User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Moving Beyond Traditional Methods for Treatment of Acne Keloidalis Nuchae
The Comparison
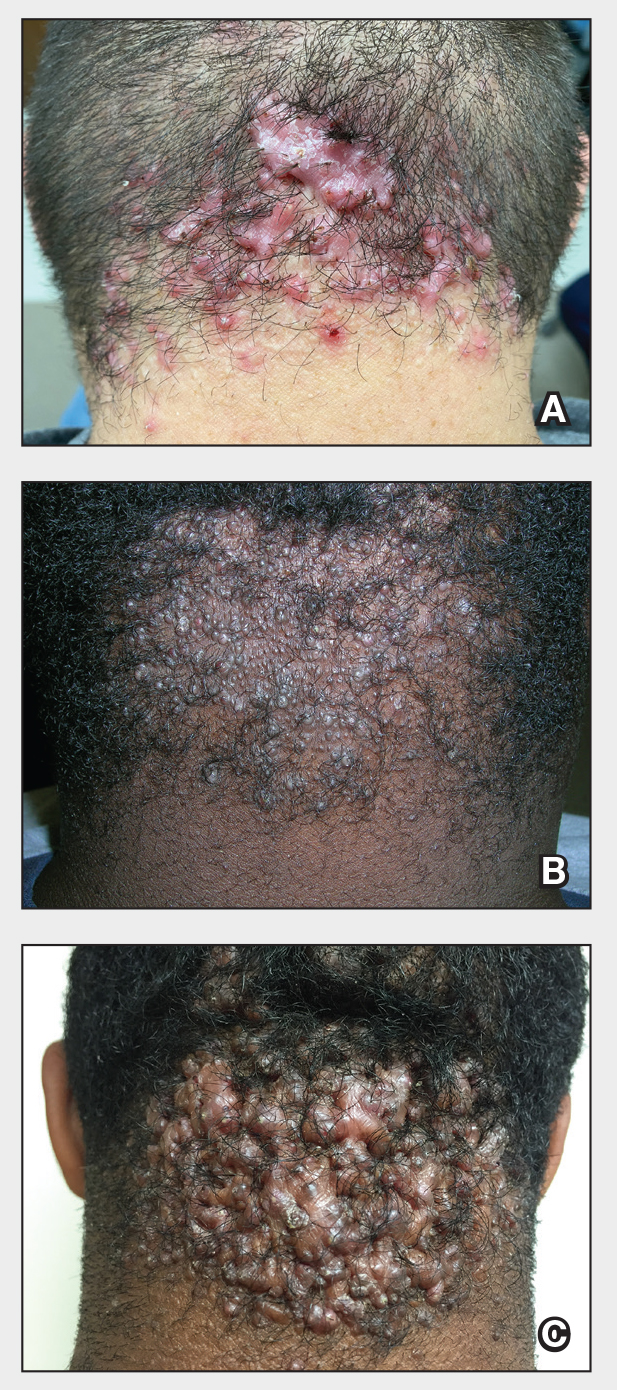
Acne keloidalis nuchae (AKN) is a chronic inflammatory condition commonly affecting the occipital scalp and posterior neck. It causes discrete or extensive fibrosing papules that may coalesce to form pronounced tumorlike masses1,2 with scarring alopecia (Figure, A–C).3 Pustules, hair tufts, secondary bacterial infections, abscesses, and sinus tracts also may occur.1 The pathogenesis of AKN has been characterized as varying stages of follicular inflammation at the infundibular and isthmus levels followed by fibrotic occlusion of the follicular lumen.4 Pruritus, pain, bleeding, oozing, and a feeling of scalp tightness may occur.1,5
Umar et al6 performed a retrospective review of 108 men with AKN—58% of African descent, 37% Hispanic, 3% Asian, and 2% Middle Eastern—and proposed a 3-tier classification system for AKN. Tier 1 focused on the distribution and sagittal spread of AKN lesions between the clinical demarcation lines of the occipital notch and posterior hairline. Tier 2 focused on the type of lesions present—discrete papules or nodules, coalescing/abutting lesions, plaques (raised, atrophic, or indurated), or dome-shaped tumoral masses. Tier 3 focused on the presence or absence of co-existing dissecting cellulitis or folliculitis decalvans.6
Epidemiology
Acne keloidalis nuchae primarily manifests in adolescent and adult men of African or Afro-Caribbean descent.7 Among African American men, the prevalence of AKN ranges from 0.5% to 13.6%.8 Similar ranges have been reported among Nigerian, South African, and West African men.1 Acne keloidalis nuchae also affects Asian and Hispanic men but rarely is seen in non-Hispanic White men or in women of any ethnicity.9,10 The male to female ratio is 20:1.1,11 Hair texture, hairstyling practices such as closely shaved or faded haircuts, and genetics likely contribute to development of AKN. Sports and occupations that require the use of headgear or a tight collar may increase the risk for AKN.12
Key clinical features in people with darker skin tones
- The lesions of AKN range in color from pink to dark brown or black. Postinflammatory hyperpigmentation or hyperchromia may be present around AKN lesions.
- Chronicity of AKN may lead to extended use of high-potency topical or intralesional corticosteroids, which causes transient or long-lasting hypopigmentation, especially in those with darker skin tones.
Worth noting
- Acne keloidalis nuchae can be disfiguring, which negatively impacts quality of life and self-esteem.12
- Some occupations (eg, military, police) have hair policies that may not be favorable to those with or at risk for AKN.
- Patients with AKN are 2 to 3 times more likely to present with metabolic syndrome, hypertension, type 2 diabetes mellitus, or obesity.13
Treatment
There are no treatments approved by the US Food and Drug Administration specifically for AKN. Treatment approaches are based on the pathophysiology, secondary impacts on the skin, and disease severity. Growing out the hair may prevent worsening and/or decrease the risk for new lesions.6
- Options include but are not limited to topical and systemic therapies (eg, topical corticosteroids, oral or topical antibiotics, isotretinoin, topical retinoids, imiquimod, pimecrolimus), light devices (eg, phototherapy, laser), ablative therapies (eg, laser, cryotherapy, radiotherapy), and surgery (eg, excision, follicular unit excision), often in combination.6,14,15
- Intralesional triamcinolone injections are considered standard of care. Adotama et al16 found that injecting triamcinolone into the deep dermis in the area of flat or papular AKN yielded better control of inflammation and decreased appearance of lesions compared with injecting individual lesions.
- For extensive AKN lesions that do not respond to less-invasive therapies, consider surgical techniques,6,17 such as follicular unit excision18 and more extensive surgical excisions building on approaches from pioneers Drs. John Kenney and Harold Pierce.19 An innovative surgical approach for removal of large AKNs is the bat excision technique—wound shape resembles a bat in a spread-eagled position—with secondary intention healing with or without debridement and/or tension sutures. The resulting linear scar acts as a new posterior hair line.20
Health disparity highlights
Access to a dermatologic or plastic surgeon with expertise in the surgical treatment of large AKNs may be challenging but is needed to reduce risk for recurrence and adverse events.
Close-cropped haircuts on the occipital scalp, which are particularly popular among men of African descent, increase the risk for AKN.5 Although this grooming style may be a personal preference, other hairstyles commonly worn by those with tightly coiled hair may be deemed “unprofessional” in society or the workplace,21 which leads to hairstyling practices that may increase the risk for AKN.
Acne keloidalis nuchae remains an understudied entity that adversely affects patients with skin of color.
- Ogunbiyi A. Acne keloidalis nuchae: prevalence, impact, and management challenges. Clin Cosmet Investig Dermatol. 2016;9:483-489. doi:10.2147/CCID.S99225
- Al Aboud DM, Badri T. Acne keloidalis nuchae. In: StatPearls [Internet]. Updated July 31, 2023. Accessed August 2, 2024. https://www.ncbi.nlm.nih.gov/books/NBK459135/ 3.
- Sperling LC, Homoky C, Pratt L, et al. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136:479-484.
- Herzberg AJ, Dinehart SM, Kerns BJ, et al. Acne keloidalis: transverse microscopy, immunohistochemistry, and electron microscopy. Am J Dermatopathol. 1990;12:109-121. doi:10.1097/00000372-199004000-00001
- Saka B, Akakpo A-S, Téclessou JN, et al. Risk factors associated with acne keloidalis nuchae in black subjects: a case-control study. Ann Dermatol Venereol. 2020;147:350-354. doi:10.1016/j.annder.2020.01.007
- Umar S, Lee DJ, Lullo JJ. A retrospective cohort study and clinical classification system of acne keloidalis nuchae. J Clin Aesthet Dermatol. 2021;14:E61-E67.
- Reja M, Silverberg NB. Acne keloidalis nuchae. In: Silverberg NB, Durán-McKinster C, Tay YK, eds. Pediatric Skin of Color. Springer; 2015:141-145. doi:10.1007/978-1-4614-6654-3_16 8.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574. doi:10.1016/s0190-9622(97)70173-7
- Umar S, Ton D, Carter MJ, et al. Unveiling a shared precursor condition for acne keloidalis nuchae and primary cicatricial alopecias. Clin Cosmet Investig Dermatol. 2023;16:2315-2327. doi:10.2147/CCID.S422310
- Na K, Oh SH, Kim SK. Acne keloidalis nuchae in Asian: a single institutional experience. PLoS One. 2017;12:e0189790. doi:10.1371/journal.pone.0189790
- Ogunbiyi A, George A. Acne keloidalis in females: case report and review of literature. J Natl Med Assoc. 2005;97:736-738.
- Alexis A, Heath CR, Halder RM. Folliculitis keloidalis nuchae and pseudofolliculitis barbae: are prevention and effective treatment within reach? Dermatol Clin. 2014;32:183-191. doi:10.1016/j.det.2013.12.001
- Kridin K, Solomon A, Tzur-Bitan D, et al. Acne keloidalis nuchae and the metabolic syndrome: a population-based study. Am J Clin Dermatol. 2020;21:733-739. doi:10.1007/s40257-020-00541-z
- Smart K, Rodriguez I, Worswick S. Comorbidities and treatment options for acne keloidalis nuchae. Dermatol Ther. Published online May 25, 2024. doi:10.1155/2024/8336926
- Callender VD, Young CM, Haverstock CL, et al. An open label study of clobetasol propionate 0.05% and betamethasone valerate 0.12% foams in the treatment of mild to moderate acne keloidalis. Cutis. 2005;75:317-321.
- Adotama P, Grullon K, Ali S, et al. How we do it: our method for triamcinolone injections of acne keloidalis nuchae. Dermatol Surg. 2023;49:713-714. doi:10.1097/DSS.0000000000003803
- Beckett N, Lawson C, Cohen G. Electrosurgical excision of acne keloidalis nuchae with secondary intention healing. J Clin Aesthet Dermatol. 2011;4:36-39.
- Esmat SM, Abdel Hay RM, Abu Zeid OM, et al. The efficacy of laser-assisted hair removal in the treatment of acne keloidalis nuchae; a pilot study. Eur J Dermatol. 2012;22:645-650. doi:10.1684/ejd.2012.1830
- Dillard AD, Quarles FN. African-American pioneers in dermatology. In: Taylor SC, Kelly AP, Lim HW, et al, eds. Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016:717-730.
- Umar S, David CV, Castillo JR, et al. Innovative surgical approaches and selection criteria of large acne keloidalis nuchae lesions. Plast Reconstr Surg Glob Open. 2019;7:E2215. doi:10.1097/GOX.0000000000002215
- Lee MS, Nambudiri VE. The CROWN act and dermatology: taking a stand against race-based hair discrimination. J Am Acad Dermatol. 2021;84:1181-1182. doi:10.1016/j.jaad.2020.11.065
The Comparison
Acne keloidalis nuchae (AKN) is a chronic inflammatory condition commonly affecting the occipital scalp and posterior neck. It causes discrete or extensive fibrosing papules that may coalesce to form pronounced tumorlike masses1,2 with scarring alopecia (Figure, A–C).3 Pustules, hair tufts, secondary bacterial infections, abscesses, and sinus tracts also may occur.1 The pathogenesis of AKN has been characterized as varying stages of follicular inflammation at the infundibular and isthmus levels followed by fibrotic occlusion of the follicular lumen.4 Pruritus, pain, bleeding, oozing, and a feeling of scalp tightness may occur.1,5
Umar et al6 performed a retrospective review of 108 men with AKN—58% of African descent, 37% Hispanic, 3% Asian, and 2% Middle Eastern—and proposed a 3-tier classification system for AKN. Tier 1 focused on the distribution and sagittal spread of AKN lesions between the clinical demarcation lines of the occipital notch and posterior hairline. Tier 2 focused on the type of lesions present—discrete papules or nodules, coalescing/abutting lesions, plaques (raised, atrophic, or indurated), or dome-shaped tumoral masses. Tier 3 focused on the presence or absence of co-existing dissecting cellulitis or folliculitis decalvans.6
Epidemiology
Acne keloidalis nuchae primarily manifests in adolescent and adult men of African or Afro-Caribbean descent.7 Among African American men, the prevalence of AKN ranges from 0.5% to 13.6%.8 Similar ranges have been reported among Nigerian, South African, and West African men.1 Acne keloidalis nuchae also affects Asian and Hispanic men but rarely is seen in non-Hispanic White men or in women of any ethnicity.9,10 The male to female ratio is 20:1.1,11 Hair texture, hairstyling practices such as closely shaved or faded haircuts, and genetics likely contribute to development of AKN. Sports and occupations that require the use of headgear or a tight collar may increase the risk for AKN.12
Key clinical features in people with darker skin tones
- The lesions of AKN range in color from pink to dark brown or black. Postinflammatory hyperpigmentation or hyperchromia may be present around AKN lesions.
- Chronicity of AKN may lead to extended use of high-potency topical or intralesional corticosteroids, which causes transient or long-lasting hypopigmentation, especially in those with darker skin tones.
Worth noting
- Acne keloidalis nuchae can be disfiguring, which negatively impacts quality of life and self-esteem.12
- Some occupations (eg, military, police) have hair policies that may not be favorable to those with or at risk for AKN.
- Patients with AKN are 2 to 3 times more likely to present with metabolic syndrome, hypertension, type 2 diabetes mellitus, or obesity.13
Treatment
There are no treatments approved by the US Food and Drug Administration specifically for AKN. Treatment approaches are based on the pathophysiology, secondary impacts on the skin, and disease severity. Growing out the hair may prevent worsening and/or decrease the risk for new lesions.6
- Options include but are not limited to topical and systemic therapies (eg, topical corticosteroids, oral or topical antibiotics, isotretinoin, topical retinoids, imiquimod, pimecrolimus), light devices (eg, phototherapy, laser), ablative therapies (eg, laser, cryotherapy, radiotherapy), and surgery (eg, excision, follicular unit excision), often in combination.6,14,15
- Intralesional triamcinolone injections are considered standard of care. Adotama et al16 found that injecting triamcinolone into the deep dermis in the area of flat or papular AKN yielded better control of inflammation and decreased appearance of lesions compared with injecting individual lesions.
- For extensive AKN lesions that do not respond to less-invasive therapies, consider surgical techniques,6,17 such as follicular unit excision18 and more extensive surgical excisions building on approaches from pioneers Drs. John Kenney and Harold Pierce.19 An innovative surgical approach for removal of large AKNs is the bat excision technique—wound shape resembles a bat in a spread-eagled position—with secondary intention healing with or without debridement and/or tension sutures. The resulting linear scar acts as a new posterior hair line.20
Health disparity highlights
Access to a dermatologic or plastic surgeon with expertise in the surgical treatment of large AKNs may be challenging but is needed to reduce risk for recurrence and adverse events.
Close-cropped haircuts on the occipital scalp, which are particularly popular among men of African descent, increase the risk for AKN.5 Although this grooming style may be a personal preference, other hairstyles commonly worn by those with tightly coiled hair may be deemed “unprofessional” in society or the workplace,21 which leads to hairstyling practices that may increase the risk for AKN.
Acne keloidalis nuchae remains an understudied entity that adversely affects patients with skin of color.
The Comparison
Acne keloidalis nuchae (AKN) is a chronic inflammatory condition commonly affecting the occipital scalp and posterior neck. It causes discrete or extensive fibrosing papules that may coalesce to form pronounced tumorlike masses1,2 with scarring alopecia (Figure, A–C).3 Pustules, hair tufts, secondary bacterial infections, abscesses, and sinus tracts also may occur.1 The pathogenesis of AKN has been characterized as varying stages of follicular inflammation at the infundibular and isthmus levels followed by fibrotic occlusion of the follicular lumen.4 Pruritus, pain, bleeding, oozing, and a feeling of scalp tightness may occur.1,5
Umar et al6 performed a retrospective review of 108 men with AKN—58% of African descent, 37% Hispanic, 3% Asian, and 2% Middle Eastern—and proposed a 3-tier classification system for AKN. Tier 1 focused on the distribution and sagittal spread of AKN lesions between the clinical demarcation lines of the occipital notch and posterior hairline. Tier 2 focused on the type of lesions present—discrete papules or nodules, coalescing/abutting lesions, plaques (raised, atrophic, or indurated), or dome-shaped tumoral masses. Tier 3 focused on the presence or absence of co-existing dissecting cellulitis or folliculitis decalvans.6
Epidemiology
Acne keloidalis nuchae primarily manifests in adolescent and adult men of African or Afro-Caribbean descent.7 Among African American men, the prevalence of AKN ranges from 0.5% to 13.6%.8 Similar ranges have been reported among Nigerian, South African, and West African men.1 Acne keloidalis nuchae also affects Asian and Hispanic men but rarely is seen in non-Hispanic White men or in women of any ethnicity.9,10 The male to female ratio is 20:1.1,11 Hair texture, hairstyling practices such as closely shaved or faded haircuts, and genetics likely contribute to development of AKN. Sports and occupations that require the use of headgear or a tight collar may increase the risk for AKN.12
Key clinical features in people with darker skin tones
- The lesions of AKN range in color from pink to dark brown or black. Postinflammatory hyperpigmentation or hyperchromia may be present around AKN lesions.
- Chronicity of AKN may lead to extended use of high-potency topical or intralesional corticosteroids, which causes transient or long-lasting hypopigmentation, especially in those with darker skin tones.
Worth noting
- Acne keloidalis nuchae can be disfiguring, which negatively impacts quality of life and self-esteem.12
- Some occupations (eg, military, police) have hair policies that may not be favorable to those with or at risk for AKN.
- Patients with AKN are 2 to 3 times more likely to present with metabolic syndrome, hypertension, type 2 diabetes mellitus, or obesity.13
Treatment
There are no treatments approved by the US Food and Drug Administration specifically for AKN. Treatment approaches are based on the pathophysiology, secondary impacts on the skin, and disease severity. Growing out the hair may prevent worsening and/or decrease the risk for new lesions.6
- Options include but are not limited to topical and systemic therapies (eg, topical corticosteroids, oral or topical antibiotics, isotretinoin, topical retinoids, imiquimod, pimecrolimus), light devices (eg, phototherapy, laser), ablative therapies (eg, laser, cryotherapy, radiotherapy), and surgery (eg, excision, follicular unit excision), often in combination.6,14,15
- Intralesional triamcinolone injections are considered standard of care. Adotama et al16 found that injecting triamcinolone into the deep dermis in the area of flat or papular AKN yielded better control of inflammation and decreased appearance of lesions compared with injecting individual lesions.
- For extensive AKN lesions that do not respond to less-invasive therapies, consider surgical techniques,6,17 such as follicular unit excision18 and more extensive surgical excisions building on approaches from pioneers Drs. John Kenney and Harold Pierce.19 An innovative surgical approach for removal of large AKNs is the bat excision technique—wound shape resembles a bat in a spread-eagled position—with secondary intention healing with or without debridement and/or tension sutures. The resulting linear scar acts as a new posterior hair line.20
Health disparity highlights
Access to a dermatologic or plastic surgeon with expertise in the surgical treatment of large AKNs may be challenging but is needed to reduce risk for recurrence and adverse events.
Close-cropped haircuts on the occipital scalp, which are particularly popular among men of African descent, increase the risk for AKN.5 Although this grooming style may be a personal preference, other hairstyles commonly worn by those with tightly coiled hair may be deemed “unprofessional” in society or the workplace,21 which leads to hairstyling practices that may increase the risk for AKN.
Acne keloidalis nuchae remains an understudied entity that adversely affects patients with skin of color.
- Ogunbiyi A. Acne keloidalis nuchae: prevalence, impact, and management challenges. Clin Cosmet Investig Dermatol. 2016;9:483-489. doi:10.2147/CCID.S99225
- Al Aboud DM, Badri T. Acne keloidalis nuchae. In: StatPearls [Internet]. Updated July 31, 2023. Accessed August 2, 2024. https://www.ncbi.nlm.nih.gov/books/NBK459135/ 3.
- Sperling LC, Homoky C, Pratt L, et al. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136:479-484.
- Herzberg AJ, Dinehart SM, Kerns BJ, et al. Acne keloidalis: transverse microscopy, immunohistochemistry, and electron microscopy. Am J Dermatopathol. 1990;12:109-121. doi:10.1097/00000372-199004000-00001
- Saka B, Akakpo A-S, Téclessou JN, et al. Risk factors associated with acne keloidalis nuchae in black subjects: a case-control study. Ann Dermatol Venereol. 2020;147:350-354. doi:10.1016/j.annder.2020.01.007
- Umar S, Lee DJ, Lullo JJ. A retrospective cohort study and clinical classification system of acne keloidalis nuchae. J Clin Aesthet Dermatol. 2021;14:E61-E67.
- Reja M, Silverberg NB. Acne keloidalis nuchae. In: Silverberg NB, Durán-McKinster C, Tay YK, eds. Pediatric Skin of Color. Springer; 2015:141-145. doi:10.1007/978-1-4614-6654-3_16 8.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574. doi:10.1016/s0190-9622(97)70173-7
- Umar S, Ton D, Carter MJ, et al. Unveiling a shared precursor condition for acne keloidalis nuchae and primary cicatricial alopecias. Clin Cosmet Investig Dermatol. 2023;16:2315-2327. doi:10.2147/CCID.S422310
- Na K, Oh SH, Kim SK. Acne keloidalis nuchae in Asian: a single institutional experience. PLoS One. 2017;12:e0189790. doi:10.1371/journal.pone.0189790
- Ogunbiyi A, George A. Acne keloidalis in females: case report and review of literature. J Natl Med Assoc. 2005;97:736-738.
- Alexis A, Heath CR, Halder RM. Folliculitis keloidalis nuchae and pseudofolliculitis barbae: are prevention and effective treatment within reach? Dermatol Clin. 2014;32:183-191. doi:10.1016/j.det.2013.12.001
- Kridin K, Solomon A, Tzur-Bitan D, et al. Acne keloidalis nuchae and the metabolic syndrome: a population-based study. Am J Clin Dermatol. 2020;21:733-739. doi:10.1007/s40257-020-00541-z
- Smart K, Rodriguez I, Worswick S. Comorbidities and treatment options for acne keloidalis nuchae. Dermatol Ther. Published online May 25, 2024. doi:10.1155/2024/8336926
- Callender VD, Young CM, Haverstock CL, et al. An open label study of clobetasol propionate 0.05% and betamethasone valerate 0.12% foams in the treatment of mild to moderate acne keloidalis. Cutis. 2005;75:317-321.
- Adotama P, Grullon K, Ali S, et al. How we do it: our method for triamcinolone injections of acne keloidalis nuchae. Dermatol Surg. 2023;49:713-714. doi:10.1097/DSS.0000000000003803
- Beckett N, Lawson C, Cohen G. Electrosurgical excision of acne keloidalis nuchae with secondary intention healing. J Clin Aesthet Dermatol. 2011;4:36-39.
- Esmat SM, Abdel Hay RM, Abu Zeid OM, et al. The efficacy of laser-assisted hair removal in the treatment of acne keloidalis nuchae; a pilot study. Eur J Dermatol. 2012;22:645-650. doi:10.1684/ejd.2012.1830
- Dillard AD, Quarles FN. African-American pioneers in dermatology. In: Taylor SC, Kelly AP, Lim HW, et al, eds. Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016:717-730.
- Umar S, David CV, Castillo JR, et al. Innovative surgical approaches and selection criteria of large acne keloidalis nuchae lesions. Plast Reconstr Surg Glob Open. 2019;7:E2215. doi:10.1097/GOX.0000000000002215
- Lee MS, Nambudiri VE. The CROWN act and dermatology: taking a stand against race-based hair discrimination. J Am Acad Dermatol. 2021;84:1181-1182. doi:10.1016/j.jaad.2020.11.065
- Ogunbiyi A. Acne keloidalis nuchae: prevalence, impact, and management challenges. Clin Cosmet Investig Dermatol. 2016;9:483-489. doi:10.2147/CCID.S99225
- Al Aboud DM, Badri T. Acne keloidalis nuchae. In: StatPearls [Internet]. Updated July 31, 2023. Accessed August 2, 2024. https://www.ncbi.nlm.nih.gov/books/NBK459135/ 3.
- Sperling LC, Homoky C, Pratt L, et al. Acne keloidalis is a form of primary scarring alopecia. Arch Dermatol. 2000;136:479-484.
- Herzberg AJ, Dinehart SM, Kerns BJ, et al. Acne keloidalis: transverse microscopy, immunohistochemistry, and electron microscopy. Am J Dermatopathol. 1990;12:109-121. doi:10.1097/00000372-199004000-00001
- Saka B, Akakpo A-S, Téclessou JN, et al. Risk factors associated with acne keloidalis nuchae in black subjects: a case-control study. Ann Dermatol Venereol. 2020;147:350-354. doi:10.1016/j.annder.2020.01.007
- Umar S, Lee DJ, Lullo JJ. A retrospective cohort study and clinical classification system of acne keloidalis nuchae. J Clin Aesthet Dermatol. 2021;14:E61-E67.
- Reja M, Silverberg NB. Acne keloidalis nuchae. In: Silverberg NB, Durán-McKinster C, Tay YK, eds. Pediatric Skin of Color. Springer; 2015:141-145. doi:10.1007/978-1-4614-6654-3_16 8.
- Knable AL Jr, Hanke CW, Gonin R. Prevalence of acne keloidalis nuchae in football players. J Am Acad Dermatol. 1997;37:570-574. doi:10.1016/s0190-9622(97)70173-7
- Umar S, Ton D, Carter MJ, et al. Unveiling a shared precursor condition for acne keloidalis nuchae and primary cicatricial alopecias. Clin Cosmet Investig Dermatol. 2023;16:2315-2327. doi:10.2147/CCID.S422310
- Na K, Oh SH, Kim SK. Acne keloidalis nuchae in Asian: a single institutional experience. PLoS One. 2017;12:e0189790. doi:10.1371/journal.pone.0189790
- Ogunbiyi A, George A. Acne keloidalis in females: case report and review of literature. J Natl Med Assoc. 2005;97:736-738.
