User login
The role of repeat uterine curettage in postmolar gestational trophoblastic neoplasia
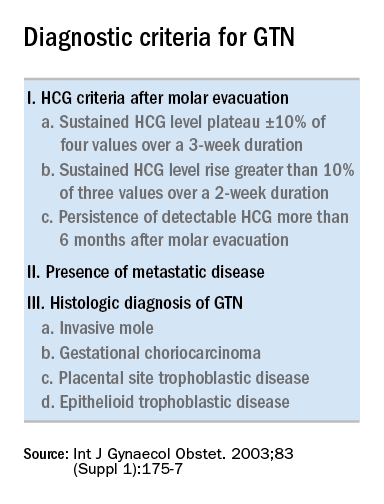
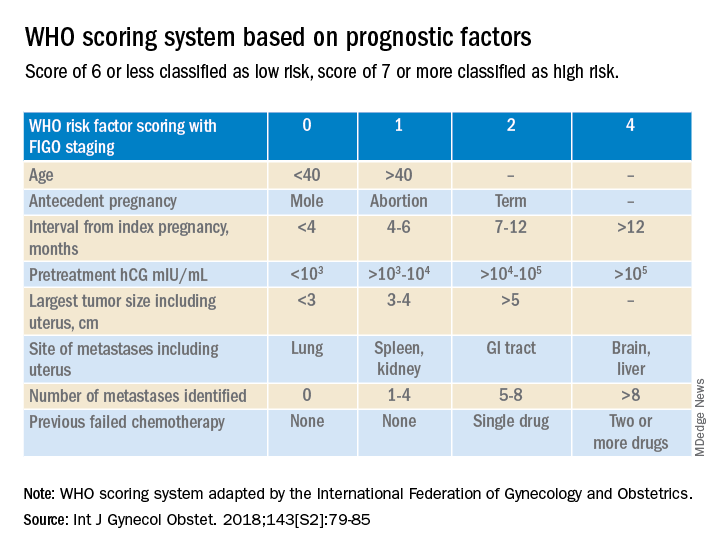
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.

More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.
More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
Trophoblastic tissue is responsible for formation of the placenta during pregnancy. Gestational trophoblastic disease (GTD), a group comprising benign (hydatidiform moles) and malignant tumors, occurs when gestational trophoblastic tissue behaves in an abnormal manner. Hydatidiform moles, which are thought to be caused by errors in fertilization, occur in approximately 1 in 1,200 pregnancies in the United States. Gestational trophoblastic neoplasia (GTN) refers to the subgroup of these trophoblastic or placental tumors with malignant behavior and includes postmolar GTN, invasive mole, gestational choriocarcinoma, placental-site trophoblastic tumor (PSTT), and epithelioid trophoblastic tumor. Postmolar GTN arises after evacuation of a molar pregnancy and is most frequently diagnosed by a plateau or increase in human chorionic gonadotropin (hCG).1 The risk of postmolar GTN is much higher after a complete mole (7%-30%) compared with a partial mole (2.5%-7.5%).2 Once postmolar GTN is diagnosed, a World Health Organization score is assigned to determine if patients have low- or high-risk disease.3 The primary treatment for most GTN is chemotherapy. A patient’s WHO score helps determine whether they would benefit from single-agent or multiagent chemotherapy. The standard of care for low-risk disease is single-agent chemotherapy with either methotrexate or actinomycin D.
The role of a second uterine curettage, after the diagnosis of low-risk postmolar GTN, has been controversial because of the limited data and disparate outcomes reported. In older retrospective series, a second curettage affected treatment or produced remission in only 9%-20% of patients and caused uterine perforation or major hemorrhage in 5%-8% of patients.4,5 Given relatively high rates of major complications compared with surgical cure or decreased chemotherapy cycles needed, only a limited number of patients seemed to benefit from a second procedure. On the other hand, an observational study of 544 patients who underwent second uterine evacuation after a presumed diagnosis of persistent GTD found that up to 60% of patients did not require chemotherapy afterward.6 Those with hCG levels greater than 1,500 IU/L or histologic evidence of GTD were less likely to have a surgical cure after second curettage. The indications for uterine evacuations were varied across these studies and make it nearly impossible to compare their results.
More recently, there have been two prospective trials that have tackled the question of the utility of second uterine evacuation in low-risk, nonmetastatic GTN. The Gynecologic Oncology Group performed a single-arm prospective study in the United States that enrolled patients with postmolar GTN to undergo second curettage as initial treatment of their disease.7 Of 60 eligible patients, 40% had a surgical cure (defined as normalization of hCG followed by at least 6 months of subsequent normal hCG values). Overall, 47% of patients were able to avoid chemotherapy. All surgical cures were seen in patients with WHO scores between 0 and 4. Importantly, three women were diagnosed with PSTT, which tends to be resistant to methotrexate and actinomycin D (treatment for nonmetastatic PSTT is definitive surgery with hysterectomy). The study found that hCG was a poor discriminator for achieving surgical cure. While age appeared to have an association with surgical cure (cure less likely for younger and older ages, younger than 19 and older than 40), patient numbers were too small to make a statistical conclusion. There were no uterine perforations and one patient had a grade 3 hemorrhage (requiring transfusion).
In the second prospective trial, performed in Iran, 62 patients were randomized to either second uterine evacuation or standard treatment after diagnosis of postmolar GTN.8 All patients in the surgical arm received a cervical ripening agent prior to their procedure, had their procedure under ultrasound guidance, and received misoprostol afterward to prevent uterine bleeding. Among those undergoing second uterine evacuation, 50% were cured (no need for chemotherapy). Among those needing chemotherapy after surgery, the mean number of cycles of chemotherapy needed (3.07 vs. 6.69) and the time it took to achieve negative hCG (3.23 vs. 9.19 weeks) were significantly less compared with patients who did not undergo surgery. hCG prior to second uterine evacuation could distinguish response to surgery compared with those needing chemotherapy (hCG of 1,983 IU/L or less was the level determined to best predict response). No complications related to surgery were reported.
Given prospective data available, second uterine evacuation for treatment of nonmetastatic, low-risk postmolar GTN is a reasonable treatment option and one that should be considered and discussed with patients given the potential to avoid chemotherapy or decrease the number of cycles needed. It may be prudent to limit the procedure to patients with an hCG less than 1,500-2,000 IU/L and to those between the ages of 20 and 40. While uterine hemorrhage and perforation have been reported in the literature, more recent data suggest low rates of these complications. Unfortunately, given the rarity of the disease and the historically controversial use of second curettage, little is known about the effects on future fertility that this procedure may have, including the development of uterine synechiae.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Ngan HY et al, FIGO Committee on Gynecologic Oncology. Int J Gynaecol Obstet. 2003 Oct;83 Suppl 1:175-7. Erratum in: Int J Gynaecol Obstet. 2021 Dec;155(3):563.
2. Soper JT. Obstet Gynecol. 2021 Feb.;137(2):355-70.
3. Ngan HY et al. Int J Gynecol Obstet. 2018;143:79-85.
4. Schlaerth JB et al. Am J Obstet Gynecol. 1990 Jun;162(6):1465-70.
5. van Trommel NE et al. Gynecol Oncol. 2005 Oct;99(1):6-13.
6. Pezeshki M et al. Gynecol Oncol. 2004 Dec;95(3):423-9.
7. Osborne RJ et al. Obstet Gynecol. 2016 Sep;128(3):535-42.
8. Ayatollahi H et al. Int J Womens Health. 2017 Sep 21;9:665-71.
High BMI linked to better survival for cancer patients treated with ICI, but for men only
That is the conclusion of a new retrospective analysis presented during a poster session given at the annual meeting of the European Society for Medical Oncology. The study sought to better understand ICI outcomes. “These are complex new treatments and, because they harness the immune system, no two patients are likely to respond in the same way. BMI has previously been associated with improved survival in patients with advanced lung cancer treated with immunotherapy. However, the reasons behind this observation, and the implications for treatment are unknown, as is whether this observation is specific for patients with only certain types of cancers,” study author Dwight Owen, MD, said in an email.
He pointed out that the retrospective nature of the findings means that they have no immediate clinical implications. “The reason for the discrepancy in males remains unclear. Although our study included a relatively large number of patients, it is a heterogenous cohort and there may be confounding factors that we haven’t recognized, so these findings need to be replicated in larger cohorts,” said Dr. Owen, a medical oncologist with The Ohio State University Comprehensive Cancer Center, Columbus.
Asked if there is a potential biological explanation for a difference between males and females, Dr. Owen said that this is an area of intense research. One recent study examined whether androgen could help explain why men are more likely than women to both develop and have more aggressive nonreproductive cancers. They concluded that androgen receptor signaling may be leading to loss of effector and proliferative potential of CD8+ T cells in the tumor microenvironment. Once exhausted, these cells do not respond well to stimulation that can occur after ICI treatment.
On the opposite end of the spectrum, cancer cachexia is also a key subject of study. It is characterized by weight loss and is associated with worse clinical outcomes. A cachexia mouse model found that weight loss can lead to more clearance of immune checkpoint antibodies.
Still, much more work needs to be done. “For now, how BMI, obesity, and cachexia relate to other factors, for instance the microbiome and tumor immunogenicity, are still not fully understood,” Dr. Owen said.
The study data
The researchers analyzed data from 688 patients with metastatic cancer treated at their center between 2011 and 2017. 94% were White and 5% were Black. 41% were female and the mean age was 61.9 years. The mean BMI was 28.8 kg/m2; 40% of patients had melanoma, 23% had non–small cell lung cancer, 10% had renal cancer, and 27% had another form of cancer.
For every unit decrease in BMI, the researchers observed a 1.8% decrease in mortality (hazard ratio, 0.982; P = .007). Patients with a BMI of 40 or above had better survival than all other patients grouped by 5 BMI increments (that is, 35-40, 30-35, etc.). When separated by sex, males had a significant decrease in mortality for every increase in BMI unit (HR, 0.964; P = .004), but there was no significant difference among women (HR, 1.003; P = .706). The relationship in men held up after adjustment for Eastern Cooperative Oncology Group score, line of therapy, and cancer type (HR, 0.979; P = .0308). The researchers also looked at a separate cohort of 185 normal weight and 15 obese (BMI ≥ 40) NSCLC patients. Median survival was 27.5 months in the obese group and 9.1 months in the normal weight group (HR, 0.474; 95% CI, 0.232-0.969).
Dr. Owen has received research funding through his institution from Bristol-Myers Squibb, Genentech, Pfizer, Palobiofarma, and Onc.AI.
That is the conclusion of a new retrospective analysis presented during a poster session given at the annual meeting of the European Society for Medical Oncology. The study sought to better understand ICI outcomes. “These are complex new treatments and, because they harness the immune system, no two patients are likely to respond in the same way. BMI has previously been associated with improved survival in patients with advanced lung cancer treated with immunotherapy. However, the reasons behind this observation, and the implications for treatment are unknown, as is whether this observation is specific for patients with only certain types of cancers,” study author Dwight Owen, MD, said in an email.
He pointed out that the retrospective nature of the findings means that they have no immediate clinical implications. “The reason for the discrepancy in males remains unclear. Although our study included a relatively large number of patients, it is a heterogenous cohort and there may be confounding factors that we haven’t recognized, so these findings need to be replicated in larger cohorts,” said Dr. Owen, a medical oncologist with The Ohio State University Comprehensive Cancer Center, Columbus.
Asked if there is a potential biological explanation for a difference between males and females, Dr. Owen said that this is an area of intense research. One recent study examined whether androgen could help explain why men are more likely than women to both develop and have more aggressive nonreproductive cancers. They concluded that androgen receptor signaling may be leading to loss of effector and proliferative potential of CD8+ T cells in the tumor microenvironment. Once exhausted, these cells do not respond well to stimulation that can occur after ICI treatment.
On the opposite end of the spectrum, cancer cachexia is also a key subject of study. It is characterized by weight loss and is associated with worse clinical outcomes. A cachexia mouse model found that weight loss can lead to more clearance of immune checkpoint antibodies.
Still, much more work needs to be done. “For now, how BMI, obesity, and cachexia relate to other factors, for instance the microbiome and tumor immunogenicity, are still not fully understood,” Dr. Owen said.
The study data
The researchers analyzed data from 688 patients with metastatic cancer treated at their center between 2011 and 2017. 94% were White and 5% were Black. 41% were female and the mean age was 61.9 years. The mean BMI was 28.8 kg/m2; 40% of patients had melanoma, 23% had non–small cell lung cancer, 10% had renal cancer, and 27% had another form of cancer.
