other tests, and yet we have primary care physicians around the country spending an hour or more per 8 hours of patient visits on this task,” she said.
‘Growing Mountain’
Sally Baxter, MD, assistant professor of ophthalmology and division chief for Ophthalmology Informatics and Data Sciences at University of California San Diego, said, “Studies like this ... are important for continuing to quantify the burden of EHR work and to evaluate potential interventions to reduce this burden and subsequent burnout.”
Baxter’s health system allows physicians to bill for asynchronous messaging when certain eligibility criteria are met. “This can deter frivolous messaging and also provide some compensation for the work involved,” she said.
“In addition, we’ve recently piloted using AI tools to help draft replies to patient messages in the EHR as another approach to tackling this important issue,” said Baxter, who wasn’t involved with the current study.
Eve Rittenberg, MD, an assistant professor at Harvard Medical School and a PCP at Brigham and Women’s Hospital Fish Center for Women’s Health, in Boston, recommended that healthcare systems “monitor EHR workload across gender, specialty, and other variables to develop equitable support and compensation models.”
Dr. Rittenberg, who wasn’t involved with the current study, said healthcare systems should consider supporting physicians by blocking out time during clinic sessions to manage their EHR work. “Cross-coverage systems are vital so that on their days off, physicians can unplug from the computer and know that their patients’ needs are being met,” she added.
This work was supported in part by the AMA Practice Transformation Initiative: EHR-Use Metrics Research which provided grant funding to several of the authors. Sinsky is employed by the AMA. Dr. Arndt and coauthors disclosed no relevant financial information. Dr. Baxter received nonfinancial support from Optonmed and Topcon for research studies and collaborated with some of the study authors on other research but not this particular study. Dr. Rittenberg received internal funding from the Brigham Care Redesign Incubator and Startup Program, Brigham and Women’s Hospital, for a previous pilot project of inbasket cross-coverage. She had no relevant current disclosures.
A version of this article appeared on Medscape.com.
If you feel like the day doesn’t hold enough hours for you to get your work done, you’re right: (EHRs).
Investigators followed 141 academic PCPs between May 2019 and March 2023 and found they spent considerably more time engaging in EHR tasks during the final year of the study than in the prepandemic period. EHR time increased by over 8% on days with scheduled appointments and almost 20% on days without scheduled appointments.
“Physicians spend an unsustainable amount of time on EHR-based work, and that amount has increased steadily from 2019 to 2023,” Christine Sinsky, MD, vice president of professional satisfaction at the American Medical Association (AMA) and the senior author of the study, told this news organization. “It is imperative for healthcare systems to develop strategies to change the overall EHR workload trajectory to minimize PCPs’ occupational stress, including improved workflows, where the work is more appropriately distributed amongst the team.”
The study was published online on January 22, 2024, in the Annals of Family Medicine.
‘Pajama Time’
Dr. Sinsky said the motivation for conducting the current study was that PCPs have reported an increase in their workload, especially EHR tasks outside of work (“pajama time”) since the onset of the pandemic.
The research followed up on a 2017 analysis from the same group and other findings showing an increase in the time physicians spend in EHR tasks and the number of Inbox messages they receive from patients seeking medical advice increased during the months following the start of the pandemic.
“As a busy practicing PCP with a large panel of patients, my sense was that the workload was increasing even more, which is what our study confirmed,” said Brian G. Arndt, MD, of the Department of Family Medicine and Community Heath at the University of Wisconsin School of Medicine and Public Health, in Madison, Wisconsin, who led the new study.
The researchers analyzed EHR usage of 141 academic PCPs practicing family medicine, internal medicine, and general pediatrics, two thirds (66.7%) of whom were female. They compared the amount of time spent on EHR tasks during four timespans:
- May 2019 to February 2020
- June 2020 to March 2021
- May 2021 to March 2022
- April 2022 to March 2023
Each PCP’s time and Inbox message volume were calculated and then normalized over 8 hours of scheduled clinic appointments.
Increased Time, Increased Burnout
The study found evidence PCPs have reduced their clinical hours in response to their growing digital workload.
“We have a serious shortage of primary care physicians,” Dr. Sinsky said. “When PCPs cut back their clinical [work] as a coping mechanism for an unmanageable workload, this further exacerbates the primary care shortage, reducing access to care for patients.”
The researchers found increases from the first prepandemic period to the final period of their study in average time that PCPs spent at the EHR per 8 hours of scheduled clinic appointments (Table).
PCPs were inundated with several types of EHR-related responsibilities, including more medical advice requests (+55.5%) and more prescription messages (+19.5%) per 8 hours of scheduled clinic appointments. On the other hand, they had slightly fewer patient calls (−10.5%) and messages concerning test results (−2.7%).
A recent study of 307 PCPs across 31 primary care practices paralleled these findings. It found that physicians spent 36.2 minutes on the EHR per visit (interquartile range, 28.9-45.7 minutes). Included were 6.2 minutes of “pajama time” per visit and 7.8 minutes on the EHR per visit.
