User login
Clinical Psychiatry News is the online destination and multimedia properties of Clinica Psychiatry News, the independent news publication for psychiatrists. Since 1971, Clinical Psychiatry News has been the leading source of news and commentary about clinical developments in psychiatry as well as health care policy and regulations that affect the physician's practice.
Dear Drupal User: You're seeing this because you're logged in to Drupal, and not redirected to MDedge.com/psychiatry.
Depression
adolescent depression
adolescent major depressive disorder
adolescent schizophrenia
adolescent with major depressive disorder
animals
autism
baby
brexpiprazole
child
child bipolar
child depression
child schizophrenia
children with bipolar disorder
children with depression
children with major depressive disorder
compulsive behaviors
cure
elderly bipolar
elderly depression
elderly major depressive disorder
elderly schizophrenia
elderly with dementia
first break
first episode
gambling
gaming
geriatric depression
geriatric major depressive disorder
geriatric schizophrenia
infant
ketamine
kid
major depressive disorder
major depressive disorder in adolescents
major depressive disorder in children
parenting
pediatric
pediatric bipolar
pediatric depression
pediatric major depressive disorder
pediatric schizophrenia
pregnancy
pregnant
rexulti
skin care
suicide
teen
wine
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-cpn')]
div[contains(@class, 'pane-pub-home-cpn')]
div[contains(@class, 'pane-pub-topic-cpn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Don’t wait for a cyberattack; know what coverage you have now
Barbara L. McAneny, MD, CEO of New Mexico Oncology Hematology Consultants, experienced a data breach about 10 years ago, when a laptop was stolen from her large practice.
She and the other physicians were upset and worried that the individual would attempt to log in to the computer system and hack their patients’ private health information.
Dr. McAneny was also worried that the practice would have to pay a hefty fine to the government for having unsecured private health information on a laptop. She could have paid from $50,000 to more than $1.9 million for lost and stolen devices (although that didn’t happen).
Dr. McAneny had a standard cyber liability benefit in her med-mal policy that covered up to $50,000 of the data breach costs. That covered the legal advice The Doctors Company provided about state and federal reporting requirements when a data breach occurs and the costs the practice incurred from mailing letters to all of its patients notifying them of the data breach, says Dr. McAneny.
“The data breach taught me a lot. Our practice spent a lot of money on increasing our internal controls, cybersecurity, and monitoring. Our IT department started testing our computer firewalls periodically, and that’s how we discovered that cybercriminals were attempting to break into our computer system at least 100 times daily,” says Dr. McAneny.
That discovery changed how she thought about insurance. “I decided the med-mal benefit wasn’t enough. I bought the best cybersecurity policy we could afford to protect against future breaches, especially malware or ransomware attacks.”
Her practice also had to make its electronic health records (EHRs) more secure to comply with the Department of Health & Human Services Office of Civil Rights standards for protected health information. The cost of increased security wasn’t covered by her cyber benefit.
Cyberattacks increasing in health care
Despite having comprehensive coverage, Dr. McAneny worries that the cybercriminals are a step ahead of the cybersecurity experts and her practice will eventually have another data breach.
“The policy only covers things that we know about today. As we upgrade our defenses, criminals are finding new ways to breach firewalls and work around our defenses,” she says.
So far this year, nearly 200 medical groups have reported cyberattacks involving 500 or more of their patients’ medical records to the federal government.
EHRs are valuable targets to cybercriminals because of the protected health information they contain. Cybercriminals grab information such as Social Security numbers, dates of birth, medical procedures and results, and in some cases billing and financial information and sell it on the dark web.
They typically bundle the information and sell it to other criminals who later use it for various kinds of fraud and extortion such as banking and credit fraud, health care fraud, identity theft, and ransom extortion.
What do most doctors have?
The vast majority (82%) of doctors polled by the Medical Group Management Association last year said they had cyber insurance, compared with 54% in 2018.
For those who answered “yes,” many said they have coverage through their malpractice insurance carrier.
David Zetter, president of Zetter HealthCare Management Consultants, recommends that physicians speak with their malpractice carrier to determine what coverage they have, if any, within their malpractice policy.
A typical cybersecurity benefit is limited to what is needed to fix and resolve the hacking incident, says Raj Shah, senior regulatory attorney and policyholder advisor at MagMutual, which insures medical practices for malpractice and cyber liability.
That usually covers investigating the cause of the breach and the extent of the damage, legal advice about federal and state reporting requirements, whether to pay a ransom, and a public relations professional to handle patient communication, says Mr. Shah.
The benefit doesn’t cover lost patient revenue when practices have to shut down their operations, the cost of replacing damaged computers, or the ransom payment, he says.
Mr. Zetter advises doctors to consider buying cybersecurity coverage. “I recommend that they speak with an insurance broker who is experienced with cybersecurity policies sold to health care professionals to determine what type of coverage and how much coverage they may need. Their malpractice carrier may also be able to provide some answers,” says Mr. Zetter.
The physician will need to be able to answer questions about their network and how many staff they have and may need to involve their IT vendor too, he adds.
How does comprehensive coverage compare?
Ransomware attacks continue to be one of the most frequent types of attacks, and the amount criminals are demanding has risen significantly. The median ransom payment was $5,000 in the fourth quarter of 2018, compared with over $300,000 during the fourth quarter of 2021.
Cybercriminals now engage in “double extortion” – demanding a ransom payment to hand over the code that will unlock their encrypted data – and then another ransom payment to not post patients’ sensitive medical information they copied onto the dark web.
Comprehensive cybersecurity insurance will cover “double extortion” payments, legal costs that may arise from defending against patient lawsuits, and the costs of meeting federal and state privacy requirements, including notifying patients of the data breach and regulatory investigations, says Michael Carr, head of risk engineering for North America for Coalition, a cyber insurance firm.
Cyber insurers also contract with vendors who sell bitcoin, which is the currency cybercriminals typically demand for ransom payments, and work with ransom negotiators.
For example, once Coalition decided to pay the ransom on behalf of a health care client, it negotiated the ransom demand down by nearly 75% from $750,000 to $200,000, and proceeded to help the company restore all of its data.
The costs to respond to the incident, to recover lost data, and to pay the extortion, together with the lost business income resulting from the incident, were covered by Coalition’s cyber insurance policy.
Other clients have had their funds retrieved before a fraudulent wire transfer was completed. “Medical practices have vendors they pay regularly. A cybercriminal may compromise your email or take over a bank account and then impersonate a vendor asking to be paid for services they didn’t provide,” says Mr. Carr.
How much coverage do you need? Cost?
Dr. McAneny has increased her cybersecurity coverage every year. “It’s expensive, but I think it’s worth it. But you can never buy enough protection due to the coverage limits.”
She worries that the costs could exceed the limits if a ransomware attack disrupts her practice for days, weeks, or longer, or if the Office for Civil Rights fines her practice $10,000 per patient chart – the practice has 100,000 health records. “That can run several millions of dollars and ruin a practice,” she says.
Health systems and hospitals need massive amounts of coverage, which often runs from $20 million to $30 million, says Mr. Shah. However, practices insured through MagMutual have lower coverage limits that range from $1 million to $5 million, he says.
“A large practice does not necessarily need more than $1,000,000 in coverage if they have limited loss in this area and strong internal processes and controls. Most large practices also have a dedicated information security director, which reduces their risk, so they may be comfortable with $1,000,000 in coverage,” says Mr. Shah.
Premiums are based on the number of patient health records per practice, which translates into higher premiums for larger practices.
Other factors that come into play include the underlying coverage, risk controls the practice has implemented, and its claims history, says Mr. Shah.
However, the cost for cyber liability insurance has increased, and practices can expect to pay higher premiums and deductibles. For example, a practice that paid $10,000 in premiums for a new policy last year will have to pay $20,000 this year, says Dan Hanson, senior vice president of management liability and client experience at Marsh & McLennon Agency, a risk management firm that sells cyber insurance policies.
“We saw 71% of our self-insured clients experience higher deductibles over last year due to increased claim activity and the lack of capacity in the market. The carriers are saying they will set limits, but you are going to pay a lot more, and you are going to participate more in losses through the higher deductibles,” says Mr. Hanson.
Are you eligible?
Cyber insurance companies have a vested interest in avoiding claims. With increasing cyberattacks and larger payouts, many insurers are requiring practices to implement some defensive measures before they insure them. Some insurers, such as Coalition, say they may still insure small practices for comprehensive coverage, but it may impact the pricing or what’s covered, says Mr. Carr.
Here are some of the security measures that cyber insurers are looking for:
- Multifactorial authentication (MFA) requires an extra layer of security to access the system. For example, when logging into your organization’s EHR platform, instead of just using a username and password to access the platform, MFA would require you to input an additional unique login credential before you can access the EHR. A secondary login credential may include security questions, a one-time PIN, or biometrics.
- Removing a terminated employee’s login credentials quickly from the computer system. “One of the most damaging and expensive types of attacks are by disgruntled employees who still have their login credentials and take revenge by logging back into the system and planting malware,” says Mr. Shah.
- Automatic system updates (patches). “Phishing email compromises usually result from a failure to fix vulnerabilities. When a system needs to restart, it should be set to automatically update any potential security loopholes within programs or products,” says Mr. Carr. The firewall settings should also be updated.
- Prior hacking incidents: Are the attackers out of your system? Once criminals hack into the system, your practice is vulnerable to repeat attacks. “If a cyberattack is not completely addressed, threat actors will maintain access to or a presence on the compromised network. In general, we will work with the insured to ensure that the initial point of compromise has been addressed and that any threat actor presence in the network has been removed,” says Mr. Carr.
When doctors compare cybersecurity policies, experts recommend avoiding companies that may offer lower prices but lack a proven track record of handling claims and do not offer resources that can detect a threat, such as ongoing network monitoring and employee training with simulated exercises.
“Practices tend to think, ‘It won’t happen to me.’ Every practice needs to take this seriously,” says Dr. McAneny.
A version of this article first appeared on Medscape.com.
Barbara L. McAneny, MD, CEO of New Mexico Oncology Hematology Consultants, experienced a data breach about 10 years ago, when a laptop was stolen from her large practice.
She and the other physicians were upset and worried that the individual would attempt to log in to the computer system and hack their patients’ private health information.
Dr. McAneny was also worried that the practice would have to pay a hefty fine to the government for having unsecured private health information on a laptop. She could have paid from $50,000 to more than $1.9 million for lost and stolen devices (although that didn’t happen).
Dr. McAneny had a standard cyber liability benefit in her med-mal policy that covered up to $50,000 of the data breach costs. That covered the legal advice The Doctors Company provided about state and federal reporting requirements when a data breach occurs and the costs the practice incurred from mailing letters to all of its patients notifying them of the data breach, says Dr. McAneny.
“The data breach taught me a lot. Our practice spent a lot of money on increasing our internal controls, cybersecurity, and monitoring. Our IT department started testing our computer firewalls periodically, and that’s how we discovered that cybercriminals were attempting to break into our computer system at least 100 times daily,” says Dr. McAneny.
That discovery changed how she thought about insurance. “I decided the med-mal benefit wasn’t enough. I bought the best cybersecurity policy we could afford to protect against future breaches, especially malware or ransomware attacks.”
Her practice also had to make its electronic health records (EHRs) more secure to comply with the Department of Health & Human Services Office of Civil Rights standards for protected health information. The cost of increased security wasn’t covered by her cyber benefit.
Cyberattacks increasing in health care
Despite having comprehensive coverage, Dr. McAneny worries that the cybercriminals are a step ahead of the cybersecurity experts and her practice will eventually have another data breach.
“The policy only covers things that we know about today. As we upgrade our defenses, criminals are finding new ways to breach firewalls and work around our defenses,” she says.
So far this year, nearly 200 medical groups have reported cyberattacks involving 500 or more of their patients’ medical records to the federal government.
EHRs are valuable targets to cybercriminals because of the protected health information they contain. Cybercriminals grab information such as Social Security numbers, dates of birth, medical procedures and results, and in some cases billing and financial information and sell it on the dark web.
They typically bundle the information and sell it to other criminals who later use it for various kinds of fraud and extortion such as banking and credit fraud, health care fraud, identity theft, and ransom extortion.
What do most doctors have?
The vast majority (82%) of doctors polled by the Medical Group Management Association last year said they had cyber insurance, compared with 54% in 2018.
For those who answered “yes,” many said they have coverage through their malpractice insurance carrier.
David Zetter, president of Zetter HealthCare Management Consultants, recommends that physicians speak with their malpractice carrier to determine what coverage they have, if any, within their malpractice policy.
A typical cybersecurity benefit is limited to what is needed to fix and resolve the hacking incident, says Raj Shah, senior regulatory attorney and policyholder advisor at MagMutual, which insures medical practices for malpractice and cyber liability.
That usually covers investigating the cause of the breach and the extent of the damage, legal advice about federal and state reporting requirements, whether to pay a ransom, and a public relations professional to handle patient communication, says Mr. Shah.
The benefit doesn’t cover lost patient revenue when practices have to shut down their operations, the cost of replacing damaged computers, or the ransom payment, he says.
Mr. Zetter advises doctors to consider buying cybersecurity coverage. “I recommend that they speak with an insurance broker who is experienced with cybersecurity policies sold to health care professionals to determine what type of coverage and how much coverage they may need. Their malpractice carrier may also be able to provide some answers,” says Mr. Zetter.
The physician will need to be able to answer questions about their network and how many staff they have and may need to involve their IT vendor too, he adds.
How does comprehensive coverage compare?
Ransomware attacks continue to be one of the most frequent types of attacks, and the amount criminals are demanding has risen significantly. The median ransom payment was $5,000 in the fourth quarter of 2018, compared with over $300,000 during the fourth quarter of 2021.
Cybercriminals now engage in “double extortion” – demanding a ransom payment to hand over the code that will unlock their encrypted data – and then another ransom payment to not post patients’ sensitive medical information they copied onto the dark web.
Comprehensive cybersecurity insurance will cover “double extortion” payments, legal costs that may arise from defending against patient lawsuits, and the costs of meeting federal and state privacy requirements, including notifying patients of the data breach and regulatory investigations, says Michael Carr, head of risk engineering for North America for Coalition, a cyber insurance firm.
Cyber insurers also contract with vendors who sell bitcoin, which is the currency cybercriminals typically demand for ransom payments, and work with ransom negotiators.
For example, once Coalition decided to pay the ransom on behalf of a health care client, it negotiated the ransom demand down by nearly 75% from $750,000 to $200,000, and proceeded to help the company restore all of its data.
