User login
Virtual ADA Scientific Sessions to offer full program
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
The American Diabetes Association’s 80th Scientific Sessions will forge ahead virtually this year in the face of the COVID-19 pandemic, with nearly all of its originally scheduled content to be presented online.
The meeting will take place online June 12-16, the same days it was slated to occur in Chicago and at the same times. All presentations were recorded in advance, but participants will be able to ask real-time questions during some sessions. Registered attendees – who paid a reduced fee – will have access to the online content for 90 days afterward.
ADA announced the shift in plans on April 3, after Chicago’s McCormick Place convention center became unavailable due to the COVID-19 pandemic. While some major medical meetings had to be canceled entirely or trimmed down online, “This is one of the international meetings that has had more time to really get ready to plan such a virtual session,” association co-president Robert H. Eckel, MD, told Medscape Medical News.
This year’s program features fewer blockbuster randomized clinical trials than in years past.
But it does offer a huge amount of clinical research focused on both type 1 and type 2 diabetes, children with diabetes, gestational diabetes, and much more. Also included are deep dives into optimal clinical translation of findings from previous cardiovascular outcomes trials (CVOTs).
Noteworthy sessions include four new automated insulin delivery system trials on Friday, new diabetes-specific data from the DAPA-HF trial on Saturday, and a debate on Sunday about the future of metformin as first-line therapy for people with established heart disease or at high risk.
And on Tuesday morning, full results from the CVOT VERTIS-CV, with the sodium-glucose cotransporter 2 (SGLT2) inhibitor ertugliflozin (Steglatro, Merck), will be reported.
Also presented on Tuesday will be the first cardiovascular and cancer outcomes from the Diabetes Prevention Program Outcomes Study (DPPOS).
The online content will cover roughly 90% of what was originally scheduled, meeting planning committee chair Jose C. Florez, MD, PhD, told Medscape Medical News.
There is no session officially addressing COVID-19, he said, because the topics were already finalized by February, but “I’m sure it will be discussed in informal exchanges ... the data are just coming out,” he said.
Florez also called attention to two symposia addressing the other major topic dominating today’s news: racial disparities. One on Friday will address that topic with regard to maternal/fetal health, and another on Monday will cover disparities in diabetes care generally.
“Both because of COVID-19 and how it has affected people with diabetes, and within that, disadvantaged people, more aggressively, and in the current context of how racism is coming to the surface, these two sessions will become very, very pertinent,” he said.
Putting the Treatment Pieces Together in Type 2 Diabetes
The Evaluation of Ertugliflozin Efficacy and Safety Cardiovascular Outcomes Trial (VERTIS-CV) session will include the major cardiovascular, metabolic, renal, and safety outcomes for that drug, along with a meta-analysis of outcomes from trials of several different SGLT2 inhibitors.
All eyes will be on the VERTIS-CV presentation because ertugliflozin broke ranks with the other drugs in this class and failed to produce statistically significant drops in the relevant endpoints, as detailed in top-line data issued by the company in April.
And the provocatively titled session, “DAPA-HF Update: Have We Lost SGLT2 inhibitors to Cardiologists?!” will include a review of the trial’s main findings presented at the European Society of Cardiology meeting in September 2019, and published a few weeks later in the New England Journal of Medicine, along with new data on patient-centered and metabolic outcomes, and diabetes prevention. An independent commentator will presumably address the session title’s question.
Eckel, who has been working to establish a new cardiometabolic medicine subspecialty, commented: “I think we have not lost it, but I think SGLT2 inhibitors are a perfect example of why we need physicians trained in this overlap of diabetes medicine and cardiology.”
And, he said, we may be coming to the end of the CVOTs trial phenomenon.
“I think unless there’s a whole new class of drugs developed, we may be done with CVOTs for dipeptidyl peptidase-4 (DPP-4) inhibitors, SGLT2 inhibitors, and glucagon-like peptide 1 (GLP-1) receptor agonists. We’ve learned a lot, and I’m not sure we need more other than mechanistic studies ... I don’t think we really know yet how SGLT2 inhibitors or GLP-1 agonists work,” Eckel said.
Metformin, on the other hand, has not been subject to a CVOT because it has been available as a generic since long before the US Food and Drug Administration mandated the CVOTs for new drugs for type 2 diabetes in 2008.
Such a trial is unlikely to be conducted at this point, but the new DPPOS data might actually come close, Florez noted.
The DPPOS is the observational follow-up of the landmark randomized DPP trial, which found that intensive lifestyle intervention and metformin reduced progression from prediabetes to type 2 diabetes.
Numerous additional outcomes have been reported over the years, but this will be the first-ever reporting of DPPOS data on both hard cardiovascular events and cancer incidence in people who have been continuously taking metformin for more than 20 years.
“There’s a lot of interest in whether metformin has an effect on cardiovascular events and cancer ... I think that’s going to be a very interesting session,” Florez said, noting that “short of a randomized clinical trial, which it’s hard to imagine would come to be, this is really, really good.”
Also examining metformin will be a debate on Sunday, “Should Metformin Be Considered First-Line Therapy for Individuals with Type 2 Diabetes With Established Arteriosclerotic Cardiovascular Disease (ASCVD) or at High Risk for ASCVD?”
And on Saturday, a debate will address another old-guard diabetes drug class, asking: “Is There a Current Place for Sulfonylureas in the Treatment of Type 2 Diabetes?”
Overall, Florez said, meeting attendees will come away with “a more clear understanding of the placement of SGLT2 inhibitors and GLP-1 agonists in the type 2 diabetes treatment algorithm.”
“What are the settings in which these [newer] drugs ought to be used, compared to the old-timers like metformin and sulfonylureas? One thing is having the trials, but the other is figuring out how you interpret these in deciding what happens at the point of care.”
Two more future-looking type 2 diabetes symposia of potential interest to clinicians are “Unraveling the Heterogeneity in Type 2 Diabetes” on Sunday and “Perspectives on the Future of Precision Diabetes Medicine — A Joint ADA/EASD Symposium” on Monday.
Type 1 Diabetes, Technology, and Kids
A symposium on Friday will feature four new clinical trials of automated insulin delivery systems for people with type 1 diabetes, the “US Advanced Hybrid Closed-Loop (AHCL) Pivotal Safety Study, FLAIR — An NIDDK-Sponsored International, Multi-site Randomized Crossover Trial of AHCL vs 670G,” the New Zealand AHCL randomized crossover trial, and the Horizon Automated Glucose Control System pre-pivotal trial data.
“Closed-loop devices are getting a lot of traction ... These trials will continue to advance the notion that these devices will narrow the glycemic range, prevent hypoglycemia, and improve quality of life because people don’t have to pay as much attention mentally to the management of the diabetes,” Florez said.
He added that although these trials “have been in the works for a while and they’re not big surprises, they continue to build a body of evidence suggesting that these devices will be part of our armamentarium in the very near future.”
And on Saturday, a debate will address the somewhat controversial question of whether continuous glucose monitoring in type 2 diabetes is worth the cost.
There will also be plenty of pediatric diabetes material presented this year, too.
On Sunday, there will be new insights from the Restoring Insulin Secretion (RISE) study, which examines prediabetes and type 2 diabetes in youth, and on Monday, 20-year data from the SEARCH for Diabetes in Youth Study will be reported.
And on Monday, the most recent findings from The Environmental Determinants of Diabetes in the Young (TEDDY) study of environmental triggers of type 1 diabetes will be presented.
All-Virtual Meeting: Pros and Cons
The all-virtual meeting format will have pluses and minuses, Eckel predicts.
Advantages include the fact that attendees don’t have to physically run from room to room or make difficult decisions about conflicting sessions.
“The fact that this meeting will be taking place in reality in terms of the timing of sessions, one can transition from one room to another in a matter of seconds if you want to,” he noted.
However, he observed, “a lot of interesting things happen in the hallways at meetings. Colleagues from around the world get together and knock heads about their ongoing research and potential collaborations can be formulated.
“Opportunities to engage with one another beyond the formality of the meeting is going to be lost to some extent.”
What’s more, the sessions will all be in Central US (Chicago) time, “So if you live in Thailand, the session may be occurring at a time when you’re in bed. If you want to see it live, then you’ve got to get up. Then you can ask a question.”
On the other hand, since all the content will be available online for 90 days, “if you want to stay in bed and you live in Thailand, you can get up a week from now during the day and log into a session you may have missed.”
Indeed, Florez said, “One silver lining of this virtual conference is that we’ve lowered the barriers for people to attend. It’s much more global. We’ve had an amazing influx of new registrants who were not planning on coming and were not registered for the original meeting and have registered since [more than 10,000 at the time of writing], and they continue to pile in.”
“We plan to reach people we haven’t reached before. The big question for ADA moving forward will be how much this can become a permanent feature, where even if we do it in person in the future, maybe we offer at least some virtual options so that our reach can go farther.”
Eckel has reported sitting on the scientific advisory board for a Kowa Company trial of pemafibrate and on an advisory board for Novo Nordisk. Florez has reported being a speaker for Novo Nordisk and receiving an honorarium from ADA for chairing the conference planning committee.
This article originally appeared on Medscape.com.
Do cinnamon supplements improve glycemic control in adults with T2DM?
EVIDENCE SUMMARY
A 2013 systematic review of 10 randomized controlled trials (RCTs) with a total of 543 patients with type 2 diabetes evaluated the effect of cinnamon (120 mg/d to 6 g/d) on measures of glycemic control.1 Study duration ranged from 4 to 18 weeks. Fasting glucose levels demonstrated small but statistically significant reductions (−24.6 mg/dL; 95% confidence interval [CI], −40.5 to −8.7 mg/dL), whereas hemoglobin A1C levels didn’t differ between treatment and control groups (−0.16%; 95% CI, −0.39% to 0.02%). Study limitations included heterogeneity of cinnamon dosing and formulation and concurrent use of oral hypoglycemic agents.
Studies of glycemic control produce mixed results
A 2012 systematic review of 10 RCTs comprising 577 patients with type 1 (72 patients) or type 2 (505 patients) diabetes evaluated the effects of cinnamon supplements (mean dose, 1.9 g/d) on glycemic control compared with placebo, active control, or no treatment.2 Study duration ranged from 4.3 to 16 weeks (mean, 10.8 weeks). Studies evaluating hemoglobin A1C lasted at least 12 weeks.
Fasting glucose as measured in 8 studies (338 patients) and hemoglobin A1C as measured in 6 studies (405 patients) didn’t differ between treatment groups (mean fasting glucose difference = −0.91 mmol/L; 95% CI, −1.93 to 0.11; mean hemoglobin A1C difference = −0.06; 95% CI, −0.29 to 0.18). The risk for bias was assessed as high or unclear in 8 studies and moderate in 2 studies.
A 2012 systematic review and meta-analysis of 6 RCTs including 435 patients with type 2 diabetes evaluated the impact of cinnamon supplements (1 to 6 g/d) on glycemic control.3 Participants consumed cinnamon for 40 to 160 days. Hemoglobin A1C decreased by 0.09% (95% CI, 0.04% to 0.14%) in 5 trials (375 patients), and fasting glucose decreased by 0.84 mmol/L (CI, 0.66 to 1.02) in 5 trials (326 patients). Study limitations included heterogeneity of cinnamon dosing and study population.
RECOMMENDATIONS
The American Diabetes Association finds insufficient evidence to support the use of herbs or spices, including cinnamon, in treating diabetes.4
Editor’s Takeaway
Meta-analyses of multiple small, lower-quality studies yield uncertain conclusions. If cinnamon does improve glycemic control, the benefit is minimal—but so is therisk.
1. Allen RW, Schwartzman E, Baker WL, et al. Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis. Ann Fam Med. 2013;11:452-459.
2. Leach MJ, Kumar S. Cinnamon for diabetes mellitus. Cochrane Database Syst Rev. 2012;(9):CD007170.
3. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: systematic review and meta-analysis. Clin Nutr. 2012;31:609-615.
4. American Diabetes Association. Standards of medical care in diabetes—2017. 4. Lifestyle management. Diabetes Care. 2017;40(suppl 1):S33-S43.
EVIDENCE SUMMARY
A 2013 systematic review of 10 randomized controlled trials (RCTs) with a total of 543 patients with type 2 diabetes evaluated the effect of cinnamon (120 mg/d to 6 g/d) on measures of glycemic control.1 Study duration ranged from 4 to 18 weeks. Fasting glucose levels demonstrated small but statistically significant reductions (−24.6 mg/dL; 95% confidence interval [CI], −40.5 to −8.7 mg/dL), whereas hemoglobin A1C levels didn’t differ between treatment and control groups (−0.16%; 95% CI, −0.39% to 0.02%). Study limitations included heterogeneity of cinnamon dosing and formulation and concurrent use of oral hypoglycemic agents.
Studies of glycemic control produce mixed results
A 2012 systematic review of 10 RCTs comprising 577 patients with type 1 (72 patients) or type 2 (505 patients) diabetes evaluated the effects of cinnamon supplements (mean dose, 1.9 g/d) on glycemic control compared with placebo, active control, or no treatment.2 Study duration ranged from 4.3 to 16 weeks (mean, 10.8 weeks). Studies evaluating hemoglobin A1C lasted at least 12 weeks.
Fasting glucose as measured in 8 studies (338 patients) and hemoglobin A1C as measured in 6 studies (405 patients) didn’t differ between treatment groups (mean fasting glucose difference = −0.91 mmol/L; 95% CI, −1.93 to 0.11; mean hemoglobin A1C difference = −0.06; 95% CI, −0.29 to 0.18). The risk for bias was assessed as high or unclear in 8 studies and moderate in 2 studies.
A 2012 systematic review and meta-analysis of 6 RCTs including 435 patients with type 2 diabetes evaluated the impact of cinnamon supplements (1 to 6 g/d) on glycemic control.3 Participants consumed cinnamon for 40 to 160 days. Hemoglobin A1C decreased by 0.09% (95% CI, 0.04% to 0.14%) in 5 trials (375 patients), and fasting glucose decreased by 0.84 mmol/L (CI, 0.66 to 1.02) in 5 trials (326 patients). Study limitations included heterogeneity of cinnamon dosing and study population.
RECOMMENDATIONS
The American Diabetes Association finds insufficient evidence to support the use of herbs or spices, including cinnamon, in treating diabetes.4
Editor’s Takeaway
Meta-analyses of multiple small, lower-quality studies yield uncertain conclusions. If cinnamon does improve glycemic control, the benefit is minimal—but so is therisk.
EVIDENCE SUMMARY
A 2013 systematic review of 10 randomized controlled trials (RCTs) with a total of 543 patients with type 2 diabetes evaluated the effect of cinnamon (120 mg/d to 6 g/d) on measures of glycemic control.1 Study duration ranged from 4 to 18 weeks. Fasting glucose levels demonstrated small but statistically significant reductions (−24.6 mg/dL; 95% confidence interval [CI], −40.5 to −8.7 mg/dL), whereas hemoglobin A1C levels didn’t differ between treatment and control groups (−0.16%; 95% CI, −0.39% to 0.02%). Study limitations included heterogeneity of cinnamon dosing and formulation and concurrent use of oral hypoglycemic agents.
Studies of glycemic control produce mixed results
A 2012 systematic review of 10 RCTs comprising 577 patients with type 1 (72 patients) or type 2 (505 patients) diabetes evaluated the effects of cinnamon supplements (mean dose, 1.9 g/d) on glycemic control compared with placebo, active control, or no treatment.2 Study duration ranged from 4.3 to 16 weeks (mean, 10.8 weeks). Studies evaluating hemoglobin A1C lasted at least 12 weeks.
Fasting glucose as measured in 8 studies (338 patients) and hemoglobin A1C as measured in 6 studies (405 patients) didn’t differ between treatment groups (mean fasting glucose difference = −0.91 mmol/L; 95% CI, −1.93 to 0.11; mean hemoglobin A1C difference = −0.06; 95% CI, −0.29 to 0.18). The risk for bias was assessed as high or unclear in 8 studies and moderate in 2 studies.
A 2012 systematic review and meta-analysis of 6 RCTs including 435 patients with type 2 diabetes evaluated the impact of cinnamon supplements (1 to 6 g/d) on glycemic control.3 Participants consumed cinnamon for 40 to 160 days. Hemoglobin A1C decreased by 0.09% (95% CI, 0.04% to 0.14%) in 5 trials (375 patients), and fasting glucose decreased by 0.84 mmol/L (CI, 0.66 to 1.02) in 5 trials (326 patients). Study limitations included heterogeneity of cinnamon dosing and study population.
RECOMMENDATIONS
The American Diabetes Association finds insufficient evidence to support the use of herbs or spices, including cinnamon, in treating diabetes.4
Editor’s Takeaway
Meta-analyses of multiple small, lower-quality studies yield uncertain conclusions. If cinnamon does improve glycemic control, the benefit is minimal—but so is therisk.
1. Allen RW, Schwartzman E, Baker WL, et al. Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis. Ann Fam Med. 2013;11:452-459.
2. Leach MJ, Kumar S. Cinnamon for diabetes mellitus. Cochrane Database Syst Rev. 2012;(9):CD007170.
3. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: systematic review and meta-analysis. Clin Nutr. 2012;31:609-615.
4. American Diabetes Association. Standards of medical care in diabetes—2017. 4. Lifestyle management. Diabetes Care. 2017;40(suppl 1):S33-S43.
1. Allen RW, Schwartzman E, Baker WL, et al. Cinnamon use in type 2 diabetes: an updated systematic review and meta-analysis. Ann Fam Med. 2013;11:452-459.
2. Leach MJ, Kumar S. Cinnamon for diabetes mellitus. Cochrane Database Syst Rev. 2012;(9):CD007170.
3. Akilen R, Tsiami A, Devendra D, et al. Cinnamon in glycaemic control: systematic review and meta-analysis. Clin Nutr. 2012;31:609-615.
4. American Diabetes Association. Standards of medical care in diabetes—2017. 4. Lifestyle management. Diabetes Care. 2017;40(suppl 1):S33-S43.
EVIDENCE-BASED ANSWER:
The answer isn’t clear. Cinnamon supplements for adults with type 2 diabetes haven’t been shown to decrease hemoglobin A1C (strength of recommendation [SOR]: C, multiple systematic reviews of disease-oriented outcomes).
Cinnamon supplements have shown inconsistent effects on fasting glucose levels (SOR: C, multiple systematic reviews and a single meta-analysis of disease-oriented outcomes). Supplements decreased fasting glucose levels in some studies, but the evidence isn’t consistent and hasn’t been correlated with clinically significant improvements in glycemic control.

Hemiballismus in Patients With Poorly Controlled Type 2 Diabetes Mellitus
Hemiballismus is an acquired hyperkinetic movement disorder characterized by unilateral, involuntary, often large-amplitude limb movements. Ballistic movements are now considered to be on the choreiform spectrum.1 Movements usually involve both the arm and leg, and in half of cases, facial movements such as tongue clucking and grimacing are seen.2,3 Presentations of hemiballismus vary in severity from intermittent to nearly continuous movements, which, in some cases, may lead to exhaustion, injury, or disability. Some patients are unable to ambulate or feed themselves with the affected limb.
