User login
Combined Pediatric Derm-Rheum Clinics Supported by Survey Respondents
TOPLINE:
.
METHODOLOGY:
- Combined pediatric dermatology-rheumatology clinics can improve patient outcomes and experiences, particularly for pediatric autoimmune conditions presenting with both cutaneous and systemic manifestations.
- The researchers surveyed 208 pediatric dermatologists working in combined pediatric dermatology-rheumatology clinics.
- A total of 13 member responses were recorded from three countries: 10 from the United States, two from Mexico, and one from Canada.
TAKEAWAY:
- Perceived benefits of combined clinics were improved patient care through coordinated treatment decisions and timely communication between providers.
- Patient satisfaction was favorable, and patients and families endorsed the combined clinic approach.
- Barriers to clinic establishment included differences in the pace between dermatology and rheumatology clinic flow, the need to generate more relative value units, resistance from colleagues, and limited time.
- Areas that needed improvement included more time for patient visits, dedicated research assistants, new patient referrals, additional patient rooms, resources for research, and patient care infrastructure.
IN PRACTICE:
The insights from this survey “will hopefully inspire further development of these combined clinics,” the authors wrote.
SOURCE:
The investigation, led by Olga S. Cherepakhin, BS, University of Washington, Seattle, Washington, was published in Pediatric Dermatology.
LIMITATIONS:
Limitations included the subjective nature, lack of some information, selection bias, and small number of respondents, and the survey reflected the perspective of the pediatric dermatologists only.
DISCLOSURES:
The study was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. One author reported full-time employment at Janssen R&D, and the other authors had no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Combined pediatric dermatology-rheumatology clinics can improve patient outcomes and experiences, particularly for pediatric autoimmune conditions presenting with both cutaneous and systemic manifestations.
- The researchers surveyed 208 pediatric dermatologists working in combined pediatric dermatology-rheumatology clinics.
- A total of 13 member responses were recorded from three countries: 10 from the United States, two from Mexico, and one from Canada.
TAKEAWAY:
- Perceived benefits of combined clinics were improved patient care through coordinated treatment decisions and timely communication between providers.
- Patient satisfaction was favorable, and patients and families endorsed the combined clinic approach.
- Barriers to clinic establishment included differences in the pace between dermatology and rheumatology clinic flow, the need to generate more relative value units, resistance from colleagues, and limited time.
- Areas that needed improvement included more time for patient visits, dedicated research assistants, new patient referrals, additional patient rooms, resources for research, and patient care infrastructure.
IN PRACTICE:
The insights from this survey “will hopefully inspire further development of these combined clinics,” the authors wrote.
SOURCE:
The investigation, led by Olga S. Cherepakhin, BS, University of Washington, Seattle, Washington, was published in Pediatric Dermatology.
LIMITATIONS:
Limitations included the subjective nature, lack of some information, selection bias, and small number of respondents, and the survey reflected the perspective of the pediatric dermatologists only.
DISCLOSURES:
The study was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. One author reported full-time employment at Janssen R&D, and the other authors had no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
.
METHODOLOGY:
- Combined pediatric dermatology-rheumatology clinics can improve patient outcomes and experiences, particularly for pediatric autoimmune conditions presenting with both cutaneous and systemic manifestations.
- The researchers surveyed 208 pediatric dermatologists working in combined pediatric dermatology-rheumatology clinics.
- A total of 13 member responses were recorded from three countries: 10 from the United States, two from Mexico, and one from Canada.
TAKEAWAY:
- Perceived benefits of combined clinics were improved patient care through coordinated treatment decisions and timely communication between providers.
- Patient satisfaction was favorable, and patients and families endorsed the combined clinic approach.
- Barriers to clinic establishment included differences in the pace between dermatology and rheumatology clinic flow, the need to generate more relative value units, resistance from colleagues, and limited time.
- Areas that needed improvement included more time for patient visits, dedicated research assistants, new patient referrals, additional patient rooms, resources for research, and patient care infrastructure.
IN PRACTICE:
The insights from this survey “will hopefully inspire further development of these combined clinics,” the authors wrote.
SOURCE:
The investigation, led by Olga S. Cherepakhin, BS, University of Washington, Seattle, Washington, was published in Pediatric Dermatology.
LIMITATIONS:
Limitations included the subjective nature, lack of some information, selection bias, and small number of respondents, and the survey reflected the perspective of the pediatric dermatologists only.
DISCLOSURES:
The study was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health. One author reported full-time employment at Janssen R&D, and the other authors had no disclosures.
A version of this article appeared on Medscape.com.
Second Ustekinumab Biosimilar Gets FDA Approval
The US Food and Drug Administration (FDA) has approved the biosimilar ustekinumab-aekn (Selarsdi) for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis in adults and pediatric patients aged 6 years or older.
This is the second ustekinumab biosimilar approved by the regulatory agency and is the second biosimilar approval in the United States for the Icelandic pharmaceutical company Alvotech in partnership with Teva Pharmaceuticals.
Ustekinumab (Stelara) is a human monoclonal antibody targeting interleukin (IL)–12 and IL-23. The drug, manufactured by Johnson & Johnson, totaled nearly $7 billion in sales in 2023 alone, according a press release.
“Bringing Selarsdi to market in the US early next year presents a significant opportunity to improve patient access to a vital biologic in inflammatory disease and contribute to the reduction of inflationary pressure in healthcare costs,” the chairman and CEO of Alvotech said in the release.
The first ustekinumab biosimilar, ustekinumab-auub (Wezlana), was approved by the FDA in on October 31, 2023 and is interchangeable with the reference product. This allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Besides psoriasis and psoriatic arthritis, ustekinumab-auub was also approved for treating moderate to severely active Crohn’s disease and ulcerative colitis. Ustekinumab-aekn does not have an interchangeability designation and was not approved for Crohn’s disease or ulcerative colitis.
The approval of ustekinumab-aekn was based on two clinical studies. A randomized, double blind, multicenter, 52-week study of 581 patients with moderate to severe plaque psoriasis demonstrated that the biosimilar was as effective as the reference product, with equivalent safety and immunogenicity profiles. A phase 1, randomized, double-blind, single-dose, parallel-group, three-arm study also compared the pharmacokinetic profile of the biosimilar to ustekinumab in 294 healthy adults.
Ustekinumab-aekn is expected to be marketed in the United States on or after February 21, 2025 per a settlement and license agreement with Johnson & Johnson.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved the biosimilar ustekinumab-aekn (Selarsdi) for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis in adults and pediatric patients aged 6 years or older.
This is the second ustekinumab biosimilar approved by the regulatory agency and is the second biosimilar approval in the United States for the Icelandic pharmaceutical company Alvotech in partnership with Teva Pharmaceuticals.
Ustekinumab (Stelara) is a human monoclonal antibody targeting interleukin (IL)–12 and IL-23. The drug, manufactured by Johnson & Johnson, totaled nearly $7 billion in sales in 2023 alone, according a press release.
“Bringing Selarsdi to market in the US early next year presents a significant opportunity to improve patient access to a vital biologic in inflammatory disease and contribute to the reduction of inflationary pressure in healthcare costs,” the chairman and CEO of Alvotech said in the release.
The first ustekinumab biosimilar, ustekinumab-auub (Wezlana), was approved by the FDA in on October 31, 2023 and is interchangeable with the reference product. This allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Besides psoriasis and psoriatic arthritis, ustekinumab-auub was also approved for treating moderate to severely active Crohn’s disease and ulcerative colitis. Ustekinumab-aekn does not have an interchangeability designation and was not approved for Crohn’s disease or ulcerative colitis.
The approval of ustekinumab-aekn was based on two clinical studies. A randomized, double blind, multicenter, 52-week study of 581 patients with moderate to severe plaque psoriasis demonstrated that the biosimilar was as effective as the reference product, with equivalent safety and immunogenicity profiles. A phase 1, randomized, double-blind, single-dose, parallel-group, three-arm study also compared the pharmacokinetic profile of the biosimilar to ustekinumab in 294 healthy adults.
Ustekinumab-aekn is expected to be marketed in the United States on or after February 21, 2025 per a settlement and license agreement with Johnson & Johnson.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved the biosimilar ustekinumab-aekn (Selarsdi) for the treatment of moderate to severe plaque psoriasis and psoriatic arthritis in adults and pediatric patients aged 6 years or older.
This is the second ustekinumab biosimilar approved by the regulatory agency and is the second biosimilar approval in the United States for the Icelandic pharmaceutical company Alvotech in partnership with Teva Pharmaceuticals.
Ustekinumab (Stelara) is a human monoclonal antibody targeting interleukin (IL)–12 and IL-23. The drug, manufactured by Johnson & Johnson, totaled nearly $7 billion in sales in 2023 alone, according a press release.
“Bringing Selarsdi to market in the US early next year presents a significant opportunity to improve patient access to a vital biologic in inflammatory disease and contribute to the reduction of inflationary pressure in healthcare costs,” the chairman and CEO of Alvotech said in the release.
The first ustekinumab biosimilar, ustekinumab-auub (Wezlana), was approved by the FDA in on October 31, 2023 and is interchangeable with the reference product. This allows pharmacists to substitute the biosimilar for the reference product without involving the prescribing clinician (according to state law). Besides psoriasis and psoriatic arthritis, ustekinumab-auub was also approved for treating moderate to severely active Crohn’s disease and ulcerative colitis. Ustekinumab-aekn does not have an interchangeability designation and was not approved for Crohn’s disease or ulcerative colitis.
The approval of ustekinumab-aekn was based on two clinical studies. A randomized, double blind, multicenter, 52-week study of 581 patients with moderate to severe plaque psoriasis demonstrated that the biosimilar was as effective as the reference product, with equivalent safety and immunogenicity profiles. A phase 1, randomized, double-blind, single-dose, parallel-group, three-arm study also compared the pharmacokinetic profile of the biosimilar to ustekinumab in 294 healthy adults.
Ustekinumab-aekn is expected to be marketed in the United States on or after February 21, 2025 per a settlement and license agreement with Johnson & Johnson.
A version of this article appeared on Medscape.com.
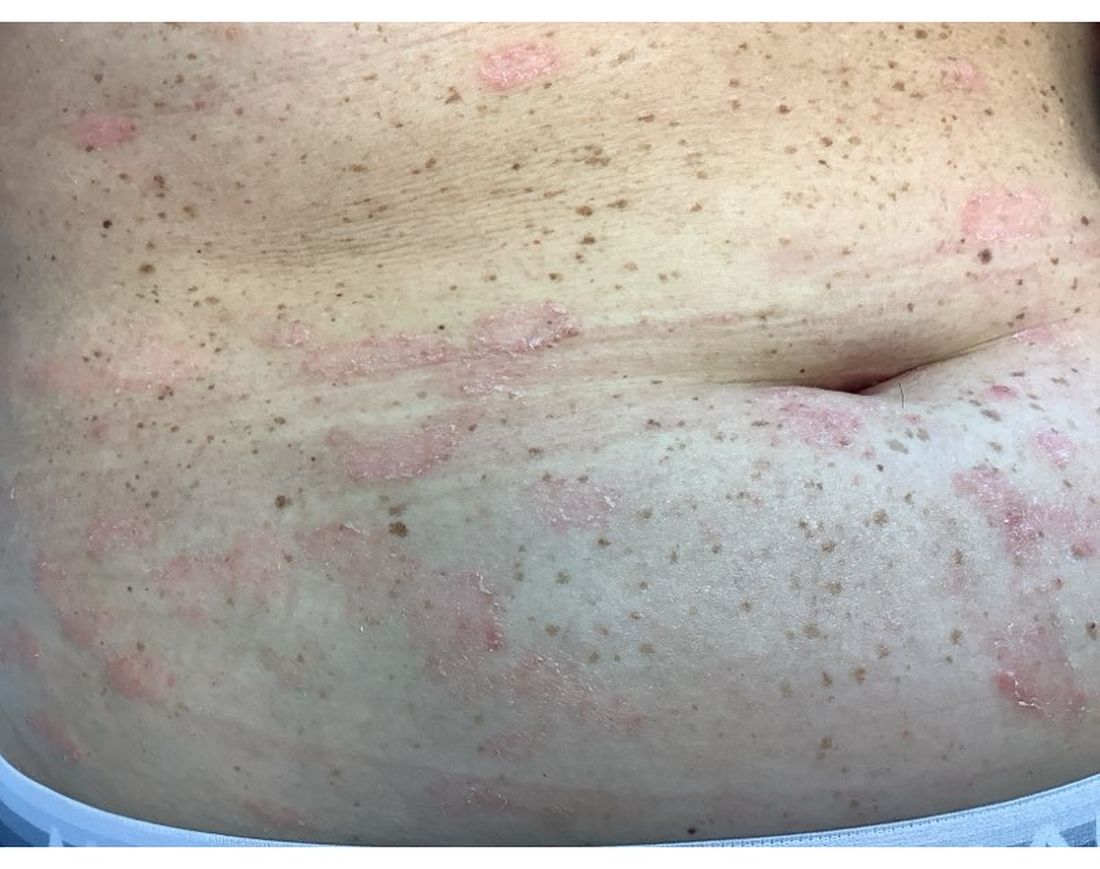
A 30-Year-Old White Female Presented With a 4-Month History of Scaly, Erythematous Patches and Plaques on Her Trunk and Extremities
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.

There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.
There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
Tumor necrosis factor (TNF)-alpha inhibitors are used to treat a variety of autoimmune conditions including psoriasis, psoriatic arthritis, rheumatoid arthritis (RA), spondyloarthritis, and inflammatory bowel disease (IBD). Interestingly, they have also been observed to cause paradoxical psoriasis with an incidence between 0.6%-5.3%, most commonly occurring in patients with underlying Crohn’s disease and rheumatoid arthritis (RA). Infliximab is the most common TNF inhibitor associated with this condition (52.6%-62.6% of cases) followed by etanercept (12%-29%). .
Psoriasis is traditionally divided into two types. Patients with type I psoriasis have a family history, develop symptoms before the age of 40 and are often positive for HLA-Cw6. Type II psoriasis is not related to HLA-Cw6, lacks a family history, and typically manifests after age 40. Psoriatic lesions are well-defined, erythematous plaques with silvery scales most commonly appearing on extensor surfaces and the scalp. Variants include nail psoriasis, pustular psoriasis, inverse psoriasis, and guttate psoriasis.
Although psoriasis is typically a clinical diagnosis, histologic examination may be used to differentiate from other dermatoses if necessary. The lesions of TNF inhibitor-induced psoriasis characteristically display patterns similar to primary psoriasis, including parakeratosis, microabscesses, and rete ridges. Eosinophilic hypersensitivity reactions and features overlapping with eczematous hypersensitivity (psoriasiform dermatitis) may also be present.
