User login
Is fructose all to blame for obesity?
A recent article hypothesized that fructose causes more metabolic disease than does sucrose when overfed in the human diet. Fructose intake as high-fructose corn syrup (HFCS) has risen since its use in soft drinks in the United States and parallels the increase in the prevalence of obesity.
The newest hypothesis regarding fructose invokes a genetic survival of the fittest rationale for how fructose-enhanced fat deposition exacerbates the increased caloric consumption from the Western diet to promote metabolic disease especially in our adolescent and young adult population. This theory suggests that fructose consumption causes low adenosine triphosphate, which stimulates energy intake causing an imbalance of energy regulation.
Ongoing interest in the association between the increased use of HFCS and the prevalence of obesity in the United States continues. The use of HFCS in sugary sweetened beverages (SSBs) has reduced the cost of these beverages because of technology in preparing HFCS from corn and the substitution of the cheaper HFCS for sugar in SSBs. Although SSBs haven’t been proven to cause obesity, there has been an increase in the risk for type 2 diabetes, cardiovascular disease (CVD), nonalcoholic fatty liver disease (NAFLD), and even cancer. Research in HFCS, weight gain, and metabolic disease continues despite little definitive evidence of causation.
The relationship between SSBs consumption and obesity has been attributed to the increase in overall total caloric intake of the diet. These liquid calories do not suppress the intake of other foods to equalize the total amount of calories ingested. This knowledge has been gleaned from work performed by R. Mattes and B. Rolls in the 1990s through the early 2000s.
This research and the current work on HFCS and metabolic disease is important because there are adolescents and young adults in the United States and globally that ingest a large amount of SSBs and therefore are at risk for metabolic disease, type 2 diabetes, NAFLD, and CVD at an early age.
, around 1970-1980.
Researchers noted the association and began to focus on potential reasons to pinpoint HFCS or fructose itself so we have a mechanism of action specific to fructose. Therefore, the public could be warned about the risk of drinking SSBs due to the HFCS and fructose ingested and the possibility of metabolic disease. Perhaps, there is a method to remove harmful HFCS from the food supply much like what has happened with industrially produced trans fatty acids. In 2018, the World Health Organization called for a total ban on trans fats due to causation of 500 million early deaths per year globally.
Similar to the process of making HFCS, most trans fats are formed through an industrial process that alters vegetable oil and creates a shelf stable inexpensive partially hydrogenated oil. Trans fats have been shown to increase low-density lipoprotein (LDL) cholesterol and decrease high-density lipoprotein (HDL) increasing the risk for myocardial infarction and stroke.
What was the pivotal moment for the ban on trans fats? It was tough convincing the scientific community and certainly the industry that trans fats were especially harmful. This is because of the dogma that margarine and Crisco oils were somehow better for you than were lard and butter. The evidence kept coming in from epidemiological studies showing that people who ate more trans fats had increased levels of LDL and decreased levels of HDL, and the dogma that saturated fat was the villain in heart disease was reinforced. Maybe that pivotal moment was when a researcher with experience testing trans fat deposition in cadavers and pigs sued the US Food and Drug Administration (FDA) for not acting on cumulative evidence sooner.
Do we have this kind of evidence to make a claim for the FDA to ban HFCS? What we have is the time course of HFCS entry into the food supply which occurred in 1970. This coincided with the growing prevalence of obesity between 1960 and 2000.
The excess energy in SSBs can provide a hedonic stimulus that overcomes the natural energy balance regulatory mechanism because SSBs excess energy comes in liquid form and may bypass the satiety signal in the hypothalamus.
We still have to prove this.
Blaming fructose in HFCS as the sole cause for the increase obesity will be much tougher than blaming trans fats for an increase in LDL cholesterol and a decrease in HDL cholesterol.
The prevalence of obesity has increased worldwide, even in countries where SSBs do not contain HFCS.
Still, the proof that HFCS can override the satiety pathway and cause excess calorie intake is intriguing and may have teeth if we can pinpoint the increase in prevalence of obesity in children and adolescents on increased ingestion of HFCS in SSBs. There is no reason nutritionally to add sugar or HFCS to liquids. Plus, if HFCS has a metabolic disadvantage then all the more reason to ban it. Then, it becomes like trans fats: a toxin in the food supply.
Dr. Apovian is a Faculty Member, Department of Medicine; Co-Director, Center for Weight Management and Wellness, Section of Endocrinology, Diabetes, and Hypertension, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts. She has disclosed financial relationships with Altimmune, Inc; Cowen and Company, LLC; Currax Pharmaceuticals, LLC; EPG Communication Holdings, Ltd; Gelesis, Srl; L-Nutra, Inc; NeuroBo Pharmaceuticals; and Novo Nordisk, Inc. She has received research grants from the National Institutes of Health; Patient-Centered Outcomes Research Institute; GI Dynamics, Inc.
A version of this article appeared on Medscape.com.
A recent article hypothesized that fructose causes more metabolic disease than does sucrose when overfed in the human diet. Fructose intake as high-fructose corn syrup (HFCS) has risen since its use in soft drinks in the United States and parallels the increase in the prevalence of obesity.
The newest hypothesis regarding fructose invokes a genetic survival of the fittest rationale for how fructose-enhanced fat deposition exacerbates the increased caloric consumption from the Western diet to promote metabolic disease especially in our adolescent and young adult population. This theory suggests that fructose consumption causes low adenosine triphosphate, which stimulates energy intake causing an imbalance of energy regulation.
Ongoing interest in the association between the increased use of HFCS and the prevalence of obesity in the United States continues. The use of HFCS in sugary sweetened beverages (SSBs) has reduced the cost of these beverages because of technology in preparing HFCS from corn and the substitution of the cheaper HFCS for sugar in SSBs. Although SSBs haven’t been proven to cause obesity, there has been an increase in the risk for type 2 diabetes, cardiovascular disease (CVD), nonalcoholic fatty liver disease (NAFLD), and even cancer. Research in HFCS, weight gain, and metabolic disease continues despite little definitive evidence of causation.
The relationship between SSBs consumption and obesity has been attributed to the increase in overall total caloric intake of the diet. These liquid calories do not suppress the intake of other foods to equalize the total amount of calories ingested. This knowledge has been gleaned from work performed by R. Mattes and B. Rolls in the 1990s through the early 2000s.
This research and the current work on HFCS and metabolic disease is important because there are adolescents and young adults in the United States and globally that ingest a large amount of SSBs and therefore are at risk for metabolic disease, type 2 diabetes, NAFLD, and CVD at an early age.
, around 1970-1980.
Researchers noted the association and began to focus on potential reasons to pinpoint HFCS or fructose itself so we have a mechanism of action specific to fructose. Therefore, the public could be warned about the risk of drinking SSBs due to the HFCS and fructose ingested and the possibility of metabolic disease. Perhaps, there is a method to remove harmful HFCS from the food supply much like what has happened with industrially produced trans fatty acids. In 2018, the World Health Organization called for a total ban on trans fats due to causation of 500 million early deaths per year globally.
Similar to the process of making HFCS, most trans fats are formed through an industrial process that alters vegetable oil and creates a shelf stable inexpensive partially hydrogenated oil. Trans fats have been shown to increase low-density lipoprotein (LDL) cholesterol and decrease high-density lipoprotein (HDL) increasing the risk for myocardial infarction and stroke.
What was the pivotal moment for the ban on trans fats? It was tough convincing the scientific community and certainly the industry that trans fats were especially harmful. This is because of the dogma that margarine and Crisco oils were somehow better for you than were lard and butter. The evidence kept coming in from epidemiological studies showing that people who ate more trans fats had increased levels of LDL and decreased levels of HDL, and the dogma that saturated fat was the villain in heart disease was reinforced. Maybe that pivotal moment was when a researcher with experience testing trans fat deposition in cadavers and pigs sued the US Food and Drug Administration (FDA) for not acting on cumulative evidence sooner.
Do we have this kind of evidence to make a claim for the FDA to ban HFCS? What we have is the time course of HFCS entry into the food supply which occurred in 1970. This coincided with the growing prevalence of obesity between 1960 and 2000.
The excess energy in SSBs can provide a hedonic stimulus that overcomes the natural energy balance regulatory mechanism because SSBs excess energy comes in liquid form and may bypass the satiety signal in the hypothalamus.
We still have to prove this.
Blaming fructose in HFCS as the sole cause for the increase obesity will be much tougher than blaming trans fats for an increase in LDL cholesterol and a decrease in HDL cholesterol.
The prevalence of obesity has increased worldwide, even in countries where SSBs do not contain HFCS.
Still, the proof that HFCS can override the satiety pathway and cause excess calorie intake is intriguing and may have teeth if we can pinpoint the increase in prevalence of obesity in children and adolescents on increased ingestion of HFCS in SSBs. There is no reason nutritionally to add sugar or HFCS to liquids. Plus, if HFCS has a metabolic disadvantage then all the more reason to ban it. Then, it becomes like trans fats: a toxin in the food supply.
Dr. Apovian is a Faculty Member, Department of Medicine; Co-Director, Center for Weight Management and Wellness, Section of Endocrinology, Diabetes, and Hypertension, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts. She has disclosed financial relationships with Altimmune, Inc; Cowen and Company, LLC; Currax Pharmaceuticals, LLC; EPG Communication Holdings, Ltd; Gelesis, Srl; L-Nutra, Inc; NeuroBo Pharmaceuticals; and Novo Nordisk, Inc. She has received research grants from the National Institutes of Health; Patient-Centered Outcomes Research Institute; GI Dynamics, Inc.
A version of this article appeared on Medscape.com.
A recent article hypothesized that fructose causes more metabolic disease than does sucrose when overfed in the human diet. Fructose intake as high-fructose corn syrup (HFCS) has risen since its use in soft drinks in the United States and parallels the increase in the prevalence of obesity.
The newest hypothesis regarding fructose invokes a genetic survival of the fittest rationale for how fructose-enhanced fat deposition exacerbates the increased caloric consumption from the Western diet to promote metabolic disease especially in our adolescent and young adult population. This theory suggests that fructose consumption causes low adenosine triphosphate, which stimulates energy intake causing an imbalance of energy regulation.
Ongoing interest in the association between the increased use of HFCS and the prevalence of obesity in the United States continues. The use of HFCS in sugary sweetened beverages (SSBs) has reduced the cost of these beverages because of technology in preparing HFCS from corn and the substitution of the cheaper HFCS for sugar in SSBs. Although SSBs haven’t been proven to cause obesity, there has been an increase in the risk for type 2 diabetes, cardiovascular disease (CVD), nonalcoholic fatty liver disease (NAFLD), and even cancer. Research in HFCS, weight gain, and metabolic disease continues despite little definitive evidence of causation.
The relationship between SSBs consumption and obesity has been attributed to the increase in overall total caloric intake of the diet. These liquid calories do not suppress the intake of other foods to equalize the total amount of calories ingested. This knowledge has been gleaned from work performed by R. Mattes and B. Rolls in the 1990s through the early 2000s.
This research and the current work on HFCS and metabolic disease is important because there are adolescents and young adults in the United States and globally that ingest a large amount of SSBs and therefore are at risk for metabolic disease, type 2 diabetes, NAFLD, and CVD at an early age.
, around 1970-1980.
Researchers noted the association and began to focus on potential reasons to pinpoint HFCS or fructose itself so we have a mechanism of action specific to fructose. Therefore, the public could be warned about the risk of drinking SSBs due to the HFCS and fructose ingested and the possibility of metabolic disease. Perhaps, there is a method to remove harmful HFCS from the food supply much like what has happened with industrially produced trans fatty acids. In 2018, the World Health Organization called for a total ban on trans fats due to causation of 500 million early deaths per year globally.
Similar to the process of making HFCS, most trans fats are formed through an industrial process that alters vegetable oil and creates a shelf stable inexpensive partially hydrogenated oil. Trans fats have been shown to increase low-density lipoprotein (LDL) cholesterol and decrease high-density lipoprotein (HDL) increasing the risk for myocardial infarction and stroke.
What was the pivotal moment for the ban on trans fats? It was tough convincing the scientific community and certainly the industry that trans fats were especially harmful. This is because of the dogma that margarine and Crisco oils were somehow better for you than were lard and butter. The evidence kept coming in from epidemiological studies showing that people who ate more trans fats had increased levels of LDL and decreased levels of HDL, and the dogma that saturated fat was the villain in heart disease was reinforced. Maybe that pivotal moment was when a researcher with experience testing trans fat deposition in cadavers and pigs sued the US Food and Drug Administration (FDA) for not acting on cumulative evidence sooner.
Do we have this kind of evidence to make a claim for the FDA to ban HFCS? What we have is the time course of HFCS entry into the food supply which occurred in 1970. This coincided with the growing prevalence of obesity between 1960 and 2000.
The excess energy in SSBs can provide a hedonic stimulus that overcomes the natural energy balance regulatory mechanism because SSBs excess energy comes in liquid form and may bypass the satiety signal in the hypothalamus.
We still have to prove this.
Blaming fructose in HFCS as the sole cause for the increase obesity will be much tougher than blaming trans fats for an increase in LDL cholesterol and a decrease in HDL cholesterol.
The prevalence of obesity has increased worldwide, even in countries where SSBs do not contain HFCS.
