User login
Tinkering With Elective Repeat Cesarean Timing Proves Tricky
MINNEAPOLIS – Shifting the timing of elective repeat cesareans to late term may have the unintended consequence of increasing the proportion of women needing an emergency cesarean section, results of a new study suggest.
Moreover, these emergency deliveries were associated with a twofold increased risk of adverse maternal and neonatal outcomes after adjustment for confounders, Jennifer Hutcheon, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.

Previous studies have established that elective repeat cesarean sections performed at early-term gestation, 37-38 weeks, have higher rates of neonatal respiratory complications than late-term deliveries at 39-41 weeks.
The American College of Obstetricians and Gynecologists (ACOG) discourages elective cesarean delivery before 39 weeks of gestation unless there is evidence of fetal lung maturity.
A recent report from the United States and a report from the Netherlands, however, indicate that 35%-55% of elective repeat cesarean deliveries are performed before 39 weeks, said Dr. Hutcheon, an epidemiologist in obstetrics and gynecology at the University of British Columbia, Vancouver.
"A better understanding of potential risks and their mechanisms is needed in order to make sure we implement preventive measures," she said.
To explore this, the researchers used the birth records of 9,206 low-risk women undergoing a planned repeat cesarean delivery in the British Columbia Perinatal Database Registry for 2008-2011, and calculated the correlation between institutional rates of early-term delivery and rates of emergency cesarean delivery for each of the 13 major obstetrical centers in British Columbia. Early term was defined as 37 weeks, 0 days, to 38 weeks, 6 days.
Adverse maternal outcome was defined as any occurrence of maternal mortality, cardiac arrest, obstetric shock, postpartum hemorrhage requiring transfusion or hysterectomy, mechanical ventilation through endotracheal tube, or severe medical morbidity. Adverse neonatal outcome was defined as any in-hospital newborn death, neonatal seizures, or respiratory morbidity requiring positive-pressure ventilation.
The analysis excluded women with suspected intrauterine growth restriction, multiples, congenital anomalies, diabetes, hypertension, or cardiac or renal disease.
In British Columbia, 55% of the elective repeat C-section deliveries were done before 39 weeks, Dr. Hutcheon said. There was considerable variation between institutions, with some centers performing only 35% of cases before 39 weeks and others 72%.
Overall, 15% of repeat cesarean deliveries in the province were performed under emergency timing. Once again, rates ranged between 35% and 72% at the different institutions.
There was a strong negative correlation between institutional rates of early-term delivery and emergency cesareans (r = –0.86; P less than .001), she said. For example, the institution with 72% of its elective repeat cesareans delivered before 39 weeks had fewer than 10% of women needing an emergency cesarean. On the other hand, the institution doing only 35% of elective cesareans before 39 weeks had one in three women going into labor and requiring emergency cesarean delivery.
In a univariate analysis, emergency cesarean delivery was associated with a significantly increased risk of adverse maternal outcome (odds ratio 2.1) and adverse neonatal outcome (OR 2.3), and a modest, nonsignificant increase in obstetrical wound infection (OR 1.4) and use of general anesthesia (OR 1.7), Dr. Hutcheon said.
In a multivariate analysis that adjusted for maternal age, body mass index, number of previous cesareans, and institutional obstetrical volume, the odds ratios were 2.1, 2.5, 1.2, and 1.8, for adverse maternal outcome, adverse neonatal outcome, obstetrical wound infection, and use of general anesthesia, respectively. All differences were significant except for obstetrical wound infection.
Dr. Hutcheon acknowledged that identifying the planned mode of delivery was challenging, and that some of the cesareans performed for an indication of "repeat" or "maternal request/VBAC [vaginal birth after cesarean] declined" may actually have been attempted vaginal deliveries.
To get a handle on this, the investigators looked at the time between hospital admission and when the delivery was actually performed. What they found was that the median interval was less than 3 hours, and was less than 4 hours for all of the cases with adverse outcomes.
"This is certainly more suggestive of a planned cesarean delivery rather than a failed VBAC attempt, where we would expect that interval to be quite a bit longer, although we can’t be sure," she said.
During a discussion of the results, an attendee asked whether it’s possible from the data to identify a "gestational sweet spot" that would reduce the risk of an emergency cesarean and yet be late enough to minimize the risk of adverse neonatal outcomes. Dr. Hutcheon said that is not possible from their data, and that this requires weighing two competing risks.
"You’re weighing a baby in the NICU [neonatal intensive care unit] and the potential for maternal complications, and those risks may be weighed differently by different people," she said, adding that this risk also varies depending on whether the delivery is at an academic center or a community hospital.
Finally, another attendee said the finding that institutions with high rates of repeat cesareans before 39 weeks are doing fewer emergency cesarean deliveries implies that obstetricians should be performing more cesareans before 39 weeks.
Dr. Hutcheon said, "I’m not trying to make the case that we should be doing more early-term elective cesarean deliveries. I think the point is more that we need to be more aware that if we’re introducing policies to try to shift the timing of delivery, this is going to be a side effect. And we need to plan for it better ... and to evaluate our policies to see if there are any adverse effects."
Perinatal Services BC sponsored the study. Dr. Hutcheon and her coauthors reported no conflicts.
MINNEAPOLIS – Shifting the timing of elective repeat cesareans to late term may have the unintended consequence of increasing the proportion of women needing an emergency cesarean section, results of a new study suggest.
Moreover, these emergency deliveries were associated with a twofold increased risk of adverse maternal and neonatal outcomes after adjustment for confounders, Jennifer Hutcheon, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
Previous studies have established that elective repeat cesarean sections performed at early-term gestation, 37-38 weeks, have higher rates of neonatal respiratory complications than late-term deliveries at 39-41 weeks.
The American College of Obstetricians and Gynecologists (ACOG) discourages elective cesarean delivery before 39 weeks of gestation unless there is evidence of fetal lung maturity.
A recent report from the United States and a report from the Netherlands, however, indicate that 35%-55% of elective repeat cesarean deliveries are performed before 39 weeks, said Dr. Hutcheon, an epidemiologist in obstetrics and gynecology at the University of British Columbia, Vancouver.
"A better understanding of potential risks and their mechanisms is needed in order to make sure we implement preventive measures," she said.
To explore this, the researchers used the birth records of 9,206 low-risk women undergoing a planned repeat cesarean delivery in the British Columbia Perinatal Database Registry for 2008-2011, and calculated the correlation between institutional rates of early-term delivery and rates of emergency cesarean delivery for each of the 13 major obstetrical centers in British Columbia. Early term was defined as 37 weeks, 0 days, to 38 weeks, 6 days.
Adverse maternal outcome was defined as any occurrence of maternal mortality, cardiac arrest, obstetric shock, postpartum hemorrhage requiring transfusion or hysterectomy, mechanical ventilation through endotracheal tube, or severe medical morbidity. Adverse neonatal outcome was defined as any in-hospital newborn death, neonatal seizures, or respiratory morbidity requiring positive-pressure ventilation.
The analysis excluded women with suspected intrauterine growth restriction, multiples, congenital anomalies, diabetes, hypertension, or cardiac or renal disease.
In British Columbia, 55% of the elective repeat C-section deliveries were done before 39 weeks, Dr. Hutcheon said. There was considerable variation between institutions, with some centers performing only 35% of cases before 39 weeks and others 72%.
Overall, 15% of repeat cesarean deliveries in the province were performed under emergency timing. Once again, rates ranged between 35% and 72% at the different institutions.
There was a strong negative correlation between institutional rates of early-term delivery and emergency cesareans (r = –0.86; P less than .001), she said. For example, the institution with 72% of its elective repeat cesareans delivered before 39 weeks had fewer than 10% of women needing an emergency cesarean. On the other hand, the institution doing only 35% of elective cesareans before 39 weeks had one in three women going into labor and requiring emergency cesarean delivery.
In a univariate analysis, emergency cesarean delivery was associated with a significantly increased risk of adverse maternal outcome (odds ratio 2.1) and adverse neonatal outcome (OR 2.3), and a modest, nonsignificant increase in obstetrical wound infection (OR 1.4) and use of general anesthesia (OR 1.7), Dr. Hutcheon said.
In a multivariate analysis that adjusted for maternal age, body mass index, number of previous cesareans, and institutional obstetrical volume, the odds ratios were 2.1, 2.5, 1.2, and 1.8, for adverse maternal outcome, adverse neonatal outcome, obstetrical wound infection, and use of general anesthesia, respectively. All differences were significant except for obstetrical wound infection.
Dr. Hutcheon acknowledged that identifying the planned mode of delivery was challenging, and that some of the cesareans performed for an indication of "repeat" or "maternal request/VBAC [vaginal birth after cesarean] declined" may actually have been attempted vaginal deliveries.
To get a handle on this, the investigators looked at the time between hospital admission and when the delivery was actually performed. What they found was that the median interval was less than 3 hours, and was less than 4 hours for all of the cases with adverse outcomes.
"This is certainly more suggestive of a planned cesarean delivery rather than a failed VBAC attempt, where we would expect that interval to be quite a bit longer, although we can’t be sure," she said.
During a discussion of the results, an attendee asked whether it’s possible from the data to identify a "gestational sweet spot" that would reduce the risk of an emergency cesarean and yet be late enough to minimize the risk of adverse neonatal outcomes. Dr. Hutcheon said that is not possible from their data, and that this requires weighing two competing risks.
"You’re weighing a baby in the NICU [neonatal intensive care unit] and the potential for maternal complications, and those risks may be weighed differently by different people," she said, adding that this risk also varies depending on whether the delivery is at an academic center or a community hospital.
Finally, another attendee said the finding that institutions with high rates of repeat cesareans before 39 weeks are doing fewer emergency cesarean deliveries implies that obstetricians should be performing more cesareans before 39 weeks.
Dr. Hutcheon said, "I’m not trying to make the case that we should be doing more early-term elective cesarean deliveries. I think the point is more that we need to be more aware that if we’re introducing policies to try to shift the timing of delivery, this is going to be a side effect. And we need to plan for it better ... and to evaluate our policies to see if there are any adverse effects."
Perinatal Services BC sponsored the study. Dr. Hutcheon and her coauthors reported no conflicts.
MINNEAPOLIS – Shifting the timing of elective repeat cesareans to late term may have the unintended consequence of increasing the proportion of women needing an emergency cesarean section, results of a new study suggest.
Moreover, these emergency deliveries were associated with a twofold increased risk of adverse maternal and neonatal outcomes after adjustment for confounders, Jennifer Hutcheon, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
Previous studies have established that elective repeat cesarean sections performed at early-term gestation, 37-38 weeks, have higher rates of neonatal respiratory complications than late-term deliveries at 39-41 weeks.
The American College of Obstetricians and Gynecologists (ACOG) discourages elective cesarean delivery before 39 weeks of gestation unless there is evidence of fetal lung maturity.
A recent report from the United States and a report from the Netherlands, however, indicate that 35%-55% of elective repeat cesarean deliveries are performed before 39 weeks, said Dr. Hutcheon, an epidemiologist in obstetrics and gynecology at the University of British Columbia, Vancouver.
"A better understanding of potential risks and their mechanisms is needed in order to make sure we implement preventive measures," she said.
To explore this, the researchers used the birth records of 9,206 low-risk women undergoing a planned repeat cesarean delivery in the British Columbia Perinatal Database Registry for 2008-2011, and calculated the correlation between institutional rates of early-term delivery and rates of emergency cesarean delivery for each of the 13 major obstetrical centers in British Columbia. Early term was defined as 37 weeks, 0 days, to 38 weeks, 6 days.
Adverse maternal outcome was defined as any occurrence of maternal mortality, cardiac arrest, obstetric shock, postpartum hemorrhage requiring transfusion or hysterectomy, mechanical ventilation through endotracheal tube, or severe medical morbidity. Adverse neonatal outcome was defined as any in-hospital newborn death, neonatal seizures, or respiratory morbidity requiring positive-pressure ventilation.
The analysis excluded women with suspected intrauterine growth restriction, multiples, congenital anomalies, diabetes, hypertension, or cardiac or renal disease.
In British Columbia, 55% of the elective repeat C-section deliveries were done before 39 weeks, Dr. Hutcheon said. There was considerable variation between institutions, with some centers performing only 35% of cases before 39 weeks and others 72%.
Overall, 15% of repeat cesarean deliveries in the province were performed under emergency timing. Once again, rates ranged between 35% and 72% at the different institutions.
There was a strong negative correlation between institutional rates of early-term delivery and emergency cesareans (r = –0.86; P less than .001), she said. For example, the institution with 72% of its elective repeat cesareans delivered before 39 weeks had fewer than 10% of women needing an emergency cesarean. On the other hand, the institution doing only 35% of elective cesareans before 39 weeks had one in three women going into labor and requiring emergency cesarean delivery.
In a univariate analysis, emergency cesarean delivery was associated with a significantly increased risk of adverse maternal outcome (odds ratio 2.1) and adverse neonatal outcome (OR 2.3), and a modest, nonsignificant increase in obstetrical wound infection (OR 1.4) and use of general anesthesia (OR 1.7), Dr. Hutcheon said.
In a multivariate analysis that adjusted for maternal age, body mass index, number of previous cesareans, and institutional obstetrical volume, the odds ratios were 2.1, 2.5, 1.2, and 1.8, for adverse maternal outcome, adverse neonatal outcome, obstetrical wound infection, and use of general anesthesia, respectively. All differences were significant except for obstetrical wound infection.
Dr. Hutcheon acknowledged that identifying the planned mode of delivery was challenging, and that some of the cesareans performed for an indication of "repeat" or "maternal request/VBAC [vaginal birth after cesarean] declined" may actually have been attempted vaginal deliveries.
To get a handle on this, the investigators looked at the time between hospital admission and when the delivery was actually performed. What they found was that the median interval was less than 3 hours, and was less than 4 hours for all of the cases with adverse outcomes.
"This is certainly more suggestive of a planned cesarean delivery rather than a failed VBAC attempt, where we would expect that interval to be quite a bit longer, although we can’t be sure," she said.
During a discussion of the results, an attendee asked whether it’s possible from the data to identify a "gestational sweet spot" that would reduce the risk of an emergency cesarean and yet be late enough to minimize the risk of adverse neonatal outcomes. Dr. Hutcheon said that is not possible from their data, and that this requires weighing two competing risks.
"You’re weighing a baby in the NICU [neonatal intensive care unit] and the potential for maternal complications, and those risks may be weighed differently by different people," she said, adding that this risk also varies depending on whether the delivery is at an academic center or a community hospital.
Finally, another attendee said the finding that institutions with high rates of repeat cesareans before 39 weeks are doing fewer emergency cesarean deliveries implies that obstetricians should be performing more cesareans before 39 weeks.
Dr. Hutcheon said, "I’m not trying to make the case that we should be doing more early-term elective cesarean deliveries. I think the point is more that we need to be more aware that if we’re introducing policies to try to shift the timing of delivery, this is going to be a side effect. And we need to plan for it better ... and to evaluate our policies to see if there are any adverse effects."
Perinatal Services BC sponsored the study. Dr. Hutcheon and her coauthors reported no conflicts.
AT THE ANNUAL MEETING OF THE SOCIETY FOR PEDIATRIC AND PERINATAL EPIDEMIOLOGIC RESEARCH

Treatment Guidelines for Thyroid Dysfunction in Pregnancy Updated
When treating women with thyroid dysfunction during and after pregnancy, clinicians should use caution interpreting serum-free thyroxine levels, use propylthiouracil as the first-line drug during for hyperthyroidism in the first trimester, and advise breastfeeding women to maintain a daily intake of 250 mcg of iodine to ensure breast milk provides 100 mcg of iodine/day to the infant.
These mark some of the changes the Endocrine Society made to its 2007 Clinical Practice Guideline (CPG) for the management of thyroid disease during pregnancy and the postpartum.

"Pregnancy may affect the course of thyroid diseases and conversely, thyroid diseases may affect the course of pregnancy," Dr. Leslie De Groot, lead researcher from the University of Rhode Island, Kingston, said in a prepared statement. "Pregnant women may be under the care of multiple health care professionals including obstetricians, nurse midwives, family practitioners and endocrinologists making the development of guidelines all the more critical."
In order to update the Endocrine Society’s 2007 CPG, Dr. De Groot and a task force of 12 other experts reviewed existing medical literature on the topic and followed the approach of the U.S. Preventive Services Task Force and the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) system to evaluate the strength of each recommendation. The effort, published online in the Aug. 12 issue of the Journal of Clinical Endocrinology & Metabolism, included collaboration with the Asia and Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society (J. Clin. Endocrinol. Metab. 2012 Aug. 1;97:2543-65 [doi: 10.1210/jc.2011-2803]).
