User login
Heat Exposure Tied to Acute Immune Changes
In this study, blood work from volunteers was examined for immune biomarkers, and the findings mapped against environmental data.
“With rising global temperatures, the association between heat exposure and a temporarily weakened response from the immune system is a concern because temperature and humidity are known to be important environmental drivers of infectious, airborne disease transmission,” lead author Daniel W. Riggs, PhD, with the Christina Lee Brown Envirome Institute, University of Louisville in Louisville, Kentucky, said in a news release.
“In this study, even exposure to relatively modest increases in temperature were associated with acute changes in immune system functioning indexed by low-grade inflammation known to be linked to cardiovascular disorders, as well as potential secondary effects on the ability to optimally protect against infection,” said Rosalind J. Wright, MD, MPH, who wasn’t involved in the study.
“Further elucidation of the effects of both acute and more prolonged heat exposures (heat waves) on immune signaling will be important given potential broad health implications beyond the heart,” said Dr. Wright, dean of public health and professor and chair, Department of Public Health, Mount Sinai Health System.
The study was presented at the American Heart Association (AHA) Epidemiology and Prevention | Lifestyle and Cardiometabolic Scientific Sessions 2024.
High Temps Hard on Multiple Organs
Extreme-heat events have been shown to increase mortality, and excessive deaths due to heat waves are overwhelmingly cardiovascular in origin. Many prior studies only considered ambient temperature, which fails to capture the actual heat stress experienced by individuals, Dr. Riggs and colleagues wrote.
They designed their study to gauge how short-term heat exposures are related to markers of inflammation and the immune response.
They recruited 624 adults (mean age 49 years, 59% women) from a neighborhood in Louisville during the summer months, when median temperatures over 24 hours were 24.5 °C (76 °F).
They obtained blood samples to measure circulating cytokines and immune cells during clinic visits. Heat metrics, collected on the same day as blood draws, included 24-hour averages of temperature, net effective temperature, and the Universal Thermal Climate Index (UTCI), a metric that incorporates temperature, humidity, wind speed, and ultraviolet radiation, to determine the physiological comfort of the human body under specific weather conditions.
The results were adjusted for multiple factors, including sex, age, race, education, body mass index, smoking status, anti-inflammatory medication use, and daily air pollution (PM 2.5).
In adjusted analyses, for every five-degree increase in UTCI, there was an increase in levels of several inflammatory markers, including monocytes (4.2%), eosinophils (9.5%), natural killer T cells (9.9%), and tumor necrosis factor-alpha (7.0%) and a decrease in infection-fighting B cells (−6.8%).
Study Raises Important Questions
“We’re finding that heat is associated with health effects across a wide range of organ systems and outcomes, but this study helps start to get at the ‘how,’” said Perry E. Sheffield, MD, MPH, with the Departments of Pediatrics and Environmental Medicine and Public Health, Icahn School of Medicine at Mount Sinai in New York City, who wasn’t involved in the study.
Dr. Sheffield said the study raises “important questions like, Does the timing of heat exposure matter (going in and out of air-conditioned spaces for example)? and Could some people be more vulnerable than others based on things like what they eat, whether they exercise, or their genetics?”
The study comes on the heels of a report released earlier this month from the World Meteorological Organization noting that climate change indicators reached record levels in 2023.
“The most critical challenges facing medicine are occurring at the intersection of climate and health, underscoring the urgent need to understand how climate-related factors, such as exposure to more extreme temperatures, shift key regulatory systems in our bodies to contribute to disease,” Dr. Wright told this news organization.
The study was supported by grants from the National Institute of Environmental Health Sciences. Dr. Riggs, Dr. Wright, and Sheffield had no relevant disclosures.
A version of this article appeared on Medscape.com.
In this study, blood work from volunteers was examined for immune biomarkers, and the findings mapped against environmental data.
“With rising global temperatures, the association between heat exposure and a temporarily weakened response from the immune system is a concern because temperature and humidity are known to be important environmental drivers of infectious, airborne disease transmission,” lead author Daniel W. Riggs, PhD, with the Christina Lee Brown Envirome Institute, University of Louisville in Louisville, Kentucky, said in a news release.
“In this study, even exposure to relatively modest increases in temperature were associated with acute changes in immune system functioning indexed by low-grade inflammation known to be linked to cardiovascular disorders, as well as potential secondary effects on the ability to optimally protect against infection,” said Rosalind J. Wright, MD, MPH, who wasn’t involved in the study.
“Further elucidation of the effects of both acute and more prolonged heat exposures (heat waves) on immune signaling will be important given potential broad health implications beyond the heart,” said Dr. Wright, dean of public health and professor and chair, Department of Public Health, Mount Sinai Health System.
The study was presented at the American Heart Association (AHA) Epidemiology and Prevention | Lifestyle and Cardiometabolic Scientific Sessions 2024.
High Temps Hard on Multiple Organs
Extreme-heat events have been shown to increase mortality, and excessive deaths due to heat waves are overwhelmingly cardiovascular in origin. Many prior studies only considered ambient temperature, which fails to capture the actual heat stress experienced by individuals, Dr. Riggs and colleagues wrote.
They designed their study to gauge how short-term heat exposures are related to markers of inflammation and the immune response.
They recruited 624 adults (mean age 49 years, 59% women) from a neighborhood in Louisville during the summer months, when median temperatures over 24 hours were 24.5 °C (76 °F).
They obtained blood samples to measure circulating cytokines and immune cells during clinic visits. Heat metrics, collected on the same day as blood draws, included 24-hour averages of temperature, net effective temperature, and the Universal Thermal Climate Index (UTCI), a metric that incorporates temperature, humidity, wind speed, and ultraviolet radiation, to determine the physiological comfort of the human body under specific weather conditions.
The results were adjusted for multiple factors, including sex, age, race, education, body mass index, smoking status, anti-inflammatory medication use, and daily air pollution (PM 2.5).
In adjusted analyses, for every five-degree increase in UTCI, there was an increase in levels of several inflammatory markers, including monocytes (4.2%), eosinophils (9.5%), natural killer T cells (9.9%), and tumor necrosis factor-alpha (7.0%) and a decrease in infection-fighting B cells (−6.8%).
Study Raises Important Questions
“We’re finding that heat is associated with health effects across a wide range of organ systems and outcomes, but this study helps start to get at the ‘how,’” said Perry E. Sheffield, MD, MPH, with the Departments of Pediatrics and Environmental Medicine and Public Health, Icahn School of Medicine at Mount Sinai in New York City, who wasn’t involved in the study.
Dr. Sheffield said the study raises “important questions like, Does the timing of heat exposure matter (going in and out of air-conditioned spaces for example)? and Could some people be more vulnerable than others based on things like what they eat, whether they exercise, or their genetics?”
The study comes on the heels of a report released earlier this month from the World Meteorological Organization noting that climate change indicators reached record levels in 2023.
“The most critical challenges facing medicine are occurring at the intersection of climate and health, underscoring the urgent need to understand how climate-related factors, such as exposure to more extreme temperatures, shift key regulatory systems in our bodies to contribute to disease,” Dr. Wright told this news organization.
The study was supported by grants from the National Institute of Environmental Health Sciences. Dr. Riggs, Dr. Wright, and Sheffield had no relevant disclosures.
A version of this article appeared on Medscape.com.
In this study, blood work from volunteers was examined for immune biomarkers, and the findings mapped against environmental data.
“With rising global temperatures, the association between heat exposure and a temporarily weakened response from the immune system is a concern because temperature and humidity are known to be important environmental drivers of infectious, airborne disease transmission,” lead author Daniel W. Riggs, PhD, with the Christina Lee Brown Envirome Institute, University of Louisville in Louisville, Kentucky, said in a news release.
“In this study, even exposure to relatively modest increases in temperature were associated with acute changes in immune system functioning indexed by low-grade inflammation known to be linked to cardiovascular disorders, as well as potential secondary effects on the ability to optimally protect against infection,” said Rosalind J. Wright, MD, MPH, who wasn’t involved in the study.
“Further elucidation of the effects of both acute and more prolonged heat exposures (heat waves) on immune signaling will be important given potential broad health implications beyond the heart,” said Dr. Wright, dean of public health and professor and chair, Department of Public Health, Mount Sinai Health System.
The study was presented at the American Heart Association (AHA) Epidemiology and Prevention | Lifestyle and Cardiometabolic Scientific Sessions 2024.
High Temps Hard on Multiple Organs
Extreme-heat events have been shown to increase mortality, and excessive deaths due to heat waves are overwhelmingly cardiovascular in origin. Many prior studies only considered ambient temperature, which fails to capture the actual heat stress experienced by individuals, Dr. Riggs and colleagues wrote.
They designed their study to gauge how short-term heat exposures are related to markers of inflammation and the immune response.
They recruited 624 adults (mean age 49 years, 59% women) from a neighborhood in Louisville during the summer months, when median temperatures over 24 hours were 24.5 °C (76 °F).
They obtained blood samples to measure circulating cytokines and immune cells during clinic visits. Heat metrics, collected on the same day as blood draws, included 24-hour averages of temperature, net effective temperature, and the Universal Thermal Climate Index (UTCI), a metric that incorporates temperature, humidity, wind speed, and ultraviolet radiation, to determine the physiological comfort of the human body under specific weather conditions.
The results were adjusted for multiple factors, including sex, age, race, education, body mass index, smoking status, anti-inflammatory medication use, and daily air pollution (PM 2.5).
In adjusted analyses, for every five-degree increase in UTCI, there was an increase in levels of several inflammatory markers, including monocytes (4.2%), eosinophils (9.5%), natural killer T cells (9.9%), and tumor necrosis factor-alpha (7.0%) and a decrease in infection-fighting B cells (−6.8%).
Study Raises Important Questions
“We’re finding that heat is associated with health effects across a wide range of organ systems and outcomes, but this study helps start to get at the ‘how,’” said Perry E. Sheffield, MD, MPH, with the Departments of Pediatrics and Environmental Medicine and Public Health, Icahn School of Medicine at Mount Sinai in New York City, who wasn’t involved in the study.
Dr. Sheffield said the study raises “important questions like, Does the timing of heat exposure matter (going in and out of air-conditioned spaces for example)? and Could some people be more vulnerable than others based on things like what they eat, whether they exercise, or their genetics?”
The study comes on the heels of a report released earlier this month from the World Meteorological Organization noting that climate change indicators reached record levels in 2023.
“The most critical challenges facing medicine are occurring at the intersection of climate and health, underscoring the urgent need to understand how climate-related factors, such as exposure to more extreme temperatures, shift key regulatory systems in our bodies to contribute to disease,” Dr. Wright told this news organization.
The study was supported by grants from the National Institute of Environmental Health Sciences. Dr. Riggs, Dr. Wright, and Sheffield had no relevant disclosures.
A version of this article appeared on Medscape.com.
Systematic Viral Testing in Emergency Departments Has Limited Benefit for General Population
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
Routine use of rapid respiratory virus testing in the emergency department (ED) appears to show limited benefit among patients with signs and symptoms of acute respiratory infection (ARI), according to a new study.
