User login
M. Alexander Otto began his reporting career early in 1999 covering the pharmaceutical industry for a national pharmacists' magazine and freelancing for the Washington Post and other newspapers. He then joined BNA, now part of Bloomberg News, covering health law and the protection of people and animals in medical research. Alex next worked for the McClatchy Company. Based on his work, Alex won a year-long Knight Science Journalism Fellowship to MIT in 2008-2009. He joined the company shortly thereafter. Alex has a newspaper journalism degree from Syracuse (N.Y.) University and a master's degree in medical science -- a physician assistant degree -- from George Washington University. Alex is based in Seattle.
Recreational marijuana use should not rule out ADHD stimulant treatment
SAN FRANCISCO – “If one is going to say ‘you need 6 months of abstinence from cannabis before I am going to treat your ADHD,’ that’s absurd. If [kids] are stoned all the time, no, but if it’s intermittent, it’s really not a factor,” according to James J. McGough, MD, director of the Attention Deficit Disorder Clinic at the University of California, Los Angeles.
There’s no evidence that ongoing stimulant treatment increases the risk of substance abuse, and “we must admit to ourselves that substance use among adolescents and young adults is normative. It happens,” even among well-adapted kids. “Think of your own past histories,” he said to an audience of psychiatrists and other medical professionals at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.

“You have” to deal with substance abuse that’s ruining lives, but otherwise, “I’m comfortable giving a prescription under some circumstances even if I know [patients] are using drugs. It’s the extent and type of [drug use] that informs if we should prescribe or not,” said Dr. McGough, also a professor of clinical psychiatry at the university, but be careful to “really document what you’re doing.”
Misuse and diversion is mostly related to performance enhancement, especially at competitive universities, or when grades head south. Children and young adults in those situations, as well as smokers, drinkers, and those with conduct disorders, “are the ones you worry about.” If a Stanford medical school student at age 27 suddenly develops a horrible problem focusing, with no past ADHD history, “I’m a little suspicious,” he said, noting that people who malinger “tend to go off the scale in terms of endorsing symptoms.”
If misuse and abuse are a concern, extended-release stimulants, as well as nonstimulants, are better options than immediate-release formulations.
Audience members also were curious about alternative approaches for ADHD, but the news wasn’t very good.
For now, there’s no brain scan, test, or lab measurement that reliably detects ADHD. Even with neuropsychiatric testing, only half of children and adolescents will have executive-functioning deficits. The problem with computerized tests, meanwhile, is that a lot of children and adolescents with ADHD have no problem focusing on computer games, so they aren’t helpful for diagnosis.
“The gold standard for ADHD assessment remains a good interview,” and documenting DSM-5 criteria, he said.
As for alternative treatments, “what studies have shown is that if you are highly invested in the treatment and not blinded” to it, “you tend to think you do better. In good studies where they look at teachers who don’t know what’s going on, it doesn’t pan out,” he said. Metanalysis of neurofeedback hasn’t shown effect, nor have computer games to train focus; kids will get better at them with practice, but they haven’t been shown to improve ADHD.
The only exception is omega-3, but the effect size is barely measurable. “If you can get the kid so swallow those fish oil things, go for it, or they can eat salmon,” Dr. McGough said.
In short, medications remain the best option for treating the core symptoms of ADHD, first with stimulants then, as needed, nonstimulants.
But “you are not meeting your patients’ needs if you are only prescribing medications,” he said. Psychosocial education, family behavioral therapy, and school interventions – even things as simple as sitting toward the front of the class and having a little more time on tests – are critical for overall improvement.
It’s also important to let patients and families know that “they don’t have to be ashamed of this,” and the patients need to know why they are taking their medication, he said.
Too often, children are started on a low dose of medication and told to come back in a month. “That’s a waste of time, because it’s a whole month when the person is probably inadequately treated,” Dr. McGough said.
Instead, he has patients titrate up at first, with advice to cut back or stop and call if there are problems. The patient returns after 3 weeks, and the most effective, best-tolerated dose is selected for treatment.
Dr. McGough disclosed relationships with Purdue, Shire, Tris, Sunovion, NeuroSigma, and Neurovance.
SAN FRANCISCO – “If one is going to say ‘you need 6 months of abstinence from cannabis before I am going to treat your ADHD,’ that’s absurd. If [kids] are stoned all the time, no, but if it’s intermittent, it’s really not a factor,” according to James J. McGough, MD, director of the Attention Deficit Disorder Clinic at the University of California, Los Angeles.
There’s no evidence that ongoing stimulant treatment increases the risk of substance abuse, and “we must admit to ourselves that substance use among adolescents and young adults is normative. It happens,” even among well-adapted kids. “Think of your own past histories,” he said to an audience of psychiatrists and other medical professionals at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“You have” to deal with substance abuse that’s ruining lives, but otherwise, “I’m comfortable giving a prescription under some circumstances even if I know [patients] are using drugs. It’s the extent and type of [drug use] that informs if we should prescribe or not,” said Dr. McGough, also a professor of clinical psychiatry at the university, but be careful to “really document what you’re doing.”
Misuse and diversion is mostly related to performance enhancement, especially at competitive universities, or when grades head south. Children and young adults in those situations, as well as smokers, drinkers, and those with conduct disorders, “are the ones you worry about.” If a Stanford medical school student at age 27 suddenly develops a horrible problem focusing, with no past ADHD history, “I’m a little suspicious,” he said, noting that people who malinger “tend to go off the scale in terms of endorsing symptoms.”
If misuse and abuse are a concern, extended-release stimulants, as well as nonstimulants, are better options than immediate-release formulations.
Audience members also were curious about alternative approaches for ADHD, but the news wasn’t very good.
For now, there’s no brain scan, test, or lab measurement that reliably detects ADHD. Even with neuropsychiatric testing, only half of children and adolescents will have executive-functioning deficits. The problem with computerized tests, meanwhile, is that a lot of children and adolescents with ADHD have no problem focusing on computer games, so they aren’t helpful for diagnosis.
“The gold standard for ADHD assessment remains a good interview,” and documenting DSM-5 criteria, he said.
As for alternative treatments, “what studies have shown is that if you are highly invested in the treatment and not blinded” to it, “you tend to think you do better. In good studies where they look at teachers who don’t know what’s going on, it doesn’t pan out,” he said. Metanalysis of neurofeedback hasn’t shown effect, nor have computer games to train focus; kids will get better at them with practice, but they haven’t been shown to improve ADHD.
The only exception is omega-3, but the effect size is barely measurable. “If you can get the kid so swallow those fish oil things, go for it, or they can eat salmon,” Dr. McGough said.
In short, medications remain the best option for treating the core symptoms of ADHD, first with stimulants then, as needed, nonstimulants.
But “you are not meeting your patients’ needs if you are only prescribing medications,” he said. Psychosocial education, family behavioral therapy, and school interventions – even things as simple as sitting toward the front of the class and having a little more time on tests – are critical for overall improvement.
It’s also important to let patients and families know that “they don’t have to be ashamed of this,” and the patients need to know why they are taking their medication, he said.
Too often, children are started on a low dose of medication and told to come back in a month. “That’s a waste of time, because it’s a whole month when the person is probably inadequately treated,” Dr. McGough said.
Instead, he has patients titrate up at first, with advice to cut back or stop and call if there are problems. The patient returns after 3 weeks, and the most effective, best-tolerated dose is selected for treatment.
Dr. McGough disclosed relationships with Purdue, Shire, Tris, Sunovion, NeuroSigma, and Neurovance.
SAN FRANCISCO – “If one is going to say ‘you need 6 months of abstinence from cannabis before I am going to treat your ADHD,’ that’s absurd. If [kids] are stoned all the time, no, but if it’s intermittent, it’s really not a factor,” according to James J. McGough, MD, director of the Attention Deficit Disorder Clinic at the University of California, Los Angeles.
There’s no evidence that ongoing stimulant treatment increases the risk of substance abuse, and “we must admit to ourselves that substance use among adolescents and young adults is normative. It happens,” even among well-adapted kids. “Think of your own past histories,” he said to an audience of psychiatrists and other medical professionals at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“You have” to deal with substance abuse that’s ruining lives, but otherwise, “I’m comfortable giving a prescription under some circumstances even if I know [patients] are using drugs. It’s the extent and type of [drug use] that informs if we should prescribe or not,” said Dr. McGough, also a professor of clinical psychiatry at the university, but be careful to “really document what you’re doing.”
Misuse and diversion is mostly related to performance enhancement, especially at competitive universities, or when grades head south. Children and young adults in those situations, as well as smokers, drinkers, and those with conduct disorders, “are the ones you worry about.” If a Stanford medical school student at age 27 suddenly develops a horrible problem focusing, with no past ADHD history, “I’m a little suspicious,” he said, noting that people who malinger “tend to go off the scale in terms of endorsing symptoms.”
If misuse and abuse are a concern, extended-release stimulants, as well as nonstimulants, are better options than immediate-release formulations.
Audience members also were curious about alternative approaches for ADHD, but the news wasn’t very good.
For now, there’s no brain scan, test, or lab measurement that reliably detects ADHD. Even with neuropsychiatric testing, only half of children and adolescents will have executive-functioning deficits. The problem with computerized tests, meanwhile, is that a lot of children and adolescents with ADHD have no problem focusing on computer games, so they aren’t helpful for diagnosis.
“The gold standard for ADHD assessment remains a good interview,” and documenting DSM-5 criteria, he said.
As for alternative treatments, “what studies have shown is that if you are highly invested in the treatment and not blinded” to it, “you tend to think you do better. In good studies where they look at teachers who don’t know what’s going on, it doesn’t pan out,” he said. Metanalysis of neurofeedback hasn’t shown effect, nor have computer games to train focus; kids will get better at them with practice, but they haven’t been shown to improve ADHD.
The only exception is omega-3, but the effect size is barely measurable. “If you can get the kid so swallow those fish oil things, go for it, or they can eat salmon,” Dr. McGough said.
In short, medications remain the best option for treating the core symptoms of ADHD, first with stimulants then, as needed, nonstimulants.
But “you are not meeting your patients’ needs if you are only prescribing medications,” he said. Psychosocial education, family behavioral therapy, and school interventions – even things as simple as sitting toward the front of the class and having a little more time on tests – are critical for overall improvement.
It’s also important to let patients and families know that “they don’t have to be ashamed of this,” and the patients need to know why they are taking their medication, he said.