- Alexis A, Heath CR, Halder RM. Folliculitis keloidalis nuchae and pseudofolliculitis barbae: are prevention and effective treatment within reach? Dermatol Clin. 2014;32:183-191. doi:10.1016/j.det.2013.12.001
- Kridin K, Solomon A, Tzur-Bitan D, et al. Acne keloidalis nuchae and the metabolic syndrome: a population-based study. Am J Clin Dermatol. 2020;21:733-739. doi:10.1007/s40257-020-00541-z
- Smart K, Rodriguez I, Worswick S. Comorbidities and treatment options for acne keloidalis nuchae. Dermatol Ther. Published online May 25, 2024. doi:10.1155/2024/8336926
- Callender VD, Young CM, Haverstock CL, et al. An open label study of clobetasol propionate 0.05% and betamethasone valerate 0.12% foams in the treatment of mild to moderate acne keloidalis. Cutis. 2005;75:317-321.
- Adotama P, Grullon K, Ali S, et al. How we do it: our method for triamcinolone injections of acne keloidalis nuchae. Dermatol Surg. 2023;49:713-714. doi:10.1097/DSS.0000000000003803
- Beckett N, Lawson C, Cohen G. Electrosurgical excision of acne keloidalis nuchae with secondary intention healing. J Clin Aesthet Dermatol. 2011;4:36-39.
- Esmat SM, Abdel Hay RM, Abu Zeid OM, et al. The efficacy of laser-assisted hair removal in the treatment of acne keloidalis nuchae; a pilot study. Eur J Dermatol. 2012;22:645-650. doi:10.1684/ejd.2012.1830
- Dillard AD, Quarles FN. African-American pioneers in dermatology. In: Taylor SC, Kelly AP, Lim HW, et al, eds. Dermatology for Skin of Color. 2nd ed. McGraw-Hill Education; 2016:717-730.
- Umar S, David CV, Castillo JR, et al. Innovative surgical approaches and selection criteria of large acne keloidalis nuchae lesions. Plast Reconstr Surg Glob Open. 2019;7:E2215. doi:10.1097/GOX.0000000000002215
- Lee MS, Nambudiri VE. The CROWN act and dermatology: taking a stand against race-based hair discrimination. J Am Acad Dermatol. 2021;84:1181-1182. doi:10.1016/j.jaad.2020.11.065

Benefits of High-Dose Vitamin D in Managing Cutaneous Adverse Events Induced by Chemotherapy and Radiation Therapy
Vitamin D (VD) regulates keratinocyte proliferation and differentiation, modulates inflammatory pathways, and protects against cellular damage in the skin. 1 In the setting of tissue injury and acute skin inflammation, active vitamin D—1,25(OH) 2 D—suppresses signaling from pro-inflammatory chemokines and cytokines such as IFN- γ and IL-17. 2,3 This suppression reduces proliferation of helper T cells (T H 1, T H 17) and B cells, decreasing tissue damage from reactive oxygen species release while enhancing secretion of the anti-inflammatory cytokine IL-10 by antigen-presenting cells. 2-4
Suboptimal VD levels have been associated with numerous health consequences including malignancy, prompting interest in VD supplementation for improving cancer-related outcomes.5 Beyond disease prognosis, high-dose VD supplementation has been suggested as a potential therapy for adverse events (AEs) related to cancer treatments. In one study, mice that received oral vitamin D3 supplementation of 11,500 IU/kg daily had fewer doxorubicin-induced cardiotoxic effects on ejection fraction (P<.0001) and stroke volume (P<.01) than mice that received VD supplementation of 1500 IU/kg daily.6
In this review, we examine the impact of chemoradiation on 25(OH)D levels—which more accurately reflects VD stores than 1,25(OH)2D levels—and the impact of suboptimal VD on cutaneous toxicities related to chemoradiation. To define the suboptimal VD threshold, we used the Endocrine Society’s clinical practice guidelines, which characterize suboptimal 25(OH)D levels as insufficiency (21–29 ng/mL [52.5–72.5 nmol/L]) or deficiency (<20 ng/mL [50 nmol/L])7; deficiency can be further categorized as severe deficiency (<12 ng/mL [30 nmol/L]).8 This review also evaluates the evidence for vitamin D3 supplementation to alleviate the cutaneous AEs of chemotherapy and radiation treatments.
Effects of Chemotherapy on Vitamin D Levels
A high prevalence of VD deficiency is seen in various cancers. In a retrospective review of 25(OH)D levels in 2098 adults with solid tumors of any stage (6% had metastatic disease [n=124]), suboptimal levels were found in 69% of patients with breast cancer (n=617), 75% with colorectal cancer (n=84), 72% with gynecologic cancer (n=65), 79% with kidney and bladder cancer (n=145), 83% with pancreatic and upper gastrointestinal tract cancer (n=178), 73% with lung cancer (n=73), 69% with prostate cancer (n=225), 61% with skin cancer (n=399), and 63% with thyroid cancer (n=172).5 Suboptimal VD also has been found in hematologic malignancies. In a prospective cohort study, mean serum 25(OH)D levels in 23 patients with recently diagnosed acute myeloid leukemia demonstrated VD deficiency (mean [SD], 18.6 [6.6] nmol/L).9 Given that many patients already exhibit a baseline VD deficiency at cancer diagnosis, it is important to understand the relationship between VD and cancer treatment modalities.5
In the United States, breast and colorectal cancers were estimated to be the first and fourth most common cancers, with 313,510 and 152,810 predicted new cases in 2024, respectively.10 This review will focus on breast and colorectal cancer when describing VD variation associated with chemotherapy exposure due to their high prevalence.
Effects of Chemotherapy on Vitamin D Levels in Breast Cancer—Breast cancer studies have shown suboptimal VD levels in 76% of females 75 years or younger with any T1, T2, or T3; N0 or N1; and M0 breast cancer, in which 38.5% (n=197) had insufficient and 37.5% (n=192) had deficient 25(OH)D levels.11 In a study of female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), VD deficiency was seen in 60% of patients not receiving VD supplementation.12,13 A systematic review that included 7 studies of different types of breast cancer suggested that circulating 25(OH)D may be associated with improved prognosis.14 Thus, studies have investigated risk factors associated with poor or worsening VD status in individuals with breast cancer, including exposure to chemotherapy and/or radiation treatment.12,15-18
A prospective cohort study assessed 25(OH)D levels in 95 patients with any breast cancer (stages I, II, IIIA, IIIB) before and after initiating chemotherapy with docetaxel, doxorubicin, epirubicin, 5-fluorouracil, or cyclophosphamide, compared with a group of 52 females without cancer.17 In the breast cancer group, approximately 80% (76/95) had suboptimal and 50% (47/95) had deficient VD levels before chemotherapy initiation (mean [SD], 54.1 [22.8] nmol/L). In the comparison group, 60% (31/52) had suboptimal and 30% (15/52) had deficient VD at baseline (mean [SD], 66.1 [23.5] nmol/L), which was higher than the breast cancer group (P=.03). A subgroup analysis excluded participants who started, stopped, or lacked data on dietary supplements containing VD (n=39); in the remaining 56 participants, a significant decrease in 25(OH)D levels was observed shortly after finishing chemotherapy compared with the prechemotherapy baseline value (mean, −7.9 nmol/L; P=.004). Notably, 6 months after chemotherapy completion, 25(OH)D levels increased (mean, +12.8 nmol/L; P<.001). Vitamin D levels remained stable in the comparison group (P=.987).17
Consistent with these findings, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of chemotherapy was associated with increased odds of 25(OH)D levels less than 20 ng/mL compared with breast cancer patients with no prior chemotherapy (odds ratio, 1.86; 95% CI, 1.03-3.38).12 Although the study data included chemotherapy history, no information was provided on specific chemotherapy agents or regimens used in this cohort, limiting the ability to detect the drugs most often implicated.
Both studies indicated a complex interplay between chemotherapy and VD levels in breast cancer patients. Although Kok et al17 suggested a transient decrease in VD levels during chemotherapy with a subsequent recovery after cessation, Fassio et al12 highlighted the increased odds of VD deficiency associated with chemotherapy. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status in breast cancer patients.
Effects of Chemotherapy on Vitamin D Levels in Colorectal Cancer—Similar to patterns seen in breast cancer, a systematic review with 6 studies of different types of colorectal cancer suggested that circulating 25(OH)D levels may be associated with prognosis.14 Studies also have investigated the relationship between colorectal chemotherapy regimens and VD status.15,16,18,19
A retrospective study assessed 25(OH)D levels in 315 patients with any colorectal cancer (stage I–IV).15 Patients were included in the analysis if they received less than 400 IU daily of VD supplementation at baseline. For the whole study sample, the mean (SD) VD level was 23.7 (13.71) ng/mL. Patients who had not received chemotherapy within 3 months of the VD level assessment were categorized as the no chemotherapy group, and the others were designated as the chemotherapy group; the latter group was exposed to various chemotherapy regimens, including combinations of irinotecan, oxaliplatin, 5-fluorouracil, leucovorin, bevacizumab, or cetuximab. Multivariate analysis showed that the chemotherapy group was 3.7 times more likely to have very low VD levels (≤15 ng/mL) compared with those in the no chemotherapy group (P<.0001).15
A separate cross-sectional study examined serum 25(OH)D concentrations in 1201 patients with any newly diagnosed colorectal carcinoma (stage I–III); 91% of cases were adenocarcinoma.18 In a multivariate analysis, chemotherapy plus surgery was associated with lower VD levels than surgery alone 6 months after diagnosis (mean, −8.74 nmol/L; 95% CI, −11.30 to −6.18 nmol/L), specifically decreasing by a mean of 6.7 nmol/L (95% CI, −9.8 to −3.8 nmol/L) after adjusting for demographic and lifestyle factors.18 However, a prospective cohort study demonstrated different findings.19 Comparing 58 patients with newly diagnosed colorectal adenocarcinoma (stages I–IV) who underwent chemotherapy and 36 patients who did not receive chemotherapy, there was no significant change in 25(OH)D levels from the time of diagnosis to 6 months later. Median VD levels decreased by 0.7 ng/mL in those who received chemotherapy, while a minimal (and not significant) increase of 1.6 ng/mL was observed in those without chemotherapy intervention (P=.26). Notably, supplementation was not restricted in this cohort, which may have resulted in higher VD levels in those taking supplements.19
Since time of year and geographic location can influence VD levels, one prospective cohort study controlled for differential sun exposure due to these factors in their analysis.16 Assessment of 25(OH)D levels was completed in 81 chemotherapy-naïve cancer patients immediately before beginning chemotherapy as well as 6 and 12 weeks into treatment. More than 8 primary cancer types were represented in this study, with breast (34% [29/81]) and colorectal (14% [12/81]) cancer being the most common, but the cancer stages of the participants were not detailed. Vitamin D levels decreased after commencing chemotherapy, with the largest drop occurring 6 weeks into treatment. From the 6- to 12-week end points, VD increased but remained below the original baseline level (baseline: mean [SD], 49.2 [22.3] nmol/L; 6 weeks: mean [SD], 40.9 [19.0] nmol/L; 12 weeks: mean [SD], 45.9 [19.7] nmol/L; P=.05).16
Although focused on breast and colorectal cancers, these studies suggest that various chemotherapy regimens may confer a higher risk for VD deficiency compared with VD status at diagnosis and/or prior to chemotherapy treatment. However, most of these studies only discussed stage-based differences, excluding analysis of the variety of cancer subtypes that comprise breast and colorectal malignancies, which may limit our ability to extrapolate from these data. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status across various primary cancer types.
Effects of Radiation Therapy on Vitamin D Levels
Unlike chemotherapy, studies on the association between radiation therapy and VD levels are minimal, with most reports in the literature discussing the use of VD to potentiate the effects of radiation therapy. In one cross-sectional analysis of 1201 patients with newly diagnosed stage I, II, or III colorectal cancer of any type (94% were adenocarcinoma), radiation plus surgery was associated with slightly lower 25(OH)D levels than surgery alone for tumor treatment 6 months after diagnosis (mean, −3.17; 95% CI, −6.07 to −0.28 nmol/L). However, after adjustment for demographic and lifestyle factors, this decrease in VD levels attributable to radiotherapy was not statistically significant compared with the surgery-only cohort (mean, −1.78; 95% CI, −5.07 to 1.52 nmol/L).18
Similarly, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of radiotherapy was not associated with a difference in serum 25(OH)D levels compared with those with breast cancer without prior radiotherapy (odds ratio, 0.90; 95% CI, 0.52-1.54).12 From the limited existing literature specifically addressing variations of VD levels with radiation, radiation therapy does not appear to significantly impact VD levels.
Vitamin D Levels and the Severity of Chemotherapy- or Radiation Therapy–Induced AEs
A prospective cohort of 241 patients did not find an increase in the incidence or severity of chemotherapy-induced cutaneous toxicities in those with suboptimal 1,25(OH)2D3 levels (≤75 nmol/L).20 Eight different primary cancer types were represented, including breast and colorectal cancer; the tumor stages of the participants were not detailed. Forty-one patients had normal 1,25(OH)2D3 levels, while the remaining 200 had suboptimal levels. There was no significant association between serum VD levels and the following dermatologic toxicities: desquamation (P=.26), xerosis (P=.15), mucositis (P=.30), or painful rash (P=.87). Surprisingly, nail changes and hand-foot reactions occurred with greater frequency in patients with normal VD levels (P=.01 and P=.03, respectively).20 Hand-foot reaction is part of the toxic erythema of chemotherapy (TEC) spectrum, which is comprised of a range of cytotoxic skin injuries that typically manifest within 2 to 3 weeks of exposure to the offending chemotherapeutic agents, often characterized by erythema, pain, swelling, and blistering, particularly in intertriginous and acral areas.21-23 Recovery from TEC generally takes at least 2 to 4 weeks and may necessitate cessation of the offending chemotherapeutic agent.21,24 Notably, this study measured 1,25(OH)2D3 levels instead of 25(OH)D levels, which may not reliably indicate body stores of VD.7,20 These results underscore the complex nature between chemotherapy and VD; however, VD levels alone do not appear to be a sufficient biomarker for predicting chemotherapy-associated cutaneous AEs.
Interestingly, radiation therapy–induced AEs may be associated with VD levels. A prospective cohort study of 98 patients with prostate, bladder, or gynecologic cancers (tumor stages were not detailed) undergoing pelvic radiotherapy found that females and males with 25(OH)D levels below a threshold of 35 and 40 nmol/L, respectively, were more likely to experience higher Radiation Therapy Oncology Group (RTOG) grade acute proctitis compared with those with VD above these thresholds.25 Specifically, VD below these thresholds was associated with increased odds of RTOG grade 2 or higher radiation-induced proctitis (OR, 3.07; 95% CI, 1.27-7.50 [P=.013]). Additionally, a weak correlation was noted between VD below these thresholds and the RTOG grade, with a Spearman correlation value of −0.189 (P=.031).25
One prospective cohort study included 28 patients with any cancer of the oral cavity, oropharynx, hypopharynx, or larynx stages II, III, or IVA; 93% (26/28) were stage III or IVA.26 The 20 (71%) patients with suboptimal 25(OH)D levels (≤75 nmol/L) experienced a higher prevalence of grade II radiation dermatitis compared with the 8 (29%) patients with optimal VD levels (χ22 =5.973; P=.0505). This pattern persisted with the severity of mucositis; patients from the suboptimal VD group presented with higher rates of grades II and III mucositis compared with the VD optimal group (χ22 =13.627; P=.0011).26 Recognizing the small cohort evaluated in the study, we highlight the importance of further studies to clarify these associations.
Chemotherapy-Induced Cutaneous Events Treated with High-Dose Vitamin D
Chemotherapeutic agents are known to induce cellular damage, resulting in a range of cutaneous AEs that can invoke discontinuation of otherwise effective chemotherapeutic interventions.27,28 Recent research has explored the potential of high-dose vitamin D3 as a therapeutic agent to mitigate cutaneous reactions.29,30
A randomized, double-blind, placebo-controlled trial investigated the use of a single high dose of oral 25(OH)D to treat topical nitrogen mustard (NM)–induced rash.29 To characterize baseline inflammatory responses from NM injury without intervention, clinical measures, serum studies, and tissue analyses from skin biopsies were performed on 28 healthy adults after exposure to topical NM—a chemotherapeutic agent classified as a DNA alkylator. Two weeks later, participants were exposed to topical NM a second time and were split into 2 groups: 14 patients received a single 200,000-IU dose of oral 25(OH)D while the other 14 participants were given a placebo. Using the inflammatory markers induced from baseline exposure to NM alone, posttreatment analysis revealed that the punch biopsies from
Although Ernst et al29 did not observe any clinically significant improvements with VD treatment, a case series of 6 patients with either glioblastoma multiforme, acute myeloid leukemia, or aplastic anemia did demonstrate clinical improvement of TEC after receiving high-dose vitamin D3.30 The mean time to onset of TEC was noted at 8.5 days following administration of the inciting chemotherapeutic agent, which included combinations of anthracycline, antimetabolite, kinase inhibitor, B-cell lymphoma 2 inhibitor, purine analogue, and alkylating agents. A combination of clinical and histologic findings was used to diagnose TEC. Baseline 25(OH)D levels were not established prior to treatment. The treatment regimen for 1 patient included 2 doses of 50,000 IU of VD spaced 1 week apart, totaling 100,000 IU, while the remaining 5 patients received a total of 200,000 IU, also split into 2 doses given 1 week apart. All patients received their first dose of VD within a week of the cutaneous eruption. Following the initial VD dose, there was a notable improvement in pain, pruritus, or swelling by the next day. Reduction in erythema also was observed within 1 to 4 days.30
No AEs associated with VD supplementation were reported, suggesting a potential beneficial role of high-dose VD in accelerating recovery from chemotherapy-induced rashes without evident safety concerns.
Radiation Therapy–Induced Cutaneous Events Treated with High-Dose Vitamin D
Radiation dermatitis is a common and often severe complication of radiation therapy that affects more than 90% of patients undergoing treatment, with half of these individuals experiencing grade 2 toxicity, according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events.31,32 Radiation damage to basal keratinocytes and hair follicle stem cells disrupts the renewal of the skin’s outer layer, while a surge of free radicals causes irreversible DNA damage.33 Symptoms of radiation dermatitis can vary from mild pink erythema to tissue ulceration and necrosis, typically within 1 to 4 weeks of radiation exposure.34 The resulting dermatitis can take 2 to 4 weeks to heal, notably impacting patient quality of life and often necessitating modifications or interruptions in cancer therapy.33
Prior studies have demonstrated the use of high-dose VD to improve the healing of UV-irradiated skin. A randomized controlled trial investigated high-dose vitamin D3 to treat experimentally induced sunburn in 20 healthy adults. Compared with those who received a placebo, participants receiving the oral dose of 200,000 IU of vitamin D3 demonstrated suppression of the pro-inflammatory mediators tumor necrosis factor α (P=.04) and inducible nitric oxide synthase (P=.02), while expression of tissue repair enhancer arginase 1 was increased (P<.005).35 The mechanism of this enhanced tissue repair was investigated using a mouse model, in which intraperitoneal 25(OH)D was administered following severe UV-induced skin injury. On immunofluorescence microscopy, mice treated with VD showed enhanced autophagy within the macrophages infiltrating UV-irradiated skin.36 The use of high-dose VD to treat UV-irradiated skin in these studies established a precedent for using VD to heal cutaneous injury caused by ionizing radiation therapy.
Some studies have focused on the role of VD for treating acute radiation dermatitis. A study of 23 patients with ductal carcinoma in situ or localized invasive ductal carcinoma breast cancer compared the effectiveness of topical calcipotriol to that of a standard hydrating ointment.37 Participants were randomized to 1 of 2 treatments before starting adjuvant radiotherapy to evaluate their potential in preventing radiation dermatitis. In 87% (20/23) of these patients, no difference in skin reaction was observed between the 2 treatments, suggesting that topical VD application may not offer any advantage over the standard hydrating ointment for the prevention of radiation dermatitis.37
Benefits of high-dose oral VD for treating radiation dermatitis also have been reported. Nguyen et al38 documented 3 cases in which patients with neuroendocrine carcinoma of the pancreas, tonsillar carcinoma, and breast cancer received 200,000 IU of oral ergocalciferol distributed over 2 doses given 7 days apart for radiation dermatitis. These patients experienced substantial improvements in pain, swelling, and redness within a week of the initial dose. Additionally, a case of radiation recall dermatitis, which occurred a week after vinorelbine chemotherapy, was treated with 2 doses totaling 100,000 IU of oral ergocalciferol. This patient also had improvement in pain and swelling but continued to have tumor-related induration and ulceration.39
Although topical VD did not show significant benefits over standard treatments for radiation dermatitis, high-dose oral VD appears promising in improving patient outcomes of pain and swelling more rapidly than current practices. Further research is needed to confirm these findings and establish standardized treatment protocols.
Final Thoughts
Suboptimal VD levels are prevalent in numerous cancer types. Chemotherapy often is associated with acute, potentially transient worsening of VD status in patients with breast and colorectal cancer. Although 25(OH)D levels have not corresponded with increased frequency of chemotherapy-related dermatologic AEs, suboptimal 25(OH)D levels appear to be associated with increased severity of radiation-induced mucositis and dermatitis.20,25,26 The use of high-dose VD as a therapeutic agent shows promise in mitigating chemotherapy-induced and radiation therapy–induced rashes in multiple cancer types with reduction of inflammatory markers and a durable anti-inflammatory impact. Although the mechanisms of cellular injury vary among chemotherapeutic agents, the anti-inflammatory and tissue repair properties of VD may make it an effective treatment for chemotherapy-induced cutaneous damage regardless of injury mechanism.2-4,35 However, reports of clinical improvement vary, and further objective studies to classify optimal dosing, administration, and outcome measures are needed. The absence of reported AEs associated with high-dose VD supplementation is encouraging, but selection of a safe and optimal dosing regimen can only occur with dedicated clinical trials.
- Bikle DD. Vitamin D and the skin: physiology and pathophysiology. Rev Endocr Metab Disord. 2012;13:3-19. doi:10.1007/s11154-011-9194-0
- Penna G, Adorini L. 1α,25-Dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164:2405-2411. doi:10.4049/jimmunol.164.5.2405
- Penna G, Amuchastegui S, Cossetti C, et al. Treatment of experimental autoimmune prostatitis in nonobese diabetic mice by the vitamin D receptor agonist elocalcitol. J Immunol. 2006;177:8504-8511. doi:10.4049/jimmunol.177.12.8504
- Heine G, Niesner U, Chang HD, et al. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur J Immunol. 2008;38:2210-2218. doi:10.1002/eji.200838216
- Hauser K, Walsh D, Shrotriya S, et al. Low 25-hydroxyvitamin D levels in people with a solid tumor cancer diagnosis: the tip of the iceberg? Support Care Cancer. 2014;22:1931-1939. doi:10.1007/s00520-014-2154-y
- Lee KJ, Wright G, Bryant H, et al. Cytoprotective effect of vitamin D on doxorubicin-induced cardiac toxicity in triple negative breast cancer. Int J Mol Sci. 2021;22:7439. doi:10.3390/ijms22147439
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-1930. doi:10.1210/jc.2011-0385
- Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74:1498-1513. doi:10.1038/s41430-020-0558-y
- Thomas X, Chelghoum Y, Fanari N, et al. Serum 25-hydroxyvitamin D levels are associated with prognosis in hematological malignancies. Hematology. 2011;16:278-283. doi:10.1179/102453311X13085644679908
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74:12-49. doi:10.3322/caac.21820
- Goodwin PJ, Ennis M, Pritchard KI, et al. Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J Clin Oncol. 2009;27:3757-3763. doi:10.1200/JCO.2008.20.0725
- Fassio A, Porciello G, Carioli G, et al. Post-diagnosis serum 25-hydroxyvitamin D concentrations in women treated for breast cancer participating in a lifestyle trial in Italy. Reumatismo. 2024;76:21-34.
- Augustin LSA, Libra M, Crispo A, et al. Low glycemic index diet, exercise and vitamin D to reduce breast cancer recurrence (DEDiCa): design of a clinical trial. BMC Cancer. 2017;17:69. doi:10.1186/s12885-017-3064-4
- Toriola AT, Nguyen N, Scheitler-Ring K, et al. Circulating 25-hydroxyvitamin D levels and prognosis among cancer patients: a systematic review. Cancer Epidemiol Biomarkers Prev. 2014;23:917-933. doi:10.1158/1055-9965.EPI-14-0053
- Fakih MG, Trump DL, Johnson CS, et al. Chemotherapy is linked to severe vitamin D deficiency in patients with colorectal cancer. Int J Colorectal Dis. 2009;24:219-224. doi:10.1007/s00384-008-0593-y
- Isenring EA, Teleni L, Woodman RJ, et al. Serum vitamin D decreases during chemotherapy: an Australian prospective cohort study. Asia Pac J Clin Nutr. 2018;27:962-967. doi:10.6133/apjcn.042018.01
- Kok DE, van den Berg MMGA, Posthuma L, et al. Changes in circulating levels of 25-hydroxyvitamin D3 in breast cancer patients receiving chemotherapy. Nutr Cancer. 2019;71:756-766. doi:10.1080/01635581.2018.1559938
- Wesselink E, Bours MJL, de Wilt JHW, et al. Chemotherapy and vitamin D supplement use are determinants of serum 25-hydroxyvitamin D levels during the first six months after colorectal cancer diagnosis. J Steroid Biochem Mol Biol. 2020;199:105577. doi:10.1016/j.jsbmb.2020.105577
- Savoie MB, Paciorek A, Zhang L, et al. Vitamin D levels in patients with colorectal cancer before and after treatment initiation. J Gastrointest Cancer. 2019;50:769-779. doi:10.1007/s12029-018-0147-7
- Kitchen D, Hughes B, Gill I, et al. The relationship between vitamin D and chemotherapy-induced toxicity—a pilot study. Br J Cancer. 2012;107:158-160. doi:10.1038/bjc.2012.194
- Demircay Z, Gürbüz O, Alpdogan TB, et al. Chemotherapy-induced acral erythema in leukemic patients: a report of 15 cases. Int J Dermatol. 1997;36:593-598. doi:10.1046/j.1365-4362.1997.00040.x
- Valks R, Fraga J, Porras-Luque J, et al. Chemotherapy-induced eccrine squamous syringometaplasia. a distinctive eruption in patients receiving hematopoietic progenitor cells. Arch Dermatol. 1997;133;873-878. doi:10.1001/archderm.133.7.873
- Webber KA, Kos L, Holland KE, et al. Intertriginous eruption associated with chemotherapy in pediatric patients. Arch Dermatol. 2007;143:67-71. doi:10.1001/archderm.143.1.67
- Hunjan MK, Nowsheen S, Ramos-Rodriguez AJ, et al. Clinical and histopathological spectrum of toxic erythema of chemotherapy in patients who have undergone allogeneic hematopoietic cell transplantation. Hematol Oncol Stem Cell Ther. 2019;12:19-25. doi:10.1016/j.hemonc.2018.09.001
- Ghorbanzadeh-Moghaddam A, Gholamrezaei A, Hemati S. Vitamin D deficiency is associated with the severity of radiation-induced proctitis in cancer patients. Int J Radiat Oncol Biol Phys. 2015;92:613-618. doi:10.1016/j.ijrobp.2015.02.011
- Bhanu A, Waghmare CM, Jain VS, et al. Serum 25-hydroxy vitamin-D levels in head and neck cancer chemoradiation therapy: potential in cancer therapeutics. Indian J Cancer. Published online February 27, 2003. doi:10.4103/ijc.ijc_358_20
- Yang B, Xie X, Wu Z, et al. DNA damage-mediated cellular senescence promotes hand-foot syndrome that can be relieved by thymidine prodrug. Genes Dis. 2022;10:2557-2571. doi:10.1016/j.gendis.2022.10.004
- Lassere Y, Hoff P. Management of hand-foot syndrome in patients treated with capecitabine (Xeloda®). Eur J Oncol Nurs. 2004;8(suppl 1):S31-S40. doi:10.1016/j.ejon.2004.06.007
- Ernst MK, Evans ST, Techner JM, et al. Vitamin D3 and deconvoluting a rash. JCI Insight. 2023;8:E163789.