Rapid viral testing wasn’t associated with reduced antibiotic use, ED length of stay, or rates of ED return visits or hospitalization. However, testing was associated with a small increase in antiviral prescriptions and a small reduction in blood tests and chest x-rays.
“Our interest in studying the benefits of rapid viral testing in emergency departments comes from a commitment to diagnostic stewardship — ensuring that the right tests are administered to the right patients at the right time while also curbing overuse,” said lead author Tilmann Schober, MD, a resident in pediatric infectious disease at McGill University and Montreal Children’s Hospital.
“Following the SARS-CoV-2 pandemic, we have seen a surge in the availability of rapid viral testing, including molecular multiplex panels,” he said. “However, the actual impact of these advancements on patient care in the ED remains uncertain.”
The study was published online on March 4, 2024, in JAMA Internal Medicine).
Rapid Viral Testing
Dr. Schober and colleagues conducted a systematic review and meta-analysis of 11 randomized clinical trials to understand whether rapid testing for respiratory viruses was associated with patient treatment in the ED.
In particular, the research team looked at whether testing in patients with suspected ARI was associated with decreased antibiotic use, ancillary tests, ED length of stay, ED return visits, hospitalization, and increased influenza antiviral treatment.
Among the trials, seven studies included molecular testing, and eight used multiplex panels, including influenza and respiratory syncytial virus (RSV), influenza/RSV/adenovirus/parainfluenza, or a panel of 15 or more respiratory viruses. No study evaluated testing for SARS-CoV-2. The research team reported risk ratios (RRs) and risk difference estimates.
In general, routine rapid viral testing was associated with higher use of influenza antivirals (RR, 1.33) and lower use of chest radiography (RR, 0.88) and blood tests (RR, 0.81). However, the magnitude of these effects was small. For instance, to achieve one additional viral prescription, 70 patients would need to be tested, and to save one x-ray, 30 patients would need to be tested.
“This suggests that, while statistically significant, the practical impact of these secondary outcomes may not justify the extensive effort and resources involved in widespread testing,” Dr. Schober said.
In addition, there was no association between rapid testing and antibiotic use (RR, 0.99), urine testing (RR, 0.95), ED length of stay (0 h), return visits (RR, 0.93), or hospitalization (RR, 1.01).
Notably, there was no association between rapid viral testing and antibiotic use in any prespecified subgroup based on age, test method, publication date, number of viral targets, risk of bias, or industry funding, the authors said. They concluded that rapid virus testing should be reserved for patients for whom the testing will change treatment, such as high-risk patients or those with severe disease.
“It’s crucial to note that our study specifically evaluated the impact of systematic testing of patients with signs and symptoms of acute respiratory infection. Our findings do not advocate against rapid respiratory virus testing in general,” Dr. Schober said. “There is well-established evidence supporting the benefits of viral testing in certain contexts, such as hospitalized patients, to guide infection control practices or in specific high-risk populations.”
Future Research
Additional studies should look at testing among subgroups, particularly those with high-risk conditions, the study authors wrote. In addition, the research team would like to study the implementation of novel diagnostic stewardship programs as compared with well-established antibiotic stewardship programs.
“Acute respiratory tract illnesses represent one of the most common reasons for being evaluated in an acute care setting, especially in pediatrics, and these visits have traditionally resulted in excessive antibiotic prescribing, despite the etiology of the infection mostly being viral,” said Suchitra Rao, MBBS, associate professor of pediatrics at the University of Colorado School of Medicine and associate medical director of infection prevention and control at Children’s Hospital Colorado, Aurora.
Dr. Rao, who wasn’t involved with this study, has surveyed ED providers about respiratory viral testing and changes in clinical decision-making. She and colleagues found that providers most commonly changed clinical decision-making while prescribing an antiviral if influenza was detected or withholding antivirals if influenza wasn’t detected.
“Multiplex testing for respiratory viruses and atypical bacteria is becoming more widespread, with newer-generation platforms having shorter turnaround times, and offers the potential to impact point-of-care decision-making,” she said. “However, these tests are expensive, and more studies are needed to explore whether respiratory pathogen panel testing in the acute care setting has an impact in terms of reduced antibiotic use as well as other outcomes, including ED visits, health-seeking behaviors, and hospitalization.”
For instance, more recent studies around SARS-CoV-2 with newer-generation panels may make a difference, as well as multiplex panels that include numerous viral targets, she said.
“Further RCTs are required to evaluate the impact of influenza/RSV/SARS-CoV-2 panels, as well as respiratory pathogen panel testing in conjunction with antimicrobial and diagnostic stewardship efforts, which have been associated with improved outcomes for other rapid molecular platforms, such as blood culture identification panels,” Rao said.
The study was funded by the Research Institute of the McGill University Health Center. Dr. Schober reported no disclosures, and several study authors reported grants or personal fees from companies outside of this research. Dr. Rao disclosed no relevant relationships.
A version of this article appeared on Medscape.com .
New Infant RSV Antibody Treatment Shows Strong Results
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
The new RSV antibody treatment for babies has been highly effective in its first season, according to a first look at data from four children’s hospitals.
Babies who received the new preventive treatment for RSV shortly after birth were 90% less likely to be severely sickened with the potentially deadly respiratory illness, according to the new estimate published by the Centers for Disease Control and Prevention. It is the first real-world evaluation of Beyfortus (the generic name is nirsevimab), which was approved by the Food and Drug Administration last July.
RSV is a seasonal illness that affects more people — particularly infants and the elderly — in the fall and winter. Symptoms are usually mild in healthy adults, but infants are particularly at risk of getting bronchiolitis, which results in exhausting wheezing and coughing in babies due to swelling in their airways and lungs. Babies who are hospitalized may need fluids and medical devices to help them breathe.
RSV peaked this season from November to January, with more than 10,000 monthly diagnoses reported to the CDC.
The new CDC analysis was conducted among about 700 babies hospitalized for severe respiratory problems from October to the end of February. Among the babies in the study, 407 were diagnosed with RSV and 292 tested negative. The researchers found that 1% of babies in the study who were diagnosed with RSV had received Beyfortus, while the remaining babies who were positive for the virus had not.
Among the babies hospitalized for other severe respiratory problems, 18% had received Beyfortus. Overall, just 59 babies among the nearly 700 in the study received Beyfortus, perhaps reflecting the short supply of the medicine the first season it was available. The report authors noted that babies in the study who did receive Beyfortus also tended to have high-risk medical conditions.
The number of babies nationwide who received Beyfortus during this first season of availability is unclear, but a January CDC survey showed that 4 in 10 parents said their babies under 8 months old had received the treatment. The Wall Street Journal reported recently that a shortage last fall resulted from underestimated demand and from production plans that were set before the CDC decided to recommend that all infants under 8 months old receive Beyfortus if their mothers did not get a maternal vaccine that can protect infants from RSV.
Both the antibody treatment for infants and the maternal vaccine were shown in clinical trials to be about 80% effective at preventing severe illness stemming from RSV.
The authors of the latest CDC report concluded that “this early estimate supports the current nirsevimab recommendation for the prevention of severe RSV disease in infants. Infants should be protected by maternal RSV vaccination or infant receipt of nirsevimab.”
A version of this article appeared on WebMD.com.
Risk for Preterm Birth Stops Maternal RSV Vaccine Trial
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
A phase 3 trial of a maternal vaccine candidate for respiratory syncytial virus (RSV) has been stopped early because the risk for preterm births is higher in the candidate vaccine group than in the placebo group.
By the time enrollment was stopped on February 25, 2022 because of the safety signal of preterm birth, 5328 pregnant women had been vaccinated, about half of the intended 10,000 enrollees. Of these, 3557 received the candidate vaccine RSV prefusion F protein–based maternal vaccine, and another 1771 received a placebo.
Data from the trial, sponsored by GSK, were immediately made available when recruitment and vaccination were stopped, and investigation of the preterm birth risk followed. Results of that analysis, led by Ilse Dieussaert, IR, vice president for vaccine development at GSK in Wavre, Belgium, are published online on March 13 in The New England Journal of Medicine.
“We have discontinued our work on this RSV maternal candidate vaccine, and we are closing out all ongoing trials with the exception of the MAT-015 follow-on study to monitor subsequent pregnancies,” a GSK spokesperson said in an interview.
The trial was conducted in pregnant women aged 18-49 years to assess the efficacy and safety of the vaccine. The women were randomly assigned 2:1 to receive the candidate vaccine or placebo between 24 and 34 weeks’ gestation.
Preterm Births
The primary outcomes were any or severe medically assessed RSV-associated lower respiratory tract infection in infants from birth to 6 months and safety in infants from birth to 12 months.
According to the data, preterm birth occurred in 6.8% of the infants in the vaccine group and in 4.9% of those in the placebo group (relative risk [RR], 1.37; 95% CI, 1.08-1.74; P = .01). Neonatal death occurred in 0.4% in the vaccine group and 0.2% in the placebo group (RR, 2.16; 95% CI, 0.62-7.56; P = .23).
To date, only one RSV vaccine (Abrysvo, Pfizer) has been approved for use during pregnancy to protect infants from RSV-associated lower respiratory tract infection.
“It was a very big deal that this trial was stopped, and the new candidate won’t get approval.” said Aaron E. Glatt, MD, chair of the Department of Medicine and chief of Infectious Diseases and Hospital Epidemiologist at Mount Sinai South Nassau in Oceanside, New York.
Only One RSV Vaccine Approved in Pregnancy
Dr. Glatt pointed out the GSK vaccine is like the maternal vaccine that did get approved. “The data clearly show that there was a slight but increased risk in preterm labor,” Dr. Glatt said, “and while not as clearly shown, there was an increase in neonatal death in the group of very small numbers, but any neonatal death is of concern.”
The implications were disturbing, he added, “You’re giving this vaccine to prevent neonatal death.” Though the Pfizer vaccine that was granted approval had a very slight increase in premature birth, the risk wasn’t statistically significant, he pointed out, “and it showed similar benefits in preventing neonatal illness, which can be fatal.”
Dr. Glatt said that there is still a lingering concern with the approved vaccine, and he explained that most clinicians will give it closer to the end of the recommended time window of 34 weeks. “This way, even if there is a slight increase in premature term labor, you’re probably not going to have a serious outcome because the baby will be far enough along.”
A difference in the incidence of preterm birth between the experimental vaccine and placebo groups was predominantly found in low- and middle-income countries, according to Dieussaert’s team, “where approximately 50% of the trial population was enrolled and where the medical need for maternal RSV vaccines is the greatest.”
The RR was 1.56 (95% CI, 1.17-2.10) for low- and middle-income countries and 1.04 (95% CI, 0.68-1.58) for high-income countries.
“If a smaller percentage of participants from low- and middle-income countries had been enrolled in our trial, the RR for preterm birth in the vaccine group as compared with the placebo group might have been reduced in the overall trial population,” they reported.