The amount of EHR time exceeded the amount of time allotted to a primary care visit (30 minutes). The authors commented that the EHR time burden “and the burnout associated with this burden represent a serious threat to the primary care physician workforce.”
“As more health systems across the country transition from fee-for-service to value-based payment arrangements, they need to balance the time PCPs and their care teams need for face-to-face care — in-person or video visits — with the increasing asynchronous care patients are seeking from us through the portal, for example, MyChart,” Dr. Arndt said.
Sinsky noted that when patients receive care from a PCP, quality is higher and costs are lower. “When access to primary care is further limited by virtue of physicians being overwhelmed by administrative work implemented via the EHR, so that they are reducing their hours, then we can expect negative consequences for patient care and costs of care.”
Tips for Reducing EHR Time
Arndt noted that some “brief investments” of time with patients “lead to high rates of return on decreased MyChart messaging.” For example, he has said to patients: “In the future, there’s no need to respond in MyChart with a ‘Thank you.’” Or “In the future, if you have questions from preappointment labs, no need to send me a separate message in MyChart prior to your visit since they’re typically just a few days out. I look closely at your labs and would always pick up the phone and call you if there was anything more urgent or pressing that needs more immediate action.”
Sinsky recommended two “high-yield opportunities” to reduce EHR-associated workload. The AMA offers a brief Inbox reduction checklist as well as a detailed toolkit to guide physicians and operational leaders in reducing the volume of unnecessary Inbox messages, she said.
Distribution of work among the team also can reduce the time physicians spent on order entry. “It doesn’t take a medical school education to enter orders for flu shots, lipid profiles, mammograms, and other tests, and yet we have primary care physicians around the country spending an hour or more per 8 hours of patient visits on this task,” she said.
‘Growing Mountain’
Sally Baxter, MD, assistant professor of ophthalmology and division chief for Ophthalmology Informatics and Data Sciences at University of California San Diego, said, “Studies like this ... are important for continuing to quantify the burden of EHR work and to evaluate potential interventions to reduce this burden and subsequent burnout.”
Baxter’s health system allows physicians to bill for asynchronous messaging when certain eligibility criteria are met. “This can deter frivolous messaging and also provide some compensation for the work involved,” she said.
“In addition, we’ve recently piloted using AI tools to help draft replies to patient messages in the EHR as another approach to tackling this important issue,” said Baxter, who wasn’t involved with the current study.
Eve Rittenberg, MD, an assistant professor at Harvard Medical School and a PCP at Brigham and Women’s Hospital Fish Center for Women’s Health, in Boston, recommended that healthcare systems “monitor EHR workload across gender, specialty, and other variables to develop equitable support and compensation models.”
Dr. Rittenberg, who wasn’t involved with the current study, said healthcare systems should consider supporting physicians by blocking out time during clinic sessions to manage their EHR work. “Cross-coverage systems are vital so that on their days off, physicians can unplug from the computer and know that their patients’ needs are being met,” she added.
This work was supported in part by the AMA Practice Transformation Initiative: EHR-Use Metrics Research which provided grant funding to several of the authors. Sinsky is employed by the AMA. Dr. Arndt and coauthors disclosed no relevant financial information. Dr. Baxter received nonfinancial support from Optonmed and Topcon for research studies and collaborated with some of the study authors on other research but not this particular study. Dr. Rittenberg received internal funding from the Brigham Care Redesign Incubator and Startup Program, Brigham and Women’s Hospital, for a previous pilot project of inbasket cross-coverage. She had no relevant current disclosures.
A version of this article appeared on Medscape.com.
VA Versus the Private Sector — No Contest? Think Again
Veterans Administration (VA) hospitals are a stepchild in the bizarre mishmash of the U.S. healthcare system. They’re best known (often justifiably so) for rather cantankerous patients, rigid rules, and other oddities (such as patients being able to go on leave and come back).
The majority of American doctors, including myself, did at least part of our training at a VA and have no shortage of stories about them. One I worked at (Omaha VA) was powered by its own nuclear reactor in the basement (no, really, it was, though sadly it’s since been taken out).

VA hospitals, in general, are no-frills — linoleum floors, no piano player in the lobby, very few private rooms, and occasionally in the news for scandals like the one at my hometown Carl T. Hayden VA hospital (I trained there, too).
Yet, . Their focus on patient care, rather than profits, allows them to run with 8% fewer administrative staff since they generally don’t have to deal with insurance billings, denials, and other paperwork (they also don’t have to deal with shareholders and investor demands or ridiculous CEO salaries, though the study didn’t address that).
On a national scale, this would mean roughly 900,000 fewer administrative jobs in the private sector. Granted, that also would mean those people would have to find other jobs, but let’s look at the patient side. If you had 900,000 fewer desk workers, you’d have the money to hire more nurses, respiratory techs, therapists, and other people directly involved in patient care. You’d also need a lot less office space, which further brings down overhead.
