User login
Eyelid Plaque May Increase Risk for Severe Atherosclerosis
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
"The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease," Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).

The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a grey-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
"The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol," wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and his colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners. The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%).
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins containing apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died. The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years' smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the "presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk," the authors concluded.
This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The study authors reported that they had no other financial disclosures.
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
"In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population," Dr. Fernandez and Dr. Thompson wrote. There are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
"Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis," they noted.
Importantly, the results of this study confirm "that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia."
However, "what do these results mean in practice?" they asked. "Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. ... Patients with xanthelasmata may therefore require more aggressive management of risk factors," they concluded.
Dr. Fernandez is a clinical cardiology fellow at the Alpert Medical School at Brown University in Providence, R.I. Dr. Thompson is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
"In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population," Dr. Fernandez and Dr. Thompson wrote. There are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
"Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis," they noted.
Importantly, the results of this study confirm "that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia."
However, "what do these results mean in practice?" they asked. "Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. ... Patients with xanthelasmata may therefore require more aggressive management of risk factors," they concluded.
Dr. Fernandez is a clinical cardiology fellow at the Alpert Medical School at Brown University in Providence, R.I. Dr. Thompson is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
In an accompanying editorial, Dr. Antonio B. Fernandez and Dr. Paul D. Thompson discussed the clinical relevance of the findings.
"In the linked prospective cohort study, Christoffersen and colleagues assess whether xanthelasmata and arcus corneae, individually and combined, predict risk of ischemic vascular disease and death in the general population," Dr. Fernandez and Dr. Thompson wrote. There are some good reasons for suspecting such a link (BMJ 2011;343:d5304).
"Both xanthelasmata and arcus corneae are composed of cholesteryl esters similar to those found in serum low-density lipoprotein cholesterol and very low-density lipoprotein cholesterol. They share similar risk factors and have pathophysiological similarities with atherosclerosis," they noted.
Importantly, the results of this study confirm "that xanthelasmata are an important predictor of cardiovascular disease events and death beyond [their] known association with hyperlipidemia."
However, "what do these results mean in practice?" they asked. "Overall, the evidence highlights the importance of a comprehensive physical examination and suggests that xanthelasmata could be used by general clinicians to help identify people at higher risk of cardiovascular disease. These people may have an enhanced biological propensity to deposition of cholesterol in vascular and soft tissue, which is not fully represented by their fasting lipid profiles. ... Patients with xanthelasmata may therefore require more aggressive management of risk factors," they concluded.
Dr. Fernandez is a clinical cardiology fellow at the Alpert Medical School at Brown University in Providence, R.I. Dr. Thompson is the director of cardiology at Hartford (Conn.) Hospital. Dr. Thompson reported significant financial relationships with several pharmaceutical companies.
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
"The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease," Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).
The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a grey-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
"The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol," wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and his colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners. The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%).
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins containing apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died. The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years' smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the "presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk," the authors concluded.
This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The study authors reported that they had no other financial disclosures.
Plaque occurring around the eyelids may offer clinicians a new way of identifying patients at an increased risk for myocardial infarction and severe atherosclerosis, a study has shown.
"The results from this study suggest that xanthelasmata are a cutaneous marker of atherosclerosis independent of lipid concentrations and thus should be considered in clinical practice as an independent and additional risk factor for myocardial infarction and ischemic heart disease," Mette Christoffersen and her coinvestigators wrote in a study published online (BMJ 2011;343:d5497).
The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study of 12,745 patients. However, on multifactorial adjustment for arcus corneae, no hazard ratios remained significant. The presence of both xanthelasmata and arcus corneae significantly increased the risk of ischemic heart disease (HR, 1.56) but not any other outcomes after multifactorial adjustment.
Xanthelasmata palpebrarum are sharply demarcated, yellowish flat plaques that appear on the upper or lower eyelids, most often near the inner canthus. Xanthelasmata represent areas of macrophages containing lipids. Arcus corneae (or arcus senilis) is a grey-white-yellowish opacity that is located near the periphery of the cornea, though separated from the limbic margin by a clear corneal zone. Arcus corneae represents deposits of cholesteryl ester–rich lipid particles. It has been suggested that xanthelasmata and arcus corneae may be markers of proatherogenic changes in the vessels and thus markers of atherosclerosis.
"The findings from our study could be of particular value in societies where access to laboratory facilities, and thus lipid profile measurement, is difficult. In this setting, presence of xanthelasmata may be a useful predictor of underlying atherosclerotic disease. An easy registration of presence of xanthelasmata along with age and sex makes it possible to assess the risk of myocardial infarction and ischemic heart disease and thus to make sure that people at increased risk are managed accordingly with lifestyle changes and treatment to reduce low-density lipoprotein cholesterol," wrote Ms. Christoffersen, a clinical biochemistry PhD student at Rigshospitalet in Copenhagen, and his colleagues.
They used data from the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978 with follow-up examinations. A total of 19,329 white women and men of Danish descent were drawn randomly from the Copenhagen Central Person Registry and invited to participate. Data came from a self-administered questionnaire, a physical examination, and blood samples.
For this analysis, the researchers included 12,745 people, for whom complete information on all relevant variables, including xanthelasmata and arcus corneae, were available at baseline. The patients were followed from baseline at the 1976-1978 examination to the end of May 2009 through the use of their unique Central Person Register number. No participants were lost to follow-up.
Trained nurses or medical laboratory technicians determined the presence of xanthelasmata and arcus corneae by careful visual inspection of the eyelids and the cornea during the physical examination. The investigators collected and verified diagnoses of MI and ischemic heart disease using ICD-8 and ICD-10 codes by reviewing all hospital admissions, diagnoses entered in the national Danish Patient Registry, all causes of death entered in the national Danish Causes of Death Registry, and medical records from hospitals and general practitioners. The prevalence of xanthelasmata was 4.4% and similar in women and men. The prevalence of arcus corneae was 24.8% overall, but was lower in women than in men (20.1% vs. 30.2%).
Potential patients with ischemic cerebrovascular disease, including ischemic stroke, were collected from the national Danish Patient Registry and the national Danish Causes of Death Registry. Hospital records were reviewed by experienced neurologists. Ankle brachial index, a drop in blood pressure in the legs that predicts severe atherosclerosis, was determined in the 2001-2003 examination of the Copenhagen City Heart Study in 2,773 participants, who had also participated in the baseline examination and had complete information on all relevant variables, including xanthelasmata and arcus corneae.
Enzymatic methods were used on fresh plasma samples to measure plasma concentrations of total cholesterol, triglycerides, and high-density lipoprotein cholesterol, the last after precipitation of lipoproteins containing apolipoprotein B.
The median follow-up was 22 years. In all, 1,872 participants developed MI, 3,699 developed ischemic heart disease, 1,498 developed ischemic strokes, 1,815 developed ischemic cerebrovascular disease, and 8,507 died. The models were adjusted for age, sex, total cholesterol, triglycerides, body mass index, hypertension, diabetes, pack-years' smoking, alcohol consumption, physical activity, postmenopausal status, hormone therapy, education, income, and family history of ischemic vascular disease.
In this population, the "presence of xanthelasmata in itself predicts risk of myocardial infarction, ischemic heart disease, severe atherosclerosis, and death in the general population independent of well-known cardiovascular risk factors, including plasma cholesterol and triglyceride concentrations. In contrast, arcus corneae is not an important independent predictor of risk," the authors concluded.
This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The study authors reported that they had no other financial disclosures.
FROM BMJ
Major Finding: The presence of xanthelasmata predicted MI (hazard ratio, 1.48); ischemic heart disease (HR, 1.39); severe atherosclerosis determined by ankle brachial index (HR, 1.69); and death (HR, 1.14), in a Danish population-based study.
Data Source: Patients were part of the Copenhagen City Heart Study, which is a prospective cardiovascular study of the Danish general population that started in 1976-1978; a total of 19,329 white women and men of Danish descent were included at baseline.
Disclosures: This study was funded by the Research Fund at Rigshospitalet, the Lundbeck Foundation, the Danish Medical Research Council, and the Danish Heart Foundation. The authors reported that they had no other financial disclosures.
Global Breast, Cervical Cancer Estimate Hits 2 Million
Cervical and breast cancer may soon be as great a cause of death as is maternal mortality in reproductive-aged women worldwide, given calculated trends from a newly released study.
The worldwide incidence of breast cancer has tripled annually since 1980, reaching 1.6 million cases in 2010; mortality from breast cancer has increased at an annual rate of 1.8%, reaching 425,000.
While the worldwide incidence of cervical cancer has increased at a slower annual rate of 0.6%, reaching more than 450,000 cases in 2010, annual mortality from cervical cancer has increased by 0.46%, reaching 200,000 cases in the same period.
"On the basis of trends recorded in this study, breast and cervical cancer are likely to soon approach maternal causes as a crucial cause of mortality in women of reproductive age in developing countries," wrote Dr. Mohammad H. Forouzanfar and his coinvestigators at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle. The study was published online in the Lancet on Sept. 14 (doi:10.1016/S0140-6736[11]61351-2).
Twice as many breast cancer cases were recorded in developing countries among women aged 15-49 years as were in developed countries. New cases of cervical cancer occurred more often in developing countries (primarily in South and East Asia, Latin America, and Africa) across all age groups, while declining in high-income countries. In developing countries, there were 367,000 cases of breast cancer and 154,000 cases of cervical cancer among women aged 15-49 years. Three-quarters (76%) of cervical cancer cases occur in developing regions. In these areas of the world, 1.7 breast and cervical cancer deaths occur for every direct or indirect obstetric maternal death.
"Our findings suggest that breast and cervical cancer in low-income countries are major causes of death for women of these ages. The UN [United Nations] High-Level Meeting on Non-Communicable Diseases should raise policy awareness of the importance of the control of breast and cervical cancer, as should policy responses to improve reproductive health," the authors argued.
"Indeed, if the trends of the past 3 decades were to continue during the next 15 years, the ratio of maternal deaths to breast and cervical cancer deaths in developing countries in the reproductive age group will decrease from 2.3 to 1.3. In view of the potential for effective health system responses, greater efforts to reduce their disease burden are an important global health priority."
The researchers used information collected through population-based cancer registries, vital registration systems with medical certification of causes of death, and various subnational and national verbal autopsy studies. Their analysis comprised four components: database development, modeling MI ratios, estimation of trends in mortality by age, and estimation of trends in incidence. The investigators incorporated different data sources in a standardized approach to use all available information for every country.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day. Other forms of cancer kill three times this number of women daily, and the number of cancer deaths is even larger in men," wrote Dr. Coebergh, an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
The study was funded by Susan G. Komen for the Cure and the Bill and Melinda Gates Foundation.
The authors reported that they have no conflicts of interest. Dr. Coebergh reported that he has no conflicts of interest.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day," Dr. Coebergh wrote.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
Jan W. Coebergh, M.D., Ph.D., is an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam. He reported that he has no conflicts of interest.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day," Dr. Coebergh wrote.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
Jan W. Coebergh, M.D., Ph.D., is an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam. He reported that he has no conflicts of interest.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day," Dr. Coebergh wrote.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
Jan W. Coebergh, M.D., Ph.D., is an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam. He reported that he has no conflicts of interest.
Cervical and breast cancer may soon be as great a cause of death as is maternal mortality in reproductive-aged women worldwide, given calculated trends from a newly released study.
The worldwide incidence of breast cancer has tripled annually since 1980, reaching 1.6 million cases in 2010; mortality from breast cancer has increased at an annual rate of 1.8%, reaching 425,000.
While the worldwide incidence of cervical cancer has increased at a slower annual rate of 0.6%, reaching more than 450,000 cases in 2010, annual mortality from cervical cancer has increased by 0.46%, reaching 200,000 cases in the same period.
"On the basis of trends recorded in this study, breast and cervical cancer are likely to soon approach maternal causes as a crucial cause of mortality in women of reproductive age in developing countries," wrote Dr. Mohammad H. Forouzanfar and his coinvestigators at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle. The study was published online in the Lancet on Sept. 14 (doi:10.1016/S0140-6736[11]61351-2).