The authors explained that the data do not reveal the cause of the higher risk for preterm birth in the vaccine group.
“We do not know what caused the signal,” the company’s spokesperson added. “GSK completed all the necessary steps of product development including preclinical toxicology studies and clinical studies in nonpregnant women prior to starting the studies in pregnant women. There were no safety signals identified in any of the earlier parts of the clinical testing. There have been no safety signals identified in the other phase 3 trials for this vaccine candidate.”
Researchers did not find a correlation between preterm births in the treatment vs control groups with gestational age at the time of vaccination or with particular vaccine clinical trial material lots, race, ethnicity, maternal smoking, alcohol consumption, body mass index, or time between study vaccination and delivery, the GSK spokesperson said.
The spokesperson noted that the halted vaccine is different from GSK’s currently approved adjuvanted RSV vaccine (Arexvy) for adults aged 60 years or older.
What’s Next for Other Vaccines
Maternal vaccines have been effective in preventing other diseases in infants, such as tetanus, influenza, and pertussis, but RSV is a very hard virus to make a vaccine for, Dr. Glatt shared.
The need is great to have more than one option for a maternal RSV vaccine, he added, to address any potential supply concerns.
“People have to realize how serious RSV can be in infants,” he said. “It can be a fatal disease. This can be a serious illness even in healthy children.”
A version of this article appeared on Medscape.com.
Postinfectious Cough: Are Treatments Ever Warranted?
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
Lingering postinfectious cough has been a concern across Canada this winter. , according to an overview published on February 12 in the Canadian Medical Association Journal
“It’s something a lot of patients are worried about: That lingering cough after a common cold or flu,” lead author Kevin Liang, MD, of the Department of Family Medicine at The University of British Columbia in Vancouver, British Columbia, Canada, told this news organization. He added that some studies show that as much as a quarter of adult patients have this complaint.
Dr. Liang and his colleagues emphasized that the diagnosis of postinfectious cough is one of exclusion. It relies on the absence of concerning physical examination findings and other “subacute cough mimics” such as asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease, or use of angiotensin-converting enzyme inhibitors.
“Pertussis should be considered in patients with a paroxysmal cough, post-tussive vomiting, and inspiratory whoop,” they added. Coughs that persist beyond 8 weeks warrant further workup such as a pulmonary function test to rule out asthma or COPD. Coughs accompanied by hemoptysis, systemic symptoms, dysphagia, excessive dyspnea, or hoarseness also warrant further workup, they added. And patients with a history of smoking or recurrent pneumonia should be followed more closely.
In the absence of red flags, Dr. Liang and coauthors advised that there is no evidence supporting pharmacologic treatment, “which is associated with harms,” such as medication adverse effects, cost, strain on the medical supply chain, and the fact that pressurized metered-dose inhalers emit powerful greenhouse gases. “A lot of patients come in looking for solutions, but really, all the evidence says the over-the-counter cough syrup just doesn’t work. Or I see clinicians prescribing inhalers or different medication that can cost hundreds of dollars, and their efficacy, at least from the literature, shows that there’s really no improvement. Time and patience are the two keys to solving this,” Dr. Liang told this news organization.
Moreover, there is a distinct absence of guidelines on this topic. The College of Family Physicians of Canada’s recent literature review cited limited data supporting a trial of inhaled corticosteroids, a bronchodilator such as ipratropium-salbutamol, or an intranasal steroid if postnasal drip is suspected. However, “there’s a high risk of bias in the study they cite from using the short-acting bronchodilators, and what it ultimately says is that in most cases, this is self-resolving by around the 20-day mark,” said Dr. Liang. “Our advice is just to err on the side of caution and just provide that information piece to the patient.”
‘Significant Nuance’
Imran Satia, MD, assistant professor of respirology at McMaster University in Hamilton, Ontario, Canada, agreed that “most people who get a viral or bacterial upper or lower respiratory tract infection will get better with time, and there is very little evidence that giving steroids, antibiotics, or cough suppressants is better than waiting it out.” There is “significant nuance” in how to manage this situation, however.
“In some patients with underlying lung disease like asthma or COPD, increasing the frequency of regular inhaled steroids, bronchodilators, oral steroids, antibiotics, and chest imaging with breathing tests may be clinically warranted, and many physicians will do this,” he told this news organization. “In some patients with refractory chronic cough, there is no underlying identifiable disease, despite completing the necessary investigations. Or coughing persists despite trials of treatment for lung diseases, nasal diseases, and stomach reflux disease. This is commonly described as cough hypersensitivity syndrome, for which therapies targeting the neuronal pathways that control coughing are needed.”
Physicians should occasionally consider trying a temporary course of a short-acting bronchodilator inhaler, said Nicholas Vozoris, MD, assistant professor and clinician investigator in respirology at the University of Toronto, Toronto, Ontario, Canada. “I think that would be a reasonable first step in a case of really bad postinfectious cough,” he told this news organization. “But in general, drug treatments are not indicated.”
Environmental Concerns
Yet some things should raise clinicians’ suspicion of more complex issues.
“A pattern of recurrent colds or bronchitis with protracted coughing afterward raises strong suspicion for asthma, which can present as repeated, prolonged respiratory exacerbations,” he said. “Unless asthma is treated with appropriate inhaler therapy on a regular basis, it will unlikely come under control.”
Dr. Vozoris added that the environmental concerns over the use of metered dose inhalers (MDIs) are minimal compared with the other sources of pollution and the risks for undertreatment. “The authors are overplaying the environmental impact of MDI, in my opinion,” he said. “Physicians already have to deal with the challenging issue of suboptimal patient adherence to inhalers, and I fear that such comments may further drive that up. Furthermore, there is also an environmental footprint with not using inhalers, as patients can then experience suboptimally controlled lung disease as a result — and then present to the ER and get admitted to hospital for exacerbations of disease, where more resources and medications are used up.”
“In addition, in patients who are immunocompromised, protracted coughing after what was thought to be a cold may be associated with an “atypical” respiratory infection, such as tuberculosis, that will require special medical treatment,” Dr. Vozoris concluded.
No funding for the review of postinfectious cough was reported. Dr. Liang and Dr. Vozoris disclosed no competing interests. Dr. Satia reported receiving funding from the ERS Respire 3 Fellowship Award, BMA James Trust Award, North-West Lung Centre Charity (Manchester), NIHR CRF Manchester, Merck MSD, AstraZeneca, and GSK. Dr. Satia also has received consulting fees from Merck MSD, Genentech, and Respiplus; as well as speaker fees from AstraZeneca, GSK, Merck MSD, Sanofi-Regeneron. Satia has served on the following task force committees: Chronic Cough (ERS), Asthma Diagnosis and Management (ERS), NEUROCOUGH (ERS CRC), and the CTS Chronic Cough working group.
A version of this article appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Bivalent Vaccines Protect Even Children Who’ve Had COVID
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.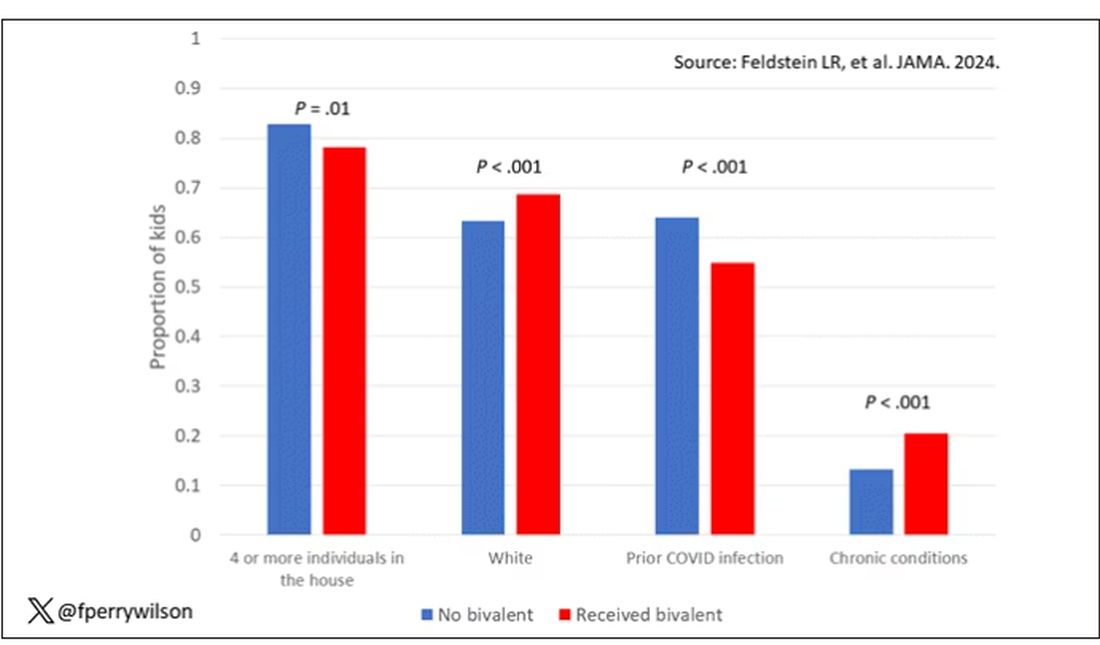
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.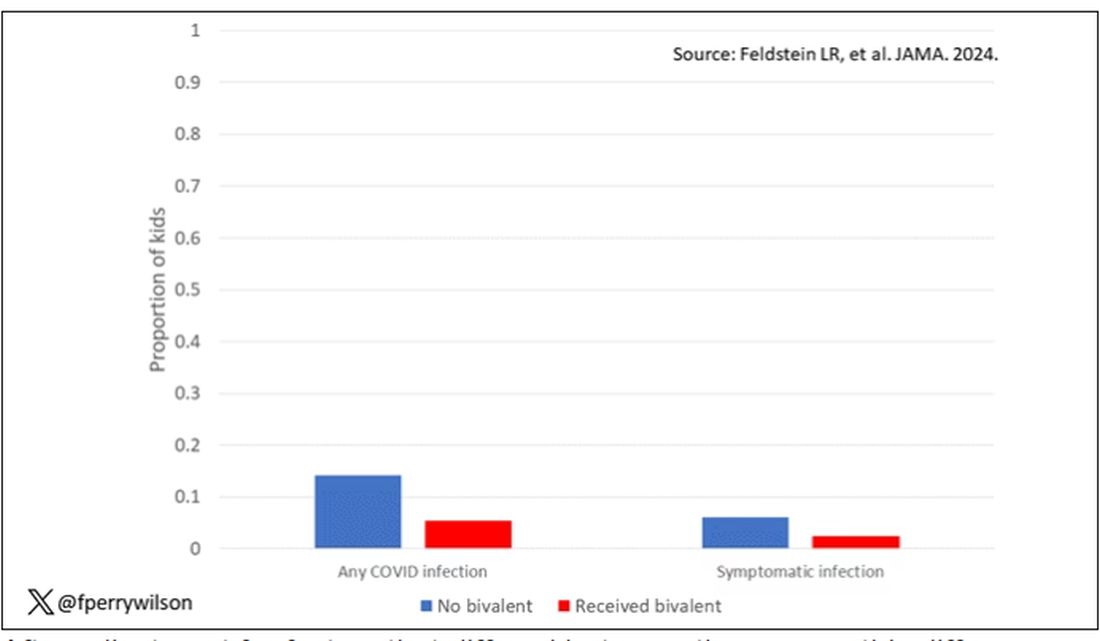
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.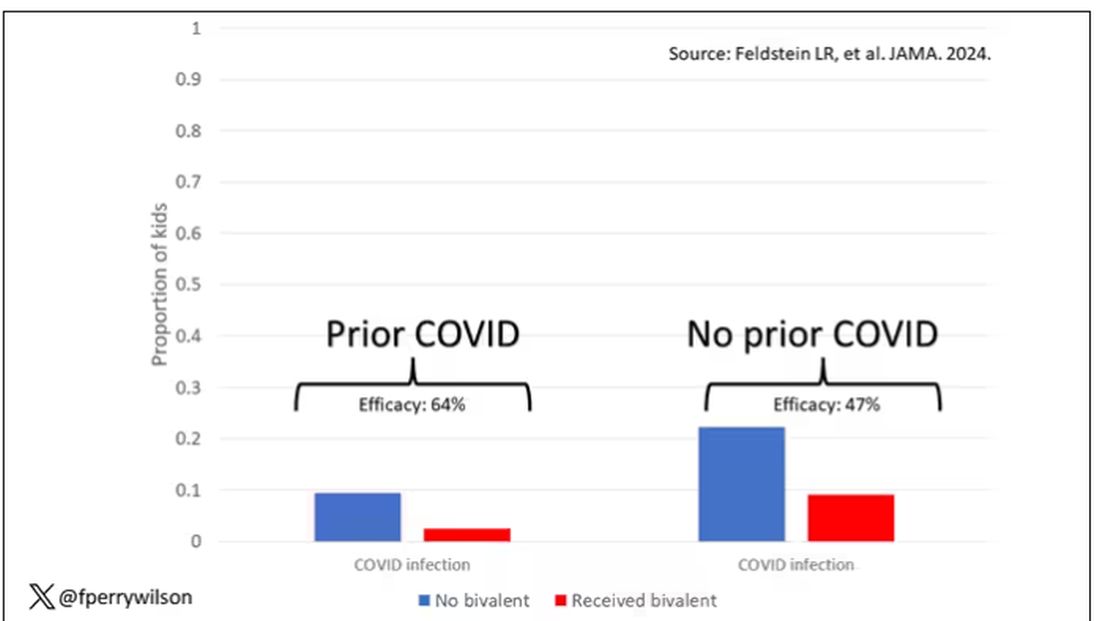
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
It was only 3 years ago when we called the pathogen we now refer to as the coronavirus “nCOV-19.” It was, in many ways, more descriptive than what we have today. The little “n” there stood for “novel” — and it was really that little “n” that caused us all the trouble.