The pathogenesis of this condition is not well understood, but theories include a variety of immune processes including interferon overproduction, interleukin and T-cell activation, and the presence of an infectious nidus. Classical psoriasis is related to type 1 interferon release, so theoretically, immunosuppression caused by TNF inhibitor treatment may permit uncontrolled production of interferons, resulting in psoriatic lesions. Another theory is that interleukin (IL)-23, a pro-inflammatory cytokine, promotes activation of T-helper 17 (Th17) cells. Th17 cells are part of the pathogenesis of primary psoriasis and other inflammatory conditions, such as RA and inflammatory bowel disease. Of note, individuals with gastrointestinal inflammatory diseases are already known to be at a greater risk for developing psoriasis. Immunosuppression caused by a TNF inhibitor may leave patients more susceptible to other infections, which may induce psoriatic plaques.
There are multiple approaches to treatment depending on the severity of the disease. If the psoriatic eruption is mild, the medication may be continued. This “treat-through” method is often considered when stopping the current immunotherapy would cause the patient significant issues. Moderate to severe cases of TNF inhibitor-induced psoriasis may warrant switching TNF inhibitor therapy or completely changing the drug class used in the treatment of the underlying autoimmune condition. Additional treatments include topical and oral steroids, UV therapy, methotrexate, cyclosporine, and acitretin.
This case and the photo were submitted by Lucas Shapiro, BS, of Nova Southeastern University College of Osteopathic Medicine, Fort Lauderdale, Florida, and Leon S. Maratchi, MD, Gastro Health, Hollywood, Florida. The column was edited by Donna Bilu Martin, MD.
Dr. Bilu Martin is a board-certified dermatologist in private practice at Premier Dermatology, MD, in Aventura, Florida. More diagnostic cases are available at mdedge.com/dermatology. To submit a case for possible publication, send an email to [email protected].
References
1. Li SJ et al. J Psoriasis Psoriatic Arthritis. 2019 Apr;4(2):70-80. doi: 10.1177/2475530318810851.
2. Lu J and Lu Y. J Transl Autoimmun. 2023 Sep 6:7:100211. doi: 10.1016/j.jtauto.2023.100211.
3. Nair PA and Badri T. Psoriasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK448194/
Lichenoid Dermatosis on the Feet
The Diagnosis: Hypertrophic Lichen Planus
Two biopsies from the left lateral foot revealed hyperkeratosis, wedge-shaped hypergranulosis, irregular acanthosis, and a bandlike lymphocytic infiltrate in the superficial dermis with a classic sawtooth pattern of the rete ridges (Figure 1). Based on the clinical findings and histopathology, the patient was diagnosed with hypertrophic lichen planus (LP) and was treated with clobetasol ointment 0.05%, which resulted in progression of the symptoms. She experienced notable improvement 3 months after adding methotrexate 12.5 mg weekly (Figure 2).

Lichen planus is an idiopathic chronic inflammatory condition of the skin and mucous membranes that classically manifests as pruritic violaceous papules and plaques, which commonly are found on the wrists, lower back, and ankles.1 The most common variants of LP are hypertrophic, linear, mucosal, actinic, follicular, pigmented, annular, atrophic, and guttate.2 The clinical presentation and biopsy results in our patient were consistent with the hypertrophic variant of LP, which is a chronic condition that most often manifests on the lower legs, especially around the ankles, as hyperkeratotic papules, plaques, and nodules.2,3 The exact pathophysiology of hypertrophic LP is unknown, but there is evidence that the immune system plays a role in its development and that the Koebner phenomenon may contribute to its exacerbation.4 There is a well-known association between LP and hepatitis. Patients with chronic LP may develop squamous cell carcinoma.4 The variants of LP can overlap and do not exist independent of one another. Recognizing the overlap in these variants allows for earlier diagnosis and therapeutic intervention of the disease process to limit disease progression and patient clinic visits and to improve patient quality of life.

The differential diagnosis for hyperkeratotic plaques of the feet and ankles can be broad and may include keratosis lichenoides chronica, palmoplantar keratoderma, palmoplantar psoriasis, or lichen amyloidosis. These conditions are classified based on various criteria that include extent of disease manifestations, morphology of palmoplantar skin involvement, inheritance patterns, and molecular pathogenesis.5 Keratosis lichenoides chronica is a rare dermatosis that presents as a distinctive seborrheic dermatitis–like facial eruption. The facial eruption is accompanied by violaceous papular and nodular lesions that appear on the extremities and trunk, typically arranged in a linear or reticular pattern.6 Palmoplantar keratoderma represents a group of acquired and hereditary conditions that are characterized by excessive thickening of the palms and soles.5 Palmoplantar psoriasis is a variant of psoriasis that affects the palms and soles and can manifest as hyperkeratosis, pustular, or mixed morphology.7 Lichen amyloidosis is a subtype of primary localized cutaneous amyloidosis that manifests as multiple pruritic, firm, hyperpigmented, hyperkeratotic papules on the shins that later coalesce in a rippled pattern.8,9
The first-line treatment for hypertrophic LP is topical corticosteroids. Alternative therapies include mycophenolate mofetil, acitretin, and intralesional corticosteroid injections.4 Treatment is similar for all of the LP variants.
- Arnold DL, Krishnamurthy K. Lichen planus. In: StatPearls. StatPearls Publishing; 2022.
- Namazi MR, Bahmani M. Diagnosis: hypertrophic lichen planus. Ann Saudi Med. 2008;28:1-2. doi:10.5144/0256-4947.2008.222
- Riahi RR, Cohen PR. Hypertrophic lichen planus mimicking verrucous lupus erythematosus. Cureus. 2018;10:e3555. doi:10.7759 /cureus.3555
- Weston G, Payette M. Update on lichen planus and its clinical variants. Int J Womens Dermatol. 2015;1:140-149. doi:10.1016/j .ijwd.2015.04.001
- Has C, Technau-Hafsi K. Palmoplantar keratodermas: clinical and genetic aspects. J Dtsch Dermatol Ges. 2016;14:123-139; quiz 140. doi:10.1111/ddg.12930
- Konstantinov KN, Søndergaard J, Izuno G, et al. Keratosis lichenoides chronica. J Am Acad Dermatol. 1998;38(2 Pt 2):306-309. doi:10.1016 /s0190-9622(98)70570-5
- Miceli A, Schmieder GJ. Palmoplantar psoriasis. In: StatPearls. StatPearls Publishing; 2023.
- Tay CH, Dacosta JL. Lichen amyloidosis—clinical study of 40 cases. Br J Dermatol. 1970;82:129-136.
- Salim T, Shenoi SD, Balachandran C, et al. Lichen amyloidosis: a study of clinical, histopathologic and immunofluorescence findings in 30 cases. Indian J Dermatol Venereol Leprol. 2005;71:166-169.
The Diagnosis: Hypertrophic Lichen Planus
Two biopsies from the left lateral foot revealed hyperkeratosis, wedge-shaped hypergranulosis, irregular acanthosis, and a bandlike lymphocytic infiltrate in the superficial dermis with a classic sawtooth pattern of the rete ridges (Figure 1). Based on the clinical findings and histopathology, the patient was diagnosed with hypertrophic lichen planus (LP) and was treated with clobetasol ointment 0.05%, which resulted in progression of the symptoms. She experienced notable improvement 3 months after adding methotrexate 12.5 mg weekly (Figure 2).
Lichen planus is an idiopathic chronic inflammatory condition of the skin and mucous membranes that classically manifests as pruritic violaceous papules and plaques, which commonly are found on the wrists, lower back, and ankles.1 The most common variants of LP are hypertrophic, linear, mucosal, actinic, follicular, pigmented, annular, atrophic, and guttate.2 The clinical presentation and biopsy results in our patient were consistent with the hypertrophic variant of LP, which is a chronic condition that most often manifests on the lower legs, especially around the ankles, as hyperkeratotic papules, plaques, and nodules.2,3 The exact pathophysiology of hypertrophic LP is unknown, but there is evidence that the immune system plays a role in its development and that the Koebner phenomenon may contribute to its exacerbation.4 There is a well-known association between LP and hepatitis. Patients with chronic LP may develop squamous cell carcinoma.4 The variants of LP can overlap and do not exist independent of one another. Recognizing the overlap in these variants allows for earlier diagnosis and therapeutic intervention of the disease process to limit disease progression and patient clinic visits and to improve patient quality of life.
The differential diagnosis for hyperkeratotic plaques of the feet and ankles can be broad and may include keratosis lichenoides chronica, palmoplantar keratoderma, palmoplantar psoriasis, or lichen amyloidosis. These conditions are classified based on various criteria that include extent of disease manifestations, morphology of palmoplantar skin involvement, inheritance patterns, and molecular pathogenesis.5 Keratosis lichenoides chronica is a rare dermatosis that presents as a distinctive seborrheic dermatitis–like facial eruption. The facial eruption is accompanied by violaceous papular and nodular lesions that appear on the extremities and trunk, typically arranged in a linear or reticular pattern.6 Palmoplantar keratoderma represents a group of acquired and hereditary conditions that are characterized by excessive thickening of the palms and soles.5 Palmoplantar psoriasis is a variant of psoriasis that affects the palms and soles and can manifest as hyperkeratosis, pustular, or mixed morphology.7 Lichen amyloidosis is a subtype of primary localized cutaneous amyloidosis that manifests as multiple pruritic, firm, hyperpigmented, hyperkeratotic papules on the shins that later coalesce in a rippled pattern.8,9
The first-line treatment for hypertrophic LP is topical corticosteroids. Alternative therapies include mycophenolate mofetil, acitretin, and intralesional corticosteroid injections.4 Treatment is similar for all of the LP variants.
The Diagnosis: Hypertrophic Lichen Planus
Two biopsies from the left lateral foot revealed hyperkeratosis, wedge-shaped hypergranulosis, irregular acanthosis, and a bandlike lymphocytic infiltrate in the superficial dermis with a classic sawtooth pattern of the rete ridges (Figure 1). Based on the clinical findings and histopathology, the patient was diagnosed with hypertrophic lichen planus (LP) and was treated with clobetasol ointment 0.05%, which resulted in progression of the symptoms. She experienced notable improvement 3 months after adding methotrexate 12.5 mg weekly (Figure 2).
Lichen planus is an idiopathic chronic inflammatory condition of the skin and mucous membranes that classically manifests as pruritic violaceous papules and plaques, which commonly are found on the wrists, lower back, and ankles.1 The most common variants of LP are hypertrophic, linear, mucosal, actinic, follicular, pigmented, annular, atrophic, and guttate.2 The clinical presentation and biopsy results in our patient were consistent with the hypertrophic variant of LP, which is a chronic condition that most often manifests on the lower legs, especially around the ankles, as hyperkeratotic papules, plaques, and nodules.2,3 The exact pathophysiology of hypertrophic LP is unknown, but there is evidence that the immune system plays a role in its development and that the Koebner phenomenon may contribute to its exacerbation.4 There is a well-known association between LP and hepatitis. Patients with chronic LP may develop squamous cell carcinoma.4 The variants of LP can overlap and do not exist independent of one another. Recognizing the overlap in these variants allows for earlier diagnosis and therapeutic intervention of the disease process to limit disease progression and patient clinic visits and to improve patient quality of life.
The differential diagnosis for hyperkeratotic plaques of the feet and ankles can be broad and may include keratosis lichenoides chronica, palmoplantar keratoderma, palmoplantar psoriasis, or lichen amyloidosis. These conditions are classified based on various criteria that include extent of disease manifestations, morphology of palmoplantar skin involvement, inheritance patterns, and molecular pathogenesis.5 Keratosis lichenoides chronica is a rare dermatosis that presents as a distinctive seborrheic dermatitis–like facial eruption. The facial eruption is accompanied by violaceous papular and nodular lesions that appear on the extremities and trunk, typically arranged in a linear or reticular pattern.6 Palmoplantar keratoderma represents a group of acquired and hereditary conditions that are characterized by excessive thickening of the palms and soles.5 Palmoplantar psoriasis is a variant of psoriasis that affects the palms and soles and can manifest as hyperkeratosis, pustular, or mixed morphology.7 Lichen amyloidosis is a subtype of primary localized cutaneous amyloidosis that manifests as multiple pruritic, firm, hyperpigmented, hyperkeratotic papules on the shins that later coalesce in a rippled pattern.8,9
The first-line treatment for hypertrophic LP is topical corticosteroids. Alternative therapies include mycophenolate mofetil, acitretin, and intralesional corticosteroid injections.4 Treatment is similar for all of the LP variants.
- Arnold DL, Krishnamurthy K. Lichen planus. In: StatPearls. StatPearls Publishing; 2022.
- Namazi MR, Bahmani M. Diagnosis: hypertrophic lichen planus. Ann Saudi Med. 2008;28:1-2. doi:10.5144/0256-4947.2008.222
- Riahi RR, Cohen PR. Hypertrophic lichen planus mimicking verrucous lupus erythematosus. Cureus. 2018;10:e3555. doi:10.7759 /cureus.3555
- Weston G, Payette M. Update on lichen planus and its clinical variants. Int J Womens Dermatol. 2015;1:140-149. doi:10.1016/j .ijwd.2015.04.001
- Has C, Technau-Hafsi K. Palmoplantar keratodermas: clinical and genetic aspects. J Dtsch Dermatol Ges. 2016;14:123-139; quiz 140. doi:10.1111/ddg.12930
- Konstantinov KN, Søndergaard J, Izuno G, et al. Keratosis lichenoides chronica. J Am Acad Dermatol. 1998;38(2 Pt 2):306-309. doi:10.1016 /s0190-9622(98)70570-5
- Miceli A, Schmieder GJ. Palmoplantar psoriasis. In: StatPearls. StatPearls Publishing; 2023.
- Tay CH, Dacosta JL. Lichen amyloidosis—clinical study of 40 cases. Br J Dermatol. 1970;82:129-136.
- Salim T, Shenoi SD, Balachandran C, et al. Lichen amyloidosis: a study of clinical, histopathologic and immunofluorescence findings in 30 cases. Indian J Dermatol Venereol Leprol. 2005;71:166-169.
- Arnold DL, Krishnamurthy K. Lichen planus. In: StatPearls. StatPearls Publishing; 2022.
- Namazi MR, Bahmani M. Diagnosis: hypertrophic lichen planus. Ann Saudi Med. 2008;28:1-2. doi:10.5144/0256-4947.2008.222
- Riahi RR, Cohen PR. Hypertrophic lichen planus mimicking verrucous lupus erythematosus. Cureus. 2018;10:e3555. doi:10.7759 /cureus.3555
- Weston G, Payette M. Update on lichen planus and its clinical variants. Int J Womens Dermatol. 2015;1:140-149. doi:10.1016/j .ijwd.2015.04.001
- Has C, Technau-Hafsi K. Palmoplantar keratodermas: clinical and genetic aspects. J Dtsch Dermatol Ges. 2016;14:123-139; quiz 140. doi:10.1111/ddg.12930
- Konstantinov KN, Søndergaard J, Izuno G, et al. Keratosis lichenoides chronica. J Am Acad Dermatol. 1998;38(2 Pt 2):306-309. doi:10.1016 /s0190-9622(98)70570-5
- Miceli A, Schmieder GJ. Palmoplantar psoriasis. In: StatPearls. StatPearls Publishing; 2023.
- Tay CH, Dacosta JL. Lichen amyloidosis—clinical study of 40 cases. Br J Dermatol. 1970;82:129-136.