Too often, children are started on a low dose of medication and told to come back in a month. “That’s a waste of time, because it’s a whole month when the person is probably inadequately treated,” Dr. McGough said.
Instead, he has patients titrate up at first, with advice to cut back or stop and call if there are problems. The patient returns after 3 weeks, and the most effective, best-tolerated dose is selected for treatment.
Dr. McGough disclosed relationships with Purdue, Shire, Tris, Sunovion, NeuroSigma, and Neurovance.
Circulating DNA catches lymphoma relapse early
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
A newer technique aimed at detect circulating tumor DNA in the blood – cancer personalized profiling by deep sequencing (CAPP-Seq) – detected recurrence of diffuse large B cell lymphoma more than 6 months earlier than radiographic findings in a study at Stanford (Calif.) University, where the technique was invented.
The findings signal another win for “liquid biopsy,” the measurement of tumor DNA circulating in the blood, which is rapidly emerging as a quick and powerful tool for the diagnosis of a range of cancers and tumor subtypes, and prediction of tumor behavior and treatment response. Investigators at Stanford and elsewhere are studying liquid biopsy not only for lymphoma, but also for colorectal, thyroid, breast, prostate, and most other cancers. The Stanford team recently reported that its circulating DNA-detecting CAPP-Seq technique also helps in lung cancer.
In the new study, Stanford used CAPP-Seq (Cancer Personalized Profiling by deep Sequencing), which it called “an ultrasensitive capture-based targeted sequencing method” to analyze 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma (DLBCL) at diagnosis and various point afterward. The team compared the results to radiologic, and other standard diagnostic and monitoring techniques (Sci Transl Med. 2016 Nov 9;8[364]:364ra155).
At diagnosis, the amount of circulating DNA (ctDNA) correlated strongly with clinical indices and was independently predictive of patient outcomes; “whereas 100% of pretreatment samples had detectable ctDNA, only 37% of samples had abnormally high serum” lactate dehydrogenase, currently the most commonly used biomarker for DLBCL, said investigators, led by research fellow Florian Scherer, MD.
The group detected ctDNA in 73% of patients (8/11) who eventually relapsed a mean of 188 days before relapse was detected by standard-of-care radiologic techniques.
CAPP-Seq identified nine patients with a particular type of activated B cell-like tumor, for whom ibrutinib (Imbruvica) is particularly effective; ctDNA also predicted the transformation of indolent follicular lymphoma to DLBCL “with high sensitivity and specificity,” the group reported.
Stanford anticipates “ctDNA will have broad utility for dissecting tumor heterogeneity within and between patients with lymphomas and other cancer types, with applications for the identification of adverse risk groups, the discovery of resistance mechanisms to diverse therapies, and the development of risk-adapted therapeutics.”
The team said its approach “outperformed immunoglobulin sequencing and radiographic imaging for the detection of minimal residual disease and facilitated noninvasive identification of emergent resistance mutations to targeted therapies.” Meanwhile, while biomarkers hold “great promise for risk stratification and therapeutic targeting,” they are “currently difficult to measure in clinical settings,” the investigators said.
Roche bought the rights to CAPP-Seq from Stanford in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consultants. Two are employees. Dr. Scherer had no disclosures. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: Major finding: Circulating tumor DNA was found in 73% of relapse patients a mean of 188 days before relapse was detected by standard-of-care radiologic techniques. Circulating tumor DNA was found in the plasma of 100% of patients at diagnosis, but only 37% had abnormally high serum lactate dehydrogenase, currently the most commonly used biomarker.
Data source: Analysis of 166 plasma and 118 tissue samples from 92 patients with diffuse large B cell lymphoma.
Disclosures: Roche bought the rights to CAPP-Seq from Stanford (Calif.) University in 2015. Several authors are coinventors on patent applications for CAPP-Seq and also Roche consults. Two are employees. The work was funded by Stanford, the American Society of Hematology, the National Cancer Institute, and others.
Marijuana calms children with autism
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.

Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.
Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
SAN FRANCISCO – About once a month, Antonio Y. Hardan, MD, and his colleagues at the Stanford (Calif.) University Autism and Developmental Disorders Clinic see an autistic child who is using or being prescribed marijuana.
“There are two types or responses we see with marijuana,” said Dr. Hardan, director of the clinic. “Most of the time, it calms the kid down for 2 or 3 hours, which is what you’d expect from marijuana. In one out of 10, I am hearing that parents see improvements in the core features of autism. We have several families who would swear by marijuana, but then 4 or 6 months later, they will change their mind and say it’s not helping as much.
Marijuana is just one of many alternatives families and doctors are trying to improve upon the usual medications and therapies for autism; the range of options being tried speaks to the desperation and frustration of families looking for help. There’s no home run so far; the common denominator for alternatives is anecdotal support but little evidence. Stanford has tried to address the evidence gap and continues to do so.
In 2012, for instance, Dr. Hardan and his colleagues reported a 33 patient study that found that N-acetylcysteine (NAC) – another hopeful candidate in recent years – might curb irritability (Biol Psychiatry. 2012 Jun 1;71[11]:956-61).
The tricky part about NAC is that it’s a dietary supplement, so you can’t be sure of what you’re getting in the store. There were questions at the talk about dose and formulations.
“The one we used in the study is made by BioAdvantex,” a Canadian company. “That’s the one that worked for us. One of the advantages is that every dose is wrapped individually.” NAC is an antioxidant, “so if you expose [it] to oxygen or light, it will get oxidized, and over time be less effective,” said Dr. Hardan, also a professor of psychiatry and behavioral sciences at the university.
Most of the time, NAC is very well tolerated, with only a little bit of flatulence and upset stomach.
Dr. Hardan and his colleagues started with 900 mg in one dose once a day for 4 weeks, then one dose twice a day for 4 weeks, followed by one dose three times daily, in children aged 2-12 years old. With experience, they are going faster now, cutting the 4 week interval to 2. “Some people are [even] more aggressive, which is okay,” he said.
Propranolol is another fashionable option, prescribed by a lot of doctors.
It’s not a new option; about 20 years ago, “we used it in very high dosages, 700-800 mg a day for self-injurious behavior. People wonder how you can go that high; above a dose of 200 mg, there is what we call an ‘escape phenomena’ where the heart will stop responding, and the effects on blood pressure and pulse are minimal,” Dr. Hardan said.
Interest in propranolol over the past 5 years has expanded to anxiety, sensory abnormalities, and other non-specific autism symptoms. “Unfortunately, there are no clinical trials to support that,” he said. The only evidence so far is from a functional MRI study in adults that suggested a little bit more efficient processing on a language task; further investigation is underway.
A lot of parents also are asking for oxytocin, and doctors are prescribing it. Someone in the audience wondered whether it had a role in everyday practice.
“Not at this time,” Dr. Hardan said. “I would suggest waiting a little bit until” results are reported from an ongoing trial. They are due soon, and there might be a subgroup of kids who benefit. Oxytocin seemed to help all-comers recognize facial cues.
Arginine vasopressin might do that, too, and be more specific for autism; Stanford is planning a study to look into it.
Attendees also wanted to know what to do about sleep problems, a common issue in autism.
“I’m aggressive in the treatment of insomnia, especially in single-parent households, because if the kid isn’t sleeping, the parent isn’t sleeping” and they may get irritable and moody, which raises the risk of abuse, Dr. Hardan said.
He starts with melatonin, 1 mg in the evening, and increases it by 1 mg every week to hit a target of 6 mg per night. He hasn’t seen much benefit of going higher. It’s important to remember that melatonin might take up to a week to see the full effect.
If melatonin fails, Dr. Hardan goes up the ladder. Diphenhydramine (Benadryl), benzodiazepines, trazodone (Oleptro), and mirtazapine (Remeron) are among the options. Rarely, there’s a need for quetiapine (Seroquel).
To counter benzodiazepine disinhibition, he asks parents to try them on a good day at home, so the effect of environmental stressors like going to the dentist can be divided out from the drug.
Dr. Hardan cautioned that there is “no evidence at this time to support the use of” lamotrigine (Lamictal). “Please don’t use it; somebody will end up developing” Stevens-Johnson syndrome. “It will be difficult to defend against that.”
Dr. Hardan is an adviser for Roche.
EXPERT ANALYSIS AT THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Guideline: Keep blood pressure below 150 mm Hg in healthy elderly
Treat to lower a persistent systolic blood pressure of 150 mm Hg or more in patients aged 60 years or older who are otherwise healthy, the American College of Physicians and the American Academy of Family Physicians recommended in a new guideline for managing blood pressure in older patients.
The recommendation was “strong,” based on high-quality evidence from the 24 studies reviewed. The groups also made a weak recommendation based on lower-quality evidence to keep systolic blood pressure below 140 mm Hg in patients aged 60 years and older who have a history of stroke, transient ischemic attack, or high cardiovascular risks.
For those patients who are otherwise well, “most patients aged 60 years or older with a SPB [systolic blood pressure] of 150 mm Hg or greater who receive antihypertensive medications will have benefit with acceptable harms and costs from treatment to a BP target of less than 150/90 mm Hg,” according to the guideline’s authors.
“Although some benefit is achieved by aiming for lower BP targets, most benefit occurs with acceptable harms and costs in the pharmacologic treatment of patients who have an SBP of 150 mm Hg or greater,” said the authors, led by Amir Qaseem, MD, PhD, ACP’s vice president of clinical policy (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Meanwhile, treating hypertension to an SBP of 130-140 mm Hg in older adults with previous transient ischemic attacks or strokes reduces stroke recurrence, according to the guideline. In addition, an SBP of less than 140 mm Hg “is a reasonable goal for some patients with increased cardiovascular risk,” including those with vascular disease, diabetes, chronic kidney disease, or metabolic syndrome.
Trials with lower BP targets had higher rates of hypotension, electrolyte abnormalities, abnormal renal function, cough, and withdrawals because of side effects.
Older “patients might theoretically benefit from more aggressive BP treatment because of higher cardiovascular risks,” the guideline authors noted. “However, they are more likely to be susceptible to serious harm[s] from higher rates of syncope and hypotension, which were seen in some trials. Moreover, the absolute benefits of more aggressive BP treatment in elderly persons, those with multimorbidity, or those who are frail are not well known, given limitations of the trials.”