"At present, with the exception of studies on iodide nutrition, only a few prospective, randomized intervention trials have been published in this area [of thyroid dysfunction during pregnancy]," the authors wrote. "We are aware of large-scale prospective intervention trials that are ongoing. Nevertheless, in the past decade many high-quality studies have modified older dogmas and profoundly changed the ways in which these patients are managed."
Key recommendations in the 2012 clinical practice guideline that differ from the 2007 version include the following:
• Use caution in the interpretation of serum-free T4 levels during pregnancy. "Each laboratory should establish trimester-specific reference ranges for pregnant women if using a free T4 assay," the authors wrote in a supplemental index in which they summarized changes between the 2007 and 2012 versions of the guideline. "The non-pregnant total T4 range (5-12 mcg/dL or 50-150 nmol/L) can be adapted in the second and third trimesters by multiplying this range by 1.5-fold. Alternatively, the free thyroxine index (‘adjusted T4’) appears to be a reliable assay during pregnancy."
• Use propylthiouracil (PTU), if available, as the first-line drug for treatment of hyperthyroidism during the first trimester. This is because of the possible association of methimazole (MMI) with congenital abnormalities. MMI "may also be prescribed if PTU is not available or if a patient cannot tolerate or has an adverse response to PTU," the authors wrote. "Recent analyses reported by the FDA indicate that PTU may rarely be associated with severe liver toxicity. For this reason, we recommend that clinicians should change treatment of patients from PTU to MMI after the completion of first trimester. Available data indicate that MMI and PTU are equally efficacious in treatment of pregnant women."
• Breastfeeding women should maintain a daily intake of 250 mcg of iodine. This ensures that breast milk provides 100 mcg iodine/day to the infant. "These changes are in response to recent publications indicating that some vitamin-mineral preparations used during pregnancy may not provide adequate iodine intake, and that iodine supplements should be continued during breastfeeding," the authors explained.
• Measure thyroid receptor antibodies (TRAb) before 22 weeks’ gestational age in a subset of mothers. This includes mothers with either current Graves’ disease, a history of Graves’ disease and treatment with 131-I (radioiodine) or thyroidectomy before pregnancy, a previous neonate with Graves’ disease, or previously elevated TRAb. This approach is recommended because thyroid receptor antibodies "freely cross the placenta and can stimulate or inhibit the fetal thyroid," the authors wrote. "Women who have negative TRAb and do not require antithyroid drugs have a very low risk of fetal or neonatal thyroid dysfunction. This change makes more explicit the timing and indications for measurement of TRAb in pregnancy."
The authors could not reach agreement on universal screening recommendations for all newly pregnant women. Some recommend screening of all pregnant women for serum TSH abnormalities by the 9th week or at the time of their first visit while others recommended neither for nor against universal screening of all pregnant women for TSH abnormalities at the time of their first visit.
Despite their differences on universal screening recommendations, the authors unanimously agreed that clinicians should perform targeted screening of high-risk women during the prenatal and perinatal periods. This includes women over age 30 years and those with a family history or autoimmune thyroid disease or hypothyroidism; a goiter; thyroid antibodies, primarily thyroid peroxidase antibodies; symptoms or clinical signs suggestive of thyroid hypofunction; type 1 diabetes mellitus, or other autoimmune disorders; those with infertility; a prior history of preterm delivery; prior therapeutic head or neck irradiation or prior thyroid surgery; and those currently receiving levothyroxine replacement.
No member of the task force disclosed relevant financial conflicts of interest.
When treating women with thyroid dysfunction during and after pregnancy, clinicians should use caution interpreting serum-free thyroxine levels, use propylthiouracil as the first-line drug during for hyperthyroidism in the first trimester, and advise breastfeeding women to maintain a daily intake of 250 mcg of iodine to ensure breast milk provides 100 mcg of iodine/day to the infant.
These mark some of the changes the Endocrine Society made to its 2007 Clinical Practice Guideline (CPG) for the management of thyroid disease during pregnancy and the postpartum.
"Pregnancy may affect the course of thyroid diseases and conversely, thyroid diseases may affect the course of pregnancy," Dr. Leslie De Groot, lead researcher from the University of Rhode Island, Kingston, said in a prepared statement. "Pregnant women may be under the care of multiple health care professionals including obstetricians, nurse midwives, family practitioners and endocrinologists making the development of guidelines all the more critical."
In order to update the Endocrine Society’s 2007 CPG, Dr. De Groot and a task force of 12 other experts reviewed existing medical literature on the topic and followed the approach of the U.S. Preventive Services Task Force and the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) system to evaluate the strength of each recommendation. The effort, published online in the Aug. 12 issue of the Journal of Clinical Endocrinology & Metabolism, included collaboration with the Asia and Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society (J. Clin. Endocrinol. Metab. 2012 Aug. 1;97:2543-65 [doi: 10.1210/jc.2011-2803]).
"At present, with the exception of studies on iodide nutrition, only a few prospective, randomized intervention trials have been published in this area [of thyroid dysfunction during pregnancy]," the authors wrote. "We are aware of large-scale prospective intervention trials that are ongoing. Nevertheless, in the past decade many high-quality studies have modified older dogmas and profoundly changed the ways in which these patients are managed."
Key recommendations in the 2012 clinical practice guideline that differ from the 2007 version include the following:
• Use caution in the interpretation of serum-free T4 levels during pregnancy. "Each laboratory should establish trimester-specific reference ranges for pregnant women if using a free T4 assay," the authors wrote in a supplemental index in which they summarized changes between the 2007 and 2012 versions of the guideline. "The non-pregnant total T4 range (5-12 mcg/dL or 50-150 nmol/L) can be adapted in the second and third trimesters by multiplying this range by 1.5-fold. Alternatively, the free thyroxine index (‘adjusted T4’) appears to be a reliable assay during pregnancy."
• Use propylthiouracil (PTU), if available, as the first-line drug for treatment of hyperthyroidism during the first trimester. This is because of the possible association of methimazole (MMI) with congenital abnormalities. MMI "may also be prescribed if PTU is not available or if a patient cannot tolerate or has an adverse response to PTU," the authors wrote. "Recent analyses reported by the FDA indicate that PTU may rarely be associated with severe liver toxicity. For this reason, we recommend that clinicians should change treatment of patients from PTU to MMI after the completion of first trimester. Available data indicate that MMI and PTU are equally efficacious in treatment of pregnant women."
• Breastfeeding women should maintain a daily intake of 250 mcg of iodine. This ensures that breast milk provides 100 mcg iodine/day to the infant. "These changes are in response to recent publications indicating that some vitamin-mineral preparations used during pregnancy may not provide adequate iodine intake, and that iodine supplements should be continued during breastfeeding," the authors explained.
• Measure thyroid receptor antibodies (TRAb) before 22 weeks’ gestational age in a subset of mothers. This includes mothers with either current Graves’ disease, a history of Graves’ disease and treatment with 131-I (radioiodine) or thyroidectomy before pregnancy, a previous neonate with Graves’ disease, or previously elevated TRAb. This approach is recommended because thyroid receptor antibodies "freely cross the placenta and can stimulate or inhibit the fetal thyroid," the authors wrote. "Women who have negative TRAb and do not require antithyroid drugs have a very low risk of fetal or neonatal thyroid dysfunction. This change makes more explicit the timing and indications for measurement of TRAb in pregnancy."
The authors could not reach agreement on universal screening recommendations for all newly pregnant women. Some recommend screening of all pregnant women for serum TSH abnormalities by the 9th week or at the time of their first visit while others recommended neither for nor against universal screening of all pregnant women for TSH abnormalities at the time of their first visit.
Despite their differences on universal screening recommendations, the authors unanimously agreed that clinicians should perform targeted screening of high-risk women during the prenatal and perinatal periods. This includes women over age 30 years and those with a family history or autoimmune thyroid disease or hypothyroidism; a goiter; thyroid antibodies, primarily thyroid peroxidase antibodies; symptoms or clinical signs suggestive of thyroid hypofunction; type 1 diabetes mellitus, or other autoimmune disorders; those with infertility; a prior history of preterm delivery; prior therapeutic head or neck irradiation or prior thyroid surgery; and those currently receiving levothyroxine replacement.
No member of the task force disclosed relevant financial conflicts of interest.
When treating women with thyroid dysfunction during and after pregnancy, clinicians should use caution interpreting serum-free thyroxine levels, use propylthiouracil as the first-line drug during for hyperthyroidism in the first trimester, and advise breastfeeding women to maintain a daily intake of 250 mcg of iodine to ensure breast milk provides 100 mcg of iodine/day to the infant.
These mark some of the changes the Endocrine Society made to its 2007 Clinical Practice Guideline (CPG) for the management of thyroid disease during pregnancy and the postpartum.
"Pregnancy may affect the course of thyroid diseases and conversely, thyroid diseases may affect the course of pregnancy," Dr. Leslie De Groot, lead researcher from the University of Rhode Island, Kingston, said in a prepared statement. "Pregnant women may be under the care of multiple health care professionals including obstetricians, nurse midwives, family practitioners and endocrinologists making the development of guidelines all the more critical."
In order to update the Endocrine Society’s 2007 CPG, Dr. De Groot and a task force of 12 other experts reviewed existing medical literature on the topic and followed the approach of the U.S. Preventive Services Task Force and the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) system to evaluate the strength of each recommendation. The effort, published online in the Aug. 12 issue of the Journal of Clinical Endocrinology & Metabolism, included collaboration with the Asia and Oceania Thyroid Association, European Thyroid Association, and Latin American Thyroid Society (J. Clin. Endocrinol. Metab. 2012 Aug. 1;97:2543-65 [doi: 10.1210/jc.2011-2803]).
"At present, with the exception of studies on iodide nutrition, only a few prospective, randomized intervention trials have been published in this area [of thyroid dysfunction during pregnancy]," the authors wrote. "We are aware of large-scale prospective intervention trials that are ongoing. Nevertheless, in the past decade many high-quality studies have modified older dogmas and profoundly changed the ways in which these patients are managed."
Key recommendations in the 2012 clinical practice guideline that differ from the 2007 version include the following:
• Use caution in the interpretation of serum-free T4 levels during pregnancy. "Each laboratory should establish trimester-specific reference ranges for pregnant women if using a free T4 assay," the authors wrote in a supplemental index in which they summarized changes between the 2007 and 2012 versions of the guideline. "The non-pregnant total T4 range (5-12 mcg/dL or 50-150 nmol/L) can be adapted in the second and third trimesters by multiplying this range by 1.5-fold. Alternatively, the free thyroxine index (‘adjusted T4’) appears to be a reliable assay during pregnancy."
• Use propylthiouracil (PTU), if available, as the first-line drug for treatment of hyperthyroidism during the first trimester. This is because of the possible association of methimazole (MMI) with congenital abnormalities. MMI "may also be prescribed if PTU is not available or if a patient cannot tolerate or has an adverse response to PTU," the authors wrote. "Recent analyses reported by the FDA indicate that PTU may rarely be associated with severe liver toxicity. For this reason, we recommend that clinicians should change treatment of patients from PTU to MMI after the completion of first trimester. Available data indicate that MMI and PTU are equally efficacious in treatment of pregnant women."
• Breastfeeding women should maintain a daily intake of 250 mcg of iodine. This ensures that breast milk provides 100 mcg iodine/day to the infant. "These changes are in response to recent publications indicating that some vitamin-mineral preparations used during pregnancy may not provide adequate iodine intake, and that iodine supplements should be continued during breastfeeding," the authors explained.
• Measure thyroid receptor antibodies (TRAb) before 22 weeks’ gestational age in a subset of mothers. This includes mothers with either current Graves’ disease, a history of Graves’ disease and treatment with 131-I (radioiodine) or thyroidectomy before pregnancy, a previous neonate with Graves’ disease, or previously elevated TRAb. This approach is recommended because thyroid receptor antibodies "freely cross the placenta and can stimulate or inhibit the fetal thyroid," the authors wrote. "Women who have negative TRAb and do not require antithyroid drugs have a very low risk of fetal or neonatal thyroid dysfunction. This change makes more explicit the timing and indications for measurement of TRAb in pregnancy."
The authors could not reach agreement on universal screening recommendations for all newly pregnant women. Some recommend screening of all pregnant women for serum TSH abnormalities by the 9th week or at the time of their first visit while others recommended neither for nor against universal screening of all pregnant women for TSH abnormalities at the time of their first visit.
Despite their differences on universal screening recommendations, the authors unanimously agreed that clinicians should perform targeted screening of high-risk women during the prenatal and perinatal periods. This includes women over age 30 years and those with a family history or autoimmune thyroid disease or hypothyroidism; a goiter; thyroid antibodies, primarily thyroid peroxidase antibodies; symptoms or clinical signs suggestive of thyroid hypofunction; type 1 diabetes mellitus, or other autoimmune disorders; those with infertility; a prior history of preterm delivery; prior therapeutic head or neck irradiation or prior thyroid surgery; and those currently receiving levothyroxine replacement.
No member of the task force disclosed relevant financial conflicts of interest.
FROM THE JOURNAL OF CLINICAL ENDOCRINOLOGY AND METABOLISM

Pregnancy-Related Cancers: Rise Is Largely Unrelated to Delayed Childbearing
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.

After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
postponing childbearing, pregnancy-associated cancer,
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
MINNEAPOLIS – Pregnancy-associated cancers are increasing, although the phenomenon of delayed childbirth is only partially responsible, researchers suggest.
From 1994 to 2008, the crude incidence of pregnancy-associated cancer increased from 112 to 192 per 100,000 pregnancies (P less than .001) in an analysis of 787,907 Australian women.
During the same period, the number of Australian mothers aged 35 years or more nearly doubled from 13% to 24%, including an increase from 2% to 4% of mothers over age 40, Christine L. Roberts, Ph.D., said at the annual meeting of the Society for Pediatric and Perinatal Epidemiologic Research.
After the cancer rate was standardized to the age of the 1994 population, however, only 14% of the increase in cancer was explained by increasing maternal age, said Dr. Roberts of the University of Sydney, New South Wales, Australia.
"Improved diagnostic techniques, detection, and interracial health services likely contribute to the unexplained portion," she said. "The increasing incidence of cancer confirmed a clinical impression that obstetricians were seeing women with cancer more frequently, although of course it remains uncommon."
The growing number of women postponing childbearing has raised concerns that the incidence of pregnancy-associated cancer would rise. The incidence is generally reported to be about 1 in 1,000 pregnancies, but estimates based largely on cancer reports have been imprecise, Dr. Roberts said.
The investigators obtained cancer and maternal information from linked cancer registry, birth, and hospital records for 1.31 million pregnancies and 1.33 million infants among 781,907 women in Australia.
During the study period, 1,798 women had a new cancer diagnosis: 499 during pregnancy and 1,299 within 12 months of delivery. This equates to 137.3 cancers per 100,000 pregnancies, Dr. Roberts said.
There were 42 cancer deaths, or 3.2 deaths per 100,000 pregnancies.
The highest proportion of cancers (14.5%) was diagnosed in the first 2 months post partum, lending support to the rationale that women and physicians may incorrectly attribute cancer-related symptoms to the physiologic changes of pregnancy and may be reluctant to use radiographs or invasive procedures during pregnancy, she observed.
The cancers were predominantly melanoma (599) or breast cancer (377), followed by thyroid/endocrine (228) and lymphohematopoietic (151) cancers.
Melanoma was twice as likely to be observed in pregnant women as in women of similar reproductive age (observed to expected ratio, 2.2), according to the authors, led by Dr. Yuen Yi (Cathy) Lee of the New South Wales Ministry of Health in North Sydney, Australia.
In prior studies, breast and thyroid cancer were the most common pregnancy-related cancers in California in the 1990s (Am. J. Obstet. Gynecol. 2003;189:1128-35), whereas more recently, melanoma and cervical cancer were the most common cancers during pregnancy in Norway (J. Clin. Oncol. 2009;27:45-51), Dr. Roberts noted.
In logistic regression analysis adjusted for age, country of birth, socioeconomic status, rural residence, parity, plurality, previous cancer, and assisted reproductive technology, significant risk factors for a pregnancy-associated cancer were previous cancer diagnosis (adjusted odds ratio, 3.8), multiple pregnancy (OR, 1.5), age 30-34 years (OR, 2.1), age 35-39 years (OR, 3.0), and age 40 years or older (OR, 3.6).
Women with a cancer diagnosis had a significantly higher risk of thromboembolic events (OR, 10.2), sepsis (OR, 4.3), and life-threatening maternal morbidity (OR, 6.9) after adjustment for maternal age, socioeconomic status, plurality, parity, previous preterm birth, diabetes, and hypertension.
A novel finding was that cancer during pregnancy also was associated with large-for-gestational age infants (OR, 1.5), said Dr. Roberts, who pointed out that large-for-gestational age is also a risk factor for pediatric cancer.
"Elevated levels of maternal hormone angiogenic factors during pregnancy may influence both infant size and tumor growth," she speculated.