Background
The 2 most common causes of hemichorea-hemiballismus are stroke and hyperglycemia, with an incidence of 4% and unknown incidence, respectively.1,3,4 Other causes include HIV, traumatic brain injury, encephalitis, vasculitis, mass effect, multiple sclerosis, and adverse drug reactions. 4-7 Acute or subacute hemiballismus is classically attributed to a lesion in subthalamic nucleus (STN), but this is true only in a minority of cases. Hemiballismus can be caused by any abnormality in various subnuclei of the basal ganglia, including the classic location in the STN, striatum, and globus pallidus.4 Evidence shows the lesions typically involve a functional network connected to the posterolateral putamen.8
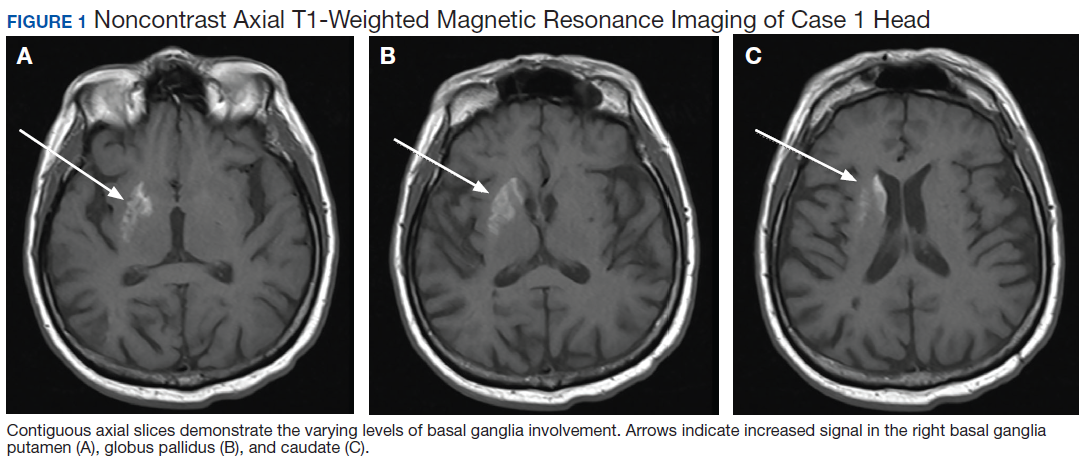
Although not commonly recognized, hyperglycemia in patients with type 2 diabetes mellitus (T2DM) is the second most common cause of hemichoreahemiballismus. 3 Over the past 90 years, numerous case reports have described patients with DM with acute and subacute onset of hemiballistic and hemichoreiform movements while in a hyperglycemic state or after its resolution. Reported cases have been limited to small numbers of patients with only a few larger-scale reviews of more than 20 patients.7,9 Most reported cases involve geriatric patients and more commonly, females of Eastern Asian descent with an average age of onset of 71 years.4,10 Patients typically present with glucose levels from 500 to 1,000 mg/dL and hemoglobin A1c (HbA1c) levels almost double the normal values. Interestingly, neuroimaging findings in these patients have consistently shown hyperintense signal in the contralateral basal ganglia on T1-weighted magnetic resonance images (MRIs). Noncontrast computed tomography (CT) shows well-defined unilateral increased density in the contralateral basal ganglia without mass effect.1,9,11
This report aims to illustrate and enhance the understanding of hemiballismus associated with hyperglycemia. One patient presented to the US Department of Veterans Affairs (VA) Bay Pines VA Healthcare System (BPVAHCS) in Florida, which motivated us to search for other similar cases. We reviewed the charts of 2 other patients who presented to BPVAHCS over the past 10 years. The first case presented with severe hyperglycemia and abnormal movements that were not clearly diagnosed as hemiballismus. MRI findings were characteristic and assisted in making the diagnosis. The second case was misdiagnosed as hemiballismus secondary to ischemic stroke. The third case was initially diagnosed as conversion disorder until movements worsened and the correct diagnosis of hyperglycemia-induced hemichorea hemiballismus was confirmed by the pathognomonic neuroimaging findings.
Case Presentations
Case 1
A 65-year-old male with a history of uncontrolled T2DM presented with repetitive twitching and kicking movements that involved his left upper and lower extremities for 3 weeks. The patient reported that he did not take his medications or follow the recommended diabetes diet. His HbA1c on admission was 12.2% with a serum glucose of 254 mg/dL. The MRI showed a hyperintense T1 signal within the right basal ganglia including the right caudate with sparing of the internal capsule (Figure 1). There was no associated mass effect or restricted diffusion. It was compatible with a diagnosis of hyperglycemia- induced hemichorea-hemiballismus. The patient was advised to resume taking glipizide 10 mg daily, metformin 1,000 mg by mouth twice daily, and to begin 10 units of 70/30 insulin aspart 15 minutes before meals twice daily, and to follow a low carbohydrate diet, with reduce dietary intake of sugar. At his 1-month follow-up visit, the patient reported an improvement in his involuntary movements. At the 5-month follow-up, the patient’s HbA1c level was 10.4% and his hyperkinetic movements had completely resolved.
Case 2
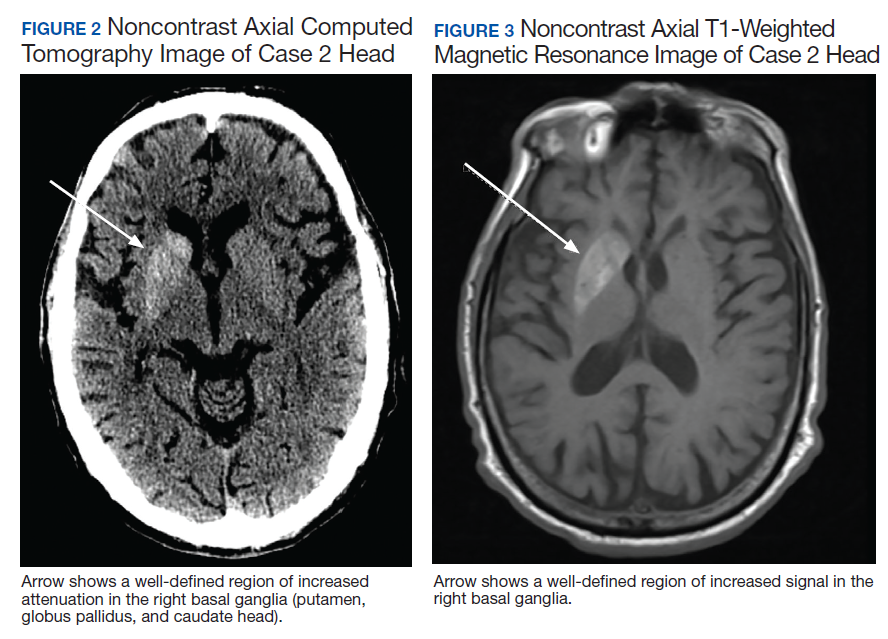
of T2DM, hypertension, and hyperlipidemia was admitted due to increased jerky movements in the left upper extremity. On admission, his vital signs were within normal limits and his physical examination demonstrated choreoathetoid movements with ballistic components of his left upper extremity. His laboratory results showed a glucose level of 528 mg/dL with a HbA1c of 16.3%. An initial CT obtained in the emergency department (ED) demonstrated a well-defined hyperdensity in the striatal (caudate and lentiform nucleus) region (Figure 2). There was no associated edema/mass effect that would be typical for an intracranial hemorrhage.
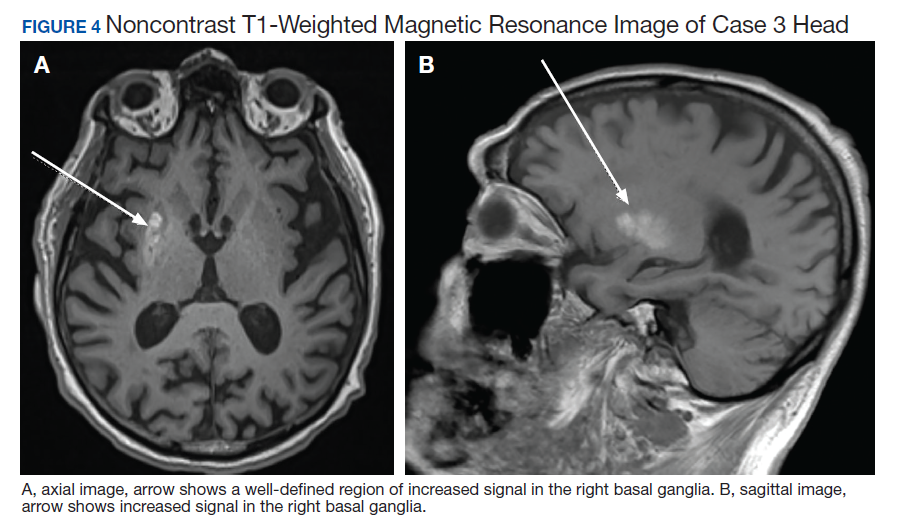
An MRI obtained 1 week later showed hyperintense TI signal corresponding to the basal ganglia (Figure 3). In addition, there was a questionable lacunar infarct in the right internal capsule. Due to lack of awareness regarding hyperglycemic associated basal ganglia changes, the patient’s movement disorder was presumed to be ischemic in etiology. The patient was prescribed oral amantadine 100 mg 3 times daily for the hemiballismus in conjunction with treatment of his T2DM. The only follow-up occurred 5 weeks later, which showed no improvement of uncontrollable movements. Imaging at that time (not available) indicated the persistence of the abnormal signal in the right basal ganglia. This patient died later that year without further follow-up.
Case 3
A 78-year-old white male with a history of syncope, transient ischemic attacks (TIAs), and poorly controlled T2DM presented with a 1-month history of progressively worsening involuntary, left-sided movements that began in his left shoulder and advanced to involve his arm, hand, and leg, and the left side of his face with grimacing and clucking of his tongue. Three weeks earlier, the patient had been discharged from the ED with a diagnosis of conversion disorder particularly because he experienced decreased movements when given a dose of Vitamin D. It was overlooked that administration of haloperidol had occurred a few hours before, and because the sounds made by his tongue were not felt to be consistent with a known movement disorder. A MRI of the brain was read as normal.
The patient returned 3 weeks later (the original presentation) due to his inability to perform activities of daily living because of his worsening involuntary movements. On admission, his HbA1c was 11.1% and his glucose was 167 mg/dL. On chart review, it was revealed that the patient’s HbA1c had been > 9% for the past 3 years with an increase from 10.1% to 11.1% in the 3 months preceding the onset of his symptoms.
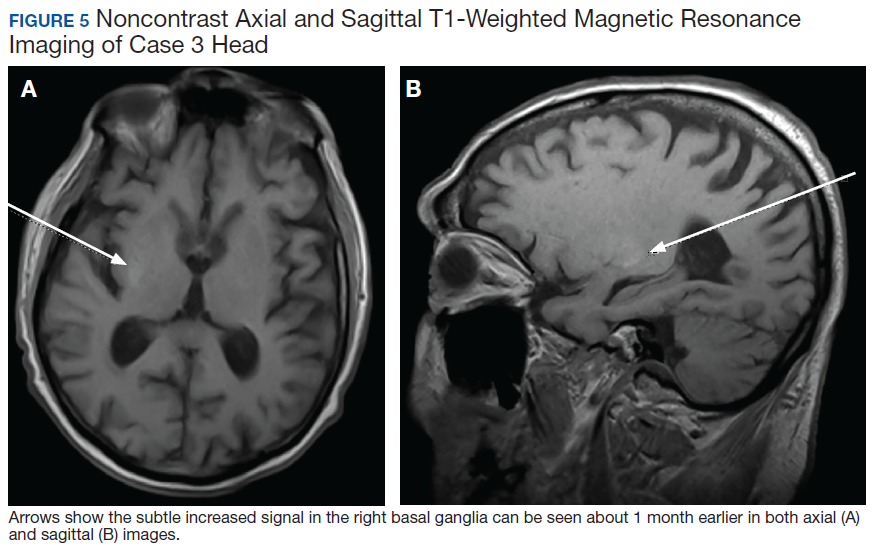
On admission a MRI showed a unilateral right-sided T1 hyperintensity in the basal ganglia, no acute ischemia (Figure 4). In retrospect, subtle increased T1 signal can be seen on the earlier MRI (Figure 5). In view of the patient’s left-sided symptoms, DM, and MRI findings, a diagnosis of hyperglycemia-induced hemichorea- hemiballismus was made as the etiology of the patient’s symptoms.
The patient was prescribed numerous medications to control his hyperkinesia including (and in combination): benztropine, gabapentin, baclofen, diphenhydramine, benzodiazepines, risperidone, olanzapine, and valproic acid, which did not control his movements. Ultimately, his hyperglycemic hemiballismus improved with tight glycemic control and oral tetrabenazine 12.5 mg twice daily. This patient underwent a protracted course of treatment with 17 days of inpatient medical admission, 3 weeks inpatient rehabilitation, and subsequent transfer to an assisted living facility.
Discussion
The 3 cases presented in this report contribute to the evidence that severe persistent hyperglycemia can result in movement disorders that mimic those seen after basal ganglia strokes. As with Case 2, past literature describes many cases of acute hyperglycemic episodes with glucose ranging from 500 to 1,000 mg/mL presenting with hemiballismus.1,3 However, there are many cases that describe hemiballismus occurring after glycemic correction, persisting despite glycemic correction, and presenting without an acute hyperglycemic episode, but in the setting of elevated HbA1c, as in Case 3.12,13 Notably, all 3 cases in this series had marked elevation in their HbA1c levels, which suggests that a more chronic hyperglycemic state or multiple shorter periods of hyperglycemia may be necessary to produce the described hyperkinetic movements.
Case reports describe the pathognomonic T1 hyperintensity of the basal ganglia that is identified in all 3 cases presented here. While the exact etiology remains unclear, the to metabolic derangements caused by hyperviscosity of the blood in the small end arteries feeding the basal ganglia.3,11 These abnormalities in turn interrupt the signaling cascade with abnormal firing rates or firing patterns, leading to reduced inhibition of the motor thalamus and ultimately present as hemiballismus.1,3,7 While most cases presented with unilateral hyperkinesis and associated contralateral basal ganglia abnormalities, there are reports of both unilateral and bilateral movements associated with bilateral basal ganglia hyperintensities on imaging. 9 The predilection for unilateral brain lesions may be explained by the varying degree of small vessel disease in different areas of the brain leading to perfusion deficits worsened by hyper viscosity. Further research into this is required to elucidate the exact pathophysiologic mechanism.
The course of disease for patients ranges from resolution within hours of tight glycemic control to persistent movements for > 3 months with a gradual improvement in severity.12,13 Treatments center on the importance of tight glycemic control to protect against the protracted course described in Case 3. Swift recognition of this rare condition is critical because improved glycemic control decreases the severity and duration of this disease. The significant disability associated with Case 3 highlights the need for prompt recognition and early, aggressive glycemic management to prevent the progression of hemiballismus. In addition to glycemic control, various CNS medications such as typical and atypical antipsychotics and tetrabenazine are firstline therapy with chemodenervation and surgical lesioning in cases unresponsive to medication therapy.
When unrecognized, hyperglycemic hemiballismus is associated with significant morbidity and mortality. The patients presented in this report were subject to either delayed diagnosis or misdiagnosis as stroke or psychiatric disorder. The rarity of the disorder, lack of evidence delineating pathogenesis and causality, low level of awareness, and varying presentations of patients all contribute to the challenge of recognizing, diagnosing, and treating hemiballismus due to hyperglycemia. This challenge can subsequently result in deteriorating symptoms, prolonged hospital stays, and unnecessary health care costs.
Conclusion
While hemiballismus due to severe persistent hyperglycemia is rare, the goal of this report is to highlight its occurrence in patients with T2DM. Further research can help develop a standardized, effective treatment strategy for these patients. Currently, lowering and maintaining appropriate glucose and HbA1c levels is the most effective treatment approach. Potential areas of research include alternative medical and surgical treatment interventions for patients while glycemic control is being achieved or for those who fail to benefit from glycemic control alone. Some success has been demonstrated with the use of antidopaminergic medications such as atypical antipsychotics and tetrabenazine and these medications should be considered when tight, sustained glycemic control alone is not successful in treating this disorder in the acute stages. Hopefully, with increasing awareness and recognition of hemiballismus related to hyperglycemia, more large-scale clinical trials can be conducted that will result in an effective treatment strategy for this devastating disorder.
1. Hawley JS, Weiner WJ. Hemiballismus: current concepts and review. Parkinsonism Relat Disord. 2012;18(2):125‐129. doi:10.1016/j.parkreldis.2011.08.015
2. Gasca-Salas C, Lang AE. Paroxysmal Hemiballism/ Hemichorea Resulting from Transient Ischemic Attacks. Mov Disord Clin Pract. 2015;3(3):303‐305. doi:10.1002/mdc3.12268
3. Garcia-Grimshaw MA, Jimenez-Ruiz A, Ornelas-Velazquez A, Luna-Armenta A, Gutierrez-Manjarrez FA. New-onset diabetes presenting as monoballism secondary to a mixed hyperglycemic crisis. Cureus. 2018;10(6):e2882. doi:10.7759/cureus.2882
4. Postuma RB, Lang AE. Hemiballism: revisiting a classic disorder. Lancet Neurol. 2003;2(11):661‐668. doi:10.1016/s1474-4422(03)00554-4
5. Gallo BV, Shulman LM, Weiner WJ, Petito CK, Berger JR. HIV encephalitis presenting with severe generalized chorea. Neurology. 1996;46(4):1163‐1165. doi:10.1212/wnl.46.4.1163
6. Provenzale JM, Glass JP. Hemiballismus: CT and MR findings. J Comput Assist Tomogr. 1995;19(4):537‐540.
7. Hodde M, Rowe KE, Surapaneni K, Terrigno P, Brighenti A, Altschuler EL. Management of severe hemiballismus: treatment challenges in the acute inpatient rehabilitation setting: a case presentation. PMR. 2017;9(7):732‐735. doi:10.1016/j.pmrj.2016.10.023
8. Laganiere S, Boes AD, Fox MD. Network localization of hemichorea-hemiballismus. Neurology. 2016;86(23):2187‐2195. doi:10.1212/WNL.0000000000002741
9. Cosentino C, Torres L, Nuñez Y, Suarez R, Velez M, Flores M. Hemichorea/hemiballism associated with hyperglycemia: report of 20 cases. Tremor Other Hyperkinet Mov (NY). 2016;6:402. doi:10.7916/D8DN454P
10. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a metaanalysis of 53 cases including four present cases. J Neurol Sci. 2002;200(1-2):57‐62. doi:10.1016/s0022-510x(02)00133-8
11. Carrion DM, Carrion AF. Non-ketotic hyperglycaemia hemichorea-hemiballismus and acute ischaemic stroke. BMJ Case Rep. 2013;2013:bcr2012008359. doi:10.1136/bcr-2012-008359
12. Cho HS, Hong CT, Chan L. Hemichorea after hyperglycemia correction: a case report and a short review of hyperglycemia-related hemichorea at the euglycemic state. Medicine (Baltimore). 2018;97(10):e0076. doi:10.1097/MD.0000000000010076
13. Lin YC, Lin YC. Prolonged hemiballism after the remission of non-ketotic hyperosmolar syndrome. BMJ Case Rep. 2012;2012:bcr0120125627. doi:10.1136/bcr.01.2012.5627
Hemiballismus is an acquired hyperkinetic movement disorder characterized by unilateral, involuntary, often large-amplitude limb movements. Ballistic movements are now considered to be on the choreiform spectrum.1 Movements usually involve both the arm and leg, and in half of cases, facial movements such as tongue clucking and grimacing are seen.2,3 Presentations of hemiballismus vary in severity from intermittent to nearly continuous movements, which, in some cases, may lead to exhaustion, injury, or disability. Some patients are unable to ambulate or feed themselves with the affected limb.