Twice as many breast cancer cases were recorded in developing countries among women aged 15-49 years as were in developed countries. New cases of cervical cancer occurred more often in developing countries (primarily in South and East Asia, Latin America, and Africa) across all age groups, while declining in high-income countries. In developing countries, there were 367,000 cases of breast cancer and 154,000 cases of cervical cancer among women aged 15-49 years. Three-quarters (76%) of cervical cancer cases occur in developing regions. In these areas of the world, 1.7 breast and cervical cancer deaths occur for every direct or indirect obstetric maternal death.
"Our findings suggest that breast and cervical cancer in low-income countries are major causes of death for women of these ages. The UN [United Nations] High-Level Meeting on Non-Communicable Diseases should raise policy awareness of the importance of the control of breast and cervical cancer, as should policy responses to improve reproductive health," the authors argued.
"Indeed, if the trends of the past 3 decades were to continue during the next 15 years, the ratio of maternal deaths to breast and cervical cancer deaths in developing countries in the reproductive age group will decrease from 2.3 to 1.3. In view of the potential for effective health system responses, greater efforts to reduce their disease burden are an important global health priority."
The researchers used information collected through population-based cancer registries, vital registration systems with medical certification of causes of death, and various subnational and national verbal autopsy studies. Their analysis comprised four components: database development, modeling MI ratios, estimation of trends in mortality by age, and estimation of trends in incidence. The investigators incorporated different data sources in a standardized approach to use all available information for every country.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day. Other forms of cancer kill three times this number of women daily, and the number of cancer deaths is even larger in men," wrote Dr. Coebergh, an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
The study was funded by Susan G. Komen for the Cure and the Bill and Melinda Gates Foundation.
The authors reported that they have no conflicts of interest. Dr. Coebergh reported that he has no conflicts of interest.
Cervical and breast cancer may soon be as great a cause of death as is maternal mortality in reproductive-aged women worldwide, given calculated trends from a newly released study.
The worldwide incidence of breast cancer has tripled annually since 1980, reaching 1.6 million cases in 2010; mortality from breast cancer has increased at an annual rate of 1.8%, reaching 425,000.
While the worldwide incidence of cervical cancer has increased at a slower annual rate of 0.6%, reaching more than 450,000 cases in 2010, annual mortality from cervical cancer has increased by 0.46%, reaching 200,000 cases in the same period.
"On the basis of trends recorded in this study, breast and cervical cancer are likely to soon approach maternal causes as a crucial cause of mortality in women of reproductive age in developing countries," wrote Dr. Mohammad H. Forouzanfar and his coinvestigators at the Institute for Health Metrics and Evaluation at the University of Washington, Seattle. The study was published online in the Lancet on Sept. 14 (doi:10.1016/S0140-6736[11]61351-2).
Twice as many breast cancer cases were recorded in developing countries among women aged 15-49 years as were in developed countries. New cases of cervical cancer occurred more often in developing countries (primarily in South and East Asia, Latin America, and Africa) across all age groups, while declining in high-income countries. In developing countries, there were 367,000 cases of breast cancer and 154,000 cases of cervical cancer among women aged 15-49 years. Three-quarters (76%) of cervical cancer cases occur in developing regions. In these areas of the world, 1.7 breast and cervical cancer deaths occur for every direct or indirect obstetric maternal death.
"Our findings suggest that breast and cervical cancer in low-income countries are major causes of death for women of these ages. The UN [United Nations] High-Level Meeting on Non-Communicable Diseases should raise policy awareness of the importance of the control of breast and cervical cancer, as should policy responses to improve reproductive health," the authors argued.
"Indeed, if the trends of the past 3 decades were to continue during the next 15 years, the ratio of maternal deaths to breast and cervical cancer deaths in developing countries in the reproductive age group will decrease from 2.3 to 1.3. In view of the potential for effective health system responses, greater efforts to reduce their disease burden are an important global health priority."
The researchers used information collected through population-based cancer registries, vital registration systems with medical certification of causes of death, and various subnational and national verbal autopsy studies. Their analysis comprised four components: database development, modeling MI ratios, estimation of trends in mortality by age, and estimation of trends in incidence. The investigators incorporated different data sources in a standardized approach to use all available information for every country.
In an accompanying commentary, epidemiologist Jan W. Coebergh described the new estimates of global breast and cervical cancer incidence and mortality as "staggering" (doi:10.1016/S0140-6736[11]61459-1).
"What would happen in response to another global problem causing morbidity and mortality of a similar magnitude? For example, the global death toll owing to breast and cervical cancer is the equivalent of six large jets crashing every day. Other forms of cancer kill three times this number of women daily, and the number of cancer deaths is even larger in men," wrote Dr. Coebergh, an epidemiologist in the department of public health at Erasmus University Medical Centre in Rotterdam.
"What will it take to instill a sense of urgency in our professional societies, academic institutions, governments, shareholders of biomedical companies, payers for health care, or society at large to end this tragic daily toll? Can we become as successful in prevention and cure of cancer as aeroplane manufacturers and the airline industry have been in improving safety in the past 80 years or so?"
Better cancer surveillance is crucial. "Improved cancer surveillance systems would also allow a detailed view of the quality of evolving clinical care, not only in different health settings and countries but also in respect of the various emerging and declining epidemics of individual cancers," he argued.
"Clearly broad actions are warranted, supported by global funds ... Nowadays, more and better research is demanded everywhere by representatives of the increasingly vocal cancer survivors’ groups. Let us listen to them more," he concluded.
The study was funded by Susan G. Komen for the Cure and the Bill and Melinda Gates Foundation.
The authors reported that they have no conflicts of interest. Dr. Coebergh reported that he has no conflicts of interest.
FROM THE LANCET
Major Finding: The worldwide incidence of breast cancer hit 1.6 million cases in 2010 and the worldwide incidence of cervical cancer reached 454,000 cases.
Data Source: An annual age-specific assessment of breast and cervical cancer in 187 countries.
Disclosures: The study was funded by Susan G Komen for Cure and the Bill and Melinda Gates Foundation. The authors reported that they have no conflicts of interest.
FDA Panel: Update Bisphosphonate Labeling
ADELPHI, MD. – Data on the safety and effectiveness of bisphosphonate drugs for the long-term treatment of osteoporosis is lacking and direly needed, according to a joint Food and Drug Administration advisory committee meeting.
Specifically, the Reproductive Health Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted 17-6 on Sept. 9 that labeling for these drugs should be changed to clarify the duration of use for this drug class.
The agency convened the joint meeting to evaluate particular concerns about the long-term use bisphosphonate drugs, given reports of atypical subtrochanteric and femoral fractures, jaw osteonecrosis, and esophageal cancer associated with bisphosphonate use.
The labels of bisphosphonate drugs – alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and zoledronic acid (Reclast) – already include "important limitation of use" information. This labeling states that the optimal duration of treatment (for an individual drug) has not been determined and that all patients on bisphosphonate therapy should be periodically reassessed for the necessity of continued therapy.
While the panel voted to clarify the label language, they were emphatic that much more data are needed to establish the long-term efficacy and safety of bisphosphonates in general and with special regard to atypical fractures, jaw osteonecrosis, and esophageal cancer.
The two committees also were asked to assess the strength of data on the long-term use of bisphosphonates; the overall risks and benefits of continuous long-term use (3-5 years or more); whether restricting the duration of use or implementing a drug holiday would be beneficial; which outcomes require further evidence; and how should this data be obtained.
The expert consensus is that existing data – some of which go out to roughly 10 years for one drug – do not address the efficacy of the long-term use of bisphosphonates. They recommended that (in no particular order) additional data are needed with regard to the occurrence of atypical fractures, osteonecrosis of the jaw, esophageal cancer, osteoporotic fracture reduction efficacy with long-term (at least 3-5 years) continuous bisphosphonate use, and the effect of a "drug holiday" on drug safety and effectiveness.
Osteoporosis currently affects approximately 10 million Americans, according to the American Society for Bone and Mineral Research. An additional 34 million have low bone mass, which may progress to osteoporosis.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although occasionally a panelist may be given a waiver, but none were given at this meeting.
ADELPHI, MD. – Data on the safety and effectiveness of bisphosphonate drugs for the long-term treatment of osteoporosis is lacking and direly needed, according to a joint Food and Drug Administration advisory committee meeting.
Specifically, the Reproductive Health Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted 17-6 on Sept. 9 that labeling for these drugs should be changed to clarify the duration of use for this drug class.
The agency convened the joint meeting to evaluate particular concerns about the long-term use bisphosphonate drugs, given reports of atypical subtrochanteric and femoral fractures, jaw osteonecrosis, and esophageal cancer associated with bisphosphonate use.
The labels of bisphosphonate drugs – alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and zoledronic acid (Reclast) – already include "important limitation of use" information. This labeling states that the optimal duration of treatment (for an individual drug) has not been determined and that all patients on bisphosphonate therapy should be periodically reassessed for the necessity of continued therapy.
While the panel voted to clarify the label language, they were emphatic that much more data are needed to establish the long-term efficacy and safety of bisphosphonates in general and with special regard to atypical fractures, jaw osteonecrosis, and esophageal cancer.
The two committees also were asked to assess the strength of data on the long-term use of bisphosphonates; the overall risks and benefits of continuous long-term use (3-5 years or more); whether restricting the duration of use or implementing a drug holiday would be beneficial; which outcomes require further evidence; and how should this data be obtained.
The expert consensus is that existing data – some of which go out to roughly 10 years for one drug – do not address the efficacy of the long-term use of bisphosphonates. They recommended that (in no particular order) additional data are needed with regard to the occurrence of atypical fractures, osteonecrosis of the jaw, esophageal cancer, osteoporotic fracture reduction efficacy with long-term (at least 3-5 years) continuous bisphosphonate use, and the effect of a "drug holiday" on drug safety and effectiveness.
Osteoporosis currently affects approximately 10 million Americans, according to the American Society for Bone and Mineral Research. An additional 34 million have low bone mass, which may progress to osteoporosis.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although occasionally a panelist may be given a waiver, but none were given at this meeting.
ADELPHI, MD. – Data on the safety and effectiveness of bisphosphonate drugs for the long-term treatment of osteoporosis is lacking and direly needed, according to a joint Food and Drug Administration advisory committee meeting.
Specifically, the Reproductive Health Drugs Advisory Committee and the Drug Safety and Risk Management Advisory Committee voted 17-6 on Sept. 9 that labeling for these drugs should be changed to clarify the duration of use for this drug class.
The agency convened the joint meeting to evaluate particular concerns about the long-term use bisphosphonate drugs, given reports of atypical subtrochanteric and femoral fractures, jaw osteonecrosis, and esophageal cancer associated with bisphosphonate use.
The labels of bisphosphonate drugs – alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and zoledronic acid (Reclast) – already include "important limitation of use" information. This labeling states that the optimal duration of treatment (for an individual drug) has not been determined and that all patients on bisphosphonate therapy should be periodically reassessed for the necessity of continued therapy.
While the panel voted to clarify the label language, they were emphatic that much more data are needed to establish the long-term efficacy and safety of bisphosphonates in general and with special regard to atypical fractures, jaw osteonecrosis, and esophageal cancer.
The two committees also were asked to assess the strength of data on the long-term use of bisphosphonates; the overall risks and benefits of continuous long-term use (3-5 years or more); whether restricting the duration of use or implementing a drug holiday would be beneficial; which outcomes require further evidence; and how should this data be obtained.
The expert consensus is that existing data – some of which go out to roughly 10 years for one drug – do not address the efficacy of the long-term use of bisphosphonates. They recommended that (in no particular order) additional data are needed with regard to the occurrence of atypical fractures, osteonecrosis of the jaw, esophageal cancer, osteoporotic fracture reduction efficacy with long-term (at least 3-5 years) continuous bisphosphonate use, and the effect of a "drug holiday" on drug safety and effectiveness.
Osteoporosis currently affects approximately 10 million Americans, according to the American Society for Bone and Mineral Research. An additional 34 million have low bone mass, which may progress to osteoporosis.
Panelists have been cleared of potential conflicts of interest related to the topic of the meeting, although occasionally a panelist may be given a waiver, but none were given at this meeting.
