User login
One in six HIV PrEP Descovy switches contraindicated
George Froehle, PA, a primary care clinician at CentraCare in rural St. Cloud, Minn., has been prescribing the HIV prevention pill tenofovir disoproxil fumarate plus emtricitabine since it was marketed by the brand name Truvada and the Food and Drug Administration approved it in 2012. But recently, he’s been having conversations with patients about the new HIV prevention pill, tenofovir alafenamide plus emtricitabine (TAF/FTC, Descovy) as well.
“They may have a friend who has heard that Descovy is newer and safer,” Mr. Froehle said. But that’s not necessarily the case, at least according to lab values. A recent study in the journal Open Forum Infectious Diseases suggests that only between 1 in 10 and 1 in 3 switches to the new formulation of HIV pre-exposure prophylaxis (PrEP) are indicated by lab work – and that nearly half of people receiving a prescription for the new version had lab results actually contraindicating the switch.
This, combined with the lower cost of generic Truvada and the steep cost of Descovy, led study coauthor and HIV PrEP prescriber Douglas Krakower, MD, and colleagues to suggest that the generic version should be standard of care for all people on PrEP unless otherwise indicated.
This just “makes good sense,” Dr. Krakower, assistant professor of medicine at Harvard Medical School, Boston, told this news organization.
“It’s important to ultimately allow for patients and providers to have access to all of the PrEP options so they can choose the best option for each person,” he said. “But our data suggest that strategies to optimize the cost-effectiveness of PrEP prescribing, such as formulary interventions and education for patients and providers, could be beneficial – as long as there is an easy mechanism for patients and providers to override restrictions when there are clinical indications.”
Current PrEP guidelines from the Centers for Disease Control and Prevention don’t list a first-line or second-line treatment for PrEP. But recent guidance issued to insurance companies by the Biden administration specifically grants insurers permission to employ stepped formularies and cost sharing.
“Since the branded version of PrEP is not specified in the [U.S. Preventive Services Task Force] recommendation, plans and issuers may cover a generic version of PrEP without cost sharing and impose cost sharing on an equivalent branded version,” the rule, issued July 19, states. “However, plans and insurers must accommodate any individual for whom a particular PrEP medication [generic or brand name] would be medically inappropriate, as determined by the individual’s health care provider, by having a mechanism for waiving the otherwise applicable cost-sharing for the brand or nonpreferred brand version.”
Both drugs have been found to be 99% effective in stopping HIV acquisition in people at risk for it. Descovy is approved specifically for gay and bisexual men, transgender women, and anyone having anal sex. Ongoing studies are looking at the effectiveness of Descovy in people having vaginal sex. Generic Truvada has been approved for all people.
The biomarkers of switching
To be clear, both medicines are exceedingly safe, said lead author and epidemiologist Julia Marcus, PhD, MPH, associate professor at Harvard Medical School. Side effects have been mild and include nausea and diarrhea in the first month. What lab work tells clinicians is the potential for physiologic changes, but those changes don’t necessarily translate to clinical events.
“When I say harmful, I mean potentially harmful,” she said in an interview. “It’s really based on these incremental changes that maybe, in the long run, could be harmful.”
But she added that there are two types of damage from medicines: “There’s potential physiological damage, but there’s also potential financial damage.” While generic Truvada has a list price as low as $30 a bottle, Descovy has a list price of up to $2,000 a month. And the push for PrEP is growing. Recently, the head of the division of HIV/AIDS at the National Institute of Allergy and Infectious Diseases urged providers to get all their “HIV-negative, at-risk patients on PrEP tomorrow,” in light of the latest HIV vaccine failure.
So Dr. Marcus and team looked at data from the 2892 people who started taking PrEP in the year before the FDA approved Descovy in October 2019. Participants accessed PrEP through Fenway Health, a Boston-area health clinic serving a largely gay, lesbian, bisexual, transgender, and otherwise queer population, and the largest PrEP prescriber in New England. They then tracked which participants switched to Descovy and correlated the switches to lab work and CDC guidance for PrEP.
What they found was that just 11.9% of participants, or 343 people, switched to the newer formulation. That’s lower than the 27.2% who switched in nationally available data, which were released at a recent HIV conference. But when Dr. Krakower and colleagues looked at whether their PrEP prescriptions were appropriate based on the patients’ lab work, the findings were mixed.
On the one hand, they showed that 24 of those 343 people who switched to Descovy had creatinine clearance levels or bone mineral density measurements low enough to make the switch a good option. But that’s just 7% of all people who switched. They then ran a secondary model, in which they broadened the criteria for a switch from strictly those lab values to conditions that might indicate borderline kidney function, which could eventually lead to kidney damage. These included diagnoses of hypertension or diabetes, or borderline creatinine levels between 60 and 70 mL/minute.
“Even when we defined clinical indications as generously as we could, we still saw that only a minority had clinical indications for switching,” said “Most of the switching to TAF/FTC was potentially unnecessary, and some of it may have been harmful for people who had cardiovascular risk factors.”
That’s because although Descovy doesn’t affect renal and bone mineral markers, it does affect cholesterol levels and weight. Aftermarket and FDA data revealed a small but noticeable increase in statin use among people taking the new brand-name PrEP pill. When Marcus and colleagues looked for those biomarkers – total cholesterol greater than200, BMI of 30 or more, LDL cholesterol of more than 160 or HDL cholesterol of less than 40 – 14% of switches fit the criteria for contraindications for Descovy. That’s 10 times the rate of potential harm in switching as there was for those who stayed on the generic Truvada and would have been better served on Descovy. That came in at just 1.4%.
“There may be many reasons why patients or providers might choose to switch that we couldn’t document in our study,” she said. For instance, the newer formulation, Descovy, is a significantly smaller pill than the generic is. Or the perception of novelty might drive some switches.
“But I think we need qualitative work to understand how these decisions are being made,” she said in an interview. “It will be important to follow these patients to see what happens in terms of clinical outcomes.”
For his part, Mr. Froehle found the study intriguing. It reflects his own thinking around the value of the newer formulation. He also prescribes for people living with HIV. For them, the benefit of the new formulation of tenofovir present in Descovy has clear clinical relevance. After all, people living with HIV can be on their drug regimens for decades.
But people on PrEP aren’t likely to be on the pills as long, and so the real benefit of the newer, more expensive formulation is less clear. And he added that he’s already getting “pushback” from some insurance companies on the name-brand version, with companies asking for proof via lab values that a person has a history of kidney impairment or bone mineral density loss.
“It doesn’t happen a ton,” he said. “But it’s starting to happen, and normally it kind of builds from there.”
So when a patient comes in and asks specifically for Descovy, he usually will talk to them about it.
“If it’s what the patient wants and insurance covers it and it’s not unsafe for them to be on it, there might not be a reason to not prescribe Descovy,” said Mr. Froehle, who served as a sub-principal investigator for the DISCOVER clinical trial that showed the new PrEP was as effective as Truvada. “But now with Truvada being generic, we will talk about Truvada as being something we start up front because it may have a lower cost and it’s cheaper to the system. Then we can always switch to Descovy as needed.”
This study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Marcus reported receiving fees from Kaiser Permanente Northern California on a research grant from Gilead Sciences. Dr. Krakower reported having conducted research that was funded by Gilead Sciences and Merck, as well as honoraria for medical education content and presentations for Medscape Medical News, MED-IQ, and DKBMed and royalties from work conducted by UpToDate. Mr. Froehle reported receiving fees from Gilead Sciences in connection with a Gilead advisory board.
A version of this article first appeared on Medscape.com.
George Froehle, PA, a primary care clinician at CentraCare in rural St. Cloud, Minn., has been prescribing the HIV prevention pill tenofovir disoproxil fumarate plus emtricitabine since it was marketed by the brand name Truvada and the Food and Drug Administration approved it in 2012. But recently, he’s been having conversations with patients about the new HIV prevention pill, tenofovir alafenamide plus emtricitabine (TAF/FTC, Descovy) as well.
“They may have a friend who has heard that Descovy is newer and safer,” Mr. Froehle said. But that’s not necessarily the case, at least according to lab values. A recent study in the journal Open Forum Infectious Diseases suggests that only between 1 in 10 and 1 in 3 switches to the new formulation of HIV pre-exposure prophylaxis (PrEP) are indicated by lab work – and that nearly half of people receiving a prescription for the new version had lab results actually contraindicating the switch.
This, combined with the lower cost of generic Truvada and the steep cost of Descovy, led study coauthor and HIV PrEP prescriber Douglas Krakower, MD, and colleagues to suggest that the generic version should be standard of care for all people on PrEP unless otherwise indicated.
This just “makes good sense,” Dr. Krakower, assistant professor of medicine at Harvard Medical School, Boston, told this news organization.
“It’s important to ultimately allow for patients and providers to have access to all of the PrEP options so they can choose the best option for each person,” he said. “But our data suggest that strategies to optimize the cost-effectiveness of PrEP prescribing, such as formulary interventions and education for patients and providers, could be beneficial – as long as there is an easy mechanism for patients and providers to override restrictions when there are clinical indications.”
Current PrEP guidelines from the Centers for Disease Control and Prevention don’t list a first-line or second-line treatment for PrEP. But recent guidance issued to insurance companies by the Biden administration specifically grants insurers permission to employ stepped formularies and cost sharing.
“Since the branded version of PrEP is not specified in the [U.S. Preventive Services Task Force] recommendation, plans and issuers may cover a generic version of PrEP without cost sharing and impose cost sharing on an equivalent branded version,” the rule, issued July 19, states. “However, plans and insurers must accommodate any individual for whom a particular PrEP medication [generic or brand name] would be medically inappropriate, as determined by the individual’s health care provider, by having a mechanism for waiving the otherwise applicable cost-sharing for the brand or nonpreferred brand version.”
Both drugs have been found to be 99% effective in stopping HIV acquisition in people at risk for it. Descovy is approved specifically for gay and bisexual men, transgender women, and anyone having anal sex. Ongoing studies are looking at the effectiveness of Descovy in people having vaginal sex. Generic Truvada has been approved for all people.
The biomarkers of switching
To be clear, both medicines are exceedingly safe, said lead author and epidemiologist Julia Marcus, PhD, MPH, associate professor at Harvard Medical School. Side effects have been mild and include nausea and diarrhea in the first month. What lab work tells clinicians is the potential for physiologic changes, but those changes don’t necessarily translate to clinical events.
“When I say harmful, I mean potentially harmful,” she said in an interview. “It’s really based on these incremental changes that maybe, in the long run, could be harmful.”
But she added that there are two types of damage from medicines: “There’s potential physiological damage, but there’s also potential financial damage.” While generic Truvada has a list price as low as $30 a bottle, Descovy has a list price of up to $2,000 a month. And the push for PrEP is growing. Recently, the head of the division of HIV/AIDS at the National Institute of Allergy and Infectious Diseases urged providers to get all their “HIV-negative, at-risk patients on PrEP tomorrow,” in light of the latest HIV vaccine failure.
So Dr. Marcus and team looked at data from the 2892 people who started taking PrEP in the year before the FDA approved Descovy in October 2019. Participants accessed PrEP through Fenway Health, a Boston-area health clinic serving a largely gay, lesbian, bisexual, transgender, and otherwise queer population, and the largest PrEP prescriber in New England. They then tracked which participants switched to Descovy and correlated the switches to lab work and CDC guidance for PrEP.
What they found was that just 11.9% of participants, or 343 people, switched to the newer formulation. That’s lower than the 27.2% who switched in nationally available data, which were released at a recent HIV conference. But when Dr. Krakower and colleagues looked at whether their PrEP prescriptions were appropriate based on the patients’ lab work, the findings were mixed.
On the one hand, they showed that 24 of those 343 people who switched to Descovy had creatinine clearance levels or bone mineral density measurements low enough to make the switch a good option. But that’s just 7% of all people who switched. They then ran a secondary model, in which they broadened the criteria for a switch from strictly those lab values to conditions that might indicate borderline kidney function, which could eventually lead to kidney damage. These included diagnoses of hypertension or diabetes, or borderline creatinine levels between 60 and 70 mL/minute.
“Even when we defined clinical indications as generously as we could, we still saw that only a minority had clinical indications for switching,” said “Most of the switching to TAF/FTC was potentially unnecessary, and some of it may have been harmful for people who had cardiovascular risk factors.”
That’s because although Descovy doesn’t affect renal and bone mineral markers, it does affect cholesterol levels and weight. Aftermarket and FDA data revealed a small but noticeable increase in statin use among people taking the new brand-name PrEP pill. When Marcus and colleagues looked for those biomarkers – total cholesterol greater than200, BMI of 30 or more, LDL cholesterol of more than 160 or HDL cholesterol of less than 40 – 14% of switches fit the criteria for contraindications for Descovy. That’s 10 times the rate of potential harm in switching as there was for those who stayed on the generic Truvada and would have been better served on Descovy. That came in at just 1.4%.
“There may be many reasons why patients or providers might choose to switch that we couldn’t document in our study,” she said. For instance, the newer formulation, Descovy, is a significantly smaller pill than the generic is. Or the perception of novelty might drive some switches.
“But I think we need qualitative work to understand how these decisions are being made,” she said in an interview. “It will be important to follow these patients to see what happens in terms of clinical outcomes.”
For his part, Mr. Froehle found the study intriguing. It reflects his own thinking around the value of the newer formulation. He also prescribes for people living with HIV. For them, the benefit of the new formulation of tenofovir present in Descovy has clear clinical relevance. After all, people living with HIV can be on their drug regimens for decades.
But people on PrEP aren’t likely to be on the pills as long, and so the real benefit of the newer, more expensive formulation is less clear. And he added that he’s already getting “pushback” from some insurance companies on the name-brand version, with companies asking for proof via lab values that a person has a history of kidney impairment or bone mineral density loss.
“It doesn’t happen a ton,” he said. “But it’s starting to happen, and normally it kind of builds from there.”
So when a patient comes in and asks specifically for Descovy, he usually will talk to them about it.
“If it’s what the patient wants and insurance covers it and it’s not unsafe for them to be on it, there might not be a reason to not prescribe Descovy,” said Mr. Froehle, who served as a sub-principal investigator for the DISCOVER clinical trial that showed the new PrEP was as effective as Truvada. “But now with Truvada being generic, we will talk about Truvada as being something we start up front because it may have a lower cost and it’s cheaper to the system. Then we can always switch to Descovy as needed.”
This study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Marcus reported receiving fees from Kaiser Permanente Northern California on a research grant from Gilead Sciences. Dr. Krakower reported having conducted research that was funded by Gilead Sciences and Merck, as well as honoraria for medical education content and presentations for Medscape Medical News, MED-IQ, and DKBMed and royalties from work conducted by UpToDate. Mr. Froehle reported receiving fees from Gilead Sciences in connection with a Gilead advisory board.