Still, the proof that HFCS can override the satiety pathway and cause excess calorie intake is intriguing and may have teeth if we can pinpoint the increase in prevalence of obesity in children and adolescents on increased ingestion of HFCS in SSBs. There is no reason nutritionally to add sugar or HFCS to liquids. Plus, if HFCS has a metabolic disadvantage then all the more reason to ban it. Then, it becomes like trans fats: a toxin in the food supply.
Dr. Apovian is a Faculty Member, Department of Medicine; Co-Director, Center for Weight Management and Wellness, Section of Endocrinology, Diabetes, and Hypertension, Brigham and Women’s Hospital, Harvard Medical School, Boston, Massachusetts. She has disclosed financial relationships with Altimmune, Inc; Cowen and Company, LLC; Currax Pharmaceuticals, LLC; EPG Communication Holdings, Ltd; Gelesis, Srl; L-Nutra, Inc; NeuroBo Pharmaceuticals; and Novo Nordisk, Inc. She has received research grants from the National Institutes of Health; Patient-Centered Outcomes Research Institute; GI Dynamics, Inc.
A version of this article appeared on Medscape.com.
Making an impact beyond medicine
across all career stages and practice settings, highlight the diversity of our membership, and build a sense of community by learning more about one another.
As physicians, we are fortunate to have the opportunity to meaningfully impact the lives of our patients through the practice of clinical medicine, or by spearheading groundbreaking research that improves patient outcomes. However, some physicians arguably make their greatest mark outside of medicine.

To close out the inaugural year of our Member Spotlight feature, we introduce you to gastroenterologist Eric Esrailian, MD, MPH, chair of the division of gastroenterology at UCLA. He is an Emmy-nominated film producer and distinguished human rights advocate. His story is inspirational, and poignantly highlights how one’s impact as a physician can extend far beyond the walls of the hospital. We hope to continue to feature exceptional individuals like Dr. Esrailian who leverage their unique talents for societal good. We appreciate your continued nominations as we plan our 2024 coverage.
Also in the December issue, we summarize the results of a pivotal, head-to-head trial of risankizumab (Skyrizi) and ustekinumab (Stelara) for Crohn’s disease, which was presented in October at United European Gastroenterology (UEG) Week in Copenhagen.
We also highlight the FDA’s recent approval of vonoprazan, a new pharmacologic treatment for erosive esophagitis expected to be available in the U.S. sometime this month. Finally, Dr. Lauren Feld explains how gastroenterologists can advocate for more robust parental leave and return to work policies at their institutions and why it matters.
We wish you all a wonderful holiday season and look forward to seeing you again in the New Year.
Megan A. Adams, MD, JD, MSc
across all career stages and practice settings, highlight the diversity of our membership, and build a sense of community by learning more about one another.
As physicians, we are fortunate to have the opportunity to meaningfully impact the lives of our patients through the practice of clinical medicine, or by spearheading groundbreaking research that improves patient outcomes. However, some physicians arguably make their greatest mark outside of medicine.
To close out the inaugural year of our Member Spotlight feature, we introduce you to gastroenterologist Eric Esrailian, MD, MPH, chair of the division of gastroenterology at UCLA. He is an Emmy-nominated film producer and distinguished human rights advocate. His story is inspirational, and poignantly highlights how one’s impact as a physician can extend far beyond the walls of the hospital. We hope to continue to feature exceptional individuals like Dr. Esrailian who leverage their unique talents for societal good. We appreciate your continued nominations as we plan our 2024 coverage.
Also in the December issue, we summarize the results of a pivotal, head-to-head trial of risankizumab (Skyrizi) and ustekinumab (Stelara) for Crohn’s disease, which was presented in October at United European Gastroenterology (UEG) Week in Copenhagen.
We also highlight the FDA’s recent approval of vonoprazan, a new pharmacologic treatment for erosive esophagitis expected to be available in the U.S. sometime this month. Finally, Dr. Lauren Feld explains how gastroenterologists can advocate for more robust parental leave and return to work policies at their institutions and why it matters.
We wish you all a wonderful holiday season and look forward to seeing you again in the New Year.
Megan A. Adams, MD, JD, MSc
across all career stages and practice settings, highlight the diversity of our membership, and build a sense of community by learning more about one another.
As physicians, we are fortunate to have the opportunity to meaningfully impact the lives of our patients through the practice of clinical medicine, or by spearheading groundbreaking research that improves patient outcomes. However, some physicians arguably make their greatest mark outside of medicine.
To close out the inaugural year of our Member Spotlight feature, we introduce you to gastroenterologist Eric Esrailian, MD, MPH, chair of the division of gastroenterology at UCLA. He is an Emmy-nominated film producer and distinguished human rights advocate. His story is inspirational, and poignantly highlights how one’s impact as a physician can extend far beyond the walls of the hospital. We hope to continue to feature exceptional individuals like Dr. Esrailian who leverage their unique talents for societal good. We appreciate your continued nominations as we plan our 2024 coverage.
Also in the December issue, we summarize the results of a pivotal, head-to-head trial of risankizumab (Skyrizi) and ustekinumab (Stelara) for Crohn’s disease, which was presented in October at United European Gastroenterology (UEG) Week in Copenhagen.
We also highlight the FDA’s recent approval of vonoprazan, a new pharmacologic treatment for erosive esophagitis expected to be available in the U.S. sometime this month. Finally, Dr. Lauren Feld explains how gastroenterologists can advocate for more robust parental leave and return to work policies at their institutions and why it matters.
We wish you all a wonderful holiday season and look forward to seeing you again in the New Year.
Megan A. Adams, MD, JD, MSc

In general, I’m happy
I’m a general neurologist. I consider myself a jack of all (or at least most) trades in my field, and a master of none.
In the April 2023 issue of JAMA Neurology there was an editorial about neurology training, with general neurology being renamed “comprehensive neurology” and a fellowship offered in practicing general neurology.
This seems rather silly to me. If 4 years of residency (1 of internship and 3 of neurology) don’t prepare you to practice general neurology, then what’s the point of residency at all? For that matter, what difference will renaming it do?

Imagine completing a 3-year internal medicine residency, then being told you need to do a fellowship in “comprehensive medicine” in order to practice. Or at least so you can add the word “comprehensive” to your shingle.
The authors bemoan the increasing number of neurology residents wanting to do fellowships and subspecialize, a situation that mirrors the general trend of people away from general medicine toward specialties.
While I agree we do need subspecialists in neurology (and currently there are at least 31 recognized, which is way more than I would have guessed), the fact is that patients, and sometimes their internists, aren’t going to be the best judge of who does or doesn’t need to see one, compared with a general neurologist.
Most of us general people can handle straightforward Parkinson’s disease, epilepsy, migraines, etc. Certainly, there are times where the condition is refractory to our care, or there’s something unusual about the case, that leads us to refer them to someone with more expertise. But isn’t that how it’s supposed to work? Like medicine in general, we need more general people than subspecialists.
Honestly, I can’t claim to be any different. Twenty-six years ago, when I finished residency, I did a clinical neurophysiology fellowship. From a practical view it was an epilepsy fellowship at my program. Some of this was an interest at the time in subspecializing, some of it was me putting off joining the “real world” of having to find a job for a year.
When I hung up my own shingle, my business card listed a subspecialty in epilepsy. Looking back years later, this wasn’t the best move. In solo practice I had no access to an epilepsy monitoring unit, vagus nerve stimulation capabilities, or epilepsy surgery at the hospital I rounded at. Not only that, I discovered it put me at a disadvantage, as internists were referring only epilepsy patients to me, and all the other stuff (which is the majority of patients) to the general (or comprehensive) neurologists around me. Which, financially, wasn’t a good thing when you’re young and starting out.
Not only that, but I discovered that I didn’t like only seeing one thing. I found it boring, and not for me.
So after a year or so, I took the word “epilepsy” off my card, left it at “general neurology,” and sent out letters reminding my referral base that I was willing to see the majority of things in my field (rare diseases, even today, I won’t attempt to handle).
So now my days are a mix of things, which I like. Neurology is enough of a specialty for me without going further up the pyramid. Having sub (and even sub-sub) specialists is important to maintain medical excellence, but we still need people willing to do general neurology, and I’m happy there.
Changing my title to “comprehensive” is unnecessary. I’m happy with what I am.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m a general neurologist. I consider myself a jack of all (or at least most) trades in my field, and a master of none.
In the April 2023 issue of JAMA Neurology there was an editorial about neurology training, with general neurology being renamed “comprehensive neurology” and a fellowship offered in practicing general neurology.
This seems rather silly to me. If 4 years of residency (1 of internship and 3 of neurology) don’t prepare you to practice general neurology, then what’s the point of residency at all? For that matter, what difference will renaming it do?
Imagine completing a 3-year internal medicine residency, then being told you need to do a fellowship in “comprehensive medicine” in order to practice. Or at least so you can add the word “comprehensive” to your shingle.
The authors bemoan the increasing number of neurology residents wanting to do fellowships and subspecialize, a situation that mirrors the general trend of people away from general medicine toward specialties.
While I agree we do need subspecialists in neurology (and currently there are at least 31 recognized, which is way more than I would have guessed), the fact is that patients, and sometimes their internists, aren’t going to be the best judge of who does or doesn’t need to see one, compared with a general neurologist.
Most of us general people can handle straightforward Parkinson’s disease, epilepsy, migraines, etc. Certainly, there are times where the condition is refractory to our care, or there’s something unusual about the case, that leads us to refer them to someone with more expertise. But isn’t that how it’s supposed to work? Like medicine in general, we need more general people than subspecialists.
Honestly, I can’t claim to be any different. Twenty-six years ago, when I finished residency, I did a clinical neurophysiology fellowship. From a practical view it was an epilepsy fellowship at my program. Some of this was an interest at the time in subspecializing, some of it was me putting off joining the “real world” of having to find a job for a year.
When I hung up my own shingle, my business card listed a subspecialty in epilepsy. Looking back years later, this wasn’t the best move. In solo practice I had no access to an epilepsy monitoring unit, vagus nerve stimulation capabilities, or epilepsy surgery at the hospital I rounded at. Not only that, I discovered it put me at a disadvantage, as internists were referring only epilepsy patients to me, and all the other stuff (which is the majority of patients) to the general (or comprehensive) neurologists around me. Which, financially, wasn’t a good thing when you’re young and starting out.
Not only that, but I discovered that I didn’t like only seeing one thing. I found it boring, and not for me.
So after a year or so, I took the word “epilepsy” off my card, left it at “general neurology,” and sent out letters reminding my referral base that I was willing to see the majority of things in my field (rare diseases, even today, I won’t attempt to handle).
So now my days are a mix of things, which I like. Neurology is enough of a specialty for me without going further up the pyramid. Having sub (and even sub-sub) specialists is important to maintain medical excellence, but we still need people willing to do general neurology, and I’m happy there.
Changing my title to “comprehensive” is unnecessary. I’m happy with what I am.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m a general neurologist. I consider myself a jack of all (or at least most) trades in my field, and a master of none.
In the April 2023 issue of JAMA Neurology there was an editorial about neurology training, with general neurology being renamed “comprehensive neurology” and a fellowship offered in practicing general neurology.
This seems rather silly to me. If 4 years of residency (1 of internship and 3 of neurology) don’t prepare you to practice general neurology, then what’s the point of residency at all? For that matter, what difference will renaming it do?
Imagine completing a 3-year internal medicine residency, then being told you need to do a fellowship in “comprehensive medicine” in order to practice. Or at least so you can add the word “comprehensive” to your shingle.
The authors bemoan the increasing number of neurology residents wanting to do fellowships and subspecialize, a situation that mirrors the general trend of people away from general medicine toward specialties.
While I agree we do need subspecialists in neurology (and currently there are at least 31 recognized, which is way more than I would have guessed), the fact is that patients, and sometimes their internists, aren’t going to be the best judge of who does or doesn’t need to see one, compared with a general neurologist.
Most of us general people can handle straightforward Parkinson’s disease, epilepsy, migraines, etc. Certainly, there are times where the condition is refractory to our care, or there’s something unusual about the case, that leads us to refer them to someone with more expertise. But isn’t that how it’s supposed to work? Like medicine in general, we need more general people than subspecialists.
Honestly, I can’t claim to be any different. Twenty-six years ago, when I finished residency, I did a clinical neurophysiology fellowship. From a practical view it was an epilepsy fellowship at my program. Some of this was an interest at the time in subspecializing, some of it was me putting off joining the “real world” of having to find a job for a year.
When I hung up my own shingle, my business card listed a subspecialty in epilepsy. Looking back years later, this wasn’t the best move. In solo practice I had no access to an epilepsy monitoring unit, vagus nerve stimulation capabilities, or epilepsy surgery at the hospital I rounded at. Not only that, I discovered it put me at a disadvantage, as internists were referring only epilepsy patients to me, and all the other stuff (which is the majority of patients) to the general (or comprehensive) neurologists around me. Which, financially, wasn’t a good thing when you’re young and starting out.
Not only that, but I discovered that I didn’t like only seeing one thing. I found it boring, and not for me.
So after a year or so, I took the word “epilepsy” off my card, left it at “general neurology,” and sent out letters reminding my referral base that I was willing to see the majority of things in my field (rare diseases, even today, I won’t attempt to handle).
So now my days are a mix of things, which I like. Neurology is enough of a specialty for me without going further up the pyramid. Having sub (and even sub-sub) specialists is important to maintain medical excellence, but we still need people willing to do general neurology, and I’m happy there.