The costs to respond to the incident, to recover lost data, and to pay the extortion, together with the lost business income resulting from the incident, were covered by Coalition’s cyber insurance policy.
Other clients have had their funds retrieved before a fraudulent wire transfer was completed. “Medical practices have vendors they pay regularly. A cybercriminal may compromise your email or take over a bank account and then impersonate a vendor asking to be paid for services they didn’t provide,” says Mr. Carr.
How much coverage do you need? Cost?
Dr. McAneny has increased her cybersecurity coverage every year. “It’s expensive, but I think it’s worth it. But you can never buy enough protection due to the coverage limits.”
She worries that the costs could exceed the limits if a ransomware attack disrupts her practice for days, weeks, or longer, or if the Office for Civil Rights fines her practice $10,000 per patient chart – the practice has 100,000 health records. “That can run several millions of dollars and ruin a practice,” she says.
Health systems and hospitals need massive amounts of coverage, which often runs from $20 million to $30 million, says Mr. Shah. However, practices insured through MagMutual have lower coverage limits that range from $1 million to $5 million, he says.
“A large practice does not necessarily need more than $1,000,000 in coverage if they have limited loss in this area and strong internal processes and controls. Most large practices also have a dedicated information security director, which reduces their risk, so they may be comfortable with $1,000,000 in coverage,” says Mr. Shah.
Premiums are based on the number of patient health records per practice, which translates into higher premiums for larger practices.
Other factors that come into play include the underlying coverage, risk controls the practice has implemented, and its claims history, says Mr. Shah.
However, the cost for cyber liability insurance has increased, and practices can expect to pay higher premiums and deductibles. For example, a practice that paid $10,000 in premiums for a new policy last year will have to pay $20,000 this year, says Dan Hanson, senior vice president of management liability and client experience at Marsh & McLennon Agency, a risk management firm that sells cyber insurance policies.
“We saw 71% of our self-insured clients experience higher deductibles over last year due to increased claim activity and the lack of capacity in the market. The carriers are saying they will set limits, but you are going to pay a lot more, and you are going to participate more in losses through the higher deductibles,” says Mr. Hanson.
Are you eligible?
Cyber insurance companies have a vested interest in avoiding claims. With increasing cyberattacks and larger payouts, many insurers are requiring practices to implement some defensive measures before they insure them. Some insurers, such as Coalition, say they may still insure small practices for comprehensive coverage, but it may impact the pricing or what’s covered, says Mr. Carr.
Here are some of the security measures that cyber insurers are looking for:
- Multifactorial authentication (MFA) requires an extra layer of security to access the system. For example, when logging into your organization’s EHR platform, instead of just using a username and password to access the platform, MFA would require you to input an additional unique login credential before you can access the EHR. A secondary login credential may include security questions, a one-time PIN, or biometrics.
- Removing a terminated employee’s login credentials quickly from the computer system. “One of the most damaging and expensive types of attacks are by disgruntled employees who still have their login credentials and take revenge by logging back into the system and planting malware,” says Mr. Shah.
- Automatic system updates (patches). “Phishing email compromises usually result from a failure to fix vulnerabilities. When a system needs to restart, it should be set to automatically update any potential security loopholes within programs or products,” says Mr. Carr. The firewall settings should also be updated.
- Prior hacking incidents: Are the attackers out of your system? Once criminals hack into the system, your practice is vulnerable to repeat attacks. “If a cyberattack is not completely addressed, threat actors will maintain access to or a presence on the compromised network. In general, we will work with the insured to ensure that the initial point of compromise has been addressed and that any threat actor presence in the network has been removed,” says Mr. Carr.
When doctors compare cybersecurity policies, experts recommend avoiding companies that may offer lower prices but lack a proven track record of handling claims and do not offer resources that can detect a threat, such as ongoing network monitoring and employee training with simulated exercises.
“Practices tend to think, ‘It won’t happen to me.’ Every practice needs to take this seriously,” says Dr. McAneny.
A version of this article first appeared on Medscape.com.
Barbara L. McAneny, MD, CEO of New Mexico Oncology Hematology Consultants, experienced a data breach about 10 years ago, when a laptop was stolen from her large practice.
She and the other physicians were upset and worried that the individual would attempt to log in to the computer system and hack their patients’ private health information.
Dr. McAneny was also worried that the practice would have to pay a hefty fine to the government for having unsecured private health information on a laptop. She could have paid from $50,000 to more than $1.9 million for lost and stolen devices (although that didn’t happen).
Dr. McAneny had a standard cyber liability benefit in her med-mal policy that covered up to $50,000 of the data breach costs. That covered the legal advice The Doctors Company provided about state and federal reporting requirements when a data breach occurs and the costs the practice incurred from mailing letters to all of its patients notifying them of the data breach, says Dr. McAneny.
“The data breach taught me a lot. Our practice spent a lot of money on increasing our internal controls, cybersecurity, and monitoring. Our IT department started testing our computer firewalls periodically, and that’s how we discovered that cybercriminals were attempting to break into our computer system at least 100 times daily,” says Dr. McAneny.
That discovery changed how she thought about insurance. “I decided the med-mal benefit wasn’t enough. I bought the best cybersecurity policy we could afford to protect against future breaches, especially malware or ransomware attacks.”
Her practice also had to make its electronic health records (EHRs) more secure to comply with the Department of Health & Human Services Office of Civil Rights standards for protected health information. The cost of increased security wasn’t covered by her cyber benefit.
Cyberattacks increasing in health care
Despite having comprehensive coverage, Dr. McAneny worries that the cybercriminals are a step ahead of the cybersecurity experts and her practice will eventually have another data breach.
“The policy only covers things that we know about today. As we upgrade our defenses, criminals are finding new ways to breach firewalls and work around our defenses,” she says.
So far this year, nearly 200 medical groups have reported cyberattacks involving 500 or more of their patients’ medical records to the federal government.
EHRs are valuable targets to cybercriminals because of the protected health information they contain. Cybercriminals grab information such as Social Security numbers, dates of birth, medical procedures and results, and in some cases billing and financial information and sell it on the dark web.
They typically bundle the information and sell it to other criminals who later use it for various kinds of fraud and extortion such as banking and credit fraud, health care fraud, identity theft, and ransom extortion.
What do most doctors have?
The vast majority (82%) of doctors polled by the Medical Group Management Association last year said they had cyber insurance, compared with 54% in 2018.
For those who answered “yes,” many said they have coverage through their malpractice insurance carrier.
David Zetter, president of Zetter HealthCare Management Consultants, recommends that physicians speak with their malpractice carrier to determine what coverage they have, if any, within their malpractice policy.
A typical cybersecurity benefit is limited to what is needed to fix and resolve the hacking incident, says Raj Shah, senior regulatory attorney and policyholder advisor at MagMutual, which insures medical practices for malpractice and cyber liability.
That usually covers investigating the cause of the breach and the extent of the damage, legal advice about federal and state reporting requirements, whether to pay a ransom, and a public relations professional to handle patient communication, says Mr. Shah.
The benefit doesn’t cover lost patient revenue when practices have to shut down their operations, the cost of replacing damaged computers, or the ransom payment, he says.
Mr. Zetter advises doctors to consider buying cybersecurity coverage. “I recommend that they speak with an insurance broker who is experienced with cybersecurity policies sold to health care professionals to determine what type of coverage and how much coverage they may need. Their malpractice carrier may also be able to provide some answers,” says Mr. Zetter.
The physician will need to be able to answer questions about their network and how many staff they have and may need to involve their IT vendor too, he adds.
How does comprehensive coverage compare?
Ransomware attacks continue to be one of the most frequent types of attacks, and the amount criminals are demanding has risen significantly. The median ransom payment was $5,000 in the fourth quarter of 2018, compared with over $300,000 during the fourth quarter of 2021.
Cybercriminals now engage in “double extortion” – demanding a ransom payment to hand over the code that will unlock their encrypted data – and then another ransom payment to not post patients’ sensitive medical information they copied onto the dark web.
Comprehensive cybersecurity insurance will cover “double extortion” payments, legal costs that may arise from defending against patient lawsuits, and the costs of meeting federal and state privacy requirements, including notifying patients of the data breach and regulatory investigations, says Michael Carr, head of risk engineering for North America for Coalition, a cyber insurance firm.
Cyber insurers also contract with vendors who sell bitcoin, which is the currency cybercriminals typically demand for ransom payments, and work with ransom negotiators.
For example, once Coalition decided to pay the ransom on behalf of a health care client, it negotiated the ransom demand down by nearly 75% from $750,000 to $200,000, and proceeded to help the company restore all of its data.
The costs to respond to the incident, to recover lost data, and to pay the extortion, together with the lost business income resulting from the incident, were covered by Coalition’s cyber insurance policy.
Other clients have had their funds retrieved before a fraudulent wire transfer was completed. “Medical practices have vendors they pay regularly. A cybercriminal may compromise your email or take over a bank account and then impersonate a vendor asking to be paid for services they didn’t provide,” says Mr. Carr.
How much coverage do you need? Cost?
Dr. McAneny has increased her cybersecurity coverage every year. “It’s expensive, but I think it’s worth it. But you can never buy enough protection due to the coverage limits.”
She worries that the costs could exceed the limits if a ransomware attack disrupts her practice for days, weeks, or longer, or if the Office for Civil Rights fines her practice $10,000 per patient chart – the practice has 100,000 health records. “That can run several millions of dollars and ruin a practice,” she says.
Health systems and hospitals need massive amounts of coverage, which often runs from $20 million to $30 million, says Mr. Shah. However, practices insured through MagMutual have lower coverage limits that range from $1 million to $5 million, he says.
“A large practice does not necessarily need more than $1,000,000 in coverage if they have limited loss in this area and strong internal processes and controls. Most large practices also have a dedicated information security director, which reduces their risk, so they may be comfortable with $1,000,000 in coverage,” says Mr. Shah.
Premiums are based on the number of patient health records per practice, which translates into higher premiums for larger practices.
Other factors that come into play include the underlying coverage, risk controls the practice has implemented, and its claims history, says Mr. Shah.
However, the cost for cyber liability insurance has increased, and practices can expect to pay higher premiums and deductibles. For example, a practice that paid $10,000 in premiums for a new policy last year will have to pay $20,000 this year, says Dan Hanson, senior vice president of management liability and client experience at Marsh & McLennon Agency, a risk management firm that sells cyber insurance policies.
“We saw 71% of our self-insured clients experience higher deductibles over last year due to increased claim activity and the lack of capacity in the market. The carriers are saying they will set limits, but you are going to pay a lot more, and you are going to participate more in losses through the higher deductibles,” says Mr. Hanson.
Are you eligible?
Cyber insurance companies have a vested interest in avoiding claims. With increasing cyberattacks and larger payouts, many insurers are requiring practices to implement some defensive measures before they insure them. Some insurers, such as Coalition, say they may still insure small practices for comprehensive coverage, but it may impact the pricing or what’s covered, says Mr. Carr.
Here are some of the security measures that cyber insurers are looking for:
- Multifactorial authentication (MFA) requires an extra layer of security to access the system. For example, when logging into your organization’s EHR platform, instead of just using a username and password to access the platform, MFA would require you to input an additional unique login credential before you can access the EHR. A secondary login credential may include security questions, a one-time PIN, or biometrics.
- Removing a terminated employee’s login credentials quickly from the computer system. “One of the most damaging and expensive types of attacks are by disgruntled employees who still have their login credentials and take revenge by logging back into the system and planting malware,” says Mr. Shah.
- Automatic system updates (patches). “Phishing email compromises usually result from a failure to fix vulnerabilities. When a system needs to restart, it should be set to automatically update any potential security loopholes within programs or products,” says Mr. Carr. The firewall settings should also be updated.
- Prior hacking incidents: Are the attackers out of your system? Once criminals hack into the system, your practice is vulnerable to repeat attacks. “If a cyberattack is not completely addressed, threat actors will maintain access to or a presence on the compromised network. In general, we will work with the insured to ensure that the initial point of compromise has been addressed and that any threat actor presence in the network has been removed,” says Mr. Carr.
When doctors compare cybersecurity policies, experts recommend avoiding companies that may offer lower prices but lack a proven track record of handling claims and do not offer resources that can detect a threat, such as ongoing network monitoring and employee training with simulated exercises.
“Practices tend to think, ‘It won’t happen to me.’ Every practice needs to take this seriously,” says Dr. McAneny.
A version of this article first appeared on Medscape.com.
Shift schedule today could worsen that stroke tomorrow
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.

In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.

A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”

KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.

Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.
In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.
A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”
KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.
Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Body clocks and the shifting risks of stroke
Health care professionals, we’re sure, are no strangers to rotating shifts. And, as practitioners of the shiftly arts, you should know new research shows that working those kinds of hours can have lasting effects on your health. And it’s all based on your sleep-wake cycle.
In a study published in Neurobiology of Sleep and Circadian Rhythms, investigators at Texas A&M University looked at the effects of working these kinds of shifts for a long period of time and then returning to a regular 24-hour cycle later in life. The study piggybacks on a previous study, which showed that rats on shift schedules had more severe stroke outcomes than those who were on a 24-hour cycle.
The current study demonstrates that working rotating shifts does have a lasting effect, by way of messing with the sleep-wake cycle. Based on the research, the rats that performed those kinds of shifts never got back to a normal schedule. When strokes occurred, outcomes were much worse, and the females had a higher mortality rate and more severe functional deficits than the males.
Now for the “good” news: Even if you’re among those who haven’t worked a rotating shift, you may not be safe either.
People who have regular working hours have a tendency to take work home and stay up late, especially with so many moving to a remote-work model. And if you’re staying up late on the weekends you’re producing what lead author David J. Earnest, PhD, called “social jet lag,” which messes with your circadian rhythm to wind you down for sleep. All of these things can lead to the same kind of effects that working rotating shifts has on your health, he said in a written statement.
How do you combat this? Dr. Earnest recommended creating a sleep schedule and setting regular mealtimes. Also ease up on high-fat foods, drinking, and smoking. The connection between your brain and gut also could play a part in how severe a stroke can be.
So continue to work hard, but not too hard.
Got 3 minutes? You got time for culture
Much like a Krabby Patty, art is good for your soul. Seriously, staring at a 500-year-old painting may not seem like much, but research has proven time and again that going to a museum and looking at paintings by long-dead artists you probably know better as pizza-eating superhero turtles improves mood, stress, and well-being.
