User login
High serum Angiopoietin 2 identified patients with HCC
Key clinical point: High serum levels of angiopoietin 2 (Ang2) levels identified patients with hepatocellular carcinoma (HCC) and predicted a shorter time to recurrence after treatment with curative intent.
Major finding: Serum Ang2 levels were significantly higher in patients with HCC vs controls (P less than .001) and patients with chronic liver disease (P less than .001). At the optimal threshold (3.5 ng/mL), sensitivity, specificity, and accuracy were 51%, 84%, and 59.5%, respectively. Higher serum Ang2 levels correlated with significantly shorter recurrence-free survival after ablation therapy, even after controlling for other prognostic factors.
Study details: The researchers reviewed medical charts and used sandwich enzyme-linked immunosorbent assay (ELISA) to measure Ang2 levels in stored serum from 275 patients with HCC, 98 patients with chronic liver disease, and 20 controls.
Disclosures: Partial funding came from the Japan Society for the Promotion of Science and the Program for Basic and Clinical Research on Hepatitis from Japan Agency for Medical Research and Development. The researchers reported having no conflicts of interest.
Source: J Ao et al. J Cancer. 2021 Mar 5. doi: 10.7150/jca.56436
Key clinical point: High serum levels of angiopoietin 2 (Ang2) levels identified patients with hepatocellular carcinoma (HCC) and predicted a shorter time to recurrence after treatment with curative intent.
Major finding: Serum Ang2 levels were significantly higher in patients with HCC vs controls (P less than .001) and patients with chronic liver disease (P less than .001). At the optimal threshold (3.5 ng/mL), sensitivity, specificity, and accuracy were 51%, 84%, and 59.5%, respectively. Higher serum Ang2 levels correlated with significantly shorter recurrence-free survival after ablation therapy, even after controlling for other prognostic factors.
Study details: The researchers reviewed medical charts and used sandwich enzyme-linked immunosorbent assay (ELISA) to measure Ang2 levels in stored serum from 275 patients with HCC, 98 patients with chronic liver disease, and 20 controls.
Disclosures: Partial funding came from the Japan Society for the Promotion of Science and the Program for Basic and Clinical Research on Hepatitis from Japan Agency for Medical Research and Development. The researchers reported having no conflicts of interest.
Source: J Ao et al. J Cancer. 2021 Mar 5. doi: 10.7150/jca.56436
Key clinical point: High serum levels of angiopoietin 2 (Ang2) levels identified patients with hepatocellular carcinoma (HCC) and predicted a shorter time to recurrence after treatment with curative intent.
Major finding: Serum Ang2 levels were significantly higher in patients with HCC vs controls (P less than .001) and patients with chronic liver disease (P less than .001). At the optimal threshold (3.5 ng/mL), sensitivity, specificity, and accuracy were 51%, 84%, and 59.5%, respectively. Higher serum Ang2 levels correlated with significantly shorter recurrence-free survival after ablation therapy, even after controlling for other prognostic factors.
Study details: The researchers reviewed medical charts and used sandwich enzyme-linked immunosorbent assay (ELISA) to measure Ang2 levels in stored serum from 275 patients with HCC, 98 patients with chronic liver disease, and 20 controls.
Disclosures: Partial funding came from the Japan Society for the Promotion of Science and the Program for Basic and Clinical Research on Hepatitis from Japan Agency for Medical Research and Development. The researchers reported having no conflicts of interest.
Source: J Ao et al. J Cancer. 2021 Mar 5. doi: 10.7150/jca.56436
Young adults with epilepsy face higher mental illness risks
Young adults with epilepsy experience higher rates of anxiety, depression, and suicidality, compared with their counterparts in the general population, a new study shows.
The findings, based on a study of 144 young adults with epilepsy (YAWE), was published recently in Epilepsy & Behavior.
“People with epilepsy (PWE) are at a significantly higher risk of experiencing mental health difficulties, compared with healthy controls and individuals with other [long-term conditions] such as asthma and diabetes,” according to Rachel Batchelor, MSc, and Michelle D. Taylor, PhD, of the University of London (England) in Surrey.
Young adulthood, which encompasses people aged 18-25 years, has been identified as “a peak age of onset for anxiety and depression,” but mental health in young adults with epilepsy in particular has not been well studied, they wrote.
The survey measured current mental health symptoms, including anxiety, depression, and suicidality, as well as sociodemographic and epilepsy-related factors, coping strategies, and social support (Epilepsy Behav. 2021 May;118:107911. doi: 10.1016/j.yebeh.2021.107911).
The average age of the respondents was 21.6 years, 61% were female, and 88% were of White British ethnicity. A total of 88 participants were single, 48 were in a relationship, and 8 were married or engaged. About one-third (38%) worked full-time, and 28.5% were full-time university students, 18.8% worked part-time, and 8.3% were unemployed and not students. The average age of seizure onset was 12.4 years.
Overall, 116 (80.6%) of the survey respondents met the criteria for anxiety, 110 (76.4%) for depression, and 51 (35.4%) for suicidality.
Ratings of all three of these conditions were significantly higher in females, compared with males, the researchers noted. Anxiety, depression, and suicidality also were rated higher for individuals who waited more than 1 year vs. less than 1 year for an epilepsy diagnosis from the time of seizure onset, for those suffering from anti-seizure medication side effects vs. no side effects, and for those with comorbid conditions vs. no comorbid conditions.
Avoidant-focused coping strategies were positively correlated with anxiety, depression, and suicidality, while problem-focused coping and meaning-focused coping were negatively correlated, the researchers said. In addition, those who reported greater levels of support from friends had lower rates of anxiety and depression, and those who reported greater levels of support from family had lower rates of suicidality.
The study findings were limited by several factors, including the relatively homogenous population, and the absence of data on current anxiety and depression medications and additional professional support, the researchers noted.
However, the results extend the research on mental health in people with epilepsy, and the study is the first known to focus on the young adult population with epilepsy, they said.
“The high rates of anxiety, depression, and suicidality underscore the need for better integration of mental health provision into epilepsy care,” the researchers wrote. “While it would be premature to base recommendations for treating anxiety, depression, and suicidality in YAWE on the current study, investigating the efficacy of psychological interventions (for example, [acceptance and commitment therapy], [compassion-focused therapy], peer support, and family-based [therapy]) designed to address the psychosocial variables shown to independently predict mental health outcomes in YAWE would be worthy future research avenues,” they concluded.
The study received no outside funding, and the researchers disclosed no financial conflicts.
Young adults with epilepsy experience higher rates of anxiety, depression, and suicidality, compared with their counterparts in the general population, a new study shows.
The findings, based on a study of 144 young adults with epilepsy (YAWE), was published recently in Epilepsy & Behavior.
“People with epilepsy (PWE) are at a significantly higher risk of experiencing mental health difficulties, compared with healthy controls and individuals with other [long-term conditions] such as asthma and diabetes,” according to Rachel Batchelor, MSc, and Michelle D. Taylor, PhD, of the University of London (England) in Surrey.
Young adulthood, which encompasses people aged 18-25 years, has been identified as “a peak age of onset for anxiety and depression,” but mental health in young adults with epilepsy in particular has not been well studied, they wrote.
The survey measured current mental health symptoms, including anxiety, depression, and suicidality, as well as sociodemographic and epilepsy-related factors, coping strategies, and social support (Epilepsy Behav. 2021 May;118:107911. doi: 10.1016/j.yebeh.2021.107911).
The average age of the respondents was 21.6 years, 61% were female, and 88% were of White British ethnicity. A total of 88 participants were single, 48 were in a relationship, and 8 were married or engaged. About one-third (38%) worked full-time, and 28.5% were full-time university students, 18.8% worked part-time, and 8.3% were unemployed and not students. The average age of seizure onset was 12.4 years.
Overall, 116 (80.6%) of the survey respondents met the criteria for anxiety, 110 (76.4%) for depression, and 51 (35.4%) for suicidality.
Ratings of all three of these conditions were significantly higher in females, compared with males, the researchers noted. Anxiety, depression, and suicidality also were rated higher for individuals who waited more than 1 year vs. less than 1 year for an epilepsy diagnosis from the time of seizure onset, for those suffering from anti-seizure medication side effects vs. no side effects, and for those with comorbid conditions vs. no comorbid conditions.
Avoidant-focused coping strategies were positively correlated with anxiety, depression, and suicidality, while problem-focused coping and meaning-focused coping were negatively correlated, the researchers said. In addition, those who reported greater levels of support from friends had lower rates of anxiety and depression, and those who reported greater levels of support from family had lower rates of suicidality.
The study findings were limited by several factors, including the relatively homogenous population, and the absence of data on current anxiety and depression medications and additional professional support, the researchers noted.
However, the results extend the research on mental health in people with epilepsy, and the study is the first known to focus on the young adult population with epilepsy, they said.
“The high rates of anxiety, depression, and suicidality underscore the need for better integration of mental health provision into epilepsy care,” the researchers wrote. “While it would be premature to base recommendations for treating anxiety, depression, and suicidality in YAWE on the current study, investigating the efficacy of psychological interventions (for example, [acceptance and commitment therapy], [compassion-focused therapy], peer support, and family-based [therapy]) designed to address the psychosocial variables shown to independently predict mental health outcomes in YAWE would be worthy future research avenues,” they concluded.
The study received no outside funding, and the researchers disclosed no financial conflicts.
Young adults with epilepsy experience higher rates of anxiety, depression, and suicidality, compared with their counterparts in the general population, a new study shows.
The findings, based on a study of 144 young adults with epilepsy (YAWE), was published recently in Epilepsy & Behavior.
“People with epilepsy (PWE) are at a significantly higher risk of experiencing mental health difficulties, compared with healthy controls and individuals with other [long-term conditions] such as asthma and diabetes,” according to Rachel Batchelor, MSc, and Michelle D. Taylor, PhD, of the University of London (England) in Surrey.
Young adulthood, which encompasses people aged 18-25 years, has been identified as “a peak age of onset for anxiety and depression,” but mental health in young adults with epilepsy in particular has not been well studied, they wrote.
The survey measured current mental health symptoms, including anxiety, depression, and suicidality, as well as sociodemographic and epilepsy-related factors, coping strategies, and social support (Epilepsy Behav. 2021 May;118:107911. doi: 10.1016/j.yebeh.2021.107911).
The average age of the respondents was 21.6 years, 61% were female, and 88% were of White British ethnicity. A total of 88 participants were single, 48 were in a relationship, and 8 were married or engaged. About one-third (38%) worked full-time, and 28.5% were full-time university students, 18.8% worked part-time, and 8.3% were unemployed and not students. The average age of seizure onset was 12.4 years.
Overall, 116 (80.6%) of the survey respondents met the criteria for anxiety, 110 (76.4%) for depression, and 51 (35.4%) for suicidality.
Ratings of all three of these conditions were significantly higher in females, compared with males, the researchers noted. Anxiety, depression, and suicidality also were rated higher for individuals who waited more than 1 year vs. less than 1 year for an epilepsy diagnosis from the time of seizure onset, for those suffering from anti-seizure medication side effects vs. no side effects, and for those with comorbid conditions vs. no comorbid conditions.
Avoidant-focused coping strategies were positively correlated with anxiety, depression, and suicidality, while problem-focused coping and meaning-focused coping were negatively correlated, the researchers said. In addition, those who reported greater levels of support from friends had lower rates of anxiety and depression, and those who reported greater levels of support from family had lower rates of suicidality.
The study findings were limited by several factors, including the relatively homogenous population, and the absence of data on current anxiety and depression medications and additional professional support, the researchers noted.