For every unit decrease in BMI, the researchers observed a 1.8% decrease in mortality (hazard ratio, 0.982; P = .007). Patients with a BMI of 40 or above had better survival than all other patients grouped by 5 BMI increments (that is, 35-40, 30-35, etc.). When separated by sex, males had a significant decrease in mortality for every increase in BMI unit (HR, 0.964; P = .004), but there was no significant difference among women (HR, 1.003; P = .706). The relationship in men held up after adjustment for Eastern Cooperative Oncology Group score, line of therapy, and cancer type (HR, 0.979; P = .0308). The researchers also looked at a separate cohort of 185 normal weight and 15 obese (BMI ≥ 40) NSCLC patients. Median survival was 27.5 months in the obese group and 9.1 months in the normal weight group (HR, 0.474; 95% CI, 0.232-0.969).
Dr. Owen has received research funding through his institution from Bristol-Myers Squibb, Genentech, Pfizer, Palobiofarma, and Onc.AI.
That is the conclusion of a new retrospective analysis presented during a poster session given at the annual meeting of the European Society for Medical Oncology. The study sought to better understand ICI outcomes. “These are complex new treatments and, because they harness the immune system, no two patients are likely to respond in the same way. BMI has previously been associated with improved survival in patients with advanced lung cancer treated with immunotherapy. However, the reasons behind this observation, and the implications for treatment are unknown, as is whether this observation is specific for patients with only certain types of cancers,” study author Dwight Owen, MD, said in an email.
He pointed out that the retrospective nature of the findings means that they have no immediate clinical implications. “The reason for the discrepancy in males remains unclear. Although our study included a relatively large number of patients, it is a heterogenous cohort and there may be confounding factors that we haven’t recognized, so these findings need to be replicated in larger cohorts,” said Dr. Owen, a medical oncologist with The Ohio State University Comprehensive Cancer Center, Columbus.
Asked if there is a potential biological explanation for a difference between males and females, Dr. Owen said that this is an area of intense research. One recent study examined whether androgen could help explain why men are more likely than women to both develop and have more aggressive nonreproductive cancers. They concluded that androgen receptor signaling may be leading to loss of effector and proliferative potential of CD8+ T cells in the tumor microenvironment. Once exhausted, these cells do not respond well to stimulation that can occur after ICI treatment.
On the opposite end of the spectrum, cancer cachexia is also a key subject of study. It is characterized by weight loss and is associated with worse clinical outcomes. A cachexia mouse model found that weight loss can lead to more clearance of immune checkpoint antibodies.
Still, much more work needs to be done. “For now, how BMI, obesity, and cachexia relate to other factors, for instance the microbiome and tumor immunogenicity, are still not fully understood,” Dr. Owen said.
The study data
The researchers analyzed data from 688 patients with metastatic cancer treated at their center between 2011 and 2017. 94% were White and 5% were Black. 41% were female and the mean age was 61.9 years. The mean BMI was 28.8 kg/m2; 40% of patients had melanoma, 23% had non–small cell lung cancer, 10% had renal cancer, and 27% had another form of cancer.
For every unit decrease in BMI, the researchers observed a 1.8% decrease in mortality (hazard ratio, 0.982; P = .007). Patients with a BMI of 40 or above had better survival than all other patients grouped by 5 BMI increments (that is, 35-40, 30-35, etc.). When separated by sex, males had a significant decrease in mortality for every increase in BMI unit (HR, 0.964; P = .004), but there was no significant difference among women (HR, 1.003; P = .706). The relationship in men held up after adjustment for Eastern Cooperative Oncology Group score, line of therapy, and cancer type (HR, 0.979; P = .0308). The researchers also looked at a separate cohort of 185 normal weight and 15 obese (BMI ≥ 40) NSCLC patients. Median survival was 27.5 months in the obese group and 9.1 months in the normal weight group (HR, 0.474; 95% CI, 0.232-0.969).
Dr. Owen has received research funding through his institution from Bristol-Myers Squibb, Genentech, Pfizer, Palobiofarma, and Onc.AI.
FROM ESMO CONGRESS 2022
Early trial supports hypofractionated radiotherapy in uterine cancer
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
Postoperative radiotherapy is a mainstay in the treatment of uterine cancer, but the typical 5-week regimen can be time-consuming and expensive. A pilot study found that delivery of approximately the same dose over just 2.5 weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, who is an associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues, and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in the hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective [compared to standard protocol], and their study cannot answer that at any rate because it was not designed to answer that question,” said Dr. Williams in an interview. She also noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is [equivalent]. Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” Dr. Williams said.
The study’s findings
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 serous or clear cell, 3 carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
FROM JAMA ONCOLOGY
A farewell to arms? Drug approvals based on single-arm trials can be flawed
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
PARIS – with results that should only be used, under certain conditions, for accelerated approvals that should then be followed by confirmatory studies.
In fact, many drugs approved over the last decade based solely on data from single-arm trials have been subsequently withdrawn when put through the rigors of a head-to-head randomized controlled trial, according to Bishal Gyawali, MD, PhD, from the department of oncology at Queen’s University, Kingston, Ont.
“Single-arm trials are not meant to provide confirmatory evidence sufficient for approval; However, that ship has sailed, and we have several drugs that are approved on the basis of single-arm trials, but we need to make sure that those approvals are accelerated or conditional approvals, not regular approval,” he said in a presentation included in a special session on drug approvals at the European Society for Medical Oncology Congress.
“We should not allow premature regular approval based on single-arm trials, because once a drug gets conditional approval, access is not an issue. Patients will have access to the drug anyway, but we should ensure that robust evidence follows, and long-term follow-up data are needed to develop confidence in the efficacy outcomes that are seen in single-arm trials,” he said.
In many cases, single-arm trials are large enough or of long enough duration that investigators could have reasonably performed a randomized controlled trial (RCT) in the first place, Dr. Gyawali added.
Why do single-arm trials?
The term “single-arm registration trial” is something of an oxymoron, he said, noting that the purpose of such trials should be whether to take the drug to a phase 3, randomized trial. But as authors of a 2019 study in JAMA Network Open showed, of a sample of phase 3 RCTs, 42% did not have a prior phase 2 trial, and 28% had a negative phase 2 trial. Single-arm trials may be acceptable for conditional drug approvals if all of the following conditions are met:
- A RCT is not possible because the disease is rare or randomization would be unethical.
- The safety of the drug is established and its potential benefits outweigh its risks.
- The drug is associated with a high and durable overall or objective response rate.
- The mechanism of action is supported by a strong scientific rationale, and if the drug may meet an unmet medical need.
Survival endpoints won’t do
Efficacy endpoints typically used in RCTs, such as progression-free survival (PFS) and overall survival (OS) can be misleading because they may be a result of the natural history of the disease and not the drug being tested, whereas ORRs are almost certainly reflective of the action of the drug itself, because spontaneous tumor regression is a rare phenomenon, Dr. Gyawali said.
He cautioned, however, that the ORR of placebo is not zero percent. For example in a 2018 study of sorafenib (Nexavar) versus placebo for advanced or refractory desmoid tumors, the ORR with the active drug was 33%, and the ORR for placebo was 20%.
It’s also open to question, he said, what constitutes an acceptably high ORR and duration of response, pointing to Food and Drug Administration accelerated approval of an indication for nivolumab (Opdivo) for treatment of patients with hepatocellular carcinoma (HCC) that had progressed on sorafenib. In the single-arm trial used as the basis for approval, the ORRs as assessed by an independent central review committee blinded to the results was 14.3%.
“So, nivolumab in hepatocellular cancer was approved on the basis of a response rate lower than that of placebo, albeit in a different tumor. But the point I’m trying to show here is we don’t have a good definition of what is a good response rate,” he said.
In July 2021, Bristol-Myers Squibb voluntarily withdrew the HCC indication for nivolumab, following negative results of the CheckMate 459 trial and a 5-4 vote against continuing the accelerated approval.
On second thought ...
Citing data compiled by Nathan I. Cherny, MD, from Shaare Zedek Medical Center, Jerusalem, Dr. Gyawali noted that 58 of 161 FDA approvals from 2017 to 2021 of drugs for adult solid tumors were based on single-arm trials. Of the 58 drugs, 39 received accelerated approvals, and 19 received regular approvals; of the 39 that received accelerated approvals, 4 were subsequently withdrawn, 8 were converted to regular approvals, and the remainder continued as accelerated approvals.
Interestingly, the median response rate among all the drugs was 40%, and did not differ between the type of approval received, suggesting that response rates are not predictive of whether a drug will receive a conditional or full-fledged go-ahead.
What’s rare and safe?
The definition of a rare disease in the United States is one that affects fewer than 40,000 per year, and in Europe it’s an incidence rate of less than 6 per 100,000 population, Dr. Gyawali noted. But he argued that even non–small cell lung cancer, the most common form of cancer in the world, could be considered rare if it is broken down into subtypes that are treated according to specific mutations that may occur in a relatively small number of patients.
He also noted that a specific drug’s safety, one of the most important criteria for granting approval to a drug based on a single-arm trial, can be difficult to judge without adequate controls for comparison.
Cherry-picking patients
Winette van der Graaf, MD, president of the European Organization for the Research and Treatment of Cancer, who attended the session where Dr. Gyawali’s presentation was played, said in an interview that clinicians should cast a critical eye on how trials are designed and conducted, including patient selection and choice of endpoints.
“One of the most obvious things to be concerned about is that we’re still having patients with good performance status enrolled, mostly PS 0 or 1, so how representative are these clinical trials for the patients we see in front of us on a daily basis?” she said.
“The other question is radiological endpoints, which we focus on with OS and PFS are most important for patients, especially if you consider that if patients may have asymptomatic disease, and we are only treating them with potentially toxic medication, what are we doing for them? Median overall survival when you look at all of these trials is only 4 months, so we really need to take into account how we affect patients in clinical trials,” she added.
Dr. van der Graaf emphasized that clinical trial investigators need to more routinely incorporate quality of life measures and other patient-reported outcomes in clinical trial results to help regulators and clinicians in practice get a better sense of the true clinical benefit of a new drug.
Dr. Gyawali did not disclose a funding source for his presentation. He reported consulting fees from Vivio Health and research grants from the American Society of Clinical Oncology. Dr. van der Graaf reported no conflicts of interest.
AT ESMO CONGRESS 2022
Time to cancer diagnoses in U.S. averages 5 months
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
Time to diagnosis is a crucial factor in cancer. Delays can lead to diagnosis at later stages and prevent optimal therapeutic strategies, both of which have the potential to reduce survival. An estimated 63%-82% of cancers get diagnosed as a result of symptom presentation, and delays in diagnosis can hamper treatment efforts. Diagnosis can be challenging because common symptoms – such as weight loss, weakness, poor appetite, and shortness of breath – are nonspecific.
A new analysis of U.S.-based data shows that the average time to diagnosis is 5.2 months for patients with solid tumors. The authors of the study call for better cancer diagnosis pathways in the U.S.
“Several countries, including the UK, Denmark, Sweden, Canada and Australia, have identified the importance and potential impact of more timely diagnosis by establishing national guidelines, special programs, and treatment pathways. However, in the U.S., there’s relatively little research and effort focused on streamlining the diagnostic pathway. Currently, the U.S. does not have established cancer diagnostic pathways that are used consistently,” Matthew Gitlin, PharmD, said during a presentation at the annual meeting of the European Society for Medical Oncology.
“That is often associated with worse clinical outcomes, increased economic burden, and decreased health related quality of life,” said Dr. Gitlin, founder and managing director of the health economics consulting firm BluePath Solutions, which conducted the analysis.
The study retrospectively examined administrative billing data drawn from the Clinformatics for Managed Markets longitudinal database. The data represent individuals in Medicare Advantage and a large, U.S.-based private insurance plan. Between 2018 and 2019, there were 458,818 cancer diagnoses. The mean age was 70.6 years and 49.6% of the patients were female. Sixty-five percent were White, 11.1% Black, 8.3% Hispanic, and 2.5% Asian. No race data were available for 13.2%. Medicare Advantage was the primary insurance carrier for 74.0%, and 24.0% had a commercial plan.
The mean time to diagnosis across all tumors was 5.2 months (standard deviation, 5.5 months). There was significant variation across different tumor types, as well as within the same tumor type. The median value was 3.9 months (interquartile range, 1.1-7.2 months).
Mean time to diagnosis ranged from 121.6 days for bladder cancer to as high as 229 days for multiple myeloma. Standard deviations were nearly as large or even larger than the mean values. The study showed that 15.8% of patients waited 6 months or longer for a diagnosis. Delays were most common in kidney cancer, colorectal cancer, gallbladder cancer, esophageal cancer, stomach cancer, lymphoma, and multiple myeloma: More than 25% of patients had a time to diagnosis of at least 6 months in these tumors.
“Although there is limited research in the published literature, our findings are consistent with that literature that does exist. Development or modification of policies, guidelines or medical interventions that streamline the diagnostic pathway are needed to optimize patient outcomes and reduce resource burden and cost to the health care system,” Dr. Gitlin said.
Previous literature on this topic has seen wide variation in how time to diagnosis is defined, and most research is conducted in high-income countries, according to Felipe Roitberg, PhD, who served as a discussant during the session. “Most of the countries and patients in need are localized in low- and middle-income countries, so that is a call to action (for more research),” said Dr. Roitberg, a clinical oncologist at Hospital Sírio Libanês in São Paulo, Brazil.