Background
The 2 most common causes of hemichorea-hemiballismus are stroke and hyperglycemia, with an incidence of 4% and unknown incidence, respectively.1,3,4 Other causes include HIV, traumatic brain injury, encephalitis, vasculitis, mass effect, multiple sclerosis, and adverse drug reactions. 4-7 Acute or subacute hemiballismus is classically attributed to a lesion in subthalamic nucleus (STN), but this is true only in a minority of cases. Hemiballismus can be caused by any abnormality in various subnuclei of the basal ganglia, including the classic location in the STN, striatum, and globus pallidus.4 Evidence shows the lesions typically involve a functional network connected to the posterolateral putamen.8
Although not commonly recognized, hyperglycemia in patients with type 2 diabetes mellitus (T2DM) is the second most common cause of hemichoreahemiballismus. 3 Over the past 90 years, numerous case reports have described patients with DM with acute and subacute onset of hemiballistic and hemichoreiform movements while in a hyperglycemic state or after its resolution. Reported cases have been limited to small numbers of patients with only a few larger-scale reviews of more than 20 patients.7,9 Most reported cases involve geriatric patients and more commonly, females of Eastern Asian descent with an average age of onset of 71 years.4,10 Patients typically present with glucose levels from 500 to 1,000 mg/dL and hemoglobin A1c (HbA1c) levels almost double the normal values. Interestingly, neuroimaging findings in these patients have consistently shown hyperintense signal in the contralateral basal ganglia on T1-weighted magnetic resonance images (MRIs). Noncontrast computed tomography (CT) shows well-defined unilateral increased density in the contralateral basal ganglia without mass effect.1,9,11
This report aims to illustrate and enhance the understanding of hemiballismus associated with hyperglycemia. One patient presented to the US Department of Veterans Affairs (VA) Bay Pines VA Healthcare System (BPVAHCS) in Florida, which motivated us to search for other similar cases. We reviewed the charts of 2 other patients who presented to BPVAHCS over the past 10 years. The first case presented with severe hyperglycemia and abnormal movements that were not clearly diagnosed as hemiballismus. MRI findings were characteristic and assisted in making the diagnosis. The second case was misdiagnosed as hemiballismus secondary to ischemic stroke. The third case was initially diagnosed as conversion disorder until movements worsened and the correct diagnosis of hyperglycemia-induced hemichorea hemiballismus was confirmed by the pathognomonic neuroimaging findings.
Case Presentations
Case 1
A 65-year-old male with a history of uncontrolled T2DM presented with repetitive twitching and kicking movements that involved his left upper and lower extremities for 3 weeks. The patient reported that he did not take his medications or follow the recommended diabetes diet. His HbA1c on admission was 12.2% with a serum glucose of 254 mg/dL. The MRI showed a hyperintense T1 signal within the right basal ganglia including the right caudate with sparing of the internal capsule (Figure 1). There was no associated mass effect or restricted diffusion. It was compatible with a diagnosis of hyperglycemia- induced hemichorea-hemiballismus. The patient was advised to resume taking glipizide 10 mg daily, metformin 1,000 mg by mouth twice daily, and to begin 10 units of 70/30 insulin aspart 15 minutes before meals twice daily, and to follow a low carbohydrate diet, with reduce dietary intake of sugar. At his 1-month follow-up visit, the patient reported an improvement in his involuntary movements. At the 5-month follow-up, the patient’s HbA1c level was 10.4% and his hyperkinetic movements had completely resolved.
Case 2
of T2DM, hypertension, and hyperlipidemia was admitted due to increased jerky movements in the left upper extremity. On admission, his vital signs were within normal limits and his physical examination demonstrated choreoathetoid movements with ballistic components of his left upper extremity. His laboratory results showed a glucose level of 528 mg/dL with a HbA1c of 16.3%. An initial CT obtained in the emergency department (ED) demonstrated a well-defined hyperdensity in the striatal (caudate and lentiform nucleus) region (Figure 2). There was no associated edema/mass effect that would be typical for an intracranial hemorrhage.
An MRI obtained 1 week later showed hyperintense TI signal corresponding to the basal ganglia (Figure 3). In addition, there was a questionable lacunar infarct in the right internal capsule. Due to lack of awareness regarding hyperglycemic associated basal ganglia changes, the patient’s movement disorder was presumed to be ischemic in etiology. The patient was prescribed oral amantadine 100 mg 3 times daily for the hemiballismus in conjunction with treatment of his T2DM. The only follow-up occurred 5 weeks later, which showed no improvement of uncontrollable movements. Imaging at that time (not available) indicated the persistence of the abnormal signal in the right basal ganglia. This patient died later that year without further follow-up.
Case 3
A 78-year-old white male with a history of syncope, transient ischemic attacks (TIAs), and poorly controlled T2DM presented with a 1-month history of progressively worsening involuntary, left-sided movements that began in his left shoulder and advanced to involve his arm, hand, and leg, and the left side of his face with grimacing and clucking of his tongue. Three weeks earlier, the patient had been discharged from the ED with a diagnosis of conversion disorder particularly because he experienced decreased movements when given a dose of Vitamin D. It was overlooked that administration of haloperidol had occurred a few hours before, and because the sounds made by his tongue were not felt to be consistent with a known movement disorder. A MRI of the brain was read as normal.
The patient returned 3 weeks later (the original presentation) due to his inability to perform activities of daily living because of his worsening involuntary movements. On admission, his HbA1c was 11.1% and his glucose was 167 mg/dL. On chart review, it was revealed that the patient’s HbA1c had been > 9% for the past 3 years with an increase from 10.1% to 11.1% in the 3 months preceding the onset of his symptoms.
On admission a MRI showed a unilateral right-sided T1 hyperintensity in the basal ganglia, no acute ischemia (Figure 4). In retrospect, subtle increased T1 signal can be seen on the earlier MRI (Figure 5). In view of the patient’s left-sided symptoms, DM, and MRI findings, a diagnosis of hyperglycemia-induced hemichorea- hemiballismus was made as the etiology of the patient’s symptoms.
The patient was prescribed numerous medications to control his hyperkinesia including (and in combination): benztropine, gabapentin, baclofen, diphenhydramine, benzodiazepines, risperidone, olanzapine, and valproic acid, which did not control his movements. Ultimately, his hyperglycemic hemiballismus improved with tight glycemic control and oral tetrabenazine 12.5 mg twice daily. This patient underwent a protracted course of treatment with 17 days of inpatient medical admission, 3 weeks inpatient rehabilitation, and subsequent transfer to an assisted living facility.
Discussion
The 3 cases presented in this report contribute to the evidence that severe persistent hyperglycemia can result in movement disorders that mimic those seen after basal ganglia strokes. As with Case 2, past literature describes many cases of acute hyperglycemic episodes with glucose ranging from 500 to 1,000 mg/mL presenting with hemiballismus.1,3 However, there are many cases that describe hemiballismus occurring after glycemic correction, persisting despite glycemic correction, and presenting without an acute hyperglycemic episode, but in the setting of elevated HbA1c, as in Case 3.12,13 Notably, all 3 cases in this series had marked elevation in their HbA1c levels, which suggests that a more chronic hyperglycemic state or multiple shorter periods of hyperglycemia may be necessary to produce the described hyperkinetic movements.
Case reports describe the pathognomonic T1 hyperintensity of the basal ganglia that is identified in all 3 cases presented here. While the exact etiology remains unclear, the to metabolic derangements caused by hyperviscosity of the blood in the small end arteries feeding the basal ganglia.3,11 These abnormalities in turn interrupt the signaling cascade with abnormal firing rates or firing patterns, leading to reduced inhibition of the motor thalamus and ultimately present as hemiballismus.1,3,7 While most cases presented with unilateral hyperkinesis and associated contralateral basal ganglia abnormalities, there are reports of both unilateral and bilateral movements associated with bilateral basal ganglia hyperintensities on imaging. 9 The predilection for unilateral brain lesions may be explained by the varying degree of small vessel disease in different areas of the brain leading to perfusion deficits worsened by hyper viscosity. Further research into this is required to elucidate the exact pathophysiologic mechanism.
The course of disease for patients ranges from resolution within hours of tight glycemic control to persistent movements for > 3 months with a gradual improvement in severity.12,13 Treatments center on the importance of tight glycemic control to protect against the protracted course described in Case 3. Swift recognition of this rare condition is critical because improved glycemic control decreases the severity and duration of this disease. The significant disability associated with Case 3 highlights the need for prompt recognition and early, aggressive glycemic management to prevent the progression of hemiballismus. In addition to glycemic control, various CNS medications such as typical and atypical antipsychotics and tetrabenazine are firstline therapy with chemodenervation and surgical lesioning in cases unresponsive to medication therapy.
When unrecognized, hyperglycemic hemiballismus is associated with significant morbidity and mortality. The patients presented in this report were subject to either delayed diagnosis or misdiagnosis as stroke or psychiatric disorder. The rarity of the disorder, lack of evidence delineating pathogenesis and causality, low level of awareness, and varying presentations of patients all contribute to the challenge of recognizing, diagnosing, and treating hemiballismus due to hyperglycemia. This challenge can subsequently result in deteriorating symptoms, prolonged hospital stays, and unnecessary health care costs.
Conclusion
While hemiballismus due to severe persistent hyperglycemia is rare, the goal of this report is to highlight its occurrence in patients with T2DM. Further research can help develop a standardized, effective treatment strategy for these patients. Currently, lowering and maintaining appropriate glucose and HbA1c levels is the most effective treatment approach. Potential areas of research include alternative medical and surgical treatment interventions for patients while glycemic control is being achieved or for those who fail to benefit from glycemic control alone. Some success has been demonstrated with the use of antidopaminergic medications such as atypical antipsychotics and tetrabenazine and these medications should be considered when tight, sustained glycemic control alone is not successful in treating this disorder in the acute stages. Hopefully, with increasing awareness and recognition of hemiballismus related to hyperglycemia, more large-scale clinical trials can be conducted that will result in an effective treatment strategy for this devastating disorder.
Hemiballismus is an acquired hyperkinetic movement disorder characterized by unilateral, involuntary, often large-amplitude limb movements. Ballistic movements are now considered to be on the choreiform spectrum.1 Movements usually involve both the arm and leg, and in half of cases, facial movements such as tongue clucking and grimacing are seen.2,3 Presentations of hemiballismus vary in severity from intermittent to nearly continuous movements, which, in some cases, may lead to exhaustion, injury, or disability. Some patients are unable to ambulate or feed themselves with the affected limb.
Background
The 2 most common causes of hemichorea-hemiballismus are stroke and hyperglycemia, with an incidence of 4% and unknown incidence, respectively.1,3,4 Other causes include HIV, traumatic brain injury, encephalitis, vasculitis, mass effect, multiple sclerosis, and adverse drug reactions. 4-7 Acute or subacute hemiballismus is classically attributed to a lesion in subthalamic nucleus (STN), but this is true only in a minority of cases. Hemiballismus can be caused by any abnormality in various subnuclei of the basal ganglia, including the classic location in the STN, striatum, and globus pallidus.4 Evidence shows the lesions typically involve a functional network connected to the posterolateral putamen.8
Although not commonly recognized, hyperglycemia in patients with type 2 diabetes mellitus (T2DM) is the second most common cause of hemichoreahemiballismus. 3 Over the past 90 years, numerous case reports have described patients with DM with acute and subacute onset of hemiballistic and hemichoreiform movements while in a hyperglycemic state or after its resolution. Reported cases have been limited to small numbers of patients with only a few larger-scale reviews of more than 20 patients.7,9 Most reported cases involve geriatric patients and more commonly, females of Eastern Asian descent with an average age of onset of 71 years.4,10 Patients typically present with glucose levels from 500 to 1,000 mg/dL and hemoglobin A1c (HbA1c) levels almost double the normal values. Interestingly, neuroimaging findings in these patients have consistently shown hyperintense signal in the contralateral basal ganglia on T1-weighted magnetic resonance images (MRIs). Noncontrast computed tomography (CT) shows well-defined unilateral increased density in the contralateral basal ganglia without mass effect.1,9,11
This report aims to illustrate and enhance the understanding of hemiballismus associated with hyperglycemia. One patient presented to the US Department of Veterans Affairs (VA) Bay Pines VA Healthcare System (BPVAHCS) in Florida, which motivated us to search for other similar cases. We reviewed the charts of 2 other patients who presented to BPVAHCS over the past 10 years. The first case presented with severe hyperglycemia and abnormal movements that were not clearly diagnosed as hemiballismus. MRI findings were characteristic and assisted in making the diagnosis. The second case was misdiagnosed as hemiballismus secondary to ischemic stroke. The third case was initially diagnosed as conversion disorder until movements worsened and the correct diagnosis of hyperglycemia-induced hemichorea hemiballismus was confirmed by the pathognomonic neuroimaging findings.
Case Presentations
Case 1
A 65-year-old male with a history of uncontrolled T2DM presented with repetitive twitching and kicking movements that involved his left upper and lower extremities for 3 weeks. The patient reported that he did not take his medications or follow the recommended diabetes diet. His HbA1c on admission was 12.2% with a serum glucose of 254 mg/dL. The MRI showed a hyperintense T1 signal within the right basal ganglia including the right caudate with sparing of the internal capsule (Figure 1). There was no associated mass effect or restricted diffusion. It was compatible with a diagnosis of hyperglycemia- induced hemichorea-hemiballismus. The patient was advised to resume taking glipizide 10 mg daily, metformin 1,000 mg by mouth twice daily, and to begin 10 units of 70/30 insulin aspart 15 minutes before meals twice daily, and to follow a low carbohydrate diet, with reduce dietary intake of sugar. At his 1-month follow-up visit, the patient reported an improvement in his involuntary movements. At the 5-month follow-up, the patient’s HbA1c level was 10.4% and his hyperkinetic movements had completely resolved.
Case 2
of T2DM, hypertension, and hyperlipidemia was admitted due to increased jerky movements in the left upper extremity. On admission, his vital signs were within normal limits and his physical examination demonstrated choreoathetoid movements with ballistic components of his left upper extremity. His laboratory results showed a glucose level of 528 mg/dL with a HbA1c of 16.3%. An initial CT obtained in the emergency department (ED) demonstrated a well-defined hyperdensity in the striatal (caudate and lentiform nucleus) region (Figure 2). There was no associated edema/mass effect that would be typical for an intracranial hemorrhage.
An MRI obtained 1 week later showed hyperintense TI signal corresponding to the basal ganglia (Figure 3). In addition, there was a questionable lacunar infarct in the right internal capsule. Due to lack of awareness regarding hyperglycemic associated basal ganglia changes, the patient’s movement disorder was presumed to be ischemic in etiology. The patient was prescribed oral amantadine 100 mg 3 times daily for the hemiballismus in conjunction with treatment of his T2DM. The only follow-up occurred 5 weeks later, which showed no improvement of uncontrollable movements. Imaging at that time (not available) indicated the persistence of the abnormal signal in the right basal ganglia. This patient died later that year without further follow-up.
Case 3
A 78-year-old white male with a history of syncope, transient ischemic attacks (TIAs), and poorly controlled T2DM presented with a 1-month history of progressively worsening involuntary, left-sided movements that began in his left shoulder and advanced to involve his arm, hand, and leg, and the left side of his face with grimacing and clucking of his tongue. Three weeks earlier, the patient had been discharged from the ED with a diagnosis of conversion disorder particularly because he experienced decreased movements when given a dose of Vitamin D. It was overlooked that administration of haloperidol had occurred a few hours before, and because the sounds made by his tongue were not felt to be consistent with a known movement disorder. A MRI of the brain was read as normal.
The patient returned 3 weeks later (the original presentation) due to his inability to perform activities of daily living because of his worsening involuntary movements. On admission, his HbA1c was 11.1% and his glucose was 167 mg/dL. On chart review, it was revealed that the patient’s HbA1c had been > 9% for the past 3 years with an increase from 10.1% to 11.1% in the 3 months preceding the onset of his symptoms.
On admission a MRI showed a unilateral right-sided T1 hyperintensity in the basal ganglia, no acute ischemia (Figure 4). In retrospect, subtle increased T1 signal can be seen on the earlier MRI (Figure 5). In view of the patient’s left-sided symptoms, DM, and MRI findings, a diagnosis of hyperglycemia-induced hemichorea- hemiballismus was made as the etiology of the patient’s symptoms.
The patient was prescribed numerous medications to control his hyperkinesia including (and in combination): benztropine, gabapentin, baclofen, diphenhydramine, benzodiazepines, risperidone, olanzapine, and valproic acid, which did not control his movements. Ultimately, his hyperglycemic hemiballismus improved with tight glycemic control and oral tetrabenazine 12.5 mg twice daily. This patient underwent a protracted course of treatment with 17 days of inpatient medical admission, 3 weeks inpatient rehabilitation, and subsequent transfer to an assisted living facility.
Discussion
The 3 cases presented in this report contribute to the evidence that severe persistent hyperglycemia can result in movement disorders that mimic those seen after basal ganglia strokes. As with Case 2, past literature describes many cases of acute hyperglycemic episodes with glucose ranging from 500 to 1,000 mg/mL presenting with hemiballismus.1,3 However, there are many cases that describe hemiballismus occurring after glycemic correction, persisting despite glycemic correction, and presenting without an acute hyperglycemic episode, but in the setting of elevated HbA1c, as in Case 3.12,13 Notably, all 3 cases in this series had marked elevation in their HbA1c levels, which suggests that a more chronic hyperglycemic state or multiple shorter periods of hyperglycemia may be necessary to produce the described hyperkinetic movements.
Case reports describe the pathognomonic T1 hyperintensity of the basal ganglia that is identified in all 3 cases presented here. While the exact etiology remains unclear, the to metabolic derangements caused by hyperviscosity of the blood in the small end arteries feeding the basal ganglia.3,11 These abnormalities in turn interrupt the signaling cascade with abnormal firing rates or firing patterns, leading to reduced inhibition of the motor thalamus and ultimately present as hemiballismus.1,3,7 While most cases presented with unilateral hyperkinesis and associated contralateral basal ganglia abnormalities, there are reports of both unilateral and bilateral movements associated with bilateral basal ganglia hyperintensities on imaging. 9 The predilection for unilateral brain lesions may be explained by the varying degree of small vessel disease in different areas of the brain leading to perfusion deficits worsened by hyper viscosity. Further research into this is required to elucidate the exact pathophysiologic mechanism.
The course of disease for patients ranges from resolution within hours of tight glycemic control to persistent movements for > 3 months with a gradual improvement in severity.12,13 Treatments center on the importance of tight glycemic control to protect against the protracted course described in Case 3. Swift recognition of this rare condition is critical because improved glycemic control decreases the severity and duration of this disease. The significant disability associated with Case 3 highlights the need for prompt recognition and early, aggressive glycemic management to prevent the progression of hemiballismus. In addition to glycemic control, various CNS medications such as typical and atypical antipsychotics and tetrabenazine are firstline therapy with chemodenervation and surgical lesioning in cases unresponsive to medication therapy.
When unrecognized, hyperglycemic hemiballismus is associated with significant morbidity and mortality. The patients presented in this report were subject to either delayed diagnosis or misdiagnosis as stroke or psychiatric disorder. The rarity of the disorder, lack of evidence delineating pathogenesis and causality, low level of awareness, and varying presentations of patients all contribute to the challenge of recognizing, diagnosing, and treating hemiballismus due to hyperglycemia. This challenge can subsequently result in deteriorating symptoms, prolonged hospital stays, and unnecessary health care costs.
Conclusion
While hemiballismus due to severe persistent hyperglycemia is rare, the goal of this report is to highlight its occurrence in patients with T2DM. Further research can help develop a standardized, effective treatment strategy for these patients. Currently, lowering and maintaining appropriate glucose and HbA1c levels is the most effective treatment approach. Potential areas of research include alternative medical and surgical treatment interventions for patients while glycemic control is being achieved or for those who fail to benefit from glycemic control alone. Some success has been demonstrated with the use of antidopaminergic medications such as atypical antipsychotics and tetrabenazine and these medications should be considered when tight, sustained glycemic control alone is not successful in treating this disorder in the acute stages. Hopefully, with increasing awareness and recognition of hemiballismus related to hyperglycemia, more large-scale clinical trials can be conducted that will result in an effective treatment strategy for this devastating disorder.