However, the results extend the research on mental health in people with epilepsy, and the study is the first known to focus on the young adult population with epilepsy, they said.
“The high rates of anxiety, depression, and suicidality underscore the need for better integration of mental health provision into epilepsy care,” the researchers wrote. “While it would be premature to base recommendations for treating anxiety, depression, and suicidality in YAWE on the current study, investigating the efficacy of psychological interventions (for example, [acceptance and commitment therapy], [compassion-focused therapy], peer support, and family-based [therapy]) designed to address the psychosocial variables shown to independently predict mental health outcomes in YAWE would be worthy future research avenues,” they concluded.
The study received no outside funding, and the researchers disclosed no financial conflicts.
FROM EPILEPSY & BEHAVIOR
High PIGC expression predicts poor liver cancer survival
Key clinical point: Among patients with hepatocellular carcinoma, overexpression of phosphatidylinositol glycan anchor biosynthesis, class C (PIGC) was linked to more aggressive disease and worse survival.
Major finding: PIGC mRNA was overexpressed in cancerous vs normal liver (P less than .0001). Among patients with liver cancer, higher PIGC expression correlated with worse overall survival (37.8 vs 71.0 months; hazard ratio [HR], 1.7, P = .003) and disease-free survival (48.4 vs 68.6 months; HR, 1.5, P = .007), and with higher tumor grade and stage, lymphatic metastasis, and TP53 mutation. In addition, liver cancer cell migration and proliferation were significantly higher in PIGC-upregulated cells, and significantly lower in PIGC-silenced cells. The PIGC mutation rate was 10%; PIGC mutation was significantly associated with higher T and M stages.
Study details: The researchers searched and analyzed bioinformatic databases and websites, such as UALCAN and cBioPortal , and performed Western blot, transwell migration assays, CCK-8 assays, and flow cytometry of cancerous and normal liver cells.
Disclosures: The Fundamental Research Funds of Wuhan University provided funding. The investigators reported having no conflicts of interest.
Source: Guo X et al. J Hepatocell Carcinoma. 2021 Apr 6. doi: 10.2147/JHC.S297601.
Key clinical point: Among patients with hepatocellular carcinoma, overexpression of phosphatidylinositol glycan anchor biosynthesis, class C (PIGC) was linked to more aggressive disease and worse survival.
Major finding: PIGC mRNA was overexpressed in cancerous vs normal liver (P less than .0001). Among patients with liver cancer, higher PIGC expression correlated with worse overall survival (37.8 vs 71.0 months; hazard ratio [HR], 1.7, P = .003) and disease-free survival (48.4 vs 68.6 months; HR, 1.5, P = .007), and with higher tumor grade and stage, lymphatic metastasis, and TP53 mutation. In addition, liver cancer cell migration and proliferation were significantly higher in PIGC-upregulated cells, and significantly lower in PIGC-silenced cells. The PIGC mutation rate was 10%; PIGC mutation was significantly associated with higher T and M stages.
Study details: The researchers searched and analyzed bioinformatic databases and websites, such as UALCAN and cBioPortal , and performed Western blot, transwell migration assays, CCK-8 assays, and flow cytometry of cancerous and normal liver cells.
Disclosures: The Fundamental Research Funds of Wuhan University provided funding. The investigators reported having no conflicts of interest.
Source: Guo X et al. J Hepatocell Carcinoma. 2021 Apr 6. doi: 10.2147/JHC.S297601.
Key clinical point: Among patients with hepatocellular carcinoma, overexpression of phosphatidylinositol glycan anchor biosynthesis, class C (PIGC) was linked to more aggressive disease and worse survival.
Major finding: PIGC mRNA was overexpressed in cancerous vs normal liver (P less than .0001). Among patients with liver cancer, higher PIGC expression correlated with worse overall survival (37.8 vs 71.0 months; hazard ratio [HR], 1.7, P = .003) and disease-free survival (48.4 vs 68.6 months; HR, 1.5, P = .007), and with higher tumor grade and stage, lymphatic metastasis, and TP53 mutation. In addition, liver cancer cell migration and proliferation were significantly higher in PIGC-upregulated cells, and significantly lower in PIGC-silenced cells. The PIGC mutation rate was 10%; PIGC mutation was significantly associated with higher T and M stages.
Study details: The researchers searched and analyzed bioinformatic databases and websites, such as UALCAN and cBioPortal , and performed Western blot, transwell migration assays, CCK-8 assays, and flow cytometry of cancerous and normal liver cells.
Disclosures: The Fundamental Research Funds of Wuhan University provided funding. The investigators reported having no conflicts of interest.
Source: Guo X et al. J Hepatocell Carcinoma. 2021 Apr 6. doi: 10.2147/JHC.S297601.
Immunotherapy takes first major step into earlier NSCLC
Immunotherapy has already had a huge impact on treatment of patients with later stages of non–small cell lung cancer (NSCLC): new clinical data are now showing benefits in patients with earlier stage disease.
Patients with stage IB-IIIA NSCLC showed a markedly improved disease-free survival (DFS) when atezolizumab (Tecentriq) was added onto adjuvant chemotherapy following resection, according to results from an interim analysis of the IMpower010 study.
Notably, the benefit with atezolizumab versus best supportive care was greatest in patients with expression of programmed death–ligand 1 (PD-L1) on their tumor, in whom the DFS improvement was a significant 34%.
This is the “first global phase 3 trial using an immune checkpoint inhibitor to show a disease-free survival outcome in early-stage NSCLC,” said lead researcher Heather Wakelee, MD, professor of medicine and chief of the division of oncology at Stanford (Calif.) University Medical Center.
She was speaking at a press briefing ahead of the American Society of Clinical Oncology annual meeting, where the results will be presented on June 6.
Dr. Wakelee added that the “planned analysis for disease-free survival and overall survival in the intention-to-treat populations will continue with longer-term follow-up.”
Asked whether the drug could be recommended for these patients based on the current results, Dr. Wakelee said that “obviously we need approval” for this use from the Food and Drug Administration, but she added that “the FDA has approved other agents, particularly most recently osimertinib [Tagrisso], based on a disease-free survival endpoint.”
These new results show that the benefit with atezolizumab plus chemotherapy is “more profound” than with chemotherapy plus best supportive care, “and therefore, to me, it would be something I would want to offer my patients in that setting.”
Dr. Wakelee also emphasized the importance of screening for lung cancer, so that the disease is detected at earlier stages “when it is potentially curable.”
She also stressed the importance of biomarker testing for patients with resected disease “to look for EGFR mutations, which can be treated with EGFR [tyrosine kinase inhibitors] and also, at some point, to check for PD-L1 ... because, in this trial, the vast majority of benefit” appeared to be in those with PD-L1 expression on their tumors.
Julie R. Gralow, MD, ASCO chief medical officer and executive vice president, said that “immune checkpoint inhibitors have certainly changed the treatment landscape for many types of cancers” and the current study “is the first time we’ve seen an immunotherapy that’s effective in treating early-stage NSCLC.”
“This is an important advance in understanding the role of immunotherapy in earlier stage lung cancer” and “potentially a step forward for many patients.”
Study details
The standard of care for many stage IB-IIIA NSCLC patients “has not changed for many years,” despite “significant progress” having been made in the treatment of more advanced disease, Dr. Wakelee commented.
Consequently, the majority of patients with resected NSCLC continue to receive adjuvant platinum-based chemotherapy, which has been shown to reduce the risk of disease recurrence by 16% in those with completely resected disease.
The new study set out to examine the benefit of adding atezolizumab to adjuvant chemotherapy in the global phase 3 IMpower010 study.
Patients had to have stage IB-IIIA NSCLC, with stage IB tumors at least 4 cm in size, and tumor tissue available for PD-L1 analysis. Following complete resection, 1,280 patients were given up to four cycles of adjuvant platinum-based chemotherapy.
Of those, 1,005 patients were then randomly assigned 1:1 to receive either 16 cycles of atezolizumab 1,200 mg IV every 3 weeks or best supportive care.
The interim results show that, after a median follow-up of 32.8 months, the addition of atezolizumab significantly reduced the risk of recurrence or death versus best supportive care in patients whose tumors had PD-L1 expression of at least 1%, at a hazard ratio of 0.66 (P = .004).
At 24 months, the DFS rate was 74.6% among patients given atezolizumab versus 61% in those receiving best supportive care, reducing to 60% and 48.2%, respectively, at 36 months.
When looking across all randomized patients, the addition of atezolizumab was associated with a smaller reduction in the risk of recurrence of death versus best supportive care, at a hazard ratio of 0.79 after a median follow-up of 32.2 months (P = .02).
On the intention to treat analysis, the reduction in the risk of recurrence or death with atezolizumab was of borderline significance, at a hazard ratio of 0.81 after a median follow-up of 32.2 months (P = .04).
Dr. Wakelee pointed out that patients with stage IB disease, who represented around 12% of those in the trial, “tend to do better and we require longer time to see some of the disease recurrence outcomes,” and so these results are “preliminary.”
She also emphasized that the overall survival data are not yet mature and survival was not formally tested in the current analysis.
In terms of safety, the adverse event profile with atezolizumab was consistent with previous reports, the investigators noted in the abstract. However, Dr. Wakelee said at the briefing that “we had to stop treatment with atezolizumab in 18% of patients because of toxicity.”
All-grade adverse events were reported in 70.7% of the best supportive care group versus 92.7% among those given atezolizumab, while grade 3-4 adverse events were reported in 11.5% and 21.8% of patients, respectively.
The study was funded by Hoffmann–La Roche. Dr. Wakelee reported relationships with AstraZeneca, Blueprint Medicines, Daiichi Sankyo, Helsinn Therapeutics, Janssen Oncology, Mirati Therapeutics, Xcovery, ACEA Biosciences, Arrys Therapeutics, AstraZeneca/MedImmune, Bristol-Myers Squibb, Celgene, Clovis Oncology, Exelixis, Genentech/Roche, Gilead Sciences, Merck, Novartis, Pharmacyclics, Seattle Genetics, and Xcovery. She also reports uncompensated relationships with Genentech/Roche, Merck, and Takeda. Dr. Gralow reported relationships with AstraZeneca, Genentech, Sandoz, and Immunomedics.
A version of this article first appeared on Medscape.com.
Immunotherapy has already had a huge impact on treatment of patients with later stages of non–small cell lung cancer (NSCLC): new clinical data are now showing benefits in patients with earlier stage disease.
Patients with stage IB-IIIA NSCLC showed a markedly improved disease-free survival (DFS) when atezolizumab (Tecentriq) was added onto adjuvant chemotherapy following resection, according to results from an interim analysis of the IMpower010 study.
Notably, the benefit with atezolizumab versus best supportive care was greatest in patients with expression of programmed death–ligand 1 (PD-L1) on their tumor, in whom the DFS improvement was a significant 34%.
This is the “first global phase 3 trial using an immune checkpoint inhibitor to show a disease-free survival outcome in early-stage NSCLC,” said lead researcher Heather Wakelee, MD, professor of medicine and chief of the division of oncology at Stanford (Calif.) University Medical Center.
She was speaking at a press briefing ahead of the American Society of Clinical Oncology annual meeting, where the results will be presented on June 6.
Dr. Wakelee added that the “planned analysis for disease-free survival and overall survival in the intention-to-treat populations will continue with longer-term follow-up.”
