User login
Music Interventions Improve Anxiety, Pain in Cancer Patients
DENVER – Playing a musical instrument, singing, or simply listening to recorded music resulted in significant reduction in anxiety scores in patients with cancer, according to a Cochrane Database systematic review and meta-analysis.
The various music interventions offered by medical staff or trained music therapists also achieved significant improvements in the secondary end points of pain, mood, and quality of life scores, according to the review by investigators in the department of creative arts therapies at Drexel University in Philadelphia.

At the annual meeting of the American Academy of Hospice and Palliative Care Medicine, Dr. Wendy Anderson highlighted the Cochrane review findings as particularly on-point for her colleagues in oncology and palliative medicine.
"In palliative care we’re always trying to make the best of a difficult situation, and sometimes the best way to do this is through a nonpharmacologic intervention, even though it means doing something outside of our comfort zone," commented Dr. Anderson of the University of California, San Francisco.
Prior studies of music interventions in patients with cancer have been quite small. The Cochrane meta-analysis was designed to yield stronger, more definitive conclusions by incorporating those small studies which were sufficiently similar to combine.
The Cochrane report included 30 randomized clinical trials in seven countries with a total of 1,891 participating patients of all ages and with all types of cancer. In all, 13 trials involved the use of trained music therapists, while in the other 17 in the intervention consisted of listening to various genres of prerecorded music selected by the patients. Sessions were typically 30-45 minutes in length. The number of sessions varied widely from study to study. Subjects in the control arm received usual care or in some studies listened to white noise through headphones.
Sixteen randomized trials assessed anxiety. Collectively they showed that music interventions achieved statistically and clinically meaningful reductions in anxiety scores, with median to large effect sizes. For example, mean scores on the State Trait Anxiety Inventory fell by a mean of 11.2 units following the various music interventions while remaining unchanged in controls.
Similarly, the reduction in pain scores and improvements in structured measures of mood and quality of life in participants in the music interventions as compared to controls were also in the moderate to large range.
"Those are important outcomes in our patients with cancer," Dr. Anderson observed.
Music therapy is an established profession. Trained music therapists can perform a detailed patient evaluation and provide a tailored music experience. Although the Drexel researchers sought to learn whether the more elaborate, active participation music interventions provided by trained music therapists result in bigger improvements in psychologic and physical outcomes than the simpler music-listening interventions offered by medical staff, the investigators found that the research database wasn’t sufficiently large to draw any conclusions on that score (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD006911]).
The Cochrane group self-rated the quality of evidence on which the music intervention meta-analysis was based as low because these were nonblinded randomized trials. Patient awareness of whether they received a music intervention may have biased the results.
"Usually a low quality of evidence would, I think, make us reluctant to admit some innovations into our practices, but what’s interesting here is there’s a low potential for harm from music, and the patients feel the music improves their symptoms. That may be enough for us to implement music interventions in our practices," Dr. Anderson concluded.
The Cochrane review was funded by the State of Pennsylvania Formula Fund.
Dr. Anderson reported having no financial conflicts.
DENVER – Playing a musical instrument, singing, or simply listening to recorded music resulted in significant reduction in anxiety scores in patients with cancer, according to a Cochrane Database systematic review and meta-analysis.
The various music interventions offered by medical staff or trained music therapists also achieved significant improvements in the secondary end points of pain, mood, and quality of life scores, according to the review by investigators in the department of creative arts therapies at Drexel University in Philadelphia.
At the annual meeting of the American Academy of Hospice and Palliative Care Medicine, Dr. Wendy Anderson highlighted the Cochrane review findings as particularly on-point for her colleagues in oncology and palliative medicine.
"In palliative care we’re always trying to make the best of a difficult situation, and sometimes the best way to do this is through a nonpharmacologic intervention, even though it means doing something outside of our comfort zone," commented Dr. Anderson of the University of California, San Francisco.
Prior studies of music interventions in patients with cancer have been quite small. The Cochrane meta-analysis was designed to yield stronger, more definitive conclusions by incorporating those small studies which were sufficiently similar to combine.
The Cochrane report included 30 randomized clinical trials in seven countries with a total of 1,891 participating patients of all ages and with all types of cancer. In all, 13 trials involved the use of trained music therapists, while in the other 17 in the intervention consisted of listening to various genres of prerecorded music selected by the patients. Sessions were typically 30-45 minutes in length. The number of sessions varied widely from study to study. Subjects in the control arm received usual care or in some studies listened to white noise through headphones.
Sixteen randomized trials assessed anxiety. Collectively they showed that music interventions achieved statistically and clinically meaningful reductions in anxiety scores, with median to large effect sizes. For example, mean scores on the State Trait Anxiety Inventory fell by a mean of 11.2 units following the various music interventions while remaining unchanged in controls.
Similarly, the reduction in pain scores and improvements in structured measures of mood and quality of life in participants in the music interventions as compared to controls were also in the moderate to large range.
"Those are important outcomes in our patients with cancer," Dr. Anderson observed.
Music therapy is an established profession. Trained music therapists can perform a detailed patient evaluation and provide a tailored music experience. Although the Drexel researchers sought to learn whether the more elaborate, active participation music interventions provided by trained music therapists result in bigger improvements in psychologic and physical outcomes than the simpler music-listening interventions offered by medical staff, the investigators found that the research database wasn’t sufficiently large to draw any conclusions on that score (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD006911]).
The Cochrane group self-rated the quality of evidence on which the music intervention meta-analysis was based as low because these were nonblinded randomized trials. Patient awareness of whether they received a music intervention may have biased the results.
"Usually a low quality of evidence would, I think, make us reluctant to admit some innovations into our practices, but what’s interesting here is there’s a low potential for harm from music, and the patients feel the music improves their symptoms. That may be enough for us to implement music interventions in our practices," Dr. Anderson concluded.
The Cochrane review was funded by the State of Pennsylvania Formula Fund.
Dr. Anderson reported having no financial conflicts.
DENVER – Playing a musical instrument, singing, or simply listening to recorded music resulted in significant reduction in anxiety scores in patients with cancer, according to a Cochrane Database systematic review and meta-analysis.
The various music interventions offered by medical staff or trained music therapists also achieved significant improvements in the secondary end points of pain, mood, and quality of life scores, according to the review by investigators in the department of creative arts therapies at Drexel University in Philadelphia.
At the annual meeting of the American Academy of Hospice and Palliative Care Medicine, Dr. Wendy Anderson highlighted the Cochrane review findings as particularly on-point for her colleagues in oncology and palliative medicine.
"In palliative care we’re always trying to make the best of a difficult situation, and sometimes the best way to do this is through a nonpharmacologic intervention, even though it means doing something outside of our comfort zone," commented Dr. Anderson of the University of California, San Francisco.
Prior studies of music interventions in patients with cancer have been quite small. The Cochrane meta-analysis was designed to yield stronger, more definitive conclusions by incorporating those small studies which were sufficiently similar to combine.
The Cochrane report included 30 randomized clinical trials in seven countries with a total of 1,891 participating patients of all ages and with all types of cancer. In all, 13 trials involved the use of trained music therapists, while in the other 17 in the intervention consisted of listening to various genres of prerecorded music selected by the patients. Sessions were typically 30-45 minutes in length. The number of sessions varied widely from study to study. Subjects in the control arm received usual care or in some studies listened to white noise through headphones.
Sixteen randomized trials assessed anxiety. Collectively they showed that music interventions achieved statistically and clinically meaningful reductions in anxiety scores, with median to large effect sizes. For example, mean scores on the State Trait Anxiety Inventory fell by a mean of 11.2 units following the various music interventions while remaining unchanged in controls.
Similarly, the reduction in pain scores and improvements in structured measures of mood and quality of life in participants in the music interventions as compared to controls were also in the moderate to large range.
"Those are important outcomes in our patients with cancer," Dr. Anderson observed.
Music therapy is an established profession. Trained music therapists can perform a detailed patient evaluation and provide a tailored music experience. Although the Drexel researchers sought to learn whether the more elaborate, active participation music interventions provided by trained music therapists result in bigger improvements in psychologic and physical outcomes than the simpler music-listening interventions offered by medical staff, the investigators found that the research database wasn’t sufficiently large to draw any conclusions on that score (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD006911]).
The Cochrane group self-rated the quality of evidence on which the music intervention meta-analysis was based as low because these were nonblinded randomized trials. Patient awareness of whether they received a music intervention may have biased the results.
"Usually a low quality of evidence would, I think, make us reluctant to admit some innovations into our practices, but what’s interesting here is there’s a low potential for harm from music, and the patients feel the music improves their symptoms. That may be enough for us to implement music interventions in our practices," Dr. Anderson concluded.
The Cochrane review was funded by the State of Pennsylvania Formula Fund.
Dr. Anderson reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL ASSEMBLY OF THE AMERICAN ACADEMY OF HOSPICE AND PALLIATIVE MEDICINE
Antinausea Gel Not Absorbed at Therapeutic Levels
DENVER – Compounded ABH gel is widely prescribed for treatment of nausea in the hospice setting. It costs less than $1 per dose. Side effects are rare. And many clinicians swear by its effectiveness, noting that the constituent medications in ABH gel – Ativan (lorazepam), Benadryl (diphenhydramine), and Haldol (haloperidol) – target different mechanisms of nausea.
There is, however, a fly in the ointment ... er, gel.
It turns out that none of the three medications in topical ABH gel are absorbed systemically in anything remotely approaching therapeutic levels, Dr. Devon S. Fletcher reported at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
"Either ABH gel doesn’t work, or the effect is attributable to placebo, or possibly a nonpharmacologic mechanism is involved, such as stimulation of the P6 acupressure point on the wrist as patients rub the gel in," said Dr. Fletcher of Virginia Commonwealth University, Richmond. "If ABH doesn’t work, using it to treat a symptom leads to unacceptable suffering and unnecessary hospitalizations," she added.
Dr. Fletcher and coworkers measured levels of the three medications contained in ABH gel in six blood samples taken serially in each of 10 healthy volunteers up to 4 hours after they rubbed 1 mL of the gel between their volar wrists for 2 minutes. That’s the standard means of administering the medication, which is self-applied every 4-6 hours in clinical practice. A 1-mL dose contains 2 mg of lorazepam, 25 mg of diphenhydramine, and 2 mg of haloperidol compounded using a popular published formula.
Both lorazepam and haloperidol were undetectable in blood samples at all times in all 10 subjects; the medications never made it past the skin barrier. The highest concentration of diphenhydramine, reached in only a single patient, was 0.3 ng at 4 hours. That translates to 0.0003 mcg/mL, roughly 1/1000th of the therapeutic level, she noted.
The study was undertaken as a prelude to a planned single-center, randomized, placebo-controlled, crossover clinical trial of ABH gel in hospice patients with nausea. Dr. Fletcher and coinvestigators still plan to conduct that trial because ABH gel has never been subjected to a prospective controlled study.