A version of this article first appeared on Medscape.com.
George Froehle, PA, a primary care clinician at CentraCare in rural St. Cloud, Minn., has been prescribing the HIV prevention pill tenofovir disoproxil fumarate plus emtricitabine since it was marketed by the brand name Truvada and the Food and Drug Administration approved it in 2012. But recently, he’s been having conversations with patients about the new HIV prevention pill, tenofovir alafenamide plus emtricitabine (TAF/FTC, Descovy) as well.
“They may have a friend who has heard that Descovy is newer and safer,” Mr. Froehle said. But that’s not necessarily the case, at least according to lab values. A recent study in the journal Open Forum Infectious Diseases suggests that only between 1 in 10 and 1 in 3 switches to the new formulation of HIV pre-exposure prophylaxis (PrEP) are indicated by lab work – and that nearly half of people receiving a prescription for the new version had lab results actually contraindicating the switch.
This, combined with the lower cost of generic Truvada and the steep cost of Descovy, led study coauthor and HIV PrEP prescriber Douglas Krakower, MD, and colleagues to suggest that the generic version should be standard of care for all people on PrEP unless otherwise indicated.
This just “makes good sense,” Dr. Krakower, assistant professor of medicine at Harvard Medical School, Boston, told this news organization.
“It’s important to ultimately allow for patients and providers to have access to all of the PrEP options so they can choose the best option for each person,” he said. “But our data suggest that strategies to optimize the cost-effectiveness of PrEP prescribing, such as formulary interventions and education for patients and providers, could be beneficial – as long as there is an easy mechanism for patients and providers to override restrictions when there are clinical indications.”
Current PrEP guidelines from the Centers for Disease Control and Prevention don’t list a first-line or second-line treatment for PrEP. But recent guidance issued to insurance companies by the Biden administration specifically grants insurers permission to employ stepped formularies and cost sharing.
“Since the branded version of PrEP is not specified in the [U.S. Preventive Services Task Force] recommendation, plans and issuers may cover a generic version of PrEP without cost sharing and impose cost sharing on an equivalent branded version,” the rule, issued July 19, states. “However, plans and insurers must accommodate any individual for whom a particular PrEP medication [generic or brand name] would be medically inappropriate, as determined by the individual’s health care provider, by having a mechanism for waiving the otherwise applicable cost-sharing for the brand or nonpreferred brand version.”
Both drugs have been found to be 99% effective in stopping HIV acquisition in people at risk for it. Descovy is approved specifically for gay and bisexual men, transgender women, and anyone having anal sex. Ongoing studies are looking at the effectiveness of Descovy in people having vaginal sex. Generic Truvada has been approved for all people.
The biomarkers of switching
To be clear, both medicines are exceedingly safe, said lead author and epidemiologist Julia Marcus, PhD, MPH, associate professor at Harvard Medical School. Side effects have been mild and include nausea and diarrhea in the first month. What lab work tells clinicians is the potential for physiologic changes, but those changes don’t necessarily translate to clinical events.
“When I say harmful, I mean potentially harmful,” she said in an interview. “It’s really based on these incremental changes that maybe, in the long run, could be harmful.”
But she added that there are two types of damage from medicines: “There’s potential physiological damage, but there’s also potential financial damage.” While generic Truvada has a list price as low as $30 a bottle, Descovy has a list price of up to $2,000 a month. And the push for PrEP is growing. Recently, the head of the division of HIV/AIDS at the National Institute of Allergy and Infectious Diseases urged providers to get all their “HIV-negative, at-risk patients on PrEP tomorrow,” in light of the latest HIV vaccine failure.
So Dr. Marcus and team looked at data from the 2892 people who started taking PrEP in the year before the FDA approved Descovy in October 2019. Participants accessed PrEP through Fenway Health, a Boston-area health clinic serving a largely gay, lesbian, bisexual, transgender, and otherwise queer population, and the largest PrEP prescriber in New England. They then tracked which participants switched to Descovy and correlated the switches to lab work and CDC guidance for PrEP.
What they found was that just 11.9% of participants, or 343 people, switched to the newer formulation. That’s lower than the 27.2% who switched in nationally available data, which were released at a recent HIV conference. But when Dr. Krakower and colleagues looked at whether their PrEP prescriptions were appropriate based on the patients’ lab work, the findings were mixed.
On the one hand, they showed that 24 of those 343 people who switched to Descovy had creatinine clearance levels or bone mineral density measurements low enough to make the switch a good option. But that’s just 7% of all people who switched. They then ran a secondary model, in which they broadened the criteria for a switch from strictly those lab values to conditions that might indicate borderline kidney function, which could eventually lead to kidney damage. These included diagnoses of hypertension or diabetes, or borderline creatinine levels between 60 and 70 mL/minute.
“Even when we defined clinical indications as generously as we could, we still saw that only a minority had clinical indications for switching,” said “Most of the switching to TAF/FTC was potentially unnecessary, and some of it may have been harmful for people who had cardiovascular risk factors.”
That’s because although Descovy doesn’t affect renal and bone mineral markers, it does affect cholesterol levels and weight. Aftermarket and FDA data revealed a small but noticeable increase in statin use among people taking the new brand-name PrEP pill. When Marcus and colleagues looked for those biomarkers – total cholesterol greater than200, BMI of 30 or more, LDL cholesterol of more than 160 or HDL cholesterol of less than 40 – 14% of switches fit the criteria for contraindications for Descovy. That’s 10 times the rate of potential harm in switching as there was for those who stayed on the generic Truvada and would have been better served on Descovy. That came in at just 1.4%.
“There may be many reasons why patients or providers might choose to switch that we couldn’t document in our study,” she said. For instance, the newer formulation, Descovy, is a significantly smaller pill than the generic is. Or the perception of novelty might drive some switches.
“But I think we need qualitative work to understand how these decisions are being made,” she said in an interview. “It will be important to follow these patients to see what happens in terms of clinical outcomes.”
For his part, Mr. Froehle found the study intriguing. It reflects his own thinking around the value of the newer formulation. He also prescribes for people living with HIV. For them, the benefit of the new formulation of tenofovir present in Descovy has clear clinical relevance. After all, people living with HIV can be on their drug regimens for decades.
But people on PrEP aren’t likely to be on the pills as long, and so the real benefit of the newer, more expensive formulation is less clear. And he added that he’s already getting “pushback” from some insurance companies on the name-brand version, with companies asking for proof via lab values that a person has a history of kidney impairment or bone mineral density loss.
“It doesn’t happen a ton,” he said. “But it’s starting to happen, and normally it kind of builds from there.”
So when a patient comes in and asks specifically for Descovy, he usually will talk to them about it.
“If it’s what the patient wants and insurance covers it and it’s not unsafe for them to be on it, there might not be a reason to not prescribe Descovy,” said Mr. Froehle, who served as a sub-principal investigator for the DISCOVER clinical trial that showed the new PrEP was as effective as Truvada. “But now with Truvada being generic, we will talk about Truvada as being something we start up front because it may have a lower cost and it’s cheaper to the system. Then we can always switch to Descovy as needed.”
This study was funded by the National Institute of Allergy and Infectious Diseases. Dr. Marcus reported receiving fees from Kaiser Permanente Northern California on a research grant from Gilead Sciences. Dr. Krakower reported having conducted research that was funded by Gilead Sciences and Merck, as well as honoraria for medical education content and presentations for Medscape Medical News, MED-IQ, and DKBMed and royalties from work conducted by UpToDate. Mr. Froehle reported receiving fees from Gilead Sciences in connection with a Gilead advisory board.
A version of this article first appeared on Medscape.com.
New virus causing ‘Alaskapox’ detected in two more cases
Both people were diagnosed after receiving urgent care in a Fairbanks-area clinic. One was a child with a sore on the left elbow, along with fever and swollen lymph nodes. And the other was an unrelated middle-aged woman with a pox mark on her leg, swollen lymph nodes, and joint pain. In both cases, symptoms improved within 3 weeks.
This isn’t the first time the so-called Alaskapox virus has been detected in the region. In 2015, a woman living near Fairbanks turned up at her doctor’s office with a single reddened pox-like mark on her upper arm and a feeling of fatigue.
Sampling of the pox mark showed that it was caused by a previously unidentified virus of the same family as smallpox and cowpox.
Five years later, another woman showed up with similar signs and symptoms, and her pox also proved to be the result of what public health experts started calling the Alaskapox virus.
In both cases, the women recovered completely.
Smallpox-like illness
Public health sleuths figured out that in three of the four cases, the patients lived in a home with a cat or cats, and one of these cats was known to hunt small animals.
Experts already knew that cats mingling in cow pastures and sickened by cattle virus had helped cowpox make the leap from bovines to humans. And just as in the case of cowpox, they suspected that cats might again be spreading this new virus to people, too.
All four of the infected people lived in sparsely populated areas amid forests. Officials laid animal traps where some of the affected people lived and identified the virus in several species of small wild animals.
The animals that turned up most often with Alaskapox were small mouse-like voles. The rodents with rounded muzzles are known for burrowing in the region. And scientists suspect the Alaskapox virus makes its way from these wild animals to humans through their pet cats or possibly by direct exposure outdoors.
None of the four people identified so far with Alaskapox knew each other or interacted, so officials also suspect that there are more cases going unrecognized, possibly because the symptoms are mild or nonexistent.
There are no documented cases of person-to-person transmission of Alaskapox, according to public health officials monitoring the small number of cases. But other pox viruses can spread by direct contact with skin lesions, so clinicians are recommending that people cover wounds with bandages. Three of the people with Alaskapox mistook their lesions at first for a bite from a spider or insect.
A version of this article first appeared on WebMD.com.
Both people were diagnosed after receiving urgent care in a Fairbanks-area clinic. One was a child with a sore on the left elbow, along with fever and swollen lymph nodes. And the other was an unrelated middle-aged woman with a pox mark on her leg, swollen lymph nodes, and joint pain. In both cases, symptoms improved within 3 weeks.
This isn’t the first time the so-called Alaskapox virus has been detected in the region. In 2015, a woman living near Fairbanks turned up at her doctor’s office with a single reddened pox-like mark on her upper arm and a feeling of fatigue.
Sampling of the pox mark showed that it was caused by a previously unidentified virus of the same family as smallpox and cowpox.
Five years later, another woman showed up with similar signs and symptoms, and her pox also proved to be the result of what public health experts started calling the Alaskapox virus.
In both cases, the women recovered completely.
Smallpox-like illness
Public health sleuths figured out that in three of the four cases, the patients lived in a home with a cat or cats, and one of these cats was known to hunt small animals.
Experts already knew that cats mingling in cow pastures and sickened by cattle virus had helped cowpox make the leap from bovines to humans. And just as in the case of cowpox, they suspected that cats might again be spreading this new virus to people, too.
All four of the infected people lived in sparsely populated areas amid forests. Officials laid animal traps where some of the affected people lived and identified the virus in several species of small wild animals.
The animals that turned up most often with Alaskapox were small mouse-like voles. The rodents with rounded muzzles are known for burrowing in the region. And scientists suspect the Alaskapox virus makes its way from these wild animals to humans through their pet cats or possibly by direct exposure outdoors.
None of the four people identified so far with Alaskapox knew each other or interacted, so officials also suspect that there are more cases going unrecognized, possibly because the symptoms are mild or nonexistent.
There are no documented cases of person-to-person transmission of Alaskapox, according to public health officials monitoring the small number of cases. But other pox viruses can spread by direct contact with skin lesions, so clinicians are recommending that people cover wounds with bandages. Three of the people with Alaskapox mistook their lesions at first for a bite from a spider or insect.
A version of this article first appeared on WebMD.com.
Both people were diagnosed after receiving urgent care in a Fairbanks-area clinic. One was a child with a sore on the left elbow, along with fever and swollen lymph nodes. And the other was an unrelated middle-aged woman with a pox mark on her leg, swollen lymph nodes, and joint pain. In both cases, symptoms improved within 3 weeks.
This isn’t the first time the so-called Alaskapox virus has been detected in the region. In 2015, a woman living near Fairbanks turned up at her doctor’s office with a single reddened pox-like mark on her upper arm and a feeling of fatigue.
Sampling of the pox mark showed that it was caused by a previously unidentified virus of the same family as smallpox and cowpox.
Five years later, another woman showed up with similar signs and symptoms, and her pox also proved to be the result of what public health experts started calling the Alaskapox virus.
In both cases, the women recovered completely.
Smallpox-like illness
Public health sleuths figured out that in three of the four cases, the patients lived in a home with a cat or cats, and one of these cats was known to hunt small animals.
Experts already knew that cats mingling in cow pastures and sickened by cattle virus had helped cowpox make the leap from bovines to humans. And just as in the case of cowpox, they suspected that cats might again be spreading this new virus to people, too.
All four of the infected people lived in sparsely populated areas amid forests. Officials laid animal traps where some of the affected people lived and identified the virus in several species of small wild animals.
The animals that turned up most often with Alaskapox were small mouse-like voles. The rodents with rounded muzzles are known for burrowing in the region. And scientists suspect the Alaskapox virus makes its way from these wild animals to humans through their pet cats or possibly by direct exposure outdoors.
None of the four people identified so far with Alaskapox knew each other or interacted, so officials also suspect that there are more cases going unrecognized, possibly because the symptoms are mild or nonexistent.
There are no documented cases of person-to-person transmission of Alaskapox, according to public health officials monitoring the small number of cases. But other pox viruses can spread by direct contact with skin lesions, so clinicians are recommending that people cover wounds with bandages. Three of the people with Alaskapox mistook their lesions at first for a bite from a spider or insect.
A version of this article first appeared on WebMD.com.
Authors’ response
My co-authors and I appreciate the excellent comments regarding our Photo Rounds column, “Foot rash and joint pain,” and would like to provide some additional detail.
After our patient’s 27-day hospital stay, he was admitted to a rehabilitation center for continued inpatient physical therapy for 14 days due to weakness and deconditioning. Following his discharge from the rehabilitation center, the patient was still confined to a wheelchair. He was prescribed an oral prednisone taper (as mentioned in our article) and celecoxib 200 mg bid and referred for outpatient physical therapy. At a follow-up appointment with the rheumatologist, he received adalimumab 80 mg followed by 40 mg every other week, which led to improvement in his range of motion and pain. Two months after outpatient physical therapy, the patient was lost to follow-up.