- Nguyen CV, Zheng L, Zhou XA, et al. High-dose vitamin d for the management of toxic erythema of chemotherapy in hospitalized patients. JAMA Dermatol. 2023;159:219-221. doi:10.1001/jamadermatol.2022.5397
- Fisher J, Scott C, Stevens R, et al. Randomized phase III study comparing best supportive care to biafine as a prophylactic agent for radiation-induced skin toxicity for women undergoing breast irradiation: Radiation Therapy Oncology Group (RTOG) 97-13. Int J Radiat Oncol Biol Phys. 2000;48:1307-1310. doi:10.1016/s0360-3016(00)00782-3
- Pignol JP, Olivotto I, Rakovitch E, et al. A multicenter randomized trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitis. J Clin Oncol. 2008;26:2085-2092. doi:10.1200/JCO.2007.15.2488
- Hymes SR, Strom EA, Fife C. Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006. J Am Acad Dermatol. 2006;54:28-46. doi:10.1016/j.jaad.2005.08.054
- Ryan JL. Ionizing radiation: the good, the bad, and the ugly. J Invest Dermatol. 2012;132(3 pt 2):985-993. doi:10.1038/jid.2011.411
- Scott JF, Das LM, Ahsanuddin S, et al. Oral vitamin D rapidly attenuates inflammation from sunburn: an interventional study. J Invest Dermatol. 2017;137:2078-2086. doi:10.1016/j.jid.2017.04.040
- Das LM, Binko AM, Traylor ZP, et al. Vitamin D improves sunburns by increasing autophagy in M2 macrophages. Autophagy. 2019;15:813-826. doi:10.1080/15548627.2019.1569298
- Nasser NJ, Fenig S, Ravid A, et al. Vitamin D ointment for prevention of radiation dermatitis in breast cancer patients. NPJ Breast Cancer. 2017;3:10. doi:10.1038/s41523-017-0006-x
- Nguyen CV, Zheng L, Lu KQ. High-dose vitamin D for the management acute radiation dermatitis. JAAD Case Rep. 2023;39:47-50. doi:10.1016/j.jdcr.2023.07.001
- Nguyen CV, Lu KQ. Vitamin D3 and its potential to ameliorate chemical and radiation-induced skin injury during cancer therapy. Disaster Med Public Health Prep. 2024;18:E4. doi:10.1017/dmp.2023.211
Vitamin D (VD) regulates keratinocyte proliferation and differentiation, modulates inflammatory pathways, and protects against cellular damage in the skin. 1 In the setting of tissue injury and acute skin inflammation, active vitamin D—1,25(OH) 2 D—suppresses signaling from pro-inflammatory chemokines and cytokines such as IFN- γ and IL-17. 2,3 This suppression reduces proliferation of helper T cells (T H 1, T H 17) and B cells, decreasing tissue damage from reactive oxygen species release while enhancing secretion of the anti-inflammatory cytokine IL-10 by antigen-presenting cells. 2-4
Suboptimal VD levels have been associated with numerous health consequences including malignancy, prompting interest in VD supplementation for improving cancer-related outcomes.5 Beyond disease prognosis, high-dose VD supplementation has been suggested as a potential therapy for adverse events (AEs) related to cancer treatments. In one study, mice that received oral vitamin D3 supplementation of 11,500 IU/kg daily had fewer doxorubicin-induced cardiotoxic effects on ejection fraction (P<.0001) and stroke volume (P<.01) than mice that received VD supplementation of 1500 IU/kg daily.6
In this review, we examine the impact of chemoradiation on 25(OH)D levels—which more accurately reflects VD stores than 1,25(OH)2D levels—and the impact of suboptimal VD on cutaneous toxicities related to chemoradiation. To define the suboptimal VD threshold, we used the Endocrine Society’s clinical practice guidelines, which characterize suboptimal 25(OH)D levels as insufficiency (21–29 ng/mL [52.5–72.5 nmol/L]) or deficiency (<20 ng/mL [50 nmol/L])7; deficiency can be further categorized as severe deficiency (<12 ng/mL [30 nmol/L]).8 This review also evaluates the evidence for vitamin D3 supplementation to alleviate the cutaneous AEs of chemotherapy and radiation treatments.
Effects of Chemotherapy on Vitamin D Levels
A high prevalence of VD deficiency is seen in various cancers. In a retrospective review of 25(OH)D levels in 2098 adults with solid tumors of any stage (6% had metastatic disease [n=124]), suboptimal levels were found in 69% of patients with breast cancer (n=617), 75% with colorectal cancer (n=84), 72% with gynecologic cancer (n=65), 79% with kidney and bladder cancer (n=145), 83% with pancreatic and upper gastrointestinal tract cancer (n=178), 73% with lung cancer (n=73), 69% with prostate cancer (n=225), 61% with skin cancer (n=399), and 63% with thyroid cancer (n=172).5 Suboptimal VD also has been found in hematologic malignancies. In a prospective cohort study, mean serum 25(OH)D levels in 23 patients with recently diagnosed acute myeloid leukemia demonstrated VD deficiency (mean [SD], 18.6 [6.6] nmol/L).9 Given that many patients already exhibit a baseline VD deficiency at cancer diagnosis, it is important to understand the relationship between VD and cancer treatment modalities.5
In the United States, breast and colorectal cancers were estimated to be the first and fourth most common cancers, with 313,510 and 152,810 predicted new cases in 2024, respectively.10 This review will focus on breast and colorectal cancer when describing VD variation associated with chemotherapy exposure due to their high prevalence.
Effects of Chemotherapy on Vitamin D Levels in Breast Cancer—Breast cancer studies have shown suboptimal VD levels in 76% of females 75 years or younger with any T1, T2, or T3; N0 or N1; and M0 breast cancer, in which 38.5% (n=197) had insufficient and 37.5% (n=192) had deficient 25(OH)D levels.11 In a study of female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), VD deficiency was seen in 60% of patients not receiving VD supplementation.12,13 A systematic review that included 7 studies of different types of breast cancer suggested that circulating 25(OH)D may be associated with improved prognosis.14 Thus, studies have investigated risk factors associated with poor or worsening VD status in individuals with breast cancer, including exposure to chemotherapy and/or radiation treatment.12,15-18
A prospective cohort study assessed 25(OH)D levels in 95 patients with any breast cancer (stages I, II, IIIA, IIIB) before and after initiating chemotherapy with docetaxel, doxorubicin, epirubicin, 5-fluorouracil, or cyclophosphamide, compared with a group of 52 females without cancer.17 In the breast cancer group, approximately 80% (76/95) had suboptimal and 50% (47/95) had deficient VD levels before chemotherapy initiation (mean [SD], 54.1 [22.8] nmol/L). In the comparison group, 60% (31/52) had suboptimal and 30% (15/52) had deficient VD at baseline (mean [SD], 66.1 [23.5] nmol/L), which was higher than the breast cancer group (P=.03). A subgroup analysis excluded participants who started, stopped, or lacked data on dietary supplements containing VD (n=39); in the remaining 56 participants, a significant decrease in 25(OH)D levels was observed shortly after finishing chemotherapy compared with the prechemotherapy baseline value (mean, −7.9 nmol/L; P=.004). Notably, 6 months after chemotherapy completion, 25(OH)D levels increased (mean, +12.8 nmol/L; P<.001). Vitamin D levels remained stable in the comparison group (P=.987).17
Consistent with these findings, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of chemotherapy was associated with increased odds of 25(OH)D levels less than 20 ng/mL compared with breast cancer patients with no prior chemotherapy (odds ratio, 1.86; 95% CI, 1.03-3.38).12 Although the study data included chemotherapy history, no information was provided on specific chemotherapy agents or regimens used in this cohort, limiting the ability to detect the drugs most often implicated.
Both studies indicated a complex interplay between chemotherapy and VD levels in breast cancer patients. Although Kok et al17 suggested a transient decrease in VD levels during chemotherapy with a subsequent recovery after cessation, Fassio et al12 highlighted the increased odds of VD deficiency associated with chemotherapy. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status in breast cancer patients.
Effects of Chemotherapy on Vitamin D Levels in Colorectal Cancer—Similar to patterns seen in breast cancer, a systematic review with 6 studies of different types of colorectal cancer suggested that circulating 25(OH)D levels may be associated with prognosis.14 Studies also have investigated the relationship between colorectal chemotherapy regimens and VD status.15,16,18,19
A retrospective study assessed 25(OH)D levels in 315 patients with any colorectal cancer (stage I–IV).15 Patients were included in the analysis if they received less than 400 IU daily of VD supplementation at baseline. For the whole study sample, the mean (SD) VD level was 23.7 (13.71) ng/mL. Patients who had not received chemotherapy within 3 months of the VD level assessment were categorized as the no chemotherapy group, and the others were designated as the chemotherapy group; the latter group was exposed to various chemotherapy regimens, including combinations of irinotecan, oxaliplatin, 5-fluorouracil, leucovorin, bevacizumab, or cetuximab. Multivariate analysis showed that the chemotherapy group was 3.7 times more likely to have very low VD levels (≤15 ng/mL) compared with those in the no chemotherapy group (P<.0001).15
A separate cross-sectional study examined serum 25(OH)D concentrations in 1201 patients with any newly diagnosed colorectal carcinoma (stage I–III); 91% of cases were adenocarcinoma.18 In a multivariate analysis, chemotherapy plus surgery was associated with lower VD levels than surgery alone 6 months after diagnosis (mean, −8.74 nmol/L; 95% CI, −11.30 to −6.18 nmol/L), specifically decreasing by a mean of 6.7 nmol/L (95% CI, −9.8 to −3.8 nmol/L) after adjusting for demographic and lifestyle factors.18 However, a prospective cohort study demonstrated different findings.19 Comparing 58 patients with newly diagnosed colorectal adenocarcinoma (stages I–IV) who underwent chemotherapy and 36 patients who did not receive chemotherapy, there was no significant change in 25(OH)D levels from the time of diagnosis to 6 months later. Median VD levels decreased by 0.7 ng/mL in those who received chemotherapy, while a minimal (and not significant) increase of 1.6 ng/mL was observed in those without chemotherapy intervention (P=.26). Notably, supplementation was not restricted in this cohort, which may have resulted in higher VD levels in those taking supplements.19
Since time of year and geographic location can influence VD levels, one prospective cohort study controlled for differential sun exposure due to these factors in their analysis.16 Assessment of 25(OH)D levels was completed in 81 chemotherapy-naïve cancer patients immediately before beginning chemotherapy as well as 6 and 12 weeks into treatment. More than 8 primary cancer types were represented in this study, with breast (34% [29/81]) and colorectal (14% [12/81]) cancer being the most common, but the cancer stages of the participants were not detailed. Vitamin D levels decreased after commencing chemotherapy, with the largest drop occurring 6 weeks into treatment. From the 6- to 12-week end points, VD increased but remained below the original baseline level (baseline: mean [SD], 49.2 [22.3] nmol/L; 6 weeks: mean [SD], 40.9 [19.0] nmol/L; 12 weeks: mean [SD], 45.9 [19.7] nmol/L; P=.05).16
Although focused on breast and colorectal cancers, these studies suggest that various chemotherapy regimens may confer a higher risk for VD deficiency compared with VD status at diagnosis and/or prior to chemotherapy treatment. However, most of these studies only discussed stage-based differences, excluding analysis of the variety of cancer subtypes that comprise breast and colorectal malignancies, which may limit our ability to extrapolate from these data. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status across various primary cancer types.
Effects of Radiation Therapy on Vitamin D Levels
Unlike chemotherapy, studies on the association between radiation therapy and VD levels are minimal, with most reports in the literature discussing the use of VD to potentiate the effects of radiation therapy. In one cross-sectional analysis of 1201 patients with newly diagnosed stage I, II, or III colorectal cancer of any type (94% were adenocarcinoma), radiation plus surgery was associated with slightly lower 25(OH)D levels than surgery alone for tumor treatment 6 months after diagnosis (mean, −3.17; 95% CI, −6.07 to −0.28 nmol/L). However, after adjustment for demographic and lifestyle factors, this decrease in VD levels attributable to radiotherapy was not statistically significant compared with the surgery-only cohort (mean, −1.78; 95% CI, −5.07 to 1.52 nmol/L).18
Similarly, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of radiotherapy was not associated with a difference in serum 25(OH)D levels compared with those with breast cancer without prior radiotherapy (odds ratio, 0.90; 95% CI, 0.52-1.54).12 From the limited existing literature specifically addressing variations of VD levels with radiation, radiation therapy does not appear to significantly impact VD levels.
Vitamin D Levels and the Severity of Chemotherapy- or Radiation Therapy–Induced AEs
A prospective cohort of 241 patients did not find an increase in the incidence or severity of chemotherapy-induced cutaneous toxicities in those with suboptimal 1,25(OH)2D3 levels (≤75 nmol/L).20 Eight different primary cancer types were represented, including breast and colorectal cancer; the tumor stages of the participants were not detailed. Forty-one patients had normal 1,25(OH)2D3 levels, while the remaining 200 had suboptimal levels. There was no significant association between serum VD levels and the following dermatologic toxicities: desquamation (P=.26), xerosis (P=.15), mucositis (P=.30), or painful rash (P=.87). Surprisingly, nail changes and hand-foot reactions occurred with greater frequency in patients with normal VD levels (P=.01 and P=.03, respectively).20 Hand-foot reaction is part of the toxic erythema of chemotherapy (TEC) spectrum, which is comprised of a range of cytotoxic skin injuries that typically manifest within 2 to 3 weeks of exposure to the offending chemotherapeutic agents, often characterized by erythema, pain, swelling, and blistering, particularly in intertriginous and acral areas.21-23 Recovery from TEC generally takes at least 2 to 4 weeks and may necessitate cessation of the offending chemotherapeutic agent.21,24 Notably, this study measured 1,25(OH)2D3 levels instead of 25(OH)D levels, which may not reliably indicate body stores of VD.7,20 These results underscore the complex nature between chemotherapy and VD; however, VD levels alone do not appear to be a sufficient biomarker for predicting chemotherapy-associated cutaneous AEs.
Interestingly, radiation therapy–induced AEs may be associated with VD levels. A prospective cohort study of 98 patients with prostate, bladder, or gynecologic cancers (tumor stages were not detailed) undergoing pelvic radiotherapy found that females and males with 25(OH)D levels below a threshold of 35 and 40 nmol/L, respectively, were more likely to experience higher Radiation Therapy Oncology Group (RTOG) grade acute proctitis compared with those with VD above these thresholds.25 Specifically, VD below these thresholds was associated with increased odds of RTOG grade 2 or higher radiation-induced proctitis (OR, 3.07; 95% CI, 1.27-7.50 [P=.013]). Additionally, a weak correlation was noted between VD below these thresholds and the RTOG grade, with a Spearman correlation value of −0.189 (P=.031).25
One prospective cohort study included 28 patients with any cancer of the oral cavity, oropharynx, hypopharynx, or larynx stages II, III, or IVA; 93% (26/28) were stage III or IVA.26 The 20 (71%) patients with suboptimal 25(OH)D levels (≤75 nmol/L) experienced a higher prevalence of grade II radiation dermatitis compared with the 8 (29%) patients with optimal VD levels (χ22 =5.973; P=.0505). This pattern persisted with the severity of mucositis; patients from the suboptimal VD group presented with higher rates of grades II and III mucositis compared with the VD optimal group (χ22 =13.627; P=.0011).26 Recognizing the small cohort evaluated in the study, we highlight the importance of further studies to clarify these associations.
Chemotherapy-Induced Cutaneous Events Treated with High-Dose Vitamin D
Chemotherapeutic agents are known to induce cellular damage, resulting in a range of cutaneous AEs that can invoke discontinuation of otherwise effective chemotherapeutic interventions.27,28 Recent research has explored the potential of high-dose vitamin D3 as a therapeutic agent to mitigate cutaneous reactions.29,30
A randomized, double-blind, placebo-controlled trial investigated the use of a single high dose of oral 25(OH)D to treat topical nitrogen mustard (NM)–induced rash.29 To characterize baseline inflammatory responses from NM injury without intervention, clinical measures, serum studies, and tissue analyses from skin biopsies were performed on 28 healthy adults after exposure to topical NM—a chemotherapeutic agent classified as a DNA alkylator. Two weeks later, participants were exposed to topical NM a second time and were split into 2 groups: 14 patients received a single 200,000-IU dose of oral 25(OH)D while the other 14 participants were given a placebo. Using the inflammatory markers induced from baseline exposure to NM alone, posttreatment analysis revealed that the punch biopsies from
Although Ernst et al29 did not observe any clinically significant improvements with VD treatment, a case series of 6 patients with either glioblastoma multiforme, acute myeloid leukemia, or aplastic anemia did demonstrate clinical improvement of TEC after receiving high-dose vitamin D3.30 The mean time to onset of TEC was noted at 8.5 days following administration of the inciting chemotherapeutic agent, which included combinations of anthracycline, antimetabolite, kinase inhibitor, B-cell lymphoma 2 inhibitor, purine analogue, and alkylating agents. A combination of clinical and histologic findings was used to diagnose TEC. Baseline 25(OH)D levels were not established prior to treatment. The treatment regimen for 1 patient included 2 doses of 50,000 IU of VD spaced 1 week apart, totaling 100,000 IU, while the remaining 5 patients received a total of 200,000 IU, also split into 2 doses given 1 week apart. All patients received their first dose of VD within a week of the cutaneous eruption. Following the initial VD dose, there was a notable improvement in pain, pruritus, or swelling by the next day. Reduction in erythema also was observed within 1 to 4 days.30
No AEs associated with VD supplementation were reported, suggesting a potential beneficial role of high-dose VD in accelerating recovery from chemotherapy-induced rashes without evident safety concerns.
Radiation Therapy–Induced Cutaneous Events Treated with High-Dose Vitamin D
Radiation dermatitis is a common and often severe complication of radiation therapy that affects more than 90% of patients undergoing treatment, with half of these individuals experiencing grade 2 toxicity, according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events.31,32 Radiation damage to basal keratinocytes and hair follicle stem cells disrupts the renewal of the skin’s outer layer, while a surge of free radicals causes irreversible DNA damage.33 Symptoms of radiation dermatitis can vary from mild pink erythema to tissue ulceration and necrosis, typically within 1 to 4 weeks of radiation exposure.34 The resulting dermatitis can take 2 to 4 weeks to heal, notably impacting patient quality of life and often necessitating modifications or interruptions in cancer therapy.33
Prior studies have demonstrated the use of high-dose VD to improve the healing of UV-irradiated skin. A randomized controlled trial investigated high-dose vitamin D3 to treat experimentally induced sunburn in 20 healthy adults. Compared with those who received a placebo, participants receiving the oral dose of 200,000 IU of vitamin D3 demonstrated suppression of the pro-inflammatory mediators tumor necrosis factor α (P=.04) and inducible nitric oxide synthase (P=.02), while expression of tissue repair enhancer arginase 1 was increased (P<.005).35 The mechanism of this enhanced tissue repair was investigated using a mouse model, in which intraperitoneal 25(OH)D was administered following severe UV-induced skin injury. On immunofluorescence microscopy, mice treated with VD showed enhanced autophagy within the macrophages infiltrating UV-irradiated skin.36 The use of high-dose VD to treat UV-irradiated skin in these studies established a precedent for using VD to heal cutaneous injury caused by ionizing radiation therapy.
Some studies have focused on the role of VD for treating acute radiation dermatitis. A study of 23 patients with ductal carcinoma in situ or localized invasive ductal carcinoma breast cancer compared the effectiveness of topical calcipotriol to that of a standard hydrating ointment.37 Participants were randomized to 1 of 2 treatments before starting adjuvant radiotherapy to evaluate their potential in preventing radiation dermatitis. In 87% (20/23) of these patients, no difference in skin reaction was observed between the 2 treatments, suggesting that topical VD application may not offer any advantage over the standard hydrating ointment for the prevention of radiation dermatitis.37
Benefits of high-dose oral VD for treating radiation dermatitis also have been reported. Nguyen et al38 documented 3 cases in which patients with neuroendocrine carcinoma of the pancreas, tonsillar carcinoma, and breast cancer received 200,000 IU of oral ergocalciferol distributed over 2 doses given 7 days apart for radiation dermatitis. These patients experienced substantial improvements in pain, swelling, and redness within a week of the initial dose. Additionally, a case of radiation recall dermatitis, which occurred a week after vinorelbine chemotherapy, was treated with 2 doses totaling 100,000 IU of oral ergocalciferol. This patient also had improvement in pain and swelling but continued to have tumor-related induration and ulceration.39
Although topical VD did not show significant benefits over standard treatments for radiation dermatitis, high-dose oral VD appears promising in improving patient outcomes of pain and swelling more rapidly than current practices. Further research is needed to confirm these findings and establish standardized treatment protocols.
Final Thoughts
Suboptimal VD levels are prevalent in numerous cancer types. Chemotherapy often is associated with acute, potentially transient worsening of VD status in patients with breast and colorectal cancer. Although 25(OH)D levels have not corresponded with increased frequency of chemotherapy-related dermatologic AEs, suboptimal 25(OH)D levels appear to be associated with increased severity of radiation-induced mucositis and dermatitis.20,25,26 The use of high-dose VD as a therapeutic agent shows promise in mitigating chemotherapy-induced and radiation therapy–induced rashes in multiple cancer types with reduction of inflammatory markers and a durable anti-inflammatory impact. Although the mechanisms of cellular injury vary among chemotherapeutic agents, the anti-inflammatory and tissue repair properties of VD may make it an effective treatment for chemotherapy-induced cutaneous damage regardless of injury mechanism.2-4,35 However, reports of clinical improvement vary, and further objective studies to classify optimal dosing, administration, and outcome measures are needed. The absence of reported AEs associated with high-dose VD supplementation is encouraging, but selection of a safe and optimal dosing regimen can only occur with dedicated clinical trials.
Vitamin D (VD) regulates keratinocyte proliferation and differentiation, modulates inflammatory pathways, and protects against cellular damage in the skin. 1 In the setting of tissue injury and acute skin inflammation, active vitamin D—1,25(OH) 2 D—suppresses signaling from pro-inflammatory chemokines and cytokines such as IFN- γ and IL-17. 2,3 This suppression reduces proliferation of helper T cells (T H 1, T H 17) and B cells, decreasing tissue damage from reactive oxygen species release while enhancing secretion of the anti-inflammatory cytokine IL-10 by antigen-presenting cells. 2-4
Suboptimal VD levels have been associated with numerous health consequences including malignancy, prompting interest in VD supplementation for improving cancer-related outcomes.5 Beyond disease prognosis, high-dose VD supplementation has been suggested as a potential therapy for adverse events (AEs) related to cancer treatments. In one study, mice that received oral vitamin D3 supplementation of 11,500 IU/kg daily had fewer doxorubicin-induced cardiotoxic effects on ejection fraction (P<.0001) and stroke volume (P<.01) than mice that received VD supplementation of 1500 IU/kg daily.6
In this review, we examine the impact of chemoradiation on 25(OH)D levels—which more accurately reflects VD stores than 1,25(OH)2D levels—and the impact of suboptimal VD on cutaneous toxicities related to chemoradiation. To define the suboptimal VD threshold, we used the Endocrine Society’s clinical practice guidelines, which characterize suboptimal 25(OH)D levels as insufficiency (21–29 ng/mL [52.5–72.5 nmol/L]) or deficiency (<20 ng/mL [50 nmol/L])7; deficiency can be further categorized as severe deficiency (<12 ng/mL [30 nmol/L]).8 This review also evaluates the evidence for vitamin D3 supplementation to alleviate the cutaneous AEs of chemotherapy and radiation treatments.
Effects of Chemotherapy on Vitamin D Levels
A high prevalence of VD deficiency is seen in various cancers. In a retrospective review of 25(OH)D levels in 2098 adults with solid tumors of any stage (6% had metastatic disease [n=124]), suboptimal levels were found in 69% of patients with breast cancer (n=617), 75% with colorectal cancer (n=84), 72% with gynecologic cancer (n=65), 79% with kidney and bladder cancer (n=145), 83% with pancreatic and upper gastrointestinal tract cancer (n=178), 73% with lung cancer (n=73), 69% with prostate cancer (n=225), 61% with skin cancer (n=399), and 63% with thyroid cancer (n=172).5 Suboptimal VD also has been found in hematologic malignancies. In a prospective cohort study, mean serum 25(OH)D levels in 23 patients with recently diagnosed acute myeloid leukemia demonstrated VD deficiency (mean [SD], 18.6 [6.6] nmol/L).9 Given that many patients already exhibit a baseline VD deficiency at cancer diagnosis, it is important to understand the relationship between VD and cancer treatment modalities.5
In the United States, breast and colorectal cancers were estimated to be the first and fourth most common cancers, with 313,510 and 152,810 predicted new cases in 2024, respectively.10 This review will focus on breast and colorectal cancer when describing VD variation associated with chemotherapy exposure due to their high prevalence.