1. Hawley JS, Weiner WJ. Hemiballismus: current concepts and review. Parkinsonism Relat Disord. 2012;18(2):125‐129. doi:10.1016/j.parkreldis.2011.08.015
2. Gasca-Salas C, Lang AE. Paroxysmal Hemiballism/ Hemichorea Resulting from Transient Ischemic Attacks. Mov Disord Clin Pract. 2015;3(3):303‐305. doi:10.1002/mdc3.12268
3. Garcia-Grimshaw MA, Jimenez-Ruiz A, Ornelas-Velazquez A, Luna-Armenta A, Gutierrez-Manjarrez FA. New-onset diabetes presenting as monoballism secondary to a mixed hyperglycemic crisis. Cureus. 2018;10(6):e2882. doi:10.7759/cureus.2882
4. Postuma RB, Lang AE. Hemiballism: revisiting a classic disorder. Lancet Neurol. 2003;2(11):661‐668. doi:10.1016/s1474-4422(03)00554-4
5. Gallo BV, Shulman LM, Weiner WJ, Petito CK, Berger JR. HIV encephalitis presenting with severe generalized chorea. Neurology. 1996;46(4):1163‐1165. doi:10.1212/wnl.46.4.1163
6. Provenzale JM, Glass JP. Hemiballismus: CT and MR findings. J Comput Assist Tomogr. 1995;19(4):537‐540.
7. Hodde M, Rowe KE, Surapaneni K, Terrigno P, Brighenti A, Altschuler EL. Management of severe hemiballismus: treatment challenges in the acute inpatient rehabilitation setting: a case presentation. PMR. 2017;9(7):732‐735. doi:10.1016/j.pmrj.2016.10.023
8. Laganiere S, Boes AD, Fox MD. Network localization of hemichorea-hemiballismus. Neurology. 2016;86(23):2187‐2195. doi:10.1212/WNL.0000000000002741
9. Cosentino C, Torres L, Nuñez Y, Suarez R, Velez M, Flores M. Hemichorea/hemiballism associated with hyperglycemia: report of 20 cases. Tremor Other Hyperkinet Mov (NY). 2016;6:402. doi:10.7916/D8DN454P
10. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a metaanalysis of 53 cases including four present cases. J Neurol Sci. 2002;200(1-2):57‐62. doi:10.1016/s0022-510x(02)00133-8
11. Carrion DM, Carrion AF. Non-ketotic hyperglycaemia hemichorea-hemiballismus and acute ischaemic stroke. BMJ Case Rep. 2013;2013:bcr2012008359. doi:10.1136/bcr-2012-008359
12. Cho HS, Hong CT, Chan L. Hemichorea after hyperglycemia correction: a case report and a short review of hyperglycemia-related hemichorea at the euglycemic state. Medicine (Baltimore). 2018;97(10):e0076. doi:10.1097/MD.0000000000010076
13. Lin YC, Lin YC. Prolonged hemiballism after the remission of non-ketotic hyperosmolar syndrome. BMJ Case Rep. 2012;2012:bcr0120125627. doi:10.1136/bcr.01.2012.5627
1. Hawley JS, Weiner WJ. Hemiballismus: current concepts and review. Parkinsonism Relat Disord. 2012;18(2):125‐129. doi:10.1016/j.parkreldis.2011.08.015
2. Gasca-Salas C, Lang AE. Paroxysmal Hemiballism/ Hemichorea Resulting from Transient Ischemic Attacks. Mov Disord Clin Pract. 2015;3(3):303‐305. doi:10.1002/mdc3.12268
3. Garcia-Grimshaw MA, Jimenez-Ruiz A, Ornelas-Velazquez A, Luna-Armenta A, Gutierrez-Manjarrez FA. New-onset diabetes presenting as monoballism secondary to a mixed hyperglycemic crisis. Cureus. 2018;10(6):e2882. doi:10.7759/cureus.2882
4. Postuma RB, Lang AE. Hemiballism: revisiting a classic disorder. Lancet Neurol. 2003;2(11):661‐668. doi:10.1016/s1474-4422(03)00554-4
5. Gallo BV, Shulman LM, Weiner WJ, Petito CK, Berger JR. HIV encephalitis presenting with severe generalized chorea. Neurology. 1996;46(4):1163‐1165. doi:10.1212/wnl.46.4.1163
6. Provenzale JM, Glass JP. Hemiballismus: CT and MR findings. J Comput Assist Tomogr. 1995;19(4):537‐540.
7. Hodde M, Rowe KE, Surapaneni K, Terrigno P, Brighenti A, Altschuler EL. Management of severe hemiballismus: treatment challenges in the acute inpatient rehabilitation setting: a case presentation. PMR. 2017;9(7):732‐735. doi:10.1016/j.pmrj.2016.10.023
8. Laganiere S, Boes AD, Fox MD. Network localization of hemichorea-hemiballismus. Neurology. 2016;86(23):2187‐2195. doi:10.1212/WNL.0000000000002741
9. Cosentino C, Torres L, Nuñez Y, Suarez R, Velez M, Flores M. Hemichorea/hemiballism associated with hyperglycemia: report of 20 cases. Tremor Other Hyperkinet Mov (NY). 2016;6:402. doi:10.7916/D8DN454P
10. Oh SH, Lee KY, Im JH, Lee MS. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a metaanalysis of 53 cases including four present cases. J Neurol Sci. 2002;200(1-2):57‐62. doi:10.1016/s0022-510x(02)00133-8
11. Carrion DM, Carrion AF. Non-ketotic hyperglycaemia hemichorea-hemiballismus and acute ischaemic stroke. BMJ Case Rep. 2013;2013:bcr2012008359. doi:10.1136/bcr-2012-008359
12. Cho HS, Hong CT, Chan L. Hemichorea after hyperglycemia correction: a case report and a short review of hyperglycemia-related hemichorea at the euglycemic state. Medicine (Baltimore). 2018;97(10):e0076. doi:10.1097/MD.0000000000010076
13. Lin YC, Lin YC. Prolonged hemiballism after the remission of non-ketotic hyperosmolar syndrome. BMJ Case Rep. 2012;2012:bcr0120125627. doi:10.1136/bcr.01.2012.5627
How old is too old for statins?
ILLUSTRATIVE CASE
Ms. M is a 76-year-old woman with well-controlled type 2 diabetes mellitus for 10 years and well-controlled mild hypertension. She is otherwise healthy, and her mother lived to age 95. Ms. M has never smoked, has no previous history of vascular/cardiovascular disease, and drinks 1 glass of wine 2 to 3 times per week. Based on the American College of Cardiology (ACC) calculator, she was started on atorvastatin years ago. Is continued use of the medication of any benefit at her current age?
The 2018 American Heart Association (AHA)/ACC/Multi-Society cholesterol guidelines do not provide primary prevention recommendations for those older than age 75 years.3 Up to age 75, the guidelines recommend that patients with type 2 diabetes and a low-density lipoprotein cholesterol (LDL-C) level ≥ 70 mg/dL, as well as those without diabetes but with an LDL-C ≥ 70 mg/dL and a 10-year atherosclerotic cardiovascular disease (ASCVD) risk ≥ 10%, be started on medium-intensity statin therapy.
A 2018 consensus panel review of the current literature, sponsored by the National Institute on Aging and the National Heart, Lung, and Blood Institute, concluded that there was insufficient evidence regarding the benefits and harms of statins in older adults, especially those with comorbidities, and that there was a paucity of evidence about statin therapy outcomes (both adverse and beneficial) relevant to older adults.4
A review of all guidelines published since 2013 revealed that only the United Kingdom’s 2014 National Institute for Health and Care Excellence (NICE) guideline provides a strong, risk-based recommendation for initiating primary prevention with statins in patients > 75 years old.5 These recommendations are based on the QRISK2 calculator (which has since been updated to the QRISK3), which assigns everyone ages > 75 years a > 10% 10-year risk score. This provides a universal statin indication for anyone in the 76-to-84 age range.6
Both the ACC/AHA and US Preventive Services Task Force guidelines clearly state that there are too few data and inadequate evidence in people older than 75 for a strong, risk-based statin recommendation.5 The Canadian Cardiovascular Society guideline takes a similar stance, emphasizing that the recommended Framingham risk model is not well validated in people > 75 years.5
STUDY SUMMARIES
Two different looks at statin use in the elderly
A retrospective cohort study (N = 46,864; median follow-up, 5.6 years) examined whether statin treatment is associated with a reduction in atherosclerotic disease and mortality in old and very old adults with and without type 2 diabetes.1 Patients were enrolled from a large, anonymized national database in Spain. The researchers looked only at first-time users of statins and those without a statin prescription within the past 18 months.
Patients with previous ASCVD, type 1 diabetes, previous lipid-lowering treatment, dementia, cancer, or paralysis were excluded, as were those who were in residential care, were on dialysis, or had received an organ transplant. Patients were stratified by age (75-84 years and ≥ 85 years), diabetes status (with or without type 2 diabetes), and statin use (nonuser or new user).
Continue to: Results
Results. For patients with type 2 diabetes, the risk of ASCVD (a composite of coronary heart disease and stroke) was lower among those who took statins than among those who did not in the 75-to-84 group (hazard ratio [HR] = 0.76; 95% confidence interval [CI], 0.65-0.89; 1-year number needed to treat [NNT] = 164). Among those who took statins, there was also lower all-cause mortality (HR = 0.84; 95% CI, 0.75-0.94; 1-year NNT = 306). In those ages ≥ 85 years with diabetes, the statin group did not have a lower risk of ASCVD (HR = 0.82; 95% CI, 0.53-1.26) or all-cause mortality (HR = 1.05; 95% CI, 0.86-1.28).
For patients ages 75 to 84 years without diabetes, there was no difference in risk between groups for ASCVD (HR = 0.94; 95% CI, 0.86–1.04) or all-cause mortality (HR = 0.98; 95% CI, 0.91-1.05). In those ages ≥ 85 years without diabetes, there was also no difference between groups for ASCVD (HR = 1; 95% CI, 0.80-1.24) or for all-cause mortality (HR = 1; 95% CI, 0.90-1.11).
A 2019 meta-analysis of randomized controlled trials (RCTs) (n = 134,537) and RCT summary data (n = 12,705) evaluated the safety and efficacy of statin therapy in patients ages ≥ 55 years.2 In the group of patients ages > 75 years (n = 14,483; median follow-up, 4.9 years), each 1 mmol/L reduction in LDL-C was associated with significant decreased risk for major vascular events (risk ratio [RR] = 0.82; 95% CI, 0.70-0.95) and for major coronary events (RR = 0.82; 95% CI, 0.70-0.96).
In subgroup analysis by the presence or absence of previous vascular disease, there was a decreased risk per 1 mmol/L LDL-C reduction of major vascular events in patients with previous vascular disease (RR = 0.85; 95% CI, 0.73-0.98); however, there was not a significant effect in patients without previous vascular disease (RR = 0.92; 95% CI, 0.73-1.16).
WHAT’S NEW
Statins may be unnecessary in older adults without ASCVD or T2DM
Statin therapy reduces the risk of ASCVD and mortality in patients ages 75 to 84 with type 2 diabetes and in patients > 75 years with known vascular disease. However, statin therapy seems to provide no benefit in patients ages > 75 years without ASCVD or in patients ages ≥ 85 years without ASCVD, regardless of type 2 diabetes status.
Continue to: CAVEATS
CAVEATS
Retrospective cohort design leaves cause and effect equivocal
Even though the first study was large (with more than 46,000 patients) and the median follow-up was 5.6 years, it was a retrospective cohort study. While there is clearly an association between statin therapy and reduced ASCVD and all-cause mortality in patients with diabetes ages 75 to 84 years, cause and effect cannot be unequivocally stated. However, the meta-analysis, which included RCTs, confirms the benefit of statins in secondary prevention for older patients.
The cohort study did not look at adverse effects from statin therapy in this age group, but the data from the 2019 meta-analysis did not reveal any significant risk of myopathy.
CHALLENGES TO IMPLEMENTATION
Guidelines are lacking and discontinuing meds requires discussion
The lack of supporting guidelines to treat this age group with statins remains the largest barrier to implementation. Many patients may already be taking a statin, so a discussion about discontinuing medication will need to be initiated.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Ramos R, Comas-Cufi M, Marti-Lluch R, et al. Statins for primary prevention of cardiovascular events and mortality in old and very old adults with and without type 2 diabetes: retrospective cohort study. BMJ. 2018;362:k3359.
2. Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomized controlled trials. Lancet. 2019;393:407-415.
3. Stone NJ, Grundy SM. The 2018 AHA/ACC/Multi-Society cholesterol guidelines: looking at past, present and future. Prog Cardiovasc Dis. 2019;62:375-383.
4. Singh S, Zieman S, Go AS, et al. Statins for primary prevention in older adults—moving towards evidence-based decision-making. J Am Geriatr Soc. 2018;66:2188-2196.
5. Mortensen MB, Falk E. Primary prevention with statins in the elderly. J Am Coll Cardiol. 2018;71:85-94.
6. ClinRisk. Welcome to the QRISK®3-2018 risk calculator. www.qrisk.org/three/. Accessed May 27, 2020.
ILLUSTRATIVE CASE
Ms. M is a 76-year-old woman with well-controlled type 2 diabetes mellitus for 10 years and well-controlled mild hypertension. She is otherwise healthy, and her mother lived to age 95. Ms. M has never smoked, has no previous history of vascular/cardiovascular disease, and drinks 1 glass of wine 2 to 3 times per week. Based on the American College of Cardiology (ACC) calculator, she was started on atorvastatin years ago. Is continued use of the medication of any benefit at her current age?
The 2018 American Heart Association (AHA)/ACC/Multi-Society cholesterol guidelines do not provide primary prevention recommendations for those older than age 75 years.3 Up to age 75, the guidelines recommend that patients with type 2 diabetes and a low-density lipoprotein cholesterol (LDL-C) level ≥ 70 mg/dL, as well as those without diabetes but with an LDL-C ≥ 70 mg/dL and a 10-year atherosclerotic cardiovascular disease (ASCVD) risk ≥ 10%, be started on medium-intensity statin therapy.
A 2018 consensus panel review of the current literature, sponsored by the National Institute on Aging and the National Heart, Lung, and Blood Institute, concluded that there was insufficient evidence regarding the benefits and harms of statins in older adults, especially those with comorbidities, and that there was a paucity of evidence about statin therapy outcomes (both adverse and beneficial) relevant to older adults.4
A review of all guidelines published since 2013 revealed that only the United Kingdom’s 2014 National Institute for Health and Care Excellence (NICE) guideline provides a strong, risk-based recommendation for initiating primary prevention with statins in patients > 75 years old.5 These recommendations are based on the QRISK2 calculator (which has since been updated to the QRISK3), which assigns everyone ages > 75 years a > 10% 10-year risk score. This provides a universal statin indication for anyone in the 76-to-84 age range.6
Both the ACC/AHA and US Preventive Services Task Force guidelines clearly state that there are too few data and inadequate evidence in people older than 75 for a strong, risk-based statin recommendation.5 The Canadian Cardiovascular Society guideline takes a similar stance, emphasizing that the recommended Framingham risk model is not well validated in people > 75 years.5
STUDY SUMMARIES
Two different looks at statin use in the elderly
A retrospective cohort study (N = 46,864; median follow-up, 5.6 years) examined whether statin treatment is associated with a reduction in atherosclerotic disease and mortality in old and very old adults with and without type 2 diabetes.1 Patients were enrolled from a large, anonymized national database in Spain. The researchers looked only at first-time users of statins and those without a statin prescription within the past 18 months.
Patients with previous ASCVD, type 1 diabetes, previous lipid-lowering treatment, dementia, cancer, or paralysis were excluded, as were those who were in residential care, were on dialysis, or had received an organ transplant. Patients were stratified by age (75-84 years and ≥ 85 years), diabetes status (with or without type 2 diabetes), and statin use (nonuser or new user).
Continue to: Results
Results. For patients with type 2 diabetes, the risk of ASCVD (a composite of coronary heart disease and stroke) was lower among those who took statins than among those who did not in the 75-to-84 group (hazard ratio [HR] = 0.76; 95% confidence interval [CI], 0.65-0.89; 1-year number needed to treat [NNT] = 164). Among those who took statins, there was also lower all-cause mortality (HR = 0.84; 95% CI, 0.75-0.94; 1-year NNT = 306). In those ages ≥ 85 years with diabetes, the statin group did not have a lower risk of ASCVD (HR = 0.82; 95% CI, 0.53-1.26) or all-cause mortality (HR = 1.05; 95% CI, 0.86-1.28).
For patients ages 75 to 84 years without diabetes, there was no difference in risk between groups for ASCVD (HR = 0.94; 95% CI, 0.86–1.04) or all-cause mortality (HR = 0.98; 95% CI, 0.91-1.05). In those ages ≥ 85 years without diabetes, there was also no difference between groups for ASCVD (HR = 1; 95% CI, 0.80-1.24) or for all-cause mortality (HR = 1; 95% CI, 0.90-1.11).
A 2019 meta-analysis of randomized controlled trials (RCTs) (n = 134,537) and RCT summary data (n = 12,705) evaluated the safety and efficacy of statin therapy in patients ages ≥ 55 years.2 In the group of patients ages > 75 years (n = 14,483; median follow-up, 4.9 years), each 1 mmol/L reduction in LDL-C was associated with significant decreased risk for major vascular events (risk ratio [RR] = 0.82; 95% CI, 0.70-0.95) and for major coronary events (RR = 0.82; 95% CI, 0.70-0.96).
In subgroup analysis by the presence or absence of previous vascular disease, there was a decreased risk per 1 mmol/L LDL-C reduction of major vascular events in patients with previous vascular disease (RR = 0.85; 95% CI, 0.73-0.98); however, there was not a significant effect in patients without previous vascular disease (RR = 0.92; 95% CI, 0.73-1.16).
WHAT’S NEW
Statins may be unnecessary in older adults without ASCVD or T2DM
Statin therapy reduces the risk of ASCVD and mortality in patients ages 75 to 84 with type 2 diabetes and in patients > 75 years with known vascular disease. However, statin therapy seems to provide no benefit in patients ages > 75 years without ASCVD or in patients ages ≥ 85 years without ASCVD, regardless of type 2 diabetes status.
Continue to: CAVEATS
CAVEATS
Retrospective cohort design leaves cause and effect equivocal
Even though the first study was large (with more than 46,000 patients) and the median follow-up was 5.6 years, it was a retrospective cohort study. While there is clearly an association between statin therapy and reduced ASCVD and all-cause mortality in patients with diabetes ages 75 to 84 years, cause and effect cannot be unequivocally stated. However, the meta-analysis, which included RCTs, confirms the benefit of statins in secondary prevention for older patients.
The cohort study did not look at adverse effects from statin therapy in this age group, but the data from the 2019 meta-analysis did not reveal any significant risk of myopathy.
CHALLENGES TO IMPLEMENTATION
Guidelines are lacking and discontinuing meds requires discussion
The lack of supporting guidelines to treat this age group with statins remains the largest barrier to implementation. Many patients may already be taking a statin, so a discussion about discontinuing medication will need to be initiated.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
Ms. M is a 76-year-old woman with well-controlled type 2 diabetes mellitus for 10 years and well-controlled mild hypertension. She is otherwise healthy, and her mother lived to age 95. Ms. M has never smoked, has no previous history of vascular/cardiovascular disease, and drinks 1 glass of wine 2 to 3 times per week. Based on the American College of Cardiology (ACC) calculator, she was started on atorvastatin years ago. Is continued use of the medication of any benefit at her current age?