The study did not look at the associations between race and time to diagnosis. “This is a source of analysis could further be explored,” said Dr. Roitberg.
He noted that the ABC-DO prospective cohort study in sub-Saharan Africa found large variations in breast cancer survival by country, and its authors predicted that downstaging and improvements in treatment could prevent up to one-third of projected breast cancer deaths over the next decade. “So these are the drivers of populational gain in terms of overall survival – not more drugs, not more services available, but coordination of services and making sure the patient has a right pathway (to diagnosis and treatment),” Dr. Roitberg said.
Dr. Gitlin has received consulting fees from GRAIL LLC, which is a subsidiary of Illumina. Dr. Roitberg has received honoraria from Boehringer Ingelheim, Sanofi, Roche, MSD Oncology, AstraZeneca, Nestle Health Science, Dr Reddy’s, and Oncologia Brazil. He has consulted for MSD Oncology. He has received research funding from Roche, Boehringer Ingelheim, MSD, Bayer, AstraZeneca, and Takeda.
FROM ESMO CONGRESS 2022
Shortened radiotherapy for endometrial cancer looks safe, questions remain
Postoperative radiotherapy is a mainstay in the treatment of endometrial cancer, but the typical 5-week regimen can be time consuming and expensive. A pilot study found that delivery of approximately the same dose over just two and a half weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective (compared to standard protocol), and their study cannot answer that at any rate because it was not designed to answer that question,” Dr. Williams said in an interview. She noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is (equivalent). Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” said Dr. Williams.
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 had serous or clear cell, 3 had carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
The study authors reported grants, consulting, and personal fees from a variety of pharmaceutical companies. Dr. Williams reported having no disclosures.
Postoperative radiotherapy is a mainstay in the treatment of endometrial cancer, but the typical 5-week regimen can be time consuming and expensive. A pilot study found that delivery of approximately the same dose over just two and a half weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective (compared to standard protocol), and their study cannot answer that at any rate because it was not designed to answer that question,” Dr. Williams said in an interview. She noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is (equivalent). Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” said Dr. Williams.
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 had serous or clear cell, 3 had carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
The study authors reported grants, consulting, and personal fees from a variety of pharmaceutical companies. Dr. Williams reported having no disclosures.
Postoperative radiotherapy is a mainstay in the treatment of endometrial cancer, but the typical 5-week regimen can be time consuming and expensive. A pilot study found that delivery of approximately the same dose over just two and a half weeks, known as hypofractionation, had good short-term toxicity outcomes.
Nevertheless, shortening the duration of radiotherapy could have benefits, especially in advanced uterine cancer, where chemotherapy is employed against distant metastases. Following surgery, there is a risk of both local recurrence and distant metastasis, complicating the choice of initial treatment. “Chemo can be several months long and radiation is typically several weeks. Therefore a shortened radiation schedule may have potential benefits, especially if there is an opportunity for this to be delivered earlier without delaying or interrupting chemotherapy, for example,” said lead study author Eric Leung, MD, associate professor of radiation oncology at the University of Toronto’s Sunnybrook Health Sciences Centre.
The research was published in JAMA Oncology.
Delivery of hypofractionation is tricky, according to Dr. Leung. “Gynecological cancer patients were treated with hypofractionation radiation to the pelvis which included the vagina, paravaginal tissues and pelvic lymph nodes. With this relatively large pelvic volume with surrounding normal tissues, this requires a highly focused radiation treatment with advanced technology,” said Dr. Leung. The study protocol employed stereotactic technique to deliver 30 Gy in 5 fractions.
Hypofractionation could be beneficial in reduction of travel time and time spent in hospital, as well as reducing financial burden and increasing quality of life. These benefits have taken on a larger role in the context of the COVID-19 pandemic.
Although the findings are encouraging, they are preliminary, according to Vonetta Williams, MD, PhD, who wrote an accompanying editorial. “I would caution that all they’ve done is presented preliminary toxicity data, so we don’t have any proof yet that it is equally effective (compared to standard protocol), and their study cannot answer that at any rate because it was not designed to answer that question,” Dr. Williams said in an interview. She noted that long-term follow-up is needed to measure bowel dysfunction, sexual dysfunction, vaginal stenosis, and other side effects.
It is also uncertain whether hypofractionated doses are actually equivalent to the standard dose. “We know that they’re roughly equivalent, but that is very much a question if they are equivalent in terms of efficacy. I don’t know that I would be confident that they are. That’s probably what would give most radiation oncologists pause, because we don’t have any data to say that it is (equivalent). Although it would be nice to shorten treatment, and I think it would certainly be better for patients, I want to caution that we want to do so once we know what the toxicity and the outcomes really are,” said Dr. Williams.
The researchers enrolled 61 patients with a median age of 66 years. Thirty-nine had endometrioid adenocarcinoma, 15 had serous or clear cell, 3 had carcinosarcoma, and 4 had dedifferentiated disease. Sixteen patients underwent sequential chemotherapy, and 9 underwent additional vault brachytherapy. Over a median follow-up of 9 months, 54% had a worst gastrointestinal side effect of grade 1, while 13% had a worst side effect of grade 2. Among worst genitourinary side effects, 41% had grade 1 and 3% had grade 2. One patient had acute grade 3 diarrhea at fraction 5, but this resolved at follow-up. One patient had diarrhea scores that were both clinically and statistically significantly worse than baseline at fraction 5, and this improved at follow-up.
Patient-reported quality of life outcomes were generally good. Of all measures, only diarrhea was clinically and statistically worse by fraction 5, and improvement was seen at 6 weeks and 3 months. Global health status was consistent throughout treatment and follow-up. There was no change in sexual and vaginal symptoms.
The study authors reported grants, consulting, and personal fees from a variety of pharmaceutical companies. Dr. Williams reported having no disclosures.
FROM JAMA ONCOLOGY
In America, cancer patients endure debt on top of disease
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
RAPID CITY, S.D. – Jeni Rae Peters would make promises to herself as she lay awake nights after being diagnosed with breast cancer two years ago.
“My kids had lost so much,” said Ms. Peters, a single mom and mental health counselor. She had just adopted two girls and was fostering four other children. “I swore I wouldn’t force them to have yet another parent.”
Multiple surgeries, radiation, and chemotherapy controlled the cancer. But, despite having insurance, Ms. Peters was left with more than $30,000 of debt, threats from bill collectors, and more anxious nights thinking of her kids. “Do I pull them out of day care? Do I stop their schooling and tutoring? Do I not help them with college?” Ms. Peters asked herself. “My doctor saved my life, but my medical bills are stealing from my children’s lives.”
Cancer kills about 600,000 people in the United States every year, making it a leading cause of death. Many more survive it, because of breakthroughs in medicines and therapies.
That’s forced patients and their families to make gut-wrenching sacrifices even as they confront a grave illness, according to a KHN-NPR investigation of America’s sprawling medical debt problem. The project shows few suffer more than those with cancer.
About two-thirds of adults with health care debt who’ve had cancer themselves or in their family have cut spending on food, clothing, or other household basics, a poll conducted by KFF for this project found. About one in four have declared bankruptcy or lost their home to eviction or foreclosure.
Other research shows that patients from minority groups are more likely to experience financial hardships caused by cancer than White patients, reinforcing racial disparities that shadow the U.S. health care system.
“It’s crippling,” said Dr. Veena Shankaran, MD, an oncologist at the University of Washington, Seattle, who began studying the financial impact of cancer after seeing patients ruined by medical bills. “Even if someone survives the cancer, they often can’t shake the debt.”
Dr. Shankaran found that cancer patients were 71% more likely than Americans without the disease to have bills in collections, face tax liens and mortgage foreclosure, or experience other financial setbacks. Analyzing bankruptcy records and cancer registries in Washington state, Dr. Shankaran and other researchers also discovered that cancer patients were 2½ times as likely to declare bankruptcy as those without the disease. And those who went bankrupt were likelier to die than cancer patients who did not.
Oncologists have a name for this: “financial toxicity,” a term that echoes the intractable vomiting, life-threatening infections, and other noxious effects of chemotherapy.
“Sometimes,” Dr. Shankaran said, “it’s tough to think about what the system puts patients through.”
Cancer diagnosis upends family
At the three-bedroom home in Rapid City that Ms. Peters shares with her children and a friend, there isn’t time most days to dwell on these worries. There are ice skating lessons and driving tests and countless meals to prepare. Teenagers drift in and out, chattering about homework and tattoos and driving.
The smallest children congregate at a small kitchen table under a wall decorated with seven old telephones. (As Ms. Peters tells it, the red one is a hotline to Santa, a green one to the Grinch, and a space shuttle–shaped phone connects to astronauts orbiting the Earth.)
Ms. Peters, 44, presides cheerfully over the chaos, directing her children with snide asides and expressions of love. She watches proudly as one teenage daughter helps another with math in the living room. Later she dances with a 5-year-old to Queen under a disco ball in the entry hall.
Ms. Peters, who sports tattoos and earlier this year dyed her hair purple, never planned to have a family. In her late 30s, she wanted to do more for her adopted community, so she took in foster children, many of whom come from the nearby Pine Ridge Indian Reservation. One of her daughters had been homeless.
“Foster kids are amazing humans,” she said. “I joke I’m the most reluctant parent of the most amazing children that have ever existed. And I get to help raise these little people to be healthy and safe.”
In spring 2020, the secure world Ms. Peters had carefully tended was shattered. As the COVID pandemic spread across the country, she was diagnosed with stage 2 breast cancer.
Within weeks, she had an intravenous port inserted into her chest. Surgeons removed both her breasts, then her ovaries after tests showed she was at risk of ovarian cancer as well.
Cancer treatment today often entails a costly, debilitating march of procedures, infusions, and radiation sessions that can exhaust patients physically and emotionally. It was scary, Ms. Peters said. But she rallied her children. “We talked a lot about how they had all lost siblings or parents or other relatives,” she said. “All I had to do was lose my boobs.”
Much harder, she said, were the endless and perplexing medical bills.
There were bills from the anesthesiologists who attended her surgeries, from the hospital, and from a surgery center. For a while, the hospital stopped sending bills. Then in April, Ms. Peters got a call one morning from a bill collector saying she owed $13,000. In total, Ms. Peters estimates her medical debts now exceed $30,000.
High costs, despite insurance
Debts of that size aren’t unusual. Nationwide, about one in five indebted adults who have had cancer or have a family member who’s been sick say they owe $10,000 or more, according to the KFF poll. Those dealing with cancer are also more likely than others with health care debt to owe large sums and to say they don’t expect to ever pay them off.
This debt has been fueled in part by the advent of lifesaving therapies that also come with eye-popping price tags. The National Cancer Institute calculated the average cost of medical care and drugs tops $42,000 in the year following a cancer diagnosis. Some treatments can exceed $1 million.
Usually, most costs are covered. But patients are increasingly on the hook for large bills because of deductibles and other health plan cost sharing. The average leukemia patient with private health insurance, for example, can expect to pay more than $5,100 in the year after diagnosis, according to an analysis by the consulting firm Milliman. Even Medicare can leave seniors with huge bills. The average blood cancer patient covered by fee-for-service Medicare can expect to pay more than $17,000 out-of-pocket in the year following diagnosis, Milliman found.
Additionally, ongoing surgeries, tests, and medications can make patients pay large out-of-pocket costs year after year. Physicians and patient advocates say this cost sharing -- originally billed as a way to encourage patients to shop for care -- is devastating. “The problem is that model doesn’t work very well with cancer,” said David Eagle, MD, an oncologist at New York Cancer & Blood Specialists.
More broadly, the KHN-NPR investigation found that about 100 million people in the United States are now in debt from medical or dental bills. Poor health is among the most powerful predictors of debt, with this debt concentrated in parts of the country with the highest levels of illness.
According to the KFF poll, 6 in 10 adults with a chronic disease such as cancer, diabetes, or heart disease or with a close family member who is sick have had some kind of health care debt in the past 5 years. The poll was designed to capture not just bills patients haven’t paid, but also other borrowing used to pay for health care, such as credit cards, payment plans, and loans from friends and family.
For her part, Ms. Peters has had seven surgeries since 2020. Through it all, she had health insurance through her employers. Ms. Peters said she knew she had to keep working or would lose coverage and face even bigger bills. Like most plans, however, hers have required she pay thousands of dollars out of pocket.
Within weeks of her diagnosis, the bills rolled in. Then collectors started calling. One call came as Ms. Peters was lying in the recovery room after her double mastectomy. “I was kind of delirious, and I thought it was my kids,” she said. “It was someone asking me to pay a medical bill.”
Ms. Peters faced more bills when she switched jobs later that year and her insurance changed. The deductible and cap on her out-of-pocket costs reset.