"This is a wake-up call that we need further testing and evaluation before introducing treatments into widespread use," the physician declared.
Several audience members rose to applaud Dr. Fletcher for what they called a long-overdue rigorous look at an extremely popular yet unexamined therapy. One physician said he’d also like to see placebo-controlled studies of phenobarbital and dexamethasone for nausea, as these agents are widely prescribed but lacking in solid data supporting efficacy. He added that his own anecdotal experience with those two drugs as antiemetic agents in the hospice setting has been disappointing.
Dr. Fletcher reported having no financial conflicts.
DENVER – Compounded ABH gel is widely prescribed for treatment of nausea in the hospice setting. It costs less than $1 per dose. Side effects are rare. And many clinicians swear by its effectiveness, noting that the constituent medications in ABH gel – Ativan (lorazepam), Benadryl (diphenhydramine), and Haldol (haloperidol) – target different mechanisms of nausea.
There is, however, a fly in the ointment ... er, gel.
It turns out that none of the three medications in topical ABH gel are absorbed systemically in anything remotely approaching therapeutic levels, Dr. Devon S. Fletcher reported at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
"Either ABH gel doesn’t work, or the effect is attributable to placebo, or possibly a nonpharmacologic mechanism is involved, such as stimulation of the P6 acupressure point on the wrist as patients rub the gel in," said Dr. Fletcher of Virginia Commonwealth University, Richmond. "If ABH doesn’t work, using it to treat a symptom leads to unacceptable suffering and unnecessary hospitalizations," she added.
Dr. Fletcher and coworkers measured levels of the three medications contained in ABH gel in six blood samples taken serially in each of 10 healthy volunteers up to 4 hours after they rubbed 1 mL of the gel between their volar wrists for 2 minutes. That’s the standard means of administering the medication, which is self-applied every 4-6 hours in clinical practice. A 1-mL dose contains 2 mg of lorazepam, 25 mg of diphenhydramine, and 2 mg of haloperidol compounded using a popular published formula.
Both lorazepam and haloperidol were undetectable in blood samples at all times in all 10 subjects; the medications never made it past the skin barrier. The highest concentration of diphenhydramine, reached in only a single patient, was 0.3 ng at 4 hours. That translates to 0.0003 mcg/mL, roughly 1/1000th of the therapeutic level, she noted.
The study was undertaken as a prelude to a planned single-center, randomized, placebo-controlled, crossover clinical trial of ABH gel in hospice patients with nausea. Dr. Fletcher and coinvestigators still plan to conduct that trial because ABH gel has never been subjected to a prospective controlled study.
"This is a wake-up call that we need further testing and evaluation before introducing treatments into widespread use," the physician declared.
Several audience members rose to applaud Dr. Fletcher for what they called a long-overdue rigorous look at an extremely popular yet unexamined therapy. One physician said he’d also like to see placebo-controlled studies of phenobarbital and dexamethasone for nausea, as these agents are widely prescribed but lacking in solid data supporting efficacy. He added that his own anecdotal experience with those two drugs as antiemetic agents in the hospice setting has been disappointing.
Dr. Fletcher reported having no financial conflicts.
DENVER – Compounded ABH gel is widely prescribed for treatment of nausea in the hospice setting. It costs less than $1 per dose. Side effects are rare. And many clinicians swear by its effectiveness, noting that the constituent medications in ABH gel – Ativan (lorazepam), Benadryl (diphenhydramine), and Haldol (haloperidol) – target different mechanisms of nausea.
There is, however, a fly in the ointment ... er, gel.
It turns out that none of the three medications in topical ABH gel are absorbed systemically in anything remotely approaching therapeutic levels, Dr. Devon S. Fletcher reported at the annual meeting of the American Academy of Hospice and Palliative Care Medicine.
"Either ABH gel doesn’t work, or the effect is attributable to placebo, or possibly a nonpharmacologic mechanism is involved, such as stimulation of the P6 acupressure point on the wrist as patients rub the gel in," said Dr. Fletcher of Virginia Commonwealth University, Richmond. "If ABH doesn’t work, using it to treat a symptom leads to unacceptable suffering and unnecessary hospitalizations," she added.
Dr. Fletcher and coworkers measured levels of the three medications contained in ABH gel in six blood samples taken serially in each of 10 healthy volunteers up to 4 hours after they rubbed 1 mL of the gel between their volar wrists for 2 minutes. That’s the standard means of administering the medication, which is self-applied every 4-6 hours in clinical practice. A 1-mL dose contains 2 mg of lorazepam, 25 mg of diphenhydramine, and 2 mg of haloperidol compounded using a popular published formula.
Both lorazepam and haloperidol were undetectable in blood samples at all times in all 10 subjects; the medications never made it past the skin barrier. The highest concentration of diphenhydramine, reached in only a single patient, was 0.3 ng at 4 hours. That translates to 0.0003 mcg/mL, roughly 1/1000th of the therapeutic level, she noted.
The study was undertaken as a prelude to a planned single-center, randomized, placebo-controlled, crossover clinical trial of ABH gel in hospice patients with nausea. Dr. Fletcher and coinvestigators still plan to conduct that trial because ABH gel has never been subjected to a prospective controlled study.
"This is a wake-up call that we need further testing and evaluation before introducing treatments into widespread use," the physician declared.
Several audience members rose to applaud Dr. Fletcher for what they called a long-overdue rigorous look at an extremely popular yet unexamined therapy. One physician said he’d also like to see placebo-controlled studies of phenobarbital and dexamethasone for nausea, as these agents are widely prescribed but lacking in solid data supporting efficacy. He added that his own anecdotal experience with those two drugs as antiemetic agents in the hospice setting has been disappointing.
Dr. Fletcher reported having no financial conflicts.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN ACADEMY OF HOSPICE AND PALLIATIVE CARE MEDICINE
'Early, Proactive' Management of Chemo Toxicites Improves QOL
Skin conditions in cancer patients can lead to a decreased quality of life because of the psychosocial impact, financial burden, poor health, and disruption of anticancer treatments, said Dr. Mario E. Lacouture at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Clinical trials are underway to address management, cost, and quality of life, but in the meantime, "an early and proactive approach toward toxicities is advisable," he said.
Dr. Lacouture, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York, discussed common cancer-associated dermatology at the seminar.
• Rashes. A RAF inhibitor–induced rash can occur within 1-2 weeks of starting treatment, Dr. Lacouture noted. This rash is associated with sensations of burning or itching in photo-exposed areas. In most cases, the rash can be managed with topical steroids and oral GABA agonists. Vemurafenib use also has been associated with rashes, as well as with photosensitivity, itching, and alopecia, he said.
In addition, mTOR inhibitor–induced rashes involving erythematous pruritic papules and ulcerlike lesions have been observed in patients on everolimus and temsirolimus.
• Skin cancers. Data from several studies suggest that the incidence of squamous cell carcinomas in patients on RAF inhibitors is 7%, and the incidence of actinic keratoses in these patients is 4%, according to Dr. Lacouture. These conditions usually develop after approximately 6 months of treatment. They can be managed by surgery or destruction; and there have been no reports of metastases.

• Hand-foot syndrome. Hand-Foot Syndrome (HFSR) is a common side effect in cancer patients that usually occurs within 45 days of starting treatment, said Dr. Lacouture. HFSR is often associated with the use of sorafenib, sunitinib, and pazopanib, and the histology of these patients shows epidermal necrosis, he noted. Patients who develop HFSR may need to temporarily reduce their medications. Additional management of HFSR includes avoiding excess pressure on the affected areas and keeping them cool and moist to reduce patient discomfort.
• Hair and nail changes. Changes in hair can occur in patients being treated with epidermal growth factor receptor inhibitors (EGFRIs), including a slower hair growth rate and alopecia, Dr. Lacouture said. Changes in hair texture such as increased brittleness and hair curling also have been observed, he said. Other hair-related adverse events can include hirsutism on the face and eyelash trichomegaly. In addition, paronychia has been observed in patients on EGFRIs for more than 6 months.
• Radiation dermatitis. Approximately 50% of cancer patients develop radiation dermatitis, including 87% of breast cancer patients, reported Dr. Lacouture. However, the treatment of radiation dermatitis remains challenging, he said. In several studies, patients who used a nonsteroidal topical, including aloe vera and trolamine, showed no significant improvement in radiation dermatitis, compared with controls. However, studies are ongoing, and significant improvements in radiation dermatitis in breast cancer patients have been seen with topical corticosteroids including mometasone, beclomethasone, and betamethasone.
Dr. Lacouture disclosed financial relationships with multiple companies including Amgen, Bristol-Myers Squibb, Genentech, GlaxoSmithKline, Merck, and Roche. SDEF and this news organization are owned by Elsevier.
Skin conditions in cancer patients can lead to a decreased quality of life because of the psychosocial impact, financial burden, poor health, and disruption of anticancer treatments, said Dr. Mario E. Lacouture at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Clinical trials are underway to address management, cost, and quality of life, but in the meantime, "an early and proactive approach toward toxicities is advisable," he said.
Dr. Lacouture, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York, discussed common cancer-associated dermatology at the seminar.
• Rashes. A RAF inhibitor–induced rash can occur within 1-2 weeks of starting treatment, Dr. Lacouture noted. This rash is associated with sensations of burning or itching in photo-exposed areas. In most cases, the rash can be managed with topical steroids and oral GABA agonists. Vemurafenib use also has been associated with rashes, as well as with photosensitivity, itching, and alopecia, he said.
In addition, mTOR inhibitor–induced rashes involving erythematous pruritic papules and ulcerlike lesions have been observed in patients on everolimus and temsirolimus.
• Skin cancers. Data from several studies suggest that the incidence of squamous cell carcinomas in patients on RAF inhibitors is 7%, and the incidence of actinic keratoses in these patients is 4%, according to Dr. Lacouture. These conditions usually develop after approximately 6 months of treatment. They can be managed by surgery or destruction; and there have been no reports of metastases.
• Hand-foot syndrome. Hand-Foot Syndrome (HFSR) is a common side effect in cancer patients that usually occurs within 45 days of starting treatment, said Dr. Lacouture. HFSR is often associated with the use of sorafenib, sunitinib, and pazopanib, and the histology of these patients shows epidermal necrosis, he noted. Patients who develop HFSR may need to temporarily reduce their medications. Additional management of HFSR includes avoiding excess pressure on the affected areas and keeping them cool and moist to reduce patient discomfort.
• Hair and nail changes. Changes in hair can occur in patients being treated with epidermal growth factor receptor inhibitors (EGFRIs), including a slower hair growth rate and alopecia, Dr. Lacouture said. Changes in hair texture such as increased brittleness and hair curling also have been observed, he said. Other hair-related adverse events can include hirsutism on the face and eyelash trichomegaly. In addition, paronychia has been observed in patients on EGFRIs for more than 6 months.