The 2018 American Heart Association (AHA)/ACC/Multi-Society cholesterol guidelines do not provide primary prevention recommendations for those older than age 75 years.3 Up to age 75, the guidelines recommend that patients with type 2 diabetes and a low-density lipoprotein cholesterol (LDL-C) level ≥ 70 mg/dL, as well as those without diabetes but with an LDL-C ≥ 70 mg/dL and a 10-year atherosclerotic cardiovascular disease (ASCVD) risk ≥ 10%, be started on medium-intensity statin therapy.
A 2018 consensus panel review of the current literature, sponsored by the National Institute on Aging and the National Heart, Lung, and Blood Institute, concluded that there was insufficient evidence regarding the benefits and harms of statins in older adults, especially those with comorbidities, and that there was a paucity of evidence about statin therapy outcomes (both adverse and beneficial) relevant to older adults.4
A review of all guidelines published since 2013 revealed that only the United Kingdom’s 2014 National Institute for Health and Care Excellence (NICE) guideline provides a strong, risk-based recommendation for initiating primary prevention with statins in patients > 75 years old.5 These recommendations are based on the QRISK2 calculator (which has since been updated to the QRISK3), which assigns everyone ages > 75 years a > 10% 10-year risk score. This provides a universal statin indication for anyone in the 76-to-84 age range.6
Both the ACC/AHA and US Preventive Services Task Force guidelines clearly state that there are too few data and inadequate evidence in people older than 75 for a strong, risk-based statin recommendation.5 The Canadian Cardiovascular Society guideline takes a similar stance, emphasizing that the recommended Framingham risk model is not well validated in people > 75 years.5
STUDY SUMMARIES
Two different looks at statin use in the elderly
A retrospective cohort study (N = 46,864; median follow-up, 5.6 years) examined whether statin treatment is associated with a reduction in atherosclerotic disease and mortality in old and very old adults with and without type 2 diabetes.1 Patients were enrolled from a large, anonymized national database in Spain. The researchers looked only at first-time users of statins and those without a statin prescription within the past 18 months.
Patients with previous ASCVD, type 1 diabetes, previous lipid-lowering treatment, dementia, cancer, or paralysis were excluded, as were those who were in residential care, were on dialysis, or had received an organ transplant. Patients were stratified by age (75-84 years and ≥ 85 years), diabetes status (with or without type 2 diabetes), and statin use (nonuser or new user).
Continue to: Results
Results. For patients with type 2 diabetes, the risk of ASCVD (a composite of coronary heart disease and stroke) was lower among those who took statins than among those who did not in the 75-to-84 group (hazard ratio [HR] = 0.76; 95% confidence interval [CI], 0.65-0.89; 1-year number needed to treat [NNT] = 164). Among those who took statins, there was also lower all-cause mortality (HR = 0.84; 95% CI, 0.75-0.94; 1-year NNT = 306). In those ages ≥ 85 years with diabetes, the statin group did not have a lower risk of ASCVD (HR = 0.82; 95% CI, 0.53-1.26) or all-cause mortality (HR = 1.05; 95% CI, 0.86-1.28).
For patients ages 75 to 84 years without diabetes, there was no difference in risk between groups for ASCVD (HR = 0.94; 95% CI, 0.86–1.04) or all-cause mortality (HR = 0.98; 95% CI, 0.91-1.05). In those ages ≥ 85 years without diabetes, there was also no difference between groups for ASCVD (HR = 1; 95% CI, 0.80-1.24) or for all-cause mortality (HR = 1; 95% CI, 0.90-1.11).
A 2019 meta-analysis of randomized controlled trials (RCTs) (n = 134,537) and RCT summary data (n = 12,705) evaluated the safety and efficacy of statin therapy in patients ages ≥ 55 years.2 In the group of patients ages > 75 years (n = 14,483; median follow-up, 4.9 years), each 1 mmol/L reduction in LDL-C was associated with significant decreased risk for major vascular events (risk ratio [RR] = 0.82; 95% CI, 0.70-0.95) and for major coronary events (RR = 0.82; 95% CI, 0.70-0.96).
In subgroup analysis by the presence or absence of previous vascular disease, there was a decreased risk per 1 mmol/L LDL-C reduction of major vascular events in patients with previous vascular disease (RR = 0.85; 95% CI, 0.73-0.98); however, there was not a significant effect in patients without previous vascular disease (RR = 0.92; 95% CI, 0.73-1.16).
WHAT’S NEW
Statins may be unnecessary in older adults without ASCVD or T2DM
Statin therapy reduces the risk of ASCVD and mortality in patients ages 75 to 84 with type 2 diabetes and in patients > 75 years with known vascular disease. However, statin therapy seems to provide no benefit in patients ages > 75 years without ASCVD or in patients ages ≥ 85 years without ASCVD, regardless of type 2 diabetes status.
Continue to: CAVEATS
CAVEATS
Retrospective cohort design leaves cause and effect equivocal
Even though the first study was large (with more than 46,000 patients) and the median follow-up was 5.6 years, it was a retrospective cohort study. While there is clearly an association between statin therapy and reduced ASCVD and all-cause mortality in patients with diabetes ages 75 to 84 years, cause and effect cannot be unequivocally stated. However, the meta-analysis, which included RCTs, confirms the benefit of statins in secondary prevention for older patients.
The cohort study did not look at adverse effects from statin therapy in this age group, but the data from the 2019 meta-analysis did not reveal any significant risk of myopathy.
CHALLENGES TO IMPLEMENTATION
Guidelines are lacking and discontinuing meds requires discussion
The lack of supporting guidelines to treat this age group with statins remains the largest barrier to implementation. Many patients may already be taking a statin, so a discussion about discontinuing medication will need to be initiated.
ACKNOWLEDGMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Ramos R, Comas-Cufi M, Marti-Lluch R, et al. Statins for primary prevention of cardiovascular events and mortality in old and very old adults with and without type 2 diabetes: retrospective cohort study. BMJ. 2018;362:k3359.
2. Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomized controlled trials. Lancet. 2019;393:407-415.
3. Stone NJ, Grundy SM. The 2018 AHA/ACC/Multi-Society cholesterol guidelines: looking at past, present and future. Prog Cardiovasc Dis. 2019;62:375-383.
4. Singh S, Zieman S, Go AS, et al. Statins for primary prevention in older adults—moving towards evidence-based decision-making. J Am Geriatr Soc. 2018;66:2188-2196.
5. Mortensen MB, Falk E. Primary prevention with statins in the elderly. J Am Coll Cardiol. 2018;71:85-94.
6. ClinRisk. Welcome to the QRISK®3-2018 risk calculator. www.qrisk.org/three/. Accessed May 27, 2020.
1. Ramos R, Comas-Cufi M, Marti-Lluch R, et al. Statins for primary prevention of cardiovascular events and mortality in old and very old adults with and without type 2 diabetes: retrospective cohort study. BMJ. 2018;362:k3359.
2. Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomized controlled trials. Lancet. 2019;393:407-415.
3. Stone NJ, Grundy SM. The 2018 AHA/ACC/Multi-Society cholesterol guidelines: looking at past, present and future. Prog Cardiovasc Dis. 2019;62:375-383.
4. Singh S, Zieman S, Go AS, et al. Statins for primary prevention in older adults—moving towards evidence-based decision-making. J Am Geriatr Soc. 2018;66:2188-2196.
5. Mortensen MB, Falk E. Primary prevention with statins in the elderly. J Am Coll Cardiol. 2018;71:85-94.
6. ClinRisk. Welcome to the QRISK®3-2018 risk calculator. www.qrisk.org/three/. Accessed May 27, 2020.
PRACTICE CHANGER
Do not start a statin in patients ages ≥ 75 years who do not have known vascular disease or type 2 diabetes; start or continue a statin in all patients ages 75 to 84 with type 2 diabetes to prevent cardiovascular events and mortality; and start or continue a statin in patients ages > 75 years who have known vascular occlusive disease.
STRENGTH OF RECOMMENDATION
B: Based on a meta-analysis of randomized controlled trials and a retrospective cohort study.
Ramos R, Comas-Cufi M, Marti-Lluch R, et al. Statins for primary prevention of cardiovascular events and mortality in old and very old adults with and without type 2 diabetes: retrospective cohort study. BMJ. 2018;362:k3359.1
Cholesterol Treatment Trialists’ Collaboration. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomized controlled trials. Lancet. 2019;393:407-415.2

First-in-class antipsychotic linked to lower cardiometabolic risk
A recently approved first-in-class antipsychotic appears to have fewer adverse cardiometabolic effects than standard care with risperidone, new research suggests.

In post hoc analyses of two short-term randomized controlled trials plus an open-label long-term study, patients with schizophrenia on lumateperone (Caplyta, Intra-Cellular Therapies) had reduced rates of metabolic syndrome, compared with their counterparts taking placebo or the antipsychotic risperidone.
In the short-term studies, rates of metabolic syndrome were similar between groups at baseline, but by the end of 4 and 6 weeks of treatment, 25% of patients taking lumateperone no longer met criteria for metabolic syndrome. A similar finding occurred in 36% of patients in the 1-year open label study.
“One of the major advantages that we found during the drug’s development was that it has a very favorable profile with regard to changes in weight, and other [parameters] associated with cardiovascular disease risk, such as elevated glucose and lipids,” study investigator Andrew Satlin, MD, chief medical officer at Intra-Cellular Therapies, New York, told this news organization.
“So we went back to our data and looked to see whether the changes that we saw had an impact on either the development or the resolution of metabolic syndrome in the patients who came into our studies,” he said.
The findings were presented at the American Society of Clinical Psychopharmacology 2020 Virtual Conference.
Reduced cholesterol
Lumateperone was approved in December by the Food and Drug Administration. The drug acts synergistically through the serotonergic, dopaminergic, and glutamatergic systems.
The short-term studies included 511 patients randomly assigned to receive lumateperone 42 mg (n = 256 patients) or risperidone 4 mg (n = 255 patients).
At baseline, rates of metabolic syndrome were 16% in the lumateperone group and 19% in the risperidone group. At the end of treatment, metabolic syndrome was less common in the lumateperone group (13%) vs. those receiving risperidone (25%).
In addition, 46% of lumateperone patients with metabolic syndrome at baseline no longer had it at the end of the study period. This compared with 25% of patients on risperidone.
The differences in metabolic syndrome conversion rates appeared to be driven by greater reductions in total cholesterol with lumateperone, compared with risperidone (–2.8 mg/dL with lumateperone vs. 4.8 mg/dL with risperidone) and triglycerides (–0.7 mg/dL with lumateperone vs. 20.4 mg/dL with risperidone).
Greater increases in blood glucose were also seen with risperidone (7.7 mg/dL) than with lumateperone (0.9 mg/dL).
The long-term study included 602 patients with stable schizophrenia. All received lumateperone 42 mg, and 197 patients (33%) had metabolic syndrome at baseline.
At the end of the 1-year study, 72 of these patients (36%) no longer met criteria for metabolic syndrome.
“Safest antipsychotic so far”
“Lumateperone seems to be the safest antipsychotic we have seen so far,” Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charité Universitatsmedizin, Berlin, who was also involved in clinical trials of lumateperone, told this news organization.
“It seems to be very safe when it comes to cardiometabolic parameters, and it shows similar reduction in symptoms as risperidone. It is certainly an agent one should consider, particularly when a patient cannot tolerate other medications or may not be in full adherence,” said Dr. Correll, who has a joint appointment as professor of psychiatry and molecular medicine at the Zucker School of Medicine at Hofstra University in Hempstead, New York.
The drug’s safety and efficacy profile would make it a good candidate in patients initiating antipsychotic treatment, but reimbursement issues may be a barrier, at least for now, he added.
He said that the drug may prevent the onset of metabolic side effects and added that once payers are willing to reimburse the drug it should become the “first-line standard of care.”
It is well known that atypical antipsychotics are associated with adverse and rapid metabolic changes. Dr. Correll noted that particularly early-phase and first-episode patients can be “very sensitive” to the side effects of these drugs and often experience rapid weight gain and other adverse metabolic changes. Lumateperone, he added, may help avoid some of this cardiometabolic risk.
Time will tell
Jessica M. Gannon, MD, a psychiatrist at the University of Pittsburgh said in commenting on the findings that the drug’s favorable metabolic profile has previously been reported.
She also noted that there has been some interest in lumateperone because of possible “downstream effects on NMDA-type glutamate receptor activity, a larger binding ratio at dopamine-2:5HT1A receptors than other atypical antipsychotics, and presynaptic D2 partial agonism and a postsynaptic D2 antagonism.”
“This latter feature may explain the reported low extrapyramidal symptom incidence in the clinical trials,” she said .
“While I think future studies and clinical use can help determine how clinically efficacious this medication will be for our patients when compared to others on the market, its favorable metabolic and EPS profile do make it of interest,” added Gannon, who was not involved in researching the drug.
The study was funded by Intra-Cellular Therapies. Dr. Satlin is chief medical officer of Intracellular Therapies. Dr. Correll has been a consultant or advisor to and has received honoraria from Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
A recently approved first-in-class antipsychotic appears to have fewer adverse cardiometabolic effects than standard care with risperidone, new research suggests.
In post hoc analyses of two short-term randomized controlled trials plus an open-label long-term study, patients with schizophrenia on lumateperone (Caplyta, Intra-Cellular Therapies) had reduced rates of metabolic syndrome, compared with their counterparts taking placebo or the antipsychotic risperidone.
In the short-term studies, rates of metabolic syndrome were similar between groups at baseline, but by the end of 4 and 6 weeks of treatment, 25% of patients taking lumateperone no longer met criteria for metabolic syndrome. A similar finding occurred in 36% of patients in the 1-year open label study.
“One of the major advantages that we found during the drug’s development was that it has a very favorable profile with regard to changes in weight, and other [parameters] associated with cardiovascular disease risk, such as elevated glucose and lipids,” study investigator Andrew Satlin, MD, chief medical officer at Intra-Cellular Therapies, New York, told this news organization.
“So we went back to our data and looked to see whether the changes that we saw had an impact on either the development or the resolution of metabolic syndrome in the patients who came into our studies,” he said.
The findings were presented at the American Society of Clinical Psychopharmacology 2020 Virtual Conference.
Reduced cholesterol
Lumateperone was approved in December by the Food and Drug Administration. The drug acts synergistically through the serotonergic, dopaminergic, and glutamatergic systems.
The short-term studies included 511 patients randomly assigned to receive lumateperone 42 mg (n = 256 patients) or risperidone 4 mg (n = 255 patients).
At baseline, rates of metabolic syndrome were 16% in the lumateperone group and 19% in the risperidone group. At the end of treatment, metabolic syndrome was less common in the lumateperone group (13%) vs. those receiving risperidone (25%).
In addition, 46% of lumateperone patients with metabolic syndrome at baseline no longer had it at the end of the study period. This compared with 25% of patients on risperidone.
The differences in metabolic syndrome conversion rates appeared to be driven by greater reductions in total cholesterol with lumateperone, compared with risperidone (–2.8 mg/dL with lumateperone vs. 4.8 mg/dL with risperidone) and triglycerides (–0.7 mg/dL with lumateperone vs. 20.4 mg/dL with risperidone).
Greater increases in blood glucose were also seen with risperidone (7.7 mg/dL) than with lumateperone (0.9 mg/dL).
The long-term study included 602 patients with stable schizophrenia. All received lumateperone 42 mg, and 197 patients (33%) had metabolic syndrome at baseline.
At the end of the 1-year study, 72 of these patients (36%) no longer met criteria for metabolic syndrome.
“Safest antipsychotic so far”
“Lumateperone seems to be the safest antipsychotic we have seen so far,” Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charité Universitatsmedizin, Berlin, who was also involved in clinical trials of lumateperone, told this news organization.
“It seems to be very safe when it comes to cardiometabolic parameters, and it shows similar reduction in symptoms as risperidone. It is certainly an agent one should consider, particularly when a patient cannot tolerate other medications or may not be in full adherence,” said Dr. Correll, who has a joint appointment as professor of psychiatry and molecular medicine at the Zucker School of Medicine at Hofstra University in Hempstead, New York.
The drug’s safety and efficacy profile would make it a good candidate in patients initiating antipsychotic treatment, but reimbursement issues may be a barrier, at least for now, he added.
He said that the drug may prevent the onset of metabolic side effects and added that once payers are willing to reimburse the drug it should become the “first-line standard of care.”
It is well known that atypical antipsychotics are associated with adverse and rapid metabolic changes. Dr. Correll noted that particularly early-phase and first-episode patients can be “very sensitive” to the side effects of these drugs and often experience rapid weight gain and other adverse metabolic changes. Lumateperone, he added, may help avoid some of this cardiometabolic risk.
Time will tell
Jessica M. Gannon, MD, a psychiatrist at the University of Pittsburgh said in commenting on the findings that the drug’s favorable metabolic profile has previously been reported.
She also noted that there has been some interest in lumateperone because of possible “downstream effects on NMDA-type glutamate receptor activity, a larger binding ratio at dopamine-2:5HT1A receptors than other atypical antipsychotics, and presynaptic D2 partial agonism and a postsynaptic D2 antagonism.”
“This latter feature may explain the reported low extrapyramidal symptom incidence in the clinical trials,” she said .
“While I think future studies and clinical use can help determine how clinically efficacious this medication will be for our patients when compared to others on the market, its favorable metabolic and EPS profile do make it of interest,” added Gannon, who was not involved in researching the drug.
The study was funded by Intra-Cellular Therapies. Dr. Satlin is chief medical officer of Intracellular Therapies. Dr. Correll has been a consultant or advisor to and has received honoraria from Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
A recently approved first-in-class antipsychotic appears to have fewer adverse cardiometabolic effects than standard care with risperidone, new research suggests.
In post hoc analyses of two short-term randomized controlled trials plus an open-label long-term study, patients with schizophrenia on lumateperone (Caplyta, Intra-Cellular Therapies) had reduced rates of metabolic syndrome, compared with their counterparts taking placebo or the antipsychotic risperidone.
In the short-term studies, rates of metabolic syndrome were similar between groups at baseline, but by the end of 4 and 6 weeks of treatment, 25% of patients taking lumateperone no longer met criteria for metabolic syndrome. A similar finding occurred in 36% of patients in the 1-year open label study.
“One of the major advantages that we found during the drug’s development was that it has a very favorable profile with regard to changes in weight, and other [parameters] associated with cardiovascular disease risk, such as elevated glucose and lipids,” study investigator Andrew Satlin, MD, chief medical officer at Intra-Cellular Therapies, New York, told this news organization.
“So we went back to our data and looked to see whether the changes that we saw had an impact on either the development or the resolution of metabolic syndrome in the patients who came into our studies,” he said.
The findings were presented at the American Society of Clinical Psychopharmacology 2020 Virtual Conference.
Reduced cholesterol
Lumateperone was approved in December by the Food and Drug Administration. The drug acts synergistically through the serotonergic, dopaminergic, and glutamatergic systems.
The short-term studies included 511 patients randomly assigned to receive lumateperone 42 mg (n = 256 patients) or risperidone 4 mg (n = 255 patients).
At baseline, rates of metabolic syndrome were 16% in the lumateperone group and 19% in the risperidone group. At the end of treatment, metabolic syndrome was less common in the lumateperone group (13%) vs. those receiving risperidone (25%).
In addition, 46% of lumateperone patients with metabolic syndrome at baseline no longer had it at the end of the study period. This compared with 25% of patients on risperidone.
The differences in metabolic syndrome conversion rates appeared to be driven by greater reductions in total cholesterol with lumateperone, compared with risperidone (–2.8 mg/dL with lumateperone vs. 4.8 mg/dL with risperidone) and triglycerides (–0.7 mg/dL with lumateperone vs. 20.4 mg/dL with risperidone).
Greater increases in blood glucose were also seen with risperidone (7.7 mg/dL) than with lumateperone (0.9 mg/dL).