In 2021, the deductible and out-of-pocket limit reset again, as they do every year for most health plans. So when Ms. Peters slipped on the ice and broke her wrist – a fracture likely made worse by chemotherapy that weakened her bones – she was charged thousands more.
This year has brought more surgeries and yet more bills, as her deductible and out-of-pocket limit reset again.
“I don’t even know anymore how much I owe,” Ms. Peters said. “Sometimes it feels like people just send me random bills. I don’t even know what they’re for.”
Making sacrifices
Before getting sick, Ms. Peters was earning about $60,000 a year. It was enough to provide for her children, she said, supplemented with a stipend she receives for foster care.
The family budget was always tight. Ms. Peters and her kids don’t take extravagant vacations. Ms. Peters doesn’t own her home and has next to no savings. Now, she said, they are living at the edge. “I keep praying there is a shoe fairy,” she said, joking about the demands of so many growing feet in her home.
Ms. Peters took on extra work to pay some of the bills. Five days a week, she works back-to-back shifts at both a mental health crisis center and a clinic where she counsels teenagers, some of whom are suicidal. In 2021, three friends on the East Coast paid off some of the debt.
But Ms. Peters’ credit score has tumbled below 600. And the bills pile high on the microwave in her kitchen. “I’m middle class,” she said. “Could I make payments on some of these? Yes, I suppose I could.”
That would require trade-offs. She could drop car insurance for her teenage daughter, who just got her license. Canceling ice skating for another daughter would yield an extra $60 a month. But Ms. Peters is reluctant. “Do you know what it feels like to be a foster kid and get a gold medal in ice skating? Do you know what kind of citizen they could become if they know they’re special?” she said. “There seems to be a myth that you can pay for it all. You can’t.”
Many cancer patients face difficult choices.
About 4 in 10 with debt have taken money out of a retirement, college, or other long-term savings account, the KFF poll found; about 3 in 10 have moved in with family or friends or made another change in their living situation.
Kashyap Patel, MD, chief executive of Carolina Blood and Cancer Care Associates, said the South Carolina practice has found patients turning to food banks and other charities to get by. One patient was living in his car. Dr. Patel estimated that half the patients need some kind of financial aid. Even then, many end up in debt.
The Leukemia & Lymphoma Society, which typically helps blood cancer patients navigate health insurance and find food, housing, and other nonmedical assistance, is hearing from more patients simply seeking cash to pay off debt, said Nikki Yuill, who oversees the group’s call center. “People tell us they won’t get follow-up care because they can’t take on more debt,” Ms. Yuill said, recalling one man who refused to call an ambulance even though he couldn’t get to the hospital. “It breaks your heart.”
Academic research has revealed widespread self-rationing by patients. For example, while nearly one in five people taking oral chemotherapy abandon treatment, about half stop when out-of-pocket costs exceed $2,000, according to a 2017 analysis.
Robin Yabroff, PhD, MBA, an epidemiologist at the American Cancer Society, said more research must be done to understand the lasting effects of medical debt on cancer survivors and their families. “What does it mean for a family if they have to liquidate savings or drain college funds or sell their home?” Dr. Yabroff said. “We just don’t know yet.”
As Ms. Peters put away bags of groceries in her kitchen, she conceded she doesn’t know what will happen to her family. Like many patients, she worries about how she’ll pay for tests and follow-up care if the cancer reappears.
She is still wading through collection notices in the mail and fielding calls from debt collectors. Ms. Peters told one that she was prepared to go to court and ask the judge to decide which of her children should be cut off from after-school activities to pay off the debts.
She asked another debt collector whether he had kids. “He told me that it had been my choice to get the surgery,” Ms. Peters recalled. “And I said: ‘Yeah, I guess I chose not to be dead.’ ”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
After cancer, abortion experience highlights post-Roe reality
The drive from Texas to the clinic in Albuquerque, N.M., took 10 hours. It was mid-April of this year. There wasn’t much to see along the mostly barren stretch, and there wasn’t much for Kailee DeSpain to do aside from think about where she was going and why.
Her husband was driving. She sensed his nervous glances toward the passenger seat where she sat struggling to quiet her thoughts.
No, she wasn’t having any pain, she told him. No, she wasn’t feeling like she did the last time or the two times before that.
This pregnancy was different. It was the first in which she feared for her own life. Her fetus – Finley – had triploidy, a rare chromosomal abnormality. Because of the condition, which affects 1%-3% of pregnancies, his heart, brain, and kidneys were not developing properly.
At 19 weeks, Finley was already struggling to draw breath from lungs squeezed inside an overcrowded chest cavity. Ms. DeSpain wanted nothing more than to carry Finley to term, hold him, meet him even for a moment before saying goodbye.
But his condition meant he would likely suffocate in utero well before that. And Ms. DeSpain knew that carrying him longer would likely raise her risk of bleeding and of her blood pressure increasing to dangerous highs.
“This could kill you,” her husband told her. “Do you realize you could die bringing a baby into this world who is not going to live? I don’t want to lose you.’”
Unlike her other pregnancies, the timing of this one and the decision she faced to end it put her health in even greater danger.
Imminent danger
On Sept. 1, 2021, a bill went into effect in Texas that banned abortions from as early as 6 weeks’ gestation. Texas Senate Bill 8 (SB8) became one of the most restrictive abortion laws in the country. It prohibited abortions whenever a fetal heartbeat, defined by lawmakers, could be detected on an ultrasound, often before many women knew they were pregnant.
The Texas abortion law was hardly the last word on the topic. Ms. DeSpain didn’t know it on her drive to New Mexico in April, but the U.S. Supreme Court was weeks away from overturning the landmark Roe v. Wade decision.
On June 24, the Supreme Court delivered its 6-3 ruling overturning Roe v. Wade, the 1973 case that granted women the right to abortion.
This decision set in motion “trigger laws” in some states – laws that essentially fully banned abortions. Those states included Ms. DeSpain’s home state of Texas, where abortion is now a felony except when the life of the mother is in peril.
However, legal definitions of what qualifies as “life-threatening” remain murky.
The law is unclear, says Lisa Harris, MD, PhD, professor in the department of obstetrics and gynecology at the University of Michigan, Ann Arbor. “What does the risk of death have to be, and how imminent must it be?” she asked in a recent editorial in the New England Journal of Medicine. Is 25% enough? 50%? Or does a woman have to be moments from dying?
“This whole thing makes me so angry,” says Shikha Jain, MD, a medical oncologist at University of Illinois Health, Chicago. “A patient may not be experiencing an emergency right now, but if we don’t take care of the situation, it may become an emergency in 2 hours or 2 days.”
Even before the Roe v. Wade decision, pregnancy had been a high-stakes endeavor for many women. In 2019, more than 750 women died from pregnancy-related events in the United States. In 2020, that number rose to 850. Each year dozens more suffer pregnancy-related events that require lifesaving interventions.
Now, in a post-Roe world, the number of maternal deaths will likely climb as more abortion bans take effect and fewer women have access to lifesaving care, experts say. A 2021 study that compared 2017 maternal mortality rates in states with different levels of abortion restrictions found that the rate of maternal mortality was almost two times higher in states that restricted abortion access compared with those that protected it – 28.5 per 100,000 women vs. 15.7.
Some women living in states with abortion bans won’t have the resources to cross state lines for care.
“This is just going to widen the health care disparities that are already so prevalent in this country,” Dr. Jain says.
Navigating a crossroads
Ms. DeSpain’s medical history reads like a checklist of pregnancy-related perils: chronic high blood pressure, persistent clotting problems, and a high risk of hemorrhage. She was also diagnosed with cervical cancer in 2020, which left her body more fragile.
Cardiovascular conditions, including hypertension and hemorrhage, are the leading causes of maternal mortality, responsible for more than one-third of pregnancy-related deaths. Preeclampsia, characterized by high blood pressure, accounts for more than 7% of maternal deaths in the United States. Although less common, genetic disorders, such as spinal muscular atrophy and triploidy, or cancer during pregnancy can put a mother and fetus at risk.
Cancer – which affects about 1 in 1,000 pregnant women and results in termination in as many as 28% of cases – brings sharp focus to the new dangers and complex decision-making patients and their doctors face as abortion bans take hold.
Before the Supreme Court decision, a pregnant woman with cancer was already facing great uncertainty. The decision to treat cancer during pregnancy involves “weighing the risk of exposing the fetus to medication vs. the risk to the mother’s untreated illness if you don’t expose the fetus to medication,” Elyce Cardonick, MD, an obstetrician at Cooper University Health Care, Camden, N.J., who specializes in high-risk pregnancies, told the National Cancer Institute.
Oncologists generally agree that it’s safe for pregnant women to receive chemotherapy during the second and third trimesters. But for women with aggressive cancers that are diagnosed in the first trimester, chemotherapy is dangerous. For women who need immunotherapy, the risks of treatment remain unclear.
In these cases, Alice S. Mims, MD, must broach the possibility of terminating the pregnancy.
“Cancer is a very urgent condition,” says Dr. Mims, a hematology specialist at the Ohio State University Comprehensive Cancer Center, Columbus, who sees patients who are pregnant. “These women may have other children at home, and they want to do their best to fight the disease so they can be around for their family long term.”
Now the changing legal landscape on abortion will put hundreds more pregnant women with cancer in danger. In a recent viewpoint article published in JAMA Oncology, Jordyn Silverstein and Katherine Van Loon, MD, MPH, estimate that during the next year, up to 420 pregnant women living in states with restricted abortion access will face threats to their cancer care and potentially their life.
“The repercussions of overturning Roe v. Wade – and the failure of the Supreme Court to provide any guidance on exceptions related to the life and health of the mother – are potentially catastrophic for a subset of women who face a life-threating diagnosis of [pregnancy-associated cancer],” they write.
The choice Ms. DeSpain faced after her cervical cancer diagnosis was different. She was not pregnant at the time, but she was at a crossroads.
Although it was caught early, the cancer was aggressive. Her oncologist recommended that she undergo a hysterectomy – the surgery that would give her the best chance for a cancer-free future. It would also mean she could no longer become pregnant.
With a less invasive procedure, on the other hand, she could still carry a child, but she would face a much greater chance that the cancer would come back.
At 27, Ms. DeSpain was not ready to close the pregnancy door. She opted for a surgery in which part of her cervix was removed, allowing her to try for another baby.
But she faced a ticking clock in the event her cancer returned.
If you want to have a baby, “try soon,” her doctor warned.
A dead end
After her cancer surgery and a third miscarriage, Ms. DeSpain and her husband were surprised and excited when in late 2021 she again became pregnant.
The first trimester seemed blissfully uneventful. As the weeks passed, Finley’s heart started to beat.
But the 16-week ultrasound signaled a turning point. The sonographer was too quiet.
“This is really bad, isn’t it?” Ms. DeSpain asked her sonographer.
The doctors told her he wouldn’t survive. Finley had no heart chambers. His heart couldn’t pump blood properly. He was missing one kidney, and his brain was split in the back. With almost no amniotic fluid, her doctor said he would likely die in utero, crushed to death without support from the protective liquid.
She fought for him anyway. She sought specialty care, followed bed rest orders, and traveled 3 hours to Houston to enroll in a clinical trial.
But every road was a dead end.
Ultimately, testing revealed Finley had triploidy, and all lines led to one point.
“There were too many things wrong, too much wrong for them to fix,” says Ms. DeSpain, recalling the news from her doctor in Houston. “I was in shock. My husband was just sitting with his hands flat on the table, staring at nothing, shaking a little bit.”
However, Finley still had a heartbeat, making an abortion after 6 weeks a felony in Texas. Even a compassionate induction was now out of the question unless her death was imminent.
Ms. DeSpain called the abortion clinic in Albuquerque and made an appointment. She would have to wait 2 weeks because of an influx of pregnant patients coming from Texas.
She welcomed the wait … just in case she changed her mind.
“At that point I wanted to carry him as far as I could,” she says.
For those 2 weeks, Ms. DeSpain remained on bed rest. She cried all day every day. She worried that Finley was experiencing pain.
Through this process, her doctor’s support helped keep her grounded.
“She cried with us in her office and said, ‘I wish that you didn’t have to go, but I think you’re doing the right thing, doing what keeps you safest,’ “ Ms. DeSpain recalls.
Ms. DeSpain declined to share the name of her doctor out of fear that even expressing compassion for a patient’s safety could put the physician in legal jeopardy and provoke harassment.
That fear is warranted. Some doctors will be forced to choose between doing what is legal – even though the law is vague – and doing what is right for patients, says law professor Jamie Abrams, who was recently diagnosed with breast cancer.
To live in a world where there’s talk of criminalizing doctors for taking care of their patients, where there’s “this national movement to position some women to be shunned and exiled for seeking care that’s right for them, their health, and might save their life is staggering and beyond comprehension,” says Ms. Abrams, professor of law at the American University Washington College of Law.
