User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Optimal rate of flow for high-flow nasal cannula in young children
Clinical question
Is there an optimal rate of flow for high-flow nasal cannula in respiratory distress?
Background
High-flow nasal cannula (HFNC) has been increasingly used to treat children with moderate to severe bronchiolitis, both in intensive care unit (ICU) settings and on inpatient wards. Studies have shown it may allow children with bronchiolitis to avoid ICU admission and intubation. In preterm infants it has been shown to decrease work of breathing. No prior studies, however, have examined optimizing the rate of flow for individual patients, and considerable heterogeneity exists in choosing initial HFNC flow rates.

Reliably measuring effort of breathing has proved challenging. Placing a manometer in the esophagus allows measurement of the pressure-rate product (PRP), a previously validated measure of effort of breathing computed by multiplying the difference between maximum and minimum esophageal pressures by the respiratory rate.1 An increasing PRP indicates increasing effort of breathing. The authors chose systems from Fisher & Paykel and Vapotherm for their testing.
Study design
Single-center prospective observational trial.
Setting
24-bed pediatric intensive care unit in a 347-bed urban free-standing children’s hospital.
Synopsis
A single center recruited patients aged 37 weeks corrected gestational age to 3 years who were admitted to the ICU with respiratory distress. Fifty-four patients met inclusion criteria and 21 were enrolled and completed the study. Prior data suggested a sample size of 20 would be sufficient to identify a clinically significant effect size. Median age was 6 months.
Thirteen patients had bronchiolitis, three had pneumonia, and five had other respiratory illnesses. Each patient received HFNC delivered by both systems in sequence with flow rates of 0.5, 1, 1.5, and 2 L/kg per minute to a maximum of 30 L/min. Following the trials, patients remained on HFNC as per usual care with twice-daily PRP measurements until weaned off HFNC.
A dose-dependent relationship existed between flow and change in PRP, with the greatest reduction in PRP at 2 L/kg per minute flow (P less than .001) and a slightly smaller but similar reduction in PRP at 1.5 L/kg per minute. When stratifying the subjects by weight, this effect was not statistically significant for patients heavier than 8 kg (P = .38), with all significant changes being in patients less than 8 kg (P less than .001) with a median drop in PRP of 25%. Further examining these younger and lighter patients, the greatest reduction in PRP was in the lightest patients (less than 5 kg).
Given the similarity in drop in PRP at 1.5 L/kg per minute and 2 L/kg per minute, the authors suggest this flow rate yields a plateau effect and minimal further improvement would be seen with increasing flow rates. A rate of 2 L/kg per minute was chosen as a maximum a priori as it was judged the highest level of HFNC patients could tolerate without worsening agitation or air leak. There was no difference seen between the two HFNC systems in the study. The authors did not report the fraction of inspired oxygen settings used, the size of HFNC cannulas, or how PRP changed over several days as HFNC was weaned.
Bottom line
The optimal HFNC rate to decrease effort of breathing for children less than 3 years old is between 1.5 and 2 L/kg/min with the greatest improvement expected in children under 5 kg.
Citation
Weiler T et al. The Relationship between High Flow Nasal Cannula Flow Rate and Effort of Breathing in Children. The Journal of Pediatrics. October 2017. doi: 10.1016/j.jpeds.2017.06.006.
Reference
1. Argent AC, Newth CJL, Klein M. The mechanics of breathing in children with acute severe croup. Intensive Care Med. 2008;34(2):324-32. doi: 10.1007/s00134-007-0910-x.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Jefferson Medical College in Philadelphia.
Clinical question
Is there an optimal rate of flow for high-flow nasal cannula in respiratory distress?
Background
High-flow nasal cannula (HFNC) has been increasingly used to treat children with moderate to severe bronchiolitis, both in intensive care unit (ICU) settings and on inpatient wards. Studies have shown it may allow children with bronchiolitis to avoid ICU admission and intubation. In preterm infants it has been shown to decrease work of breathing. No prior studies, however, have examined optimizing the rate of flow for individual patients, and considerable heterogeneity exists in choosing initial HFNC flow rates.
Reliably measuring effort of breathing has proved challenging. Placing a manometer in the esophagus allows measurement of the pressure-rate product (PRP), a previously validated measure of effort of breathing computed by multiplying the difference between maximum and minimum esophageal pressures by the respiratory rate.1 An increasing PRP indicates increasing effort of breathing. The authors chose systems from Fisher & Paykel and Vapotherm for their testing.
Study design
Single-center prospective observational trial.
Setting
24-bed pediatric intensive care unit in a 347-bed urban free-standing children’s hospital.
Synopsis
A single center recruited patients aged 37 weeks corrected gestational age to 3 years who were admitted to the ICU with respiratory distress. Fifty-four patients met inclusion criteria and 21 were enrolled and completed the study. Prior data suggested a sample size of 20 would be sufficient to identify a clinically significant effect size. Median age was 6 months.
Thirteen patients had bronchiolitis, three had pneumonia, and five had other respiratory illnesses. Each patient received HFNC delivered by both systems in sequence with flow rates of 0.5, 1, 1.5, and 2 L/kg per minute to a maximum of 30 L/min. Following the trials, patients remained on HFNC as per usual care with twice-daily PRP measurements until weaned off HFNC.
A dose-dependent relationship existed between flow and change in PRP, with the greatest reduction in PRP at 2 L/kg per minute flow (P less than .001) and a slightly smaller but similar reduction in PRP at 1.5 L/kg per minute. When stratifying the subjects by weight, this effect was not statistically significant for patients heavier than 8 kg (P = .38), with all significant changes being in patients less than 8 kg (P less than .001) with a median drop in PRP of 25%. Further examining these younger and lighter patients, the greatest reduction in PRP was in the lightest patients (less than 5 kg).
Given the similarity in drop in PRP at 1.5 L/kg per minute and 2 L/kg per minute, the authors suggest this flow rate yields a plateau effect and minimal further improvement would be seen with increasing flow rates. A rate of 2 L/kg per minute was chosen as a maximum a priori as it was judged the highest level of HFNC patients could tolerate without worsening agitation or air leak. There was no difference seen between the two HFNC systems in the study. The authors did not report the fraction of inspired oxygen settings used, the size of HFNC cannulas, or how PRP changed over several days as HFNC was weaned.
Bottom line
The optimal HFNC rate to decrease effort of breathing for children less than 3 years old is between 1.5 and 2 L/kg/min with the greatest improvement expected in children under 5 kg.
Citation
Weiler T et al. The Relationship between High Flow Nasal Cannula Flow Rate and Effort of Breathing in Children. The Journal of Pediatrics. October 2017. doi: 10.1016/j.jpeds.2017.06.006.
Reference
1. Argent AC, Newth CJL, Klein M. The mechanics of breathing in children with acute severe croup. Intensive Care Med. 2008;34(2):324-32. doi: 10.1007/s00134-007-0910-x.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Jefferson Medical College in Philadelphia.
Clinical question
Is there an optimal rate of flow for high-flow nasal cannula in respiratory distress?
Background
High-flow nasal cannula (HFNC) has been increasingly used to treat children with moderate to severe bronchiolitis, both in intensive care unit (ICU) settings and on inpatient wards. Studies have shown it may allow children with bronchiolitis to avoid ICU admission and intubation. In preterm infants it has been shown to decrease work of breathing. No prior studies, however, have examined optimizing the rate of flow for individual patients, and considerable heterogeneity exists in choosing initial HFNC flow rates.
Reliably measuring effort of breathing has proved challenging. Placing a manometer in the esophagus allows measurement of the pressure-rate product (PRP), a previously validated measure of effort of breathing computed by multiplying the difference between maximum and minimum esophageal pressures by the respiratory rate.1 An increasing PRP indicates increasing effort of breathing. The authors chose systems from Fisher & Paykel and Vapotherm for their testing.
Study design
Single-center prospective observational trial.
Setting
24-bed pediatric intensive care unit in a 347-bed urban free-standing children’s hospital.
Synopsis
A single center recruited patients aged 37 weeks corrected gestational age to 3 years who were admitted to the ICU with respiratory distress. Fifty-four patients met inclusion criteria and 21 were enrolled and completed the study. Prior data suggested a sample size of 20 would be sufficient to identify a clinically significant effect size. Median age was 6 months.
Thirteen patients had bronchiolitis, three had pneumonia, and five had other respiratory illnesses. Each patient received HFNC delivered by both systems in sequence with flow rates of 0.5, 1, 1.5, and 2 L/kg per minute to a maximum of 30 L/min. Following the trials, patients remained on HFNC as per usual care with twice-daily PRP measurements until weaned off HFNC.
A dose-dependent relationship existed between flow and change in PRP, with the greatest reduction in PRP at 2 L/kg per minute flow (P less than .001) and a slightly smaller but similar reduction in PRP at 1.5 L/kg per minute. When stratifying the subjects by weight, this effect was not statistically significant for patients heavier than 8 kg (P = .38), with all significant changes being in patients less than 8 kg (P less than .001) with a median drop in PRP of 25%. Further examining these younger and lighter patients, the greatest reduction in PRP was in the lightest patients (less than 5 kg).
Given the similarity in drop in PRP at 1.5 L/kg per minute and 2 L/kg per minute, the authors suggest this flow rate yields a plateau effect and minimal further improvement would be seen with increasing flow rates. A rate of 2 L/kg per minute was chosen as a maximum a priori as it was judged the highest level of HFNC patients could tolerate without worsening agitation or air leak. There was no difference seen between the two HFNC systems in the study. The authors did not report the fraction of inspired oxygen settings used, the size of HFNC cannulas, or how PRP changed over several days as HFNC was weaned.
Bottom line
The optimal HFNC rate to decrease effort of breathing for children less than 3 years old is between 1.5 and 2 L/kg/min with the greatest improvement expected in children under 5 kg.
Citation
Weiler T et al. The Relationship between High Flow Nasal Cannula Flow Rate and Effort of Breathing in Children. The Journal of Pediatrics. October 2017. doi: 10.1016/j.jpeds.2017.06.006.
Reference
1. Argent AC, Newth CJL, Klein M. The mechanics of breathing in children with acute severe croup. Intensive Care Med. 2008;34(2):324-32. doi: 10.1007/s00134-007-0910-x.
Dr. Stubblefield is a pediatric hospitalist at Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del., and clinical assistant professor of pediatrics at Jefferson Medical College in Philadelphia.
Phoenix Children’s Hospital integrates care from ground up
About 4 years ago, officials at Phoenix Children’s Hospital stopped and took a look around. The adult health care landscape was zooming toward value-based models and integrating care so that previously separate components were now working together. The health of whole populations mattered more than ever.
But their hospital, they found, accounted for just 9% of the “care touches” – interactions between a patient and a doctor – of their half-million pediatric population. They were not working closely with primary care doctors and independent specialists. Patients would come to the hospital, get treated, and then – poof, they were gone. The hospital came to a realization that there was a better way to provide care.

They began a process that led to what appears to be a “first-of-its-kind” model, an integrated care network created from the ground up by a hospital venturing out into the community and actively recruiting private primary care doctors and specialists. Now, more than 1,000 physicians from more than 100 practices in the Phoenix metro area are part of the network, joined with the hospital through contracts laden with incentives for meeting care and wellness goals. When good care is being given, the network gets paid, and everyone benefits financially.
“It’s amazing the difference we’re able to provide when we start linking together what used to be very disparate systems,” Mr. Johnson said.
Here are some features of the network:
Every group and practice, including the hospital, is now sharing their data. When a child shows up at the ER, the ER doctor can quickly see things like who the primary care doctor is, allergies, medications, and care history.
- Targets such as asthma control, providing basic wellness exams, and following patients appropriately, are tied to financial rewards.
- Children with complex or special health care needs, and patients who are high utilizers, have a care coordinator assigned to look more closely at their cases.
- A corporate entity created by the hospital and its independent community physician partners has a doctor-heavy board of directors composed of community primary care physicians, specialists, hospital-employed physicians, and hospital administrators.
Some of the care improvements have been dramatic, Mr. Johnson said. One teenager had made 55 ER visits and 21 inpatient visits over 9 months, but the pattern went unnoticed. With new tools – reports drawn from hospital records, insurance records, and records from other doctor visits – the problem became apparent. A care coordinator found that the mother didn’t quite understand how to administer the boy’s medication, prompting repeated medical crises and hundred of thousands of dollars in unnecessary costs. The teenager has since re-enrolled in school and has had no more hospital admissions, Johnson said.
He said that, at first, many community doctors had a “real skepticism” of being too closely tied to a hospital financially, but now doctors are getting in touch with the network about joining.
“There’s a leap of faith that has to happen in the initial stages,” he said. “When you get the insurance companies at the table to really work with you to build the right incentives around truly impactful and quality care, you can really start to move the needle. When you see – with data – that what you’re doing is having success, and they see the additional money coming from the incentives, that really helps.”
Amy Knight, MHA, chief operating officer of the Washington-based Children’s Hospital Association, said that, while other children’s hospitals have migrated toward more integrated care, they either haven’t needed to recruit community physicians as they have in Phoenix, because they already employed many primary care physicians, or market conditions have been such that they haven’t expanded as quickly.
“Phoenix saw a huge opportunity and was very smart about how they approached their own market,” she said. “They are definitely on the front end, the cutting edge of doing that.”
Since its network has expanded, Phoenix Children’s has hosted visitors who hope to draw lessons from their experience, she said.
“I think what most people go away with is: ‘Very interesting, very cool – not sure it would work in our market,’” she said. Still, lessons on thinking about risk and building a governance structure are widely applicable, she said.
“The house may look a little bit different, but some of the things you’re doing inside it may actually all look the same,” Ms. Knight said.
She expects a continued move toward more integrated care networks, despite the on-again, off-again political talk about repealing and replacing the Affordable Care Act.
“There’s probably some people stepping back in hesitancy, but I don’t think that the political discourse right now will necessarily change the trajectory that we’re on.”
About 4 years ago, officials at Phoenix Children’s Hospital stopped and took a look around. The adult health care landscape was zooming toward value-based models and integrating care so that previously separate components were now working together. The health of whole populations mattered more than ever.
But their hospital, they found, accounted for just 9% of the “care touches” – interactions between a patient and a doctor – of their half-million pediatric population. They were not working closely with primary care doctors and independent specialists. Patients would come to the hospital, get treated, and then – poof, they were gone. The hospital came to a realization that there was a better way to provide care.
They began a process that led to what appears to be a “first-of-its-kind” model, an integrated care network created from the ground up by a hospital venturing out into the community and actively recruiting private primary care doctors and specialists. Now, more than 1,000 physicians from more than 100 practices in the Phoenix metro area are part of the network, joined with the hospital through contracts laden with incentives for meeting care and wellness goals. When good care is being given, the network gets paid, and everyone benefits financially.