- Salim T, Shenoi SD, Balachandran C, et al. Lichen amyloidosis: a study of clinical, histopathologic and immunofluorescence findings in 30 cases. Indian J Dermatol Venereol Leprol. 2005;71:166-169.
An 83-year-old woman presented for evaluation of hyperkeratotic plaques on the medial and lateral aspects of the left heel (top). Physical examination also revealed onychodystrophy of the toenails on the halluces (bottom). A crusted friable plaque on the lower lip and white plaques with peripheral reticulation and erosions on the buccal mucosa also were present. The patient had a history of nummular eczema, stasis dermatitis, and hand dermatitis. She denied a history of cold sores.


Approval of Spesolimab for Generalized Pustular Psoriasis Expanded
The in adults and in pediatric patients aged ≥ 12 years who weigh ≥ 40 kg, according to an announcement from the manufacturer.
This is an expanded indication for spesolimab-sbzo, first approved in September 2022 for treating GPP flares. Developed by Boehringer Ingelheim and marketed under the name Spevigo, the product is an injectable antibody that blocks the IL-36 receptor, a key part of the pathway shown to be involved in the cause of GPP, which is rare and is a potentially-life-threatening disease.
According to a press release from the company, the FDA’s approval of the expanded indication was based on the results of a 48-week clinical trial of 123 patients (Effisayil 2), which showed that individuals who received spesolimab experienced a significant 84% reduction in GPP flares compared with those who received placebo. Among 30 study participants who received a high treatment dose, no flares were observed after week 4. Among all patients who received spesolimab-sbzo, treatment was associated with an increased incidence (defined as ≥ 9 cases per 100 patient-years) of injection site reactions, urinary tract infections, arthralgia, and pruritus compared with placebo.
Spesolimab-sbzo is currently available in 48 countries, according to the Boehringer Ingelheim release, which states that the approval makes it the first targeted therapy that is available for the acute and chronic treatment of patients with GPP.
A version of this article appeared on Medscape.com.
The in adults and in pediatric patients aged ≥ 12 years who weigh ≥ 40 kg, according to an announcement from the manufacturer.
This is an expanded indication for spesolimab-sbzo, first approved in September 2022 for treating GPP flares. Developed by Boehringer Ingelheim and marketed under the name Spevigo, the product is an injectable antibody that blocks the IL-36 receptor, a key part of the pathway shown to be involved in the cause of GPP, which is rare and is a potentially-life-threatening disease.
According to a press release from the company, the FDA’s approval of the expanded indication was based on the results of a 48-week clinical trial of 123 patients (Effisayil 2), which showed that individuals who received spesolimab experienced a significant 84% reduction in GPP flares compared with those who received placebo. Among 30 study participants who received a high treatment dose, no flares were observed after week 4. Among all patients who received spesolimab-sbzo, treatment was associated with an increased incidence (defined as ≥ 9 cases per 100 patient-years) of injection site reactions, urinary tract infections, arthralgia, and pruritus compared with placebo.
Spesolimab-sbzo is currently available in 48 countries, according to the Boehringer Ingelheim release, which states that the approval makes it the first targeted therapy that is available for the acute and chronic treatment of patients with GPP.
A version of this article appeared on Medscape.com.
The in adults and in pediatric patients aged ≥ 12 years who weigh ≥ 40 kg, according to an announcement from the manufacturer.
This is an expanded indication for spesolimab-sbzo, first approved in September 2022 for treating GPP flares. Developed by Boehringer Ingelheim and marketed under the name Spevigo, the product is an injectable antibody that blocks the IL-36 receptor, a key part of the pathway shown to be involved in the cause of GPP, which is rare and is a potentially-life-threatening disease.
According to a press release from the company, the FDA’s approval of the expanded indication was based on the results of a 48-week clinical trial of 123 patients (Effisayil 2), which showed that individuals who received spesolimab experienced a significant 84% reduction in GPP flares compared with those who received placebo. Among 30 study participants who received a high treatment dose, no flares were observed after week 4. Among all patients who received spesolimab-sbzo, treatment was associated with an increased incidence (defined as ≥ 9 cases per 100 patient-years) of injection site reactions, urinary tract infections, arthralgia, and pruritus compared with placebo.
Spesolimab-sbzo is currently available in 48 countries, according to the Boehringer Ingelheim release, which states that the approval makes it the first targeted therapy that is available for the acute and chronic treatment of patients with GPP.
A version of this article appeared on Medscape.com.
LITE Study Provides Encouraging Data on Home-Based Phototherapy for Psoriasis
SAN DIEGO — and Dermatology Life Quality Index (DLQI) scores, results from a pragmatic, multicenter study showed.
“In 2024, we have a lot of ways to treat moderate-to-severe psoriasis, and phototherapy remains relevant,” lead investigator Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, told attendees of a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.

“Office phototherapy is 10 to 100 times less expensive than biologics for psoriasis, and in head-to-head trials, it’s about as effective as adalimumab and achieves better patient-reported outcomes. It may have some cardiovascular benefits by lowering IL-6 and improving HDL-P,” he said. “And, compared to secukinumab, it has no risk of infection.”
Although phototherapy is a preferred as a treatment by patients with psoriasis, he continued, inconvenience of traveling to a clinician’s office for the treatment and lack of coverage by health insurance plans remain major barriers to this option. According to Dr. Gelfand, office-based phototherapy is not available in 90% of counties in the United States, “and a lack of US data has resulted in many insurance companies not covering home phototherapy. As a result, many providers are uncertain about prescribing it.”
LITE Study Data
In 2019, Dr. Gelfand and colleagues Light Treatment Effectiveness (LITE) study, a patient-centered study that tested the hypothesis that narrowband UVB phototherapy of psoriasis at home is non-inferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. The co-primary outcomes were a PGA score of 0/1 (clear, almost clear) and a DLQI score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. New or established patients to the practices were accepted into the trial, while those treated with phototherapy within 14 days before the baseline visit were not. These entry criteria “are highly pragmatic and reflect routine clinical practice,” he said.
The researchers evenly stratified patients by skin types I and II, III and IV, and V and VI. They collected data from medical records or from an app on the patient’s cell phone, which captured the DLQI data. Study participants were randomly assigned 1:1 to office- or home-based phototherapy for 12 weeks at doses recommended in the 2019 AAD-National Psoriasis Foundation guidelines. This was followed by a 12-week observation period, which ended at 24 weeks.
At baseline, the mean DLQI score of patients was 12.2, the mean PGA score was 3, and their mean body surface area affected was 12.5%. “These patients had pretty severe disease, long-standing disease, and about 12% were on biologics or nonbiologic systemic therapy during the study,” said Dr. Gelfand, also the director of the Psoriasis and Phototherapy Treatment Center at Penn. In addition, he said, “the average round-trip to receive phototherapy in the office was about 60 minutes.”
An Improvement in Health Equity
Following treatment at 12 weeks, 25.6% of patients in the office-based phototherapy group achieved a PGA of 0/1, compared with 32.8% of patients in the home-based phototherapy group (P >.0001 for non-inferiority). Similarly, 33.6% of patients in the office-based phototherapy group achieved a score of 5 or less on the DLQI, compared with 52.4% of patients in the home-based phototherapy group (P >.0001 for non-inferiority).
In subgroup analyses, patients with darkly pigmented skin did especially well on home phototherapy relative to office treatment. “This finding is an example of how the LITE study was specifically designed to improve health equity through an intentionally inclusive approach,” Dr. Gelfand said. Perhaps not surprisingly, patients in the home-based phototherapy arm were more adherent to treatment compared with those in the office-based arm (a mean of 26.8 sessions during the study period, compared with a mean of 17.9, respectively; P < .0001). “They also had higher cumulative doses of phototherapy and therefore higher episodes of treatments with erythema,” he noted.
Among patients who reported “itchy, sore, painful, or stinging” skin in the previous week, 63% characterized the degree of discomfort as “not at all or a little,” while 28% said “a lot,” and 9% said “very much.” No patients withdrew or stopped phototherapy during the trial because of treatment-related side effects, “so it’s very well tolerated,” Dr. Gelfand said.
“If a patient never had phototherapy before, they did just as well at home as they did in the office. This suggests that there’s no reason to insist that a patient use office-based phototherapy before using home phototherapy.”
The researchers studied the efficacy of narrow-band UVB in patients who had at least two treatments per week for 12 weeks. In this subgroup of patients, 60% achieved clear or almost clear skin and nearly 50% achieved the equivalent of a Psoriasis Area and Severity Index (PASI) 90 score.
“Home phototherapy is clearly non-inferior to office-based phototherapy across all skin types and both primary outcomes, PGA and DLQI, and both have excellent effectiveness and safety in real-world settings,” Dr. Gelfand concluded. “These data support the use of home phototherapy as a first-line treatment option for psoriasis, including those with no prior phototherapy experience.”
LITE Study Described as “Groundbreaking”
One of the session moderators, dermatologist Andrew Blauvelt, MD, MBA, of the Oregon Medical Research Center, Portland, asked about the impact that lockdowns during the early phase of the COVID-19 pandemic had on the trial. “The study shut down for a couple weeks during the initial lockdown, but we got back up and running pretty quickly,” Dr. Gelfand responded. “We didn’t study that specific period of time, but the study was going on well before COVID and well after COVID restrictions were lifted. We’ll have to analyze that period of time you question but I suspect that it’s not driving the results we see.”
Asked to comment, Henry W. Lim, MD, a dermatologist with Henry Ford Health in Detroit, characterized the findings of the study as “groundbreaking, because it looked at a real-life situation in the use of phototherapy at home vs in the office, showing that the home phototherapy is not inferior to office-based phototherapy.”

This is important, he continued, “because it can inform payers to approve home phototherapy equipment for patients, because it’s much more convenient and it definitely works. The other strong point of the study is that it included patients of different skin types,” he said in an interview at the meeting.
The study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices. Dr. Gelfand reported no relevant financial relationships. Dr. Blauvelt disclosed conflicts of interest from many pharmaceutical companies. Dr. Lim disclosed conflicts of interest from many pharmaceutical companies.
A version of this article appeared on Medscape.com.
SAN DIEGO — and Dermatology Life Quality Index (DLQI) scores, results from a pragmatic, multicenter study showed.
“In 2024, we have a lot of ways to treat moderate-to-severe psoriasis, and phototherapy remains relevant,” lead investigator Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, told attendees of a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.
“Office phototherapy is 10 to 100 times less expensive than biologics for psoriasis, and in head-to-head trials, it’s about as effective as adalimumab and achieves better patient-reported outcomes. It may have some cardiovascular benefits by lowering IL-6 and improving HDL-P,” he said. “And, compared to secukinumab, it has no risk of infection.”
Although phototherapy is a preferred as a treatment by patients with psoriasis, he continued, inconvenience of traveling to a clinician’s office for the treatment and lack of coverage by health insurance plans remain major barriers to this option. According to Dr. Gelfand, office-based phototherapy is not available in 90% of counties in the United States, “and a lack of US data has resulted in many insurance companies not covering home phototherapy. As a result, many providers are uncertain about prescribing it.”
LITE Study Data
In 2019, Dr. Gelfand and colleagues Light Treatment Effectiveness (LITE) study, a patient-centered study that tested the hypothesis that narrowband UVB phototherapy of psoriasis at home is non-inferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. The co-primary outcomes were a PGA score of 0/1 (clear, almost clear) and a DLQI score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. New or established patients to the practices were accepted into the trial, while those treated with phototherapy within 14 days before the baseline visit were not. These entry criteria “are highly pragmatic and reflect routine clinical practice,” he said.
The researchers evenly stratified patients by skin types I and II, III and IV, and V and VI. They collected data from medical records or from an app on the patient’s cell phone, which captured the DLQI data. Study participants were randomly assigned 1:1 to office- or home-based phototherapy for 12 weeks at doses recommended in the 2019 AAD-National Psoriasis Foundation guidelines. This was followed by a 12-week observation period, which ended at 24 weeks.
At baseline, the mean DLQI score of patients was 12.2, the mean PGA score was 3, and their mean body surface area affected was 12.5%. “These patients had pretty severe disease, long-standing disease, and about 12% were on biologics or nonbiologic systemic therapy during the study,” said Dr. Gelfand, also the director of the Psoriasis and Phototherapy Treatment Center at Penn. In addition, he said, “the average round-trip to receive phototherapy in the office was about 60 minutes.”
An Improvement in Health Equity
Following treatment at 12 weeks, 25.6% of patients in the office-based phototherapy group achieved a PGA of 0/1, compared with 32.8% of patients in the home-based phototherapy group (P >.0001 for non-inferiority). Similarly, 33.6% of patients in the office-based phototherapy group achieved a score of 5 or less on the DLQI, compared with 52.4% of patients in the home-based phototherapy group (P >.0001 for non-inferiority).
In subgroup analyses, patients with darkly pigmented skin did especially well on home phototherapy relative to office treatment. “This finding is an example of how the LITE study was specifically designed to improve health equity through an intentionally inclusive approach,” Dr. Gelfand said. Perhaps not surprisingly, patients in the home-based phototherapy arm were more adherent to treatment compared with those in the office-based arm (a mean of 26.8 sessions during the study period, compared with a mean of 17.9, respectively; P < .0001). “They also had higher cumulative doses of phototherapy and therefore higher episodes of treatments with erythema,” he noted.
Among patients who reported “itchy, sore, painful, or stinging” skin in the previous week, 63% characterized the degree of discomfort as “not at all or a little,” while 28% said “a lot,” and 9% said “very much.” No patients withdrew or stopped phototherapy during the trial because of treatment-related side effects, “so it’s very well tolerated,” Dr. Gelfand said.
“If a patient never had phototherapy before, they did just as well at home as they did in the office. This suggests that there’s no reason to insist that a patient use office-based phototherapy before using home phototherapy.”
The researchers studied the efficacy of narrow-band UVB in patients who had at least two treatments per week for 12 weeks. In this subgroup of patients, 60% achieved clear or almost clear skin and nearly 50% achieved the equivalent of a Psoriasis Area and Severity Index (PASI) 90 score.
“Home phototherapy is clearly non-inferior to office-based phototherapy across all skin types and both primary outcomes, PGA and DLQI, and both have excellent effectiveness and safety in real-world settings,” Dr. Gelfand concluded. “These data support the use of home phototherapy as a first-line treatment option for psoriasis, including those with no prior phototherapy experience.”
LITE Study Described as “Groundbreaking”
One of the session moderators, dermatologist Andrew Blauvelt, MD, MBA, of the Oregon Medical Research Center, Portland, asked about the impact that lockdowns during the early phase of the COVID-19 pandemic had on the trial. “The study shut down for a couple weeks during the initial lockdown, but we got back up and running pretty quickly,” Dr. Gelfand responded. “We didn’t study that specific period of time, but the study was going on well before COVID and well after COVID restrictions were lifted. We’ll have to analyze that period of time you question but I suspect that it’s not driving the results we see.”
Asked to comment, Henry W. Lim, MD, a dermatologist with Henry Ford Health in Detroit, characterized the findings of the study as “groundbreaking, because it looked at a real-life situation in the use of phototherapy at home vs in the office, showing that the home phototherapy is not inferior to office-based phototherapy.”