We agree with Dr. Hahn et al that many of these patients with chlamydia-associated ReA become “long-haulers.” In medicine—especially when rare diseases are considered—we must often make decisions without perfect science. The studies referenced by Dr. Hahn et al suggest that combinations of doxycycline and rifampin or azithromycin and rifampin may treat not only chlamydial infection, but ReA and associated cutaneous disease, as well.1,2 While these studies are small in size, larger studies may never be funded. We agree that combination therapy should be considered in this population of patients.
Hannah R. Badon, MD
Ross L. Pearlman, MD
Robert T. Brodell, MD
Jackson, MS
1. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
2. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
My co-authors and I appreciate the excellent comments regarding our Photo Rounds column, “Foot rash and joint pain,” and would like to provide some additional detail.
After our patient’s 27-day hospital stay, he was admitted to a rehabilitation center for continued inpatient physical therapy for 14 days due to weakness and deconditioning. Following his discharge from the rehabilitation center, the patient was still confined to a wheelchair. He was prescribed an oral prednisone taper (as mentioned in our article) and celecoxib 200 mg bid and referred for outpatient physical therapy. At a follow-up appointment with the rheumatologist, he received adalimumab 80 mg followed by 40 mg every other week, which led to improvement in his range of motion and pain. Two months after outpatient physical therapy, the patient was lost to follow-up.
We agree with Dr. Hahn et al that many of these patients with chlamydia-associated ReA become “long-haulers.” In medicine—especially when rare diseases are considered—we must often make decisions without perfect science. The studies referenced by Dr. Hahn et al suggest that combinations of doxycycline and rifampin or azithromycin and rifampin may treat not only chlamydial infection, but ReA and associated cutaneous disease, as well.1,2 While these studies are small in size, larger studies may never be funded. We agree that combination therapy should be considered in this population of patients.
Hannah R. Badon, MD
Ross L. Pearlman, MD
Robert T. Brodell, MD
Jackson, MS
My co-authors and I appreciate the excellent comments regarding our Photo Rounds column, “Foot rash and joint pain,” and would like to provide some additional detail.
After our patient’s 27-day hospital stay, he was admitted to a rehabilitation center for continued inpatient physical therapy for 14 days due to weakness and deconditioning. Following his discharge from the rehabilitation center, the patient was still confined to a wheelchair. He was prescribed an oral prednisone taper (as mentioned in our article) and celecoxib 200 mg bid and referred for outpatient physical therapy. At a follow-up appointment with the rheumatologist, he received adalimumab 80 mg followed by 40 mg every other week, which led to improvement in his range of motion and pain. Two months after outpatient physical therapy, the patient was lost to follow-up.
We agree with Dr. Hahn et al that many of these patients with chlamydia-associated ReA become “long-haulers.” In medicine—especially when rare diseases are considered—we must often make decisions without perfect science. The studies referenced by Dr. Hahn et al suggest that combinations of doxycycline and rifampin or azithromycin and rifampin may treat not only chlamydial infection, but ReA and associated cutaneous disease, as well.1,2 While these studies are small in size, larger studies may never be funded. We agree that combination therapy should be considered in this population of patients.
Hannah R. Badon, MD
Ross L. Pearlman, MD
Robert T. Brodell, MD
Jackson, MS
1. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
2. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
1. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
2. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
How best to treat “long-haulers” with reactive arthritis?
In the June Photo Rounds column, “Foot rash and joint pain” (J Fam Pract. 2021;70:249-251), Badon et al presented a case of chlamydia-associated reactive arthritis (ReA), formerly called Reiter syndrome, in a 21-year-old man following Chlamydia trachomatis urethritis. We would like to point out that, contrary to the conventional definition of ReA, in which the causative pathogen can’t be cultured from the affected joints,1 chlamydia-associated ReA is associated with evidence of chronic joint infection that, while not cultivable, can be confirmed by real-time polymerase chain reaction testing of metabolically active pathogens in synovial tissue and/or fluid.2
C trachomatis and C pneumoniae are the most frequent causative pathogens to elicit ReA.3 Short-course antibiotics and anti-inflammatory treatments can palliate ReA, but these treatments often do not provide a cure.3 Two controlled clinical trials demonstrated that chlamydia-associated ReA can be treated successfully with longer-term combination antibiotic therapy.4,5 ReA is usually diagnosed in the acute stage (first 6 months) and can become chronic in 30% of cases.6 It would be interesting to know the long-term treatment and outcome data for the case patient.
David L. Hahn, MD, MS
Alan P. Hudson, PhD
Charles Stratton, MD
Wilmore Webley, PhD
Judith Whittum-Hudson, PhD
1. Yu D, van Tubergenm A. Reactive arthritis. UpToDate. Updated 2021. Accessed August 10, 2021. www.uptodate.com/contents/reactive-arthritis
2. Gérard HC, Carter JD, Hudson AP. Chlamydia trachomatis is present and metabolically active during the remitting phase in synovial tissues from patients with chronic chlamydia-induced reactive arthritis. Am J Med Sci. 2013;346:22-25. doi: 10.1097/MAJ.0b013e3182648740
3. Zeidler H, Hudson AP. New insights into chlamydia and arthritis. Promise of a cure? Ann Rheum Dis. 2014;73:637-644. doi: 10.1136/annrheumdis-2013-204110
4. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
5. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
6. Carter JD, Inman RD, Whittum-Hudson J, et al. Chlamydia and chronic arthritis. Ann Med. 2012;44:784-792. doi: 10.3109/07853890.2011.606830
In the June Photo Rounds column, “Foot rash and joint pain” (J Fam Pract. 2021;70:249-251), Badon et al presented a case of chlamydia-associated reactive arthritis (ReA), formerly called Reiter syndrome, in a 21-year-old man following Chlamydia trachomatis urethritis. We would like to point out that, contrary to the conventional definition of ReA, in which the causative pathogen can’t be cultured from the affected joints,1 chlamydia-associated ReA is associated with evidence of chronic joint infection that, while not cultivable, can be confirmed by real-time polymerase chain reaction testing of metabolically active pathogens in synovial tissue and/or fluid.2
C trachomatis and C pneumoniae are the most frequent causative pathogens to elicit ReA.3 Short-course antibiotics and anti-inflammatory treatments can palliate ReA, but these treatments often do not provide a cure.3 Two controlled clinical trials demonstrated that chlamydia-associated ReA can be treated successfully with longer-term combination antibiotic therapy.4,5 ReA is usually diagnosed in the acute stage (first 6 months) and can become chronic in 30% of cases.6 It would be interesting to know the long-term treatment and outcome data for the case patient.
David L. Hahn, MD, MS
Alan P. Hudson, PhD
Charles Stratton, MD
Wilmore Webley, PhD
Judith Whittum-Hudson, PhD
In the June Photo Rounds column, “Foot rash and joint pain” (J Fam Pract. 2021;70:249-251), Badon et al presented a case of chlamydia-associated reactive arthritis (ReA), formerly called Reiter syndrome, in a 21-year-old man following Chlamydia trachomatis urethritis. We would like to point out that, contrary to the conventional definition of ReA, in which the causative pathogen can’t be cultured from the affected joints,1 chlamydia-associated ReA is associated with evidence of chronic joint infection that, while not cultivable, can be confirmed by real-time polymerase chain reaction testing of metabolically active pathogens in synovial tissue and/or fluid.2
C trachomatis and C pneumoniae are the most frequent causative pathogens to elicit ReA.3 Short-course antibiotics and anti-inflammatory treatments can palliate ReA, but these treatments often do not provide a cure.3 Two controlled clinical trials demonstrated that chlamydia-associated ReA can be treated successfully with longer-term combination antibiotic therapy.4,5 ReA is usually diagnosed in the acute stage (first 6 months) and can become chronic in 30% of cases.6 It would be interesting to know the long-term treatment and outcome data for the case patient.
David L. Hahn, MD, MS
Alan P. Hudson, PhD
Charles Stratton, MD
Wilmore Webley, PhD
Judith Whittum-Hudson, PhD
1. Yu D, van Tubergenm A. Reactive arthritis. UpToDate. Updated 2021. Accessed August 10, 2021. www.uptodate.com/contents/reactive-arthritis
2. Gérard HC, Carter JD, Hudson AP. Chlamydia trachomatis is present and metabolically active during the remitting phase in synovial tissues from patients with chronic chlamydia-induced reactive arthritis. Am J Med Sci. 2013;346:22-25. doi: 10.1097/MAJ.0b013e3182648740
3. Zeidler H, Hudson AP. New insights into chlamydia and arthritis. Promise of a cure? Ann Rheum Dis. 2014;73:637-644. doi: 10.1136/annrheumdis-2013-204110
4. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
5. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
6. Carter JD, Inman RD, Whittum-Hudson J, et al. Chlamydia and chronic arthritis. Ann Med. 2012;44:784-792. doi: 10.3109/07853890.2011.606830
1. Yu D, van Tubergenm A. Reactive arthritis. UpToDate. Updated 2021. Accessed August 10, 2021. www.uptodate.com/contents/reactive-arthritis
2. Gérard HC, Carter JD, Hudson AP. Chlamydia trachomatis is present and metabolically active during the remitting phase in synovial tissues from patients with chronic chlamydia-induced reactive arthritis. Am J Med Sci. 2013;346:22-25. doi: 10.1097/MAJ.0b013e3182648740
3. Zeidler H, Hudson AP. New insights into chlamydia and arthritis. Promise of a cure? Ann Rheum Dis. 2014;73:637-644. doi: 10.1136/annrheumdis-2013-204110
4. Carter JD, Valeriano J, Vasey FB. Doxycycline versus doxycycline and rifampin in undifferentiated spondyloarthropathy, with special reference to chlamydia-induced arthritis. A prospective, randomized 9-month comparison. J Rheumatol. 2004;31:1973-1980.
5. Carter JD, Espinoza LR, Inman RD, et al. Combination antibiotics as a treatment for chronic Chlamydia-induced reactive arthritis: a double-blind, placebo-controlled, prospective trial. Arthritis Rheum. 2010;62:1298-1307. doi: 10.1002/art.27394
6. Carter JD, Inman RD, Whittum-Hudson J, et al. Chlamydia and chronic arthritis. Ann Med. 2012;44:784-792. doi: 10.3109/07853890.2011.606830
COVID-detecting dogs pilot first airport program
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
If she identifies a specific scent, she’ll let her handler know simply by sitting down. When this good girl sits, that means Cobra has detected an olfactory signal of the coronavirus, the virus that causes COVID-19.
Cobra, a Belgian Malinois, is one of two canines – her partner is One Betta, a Dutch shepherd – working this checkpoint at Miami International. They are part of a pilot program with the Global Forensic and Justice Center at Florida International University, using the detection dogs as a quick screen for people who have COVID-19.
Their detection rate is high, at more than 98%, and the program has been such a success that it’s being extended for another month at the airport.
If these two dogs continue to accurately detect COVID-19, they and other canines with similar training could be deployed to other places with lots of people coming and going at once, including other airports or even schools. In fact, COVID-sniffing dogs are in use in some university classrooms already.
But building up a big brigade of live animals as disease detectors involves some thorny issues, including where the animals retire once their careers are complete.
“When COVID first arose, we said let’s see if we can train these two dogs on either the virus or the odor of COVID-19,” says Kenneth Furton, PhD, a professor of chemistry and biochemistry, provost, and executive vice president at Florida International University.
His team had completed a study with what he calls “medical detector dogs,” animals that might be able to detect the odor of someone having a seizure. That led them to see how well the animals could detect other kinds of disorders.
Training a dog to sniff out specific odors starts with getting them to understand the task in general. Dr. Furton says that the animals first are trained to grasp that their job is to detect one odor among many. Once the dogs grasp that, they can be trained on just about any specific odor.
In fact, in addition to detecting seizures, dogs reportedly have been able to identify diabetes and even some cancers, such as ovarian cancer.
Dr. Furton says he’s not aware of any previous use of dogs to screen for infectious disease. That may simply be because nothing recently has struck with the global ferocity of COVID, driving humans to turn to their best friends for help.
Cobra and One Betta got their start learning to identify the presence of laurel wilt, a fungus that attacks avocado trees and kills them, costing Florida growers millions. With that expertise under their collars, the two dogs need only a few weeks to get good at detecting other smells assigned to them.
Training the dogs, safely
To train Cobra and One Betta on COVID-19 odors, Dr. Furton’s team first acquired mask samples from people hospitalized with COVID and people who did not have the disease. In battling the viruses, people produce certain chemicals that they exhale every time they breathe. When Dr. Furton and his colleagues compared the exhaled components trapped in the masks, they found differences between masks from people with COVID and those without.
Having confirmed that exhalations can be COVID-specific, the research team trained four dogs – Cobra, One Betta, Hubble, and Max – to detect masks from people with COVID among an assortment of mask choices. Before this step, though, the researchers made sure that any trace of active virus was destroyed by ultraviolet light so that the dogs would not be infected.
Each time the dogs accurately selected a mask from a COVID patient, their reward was access to a favorite toy: A red ball to chew on. Although all four dogs performed very well, yes, they did, Cobra and One Betta showed the most accuracy, outperforming their training colleagues. From their training scores, Cobra ranked first, with 99.45% accuracy. Despite her name, says Dr. Furton, One Betta was “not one better,” coming in second at 98.1%, which is still quite high.
Both dogs are good at their airport screening duties. If one of them sits after sniffing a mask at the checkpoint, the next step is for the mask owner to be tested.
From Aug. 23 to Sept. 8, the two canines screened 1,093 people during 8 working days, alerting on only one case, according to Greg Chin, communications director for the Miami-Dade Aviation Department. That person had tested positive for COVID 2 weeks earlier and was returning to work after quarantine, and their rapid test after the dog alerted was negative.
Dr. Furton says that there are some reports of dogs also alerting before tests can show a positive result, suggesting the dogs’ odor detection can be more precise. They hope to expand their study to see how tight the window of dog-based detection is.
For now, the detector dogs are doing so well that the program has been extended for 30 more days, Mr. Chin says.
As promising as this seems, using dogs for screening carries some logistical and ethical tangles. Training a canine army to deploy for high-volume detection points means that once the work is done, a whole lot of dogs will need a safe place to retire. In addition, the initial training takes several months, says Dr. Furton, whereas if a device were developed for screening, manufacturing could likely be ramped up quickly to meet demand.
The dogs might not need to retire right away, though.
“We envision that they could be redeployed to another type of detection for another infectious disease” if the need arises, Dr. Furton says. But in the end, when working with dogs, he says, there is “a moral connection that you don’t have to deal with using instruments.”
Although the pilot screening at Miami International is the first airport test, the dogs have also done this work in other venues, including at a state emergency operations center in Florida and in some university classrooms, says Dr. Furton.