Ms. Abrams, who was diagnosed with hormone receptor–positive invasive breast cancer the same day she read the leaked Supreme Court draft on the decision to end of Roe v. Wade, said that “overnight, I became a person who would need an abortion if I became pregnant, because my treatment would compromise a healthy birth or delay necessary cancer care.” Ms. Abrams was also told she could no longer use hormonal contraception.
Dr. Harris’s advice to clinicians is to try to do what they feel is best for patients, including referring them to centers that have legal resources and protections regarding abortions.
Dr. Mims agrees and recommends that doctors reach out to those with more resources and legal backing for support. “I would advise doctors in [states with restrictive laws] to familiarize themselves with available resources and organizations taking action to deal with questionable cases,” Dr. Mims says.
‘Baby killers work here’
Following her 10-hour drive to Albuquerque, Ms. DeSpain encountered lines of protesters at the clinic. They were holding signs that said, “Abortion is murder,” and “Baby killers work here.”
“Please don’t kill your baby – we have resources for you,” a woman screeched through a megaphone as Ms. DeSpain, nearly 20 weeks’ pregnant, stepped out of the car to enter the clinic.
“I remember turning around, looking at her and making eye contact, and yelling back, ‘My baby has triploidy – he is dying! He is going to suffocate if I carry him full term. You don’t know what you’re talking about!’ “
A nurse held her hand during the procedure.
“He said, ‘You’re doing great, you’re okay,’ “ she recalls. She knew there was a chance that Finley’s face would be crushed by contractions during labor because of the lack of amniotic fluid, but she hoped not. Ms. DeSpain longed for a photo.
There was no photo to take home the next day, but Ms. DeSpain did receive Finley’s footprints, and his heartbeat – as captured by the specialty team in Houston – lives on in a stuffed giraffe.
His ashes arrived a few weeks later.
By then, the Supreme Court draft had been leaked. Ms. DeSpain knew her predicament in Texas would soon affect women across the United States and make any future pregnancy attempt for her even more risky.
The weeks and months that followed were a blur of grief, anger, and medical testing.
But she received some good news. A second triploidy pregnancy was extremely unlikely.
Several weeks later, Ms. DeSpain got more good news.
“I had a follow-up cancer appointment, and everything was completely clear,” she says.
She remains hopeful that she will be able to give birth, but her doctor cautioned that it’s no longer safe to become pregnant in Texas.
“I need you to understand that if you get pregnant and you have complications, we can’t intervene unless the baby doesn’t have a heartbeat, even if it would save your life,” Ms. DeSpain recalls her doctor saying.
If Texas remains a dangerous place to be pregnant, Ms. DeSpain and her husband will have to move.
For now, Ms. DeSpain wants people to know her story and to continue to fight for her right to govern her body.
In a public post to Facebook, she laid bare her pregnancy journey.
“No one should have to share a story like mine to justify abortion,” she wrote. “My choice is not yours to judge, and my rights are not yours to gleefully take away.”
Ms. Abrams, Ms. DeSpain, Dr. Harris, Dr. Jain, and Dr. Mims have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The drive from Texas to the clinic in Albuquerque, N.M., took 10 hours. It was mid-April of this year. There wasn’t much to see along the mostly barren stretch, and there wasn’t much for Kailee DeSpain to do aside from think about where she was going and why.
Her husband was driving. She sensed his nervous glances toward the passenger seat where she sat struggling to quiet her thoughts.
No, she wasn’t having any pain, she told him. No, she wasn’t feeling like she did the last time or the two times before that.
This pregnancy was different. It was the first in which she feared for her own life. Her fetus – Finley – had triploidy, a rare chromosomal abnormality. Because of the condition, which affects 1%-3% of pregnancies, his heart, brain, and kidneys were not developing properly.
At 19 weeks, Finley was already struggling to draw breath from lungs squeezed inside an overcrowded chest cavity. Ms. DeSpain wanted nothing more than to carry Finley to term, hold him, meet him even for a moment before saying goodbye.
But his condition meant he would likely suffocate in utero well before that. And Ms. DeSpain knew that carrying him longer would likely raise her risk of bleeding and of her blood pressure increasing to dangerous highs.
“This could kill you,” her husband told her. “Do you realize you could die bringing a baby into this world who is not going to live? I don’t want to lose you.’”
Unlike her other pregnancies, the timing of this one and the decision she faced to end it put her health in even greater danger.
Imminent danger
On Sept. 1, 2021, a bill went into effect in Texas that banned abortions from as early as 6 weeks’ gestation. Texas Senate Bill 8 (SB8) became one of the most restrictive abortion laws in the country. It prohibited abortions whenever a fetal heartbeat, defined by lawmakers, could be detected on an ultrasound, often before many women knew they were pregnant.
The Texas abortion law was hardly the last word on the topic. Ms. DeSpain didn’t know it on her drive to New Mexico in April, but the U.S. Supreme Court was weeks away from overturning the landmark Roe v. Wade decision.
On June 24, the Supreme Court delivered its 6-3 ruling overturning Roe v. Wade, the 1973 case that granted women the right to abortion.
This decision set in motion “trigger laws” in some states – laws that essentially fully banned abortions. Those states included Ms. DeSpain’s home state of Texas, where abortion is now a felony except when the life of the mother is in peril.
However, legal definitions of what qualifies as “life-threatening” remain murky.
The law is unclear, says Lisa Harris, MD, PhD, professor in the department of obstetrics and gynecology at the University of Michigan, Ann Arbor. “What does the risk of death have to be, and how imminent must it be?” she asked in a recent editorial in the New England Journal of Medicine. Is 25% enough? 50%? Or does a woman have to be moments from dying?
“This whole thing makes me so angry,” says Shikha Jain, MD, a medical oncologist at University of Illinois Health, Chicago. “A patient may not be experiencing an emergency right now, but if we don’t take care of the situation, it may become an emergency in 2 hours or 2 days.”
Even before the Roe v. Wade decision, pregnancy had been a high-stakes endeavor for many women. In 2019, more than 750 women died from pregnancy-related events in the United States. In 2020, that number rose to 850. Each year dozens more suffer pregnancy-related events that require lifesaving interventions.
Now, in a post-Roe world, the number of maternal deaths will likely climb as more abortion bans take effect and fewer women have access to lifesaving care, experts say. A 2021 study that compared 2017 maternal mortality rates in states with different levels of abortion restrictions found that the rate of maternal mortality was almost two times higher in states that restricted abortion access compared with those that protected it – 28.5 per 100,000 women vs. 15.7.
Some women living in states with abortion bans won’t have the resources to cross state lines for care.
“This is just going to widen the health care disparities that are already so prevalent in this country,” Dr. Jain says.
Navigating a crossroads
Ms. DeSpain’s medical history reads like a checklist of pregnancy-related perils: chronic high blood pressure, persistent clotting problems, and a high risk of hemorrhage. She was also diagnosed with cervical cancer in 2020, which left her body more fragile.
Cardiovascular conditions, including hypertension and hemorrhage, are the leading causes of maternal mortality, responsible for more than one-third of pregnancy-related deaths. Preeclampsia, characterized by high blood pressure, accounts for more than 7% of maternal deaths in the United States. Although less common, genetic disorders, such as spinal muscular atrophy and triploidy, or cancer during pregnancy can put a mother and fetus at risk.
Cancer – which affects about 1 in 1,000 pregnant women and results in termination in as many as 28% of cases – brings sharp focus to the new dangers and complex decision-making patients and their doctors face as abortion bans take hold.
Before the Supreme Court decision, a pregnant woman with cancer was already facing great uncertainty. The decision to treat cancer during pregnancy involves “weighing the risk of exposing the fetus to medication vs. the risk to the mother’s untreated illness if you don’t expose the fetus to medication,” Elyce Cardonick, MD, an obstetrician at Cooper University Health Care, Camden, N.J., who specializes in high-risk pregnancies, told the National Cancer Institute.
Oncologists generally agree that it’s safe for pregnant women to receive chemotherapy during the second and third trimesters. But for women with aggressive cancers that are diagnosed in the first trimester, chemotherapy is dangerous. For women who need immunotherapy, the risks of treatment remain unclear.
In these cases, Alice S. Mims, MD, must broach the possibility of terminating the pregnancy.
“Cancer is a very urgent condition,” says Dr. Mims, a hematology specialist at the Ohio State University Comprehensive Cancer Center, Columbus, who sees patients who are pregnant. “These women may have other children at home, and they want to do their best to fight the disease so they can be around for their family long term.”
Now the changing legal landscape on abortion will put hundreds more pregnant women with cancer in danger. In a recent viewpoint article published in JAMA Oncology, Jordyn Silverstein and Katherine Van Loon, MD, MPH, estimate that during the next year, up to 420 pregnant women living in states with restricted abortion access will face threats to their cancer care and potentially their life.
“The repercussions of overturning Roe v. Wade – and the failure of the Supreme Court to provide any guidance on exceptions related to the life and health of the mother – are potentially catastrophic for a subset of women who face a life-threating diagnosis of [pregnancy-associated cancer],” they write.
The choice Ms. DeSpain faced after her cervical cancer diagnosis was different. She was not pregnant at the time, but she was at a crossroads.
Although it was caught early, the cancer was aggressive. Her oncologist recommended that she undergo a hysterectomy – the surgery that would give her the best chance for a cancer-free future. It would also mean she could no longer become pregnant.
With a less invasive procedure, on the other hand, she could still carry a child, but she would face a much greater chance that the cancer would come back.
At 27, Ms. DeSpain was not ready to close the pregnancy door. She opted for a surgery in which part of her cervix was removed, allowing her to try for another baby.
But she faced a ticking clock in the event her cancer returned.
If you want to have a baby, “try soon,” her doctor warned.
A dead end
After her cancer surgery and a third miscarriage, Ms. DeSpain and her husband were surprised and excited when in late 2021 she again became pregnant.
The first trimester seemed blissfully uneventful. As the weeks passed, Finley’s heart started to beat.
But the 16-week ultrasound signaled a turning point. The sonographer was too quiet.
“This is really bad, isn’t it?” Ms. DeSpain asked her sonographer.
The doctors told her he wouldn’t survive. Finley had no heart chambers. His heart couldn’t pump blood properly. He was missing one kidney, and his brain was split in the back. With almost no amniotic fluid, her doctor said he would likely die in utero, crushed to death without support from the protective liquid.
She fought for him anyway. She sought specialty care, followed bed rest orders, and traveled 3 hours to Houston to enroll in a clinical trial.
But every road was a dead end.
Ultimately, testing revealed Finley had triploidy, and all lines led to one point.
“There were too many things wrong, too much wrong for them to fix,” says Ms. DeSpain, recalling the news from her doctor in Houston. “I was in shock. My husband was just sitting with his hands flat on the table, staring at nothing, shaking a little bit.”
However, Finley still had a heartbeat, making an abortion after 6 weeks a felony in Texas. Even a compassionate induction was now out of the question unless her death was imminent.
Ms. DeSpain called the abortion clinic in Albuquerque and made an appointment. She would have to wait 2 weeks because of an influx of pregnant patients coming from Texas.
She welcomed the wait … just in case she changed her mind.
“At that point I wanted to carry him as far as I could,” she says.
For those 2 weeks, Ms. DeSpain remained on bed rest. She cried all day every day. She worried that Finley was experiencing pain.
Through this process, her doctor’s support helped keep her grounded.
“She cried with us in her office and said, ‘I wish that you didn’t have to go, but I think you’re doing the right thing, doing what keeps you safest,’ “ Ms. DeSpain recalls.
Ms. DeSpain declined to share the name of her doctor out of fear that even expressing compassion for a patient’s safety could put the physician in legal jeopardy and provoke harassment.
That fear is warranted. Some doctors will be forced to choose between doing what is legal – even though the law is vague – and doing what is right for patients, says law professor Jamie Abrams, who was recently diagnosed with breast cancer.
To live in a world where there’s talk of criminalizing doctors for taking care of their patients, where there’s “this national movement to position some women to be shunned and exiled for seeking care that’s right for them, their health, and might save their life is staggering and beyond comprehension,” says Ms. Abrams, professor of law at the American University Washington College of Law.
Ms. Abrams, who was diagnosed with hormone receptor–positive invasive breast cancer the same day she read the leaked Supreme Court draft on the decision to end of Roe v. Wade, said that “overnight, I became a person who would need an abortion if I became pregnant, because my treatment would compromise a healthy birth or delay necessary cancer care.” Ms. Abrams was also told she could no longer use hormonal contraception.
Dr. Harris’s advice to clinicians is to try to do what they feel is best for patients, including referring them to centers that have legal resources and protections regarding abortions.
Dr. Mims agrees and recommends that doctors reach out to those with more resources and legal backing for support. “I would advise doctors in [states with restrictive laws] to familiarize themselves with available resources and organizations taking action to deal with questionable cases,” Dr. Mims says.
‘Baby killers work here’
Following her 10-hour drive to Albuquerque, Ms. DeSpain encountered lines of protesters at the clinic. They were holding signs that said, “Abortion is murder,” and “Baby killers work here.”