• Radiation dermatitis. Approximately 50% of cancer patients develop radiation dermatitis, including 87% of breast cancer patients, reported Dr. Lacouture. However, the treatment of radiation dermatitis remains challenging, he said. In several studies, patients who used a nonsteroidal topical, including aloe vera and trolamine, showed no significant improvement in radiation dermatitis, compared with controls. However, studies are ongoing, and significant improvements in radiation dermatitis in breast cancer patients have been seen with topical corticosteroids including mometasone, beclomethasone, and betamethasone.
Dr. Lacouture disclosed financial relationships with multiple companies including Amgen, Bristol-Myers Squibb, Genentech, GlaxoSmithKline, Merck, and Roche. SDEF and this news organization are owned by Elsevier.
Skin conditions in cancer patients can lead to a decreased quality of life because of the psychosocial impact, financial burden, poor health, and disruption of anticancer treatments, said Dr. Mario E. Lacouture at the annual Hawaii Dermatology Seminar sponsored by Skin Disease Education Foundation (SDEF).
Clinical trials are underway to address management, cost, and quality of life, but in the meantime, "an early and proactive approach toward toxicities is advisable," he said.
Dr. Lacouture, a dermatologist at Memorial Sloan-Kettering Cancer Center in New York, discussed common cancer-associated dermatology at the seminar.
• Rashes. A RAF inhibitor–induced rash can occur within 1-2 weeks of starting treatment, Dr. Lacouture noted. This rash is associated with sensations of burning or itching in photo-exposed areas. In most cases, the rash can be managed with topical steroids and oral GABA agonists. Vemurafenib use also has been associated with rashes, as well as with photosensitivity, itching, and alopecia, he said.
In addition, mTOR inhibitor–induced rashes involving erythematous pruritic papules and ulcerlike lesions have been observed in patients on everolimus and temsirolimus.
• Skin cancers. Data from several studies suggest that the incidence of squamous cell carcinomas in patients on RAF inhibitors is 7%, and the incidence of actinic keratoses in these patients is 4%, according to Dr. Lacouture. These conditions usually develop after approximately 6 months of treatment. They can be managed by surgery or destruction; and there have been no reports of metastases.
• Hand-foot syndrome. Hand-Foot Syndrome (HFSR) is a common side effect in cancer patients that usually occurs within 45 days of starting treatment, said Dr. Lacouture. HFSR is often associated with the use of sorafenib, sunitinib, and pazopanib, and the histology of these patients shows epidermal necrosis, he noted. Patients who develop HFSR may need to temporarily reduce their medications. Additional management of HFSR includes avoiding excess pressure on the affected areas and keeping them cool and moist to reduce patient discomfort.
• Hair and nail changes. Changes in hair can occur in patients being treated with epidermal growth factor receptor inhibitors (EGFRIs), including a slower hair growth rate and alopecia, Dr. Lacouture said. Changes in hair texture such as increased brittleness and hair curling also have been observed, he said. Other hair-related adverse events can include hirsutism on the face and eyelash trichomegaly. In addition, paronychia has been observed in patients on EGFRIs for more than 6 months.
• Radiation dermatitis. Approximately 50% of cancer patients develop radiation dermatitis, including 87% of breast cancer patients, reported Dr. Lacouture. However, the treatment of radiation dermatitis remains challenging, he said. In several studies, patients who used a nonsteroidal topical, including aloe vera and trolamine, showed no significant improvement in radiation dermatitis, compared with controls. However, studies are ongoing, and significant improvements in radiation dermatitis in breast cancer patients have been seen with topical corticosteroids including mometasone, beclomethasone, and betamethasone.
Dr. Lacouture disclosed financial relationships with multiple companies including Amgen, Bristol-Myers Squibb, Genentech, GlaxoSmithKline, Merck, and Roche. SDEF and this news organization are owned by Elsevier.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR
Infrared Imaging Eyes Mucositis After Head & Neck Radiation
PHOENIX – Thermal imaging was able to detect small and early changes in the temperature of mucosal surfaces – a possible predictor of the development of mucositis – among 34 patients who were treated with chemoradiotherapy for locally advanced squamous cell carcinoma of the head and neck.
"Detection of these early changes using sensitive thermal imaging technology would allow identification of patients who will require more intensive supportive care," said Dr. Ezra Cohen, who presented the pilot study at the head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
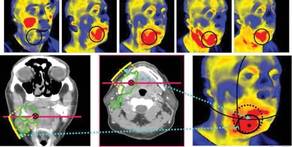
Radiotherapy-associated mucositis manifests initially as erythematous areas in the treatment field, which are accompanied by an intense inflammatory response histologically. Thus, Dr. Cohen and his associates had hypothesized that patients destined to display severe mucocutaneous toxicity would demonstrate greater alterations in thermal intensity early in therapy, compared with identically treated counterparts who do not subsequently develop the toxicity.
The researchers further hypothesized that they could measure those changes with infrared thermal imaging, a noninvasive technique that allows visualization and quantification of changes in skin or mucosal surface temperature.
The 34 patients (28 male, mean age 58 years) in the pilot study were treated with identical chemoradiotherapy regimens of 5-fluorouracil and hydroxyurea with a median radiation dose of 74 Gy for cancers of the oral cavity or oropharynx.
Using a portable device developed at Argonne National Laboratory in Illinois, the investigators conducted noninvasive baseline and weekly thermal imaging. The device detects infrared light naturally emitted from the skin or mucosal surface and generates an electrical signal, which is amplified and converted into digital data flow that is visualized in color on a monitor.
Grade 3 mucositis based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events v3.0 was observed in 53% of the patients, and dermatitis in 21%. All patients displayed an increase in temperature within the radiation field.
Investigators charted a statistically significant positive association between an early rise in temperature in oral mucous membranes when compared with a reference area and mucositis grade (P = .03). For every 1 C increase in temperature, compared with the reference (temperature near the medial angle of one eye), there was a 0.157 increase in average subsequent mucositis grade, reported Dr. Cohen, codirector of the head and neck cancer program at the University of Chicago.
Mucositis and its clinical sequelae are consistently reported as the most clinically significant acute toxicity in the treatment of locally advanced squamous cell carcinoma of the head and neck with chemoradiotherapy, according to Dr. Cohen, who also chaired the meeting. Patient to patient variability in mucositis is related to radiotherapy dosing, fractionation, and volumes, but there also appear to be individual differences in "normal tissue tolerance," even among patients on the same treatment regimen, he said.
"Larger studies with greater dynamic ranges in mucositis scoring are warranted to evaluate whether this tool can help predict which patients would be in need of early intervention to prevent acute complications," he said.
The study was funded by the National Institutes of Health and the University of Chicago Comprehensive Cancer Center. Dr. Cohen and his associates said they had no relevant financial disclosures.
PHOENIX – Thermal imaging was able to detect small and early changes in the temperature of mucosal surfaces – a possible predictor of the development of mucositis – among 34 patients who were treated with chemoradiotherapy for locally advanced squamous cell carcinoma of the head and neck.
"Detection of these early changes using sensitive thermal imaging technology would allow identification of patients who will require more intensive supportive care," said Dr. Ezra Cohen, who presented the pilot study at the head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
Radiotherapy-associated mucositis manifests initially as erythematous areas in the treatment field, which are accompanied by an intense inflammatory response histologically. Thus, Dr. Cohen and his associates had hypothesized that patients destined to display severe mucocutaneous toxicity would demonstrate greater alterations in thermal intensity early in therapy, compared with identically treated counterparts who do not subsequently develop the toxicity.
The researchers further hypothesized that they could measure those changes with infrared thermal imaging, a noninvasive technique that allows visualization and quantification of changes in skin or mucosal surface temperature.
The 34 patients (28 male, mean age 58 years) in the pilot study were treated with identical chemoradiotherapy regimens of 5-fluorouracil and hydroxyurea with a median radiation dose of 74 Gy for cancers of the oral cavity or oropharynx.
Using a portable device developed at Argonne National Laboratory in Illinois, the investigators conducted noninvasive baseline and weekly thermal imaging. The device detects infrared light naturally emitted from the skin or mucosal surface and generates an electrical signal, which is amplified and converted into digital data flow that is visualized in color on a monitor.
Grade 3 mucositis based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events v3.0 was observed in 53% of the patients, and dermatitis in 21%. All patients displayed an increase in temperature within the radiation field.
Investigators charted a statistically significant positive association between an early rise in temperature in oral mucous membranes when compared with a reference area and mucositis grade (P = .03). For every 1 C increase in temperature, compared with the reference (temperature near the medial angle of one eye), there was a 0.157 increase in average subsequent mucositis grade, reported Dr. Cohen, codirector of the head and neck cancer program at the University of Chicago.
Mucositis and its clinical sequelae are consistently reported as the most clinically significant acute toxicity in the treatment of locally advanced squamous cell carcinoma of the head and neck with chemoradiotherapy, according to Dr. Cohen, who also chaired the meeting. Patient to patient variability in mucositis is related to radiotherapy dosing, fractionation, and volumes, but there also appear to be individual differences in "normal tissue tolerance," even among patients on the same treatment regimen, he said.
"Larger studies with greater dynamic ranges in mucositis scoring are warranted to evaluate whether this tool can help predict which patients would be in need of early intervention to prevent acute complications," he said.
The study was funded by the National Institutes of Health and the University of Chicago Comprehensive Cancer Center. Dr. Cohen and his associates said they had no relevant financial disclosures.
PHOENIX – Thermal imaging was able to detect small and early changes in the temperature of mucosal surfaces – a possible predictor of the development of mucositis – among 34 patients who were treated with chemoradiotherapy for locally advanced squamous cell carcinoma of the head and neck.
"Detection of these early changes using sensitive thermal imaging technology would allow identification of patients who will require more intensive supportive care," said Dr. Ezra Cohen, who presented the pilot study at the head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
Radiotherapy-associated mucositis manifests initially as erythematous areas in the treatment field, which are accompanied by an intense inflammatory response histologically. Thus, Dr. Cohen and his associates had hypothesized that patients destined to display severe mucocutaneous toxicity would demonstrate greater alterations in thermal intensity early in therapy, compared with identically treated counterparts who do not subsequently develop the toxicity.
The researchers further hypothesized that they could measure those changes with infrared thermal imaging, a noninvasive technique that allows visualization and quantification of changes in skin or mucosal surface temperature.
The 34 patients (28 male, mean age 58 years) in the pilot study were treated with identical chemoradiotherapy regimens of 5-fluorouracil and hydroxyurea with a median radiation dose of 74 Gy for cancers of the oral cavity or oropharynx.
Using a portable device developed at Argonne National Laboratory in Illinois, the investigators conducted noninvasive baseline and weekly thermal imaging. The device detects infrared light naturally emitted from the skin or mucosal surface and generates an electrical signal, which is amplified and converted into digital data flow that is visualized in color on a monitor.