A version of this article first appeared on WebMD.com.
COVID-19 causes major interruption in global HIV progress
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“We’ve been set back by COVID but we’ve seen remarkable resilience, a lot of innovation and creativity,” Siobhan Crowley MD, head of HIV at the Global Fund, said in an interview.
“If you consider that 21.9 million people are getting antiretrovirals at this point through the Global Fund, I think that needs to be appreciated. Ten years ago, that wouldn’t have been the case; all of those people would have disappeared into the ethers,” she said.
Through close partnerships with the U.S. Agency for International Development, the U.S. President’s Emergency Plan for AIDS Relief, and other Western countries and organizations, the Global Fund has invested $22.7 billion in programs to prevent and treat HIV and AIDS, and $3.8 billion in tuberculosis (TB)/HIV programs, according to the organization’s 2021 Results Report.
But the report also underscores the significant effect that the COVID-19 pandemic has had on funded countries’ progress toward achieving renewed 90-90-90 targets for HIV testing/diagnosis, treatment, and viral suppression by 2030.
The setbacks have been challenging and have touched nearly every service from prevention to treatment. According to the report, between 2019 and 2020:
- Voluntary male circumcision declined by 27%.
- Numbers reached by HIV prevention programs fell by 11%.
- 4.5% fewer mothers received medications to prevent HIV transmission to their babies.
- HIV testing services, including initiation, decreased by 22%.
The numbers tell only a part of the story, according to Dr. Crowley.
“We put in place an emergency mechanism to make funds available for countries to do everything except vaccines in support of COVID,” Dr. Crowley explained. (As of August 2021, these funds had been allocated to 107 countries and 16 multicountry programs.)
Countries were advised that they could use the emergency funds three different ways: 1) for COVID-specific purposes (e.g., diagnostics, oxygen, personal protective equipment; 2) to support mitigation strategies geared toward protecting existing HIV, tuberculosis, and malaria programs and getting them back on track; and 3) for so-called “health system fixes,” such as investing in data systems to track COVID, HIV, and other core diseases, as well as the community workforce.
With regard to HIV, each country supported by the Global Fund was asked to ensure that multimonth (3-6 months) dispensing was implemented and/or accelerated so that patients could avoid congested facilities, and, wherever possible, that drugs were delivered or accessed outside the facility. One example of the success of this effort was found in South Africa, where the number of people on antiretrovirals increased almost threefold, from 1.2 million to 4.2 million people.
Countries also were asked to adapt HIV testing procedures by, for example, moving organized testing out of the facilities and into neighborhoods to meet people where they are. Rapid diagnostic testing and triage care linkage using technologies such as WhatsApp were the result, as were opportunities for home testing which, Dr. Crowley noted, remains a critical component of the overall strategy.
“The self-test is important for two reasons, not just because you are trying to find people with HIV, but also, when people know that they’re negative, they know what they can or should do to stay negative,” she said. “It’s quite a powerful motivator.”
Self-testing might also help countries motivate the 6 million people who know that they have HIV but are not on treatment. But there are still 4.1 million residing in these countries who aren’t aware that they are infected, according to the report. This figure is especially troubling, considering that some may also be harboring TB coinfections, including multidrug-resistant TB (MDR-TB).
The imperfect storm globally and in the U.S.
“One of the things that was striking in the report was the decline in the number of people reached with testing and prevention services,” Chris Beyrer, MD, MPH, the Desmond M. Tutu Professor of Public Health and Human Rights at the Johns Hopkins Bloomberg School of Public Health in Baltimore, said in an interview. Dr. Beyrer was not involved in the report’s development.
“You know, a 10% decline in 1 year to reach people in need is substantial,” he said. “Let’s say it continues; many people are predicting that we won’t have reasonable coverage for low-income countries with COVID until 2023. That adds up to a substantial decline in people reached with these services.”
Dr. Beyrer also expressed concern about the convergence of HIV and TB in already overburdened, fragile health care systems. “Globally, the No. 1 cause of death for people living with HIV is TB, and of course, it’s highly transmissible. So, in many high-burden countries, children are exposed, typically from household members early on, and so the number of people with latent TB infection is just enormous.
“If you look at the report, the worst outcomes are MDR-TB. Those multidrug-resistant and extensively-drug-resistant strains are really a threat to everybody,” Dr. Beyrer said.
But it’s not time for U.S. providers to rest on their laurels either. Dr. Beyrer noted that the 22% decline in HIV testing reported by the Global Fund is similar to what has been happening in the United States with elective procedures such as HIV testing and even preventive procedures like medical male circumcision.
“It’s very clear here in the Global Fund data that the majority of new infections worldwide are in key populations [that] include gay and bisexual men, men who have sex with men, transgender women who have sex with men, people who inject drugs, and sex workers of all genders. Those are people who already faced barriers to health care access and were made worse by COVID.”
Dr. Beyrer noted that, according to the Centers for Disease Control and Prevention, in 2019 in the United States, 68% of new HIV infections occurred in gay and bisexual men, and the effect that COVID-19 will have is still unknown. He also noted the similarity between the most marginalized populations in the Global Fund report and African American men, who have not realized the same increase in the use of preexposure prophylaxis or the same decline in new infections as have their White counterparts.
“It’s also where we are seeing the worst of COVID, low immunization coverage, and high rates of hospitalization and death. ... It’s a dark, dark time for many,” Dr. Crowley said. “And there has also been some amazing resilience and adaptation. The weird thing is, the HIV platform is a natural platform; I mean, if we can keep 21.9 million people on treatment, we can probably deliver them a COVID test and a vaccine.”
Dr. Crowley and Dr. Beyrer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Should hospitalists use albumin to treat non-SBP infections in patients with cirrhosis?
Caution is advised in patients at risk of pulmonary edema
Case
A 56 year-old male with hypertension, alcohol use disorder, stage II chronic kidney disease, and biopsy-proven cirrhosis presents with fever and chills, pyuria, flank pain, and an acute kidney injury concerning for pyelonephritis. Is there a benefit in treating with albumin in addition to guideline-based antibiotics?
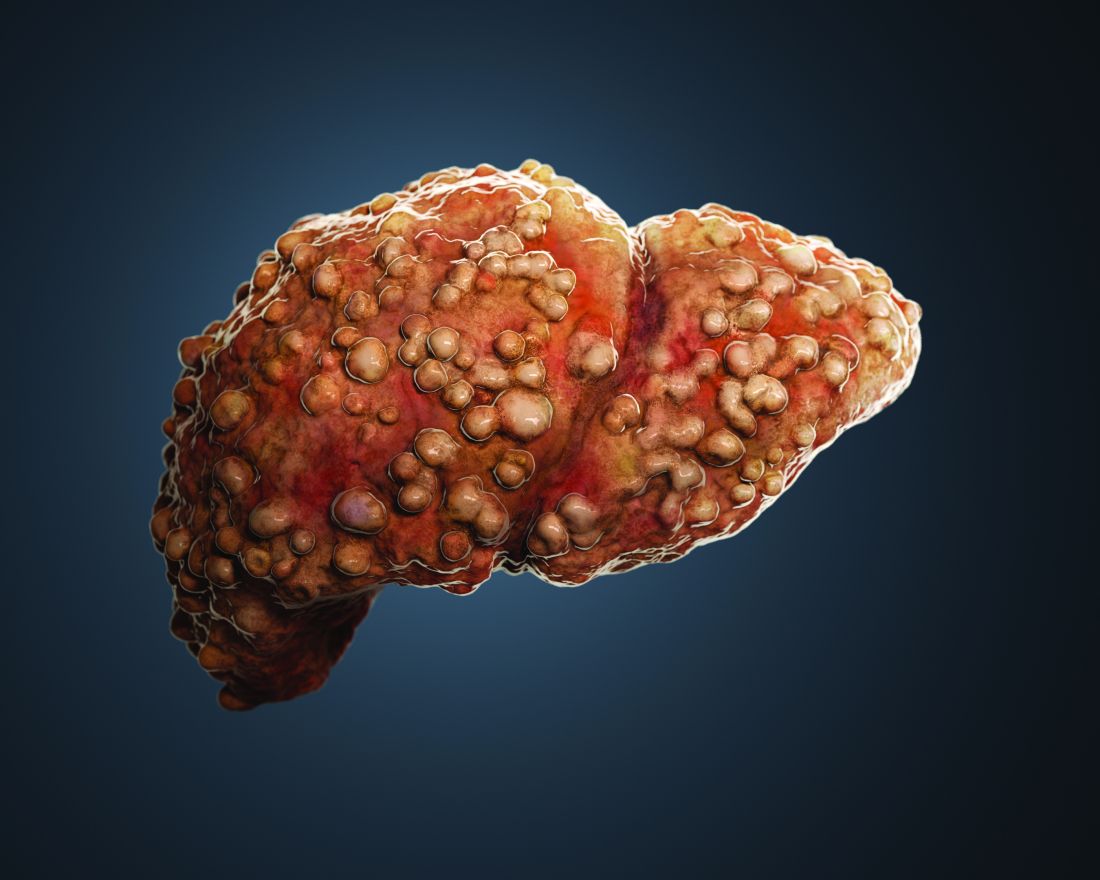
Brief overview of the issue
Albumin is a negatively charged human protein produced by the liver. Albumin comprises 50% of plasma protein and over 75% of plasma oncotic pressure.1 It was first used at Walter Reed Hospital in 1940 and subsequently for burn injuries after the attack on Pearl Harbor in 1941.2

Albumin serves several important physiologic functions including maintaining oncotic pressure, endothelial support, antioxidation, nitrogen oxide scavenging, and buffering and transport of solutes and drugs, including antibiotics. In cirrhosis, albumin is diluted due to sodium and water retention. There is increased redistribution, decreased synthesis by the liver, and impaired albumin molecule binding.3
For patients with liver disease, per the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD), albumin should be administered to prevent post paracentesis circulatory dysfunction after large volume paracentesis, to prevent renal failure and mortality in the setting of spontaneous bacterial peritonitis (SBP), and in the diagnosis and treatment of hepatorenal syndrome (HRS) type I to potentially improve mortality.4,5 Beyond these three guideline-based indications, other uses for albumin for patients with liver disease have been proposed, including treatment of hyponatremia, posttransplant fluid resuscitation, diuretic unresponsive ascites, and long-term management of cirrhosis. There has yet to be strong evidence supporting these additional indications. However, given the known benefits of albumin in patients with SBP, there has been recent research into treatment of non-SBP infections, including urinary tract infections.
Overview of the data
There have been three randomized controlled trials (RCTs) regarding albumin administration for the treatment of non-SBP infections for hospitalized patients with cirrhosis. All three trials randomized patients to a treatment arm of albumin and antibiotics versus a control group of antibiotics alone. The treatment protocol prescribed 20% albumin with 1.5 g/kg on day 1 and 1.0 g/kg on day 3. The most common infections studied were pneumonia and urinary tract infection. These RCTs found that albumin administration was associated with improved renal and/or circulatory function, but not with a reduction in mortality.

First, there was a single center RCT by Guevara et al. in 2012 of 110 patients with cirrhosis and infection based on SIRS criteria.6 The primary outcome was 90-day survival with secondary outcomes of renal failure development, renal function at days 3,7 and 14, and circulatory function measured by plasma renin, aldosterone, and norepinephrine. Renal function and circulatory function improved in the albumin group, but not mortality. In a multivariable regression analysis, albumin was statistically predictive of survival (hazard ratio of 0.294).
Second, there was a multicenter RCT by Thévenot et al. in 2015 of 193 patients.7 The primary outcome was 90-day renal failure and the secondary outcome was 90-day survival. Renal failure was chosen as the primary endpoint because of its association with survival in this patient population. The treatment group had delayed onset of renal failure, but no difference in the development of 90-day renal failure or 90-day mortality rate. Notably, eight patients (8.3%) in the albumin group developed pulmonary edema with two deaths. This led the oversight committee to prematurely terminate the study.
Third and most recently, there was a multicenter RCT by Fernández et al. in 2019 of 118 patients.8 The primary outcome was in-hospital mortality, with secondary outcomes of circulatory dysfunction measured by plasma renin concentration, systemic inflammation measured by plasma IL-6 and biomarkers, complications including acute-on-chronic liver failure (ACLF) and nosocomial bacterial infections, and 90-day mortality. Between the albumin and control group, there were no differences in in-hospital mortality (13.1% vs. 10.5%, P > .66), inflammation, circulatory dysfunction, or liver severity. However, a significantly higher proportion of patients in the albumin group had resolution of their ACLF (82.3% vs. 33.3%, P = .003) and a lower proportion developed nosocomial infections (6.6% vs. 24.6%, P = .007). A major weakness of this study was that patients in the albumin group had a higher combined rate of ACLF and kidney dysfunction (44.3% vs. 24.6%, P = .02).
Beyond these three randomized controlled trials, there was a study on the long-term administration of albumin for patients with cirrhosis and ascites. Patients who received twice weekly albumin infusions had a lower 2-year mortality rate and a reduction in the incidence of both SBP and non-SBP infections.9 Another long-term study of albumin administration found similar results with greater 18-month survival and fewer non-SBP infections.10 A trial looking at inflammation in patients without bacterial infections and in biobanked samples from cirrhotic patients with bacterial infections found that treatment with albumin reduced systemic inflammation.11
In summary, the three RCTs looked at comparable patients with cirrhosis and a non-SBP infection and all underwent similar treatment protocols with 20% albumin dosed at 1.5 g/kg on day 1 and 1.0 g/kg on day 3. All studies evaluated mortality in either the primary or secondary outcome, and none found significant differences in mortality between treatment and control groups. Each study also evaluated and found improvement in renal and/or circulatory function. Fernández et al. also found increased resolution of ACLF, fewer nosocomial infections, and reduction in some inflammatory markers. However, all studies had relatively small sample sizes that were underpowered to detect mortality differences. Furthermore, randomization did not lead to well-matched groups, with the treatment group patients in the Fernández study having higher rates of ACLF and kidney dysfunction.
The data suggest that albumin may be beneficial in improving renal and circulatory function. In select patients with ACLF and elevated serum creatinine, albumin treatment may be considered. There has been discussion about the use of albumin preferentially in patients with subdiaphragmatic bacterial infections, most related to increased risk of renal failure such as biliary and urinary tract infections.12 The authors of these studies also note that albumin may be more beneficial in patients with higher baseline creatinine. Caution is warranted for patients with impaired cardiac function or poor respiratory status given the possibility of pulmonary edema. Finally, the high cost of albumin in many medical centers is a major limitation of this treatment approach.