Changing my title to “comprehensive” is unnecessary. I’m happy with what I am.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Quitting medical school
A few weeks ago I shared by concerns about the dwindling numbers of primary care physicians. The early exodus of practicing providers and an obvious disinterest by future physicians in what they see as the unpalatable work/life balance of frontline hands-on medicine are among the causes.
A recent study published in the journal Pediatrics highlights personal finance as a contributor to the drain on the primary care workforce. The investigators found “high self-reported educational debt ($200,000 to < $300,000) was positively associated with training in a positive lifetime earnings potential subspecialty.” In other words, why would a physician who was burdened with student loans enter a subspecialty that would limit his or her ability to pay it off? I suspect that money has always been a factor in career selection, but the ballooning cost of college and medical school has certainly not nudged graduates toward the low lifetime earnings potential of primary care pediatrics.

Another recently released survey adds the perspective of current medical school students to the murky future of the primary health care workforce. The Clinician of the Future 2023: Education Edition, published by Elsevier Health, reports on insights of more than 2,000 nursing and medical school student from around the world. The headline shocker was that while across the board a not surprising 12% of medical students were considering quitting their studies, in the United States this number was 25%.
Overall, more than 60% of the students worried about their future income, how workforce shortages would effect them and whether they would join the ranks of those clinicians suffering from burnout. While the students surveyed acknowledged that artificial intelligence could have some negative repercussions, 62% were excited about its use in their education. Similarly, they anticipated the positive contribution of digital technology while acknowledging its potential downsides.
Given the current mental health climate in this country, I was not surprised that almost a quarter of medical students in this country are considering quitting school. I would like to see a larger sample surveyed and repeated over time. But, the discrepancy between the United States and the rest of the world is troubling.
The number that really jumped out at me was that 54% of medical students (nurses, 62%) viewed “ their current studies as a stepping-stone toward a broader career in health care.” As an example, the authors quoted one medical student who plans to “look for other possibilities where I don’t directly treat patients.”
Whether this disinterest in direct patient care is an attitude that preceded their entry into medical school or a change reflecting a major reversal induced by the realty of face-to-face patient encounters in school was not addressed in the survey. I think the general population would be surprised and maybe disappointed to learn that half the students in medical school weren’t planning on seeing patients.
I went off to medical school with a rather naive Norman Rockwellian view of a physician. I was a little surprised that a few of my classmates seemed to be gravitating toward administrative and research careers, but by far most of us were heading toward opportunities that would place us face to face with patients. Some would become specialists but primary care still had an appeal for many of us.
In my last letter about primary care training, I suggested that traditional medical school was probably a poor investment for the person who shares a bit of my old-school image of the primary care physician. In addition to cost and the time invested, the curriculum would likely be overly broad and deep and not terribly applicable to the patient mix he or she would eventually be seeing. This global survey may suggest that medical students have already discovered, or are just now discovering, this mismatch between medical school and the realities of primary care.
Our challenge is to first deal with deterrent of student debt and then to develop a new, affordable and efficient pathway to primary care that attracts those people who are looking for a face to face style of medicine on the front line. The patients know we need specialists and administrators but they also want a bit more of Norman Rockwell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A few weeks ago I shared by concerns about the dwindling numbers of primary care physicians. The early exodus of practicing providers and an obvious disinterest by future physicians in what they see as the unpalatable work/life balance of frontline hands-on medicine are among the causes.
A recent study published in the journal Pediatrics highlights personal finance as a contributor to the drain on the primary care workforce. The investigators found “high self-reported educational debt ($200,000 to < $300,000) was positively associated with training in a positive lifetime earnings potential subspecialty.” In other words, why would a physician who was burdened with student loans enter a subspecialty that would limit his or her ability to pay it off? I suspect that money has always been a factor in career selection, but the ballooning cost of college and medical school has certainly not nudged graduates toward the low lifetime earnings potential of primary care pediatrics.
Another recently released survey adds the perspective of current medical school students to the murky future of the primary health care workforce. The Clinician of the Future 2023: Education Edition, published by Elsevier Health, reports on insights of more than 2,000 nursing and medical school student from around the world. The headline shocker was that while across the board a not surprising 12% of medical students were considering quitting their studies, in the United States this number was 25%.
Overall, more than 60% of the students worried about their future income, how workforce shortages would effect them and whether they would join the ranks of those clinicians suffering from burnout. While the students surveyed acknowledged that artificial intelligence could have some negative repercussions, 62% were excited about its use in their education. Similarly, they anticipated the positive contribution of digital technology while acknowledging its potential downsides.
Given the current mental health climate in this country, I was not surprised that almost a quarter of medical students in this country are considering quitting school. I would like to see a larger sample surveyed and repeated over time. But, the discrepancy between the United States and the rest of the world is troubling.
The number that really jumped out at me was that 54% of medical students (nurses, 62%) viewed “ their current studies as a stepping-stone toward a broader career in health care.” As an example, the authors quoted one medical student who plans to “look for other possibilities where I don’t directly treat patients.”
Whether this disinterest in direct patient care is an attitude that preceded their entry into medical school or a change reflecting a major reversal induced by the realty of face-to-face patient encounters in school was not addressed in the survey. I think the general population would be surprised and maybe disappointed to learn that half the students in medical school weren’t planning on seeing patients.
I went off to medical school with a rather naive Norman Rockwellian view of a physician. I was a little surprised that a few of my classmates seemed to be gravitating toward administrative and research careers, but by far most of us were heading toward opportunities that would place us face to face with patients. Some would become specialists but primary care still had an appeal for many of us.
In my last letter about primary care training, I suggested that traditional medical school was probably a poor investment for the person who shares a bit of my old-school image of the primary care physician. In addition to cost and the time invested, the curriculum would likely be overly broad and deep and not terribly applicable to the patient mix he or she would eventually be seeing. This global survey may suggest that medical students have already discovered, or are just now discovering, this mismatch between medical school and the realities of primary care.
Our challenge is to first deal with deterrent of student debt and then to develop a new, affordable and efficient pathway to primary care that attracts those people who are looking for a face to face style of medicine on the front line. The patients know we need specialists and administrators but they also want a bit more of Norman Rockwell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A few weeks ago I shared by concerns about the dwindling numbers of primary care physicians. The early exodus of practicing providers and an obvious disinterest by future physicians in what they see as the unpalatable work/life balance of frontline hands-on medicine are among the causes.
A recent study published in the journal Pediatrics highlights personal finance as a contributor to the drain on the primary care workforce. The investigators found “high self-reported educational debt ($200,000 to < $300,000) was positively associated with training in a positive lifetime earnings potential subspecialty.” In other words, why would a physician who was burdened with student loans enter a subspecialty that would limit his or her ability to pay it off? I suspect that money has always been a factor in career selection, but the ballooning cost of college and medical school has certainly not nudged graduates toward the low lifetime earnings potential of primary care pediatrics.
Another recently released survey adds the perspective of current medical school students to the murky future of the primary health care workforce. The Clinician of the Future 2023: Education Edition, published by Elsevier Health, reports on insights of more than 2,000 nursing and medical school student from around the world. The headline shocker was that while across the board a not surprising 12% of medical students were considering quitting their studies, in the United States this number was 25%.
Overall, more than 60% of the students worried about their future income, how workforce shortages would effect them and whether they would join the ranks of those clinicians suffering from burnout. While the students surveyed acknowledged that artificial intelligence could have some negative repercussions, 62% were excited about its use in their education. Similarly, they anticipated the positive contribution of digital technology while acknowledging its potential downsides.
Given the current mental health climate in this country, I was not surprised that almost a quarter of medical students in this country are considering quitting school. I would like to see a larger sample surveyed and repeated over time. But, the discrepancy between the United States and the rest of the world is troubling.
The number that really jumped out at me was that 54% of medical students (nurses, 62%) viewed “ their current studies as a stepping-stone toward a broader career in health care.” As an example, the authors quoted one medical student who plans to “look for other possibilities where I don’t directly treat patients.”
Whether this disinterest in direct patient care is an attitude that preceded their entry into medical school or a change reflecting a major reversal induced by the realty of face-to-face patient encounters in school was not addressed in the survey. I think the general population would be surprised and maybe disappointed to learn that half the students in medical school weren’t planning on seeing patients.
I went off to medical school with a rather naive Norman Rockwellian view of a physician. I was a little surprised that a few of my classmates seemed to be gravitating toward administrative and research careers, but by far most of us were heading toward opportunities that would place us face to face with patients. Some would become specialists but primary care still had an appeal for many of us.
In my last letter about primary care training, I suggested that traditional medical school was probably a poor investment for the person who shares a bit of my old-school image of the primary care physician. In addition to cost and the time invested, the curriculum would likely be overly broad and deep and not terribly applicable to the patient mix he or she would eventually be seeing. This global survey may suggest that medical students have already discovered, or are just now discovering, this mismatch between medical school and the realities of primary care.
Our challenge is to first deal with deterrent of student debt and then to develop a new, affordable and efficient pathway to primary care that attracts those people who are looking for a face to face style of medicine on the front line. The patients know we need specialists and administrators but they also want a bit more of Norman Rockwell.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Is air filtration the best public health intervention against respiratory viruses?
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.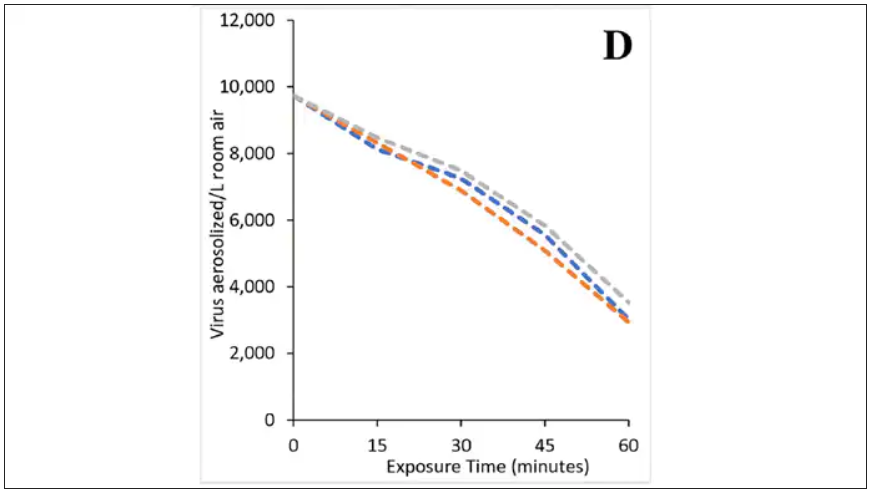
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
When it comes to the public health fight against respiratory viruses – COVID, flu, RSV, and so on – it has always struck me as strange how staunchly basically any intervention is opposed. Masking was, of course, the prototypical entrenched warfare of opposing ideologies, with advocates pointing to studies suggesting the efficacy of masking to prevent transmission and advocating for broad masking recommendations, and detractors citing studies that suggested masks were ineffective and characterizing masking policies as fascist overreach. I’ll admit that I was always perplexed by this a bit, as that particular intervention seemed so benign – a bit annoying, I guess, but not crazy.
I have come to appreciate what I call status quo bias, which is the tendency to reject any policy, advice, or intervention that would force you, as an individual, to change your usual behavior. We just don’t like to do that. It has made me think that the most successful public health interventions might be the ones that take the individual out of the loop. And air quality control seems an ideal fit here. Here is a potential intervention where you, the individual, have to do precisely nothing. The status quo is preserved. We just, you know, have cleaner indoor air.
But even the suggestion of air treatment systems as a bulwark against respiratory virus transmission has been met with not just skepticism but cynicism, and perhaps even defeatism. It seems that there are those out there who think there really is nothing we can do. Sickness is interpreted in a Calvinistic framework: You become ill because it is your pre-destiny. But maybe air treatment could actually work. It seems like it might, if a new paper from PLOS One is to be believed.
What we’re talking about is a study titled “Bipolar Ionization Rapidly Inactivates Real-World, Airborne Concentrations of Infective Respiratory Viruses” – a highly controlled, laboratory-based analysis of a bipolar ionization system which seems to rapidly reduce viral counts in the air.
The proposed mechanism of action is pretty simple. The ionization system – which, don’t worry, has been shown not to produce ozone – spits out positively and negatively charged particles, which float around the test chamber, designed to look like a pretty standard room that you might find in an office or a school.
Virus is then injected into the chamber through an aerosolization machine, to achieve concentrations on the order of what you might get standing within 6 feet or so of someone actively infected with COVID while they are breathing and talking.
The idea is that those ions stick to the virus particles, similar to how a balloon sticks to the wall after you rub it on your hair, and that tends to cause them to clump together and settle on surfaces more rapidly, and thus get farther away from their ports of entry to the human system: nose, mouth, and eyes. But the ions may also interfere with viruses’ ability to bind to cellular receptors, even in the air.
To quantify viral infectivity, the researchers used a biological system. Basically, you take air samples and expose a petri dish of cells to them and see how many cells die. Fewer cells dying, less infective. Under control conditions, you can see that virus infectivity does decrease over time. Time zero here is the end of a SARS-CoV-2 aerosolization.
This may simply reflect the fact that virus particles settle out of the air. But As you can see, within about an hour, you have almost no infective virus detectable. That’s fairly impressive.
