User login
Treatment of Melasma Using Tranexamic Acid: What’s Known and What’s Next
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
Tranexamic acid is a synthetic lysine derivative that inhibits plasminogen activation by blocking lysine-binding sites on the plasminogen molecule. Although the US Food and Drug Administration–approved indications for tranexamic acid include treatment of patients with menorrhagia and reduction or prevention of hemorrhage in patients with hemophilia undergoing tooth extraction, the potential efficacy of tranexamic acid in the treatment of melasma has been consistently reported since the 1980s.1
Tranexamic acid exerts effects on pigmentation via its inhibitory effects on UV light–induced plasminogen activator and plasmin activity.2 UV radiation induces the synthesis of plasminogen activator by keratinocytes, which results in increased conversion of plasminogen to plasmin. Plasminogen activator induces tyrosinase activity, resulting in increased melanin synthesis. The presence of plasmin results in increased production of both arachidonic acid and fibroblast growth factor, which stimulate melanogenesis and neovascularization, respectively.3 By inhibiting plasminogen activation, tranexamic acid mitigates UV radiation–induced melanogenesis and neovascularization. In treated guinea pig skin, application of topical tranexamic acid following UV radiation exposure inhibited the development of expected skin hyperpigmentation and also reduced tyrosinase activity.4,5
The largest study on the use of oral tranexamic acid for treatment of melasma was a retrospective chart review of 561 melasma patients treated with tranexamic acid at a single center in Singapore.6 More than 90% of patients received prior treatment of their melasma, including bleaching creams and energy-based treatment. Among patients who received oral tranexamic acid over a 4-month period, 90% of patients demonstrated improvement in their melasma severity. Side effects were experienced by 7% of patients; the most common side effects were abdominal bloating and pain (experienced by 2% of patients). Notably, 1 patient developed deep vein thrombosis during treatment and subsequently was found to have protein S deficiency.6
Although the daily doses of tranexamic acid for the treatment of menorrhagia and perioperative hemophilia patients are 3900 mg and 30 to 40 mg/kg, respectively, effective daily doses reported for the treatment of melasma have ranged from the initial report of efficacy at 750 to 1500 mg to subsequent reports of improvement at daily doses of 500 mg.1,2,6-8
Challenges to the use of tranexamic acid for melasma treatment in the United States include the medicolegal environment, specifically the risks associated with using a systemic procoagulant medication for a cosmetic indication. Patients should be screened and counseled on the risks of developing deep vein thrombosis and pulmonary embolism prior to initiating treatment. Cost and accessibility also may limit the use of tranexamic acid in the United States. Tranexamic acid is available for off-label use in the United States with a prescription in the form of 650-mg tablets that can be split by patients to approximate twice-daily 325 mg dosing. This cosmetic indication poses an out-of-pocket cost to patients of over $110 per month or as low as $48 per month with a coupon at the time of publication.9
Given the potential for serious adverse effects with the use of systemic tranexamic acid, there has been interest in formulating and evaluating topical tranexamic acid for cosmetic indications.10-13 Topical tranexamic acid has been used alone and in conjunction with modalities to increase uptake, including intradermal injection, microneedling, and fractionated CO2 laser.12-14 Although these reports show initial promise, the currently available data are limited by small sample sizes, short treatment durations, lack of dose comparisons, and lack of short-term or long-term follow-up data. In addition to addressing these knowledge gaps in our understanding of topical tranexamic acid as a treatment option for melasma, further studies on the minimum systemic dose may address the downside of cost and potential for complications that may limit use of this medication in the United States.
The potential uses for tranexamic acid extend to the treatment of postinflammatory hyperpigmentation and rosacea. Melanocytes cultured in media conditioned by fractionated CO2 laser–treated keratinocytes were found to have decreased tyrosinase activity and reduced melanin content when treated with tranexamic acid, suggesting the potential role for tranexamic acid to be used postprocedurally to reduce the risk for postinflammatory hyperpigmentation in prone skin types.15 Oral and topical tranexamic acid also have been reported to improve the appearance of erythematotelangiectatic rosacea, potentially relating to the inhibitory effects of tranexamic acid on neovascularization.3,16,17 Although larger-scale controlled studies are required for further investigation of tranexamic acid for these indications, it has shown early promise as an adjunctive treatment for several dermatologic disorders, including melasma, and warrants further characterization as a potential therapeutic option.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res. 1988;30:676-680.
- Tse TW, Hui E. Tranexamic acid: an important adjuvant in the treatment of melasma. J Cosmet Dermatol. 2013;12:57-66.
- Sundbeck A, Karlsson L, Lilja J, et al. Inhibition of tumour vascularization by tranexamic acid. experimental studies on possible mechanisms. Anticancer Res. 1981;1:299-304.
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B. 1998;47:136-141.
- Li D, Shi Y, Li M, et al. Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs. Eur J Dermatol. 2010;20:289-292.
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol. 2016;75:385-392.
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781.
- Perper M, Eber AE, Fayne R, et al. Tranexamic acid in the treatment of melasma: a review of the literature. Am J Clin Dermatol. 2017;18:373-381.