Application of data to our patient
Our patient has cirrhosis and is acutely presenting with pyelonephritis and acute kidney injury. He has no baseline pulmonary disease or oxygen requirement. His recent transthoracic echocardiogram is reviewed and he has no evidence of cardiac disease.
Because he has an elevated creatinine, an infectious process associated with progressive renal failure, and is not at an elevated baseline risk of developing pulmonary edema, albumin would be reasonable to administer at 1.5 g/kg on day 1 and 1.0 g/kg on day 3 of hospitalization.
Bottom line
In certain patients with cirrhosis and a non-SBP infection, the use of albumin to help improve renal and circulatory function is reasonable. There is no evidence that albumin will improve mortality and caution is warranted for patients at risk for pulmonary edema.
Dr. Rambachan is an academic hospital medicine fellow at the University of California, San Francisco.
References
1. Caironi P and Gattinoni L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus. 2009;7(4):259-67. doi: 10.2450/2009.0002-09.
2. Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
3. Walayat S et al. Role of albumin in cirrhosis: from a hospitalist’s perspective. J Community Hosp Intern Med Perspect. 2017;7(1):8-14. 2017 Mar 31. doi: 10.1080/20009666.2017.1302704.
4. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
5. European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis [published correction appears in J Hepatol. 2018 Nov;69(5):1207]. J Hepatol. 2018 Aug;69(2):406-60. doi: 10.1016/j.jhep.2018.03.024.
6. Guevara M et al. Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis. A randomized, controlled study. J Hepatol. 2012 Oct;57(4):759-65. doi: 10.1016/j.jhep.2012.06.013.
7. Thévenot T et al. Effect of albumin in cirrhotic patients with infection other than spontaneous bacterial peritonitis. A randomized trial. J Hepatol. 2015 Apr;62(4):822-30. doi: 10.1016/j.jhep.2014.11.017.
8. Fernández J et al. Efficacy of albumin treatment for patients with cirrhosis and infections unrelated to spontaneous bacterial peritonitis. Clin Gastroenterol Hepatol. 2020 Apr;18(4):963-73.e14. doi: 10.1016/j.c gh.2019.07.055.
9. Di Pascoli M et al. Long-term administration of human albumin improves survival in patients with cirrhosis and refractory ascites. Liver Int. 2019 Jan;39(1):98-105. doi: 10.1111/liv.13968.
10. Caraceni P et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial [published correction appears in Lancet. 2018 Aug 4;392(10145):386]. Lancet. 2018 June;391(10138):2417-29. doi: 10.1016/S0140-6736(18)30840-7.
11. Fernández J et al. Effects of albumin treatment on systemic and portal hemodynamics and systemic inflammation in patients with decompensated cirrhosis. Gastroenterology. 2019 July;157(1):149-62. doi: 10.1053/j.gastro.2019.03.021.
12. Fasolato S et al. Renal failure and bacterial infections in patients with cirrhosis: Epidemiology and clinical features. Hepatology. 2007;45(1):223-9. doi: 10.1002/hep.21443.
Key points
- In patients with spontaneous bacterial peritonitis, hepatorenal syndrome, and for large volume paracentesis, albumin improves outcomes and is recommended by guidelines.
- In patients with cirrhosis and a non-SBP infection, there is some evidence that albumin may improve renal and circulatory function.
- Clinicians should be cautious about albumin use in patients at an elevated risk for development of pulmonary edema.
Quiz
Which of the following is not a guideline-recommended use of albumin for patients with cirrhosis?
A. Treatment of type 1 hepatorenal syndrome
B. Treatment of spontaneous bacterial peritonitis
C. To correct plasma albumin < 2.5 g/dL in nontransplant patients
D. Post large-volume paracentesis
The answer is C. Per the EASL and AASLD, A,B, and D are recommended. There is not strong evidence to support administering albumin to correct low plasma albumin.
Additional reading
- Bernardi M et al. Albumin in decompensated cirrhosis: new concepts and perspectives. Gut. 2020 June;69(6):1127-38. doi: 10.1136/gutjnl-2019-318843.
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
- Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019 June;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
Caution is advised in patients at risk of pulmonary edema
Caution is advised in patients at risk of pulmonary edema
Case
A 56 year-old male with hypertension, alcohol use disorder, stage II chronic kidney disease, and biopsy-proven cirrhosis presents with fever and chills, pyuria, flank pain, and an acute kidney injury concerning for pyelonephritis. Is there a benefit in treating with albumin in addition to guideline-based antibiotics?
Brief overview of the issue
Albumin is a negatively charged human protein produced by the liver. Albumin comprises 50% of plasma protein and over 75% of plasma oncotic pressure.1 It was first used at Walter Reed Hospital in 1940 and subsequently for burn injuries after the attack on Pearl Harbor in 1941.2
Albumin serves several important physiologic functions including maintaining oncotic pressure, endothelial support, antioxidation, nitrogen oxide scavenging, and buffering and transport of solutes and drugs, including antibiotics. In cirrhosis, albumin is diluted due to sodium and water retention. There is increased redistribution, decreased synthesis by the liver, and impaired albumin molecule binding.3
For patients with liver disease, per the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD), albumin should be administered to prevent post paracentesis circulatory dysfunction after large volume paracentesis, to prevent renal failure and mortality in the setting of spontaneous bacterial peritonitis (SBP), and in the diagnosis and treatment of hepatorenal syndrome (HRS) type I to potentially improve mortality.4,5 Beyond these three guideline-based indications, other uses for albumin for patients with liver disease have been proposed, including treatment of hyponatremia, posttransplant fluid resuscitation, diuretic unresponsive ascites, and long-term management of cirrhosis. There has yet to be strong evidence supporting these additional indications. However, given the known benefits of albumin in patients with SBP, there has been recent research into treatment of non-SBP infections, including urinary tract infections.
Overview of the data
There have been three randomized controlled trials (RCTs) regarding albumin administration for the treatment of non-SBP infections for hospitalized patients with cirrhosis. All three trials randomized patients to a treatment arm of albumin and antibiotics versus a control group of antibiotics alone. The treatment protocol prescribed 20% albumin with 1.5 g/kg on day 1 and 1.0 g/kg on day 3. The most common infections studied were pneumonia and urinary tract infection. These RCTs found that albumin administration was associated with improved renal and/or circulatory function, but not with a reduction in mortality.
First, there was a single center RCT by Guevara et al. in 2012 of 110 patients with cirrhosis and infection based on SIRS criteria.6 The primary outcome was 90-day survival with secondary outcomes of renal failure development, renal function at days 3,7 and 14, and circulatory function measured by plasma renin, aldosterone, and norepinephrine. Renal function and circulatory function improved in the albumin group, but not mortality. In a multivariable regression analysis, albumin was statistically predictive of survival (hazard ratio of 0.294).
Second, there was a multicenter RCT by Thévenot et al. in 2015 of 193 patients.7 The primary outcome was 90-day renal failure and the secondary outcome was 90-day survival. Renal failure was chosen as the primary endpoint because of its association with survival in this patient population. The treatment group had delayed onset of renal failure, but no difference in the development of 90-day renal failure or 90-day mortality rate. Notably, eight patients (8.3%) in the albumin group developed pulmonary edema with two deaths. This led the oversight committee to prematurely terminate the study.
Third and most recently, there was a multicenter RCT by Fernández et al. in 2019 of 118 patients.8 The primary outcome was in-hospital mortality, with secondary outcomes of circulatory dysfunction measured by plasma renin concentration, systemic inflammation measured by plasma IL-6 and biomarkers, complications including acute-on-chronic liver failure (ACLF) and nosocomial bacterial infections, and 90-day mortality. Between the albumin and control group, there were no differences in in-hospital mortality (13.1% vs. 10.5%, P > .66), inflammation, circulatory dysfunction, or liver severity. However, a significantly higher proportion of patients in the albumin group had resolution of their ACLF (82.3% vs. 33.3%, P = .003) and a lower proportion developed nosocomial infections (6.6% vs. 24.6%, P = .007). A major weakness of this study was that patients in the albumin group had a higher combined rate of ACLF and kidney dysfunction (44.3% vs. 24.6%, P = .02).
Beyond these three randomized controlled trials, there was a study on the long-term administration of albumin for patients with cirrhosis and ascites. Patients who received twice weekly albumin infusions had a lower 2-year mortality rate and a reduction in the incidence of both SBP and non-SBP infections.9 Another long-term study of albumin administration found similar results with greater 18-month survival and fewer non-SBP infections.10 A trial looking at inflammation in patients without bacterial infections and in biobanked samples from cirrhotic patients with bacterial infections found that treatment with albumin reduced systemic inflammation.11
In summary, the three RCTs looked at comparable patients with cirrhosis and a non-SBP infection and all underwent similar treatment protocols with 20% albumin dosed at 1.5 g/kg on day 1 and 1.0 g/kg on day 3. All studies evaluated mortality in either the primary or secondary outcome, and none found significant differences in mortality between treatment and control groups. Each study also evaluated and found improvement in renal and/or circulatory function. Fernández et al. also found increased resolution of ACLF, fewer nosocomial infections, and reduction in some inflammatory markers. However, all studies had relatively small sample sizes that were underpowered to detect mortality differences. Furthermore, randomization did not lead to well-matched groups, with the treatment group patients in the Fernández study having higher rates of ACLF and kidney dysfunction.
The data suggest that albumin may be beneficial in improving renal and circulatory function. In select patients with ACLF and elevated serum creatinine, albumin treatment may be considered. There has been discussion about the use of albumin preferentially in patients with subdiaphragmatic bacterial infections, most related to increased risk of renal failure such as biliary and urinary tract infections.12 The authors of these studies also note that albumin may be more beneficial in patients with higher baseline creatinine. Caution is warranted for patients with impaired cardiac function or poor respiratory status given the possibility of pulmonary edema. Finally, the high cost of albumin in many medical centers is a major limitation of this treatment approach.
Application of data to our patient
Our patient has cirrhosis and is acutely presenting with pyelonephritis and acute kidney injury. He has no baseline pulmonary disease or oxygen requirement. His recent transthoracic echocardiogram is reviewed and he has no evidence of cardiac disease.
Because he has an elevated creatinine, an infectious process associated with progressive renal failure, and is not at an elevated baseline risk of developing pulmonary edema, albumin would be reasonable to administer at 1.5 g/kg on day 1 and 1.0 g/kg on day 3 of hospitalization.
Bottom line
In certain patients with cirrhosis and a non-SBP infection, the use of albumin to help improve renal and circulatory function is reasonable. There is no evidence that albumin will improve mortality and caution is warranted for patients at risk for pulmonary edema.
Dr. Rambachan is an academic hospital medicine fellow at the University of California, San Francisco.
References
1. Caironi P and Gattinoni L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus. 2009;7(4):259-67. doi: 10.2450/2009.0002-09.
2. Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
3. Walayat S et al. Role of albumin in cirrhosis: from a hospitalist’s perspective. J Community Hosp Intern Med Perspect. 2017;7(1):8-14. 2017 Mar 31. doi: 10.1080/20009666.2017.1302704.
4. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
5. European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis [published correction appears in J Hepatol. 2018 Nov;69(5):1207]. J Hepatol. 2018 Aug;69(2):406-60. doi: 10.1016/j.jhep.2018.03.024.
6. Guevara M et al. Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis. A randomized, controlled study. J Hepatol. 2012 Oct;57(4):759-65. doi: 10.1016/j.jhep.2012.06.013.
7. Thévenot T et al. Effect of albumin in cirrhotic patients with infection other than spontaneous bacterial peritonitis. A randomized trial. J Hepatol. 2015 Apr;62(4):822-30. doi: 10.1016/j.jhep.2014.11.017.
8. Fernández J et al. Efficacy of albumin treatment for patients with cirrhosis and infections unrelated to spontaneous bacterial peritonitis. Clin Gastroenterol Hepatol. 2020 Apr;18(4):963-73.e14. doi: 10.1016/j.c gh.2019.07.055.
9. Di Pascoli M et al. Long-term administration of human albumin improves survival in patients with cirrhosis and refractory ascites. Liver Int. 2019 Jan;39(1):98-105. doi: 10.1111/liv.13968.
10. Caraceni P et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial [published correction appears in Lancet. 2018 Aug 4;392(10145):386]. Lancet. 2018 June;391(10138):2417-29. doi: 10.1016/S0140-6736(18)30840-7.
11. Fernández J et al. Effects of albumin treatment on systemic and portal hemodynamics and systemic inflammation in patients with decompensated cirrhosis. Gastroenterology. 2019 July;157(1):149-62. doi: 10.1053/j.gastro.2019.03.021.
12. Fasolato S et al. Renal failure and bacterial infections in patients with cirrhosis: Epidemiology and clinical features. Hepatology. 2007;45(1):223-9. doi: 10.1002/hep.21443.
Key points
- In patients with spontaneous bacterial peritonitis, hepatorenal syndrome, and for large volume paracentesis, albumin improves outcomes and is recommended by guidelines.
- In patients with cirrhosis and a non-SBP infection, there is some evidence that albumin may improve renal and circulatory function.
- Clinicians should be cautious about albumin use in patients at an elevated risk for development of pulmonary edema.
Quiz
Which of the following is not a guideline-recommended use of albumin for patients with cirrhosis?
A. Treatment of type 1 hepatorenal syndrome
B. Treatment of spontaneous bacterial peritonitis
C. To correct plasma albumin < 2.5 g/dL in nontransplant patients
D. Post large-volume paracentesis
The answer is C. Per the EASL and AASLD, A,B, and D are recommended. There is not strong evidence to support administering albumin to correct low plasma albumin.
Additional reading
- Bernardi M et al. Albumin in decompensated cirrhosis: new concepts and perspectives. Gut. 2020 June;69(6):1127-38. doi: 10.1136/gutjnl-2019-318843.
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
- Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019 June;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
Case
A 56 year-old male with hypertension, alcohol use disorder, stage II chronic kidney disease, and biopsy-proven cirrhosis presents with fever and chills, pyuria, flank pain, and an acute kidney injury concerning for pyelonephritis. Is there a benefit in treating with albumin in addition to guideline-based antibiotics?