Now, I’m not saying that this is a panacea, but it is certainly worth considering the use of technologies like these if we are going to revamp the infrastructure of our offices and schools. And, of course, it would be nice to see this tested in a rigorous clinical trial with actual infected people, not cells, as the outcome. But I continue to be encouraged by interventions like this which, to be honest, ask very little of us as individuals. Maybe it’s time we accept the things, or people, that we cannot change.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Physicians: Don’t ignore sexuality in your dying patients
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
I have a long history of being interested in conversations that others avoid. In medical school, I felt that we didn’t talk enough about death, so I organized a lecture series on end-of-life care for my fellow students. Now, as a sexual medicine specialist, I have other conversations from which many medical providers shy away. So, buckle up!
A key question in palliative care is: How do you want to live the life you have left? And where does the wide range of human pleasures fit in? In her book The Pleasure Zone, sex therapist Stella Resnick describes eight kinds of pleasure:
- pain relief
- play, humor, movement, and sound
- mental
- emotional
- sensual
- spiritual
- primal (just being)
- sexual
At the end of life, both medically and culturally, we pay attention to many of these pleasures. But sexuality is often ignored.
Sexuality – which can be defined as the experience of oneself as a sexual being – may include how sex is experienced in relationships or with oneself, sexual orientation, body image, gender expression and identity, as well as sexual satisfaction and pleasure. People may have different priorities at different times regarding their sexuality, but sexuality is a key aspect of feeling fully alive and human across the lifespan. At the end of life, sexuality, sexual expression, and physical connection may play even more important roles than previously.
‘I just want to be able to have sex with my husband again’
Z was a 75-year-old woman who came to me for help with vaginal stenosis. Her cancer treatments were not going well. I asked her one of my typical questions: “What does sex mean to you?”
Sexual pleasure was “glue” – a critical way for her to connect with her sense of self and with her husband, a man of few words. She described transcendent experiences with partnered sex during her life. Finally, she explained, she was saddened by the idea of not experiencing that again before she died.
As medical providers, we don’t all need to be sex experts, but our patients should be able to have open and shame-free conversations with us about these issues at all stages of life. Up to 86% of palliative care patients want the chance to discuss their sexual concerns with a skilled clinician, and many consider this issue important to their psychological well-being. And yet, 91% reported that sexuality had not been addressed in their care.
In a Canadian study of 10 palliative care patients (and their partners), all but one felt that their medical providers should initiate conversations about sexuality and the effect of illness on sexual experience. They felt that this communication should be an integral component of care. The one person who disagreed said it was appropriate for clinicians to ask patients whether they wanted to talk about sexuality.
Before this study, sexuality had been discussed with only one participant. Here’s the magic part: Several of the patients reported that the study itself was therapeutic. This is my clinical experience as well. More often than not, open and shame-free clinical discussions about sexuality led to patients reflecting: “I’ve never been able to say this to another person, and now I feel so much better.”
One study of palliative care nurses found that while the nurses acknowledged the importance of addressing sexuality, their way of addressing sexuality followed cultural myths and norms or relied on their own experience rather than knowledge-based guidelines. Why? One explanation could be that clinicians raised and educated in North America probably did not get adequate training on this topic. We need to do better.
Second, cultural concepts that equate sexuality with healthy and able bodies who are partnered, young, cisgender, and heterosexual make it hard to conceive of how to relate sexuality to other bodies. We’ve been steeped in the biases of our culture.
Some medical providers avoid the topic because they feel vulnerable, fearful that a conversation about sexuality with a patient will reveal something about themselves. Others may simply deny the possibility that sexual function changes in the face of serious illness or that this could be a priority for their patients. Of course, we have a million other things to talk about – I get it.
Views on sex and sexuality affect how clinicians approach these conversations as well. A study of palliative care professionals described themes among those who did and did not address the topic. The professionals who did not discuss sexuality endorsed a narrow definition of sex based on genital sexual acts between two partners, usually heterosexual. Among these clinicians, when the issue came up, patients had raised the topic. They talked about sex using jokes and euphemisms (“are you still enjoying ‘good moments’ with your partner?”), perhaps to ease their own discomfort.
On the other hand, professionals who more frequently discussed sexuality with their patients endorsed a more holistic concept of sexuality: including genital and nongenital contact as well as nonphysical components like verbal communication and emotions. These clinicians found sexuality applicable to all individuals across the lifespan. They were more likely to initiate discussions about the effect of medications or illness on sexual function and address the need for equipment, such as a larger hospital bed.
I’m hoping that you might one day find yourself in the second group. Our patients at the end of life need our help in accessing the full range of pleasure in their lives. We need better medical education on how to help with sexual concerns when they arise (an article for another day), but we can start right now by simply initiating open, shame-free sexual health conversations. This is often the most important therapeutic intervention.
Dr. Kranz, Clinical Assistant Professor of Obstetrics/Gynecology and Family Medicine, University of Rochester (N.Y.) Medical Center, has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Is metabolically healthy obesity an ‘illusion’?
I cock my head at my “new” patient, Sherri, who heads into my consultation room at 8:30 on a rainy Monday morning. She looks vaguely familiar but I can’t quite place her face. “Dr. Messer,” she cries, “don’t you remember me? I was one of your very first patients 15 years ago in Westchester. You had just finished training.” Suddenly it all comes back to me.
Meeting Sherri reminded me of the lesson in humility that my mentor, Dr. Alice Levine, taught our crowded lecture hall so many years ago. Once upon a time, she prided herself on being an infinitely important doctor. One day, she met a patient with empty sella syndrome (literally missing his whole pituitary gland – MRI proven). She fully expected to swoop in to save the patient’s life by expertly replacing each absconded pituitary hormone, but to her shock and delight, an invisible little sliver of pituitary left in his brain allowed him to magically eek out completely normal hormone levels.
Sherri walked into my office so many years ago with a body mass index in the mid-40s. In laymen’s terms, she was morbidly obese. I settled in to discuss her hypertension, diabetes, high cholesterol, fatty liver, polycystic ovary syndrome, etc., but to my shock and delight, her blood pressure and blood work were completely normal. I struggled to keep a neutral face. She was there to discuss hair loss. I had just met my first patient with metabolically healthy obesity (MHO), and I was floored.
Fast-forward 15 years. Sherri sits down across the desk from me and hands me her blood work. Her formerly pristine labs are now peppered with red exclamation points and critically high lab values. Sherri had transitioned from MHO to metabolically unhealthy obesity (MUO).
Early clinical trials concluded that it was possible to have obesity but be metabolically healthy. Approximately 15% of patients living with obesity lack any of the comorbidities typically associated with this phenotype. These findings contributed to the de-emphasis on obesity as a true disease state.
In retrospect, the MHO subtype appears to be much more common in the younger and more active population and is typically quite transient. A new study published in Diabetes, Obesity and Metabolism revealed that people with MHO are 1.5 times more likely to develop diabetes vs. metabolically healthy normal-weight individuals. In addition, people living with obesity and no known metabolic complications still had a 50% higher risk for coronary artery disease. The study also showed that over 50% of people initially characterized as MHO eventually became MUO after a 16-year follow-up.
So once again, all roads lead to semaglutide (Wegovy), the most effective U.S. Food and Drug Administration–approved weight loss medication to date. The incretin class of medications not only helps patients lose 15% or more of their body weight, but it also helps reverse insulin resistance, lower the risk for heart disease, melt away fatty liver, and lower cholesterol levels and blood pressures. While an emphasis on lifestyle changes is always important, these medications are critical adjuncts to conventional therapies.
Fifteen years ago, I discussed her hair loss for 45 minutes and never mentioned the looming issue. Of course, back then there was no semaglutide or tirzepatide, which was just approved for obesity.
Sherri left our most recent visit with a prescription for Wegovy as well as appointments with a complimentary trainer and dietitian. Now that we have the tools we need, let’s commit to helping our patients achieve true metabolic health. Unlike the magical pituitary patient, metabolically healthy obesity is an illusion – and we owe it to our patients to treat it as such.
Dr. Messer is a clinical assistant professor at Mount Sinai School of Medicine, New York, and an associate professor at Hofstra University, Hempstead, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
I cock my head at my “new” patient, Sherri, who heads into my consultation room at 8:30 on a rainy Monday morning. She looks vaguely familiar but I can’t quite place her face. “Dr. Messer,” she cries, “don’t you remember me? I was one of your very first patients 15 years ago in Westchester. You had just finished training.” Suddenly it all comes back to me.
Meeting Sherri reminded me of the lesson in humility that my mentor, Dr. Alice Levine, taught our crowded lecture hall so many years ago. Once upon a time, she prided herself on being an infinitely important doctor. One day, she met a patient with empty sella syndrome (literally missing his whole pituitary gland – MRI proven). She fully expected to swoop in to save the patient’s life by expertly replacing each absconded pituitary hormone, but to her shock and delight, an invisible little sliver of pituitary left in his brain allowed him to magically eek out completely normal hormone levels.
Sherri walked into my office so many years ago with a body mass index in the mid-40s. In laymen’s terms, she was morbidly obese. I settled in to discuss her hypertension, diabetes, high cholesterol, fatty liver, polycystic ovary syndrome, etc., but to my shock and delight, her blood pressure and blood work were completely normal. I struggled to keep a neutral face. She was there to discuss hair loss. I had just met my first patient with metabolically healthy obesity (MHO), and I was floored.
Fast-forward 15 years. Sherri sits down across the desk from me and hands me her blood work. Her formerly pristine labs are now peppered with red exclamation points and critically high lab values. Sherri had transitioned from MHO to metabolically unhealthy obesity (MUO).
Early clinical trials concluded that it was possible to have obesity but be metabolically healthy. Approximately 15% of patients living with obesity lack any of the comorbidities typically associated with this phenotype. These findings contributed to the de-emphasis on obesity as a true disease state.
In retrospect, the MHO subtype appears to be much more common in the younger and more active population and is typically quite transient. A new study published in Diabetes, Obesity and Metabolism revealed that people with MHO are 1.5 times more likely to develop diabetes vs. metabolically healthy normal-weight individuals. In addition, people living with obesity and no known metabolic complications still had a 50% higher risk for coronary artery disease. The study also showed that over 50% of people initially characterized as MHO eventually became MUO after a 16-year follow-up.
So once again, all roads lead to semaglutide (Wegovy), the most effective U.S. Food and Drug Administration–approved weight loss medication to date. The incretin class of medications not only helps patients lose 15% or more of their body weight, but it also helps reverse insulin resistance, lower the risk for heart disease, melt away fatty liver, and lower cholesterol levels and blood pressures. While an emphasis on lifestyle changes is always important, these medications are critical adjuncts to conventional therapies.
Fifteen years ago, I discussed her hair loss for 45 minutes and never mentioned the looming issue. Of course, back then there was no semaglutide or tirzepatide, which was just approved for obesity.
Sherri left our most recent visit with a prescription for Wegovy as well as appointments with a complimentary trainer and dietitian. Now that we have the tools we need, let’s commit to helping our patients achieve true metabolic health. Unlike the magical pituitary patient, metabolically healthy obesity is an illusion – and we owe it to our patients to treat it as such.
Dr. Messer is a clinical assistant professor at Mount Sinai School of Medicine, New York, and an associate professor at Hofstra University, Hempstead, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
I cock my head at my “new” patient, Sherri, who heads into my consultation room at 8:30 on a rainy Monday morning. She looks vaguely familiar but I can’t quite place her face. “Dr. Messer,” she cries, “don’t you remember me? I was one of your very first patients 15 years ago in Westchester. You had just finished training.” Suddenly it all comes back to me.
Meeting Sherri reminded me of the lesson in humility that my mentor, Dr. Alice Levine, taught our crowded lecture hall so many years ago. Once upon a time, she prided herself on being an infinitely important doctor. One day, she met a patient with empty sella syndrome (literally missing his whole pituitary gland – MRI proven). She fully expected to swoop in to save the patient’s life by expertly replacing each absconded pituitary hormone, but to her shock and delight, an invisible little sliver of pituitary left in his brain allowed him to magically eek out completely normal hormone levels.
Sherri walked into my office so many years ago with a body mass index in the mid-40s. In laymen’s terms, she was morbidly obese. I settled in to discuss her hypertension, diabetes, high cholesterol, fatty liver, polycystic ovary syndrome, etc., but to my shock and delight, her blood pressure and blood work were completely normal. I struggled to keep a neutral face. She was there to discuss hair loss. I had just met my first patient with metabolically healthy obesity (MHO), and I was floored.
Fast-forward 15 years. Sherri sits down across the desk from me and hands me her blood work. Her formerly pristine labs are now peppered with red exclamation points and critically high lab values. Sherri had transitioned from MHO to metabolically unhealthy obesity (MUO).
Early clinical trials concluded that it was possible to have obesity but be metabolically healthy. Approximately 15% of patients living with obesity lack any of the comorbidities typically associated with this phenotype. These findings contributed to the de-emphasis on obesity as a true disease state.
In retrospect, the MHO subtype appears to be much more common in the younger and more active population and is typically quite transient. A new study published in Diabetes, Obesity and Metabolism revealed that people with MHO are 1.5 times more likely to develop diabetes vs. metabolically healthy normal-weight individuals. In addition, people living with obesity and no known metabolic complications still had a 50% higher risk for coronary artery disease. The study also showed that over 50% of people initially characterized as MHO eventually became MUO after a 16-year follow-up.