This is important, he continued, “because it can inform payers to approve home phototherapy equipment for patients, because it’s much more convenient and it definitely works. The other strong point of the study is that it included patients of different skin types,” he said in an interview at the meeting.
The study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices. Dr. Gelfand reported no relevant financial relationships. Dr. Blauvelt disclosed conflicts of interest from many pharmaceutical companies. Dr. Lim disclosed conflicts of interest from many pharmaceutical companies.
A version of this article appeared on Medscape.com.
SAN DIEGO — and Dermatology Life Quality Index (DLQI) scores, results from a pragmatic, multicenter study showed.
“In 2024, we have a lot of ways to treat moderate-to-severe psoriasis, and phototherapy remains relevant,” lead investigator Joel M. Gelfand, MD, professor of dermatology and epidemiology at the University of Pennsylvania in Philadelphia, told attendees of a late-breaking abstract session at the annual meeting of the American Academy of Dermatology.
“Office phototherapy is 10 to 100 times less expensive than biologics for psoriasis, and in head-to-head trials, it’s about as effective as adalimumab and achieves better patient-reported outcomes. It may have some cardiovascular benefits by lowering IL-6 and improving HDL-P,” he said. “And, compared to secukinumab, it has no risk of infection.”
Although phototherapy is a preferred as a treatment by patients with psoriasis, he continued, inconvenience of traveling to a clinician’s office for the treatment and lack of coverage by health insurance plans remain major barriers to this option. According to Dr. Gelfand, office-based phototherapy is not available in 90% of counties in the United States, “and a lack of US data has resulted in many insurance companies not covering home phototherapy. As a result, many providers are uncertain about prescribing it.”
LITE Study Data
In 2019, Dr. Gelfand and colleagues Light Treatment Effectiveness (LITE) study, a patient-centered study that tested the hypothesis that narrowband UVB phototherapy of psoriasis at home is non-inferior to office treatment, based on outcomes that matter to patients, clinicians, and payers. The co-primary outcomes were a PGA score of 0/1 (clear, almost clear) and a DLQI score of 5 or less (small, no effect on health-related quality of life).
Dr. Gelfand and colleagues at 42 sites in the United States enrolled 783 patients aged 12 years and older who had plaque or guttate psoriasis and were candidates for phototherapy at home or in an office setting. New or established patients to the practices were accepted into the trial, while those treated with phototherapy within 14 days before the baseline visit were not. These entry criteria “are highly pragmatic and reflect routine clinical practice,” he said.
The researchers evenly stratified patients by skin types I and II, III and IV, and V and VI. They collected data from medical records or from an app on the patient’s cell phone, which captured the DLQI data. Study participants were randomly assigned 1:1 to office- or home-based phototherapy for 12 weeks at doses recommended in the 2019 AAD-National Psoriasis Foundation guidelines. This was followed by a 12-week observation period, which ended at 24 weeks.
At baseline, the mean DLQI score of patients was 12.2, the mean PGA score was 3, and their mean body surface area affected was 12.5%. “These patients had pretty severe disease, long-standing disease, and about 12% were on biologics or nonbiologic systemic therapy during the study,” said Dr. Gelfand, also the director of the Psoriasis and Phototherapy Treatment Center at Penn. In addition, he said, “the average round-trip to receive phototherapy in the office was about 60 minutes.”
An Improvement in Health Equity
Following treatment at 12 weeks, 25.6% of patients in the office-based phototherapy group achieved a PGA of 0/1, compared with 32.8% of patients in the home-based phototherapy group (P >.0001 for non-inferiority). Similarly, 33.6% of patients in the office-based phototherapy group achieved a score of 5 or less on the DLQI, compared with 52.4% of patients in the home-based phototherapy group (P >.0001 for non-inferiority).
In subgroup analyses, patients with darkly pigmented skin did especially well on home phototherapy relative to office treatment. “This finding is an example of how the LITE study was specifically designed to improve health equity through an intentionally inclusive approach,” Dr. Gelfand said. Perhaps not surprisingly, patients in the home-based phototherapy arm were more adherent to treatment compared with those in the office-based arm (a mean of 26.8 sessions during the study period, compared with a mean of 17.9, respectively; P < .0001). “They also had higher cumulative doses of phototherapy and therefore higher episodes of treatments with erythema,” he noted.
Among patients who reported “itchy, sore, painful, or stinging” skin in the previous week, 63% characterized the degree of discomfort as “not at all or a little,” while 28% said “a lot,” and 9% said “very much.” No patients withdrew or stopped phototherapy during the trial because of treatment-related side effects, “so it’s very well tolerated,” Dr. Gelfand said.
“If a patient never had phototherapy before, they did just as well at home as they did in the office. This suggests that there’s no reason to insist that a patient use office-based phototherapy before using home phototherapy.”
The researchers studied the efficacy of narrow-band UVB in patients who had at least two treatments per week for 12 weeks. In this subgroup of patients, 60% achieved clear or almost clear skin and nearly 50% achieved the equivalent of a Psoriasis Area and Severity Index (PASI) 90 score.
“Home phototherapy is clearly non-inferior to office-based phototherapy across all skin types and both primary outcomes, PGA and DLQI, and both have excellent effectiveness and safety in real-world settings,” Dr. Gelfand concluded. “These data support the use of home phototherapy as a first-line treatment option for psoriasis, including those with no prior phototherapy experience.”
LITE Study Described as “Groundbreaking”
One of the session moderators, dermatologist Andrew Blauvelt, MD, MBA, of the Oregon Medical Research Center, Portland, asked about the impact that lockdowns during the early phase of the COVID-19 pandemic had on the trial. “The study shut down for a couple weeks during the initial lockdown, but we got back up and running pretty quickly,” Dr. Gelfand responded. “We didn’t study that specific period of time, but the study was going on well before COVID and well after COVID restrictions were lifted. We’ll have to analyze that period of time you question but I suspect that it’s not driving the results we see.”
Asked to comment, Henry W. Lim, MD, a dermatologist with Henry Ford Health in Detroit, characterized the findings of the study as “groundbreaking, because it looked at a real-life situation in the use of phototherapy at home vs in the office, showing that the home phototherapy is not inferior to office-based phototherapy.”
This is important, he continued, “because it can inform payers to approve home phototherapy equipment for patients, because it’s much more convenient and it definitely works. The other strong point of the study is that it included patients of different skin types,” he said in an interview at the meeting.
The study was funded by the Patient-Centered Outcomes Research Institute. Research partners included the National Psoriasis Foundation and Daavlin, which provided the home phototherapy machines and covered the cost of shipping the devices. Dr. Gelfand reported no relevant financial relationships. Dr. Blauvelt disclosed conflicts of interest from many pharmaceutical companies. Dr. Lim disclosed conflicts of interest from many pharmaceutical companies.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Immunomodulators Do Not Affect COVID-19 Vaccine Efficacy
TOPLINE:
The results of a recent study suggest that biologics and small molecule inhibitors (SMIs) do not impair the protective effect of COVID-19 vaccine against hospitalization in patients with psoriasis and hidradenitis suppurativa (HS).
METHODOLOGY:
- It remains unknown whether immunomodulatory therapies impair COVID-19 vaccine efficacy and increase hospitalization rates linked to COVID-19 in patients with inflammatory skin conditions such as psoriasis or HS.
- Researchers conducted a cross-sectional study using data from the Epic Cosmos database from January 2020 to October 2023, identifying 30,845 patients with psoriasis or HS.
- Overall, 22,293 patients with documented completion of their primary COVID-19 vaccine series were included in the analysis.
- Of the vaccinated patients, they compared 7046 patients with psoriasis on SMIs and 2033 with psoriasis or HS on biologics with 13,214 patients who did not receive biologics or SMIs.
- The primary outcome was the COVID-19 hospitalization rate.
- Treatment with biologics did not increase COVID-19-related hospitalization rates in vaccinated patients with psoriasis or HS (hospitalization rate, 6.0% for both those taking and those not taking a biologic; P > .99).
- Similarly, hospitalization rates did not significantly differ between vaccinated patients who received SMIs vs those who did not (7.1% vs 6.0%; P = .0596).
IN PRACTICE:
These findings “encourage dermatologists to continue treating [psoriasis]/HS confidently despite the ongoing COVID-19 pandemic,” the authors concluded.
SOURCE:
The study led by Bella R. Lee from Ohio State University Wexner Medical Center, Columbus, was published online on March 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Multivariable adjustments could not be performed in this study due to unavailability of individual-level data, and hospital admissions that occurred outside the Epic system were not captured.
DISCLOSURES:
The study did not receive any funding. All authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
The results of a recent study suggest that biologics and small molecule inhibitors (SMIs) do not impair the protective effect of COVID-19 vaccine against hospitalization in patients with psoriasis and hidradenitis suppurativa (HS).
METHODOLOGY:
- It remains unknown whether immunomodulatory therapies impair COVID-19 vaccine efficacy and increase hospitalization rates linked to COVID-19 in patients with inflammatory skin conditions such as psoriasis or HS.
- Researchers conducted a cross-sectional study using data from the Epic Cosmos database from January 2020 to October 2023, identifying 30,845 patients with psoriasis or HS.
- Overall, 22,293 patients with documented completion of their primary COVID-19 vaccine series were included in the analysis.
- Of the vaccinated patients, they compared 7046 patients with psoriasis on SMIs and 2033 with psoriasis or HS on biologics with 13,214 patients who did not receive biologics or SMIs.
- The primary outcome was the COVID-19 hospitalization rate.
- Treatment with biologics did not increase COVID-19-related hospitalization rates in vaccinated patients with psoriasis or HS (hospitalization rate, 6.0% for both those taking and those not taking a biologic; P > .99).
- Similarly, hospitalization rates did not significantly differ between vaccinated patients who received SMIs vs those who did not (7.1% vs 6.0%; P = .0596).
IN PRACTICE:
These findings “encourage dermatologists to continue treating [psoriasis]/HS confidently despite the ongoing COVID-19 pandemic,” the authors concluded.
SOURCE:
The study led by Bella R. Lee from Ohio State University Wexner Medical Center, Columbus, was published online on March 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Multivariable adjustments could not be performed in this study due to unavailability of individual-level data, and hospital admissions that occurred outside the Epic system were not captured.
DISCLOSURES:
The study did not receive any funding. All authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
The results of a recent study suggest that biologics and small molecule inhibitors (SMIs) do not impair the protective effect of COVID-19 vaccine against hospitalization in patients with psoriasis and hidradenitis suppurativa (HS).
METHODOLOGY:
- It remains unknown whether immunomodulatory therapies impair COVID-19 vaccine efficacy and increase hospitalization rates linked to COVID-19 in patients with inflammatory skin conditions such as psoriasis or HS.
- Researchers conducted a cross-sectional study using data from the Epic Cosmos database from January 2020 to October 2023, identifying 30,845 patients with psoriasis or HS.
- Overall, 22,293 patients with documented completion of their primary COVID-19 vaccine series were included in the analysis.
- Of the vaccinated patients, they compared 7046 patients with psoriasis on SMIs and 2033 with psoriasis or HS on biologics with 13,214 patients who did not receive biologics or SMIs.
- The primary outcome was the COVID-19 hospitalization rate.
- Treatment with biologics did not increase COVID-19-related hospitalization rates in vaccinated patients with psoriasis or HS (hospitalization rate, 6.0% for both those taking and those not taking a biologic; P > .99).
- Similarly, hospitalization rates did not significantly differ between vaccinated patients who received SMIs vs those who did not (7.1% vs 6.0%; P = .0596).
IN PRACTICE:
These findings “encourage dermatologists to continue treating [psoriasis]/HS confidently despite the ongoing COVID-19 pandemic,” the authors concluded.
SOURCE:
The study led by Bella R. Lee from Ohio State University Wexner Medical Center, Columbus, was published online on March 13, 2024, in the Journal of the American Academy of Dermatology.
LIMITATIONS:
Multivariable adjustments could not be performed in this study due to unavailability of individual-level data, and hospital admissions that occurred outside the Epic system were not captured.
DISCLOSURES:
The study did not receive any funding. All authors declared no conflicts of interest.
A version of this article appeared on Medscape.com.
Sustained Control Reported for Anti–IL-17, Anti–IL-23 Psoriasis Treatments
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
SAN DIEGO — , but late-breaker data presented at the annual meeting of the American Academy of Dermatology show that these types of responses are sustained for as long as patients have remained on therapy.
Of the two, the longer follow up is with the IL-17 inhibitor bimekizumab (Bimzelx). In a 4-year open-label extension study, the Psoriasis Area and Severity Index (PASI) 90 rate was approximately 85% in treated patients, according to Mark Lebwohl, MD, professor and chairman emeritus of the Department of Dermatology, Icahn School of Medicine at Mount Sinai in New York City
A PASI 90 score signifies that 90% of skin surface area is cleared. The proportion of patients who achieved a PASI 100 score, signifying total clearance, approached 70% at 4 years in the group with the greatest response. PASI 90 and PASI 100 rates at this point were only modestly lower than those reported at the end of the double-blind phase 3 trial when evaluated 3 years earlier.
Follow-up with a novel oral anti-IL-23 inhibitor JNJ-2113 (JNJ-77242113) was only 52 weeks, far shorter. But again, the response for the most effective dose at the end of this period was essentially unchanged from that at 16 weeks. Among those on the highest and most effective test dose of once-daily 100 mg, the PASI 90 at 1 year was 64.3%, a rate that was essentially unchanged from week 16.
No Apparent Loss of Benefit Over Time
“We can really look at those dose-response curves and see that there is, overall, a maintenance of response,” reported Laura K. Ferris, MD, PhD, professor and director of clinical trials, Department of Dermatology, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania. In her presentation of the data, she showed similar sustained control for the most effective doses of JNJ-2113 for multiple clinical outcomes, including an investigator’s global assessment (IGA) score of 0 or 1, also signifying clear or near clear skin.
Bimekizumab, a monoclonal antibody that inhibits both IL-17A and IL-17F, is already approved for the treatment of plaque psoriasis. The 52-week BE SURE trial, which provided the 478 patients who entered into the BE BRIGHT open label extension study, was published in The New England Journal of Medicine in July 2021.
In the 4-year data reported by Dr. Lebwohl, three groups were compared: Those initially randomized to an every-4-week dosing schedule of bimekizumab over the course of the 52-week BE SURE trial; those randomized to an every-4-week bimekizumab schedule who were then subsequently switched to an every-8-week schedule; and those initiated on the TNF-inhibitor adalimumab (Humira) and were then switched at week 24 to every-4-week bimekizumab.
The PASI 90 responses at 52 weeks in these three groups, respectively, were 91.2%, 89.3%, and 95.2%. At 4 years, this almost clear response was observed in 82.4%, 83.2%, and 87.6%, respectively. At 52 weeks, the PASI 100 responses in these three groups, respectively, were 75.3%, 74.2%, and 72.9%. At 4 years, 61.9%, 58.5%, and 69.5% still had complete skin clearance.