FROM A JOINT FDA ADVISORY COMMITTEE MEETING
Multiple Sclerosis Does Not Hurt Pregnancy, Birth Outcomes
Women with multiple sclerosis can be reassured that should they choose to become pregnant, they are generally not at any greater risk of adverse pregnancy or birth outcomes than are similar women without the disease, according to a retrospective cohort study.
The findings should have important clinical implications for this group of patients, because about three-quarters of people with MS are women and the clinical onset of the disease most often occurs in early adulthood, just when many are considering starting a family, Mia L. van der Kop and her coauthors wrote.
Studies have shown that one-fifth to one-third of women with MS bear children after disease onset.
Ms. van der Kop and her coinvestigators at the University of British Columbia, Vancouver, linked clinical data from the British Columbia (BC) MS clinics' database with outcomes data from the BC Perinatal Database Registry (BCPDR) to examine whether maternal MS was associated with adverse neonatal and delivery outcomes and what factors, if any, were associated with risk (Ann. Neurol. 2011 June 27 [doi: 10.1002/ana.22483]).
Of 7,056 female patients who were registered at one of the four MS clinics in BC from 1980 through 2008, the investigators found links for 321 women (432 births) with laboratory-supported or clinically definite MS whose with births occurred between April 1998 and March 2009 in the BCPDR. These births were compared with 2,975 births from a random sample of 2,958 women in the general population who were frequency-matched for age, local health authority, and delivery year. The clinics' database is estimated to capture 80% of the MS population in BC. Patients' names and dates of birth were used to confirm the accuracy of linkage.
A greater proportion of births in the MS group were to women who were nulliparous, primigravid, hypertensive, or had smoked during pregnancy. A greater proportion of births in the comparison group were to mothers with diabetes during pregnancy and a history of multiple therapeutic abortions.
Maternal MS was not associated with assisted vaginal delivery (odds ratio, 0.78) or cesarean section (OR, 0.94). The proportion of elective cesarean sections was similar in both the MS and comparison groups (18.6% vs. 16.1%, respectively), and the indication for cesarean delivery did not differ between groups. Delivery outcomes were not associated with either an older age at MS onset or longer duration.
The degree of disability in MS mothers was not significantly associated with higher odds of a cesarean section or an assisted vaginal delivery, compared with women with a normal neurologic exam.
Among nulliparous women, there was no significant difference in the median duration of the second stage of labor between those with MS and those in the comparison group. Duration of the second stage of labor was not associated with age at MS onset.
This study was supported by the Canadian Institutes of Health Research. All of the authors reported having significant ties to disease advocacy- or government-based groups, research groups, or pharmaceutical companies.
Women with multiple sclerosis can be reassured that should they choose to become pregnant, they are generally not at any greater risk of adverse pregnancy or birth outcomes than are similar women without the disease, according to a retrospective cohort study.
The findings should have important clinical implications for this group of patients, because about three-quarters of people with MS are women and the clinical onset of the disease most often occurs in early adulthood, just when many are considering starting a family, Mia L. van der Kop and her coauthors wrote.
Studies have shown that one-fifth to one-third of women with MS bear children after disease onset.
Ms. van der Kop and her coinvestigators at the University of British Columbia, Vancouver, linked clinical data from the British Columbia (BC) MS clinics' database with outcomes data from the BC Perinatal Database Registry (BCPDR) to examine whether maternal MS was associated with adverse neonatal and delivery outcomes and what factors, if any, were associated with risk (Ann. Neurol. 2011 June 27 [doi: 10.1002/ana.22483]).
Of 7,056 female patients who were registered at one of the four MS clinics in BC from 1980 through 2008, the investigators found links for 321 women (432 births) with laboratory-supported or clinically definite MS whose with births occurred between April 1998 and March 2009 in the BCPDR. These births were compared with 2,975 births from a random sample of 2,958 women in the general population who were frequency-matched for age, local health authority, and delivery year. The clinics' database is estimated to capture 80% of the MS population in BC. Patients' names and dates of birth were used to confirm the accuracy of linkage.
A greater proportion of births in the MS group were to women who were nulliparous, primigravid, hypertensive, or had smoked during pregnancy. A greater proportion of births in the comparison group were to mothers with diabetes during pregnancy and a history of multiple therapeutic abortions.
Maternal MS was not associated with assisted vaginal delivery (odds ratio, 0.78) or cesarean section (OR, 0.94). The proportion of elective cesarean sections was similar in both the MS and comparison groups (18.6% vs. 16.1%, respectively), and the indication for cesarean delivery did not differ between groups. Delivery outcomes were not associated with either an older age at MS onset or longer duration.
The degree of disability in MS mothers was not significantly associated with higher odds of a cesarean section or an assisted vaginal delivery, compared with women with a normal neurologic exam.
Among nulliparous women, there was no significant difference in the median duration of the second stage of labor between those with MS and those in the comparison group. Duration of the second stage of labor was not associated with age at MS onset.
This study was supported by the Canadian Institutes of Health Research. All of the authors reported having significant ties to disease advocacy- or government-based groups, research groups, or pharmaceutical companies.
Women with multiple sclerosis can be reassured that should they choose to become pregnant, they are generally not at any greater risk of adverse pregnancy or birth outcomes than are similar women without the disease, according to a retrospective cohort study.
The findings should have important clinical implications for this group of patients, because about three-quarters of people with MS are women and the clinical onset of the disease most often occurs in early adulthood, just when many are considering starting a family, Mia L. van der Kop and her coauthors wrote.
Studies have shown that one-fifth to one-third of women with MS bear children after disease onset.
Ms. van der Kop and her coinvestigators at the University of British Columbia, Vancouver, linked clinical data from the British Columbia (BC) MS clinics' database with outcomes data from the BC Perinatal Database Registry (BCPDR) to examine whether maternal MS was associated with adverse neonatal and delivery outcomes and what factors, if any, were associated with risk (Ann. Neurol. 2011 June 27 [doi: 10.1002/ana.22483]).
Of 7,056 female patients who were registered at one of the four MS clinics in BC from 1980 through 2008, the investigators found links for 321 women (432 births) with laboratory-supported or clinically definite MS whose with births occurred between April 1998 and March 2009 in the BCPDR. These births were compared with 2,975 births from a random sample of 2,958 women in the general population who were frequency-matched for age, local health authority, and delivery year. The clinics' database is estimated to capture 80% of the MS population in BC. Patients' names and dates of birth were used to confirm the accuracy of linkage.
A greater proportion of births in the MS group were to women who were nulliparous, primigravid, hypertensive, or had smoked during pregnancy. A greater proportion of births in the comparison group were to mothers with diabetes during pregnancy and a history of multiple therapeutic abortions.
Maternal MS was not associated with assisted vaginal delivery (odds ratio, 0.78) or cesarean section (OR, 0.94). The proportion of elective cesarean sections was similar in both the MS and comparison groups (18.6% vs. 16.1%, respectively), and the indication for cesarean delivery did not differ between groups. Delivery outcomes were not associated with either an older age at MS onset or longer duration.
The degree of disability in MS mothers was not significantly associated with higher odds of a cesarean section or an assisted vaginal delivery, compared with women with a normal neurologic exam.
Among nulliparous women, there was no significant difference in the median duration of the second stage of labor between those with MS and those in the comparison group. Duration of the second stage of labor was not associated with age at MS onset.
This study was supported by the Canadian Institutes of Health Research. All of the authors reported having significant ties to disease advocacy- or government-based groups, research groups, or pharmaceutical companies.
Test Neurocognitive Skills in PHACE Syndrome Patients
BALTIMORE – Preliminary data from a small study suggest that children with PHACE syndrome are at high risk for both motor and speech delay, and should be closely evaluated so that early interventions can be started to improve outcomes.
Dr. Anna M. Juern and her coinvestigators at the Children’s Hospital of Wisconsin in Milwaukee reported on 15 children with definite or probable PHACE syndrome in an ongoing, prospective study. PHACE syndrome affects a subgroup of patients with infantile hemangioma who exhibit additional associated structural anomalies of the brain (posterior fossa), cerebral vasculature, eyes, aorta, and chest wall. (PHACE is an acronym for posterior fossa, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and eye abnormalities.)
Despite improved clinical recognition of PHACE syndrome, longitudinal studies of outcome and natural history have never been conducted. A clear clinical gap exists in the ability of physicians to provide an informed prognosis to PHACE patients based on the specific types and numbers of anomalies detected at the time of diagnosis. Given the wide range of cerebrovascular and central nervous system anomalies observed in PHACE, these children have many potential causes of neurocognitive impairment, according to Dr. Juern, who is a resident at the hospital.
Recent research has suggested that this syndrome is more common than previously thought. Some children with PHACE do quite well, whereas others suffer from epilepsy, mental retardation, and devastating arterial ischemic strokes. Epilepsy, developmental delay, and recurrent headaches appear to be the most common neurologic signs and symptoms,
For their study, Dr. Juern and her colleagues "hypothesize that certain risk factors, such as hemangioma size, previous pharmacologic intervention, cerebral anomalies, cerebellar anomalies, and cerebrovascular anomalies predispose patients to neurodevelopmental delay."
In a poster presented at the annual meeting of the Society for Pediatric Dermatology, they reported that 13 of the 15 children enrolled in the study so far (including 14 with definite PHACE and 1 with probable PHACE) have required special services. More than 70% had prior physical therapy and participated in "Birth to 3," Wisconsin’s early intervention program. Half of the children are currently receiving speech therapy. On a test of fine motor skills using the dominant hand, a majority scored below average. In addition, more than half of the children scored in the below-average or borderline range on a computerized test of sustained attention; 40% of patients scored below average on a subtest assessing word structure.
The study cohort comprises 13 girls and 2 boys. The average age at the time of testing was 5 years (range, 4-6 years). "This age range represents a critical period, as it is the time [when most children] enter the formal education system and allows for a more thorough evaluation of neurocognitive skills than what is possible with younger children," according to Dr. Juern.
One patient had suffered an acute ischemic stroke during infancy, and two additional patients showing evidence of infarct on imaging. All patients received a systemic therapy for the treatment of their hemangiomas, such as interferon-alpha, corticosteroids, and vincristine.
The investigators are using a standardized electronic data collection form to record demographic data, clinical features, and dose and duration of therapy for infantile hemangioma. All children must undergo a standard evaluation (echocardiography, brain MRI, and MR angiography of the head and neck) prior to study enrollment. A pediatric dermatologist and a pediatric neurologist perform a physical exam, obtain a detailed medical history, and review all neuroimaging.
Patients also are administered standardized instruments by a pediatric psychologist to measure verbal reasoning; executive functioning; motor, attention, visual-spatial, and language skills; and verbal and nonverbal memory.
Dr. Juern did not report whether she has any relevant disclosures.
BALTIMORE – Preliminary data from a small study suggest that children with PHACE syndrome are at high risk for both motor and speech delay, and should be closely evaluated so that early interventions can be started to improve outcomes.
Dr. Anna M. Juern and her coinvestigators at the Children’s Hospital of Wisconsin in Milwaukee reported on 15 children with definite or probable PHACE syndrome in an ongoing, prospective study. PHACE syndrome affects a subgroup of patients with infantile hemangioma who exhibit additional associated structural anomalies of the brain (posterior fossa), cerebral vasculature, eyes, aorta, and chest wall. (PHACE is an acronym for posterior fossa, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and eye abnormalities.)
Despite improved clinical recognition of PHACE syndrome, longitudinal studies of outcome and natural history have never been conducted. A clear clinical gap exists in the ability of physicians to provide an informed prognosis to PHACE patients based on the specific types and numbers of anomalies detected at the time of diagnosis. Given the wide range of cerebrovascular and central nervous system anomalies observed in PHACE, these children have many potential causes of neurocognitive impairment, according to Dr. Juern, who is a resident at the hospital.
Recent research has suggested that this syndrome is more common than previously thought. Some children with PHACE do quite well, whereas others suffer from epilepsy, mental retardation, and devastating arterial ischemic strokes. Epilepsy, developmental delay, and recurrent headaches appear to be the most common neurologic signs and symptoms,
For their study, Dr. Juern and her colleagues "hypothesize that certain risk factors, such as hemangioma size, previous pharmacologic intervention, cerebral anomalies, cerebellar anomalies, and cerebrovascular anomalies predispose patients to neurodevelopmental delay."