The advice is based on 21 randomized, controlled trials of hypertension treatment intensity through September 2016, plus three observational studies of harms. Antihypertensive selection varied widely across the studies. The guideline notes the various lifestyle and pharmacy options, but did not recommend any specific treatment.
Nine trials provided high-strength evidence that BP control to less than 150/90 mm Hg reduces mortality (relative risk, 0.90; 95% confidence interval, 0.83-0.98), cardiac events (RR, 0.77; 95% CI, 0.68-0.89), and stroke (RR, 0.74; 95% CI, 0.65-0.84), according to the evidence review (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Low- to moderate-strength evidence suggested targets at or below 140/85 mm Hg in older people, but there was only a modest decrease in cardiac events (RR, 0.82; 95% CI, 0.64-1.00) and stroke (RR, 0.79; 95% CI, 0.59-0.99), and a statistically insignificant trend toward fewer deaths (RR, 0.86; 95% CI, 0.69-1.06).
Evidence was insufficient for targeting treatment according to diastolic BP.
Patients have to be involved with decisions about BP targets. Ongoing discussions about the risks and benefits of target options need to be a part of routine care, the guideline authors said.
The work was funded by ACP and the U.S. Department of Veterans Affairs. The authors had no disclosures.
To prevent hypertension-related morbidity and mortality, providers should develop an office-based program with the following features:
• High-fidelity BP measurement support, including office BP measurement by well-trained staff, resources to train patients in home monitoring or making ambulatory BP monitoring available, and ongoing quality assurance efforts.
• Routine assessment of global CVD risk in all patients 40 years or older, as well as in younger patients with multiple risk factors or extreme elevations of a single risk factor.
• Provider training in shared decision making for hypertension treatment and CVD risk reduction.
• A registry to track patients who receive hypertension treatment.
• Nonvisit-based follow-up for patients with moderate to severe hypertension who have had treatment initiation or changes.
Such programs, when implemented, have been associated with large improvements in BP control.
Michael Pignone, MD , is the chair of internal medicine at the University of Texas, Austin. Anthony Viera, MD , is the director of the hypertension research program at the University of North Carolina at Chapel Hill. They had no commercial disclosures and made these recommendations in an editorial (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M17-0034 ).
To prevent hypertension-related morbidity and mortality, providers should develop an office-based program with the following features:
• High-fidelity BP measurement support, including office BP measurement by well-trained staff, resources to train patients in home monitoring or making ambulatory BP monitoring available, and ongoing quality assurance efforts.
• Routine assessment of global CVD risk in all patients 40 years or older, as well as in younger patients with multiple risk factors or extreme elevations of a single risk factor.
• Provider training in shared decision making for hypertension treatment and CVD risk reduction.
• A registry to track patients who receive hypertension treatment.
• Nonvisit-based follow-up for patients with moderate to severe hypertension who have had treatment initiation or changes.
Such programs, when implemented, have been associated with large improvements in BP control.
Michael Pignone, MD , is the chair of internal medicine at the University of Texas, Austin. Anthony Viera, MD , is the director of the hypertension research program at the University of North Carolina at Chapel Hill. They had no commercial disclosures and made these recommendations in an editorial (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M17-0034 ).
To prevent hypertension-related morbidity and mortality, providers should develop an office-based program with the following features:
• High-fidelity BP measurement support, including office BP measurement by well-trained staff, resources to train patients in home monitoring or making ambulatory BP monitoring available, and ongoing quality assurance efforts.
• Routine assessment of global CVD risk in all patients 40 years or older, as well as in younger patients with multiple risk factors or extreme elevations of a single risk factor.
• Provider training in shared decision making for hypertension treatment and CVD risk reduction.
• A registry to track patients who receive hypertension treatment.
• Nonvisit-based follow-up for patients with moderate to severe hypertension who have had treatment initiation or changes.
Such programs, when implemented, have been associated with large improvements in BP control.
Michael Pignone, MD , is the chair of internal medicine at the University of Texas, Austin. Anthony Viera, MD , is the director of the hypertension research program at the University of North Carolina at Chapel Hill. They had no commercial disclosures and made these recommendations in an editorial (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M17-0034 ).
Treat to lower a persistent systolic blood pressure of 150 mm Hg or more in patients aged 60 years or older who are otherwise healthy, the American College of Physicians and the American Academy of Family Physicians recommended in a new guideline for managing blood pressure in older patients.
The recommendation was “strong,” based on high-quality evidence from the 24 studies reviewed. The groups also made a weak recommendation based on lower-quality evidence to keep systolic blood pressure below 140 mm Hg in patients aged 60 years and older who have a history of stroke, transient ischemic attack, or high cardiovascular risks.
For those patients who are otherwise well, “most patients aged 60 years or older with a SPB [systolic blood pressure] of 150 mm Hg or greater who receive antihypertensive medications will have benefit with acceptable harms and costs from treatment to a BP target of less than 150/90 mm Hg,” according to the guideline’s authors.
“Although some benefit is achieved by aiming for lower BP targets, most benefit occurs with acceptable harms and costs in the pharmacologic treatment of patients who have an SBP of 150 mm Hg or greater,” said the authors, led by Amir Qaseem, MD, PhD, ACP’s vice president of clinical policy (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Meanwhile, treating hypertension to an SBP of 130-140 mm Hg in older adults with previous transient ischemic attacks or strokes reduces stroke recurrence, according to the guideline. In addition, an SBP of less than 140 mm Hg “is a reasonable goal for some patients with increased cardiovascular risk,” including those with vascular disease, diabetes, chronic kidney disease, or metabolic syndrome.
Trials with lower BP targets had higher rates of hypotension, electrolyte abnormalities, abnormal renal function, cough, and withdrawals because of side effects.
Older “patients might theoretically benefit from more aggressive BP treatment because of higher cardiovascular risks,” the guideline authors noted. “However, they are more likely to be susceptible to serious harm[s] from higher rates of syncope and hypotension, which were seen in some trials. Moreover, the absolute benefits of more aggressive BP treatment in elderly persons, those with multimorbidity, or those who are frail are not well known, given limitations of the trials.”
The advice is based on 21 randomized, controlled trials of hypertension treatment intensity through September 2016, plus three observational studies of harms. Antihypertensive selection varied widely across the studies. The guideline notes the various lifestyle and pharmacy options, but did not recommend any specific treatment.
Nine trials provided high-strength evidence that BP control to less than 150/90 mm Hg reduces mortality (relative risk, 0.90; 95% confidence interval, 0.83-0.98), cardiac events (RR, 0.77; 95% CI, 0.68-0.89), and stroke (RR, 0.74; 95% CI, 0.65-0.84), according to the evidence review (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Low- to moderate-strength evidence suggested targets at or below 140/85 mm Hg in older people, but there was only a modest decrease in cardiac events (RR, 0.82; 95% CI, 0.64-1.00) and stroke (RR, 0.79; 95% CI, 0.59-0.99), and a statistically insignificant trend toward fewer deaths (RR, 0.86; 95% CI, 0.69-1.06).
Evidence was insufficient for targeting treatment according to diastolic BP.
Patients have to be involved with decisions about BP targets. Ongoing discussions about the risks and benefits of target options need to be a part of routine care, the guideline authors said.
The work was funded by ACP and the U.S. Department of Veterans Affairs. The authors had no disclosures.
Treat to lower a persistent systolic blood pressure of 150 mm Hg or more in patients aged 60 years or older who are otherwise healthy, the American College of Physicians and the American Academy of Family Physicians recommended in a new guideline for managing blood pressure in older patients.
The recommendation was “strong,” based on high-quality evidence from the 24 studies reviewed. The groups also made a weak recommendation based on lower-quality evidence to keep systolic blood pressure below 140 mm Hg in patients aged 60 years and older who have a history of stroke, transient ischemic attack, or high cardiovascular risks.
For those patients who are otherwise well, “most patients aged 60 years or older with a SPB [systolic blood pressure] of 150 mm Hg or greater who receive antihypertensive medications will have benefit with acceptable harms and costs from treatment to a BP target of less than 150/90 mm Hg,” according to the guideline’s authors.
“Although some benefit is achieved by aiming for lower BP targets, most benefit occurs with acceptable harms and costs in the pharmacologic treatment of patients who have an SBP of 150 mm Hg or greater,” said the authors, led by Amir Qaseem, MD, PhD, ACP’s vice president of clinical policy (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Meanwhile, treating hypertension to an SBP of 130-140 mm Hg in older adults with previous transient ischemic attacks or strokes reduces stroke recurrence, according to the guideline. In addition, an SBP of less than 140 mm Hg “is a reasonable goal for some patients with increased cardiovascular risk,” including those with vascular disease, diabetes, chronic kidney disease, or metabolic syndrome.
Trials with lower BP targets had higher rates of hypotension, electrolyte abnormalities, abnormal renal function, cough, and withdrawals because of side effects.
Older “patients might theoretically benefit from more aggressive BP treatment because of higher cardiovascular risks,” the guideline authors noted. “However, they are more likely to be susceptible to serious harm[s] from higher rates of syncope and hypotension, which were seen in some trials. Moreover, the absolute benefits of more aggressive BP treatment in elderly persons, those with multimorbidity, or those who are frail are not well known, given limitations of the trials.”
The advice is based on 21 randomized, controlled trials of hypertension treatment intensity through September 2016, plus three observational studies of harms. Antihypertensive selection varied widely across the studies. The guideline notes the various lifestyle and pharmacy options, but did not recommend any specific treatment.
Nine trials provided high-strength evidence that BP control to less than 150/90 mm Hg reduces mortality (relative risk, 0.90; 95% confidence interval, 0.83-0.98), cardiac events (RR, 0.77; 95% CI, 0.68-0.89), and stroke (RR, 0.74; 95% CI, 0.65-0.84), according to the evidence review (Ann Intern Med. 2017 Jan 17. doi: 10.7326/M16-1754).
Low- to moderate-strength evidence suggested targets at or below 140/85 mm Hg in older people, but there was only a modest decrease in cardiac events (RR, 0.82; 95% CI, 0.64-1.00) and stroke (RR, 0.79; 95% CI, 0.59-0.99), and a statistically insignificant trend toward fewer deaths (RR, 0.86; 95% CI, 0.69-1.06).
Evidence was insufficient for targeting treatment according to diastolic BP.
Patients have to be involved with decisions about BP targets. Ongoing discussions about the risks and benefits of target options need to be a part of routine care, the guideline authors said.
The work was funded by ACP and the U.S. Department of Veterans Affairs. The authors had no disclosures.