Bimekizumab was well tolerated during the randomized trial, reported Dr. Lebwohl. The rates of nasopharyngitis and oral candidiasis, which were observed in approximately 12% and 8%, respectively, of treated patients during the randomized phase remained at about the same level in the long-term follow up. There were no new safety signals, he said.
JNJ-2113 Is First Potential Oral IL-23 Inhibitor
JNJ-2113 is a first-in-class oral peptide that binds to the IL-23 receptor, blocking the IL-23 signaling pathway. If approved, it would be the first oral therapy targeting IL-23. The 16-week outcomes of the dose-finding FRONTIER 1 phase 2b trial were published in The New England Journal of Medicine earlier this year. The primary endpoint was PASI 75, achieved by 79% of those on the 100 mg twice daily dose at week 16, vs 9% on placebo, and at 52 weeks, was 76%.
“The proportion of patients achieving the FRONTIER 1 primary endpoint was maintained from week 16 to the end of week 52 in the extension study,” Dr. Ferris said, but further pointed out that rates of near or complete clearance achieved at week 16 were also essentially unchanged at week 52. This was true of PASI scores and IGA.
Clearance of psoriatic lesions on the scalp was particularly impressive. By scalp-specific IGA, rates of clear or near clear (0/1) were not just maintained but improved over the course of follow-up, reaching 75.1% at 52 weeks in the highest dose group, she said.
JNJ-2113 was well tolerated in FRONTIER 1 and remained so during long-term follow-up, in the FRONTIER 2 extension study, according to Dr. Ferris. The most common complaints with JNJ-2113, such as nasopharyngitis (18.1% vs 25.7% in placebo), did not appear to differ significantly from placebo and the treatment remained well tolerated over the course of the extended follow-up.
There are limited direct comparisons of different biologics active in the treatment of plaque psoriasis for efficacy and safety, but these data appear to show a depth and durability of benefit for psoriasis that is exceptional, Dr. Lebwohl told this news organization. “The PASI 100 scores achieved by bimekizumab exceed anything we have seen to date,” he said. “And the durability of those exceedingly high scores is remarkable.”
Dr. Lebwohl reports financial relationships with approximately 40 pharmaceutical companies, including UCB Pharma, which developed bimekizumab. Dr. Ferris reports financial relationships with more than 20 pharmaceutical companies, including Janssen, which is developing JNJ-2113.
A version of this article appeared on Medscape.com.
FROM AAD 2024
Depression As a Potential Contributing Factor in Hidradenitis Suppurativa and Associated Racial Gaps
Hidradenitis suppurativa (HS)—a chronic, relapsing, inflammatory disorder involving terminal hair follicles in apocrine gland–rich skin—manifests as tender inflamed nodules that transform into abscesses, sinus tracts, and scarring.1,2 The etiology of HS is multifactorial, encompassing lifestyle, microbiota, hormonal status, and genetic and environmental factors. These factors activate the immune system around the terminal hair follicles and lead to hyperkeratosis of the infundibulum of the hair follicles in intertriginous regions. This progresses to follicular occlusion, stasis, and eventual rupture. Bacterial multiplication within the plugged pilosebaceous units further boosts immune activation. Resident and migrated cells of the innate and adaptive immune system then release proinflammatory cytokines such as tumor necrosis factor, IL-1β, and IL-17, which further enhance immune cell influx and inflammation.3,4 This aberrant immune response propagates the production of deep-seated inflammatory nodules and abscesses.3-8
The estimated prevalence of HS is 1% worldwide.9 It is more prevalent in female and Black patients (0.30%) than White patients (0.09%) and is intermediate in prevalence in the biracial population (0.22%).10 Hidradenitis suppurativa is thought to be associated with lower socioeconomic status (SES). In a retrospective analysis of HS patients (N=375), approximately one-third of patients were Black, had advanced disease, and had a notably lower SES.11 Furthermore, HS has been reported to be associated with systemic inflammation and comorbidities such as morbid obesity (38.3%) and hypertension (39.6%) as well as other metabolic syndrome–related disorders and depression (48.1%).1
Hidradenitis suppurativa may contribute to the risk for depression through its substantial impact on health-related quality of life, which culminates in social withdrawal, unemployment, and suicidal thoughts.12 The high prevalence of depression in individuals with HS1 and its association with systemic inflammation13 increases the likelihood that a common genetic predisposition also may exist between both conditions. Because depression frequently has been discovered as a concomitant diagnosis in patients with HS, we hypothesize that a shared genetic susceptibility also may exist between the 2 disorders. Our study sought to explore data on the co-occurrence of depression with HS, including its demographics and racial data.
Methods
We conducted a PubMed search of articles indexed for MEDLINE as well as Google Scholar using the terms depression and hidradenitis suppurativa to obtain all research articles published from 2000 to 2022. Articles were selected based on relevance to the topic of exploration. English-language articles that directly addressed the epidemiology, etiology, pathophysiology, and co-occurrence of both depression and HS with numerical data were included. Articles were excluded if they did not explore the information of interest on these 2 disorders or did not contain clear statistical data of patients with the 2 concurrent medical conditions.
Results
Twenty-two cross-sectional, prospective, and retrospective studies that fit the search criteria were identified and included in the analysis (eTable).1,14-34 Sixteen (72.7%) studies were cross-sectional, 5 (22.7%) were retrospective, and only 1 (4.5%) was a prospective study. Only 6 of the studies provided racial data,1,14,17,26,28,32 and of them, 4 had predominately White patients,1,14,26,32 whereas the other 2 had predominantly Black patients.17,28


Hidradenitis suppurativa was found to coexist with depression in all the studies, with a prevalence of 1.2% to 48.1%. There also was a higher prevalence of depression in HS patients than in the control patients without HS. Furthermore, a recent study by Wright and colleagues14 stratified the depression prevalence data by age and found a higher prevalence of depression in adults vs children with HS (30% vs 12%).
Comment
Major depression—a chronic and debilitating illness—is the chief cause of disability globally and in the United States alone and has a global lifetime prevalence of 17%.35 In a study of 388 patients diagnosed with depression and 404 community-matched controls who were observed for 10 years, depressed patients had a two-thirds higher likelihood of developing a serious physical illness than controls. The depression-associated elevated risk for serious physical illness persisted after controlling for confounding variables such as alcohol abuse, smoking, and level of physical activity.36 Studies also have demonstrated that HS is more prevalent in Black individuals10 and in individuals of low SES,37 who are mostly the Black and Hispanic populations that experience the highest burden of racial microaggression38 and disparities in health access and outcomes.39,40 The severity and chronicity of major depressive disorder also is higher in Black patients compared with White patients (57% vs 39%).41 Because major depression and HS are most common among Black patients who experience the highest-burden negative financial and health disparities, there may be a shared genetic disposition to both medical conditions.
Moreover, the common detrimental lifestyle choices associated with patients with depression and HS also suggest the possibility of a collective genetic susceptibility. Patients with depression also report increased consumption of alcohol, tobacco, and illicit substances; sedentary lifestyle leading to obesity; and poor compliance with prescribed medical treatment.42 Smoking and obesity are known contributors to the pathogenesis of HS, and their modification also is known to positively impact the disease course. In a retrospective single-cohort study, 50% of obese HS patients (n=35) reported a substantial decrease in disease severity after a reduction of more than 15% in body mass index over 2 years following bariatric surgery (n=35).43 Patients with HS also have reported disease remission following extensive weight loss.44 In addition, evidence has supported smoking cessation in improving the disease course of HS.43 Because these detrimental lifestyle choices are prevalent in both patients with HS and those with depression, a co-genetic susceptibility also may exist.
Furthermore, depression is characterized by a persistent inflammatory state,13,45 similar to HS.46 Elevated levels of a variety of inflammatory markers, such as C-reactive protein (CRP), IL-6, and soluble intercellular adhesion molecule 1, have been reported in patients with depression compared with healthy controls.13,45 Further analysis found a positive correlation and a strong association between depression and these inflammatory markers.47 Moreover, adipokines regulate inflammatory responses, and adipokines play a role in the pathogenesis of HS. Adipokine levels such as elevated omentin-1 (a recently identified adipokine) were found to be altered in patients with HS compared with controls.48 Results from clinical studies and meta-analyses of patients with depression also have demonstrated that adipokines are dysregulated in this population,49,50 which may be another potential genetic link between depression and HS.
In addition, genetic susceptibility to depression and HS may be shared because the inflammatory markers that have a strong association with depression also have been found to play an important role in HS treatment and disease severity prediction. In a retrospective cohort study of 404 patients, CRP or IL-6 levels were found to be reliable predictors of HS disease severity, which may explain why anti–tumor necrosis factor antibody regimens such as adalimumab and infliximab have clinically ameliorated disease activity in several cases of HS.51 In a study evaluating these drugs, high baseline levels of high-sensitivity CRP and IL-6 were predictive of patient response to infliximab.52 In a meta-analysis evaluating 20,791 participants, an association was found between concurrent depression and CRP. Furthermore, inflammation measured by high levels of CRP or IL-6 was observed to predict future depression.53 If the same inflammatory markers—CRP and IL-6—both play a major role in the disease activity of depression and HS, then a concurrent genetic predisposition may exist.
Conclusion
Understanding the comorbidities, etiologies, and risk factors for the development and progression of HS is an important step toward improved disease management. Available studies on comorbid depression in HS largely involve White patients, and more studies are needed in patients with skin of color, particularly the Black population, who have the highest prevalence of HS.10 Given the evidence for an association between depression and HS, we suggest a large-scale investigation of this patient population that includes a complete medical history, onset of HS in comparison to the onset of depression, and specific measures of disease progress and lifetime management of depression, which may help to increase knowledge about the role of depression in HS and encourage more research in this area. If shared genetic susceptibility is established, aggressive management of depression in patients at risk for HS may reduce disease incidence and severity as well as the psychological burden on patients.
- Crowley JJ, Mekkes JR, Zouboulis CC, et al. Association of hidradenitis suppurativa disease severity with increased risk for systemic comorbidities. Br J Dermatol. 2014;171:1561-1565.
- Napolitano M, Megna M, Timoshchuk EA, et al. Hidradenitis suppurativa: from pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. 2017;10:105-115.
- Sabat R, Jemec GBE, Matusiak Ł, et al. Hidradenitis suppurativa. Nat Rev Dis Prim. 2020;6:1-20.
- Wolk K, Warszawska K, Hoeflich C, et al. Deficiency of IL-22 contributes to a chronic inflammatory disease: pathogenetic mechanisms in acne inversa. J Immunol. 2011;186:1228-1239.
- von Laffert M, Helmbold P, Wohlrab J, et al. Hidradenitis suppurativa (acne inversa): early inflammatory events at terminal follicles and at interfollicular epidermis. Exp Dermatol. 2010;19:533-537.
- Van Der Zee HH, De Ruiter L, Van Den Broecke DG, et al. Elevated levels of tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-10 in hidradenitis suppurativa skin: a rationale for targeting TNF-α and IL-1β. Br J Dermatol. 2011;164:1292-1298.
- Schlapbach C, Hänni T, Yawalkar N, et al. Expression of the IL-23/Th17 pathway in lesions of hidradenitis suppurativa. J Am Acad Dermatol. 2011;65:790-798.
- Kelly G, Hughes R, McGarry T, et al. Dysregulated cytokine expression in lesional and nonlesional skin in hidradenitis suppurativa. Br J Dermatol. 2015;173:1431-1439.
- Jemec GBE, Kimball AB. Hidradenitis suppurativa: epidemiology and scope of the problem. J Am Acad Dermatol. 2015;73(5 Suppl 1):S4-S7.
- Garg A, Kirby JS, Lavian J, et al. Sex- and age-adjusted population analysis of prevalence estimates for hidradenitis suppurativa in the United States. JAMA Dermatol. 2017;153:760-764.
- Soliman YS, Hoffman LK, Guzman AK, et al. African American patients with hidradenitis suppurativa have significant health care disparities: a retrospective study. J Cutan Med Surg. 2019;23:334-336.
- Garg A, Malviya N, Strunk A, et al. Comorbidity screening in hidradenitis suppurativa: evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J Am Acad Dermatol. 2022;86:1092-1101.
- Beatriz Currier M, Nemeroff CB. Inflammation and mood disorders: proinflammatory cytokines and the pathogenesis of depression. Antiinflamm Antiallergy Agents Med Chem. 2012;9:212-220.
- Wright S, Strunk A, Garg A. Prevalence of depression among children, adolescents, and adults with hidradenitis suppurativa. J Am Acad Dermatol. 2022;86:55-60.
- Sampogna F, Fania L, Mastroeni S, et al. Correlation between depression, quality of life and clinical severity in patients with hidradenitis suppurativa. Acta Derm Venereol. 2020;100:1-6.
- Theut Riis P, Pedersen OB, Sigsgaard V, et al. Prevalence of patients with self-reported hidradenitis suppurativa in a cohort of Danish blood donors: a cross-sectional study. Br J Dermatol. 2019;180:774-781.
- Senthilnathan A, Kolli SS, Cardwell LA, et al. Depression in hidradenitis suppurativa. Br J Dermatol. 2019;181:1087-1088.
- Pavon Blanco A, Turner MA, Petrof G, et al. To what extent do disease severity and illness perceptions explain depression, anxiety and quality of life in hidradenitis suppurativa? Br J Dermatol. 2019;180:338-345.
- Butt M, Sisic M, Silva C, et al. The associations of depression and coping methods on health-related quality of life for those with hidradenitis suppurativa. J Am Acad Dermatol. 2019;80:1137-1139.
- Calao M, Wilson JL, Spelman L, et al. Hidradenitis suppurativa (HS) prevalence, demographics and management pathways in Australia: a population-based cross-sectional study. PLoS One. 2018;13:e0200683.
- Ingram JR, Jenkins-Jones S, Knipe DW, et al. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa. Br J Dermatol. 2018;178:917-924.
- Kimball AB, Sundaram M, Gauthier G, et al. The comorbidity burden of hidradenitis suppurativa in the United States: a claims data analysis. Dermatol Ther (Heidelb). 2018;8:557.
- Thorlacius L, Cohen AD, Gislason GH, et al. Increased suicide risk in patients with hidradenitis suppurativa. J Invest Dermatol. 2018;138:52-57.
- Tiri H, Jokelainen J, Timonen M, et al. Somatic and psychiatric comorbidities of hidradenitis suppurativa in children and adolescents. J Am Acad Dermatol. 2018;79:514-519.
- Huilaja L, Tiri H, Jokelainen J, et al. Patients with hidradenitis suppurativa have a high psychiatric disease burden: a Finnish nationwide registry study. J Invest Dermatol. 2018;138:46-51.
- Kirby JS, Butt M, Esmann S, et al. Association of resilience with depression and health-related quality of life for patients with hidradenitis suppurativa. JAMA Dermatol. 2017;153:1263.
- Egeberg A, Gislason GH, Hansen PR. Risk of major adverse cardiovascular events and all-cause mortality in patients with hidradenitis suppurativa. JAMA Dermatol. 2016;152:429-434.