Grade 3 mucositis based on the National Cancer Institute’s Common Terminology Criteria for Adverse Events v3.0 was observed in 53% of the patients, and dermatitis in 21%. All patients displayed an increase in temperature within the radiation field.
Investigators charted a statistically significant positive association between an early rise in temperature in oral mucous membranes when compared with a reference area and mucositis grade (P = .03). For every 1 C increase in temperature, compared with the reference (temperature near the medial angle of one eye), there was a 0.157 increase in average subsequent mucositis grade, reported Dr. Cohen, codirector of the head and neck cancer program at the University of Chicago.
Mucositis and its clinical sequelae are consistently reported as the most clinically significant acute toxicity in the treatment of locally advanced squamous cell carcinoma of the head and neck with chemoradiotherapy, according to Dr. Cohen, who also chaired the meeting. Patient to patient variability in mucositis is related to radiotherapy dosing, fractionation, and volumes, but there also appear to be individual differences in "normal tissue tolerance," even among patients on the same treatment regimen, he said.
"Larger studies with greater dynamic ranges in mucositis scoring are warranted to evaluate whether this tool can help predict which patients would be in need of early intervention to prevent acute complications," he said.
The study was funded by the National Institutes of Health and the University of Chicago Comprehensive Cancer Center. Dr. Cohen and his associates said they had no relevant financial disclosures.
FROM A HEAD AND NECK CANCER SYMPOSIUM SPONSORED BY THE AMERICAN SOCIETY FOR RADIATION ONCOLOGY
Major Finding: For every 1 C increase in temperature, compared with the reference (temperature near the medial angle of one eye), there was a 0.157 increase in average subsequent mucositis.
Data Source: Data come from a pilot study of functional infrared imaging in 34 patients with locally advanced head and neck cancer who were treated with chemoradiotherapy.
Disclosures: The study was funded by the National Institutes of Health and the University of Chicago Comprehensive Cancer Center. Dr. Cohen and his associates said they had no relevant financial disclosures.
ASCO Urges Early Palliative Care in Metastatic Cancers
Compelling evidence from a recent randomized trial has prompted the American Society for Clinical Oncology to recommend that palliative care be integrated early on into standard cancer therapies for patients with metastatic cancers or a high burden of cancer symptoms.
Potentially practice changing, the opinion is based on the best currently available clinical evidence. Palliative care is typically relegated to the final days of life of patients with advanced metastatic cancers, as it is provided only after all other options have failed.
Authors of the opinion, intended to offer guidance to oncologists on this issue, cite a study published in 2010 (N. Engl. J. Med. 2010;363:733-42). The study showed that patients who were randomized to palliative care plus standard therapy for metastatic non–small cell lung cancer (NSCLC) had significantly longer overall survival than did patients randomized to standard care alone, (11.6 vs. 8.9 months, P = .02), even though the palliative care group had less aggressive end-of-life care.
Patients receiving palliative care also had significantly better quality of life scores on a standardized assessment scale, and significantly fewer had depressive symptoms, compared with patients on standard care.

"While a survival benefit from early involvement of palliative care has not yet been demonstrated in other oncology settings, substantial evidence demonstrates that palliative care – when combined with standard cancer care or as the main focus of care – leads to better patient and caregiver outcomes. These include improvement in symptoms, quality of life, and patient satisfaction, with reduced caregiver burden," wrote Dr. Thomas J. Smith and his colleagues in an American Society of Clinical Oncology (ASCO) provisional clinical opinion published online Feb. 6 in the Journal of Clinical Oncology (doi:10.1200/JCO.2011.38.5161).
Palliative care also eases patients and families through the anguish of dashed hopes and has the potential to reduce costs by limiting expensive but often futile intensive hospital-based services, the authors wrote.
"All the data suggest that there’s absolutely no harm from earlier integration of hospice and palliative medicine into patient care. A couple of trials have shown improved survival, and there are very good data from observational studies that people who use hospice actually live longer," Dr. Smith said in an interview. He is director of palliative care for Johns Hopkins University and Hopkins’ Sidney Kimmel Comprehensive Cancer Center in Baltimore.

"I think that ASCO is sending a really strong message to oncologists that we need to do more than we’re currently doing and that comprehensive cancer care needs to included supportive care on top of cancer-directed therapy," said Dr. Jennifer S. Temel, clinical director of thoracic oncology at Massachusetts General Hospital in Boston, and lead author of the randomized trial mentioned earlier.
She noted, however, that the study was not powered to detect an overall survival benefit. "All we were hoping for was that early palliative care didn’t lead to a survival detriment ... people could have been concerned that because of the involvement of palliative care, patients would receive less-intensive therapy and have shorter survival," Dr. Temel said. "I’m just very happy that’s not what we saw, but whether the survival benefit we saw was real and will be replicated, we'll have to wait and see."
The primary value of the study, she added, is that it demonstrated distinct benefits of palliative care on patient mood and quality of life.
The Will but Not the Way?
But many oncology practices, particularly those in community settings, may not have the resources to provide a full complement of palliative care services, said an oncologist in community-based practice.
"Those types of palliative care options are not widely available, and they certainly aren’t available in smaller communities," said Dr. Patrick Cobb, managing partner at the Frontier Cancer Center in Billings, Mont.

Services required for effective palliative care, such as patient and family counseling, are not typically reimbursed under current payments systems. In addition, palliative care reimbursement is often an "either/or" proposition: insurers pay for either therapeutic services or hospice care, but not both, said Dr. Cobb, former president of the Community Oncology Alliance.
He added that the so-called Stark law – actually a set of provisions in federal law governing the ability of clinicians to refer patients to clinical or diagnostic facilities in which the clinician has a financial interest – is another barrier to palliative care in the community, particularly in rural areas where the population may not be large enough to support separate palliative care facilities or programs.
Dr. Amy P. Abernethy, medical director of oncology quality, outcomes and patient-centered care in the Duke University Health System, Durham, N.C., and a coauthor of the ASCO provisional clinical opinion, agrees that there are multiple impediments to reimbursement of palliative care.
"The Stark law is one impediment; a second is that the reimbursement mechanisms that are clear in hospice aren’t necessarily as clear in community-based care, and then there are workforce issues. Right now, we have only a finite number of palliative care practitioners, and we only have a finite number of blocks in our graduate training programs, and we're not going to be able, using those slots, to train enough palliative care docs to fill the need that's highlighted in this provisional clinical opinion," she said.
Insurers, Younger Clinicians May Be Open to Change
Insurers seem to be coming around to the idea that palliative care can mean better patient care, however, said Dr Smith.
He points to Aetna, which has a "Compassionate Care" program in which specially trained triage nurses coordinate care, identify resources, and help manage palliative care and hospice benefits for patients with terminal illnesses and their families.
Clinicians in training or new to practice are also more comfortable with the idea of advance directives, palliative care, and hospice than are their more seasoned colleagues who were trained to never give up, Dr. Smith added.
Dr. Abernethy agreed: "What we’re seeing is that young physicians totally get this. Probably because they haven’t grown up in a world where the only thing you focus on is survival, they’ve understood the language of focusing on quality of life from the time they were first exposed to what medicine is," she said.
Randomized Trials Show Benefits, No Harm
In their provisional opinion, the researchers reviewed the study by Dr. Temel and her colleagues, as well as six other randomized controlled trials looking at palliative care in patients with various terminal illnesses; two of the seven total studies evaluated palliative care in cancer patients exclusively, whereas others included diagnoses such as heart failure and advanced chronic obstructive pulmonary disease.
They found that "overall, the addition of palliative care interventions to standard oncology care delivered via different models to patients with cancer provided evidence of benefit. No harm to any patient was observed in any trial, even with discussions of end-of-life planning, such as hospice and advance directives."
There were statistically significant improvements in symptoms with palliative care in 2 of 5 clinical trials that measured such changes, and improvements in quality-of-life measures in 2 of 5 trials. Additionally, in 2 of 3 trials palliative care was associated with improved satisfaction of patients and caregivers, the consensus panel found.
The studies also showed, to varying degrees, improvements in patient mood and a reduction in costs, in one study (J. Am. Geriatr. Soc. 2007;55:993-1000) from $20,222 for usual care to $12,670 for palliative care (P = .03), and in a second study (J. Palliat. Med. 2008;11:180-90) from a total mean of $21,252 for usual care to $14,486 for interdisciplinary palliative care (P less than .001). The latter study also found savings of nearly $5,000 per patient in staffing costs with palliative care.
"Therefore, most trials showed benefits ranging from equal to improved overall survival, reduced depression, improved caregiver and/or patient quality of life, and overall lower resource use and cost because end-of-life hospitalizations were avoided," the opinion authors wrote.
All physicians interviewed for this article reported that they did not have financial conflicts of interest.
Click here to see earlier coverage of this subject and a video of Dr. Temel discussing results of the randomized trial.
Compelling evidence from a recent randomized trial has prompted the American Society for Clinical Oncology to recommend that palliative care be integrated early on into standard cancer therapies for patients with metastatic cancers or a high burden of cancer symptoms.
Potentially practice changing, the opinion is based on the best currently available clinical evidence. Palliative care is typically relegated to the final days of life of patients with advanced metastatic cancers, as it is provided only after all other options have failed.
Authors of the opinion, intended to offer guidance to oncologists on this issue, cite a study published in 2010 (N. Engl. J. Med. 2010;363:733-42). The study showed that patients who were randomized to palliative care plus standard therapy for metastatic non–small cell lung cancer (NSCLC) had significantly longer overall survival than did patients randomized to standard care alone, (11.6 vs. 8.9 months, P = .02), even though the palliative care group had less aggressive end-of-life care.
Patients receiving palliative care also had significantly better quality of life scores on a standardized assessment scale, and significantly fewer had depressive symptoms, compared with patients on standard care.
"While a survival benefit from early involvement of palliative care has not yet been demonstrated in other oncology settings, substantial evidence demonstrates that palliative care – when combined with standard cancer care or as the main focus of care – leads to better patient and caregiver outcomes. These include improvement in symptoms, quality of life, and patient satisfaction, with reduced caregiver burden," wrote Dr. Thomas J. Smith and his colleagues in an American Society of Clinical Oncology (ASCO) provisional clinical opinion published online Feb. 6 in the Journal of Clinical Oncology (doi:10.1200/JCO.2011.38.5161).
Palliative care also eases patients and families through the anguish of dashed hopes and has the potential to reduce costs by limiting expensive but often futile intensive hospital-based services, the authors wrote.
"All the data suggest that there’s absolutely no harm from earlier integration of hospice and palliative medicine into patient care. A couple of trials have shown improved survival, and there are very good data from observational studies that people who use hospice actually live longer," Dr. Smith said in an interview. He is director of palliative care for Johns Hopkins University and Hopkins’ Sidney Kimmel Comprehensive Cancer Center in Baltimore.