You see, coronaviruses themselves were not really new to us. Understudied, perhaps, but with four strains running around the globe at any time giving rise to the common cold, these were viruses our bodies understood.
But Instead of acting like a cold, it acted like nothing we had seen before, at least in our lifetime. The story of the pandemic is very much a bildungsroman of our immune systems — a story of how our immunity grew up.
The difference between the start of 2020 and now, when infections with the coronavirus remain common but not as deadly, can be measured in terms of immune education. Some of our immune systems were educated by infection, some by vaccination, and many by both.
When the first vaccines emerged in December 2020, the opportunity to educate our immune systems was still huge. Though, at the time, an estimated 20 million had been infected in the US and 350,000 had died, there was a large population that remained immunologically naive. I was one of them.
If 2020 into early 2021 was the era of immune education, the postvaccine period was the era of the variant. From one COVID strain to two, to five, to innumerable, our immune memory — trained on a specific version of the virus or its spike protein — became imperfect again. Not naive; these variants were not “novel” in the way COVID-19 was novel, but they were different. And different enough to cause infection.
Following the playbook of another virus that loves to come dressed up in different outfits, the flu virus, we find ourselves in the booster era — a world where yearly doses of a vaccine, ideally matched to the variants circulating when the vaccine is given, are the recommendation if not the norm.
But questions remain about the vaccination program, particularly around who should get it. And two populations with big question marks over their heads are (1) people who have already been infected and (2) kids, because their risk for bad outcomes is so much lower.
This week, we finally have some evidence that can shed light on these questions. The study under the spotlight is this one, appearing in JAMA, which tries to analyze the ability of the bivalent vaccine — that’s the second one to come out, around September 2022 — to protect kids from COVID-19.
Now, right off the bat, this was not a randomized trial. The studies that established the viability of the mRNA vaccine platform were; they happened before the vaccine was authorized. But trials of the bivalent vaccine were mostly limited to proving immune response, not protection from disease.
Nevertheless, with some good observational methods and some statistics, we can try to tease out whether bivalent vaccines in kids worked.
The study combines three prospective cohort studies. The details are in the paper, but what you need to know is that the special sauce of these studies was that the kids were tested for COVID-19 on a weekly basis, whether they had symptoms or not. This is critical because asymptomatic infections can transmit COVID-19.
Let’s do the variables of interest. First and foremost, the bivalent vaccine. Some of these kids got the bivalent vaccine, some didn’t. Other key variables include prior vaccination with the monovalent vaccine. Some had been vaccinated with the monovalent vaccine before, some hadn’t. And, of course, prior infection. Some had been infected before (based on either nasal swabs or blood tests).
Let’s focus first on the primary exposure of interest: getting that bivalent vaccine. Again, this was not randomly assigned; kids who got the bivalent vaccine were different from those who did not. In general, they lived in smaller households, they were more likely to be White, less likely to have had a prior COVID infection, and quite a bit more likely to have at least one chronic condition.
To me, this constellation of factors describes a slightly higher-risk group; it makes sense that they were more likely to get the second vaccine.
Given those factors, what were the rates of COVID infection? After nearly a year of follow-up, around 15% of the kids who hadn’t received the bivalent vaccine got infected compared with 5% of the vaccinated kids. Symptomatic infections represented roughly half of all infections in both groups.
After adjustment for factors that differed between the groups, this difference translated into a vaccine efficacy of about 50% in this population. That’s our first data point. Yes, the bivalent vaccine worked. Not amazingly, of course. But it worked.
What about the kids who had had a prior COVID infection? Somewhat surprisingly, the vaccine was just as effective in this population, despite the fact that their immune systems already had some knowledge of COVID. Ten percent of unvaccinated kids got infected, even though they had been infected before. Just 2.5% of kids who received the bivalent vaccine got infected, suggesting some synergy between prior infection and vaccination.
These data suggest that the bivalent vaccine did reduce the risk for COVID infection in kids. All good. But the piece still missing is how severe these infections were. It doesn’t appear that any of the 426 infections documented in this study resulted in hospitalization or death, fortunately. And no data are presented on the incidence of multisystem inflammatory syndrome of children, though given the rarity, I’d be surprised if any of these kids have this either.
So where are we? Well, it seems that the narrative out there that says “the vaccines don’t work” or “the vaccines don’t work if you’ve already been infected” is probably not true. They do work. This study and others in adults show that. If they work to reduce infections, as this study shows, they will also work to reduce deaths. It’s just that death is fortunately so rare in children that the number needed to vaccinate to prevent one death is very large. In that situation, the decision to vaccinate comes down to the risks associated with vaccination. So far, those risk seem very minimal.
Perhaps falling into a flu-like yearly vaccination schedule is not simply the result of old habits dying hard. Maybe it’s actually not a bad idea.
Dr. F. Perry Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
SARS-CoV-2 a Possible Trigger for Achalasia
TOPLINE:
METHODOLOGY:
- The etiology of achalasia is unclear. Studies have suggested an immune reaction to viral infections, including SARS-CoV-2, as a potential cause.
- Researchers studied four adults who developed achalasia within 5 months of SARS-CoV-2 infection (group 1), six with longstanding achalasia predating SARS-CoV-2 infection (group 2), and two with longstanding achalasia with no known SARS-CoV-2 infection (group 3).
- They tested for the presence of SARS-CoV-2 nucleocapsid (N) and spike (S) proteins, as well as inflammatory markers, in esophageal muscle tissue isolated from the participants.
TAKEAWAY:
- Group 1 patients (confirmed or suspected post–COVID-19 achalasia) had the highest levels of the N protein in all four cases and higher levels of the S protein in the two confirmed cases. No N or S protein was detected in group 3.
- The presence of mRNA for SARS-CoV-2 N protein correlated with a significant increase in the inflammatory markers of NOD-like receptor family pyrin domain-containing 3 and tumor necrosis factor. There were no differences in interleukin 18 in groups 1 and 2.
- The S protein was detected in all muscle tissue samples from group 1. It was also detected in some (but not all) samples from group 2 and to a much lesser degree. The presence of S protein was irrespective of the SARS-CoV-2 vaccination status.
IN PRACTICE:
“Our findings not only show the continued presence of SARS-CoV-2 proteins in esophageal muscle tissue isolated from subjects with achalasia post infection, but they further correlate this with the presence of a sustained inflammatory response,” the authors wrote.
SOURCE:
The study, with first author Salih Samo, MD, MS, Division of Gastroenterology, Hepatology, and Motility, University of Kansas School of Medicine, Kansas City, Kansas, was published online on January 24, 2024, in the American Journal of Gastroenterology.
LIMITATIONS:
The sample size was small, and it was not known which SARS-CoV-2 variant each patient had. The study cannot definitively confirm that SARS-CoV-2 is causative for achalasia.
DISCLOSURES:
The study had no specific funding. Samo reported relationships with Castle Biosciences, Sanofi, Evoke, and EndoGastric Solutions.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The etiology of achalasia is unclear. Studies have suggested an immune reaction to viral infections, including SARS-CoV-2, as a potential cause.
- Researchers studied four adults who developed achalasia within 5 months of SARS-CoV-2 infection (group 1), six with longstanding achalasia predating SARS-CoV-2 infection (group 2), and two with longstanding achalasia with no known SARS-CoV-2 infection (group 3).
- They tested for the presence of SARS-CoV-2 nucleocapsid (N) and spike (S) proteins, as well as inflammatory markers, in esophageal muscle tissue isolated from the participants.
TAKEAWAY:
- Group 1 patients (confirmed or suspected post–COVID-19 achalasia) had the highest levels of the N protein in all four cases and higher levels of the S protein in the two confirmed cases. No N or S protein was detected in group 3.
- The presence of mRNA for SARS-CoV-2 N protein correlated with a significant increase in the inflammatory markers of NOD-like receptor family pyrin domain-containing 3 and tumor necrosis factor. There were no differences in interleukin 18 in groups 1 and 2.