Effects of Chemotherapy on Vitamin D Levels in Breast Cancer—Breast cancer studies have shown suboptimal VD levels in 76% of females 75 years or younger with any T1, T2, or T3; N0 or N1; and M0 breast cancer, in which 38.5% (n=197) had insufficient and 37.5% (n=192) had deficient 25(OH)D levels.11 In a study of female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), VD deficiency was seen in 60% of patients not receiving VD supplementation.12,13 A systematic review that included 7 studies of different types of breast cancer suggested that circulating 25(OH)D may be associated with improved prognosis.14 Thus, studies have investigated risk factors associated with poor or worsening VD status in individuals with breast cancer, including exposure to chemotherapy and/or radiation treatment.12,15-18
A prospective cohort study assessed 25(OH)D levels in 95 patients with any breast cancer (stages I, II, IIIA, IIIB) before and after initiating chemotherapy with docetaxel, doxorubicin, epirubicin, 5-fluorouracil, or cyclophosphamide, compared with a group of 52 females without cancer.17 In the breast cancer group, approximately 80% (76/95) had suboptimal and 50% (47/95) had deficient VD levels before chemotherapy initiation (mean [SD], 54.1 [22.8] nmol/L). In the comparison group, 60% (31/52) had suboptimal and 30% (15/52) had deficient VD at baseline (mean [SD], 66.1 [23.5] nmol/L), which was higher than the breast cancer group (P=.03). A subgroup analysis excluded participants who started, stopped, or lacked data on dietary supplements containing VD (n=39); in the remaining 56 participants, a significant decrease in 25(OH)D levels was observed shortly after finishing chemotherapy compared with the prechemotherapy baseline value (mean, −7.9 nmol/L; P=.004). Notably, 6 months after chemotherapy completion, 25(OH)D levels increased (mean, +12.8 nmol/L; P<.001). Vitamin D levels remained stable in the comparison group (P=.987).17
Consistent with these findings, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of chemotherapy was associated with increased odds of 25(OH)D levels less than 20 ng/mL compared with breast cancer patients with no prior chemotherapy (odds ratio, 1.86; 95% CI, 1.03-3.38).12 Although the study data included chemotherapy history, no information was provided on specific chemotherapy agents or regimens used in this cohort, limiting the ability to detect the drugs most often implicated.
Both studies indicated a complex interplay between chemotherapy and VD levels in breast cancer patients. Although Kok et al17 suggested a transient decrease in VD levels during chemotherapy with a subsequent recovery after cessation, Fassio et al12 highlighted the increased odds of VD deficiency associated with chemotherapy. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status in breast cancer patients.
Effects of Chemotherapy on Vitamin D Levels in Colorectal Cancer—Similar to patterns seen in breast cancer, a systematic review with 6 studies of different types of colorectal cancer suggested that circulating 25(OH)D levels may be associated with prognosis.14 Studies also have investigated the relationship between colorectal chemotherapy regimens and VD status.15,16,18,19
A retrospective study assessed 25(OH)D levels in 315 patients with any colorectal cancer (stage I–IV).15 Patients were included in the analysis if they received less than 400 IU daily of VD supplementation at baseline. For the whole study sample, the mean (SD) VD level was 23.7 (13.71) ng/mL. Patients who had not received chemotherapy within 3 months of the VD level assessment were categorized as the no chemotherapy group, and the others were designated as the chemotherapy group; the latter group was exposed to various chemotherapy regimens, including combinations of irinotecan, oxaliplatin, 5-fluorouracil, leucovorin, bevacizumab, or cetuximab. Multivariate analysis showed that the chemotherapy group was 3.7 times more likely to have very low VD levels (≤15 ng/mL) compared with those in the no chemotherapy group (P<.0001).15
A separate cross-sectional study examined serum 25(OH)D concentrations in 1201 patients with any newly diagnosed colorectal carcinoma (stage I–III); 91% of cases were adenocarcinoma.18 In a multivariate analysis, chemotherapy plus surgery was associated with lower VD levels than surgery alone 6 months after diagnosis (mean, −8.74 nmol/L; 95% CI, −11.30 to −6.18 nmol/L), specifically decreasing by a mean of 6.7 nmol/L (95% CI, −9.8 to −3.8 nmol/L) after adjusting for demographic and lifestyle factors.18 However, a prospective cohort study demonstrated different findings.19 Comparing 58 patients with newly diagnosed colorectal adenocarcinoma (stages I–IV) who underwent chemotherapy and 36 patients who did not receive chemotherapy, there was no significant change in 25(OH)D levels from the time of diagnosis to 6 months later. Median VD levels decreased by 0.7 ng/mL in those who received chemotherapy, while a minimal (and not significant) increase of 1.6 ng/mL was observed in those without chemotherapy intervention (P=.26). Notably, supplementation was not restricted in this cohort, which may have resulted in higher VD levels in those taking supplements.19
Since time of year and geographic location can influence VD levels, one prospective cohort study controlled for differential sun exposure due to these factors in their analysis.16 Assessment of 25(OH)D levels was completed in 81 chemotherapy-naïve cancer patients immediately before beginning chemotherapy as well as 6 and 12 weeks into treatment. More than 8 primary cancer types were represented in this study, with breast (34% [29/81]) and colorectal (14% [12/81]) cancer being the most common, but the cancer stages of the participants were not detailed. Vitamin D levels decreased after commencing chemotherapy, with the largest drop occurring 6 weeks into treatment. From the 6- to 12-week end points, VD increased but remained below the original baseline level (baseline: mean [SD], 49.2 [22.3] nmol/L; 6 weeks: mean [SD], 40.9 [19.0] nmol/L; 12 weeks: mean [SD], 45.9 [19.7] nmol/L; P=.05).16
Although focused on breast and colorectal cancers, these studies suggest that various chemotherapy regimens may confer a higher risk for VD deficiency compared with VD status at diagnosis and/or prior to chemotherapy treatment. However, most of these studies only discussed stage-based differences, excluding analysis of the variety of cancer subtypes that comprise breast and colorectal malignancies, which may limit our ability to extrapolate from these data. Ultimately, larger randomized controlled trials are needed to better understand the relationship between chemotherapy and VD status across various primary cancer types.
Effects of Radiation Therapy on Vitamin D Levels
Unlike chemotherapy, studies on the association between radiation therapy and VD levels are minimal, with most reports in the literature discussing the use of VD to potentiate the effects of radiation therapy. In one cross-sectional analysis of 1201 patients with newly diagnosed stage I, II, or III colorectal cancer of any type (94% were adenocarcinoma), radiation plus surgery was associated with slightly lower 25(OH)D levels than surgery alone for tumor treatment 6 months after diagnosis (mean, −3.17; 95% CI, −6.07 to −0.28 nmol/L). However, after adjustment for demographic and lifestyle factors, this decrease in VD levels attributable to radiotherapy was not statistically significant compared with the surgery-only cohort (mean, −1.78; 95% CI, −5.07 to 1.52 nmol/L).18
Similarly, a cross-sectional study assessing VD status in 394 female patients with primary breast cancer (stage I, II, or III and T1 with high Ki67 expression [≥30%], T2, or T3), found that a history of radiotherapy was not associated with a difference in serum 25(OH)D levels compared with those with breast cancer without prior radiotherapy (odds ratio, 0.90; 95% CI, 0.52-1.54).12 From the limited existing literature specifically addressing variations of VD levels with radiation, radiation therapy does not appear to significantly impact VD levels.
Vitamin D Levels and the Severity of Chemotherapy- or Radiation Therapy–Induced AEs
A prospective cohort of 241 patients did not find an increase in the incidence or severity of chemotherapy-induced cutaneous toxicities in those with suboptimal 1,25(OH)2D3 levels (≤75 nmol/L).20 Eight different primary cancer types were represented, including breast and colorectal cancer; the tumor stages of the participants were not detailed. Forty-one patients had normal 1,25(OH)2D3 levels, while the remaining 200 had suboptimal levels. There was no significant association between serum VD levels and the following dermatologic toxicities: desquamation (P=.26), xerosis (P=.15), mucositis (P=.30), or painful rash (P=.87). Surprisingly, nail changes and hand-foot reactions occurred with greater frequency in patients with normal VD levels (P=.01 and P=.03, respectively).20 Hand-foot reaction is part of the toxic erythema of chemotherapy (TEC) spectrum, which is comprised of a range of cytotoxic skin injuries that typically manifest within 2 to 3 weeks of exposure to the offending chemotherapeutic agents, often characterized by erythema, pain, swelling, and blistering, particularly in intertriginous and acral areas.21-23 Recovery from TEC generally takes at least 2 to 4 weeks and may necessitate cessation of the offending chemotherapeutic agent.21,24 Notably, this study measured 1,25(OH)2D3 levels instead of 25(OH)D levels, which may not reliably indicate body stores of VD.7,20 These results underscore the complex nature between chemotherapy and VD; however, VD levels alone do not appear to be a sufficient biomarker for predicting chemotherapy-associated cutaneous AEs.
Interestingly, radiation therapy–induced AEs may be associated with VD levels. A prospective cohort study of 98 patients with prostate, bladder, or gynecologic cancers (tumor stages were not detailed) undergoing pelvic radiotherapy found that females and males with 25(OH)D levels below a threshold of 35 and 40 nmol/L, respectively, were more likely to experience higher Radiation Therapy Oncology Group (RTOG) grade acute proctitis compared with those with VD above these thresholds.25 Specifically, VD below these thresholds was associated with increased odds of RTOG grade 2 or higher radiation-induced proctitis (OR, 3.07; 95% CI, 1.27-7.50 [P=.013]). Additionally, a weak correlation was noted between VD below these thresholds and the RTOG grade, with a Spearman correlation value of −0.189 (P=.031).25
One prospective cohort study included 28 patients with any cancer of the oral cavity, oropharynx, hypopharynx, or larynx stages II, III, or IVA; 93% (26/28) were stage III or IVA.26 The 20 (71%) patients with suboptimal 25(OH)D levels (≤75 nmol/L) experienced a higher prevalence of grade II radiation dermatitis compared with the 8 (29%) patients with optimal VD levels (χ22 =5.973; P=.0505). This pattern persisted with the severity of mucositis; patients from the suboptimal VD group presented with higher rates of grades II and III mucositis compared with the VD optimal group (χ22 =13.627; P=.0011).26 Recognizing the small cohort evaluated in the study, we highlight the importance of further studies to clarify these associations.
Chemotherapy-Induced Cutaneous Events Treated with High-Dose Vitamin D
Chemotherapeutic agents are known to induce cellular damage, resulting in a range of cutaneous AEs that can invoke discontinuation of otherwise effective chemotherapeutic interventions.27,28 Recent research has explored the potential of high-dose vitamin D3 as a therapeutic agent to mitigate cutaneous reactions.29,30
A randomized, double-blind, placebo-controlled trial investigated the use of a single high dose of oral 25(OH)D to treat topical nitrogen mustard (NM)–induced rash.29 To characterize baseline inflammatory responses from NM injury without intervention, clinical measures, serum studies, and tissue analyses from skin biopsies were performed on 28 healthy adults after exposure to topical NM—a chemotherapeutic agent classified as a DNA alkylator. Two weeks later, participants were exposed to topical NM a second time and were split into 2 groups: 14 patients received a single 200,000-IU dose of oral 25(OH)D while the other 14 participants were given a placebo. Using the inflammatory markers induced from baseline exposure to NM alone, posttreatment analysis revealed that the punch biopsies from
Although Ernst et al29 did not observe any clinically significant improvements with VD treatment, a case series of 6 patients with either glioblastoma multiforme, acute myeloid leukemia, or aplastic anemia did demonstrate clinical improvement of TEC after receiving high-dose vitamin D3.30 The mean time to onset of TEC was noted at 8.5 days following administration of the inciting chemotherapeutic agent, which included combinations of anthracycline, antimetabolite, kinase inhibitor, B-cell lymphoma 2 inhibitor, purine analogue, and alkylating agents. A combination of clinical and histologic findings was used to diagnose TEC. Baseline 25(OH)D levels were not established prior to treatment. The treatment regimen for 1 patient included 2 doses of 50,000 IU of VD spaced 1 week apart, totaling 100,000 IU, while the remaining 5 patients received a total of 200,000 IU, also split into 2 doses given 1 week apart. All patients received their first dose of VD within a week of the cutaneous eruption. Following the initial VD dose, there was a notable improvement in pain, pruritus, or swelling by the next day. Reduction in erythema also was observed within 1 to 4 days.30
No AEs associated with VD supplementation were reported, suggesting a potential beneficial role of high-dose VD in accelerating recovery from chemotherapy-induced rashes without evident safety concerns.
Radiation Therapy–Induced Cutaneous Events Treated with High-Dose Vitamin D
Radiation dermatitis is a common and often severe complication of radiation therapy that affects more than 90% of patients undergoing treatment, with half of these individuals experiencing grade 2 toxicity, according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events.31,32 Radiation damage to basal keratinocytes and hair follicle stem cells disrupts the renewal of the skin’s outer layer, while a surge of free radicals causes irreversible DNA damage.33 Symptoms of radiation dermatitis can vary from mild pink erythema to tissue ulceration and necrosis, typically within 1 to 4 weeks of radiation exposure.34 The resulting dermatitis can take 2 to 4 weeks to heal, notably impacting patient quality of life and often necessitating modifications or interruptions in cancer therapy.33
Prior studies have demonstrated the use of high-dose VD to improve the healing of UV-irradiated skin. A randomized controlled trial investigated high-dose vitamin D3 to treat experimentally induced sunburn in 20 healthy adults. Compared with those who received a placebo, participants receiving the oral dose of 200,000 IU of vitamin D3 demonstrated suppression of the pro-inflammatory mediators tumor necrosis factor α (P=.04) and inducible nitric oxide synthase (P=.02), while expression of tissue repair enhancer arginase 1 was increased (P<.005).35 The mechanism of this enhanced tissue repair was investigated using a mouse model, in which intraperitoneal 25(OH)D was administered following severe UV-induced skin injury. On immunofluorescence microscopy, mice treated with VD showed enhanced autophagy within the macrophages infiltrating UV-irradiated skin.36 The use of high-dose VD to treat UV-irradiated skin in these studies established a precedent for using VD to heal cutaneous injury caused by ionizing radiation therapy.
Some studies have focused on the role of VD for treating acute radiation dermatitis. A study of 23 patients with ductal carcinoma in situ or localized invasive ductal carcinoma breast cancer compared the effectiveness of topical calcipotriol to that of a standard hydrating ointment.37 Participants were randomized to 1 of 2 treatments before starting adjuvant radiotherapy to evaluate their potential in preventing radiation dermatitis. In 87% (20/23) of these patients, no difference in skin reaction was observed between the 2 treatments, suggesting that topical VD application may not offer any advantage over the standard hydrating ointment for the prevention of radiation dermatitis.37
Benefits of high-dose oral VD for treating radiation dermatitis also have been reported. Nguyen et al38 documented 3 cases in which patients with neuroendocrine carcinoma of the pancreas, tonsillar carcinoma, and breast cancer received 200,000 IU of oral ergocalciferol distributed over 2 doses given 7 days apart for radiation dermatitis. These patients experienced substantial improvements in pain, swelling, and redness within a week of the initial dose. Additionally, a case of radiation recall dermatitis, which occurred a week after vinorelbine chemotherapy, was treated with 2 doses totaling 100,000 IU of oral ergocalciferol. This patient also had improvement in pain and swelling but continued to have tumor-related induration and ulceration.39
Although topical VD did not show significant benefits over standard treatments for radiation dermatitis, high-dose oral VD appears promising in improving patient outcomes of pain and swelling more rapidly than current practices. Further research is needed to confirm these findings and establish standardized treatment protocols.
Final Thoughts
Suboptimal VD levels are prevalent in numerous cancer types. Chemotherapy often is associated with acute, potentially transient worsening of VD status in patients with breast and colorectal cancer. Although 25(OH)D levels have not corresponded with increased frequency of chemotherapy-related dermatologic AEs, suboptimal 25(OH)D levels appear to be associated with increased severity of radiation-induced mucositis and dermatitis.20,25,26 The use of high-dose VD as a therapeutic agent shows promise in mitigating chemotherapy-induced and radiation therapy–induced rashes in multiple cancer types with reduction of inflammatory markers and a durable anti-inflammatory impact. Although the mechanisms of cellular injury vary among chemotherapeutic agents, the anti-inflammatory and tissue repair properties of VD may make it an effective treatment for chemotherapy-induced cutaneous damage regardless of injury mechanism.2-4,35 However, reports of clinical improvement vary, and further objective studies to classify optimal dosing, administration, and outcome measures are needed. The absence of reported AEs associated with high-dose VD supplementation is encouraging, but selection of a safe and optimal dosing regimen can only occur with dedicated clinical trials.
- Bikle DD. Vitamin D and the skin: physiology and pathophysiology. Rev Endocr Metab Disord. 2012;13:3-19. doi:10.1007/s11154-011-9194-0
- Penna G, Adorini L. 1α,25-Dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164:2405-2411. doi:10.4049/jimmunol.164.5.2405
- Penna G, Amuchastegui S, Cossetti C, et al. Treatment of experimental autoimmune prostatitis in nonobese diabetic mice by the vitamin D receptor agonist elocalcitol. J Immunol. 2006;177:8504-8511. doi:10.4049/jimmunol.177.12.8504
- Heine G, Niesner U, Chang HD, et al. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur J Immunol. 2008;38:2210-2218. doi:10.1002/eji.200838216
- Hauser K, Walsh D, Shrotriya S, et al. Low 25-hydroxyvitamin D levels in people with a solid tumor cancer diagnosis: the tip of the iceberg? Support Care Cancer. 2014;22:1931-1939. doi:10.1007/s00520-014-2154-y
- Lee KJ, Wright G, Bryant H, et al. Cytoprotective effect of vitamin D on doxorubicin-induced cardiac toxicity in triple negative breast cancer. Int J Mol Sci. 2021;22:7439. doi:10.3390/ijms22147439
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-1930. doi:10.1210/jc.2011-0385
- Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74:1498-1513. doi:10.1038/s41430-020-0558-y
- Thomas X, Chelghoum Y, Fanari N, et al. Serum 25-hydroxyvitamin D levels are associated with prognosis in hematological malignancies. Hematology. 2011;16:278-283. doi:10.1179/102453311X13085644679908
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74:12-49. doi:10.3322/caac.21820
- Goodwin PJ, Ennis M, Pritchard KI, et al. Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J Clin Oncol. 2009;27:3757-3763. doi:10.1200/JCO.2008.20.0725
- Fassio A, Porciello G, Carioli G, et al. Post-diagnosis serum 25-hydroxyvitamin D concentrations in women treated for breast cancer participating in a lifestyle trial in Italy. Reumatismo. 2024;76:21-34.
- Augustin LSA, Libra M, Crispo A, et al. Low glycemic index diet, exercise and vitamin D to reduce breast cancer recurrence (DEDiCa): design of a clinical trial. BMC Cancer. 2017;17:69. doi:10.1186/s12885-017-3064-4
- Toriola AT, Nguyen N, Scheitler-Ring K, et al. Circulating 25-hydroxyvitamin D levels and prognosis among cancer patients: a systematic review. Cancer Epidemiol Biomarkers Prev. 2014;23:917-933. doi:10.1158/1055-9965.EPI-14-0053
- Fakih MG, Trump DL, Johnson CS, et al. Chemotherapy is linked to severe vitamin D deficiency in patients with colorectal cancer. Int J Colorectal Dis. 2009;24:219-224. doi:10.1007/s00384-008-0593-y
- Isenring EA, Teleni L, Woodman RJ, et al. Serum vitamin D decreases during chemotherapy: an Australian prospective cohort study. Asia Pac J Clin Nutr. 2018;27:962-967. doi:10.6133/apjcn.042018.01
- Kok DE, van den Berg MMGA, Posthuma L, et al. Changes in circulating levels of 25-hydroxyvitamin D3 in breast cancer patients receiving chemotherapy. Nutr Cancer. 2019;71:756-766. doi:10.1080/01635581.2018.1559938
- Wesselink E, Bours MJL, de Wilt JHW, et al. Chemotherapy and vitamin D supplement use are determinants of serum 25-hydroxyvitamin D levels during the first six months after colorectal cancer diagnosis. J Steroid Biochem Mol Biol. 2020;199:105577. doi:10.1016/j.jsbmb.2020.105577
- Savoie MB, Paciorek A, Zhang L, et al. Vitamin D levels in patients with colorectal cancer before and after treatment initiation. J Gastrointest Cancer. 2019;50:769-779. doi:10.1007/s12029-018-0147-7
- Kitchen D, Hughes B, Gill I, et al. The relationship between vitamin D and chemotherapy-induced toxicity—a pilot study. Br J Cancer. 2012;107:158-160. doi:10.1038/bjc.2012.194
- Demircay Z, Gürbüz O, Alpdogan TB, et al. Chemotherapy-induced acral erythema in leukemic patients: a report of 15 cases. Int J Dermatol. 1997;36:593-598. doi:10.1046/j.1365-4362.1997.00040.x
- Valks R, Fraga J, Porras-Luque J, et al. Chemotherapy-induced eccrine squamous syringometaplasia. a distinctive eruption in patients receiving hematopoietic progenitor cells. Arch Dermatol. 1997;133;873-878. doi:10.1001/archderm.133.7.873
- Webber KA, Kos L, Holland KE, et al. Intertriginous eruption associated with chemotherapy in pediatric patients. Arch Dermatol. 2007;143:67-71. doi:10.1001/archderm.143.1.67
- Hunjan MK, Nowsheen S, Ramos-Rodriguez AJ, et al. Clinical and histopathological spectrum of toxic erythema of chemotherapy in patients who have undergone allogeneic hematopoietic cell transplantation. Hematol Oncol Stem Cell Ther. 2019;12:19-25. doi:10.1016/j.hemonc.2018.09.001
- Ghorbanzadeh-Moghaddam A, Gholamrezaei A, Hemati S. Vitamin D deficiency is associated with the severity of radiation-induced proctitis in cancer patients. Int J Radiat Oncol Biol Phys. 2015;92:613-618. doi:10.1016/j.ijrobp.2015.02.011
- Bhanu A, Waghmare CM, Jain VS, et al. Serum 25-hydroxy vitamin-D levels in head and neck cancer chemoradiation therapy: potential in cancer therapeutics. Indian J Cancer. Published online February 27, 2003. doi:10.4103/ijc.ijc_358_20
- Yang B, Xie X, Wu Z, et al. DNA damage-mediated cellular senescence promotes hand-foot syndrome that can be relieved by thymidine prodrug. Genes Dis. 2022;10:2557-2571. doi:10.1016/j.gendis.2022.10.004
- Lassere Y, Hoff P. Management of hand-foot syndrome in patients treated with capecitabine (Xeloda®). Eur J Oncol Nurs. 2004;8(suppl 1):S31-S40. doi:10.1016/j.ejon.2004.06.007
- Ernst MK, Evans ST, Techner JM, et al. Vitamin D3 and deconvoluting a rash. JCI Insight. 2023;8:E163789.
- Nguyen CV, Zheng L, Zhou XA, et al. High-dose vitamin d for the management of toxic erythema of chemotherapy in hospitalized patients. JAMA Dermatol. 2023;159:219-221. doi:10.1001/jamadermatol.2022.5397
- Fisher J, Scott C, Stevens R, et al. Randomized phase III study comparing best supportive care to biafine as a prophylactic agent for radiation-induced skin toxicity for women undergoing breast irradiation: Radiation Therapy Oncology Group (RTOG) 97-13. Int J Radiat Oncol Biol Phys. 2000;48:1307-1310. doi:10.1016/s0360-3016(00)00782-3
- Pignol JP, Olivotto I, Rakovitch E, et al. A multicenter randomized trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitis. J Clin Oncol. 2008;26:2085-2092. doi:10.1200/JCO.2007.15.2488
- Hymes SR, Strom EA, Fife C. Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006. J Am Acad Dermatol. 2006;54:28-46. doi:10.1016/j.jaad.2005.08.054
- Ryan JL. Ionizing radiation: the good, the bad, and the ugly. J Invest Dermatol. 2012;132(3 pt 2):985-993. doi:10.1038/jid.2011.411
- Scott JF, Das LM, Ahsanuddin S, et al. Oral vitamin D rapidly attenuates inflammation from sunburn: an interventional study. J Invest Dermatol. 2017;137:2078-2086. doi:10.1016/j.jid.2017.04.040
- Das LM, Binko AM, Traylor ZP, et al. Vitamin D improves sunburns by increasing autophagy in M2 macrophages. Autophagy. 2019;15:813-826. doi:10.1080/15548627.2019.1569298
- Nasser NJ, Fenig S, Ravid A, et al. Vitamin D ointment for prevention of radiation dermatitis in breast cancer patients. NPJ Breast Cancer. 2017;3:10. doi:10.1038/s41523-017-0006-x
- Nguyen CV, Zheng L, Lu KQ. High-dose vitamin D for the management acute radiation dermatitis. JAAD Case Rep. 2023;39:47-50. doi:10.1016/j.jdcr.2023.07.001
- Nguyen CV, Lu KQ. Vitamin D3 and its potential to ameliorate chemical and radiation-induced skin injury during cancer therapy. Disaster Med Public Health Prep. 2024;18:E4. doi:10.1017/dmp.2023.211
- Bikle DD. Vitamin D and the skin: physiology and pathophysiology. Rev Endocr Metab Disord. 2012;13:3-19. doi:10.1007/s11154-011-9194-0
- Penna G, Adorini L. 1α,25-Dihydroxyvitamin D3 inhibits differentiation, maturation, activation, and survival of dendritic cells leading to impaired alloreactive T cell activation. J Immunol. 2000;164:2405-2411. doi:10.4049/jimmunol.164.5.2405
- Penna G, Amuchastegui S, Cossetti C, et al. Treatment of experimental autoimmune prostatitis in nonobese diabetic mice by the vitamin D receptor agonist elocalcitol. J Immunol. 2006;177:8504-8511. doi:10.4049/jimmunol.177.12.8504
- Heine G, Niesner U, Chang HD, et al. 1,25-dihydroxyvitamin D3 promotes IL-10 production in human B cells. Eur J Immunol. 2008;38:2210-2218. doi:10.1002/eji.200838216
- Hauser K, Walsh D, Shrotriya S, et al. Low 25-hydroxyvitamin D levels in people with a solid tumor cancer diagnosis: the tip of the iceberg? Support Care Cancer. 2014;22:1931-1939. doi:10.1007/s00520-014-2154-y
- Lee KJ, Wright G, Bryant H, et al. Cytoprotective effect of vitamin D on doxorubicin-induced cardiac toxicity in triple negative breast cancer. Int J Mol Sci. 2021;22:7439. doi:10.3390/ijms22147439
- Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911-1930. doi:10.1210/jc.2011-0385
- Amrein K, Scherkl M, Hoffmann M, et al. Vitamin D deficiency 2.0: an update on the current status worldwide. Eur J Clin Nutr. 2020;74:1498-1513. doi:10.1038/s41430-020-0558-y
- Thomas X, Chelghoum Y, Fanari N, et al. Serum 25-hydroxyvitamin D levels are associated with prognosis in hematological malignancies. Hematology. 2011;16:278-283. doi:10.1179/102453311X13085644679908
- Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74:12-49. doi:10.3322/caac.21820
- Goodwin PJ, Ennis M, Pritchard KI, et al. Prognostic effects of 25-hydroxyvitamin D levels in early breast cancer. J Clin Oncol. 2009;27:3757-3763. doi:10.1200/JCO.2008.20.0725
- Fassio A, Porciello G, Carioli G, et al. Post-diagnosis serum 25-hydroxyvitamin D concentrations in women treated for breast cancer participating in a lifestyle trial in Italy. Reumatismo. 2024;76:21-34.