- Tranexamic acid. GoodRx website. https://www.goodrx.com/tranexamic-acid. Accessed February 2, 2018.
- Kim SJ, Park JY, Shibata T, et al. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol. 2016;41:480-485.
- Ebrahimi B, Naeini FF. Topical tranexamic acid as a promising treatment for melasma. J Res Med Sci. 2014;19:753-757.
- Xu Y, Ma R, Juliandri J, et al. Efficacy of functional microarray of microneedles combined with topical tranexamic acid for melasma: a randomized, self-controlled, split-face study. Medicine (Baltimore). 2017;96(19):e6897.
- Hsiao CY, Sung HC, Hu S, et al. Fractional CO2 laser treatment to enhance skin permeation of tranexamic acid with minimal skin disruption. Dermatology (Basel). 2015;230:269-275.
- Saki N, Darayesh M, Heiran A. Comparing the efficacy of topical hydroquinone 2% versus intradermal tranexamic acid microinjections in treating melasma: a split-face controlled trial [published online November 9, 2017]. J Dermatolog Treat. doi:10.1080/09546634.2017.1392476.
- Kim MS, Bang SH, Kim JH, et al. Tranexamic acid diminishes laser-induced melanogenesis. Ann Dermatol. 2015;27:250-256.
- Kim MS, Chang SE, Haw S, et al. Tranexamic acid solution soaking is an excellent approach for rosacea patients: a preliminary observation in six patients. J Dermatol. 2013;40:70-71.
- Kwon HJ, Suh JH, Ko EJ, et al. Combination treatment of propranolol, minocycline, and tranexamic acid for effective control of rosacea [published online November 26, 2017]. Dermatol Ther. doi:10.1111/dth.12439.
Resident Pearl
- Oral tranexamic acid is an antifibrinolytic agent that can be used off-label for the treatment of melasma.

Late-breaking research presented at AAD on Saturday February 17
Dermatology News will be on site later this week at the annual meeting of the American Academy of Dermatology in San Diego. Look for the latest news and video interviews from the meeting in medical, surgical, and aesthetic dermatology at edermatologynews.com starting Friday February 16.
Coverage will include the late-breaker sessions, which will be presented on Saturday February 17.

Check out another late-breaking session – on basic science, cutaneous oncology, and pathology – which will include presentations on the growing burden of melanoma, the incidence of Merkel cell carcinoma in the United States, and the inverse genetic risk between vitiligo and cutaneous melanoma.
Find out more about these and other sessions at the official 2018 AAD Annual Meeting’s page.
Dermatology News will be on site later this week at the annual meeting of the American Academy of Dermatology in San Diego. Look for the latest news and video interviews from the meeting in medical, surgical, and aesthetic dermatology at edermatologynews.com starting Friday February 16.
Coverage will include the late-breaker sessions, which will be presented on Saturday February 17.
Check out another late-breaking session – on basic science, cutaneous oncology, and pathology – which will include presentations on the growing burden of melanoma, the incidence of Merkel cell carcinoma in the United States, and the inverse genetic risk between vitiligo and cutaneous melanoma.
Find out more about these and other sessions at the official 2018 AAD Annual Meeting’s page.
Dermatology News will be on site later this week at the annual meeting of the American Academy of Dermatology in San Diego. Look for the latest news and video interviews from the meeting in medical, surgical, and aesthetic dermatology at edermatologynews.com starting Friday February 16.
Coverage will include the late-breaker sessions, which will be presented on Saturday February 17.
Check out another late-breaking session – on basic science, cutaneous oncology, and pathology – which will include presentations on the growing burden of melanoma, the incidence of Merkel cell carcinoma in the United States, and the inverse genetic risk between vitiligo and cutaneous melanoma.
Find out more about these and other sessions at the official 2018 AAD Annual Meeting’s page.
Pearls in Dermatology: 2017
The Pearls in Dermatology collection consists of our popular pearls from the year in one convenient file. Topics include:
- Nail psoriasis and psoriasis on the hands and feet
- Genital wart treatment
- Isotretinoin for acne
- Cosmeceuticals for rosacea
- Surgical technique with the flexible scalpel blade
Editor’s Commentary provided by Vincent A. DeLeo, MD, Editor-in-Chief, Cutis.
Save this collection, print it, and/or share it with your colleagues. We hope this comprehensive collection will positively impact how you manage patients.

The Pearls in Dermatology collection consists of our popular pearls from the year in one convenient file. Topics include:
- Nail psoriasis and psoriasis on the hands and feet
- Genital wart treatment
- Isotretinoin for acne
- Cosmeceuticals for rosacea
- Surgical technique with the flexible scalpel blade
Editor’s Commentary provided by Vincent A. DeLeo, MD, Editor-in-Chief, Cutis.
Save this collection, print it, and/or share it with your colleagues. We hope this comprehensive collection will positively impact how you manage patients.