In a poster presented at the annual meeting of the Society for Pediatric Dermatology, they reported that 13 of the 15 children enrolled in the study so far (including 14 with definite PHACE and 1 with probable PHACE) have required special services. More than 70% had prior physical therapy and participated in "Birth to 3," Wisconsin’s early intervention program. Half of the children are currently receiving speech therapy. On a test of fine motor skills using the dominant hand, a majority scored below average. In addition, more than half of the children scored in the below-average or borderline range on a computerized test of sustained attention; 40% of patients scored below average on a subtest assessing word structure.
The study cohort comprises 13 girls and 2 boys. The average age at the time of testing was 5 years (range, 4-6 years). "This age range represents a critical period, as it is the time [when most children] enter the formal education system and allows for a more thorough evaluation of neurocognitive skills than what is possible with younger children," according to Dr. Juern.
One patient had suffered an acute ischemic stroke during infancy, and two additional patients showing evidence of infarct on imaging. All patients received a systemic therapy for the treatment of their hemangiomas, such as interferon-alpha, corticosteroids, and vincristine.
The investigators are using a standardized electronic data collection form to record demographic data, clinical features, and dose and duration of therapy for infantile hemangioma. All children must undergo a standard evaluation (echocardiography, brain MRI, and MR angiography of the head and neck) prior to study enrollment. A pediatric dermatologist and a pediatric neurologist perform a physical exam, obtain a detailed medical history, and review all neuroimaging.
Patients also are administered standardized instruments by a pediatric psychologist to measure verbal reasoning; executive functioning; motor, attention, visual-spatial, and language skills; and verbal and nonverbal memory.
Dr. Juern did not report whether she has any relevant disclosures.
BALTIMORE – Preliminary data from a small study suggest that children with PHACE syndrome are at high risk for both motor and speech delay, and should be closely evaluated so that early interventions can be started to improve outcomes.
Dr. Anna M. Juern and her coinvestigators at the Children’s Hospital of Wisconsin in Milwaukee reported on 15 children with definite or probable PHACE syndrome in an ongoing, prospective study. PHACE syndrome affects a subgroup of patients with infantile hemangioma who exhibit additional associated structural anomalies of the brain (posterior fossa), cerebral vasculature, eyes, aorta, and chest wall. (PHACE is an acronym for posterior fossa, hemangioma, arterial lesions, cardiac abnormalities/aortic coarctation, and eye abnormalities.)
Despite improved clinical recognition of PHACE syndrome, longitudinal studies of outcome and natural history have never been conducted. A clear clinical gap exists in the ability of physicians to provide an informed prognosis to PHACE patients based on the specific types and numbers of anomalies detected at the time of diagnosis. Given the wide range of cerebrovascular and central nervous system anomalies observed in PHACE, these children have many potential causes of neurocognitive impairment, according to Dr. Juern, who is a resident at the hospital.
Recent research has suggested that this syndrome is more common than previously thought. Some children with PHACE do quite well, whereas others suffer from epilepsy, mental retardation, and devastating arterial ischemic strokes. Epilepsy, developmental delay, and recurrent headaches appear to be the most common neurologic signs and symptoms,
For their study, Dr. Juern and her colleagues "hypothesize that certain risk factors, such as hemangioma size, previous pharmacologic intervention, cerebral anomalies, cerebellar anomalies, and cerebrovascular anomalies predispose patients to neurodevelopmental delay."
In a poster presented at the annual meeting of the Society for Pediatric Dermatology, they reported that 13 of the 15 children enrolled in the study so far (including 14 with definite PHACE and 1 with probable PHACE) have required special services. More than 70% had prior physical therapy and participated in "Birth to 3," Wisconsin’s early intervention program. Half of the children are currently receiving speech therapy. On a test of fine motor skills using the dominant hand, a majority scored below average. In addition, more than half of the children scored in the below-average or borderline range on a computerized test of sustained attention; 40% of patients scored below average on a subtest assessing word structure.
The study cohort comprises 13 girls and 2 boys. The average age at the time of testing was 5 years (range, 4-6 years). "This age range represents a critical period, as it is the time [when most children] enter the formal education system and allows for a more thorough evaluation of neurocognitive skills than what is possible with younger children," according to Dr. Juern.
One patient had suffered an acute ischemic stroke during infancy, and two additional patients showing evidence of infarct on imaging. All patients received a systemic therapy for the treatment of their hemangiomas, such as interferon-alpha, corticosteroids, and vincristine.
The investigators are using a standardized electronic data collection form to record demographic data, clinical features, and dose and duration of therapy for infantile hemangioma. All children must undergo a standard evaluation (echocardiography, brain MRI, and MR angiography of the head and neck) prior to study enrollment. A pediatric dermatologist and a pediatric neurologist perform a physical exam, obtain a detailed medical history, and review all neuroimaging.
Patients also are administered standardized instruments by a pediatric psychologist to measure verbal reasoning; executive functioning; motor, attention, visual-spatial, and language skills; and verbal and nonverbal memory.
Dr. Juern did not report whether she has any relevant disclosures.
FROM THE ANNUAL MEETING OF THE SOCIETY FOR PEDIATRIC DERMATOLOGY
Major Finding: Special services, including speech and physical therapy, have been required by 13 of 15 patients with PHACE syndrome.
Data Source: Preliminary data from an ongoing, prospective study of 15 patients aged 4-6 years.
Disclosures: Dr. Juern did not report whether she has any relevant disclosures.
Liraglutide Improves Glucose Control in Type 1 Diabetes
Major Finding: Eight patients who continued liraglutide treatment for 24 weeks lost a significant amount of weight, down from a mean of 68 kg to 63.5 kg. Mean hemoglobin A1c also dropped significantly from 6.5% to 6.1%. Mean basal insulin dropped by 48%, and mean bolus dropped by 42% as well.
Data Source: A prospective study of 14 patients with type 1 diabetes; eight patients were treated for a total of 24 weeks.
Disclosures: Two of the authors have significant financial relationships with several pharmaceutical companies, but not with Novo Nordisk, the makers of liraglutide. The remaining authors, including Dr. Varanasi, reported that they have no relevant financial disclosures.
BOSTON – Use of the type 2 medication liraglutide helped control glycemic oscillations in type 1 diabetes, significantly lowered hemoglobin A1c levels, and was associated with weight loss, a small study has shown.
The net effect is not only an improvement in mean fasting and weekly glucose concentrations, but also “you have a remarkable effect on the oscillations of glucose,” seen among type 1 diabetic patients, Dr. Paresh Dandona said at the meeting.
Liraglutide (Vitoza), made by Novo Nordisk, is a glucagonlike peptide-1 (GLP-1) receptor agonist that is currently approved for use as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. As a GLP-1 analogue, liraglutide stimulates the release of insulin in response to elevated levels of blood sugar. It also inhibits the release of glucagon following meals, slowing the rate of food absorption from the gut into the bloodstream.
At the meeting, Dr. Ajay Varanasi reported the results of a prospective study in which 14 patients (9 male) with type 1 diabetes all used liraglutide.
Treatment for six of the patients involved a 1-week pretreatment period to optimize glycemic control, 1 week of liraglutide therapy, and 1 week post treatment. Eight additional patients also had a 1-week pretreatment period, followed by a 22-week period of liraglutide therapy, and a 1-week posttreatment period, for a total of 24 weeks.
During treatment, patients were instructed to inject 0.6 mg of liraglutide subcutaneously every day. At the onset of treatment, patients were advised to reduce their basal insulin by a quarter and bolus by a third. “This was to avoid hypoglycemia,” explained Dr. Varanasi, the lead author, who is with the division of endocrinology and metabolism at the State University of New York at Buffalo. The eight patients treated for 24 weeks were advised to increase the daily dose of liraglutide to 1.2 mg after the first week and again to 1.8 mg after 2 weeks.
At baseline, the mean patient age was 40 years and the mean BMI was 24 kg/m
During the first week of treatment, despite the reduction in insulin, there was a significant reduction in mean fasting glucose and mean weekly blood glucose.
Most interestingly, said Dr. Varanasi, the mean weekly standard deviations in insulin concentrations were significantly reduced with treatment.
“Even in a reasonably well-controlled [type 1] diabetic with an HbA1c of around 7% or less, there is [usually] a massive vacillation in insulin concentrations,” observed Dr. Dandona, the principal investigator, who is chief of the division of endocrinology at the State University of New York at Buffalo.
The eight patients on longer-term therapy lost a significant amount of weight – down from a mean of 68 kg to 63.5 kg. The mean HbA1c level dropped from 6.5% to 6.1%, which also was significant. Mean basal insulin dropped by 48%, and mean bolus dropped by 42%. The decrease in mean blood glucose was significantly reduced within the 24-48 hours. “This tells us that the response is pretty quick. And the mean standard deviation values were reduced within 48 hours,” Dr. Varanasi noted.
Regarding the mechanism of action, Dr. Varanasi hypothesized that liraglutide may decrease the concentration of glucagon secreted after meals. Another theory is that the decrease in postprandial glucose excursion may be the result of slower gastric emptying, which is known to occur with liraglutide. The weight loss seen in patients on liraglutide may have also contributed to improved glycemic control.
Major Finding: Eight patients who continued liraglutide treatment for 24 weeks lost a significant amount of weight, down from a mean of 68 kg to 63.5 kg. Mean hemoglobin A1c also dropped significantly from 6.5% to 6.1%. Mean basal insulin dropped by 48%, and mean bolus dropped by 42% as well.
Data Source: A prospective study of 14 patients with type 1 diabetes; eight patients were treated for a total of 24 weeks.
Disclosures: Two of the authors have significant financial relationships with several pharmaceutical companies, but not with Novo Nordisk, the makers of liraglutide. The remaining authors, including Dr. Varanasi, reported that they have no relevant financial disclosures.
BOSTON – Use of the type 2 medication liraglutide helped control glycemic oscillations in type 1 diabetes, significantly lowered hemoglobin A1c levels, and was associated with weight loss, a small study has shown.
The net effect is not only an improvement in mean fasting and weekly glucose concentrations, but also “you have a remarkable effect on the oscillations of glucose,” seen among type 1 diabetic patients, Dr. Paresh Dandona said at the meeting.
Liraglutide (Vitoza), made by Novo Nordisk, is a glucagonlike peptide-1 (GLP-1) receptor agonist that is currently approved for use as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. As a GLP-1 analogue, liraglutide stimulates the release of insulin in response to elevated levels of blood sugar. It also inhibits the release of glucagon following meals, slowing the rate of food absorption from the gut into the bloodstream.
At the meeting, Dr. Ajay Varanasi reported the results of a prospective study in which 14 patients (9 male) with type 1 diabetes all used liraglutide.
Treatment for six of the patients involved a 1-week pretreatment period to optimize glycemic control, 1 week of liraglutide therapy, and 1 week post treatment. Eight additional patients also had a 1-week pretreatment period, followed by a 22-week period of liraglutide therapy, and a 1-week posttreatment period, for a total of 24 weeks.
During treatment, patients were instructed to inject 0.6 mg of liraglutide subcutaneously every day. At the onset of treatment, patients were advised to reduce their basal insulin by a quarter and bolus by a third. “This was to avoid hypoglycemia,” explained Dr. Varanasi, the lead author, who is with the division of endocrinology and metabolism at the State University of New York at Buffalo. The eight patients treated for 24 weeks were advised to increase the daily dose of liraglutide to 1.2 mg after the first week and again to 1.8 mg after 2 weeks.
At baseline, the mean patient age was 40 years and the mean BMI was 24 kg/m
During the first week of treatment, despite the reduction in insulin, there was a significant reduction in mean fasting glucose and mean weekly blood glucose.
Most interestingly, said Dr. Varanasi, the mean weekly standard deviations in insulin concentrations were significantly reduced with treatment.