- Augustin LSA, Libra M, Crispo A, et al. Low glycemic index diet, exercise and vitamin D to reduce breast cancer recurrence (DEDiCa): design of a clinical trial. BMC Cancer. 2017;17:69. doi:10.1186/s12885-017-3064-4
- Toriola AT, Nguyen N, Scheitler-Ring K, et al. Circulating 25-hydroxyvitamin D levels and prognosis among cancer patients: a systematic review. Cancer Epidemiol Biomarkers Prev. 2014;23:917-933. doi:10.1158/1055-9965.EPI-14-0053
- Fakih MG, Trump DL, Johnson CS, et al. Chemotherapy is linked to severe vitamin D deficiency in patients with colorectal cancer. Int J Colorectal Dis. 2009;24:219-224. doi:10.1007/s00384-008-0593-y
- Isenring EA, Teleni L, Woodman RJ, et al. Serum vitamin D decreases during chemotherapy: an Australian prospective cohort study. Asia Pac J Clin Nutr. 2018;27:962-967. doi:10.6133/apjcn.042018.01
- Kok DE, van den Berg MMGA, Posthuma L, et al. Changes in circulating levels of 25-hydroxyvitamin D3 in breast cancer patients receiving chemotherapy. Nutr Cancer. 2019;71:756-766. doi:10.1080/01635581.2018.1559938
- Wesselink E, Bours MJL, de Wilt JHW, et al. Chemotherapy and vitamin D supplement use are determinants of serum 25-hydroxyvitamin D levels during the first six months after colorectal cancer diagnosis. J Steroid Biochem Mol Biol. 2020;199:105577. doi:10.1016/j.jsbmb.2020.105577
- Savoie MB, Paciorek A, Zhang L, et al. Vitamin D levels in patients with colorectal cancer before and after treatment initiation. J Gastrointest Cancer. 2019;50:769-779. doi:10.1007/s12029-018-0147-7
- Kitchen D, Hughes B, Gill I, et al. The relationship between vitamin D and chemotherapy-induced toxicity—a pilot study. Br J Cancer. 2012;107:158-160. doi:10.1038/bjc.2012.194
- Demircay Z, Gürbüz O, Alpdogan TB, et al. Chemotherapy-induced acral erythema in leukemic patients: a report of 15 cases. Int J Dermatol. 1997;36:593-598. doi:10.1046/j.1365-4362.1997.00040.x
- Valks R, Fraga J, Porras-Luque J, et al. Chemotherapy-induced eccrine squamous syringometaplasia. a distinctive eruption in patients receiving hematopoietic progenitor cells. Arch Dermatol. 1997;133;873-878. doi:10.1001/archderm.133.7.873
- Webber KA, Kos L, Holland KE, et al. Intertriginous eruption associated with chemotherapy in pediatric patients. Arch Dermatol. 2007;143:67-71. doi:10.1001/archderm.143.1.67
- Hunjan MK, Nowsheen S, Ramos-Rodriguez AJ, et al. Clinical and histopathological spectrum of toxic erythema of chemotherapy in patients who have undergone allogeneic hematopoietic cell transplantation. Hematol Oncol Stem Cell Ther. 2019;12:19-25. doi:10.1016/j.hemonc.2018.09.001
- Ghorbanzadeh-Moghaddam A, Gholamrezaei A, Hemati S. Vitamin D deficiency is associated with the severity of radiation-induced proctitis in cancer patients. Int J Radiat Oncol Biol Phys. 2015;92:613-618. doi:10.1016/j.ijrobp.2015.02.011
- Bhanu A, Waghmare CM, Jain VS, et al. Serum 25-hydroxy vitamin-D levels in head and neck cancer chemoradiation therapy: potential in cancer therapeutics. Indian J Cancer. Published online February 27, 2003. doi:10.4103/ijc.ijc_358_20
- Yang B, Xie X, Wu Z, et al. DNA damage-mediated cellular senescence promotes hand-foot syndrome that can be relieved by thymidine prodrug. Genes Dis. 2022;10:2557-2571. doi:10.1016/j.gendis.2022.10.004
- Lassere Y, Hoff P. Management of hand-foot syndrome in patients treated with capecitabine (Xeloda®). Eur J Oncol Nurs. 2004;8(suppl 1):S31-S40. doi:10.1016/j.ejon.2004.06.007
- Ernst MK, Evans ST, Techner JM, et al. Vitamin D3 and deconvoluting a rash. JCI Insight. 2023;8:E163789.
- Nguyen CV, Zheng L, Zhou XA, et al. High-dose vitamin d for the management of toxic erythema of chemotherapy in hospitalized patients. JAMA Dermatol. 2023;159:219-221. doi:10.1001/jamadermatol.2022.5397
- Fisher J, Scott C, Stevens R, et al. Randomized phase III study comparing best supportive care to biafine as a prophylactic agent for radiation-induced skin toxicity for women undergoing breast irradiation: Radiation Therapy Oncology Group (RTOG) 97-13. Int J Radiat Oncol Biol Phys. 2000;48:1307-1310. doi:10.1016/s0360-3016(00)00782-3
- Pignol JP, Olivotto I, Rakovitch E, et al. A multicenter randomized trial of breast intensity-modulated radiation therapy to reduce acute radiation dermatitis. J Clin Oncol. 2008;26:2085-2092. doi:10.1200/JCO.2007.15.2488
- Hymes SR, Strom EA, Fife C. Radiation dermatitis: clinical presentation, pathophysiology, and treatment 2006. J Am Acad Dermatol. 2006;54:28-46. doi:10.1016/j.jaad.2005.08.054
- Ryan JL. Ionizing radiation: the good, the bad, and the ugly. J Invest Dermatol. 2012;132(3 pt 2):985-993. doi:10.1038/jid.2011.411
- Scott JF, Das LM, Ahsanuddin S, et al. Oral vitamin D rapidly attenuates inflammation from sunburn: an interventional study. J Invest Dermatol. 2017;137:2078-2086. doi:10.1016/j.jid.2017.04.040
- Das LM, Binko AM, Traylor ZP, et al. Vitamin D improves sunburns by increasing autophagy in M2 macrophages. Autophagy. 2019;15:813-826. doi:10.1080/15548627.2019.1569298
- Nasser NJ, Fenig S, Ravid A, et al. Vitamin D ointment for prevention of radiation dermatitis in breast cancer patients. NPJ Breast Cancer. 2017;3:10. doi:10.1038/s41523-017-0006-x
- Nguyen CV, Zheng L, Lu KQ. High-dose vitamin D for the management acute radiation dermatitis. JAAD Case Rep. 2023;39:47-50. doi:10.1016/j.jdcr.2023.07.001
- Nguyen CV, Lu KQ. Vitamin D3 and its potential to ameliorate chemical and radiation-induced skin injury during cancer therapy. Disaster Med Public Health Prep. 2024;18:E4. doi:10.1017/dmp.2023.211
Practice Points
- High-dose vitamin D supplementation may be considered in the management of cutaneous injury from chemotherapy or ionizing radiation.
- Optimal dosing has not been established, so patients given high-dose vitamin D supplementation should have close clinical follow-up; however, adverse events from high-dose vitamin D supplementation have not been reported.
Is Frontal Fibrosing Alopecia Connected to Sunscreen Usage?
Frontal fibrosing alopecia (FFA) has become increasingly common since it was first described in 1994.1 A positive correlation between FFA and the use of sunscreens was reported in an observational study.2 The geographic distribution of this association has spanned the United Kingdom (UK), Europe, and Asia, though data from the United States are lacking. Various international studies have demonstrated an association between FFA and sunscreen use, further exemplifying this stark contrast.
In the United Kingdom (UK), Aldoori et al2 found that women who used sunscreen at least twice weekly had 2 times the likelihood of developing FFA compared with women who did not use sunscreen regularly. Kidambi et al3 found similar results in UK men with FFA who had higher rates of primary sunscreen use and higher rates of at least twice-weekly use of facial moisturizer with unspecified sunscreen content.
These associations between FFA and sunscreen use are not unique to the UK. A study conducted in Spain identified a statistical association between FFA and use of facial sunscreen in women (odds ratio, 1.6 [95% CI, 1.06-2.41]) and men (odds ratio, 1.84 [95% CI, 1.04-3.23]).4 In Thailand, FFA was nearly twice as likely to be present in patients with regular sunscreen use compared to controls who did not apply sunscreen regularly.5 Interestingly, a Brazilian study showed no connection between sunscreen use and FFA. Instead, FFA was associated with hair straightening with formalin or use of facial soap orfacial moisturizer.6 An international systematic review of 1248 patients with FFA and 1459 controls determined that sunscreen users were 2.21 times more likely to develop FFA than their counterparts who did not use sunscreen regularly.7
Quite glaring is the lack of data from the United States, which could be used to compare FFA and sunscreen associations to other nations. It is possible that certain regions of the world such as the United States may not have an increased risk for FFA in sunscreen users due to other environmental factors, differing sunscreen application practices, or differing chemical ingredients. At the same time, many other countries cannot afford or lack access to sunscreens or facial moisturizers, which is an additional variable that may complicate this association. These populations need to be studied to determine whether they are as susceptible to FFA as those who use sunscreen regularly around the world.
Another underlying factor supporting this association is the inherent need for sunscreen use. For instance, research has shown that patients with FFA had higher rates of actinic skin damage, which could explain increased sunscreen use.8
To make more clear and distinct claims, further studies are needed in regions that are known to use sunscreen extensively (eg, United States) to compare with their European, Asian, and South American counterparts. Moreover, it also is important to study regions where sunscreen access is limited and whether there is FFA development in these populations.
Given the potential association between sunscreen use and FFA, dermatologists can take a cautious approach tailored to the patient by recommending noncomedogenic mineral sunscreens with zinc or titanium oxide, which are less irritating than chemical sunscreens. Avoidance of sunscreen application to the hairline and use of additional sun-protection methods such as broad-brimmed hats also should be emphasized.
- Kossard S. Postmenopausal frontal fibrosing alopecia: scarring alopecia in a pattern distribution. Arch Dermatol. 1994;130:770-774. doi:10.1001/archderm.1994.01690060100013
- Aldoori N, Dobson K, Holden CR, et al. Frontal fibrosing alopecia: possible association with leave-on facial skin care products and sunscreens: a questionnaire study. Br J Dermatol. 2016;175:762-767.
- Kidambi AD, Dobson K, Holmes S, et al. Frontal fibrosing alopecia in men: an association with leave-on facial cosmetics and sunscreens. Br J Dermatol. 2020;175:61-67.
- Moreno-Arrones OM, Saceda-Corralo D, Rodrigues-Barata AR, et al. Risk factors associated with frontal fibrosing alopecia: a multicentre case-control study. Clin Exp Dermatol. 2019;44:404-410. doi:10.1111/ced.13785
- Leecharoen W, Thanomkitti K, Thuangtong R, et al. Use of facial care products and frontal fibrosing alopecia: coincidence or true association? J Dermatol. 2021;48:1557-1563.
- Müller Ramos P, Anzai A, Duque-Estrada B, et al. Risk factors for frontal fibrosing alopecia: a case-control study in a multiracial population. J Am Acad Dermatol. 2021;84:712-718. doi:10.1016/j.jaad.2020.08.07
- Kam O, Na S, Guo W, et al. Frontal fibrosing alopecia and personal care product use: a systematic review and meta-analysis. Arch Dermatol Res. 2023;315:2313-2331. doi:10.1007/s00403-023-02604-7
- Porriño-Bustamante ML, Montero-Vílchez T, Pinedo-Moraleda FJ, et al. Frontal fibrosing alopecia and sunscreen use: a cross-sectionalstudy of actinic damage. Acta Derm Venereol. Published online August 11, 2022. doi:10.2340/actadv.v102.306
Frontal fibrosing alopecia (FFA) has become increasingly common since it was first described in 1994.1 A positive correlation between FFA and the use of sunscreens was reported in an observational study.2 The geographic distribution of this association has spanned the United Kingdom (UK), Europe, and Asia, though data from the United States are lacking. Various international studies have demonstrated an association between FFA and sunscreen use, further exemplifying this stark contrast.
In the United Kingdom (UK), Aldoori et al2 found that women who used sunscreen at least twice weekly had 2 times the likelihood of developing FFA compared with women who did not use sunscreen regularly. Kidambi et al3 found similar results in UK men with FFA who had higher rates of primary sunscreen use and higher rates of at least twice-weekly use of facial moisturizer with unspecified sunscreen content.
These associations between FFA and sunscreen use are not unique to the UK. A study conducted in Spain identified a statistical association between FFA and use of facial sunscreen in women (odds ratio, 1.6 [95% CI, 1.06-2.41]) and men (odds ratio, 1.84 [95% CI, 1.04-3.23]).4 In Thailand, FFA was nearly twice as likely to be present in patients with regular sunscreen use compared to controls who did not apply sunscreen regularly.5 Interestingly, a Brazilian study showed no connection between sunscreen use and FFA. Instead, FFA was associated with hair straightening with formalin or use of facial soap orfacial moisturizer.6 An international systematic review of 1248 patients with FFA and 1459 controls determined that sunscreen users were 2.21 times more likely to develop FFA than their counterparts who did not use sunscreen regularly.7
Quite glaring is the lack of data from the United States, which could be used to compare FFA and sunscreen associations to other nations. It is possible that certain regions of the world such as the United States may not have an increased risk for FFA in sunscreen users due to other environmental factors, differing sunscreen application practices, or differing chemical ingredients. At the same time, many other countries cannot afford or lack access to sunscreens or facial moisturizers, which is an additional variable that may complicate this association. These populations need to be studied to determine whether they are as susceptible to FFA as those who use sunscreen regularly around the world.
Another underlying factor supporting this association is the inherent need for sunscreen use. For instance, research has shown that patients with FFA had higher rates of actinic skin damage, which could explain increased sunscreen use.8
To make more clear and distinct claims, further studies are needed in regions that are known to use sunscreen extensively (eg, United States) to compare with their European, Asian, and South American counterparts. Moreover, it also is important to study regions where sunscreen access is limited and whether there is FFA development in these populations.
Given the potential association between sunscreen use and FFA, dermatologists can take a cautious approach tailored to the patient by recommending noncomedogenic mineral sunscreens with zinc or titanium oxide, which are less irritating than chemical sunscreens. Avoidance of sunscreen application to the hairline and use of additional sun-protection methods such as broad-brimmed hats also should be emphasized.
Frontal fibrosing alopecia (FFA) has become increasingly common since it was first described in 1994.1 A positive correlation between FFA and the use of sunscreens was reported in an observational study.2 The geographic distribution of this association has spanned the United Kingdom (UK), Europe, and Asia, though data from the United States are lacking. Various international studies have demonstrated an association between FFA and sunscreen use, further exemplifying this stark contrast.
In the United Kingdom (UK), Aldoori et al2 found that women who used sunscreen at least twice weekly had 2 times the likelihood of developing FFA compared with women who did not use sunscreen regularly. Kidambi et al3 found similar results in UK men with FFA who had higher rates of primary sunscreen use and higher rates of at least twice-weekly use of facial moisturizer with unspecified sunscreen content.
These associations between FFA and sunscreen use are not unique to the UK. A study conducted in Spain identified a statistical association between FFA and use of facial sunscreen in women (odds ratio, 1.6 [95% CI, 1.06-2.41]) and men (odds ratio, 1.84 [95% CI, 1.04-3.23]).4 In Thailand, FFA was nearly twice as likely to be present in patients with regular sunscreen use compared to controls who did not apply sunscreen regularly.5 Interestingly, a Brazilian study showed no connection between sunscreen use and FFA. Instead, FFA was associated with hair straightening with formalin or use of facial soap orfacial moisturizer.6 An international systematic review of 1248 patients with FFA and 1459 controls determined that sunscreen users were 2.21 times more likely to develop FFA than their counterparts who did not use sunscreen regularly.7
Quite glaring is the lack of data from the United States, which could be used to compare FFA and sunscreen associations to other nations. It is possible that certain regions of the world such as the United States may not have an increased risk for FFA in sunscreen users due to other environmental factors, differing sunscreen application practices, or differing chemical ingredients. At the same time, many other countries cannot afford or lack access to sunscreens or facial moisturizers, which is an additional variable that may complicate this association. These populations need to be studied to determine whether they are as susceptible to FFA as those who use sunscreen regularly around the world.
Another underlying factor supporting this association is the inherent need for sunscreen use. For instance, research has shown that patients with FFA had higher rates of actinic skin damage, which could explain increased sunscreen use.8
To make more clear and distinct claims, further studies are needed in regions that are known to use sunscreen extensively (eg, United States) to compare with their European, Asian, and South American counterparts. Moreover, it also is important to study regions where sunscreen access is limited and whether there is FFA development in these populations.
Given the potential association between sunscreen use and FFA, dermatologists can take a cautious approach tailored to the patient by recommending noncomedogenic mineral sunscreens with zinc or titanium oxide, which are less irritating than chemical sunscreens. Avoidance of sunscreen application to the hairline and use of additional sun-protection methods such as broad-brimmed hats also should be emphasized.
- Kossard S. Postmenopausal frontal fibrosing alopecia: scarring alopecia in a pattern distribution. Arch Dermatol. 1994;130:770-774. doi:10.1001/archderm.1994.01690060100013
- Aldoori N, Dobson K, Holden CR, et al. Frontal fibrosing alopecia: possible association with leave-on facial skin care products and sunscreens: a questionnaire study. Br J Dermatol. 2016;175:762-767.
- Kidambi AD, Dobson K, Holmes S, et al. Frontal fibrosing alopecia in men: an association with leave-on facial cosmetics and sunscreens. Br J Dermatol. 2020;175:61-67.
- Moreno-Arrones OM, Saceda-Corralo D, Rodrigues-Barata AR, et al. Risk factors associated with frontal fibrosing alopecia: a multicentre case-control study. Clin Exp Dermatol. 2019;44:404-410. doi:10.1111/ced.13785
- Leecharoen W, Thanomkitti K, Thuangtong R, et al. Use of facial care products and frontal fibrosing alopecia: coincidence or true association? J Dermatol. 2021;48:1557-1563.
- Müller Ramos P, Anzai A, Duque-Estrada B, et al. Risk factors for frontal fibrosing alopecia: a case-control study in a multiracial population. J Am Acad Dermatol. 2021;84:712-718. doi:10.1016/j.jaad.2020.08.07
- Kam O, Na S, Guo W, et al. Frontal fibrosing alopecia and personal care product use: a systematic review and meta-analysis. Arch Dermatol Res. 2023;315:2313-2331. doi:10.1007/s00403-023-02604-7
- Porriño-Bustamante ML, Montero-Vílchez T, Pinedo-Moraleda FJ, et al. Frontal fibrosing alopecia and sunscreen use: a cross-sectionalstudy of actinic damage. Acta Derm Venereol. Published online August 11, 2022. doi:10.2340/actadv.v102.306
- Kossard S. Postmenopausal frontal fibrosing alopecia: scarring alopecia in a pattern distribution. Arch Dermatol. 1994;130:770-774. doi:10.1001/archderm.1994.01690060100013
- Aldoori N, Dobson K, Holden CR, et al. Frontal fibrosing alopecia: possible association with leave-on facial skin care products and sunscreens: a questionnaire study. Br J Dermatol. 2016;175:762-767.
- Kidambi AD, Dobson K, Holmes S, et al. Frontal fibrosing alopecia in men: an association with leave-on facial cosmetics and sunscreens. Br J Dermatol. 2020;175:61-67.
- Moreno-Arrones OM, Saceda-Corralo D, Rodrigues-Barata AR, et al. Risk factors associated with frontal fibrosing alopecia: a multicentre case-control study. Clin Exp Dermatol. 2019;44:404-410. doi:10.1111/ced.13785
- Leecharoen W, Thanomkitti K, Thuangtong R, et al. Use of facial care products and frontal fibrosing alopecia: coincidence or true association? J Dermatol. 2021;48:1557-1563.
- Müller Ramos P, Anzai A, Duque-Estrada B, et al. Risk factors for frontal fibrosing alopecia: a case-control study in a multiracial population. J Am Acad Dermatol. 2021;84:712-718. doi:10.1016/j.jaad.2020.08.07
- Kam O, Na S, Guo W, et al. Frontal fibrosing alopecia and personal care product use: a systematic review and meta-analysis. Arch Dermatol Res. 2023;315:2313-2331. doi:10.1007/s00403-023-02604-7
- Porriño-Bustamante ML, Montero-Vílchez T, Pinedo-Moraleda FJ, et al. Frontal fibrosing alopecia and sunscreen use: a cross-sectionalstudy of actinic damage. Acta Derm Venereol. Published online August 11, 2022. doi:10.2340/actadv.v102.306
Does Omalizumab Cause Atopic Dermatitis Flare-Ups?
To the Editor:
We read with interest the case reported by Yanovsky et al1 (Cutis. 2023;112:E23-E25). We thank the authors for updating our knowledge about atopic dermatitis (AD) and omalizumab and improving our understanding of the various wanted and unwanted effects that may manifest with omalizumab. We wish to clarify a few points on omalizumab use.
First, Yanovsky et al1 reported that their patient’s AD flares occurred within a few days after omalizumab injections to control asthma, possibly because omalizumab may have caused a paradoxical increase in sensitivity to other cytokines such as IL-33 in basophils and increased IL-4/IL-13 production in the skin. The authors cited Imai2 to explain that IL-33 plays a role in the pathogenesis of AD, increases itching, and disrupts the skin barrier. However, Imai2 did not discuss a relationship with omalizumab. As a recombinant humanized IgG1 monoclonal anti-IgE antibody, omalizumab works by interacting with the high-affinity receptor Fc epsilon RI that typically is found on eosinophils, mast cells, and basophils and plays a critical role in preventing the allergic cascade.3 We could not find any studies in the literature regarding omalizumab having a specific effect on the skin, causing cytokine imbalance, or increasing IL-4/IL-13 levels.
Second, the case report indicated that AD lesions improved with the biologic dupilumab,1 which seems amazing. Dupilumab is a monoclonal antibody used in patients with moderate to severe AD that blocks IL-4/IL-13 signaling and thus inhibits receptor signaling downstream of the Janus kinase signal transducer and activator of transcription protein pathway.4 It also has been shown to be beneficial in children with moderate to severe uncontrolled asthma.5 In vivo studies are needed to learn about the effects of these biologics on asthma and AD, whose complex immunologic effects are increasingly well understood by real patient experience.
Third, omalizumab has been found to relieve AD, not exacerbate it, in our own experience with 7 patients (unpublished data, 2024) and randomized controlled trials.6
Fourth, Yanovsky et al1 reported that the patient’s lesions flared up within a few days after taking omalizumab, which suggests a non-IgE delayed reaction. Could this reaction be related to polysorbate 20 used as an excipient in the commercial preparation? When we examined both preparations, the presence of polysorbate 80 in dupilumab was noteworthy,7 unlike omalizumab. We suggest the authors perform a patch test including polysorbate 20 and polysorbate 80.
Finally, the authors mentioned that omalizumab may cause a paradoxical exacerbation of AD in certain patients, as in tumor necrosis factor α inhibitor–induced psoriasis.8 This has been reported,8 but tumor necrosis factor α inhibitors are cytokine inhibitors and can lead to cytokine imbalance, while omalizumab is an IgE inhibitor.
Yanovsky et al1 described AD flares as “triggered by omalizumab,” which we believe was not the case. Because this patient had chronic AD, other causes of AD exacerbation in this patient could include stress or infection. Also, when they say that AD is triggered or induced, it implies that they are attributing the occurrence/development of AD in this patient to omalizumab. Of course, this also is not true.
Author’s Response
Thank you for your thoughtful comments. Although we agree that we cannot prove omalizumab was the cause of our patient’s AD flares, the new onset of severely worsening disease that was exacerbated by each dose of omalizumab as well as subsequent resolution upon switching to dupilumab was highly suggestive for a causal relationship. Our goal was to alert physicians to the possibility of this phenomenon and to encourage further study.
Karen A. Chernoff, MD
From the Department of Dermatology, Weill Cornell Medical College, New York, New York.
The author has no relevant financial disclosures to report.
- Yanovsky RL, Mitre M, Chernoff KA. Atopic dermatitis triggered by omalizumab and treated with dupilumab. Cutis. 2023;112:E23-E25. 2. Imai Y. Interleukin-33 in atopic dermatitis. J Dermatol Sci. 2019;96:2-7.
- Kumar C, Zito PM. Omalizumab. In: StatPearls [internet]. StatPearls Publishing; 2024.
- Seegräber M, Srour J, Walter A, et al. Dupilumab for treatment of atopic dermatitis. Expert Rev Clin Pharmacol. 2018;11:467-474.
- Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. N Engl J Med. 2021;385:2230-2240.
- Chan SMH, Cro S, Cornelius V, et al. Omalizumab for severe atopic dermatitis in 4- to 19-year-olds: the ADAPT RCT. National Institute for Health and Care Research; May 2022.
- Sumi T, Nagahisa Y, Matsuura K, et al. Delayed local reaction at a previous injection site reaction with dupilumab. Respirol Case Rep. 2021;9:E0852.
- Lian N, Zhang L, Chen M. Tumor necrosis factors-α inhibition-induced paradoxical psoriasis: a case series and literature review. Dermatol Ther. 2020;33:e14225.
To the Editor:
We read with interest the case reported by Yanovsky et al1 (Cutis. 2023;112:E23-E25). We thank the authors for updating our knowledge about atopic dermatitis (AD) and omalizumab and improving our understanding of the various wanted and unwanted effects that may manifest with omalizumab. We wish to clarify a few points on omalizumab use.
First, Yanovsky et al1 reported that their patient’s AD flares occurred within a few days after omalizumab injections to control asthma, possibly because omalizumab may have caused a paradoxical increase in sensitivity to other cytokines such as IL-33 in basophils and increased IL-4/IL-13 production in the skin. The authors cited Imai2 to explain that IL-33 plays a role in the pathogenesis of AD, increases itching, and disrupts the skin barrier. However, Imai2 did not discuss a relationship with omalizumab. As a recombinant humanized IgG1 monoclonal anti-IgE antibody, omalizumab works by interacting with the high-affinity receptor Fc epsilon RI that typically is found on eosinophils, mast cells, and basophils and plays a critical role in preventing the allergic cascade.3 We could not find any studies in the literature regarding omalizumab having a specific effect on the skin, causing cytokine imbalance, or increasing IL-4/IL-13 levels.
Second, the case report indicated that AD lesions improved with the biologic dupilumab,1 which seems amazing. Dupilumab is a monoclonal antibody used in patients with moderate to severe AD that blocks IL-4/IL-13 signaling and thus inhibits receptor signaling downstream of the Janus kinase signal transducer and activator of transcription protein pathway.4 It also has been shown to be beneficial in children with moderate to severe uncontrolled asthma.5 In vivo studies are needed to learn about the effects of these biologics on asthma and AD, whose complex immunologic effects are increasingly well understood by real patient experience.