"I think that ASCO is sending a really strong message to oncologists that we need to do more than we’re currently doing and that comprehensive cancer care needs to included supportive care on top of cancer-directed therapy," said Dr. Jennifer S. Temel, clinical director of thoracic oncology at Massachusetts General Hospital in Boston, and lead author of the randomized trial mentioned earlier.
She noted, however, that the study was not powered to detect an overall survival benefit. "All we were hoping for was that early palliative care didn’t lead to a survival detriment ... people could have been concerned that because of the involvement of palliative care, patients would receive less-intensive therapy and have shorter survival," Dr. Temel said. "I’m just very happy that’s not what we saw, but whether the survival benefit we saw was real and will be replicated, we'll have to wait and see."
The primary value of the study, she added, is that it demonstrated distinct benefits of palliative care on patient mood and quality of life.
The Will but Not the Way?
But many oncology practices, particularly those in community settings, may not have the resources to provide a full complement of palliative care services, said an oncologist in community-based practice.
"Those types of palliative care options are not widely available, and they certainly aren’t available in smaller communities," said Dr. Patrick Cobb, managing partner at the Frontier Cancer Center in Billings, Mont.
Services required for effective palliative care, such as patient and family counseling, are not typically reimbursed under current payments systems. In addition, palliative care reimbursement is often an "either/or" proposition: insurers pay for either therapeutic services or hospice care, but not both, said Dr. Cobb, former president of the Community Oncology Alliance.
He added that the so-called Stark law – actually a set of provisions in federal law governing the ability of clinicians to refer patients to clinical or diagnostic facilities in which the clinician has a financial interest – is another barrier to palliative care in the community, particularly in rural areas where the population may not be large enough to support separate palliative care facilities or programs.
Dr. Amy P. Abernethy, medical director of oncology quality, outcomes and patient-centered care in the Duke University Health System, Durham, N.C., and a coauthor of the ASCO provisional clinical opinion, agrees that there are multiple impediments to reimbursement of palliative care.
"The Stark law is one impediment; a second is that the reimbursement mechanisms that are clear in hospice aren’t necessarily as clear in community-based care, and then there are workforce issues. Right now, we have only a finite number of palliative care practitioners, and we only have a finite number of blocks in our graduate training programs, and we're not going to be able, using those slots, to train enough palliative care docs to fill the need that's highlighted in this provisional clinical opinion," she said.
Insurers, Younger Clinicians May Be Open to Change
Insurers seem to be coming around to the idea that palliative care can mean better patient care, however, said Dr Smith.
He points to Aetna, which has a "Compassionate Care" program in which specially trained triage nurses coordinate care, identify resources, and help manage palliative care and hospice benefits for patients with terminal illnesses and their families.
Clinicians in training or new to practice are also more comfortable with the idea of advance directives, palliative care, and hospice than are their more seasoned colleagues who were trained to never give up, Dr. Smith added.
Dr. Abernethy agreed: "What we’re seeing is that young physicians totally get this. Probably because they haven’t grown up in a world where the only thing you focus on is survival, they’ve understood the language of focusing on quality of life from the time they were first exposed to what medicine is," she said.
Randomized Trials Show Benefits, No Harm
In their provisional opinion, the researchers reviewed the study by Dr. Temel and her colleagues, as well as six other randomized controlled trials looking at palliative care in patients with various terminal illnesses; two of the seven total studies evaluated palliative care in cancer patients exclusively, whereas others included diagnoses such as heart failure and advanced chronic obstructive pulmonary disease.
They found that "overall, the addition of palliative care interventions to standard oncology care delivered via different models to patients with cancer provided evidence of benefit. No harm to any patient was observed in any trial, even with discussions of end-of-life planning, such as hospice and advance directives."
There were statistically significant improvements in symptoms with palliative care in 2 of 5 clinical trials that measured such changes, and improvements in quality-of-life measures in 2 of 5 trials. Additionally, in 2 of 3 trials palliative care was associated with improved satisfaction of patients and caregivers, the consensus panel found.
The studies also showed, to varying degrees, improvements in patient mood and a reduction in costs, in one study (J. Am. Geriatr. Soc. 2007;55:993-1000) from $20,222 for usual care to $12,670 for palliative care (P = .03), and in a second study (J. Palliat. Med. 2008;11:180-90) from a total mean of $21,252 for usual care to $14,486 for interdisciplinary palliative care (P less than .001). The latter study also found savings of nearly $5,000 per patient in staffing costs with palliative care.
"Therefore, most trials showed benefits ranging from equal to improved overall survival, reduced depression, improved caregiver and/or patient quality of life, and overall lower resource use and cost because end-of-life hospitalizations were avoided," the opinion authors wrote.
All physicians interviewed for this article reported that they did not have financial conflicts of interest.
Click here to see earlier coverage of this subject and a video of Dr. Temel discussing results of the randomized trial.
Compelling evidence from a recent randomized trial has prompted the American Society for Clinical Oncology to recommend that palliative care be integrated early on into standard cancer therapies for patients with metastatic cancers or a high burden of cancer symptoms.
Potentially practice changing, the opinion is based on the best currently available clinical evidence. Palliative care is typically relegated to the final days of life of patients with advanced metastatic cancers, as it is provided only after all other options have failed.
Authors of the opinion, intended to offer guidance to oncologists on this issue, cite a study published in 2010 (N. Engl. J. Med. 2010;363:733-42). The study showed that patients who were randomized to palliative care plus standard therapy for metastatic non–small cell lung cancer (NSCLC) had significantly longer overall survival than did patients randomized to standard care alone, (11.6 vs. 8.9 months, P = .02), even though the palliative care group had less aggressive end-of-life care.
Patients receiving palliative care also had significantly better quality of life scores on a standardized assessment scale, and significantly fewer had depressive symptoms, compared with patients on standard care.
"While a survival benefit from early involvement of palliative care has not yet been demonstrated in other oncology settings, substantial evidence demonstrates that palliative care – when combined with standard cancer care or as the main focus of care – leads to better patient and caregiver outcomes. These include improvement in symptoms, quality of life, and patient satisfaction, with reduced caregiver burden," wrote Dr. Thomas J. Smith and his colleagues in an American Society of Clinical Oncology (ASCO) provisional clinical opinion published online Feb. 6 in the Journal of Clinical Oncology (doi:10.1200/JCO.2011.38.5161).
Palliative care also eases patients and families through the anguish of dashed hopes and has the potential to reduce costs by limiting expensive but often futile intensive hospital-based services, the authors wrote.
"All the data suggest that there’s absolutely no harm from earlier integration of hospice and palliative medicine into patient care. A couple of trials have shown improved survival, and there are very good data from observational studies that people who use hospice actually live longer," Dr. Smith said in an interview. He is director of palliative care for Johns Hopkins University and Hopkins’ Sidney Kimmel Comprehensive Cancer Center in Baltimore.
"I think that ASCO is sending a really strong message to oncologists that we need to do more than we’re currently doing and that comprehensive cancer care needs to included supportive care on top of cancer-directed therapy," said Dr. Jennifer S. Temel, clinical director of thoracic oncology at Massachusetts General Hospital in Boston, and lead author of the randomized trial mentioned earlier.
She noted, however, that the study was not powered to detect an overall survival benefit. "All we were hoping for was that early palliative care didn’t lead to a survival detriment ... people could have been concerned that because of the involvement of palliative care, patients would receive less-intensive therapy and have shorter survival," Dr. Temel said. "I’m just very happy that’s not what we saw, but whether the survival benefit we saw was real and will be replicated, we'll have to wait and see."
The primary value of the study, she added, is that it demonstrated distinct benefits of palliative care on patient mood and quality of life.
The Will but Not the Way?
But many oncology practices, particularly those in community settings, may not have the resources to provide a full complement of palliative care services, said an oncologist in community-based practice.
"Those types of palliative care options are not widely available, and they certainly aren’t available in smaller communities," said Dr. Patrick Cobb, managing partner at the Frontier Cancer Center in Billings, Mont.
Services required for effective palliative care, such as patient and family counseling, are not typically reimbursed under current payments systems. In addition, palliative care reimbursement is often an "either/or" proposition: insurers pay for either therapeutic services or hospice care, but not both, said Dr. Cobb, former president of the Community Oncology Alliance.
He added that the so-called Stark law – actually a set of provisions in federal law governing the ability of clinicians to refer patients to clinical or diagnostic facilities in which the clinician has a financial interest – is another barrier to palliative care in the community, particularly in rural areas where the population may not be large enough to support separate palliative care facilities or programs.
Dr. Amy P. Abernethy, medical director of oncology quality, outcomes and patient-centered care in the Duke University Health System, Durham, N.C., and a coauthor of the ASCO provisional clinical opinion, agrees that there are multiple impediments to reimbursement of palliative care.
"The Stark law is one impediment; a second is that the reimbursement mechanisms that are clear in hospice aren’t necessarily as clear in community-based care, and then there are workforce issues. Right now, we have only a finite number of palliative care practitioners, and we only have a finite number of blocks in our graduate training programs, and we're not going to be able, using those slots, to train enough palliative care docs to fill the need that's highlighted in this provisional clinical opinion," she said.
Insurers, Younger Clinicians May Be Open to Change
Insurers seem to be coming around to the idea that palliative care can mean better patient care, however, said Dr Smith.
He points to Aetna, which has a "Compassionate Care" program in which specially trained triage nurses coordinate care, identify resources, and help manage palliative care and hospice benefits for patients with terminal illnesses and their families.
Clinicians in training or new to practice are also more comfortable with the idea of advance directives, palliative care, and hospice than are their more seasoned colleagues who were trained to never give up, Dr. Smith added.
Dr. Abernethy agreed: "What we’re seeing is that young physicians totally get this. Probably because they haven’t grown up in a world where the only thing you focus on is survival, they’ve understood the language of focusing on quality of life from the time they were first exposed to what medicine is," she said.
Randomized Trials Show Benefits, No Harm
In their provisional opinion, the researchers reviewed the study by Dr. Temel and her colleagues, as well as six other randomized controlled trials looking at palliative care in patients with various terminal illnesses; two of the seven total studies evaluated palliative care in cancer patients exclusively, whereas others included diagnoses such as heart failure and advanced chronic obstructive pulmonary disease.
They found that "overall, the addition of palliative care interventions to standard oncology care delivered via different models to patients with cancer provided evidence of benefit. No harm to any patient was observed in any trial, even with discussions of end-of-life planning, such as hospice and advance directives."
There were statistically significant improvements in symptoms with palliative care in 2 of 5 clinical trials that measured such changes, and improvements in quality-of-life measures in 2 of 5 trials. Additionally, in 2 of 3 trials palliative care was associated with improved satisfaction of patients and caregivers, the consensus panel found.
The studies also showed, to varying degrees, improvements in patient mood and a reduction in costs, in one study (J. Am. Geriatr. Soc. 2007;55:993-1000) from $20,222 for usual care to $12,670 for palliative care (P = .03), and in a second study (J. Palliat. Med. 2008;11:180-90) from a total mean of $21,252 for usual care to $14,486 for interdisciplinary palliative care (P less than .001). The latter study also found savings of nearly $5,000 per patient in staffing costs with palliative care.