Brief overview of the issue
Albumin is a negatively charged human protein produced by the liver. Albumin comprises 50% of plasma protein and over 75% of plasma oncotic pressure.1 It was first used at Walter Reed Hospital in 1940 and subsequently for burn injuries after the attack on Pearl Harbor in 1941.2
Albumin serves several important physiologic functions including maintaining oncotic pressure, endothelial support, antioxidation, nitrogen oxide scavenging, and buffering and transport of solutes and drugs, including antibiotics. In cirrhosis, albumin is diluted due to sodium and water retention. There is increased redistribution, decreased synthesis by the liver, and impaired albumin molecule binding.3
For patients with liver disease, per the European Association for the Study of the Liver (EASL) and the American Association for the Study of Liver Diseases (AASLD), albumin should be administered to prevent post paracentesis circulatory dysfunction after large volume paracentesis, to prevent renal failure and mortality in the setting of spontaneous bacterial peritonitis (SBP), and in the diagnosis and treatment of hepatorenal syndrome (HRS) type I to potentially improve mortality.4,5 Beyond these three guideline-based indications, other uses for albumin for patients with liver disease have been proposed, including treatment of hyponatremia, posttransplant fluid resuscitation, diuretic unresponsive ascites, and long-term management of cirrhosis. There has yet to be strong evidence supporting these additional indications. However, given the known benefits of albumin in patients with SBP, there has been recent research into treatment of non-SBP infections, including urinary tract infections.
Overview of the data
There have been three randomized controlled trials (RCTs) regarding albumin administration for the treatment of non-SBP infections for hospitalized patients with cirrhosis. All three trials randomized patients to a treatment arm of albumin and antibiotics versus a control group of antibiotics alone. The treatment protocol prescribed 20% albumin with 1.5 g/kg on day 1 and 1.0 g/kg on day 3. The most common infections studied were pneumonia and urinary tract infection. These RCTs found that albumin administration was associated with improved renal and/or circulatory function, but not with a reduction in mortality.
First, there was a single center RCT by Guevara et al. in 2012 of 110 patients with cirrhosis and infection based on SIRS criteria.6 The primary outcome was 90-day survival with secondary outcomes of renal failure development, renal function at days 3,7 and 14, and circulatory function measured by plasma renin, aldosterone, and norepinephrine. Renal function and circulatory function improved in the albumin group, but not mortality. In a multivariable regression analysis, albumin was statistically predictive of survival (hazard ratio of 0.294).
Second, there was a multicenter RCT by Thévenot et al. in 2015 of 193 patients.7 The primary outcome was 90-day renal failure and the secondary outcome was 90-day survival. Renal failure was chosen as the primary endpoint because of its association with survival in this patient population. The treatment group had delayed onset of renal failure, but no difference in the development of 90-day renal failure or 90-day mortality rate. Notably, eight patients (8.3%) in the albumin group developed pulmonary edema with two deaths. This led the oversight committee to prematurely terminate the study.
Third and most recently, there was a multicenter RCT by Fernández et al. in 2019 of 118 patients.8 The primary outcome was in-hospital mortality, with secondary outcomes of circulatory dysfunction measured by plasma renin concentration, systemic inflammation measured by plasma IL-6 and biomarkers, complications including acute-on-chronic liver failure (ACLF) and nosocomial bacterial infections, and 90-day mortality. Between the albumin and control group, there were no differences in in-hospital mortality (13.1% vs. 10.5%, P > .66), inflammation, circulatory dysfunction, or liver severity. However, a significantly higher proportion of patients in the albumin group had resolution of their ACLF (82.3% vs. 33.3%, P = .003) and a lower proportion developed nosocomial infections (6.6% vs. 24.6%, P = .007). A major weakness of this study was that patients in the albumin group had a higher combined rate of ACLF and kidney dysfunction (44.3% vs. 24.6%, P = .02).
Beyond these three randomized controlled trials, there was a study on the long-term administration of albumin for patients with cirrhosis and ascites. Patients who received twice weekly albumin infusions had a lower 2-year mortality rate and a reduction in the incidence of both SBP and non-SBP infections.9 Another long-term study of albumin administration found similar results with greater 18-month survival and fewer non-SBP infections.10 A trial looking at inflammation in patients without bacterial infections and in biobanked samples from cirrhotic patients with bacterial infections found that treatment with albumin reduced systemic inflammation.11
In summary, the three RCTs looked at comparable patients with cirrhosis and a non-SBP infection and all underwent similar treatment protocols with 20% albumin dosed at 1.5 g/kg on day 1 and 1.0 g/kg on day 3. All studies evaluated mortality in either the primary or secondary outcome, and none found significant differences in mortality between treatment and control groups. Each study also evaluated and found improvement in renal and/or circulatory function. Fernández et al. also found increased resolution of ACLF, fewer nosocomial infections, and reduction in some inflammatory markers. However, all studies had relatively small sample sizes that were underpowered to detect mortality differences. Furthermore, randomization did not lead to well-matched groups, with the treatment group patients in the Fernández study having higher rates of ACLF and kidney dysfunction.
The data suggest that albumin may be beneficial in improving renal and circulatory function. In select patients with ACLF and elevated serum creatinine, albumin treatment may be considered. There has been discussion about the use of albumin preferentially in patients with subdiaphragmatic bacterial infections, most related to increased risk of renal failure such as biliary and urinary tract infections.12 The authors of these studies also note that albumin may be more beneficial in patients with higher baseline creatinine. Caution is warranted for patients with impaired cardiac function or poor respiratory status given the possibility of pulmonary edema. Finally, the high cost of albumin in many medical centers is a major limitation of this treatment approach.
Application of data to our patient
Our patient has cirrhosis and is acutely presenting with pyelonephritis and acute kidney injury. He has no baseline pulmonary disease or oxygen requirement. His recent transthoracic echocardiogram is reviewed and he has no evidence of cardiac disease.
Because he has an elevated creatinine, an infectious process associated with progressive renal failure, and is not at an elevated baseline risk of developing pulmonary edema, albumin would be reasonable to administer at 1.5 g/kg on day 1 and 1.0 g/kg on day 3 of hospitalization.
Bottom line
In certain patients with cirrhosis and a non-SBP infection, the use of albumin to help improve renal and circulatory function is reasonable. There is no evidence that albumin will improve mortality and caution is warranted for patients at risk for pulmonary edema.
Dr. Rambachan is an academic hospital medicine fellow at the University of California, San Francisco.
References
1. Caironi P and Gattinoni L. The clinical use of albumin: the point of view of a specialist in intensive care. Blood Transfus. 2009;7(4):259-67. doi: 10.2450/2009.0002-09.
2. Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
3. Walayat S et al. Role of albumin in cirrhosis: from a hospitalist’s perspective. J Community Hosp Intern Med Perspect. 2017;7(1):8-14. 2017 Mar 31. doi: 10.1080/20009666.2017.1302704.
4. Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
5. European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis [published correction appears in J Hepatol. 2018 Nov;69(5):1207]. J Hepatol. 2018 Aug;69(2):406-60. doi: 10.1016/j.jhep.2018.03.024.
6. Guevara M et al. Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis. A randomized, controlled study. J Hepatol. 2012 Oct;57(4):759-65. doi: 10.1016/j.jhep.2012.06.013.
7. Thévenot T et al. Effect of albumin in cirrhotic patients with infection other than spontaneous bacterial peritonitis. A randomized trial. J Hepatol. 2015 Apr;62(4):822-30. doi: 10.1016/j.jhep.2014.11.017.
8. Fernández J et al. Efficacy of albumin treatment for patients with cirrhosis and infections unrelated to spontaneous bacterial peritonitis. Clin Gastroenterol Hepatol. 2020 Apr;18(4):963-73.e14. doi: 10.1016/j.c gh.2019.07.055.
9. Di Pascoli M et al. Long-term administration of human albumin improves survival in patients with cirrhosis and refractory ascites. Liver Int. 2019 Jan;39(1):98-105. doi: 10.1111/liv.13968.
10. Caraceni P et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial [published correction appears in Lancet. 2018 Aug 4;392(10145):386]. Lancet. 2018 June;391(10138):2417-29. doi: 10.1016/S0140-6736(18)30840-7.
11. Fernández J et al. Effects of albumin treatment on systemic and portal hemodynamics and systemic inflammation in patients with decompensated cirrhosis. Gastroenterology. 2019 July;157(1):149-62. doi: 10.1053/j.gastro.2019.03.021.
12. Fasolato S et al. Renal failure and bacterial infections in patients with cirrhosis: Epidemiology and clinical features. Hepatology. 2007;45(1):223-9. doi: 10.1002/hep.21443.
Key points
- In patients with spontaneous bacterial peritonitis, hepatorenal syndrome, and for large volume paracentesis, albumin improves outcomes and is recommended by guidelines.
- In patients with cirrhosis and a non-SBP infection, there is some evidence that albumin may improve renal and circulatory function.
- Clinicians should be cautious about albumin use in patients at an elevated risk for development of pulmonary edema.
Quiz
Which of the following is not a guideline-recommended use of albumin for patients with cirrhosis?
A. Treatment of type 1 hepatorenal syndrome
B. Treatment of spontaneous bacterial peritonitis
C. To correct plasma albumin < 2.5 g/dL in nontransplant patients
D. Post large-volume paracentesis
The answer is C. Per the EASL and AASLD, A,B, and D are recommended. There is not strong evidence to support administering albumin to correct low plasma albumin.
Additional reading
- Bernardi M et al. Albumin in decompensated cirrhosis: new concepts and perspectives. Gut. 2020 June;69(6):1127-38. doi: 10.1136/gutjnl-2019-318843.
- Runyon BA; AASLD. Introduction to the revised American Association for the Study of Liver Diseases Practice Guideline [for the] management of adult patients with ascites due to cirrhosis 2012. Hepatology. 2013 Apr;57(4):1651-3. doi: 10.1002/hep.26359.
- Paine CH et al. Albumin in cirrhosis: More than a colloid. Curr Treat Options Gastroenterol. 2019 June;17(2):231-43. doi: 10.1007/s11938-019-00227-4.
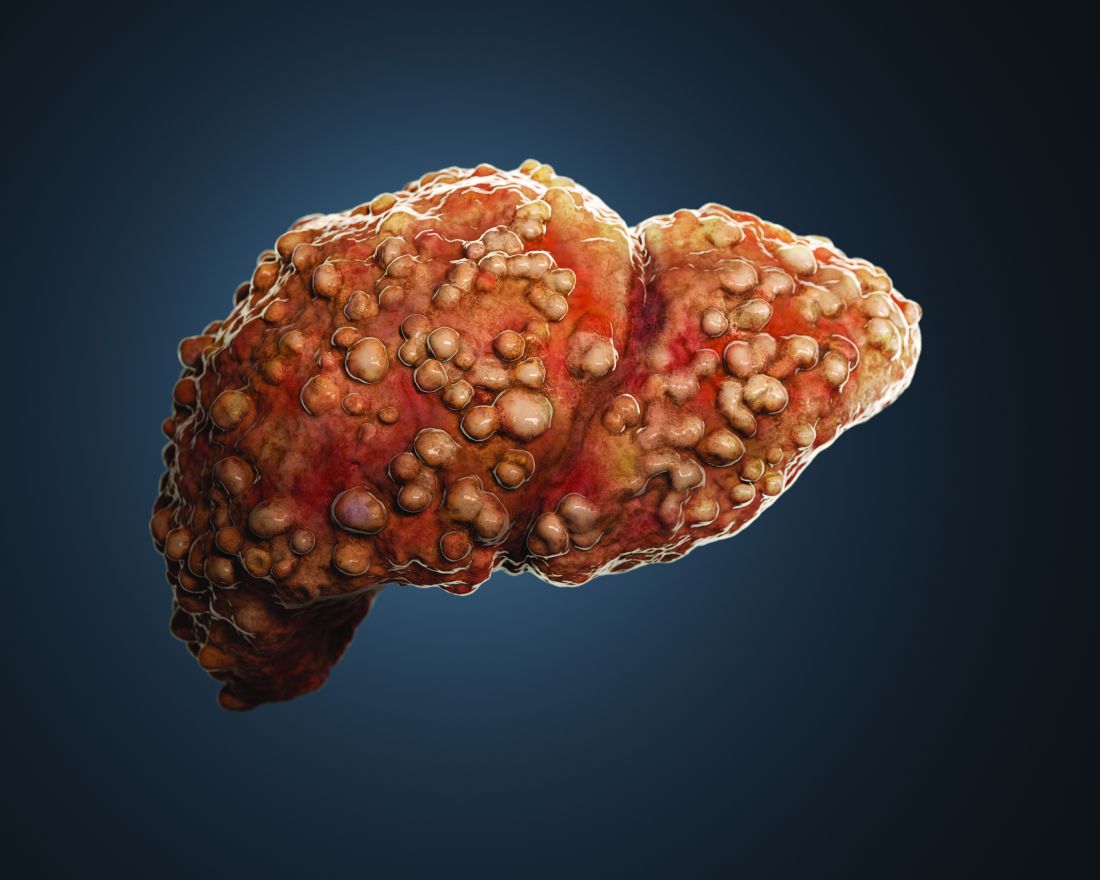
Decline in child COVID may signal end of latest surge
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.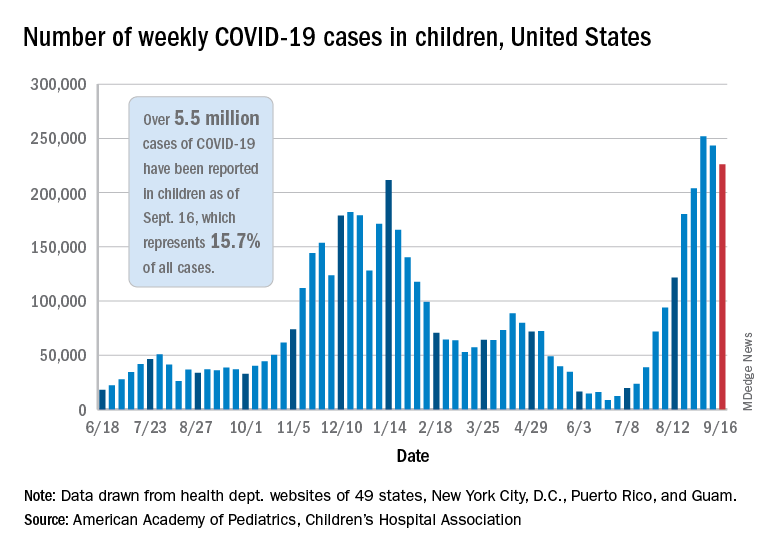
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
A second consecutive week of falling COVID-19 cases in children, along with continued declines in new admissions, may indicate that the latest surge has peaked.
Children made up over 25% of all new cases each week over that 3-week period covering the end of August and the first half of September, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
New hospitalizations in children aged 0-17 years peaked on Sept. 4 – when the rate reached 0.51 per 100,000 population – and were down to 0.47 as of Sept. 11, the latest date for which data should be considered reliable, the Centers for Disease Control and Prevention said.