Part of the problem is that a lot of the current medical business is in marketing — how many ads do you see each day for different hospitals in your area? — and upcoding to extract more money from each billing. Neither of these has any clinical value on the patient side of things.
You don’t have to look back too far (2020) for the study that found U.S. healthcare spent four times as much money ($812 billion) per capita than our northern neighbors.
And, for all the jokes we make about the VA (myself included), a study last year found its care was on par (or even better than) most hospitals .
I’m not saying the VA is perfect. All of us who worked there can think of times it wasn’t. But we also remember plenty of issues we’ve had at other places we’ve practiced, too.
Maybe it’s time to stop laughing at the VA and realize they’re doing something right — and learn from it to make healthcare better at the other 6,000 or so hospitals in the U.S.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Veterans Administration (VA) hospitals are a stepchild in the bizarre mishmash of the U.S. healthcare system. They’re best known (often justifiably so) for rather cantankerous patients, rigid rules, and other oddities (such as patients being able to go on leave and come back).
The majority of American doctors, including myself, did at least part of our training at a VA and have no shortage of stories about them. One I worked at (Omaha VA) was powered by its own nuclear reactor in the basement (no, really, it was, though sadly it’s since been taken out).
VA hospitals, in general, are no-frills — linoleum floors, no piano player in the lobby, very few private rooms, and occasionally in the news for scandals like the one at my hometown Carl T. Hayden VA hospital (I trained there, too).
Yet, . Their focus on patient care, rather than profits, allows them to run with 8% fewer administrative staff since they generally don’t have to deal with insurance billings, denials, and other paperwork (they also don’t have to deal with shareholders and investor demands or ridiculous CEO salaries, though the study didn’t address that).
On a national scale, this would mean roughly 900,000 fewer administrative jobs in the private sector. Granted, that also would mean those people would have to find other jobs, but let’s look at the patient side. If you had 900,000 fewer desk workers, you’d have the money to hire more nurses, respiratory techs, therapists, and other people directly involved in patient care. You’d also need a lot less office space, which further brings down overhead.
Part of the problem is that a lot of the current medical business is in marketing — how many ads do you see each day for different hospitals in your area? — and upcoding to extract more money from each billing. Neither of these has any clinical value on the patient side of things.
You don’t have to look back too far (2020) for the study that found U.S. healthcare spent four times as much money ($812 billion) per capita than our northern neighbors.
And, for all the jokes we make about the VA (myself included), a study last year found its care was on par (or even better than) most hospitals .
I’m not saying the VA is perfect. All of us who worked there can think of times it wasn’t. But we also remember plenty of issues we’ve had at other places we’ve practiced, too.
Maybe it’s time to stop laughing at the VA and realize they’re doing something right — and learn from it to make healthcare better at the other 6,000 or so hospitals in the U.S.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Veterans Administration (VA) hospitals are a stepchild in the bizarre mishmash of the U.S. healthcare system. They’re best known (often justifiably so) for rather cantankerous patients, rigid rules, and other oddities (such as patients being able to go on leave and come back).
The majority of American doctors, including myself, did at least part of our training at a VA and have no shortage of stories about them. One I worked at (Omaha VA) was powered by its own nuclear reactor in the basement (no, really, it was, though sadly it’s since been taken out).
VA hospitals, in general, are no-frills — linoleum floors, no piano player in the lobby, very few private rooms, and occasionally in the news for scandals like the one at my hometown Carl T. Hayden VA hospital (I trained there, too).
Yet, . Their focus on patient care, rather than profits, allows them to run with 8% fewer administrative staff since they generally don’t have to deal with insurance billings, denials, and other paperwork (they also don’t have to deal with shareholders and investor demands or ridiculous CEO salaries, though the study didn’t address that).
On a national scale, this would mean roughly 900,000 fewer administrative jobs in the private sector. Granted, that also would mean those people would have to find other jobs, but let’s look at the patient side. If you had 900,000 fewer desk workers, you’d have the money to hire more nurses, respiratory techs, therapists, and other people directly involved in patient care. You’d also need a lot less office space, which further brings down overhead.
Part of the problem is that a lot of the current medical business is in marketing — how many ads do you see each day for different hospitals in your area? — and upcoding to extract more money from each billing. Neither of these has any clinical value on the patient side of things.
You don’t have to look back too far (2020) for the study that found U.S. healthcare spent four times as much money ($812 billion) per capita than our northern neighbors.
And, for all the jokes we make about the VA (myself included), a study last year found its care was on par (or even better than) most hospitals .
I’m not saying the VA is perfect. All of us who worked there can think of times it wasn’t. But we also remember plenty of issues we’ve had at other places we’ve practiced, too.
Maybe it’s time to stop laughing at the VA and realize they’re doing something right — and learn from it to make healthcare better at the other 6,000 or so hospitals in the U.S.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.