“It’s amazing the difference we’re able to provide when we start linking together what used to be very disparate systems,” Mr. Johnson said.
Here are some features of the network:
Every group and practice, including the hospital, is now sharing their data. When a child shows up at the ER, the ER doctor can quickly see things like who the primary care doctor is, allergies, medications, and care history.
- Targets such as asthma control, providing basic wellness exams, and following patients appropriately, are tied to financial rewards.
- Children with complex or special health care needs, and patients who are high utilizers, have a care coordinator assigned to look more closely at their cases.
- A corporate entity created by the hospital and its independent community physician partners has a doctor-heavy board of directors composed of community primary care physicians, specialists, hospital-employed physicians, and hospital administrators.
Some of the care improvements have been dramatic, Mr. Johnson said. One teenager had made 55 ER visits and 21 inpatient visits over 9 months, but the pattern went unnoticed. With new tools – reports drawn from hospital records, insurance records, and records from other doctor visits – the problem became apparent. A care coordinator found that the mother didn’t quite understand how to administer the boy’s medication, prompting repeated medical crises and hundred of thousands of dollars in unnecessary costs. The teenager has since re-enrolled in school and has had no more hospital admissions, Johnson said.
He said that, at first, many community doctors had a “real skepticism” of being too closely tied to a hospital financially, but now doctors are getting in touch with the network about joining.
“There’s a leap of faith that has to happen in the initial stages,” he said. “When you get the insurance companies at the table to really work with you to build the right incentives around truly impactful and quality care, you can really start to move the needle. When you see – with data – that what you’re doing is having success, and they see the additional money coming from the incentives, that really helps.”
Amy Knight, MHA, chief operating officer of the Washington-based Children’s Hospital Association, said that, while other children’s hospitals have migrated toward more integrated care, they either haven’t needed to recruit community physicians as they have in Phoenix, because they already employed many primary care physicians, or market conditions have been such that they haven’t expanded as quickly.
“Phoenix saw a huge opportunity and was very smart about how they approached their own market,” she said. “They are definitely on the front end, the cutting edge of doing that.”
Since its network has expanded, Phoenix Children’s has hosted visitors who hope to draw lessons from their experience, she said.
“I think what most people go away with is: ‘Very interesting, very cool – not sure it would work in our market,’” she said. Still, lessons on thinking about risk and building a governance structure are widely applicable, she said.
“The house may look a little bit different, but some of the things you’re doing inside it may actually all look the same,” Ms. Knight said.
She expects a continued move toward more integrated care networks, despite the on-again, off-again political talk about repealing and replacing the Affordable Care Act.
“There’s probably some people stepping back in hesitancy, but I don’t think that the political discourse right now will necessarily change the trajectory that we’re on.”
About 4 years ago, officials at Phoenix Children’s Hospital stopped and took a look around. The adult health care landscape was zooming toward value-based models and integrating care so that previously separate components were now working together. The health of whole populations mattered more than ever.
But their hospital, they found, accounted for just 9% of the “care touches” – interactions between a patient and a doctor – of their half-million pediatric population. They were not working closely with primary care doctors and independent specialists. Patients would come to the hospital, get treated, and then – poof, they were gone. The hospital came to a realization that there was a better way to provide care.
They began a process that led to what appears to be a “first-of-its-kind” model, an integrated care network created from the ground up by a hospital venturing out into the community and actively recruiting private primary care doctors and specialists. Now, more than 1,000 physicians from more than 100 practices in the Phoenix metro area are part of the network, joined with the hospital through contracts laden with incentives for meeting care and wellness goals. When good care is being given, the network gets paid, and everyone benefits financially.
“It’s amazing the difference we’re able to provide when we start linking together what used to be very disparate systems,” Mr. Johnson said.
Here are some features of the network:
Every group and practice, including the hospital, is now sharing their data. When a child shows up at the ER, the ER doctor can quickly see things like who the primary care doctor is, allergies, medications, and care history.
- Targets such as asthma control, providing basic wellness exams, and following patients appropriately, are tied to financial rewards.
- Children with complex or special health care needs, and patients who are high utilizers, have a care coordinator assigned to look more closely at their cases.
- A corporate entity created by the hospital and its independent community physician partners has a doctor-heavy board of directors composed of community primary care physicians, specialists, hospital-employed physicians, and hospital administrators.
Some of the care improvements have been dramatic, Mr. Johnson said. One teenager had made 55 ER visits and 21 inpatient visits over 9 months, but the pattern went unnoticed. With new tools – reports drawn from hospital records, insurance records, and records from other doctor visits – the problem became apparent. A care coordinator found that the mother didn’t quite understand how to administer the boy’s medication, prompting repeated medical crises and hundred of thousands of dollars in unnecessary costs. The teenager has since re-enrolled in school and has had no more hospital admissions, Johnson said.
He said that, at first, many community doctors had a “real skepticism” of being too closely tied to a hospital financially, but now doctors are getting in touch with the network about joining.
“There’s a leap of faith that has to happen in the initial stages,” he said. “When you get the insurance companies at the table to really work with you to build the right incentives around truly impactful and quality care, you can really start to move the needle. When you see – with data – that what you’re doing is having success, and they see the additional money coming from the incentives, that really helps.”
Amy Knight, MHA, chief operating officer of the Washington-based Children’s Hospital Association, said that, while other children’s hospitals have migrated toward more integrated care, they either haven’t needed to recruit community physicians as they have in Phoenix, because they already employed many primary care physicians, or market conditions have been such that they haven’t expanded as quickly.
“Phoenix saw a huge opportunity and was very smart about how they approached their own market,” she said. “They are definitely on the front end, the cutting edge of doing that.”
Since its network has expanded, Phoenix Children’s has hosted visitors who hope to draw lessons from their experience, she said.
“I think what most people go away with is: ‘Very interesting, very cool – not sure it would work in our market,’” she said. Still, lessons on thinking about risk and building a governance structure are widely applicable, she said.
“The house may look a little bit different, but some of the things you’re doing inside it may actually all look the same,” Ms. Knight said.
She expects a continued move toward more integrated care networks, despite the on-again, off-again political talk about repealing and replacing the Affordable Care Act.
“There’s probably some people stepping back in hesitancy, but I don’t think that the political discourse right now will necessarily change the trajectory that we’re on.”
Sexual harassment
Question: A medical assistant alleged that Dr. Y sexually harassed her by sending anonymous gifts and messages such as, “you’re gorgeous,” and “I love your figure.” It was a repeat of Dr. Y’s previous behavior pattern directed at a different worker, who had lodged a complaint with the human resources department. The medical assistant now files a sexual harassment action under Title VII of the federal Civil Rights Act of 1964 against the health care institution, alleging a hostile work environment.
Which of the following is false?
A. Sexual harassment is a form of sexual misconduct regulated by state medical boards.
B. Mere words, without physical action, may suffice to be deemed sexual harassment.
C. A hostile environment arises when offensive conduct is so severe and pervasive as to amount to job discrimination.
D. Sexual harassment is a civil rights violation unique to the workplace.
E. Liability may attach to the supervisor, institution, or the harasser.
Answer: D. This hypothetical is modified from an actual Connecticut case that was recently decided in favor of the plaintiff.1 In that case, which involved a dentist, the federal Second Circuit unanimously rejected the University of Connecticut Health Center’s appeal against a jury’s verdict holding it responsible for its employee’s sexual harassment of a coworker, who was awarded $125,000. It ruled that the health center should have known of its employee’s harassing behavior.
Sexual harassment, a current hot topic, is pervasive, affecting a diversity of individuals in the fields of media, sports, politics, judiciary, education, entertainment, and others. The medical profession is no exception, and studies indicate that sexual harassment affects patients and physicians alike, occurring in hospitals, private offices, and academic centers.
In a large questionnaire study involving 4,501 female physicians, the authors found a prevalence rate of 47.7%. Harassment was more common while in medical school or during internship, residency, or fellowship than in practice.2 Patients may be the harassers. In 599 of the 1,064 licensed female family physicians in Ontario, more than 75% reported sexual harassment by patients at some time during their careers, either in their own offices by their own patients, or in settings such as emergency departments and clinics, where unknown patients presented an even higher risk.3
When physicians sexually harass fellow workers such as nurses, they distract their victims from providing attentive and competent care. In a review of the subject, researchers cited a study of 188 critical care nurses in hospitals, where nearly half (46%) reported experiencing sexual harassment that included “offensive sexual remarks, unwanted physical contact, unwanted nonverbal attention, requests for unwanted dates, sexual propositions, and physical assault.”4 To this list must now be added misconduct via the use of social media. In the study, physicians (82%), coworkers (20%), and immediate supervisors (7%) accounted for most of the incidents.
Neglecting to look seriously into complaints or to monitor and remedy the situation may create a hostile environment and trigger liability.
An example is the recent well-publicized case of Olympics team physician Dr. Larry Nassar, who was also a faculty member at Michigan State University. Olympic gold medalist McKayla Maroney named both the university and the U.S. Olympic Committee as codefendants in a lawsuit alleging that the institutions failed to properly investigate the team doctor’s criminal sexual conduct.
In Anania v. Daubenspeck Chiropractic, two employees of a chiropractor alleged that his patients sexually harassed them, but he did not remedy the situation.5 The trial court initially dismissed their lawsuit, holding that Ohio law did not recognize a cause of action for sexual harassment by a nonemployee patient, and that liability for sexual harassment can only exist in the context of respondeat superior (employer-employee) liability.
However, the court of appeals held that so long as the chiropractor knew or should have known of the harassment, and failed to take corrective action, he could be liable for allowing a hostile environment to exist.
Negligent supervision is another favorite plaintiff’s cause of action. In Doe v. Borromeo, a patient sought to hold the hospital liable for sexual assault by a physician during a medical exam.6 The lower state court had summarily dismissed the case, which was based on vicarious liability, but the state court of appeals reversed, finding the patient’s complaint against the hospital included a negligent supervision claim.
The appeals court reasoned that this was distinguishable from one based upon vicarious liability, so long as the supervising entity had a duty to protect the victim – and such a duty can only be established if the supervising entity knew or should have known of the existence of the harasser’s propensities, if any, to commit criminal and tortious acts.
Sexual harassment is a form of sex discrimination under Title VII of the Civil Rights Act of 1964, which is enforced by the Equal Employment Opportunity Commission. The commission’s website explains the law in clear and simple language:
“It is unlawful to harass a person (an applicant or employee) because of that person’s sex. Harassment can include ‘sexual harassment’ or unwelcome sexual advances, requests for sexual favors, and other verbal or physical harassment of a sexual nature. Harassment does not have to be of a sexual nature, however, and can include offensive remarks about a person’s sex.
“For example, it is illegal to harass a woman by making offensive comments about women in general. Both victim and the harasser can be either a woman or a man, and the victim and harasser can be the same sex.
“Although the law doesn’t prohibit simple teasing, offhand comments, or isolated incidents that are not very serious, harassment is illegal when it is so frequent or severe that it creates a hostile or offensive work environment or when it results in an adverse employment decision (such as the victim being fired or demoted). The harasser can be the victim’s supervisor, a supervisor in another area, a coworker, or someone who is not an employee of the employer, such as a client or customer.”7
For sexual harassment to occur, the aggrieved party must either show a “hostile environment” or “quid pro quo” situation.
In a hostile environment case, the harassment is serious and persistent, creating unacceptable and offensive work conditions. The plaintiff has to show that the employer knew or should have known of the situation but failed to remedy it.
The “quid pro quo” type of case requires a showing that a person in authority conditioned some aspect of the employee’s employment, such as promotion or retention, upon a sexual favor or relationship.
The U.S. Supreme Court has both clarified and muddied the law’s position on these two previously distinct types of sexual harassment.
In the landmark case of Burlington Industries v. Ellerth, the plaintiff, who was a salesperson, alleged that a supervisor made advances to her and threatened to deny her certain job benefits if she did not cooperate.8 The threats were never carried out, and she was in fact promoted; but her lawsuit alleged that the harassment caused her resignation and amounted to a “constructive” discharge.
Likewise, in Faragher v. City of Boca Raton, the plaintiff, employed as a lifeguard, alleged that her work environment was riddled with crude remarks and obscenities.9 One of the two supervisors reportedly once said to Faragher, “Date me or clean toilets for a year.” Another lifeguard had previously lodged similar complaints. The plaintiff ultimately resigned and brought suit.
The U.S. Supreme Court characterized both of these as “hostile environment” rather than “quid pro quo” cases, because the plaintiffs did not suffer any direct adverse job action. In its decisions, the court defined the scope of liability and affirmative defenses, holding that employers can be subject to vicarious liability when supervisors create actionable hostile work environments.
In other cases, the Supreme Court has ruled for the use of “the reasonable person in the plaintiff’s position” standard in judging the severity of sexual harassment. The court has also held that the genders of the harasser and the harassed employee are not material in determining whether sexual harassment has occurred.
A physician can be accused of harassing an employee, a nurse, an assistant, a fellow worker, a third party, or a patient. Focusing on misconduct within the doctor-patient relationship, the Federation of State Medical Boards adopted in May 2006 a policy entitled “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”10
Although it did not use the term sexual harassment, the policy emphasized that physician sexual misconduct may include behavior that is verbal or physical, and may include expressions of thoughts and feelings or gestures that are sexual. It used the term “sexual impropriety” to denote behavior, gestures, or expressions that are seductive, sexually suggestive, disrespectful of patient privacy, or sexually demeaning to a patient. Together with “sexual violation,” a term the FSMB used when referring to physical sexual contact, they form the basis for disciplinary action by a state medical board.
Caveat: When performing a physical exam, physicians should always use good judgment and sensitivity, relying on the presence of a medical assistant to ensure patient comfort and to alleviate possible embarrassment or anxiety.
Under the federal EEOC rules, the employer rather than the harasser is the defendant. But there are other legal recourses, including tort and criminal actions, that directly target the harasser. Successful plaintiffs may be awarded lost wages, as well as damages for emotional distress, medical expenses, and punitive damages. They may also recover attorney fees.
In one case, a psychiatric nurse was awarded $1.2 million (later reduced to $850,000); in another, a nurse successfully sued a physician’s medical practice and received $150,000 in damages.4 And in an unusual case, a plaintiff was awarded only $1 in damages, but her counsel was paid $41,598 in fees.11 For the practicing doctor, medical board sanction, notoriety, and loss of professional standing and privileges constitute additional costs.
The medical profession is as susceptible as any other – perhaps more so – to allegations of sexual harassment. The magic words for actionable sexual harassment are severe, pervasive, and unwelcome. Although laws in the workplace generally do not prohibit simple teasing, offhand comments, or minor isolated incidents, the line separating these behaviors from bona fide sexual harassment is thin.