The CDC’s data largely agree with the AAP/CHA report, showing that cases peaked during the week of Aug. 22-28. Cases per 100,000 for children that week looked like this: 154.7 (age 0-4 years), 276.6 (5-11 years), 320.0 (12-15), and 334.1 (16-17). The highest rates that week among adults were 288.6 per 100,000 in 30- to 39-year-olds and 286.5 for those aged 18-29, the CDC said on its COVID Data Tracker.
By the week of Sept. 5-11 – reporting delays can affect more recent data – the rates in children were down more than 20% in each of the four age groups, according to the CDC.
Vaccinations among children, unfortunately, continue to decline. Vaccine initiations for 12- to 15-year-olds slipped from 199,000 (Sept. 7-13) to 179,000 during the week of Sept. 14-20, while the 16- to 17-year-olds went from almost 83,000 down to 75,000. Initiations have dropped for 6 straight weeks in both age groups, based on the CDC data.
Despite those declines, however, the 16- and 17-year-olds just passed a couple of vaccination milestones. More than 60% – 60.9%, to be exact – have now received at least one dose of COVID vaccine, and 50.3% can be considered fully vaccinated. For those aged 12-15, the corresponding figures are 53.1% and 42.0%, the CDC reported.
When children under age 12 years are included – through clinical trial involvement or incorrect birth dates – the CDC data put the total count of Americans under age 18 who have received at least one dose of vaccine at almost 12.8 million, with vaccination complete in 10.3 million.
Total cases, as calculated by the APA and CHA, are now over 5.5 million, although that figure includes cases in individuals as old as 20 years, since many states differ from the CDC on the age range for a child. The CDC’s COVID Data Tracker put the total for children aged 0-17 at nearly 4.6 million.
The total number of COVID-related deaths in children is 480 as of Sept. 16, the AAP and CHA said, based on data from 45 states, New York, City, Puerto Rico, and Guam, but the CDC provides a higher number, 548, since the pandemic began. Children aged 0-4 years represent the largest share (32.3%) of those 548 deaths, followed by the 12- to 15-year-olds (26.5%), based on the CDC data.
Adolescent immunizations and protecting our children from COVID-19
I began thinking of a topic for this column weeks ago determined to discuss anything except COVID-19. Yet, news reports from all sources blasted daily reminders of rising COVID-19 cases overall and specifically in children.

In August, school resumed for many of our patients and the battle over mandating masks for school attendance was in full swing. The fact that it is a Centers for Disease Control and Prevention recommendation supported by both the American Academy of Pediatrics and the Pediatric Infectious Disease Society fell on deaf ears. One day, I heard a report that over 25,000 students attending Texas public schools were diagnosed with COVID-19 between Aug. 23 and Aug. 29. This peak in activity occurred just 2 weeks after the start of school and led to the closure of 45 school districts. Texas does not have a monopoly on these rising cases. Delta, a more contagious variant, began circulating in June 2021 and by July it was the most predominant. Emergency department visits and hospitalizations have increased nationwide. During the latter 2 weeks of August 2021, COVID-19–related ED visits and hospitalizations for persons aged 0-17 years were 3.4 and 3.7 times higher in states with the lowest vaccination coverage, compared with states with high vaccination coverage (MMWR Morb Mortal Wkly Rep. 2021;70:1249-54). Specifically, the rates of hospitalization the week ending Aug. 14, 2021, were nearly 5 times the rates for the week ending June 26, 2021, for 0- to 17-year-olds and nearly 10 times the rates for children 0-4 years of age. Hospitalization rates were 10.1 times higher for unimmunized adolescents than for fully vaccinated ones (MMWR Morb Mortal Wkly Rep. 2021;70:1255-60).
Multiple elected state leaders have opposed interventions such as mandating masks in school, and our children are paying for it. These leaders have relinquished their responsibility to local school boards. Several have reinforced the no-mask mandate while others have had the courage and insight to ignore state government leaders and have established mask mandates.
How is this lack of enforcement of national recommendations affecting our patients? Let’s look at two neighboring school districts in Texas. School districts have COVID-19 dashboards that are updated daily and accessible to the general public. School District A requires masks for school entry. It serves 196,171 students and has 27,195 teachers and staff. Since school opened in August, 1,606 cumulative cases of COVID-19 in students (0.8%) and 282 in staff (1%) have been reported. Fifty-five percent of the student cases occurred in elementary schools. In contrast, School District B located in the adjacent county serves 64,517 students and has 3,906 teachers and staff with no mask mandate. Since August, there have been 4,506 cumulative COVID-19 cases in students (6.9%) and 578 (14.7%) in staff. Information regarding the specific school type was not provided; however, the dashboard indicates that 2,924 cases (64.8%) occurred in children younger than 11 years of age. County data indicate 62% of those older than 12 years of age were fully vaccinated in District A, compared with 54% of persons older than 12 years in District B. The county COVID-19 positivity rate in District A is 17.6% and in District B it is 20%. Both counties are experiencing increased COVID-19 activity yet have had strikingly different outcomes in the student/staff population. While supporting the case for wearing masks to prevent disease transmission, one can’t ignore the adolescents who were infected and vaccine eligible (District A: 706; District B: 1,582). Their vaccination status could not be determined.
As pediatricians we have played an integral part in the elimination of diseases through educating and administering vaccinations. Adolescents are relatively healthy, thus limiting the number of encounters with them. The majority complete the 11-year visit; however, many fail to return for the 16- to 18-year visit.
So how are we doing? CDC data from 10 U.S. jurisdictions demonstrated a substantial decrease in vaccine administration between March and May of 2020, compared with the same period in 2018 and 2019. A decline was anticipated because of the nationwide lockdown. Doses of HPV administered declined almost 64% and 71% for 9- to 12-year-olds and 13- to 17-year-olds, respectively. Tdap administration declined 66% and 61% for the same respective age groups. Although administered doses increased between June and September of 2020, it was not sufficient to achieve catch-up coverage. Compared to the same period in 2018-2019, administration of the HPV vaccine declined 12.8% and 28% (ages 9-12 and ages 13-17) and for Tdap it was 21% and 30% lower (ages 9-12 and ages 13-17) (MMWR Morb Mortal Wkly Rep. 2021;70:840-5).
Now, we have another adolescent vaccine to discuss and encourage our patients to receive. We also need to address their concerns and/or to at least direct them to a reliable source to obtain accurate information. For the first time, a recommended vaccine may not be available at their medical home. Many don’t know where to go to receive it (http://www.vaccines.gov). Results of a Kaiser Family Foundation COVID-19 survey (August 2021) indicated that parents trusted their pediatricians most often (78%) for vaccine advice. The respondents voiced concern about trusting the location where the child would be immunized and long-term effects especially related to fertility. Parents who received communications regarding the benefits of vaccination were twice as likely to have their adolescents immunized. Finally, remember: Like parent, like child. An immunized parent is more likely to immunize the adolescent. (See Fig. 1.)
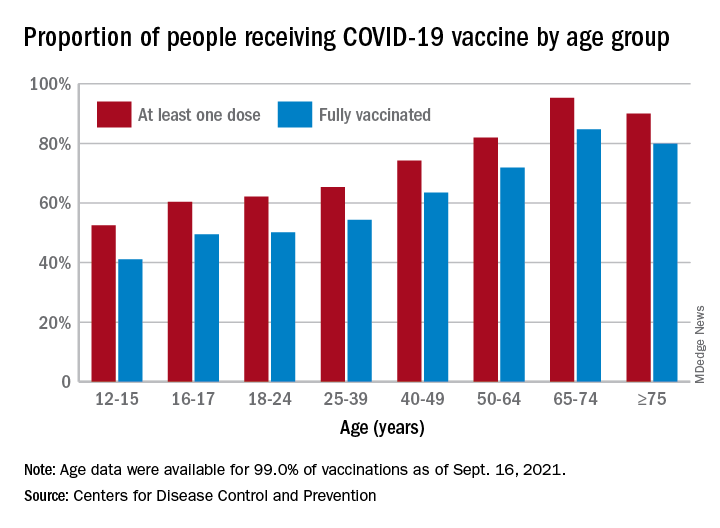
It is beyond the scope of this column to discuss the psychosocial aspects of this disease: children experiencing the death of teachers, classmates, family members, and those viewing the vitriol between pro- and antimask proponents often exhibited on school premises. And let’s not forget the child who wants to wear a mask but may be ostracized or bullied for doing so.
Our job is to do our very best to advocate for and to protect our patients by promoting mandatory masks at schools and encouraging vaccination of adolescents as we patiently wait for vaccines to become available for all of our children.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
I began thinking of a topic for this column weeks ago determined to discuss anything except COVID-19. Yet, news reports from all sources blasted daily reminders of rising COVID-19 cases overall and specifically in children.
In August, school resumed for many of our patients and the battle over mandating masks for school attendance was in full swing. The fact that it is a Centers for Disease Control and Prevention recommendation supported by both the American Academy of Pediatrics and the Pediatric Infectious Disease Society fell on deaf ears. One day, I heard a report that over 25,000 students attending Texas public schools were diagnosed with COVID-19 between Aug. 23 and Aug. 29. This peak in activity occurred just 2 weeks after the start of school and led to the closure of 45 school districts. Texas does not have a monopoly on these rising cases. Delta, a more contagious variant, began circulating in June 2021 and by July it was the most predominant. Emergency department visits and hospitalizations have increased nationwide. During the latter 2 weeks of August 2021, COVID-19–related ED visits and hospitalizations for persons aged 0-17 years were 3.4 and 3.7 times higher in states with the lowest vaccination coverage, compared with states with high vaccination coverage (MMWR Morb Mortal Wkly Rep. 2021;70:1249-54). Specifically, the rates of hospitalization the week ending Aug. 14, 2021, were nearly 5 times the rates for the week ending June 26, 2021, for 0- to 17-year-olds and nearly 10 times the rates for children 0-4 years of age. Hospitalization rates were 10.1 times higher for unimmunized adolescents than for fully vaccinated ones (MMWR Morb Mortal Wkly Rep. 2021;70:1255-60).
Multiple elected state leaders have opposed interventions such as mandating masks in school, and our children are paying for it. These leaders have relinquished their responsibility to local school boards. Several have reinforced the no-mask mandate while others have had the courage and insight to ignore state government leaders and have established mask mandates.
How is this lack of enforcement of national recommendations affecting our patients? Let’s look at two neighboring school districts in Texas. School districts have COVID-19 dashboards that are updated daily and accessible to the general public. School District A requires masks for school entry. It serves 196,171 students and has 27,195 teachers and staff. Since school opened in August, 1,606 cumulative cases of COVID-19 in students (0.8%) and 282 in staff (1%) have been reported. Fifty-five percent of the student cases occurred in elementary schools. In contrast, School District B located in the adjacent county serves 64,517 students and has 3,906 teachers and staff with no mask mandate. Since August, there have been 4,506 cumulative COVID-19 cases in students (6.9%) and 578 (14.7%) in staff. Information regarding the specific school type was not provided; however, the dashboard indicates that 2,924 cases (64.8%) occurred in children younger than 11 years of age. County data indicate 62% of those older than 12 years of age were fully vaccinated in District A, compared with 54% of persons older than 12 years in District B. The county COVID-19 positivity rate in District A is 17.6% and in District B it is 20%. Both counties are experiencing increased COVID-19 activity yet have had strikingly different outcomes in the student/staff population. While supporting the case for wearing masks to prevent disease transmission, one can’t ignore the adolescents who were infected and vaccine eligible (District A: 706; District B: 1,582). Their vaccination status could not be determined.
As pediatricians we have played an integral part in the elimination of diseases through educating and administering vaccinations. Adolescents are relatively healthy, thus limiting the number of encounters with them. The majority complete the 11-year visit; however, many fail to return for the 16- to 18-year visit.
So how are we doing? CDC data from 10 U.S. jurisdictions demonstrated a substantial decrease in vaccine administration between March and May of 2020, compared with the same period in 2018 and 2019. A decline was anticipated because of the nationwide lockdown. Doses of HPV administered declined almost 64% and 71% for 9- to 12-year-olds and 13- to 17-year-olds, respectively. Tdap administration declined 66% and 61% for the same respective age groups. Although administered doses increased between June and September of 2020, it was not sufficient to achieve catch-up coverage. Compared to the same period in 2018-2019, administration of the HPV vaccine declined 12.8% and 28% (ages 9-12 and ages 13-17) and for Tdap it was 21% and 30% lower (ages 9-12 and ages 13-17) (MMWR Morb Mortal Wkly Rep. 2021;70:840-5).
Now, we have another adolescent vaccine to discuss and encourage our patients to receive. We also need to address their concerns and/or to at least direct them to a reliable source to obtain accurate information. For the first time, a recommended vaccine may not be available at their medical home. Many don’t know where to go to receive it (http://www.vaccines.gov). Results of a Kaiser Family Foundation COVID-19 survey (August 2021) indicated that parents trusted their pediatricians most often (78%) for vaccine advice. The respondents voiced concern about trusting the location where the child would be immunized and long-term effects especially related to fertility. Parents who received communications regarding the benefits of vaccination were twice as likely to have their adolescents immunized. Finally, remember: Like parent, like child. An immunized parent is more likely to immunize the adolescent. (See Fig. 1.)
It is beyond the scope of this column to discuss the psychosocial aspects of this disease: children experiencing the death of teachers, classmates, family members, and those viewing the vitriol between pro- and antimask proponents often exhibited on school premises. And let’s not forget the child who wants to wear a mask but may be ostracized or bullied for doing so.
Our job is to do our very best to advocate for and to protect our patients by promoting mandatory masks at schools and encouraging vaccination of adolescents as we patiently wait for vaccines to become available for all of our children.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
I began thinking of a topic for this column weeks ago determined to discuss anything except COVID-19. Yet, news reports from all sources blasted daily reminders of rising COVID-19 cases overall and specifically in children.
In August, school resumed for many of our patients and the battle over mandating masks for school attendance was in full swing. The fact that it is a Centers for Disease Control and Prevention recommendation supported by both the American Academy of Pediatrics and the Pediatric Infectious Disease Society fell on deaf ears. One day, I heard a report that over 25,000 students attending Texas public schools were diagnosed with COVID-19 between Aug. 23 and Aug. 29. This peak in activity occurred just 2 weeks after the start of school and led to the closure of 45 school districts. Texas does not have a monopoly on these rising cases. Delta, a more contagious variant, began circulating in June 2021 and by July it was the most predominant. Emergency department visits and hospitalizations have increased nationwide. During the latter 2 weeks of August 2021, COVID-19–related ED visits and hospitalizations for persons aged 0-17 years were 3.4 and 3.7 times higher in states with the lowest vaccination coverage, compared with states with high vaccination coverage (MMWR Morb Mortal Wkly Rep. 2021;70:1249-54). Specifically, the rates of hospitalization the week ending Aug. 14, 2021, were nearly 5 times the rates for the week ending June 26, 2021, for 0- to 17-year-olds and nearly 10 times the rates for children 0-4 years of age. Hospitalization rates were 10.1 times higher for unimmunized adolescents than for fully vaccinated ones (MMWR Morb Mortal Wkly Rep. 2021;70:1255-60).