“Even in a reasonably well-controlled [type 1] diabetic with an HbA1c of around 7% or less, there is [usually] a massive vacillation in insulin concentrations,” observed Dr. Dandona, the principal investigator, who is chief of the division of endocrinology at the State University of New York at Buffalo.
The eight patients on longer-term therapy lost a significant amount of weight – down from a mean of 68 kg to 63.5 kg. The mean HbA1c level dropped from 6.5% to 6.1%, which also was significant. Mean basal insulin dropped by 48%, and mean bolus dropped by 42%. The decrease in mean blood glucose was significantly reduced within the 24-48 hours. “This tells us that the response is pretty quick. And the mean standard deviation values were reduced within 48 hours,” Dr. Varanasi noted.
Regarding the mechanism of action, Dr. Varanasi hypothesized that liraglutide may decrease the concentration of glucagon secreted after meals. Another theory is that the decrease in postprandial glucose excursion may be the result of slower gastric emptying, which is known to occur with liraglutide. The weight loss seen in patients on liraglutide may have also contributed to improved glycemic control.
Major Finding: Eight patients who continued liraglutide treatment for 24 weeks lost a significant amount of weight, down from a mean of 68 kg to 63.5 kg. Mean hemoglobin A1c also dropped significantly from 6.5% to 6.1%. Mean basal insulin dropped by 48%, and mean bolus dropped by 42% as well.
Data Source: A prospective study of 14 patients with type 1 diabetes; eight patients were treated for a total of 24 weeks.
Disclosures: Two of the authors have significant financial relationships with several pharmaceutical companies, but not with Novo Nordisk, the makers of liraglutide. The remaining authors, including Dr. Varanasi, reported that they have no relevant financial disclosures.
BOSTON – Use of the type 2 medication liraglutide helped control glycemic oscillations in type 1 diabetes, significantly lowered hemoglobin A1c levels, and was associated with weight loss, a small study has shown.
The net effect is not only an improvement in mean fasting and weekly glucose concentrations, but also “you have a remarkable effect on the oscillations of glucose,” seen among type 1 diabetic patients, Dr. Paresh Dandona said at the meeting.
Liraglutide (Vitoza), made by Novo Nordisk, is a glucagonlike peptide-1 (GLP-1) receptor agonist that is currently approved for use as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus. As a GLP-1 analogue, liraglutide stimulates the release of insulin in response to elevated levels of blood sugar. It also inhibits the release of glucagon following meals, slowing the rate of food absorption from the gut into the bloodstream.
At the meeting, Dr. Ajay Varanasi reported the results of a prospective study in which 14 patients (9 male) with type 1 diabetes all used liraglutide.
Treatment for six of the patients involved a 1-week pretreatment period to optimize glycemic control, 1 week of liraglutide therapy, and 1 week post treatment. Eight additional patients also had a 1-week pretreatment period, followed by a 22-week period of liraglutide therapy, and a 1-week posttreatment period, for a total of 24 weeks.
During treatment, patients were instructed to inject 0.6 mg of liraglutide subcutaneously every day. At the onset of treatment, patients were advised to reduce their basal insulin by a quarter and bolus by a third. “This was to avoid hypoglycemia,” explained Dr. Varanasi, the lead author, who is with the division of endocrinology and metabolism at the State University of New York at Buffalo. The eight patients treated for 24 weeks were advised to increase the daily dose of liraglutide to 1.2 mg after the first week and again to 1.8 mg after 2 weeks.
At baseline, the mean patient age was 40 years and the mean BMI was 24 kg/m
During the first week of treatment, despite the reduction in insulin, there was a significant reduction in mean fasting glucose and mean weekly blood glucose.
Most interestingly, said Dr. Varanasi, the mean weekly standard deviations in insulin concentrations were significantly reduced with treatment.
“Even in a reasonably well-controlled [type 1] diabetic with an HbA1c of around 7% or less, there is [usually] a massive vacillation in insulin concentrations,” observed Dr. Dandona, the principal investigator, who is chief of the division of endocrinology at the State University of New York at Buffalo.
The eight patients on longer-term therapy lost a significant amount of weight – down from a mean of 68 kg to 63.5 kg. The mean HbA1c level dropped from 6.5% to 6.1%, which also was significant. Mean basal insulin dropped by 48%, and mean bolus dropped by 42%. The decrease in mean blood glucose was significantly reduced within the 24-48 hours. “This tells us that the response is pretty quick. And the mean standard deviation values were reduced within 48 hours,” Dr. Varanasi noted.
Regarding the mechanism of action, Dr. Varanasi hypothesized that liraglutide may decrease the concentration of glucagon secreted after meals. Another theory is that the decrease in postprandial glucose excursion may be the result of slower gastric emptying, which is known to occur with liraglutide. The weight loss seen in patients on liraglutide may have also contributed to improved glycemic control.
From the Annual Meeting of the Endocrine Society
Facial Wrinkles May Signal Bone Mineral Loss
Major Finding: The worse the skin wrinkles were in terms of depth and number, the lower BMD was in that individual.
Data Source: A skin ancillary study of 114 women also enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
Disclosures: Dr. Pal and her coinvestigators reported that they have no relevant financial relationships.
BOSTON – Skin wrinkling and rigidity could give physicians a clue to bone mineral density, at least among early postmenopausal women.
“In the women that we're talking about, skin wrinkling and skin rigidity – features that are easily appreciable across the table when you are looking at the patient – tie in with bone mineral density as assessed by clinical gold standards, such as dual x-ray absorptiometry,” Dr. Lubna Pal said at the meeting.
The researchers explored possible relationships between skin wrinkling/rigidity and bone mineral density (BMD) in a cohort of early menopausal women who were enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
The skin ancillary study to the ongoing Kronos clinical trial included 114 women who had their last menstrual period within the past 3 years. Most of the participants were white, although 30% were not. Cross-sectional baseline data were used, said Dr. Pal, a reproductive endocrinologist at Yale University, New Haven, Conn.
Skin wrinkles were assessed at 11 sites on the face and neck using the validated Lemperle wrinkle scale. Skin rigidity was assessed at the forehead and cheek using a durometer. Participants also underwent BMD assessment by dual-energy x-ray absorptiometry at the lumbar spine, left hip, and total body. The patients also underwent quantitative heel ultrasound.
Stepwise multivariable linear regression analyses explored the relationship between skin parameters and BMD. Covariates included age, body mass, race/ethnicity, age at menopause, history of smoking, multivitamin intake, and enrollment site.
The researchers found that skin wrinkle severity correlates with BMD. In particular, when wrinkles are severe, BMD is low.
“Our hypothesis, I'm very pleased to say, was substantiated by these findings,” said Dr. Pal. “But we are really seeing the tip of the iceberg here. This is a tantalizing association.
“The quest for all of us really is, can we pick out markers in a cost-effective manner that may translate into overall risk detection that would prevent [fractures]?” she added.
Why look at skin wrinkles and bone density? “Well, when you look at the architecture of the skeleton and the architecture of the skin, about 90% of shared properties within tissues exist, which are the protein building blocks,” Dr. Pal said.
In the skeleton, bone mineral must be deposited on some struts, and proteins provide that infrastructure, she explained. So, loss of protein in the skeleton translates into increased skeletal fragility. That structural deterioration is also seen in the skin. “As we age, the protein texture in our dermis and the deeper layers of our skin also deteriorate,” Dr. Pal noted.
Major Finding: The worse the skin wrinkles were in terms of depth and number, the lower BMD was in that individual.
Data Source: A skin ancillary study of 114 women also enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
Disclosures: Dr. Pal and her coinvestigators reported that they have no relevant financial relationships.
BOSTON – Skin wrinkling and rigidity could give physicians a clue to bone mineral density, at least among early postmenopausal women.
“In the women that we're talking about, skin wrinkling and skin rigidity – features that are easily appreciable across the table when you are looking at the patient – tie in with bone mineral density as assessed by clinical gold standards, such as dual x-ray absorptiometry,” Dr. Lubna Pal said at the meeting.
The researchers explored possible relationships between skin wrinkling/rigidity and bone mineral density (BMD) in a cohort of early menopausal women who were enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
The skin ancillary study to the ongoing Kronos clinical trial included 114 women who had their last menstrual period within the past 3 years. Most of the participants were white, although 30% were not. Cross-sectional baseline data were used, said Dr. Pal, a reproductive endocrinologist at Yale University, New Haven, Conn.
Skin wrinkles were assessed at 11 sites on the face and neck using the validated Lemperle wrinkle scale. Skin rigidity was assessed at the forehead and cheek using a durometer. Participants also underwent BMD assessment by dual-energy x-ray absorptiometry at the lumbar spine, left hip, and total body. The patients also underwent quantitative heel ultrasound.
Stepwise multivariable linear regression analyses explored the relationship between skin parameters and BMD. Covariates included age, body mass, race/ethnicity, age at menopause, history of smoking, multivitamin intake, and enrollment site.
The researchers found that skin wrinkle severity correlates with BMD. In particular, when wrinkles are severe, BMD is low.
“Our hypothesis, I'm very pleased to say, was substantiated by these findings,” said Dr. Pal. “But we are really seeing the tip of the iceberg here. This is a tantalizing association.
“The quest for all of us really is, can we pick out markers in a cost-effective manner that may translate into overall risk detection that would prevent [fractures]?” she added.
Why look at skin wrinkles and bone density? “Well, when you look at the architecture of the skeleton and the architecture of the skin, about 90% of shared properties within tissues exist, which are the protein building blocks,” Dr. Pal said.
In the skeleton, bone mineral must be deposited on some struts, and proteins provide that infrastructure, she explained. So, loss of protein in the skeleton translates into increased skeletal fragility. That structural deterioration is also seen in the skin. “As we age, the protein texture in our dermis and the deeper layers of our skin also deteriorate,” Dr. Pal noted.
Major Finding: The worse the skin wrinkles were in terms of depth and number, the lower BMD was in that individual.
Data Source: A skin ancillary study of 114 women also enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
Disclosures: Dr. Pal and her coinvestigators reported that they have no relevant financial relationships.
BOSTON – Skin wrinkling and rigidity could give physicians a clue to bone mineral density, at least among early postmenopausal women.
“In the women that we're talking about, skin wrinkling and skin rigidity – features that are easily appreciable across the table when you are looking at the patient – tie in with bone mineral density as assessed by clinical gold standards, such as dual x-ray absorptiometry,” Dr. Lubna Pal said at the meeting.
The researchers explored possible relationships between skin wrinkling/rigidity and bone mineral density (BMD) in a cohort of early menopausal women who were enrolled in the Kronos Early Estrogen Prevention Study, a longitudinal trial of menopausal hormone therapy.
The skin ancillary study to the ongoing Kronos clinical trial included 114 women who had their last menstrual period within the past 3 years. Most of the participants were white, although 30% were not. Cross-sectional baseline data were used, said Dr. Pal, a reproductive endocrinologist at Yale University, New Haven, Conn.
Skin wrinkles were assessed at 11 sites on the face and neck using the validated Lemperle wrinkle scale. Skin rigidity was assessed at the forehead and cheek using a durometer. Participants also underwent BMD assessment by dual-energy x-ray absorptiometry at the lumbar spine, left hip, and total body. The patients also underwent quantitative heel ultrasound.
Stepwise multivariable linear regression analyses explored the relationship between skin parameters and BMD. Covariates included age, body mass, race/ethnicity, age at menopause, history of smoking, multivitamin intake, and enrollment site.
The researchers found that skin wrinkle severity correlates with BMD. In particular, when wrinkles are severe, BMD is low.
“Our hypothesis, I'm very pleased to say, was substantiated by these findings,” said Dr. Pal. “But we are really seeing the tip of the iceberg here. This is a tantalizing association.
“The quest for all of us really is, can we pick out markers in a cost-effective manner that may translate into overall risk detection that would prevent [fractures]?” she added.
Why look at skin wrinkles and bone density? “Well, when you look at the architecture of the skeleton and the architecture of the skin, about 90% of shared properties within tissues exist, which are the protein building blocks,” Dr. Pal said.
In the skeleton, bone mineral must be deposited on some struts, and proteins provide that infrastructure, she explained. So, loss of protein in the skeleton translates into increased skeletal fragility. That structural deterioration is also seen in the skin. “As we age, the protein texture in our dermis and the deeper layers of our skin also deteriorate,” Dr. Pal noted.