- The S protein was detected in all muscle tissue samples from group 1. It was also detected in some (but not all) samples from group 2 and to a much lesser degree. The presence of S protein was irrespective of the SARS-CoV-2 vaccination status.
IN PRACTICE:
“Our findings not only show the continued presence of SARS-CoV-2 proteins in esophageal muscle tissue isolated from subjects with achalasia post infection, but they further correlate this with the presence of a sustained inflammatory response,” the authors wrote.
SOURCE:
The study, with first author Salih Samo, MD, MS, Division of Gastroenterology, Hepatology, and Motility, University of Kansas School of Medicine, Kansas City, Kansas, was published online on January 24, 2024, in the American Journal of Gastroenterology.
LIMITATIONS:
The sample size was small, and it was not known which SARS-CoV-2 variant each patient had. The study cannot definitively confirm that SARS-CoV-2 is causative for achalasia.
DISCLOSURES:
The study had no specific funding. Samo reported relationships with Castle Biosciences, Sanofi, Evoke, and EndoGastric Solutions.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- The etiology of achalasia is unclear. Studies have suggested an immune reaction to viral infections, including SARS-CoV-2, as a potential cause.
- Researchers studied four adults who developed achalasia within 5 months of SARS-CoV-2 infection (group 1), six with longstanding achalasia predating SARS-CoV-2 infection (group 2), and two with longstanding achalasia with no known SARS-CoV-2 infection (group 3).
- They tested for the presence of SARS-CoV-2 nucleocapsid (N) and spike (S) proteins, as well as inflammatory markers, in esophageal muscle tissue isolated from the participants.
TAKEAWAY:
- Group 1 patients (confirmed or suspected post–COVID-19 achalasia) had the highest levels of the N protein in all four cases and higher levels of the S protein in the two confirmed cases. No N or S protein was detected in group 3.
- The presence of mRNA for SARS-CoV-2 N protein correlated with a significant increase in the inflammatory markers of NOD-like receptor family pyrin domain-containing 3 and tumor necrosis factor. There were no differences in interleukin 18 in groups 1 and 2.
- The S protein was detected in all muscle tissue samples from group 1. It was also detected in some (but not all) samples from group 2 and to a much lesser degree. The presence of S protein was irrespective of the SARS-CoV-2 vaccination status.
IN PRACTICE:
“Our findings not only show the continued presence of SARS-CoV-2 proteins in esophageal muscle tissue isolated from subjects with achalasia post infection, but they further correlate this with the presence of a sustained inflammatory response,” the authors wrote.
SOURCE:
The study, with first author Salih Samo, MD, MS, Division of Gastroenterology, Hepatology, and Motility, University of Kansas School of Medicine, Kansas City, Kansas, was published online on January 24, 2024, in the American Journal of Gastroenterology.
LIMITATIONS:
The sample size was small, and it was not known which SARS-CoV-2 variant each patient had. The study cannot definitively confirm that SARS-CoV-2 is causative for achalasia.
DISCLOSURES:
The study had no specific funding. Samo reported relationships with Castle Biosciences, Sanofi, Evoke, and EndoGastric Solutions.
A version of this article appeared on Medscape.com.
Healthcare Workers Face Increased Risks During the Pandemic
Healthcare workers have been at an increased risk for SARS-CoV-2 infection and mental distress such as anxiety and depression during the pandemic, according to new research.
The risk for infection was higher among healthcare workers in the first two waves of the pandemic and again during the fifth wave.
“Previous publications, including ours, suggested that the main problem was in the early weeks and months of the pandemic, but this paper shows that it continued until the later stages,” senior author Nicola Cherry, MD, an occupational epidemiologist at the University of Alberta in Edmonton, Canada, told this news organization.
The findings were published in the Canadian Journal of Public Health.
Wave Upon Wave
In the current study, the investigators sought to compare the risk for SARS-CoV-2 infection and mental distress among healthcare workers and among community referents (CRs). They examined the following waves of the COVID-19 pandemic:
- Wave 1: From March to June 2020 (4 months).
- Wave 2: From July 2020 to February 2021 (8 months).
- Wave 3: From March to June 2021 (4 months).
- Wave 4: From July to October 2021 (4 months).
- Wave 5 (Omicron): From November 2021 to March 2022 (5 months).
Healthcare workers in Alberta were asked at recruitment for consent to match their individual records to the Alberta Administrative Health Database. As the pandemic progressed, participants were also asked for consent to be linked to COVID-19 immunization records maintained by the provinces, as well as for the results of all polymerase chain reaction (PCR) testing for the SARS-CoV-2 virus.
The investigators matched 2959 healthcare workers to 14,546 CRs according to their age, sex, geographic location in Alberta, and number of physician claims from April 1, 2019, to March 31, 2020.
Incident SARS-CoV-2 infection was examined using PCR testing and the first date of a physician consultation at which the code for SARS-CoV-2 infection had been recorded. Mental health disorders were identified from physician records. They included anxiety disorders, stress and adjustment reactions, and depressive disorders.
Most (79.5%) of the healthcare workers were registered nurses, followed by physicians (16.1%), healthcare aides (2.4%), and licensed practical nurses (2.0%). Most participants (87.5%) were female. The median age at recruitment was 44 years.
Healthcare workers were at a greater risk for COVID-19 overall, with the first SARS-CoV-2 infection defined from either PCR tests (odds ratio [OR], 1.96) or from physician records (OR, 1.33). They were also at an increased risk for anxiety (adjusted OR, 1.25; P < .001), stress/adjustment reaction (adjusted OR, 1.52; P < .001), and depressive condition (adjusted OR, 1.39; P < .001). Moreover, the excess risks for stress/adjustment reactions and depressive conditions increased with successive waves during the pandemic, peaking in the fourth wave and continuing in the fifth wave.
“Although the increase was less in the middle of the phases of the pandemic, it came back with a vengeance during the last phase, which was the Omicron phase,” said Dr. Cherry.
“Employers of healthcare workers can’t assume that everything is now under control, that they know what they’re doing, and that there is no risk. We are now having some increases in COVID. It’s going to go on. The pandemic is not over in that sense, and infection control continues to be major,” she added.
The finding that mental health worsened among healthcare workers was not surprising, Dr. Cherry said. Even before the pandemic, studies had shown that healthcare workers were at a greater risk for depression than the population overall.
“There is a lot of need for care in mental health support of healthcare workers, whether during a pandemic or not,” said Dr. Cherry.
Nurses Are Suffering
Commenting on the research for this news organization, Farinaz Havaei, PhD, RN, assistant professor of nursing at the University of British Columbia in Vancouver, Canada, said, “This is a very important and timely study that draws on objective clinical and administrative data, as opposed to healthcare workers’ subjective reports.” Dr. Havaei did not participate in the research.
Overall, the findings are consistent with previous research that drew upon healthcare workers’ reports. They speak to the chronic and cumulative impact of COVID-19 and its associated stressors on the mental health and well-being of healthcare workers, said Dr. Havaei.
“The likelihood of stress/adjustment reaction and depression showed a relatively steady increase with increasing COVID-19 waves. This increase can likely be explained by healthcare workers’ depleting emotional reserves for coping with chronic workplace stressors such as concerns about exposure to COVID-19, inadequate staffing, and work overload,” she said. Witnessing the suffering and trauma of patients and their families likely added to this risk.
Dr. Havaei also pointed out that most of the study participants were nurses. The findings are consistent with prepandemic research that showed that the suboptimal conditions that nurses increasingly faced resulted in high levels of exhaustion and burnout.
“While I agree with the authors’ call for more mental health support for healthcare workers, I think prevention efforts that address the root cause of the problem should be prioritized,” she said.
From Heroes to Zeros
The same phenomena have been observed in the United States, said John Q. Young, MD, MPP, PhD, professor and chair of psychiatry at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. In various studies, Dr. Young and his colleagues have reported a strong association between exposure to the stressors of the pandemic and subsequent development of depression, anxiety, and posttraumatic stress disorder (PTSD) among healthcare workers.
“The findings from Alberta are remarkably consistent. In the beginning of the pandemic, there was a lot of acknowledgment of the work healthcare workers were doing. The fire department clapping as you leave work at night, being called heroes, even though a lot of healthcare workers feel uncomfortable with the hero language because they don’t feel like heroes. Yes, they’re afraid, but they are going to do what they need to do and help,” he said.
But as the pandemic continued, public sentiment changed, Dr. Young said. “They’ve gone from heroes to zeros. Now we are seeing the accumulated, chronic effects over months and years, and these are significant. Our healthcare workforce is vulnerable now. The reserves are low. There are serious shortages in nursing, with more retirements and more people leaving the field,” he said.
As part of a campaign to help healthcare workers cope, psychiatrists at Northwell Health have started a program called Stress First Aid at their Center for Traumatic Stress Response Resilience, where they train nurses, physicians, and other healthcare staff to use basic tools to recognize and respond to stress and distress in themselves and in their colleagues, said Dr. Young.
“For those healthcare workers who find that they are struggling and need more support, there is resilience coaching, which is one-on-one support. For those who need more clinical attention, there is a clinical program where our healthcare workers can meet with a psychologist, psychiatrist, or a therapist, to work through depression, PTSD, and anxiety. We didn’t have this before the pandemic, but it is now a big focus for our workforce,” he said. “We are trying to build resilience. The trauma is real.”
The study was supported by the College of Physicians and Surgeons of Alberta, the Canadian Institutes of Health Research, and the Canadian Immunology Task Force. Dr. Cherry and Dr. Havaei reported no relevant financial relationships. Dr. Young reported that he is senior vice president of behavioral health at Northwell.
A version of this article appeared on Medscape.com.
Healthcare workers have been at an increased risk for SARS-CoV-2 infection and mental distress such as anxiety and depression during the pandemic, according to new research.
The risk for infection was higher among healthcare workers in the first two waves of the pandemic and again during the fifth wave.
“Previous publications, including ours, suggested that the main problem was in the early weeks and months of the pandemic, but this paper shows that it continued until the later stages,” senior author Nicola Cherry, MD, an occupational epidemiologist at the University of Alberta in Edmonton, Canada, told this news organization.
The findings were published in the Canadian Journal of Public Health.
Wave Upon Wave
In the current study, the investigators sought to compare the risk for SARS-CoV-2 infection and mental distress among healthcare workers and among community referents (CRs). They examined the following waves of the COVID-19 pandemic:
- Wave 1: From March to June 2020 (4 months).
- Wave 2: From July 2020 to February 2021 (8 months).
- Wave 3: From March to June 2021 (4 months).
- Wave 4: From July to October 2021 (4 months).
- Wave 5 (Omicron): From November 2021 to March 2022 (5 months).
Healthcare workers in Alberta were asked at recruitment for consent to match their individual records to the Alberta Administrative Health Database. As the pandemic progressed, participants were also asked for consent to be linked to COVID-19 immunization records maintained by the provinces, as well as for the results of all polymerase chain reaction (PCR) testing for the SARS-CoV-2 virus.