Left ventricle dose predicts heart events after BC radiation
The risk of acute coronary events following radiotherapy for breast cancer is better predicted by the volume of the left ventricle that received 5 Gy than by the mean dose of radiation to the heart, according to a Dutch investigation of 910 women who underwent radiation treatment following breast-conserving surgery.
The finding follows up a 2013 report that found that the risk of acute coronary events (ACE) after breast cancer (BC) radiation could be predicted by the mean radiation heart dose (MHD), the presence of cardiac risk factors, and age (N Engl J Med. 2013 Mar 14;368[11]:987-98. doi: 0.1056/NEJMoa1209825).
The new study validated those findings, but also found that risk prediction was better when mean heart dose (MHD) was replaced by the volume of the left ventricle receiving 5 Gy (LV-V5); the substitution improved the c-statistic to 0.80 (95% confidence interval, 0.72-0.88). Using a weighted ACE risk score based on baseline diabetes, hypertension, and ischemic event history – instead of the risk factor yes-or-no approach from 2013 – further improved predictive power, with a c-statistic of 0.83 (95% CI, 0.75-0.91). Anything over a c-statistic of 0.8 is considered strong; 0.5 is chance, 1.0 is perfect prediction.
For instance, a 70-year-old woman with an LV-V5 of 50% and no cardiac risk factors had an excess ACE risk in the new system of 2.52% within 9 years of radiotherapy (RT). If she had a history of ischemic heart disease, the excess risk increased to 8.42%, the investigators said (J Clin Oncol. 2017 Jan 17. doi: 10.1200/JCO.2016.69.8480).
“Model performance was significantly improved by replacing MHD with LV-V5 and using the weighted ACE risk score.” However, “because we were not able to externally validate the LV-V5 model, this model” requires validation “before it can be used in routine clinical practice,” said investigators, led by Veerle van den Bogaard, MD, of the University of Groningen, the Netherlands.
The women were a median of 59 years old, and they were followed for a median of 7.6 years, with a range of 0.1-10.1 years. Radiation dose information was derived from CT planning scans. The median MHD was 2.37 Gy.
Thirty patients (3.3%) had an ACE, defined as myocardial infarction, coronary revascularization, or death due to ischemic heart disease; 17 had events in the first 5 years. The 5- and 9-year cumulative ACE incidences were 1.9% and 3.9%. Ten of the 30 women died from their cardiac complication.
The model predicted a cumulative ACE incidence at 9 years of 3.5%, which was in line with the observed rate of 3.9%. The excess cumulative risk related to RT was 1.13%. Overall, about 10 patients had an ACE that could be attributed to RT. The cumulative incidence of ACE increased by 16.5% per Gy (95% CI, 0.6-35.0; P = .042). The findings were consistent with the 2013 study.
ACE incidence was not significantly associated with the maximum dose of radiation to the heart.
LV-V5 was the most important prognostic dose-volume parameter associated with the cumulative incidence of ACE, with a hazard ratio of 1.016 (95% CI, 1.002-1.030; P = .016). “Because of this strong association, we chose to include LV-V5 in the model,” the investigators said.
There was no external funding. The lead investigator had no disclosures, but two authors reported institutional research funding from Philips, Roche, and other companies. One was an advisor and speaker for IBA.
The limitations of this study are substantial. As the authors note, their work was based on only a small number of events, and their length of follow-up prevented them from being able to examine risk in the period of 10 years and beyond.
Also, the likelihood is high that the risk of radiation-induced heart disease can be reduced below that seen in the study. Cardiac exposure in many recent studies has been lower. Techniques such as deep inspiration breath holding or treatment in the prone position often can further decrease this exposure. Several randomized trials comparing partial-breast with whole-breast irradiation have found equal local control rates with both approaches, strongly suggesting that judicious individualization of field borders and cardiac blocks are unlikely to compromise outcome for selected patients treated with partial mastectomy.
Nonetheless, at some point, compromising coverage of the breast, chest wall, or nodal target volumes because an arbitrary threshold of a cardiac dose-volume parameter has been exceeded may be dangerous. Computer programs can likely be created to perform calculations of an individual’s excess risk of cardiac events or death in relation to dose-volume and clinical parameters, although I suspect it will be some years before they provide sufficiently validated, narrow estimates of risk to be clinically useful. Perhaps by then we will also have better ways to explain such sobering decisions to patients.
Abram Recht, MD , is a professor of radiation oncology at Harvard Medical School, Boston. He is also an advisor for CareCore and US Oncology, and receives institutional research funding form Genomic Health. He made his comments in an editorial (J Clin Oncol. 2017 Jan 17. doi: 0.1200/JCO.2016.71.4113 ).
The limitations of this study are substantial. As the authors note, their work was based on only a small number of events, and their length of follow-up prevented them from being able to examine risk in the period of 10 years and beyond.
Also, the likelihood is high that the risk of radiation-induced heart disease can be reduced below that seen in the study. Cardiac exposure in many recent studies has been lower. Techniques such as deep inspiration breath holding or treatment in the prone position often can further decrease this exposure. Several randomized trials comparing partial-breast with whole-breast irradiation have found equal local control rates with both approaches, strongly suggesting that judicious individualization of field borders and cardiac blocks are unlikely to compromise outcome for selected patients treated with partial mastectomy.
Nonetheless, at some point, compromising coverage of the breast, chest wall, or nodal target volumes because an arbitrary threshold of a cardiac dose-volume parameter has been exceeded may be dangerous. Computer programs can likely be created to perform calculations of an individual’s excess risk of cardiac events or death in relation to dose-volume and clinical parameters, although I suspect it will be some years before they provide sufficiently validated, narrow estimates of risk to be clinically useful. Perhaps by then we will also have better ways to explain such sobering decisions to patients.
Abram Recht, MD , is a professor of radiation oncology at Harvard Medical School, Boston. He is also an advisor for CareCore and US Oncology, and receives institutional research funding form Genomic Health. He made his comments in an editorial (J Clin Oncol. 2017 Jan 17. doi: 0.1200/JCO.2016.71.4113 ).
The limitations of this study are substantial. As the authors note, their work was based on only a small number of events, and their length of follow-up prevented them from being able to examine risk in the period of 10 years and beyond.
Also, the likelihood is high that the risk of radiation-induced heart disease can be reduced below that seen in the study. Cardiac exposure in many recent studies has been lower. Techniques such as deep inspiration breath holding or treatment in the prone position often can further decrease this exposure. Several randomized trials comparing partial-breast with whole-breast irradiation have found equal local control rates with both approaches, strongly suggesting that judicious individualization of field borders and cardiac blocks are unlikely to compromise outcome for selected patients treated with partial mastectomy.
Nonetheless, at some point, compromising coverage of the breast, chest wall, or nodal target volumes because an arbitrary threshold of a cardiac dose-volume parameter has been exceeded may be dangerous. Computer programs can likely be created to perform calculations of an individual’s excess risk of cardiac events or death in relation to dose-volume and clinical parameters, although I suspect it will be some years before they provide sufficiently validated, narrow estimates of risk to be clinically useful. Perhaps by then we will also have better ways to explain such sobering decisions to patients.
Abram Recht, MD , is a professor of radiation oncology at Harvard Medical School, Boston. He is also an advisor for CareCore and US Oncology, and receives institutional research funding form Genomic Health. He made his comments in an editorial (J Clin Oncol. 2017 Jan 17. doi: 0.1200/JCO.2016.71.4113 ).
The risk of acute coronary events following radiotherapy for breast cancer is better predicted by the volume of the left ventricle that received 5 Gy than by the mean dose of radiation to the heart, according to a Dutch investigation of 910 women who underwent radiation treatment following breast-conserving surgery.
The finding follows up a 2013 report that found that the risk of acute coronary events (ACE) after breast cancer (BC) radiation could be predicted by the mean radiation heart dose (MHD), the presence of cardiac risk factors, and age (N Engl J Med. 2013 Mar 14;368[11]:987-98. doi: 0.1056/NEJMoa1209825).
The new study validated those findings, but also found that risk prediction was better when mean heart dose (MHD) was replaced by the volume of the left ventricle receiving 5 Gy (LV-V5); the substitution improved the c-statistic to 0.80 (95% confidence interval, 0.72-0.88). Using a weighted ACE risk score based on baseline diabetes, hypertension, and ischemic event history – instead of the risk factor yes-or-no approach from 2013 – further improved predictive power, with a c-statistic of 0.83 (95% CI, 0.75-0.91). Anything over a c-statistic of 0.8 is considered strong; 0.5 is chance, 1.0 is perfect prediction.
For instance, a 70-year-old woman with an LV-V5 of 50% and no cardiac risk factors had an excess ACE risk in the new system of 2.52% within 9 years of radiotherapy (RT). If she had a history of ischemic heart disease, the excess risk increased to 8.42%, the investigators said (J Clin Oncol. 2017 Jan 17. doi: 10.1200/JCO.2016.69.8480).
“Model performance was significantly improved by replacing MHD with LV-V5 and using the weighted ACE risk score.” However, “because we were not able to externally validate the LV-V5 model, this model” requires validation “before it can be used in routine clinical practice,” said investigators, led by Veerle van den Bogaard, MD, of the University of Groningen, the Netherlands.
The women were a median of 59 years old, and they were followed for a median of 7.6 years, with a range of 0.1-10.1 years. Radiation dose information was derived from CT planning scans. The median MHD was 2.37 Gy.
Thirty patients (3.3%) had an ACE, defined as myocardial infarction, coronary revascularization, or death due to ischemic heart disease; 17 had events in the first 5 years. The 5- and 9-year cumulative ACE incidences were 1.9% and 3.9%. Ten of the 30 women died from their cardiac complication.
The model predicted a cumulative ACE incidence at 9 years of 3.5%, which was in line with the observed rate of 3.9%. The excess cumulative risk related to RT was 1.13%. Overall, about 10 patients had an ACE that could be attributed to RT. The cumulative incidence of ACE increased by 16.5% per Gy (95% CI, 0.6-35.0; P = .042). The findings were consistent with the 2013 study.
ACE incidence was not significantly associated with the maximum dose of radiation to the heart.
LV-V5 was the most important prognostic dose-volume parameter associated with the cumulative incidence of ACE, with a hazard ratio of 1.016 (95% CI, 1.002-1.030; P = .016). “Because of this strong association, we chose to include LV-V5 in the model,” the investigators said.
There was no external funding. The lead investigator had no disclosures, but two authors reported institutional research funding from Philips, Roche, and other companies. One was an advisor and speaker for IBA.
The risk of acute coronary events following radiotherapy for breast cancer is better predicted by the volume of the left ventricle that received 5 Gy than by the mean dose of radiation to the heart, according to a Dutch investigation of 910 women who underwent radiation treatment following breast-conserving surgery.
The finding follows up a 2013 report that found that the risk of acute coronary events (ACE) after breast cancer (BC) radiation could be predicted by the mean radiation heart dose (MHD), the presence of cardiac risk factors, and age (N Engl J Med. 2013 Mar 14;368[11]:987-98. doi: 0.1056/NEJMoa1209825).
The new study validated those findings, but also found that risk prediction was better when mean heart dose (MHD) was replaced by the volume of the left ventricle receiving 5 Gy (LV-V5); the substitution improved the c-statistic to 0.80 (95% confidence interval, 0.72-0.88). Using a weighted ACE risk score based on baseline diabetes, hypertension, and ischemic event history – instead of the risk factor yes-or-no approach from 2013 – further improved predictive power, with a c-statistic of 0.83 (95% CI, 0.75-0.91). Anything over a c-statistic of 0.8 is considered strong; 0.5 is chance, 1.0 is perfect prediction.
For instance, a 70-year-old woman with an LV-V5 of 50% and no cardiac risk factors had an excess ACE risk in the new system of 2.52% within 9 years of radiotherapy (RT). If she had a history of ischemic heart disease, the excess risk increased to 8.42%, the investigators said (J Clin Oncol. 2017 Jan 17. doi: 10.1200/JCO.2016.69.8480).
“Model performance was significantly improved by replacing MHD with LV-V5 and using the weighted ACE risk score.” However, “because we were not able to externally validate the LV-V5 model, this model” requires validation “before it can be used in routine clinical practice,” said investigators, led by Veerle van den Bogaard, MD, of the University of Groningen, the Netherlands.
The women were a median of 59 years old, and they were followed for a median of 7.6 years, with a range of 0.1-10.1 years. Radiation dose information was derived from CT planning scans. The median MHD was 2.37 Gy.
Thirty patients (3.3%) had an ACE, defined as myocardial infarction, coronary revascularization, or death due to ischemic heart disease; 17 had events in the first 5 years. The 5- and 9-year cumulative ACE incidences were 1.9% and 3.9%. Ten of the 30 women died from their cardiac complication.
The model predicted a cumulative ACE incidence at 9 years of 3.5%, which was in line with the observed rate of 3.9%. The excess cumulative risk related to RT was 1.13%. Overall, about 10 patients had an ACE that could be attributed to RT. The cumulative incidence of ACE increased by 16.5% per Gy (95% CI, 0.6-35.0; P = .042). The findings were consistent with the 2013 study.
ACE incidence was not significantly associated with the maximum dose of radiation to the heart.
LV-V5 was the most important prognostic dose-volume parameter associated with the cumulative incidence of ACE, with a hazard ratio of 1.016 (95% CI, 1.002-1.030; P = .016). “Because of this strong association, we chose to include LV-V5 in the model,” the investigators said.
There was no external funding. The lead investigator had no disclosures, but two authors reported institutional research funding from Philips, Roche, and other companies. One was an advisor and speaker for IBA.
FROM THE JOURNAL OF CLINICAL ONCOLOGY
Key clinical point:
Major finding: Replacing the mean heart dose with the volume of the left ventricle receiving 5 Gy improves the predictive c-statistic to 0.80.
Data source: Investigation of 910 women who underwent radiation treatment following breast-conserving surgery.
Disclosures: There was no external funding. The lead investigator had no disclosures, but two authors reported institutional research funding from Philips, Roche, and other companies. One was an advisor and speaker for IBA.
Switch from fingolimod to alemtuzumab might trigger MS relapse
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
FROM NEUROLOGY: NEUROIMMUNOLOGY AND NEUROINFLAMMATION
Cutaneous eruption reported in pregnant woman with locally acquired Zika virus
Zika presented in a young, pregnant Florida woman as erythematous follicular macules and papules on the trunk and arms, scattered tender pink papules on the palms, and a few petechiae on the hard palate, according to a Jan. 11 report in the New England Journal of Medicine.
The report advises how Zika virus may present during pregnancy. “Medical providers on the front line should be aware of the constellation of symptoms in patients reporting travel to endemic areas, including areas in Southern Florida, where other non–travel-associated cases have been confirmed,” wrote investigators led by Lucy Chen, MD, of the University of Miami (N Engl J Med. 2017 Jan 11. doi: 10.1056/NEJMc1610614).
Zika virus RNA was detected in the woman’s urine and serum specimens with the use of reverse-transcriptase polymerase chain reaction and persisted for 2 weeks in urine samples and for 6 weeks in serum samples. On histopathology, skin lesions revealed a mild perivascular lymphocytic infiltration in the upper dermis, admixed with some neutrophils. Liver and renal functions were normal.
Fetal ultrasonography performed on the day of presentation showed an estimated fetal weight of 644 g (53rd percentile), an estimated head circumference of 221 mm (63rd percentile), and normal intracranial anatomy. Fevers and rash subsided after 3 days of supportive care. Screening for measles, varicella, rubella, syphilis, Epstein-Barr virus, influenza, hepatitis B, hepatitis C, mumps, and dengue was unrevealing.
An initial IgM test on July 7 was negative; seroconversion occurred 1 week after presentation and remained positive through delivery.
A full-term infant weighing 2,990 g was delivered vaginally. Neonatal ultrasonography and magnetic resonance imaging of the head showed a normal head size and intracranial anatomy, with no calcifications. Placental tissue was negative for Zika virus, and neonatal laboratory testing revealed no evidence of infection.
The case was confirmed by the Miami-Dade County Department of Health as the first non–travel-associated Zika infection in the United States.
The investigators reported having no relevant financial disclosures.
Zika presented in a young, pregnant Florida woman as erythematous follicular macules and papules on the trunk and arms, scattered tender pink papules on the palms, and a few petechiae on the hard palate, according to a Jan. 11 report in the New England Journal of Medicine.
The report advises how Zika virus may present during pregnancy. “Medical providers on the front line should be aware of the constellation of symptoms in patients reporting travel to endemic areas, including areas in Southern Florida, where other non–travel-associated cases have been confirmed,” wrote investigators led by Lucy Chen, MD, of the University of Miami (N Engl J Med. 2017 Jan 11. doi: 10.1056/NEJMc1610614).
Zika virus RNA was detected in the woman’s urine and serum specimens with the use of reverse-transcriptase polymerase chain reaction and persisted for 2 weeks in urine samples and for 6 weeks in serum samples. On histopathology, skin lesions revealed a mild perivascular lymphocytic infiltration in the upper dermis, admixed with some neutrophils. Liver and renal functions were normal.
Fetal ultrasonography performed on the day of presentation showed an estimated fetal weight of 644 g (53rd percentile), an estimated head circumference of 221 mm (63rd percentile), and normal intracranial anatomy. Fevers and rash subsided after 3 days of supportive care. Screening for measles, varicella, rubella, syphilis, Epstein-Barr virus, influenza, hepatitis B, hepatitis C, mumps, and dengue was unrevealing.
An initial IgM test on July 7 was negative; seroconversion occurred 1 week after presentation and remained positive through delivery.
A full-term infant weighing 2,990 g was delivered vaginally. Neonatal ultrasonography and magnetic resonance imaging of the head showed a normal head size and intracranial anatomy, with no calcifications. Placental tissue was negative for Zika virus, and neonatal laboratory testing revealed no evidence of infection.
The case was confirmed by the Miami-Dade County Department of Health as the first non–travel-associated Zika infection in the United States.
The investigators reported having no relevant financial disclosures.
Zika presented in a young, pregnant Florida woman as erythematous follicular macules and papules on the trunk and arms, scattered tender pink papules on the palms, and a few petechiae on the hard palate, according to a Jan. 11 report in the New England Journal of Medicine.
The report advises how Zika virus may present during pregnancy. “Medical providers on the front line should be aware of the constellation of symptoms in patients reporting travel to endemic areas, including areas in Southern Florida, where other non–travel-associated cases have been confirmed,” wrote investigators led by Lucy Chen, MD, of the University of Miami (N Engl J Med. 2017 Jan 11. doi: 10.1056/NEJMc1610614).
Zika virus RNA was detected in the woman’s urine and serum specimens with the use of reverse-transcriptase polymerase chain reaction and persisted for 2 weeks in urine samples and for 6 weeks in serum samples. On histopathology, skin lesions revealed a mild perivascular lymphocytic infiltration in the upper dermis, admixed with some neutrophils. Liver and renal functions were normal.
Fetal ultrasonography performed on the day of presentation showed an estimated fetal weight of 644 g (53rd percentile), an estimated head circumference of 221 mm (63rd percentile), and normal intracranial anatomy. Fevers and rash subsided after 3 days of supportive care. Screening for measles, varicella, rubella, syphilis, Epstein-Barr virus, influenza, hepatitis B, hepatitis C, mumps, and dengue was unrevealing.
An initial IgM test on July 7 was negative; seroconversion occurred 1 week after presentation and remained positive through delivery.
A full-term infant weighing 2,990 g was delivered vaginally. Neonatal ultrasonography and magnetic resonance imaging of the head showed a normal head size and intracranial anatomy, with no calcifications. Placental tissue was negative for Zika virus, and neonatal laboratory testing revealed no evidence of infection.
The case was confirmed by the Miami-Dade County Department of Health as the first non–travel-associated Zika infection in the United States.
The investigators reported having no relevant financial disclosures.
Type 2 risk increases with number of GDM pregnancies
In women with prior mild gestational diabetes, subsequent pregnancies did not increase the frequency of metabolic syndrome but did increase the risk of type 2 diabetes, according to a review of 426 women 5-10 years after a GDM pregnancy.
The risk of diabetes was greatest if additional pregnancies were also complicated by mild gestational diabetes mellitus (GDM).
The investigators assessed women 5-10 years after they participated in a mild GDM treatment study. The goal was to assess the impact of subsequent pregnancies on cardiometabolic risks. GDM is a known risk factor for type 2 diabetes and metabolic syndrome, but it hasn’t been clear until know how subsequent pregnancies influence the risk, said investigators led by Michael Varner, MD, a professor at the University of Utah School of Medicine, Salt Lake City (Obstet Gynecol 2017;129:273-80).
Echoing previous studies of mild GDM, about a third of the women had metabolic syndrome at follow-up, but the number of subsequent pregnancies didn’t seem to make a difference. Among the 212 women with no additional pregnancies, 34% had metabolic syndrome; among the 143 with one pregnancy, 33% had metabolic syndrome; and among the 71 with two or more, 30% had metabolic syndrome, as defined by American Heart Association and National Heart, Lung, and Blood Institute criteria.
“Although we observed a high overall frequency of metabolic syndrome in our cohort, our data suggest that subsequent pregnancies do not increase a woman’s risk of developing metabolic syndrome,” Dr. Varner and his colleagues said.
However, subsequent pregnancies did affect diabetes risk; 5.2% of women with no additional pregnancies had diabetes at follow-up, versus 10.5% of women with one additional pregnancy and 11.3% of those with two or more. The risk of diabetes was greatest if a subsequent pregnancy was complicated by GDM (relative risk, 3.75; 95% confidence interval, 1.60-8.82), as was the case for about a third of the women who had additional pregnancies.
“The association with diabetes was driven mostly by subsequent pregnancy complicated with GDM,” the investigators said.
The findings “could be consistent with either a stronger genetic or an environmental predisposition to type II diabetes, [but] could also represent confounders that were not measured in this prospective observational follow-up study. ... Our data are limited ... by the fact that we do not know how many patients had metabolic syndrome at the time of the index pregnancy,” they said.
At follow-up during Feb. 2012-Sept. 2013, women with no additional pregnancies were a median 38 years old; women who had one pregnancy were a median of 35 years, and those with two or more a median of 33 years. The interval from participation in the parent study to participation in the follow-up study was 7 years in women with no or one additional pregnancy, and 8 years for women with two or more. There were no other significant differences among the groups. The average body mass index was about 29 kg/m2; 59% of the women were Hispanic.
The National Institutes of Health funded the work. The authors had no disclosures.
In women with prior mild gestational diabetes, subsequent pregnancies did not increase the frequency of metabolic syndrome but did increase the risk of type 2 diabetes, according to a review of 426 women 5-10 years after a GDM pregnancy.
The risk of diabetes was greatest if additional pregnancies were also complicated by mild gestational diabetes mellitus (GDM).
The investigators assessed women 5-10 years after they participated in a mild GDM treatment study. The goal was to assess the impact of subsequent pregnancies on cardiometabolic risks. GDM is a known risk factor for type 2 diabetes and metabolic syndrome, but it hasn’t been clear until know how subsequent pregnancies influence the risk, said investigators led by Michael Varner, MD, a professor at the University of Utah School of Medicine, Salt Lake City (Obstet Gynecol 2017;129:273-80).
Echoing previous studies of mild GDM, about a third of the women had metabolic syndrome at follow-up, but the number of subsequent pregnancies didn’t seem to make a difference. Among the 212 women with no additional pregnancies, 34% had metabolic syndrome; among the 143 with one pregnancy, 33% had metabolic syndrome; and among the 71 with two or more, 30% had metabolic syndrome, as defined by American Heart Association and National Heart, Lung, and Blood Institute criteria.
“Although we observed a high overall frequency of metabolic syndrome in our cohort, our data suggest that subsequent pregnancies do not increase a woman’s risk of developing metabolic syndrome,” Dr. Varner and his colleagues said.
However, subsequent pregnancies did affect diabetes risk; 5.2% of women with no additional pregnancies had diabetes at follow-up, versus 10.5% of women with one additional pregnancy and 11.3% of those with two or more. The risk of diabetes was greatest if a subsequent pregnancy was complicated by GDM (relative risk, 3.75; 95% confidence interval, 1.60-8.82), as was the case for about a third of the women who had additional pregnancies.
“The association with diabetes was driven mostly by subsequent pregnancy complicated with GDM,” the investigators said.
The findings “could be consistent with either a stronger genetic or an environmental predisposition to type II diabetes, [but] could also represent confounders that were not measured in this prospective observational follow-up study. ... Our data are limited ... by the fact that we do not know how many patients had metabolic syndrome at the time of the index pregnancy,” they said.
At follow-up during Feb. 2012-Sept. 2013, women with no additional pregnancies were a median 38 years old; women who had one pregnancy were a median of 35 years, and those with two or more a median of 33 years. The interval from participation in the parent study to participation in the follow-up study was 7 years in women with no or one additional pregnancy, and 8 years for women with two or more. There were no other significant differences among the groups. The average body mass index was about 29 kg/m2; 59% of the women were Hispanic.
The National Institutes of Health funded the work. The authors had no disclosures.
In women with prior mild gestational diabetes, subsequent pregnancies did not increase the frequency of metabolic syndrome but did increase the risk of type 2 diabetes, according to a review of 426 women 5-10 years after a GDM pregnancy.
The risk of diabetes was greatest if additional pregnancies were also complicated by mild gestational diabetes mellitus (GDM).
The investigators assessed women 5-10 years after they participated in a mild GDM treatment study. The goal was to assess the impact of subsequent pregnancies on cardiometabolic risks. GDM is a known risk factor for type 2 diabetes and metabolic syndrome, but it hasn’t been clear until know how subsequent pregnancies influence the risk, said investigators led by Michael Varner, MD, a professor at the University of Utah School of Medicine, Salt Lake City (Obstet Gynecol 2017;129:273-80).
Echoing previous studies of mild GDM, about a third of the women had metabolic syndrome at follow-up, but the number of subsequent pregnancies didn’t seem to make a difference. Among the 212 women with no additional pregnancies, 34% had metabolic syndrome; among the 143 with one pregnancy, 33% had metabolic syndrome; and among the 71 with two or more, 30% had metabolic syndrome, as defined by American Heart Association and National Heart, Lung, and Blood Institute criteria.
“Although we observed a high overall frequency of metabolic syndrome in our cohort, our data suggest that subsequent pregnancies do not increase a woman’s risk of developing metabolic syndrome,” Dr. Varner and his colleagues said.
However, subsequent pregnancies did affect diabetes risk; 5.2% of women with no additional pregnancies had diabetes at follow-up, versus 10.5% of women with one additional pregnancy and 11.3% of those with two or more. The risk of diabetes was greatest if a subsequent pregnancy was complicated by GDM (relative risk, 3.75; 95% confidence interval, 1.60-8.82), as was the case for about a third of the women who had additional pregnancies.
“The association with diabetes was driven mostly by subsequent pregnancy complicated with GDM,” the investigators said.
The findings “could be consistent with either a stronger genetic or an environmental predisposition to type II diabetes, [but] could also represent confounders that were not measured in this prospective observational follow-up study. ... Our data are limited ... by the fact that we do not know how many patients had metabolic syndrome at the time of the index pregnancy,” they said.
At follow-up during Feb. 2012-Sept. 2013, women with no additional pregnancies were a median 38 years old; women who had one pregnancy were a median of 35 years, and those with two or more a median of 33 years. The interval from participation in the parent study to participation in the follow-up study was 7 years in women with no or one additional pregnancy, and 8 years for women with two or more. There were no other significant differences among the groups. The average body mass index was about 29 kg/m2; 59% of the women were Hispanic.
The National Institutes of Health funded the work. The authors had no disclosures.
Key clinical point:
Major finding: The risk of diabetes was greatest if a subsequent pregnancy was complicated by GDM (RR, 3.75; 95% CI, 1.60-8.82).
Data source: Review of subsequent pregnancies in 426 women 5-10 years after a GDM pregnancy
Disclosures: The National Institutes of Health funded the work. The authors had no disclosures.
AKT inhibition not superior to everolimus for RCC
The AKT inhibitor MK-2206 was not superior to everolimus (Afinitor) for patients with metastatic renal cell carcinoma refractory to vascular endothelial growth factor inhibitors, according to a phase II trial from the University of Texas MD Anderson Cancer Center, Houston.
Median progression-free survival was 3.68 months in the 29 patients randomized to MK-2206, versus 5.98 months in the 14 randomized to everolimus, leading to closure of the study, reported Eric Jonasch, MD, of the department of genitourinary medical oncology at MD Anderson, and his associates.
However, dichotomous response rate profiles were seen in the MK-2206 arm with one complete response and three partial responses in the MK-2206 arm versus none in the everolimus arm.
“Whereas patients treated with everolimus for the large part had minimal changes in tumor size, MK-2206 induced a fairly dichotomous response dynamic, with [a few] patients demonstrating profound response, [but] a number of patients exhibiting rapid growth,” Dr. Jonasch and associates said (Ann Oncol. 2017 Jan 3. pii: mdw676. doi: 10.1093/annonc/mdw676).
Several studies have shown that upregulation of the PI3K/AKT pathway is associated with poor prognosis in renal cell carcinoma (RCC), making the pathway an attractive target for therapeutic intervention. The trial “results indicate that potential exists for effective blockade of the PI3K pathway in patients with RCC, but considerable work is required to better understand the nuances of this pathway before we can consistently modulate it to benefit patients with RCC,” the investigators said.
Molecular analysis failed to find a biomarker for response, but did demonstrate that deleterious tumor protein 53 or ataxia telangiectasia mutations or deletions were associated with poor prognosis. Among patients who progressed, 57.1% had TP53 or ATM aberrations; TP53 and ATM defects were absent in patients who did not progress.
Malfunction of DNA repair driven by TP53 and ATM gene modifications, the group said, “are associated with early disease progression, indicating that dysregulation of DNA repair is associated with a more aggressive tumor phenotype in RCC ... This subcategory of patients clearly needs new approaches based on our emerging understanding of the significance of TP53 mutations in RCC biology.”
MK-2206 induced significantly more rash and pruritus than did everolimus, with dose reduction in 37.9% of MK-2206 versus 21.4% of everolimus patients.
Subjects were a median of 63.5 years old in the everolimus group and 59 years in the MK-2206 group. The majority of patients were white men. More than 65% of the patients had performance status 1 and around 60% were in the Memorial Sloan Kettering Cancer Center intermediate risk group. The majority of patients in both treatment arms had clear cell histology; 57.1% (8) in the everolimus group and 82.8% (24) in the MK-2206 group had lung metastasis; half of the everolimus and 59% (17) of MK-2206 subjects were previously treated with sunitinib (Sutent).
The National Institutes of Health funded the work. The authors reported no conflicts of interest.
The AKT inhibitor MK-2206 was not superior to everolimus (Afinitor) for patients with metastatic renal cell carcinoma refractory to vascular endothelial growth factor inhibitors, according to a phase II trial from the University of Texas MD Anderson Cancer Center, Houston.
Median progression-free survival was 3.68 months in the 29 patients randomized to MK-2206, versus 5.98 months in the 14 randomized to everolimus, leading to closure of the study, reported Eric Jonasch, MD, of the department of genitourinary medical oncology at MD Anderson, and his associates.
However, dichotomous response rate profiles were seen in the MK-2206 arm with one complete response and three partial responses in the MK-2206 arm versus none in the everolimus arm.
“Whereas patients treated with everolimus for the large part had minimal changes in tumor size, MK-2206 induced a fairly dichotomous response dynamic, with [a few] patients demonstrating profound response, [but] a number of patients exhibiting rapid growth,” Dr. Jonasch and associates said (Ann Oncol. 2017 Jan 3. pii: mdw676. doi: 10.1093/annonc/mdw676).
Several studies have shown that upregulation of the PI3K/AKT pathway is associated with poor prognosis in renal cell carcinoma (RCC), making the pathway an attractive target for therapeutic intervention. The trial “results indicate that potential exists for effective blockade of the PI3K pathway in patients with RCC, but considerable work is required to better understand the nuances of this pathway before we can consistently modulate it to benefit patients with RCC,” the investigators said.
Molecular analysis failed to find a biomarker for response, but did demonstrate that deleterious tumor protein 53 or ataxia telangiectasia mutations or deletions were associated with poor prognosis. Among patients who progressed, 57.1% had TP53 or ATM aberrations; TP53 and ATM defects were absent in patients who did not progress.
Malfunction of DNA repair driven by TP53 and ATM gene modifications, the group said, “are associated with early disease progression, indicating that dysregulation of DNA repair is associated with a more aggressive tumor phenotype in RCC ... This subcategory of patients clearly needs new approaches based on our emerging understanding of the significance of TP53 mutations in RCC biology.”
MK-2206 induced significantly more rash and pruritus than did everolimus, with dose reduction in 37.9% of MK-2206 versus 21.4% of everolimus patients.
Subjects were a median of 63.5 years old in the everolimus group and 59 years in the MK-2206 group. The majority of patients were white men. More than 65% of the patients had performance status 1 and around 60% were in the Memorial Sloan Kettering Cancer Center intermediate risk group. The majority of patients in both treatment arms had clear cell histology; 57.1% (8) in the everolimus group and 82.8% (24) in the MK-2206 group had lung metastasis; half of the everolimus and 59% (17) of MK-2206 subjects were previously treated with sunitinib (Sutent).
The National Institutes of Health funded the work. The authors reported no conflicts of interest.
The AKT inhibitor MK-2206 was not superior to everolimus (Afinitor) for patients with metastatic renal cell carcinoma refractory to vascular endothelial growth factor inhibitors, according to a phase II trial from the University of Texas MD Anderson Cancer Center, Houston.
Median progression-free survival was 3.68 months in the 29 patients randomized to MK-2206, versus 5.98 months in the 14 randomized to everolimus, leading to closure of the study, reported Eric Jonasch, MD, of the department of genitourinary medical oncology at MD Anderson, and his associates.
However, dichotomous response rate profiles were seen in the MK-2206 arm with one complete response and three partial responses in the MK-2206 arm versus none in the everolimus arm.
“Whereas patients treated with everolimus for the large part had minimal changes in tumor size, MK-2206 induced a fairly dichotomous response dynamic, with [a few] patients demonstrating profound response, [but] a number of patients exhibiting rapid growth,” Dr. Jonasch and associates said (Ann Oncol. 2017 Jan 3. pii: mdw676. doi: 10.1093/annonc/mdw676).
Several studies have shown that upregulation of the PI3K/AKT pathway is associated with poor prognosis in renal cell carcinoma (RCC), making the pathway an attractive target for therapeutic intervention. The trial “results indicate that potential exists for effective blockade of the PI3K pathway in patients with RCC, but considerable work is required to better understand the nuances of this pathway before we can consistently modulate it to benefit patients with RCC,” the investigators said.
Molecular analysis failed to find a biomarker for response, but did demonstrate that deleterious tumor protein 53 or ataxia telangiectasia mutations or deletions were associated with poor prognosis. Among patients who progressed, 57.1% had TP53 or ATM aberrations; TP53 and ATM defects were absent in patients who did not progress.
Malfunction of DNA repair driven by TP53 and ATM gene modifications, the group said, “are associated with early disease progression, indicating that dysregulation of DNA repair is associated with a more aggressive tumor phenotype in RCC ... This subcategory of patients clearly needs new approaches based on our emerging understanding of the significance of TP53 mutations in RCC biology.”
MK-2206 induced significantly more rash and pruritus than did everolimus, with dose reduction in 37.9% of MK-2206 versus 21.4% of everolimus patients.
Subjects were a median of 63.5 years old in the everolimus group and 59 years in the MK-2206 group. The majority of patients were white men. More than 65% of the patients had performance status 1 and around 60% were in the Memorial Sloan Kettering Cancer Center intermediate risk group. The majority of patients in both treatment arms had clear cell histology; 57.1% (8) in the everolimus group and 82.8% (24) in the MK-2206 group had lung metastasis; half of the everolimus and 59% (17) of MK-2206 subjects were previously treated with sunitinib (Sutent).
The National Institutes of Health funded the work. The authors reported no conflicts of interest.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point:
Major finding: Progression-free survival was a median of 3.68 months in the 29 patients randomized to MK-2206, versus 5.98 months in the 14 randomized to everolimus.
Data source: Phase II trial with 43 patients.
Disclosures: The National Institutes of Health funded the work. The authors reported no conflicts of interest.
Giant cell arteritis independently raises risk for venous thromboembolism
The risk of venous thromboembolism increases markedly shortly before the diagnosis of giant cell arteritis regardless of glucocorticoid exposure, peaks at the time of diagnosis, and then progressively declines, according to a matched cohort review involving more than 6,000 arteritis patients.
It’s not been clear until now if the recently recognized risk of venous thromboembolism (VTE) in giant cell arteritis (GCA) was due to the disease itself, or the glucocorticoids used to treat it. “Because inflammation in GCA spares the venous circulation, our finding that patients are at greatest risk of VTE in the period surrounding GCA diagnosis (when inflammation is at its highest level), and the demonstration that this risk is not associated with the use of glucocorticoids, suggest that immunothrombosis could play a pathogenic role,” said investigators led by Sebastian Unizony, MD, of Massachusetts General Hospital, Boston (Arthritis Rheumatol. 2017 Jan;69[1]:176-84).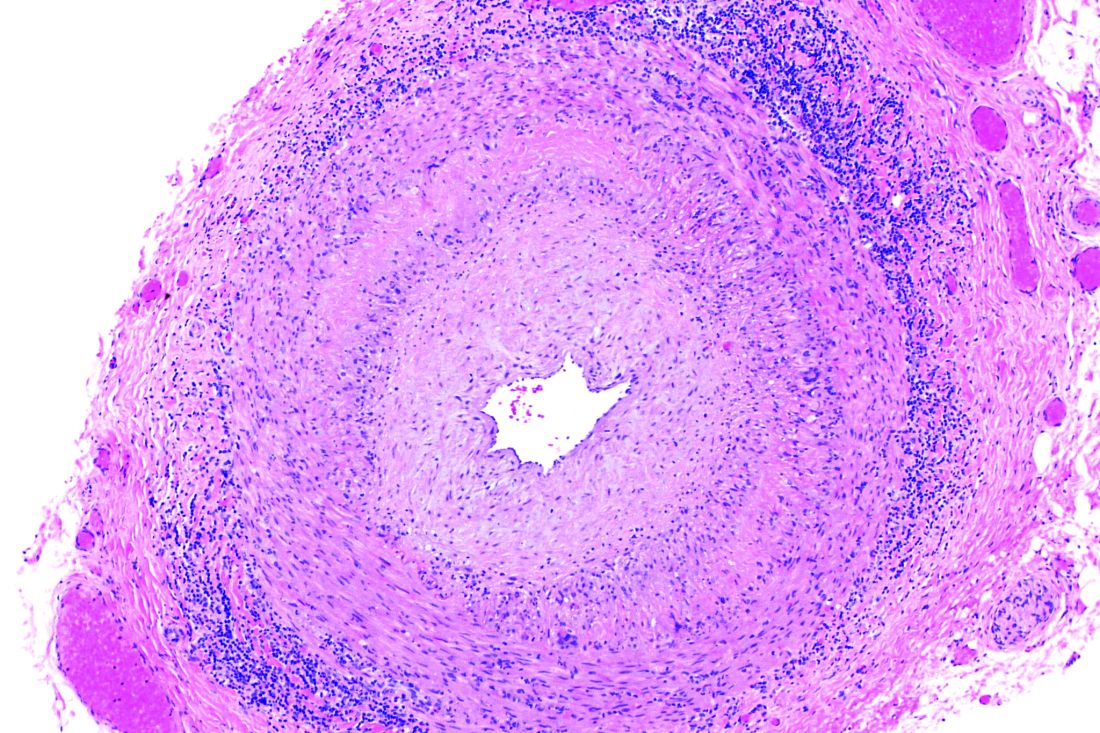
The report was short on advice about what to do to prevent VTE in GCA, but the investigators did recommend “adequate monitoring ... for early recognition of this potentially serious complication.”
The team used a British medical record database covering 1990-2013 to compare 6,441 patients with new-onset GCA to 63,985 controls without GCA matched for age, sex, and date of study entry. VTE was defined as pulmonary embolism and/or deep vein thrombosis.
The incidence of VTE shortly before diagnosis was 4.2 cases per 1,000 person-years in the GCA group, but 2.3 cases per 1,000 person-years among controls. It was about the same when the analysis was limited to GCA patients not exposed to oral glucocorticoids before diagnosis: 4.0 cases versus 2.2 cases in the control group per 1,000 person-years. The finding was key to the conclusion that GCA is an independent VTE risk factor.
During the 12, 9, 6, and 3 months leading up to GCA diagnosis, the relative risks for VTE among patients not treated with glucocorticoids – versus controls – were 1.8, 2.2, 2.4, and 3.6. In the first 3, 6, 12, 24, 48, and 96 months after GCA diagnosis, when virtually all patients were on glucocorticoids at least for the first 6 months, the relative risks for VTE were 9.9, 7.7, 5.9, 4.4, 3.3, 2.4; the last risk score of 2.4 indicated that GCA patients were still slightly more likely than controls to have a VTE even 8 years after diagnosis.
The mean age of patients in the study was 73 years, and 70% of the subjects were women. GCA patients were more likely than were controls to be smokers and to have cardiovascular disease. Also, a greater proportion of GCA patients used aspirin and had recent surgery and hospitalizations. There was no difference in body mass index (mean in both groups 27 kg/m2) or the prevalence of fracture, trauma, or cancer between the groups.
The National Institutes of Health funded the work. There was no disclosure information in the report.
Whether these findings have implications for treatment is unclear. Should a patient with GCA who sustains a VTE early in the course of disease receive anticoagulation short term, with the thought that the VTE was provoked by a risk factor that has been neutralized? Or should treatment be long term, out of concern that the risk factor is still present? Does this finding bear on the controversial question of whether a patient with GCA should receive aspirin?
[A] robust finding of the analysis is that the risk of a first VTE declines steadily over at least the first 2 years after diagnosis of GCA. However, the problem of distinguishing the effects of disease from the effects of treatment has returned. All patients with GCA are now receiving corticosteroids, at least during the period of very high risk in the first 6 months after diagnosis, and one can expect that the average severity of inflammation and average dose of prednisone/prednisolone will decline in parallel. The steadily declining risk of VTE for at least 1 year after diagnosis suggests that both GCA and corticosteroids increase the risk of VTE. It remains impossible to prove or disprove that hypothesis or to estimate the independent risks conferred by the disease and its treatment.
Having GCA probably increases the risk of VTE at least for the first 24 months after diagnosis and the beginning of treatment, but after 24 months, it is unclear. The clinician will still need to make a guess regarding duration of anticoagulation.
Paul Monach, MD, PhD, is a vasculitis specialist at Boston University. He made his comments in an accompanying editorial (Arthritis Rheumatol. 2017 Jan;69[1]:3-5).
Whether these findings have implications for treatment is unclear. Should a patient with GCA who sustains a VTE early in the course of disease receive anticoagulation short term, with the thought that the VTE was provoked by a risk factor that has been neutralized? Or should treatment be long term, out of concern that the risk factor is still present? Does this finding bear on the controversial question of whether a patient with GCA should receive aspirin?
[A] robust finding of the analysis is that the risk of a first VTE declines steadily over at least the first 2 years after diagnosis of GCA. However, the problem of distinguishing the effects of disease from the effects of treatment has returned. All patients with GCA are now receiving corticosteroids, at least during the period of very high risk in the first 6 months after diagnosis, and one can expect that the average severity of inflammation and average dose of prednisone/prednisolone will decline in parallel. The steadily declining risk of VTE for at least 1 year after diagnosis suggests that both GCA and corticosteroids increase the risk of VTE. It remains impossible to prove or disprove that hypothesis or to estimate the independent risks conferred by the disease and its treatment.
Having GCA probably increases the risk of VTE at least for the first 24 months after diagnosis and the beginning of treatment, but after 24 months, it is unclear. The clinician will still need to make a guess regarding duration of anticoagulation.
Paul Monach, MD, PhD, is a vasculitis specialist at Boston University. He made his comments in an accompanying editorial (Arthritis Rheumatol. 2017 Jan;69[1]:3-5).
Whether these findings have implications for treatment is unclear. Should a patient with GCA who sustains a VTE early in the course of disease receive anticoagulation short term, with the thought that the VTE was provoked by a risk factor that has been neutralized? Or should treatment be long term, out of concern that the risk factor is still present? Does this finding bear on the controversial question of whether a patient with GCA should receive aspirin?
[A] robust finding of the analysis is that the risk of a first VTE declines steadily over at least the first 2 years after diagnosis of GCA. However, the problem of distinguishing the effects of disease from the effects of treatment has returned. All patients with GCA are now receiving corticosteroids, at least during the period of very high risk in the first 6 months after diagnosis, and one can expect that the average severity of inflammation and average dose of prednisone/prednisolone will decline in parallel. The steadily declining risk of VTE for at least 1 year after diagnosis suggests that both GCA and corticosteroids increase the risk of VTE. It remains impossible to prove or disprove that hypothesis or to estimate the independent risks conferred by the disease and its treatment.
Having GCA probably increases the risk of VTE at least for the first 24 months after diagnosis and the beginning of treatment, but after 24 months, it is unclear. The clinician will still need to make a guess regarding duration of anticoagulation.
Paul Monach, MD, PhD, is a vasculitis specialist at Boston University. He made his comments in an accompanying editorial (Arthritis Rheumatol. 2017 Jan;69[1]:3-5).
The risk of venous thromboembolism increases markedly shortly before the diagnosis of giant cell arteritis regardless of glucocorticoid exposure, peaks at the time of diagnosis, and then progressively declines, according to a matched cohort review involving more than 6,000 arteritis patients.
It’s not been clear until now if the recently recognized risk of venous thromboembolism (VTE) in giant cell arteritis (GCA) was due to the disease itself, or the glucocorticoids used to treat it. “Because inflammation in GCA spares the venous circulation, our finding that patients are at greatest risk of VTE in the period surrounding GCA diagnosis (when inflammation is at its highest level), and the demonstration that this risk is not associated with the use of glucocorticoids, suggest that immunothrombosis could play a pathogenic role,” said investigators led by Sebastian Unizony, MD, of Massachusetts General Hospital, Boston (Arthritis Rheumatol. 2017 Jan;69[1]:176-84).
The report was short on advice about what to do to prevent VTE in GCA, but the investigators did recommend “adequate monitoring ... for early recognition of this potentially serious complication.”
The team used a British medical record database covering 1990-2013 to compare 6,441 patients with new-onset GCA to 63,985 controls without GCA matched for age, sex, and date of study entry. VTE was defined as pulmonary embolism and/or deep vein thrombosis.
The incidence of VTE shortly before diagnosis was 4.2 cases per 1,000 person-years in the GCA group, but 2.3 cases per 1,000 person-years among controls. It was about the same when the analysis was limited to GCA patients not exposed to oral glucocorticoids before diagnosis: 4.0 cases versus 2.2 cases in the control group per 1,000 person-years. The finding was key to the conclusion that GCA is an independent VTE risk factor.
During the 12, 9, 6, and 3 months leading up to GCA diagnosis, the relative risks for VTE among patients not treated with glucocorticoids – versus controls – were 1.8, 2.2, 2.4, and 3.6. In the first 3, 6, 12, 24, 48, and 96 months after GCA diagnosis, when virtually all patients were on glucocorticoids at least for the first 6 months, the relative risks for VTE were 9.9, 7.7, 5.9, 4.4, 3.3, 2.4; the last risk score of 2.4 indicated that GCA patients were still slightly more likely than controls to have a VTE even 8 years after diagnosis.
The mean age of patients in the study was 73 years, and 70% of the subjects were women. GCA patients were more likely than were controls to be smokers and to have cardiovascular disease. Also, a greater proportion of GCA patients used aspirin and had recent surgery and hospitalizations. There was no difference in body mass index (mean in both groups 27 kg/m2) or the prevalence of fracture, trauma, or cancer between the groups.
The National Institutes of Health funded the work. There was no disclosure information in the report.
The risk of venous thromboembolism increases markedly shortly before the diagnosis of giant cell arteritis regardless of glucocorticoid exposure, peaks at the time of diagnosis, and then progressively declines, according to a matched cohort review involving more than 6,000 arteritis patients.
It’s not been clear until now if the recently recognized risk of venous thromboembolism (VTE) in giant cell arteritis (GCA) was due to the disease itself, or the glucocorticoids used to treat it. “Because inflammation in GCA spares the venous circulation, our finding that patients are at greatest risk of VTE in the period surrounding GCA diagnosis (when inflammation is at its highest level), and the demonstration that this risk is not associated with the use of glucocorticoids, suggest that immunothrombosis could play a pathogenic role,” said investigators led by Sebastian Unizony, MD, of Massachusetts General Hospital, Boston (Arthritis Rheumatol. 2017 Jan;69[1]:176-84).
The report was short on advice about what to do to prevent VTE in GCA, but the investigators did recommend “adequate monitoring ... for early recognition of this potentially serious complication.”
The team used a British medical record database covering 1990-2013 to compare 6,441 patients with new-onset GCA to 63,985 controls without GCA matched for age, sex, and date of study entry. VTE was defined as pulmonary embolism and/or deep vein thrombosis.
The incidence of VTE shortly before diagnosis was 4.2 cases per 1,000 person-years in the GCA group, but 2.3 cases per 1,000 person-years among controls. It was about the same when the analysis was limited to GCA patients not exposed to oral glucocorticoids before diagnosis: 4.0 cases versus 2.2 cases in the control group per 1,000 person-years. The finding was key to the conclusion that GCA is an independent VTE risk factor.
During the 12, 9, 6, and 3 months leading up to GCA diagnosis, the relative risks for VTE among patients not treated with glucocorticoids – versus controls – were 1.8, 2.2, 2.4, and 3.6. In the first 3, 6, 12, 24, 48, and 96 months after GCA diagnosis, when virtually all patients were on glucocorticoids at least for the first 6 months, the relative risks for VTE were 9.9, 7.7, 5.9, 4.4, 3.3, 2.4; the last risk score of 2.4 indicated that GCA patients were still slightly more likely than controls to have a VTE even 8 years after diagnosis.
The mean age of patients in the study was 73 years, and 70% of the subjects were women. GCA patients were more likely than were controls to be smokers and to have cardiovascular disease. Also, a greater proportion of GCA patients used aspirin and had recent surgery and hospitalizations. There was no difference in body mass index (mean in both groups 27 kg/m2) or the prevalence of fracture, trauma, or cancer between the groups.
The National Institutes of Health funded the work. There was no disclosure information in the report.
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point:
Major finding: In the 12, 9, 6, and 3 months before GCA diagnosis, the relative risks for VTE among patients not treated with glucocorticoids – versus controls without GCA – were 1.8, 2.2, 2.4, and 3.6.
Data source: Matched cohort review involving more than 6,000 arteritis patients.
Disclosures: The National Institutes of Health funded the work. There was no disclosure information in the report.