Asked whether the drug could be recommended for these patients based on the current results, Dr. Wakelee said that “obviously we need approval” for this use from the Food and Drug Administration, but she added that “the FDA has approved other agents, particularly most recently osimertinib [Tagrisso], based on a disease-free survival endpoint.”
These new results show that the benefit with atezolizumab plus chemotherapy is “more profound” than with chemotherapy plus best supportive care, “and therefore, to me, it would be something I would want to offer my patients in that setting.”
Dr. Wakelee also emphasized the importance of screening for lung cancer, so that the disease is detected at earlier stages “when it is potentially curable.”
She also stressed the importance of biomarker testing for patients with resected disease “to look for EGFR mutations, which can be treated with EGFR [tyrosine kinase inhibitors] and also, at some point, to check for PD-L1 ... because, in this trial, the vast majority of benefit” appeared to be in those with PD-L1 expression on their tumors.
Julie R. Gralow, MD, ASCO chief medical officer and executive vice president, said that “immune checkpoint inhibitors have certainly changed the treatment landscape for many types of cancers” and the current study “is the first time we’ve seen an immunotherapy that’s effective in treating early-stage NSCLC.”
“This is an important advance in understanding the role of immunotherapy in earlier stage lung cancer” and “potentially a step forward for many patients.”
Study details
The standard of care for many stage IB-IIIA NSCLC patients “has not changed for many years,” despite “significant progress” having been made in the treatment of more advanced disease, Dr. Wakelee commented.
Consequently, the majority of patients with resected NSCLC continue to receive adjuvant platinum-based chemotherapy, which has been shown to reduce the risk of disease recurrence by 16% in those with completely resected disease.
The new study set out to examine the benefit of adding atezolizumab to adjuvant chemotherapy in the global phase 3 IMpower010 study.
Patients had to have stage IB-IIIA NSCLC, with stage IB tumors at least 4 cm in size, and tumor tissue available for PD-L1 analysis. Following complete resection, 1,280 patients were given up to four cycles of adjuvant platinum-based chemotherapy.
Of those, 1,005 patients were then randomly assigned 1:1 to receive either 16 cycles of atezolizumab 1,200 mg IV every 3 weeks or best supportive care.
The interim results show that, after a median follow-up of 32.8 months, the addition of atezolizumab significantly reduced the risk of recurrence or death versus best supportive care in patients whose tumors had PD-L1 expression of at least 1%, at a hazard ratio of 0.66 (P = .004).
At 24 months, the DFS rate was 74.6% among patients given atezolizumab versus 61% in those receiving best supportive care, reducing to 60% and 48.2%, respectively, at 36 months.
When looking across all randomized patients, the addition of atezolizumab was associated with a smaller reduction in the risk of recurrence of death versus best supportive care, at a hazard ratio of 0.79 after a median follow-up of 32.2 months (P = .02).
On the intention to treat analysis, the reduction in the risk of recurrence or death with atezolizumab was of borderline significance, at a hazard ratio of 0.81 after a median follow-up of 32.2 months (P = .04).
Dr. Wakelee pointed out that patients with stage IB disease, who represented around 12% of those in the trial, “tend to do better and we require longer time to see some of the disease recurrence outcomes,” and so these results are “preliminary.”
She also emphasized that the overall survival data are not yet mature and survival was not formally tested in the current analysis.
In terms of safety, the adverse event profile with atezolizumab was consistent with previous reports, the investigators noted in the abstract. However, Dr. Wakelee said at the briefing that “we had to stop treatment with atezolizumab in 18% of patients because of toxicity.”
All-grade adverse events were reported in 70.7% of the best supportive care group versus 92.7% among those given atezolizumab, while grade 3-4 adverse events were reported in 11.5% and 21.8% of patients, respectively.
The study was funded by Hoffmann–La Roche. Dr. Wakelee reported relationships with AstraZeneca, Blueprint Medicines, Daiichi Sankyo, Helsinn Therapeutics, Janssen Oncology, Mirati Therapeutics, Xcovery, ACEA Biosciences, Arrys Therapeutics, AstraZeneca/MedImmune, Bristol-Myers Squibb, Celgene, Clovis Oncology, Exelixis, Genentech/Roche, Gilead Sciences, Merck, Novartis, Pharmacyclics, Seattle Genetics, and Xcovery. She also reports uncompensated relationships with Genentech/Roche, Merck, and Takeda. Dr. Gralow reported relationships with AstraZeneca, Genentech, Sandoz, and Immunomedics.
A version of this article first appeared on Medscape.com.
Immunotherapy has already had a huge impact on treatment of patients with later stages of non–small cell lung cancer (NSCLC): new clinical data are now showing benefits in patients with earlier stage disease.
Patients with stage IB-IIIA NSCLC showed a markedly improved disease-free survival (DFS) when atezolizumab (Tecentriq) was added onto adjuvant chemotherapy following resection, according to results from an interim analysis of the IMpower010 study.
Notably, the benefit with atezolizumab versus best supportive care was greatest in patients with expression of programmed death–ligand 1 (PD-L1) on their tumor, in whom the DFS improvement was a significant 34%.
This is the “first global phase 3 trial using an immune checkpoint inhibitor to show a disease-free survival outcome in early-stage NSCLC,” said lead researcher Heather Wakelee, MD, professor of medicine and chief of the division of oncology at Stanford (Calif.) University Medical Center.
She was speaking at a press briefing ahead of the American Society of Clinical Oncology annual meeting, where the results will be presented on June 6.
Dr. Wakelee added that the “planned analysis for disease-free survival and overall survival in the intention-to-treat populations will continue with longer-term follow-up.”
Asked whether the drug could be recommended for these patients based on the current results, Dr. Wakelee said that “obviously we need approval” for this use from the Food and Drug Administration, but she added that “the FDA has approved other agents, particularly most recently osimertinib [Tagrisso], based on a disease-free survival endpoint.”
These new results show that the benefit with atezolizumab plus chemotherapy is “more profound” than with chemotherapy plus best supportive care, “and therefore, to me, it would be something I would want to offer my patients in that setting.”
Dr. Wakelee also emphasized the importance of screening for lung cancer, so that the disease is detected at earlier stages “when it is potentially curable.”
She also stressed the importance of biomarker testing for patients with resected disease “to look for EGFR mutations, which can be treated with EGFR [tyrosine kinase inhibitors] and also, at some point, to check for PD-L1 ... because, in this trial, the vast majority of benefit” appeared to be in those with PD-L1 expression on their tumors.
Julie R. Gralow, MD, ASCO chief medical officer and executive vice president, said that “immune checkpoint inhibitors have certainly changed the treatment landscape for many types of cancers” and the current study “is the first time we’ve seen an immunotherapy that’s effective in treating early-stage NSCLC.”
“This is an important advance in understanding the role of immunotherapy in earlier stage lung cancer” and “potentially a step forward for many patients.”
Study details
The standard of care for many stage IB-IIIA NSCLC patients “has not changed for many years,” despite “significant progress” having been made in the treatment of more advanced disease, Dr. Wakelee commented.
Consequently, the majority of patients with resected NSCLC continue to receive adjuvant platinum-based chemotherapy, which has been shown to reduce the risk of disease recurrence by 16% in those with completely resected disease.
The new study set out to examine the benefit of adding atezolizumab to adjuvant chemotherapy in the global phase 3 IMpower010 study.
Patients had to have stage IB-IIIA NSCLC, with stage IB tumors at least 4 cm in size, and tumor tissue available for PD-L1 analysis. Following complete resection, 1,280 patients were given up to four cycles of adjuvant platinum-based chemotherapy.
Of those, 1,005 patients were then randomly assigned 1:1 to receive either 16 cycles of atezolizumab 1,200 mg IV every 3 weeks or best supportive care.
The interim results show that, after a median follow-up of 32.8 months, the addition of atezolizumab significantly reduced the risk of recurrence or death versus best supportive care in patients whose tumors had PD-L1 expression of at least 1%, at a hazard ratio of 0.66 (P = .004).
At 24 months, the DFS rate was 74.6% among patients given atezolizumab versus 61% in those receiving best supportive care, reducing to 60% and 48.2%, respectively, at 36 months.
When looking across all randomized patients, the addition of atezolizumab was associated with a smaller reduction in the risk of recurrence of death versus best supportive care, at a hazard ratio of 0.79 after a median follow-up of 32.2 months (P = .02).
On the intention to treat analysis, the reduction in the risk of recurrence or death with atezolizumab was of borderline significance, at a hazard ratio of 0.81 after a median follow-up of 32.2 months (P = .04).
Dr. Wakelee pointed out that patients with stage IB disease, who represented around 12% of those in the trial, “tend to do better and we require longer time to see some of the disease recurrence outcomes,” and so these results are “preliminary.”
She also emphasized that the overall survival data are not yet mature and survival was not formally tested in the current analysis.
In terms of safety, the adverse event profile with atezolizumab was consistent with previous reports, the investigators noted in the abstract. However, Dr. Wakelee said at the briefing that “we had to stop treatment with atezolizumab in 18% of patients because of toxicity.”
All-grade adverse events were reported in 70.7% of the best supportive care group versus 92.7% among those given atezolizumab, while grade 3-4 adverse events were reported in 11.5% and 21.8% of patients, respectively.
The study was funded by Hoffmann–La Roche. Dr. Wakelee reported relationships with AstraZeneca, Blueprint Medicines, Daiichi Sankyo, Helsinn Therapeutics, Janssen Oncology, Mirati Therapeutics, Xcovery, ACEA Biosciences, Arrys Therapeutics, AstraZeneca/MedImmune, Bristol-Myers Squibb, Celgene, Clovis Oncology, Exelixis, Genentech/Roche, Gilead Sciences, Merck, Novartis, Pharmacyclics, Seattle Genetics, and Xcovery. She also reports uncompensated relationships with Genentech/Roche, Merck, and Takeda. Dr. Gralow reported relationships with AstraZeneca, Genentech, Sandoz, and Immunomedics.
A version of this article first appeared on Medscape.com.
Medication overuse headache: Preventive treatment with or without detoxification?

The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
The goal of treating medication overuse headache is obvious: ceasing overuse of the medication in question in an effort to return to a headache pattern that is episodic and better managed. Although guidelines suggest withdrawal of the overused medication and initiating preventive treatment, there is debate about this approach versus withdrawal alone or preventive treatment without ceasing the overused medication. A recently published randomized trial from Carlsen and colleagues evaluated 3 treatment methods: 1) withdrawal plus preventive treatment; 2) preventive treatment only; and 3) withdrawal followed by optional preventive treatment 2 months after withdrawal. Investigators found all 3 approaches effective, but participants who underwent withdrawal plus preventive care saw their headache days reduced by 12.3 days, versus 9.9 days in the preventive-only group and 8.5 days in the withdrawal/optional preventive follow-up treatment contingent. No statistically significant differences were seen between the groups in terms of migraine days, days with short-term medication use, and headache pain intensity.
Particularly noteworthy was the finding that individuals treated with withdrawal plus preventive treatment were significantly more likely to achieve remission. Specifically, nearly 75% returned to experiencing episodic headache, compared with 60% in the preventive group and 42% in the withdrawal contingent. Nearly all (97%) of those on the withdrawal plus preventive regimen were cured of medication overuse headache, versus 90% (withdrawal) and 74% (preventive).
The bottom line: Individuals undergoing withdrawal plus preventive treatment were 30% more likely to be cured of medication overuse headache. Thus, it appears that detoxification is key.
Or is it?
On the one hand…
In studies, withdrawal from the offending medication is linked with substantial improvement in headache days. Additionally, individuals who previously responded poorly to preventive treatment fared better with such treatment after detoxification.