The investigators matched 2959 healthcare workers to 14,546 CRs according to their age, sex, geographic location in Alberta, and number of physician claims from April 1, 2019, to March 31, 2020.
Incident SARS-CoV-2 infection was examined using PCR testing and the first date of a physician consultation at which the code for SARS-CoV-2 infection had been recorded. Mental health disorders were identified from physician records. They included anxiety disorders, stress and adjustment reactions, and depressive disorders.
Most (79.5%) of the healthcare workers were registered nurses, followed by physicians (16.1%), healthcare aides (2.4%), and licensed practical nurses (2.0%). Most participants (87.5%) were female. The median age at recruitment was 44 years.
Healthcare workers were at a greater risk for COVID-19 overall, with the first SARS-CoV-2 infection defined from either PCR tests (odds ratio [OR], 1.96) or from physician records (OR, 1.33). They were also at an increased risk for anxiety (adjusted OR, 1.25; P < .001), stress/adjustment reaction (adjusted OR, 1.52; P < .001), and depressive condition (adjusted OR, 1.39; P < .001). Moreover, the excess risks for stress/adjustment reactions and depressive conditions increased with successive waves during the pandemic, peaking in the fourth wave and continuing in the fifth wave.
“Although the increase was less in the middle of the phases of the pandemic, it came back with a vengeance during the last phase, which was the Omicron phase,” said Dr. Cherry.
“Employers of healthcare workers can’t assume that everything is now under control, that they know what they’re doing, and that there is no risk. We are now having some increases in COVID. It’s going to go on. The pandemic is not over in that sense, and infection control continues to be major,” she added.
The finding that mental health worsened among healthcare workers was not surprising, Dr. Cherry said. Even before the pandemic, studies had shown that healthcare workers were at a greater risk for depression than the population overall.
“There is a lot of need for care in mental health support of healthcare workers, whether during a pandemic or not,” said Dr. Cherry.
Nurses Are Suffering
Commenting on the research for this news organization, Farinaz Havaei, PhD, RN, assistant professor of nursing at the University of British Columbia in Vancouver, Canada, said, “This is a very important and timely study that draws on objective clinical and administrative data, as opposed to healthcare workers’ subjective reports.” Dr. Havaei did not participate in the research.
Overall, the findings are consistent with previous research that drew upon healthcare workers’ reports. They speak to the chronic and cumulative impact of COVID-19 and its associated stressors on the mental health and well-being of healthcare workers, said Dr. Havaei.
“The likelihood of stress/adjustment reaction and depression showed a relatively steady increase with increasing COVID-19 waves. This increase can likely be explained by healthcare workers’ depleting emotional reserves for coping with chronic workplace stressors such as concerns about exposure to COVID-19, inadequate staffing, and work overload,” she said. Witnessing the suffering and trauma of patients and their families likely added to this risk.
Dr. Havaei also pointed out that most of the study participants were nurses. The findings are consistent with prepandemic research that showed that the suboptimal conditions that nurses increasingly faced resulted in high levels of exhaustion and burnout.
“While I agree with the authors’ call for more mental health support for healthcare workers, I think prevention efforts that address the root cause of the problem should be prioritized,” she said.
From Heroes to Zeros
The same phenomena have been observed in the United States, said John Q. Young, MD, MPP, PhD, professor and chair of psychiatry at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. In various studies, Dr. Young and his colleagues have reported a strong association between exposure to the stressors of the pandemic and subsequent development of depression, anxiety, and posttraumatic stress disorder (PTSD) among healthcare workers.
“The findings from Alberta are remarkably consistent. In the beginning of the pandemic, there was a lot of acknowledgment of the work healthcare workers were doing. The fire department clapping as you leave work at night, being called heroes, even though a lot of healthcare workers feel uncomfortable with the hero language because they don’t feel like heroes. Yes, they’re afraid, but they are going to do what they need to do and help,” he said.
But as the pandemic continued, public sentiment changed, Dr. Young said. “They’ve gone from heroes to zeros. Now we are seeing the accumulated, chronic effects over months and years, and these are significant. Our healthcare workforce is vulnerable now. The reserves are low. There are serious shortages in nursing, with more retirements and more people leaving the field,” he said.
As part of a campaign to help healthcare workers cope, psychiatrists at Northwell Health have started a program called Stress First Aid at their Center for Traumatic Stress Response Resilience, where they train nurses, physicians, and other healthcare staff to use basic tools to recognize and respond to stress and distress in themselves and in their colleagues, said Dr. Young.
“For those healthcare workers who find that they are struggling and need more support, there is resilience coaching, which is one-on-one support. For those who need more clinical attention, there is a clinical program where our healthcare workers can meet with a psychologist, psychiatrist, or a therapist, to work through depression, PTSD, and anxiety. We didn’t have this before the pandemic, but it is now a big focus for our workforce,” he said. “We are trying to build resilience. The trauma is real.”
The study was supported by the College of Physicians and Surgeons of Alberta, the Canadian Institutes of Health Research, and the Canadian Immunology Task Force. Dr. Cherry and Dr. Havaei reported no relevant financial relationships. Dr. Young reported that he is senior vice president of behavioral health at Northwell.
A version of this article appeared on Medscape.com.
Healthcare workers have been at an increased risk for SARS-CoV-2 infection and mental distress such as anxiety and depression during the pandemic, according to new research.
The risk for infection was higher among healthcare workers in the first two waves of the pandemic and again during the fifth wave.
“Previous publications, including ours, suggested that the main problem was in the early weeks and months of the pandemic, but this paper shows that it continued until the later stages,” senior author Nicola Cherry, MD, an occupational epidemiologist at the University of Alberta in Edmonton, Canada, told this news organization.
The findings were published in the Canadian Journal of Public Health.
Wave Upon Wave
In the current study, the investigators sought to compare the risk for SARS-CoV-2 infection and mental distress among healthcare workers and among community referents (CRs). They examined the following waves of the COVID-19 pandemic:
- Wave 1: From March to June 2020 (4 months).
- Wave 2: From July 2020 to February 2021 (8 months).
- Wave 3: From March to June 2021 (4 months).
- Wave 4: From July to October 2021 (4 months).
- Wave 5 (Omicron): From November 2021 to March 2022 (5 months).
Healthcare workers in Alberta were asked at recruitment for consent to match their individual records to the Alberta Administrative Health Database. As the pandemic progressed, participants were also asked for consent to be linked to COVID-19 immunization records maintained by the provinces, as well as for the results of all polymerase chain reaction (PCR) testing for the SARS-CoV-2 virus.
The investigators matched 2959 healthcare workers to 14,546 CRs according to their age, sex, geographic location in Alberta, and number of physician claims from April 1, 2019, to March 31, 2020.
Incident SARS-CoV-2 infection was examined using PCR testing and the first date of a physician consultation at which the code for SARS-CoV-2 infection had been recorded. Mental health disorders were identified from physician records. They included anxiety disorders, stress and adjustment reactions, and depressive disorders.
Most (79.5%) of the healthcare workers were registered nurses, followed by physicians (16.1%), healthcare aides (2.4%), and licensed practical nurses (2.0%). Most participants (87.5%) were female. The median age at recruitment was 44 years.
Healthcare workers were at a greater risk for COVID-19 overall, with the first SARS-CoV-2 infection defined from either PCR tests (odds ratio [OR], 1.96) or from physician records (OR, 1.33). They were also at an increased risk for anxiety (adjusted OR, 1.25; P < .001), stress/adjustment reaction (adjusted OR, 1.52; P < .001), and depressive condition (adjusted OR, 1.39; P < .001). Moreover, the excess risks for stress/adjustment reactions and depressive conditions increased with successive waves during the pandemic, peaking in the fourth wave and continuing in the fifth wave.
“Although the increase was less in the middle of the phases of the pandemic, it came back with a vengeance during the last phase, which was the Omicron phase,” said Dr. Cherry.
“Employers of healthcare workers can’t assume that everything is now under control, that they know what they’re doing, and that there is no risk. We are now having some increases in COVID. It’s going to go on. The pandemic is not over in that sense, and infection control continues to be major,” she added.
The finding that mental health worsened among healthcare workers was not surprising, Dr. Cherry said. Even before the pandemic, studies had shown that healthcare workers were at a greater risk for depression than the population overall.
“There is a lot of need for care in mental health support of healthcare workers, whether during a pandemic or not,” said Dr. Cherry.
Nurses Are Suffering
Commenting on the research for this news organization, Farinaz Havaei, PhD, RN, assistant professor of nursing at the University of British Columbia in Vancouver, Canada, said, “This is a very important and timely study that draws on objective clinical and administrative data, as opposed to healthcare workers’ subjective reports.” Dr. Havaei did not participate in the research.
Overall, the findings are consistent with previous research that drew upon healthcare workers’ reports. They speak to the chronic and cumulative impact of COVID-19 and its associated stressors on the mental health and well-being of healthcare workers, said Dr. Havaei.
“The likelihood of stress/adjustment reaction and depression showed a relatively steady increase with increasing COVID-19 waves. This increase can likely be explained by healthcare workers’ depleting emotional reserves for coping with chronic workplace stressors such as concerns about exposure to COVID-19, inadequate staffing, and work overload,” she said. Witnessing the suffering and trauma of patients and their families likely added to this risk.
Dr. Havaei also pointed out that most of the study participants were nurses. The findings are consistent with prepandemic research that showed that the suboptimal conditions that nurses increasingly faced resulted in high levels of exhaustion and burnout.
“While I agree with the authors’ call for more mental health support for healthcare workers, I think prevention efforts that address the root cause of the problem should be prioritized,” she said.
From Heroes to Zeros
The same phenomena have been observed in the United States, said John Q. Young, MD, MPP, PhD, professor and chair of psychiatry at the Donald and Barbara Zucker School of Medicine at Hofstra/Northwell in Hempstead, New York. In various studies, Dr. Young and his colleagues have reported a strong association between exposure to the stressors of the pandemic and subsequent development of depression, anxiety, and posttraumatic stress disorder (PTSD) among healthcare workers.
“The findings from Alberta are remarkably consistent. In the beginning of the pandemic, there was a lot of acknowledgment of the work healthcare workers were doing. The fire department clapping as you leave work at night, being called heroes, even though a lot of healthcare workers feel uncomfortable with the hero language because they don’t feel like heroes. Yes, they’re afraid, but they are going to do what they need to do and help,” he said.
But as the pandemic continued, public sentiment changed, Dr. Young said. “They’ve gone from heroes to zeros. Now we are seeing the accumulated, chronic effects over months and years, and these are significant. Our healthcare workforce is vulnerable now. The reserves are low. There are serious shortages in nursing, with more retirements and more people leaving the field,” he said.
As part of a campaign to help healthcare workers cope, psychiatrists at Northwell Health have started a program called Stress First Aid at their Center for Traumatic Stress Response Resilience, where they train nurses, physicians, and other healthcare staff to use basic tools to recognize and respond to stress and distress in themselves and in their colleagues, said Dr. Young.