A couple of years ago, however, museums and art galleries ran into a big virus-shaped problem. You may have heard of it. All of a sudden it became a very bad idea for people to gather together in one building and huddle around the Mona Lisa, which, by the way, is a lot smaller in person than you might expect. But, rather than sit around with a bunch of priceless art for an indeterminate amount of time, museums brought their exhibits to the Internet so that people from all over the world could see great works from their couches.
This is absolutely a good thing for public access, but do these virtual art exhibits provide the same health benefits as going to a museum in person? That’s what a group of European researchers aimed to find out, and in a study published in Frontiers of Psychology, that’s exactly what they found.
Their directive to the 84 study participants was simple: Take a well-being survey, engage with either of a pair of online exhibits (a Monet painting and a display of Japanese culinary traditions) for just 3 minutes, then take another well-being assessment. The results were quite clear: Even just a couple of minutes of viewing art online improved all the well-being categories on the survey, such as lowering anxiety, negative mood, and loneliness, as well as increasing subjective well-being. Also, the more beautiful or meaningful a person found the art, the more their mood and well-being improved.
The researchers noted that these results could help access in places where access to art is limited, such as waiting rooms, hospitals, and rural areas. Let’s just hope it sticks to that, and that big businesses don’t take notice. Just imagine them plastering ads with classic Renaissance artworks. After all, art makes you feel good, and you know what else feels good on a hot summer day? An ice-cold Coca-Cola! By the way, we’re taking offers, advertising agencies. The LOTME staff can absolutely be bought.
Appetite for etymology
Today on “It’s a Thing,” we examine various states of hunger and what they should be called. Our first guest is that historically hungry royal person, King Henry VIII of England. Your majesty, have you ever been “hangry?”
KH8: First, let me thank you for inviting me on the show, Maurice. I’m a huge fan. A recent study done in the United Kingdom and Austria showed that “hunger is associated with greater levels of anger and irritability, as well as lower levels of pleasure,” according to a Eurekalert statement. So, yes, I have been “hangry.”
Maurice: Now to our next guest. Martha Stewart, can you add anything about that study?
Martha: Happy to, Maurice. The 64 participants used a smartphone app to record their hunger levels and emotional states five times a day for 21 days. It’s the first time that “hanger” was studied outside a lab, and it showed that hunger “was associated with 37% of the variance in irritability, 34% of the variance in anger, and 38% of the variance in pleasure recorded by the participants,” the investigators said in that statement.
Maurice: It’s official, then. Hangry is a thing, and we don’t need to put it in quotes anymore. Now let’s meet our third and final guest, Betty Crocker. Betty, I’m told you have a study to plug.
Betty: That’s right, Mo. Researchers at Tel Aviv University looked at survey data from almost 3,000 men and women and found that men ate 17% more food during the warmer months (March to September) than they did the rest of the year. Among women, however, caloric intake did not change.
KH8: I saw that study. Didn’t they put 27 people out in the sun and then take blood samples?
Betty: Indeed they did, Hank. After 25 minutes of sun exposure, the 13 men felt hungrier than before, but the 14 women did not. The men also had higher levels of ghrelin, an appetite-stimulating hormone, than the women.
Maurice: To sum all this up, then, we’ve got angry and hungry officially combining to make hangry, and now it looks like the sun is causing hunger in men, which makes them … sungry?
Martha: It’s a thing.
Chicken cutlets with a side of COVID
You stopped at the drive through at McDonald’s on the way home from work, and while you’re looking for something sweet in the refrigerator for dessert, you see that chicken breast that expires today.
Freezing meat that’s about to expire might be your go-to so it doesn’t go to waste, but it’s been found that SARS-CoV-2 can live in meat that’s been in the refrigerator or freezer for more than a month.
Researchers exposed chicken, beef, pork, and salmon to surrogate viruses that are similar to COVID but not as harmful and stored them in freezers at –4° F and in the refrigerator at 39.2° F. “We even found that the viruses could be cultured after [being frozen for] that length of time,” lead author Emily Bailey, PhD, of Campbell University in Buies Creek, N.C., said in Study Finds.
The team began its research after hearing of COVID-19 outbreaks where there were no reports of community transmission, such as in Southeast Asia. Tracing eventually led to packaged meats as the culprits in those cases. SARS-CoV-2 is able to replicate in the gut, as well as the respiratory tract, so it could affect the gut before respiratory symptoms start. It is crucial to ensure cross contamination doesn’t occur, and inadequate sanitation prior to packaging needs to be addressed, the investigators said.
Honestly, we didn’t think anything could survive in a freezer for that long, but SARS-CoV-2 is a fighter.
Inflammatory profiles impact major depressive disorder
Early onset of disease in patients with major depressive disorder may be linked to a specific inflammatory profile, based on data from 234 individuals.
Major depressive disorder (MDD) remains common, and evidence suggests that it is increasing among younger individuals, but data on early-onset MDD in adults are limited, Ana Paula Anzolin, a graduate student at the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil, and colleagues wrote.
Although previous studies have shown abnormal cytokine production in patients with MDD, the impact of inflammation on MDD and disease onset and progression remains unclear, they said.
In a study published in Psychiatry Research, the authors identified outpatients aged 18-85 years with confirmed MDD and scores of at least 8 on the HAM-D scale who were undergoing treatment at a single center. Early onset was defined as a diagnosis of MDD before age 30 years (99 patients) and late onset was defined as a diagnosis at age 30 years and older (135 patients). The researchers measured levels of interleukin-6, IL-1 beta, IL-10, and tumor necrosis factor alpha (TNF-alpha).
Overall, the level of cytokine profiles in early- versus late-onset disease was significantly higher for IL-1B and TNF-alpha (P < .001 for both). The significant difference between early- and late-onset disease remained regardless of comorbidity with autoimmune diseases, the researchers noted.
IL-6 levels were higher in the early-onset group and IL-10 levels were higher in the late-onset group, but these differences were not significant.
the researchers wrote.
The results also support findings from previous studies that suggest a divergence between early- and late adult–onset depression, they said. More research on early-onset MDD in adults is needed, as these patients tend to have more severe symptoms, more medical and psychiatric comorbidities, and an increased risk of depressive episodes and suicide attempts.
The study findings were limited by several factors including the lack of a control group, the retrospective assessment of disease onset, and the limited cytokines studied, which do not reflect changes in the entire immune network response, the researchers noted.
However, the study is the first known to examine the association of serum cytokines and early- and late-onset MDD in adults, and the results support the use of IL-1B and TNF-alpha as potential treatment targets in the development of new therapies for MDD, they concluded.
The study was supported by the Fundo de Incentivo à Pesquisa – Hospital de Clínicas de Porto Alegre, the Conselho Nacional de Desenvolvimento Científico e Tecnológico, and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The researchers had no financial conflicts to disclose.
Early onset of disease in patients with major depressive disorder may be linked to a specific inflammatory profile, based on data from 234 individuals.
Major depressive disorder (MDD) remains common, and evidence suggests that it is increasing among younger individuals, but data on early-onset MDD in adults are limited, Ana Paula Anzolin, a graduate student at the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil, and colleagues wrote.
Although previous studies have shown abnormal cytokine production in patients with MDD, the impact of inflammation on MDD and disease onset and progression remains unclear, they said.
In a study published in Psychiatry Research, the authors identified outpatients aged 18-85 years with confirmed MDD and scores of at least 8 on the HAM-D scale who were undergoing treatment at a single center. Early onset was defined as a diagnosis of MDD before age 30 years (99 patients) and late onset was defined as a diagnosis at age 30 years and older (135 patients). The researchers measured levels of interleukin-6, IL-1 beta, IL-10, and tumor necrosis factor alpha (TNF-alpha).
Overall, the level of cytokine profiles in early- versus late-onset disease was significantly higher for IL-1B and TNF-alpha (P < .001 for both). The significant difference between early- and late-onset disease remained regardless of comorbidity with autoimmune diseases, the researchers noted.
IL-6 levels were higher in the early-onset group and IL-10 levels were higher in the late-onset group, but these differences were not significant.
the researchers wrote.
The results also support findings from previous studies that suggest a divergence between early- and late adult–onset depression, they said. More research on early-onset MDD in adults is needed, as these patients tend to have more severe symptoms, more medical and psychiatric comorbidities, and an increased risk of depressive episodes and suicide attempts.
The study findings were limited by several factors including the lack of a control group, the retrospective assessment of disease onset, and the limited cytokines studied, which do not reflect changes in the entire immune network response, the researchers noted.
However, the study is the first known to examine the association of serum cytokines and early- and late-onset MDD in adults, and the results support the use of IL-1B and TNF-alpha as potential treatment targets in the development of new therapies for MDD, they concluded.
The study was supported by the Fundo de Incentivo à Pesquisa – Hospital de Clínicas de Porto Alegre, the Conselho Nacional de Desenvolvimento Científico e Tecnológico, and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The researchers had no financial conflicts to disclose.
Early onset of disease in patients with major depressive disorder may be linked to a specific inflammatory profile, based on data from 234 individuals.
Major depressive disorder (MDD) remains common, and evidence suggests that it is increasing among younger individuals, but data on early-onset MDD in adults are limited, Ana Paula Anzolin, a graduate student at the Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil, and colleagues wrote.
Although previous studies have shown abnormal cytokine production in patients with MDD, the impact of inflammation on MDD and disease onset and progression remains unclear, they said.
In a study published in Psychiatry Research, the authors identified outpatients aged 18-85 years with confirmed MDD and scores of at least 8 on the HAM-D scale who were undergoing treatment at a single center. Early onset was defined as a diagnosis of MDD before age 30 years (99 patients) and late onset was defined as a diagnosis at age 30 years and older (135 patients). The researchers measured levels of interleukin-6, IL-1 beta, IL-10, and tumor necrosis factor alpha (TNF-alpha).
Overall, the level of cytokine profiles in early- versus late-onset disease was significantly higher for IL-1B and TNF-alpha (P < .001 for both). The significant difference between early- and late-onset disease remained regardless of comorbidity with autoimmune diseases, the researchers noted.
IL-6 levels were higher in the early-onset group and IL-10 levels were higher in the late-onset group, but these differences were not significant.
the researchers wrote.
The results also support findings from previous studies that suggest a divergence between early- and late adult–onset depression, they said. More research on early-onset MDD in adults is needed, as these patients tend to have more severe symptoms, more medical and psychiatric comorbidities, and an increased risk of depressive episodes and suicide attempts.
The study findings were limited by several factors including the lack of a control group, the retrospective assessment of disease onset, and the limited cytokines studied, which do not reflect changes in the entire immune network response, the researchers noted.
However, the study is the first known to examine the association of serum cytokines and early- and late-onset MDD in adults, and the results support the use of IL-1B and TNF-alpha as potential treatment targets in the development of new therapies for MDD, they concluded.
The study was supported by the Fundo de Incentivo à Pesquisa – Hospital de Clínicas de Porto Alegre, the Conselho Nacional de Desenvolvimento Científico e Tecnológico, and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The researchers had no financial conflicts to disclose.
FROM PSYCHIATRY RESEARCH
The heartache of bereavement can be fatal in heart failure
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
that points to the need for greater integration of psychosocial risk factors in the treatment of HF.
The adjusted relative risk of dying was nearly 30% higher among bereaved patients with HF (1.29; 95% confidence interval, 1.27-1.30) and slightly higher for those grieving the loss of more than one family member (RR, 1.35).
The highest risk was in the first week after the loss (RR, 1.78) but persisted after 5 years of follow-up (RR, 1.30).
“Heart failure is a very difficult condition and has a very poor prognosis comparable to many, many cancers,” senior author Krisztina László, PhD, Karolinska Institutet, Stockholm, said in an interview. “So it’s important for us to be aware of these increased risks and to understand them better.”
The early risk for death could be related to stress-induced cardiomyopathy, or Takotsubo syndrome, as well as activation of the hypothalamic-pituitary-adrenal axis, the renin-angiotensin-aldosterone system, and sympathetic nervous system, she explained. Higher long-term risks may reflect chronic stress, leading to poorly managed disease and an unhealthy lifestyle.
“If we understand better the underlying mechanisms maybe we can give more specific advice,” Dr. László said. “At this stage, I think having an awareness of the risk and trying to follow patients or at least not let them fall out of usual care, asking questions, trying to understand what their needs are, maybe that is what we can do well.”
A recent position paper by the European Association of Preventive Cardiology pointed out that psychosocial risk factors, like depression and social isolation, can exacerbate heart failure and calls for better integration of psychosocial factors in the treatment of patients with chronic HF.
“We don’t do a very good job of it, but I think they are very important,” observed Stuart D. Russell, MD, a professor of medicine who specializes in advanced HF at Duke University, Durham, N.C., and was not involved in the study.
“When we hear about a spouse dying, we might call and give condolences, but it’s probably a group of patients that for the next 6 months or so we need to watch more closely and see if there are things we can impact both medically as well as socially to perhaps prevent some of this increase in mortality,” he told this news organization.
Although several studies have linked bereavement with adverse health outcomes, this is just one of two studies to look specifically at its role in HF prognosis, Dr. László noted. A 2013 study of 66,000 male veterans reported that widowers had nearly a 38% higher all-cause mortality risk than did married veterans.
The present study extends those findings to 490,527 patients in the Swedish Heart Failure Registry between 2000 and 2018 and/or in the Swedish Patient Register with a primary diagnosis of HF between 1987 and 2018. During a mean follow-up of 3.7 years, 12% of participants had a family member die, and 383,674 participants died.
Results showed the HF mortality risk increased 10% after the death of a child, 20% with the death of a spouse/partner, 13% with a sibling’s death, and 5% with the death of a grandchild.
No increased risk was seen after the death of a parent, which is likely owed to a median patient age of about 75 years and “is in line with our expectations of the life cycle,” Dr. László said.
An association between bereavement and mortality risk was observed in cases of loss caused by cardiovascular disease (RR, 1.34) and other natural causes (RR, 1.27) but also in cases of unnatural deaths, such as suicide (RR, 1.13).
The overall findings were similar regardless of left ventricular ejection fraction and New York Heart Association functional class and were not affected by sex or country of birth.
Dr. Russell agreed that the death of a parent would be expected among these older patients with HF but said that “if the mechanism of this truly is kind of this increased stress hormones and Takotsubo-type mechanism, you’d think it would be worse if it was your kid that died. That shocked me a bit.”
The strong association between mortality and the loss of a spouse or partner was not surprising, given that they’re an important source of mutual social support, he added.