Dr. Roberts said there is an Australian national policy on cervical screening recommending that Pap smears be offered to every woman presenting for antenatal care who has not had cervical screening within the past 2 years; however, this was introduced in 2008 at the end of the study period. "We are not aware of other policies for screening during pregnancy," she added.
Full details of the study are expected to be published in the coming weeks (BJOG 2012 [doi: 10.111/j.1471-0528.2012.03475.x]).
The authors report no conflicts of interest.
postponing childbearing, pregnancy-associated cancer,
postponing childbearing, pregnancy-associated cancer,
AT THE ANNUAL MEETING OF THE SOCIETY FOR PEDIATRIC AND PERINATAL EPIDEMIOLOGIC RESEARCH

Postpartum Glucose Won't Predict 6-Week Diabetes
PHILADELPHIA – An elevated postpartum fasting blood sugar does not predict type 2 diabetes in women who had gestational diabetes.
Out of nine women with an elevated fasting glucose after giving birth, only two went on to a diagnosis of type 2 diabetes 6 weeks later, Dr. Hilary Roeder said at the annual scientific sessions of the American Diabetes Association.
"That means that if we had used the postpartum glucose value as a diagnostic tool, seven women would have been misdiagnosed," Dr. Roeder, an ob.gyn. at Scripps Health in San Diego, said in an interview. "We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
For women with gestational diabetes, an oral glucose tolerance test should be done 6 weeks after delivery, the American Diabetes Association recommends. But some new mothers don’t make it back to the doctor at that time, Dr. Roeder said.
"We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
"The problem with formal screening at the 6-week postpartum appointment is that patients don’t always come back for this visit," she said. "They get busy with the new baby or have already gone back to work and they don’t follow up. Or if they do, they often are not fasting – a requirement to perform formal screening for type 2 diabetes. Our thought was that if we could diagnose them prior to discharge from the hospital, we could set up a follow-up visit with a primary care physician or an endocrinologist so they can get proper care."
She employed a retrospective cohort study to determine whether postpartum glucose on the day of delivery was associated with a later type 2 diabetes diagnosis. Although there were 545 patients with gestational diabetes in the records, only 165 (30%) had a formal diabetes screen at 6 weeks – illustrating the poor rate of follow-up in the cohort.
Of those who were tested at 6 weeks, 111 also had a postpartum fasting glucose available for review. The patients had a mean age of 32 years, with a mean body mass index of 31 kg/m2. They had a mean gestation of 25 weeks when diagnosed with gestational diabetes.
Nine of those with a postpartum test had glucose levels above 126 mg/dL. But 6 weeks later, only two of those women were found to have type 2 diabetes.
When Dr. Roeder compared the postpartum glucose levels between patients, she found no significant difference between those who developed type 2 diabetes and those who did not. In fact, had the diagnosis been made immediately post partum, six additional women who did develop diabetes would have been missed, as their blood sugar was less than 126 mg/dL after delivery.
Overall, postpartum blood glucose levels were significantly higher than 6-week levels (mean 101 mg/dL vs. 93 mg/dL). Dr. Roeder said she believes human placental lactogen and other placentally-derived hormones could be responsible for this in part. The hormones keep glucose in the maternal bloodstream, making it more available for fetal metabolism. This results in higher maternal glucose levels, which take some time after birth to decline.
"Even though the placenta has been removed, the hormones are still circulating for an indefinite time after birth," she said.
Because immediate postpartum testing does not appear helpful, Dr. Roeder said it’s critical that women with gestational diabetes attend their 6-week checkup and have a full diabetes screen.
"We really need to impress upon our patients how important this visit is to their future health."
Dr. Roeder had no financial disclosures.
PHILADELPHIA – An elevated postpartum fasting blood sugar does not predict type 2 diabetes in women who had gestational diabetes.
Out of nine women with an elevated fasting glucose after giving birth, only two went on to a diagnosis of type 2 diabetes 6 weeks later, Dr. Hilary Roeder said at the annual scientific sessions of the American Diabetes Association.
"That means that if we had used the postpartum glucose value as a diagnostic tool, seven women would have been misdiagnosed," Dr. Roeder, an ob.gyn. at Scripps Health in San Diego, said in an interview. "We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
For women with gestational diabetes, an oral glucose tolerance test should be done 6 weeks after delivery, the American Diabetes Association recommends. But some new mothers don’t make it back to the doctor at that time, Dr. Roeder said.
"We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
"The problem with formal screening at the 6-week postpartum appointment is that patients don’t always come back for this visit," she said. "They get busy with the new baby or have already gone back to work and they don’t follow up. Or if they do, they often are not fasting – a requirement to perform formal screening for type 2 diabetes. Our thought was that if we could diagnose them prior to discharge from the hospital, we could set up a follow-up visit with a primary care physician or an endocrinologist so they can get proper care."
She employed a retrospective cohort study to determine whether postpartum glucose on the day of delivery was associated with a later type 2 diabetes diagnosis. Although there were 545 patients with gestational diabetes in the records, only 165 (30%) had a formal diabetes screen at 6 weeks – illustrating the poor rate of follow-up in the cohort.
Of those who were tested at 6 weeks, 111 also had a postpartum fasting glucose available for review. The patients had a mean age of 32 years, with a mean body mass index of 31 kg/m2. They had a mean gestation of 25 weeks when diagnosed with gestational diabetes.
Nine of those with a postpartum test had glucose levels above 126 mg/dL. But 6 weeks later, only two of those women were found to have type 2 diabetes.
When Dr. Roeder compared the postpartum glucose levels between patients, she found no significant difference between those who developed type 2 diabetes and those who did not. In fact, had the diagnosis been made immediately post partum, six additional women who did develop diabetes would have been missed, as their blood sugar was less than 126 mg/dL after delivery.
Overall, postpartum blood glucose levels were significantly higher than 6-week levels (mean 101 mg/dL vs. 93 mg/dL). Dr. Roeder said she believes human placental lactogen and other placentally-derived hormones could be responsible for this in part. The hormones keep glucose in the maternal bloodstream, making it more available for fetal metabolism. This results in higher maternal glucose levels, which take some time after birth to decline.
"Even though the placenta has been removed, the hormones are still circulating for an indefinite time after birth," she said.
Because immediate postpartum testing does not appear helpful, Dr. Roeder said it’s critical that women with gestational diabetes attend their 6-week checkup and have a full diabetes screen.
"We really need to impress upon our patients how important this visit is to their future health."
Dr. Roeder had no financial disclosures.
PHILADELPHIA – An elevated postpartum fasting blood sugar does not predict type 2 diabetes in women who had gestational diabetes.
Out of nine women with an elevated fasting glucose after giving birth, only two went on to a diagnosis of type 2 diabetes 6 weeks later, Dr. Hilary Roeder said at the annual scientific sessions of the American Diabetes Association.
"That means that if we had used the postpartum glucose value as a diagnostic tool, seven women would have been misdiagnosed," Dr. Roeder, an ob.gyn. at Scripps Health in San Diego, said in an interview. "We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
For women with gestational diabetes, an oral glucose tolerance test should be done 6 weeks after delivery, the American Diabetes Association recommends. But some new mothers don’t make it back to the doctor at that time, Dr. Roeder said.
"We still have no good way to know specifically which women with gestational diabetes will subsequently develop type 2 diabetes."
"The problem with formal screening at the 6-week postpartum appointment is that patients don’t always come back for this visit," she said. "They get busy with the new baby or have already gone back to work and they don’t follow up. Or if they do, they often are not fasting – a requirement to perform formal screening for type 2 diabetes. Our thought was that if we could diagnose them prior to discharge from the hospital, we could set up a follow-up visit with a primary care physician or an endocrinologist so they can get proper care."
She employed a retrospective cohort study to determine whether postpartum glucose on the day of delivery was associated with a later type 2 diabetes diagnosis. Although there were 545 patients with gestational diabetes in the records, only 165 (30%) had a formal diabetes screen at 6 weeks – illustrating the poor rate of follow-up in the cohort.
Of those who were tested at 6 weeks, 111 also had a postpartum fasting glucose available for review. The patients had a mean age of 32 years, with a mean body mass index of 31 kg/m2. They had a mean gestation of 25 weeks when diagnosed with gestational diabetes.
Nine of those with a postpartum test had glucose levels above 126 mg/dL. But 6 weeks later, only two of those women were found to have type 2 diabetes.
When Dr. Roeder compared the postpartum glucose levels between patients, she found no significant difference between those who developed type 2 diabetes and those who did not. In fact, had the diagnosis been made immediately post partum, six additional women who did develop diabetes would have been missed, as their blood sugar was less than 126 mg/dL after delivery.
Overall, postpartum blood glucose levels were significantly higher than 6-week levels (mean 101 mg/dL vs. 93 mg/dL). Dr. Roeder said she believes human placental lactogen and other placentally-derived hormones could be responsible for this in part. The hormones keep glucose in the maternal bloodstream, making it more available for fetal metabolism. This results in higher maternal glucose levels, which take some time after birth to decline.
"Even though the placenta has been removed, the hormones are still circulating for an indefinite time after birth," she said.
Because immediate postpartum testing does not appear helpful, Dr. Roeder said it’s critical that women with gestational diabetes attend their 6-week checkup and have a full diabetes screen.
"We really need to impress upon our patients how important this visit is to their future health."
Dr. Roeder had no financial disclosures.
AT THE ANNUAL MEETING OF THE AMERICAN DIABETES ASSOCIATION
Major Finding: Of nine women with gestational diabetes and elevated postpartum blood glucose, only two were diagnosed with type 2 diabetes at 6 weeks. Six women with lower postpartum glucose ended up with a diabetes diagnosis at the 6-week checkup.
Data Source: This was a retrospective study of 545 women with gestational diabetes.
Disclosures: Dr. Roeder had no disclosures.
A Case of Suspected Appendicitis
Prolonged delivery: child with CP awarded $70M … and more

AFTER MORE THAN 4 HOURS of second-stage labor followed by prolonged pushing and crowning, the baby was born depressed. Later, the child was found to have cerebral palsy.
PARENTS’ CLAIM The ObGyn was negligent in failing to perform an episiotomy, not attempting vacuum extraction, and not using forceps to assist delivery. Although fetal heart-rate monitoring results deteriorated, the ObGyn did not assess contractions for 30 minutes at one point. Hospital staff members were unable to adequately intubate or ventilate the newborn. The hospital staff disposed of the baby’s cord blood. Records were altered.
The parents’ counsel proposed that the defendants’ insurance company refused all settlement efforts prior to trial because the case venue was known to be conservative regarding jury verdicts.
DEFENDANTS’ DEFENSE The hospital and the ObGyn were not negligent; the mother and baby received proper care. Hospital staff acted appropriately.
VERDICT During the trial, the hospital settled for an undisclosed amount. An additional $2 million was offered on behalf of the ObGyn later in the trial, but the parents refused settlement at that time.
A California jury returned a $74.525 million verdict against the ObGyn. The child was awarded $70.725 million for medical expenses, lost earnings, and damages. The parents were awarded $3.8 million for emotional distress.
Was ectopic pregnancy missed?
A WOMAN IN SEVERE ABDOMINAL PAIN saw her internist. CT scans revealed a right ovarian cyst. When pain continued, she saw her ObGyn 3 weeks later, and her bowel was full of hard stool. Ultrasonography (US) showed a multicystic right ovary and a thin endometrial stripe. She was taking birth control pills and her husband had a vasectomy. She was told her abdominal pain was from constipation and ovarian cysts. A week later, she had laparoscopic surgery to remove an ectopic pregnancy.
PATIENT’S CLAIM The ObGyn did not perform a pregnancy test, and did not diagnose an ectopic pregnancy in a timely manner. An earlier diagnosis would have allowed medical rather than surgical resolution.
PHYSICIAN’S DEFENSE It was too early to determine if the pregnancy was intrauterine or ectopic. An earlier diagnosis would have resulted in laparoscopic surgery rather than medical treatment, as the medication (methotrexate) can cause increased pain.
VERDICT An Illinois defense verdict was returned.
Foreshortened vagina inhibits intercourse
A 65-YEAR-OLD WOMAN underwent anterior and posterior colphorrhaphy to repair a cystocele and rectocele, sacrospinous ligament fixation for vaginal prolapse, and a TVT mid-urethral suspension procedure to correct stress urinary incontinence. During two follow-up visits, the gynecologist determined that she was healing normally.
Within the next few weeks, the patient came to believe that her vagina had been sewn shut. She did not return to her gynecologist, but sought treatment with another physician 6 months later. It was determined that she had a stenotic and foreshortened vagina.
PATIENT’S CLAIM Too much vaginal tissue was removed during surgery.
PHYSICIAN’S DEFENSE The stenotic and foreshortened vagina was an unexpected result of the healing process after surgery.
VERDICT An Illinois defense verdict was returned.
Hydrocephalus in utero not seen until too late
A WOMAN HAD PRENATAL TREATMENT at a federally funded health clinic. A certified nurse midwife (CNM) ordered second-trimester US, with normal results. During the third trimester, the mother switched to a private ObGyn who ordered testing. US indicated the fetus was hydrocephalic. The child was born with cognitive disabilities and will need lifelong care.
PARENTS’ CLAIM The CNM ordered US too early in the pregnancy to be of diagnostic value; no further testing was undertaken. When hydrocephalus was seen, an abortion was not legally available because of fetal age.
DEFENDANT’S DEFENSE Even if US had been performed later in the second trimester, the defect would not have shown.
VERDICT A $4 million New Jersey settlement was reached.

WHEN SHOULDER DYSTOCIA WAS ENCOUNTERED, the ObGyn used standard maneuvers to deliver the child. The baby suffered a severe brachial plexus injury with rupture of C7 nerve and avulsions at C8 and T1.
Nerve-graft surgery at 6 months and tendon transfer surgery at 2 years resulted in recovery of good shoulder and elbow function, but the child has inadequate use of his wrist and hand. Additional surgeries are planned.
PARENTS’ CLAIM The ObGyn did not inform the mother that she was at risk for shoulder dystocia, nor did he discuss cesarean delivery. The mother’s risk factors included short stature, gestational diabetes, excessive weight gain during pregnancy, and two previous deliveries that involved vacuum assistance and a broken clavicle. The ObGyn applied excessive traction to the fetal head during delivery.
PHYSICIAN’S DEFENSE The mother’s risk factors were not severe enough to consider the chance of shoulder dystocia. The baby’s injuries were due to the normal forces of labor. Traction placed on the baby’s head during delivery was gentle and appropriate.
VERDICT A $5.5 million Iowa verdict was returned.
Faulty testing: baby has Down syndrome
AT 13 WEEKS’ GESTATION, a 34-year-old woman underwent chorionic villus sampling (CVS) at a maternal-fetal medicine center. Results showed a normal chromosomal profile. Later, two sonograms indicated possible Down syndrome. The parents were assured that the baby did not have a genetic disorder; amniocentesis was never suggested.
A week before the baby’s birth, the parents were told the child has Down syndrome.
PARENTS’ CLAIM Maternal tissue, not fetal tissue, had been removed and tested during CVS. The parents would have aborted the fetus had they known she had Down syndrome.
DEFENDANTS’ DEFENSE CVS was properly administered.
VERDICT A $3 million Missouri verdict was returned against the center where the testing was performed.
Why did the uterus seem to be growing?
A 52-YEAR-OLD WOMAN’S UTERUS was larger than normal in February 2007. By November 2008, her uterus was the size of a 14-week gestation. In September 2009, she complained of abdominal discomfort. Her uterus was larger than at the previous visit. The gynecologist suggested a hysterectomy, but nothing was scheduled.
In November 2009, she reported increasing pelvic pressure; her uterus was the size of an 18-week gestation. US and MRI showed large masses on both ovaries although the uterus had no masses or fibroids within it. A gynecologic oncologist performed abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral peri-aortic lymph node dissection. Pathology returned a diagnosis of ovarian cancer. The patient underwent chemotherapy.
PATIENT’S CLAIM The gynecologist was negligent in not ordering testing in 2007 when the larger-than-normal uterus was first detected, or in subsequent visits through September 2009. A more timely reaction would have given her an opportunity to treat the cancer at an earlier stage.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $650,000 Maryland settlement was reached.
Erb’s palsy after shoulder dystocia
DURING VAGINAL DELIVERY, the ObGyn encountered shoulder dystocia. The child suffered a brachial plexus injury and has Erb’s palsy. There was some improvement after two operations, but she still has muscle weakness, arm-length discrepancy, and limited range of motion.
PARENTS’ CLAIM The ObGyn applied excessive downward traction on the baby’s head when her left shoulder could not pass under the pubic bone.
PHYSICIAN’S DEFENSE The injury was caused by uterine contractions and maternal pushing. Proper maneuvers and gentle pressure were used.