"Therefore, most trials showed benefits ranging from equal to improved overall survival, reduced depression, improved caregiver and/or patient quality of life, and overall lower resource use and cost because end-of-life hospitalizations were avoided," the opinion authors wrote.
All physicians interviewed for this article reported that they did not have financial conflicts of interest.
Click here to see earlier coverage of this subject and a video of Dr. Temel discussing results of the randomized trial.
Hospitalist/Palliative-Care Collaboration Aims to Reduce Readmissions
A poster presented at the Center to Advance Palliative Care national seminar in San Diego in November described a growing collaboration between the HM service and the palliative-care team at a Wisconsin medical center as part of efforts to control readmissions using tools from SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions).
On admission to 227-bed Aurora West Allis (Wis.) Medical Center, all patients assigned to a hospitalist are assessed for readmission risk factors. If a risk factor is identified, the hospital has established a set of specific interventions, including a palliative-care consultation.
“Basically, we took the BOOST tools and developed a physician action plan behind those risk factors,” says Andrew McDonagh, MD, head of the center’s hospitalist service.
Dr. McDonagh started Aurora West Allis’ HM service in 2008, and Timothy Jessick, DO, initiated the palliative-care service in 2010. “As our programs grew together, it became apparent that there were significant synergies between the two specialties, so we took the opportunity to work together in several ways,” Dr. McDonagh says.
A Palliative Care Quality Indicators Checklist, which looks for four key clinical indicators, triggers hospitalists and unit nurses to order the palliative consult. If an elderly patient has multiple admissions for the same diagnosis, the second admission triggers a geriatric consultation, and the third admission gets a palliative-care consult.
Hospitalists at the medical center are given education and modeling on how to hold family conferences with patients and their families to elicit their goals of care. Collaboration between HM and palliative care is spreading to the hospital’s ICUs, to patients transitioning out of the hospital to nursing homes, and to two other Aurora hospitals in the Milwaukee area, Dr. McDonagh explains. Since the BOOST tools have been implemented, preliminary evidence points to reduced readmissions, increased patient satisfaction, and increased palliative-care consults at the hospital.
“In the future, doing our job well as hospitalists will be more than just addressing medical needs but tailoring our care plans to the individual patient. Palliative care helps us better define appropriate care for these patients, looking beyond the trees for the forest,” he says. “I believe I’m a better clinician for being part of this relationship.”
A poster presented at the Center to Advance Palliative Care national seminar in San Diego in November described a growing collaboration between the HM service and the palliative-care team at a Wisconsin medical center as part of efforts to control readmissions using tools from SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions).
On admission to 227-bed Aurora West Allis (Wis.) Medical Center, all patients assigned to a hospitalist are assessed for readmission risk factors. If a risk factor is identified, the hospital has established a set of specific interventions, including a palliative-care consultation.
“Basically, we took the BOOST tools and developed a physician action plan behind those risk factors,” says Andrew McDonagh, MD, head of the center’s hospitalist service.
Dr. McDonagh started Aurora West Allis’ HM service in 2008, and Timothy Jessick, DO, initiated the palliative-care service in 2010. “As our programs grew together, it became apparent that there were significant synergies between the two specialties, so we took the opportunity to work together in several ways,” Dr. McDonagh says.
A Palliative Care Quality Indicators Checklist, which looks for four key clinical indicators, triggers hospitalists and unit nurses to order the palliative consult. If an elderly patient has multiple admissions for the same diagnosis, the second admission triggers a geriatric consultation, and the third admission gets a palliative-care consult.
Hospitalists at the medical center are given education and modeling on how to hold family conferences with patients and their families to elicit their goals of care. Collaboration between HM and palliative care is spreading to the hospital’s ICUs, to patients transitioning out of the hospital to nursing homes, and to two other Aurora hospitals in the Milwaukee area, Dr. McDonagh explains. Since the BOOST tools have been implemented, preliminary evidence points to reduced readmissions, increased patient satisfaction, and increased palliative-care consults at the hospital.
“In the future, doing our job well as hospitalists will be more than just addressing medical needs but tailoring our care plans to the individual patient. Palliative care helps us better define appropriate care for these patients, looking beyond the trees for the forest,” he says. “I believe I’m a better clinician for being part of this relationship.”
A poster presented at the Center to Advance Palliative Care national seminar in San Diego in November described a growing collaboration between the HM service and the palliative-care team at a Wisconsin medical center as part of efforts to control readmissions using tools from SHM’s Project BOOST (Better Outcomes for Older Adults through Safe Transitions).
On admission to 227-bed Aurora West Allis (Wis.) Medical Center, all patients assigned to a hospitalist are assessed for readmission risk factors. If a risk factor is identified, the hospital has established a set of specific interventions, including a palliative-care consultation.
“Basically, we took the BOOST tools and developed a physician action plan behind those risk factors,” says Andrew McDonagh, MD, head of the center’s hospitalist service.
Dr. McDonagh started Aurora West Allis’ HM service in 2008, and Timothy Jessick, DO, initiated the palliative-care service in 2010. “As our programs grew together, it became apparent that there were significant synergies between the two specialties, so we took the opportunity to work together in several ways,” Dr. McDonagh says.
A Palliative Care Quality Indicators Checklist, which looks for four key clinical indicators, triggers hospitalists and unit nurses to order the palliative consult. If an elderly patient has multiple admissions for the same diagnosis, the second admission triggers a geriatric consultation, and the third admission gets a palliative-care consult.
Hospitalists at the medical center are given education and modeling on how to hold family conferences with patients and their families to elicit their goals of care. Collaboration between HM and palliative care is spreading to the hospital’s ICUs, to patients transitioning out of the hospital to nursing homes, and to two other Aurora hospitals in the Milwaukee area, Dr. McDonagh explains. Since the BOOST tools have been implemented, preliminary evidence points to reduced readmissions, increased patient satisfaction, and increased palliative-care consults at the hospital.
“In the future, doing our job well as hospitalists will be more than just addressing medical needs but tailoring our care plans to the individual patient. Palliative care helps us better define appropriate care for these patients, looking beyond the trees for the forest,” he says. “I believe I’m a better clinician for being part of this relationship.”
Palliative Care ‘Report Card’ Released
The Center to Advance Palliative Care recently issued its 2011 state-by-state report card, “America’s Care of Serious Illness”
(www.capc.org/reportcard), counting the proportion of each state’s hospitals with access to organized palliative-care programs. Eight states and the District of Columbia received “A” grades, as 80% of their acute-care hospitals also provided palliative-care services. Two states, Delaware and Mississippi, received “F” grades, as their hospitals hit only 20%.
The authors say palliative-care teams can reduce suffering and distress among patients with serious illnesses, regardless of age or disease state, improve communication, and reduce unwanted medical interventions. According to the most recent survey by the American Hospital Association, 1,894 U.S. hospitals have palliative-care programs, including 85% of those with 300 beds or more.
The Center to Advance Palliative Care recently issued its 2011 state-by-state report card, “America’s Care of Serious Illness”
(www.capc.org/reportcard), counting the proportion of each state’s hospitals with access to organized palliative-care programs. Eight states and the District of Columbia received “A” grades, as 80% of their acute-care hospitals also provided palliative-care services. Two states, Delaware and Mississippi, received “F” grades, as their hospitals hit only 20%.
The authors say palliative-care teams can reduce suffering and distress among patients with serious illnesses, regardless of age or disease state, improve communication, and reduce unwanted medical interventions. According to the most recent survey by the American Hospital Association, 1,894 U.S. hospitals have palliative-care programs, including 85% of those with 300 beds or more.
The Center to Advance Palliative Care recently issued its 2011 state-by-state report card, “America’s Care of Serious Illness”
(www.capc.org/reportcard), counting the proportion of each state’s hospitals with access to organized palliative-care programs. Eight states and the District of Columbia received “A” grades, as 80% of their acute-care hospitals also provided palliative-care services. Two states, Delaware and Mississippi, received “F” grades, as their hospitals hit only 20%.
The authors say palliative-care teams can reduce suffering and distress among patients with serious illnesses, regardless of age or disease state, improve communication, and reduce unwanted medical interventions. According to the most recent survey by the American Hospital Association, 1,894 U.S. hospitals have palliative-care programs, including 85% of those with 300 beds or more.
Think Smart to Improve the Safety of Patient-Controlled Analgesia
How often do errors with patient-controlled analgesia occur? More often than we know, research suggests.
Researchers who studied more than 900,000 medication record errors say that the 1% of errors related to patient-controlled analgesia (PCA) is probably just the tip of the iceberg. Although 1% may seem insignificant, this analysis was based on the voluntary medication error reporting, says lead researcher Rodney Hicks, Ph.D., who at that time of the study was manager, patient safety research and practice, U.S. Pharmacopeia.

"Although generalization of voluntary reported findings to the general population should be done cautiously," he points out, that "the general rule of thumb is that for every reported event, there can be between 300-1,000 unreported events."
This rule of thumb, based on 9,571 reported events, would mean that between 2.8 million and 9.6 million total events (unreported & reported) occurred over the 5-year period from July 1, 2000, to June 30, 2005. On an annualized basis, this would mean that about 600,000-2 million events/year could involve PCA.
These numbers are unacceptable in what should be an era of increasing patient safety. Says Dr. Hicks, "Further study would need to be done to ascertain the total number of PCA events, but the problem is extensive in my opinion." The picture is already pretty clear, but there is more to the data.
When the study looked at the number of events that caused harm, there were 624 records of PCA associated with harm, corresponding to 6.5% of the patients. Again, while 6.5% may seem small, as the study found, "By comparison, during the same period, only 1.5% of all other errors reported to MedMarx led to harm. This represents a fourfold higher relative risk of harm for PCA events."
"All health care disciplines were implicated in the errors, including physicians, pharmacists, and nurses" he said. "Therefore, it will take an interdisciplinary team to resolve the problems."

Dr. Hicks’ retrospective study of the magnitude, frequency, and nature of nonharmful and harmful medication errors associated with patient-controlled analgesia covered a 5-year review period with 919,241 medication errors records from 801 reporting health care facilities. The analysis was based on the international voluntary medication error reporting program, MedMarx. Dr. Hicks is now a professor a Western University College of Graduate Nursing, Pomona, Calif.
"Our analysis was in no means trying to discourage the use of PCA pumps. Many studies have shown the benefits of using PCA, including improved pain management, better utilization of nursing resources, increased patient satisfaction, and improved pulmonary function.
"However, this is clearly an indication that standardization needs to occur and organizations should invest in training and policies and procedures as well as equipment – all areas to promote safety."
Moreover, although elimination of error is critical, studies have shown even a correctly programmed PCA pump poses patient safety risks.