So once again, all roads lead to semaglutide (Wegovy), the most effective U.S. Food and Drug Administration–approved weight loss medication to date. The incretin class of medications not only helps patients lose 15% or more of their body weight, but it also helps reverse insulin resistance, lower the risk for heart disease, melt away fatty liver, and lower cholesterol levels and blood pressures. While an emphasis on lifestyle changes is always important, these medications are critical adjuncts to conventional therapies.
Fifteen years ago, I discussed her hair loss for 45 minutes and never mentioned the looming issue. Of course, back then there was no semaglutide or tirzepatide, which was just approved for obesity.
Sherri left our most recent visit with a prescription for Wegovy as well as appointments with a complimentary trainer and dietitian. Now that we have the tools we need, let’s commit to helping our patients achieve true metabolic health. Unlike the magical pituitary patient, metabolically healthy obesity is an illusion – and we owe it to our patients to treat it as such.
Dr. Messer is a clinical assistant professor at Mount Sinai School of Medicine, New York, and an associate professor at Hofstra University, Hempstead, N.Y. She disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Fatal and nonfatal injuries
I suspect that, like me, you were saddened, but maybe not shocked, to learn that firearm-related fatalities have recently surpassed motor vehicle–related fatalities as the leading cause of death among children. For those of us living in Maine, this revelation came at a particularly difficult time. The body of the presumed shooter in the Lewiston massacre was found less than 10 miles from where I am writing you this letter. There is a good chance he may have been a former patient of mine, but I no longer have access to my records to confirm that.
This reshuffling at the top of the list of mortality causes is just one example of the shifting trends that have occurred in pediatric fatality statistics. In a recent analysis of the Centers for Disease Control and Prevention statistics published in Pediatrics investigators discovered that while, in general, fatal injuries have increased over the study period (2011-2021) nonfatal injuries have decreased.
We should no longer be surprised to learn that firearm-related deaths increased more than 87%. Fatal drug poisoning was up 133% and suffocation-related deaths increased 12.5% over that 10-year period. Given this profile of fatalities, it shouldn’t surprise us that nonfatal injuries due to firearms, poisoning, and self-harm also increased.
However, nonfatal injuries in other broad categories decreased: falls were down 52.8%, overexertion 63%, struck by [something or someone] 47.3%, motor vehicle occupant 36.7%, and cut pierce 36.7%. Nonfatal drownings were unchanged.
Diverging trends
What are we to make of these diverging trends? I suspect that when it comes to both firearms and drug poisonings, both fatal and nonfatal, children are now living in an environment in which the sheer volume of guns and drugs have grown the point, and will continue to grow, that contact and its consequences will continue to increase until we reach a saturation point at some unpredictable point in the future. There still may be some opportunities to curb the flow of drugs. But, I am afraid when it comes to firearms, that ship has sailed. We may have a chance to curb assault weapons, but hand guns have become ubiquitous to the point that they will continue to be a threat to children.
The increase in self-harm injuries is clearly a reflection of the increase in pediatric and adolescent mental health disturbances, which in turn is a reflection of the gloom hanging over the population in general.
But, what’s going on with the decrease in nonfatal injuries caused by falls, overexertion, struck by, and cut pierce? Is this a bit of sunshine in an otherwise cloudy picture? The authors of the paper see it as a reflection of our “public health interventions targeting pediatric safety partnered with technological advancement and legislative requirements.” Maybe when we are talking about booster seats and other automotive safety advancements. But I’m not so sure we should be too vigorous as we pat ourselves on the back.
On the other hand, aren’t these decreases in injuries related to activity just more evidence of our increasingly sedentary pediatric population? Falling off the couch seldom creates an injury that generates an ED statistic. Myopia and obesity related to excess screen time doesn’t trigger data points in this study. Overexertion injuries are down. We already know the consequences of underexertion are up.
I’m not sure we need to cut back on our efforts at injury prevention but I worry that we may run the risk of discouraging healthy activity if we aren’t careful with our voices of caution.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I suspect that, like me, you were saddened, but maybe not shocked, to learn that firearm-related fatalities have recently surpassed motor vehicle–related fatalities as the leading cause of death among children. For those of us living in Maine, this revelation came at a particularly difficult time. The body of the presumed shooter in the Lewiston massacre was found less than 10 miles from where I am writing you this letter. There is a good chance he may have been a former patient of mine, but I no longer have access to my records to confirm that.
This reshuffling at the top of the list of mortality causes is just one example of the shifting trends that have occurred in pediatric fatality statistics. In a recent analysis of the Centers for Disease Control and Prevention statistics published in Pediatrics investigators discovered that while, in general, fatal injuries have increased over the study period (2011-2021) nonfatal injuries have decreased.
We should no longer be surprised to learn that firearm-related deaths increased more than 87%. Fatal drug poisoning was up 133% and suffocation-related deaths increased 12.5% over that 10-year period. Given this profile of fatalities, it shouldn’t surprise us that nonfatal injuries due to firearms, poisoning, and self-harm also increased.
However, nonfatal injuries in other broad categories decreased: falls were down 52.8%, overexertion 63%, struck by [something or someone] 47.3%, motor vehicle occupant 36.7%, and cut pierce 36.7%. Nonfatal drownings were unchanged.
Diverging trends
What are we to make of these diverging trends? I suspect that when it comes to both firearms and drug poisonings, both fatal and nonfatal, children are now living in an environment in which the sheer volume of guns and drugs have grown the point, and will continue to grow, that contact and its consequences will continue to increase until we reach a saturation point at some unpredictable point in the future. There still may be some opportunities to curb the flow of drugs. But, I am afraid when it comes to firearms, that ship has sailed. We may have a chance to curb assault weapons, but hand guns have become ubiquitous to the point that they will continue to be a threat to children.
The increase in self-harm injuries is clearly a reflection of the increase in pediatric and adolescent mental health disturbances, which in turn is a reflection of the gloom hanging over the population in general.
But, what’s going on with the decrease in nonfatal injuries caused by falls, overexertion, struck by, and cut pierce? Is this a bit of sunshine in an otherwise cloudy picture? The authors of the paper see it as a reflection of our “public health interventions targeting pediatric safety partnered with technological advancement and legislative requirements.” Maybe when we are talking about booster seats and other automotive safety advancements. But I’m not so sure we should be too vigorous as we pat ourselves on the back.
On the other hand, aren’t these decreases in injuries related to activity just more evidence of our increasingly sedentary pediatric population? Falling off the couch seldom creates an injury that generates an ED statistic. Myopia and obesity related to excess screen time doesn’t trigger data points in this study. Overexertion injuries are down. We already know the consequences of underexertion are up.
I’m not sure we need to cut back on our efforts at injury prevention but I worry that we may run the risk of discouraging healthy activity if we aren’t careful with our voices of caution.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
I suspect that, like me, you were saddened, but maybe not shocked, to learn that firearm-related fatalities have recently surpassed motor vehicle–related fatalities as the leading cause of death among children. For those of us living in Maine, this revelation came at a particularly difficult time. The body of the presumed shooter in the Lewiston massacre was found less than 10 miles from where I am writing you this letter. There is a good chance he may have been a former patient of mine, but I no longer have access to my records to confirm that.
This reshuffling at the top of the list of mortality causes is just one example of the shifting trends that have occurred in pediatric fatality statistics. In a recent analysis of the Centers for Disease Control and Prevention statistics published in Pediatrics investigators discovered that while, in general, fatal injuries have increased over the study period (2011-2021) nonfatal injuries have decreased.
We should no longer be surprised to learn that firearm-related deaths increased more than 87%. Fatal drug poisoning was up 133% and suffocation-related deaths increased 12.5% over that 10-year period. Given this profile of fatalities, it shouldn’t surprise us that nonfatal injuries due to firearms, poisoning, and self-harm also increased.
However, nonfatal injuries in other broad categories decreased: falls were down 52.8%, overexertion 63%, struck by [something or someone] 47.3%, motor vehicle occupant 36.7%, and cut pierce 36.7%. Nonfatal drownings were unchanged.
Diverging trends
What are we to make of these diverging trends? I suspect that when it comes to both firearms and drug poisonings, both fatal and nonfatal, children are now living in an environment in which the sheer volume of guns and drugs have grown the point, and will continue to grow, that contact and its consequences will continue to increase until we reach a saturation point at some unpredictable point in the future. There still may be some opportunities to curb the flow of drugs. But, I am afraid when it comes to firearms, that ship has sailed. We may have a chance to curb assault weapons, but hand guns have become ubiquitous to the point that they will continue to be a threat to children.
The increase in self-harm injuries is clearly a reflection of the increase in pediatric and adolescent mental health disturbances, which in turn is a reflection of the gloom hanging over the population in general.
But, what’s going on with the decrease in nonfatal injuries caused by falls, overexertion, struck by, and cut pierce? Is this a bit of sunshine in an otherwise cloudy picture? The authors of the paper see it as a reflection of our “public health interventions targeting pediatric safety partnered with technological advancement and legislative requirements.” Maybe when we are talking about booster seats and other automotive safety advancements. But I’m not so sure we should be too vigorous as we pat ourselves on the back.
On the other hand, aren’t these decreases in injuries related to activity just more evidence of our increasingly sedentary pediatric population? Falling off the couch seldom creates an injury that generates an ED statistic. Myopia and obesity related to excess screen time doesn’t trigger data points in this study. Overexertion injuries are down. We already know the consequences of underexertion are up.
I’m not sure we need to cut back on our efforts at injury prevention but I worry that we may run the risk of discouraging healthy activity if we aren’t careful with our voices of caution.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Staying in my lane
In one of my favorite fall rituals, I fired up my hot tub. In Phoenix the months for relaxing in one are limited, so I try to enjoy it when I can.
It’s a routine I know well. Remove the coverings it’s been hiding under for the 8-month Phoenix summer. Clean out the dust, dead bugs, leaves. Connect the pipes and hoses, tighten the clamps, and begin filling it with water. A pinch of water softener, a dash of chlorine, plug in the motor, and stir.
After a few minutes of running, however, I noticed water starting to come out from under the motor unit. That ain’t good. I checked the fittings to make sure everything was in place and tight. They were. So the problem was somewhere inside the motor.
I unplugged the hot tub and went to my computer. Using the ever-popular Google, I looked at diagrams of motor plumbing and wiring, then watched several DIY videos on YouTube.
After about an hour of this I got some screwdrivers, went back out to the hot tub, stared at it for a few minutes ... then I realized I was out of my league and called a repair service.
I’m a neurologist. I hope I’m a decent one. But I’m not a hot tub mechanic anymore than I am a neurosurgeon. Or, as Bones McCoy would have said, “Dammit, Jim, I’m a doctor, not a spa repairman.” Either way, I was out of my league and I knew it. My taking the motor apart – while certainly feasible – was more likely to make things worse.
Unfortunately, not everyone feels the same way. Although I spent quite a few years learning to be a neurologist, it’s amazing how many people feel that, after a similar time on Google, they’re qualified to diagnose and treat neurological (or any medical) conditions. They know what they have, what tests need to be done, and which medications should be prescribed. They only need me to rubber stamp their plan, since their insurance won’t take orders from them. (They often won’t take orders from me, either, but that’s another matter).
While occasionally they’re correct, most of the time I have to politely explain why I disagree with them, or why other possibilities have to be considered and treated. No one is forcing them to follow my plan, but if they aren’t happy with it, they’ll have to find another neurologist. I have to go with my education and experience over theirs. I mean, this is my job. I’ve been doing it for more than 25 years.
I’m sure if the hot tub mechanic showed up and I told him where and how to fix the problem he’d wonder what my qualifications were. I may be right, but I may be crazy (or at least wrong).
Unlike medicine, there’s nothing to keep me from trying to fix the hot tub myself, except my own awareness that I have no practical idea how to do so.
I try my best not to practice outside of my field. Google isn’t going to make me a cardiologist any more than it will let me fix hot tubs.
I’m all for knowledge, but it also has its limits. Why some patients think the Internet is a good substitute for 9 years of education and 25 years of ongoing experience, I have no idea.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In one of my favorite fall rituals, I fired up my hot tub. In Phoenix the months for relaxing in one are limited, so I try to enjoy it when I can.
It’s a routine I know well. Remove the coverings it’s been hiding under for the 8-month Phoenix summer. Clean out the dust, dead bugs, leaves. Connect the pipes and hoses, tighten the clamps, and begin filling it with water. A pinch of water softener, a dash of chlorine, plug in the motor, and stir.
After a few minutes of running, however, I noticed water starting to come out from under the motor unit. That ain’t good. I checked the fittings to make sure everything was in place and tight. They were. So the problem was somewhere inside the motor.
I unplugged the hot tub and went to my computer. Using the ever-popular Google, I looked at diagrams of motor plumbing and wiring, then watched several DIY videos on YouTube.
After about an hour of this I got some screwdrivers, went back out to the hot tub, stared at it for a few minutes ... then I realized I was out of my league and called a repair service.
I’m a neurologist. I hope I’m a decent one. But I’m not a hot tub mechanic anymore than I am a neurosurgeon. Or, as Bones McCoy would have said, “Dammit, Jim, I’m a doctor, not a spa repairman.” Either way, I was out of my league and I knew it. My taking the motor apart – while certainly feasible – was more likely to make things worse.