- Vangipuram R, Vaidya T, Jandarov R, et al. Factors contributing to depression and chronic pain in patients with hidradenitis suppurativa: results from a single-center retrospective review. Dermatology. 2016;232:692-695.
- Rayner L, Jackson K, Turner M, et al. Integrated mental health assessment in a tertiary medical dermatology service: feasibility and the prevalence of common mental disorder. Br J Dermatol. 2015;173:201.
- Shavit E, Dreiher J, Freud T, et al. Psychiatric comorbidities in 3207 patients with hidradenitis suppurativa [published online June 9, 2014]. J Eur Acad Dermatol Venereol. 2015;29:371-376.
- Kurek A, Johanne Peters EM, Sabat R, et al. Depression is a frequent co-morbidity in patients with acne inversa. J Dtsch Dermatol Ges. 2013;11:743-749.
- Vazquez BG, Alikhan A, Weaver AL, et al. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133:97.
- Onderdijk AJ, Van Der Zee HH, Esmann S, et al. Depression in patients with hidradenitis suppurativa [published online February 20, 2012]. J Eur Acad Dermatol Venereol. 2013;27:473-478.
- Matusiak Ł, Bieniek A, Szepietowski JC. Psychophysical aspects of hidradenitis suppurativa. Acta Derm Venereol. 2010;90:264-268.
- Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617-627.
- Holahan CJ, Pahl SA, Cronkite RC, et al. Depression and vulnerability to incident physical illness across 10 years. J Affect Disord. 2009;123:222-229.
- Deckers IE, Janse IC, van der Zee HH, et al. Hidradenitis suppurativa (HS) is associated with low socioeconomic status (SES): a cross-sectional reference study. J Am Acad Dermatol. 2016;75:755-759.e1.
- Williams MT, Skinta MD, Kanter JW, et al. A qualitative study of microaggressions against African Americans on predominantly White campuses. BMC Psychol. 2020;8:1-13.
- Dunlop DD, Song J, Lyons JS, et al. Racial/ethnic differences in rates of depression among preretirement adults. Am J Public Health. 2003;93:1945-1952.
- Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: patterns and prospects. Health Psychol. 2016;35:407-411.
- Williams DR, González HM, Neighbors H, et al. Prevalence and distribution of major depressive disorder in African Americans, Caribbean Blacks, and Non-Hispanic Whites: results from the National Survey of American Life. Arch Gen Psychiatry. 2007;64:305-315.
- Druss BG, Bradford DW, Rosenheck RA, et al. Mental disorders and use of cardiovascular procedures after myocardial infarction. JAMA. 2000;283:506-511.
- Kromann CB, Deckers IE, Esmann S, et al. Risk factors, clinical course and long-term prognosis in hidradenitis suppurativa: a cross-sectional study. Br J Dermatol. 2014;171:819-824.
- Sivanand A, Gulliver WP, Josan CK, et al. Weight loss and dietary interventions for hidradenitis suppurativa: a systematic review. J Cutan Med Surg . 2020;24:64-72.
- Raedler TJ. Inflammatory mechanisms in major depressive disorder. Curr Opin Psychiatry. 2011;24:519-525.
- Rocha VZ, Libby P. Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol. 2009;6:399-409.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol. 2009;103:755-761.
- González-López MA, Ocejo-Viñals JG, Mata C, et al. Evaluation of serum omentin-1 and apelin concentrations in patients with hidradenitis suppurativa. Postepy Dermatol Alergol. 2021;38:450-454.
- Taylor VH, Macqueen GM. The role of adipokines in understanding the associations between obesity and depression. J Obes. 2010;2010:748048.
- Setayesh L, Ebrahimi R, Pooyan S, et al. The possible mediatory role of adipokines in the association between low carbohydrate diet and depressive symptoms among overweight and obese women. PLoS One. 2021;16:e0257275 .
- Andriano TM, Benesh G, Babbush KM, et al. Serum inflammatory markers and leukocyte profiles accurately describe hidradenitis suppurativa disease severity. Int J Dermatol. 2022;61:1270-1275.
- Montaudié H, Seitz-Polski B, Cornille A, et al. Interleukin 6 and high-sensitivity C-reactive protein are potential predictive markers of response to infliximab in hidradenitis suppurativa. J Am Acad Dermatol. 2017;6:156-158.
- Colasanto M, Madigan S, Korczak DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. 2020;277:940-948.
Hidradenitis suppurativa (HS)—a chronic, relapsing, inflammatory disorder involving terminal hair follicles in apocrine gland–rich skin—manifests as tender inflamed nodules that transform into abscesses, sinus tracts, and scarring.1,2 The etiology of HS is multifactorial, encompassing lifestyle, microbiota, hormonal status, and genetic and environmental factors. These factors activate the immune system around the terminal hair follicles and lead to hyperkeratosis of the infundibulum of the hair follicles in intertriginous regions. This progresses to follicular occlusion, stasis, and eventual rupture. Bacterial multiplication within the plugged pilosebaceous units further boosts immune activation. Resident and migrated cells of the innate and adaptive immune system then release proinflammatory cytokines such as tumor necrosis factor, IL-1β, and IL-17, which further enhance immune cell influx and inflammation.3,4 This aberrant immune response propagates the production of deep-seated inflammatory nodules and abscesses.3-8
The estimated prevalence of HS is 1% worldwide.9 It is more prevalent in female and Black patients (0.30%) than White patients (0.09%) and is intermediate in prevalence in the biracial population (0.22%).10 Hidradenitis suppurativa is thought to be associated with lower socioeconomic status (SES). In a retrospective analysis of HS patients (N=375), approximately one-third of patients were Black, had advanced disease, and had a notably lower SES.11 Furthermore, HS has been reported to be associated with systemic inflammation and comorbidities such as morbid obesity (38.3%) and hypertension (39.6%) as well as other metabolic syndrome–related disorders and depression (48.1%).1
Hidradenitis suppurativa may contribute to the risk for depression through its substantial impact on health-related quality of life, which culminates in social withdrawal, unemployment, and suicidal thoughts.12 The high prevalence of depression in individuals with HS1 and its association with systemic inflammation13 increases the likelihood that a common genetic predisposition also may exist between both conditions. Because depression frequently has been discovered as a concomitant diagnosis in patients with HS, we hypothesize that a shared genetic susceptibility also may exist between the 2 disorders. Our study sought to explore data on the co-occurrence of depression with HS, including its demographics and racial data.
Methods
We conducted a PubMed search of articles indexed for MEDLINE as well as Google Scholar using the terms depression and hidradenitis suppurativa to obtain all research articles published from 2000 to 2022. Articles were selected based on relevance to the topic of exploration. English-language articles that directly addressed the epidemiology, etiology, pathophysiology, and co-occurrence of both depression and HS with numerical data were included. Articles were excluded if they did not explore the information of interest on these 2 disorders or did not contain clear statistical data of patients with the 2 concurrent medical conditions.
Results
Twenty-two cross-sectional, prospective, and retrospective studies that fit the search criteria were identified and included in the analysis (eTable).1,14-34 Sixteen (72.7%) studies were cross-sectional, 5 (22.7%) were retrospective, and only 1 (4.5%) was a prospective study. Only 6 of the studies provided racial data,1,14,17,26,28,32 and of them, 4 had predominately White patients,1,14,26,32 whereas the other 2 had predominantly Black patients.17,28
Hidradenitis suppurativa was found to coexist with depression in all the studies, with a prevalence of 1.2% to 48.1%. There also was a higher prevalence of depression in HS patients than in the control patients without HS. Furthermore, a recent study by Wright and colleagues14 stratified the depression prevalence data by age and found a higher prevalence of depression in adults vs children with HS (30% vs 12%).
Comment
Major depression—a chronic and debilitating illness—is the chief cause of disability globally and in the United States alone and has a global lifetime prevalence of 17%.35 In a study of 388 patients diagnosed with depression and 404 community-matched controls who were observed for 10 years, depressed patients had a two-thirds higher likelihood of developing a serious physical illness than controls. The depression-associated elevated risk for serious physical illness persisted after controlling for confounding variables such as alcohol abuse, smoking, and level of physical activity.36 Studies also have demonstrated that HS is more prevalent in Black individuals10 and in individuals of low SES,37 who are mostly the Black and Hispanic populations that experience the highest burden of racial microaggression38 and disparities in health access and outcomes.39,40 The severity and chronicity of major depressive disorder also is higher in Black patients compared with White patients (57% vs 39%).41 Because major depression and HS are most common among Black patients who experience the highest-burden negative financial and health disparities, there may be a shared genetic disposition to both medical conditions.
Moreover, the common detrimental lifestyle choices associated with patients with depression and HS also suggest the possibility of a collective genetic susceptibility. Patients with depression also report increased consumption of alcohol, tobacco, and illicit substances; sedentary lifestyle leading to obesity; and poor compliance with prescribed medical treatment.42 Smoking and obesity are known contributors to the pathogenesis of HS, and their modification also is known to positively impact the disease course. In a retrospective single-cohort study, 50% of obese HS patients (n=35) reported a substantial decrease in disease severity after a reduction of more than 15% in body mass index over 2 years following bariatric surgery (n=35).43 Patients with HS also have reported disease remission following extensive weight loss.44 In addition, evidence has supported smoking cessation in improving the disease course of HS.43 Because these detrimental lifestyle choices are prevalent in both patients with HS and those with depression, a co-genetic susceptibility also may exist.
Furthermore, depression is characterized by a persistent inflammatory state,13,45 similar to HS.46 Elevated levels of a variety of inflammatory markers, such as C-reactive protein (CRP), IL-6, and soluble intercellular adhesion molecule 1, have been reported in patients with depression compared with healthy controls.13,45 Further analysis found a positive correlation and a strong association between depression and these inflammatory markers.47 Moreover, adipokines regulate inflammatory responses, and adipokines play a role in the pathogenesis of HS. Adipokine levels such as elevated omentin-1 (a recently identified adipokine) were found to be altered in patients with HS compared with controls.48 Results from clinical studies and meta-analyses of patients with depression also have demonstrated that adipokines are dysregulated in this population,49,50 which may be another potential genetic link between depression and HS.
In addition, genetic susceptibility to depression and HS may be shared because the inflammatory markers that have a strong association with depression also have been found to play an important role in HS treatment and disease severity prediction. In a retrospective cohort study of 404 patients, CRP or IL-6 levels were found to be reliable predictors of HS disease severity, which may explain why anti–tumor necrosis factor antibody regimens such as adalimumab and infliximab have clinically ameliorated disease activity in several cases of HS.51 In a study evaluating these drugs, high baseline levels of high-sensitivity CRP and IL-6 were predictive of patient response to infliximab.52 In a meta-analysis evaluating 20,791 participants, an association was found between concurrent depression and CRP. Furthermore, inflammation measured by high levels of CRP or IL-6 was observed to predict future depression.53 If the same inflammatory markers—CRP and IL-6—both play a major role in the disease activity of depression and HS, then a concurrent genetic predisposition may exist.
Conclusion
Understanding the comorbidities, etiologies, and risk factors for the development and progression of HS is an important step toward improved disease management. Available studies on comorbid depression in HS largely involve White patients, and more studies are needed in patients with skin of color, particularly the Black population, who have the highest prevalence of HS.10 Given the evidence for an association between depression and HS, we suggest a large-scale investigation of this patient population that includes a complete medical history, onset of HS in comparison to the onset of depression, and specific measures of disease progress and lifetime management of depression, which may help to increase knowledge about the role of depression in HS and encourage more research in this area. If shared genetic susceptibility is established, aggressive management of depression in patients at risk for HS may reduce disease incidence and severity as well as the psychological burden on patients.
Hidradenitis suppurativa (HS)—a chronic, relapsing, inflammatory disorder involving terminal hair follicles in apocrine gland–rich skin—manifests as tender inflamed nodules that transform into abscesses, sinus tracts, and scarring.1,2 The etiology of HS is multifactorial, encompassing lifestyle, microbiota, hormonal status, and genetic and environmental factors. These factors activate the immune system around the terminal hair follicles and lead to hyperkeratosis of the infundibulum of the hair follicles in intertriginous regions. This progresses to follicular occlusion, stasis, and eventual rupture. Bacterial multiplication within the plugged pilosebaceous units further boosts immune activation. Resident and migrated cells of the innate and adaptive immune system then release proinflammatory cytokines such as tumor necrosis factor, IL-1β, and IL-17, which further enhance immune cell influx and inflammation.3,4 This aberrant immune response propagates the production of deep-seated inflammatory nodules and abscesses.3-8
The estimated prevalence of HS is 1% worldwide.9 It is more prevalent in female and Black patients (0.30%) than White patients (0.09%) and is intermediate in prevalence in the biracial population (0.22%).10 Hidradenitis suppurativa is thought to be associated with lower socioeconomic status (SES). In a retrospective analysis of HS patients (N=375), approximately one-third of patients were Black, had advanced disease, and had a notably lower SES.11 Furthermore, HS has been reported to be associated with systemic inflammation and comorbidities such as morbid obesity (38.3%) and hypertension (39.6%) as well as other metabolic syndrome–related disorders and depression (48.1%).1
Hidradenitis suppurativa may contribute to the risk for depression through its substantial impact on health-related quality of life, which culminates in social withdrawal, unemployment, and suicidal thoughts.12 The high prevalence of depression in individuals with HS1 and its association with systemic inflammation13 increases the likelihood that a common genetic predisposition also may exist between both conditions. Because depression frequently has been discovered as a concomitant diagnosis in patients with HS, we hypothesize that a shared genetic susceptibility also may exist between the 2 disorders. Our study sought to explore data on the co-occurrence of depression with HS, including its demographics and racial data.
Methods
We conducted a PubMed search of articles indexed for MEDLINE as well as Google Scholar using the terms depression and hidradenitis suppurativa to obtain all research articles published from 2000 to 2022. Articles were selected based on relevance to the topic of exploration. English-language articles that directly addressed the epidemiology, etiology, pathophysiology, and co-occurrence of both depression and HS with numerical data were included. Articles were excluded if they did not explore the information of interest on these 2 disorders or did not contain clear statistical data of patients with the 2 concurrent medical conditions.
Results
Twenty-two cross-sectional, prospective, and retrospective studies that fit the search criteria were identified and included in the analysis (eTable).1,14-34 Sixteen (72.7%) studies were cross-sectional, 5 (22.7%) were retrospective, and only 1 (4.5%) was a prospective study. Only 6 of the studies provided racial data,1,14,17,26,28,32 and of them, 4 had predominately White patients,1,14,26,32 whereas the other 2 had predominantly Black patients.17,28
Hidradenitis suppurativa was found to coexist with depression in all the studies, with a prevalence of 1.2% to 48.1%. There also was a higher prevalence of depression in HS patients than in the control patients without HS. Furthermore, a recent study by Wright and colleagues14 stratified the depression prevalence data by age and found a higher prevalence of depression in adults vs children with HS (30% vs 12%).