Multiple elected state leaders have opposed interventions such as mandating masks in school, and our children are paying for it. These leaders have relinquished their responsibility to local school boards. Several have reinforced the no-mask mandate while others have had the courage and insight to ignore state government leaders and have established mask mandates.
How is this lack of enforcement of national recommendations affecting our patients? Let’s look at two neighboring school districts in Texas. School districts have COVID-19 dashboards that are updated daily and accessible to the general public. School District A requires masks for school entry. It serves 196,171 students and has 27,195 teachers and staff. Since school opened in August, 1,606 cumulative cases of COVID-19 in students (0.8%) and 282 in staff (1%) have been reported. Fifty-five percent of the student cases occurred in elementary schools. In contrast, School District B located in the adjacent county serves 64,517 students and has 3,906 teachers and staff with no mask mandate. Since August, there have been 4,506 cumulative COVID-19 cases in students (6.9%) and 578 (14.7%) in staff. Information regarding the specific school type was not provided; however, the dashboard indicates that 2,924 cases (64.8%) occurred in children younger than 11 years of age. County data indicate 62% of those older than 12 years of age were fully vaccinated in District A, compared with 54% of persons older than 12 years in District B. The county COVID-19 positivity rate in District A is 17.6% and in District B it is 20%. Both counties are experiencing increased COVID-19 activity yet have had strikingly different outcomes in the student/staff population. While supporting the case for wearing masks to prevent disease transmission, one can’t ignore the adolescents who were infected and vaccine eligible (District A: 706; District B: 1,582). Their vaccination status could not be determined.
As pediatricians we have played an integral part in the elimination of diseases through educating and administering vaccinations. Adolescents are relatively healthy, thus limiting the number of encounters with them. The majority complete the 11-year visit; however, many fail to return for the 16- to 18-year visit.
So how are we doing? CDC data from 10 U.S. jurisdictions demonstrated a substantial decrease in vaccine administration between March and May of 2020, compared with the same period in 2018 and 2019. A decline was anticipated because of the nationwide lockdown. Doses of HPV administered declined almost 64% and 71% for 9- to 12-year-olds and 13- to 17-year-olds, respectively. Tdap administration declined 66% and 61% for the same respective age groups. Although administered doses increased between June and September of 2020, it was not sufficient to achieve catch-up coverage. Compared to the same period in 2018-2019, administration of the HPV vaccine declined 12.8% and 28% (ages 9-12 and ages 13-17) and for Tdap it was 21% and 30% lower (ages 9-12 and ages 13-17) (MMWR Morb Mortal Wkly Rep. 2021;70:840-5).
Now, we have another adolescent vaccine to discuss and encourage our patients to receive. We also need to address their concerns and/or to at least direct them to a reliable source to obtain accurate information. For the first time, a recommended vaccine may not be available at their medical home. Many don’t know where to go to receive it (http://www.vaccines.gov). Results of a Kaiser Family Foundation COVID-19 survey (August 2021) indicated that parents trusted their pediatricians most often (78%) for vaccine advice. The respondents voiced concern about trusting the location where the child would be immunized and long-term effects especially related to fertility. Parents who received communications regarding the benefits of vaccination were twice as likely to have their adolescents immunized. Finally, remember: Like parent, like child. An immunized parent is more likely to immunize the adolescent. (See Fig. 1.)
It is beyond the scope of this column to discuss the psychosocial aspects of this disease: children experiencing the death of teachers, classmates, family members, and those viewing the vitriol between pro- and antimask proponents often exhibited on school premises. And let’s not forget the child who wants to wear a mask but may be ostracized or bullied for doing so.
Our job is to do our very best to advocate for and to protect our patients by promoting mandatory masks at schools and encouraging vaccination of adolescents as we patiently wait for vaccines to become available for all of our children.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures.
Patient risk-benefit thresholds for antibiotic use in dermatologic surgery vary widely
(SSI) and had negligible side effects, in a prospective multicenter study.

In addition, a similar proportion of patients preferred to take an antibiotic if there was no SSI reduction and a high risk of adverse events.
Those are two key findings from the study aimed at understanding patient preferences for prophylactic oral antibiotic use following dermatologic surgery, which was published in Dermatologic Surgery.
“Patient risk-benefit thresholds for using antibiotics vary considerably,” the study’s corresponding author, Jeremy R. Etzkorn, MD, MS, of the department of dermatology at the Hospital of the University of Pennsylvania, Philadelphia, told this news organization. “Physicians should appreciate and consider the variation between patients before deciding to send in a prescription after skin surgery.”
To investigate patient preferences about taking antibiotics to prevent SSI relative to antibiotic efficacy and antibiotic-associated adverse drug reactions, Dr. Etzkorn and colleagues at six U.S. medical centers prospectively administered a web-based survey and discrete choice experiment to 388 adults including dermatologic surgery patients and their family members, as well as health care workers (defined as dermatologic surgery patients who work in health care, individuals who work in health care and are accompanying patients to their surgery, or staff in the dermatology clinic.) “A lot has been published about physician preferences and practice patterns with respect to antibiotic prescribing after dermatologic surgery,” Dr. Etzkorn noted. “This is the first study to evaluate patient preferences in a rigorous way.”
He and his coinvestigators used a technique from marketing and product research (conjoint analysis/discrete choice experiments) to quantify what patients think about using antibiotics and what trade-offs they are – or are not – willing to make to reduce their risk of infection.
Nearly half of the respondents (47%) were patients, 29% were family members of patients, 19% were health care workers, and the rest were described as patient caregivers or “other.” More than half (59%) were female, the mean age at surgery was 59 years, and 69% had college or postgraduate degrees.
More than half of respondents (55%) would choose to take an antibiotic if it reduced the SSI rate from 5% to 2.5% and if the risk of adverse drug reactions was low (defined as a 1% risk gastrointestinal upset, 0.5% risk itchy skin rash, and 0.01% risk ED visit). Even if an antibiotic could eliminate SSI risk entirely and had a low adverse drug reaction profile, 27% of respondents preferred not to take prophylactic oral antibiotics.
A subgroup analysis revealed that only 21% of health care workers would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 41% of those who do not work in health care. Respondent age also drove treatment choice. For example, only 33% of respondents younger than age 65 would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 45% of those aged 65 years and older.
“We knew patients would likely trade some antibiotic efficacy for some side effects, just as one would trade price for features when shopping for a car,” Dr. Etzkorn said. “We were shocked to see that over a quarter – 27% – of respondents preferred to not take antibiotics even if they were able to prevent all infections and had minimal side effects.”
“It’s interesting that between 27% [and] 55% of patients preferred no operative antibiotic prophylaxis despite a theoretical 100% cure rate for surgical-site infections,” said Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study results.
“I think this mirrors dermatologist’s preferences, as a majority also prefer not to prescribe postoperative antibiotic therapy, unless operating in an area of or a patient with a high risk for infection. It would also be interesting to see if a less educated population would also have similar preferences.”
Dr. Etzkorn acknowledged certain limitations of the study, including that while it evaluated patient reported preferences, it did not include all possible risks and benefits, and “it does not measure actual patient behaviors.”
The researchers reported having no relevant financial disclosures. Dr. Etzkorn disclosed that he serves as a data safety monitoring board member for a clinical trial of Replimmune. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
(SSI) and had negligible side effects, in a prospective multicenter study.
In addition, a similar proportion of patients preferred to take an antibiotic if there was no SSI reduction and a high risk of adverse events.
Those are two key findings from the study aimed at understanding patient preferences for prophylactic oral antibiotic use following dermatologic surgery, which was published in Dermatologic Surgery.
“Patient risk-benefit thresholds for using antibiotics vary considerably,” the study’s corresponding author, Jeremy R. Etzkorn, MD, MS, of the department of dermatology at the Hospital of the University of Pennsylvania, Philadelphia, told this news organization. “Physicians should appreciate and consider the variation between patients before deciding to send in a prescription after skin surgery.”
To investigate patient preferences about taking antibiotics to prevent SSI relative to antibiotic efficacy and antibiotic-associated adverse drug reactions, Dr. Etzkorn and colleagues at six U.S. medical centers prospectively administered a web-based survey and discrete choice experiment to 388 adults including dermatologic surgery patients and their family members, as well as health care workers (defined as dermatologic surgery patients who work in health care, individuals who work in health care and are accompanying patients to their surgery, or staff in the dermatology clinic.) “A lot has been published about physician preferences and practice patterns with respect to antibiotic prescribing after dermatologic surgery,” Dr. Etzkorn noted. “This is the first study to evaluate patient preferences in a rigorous way.”
He and his coinvestigators used a technique from marketing and product research (conjoint analysis/discrete choice experiments) to quantify what patients think about using antibiotics and what trade-offs they are – or are not – willing to make to reduce their risk of infection.
Nearly half of the respondents (47%) were patients, 29% were family members of patients, 19% were health care workers, and the rest were described as patient caregivers or “other.” More than half (59%) were female, the mean age at surgery was 59 years, and 69% had college or postgraduate degrees.
More than half of respondents (55%) would choose to take an antibiotic if it reduced the SSI rate from 5% to 2.5% and if the risk of adverse drug reactions was low (defined as a 1% risk gastrointestinal upset, 0.5% risk itchy skin rash, and 0.01% risk ED visit). Even if an antibiotic could eliminate SSI risk entirely and had a low adverse drug reaction profile, 27% of respondents preferred not to take prophylactic oral antibiotics.
A subgroup analysis revealed that only 21% of health care workers would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 41% of those who do not work in health care. Respondent age also drove treatment choice. For example, only 33% of respondents younger than age 65 would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 45% of those aged 65 years and older.
“We knew patients would likely trade some antibiotic efficacy for some side effects, just as one would trade price for features when shopping for a car,” Dr. Etzkorn said. “We were shocked to see that over a quarter – 27% – of respondents preferred to not take antibiotics even if they were able to prevent all infections and had minimal side effects.”
“It’s interesting that between 27% [and] 55% of patients preferred no operative antibiotic prophylaxis despite a theoretical 100% cure rate for surgical-site infections,” said Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study results.
“I think this mirrors dermatologist’s preferences, as a majority also prefer not to prescribe postoperative antibiotic therapy, unless operating in an area of or a patient with a high risk for infection. It would also be interesting to see if a less educated population would also have similar preferences.”
Dr. Etzkorn acknowledged certain limitations of the study, including that while it evaluated patient reported preferences, it did not include all possible risks and benefits, and “it does not measure actual patient behaviors.”
The researchers reported having no relevant financial disclosures. Dr. Etzkorn disclosed that he serves as a data safety monitoring board member for a clinical trial of Replimmune. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
(SSI) and had negligible side effects, in a prospective multicenter study.
In addition, a similar proportion of patients preferred to take an antibiotic if there was no SSI reduction and a high risk of adverse events.
Those are two key findings from the study aimed at understanding patient preferences for prophylactic oral antibiotic use following dermatologic surgery, which was published in Dermatologic Surgery.
“Patient risk-benefit thresholds for using antibiotics vary considerably,” the study’s corresponding author, Jeremy R. Etzkorn, MD, MS, of the department of dermatology at the Hospital of the University of Pennsylvania, Philadelphia, told this news organization. “Physicians should appreciate and consider the variation between patients before deciding to send in a prescription after skin surgery.”
To investigate patient preferences about taking antibiotics to prevent SSI relative to antibiotic efficacy and antibiotic-associated adverse drug reactions, Dr. Etzkorn and colleagues at six U.S. medical centers prospectively administered a web-based survey and discrete choice experiment to 388 adults including dermatologic surgery patients and their family members, as well as health care workers (defined as dermatologic surgery patients who work in health care, individuals who work in health care and are accompanying patients to their surgery, or staff in the dermatology clinic.) “A lot has been published about physician preferences and practice patterns with respect to antibiotic prescribing after dermatologic surgery,” Dr. Etzkorn noted. “This is the first study to evaluate patient preferences in a rigorous way.”
He and his coinvestigators used a technique from marketing and product research (conjoint analysis/discrete choice experiments) to quantify what patients think about using antibiotics and what trade-offs they are – or are not – willing to make to reduce their risk of infection.
Nearly half of the respondents (47%) were patients, 29% were family members of patients, 19% were health care workers, and the rest were described as patient caregivers or “other.” More than half (59%) were female, the mean age at surgery was 59 years, and 69% had college or postgraduate degrees.
More than half of respondents (55%) would choose to take an antibiotic if it reduced the SSI rate from 5% to 2.5% and if the risk of adverse drug reactions was low (defined as a 1% risk gastrointestinal upset, 0.5% risk itchy skin rash, and 0.01% risk ED visit). Even if an antibiotic could eliminate SSI risk entirely and had a low adverse drug reaction profile, 27% of respondents preferred not to take prophylactic oral antibiotics.
A subgroup analysis revealed that only 21% of health care workers would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 41% of those who do not work in health care. Respondent age also drove treatment choice. For example, only 33% of respondents younger than age 65 would choose a moderate efficacy antibiotic (2.5% SSI risk) with a high adverse effect profile, compared with 45% of those aged 65 years and older.
“We knew patients would likely trade some antibiotic efficacy for some side effects, just as one would trade price for features when shopping for a car,” Dr. Etzkorn said. “We were shocked to see that over a quarter – 27% – of respondents preferred to not take antibiotics even if they were able to prevent all infections and had minimal side effects.”
“It’s interesting that between 27% [and] 55% of patients preferred no operative antibiotic prophylaxis despite a theoretical 100% cure rate for surgical-site infections,” said Lawrence J. Green, MD, clinical professor of dermatology at George Washington University, Washington, who was asked to comment on the study results.
“I think this mirrors dermatologist’s preferences, as a majority also prefer not to prescribe postoperative antibiotic therapy, unless operating in an area of or a patient with a high risk for infection. It would also be interesting to see if a less educated population would also have similar preferences.”
Dr. Etzkorn acknowledged certain limitations of the study, including that while it evaluated patient reported preferences, it did not include all possible risks and benefits, and “it does not measure actual patient behaviors.”
The researchers reported having no relevant financial disclosures. Dr. Etzkorn disclosed that he serves as a data safety monitoring board member for a clinical trial of Replimmune. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
FROM DERMATOLOGIC SURGERY