The Annual Meeting of the Endocrine Society
Carvedilol Cut Intradialytic HT
NEW YORK – Patients treated with carvedilol not only had a reduced frequency of intradialytic hypertension, but also showed improvements in endothelial cell function, in a small study.
After 8 weeks of treatment with carvedilol, mean systolic postdialysis blood pressure dropped from 159 mm Hg at baseline to 142 mm Hg, reported Dr. Julia Inrig of the University of Texas Southwestern Medical Center in Dallas.
We are “very interested in this phenomenon of intradialytic hypertension,” she said at the meeting. When most patients come for dialysis, there is a gradual reduction in their systolic blood pressure. “However, up to 20% of patients have this gradual increase in their systolic blood pressure during their dialysis. So they leave their dialysis session much more hypertensive than when they showed up, despite similar amounts of fluid removed.”
In addition, “we've identified that this is an important prognostic indicator.” In a cohort of 450 dialysis patients, those with increased BP during dialysis were nearly twice as likely to be hospitalized or die by 6 months (Kidney Int. 2007;71:454-61).
The researchers in the Mechanisms and Treatment of Intradialytic Hypertension (MATCH) pilot study prospectively enrolled 25 hemodialysis patients with intradialytic hypertension into an open-label intervention study. Once patients were accepted into the study, they underwent baseline testing, including 44-hour ambulatory blood pressure, lipids, albumin, sodium, and C-reactive protein, as well as postdialysis endothelin-1, asymmetric dimethylarginine, endothelial progenitor cells, pulse-wave velocity, and brachial artery flow. In 8 weeks, the baseline lab work was repeated.
Patients were started on carvedilol 6.25 mg twice daily, and eventually titrated to 50 mg twice daily. “Our goal was to reach a delta [systolic] blood pressure less than zero with regard to their postdialysis blood pressure no longer increasing,” said Dr. Inrig. However, she and her colleagues were also targeting a postdialysis systolic BP of less than 130 mm Hg as an alternative goal.
The average patient age was 54 years, and the group was 80% male. Roughly two-thirds of the population was Hispanic (64%), and more than a third was black (36%). Almost all (88%) had diabetes, and 32% had cardiovascular disease. Many were on ACE inhibitors or angiotensin II receptor blockers (64%), beta-blockers (68%), or calcium channel blockers (60%) at baseline.
Mean predialysis BP was roughly the same regardless of carvedilol treatment (144 mm Hg vs. 146 mm Hg). The frequency of intradialytic hypertension declined from 77% of hemodialysis sessions at baseline to 28% by the study's end, a significant difference.
Carvedilol treatment showed a trend toward improvement of brachial artery flow–mediated dilation. However there was no change in C-reactive protein or pulse-wave velocity.
“With regard to safety, patients tolerated carvedilol fairly well,” said Dr. Inrig. There was a low incidence of side effects.
Dr. Inrig has received an investigator-initiated research grant from Genzyme, and has participated in industry-sponsored research for Keryx Biopharmaceuticals.
NEW YORK – Patients treated with carvedilol not only had a reduced frequency of intradialytic hypertension, but also showed improvements in endothelial cell function, in a small study.
After 8 weeks of treatment with carvedilol, mean systolic postdialysis blood pressure dropped from 159 mm Hg at baseline to 142 mm Hg, reported Dr. Julia Inrig of the University of Texas Southwestern Medical Center in Dallas.
We are “very interested in this phenomenon of intradialytic hypertension,” she said at the meeting. When most patients come for dialysis, there is a gradual reduction in their systolic blood pressure. “However, up to 20% of patients have this gradual increase in their systolic blood pressure during their dialysis. So they leave their dialysis session much more hypertensive than when they showed up, despite similar amounts of fluid removed.”
In addition, “we've identified that this is an important prognostic indicator.” In a cohort of 450 dialysis patients, those with increased BP during dialysis were nearly twice as likely to be hospitalized or die by 6 months (Kidney Int. 2007;71:454-61).
The researchers in the Mechanisms and Treatment of Intradialytic Hypertension (MATCH) pilot study prospectively enrolled 25 hemodialysis patients with intradialytic hypertension into an open-label intervention study. Once patients were accepted into the study, they underwent baseline testing, including 44-hour ambulatory blood pressure, lipids, albumin, sodium, and C-reactive protein, as well as postdialysis endothelin-1, asymmetric dimethylarginine, endothelial progenitor cells, pulse-wave velocity, and brachial artery flow. In 8 weeks, the baseline lab work was repeated.
Patients were started on carvedilol 6.25 mg twice daily, and eventually titrated to 50 mg twice daily. “Our goal was to reach a delta [systolic] blood pressure less than zero with regard to their postdialysis blood pressure no longer increasing,” said Dr. Inrig. However, she and her colleagues were also targeting a postdialysis systolic BP of less than 130 mm Hg as an alternative goal.
The average patient age was 54 years, and the group was 80% male. Roughly two-thirds of the population was Hispanic (64%), and more than a third was black (36%). Almost all (88%) had diabetes, and 32% had cardiovascular disease. Many were on ACE inhibitors or angiotensin II receptor blockers (64%), beta-blockers (68%), or calcium channel blockers (60%) at baseline.
Mean predialysis BP was roughly the same regardless of carvedilol treatment (144 mm Hg vs. 146 mm Hg). The frequency of intradialytic hypertension declined from 77% of hemodialysis sessions at baseline to 28% by the study's end, a significant difference.
Carvedilol treatment showed a trend toward improvement of brachial artery flow–mediated dilation. However there was no change in C-reactive protein or pulse-wave velocity.
“With regard to safety, patients tolerated carvedilol fairly well,” said Dr. Inrig. There was a low incidence of side effects.
Dr. Inrig has received an investigator-initiated research grant from Genzyme, and has participated in industry-sponsored research for Keryx Biopharmaceuticals.
NEW YORK – Patients treated with carvedilol not only had a reduced frequency of intradialytic hypertension, but also showed improvements in endothelial cell function, in a small study.
After 8 weeks of treatment with carvedilol, mean systolic postdialysis blood pressure dropped from 159 mm Hg at baseline to 142 mm Hg, reported Dr. Julia Inrig of the University of Texas Southwestern Medical Center in Dallas.
We are “very interested in this phenomenon of intradialytic hypertension,” she said at the meeting. When most patients come for dialysis, there is a gradual reduction in their systolic blood pressure. “However, up to 20% of patients have this gradual increase in their systolic blood pressure during their dialysis. So they leave their dialysis session much more hypertensive than when they showed up, despite similar amounts of fluid removed.”
In addition, “we've identified that this is an important prognostic indicator.” In a cohort of 450 dialysis patients, those with increased BP during dialysis were nearly twice as likely to be hospitalized or die by 6 months (Kidney Int. 2007;71:454-61).
The researchers in the Mechanisms and Treatment of Intradialytic Hypertension (MATCH) pilot study prospectively enrolled 25 hemodialysis patients with intradialytic hypertension into an open-label intervention study. Once patients were accepted into the study, they underwent baseline testing, including 44-hour ambulatory blood pressure, lipids, albumin, sodium, and C-reactive protein, as well as postdialysis endothelin-1, asymmetric dimethylarginine, endothelial progenitor cells, pulse-wave velocity, and brachial artery flow. In 8 weeks, the baseline lab work was repeated.
Patients were started on carvedilol 6.25 mg twice daily, and eventually titrated to 50 mg twice daily. “Our goal was to reach a delta [systolic] blood pressure less than zero with regard to their postdialysis blood pressure no longer increasing,” said Dr. Inrig. However, she and her colleagues were also targeting a postdialysis systolic BP of less than 130 mm Hg as an alternative goal.
The average patient age was 54 years, and the group was 80% male. Roughly two-thirds of the population was Hispanic (64%), and more than a third was black (36%). Almost all (88%) had diabetes, and 32% had cardiovascular disease. Many were on ACE inhibitors or angiotensin II receptor blockers (64%), beta-blockers (68%), or calcium channel blockers (60%) at baseline.
Mean predialysis BP was roughly the same regardless of carvedilol treatment (144 mm Hg vs. 146 mm Hg). The frequency of intradialytic hypertension declined from 77% of hemodialysis sessions at baseline to 28% by the study's end, a significant difference.
Carvedilol treatment showed a trend toward improvement of brachial artery flow–mediated dilation. However there was no change in C-reactive protein or pulse-wave velocity.
“With regard to safety, patients tolerated carvedilol fairly well,” said Dr. Inrig. There was a low incidence of side effects.
Dr. Inrig has received an investigator-initiated research grant from Genzyme, and has participated in industry-sponsored research for Keryx Biopharmaceuticals.
Methamphetamines Linked With Parkinson's Disease
Methamphetamine use may increase an individual’s relative risk of developing Parkinson’s disease by as much as 76%, based on the results of a large retrospective database study.
"Our epidemiological data showing, in hospitalized methamphetamine users, increased risk of subsequent diagnosis of PD [Parkinson’s disease] in hospitalization or death records provides support to the long-hypothesized notion, based on animal data, that methamphetamine exposure might lead to enduring damage of brain dopamine neurons in humans," Dr. Russell C. Callaghan and his coinvestigators wrote in Drug and Alcohol Dependence.
More than 30 years ago, researchers discovered that methamphetamine and its metabolite amphetamine can harm brain dopamine neurons in animal testing. The animal findings raise the concern that use of methamphetamine might damage dopamine neurons in humans and thereby increase the risk of developing PD.
To assess the risk of PD among patients who had used methamphetamine and amphetamine-like drugs, the investigators searched hospital inpatient admission data from 1990 until 2005 from the Patient Discharge Database of the California Office of Statewide Health Planning and Development. These data contain records with demographic information and diagnoses for each inpatient discharged from a California-licensed hospital, including general acute care, acute psychiatric care, chemical dependency recovery, and psychiatric health facilities. The inpatient data were then linked to death records from the California Vital Statistics Database.
Dr. Callaghan of the Centre for Addiction and Mental Health, Toronto, and his associates pulled together three cohorts for the study: 207,831 patients admitted for appendicitis, 35,335 patients admitted for a cocaine-related ICD-9 code, and 40,472 patients admitted for ICD-9 codes related to amphetamine or other psychostimulants (Drug Alcohol Depend. 2011 [doi:10.1016/j.drugalcdep.2011.06.013]).
Patients in the appendicitis group had to be at least 30 years old with a diagnosis of an appendicitis-related condition. They could have no recorded indications or signs of PD or methamphetamine or cocaine use.
Likewise, patients in the cocaine group had to be at least 30 years old and had an ICD-9 code related to cocaine dependence, abuse, or poisoning. They could have no recorded indications or signs of PD, other alcohol or drug use, or HIV.
For the methamphetamine group, the researchers noted that it is not possible to distinguish between methamphetamine and other amphetamine-like stimulants based on ICD-9 codes. However, based on previous studies "we argue that it is reasonable to expect that the bulk of the admissions in our study are specific to methamphetamine."
The methamphetamine cohort had a significantly greater risk of a PD outcome – with a hazard ratio 1.76 – than did the appendicitis group. A PD outcome was measured as an inpatient admission with a diagnosis of PD or an underlying cause of death listed as PD. This result was based on a competing risks analysis using a 1:1 matched sample.
The increased risk "means that if we followed 10,000 methamphetamine users (at least 30 years of age) and 10,000 people of similar age, race, and sex from a California population-based sample for 10 years, we would expect approximately 21 cases of PD in the methamphetamine group and approximately 12 in the population group."
Similarly, the methamphetamine group had a greater risk of developing PD than did the cocaine group (hazard ratio, 2.41). But the cocaine group did not have a higher risk of developing PD than did the appendicitis group (HR, 1.04).
One important limitation of the study is its lack of information on the age of initiation, frequency, dose, or duration of drug use. "Nevertheless, it is reasonable to assume that the drug users in our study were, for the most part, ‘moderate to heavy’ stimulant users having clinically significant problems as indicated by a formal hospital diagnosis of a methamphetamine-use disorder," the investigators concluded.