Third, omalizumab has been found to relieve AD, not exacerbate it, in our own experience with 7 patients (unpublished data, 2024) and randomized controlled trials.6
Fourth, Yanovsky et al1 reported that the patient’s lesions flared up within a few days after taking omalizumab, which suggests a non-IgE delayed reaction. Could this reaction be related to polysorbate 20 used as an excipient in the commercial preparation? When we examined both preparations, the presence of polysorbate 80 in dupilumab was noteworthy,7 unlike omalizumab. We suggest the authors perform a patch test including polysorbate 20 and polysorbate 80.
Finally, the authors mentioned that omalizumab may cause a paradoxical exacerbation of AD in certain patients, as in tumor necrosis factor α inhibitor–induced psoriasis.8 This has been reported,8 but tumor necrosis factor α inhibitors are cytokine inhibitors and can lead to cytokine imbalance, while omalizumab is an IgE inhibitor.
Yanovsky et al1 described AD flares as “triggered by omalizumab,” which we believe was not the case. Because this patient had chronic AD, other causes of AD exacerbation in this patient could include stress or infection. Also, when they say that AD is triggered or induced, it implies that they are attributing the occurrence/development of AD in this patient to omalizumab. Of course, this also is not true.
Author’s Response
Thank you for your thoughtful comments. Although we agree that we cannot prove omalizumab was the cause of our patient’s AD flares, the new onset of severely worsening disease that was exacerbated by each dose of omalizumab as well as subsequent resolution upon switching to dupilumab was highly suggestive for a causal relationship. Our goal was to alert physicians to the possibility of this phenomenon and to encourage further study.
Karen A. Chernoff, MD
From the Department of Dermatology, Weill Cornell Medical College, New York, New York.
The author has no relevant financial disclosures to report.
To the Editor:
We read with interest the case reported by Yanovsky et al1 (Cutis. 2023;112:E23-E25). We thank the authors for updating our knowledge about atopic dermatitis (AD) and omalizumab and improving our understanding of the various wanted and unwanted effects that may manifest with omalizumab. We wish to clarify a few points on omalizumab use.
First, Yanovsky et al1 reported that their patient’s AD flares occurred within a few days after omalizumab injections to control asthma, possibly because omalizumab may have caused a paradoxical increase in sensitivity to other cytokines such as IL-33 in basophils and increased IL-4/IL-13 production in the skin. The authors cited Imai2 to explain that IL-33 plays a role in the pathogenesis of AD, increases itching, and disrupts the skin barrier. However, Imai2 did not discuss a relationship with omalizumab. As a recombinant humanized IgG1 monoclonal anti-IgE antibody, omalizumab works by interacting with the high-affinity receptor Fc epsilon RI that typically is found on eosinophils, mast cells, and basophils and plays a critical role in preventing the allergic cascade.3 We could not find any studies in the literature regarding omalizumab having a specific effect on the skin, causing cytokine imbalance, or increasing IL-4/IL-13 levels.
Second, the case report indicated that AD lesions improved with the biologic dupilumab,1 which seems amazing. Dupilumab is a monoclonal antibody used in patients with moderate to severe AD that blocks IL-4/IL-13 signaling and thus inhibits receptor signaling downstream of the Janus kinase signal transducer and activator of transcription protein pathway.4 It also has been shown to be beneficial in children with moderate to severe uncontrolled asthma.5 In vivo studies are needed to learn about the effects of these biologics on asthma and AD, whose complex immunologic effects are increasingly well understood by real patient experience.
Third, omalizumab has been found to relieve AD, not exacerbate it, in our own experience with 7 patients (unpublished data, 2024) and randomized controlled trials.6
Fourth, Yanovsky et al1 reported that the patient’s lesions flared up within a few days after taking omalizumab, which suggests a non-IgE delayed reaction. Could this reaction be related to polysorbate 20 used as an excipient in the commercial preparation? When we examined both preparations, the presence of polysorbate 80 in dupilumab was noteworthy,7 unlike omalizumab. We suggest the authors perform a patch test including polysorbate 20 and polysorbate 80.
Finally, the authors mentioned that omalizumab may cause a paradoxical exacerbation of AD in certain patients, as in tumor necrosis factor α inhibitor–induced psoriasis.8 This has been reported,8 but tumor necrosis factor α inhibitors are cytokine inhibitors and can lead to cytokine imbalance, while omalizumab is an IgE inhibitor.
Yanovsky et al1 described AD flares as “triggered by omalizumab,” which we believe was not the case. Because this patient had chronic AD, other causes of AD exacerbation in this patient could include stress or infection. Also, when they say that AD is triggered or induced, it implies that they are attributing the occurrence/development of AD in this patient to omalizumab. Of course, this also is not true.
Author’s Response
Thank you for your thoughtful comments. Although we agree that we cannot prove omalizumab was the cause of our patient’s AD flares, the new onset of severely worsening disease that was exacerbated by each dose of omalizumab as well as subsequent resolution upon switching to dupilumab was highly suggestive for a causal relationship. Our goal was to alert physicians to the possibility of this phenomenon and to encourage further study.
Karen A. Chernoff, MD
From the Department of Dermatology, Weill Cornell Medical College, New York, New York.
The author has no relevant financial disclosures to report.
- Yanovsky RL, Mitre M, Chernoff KA. Atopic dermatitis triggered by omalizumab and treated with dupilumab. Cutis. 2023;112:E23-E25. 2. Imai Y. Interleukin-33 in atopic dermatitis. J Dermatol Sci. 2019;96:2-7.
- Kumar C, Zito PM. Omalizumab. In: StatPearls [internet]. StatPearls Publishing; 2024.
- Seegräber M, Srour J, Walter A, et al. Dupilumab for treatment of atopic dermatitis. Expert Rev Clin Pharmacol. 2018;11:467-474.
- Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. N Engl J Med. 2021;385:2230-2240.
- Chan SMH, Cro S, Cornelius V, et al. Omalizumab for severe atopic dermatitis in 4- to 19-year-olds: the ADAPT RCT. National Institute for Health and Care Research; May 2022.
- Sumi T, Nagahisa Y, Matsuura K, et al. Delayed local reaction at a previous injection site reaction with dupilumab. Respirol Case Rep. 2021;9:E0852.
- Lian N, Zhang L, Chen M. Tumor necrosis factors-α inhibition-induced paradoxical psoriasis: a case series and literature review. Dermatol Ther. 2020;33:e14225.
- Yanovsky RL, Mitre M, Chernoff KA. Atopic dermatitis triggered by omalizumab and treated with dupilumab. Cutis. 2023;112:E23-E25. 2. Imai Y. Interleukin-33 in atopic dermatitis. J Dermatol Sci. 2019;96:2-7.
- Kumar C, Zito PM. Omalizumab. In: StatPearls [internet]. StatPearls Publishing; 2024.
- Seegräber M, Srour J, Walter A, et al. Dupilumab for treatment of atopic dermatitis. Expert Rev Clin Pharmacol. 2018;11:467-474.
- Bacharier LB, Maspero JF, Katelaris CH, et al. Dupilumab in children with uncontrolled moderate-to-severe asthma. N Engl J Med. 2021;385:2230-2240.
- Chan SMH, Cro S, Cornelius V, et al. Omalizumab for severe atopic dermatitis in 4- to 19-year-olds: the ADAPT RCT. National Institute for Health and Care Research; May 2022.
- Sumi T, Nagahisa Y, Matsuura K, et al. Delayed local reaction at a previous injection site reaction with dupilumab. Respirol Case Rep. 2021;9:E0852.
- Lian N, Zhang L, Chen M. Tumor necrosis factors-α inhibition-induced paradoxical psoriasis: a case series and literature review. Dermatol Ther. 2020;33:e14225.
Mental Health Services: The Missing Piece or Missing Peace for Patients With Atopic Dermatitis
There is a well-established connection between the mind and the skin, and it is clear that this relationship is bidirectional—not only does skin disease increase the risk for depression, anxiety, sleep disturbance, and suicidality, but psychologic stress actually can worsen skin disease through multiple mechanisms, including direct damage to the skin barrier.1,2 Psychologic stress also impacts the microbiome, another critical driver of skin disease.3,4 The concept of the itch-scratch cycle vividly illustrates the vicious interplay between the mind and body in atopic dermatitis (AD).
However, patients with AD are not the only ones impacted—caregivers also experience psychologic stress. Remarkably, one study of patients with AD and their caregivers found that the caregivers actually reported significantly worse mental health and anxiety (P=.01 and P=.03, respectively) than patients themselves, even when controlling for the severity of disease.5
Thus, it would seem obvious for mental health to be a central component of AD care—to improve patient and caregiver quality of life while also improving symptoms. Research has actually borne this out, with one systematic review and meta-analysis concluding that psychological intervention has a beneficial effect on AD,6 and another that the addition of psychological and educational interventions to conventional treatment provided better therapeutic results in alleviating eczema severity and psychological symptoms.7 One study demonstrated that patients with AD who received cognitive behavioral therapy via the internet displayed a statistically significant improvement in their disease (P<.001) as measured by the Patient-Oriented Eczema Measure compared with those in the control group who received standard care alone. They also reported improvements in perceived stress, sleep problems, and depression in the intervention group that were sustained at 1-year follow-up.8 These findings are particularly impactful because clinical results were achieved while leveraging an internet-based approach to therapy.
Regrettably, despite the preponderance of evidence supporting the connection between mental health and AD, there remain considerable unmet needs. A recent cross-sectional survey of 954 adults with AD and caregivers of children with AD (N=954) conducted by the National Eczema Association found that half of patients were never asked about mental health during any of their visits, and of those referred for mental health resources, only 57% utilized the recommended services.9 Importantly, patients aged 18 to 34 years reported wanting to be asked about mental health. Of those who did receive referrals, most were for counseling services (23%), followed by alternative mental health therapy such as music or art therapy (15%), cognitive behavioral therapy (13%), or peer/social support groups (12%). Approximately 10% reported receiving a pamphlet or a brochure only.9
Physicians who treat patients with AD can and must do better, but first we must explore why these referral rates are so low. As with many complex problems, there is unlikely to be one simple unifying reason. As expected, the answer is nuanced and multifaceted, and—most importantly—staggeringly incomplete.
For starters, mental health interventions rarely are as easy as applying a cream or taking a pill. Hedman-Lagerlöf et al8 specifically pointed out that although their approach—using internet-based cognitive behavioral therapy—was explicitly designed to be more accessible with fewer resources, it required approximately 35 hours of treatment over 12 weeks, requiring both substantial time and commitment from patients who often are already burned out and exhausted due to AD. They even underscored that the most commonly reported adverse effect of therapy was increased stress or worry, making it a difficult sell.8
Even before most patients have a chance to consider the time required and the potential adverse effects of mental health interventions for AD, greater hurdles exist. Finances, medical insurance, and wait times were highlighted as barriers to care in a systematic review.10 These are deep-seated problems in the United States; while they may be surmountable in certain geographic areas, the frequency with which these concerns arise means that it does not take too many failed attempts at referring patients for mental health services before clinicians just give up—similar to any form of operant conditioning.
A more elusive concept is stigmatization. Although it may not be quantifiable, the idea is that patients may encounter additional challenges when seeking mental health care, either because the interactions themselves may worsen their symptoms (eg, increased anxiety) or they may be more likely to have a negative perception of the experience.11 A 2020 systematic review of barriers to addressing common mental health problems found that stigma was the most prominent barrier in adolescents, with the second most prominent being negative attitudes and beliefs about mental health services and professionals.12 As a clinician, I can attest that I have sometimes detected skepticism when I have suggested mental health services to patients and have even been asked outright if I thought the problem was all in their head. My patients with AD generally have been much more open to the idea of mental health support, especially after I explain the powerful mind-body connection, than patients with other conditions—most notably delusions of parasitosis—who have been much more dismissive of such overtures. An oft-cited paper from 1976 frames the problem perfectly, describing what can happen after a referral for mental health services.13 The authors stated that the suggestion of mental health makes patients feel that the dermatologist does not believe them in the first place. Beyond this, the authors pointed out that referring the patient elsewhere reduces their hopes for dermatologic treatment.13
Knowing now—perhaps more than ever before—that the mind and skin are intimately connected compels us to solve these problems and find ways around these obstacles. Selecting the optimal forms of mental health services for each patient, having the structural support of the health care system, and winning the trust of patients and caregivers while combating stigma are undoubtedly tall orders; however, understanding the stakes for patients with AD, their caregivers, and society as a whole should inspire us to keep pushing forward.
- Nicholas MN, Gooderham MJ. Atopic dermatitis, depression, and suicidality. J Cutan Med Surg. 2017;21:237-242. doi:10.1177/1203475416685078
- aarouf M, Maarouf CL, Yosipovitch G, et al. The impact of stress on epidermal barrier function: an evidence‐based review. Br J Dermatol. 2019;181:1129-1137.
- Prescott SL, Larcombe DL, Logan AC, et al. The skin microbiome: impact of modern environments on skin ecology, barrier integrity, and systemic immune programming. World Allergy Organ J. 2017;10:29.
- Zhang XE, Zheng P, Ye SZ, et al. Microbiome: role in inflammatory skin diseases. J Inflamm Res. 2024;17:1057-1082.
- Chong AC, Schwartz A, Lang J, et al. Patients’ and caregivers’ preferences for mental health care and support in atopic dermatitis. Dermatitis. 2024;35(suppl 1):S70-S76.
- Chida Y, Steptoe A, Hirakawa N, et al. The effects of psychological intervention on atopic dermatitis. a systematic review and meta-analysis. Int Arch Allergy Immunol. 2007;144:1-9.
- Hashimoto K, Ogawa Y, Takeshima N, et al. Psychological and educational interventions for atopic dermatitis in adults: a systematic review and meta-analysis. Behav Change. 2017;34:48-65.
- Hedman-Lagerlöf E, Fust J, Axelsson E, et al. Internet-delivered cognitive behavior therapy for atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2021;157:796-804. doi:10.1001/jamadermatol.2021.1450
- Chatrath S, Loiselle AR, Johnson JK, et al. Evaluating mental health support by healthcare providers for patients with atopic dermatitis: a cross‐sectional survey. Skin Health Dis. Published online June 15, 2024. doi:10.1002/ski2.408
- Toy J, Gregory A, Rehmus W. Barriers to healthcare access in pediatric dermatology: a systematic review. Pediatr Dermatol. 2021;38(suppl 2):13-19.
- Borba CPC, DePadilla L, McCarty FA, et al. A qualitative study examining the perceived barriers and facilitators to medical healthcare services among women with a serious mental illness. Womens Health Issues. 2012;22:E217-E224.
- Aguirre Velasco A, Cruz ISS, Billings J, et al. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? a systematic review. BMC Psychiatry. 2020;20:293.
- Gould WM, Gragg TM. Delusions of parasitosis. an approach to the problem. Arch Dermatol. 1976;112:1745-1748.
There is a well-established connection between the mind and the skin, and it is clear that this relationship is bidirectional—not only does skin disease increase the risk for depression, anxiety, sleep disturbance, and suicidality, but psychologic stress actually can worsen skin disease through multiple mechanisms, including direct damage to the skin barrier.1,2 Psychologic stress also impacts the microbiome, another critical driver of skin disease.3,4 The concept of the itch-scratch cycle vividly illustrates the vicious interplay between the mind and body in atopic dermatitis (AD).
However, patients with AD are not the only ones impacted—caregivers also experience psychologic stress. Remarkably, one study of patients with AD and their caregivers found that the caregivers actually reported significantly worse mental health and anxiety (P=.01 and P=.03, respectively) than patients themselves, even when controlling for the severity of disease.5
Thus, it would seem obvious for mental health to be a central component of AD care—to improve patient and caregiver quality of life while also improving symptoms. Research has actually borne this out, with one systematic review and meta-analysis concluding that psychological intervention has a beneficial effect on AD,6 and another that the addition of psychological and educational interventions to conventional treatment provided better therapeutic results in alleviating eczema severity and psychological symptoms.7 One study demonstrated that patients with AD who received cognitive behavioral therapy via the internet displayed a statistically significant improvement in their disease (P<.001) as measured by the Patient-Oriented Eczema Measure compared with those in the control group who received standard care alone. They also reported improvements in perceived stress, sleep problems, and depression in the intervention group that were sustained at 1-year follow-up.8 These findings are particularly impactful because clinical results were achieved while leveraging an internet-based approach to therapy.
Regrettably, despite the preponderance of evidence supporting the connection between mental health and AD, there remain considerable unmet needs. A recent cross-sectional survey of 954 adults with AD and caregivers of children with AD (N=954) conducted by the National Eczema Association found that half of patients were never asked about mental health during any of their visits, and of those referred for mental health resources, only 57% utilized the recommended services.9 Importantly, patients aged 18 to 34 years reported wanting to be asked about mental health. Of those who did receive referrals, most were for counseling services (23%), followed by alternative mental health therapy such as music or art therapy (15%), cognitive behavioral therapy (13%), or peer/social support groups (12%). Approximately 10% reported receiving a pamphlet or a brochure only.9
Physicians who treat patients with AD can and must do better, but first we must explore why these referral rates are so low. As with many complex problems, there is unlikely to be one simple unifying reason. As expected, the answer is nuanced and multifaceted, and—most importantly—staggeringly incomplete.
For starters, mental health interventions rarely are as easy as applying a cream or taking a pill. Hedman-Lagerlöf et al8 specifically pointed out that although their approach—using internet-based cognitive behavioral therapy—was explicitly designed to be more accessible with fewer resources, it required approximately 35 hours of treatment over 12 weeks, requiring both substantial time and commitment from patients who often are already burned out and exhausted due to AD. They even underscored that the most commonly reported adverse effect of therapy was increased stress or worry, making it a difficult sell.8
Even before most patients have a chance to consider the time required and the potential adverse effects of mental health interventions for AD, greater hurdles exist. Finances, medical insurance, and wait times were highlighted as barriers to care in a systematic review.10 These are deep-seated problems in the United States; while they may be surmountable in certain geographic areas, the frequency with which these concerns arise means that it does not take too many failed attempts at referring patients for mental health services before clinicians just give up—similar to any form of operant conditioning.
A more elusive concept is stigmatization. Although it may not be quantifiable, the idea is that patients may encounter additional challenges when seeking mental health care, either because the interactions themselves may worsen their symptoms (eg, increased anxiety) or they may be more likely to have a negative perception of the experience.11 A 2020 systematic review of barriers to addressing common mental health problems found that stigma was the most prominent barrier in adolescents, with the second most prominent being negative attitudes and beliefs about mental health services and professionals.12 As a clinician, I can attest that I have sometimes detected skepticism when I have suggested mental health services to patients and have even been asked outright if I thought the problem was all in their head. My patients with AD generally have been much more open to the idea of mental health support, especially after I explain the powerful mind-body connection, than patients with other conditions—most notably delusions of parasitosis—who have been much more dismissive of such overtures. An oft-cited paper from 1976 frames the problem perfectly, describing what can happen after a referral for mental health services.13 The authors stated that the suggestion of mental health makes patients feel that the dermatologist does not believe them in the first place. Beyond this, the authors pointed out that referring the patient elsewhere reduces their hopes for dermatologic treatment.13
Knowing now—perhaps more than ever before—that the mind and skin are intimately connected compels us to solve these problems and find ways around these obstacles. Selecting the optimal forms of mental health services for each patient, having the structural support of the health care system, and winning the trust of patients and caregivers while combating stigma are undoubtedly tall orders; however, understanding the stakes for patients with AD, their caregivers, and society as a whole should inspire us to keep pushing forward.
There is a well-established connection between the mind and the skin, and it is clear that this relationship is bidirectional—not only does skin disease increase the risk for depression, anxiety, sleep disturbance, and suicidality, but psychologic stress actually can worsen skin disease through multiple mechanisms, including direct damage to the skin barrier.1,2 Psychologic stress also impacts the microbiome, another critical driver of skin disease.3,4 The concept of the itch-scratch cycle vividly illustrates the vicious interplay between the mind and body in atopic dermatitis (AD).
However, patients with AD are not the only ones impacted—caregivers also experience psychologic stress. Remarkably, one study of patients with AD and their caregivers found that the caregivers actually reported significantly worse mental health and anxiety (P=.01 and P=.03, respectively) than patients themselves, even when controlling for the severity of disease.5
Thus, it would seem obvious for mental health to be a central component of AD care—to improve patient and caregiver quality of life while also improving symptoms. Research has actually borne this out, with one systematic review and meta-analysis concluding that psychological intervention has a beneficial effect on AD,6 and another that the addition of psychological and educational interventions to conventional treatment provided better therapeutic results in alleviating eczema severity and psychological symptoms.7 One study demonstrated that patients with AD who received cognitive behavioral therapy via the internet displayed a statistically significant improvement in their disease (P<.001) as measured by the Patient-Oriented Eczema Measure compared with those in the control group who received standard care alone. They also reported improvements in perceived stress, sleep problems, and depression in the intervention group that were sustained at 1-year follow-up.8 These findings are particularly impactful because clinical results were achieved while leveraging an internet-based approach to therapy.
Regrettably, despite the preponderance of evidence supporting the connection between mental health and AD, there remain considerable unmet needs. A recent cross-sectional survey of 954 adults with AD and caregivers of children with AD (N=954) conducted by the National Eczema Association found that half of patients were never asked about mental health during any of their visits, and of those referred for mental health resources, only 57% utilized the recommended services.9 Importantly, patients aged 18 to 34 years reported wanting to be asked about mental health. Of those who did receive referrals, most were for counseling services (23%), followed by alternative mental health therapy such as music or art therapy (15%), cognitive behavioral therapy (13%), or peer/social support groups (12%). Approximately 10% reported receiving a pamphlet or a brochure only.9
Physicians who treat patients with AD can and must do better, but first we must explore why these referral rates are so low. As with many complex problems, there is unlikely to be one simple unifying reason. As expected, the answer is nuanced and multifaceted, and—most importantly—staggeringly incomplete.
For starters, mental health interventions rarely are as easy as applying a cream or taking a pill. Hedman-Lagerlöf et al8 specifically pointed out that although their approach—using internet-based cognitive behavioral therapy—was explicitly designed to be more accessible with fewer resources, it required approximately 35 hours of treatment over 12 weeks, requiring both substantial time and commitment from patients who often are already burned out and exhausted due to AD. They even underscored that the most commonly reported adverse effect of therapy was increased stress or worry, making it a difficult sell.8
Even before most patients have a chance to consider the time required and the potential adverse effects of mental health interventions for AD, greater hurdles exist. Finances, medical insurance, and wait times were highlighted as barriers to care in a systematic review.10 These are deep-seated problems in the United States; while they may be surmountable in certain geographic areas, the frequency with which these concerns arise means that it does not take too many failed attempts at referring patients for mental health services before clinicians just give up—similar to any form of operant conditioning.
A more elusive concept is stigmatization. Although it may not be quantifiable, the idea is that patients may encounter additional challenges when seeking mental health care, either because the interactions themselves may worsen their symptoms (eg, increased anxiety) or they may be more likely to have a negative perception of the experience.11 A 2020 systematic review of barriers to addressing common mental health problems found that stigma was the most prominent barrier in adolescents, with the second most prominent being negative attitudes and beliefs about mental health services and professionals.12 As a clinician, I can attest that I have sometimes detected skepticism when I have suggested mental health services to patients and have even been asked outright if I thought the problem was all in their head. My patients with AD generally have been much more open to the idea of mental health support, especially after I explain the powerful mind-body connection, than patients with other conditions—most notably delusions of parasitosis—who have been much more dismissive of such overtures. An oft-cited paper from 1976 frames the problem perfectly, describing what can happen after a referral for mental health services.13 The authors stated that the suggestion of mental health makes patients feel that the dermatologist does not believe them in the first place. Beyond this, the authors pointed out that referring the patient elsewhere reduces their hopes for dermatologic treatment.13
Knowing now—perhaps more than ever before—that the mind and skin are intimately connected compels us to solve these problems and find ways around these obstacles. Selecting the optimal forms of mental health services for each patient, having the structural support of the health care system, and winning the trust of patients and caregivers while combating stigma are undoubtedly tall orders; however, understanding the stakes for patients with AD, their caregivers, and society as a whole should inspire us to keep pushing forward.
- Nicholas MN, Gooderham MJ. Atopic dermatitis, depression, and suicidality. J Cutan Med Surg. 2017;21:237-242. doi:10.1177/1203475416685078
- aarouf M, Maarouf CL, Yosipovitch G, et al. The impact of stress on epidermal barrier function: an evidence‐based review. Br J Dermatol. 2019;181:1129-1137.
- Prescott SL, Larcombe DL, Logan AC, et al. The skin microbiome: impact of modern environments on skin ecology, barrier integrity, and systemic immune programming. World Allergy Organ J. 2017;10:29.
- Zhang XE, Zheng P, Ye SZ, et al. Microbiome: role in inflammatory skin diseases. J Inflamm Res. 2024;17:1057-1082.
- Chong AC, Schwartz A, Lang J, et al. Patients’ and caregivers’ preferences for mental health care and support in atopic dermatitis. Dermatitis. 2024;35(suppl 1):S70-S76.
- Chida Y, Steptoe A, Hirakawa N, et al. The effects of psychological intervention on atopic dermatitis. a systematic review and meta-analysis. Int Arch Allergy Immunol. 2007;144:1-9.
- Hashimoto K, Ogawa Y, Takeshima N, et al. Psychological and educational interventions for atopic dermatitis in adults: a systematic review and meta-analysis. Behav Change. 2017;34:48-65.
- Hedman-Lagerlöf E, Fust J, Axelsson E, et al. Internet-delivered cognitive behavior therapy for atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2021;157:796-804. doi:10.1001/jamadermatol.2021.1450
- Chatrath S, Loiselle AR, Johnson JK, et al. Evaluating mental health support by healthcare providers for patients with atopic dermatitis: a cross‐sectional survey. Skin Health Dis. Published online June 15, 2024. doi:10.1002/ski2.408
- Toy J, Gregory A, Rehmus W. Barriers to healthcare access in pediatric dermatology: a systematic review. Pediatr Dermatol. 2021;38(suppl 2):13-19.
- Borba CPC, DePadilla L, McCarty FA, et al. A qualitative study examining the perceived barriers and facilitators to medical healthcare services among women with a serious mental illness. Womens Health Issues. 2012;22:E217-E224.
- Aguirre Velasco A, Cruz ISS, Billings J, et al. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? a systematic review. BMC Psychiatry. 2020;20:293.
- Gould WM, Gragg TM. Delusions of parasitosis. an approach to the problem. Arch Dermatol. 1976;112:1745-1748.
- Nicholas MN, Gooderham MJ. Atopic dermatitis, depression, and suicidality. J Cutan Med Surg. 2017;21:237-242. doi:10.1177/1203475416685078
- aarouf M, Maarouf CL, Yosipovitch G, et al. The impact of stress on epidermal barrier function: an evidence‐based review. Br J Dermatol. 2019;181:1129-1137.
- Prescott SL, Larcombe DL, Logan AC, et al. The skin microbiome: impact of modern environments on skin ecology, barrier integrity, and systemic immune programming. World Allergy Organ J. 2017;10:29.