Unfortunately, not everyone feels the same way. Although I spent quite a few years learning to be a neurologist, it’s amazing how many people feel that, after a similar time on Google, they’re qualified to diagnose and treat neurological (or any medical) conditions. They know what they have, what tests need to be done, and which medications should be prescribed. They only need me to rubber stamp their plan, since their insurance won’t take orders from them. (They often won’t take orders from me, either, but that’s another matter).
While occasionally they’re correct, most of the time I have to politely explain why I disagree with them, or why other possibilities have to be considered and treated. No one is forcing them to follow my plan, but if they aren’t happy with it, they’ll have to find another neurologist. I have to go with my education and experience over theirs. I mean, this is my job. I’ve been doing it for more than 25 years.
I’m sure if the hot tub mechanic showed up and I told him where and how to fix the problem he’d wonder what my qualifications were. I may be right, but I may be crazy (or at least wrong).
Unlike medicine, there’s nothing to keep me from trying to fix the hot tub myself, except my own awareness that I have no practical idea how to do so.
I try my best not to practice outside of my field. Google isn’t going to make me a cardiologist any more than it will let me fix hot tubs.
I’m all for knowledge, but it also has its limits. Why some patients think the Internet is a good substitute for 9 years of education and 25 years of ongoing experience, I have no idea.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
In one of my favorite fall rituals, I fired up my hot tub. In Phoenix the months for relaxing in one are limited, so I try to enjoy it when I can.
It’s a routine I know well. Remove the coverings it’s been hiding under for the 8-month Phoenix summer. Clean out the dust, dead bugs, leaves. Connect the pipes and hoses, tighten the clamps, and begin filling it with water. A pinch of water softener, a dash of chlorine, plug in the motor, and stir.
After a few minutes of running, however, I noticed water starting to come out from under the motor unit. That ain’t good. I checked the fittings to make sure everything was in place and tight. They were. So the problem was somewhere inside the motor.
I unplugged the hot tub and went to my computer. Using the ever-popular Google, I looked at diagrams of motor plumbing and wiring, then watched several DIY videos on YouTube.
After about an hour of this I got some screwdrivers, went back out to the hot tub, stared at it for a few minutes ... then I realized I was out of my league and called a repair service.
I’m a neurologist. I hope I’m a decent one. But I’m not a hot tub mechanic anymore than I am a neurosurgeon. Or, as Bones McCoy would have said, “Dammit, Jim, I’m a doctor, not a spa repairman.” Either way, I was out of my league and I knew it. My taking the motor apart – while certainly feasible – was more likely to make things worse.
Unfortunately, not everyone feels the same way. Although I spent quite a few years learning to be a neurologist, it’s amazing how many people feel that, after a similar time on Google, they’re qualified to diagnose and treat neurological (or any medical) conditions. They know what they have, what tests need to be done, and which medications should be prescribed. They only need me to rubber stamp their plan, since their insurance won’t take orders from them. (They often won’t take orders from me, either, but that’s another matter).
While occasionally they’re correct, most of the time I have to politely explain why I disagree with them, or why other possibilities have to be considered and treated. No one is forcing them to follow my plan, but if they aren’t happy with it, they’ll have to find another neurologist. I have to go with my education and experience over theirs. I mean, this is my job. I’ve been doing it for more than 25 years.
I’m sure if the hot tub mechanic showed up and I told him where and how to fix the problem he’d wonder what my qualifications were. I may be right, but I may be crazy (or at least wrong).
Unlike medicine, there’s nothing to keep me from trying to fix the hot tub myself, except my own awareness that I have no practical idea how to do so.
I try my best not to practice outside of my field. Google isn’t going to make me a cardiologist any more than it will let me fix hot tubs.
I’m all for knowledge, but it also has its limits. Why some patients think the Internet is a good substitute for 9 years of education and 25 years of ongoing experience, I have no idea.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Is most Parkinson’s disease man-made and therefore preventable?
This transcript has been edited for clarity.
Indu Subramanian, MD: It’s my pleasure to have Ray Dorsey on our program today. Ray is a professor of neurology at the University of Rochester and has been doing some amazing advocacy work in largely the space of trying to end Parkinson’s disease.
E. Ray Dorsey, MD: Thanks very much for having me, Indu. I’m delighted to be with you.
Trichloroethylene and PD
Dr. Subramanian: I wanted to first that we talk about as something that is in pretty much everywhere. This paper came out, and you wrote a commentary in JAMA Neurology as well. Perhaps we can summarize the paper and its findings.
Dr. Dorsey: Like most people, I didn’t know what TCE was until about 5 or 6 years ago. TCE is a very simple molecule. It’s got six atoms – two carbon atoms, one hydrogen atom, and three chlorine atoms — hence, its name “trichloroethylene.” There’s a very similar chemical called perchloroethylene, which is widely used in dry cleaning. It’s got one additional chlorine atom, and the prefix “per-” means “four.” I’ll talk about TCE predominantly, but both of these chemicals probably have similar toxicity with respect to Parkinson’s disease.
Research done by Dr. Carlie Tanner and Dr. Sam Goldman about a decade ago showed that in twins who were exposed to this through their work (it’s widely used as a degreasing agent) or hobbies (it’s used in printing and painting, by varnish workers, or by anyone that needs it as a solvent) had a 500% increased risk of developing Parkinson’s disease. Importantly, in that study, they showed that there was a lag time of 10-40 years between exposure to that chemical and the diagnosis of the disease. Because TCE was so widely used, they said that public health implications could be substantial.
What’s Camp Lejeune? Camp Lejeune is a Marine base in North Carolina where many Marines are trained. Between 1953 and 1987 at that Marine base, the drinking water was contaminated with TCE, perchloroethylene, and other toxic chemicals. The reason Camp Lejeune is so infamous is because the Marines knew about the contamination for many years and covered it up.
Indeed, this story only came to the forefront because Jennie Ensminger, the daughter of a Marine drill instructor, developed leukemia at age 6 and died at age 9. Her father, Jerry Ensminger, a retired master sergeant, found out after the fact that these cancer-causing chemicals, including TCE, a known carcinogen, were found at the Marine base and could be an explanation for why his daughter developed and died of leukemia.
Dr. Sam Goldman and Dr. Carlie Tanner and colleagues from UCSF looked at the rates of Parkinson’s among Marines who served at Camp Lejeune during the 1970s and compared that with rates in Marines who served Camp Pendleton on the West Coast. It turned out that the Marines who served at Camp Lejeune had a 70% higher risk of developing Parkinson’s disease than the Marines who served at Camp Pendleton.
Importantly, these Marines, by definition, were healthy. They were young. They were only 20 years old, on average, when they were at Camp Lejeune. They stayed at a Marine base for a short period of time, so on average, they were only there for 2 years. Yet 30 years later, they had a 70% increased risk of developing Parkinson’s disease.
Ending Parkinson’s disease
Dr. Subramanian: Wow, that’s pretty profound. You’ve done a large amount of work, and in fact you, along with some of our colleagues wrote a book about ending Parkinson’s disease. I read that book when it came out a couple of years ago, and I was really struck by a few things. Parkinson’s has doubled in the past 40 years and is going to double again in the next 20 years. Can you tell me a little bit about that statistic and why that is? It’s not just because people are aging. What is the sense of that? How do we interpret that?
Dr. Dorsey: According to the Global Burden of Disease study, which I was fortunate to be part of, the number of people with Parkinson’s disease has more than doubled in the past 25 years. A conservative projection based on aging alone suggests that it’s going to double again unless we change something about it. It’s now the world’s fastest-growing brain disease, and it is growing faster than can be explained by aging alone.
If you look at the map of Parkinson’s disease, if you thought it was purely genetic, you would have a relatively uniform map of rates of Parkinson’s disease. In fact, we don’t see that. Rates of Parkinson’s are five times higher in industrialized parts of the world, like the United States and Canada, than they are in sub-Saharan Africa. Rates of Parkinson’s disease are increasing most rapidly in areas of world that are undergoing the most rapid industrialization, such as India and China, where adjusted for age, the rates of Parkinson’s have more than doubled in the past 25 years.
The thesis of our book is that much of Parkinson’s disease is man-made. Work done by your colleagues at UCLA, including Jeff Bronstein and Beate Ritz, have demonstrated that air pollution and certain pesticides are likely fueling the rise of Parkinson’s disease.
Given that in the United States, rates of Parkinson’s disease are actually higher in urban and suburban areas than they are in rural areas, I think that this dry-cleaning chemical – which was widely used in the 1970s in everything from typewriter correction fluid to decaffeinated coffee and [over] 2 pounds per American [was produced] – could be one of the most important causes or contributing factors to Parkinson’s disease.
What to tell patients
Dr. Subramanian: For the general neurologists or practitioners out there watching this, what can they do? If you have a patient whom you suspect may have been exposed to toxins, what should we tell people who aren’t patients yet who are at risk? What are some things that you think would be helpful?
Dr. Dorsey: I think one of the shortcomings of American medicine is that we often just go from diagnosis to treatment. You’re depressed, you get an antidepressant; you have Parkinson’s disease, you get levodopa; you have seizures, you get put on an antiepileptic medication.
I think we need to spend a couple of minutes at least, maybe at the beginning, to go to the diagnosis of the condition and why you have this disease. If you just do a brief occupational history, after you start the exam – things like finding out what people do for a living or did for a living or how they spend their time – I think you’ll find many of these risk factors are actually present.
It’s pretty easy to identify whether people grew up in a rural area and drank well water, which is prone to be contaminated with pesticides. We know that people who drink [contaminated] well water have about a 75% increased risk of developing Parkinson’s disease. I think you can find for people, especially when they grew up, when they were young, that the most relevant exposure might be that when people were young children.
It’s a little bit harder to identify all exposure to TCE. The Marines at Camp Lejeune didn’t know they were drinking the water that was contaminated with this and only found out about it after the fact because Jerry Ensminger launched a 26-year campaign to bring justice for the Marines and their dependents.
Some people who know that they work with chemicals or with solvents might know about this. In New York City, these chemicals are widely used in dry cleaning. They’re readily volatile. These chemicals can evaporate from dry-cleaning buildings and go into the indoor air of apartments above dry cleaners, for example, in New York City. That can be in toxic levels. These readily dissolve in fat, hence their use in degreasing.
There have been studies, for example, in Germany, that found that supermarkets that are simply near a dry cleaner will have TCE or perchloroethylene in the butter and the cheese that they’re selling.
It gets even worse. For example, you bring your daughter into the dry-cleaning building and she’s eating an ice cream cone. When she leaves, she’s eating perchloroethylene and TCE.
It’s a little bit harder to find it, but I think it’s relevant because some people might be still being exposed and some people might still be drinking well water and they rarely have their well tested. For those people, I recommend they get their well tested and I recommend all my patients to get a carbon filter to decrease exposure to pesticides and chemicals. A carbon filter is just like what Brita and Pure and other brands are.
Because they’re chemicals known to cause cancer, I get a little bit concerned about cancer screening. This is most strongly tied to non-Hodgkin lymphoma, liver cancer, and renal cancer. It’s also linked to multiple myeloma, prostate cancer, probably brain cancer, and probably breast cancer, especially in men.
I tell people to be concerned about those, and then I tell people to avoid pesticides if they have Parkinson’s disease in all its forms, not only in the drinking water but in the produce you buy, the food you eat, what you put on your lawn, what’s on the golf course where you play, and the like.
Dr. Subramanian: I would say, just from the wellness perspective, if people are at risk for degenerative disease in terms of their brain health, things like sleep, mind-body practices, exercise, diet (Mediterranean or organic, if you can), and avoiding pesticides are all important. Social connection is important as well – the things that we think are helpful in general as people age and to prevent Alzheimer’s and other things like that.
Dr. Dorsey: These are fantastic ways to modify disease course. The evidence for them is only increasing. There’s an analogy I like to use. If someone is diagnosed with lung cancer, the first thing we tell them to do is to stop smoking. If someone’s diagnosed with Parkinson’s, we don’t tell them to stop getting exposure to pesticides. We don’t tell them to stop dry cleaning their clothes. We don’t tell them to avoid air pollution. These are all risk factors that are increasingly well established for Parkinson’s disease.
I think Parkinson’s disease, fundamentally for the vast majority of people, is an entirely preventable disease. We’re not taking actions to prevent people from getting this very disabling and very deadly disease.
Advocacy work
Dr. Subramanian: You and I are quite interested in the sense of being advocates as neurologists, and I think it fuels our passion and helps us to wake up every morning feeling like we have something that is meaningful and purposeful in our lives. Could you describe this as your passion and how it may prevent burnout and what it’s given you as a neurologist?
Dr. Dorsey: The credit for much of this is Dr. Carlie Tanner at UC San Francisco. I had the gift of sabbatical and I started reading the literature, I started reading her literature, and I came away with that, over the past 25 years, she detailed these environmental risk factors that are linked to Parkinson’s disease. Pesticides, these dry-cleaning chemicals, and air pollution. When I read it, I just realized that this was the case.
The same time I was reading her work, I read this book called “How to Survive a Plague,” by David France, who was a member of a group called Act Up, which was a group of men in New York City who reacted to the emergence of HIV in the 1980s. If you remember the 1980s, there was no federal response to HIV. People were blamed for the diseases that they were developing. It was only because brave men and women in New York City and in San Francisco banded together and organized that they changed the course of HIV.