VERDICT A $1.34 million New Jersey verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
AFTER MORE THAN 4 HOURS of second-stage labor followed by prolonged pushing and crowning, the baby was born depressed. Later, the child was found to have cerebral palsy.
PARENTS’ CLAIM The ObGyn was negligent in failing to perform an episiotomy, not attempting vacuum extraction, and not using forceps to assist delivery. Although fetal heart-rate monitoring results deteriorated, the ObGyn did not assess contractions for 30 minutes at one point. Hospital staff members were unable to adequately intubate or ventilate the newborn. The hospital staff disposed of the baby’s cord blood. Records were altered.
The parents’ counsel proposed that the defendants’ insurance company refused all settlement efforts prior to trial because the case venue was known to be conservative regarding jury verdicts.
DEFENDANTS’ DEFENSE The hospital and the ObGyn were not negligent; the mother and baby received proper care. Hospital staff acted appropriately.
VERDICT During the trial, the hospital settled for an undisclosed amount. An additional $2 million was offered on behalf of the ObGyn later in the trial, but the parents refused settlement at that time.
A California jury returned a $74.525 million verdict against the ObGyn. The child was awarded $70.725 million for medical expenses, lost earnings, and damages. The parents were awarded $3.8 million for emotional distress.
Was ectopic pregnancy missed?
A WOMAN IN SEVERE ABDOMINAL PAIN saw her internist. CT scans revealed a right ovarian cyst. When pain continued, she saw her ObGyn 3 weeks later, and her bowel was full of hard stool. Ultrasonography (US) showed a multicystic right ovary and a thin endometrial stripe. She was taking birth control pills and her husband had a vasectomy. She was told her abdominal pain was from constipation and ovarian cysts. A week later, she had laparoscopic surgery to remove an ectopic pregnancy.
PATIENT’S CLAIM The ObGyn did not perform a pregnancy test, and did not diagnose an ectopic pregnancy in a timely manner. An earlier diagnosis would have allowed medical rather than surgical resolution.
PHYSICIAN’S DEFENSE It was too early to determine if the pregnancy was intrauterine or ectopic. An earlier diagnosis would have resulted in laparoscopic surgery rather than medical treatment, as the medication (methotrexate) can cause increased pain.
VERDICT An Illinois defense verdict was returned.
Foreshortened vagina inhibits intercourse
A 65-YEAR-OLD WOMAN underwent anterior and posterior colphorrhaphy to repair a cystocele and rectocele, sacrospinous ligament fixation for vaginal prolapse, and a TVT mid-urethral suspension procedure to correct stress urinary incontinence. During two follow-up visits, the gynecologist determined that she was healing normally.
Within the next few weeks, the patient came to believe that her vagina had been sewn shut. She did not return to her gynecologist, but sought treatment with another physician 6 months later. It was determined that she had a stenotic and foreshortened vagina.
PATIENT’S CLAIM Too much vaginal tissue was removed during surgery.
PHYSICIAN’S DEFENSE The stenotic and foreshortened vagina was an unexpected result of the healing process after surgery.
VERDICT An Illinois defense verdict was returned.
Hydrocephalus in utero not seen until too late
A WOMAN HAD PRENATAL TREATMENT at a federally funded health clinic. A certified nurse midwife (CNM) ordered second-trimester US, with normal results. During the third trimester, the mother switched to a private ObGyn who ordered testing. US indicated the fetus was hydrocephalic. The child was born with cognitive disabilities and will need lifelong care.
PARENTS’ CLAIM The CNM ordered US too early in the pregnancy to be of diagnostic value; no further testing was undertaken. When hydrocephalus was seen, an abortion was not legally available because of fetal age.
DEFENDANT’S DEFENSE Even if US had been performed later in the second trimester, the defect would not have shown.
VERDICT A $4 million New Jersey settlement was reached.
WHEN SHOULDER DYSTOCIA WAS ENCOUNTERED, the ObGyn used standard maneuvers to deliver the child. The baby suffered a severe brachial plexus injury with rupture of C7 nerve and avulsions at C8 and T1.
Nerve-graft surgery at 6 months and tendon transfer surgery at 2 years resulted in recovery of good shoulder and elbow function, but the child has inadequate use of his wrist and hand. Additional surgeries are planned.
PARENTS’ CLAIM The ObGyn did not inform the mother that she was at risk for shoulder dystocia, nor did he discuss cesarean delivery. The mother’s risk factors included short stature, gestational diabetes, excessive weight gain during pregnancy, and two previous deliveries that involved vacuum assistance and a broken clavicle. The ObGyn applied excessive traction to the fetal head during delivery.
PHYSICIAN’S DEFENSE The mother’s risk factors were not severe enough to consider the chance of shoulder dystocia. The baby’s injuries were due to the normal forces of labor. Traction placed on the baby’s head during delivery was gentle and appropriate.
VERDICT A $5.5 million Iowa verdict was returned.
Faulty testing: baby has Down syndrome
AT 13 WEEKS’ GESTATION, a 34-year-old woman underwent chorionic villus sampling (CVS) at a maternal-fetal medicine center. Results showed a normal chromosomal profile. Later, two sonograms indicated possible Down syndrome. The parents were assured that the baby did not have a genetic disorder; amniocentesis was never suggested.
A week before the baby’s birth, the parents were told the child has Down syndrome.
PARENTS’ CLAIM Maternal tissue, not fetal tissue, had been removed and tested during CVS. The parents would have aborted the fetus had they known she had Down syndrome.
DEFENDANTS’ DEFENSE CVS was properly administered.
VERDICT A $3 million Missouri verdict was returned against the center where the testing was performed.
Why did the uterus seem to be growing?
A 52-YEAR-OLD WOMAN’S UTERUS was larger than normal in February 2007. By November 2008, her uterus was the size of a 14-week gestation. In September 2009, she complained of abdominal discomfort. Her uterus was larger than at the previous visit. The gynecologist suggested a hysterectomy, but nothing was scheduled.
In November 2009, she reported increasing pelvic pressure; her uterus was the size of an 18-week gestation. US and MRI showed large masses on both ovaries although the uterus had no masses or fibroids within it. A gynecologic oncologist performed abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral peri-aortic lymph node dissection. Pathology returned a diagnosis of ovarian cancer. The patient underwent chemotherapy.
PATIENT’S CLAIM The gynecologist was negligent in not ordering testing in 2007 when the larger-than-normal uterus was first detected, or in subsequent visits through September 2009. A more timely reaction would have given her an opportunity to treat the cancer at an earlier stage.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $650,000 Maryland settlement was reached.
Erb’s palsy after shoulder dystocia
DURING VAGINAL DELIVERY, the ObGyn encountered shoulder dystocia. The child suffered a brachial plexus injury and has Erb’s palsy. There was some improvement after two operations, but she still has muscle weakness, arm-length discrepancy, and limited range of motion.
PARENTS’ CLAIM The ObGyn applied excessive downward traction on the baby’s head when her left shoulder could not pass under the pubic bone.
PHYSICIAN’S DEFENSE The injury was caused by uterine contractions and maternal pushing. Proper maneuvers and gentle pressure were used.
VERDICT A $1.34 million New Jersey verdict was returned.
AFTER MORE THAN 4 HOURS of second-stage labor followed by prolonged pushing and crowning, the baby was born depressed. Later, the child was found to have cerebral palsy.
PARENTS’ CLAIM The ObGyn was negligent in failing to perform an episiotomy, not attempting vacuum extraction, and not using forceps to assist delivery. Although fetal heart-rate monitoring results deteriorated, the ObGyn did not assess contractions for 30 minutes at one point. Hospital staff members were unable to adequately intubate or ventilate the newborn. The hospital staff disposed of the baby’s cord blood. Records were altered.
The parents’ counsel proposed that the defendants’ insurance company refused all settlement efforts prior to trial because the case venue was known to be conservative regarding jury verdicts.
DEFENDANTS’ DEFENSE The hospital and the ObGyn were not negligent; the mother and baby received proper care. Hospital staff acted appropriately.
VERDICT During the trial, the hospital settled for an undisclosed amount. An additional $2 million was offered on behalf of the ObGyn later in the trial, but the parents refused settlement at that time.
A California jury returned a $74.525 million verdict against the ObGyn. The child was awarded $70.725 million for medical expenses, lost earnings, and damages. The parents were awarded $3.8 million for emotional distress.
Was ectopic pregnancy missed?
A WOMAN IN SEVERE ABDOMINAL PAIN saw her internist. CT scans revealed a right ovarian cyst. When pain continued, she saw her ObGyn 3 weeks later, and her bowel was full of hard stool. Ultrasonography (US) showed a multicystic right ovary and a thin endometrial stripe. She was taking birth control pills and her husband had a vasectomy. She was told her abdominal pain was from constipation and ovarian cysts. A week later, she had laparoscopic surgery to remove an ectopic pregnancy.
PATIENT’S CLAIM The ObGyn did not perform a pregnancy test, and did not diagnose an ectopic pregnancy in a timely manner. An earlier diagnosis would have allowed medical rather than surgical resolution.
PHYSICIAN’S DEFENSE It was too early to determine if the pregnancy was intrauterine or ectopic. An earlier diagnosis would have resulted in laparoscopic surgery rather than medical treatment, as the medication (methotrexate) can cause increased pain.
VERDICT An Illinois defense verdict was returned.
Foreshortened vagina inhibits intercourse
A 65-YEAR-OLD WOMAN underwent anterior and posterior colphorrhaphy to repair a cystocele and rectocele, sacrospinous ligament fixation for vaginal prolapse, and a TVT mid-urethral suspension procedure to correct stress urinary incontinence. During two follow-up visits, the gynecologist determined that she was healing normally.
Within the next few weeks, the patient came to believe that her vagina had been sewn shut. She did not return to her gynecologist, but sought treatment with another physician 6 months later. It was determined that she had a stenotic and foreshortened vagina.
PATIENT’S CLAIM Too much vaginal tissue was removed during surgery.
PHYSICIAN’S DEFENSE The stenotic and foreshortened vagina was an unexpected result of the healing process after surgery.
VERDICT An Illinois defense verdict was returned.
Hydrocephalus in utero not seen until too late
A WOMAN HAD PRENATAL TREATMENT at a federally funded health clinic. A certified nurse midwife (CNM) ordered second-trimester US, with normal results. During the third trimester, the mother switched to a private ObGyn who ordered testing. US indicated the fetus was hydrocephalic. The child was born with cognitive disabilities and will need lifelong care.
PARENTS’ CLAIM The CNM ordered US too early in the pregnancy to be of diagnostic value; no further testing was undertaken. When hydrocephalus was seen, an abortion was not legally available because of fetal age.
DEFENDANT’S DEFENSE Even if US had been performed later in the second trimester, the defect would not have shown.
VERDICT A $4 million New Jersey settlement was reached.
WHEN SHOULDER DYSTOCIA WAS ENCOUNTERED, the ObGyn used standard maneuvers to deliver the child. The baby suffered a severe brachial plexus injury with rupture of C7 nerve and avulsions at C8 and T1.
Nerve-graft surgery at 6 months and tendon transfer surgery at 2 years resulted in recovery of good shoulder and elbow function, but the child has inadequate use of his wrist and hand. Additional surgeries are planned.
PARENTS’ CLAIM The ObGyn did not inform the mother that she was at risk for shoulder dystocia, nor did he discuss cesarean delivery. The mother’s risk factors included short stature, gestational diabetes, excessive weight gain during pregnancy, and two previous deliveries that involved vacuum assistance and a broken clavicle. The ObGyn applied excessive traction to the fetal head during delivery.
PHYSICIAN’S DEFENSE The mother’s risk factors were not severe enough to consider the chance of shoulder dystocia. The baby’s injuries were due to the normal forces of labor. Traction placed on the baby’s head during delivery was gentle and appropriate.
VERDICT A $5.5 million Iowa verdict was returned.
Faulty testing: baby has Down syndrome
AT 13 WEEKS’ GESTATION, a 34-year-old woman underwent chorionic villus sampling (CVS) at a maternal-fetal medicine center. Results showed a normal chromosomal profile. Later, two sonograms indicated possible Down syndrome. The parents were assured that the baby did not have a genetic disorder; amniocentesis was never suggested.
A week before the baby’s birth, the parents were told the child has Down syndrome.
PARENTS’ CLAIM Maternal tissue, not fetal tissue, had been removed and tested during CVS. The parents would have aborted the fetus had they known she had Down syndrome.
DEFENDANTS’ DEFENSE CVS was properly administered.
VERDICT A $3 million Missouri verdict was returned against the center where the testing was performed.
Why did the uterus seem to be growing?
A 52-YEAR-OLD WOMAN’S UTERUS was larger than normal in February 2007. By November 2008, her uterus was the size of a 14-week gestation. In September 2009, she complained of abdominal discomfort. Her uterus was larger than at the previous visit. The gynecologist suggested a hysterectomy, but nothing was scheduled.
In November 2009, she reported increasing pelvic pressure; her uterus was the size of an 18-week gestation. US and MRI showed large masses on both ovaries although the uterus had no masses or fibroids within it. A gynecologic oncologist performed abdominal hysterectomy with bilateral salpingo-oophorectomy and bilateral peri-aortic lymph node dissection. Pathology returned a diagnosis of ovarian cancer. The patient underwent chemotherapy.
PATIENT’S CLAIM The gynecologist was negligent in not ordering testing in 2007 when the larger-than-normal uterus was first detected, or in subsequent visits through September 2009. A more timely reaction would have given her an opportunity to treat the cancer at an earlier stage.
PHYSICIAN’S DEFENSE The case was settled before trial.
VERDICT A $650,000 Maryland settlement was reached.
Erb’s palsy after shoulder dystocia
DURING VAGINAL DELIVERY, the ObGyn encountered shoulder dystocia. The child suffered a brachial plexus injury and has Erb’s palsy. There was some improvement after two operations, but she still has muscle weakness, arm-length discrepancy, and limited range of motion.
PARENTS’ CLAIM The ObGyn applied excessive downward traction on the baby’s head when her left shoulder could not pass under the pubic bone.
PHYSICIAN’S DEFENSE The injury was caused by uterine contractions and maternal pushing. Proper maneuvers and gentle pressure were used.
VERDICT A $1.34 million New Jersey verdict was returned.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
We want to hear from you! Tell us what you think.
PRODUCT UPDATE
AIRSTRIP OB: MOBILE ACCESS TO FETAL HEART-RATE MONITORS
AirStrip OB, the first app to receive FDA medical device clearance, enables ObGyns to remotely view up to 4 hours of data from fetal heart-rate monitors. With access to fetal heartbeats, maternal contraction patterns, vital signs, and nursing notes, physicians can communicate with L&D staff to respond quickly when clinical attention is needed. AirStrip OB from AirStrip Technologies is available for iPhone, Android, BlackBerry, and several Windows Mobile devices, and is HIPAA compliant.
FOR MORE INFORMATION, VISIT www.airstriptech.com
MENOPAUSAL SYMPTOMS RELIEVED WITH METAGENICS’ ESTROVERA™
ERr 731, the key ingredient in the supplement Estrovera, is an extract of Siberian rhubarb root that Metagenics claims provides effective relief for menopausal hot flashes comparable to conventional hormone therapies, but without the associated potential adverse side effects of estrogen. In published clinical studies, ERr 731 has been shown to significantly reduce the number and severity of hot flashes, night sweats, and other menopausal symptoms. Estrovera is not FDA approved.
FOR MORE INFORMATION, VISIT www.metagenics.com
EATING DISORDERS—AN ONLINE TRAINING MODULE FROM THE AMA
The American Medical Association offers an online training module to help physicians better screen for and manage eating disorders. Early intervention and communication has proven highly effective in combating these diseases. This CME resource will help physicians improve the process of identification, treatment, and management of these mental illnesses.
FOR MORE INFORMATION, VISIT www.ama-cmeonline.com/eating_disorders
RENESSA® IN-OFFICE PROCEDURE FOR SUI: A NONSURGICAL APPROACH
Renessa, developed by Novasys Medical, treats the most common type of incontinence, stress urinary incontinence (SUI), in a single, in-office, 20-minute procedure. This FDA approved, nonsurgical option uses radiofrequency energy to gently heat the tissue of the urethra near the bladder and activate a natural collagen regeneration process that firms the tissue. Renessa has been found to reduce or eliminate urine leakage during routine activities such as laughing, coughing, or sneezing without the use of mesh, implants, or foreign materials.
FOR MORE INFORMATION, VISIT www.renessa.com
HEALTHTAP: A MOBILE HEALTH PLATFORM THAT CONNECTS PATIENTS TO PHYSICIANS
HealthTap is a new comprehensive, consumer-facing mobile health platform. Using a free app, patients can connect with a Medical Expert Network of 12,000 US-licensed physicians via phone or messaging. Also available are doctor-to-doctor ratings and up-to-date health information. Premium features (for payment) include secure “Private Health Conversations” and storage of health records. Available for iPhone, iPad, and Android.