The long-term study included 602 patients with stable schizophrenia. All received lumateperone 42 mg, and 197 patients (33%) had metabolic syndrome at baseline.
At the end of the 1-year study, 72 of these patients (36%) no longer met criteria for metabolic syndrome.
“Safest antipsychotic so far”
“Lumateperone seems to be the safest antipsychotic we have seen so far,” Christoph U. Correll, MD, professor of child and adolescent psychiatry, Charité Universitatsmedizin, Berlin, who was also involved in clinical trials of lumateperone, told this news organization.
“It seems to be very safe when it comes to cardiometabolic parameters, and it shows similar reduction in symptoms as risperidone. It is certainly an agent one should consider, particularly when a patient cannot tolerate other medications or may not be in full adherence,” said Dr. Correll, who has a joint appointment as professor of psychiatry and molecular medicine at the Zucker School of Medicine at Hofstra University in Hempstead, New York.
The drug’s safety and efficacy profile would make it a good candidate in patients initiating antipsychotic treatment, but reimbursement issues may be a barrier, at least for now, he added.
He said that the drug may prevent the onset of metabolic side effects and added that once payers are willing to reimburse the drug it should become the “first-line standard of care.”
It is well known that atypical antipsychotics are associated with adverse and rapid metabolic changes. Dr. Correll noted that particularly early-phase and first-episode patients can be “very sensitive” to the side effects of these drugs and often experience rapid weight gain and other adverse metabolic changes. Lumateperone, he added, may help avoid some of this cardiometabolic risk.
Time will tell
Jessica M. Gannon, MD, a psychiatrist at the University of Pittsburgh said in commenting on the findings that the drug’s favorable metabolic profile has previously been reported.
She also noted that there has been some interest in lumateperone because of possible “downstream effects on NMDA-type glutamate receptor activity, a larger binding ratio at dopamine-2:5HT1A receptors than other atypical antipsychotics, and presynaptic D2 partial agonism and a postsynaptic D2 antagonism.”
“This latter feature may explain the reported low extrapyramidal symptom incidence in the clinical trials,” she said .
“While I think future studies and clinical use can help determine how clinically efficacious this medication will be for our patients when compared to others on the market, its favorable metabolic and EPS profile do make it of interest,” added Gannon, who was not involved in researching the drug.
The study was funded by Intra-Cellular Therapies. Dr. Satlin is chief medical officer of Intracellular Therapies. Dr. Correll has been a consultant or advisor to and has received honoraria from Acadia, Alkermes, Allergan, Angelini, Axsome, Gedeon Richter, Gerson Lehrman Group, Intra-Cellular Therapies, Janssen/J&J, LB Pharma, Lundbeck, MedAvante-ProPhase, Medscape, Neurocrine, Noven, Otsuka, Pfizer, Recordati, Rovi, Sumitomo Dainippon, Sunovion, Supernus, Takeda, and Teva.
A version of this article originally appeared on Medscape.com.
High out-of-pocket costs for type 1 diabetes patients: It’s not just insulin
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
For privately insured individuals with type 1 diabetes in the United States, out-of-pocket costs for insulin are typically lower than for other diabetes-related supplies. But overall out-of-pocket expenditure – taking into account everything that is needed to manage diabetes – is still very high.
Indeed, insulin costs have remained relatively stable over time in such private insurance plans, according to another analysis that looked at all types of diabetes.
Those are the findings of two separate research letters published June 1 in JAMA Internal Medicine.
The first research letter examined all costs for privately insured patients with type 1 diabetes, finding a mean out-of-pocket spend of approximately $2,500 a year.
“Insulin is the difference between life and death for patients with type 1 diabetes, and efforts to make it more affordable are critical,” said lead author of the first letter, Kao-Ping Chua, MD, PhD, of the department of pediatrics, University of Michigan, Ann Arbor.
“However, our study shows that even if insulin were free, families would still have substantial out-of-pocket costs for other health care,” he noted in a press release from his institution.
The other research letter examined trends in insulin out-of-pocket costs in 2006-2017 among U.S. patients with any type of diabetes who had different types of private health insurance plans. The study was by Amir Meiri, MD, of Harvard Pilgrim Health Care Institute, Harvard Medical School, Boston, and colleagues.
Although the study showed relatively stable costs associated with insulin for many privately insured patients with diabetes over the time period examined, “monthly out-of-pocket payments” may still “be burdensome for low-income individuals,” the authors said.
Writing in an accompanying editorial, Laura M. Nally, MD, and Kasia J. Lipska, MD, both of Yale University, New Haven, Conn., agreed that “insulin is only one component of diabetes management.”
Yet they stressed: “Diabetes does not selectively occur among individuals who can afford insulin and who have health insurance; it affects people regardless of their socioeconomic status.”
“The federal health care system should urgently act to make insulin, diabetes-related supplies, and other health care services affordable and available to everyone who needs them.”
Out-of-pocket costs for supplies higher than for insulin
Dr. Chua and colleagues compared out-of-pocket costs for insulin with those for other diabetes-related items, including insulin pump supplies, and glucose meters/continuous monitors, for privately insured patients with type 1 diabetes during 2018.
They included data for 65,192 patients aged 1-64 years with type 1 diabetes who had employer-sponsored coverage from medium to large firms.
The population included children of employees (12%), and 22.5% of patients had enrolled in high-deductible ($1,350 individual/$2,700 family) private plans. Overall, 56.8% used insulin pumps and/or continuous glucose monitors (CGMs).
Annual out-of-pocket spending was lower for insulin ($435) than other diabetes-related supplies ($490), including insulin pump supplies, continuous and fingerstick glucose monitoring equipment, urine testing strips, pen needles, and syringes.
Mean annual overall out-of-pocket spending was $2,414, but this varied widely.
For 8% of the population spending exceeded $5,000. Insulin accounted for just 18% of overall out-of-pocket spending.
Not surprisingly, out-of-pocket spending increased with the sophistication of the diabetes technology used, ranging from just $79 for those using injections and fingerstick monitoring to $1,037 for those using both insulin pumps and CGMs.
In general, for children, out-of-pocket costs of diabetes-related supplies were considerably higher than for insulin ($823 vs. $497), while for adults the two were similar ($445 vs. $427).
“These technologies can improve quality of life and improve diabetes control for all patients, but can be especially important to the families of children with type 1 diabetes,” Dr. Chua said.
Also not surprisingly, those with high-deductible plans had greater out-of-pocket costs in each category ($3,132 vs. $2,205 overall).
Dr. Chua said the study’s findings are particularly timely given recent efforts by states and insurers to cap out-of-pocket costs for insulin, calling these “important first steps.”
But there is still a long way to go, he said.
“Policymakers should improve the affordability of all care for type 1 diabetes,” Dr. Chua noted.
Dr. Nally and Dr. Lipska agreed.
“Although capping insulin copayments is a step in the right direction, such a state law does not protect many individuals with federally regulated insurance plans, with Medicare, or without any insurance,” they noted.
“In addition, insulin copayment caps do little to ease the financial burden of paying for diabetes-related supplies or other healthcare services,” they pointed out.
Private plans shield members from out-of-pocket insulin costs
The other study examined out-of-pocket spending for 10,954,436 insulin claims for 612,071 unique patients with diabetes (either type) in different types of private commercial health plans during 2006-2017:
- High-deductible health plans (HDHP) with a health savings account (HSA), which have high medication costs because they require payment of the full reimbursement price until the annual deductible is reached (7% of claims).
- Plans with health reimbursement arrangement (HRA), which typically have tiered drug copayments and members can use their reimbursement accounts to pay for medical expenses (4% of claims).
- No-account plans (without an HSA) that also typically have tiered drug copayments (80% of claims).
The price of insulin per patient per month rose from $143 in 2006 to $280 in 2012 to $394 in 2017.
However, the share of the insulin price per member per month paid by the patient actually declined from 24% in 2006 to 16% in 2012 to just 10% in 2017.
Because of the increase in insulin price, those corresponding costs still rose from $52 in 2006 to $72 in 2012, but then dropped to $64 in 2017.
By plan type, out-of-pocket costs per member per month were lowest for those no-account plans (from $52 in 2006 to $48 in 2017) and highest for those with HDHP HSA plans ($93 in 2006 to $141 in 2017).
“The data suggest that privately insured patients have been relatively shielded from insulin price increases and that commercial health insurers have accommodated higher insulin prices by increasing premiums or deductibles for all members,” Dr. Meiri and colleagues write.
Most vulnerable missing from study: COVID-19 will strike further blow
Although generally agreeing with this conclusion, Dr. Nally and Dr. Lipska nevertheless faulted the data from Dr. Meiri and colleagues on several counts.
First, they reiterated that the population was limited to those with private insurance plans, and therefore “the groups most vulnerable to high insulin costs may be missing from the study.”
Also, the data do not capture all sources of out-of-pocket insulin spending for people with high copayments, such as the federal 340B Drug Pricing Program, GoodRx, or drug manufacturer discounts.
Moreover, the editorialists noted, the study assessed only mean out-of-pocket costs without assessing differences in spending across individuals.
And, Dr. Nally and Dr. Lipska pointed out, the data do not account for rebates and discounts negotiated between pharmacy benefit managers and drug manufacturers. “As a result, these data on health plan spending on insulin may overestimate the net health plan expenditures,” they wrote.
Dr. Chua also warned that the COVID-19 pandemic has had a major adverse impact on the diabetes community.
“Many people with private insurance have lost their jobs and insurance coverage ... This may put health care like insulin and diabetes-related supplies out of reach,” he said.
Dr. Chua has reported receiving support from the National Institute on Drug Abuse. Dr. Meiri has reported receiving grants from the Centers for Disease Control and Prevention and the National Institute of Diabetes and Digestive and Kidney Diseases for the study. Dr. Nally has reported receiving a grant from Novo Nordisk outside the submitted work. Dr. Lipska has reported receiving support from the Centers for Medicare & Medicaid Services and the National Institutes of Health.
A version of this article originally appeared on Medscape.com.
10% with diabetes hospitalized for COVID-19 die within a week
Data from the CORONADO (French Coronavirus SARS-CoV-2 and Diabetes Outcomes) study also revealed that body mass index (BMI) was independently associated with death or intubation at 7 days, while A1c and use of renin-angiotensin-aldosterone system (RAAS) blockers and dipeptidyl peptidase–4 inhibitors were not.
The presence of diabetes-related complications and older age also increased the risk of death.
The findings were published online Diabetologia by Bertrand Cariou, MD, PhD, of the department of endocrinology at the Hôpital Guillaume et René Laennec in Nantes, France, and colleagues.
First study to examine specific characteristics at time of admission
Previous studies have linked diabetes to worse outcomes in COVID-19, but this is the first to examine specific characteristics before and at the time of hospital admission that predict worse outcomes among people with diabetes, study coauthor Samy Hadjadj, MD, PhD, said in an interview.
“Before the CORONADO study it was ‘all diabetes [patients] are the same.’ Now we can surely consider more precisely the risk, taking age, sex, BMI, complications, and [obstructive sleep apnea] as clear ‘very high-risk situations,’” said Dr. Hadjadj, of the same institution as Dr. Cariou.
Another clinical message, Dr. Hadjadj said, is that, “even in diabetes, each increase in BMI is associated with an increase in the risk of intubation and/or death in the 7 days following admission for COVID-19. So let’s target this population as a really important population to keep social distancing and stay alert on avoiding the virus.”
But he urged caution regarding the A1c finding. “A1c might be associated with admission to hospital but other factors far beyond A1c drive the prognosis as soon as a patient is admitted. It’s surprising but reasonable speculation can explain this.”
And Dr. Hadjadj said that no obvious signals were identified with regard to medication use.
“Insulin is not suspected of having adverse effects closely related to COVID-19. RAAS blockers are not deleterious but indicative of hypertension, which is a comorbidity even in diabetes patients,” he said. (None of the patients studied were taking sodium-glucose cotransporter 2 inhibitors or glucagonlike peptide receptor agonists.)
Yet again, high BMI emerges as a major risk factor
The study included 1,317 patients with diabetes and confirmed COVID-19 admitted to 53 French hospitals during March 10-31, 2020. Participants included 88.5% with type 2 diabetes, 3% with type 1 diabetes, and 3.1% newly diagnosed on admission. Mean age was 69.8 years.
Diabetes-related disorders on admission were reported in 11.1% of participants overall. These included 132 episodes of severe hyperglycemia, including 40 of ketosis, of which 19 were ketoacidosis, and 14 hypoglycemic events. Severe anorexia was reported in 6.3%.
The composite primary endpoint, tracheal intubation for mechanical ventilation and/or death within 7 days of admission, occurred in 29% of patients (n = 382).
Of the secondary outcomes, 31.1% (n = 410) were admitted to ICUs within 7 days of hospital admission, including 20.3% (n = 267) who required tracheal intubation for mechanical ventilation.
On day 7, 10.6% (n = 140) had died and 18.0% (n = 237) were discharged.
In the univariate analysis, the primary outcome was more frequent in men (69.1% vs. 63.2%; P = .0420) and those taking RAAS blockers (61.5% vs. 55.3%; P = .0386). Median BMI was significantly higher in those in whom the primary outcome occurred (29.1 vs 28.1 kg/m2; P = .0009),
Other characteristics prior to admission associated with risk of death on day 7 included age, hypertension, micro- and macrovascular diabetes-related complications, and comorbidities such as heart failure and treated obstructive sleep apnea.
Over 40% of those admitted had such complications. Of the patients analyzed, microvascular complications (eye, kidney, and neuropathy) were present in 47% and macrovascular complications (arteries of the heart, brain, and legs) were present in 41%.
Encouragingly, there were no deaths in patients aged under 65 years with type 1 diabetes, but only 39 participants had type 1 diabetes. Other work is ongoing to establish the effect of COVID-19 in this specific population, the researchers wrote.
Among prior medications, metformin use was lower in people who died, while insulin use, RAAS blockers, beta-blockers, loop diuretics, and mineralocorticoid-receptor antagonists were associated with death on day 7. The medication findings didn’t reach statistical significance, however.
When asked about the hint of a protective effect of metformin (odds ratio, 0.80; P = .4532), given that some experts have advised stopping it in the setting of COVID-19 because of the risk of lactic acidosis, Dr. Hadjadj said he wouldn’t necessarily stop it in all patients with COVID-19, but said, “let’s stop it in cases of severe condition.”
Analysis ongoing, ‘some new messages might pop up’
After adjustment for age and sex, BMI was significantly and positively associated with the primary outcome (P = .0001) but not with death on day 7 (P = .1488), and A1c wasn’t associated with either outcome.
In a multivariable analysis that included characteristics prior to admission, BMI remained the only independent preadmission predictor associated with the primary outcome (adjusted odds ratio, 1.28), while factors independently associated with risk of death on day 7 included age, diabetes complication history, and treated obstructive sleep apnea.
And after adjustment for age and sex, admission plasma glucose level was significantly and positively associated with both the primary outcome (P = .0001) and death on day 7 (P = .0059).
In the multivariate analysis, admission characteristics that predicted the primary outcome were dyspnea, lymphopenia, increased AST, and increased C-reactive protein.
Dr. Hadjadj said his team is now “focusing on specific risk factors such as obesity, age, vascular complications, medications ... to perform some deeper analyses.”
“We look forward to analyzing the data on in-hospital stay up to day 28 after admission. Some new messages might well pop up,” he added.
But in the meantime, “Elderly populations with long-term diabetes with advanced diabetes-related complications and/or treated obstructive sleep apnea were particularly at risk of early death and might require specific management to avoid infection with the novel coronavirus,” the researchers stressed.
The study received funding from the Fondation Francophone de Recherche sur le Diabète and was supported by Novo Nordisk, MSD, Abbott, AstraZeneca, Lilly, and the Fédération Française des Diabétiques; Société Francophone du Diabète; and Air Liquide Healthcare International. Dr. Hadjadj reported receiving grants, personal fees, and/or nonfinancial support from AstraZeneca, Bayer, Boehringer Ingelheim, Dinno Santé, Eli Lilly, LVL, MSD, Novartis, Pierre Fabre Santé, Sanofi, Servier, and Valbiotis.
A version of this article originally appeared on Medscape.com.
Data from the CORONADO (French Coronavirus SARS-CoV-2 and Diabetes Outcomes) study also revealed that body mass index (BMI) was independently associated with death or intubation at 7 days, while A1c and use of renin-angiotensin-aldosterone system (RAAS) blockers and dipeptidyl peptidase–4 inhibitors were not.
The presence of diabetes-related complications and older age also increased the risk of death.
The findings were published online Diabetologia by Bertrand Cariou, MD, PhD, of the department of endocrinology at the Hôpital Guillaume et René Laennec in Nantes, France, and colleagues.
First study to examine specific characteristics at time of admission
Previous studies have linked diabetes to worse outcomes in COVID-19, but this is the first to examine specific characteristics before and at the time of hospital admission that predict worse outcomes among people with diabetes, study coauthor Samy Hadjadj, MD, PhD, said in an interview.
“Before the CORONADO study it was ‘all diabetes [patients] are the same.’ Now we can surely consider more precisely the risk, taking age, sex, BMI, complications, and [obstructive sleep apnea] as clear ‘very high-risk situations,’” said Dr. Hadjadj, of the same institution as Dr. Cariou.
Another clinical message, Dr. Hadjadj said, is that, “even in diabetes, each increase in BMI is associated with an increase in the risk of intubation and/or death in the 7 days following admission for COVID-19. So let’s target this population as a really important population to keep social distancing and stay alert on avoiding the virus.”
But he urged caution regarding the A1c finding. “A1c might be associated with admission to hospital but other factors far beyond A1c drive the prognosis as soon as a patient is admitted. It’s surprising but reasonable speculation can explain this.”
And Dr. Hadjadj said that no obvious signals were identified with regard to medication use.
“Insulin is not suspected of having adverse effects closely related to COVID-19. RAAS blockers are not deleterious but indicative of hypertension, which is a comorbidity even in diabetes patients,” he said. (None of the patients studied were taking sodium-glucose cotransporter 2 inhibitors or glucagonlike peptide receptor agonists.)
Yet again, high BMI emerges as a major risk factor
The study included 1,317 patients with diabetes and confirmed COVID-19 admitted to 53 French hospitals during March 10-31, 2020. Participants included 88.5% with type 2 diabetes, 3% with type 1 diabetes, and 3.1% newly diagnosed on admission. Mean age was 69.8 years.
Diabetes-related disorders on admission were reported in 11.1% of participants overall. These included 132 episodes of severe hyperglycemia, including 40 of ketosis, of which 19 were ketoacidosis, and 14 hypoglycemic events. Severe anorexia was reported in 6.3%.
The composite primary endpoint, tracheal intubation for mechanical ventilation and/or death within 7 days of admission, occurred in 29% of patients (n = 382).
Of the secondary outcomes, 31.1% (n = 410) were admitted to ICUs within 7 days of hospital admission, including 20.3% (n = 267) who required tracheal intubation for mechanical ventilation.
On day 7, 10.6% (n = 140) had died and 18.0% (n = 237) were discharged.
In the univariate analysis, the primary outcome was more frequent in men (69.1% vs. 63.2%; P = .0420) and those taking RAAS blockers (61.5% vs. 55.3%; P = .0386). Median BMI was significantly higher in those in whom the primary outcome occurred (29.1 vs 28.1 kg/m2; P = .0009),
Other characteristics prior to admission associated with risk of death on day 7 included age, hypertension, micro- and macrovascular diabetes-related complications, and comorbidities such as heart failure and treated obstructive sleep apnea.
Over 40% of those admitted had such complications. Of the patients analyzed, microvascular complications (eye, kidney, and neuropathy) were present in 47% and macrovascular complications (arteries of the heart, brain, and legs) were present in 41%.