- Zhang XE, Zheng P, Ye SZ, et al. Microbiome: role in inflammatory skin diseases. J Inflamm Res. 2024;17:1057-1082.
- Chong AC, Schwartz A, Lang J, et al. Patients’ and caregivers’ preferences for mental health care and support in atopic dermatitis. Dermatitis. 2024;35(suppl 1):S70-S76.
- Chida Y, Steptoe A, Hirakawa N, et al. The effects of psychological intervention on atopic dermatitis. a systematic review and meta-analysis. Int Arch Allergy Immunol. 2007;144:1-9.
- Hashimoto K, Ogawa Y, Takeshima N, et al. Psychological and educational interventions for atopic dermatitis in adults: a systematic review and meta-analysis. Behav Change. 2017;34:48-65.
- Hedman-Lagerlöf E, Fust J, Axelsson E, et al. Internet-delivered cognitive behavior therapy for atopic dermatitis: a randomized clinical trial. JAMA Dermatol. 2021;157:796-804. doi:10.1001/jamadermatol.2021.1450
- Chatrath S, Loiselle AR, Johnson JK, et al. Evaluating mental health support by healthcare providers for patients with atopic dermatitis: a cross‐sectional survey. Skin Health Dis. Published online June 15, 2024. doi:10.1002/ski2.408
- Toy J, Gregory A, Rehmus W. Barriers to healthcare access in pediatric dermatology: a systematic review. Pediatr Dermatol. 2021;38(suppl 2):13-19.
- Borba CPC, DePadilla L, McCarty FA, et al. A qualitative study examining the perceived barriers and facilitators to medical healthcare services among women with a serious mental illness. Womens Health Issues. 2012;22:E217-E224.
- Aguirre Velasco A, Cruz ISS, Billings J, et al. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? a systematic review. BMC Psychiatry. 2020;20:293.
- Gould WM, Gragg TM. Delusions of parasitosis. an approach to the problem. Arch Dermatol. 1976;112:1745-1748.
Practice Points
- The mind-body connection plays a role in many conditions, including atopic dermatitis.
- Atopic dermatitis can make patients feel anxious, stressed, and depressed; at the same time, those feelings can lead to worsening of the condition.
- There are many barriers to getting mental health care in the United States, from financial constraints to stigmatization.
- Mental health is part of overall health and should be more highly prioritized by all physicians.

Why More Doctors Are Joining Unions
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
With huge shifts over the past decade in the way doctors are employed — half of all doctors now work for a health system or large medical group — the idea of unionizing is not only being explored but gaining traction within the profession. In fact, 8% of the physician workforce (or 70,000 physicians) belong to a union, according to statistics gathered in 2022.
Exact numbers are hard to come by, and, interestingly, although the American Medical Association (AMA) “ supports the right of physicians to engage in collective bargaining,” the organization doesn’t track union membership among physicians, according to an AMA spokesperson.
Forming a Union
One challenge is that forming a union is not only time-consuming but also difficult, owing to several barriers. For starters, the laws dictating unionization differ by state, and the rules governing unionization vary if a hospital is public or private. If there’s enough momentum from doctors leading unionization efforts, approval from hospital leaders is required before an official election can be requested from the National Labor Relations Board.
That said, for doctors who are in a union — the two most popular are the Union of American Physicians and Dentists and the Doctors Council branch of the Service Employees International Union (SEIU)—the benefits are immense, especially because union members can focus on what matters, such as providing the best patient care possible.
, reported WBUR in Boston.
Belonging Matters
“When you build a relationship with your patients, it’s special, and that connection isn’t replaceable,” said Nicholas VenOsdel, MD, a pediatrician at Allina Health Primary Care in Hastings, Minnesota, and a union member of the Doctors Council. “However, a lot of us have felt like that hasn’t been respected as the climate of healthcare has changed so fast.”
In fact, autonomy over how much time doctors spend with patients is driving a lot of interest in unionization.
“We don’t necessarily have that autonomy now,” said Amber Higgins, MD, an emergency physician and an obstetrician at ChristianaCare, a hospital network in Newark, Delaware, and a member of the Doctors Council. “There are so many other demands, whether it’s billing, patient documentation, or other demands from the employer, and all of that takes time away from patient care.”
Another primary driver of physician unionization is the physician burnout epidemic. Physicians collectively complain that they spend more time on electronic health record documentation and bureaucratic administration. Yet if unions can improve these working conditions, the benefit to physicians and their patients would be a welcome change.
Union members are bullish and believe that having a cohesive voice will make a difference.
“We need to use our collective voices to get back to focusing on patient care instead of staring at a computer screen for 80% of the day,” Dr. Higgins told this news organization. “So much of medicine involves getting to the correct diagnosis, listening to patients, observing them, and building a relationship with them. We need time to build that.”
With corporate consolidation and a profit-driven mandate by healthcare systems, doctors are increasingly frustrated and feel that their voices haven’t been heard enough when it comes to issues like workplace safety, working hours, and benefits, said Stuart Bussey, MD, JD, a family practice physician and president of the Union of American Physicians and Dentists in Sacramento, California.
However, he adds that urging doctors to join together to fight for a better working environment hasn’t been easy.
“Doctors are individualists, and they don’t know how to work in packs like hospital administrators do,” said Dr. Bussey. “They’re hard to organize, but I want them to understand that unless they join hands, sign petitions, and speak as one voice, they’re going to lose out on an amazing opportunity.”
Overcoming Misperceptions About Unions
One barrier to doctors getting involved is the sentiment that unions might do the opposite of what’s intended — that is, they might further reduce a doctor’s autonomy and work flexibility. Or there may be a perception that the drive to join a union is predicated on making more money.
Though he’s now in a union, Dr. VenOsdel, who has been in a hospital-based practice for 7 years, admits that he initially felt very differently about unions than he does today.
“Even though I have family members in healthcare unions, I had a neutral to even slightly negative view of unions,” said Dr. VenOsdel. “It took me working directly with the Minnesota Nurses Association and the Doctors Council to learn the other side of the story.”
Armed with more information, he began lobbying for stricter rules about how his state’s large healthcare systems were closing hospitals and ending much-needed community services.
“I remember standing at the Capitol in Minnesota and telling one of the members that I once felt negatively about unions,” he added. “I realized then that I only knew what employers were telling me via such things as emails about strikes — that information was all being shared from the employers’ perspective.”
The other misperception is that unions only exist to argue against management, including against colleagues who are also part of the management structure, said Dr. Higgins.
“Some doctors perceive being in a union as ‘how can those same leaders also be in a union,’” she said. She feels that they currently don’t have leadership representing them that can help with such things as restructuring their support teams or getting them help with certain tasks. “That’s another way unions can help.”
Social Justice Plays a Role
For Dr. VenOsdel, being part of a union has helped him return to what he calls the “art” of medicine.
“Philosophically, the union gave me an option for change in what felt like a hopeless situation,” he said. “It wasn’t just that I was tossing the keys to someone else and saying, ‘I can’t fix this.’ Instead, we’re taking the reins back and fixing things ourselves.”
Bussey argues that as the uneven balance between administrators and providers in many healthcare organizations grows, the time to consider forming a union is now.
“We’re in a $4 trillion medical industrial revolution,” he said. “Administrators and bureaucrats are multiplying 30-fold times vs providers, and most of that $4 trillion supports things that don’t contribute to the doctor-patient relationship.”
Furthermore, union proponents say that where a one-on-one relationship between doctor and patient once existed, that has now been “triangulated” to include administrators.
“We’ve lost power in every way,” Dr. Bussey said. “We have the degrees, the liability, and the knowledge — we should have more power to make our workplaces safer and better.”
Ultimately, for some unionized doctors, the very holding of a union card is rooted in supporting social justice issues.
“When doctors realize how powerful a tool a union can be for social justice and change, this will alter perceptions of unions within our profession,” Dr. VenOsdel said. “Our union helps give us a voice to stand up for other staff who aren’t unionized and, most importantly, to stand up for the patients who need us.”
A version of this article first appeared on Medscape.com.
Acne: Positive Outcomes Described With Laser Treatment
CARLSBAD, CALIF. — at 1 year.
“Combining the AviClear with medical therapy and energy-based devices provides the best outcomes,” Dr. Moradzadeh, who practices facial and plastic surgery in Beverly Hills, California, said at the Controversies & Conversations in Laser & Cosmetic Surgery annual symposium. “You have to do all 300 pulses per treatment, and you do need to use settings of 19.5-21.5 J/cm2 to get a great result.”

AviClear became the first 1726-nm laser cleared by the FDA for the treatment of mild to severe acne vulgaris, followed a few months later by clearance of the 1926-nm laser, the Accure Acne Laser System. But few long-term “real-world” studies of these two devices exist, according to Dr. Moradzadeh.
The protocol for Dr. Moradzadeh’s study included three AviClear treatments spaced 3-4 weeks apart combined with medical therapy and other energy-based devices such as a near-infrared Nd:YAG laser (Laser Genesis) and a non-ablative fractional laser (LaseMD Ultra), with follow-up at 1 month, 3 months, 6 months, 1 year, 1.5 years, and 2 years. Pain management options included acetaminophen, a numbing cream, and pre- and post-contact cooling.
Of the 100 patients, 90 were clear at 1 year, six patients were almost clear at 1 year, three patients were nonresponders, and one patient was lost to follow-up, Dr. Moradzadeh reported. “Two of the three nonresponders did not receive the full 300 pulses per treatment,” but all three cleared with isotretinoin treatment, he said. “What we now know from talking with other providers is that you really have to do all 300 pulses to get the best results.”
Of the 90 patients who achieved clearance, 80 remained clear at 1.5-2 years, and 10 are almost clear or have mild acne. “Of these, eight are adult females with hormonal acne and two are teenage males,” he said. “All 10 cleared with a fourth AviClear treatment and lifestyle modifications that included the elimination of whey, creatine, and skin care products containing vitamin E combined with vitamin C.”
During a question-and-answer session following the presentation, Jeffrey Dover, MD, director of SkinCare Physicians in Chestnut Hill, Massachusetts, said that general dermatologists have been slow to adopt the AviClear and Accure devices for treating patients with acne “because, for the most part, they are experts at treating acne with all the tools they have. They’re not used to using devices. They’re not used to having patients pay out of pocket for a treatment that is not covered by insurance. They don’t feel comfortable with that discussion.”
For example, the 14 dermatologists at SkinCare Physicians “almost never prescribe the 1726-nm devices for acne because it’s not in their sweet spot,” Dr. Dover continued, noting that one issue is that acne experts want more data.
In the experience of Nazanin Saedi, MD, clinical associate professor of dermatology at Thomas Jefferson University, Philadelphia, the 1726-nm laser devices for acne “fit nicely for women of childbearing age who have acne and don’t want to go on Accutane [isotretinoin], and also for teenagers who are either going to be noncompliant with Accutane or their parents are worried about side effects and the potential impacts on growth,” she said at the meeting. “That’s where we’ve found patients coming in wanting to do these treatments, and how it offers something that the medical treatments are lacking.”
Regarding concerns about out-of-pocket costs for AviClear or Accure treatments, Roy G. Geronemus, MD, who directs the Laser & Skin Surgery Center of New York, New York City, advised considering the long-term benefits. “If you calculate it out, it really is cost-effective to use the 1726-nm devices if you consider the copays, the cost of over-the-counter topicals, as well as the cost of prescription medications,” Dr. Geronemus said. “Over the long term, you are saving money for the patient.”
Dr. Dover acknowledged that was “a valid and important point,” but said that when the topic is discussed with general dermatologists who treat a lot of patients with acne, “they say patients are more willing to pay a copay [for a prescription] ... than write a check for $800 or $1000 per visit.”
The recently updated American Academy of Dermatology’s guidelines of care for the management of acne vulgaris, published in January 2024, characterized the available evidence as “insufficient” to develop a recommendation on the use of laser and light-based devices for the treatment of acne. Although the 1726-nm laser was cleared by the FDA for acne treatment in 2022, the authors of the guidelines wrote that “its evidence was not evaluated in the current guidelines due to lack of a randomized, controlled trial.”
Dr. Moradzadeh disclosed that he is a key opinion leader for Acclaro, Benev, Lutronic, Sofwave, and Cutera, the manufacturer for AviClear. Dr. Dover reported that he is a consultant for Cutera and performs research for the company. Dr. Saedi disclosed that she is a consultant to, a member of the advisory board for, and/or has received equipment and research support from many device and pharmaceutical companies. Dr. Geronemus disclosed that he is a member of the medical advisory board for and/or is an investigator for many device and pharmaceutical companies, including Accure. He also holds stock in the company.
A version of this article first appeared on Medscape.com.
CARLSBAD, CALIF. — at 1 year.
“Combining the AviClear with medical therapy and energy-based devices provides the best outcomes,” Dr. Moradzadeh, who practices facial and plastic surgery in Beverly Hills, California, said at the Controversies & Conversations in Laser & Cosmetic Surgery annual symposium. “You have to do all 300 pulses per treatment, and you do need to use settings of 19.5-21.5 J/cm2 to get a great result.”
AviClear became the first 1726-nm laser cleared by the FDA for the treatment of mild to severe acne vulgaris, followed a few months later by clearance of the 1926-nm laser, the Accure Acne Laser System. But few long-term “real-world” studies of these two devices exist, according to Dr. Moradzadeh.
The protocol for Dr. Moradzadeh’s study included three AviClear treatments spaced 3-4 weeks apart combined with medical therapy and other energy-based devices such as a near-infrared Nd:YAG laser (Laser Genesis) and a non-ablative fractional laser (LaseMD Ultra), with follow-up at 1 month, 3 months, 6 months, 1 year, 1.5 years, and 2 years. Pain management options included acetaminophen, a numbing cream, and pre- and post-contact cooling.
Of the 100 patients, 90 were clear at 1 year, six patients were almost clear at 1 year, three patients were nonresponders, and one patient was lost to follow-up, Dr. Moradzadeh reported. “Two of the three nonresponders did not receive the full 300 pulses per treatment,” but all three cleared with isotretinoin treatment, he said. “What we now know from talking with other providers is that you really have to do all 300 pulses to get the best results.”
Of the 90 patients who achieved clearance, 80 remained clear at 1.5-2 years, and 10 are almost clear or have mild acne. “Of these, eight are adult females with hormonal acne and two are teenage males,” he said. “All 10 cleared with a fourth AviClear treatment and lifestyle modifications that included the elimination of whey, creatine, and skin care products containing vitamin E combined with vitamin C.”
During a question-and-answer session following the presentation, Jeffrey Dover, MD, director of SkinCare Physicians in Chestnut Hill, Massachusetts, said that general dermatologists have been slow to adopt the AviClear and Accure devices for treating patients with acne “because, for the most part, they are experts at treating acne with all the tools they have. They’re not used to using devices. They’re not used to having patients pay out of pocket for a treatment that is not covered by insurance. They don’t feel comfortable with that discussion.”
For example, the 14 dermatologists at SkinCare Physicians “almost never prescribe the 1726-nm devices for acne because it’s not in their sweet spot,” Dr. Dover continued, noting that one issue is that acne experts want more data.
In the experience of Nazanin Saedi, MD, clinical associate professor of dermatology at Thomas Jefferson University, Philadelphia, the 1726-nm laser devices for acne “fit nicely for women of childbearing age who have acne and don’t want to go on Accutane [isotretinoin], and also for teenagers who are either going to be noncompliant with Accutane or their parents are worried about side effects and the potential impacts on growth,” she said at the meeting. “That’s where we’ve found patients coming in wanting to do these treatments, and how it offers something that the medical treatments are lacking.”
Regarding concerns about out-of-pocket costs for AviClear or Accure treatments, Roy G. Geronemus, MD, who directs the Laser & Skin Surgery Center of New York, New York City, advised considering the long-term benefits. “If you calculate it out, it really is cost-effective to use the 1726-nm devices if you consider the copays, the cost of over-the-counter topicals, as well as the cost of prescription medications,” Dr. Geronemus said. “Over the long term, you are saving money for the patient.”
Dr. Dover acknowledged that was “a valid and important point,” but said that when the topic is discussed with general dermatologists who treat a lot of patients with acne, “they say patients are more willing to pay a copay [for a prescription] ... than write a check for $800 or $1000 per visit.”
The recently updated American Academy of Dermatology’s guidelines of care for the management of acne vulgaris, published in January 2024, characterized the available evidence as “insufficient” to develop a recommendation on the use of laser and light-based devices for the treatment of acne. Although the 1726-nm laser was cleared by the FDA for acne treatment in 2022, the authors of the guidelines wrote that “its evidence was not evaluated in the current guidelines due to lack of a randomized, controlled trial.”
Dr. Moradzadeh disclosed that he is a key opinion leader for Acclaro, Benev, Lutronic, Sofwave, and Cutera, the manufacturer for AviClear. Dr. Dover reported that he is a consultant for Cutera and performs research for the company. Dr. Saedi disclosed that she is a consultant to, a member of the advisory board for, and/or has received equipment and research support from many device and pharmaceutical companies. Dr. Geronemus disclosed that he is a member of the medical advisory board for and/or is an investigator for many device and pharmaceutical companies, including Accure. He also holds stock in the company.
A version of this article first appeared on Medscape.com.
CARLSBAD, CALIF. — at 1 year.
“Combining the AviClear with medical therapy and energy-based devices provides the best outcomes,” Dr. Moradzadeh, who practices facial and plastic surgery in Beverly Hills, California, said at the Controversies & Conversations in Laser & Cosmetic Surgery annual symposium. “You have to do all 300 pulses per treatment, and you do need to use settings of 19.5-21.5 J/cm2 to get a great result.”
AviClear became the first 1726-nm laser cleared by the FDA for the treatment of mild to severe acne vulgaris, followed a few months later by clearance of the 1926-nm laser, the Accure Acne Laser System. But few long-term “real-world” studies of these two devices exist, according to Dr. Moradzadeh.
The protocol for Dr. Moradzadeh’s study included three AviClear treatments spaced 3-4 weeks apart combined with medical therapy and other energy-based devices such as a near-infrared Nd:YAG laser (Laser Genesis) and a non-ablative fractional laser (LaseMD Ultra), with follow-up at 1 month, 3 months, 6 months, 1 year, 1.5 years, and 2 years. Pain management options included acetaminophen, a numbing cream, and pre- and post-contact cooling.
Of the 100 patients, 90 were clear at 1 year, six patients were almost clear at 1 year, three patients were nonresponders, and one patient was lost to follow-up, Dr. Moradzadeh reported. “Two of the three nonresponders did not receive the full 300 pulses per treatment,” but all three cleared with isotretinoin treatment, he said. “What we now know from talking with other providers is that you really have to do all 300 pulses to get the best results.”
Of the 90 patients who achieved clearance, 80 remained clear at 1.5-2 years, and 10 are almost clear or have mild acne. “Of these, eight are adult females with hormonal acne and two are teenage males,” he said. “All 10 cleared with a fourth AviClear treatment and lifestyle modifications that included the elimination of whey, creatine, and skin care products containing vitamin E combined with vitamin C.”
During a question-and-answer session following the presentation, Jeffrey Dover, MD, director of SkinCare Physicians in Chestnut Hill, Massachusetts, said that general dermatologists have been slow to adopt the AviClear and Accure devices for treating patients with acne “because, for the most part, they are experts at treating acne with all the tools they have. They’re not used to using devices. They’re not used to having patients pay out of pocket for a treatment that is not covered by insurance. They don’t feel comfortable with that discussion.”
For example, the 14 dermatologists at SkinCare Physicians “almost never prescribe the 1726-nm devices for acne because it’s not in their sweet spot,” Dr. Dover continued, noting that one issue is that acne experts want more data.
In the experience of Nazanin Saedi, MD, clinical associate professor of dermatology at Thomas Jefferson University, Philadelphia, the 1726-nm laser devices for acne “fit nicely for women of childbearing age who have acne and don’t want to go on Accutane [isotretinoin], and also for teenagers who are either going to be noncompliant with Accutane or their parents are worried about side effects and the potential impacts on growth,” she said at the meeting. “That’s where we’ve found patients coming in wanting to do these treatments, and how it offers something that the medical treatments are lacking.”
Regarding concerns about out-of-pocket costs for AviClear or Accure treatments, Roy G. Geronemus, MD, who directs the Laser & Skin Surgery Center of New York, New York City, advised considering the long-term benefits. “If you calculate it out, it really is cost-effective to use the 1726-nm devices if you consider the copays, the cost of over-the-counter topicals, as well as the cost of prescription medications,” Dr. Geronemus said. “Over the long term, you are saving money for the patient.”
Dr. Dover acknowledged that was “a valid and important point,” but said that when the topic is discussed with general dermatologists who treat a lot of patients with acne, “they say patients are more willing to pay a copay [for a prescription] ... than write a check for $800 or $1000 per visit.”
The recently updated American Academy of Dermatology’s guidelines of care for the management of acne vulgaris, published in January 2024, characterized the available evidence as “insufficient” to develop a recommendation on the use of laser and light-based devices for the treatment of acne. Although the 1726-nm laser was cleared by the FDA for acne treatment in 2022, the authors of the guidelines wrote that “its evidence was not evaluated in the current guidelines due to lack of a randomized, controlled trial.”
Dr. Moradzadeh disclosed that he is a key opinion leader for Acclaro, Benev, Lutronic, Sofwave, and Cutera, the manufacturer for AviClear. Dr. Dover reported that he is a consultant for Cutera and performs research for the company. Dr. Saedi disclosed that she is a consultant to, a member of the advisory board for, and/or has received equipment and research support from many device and pharmaceutical companies. Dr. Geronemus disclosed that he is a member of the medical advisory board for and/or is an investigator for many device and pharmaceutical companies, including Accure. He also holds stock in the company.
A version of this article first appeared on Medscape.com.
Topical Tapinarof and Roflumilast for Psoriasis: Where Do they Fit In?
HUNTINGTON BEACH, CALIF. — The Food and Drug Administration and alternative medicine modalities for psoriasis severity measures were published in 2021, leaving some clinicians to wonder how these two newcomer drugs fit into their clinical practice.
At the annual meeting of the Pacific Dermatologic Association, Jashin J. Wu, MD, one of the authors of the guidelines and a voluntary associate professor of dermatology at the University of Miami, Coral Gables, Florida, proposed that tapinarof 1% cream and roflumilast 0.3% cream be considered first-line treatments for mild psoriasis. “The reason is because they’re very fast-acting, effective,” and result in a large improvement over steroids, Dr. Wu said. “You don’t have to worry about steroid atrophy, and it eliminates the need to use many different agents for different parts of the body necessarily, such as a weaker steroid for the face and sensitive areas. It also eliminates the need for patients to switch out steroids, such as 2 weeks on and 2 weeks off.”

Tapinarof 1% cream (Vtama) was approved in May 2022, for the topical treatment of plaque psoriasis in adults, and is under FDA review for treating atopic dermatitis (AD). “It’s once a day application, which is nice,” Dr. Wu said. “It is a first-in-class topical aryl hydrocarbon receptor agonist that can be used for the intertriginous areas. That’s where I find it helpful.”
Roflumilast 0.3% cream (Zoryve), a phosphodiesterase-4 inhibitor, was approved in July 2022 for the treatment of plaque psoriasis, including intertriginous areas, in patients aged 12 years and older. It was subsequently approved for treating plaque psoriasis in patients 6 years and older. (Roflumilast 0.15% cream is approved for mild to moderate AD in people aged 6 years or older, and roflumilast 0.3% topical foam is approved for seborrheic dermatitis in adults and children 9 years of age and older.)
The drug is contraindicated for use in patients with certain liver problems. “Patients are not going to be eating tubes of this drug, so I wouldn’t worry about that too much, but be aware if the pharmacist raises a concern about this,” Dr. Wu said.
Dr. Wu disclosed that he is or has been a consultant, investigator, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Codex Labs, Dermavant, DermTech, Dr. Reddy’s Laboratories, Eli Lilly, EPI Health, Galderma, Incyte, Janssen, LEO Pharma, Mindera, Novartis, Pfizer, Regeneron, Samsung Bioepis, Sanofi Genzyme, Solius, Sun Pharmaceuticals, UCB, and Zerigo Health.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — The Food and Drug Administration and alternative medicine modalities for psoriasis severity measures were published in 2021, leaving some clinicians to wonder how these two newcomer drugs fit into their clinical practice.
At the annual meeting of the Pacific Dermatologic Association, Jashin J. Wu, MD, one of the authors of the guidelines and a voluntary associate professor of dermatology at the University of Miami, Coral Gables, Florida, proposed that tapinarof 1% cream and roflumilast 0.3% cream be considered first-line treatments for mild psoriasis. “The reason is because they’re very fast-acting, effective,” and result in a large improvement over steroids, Dr. Wu said. “You don’t have to worry about steroid atrophy, and it eliminates the need to use many different agents for different parts of the body necessarily, such as a weaker steroid for the face and sensitive areas. It also eliminates the need for patients to switch out steroids, such as 2 weeks on and 2 weeks off.”
Tapinarof 1% cream (Vtama) was approved in May 2022, for the topical treatment of plaque psoriasis in adults, and is under FDA review for treating atopic dermatitis (AD). “It’s once a day application, which is nice,” Dr. Wu said. “It is a first-in-class topical aryl hydrocarbon receptor agonist that can be used for the intertriginous areas. That’s where I find it helpful.”
Roflumilast 0.3% cream (Zoryve), a phosphodiesterase-4 inhibitor, was approved in July 2022 for the treatment of plaque psoriasis, including intertriginous areas, in patients aged 12 years and older. It was subsequently approved for treating plaque psoriasis in patients 6 years and older. (Roflumilast 0.15% cream is approved for mild to moderate AD in people aged 6 years or older, and roflumilast 0.3% topical foam is approved for seborrheic dermatitis in adults and children 9 years of age and older.)
The drug is contraindicated for use in patients with certain liver problems. “Patients are not going to be eating tubes of this drug, so I wouldn’t worry about that too much, but be aware if the pharmacist raises a concern about this,” Dr. Wu said.
Dr. Wu disclosed that he is or has been a consultant, investigator, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Codex Labs, Dermavant, DermTech, Dr. Reddy’s Laboratories, Eli Lilly, EPI Health, Galderma, Incyte, Janssen, LEO Pharma, Mindera, Novartis, Pfizer, Regeneron, Samsung Bioepis, Sanofi Genzyme, Solius, Sun Pharmaceuticals, UCB, and Zerigo Health.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — The Food and Drug Administration and alternative medicine modalities for psoriasis severity measures were published in 2021, leaving some clinicians to wonder how these two newcomer drugs fit into their clinical practice.
At the annual meeting of the Pacific Dermatologic Association, Jashin J. Wu, MD, one of the authors of the guidelines and a voluntary associate professor of dermatology at the University of Miami, Coral Gables, Florida, proposed that tapinarof 1% cream and roflumilast 0.3% cream be considered first-line treatments for mild psoriasis. “The reason is because they’re very fast-acting, effective,” and result in a large improvement over steroids, Dr. Wu said. “You don’t have to worry about steroid atrophy, and it eliminates the need to use many different agents for different parts of the body necessarily, such as a weaker steroid for the face and sensitive areas. It also eliminates the need for patients to switch out steroids, such as 2 weeks on and 2 weeks off.”