FOR MORE INFORMATION, VISIT www.healthtap.com
VITERA HEALTHCARE SOLUTIONS FOR EHR AND PRACTICE MANAGEMENT
Vitera Healthcare Solutions is a provider of electronic health records (EHR) and practice management software and services. The Intergy v8.00 contains a refreshed user interface for EHR, a new claim management module, a physician portal, a scheduling tool, online management of referrals and reports for radiology and imaging centers, patient charts with one-click access, and additional state-of-the-art features.
FOR MORE INFORMATION, VISIT www.viterahealthcare.com
AIRSTRIP OB: MOBILE ACCESS TO FETAL HEART-RATE MONITORS
AirStrip OB, the first app to receive FDA medical device clearance, enables ObGyns to remotely view up to 4 hours of data from fetal heart-rate monitors. With access to fetal heartbeats, maternal contraction patterns, vital signs, and nursing notes, physicians can communicate with L&D staff to respond quickly when clinical attention is needed. AirStrip OB from AirStrip Technologies is available for iPhone, Android, BlackBerry, and several Windows Mobile devices, and is HIPAA compliant.
FOR MORE INFORMATION, VISIT www.airstriptech.com
MENOPAUSAL SYMPTOMS RELIEVED WITH METAGENICS’ ESTROVERA™
ERr 731, the key ingredient in the supplement Estrovera, is an extract of Siberian rhubarb root that Metagenics claims provides effective relief for menopausal hot flashes comparable to conventional hormone therapies, but without the associated potential adverse side effects of estrogen. In published clinical studies, ERr 731 has been shown to significantly reduce the number and severity of hot flashes, night sweats, and other menopausal symptoms. Estrovera is not FDA approved.
FOR MORE INFORMATION, VISIT www.metagenics.com
EATING DISORDERS—AN ONLINE TRAINING MODULE FROM THE AMA
The American Medical Association offers an online training module to help physicians better screen for and manage eating disorders. Early intervention and communication has proven highly effective in combating these diseases. This CME resource will help physicians improve the process of identification, treatment, and management of these mental illnesses.
FOR MORE INFORMATION, VISIT www.ama-cmeonline.com/eating_disorders
RENESSA® IN-OFFICE PROCEDURE FOR SUI: A NONSURGICAL APPROACH
Renessa, developed by Novasys Medical, treats the most common type of incontinence, stress urinary incontinence (SUI), in a single, in-office, 20-minute procedure. This FDA approved, nonsurgical option uses radiofrequency energy to gently heat the tissue of the urethra near the bladder and activate a natural collagen regeneration process that firms the tissue. Renessa has been found to reduce or eliminate urine leakage during routine activities such as laughing, coughing, or sneezing without the use of mesh, implants, or foreign materials.
FOR MORE INFORMATION, VISIT www.renessa.com
HEALTHTAP: A MOBILE HEALTH PLATFORM THAT CONNECTS PATIENTS TO PHYSICIANS
HealthTap is a new comprehensive, consumer-facing mobile health platform. Using a free app, patients can connect with a Medical Expert Network of 12,000 US-licensed physicians via phone or messaging. Also available are doctor-to-doctor ratings and up-to-date health information. Premium features (for payment) include secure “Private Health Conversations” and storage of health records. Available for iPhone, iPad, and Android.
FOR MORE INFORMATION, VISIT www.healthtap.com
VITERA HEALTHCARE SOLUTIONS FOR EHR AND PRACTICE MANAGEMENT
Vitera Healthcare Solutions is a provider of electronic health records (EHR) and practice management software and services. The Intergy v8.00 contains a refreshed user interface for EHR, a new claim management module, a physician portal, a scheduling tool, online management of referrals and reports for radiology and imaging centers, patient charts with one-click access, and additional state-of-the-art features.
FOR MORE INFORMATION, VISIT www.viterahealthcare.com
AIRSTRIP OB: MOBILE ACCESS TO FETAL HEART-RATE MONITORS
AirStrip OB, the first app to receive FDA medical device clearance, enables ObGyns to remotely view up to 4 hours of data from fetal heart-rate monitors. With access to fetal heartbeats, maternal contraction patterns, vital signs, and nursing notes, physicians can communicate with L&D staff to respond quickly when clinical attention is needed. AirStrip OB from AirStrip Technologies is available for iPhone, Android, BlackBerry, and several Windows Mobile devices, and is HIPAA compliant.
FOR MORE INFORMATION, VISIT www.airstriptech.com
MENOPAUSAL SYMPTOMS RELIEVED WITH METAGENICS’ ESTROVERA™
ERr 731, the key ingredient in the supplement Estrovera, is an extract of Siberian rhubarb root that Metagenics claims provides effective relief for menopausal hot flashes comparable to conventional hormone therapies, but without the associated potential adverse side effects of estrogen. In published clinical studies, ERr 731 has been shown to significantly reduce the number and severity of hot flashes, night sweats, and other menopausal symptoms. Estrovera is not FDA approved.
FOR MORE INFORMATION, VISIT www.metagenics.com
EATING DISORDERS—AN ONLINE TRAINING MODULE FROM THE AMA
The American Medical Association offers an online training module to help physicians better screen for and manage eating disorders. Early intervention and communication has proven highly effective in combating these diseases. This CME resource will help physicians improve the process of identification, treatment, and management of these mental illnesses.
FOR MORE INFORMATION, VISIT www.ama-cmeonline.com/eating_disorders
RENESSA® IN-OFFICE PROCEDURE FOR SUI: A NONSURGICAL APPROACH
Renessa, developed by Novasys Medical, treats the most common type of incontinence, stress urinary incontinence (SUI), in a single, in-office, 20-minute procedure. This FDA approved, nonsurgical option uses radiofrequency energy to gently heat the tissue of the urethra near the bladder and activate a natural collagen regeneration process that firms the tissue. Renessa has been found to reduce or eliminate urine leakage during routine activities such as laughing, coughing, or sneezing without the use of mesh, implants, or foreign materials.
FOR MORE INFORMATION, VISIT www.renessa.com
HEALTHTAP: A MOBILE HEALTH PLATFORM THAT CONNECTS PATIENTS TO PHYSICIANS
HealthTap is a new comprehensive, consumer-facing mobile health platform. Using a free app, patients can connect with a Medical Expert Network of 12,000 US-licensed physicians via phone or messaging. Also available are doctor-to-doctor ratings and up-to-date health information. Premium features (for payment) include secure “Private Health Conversations” and storage of health records. Available for iPhone, iPad, and Android.
FOR MORE INFORMATION, VISIT www.healthtap.com
VITERA HEALTHCARE SOLUTIONS FOR EHR AND PRACTICE MANAGEMENT
Vitera Healthcare Solutions is a provider of electronic health records (EHR) and practice management software and services. The Intergy v8.00 contains a refreshed user interface for EHR, a new claim management module, a physician portal, a scheduling tool, online management of referrals and reports for radiology and imaging centers, patient charts with one-click access, and additional state-of-the-art features.
FOR MORE INFORMATION, VISIT www.viterahealthcare.com
Does mediolateral episiotomy reduce the risk of anal sphincter injury in operative vaginal delivery?
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
Stop performing median episiotomy!
Robert L. Barbieri, MD (Editorial, April 2012)
Episiotomy is an incision into the perineal body that is made during the second stage of labor to expedite delivery. Despite guidelines recommending restrictions on its use, episiotomy is still performed in more than 25% of vaginal deliveries in the United States. Suggested benefits include a shortened second stage of labor, the substitution of a straight surgical incision for a ragged spontaneous tear, and a reduced incidence of severe perineal injury and resultant pelvic floor dysfunction. Few data support these assertions, however.
Episiotomy is no OASIS
Absolute indications for episiotomy have yet to be established. Although there is general agreement that episiotomy may be indicated in select circumstances (such as to expedite delivery in the setting of nonreassuring fetal testing in the second stage of labor, shoulder dystocia, or at the time of operative vaginal delivery), routine use is discouraged.1,2 Besides the lack of data showing its benefit, episiotomy is associated with several potential complications, including increased blood loss, fetal injury, and localized pain. In contrast to the stated goal of reducing perineal trauma, episiotomy is associated with an increased incidence of third- or fourth-degree perineal lacerations,3,4 referred to in this study as obstetric anal sphincter injuries (OASIS).
Third- or fourth-degree tears are identified clinically at the time of vaginal delivery in 0.6% to 9% of patients.4 Studies using two-dimensional endoanal ultrasonography suggest that the true incidence of rectal injury is probably closer to 11%.5 Such injuries are associated with an increased risk of subsequent urinary or fecal incontinence (or both) and pelvic organ prolapse.
If episiotomy is indicated, how should it be performed?
There are two main types of episiotomy: median (favored in the United States) and mediolateral episiotomy. Complications—especially OASIS—are more common with median episiotomy,3,6,7 which involves a vertical midline incision from the posterior fourchette toward the rectum. Mediolateral episiotomy (favored in Europe), refers to an incision performed at a 45° angle from the posterior fourchette. OASIS is more common after median episiotomy, compared with the mediolateral approach.4,6 What is not yet clear is whether mediolateral episiotomy actually protects against OASIS.
Details of the study
de Vogel and colleagues evaluated the frequency of OASIS in women at high risk—specifically, those undergoing operative vaginal delivery; they also sought to determine whether mediolateral episiotomy is protective against OASIS. To this end, they performed a retrospective analysis of 2,861 consecutive women who delivered a singleton liveborn infant at term by vacuum, forceps, or both, from 2001–2009. Women were identified through the Netherlands Perinatal Registry, a voluntary reporting national database that includes approximately 96% of the 190,000 births that occur after 16 weeks’ gestation each year in the Netherlands. Exclusion criteria included multiple gestation, breech presentation, and use of median episiotomy.
The overall frequency of OASIS was 5.7% (162 cases among 2,861 deliveries). After logistic-regression modeling, a number of variables were significantly associated with OASIS, all of which have been identified previously: forceps delivery, occiput posterior position, primiparity, and epidural anesthesia. Women with a mediolateral episiotomy were at a significantly lower risk for OASIS, compared with women without mediolateral episiotomy (3.5% vs 15.6%, respectively; P<.001). Further analysis suggested that 8.6 mediolateral episiotomies would be needed to prevent one OASIS during vacuum extraction, whereas 5.2 procedures would be necessary to prevent one OASIS during forceps delivery. de Vogel and colleagues concluded that mediolateral episiotomy should be performed during all operative vaginal deliveries to reduce the incidence of OASIS.
Although this study included a large sample from a well-established and validated dataset (collected prospectively), it was, by design, retrospective. There was no standardization of when or how to cut the mediolateral episiotomy. However, many of these uncontrolled variables (such as cutting an episiotomy that is more median than mediolateral or cutting an episiotomy only in women who appear to be at imminent risk of sustaining a perineal laceration) would increase—not decrease—the risk of severe perineal injury. This fact suggests that the protective effect of mediolateral episiotomy may be even more dramatic than the sixfold protection reported in this study.
This study focused on women who underwent operative vaginal delivery. It remains controversial whether mediolateral episiotomy is protective in women who have a spontaneous (noninstrumental) vaginal delivery.
The study also lacks follow-up data on how many women with OASIS went on to develop fecal or urinary incontinence or pelvic organ prolapse. However, a third- or fourth-degree perineal laceration is serious enough that it can serve as an acceptable primary outcome measure even in the absence of long-term functional data.
In this study, use of median episiotomy was an exclusion, mostly likely because it is rarely performed in Europe.
While the battle over “to cut or not to cut” continues to rage, one fact is clear: median episiotomy should be abandoned. If you are going to perform episiotomy, make it mediolateral. According to this report, accoucheurs should consider cutting a mediolateral episiotomy for perineal protection each time they perform operative vaginal delivery.
ERROL R. NORWITZ, MD, PHD
After reading this article, and Dr. Barbieri’s April Editorial, we want to know if these articles have changed your practice. If you were faced with a difficult vaginal delivery, would you use a median or mediolateral episiotomy incision? Why?
We want to hear from you! Tell us what you think.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
1. Hartmann K, Viswanathan M, Palmieri R, Gartlehner G, Thorp J, Lohr KN. Outcomes of routine episiotomy: a systematic review. JAMA. 2005;293(17):2141-2148.
2. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;(1):CD000081.-
3. Helwig JT, Thorp JM, Jr, Bowes WA, Jr. Does midline episiotomy increase the risk of third- and fourth-degree lacerations in operative vaginal deliveries? Obstet Gynecol. 1993;82(2):276-279.
4. Dudding TC, Vaizey C, Kamm MA. Obstetric anal sphincter injury: incidence, risk factors, and management. Ann Surg. 2008;247(2):224-237.
5. Williams AB, Bartram CI, Halligan S, Spencer JA, Nicholls RJ, Kmiot WA. Anal sphincter damage after vaginal delivery using three-dimensional endosonography. Obstet Gynecol. 2001;97(5 Pt 1):770-775.
6. Coats PM, Chan KK, Wilkins M, Beard RJ. A comparison between midline and mediolateral episiotomies. Br J Obstet Gynaecol. 1980;87(5):408-412.
7. Kudish B, Blackwell S, McNeeley SG, et al. Operative vaginal delivery and midline episiotomy: a bad combination for the perineum. Am J Obstet Gynecol. 2006;195(3):749-754.
Thiopurines for Inflammatory Bowel Disease
The thiopurines – 6-mercaptopurine and azathioprine, which is metabolized to 6-mercaptopurine – are highly effective medications for treating inflammatory bowel disease, a diagnosis with a peak incidence during childbearing age. IBD, therefore, is quite common among pregnant women and is associated with an increased risk of miscarriage, prematurity, and low birth weight.
The use of these drugs during pregnancy has been a concern, because they are cytotoxic antimetabolites that are also used as anticancer drugs, albeit at higher doses than those used for IBD. Moreover, animal studies have consistently found an increased risk of malformations with exposure to high doses of these drugs.
As early as 20 years ago in J.L. Schardein’s book, "Chemically Induced Birth Defects" (New York: Marcel Dekker, Inc, 1993) on the safety of drugs in pregnancy, the author noted that while published case reports typically report adverse outcomes, he had collected over 90 cases of babies exposed to thiopurines during the first trimester with no evidence of malformations. This raised the question of whether reports of malformations associated with prenatal exposure had been missed, or whether prenatal exposure to the drug – at the levels used to treat IBD – is not associated with an increased malformation rate.
Nevertheless, over the past 2 decades, the inclination has been not to use these two drugs during pregnancy if possible, and human studies evaluating their reproductive safety have been limited and have produced conflicting results. However half of all pregnancies are unplanned, and for some women, physicians feel that it is important to continue treatment, despite the uncertainty about potential fetal risks. Hence the need for authoritative data on fetal safety is paramount.
At Motherisk, we receive many calls from women with IBD and their health care providers about the safety of these two drugs in pregnancy, so we embarked on a systematic review of the available studies.
The meta-analysis of all available observational cohort studies included studies that compared women with IBD who were treated with a thiopurine vs. disease-matched controls who were not on a thiopurine; studies that compared women who were treated with a thiopurine for any diagnosis; and studies that included both comparisons.
One of the main findings was that women with IBD who continued treatment with azathioprine (Imuran) or 6-mercaptourine during pregnancy had a significantly greater risk of having a premature baby, compared with untreated disease-matched controls and disease-matched controls who were on other IBD treatments. The risk of preterm birth was also higher among women who were treated with a thiopurine for any indication, compared with the healthy controls.
Because a thiopurine is used to treat a woman with active disease, this finding is consistent with the fact that active disease is also associated with an increased risk for preterm birth, suggesting that it’s not necessarily the medicine but the condition itself that may result in preterm delivery.
There was no significant difference in the risk of congenital malformations or low birth weight among the women with IBD who were treated with a thiopurine and women with IBD who were not treated with these medications. But the risk of malformations or low birth weight was increased significantly among the women with IBD who were treated with a thiopurine, compared with healthy controls. These findings again suggest that the increased risk has more to do with the condition, and not with exposure to a thiopurine.
Because most of the studies in the meta-analysis did not include specific information on disease activity among the pregnant women with IBD, studies in the future should do so. The results of our analysis suggest that the benefits of treatment outweigh the possible risks during pregnancy.
Another consideration is that these are among the drugs used to treat IBD that have replaced corticosteroids, which have significant maternal side effects and an increased, established small risk of oral clefts with first trimester exposure.
The benefit of treatment with a thiopurine must be balanced against the risk of not treating the mother, keeping in mind that maintaining disease remission in pregnancy is critical for a positive outcome for the baby.
Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. He also holds the Ivey Chair in Molecular Toxicology at the department of medicine, University of Western Ontario, London. Dr. Koren reported that he had no relevant financial disclosures. E-mail him at [email protected].