"While our study does raise the question of whether licit amphetamines might also increase the risk of Parkinson’s disease, it is important to emphasize that our findings might not at all relate to those individuals who take much lower doses of amphetamine drugs for therapeutic purposes (e.g., for ADHD)."
All of the authors reported that they have no conflicts of interest.
Over the last 10 years, there have been a number of
studies that support the hypothesis that amphetamine use is a risk factor for
Parkinson’s disease. This is a very large retrospective study in a special
group of amphetamine-exposed patients that strongly supports that hypothesis.
This study compared the
rate of Parkinson’s disease in patients previously hospitalized with a
diagnosis of amphetamine or methamphetamine use with the rate of Parkinson’s
disease in patients previously hospitalized for appendicitis. They found a 76%
increased risk of developing Parkinson’s disease.
The strength of this study
is the large number of patients who have a hospital diagnosis of amphetamine
use. A weakness is that we don’t have a sense of the duration and the dose of
amphetamine used by the patients – because they’re recreational users. The
authors assert that those in the meth/amphetamine group were
‘moderate-to-heavy’ users of amphetamines but detailed information is not
available.
Because of the limitations
of the study, we don’t know how many exposures and at what dose methamphetamine
is likely to increase the risk of developing Parkinson’s disease.
While this study provides
solid support for methamphetamine exposure as an environmental risk factor for
Parkinson’s disease, many scientists believe there are other environmental
factors to be discovered. We are
particularly interested in identifying agents that can be controlled, such as
avoiding methamphetamine exposure.
Dr. Chad Christine is
an associate professor of neurology at the University
of California, San Francisco. He reported that he has no
financial conflicts of interest.
Over the last 10 years, there have been a number of
studies that support the hypothesis that amphetamine use is a risk factor for
Parkinson’s disease. This is a very large retrospective study in a special
group of amphetamine-exposed patients that strongly supports that hypothesis.
This study compared the
rate of Parkinson’s disease in patients previously hospitalized with a
diagnosis of amphetamine or methamphetamine use with the rate of Parkinson’s
disease in patients previously hospitalized for appendicitis. They found a 76%
increased risk of developing Parkinson’s disease.
The strength of this study
is the large number of patients who have a hospital diagnosis of amphetamine
use. A weakness is that we don’t have a sense of the duration and the dose of
amphetamine used by the patients – because they’re recreational users. The
authors assert that those in the meth/amphetamine group were
‘moderate-to-heavy’ users of amphetamines but detailed information is not
available.
Because of the limitations
of the study, we don’t know how many exposures and at what dose methamphetamine
is likely to increase the risk of developing Parkinson’s disease.
While this study provides
solid support for methamphetamine exposure as an environmental risk factor for
Parkinson’s disease, many scientists believe there are other environmental
factors to be discovered. We are
particularly interested in identifying agents that can be controlled, such as
avoiding methamphetamine exposure.
Dr. Chad Christine is
an associate professor of neurology at the University
of California, San Francisco. He reported that he has no
financial conflicts of interest.
Over the last 10 years, there have been a number of
studies that support the hypothesis that amphetamine use is a risk factor for
Parkinson’s disease. This is a very large retrospective study in a special
group of amphetamine-exposed patients that strongly supports that hypothesis.
This study compared the
rate of Parkinson’s disease in patients previously hospitalized with a
diagnosis of amphetamine or methamphetamine use with the rate of Parkinson’s
disease in patients previously hospitalized for appendicitis. They found a 76%
increased risk of developing Parkinson’s disease.
The strength of this study
is the large number of patients who have a hospital diagnosis of amphetamine
use. A weakness is that we don’t have a sense of the duration and the dose of
amphetamine used by the patients – because they’re recreational users. The
authors assert that those in the meth/amphetamine group were
‘moderate-to-heavy’ users of amphetamines but detailed information is not
available.
Because of the limitations
of the study, we don’t know how many exposures and at what dose methamphetamine
is likely to increase the risk of developing Parkinson’s disease.
While this study provides
solid support for methamphetamine exposure as an environmental risk factor for
Parkinson’s disease, many scientists believe there are other environmental
factors to be discovered. We are
particularly interested in identifying agents that can be controlled, such as
avoiding methamphetamine exposure.
Dr. Chad Christine is
an associate professor of neurology at the University
of California, San Francisco. He reported that he has no
financial conflicts of interest.
Methamphetamine use may increase an individual’s relative risk of developing Parkinson’s disease by as much as 76%, based on the results of a large retrospective database study.
"Our epidemiological data showing, in hospitalized methamphetamine users, increased risk of subsequent diagnosis of PD [Parkinson’s disease] in hospitalization or death records provides support to the long-hypothesized notion, based on animal data, that methamphetamine exposure might lead to enduring damage of brain dopamine neurons in humans," Dr. Russell C. Callaghan and his coinvestigators wrote in Drug and Alcohol Dependence.
More than 30 years ago, researchers discovered that methamphetamine and its metabolite amphetamine can harm brain dopamine neurons in animal testing. The animal findings raise the concern that use of methamphetamine might damage dopamine neurons in humans and thereby increase the risk of developing PD.
To assess the risk of PD among patients who had used methamphetamine and amphetamine-like drugs, the investigators searched hospital inpatient admission data from 1990 until 2005 from the Patient Discharge Database of the California Office of Statewide Health Planning and Development. These data contain records with demographic information and diagnoses for each inpatient discharged from a California-licensed hospital, including general acute care, acute psychiatric care, chemical dependency recovery, and psychiatric health facilities. The inpatient data were then linked to death records from the California Vital Statistics Database.
Dr. Callaghan of the Centre for Addiction and Mental Health, Toronto, and his associates pulled together three cohorts for the study: 207,831 patients admitted for appendicitis, 35,335 patients admitted for a cocaine-related ICD-9 code, and 40,472 patients admitted for ICD-9 codes related to amphetamine or other psychostimulants (Drug Alcohol Depend. 2011 [doi:10.1016/j.drugalcdep.2011.06.013]).
Patients in the appendicitis group had to be at least 30 years old with a diagnosis of an appendicitis-related condition. They could have no recorded indications or signs of PD or methamphetamine or cocaine use.
Likewise, patients in the cocaine group had to be at least 30 years old and had an ICD-9 code related to cocaine dependence, abuse, or poisoning. They could have no recorded indications or signs of PD, other alcohol or drug use, or HIV.
For the methamphetamine group, the researchers noted that it is not possible to distinguish between methamphetamine and other amphetamine-like stimulants based on ICD-9 codes. However, based on previous studies "we argue that it is reasonable to expect that the bulk of the admissions in our study are specific to methamphetamine."
The methamphetamine cohort had a significantly greater risk of a PD outcome – with a hazard ratio 1.76 – than did the appendicitis group. A PD outcome was measured as an inpatient admission with a diagnosis of PD or an underlying cause of death listed as PD. This result was based on a competing risks analysis using a 1:1 matched sample.
The increased risk "means that if we followed 10,000 methamphetamine users (at least 30 years of age) and 10,000 people of similar age, race, and sex from a California population-based sample for 10 years, we would expect approximately 21 cases of PD in the methamphetamine group and approximately 12 in the population group."
Similarly, the methamphetamine group had a greater risk of developing PD than did the cocaine group (hazard ratio, 2.41). But the cocaine group did not have a higher risk of developing PD than did the appendicitis group (HR, 1.04).
One important limitation of the study is its lack of information on the age of initiation, frequency, dose, or duration of drug use. "Nevertheless, it is reasonable to assume that the drug users in our study were, for the most part, ‘moderate to heavy’ stimulant users having clinically significant problems as indicated by a formal hospital diagnosis of a methamphetamine-use disorder," the investigators concluded.
"While our study does raise the question of whether licit amphetamines might also increase the risk of Parkinson’s disease, it is important to emphasize that our findings might not at all relate to those individuals who take much lower doses of amphetamine drugs for therapeutic purposes (e.g., for ADHD)."
All of the authors reported that they have no conflicts of interest.
Methamphetamine use may increase an individual’s relative risk of developing Parkinson’s disease by as much as 76%, based on the results of a large retrospective database study.
"Our epidemiological data showing, in hospitalized methamphetamine users, increased risk of subsequent diagnosis of PD [Parkinson’s disease] in hospitalization or death records provides support to the long-hypothesized notion, based on animal data, that methamphetamine exposure might lead to enduring damage of brain dopamine neurons in humans," Dr. Russell C. Callaghan and his coinvestigators wrote in Drug and Alcohol Dependence.
More than 30 years ago, researchers discovered that methamphetamine and its metabolite amphetamine can harm brain dopamine neurons in animal testing. The animal findings raise the concern that use of methamphetamine might damage dopamine neurons in humans and thereby increase the risk of developing PD.
To assess the risk of PD among patients who had used methamphetamine and amphetamine-like drugs, the investigators searched hospital inpatient admission data from 1990 until 2005 from the Patient Discharge Database of the California Office of Statewide Health Planning and Development. These data contain records with demographic information and diagnoses for each inpatient discharged from a California-licensed hospital, including general acute care, acute psychiatric care, chemical dependency recovery, and psychiatric health facilities. The inpatient data were then linked to death records from the California Vital Statistics Database.
Dr. Callaghan of the Centre for Addiction and Mental Health, Toronto, and his associates pulled together three cohorts for the study: 207,831 patients admitted for appendicitis, 35,335 patients admitted for a cocaine-related ICD-9 code, and 40,472 patients admitted for ICD-9 codes related to amphetamine or other psychostimulants (Drug Alcohol Depend. 2011 [doi:10.1016/j.drugalcdep.2011.06.013]).
Patients in the appendicitis group had to be at least 30 years old with a diagnosis of an appendicitis-related condition. They could have no recorded indications or signs of PD or methamphetamine or cocaine use.
Likewise, patients in the cocaine group had to be at least 30 years old and had an ICD-9 code related to cocaine dependence, abuse, or poisoning. They could have no recorded indications or signs of PD, other alcohol or drug use, or HIV.
For the methamphetamine group, the researchers noted that it is not possible to distinguish between methamphetamine and other amphetamine-like stimulants based on ICD-9 codes. However, based on previous studies "we argue that it is reasonable to expect that the bulk of the admissions in our study are specific to methamphetamine."
The methamphetamine cohort had a significantly greater risk of a PD outcome – with a hazard ratio 1.76 – than did the appendicitis group. A PD outcome was measured as an inpatient admission with a diagnosis of PD or an underlying cause of death listed as PD. This result was based on a competing risks analysis using a 1:1 matched sample.
The increased risk "means that if we followed 10,000 methamphetamine users (at least 30 years of age) and 10,000 people of similar age, race, and sex from a California population-based sample for 10 years, we would expect approximately 21 cases of PD in the methamphetamine group and approximately 12 in the population group."
Similarly, the methamphetamine group had a greater risk of developing PD than did the cocaine group (hazard ratio, 2.41). But the cocaine group did not have a higher risk of developing PD than did the appendicitis group (HR, 1.04).
One important limitation of the study is its lack of information on the age of initiation, frequency, dose, or duration of drug use. "Nevertheless, it is reasonable to assume that the drug users in our study were, for the most part, ‘moderate to heavy’ stimulant users having clinically significant problems as indicated by a formal hospital diagnosis of a methamphetamine-use disorder," the investigators concluded.
"While our study does raise the question of whether licit amphetamines might also increase the risk of Parkinson’s disease, it is important to emphasize that our findings might not at all relate to those individuals who take much lower doses of amphetamine drugs for therapeutic purposes (e.g., for ADHD)."
All of the authors reported that they have no conflicts of interest.
FROM DRUG AND ALCOHOL DEPENDENCE
Major Finding: The use of methamphetamine may increase the risk of developing Parkinson’s disease by 76%.
Data Source: Database study of almost 300,000 patients.
Disclosures: All of the authors reported that they have no conflicts of interest.
Symptom Improvement Observed After Venoplasty in MS Patients
CHICAGO – Preliminary data from a series of multiple sclerosis patients who underwent percutaneous transluminal venoplasty to treat chronic cerebrospinal venous insufficiency suggest that the treatment was safe and offered significant disease-specific and quality of life improvements.