“For those healthcare workers who find that they are struggling and need more support, there is resilience coaching, which is one-on-one support. For those who need more clinical attention, there is a clinical program where our healthcare workers can meet with a psychologist, psychiatrist, or a therapist, to work through depression, PTSD, and anxiety. We didn’t have this before the pandemic, but it is now a big focus for our workforce,” he said. “We are trying to build resilience. The trauma is real.”
The study was supported by the College of Physicians and Surgeons of Alberta, the Canadian Institutes of Health Research, and the Canadian Immunology Task Force. Dr. Cherry and Dr. Havaei reported no relevant financial relationships. Dr. Young reported that he is senior vice president of behavioral health at Northwell.
A version of this article appeared on Medscape.com.
FROM THE CANADIAN JOURNAL OF PUBLIC HEALTH
Respiratory Virus Surge: Diagnosing COVID-19 vs RSV, Flu
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
Amid the current wave of winter respiratory virus cases, influenza (types A and B) leads the way with the highest number of emergency room visits, followed closely by COVID-19, thanks to the JN.1 variant, and respiratory syncytial virus (RSV). With various similarities and differences in disease presentations, how challenging is it for physician’s to distinguish between, diagnose, and treat COVID-19 vs RSV and influenza?
While these three respiratory viruses often have similar presentations, you may often find that patients with COVID-19 experience more fever, dry cough, and labored breathing, according to Cyrus Munguti, MD, assistant professor of medicine at KU Medical Center and hospitalist at Wesley Medical Center, Wichita, Kansas.
“COVID-19 patients tend to have trouble breathing because the alveoli are affected and get inflammation and fluid accumulating in the lungs, and they end up having little to no oxygen,” said Dr. Munguti. “When we check their vital signs, patients with COVID tend to have hypoxemia [meaning saturations are less than 88% or 90% depending on the guidelines you follow].”
Patients with RSV and influenza tend to have more upper respiratory symptoms, like runny nose, sternutation — which later can progress to a cough in the upper airways, Dr. Munguti said. Unlike with COVID-19, patients with RSV and influenza — generally until they are very sick — often do not experience hypoxemia.
Inflammation in the airways can form as a result of all three viruses. Furthermore, bacteria that live in these airways could lead to a secondary bacterial infection in the upper respiratory and lower respiratory tracts — which could then cause pneumonia, Dr. Munguti said.
Another note: , according to Panagis Galiatsatos, MD, pulmonologist and associate professor at Johns Hopkins Medicine. “The Alpha through Delta variants really were a lot more lung tissue invading,” Dr. Galiatsatos said. “With the COVID-19 Omicron family — its capabilities are similar to what flu and RSV have done over the years. It’s more airway-invading.”
It’s critical to understand that diagnosing these diseases based on symptoms alone can be quite fickle, according to Dr. Galiatsatos. Objective tests, either at home or in a laboratory, are preferred. This is largely because disease presentation can depend on the host factor that the virus enters into, said Dr. Galiatsatos. For example, virus symptoms may look different for a patient with asthma and for someone with heart disease.
With children being among the most vulnerable for severe respiratory illness, testing and treatment are paramount and can be quite accurate in seasons where respiratory viruses thrive, according to Stan Spinner, MD, chief medical officer at Texas Children’s Pediatrics and Urgent Care. “When individuals are tested for either of these conditions when the prevalence in the community is low, we tend to see false positive results.”
Texas Children’s Pediatrics and Urgent Care’s 12 sites offer COVID-19 and influenza antigen tests that have results ready in around 10 minutes. RSV testing, on the other hand, is limited to around half of the Texas Children’s Pediatrics and none of the urgent care locations, as the test can only be administered through a nasal swab conducted by a physician. As there is no specific treatment or therapy for RSV, the benefits of RSV testing can actually be quite low — often leading to frustrated parents regarding next steps after diagnosis.
“There are a number of respiratory viruses that may present with similar symptoms as RSV, and some of these viruses may even lead to much of the same adverse outcomes as the RSV virus,” Dr. Galiatsatos said. “Consequently, our physicians need to help parents understand this and give them guidance as to when to seek medical attention for worsening symptoms.”
There are two new RSV immunizations to treat certain demographics of patients, Dr. Spinner added. One is an RSV vaccine for infants under 8 months old, though there is limited supply. There is also an RSV vaccine available for pregnant women (between 32 and 36 weeks gestation) that has proved to be effective in fending off RSV infections in newborns up to 6 months old.
Physicians should remain diligent in stressing to patients that vaccinations against COVID-19 and influenza play a key role in keeping their families safe during seasons of staggering respiratory infections.
“These vaccines are extremely safe, and while they may not always prevent infection, these vaccines are extremely effective in preventing more serious consequences, such as hospitalization or death,” Dr. Galiatsatos said.
A version of this article appeared on Medscape.com.
New Insights, New Standards: How 2023 Changed Care for Internists
The past year brought major changes in preventive standards for anxiety, HIV, and RSV along with new guidelines for the treatment of atrial fibrillation. For insight into the effect on internal medicine, we turned to Sarah Candler, MD, MPH, a Houston internist who specializes in the care of high-risk older adults.
Q: Which new prevention guidelines had the most impact on you over the past year?
A: I’m a primary care doctor, and most of the internal medicine updates that are interesting to me focus on how we can keep people from getting sick in the first place. That’s especially important in light of the fact that we had a decrease in life expectancy of 2 years [it finally rose slightly in 2022] and widening of the gender gap in life expectancy for men and women.
I’m excited to see new recommendations from the U.S. Preventive Services Task Force, including a new one about using PREP [pre-exposure prophylaxis] to preventively treat anyone who’s at risk for getting HIV. That’s a big one because it’s one of the first times that we’ve identified at-risk groups for screening based on social risk factors, not gender, age, or genetics.
The new recommendation is PREP for anyone who’s at risk for getting HIV because they have a partner with HIV, had an sexually transmitted infection in the last 6 months, or a history of inconsistent or no condom use with partners with unknown HIV status.
PREP therapy is something that most primary care physicians can either do or learn how to do pretty easily. But the treatment does require maintenance and monitoring.
Q: How firm is this recommendation?
A: The task force gives different grades for their recommendations based on how strong the evidence is. For the guidelines about PREP, they give a grade of A. That means this is top of the class: You should definitely do this.
Q: What are the best strategies to ask patients personal questions about their sex lives in order to evaluate their risk?
A: A lot of internal medicine physicians are getting pretty good at this. We see it as part of our job just the same way as we asked things like, “How often are you walking?” and “Have you been feeling down?”
There’s no one right way to have a conversation like that. But it’s key to say, as I do to my patients, that “I’m not here to judge anything. I am truly here to gather information and make recommendations to you as a partner in your care.”
Q: What other guidelines made an impact in 2023?
A: The U.S. Preventive Services Task Force made a recommendation to screen adults aged 18-64 for anxiety, and this guidance got a B grade. [The task force said there’s not enough evidence to support routine anxiety screening in adults 65 and older.]
The new recommendations is a sign that we’re doing a better job at making treatment of those diseases more acceptable. This is also another example of the medical community recognizing that internal medicine physicians are pretty good at identifying and treating mental health.
Q: How do you figure out whether to treat depression/anxiety yourself or refer patients to specialists?
A: As a primary care physician, I feel comfortable diagnosing and managing some mental health disease in my own practice. There are FDA-approved medications for both anxiety and depression that are easily managed by a primary care physician.
And there’s something to the therapeutic relationship, to naming and identifying these conditions with your patients. Some patients feel a bit of relief just knowing that they have a diagnosis.
Q: What should internists know about the new CDC guidelines that promote discussing RSV vaccines with patients who are over 60?
A: The vaccines are recommended for folks who have underlying conditions like lung disease or heart disease. Those are the ones who end up getting really, really sick. There are two adult vaccines that are available, and there’s not a preference for one over the other.
The vaccines are both protein-based, like the old-school versions of vaccines, not the mRNA vaccines that we’ve all been hearing more about through COVID. Anybody who’s reluctant to take an mRNA vaccine can rest assured that the RSV is not protein-based. And they are single-dose vaccines, which is helpful.
Q: What else should internists know about that was new in 2023?
A: I’m super excited about how cardiologists are thinking about atrial fibrillation. In 2023, the American College of Cardiology and the American Heart Association came up with a giant overhaul of how they look at atrial fibrillation. They classify it in stages and allows us to think about stopping it before it starts.
They’re talking about something they’re calling preclinical or subclinical atrial fibrillation, which you may detect on wearables like somebody’s watch or another tool used to monitor heart rate or exercise. It might be the first harbinger that there’s something wrong with the heart rate, and they may not even have symptoms of it. [A 2023 study in The New England Journal of Medicine linked the anticoagulant apixaban, or Eliquis, to a 37% lower risk of stroke and systemic embolism rates in older patients with subclinical atrial fibrillation but an 80% higher risk of major bleeding vs. aspirin therapy.]
And they’re now recommending early rhythm control.
Q: What does early rhythm control mean for patients and physicians?
A: For the longest time, we have thought about atrial fibrillation treatment in terms of rate control and not worrying too much about the rhythm. But now we recognize that it’s actually really important that we get the rhythm under control because physical changes to the heart can lead to permanent damage.
So now they’re recommending catheter ablation as first-line therapy in some patients as a class 1 recommendation because heart function is already decreased. Improving the ability of the heart to beat with a regular rhythm can lead to improvement of function. This was unheard of even 5 years ago.
Q: Should internists be more willing to refer patients with atrial fibrillation to cardiologists?
A: Yes, I think so. One of the biggest changes for me is that I am going to refer new diagnoses of atrial fibrillation to a cardiologist. And I’m going to ask patients if they have wearable devices because sometimes those things might tell me about something like subclinical atrial fibrillation.
Q: There’s also detailed data about atrial fibrillation risk factors, which include older age, smoking, sedentary lifestyle, alcohol use, diabetes, height, obesity, diabetes, and others. Is this information useful?
A: It’s a really great tool to have in the arsenal because it helps me have shared decision-making conversations with my patients in a way that’s much more convincing. A patient might say, “Why do you care if I drink so much? My liver levels are fine.” And I can say, “It’s going to be a risk factor for having problems with your heart.”
For better or worse, people really take the heart very seriously, I am an internal medicine physician, so I love all the organs equally. But man, people get pretty scared when you tell them something can affect their heart. So when I talk to patients about their risk factors, it’s going to really be helpful that I can remind them of the impact that some of these lifestyle behaviors can have on their heart health.
Dr. Candler has no disclosures.
The past year brought major changes in preventive standards for anxiety, HIV, and RSV along with new guidelines for the treatment of atrial fibrillation. For insight into the effect on internal medicine, we turned to Sarah Candler, MD, MPH, a Houston internist who specializes in the care of high-risk older adults.
Q: Which new prevention guidelines had the most impact on you over the past year?
A: I’m a primary care doctor, and most of the internal medicine updates that are interesting to me focus on how we can keep people from getting sick in the first place. That’s especially important in light of the fact that we had a decrease in life expectancy of 2 years [it finally rose slightly in 2022] and widening of the gender gap in life expectancy for men and women.