“If it’s a 75-year-old whose spouse dies, we need to make sure that we have the children’s phone number or other people that we can reach out to and say: ‘Can you check on them?’ ” he said. “And we need to make sure that somebody else is coming in with them because I would guess that probably at least half of what patients hear in a clinic visit goes in one ear and out the other and it’s going to make that much better. So we need to find who that new support person is for the patient.”
Asked whether there are efforts underway to incorporate psychosocial factors into current U.S. guidelines, Dr. Russell replied, “certainly within heart failure, I don’t think we’re really discussing it and, that may be the best part of this paper. It really makes us think about a different way of approaching these older patients.”
Dr. László said that future studies are needed to investigate whether less severe sources of stress may also contribute to poor HF prognosis.
“In our population, 12% of patients were affected, which is quite high, but there are patients with heart failure who experience on a daily basis other sources of stress, which are less severe but chronic and affect large numbers,” she said. “This may also have important public health implications and will be an important next step.”
The authors noted that they were unable to eliminate residual confounding by genetic factors or unmeasured socioeconomic-, lifestyle-, or health-related factors shared by family members. Other limitations are limited power to detect a modest effect in some of the subanalyses and that the findings may be generalizable only to countries with social and cultural contexts and health-related factors similar to those of Sweden.
The study was supported by grants from the Swedish Council for Working Life and Social Research, the Karolinska Institutet’s Research Foundation, and the China Scholarship Council. Dr. László is also supported by a grant from the Heart and Lung Foundation. All other authors and Dr. Russell reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JACC: HEART FAILURE
Inflation and health care: The prognosis for doctors
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Rampant inflation doesn’t just mean a spike in everyday expenses like gas and groceries. It’s also bound to have a significant impact on the cost of health care – and on your practice. A recent report from McKinsey & Company predicts that the current inflationary spiral will force health care providers to charge higher reimbursement rates, and those costs inevitably will be passed along to both employers and consumers. Bottom line: Your patients will likely have to pay more out of pocket.
How, precisely, will inflation affect your practice, and what’s the best way to minimize the damage?
Step 1: Maintain operational standards
“Based on the conversations we’ve had with our physician clients that own practices, we see the potential for cost inflation to outrun revenue inflation over the next year,” said Michael Ashley Schulman, CFA, partner and chief investment officer at Running Point Capital, El Segundo, Calif. “Staff wages, as well as office equipment and medical supply costs, are increasing faster than insurance and Medicare/Medicaid reimbursement amounts.” Even so, topflight employees are essential to keep your practice running smoothly. Prioritize excellent nursing. Instead of adding a new hire, compensate your best nurse as well as possible. The same goes for an efficient office manager: On that front, too, you should go the extra mile, even if it means trimming expenses elsewhere.
Step 2: Plan ahead for insurance challenges
Many insurers, including Medicare, set health care costs a year in advance, based on projected growth. This means insurance payouts will stay largely the same for the time being. “Almost all physicians employed by large groups won’t see costs due to inflation rise until next year,” said Mark V. Pauly, PhD, Bendheim Professor in the department of health care management at the University of Pennsylvania, Philadelphia. “For self-employed physicians, there will also be a cushion.”
“The big issue with inflation is that more patients will likely be underinsured,” said Tiffany Johnson, MBA, CFP, co-CEO and financial advisor at Piece of Wealth Planning in Atlanta. “With more out-of-pocket costs ... these patients may not seek out medical treatment or go to see a specialist if they do not believe it is necessary.” A new study from Johns Hopkins found that patients under financial pressure often delay or forgo medical treatment because of food insecurity. Compassionate care is the solution: Direct these patients to financial aid and other resources they may qualify for. That way, they can continue to receive the care they need from you, and your need to pass on costs may be lower.
Step 3: Rely on your affiliated health care organization
These are tough times when it comes to expansion. “Since we are in an environment where inflation and interest rates are both high, it will be much harder for physicians to have the capital to invest in new technology to grow or advance their practice,” Ms. Johnson said. With that in mind, keep the lines of communication between you and your affiliated hospital/health care organization more open than ever. Combining practices with another doctor is one way to increase revenue; you might ask if any affiliated doctors are seeking to team up. It’s also vital to attend meetings and pay close attention to budget cuts your organization may be making. And don’t be shy about asking your administrator for profit-boosting recommendations.
Step 4: Revisit vendor relationships
Find out if your vendors will continue to supply you with the goods you need at reasonable rates, and switch now if they won’t. Be proactive. “Test new medical suppliers,” Mr. Schulman advised. “Reread equipment leasing contracts to check if the interest rates have increased. See if buyout, prepay, or refinancing options are more economical. Also, investigate [bringing down] your rental expense by reducing square footage or moving to a lower-cost location.” In light of ongoing supply chain issues, it’s wise to consider alternative products. But stay focused on quality – you don’t want to be stuck with cheap, possibly defective equipment. Spend where it’s essential and cut the fat somewhere else.
Step 5: Don’t waste your assets
Analyze your budget in minute detail. “Now is the time to review your current inventory and overhead costs,” Ms. Johnson said. “Many physicians let their office staff handle the restocking of inventory and office supplies. While this can be efficient for their practice, it also leaves room for unnecessary business expenses.” Take a cold, hard look at your supply closet – what’s in there that you can live without? Don’t reorder it. Then seek out any revenue stream you may be overlooking. “It’s important to review billing to make sure all the services are reimbursable,” Ms. Johnson added. Small mistakes can yield dividends if you find them.
Step 6: Be poised to pivot
Get creative. “To minimize a profit decline, use video consulting – it’s more efficient and less equipment intensive,” Mr. Schulman said. “Look at how remote work and flexible hours can maximize the work your practice accomplishes while cutting office costs.”
Ms. Johnson suggests adding concierge services, noting that “concierge doctors offer personalized care and direct access for an up-front fee.” With this approach, you may see fewer patients, but your payout paperwork will decrease, and that up-front fee can be profitable. Another outside-the-box idea: Start making house calls. A Scripps study found that home health visits requested via app can result in patient care delivered by a doctor and medical assistant in less than 2 hours. House calls can be an effective and profitable solution when it comes to providing nonemergency care and preventive treatment to patients who aren’t mobile, not to mention patients who just appreciate the convenience.
Step 7: Maintain transparency
Any economic changes your practice will implement must be communicated to your staff and patients clearly and directly. Keep everyone in the loop and be ready to answer questions immediately. Show those you work with and care for that, regardless of the economy, it’s they who matter to you most. That simple reassurance will prove invaluable.
A version of this article first appeared on Medscape.com.
Many sources of PTSD are cause for concern
A few weeks ago, right after 19 children and two adults were killed by a gunman in Uvalde, Texas, Americans were really on edge. Many people I know became hypervigilant while going about activities previously thought of as routine, such as waiting for a subway or going to a grocery store.
On top of that, we are still facing the ongoing COVID-19 pandemic. Despite vaccines and therapeutics, the United States is still losing more than 300 people each day to the virus. Many people who have tested positive have continued to experience debilitating long-haul symptoms many months after testing negative, and I believe not knowing what your future life will bring from this terrible illness could lead some to posttraumatic stress disorder.
In addition to constant updates about COVID, we are getting almost daily reports about monkeypox. In New York state, medical professionals and institutions receive regular, almost weekly, information about the spread of influenza. But where are the reports and treatment approaches for PTSD, which would not only increase awareness but also lead to more care?

Some might believe that I am obsessed with PTSD, since I’ve written a great deal on the subject, particularly “underdiagnosed” PTSD. The key question I have is:
We know the signs and symptoms of PTSD. They include flashbacks, intrusive recollections, physical distress related to stimuli related to the trauma, insomnia, social isolation, avoidance of certain situations, negative thinking, and hyperarousal – coupled with anxiety and depression. PTSD can be a great masquerader. It can be triggered by many events, large and small, and all too often will masquerade as general anxiety or existential despair and depression. Too often, PTSD is undiagnosed or unrecognized completely. PTSD is also a costly disease that is an enormous economic burden on the U.S. economy.
As clinicians, we must be aware of the more subtle events that may trigger PTSD. We must think beyond ICD codes and DSM criteria and realize that each individual processes an event or a series of events differently. For example, seriously ill people in ICUs or undergoing critical care have been known to experience PTSD well beyond their physical recovery (J Crit Care. 2017 Dec. doi: 10.1016/j.jcrc.2017.06.014). Years after the Sept. 11, 2001, World Trade Center disaster, many are still suffering from PTSD symptoms (Biol Psychiatry. 2020 May 1. doi: 10.1016/j.biopsych.2020.02.817).
Again, in some cases, not knowing what the future may bring regarding life itself can lead to PTSD. I have treated patients who have lost jobs and experienced devastating social and financial losses, which were perceived as a separation from “life as they know it.” These can be precursors to PTSD for some who are sensitive to the disorder.
Intergenerational trauma is also a real phenomenon to which we must be attuned. I have treated two adult children of Holocaust survivors, both born in America well after World War II, who developed PTSD after hearing family recollections over and over about the brutality suffered by relatives, combined with watching films about people sent to concentration camps. Both of those patients self-diagnosed their symptoms as depression. Research shows that Holocaust traumatization can affect three generations (J Anxiety Disord. 2021 Jun. doi: 10.1016/j.janxdis.2021.102401).
In light of the high incidence of traumatic events affecting millions directly, more codified treatment approaches are needed that can be used both for individuals and for those in group settings.
To date, the best treatment rests with cognitive-behavioral therapy (CBT) and guided imagery coupled with relaxation techniques and the various types of in vivo exposure therapy, which I prefer to in vitro or flooding care. In terms of medication management, the U.S. Food and Drug Administration has approved only two antidepressant medications for PTSD, sertraline (Zoloft) and paroxetine (Paxil), although other selective serotonin reuptake inhibitors have been used off- label, and prazosin, a hypertensive medication, has been used off-label for PTSD-related insomnia and nightmares (Prim Care Companion CNS Disord. 2012 Mar 22. doi: 10.4088/PCC.11r01222). Thus, the limited number of choices for medication management means more research is needed so that more medications are developed that are more precisely directed at PTSD treatment.
Implications for society at large
In a recent article published in the Journal of Clinical Psychiatry (2022 Apr 25. doi: 10.4088/JCP.21m14116), authors Lori L. Davis and colleagues point out that the economic burden of PTSD goes beyond health care costs and rivals the costs of other mental illnesses, including depression and anxiety. In the process, Dr. Davis and colleagues note, unemployment caused by job loss, disability, homelessness, substance use, disordered care, as well as premature mortality, all contribute to this severe burden, going beyond PTSD itself.
This study shows that the annual economic burden of PTSD is $232 billion. Most of that burden is attributed to the civilian population, which they suggest to be $189.5 billion, or 82%.
After reading that article, it became clear to me that my “obsession” with PTSD is not really an obsession at all. Rather, it is a true concern that, against the backdrop of long COVID, gun violence, political and economic turmoil, and other factors, it is important that clinicians understand how to recognize and treat PTSD. The stakes have never been higher.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
A few weeks ago, right after 19 children and two adults were killed by a gunman in Uvalde, Texas, Americans were really on edge. Many people I know became hypervigilant while going about activities previously thought of as routine, such as waiting for a subway or going to a grocery store.
On top of that, we are still facing the ongoing COVID-19 pandemic. Despite vaccines and therapeutics, the United States is still losing more than 300 people each day to the virus. Many people who have tested positive have continued to experience debilitating long-haul symptoms many months after testing negative, and I believe not knowing what your future life will bring from this terrible illness could lead some to posttraumatic stress disorder.
In addition to constant updates about COVID, we are getting almost daily reports about monkeypox. In New York state, medical professionals and institutions receive regular, almost weekly, information about the spread of influenza. But where are the reports and treatment approaches for PTSD, which would not only increase awareness but also lead to more care?
Some might believe that I am obsessed with PTSD, since I’ve written a great deal on the subject, particularly “underdiagnosed” PTSD. The key question I have is:
We know the signs and symptoms of PTSD. They include flashbacks, intrusive recollections, physical distress related to stimuli related to the trauma, insomnia, social isolation, avoidance of certain situations, negative thinking, and hyperarousal – coupled with anxiety and depression. PTSD can be a great masquerader. It can be triggered by many events, large and small, and all too often will masquerade as general anxiety or existential despair and depression. Too often, PTSD is undiagnosed or unrecognized completely. PTSD is also a costly disease that is an enormous economic burden on the U.S. economy.
As clinicians, we must be aware of the more subtle events that may trigger PTSD. We must think beyond ICD codes and DSM criteria and realize that each individual processes an event or a series of events differently. For example, seriously ill people in ICUs or undergoing critical care have been known to experience PTSD well beyond their physical recovery (J Crit Care. 2017 Dec. doi: 10.1016/j.jcrc.2017.06.014). Years after the Sept. 11, 2001, World Trade Center disaster, many are still suffering from PTSD symptoms (Biol Psychiatry. 2020 May 1. doi: 10.1016/j.biopsych.2020.02.817).
Again, in some cases, not knowing what the future may bring regarding life itself can lead to PTSD. I have treated patients who have lost jobs and experienced devastating social and financial losses, which were perceived as a separation from “life as they know it.” These can be precursors to PTSD for some who are sensitive to the disorder.
Intergenerational trauma is also a real phenomenon to which we must be attuned. I have treated two adult children of Holocaust survivors, both born in America well after World War II, who developed PTSD after hearing family recollections over and over about the brutality suffered by relatives, combined with watching films about people sent to concentration camps. Both of those patients self-diagnosed their symptoms as depression. Research shows that Holocaust traumatization can affect three generations (J Anxiety Disord. 2021 Jun. doi: 10.1016/j.janxdis.2021.102401).
In light of the high incidence of traumatic events affecting millions directly, more codified treatment approaches are needed that can be used both for individuals and for those in group settings.
To date, the best treatment rests with cognitive-behavioral therapy (CBT) and guided imagery coupled with relaxation techniques and the various types of in vivo exposure therapy, which I prefer to in vitro or flooding care. In terms of medication management, the U.S. Food and Drug Administration has approved only two antidepressant medications for PTSD, sertraline (Zoloft) and paroxetine (Paxil), although other selective serotonin reuptake inhibitors have been used off- label, and prazosin, a hypertensive medication, has been used off-label for PTSD-related insomnia and nightmares (Prim Care Companion CNS Disord. 2012 Mar 22. doi: 10.4088/PCC.11r01222). Thus, the limited number of choices for medication management means more research is needed so that more medications are developed that are more precisely directed at PTSD treatment.