The results of the controversial treatment on 125 patients in the series will need to be validated with future randomized, blinded, controlled trials that evaluate endovascular and surgical options, Dr. Manish Mehta said at the Vascular Annual Meeting.
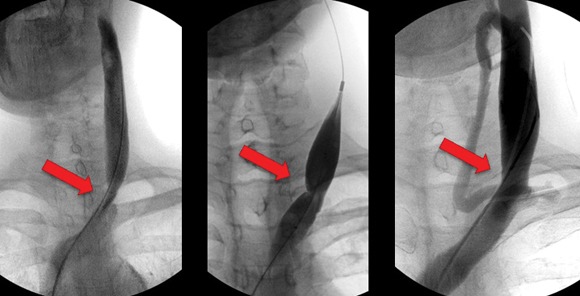
The patient series follows Dr. Paolo Zamboni’s identification in 2009 of stenoses in the internal jugular veins and azygous vein of patients with MS (J. Neurol. Neurosurg. Psychiatry 2009;80:392-9).
"Dr. Zamboni’s theory has been that stasis of blood can cause reflux, and reflux can cause propagation and [can] break down the blood-brain barrier," Dr. Mehta said. The resulting microbleeds can allow red blood cells to escape into the brain matter, leading to hemosiderin deposits that can act as the inflammatory mediators of an autoimmune response, he said.
Although Dr. Zamboni, a vascular surgeon and professor of surgery at the University of Ferrara (Italy), observed a strong association between chronic cerebrospinal venous insufficiency (CCSVI) and MS, it is unclear if the relationship between CCSVI and MS is causative, or if CCSVI might play a role in the etiology of the disease.
In 2009, Dr. Zamboni also reported on a series of 65 patients who had significant improvements in functional composite scores and quality of life at 1 year (J. Vasc. Surg. 2009;50;1348-58.e1-3).
The preliminary data that Dr. Mehta presented at the meeting came from the LIBERATION study, which is designed to assess the utility of percutaneous transluminal venoplasty for individuals with CCSVI and MS. It’s a prospective, randomized, double-blind study that is currently enrolling 600 patients.
Because there is a learning curve involved with the assessment and technique, the researchers included a prospective longitudinal arm as part of the study. Dr. Mehta of the Albany (N.Y.) Medical College and the director of endovascular services for the Vascular Group PLLC, presented preliminary results on this group of patients.

In the study, investigators performed venograms to identify stenoses of 50% or greater in internal jugular and azygous veins in the patients, all of whom underwent venoplasty. Neurologists and other clinicians evaluated the patients at baseline, and then at 1 month, 3 months, and every 6 months thereafter.
The 125 patients included in the study had a mean age of 47 years, and 62% were female. Relapsing-remitting MS accounted for 54% of the patients, followed by secondary-progressive MS in 34% and primary-progressive MS in 12%.
The patients had a total of 230 lesions altogether, 90% of which involved the internal jugular veins; the majority of these were at the origin. The remaining 10% of patients had stenoses in their azygous veins.
The mean degree of occlusion was about 80%, with approximately 1.8 lesions per patient. Immediate success (defined as less than 20% residual stenosis) occurred in 82%. The remaining patients underwent a second venoplasty without stenting.
In all, 79 patients were available for follow-up at a mean of 4.5 years. Restenosis of 50% occurred in eight of these patients, occlusions occurred in two patients, and one patient had new-onset atrial fibrillation.
The investigators reassessed 48 patients with the EDSS (Extended Disability Status Scale) following initial baseline testing. From before to after the procedure, "there was a statistical improvement. Improvements occurred in each of the MS types, except in primary progressive MS," Dr. Mehta said.
Reevaluations of 79 patients who performed a timed 25-foot walk at baseline showed a significant improvement in walking speed. In terms of MS quality of life, from before to after the procedure "there were significant improvements in physical and mental ability. There clearly seems to be a trend. In the modified fatigue impact score, there also seems to be a clear improvement," he said.
Dr. Mehta also said that there was a trend toward improvement in balance, lower-extremity weakness, incontinence, coordination, and vertigo in more than 80% of patients.
Dr. Mehta and his colleagues reported that they each had several significant financial relationships with device manufacturers.
CHICAGO – Preliminary data from a series of multiple sclerosis patients who underwent percutaneous transluminal venoplasty to treat chronic cerebrospinal venous insufficiency suggest that the treatment was safe and offered significant disease-specific and quality of life improvements.
The results of the controversial treatment on 125 patients in the series will need to be validated with future randomized, blinded, controlled trials that evaluate endovascular and surgical options, Dr. Manish Mehta said at the Vascular Annual Meeting.
The patient series follows Dr. Paolo Zamboni’s identification in 2009 of stenoses in the internal jugular veins and azygous vein of patients with MS (J. Neurol. Neurosurg. Psychiatry 2009;80:392-9).
"Dr. Zamboni’s theory has been that stasis of blood can cause reflux, and reflux can cause propagation and [can] break down the blood-brain barrier," Dr. Mehta said. The resulting microbleeds can allow red blood cells to escape into the brain matter, leading to hemosiderin deposits that can act as the inflammatory mediators of an autoimmune response, he said.
Although Dr. Zamboni, a vascular surgeon and professor of surgery at the University of Ferrara (Italy), observed a strong association between chronic cerebrospinal venous insufficiency (CCSVI) and MS, it is unclear if the relationship between CCSVI and MS is causative, or if CCSVI might play a role in the etiology of the disease.
In 2009, Dr. Zamboni also reported on a series of 65 patients who had significant improvements in functional composite scores and quality of life at 1 year (J. Vasc. Surg. 2009;50;1348-58.e1-3).
The preliminary data that Dr. Mehta presented at the meeting came from the LIBERATION study, which is designed to assess the utility of percutaneous transluminal venoplasty for individuals with CCSVI and MS. It’s a prospective, randomized, double-blind study that is currently enrolling 600 patients.
Because there is a learning curve involved with the assessment and technique, the researchers included a prospective longitudinal arm as part of the study. Dr. Mehta of the Albany (N.Y.) Medical College and the director of endovascular services for the Vascular Group PLLC, presented preliminary results on this group of patients.
In the study, investigators performed venograms to identify stenoses of 50% or greater in internal jugular and azygous veins in the patients, all of whom underwent venoplasty. Neurologists and other clinicians evaluated the patients at baseline, and then at 1 month, 3 months, and every 6 months thereafter.
The 125 patients included in the study had a mean age of 47 years, and 62% were female. Relapsing-remitting MS accounted for 54% of the patients, followed by secondary-progressive MS in 34% and primary-progressive MS in 12%.
The patients had a total of 230 lesions altogether, 90% of which involved the internal jugular veins; the majority of these were at the origin. The remaining 10% of patients had stenoses in their azygous veins.
The mean degree of occlusion was about 80%, with approximately 1.8 lesions per patient. Immediate success (defined as less than 20% residual stenosis) occurred in 82%. The remaining patients underwent a second venoplasty without stenting.
In all, 79 patients were available for follow-up at a mean of 4.5 years. Restenosis of 50% occurred in eight of these patients, occlusions occurred in two patients, and one patient had new-onset atrial fibrillation.
The investigators reassessed 48 patients with the EDSS (Extended Disability Status Scale) following initial baseline testing. From before to after the procedure, "there was a statistical improvement. Improvements occurred in each of the MS types, except in primary progressive MS," Dr. Mehta said.
Reevaluations of 79 patients who performed a timed 25-foot walk at baseline showed a significant improvement in walking speed. In terms of MS quality of life, from before to after the procedure "there were significant improvements in physical and mental ability. There clearly seems to be a trend. In the modified fatigue impact score, there also seems to be a clear improvement," he said.
Dr. Mehta also said that there was a trend toward improvement in balance, lower-extremity weakness, incontinence, coordination, and vertigo in more than 80% of patients.
Dr. Mehta and his colleagues reported that they each had several significant financial relationships with device manufacturers.
CHICAGO – Preliminary data from a series of multiple sclerosis patients who underwent percutaneous transluminal venoplasty to treat chronic cerebrospinal venous insufficiency suggest that the treatment was safe and offered significant disease-specific and quality of life improvements.
The results of the controversial treatment on 125 patients in the series will need to be validated with future randomized, blinded, controlled trials that evaluate endovascular and surgical options, Dr. Manish Mehta said at the Vascular Annual Meeting.
The patient series follows Dr. Paolo Zamboni’s identification in 2009 of stenoses in the internal jugular veins and azygous vein of patients with MS (J. Neurol. Neurosurg. Psychiatry 2009;80:392-9).
"Dr. Zamboni’s theory has been that stasis of blood can cause reflux, and reflux can cause propagation and [can] break down the blood-brain barrier," Dr. Mehta said. The resulting microbleeds can allow red blood cells to escape into the brain matter, leading to hemosiderin deposits that can act as the inflammatory mediators of an autoimmune response, he said.
Although Dr. Zamboni, a vascular surgeon and professor of surgery at the University of Ferrara (Italy), observed a strong association between chronic cerebrospinal venous insufficiency (CCSVI) and MS, it is unclear if the relationship between CCSVI and MS is causative, or if CCSVI might play a role in the etiology of the disease.
In 2009, Dr. Zamboni also reported on a series of 65 patients who had significant improvements in functional composite scores and quality of life at 1 year (J. Vasc. Surg. 2009;50;1348-58.e1-3).
The preliminary data that Dr. Mehta presented at the meeting came from the LIBERATION study, which is designed to assess the utility of percutaneous transluminal venoplasty for individuals with CCSVI and MS. It’s a prospective, randomized, double-blind study that is currently enrolling 600 patients.
Because there is a learning curve involved with the assessment and technique, the researchers included a prospective longitudinal arm as part of the study. Dr. Mehta of the Albany (N.Y.) Medical College and the director of endovascular services for the Vascular Group PLLC, presented preliminary results on this group of patients.
In the study, investigators performed venograms to identify stenoses of 50% or greater in internal jugular and azygous veins in the patients, all of whom underwent venoplasty. Neurologists and other clinicians evaluated the patients at baseline, and then at 1 month, 3 months, and every 6 months thereafter.
The 125 patients included in the study had a mean age of 47 years, and 62% were female. Relapsing-remitting MS accounted for 54% of the patients, followed by secondary-progressive MS in 34% and primary-progressive MS in 12%.
The patients had a total of 230 lesions altogether, 90% of which involved the internal jugular veins; the majority of these were at the origin. The remaining 10% of patients had stenoses in their azygous veins.
The mean degree of occlusion was about 80%, with approximately 1.8 lesions per patient. Immediate success (defined as less than 20% residual stenosis) occurred in 82%. The remaining patients underwent a second venoplasty without stenting.
In all, 79 patients were available for follow-up at a mean of 4.5 years. Restenosis of 50% occurred in eight of these patients, occlusions occurred in two patients, and one patient had new-onset atrial fibrillation.
The investigators reassessed 48 patients with the EDSS (Extended Disability Status Scale) following initial baseline testing. From before to after the procedure, "there was a statistical improvement. Improvements occurred in each of the MS types, except in primary progressive MS," Dr. Mehta said.
Reevaluations of 79 patients who performed a timed 25-foot walk at baseline showed a significant improvement in walking speed. In terms of MS quality of life, from before to after the procedure "there were significant improvements in physical and mental ability. There clearly seems to be a trend. In the modified fatigue impact score, there also seems to be a clear improvement," he said.
Dr. Mehta also said that there was a trend toward improvement in balance, lower-extremity weakness, incontinence, coordination, and vertigo in more than 80% of patients.
Dr. Mehta and his colleagues reported that they each had several significant financial relationships with device manufacturers.
FROM THE VASCULAR ANNUAL MEETING
Major Finding: Residual stenosis of less than 20% (defined as immediate success) was observed in 82% of patients.
Data Source: A series of 125 patients with multiple sclerosis who were identified by venogram to have internal jugular and/or azygous veins with stenoses of 50% or greater.
Disclosures: Dr. Mehta and his colleagues reported that they each had several significant financial relationships with device manufacturers.