The Pearls in Dermatology collection consists of our popular pearls from the year in one convenient file. Topics include:
- Nail psoriasis and psoriasis on the hands and feet
- Genital wart treatment
- Isotretinoin for acne
- Cosmeceuticals for rosacea
- Surgical technique with the flexible scalpel blade
Editor’s Commentary provided by Vincent A. DeLeo, MD, Editor-in-Chief, Cutis.
Save this collection, print it, and/or share it with your colleagues. We hope this comprehensive collection will positively impact how you manage patients.
Obesity an independent risk factor for rosacea in cohort study of U.S. women
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
Obesity was associated with a significantly higher risk of rosacea, compared with a healthy weight, particularly when the weight was gained after age 18 years, according to an analysis of data from the Nurses Health Study II.
Investigators evaluated data on 89,886 women in the U.S. study from 1991 through 2005 – 5,249 diagnosed with rosacea – over 14 years to determine what, if any, relationship existed between body mass index (BMI) and rosacea risk.
As BMI increased, the risk of rosacea increased: Compared with participants with a BMI of 21.0 to 22.9 kg/m2 (considered a healthy weight), the risk of rosacea for those with a BMI of 25.0-29.9 (overweight) was 11% greater (95% confidence interval, 1.02-1.21), and among those with a BMI of 30.0-34.9, was 21% greater (95% CI, 1.09-1.34). The risk was 48% greater among those with a BMI of 35 or above (95% CI, 1.33-1.64). (A BMI over 30 is considered obese). The results were published in the December issue of the Journal of the American Academy of Dermatology.
The association between weight and rosacea risk was only significant after age 18 years, when the risk of rosacea increased 4% for every 10 pounds of weight gain, even after adjusting for BMI.
The investigators also found a significant relationship between waist circumference and rosacea risk that was independent of BMI, with the highest quintile of waist circumference associated with a 32% greater risk of rosacea, compared with the lowest quintile. Similarly, the highest quintile of hip circumference was associated with a 38% higher risk of rosacea, also independent of BMI. However there was no association between waist-to-hip ratio and rosacea risk.
While there were associations between the risk of rosacea and smoking, alcohol intake, and physical activity, the relationship between BMI and rosacea risk was not modified by these other risk factors.
Suyun Li, PhD, of the Guangzhou (China) Medical University School of Public Health and coauthors from the department of dermatology, Brown University, Providence, R.I.; and Brigham and Women’s Hospital, Boston, wrote that previous epidemiologic studies examining the interaction between obesity and rosacea have shown inconsistent results. Longitudinal studies on the issue had focused only on BMI and ignored other measures of central obesity.
“To our knowledge, this is the first cohort study on the association between obesity and risk for incident rosacea,” they wrote. “The study contributes to the understanding of rosacea etiology and informs clinical practice related to rosacea prevention and patient care.”
They suggested a number of different mechanisms that might explain how obesity increases the risk of rosacea, including the chronic, low-grade inflammatory state associated with obesity. “Adiposity can augment proinflammatory cytokine expression, such as interleukin 6 and tumor necrosis factor–alpha, both relevant to rosacea pathophysiology,” they noted. “Vascular changes associated with obesity might be another mechanism, considering obesity can lead to abnormalities of vascular function and structure, which might lead to the vasodilatation in rosacea.”
In the NHS II study, data are collected every 2 years, which the authors said ensured they had the most up-to-date information. While rosacea diagnoses relied on self-report, the authors said the study participants – nurses – were likely to have a high validity of self-reporting of rosacea. They acknowledged, however, that the lack of information on rosacea subtypes was a limitation of the study.
The study was supported by the department of dermatology, Brown University and a Nurses’ Health Study II grant. Dr. Li was supported by a research grant from the National Rosacea Society and the Dermatology Foundation. Another author declared having served as an investigator and receiving research funds from Sanofi and Regeneron; serving as a consultant for Sanofi and RTI Health Solutions, and having received honoraria from Astellas Canada, Prime, and Spire Learning. The remaining three authors had no disclosures.
SOURCE: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
FROM JAAD
Key clinical point: independent of other risk factors such as smoking and alcohol intake.
Major finding: A BMI greater than 35 is associated with a 48% higher risk of rosacea, compared with a BMI of 21.
Data source: Information on rosacea diagnoses among 89,886 Nurses’ Health Study II participants.
Disclosures: The study was supported by the Warren Alpert Medical School of Brown University and a Nurses’ Health Study II grant. One author was supported by a research grant from the National Rosacea Society and the Dermatology Foundation; another author declared research funding, consultancies, and honoraria from the pharmaceutical industry.
Source: Li S et al. J Am Acad Dermatol. 2017 Dec;77(6):1083-7.E5.
Rare epidermotropic MZL yields to rituximab
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
Epidermotropic marginal zone lymphoma (MZL), a rare cutaneous B-cell lymphoma identified in only eight patients to date, appears to be responsive to rituximab, according to authors of a case report.