I’m excited to see new recommendations from the U.S. Preventive Services Task Force, including a new one about using PREP [pre-exposure prophylaxis] to preventively treat anyone who’s at risk for getting HIV. That’s a big one because it’s one of the first times that we’ve identified at-risk groups for screening based on social risk factors, not gender, age, or genetics.
The new recommendation is PREP for anyone who’s at risk for getting HIV because they have a partner with HIV, had an sexually transmitted infection in the last 6 months, or a history of inconsistent or no condom use with partners with unknown HIV status.
PREP therapy is something that most primary care physicians can either do or learn how to do pretty easily. But the treatment does require maintenance and monitoring.
Q: How firm is this recommendation?
A: The task force gives different grades for their recommendations based on how strong the evidence is. For the guidelines about PREP, they give a grade of A. That means this is top of the class: You should definitely do this.
Q: What are the best strategies to ask patients personal questions about their sex lives in order to evaluate their risk?
A: A lot of internal medicine physicians are getting pretty good at this. We see it as part of our job just the same way as we asked things like, “How often are you walking?” and “Have you been feeling down?”
There’s no one right way to have a conversation like that. But it’s key to say, as I do to my patients, that “I’m not here to judge anything. I am truly here to gather information and make recommendations to you as a partner in your care.”
Q: What other guidelines made an impact in 2023?
A: The U.S. Preventive Services Task Force made a recommendation to screen adults aged 18-64 for anxiety, and this guidance got a B grade. [The task force said there’s not enough evidence to support routine anxiety screening in adults 65 and older.]
The new recommendations is a sign that we’re doing a better job at making treatment of those diseases more acceptable. This is also another example of the medical community recognizing that internal medicine physicians are pretty good at identifying and treating mental health.
Q: How do you figure out whether to treat depression/anxiety yourself or refer patients to specialists?
A: As a primary care physician, I feel comfortable diagnosing and managing some mental health disease in my own practice. There are FDA-approved medications for both anxiety and depression that are easily managed by a primary care physician.
And there’s something to the therapeutic relationship, to naming and identifying these conditions with your patients. Some patients feel a bit of relief just knowing that they have a diagnosis.
Q: What should internists know about the new CDC guidelines that promote discussing RSV vaccines with patients who are over 60?
A: The vaccines are recommended for folks who have underlying conditions like lung disease or heart disease. Those are the ones who end up getting really, really sick. There are two adult vaccines that are available, and there’s not a preference for one over the other.
The vaccines are both protein-based, like the old-school versions of vaccines, not the mRNA vaccines that we’ve all been hearing more about through COVID. Anybody who’s reluctant to take an mRNA vaccine can rest assured that the RSV is not protein-based. And they are single-dose vaccines, which is helpful.
Q: What else should internists know about that was new in 2023?
A: I’m super excited about how cardiologists are thinking about atrial fibrillation. In 2023, the American College of Cardiology and the American Heart Association came up with a giant overhaul of how they look at atrial fibrillation. They classify it in stages and allows us to think about stopping it before it starts.
They’re talking about something they’re calling preclinical or subclinical atrial fibrillation, which you may detect on wearables like somebody’s watch or another tool used to monitor heart rate or exercise. It might be the first harbinger that there’s something wrong with the heart rate, and they may not even have symptoms of it. [A 2023 study in The New England Journal of Medicine linked the anticoagulant apixaban, or Eliquis, to a 37% lower risk of stroke and systemic embolism rates in older patients with subclinical atrial fibrillation but an 80% higher risk of major bleeding vs. aspirin therapy.]
And they’re now recommending early rhythm control.
Q: What does early rhythm control mean for patients and physicians?
A: For the longest time, we have thought about atrial fibrillation treatment in terms of rate control and not worrying too much about the rhythm. But now we recognize that it’s actually really important that we get the rhythm under control because physical changes to the heart can lead to permanent damage.
So now they’re recommending catheter ablation as first-line therapy in some patients as a class 1 recommendation because heart function is already decreased. Improving the ability of the heart to beat with a regular rhythm can lead to improvement of function. This was unheard of even 5 years ago.
Q: Should internists be more willing to refer patients with atrial fibrillation to cardiologists?
A: Yes, I think so. One of the biggest changes for me is that I am going to refer new diagnoses of atrial fibrillation to a cardiologist. And I’m going to ask patients if they have wearable devices because sometimes those things might tell me about something like subclinical atrial fibrillation.
Q: There’s also detailed data about atrial fibrillation risk factors, which include older age, smoking, sedentary lifestyle, alcohol use, diabetes, height, obesity, diabetes, and others. Is this information useful?
A: It’s a really great tool to have in the arsenal because it helps me have shared decision-making conversations with my patients in a way that’s much more convincing. A patient might say, “Why do you care if I drink so much? My liver levels are fine.” And I can say, “It’s going to be a risk factor for having problems with your heart.”
For better or worse, people really take the heart very seriously, I am an internal medicine physician, so I love all the organs equally. But man, people get pretty scared when you tell them something can affect their heart. So when I talk to patients about their risk factors, it’s going to really be helpful that I can remind them of the impact that some of these lifestyle behaviors can have on their heart health.
Dr. Candler has no disclosures.
The past year brought major changes in preventive standards for anxiety, HIV, and RSV along with new guidelines for the treatment of atrial fibrillation. For insight into the effect on internal medicine, we turned to Sarah Candler, MD, MPH, a Houston internist who specializes in the care of high-risk older adults.
Q: Which new prevention guidelines had the most impact on you over the past year?
A: I’m a primary care doctor, and most of the internal medicine updates that are interesting to me focus on how we can keep people from getting sick in the first place. That’s especially important in light of the fact that we had a decrease in life expectancy of 2 years [it finally rose slightly in 2022] and widening of the gender gap in life expectancy for men and women.
I’m excited to see new recommendations from the U.S. Preventive Services Task Force, including a new one about using PREP [pre-exposure prophylaxis] to preventively treat anyone who’s at risk for getting HIV. That’s a big one because it’s one of the first times that we’ve identified at-risk groups for screening based on social risk factors, not gender, age, or genetics.
The new recommendation is PREP for anyone who’s at risk for getting HIV because they have a partner with HIV, had an sexually transmitted infection in the last 6 months, or a history of inconsistent or no condom use with partners with unknown HIV status.
PREP therapy is something that most primary care physicians can either do or learn how to do pretty easily. But the treatment does require maintenance and monitoring.
Q: How firm is this recommendation?
A: The task force gives different grades for their recommendations based on how strong the evidence is. For the guidelines about PREP, they give a grade of A. That means this is top of the class: You should definitely do this.
Q: What are the best strategies to ask patients personal questions about their sex lives in order to evaluate their risk?
A: A lot of internal medicine physicians are getting pretty good at this. We see it as part of our job just the same way as we asked things like, “How often are you walking?” and “Have you been feeling down?”
There’s no one right way to have a conversation like that. But it’s key to say, as I do to my patients, that “I’m not here to judge anything. I am truly here to gather information and make recommendations to you as a partner in your care.”
Q: What other guidelines made an impact in 2023?
A: The U.S. Preventive Services Task Force made a recommendation to screen adults aged 18-64 for anxiety, and this guidance got a B grade. [The task force said there’s not enough evidence to support routine anxiety screening in adults 65 and older.]
The new recommendations is a sign that we’re doing a better job at making treatment of those diseases more acceptable. This is also another example of the medical community recognizing that internal medicine physicians are pretty good at identifying and treating mental health.
Q: How do you figure out whether to treat depression/anxiety yourself or refer patients to specialists?
A: As a primary care physician, I feel comfortable diagnosing and managing some mental health disease in my own practice. There are FDA-approved medications for both anxiety and depression that are easily managed by a primary care physician.
And there’s something to the therapeutic relationship, to naming and identifying these conditions with your patients. Some patients feel a bit of relief just knowing that they have a diagnosis.
Q: What should internists know about the new CDC guidelines that promote discussing RSV vaccines with patients who are over 60?
A: The vaccines are recommended for folks who have underlying conditions like lung disease or heart disease. Those are the ones who end up getting really, really sick. There are two adult vaccines that are available, and there’s not a preference for one over the other.
The vaccines are both protein-based, like the old-school versions of vaccines, not the mRNA vaccines that we’ve all been hearing more about through COVID. Anybody who’s reluctant to take an mRNA vaccine can rest assured that the RSV is not protein-based. And they are single-dose vaccines, which is helpful.
Q: What else should internists know about that was new in 2023?
A: I’m super excited about how cardiologists are thinking about atrial fibrillation. In 2023, the American College of Cardiology and the American Heart Association came up with a giant overhaul of how they look at atrial fibrillation. They classify it in stages and allows us to think about stopping it before it starts.
They’re talking about something they’re calling preclinical or subclinical atrial fibrillation, which you may detect on wearables like somebody’s watch or another tool used to monitor heart rate or exercise. It might be the first harbinger that there’s something wrong with the heart rate, and they may not even have symptoms of it. [A 2023 study in The New England Journal of Medicine linked the anticoagulant apixaban, or Eliquis, to a 37% lower risk of stroke and systemic embolism rates in older patients with subclinical atrial fibrillation but an 80% higher risk of major bleeding vs. aspirin therapy.]
And they’re now recommending early rhythm control.
Q: What does early rhythm control mean for patients and physicians?
A: For the longest time, we have thought about atrial fibrillation treatment in terms of rate control and not worrying too much about the rhythm. But now we recognize that it’s actually really important that we get the rhythm under control because physical changes to the heart can lead to permanent damage.
So now they’re recommending catheter ablation as first-line therapy in some patients as a class 1 recommendation because heart function is already decreased. Improving the ability of the heart to beat with a regular rhythm can lead to improvement of function. This was unheard of even 5 years ago.
Q: Should internists be more willing to refer patients with atrial fibrillation to cardiologists?
A: Yes, I think so. One of the biggest changes for me is that I am going to refer new diagnoses of atrial fibrillation to a cardiologist. And I’m going to ask patients if they have wearable devices because sometimes those things might tell me about something like subclinical atrial fibrillation.
Q: There’s also detailed data about atrial fibrillation risk factors, which include older age, smoking, sedentary lifestyle, alcohol use, diabetes, height, obesity, diabetes, and others. Is this information useful?
A: It’s a really great tool to have in the arsenal because it helps me have shared decision-making conversations with my patients in a way that’s much more convincing. A patient might say, “Why do you care if I drink so much? My liver levels are fine.” And I can say, “It’s going to be a risk factor for having problems with your heart.”
For better or worse, people really take the heart very seriously, I am an internal medicine physician, so I love all the organs equally. But man, people get pretty scared when you tell them something can affect their heart. So when I talk to patients about their risk factors, it’s going to really be helpful that I can remind them of the impact that some of these lifestyle behaviors can have on their heart health.
Dr. Candler has no disclosures.