Erring on the side of strict and sober professional propriety seems prudent, given the current climate of zero tolerance.

References
1. MacCluskey v. University of Connecticut Health Center, United States Court of Appeals, Second Circuit, No. 17-0807-cv, Dec. 19, 2017.
2. Arch Intern Med. 1998 Feb 23;158(4):352-8.
3. N Engl J Med. 1993 Dec 23;329(26):1936-9.
4. J Nurs Care Qual. 2004 Jul-Sep;19(3):234-41.
5. Anania v. Daubenspeck Chiropractic, 718 N.E. 2d 480 (Ohio 1998).
6. Doe v. Borromeo, Nos. 305162, 305163 (Mich. Ct. App. Sept. 20, 2012).
7. Available at https://www.eeoc.gov/laws/types/sexual_harassment.cfm.
8. Burlington Industries, Inc. v. Ellerth, 524 US 742 (1998).
9. Faragher v. City of Boca Raton, 524 U.S. 775 (1998).
10. Federation of State Medical Boards, “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”
11. J Healthc Risk Manag. 1999 Summer;19(3):14-25.
Question: A medical assistant alleged that Dr. Y sexually harassed her by sending anonymous gifts and messages such as, “you’re gorgeous,” and “I love your figure.” It was a repeat of Dr. Y’s previous behavior pattern directed at a different worker, who had lodged a complaint with the human resources department. The medical assistant now files a sexual harassment action under Title VII of the federal Civil Rights Act of 1964 against the health care institution, alleging a hostile work environment.
Which of the following is false?
A. Sexual harassment is a form of sexual misconduct regulated by state medical boards.
B. Mere words, without physical action, may suffice to be deemed sexual harassment.
C. A hostile environment arises when offensive conduct is so severe and pervasive as to amount to job discrimination.
D. Sexual harassment is a civil rights violation unique to the workplace.
E. Liability may attach to the supervisor, institution, or the harasser.
Answer: D. This hypothetical is modified from an actual Connecticut case that was recently decided in favor of the plaintiff.1 In that case, which involved a dentist, the federal Second Circuit unanimously rejected the University of Connecticut Health Center’s appeal against a jury’s verdict holding it responsible for its employee’s sexual harassment of a coworker, who was awarded $125,000. It ruled that the health center should have known of its employee’s harassing behavior.
Sexual harassment, a current hot topic, is pervasive, affecting a diversity of individuals in the fields of media, sports, politics, judiciary, education, entertainment, and others. The medical profession is no exception, and studies indicate that sexual harassment affects patients and physicians alike, occurring in hospitals, private offices, and academic centers.
In a large questionnaire study involving 4,501 female physicians, the authors found a prevalence rate of 47.7%. Harassment was more common while in medical school or during internship, residency, or fellowship than in practice.2 Patients may be the harassers. In 599 of the 1,064 licensed female family physicians in Ontario, more than 75% reported sexual harassment by patients at some time during their careers, either in their own offices by their own patients, or in settings such as emergency departments and clinics, where unknown patients presented an even higher risk.3
When physicians sexually harass fellow workers such as nurses, they distract their victims from providing attentive and competent care. In a review of the subject, researchers cited a study of 188 critical care nurses in hospitals, where nearly half (46%) reported experiencing sexual harassment that included “offensive sexual remarks, unwanted physical contact, unwanted nonverbal attention, requests for unwanted dates, sexual propositions, and physical assault.”4 To this list must now be added misconduct via the use of social media. In the study, physicians (82%), coworkers (20%), and immediate supervisors (7%) accounted for most of the incidents.
Neglecting to look seriously into complaints or to monitor and remedy the situation may create a hostile environment and trigger liability.
An example is the recent well-publicized case of Olympics team physician Dr. Larry Nassar, who was also a faculty member at Michigan State University. Olympic gold medalist McKayla Maroney named both the university and the U.S. Olympic Committee as codefendants in a lawsuit alleging that the institutions failed to properly investigate the team doctor’s criminal sexual conduct.
In Anania v. Daubenspeck Chiropractic, two employees of a chiropractor alleged that his patients sexually harassed them, but he did not remedy the situation.5 The trial court initially dismissed their lawsuit, holding that Ohio law did not recognize a cause of action for sexual harassment by a nonemployee patient, and that liability for sexual harassment can only exist in the context of respondeat superior (employer-employee) liability.
However, the court of appeals held that so long as the chiropractor knew or should have known of the harassment, and failed to take corrective action, he could be liable for allowing a hostile environment to exist.
Negligent supervision is another favorite plaintiff’s cause of action. In Doe v. Borromeo, a patient sought to hold the hospital liable for sexual assault by a physician during a medical exam.6 The lower state court had summarily dismissed the case, which was based on vicarious liability, but the state court of appeals reversed, finding the patient’s complaint against the hospital included a negligent supervision claim.
The appeals court reasoned that this was distinguishable from one based upon vicarious liability, so long as the supervising entity had a duty to protect the victim – and such a duty can only be established if the supervising entity knew or should have known of the existence of the harasser’s propensities, if any, to commit criminal and tortious acts.
Sexual harassment is a form of sex discrimination under Title VII of the Civil Rights Act of 1964, which is enforced by the Equal Employment Opportunity Commission. The commission’s website explains the law in clear and simple language:
“It is unlawful to harass a person (an applicant or employee) because of that person’s sex. Harassment can include ‘sexual harassment’ or unwelcome sexual advances, requests for sexual favors, and other verbal or physical harassment of a sexual nature. Harassment does not have to be of a sexual nature, however, and can include offensive remarks about a person’s sex.
“For example, it is illegal to harass a woman by making offensive comments about women in general. Both victim and the harasser can be either a woman or a man, and the victim and harasser can be the same sex.
“Although the law doesn’t prohibit simple teasing, offhand comments, or isolated incidents that are not very serious, harassment is illegal when it is so frequent or severe that it creates a hostile or offensive work environment or when it results in an adverse employment decision (such as the victim being fired or demoted). The harasser can be the victim’s supervisor, a supervisor in another area, a coworker, or someone who is not an employee of the employer, such as a client or customer.”7
For sexual harassment to occur, the aggrieved party must either show a “hostile environment” or “quid pro quo” situation.
In a hostile environment case, the harassment is serious and persistent, creating unacceptable and offensive work conditions. The plaintiff has to show that the employer knew or should have known of the situation but failed to remedy it.
The “quid pro quo” type of case requires a showing that a person in authority conditioned some aspect of the employee’s employment, such as promotion or retention, upon a sexual favor or relationship.
The U.S. Supreme Court has both clarified and muddied the law’s position on these two previously distinct types of sexual harassment.
In the landmark case of Burlington Industries v. Ellerth, the plaintiff, who was a salesperson, alleged that a supervisor made advances to her and threatened to deny her certain job benefits if she did not cooperate.8 The threats were never carried out, and she was in fact promoted; but her lawsuit alleged that the harassment caused her resignation and amounted to a “constructive” discharge.
Likewise, in Faragher v. City of Boca Raton, the plaintiff, employed as a lifeguard, alleged that her work environment was riddled with crude remarks and obscenities.9 One of the two supervisors reportedly once said to Faragher, “Date me or clean toilets for a year.” Another lifeguard had previously lodged similar complaints. The plaintiff ultimately resigned and brought suit.
The U.S. Supreme Court characterized both of these as “hostile environment” rather than “quid pro quo” cases, because the plaintiffs did not suffer any direct adverse job action. In its decisions, the court defined the scope of liability and affirmative defenses, holding that employers can be subject to vicarious liability when supervisors create actionable hostile work environments.
In other cases, the Supreme Court has ruled for the use of “the reasonable person in the plaintiff’s position” standard in judging the severity of sexual harassment. The court has also held that the genders of the harasser and the harassed employee are not material in determining whether sexual harassment has occurred.
A physician can be accused of harassing an employee, a nurse, an assistant, a fellow worker, a third party, or a patient. Focusing on misconduct within the doctor-patient relationship, the Federation of State Medical Boards adopted in May 2006 a policy entitled “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”10
Although it did not use the term sexual harassment, the policy emphasized that physician sexual misconduct may include behavior that is verbal or physical, and may include expressions of thoughts and feelings or gestures that are sexual. It used the term “sexual impropriety” to denote behavior, gestures, or expressions that are seductive, sexually suggestive, disrespectful of patient privacy, or sexually demeaning to a patient. Together with “sexual violation,” a term the FSMB used when referring to physical sexual contact, they form the basis for disciplinary action by a state medical board.
Caveat: When performing a physical exam, physicians should always use good judgment and sensitivity, relying on the presence of a medical assistant to ensure patient comfort and to alleviate possible embarrassment or anxiety.
Under the federal EEOC rules, the employer rather than the harasser is the defendant. But there are other legal recourses, including tort and criminal actions, that directly target the harasser. Successful plaintiffs may be awarded lost wages, as well as damages for emotional distress, medical expenses, and punitive damages. They may also recover attorney fees.
In one case, a psychiatric nurse was awarded $1.2 million (later reduced to $850,000); in another, a nurse successfully sued a physician’s medical practice and received $150,000 in damages.4 And in an unusual case, a plaintiff was awarded only $1 in damages, but her counsel was paid $41,598 in fees.11 For the practicing doctor, medical board sanction, notoriety, and loss of professional standing and privileges constitute additional costs.
The medical profession is as susceptible as any other – perhaps more so – to allegations of sexual harassment. The magic words for actionable sexual harassment are severe, pervasive, and unwelcome. Although laws in the workplace generally do not prohibit simple teasing, offhand comments, or minor isolated incidents, the line separating these behaviors from bona fide sexual harassment is thin.
Erring on the side of strict and sober professional propriety seems prudent, given the current climate of zero tolerance.
References
1. MacCluskey v. University of Connecticut Health Center, United States Court of Appeals, Second Circuit, No. 17-0807-cv, Dec. 19, 2017.
2. Arch Intern Med. 1998 Feb 23;158(4):352-8.
3. N Engl J Med. 1993 Dec 23;329(26):1936-9.
4. J Nurs Care Qual. 2004 Jul-Sep;19(3):234-41.
5. Anania v. Daubenspeck Chiropractic, 718 N.E. 2d 480 (Ohio 1998).
6. Doe v. Borromeo, Nos. 305162, 305163 (Mich. Ct. App. Sept. 20, 2012).
7. Available at https://www.eeoc.gov/laws/types/sexual_harassment.cfm.
8. Burlington Industries, Inc. v. Ellerth, 524 US 742 (1998).
9. Faragher v. City of Boca Raton, 524 U.S. 775 (1998).
10. Federation of State Medical Boards, “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”
11. J Healthc Risk Manag. 1999 Summer;19(3):14-25.
Question: A medical assistant alleged that Dr. Y sexually harassed her by sending anonymous gifts and messages such as, “you’re gorgeous,” and “I love your figure.” It was a repeat of Dr. Y’s previous behavior pattern directed at a different worker, who had lodged a complaint with the human resources department. The medical assistant now files a sexual harassment action under Title VII of the federal Civil Rights Act of 1964 against the health care institution, alleging a hostile work environment.
Which of the following is false?
A. Sexual harassment is a form of sexual misconduct regulated by state medical boards.
B. Mere words, without physical action, may suffice to be deemed sexual harassment.
C. A hostile environment arises when offensive conduct is so severe and pervasive as to amount to job discrimination.
D. Sexual harassment is a civil rights violation unique to the workplace.
E. Liability may attach to the supervisor, institution, or the harasser.
Answer: D. This hypothetical is modified from an actual Connecticut case that was recently decided in favor of the plaintiff.1 In that case, which involved a dentist, the federal Second Circuit unanimously rejected the University of Connecticut Health Center’s appeal against a jury’s verdict holding it responsible for its employee’s sexual harassment of a coworker, who was awarded $125,000. It ruled that the health center should have known of its employee’s harassing behavior.
Sexual harassment, a current hot topic, is pervasive, affecting a diversity of individuals in the fields of media, sports, politics, judiciary, education, entertainment, and others. The medical profession is no exception, and studies indicate that sexual harassment affects patients and physicians alike, occurring in hospitals, private offices, and academic centers.
In a large questionnaire study involving 4,501 female physicians, the authors found a prevalence rate of 47.7%. Harassment was more common while in medical school or during internship, residency, or fellowship than in practice.2 Patients may be the harassers. In 599 of the 1,064 licensed female family physicians in Ontario, more than 75% reported sexual harassment by patients at some time during their careers, either in their own offices by their own patients, or in settings such as emergency departments and clinics, where unknown patients presented an even higher risk.3
When physicians sexually harass fellow workers such as nurses, they distract their victims from providing attentive and competent care. In a review of the subject, researchers cited a study of 188 critical care nurses in hospitals, where nearly half (46%) reported experiencing sexual harassment that included “offensive sexual remarks, unwanted physical contact, unwanted nonverbal attention, requests for unwanted dates, sexual propositions, and physical assault.”4 To this list must now be added misconduct via the use of social media. In the study, physicians (82%), coworkers (20%), and immediate supervisors (7%) accounted for most of the incidents.
Neglecting to look seriously into complaints or to monitor and remedy the situation may create a hostile environment and trigger liability.
An example is the recent well-publicized case of Olympics team physician Dr. Larry Nassar, who was also a faculty member at Michigan State University. Olympic gold medalist McKayla Maroney named both the university and the U.S. Olympic Committee as codefendants in a lawsuit alleging that the institutions failed to properly investigate the team doctor’s criminal sexual conduct.
In Anania v. Daubenspeck Chiropractic, two employees of a chiropractor alleged that his patients sexually harassed them, but he did not remedy the situation.5 The trial court initially dismissed their lawsuit, holding that Ohio law did not recognize a cause of action for sexual harassment by a nonemployee patient, and that liability for sexual harassment can only exist in the context of respondeat superior (employer-employee) liability.
However, the court of appeals held that so long as the chiropractor knew or should have known of the harassment, and failed to take corrective action, he could be liable for allowing a hostile environment to exist.
Negligent supervision is another favorite plaintiff’s cause of action. In Doe v. Borromeo, a patient sought to hold the hospital liable for sexual assault by a physician during a medical exam.6 The lower state court had summarily dismissed the case, which was based on vicarious liability, but the state court of appeals reversed, finding the patient’s complaint against the hospital included a negligent supervision claim.
The appeals court reasoned that this was distinguishable from one based upon vicarious liability, so long as the supervising entity had a duty to protect the victim – and such a duty can only be established if the supervising entity knew or should have known of the existence of the harasser’s propensities, if any, to commit criminal and tortious acts.