The thiopurines – 6-mercaptopurine and azathioprine, which is metabolized to 6-mercaptopurine – are highly effective medications for treating inflammatory bowel disease, a diagnosis with a peak incidence during childbearing age. IBD, therefore, is quite common among pregnant women and is associated with an increased risk of miscarriage, prematurity, and low birth weight.
The use of these drugs during pregnancy has been a concern, because they are cytotoxic antimetabolites that are also used as anticancer drugs, albeit at higher doses than those used for IBD. Moreover, animal studies have consistently found an increased risk of malformations with exposure to high doses of these drugs.
As early as 20 years ago in J.L. Schardein’s book, "Chemically Induced Birth Defects" (New York: Marcel Dekker, Inc, 1993) on the safety of drugs in pregnancy, the author noted that while published case reports typically report adverse outcomes, he had collected over 90 cases of babies exposed to thiopurines during the first trimester with no evidence of malformations. This raised the question of whether reports of malformations associated with prenatal exposure had been missed, or whether prenatal exposure to the drug – at the levels used to treat IBD – is not associated with an increased malformation rate.
Nevertheless, over the past 2 decades, the inclination has been not to use these two drugs during pregnancy if possible, and human studies evaluating their reproductive safety have been limited and have produced conflicting results. However half of all pregnancies are unplanned, and for some women, physicians feel that it is important to continue treatment, despite the uncertainty about potential fetal risks. Hence the need for authoritative data on fetal safety is paramount.
At Motherisk, we receive many calls from women with IBD and their health care providers about the safety of these two drugs in pregnancy, so we embarked on a systematic review of the available studies.
The meta-analysis of all available observational cohort studies included studies that compared women with IBD who were treated with a thiopurine vs. disease-matched controls who were not on a thiopurine; studies that compared women who were treated with a thiopurine for any diagnosis; and studies that included both comparisons.
One of the main findings was that women with IBD who continued treatment with azathioprine (Imuran) or 6-mercaptourine during pregnancy had a significantly greater risk of having a premature baby, compared with untreated disease-matched controls and disease-matched controls who were on other IBD treatments. The risk of preterm birth was also higher among women who were treated with a thiopurine for any indication, compared with the healthy controls.
Because a thiopurine is used to treat a woman with active disease, this finding is consistent with the fact that active disease is also associated with an increased risk for preterm birth, suggesting that it’s not necessarily the medicine but the condition itself that may result in preterm delivery.
There was no significant difference in the risk of congenital malformations or low birth weight among the women with IBD who were treated with a thiopurine and women with IBD who were not treated with these medications. But the risk of malformations or low birth weight was increased significantly among the women with IBD who were treated with a thiopurine, compared with healthy controls. These findings again suggest that the increased risk has more to do with the condition, and not with exposure to a thiopurine.
Because most of the studies in the meta-analysis did not include specific information on disease activity among the pregnant women with IBD, studies in the future should do so. The results of our analysis suggest that the benefits of treatment outweigh the possible risks during pregnancy.
Another consideration is that these are among the drugs used to treat IBD that have replaced corticosteroids, which have significant maternal side effects and an increased, established small risk of oral clefts with first trimester exposure.
The benefit of treatment with a thiopurine must be balanced against the risk of not treating the mother, keeping in mind that maintaining disease remission in pregnancy is critical for a positive outcome for the baby.
Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. He also holds the Ivey Chair in Molecular Toxicology at the department of medicine, University of Western Ontario, London. Dr. Koren reported that he had no relevant financial disclosures. E-mail him at [email protected].
The thiopurines – 6-mercaptopurine and azathioprine, which is metabolized to 6-mercaptopurine – are highly effective medications for treating inflammatory bowel disease, a diagnosis with a peak incidence during childbearing age. IBD, therefore, is quite common among pregnant women and is associated with an increased risk of miscarriage, prematurity, and low birth weight.
The use of these drugs during pregnancy has been a concern, because they are cytotoxic antimetabolites that are also used as anticancer drugs, albeit at higher doses than those used for IBD. Moreover, animal studies have consistently found an increased risk of malformations with exposure to high doses of these drugs.
As early as 20 years ago in J.L. Schardein’s book, "Chemically Induced Birth Defects" (New York: Marcel Dekker, Inc, 1993) on the safety of drugs in pregnancy, the author noted that while published case reports typically report adverse outcomes, he had collected over 90 cases of babies exposed to thiopurines during the first trimester with no evidence of malformations. This raised the question of whether reports of malformations associated with prenatal exposure had been missed, or whether prenatal exposure to the drug – at the levels used to treat IBD – is not associated with an increased malformation rate.
Nevertheless, over the past 2 decades, the inclination has been not to use these two drugs during pregnancy if possible, and human studies evaluating their reproductive safety have been limited and have produced conflicting results. However half of all pregnancies are unplanned, and for some women, physicians feel that it is important to continue treatment, despite the uncertainty about potential fetal risks. Hence the need for authoritative data on fetal safety is paramount.
At Motherisk, we receive many calls from women with IBD and their health care providers about the safety of these two drugs in pregnancy, so we embarked on a systematic review of the available studies.
The meta-analysis of all available observational cohort studies included studies that compared women with IBD who were treated with a thiopurine vs. disease-matched controls who were not on a thiopurine; studies that compared women who were treated with a thiopurine for any diagnosis; and studies that included both comparisons.
One of the main findings was that women with IBD who continued treatment with azathioprine (Imuran) or 6-mercaptourine during pregnancy had a significantly greater risk of having a premature baby, compared with untreated disease-matched controls and disease-matched controls who were on other IBD treatments. The risk of preterm birth was also higher among women who were treated with a thiopurine for any indication, compared with the healthy controls.
Because a thiopurine is used to treat a woman with active disease, this finding is consistent with the fact that active disease is also associated with an increased risk for preterm birth, suggesting that it’s not necessarily the medicine but the condition itself that may result in preterm delivery.
There was no significant difference in the risk of congenital malformations or low birth weight among the women with IBD who were treated with a thiopurine and women with IBD who were not treated with these medications. But the risk of malformations or low birth weight was increased significantly among the women with IBD who were treated with a thiopurine, compared with healthy controls. These findings again suggest that the increased risk has more to do with the condition, and not with exposure to a thiopurine.
Because most of the studies in the meta-analysis did not include specific information on disease activity among the pregnant women with IBD, studies in the future should do so. The results of our analysis suggest that the benefits of treatment outweigh the possible risks during pregnancy.
Another consideration is that these are among the drugs used to treat IBD that have replaced corticosteroids, which have significant maternal side effects and an increased, established small risk of oral clefts with first trimester exposure.
The benefit of treatment with a thiopurine must be balanced against the risk of not treating the mother, keeping in mind that maintaining disease remission in pregnancy is critical for a positive outcome for the baby.
Dr. Koren is professor of pediatrics, pharmacology, pharmacy, and medical genetics at the University of Toronto. He heads the Research Leadership for Better Pharmacotherapy During Pregnancy and Lactation at the Hospital for Sick Children, Toronto, where he is director of the Motherisk program. He also holds the Ivey Chair in Molecular Toxicology at the department of medicine, University of Western Ontario, London. Dr. Koren reported that he had no relevant financial disclosures. E-mail him at [email protected].
Twins
Pregnancies involving multiple births are an increasingly prevalent phenomenon in most obstetrical practices, with twin gestations now accounting for more than 3% of all births in the United States.
The incidence of twinning is attributable to two main social factors: older maternal age at childbirth, which is responsible for a third of the increase, and the increased use of assisted reproductive technology (ART), which is responsible for the other two-thirds.

Although refinements in ART and recommendations to limit the number of embryos transferred during in vitro procedures have led to reductions in the number of higher-order multiples, twin gestations are still common, occurring in up to one-third of IVF pregnancies. Ovulation induction, which is a much more commonly used ART procedure, is also associated with twinning rates of 5%-10%.
What must be appreciated is the reality that twin gestations carry significant risks and contribute disproportionately to our national rates of perinatal morbidity and mortality. Although twin gestations represent just over 3% of all live births, they account for 15% of all early preterm births and 25% of all very-low birth weight infants.
Approximately 15% of all neonates with respiratory distress syndrome are twins, and twins account for 12% of all cases of grade III or IV intraventricular hemorrhage. Of all neonatal deaths in the United States, approximately 15% are twins. Moreover, approximately 10% of all stillbirths in the United States are twins.
In short, twin gestations are one of the most common high-risk conditions in obstetrical practice. Twin pregnancies are usually exciting for parents and their families, but it is important to reflect on the significant risks they can present, and to consider how these pregnancies can be optimally managed in order to reduce these risks.
No Simple Diagnosis
The first step in the optimal management of twins is to make the early diagnosis of chorionicity. The American Journal of Obstetrics & Gynecology ran a striking editorial about the significance of establishing chorionicity by first-trimester ultrasound in multiple gestations. The editorial’s authors, Dr. Kenneth J. Moise Jr. and Dr. Anthony Johnson, reflected on a talk given by Dr. Krypos Nicolaides of King’s College London, in which he broke away from his discussion of fetal therapy, paused, and made the following statement:
"There is NO diagnosis of twins. There are only monochorionic twins or dichorionic twins. This diagnosis should be written in capital red letters across the top of the patient’s chart." (Am. J. Obstet. Gynecol. 2010;203:1-2).
It could not have been better stated. It is not appropriate in obstetrical medicine to make a simple diagnosis of "twins" any longer. Early identification of whether a twin gestation involves either a monochorionic, single-placenta placentation, or a dichorionic, dual-placenta placentation is essential for accurate risk assessment and optimal antepartum management. Monochorionic pregnancies, which represent just over 20% of all twin gestations, are at much greater risk for miscarriage, congenital anomalies, growth abnormalities (including twin-to-twin transfusion syndrome), preterm birth, stillbirth, and neurodevelopmental abnormalities.
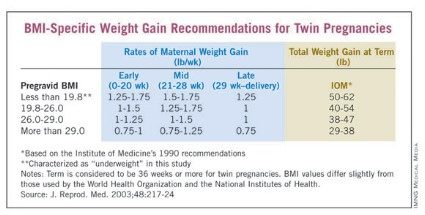
Determining this single feature – the chorionicity of the twin gestations – will thus shape a host of decisions, from the frequency of ultrasound examinations to the type of late-pregnancy surveillance and the timing of delivery.
With proper training, chorionicity can be determined with almost 100% accuracy in the first trimester, and if a patient doesn’t present in the first trimester, it still can be determined in the second trimester with an accuracy approaching 100% using a variety of ultrasound markers and parameters.
Optimizing Nutrition
I firmly believe that maximizing the mother’s nutrition is one of the most important determinants of a healthy outcome in a twin pregnancy.
In its 2009 report titled "Weight Gain During Pregnancy: Reexamining the Guidelines," the Institute of Medicine for the first time offered body mass index–specific recommendations for women with multiple gestations. The IOM has long had recommendations for singleton pregnancies based on pregravid BMI status, but this latest report marked the first time that multiple pregnancies were addressed in such detail.
Clearly, our knowledge base has advanced. During the 1990s and 2000s, a number of investigators – most notably Barbara Luke, Sc.D., currently a professor of obstetrics, gynecology, and reproductive biology at Michigan State University, East Lansing – have published articles on the role of nutrition and weight gain in women with multiple gestations, and the relationship of these factors to pregnancy outcomes. Studies have demonstrated the critical effect that appropriate maternal weight gain and optimal nutrition have on twin fetal growth, birth weight, length of gestation, and other outcomes.
Surprisingly, the IOM consensus panel did not issue recommendations for women who are underweight, citing a lack of evidence. I believe there is clear epidemiologic evidence, however, that women with twin pregnancies who are underweight before pregnancy and have poor gestational weight gain are at the highest risk for poor outcomes.
In a 2003 report, Dr. Luke and a team of investigators, myself included, developed BMI-specific weight gain guidelines for optimal birth weights in twin pregnancies. Our weight gain curves and recommendations, which were based on a multi-institution cohort study of 2,324 twin pregnancies, are similar to the IOM’s guidelines. We also addressed the category of underweight women, however, and advised a gain of 50-62 pounds for these women. (See box.)
Women with a pregravid underweight status who had a total weight gain within this range experienced optimal fetal growth and birth weight. (J. Reprod. Med. 2003;48:217-24).
In a separate follow-up study of the value of using these BMI-specific weight gain goals, Dr. William Goodnight and I found that in our twins clinic, women who failed to achieve their BMI-specific weight-gain goals had a lower birth weight by nearly 200 g per twin and a length of gestation that was 1 week shorter than that of women who met weight gain goals (Am. J. Obstet. Gynecol. 2006;195[suppl]:S121).
As we described in a review published in 2009, achieving twin weight-gain goals should be part of a comprehensive approach to nutrition that also includes an appropriate caloric intake (3,000-4,000 kcal/day in underweight to normal weight women); supplementation with calcium, magnesium, folate, and zinc (beyond a usual prenatal vitamin); and a nutrient-dense diet that is high in iron-rich proteins and omega-3 fatty acids (Obstet. Gynecol. 2009;114:1121-34). In our practice, we emphasize the value of meat protein and of low-mercury fish.
Dr. Luke, who has coauthored a book with Tamara Eberlein that we often recommend to our patients, titled "When Youre Expecting Twins, Triplets or Quads" (New York: HarperCollins, 2011), has best demonstrated the extent to which intensive nutritional counseling and follow-up pays off in twin pregnancies.
In a cohort study published in 2003, she enrolled 190 women with twin pregnancies in a specialized prenatal program that involved twice-monthly visits for nutritional counseling and monitoring. Women were prescribed a diet of 3,000-4,000 kcal/day, with 20% of calories from protein, 40% from carbohydrates, and 40% from fat, as well as multimineral supplementation. The women were monitored for adequate weight gain and had serial ultrasound assessments.
Compared with 339 women with twin pregnancies who were followed by their physicians at the University of Michigan but not enrolled in the program, the program participants had significantly longer gestations (about a week), higher birth weights (220 g), a 23% reduction in preterm births, and significant reductions in preterm premature rupture of membranes, preterm labor, preeclampsia, ICU admission, and other poor outcomes.
Overall, the incidence of major neonatal morbidity was 17% for the nutritional program participants, compared with 32% for those women who did not receive the specialized care (Am. J. Obstet. Gynecol. 2003;189:934-8).
Measuring Cervical Length
One of the major clinical concerns with any twin pregnancy is the prevention of preterm birth and, by extension, the identification of those women with twins who, within this broader high-risk category, are at greatest risk for preterm birth.
Since the mid-1990s, research has shown that a short cervix detected in the midtrimester (defined as 16-24 weeks) by transvaginal ultrasound is a powerful predictor of preterm birth in women with either singleton or twin gestations. Studies of twin gestations have shown that as cervical length shortens to 25 mm or less, the risk of subsequent preterm birth (defined less than 34 weeks) rises dramatically.
In a report on twin pregnancies from the Maternal-Fetal Medicine Units Network of the Eunice Kennedy Shriver National Institute of Child Health and Human Development, for instance, Dr. R.L. Goldenberg and associates demonstrated that cervical length less than or equal to 25 mm at 24 weeks was the best predictor of spontaneous preterm birth. In fact, of all 50 potential risk factors that were studied, a short cervix was the only factor that was consistently associated with preterm birth. The investigators also noted that this shorter cervical length was more common at both 24 and 28 weeks in twins, compared with singleton pregnancies (Am. J. Obstet. Gynecol. 1996;175:1047-53).
Through the 1990s and the next decade, investigators searched for a viable intervention. However, in numerous studies, the use of cerclage in mothers of twins with a short cervix was found to be of no benefit. Prophylactic tocolysis also failed to prevent preterm birth in published studies.
The use of bed rest has remained controversial. It is commonly prescribed to prevent preterm birth in women with a twin gestation and a short cervix, despite the fact that we have no published data demonstrating its effectiveness in prolonging pregnancy. Personally, I believe that bed rest can reduce the frequency of uterine contractions and help protect the cervix from the weight of the pregnancy.
Interest in the treatment of twin pregnancies with progesterone had waned after 2007, when a National Institutes of Health multicenter, randomized trial of injectable progesterone reported that 17-alpha-hydroxyprogesterone caproate did not reduce the rate of twin preterm birth (N. Engl. J. Med. 2007;357:454-61).
However, progesterone recently has reemerged as a treatment for women who are at higher risk of preterm birth, based on the publication this year of Dr. Roberto Romero’s review and meta-analysis of vaginal progesterone for women with a sonographic short cervix (Am. J. Obstet. Gynecol. 2012;206:124.e1-19). Indeed, this review provides the first evidence of a beneficial effect in women with a short cervix who are carrying a twin gestation. The meta-analysis covered five prospective, randomized trials of vaginal progesterone with a total of 775 women who had a sonographically confirmed short cervix (25 mm or less) in the midtrimester. The vast majority of women in these studies carried singleton pregnancies, but two of the studies enrolled twin as well as singleton gestations, and one of the five studies – albeit a small one – focused solely on twin pregnancies.