Implications for society at large
In a recent article published in the Journal of Clinical Psychiatry (2022 Apr 25. doi: 10.4088/JCP.21m14116), authors Lori L. Davis and colleagues point out that the economic burden of PTSD goes beyond health care costs and rivals the costs of other mental illnesses, including depression and anxiety. In the process, Dr. Davis and colleagues note, unemployment caused by job loss, disability, homelessness, substance use, disordered care, as well as premature mortality, all contribute to this severe burden, going beyond PTSD itself.
This study shows that the annual economic burden of PTSD is $232 billion. Most of that burden is attributed to the civilian population, which they suggest to be $189.5 billion, or 82%.
After reading that article, it became clear to me that my “obsession” with PTSD is not really an obsession at all. Rather, it is a true concern that, against the backdrop of long COVID, gun violence, political and economic turmoil, and other factors, it is important that clinicians understand how to recognize and treat PTSD. The stakes have never been higher.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
A few weeks ago, right after 19 children and two adults were killed by a gunman in Uvalde, Texas, Americans were really on edge. Many people I know became hypervigilant while going about activities previously thought of as routine, such as waiting for a subway or going to a grocery store.
On top of that, we are still facing the ongoing COVID-19 pandemic. Despite vaccines and therapeutics, the United States is still losing more than 300 people each day to the virus. Many people who have tested positive have continued to experience debilitating long-haul symptoms many months after testing negative, and I believe not knowing what your future life will bring from this terrible illness could lead some to posttraumatic stress disorder.
In addition to constant updates about COVID, we are getting almost daily reports about monkeypox. In New York state, medical professionals and institutions receive regular, almost weekly, information about the spread of influenza. But where are the reports and treatment approaches for PTSD, which would not only increase awareness but also lead to more care?
Some might believe that I am obsessed with PTSD, since I’ve written a great deal on the subject, particularly “underdiagnosed” PTSD. The key question I have is:
We know the signs and symptoms of PTSD. They include flashbacks, intrusive recollections, physical distress related to stimuli related to the trauma, insomnia, social isolation, avoidance of certain situations, negative thinking, and hyperarousal – coupled with anxiety and depression. PTSD can be a great masquerader. It can be triggered by many events, large and small, and all too often will masquerade as general anxiety or existential despair and depression. Too often, PTSD is undiagnosed or unrecognized completely. PTSD is also a costly disease that is an enormous economic burden on the U.S. economy.
As clinicians, we must be aware of the more subtle events that may trigger PTSD. We must think beyond ICD codes and DSM criteria and realize that each individual processes an event or a series of events differently. For example, seriously ill people in ICUs or undergoing critical care have been known to experience PTSD well beyond their physical recovery (J Crit Care. 2017 Dec. doi: 10.1016/j.jcrc.2017.06.014). Years after the Sept. 11, 2001, World Trade Center disaster, many are still suffering from PTSD symptoms (Biol Psychiatry. 2020 May 1. doi: 10.1016/j.biopsych.2020.02.817).
Again, in some cases, not knowing what the future may bring regarding life itself can lead to PTSD. I have treated patients who have lost jobs and experienced devastating social and financial losses, which were perceived as a separation from “life as they know it.” These can be precursors to PTSD for some who are sensitive to the disorder.
Intergenerational trauma is also a real phenomenon to which we must be attuned. I have treated two adult children of Holocaust survivors, both born in America well after World War II, who developed PTSD after hearing family recollections over and over about the brutality suffered by relatives, combined with watching films about people sent to concentration camps. Both of those patients self-diagnosed their symptoms as depression. Research shows that Holocaust traumatization can affect three generations (J Anxiety Disord. 2021 Jun. doi: 10.1016/j.janxdis.2021.102401).
In light of the high incidence of traumatic events affecting millions directly, more codified treatment approaches are needed that can be used both for individuals and for those in group settings.
To date, the best treatment rests with cognitive-behavioral therapy (CBT) and guided imagery coupled with relaxation techniques and the various types of in vivo exposure therapy, which I prefer to in vitro or flooding care. In terms of medication management, the U.S. Food and Drug Administration has approved only two antidepressant medications for PTSD, sertraline (Zoloft) and paroxetine (Paxil), although other selective serotonin reuptake inhibitors have been used off- label, and prazosin, a hypertensive medication, has been used off-label for PTSD-related insomnia and nightmares (Prim Care Companion CNS Disord. 2012 Mar 22. doi: 10.4088/PCC.11r01222). Thus, the limited number of choices for medication management means more research is needed so that more medications are developed that are more precisely directed at PTSD treatment.
Implications for society at large
In a recent article published in the Journal of Clinical Psychiatry (2022 Apr 25. doi: 10.4088/JCP.21m14116), authors Lori L. Davis and colleagues point out that the economic burden of PTSD goes beyond health care costs and rivals the costs of other mental illnesses, including depression and anxiety. In the process, Dr. Davis and colleagues note, unemployment caused by job loss, disability, homelessness, substance use, disordered care, as well as premature mortality, all contribute to this severe burden, going beyond PTSD itself.
This study shows that the annual economic burden of PTSD is $232 billion. Most of that burden is attributed to the civilian population, which they suggest to be $189.5 billion, or 82%.
After reading that article, it became clear to me that my “obsession” with PTSD is not really an obsession at all. Rather, it is a true concern that, against the backdrop of long COVID, gun violence, political and economic turmoil, and other factors, it is important that clinicians understand how to recognize and treat PTSD. The stakes have never been higher.
Dr. London is a practicing psychiatrist and has been a newspaper columnist for 35 years, specializing in and writing about short-term therapy, including cognitive-behavioral therapy and guided imagery. He is author of “Find Freedom Fast” (New York: Kettlehole Publishing, 2019). He has no conflicts of interest.
Depression screens do not reduce suicidal acts in teens: Study
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Screening adolescents for signs of depression does not reduce their emergency department visits, hospitalizations, or treatment for suicidal behaviors, according to research published in Preventive Medicine. Adolescents who underwent a depression screening were just as likely to need these services as those who did not.
In 2016, the U.S. Preventive Services Task Force recommended that adolescents aged 12-18 years be screened for major depressive disorder, provided that effective treatment options and follow-up strategies are in place.
“The main goal of depression screening is really to reduce adverse psychiatric outcomes. But I think a collateral hope is that, in reducing these adverse psychiatric outcomes, you would also reduce avoidable health services use,” such as ED visits or hospitalizations, said Kira Riehm, PhD, a postdoctoral fellow in epidemiology at Columbia University, New York, who led the research. Dr. Riehm designed the new study, which was part of her doctoral work at Johns Hopkins University, Baltimore, to test this premise.
Dr. Riehm and colleagues compared 14,433 adolescents aged 12-18 years who were screened for depression at least once during a wellness visit from 2014 to 2017 to 43,299 adolescents who were not screened for depression during such visits. Depression screenings were interspersed among a total of 281,463 adolescent wellness visits from 2014 to 2017, which represented 5% of all visits.
The researchers used diagnostic codes from a database of insurance claims to determine who had undergone depression screening. They then compared use of ED services, inpatient hospitalizations, and the number of treatments for suicidal behaviors between the two groups for the 2 years following the wellness visit.
The average age of the adolescents who underwent screening was 13-14 years, as was the average age of adolescents who were not screened. Both groups were evenly matched with respect to being male or female.
The researchers estimated that a high majority of adolescents in the sample were White (83%). Black persons represented 7% of the sample; Hispanic/Latino, 5%; and Asian, 3%. Insurance claims don’t always include racial and ethnicity data, Dr. Riehm said, so her group statistically imputed these proportions. The claims data also do not include details about which type of screening tool was used or the results of the screening, such as whether a teen exhibited mild or severe depression.
Adolescents in both groups were just as likely to go to the ED for any reason, be admitted to the hospital for any reason, or undergo treatment for suicidal behaviors. The researchers observed a slight association between being screened for depression and going to the ED specifically for a mental health reason (relative risk, 1.16; 95% confidence interval, 1.00-1.33). The sex of the adolescents had no bearing on whether they used these services.
“I think people think of [depression screening] as one event. But in reality, screening is a series of different events that all have to be happening in order for a screening program to work,” Dr. Riehm told this news organization.
These events could include ensuring that adolescents who exhibit signs of depression receive a proper assessment, receive medications if needed, and have access to psychotherapists who can help them. Without these supports in place, she said, a one-off depression screening may have limited benefit.
“There’s a lot of places where people could drop out of that care continuum,” Dr. Riehm said.
“One-time screening may not be enough,” said Trân Đoàn, PhD, MPH, a postdoctoral researcher in the University of Pittsburgh department of pediatrics.
Dr. Đoàn, who was not involved in the research, noted that the American Academy of Pediatrics recommends annual screening of all adolescents for depressive symptoms. Given that only 5% of the visits in this sample included any kind of depression screening, Dr. Đoàn said, some pediatric practices may not have felt they had the resources to adequately address positive screenings for depression.
Both Dr. Riehm and Dr. Đoàn are focusing on the link between depression screening and health outcomes. In her own doctoral work at the University of Michigan, Dr. Đoàn modeled the effects of universal annual depression screening in primary care settings on the health status of people aged 12-22 years. She is currently preparing this work for publication.
“I did find that, over the long term, there is improvement in health outcomes if we were to screen on an annual basis,” provided improved screening is coupled with comprehensive treatment plans, Dr. Đoàn said. The model’s health outcomes measures included an increase in life expectancy as well as a greater proportion of depression-free days among adolescents who receive appropriate treatment.
Dr. Riehm and Dr. Đoàn disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PREVENTIVE MEDICINE
Sleep-deprived physicians less empathetic to patient pain?
new research suggests.
In the first of two studies, resident physicians were presented with two hypothetical scenarios involving a patient who complains of pain. They were asked about their likelihood of prescribing pain medication. The test was given to one group of residents who were just starting their day and to another group who were at the end of their night shift after being on call for 26 hours.
Results showed that the night shift residents were less likely than their daytime counterparts to say they would prescribe pain medication to the patients.
In further analysis of discharge notes from more than 13,000 electronic records of patients presenting with pain complaints at hospitals in Israel and the United States, the likelihood of an analgesic being prescribed during the night shift was 11% lower in Israel and 9% lower in the United States, compared with the day shift.
“Pain management is a major challenge, and a doctor’s perception of a patient’s subjective pain is susceptible to bias,” coinvestigator David Gozal, MD, the Marie M. and Harry L. Smith Endowed Chair of Child Health, University of Missouri–Columbia, said in a press release.
“This study demonstrated that night shift work is an important and previously unrecognized source of bias in pain management, likely stemming from impaired perception of pain,” Dr. Gozal added.
The findings were published online in the Proceedings of the National Academy of Sciences.
‘Directional’ differences
Senior investigator Alex Gileles-Hillel, MD, senior pediatric pulmonologist and sleep researcher at Hadassah University Medical Center, Jerusalem, said in an interview that physicians must make “complex assessments of patients’ subjective pain experience” – and the “subjective nature of pain management decisions can give rise to various biases.”
Dr. Gileles-Hillel has previously researched the cognitive toll of night shift work on physicians.
“It’s pretty established, for example, not to drive when sleep deprived because cognition is impaired,” he said. The current study explored whether sleep deprivation could affect areas other than cognition, including emotions and empathy.
The researchers used “two complementary approaches.” First, they administered tests to measure empathy and pain management decisions in 67 resident physicians at Hadassah Medical Centers either following a 26-hour night shift that began at 8:00 a.m. the day before (n = 36) or immediately before starting the workday (n = 31).
There were no significant differences in demographic, sleep, or burnout measures between the two groups, except that night shift physicians had slept less than those in the daytime group (2.93 vs. 5.96 hours).
Participants completed two tasks. In the empathy-for-pain task, they rated their emotional reactions to pictures of individuals in pain. In the empathy accuracy task, they were asked to assess the feelings of videotaped individuals telling emotional stories.
They were then presented with two clinical scenarios: a female patient with a headache and a male patient with a backache. Following that, they were asked to assess the magnitude of the patients’ pain and how likely they would be to prescribe pain medication.
In the empathy-for-pain task, physicians’ empathy scores were significantly lower in the night shift group than in the day group (difference, –0.83; 95% CI, –1.55 to –0.10; P = .026). There were no significant differences between the groups in the empathy accuracy task.
In both scenarios, physicians in the night shift group assessed the patient’s pain as weaker in comparison with physicians in the day group. There was a statistically significant difference in the headache scenario but not the backache scenario.
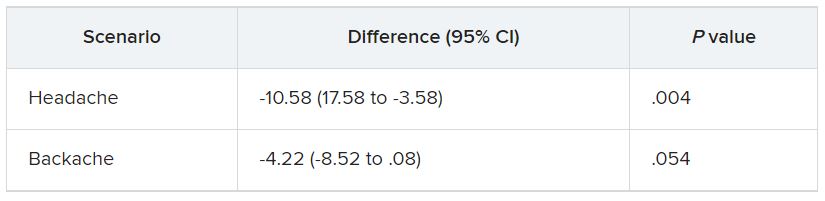
In the headache scenario, the propensity of the physicians to prescribe analgesics was “directionally lower” but did not reach statistical significance. In the backache scenario, there was no significant difference between the groups’ prescribing propensities.
In both scenarios, pain assessment was positively correlated with the propensity to prescribe analgesics.
Despite the lack of statistical significance, the findings “documented a negative effect of night shift work on physician empathy for pain and a positive association between physician assessment of patient pain and the propensity to prescribe analgesics,” the investigators wrote.
Need for naps?
The researchers then analyzed analgesic prescription patterns drawn from three datasets of discharge notes of patients presenting to the emergency department with pain complaints (n = 13,482) at two branches of Hadassah-Hebrew University Medical Center and the University of Missouri Health Center.
The researchers collected data, including discharge time, medications patients were prescribed upon discharge, and patients’ subjective pain rating on a scale of 0-10 on a visual analogue scale (VAS).
Although patients’ VAS scores did not differ with respect to time or shift, patients were discharged with significantly less prescribed analgesics during the night shift in comparison with the day shift.