Sexual harassment is a form of sex discrimination under Title VII of the Civil Rights Act of 1964, which is enforced by the Equal Employment Opportunity Commission. The commission’s website explains the law in clear and simple language:
“It is unlawful to harass a person (an applicant or employee) because of that person’s sex. Harassment can include ‘sexual harassment’ or unwelcome sexual advances, requests for sexual favors, and other verbal or physical harassment of a sexual nature. Harassment does not have to be of a sexual nature, however, and can include offensive remarks about a person’s sex.
“For example, it is illegal to harass a woman by making offensive comments about women in general. Both victim and the harasser can be either a woman or a man, and the victim and harasser can be the same sex.
“Although the law doesn’t prohibit simple teasing, offhand comments, or isolated incidents that are not very serious, harassment is illegal when it is so frequent or severe that it creates a hostile or offensive work environment or when it results in an adverse employment decision (such as the victim being fired or demoted). The harasser can be the victim’s supervisor, a supervisor in another area, a coworker, or someone who is not an employee of the employer, such as a client or customer.”7
For sexual harassment to occur, the aggrieved party must either show a “hostile environment” or “quid pro quo” situation.
In a hostile environment case, the harassment is serious and persistent, creating unacceptable and offensive work conditions. The plaintiff has to show that the employer knew or should have known of the situation but failed to remedy it.
The “quid pro quo” type of case requires a showing that a person in authority conditioned some aspect of the employee’s employment, such as promotion or retention, upon a sexual favor or relationship.
The U.S. Supreme Court has both clarified and muddied the law’s position on these two previously distinct types of sexual harassment.
In the landmark case of Burlington Industries v. Ellerth, the plaintiff, who was a salesperson, alleged that a supervisor made advances to her and threatened to deny her certain job benefits if she did not cooperate.8 The threats were never carried out, and she was in fact promoted; but her lawsuit alleged that the harassment caused her resignation and amounted to a “constructive” discharge.
Likewise, in Faragher v. City of Boca Raton, the plaintiff, employed as a lifeguard, alleged that her work environment was riddled with crude remarks and obscenities.9 One of the two supervisors reportedly once said to Faragher, “Date me or clean toilets for a year.” Another lifeguard had previously lodged similar complaints. The plaintiff ultimately resigned and brought suit.
The U.S. Supreme Court characterized both of these as “hostile environment” rather than “quid pro quo” cases, because the plaintiffs did not suffer any direct adverse job action. In its decisions, the court defined the scope of liability and affirmative defenses, holding that employers can be subject to vicarious liability when supervisors create actionable hostile work environments.
In other cases, the Supreme Court has ruled for the use of “the reasonable person in the plaintiff’s position” standard in judging the severity of sexual harassment. The court has also held that the genders of the harasser and the harassed employee are not material in determining whether sexual harassment has occurred.
A physician can be accused of harassing an employee, a nurse, an assistant, a fellow worker, a third party, or a patient. Focusing on misconduct within the doctor-patient relationship, the Federation of State Medical Boards adopted in May 2006 a policy entitled “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”10
Although it did not use the term sexual harassment, the policy emphasized that physician sexual misconduct may include behavior that is verbal or physical, and may include expressions of thoughts and feelings or gestures that are sexual. It used the term “sexual impropriety” to denote behavior, gestures, or expressions that are seductive, sexually suggestive, disrespectful of patient privacy, or sexually demeaning to a patient. Together with “sexual violation,” a term the FSMB used when referring to physical sexual contact, they form the basis for disciplinary action by a state medical board.
Caveat: When performing a physical exam, physicians should always use good judgment and sensitivity, relying on the presence of a medical assistant to ensure patient comfort and to alleviate possible embarrassment or anxiety.
Under the federal EEOC rules, the employer rather than the harasser is the defendant. But there are other legal recourses, including tort and criminal actions, that directly target the harasser. Successful plaintiffs may be awarded lost wages, as well as damages for emotional distress, medical expenses, and punitive damages. They may also recover attorney fees.
In one case, a psychiatric nurse was awarded $1.2 million (later reduced to $850,000); in another, a nurse successfully sued a physician’s medical practice and received $150,000 in damages.4 And in an unusual case, a plaintiff was awarded only $1 in damages, but her counsel was paid $41,598 in fees.11 For the practicing doctor, medical board sanction, notoriety, and loss of professional standing and privileges constitute additional costs.
The medical profession is as susceptible as any other – perhaps more so – to allegations of sexual harassment. The magic words for actionable sexual harassment are severe, pervasive, and unwelcome. Although laws in the workplace generally do not prohibit simple teasing, offhand comments, or minor isolated incidents, the line separating these behaviors from bona fide sexual harassment is thin.
Erring on the side of strict and sober professional propriety seems prudent, given the current climate of zero tolerance.
References
1. MacCluskey v. University of Connecticut Health Center, United States Court of Appeals, Second Circuit, No. 17-0807-cv, Dec. 19, 2017.
2. Arch Intern Med. 1998 Feb 23;158(4):352-8.
3. N Engl J Med. 1993 Dec 23;329(26):1936-9.
4. J Nurs Care Qual. 2004 Jul-Sep;19(3):234-41.
5. Anania v. Daubenspeck Chiropractic, 718 N.E. 2d 480 (Ohio 1998).
6. Doe v. Borromeo, Nos. 305162, 305163 (Mich. Ct. App. Sept. 20, 2012).
7. Available at https://www.eeoc.gov/laws/types/sexual_harassment.cfm.
8. Burlington Industries, Inc. v. Ellerth, 524 US 742 (1998).
9. Faragher v. City of Boca Raton, 524 U.S. 775 (1998).
10. Federation of State Medical Boards, “Addressing Sexual Boundaries: Guidelines for State Medical Boards.”
11. J Healthc Risk Manag. 1999 Summer;19(3):14-25.
A love of teaching: James Kim, MD
While James Kim, MD, did not originally begin medical school with a plan to become a hospitalist, he has embraced his current role wholeheartedly.
Since becoming board certified in both internal medicine and infectious diseases, Dr. Kim has welcomed the opportunity to be part of hospital medicine, which gives him the opportunity to pursue his other passion: teaching and mentoring.

“It’s not just what you know but how you convey what you know to other people,” said Dr. Kim. “While you might get useful information from a didactic teaching style, it’s important to ask questions to encourage the learner to think about not only what the right answer is but also what’s the thought process required to get the answer.”
As one of the newest additions to the editorial advisory board of The Hospitalist, Dr. Kim took time to tell us more about himself in a recent interview.
QUESTION: How did you find your career path in medicine?
ANSWER: I originally went into medical school thinking I was going to do pediatrics, but then I realized that I really enjoy talking to people and that I like the process of thinking through diagnoses, managing patients, and learning about what makes their circumstances unique.
Q: How did you get into hospital medicine?
A: When I finished my internal medicine residency, I thought I was going to do medical missions. However, I realized along the way that the care you need to provide in order to really make a difference in other countries requires a constant presence there – not just a week or two. So after my fellowship, I was searching for jobs and found a hospitalist position at the University of California, Los Angeles. When I saw it, I thought ‘Wow, I really miss doing inpatient medicine.’
Q: Since you started, what have been some of your favorite parts of hospital medicine?
A: When people come to you in the hospital setting, they are usually pretty sick. It is very satisfying when, through the course of a person’s hospital stay, we are able to come up with a plan that can get them acutely better.
Q: What do you think is the hardest part of hospital medicine?
A: I think one of the things that is most frustrating is when we are placed into a situation in which we are not necessarily doing medical work for a patient but are doing something more like social work. For instance, there are cases in which patients can not be on their own in the community, and there’s no family to take them in, so the hospital, on behalf of the state, has to take them in.
Q: What else do you do outside of hospitalist work?
A: Since I’ve finished medical school, I’ve always been in some kind of academia, which is not something I would have expected. But as time has gone by, I have really come to appreciate being in academia. I really enjoy teaching, and I also think that an academic institution kind of keeps me on my toes. I’m involved with interprofessional education at Emory, with teaching medical students, interns, and residents when I’m on teaching service, and obviously now I’m on The Hospitalist editorial board. I’m looking forward to keeping abreast of what’s hot in the world of hospital medicine.
Q: What are you excited about bringing to The Hospitalist editorial board?
A: I want to try to contribute ideas. I feel that even in my short time at Emory, I’ve gotten to know a few people who might be good resources for reporters to interview or even who might write articles themselves. I also think that seeing what is trending in the world of hospital medicine is a nice way of understanding the future direction of hospital medicine.
Q: What have you seen as being the biggest change in hospital medicine since you started?
A: I feel as though I’ve kept my head down and plowed forward through the first part of my career, but I think that, more than anything else, what I’ve noticed is bigger shifts within health care itself. I know that there’s a lot of consolidation going on. I think that there are many questions that are going to come up about how do we manage a health care system as complicated as America’s and how do we deliver optimal care to people especially when sometimes we end up in situations in which we don’t have all the resources that we would want to have because of circumstances.
Q: Do you see anything in particular on the horizon for hospital medicine?
A: I’ve noticed that there’s been more “hospitalist-ization” – if that’s even a term – of other medical services. At our institution, we already have an acute care service that is basically hospital medicine for general surgery. I think another thing that’s been kind of a hot topic recently is a point-of-care testing, including ultrasounds for line placements.
Q: Where do you see yourself in 10 years?
A: I really enjoy my work at Emory. I want to find more opportunities to teach. For example, I’ve already gotten involved in teaching physician assistant students about how to perform interviews and deliver presentations for attendings. A lot of serendipitous things have happened to me over time, so I think I will continue to teach, but I’m open to those opportunities that present themselves in the future.
Q: What’s the best book you’ve read recently and why?
A: “The Hero with a Thousand Faces,” by Joseph Campbell. This is a very well-known book – I think George Lucas made reference to it when he was writing Star Wars – but I think it was a great literary way to examine the hero’s journey. Once you read the book, and you then watch any kind of movie or read any other kind of adventure narrative, you can’t miss the pattern.
While James Kim, MD, did not originally begin medical school with a plan to become a hospitalist, he has embraced his current role wholeheartedly.
Since becoming board certified in both internal medicine and infectious diseases, Dr. Kim has welcomed the opportunity to be part of hospital medicine, which gives him the opportunity to pursue his other passion: teaching and mentoring.
“It’s not just what you know but how you convey what you know to other people,” said Dr. Kim. “While you might get useful information from a didactic teaching style, it’s important to ask questions to encourage the learner to think about not only what the right answer is but also what’s the thought process required to get the answer.”
As one of the newest additions to the editorial advisory board of The Hospitalist, Dr. Kim took time to tell us more about himself in a recent interview.
QUESTION: How did you find your career path in medicine?
ANSWER: I originally went into medical school thinking I was going to do pediatrics, but then I realized that I really enjoy talking to people and that I like the process of thinking through diagnoses, managing patients, and learning about what makes their circumstances unique.
Q: How did you get into hospital medicine?
A: When I finished my internal medicine residency, I thought I was going to do medical missions. However, I realized along the way that the care you need to provide in order to really make a difference in other countries requires a constant presence there – not just a week or two. So after my fellowship, I was searching for jobs and found a hospitalist position at the University of California, Los Angeles. When I saw it, I thought ‘Wow, I really miss doing inpatient medicine.’
Q: Since you started, what have been some of your favorite parts of hospital medicine?
A: When people come to you in the hospital setting, they are usually pretty sick. It is very satisfying when, through the course of a person’s hospital stay, we are able to come up with a plan that can get them acutely better.
Q: What do you think is the hardest part of hospital medicine?
A: I think one of the things that is most frustrating is when we are placed into a situation in which we are not necessarily doing medical work for a patient but are doing something more like social work. For instance, there are cases in which patients can not be on their own in the community, and there’s no family to take them in, so the hospital, on behalf of the state, has to take them in.
Q: What else do you do outside of hospitalist work?
A: Since I’ve finished medical school, I’ve always been in some kind of academia, which is not something I would have expected. But as time has gone by, I have really come to appreciate being in academia. I really enjoy teaching, and I also think that an academic institution kind of keeps me on my toes. I’m involved with interprofessional education at Emory, with teaching medical students, interns, and residents when I’m on teaching service, and obviously now I’m on The Hospitalist editorial board. I’m looking forward to keeping abreast of what’s hot in the world of hospital medicine.
Q: What are you excited about bringing to The Hospitalist editorial board?
A: I want to try to contribute ideas. I feel that even in my short time at Emory, I’ve gotten to know a few people who might be good resources for reporters to interview or even who might write articles themselves. I also think that seeing what is trending in the world of hospital medicine is a nice way of understanding the future direction of hospital medicine.
Q: What have you seen as being the biggest change in hospital medicine since you started?
A: I feel as though I’ve kept my head down and plowed forward through the first part of my career, but I think that, more than anything else, what I’ve noticed is bigger shifts within health care itself. I know that there’s a lot of consolidation going on. I think that there are many questions that are going to come up about how do we manage a health care system as complicated as America’s and how do we deliver optimal care to people especially when sometimes we end up in situations in which we don’t have all the resources that we would want to have because of circumstances.
Q: Do you see anything in particular on the horizon for hospital medicine?
A: I’ve noticed that there’s been more “hospitalist-ization” – if that’s even a term – of other medical services. At our institution, we already have an acute care service that is basically hospital medicine for general surgery. I think another thing that’s been kind of a hot topic recently is a point-of-care testing, including ultrasounds for line placements.
Q: Where do you see yourself in 10 years?
A: I really enjoy my work at Emory. I want to find more opportunities to teach. For example, I’ve already gotten involved in teaching physician assistant students about how to perform interviews and deliver presentations for attendings. A lot of serendipitous things have happened to me over time, so I think I will continue to teach, but I’m open to those opportunities that present themselves in the future.
Q: What’s the best book you’ve read recently and why?
A: “The Hero with a Thousand Faces,” by Joseph Campbell. This is a very well-known book – I think George Lucas made reference to it when he was writing Star Wars – but I think it was a great literary way to examine the hero’s journey. Once you read the book, and you then watch any kind of movie or read any other kind of adventure narrative, you can’t miss the pattern.
While James Kim, MD, did not originally begin medical school with a plan to become a hospitalist, he has embraced his current role wholeheartedly.
Since becoming board certified in both internal medicine and infectious diseases, Dr. Kim has welcomed the opportunity to be part of hospital medicine, which gives him the opportunity to pursue his other passion: teaching and mentoring.
“It’s not just what you know but how you convey what you know to other people,” said Dr. Kim. “While you might get useful information from a didactic teaching style, it’s important to ask questions to encourage the learner to think about not only what the right answer is but also what’s the thought process required to get the answer.”
As one of the newest additions to the editorial advisory board of The Hospitalist, Dr. Kim took time to tell us more about himself in a recent interview.