Overall, treatment with vaginal progesterone was associated with a highly significant 42% reduction in the rate of preterm birth at less than 33 weeks. Among twin gestations specifically, the reduction in preterm birth was 30% – a meaningful trend, but not statistically significant. When it came to neonatal morbidity and mortality, however, the effect of vaginal progesterone among twin gestations was far more striking: The group that received vaginal progesterone had a 48% reduction in the risk of composite neonatal morbidity and mortality.
Admittedly, a primary randomized, controlled trial in twin gestations is still needed. In the meantime, however, given the tremendous risk faced by women with a twin gestation and a short cervix, and the lack of any other proven treatment, I believe that vaginal progesterone (Prometrium, in either a 200-mg suppository or 90-mg gel) is an appropriate treatment for this condition.
In our practice, we routinely perform transvaginal cervical-length measurements with our twin pregnancies at the time of their anatomical survey at 18-20 weeks, and then every 2-4 weeks (depending on how short the cervix is) up to 26-28 weeks. If a short cervix is diagnosed, we restrict activity and start vaginal progesterone.
Surveillance, Delivery
Careful surveillance during the late gestational period is critical, as twins – particularly monochorionic twins – are at increased risk of growth restriction or growth discordancy, and have an increased risk of developing abnormalities in amniotic fluid volume. Compared with singletons, twins also are at increased risk of stillbirth in the third trimester; this risk, again, appears to be higher for monochorionic gestations.
We perform routine ultrasound evaluations every 3 weeks for our monochorionic twins and every 4 weeks for our dichorionic twins, in the absence of any abnormalities. If abnormalities in growth are suspected with standard ultrasound evaluation, we add umbilical artery Doppler studies to further assess well-being. We also routinely institute fetal nonstress testing at 32 weeks’ gestation for monochorionic twins and at 34 weeks for our dichorionic twins. Additional strategies are employed as necessary.
The overall risk of stillbirth for twin gestations is 0.2%-0.4% per week after 32 weeks’ gestation, and rises further beyond 38 weeks – a risk that makes surveillance critical.
Some investigators, however, have recently reported higher-than-expected stillbirth rates for "apparently uncomplicated" monochorionic twin gestations. This risk has ranged from 1% to 4% at 32 and 38 weeks’ gestation in various reports.
These studies were debated as part of a workshop held in 2011 by the National Institutes of Health and the Society for Maternal-Fetal Medicine on the "Timing of Indicated Late Preterm and Early Term Births." The findings of the higher stillbirth rates remain controversial, but on the basis of these concerns, it was recommended that monochorionic twins – even "uncomplicated" cases – should be offered elective delivery at 34-37 weeks’ gestation, with decisions made after careful discussion and informed consent.
Uncomplicated dichorionic twins, on the other hand, appear to have optimal outcomes when delivered at 38 weeks’ gestation (Obstet. Gynecol. 2011;118:323-3; Semin. Perinatol. 2011;35:277-85).
Recommended surveillance and delivery of monoamniotic twins – a rare but serious type of monochorionic twin gestation – has evolved recently in favor of intensive inpatient monitoring.
The benefits of hospitalization were demonstrated most strikingly in a multicenter cohort study that compared 43 women who were admitted at a median gestational age of 26.5 weeks for inpatient fetal testing two to three times daily vs. 44 women who were followed as outpatients with fetal testing one to three times weekly.
There were no stillbirths in the hospitalized group, but there was a 15% stillbirth rate in the outpatient group. The inpatient group also had significant improvements in birth weight, gestational age at delivery, and neonatal morbidity (Am. J. Obstet. Gynecol. 2005;192:96-101).
This and other evidence suggests that mothers of monoamniotic twins have the best possible outcome when their pregnancies are managed in a hospital setting with fetal monitoring two to three times a day, starting at 24-26 weeks’ gestation, with delivery timed between 32 and 34 weeks’ gestation. This was among the conclusions of the 2011 NIH-SMFM workshop.
Specialized Care
A final consideration regarding the antepartum care of multiples would be the benefit that might be achieved by establishing a specialized twins clinic.
The literature includes numerous reports, including one of our own (Semin. Perinatol 1995;19:387-403), describing improved perinatal outcomes for twins who are cared for by multidisciplinary teams using best practice protocols. Our team includes an obstetrician, a certified nurse-midwife, a nutritionist, an ultrasonographer, and a perinatal nurse.
In our experience, this approach significantly reduces perinatal mortality, primarily by reducing preterm premature rupture of membranes and very low birth weight delivery.
Dr. Newman is currently a professor and the Maas Chair for Reproductive Sciences in the department of obstetrics and gynecology, and vice chairman for academic affairs and women’s health research at the Medical University of South Carolina, Charleston. He established a multidisciplinary twins clinic in 1989 and since then has provided care for more than 1,000 women with twins. Dr. Rogers said he has no relevant financial disclosures.
Pregnancies involving multiple births are an increasingly prevalent phenomenon in most obstetrical practices, with twin gestations now accounting for more than 3% of all births in the United States.
The incidence of twinning is attributable to two main social factors: older maternal age at childbirth, which is responsible for a third of the increase, and the increased use of assisted reproductive technology (ART), which is responsible for the other two-thirds.
Although refinements in ART and recommendations to limit the number of embryos transferred during in vitro procedures have led to reductions in the number of higher-order multiples, twin gestations are still common, occurring in up to one-third of IVF pregnancies. Ovulation induction, which is a much more commonly used ART procedure, is also associated with twinning rates of 5%-10%.
What must be appreciated is the reality that twin gestations carry significant risks and contribute disproportionately to our national rates of perinatal morbidity and mortality. Although twin gestations represent just over 3% of all live births, they account for 15% of all early preterm births and 25% of all very-low birth weight infants.
Approximately 15% of all neonates with respiratory distress syndrome are twins, and twins account for 12% of all cases of grade III or IV intraventricular hemorrhage. Of all neonatal deaths in the United States, approximately 15% are twins. Moreover, approximately 10% of all stillbirths in the United States are twins.
In short, twin gestations are one of the most common high-risk conditions in obstetrical practice. Twin pregnancies are usually exciting for parents and their families, but it is important to reflect on the significant risks they can present, and to consider how these pregnancies can be optimally managed in order to reduce these risks.
No Simple Diagnosis
The first step in the optimal management of twins is to make the early diagnosis of chorionicity. The American Journal of Obstetrics & Gynecology ran a striking editorial about the significance of establishing chorionicity by first-trimester ultrasound in multiple gestations. The editorial’s authors, Dr. Kenneth J. Moise Jr. and Dr. Anthony Johnson, reflected on a talk given by Dr. Krypos Nicolaides of King’s College London, in which he broke away from his discussion of fetal therapy, paused, and made the following statement:
"There is NO diagnosis of twins. There are only monochorionic twins or dichorionic twins. This diagnosis should be written in capital red letters across the top of the patient’s chart." (Am. J. Obstet. Gynecol. 2010;203:1-2).
It could not have been better stated. It is not appropriate in obstetrical medicine to make a simple diagnosis of "twins" any longer. Early identification of whether a twin gestation involves either a monochorionic, single-placenta placentation, or a dichorionic, dual-placenta placentation is essential for accurate risk assessment and optimal antepartum management. Monochorionic pregnancies, which represent just over 20% of all twin gestations, are at much greater risk for miscarriage, congenital anomalies, growth abnormalities (including twin-to-twin transfusion syndrome), preterm birth, stillbirth, and neurodevelopmental abnormalities.
Determining this single feature – the chorionicity of the twin gestations – will thus shape a host of decisions, from the frequency of ultrasound examinations to the type of late-pregnancy surveillance and the timing of delivery.
With proper training, chorionicity can be determined with almost 100% accuracy in the first trimester, and if a patient doesn’t present in the first trimester, it still can be determined in the second trimester with an accuracy approaching 100% using a variety of ultrasound markers and parameters.
Optimizing Nutrition
I firmly believe that maximizing the mother’s nutrition is one of the most important determinants of a healthy outcome in a twin pregnancy.
In its 2009 report titled "Weight Gain During Pregnancy: Reexamining the Guidelines," the Institute of Medicine for the first time offered body mass index–specific recommendations for women with multiple gestations. The IOM has long had recommendations for singleton pregnancies based on pregravid BMI status, but this latest report marked the first time that multiple pregnancies were addressed in such detail.
Clearly, our knowledge base has advanced. During the 1990s and 2000s, a number of investigators – most notably Barbara Luke, Sc.D., currently a professor of obstetrics, gynecology, and reproductive biology at Michigan State University, East Lansing – have published articles on the role of nutrition and weight gain in women with multiple gestations, and the relationship of these factors to pregnancy outcomes. Studies have demonstrated the critical effect that appropriate maternal weight gain and optimal nutrition have on twin fetal growth, birth weight, length of gestation, and other outcomes.
Surprisingly, the IOM consensus panel did not issue recommendations for women who are underweight, citing a lack of evidence. I believe there is clear epidemiologic evidence, however, that women with twin pregnancies who are underweight before pregnancy and have poor gestational weight gain are at the highest risk for poor outcomes.
In a 2003 report, Dr. Luke and a team of investigators, myself included, developed BMI-specific weight gain guidelines for optimal birth weights in twin pregnancies. Our weight gain curves and recommendations, which were based on a multi-institution cohort study of 2,324 twin pregnancies, are similar to the IOM’s guidelines. We also addressed the category of underweight women, however, and advised a gain of 50-62 pounds for these women. (See box.)
Women with a pregravid underweight status who had a total weight gain within this range experienced optimal fetal growth and birth weight. (J. Reprod. Med. 2003;48:217-24).
In a separate follow-up study of the value of using these BMI-specific weight gain goals, Dr. William Goodnight and I found that in our twins clinic, women who failed to achieve their BMI-specific weight-gain goals had a lower birth weight by nearly 200 g per twin and a length of gestation that was 1 week shorter than that of women who met weight gain goals (Am. J. Obstet. Gynecol. 2006;195[suppl]:S121).
As we described in a review published in 2009, achieving twin weight-gain goals should be part of a comprehensive approach to nutrition that also includes an appropriate caloric intake (3,000-4,000 kcal/day in underweight to normal weight women); supplementation with calcium, magnesium, folate, and zinc (beyond a usual prenatal vitamin); and a nutrient-dense diet that is high in iron-rich proteins and omega-3 fatty acids (Obstet. Gynecol. 2009;114:1121-34). In our practice, we emphasize the value of meat protein and of low-mercury fish.
Dr. Luke, who has coauthored a book with Tamara Eberlein that we often recommend to our patients, titled "When Youre Expecting Twins, Triplets or Quads" (New York: HarperCollins, 2011), has best demonstrated the extent to which intensive nutritional counseling and follow-up pays off in twin pregnancies.
In a cohort study published in 2003, she enrolled 190 women with twin pregnancies in a specialized prenatal program that involved twice-monthly visits for nutritional counseling and monitoring. Women were prescribed a diet of 3,000-4,000 kcal/day, with 20% of calories from protein, 40% from carbohydrates, and 40% from fat, as well as multimineral supplementation. The women were monitored for adequate weight gain and had serial ultrasound assessments.
Compared with 339 women with twin pregnancies who were followed by their physicians at the University of Michigan but not enrolled in the program, the program participants had significantly longer gestations (about a week), higher birth weights (220 g), a 23% reduction in preterm births, and significant reductions in preterm premature rupture of membranes, preterm labor, preeclampsia, ICU admission, and other poor outcomes.
Overall, the incidence of major neonatal morbidity was 17% for the nutritional program participants, compared with 32% for those women who did not receive the specialized care (Am. J. Obstet. Gynecol. 2003;189:934-8).
Measuring Cervical Length
One of the major clinical concerns with any twin pregnancy is the prevention of preterm birth and, by extension, the identification of those women with twins who, within this broader high-risk category, are at greatest risk for preterm birth.
Since the mid-1990s, research has shown that a short cervix detected in the midtrimester (defined as 16-24 weeks) by transvaginal ultrasound is a powerful predictor of preterm birth in women with either singleton or twin gestations. Studies of twin gestations have shown that as cervical length shortens to 25 mm or less, the risk of subsequent preterm birth (defined less than 34 weeks) rises dramatically.
In a report on twin pregnancies from the Maternal-Fetal Medicine Units Network of the Eunice Kennedy Shriver National Institute of Child Health and Human Development, for instance, Dr. R.L. Goldenberg and associates demonstrated that cervical length less than or equal to 25 mm at 24 weeks was the best predictor of spontaneous preterm birth. In fact, of all 50 potential risk factors that were studied, a short cervix was the only factor that was consistently associated with preterm birth. The investigators also noted that this shorter cervical length was more common at both 24 and 28 weeks in twins, compared with singleton pregnancies (Am. J. Obstet. Gynecol. 1996;175:1047-53).
Through the 1990s and the next decade, investigators searched for a viable intervention. However, in numerous studies, the use of cerclage in mothers of twins with a short cervix was found to be of no benefit. Prophylactic tocolysis also failed to prevent preterm birth in published studies.
The use of bed rest has remained controversial. It is commonly prescribed to prevent preterm birth in women with a twin gestation and a short cervix, despite the fact that we have no published data demonstrating its effectiveness in prolonging pregnancy. Personally, I believe that bed rest can reduce the frequency of uterine contractions and help protect the cervix from the weight of the pregnancy.
Interest in the treatment of twin pregnancies with progesterone had waned after 2007, when a National Institutes of Health multicenter, randomized trial of injectable progesterone reported that 17-alpha-hydroxyprogesterone caproate did not reduce the rate of twin preterm birth (N. Engl. J. Med. 2007;357:454-61).
However, progesterone recently has reemerged as a treatment for women who are at higher risk of preterm birth, based on the publication this year of Dr. Roberto Romero’s review and meta-analysis of vaginal progesterone for women with a sonographic short cervix (Am. J. Obstet. Gynecol. 2012;206:124.e1-19). Indeed, this review provides the first evidence of a beneficial effect in women with a short cervix who are carrying a twin gestation. The meta-analysis covered five prospective, randomized trials of vaginal progesterone with a total of 775 women who had a sonographically confirmed short cervix (25 mm or less) in the midtrimester. The vast majority of women in these studies carried singleton pregnancies, but two of the studies enrolled twin as well as singleton gestations, and one of the five studies – albeit a small one – focused solely on twin pregnancies.
Overall, treatment with vaginal progesterone was associated with a highly significant 42% reduction in the rate of preterm birth at less than 33 weeks. Among twin gestations specifically, the reduction in preterm birth was 30% – a meaningful trend, but not statistically significant. When it came to neonatal morbidity and mortality, however, the effect of vaginal progesterone among twin gestations was far more striking: The group that received vaginal progesterone had a 48% reduction in the risk of composite neonatal morbidity and mortality.
Admittedly, a primary randomized, controlled trial in twin gestations is still needed. In the meantime, however, given the tremendous risk faced by women with a twin gestation and a short cervix, and the lack of any other proven treatment, I believe that vaginal progesterone (Prometrium, in either a 200-mg suppository or 90-mg gel) is an appropriate treatment for this condition.
In our practice, we routinely perform transvaginal cervical-length measurements with our twin pregnancies at the time of their anatomical survey at 18-20 weeks, and then every 2-4 weeks (depending on how short the cervix is) up to 26-28 weeks. If a short cervix is diagnosed, we restrict activity and start vaginal progesterone.
Surveillance, Delivery
Careful surveillance during the late gestational period is critical, as twins – particularly monochorionic twins – are at increased risk of growth restriction or growth discordancy, and have an increased risk of developing abnormalities in amniotic fluid volume. Compared with singletons, twins also are at increased risk of stillbirth in the third trimester; this risk, again, appears to be higher for monochorionic gestations.
We perform routine ultrasound evaluations every 3 weeks for our monochorionic twins and every 4 weeks for our dichorionic twins, in the absence of any abnormalities. If abnormalities in growth are suspected with standard ultrasound evaluation, we add umbilical artery Doppler studies to further assess well-being. We also routinely institute fetal nonstress testing at 32 weeks’ gestation for monochorionic twins and at 34 weeks for our dichorionic twins. Additional strategies are employed as necessary.
The overall risk of stillbirth for twin gestations is 0.2%-0.4% per week after 32 weeks’ gestation, and rises further beyond 38 weeks – a risk that makes surveillance critical.
Some investigators, however, have recently reported higher-than-expected stillbirth rates for "apparently uncomplicated" monochorionic twin gestations. This risk has ranged from 1% to 4% at 32 and 38 weeks’ gestation in various reports.