Comment
Major depression—a chronic and debilitating illness—is the chief cause of disability globally and in the United States alone and has a global lifetime prevalence of 17%.35 In a study of 388 patients diagnosed with depression and 404 community-matched controls who were observed for 10 years, depressed patients had a two-thirds higher likelihood of developing a serious physical illness than controls. The depression-associated elevated risk for serious physical illness persisted after controlling for confounding variables such as alcohol abuse, smoking, and level of physical activity.36 Studies also have demonstrated that HS is more prevalent in Black individuals10 and in individuals of low SES,37 who are mostly the Black and Hispanic populations that experience the highest burden of racial microaggression38 and disparities in health access and outcomes.39,40 The severity and chronicity of major depressive disorder also is higher in Black patients compared with White patients (57% vs 39%).41 Because major depression and HS are most common among Black patients who experience the highest-burden negative financial and health disparities, there may be a shared genetic disposition to both medical conditions.
Moreover, the common detrimental lifestyle choices associated with patients with depression and HS also suggest the possibility of a collective genetic susceptibility. Patients with depression also report increased consumption of alcohol, tobacco, and illicit substances; sedentary lifestyle leading to obesity; and poor compliance with prescribed medical treatment.42 Smoking and obesity are known contributors to the pathogenesis of HS, and their modification also is known to positively impact the disease course. In a retrospective single-cohort study, 50% of obese HS patients (n=35) reported a substantial decrease in disease severity after a reduction of more than 15% in body mass index over 2 years following bariatric surgery (n=35).43 Patients with HS also have reported disease remission following extensive weight loss.44 In addition, evidence has supported smoking cessation in improving the disease course of HS.43 Because these detrimental lifestyle choices are prevalent in both patients with HS and those with depression, a co-genetic susceptibility also may exist.
Furthermore, depression is characterized by a persistent inflammatory state,13,45 similar to HS.46 Elevated levels of a variety of inflammatory markers, such as C-reactive protein (CRP), IL-6, and soluble intercellular adhesion molecule 1, have been reported in patients with depression compared with healthy controls.13,45 Further analysis found a positive correlation and a strong association between depression and these inflammatory markers.47 Moreover, adipokines regulate inflammatory responses, and adipokines play a role in the pathogenesis of HS. Adipokine levels such as elevated omentin-1 (a recently identified adipokine) were found to be altered in patients with HS compared with controls.48 Results from clinical studies and meta-analyses of patients with depression also have demonstrated that adipokines are dysregulated in this population,49,50 which may be another potential genetic link between depression and HS.
In addition, genetic susceptibility to depression and HS may be shared because the inflammatory markers that have a strong association with depression also have been found to play an important role in HS treatment and disease severity prediction. In a retrospective cohort study of 404 patients, CRP or IL-6 levels were found to be reliable predictors of HS disease severity, which may explain why anti–tumor necrosis factor antibody regimens such as adalimumab and infliximab have clinically ameliorated disease activity in several cases of HS.51 In a study evaluating these drugs, high baseline levels of high-sensitivity CRP and IL-6 were predictive of patient response to infliximab.52 In a meta-analysis evaluating 20,791 participants, an association was found between concurrent depression and CRP. Furthermore, inflammation measured by high levels of CRP or IL-6 was observed to predict future depression.53 If the same inflammatory markers—CRP and IL-6—both play a major role in the disease activity of depression and HS, then a concurrent genetic predisposition may exist.
Conclusion
Understanding the comorbidities, etiologies, and risk factors for the development and progression of HS is an important step toward improved disease management. Available studies on comorbid depression in HS largely involve White patients, and more studies are needed in patients with skin of color, particularly the Black population, who have the highest prevalence of HS.10 Given the evidence for an association between depression and HS, we suggest a large-scale investigation of this patient population that includes a complete medical history, onset of HS in comparison to the onset of depression, and specific measures of disease progress and lifetime management of depression, which may help to increase knowledge about the role of depression in HS and encourage more research in this area. If shared genetic susceptibility is established, aggressive management of depression in patients at risk for HS may reduce disease incidence and severity as well as the psychological burden on patients.
- Crowley JJ, Mekkes JR, Zouboulis CC, et al. Association of hidradenitis suppurativa disease severity with increased risk for systemic comorbidities. Br J Dermatol. 2014;171:1561-1565.
- Napolitano M, Megna M, Timoshchuk EA, et al. Hidradenitis suppurativa: from pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. 2017;10:105-115.
- Sabat R, Jemec GBE, Matusiak Ł, et al. Hidradenitis suppurativa. Nat Rev Dis Prim. 2020;6:1-20.
- Wolk K, Warszawska K, Hoeflich C, et al. Deficiency of IL-22 contributes to a chronic inflammatory disease: pathogenetic mechanisms in acne inversa. J Immunol. 2011;186:1228-1239.
- von Laffert M, Helmbold P, Wohlrab J, et al. Hidradenitis suppurativa (acne inversa): early inflammatory events at terminal follicles and at interfollicular epidermis. Exp Dermatol. 2010;19:533-537.
- Van Der Zee HH, De Ruiter L, Van Den Broecke DG, et al. Elevated levels of tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-10 in hidradenitis suppurativa skin: a rationale for targeting TNF-α and IL-1β. Br J Dermatol. 2011;164:1292-1298.
- Schlapbach C, Hänni T, Yawalkar N, et al. Expression of the IL-23/Th17 pathway in lesions of hidradenitis suppurativa. J Am Acad Dermatol. 2011;65:790-798.
- Kelly G, Hughes R, McGarry T, et al. Dysregulated cytokine expression in lesional and nonlesional skin in hidradenitis suppurativa. Br J Dermatol. 2015;173:1431-1439.
- Jemec GBE, Kimball AB. Hidradenitis suppurativa: epidemiology and scope of the problem. J Am Acad Dermatol. 2015;73(5 Suppl 1):S4-S7.
- Garg A, Kirby JS, Lavian J, et al. Sex- and age-adjusted population analysis of prevalence estimates for hidradenitis suppurativa in the United States. JAMA Dermatol. 2017;153:760-764.
- Soliman YS, Hoffman LK, Guzman AK, et al. African American patients with hidradenitis suppurativa have significant health care disparities: a retrospective study. J Cutan Med Surg. 2019;23:334-336.
- Garg A, Malviya N, Strunk A, et al. Comorbidity screening in hidradenitis suppurativa: evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J Am Acad Dermatol. 2022;86:1092-1101.
- Beatriz Currier M, Nemeroff CB. Inflammation and mood disorders: proinflammatory cytokines and the pathogenesis of depression. Antiinflamm Antiallergy Agents Med Chem. 2012;9:212-220.
- Wright S, Strunk A, Garg A. Prevalence of depression among children, adolescents, and adults with hidradenitis suppurativa. J Am Acad Dermatol. 2022;86:55-60.
- Sampogna F, Fania L, Mastroeni S, et al. Correlation between depression, quality of life and clinical severity in patients with hidradenitis suppurativa. Acta Derm Venereol. 2020;100:1-6.
- Theut Riis P, Pedersen OB, Sigsgaard V, et al. Prevalence of patients with self-reported hidradenitis suppurativa in a cohort of Danish blood donors: a cross-sectional study. Br J Dermatol. 2019;180:774-781.
- Senthilnathan A, Kolli SS, Cardwell LA, et al. Depression in hidradenitis suppurativa. Br J Dermatol. 2019;181:1087-1088.
- Pavon Blanco A, Turner MA, Petrof G, et al. To what extent do disease severity and illness perceptions explain depression, anxiety and quality of life in hidradenitis suppurativa? Br J Dermatol. 2019;180:338-345.
- Butt M, Sisic M, Silva C, et al. The associations of depression and coping methods on health-related quality of life for those with hidradenitis suppurativa. J Am Acad Dermatol. 2019;80:1137-1139.
- Calao M, Wilson JL, Spelman L, et al. Hidradenitis suppurativa (HS) prevalence, demographics and management pathways in Australia: a population-based cross-sectional study. PLoS One. 2018;13:e0200683.
- Ingram JR, Jenkins-Jones S, Knipe DW, et al. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa. Br J Dermatol. 2018;178:917-924.
- Kimball AB, Sundaram M, Gauthier G, et al. The comorbidity burden of hidradenitis suppurativa in the United States: a claims data analysis. Dermatol Ther (Heidelb). 2018;8:557.
- Thorlacius L, Cohen AD, Gislason GH, et al. Increased suicide risk in patients with hidradenitis suppurativa. J Invest Dermatol. 2018;138:52-57.
- Tiri H, Jokelainen J, Timonen M, et al. Somatic and psychiatric comorbidities of hidradenitis suppurativa in children and adolescents. J Am Acad Dermatol. 2018;79:514-519.
- Huilaja L, Tiri H, Jokelainen J, et al. Patients with hidradenitis suppurativa have a high psychiatric disease burden: a Finnish nationwide registry study. J Invest Dermatol. 2018;138:46-51.
- Kirby JS, Butt M, Esmann S, et al. Association of resilience with depression and health-related quality of life for patients with hidradenitis suppurativa. JAMA Dermatol. 2017;153:1263.
- Egeberg A, Gislason GH, Hansen PR. Risk of major adverse cardiovascular events and all-cause mortality in patients with hidradenitis suppurativa. JAMA Dermatol. 2016;152:429-434.
- Vangipuram R, Vaidya T, Jandarov R, et al. Factors contributing to depression and chronic pain in patients with hidradenitis suppurativa: results from a single-center retrospective review. Dermatology. 2016;232:692-695.
- Rayner L, Jackson K, Turner M, et al. Integrated mental health assessment in a tertiary medical dermatology service: feasibility and the prevalence of common mental disorder. Br J Dermatol. 2015;173:201.
- Shavit E, Dreiher J, Freud T, et al. Psychiatric comorbidities in 3207 patients with hidradenitis suppurativa [published online June 9, 2014]. J Eur Acad Dermatol Venereol. 2015;29:371-376.
- Kurek A, Johanne Peters EM, Sabat R, et al. Depression is a frequent co-morbidity in patients with acne inversa. J Dtsch Dermatol Ges. 2013;11:743-749.
- Vazquez BG, Alikhan A, Weaver AL, et al. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133:97.
- Onderdijk AJ, Van Der Zee HH, Esmann S, et al. Depression in patients with hidradenitis suppurativa [published online February 20, 2012]. J Eur Acad Dermatol Venereol. 2013;27:473-478.
- Matusiak Ł, Bieniek A, Szepietowski JC. Psychophysical aspects of hidradenitis suppurativa. Acta Derm Venereol. 2010;90:264-268.
- Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617-627.
- Holahan CJ, Pahl SA, Cronkite RC, et al. Depression and vulnerability to incident physical illness across 10 years. J Affect Disord. 2009;123:222-229.
- Deckers IE, Janse IC, van der Zee HH, et al. Hidradenitis suppurativa (HS) is associated with low socioeconomic status (SES): a cross-sectional reference study. J Am Acad Dermatol. 2016;75:755-759.e1.
- Williams MT, Skinta MD, Kanter JW, et al. A qualitative study of microaggressions against African Americans on predominantly White campuses. BMC Psychol. 2020;8:1-13.
- Dunlop DD, Song J, Lyons JS, et al. Racial/ethnic differences in rates of depression among preretirement adults. Am J Public Health. 2003;93:1945-1952.
- Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: patterns and prospects. Health Psychol. 2016;35:407-411.
- Williams DR, González HM, Neighbors H, et al. Prevalence and distribution of major depressive disorder in African Americans, Caribbean Blacks, and Non-Hispanic Whites: results from the National Survey of American Life. Arch Gen Psychiatry. 2007;64:305-315.
- Druss BG, Bradford DW, Rosenheck RA, et al. Mental disorders and use of cardiovascular procedures after myocardial infarction. JAMA. 2000;283:506-511.
- Kromann CB, Deckers IE, Esmann S, et al. Risk factors, clinical course and long-term prognosis in hidradenitis suppurativa: a cross-sectional study. Br J Dermatol. 2014;171:819-824.
- Sivanand A, Gulliver WP, Josan CK, et al. Weight loss and dietary interventions for hidradenitis suppurativa: a systematic review. J Cutan Med Surg . 2020;24:64-72.
- Raedler TJ. Inflammatory mechanisms in major depressive disorder. Curr Opin Psychiatry. 2011;24:519-525.
- Rocha VZ, Libby P. Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol. 2009;6:399-409.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol. 2009;103:755-761.
- González-López MA, Ocejo-Viñals JG, Mata C, et al. Evaluation of serum omentin-1 and apelin concentrations in patients with hidradenitis suppurativa. Postepy Dermatol Alergol. 2021;38:450-454.
- Taylor VH, Macqueen GM. The role of adipokines in understanding the associations between obesity and depression. J Obes. 2010;2010:748048.
- Setayesh L, Ebrahimi R, Pooyan S, et al. The possible mediatory role of adipokines in the association between low carbohydrate diet and depressive symptoms among overweight and obese women. PLoS One. 2021;16:e0257275 .
- Andriano TM, Benesh G, Babbush KM, et al. Serum inflammatory markers and leukocyte profiles accurately describe hidradenitis suppurativa disease severity. Int J Dermatol. 2022;61:1270-1275.
- Montaudié H, Seitz-Polski B, Cornille A, et al. Interleukin 6 and high-sensitivity C-reactive protein are potential predictive markers of response to infliximab in hidradenitis suppurativa. J Am Acad Dermatol. 2017;6:156-158.
- Colasanto M, Madigan S, Korczak DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. 2020;277:940-948.
- Crowley JJ, Mekkes JR, Zouboulis CC, et al. Association of hidradenitis suppurativa disease severity with increased risk for systemic comorbidities. Br J Dermatol. 2014;171:1561-1565.
- Napolitano M, Megna M, Timoshchuk EA, et al. Hidradenitis suppurativa: from pathogenesis to diagnosis and treatment. Clin Cosmet Investig Dermatol. 2017;10:105-115.
- Sabat R, Jemec GBE, Matusiak Ł, et al. Hidradenitis suppurativa. Nat Rev Dis Prim. 2020;6:1-20.
- Wolk K, Warszawska K, Hoeflich C, et al. Deficiency of IL-22 contributes to a chronic inflammatory disease: pathogenetic mechanisms in acne inversa. J Immunol. 2011;186:1228-1239.
- von Laffert M, Helmbold P, Wohlrab J, et al. Hidradenitis suppurativa (acne inversa): early inflammatory events at terminal follicles and at interfollicular epidermis. Exp Dermatol. 2010;19:533-537.
- Van Der Zee HH, De Ruiter L, Van Den Broecke DG, et al. Elevated levels of tumour necrosis factor (TNF)-α, interleukin (IL)-1β and IL-10 in hidradenitis suppurativa skin: a rationale for targeting TNF-α and IL-1β. Br J Dermatol. 2011;164:1292-1298.
- Schlapbach C, Hänni T, Yawalkar N, et al. Expression of the IL-23/Th17 pathway in lesions of hidradenitis suppurativa. J Am Acad Dermatol. 2011;65:790-798.
- Kelly G, Hughes R, McGarry T, et al. Dysregulated cytokine expression in lesional and nonlesional skin in hidradenitis suppurativa. Br J Dermatol. 2015;173:1431-1439.