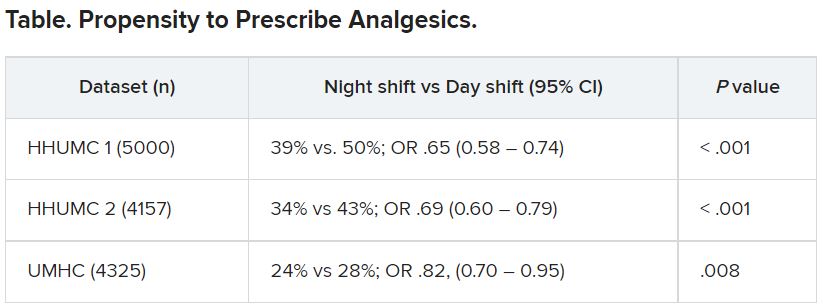
No similar differences in prescriptions between night shifts and day shifts were found for nonanalgesic medications, such as for diabetes or blood pressure. This suggests “the effect was specific to pain,” Dr. Gileles-Hillel said.
The pattern remained significant after controlling for potential confounders, including patient and physician variables and emergency department characteristics.
In addition, patients seen during night shifts received fewer analgesics, particularly opioids, than recommended by the World Health Organization for pain management.
“The first study enabled us to measure empathy for pain directly and examine our hypothesis in a controlled environment, while the second enabled us to test the implications by examining real-life pain management decisions,” Dr. Gileles-Hillel said.
“Physicians need to be aware of this,” he noted. “I try to be aware when I’m taking calls [at night] that I’m less empathetic to others and I might be more brief or angry with others.”
On a “house management level, perhaps institutions should try to schedule naps either before or during overnight call. A nap might give a boost and reboot not only to cognitive but also to emotional resources,” Dr. Gileles-Hillel added.
Compromised safety
In a comment, Eti Ben Simon, PhD, a postdoctoral fellow at the Center for Human Sleep Science, University of California, Berkeley, called the study “an important contribution to a growing list of studies that reveal how long night shifts reduce overall safety” for both patients and clinicians.
“It’s time to abandon the notion that the human brain can function as normal after being deprived of sleep for 24 hours,” said Dr. Ben Simon, who was not involved with the research.
“This is especially true in medicine, where we trust others to take care of us and feel our pain. These functions are simply not possible without adequate sleep,” she added.
Also commenting, Kannan Ramar, MD, president of the American Academy of Sleep Medicine, suggested that being cognizant of these findings “may help providers to mitigate this bias” of underprescribing pain medications when treating their patients.
Dr. Ramar, who is also a critical care specialist, pulmonologist, and sleep medicine specialist at Mayo Clinic, Rochester, Minn., was not involved with the research.
He noted that “further studies that systematically evaluate this further in a prospective and blinded way will be important.”
The research was supported in part by grants from the Israel Science Foundation, Joy Ventures, the Recanati Fund at the Jerusalem School of Business at the Hebrew University, and a fellowship from the Azrieli Foundation and received grant support to various investigators from the NIH, the Leda J. Sears Foundation, and the University of Missouri. The investigators, Ramar, and Ben Simon have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
In the first of two studies, resident physicians were presented with two hypothetical scenarios involving a patient who complains of pain. They were asked about their likelihood of prescribing pain medication. The test was given to one group of residents who were just starting their day and to another group who were at the end of their night shift after being on call for 26 hours.
Results showed that the night shift residents were less likely than their daytime counterparts to say they would prescribe pain medication to the patients.
In further analysis of discharge notes from more than 13,000 electronic records of patients presenting with pain complaints at hospitals in Israel and the United States, the likelihood of an analgesic being prescribed during the night shift was 11% lower in Israel and 9% lower in the United States, compared with the day shift.
“Pain management is a major challenge, and a doctor’s perception of a patient’s subjective pain is susceptible to bias,” coinvestigator David Gozal, MD, the Marie M. and Harry L. Smith Endowed Chair of Child Health, University of Missouri–Columbia, said in a press release.
“This study demonstrated that night shift work is an important and previously unrecognized source of bias in pain management, likely stemming from impaired perception of pain,” Dr. Gozal added.
The findings were published online in the Proceedings of the National Academy of Sciences.
‘Directional’ differences
Senior investigator Alex Gileles-Hillel, MD, senior pediatric pulmonologist and sleep researcher at Hadassah University Medical Center, Jerusalem, said in an interview that physicians must make “complex assessments of patients’ subjective pain experience” – and the “subjective nature of pain management decisions can give rise to various biases.”
Dr. Gileles-Hillel has previously researched the cognitive toll of night shift work on physicians.
“It’s pretty established, for example, not to drive when sleep deprived because cognition is impaired,” he said. The current study explored whether sleep deprivation could affect areas other than cognition, including emotions and empathy.
The researchers used “two complementary approaches.” First, they administered tests to measure empathy and pain management decisions in 67 resident physicians at Hadassah Medical Centers either following a 26-hour night shift that began at 8:00 a.m. the day before (n = 36) or immediately before starting the workday (n = 31).
There were no significant differences in demographic, sleep, or burnout measures between the two groups, except that night shift physicians had slept less than those in the daytime group (2.93 vs. 5.96 hours).
Participants completed two tasks. In the empathy-for-pain task, they rated their emotional reactions to pictures of individuals in pain. In the empathy accuracy task, they were asked to assess the feelings of videotaped individuals telling emotional stories.
They were then presented with two clinical scenarios: a female patient with a headache and a male patient with a backache. Following that, they were asked to assess the magnitude of the patients’ pain and how likely they would be to prescribe pain medication.
In the empathy-for-pain task, physicians’ empathy scores were significantly lower in the night shift group than in the day group (difference, –0.83; 95% CI, –1.55 to –0.10; P = .026). There were no significant differences between the groups in the empathy accuracy task.
In both scenarios, physicians in the night shift group assessed the patient’s pain as weaker in comparison with physicians in the day group. There was a statistically significant difference in the headache scenario but not the backache scenario.
In the headache scenario, the propensity of the physicians to prescribe analgesics was “directionally lower” but did not reach statistical significance. In the backache scenario, there was no significant difference between the groups’ prescribing propensities.
In both scenarios, pain assessment was positively correlated with the propensity to prescribe analgesics.
Despite the lack of statistical significance, the findings “documented a negative effect of night shift work on physician empathy for pain and a positive association between physician assessment of patient pain and the propensity to prescribe analgesics,” the investigators wrote.
Need for naps?
The researchers then analyzed analgesic prescription patterns drawn from three datasets of discharge notes of patients presenting to the emergency department with pain complaints (n = 13,482) at two branches of Hadassah-Hebrew University Medical Center and the University of Missouri Health Center.
The researchers collected data, including discharge time, medications patients were prescribed upon discharge, and patients’ subjective pain rating on a scale of 0-10 on a visual analogue scale (VAS).
Although patients’ VAS scores did not differ with respect to time or shift, patients were discharged with significantly less prescribed analgesics during the night shift in comparison with the day shift.
No similar differences in prescriptions between night shifts and day shifts were found for nonanalgesic medications, such as for diabetes or blood pressure. This suggests “the effect was specific to pain,” Dr. Gileles-Hillel said.
The pattern remained significant after controlling for potential confounders, including patient and physician variables and emergency department characteristics.
In addition, patients seen during night shifts received fewer analgesics, particularly opioids, than recommended by the World Health Organization for pain management.
“The first study enabled us to measure empathy for pain directly and examine our hypothesis in a controlled environment, while the second enabled us to test the implications by examining real-life pain management decisions,” Dr. Gileles-Hillel said.
“Physicians need to be aware of this,” he noted. “I try to be aware when I’m taking calls [at night] that I’m less empathetic to others and I might be more brief or angry with others.”
On a “house management level, perhaps institutions should try to schedule naps either before or during overnight call. A nap might give a boost and reboot not only to cognitive but also to emotional resources,” Dr. Gileles-Hillel added.
Compromised safety
In a comment, Eti Ben Simon, PhD, a postdoctoral fellow at the Center for Human Sleep Science, University of California, Berkeley, called the study “an important contribution to a growing list of studies that reveal how long night shifts reduce overall safety” for both patients and clinicians.
“It’s time to abandon the notion that the human brain can function as normal after being deprived of sleep for 24 hours,” said Dr. Ben Simon, who was not involved with the research.
“This is especially true in medicine, where we trust others to take care of us and feel our pain. These functions are simply not possible without adequate sleep,” she added.
Also commenting, Kannan Ramar, MD, president of the American Academy of Sleep Medicine, suggested that being cognizant of these findings “may help providers to mitigate this bias” of underprescribing pain medications when treating their patients.
Dr. Ramar, who is also a critical care specialist, pulmonologist, and sleep medicine specialist at Mayo Clinic, Rochester, Minn., was not involved with the research.
He noted that “further studies that systematically evaluate this further in a prospective and blinded way will be important.”
The research was supported in part by grants from the Israel Science Foundation, Joy Ventures, the Recanati Fund at the Jerusalem School of Business at the Hebrew University, and a fellowship from the Azrieli Foundation and received grant support to various investigators from the NIH, the Leda J. Sears Foundation, and the University of Missouri. The investigators, Ramar, and Ben Simon have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
new research suggests.
In the first of two studies, resident physicians were presented with two hypothetical scenarios involving a patient who complains of pain. They were asked about their likelihood of prescribing pain medication. The test was given to one group of residents who were just starting their day and to another group who were at the end of their night shift after being on call for 26 hours.
Results showed that the night shift residents were less likely than their daytime counterparts to say they would prescribe pain medication to the patients.
In further analysis of discharge notes from more than 13,000 electronic records of patients presenting with pain complaints at hospitals in Israel and the United States, the likelihood of an analgesic being prescribed during the night shift was 11% lower in Israel and 9% lower in the United States, compared with the day shift.
“Pain management is a major challenge, and a doctor’s perception of a patient’s subjective pain is susceptible to bias,” coinvestigator David Gozal, MD, the Marie M. and Harry L. Smith Endowed Chair of Child Health, University of Missouri–Columbia, said in a press release.
“This study demonstrated that night shift work is an important and previously unrecognized source of bias in pain management, likely stemming from impaired perception of pain,” Dr. Gozal added.
The findings were published online in the Proceedings of the National Academy of Sciences.
‘Directional’ differences
Senior investigator Alex Gileles-Hillel, MD, senior pediatric pulmonologist and sleep researcher at Hadassah University Medical Center, Jerusalem, said in an interview that physicians must make “complex assessments of patients’ subjective pain experience” – and the “subjective nature of pain management decisions can give rise to various biases.”
Dr. Gileles-Hillel has previously researched the cognitive toll of night shift work on physicians.
“It’s pretty established, for example, not to drive when sleep deprived because cognition is impaired,” he said. The current study explored whether sleep deprivation could affect areas other than cognition, including emotions and empathy.
The researchers used “two complementary approaches.” First, they administered tests to measure empathy and pain management decisions in 67 resident physicians at Hadassah Medical Centers either following a 26-hour night shift that began at 8:00 a.m. the day before (n = 36) or immediately before starting the workday (n = 31).
There were no significant differences in demographic, sleep, or burnout measures between the two groups, except that night shift physicians had slept less than those in the daytime group (2.93 vs. 5.96 hours).
Participants completed two tasks. In the empathy-for-pain task, they rated their emotional reactions to pictures of individuals in pain. In the empathy accuracy task, they were asked to assess the feelings of videotaped individuals telling emotional stories.
They were then presented with two clinical scenarios: a female patient with a headache and a male patient with a backache. Following that, they were asked to assess the magnitude of the patients’ pain and how likely they would be to prescribe pain medication.
In the empathy-for-pain task, physicians’ empathy scores were significantly lower in the night shift group than in the day group (difference, –0.83; 95% CI, –1.55 to –0.10; P = .026). There were no significant differences between the groups in the empathy accuracy task.
In both scenarios, physicians in the night shift group assessed the patient’s pain as weaker in comparison with physicians in the day group. There was a statistically significant difference in the headache scenario but not the backache scenario.
In the headache scenario, the propensity of the physicians to prescribe analgesics was “directionally lower” but did not reach statistical significance. In the backache scenario, there was no significant difference between the groups’ prescribing propensities.
In both scenarios, pain assessment was positively correlated with the propensity to prescribe analgesics.
Despite the lack of statistical significance, the findings “documented a negative effect of night shift work on physician empathy for pain and a positive association between physician assessment of patient pain and the propensity to prescribe analgesics,” the investigators wrote.
Need for naps?
The researchers then analyzed analgesic prescription patterns drawn from three datasets of discharge notes of patients presenting to the emergency department with pain complaints (n = 13,482) at two branches of Hadassah-Hebrew University Medical Center and the University of Missouri Health Center.
The researchers collected data, including discharge time, medications patients were prescribed upon discharge, and patients’ subjective pain rating on a scale of 0-10 on a visual analogue scale (VAS).
Although patients’ VAS scores did not differ with respect to time or shift, patients were discharged with significantly less prescribed analgesics during the night shift in comparison with the day shift.
No similar differences in prescriptions between night shifts and day shifts were found for nonanalgesic medications, such as for diabetes or blood pressure. This suggests “the effect was specific to pain,” Dr. Gileles-Hillel said.
The pattern remained significant after controlling for potential confounders, including patient and physician variables and emergency department characteristics.
In addition, patients seen during night shifts received fewer analgesics, particularly opioids, than recommended by the World Health Organization for pain management.
“The first study enabled us to measure empathy for pain directly and examine our hypothesis in a controlled environment, while the second enabled us to test the implications by examining real-life pain management decisions,” Dr. Gileles-Hillel said.
“Physicians need to be aware of this,” he noted. “I try to be aware when I’m taking calls [at night] that I’m less empathetic to others and I might be more brief or angry with others.”
On a “house management level, perhaps institutions should try to schedule naps either before or during overnight call. A nap might give a boost and reboot not only to cognitive but also to emotional resources,” Dr. Gileles-Hillel added.
Compromised safety
In a comment, Eti Ben Simon, PhD, a postdoctoral fellow at the Center for Human Sleep Science, University of California, Berkeley, called the study “an important contribution to a growing list of studies that reveal how long night shifts reduce overall safety” for both patients and clinicians.
“It’s time to abandon the notion that the human brain can function as normal after being deprived of sleep for 24 hours,” said Dr. Ben Simon, who was not involved with the research.
“This is especially true in medicine, where we trust others to take care of us and feel our pain. These functions are simply not possible without adequate sleep,” she added.
Also commenting, Kannan Ramar, MD, president of the American Academy of Sleep Medicine, suggested that being cognizant of these findings “may help providers to mitigate this bias” of underprescribing pain medications when treating their patients.