They didn’t just do it for themselves. They did it for all of us. You and I and many people may not have HIV because of their courage. They made HIV a treatable condition. It’s actually more treatable than Parkinson’s disease. It’s associated with a near-normal life expectancy. They also made it a preventable disease. Thousands, if not millions, of us don’t have HIV because of their work. It’s an increasingly less common disease. Rates of HIV are actually decreasing, which is something that you or I would never have expected when we were in medical training.
I can’t think of a better outcome for a neurologist or any physician than to make the diseases that they’re caring for nonexistent ... than if we lived in a world that didn’t have HIV, we lived in a world where lung cancer largely didn’t exist. We’ve had worlds in the past where Parkinson’s probably didn’t exist or existed in extremely small numbers. That might be true for diffuse Lewy body disease and others, and if these diseases are preventable, we can take actions as individuals and as a society to lower our risk.
What a wonderful gift for future generations and many generations to come, hopefully, to live in a world that’s largely devoid of Parkinson’s disease. Just like we live in a world free of typhus. We live in a world free of smallpox. We live in a world where polio is extraordinarily uncommon. We don’t even have treatments for polio because we just don’t have polio. I think we can do the same thing for Parkinson’s disease for the vast majority.
Dr. Subramanian: Thank you so much, Ray, for your advocacy. We’re getting to the point in neurology, which is exciting to me, of possibly primary prevention of some of these disorders. I think we have a role in that, which is exciting for the future.
Dr. Dorsey: Absolutely.
Dr. Subramanian is clinical professor, department of neurology, University of California Los Angeles, and director of PADRECC (Parkinson’s Disease Research, Education, and Clinical Centers), West Los Angeles Veterans Association, Los Angeles. She disclosed ties with Acorda Pharma. Dr. Dorsey is the David M. Levy Professor of Neurology, University of Rochester (N.Y.). He disclosed ties to Abbott, AbbVie, Acadia, Acorda Therapeutics, Averitas Pharma, Biogen, BioSensics, Boehringer Ingelheim, Burroughs Wellcome Fund, Caraway Therapeutics, CuraSen, DConsult2, Denali Therapeutics, Eli Lilly, Genentech, Health & Wellness Partners, HMP Education, Included Health, Karger, KOL Groups, Life Sciences, Mediflix, Medrhythms, Merck; MJH Holdings, North American Center for Continuing Medical Education, Novartis, Otsuka, Pfizer, Photopharmics, Praxis Medicine, Roche, Safra Foundation, Sanofi, Seelos Therapeutics, SemCap, Spark Therapeutics, Springer Healthcare, Synapticure, Theravance Biopharmaceuticals, and WebMD.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Indu Subramanian, MD: It’s my pleasure to have Ray Dorsey on our program today. Ray is a professor of neurology at the University of Rochester and has been doing some amazing advocacy work in largely the space of trying to end Parkinson’s disease.
E. Ray Dorsey, MD: Thanks very much for having me, Indu. I’m delighted to be with you.
Trichloroethylene and PD
Dr. Subramanian: I wanted to first that we talk about as something that is in pretty much everywhere. This paper came out, and you wrote a commentary in JAMA Neurology as well. Perhaps we can summarize the paper and its findings.
Dr. Dorsey: Like most people, I didn’t know what TCE was until about 5 or 6 years ago. TCE is a very simple molecule. It’s got six atoms – two carbon atoms, one hydrogen atom, and three chlorine atoms — hence, its name “trichloroethylene.” There’s a very similar chemical called perchloroethylene, which is widely used in dry cleaning. It’s got one additional chlorine atom, and the prefix “per-” means “four.” I’ll talk about TCE predominantly, but both of these chemicals probably have similar toxicity with respect to Parkinson’s disease.
Research done by Dr. Carlie Tanner and Dr. Sam Goldman about a decade ago showed that in twins who were exposed to this through their work (it’s widely used as a degreasing agent) or hobbies (it’s used in printing and painting, by varnish workers, or by anyone that needs it as a solvent) had a 500% increased risk of developing Parkinson’s disease. Importantly, in that study, they showed that there was a lag time of 10-40 years between exposure to that chemical and the diagnosis of the disease. Because TCE was so widely used, they said that public health implications could be substantial.
What’s Camp Lejeune? Camp Lejeune is a Marine base in North Carolina where many Marines are trained. Between 1953 and 1987 at that Marine base, the drinking water was contaminated with TCE, perchloroethylene, and other toxic chemicals. The reason Camp Lejeune is so infamous is because the Marines knew about the contamination for many years and covered it up.
Indeed, this story only came to the forefront because Jennie Ensminger, the daughter of a Marine drill instructor, developed leukemia at age 6 and died at age 9. Her father, Jerry Ensminger, a retired master sergeant, found out after the fact that these cancer-causing chemicals, including TCE, a known carcinogen, were found at the Marine base and could be an explanation for why his daughter developed and died of leukemia.
Dr. Sam Goldman and Dr. Carlie Tanner and colleagues from UCSF looked at the rates of Parkinson’s among Marines who served at Camp Lejeune during the 1970s and compared that with rates in Marines who served Camp Pendleton on the West Coast. It turned out that the Marines who served at Camp Lejeune had a 70% higher risk of developing Parkinson’s disease than the Marines who served at Camp Pendleton.
Importantly, these Marines, by definition, were healthy. They were young. They were only 20 years old, on average, when they were at Camp Lejeune. They stayed at a Marine base for a short period of time, so on average, they were only there for 2 years. Yet 30 years later, they had a 70% increased risk of developing Parkinson’s disease.
Ending Parkinson’s disease
Dr. Subramanian: Wow, that’s pretty profound. You’ve done a large amount of work, and in fact you, along with some of our colleagues wrote a book about ending Parkinson’s disease. I read that book when it came out a couple of years ago, and I was really struck by a few things. Parkinson’s has doubled in the past 40 years and is going to double again in the next 20 years. Can you tell me a little bit about that statistic and why that is? It’s not just because people are aging. What is the sense of that? How do we interpret that?
Dr. Dorsey: According to the Global Burden of Disease study, which I was fortunate to be part of, the number of people with Parkinson’s disease has more than doubled in the past 25 years. A conservative projection based on aging alone suggests that it’s going to double again unless we change something about it. It’s now the world’s fastest-growing brain disease, and it is growing faster than can be explained by aging alone.
If you look at the map of Parkinson’s disease, if you thought it was purely genetic, you would have a relatively uniform map of rates of Parkinson’s disease. In fact, we don’t see that. Rates of Parkinson’s are five times higher in industrialized parts of the world, like the United States and Canada, than they are in sub-Saharan Africa. Rates of Parkinson’s disease are increasing most rapidly in areas of world that are undergoing the most rapid industrialization, such as India and China, where adjusted for age, the rates of Parkinson’s have more than doubled in the past 25 years.
The thesis of our book is that much of Parkinson’s disease is man-made. Work done by your colleagues at UCLA, including Jeff Bronstein and Beate Ritz, have demonstrated that air pollution and certain pesticides are likely fueling the rise of Parkinson’s disease.
Given that in the United States, rates of Parkinson’s disease are actually higher in urban and suburban areas than they are in rural areas, I think that this dry-cleaning chemical – which was widely used in the 1970s in everything from typewriter correction fluid to decaffeinated coffee and [over] 2 pounds per American [was produced] – could be one of the most important causes or contributing factors to Parkinson’s disease.
What to tell patients
Dr. Subramanian: For the general neurologists or practitioners out there watching this, what can they do? If you have a patient whom you suspect may have been exposed to toxins, what should we tell people who aren’t patients yet who are at risk? What are some things that you think would be helpful?
Dr. Dorsey: I think one of the shortcomings of American medicine is that we often just go from diagnosis to treatment. You’re depressed, you get an antidepressant; you have Parkinson’s disease, you get levodopa; you have seizures, you get put on an antiepileptic medication.
I think we need to spend a couple of minutes at least, maybe at the beginning, to go to the diagnosis of the condition and why you have this disease. If you just do a brief occupational history, after you start the exam – things like finding out what people do for a living or did for a living or how they spend their time – I think you’ll find many of these risk factors are actually present.
It’s pretty easy to identify whether people grew up in a rural area and drank well water, which is prone to be contaminated with pesticides. We know that people who drink [contaminated] well water have about a 75% increased risk of developing Parkinson’s disease. I think you can find for people, especially when they grew up, when they were young, that the most relevant exposure might be that when people were young children.
It’s a little bit harder to identify all exposure to TCE. The Marines at Camp Lejeune didn’t know they were drinking the water that was contaminated with this and only found out about it after the fact because Jerry Ensminger launched a 26-year campaign to bring justice for the Marines and their dependents.
Some people who know that they work with chemicals or with solvents might know about this. In New York City, these chemicals are widely used in dry cleaning. They’re readily volatile. These chemicals can evaporate from dry-cleaning buildings and go into the indoor air of apartments above dry cleaners, for example, in New York City. That can be in toxic levels. These readily dissolve in fat, hence their use in degreasing.
There have been studies, for example, in Germany, that found that supermarkets that are simply near a dry cleaner will have TCE or perchloroethylene in the butter and the cheese that they’re selling.
It gets even worse. For example, you bring your daughter into the dry-cleaning building and she’s eating an ice cream cone. When she leaves, she’s eating perchloroethylene and TCE.
It’s a little bit harder to find it, but I think it’s relevant because some people might be still being exposed and some people might still be drinking well water and they rarely have their well tested. For those people, I recommend they get their well tested and I recommend all my patients to get a carbon filter to decrease exposure to pesticides and chemicals. A carbon filter is just like what Brita and Pure and other brands are.
Because they’re chemicals known to cause cancer, I get a little bit concerned about cancer screening. This is most strongly tied to non-Hodgkin lymphoma, liver cancer, and renal cancer. It’s also linked to multiple myeloma, prostate cancer, probably brain cancer, and probably breast cancer, especially in men.
I tell people to be concerned about those, and then I tell people to avoid pesticides if they have Parkinson’s disease in all its forms, not only in the drinking water but in the produce you buy, the food you eat, what you put on your lawn, what’s on the golf course where you play, and the like.
Dr. Subramanian: I would say, just from the wellness perspective, if people are at risk for degenerative disease in terms of their brain health, things like sleep, mind-body practices, exercise, diet (Mediterranean or organic, if you can), and avoiding pesticides are all important. Social connection is important as well – the things that we think are helpful in general as people age and to prevent Alzheimer’s and other things like that.
Dr. Dorsey: These are fantastic ways to modify disease course. The evidence for them is only increasing. There’s an analogy I like to use. If someone is diagnosed with lung cancer, the first thing we tell them to do is to stop smoking. If someone’s diagnosed with Parkinson’s, we don’t tell them to stop getting exposure to pesticides. We don’t tell them to stop dry cleaning their clothes. We don’t tell them to avoid air pollution. These are all risk factors that are increasingly well established for Parkinson’s disease.
I think Parkinson’s disease, fundamentally for the vast majority of people, is an entirely preventable disease. We’re not taking actions to prevent people from getting this very disabling and very deadly disease.
Advocacy work
Dr. Subramanian: You and I are quite interested in the sense of being advocates as neurologists, and I think it fuels our passion and helps us to wake up every morning feeling like we have something that is meaningful and purposeful in our lives. Could you describe this as your passion and how it may prevent burnout and what it’s given you as a neurologist?
Dr. Dorsey: The credit for much of this is Dr. Carlie Tanner at UC San Francisco. I had the gift of sabbatical and I started reading the literature, I started reading her literature, and I came away with that, over the past 25 years, she detailed these environmental risk factors that are linked to Parkinson’s disease. Pesticides, these dry-cleaning chemicals, and air pollution. When I read it, I just realized that this was the case.
The same time I was reading her work, I read this book called “How to Survive a Plague,” by David France, who was a member of a group called Act Up, which was a group of men in New York City who reacted to the emergence of HIV in the 1980s. If you remember the 1980s, there was no federal response to HIV. People were blamed for the diseases that they were developing. It was only because brave men and women in New York City and in San Francisco banded together and organized that they changed the course of HIV.
They didn’t just do it for themselves. They did it for all of us. You and I and many people may not have HIV because of their courage. They made HIV a treatable condition. It’s actually more treatable than Parkinson’s disease. It’s associated with a near-normal life expectancy. They also made it a preventable disease. Thousands, if not millions, of us don’t have HIV because of their work. It’s an increasingly less common disease. Rates of HIV are actually decreasing, which is something that you or I would never have expected when we were in medical training.
I can’t think of a better outcome for a neurologist or any physician than to make the diseases that they’re caring for nonexistent ... than if we lived in a world that didn’t have HIV, we lived in a world where lung cancer largely didn’t exist. We’ve had worlds in the past where Parkinson’s probably didn’t exist or existed in extremely small numbers. That might be true for diffuse Lewy body disease and others, and if these diseases are preventable, we can take actions as individuals and as a society to lower our risk.
What a wonderful gift for future generations and many generations to come, hopefully, to live in a world that’s largely devoid of Parkinson’s disease. Just like we live in a world free of typhus. We live in a world free of smallpox. We live in a world where polio is extraordinarily uncommon. We don’t even have treatments for polio because we just don’t have polio. I think we can do the same thing for Parkinson’s disease for the vast majority.
Dr. Subramanian: Thank you so much, Ray, for your advocacy. We’re getting to the point in neurology, which is exciting to me, of possibly primary prevention of some of these disorders. I think we have a role in that, which is exciting for the future.