Encouragingly, there were no deaths in patients aged under 65 years with type 1 diabetes, but only 39 participants had type 1 diabetes. Other work is ongoing to establish the effect of COVID-19 in this specific population, the researchers wrote.
Among prior medications, metformin use was lower in people who died, while insulin use, RAAS blockers, beta-blockers, loop diuretics, and mineralocorticoid-receptor antagonists were associated with death on day 7. The medication findings didn’t reach statistical significance, however.
When asked about the hint of a protective effect of metformin (odds ratio, 0.80; P = .4532), given that some experts have advised stopping it in the setting of COVID-19 because of the risk of lactic acidosis, Dr. Hadjadj said he wouldn’t necessarily stop it in all patients with COVID-19, but said, “let’s stop it in cases of severe condition.”
Analysis ongoing, ‘some new messages might pop up’
After adjustment for age and sex, BMI was significantly and positively associated with the primary outcome (P = .0001) but not with death on day 7 (P = .1488), and A1c wasn’t associated with either outcome.
In a multivariable analysis that included characteristics prior to admission, BMI remained the only independent preadmission predictor associated with the primary outcome (adjusted odds ratio, 1.28), while factors independently associated with risk of death on day 7 included age, diabetes complication history, and treated obstructive sleep apnea.
And after adjustment for age and sex, admission plasma glucose level was significantly and positively associated with both the primary outcome (P = .0001) and death on day 7 (P = .0059).
In the multivariate analysis, admission characteristics that predicted the primary outcome were dyspnea, lymphopenia, increased AST, and increased C-reactive protein.
Dr. Hadjadj said his team is now “focusing on specific risk factors such as obesity, age, vascular complications, medications ... to perform some deeper analyses.”
“We look forward to analyzing the data on in-hospital stay up to day 28 after admission. Some new messages might well pop up,” he added.
But in the meantime, “Elderly populations with long-term diabetes with advanced diabetes-related complications and/or treated obstructive sleep apnea were particularly at risk of early death and might require specific management to avoid infection with the novel coronavirus,” the researchers stressed.
The study received funding from the Fondation Francophone de Recherche sur le Diabète and was supported by Novo Nordisk, MSD, Abbott, AstraZeneca, Lilly, and the Fédération Française des Diabétiques; Société Francophone du Diabète; and Air Liquide Healthcare International. Dr. Hadjadj reported receiving grants, personal fees, and/or nonfinancial support from AstraZeneca, Bayer, Boehringer Ingelheim, Dinno Santé, Eli Lilly, LVL, MSD, Novartis, Pierre Fabre Santé, Sanofi, Servier, and Valbiotis.
A version of this article originally appeared on Medscape.com.
Data from the CORONADO (French Coronavirus SARS-CoV-2 and Diabetes Outcomes) study also revealed that body mass index (BMI) was independently associated with death or intubation at 7 days, while A1c and use of renin-angiotensin-aldosterone system (RAAS) blockers and dipeptidyl peptidase–4 inhibitors were not.
The presence of diabetes-related complications and older age also increased the risk of death.
The findings were published online Diabetologia by Bertrand Cariou, MD, PhD, of the department of endocrinology at the Hôpital Guillaume et René Laennec in Nantes, France, and colleagues.
First study to examine specific characteristics at time of admission
Previous studies have linked diabetes to worse outcomes in COVID-19, but this is the first to examine specific characteristics before and at the time of hospital admission that predict worse outcomes among people with diabetes, study coauthor Samy Hadjadj, MD, PhD, said in an interview.
“Before the CORONADO study it was ‘all diabetes [patients] are the same.’ Now we can surely consider more precisely the risk, taking age, sex, BMI, complications, and [obstructive sleep apnea] as clear ‘very high-risk situations,’” said Dr. Hadjadj, of the same institution as Dr. Cariou.
Another clinical message, Dr. Hadjadj said, is that, “even in diabetes, each increase in BMI is associated with an increase in the risk of intubation and/or death in the 7 days following admission for COVID-19. So let’s target this population as a really important population to keep social distancing and stay alert on avoiding the virus.”
But he urged caution regarding the A1c finding. “A1c might be associated with admission to hospital but other factors far beyond A1c drive the prognosis as soon as a patient is admitted. It’s surprising but reasonable speculation can explain this.”
And Dr. Hadjadj said that no obvious signals were identified with regard to medication use.
“Insulin is not suspected of having adverse effects closely related to COVID-19. RAAS blockers are not deleterious but indicative of hypertension, which is a comorbidity even in diabetes patients,” he said. (None of the patients studied were taking sodium-glucose cotransporter 2 inhibitors or glucagonlike peptide receptor agonists.)
Yet again, high BMI emerges as a major risk factor
The study included 1,317 patients with diabetes and confirmed COVID-19 admitted to 53 French hospitals during March 10-31, 2020. Participants included 88.5% with type 2 diabetes, 3% with type 1 diabetes, and 3.1% newly diagnosed on admission. Mean age was 69.8 years.
Diabetes-related disorders on admission were reported in 11.1% of participants overall. These included 132 episodes of severe hyperglycemia, including 40 of ketosis, of which 19 were ketoacidosis, and 14 hypoglycemic events. Severe anorexia was reported in 6.3%.
The composite primary endpoint, tracheal intubation for mechanical ventilation and/or death within 7 days of admission, occurred in 29% of patients (n = 382).
Of the secondary outcomes, 31.1% (n = 410) were admitted to ICUs within 7 days of hospital admission, including 20.3% (n = 267) who required tracheal intubation for mechanical ventilation.
On day 7, 10.6% (n = 140) had died and 18.0% (n = 237) were discharged.
In the univariate analysis, the primary outcome was more frequent in men (69.1% vs. 63.2%; P = .0420) and those taking RAAS blockers (61.5% vs. 55.3%; P = .0386). Median BMI was significantly higher in those in whom the primary outcome occurred (29.1 vs 28.1 kg/m2; P = .0009),
Other characteristics prior to admission associated with risk of death on day 7 included age, hypertension, micro- and macrovascular diabetes-related complications, and comorbidities such as heart failure and treated obstructive sleep apnea.
Over 40% of those admitted had such complications. Of the patients analyzed, microvascular complications (eye, kidney, and neuropathy) were present in 47% and macrovascular complications (arteries of the heart, brain, and legs) were present in 41%.
Encouragingly, there were no deaths in patients aged under 65 years with type 1 diabetes, but only 39 participants had type 1 diabetes. Other work is ongoing to establish the effect of COVID-19 in this specific population, the researchers wrote.
Among prior medications, metformin use was lower in people who died, while insulin use, RAAS blockers, beta-blockers, loop diuretics, and mineralocorticoid-receptor antagonists were associated with death on day 7. The medication findings didn’t reach statistical significance, however.
When asked about the hint of a protective effect of metformin (odds ratio, 0.80; P = .4532), given that some experts have advised stopping it in the setting of COVID-19 because of the risk of lactic acidosis, Dr. Hadjadj said he wouldn’t necessarily stop it in all patients with COVID-19, but said, “let’s stop it in cases of severe condition.”
Analysis ongoing, ‘some new messages might pop up’
After adjustment for age and sex, BMI was significantly and positively associated with the primary outcome (P = .0001) but not with death on day 7 (P = .1488), and A1c wasn’t associated with either outcome.
In a multivariable analysis that included characteristics prior to admission, BMI remained the only independent preadmission predictor associated with the primary outcome (adjusted odds ratio, 1.28), while factors independently associated with risk of death on day 7 included age, diabetes complication history, and treated obstructive sleep apnea.
And after adjustment for age and sex, admission plasma glucose level was significantly and positively associated with both the primary outcome (P = .0001) and death on day 7 (P = .0059).
In the multivariate analysis, admission characteristics that predicted the primary outcome were dyspnea, lymphopenia, increased AST, and increased C-reactive protein.
Dr. Hadjadj said his team is now “focusing on specific risk factors such as obesity, age, vascular complications, medications ... to perform some deeper analyses.”
“We look forward to analyzing the data on in-hospital stay up to day 28 after admission. Some new messages might well pop up,” he added.
But in the meantime, “Elderly populations with long-term diabetes with advanced diabetes-related complications and/or treated obstructive sleep apnea were particularly at risk of early death and might require specific management to avoid infection with the novel coronavirus,” the researchers stressed.
The study received funding from the Fondation Francophone de Recherche sur le Diabète and was supported by Novo Nordisk, MSD, Abbott, AstraZeneca, Lilly, and the Fédération Française des Diabétiques; Société Francophone du Diabète; and Air Liquide Healthcare International. Dr. Hadjadj reported receiving grants, personal fees, and/or nonfinancial support from AstraZeneca, Bayer, Boehringer Ingelheim, Dinno Santé, Eli Lilly, LVL, MSD, Novartis, Pierre Fabre Santé, Sanofi, Servier, and Valbiotis.
A version of this article originally appeared on Medscape.com.
FDA recalls extended-release metformin due to NDMA impurities
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
The US Food and Drug Administration (FDA) has recommended voluntary recall of certain extended-release (ER) versions of metformin because testing has revealed excessive levels of N-nitrosodimethylamine (NDMA) in these products.
Metformin is the most commonly prescribed drug used to treat type 2 diabetes worldwide.
NDMA is a contaminant with the potential to be carcinogenic if there is exposure to above-acceptable levels over the long-term.
Five pharmaceutical firms in particular are being contacted by the FDA with notices (posted on the FDA website) recommending they voluntarily recall their products. At the time of writing, only one was listed, Apotex Corp and its metformin hydrochloride ER tablets, USP 500 mg.
The recall does not apply to immediate-release metformin products, the most commonly prescribed ones for diabetes, the agency stresses.
It also recommends that clinicians continue to prescribe metformin when clinically appropriate.
In late 2019, the FDA announced it had become aware of NDMA in some metformin products in other countries. The agency immediately began testing to determine whether the metformin in the US supply was at risk, as part of the ongoing investigation into nitrosamine impurities across medication types, which included recalls of hypertension and heartburn medications within the past 2 years.
By February 2020, the agency had identified very low levels of NDMA in some samples, but at that time, no FDA-tested sample of metformin exceeded the acceptable intake limit for NDMA, as reported by Medscape Medical News.
“Now that we have identified some metformin products that do not meet our standards, we’re taking action. As we have been doing since this impurity was first identified, we will communicate as new scientific information becomes available and will take further action, if appropriate,” Patrizia Cavazzoni, MD, acting director of the FDA Center for Drug Evaluation and Research, said in a press release.
Requests for recall apply only to affected products
The recall was instigated after the FDA became aware of reports of higher levels of NDMA in certain ER formulations of metformin through a citizen petition filed by a private laboratory. The agency confirmed unacceptable NDMA levels in some, but not all, of those lots.
“In other instances, our laboratory detected NDMA in lots that the private laboratory did not,” it notes.
The FDA says it is working closely with manufacturers of the recalled tablets to identify the source of the NDMA impurity and ensure appropriate testing is carried out.
Elevated levels of NDMA have been found in some finished-dose tablets of the ER formulations but NDMA has not been detected in samples of the metformin active pharmaceutical ingredient.
The FDA also stresses there are many other additional manufacturers that supply metformin ER products to much of the US market, and they are not being asked to recall their products.
Work is also ongoing to determine whether the drug recalls will result in shortages, and if so, the agency says it will collaborate with manufacturers to prevent or reduce any impact of shortages.
“We understand that patients may have concerns about possible impurities in their medicines and want to assure the public that we have been looking closely at this problem over many months in order to provide patients and healthcare professionals with clear and accurate answers,” Cavazzoni said.
For more information about NDMA, visit the FDA nitrosamines web page.
This article first appeared on Medscape.com.
‘The story unfolding is worrisome’ for diabetes and COVID-19
The American Diabetes Association has dedicated a whole section of its journal, Diabetes Care, to the topic of “Diabetes and COVID-19,” publishing a range of articles with new data to help guide physicians in caring for patients.
“Certain groups are more vulnerable to COVID-19, notably older people and those with underlying medical conditions. Because diabetes is one of the conditions associated with high risk, the diabetes community urgently needs to know more about COVID-19 and its effects on people with diabetes,” an introductory commentary noted.
Entitled “COVID-19 in people with diabetes: Urgently needed lessons from early reports,” the commentary is penned by the journal’s editor-in-chief, Matthew Riddle, MD, of Oregon Health & Science University, Portland, and colleagues.
Also writing in the same issue, William T. Cefalu, MD, and colleagues from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) noted it is known that the SARS-CoV-2 virus enters cells via the angiotensin-converting enzyme 2 (ACE-2) receptor. The ACE-2 receptor is known to be in the lungs and upper respiratory tract, “but we also know that it is expressed in other tissues such as heart, small and large intestines, and pancreas,” they wrote, and also “in the kidney.”
Hence, there are emerging reports of acute kidney injury resulting from COVID-19, as well as the impact on many other endocrine/metabolic and gastrointestinal outcomes.
“Pilot clinical studies (observational and interventional) are needed that will support the understanding or treatment of COVID-19–related diseases within the mission of the NIDDK,” they stated.
Although rapidly collected, data “offer important clues”
Some of the new ground covered in the journal articles includes an analysis of COVID-19 outcomes by type of glucose-lowering medication; remote glucose monitoring in hospitalized patients with COVID-19; a suggested approach to cardiovascular risk management in the COVID-19 era, as already reported by Medscape Medical News; and the diagnosis and management of gestational diabetes during the pandemic.
Other articles provide new data for previously reported phenomena, including obesity as a risk factor for worse COVID-19 outcomes and the role of inpatient glycemic control on COVID-19 outcomes.
“The data reported in these articles were rapidly collected and analyzed, in most cases under urgent and stressful conditions,” Dr. Riddle and colleagues cautioned. “Thus, some of the analyses are understandably limited due to missing data, incomplete follow-up, and inability to identify infected but asymptomatic patients.”
Even so, they wrote, some points are clear. “The consistency of findings in these rapidly published reports is reassuring in terms of scientific validity, but the story unfolding is worrisome.”
Specifically, while diabetes does not appear to increase the likelihood of SARS-CoV-2 infection, progression to severe illness is more likely in people with diabetes and COVID-19: They are two to three times as likely to require intensive care, and to die, compared with those infected but without diabetes.
“Neither the mechanisms underlying the increased risk nor the best interventions to limit it have yet been defined, but the studies in this collection of articles offer important clues,” Dr. Riddle and colleagues wrote.
Existing insulin use linked to COVID-19 death risk
One of the articles is a retrospective study of 904 hospitalized COVID-19 patients by Yuchen Chen, MD, of the Huazhong University of Science and Technology, Wuhan, China, and colleagues.
Among the 136 patients with diabetes, risk factors for mortality included older age (adjusted odds ratio, 1.09 per year increase; P = .001) elevated C-reactive protein (aOR, 1.12; P = .043), and insulin use (aOR, 3.58; P = .009).
“Attention needs to be paid to patients with diabetes and COVID-19 who use insulin,” the Chinese authors wrote. “Whether this was due to effects of insulin itself or to characteristics of the patients for whom it was prescribed is not clear,” Dr. Riddle and colleagues noted.
Dr. Chen and colleagues also found no difference in clinical outcomes between those diabetes patients with COVID-19 who were taking an ACE inhibitor or angiotensin II type I receptor blocker, compared with those who did not, which supports existing recommendations to continue use of this type of medication.
Remote glucose monitoring a novel tool for COVID-19 isolation
Another publication, by Gilat Shehav-Zaltzman of Sheba Medical Center, Tel Hashomer, Israel, and colleagues, describes the use of remote continuous glucose monitoring (CGM) in two hospitalized COVID-19 patients who were in isolation – one with type 1 diabetes and the other with type 2 diabetes – treated with basal-bolus insulin.
Using Medtronic CGM systems, the hospital staff was able to view patients’ real-time data uploaded to the Web from computer terminals in virus-free areas outside the patients’ rooms. The hospital’s endocrinology team had trained the intensive care staff on how to replace the sensors weekly and calibrate them twice daily.
“Converting a personal CGM system originally designed for diabetes self-management to team-based, real-time remote glucose monitoring offers a novel tool for inpatient diabetes control in COVID-19 isolation facilities,” the authors wrote.
“Such a solution in addition to ongoing remotely monitored clinical parameters (such as pulse rate, electrocardiogram, and oxygen saturation) adds to quality of diabetes care while minimizing risk of staff exposure and burden,” they observed.
Dr. Riddle and colleagues concurred: “Newer methods of remotely monitoring glucose patterns could be uniquely helpful.”
Key question: Does glycemic management make a difference?
With regard to the important issue of in-hospital control of glucose, Celestino Sardu, MD, PhD, of the University of Campania Luigi Vanvitelli, Naples, Italy, and colleagues reported on 59 patients hospitalized with confirmed COVID-19 and moderately severe pneumonia.
They were categorized as normoglycemic (n = 34) or hyperglycemic (n = 25), as well as with or without diabetes, on the basis of a diagnosis preceding the current illness. Of the 25 patients with hyperglycemia, 15 patients were treated with insulin infusion and 10 patients were not.
In a risk-adjusted analysis, both patients with hyperglycemia and patients with diabetes had a higher risk of severe disease than did those without diabetes and with normoglycemia. Patients with hyperglycemia treated with insulin infusion had a lower risk of severe disease than did patients who didn’t receive an insulin infusion.
And although they noted limitations, the authors wrote, “Our data evidenced that optimal glucose control in the immediate postadmission period for almost 18 days was associated with a significant reduction of inflammatory cytokines and procoagulative status.”
Dr. Riddle and colleagues wrote that the findings of this unrandomized comparison were interpreted “as suggesting that insulin infusion may improve outcomes.”
“If the benefits of seeking excellent glycemic control by this means are confirmed, close monitoring of glucose levels will be essential.”
More on obesity and COVID-19, this time from China
Because it has become increasingly clear that obesity is a risk factor for severe COVID-19, new data from China – where this was less apparent initially – support observations in Europe and the United States.
An article by Qingxian Cai, PhD, of Southern University of Science and Technology, Shenzhen, Guangdong, China, and colleagues looks at this. They found that, among 383 hospitalized patients with COVID-19, the 41 patients with obesity (defined as a body mass index ≥ 28 kg/m2) were significantly more likely to progress to severe disease compared with the 203 patients classified as having normal weight (BMI, 18.5-23.9), with an odds ratio of 3.4.
A similar finding comes from Feng Gao, MD, PhD, of the First Affiliated Hospital of Wenzhou (China) Medical University and colleagues, who studied 75 patients hospitalized with confirmed COVID-19 and obesity (defined as a BMI > 25 in this Asian population) to 75 patients without obesity matched by age and sex. After adjustment for clinical characteristics including the presence of diabetes, those with obesity had a threefold greater risk of progression to severe or critical COVID-19 status, with a nearly linear relationship.
Emerging from the crisis: Protect the vulnerable, increase knowledge base
As the research community emerges from the crisis, “there should be renewed efforts for multidisciplinary research ... aimed at greatly increasing the knowledge base to understand how ... the current COVID-19 threat” affects “both healthy people and people with chronic diseases and conditions,” Dr. Cefalu and colleagues concluded in their commentary.
Dr. Riddle and coauthors agreed: “We will enter a longer interval in which we must continue to support the most vulnerable populations – especially older people, those with diabetes or obesity, and those who lack the resources to limit day-to-day exposure to infection. We hope a growing sense of community will help in this task.”
Dr. Riddle has reported receiving research grant support through Oregon Health & Science University from AstraZeneca, Eli Lilly, and Novo Nordisk, and honoraria for consulting from Adocia, AstraZeneca, Eli Lilly, GlaxoSmithKline, Novo Nordisk, Sanofi, and Theracos. Dr. Cefalu has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The American Diabetes Association has dedicated a whole section of its journal, Diabetes Care, to the topic of “Diabetes and COVID-19,” publishing a range of articles with new data to help guide physicians in caring for patients.