Appropriate doses of opiates can suppress respiration and decrease heart rate and blood pressure. Episodes of bradypnea and desaturation can escalate to respiratory depression requiring rescue, according to come via Ray Maddox, Pharm. D., of St. Joseph’s/Candler Health System and his colleagues, who studied an intravenous infusion safety initiative at the 644-bed, tertiary-care, magnet system to evaluate how "smart" technology can help avert high-risk adverse drug events and improve patient outcomes.
These investigators further point out that the success rate for in-hospital cardiopulmonary resuscitation remains less than one in five patients. If detected early, most cases of opioid-induced respiratory depression can be treated with naloxone. However, severe cases can be fatal. The risk of patient harm from medication errors with PCA pumps is 3.5 times the risk from any other type of medication administration error.
The researchers recommend the following: "Capnographic monitoring – measurements of ventilation using respiration and exhaled carbon dioxide – is particularly important because it can provide an earlier warning of respiratory depression than pulse oximetry in some patient populations."
In short, although there are many benefits to PCA usage, for improved patient safety, reduce the risks and monitor continuously to detect respiratory depression events.
With the desire to reduce errors and improve patient safety with the use of patient-controlled analgesia, a safety checklist is being developed by the Physician-Patient Alliance for Health and Safety. For more on this initiative, contact Michael Wong [email protected].
The Physician-Patient Alliance for Health & Safety is an advocacy group devoted to improving patient health and safety. PPAHS comprises physicians, patients, individuals, and organizations. PPAHS reports having no financial conflicts of interest and not having received funding or grants. It recently conducted a survey on the American Society of Anesthesiologists Standards & Anesthesia Patient Safety Foundation Recommendations, available online. PPAHS welcomes inquiries regarding financial assistance to implement the safety checklist initiative.
How often do errors with patient-controlled analgesia occur? More often than we know, research suggests.
Researchers who studied more than 900,000 medication record errors say that the 1% of errors related to patient-controlled analgesia (PCA) is probably just the tip of the iceberg. Although 1% may seem insignificant, this analysis was based on the voluntary medication error reporting, says lead researcher Rodney Hicks, Ph.D., who at that time of the study was manager, patient safety research and practice, U.S. Pharmacopeia.
"Although generalization of voluntary reported findings to the general population should be done cautiously," he points out, that "the general rule of thumb is that for every reported event, there can be between 300-1,000 unreported events."
This rule of thumb, based on 9,571 reported events, would mean that between 2.8 million and 9.6 million total events (unreported & reported) occurred over the 5-year period from July 1, 2000, to June 30, 2005. On an annualized basis, this would mean that about 600,000-2 million events/year could involve PCA.
These numbers are unacceptable in what should be an era of increasing patient safety. Says Dr. Hicks, "Further study would need to be done to ascertain the total number of PCA events, but the problem is extensive in my opinion." The picture is already pretty clear, but there is more to the data.
When the study looked at the number of events that caused harm, there were 624 records of PCA associated with harm, corresponding to 6.5% of the patients. Again, while 6.5% may seem small, as the study found, "By comparison, during the same period, only 1.5% of all other errors reported to MedMarx led to harm. This represents a fourfold higher relative risk of harm for PCA events."
"All health care disciplines were implicated in the errors, including physicians, pharmacists, and nurses" he said. "Therefore, it will take an interdisciplinary team to resolve the problems."
Dr. Hicks’ retrospective study of the magnitude, frequency, and nature of nonharmful and harmful medication errors associated with patient-controlled analgesia covered a 5-year review period with 919,241 medication errors records from 801 reporting health care facilities. The analysis was based on the international voluntary medication error reporting program, MedMarx. Dr. Hicks is now a professor a Western University College of Graduate Nursing, Pomona, Calif.
"Our analysis was in no means trying to discourage the use of PCA pumps. Many studies have shown the benefits of using PCA, including improved pain management, better utilization of nursing resources, increased patient satisfaction, and improved pulmonary function.
"However, this is clearly an indication that standardization needs to occur and organizations should invest in training and policies and procedures as well as equipment – all areas to promote safety."
Moreover, although elimination of error is critical, studies have shown even a correctly programmed PCA pump poses patient safety risks.
Appropriate doses of opiates can suppress respiration and decrease heart rate and blood pressure. Episodes of bradypnea and desaturation can escalate to respiratory depression requiring rescue, according to come via Ray Maddox, Pharm. D., of St. Joseph’s/Candler Health System and his colleagues, who studied an intravenous infusion safety initiative at the 644-bed, tertiary-care, magnet system to evaluate how "smart" technology can help avert high-risk adverse drug events and improve patient outcomes.
These investigators further point out that the success rate for in-hospital cardiopulmonary resuscitation remains less than one in five patients. If detected early, most cases of opioid-induced respiratory depression can be treated with naloxone. However, severe cases can be fatal. The risk of patient harm from medication errors with PCA pumps is 3.5 times the risk from any other type of medication administration error.
The researchers recommend the following: "Capnographic monitoring – measurements of ventilation using respiration and exhaled carbon dioxide – is particularly important because it can provide an earlier warning of respiratory depression than pulse oximetry in some patient populations."
In short, although there are many benefits to PCA usage, for improved patient safety, reduce the risks and monitor continuously to detect respiratory depression events.
With the desire to reduce errors and improve patient safety with the use of patient-controlled analgesia, a safety checklist is being developed by the Physician-Patient Alliance for Health and Safety. For more on this initiative, contact Michael Wong [email protected].
The Physician-Patient Alliance for Health & Safety is an advocacy group devoted to improving patient health and safety. PPAHS comprises physicians, patients, individuals, and organizations. PPAHS reports having no financial conflicts of interest and not having received funding or grants. It recently conducted a survey on the American Society of Anesthesiologists Standards & Anesthesia Patient Safety Foundation Recommendations, available online. PPAHS welcomes inquiries regarding financial assistance to implement the safety checklist initiative.
How often do errors with patient-controlled analgesia occur? More often than we know, research suggests.
Researchers who studied more than 900,000 medication record errors say that the 1% of errors related to patient-controlled analgesia (PCA) is probably just the tip of the iceberg. Although 1% may seem insignificant, this analysis was based on the voluntary medication error reporting, says lead researcher Rodney Hicks, Ph.D., who at that time of the study was manager, patient safety research and practice, U.S. Pharmacopeia.
"Although generalization of voluntary reported findings to the general population should be done cautiously," he points out, that "the general rule of thumb is that for every reported event, there can be between 300-1,000 unreported events."
This rule of thumb, based on 9,571 reported events, would mean that between 2.8 million and 9.6 million total events (unreported & reported) occurred over the 5-year period from July 1, 2000, to June 30, 2005. On an annualized basis, this would mean that about 600,000-2 million events/year could involve PCA.
These numbers are unacceptable in what should be an era of increasing patient safety. Says Dr. Hicks, "Further study would need to be done to ascertain the total number of PCA events, but the problem is extensive in my opinion." The picture is already pretty clear, but there is more to the data.
When the study looked at the number of events that caused harm, there were 624 records of PCA associated with harm, corresponding to 6.5% of the patients. Again, while 6.5% may seem small, as the study found, "By comparison, during the same period, only 1.5% of all other errors reported to MedMarx led to harm. This represents a fourfold higher relative risk of harm for PCA events."
"All health care disciplines were implicated in the errors, including physicians, pharmacists, and nurses" he said. "Therefore, it will take an interdisciplinary team to resolve the problems."
Dr. Hicks’ retrospective study of the magnitude, frequency, and nature of nonharmful and harmful medication errors associated with patient-controlled analgesia covered a 5-year review period with 919,241 medication errors records from 801 reporting health care facilities. The analysis was based on the international voluntary medication error reporting program, MedMarx. Dr. Hicks is now a professor a Western University College of Graduate Nursing, Pomona, Calif.
"Our analysis was in no means trying to discourage the use of PCA pumps. Many studies have shown the benefits of using PCA, including improved pain management, better utilization of nursing resources, increased patient satisfaction, and improved pulmonary function.
"However, this is clearly an indication that standardization needs to occur and organizations should invest in training and policies and procedures as well as equipment – all areas to promote safety."
Moreover, although elimination of error is critical, studies have shown even a correctly programmed PCA pump poses patient safety risks.
Appropriate doses of opiates can suppress respiration and decrease heart rate and blood pressure. Episodes of bradypnea and desaturation can escalate to respiratory depression requiring rescue, according to come via Ray Maddox, Pharm. D., of St. Joseph’s/Candler Health System and his colleagues, who studied an intravenous infusion safety initiative at the 644-bed, tertiary-care, magnet system to evaluate how "smart" technology can help avert high-risk adverse drug events and improve patient outcomes.
These investigators further point out that the success rate for in-hospital cardiopulmonary resuscitation remains less than one in five patients. If detected early, most cases of opioid-induced respiratory depression can be treated with naloxone. However, severe cases can be fatal. The risk of patient harm from medication errors with PCA pumps is 3.5 times the risk from any other type of medication administration error.
The researchers recommend the following: "Capnographic monitoring – measurements of ventilation using respiration and exhaled carbon dioxide – is particularly important because it can provide an earlier warning of respiratory depression than pulse oximetry in some patient populations."
In short, although there are many benefits to PCA usage, for improved patient safety, reduce the risks and monitor continuously to detect respiratory depression events.
With the desire to reduce errors and improve patient safety with the use of patient-controlled analgesia, a safety checklist is being developed by the Physician-Patient Alliance for Health and Safety. For more on this initiative, contact Michael Wong [email protected].
The Physician-Patient Alliance for Health & Safety is an advocacy group devoted to improving patient health and safety. PPAHS comprises physicians, patients, individuals, and organizations. PPAHS reports having no financial conflicts of interest and not having received funding or grants. It recently conducted a survey on the American Society of Anesthesiologists Standards & Anesthesia Patient Safety Foundation Recommendations, available online. PPAHS welcomes inquiries regarding financial assistance to implement the safety checklist initiative.
Discussing End-of-Life Planning with Patients
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Talking about end-of-life planning might not be so simple. Data suggests that patients want to know more about their prognosis, but sometimes physicians aren't sure how to bring up the discussion. Four supportive oncology experts discuss the importance and challenges of end-of-life planning during the 7th annual Chicago Supportive Oncology Conference.
Fostering Meaningful Communication at Life's End
HONOLULU – What do patients in the ICU want at the end of life?
Research has shown that pain control typically ranks at the top of the list, "but they also want to avoid inappropriate prolongation of dying," Dr. Richard Mularski said at the annual meeting of the American College of Chest Physicians.

Patients "want to achieve a sense of control at the end of life," continued Dr. Mularski, a pulmonologist who is a clinical investigator with the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore. "They don’t want to be a burden on their family. We have to offer professional help, which primarily comes from talking with our patients and providing opportunities to strengthen relationships with loved ones. This might mean backing off on sedatives and pain medications so that patients and loved ones can interact before withdrawal of life support."