- Jemec GBE, Kimball AB. Hidradenitis suppurativa: epidemiology and scope of the problem. J Am Acad Dermatol. 2015;73(5 Suppl 1):S4-S7.
- Garg A, Kirby JS, Lavian J, et al. Sex- and age-adjusted population analysis of prevalence estimates for hidradenitis suppurativa in the United States. JAMA Dermatol. 2017;153:760-764.
- Soliman YS, Hoffman LK, Guzman AK, et al. African American patients with hidradenitis suppurativa have significant health care disparities: a retrospective study. J Cutan Med Surg. 2019;23:334-336.
- Garg A, Malviya N, Strunk A, et al. Comorbidity screening in hidradenitis suppurativa: evidence-based recommendations from the US and Canadian Hidradenitis Suppurativa Foundations. J Am Acad Dermatol. 2022;86:1092-1101.
- Beatriz Currier M, Nemeroff CB. Inflammation and mood disorders: proinflammatory cytokines and the pathogenesis of depression. Antiinflamm Antiallergy Agents Med Chem. 2012;9:212-220.
- Wright S, Strunk A, Garg A. Prevalence of depression among children, adolescents, and adults with hidradenitis suppurativa. J Am Acad Dermatol. 2022;86:55-60.
- Sampogna F, Fania L, Mastroeni S, et al. Correlation between depression, quality of life and clinical severity in patients with hidradenitis suppurativa. Acta Derm Venereol. 2020;100:1-6.
- Theut Riis P, Pedersen OB, Sigsgaard V, et al. Prevalence of patients with self-reported hidradenitis suppurativa in a cohort of Danish blood donors: a cross-sectional study. Br J Dermatol. 2019;180:774-781.
- Senthilnathan A, Kolli SS, Cardwell LA, et al. Depression in hidradenitis suppurativa. Br J Dermatol. 2019;181:1087-1088.
- Pavon Blanco A, Turner MA, Petrof G, et al. To what extent do disease severity and illness perceptions explain depression, anxiety and quality of life in hidradenitis suppurativa? Br J Dermatol. 2019;180:338-345.
- Butt M, Sisic M, Silva C, et al. The associations of depression and coping methods on health-related quality of life for those with hidradenitis suppurativa. J Am Acad Dermatol. 2019;80:1137-1139.
- Calao M, Wilson JL, Spelman L, et al. Hidradenitis suppurativa (HS) prevalence, demographics and management pathways in Australia: a population-based cross-sectional study. PLoS One. 2018;13:e0200683.
- Ingram JR, Jenkins-Jones S, Knipe DW, et al. Population-based Clinical Practice Research Datalink study using algorithm modelling to identify the true burden of hidradenitis suppurativa. Br J Dermatol. 2018;178:917-924.
- Kimball AB, Sundaram M, Gauthier G, et al. The comorbidity burden of hidradenitis suppurativa in the United States: a claims data analysis. Dermatol Ther (Heidelb). 2018;8:557.
- Thorlacius L, Cohen AD, Gislason GH, et al. Increased suicide risk in patients with hidradenitis suppurativa. J Invest Dermatol. 2018;138:52-57.
- Tiri H, Jokelainen J, Timonen M, et al. Somatic and psychiatric comorbidities of hidradenitis suppurativa in children and adolescents. J Am Acad Dermatol. 2018;79:514-519.
- Huilaja L, Tiri H, Jokelainen J, et al. Patients with hidradenitis suppurativa have a high psychiatric disease burden: a Finnish nationwide registry study. J Invest Dermatol. 2018;138:46-51.
- Kirby JS, Butt M, Esmann S, et al. Association of resilience with depression and health-related quality of life for patients with hidradenitis suppurativa. JAMA Dermatol. 2017;153:1263.
- Egeberg A, Gislason GH, Hansen PR. Risk of major adverse cardiovascular events and all-cause mortality in patients with hidradenitis suppurativa. JAMA Dermatol. 2016;152:429-434.
- Vangipuram R, Vaidya T, Jandarov R, et al. Factors contributing to depression and chronic pain in patients with hidradenitis suppurativa: results from a single-center retrospective review. Dermatology. 2016;232:692-695.
- Rayner L, Jackson K, Turner M, et al. Integrated mental health assessment in a tertiary medical dermatology service: feasibility and the prevalence of common mental disorder. Br J Dermatol. 2015;173:201.
- Shavit E, Dreiher J, Freud T, et al. Psychiatric comorbidities in 3207 patients with hidradenitis suppurativa [published online June 9, 2014]. J Eur Acad Dermatol Venereol. 2015;29:371-376.
- Kurek A, Johanne Peters EM, Sabat R, et al. Depression is a frequent co-morbidity in patients with acne inversa. J Dtsch Dermatol Ges. 2013;11:743-749.
- Vazquez BG, Alikhan A, Weaver AL, et al. Incidence of hidradenitis suppurativa and associated factors: a population-based study of Olmsted County, Minnesota. J Invest Dermatol. 2013;133:97.
- Onderdijk AJ, Van Der Zee HH, Esmann S, et al. Depression in patients with hidradenitis suppurativa [published online February 20, 2012]. J Eur Acad Dermatol Venereol. 2013;27:473-478.
- Matusiak Ł, Bieniek A, Szepietowski JC. Psychophysical aspects of hidradenitis suppurativa. Acta Derm Venereol. 2010;90:264-268.
- Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62:617-627.
- Holahan CJ, Pahl SA, Cronkite RC, et al. Depression and vulnerability to incident physical illness across 10 years. J Affect Disord. 2009;123:222-229.
- Deckers IE, Janse IC, van der Zee HH, et al. Hidradenitis suppurativa (HS) is associated with low socioeconomic status (SES): a cross-sectional reference study. J Am Acad Dermatol. 2016;75:755-759.e1.
- Williams MT, Skinta MD, Kanter JW, et al. A qualitative study of microaggressions against African Americans on predominantly White campuses. BMC Psychol. 2020;8:1-13.
- Dunlop DD, Song J, Lyons JS, et al. Racial/ethnic differences in rates of depression among preretirement adults. Am J Public Health. 2003;93:1945-1952.
- Williams DR, Priest N, Anderson NB. Understanding associations among race, socioeconomic status, and health: patterns and prospects. Health Psychol. 2016;35:407-411.
- Williams DR, González HM, Neighbors H, et al. Prevalence and distribution of major depressive disorder in African Americans, Caribbean Blacks, and Non-Hispanic Whites: results from the National Survey of American Life. Arch Gen Psychiatry. 2007;64:305-315.
- Druss BG, Bradford DW, Rosenheck RA, et al. Mental disorders and use of cardiovascular procedures after myocardial infarction. JAMA. 2000;283:506-511.
- Kromann CB, Deckers IE, Esmann S, et al. Risk factors, clinical course and long-term prognosis in hidradenitis suppurativa: a cross-sectional study. Br J Dermatol. 2014;171:819-824.
- Sivanand A, Gulliver WP, Josan CK, et al. Weight loss and dietary interventions for hidradenitis suppurativa: a systematic review. J Cutan Med Surg . 2020;24:64-72.
- Raedler TJ. Inflammatory mechanisms in major depressive disorder. Curr Opin Psychiatry. 2011;24:519-525.
- Rocha VZ, Libby P. Obesity, inflammation, and atherosclerosis. Nat Rev Cardiol. 2009;6:399-409.
- Davidson KW, Schwartz JE, Kirkland SA, et al. Relation of inflammation to depression and incident coronary heart disease (from the Canadian Nova Scotia Health Survey [NSHS95] Prospective Population Study). Am J Cardiol. 2009;103:755-761.
- González-López MA, Ocejo-Viñals JG, Mata C, et al. Evaluation of serum omentin-1 and apelin concentrations in patients with hidradenitis suppurativa. Postepy Dermatol Alergol. 2021;38:450-454.
- Taylor VH, Macqueen GM. The role of adipokines in understanding the associations between obesity and depression. J Obes. 2010;2010:748048.
- Setayesh L, Ebrahimi R, Pooyan S, et al. The possible mediatory role of adipokines in the association between low carbohydrate diet and depressive symptoms among overweight and obese women. PLoS One. 2021;16:e0257275 .
- Andriano TM, Benesh G, Babbush KM, et al. Serum inflammatory markers and leukocyte profiles accurately describe hidradenitis suppurativa disease severity. Int J Dermatol. 2022;61:1270-1275.
- Montaudié H, Seitz-Polski B, Cornille A, et al. Interleukin 6 and high-sensitivity C-reactive protein are potential predictive markers of response to infliximab in hidradenitis suppurativa. J Am Acad Dermatol. 2017;6:156-158.
- Colasanto M, Madigan S, Korczak DJ. Depression and inflammation among children and adolescents: a meta-analysis. J Affect Disord. 2020;277:940-948.
Practice Points
- Hidradenitis suppurativa (HS) is known to be associated with systemic inflammation and comorbidities, including depression.
- Depression may be a potential contributing factor to HS in affected patients, and studies on HS with comorbid depression in patients with skin of color are lacking.
How Good are Tools to Screen for Spondyloarthritis in Patients With Psoriasis, Uveitis, IBD?
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.
Tools to screen for spondyloarthritis (SpA) among people with the extra-musculoskeletal conditions that commonly co-occur with SpA — psoriasis, uveitis, and inflammatory bowel disease (IBD) — show potential for their use in target populations but have limited generalizability for patients at risk for SpA, according to findings from a scoping review of 18 tools.
Prior to the review comparing available tools, first author Vartika Kesarwani, MBBS, of the University of Connecticut, Farmington, and colleagues wrote that the performance of SpA screening tools in dermatology, ophthalmology, and gastroenterology contexts had not been evaluated.
“Given the evolving landscape of therapeutics for spondyloarthritis, recognizing the full spectrum of disease manifestations in individual patients becomes increasingly important. This knowledge can inform treatment decisions, potentially altering the course of the disease,” corresponding author Joerg Ermann, MD, of Brigham and Women’s Hospital, Boston, said in an interview.
In the study, published on February 1 in Arthritis Care & Research, the investigators identified 13 SpA screening tools for psoriasis (screening specifically for psoriatic arthritis), two for uveitis, and three for IBD. All tools with the exception of one for uveitis were patient-oriented questionnaires with an average completion time of less than 5 minutes.
Overall, the researchers found significant variability in the nature of the questions used to identify clinical features of SpA; 15 tools included at least one question on back pain or stiffness; 16 tools had at least one question on joint pain, swelling, or inflammation; 10 included questions about heel or elbow pain; and 10 included questions about swelling of digits.
All 13 of the psoriasis tools were screened for peripheral arthritis, while 10 screened for axial involvement, eight screened for enthesitis, and eight screened for dactylitis.
All three of the IBD tools were screened for axial involvement and peripheral arthritis, and two were screened for enthesitis and dactylitis.
Both of the uveitis tools were screened for axial involvement, but neither was screened for peripheral arthritis, enthesitis, or dactylitis.
Sensitivities in the primary validation groups were similar for the 16 tools for which sensitivities were reported, ranging mainly from 82% to 92% for 11 psoriasis tools, 91% to 96% for uveitis tools, and 83% to 93% for IBD tools.
Specificities for psoriasis tools ranged from 69% to 83% for all but two of the tools, which was 46% for one and 35%-89% for another across three geographical cohorts. For uveitis tools, specificities were 91%-97% for uveitis tools, and for IBD tools, 77%-90%. Most of the secondary validations involved psoriasis tools, and these were generally lower and also more variable.
The Case for a Generic Tool
The relatively few SpA tools for patients with uveitis and IBD, compared with psoriasis, may be attributable to a lack of awareness of the association between these conditions on the part of ophthalmologists and gastroenterologists, the researchers wrote in their discussion. Therefore, a generic SpA screening tool that could apply to any extra-articular manifestation might increase screening across clinical settings and streamline rheumatology referrals, they noted.
The review’s findings were limited by several factors, including the inclusion of only articles in English and the relatively few tools for uveitis and IBD patients, the researchers noted.
The findings suggested that although the performances of the tools are similar, their degree of variability supports the value of a generic tool, they concluded.
Streamlining to Increase Screening
“Compared to the large amount of research in psoriasis and psoriatic arthritis, relatively little has been done with regard to screening for spondyloarthritis in patients with uveitis or IBD,” Dr. Ermann told this news organization. “Despite the numerous screening tools developed for psoriatic arthritis, no ideal screening tool has emerged, and the implementation of effective screening strategies in clinical practice is challenging,” he said. In the current study, the compartmentalization of research into individual conditions like psoriasis, uveitis, and IBD was notable despite the interconnected nature of these conditions with SpA, he added.
In practice, Dr. Ermann advised clinicians to maintain a high index of suspicion for SpA in patients presenting with psoriasis, uveitis, or IBD and proactively ask patients about symptoms outside their primary specialty.
“Future research should focus on developing a universal spondyloarthritis screening tool that is comprehensive, easily understandable, and can be used across various clinical settings,” he said.
Need for Early Identification and Closer Collaboration
A delay in SpA diagnosis of as little as 6 months can lead to worse outcomes, Rebecca Haberman, MD, a rheumatologist at NYU Langone Health, New York City, said in an interview. “Patients with these conditions may first present to dermatologists, gastroenterologists, and/or ophthalmologists before rheumatologic evaluation. If we can identify these patients early at this stage, we might be able to improve outcomes, but the question remains of how we get these patients to the proper care,” she said.
The review examined the currently available screening tools for use in patients with psoriasis, IBD, and uveitis and highlights the heterogeneity of these tools in terms of use and disease characteristics, as well as the lack of tools for use in gastroenterology and ophthalmology offices, Dr. Haberman said.
The review “proposes several important ideas, such as creating a unified screening tool that can be used across diseases and fields, to reduce confusion by providers and help provide standardization of the referral process to rheumatologists,” she said.
“Even though SpA is prevalent in many patients with psoriasis, IBD, and uveitis, it remains very underdiagnosed, and often referrals to rheumatologists are not made,” Dr. Haberman told this news organization. Diagnostic challenges likely include SpA’s heterogeneous presentation, the specialists’ lack of knowledge regarding the connection between these conditions and joint disease, and time pressures in clinical settings, she said.
“Other practitioners are not always trained to ask about joint pain and often have limited time in their exams to ask additional questions. To overcome this, more collaboration is needed between dermatologists, gastroenterologists, ophthalmologists, and rheumatologists, as many of our diseases live in the same family,” Dr. Haberman said.
Improving clinician education and creating relationships can help facilitate questions and referrals, she said. Short, effective screening tools that can be filled out by the patient may also help overcome specialists’ discomfort about asking musculoskeletal-related questions and would save time in the clinical visit, she said.
More research is needed to identify the best screening tools and questions and which are the most highly sensitive and specific, Dr. Haberman said. “This will allow for rheumatologists to see patients who may have SpA earlier in their course without overwhelming the system with new referrals.” In addition, more work is needed on how and whether screening tools are being used in clinical practice, not just in research studies, she said.
The study was supported by a grant from the National Institutes of Health/National Institute of Arthritis and Musculoskeletal and Skin Diseases. The researchers and Dr. Haberman had no financial conflicts to disclose.
A version of this article appeared on Medscape.com.