Tapinarof 1% cream (Vtama) was approved in May 2022, for the topical treatment of plaque psoriasis in adults, and is under FDA review for treating atopic dermatitis (AD). “It’s once a day application, which is nice,” Dr. Wu said. “It is a first-in-class topical aryl hydrocarbon receptor agonist that can be used for the intertriginous areas. That’s where I find it helpful.”
Roflumilast 0.3% cream (Zoryve), a phosphodiesterase-4 inhibitor, was approved in July 2022 for the treatment of plaque psoriasis, including intertriginous areas, in patients aged 12 years and older. It was subsequently approved for treating plaque psoriasis in patients 6 years and older. (Roflumilast 0.15% cream is approved for mild to moderate AD in people aged 6 years or older, and roflumilast 0.3% topical foam is approved for seborrheic dermatitis in adults and children 9 years of age and older.)
The drug is contraindicated for use in patients with certain liver problems. “Patients are not going to be eating tubes of this drug, so I wouldn’t worry about that too much, but be aware if the pharmacist raises a concern about this,” Dr. Wu said.
Dr. Wu disclosed that he is or has been a consultant, investigator, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Codex Labs, Dermavant, DermTech, Dr. Reddy’s Laboratories, Eli Lilly, EPI Health, Galderma, Incyte, Janssen, LEO Pharma, Mindera, Novartis, Pfizer, Regeneron, Samsung Bioepis, Sanofi Genzyme, Solius, Sun Pharmaceuticals, UCB, and Zerigo Health.
A version of this article first appeared on Medscape.com.
FROM PDA 2024
Topical Treatment Provides a Noninvasive Option for Pyogenic Granuloma in Children
HUNTINGTON BEACH, CALIF. — Mounting according to Julie Dhossche, MD.
A PG is a common, benign vascular tumor that often occurs in children under 5 years of age, “usually in a very inconvenient spot, like the cheek,” Dr. Dhossche, a pediatric dermatologist at Oregon Health & Science University (OHSU), Portland, said at the annual meeting of the Pacific Dermatologic Association. “It can bleed a lot. Often, parents take their child to the emergency department for unstoppable bleeding. Our first-line treatment is often surgical: shave removal, electrocautery, or excision.”
Several case reports about the use of the topical form of timolol, a nonselective beta-adrenergic antagonist, for PG have been published in the medical literature including a case series of seven patients (six were treated with topical timolol). The authors of the case series hypothesized that a beta-blocker may be effective for PGs by causing vasoconstriction that stops bleeding.
In addition, Dr. Dhossche and colleagues retrospectively evaluated 92 children with a mean age of 4.5 years who were treated with topical timolol for PG at OHSU from 2010 to 2020. The results were presented in an abstract at the 2022 Pediatric Dermatology Research Alliance annual conference.
At the initial visit, 80 of 92 (87%) children were treated with timolol only, 6 of 92 (6.5%) underwent a procedure, and 6 of 92 (6.5%) were treated with timolol and a procedure. The researchers observed that of the 80 patients who received timolol monotherapy, 42 (52.5%) were spared a procedural intervention. “So, we have had some success with this,” she said. “It can also help with bleeding episodes if you are waiting for a procedure.”
Surgery May Still Be Needed
For PGs, she applies one drop of timolol to the lesion under occlusion with DuoDERM or a similar dressing, which is repeated every 1-3 days depending on how long the dressing stays on. “It may take 3-4 months of this treatment to clear,” she said.
If topical timolol doesn’t stop the PG from bleeding, or if parents elect for surgical removal, “some tears [during removal of the lesion] may be inevitable,” Dr. Dhossche said. “My goal is to make it as good of an experience as it can be, by being very confident and offering lots of smiles, pretreatment with topical lidocaine for 20-30 minutes, icing, and formulating an alliance with parents” to help calm nerves, “knowing if that doesn’t work, I might need help from my colleagues in pediatric sedation.”
Choice of language matters when describing to children what to expect during a procedure, she continued. For example, instead of saying, “it will feel like a bee sting,” say, “some kids say it is uncomfortable like a pinch and some kids say it’s not so bad.” And, when describing the size of a needle or an incision, instead of saying, “it’s as big as ...” say, “it’s as small as ...”
As described in a 2020 paper published in Pediatric Dermatology, proper comfort positioning of children during in-office dermatologic procedures is also key, which can include having the parent or caregiver hug a child during removal of a PG, Dr. Dhossche said. “You want to optimize distractions for the patient while you do the procedure. This is the time to bring out your iPhone, iPad, or enlist help from a certified child life specialist if you have one at your institution.”
When she administers injections to children, “I don’t lie about the shot, but I do hide the actual needle from sight, if possible,” she said. “I’ll say, ‘you’ll feel a pinch.’ Vibration tools can help while you’re injecting.” She showed an image of a vibrating light-up children’s toothbrush she found on Amazon for $10 “that has served me well. It’s also kind of a tension diffuser.”
Dr. Dhossche reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — Mounting according to Julie Dhossche, MD.
A PG is a common, benign vascular tumor that often occurs in children under 5 years of age, “usually in a very inconvenient spot, like the cheek,” Dr. Dhossche, a pediatric dermatologist at Oregon Health & Science University (OHSU), Portland, said at the annual meeting of the Pacific Dermatologic Association. “It can bleed a lot. Often, parents take their child to the emergency department for unstoppable bleeding. Our first-line treatment is often surgical: shave removal, electrocautery, or excision.”
Several case reports about the use of the topical form of timolol, a nonselective beta-adrenergic antagonist, for PG have been published in the medical literature including a case series of seven patients (six were treated with topical timolol). The authors of the case series hypothesized that a beta-blocker may be effective for PGs by causing vasoconstriction that stops bleeding.
In addition, Dr. Dhossche and colleagues retrospectively evaluated 92 children with a mean age of 4.5 years who were treated with topical timolol for PG at OHSU from 2010 to 2020. The results were presented in an abstract at the 2022 Pediatric Dermatology Research Alliance annual conference.
At the initial visit, 80 of 92 (87%) children were treated with timolol only, 6 of 92 (6.5%) underwent a procedure, and 6 of 92 (6.5%) were treated with timolol and a procedure. The researchers observed that of the 80 patients who received timolol monotherapy, 42 (52.5%) were spared a procedural intervention. “So, we have had some success with this,” she said. “It can also help with bleeding episodes if you are waiting for a procedure.”
Surgery May Still Be Needed
For PGs, she applies one drop of timolol to the lesion under occlusion with DuoDERM or a similar dressing, which is repeated every 1-3 days depending on how long the dressing stays on. “It may take 3-4 months of this treatment to clear,” she said.
If topical timolol doesn’t stop the PG from bleeding, or if parents elect for surgical removal, “some tears [during removal of the lesion] may be inevitable,” Dr. Dhossche said. “My goal is to make it as good of an experience as it can be, by being very confident and offering lots of smiles, pretreatment with topical lidocaine for 20-30 minutes, icing, and formulating an alliance with parents” to help calm nerves, “knowing if that doesn’t work, I might need help from my colleagues in pediatric sedation.”
Choice of language matters when describing to children what to expect during a procedure, she continued. For example, instead of saying, “it will feel like a bee sting,” say, “some kids say it is uncomfortable like a pinch and some kids say it’s not so bad.” And, when describing the size of a needle or an incision, instead of saying, “it’s as big as ...” say, “it’s as small as ...”
As described in a 2020 paper published in Pediatric Dermatology, proper comfort positioning of children during in-office dermatologic procedures is also key, which can include having the parent or caregiver hug a child during removal of a PG, Dr. Dhossche said. “You want to optimize distractions for the patient while you do the procedure. This is the time to bring out your iPhone, iPad, or enlist help from a certified child life specialist if you have one at your institution.”
When she administers injections to children, “I don’t lie about the shot, but I do hide the actual needle from sight, if possible,” she said. “I’ll say, ‘you’ll feel a pinch.’ Vibration tools can help while you’re injecting.” She showed an image of a vibrating light-up children’s toothbrush she found on Amazon for $10 “that has served me well. It’s also kind of a tension diffuser.”
Dr. Dhossche reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIF. — Mounting according to Julie Dhossche, MD.
A PG is a common, benign vascular tumor that often occurs in children under 5 years of age, “usually in a very inconvenient spot, like the cheek,” Dr. Dhossche, a pediatric dermatologist at Oregon Health & Science University (OHSU), Portland, said at the annual meeting of the Pacific Dermatologic Association. “It can bleed a lot. Often, parents take their child to the emergency department for unstoppable bleeding. Our first-line treatment is often surgical: shave removal, electrocautery, or excision.”
Several case reports about the use of the topical form of timolol, a nonselective beta-adrenergic antagonist, for PG have been published in the medical literature including a case series of seven patients (six were treated with topical timolol). The authors of the case series hypothesized that a beta-blocker may be effective for PGs by causing vasoconstriction that stops bleeding.
In addition, Dr. Dhossche and colleagues retrospectively evaluated 92 children with a mean age of 4.5 years who were treated with topical timolol for PG at OHSU from 2010 to 2020. The results were presented in an abstract at the 2022 Pediatric Dermatology Research Alliance annual conference.
At the initial visit, 80 of 92 (87%) children were treated with timolol only, 6 of 92 (6.5%) underwent a procedure, and 6 of 92 (6.5%) were treated with timolol and a procedure. The researchers observed that of the 80 patients who received timolol monotherapy, 42 (52.5%) were spared a procedural intervention. “So, we have had some success with this,” she said. “It can also help with bleeding episodes if you are waiting for a procedure.”
Surgery May Still Be Needed
For PGs, she applies one drop of timolol to the lesion under occlusion with DuoDERM or a similar dressing, which is repeated every 1-3 days depending on how long the dressing stays on. “It may take 3-4 months of this treatment to clear,” she said.
If topical timolol doesn’t stop the PG from bleeding, or if parents elect for surgical removal, “some tears [during removal of the lesion] may be inevitable,” Dr. Dhossche said. “My goal is to make it as good of an experience as it can be, by being very confident and offering lots of smiles, pretreatment with topical lidocaine for 20-30 minutes, icing, and formulating an alliance with parents” to help calm nerves, “knowing if that doesn’t work, I might need help from my colleagues in pediatric sedation.”
Choice of language matters when describing to children what to expect during a procedure, she continued. For example, instead of saying, “it will feel like a bee sting,” say, “some kids say it is uncomfortable like a pinch and some kids say it’s not so bad.” And, when describing the size of a needle or an incision, instead of saying, “it’s as big as ...” say, “it’s as small as ...”
As described in a 2020 paper published in Pediatric Dermatology, proper comfort positioning of children during in-office dermatologic procedures is also key, which can include having the parent or caregiver hug a child during removal of a PG, Dr. Dhossche said. “You want to optimize distractions for the patient while you do the procedure. This is the time to bring out your iPhone, iPad, or enlist help from a certified child life specialist if you have one at your institution.”
When she administers injections to children, “I don’t lie about the shot, but I do hide the actual needle from sight, if possible,” she said. “I’ll say, ‘you’ll feel a pinch.’ Vibration tools can help while you’re injecting.” She showed an image of a vibrating light-up children’s toothbrush she found on Amazon for $10 “that has served me well. It’s also kind of a tension diffuser.”
Dr. Dhossche reported having no financial disclosures.
A version of this article first appeared on Medscape.com.
FROM PDA 2024
Managing Vitiligo: Combination Therapies, New Treatments
HUNTINGTON BEACH, CALIFORNIA — When patients with vitiligo see Jessica Shiu, MD, PhD, for the first time, some mention that prior healthcare providers have told them that vitiligo is merely a cosmetic issue — much to her dismay.
“Vitiligo is not a cosmetic disease,” Dr. Shiu, assistant professor of dermatology at the University of California, Irvine, said at the annual meeting of the Pacific Dermatologic Association. “It is associated with significant depression, stigmatization, and low self-esteem. I have patients who say that vitiligo has affected their marriage ... In certain cultures, it also affects their job prospects.”
As the most common pigmentary disorder, vitiligo is an autoimmune condition that often results in the recruitment of CD8+ T cells into the skin. These cells destroy melanocytes, depleting melanocytes in the epidermis. “Over time, this results in milky white patches of skin that we often see in our patients,” Dr. Shiu said.
“Depending on the site that is involved, the nonsegmental form can be further divided into focal, acrofacial, mucosal, generalized, and universal subtypes,” she said. The first step in your initial management is to determine if the vitiligo is active or stable, which can be challenging. Clinical signs of active disease include the presence of trichome vitiligo, confetti vitiligo, and koebnerization.
“Another sign of active disease is when patients tell you that their vitiligo is expanding rapidly,” Dr. Shiu added. “Stable vitiligo is more difficult to define. Many patients think their lesions don’t change, but we’re now appreciating that there can be some sites in those patients such as the hands and feet that are more susceptible to change in activity.” In general, she noted, vitiligo is considered stable when there is no change in activity for at least 12 months, and “lesions are usually completely depigmented with sharp borders.”
The level of vitiligo disease activity drives medical management. For patients with nonsegmental vitiligo who have clinical signs of active disease, the first goal is to stabilize the active disease and stop further spread of depigmentation. “This is key because losing pigment can occur very quickly, but gaining pigment back is a very slow process,” she said. Stabilization involves suppressing immune responses with topical steroids, topical calcineurin inhibitors, or 1.5% ruxolitinib cream, a JAK inhibitor that became the first Food and Drug Administration (FDA)–approved pharmacologic treatment for nonsegmental vitiligo, in 2022, for patients aged 12 years or older.
“The choice here depends somewhat on insurance coverage and shared decision-making with the patient,” Dr. Shiu said. Meanwhile, clinical trials evaluating the effect of the oral JAK inhibitors ritlecitinib, upadacitinib, povorcitinib, and baricitinib on vitiligo are underway.
Combining Phototherapy With Topical Treatment
A mainstay therapy for nonsegmental vitiligo is phototherapy, which can induce the migration of melanocyte stem cells from hair follicles. “There’s good data to show that combining topical treatment with phototherapy can augment the repigmentation that you see,” she said. “So if it’s possible, try to add phototherapy for your vitiligo patients, but sometimes, logistics for that are a challenge.”
Discussing treatment expectations with patients is key because it can take up to 1 year to see a significant response with topical immunosuppressants and narrowband ultraviolet B treatment. The head and neck areas are often the first sites to repigment, she said, followed by the extremities or the trunk. “The hands and feet are generally last; they are usually the most stubborn areas,” Dr. Shiu said. “Even when you do see repigmentation, it usually happens on the dorsal surfaces. The tips of the fingers and toes are difficult to repigment. Luckily, the face is one of the top responders, so that helps a lot.”
While some treatment efforts result in “complete and beautiful” repigmentation, she added, many yield uneven and incomplete results. “We don’t understand why repigmentation occurs in some areas but not in others,” she said. “We don’t have any biomarkers for treatment response. That is something we are looking into.”
For a patient with rapidly progressing active disease, consider an oral steroid mini-pulse 2 consecutive days per week for a maximum of 3-6 months. “I usually recommend that patients do this on Saturday and Sunday,” Dr. Shiu said. “Studies have shown this strategy can halt progression in 85%-91% of cases if patients are on it for at least 3 months.”
Relapse after successful repigmentation occurs in about 40% of cases following discontinuation of treatment, so she recommends biweekly application of 0.1% tacrolimus ointment as maintenance therapy. “Studies have shown this is enough to decrease the relapse rate to around 9%,” she said.
Tissue, Cellular Grafts
Surgical repigmentation strategies rely on transplanting normal skin to areas affected by vitiligo. In general, more than 50% of patients achieve more than 80% repigmentation. Options are divided into tissue grafts vs cellular grafts. “The old methods are tissue grafting such as punch grafting, tissue blister grafting, and spit thickness grafting, which can treat limited areas of skin,” Dr. Shiu said. Newer approaches include cellular grafting using the melanocyte-keratinocyte transplantation procedure, which can treat larger areas of skin.
The main drawback of this approach is that it is expensive and there is no insurance code for it, “but I hope that this becomes an option for our patients in the future because data indicate that repigmentation is maintained for up to 72 months after treatment,” she said.
In June 2023, an autologous cell harvesting device known as RECELL received FDA approval for repigmentation of stable vitiligo lesions. According to a press release from the manufacturer, AVITA Medical, a clinician “prepares and delivers autologous skin cells from pigmented skin to stable depigmented areas, offering a safe and effective treatment for vitiligo.”
Dr. Shiu disclosed that she received research support from AbbVie.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIFORNIA — When patients with vitiligo see Jessica Shiu, MD, PhD, for the first time, some mention that prior healthcare providers have told them that vitiligo is merely a cosmetic issue — much to her dismay.
“Vitiligo is not a cosmetic disease,” Dr. Shiu, assistant professor of dermatology at the University of California, Irvine, said at the annual meeting of the Pacific Dermatologic Association. “It is associated with significant depression, stigmatization, and low self-esteem. I have patients who say that vitiligo has affected their marriage ... In certain cultures, it also affects their job prospects.”
As the most common pigmentary disorder, vitiligo is an autoimmune condition that often results in the recruitment of CD8+ T cells into the skin. These cells destroy melanocytes, depleting melanocytes in the epidermis. “Over time, this results in milky white patches of skin that we often see in our patients,” Dr. Shiu said.
“Depending on the site that is involved, the nonsegmental form can be further divided into focal, acrofacial, mucosal, generalized, and universal subtypes,” she said. The first step in your initial management is to determine if the vitiligo is active or stable, which can be challenging. Clinical signs of active disease include the presence of trichome vitiligo, confetti vitiligo, and koebnerization.
“Another sign of active disease is when patients tell you that their vitiligo is expanding rapidly,” Dr. Shiu added. “Stable vitiligo is more difficult to define. Many patients think their lesions don’t change, but we’re now appreciating that there can be some sites in those patients such as the hands and feet that are more susceptible to change in activity.” In general, she noted, vitiligo is considered stable when there is no change in activity for at least 12 months, and “lesions are usually completely depigmented with sharp borders.”
The level of vitiligo disease activity drives medical management. For patients with nonsegmental vitiligo who have clinical signs of active disease, the first goal is to stabilize the active disease and stop further spread of depigmentation. “This is key because losing pigment can occur very quickly, but gaining pigment back is a very slow process,” she said. Stabilization involves suppressing immune responses with topical steroids, topical calcineurin inhibitors, or 1.5% ruxolitinib cream, a JAK inhibitor that became the first Food and Drug Administration (FDA)–approved pharmacologic treatment for nonsegmental vitiligo, in 2022, for patients aged 12 years or older.
“The choice here depends somewhat on insurance coverage and shared decision-making with the patient,” Dr. Shiu said. Meanwhile, clinical trials evaluating the effect of the oral JAK inhibitors ritlecitinib, upadacitinib, povorcitinib, and baricitinib on vitiligo are underway.
Combining Phototherapy With Topical Treatment
A mainstay therapy for nonsegmental vitiligo is phototherapy, which can induce the migration of melanocyte stem cells from hair follicles. “There’s good data to show that combining topical treatment with phototherapy can augment the repigmentation that you see,” she said. “So if it’s possible, try to add phototherapy for your vitiligo patients, but sometimes, logistics for that are a challenge.”
Discussing treatment expectations with patients is key because it can take up to 1 year to see a significant response with topical immunosuppressants and narrowband ultraviolet B treatment. The head and neck areas are often the first sites to repigment, she said, followed by the extremities or the trunk. “The hands and feet are generally last; they are usually the most stubborn areas,” Dr. Shiu said. “Even when you do see repigmentation, it usually happens on the dorsal surfaces. The tips of the fingers and toes are difficult to repigment. Luckily, the face is one of the top responders, so that helps a lot.”
While some treatment efforts result in “complete and beautiful” repigmentation, she added, many yield uneven and incomplete results. “We don’t understand why repigmentation occurs in some areas but not in others,” she said. “We don’t have any biomarkers for treatment response. That is something we are looking into.”
For a patient with rapidly progressing active disease, consider an oral steroid mini-pulse 2 consecutive days per week for a maximum of 3-6 months. “I usually recommend that patients do this on Saturday and Sunday,” Dr. Shiu said. “Studies have shown this strategy can halt progression in 85%-91% of cases if patients are on it for at least 3 months.”
Relapse after successful repigmentation occurs in about 40% of cases following discontinuation of treatment, so she recommends biweekly application of 0.1% tacrolimus ointment as maintenance therapy. “Studies have shown this is enough to decrease the relapse rate to around 9%,” she said.
Tissue, Cellular Grafts
Surgical repigmentation strategies rely on transplanting normal skin to areas affected by vitiligo. In general, more than 50% of patients achieve more than 80% repigmentation. Options are divided into tissue grafts vs cellular grafts. “The old methods are tissue grafting such as punch grafting, tissue blister grafting, and spit thickness grafting, which can treat limited areas of skin,” Dr. Shiu said. Newer approaches include cellular grafting using the melanocyte-keratinocyte transplantation procedure, which can treat larger areas of skin.
The main drawback of this approach is that it is expensive and there is no insurance code for it, “but I hope that this becomes an option for our patients in the future because data indicate that repigmentation is maintained for up to 72 months after treatment,” she said.
In June 2023, an autologous cell harvesting device known as RECELL received FDA approval for repigmentation of stable vitiligo lesions. According to a press release from the manufacturer, AVITA Medical, a clinician “prepares and delivers autologous skin cells from pigmented skin to stable depigmented areas, offering a safe and effective treatment for vitiligo.”
Dr. Shiu disclosed that she received research support from AbbVie.
A version of this article first appeared on Medscape.com.
HUNTINGTON BEACH, CALIFORNIA — When patients with vitiligo see Jessica Shiu, MD, PhD, for the first time, some mention that prior healthcare providers have told them that vitiligo is merely a cosmetic issue — much to her dismay.
“Vitiligo is not a cosmetic disease,” Dr. Shiu, assistant professor of dermatology at the University of California, Irvine, said at the annual meeting of the Pacific Dermatologic Association. “It is associated with significant depression, stigmatization, and low self-esteem. I have patients who say that vitiligo has affected their marriage ... In certain cultures, it also affects their job prospects.”
As the most common pigmentary disorder, vitiligo is an autoimmune condition that often results in the recruitment of CD8+ T cells into the skin. These cells destroy melanocytes, depleting melanocytes in the epidermis. “Over time, this results in milky white patches of skin that we often see in our patients,” Dr. Shiu said.
“Depending on the site that is involved, the nonsegmental form can be further divided into focal, acrofacial, mucosal, generalized, and universal subtypes,” she said. The first step in your initial management is to determine if the vitiligo is active or stable, which can be challenging. Clinical signs of active disease include the presence of trichome vitiligo, confetti vitiligo, and koebnerization.
“Another sign of active disease is when patients tell you that their vitiligo is expanding rapidly,” Dr. Shiu added. “Stable vitiligo is more difficult to define. Many patients think their lesions don’t change, but we’re now appreciating that there can be some sites in those patients such as the hands and feet that are more susceptible to change in activity.” In general, she noted, vitiligo is considered stable when there is no change in activity for at least 12 months, and “lesions are usually completely depigmented with sharp borders.”
The level of vitiligo disease activity drives medical management. For patients with nonsegmental vitiligo who have clinical signs of active disease, the first goal is to stabilize the active disease and stop further spread of depigmentation. “This is key because losing pigment can occur very quickly, but gaining pigment back is a very slow process,” she said. Stabilization involves suppressing immune responses with topical steroids, topical calcineurin inhibitors, or 1.5% ruxolitinib cream, a JAK inhibitor that became the first Food and Drug Administration (FDA)–approved pharmacologic treatment for nonsegmental vitiligo, in 2022, for patients aged 12 years or older.
“The choice here depends somewhat on insurance coverage and shared decision-making with the patient,” Dr. Shiu said. Meanwhile, clinical trials evaluating the effect of the oral JAK inhibitors ritlecitinib, upadacitinib, povorcitinib, and baricitinib on vitiligo are underway.
Combining Phototherapy With Topical Treatment
A mainstay therapy for nonsegmental vitiligo is phototherapy, which can induce the migration of melanocyte stem cells from hair follicles. “There’s good data to show that combining topical treatment with phototherapy can augment the repigmentation that you see,” she said. “So if it’s possible, try to add phototherapy for your vitiligo patients, but sometimes, logistics for that are a challenge.”
Discussing treatment expectations with patients is key because it can take up to 1 year to see a significant response with topical immunosuppressants and narrowband ultraviolet B treatment. The head and neck areas are often the first sites to repigment, she said, followed by the extremities or the trunk. “The hands and feet are generally last; they are usually the most stubborn areas,” Dr. Shiu said. “Even when you do see repigmentation, it usually happens on the dorsal surfaces. The tips of the fingers and toes are difficult to repigment. Luckily, the face is one of the top responders, so that helps a lot.”
While some treatment efforts result in “complete and beautiful” repigmentation, she added, many yield uneven and incomplete results. “We don’t understand why repigmentation occurs in some areas but not in others,” she said. “We don’t have any biomarkers for treatment response. That is something we are looking into.”
For a patient with rapidly progressing active disease, consider an oral steroid mini-pulse 2 consecutive days per week for a maximum of 3-6 months. “I usually recommend that patients do this on Saturday and Sunday,” Dr. Shiu said. “Studies have shown this strategy can halt progression in 85%-91% of cases if patients are on it for at least 3 months.”
Relapse after successful repigmentation occurs in about 40% of cases following discontinuation of treatment, so she recommends biweekly application of 0.1% tacrolimus ointment as maintenance therapy. “Studies have shown this is enough to decrease the relapse rate to around 9%,” she said.
Tissue, Cellular Grafts
Surgical repigmentation strategies rely on transplanting normal skin to areas affected by vitiligo. In general, more than 50% of patients achieve more than 80% repigmentation. Options are divided into tissue grafts vs cellular grafts. “The old methods are tissue grafting such as punch grafting, tissue blister grafting, and spit thickness grafting, which can treat limited areas of skin,” Dr. Shiu said. Newer approaches include cellular grafting using the melanocyte-keratinocyte transplantation procedure, which can treat larger areas of skin.
The main drawback of this approach is that it is expensive and there is no insurance code for it, “but I hope that this becomes an option for our patients in the future because data indicate that repigmentation is maintained for up to 72 months after treatment,” she said.
In June 2023, an autologous cell harvesting device known as RECELL received FDA approval for repigmentation of stable vitiligo lesions. According to a press release from the manufacturer, AVITA Medical, a clinician “prepares and delivers autologous skin cells from pigmented skin to stable depigmented areas, offering a safe and effective treatment for vitiligo.”
Dr. Shiu disclosed that she received research support from AbbVie.
A version of this article first appeared on Medscape.com.
FROM PDA 2024