A 69-year-old man who presented with a generalized papulosquamous eruption that was eventually diagnosed as epidermotropic MZL achieved a near total remission within 3 months of receiving four total weekly rituximab infusions, reported Cynthia M. Magro, MD, from Cornell University, New York, and her colleagues from the University of Arizona, Tucson (JAAD Case Rep. 2017 Sep 23;3[6]:474-6).
“Epidermotropic MZL represents a distinctive nosologic B-cell lymphoma that should be considered a diagnostic possibility in older men who present with an unexplained papulosquamous eruption resembling pityriasis rosea,” the researchers wrote.
“Epidermotropism refers to a state of abnormal colonization of the epidermis by leukocytes, which often reflects a clonal T-cell or monocyte dyscrasia. Epidermotropism is a distinctive pattern of passive migration into epithelial structures that is not otherwise attributable to the normal function of innate and adaptive immunity,” the researchers explained.
They described the case of the aforementioned patient, who presented with asymptomatic indurated, red-to-brown papules and plaques on his chest, abdomen, back, and buttocks, which gave the clinical impression of pityriasis rosea or a similarly appearing drug reaction.
Histopathologic examination of two biopsied lesions “demonstrated a dense superficial lymphocytic infiltrate that expanded and effaced the papillary and superficial reticular dermis.”
After epidermotropic MZL was diagnosed, the patient was evaluated for systemic disease with a bone marrow biopsy, which revealed a low-grade B-cell lymphoproliferative disorder, and with a PET scan showing lymphomatous infiltration of the spleen. The patient was treated with four weekly infusions of rituximab 375 mg/m2.
“Within 3 months, he experienced marked regression of his cutaneous disease. Repeat radiographic imaging found an interval decrease in the size of his spleen, signifying an objective response. Since achieving near total clinical remission, the patient remains under the close observation of medical oncology services,” the researchers wrote.
The investigators noted that if histopathology is the only method used to diagnosis the condition, epidermotropic MZL could be mistaken for a T-cell lymphoproliferative disorder, such as mycosis fungoides, because of the similar architecture at low resolution.
“In these settings, immunohistochemical staining for B-cell markers represents an indispensable diagnostic test,” they wrote.
The researchers reported having no conflicts of interest.
FROM JAAD CASE REPORTS
Key clinical point: Epidermotropic marginal zone lymphoma, a very rare B-cell disorder, can be effectively treated with rituximab.
Major finding: A patient with epidermotropic MZL had a near complete response to rituximab within 3 months.
Data source: Case study of a 69-year-old man presenting with an otherwise asymptomatic diffuse dermatologic eruption.
Disclosures: The researchers reported no conflicts of interest.
Recommending efficacious cleansers for your patients
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates

Reference
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates
Reference
Cleansing is one of the most important steps in any skin care routine, but the surfeit of products on the market can lead to patients selecting an inappropriate cleanser for their skin type. This can engender various adverse cutaneous effects, including xerosis, flaking, acne, and flare-ups of chronic skin conditions such as eczema and rosacea. For example, acne medications are better tolerated when the proper cleanser is used. Cleanser choice is particularly important for individuals with dry skin who have an impaired barrier and those with sensitive skin who are susceptible to inflammation. The following discussion focuses on the factors that practitioners should address with patients when recommending cleansing products to help them maximize their outcomes and maintain clear, healthy-looking skin.
TYPES OF CLEANSERS
Foaming agents
Anionic surface acting agents (surfactants or detergents) produce foam and display the greatest cleansing potency. (Table 1). Because these detergents remove lipids from the skin’s surface and protective bilayer membrane barrier, they should only be used only by individuals with increased sebum production. Ingredients in this category injure the skin barrier and make the skin more susceptible to irritant reactions.1 For example, the widely used compound sodium lauryl sulfate (SLS), which strips lipids from the skin, irritates the skin to such an extent that it is used in research labs to hinder the skin barrier to test “barrier repair products.” The “sulfate- free” trend originates from the irritation caused by SLS. The barrier disruption caused by SLS can be used to intentionally damage the skin barrier to allow increased penetration of chemical peeling products and other therapeutic agents. An alternative to SLS is sodium laureth sulfate (or sodium lauryl ether sulfate, also known as SLES), which exhibits foaming attributes but is less likely than SLS to cause irritation. We often use a foaming cleanser in our practice prior to injectable procedures to ensure that makeup and debris are removed from the skin, and to decrease the time needed for topical lidocaine to penetrate into the skin. If you adopt this strategy, you should follow the injectable procedure with a barrier repair moisturizer.
Nonfoaming agents
These agents were developed through efforts to reduce detergent irritancy. This class of cleansers includes superfatted soaps, combination bars (“combars”), syndet bars (composed of synthetic surfactants) and compounds that deposit lipids on the skin, such as creams, lotions and oils. Cream, milk, cold creams, and oil cleansers fall into this category. These products usually have a neutral pH, and include ingredients such as alkyl glyceryl, ether sulfonate, alpha olefin sulfonates, betaines, sulfosuccinates, sodium cocoyl monoglyceride sulfate, and sodium cocoyl isethionate. Organic nonfoaming agents are also available, and may include saponins, a large family of structurally related compounds derived from plant, and sucrose laurate. Nonfoaming cleansers are most appropriate for dry skin types. Oily skin types often report that they “do not feel clean” when they use these cleansers.
Hydroxy acid cleansers
Alpha hydroxy acids (AHAs) are well suited for use by individuals with dry skin because hydroxy acids act as humectants (water-soluble materials with high water absorption capabilities). These hydrophilic cleansers provide exfoliation, and are appropriate for individuals with dry skin and acne because their low pH contributes to an inhospitable microbiome for Propionibacterium acnes, making it harder for the bacteria to thrive. Importantly, the exfoliating activity imparted by hydroxy acids sets the stage for better penetration into the stratum corneum by ingredients applied subsequent to the cleanser. Alpha hydroxy acid cleansers do not dry out the skin the way that salicylic acid cleansers do because their hydrophilic nature makes them unable to penetrate through sebum.
Salicylic acid (SA) cleansers are a member of the aspirin family and therefore confer anti-inflammatory properties. Salicylic acid is lipophilic and can penetrate through the sebum derived lipids into pores. They are the most effective cleansers to unclog pores. Therefore, SA cleansers are ideal for use by individuals with oily, sensitive skin prone to acne, seborrheic dermatitis, or rosacea. The exfoliation yielded by salicylic acid also enhances skin barrier penetration by ingredients applied after its use and is well tolerated by individuals with oily skin. Dry skin types, especially those on retinoids and benzoyl peroxide, will not tolerate SA as well as they will AHA cleansers.
Antibacterial cleansers
Antibacterial cleansers contain ingredients that reduce P. acnes and other types of bacteria on the skin. These products include benzoyl peroxide (BP), silver, hypochlorous acid, and sodium hypochlorite. Benzoyl peroxide can be highly irritating and is not well tolerated by patients with dry skin. Silver has a long history, having been used as an antibacterial agent since the times of King Herod. On the other hand, hypochlorous acid and sodium hypochlorite are novel entrants in the cleansing realm, particularly for individuals with acne. In fact, sodium hypochlorite is formulated to be mild enough for daily use while still sufficiently effective for acne-prone skin.
CLEANSER CHOICE BY SKIN ISSUE
Acne
Recommending the right cleanser for acne-prone skin first depends on whether the patient has oily or dry skin. Individuals with dry skin and acne cannot tolerate drying acne medications. Choosing the correct cleanser and moisturizer can help acne patients be more compliant with the acne treatment plan because of fewer side effects. Dry skin acne types often need two different cleansers. For the morning cleanser, AHA cleansers such as glycolic acid are effective at managing dry. acne-prone skin because glycolic acid has a relatively low pH. P. acnes is less likely to grow on skin with a lower pH.
Hydroxy acids help prevent clogged pores and exfoliate dead skin, which helps prevent acne comedones. Glycolic acid also serves as a humectant ingredient. Creamy cleansers should be used once daily, preferably at night for patients who use makeup since these products are effective at makeup removal. Foaming cleansers should never be used on dry, acne-prone skin. Individuals with the acne subtype of sensitive skin should avoid using scrubs, loofahs, and other forms of mechanical exfoliation.
Patients with oily skin and acne are easier to treat than are dry types because they can better tolerate acne medications. I recommend a salicylic acid cleanser in the morning to unclog pores. The anti-inflammatory properties of salicylic acid help prevent the formation of papules and pustules that characterize acne. Twice-daily use of salicylic acid by patients with oily skin and acne may feel too drying when combined with acne medications such as a retinoid and benzoyl peroxide. If this is the case, a foaming cleanser can be used in the evening to remove dirt, makeup, sunscreen, and debris that can clog pores and exacerbate acne.
Rosacea
Most dry skin type rosacea patients flush red when they wash their face, even if they only use water. The friction alone is enough to cause them to react. Rosacea patients can skip the morning cleanse to help reduce this skin irritation and flushing. Instead they should apply their a.m. anti-redness products followed by a sunscreen appropriate for their skin type. In the evening, a soothing, nonfoaming cleanser with anti-inflammatory ingredients is the best choice to remove makeup, sunscreen, and any built-up dirt or bacteria from the skin’s surface. This should be followed by an anti-redness product that targets the inflammation caused by rosacea.
Anti-inflammatory ingredients that can be found in soothing cleansers and moisturizers for rosacea prone skin include argan oil, green tea, feverfew, chamomile, licorice extract, and aloe.
Patients with very oily skin who have rosacea need to cleanse twice daily to remove excess oil to prevent comedones and acne lesions. A foaming cleanser that contains anti-inflammatory ingredients such as green tea, feverfew, licorice extract, aloe, niacinamide, green tea, and salicylic acid are a good choice for oily rosacea prone skin types.
All rosacea patients should be counseled to avoid mechanical exfoliation, including cleansing scrubs, chemical exfoliants, and abrasive loofahs or cloths.
Eczema
Patients with eczema should choose the same nonfoaming cleansers recommended for dry skin. For patients with frequent skin infections, hypochlorite and silver are beneficial ingredients found in cleansers to help decrease skin bacteria and prevent infections. Foaming cleansers should never be used in eczema prone types.
Conclusion
Cleansers play an important role in skin care because they affect the skin barrier, pH of the skin, presence of bacteria, condition of the pores, and penetration of the post cleanser–applied ingredients. Knowing which cleansing product to use based on a patient’s skin type is critical to recommending the proper ingredients so that patients can achieve and maintain healthy skin.
Table 1. Ingredients used in foaming cleansers
Acyl glycinates
Acylglutamates
Alkyl acyl isethionates
Alkyl carboxylates
Alkyl ether sulfates
Alkyl ethoxy sulfates
Alkyl phosphates
Alkyl sulfates
Alkyl sulfonates
Alkyl sulfosuccinates
Alkyl taurates
Reference
New standard classification, pathophysiology of rosacea announced
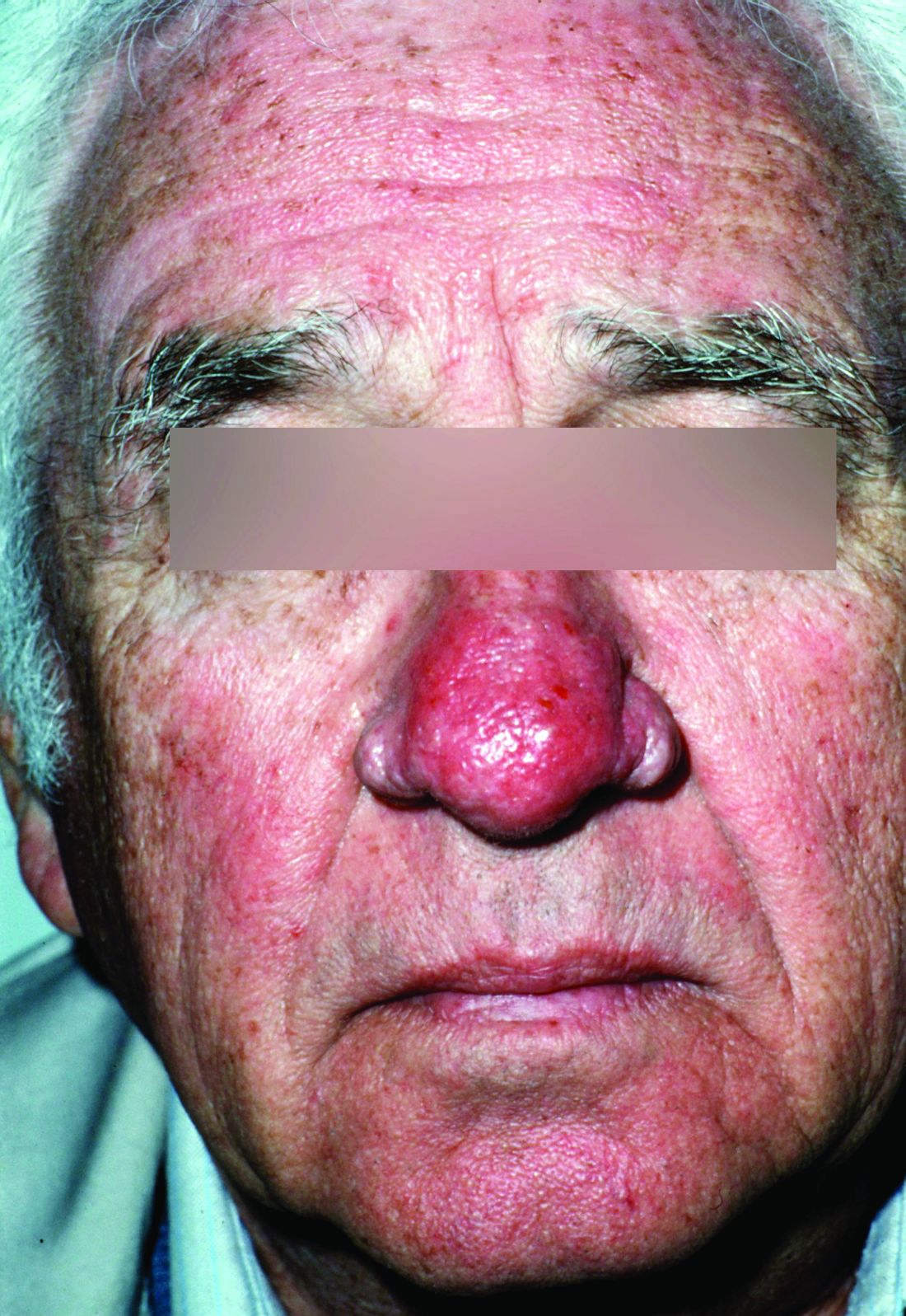
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).

Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
Rosacea’s phenotypes may occur in different combinations and at different times, but all are considered to be “manifestations of the same underlying inflammatory continuum,” the expert panel wrote (J Am Acad Dermatol. 2017. doi: 10.1016/j.jaad.2017.08.037).
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY

VIDEO: Rosacea patients no longer considered in ‘buckets’
LAS VEGAS – Clinicians are starting to see and treat rosacea differently, Julie Harper, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
“For a long time, we thought about putting rosacea patients into buckets,” based on the predominant type of rosacea they had, such as papulopustular, ocular, or erythematotelangiectatic rosacea, but “what we find is that people have pieces and parts of all of those,” she commented.
In the interview, Dr. Harper, a dermatologist in private practice in Birmingham, Ala., emphasized the importance of directing treatment to all aspects of an individual patient’s rosacea, using combinations of treatments that are approved by the Food and Drug Administration, “or at least proven to be effective for these different parts” of the disease. “That’s something that’s really new in our thinking,” she said.
Dr. Harper disclosed relationships with multiple companies including Allergan, Bayer, Galderma, La Roche-Posay, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Clinicians are starting to see and treat rosacea differently, Julie Harper, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
“For a long time, we thought about putting rosacea patients into buckets,” based on the predominant type of rosacea they had, such as papulopustular, ocular, or erythematotelangiectatic rosacea, but “what we find is that people have pieces and parts of all of those,” she commented.
In the interview, Dr. Harper, a dermatologist in private practice in Birmingham, Ala., emphasized the importance of directing treatment to all aspects of an individual patient’s rosacea, using combinations of treatments that are approved by the Food and Drug Administration, “or at least proven to be effective for these different parts” of the disease. “That’s something that’s really new in our thinking,” she said.
Dr. Harper disclosed relationships with multiple companies including Allergan, Bayer, Galderma, La Roche-Posay, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
LAS VEGAS – Clinicians are starting to see and treat rosacea differently, Julie Harper, MD, said in a video interview at Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
“For a long time, we thought about putting rosacea patients into buckets,” based on the predominant type of rosacea they had, such as papulopustular, ocular, or erythematotelangiectatic rosacea, but “what we find is that people have pieces and parts of all of those,” she commented.
In the interview, Dr. Harper, a dermatologist in private practice in Birmingham, Ala., emphasized the importance of directing treatment to all aspects of an individual patient’s rosacea, using combinations of treatments that are approved by the Food and Drug Administration, “or at least proven to be effective for these different parts” of the disease. “That’s something that’s really new in our thinking,” she said.
Dr. Harper disclosed relationships with multiple companies including Allergan, Bayer, Galderma, La Roche-Posay, Promius, and Valeant.
SDEF and this news organization are owned by the same parent company.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR
Don’t overlook all options for ocular rosacea
Managing ocular rosacea often includes a combination of oral and topical treatments, and some patients find relief with natural strategies such as warm compresses and eyelid massage, Julie C. Harper, MD, said at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Ocular rosacea can present in several forms, including sties on the eyelids, blepharitis with chalazia and telangiectasia, and “meibomian inspissation visible as pale streaks perpendicular to the lid margin,” according to a 2016 review article she cited (Clin Dermatol. 2016 Mar-Apr;34[2]:146-50).

The most common symptoms at baseline were burning, stinging, and light sensitivity. At baseline, all the cyclosporine-treated patients had burning, stinging, and light sensitivity, which dropped to 21%, 47%, and 10.5% of the patients, respectively, after 3 months of twice-daily topical treatment. In the study, all patients also were administering artificial eye drops daily.
The patients treated with doxycycline also showed improvement in these three symptoms after 3 months of treatment, but not to the same degree: At 3 months, 74% still had burning and stinging, from 100% at baseline. Almost 95% had light sensitivity at baseline, dropping to 21% after 3 months of treatment.
When treating patients with ocular rosacea, “the greatest challenge is that we don’t have any medications that are Food and Drug Administration–approved for this indication,” Dr. Harper said in an interview.
In the interview, she provided the following pearl: “Always ask about eye involvement in rosacea patients; they won’t volunteer information because they think it is unrelated. Teach patients about lid care (lid massage and artificial tears). This is analogous to good skin care in cutaneous rosacea.”
Dr. Harper disclosed serving as a speaker/adviser for Allergan, Bayer, and Galderma, and receiving research support from Bayer. SDEF and this news organization are owned by the same parent company.
Managing ocular rosacea often includes a combination of oral and topical treatments, and some patients find relief with natural strategies such as warm compresses and eyelid massage, Julie C. Harper, MD, said at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Ocular rosacea can present in several forms, including sties on the eyelids, blepharitis with chalazia and telangiectasia, and “meibomian inspissation visible as pale streaks perpendicular to the lid margin,” according to a 2016 review article she cited (Clin Dermatol. 2016 Mar-Apr;34[2]:146-50).
The most common symptoms at baseline were burning, stinging, and light sensitivity. At baseline, all the cyclosporine-treated patients had burning, stinging, and light sensitivity, which dropped to 21%, 47%, and 10.5% of the patients, respectively, after 3 months of twice-daily topical treatment. In the study, all patients also were administering artificial eye drops daily.
The patients treated with doxycycline also showed improvement in these three symptoms after 3 months of treatment, but not to the same degree: At 3 months, 74% still had burning and stinging, from 100% at baseline. Almost 95% had light sensitivity at baseline, dropping to 21% after 3 months of treatment.
When treating patients with ocular rosacea, “the greatest challenge is that we don’t have any medications that are Food and Drug Administration–approved for this indication,” Dr. Harper said in an interview.
In the interview, she provided the following pearl: “Always ask about eye involvement in rosacea patients; they won’t volunteer information because they think it is unrelated. Teach patients about lid care (lid massage and artificial tears). This is analogous to good skin care in cutaneous rosacea.”
Dr. Harper disclosed serving as a speaker/adviser for Allergan, Bayer, and Galderma, and receiving research support from Bayer. SDEF and this news organization are owned by the same parent company.
Managing ocular rosacea often includes a combination of oral and topical treatments, and some patients find relief with natural strategies such as warm compresses and eyelid massage, Julie C. Harper, MD, said at the Skin Disease Education Foundation’s annual Las Vegas Dermatology Seminar.
Ocular rosacea can present in several forms, including sties on the eyelids, blepharitis with chalazia and telangiectasia, and “meibomian inspissation visible as pale streaks perpendicular to the lid margin,” according to a 2016 review article she cited (Clin Dermatol. 2016 Mar-Apr;34[2]:146-50).
The most common symptoms at baseline were burning, stinging, and light sensitivity. At baseline, all the cyclosporine-treated patients had burning, stinging, and light sensitivity, which dropped to 21%, 47%, and 10.5% of the patients, respectively, after 3 months of twice-daily topical treatment. In the study, all patients also were administering artificial eye drops daily.
The patients treated with doxycycline also showed improvement in these three symptoms after 3 months of treatment, but not to the same degree: At 3 months, 74% still had burning and stinging, from 100% at baseline. Almost 95% had light sensitivity at baseline, dropping to 21% after 3 months of treatment.
When treating patients with ocular rosacea, “the greatest challenge is that we don’t have any medications that are Food and Drug Administration–approved for this indication,” Dr. Harper said in an interview.
In the interview, she provided the following pearl: “Always ask about eye involvement in rosacea patients; they won’t volunteer information because they think it is unrelated. Teach patients about lid care (lid massage and artificial tears). This is analogous to good skin care in cutaneous rosacea.”
Dr. Harper disclosed serving as a speaker/adviser for Allergan, Bayer, and Galderma, and receiving research support from Bayer. SDEF and this news organization are owned by the same parent company.
AT SDEF LAS VEGAS DERMATOLOGY SEMINAR
Rosacea patients host the most mites
Infestation with Demodex mites was significantly more common in patients with rosacea compared with healthy controls, based on data from a meta-analysis of 1,513 adults with rosacea. The findings were published in the September issue of the Journal of the American Academy of Dermatology.
The cause of rosacea remains unclear and differs within subgroups, but previous studies have suggested an association between rosacea and the presence of Demodex mites, wrote Yin-Shuo Chang, MD, and Yu-Chen Huang, MD, both of Taipei Medical University, Taiwan (J Am Acad Dermatol. 2017; 77[3]:441-7).


The researchers had no financial conflicts to disclose.
Find the full study online here: http://www.jaad.org/article/S0190-9622(17)30429-2/fulltext.
Infestation with Demodex mites was significantly more common in patients with rosacea compared with healthy controls, based on data from a meta-analysis of 1,513 adults with rosacea. The findings were published in the September issue of the Journal of the American Academy of Dermatology.
The cause of rosacea remains unclear and differs within subgroups, but previous studies have suggested an association between rosacea and the presence of Demodex mites, wrote Yin-Shuo Chang, MD, and Yu-Chen Huang, MD, both of Taipei Medical University, Taiwan (J Am Acad Dermatol. 2017; 77[3]:441-7).
The researchers had no financial conflicts to disclose.
Find the full study online here: http://www.jaad.org/article/S0190-9622(17)30429-2/fulltext.
Infestation with Demodex mites was significantly more common in patients with rosacea compared with healthy controls, based on data from a meta-analysis of 1,513 adults with rosacea. The findings were published in the September issue of the Journal of the American Academy of Dermatology.
The cause of rosacea remains unclear and differs within subgroups, but previous studies have suggested an association between rosacea and the presence of Demodex mites, wrote Yin-Shuo Chang, MD, and Yu-Chen Huang, MD, both of Taipei Medical University, Taiwan (J Am Acad Dermatol. 2017; 77[3]:441-7).
The researchers had no financial conflicts to disclose.
Find the full study online here: http://www.jaad.org/article/S0190-9622(17)30429-2/fulltext.
FROM JAAD
Key clinical point: Demodex mite infestations are significantly associated with rosacea.
Major finding: Rosacea patients were 9 times more likely to experience Demodex mite infestations compared with healthy controls.
Data source: The data come from a meta-analysis of 1,513 adults with rosacea.
Disclosures: The researchers had no financial conflicts to disclose.