“Please don’t kill your baby – we have resources for you,” a woman screeched through a megaphone as Ms. DeSpain, nearly 20 weeks’ pregnant, stepped out of the car to enter the clinic.
“I remember turning around, looking at her and making eye contact, and yelling back, ‘My baby has triploidy – he is dying! He is going to suffocate if I carry him full term. You don’t know what you’re talking about!’ “
A nurse held her hand during the procedure.
“He said, ‘You’re doing great, you’re okay,’ “ she recalls. She knew there was a chance that Finley’s face would be crushed by contractions during labor because of the lack of amniotic fluid, but she hoped not. Ms. DeSpain longed for a photo.
There was no photo to take home the next day, but Ms. DeSpain did receive Finley’s footprints, and his heartbeat – as captured by the specialty team in Houston – lives on in a stuffed giraffe.
His ashes arrived a few weeks later.
By then, the Supreme Court draft had been leaked. Ms. DeSpain knew her predicament in Texas would soon affect women across the United States and make any future pregnancy attempt for her even more risky.
The weeks and months that followed were a blur of grief, anger, and medical testing.
But she received some good news. A second triploidy pregnancy was extremely unlikely.
Several weeks later, Ms. DeSpain got more good news.
“I had a follow-up cancer appointment, and everything was completely clear,” she says.
She remains hopeful that she will be able to give birth, but her doctor cautioned that it’s no longer safe to become pregnant in Texas.
“I need you to understand that if you get pregnant and you have complications, we can’t intervene unless the baby doesn’t have a heartbeat, even if it would save your life,” Ms. DeSpain recalls her doctor saying.
If Texas remains a dangerous place to be pregnant, Ms. DeSpain and her husband will have to move.
For now, Ms. DeSpain wants people to know her story and to continue to fight for her right to govern her body.
In a public post to Facebook, she laid bare her pregnancy journey.
“No one should have to share a story like mine to justify abortion,” she wrote. “My choice is not yours to judge, and my rights are not yours to gleefully take away.”
Ms. Abrams, Ms. DeSpain, Dr. Harris, Dr. Jain, and Dr. Mims have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The drive from Texas to the clinic in Albuquerque, N.M., took 10 hours. It was mid-April of this year. There wasn’t much to see along the mostly barren stretch, and there wasn’t much for Kailee DeSpain to do aside from think about where she was going and why.
Her husband was driving. She sensed his nervous glances toward the passenger seat where she sat struggling to quiet her thoughts.
No, she wasn’t having any pain, she told him. No, she wasn’t feeling like she did the last time or the two times before that.
This pregnancy was different. It was the first in which she feared for her own life. Her fetus – Finley – had triploidy, a rare chromosomal abnormality. Because of the condition, which affects 1%-3% of pregnancies, his heart, brain, and kidneys were not developing properly.
At 19 weeks, Finley was already struggling to draw breath from lungs squeezed inside an overcrowded chest cavity. Ms. DeSpain wanted nothing more than to carry Finley to term, hold him, meet him even for a moment before saying goodbye.
But his condition meant he would likely suffocate in utero well before that. And Ms. DeSpain knew that carrying him longer would likely raise her risk of bleeding and of her blood pressure increasing to dangerous highs.
“This could kill you,” her husband told her. “Do you realize you could die bringing a baby into this world who is not going to live? I don’t want to lose you.’”
Unlike her other pregnancies, the timing of this one and the decision she faced to end it put her health in even greater danger.
Imminent danger
On Sept. 1, 2021, a bill went into effect in Texas that banned abortions from as early as 6 weeks’ gestation. Texas Senate Bill 8 (SB8) became one of the most restrictive abortion laws in the country. It prohibited abortions whenever a fetal heartbeat, defined by lawmakers, could be detected on an ultrasound, often before many women knew they were pregnant.
The Texas abortion law was hardly the last word on the topic. Ms. DeSpain didn’t know it on her drive to New Mexico in April, but the U.S. Supreme Court was weeks away from overturning the landmark Roe v. Wade decision.
On June 24, the Supreme Court delivered its 6-3 ruling overturning Roe v. Wade, the 1973 case that granted women the right to abortion.
This decision set in motion “trigger laws” in some states – laws that essentially fully banned abortions. Those states included Ms. DeSpain’s home state of Texas, where abortion is now a felony except when the life of the mother is in peril.
However, legal definitions of what qualifies as “life-threatening” remain murky.
The law is unclear, says Lisa Harris, MD, PhD, professor in the department of obstetrics and gynecology at the University of Michigan, Ann Arbor. “What does the risk of death have to be, and how imminent must it be?” she asked in a recent editorial in the New England Journal of Medicine. Is 25% enough? 50%? Or does a woman have to be moments from dying?
“This whole thing makes me so angry,” says Shikha Jain, MD, a medical oncologist at University of Illinois Health, Chicago. “A patient may not be experiencing an emergency right now, but if we don’t take care of the situation, it may become an emergency in 2 hours or 2 days.”
Even before the Roe v. Wade decision, pregnancy had been a high-stakes endeavor for many women. In 2019, more than 750 women died from pregnancy-related events in the United States. In 2020, that number rose to 850. Each year dozens more suffer pregnancy-related events that require lifesaving interventions.
Now, in a post-Roe world, the number of maternal deaths will likely climb as more abortion bans take effect and fewer women have access to lifesaving care, experts say. A 2021 study that compared 2017 maternal mortality rates in states with different levels of abortion restrictions found that the rate of maternal mortality was almost two times higher in states that restricted abortion access compared with those that protected it – 28.5 per 100,000 women vs. 15.7.
Some women living in states with abortion bans won’t have the resources to cross state lines for care.
“This is just going to widen the health care disparities that are already so prevalent in this country,” Dr. Jain says.
Navigating a crossroads
Ms. DeSpain’s medical history reads like a checklist of pregnancy-related perils: chronic high blood pressure, persistent clotting problems, and a high risk of hemorrhage. She was also diagnosed with cervical cancer in 2020, which left her body more fragile.
Cardiovascular conditions, including hypertension and hemorrhage, are the leading causes of maternal mortality, responsible for more than one-third of pregnancy-related deaths. Preeclampsia, characterized by high blood pressure, accounts for more than 7% of maternal deaths in the United States. Although less common, genetic disorders, such as spinal muscular atrophy and triploidy, or cancer during pregnancy can put a mother and fetus at risk.
Cancer – which affects about 1 in 1,000 pregnant women and results in termination in as many as 28% of cases – brings sharp focus to the new dangers and complex decision-making patients and their doctors face as abortion bans take hold.
Before the Supreme Court decision, a pregnant woman with cancer was already facing great uncertainty. The decision to treat cancer during pregnancy involves “weighing the risk of exposing the fetus to medication vs. the risk to the mother’s untreated illness if you don’t expose the fetus to medication,” Elyce Cardonick, MD, an obstetrician at Cooper University Health Care, Camden, N.J., who specializes in high-risk pregnancies, told the National Cancer Institute.
Oncologists generally agree that it’s safe for pregnant women to receive chemotherapy during the second and third trimesters. But for women with aggressive cancers that are diagnosed in the first trimester, chemotherapy is dangerous. For women who need immunotherapy, the risks of treatment remain unclear.
In these cases, Alice S. Mims, MD, must broach the possibility of terminating the pregnancy.
“Cancer is a very urgent condition,” says Dr. Mims, a hematology specialist at the Ohio State University Comprehensive Cancer Center, Columbus, who sees patients who are pregnant. “These women may have other children at home, and they want to do their best to fight the disease so they can be around for their family long term.”
Now the changing legal landscape on abortion will put hundreds more pregnant women with cancer in danger. In a recent viewpoint article published in JAMA Oncology, Jordyn Silverstein and Katherine Van Loon, MD, MPH, estimate that during the next year, up to 420 pregnant women living in states with restricted abortion access will face threats to their cancer care and potentially their life.
“The repercussions of overturning Roe v. Wade – and the failure of the Supreme Court to provide any guidance on exceptions related to the life and health of the mother – are potentially catastrophic for a subset of women who face a life-threating diagnosis of [pregnancy-associated cancer],” they write.
The choice Ms. DeSpain faced after her cervical cancer diagnosis was different. She was not pregnant at the time, but she was at a crossroads.
Although it was caught early, the cancer was aggressive. Her oncologist recommended that she undergo a hysterectomy – the surgery that would give her the best chance for a cancer-free future. It would also mean she could no longer become pregnant.
With a less invasive procedure, on the other hand, she could still carry a child, but she would face a much greater chance that the cancer would come back.
At 27, Ms. DeSpain was not ready to close the pregnancy door. She opted for a surgery in which part of her cervix was removed, allowing her to try for another baby.
But she faced a ticking clock in the event her cancer returned.
If you want to have a baby, “try soon,” her doctor warned.
A dead end
After her cancer surgery and a third miscarriage, Ms. DeSpain and her husband were surprised and excited when in late 2021 she again became pregnant.
The first trimester seemed blissfully uneventful. As the weeks passed, Finley’s heart started to beat.
But the 16-week ultrasound signaled a turning point. The sonographer was too quiet.
“This is really bad, isn’t it?” Ms. DeSpain asked her sonographer.
The doctors told her he wouldn’t survive. Finley had no heart chambers. His heart couldn’t pump blood properly. He was missing one kidney, and his brain was split in the back. With almost no amniotic fluid, her doctor said he would likely die in utero, crushed to death without support from the protective liquid.
She fought for him anyway. She sought specialty care, followed bed rest orders, and traveled 3 hours to Houston to enroll in a clinical trial.
But every road was a dead end.
Ultimately, testing revealed Finley had triploidy, and all lines led to one point.
“There were too many things wrong, too much wrong for them to fix,” says Ms. DeSpain, recalling the news from her doctor in Houston. “I was in shock. My husband was just sitting with his hands flat on the table, staring at nothing, shaking a little bit.”
However, Finley still had a heartbeat, making an abortion after 6 weeks a felony in Texas. Even a compassionate induction was now out of the question unless her death was imminent.
Ms. DeSpain called the abortion clinic in Albuquerque and made an appointment. She would have to wait 2 weeks because of an influx of pregnant patients coming from Texas.
She welcomed the wait … just in case she changed her mind.
“At that point I wanted to carry him as far as I could,” she says.
For those 2 weeks, Ms. DeSpain remained on bed rest. She cried all day every day. She worried that Finley was experiencing pain.
Through this process, her doctor’s support helped keep her grounded.
“She cried with us in her office and said, ‘I wish that you didn’t have to go, but I think you’re doing the right thing, doing what keeps you safest,’ “ Ms. DeSpain recalls.
Ms. DeSpain declined to share the name of her doctor out of fear that even expressing compassion for a patient’s safety could put the physician in legal jeopardy and provoke harassment.
That fear is warranted. Some doctors will be forced to choose between doing what is legal – even though the law is vague – and doing what is right for patients, says law professor Jamie Abrams, who was recently diagnosed with breast cancer.
To live in a world where there’s talk of criminalizing doctors for taking care of their patients, where there’s “this national movement to position some women to be shunned and exiled for seeking care that’s right for them, their health, and might save their life is staggering and beyond comprehension,” says Ms. Abrams, professor of law at the American University Washington College of Law.
Ms. Abrams, who was diagnosed with hormone receptor–positive invasive breast cancer the same day she read the leaked Supreme Court draft on the decision to end of Roe v. Wade, said that “overnight, I became a person who would need an abortion if I became pregnant, because my treatment would compromise a healthy birth or delay necessary cancer care.” Ms. Abrams was also told she could no longer use hormonal contraception.
Dr. Harris’s advice to clinicians is to try to do what they feel is best for patients, including referring them to centers that have legal resources and protections regarding abortions.
Dr. Mims agrees and recommends that doctors reach out to those with more resources and legal backing for support. “I would advise doctors in [states with restrictive laws] to familiarize themselves with available resources and organizations taking action to deal with questionable cases,” Dr. Mims says.
‘Baby killers work here’
Following her 10-hour drive to Albuquerque, Ms. DeSpain encountered lines of protesters at the clinic. They were holding signs that said, “Abortion is murder,” and “Baby killers work here.”
“Please don’t kill your baby – we have resources for you,” a woman screeched through a megaphone as Ms. DeSpain, nearly 20 weeks’ pregnant, stepped out of the car to enter the clinic.
“I remember turning around, looking at her and making eye contact, and yelling back, ‘My baby has triploidy – he is dying! He is going to suffocate if I carry him full term. You don’t know what you’re talking about!’ “
A nurse held her hand during the procedure.
“He said, ‘You’re doing great, you’re okay,’ “ she recalls. She knew there was a chance that Finley’s face would be crushed by contractions during labor because of the lack of amniotic fluid, but she hoped not. Ms. DeSpain longed for a photo.
There was no photo to take home the next day, but Ms. DeSpain did receive Finley’s footprints, and his heartbeat – as captured by the specialty team in Houston – lives on in a stuffed giraffe.