Dr. Dorsey: Absolutely.
Dr. Subramanian is clinical professor, department of neurology, University of California Los Angeles, and director of PADRECC (Parkinson’s Disease Research, Education, and Clinical Centers), West Los Angeles Veterans Association, Los Angeles. She disclosed ties with Acorda Pharma. Dr. Dorsey is the David M. Levy Professor of Neurology, University of Rochester (N.Y.). He disclosed ties to Abbott, AbbVie, Acadia, Acorda Therapeutics, Averitas Pharma, Biogen, BioSensics, Boehringer Ingelheim, Burroughs Wellcome Fund, Caraway Therapeutics, CuraSen, DConsult2, Denali Therapeutics, Eli Lilly, Genentech, Health & Wellness Partners, HMP Education, Included Health, Karger, KOL Groups, Life Sciences, Mediflix, Medrhythms, Merck; MJH Holdings, North American Center for Continuing Medical Education, Novartis, Otsuka, Pfizer, Photopharmics, Praxis Medicine, Roche, Safra Foundation, Sanofi, Seelos Therapeutics, SemCap, Spark Therapeutics, Springer Healthcare, Synapticure, Theravance Biopharmaceuticals, and WebMD.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
Indu Subramanian, MD: It’s my pleasure to have Ray Dorsey on our program today. Ray is a professor of neurology at the University of Rochester and has been doing some amazing advocacy work in largely the space of trying to end Parkinson’s disease.
E. Ray Dorsey, MD: Thanks very much for having me, Indu. I’m delighted to be with you.
Trichloroethylene and PD
Dr. Subramanian: I wanted to first that we talk about as something that is in pretty much everywhere. This paper came out, and you wrote a commentary in JAMA Neurology as well. Perhaps we can summarize the paper and its findings.
Dr. Dorsey: Like most people, I didn’t know what TCE was until about 5 or 6 years ago. TCE is a very simple molecule. It’s got six atoms – two carbon atoms, one hydrogen atom, and three chlorine atoms — hence, its name “trichloroethylene.” There’s a very similar chemical called perchloroethylene, which is widely used in dry cleaning. It’s got one additional chlorine atom, and the prefix “per-” means “four.” I’ll talk about TCE predominantly, but both of these chemicals probably have similar toxicity with respect to Parkinson’s disease.
Research done by Dr. Carlie Tanner and Dr. Sam Goldman about a decade ago showed that in twins who were exposed to this through their work (it’s widely used as a degreasing agent) or hobbies (it’s used in printing and painting, by varnish workers, or by anyone that needs it as a solvent) had a 500% increased risk of developing Parkinson’s disease. Importantly, in that study, they showed that there was a lag time of 10-40 years between exposure to that chemical and the diagnosis of the disease. Because TCE was so widely used, they said that public health implications could be substantial.
What’s Camp Lejeune? Camp Lejeune is a Marine base in North Carolina where many Marines are trained. Between 1953 and 1987 at that Marine base, the drinking water was contaminated with TCE, perchloroethylene, and other toxic chemicals. The reason Camp Lejeune is so infamous is because the Marines knew about the contamination for many years and covered it up.
Indeed, this story only came to the forefront because Jennie Ensminger, the daughter of a Marine drill instructor, developed leukemia at age 6 and died at age 9. Her father, Jerry Ensminger, a retired master sergeant, found out after the fact that these cancer-causing chemicals, including TCE, a known carcinogen, were found at the Marine base and could be an explanation for why his daughter developed and died of leukemia.
Dr. Sam Goldman and Dr. Carlie Tanner and colleagues from UCSF looked at the rates of Parkinson’s among Marines who served at Camp Lejeune during the 1970s and compared that with rates in Marines who served Camp Pendleton on the West Coast. It turned out that the Marines who served at Camp Lejeune had a 70% higher risk of developing Parkinson’s disease than the Marines who served at Camp Pendleton.
Importantly, these Marines, by definition, were healthy. They were young. They were only 20 years old, on average, when they were at Camp Lejeune. They stayed at a Marine base for a short period of time, so on average, they were only there for 2 years. Yet 30 years later, they had a 70% increased risk of developing Parkinson’s disease.
Ending Parkinson’s disease
Dr. Subramanian: Wow, that’s pretty profound. You’ve done a large amount of work, and in fact you, along with some of our colleagues wrote a book about ending Parkinson’s disease. I read that book when it came out a couple of years ago, and I was really struck by a few things. Parkinson’s has doubled in the past 40 years and is going to double again in the next 20 years. Can you tell me a little bit about that statistic and why that is? It’s not just because people are aging. What is the sense of that? How do we interpret that?
Dr. Dorsey: According to the Global Burden of Disease study, which I was fortunate to be part of, the number of people with Parkinson’s disease has more than doubled in the past 25 years. A conservative projection based on aging alone suggests that it’s going to double again unless we change something about it. It’s now the world’s fastest-growing brain disease, and it is growing faster than can be explained by aging alone.
If you look at the map of Parkinson’s disease, if you thought it was purely genetic, you would have a relatively uniform map of rates of Parkinson’s disease. In fact, we don’t see that. Rates of Parkinson’s are five times higher in industrialized parts of the world, like the United States and Canada, than they are in sub-Saharan Africa. Rates of Parkinson’s disease are increasing most rapidly in areas of world that are undergoing the most rapid industrialization, such as India and China, where adjusted for age, the rates of Parkinson’s have more than doubled in the past 25 years.
The thesis of our book is that much of Parkinson’s disease is man-made. Work done by your colleagues at UCLA, including Jeff Bronstein and Beate Ritz, have demonstrated that air pollution and certain pesticides are likely fueling the rise of Parkinson’s disease.
Given that in the United States, rates of Parkinson’s disease are actually higher in urban and suburban areas than they are in rural areas, I think that this dry-cleaning chemical – which was widely used in the 1970s in everything from typewriter correction fluid to decaffeinated coffee and [over] 2 pounds per American [was produced] – could be one of the most important causes or contributing factors to Parkinson’s disease.
What to tell patients
Dr. Subramanian: For the general neurologists or practitioners out there watching this, what can they do? If you have a patient whom you suspect may have been exposed to toxins, what should we tell people who aren’t patients yet who are at risk? What are some things that you think would be helpful?
Dr. Dorsey: I think one of the shortcomings of American medicine is that we often just go from diagnosis to treatment. You’re depressed, you get an antidepressant; you have Parkinson’s disease, you get levodopa; you have seizures, you get put on an antiepileptic medication.
I think we need to spend a couple of minutes at least, maybe at the beginning, to go to the diagnosis of the condition and why you have this disease. If you just do a brief occupational history, after you start the exam – things like finding out what people do for a living or did for a living or how they spend their time – I think you’ll find many of these risk factors are actually present.
It’s pretty easy to identify whether people grew up in a rural area and drank well water, which is prone to be contaminated with pesticides. We know that people who drink [contaminated] well water have about a 75% increased risk of developing Parkinson’s disease. I think you can find for people, especially when they grew up, when they were young, that the most relevant exposure might be that when people were young children.
It’s a little bit harder to identify all exposure to TCE. The Marines at Camp Lejeune didn’t know they were drinking the water that was contaminated with this and only found out about it after the fact because Jerry Ensminger launched a 26-year campaign to bring justice for the Marines and their dependents.
Some people who know that they work with chemicals or with solvents might know about this. In New York City, these chemicals are widely used in dry cleaning. They’re readily volatile. These chemicals can evaporate from dry-cleaning buildings and go into the indoor air of apartments above dry cleaners, for example, in New York City. That can be in toxic levels. These readily dissolve in fat, hence their use in degreasing.
There have been studies, for example, in Germany, that found that supermarkets that are simply near a dry cleaner will have TCE or perchloroethylene in the butter and the cheese that they’re selling.
It gets even worse. For example, you bring your daughter into the dry-cleaning building and she’s eating an ice cream cone. When she leaves, she’s eating perchloroethylene and TCE.
It’s a little bit harder to find it, but I think it’s relevant because some people might be still being exposed and some people might still be drinking well water and they rarely have their well tested. For those people, I recommend they get their well tested and I recommend all my patients to get a carbon filter to decrease exposure to pesticides and chemicals. A carbon filter is just like what Brita and Pure and other brands are.
Because they’re chemicals known to cause cancer, I get a little bit concerned about cancer screening. This is most strongly tied to non-Hodgkin lymphoma, liver cancer, and renal cancer. It’s also linked to multiple myeloma, prostate cancer, probably brain cancer, and probably breast cancer, especially in men.
I tell people to be concerned about those, and then I tell people to avoid pesticides if they have Parkinson’s disease in all its forms, not only in the drinking water but in the produce you buy, the food you eat, what you put on your lawn, what’s on the golf course where you play, and the like.
Dr. Subramanian: I would say, just from the wellness perspective, if people are at risk for degenerative disease in terms of their brain health, things like sleep, mind-body practices, exercise, diet (Mediterranean or organic, if you can), and avoiding pesticides are all important. Social connection is important as well – the things that we think are helpful in general as people age and to prevent Alzheimer’s and other things like that.
Dr. Dorsey: These are fantastic ways to modify disease course. The evidence for them is only increasing. There’s an analogy I like to use. If someone is diagnosed with lung cancer, the first thing we tell them to do is to stop smoking. If someone’s diagnosed with Parkinson’s, we don’t tell them to stop getting exposure to pesticides. We don’t tell them to stop dry cleaning their clothes. We don’t tell them to avoid air pollution. These are all risk factors that are increasingly well established for Parkinson’s disease.
I think Parkinson’s disease, fundamentally for the vast majority of people, is an entirely preventable disease. We’re not taking actions to prevent people from getting this very disabling and very deadly disease.
Advocacy work
Dr. Subramanian: You and I are quite interested in the sense of being advocates as neurologists, and I think it fuels our passion and helps us to wake up every morning feeling like we have something that is meaningful and purposeful in our lives. Could you describe this as your passion and how it may prevent burnout and what it’s given you as a neurologist?
Dr. Dorsey: The credit for much of this is Dr. Carlie Tanner at UC San Francisco. I had the gift of sabbatical and I started reading the literature, I started reading her literature, and I came away with that, over the past 25 years, she detailed these environmental risk factors that are linked to Parkinson’s disease. Pesticides, these dry-cleaning chemicals, and air pollution. When I read it, I just realized that this was the case.
The same time I was reading her work, I read this book called “How to Survive a Plague,” by David France, who was a member of a group called Act Up, which was a group of men in New York City who reacted to the emergence of HIV in the 1980s. If you remember the 1980s, there was no federal response to HIV. People were blamed for the diseases that they were developing. It was only because brave men and women in New York City and in San Francisco banded together and organized that they changed the course of HIV.
They didn’t just do it for themselves. They did it for all of us. You and I and many people may not have HIV because of their courage. They made HIV a treatable condition. It’s actually more treatable than Parkinson’s disease. It’s associated with a near-normal life expectancy. They also made it a preventable disease. Thousands, if not millions, of us don’t have HIV because of their work. It’s an increasingly less common disease. Rates of HIV are actually decreasing, which is something that you or I would never have expected when we were in medical training.
I can’t think of a better outcome for a neurologist or any physician than to make the diseases that they’re caring for nonexistent ... than if we lived in a world that didn’t have HIV, we lived in a world where lung cancer largely didn’t exist. We’ve had worlds in the past where Parkinson’s probably didn’t exist or existed in extremely small numbers. That might be true for diffuse Lewy body disease and others, and if these diseases are preventable, we can take actions as individuals and as a society to lower our risk.
What a wonderful gift for future generations and many generations to come, hopefully, to live in a world that’s largely devoid of Parkinson’s disease. Just like we live in a world free of typhus. We live in a world free of smallpox. We live in a world where polio is extraordinarily uncommon. We don’t even have treatments for polio because we just don’t have polio. I think we can do the same thing for Parkinson’s disease for the vast majority.
Dr. Subramanian: Thank you so much, Ray, for your advocacy. We’re getting to the point in neurology, which is exciting to me, of possibly primary prevention of some of these disorders. I think we have a role in that, which is exciting for the future.
Dr. Dorsey: Absolutely.
Dr. Subramanian is clinical professor, department of neurology, University of California Los Angeles, and director of PADRECC (Parkinson’s Disease Research, Education, and Clinical Centers), West Los Angeles Veterans Association, Los Angeles. She disclosed ties with Acorda Pharma. Dr. Dorsey is the David M. Levy Professor of Neurology, University of Rochester (N.Y.). He disclosed ties to Abbott, AbbVie, Acadia, Acorda Therapeutics, Averitas Pharma, Biogen, BioSensics, Boehringer Ingelheim, Burroughs Wellcome Fund, Caraway Therapeutics, CuraSen, DConsult2, Denali Therapeutics, Eli Lilly, Genentech, Health & Wellness Partners, HMP Education, Included Health, Karger, KOL Groups, Life Sciences, Mediflix, Medrhythms, Merck; MJH Holdings, North American Center for Continuing Medical Education, Novartis, Otsuka, Pfizer, Photopharmics, Praxis Medicine, Roche, Safra Foundation, Sanofi, Seelos Therapeutics, SemCap, Spark Therapeutics, Springer Healthcare, Synapticure, Theravance Biopharmaceuticals, and WebMD.
A version of this article appeared on Medscape.com.