“Certain groups are more vulnerable to COVID-19, notably older people and those with underlying medical conditions. Because diabetes is one of the conditions associated with high risk, the diabetes community urgently needs to know more about COVID-19 and its effects on people with diabetes,” an introductory commentary noted.
Entitled “COVID-19 in people with diabetes: Urgently needed lessons from early reports,” the commentary is penned by the journal’s editor-in-chief, Matthew Riddle, MD, of Oregon Health & Science University, Portland, and colleagues.
Also writing in the same issue, William T. Cefalu, MD, and colleagues from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) noted it is known that the SARS-CoV-2 virus enters cells via the angiotensin-converting enzyme 2 (ACE-2) receptor. The ACE-2 receptor is known to be in the lungs and upper respiratory tract, “but we also know that it is expressed in other tissues such as heart, small and large intestines, and pancreas,” they wrote, and also “in the kidney.”
Hence, there are emerging reports of acute kidney injury resulting from COVID-19, as well as the impact on many other endocrine/metabolic and gastrointestinal outcomes.
“Pilot clinical studies (observational and interventional) are needed that will support the understanding or treatment of COVID-19–related diseases within the mission of the NIDDK,” they stated.
Although rapidly collected, data “offer important clues”
Some of the new ground covered in the journal articles includes an analysis of COVID-19 outcomes by type of glucose-lowering medication; remote glucose monitoring in hospitalized patients with COVID-19; a suggested approach to cardiovascular risk management in the COVID-19 era, as already reported by Medscape Medical News; and the diagnosis and management of gestational diabetes during the pandemic.
Other articles provide new data for previously reported phenomena, including obesity as a risk factor for worse COVID-19 outcomes and the role of inpatient glycemic control on COVID-19 outcomes.
“The data reported in these articles were rapidly collected and analyzed, in most cases under urgent and stressful conditions,” Dr. Riddle and colleagues cautioned. “Thus, some of the analyses are understandably limited due to missing data, incomplete follow-up, and inability to identify infected but asymptomatic patients.”
Even so, they wrote, some points are clear. “The consistency of findings in these rapidly published reports is reassuring in terms of scientific validity, but the story unfolding is worrisome.”
Specifically, while diabetes does not appear to increase the likelihood of SARS-CoV-2 infection, progression to severe illness is more likely in people with diabetes and COVID-19: They are two to three times as likely to require intensive care, and to die, compared with those infected but without diabetes.
“Neither the mechanisms underlying the increased risk nor the best interventions to limit it have yet been defined, but the studies in this collection of articles offer important clues,” Dr. Riddle and colleagues wrote.
Existing insulin use linked to COVID-19 death risk
One of the articles is a retrospective study of 904 hospitalized COVID-19 patients by Yuchen Chen, MD, of the Huazhong University of Science and Technology, Wuhan, China, and colleagues.
Among the 136 patients with diabetes, risk factors for mortality included older age (adjusted odds ratio, 1.09 per year increase; P = .001) elevated C-reactive protein (aOR, 1.12; P = .043), and insulin use (aOR, 3.58; P = .009).
“Attention needs to be paid to patients with diabetes and COVID-19 who use insulin,” the Chinese authors wrote. “Whether this was due to effects of insulin itself or to characteristics of the patients for whom it was prescribed is not clear,” Dr. Riddle and colleagues noted.
Dr. Chen and colleagues also found no difference in clinical outcomes between those diabetes patients with COVID-19 who were taking an ACE inhibitor or angiotensin II type I receptor blocker, compared with those who did not, which supports existing recommendations to continue use of this type of medication.
Remote glucose monitoring a novel tool for COVID-19 isolation
Another publication, by Gilat Shehav-Zaltzman of Sheba Medical Center, Tel Hashomer, Israel, and colleagues, describes the use of remote continuous glucose monitoring (CGM) in two hospitalized COVID-19 patients who were in isolation – one with type 1 diabetes and the other with type 2 diabetes – treated with basal-bolus insulin.
Using Medtronic CGM systems, the hospital staff was able to view patients’ real-time data uploaded to the Web from computer terminals in virus-free areas outside the patients’ rooms. The hospital’s endocrinology team had trained the intensive care staff on how to replace the sensors weekly and calibrate them twice daily.
“Converting a personal CGM system originally designed for diabetes self-management to team-based, real-time remote glucose monitoring offers a novel tool for inpatient diabetes control in COVID-19 isolation facilities,” the authors wrote.
“Such a solution in addition to ongoing remotely monitored clinical parameters (such as pulse rate, electrocardiogram, and oxygen saturation) adds to quality of diabetes care while minimizing risk of staff exposure and burden,” they observed.
Dr. Riddle and colleagues concurred: “Newer methods of remotely monitoring glucose patterns could be uniquely helpful.”
Key question: Does glycemic management make a difference?
With regard to the important issue of in-hospital control of glucose, Celestino Sardu, MD, PhD, of the University of Campania Luigi Vanvitelli, Naples, Italy, and colleagues reported on 59 patients hospitalized with confirmed COVID-19 and moderately severe pneumonia.
They were categorized as normoglycemic (n = 34) or hyperglycemic (n = 25), as well as with or without diabetes, on the basis of a diagnosis preceding the current illness. Of the 25 patients with hyperglycemia, 15 patients were treated with insulin infusion and 10 patients were not.
In a risk-adjusted analysis, both patients with hyperglycemia and patients with diabetes had a higher risk of severe disease than did those without diabetes and with normoglycemia. Patients with hyperglycemia treated with insulin infusion had a lower risk of severe disease than did patients who didn’t receive an insulin infusion.
And although they noted limitations, the authors wrote, “Our data evidenced that optimal glucose control in the immediate postadmission period for almost 18 days was associated with a significant reduction of inflammatory cytokines and procoagulative status.”
Dr. Riddle and colleagues wrote that the findings of this unrandomized comparison were interpreted “as suggesting that insulin infusion may improve outcomes.”
“If the benefits of seeking excellent glycemic control by this means are confirmed, close monitoring of glucose levels will be essential.”
More on obesity and COVID-19, this time from China
Because it has become increasingly clear that obesity is a risk factor for severe COVID-19, new data from China – where this was less apparent initially – support observations in Europe and the United States.
An article by Qingxian Cai, PhD, of Southern University of Science and Technology, Shenzhen, Guangdong, China, and colleagues looks at this. They found that, among 383 hospitalized patients with COVID-19, the 41 patients with obesity (defined as a body mass index ≥ 28 kg/m2) were significantly more likely to progress to severe disease compared with the 203 patients classified as having normal weight (BMI, 18.5-23.9), with an odds ratio of 3.4.
A similar finding comes from Feng Gao, MD, PhD, of the First Affiliated Hospital of Wenzhou (China) Medical University and colleagues, who studied 75 patients hospitalized with confirmed COVID-19 and obesity (defined as a BMI > 25 in this Asian population) to 75 patients without obesity matched by age and sex. After adjustment for clinical characteristics including the presence of diabetes, those with obesity had a threefold greater risk of progression to severe or critical COVID-19 status, with a nearly linear relationship.
Emerging from the crisis: Protect the vulnerable, increase knowledge base
As the research community emerges from the crisis, “there should be renewed efforts for multidisciplinary research ... aimed at greatly increasing the knowledge base to understand how ... the current COVID-19 threat” affects “both healthy people and people with chronic diseases and conditions,” Dr. Cefalu and colleagues concluded in their commentary.
Dr. Riddle and coauthors agreed: “We will enter a longer interval in which we must continue to support the most vulnerable populations – especially older people, those with diabetes or obesity, and those who lack the resources to limit day-to-day exposure to infection. We hope a growing sense of community will help in this task.”
Dr. Riddle has reported receiving research grant support through Oregon Health & Science University from AstraZeneca, Eli Lilly, and Novo Nordisk, and honoraria for consulting from Adocia, AstraZeneca, Eli Lilly, GlaxoSmithKline, Novo Nordisk, Sanofi, and Theracos. Dr. Cefalu has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
The American Diabetes Association has dedicated a whole section of its journal, Diabetes Care, to the topic of “Diabetes and COVID-19,” publishing a range of articles with new data to help guide physicians in caring for patients.
“Certain groups are more vulnerable to COVID-19, notably older people and those with underlying medical conditions. Because diabetes is one of the conditions associated with high risk, the diabetes community urgently needs to know more about COVID-19 and its effects on people with diabetes,” an introductory commentary noted.
Entitled “COVID-19 in people with diabetes: Urgently needed lessons from early reports,” the commentary is penned by the journal’s editor-in-chief, Matthew Riddle, MD, of Oregon Health & Science University, Portland, and colleagues.
Also writing in the same issue, William T. Cefalu, MD, and colleagues from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) noted it is known that the SARS-CoV-2 virus enters cells via the angiotensin-converting enzyme 2 (ACE-2) receptor. The ACE-2 receptor is known to be in the lungs and upper respiratory tract, “but we also know that it is expressed in other tissues such as heart, small and large intestines, and pancreas,” they wrote, and also “in the kidney.”
Hence, there are emerging reports of acute kidney injury resulting from COVID-19, as well as the impact on many other endocrine/metabolic and gastrointestinal outcomes.
“Pilot clinical studies (observational and interventional) are needed that will support the understanding or treatment of COVID-19–related diseases within the mission of the NIDDK,” they stated.
Although rapidly collected, data “offer important clues”
Some of the new ground covered in the journal articles includes an analysis of COVID-19 outcomes by type of glucose-lowering medication; remote glucose monitoring in hospitalized patients with COVID-19; a suggested approach to cardiovascular risk management in the COVID-19 era, as already reported by Medscape Medical News; and the diagnosis and management of gestational diabetes during the pandemic.
Other articles provide new data for previously reported phenomena, including obesity as a risk factor for worse COVID-19 outcomes and the role of inpatient glycemic control on COVID-19 outcomes.
“The data reported in these articles were rapidly collected and analyzed, in most cases under urgent and stressful conditions,” Dr. Riddle and colleagues cautioned. “Thus, some of the analyses are understandably limited due to missing data, incomplete follow-up, and inability to identify infected but asymptomatic patients.”
Even so, they wrote, some points are clear. “The consistency of findings in these rapidly published reports is reassuring in terms of scientific validity, but the story unfolding is worrisome.”
Specifically, while diabetes does not appear to increase the likelihood of SARS-CoV-2 infection, progression to severe illness is more likely in people with diabetes and COVID-19: They are two to three times as likely to require intensive care, and to die, compared with those infected but without diabetes.
“Neither the mechanisms underlying the increased risk nor the best interventions to limit it have yet been defined, but the studies in this collection of articles offer important clues,” Dr. Riddle and colleagues wrote.
Existing insulin use linked to COVID-19 death risk
One of the articles is a retrospective study of 904 hospitalized COVID-19 patients by Yuchen Chen, MD, of the Huazhong University of Science and Technology, Wuhan, China, and colleagues.
Among the 136 patients with diabetes, risk factors for mortality included older age (adjusted odds ratio, 1.09 per year increase; P = .001) elevated C-reactive protein (aOR, 1.12; P = .043), and insulin use (aOR, 3.58; P = .009).
“Attention needs to be paid to patients with diabetes and COVID-19 who use insulin,” the Chinese authors wrote. “Whether this was due to effects of insulin itself or to characteristics of the patients for whom it was prescribed is not clear,” Dr. Riddle and colleagues noted.
Dr. Chen and colleagues also found no difference in clinical outcomes between those diabetes patients with COVID-19 who were taking an ACE inhibitor or angiotensin II type I receptor blocker, compared with those who did not, which supports existing recommendations to continue use of this type of medication.
Remote glucose monitoring a novel tool for COVID-19 isolation
Another publication, by Gilat Shehav-Zaltzman of Sheba Medical Center, Tel Hashomer, Israel, and colleagues, describes the use of remote continuous glucose monitoring (CGM) in two hospitalized COVID-19 patients who were in isolation – one with type 1 diabetes and the other with type 2 diabetes – treated with basal-bolus insulin.
Using Medtronic CGM systems, the hospital staff was able to view patients’ real-time data uploaded to the Web from computer terminals in virus-free areas outside the patients’ rooms. The hospital’s endocrinology team had trained the intensive care staff on how to replace the sensors weekly and calibrate them twice daily.
“Converting a personal CGM system originally designed for diabetes self-management to team-based, real-time remote glucose monitoring offers a novel tool for inpatient diabetes control in COVID-19 isolation facilities,” the authors wrote.
“Such a solution in addition to ongoing remotely monitored clinical parameters (such as pulse rate, electrocardiogram, and oxygen saturation) adds to quality of diabetes care while minimizing risk of staff exposure and burden,” they observed.
Dr. Riddle and colleagues concurred: “Newer methods of remotely monitoring glucose patterns could be uniquely helpful.”
Key question: Does glycemic management make a difference?
With regard to the important issue of in-hospital control of glucose, Celestino Sardu, MD, PhD, of the University of Campania Luigi Vanvitelli, Naples, Italy, and colleagues reported on 59 patients hospitalized with confirmed COVID-19 and moderately severe pneumonia.
They were categorized as normoglycemic (n = 34) or hyperglycemic (n = 25), as well as with or without diabetes, on the basis of a diagnosis preceding the current illness. Of the 25 patients with hyperglycemia, 15 patients were treated with insulin infusion and 10 patients were not.
In a risk-adjusted analysis, both patients with hyperglycemia and patients with diabetes had a higher risk of severe disease than did those without diabetes and with normoglycemia. Patients with hyperglycemia treated with insulin infusion had a lower risk of severe disease than did patients who didn’t receive an insulin infusion.
And although they noted limitations, the authors wrote, “Our data evidenced that optimal glucose control in the immediate postadmission period for almost 18 days was associated with a significant reduction of inflammatory cytokines and procoagulative status.”
Dr. Riddle and colleagues wrote that the findings of this unrandomized comparison were interpreted “as suggesting that insulin infusion may improve outcomes.”
“If the benefits of seeking excellent glycemic control by this means are confirmed, close monitoring of glucose levels will be essential.”
More on obesity and COVID-19, this time from China
Because it has become increasingly clear that obesity is a risk factor for severe COVID-19, new data from China – where this was less apparent initially – support observations in Europe and the United States.
An article by Qingxian Cai, PhD, of Southern University of Science and Technology, Shenzhen, Guangdong, China, and colleagues looks at this. They found that, among 383 hospitalized patients with COVID-19, the 41 patients with obesity (defined as a body mass index ≥ 28 kg/m2) were significantly more likely to progress to severe disease compared with the 203 patients classified as having normal weight (BMI, 18.5-23.9), with an odds ratio of 3.4.
A similar finding comes from Feng Gao, MD, PhD, of the First Affiliated Hospital of Wenzhou (China) Medical University and colleagues, who studied 75 patients hospitalized with confirmed COVID-19 and obesity (defined as a BMI > 25 in this Asian population) to 75 patients without obesity matched by age and sex. After adjustment for clinical characteristics including the presence of diabetes, those with obesity had a threefold greater risk of progression to severe or critical COVID-19 status, with a nearly linear relationship.
Emerging from the crisis: Protect the vulnerable, increase knowledge base
As the research community emerges from the crisis, “there should be renewed efforts for multidisciplinary research ... aimed at greatly increasing the knowledge base to understand how ... the current COVID-19 threat” affects “both healthy people and people with chronic diseases and conditions,” Dr. Cefalu and colleagues concluded in their commentary.
Dr. Riddle and coauthors agreed: “We will enter a longer interval in which we must continue to support the most vulnerable populations – especially older people, those with diabetes or obesity, and those who lack the resources to limit day-to-day exposure to infection. We hope a growing sense of community will help in this task.”
Dr. Riddle has reported receiving research grant support through Oregon Health & Science University from AstraZeneca, Eli Lilly, and Novo Nordisk, and honoraria for consulting from Adocia, AstraZeneca, Eli Lilly, GlaxoSmithKline, Novo Nordisk, Sanofi, and Theracos. Dr. Cefalu has reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Medicare will offer a $35/month insulin-cost cap in 2021
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.
U.S. Medicare beneficiaries with diabetes will be able to cap their out-of-pocket cost for insulin at no more than $35/month starting in January 2021 under a new coverage option in the Senior Savings Model, according to program details released by the Centers for Medicare & Medicaid Services on May 26.
This facet of the Senior Savings Model for Medicare drug benefits depends on voluntary participation by insurers offering Part D (drug) coverage to Medicare beneficiaries. As of May 26, 2020, 88 insurers had agreed to participate with a total of roughly 1,750 different drug-coverage plan options with this benefit starting next year, either as part of standalone Part D policies or as part of Medicare Advantage, or “enhanced” plans with drug coverage, said Seema Verma, administrator of the CMS, during a press conference.
Beneficiaries who opt for Part D coverage with this benefit will see a cap at $35 a month for their out-of-pocket insulin costs regardless of what phase of drug coverage they are in during the course of a benefit year: the 100% responsibility phase until their annual plan deductible is met, their initial coverage phase, their coverage gap phase (which kicks in after a total of $4,020 is spent on all prescription drugs), and the catastrophic coverage phase.
A recently published analysis of average, annual, out-of-pocket insulin costs for U.S. Medicare beneficiaries with “typical” Part D plans during 2019 found that, under this four-phase pricing scheme, the 1-year total cost to patients for their insulin came to just over $1,140 (N Engl J Med. 2020 May 14;382[20]:1878-80). For 2021 participants in the new model, annual out-of-pocket cost should be no greater than $420, and could possibly be less as the $35/month rate is not set but a cost ceiling.
A written statement from CMS about the new program predicted an average, estimated out-of-pocket cost savings of $446 per beneficiary. In addition to reducing overall out-of-pocket costs, another goal of the program is to give beneficiaries month-to-month consistency in their insulin costs. Under current coverage rules, costs fluctuate from month to month depending on the phase of coverage a beneficiary qualifies for at a given time.
The change to insulin copays in 2021 for beneficiaries in participating plans will cover “all common forms of insulin,” said Ms. Verma during the press conference. “If it goes well, we’ll extend that to other drugs,” she added. “We’re starting with insulin, but depending on the progress of this, we will consider offering this flexibility to manufacturers and plans with other drugs, depending on the results. We think that this creates a foundation and a platform to fix things, some of the problems that we have in the Part D plans. It’s time for that program to be updated. A lot of the provisions just don’t work anymore, and it’s standing in the way of free-market completion and negotiation that can lower prices for seniors.”
But “only 54% of all Medicare beneficiaries are enrolled in enhanced plans that are eligible to participate in the model, and only 44% of those plans have agreed to participate,” according to a statement from Public Citizen, a consumer-rights group based in Washington. Furthermore, the statement’s author, Peter Maybarduk, director of the organizations Access to Medicines Program, cited an analysis by Public Citizen that found that the program did nothing prevent pharmaceutical corporations from setting exorbitant prices for insulin. He added that the plan leaves out younger patients with diabetes, many of whom have been forced to ration their insulin because of the “outrageous insulin price gouging.”
CMS also recently announced on May 22 that it had finalized a rule that allows for expanded use of telehealth consultations for beneficiaries in Advantage programs. The agency said that telehealth consults had become possible for a variety of medical subspecialties, including endocrinology, dermatology, cardiology, gynecology, psychiatry, and primary care. In March, CMS announced a waiver to its prior rules on use of telehealth consults effective March 6, 2020. Kellyanne Conway, a senior counselor to President Donald Trump, said during the May 26 press conference that Medicare-covered telehealth visits rose from about 12,000 per week prior to issuance of the waiver to “well into the six figures,” in recent weeks.