His ashes arrived a few weeks later.
By then, the Supreme Court draft had been leaked. Ms. DeSpain knew her predicament in Texas would soon affect women across the United States and make any future pregnancy attempt for her even more risky.
The weeks and months that followed were a blur of grief, anger, and medical testing.
But she received some good news. A second triploidy pregnancy was extremely unlikely.
Several weeks later, Ms. DeSpain got more good news.
“I had a follow-up cancer appointment, and everything was completely clear,” she says.
She remains hopeful that she will be able to give birth, but her doctor cautioned that it’s no longer safe to become pregnant in Texas.
“I need you to understand that if you get pregnant and you have complications, we can’t intervene unless the baby doesn’t have a heartbeat, even if it would save your life,” Ms. DeSpain recalls her doctor saying.
If Texas remains a dangerous place to be pregnant, Ms. DeSpain and her husband will have to move.
For now, Ms. DeSpain wants people to know her story and to continue to fight for her right to govern her body.
In a public post to Facebook, she laid bare her pregnancy journey.
“No one should have to share a story like mine to justify abortion,” she wrote. “My choice is not yours to judge, and my rights are not yours to gleefully take away.”
Ms. Abrams, Ms. DeSpain, Dr. Harris, Dr. Jain, and Dr. Mims have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Estrogen replacement therapy in endometrial cancer survivors
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.
If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.
If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
In the United States, uterine cancer is the fourth most common cancer among women, behind breast, lung/bronchus, and colorectal cancer. There are expected to be almost 66,000 new cases of uterine cancer in 2022.1 The majority of uterine cancers are endometrioid in histology and tend to be low grade, diagnosed at an early stage, and have a good prognosis. While our molecular understanding of endometrial cancers (EC) has changed significantly in recent years, low-grade endometrioid adenocarcinomas have historically been described as type 1 ECs. Type 1 ECs are typically caused by excess estrogen exposure (often unopposed or lacking progesterone protection) and are preceded by endometrial hyperplasia. Excess estrogen can come from exogenous sources (such as unopposed estrogen replacement therapy or tamoxifen, a commonly used treatment in estrogen receptor–positive breast cancer that acts as an estrogen agonist in the endometrium in postmenopausal patients) or endogenous ones (such as obesity).
Peripheral adipose tissue converts androgens into estrogens; paired with the decreased levels of sex hormone–binding globulin seen in obesity, there is more unbound or free serum estrogen (specifically estradiol) in obese women. Estrogen acts on the endometrium to cause proliferation and, if unopposed or imbalanced in relation to progesterone exposure, can ultimately lead to hyperplasia and malignancy.
If excess and unopposed estrogen exposure are major risk factors for the development of EC, is it safe to consider estrogen replacement therapy (ERT) in patients after EC treatment?
The short answer is the data are limited, but in a patient with a history of low-risk early-stage EC who undergoes appropriate counseling, it is likely safe to consider ERT.
Among EC survivors, there has been only one prospective randomized controlled trial that assessed the effect of recurrence rate and survival in women on ERT after EC treatment.2 Patients with stage I or occult stage II endometrial adenocarcinoma treated with at least a total hysterectomy and bilateral salpingo-oophorectomy were randomized to ERT versus placebo for 3 years of treatment, with therapy starting once recovered and within 20 weeks after surgery. Trial participation required an indication for ERT, such as vasomotor symptoms, vaginal atrophy, or increased risk of cardiovascular disease or osteoporosis.
The trial accrued 1,236 patients, falling short of its goal of 2,108 patients after enrollment decreased following the publication of the Women’s Health Initiative results in 2002. This publication prompted a review of the ERT study protocol that found that between decreased accrual and lower than expected recurrence rate, goal accrual would be impossible. Of those enrolled, participants were overwhelmingly white (84%-85%), 41-70 years old (80%-82%), and had stage IA or IB disease (88%). Median follow-up was almost 3 years.
Twenty-six (2.1%) patients experienced cancer recurrence, with similar rates in both groups. Three-year progression-free and overall survival were high overall among all study participants (94.8% and 96.5%). Unfortunately, because the study was closed early, definitive conclusions about the noninferiority of ERT versus placebo regarding oncologic outcomes in early-stage endometrial adenocarcinoma could not be made.
A subsequent meta-analysis looked at the effect of hormone therapy (HT) on recurrence rate in EC survivors.3 Five observational studies were included along with the previously discussed randomized controlled trial. Among 1,975 participants across six studies, there were cancer recurrences in 19 of 896 (2.1%) HT users and 64 of 1,079 (5.9%) controls. HT did not negatively affect cancer recurrence or overall survival. There was significant heterogeneity between studies as to dosing, duration, and type of HT given (some used estrogen-only replacement, others used estrogen and progesterone replacement, and some used both estrogen only and the combination of estrogen and progesterone replacement). Among the five nonrandomized studies included, a protective effect of combined HT on EC recurrence was noted. One study included patients with stage III disease, but only four patients received HT in this cohort.
Given the data we have, ERT does not appear to significantly affect oncologic outcomes in low-risk, early-stage EC survivors. We do not have data to support this same assertion in more advanced, high-risk disease. Before initiation of any ERT in an EC survivor, there should be a detailed discussion to weigh the risks and benefits of starting therapy. The goal of treatment should be to use the lowest dose of ERT possible to treat symptoms, with planned surveillance visits for symptom check-in and assessment of readiness to start tapering treatment.
Footnote: vaginal estrogen therapy
There are no randomized trials assessing the safety of vaginal estrogen preparations or their effect on oncologic outcomes in EC survivors. Observational data from the Women’s Health Initiative showed no increased risk of endometrial cancer in patients who used vaginal estrogen with an intact uterus.4 A recently published retrospective study among 244 gynecologic cancer survivors found low rates of disease recurrence and adverse outcomes among women who used vaginal estrogen for genitourinary symptoms.5 Among EC survivors, the incidence of recurrence was 2.4% for patients with stage I/II disease and 4.3% for stage III/IV disease, with a median follow-up of 80.2 months. While there appears to be some systemic absorption with vaginal estrogen use, this can be quite challenging to measure because of the current sensitivity of serum estradiol and estrone assays. Given the significantly lower serum levels with vaginal estrogen preparations compared with ERT, vaginal estrogen use appears to be safe in EC survivors.
Dr. Tucker is assistant professor of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Cancer Stat Facts: Uterine Cancer. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Accessed 12 Aug. 2022. https://seer.cancer.gov/statfacts/html/corp.html.
2. Barakat RR et al. J Clin Oncol. 2006;24(4):587-92.
3. Shim SH et al. Eur J Cancer. 2014;50(9):1628-37.
4. Crandall CJ et al. Menopause. 2018 Jan;25(1):11-20.
5. Chambers LM et al. Int J Gynecol Cancer. 2020 Apr;30(4):515-24.
Getting cancer research on track again may require a ‘behemoth’ effort
In 2016, as vice president, Joe Biden launched the Cancer Moonshot program just 1 year after his son Beau died from glioblastoma multiforme. His objective, he said, was to “cure” cancer, but to get close to that goal, to get cancer research just back up to pre-COVID-19 pandemic levels.
There has been a significant decrease in the launch of new clinical trials for cancer and biologic therapies since 2020. “That can affect every aspect of our research operation. It really affected our capacity to continue to move forward at a fast pace. It will require a behemoth effort to get back to pre-COVID times,” said Tanios S. Bekaii-Saab, MD, leader of the gastrointestinal cancer program at Mayo Clinic in Phoenix.
Congress passed the 21st Century Cures Act in 2016 authorizing $1.8 billion for Cancer Moonshot over 7 years. More recently, the program received $194 million from the $6.9 billion National Cancer Institute budget in FY 2022.
Joseph Alvarnas, MD, a hematologist oncologist and vice president of government affairs at City of Hope, Duarte, Calif., sees the Moonshot budget as a potential shortcoming.
“The priorities are well founded and based on what we would think are the most important things to cover, but, if we’re going to achieve these extraordinarily ambitious goals of halving cancer mortality and serving communities more equitably, it’s going to need more funding positioned at making these things real,” he said.
Moonshot is being positioned as an opportunity to double down on efforts started in 2016, but treating cancer is complex and goes well beyond funding new research.
“We know that we have amazing research and progress around innovations that will drive us toward the goal of reducing the death rate from cancer. But we also know that we have tools that aren’t reaching all parts of the country, so we have a great opportunity to make sure that we’re doing all we can to prevent, detect and treat cancer,” Dr. Carnival said.
Can cancer be cured?
The Biden administration relaunched Moonshot in 2022 with newly defined goals: Cut the rate of cancer-related deaths in half within 25 years; improve the experience of people with cancer, cancer survivors, and their families; and “end cancer as we know it,” President Biden said in a press conference in February.
Cancer is the second leading cause of death in the United States after heart disease, but it may indeed be possible to cut the total number of cancer-related deaths in half over the next 25 years.
“As a hematologist who’s been involved in both research and clinical care, I think it’s important to realize this is actually doable. Between 1990 and 2020 cancer mortality rates decreased by 31%, and in the last American Cancer Society’s annual report, mortality rates dropped by the largest percentages for 2 consecutive years in a row. The question shifts now from ‘Is this possible? to ‘How do we ensure that it’s possible?’ The spirit of Cancer Moonshot 2.0 is identifying the multiple paths to move this effort forward,” Dr. Alvarnas said.
But without a significant infusion of cash for research, it’s doubtful cancer-related deaths will drop by 50% over the next 25 years.
“There are a lot of big and lofty goals in Cancer Moonshot, and the words ‘ending cancer,’ well those are big words,” Dr. Bekaii-Saab said. “The reality is how do we measure in 25 years the impact of this today? I think it will require significantly more funding over the next few years to achieve the goals set by the Moonshot. Otherwise it will be a 7-year done deal that will accrue a lot of great numbers but won’t make a dent in those goals for the next 25 years. To stop it at some point and not invest more into it, we will probably lose most of the benefit.”
Closing the loop on data sharing
Moonshot has been instrumental in fostering research collaborations by encouraging data sharing among scientists.
“It also brought together a new way for the National Cancer Institute and Department of Energy to drive progress on some of the big data initiatives. The initial Cancer Moonshot infused a sense of urgency and hope into this effort,” said Danielle Carnival, PhD, coordinator of Cancer Moonshot.
Between 2017 and 2022, Cancer Moonshot created more than 70 consortiums or programs, and funded about 240 research projects. Its fundamental goals of improving data sharing and encouraging collaboration are very important, Dr. Bekaii-Saab said.
“Because, historically, what happens with cancer is that researchers compete for resources...and they become very protective of their data. Sharing gets more difficult, collaborations become more onerous, and it becomes counterproductive,” he said.
Dr. Bekaii-Saab highlighted two networks created specifically for data sharing. They include the Human Tumor Atlas for cellular, morphological, and molecular tumor data, and PDXNet, a patient derived xenograft research network.
A shift in funding priorities?
Cancer funding has been stagnant for years. When adjusted for growth, it hasn’t had a significant infusion of funding since at least 2003—at least in relative terms, Dr. Bekaii-Saab said. “This affects a lot of the things we do, including NCI-funded clinical trials. It pushes us to work with the private sector, which is not necessarily a detriment, but it doesn’t advance the academic mission at the same level. So, overall, I wouldn’t call it tragic, but I do think we’re falling behind,” he said.
“I think when we do the process for the budget for FY24 and after we’ve had time to really explore the best ideas and build the foundation for some of these new aspects of the Cancer Moonshot, we hope to have something more concrete going toward these efforts,” Dr. Carnival said.
But in addition to funding, Dr. Alvarnas says, it is equally important to address gaps in care. Not all patients have access to existing cancer treatments.
“The great challenge to us in the 2020s is not only about developing new and more effective technologies, but also in doing a better job of getting existing life-saving treatments into the hands of underserved populations. One of the really positive challenges set forth by the Biden administration is the idea that financing care equity is as important, if not more so, than advancing technologies. If there’s been stagnation, it’s because from a government and resourcing point of view, that priority has been ineffectively supported financially.”
The pandemic stymies cancer research
The pandemic has had a significant impact on cancer research. As in other fields, it disrupted ongoing research, but it may have also contributed to the loss of employees who resigned in what’s been called the “Great Resignation.” “A lot of employees just decided to change jobs in the middle of the pandemic, which led to a cancer research staffing crisis,” Dr. Bekaii-Saab said.
“We all recognized that turning so much of the attention of the entire biomedical research engine and health system to the COVID-19 pandemic would have an impact across cancer research, screenings and care,” Dr. Carnival said. “There is work to do to get us back to whole, but from a research perspective, we’ve seen a reorientation of the trial networks we were using for COVID-19 research, back to their initial purpose. Some of those are cancer and oncology networks, so we’re excited about that and fully believe that we can catch up.”