Dr. Mularski highlighted four key points from a 2009 consensus statement he helped to create on pain management during the palliative and end-of-life experience in the ICU (Chest 2009;135:1360-9). The first point reads that all ICU patients "experience opportunities for discomfort and suffering regardless of prognosis or goals, thus palliative therapy is a requisite approach for every patient, of which pain management is a principal component."
According to the second, third, and fourth key points, "for those dying in the ICU, an explicit shift in management to comfort-oriented care is often warranted and may be the most beneficial treatment the health-care team can offer; communication and cultural sensitivity with the patient-family unit is a principal approach for optimizing palliative and pain management as part of comprehensive ICU care, [and] ethical and legal misconceptions about the escalation of opiates and other palliative therapies should not be barriers to appropriate care, provided the intention of treatment is alleviation of pain and suffering."
Communicating effectively with the patient and family about prognosis in the critical care setting can be difficult "because we’re often limited by what treatments or interventions we can make," Dr. Mularski said. "This creates a certain tension: Patients have a widespread and deeply held desire not to be dead. We have to try to focus on that desire and acknowledge our limitations. Data show we don’t really prognosticate when death will occur very well."
"For those dying in the ICU, an explicit shift in management to comfort-oriented care ... may be the most beneficial treatment the health-care team can offer."
The potential for limited treatment options is only part of the problem. A trial conducted in a university-affiliated ICU found that 54% of families fail to comprehend a diagnosis, a prognosis, or treatment options (Crit. Care Med. 2000;28:3044-9). "We also know that family members experience a fair amount of moderate to severe posttraumatic stress," Dr. Mularski added. "This stress is increased when we provide inadequate information. We have to be careful not to use phrases that suggest abandonment or a failure of medicine to care, such as ‘there’s nothing more we can do,’ or ‘we have nothing to offer.’ We have plenty to offer. Palliative care may be the most important thing we have to offer at the end of life."
Key factors in shared decision making between clinicians and families about end-of-life care include prognosis, level of certainty "which may not be there," and family preferences. "The role of the patient and family is to help us understand patient values and preferences, and for us as clinicians to indicate which treatments might be concurrent with those values and preferences," Dr. Mularski said.
In a 2008 article, "Practical Guidance for Evidence-Based ICU Family Conferences," Dr. J. Randall Curtis and Dr. Douglas B. White offered a five-step approach to improving communication in the ICU with families (Chest 2008;134:835-43). It centers on the mnemonic "VALUE," which stands for value family statements, acknowledge family emotions, listen to the family, understand the patient as a person, and elicit family questions.
At Kaiser Permanente Northwest, Dr. Mularski and his colleagues created pocket cards for critical care staff that contain the VALUE mnemonic to remind them of how to best interact with families of patients in the ICU. He also recommends the book by Dr. Anthony L. Back and colleagues, "Mastering Communication with Seriously Ill Patients: Balancing Honesty with Empathy and Hope" (New York: Cambridge University Press, 2009).
Dr. Mularski disclosed that he has received research funding from several agencies including the Agency for Healthcare Research and Quality, National Cancer Institute, National Quality Forum, and Robert Wood Johnson Foundation. He also has received research support from Novartis and Spiration for unrelated work in chronic obstructive pulmonary disorder.
HONOLULU – What do patients in the ICU want at the end of life?
Research has shown that pain control typically ranks at the top of the list, "but they also want to avoid inappropriate prolongation of dying," Dr. Richard Mularski said at the annual meeting of the American College of Chest Physicians.
Patients "want to achieve a sense of control at the end of life," continued Dr. Mularski, a pulmonologist who is a clinical investigator with the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore. "They don’t want to be a burden on their family. We have to offer professional help, which primarily comes from talking with our patients and providing opportunities to strengthen relationships with loved ones. This might mean backing off on sedatives and pain medications so that patients and loved ones can interact before withdrawal of life support."
Dr. Mularski highlighted four key points from a 2009 consensus statement he helped to create on pain management during the palliative and end-of-life experience in the ICU (Chest 2009;135:1360-9). The first point reads that all ICU patients "experience opportunities for discomfort and suffering regardless of prognosis or goals, thus palliative therapy is a requisite approach for every patient, of which pain management is a principal component."
According to the second, third, and fourth key points, "for those dying in the ICU, an explicit shift in management to comfort-oriented care is often warranted and may be the most beneficial treatment the health-care team can offer; communication and cultural sensitivity with the patient-family unit is a principal approach for optimizing palliative and pain management as part of comprehensive ICU care, [and] ethical and legal misconceptions about the escalation of opiates and other palliative therapies should not be barriers to appropriate care, provided the intention of treatment is alleviation of pain and suffering."
Communicating effectively with the patient and family about prognosis in the critical care setting can be difficult "because we’re often limited by what treatments or interventions we can make," Dr. Mularski said. "This creates a certain tension: Patients have a widespread and deeply held desire not to be dead. We have to try to focus on that desire and acknowledge our limitations. Data show we don’t really prognosticate when death will occur very well."
"For those dying in the ICU, an explicit shift in management to comfort-oriented care ... may be the most beneficial treatment the health-care team can offer."
The potential for limited treatment options is only part of the problem. A trial conducted in a university-affiliated ICU found that 54% of families fail to comprehend a diagnosis, a prognosis, or treatment options (Crit. Care Med. 2000;28:3044-9). "We also know that family members experience a fair amount of moderate to severe posttraumatic stress," Dr. Mularski added. "This stress is increased when we provide inadequate information. We have to be careful not to use phrases that suggest abandonment or a failure of medicine to care, such as ‘there’s nothing more we can do,’ or ‘we have nothing to offer.’ We have plenty to offer. Palliative care may be the most important thing we have to offer at the end of life."
Key factors in shared decision making between clinicians and families about end-of-life care include prognosis, level of certainty "which may not be there," and family preferences. "The role of the patient and family is to help us understand patient values and preferences, and for us as clinicians to indicate which treatments might be concurrent with those values and preferences," Dr. Mularski said.
In a 2008 article, "Practical Guidance for Evidence-Based ICU Family Conferences," Dr. J. Randall Curtis and Dr. Douglas B. White offered a five-step approach to improving communication in the ICU with families (Chest 2008;134:835-43). It centers on the mnemonic "VALUE," which stands for value family statements, acknowledge family emotions, listen to the family, understand the patient as a person, and elicit family questions.
At Kaiser Permanente Northwest, Dr. Mularski and his colleagues created pocket cards for critical care staff that contain the VALUE mnemonic to remind them of how to best interact with families of patients in the ICU. He also recommends the book by Dr. Anthony L. Back and colleagues, "Mastering Communication with Seriously Ill Patients: Balancing Honesty with Empathy and Hope" (New York: Cambridge University Press, 2009).
Dr. Mularski disclosed that he has received research funding from several agencies including the Agency for Healthcare Research and Quality, National Cancer Institute, National Quality Forum, and Robert Wood Johnson Foundation. He also has received research support from Novartis and Spiration for unrelated work in chronic obstructive pulmonary disorder.
HONOLULU – What do patients in the ICU want at the end of life?
Research has shown that pain control typically ranks at the top of the list, "but they also want to avoid inappropriate prolongation of dying," Dr. Richard Mularski said at the annual meeting of the American College of Chest Physicians.
Patients "want to achieve a sense of control at the end of life," continued Dr. Mularski, a pulmonologist who is a clinical investigator with the Center for Health Research at Kaiser Permanente Northwest, Portland, Ore. "They don’t want to be a burden on their family. We have to offer professional help, which primarily comes from talking with our patients and providing opportunities to strengthen relationships with loved ones. This might mean backing off on sedatives and pain medications so that patients and loved ones can interact before withdrawal of life support."
Dr. Mularski highlighted four key points from a 2009 consensus statement he helped to create on pain management during the palliative and end-of-life experience in the ICU (Chest 2009;135:1360-9). The first point reads that all ICU patients "experience opportunities for discomfort and suffering regardless of prognosis or goals, thus palliative therapy is a requisite approach for every patient, of which pain management is a principal component."
According to the second, third, and fourth key points, "for those dying in the ICU, an explicit shift in management to comfort-oriented care is often warranted and may be the most beneficial treatment the health-care team can offer; communication and cultural sensitivity with the patient-family unit is a principal approach for optimizing palliative and pain management as part of comprehensive ICU care, [and] ethical and legal misconceptions about the escalation of opiates and other palliative therapies should not be barriers to appropriate care, provided the intention of treatment is alleviation of pain and suffering."
Communicating effectively with the patient and family about prognosis in the critical care setting can be difficult "because we’re often limited by what treatments or interventions we can make," Dr. Mularski said. "This creates a certain tension: Patients have a widespread and deeply held desire not to be dead. We have to try to focus on that desire and acknowledge our limitations. Data show we don’t really prognosticate when death will occur very well."
"For those dying in the ICU, an explicit shift in management to comfort-oriented care ... may be the most beneficial treatment the health-care team can offer."
The potential for limited treatment options is only part of the problem. A trial conducted in a university-affiliated ICU found that 54% of families fail to comprehend a diagnosis, a prognosis, or treatment options (Crit. Care Med. 2000;28:3044-9). "We also know that family members experience a fair amount of moderate to severe posttraumatic stress," Dr. Mularski added. "This stress is increased when we provide inadequate information. We have to be careful not to use phrases that suggest abandonment or a failure of medicine to care, such as ‘there’s nothing more we can do,’ or ‘we have nothing to offer.’ We have plenty to offer. Palliative care may be the most important thing we have to offer at the end of life."
Key factors in shared decision making between clinicians and families about end-of-life care include prognosis, level of certainty "which may not be there," and family preferences. "The role of the patient and family is to help us understand patient values and preferences, and for us as clinicians to indicate which treatments might be concurrent with those values and preferences," Dr. Mularski said.
In a 2008 article, "Practical Guidance for Evidence-Based ICU Family Conferences," Dr. J. Randall Curtis and Dr. Douglas B. White offered a five-step approach to improving communication in the ICU with families (Chest 2008;134:835-43). It centers on the mnemonic "VALUE," which stands for value family statements, acknowledge family emotions, listen to the family, understand the patient as a person, and elicit family questions.
At Kaiser Permanente Northwest, Dr. Mularski and his colleagues created pocket cards for critical care staff that contain the VALUE mnemonic to remind them of how to best interact with families of patients in the ICU. He also recommends the book by Dr. Anthony L. Back and colleagues, "Mastering Communication with Seriously Ill Patients: Balancing Honesty with Empathy and Hope" (New York: Cambridge University Press, 2009).
Dr. Mularski disclosed that he has received research funding from several agencies including the Agency for Healthcare Research and Quality, National Cancer Institute, National Quality Forum, and Robert Wood Johnson Foundation. He also has received research support from Novartis and Spiration for unrelated work in chronic obstructive pulmonary disorder.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF CHEST PHYSICIANS