These studies were debated as part of a workshop held in 2011 by the National Institutes of Health and the Society for Maternal-Fetal Medicine on the "Timing of Indicated Late Preterm and Early Term Births." The findings of the higher stillbirth rates remain controversial, but on the basis of these concerns, it was recommended that monochorionic twins – even "uncomplicated" cases – should be offered elective delivery at 34-37 weeks’ gestation, with decisions made after careful discussion and informed consent.
Uncomplicated dichorionic twins, on the other hand, appear to have optimal outcomes when delivered at 38 weeks’ gestation (Obstet. Gynecol. 2011;118:323-3; Semin. Perinatol. 2011;35:277-85).
Recommended surveillance and delivery of monoamniotic twins – a rare but serious type of monochorionic twin gestation – has evolved recently in favor of intensive inpatient monitoring.
The benefits of hospitalization were demonstrated most strikingly in a multicenter cohort study that compared 43 women who were admitted at a median gestational age of 26.5 weeks for inpatient fetal testing two to three times daily vs. 44 women who were followed as outpatients with fetal testing one to three times weekly.
There were no stillbirths in the hospitalized group, but there was a 15% stillbirth rate in the outpatient group. The inpatient group also had significant improvements in birth weight, gestational age at delivery, and neonatal morbidity (Am. J. Obstet. Gynecol. 2005;192:96-101).
This and other evidence suggests that mothers of monoamniotic twins have the best possible outcome when their pregnancies are managed in a hospital setting with fetal monitoring two to three times a day, starting at 24-26 weeks’ gestation, with delivery timed between 32 and 34 weeks’ gestation. This was among the conclusions of the 2011 NIH-SMFM workshop.
Specialized Care
A final consideration regarding the antepartum care of multiples would be the benefit that might be achieved by establishing a specialized twins clinic.
The literature includes numerous reports, including one of our own (Semin. Perinatol 1995;19:387-403), describing improved perinatal outcomes for twins who are cared for by multidisciplinary teams using best practice protocols. Our team includes an obstetrician, a certified nurse-midwife, a nutritionist, an ultrasonographer, and a perinatal nurse.
In our experience, this approach significantly reduces perinatal mortality, primarily by reducing preterm premature rupture of membranes and very low birth weight delivery.
Dr. Newman is currently a professor and the Maas Chair for Reproductive Sciences in the department of obstetrics and gynecology, and vice chairman for academic affairs and women’s health research at the Medical University of South Carolina, Charleston. He established a multidisciplinary twins clinic in 1989 and since then has provided care for more than 1,000 women with twins. Dr. Rogers said he has no relevant financial disclosures.
Pregnancies involving multiple births are an increasingly prevalent phenomenon in most obstetrical practices, with twin gestations now accounting for more than 3% of all births in the United States.
The incidence of twinning is attributable to two main social factors: older maternal age at childbirth, which is responsible for a third of the increase, and the increased use of assisted reproductive technology (ART), which is responsible for the other two-thirds.
Although refinements in ART and recommendations to limit the number of embryos transferred during in vitro procedures have led to reductions in the number of higher-order multiples, twin gestations are still common, occurring in up to one-third of IVF pregnancies. Ovulation induction, which is a much more commonly used ART procedure, is also associated with twinning rates of 5%-10%.
What must be appreciated is the reality that twin gestations carry significant risks and contribute disproportionately to our national rates of perinatal morbidity and mortality. Although twin gestations represent just over 3% of all live births, they account for 15% of all early preterm births and 25% of all very-low birth weight infants.
Approximately 15% of all neonates with respiratory distress syndrome are twins, and twins account for 12% of all cases of grade III or IV intraventricular hemorrhage. Of all neonatal deaths in the United States, approximately 15% are twins. Moreover, approximately 10% of all stillbirths in the United States are twins.
In short, twin gestations are one of the most common high-risk conditions in obstetrical practice. Twin pregnancies are usually exciting for parents and their families, but it is important to reflect on the significant risks they can present, and to consider how these pregnancies can be optimally managed in order to reduce these risks.
No Simple Diagnosis
The first step in the optimal management of twins is to make the early diagnosis of chorionicity. The American Journal of Obstetrics & Gynecology ran a striking editorial about the significance of establishing chorionicity by first-trimester ultrasound in multiple gestations. The editorial’s authors, Dr. Kenneth J. Moise Jr. and Dr. Anthony Johnson, reflected on a talk given by Dr. Krypos Nicolaides of King’s College London, in which he broke away from his discussion of fetal therapy, paused, and made the following statement:
"There is NO diagnosis of twins. There are only monochorionic twins or dichorionic twins. This diagnosis should be written in capital red letters across the top of the patient’s chart." (Am. J. Obstet. Gynecol. 2010;203:1-2).
It could not have been better stated. It is not appropriate in obstetrical medicine to make a simple diagnosis of "twins" any longer. Early identification of whether a twin gestation involves either a monochorionic, single-placenta placentation, or a dichorionic, dual-placenta placentation is essential for accurate risk assessment and optimal antepartum management. Monochorionic pregnancies, which represent just over 20% of all twin gestations, are at much greater risk for miscarriage, congenital anomalies, growth abnormalities (including twin-to-twin transfusion syndrome), preterm birth, stillbirth, and neurodevelopmental abnormalities.
Determining this single feature – the chorionicity of the twin gestations – will thus shape a host of decisions, from the frequency of ultrasound examinations to the type of late-pregnancy surveillance and the timing of delivery.
With proper training, chorionicity can be determined with almost 100% accuracy in the first trimester, and if a patient doesn’t present in the first trimester, it still can be determined in the second trimester with an accuracy approaching 100% using a variety of ultrasound markers and parameters.
Optimizing Nutrition
I firmly believe that maximizing the mother’s nutrition is one of the most important determinants of a healthy outcome in a twin pregnancy.
In its 2009 report titled "Weight Gain During Pregnancy: Reexamining the Guidelines," the Institute of Medicine for the first time offered body mass index–specific recommendations for women with multiple gestations. The IOM has long had recommendations for singleton pregnancies based on pregravid BMI status, but this latest report marked the first time that multiple pregnancies were addressed in such detail.
Clearly, our knowledge base has advanced. During the 1990s and 2000s, a number of investigators – most notably Barbara Luke, Sc.D., currently a professor of obstetrics, gynecology, and reproductive biology at Michigan State University, East Lansing – have published articles on the role of nutrition and weight gain in women with multiple gestations, and the relationship of these factors to pregnancy outcomes. Studies have demonstrated the critical effect that appropriate maternal weight gain and optimal nutrition have on twin fetal growth, birth weight, length of gestation, and other outcomes.
Surprisingly, the IOM consensus panel did not issue recommendations for women who are underweight, citing a lack of evidence. I believe there is clear epidemiologic evidence, however, that women with twin pregnancies who are underweight before pregnancy and have poor gestational weight gain are at the highest risk for poor outcomes.
In a 2003 report, Dr. Luke and a team of investigators, myself included, developed BMI-specific weight gain guidelines for optimal birth weights in twin pregnancies. Our weight gain curves and recommendations, which were based on a multi-institution cohort study of 2,324 twin pregnancies, are similar to the IOM’s guidelines. We also addressed the category of underweight women, however, and advised a gain of 50-62 pounds for these women. (See box.)
Women with a pregravid underweight status who had a total weight gain within this range experienced optimal fetal growth and birth weight. (J. Reprod. Med. 2003;48:217-24).
In a separate follow-up study of the value of using these BMI-specific weight gain goals, Dr. William Goodnight and I found that in our twins clinic, women who failed to achieve their BMI-specific weight-gain goals had a lower birth weight by nearly 200 g per twin and a length of gestation that was 1 week shorter than that of women who met weight gain goals (Am. J. Obstet. Gynecol. 2006;195[suppl]:S121).
As we described in a review published in 2009, achieving twin weight-gain goals should be part of a comprehensive approach to nutrition that also includes an appropriate caloric intake (3,000-4,000 kcal/day in underweight to normal weight women); supplementation with calcium, magnesium, folate, and zinc (beyond a usual prenatal vitamin); and a nutrient-dense diet that is high in iron-rich proteins and omega-3 fatty acids (Obstet. Gynecol. 2009;114:1121-34). In our practice, we emphasize the value of meat protein and of low-mercury fish.
Dr. Luke, who has coauthored a book with Tamara Eberlein that we often recommend to our patients, titled "When Youre Expecting Twins, Triplets or Quads" (New York: HarperCollins, 2011), has best demonstrated the extent to which intensive nutritional counseling and follow-up pays off in twin pregnancies.
In a cohort study published in 2003, she enrolled 190 women with twin pregnancies in a specialized prenatal program that involved twice-monthly visits for nutritional counseling and monitoring. Women were prescribed a diet of 3,000-4,000 kcal/day, with 20% of calories from protein, 40% from carbohydrates, and 40% from fat, as well as multimineral supplementation. The women were monitored for adequate weight gain and had serial ultrasound assessments.
Compared with 339 women with twin pregnancies who were followed by their physicians at the University of Michigan but not enrolled in the program, the program participants had significantly longer gestations (about a week), higher birth weights (220 g), a 23% reduction in preterm births, and significant reductions in preterm premature rupture of membranes, preterm labor, preeclampsia, ICU admission, and other poor outcomes.
Overall, the incidence of major neonatal morbidity was 17% for the nutritional program participants, compared with 32% for those women who did not receive the specialized care (Am. J. Obstet. Gynecol. 2003;189:934-8).
Measuring Cervical Length
One of the major clinical concerns with any twin pregnancy is the prevention of preterm birth and, by extension, the identification of those women with twins who, within this broader high-risk category, are at greatest risk for preterm birth.
Since the mid-1990s, research has shown that a short cervix detected in the midtrimester (defined as 16-24 weeks) by transvaginal ultrasound is a powerful predictor of preterm birth in women with either singleton or twin gestations. Studies of twin gestations have shown that as cervical length shortens to 25 mm or less, the risk of subsequent preterm birth (defined less than 34 weeks) rises dramatically.
In a report on twin pregnancies from the Maternal-Fetal Medicine Units Network of the Eunice Kennedy Shriver National Institute of Child Health and Human Development, for instance, Dr. R.L. Goldenberg and associates demonstrated that cervical length less than or equal to 25 mm at 24 weeks was the best predictor of spontaneous preterm birth. In fact, of all 50 potential risk factors that were studied, a short cervix was the only factor that was consistently associated with preterm birth. The investigators also noted that this shorter cervical length was more common at both 24 and 28 weeks in twins, compared with singleton pregnancies (Am. J. Obstet. Gynecol. 1996;175:1047-53).
Through the 1990s and the next decade, investigators searched for a viable intervention. However, in numerous studies, the use of cerclage in mothers of twins with a short cervix was found to be of no benefit. Prophylactic tocolysis also failed to prevent preterm birth in published studies.
The use of bed rest has remained controversial. It is commonly prescribed to prevent preterm birth in women with a twin gestation and a short cervix, despite the fact that we have no published data demonstrating its effectiveness in prolonging pregnancy. Personally, I believe that bed rest can reduce the frequency of uterine contractions and help protect the cervix from the weight of the pregnancy.
Interest in the treatment of twin pregnancies with progesterone had waned after 2007, when a National Institutes of Health multicenter, randomized trial of injectable progesterone reported that 17-alpha-hydroxyprogesterone caproate did not reduce the rate of twin preterm birth (N. Engl. J. Med. 2007;357:454-61).
However, progesterone recently has reemerged as a treatment for women who are at higher risk of preterm birth, based on the publication this year of Dr. Roberto Romero’s review and meta-analysis of vaginal progesterone for women with a sonographic short cervix (Am. J. Obstet. Gynecol. 2012;206:124.e1-19). Indeed, this review provides the first evidence of a beneficial effect in women with a short cervix who are carrying a twin gestation. The meta-analysis covered five prospective, randomized trials of vaginal progesterone with a total of 775 women who had a sonographically confirmed short cervix (25 mm or less) in the midtrimester. The vast majority of women in these studies carried singleton pregnancies, but two of the studies enrolled twin as well as singleton gestations, and one of the five studies – albeit a small one – focused solely on twin pregnancies.
Overall, treatment with vaginal progesterone was associated with a highly significant 42% reduction in the rate of preterm birth at less than 33 weeks. Among twin gestations specifically, the reduction in preterm birth was 30% – a meaningful trend, but not statistically significant. When it came to neonatal morbidity and mortality, however, the effect of vaginal progesterone among twin gestations was far more striking: The group that received vaginal progesterone had a 48% reduction in the risk of composite neonatal morbidity and mortality.
Admittedly, a primary randomized, controlled trial in twin gestations is still needed. In the meantime, however, given the tremendous risk faced by women with a twin gestation and a short cervix, and the lack of any other proven treatment, I believe that vaginal progesterone (Prometrium, in either a 200-mg suppository or 90-mg gel) is an appropriate treatment for this condition.
In our practice, we routinely perform transvaginal cervical-length measurements with our twin pregnancies at the time of their anatomical survey at 18-20 weeks, and then every 2-4 weeks (depending on how short the cervix is) up to 26-28 weeks. If a short cervix is diagnosed, we restrict activity and start vaginal progesterone.
Surveillance, Delivery
Careful surveillance during the late gestational period is critical, as twins – particularly monochorionic twins – are at increased risk of growth restriction or growth discordancy, and have an increased risk of developing abnormalities in amniotic fluid volume. Compared with singletons, twins also are at increased risk of stillbirth in the third trimester; this risk, again, appears to be higher for monochorionic gestations.
We perform routine ultrasound evaluations every 3 weeks for our monochorionic twins and every 4 weeks for our dichorionic twins, in the absence of any abnormalities. If abnormalities in growth are suspected with standard ultrasound evaluation, we add umbilical artery Doppler studies to further assess well-being. We also routinely institute fetal nonstress testing at 32 weeks’ gestation for monochorionic twins and at 34 weeks for our dichorionic twins. Additional strategies are employed as necessary.
The overall risk of stillbirth for twin gestations is 0.2%-0.4% per week after 32 weeks’ gestation, and rises further beyond 38 weeks – a risk that makes surveillance critical.
Some investigators, however, have recently reported higher-than-expected stillbirth rates for "apparently uncomplicated" monochorionic twin gestations. This risk has ranged from 1% to 4% at 32 and 38 weeks’ gestation in various reports.
These studies were debated as part of a workshop held in 2011 by the National Institutes of Health and the Society for Maternal-Fetal Medicine on the "Timing of Indicated Late Preterm and Early Term Births." The findings of the higher stillbirth rates remain controversial, but on the basis of these concerns, it was recommended that monochorionic twins – even "uncomplicated" cases – should be offered elective delivery at 34-37 weeks’ gestation, with decisions made after careful discussion and informed consent.
Uncomplicated dichorionic twins, on the other hand, appear to have optimal outcomes when delivered at 38 weeks’ gestation (Obstet. Gynecol. 2011;118:323-3; Semin. Perinatol. 2011;35:277-85).
Recommended surveillance and delivery of monoamniotic twins – a rare but serious type of monochorionic twin gestation – has evolved recently in favor of intensive inpatient monitoring.
The benefits of hospitalization were demonstrated most strikingly in a multicenter cohort study that compared 43 women who were admitted at a median gestational age of 26.5 weeks for inpatient fetal testing two to three times daily vs. 44 women who were followed as outpatients with fetal testing one to three times weekly.
There were no stillbirths in the hospitalized group, but there was a 15% stillbirth rate in the outpatient group. The inpatient group also had significant improvements in birth weight, gestational age at delivery, and neonatal morbidity (Am. J. Obstet. Gynecol. 2005;192:96-101).
This and other evidence suggests that mothers of monoamniotic twins have the best possible outcome when their pregnancies are managed in a hospital setting with fetal monitoring two to three times a day, starting at 24-26 weeks’ gestation, with delivery timed between 32 and 34 weeks’ gestation. This was among the conclusions of the 2011 NIH-SMFM workshop.
Specialized Care
A final consideration regarding the antepartum care of multiples would be the benefit that might be achieved by establishing a specialized twins clinic.
The literature includes numerous reports, including one of our own (Semin. Perinatol 1995;19:387-403), describing improved perinatal outcomes for twins who are cared for by multidisciplinary teams using best practice protocols. Our team includes an obstetrician, a certified nurse-midwife, a nutritionist, an ultrasonographer, and a perinatal nurse.
In our experience, this approach significantly reduces perinatal mortality, primarily by reducing preterm premature rupture of membranes and very low birth weight delivery.
Dr. Newman is currently a professor and the Maas Chair for Reproductive Sciences in the department of obstetrics and gynecology, and vice chairman for academic affairs and women’s health research at the Medical University of South Carolina, Charleston. He established a multidisciplinary twins clinic in 1989 and since then has provided care for more than 1,000 women with twins. Dr. Rogers said he has no relevant financial disclosures.