But then there’s also the impact the pandemic has had on cancer patients who delayed their care at the primary level. This, Dr. Bekaii-Saab fears, will lead to more patients presenting with more advanced disease in years to come. “One of the biggest problems was that a lot of patients delayed their care at the primary level. My biggest concern is that in the years to come we will see a lot more patients presenting with more advanced cancer.”
In 2016, as vice president, Joe Biden launched the Cancer Moonshot program just 1 year after his son Beau died from glioblastoma multiforme. His objective, he said, was to “cure” cancer, but to get close to that goal, to get cancer research just back up to pre-COVID-19 pandemic levels.
There has been a significant decrease in the launch of new clinical trials for cancer and biologic therapies since 2020. “That can affect every aspect of our research operation. It really affected our capacity to continue to move forward at a fast pace. It will require a behemoth effort to get back to pre-COVID times,” said Tanios S. Bekaii-Saab, MD, leader of the gastrointestinal cancer program at Mayo Clinic in Phoenix.
Congress passed the 21st Century Cures Act in 2016 authorizing $1.8 billion for Cancer Moonshot over 7 years. More recently, the program received $194 million from the $6.9 billion National Cancer Institute budget in FY 2022.
Joseph Alvarnas, MD, a hematologist oncologist and vice president of government affairs at City of Hope, Duarte, Calif., sees the Moonshot budget as a potential shortcoming.
“The priorities are well founded and based on what we would think are the most important things to cover, but, if we’re going to achieve these extraordinarily ambitious goals of halving cancer mortality and serving communities more equitably, it’s going to need more funding positioned at making these things real,” he said.
Moonshot is being positioned as an opportunity to double down on efforts started in 2016, but treating cancer is complex and goes well beyond funding new research.
“We know that we have amazing research and progress around innovations that will drive us toward the goal of reducing the death rate from cancer. But we also know that we have tools that aren’t reaching all parts of the country, so we have a great opportunity to make sure that we’re doing all we can to prevent, detect and treat cancer,” Dr. Carnival said.
Can cancer be cured?
The Biden administration relaunched Moonshot in 2022 with newly defined goals: Cut the rate of cancer-related deaths in half within 25 years; improve the experience of people with cancer, cancer survivors, and their families; and “end cancer as we know it,” President Biden said in a press conference in February.
Cancer is the second leading cause of death in the United States after heart disease, but it may indeed be possible to cut the total number of cancer-related deaths in half over the next 25 years.
“As a hematologist who’s been involved in both research and clinical care, I think it’s important to realize this is actually doable. Between 1990 and 2020 cancer mortality rates decreased by 31%, and in the last American Cancer Society’s annual report, mortality rates dropped by the largest percentages for 2 consecutive years in a row. The question shifts now from ‘Is this possible? to ‘How do we ensure that it’s possible?’ The spirit of Cancer Moonshot 2.0 is identifying the multiple paths to move this effort forward,” Dr. Alvarnas said.
But without a significant infusion of cash for research, it’s doubtful cancer-related deaths will drop by 50% over the next 25 years.
“There are a lot of big and lofty goals in Cancer Moonshot, and the words ‘ending cancer,’ well those are big words,” Dr. Bekaii-Saab said. “The reality is how do we measure in 25 years the impact of this today? I think it will require significantly more funding over the next few years to achieve the goals set by the Moonshot. Otherwise it will be a 7-year done deal that will accrue a lot of great numbers but won’t make a dent in those goals for the next 25 years. To stop it at some point and not invest more into it, we will probably lose most of the benefit.”
Closing the loop on data sharing
Moonshot has been instrumental in fostering research collaborations by encouraging data sharing among scientists.
“It also brought together a new way for the National Cancer Institute and Department of Energy to drive progress on some of the big data initiatives. The initial Cancer Moonshot infused a sense of urgency and hope into this effort,” said Danielle Carnival, PhD, coordinator of Cancer Moonshot.
Between 2017 and 2022, Cancer Moonshot created more than 70 consortiums or programs, and funded about 240 research projects. Its fundamental goals of improving data sharing and encouraging collaboration are very important, Dr. Bekaii-Saab said.
“Because, historically, what happens with cancer is that researchers compete for resources...and they become very protective of their data. Sharing gets more difficult, collaborations become more onerous, and it becomes counterproductive,” he said.
Dr. Bekaii-Saab highlighted two networks created specifically for data sharing. They include the Human Tumor Atlas for cellular, morphological, and molecular tumor data, and PDXNet, a patient derived xenograft research network.
A shift in funding priorities?
Cancer funding has been stagnant for years. When adjusted for growth, it hasn’t had a significant infusion of funding since at least 2003—at least in relative terms, Dr. Bekaii-Saab said. “This affects a lot of the things we do, including NCI-funded clinical trials. It pushes us to work with the private sector, which is not necessarily a detriment, but it doesn’t advance the academic mission at the same level. So, overall, I wouldn’t call it tragic, but I do think we’re falling behind,” he said.
“I think when we do the process for the budget for FY24 and after we’ve had time to really explore the best ideas and build the foundation for some of these new aspects of the Cancer Moonshot, we hope to have something more concrete going toward these efforts,” Dr. Carnival said.
But in addition to funding, Dr. Alvarnas says, it is equally important to address gaps in care. Not all patients have access to existing cancer treatments.
“The great challenge to us in the 2020s is not only about developing new and more effective technologies, but also in doing a better job of getting existing life-saving treatments into the hands of underserved populations. One of the really positive challenges set forth by the Biden administration is the idea that financing care equity is as important, if not more so, than advancing technologies. If there’s been stagnation, it’s because from a government and resourcing point of view, that priority has been ineffectively supported financially.”
The pandemic stymies cancer research
The pandemic has had a significant impact on cancer research. As in other fields, it disrupted ongoing research, but it may have also contributed to the loss of employees who resigned in what’s been called the “Great Resignation.” “A lot of employees just decided to change jobs in the middle of the pandemic, which led to a cancer research staffing crisis,” Dr. Bekaii-Saab said.
“We all recognized that turning so much of the attention of the entire biomedical research engine and health system to the COVID-19 pandemic would have an impact across cancer research, screenings and care,” Dr. Carnival said. “There is work to do to get us back to whole, but from a research perspective, we’ve seen a reorientation of the trial networks we were using for COVID-19 research, back to their initial purpose. Some of those are cancer and oncology networks, so we’re excited about that and fully believe that we can catch up.”
But then there’s also the impact the pandemic has had on cancer patients who delayed their care at the primary level. This, Dr. Bekaii-Saab fears, will lead to more patients presenting with more advanced disease in years to come. “One of the biggest problems was that a lot of patients delayed their care at the primary level. My biggest concern is that in the years to come we will see a lot more patients presenting with more advanced cancer.”
In 2016, as vice president, Joe Biden launched the Cancer Moonshot program just 1 year after his son Beau died from glioblastoma multiforme. His objective, he said, was to “cure” cancer, but to get close to that goal, to get cancer research just back up to pre-COVID-19 pandemic levels.
There has been a significant decrease in the launch of new clinical trials for cancer and biologic therapies since 2020. “That can affect every aspect of our research operation. It really affected our capacity to continue to move forward at a fast pace. It will require a behemoth effort to get back to pre-COVID times,” said Tanios S. Bekaii-Saab, MD, leader of the gastrointestinal cancer program at Mayo Clinic in Phoenix.
Congress passed the 21st Century Cures Act in 2016 authorizing $1.8 billion for Cancer Moonshot over 7 years. More recently, the program received $194 million from the $6.9 billion National Cancer Institute budget in FY 2022.
Joseph Alvarnas, MD, a hematologist oncologist and vice president of government affairs at City of Hope, Duarte, Calif., sees the Moonshot budget as a potential shortcoming.
“The priorities are well founded and based on what we would think are the most important things to cover, but, if we’re going to achieve these extraordinarily ambitious goals of halving cancer mortality and serving communities more equitably, it’s going to need more funding positioned at making these things real,” he said.
Moonshot is being positioned as an opportunity to double down on efforts started in 2016, but treating cancer is complex and goes well beyond funding new research.
“We know that we have amazing research and progress around innovations that will drive us toward the goal of reducing the death rate from cancer. But we also know that we have tools that aren’t reaching all parts of the country, so we have a great opportunity to make sure that we’re doing all we can to prevent, detect and treat cancer,” Dr. Carnival said.
Can cancer be cured?
The Biden administration relaunched Moonshot in 2022 with newly defined goals: Cut the rate of cancer-related deaths in half within 25 years; improve the experience of people with cancer, cancer survivors, and their families; and “end cancer as we know it,” President Biden said in a press conference in February.
Cancer is the second leading cause of death in the United States after heart disease, but it may indeed be possible to cut the total number of cancer-related deaths in half over the next 25 years.
“As a hematologist who’s been involved in both research and clinical care, I think it’s important to realize this is actually doable. Between 1990 and 2020 cancer mortality rates decreased by 31%, and in the last American Cancer Society’s annual report, mortality rates dropped by the largest percentages for 2 consecutive years in a row. The question shifts now from ‘Is this possible? to ‘How do we ensure that it’s possible?’ The spirit of Cancer Moonshot 2.0 is identifying the multiple paths to move this effort forward,” Dr. Alvarnas said.
But without a significant infusion of cash for research, it’s doubtful cancer-related deaths will drop by 50% over the next 25 years.
“There are a lot of big and lofty goals in Cancer Moonshot, and the words ‘ending cancer,’ well those are big words,” Dr. Bekaii-Saab said. “The reality is how do we measure in 25 years the impact of this today? I think it will require significantly more funding over the next few years to achieve the goals set by the Moonshot. Otherwise it will be a 7-year done deal that will accrue a lot of great numbers but won’t make a dent in those goals for the next 25 years. To stop it at some point and not invest more into it, we will probably lose most of the benefit.”
Closing the loop on data sharing
Moonshot has been instrumental in fostering research collaborations by encouraging data sharing among scientists.
“It also brought together a new way for the National Cancer Institute and Department of Energy to drive progress on some of the big data initiatives. The initial Cancer Moonshot infused a sense of urgency and hope into this effort,” said Danielle Carnival, PhD, coordinator of Cancer Moonshot.
Between 2017 and 2022, Cancer Moonshot created more than 70 consortiums or programs, and funded about 240 research projects. Its fundamental goals of improving data sharing and encouraging collaboration are very important, Dr. Bekaii-Saab said.
“Because, historically, what happens with cancer is that researchers compete for resources...and they become very protective of their data. Sharing gets more difficult, collaborations become more onerous, and it becomes counterproductive,” he said.
Dr. Bekaii-Saab highlighted two networks created specifically for data sharing. They include the Human Tumor Atlas for cellular, morphological, and molecular tumor data, and PDXNet, a patient derived xenograft research network.
A shift in funding priorities?
Cancer funding has been stagnant for years. When adjusted for growth, it hasn’t had a significant infusion of funding since at least 2003—at least in relative terms, Dr. Bekaii-Saab said. “This affects a lot of the things we do, including NCI-funded clinical trials. It pushes us to work with the private sector, which is not necessarily a detriment, but it doesn’t advance the academic mission at the same level. So, overall, I wouldn’t call it tragic, but I do think we’re falling behind,” he said.
“I think when we do the process for the budget for FY24 and after we’ve had time to really explore the best ideas and build the foundation for some of these new aspects of the Cancer Moonshot, we hope to have something more concrete going toward these efforts,” Dr. Carnival said.
But in addition to funding, Dr. Alvarnas says, it is equally important to address gaps in care. Not all patients have access to existing cancer treatments.
“The great challenge to us in the 2020s is not only about developing new and more effective technologies, but also in doing a better job of getting existing life-saving treatments into the hands of underserved populations. One of the really positive challenges set forth by the Biden administration is the idea that financing care equity is as important, if not more so, than advancing technologies. If there’s been stagnation, it’s because from a government and resourcing point of view, that priority has been ineffectively supported financially.”
The pandemic stymies cancer research
The pandemic has had a significant impact on cancer research. As in other fields, it disrupted ongoing research, but it may have also contributed to the loss of employees who resigned in what’s been called the “Great Resignation.” “A lot of employees just decided to change jobs in the middle of the pandemic, which led to a cancer research staffing crisis,” Dr. Bekaii-Saab said.
“We all recognized that turning so much of the attention of the entire biomedical research engine and health system to the COVID-19 pandemic would have an impact across cancer research, screenings and care,” Dr. Carnival said. “There is work to do to get us back to whole, but from a research perspective, we’ve seen a reorientation of the trial networks we were using for COVID-19 research, back to their initial purpose. Some of those are cancer and oncology networks, so we’re excited about that and fully believe that we can catch up.”
But then there’s also the impact the pandemic has had on cancer patients who delayed their care at the primary level. This, Dr. Bekaii-Saab fears, will lead to more patients presenting with more advanced disease in years to come. “One of the biggest problems was that a lot of patients delayed their care at the primary level. My biggest concern is that in the years to come we will see a lot more patients presenting with more advanced cancer.”