Dr. Ramar, who is also a critical care specialist, pulmonologist, and sleep medicine specialist at Mayo Clinic, Rochester, Minn., was not involved with the research.
He noted that “further studies that systematically evaluate this further in a prospective and blinded way will be important.”
The research was supported in part by grants from the Israel Science Foundation, Joy Ventures, the Recanati Fund at the Jerusalem School of Business at the Hebrew University, and a fellowship from the Azrieli Foundation and received grant support to various investigators from the NIH, the Leda J. Sears Foundation, and the University of Missouri. The investigators, Ramar, and Ben Simon have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCES
Docs reveal perils of giving medical advice to friends and family
Stephen Pribut, DPM, a sports medicine podiatrist based in Washington, has had many friends or family members ask him for medical advice. It’s a scenario every doctor will face at one point or another in their careers, and it’s never an easy one.
Dr. Pribut received a call from a friend about a sore shoulder from swimming, saying that his doctor had dismissed the potential for a rotator cuff injury. “Months later, images revealed it was a rotator cuff tear and he wanted my advice,” says Dr. Pribut.
Not being a shoulder specialist, Dr. Pribut limited his input. “I told him to consider a good physical therapist or a shoulder specialist and gave him some alternative strokes for swimming that hopefully wouldn’t aggravate the injury,” he explains.
But he admits some situations are challenging. “I had a relative asking about a third party with an ankle injury. I advised he hold off on using a balance board until things healed, and to make sure he went to see a specialist. Unfortunately, he went to his general practitioner who likely knows nothing about ankle anatomy,” says Dr. Pribut.
“I finally saw a photo, which revealed swelling higher up on the ankle and no evidence of a hematoma – much lower than we would see in an ankle ligament injury. I would like him to see a sports podiatrist or foot and ankle orthopedist, but now I have to stay calm when the advice isn’t followed,” he says.
When asked, “Do you give medical advice to your friends?” 96% of respondents answered yes.
Yazan Abou-Ismail, MD, assistant professor of medicine in the division of hematology at the University of Utah, Salt Lake City, has often faced questions from friends and family, particularly throughout the COVID-19 pandemic. “How you respond is something all physicians need to analyze carefully,” he says. “I get questions on a regular basis, but this greatly increased with COVID.”
“Sharing general information is okay, and it’s even a requirement that we educate on such topics,” says Dr. Abou-Ismail. “But if someone knows they have COVID, for instance, and wants advice on how to proceed, it’s important to send them to their primary care physician for an evaluation rather than give them instructions on care.”
Dr. Abou-Ismail says that most “curbside consulting” equates to lack of an ethical follow-up. “If you gave medical advice without having assessed them, you’re lacking the medical history, a physical exam, and you should not be giving advice,” he says. “This applies to follow-ups, too.”
Throughout the pandemic, Dr. Abou-Ismail’s requests for advice on COVID even extended to online inquiries, often from strangers. “This is not a place to do a formal assessment,” he reminds. “But there are certain types of advice you can offer appropriately.”
Dr. Abou-Ismail considers safe advice to be simple public health messages that stay far out of specifics. Things like “don’t smoke,” or “eat a healthy diet,” and “get enough sleep,” fall into this safety zone. Even, “What is XYZ disease?” or “How do COVID vaccines work?” are topics he says he answers comfortably.
“But telling someone you need a specific treatment for a condition is inappropriate,” he explains. “This is a general way of practicing medicine – your advice should never venture into the potential of doing harm.”
This approach is exactly in line with legal advice, according to Jeff Caesar Chukwuma, founder and senior partner at Chukwuma Law Group, Miami. “It doesn’t mean that doctors should never give medical advice to friends or family, but if they do, they should make sure to take several precautions to protect both themselves and their family and friends,” he says.
When the request for medical advice from an acquaintance migrates into areas in which a physician is not a specialist, sharing recommendations gets even trickier – and more ethically questionable.
Says Mr. Chukwuma, “Doctors should avoid giving advice in areas outside their area of expertise to lower the possibility of providing erroneous or harmful information,” he says.
How to stay safe when asked for advice
The American Medical Association has weighed in on the topic. In the Code of Medical Ethics Opinion 1.2.1, the AMA states that, “Treating oneself or a member of one’s own family poses several challenges for physicians, including concerns about professional objectivity, patient autonomy, and informed consent.”
What about friends or acquaintances, however?
Even so, some respondents voiced their concerns with the scenario. Responses like, “Due to ethics, I would prefer they go and get first, second, and third opinions,” and “Usually the medical advice is very basic first aid (often mental health first aid), and if it’s anything remotely more complicated, I direct them to the appropriate provider.”
The AMA places advising friends in the same basket as advising and treating family members or oneself. In an article appearing in the AMA Journal of Ethics, Horacio Hojman, MD, of Tufts University School of Medicine, Boston, weighed in: “First and foremost, patients deserve objectivity from their doctors. When a physician is emotionally involved with a patient, that physician’s objectivity can be called into question.”
Why is medical advice so thorny when dealing with friends or relatives?
In some cases, a physician might not ask a friend relevant personal questions about his or her medical history, for instance. Or the friend might not want to share details with the doctor. In either case, the lack of information exchange can lead to improper advice.
The issue of giving medical advice to friends, family, and acquaintances can also wade into legal territory. “Personally or professionally, trust is the decisive factor that puts us at ease with the people we surround ourselves with,” says Mr. Chukwuma. “Nowhere is this truer than in medicine, where we approach doctors with some of the most sensitive matters in our lives and entrust our care to them, especially when the physician in question is a close friend or family member.”
Mr. Chukwuma points out that, while there are few strict legal prohibitions against doctors providing care or advice to family and friends, the AMA’s code of ethics states that such action should be reserved for rare situations, such as emergency settings or isolated settings where there is no other qualified physician available, or for minor, not long-term problems.
This was part of the equation for Dr. Pribut when helping his mother navigate her treatment for breast cancer. “With close relatives, offering advice and help can be very hard,” he says.
“This is to protect both patients and doctors,” says Mr. Chukwuma. “Although seeking advice from a family member or friend who is a doctor may be more convenient for a patient, they run the risk of receiving inadequate care by not going in for a formal medical visit complete with tests, medical examination, and follow-up care.”
Mr. Chukwuma offers guidance on how to share medical advice ethically and legally with family, friends, and acquaintances. “First, as much as possible, speak to general medical facts and knowledge rather than comment directly on the patient’s particular situation,” he says. “In the absence of thorough examination and tests, the doctor’s knowledge of a patient’s condition is limited, therefore, you should take care not to provide seemingly definitive answers on that patient’s unique condition in situations where they can’t rely on data to back up their advice and recommendations.”
The AMA’s Journal of Ethics article shares these tips for staying on the right side of the ethical line when dealing with friends and family members:
- Politely decline.
- Offer other forms of assistance – this might help a friend find the right qualified physician – as Dr. Pribut tends to do. Maybe help in navigating the sometimes-confusing health care system.
- Don’t hesitate in an emergency – the old “is there a doctor on board,” scenario on a plane when someone is in distress is a perfectly acceptable, and recommended, time to step in, even if it is a friend or family member.
Dr. Pribut, a long-time veteran of the tricky medical waters involving friends and family, has this to offer: “Be cautious and always stay in the realm of what you know,” he says. “Always encourage people to seek an opinion from a qualified doctor. Help them find a reputable doctor if that’s useful.”
Mr. Chukwuma adds also that doctors should stand firm when pushed by a friend or family member, especially when offering advice, even if it’s in the form of general education. “The doctor should make it clear to the family member or friend that their advice in no way takes the place of actual treatment or examination by a medical professional and that, if need be, the patient should seek formal medical help from another doctor, ideally one not related to or friends with the patient,” he says.
A version of this article first appeared on Medscape.com.
Stephen Pribut, DPM, a sports medicine podiatrist based in Washington, has had many friends or family members ask him for medical advice. It’s a scenario every doctor will face at one point or another in their careers, and it’s never an easy one.
Dr. Pribut received a call from a friend about a sore shoulder from swimming, saying that his doctor had dismissed the potential for a rotator cuff injury. “Months later, images revealed it was a rotator cuff tear and he wanted my advice,” says Dr. Pribut.
Not being a shoulder specialist, Dr. Pribut limited his input. “I told him to consider a good physical therapist or a shoulder specialist and gave him some alternative strokes for swimming that hopefully wouldn’t aggravate the injury,” he explains.
But he admits some situations are challenging. “I had a relative asking about a third party with an ankle injury. I advised he hold off on using a balance board until things healed, and to make sure he went to see a specialist. Unfortunately, he went to his general practitioner who likely knows nothing about ankle anatomy,” says Dr. Pribut.
“I finally saw a photo, which revealed swelling higher up on the ankle and no evidence of a hematoma – much lower than we would see in an ankle ligament injury. I would like him to see a sports podiatrist or foot and ankle orthopedist, but now I have to stay calm when the advice isn’t followed,” he says.
When asked, “Do you give medical advice to your friends?” 96% of respondents answered yes.
Yazan Abou-Ismail, MD, assistant professor of medicine in the division of hematology at the University of Utah, Salt Lake City, has often faced questions from friends and family, particularly throughout the COVID-19 pandemic. “How you respond is something all physicians need to analyze carefully,” he says. “I get questions on a regular basis, but this greatly increased with COVID.”
“Sharing general information is okay, and it’s even a requirement that we educate on such topics,” says Dr. Abou-Ismail. “But if someone knows they have COVID, for instance, and wants advice on how to proceed, it’s important to send them to their primary care physician for an evaluation rather than give them instructions on care.”
Dr. Abou-Ismail says that most “curbside consulting” equates to lack of an ethical follow-up. “If you gave medical advice without having assessed them, you’re lacking the medical history, a physical exam, and you should not be giving advice,” he says. “This applies to follow-ups, too.”
Throughout the pandemic, Dr. Abou-Ismail’s requests for advice on COVID even extended to online inquiries, often from strangers. “This is not a place to do a formal assessment,” he reminds. “But there are certain types of advice you can offer appropriately.”
Dr. Abou-Ismail considers safe advice to be simple public health messages that stay far out of specifics. Things like “don’t smoke,” or “eat a healthy diet,” and “get enough sleep,” fall into this safety zone. Even, “What is XYZ disease?” or “How do COVID vaccines work?” are topics he says he answers comfortably.
“But telling someone you need a specific treatment for a condition is inappropriate,” he explains. “This is a general way of practicing medicine – your advice should never venture into the potential of doing harm.”
This approach is exactly in line with legal advice, according to Jeff Caesar Chukwuma, founder and senior partner at Chukwuma Law Group, Miami. “It doesn’t mean that doctors should never give medical advice to friends or family, but if they do, they should make sure to take several precautions to protect both themselves and their family and friends,” he says.
When the request for medical advice from an acquaintance migrates into areas in which a physician is not a specialist, sharing recommendations gets even trickier – and more ethically questionable.
Says Mr. Chukwuma, “Doctors should avoid giving advice in areas outside their area of expertise to lower the possibility of providing erroneous or harmful information,” he says.
How to stay safe when asked for advice
The American Medical Association has weighed in on the topic. In the Code of Medical Ethics Opinion 1.2.1, the AMA states that, “Treating oneself or a member of one’s own family poses several challenges for physicians, including concerns about professional objectivity, patient autonomy, and informed consent.”
What about friends or acquaintances, however?
Even so, some respondents voiced their concerns with the scenario. Responses like, “Due to ethics, I would prefer they go and get first, second, and third opinions,” and “Usually the medical advice is very basic first aid (often mental health first aid), and if it’s anything remotely more complicated, I direct them to the appropriate provider.”
The AMA places advising friends in the same basket as advising and treating family members or oneself. In an article appearing in the AMA Journal of Ethics, Horacio Hojman, MD, of Tufts University School of Medicine, Boston, weighed in: “First and foremost, patients deserve objectivity from their doctors. When a physician is emotionally involved with a patient, that physician’s objectivity can be called into question.”
Why is medical advice so thorny when dealing with friends or relatives?
In some cases, a physician might not ask a friend relevant personal questions about his or her medical history, for instance. Or the friend might not want to share details with the doctor. In either case, the lack of information exchange can lead to improper advice.
The issue of giving medical advice to friends, family, and acquaintances can also wade into legal territory. “Personally or professionally, trust is the decisive factor that puts us at ease with the people we surround ourselves with,” says Mr. Chukwuma. “Nowhere is this truer than in medicine, where we approach doctors with some of the most sensitive matters in our lives and entrust our care to them, especially when the physician in question is a close friend or family member.”
Mr. Chukwuma points out that, while there are few strict legal prohibitions against doctors providing care or advice to family and friends, the AMA’s code of ethics states that such action should be reserved for rare situations, such as emergency settings or isolated settings where there is no other qualified physician available, or for minor, not long-term problems.
This was part of the equation for Dr. Pribut when helping his mother navigate her treatment for breast cancer. “With close relatives, offering advice and help can be very hard,” he says.
“This is to protect both patients and doctors,” says Mr. Chukwuma. “Although seeking advice from a family member or friend who is a doctor may be more convenient for a patient, they run the risk of receiving inadequate care by not going in for a formal medical visit complete with tests, medical examination, and follow-up care.”
Mr. Chukwuma offers guidance on how to share medical advice ethically and legally with family, friends, and acquaintances. “First, as much as possible, speak to general medical facts and knowledge rather than comment directly on the patient’s particular situation,” he says. “In the absence of thorough examination and tests, the doctor’s knowledge of a patient’s condition is limited, therefore, you should take care not to provide seemingly definitive answers on that patient’s unique condition in situations where they can’t rely on data to back up their advice and recommendations.”
The AMA’s Journal of Ethics article shares these tips for staying on the right side of the ethical line when dealing with friends and family members:
- Politely decline.
- Offer other forms of assistance – this might help a friend find the right qualified physician – as Dr. Pribut tends to do. Maybe help in navigating the sometimes-confusing health care system.
- Don’t hesitate in an emergency – the old “is there a doctor on board,” scenario on a plane when someone is in distress is a perfectly acceptable, and recommended, time to step in, even if it is a friend or family member.
Dr. Pribut, a long-time veteran of the tricky medical waters involving friends and family, has this to offer: “Be cautious and always stay in the realm of what you know,” he says. “Always encourage people to seek an opinion from a qualified doctor. Help them find a reputable doctor if that’s useful.”