QUESTION: How did you find your career path in medicine?
ANSWER: I originally went into medical school thinking I was going to do pediatrics, but then I realized that I really enjoy talking to people and that I like the process of thinking through diagnoses, managing patients, and learning about what makes their circumstances unique.
Q: How did you get into hospital medicine?
A: When I finished my internal medicine residency, I thought I was going to do medical missions. However, I realized along the way that the care you need to provide in order to really make a difference in other countries requires a constant presence there – not just a week or two. So after my fellowship, I was searching for jobs and found a hospitalist position at the University of California, Los Angeles. When I saw it, I thought ‘Wow, I really miss doing inpatient medicine.’
Q: Since you started, what have been some of your favorite parts of hospital medicine?
A: When people come to you in the hospital setting, they are usually pretty sick. It is very satisfying when, through the course of a person’s hospital stay, we are able to come up with a plan that can get them acutely better.
Q: What do you think is the hardest part of hospital medicine?
A: I think one of the things that is most frustrating is when we are placed into a situation in which we are not necessarily doing medical work for a patient but are doing something more like social work. For instance, there are cases in which patients can not be on their own in the community, and there’s no family to take them in, so the hospital, on behalf of the state, has to take them in.
Q: What else do you do outside of hospitalist work?
A: Since I’ve finished medical school, I’ve always been in some kind of academia, which is not something I would have expected. But as time has gone by, I have really come to appreciate being in academia. I really enjoy teaching, and I also think that an academic institution kind of keeps me on my toes. I’m involved with interprofessional education at Emory, with teaching medical students, interns, and residents when I’m on teaching service, and obviously now I’m on The Hospitalist editorial board. I’m looking forward to keeping abreast of what’s hot in the world of hospital medicine.
Q: What are you excited about bringing to The Hospitalist editorial board?
A: I want to try to contribute ideas. I feel that even in my short time at Emory, I’ve gotten to know a few people who might be good resources for reporters to interview or even who might write articles themselves. I also think that seeing what is trending in the world of hospital medicine is a nice way of understanding the future direction of hospital medicine.
Q: What have you seen as being the biggest change in hospital medicine since you started?
A: I feel as though I’ve kept my head down and plowed forward through the first part of my career, but I think that, more than anything else, what I’ve noticed is bigger shifts within health care itself. I know that there’s a lot of consolidation going on. I think that there are many questions that are going to come up about how do we manage a health care system as complicated as America’s and how do we deliver optimal care to people especially when sometimes we end up in situations in which we don’t have all the resources that we would want to have because of circumstances.
Q: Do you see anything in particular on the horizon for hospital medicine?
A: I’ve noticed that there’s been more “hospitalist-ization” – if that’s even a term – of other medical services. At our institution, we already have an acute care service that is basically hospital medicine for general surgery. I think another thing that’s been kind of a hot topic recently is a point-of-care testing, including ultrasounds for line placements.
Q: Where do you see yourself in 10 years?
A: I really enjoy my work at Emory. I want to find more opportunities to teach. For example, I’ve already gotten involved in teaching physician assistant students about how to perform interviews and deliver presentations for attendings. A lot of serendipitous things have happened to me over time, so I think I will continue to teach, but I’m open to those opportunities that present themselves in the future.
Q: What’s the best book you’ve read recently and why?
A: “The Hero with a Thousand Faces,” by Joseph Campbell. This is a very well-known book – I think George Lucas made reference to it when he was writing Star Wars – but I think it was a great literary way to examine the hero’s journey. Once you read the book, and you then watch any kind of movie or read any other kind of adventure narrative, you can’t miss the pattern.
Homelessness: Whose job is it?
Despite programs to end homelessness, it remains a substantial and growing problem in many cities in the United States.1,2 In 2016, there were an estimated 10,550 homeless people living in my home state of Colorado, a 6% increase from the prior year.2 A recent point-estimate study found that there were more than 5,000 homeless individuals in the Denver metropolitan area on a single night in January 2017.3 Because of the relative scarcity of housing, a growing number of cities like Denver now utilize a practice known as vulnerability indexing to prioritize homeless persons at high risk of mortality from medical conditions for placement in permanent supportive housing.4

Although hospitalists like myself frequently care for vulnerable homeless patients in the hospital, most have little formal training in how best to care for and advocate for these individuals beyond treating their acute medical need, and little direct contact with community organizations with expertise in doing so. Instead, we have learned informally through experience. Hospital providers are often frustrated by the perceived lack of services and support available to these patients, and there is substantial variability in the extent to which providers engage patients and community partners during and after hospitalization. Despite the growing practice of vulnerability indexing in the community, hospital-based providers do not routinely assess vulnerability with respect to housing. Previous research indicates that housing status is assessed in only a minority of homeless patients during their hospital stay.12 Thus, hospitalization often represents a missed opportunity to identify vulnerability and utilize it to connect patients with housing and other resources.
Addressing the significant known health disparities faced by homeless persons is one of the greatest health equity challenges of our time.13 We need better ways of understanding, identifying, and addressing vulnerability among homeless patients who are hospitalized, paired with improved integration with local community organizations. This will require moving beyond the idea that homelessness is the social worker’s job to one of shared responsibility and advocacy.
Collaborative research and other partnerships that engage both community organizations and individuals affected by homelessness are crucial to further understand the specific needs, barriers, challenges, and opportunities for improving hospital care and care transitions in this population. As well-respected community members and systems thinkers who witness these inequities on a daily basis, hospitalists are well positioned to help lead this work.
Dr. Stella is a hospitalist at Denver Health and Hospital Authority, and an associate professor of medicine at the University of Colorado. She is a member of The Hospitalist editorial advisory board.
References
1. Ending Chronic Homelessness. (Aug 2017). U.S. Interagency Council on Homelessness. Available at: https://www.usich.gov/goals/chronicsness. Accessed: Oct 21, 2017.
2. 2016 Annual Homeless Assessment Report (AHAR) to Congress. (Nov 2016). U.S. Department of Housing and Urban Development Office of Community Planning and Development, Part 1. Available at: https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Accessed: Oct 21, 2017.
3. 2017 Point-In-Time Report, Seven-County Metro Denver Region. Metro Denver Homeless Initiative. Available at: http://www.mdhi.org/2017_pit. Accessed Oct 22, 2017.
4. Henwood BF et al. Examining mortality among formerly homeless adults enrolled in Housing First: An observational study. BMC Public Health. 2015;15:1209.
5. Weinstein LC et al. Moving from street to home: Health status of entrants to a Housing First program. J Prim Care Community Health. 2011;2:11–5.
6. Kushel MB et al. Factors associated with the health care utilization of homeless persons. JAMA. 2001;285(2):200-6.
7. Kushel MB et al. Emergency department use among the homeless and marginally housed: Results from a community-based study. Am J Public Health. 2002;92(5):778-84.
8. Baggett TP et al. Mortality among homeless adults in Boston: Shifts in causes of death over a 15-year period. JAMA Intern Med. 2013 Feb 11;173(3):189–95.
9. Johnson et al. For many patients who use large amounts of health care services, the need is intense yet temporary. Health Aff (Millwood). 2015 Aug;34(8):1312-9.
10. Durfee J et al. The impact of tailored intervention services on charges and mortality for adult super-utilizers. Healthc (Amst). 2017 Aug 25. pii: S2213-0764(17)30057-X. doi: 10.1016/j.hjdsi.2017.08.004. [Epub ahead of print]
11. Rinehart DJ et al. Identifying subgroups of adult super utilizers in an urban safety-net system using latent class analysis: Implications for clinical practice. Med Care. 2016 Sep 14. doi: 10.1097/MLR.0000000000000628. [Epub ahead of print]
12. Greysen RS et al. Understanding transitions of care from hospital to homeless shelter: A mixed-methods, community-based participatory approach. J Gen Intern Med. 2012;27(11):1484-91.
13. National Health Care for the Homeless Council. (Oct 2012). Improving Care Transitions for People Experiencing Homelessness. (Lead author: Sabrina Edgington, policy and program specialist.) Available at: www.nhchc.org/wp-content/uploads/2012/12/Policy_Brief_Care_Transitions.pdf. Accessed Oct 21, 2017.
14. Koh HK et al. Improving healthcare for homeless people. JAMA. 2016;316(24):2586-7.
Despite programs to end homelessness, it remains a substantial and growing problem in many cities in the United States.1,2 In 2016, there were an estimated 10,550 homeless people living in my home state of Colorado, a 6% increase from the prior year.2 A recent point-estimate study found that there were more than 5,000 homeless individuals in the Denver metropolitan area on a single night in January 2017.3 Because of the relative scarcity of housing, a growing number of cities like Denver now utilize a practice known as vulnerability indexing to prioritize homeless persons at high risk of mortality from medical conditions for placement in permanent supportive housing.4
Although hospitalists like myself frequently care for vulnerable homeless patients in the hospital, most have little formal training in how best to care for and advocate for these individuals beyond treating their acute medical need, and little direct contact with community organizations with expertise in doing so. Instead, we have learned informally through experience. Hospital providers are often frustrated by the perceived lack of services and support available to these patients, and there is substantial variability in the extent to which providers engage patients and community partners during and after hospitalization. Despite the growing practice of vulnerability indexing in the community, hospital-based providers do not routinely assess vulnerability with respect to housing. Previous research indicates that housing status is assessed in only a minority of homeless patients during their hospital stay.12 Thus, hospitalization often represents a missed opportunity to identify vulnerability and utilize it to connect patients with housing and other resources.
Addressing the significant known health disparities faced by homeless persons is one of the greatest health equity challenges of our time.13 We need better ways of understanding, identifying, and addressing vulnerability among homeless patients who are hospitalized, paired with improved integration with local community organizations. This will require moving beyond the idea that homelessness is the social worker’s job to one of shared responsibility and advocacy.
Collaborative research and other partnerships that engage both community organizations and individuals affected by homelessness are crucial to further understand the specific needs, barriers, challenges, and opportunities for improving hospital care and care transitions in this population. As well-respected community members and systems thinkers who witness these inequities on a daily basis, hospitalists are well positioned to help lead this work.
Dr. Stella is a hospitalist at Denver Health and Hospital Authority, and an associate professor of medicine at the University of Colorado. She is a member of The Hospitalist editorial advisory board.
References
1. Ending Chronic Homelessness. (Aug 2017). U.S. Interagency Council on Homelessness. Available at: https://www.usich.gov/goals/chronicsness. Accessed: Oct 21, 2017.
2. 2016 Annual Homeless Assessment Report (AHAR) to Congress. (Nov 2016). U.S. Department of Housing and Urban Development Office of Community Planning and Development, Part 1. Available at: https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Accessed: Oct 21, 2017.
3. 2017 Point-In-Time Report, Seven-County Metro Denver Region. Metro Denver Homeless Initiative. Available at: http://www.mdhi.org/2017_pit. Accessed Oct 22, 2017.
4. Henwood BF et al. Examining mortality among formerly homeless adults enrolled in Housing First: An observational study. BMC Public Health. 2015;15:1209.
5. Weinstein LC et al. Moving from street to home: Health status of entrants to a Housing First program. J Prim Care Community Health. 2011;2:11–5.
6. Kushel MB et al. Factors associated with the health care utilization of homeless persons. JAMA. 2001;285(2):200-6.
7. Kushel MB et al. Emergency department use among the homeless and marginally housed: Results from a community-based study. Am J Public Health. 2002;92(5):778-84.
8. Baggett TP et al. Mortality among homeless adults in Boston: Shifts in causes of death over a 15-year period. JAMA Intern Med. 2013 Feb 11;173(3):189–95.
9. Johnson et al. For many patients who use large amounts of health care services, the need is intense yet temporary. Health Aff (Millwood). 2015 Aug;34(8):1312-9.
10. Durfee J et al. The impact of tailored intervention services on charges and mortality for adult super-utilizers. Healthc (Amst). 2017 Aug 25. pii: S2213-0764(17)30057-X. doi: 10.1016/j.hjdsi.2017.08.004. [Epub ahead of print]
11. Rinehart DJ et al. Identifying subgroups of adult super utilizers in an urban safety-net system using latent class analysis: Implications for clinical practice. Med Care. 2016 Sep 14. doi: 10.1097/MLR.0000000000000628. [Epub ahead of print]
12. Greysen RS et al. Understanding transitions of care from hospital to homeless shelter: A mixed-methods, community-based participatory approach. J Gen Intern Med. 2012;27(11):1484-91.
13. National Health Care for the Homeless Council. (Oct 2012). Improving Care Transitions for People Experiencing Homelessness. (Lead author: Sabrina Edgington, policy and program specialist.) Available at: www.nhchc.org/wp-content/uploads/2012/12/Policy_Brief_Care_Transitions.pdf. Accessed Oct 21, 2017.
14. Koh HK et al. Improving healthcare for homeless people. JAMA. 2016;316(24):2586-7.
Despite programs to end homelessness, it remains a substantial and growing problem in many cities in the United States.1,2 In 2016, there were an estimated 10,550 homeless people living in my home state of Colorado, a 6% increase from the prior year.2 A recent point-estimate study found that there were more than 5,000 homeless individuals in the Denver metropolitan area on a single night in January 2017.3 Because of the relative scarcity of housing, a growing number of cities like Denver now utilize a practice known as vulnerability indexing to prioritize homeless persons at high risk of mortality from medical conditions for placement in permanent supportive housing.4
Although hospitalists like myself frequently care for vulnerable homeless patients in the hospital, most have little formal training in how best to care for and advocate for these individuals beyond treating their acute medical need, and little direct contact with community organizations with expertise in doing so. Instead, we have learned informally through experience. Hospital providers are often frustrated by the perceived lack of services and support available to these patients, and there is substantial variability in the extent to which providers engage patients and community partners during and after hospitalization. Despite the growing practice of vulnerability indexing in the community, hospital-based providers do not routinely assess vulnerability with respect to housing. Previous research indicates that housing status is assessed in only a minority of homeless patients during their hospital stay.12 Thus, hospitalization often represents a missed opportunity to identify vulnerability and utilize it to connect patients with housing and other resources.
Addressing the significant known health disparities faced by homeless persons is one of the greatest health equity challenges of our time.13 We need better ways of understanding, identifying, and addressing vulnerability among homeless patients who are hospitalized, paired with improved integration with local community organizations. This will require moving beyond the idea that homelessness is the social worker’s job to one of shared responsibility and advocacy.
Collaborative research and other partnerships that engage both community organizations and individuals affected by homelessness are crucial to further understand the specific needs, barriers, challenges, and opportunities for improving hospital care and care transitions in this population. As well-respected community members and systems thinkers who witness these inequities on a daily basis, hospitalists are well positioned to help lead this work.
Dr. Stella is a hospitalist at Denver Health and Hospital Authority, and an associate professor of medicine at the University of Colorado. She is a member of The Hospitalist editorial advisory board.
References
1. Ending Chronic Homelessness. (Aug 2017). U.S. Interagency Council on Homelessness. Available at: https://www.usich.gov/goals/chronicsness. Accessed: Oct 21, 2017.
2. 2016 Annual Homeless Assessment Report (AHAR) to Congress. (Nov 2016). U.S. Department of Housing and Urban Development Office of Community Planning and Development, Part 1. Available at: https://www.hudexchange.info/resources/documents/2016-AHAR-Part-1.pdf. Accessed: Oct 21, 2017.
3. 2017 Point-In-Time Report, Seven-County Metro Denver Region. Metro Denver Homeless Initiative. Available at: http://www.mdhi.org/2017_pit. Accessed Oct 22, 2017.
4. Henwood BF et al. Examining mortality among formerly homeless adults enrolled in Housing First: An observational study. BMC Public Health. 2015;15:1209.
5. Weinstein LC et al. Moving from street to home: Health status of entrants to a Housing First program. J Prim Care Community Health. 2011;2:11–5.
6. Kushel MB et al. Factors associated with the health care utilization of homeless persons. JAMA. 2001;285(2):200-6.
7. Kushel MB et al. Emergency department use among the homeless and marginally housed: Results from a community-based study. Am J Public Health. 2002;92(5):778-84.
8. Baggett TP et al. Mortality among homeless adults in Boston: Shifts in causes of death over a 15-year period. JAMA Intern Med. 2013 Feb 11;173(3):189–95.
9. Johnson et al. For many patients who use large amounts of health care services, the need is intense yet temporary. Health Aff (Millwood). 2015 Aug;34(8):1312-9.
10. Durfee J et al. The impact of tailored intervention services on charges and mortality for adult super-utilizers. Healthc (Amst). 2017 Aug 25. pii: S2213-0764(17)30057-X. doi: 10.1016/j.hjdsi.2017.08.004. [Epub ahead of print]
11. Rinehart DJ et al. Identifying subgroups of adult super utilizers in an urban safety-net system using latent class analysis: Implications for clinical practice. Med Care. 2016 Sep 14. doi: 10.1097/MLR.0000000000000628. [Epub ahead of print]
12. Greysen RS et al. Understanding transitions of care from hospital to homeless shelter: A mixed-methods, community-based participatory approach. J Gen Intern Med. 2012;27(11):1484-91.
13. National Health Care for the Homeless Council. (Oct 2012). Improving Care Transitions for People Experiencing Homelessness. (Lead author: Sabrina Edgington, policy and program specialist.) Available at: www.nhchc.org/wp-content/uploads/2012/12/Policy_Brief_Care_Transitions.pdf. Accessed Oct 21, 2017.
14. Koh HK et al. Improving healthcare for homeless people. JAMA. 2016;316(24):2586-7.
How to manage a patient presenting with syncope
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview

The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2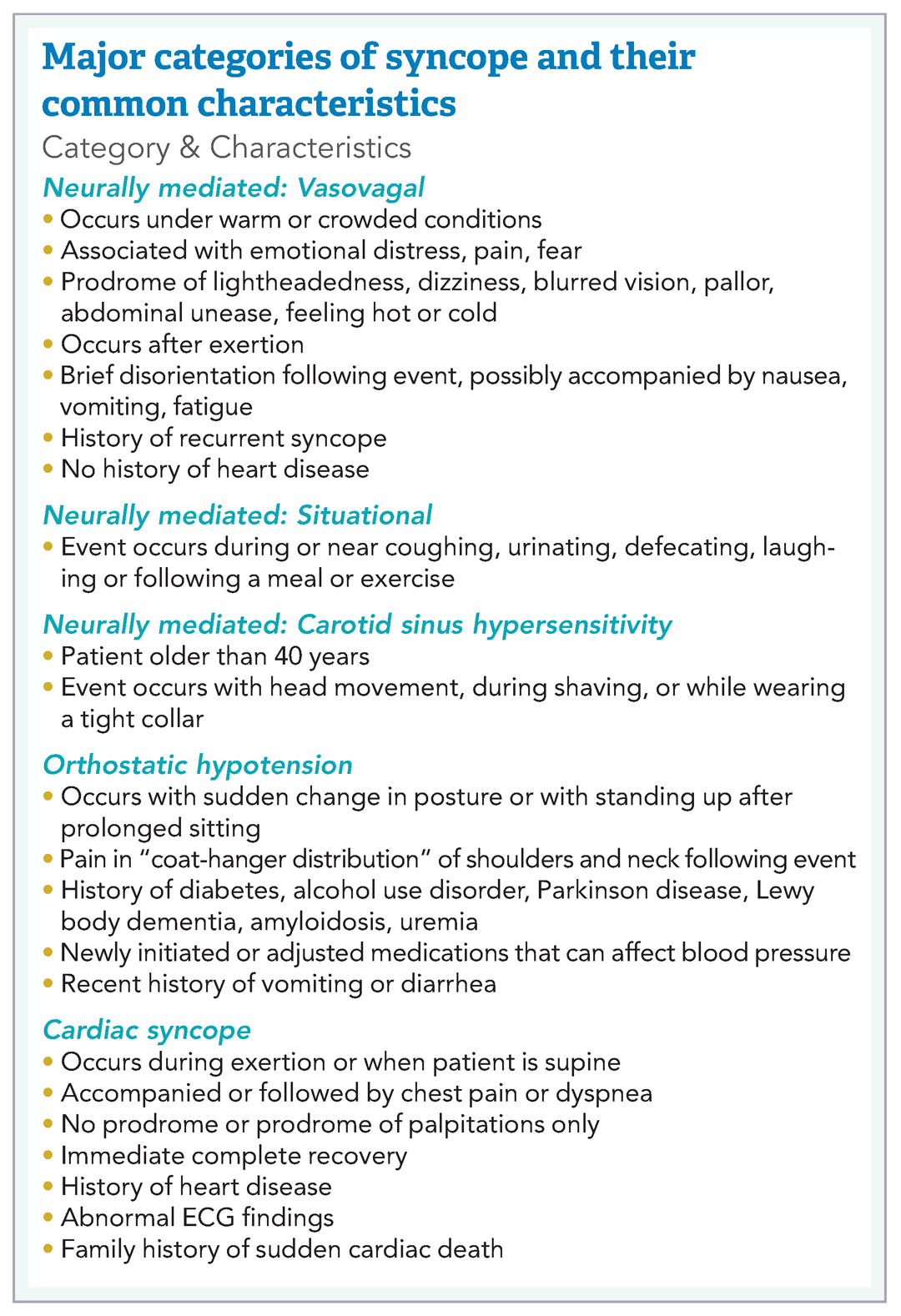
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.

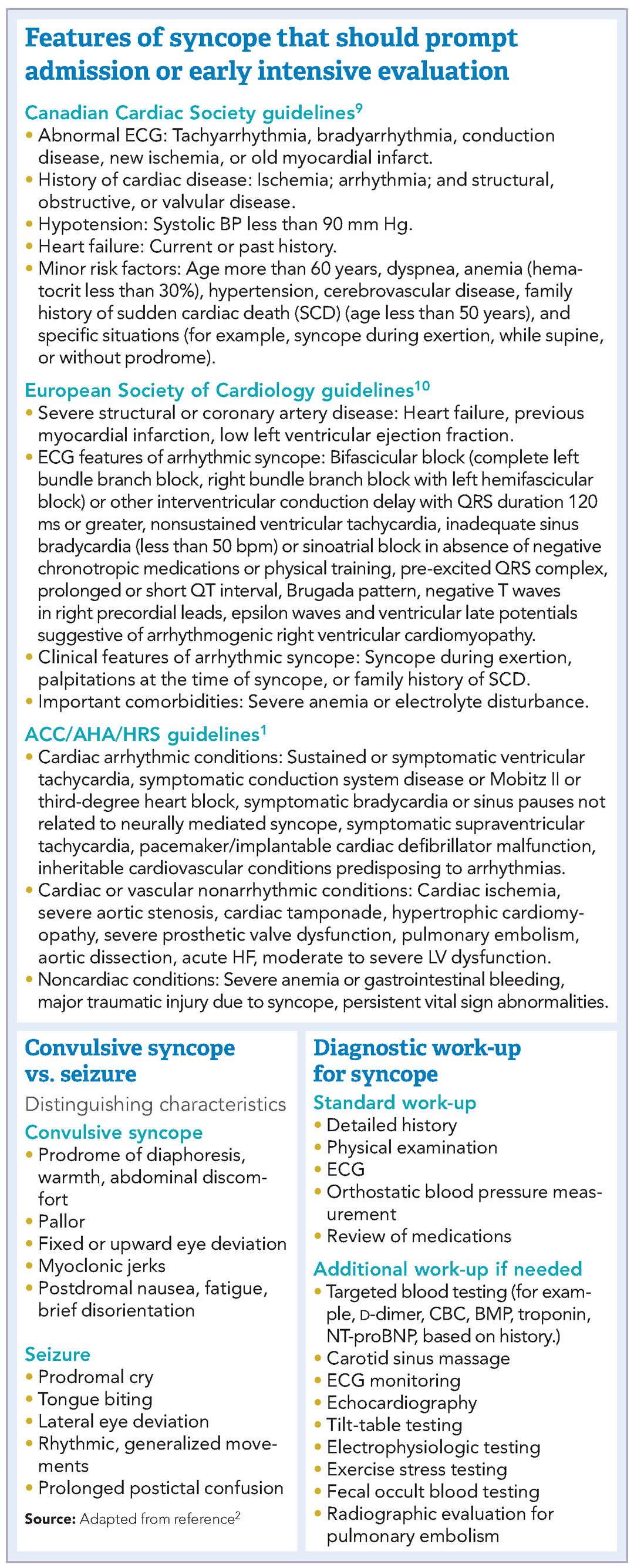
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.

Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
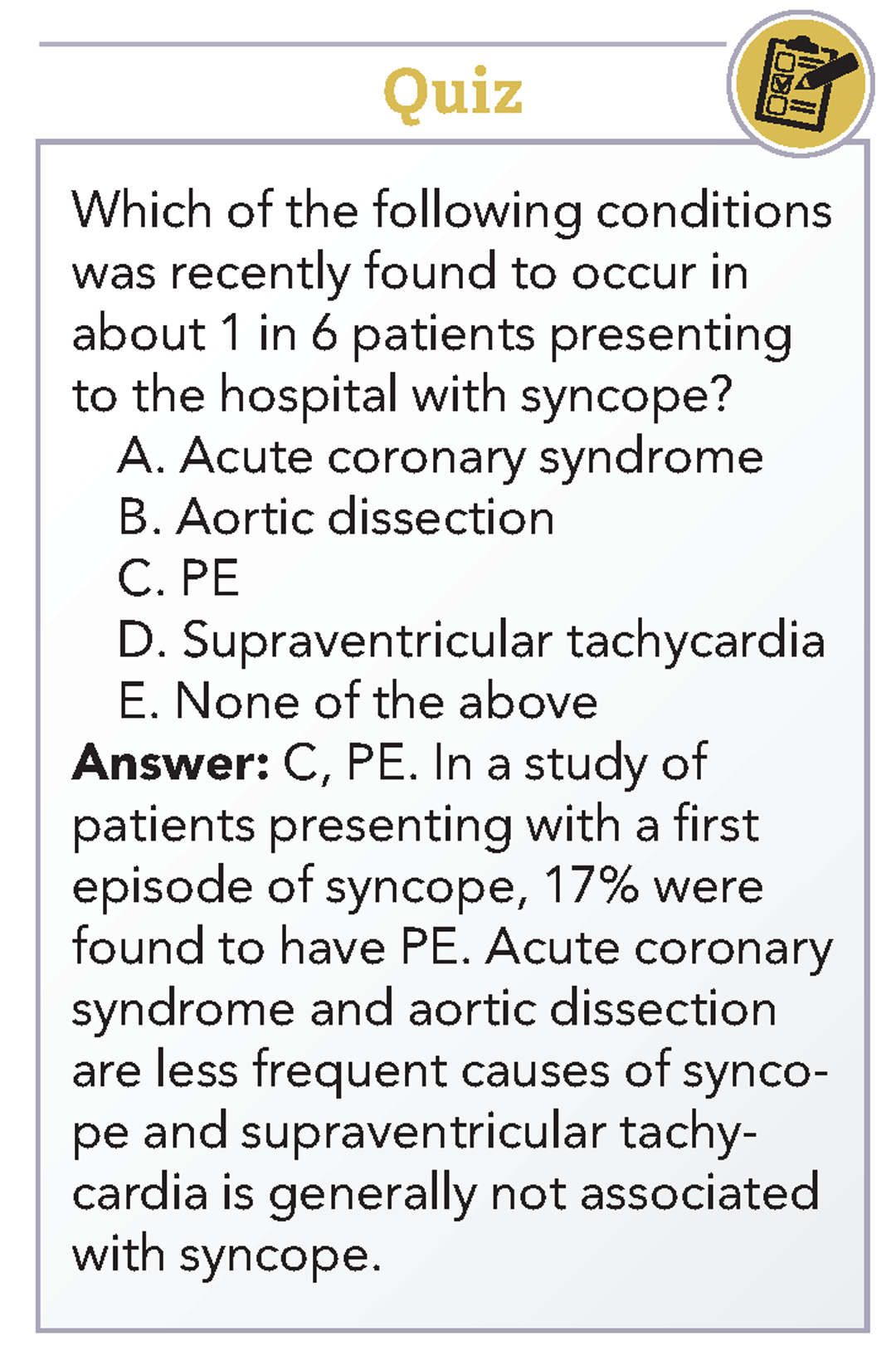
Bottom Line
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview
The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.
Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
Bottom Line
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Case
A 38-year-old construction worker without significant medical history presents following witnessed syncope at her job, after standing for at least 2 hours on a particularly warm day. She reported an episode of syncope under similar circumstances 2 months prior. With each episode, she experienced “tunneling” of peripheral vision, then loss of consciousness without palpitations or incontinence. Her physical exam, vital signs (including orthostatic blood pressures), labs, and ECG were unremarkable.
Brief overview
The American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines define syncope as “a symptom that presents with an abrupt, transient, complete loss of consciousness, associated with inability to maintain postural tone, with rapid and spontaneous recovery” with cerebral hypoperfusion as the presumed mechanism.1 Furthermore, “there should not be clinical features of other nonsyncope causes of loss of consciousness, such as seizure, antecedent head trauma, or apparent loss of consciousness (that is, pseudosyncope).”1
A careful history revolving around the patient’s behavior prior to, during, and following the event, a thorough past medical history, and a review of current medications are essential. Potential obstacles in obtaining details of the event include lack of witnesses, patient’s inability to recall the experience, and inaccurate description of convulsive syncope as a “seizure” by bystanders.2
Overview of data
Obtaining a detailed history is crucial to understanding both the etiology of the syncopal event and determining which patients are at high risk for adverse outcomes. The etiology of syncope can be determined by history alone in 26% of patients younger than 65 years.3 Data on the prevalence of syncope by cause varies widely. As a general rule, in younger patients, especially those under 40 years of age, neurally mediated syncope is most common. As patients age, orthostatic hypotension and cardiac causes (including arrhythmias and structural diseases) occur more frequently, though neurally mediated syncope is still the most common.
Many of these predictors, however, would raise the clinical suspicion of most hospitalists for adverse outcomes in their hospitalized patients independent of the presence or absence of syncope. In fact, a meta-analysis has concluded that “None of the evaluated prediction tools (SFSR, EGSYS) performed better than clinical judgment in identifying serious outcomes during emergency department stay, and at 10 and 30 days after syncope.”6
Once the patient is hospitalized, further evaluation should be based on a careful history and physical examination. Standard evaluation also includes careful review of medications, an ECG to exclude findings suggestive of arrhythmias as well as structural or coronary artery disease, and orthostatic blood pressure measurements.1 Additional tests should be considered as deemed appropriate. For example, in patients over 40 years of age without history of carotid artery disease or stroke and in whom no carotid artery bruit is appreciated, a carotid sinus massage may be considered. The correct technique is to massage the sinus on the right then left, each for 5 seconds in both supine and standing positions with continuous heart rate and frequent blood pressure monitoring. Reproduction of syncope, especially concurrent with a cardiac pause of greater than 3 seconds and a systolic blood pressure drop of greater than 50 mmHg, is considered a positive test. Tilt-table testing should be considered in those for whom neurally mediated syncope is suspected but not confirmed, or in patients who might benefit from further elucidation of their prodromal symptoms.
Of note, a study recently published in the New England Journal of Medicine suggests that the prevalence of PE in patients (median age, 80 years) presenting with a first episode of syncope was 17%, a rate that is substantially higher than historically presumed.8 Although the prevalence of PE was highest among patients presenting with syncope of unclear origin (25%), nearly 13% of patients with other explanations for syncope also had PE.
Application of data
Bottom Line
Dr. Roberts, Dr. Krason, and Dr. Manian are hospitalists at Massachusetts General Hospital in Boston.
References
1. Shen W-K et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope. J Am Coll Cardiol. 2017 Aug 1;70(5):e39-e110.
2. Sheldon R. How to differentiate syncope from seizure. Cardiol Clin. 2015 Aug;33(3):377-85.
3. Del Rosso A et al. Relation of clinical presentation of syncope to the age of patients. Am J Cardiol. 2005 Nov 15;96(10):1431-5.
4. Blanc JJ. Syncope: Definition, epidemiology, and classification. Cardiol Clin. 2015 Aug;33(3):341-5.
5. Matthews IG et al. Syncope in the older person. Cardiol Clin. 2015 Aug;33(3):411-21.
6. Costantino G et al. Syncope risk stratification tools vs clinical judgment: An individual patient data meta-analysis. Am J Med. 2014 Nov;127(11):1126.e13-25.
7. Chiu DT et al. Are echocardiography, telemetry, ambulatory electrocardiography monitoring, and cardiac enzymes in emergency department patients presenting with syncope useful tests? A preliminary investigation. J Emerg Med. 2014;47:113-8.
8. Prandoni P et al. Prevalence of pulmonary embolism among patients hospitalized for syncope. N Engl J Med. 2016 Oct;375(20):1524-31.
9. Sheldon RS et al. Standardized approaches to the investigation of syncope: Canadian Cardiovascular Society position paper. Can J Cardiol. 2011 Mar-Apr;27(2):246-253.
10. Moya A et al. Guidelines for the diagnosis and management of syncope (version 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J. 2009 Nov;30(21):2631-71.
Additional reading
1. Brignole M, Hamdan MH. New concepts in the assessment of syncope. J Am Coll Cardiol. 2012 May; 59(18):1583-91.
2. Rosanio S et al. Syncope in adults: systematic review and proposal of a diagnostic and therapeutic algorithm. Int J Cardiol. 2013 Jan;162(3):149-57.
Analysis: Hospital pay for performance not significantly improving Medicare outcomes
for Medicare beneficiaries, according to an analysis of Medicare claims data.
“No evidence that hospitals [that were] operating under pay for performance programs for more than a decade had better process scores or lower mortality than other hospitals was found,” Igna Bonfrer, PhD, of Erasmus University, Rotterdam, the Netherlands, and colleagues wrote in a study published Jan. 4, 2018, in BMJ.
Researchers looked at Medicare claims data from nearly 1.4 million patients aged 65 years and older across 1,189 hospitals. That total included 214 hospitals that were early adopters of pay for performance (PFP) programs, including the Hospital Quality Incentive Demonstration (HQID) and the current Hospital Value-Based Purchasing (HVBP) program, and 975 hospitals that adopted the programs at a later date. The study authors examined clinical process scores and 30-day mortality rates from 2003 to 2013.
Hospitals that were early adopters of a PFP program typically started from a higher baseline process measure score (91.5), compared with late adopters (89.9).
However, improvements among the early adopters “were smaller during the HQID period, although early adopters continued to perform at a slightly higher level than the late adopters during the pre-HVBP period,” the researchers explained. “Over the HVBP period, early and late adopters no longer differed in their clinical process scores.”
Indeed, a ceiling was ultimately reached, with early and late adopters approaching the same level (98.5 vs. 98.2).
For the 30-day mortality rates, both groups “started from a similar baseline (14.9% and 14.8% for the early and late adopters in the fourth quarter of 2003) and ended at the same rate of 9.9% for both groups in the fourth quarter of 2013,” Dr. Bonfrer and colleagues wrote.
The researchers suggested that the programs did not yield better results because of small financial incentives, coupled with program complexities that made it “difficult for hospitals to meaningfully engage in the program.” They also suggested that having to wait until year end to receive any financial incentives could have limited the impact.
“We found that hospitals that have been under financial incentives for more than a decade have not been able to reduce patient mortality more than late adopters, which had only been under financial incentives for less than 3 years,” the researchers concluded. “Given its cost, policymakers in the [United States] should consider one of two things: revise the current program or potentially end it.”
The changes suggested include increasing financial incentives and focusing on process measures that matter most to patients (mortality, patient experience, and functional status), rather than the current measure set that is larger and more difficult to track.
The researchers did not report any financial conflicts of interest.
SOURCE: Dr. Igna Bonfrer et al. BMJ 2018;360:j5622.

for Medicare beneficiaries, according to an analysis of Medicare claims data.
“No evidence that hospitals [that were] operating under pay for performance programs for more than a decade had better process scores or lower mortality than other hospitals was found,” Igna Bonfrer, PhD, of Erasmus University, Rotterdam, the Netherlands, and colleagues wrote in a study published Jan. 4, 2018, in BMJ.
Researchers looked at Medicare claims data from nearly 1.4 million patients aged 65 years and older across 1,189 hospitals. That total included 214 hospitals that were early adopters of pay for performance (PFP) programs, including the Hospital Quality Incentive Demonstration (HQID) and the current Hospital Value-Based Purchasing (HVBP) program, and 975 hospitals that adopted the programs at a later date. The study authors examined clinical process scores and 30-day mortality rates from 2003 to 2013.
Hospitals that were early adopters of a PFP program typically started from a higher baseline process measure score (91.5), compared with late adopters (89.9).
However, improvements among the early adopters “were smaller during the HQID period, although early adopters continued to perform at a slightly higher level than the late adopters during the pre-HVBP period,” the researchers explained. “Over the HVBP period, early and late adopters no longer differed in their clinical process scores.”
Indeed, a ceiling was ultimately reached, with early and late adopters approaching the same level (98.5 vs. 98.2).
For the 30-day mortality rates, both groups “started from a similar baseline (14.9% and 14.8% for the early and late adopters in the fourth quarter of 2003) and ended at the same rate of 9.9% for both groups in the fourth quarter of 2013,” Dr. Bonfrer and colleagues wrote.
The researchers suggested that the programs did not yield better results because of small financial incentives, coupled with program complexities that made it “difficult for hospitals to meaningfully engage in the program.” They also suggested that having to wait until year end to receive any financial incentives could have limited the impact.
“We found that hospitals that have been under financial incentives for more than a decade have not been able to reduce patient mortality more than late adopters, which had only been under financial incentives for less than 3 years,” the researchers concluded. “Given its cost, policymakers in the [United States] should consider one of two things: revise the current program or potentially end it.”
The changes suggested include increasing financial incentives and focusing on process measures that matter most to patients (mortality, patient experience, and functional status), rather than the current measure set that is larger and more difficult to track.
The researchers did not report any financial conflicts of interest.
SOURCE: Dr. Igna Bonfrer et al. BMJ 2018;360:j5622.
for Medicare beneficiaries, according to an analysis of Medicare claims data.
“No evidence that hospitals [that were] operating under pay for performance programs for more than a decade had better process scores or lower mortality than other hospitals was found,” Igna Bonfrer, PhD, of Erasmus University, Rotterdam, the Netherlands, and colleagues wrote in a study published Jan. 4, 2018, in BMJ.
Researchers looked at Medicare claims data from nearly 1.4 million patients aged 65 years and older across 1,189 hospitals. That total included 214 hospitals that were early adopters of pay for performance (PFP) programs, including the Hospital Quality Incentive Demonstration (HQID) and the current Hospital Value-Based Purchasing (HVBP) program, and 975 hospitals that adopted the programs at a later date. The study authors examined clinical process scores and 30-day mortality rates from 2003 to 2013.
Hospitals that were early adopters of a PFP program typically started from a higher baseline process measure score (91.5), compared with late adopters (89.9).
However, improvements among the early adopters “were smaller during the HQID period, although early adopters continued to perform at a slightly higher level than the late adopters during the pre-HVBP period,” the researchers explained. “Over the HVBP period, early and late adopters no longer differed in their clinical process scores.”
Indeed, a ceiling was ultimately reached, with early and late adopters approaching the same level (98.5 vs. 98.2).
For the 30-day mortality rates, both groups “started from a similar baseline (14.9% and 14.8% for the early and late adopters in the fourth quarter of 2003) and ended at the same rate of 9.9% for both groups in the fourth quarter of 2013,” Dr. Bonfrer and colleagues wrote.
The researchers suggested that the programs did not yield better results because of small financial incentives, coupled with program complexities that made it “difficult for hospitals to meaningfully engage in the program.” They also suggested that having to wait until year end to receive any financial incentives could have limited the impact.
“We found that hospitals that have been under financial incentives for more than a decade have not been able to reduce patient mortality more than late adopters, which had only been under financial incentives for less than 3 years,” the researchers concluded. “Given its cost, policymakers in the [United States] should consider one of two things: revise the current program or potentially end it.”
The changes suggested include increasing financial incentives and focusing on process measures that matter most to patients (mortality, patient experience, and functional status), rather than the current measure set that is larger and more difficult to track.
The researchers did not report any financial conflicts of interest.
SOURCE: Dr. Igna Bonfrer et al. BMJ 2018;360:j5622.
FROM BMJ
Thrombectomy shines in presence of a clinical deficit and imaging mismatch
, according to Raul G. Nogueira, MD, and his DAWN trial coinvestigators.
A total of 206 patients who had experienced occlusion of the intracranial internal carotid artery or proximal middle cerebral artery in the past 6-24 hours were included in the study – 107 receiving thrombectomy with the Trevo device plus standard care and 99 receiving standard care alone. After 90 days of treatment, the mean utility-weighted modified Rankin scale score for patients who received thrombectomy was 5.5, compared with 3.4 in the control group. The rate of functional independence was 49% in the thrombectomy group and 13% in the control group.

“Further studies are needed to establish the prevalence of patients who would be eligible for thrombectomy among the entire population of patients with ischemic stroke. Further studies are also needed to determine whether late thrombectomy has a benefit when more widely available imaging techniques are used to estimate the infarct volume at presentation, such as assessment of the extent of hypodensity on non–contrast-enhanced CT,” the investigators noted.
SOURCE: Nogueira R et al. N Engl J Med. 2018;378:11-21
, according to Raul G. Nogueira, MD, and his DAWN trial coinvestigators.
A total of 206 patients who had experienced occlusion of the intracranial internal carotid artery or proximal middle cerebral artery in the past 6-24 hours were included in the study – 107 receiving thrombectomy with the Trevo device plus standard care and 99 receiving standard care alone. After 90 days of treatment, the mean utility-weighted modified Rankin scale score for patients who received thrombectomy was 5.5, compared with 3.4 in the control group. The rate of functional independence was 49% in the thrombectomy group and 13% in the control group.
“Further studies are needed to establish the prevalence of patients who would be eligible for thrombectomy among the entire population of patients with ischemic stroke. Further studies are also needed to determine whether late thrombectomy has a benefit when more widely available imaging techniques are used to estimate the infarct volume at presentation, such as assessment of the extent of hypodensity on non–contrast-enhanced CT,” the investigators noted.
SOURCE: Nogueira R et al. N Engl J Med. 2018;378:11-21
, according to Raul G. Nogueira, MD, and his DAWN trial coinvestigators.
A total of 206 patients who had experienced occlusion of the intracranial internal carotid artery or proximal middle cerebral artery in the past 6-24 hours were included in the study – 107 receiving thrombectomy with the Trevo device plus standard care and 99 receiving standard care alone. After 90 days of treatment, the mean utility-weighted modified Rankin scale score for patients who received thrombectomy was 5.5, compared with 3.4 in the control group. The rate of functional independence was 49% in the thrombectomy group and 13% in the control group.
“Further studies are needed to establish the prevalence of patients who would be eligible for thrombectomy among the entire population of patients with ischemic stroke. Further studies are also needed to determine whether late thrombectomy has a benefit when more widely available imaging techniques are used to estimate the infarct volume at presentation, such as assessment of the extent of hypodensity on non–contrast-enhanced CT,” the investigators noted.
SOURCE: Nogueira R et al. N Engl J Med. 2018;378:11-21
FROM NEW ENGLAND JOURNAL OF MEDICINE
More thoughts about hospitalist burnout
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.

Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.
Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
I wrote about physician burnout and well-being in the July 2017 version of this column, and am still thinking a great deal about those issues. In the past 6 months, I can’t identify anything that strikes me as a real breakthrough in addressing these issues. However, the ever-increasing attention and resources directed at physician burnout and wellness, on both a local and national level, strike me as reason for cautious optimism.
A chief wellness officer
In summer 2017, Stanford University created a new physician executive role called chief wellness officer (CWO). As far as I am aware, this is the first such position connected with a hospital or medical school. It will be interesting to see if other organizations create similar positions, although I suspect that in places where it is explicitly recognized as a priority, responsibility for this work will be one of the many duties of a chief medical officer or other such executive, and not a position devoted solely to wellness. Interestingly, an Internet search revealed that some non–health care businesses have executive positions with that title, though the role seems focused more on physical health – as in exercise and smoking cessation – than emotional well-being and burnout.
According to a statement on the Stanford Medicine website, the new CWO will work with colleagues to continue “building on its innovative WellMD Center , which was established in 2016. The center has engaged more than 200 physicians through programs focusing on peer support, stress reduction, and ways to cultivate compassion and resilience, as well as a literature and a dinner series in which physicians explore the challenges and rewards of being a doctor. The center also aims to relieve some of the burden on physicians by improving efficiency and simplifying workplace systems, such as electronic medical records.”
A national conference
Over the last 2 or 3 years many, if not most, physician conferences, including the SHM annual conference, have added some content around physician burnout and well-being. But for the first time I’m aware of, an entire conference, the American Conference on Physician Health, addressed these topics in San Francisco in October 2017, and attracted 425 attendees along with an all-star faculty. I couldn’t attend myself, but found a reporter’s summary informative and I recommend it.
While the summary didn’t suggest the conference provided a cure or simple path to improvement, I’m encouraged that the topic has attracted the attention of some pretty smart people. If there is a second edition of this conference, I’ll try hard to attend.
Worthwhile web resources
The home page of Stanford’s WellMD Center provides a continuously updated list of recent research publications on physician health and links to many other resources, and is worth bookmarking.
Another great educational resource for physician wellness is the AMA’s STEPS Forward, a site devoted to practice improvement that provides guidance on patient care, work flow and process, leading change, technology and finance, as well as professional well-being. Of the five separate education modules in the latter category, I found the one on “Preventing Physician Burnout” especially informative. The site is free, doesn’t require an AMA membership, and can provide CME credit.
Making a difference locally: Individuals
Surveys, research, and the experience of experts available via the above resources and others are very valuable, but may be hard to translate into action for you and your fellow local caregivers. My sense is that many hospitalists address their own work-related distress by simply working less in total – reducing their full-time equivalents. That may be the most tangible and accessible intervention, and undeniably the right thing to do in some cases. But it isn’t an ideal approach for our field, which faces chronic staffing shortages. And it doesn’t do anything to change the average level of distress of a day of work. I worry that many people will find disappointment if working fewer shifts is their only burnout mitigation strategy.
Ensuring that you have some work-related interest outside of direct patient care, such as being the local electronic health record expert, or even the person leading formation of a support committee, can be really valuable. I first addressed this topic in the June 2011 issue of The Hospitalist, and there is a long list of things to consider: mindfulness, practicing “ self-compassion ,” cultivating deeper social connections in and out of the workplace, etc. Ultimately, each of us will have to choose our own path, and for some that should include professional help, e.g., from a mental health care provider.
But as a colleague once put it, a focus on changing ourselves is akin to just learning to take a punch better. A worthwhile endeavor, but it’s also necessary to try to decrease the number of punches thrown our way.
Making a difference locally: Medical staff
I’m part of the Provider Support Committee at my hospital, and I have concluded that nearly every hospital should have a group like this. Our own committee was modeled after the support committee at a hospital five miles away, and both groups see value in collaborating in our efforts. In fact, a person from each hospital’s committee serves on the committee at the other hospital.
These committees have popped up in other institutions, and many have been at it longer than at my hospital. But they all seem to share a mission of developing and implementing programs to position caregivers to thrive in their work, increase resilience, and reduce their risk of burnout. Some interventions are focused on making changes to an EHR, work schedules, work flows, or even staffing levels (i.e., reducing the “number of punches”). Other efforts are directed toward establishing groups that support personal reflection and/or social connections among providers.
A review of activities undertaken by seven different organizations is available at the AMA STEPS forward Preventing Physician Burnout website (click on “STEPS in practice.”)
Dr. Nelson has had a career in clinical practice as a hospitalist starting in 1988. He is cofounder and past president of SHM, and principal in Nelson Flores Hospital Medicine Consultants. He is codirector for SHM’s practice management courses. Contact him at [email protected]
Choosing location after discharge wisely
Of all the care decisions we make during a hospital stay, perhaps the one with the biggest implications for cost and quality is the one determining the location to which we send the patient after discharge.
Yet ironically, we haven’t typically participated in this decision, but instead have left it up to case managers and others to work with patients to determine discharge location. This is a missed opportunity, as patients first look to their doctor for guidance on this decision. Absent such guidance, they turn to other care team members for the conversation. With a principal focus on hospital length of stay, we have prioritized when patients are ready to leave over where they go after they leave.

In terms of cost during hospitalization and for the 30 days after discharge, for common conditions such as pneumonia, heart failure, COPD, or major joint replacement, Medicare spends nearly as much on postacute care – home health, skilled nursing facilities, inpatient rehabilitation, long-term acute care hospitals – as for hospital care.1 Further, an Institute of Medicine analysis showed that geographic variation in postacute care spending is responsible for three-quarters of all variation in Medicare spending.2 Such variation raises questions about the rigor with which postacute care decisions are made by hospital teams.
Perhaps most striking of all, hospitalist care (versus that of traditional primary care providers) has been associated with excess discharge rates to skilled nursing facilities, and savings that accrue under hospitalists during hospitalization are more than outweighed by spending on care during the postacute period.3
All of this leads me to my point: Hospitalists and inpatient teams need a defined process for selecting the most appropriate discharge location. Such a location should ideally be the least restrictive location suitable for a patient’s needs. In the box below, I propose a framework for the process. The domains listed in the box should be evaluated and discussed by the team, with early input and final approval by the patient and caregiver(s). The domains listed are not intended to be an exhaustive list, but rather to serve as the basis for discussion during discharge team rounds.
Identifying patient factors informing an optimal discharge location may represent a new skill set for many hospitalists and underscores the value of collaboration with team members who can provide needed information. In April, the Society of Hospital Medicine published the Revised Core Competencies in Hospital Medicine. In the Care of the Older Patient section, the authors state that hospitalists should be able to “describe postacute care options that can enable older patients to regain functional capacity.”4 Inherent in this competency is an understanding of not only patient factors in postacute care location decisions, but also the differing capabilities of home health agencies, skilled nursing facilities, inpatient rehabilitation facilities, and long-term acute care hospitals.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected].
References
1. Mechanic R. Post-acute care – the next frontier for controlling Medicare spending. N Engl J Med. 2014;370:692-4.
2. Newhouse JP, et al. Geographic variation in Medicare services. N Engl J Med. 2013;368:1465-8.
3. Kuo YF, et al. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-9.
4. Nichani S, et al. Core Competencies in Hospital Medicine 2017 Revision. Section 3: Healthcare Systems. J Hosp Med. 2017 April;12(1):S55-S82.
Framework for Selecting Appropriate Discharge Location
Patient Independence
- Can the patient perform activities of daily living?
- Can the patient ambulate?
- Is there cognitive impairment?
Caregiver Availability
- If the patient needs it, is a caregiver who is capable and reliable available? If so, to what extent is s/he available?
Therapy Needs
- Does the patient require PT, OT, and/or ST?
- How much and for how long?
Skilled Nursing Needs
- What, if anything, does the patient require in this area? For example, a new PEG tube, wound care, IV therapies, etc.
Social Factors
- Is there access to transportation, food, and safe housing?
Home Factors
- Are there stairs to enter the house or to get to the bedroom or bathroom?
- Has the home been modified to accommodate special needs? Is the home inhabitable?
Of all the care decisions we make during a hospital stay, perhaps the one with the biggest implications for cost and quality is the one determining the location to which we send the patient after discharge.
Yet ironically, we haven’t typically participated in this decision, but instead have left it up to case managers and others to work with patients to determine discharge location. This is a missed opportunity, as patients first look to their doctor for guidance on this decision. Absent such guidance, they turn to other care team members for the conversation. With a principal focus on hospital length of stay, we have prioritized when patients are ready to leave over where they go after they leave.
In terms of cost during hospitalization and for the 30 days after discharge, for common conditions such as pneumonia, heart failure, COPD, or major joint replacement, Medicare spends nearly as much on postacute care – home health, skilled nursing facilities, inpatient rehabilitation, long-term acute care hospitals – as for hospital care.1 Further, an Institute of Medicine analysis showed that geographic variation in postacute care spending is responsible for three-quarters of all variation in Medicare spending.2 Such variation raises questions about the rigor with which postacute care decisions are made by hospital teams.
Perhaps most striking of all, hospitalist care (versus that of traditional primary care providers) has been associated with excess discharge rates to skilled nursing facilities, and savings that accrue under hospitalists during hospitalization are more than outweighed by spending on care during the postacute period.3
All of this leads me to my point: Hospitalists and inpatient teams need a defined process for selecting the most appropriate discharge location. Such a location should ideally be the least restrictive location suitable for a patient’s needs. In the box below, I propose a framework for the process. The domains listed in the box should be evaluated and discussed by the team, with early input and final approval by the patient and caregiver(s). The domains listed are not intended to be an exhaustive list, but rather to serve as the basis for discussion during discharge team rounds.
Identifying patient factors informing an optimal discharge location may represent a new skill set for many hospitalists and underscores the value of collaboration with team members who can provide needed information. In April, the Society of Hospital Medicine published the Revised Core Competencies in Hospital Medicine. In the Care of the Older Patient section, the authors state that hospitalists should be able to “describe postacute care options that can enable older patients to regain functional capacity.”4 Inherent in this competency is an understanding of not only patient factors in postacute care location decisions, but also the differing capabilities of home health agencies, skilled nursing facilities, inpatient rehabilitation facilities, and long-term acute care hospitals.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected].
References
1. Mechanic R. Post-acute care – the next frontier for controlling Medicare spending. N Engl J Med. 2014;370:692-4.
2. Newhouse JP, et al. Geographic variation in Medicare services. N Engl J Med. 2013;368:1465-8.
3. Kuo YF, et al. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-9.
4. Nichani S, et al. Core Competencies in Hospital Medicine 2017 Revision. Section 3: Healthcare Systems. J Hosp Med. 2017 April;12(1):S55-S82.
Framework for Selecting Appropriate Discharge Location
Patient Independence
- Can the patient perform activities of daily living?
- Can the patient ambulate?
- Is there cognitive impairment?
Caregiver Availability
- If the patient needs it, is a caregiver who is capable and reliable available? If so, to what extent is s/he available?
Therapy Needs
- Does the patient require PT, OT, and/or ST?
- How much and for how long?
Skilled Nursing Needs
- What, if anything, does the patient require in this area? For example, a new PEG tube, wound care, IV therapies, etc.
Social Factors
- Is there access to transportation, food, and safe housing?
Home Factors
- Are there stairs to enter the house or to get to the bedroom or bathroom?
- Has the home been modified to accommodate special needs? Is the home inhabitable?
Of all the care decisions we make during a hospital stay, perhaps the one with the biggest implications for cost and quality is the one determining the location to which we send the patient after discharge.
Yet ironically, we haven’t typically participated in this decision, but instead have left it up to case managers and others to work with patients to determine discharge location. This is a missed opportunity, as patients first look to their doctor for guidance on this decision. Absent such guidance, they turn to other care team members for the conversation. With a principal focus on hospital length of stay, we have prioritized when patients are ready to leave over where they go after they leave.
In terms of cost during hospitalization and for the 30 days after discharge, for common conditions such as pneumonia, heart failure, COPD, or major joint replacement, Medicare spends nearly as much on postacute care – home health, skilled nursing facilities, inpatient rehabilitation, long-term acute care hospitals – as for hospital care.1 Further, an Institute of Medicine analysis showed that geographic variation in postacute care spending is responsible for three-quarters of all variation in Medicare spending.2 Such variation raises questions about the rigor with which postacute care decisions are made by hospital teams.
Perhaps most striking of all, hospitalist care (versus that of traditional primary care providers) has been associated with excess discharge rates to skilled nursing facilities, and savings that accrue under hospitalists during hospitalization are more than outweighed by spending on care during the postacute period.3
All of this leads me to my point: Hospitalists and inpatient teams need a defined process for selecting the most appropriate discharge location. Such a location should ideally be the least restrictive location suitable for a patient’s needs. In the box below, I propose a framework for the process. The domains listed in the box should be evaluated and discussed by the team, with early input and final approval by the patient and caregiver(s). The domains listed are not intended to be an exhaustive list, but rather to serve as the basis for discussion during discharge team rounds.
Identifying patient factors informing an optimal discharge location may represent a new skill set for many hospitalists and underscores the value of collaboration with team members who can provide needed information. In April, the Society of Hospital Medicine published the Revised Core Competencies in Hospital Medicine. In the Care of the Older Patient section, the authors state that hospitalists should be able to “describe postacute care options that can enable older patients to regain functional capacity.”4 Inherent in this competency is an understanding of not only patient factors in postacute care location decisions, but also the differing capabilities of home health agencies, skilled nursing facilities, inpatient rehabilitation facilities, and long-term acute care hospitals.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn., and cofounder and past president of the Society of Hospital Medicine. Contact him at [email protected].
References
1. Mechanic R. Post-acute care – the next frontier for controlling Medicare spending. N Engl J Med. 2014;370:692-4.
2. Newhouse JP, et al. Geographic variation in Medicare services. N Engl J Med. 2013;368:1465-8.
3. Kuo YF, et al. Association of hospitalist care with medical utilization after discharge: evidence of cost shift from a cohort study. Ann Intern Med. 2011;155(3):152-9.
4. Nichani S, et al. Core Competencies in Hospital Medicine 2017 Revision. Section 3: Healthcare Systems. J Hosp Med. 2017 April;12(1):S55-S82.
Framework for Selecting Appropriate Discharge Location
Patient Independence
- Can the patient perform activities of daily living?
- Can the patient ambulate?
- Is there cognitive impairment?
Caregiver Availability
- If the patient needs it, is a caregiver who is capable and reliable available? If so, to what extent is s/he available?
Therapy Needs
- Does the patient require PT, OT, and/or ST?
- How much and for how long?
Skilled Nursing Needs
- What, if anything, does the patient require in this area? For example, a new PEG tube, wound care, IV therapies, etc.
Social Factors
- Is there access to transportation, food, and safe housing?
Home Factors
- Are there stairs to enter the house or to get to the bedroom or bathroom?
- Has the home been modified to accommodate special needs? Is the home inhabitable?