When treating medication overuse headache using the detoxification and preventive care approach, Sun-Edelstein and colleagues outline these important steps:
- Educate your patients and their family/caregivers about the detoxification process
- Wean patient off the offending medication with a goal of complete detoxification
- Initiate preventive medical therapy or behavioral/non-drug strategies
- Establish clear limits on acute medication intake
- Arrange for regular follow-up to minimize or prevent relapse
While on the other hand…
Even though guidelines recommend detoxification, there is data supporting the concept of initiating preventive treatment without detoxification. A randomized, double-blind, placebo-controlled trial by Mei and colleagues found that 100 mg per day of topiramate led to a significant reduction in headache days and average amount of acute medication intake, versus placebo. However, treatment completion rates were low, leading Sun-Edelstein and colleagues to surmise that topiramate without detoxification would probably not have had a high success rate in practice.
Meanwhile, onabotulinumtoxin A was found in the PREEMPT trials conducted by Dodick and colleagues to reduce the number of headache days, migraine days, and moderate/severe headache days, compared with placebo, at week 24. Disappointingly, researchers found that acute medication frequency was not reduced in the overall treatment group, but they did note a significant reduction in the subgroup that was taking triptans. Moreover, a follow-up analysis by Aurora and colleagues involving 32 weeks of open-label treatment with onabotulinumtoxin A following the 24-week randomized study revealed significant reductions in acute headache days at 56 weeks.
Using anti-CGRPs without acute medication withdrawal
More recently, strong evidence is emerging about the value of using anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies without acute medication withdrawal. The findings involve 4 anti-CGRP medications.
Erenumab: A subgroup analysis of a randomized, double-blind, placebo-controlled parallel-group trial by Tepper and colleagues showed that erenumab reduced frequency of migraine at 3 months in participants with chronic migraine and medication overuse. Patients receiving either 70 or 140 mg of erenumab saw their migraine frequency reduced by an average of 6.6 days, versus 3.5 days in the placebo group.
Additionally, a significantly greater number of patients in the treatment groups stopped overusing medication, and did so early, which led to improved patient-reported outcomes. Acute migraine-specific medication treatment days were reduced by an average of 5.4 days in the 70 mg group, 4.9 days in the 140 mg contingent, and 2.9 days in those who received placebo.
Overall, consistent improvement in measures of impact, disability and health-related quality of life were seen in individuals’ treatment with erenumab.
Galcanezumab: A post-hoc analysis of pooled data from the phase 3 EVOLVE-1 and EVOLVE-2 studies, as well as the phase 3 REGAIN trial found that in participants with medication overuse, 120 mg and 240 mg doses of galcanezumab cut the number of average migraine days and decreased medication overuse. Average migraine days were lowered in EVOLVE participants by 6.26 days in the 120 mg group, 5.77 days in the 240 mg contingent, and 2.71 in those who received placebo. In REGAIN, these numbers were 4.78, 4.51, and 2.25, respectively. Average monthly medication use rates in EVOLVE were 6.2%, 7.9%, and 15.9%, respectively; in REGAIN they were 24.3%, 23.1%, and 40.6%, respectively.
Notably, though the study demonstrated galcanezumab’s efficacy in those with and without medication overuse, improvement was more pronounced in patients with medication overuse.
Fremanezumab: In an analysis by Silberstein and colleagues, significantly more patients who received quarterly or monthly injections of fremanezumab reported no medication overuse during the 3-month study, versus placebo. Specifically, 61% of participants who received monthly injections of fremanezumab and 55% of those who took quarterly injections reported no medication overuse. Among those receiving placebo, only 46% reverted to no overuse. The effect was seen as early as week 4. Additionally, among patients with medication overuse at baseline, the number of days with acute medication use was significantly lower in the treatment groups versus placebo—1.8 days lower in the quarterly group and 2.8 days in the monthly contingent.
A subsequent post-hoc analysis presented at the 2019 American Headache Society (AHS) Annual Scientific Meeting showed that the benefits were sustained over time and the medication was effective in difficult cases. Continued treatment with either quarterly or monthly dosing resulted in a reduced number of headache days, acute medication overuse headache, and headache-related disability, compared with baseline measures. Notably, about 6 in every 10 individuals with medication overuse at baseline who received fremanezumab reverted to no acute medication overuse at 6 months. This effect was maintained through 1 year of treatment.
Eptinezumab: In PROMISE-2, a post-hoc analysis of the phase 3 trials evaluating quarterly IV infusions of eptinezumab 100 mg and 300 mg, Lipton and colleagues reported that participants with chronic migraine and medication overuse experienced greater reductions in monthly migraine days during weeks 1 through 12, versus placebo (100 mg, 7.7 days; 300 mg, 8.2 days; placebo, 5.6 days). Benefits, seen as early as the day after dosing, were generally maintained or improved over 24 weeks.
Acute care medication use was reduced by about 50% in the treatment group versus roughly 25% in the placebo contingent. Most encouraging was the finding that about one-third of individuals in the treatment cohort experienced 6 months without medication overuse and below the chronic migraine diagnostic threshold; only 10% of patients who received placebo resolved in this way. Consistent improvement across patient-reported outcomes was also observed in the treatment group versus placebo.
While the studies involving topiramate, onabotulinumtoxin A, and the anti-CGRP monoclonal antibodies suggest that preventive treatment alone may effectively treat acute medical overuse and medication overuse headache, it is the data behind the anti-CGRP treatments that seem to be most compelling and causing conventional thinking to be challenged. These medications appear to be able to convert individuals with chronic migraine and medication overuse, out of overuse and back to episodic migraine. Moreover, results show they may be able to reduce acute medication use in episodic migraine, which reduces the risk of the headache sufferer transforming to chronic migraine. It is worth considering this approach in patients’ overuse acute care medication, as well as those in whom discontinuation may otherwise prove difficult without concurrent preventive treatment.
The emerging role of gepants
Availability of the so-called “gepants”—small molecule CGRP receptor agonists—is shedding additional light on management of medication overuse headache and pointing to the future. Gepants—which include ubrogepant, rimegepant, and atogepant—have been shown in early data to have a preventive effect when used regularly. Thus, it is much less likely that their use will lead to excess use and medication overuse headache.
Preclinical data demonstrated that continued use of ubrogepant does not appear to produce early or latent trigeminal sensory sensitization. Meanwhile, rimegepant, when used every other day, and as needed for acute treatment of migraine in individuals suffering from moderate-to-high frequency episodic migraine, resulted in reductions in monthly migraine days. The preventive effects appear to be rapid and sustained. And in a phase 3 trial, atogepant demonstrated efficacy at doses of 10 mg, 30 mg, and 60 mg twice a day, compared with placebo over 12 weeks.
It is important to note that the link between the gepants and medication overuse and medication overuse headache have not yet been studied. Still, it is encouraging to see that migraine frequency improves and medication use days are reduced when gepants are taken preventively. Thus, gepants could emerge as a preferred approach for acute or preventive treatment in individuals who have or are at risk of developing medication overuse headache.
First issue vs. April 2021 issue: Much has changed since 1971
For the first readers of Family Practice News, it started with this: “How safe is the pill? An extensive epidemiologic study being carried out in the United Kingdom by the Royal College of General Practitioners is expected to provide definitive answers to this question within the next few years.”
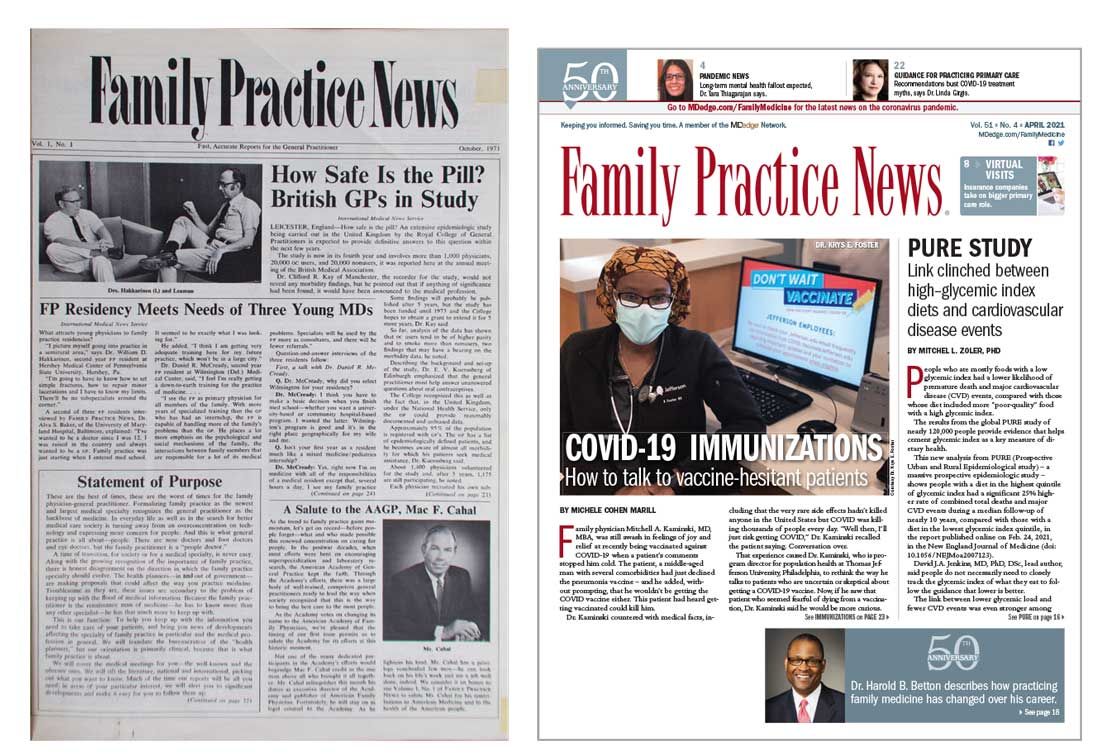
That was the first paragraph of the lead article on the front page of our very first issue, published in October 1971. The report on oral contraceptives, coming from the annual meeting of the British Medical Association in Leicester, largely focused on recruiting – noting that “all women in the study are married” – and data-gathering methods.
That first issue also covered such topics as the effect of “early and frequent coitus” on cervical dysplasia incidence (p. 4), breast cancer in men (p. 13), and treatment of prostate inflammation in patients with impotence (p. 34).
Our April 2021 issue included five articles related to the COVID-19 pandemic, starting on the front page and featuring a photo – a physician sitting at a computer, wearing a mask – and a topic – vaccine-hesitant patients.
Business of medicine today vs. in 1971
At the time of publication of our first issue the United States was in the midst of a 90-day freeze on wages and prices ordered by President Richard Nixon. Two articles in that first issue discussed the subject: “Freeze clouds future of health insurance plans” and “Freeze lets physicians ‘stabilize’ office fees.”
Besides COVID-19, here are some other topics covered in April 2021 but not in 1971: lessons learned from an electronic health records conversion, competition for physicians in the form of a “virtual primary care service” offered by United Healthcare, and the sleep effects of smartphone “addiction.”
Technology, clearly, plays a much larger role in physicians’ lives these days.
Similarities between issues
Not everything has changed, of course. We were informing physicians about heart disease in 1971 with “Primary MD can treat most vascular cases” and “Job satisfaction can help prevent heart disease.”
A look at the latest issue uncovered “Link clinched between high-glycemic index diets and cardiovascular disease events” and “Ultraprocessed ‘healthy’ foods raise cardiovascular disease events risk.” Diabetes is another topic that we have began covering since day one and continue to consider to be relevant to practicing family medicine. “Family attitude key to diabetic’s state” was published in our first issue and “Type 1 diabetes prevention moves toward reality as studies published” ran in our April 2021 issue.
The photos in that first issue, however, present a somewhat jarring counterpoint to our latest issue. The faces that look back from 50 years ago are men’s faces: 29 men, to be exact. There were no photos of women physicians in that issue.
That was not the case in April of 2021. Of the 26 physicians or research scientists who appeared in photos in that issue, 8 were women. Plus, three of those women appeared on the cover.
Among the photos from 1971 were 6 of the 14 founding members of our editorial advisory board, who were, again, all men. Our current board consists of 13 men and 8 women.
Times have changed.
This article was updated 5/27/21.
For the first readers of Family Practice News, it started with this: “How safe is the pill? An extensive epidemiologic study being carried out in the United Kingdom by the Royal College of General Practitioners is expected to provide definitive answers to this question within the next few years.”
That was the first paragraph of the lead article on the front page of our very first issue, published in October 1971. The report on oral contraceptives, coming from the annual meeting of the British Medical Association in Leicester, largely focused on recruiting – noting that “all women in the study are married” – and data-gathering methods.
That first issue also covered such topics as the effect of “early and frequent coitus” on cervical dysplasia incidence (p. 4), breast cancer in men (p. 13), and treatment of prostate inflammation in patients with impotence (p. 34).
Our April 2021 issue included five articles related to the COVID-19 pandemic, starting on the front page and featuring a photo – a physician sitting at a computer, wearing a mask – and a topic – vaccine-hesitant patients.
Business of medicine today vs. in 1971
At the time of publication of our first issue the United States was in the midst of a 90-day freeze on wages and prices ordered by President Richard Nixon. Two articles in that first issue discussed the subject: “Freeze clouds future of health insurance plans” and “Freeze lets physicians ‘stabilize’ office fees.”
Besides COVID-19, here are some other topics covered in April 2021 but not in 1971: lessons learned from an electronic health records conversion, competition for physicians in the form of a “virtual primary care service” offered by United Healthcare, and the sleep effects of smartphone “addiction.”
Technology, clearly, plays a much larger role in physicians’ lives these days.
Similarities between issues
Not everything has changed, of course. We were informing physicians about heart disease in 1971 with “Primary MD can treat most vascular cases” and “Job satisfaction can help prevent heart disease.”
A look at the latest issue uncovered “Link clinched between high-glycemic index diets and cardiovascular disease events” and “Ultraprocessed ‘healthy’ foods raise cardiovascular disease events risk.” Diabetes is another topic that we have began covering since day one and continue to consider to be relevant to practicing family medicine. “Family attitude key to diabetic’s state” was published in our first issue and “Type 1 diabetes prevention moves toward reality as studies published” ran in our April 2021 issue.
The photos in that first issue, however, present a somewhat jarring counterpoint to our latest issue. The faces that look back from 50 years ago are men’s faces: 29 men, to be exact. There were no photos of women physicians in that issue.
That was not the case in April of 2021. Of the 26 physicians or research scientists who appeared in photos in that issue, 8 were women. Plus, three of those women appeared on the cover.
Among the photos from 1971 were 6 of the 14 founding members of our editorial advisory board, who were, again, all men. Our current board consists of 13 men and 8 women.
Times have changed.
This article was updated 5/27/21.
For the first readers of Family Practice News, it started with this: “How safe is the pill? An extensive epidemiologic study being carried out in the United Kingdom by the Royal College of General Practitioners is expected to provide definitive answers to this question within the next few years.”
That was the first paragraph of the lead article on the front page of our very first issue, published in October 1971. The report on oral contraceptives, coming from the annual meeting of the British Medical Association in Leicester, largely focused on recruiting – noting that “all women in the study are married” – and data-gathering methods.
That first issue also covered such topics as the effect of “early and frequent coitus” on cervical dysplasia incidence (p. 4), breast cancer in men (p. 13), and treatment of prostate inflammation in patients with impotence (p. 34).
Our April 2021 issue included five articles related to the COVID-19 pandemic, starting on the front page and featuring a photo – a physician sitting at a computer, wearing a mask – and a topic – vaccine-hesitant patients.
Business of medicine today vs. in 1971
At the time of publication of our first issue the United States was in the midst of a 90-day freeze on wages and prices ordered by President Richard Nixon. Two articles in that first issue discussed the subject: “Freeze clouds future of health insurance plans” and “Freeze lets physicians ‘stabilize’ office fees.”
Besides COVID-19, here are some other topics covered in April 2021 but not in 1971: lessons learned from an electronic health records conversion, competition for physicians in the form of a “virtual primary care service” offered by United Healthcare, and the sleep effects of smartphone “addiction.”
Technology, clearly, plays a much larger role in physicians’ lives these days.
Similarities between issues
Not everything has changed, of course. We were informing physicians about heart disease in 1971 with “Primary MD can treat most vascular cases” and “Job satisfaction can help prevent heart disease.”
A look at the latest issue uncovered “Link clinched between high-glycemic index diets and cardiovascular disease events” and “Ultraprocessed ‘healthy’ foods raise cardiovascular disease events risk.” Diabetes is another topic that we have began covering since day one and continue to consider to be relevant to practicing family medicine. “Family attitude key to diabetic’s state” was published in our first issue and “Type 1 diabetes prevention moves toward reality as studies published” ran in our April 2021 issue.
The photos in that first issue, however, present a somewhat jarring counterpoint to our latest issue. The faces that look back from 50 years ago are men’s faces: 29 men, to be exact. There were no photos of women physicians in that issue.
That was not the case in April of 2021. Of the 26 physicians or research scientists who appeared in photos in that issue, 8 were women. Plus, three of those women appeared on the cover.
Among the photos from 1971 were 6 of the 14 founding members of our editorial advisory board, who were, again, all men. Our current board consists of 13 men and 8 women.
Times have changed.
This article was updated 5/27/21.
Rituximab superior to mycophenolate mofetil in pemphigus vulgaris study
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.

Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.
Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
Mycophenolate mofetil, commonly used as a first-line corticosteroid-sparing agent for moderate to severe cases of the autoimmune blistering skin condition pemphigus vulgaris, has been found to be inferior to the biologic agent rituximab.
Mycophenolate mofetil is widely accepted as a first-in-line corticosteroid-sparing agent for pemphigus vulgaris, but few studies have compared the effectiveness of the two treatments for pemphigus vulgaris. The European Academy of Dermatology and Venereology recommends rituximab (Rituxan), a CD20 inhibitor, as first-line treatment for patients with new-onset cases of moderate to severe intensity or for patients who fail to achieve clinical remission with systemic corticosteroids with or without other immunosuppressive treatments.
In the current study, published online on May 19, 2021, in the New England Journal of Medicine, researchers led by Victoria P. Werth, MD, professor of dermatology at the University of Pennsylvania, Philadelphia, conducted a randomized, controlled trial of 135 patients (mean age, 48 years; 53% women) with moderate to severe pemphigus vulgaris with 67 receiving rituximab and 68 receiving mycophenolate mofetil (99% of patients in the rituximab group and 85% of patients in the mycophenolate mofetil group completed the trial).
Patients in the rituximab group received 1,000 mg of IV rituximab on days 1, 15, 168, and 182 of the study, plus twice-daily oral placebo. Intravenous methylprednisolone at 100 mg was administered before each rituximab infusion to reduce infusion-related reactions. Patients in the second group were given mycophenolate mofetil orally twice daily, starting at 1 g/day in divided doses and adjusted to 2 g/day in divided doses by week 2. They also received placebo infusions on days 1, 15, 168, and 182 of the study.
Patients in both groups received oral glucocorticoids throughout the course of the trial: an average of 3,545 mg for the rituximab treatment group and a cumulative dose of 5,140 mg for the group treated with mycophenolate mofetil, a statistically significant difference (P < .001). Outcomes based on 62 patients treated with rituximab and 63 on MMF, a modified intention-to-treat group.
By week 52, 25 patients (40%) who were treated with rituximab experienced complete sustained remission (the primary endpoint), compared with 6 patients (10%) in the mycophenolate mofetil group (95% confidence interval, 15-45, P < .001).
Only six patients in the rituximab group experienced a disease flare as compared with 44 patients in the mycophenolate mofetil group (adjusted rate ratio, 0.12; 95% CI, 0.05-0.29; P < .001). Serious adverse events occurred in 15 of 67 patients (22%) in the rituximab group and in 10 of 68 (15%) in the mycophenolate mofetil group with 3 patients in the rituximab group and 26 in the mycophenolate mofetil receiving rescue therapy.
Second to remission, the goal of treatment for pemphigus vulgaris is to reduce the use of glucocorticoids, Dr. Werth and colleagues wrote, adding: “The results of this trial showed that rituximab was superior to mycophenolate mofetil in producing sustained complete remission over 52 weeks among patients with moderate to severe pemphigus vulgaris. Rituximab had a greater glucocorticoid-sparing effect than mycophenolate mofetil, but more patients in this group had serious adverse events.”
Most adverse events in the rituximab group were limited to infusion-related reactions, but serious adverse events occurred in 15 patients (including pneumonia and upper respiratory tract infection, cellulitis and acute pyelonephritis, viral pneumonia, and skin infection). Ten patients in the mycophenolate mofetil group experienced serious adverse events (pneumonia and influenza, cellulitis and sepsis, herpes zoster, and pyelonephritis).
The current study had several limitations, primarily its small size. Plus, the authors noted a short follow-up period after glucocorticoids were stopped.
Mycophenolate mofetil, along with immunosuppressants, is approved in the United States as a treatment for organ rejection in patients who have received kidney, heart or liver transplants. But it is also used off label for pemphigus vulgaris and in rheumatology as a treatment for lupus, rheumatoid arthritis, vasculitis, inflammatory bowel disease (Crohn’s disease), inflammatory eye disease (uveitis) as well as kidney and skin disorders.
In the 2018 treatment guidelines for pemphigus by the European Dermatology Forum and the EADV, mycophenolate mofetil is recommended as a first-line corticosteroid sparing agent for pemphigus vulgaris.
Rituximab was approved in 2018 as the first biologic therapy for patients with pemphigus vulgaris and is currently recommended as a treatment for patients with pemphigus. But how well it works in comparison with the long-established mycophenolate mofetil hasn’t been extensively studied.
Other smaller studies show that mycophenolate mofetil has a treatment effect, but those studies were small. The Ritux 3 trial, published in The Lancet showed that rituximab plus glucocorticoids as opposed to glucocorticoids alone was beneficial in treating pemphigus.
“Rituximab has moved toward first-line therapy for moderate to severe pemphigus as recommended by an international panel of experts,” Dr. Werth said in an interview.
In her practice, Dr. Werth said that she has observed similar outcomes in clinical practice for patients prescribed oral mycophenolate mofetil. “Patients take a long time to get to remission and frequently end up staying on prednisone and long-term mycophenolate mofetil,” she said. She uses mycophenolate mofetil less often since rituximab has been shown to be effective for many patients, but mycophenolate mofetil “still has a place for patients who don’t want, or can’t tolerate, rituximab, or for cases in which rituximab doesn’t work.”
This study was supported by a grant from Hoffmann–La Roche. Dr. Werth disclosed having served as a consultant to Genentech on pemphigus, and that the University of Pennsylvania has received a grant/contract to perform a rituximab–mycophenolate mofetil trial for pemphigus vulgaris.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Unhealthy drinking may worsen after weight loss surgery
Internal medicine primarily affords us the skill to cope with disorders of chronicity that rarely disappear. For every pneumococcal pneumonia we eradicate, we have multiple patients with HIV who will be treated indefinitely. Diabetes, once a lethal disease, is now a chronic condition for most patients, and even with treatment the trajectory is usually one of progression.

One gratifying exception in my professional lifetime has been the introduction of gastric surgeries that reduce morbidity and seem to extend the life span of those who successfully undergo these procedures. The Roux-en-Y gastric bypass and sleeve gastrectomy have kept thousands of patients in better health for many years, giving them a second chance. For a subset, however, this second chance comes with a stumbling block of substance use – most notably alcohol – that exceeds their preoperative use.
Increased alcohol use after surgery
A group affiliated with the Department of Veterans Affairs (VA) recently reviewed the large central database to identify changes in alcohol consumption among patients who had undergone successful bariatric surgery. The VA regularly administers the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), a survey validated as a reliable estimate of individual alcohol consumption. It is inserted into the VA electronic health record where it can be readily retrieved. By matching these survey results with individuals who underwent bariatric surgery at the VA and survived at least 8 years post op, the authors were able to follow trends in alcohol consumption, beginning 2 years before surgery through 8 years after.
Using the same database, the authors identified a larger number of nonoperative control patients with slightly less obesity but otherwise matched for several elements of comorbidity, such as hypertension, certain psychiatric disorders, and personal habits, including alcohol consumption.
Alcohol use was categorized as none, minor social use, and “unhealthy” use. Among those with no or minor social use preoperatively, 4% converted to unhealthy use at 3 years and about 5% at 8 years, significantly more than in the nonoperative control group. Those who had gastric bypass had somewhat more conversion than did those who had sleeve gastrectomy, though not significantly so.
Patients with an alcohol concern preoperatively took an interesting course. Consumption declined from 2 years pre op to the year of surgery, suggesting that curtailing its use may have been a surgical precondition. Postoperatively, they returned to unhealthy drinking levels. Those who underwent the sleeve gastrectomy consumed about the same amount of alcohol as did their matched nonoperative controls, but those who underwent bypass increased their baseline unhealthy use beyond that of the controls.
Because total abstinence is often the recommendation for treating alcoholism, the research group assessed how adherent the excessive drinkers were to abstinence. In anticipation of surgery, the rates of abstinence increased until the year of surgery, but by 3 years post op, consumption was often up to unhealthy levels, though no more than that of control participants with preexisting drinking problems.
Smoking and illicit drug use
Although increased alcohol consumption has generated the most studies, some attention has been given to smoking and illicit drug use, which may also increase over time.
One small study looked at composite tobacco, alcohol, and drug use pre- and postoperatively over 2 years, using population data. The authors found a parallel pattern of users voluntarily reducing their substance use in anticipation of surgery but relapsing as the procedure made them more functional and perhaps more independent. Of the substances people resumed, alcohol by far involved the largest increase in use from the preoperative baseline.
These studies, as important as they are, reveal what happened more effectively than they disclose why it happened. The latter requires some clinical experience. Curtailing cigarettes and alcohol use preoperatively may have been done to stay in the good graces of the surgeon. Many patients may have seen this as their path to a second chance that they intended to maintain.
The incentive to proceed to surgical weight loss, which incurs a measure of risk and forces changes in long ingrained eating habits, involves avoiding future morbidity and promoting longevity. Thus, the postoperative behaviors that threaten the long-term goal need to become a component of ongoing follow-up.
The acquisition of adverse behaviors not present preoperatively seems more difficult to sort out, and obligates those of us following these patients to ask about changes in alcohol use and provide resources for them should they need intervention.
Dr. Plotzker is a retired endocrinologist with 40 years of experience treating patients in both private practice and hospital settings.
A version of this article first appeared on Medscape.com.
Internal medicine primarily affords us the skill to cope with disorders of chronicity that rarely disappear. For every pneumococcal pneumonia we eradicate, we have multiple patients with HIV who will be treated indefinitely. Diabetes, once a lethal disease, is now a chronic condition for most patients, and even with treatment the trajectory is usually one of progression.
One gratifying exception in my professional lifetime has been the introduction of gastric surgeries that reduce morbidity and seem to extend the life span of those who successfully undergo these procedures. The Roux-en-Y gastric bypass and sleeve gastrectomy have kept thousands of patients in better health for many years, giving them a second chance. For a subset, however, this second chance comes with a stumbling block of substance use – most notably alcohol – that exceeds their preoperative use.
Increased alcohol use after surgery
A group affiliated with the Department of Veterans Affairs (VA) recently reviewed the large central database to identify changes in alcohol consumption among patients who had undergone successful bariatric surgery. The VA regularly administers the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), a survey validated as a reliable estimate of individual alcohol consumption. It is inserted into the VA electronic health record where it can be readily retrieved. By matching these survey results with individuals who underwent bariatric surgery at the VA and survived at least 8 years post op, the authors were able to follow trends in alcohol consumption, beginning 2 years before surgery through 8 years after.
Using the same database, the authors identified a larger number of nonoperative control patients with slightly less obesity but otherwise matched for several elements of comorbidity, such as hypertension, certain psychiatric disorders, and personal habits, including alcohol consumption.
Alcohol use was categorized as none, minor social use, and “unhealthy” use. Among those with no or minor social use preoperatively, 4% converted to unhealthy use at 3 years and about 5% at 8 years, significantly more than in the nonoperative control group. Those who had gastric bypass had somewhat more conversion than did those who had sleeve gastrectomy, though not significantly so.
Patients with an alcohol concern preoperatively took an interesting course. Consumption declined from 2 years pre op to the year of surgery, suggesting that curtailing its use may have been a surgical precondition. Postoperatively, they returned to unhealthy drinking levels. Those who underwent the sleeve gastrectomy consumed about the same amount of alcohol as did their matched nonoperative controls, but those who underwent bypass increased their baseline unhealthy use beyond that of the controls.
Because total abstinence is often the recommendation for treating alcoholism, the research group assessed how adherent the excessive drinkers were to abstinence. In anticipation of surgery, the rates of abstinence increased until the year of surgery, but by 3 years post op, consumption was often up to unhealthy levels, though no more than that of control participants with preexisting drinking problems.
Smoking and illicit drug use
Although increased alcohol consumption has generated the most studies, some attention has been given to smoking and illicit drug use, which may also increase over time.
One small study looked at composite tobacco, alcohol, and drug use pre- and postoperatively over 2 years, using population data. The authors found a parallel pattern of users voluntarily reducing their substance use in anticipation of surgery but relapsing as the procedure made them more functional and perhaps more independent. Of the substances people resumed, alcohol by far involved the largest increase in use from the preoperative baseline.
These studies, as important as they are, reveal what happened more effectively than they disclose why it happened. The latter requires some clinical experience. Curtailing cigarettes and alcohol use preoperatively may have been done to stay in the good graces of the surgeon. Many patients may have seen this as their path to a second chance that they intended to maintain.
The incentive to proceed to surgical weight loss, which incurs a measure of risk and forces changes in long ingrained eating habits, involves avoiding future morbidity and promoting longevity. Thus, the postoperative behaviors that threaten the long-term goal need to become a component of ongoing follow-up.
The acquisition of adverse behaviors not present preoperatively seems more difficult to sort out, and obligates those of us following these patients to ask about changes in alcohol use and provide resources for them should they need intervention.
Dr. Plotzker is a retired endocrinologist with 40 years of experience treating patients in both private practice and hospital settings.
A version of this article first appeared on Medscape.com.
Internal medicine primarily affords us the skill to cope with disorders of chronicity that rarely disappear. For every pneumococcal pneumonia we eradicate, we have multiple patients with HIV who will be treated indefinitely. Diabetes, once a lethal disease, is now a chronic condition for most patients, and even with treatment the trajectory is usually one of progression.
One gratifying exception in my professional lifetime has been the introduction of gastric surgeries that reduce morbidity and seem to extend the life span of those who successfully undergo these procedures. The Roux-en-Y gastric bypass and sleeve gastrectomy have kept thousands of patients in better health for many years, giving them a second chance. For a subset, however, this second chance comes with a stumbling block of substance use – most notably alcohol – that exceeds their preoperative use.
Increased alcohol use after surgery
A group affiliated with the Department of Veterans Affairs (VA) recently reviewed the large central database to identify changes in alcohol consumption among patients who had undergone successful bariatric surgery. The VA regularly administers the Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), a survey validated as a reliable estimate of individual alcohol consumption. It is inserted into the VA electronic health record where it can be readily retrieved. By matching these survey results with individuals who underwent bariatric surgery at the VA and survived at least 8 years post op, the authors were able to follow trends in alcohol consumption, beginning 2 years before surgery through 8 years after.
Using the same database, the authors identified a larger number of nonoperative control patients with slightly less obesity but otherwise matched for several elements of comorbidity, such as hypertension, certain psychiatric disorders, and personal habits, including alcohol consumption.
Alcohol use was categorized as none, minor social use, and “unhealthy” use. Among those with no or minor social use preoperatively, 4% converted to unhealthy use at 3 years and about 5% at 8 years, significantly more than in the nonoperative control group. Those who had gastric bypass had somewhat more conversion than did those who had sleeve gastrectomy, though not significantly so.
Patients with an alcohol concern preoperatively took an interesting course. Consumption declined from 2 years pre op to the year of surgery, suggesting that curtailing its use may have been a surgical precondition. Postoperatively, they returned to unhealthy drinking levels. Those who underwent the sleeve gastrectomy consumed about the same amount of alcohol as did their matched nonoperative controls, but those who underwent bypass increased their baseline unhealthy use beyond that of the controls.
Because total abstinence is often the recommendation for treating alcoholism, the research group assessed how adherent the excessive drinkers were to abstinence. In anticipation of surgery, the rates of abstinence increased until the year of surgery, but by 3 years post op, consumption was often up to unhealthy levels, though no more than that of control participants with preexisting drinking problems.
Smoking and illicit drug use
Although increased alcohol consumption has generated the most studies, some attention has been given to smoking and illicit drug use, which may also increase over time.
One small study looked at composite tobacco, alcohol, and drug use pre- and postoperatively over 2 years, using population data. The authors found a parallel pattern of users voluntarily reducing their substance use in anticipation of surgery but relapsing as the procedure made them more functional and perhaps more independent. Of the substances people resumed, alcohol by far involved the largest increase in use from the preoperative baseline.
These studies, as important as they are, reveal what happened more effectively than they disclose why it happened. The latter requires some clinical experience. Curtailing cigarettes and alcohol use preoperatively may have been done to stay in the good graces of the surgeon. Many patients may have seen this as their path to a second chance that they intended to maintain.
The incentive to proceed to surgical weight loss, which incurs a measure of risk and forces changes in long ingrained eating habits, involves avoiding future morbidity and promoting longevity. Thus, the postoperative behaviors that threaten the long-term goal need to become a component of ongoing follow-up.
The acquisition of adverse behaviors not present preoperatively seems more difficult to sort out, and obligates those of us following these patients to ask about changes in alcohol use and provide resources for them should they need intervention.
Dr. Plotzker is a retired endocrinologist with 40 years of experience treating patients in both private practice and hospital settings.
A version of this article first appeared on Medscape.com.
Obesity hope as neuropeptide Y blocker turns white fat to brown
A peripherally-acting substance that boosts energy expenditure and reduces fat mass has the potential to become an obesity treatment that doesn’t produce cardiovascular or psychiatric side effects, scientists say.
The agent, BIBO3304, is a selective antagonist of the neuropeptide Y1 receptor, which is elevated in the fat tissue of individuals with obesity, resulting in reduced fat accumulation. It was originally developed more than 25 years ago by scientists at Boehringer Ingelheim, who had thought that it would reduce appetite by targeting Y1 receptors in the brain. But when it didn’t cross the blood-brain barrier as an oral drug, the company abandoned it.
Now a series of experiments by Chenxu Yan, of the Garvan Institute of Medical Research, St. Vincent’s Hospital, Sydney, and colleagues have shown that “BIBO” works directly on Y1 receptors in the periphery to turn fat-storing white fat cells into heat-generating brown-like fat tissue, thereby enhancing energy expenditure.
The data were published online May 11 in Nature Communications.
Drug’s lack of effect on the brain turns out to be a positive
“Rather than just having the cells store fat, we change their characteristics so that most of the excess energy gets burned and produces heat instead of being stored as fat. BIBO programs the cell toward a more heat-producing cell rather than a fat-storing cell,” study coauthor Herbert Herzog, PhD, of the Garvan Institute, said in an interview.
Importantly, he said, the lack of effect on the brain that caused the drug’s initial developer to abandon it turns out to be a positive.
“As we looked at fat specifically, and we didn’t want to have any interference with the brain, this seems to work out as a real advantage … It has the desired effect of blocking fat accumulation but has the enormous benefit of not interfering with any brain function. That’s why so many of the obesity drugs that were on the market were taken off, because of the side effects they caused in the brain on mood and cardiovascular control. It’s a completely different ball game.”
The problem now, he said, is that because BIBO is off-patent, no pharmaceutical company is currently willing to invest in its development as a peripherally acting weight-loss drug, despite its potential advantages.
“We’re trying to find some interested party to help us get this to the clinical setting. We’re basic scientists. We need big money. We can do small-scale studies to get proof of principle. Hopefully, if that’s interesting, some bigger company will come along,” said Dr. Herzog.
Experiments in mice, human tissues demonstrate principle
In the series of studies, investigators fed genetically inbred mice a high-fat, high-sugar diet while giving BIBO to half of them. Over 8 weeks, the mice given BIBO had 40% less gain in fat mass compared to those overfed without the drug, despite them all eating the same amount.
Using a noninvasive infrared camera to measure skin surface temperature above brown adipose tissue, they found that the temperature was significantly increased with BIBO, independent of the weight of the brown fat.
This suggests that the thermogenesis of the brown fat is significantly contributing to whole-body energy expenditure. “With the drug, the mice have far greater energy expenditure measured by heat production,” Dr. Herzog explained.
In vitro experiments showed that Y1R blockade by BIBO induced “beigeing” of white fat deposits into more heat-producing brown fat. The body temperature increase is about 0.1-0.2ºC. “That’s a tiny amount, but it actually requires quite a lot of energy,” he said.
Experiments using fat tissue taken from obese and normal-weight humans showed the same thermogenesis with BIBO. “It’s such a fundamental process [that] you wouldn’t expect it to differ. The same mechanism is even found in flies and primitive worms,” he noted.
Neuropeptide Y receptor blockage: A treatment for many ills?
Previously, Dr. Herzog and colleagues found that blockade of the neuropeptide Y1 receptor also increases bone mass in mice.
“It’s a modest effect, but there’s nothing out there at the moment that really improves bone mass. If you can stop osteoporosis, that’s a benefit on its own,” he said.
Now they hope to study BIBO’s vasodilatory properties as a potential treatment for hypertension, if they get the funding.
Dr. Herzog is hopeful, as obesity, osteoporosis, and hypertension are all chronic conditions. “Having one drug that benefits them all would surely be of interest to clinicians and drug companies,” he observed.
Dr. Yan and Dr. Herzog have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A peripherally-acting substance that boosts energy expenditure and reduces fat mass has the potential to become an obesity treatment that doesn’t produce cardiovascular or psychiatric side effects, scientists say.
The agent, BIBO3304, is a selective antagonist of the neuropeptide Y1 receptor, which is elevated in the fat tissue of individuals with obesity, resulting in reduced fat accumulation. It was originally developed more than 25 years ago by scientists at Boehringer Ingelheim, who had thought that it would reduce appetite by targeting Y1 receptors in the brain. But when it didn’t cross the blood-brain barrier as an oral drug, the company abandoned it.
Now a series of experiments by Chenxu Yan, of the Garvan Institute of Medical Research, St. Vincent’s Hospital, Sydney, and colleagues have shown that “BIBO” works directly on Y1 receptors in the periphery to turn fat-storing white fat cells into heat-generating brown-like fat tissue, thereby enhancing energy expenditure.
The data were published online May 11 in Nature Communications.
Drug’s lack of effect on the brain turns out to be a positive
“Rather than just having the cells store fat, we change their characteristics so that most of the excess energy gets burned and produces heat instead of being stored as fat. BIBO programs the cell toward a more heat-producing cell rather than a fat-storing cell,” study coauthor Herbert Herzog, PhD, of the Garvan Institute, said in an interview.
Importantly, he said, the lack of effect on the brain that caused the drug’s initial developer to abandon it turns out to be a positive.
“As we looked at fat specifically, and we didn’t want to have any interference with the brain, this seems to work out as a real advantage … It has the desired effect of blocking fat accumulation but has the enormous benefit of not interfering with any brain function. That’s why so many of the obesity drugs that were on the market were taken off, because of the side effects they caused in the brain on mood and cardiovascular control. It’s a completely different ball game.”
The problem now, he said, is that because BIBO is off-patent, no pharmaceutical company is currently willing to invest in its development as a peripherally acting weight-loss drug, despite its potential advantages.
“We’re trying to find some interested party to help us get this to the clinical setting. We’re basic scientists. We need big money. We can do small-scale studies to get proof of principle. Hopefully, if that’s interesting, some bigger company will come along,” said Dr. Herzog.
Experiments in mice, human tissues demonstrate principle
In the series of studies, investigators fed genetically inbred mice a high-fat, high-sugar diet while giving BIBO to half of them. Over 8 weeks, the mice given BIBO had 40% less gain in fat mass compared to those overfed without the drug, despite them all eating the same amount.
Using a noninvasive infrared camera to measure skin surface temperature above brown adipose tissue, they found that the temperature was significantly increased with BIBO, independent of the weight of the brown fat.
This suggests that the thermogenesis of the brown fat is significantly contributing to whole-body energy expenditure. “With the drug, the mice have far greater energy expenditure measured by heat production,” Dr. Herzog explained.
In vitro experiments showed that Y1R blockade by BIBO induced “beigeing” of white fat deposits into more heat-producing brown fat. The body temperature increase is about 0.1-0.2ºC. “That’s a tiny amount, but it actually requires quite a lot of energy,” he said.
Experiments using fat tissue taken from obese and normal-weight humans showed the same thermogenesis with BIBO. “It’s such a fundamental process [that] you wouldn’t expect it to differ. The same mechanism is even found in flies and primitive worms,” he noted.
Neuropeptide Y receptor blockage: A treatment for many ills?
Previously, Dr. Herzog and colleagues found that blockade of the neuropeptide Y1 receptor also increases bone mass in mice.
“It’s a modest effect, but there’s nothing out there at the moment that really improves bone mass. If you can stop osteoporosis, that’s a benefit on its own,” he said.
Now they hope to study BIBO’s vasodilatory properties as a potential treatment for hypertension, if they get the funding.
Dr. Herzog is hopeful, as obesity, osteoporosis, and hypertension are all chronic conditions. “Having one drug that benefits them all would surely be of interest to clinicians and drug companies,” he observed.
Dr. Yan and Dr. Herzog have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A peripherally-acting substance that boosts energy expenditure and reduces fat mass has the potential to become an obesity treatment that doesn’t produce cardiovascular or psychiatric side effects, scientists say.
The agent, BIBO3304, is a selective antagonist of the neuropeptide Y1 receptor, which is elevated in the fat tissue of individuals with obesity, resulting in reduced fat accumulation. It was originally developed more than 25 years ago by scientists at Boehringer Ingelheim, who had thought that it would reduce appetite by targeting Y1 receptors in the brain. But when it didn’t cross the blood-brain barrier as an oral drug, the company abandoned it.
Now a series of experiments by Chenxu Yan, of the Garvan Institute of Medical Research, St. Vincent’s Hospital, Sydney, and colleagues have shown that “BIBO” works directly on Y1 receptors in the periphery to turn fat-storing white fat cells into heat-generating brown-like fat tissue, thereby enhancing energy expenditure.
The data were published online May 11 in Nature Communications.
Drug’s lack of effect on the brain turns out to be a positive
“Rather than just having the cells store fat, we change their characteristics so that most of the excess energy gets burned and produces heat instead of being stored as fat. BIBO programs the cell toward a more heat-producing cell rather than a fat-storing cell,” study coauthor Herbert Herzog, PhD, of the Garvan Institute, said in an interview.
Importantly, he said, the lack of effect on the brain that caused the drug’s initial developer to abandon it turns out to be a positive.
“As we looked at fat specifically, and we didn’t want to have any interference with the brain, this seems to work out as a real advantage … It has the desired effect of blocking fat accumulation but has the enormous benefit of not interfering with any brain function. That’s why so many of the obesity drugs that were on the market were taken off, because of the side effects they caused in the brain on mood and cardiovascular control. It’s a completely different ball game.”
The problem now, he said, is that because BIBO is off-patent, no pharmaceutical company is currently willing to invest in its development as a peripherally acting weight-loss drug, despite its potential advantages.
“We’re trying to find some interested party to help us get this to the clinical setting. We’re basic scientists. We need big money. We can do small-scale studies to get proof of principle. Hopefully, if that’s interesting, some bigger company will come along,” said Dr. Herzog.
Experiments in mice, human tissues demonstrate principle
In the series of studies, investigators fed genetically inbred mice a high-fat, high-sugar diet while giving BIBO to half of them. Over 8 weeks, the mice given BIBO had 40% less gain in fat mass compared to those overfed without the drug, despite them all eating the same amount.
Using a noninvasive infrared camera to measure skin surface temperature above brown adipose tissue, they found that the temperature was significantly increased with BIBO, independent of the weight of the brown fat.
This suggests that the thermogenesis of the brown fat is significantly contributing to whole-body energy expenditure. “With the drug, the mice have far greater energy expenditure measured by heat production,” Dr. Herzog explained.
In vitro experiments showed that Y1R blockade by BIBO induced “beigeing” of white fat deposits into more heat-producing brown fat. The body temperature increase is about 0.1-0.2ºC. “That’s a tiny amount, but it actually requires quite a lot of energy,” he said.
Experiments using fat tissue taken from obese and normal-weight humans showed the same thermogenesis with BIBO. “It’s such a fundamental process [that] you wouldn’t expect it to differ. The same mechanism is even found in flies and primitive worms,” he noted.
Neuropeptide Y receptor blockage: A treatment for many ills?
Previously, Dr. Herzog and colleagues found that blockade of the neuropeptide Y1 receptor also increases bone mass in mice.
“It’s a modest effect, but there’s nothing out there at the moment that really improves bone mass. If you can stop osteoporosis, that’s a benefit on its own,” he said.
Now they hope to study BIBO’s vasodilatory properties as a potential treatment for hypertension, if they get the funding.
Dr. Herzog is hopeful, as obesity, osteoporosis, and hypertension are all chronic conditions. “Having one drug that benefits them all would surely be of interest to clinicians and drug companies,” he observed.
Dr. Yan and Dr. Herzog have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FDA OKs nivolumab after surgery for esophageal or GEJ cancer: Practice-changing use of immunotherapy
The Food and Drug Administration has approved the adjuvant use of nivolumab (Opdivo) in patients with resected esophageal or gastroesophageal junction (GEJ) cancer who have received neoadjuvant chemoradiotherapy and have residual pathological disease following surgery.
The approval addresses an unmet need among these patients, who have a high risk of recurrence but for whom surveillance is the only current management option after the above-described standard treatment, according to experts.
The FDA’s approval is based on results from the CheckMate 577 study, which showed a significant improvement in disease-free survival compared with placebo.
This was described as “a practice-changing trial in the treatment of esophageal cancer” by David H. Ilson, MD, PhD, Memorial Sloan Kettering Cancer Center, New York, in an editorial in The New England Journal of Medicine that accompanied the published study results.
“The trial shows the first true advance in the adjuvant therapy of esophageal cancer in recent years,” wrote Dr. Ilson.
In the randomized, double-blind, phase 3 trial, patients with resected stage II or III esophageal or GEJ cancer were randomly assigned in a 2:1 ratio to receive nivolumab (at a dose of 240 mg every 2 weeks for 16 weeks, followed by a dose of 480 mg every 4 weeks) or placebo. The maximum duration of the intervention period was 1 year.
All of these patients had received neoadjuvant chemoradiotherapy and had residual pathological disease, as noted in the new indication. Patients were enrolled regardless of programmed death ligand 1 (PD-L1) expression.
For the primary endpoint of disease-free survival, the median was 22.4 months for the nivolumab group (n = 532) versus 11.0 months for the placebo group (n = 262; hazard ratio [HR] for disease recurrence or death, 0.69; 96.4% confidence interval [CI], 0.56-0.86; P < .001).
The median follow-up was 24.4 months.
Disease-free survival favored nivolumab across multiple preplanned subgroups.
However, as Dr. Ilson noted in the editorial, the efficacy of nivolumab varied, with more benefit seen for patients with squamous cell cancer (HR, 0.61) than for those with adenocarcinoma (HR, 0.75). Patients with esophageal tumors also had greater benefit (HR, 0.61) than did those with GEJ tumors (HR, 0.87).
There was benefit in patients with node-negative disease (HR, 0.74) and node-positive disease (HR, 0.67) and benefit in patients with tumors that were PD-L1–negative (HR, 0.73) and PD-L1–positive (HR, 0.75).
There were fewer distant recurrences in the nivolumab group than in the placebo group (29% vs. 39%) and fewer locoregional recurrences (12% vs. 17%).
No new safety signals were observed, and 9% of the nivolumab patients discontinued the drug because of treatment-related adverse events versus 3% of placebo patients. In addition, a 1-year course of adjuvant nivolumab did not negatively impact patient-reported quality of life, the trialists reported.
Grade 3 or 4 adverse events of any cause were more frequent in the nivolumab group versus the placebo group (34% vs. 32%) as were those related to the intervention (13% vs. 6%).
Although overall survival data are not mature, “the doubling of median disease-free survival will almost certainly translate into an overall survival benefit,” Dr. Ilson wrote.
Notably, the trial’s original co-primary endpoint was overall survival, but was dropped to a secondary endpoint after enrollment “challenges.”
When the now-published data were first presented at the 2020 annual meeting of the European Society for Medical Oncology, the invited discussant, Andrés Cervantes, MD, PhD, University of Valencia, Spain, raised several issues with the trial.
Preoperative chemoradiation is not “universally accepted” as the standard of care in this setting, said Dr. Cervantes, president-elect of ESMO.
Dr. Ilson acknowledged as much. “A debate is ongoing about whether chemotherapy alone or combined chemoradiotherapy is the preferred treatment for esophageal cancer before surgery,” he wrote.
In addition, Dr. Cervantes noted that disease-free survival is not currently validated as a major endpoint in gastroesophageal cancers, and the median follow-up was short.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the adjuvant use of nivolumab (Opdivo) in patients with resected esophageal or gastroesophageal junction (GEJ) cancer who have received neoadjuvant chemoradiotherapy and have residual pathological disease following surgery.
The approval addresses an unmet need among these patients, who have a high risk of recurrence but for whom surveillance is the only current management option after the above-described standard treatment, according to experts.
The FDA’s approval is based on results from the CheckMate 577 study, which showed a significant improvement in disease-free survival compared with placebo.
This was described as “a practice-changing trial in the treatment of esophageal cancer” by David H. Ilson, MD, PhD, Memorial Sloan Kettering Cancer Center, New York, in an editorial in The New England Journal of Medicine that accompanied the published study results.
“The trial shows the first true advance in the adjuvant therapy of esophageal cancer in recent years,” wrote Dr. Ilson.
In the randomized, double-blind, phase 3 trial, patients with resected stage II or III esophageal or GEJ cancer were randomly assigned in a 2:1 ratio to receive nivolumab (at a dose of 240 mg every 2 weeks for 16 weeks, followed by a dose of 480 mg every 4 weeks) or placebo. The maximum duration of the intervention period was 1 year.
All of these patients had received neoadjuvant chemoradiotherapy and had residual pathological disease, as noted in the new indication. Patients were enrolled regardless of programmed death ligand 1 (PD-L1) expression.
For the primary endpoint of disease-free survival, the median was 22.4 months for the nivolumab group (n = 532) versus 11.0 months for the placebo group (n = 262; hazard ratio [HR] for disease recurrence or death, 0.69; 96.4% confidence interval [CI], 0.56-0.86; P < .001).
The median follow-up was 24.4 months.
Disease-free survival favored nivolumab across multiple preplanned subgroups.
However, as Dr. Ilson noted in the editorial, the efficacy of nivolumab varied, with more benefit seen for patients with squamous cell cancer (HR, 0.61) than for those with adenocarcinoma (HR, 0.75). Patients with esophageal tumors also had greater benefit (HR, 0.61) than did those with GEJ tumors (HR, 0.87).
There was benefit in patients with node-negative disease (HR, 0.74) and node-positive disease (HR, 0.67) and benefit in patients with tumors that were PD-L1–negative (HR, 0.73) and PD-L1–positive (HR, 0.75).
There were fewer distant recurrences in the nivolumab group than in the placebo group (29% vs. 39%) and fewer locoregional recurrences (12% vs. 17%).
No new safety signals were observed, and 9% of the nivolumab patients discontinued the drug because of treatment-related adverse events versus 3% of placebo patients. In addition, a 1-year course of adjuvant nivolumab did not negatively impact patient-reported quality of life, the trialists reported.
Grade 3 or 4 adverse events of any cause were more frequent in the nivolumab group versus the placebo group (34% vs. 32%) as were those related to the intervention (13% vs. 6%).
Although overall survival data are not mature, “the doubling of median disease-free survival will almost certainly translate into an overall survival benefit,” Dr. Ilson wrote.
Notably, the trial’s original co-primary endpoint was overall survival, but was dropped to a secondary endpoint after enrollment “challenges.”
When the now-published data were first presented at the 2020 annual meeting of the European Society for Medical Oncology, the invited discussant, Andrés Cervantes, MD, PhD, University of Valencia, Spain, raised several issues with the trial.
Preoperative chemoradiation is not “universally accepted” as the standard of care in this setting, said Dr. Cervantes, president-elect of ESMO.
Dr. Ilson acknowledged as much. “A debate is ongoing about whether chemotherapy alone or combined chemoradiotherapy is the preferred treatment for esophageal cancer before surgery,” he wrote.
In addition, Dr. Cervantes noted that disease-free survival is not currently validated as a major endpoint in gastroesophageal cancers, and the median follow-up was short.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the adjuvant use of nivolumab (Opdivo) in patients with resected esophageal or gastroesophageal junction (GEJ) cancer who have received neoadjuvant chemoradiotherapy and have residual pathological disease following surgery.
The approval addresses an unmet need among these patients, who have a high risk of recurrence but for whom surveillance is the only current management option after the above-described standard treatment, according to experts.
The FDA’s approval is based on results from the CheckMate 577 study, which showed a significant improvement in disease-free survival compared with placebo.
This was described as “a practice-changing trial in the treatment of esophageal cancer” by David H. Ilson, MD, PhD, Memorial Sloan Kettering Cancer Center, New York, in an editorial in The New England Journal of Medicine that accompanied the published study results.
“The trial shows the first true advance in the adjuvant therapy of esophageal cancer in recent years,” wrote Dr. Ilson.
In the randomized, double-blind, phase 3 trial, patients with resected stage II or III esophageal or GEJ cancer were randomly assigned in a 2:1 ratio to receive nivolumab (at a dose of 240 mg every 2 weeks for 16 weeks, followed by a dose of 480 mg every 4 weeks) or placebo. The maximum duration of the intervention period was 1 year.
All of these patients had received neoadjuvant chemoradiotherapy and had residual pathological disease, as noted in the new indication. Patients were enrolled regardless of programmed death ligand 1 (PD-L1) expression.
For the primary endpoint of disease-free survival, the median was 22.4 months for the nivolumab group (n = 532) versus 11.0 months for the placebo group (n = 262; hazard ratio [HR] for disease recurrence or death, 0.69; 96.4% confidence interval [CI], 0.56-0.86; P < .001).
The median follow-up was 24.4 months.
Disease-free survival favored nivolumab across multiple preplanned subgroups.
However, as Dr. Ilson noted in the editorial, the efficacy of nivolumab varied, with more benefit seen for patients with squamous cell cancer (HR, 0.61) than for those with adenocarcinoma (HR, 0.75). Patients with esophageal tumors also had greater benefit (HR, 0.61) than did those with GEJ tumors (HR, 0.87).
There was benefit in patients with node-negative disease (HR, 0.74) and node-positive disease (HR, 0.67) and benefit in patients with tumors that were PD-L1–negative (HR, 0.73) and PD-L1–positive (HR, 0.75).
There were fewer distant recurrences in the nivolumab group than in the placebo group (29% vs. 39%) and fewer locoregional recurrences (12% vs. 17%).
No new safety signals were observed, and 9% of the nivolumab patients discontinued the drug because of treatment-related adverse events versus 3% of placebo patients. In addition, a 1-year course of adjuvant nivolumab did not negatively impact patient-reported quality of life, the trialists reported.
Grade 3 or 4 adverse events of any cause were more frequent in the nivolumab group versus the placebo group (34% vs. 32%) as were those related to the intervention (13% vs. 6%).
Although overall survival data are not mature, “the doubling of median disease-free survival will almost certainly translate into an overall survival benefit,” Dr. Ilson wrote.
Notably, the trial’s original co-primary endpoint was overall survival, but was dropped to a secondary endpoint after enrollment “challenges.”
When the now-published data were first presented at the 2020 annual meeting of the European Society for Medical Oncology, the invited discussant, Andrés Cervantes, MD, PhD, University of Valencia, Spain, raised several issues with the trial.
Preoperative chemoradiation is not “universally accepted” as the standard of care in this setting, said Dr. Cervantes, president-elect of ESMO.
Dr. Ilson acknowledged as much. “A debate is ongoing about whether chemotherapy alone or combined chemoradiotherapy is the preferred treatment for esophageal cancer before surgery,” he wrote.
In addition, Dr. Cervantes noted that disease-free survival is not currently validated as a major endpoint in gastroesophageal cancers, and the median follow-up was short.
A version of this article first appeared on Medscape.com.