Mr. Chukwuma adds also that doctors should stand firm when pushed by a friend or family member, especially when offering advice, even if it’s in the form of general education. “The doctor should make it clear to the family member or friend that their advice in no way takes the place of actual treatment or examination by a medical professional and that, if need be, the patient should seek formal medical help from another doctor, ideally one not related to or friends with the patient,” he says.
A version of this article first appeared on Medscape.com.
Stephen Pribut, DPM, a sports medicine podiatrist based in Washington, has had many friends or family members ask him for medical advice. It’s a scenario every doctor will face at one point or another in their careers, and it’s never an easy one.
Dr. Pribut received a call from a friend about a sore shoulder from swimming, saying that his doctor had dismissed the potential for a rotator cuff injury. “Months later, images revealed it was a rotator cuff tear and he wanted my advice,” says Dr. Pribut.
Not being a shoulder specialist, Dr. Pribut limited his input. “I told him to consider a good physical therapist or a shoulder specialist and gave him some alternative strokes for swimming that hopefully wouldn’t aggravate the injury,” he explains.
But he admits some situations are challenging. “I had a relative asking about a third party with an ankle injury. I advised he hold off on using a balance board until things healed, and to make sure he went to see a specialist. Unfortunately, he went to his general practitioner who likely knows nothing about ankle anatomy,” says Dr. Pribut.
“I finally saw a photo, which revealed swelling higher up on the ankle and no evidence of a hematoma – much lower than we would see in an ankle ligament injury. I would like him to see a sports podiatrist or foot and ankle orthopedist, but now I have to stay calm when the advice isn’t followed,” he says.
When asked, “Do you give medical advice to your friends?” 96% of respondents answered yes.
Yazan Abou-Ismail, MD, assistant professor of medicine in the division of hematology at the University of Utah, Salt Lake City, has often faced questions from friends and family, particularly throughout the COVID-19 pandemic. “How you respond is something all physicians need to analyze carefully,” he says. “I get questions on a regular basis, but this greatly increased with COVID.”
“Sharing general information is okay, and it’s even a requirement that we educate on such topics,” says Dr. Abou-Ismail. “But if someone knows they have COVID, for instance, and wants advice on how to proceed, it’s important to send them to their primary care physician for an evaluation rather than give them instructions on care.”
Dr. Abou-Ismail says that most “curbside consulting” equates to lack of an ethical follow-up. “If you gave medical advice without having assessed them, you’re lacking the medical history, a physical exam, and you should not be giving advice,” he says. “This applies to follow-ups, too.”
Throughout the pandemic, Dr. Abou-Ismail’s requests for advice on COVID even extended to online inquiries, often from strangers. “This is not a place to do a formal assessment,” he reminds. “But there are certain types of advice you can offer appropriately.”
Dr. Abou-Ismail considers safe advice to be simple public health messages that stay far out of specifics. Things like “don’t smoke,” or “eat a healthy diet,” and “get enough sleep,” fall into this safety zone. Even, “What is XYZ disease?” or “How do COVID vaccines work?” are topics he says he answers comfortably.
“But telling someone you need a specific treatment for a condition is inappropriate,” he explains. “This is a general way of practicing medicine – your advice should never venture into the potential of doing harm.”
This approach is exactly in line with legal advice, according to Jeff Caesar Chukwuma, founder and senior partner at Chukwuma Law Group, Miami. “It doesn’t mean that doctors should never give medical advice to friends or family, but if they do, they should make sure to take several precautions to protect both themselves and their family and friends,” he says.
When the request for medical advice from an acquaintance migrates into areas in which a physician is not a specialist, sharing recommendations gets even trickier – and more ethically questionable.
Says Mr. Chukwuma, “Doctors should avoid giving advice in areas outside their area of expertise to lower the possibility of providing erroneous or harmful information,” he says.
How to stay safe when asked for advice
The American Medical Association has weighed in on the topic. In the Code of Medical Ethics Opinion 1.2.1, the AMA states that, “Treating oneself or a member of one’s own family poses several challenges for physicians, including concerns about professional objectivity, patient autonomy, and informed consent.”
What about friends or acquaintances, however?
Even so, some respondents voiced their concerns with the scenario. Responses like, “Due to ethics, I would prefer they go and get first, second, and third opinions,” and “Usually the medical advice is very basic first aid (often mental health first aid), and if it’s anything remotely more complicated, I direct them to the appropriate provider.”
The AMA places advising friends in the same basket as advising and treating family members or oneself. In an article appearing in the AMA Journal of Ethics, Horacio Hojman, MD, of Tufts University School of Medicine, Boston, weighed in: “First and foremost, patients deserve objectivity from their doctors. When a physician is emotionally involved with a patient, that physician’s objectivity can be called into question.”
Why is medical advice so thorny when dealing with friends or relatives?
In some cases, a physician might not ask a friend relevant personal questions about his or her medical history, for instance. Or the friend might not want to share details with the doctor. In either case, the lack of information exchange can lead to improper advice.
The issue of giving medical advice to friends, family, and acquaintances can also wade into legal territory. “Personally or professionally, trust is the decisive factor that puts us at ease with the people we surround ourselves with,” says Mr. Chukwuma. “Nowhere is this truer than in medicine, where we approach doctors with some of the most sensitive matters in our lives and entrust our care to them, especially when the physician in question is a close friend or family member.”
Mr. Chukwuma points out that, while there are few strict legal prohibitions against doctors providing care or advice to family and friends, the AMA’s code of ethics states that such action should be reserved for rare situations, such as emergency settings or isolated settings where there is no other qualified physician available, or for minor, not long-term problems.
This was part of the equation for Dr. Pribut when helping his mother navigate her treatment for breast cancer. “With close relatives, offering advice and help can be very hard,” he says.
“This is to protect both patients and doctors,” says Mr. Chukwuma. “Although seeking advice from a family member or friend who is a doctor may be more convenient for a patient, they run the risk of receiving inadequate care by not going in for a formal medical visit complete with tests, medical examination, and follow-up care.”
Mr. Chukwuma offers guidance on how to share medical advice ethically and legally with family, friends, and acquaintances. “First, as much as possible, speak to general medical facts and knowledge rather than comment directly on the patient’s particular situation,” he says. “In the absence of thorough examination and tests, the doctor’s knowledge of a patient’s condition is limited, therefore, you should take care not to provide seemingly definitive answers on that patient’s unique condition in situations where they can’t rely on data to back up their advice and recommendations.”
The AMA’s Journal of Ethics article shares these tips for staying on the right side of the ethical line when dealing with friends and family members:
- Politely decline.
- Offer other forms of assistance – this might help a friend find the right qualified physician – as Dr. Pribut tends to do. Maybe help in navigating the sometimes-confusing health care system.
- Don’t hesitate in an emergency – the old “is there a doctor on board,” scenario on a plane when someone is in distress is a perfectly acceptable, and recommended, time to step in, even if it is a friend or family member.
Dr. Pribut, a long-time veteran of the tricky medical waters involving friends and family, has this to offer: “Be cautious and always stay in the realm of what you know,” he says. “Always encourage people to seek an opinion from a qualified doctor. Help them find a reputable doctor if that’s useful.”
Mr. Chukwuma adds also that doctors should stand firm when pushed by a friend or family member, especially when offering advice, even if it’s in the form of general education. “The doctor should make it clear to the family member or friend that their advice in no way takes the place of actual treatment or examination by a medical professional and that, if need be, the patient should seek formal medical help from another doctor, ideally one not related to or friends with the patient,” he says.
A version of this article first appeared on Medscape.com.
Compulsivity contributes to poor outcomes in body-focused repetitive behaviors
Although body-focused repetitive behaviors (BFRBs), specifically trichotillomania and skin-picking disorder, are similar in clinical presentation to aspects of obsessive-compulsive disorder (OCD), the role of compulsivity in TTM and SPD has not been well studied, wrote Jon E. Grant, MD, of the University of Chicago and colleagues.
In a study published in the Journal of Psychiatric Research, the authors recruited 69 women and 22 men who met DSM-5 criteria for TTM and SPD. Participants completed diagnostic interviews, symptom inventories, and measures of disability/functioning. Compulsivity was measured using the 15-item Cambridge-Chicago Compulsivity Trait Scale (CHI-T). The average age of the participants was 30.9 years; 48 had TTM, 37 had SPD, and 2 had both conditions.

Overall, total CHI-T scores were significantly correlated with worse disability and quality of life, based on the Quality of Life Inventory (P = .0278) and the Sheehan Disability Scale (P = .0085) but not with severity of TTM or SPD symptoms. TTM and SPD symptoms were assessed using the Massachusetts General Hospital Hair Pulling Scale and the Skin Picking Symptom Symptom Assessment Scale.
“In the current study, we did not find a link between conventional symptom severity measures for BFRBs and disability or quality of life, whereas trans-diagnostic compulsivity did correlate with these clinically important parameters,” the researchers wrote in their discussion. “These findings might suggest the current symptom measures for BFRBs are not including an important aspect of the disease and that a fuller understanding of these symptoms requires measurement of compulsivity. Including validated measures of compulsivity in clinical trials of therapy or medication would also seem to be important for future work,” they said.
The study findings were limited by several factors including the use of a community sample that may not generalize to a clinical setting, the researchers noted. Other limitations include the cross-sectional design, which prevents conclusions about causality, the lack of a control group, and the relatively small sample size, they said.
However, the study is the first known to use a validated compulsivity measure to assess BFRBs, and the results suggest a clinically relevant impact of compulsivity on both psychosocial dysfunction and poor quality of life in this patient population, with possible implications for treatment, the researchers wrote.
The study received no outside funding. Lead author Dr. Grant disclosed research grants from Otsuka and Biohaven Pharmaceuticals, yearly compensation from Springer Publishing for acting as editor in chief of the Journal of Gambling Studies, and royalties from Oxford University Press, American Psychiatric Publishing, Norton Press, and McGraw Hill.
Although body-focused repetitive behaviors (BFRBs), specifically trichotillomania and skin-picking disorder, are similar in clinical presentation to aspects of obsessive-compulsive disorder (OCD), the role of compulsivity in TTM and SPD has not been well studied, wrote Jon E. Grant, MD, of the University of Chicago and colleagues.
In a study published in the Journal of Psychiatric Research, the authors recruited 69 women and 22 men who met DSM-5 criteria for TTM and SPD. Participants completed diagnostic interviews, symptom inventories, and measures of disability/functioning. Compulsivity was measured using the 15-item Cambridge-Chicago Compulsivity Trait Scale (CHI-T). The average age of the participants was 30.9 years; 48 had TTM, 37 had SPD, and 2 had both conditions.
Overall, total CHI-T scores were significantly correlated with worse disability and quality of life, based on the Quality of Life Inventory (P = .0278) and the Sheehan Disability Scale (P = .0085) but not with severity of TTM or SPD symptoms. TTM and SPD symptoms were assessed using the Massachusetts General Hospital Hair Pulling Scale and the Skin Picking Symptom Symptom Assessment Scale.
“In the current study, we did not find a link between conventional symptom severity measures for BFRBs and disability or quality of life, whereas trans-diagnostic compulsivity did correlate with these clinically important parameters,” the researchers wrote in their discussion. “These findings might suggest the current symptom measures for BFRBs are not including an important aspect of the disease and that a fuller understanding of these symptoms requires measurement of compulsivity. Including validated measures of compulsivity in clinical trials of therapy or medication would also seem to be important for future work,” they said.
The study findings were limited by several factors including the use of a community sample that may not generalize to a clinical setting, the researchers noted. Other limitations include the cross-sectional design, which prevents conclusions about causality, the lack of a control group, and the relatively small sample size, they said.
However, the study is the first known to use a validated compulsivity measure to assess BFRBs, and the results suggest a clinically relevant impact of compulsivity on both psychosocial dysfunction and poor quality of life in this patient population, with possible implications for treatment, the researchers wrote.
The study received no outside funding. Lead author Dr. Grant disclosed research grants from Otsuka and Biohaven Pharmaceuticals, yearly compensation from Springer Publishing for acting as editor in chief of the Journal of Gambling Studies, and royalties from Oxford University Press, American Psychiatric Publishing, Norton Press, and McGraw Hill.
Although body-focused repetitive behaviors (BFRBs), specifically trichotillomania and skin-picking disorder, are similar in clinical presentation to aspects of obsessive-compulsive disorder (OCD), the role of compulsivity in TTM and SPD has not been well studied, wrote Jon E. Grant, MD, of the University of Chicago and colleagues.
In a study published in the Journal of Psychiatric Research, the authors recruited 69 women and 22 men who met DSM-5 criteria for TTM and SPD. Participants completed diagnostic interviews, symptom inventories, and measures of disability/functioning. Compulsivity was measured using the 15-item Cambridge-Chicago Compulsivity Trait Scale (CHI-T). The average age of the participants was 30.9 years; 48 had TTM, 37 had SPD, and 2 had both conditions.
Overall, total CHI-T scores were significantly correlated with worse disability and quality of life, based on the Quality of Life Inventory (P = .0278) and the Sheehan Disability Scale (P = .0085) but not with severity of TTM or SPD symptoms. TTM and SPD symptoms were assessed using the Massachusetts General Hospital Hair Pulling Scale and the Skin Picking Symptom Symptom Assessment Scale.
“In the current study, we did not find a link between conventional symptom severity measures for BFRBs and disability or quality of life, whereas trans-diagnostic compulsivity did correlate with these clinically important parameters,” the researchers wrote in their discussion. “These findings might suggest the current symptom measures for BFRBs are not including an important aspect of the disease and that a fuller understanding of these symptoms requires measurement of compulsivity. Including validated measures of compulsivity in clinical trials of therapy or medication would also seem to be important for future work,” they said.
The study findings were limited by several factors including the use of a community sample that may not generalize to a clinical setting, the researchers noted. Other limitations include the cross-sectional design, which prevents conclusions about causality, the lack of a control group, and the relatively small sample size, they said.
However, the study is the first known to use a validated compulsivity measure to assess BFRBs, and the results suggest a clinically relevant impact of compulsivity on both psychosocial dysfunction and poor quality of life in this patient population, with possible implications for treatment, the researchers wrote.
The study received no outside funding. Lead author Dr. Grant disclosed research grants from Otsuka and Biohaven Pharmaceuticals, yearly compensation from Springer Publishing for acting as editor in chief of the Journal of Gambling Studies, and royalties from Oxford University Press, American Psychiatric Publishing, Norton Press, and McGraw Hill.
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH