User login
Does childhood eczema mean food allergies forever?
Atopic dermatitis at 1 year is linked with persistent food allergies. The incidence of treated depression is nearly 100% higher in patients with multiple sclerosis. Infective endocarditis isn’t what it used to be. And dog walking may pose a fracture danger for your elderly patients.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Atopic dermatitis at 1 year is linked with persistent food allergies. The incidence of treated depression is nearly 100% higher in patients with multiple sclerosis. Infective endocarditis isn’t what it used to be. And dog walking may pose a fracture danger for your elderly patients.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify
Atopic dermatitis at 1 year is linked with persistent food allergies. The incidence of treated depression is nearly 100% higher in patients with multiple sclerosis. Infective endocarditis isn’t what it used to be. And dog walking may pose a fracture danger for your elderly patients.
Amazon Alexa
Apple Podcasts
Google Podcasts
Spotify

Are You Sitting Down for This?
Not all sedentary behavior is equal, say researchers from Universidad Autónoma de Madrid in Spain, who evaluated the sedentary habits of 5,459 women and 4,740 men.
The researchers note that several studies have found that, unlike, for example, computer use and reading, TV watching is consistently associated with adverse health outcomes, such as metabolic syndrome, obesity, and diabetes mellitus (DM). But different sedentary behaviors (SBs) have different health effects, they add. They cite research that suggests TV and other “passive” SBs (eg, listening or talking while sitting) could be more harmful than “mentally active” SBs, such as computer use and reading. In this study, “passive” sedentary time, such as TV watching, was associated with less recreational activity and higher body weight. Time at the computer and reading were linked to more recreational physical activity but less light-intensity activity at home.
Moreover, each type of SB has a distinct demographic and lifestyle profile, the researchers say. Older age, lower education, unhealthy lifestyle (smoking, worse diet, less physical activity, higher BMI) and chronic morbidity, such as DM or osteomuscular disease, were linked to more TV time. Longer time at the computer or in commuting was linked to younger age, male gender, higher education, and a sedentary job.
Watching TV had no association with total time spent on the rest of leisure-time SBs. The researchers also found that “mentally active” SBs, such as using the computer and reading, tend to cluster.
Many studies have looked at the effects of and connections between SB, lifestyle choices, and health. The researchers of this study say theirs extends knowledge in the field by considering more types of SB (using the computer, commuting, lying in the sun, listening to music, and reading). To their knowledge, they say, no previous study on a representative sample of an entire country has examined the association between TV watching time and the rest of SB, or has reported the full profile of sociodemographic, lifestyle, and health variables associated with each type of SB.
Watching TV was the predominant SB (45% of total sitting time), followed by sitting at the computer (23%), reading (15%), and commuting (12%). The participants spent a mean of 1.96 hours a day watching TV, vs > 1 hour for the other behaviors.
Not all sedentary behavior is equal, say researchers from Universidad Autónoma de Madrid in Spain, who evaluated the sedentary habits of 5,459 women and 4,740 men.
The researchers note that several studies have found that, unlike, for example, computer use and reading, TV watching is consistently associated with adverse health outcomes, such as metabolic syndrome, obesity, and diabetes mellitus (DM). But different sedentary behaviors (SBs) have different health effects, they add. They cite research that suggests TV and other “passive” SBs (eg, listening or talking while sitting) could be more harmful than “mentally active” SBs, such as computer use and reading. In this study, “passive” sedentary time, such as TV watching, was associated with less recreational activity and higher body weight. Time at the computer and reading were linked to more recreational physical activity but less light-intensity activity at home.
Moreover, each type of SB has a distinct demographic and lifestyle profile, the researchers say. Older age, lower education, unhealthy lifestyle (smoking, worse diet, less physical activity, higher BMI) and chronic morbidity, such as DM or osteomuscular disease, were linked to more TV time. Longer time at the computer or in commuting was linked to younger age, male gender, higher education, and a sedentary job.
Watching TV had no association with total time spent on the rest of leisure-time SBs. The researchers also found that “mentally active” SBs, such as using the computer and reading, tend to cluster.
Many studies have looked at the effects of and connections between SB, lifestyle choices, and health. The researchers of this study say theirs extends knowledge in the field by considering more types of SB (using the computer, commuting, lying in the sun, listening to music, and reading). To their knowledge, they say, no previous study on a representative sample of an entire country has examined the association between TV watching time and the rest of SB, or has reported the full profile of sociodemographic, lifestyle, and health variables associated with each type of SB.
Watching TV was the predominant SB (45% of total sitting time), followed by sitting at the computer (23%), reading (15%), and commuting (12%). The participants spent a mean of 1.96 hours a day watching TV, vs > 1 hour for the other behaviors.
Not all sedentary behavior is equal, say researchers from Universidad Autónoma de Madrid in Spain, who evaluated the sedentary habits of 5,459 women and 4,740 men.
The researchers note that several studies have found that, unlike, for example, computer use and reading, TV watching is consistently associated with adverse health outcomes, such as metabolic syndrome, obesity, and diabetes mellitus (DM). But different sedentary behaviors (SBs) have different health effects, they add. They cite research that suggests TV and other “passive” SBs (eg, listening or talking while sitting) could be more harmful than “mentally active” SBs, such as computer use and reading. In this study, “passive” sedentary time, such as TV watching, was associated with less recreational activity and higher body weight. Time at the computer and reading were linked to more recreational physical activity but less light-intensity activity at home.
Moreover, each type of SB has a distinct demographic and lifestyle profile, the researchers say. Older age, lower education, unhealthy lifestyle (smoking, worse diet, less physical activity, higher BMI) and chronic morbidity, such as DM or osteomuscular disease, were linked to more TV time. Longer time at the computer or in commuting was linked to younger age, male gender, higher education, and a sedentary job.
Watching TV had no association with total time spent on the rest of leisure-time SBs. The researchers also found that “mentally active” SBs, such as using the computer and reading, tend to cluster.
Many studies have looked at the effects of and connections between SB, lifestyle choices, and health. The researchers of this study say theirs extends knowledge in the field by considering more types of SB (using the computer, commuting, lying in the sun, listening to music, and reading). To their knowledge, they say, no previous study on a representative sample of an entire country has examined the association between TV watching time and the rest of SB, or has reported the full profile of sociodemographic, lifestyle, and health variables associated with each type of SB.
Watching TV was the predominant SB (45% of total sitting time), followed by sitting at the computer (23%), reading (15%), and commuting (12%). The participants spent a mean of 1.96 hours a day watching TV, vs > 1 hour for the other behaviors.
Police department offers mental health care for officers
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.

Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.

A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.
Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.
A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
Police officers often are criticized for the way they respond to people with serious mental illness. A police department in Florida is addressing this issue by hiring a licensed clinical psychologist and making her available to officers on a 24/7 basis, an ABC-TV affiliate reported. “The goal is they come in, they work on what they need to; we get them right, we get them good so that they can go back out and do what they need to do – and then they check in as needed,” Brandy Benson, PsyD, said in the report. The meetings take place in her office and not the police station, which allows officers to maintain confidentiality. Each officer is allotted a set number of free sessions for each issue that is fueling their distress. Issues can range from depression to anxiety to marital problems. The aim is prevention – not reaction to whatever has happened. Getting at the root cause can prevent spillover on the job, which in turn, can prove disastrous for officers, the people they serve, and their families. “It’s okay to go through those emotions, but you don’t want to tie those emotions up because sooner or later it’s going to pop and we want to make sure we address that issue before it goes ‘pop,’ ” said St. Petersburg Police Chief Anthony Holloway. WFTS-TV, Tampa Bay, Fla.
Two women have embarked on their self-described “joy tour” to raise awareness about suicide prevention. Shontice McKenzie and Cedrica Mitchell are on the road with the intention of visiting every state, according to an article on thefix.com, a website that focuses on addiction and recovery. The tour is the brainchild of Ms. McKenzie and is funded by her nonprofit H.U.M.A.N.I.T.Y. 360. During their month-long extended stops in Virginia, North Carolina, South Carolina, Georgia, Florida, and a just-completed stay in Alabama, the women are speaking and providing positive outlets to those in turmoil and contemplating suicide, thefix reported, based on a post on al.com. The choice of Alabama as one of the first stops on the planned nationwide tour was deliberate. The suicide rate in the state has been higher than the national average for nearly 3 decades – 16.2/100,000, compared with 13.9/100,000 nationally. Suicide is the second-leading cause of death of those aged 10-14 years in Alabama. Ms. McKenzie and Ms. Mitchell want to see the stigma surrounding mental illness removed. “We have met so many families who are still in denial about a family member who completed the act of suicide because they don’t want the backlash from the public,” Ms. McKenzie said. “They should have received more support around the topic. Then we can prevent suicides. That’s what the Joy Tour is about.” The end of each state visit includes what the two call a “joy jam” – a free event where people can eat, get information on mental health resources in their area, and learn how to incorporate mental health care into their everyday lives. The tour is slated to wrap up in 2023 in Hawaii. Thefix.com.
An editorial in the Winston-Salem (N.C.) Journal has backed a recently introduced bill in the state legislature that would open the door for mental health screenings for public school students. “This legislation is a worthwhile step in tackling the problem of school shootings as well as other problems that can arise among our children. It should work well in conjunction with other efforts, such as increased school security and gun-law reform,” the paper’s editorial board wrote. The bill would trigger a study by the North Carolina Department of Health and Human Services to come up with a screening system that would identify school children at risk of harming themselves or others. The idea is that all students would be screened initially. “We have nothing that determines if a child has a mental health concern ... to the point they could be contemplating harming themselves or others,” said state Rep. John Torbett, the bill’s main sponsor. “This bill would bring smart people together for determining the appropriate criteria.” One of the bill’s cosponsors, Rep. Debra Forsyth, said school counselors tell her that most of their time is spent dealing with students with emotional and mental issues. “When we were studying the impact of [math and reading standards] a few years back, many parents complained about emotional stress in very young children, so issues can obviously arise at an early age,” Ms. Forsyth said in the article. “Our children are facing pressures from all sides – increased testing, peer pressure, and economic difficulties. They’re not receiving the best resources we could provide. It’s about time they received a helping hand.” Winston-Salem Journal.
A mental health facility has opened in southeast Fresno, Calif., that seeks to provide a bridge for people experiencing a mental health crisis and need a place to live, according to a report by ABC affiliate KFSN. The $5 million, 12,000-square-foot, 16-bed facility is an alternative to hospitalization, said Gerardo Puga-Cervantes, an administrator at the facility. “A facility like this creates a stepping-stone that’s closer to the ones before and after, so when a person is making that pathway toward recovery, it’s not a Grand Canyon they have to leap to get that recovery. It’s really a clear pathway,” said Fresno County Behavioral Health Director Dawan Utecht. The facility, called the Fresno Crisis Residential Treatment Center, will provide psychiatric support to residents and will aim to serve hundreds of people each year. To get into the center, patients must be referred by the county’s behavioral health department. Next, the department hopes to provide residential housing for those who leave the facility. ABC30 Action News/KFSN-TV.
A former dairy farm reincarnated as a school called Green Chimneys in Putnam County, N.Y., is helping children with special needs find solace, the New York Times reported. Aside from usual pigs and goats, the farm’s denizens include more exotic critters, such as camels, an emu, peacocks, miniature horses and donkeys, owls, falcons, and a condor. “Green Chimneys’ approach focuses on an awareness of how trauma impacts human and animal lives, that a healing setting can benefit both, and that there is a broader parallel between human, animal, environmental, and societal well-being,” according to the school’s website. The article describes the experience of 8-year-old Xander DeLeon, who was diagnosed with attention-deficit/hyperactivity disorder and dyslexia, and experienced rages and absences while attending a charter school in Manhattan. Now he is pulling down As and Bs. “The school staff tell him that he won’t be able to work on the farm if he doesn’t continue to do well in school,” said Leslie DeLeon, Xander’s mother. The philosophy is that caring for animals can be a means to confidence and social skills for emotionally challenged children. The day and residential facility now has two campuses in Brewster and Carmel, N.Y., more than 240 students, and about the same number of animals. “There has been a lot of research on pets at home and how healthy it is in the past 10 years,” said Steven Klee, PhD, director of clinical and medical services at Green Chimneys. Yet, as he first became aware of the use of animal intervention for special-needs children, even he was skeptical. “When you have traditional training as a psychologist, you never think about doing anything outside of the office,” Dr. Klee said. But Dr. Klee was converted. “Animals in a sense are purer, more consistent, more accepting. You are kind to the animals; they show their appreciation.” New York Times.
Novel RA strategy: Target first-line biologics for likely methotrexate nonresponders
MAUI, HAWAII – An ongoing proof-of-concept study in the United Kingdom uses T-cell subset analysis to identify those patients with early rheumatoid arthritis who are unlikely to experience remission with methotrexate alone and therefore warrant more potent first-line therapy with a tumor necrosis factor (TNF) inhibitor in combination with methotrexate, Paul Emery, MD, said at the 2019 Rheumatology Winter Clinical Symposium.

“When we get the readout from this study, if we get the results we expect, we could actually put it to the National Health Service that it would be cost saving to use biologics as first-line therapy in a proportion, which will be about 40% of patients. But we won’t necessarily need to use them for a year, and we’ll get a 70%-plus remission rate, which I think is the sort of level we should be asking for in our patients,” according to Dr. Emery, professor of rheumatology and director of the University of Leeds (England) Musculoskeletal Biomedical Research Center.
This proof-of-concept study capitalizes on earlier work by Dr. Emery and coinvestigators, who showed in 70 patients with early rheumatoid arthritis given methotrexate as their first-ever disease-modifying antirheumatic drug (DMARD) that those with a normal pretreatment frequency of naive CD4+ T cells had an 83% remission rate at 6 months as defined by a Disease Activity Score in 28 joints (DAS28) of less than 2.6. In contrast, only 21% of those with a reduced naive CD4+ T-cell frequency experienced remission when compared with healthy controls. In an analysis adjusted for age and the presence of anti–citrullinated protein antibodies (ACPA), a normal baseline naive CD4+ T-cell frequency was associated with a 5.9-fold increased likelihood of remission on methotrexate (Ann Rheum Dis. 2014 Nov;73[11]:2047-53).
In the new proof-of-concept study, DMARD-naive, ACPA-positive patients with early RA undergo T-cell subset quantification by flow cytometry. Thirty patients with a normal test result are assigned to methotrexate with treat-to-target dose escalation. Based upon the investigators’ earlier work, it’s anticipated that about 80% of these patients will be in remission at 6 months.
Sixty patients with an abnormal baseline T-cell test result are being randomized to methotrexate plus either placebo or biosimilar etanercept. Again based upon the earlier study, the expected remission rate at 6 months in the methotrexate-plus-placebo group is about 20%. In contrast, the anticipated remission rate in the patients on an anti-TNF biologic plus methotrexate as first-line therapy is about 70% on the basis of the results of previous clinical trials, including PRIZE (N Engl J Med. 2014 Nov 6;371[19]:1781-92) and COMET (Ann Rheum Dis. 2012 Jun;71[6]:989-92).
Meanwhile, the price tag for biosimilar TNF inhibitors in the United Kingdom has come down to the point that routine across-the-board use of biologics as first-line therapy is arguably cost effective, a situation Dr. Emery described as hitherto “the unthinkable.”
The cost of biosimilar adalimumab in the coming year will be less than $3,000 annually in the U.K. health care system. So if 100 patients with early RA and no contraindication to biologic therapy are placed on biosimilar adalimumab and methotrexate for 1 year, the total cost for the biologic in this cohort will be less than $300,000, and roughly 70 of the 100 patients will have achieved remission. This approach makes much more sense than current standard practice, which is to reserve biologics as second-line therapy for patients who have failed to achieve remission on nonbiologic DMARDs, thereby allowing their joint damage to advance in the interim to the point that they need to stay on biologic therapy for decades, the rheumatologist argued.
“Once one accepts that remission has become the aim of therapy, then the facts, I think, speak for themselves: There’s absolutely no doubt that the rate of remission is best with the first DMARD. So if our aim is remission, we should use that one opportunity with the best agent first, because we’re not going to get the same response later,” Dr. Emery said.
Also, “there’s no doubt” that the dose of biologics can be halved with no loss of efficacy in patients who achieve remission on full-dose therapy, as previously demonstrated in PRIZE and other trials. This strategy further reduces the overall cost of biologic therapy, he added.
Dr. Emery, who recently received the Order of the British Empire from Queen Elizabeth personally in recognition of his career achievements in rheumatology, reported having no financial conflicts of interest regarding his presentation.
MAUI, HAWAII – An ongoing proof-of-concept study in the United Kingdom uses T-cell subset analysis to identify those patients with early rheumatoid arthritis who are unlikely to experience remission with methotrexate alone and therefore warrant more potent first-line therapy with a tumor necrosis factor (TNF) inhibitor in combination with methotrexate, Paul Emery, MD, said at the 2019 Rheumatology Winter Clinical Symposium.
“When we get the readout from this study, if we get the results we expect, we could actually put it to the National Health Service that it would be cost saving to use biologics as first-line therapy in a proportion, which will be about 40% of patients. But we won’t necessarily need to use them for a year, and we’ll get a 70%-plus remission rate, which I think is the sort of level we should be asking for in our patients,” according to Dr. Emery, professor of rheumatology and director of the University of Leeds (England) Musculoskeletal Biomedical Research Center.
This proof-of-concept study capitalizes on earlier work by Dr. Emery and coinvestigators, who showed in 70 patients with early rheumatoid arthritis given methotrexate as their first-ever disease-modifying antirheumatic drug (DMARD) that those with a normal pretreatment frequency of naive CD4+ T cells had an 83% remission rate at 6 months as defined by a Disease Activity Score in 28 joints (DAS28) of less than 2.6. In contrast, only 21% of those with a reduced naive CD4+ T-cell frequency experienced remission when compared with healthy controls. In an analysis adjusted for age and the presence of anti–citrullinated protein antibodies (ACPA), a normal baseline naive CD4+ T-cell frequency was associated with a 5.9-fold increased likelihood of remission on methotrexate (Ann Rheum Dis. 2014 Nov;73[11]:2047-53).
In the new proof-of-concept study, DMARD-naive, ACPA-positive patients with early RA undergo T-cell subset quantification by flow cytometry. Thirty patients with a normal test result are assigned to methotrexate with treat-to-target dose escalation. Based upon the investigators’ earlier work, it’s anticipated that about 80% of these patients will be in remission at 6 months.
Sixty patients with an abnormal baseline T-cell test result are being randomized to methotrexate plus either placebo or biosimilar etanercept. Again based upon the earlier study, the expected remission rate at 6 months in the methotrexate-plus-placebo group is about 20%. In contrast, the anticipated remission rate in the patients on an anti-TNF biologic plus methotrexate as first-line therapy is about 70% on the basis of the results of previous clinical trials, including PRIZE (N Engl J Med. 2014 Nov 6;371[19]:1781-92) and COMET (Ann Rheum Dis. 2012 Jun;71[6]:989-92).
Meanwhile, the price tag for biosimilar TNF inhibitors in the United Kingdom has come down to the point that routine across-the-board use of biologics as first-line therapy is arguably cost effective, a situation Dr. Emery described as hitherto “the unthinkable.”
The cost of biosimilar adalimumab in the coming year will be less than $3,000 annually in the U.K. health care system. So if 100 patients with early RA and no contraindication to biologic therapy are placed on biosimilar adalimumab and methotrexate for 1 year, the total cost for the biologic in this cohort will be less than $300,000, and roughly 70 of the 100 patients will have achieved remission. This approach makes much more sense than current standard practice, which is to reserve biologics as second-line therapy for patients who have failed to achieve remission on nonbiologic DMARDs, thereby allowing their joint damage to advance in the interim to the point that they need to stay on biologic therapy for decades, the rheumatologist argued.
“Once one accepts that remission has become the aim of therapy, then the facts, I think, speak for themselves: There’s absolutely no doubt that the rate of remission is best with the first DMARD. So if our aim is remission, we should use that one opportunity with the best agent first, because we’re not going to get the same response later,” Dr. Emery said.
Also, “there’s no doubt” that the dose of biologics can be halved with no loss of efficacy in patients who achieve remission on full-dose therapy, as previously demonstrated in PRIZE and other trials. This strategy further reduces the overall cost of biologic therapy, he added.
Dr. Emery, who recently received the Order of the British Empire from Queen Elizabeth personally in recognition of his career achievements in rheumatology, reported having no financial conflicts of interest regarding his presentation.
MAUI, HAWAII – An ongoing proof-of-concept study in the United Kingdom uses T-cell subset analysis to identify those patients with early rheumatoid arthritis who are unlikely to experience remission with methotrexate alone and therefore warrant more potent first-line therapy with a tumor necrosis factor (TNF) inhibitor in combination with methotrexate, Paul Emery, MD, said at the 2019 Rheumatology Winter Clinical Symposium.
“When we get the readout from this study, if we get the results we expect, we could actually put it to the National Health Service that it would be cost saving to use biologics as first-line therapy in a proportion, which will be about 40% of patients. But we won’t necessarily need to use them for a year, and we’ll get a 70%-plus remission rate, which I think is the sort of level we should be asking for in our patients,” according to Dr. Emery, professor of rheumatology and director of the University of Leeds (England) Musculoskeletal Biomedical Research Center.
This proof-of-concept study capitalizes on earlier work by Dr. Emery and coinvestigators, who showed in 70 patients with early rheumatoid arthritis given methotrexate as their first-ever disease-modifying antirheumatic drug (DMARD) that those with a normal pretreatment frequency of naive CD4+ T cells had an 83% remission rate at 6 months as defined by a Disease Activity Score in 28 joints (DAS28) of less than 2.6. In contrast, only 21% of those with a reduced naive CD4+ T-cell frequency experienced remission when compared with healthy controls. In an analysis adjusted for age and the presence of anti–citrullinated protein antibodies (ACPA), a normal baseline naive CD4+ T-cell frequency was associated with a 5.9-fold increased likelihood of remission on methotrexate (Ann Rheum Dis. 2014 Nov;73[11]:2047-53).
In the new proof-of-concept study, DMARD-naive, ACPA-positive patients with early RA undergo T-cell subset quantification by flow cytometry. Thirty patients with a normal test result are assigned to methotrexate with treat-to-target dose escalation. Based upon the investigators’ earlier work, it’s anticipated that about 80% of these patients will be in remission at 6 months.
Sixty patients with an abnormal baseline T-cell test result are being randomized to methotrexate plus either placebo or biosimilar etanercept. Again based upon the earlier study, the expected remission rate at 6 months in the methotrexate-plus-placebo group is about 20%. In contrast, the anticipated remission rate in the patients on an anti-TNF biologic plus methotrexate as first-line therapy is about 70% on the basis of the results of previous clinical trials, including PRIZE (N Engl J Med. 2014 Nov 6;371[19]:1781-92) and COMET (Ann Rheum Dis. 2012 Jun;71[6]:989-92).
Meanwhile, the price tag for biosimilar TNF inhibitors in the United Kingdom has come down to the point that routine across-the-board use of biologics as first-line therapy is arguably cost effective, a situation Dr. Emery described as hitherto “the unthinkable.”
The cost of biosimilar adalimumab in the coming year will be less than $3,000 annually in the U.K. health care system. So if 100 patients with early RA and no contraindication to biologic therapy are placed on biosimilar adalimumab and methotrexate for 1 year, the total cost for the biologic in this cohort will be less than $300,000, and roughly 70 of the 100 patients will have achieved remission. This approach makes much more sense than current standard practice, which is to reserve biologics as second-line therapy for patients who have failed to achieve remission on nonbiologic DMARDs, thereby allowing their joint damage to advance in the interim to the point that they need to stay on biologic therapy for decades, the rheumatologist argued.
“Once one accepts that remission has become the aim of therapy, then the facts, I think, speak for themselves: There’s absolutely no doubt that the rate of remission is best with the first DMARD. So if our aim is remission, we should use that one opportunity with the best agent first, because we’re not going to get the same response later,” Dr. Emery said.
Also, “there’s no doubt” that the dose of biologics can be halved with no loss of efficacy in patients who achieve remission on full-dose therapy, as previously demonstrated in PRIZE and other trials. This strategy further reduces the overall cost of biologic therapy, he added.
Dr. Emery, who recently received the Order of the British Empire from Queen Elizabeth personally in recognition of his career achievements in rheumatology, reported having no financial conflicts of interest regarding his presentation.
REPORTING FROM RWCS 2019
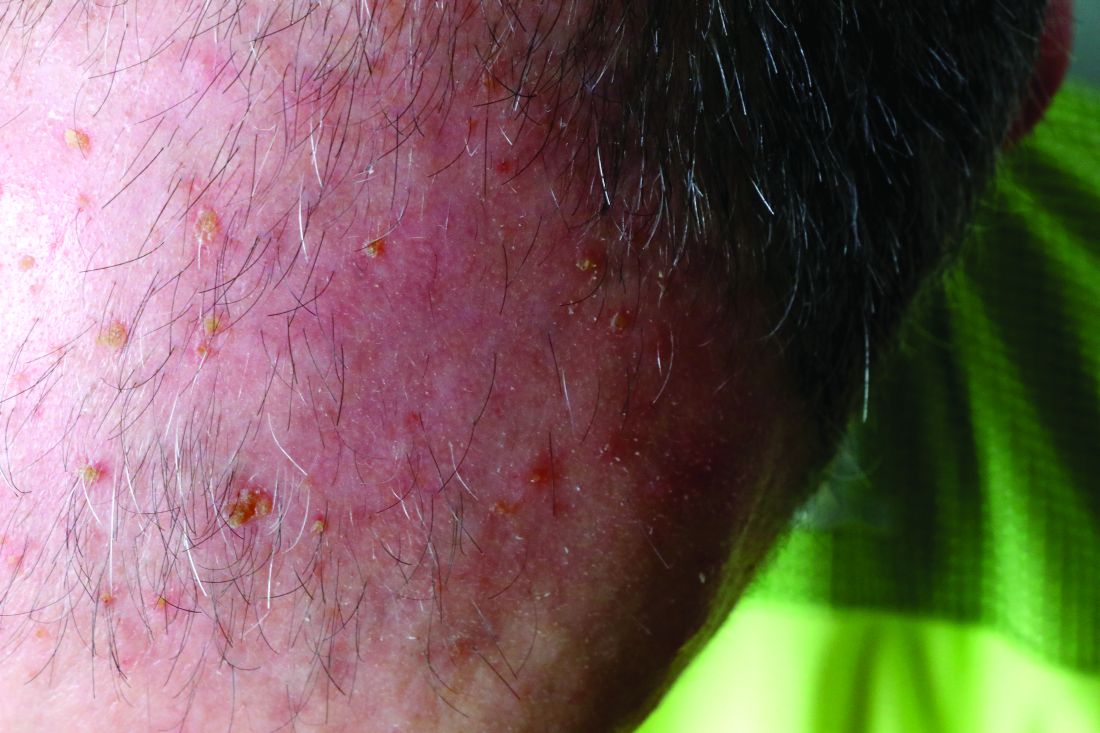
Fluorouracil beats other actinic keratosis treatments in head-to-head trial
A head-to-head comparison of four commonly used field-directed treatments for actinic keratosis (AK) found that 5% fluorouracil cream was the most effective at reducing the size of lesions.

In a study published in the March 7 issue of the New England Journal of Medicine, researchers reported the outcomes of a multicenter, single-blind trial in 602 patients with five or more AK lesions in one continuous area on the head measuring 25-100 cm2. Patients were randomized to treatment with either 5% fluorouracil cream, 5% imiquimod cream, methyl aminolevulinate photodynamic therapy (MAL-PDT), or 0.015% ingenol mebutate gel.
Overall, 74.7% of patients who received fluorouracil cream achieved treatment success – defined as at least a 75% reduction in lesion size at 12 months after the end of treatment – compared with 53.9% of patients treated with imiquimod, 37.7% of those treated with MAL-PDT, and 28.9% of those treated with ingenol mebutate. The differences between fluorouracil and the other treatments was significant.
Maud H.E. Jansen, MD, and Janneke P.H.M. Kessels, MD, of the department of dermatology at Maastricht (the Netherlands) University Medical Center and their coauthors pointed out that, while there was plenty of literature about different AK treatments, there were few head-to-head comparisons and many studies were underpowered or had different outcome measures.
Even when the analysis was restricted to patients with grade I or II lesions, fluorouracil remained the most effective treatment, with 75.3% of patients achieving treatment success, compared with 52.6% with imiquimod, 38.7% with MAL-PDT, and 30.2% with ingenol mebutate.
There were not enough patients with more severe grade III lesions to enable a separate analysis of their outcomes; 49 (7.9%) of patients in the study had at least one grade III lesion.
The authors noted that many previous studies had excluded patients with grade III lesions. “Exclusion of patients with grade III lesions was associated with slightly higher rates of success in the fluorouracil, MAL-PDT, and ingenol mebutate groups than the rates in the unrestricted analysis,” they wrote. The inclusion of patients with grade III AK lesions in this trial made it “more representative of patients seen in daily practice,” they added.
Treatment failure – less than 75% clearance of actinic keratosis at 3 months after the final treatment – was seen after one treatment cycle in 14.8% of patients treated with fluorouracil, 37.2% of patients on imiquimod, 34.6% of patients given photodynamic therapy, and 47.8% of patients on ingenol mebutate therapy.
All these patients were offered a second treatment cycle, but those treated with imiquimod, PDT, and ingenol mebutate were less likely to undergo a second treatment.
The authors suggested that the higher proportion of patients in the fluorouracil group who were willing to undergo a second round of therapy suggests they may have experienced less discomfort and inconvenience with the therapy to begin with, compared with those treated with the other regimens.
Full adherence to treatment was more common in the ingenol mebutate (98.7% of patients) and MAL-PDT (96.8%) groups, compared with the fluorouracil (88.7%) and imiquimod (88.2%) groups. However, patients in the fluorouracil group reported greater levels of patient satisfaction and improvements in health-related quality of life than did patients in the other treatment arms of the study.
No serious adverse events were reported with any of the treatments, and no patients stopped treatment because of adverse events. However, reports of moderate or severe crusts were highest among patients treated with imiquimod, and moderate to severe vesicles or bullae were highest among those treated with ingenol mebutate. Severe pain and severe burning sensation were significantly more common among those treated with MAL-PDT.
While the study had some limitations, the results “could affect treatment choices in both dermatology and primary care,” the authors wrote, pointing out how common AKs are in practice, accounting for 5 million dermatology visits in the United States every year. When considering treatment costs, “fluorouracil is also the most attractive option,” they added. “It is expected that a substantial cost reduction could be achieved with more uniformity in care and the choice for effective therapy.”
The study was supported by the Netherlands Organization for Health Research and Development. Five of the 11 authors declared conference costs, advisory board fees, or trial supplies from private industry, including from manufacturers of some of the products in the study. The remaining authors had no disclosures.
SOURCE: Jansen M et al. N Engl J Med. 2019;380:935-46.
A head-to-head comparison of four commonly used field-directed treatments for actinic keratosis (AK) found that 5% fluorouracil cream was the most effective at reducing the size of lesions.
In a study published in the March 7 issue of the New England Journal of Medicine, researchers reported the outcomes of a multicenter, single-blind trial in 602 patients with five or more AK lesions in one continuous area on the head measuring 25-100 cm2. Patients were randomized to treatment with either 5% fluorouracil cream, 5% imiquimod cream, methyl aminolevulinate photodynamic therapy (MAL-PDT), or 0.015% ingenol mebutate gel.
Overall, 74.7% of patients who received fluorouracil cream achieved treatment success – defined as at least a 75% reduction in lesion size at 12 months after the end of treatment – compared with 53.9% of patients treated with imiquimod, 37.7% of those treated with MAL-PDT, and 28.9% of those treated with ingenol mebutate. The differences between fluorouracil and the other treatments was significant.
Maud H.E. Jansen, MD, and Janneke P.H.M. Kessels, MD, of the department of dermatology at Maastricht (the Netherlands) University Medical Center and their coauthors pointed out that, while there was plenty of literature about different AK treatments, there were few head-to-head comparisons and many studies were underpowered or had different outcome measures.
Even when the analysis was restricted to patients with grade I or II lesions, fluorouracil remained the most effective treatment, with 75.3% of patients achieving treatment success, compared with 52.6% with imiquimod, 38.7% with MAL-PDT, and 30.2% with ingenol mebutate.
There were not enough patients with more severe grade III lesions to enable a separate analysis of their outcomes; 49 (7.9%) of patients in the study had at least one grade III lesion.
The authors noted that many previous studies had excluded patients with grade III lesions. “Exclusion of patients with grade III lesions was associated with slightly higher rates of success in the fluorouracil, MAL-PDT, and ingenol mebutate groups than the rates in the unrestricted analysis,” they wrote. The inclusion of patients with grade III AK lesions in this trial made it “more representative of patients seen in daily practice,” they added.
Treatment failure – less than 75% clearance of actinic keratosis at 3 months after the final treatment – was seen after one treatment cycle in 14.8% of patients treated with fluorouracil, 37.2% of patients on imiquimod, 34.6% of patients given photodynamic therapy, and 47.8% of patients on ingenol mebutate therapy.
All these patients were offered a second treatment cycle, but those treated with imiquimod, PDT, and ingenol mebutate were less likely to undergo a second treatment.
The authors suggested that the higher proportion of patients in the fluorouracil group who were willing to undergo a second round of therapy suggests they may have experienced less discomfort and inconvenience with the therapy to begin with, compared with those treated with the other regimens.
Full adherence to treatment was more common in the ingenol mebutate (98.7% of patients) and MAL-PDT (96.8%) groups, compared with the fluorouracil (88.7%) and imiquimod (88.2%) groups. However, patients in the fluorouracil group reported greater levels of patient satisfaction and improvements in health-related quality of life than did patients in the other treatment arms of the study.
No serious adverse events were reported with any of the treatments, and no patients stopped treatment because of adverse events. However, reports of moderate or severe crusts were highest among patients treated with imiquimod, and moderate to severe vesicles or bullae were highest among those treated with ingenol mebutate. Severe pain and severe burning sensation were significantly more common among those treated with MAL-PDT.
While the study had some limitations, the results “could affect treatment choices in both dermatology and primary care,” the authors wrote, pointing out how common AKs are in practice, accounting for 5 million dermatology visits in the United States every year. When considering treatment costs, “fluorouracil is also the most attractive option,” they added. “It is expected that a substantial cost reduction could be achieved with more uniformity in care and the choice for effective therapy.”
The study was supported by the Netherlands Organization for Health Research and Development. Five of the 11 authors declared conference costs, advisory board fees, or trial supplies from private industry, including from manufacturers of some of the products in the study. The remaining authors had no disclosures.
SOURCE: Jansen M et al. N Engl J Med. 2019;380:935-46.
A head-to-head comparison of four commonly used field-directed treatments for actinic keratosis (AK) found that 5% fluorouracil cream was the most effective at reducing the size of lesions.
In a study published in the March 7 issue of the New England Journal of Medicine, researchers reported the outcomes of a multicenter, single-blind trial in 602 patients with five or more AK lesions in one continuous area on the head measuring 25-100 cm2. Patients were randomized to treatment with either 5% fluorouracil cream, 5% imiquimod cream, methyl aminolevulinate photodynamic therapy (MAL-PDT), or 0.015% ingenol mebutate gel.
Overall, 74.7% of patients who received fluorouracil cream achieved treatment success – defined as at least a 75% reduction in lesion size at 12 months after the end of treatment – compared with 53.9% of patients treated with imiquimod, 37.7% of those treated with MAL-PDT, and 28.9% of those treated with ingenol mebutate. The differences between fluorouracil and the other treatments was significant.
Maud H.E. Jansen, MD, and Janneke P.H.M. Kessels, MD, of the department of dermatology at Maastricht (the Netherlands) University Medical Center and their coauthors pointed out that, while there was plenty of literature about different AK treatments, there were few head-to-head comparisons and many studies were underpowered or had different outcome measures.
Even when the analysis was restricted to patients with grade I or II lesions, fluorouracil remained the most effective treatment, with 75.3% of patients achieving treatment success, compared with 52.6% with imiquimod, 38.7% with MAL-PDT, and 30.2% with ingenol mebutate.
There were not enough patients with more severe grade III lesions to enable a separate analysis of their outcomes; 49 (7.9%) of patients in the study had at least one grade III lesion.
The authors noted that many previous studies had excluded patients with grade III lesions. “Exclusion of patients with grade III lesions was associated with slightly higher rates of success in the fluorouracil, MAL-PDT, and ingenol mebutate groups than the rates in the unrestricted analysis,” they wrote. The inclusion of patients with grade III AK lesions in this trial made it “more representative of patients seen in daily practice,” they added.
Treatment failure – less than 75% clearance of actinic keratosis at 3 months after the final treatment – was seen after one treatment cycle in 14.8% of patients treated with fluorouracil, 37.2% of patients on imiquimod, 34.6% of patients given photodynamic therapy, and 47.8% of patients on ingenol mebutate therapy.
All these patients were offered a second treatment cycle, but those treated with imiquimod, PDT, and ingenol mebutate were less likely to undergo a second treatment.
The authors suggested that the higher proportion of patients in the fluorouracil group who were willing to undergo a second round of therapy suggests they may have experienced less discomfort and inconvenience with the therapy to begin with, compared with those treated with the other regimens.
Full adherence to treatment was more common in the ingenol mebutate (98.7% of patients) and MAL-PDT (96.8%) groups, compared with the fluorouracil (88.7%) and imiquimod (88.2%) groups. However, patients in the fluorouracil group reported greater levels of patient satisfaction and improvements in health-related quality of life than did patients in the other treatment arms of the study.
No serious adverse events were reported with any of the treatments, and no patients stopped treatment because of adverse events. However, reports of moderate or severe crusts were highest among patients treated with imiquimod, and moderate to severe vesicles or bullae were highest among those treated with ingenol mebutate. Severe pain and severe burning sensation were significantly more common among those treated with MAL-PDT.
While the study had some limitations, the results “could affect treatment choices in both dermatology and primary care,” the authors wrote, pointing out how common AKs are in practice, accounting for 5 million dermatology visits in the United States every year. When considering treatment costs, “fluorouracil is also the most attractive option,” they added. “It is expected that a substantial cost reduction could be achieved with more uniformity in care and the choice for effective therapy.”
The study was supported by the Netherlands Organization for Health Research and Development. Five of the 11 authors declared conference costs, advisory board fees, or trial supplies from private industry, including from manufacturers of some of the products in the study. The remaining authors had no disclosures.
SOURCE: Jansen M et al. N Engl J Med. 2019;380:935-46.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Forget what you learned about infective endocarditis
This week in MDedge Cardiocast: Infective endocarditis isn’t what it used to be, there’s a new, lower goal for Americans’ dietary intake of sodium, a drug to treat multiple myeloma also raises heart failure risk, and Big Pharma says it can’t drop drug list prices alone.
Amazon Alexa
Apple Podcasts
Google Podcasts
TuneIn
This week in MDedge Cardiocast: Infective endocarditis isn’t what it used to be, there’s a new, lower goal for Americans’ dietary intake of sodium, a drug to treat multiple myeloma also raises heart failure risk, and Big Pharma says it can’t drop drug list prices alone.
Amazon Alexa
Apple Podcasts
Google Podcasts
TuneIn
This week in MDedge Cardiocast: Infective endocarditis isn’t what it used to be, there’s a new, lower goal for Americans’ dietary intake of sodium, a drug to treat multiple myeloma also raises heart failure risk, and Big Pharma says it can’t drop drug list prices alone.
Amazon Alexa
Apple Podcasts
Google Podcasts
TuneIn

FDA approves liquid colchicine for gout
for prophylaxis of gout flares in adults, according to a statement from Romeg Therapeutics.

Colchicine has been used in capsule and tablet forms to treat this form of arthritis for decades. An advantage to the new formulation is that it allows physicians to “easily make dose adjustments,” according to the statement.
“Existing therapies do not adequately address the physician’s need to adjust dosages of colchicine to manage the toxicity profile for patients with renal and liver impairments, side effects, common drug-to-drug interactions, and age-related health disorders,” said Naomi Vishnupad, PhD, chief scientific officer of Romeg Therapeutics, in the statement.
According to the prescribing information for the drug on the FDA website, this formulation is indicated for prophylaxis rather than acute treatment of gout flares because the safety profile of acute treatment with it has not yet been studied. It is contraindicated in patients with hepatic and/or renal impairment. Gastrointestinal symptoms were the most commonly reported adverse reactions.
The drug is expected to be available this summer.
for prophylaxis of gout flares in adults, according to a statement from Romeg Therapeutics.
Colchicine has been used in capsule and tablet forms to treat this form of arthritis for decades. An advantage to the new formulation is that it allows physicians to “easily make dose adjustments,” according to the statement.
“Existing therapies do not adequately address the physician’s need to adjust dosages of colchicine to manage the toxicity profile for patients with renal and liver impairments, side effects, common drug-to-drug interactions, and age-related health disorders,” said Naomi Vishnupad, PhD, chief scientific officer of Romeg Therapeutics, in the statement.
According to the prescribing information for the drug on the FDA website, this formulation is indicated for prophylaxis rather than acute treatment of gout flares because the safety profile of acute treatment with it has not yet been studied. It is contraindicated in patients with hepatic and/or renal impairment. Gastrointestinal symptoms were the most commonly reported adverse reactions.
The drug is expected to be available this summer.
for prophylaxis of gout flares in adults, according to a statement from Romeg Therapeutics.
Colchicine has been used in capsule and tablet forms to treat this form of arthritis for decades. An advantage to the new formulation is that it allows physicians to “easily make dose adjustments,” according to the statement.
“Existing therapies do not adequately address the physician’s need to adjust dosages of colchicine to manage the toxicity profile for patients with renal and liver impairments, side effects, common drug-to-drug interactions, and age-related health disorders,” said Naomi Vishnupad, PhD, chief scientific officer of Romeg Therapeutics, in the statement.
According to the prescribing information for the drug on the FDA website, this formulation is indicated for prophylaxis rather than acute treatment of gout flares because the safety profile of acute treatment with it has not yet been studied. It is contraindicated in patients with hepatic and/or renal impairment. Gastrointestinal symptoms were the most commonly reported adverse reactions.
The drug is expected to be available this summer.
One-time, universal hepatitis C testing cost effective, researchers say
Universal one-time screening for hepatitis C virus infection is cost effective, compared with birth cohort screening alone, according to the results of a study published in Clinical Gastroenterology and Hepatology.
The Centers for Disease Control and Prevention and the U.S. Preventive Services Task Force recommend testing all individuals born between 1945 and 1965 in addition to injection drug users and other high-risk individuals. But so-called birth cohort screening does not reflect the recent spike in hepatitis C virus (HCV) cases among younger persons in the United States, nor the current recommendation to treat nearly all chronic HCV cases, wrote Mark H. Eckman, MD, of the University of Cincinnati, and his associates.
Using a computer program called Decision Maker, they modeled the cost-effectiveness of universal one-time testing, birth cohort screening, and no screening based on quality-adjusted life-years (QALYS) and 2017 U.S. dollars. They assumed that all HCV-infected patients were treatment naive, treatment eligible, and asymptomatic (for example, had no decompensated cirrhosis). They used efficacy data from the ASTRAL trials of sofosbuvir-velpatasvir as well as the ENDURANCE, SURVEYOR, and EXPEDITION trials of glecaprevir-pibrentasvir. In the model, patients who did not achieve a sustained viral response to treatment went on to complete a 12-week triple direct-acting antiviral (DAA) regimen (sofosbuvir, velpatasvir, and voxilaprevir).
Based on these assumptions, universal one-time screening and treatment of infected individuals cost less than $50,000 per QALY gained, making it highly cost effective, compared with no screening, the investigators wrote. Universal screening also was highly cost effective when compared with birth cohort screening, costing $11,378 for each QALY gained.
“Analyses performed during the era of first-generation DAAs and interferon-based treatment regimens found birth-cohort screening to be ‘cost effective,’ ” the researchers wrote. “However, the availability of a new generation of highly effective, non–interferon-based oral regimens, with fewer side effects and shorter treatment courses, has altered the dynamic around the question of screening.” They pointed to another recent study in which universal one-time HCV testing was more cost effective than birth cohort screening.
Such findings have spurred experts to revisit guidelines on HCV screening, but universal testing is controversial when some states, counties, and communities have a low HCV prevalence. In the model, universal one-time HCV screening was cost effective (less than $50,000 per QALY gained), compared with birth cohort screening as long as prevalence exceeded 0.07% among adults not born between 1945 and 1965. The current prevalence estimate in this group is 0.29%, which is probably low because it does not account for the rising incidence among younger adults, the researchers wrote. In an ideal world, all clinics and hospitals would implement an HCV testing program, but in the real world of scarce resources, “data regarding the cost-effectiveness threshold can guide local policy decisions by directing testing services to settings in which they generate sufficient benefit for the cost.”
Partial funding came from the National Foundation for the Centers for Disease Control and Prevention (CDC Foundation), with funding provided through multiple donors to the CDC Foundation’s Viral Hepatitis Action Coalition. Dr. Eckman reported grant support from Merck and one coinvestigator reported ties to AbbVie, Gilead, Merck, and several other pharmaceutical companies.
SOURCE: Eckman MH et al. Clin Gastroenterol Hepatol. 2018 Sep 7. doi: 10.1016/j.cgh.2018.08.080.
Universal one-time screening for hepatitis C virus infection is cost effective, compared with birth cohort screening alone, according to the results of a study published in Clinical Gastroenterology and Hepatology.
The Centers for Disease Control and Prevention and the U.S. Preventive Services Task Force recommend testing all individuals born between 1945 and 1965 in addition to injection drug users and other high-risk individuals. But so-called birth cohort screening does not reflect the recent spike in hepatitis C virus (HCV) cases among younger persons in the United States, nor the current recommendation to treat nearly all chronic HCV cases, wrote Mark H. Eckman, MD, of the University of Cincinnati, and his associates.
Using a computer program called Decision Maker, they modeled the cost-effectiveness of universal one-time testing, birth cohort screening, and no screening based on quality-adjusted life-years (QALYS) and 2017 U.S. dollars. They assumed that all HCV-infected patients were treatment naive, treatment eligible, and asymptomatic (for example, had no decompensated cirrhosis). They used efficacy data from the ASTRAL trials of sofosbuvir-velpatasvir as well as the ENDURANCE, SURVEYOR, and EXPEDITION trials of glecaprevir-pibrentasvir. In the model, patients who did not achieve a sustained viral response to treatment went on to complete a 12-week triple direct-acting antiviral (DAA) regimen (sofosbuvir, velpatasvir, and voxilaprevir).
Based on these assumptions, universal one-time screening and treatment of infected individuals cost less than $50,000 per QALY gained, making it highly cost effective, compared with no screening, the investigators wrote. Universal screening also was highly cost effective when compared with birth cohort screening, costing $11,378 for each QALY gained.
“Analyses performed during the era of first-generation DAAs and interferon-based treatment regimens found birth-cohort screening to be ‘cost effective,’ ” the researchers wrote. “However, the availability of a new generation of highly effective, non–interferon-based oral regimens, with fewer side effects and shorter treatment courses, has altered the dynamic around the question of screening.” They pointed to another recent study in which universal one-time HCV testing was more cost effective than birth cohort screening.
Such findings have spurred experts to revisit guidelines on HCV screening, but universal testing is controversial when some states, counties, and communities have a low HCV prevalence. In the model, universal one-time HCV screening was cost effective (less than $50,000 per QALY gained), compared with birth cohort screening as long as prevalence exceeded 0.07% among adults not born between 1945 and 1965. The current prevalence estimate in this group is 0.29%, which is probably low because it does not account for the rising incidence among younger adults, the researchers wrote. In an ideal world, all clinics and hospitals would implement an HCV testing program, but in the real world of scarce resources, “data regarding the cost-effectiveness threshold can guide local policy decisions by directing testing services to settings in which they generate sufficient benefit for the cost.”
Partial funding came from the National Foundation for the Centers for Disease Control and Prevention (CDC Foundation), with funding provided through multiple donors to the CDC Foundation’s Viral Hepatitis Action Coalition. Dr. Eckman reported grant support from Merck and one coinvestigator reported ties to AbbVie, Gilead, Merck, and several other pharmaceutical companies.
SOURCE: Eckman MH et al. Clin Gastroenterol Hepatol. 2018 Sep 7. doi: 10.1016/j.cgh.2018.08.080.
Universal one-time screening for hepatitis C virus infection is cost effective, compared with birth cohort screening alone, according to the results of a study published in Clinical Gastroenterology and Hepatology.
The Centers for Disease Control and Prevention and the U.S. Preventive Services Task Force recommend testing all individuals born between 1945 and 1965 in addition to injection drug users and other high-risk individuals. But so-called birth cohort screening does not reflect the recent spike in hepatitis C virus (HCV) cases among younger persons in the United States, nor the current recommendation to treat nearly all chronic HCV cases, wrote Mark H. Eckman, MD, of the University of Cincinnati, and his associates.
Using a computer program called Decision Maker, they modeled the cost-effectiveness of universal one-time testing, birth cohort screening, and no screening based on quality-adjusted life-years (QALYS) and 2017 U.S. dollars. They assumed that all HCV-infected patients were treatment naive, treatment eligible, and asymptomatic (for example, had no decompensated cirrhosis). They used efficacy data from the ASTRAL trials of sofosbuvir-velpatasvir as well as the ENDURANCE, SURVEYOR, and EXPEDITION trials of glecaprevir-pibrentasvir. In the model, patients who did not achieve a sustained viral response to treatment went on to complete a 12-week triple direct-acting antiviral (DAA) regimen (sofosbuvir, velpatasvir, and voxilaprevir).
Based on these assumptions, universal one-time screening and treatment of infected individuals cost less than $50,000 per QALY gained, making it highly cost effective, compared with no screening, the investigators wrote. Universal screening also was highly cost effective when compared with birth cohort screening, costing $11,378 for each QALY gained.
“Analyses performed during the era of first-generation DAAs and interferon-based treatment regimens found birth-cohort screening to be ‘cost effective,’ ” the researchers wrote. “However, the availability of a new generation of highly effective, non–interferon-based oral regimens, with fewer side effects and shorter treatment courses, has altered the dynamic around the question of screening.” They pointed to another recent study in which universal one-time HCV testing was more cost effective than birth cohort screening.
Such findings have spurred experts to revisit guidelines on HCV screening, but universal testing is controversial when some states, counties, and communities have a low HCV prevalence. In the model, universal one-time HCV screening was cost effective (less than $50,000 per QALY gained), compared with birth cohort screening as long as prevalence exceeded 0.07% among adults not born between 1945 and 1965. The current prevalence estimate in this group is 0.29%, which is probably low because it does not account for the rising incidence among younger adults, the researchers wrote. In an ideal world, all clinics and hospitals would implement an HCV testing program, but in the real world of scarce resources, “data regarding the cost-effectiveness threshold can guide local policy decisions by directing testing services to settings in which they generate sufficient benefit for the cost.”
Partial funding came from the National Foundation for the Centers for Disease Control and Prevention (CDC Foundation), with funding provided through multiple donors to the CDC Foundation’s Viral Hepatitis Action Coalition. Dr. Eckman reported grant support from Merck and one coinvestigator reported ties to AbbVie, Gilead, Merck, and several other pharmaceutical companies.
SOURCE: Eckman MH et al. Clin Gastroenterol Hepatol. 2018 Sep 7. doi: 10.1016/j.cgh.2018.08.080.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Poor COPD management might increase MI risk in HIV
SEATTLE – Chronic obstructive pulmonary disease is independently associated with an increased risk of myocardial infarction in people with HIV, according to a report at the Conference on Retroviruses and Opportunistic Infections.

Chronic obstructive pulmonary disease (COPD) is known to increase the risk of myocardial infarction (MI) in the general population, but hadn’t been shown until now to do the same in HIV. The study raises the question of whether COPD is being managed adequately in patients with the virus, according to study lead Kristina Crothers, MD, associate professor in the division of pulmonary, critical care & sleep medicine at the University of Washington, Seattle.
The investigators reviewed 25,509 HIV patients in the Center for AIDS Research Network of Integrated Clinical Systems cohort, a large electronic database of HIV-infected people. They defined COPD by diagnostic codes and inhaler prescriptions. MIs were adjudicated by review.
The team identified 423 subjects with moderate to severe COPD, and 698 who had MIs, including 339 type 1 MIs (T1MI) from a ruptured plaque (54%), and 294 (46%) type 2 heart attacks (T2MI) from a supply-demand mismatch due to sepsis or some other problem. In general, T2MIs are far more common in people with HIV.
COPD was associated with a greater than twofold increased risk of MI after adjustment for age, sex, viral load, nadir CD4 count, hypertension, and other confounders. The risk dropped slightly when smoking – both current smoking and pack years – was added to the model (adjusted hazard ratio 1.88, 95% confidence interval, 1.34-2.63).
The association was particularly strong for T2MI, especially in the setting of bacteremia and sepsis, and unlike T1MI, it remained significant after adjustment for smoking.
The study establishes a link between COPD and MI in HIV, but it could not answer what’s going on. Chronic inflammation from the virus could be at play, but the team also found hints of inadequate COPD management.
“About 60% of patients were on inhalers ... but only about 25% of them were on long-acting inhalers. 75% were only on short-acting.” That’s a problem because long-acting inhalers are needed to control exacerbations, Dr. Crothers said.
The study didn’t capture exacerbation rates, but increased rates could help explain the MI risk. Increased rates of pneumonia could as well, since pneumonia is a common cause of sepsis.
“We need to better manage complications of COPD in this population. I think optimizing long-term COPD management could have many beneficial effects,” Dr. Crothers said.
The National Institutes of Health funded the work. Dr. Crothers had no disclosures.
SOURCE: Crothers K et al. CROI 2019, Abstract 31.
SEATTLE – Chronic obstructive pulmonary disease is independently associated with an increased risk of myocardial infarction in people with HIV, according to a report at the Conference on Retroviruses and Opportunistic Infections.
Chronic obstructive pulmonary disease (COPD) is known to increase the risk of myocardial infarction (MI) in the general population, but hadn’t been shown until now to do the same in HIV. The study raises the question of whether COPD is being managed adequately in patients with the virus, according to study lead Kristina Crothers, MD, associate professor in the division of pulmonary, critical care & sleep medicine at the University of Washington, Seattle.
The investigators reviewed 25,509 HIV patients in the Center for AIDS Research Network of Integrated Clinical Systems cohort, a large electronic database of HIV-infected people. They defined COPD by diagnostic codes and inhaler prescriptions. MIs were adjudicated by review.
The team identified 423 subjects with moderate to severe COPD, and 698 who had MIs, including 339 type 1 MIs (T1MI) from a ruptured plaque (54%), and 294 (46%) type 2 heart attacks (T2MI) from a supply-demand mismatch due to sepsis or some other problem. In general, T2MIs are far more common in people with HIV.
COPD was associated with a greater than twofold increased risk of MI after adjustment for age, sex, viral load, nadir CD4 count, hypertension, and other confounders. The risk dropped slightly when smoking – both current smoking and pack years – was added to the model (adjusted hazard ratio 1.88, 95% confidence interval, 1.34-2.63).
The association was particularly strong for T2MI, especially in the setting of bacteremia and sepsis, and unlike T1MI, it remained significant after adjustment for smoking.
The study establishes a link between COPD and MI in HIV, but it could not answer what’s going on. Chronic inflammation from the virus could be at play, but the team also found hints of inadequate COPD management.
“About 60% of patients were on inhalers ... but only about 25% of them were on long-acting inhalers. 75% were only on short-acting.” That’s a problem because long-acting inhalers are needed to control exacerbations, Dr. Crothers said.
The study didn’t capture exacerbation rates, but increased rates could help explain the MI risk. Increased rates of pneumonia could as well, since pneumonia is a common cause of sepsis.
“We need to better manage complications of COPD in this population. I think optimizing long-term COPD management could have many beneficial effects,” Dr. Crothers said.
The National Institutes of Health funded the work. Dr. Crothers had no disclosures.
SOURCE: Crothers K et al. CROI 2019, Abstract 31.
SEATTLE – Chronic obstructive pulmonary disease is independently associated with an increased risk of myocardial infarction in people with HIV, according to a report at the Conference on Retroviruses and Opportunistic Infections.
Chronic obstructive pulmonary disease (COPD) is known to increase the risk of myocardial infarction (MI) in the general population, but hadn’t been shown until now to do the same in HIV. The study raises the question of whether COPD is being managed adequately in patients with the virus, according to study lead Kristina Crothers, MD, associate professor in the division of pulmonary, critical care & sleep medicine at the University of Washington, Seattle.
The investigators reviewed 25,509 HIV patients in the Center for AIDS Research Network of Integrated Clinical Systems cohort, a large electronic database of HIV-infected people. They defined COPD by diagnostic codes and inhaler prescriptions. MIs were adjudicated by review.
The team identified 423 subjects with moderate to severe COPD, and 698 who had MIs, including 339 type 1 MIs (T1MI) from a ruptured plaque (54%), and 294 (46%) type 2 heart attacks (T2MI) from a supply-demand mismatch due to sepsis or some other problem. In general, T2MIs are far more common in people with HIV.
COPD was associated with a greater than twofold increased risk of MI after adjustment for age, sex, viral load, nadir CD4 count, hypertension, and other confounders. The risk dropped slightly when smoking – both current smoking and pack years – was added to the model (adjusted hazard ratio 1.88, 95% confidence interval, 1.34-2.63).
The association was particularly strong for T2MI, especially in the setting of bacteremia and sepsis, and unlike T1MI, it remained significant after adjustment for smoking.
The study establishes a link between COPD and MI in HIV, but it could not answer what’s going on. Chronic inflammation from the virus could be at play, but the team also found hints of inadequate COPD management.
“About 60% of patients were on inhalers ... but only about 25% of them were on long-acting inhalers. 75% were only on short-acting.” That’s a problem because long-acting inhalers are needed to control exacerbations, Dr. Crothers said.
The study didn’t capture exacerbation rates, but increased rates could help explain the MI risk. Increased rates of pneumonia could as well, since pneumonia is a common cause of sepsis.
“We need to better manage complications of COPD in this population. I think optimizing long-term COPD management could have many beneficial effects,” Dr. Crothers said.
The National Institutes of Health funded the work. Dr. Crothers had no disclosures.
SOURCE: Crothers K et al. CROI 2019, Abstract 31.
REPORTING FROM CROI 2019
Higher dose of checkpoint inhibitor every 4 weeks feasible in NSCLC
SAN FRANCISCO – For patients with advanced non–small cell lung cancer (NSCLC) who previously had disease control with the checkpoint inhibitor nivolumab (Opdivo), second-line nivolumab at a higher dose every 4 weeks appeared to be comparable in efficacy and safety with standard-dose nivolumab every 2 weeks.
The key word in that last sentence is “appeared,” because the Checkmate 384 trial that was designed to show noninferiority of the every-4-weeks regimen lacked the statistical muscle to get the job done, reported Edward B. Garon, MD, from the University of California, Los Angeles.
“In many respects, extending the dosing frequency of nivolumab fulfills some of the promise of immunotherapy: The idea that we would be able to decrease the medicalization of the lives of our patients. For some people this would lead to them being able to resume a more normal work schedule, and for other people it would allow them to do things for fun, like travel on trips that would take longer than a couple of weeks,” he said at the American Society of Clinical Oncology (ASCO) – Society for Immunotherapy of Cancer (SITC): Clinical Immuno-Oncology Symposium.
However, because of difficulties in recruitment, the investigators had to stop enrollment early and settle for a sample size of 363 patients, instead of the 600 planned that would be necessary to meet a 10% noninferiority margin and one-sided 95% confidence interval. Thus, the trial analysis can only be reported as descriptive rather than definitive, Dr. Garon acknowledged.
Nivolumab is approved at a fixed dose of 240 mg every 2 weeks for the treatment of multiple tumor types in several different nations, and in the United States and Canada it is approved at a dose of 480 mg every 4 weeks for the treatment of NSCLC.
The CheckMate 384 study enrolled patients with advanced or metastatic NSCLC who had received 3 mg/kg or 240 mg of nivolumab every 2 weeks for up to 1 year. The patients had to have had relatively good performance status (Eastern Cooperative Oncology Group 0-2) and two consecutive assessments of either complete response, partial response, or stable disease.
The patients were stratified by tumor histology (squamous or nonsquamous) and response to prior nivolumab therapy at randomization, and were then randomized to receive nivolumab 240 mg every 2 weeks or 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
Dr. Garon presented an interim analysis including data on 329 of the 363 patients; the final analysis will occur after all patients have had a minimum of 12 months of follow-up. Here, he reported on 6-month progression-free survival, a coprimary endpoint with 12-month PFS.
After a median follow-up of 9.5 months in the Q4-week group and 10.2 months in the Q2-week group, the 6-month PFS rates were identical between the two dosing strategies, at 72%. The median PFS was 12.1 months and 12.2 months, respectively.
“Although the study is no longer formally powered to show noninferiority, there’s certainly nothing in these curves that makes me concerned that this 480 mg every-4-week dose would be inferior,” Dr. Garon said.
There was a slightly higher rate of treatment-related adverse events of any grade in the lower, more frequent dose group: 48% in the Q4-week versus 61% in the Q2-week arm. The respective rates of grade 3 or 4 adverse events were 8% and 12%. Rates of serious adverse events and events leading to treatment discontinuation were similar between the group; there were no treatment-related deaths.
The investigators hypothesize that the higher rate of overall events in the lower-dose group may be attributable to more frequent visits and more opportunities to report adverse events, Dr. Garon said.
“Overall, the clinical data are in agreement with the pharmacokinetic modeling and give further evidence for this 480 mg every 4 week nivolumab dosing option,” he concluded.
The study was supported by Bristol-Myers Squibb. Dr. Garon reported receiving research support from Bristol-Myers Squibb and others and consulting fees from Dracen Pharmaceuticals.
SOURCE: Garon EB et al. ASCO-SITC, Abstract 100.
SAN FRANCISCO – For patients with advanced non–small cell lung cancer (NSCLC) who previously had disease control with the checkpoint inhibitor nivolumab (Opdivo), second-line nivolumab at a higher dose every 4 weeks appeared to be comparable in efficacy and safety with standard-dose nivolumab every 2 weeks.
The key word in that last sentence is “appeared,” because the Checkmate 384 trial that was designed to show noninferiority of the every-4-weeks regimen lacked the statistical muscle to get the job done, reported Edward B. Garon, MD, from the University of California, Los Angeles.
“In many respects, extending the dosing frequency of nivolumab fulfills some of the promise of immunotherapy: The idea that we would be able to decrease the medicalization of the lives of our patients. For some people this would lead to them being able to resume a more normal work schedule, and for other people it would allow them to do things for fun, like travel on trips that would take longer than a couple of weeks,” he said at the American Society of Clinical Oncology (ASCO) – Society for Immunotherapy of Cancer (SITC): Clinical Immuno-Oncology Symposium.
However, because of difficulties in recruitment, the investigators had to stop enrollment early and settle for a sample size of 363 patients, instead of the 600 planned that would be necessary to meet a 10% noninferiority margin and one-sided 95% confidence interval. Thus, the trial analysis can only be reported as descriptive rather than definitive, Dr. Garon acknowledged.
Nivolumab is approved at a fixed dose of 240 mg every 2 weeks for the treatment of multiple tumor types in several different nations, and in the United States and Canada it is approved at a dose of 480 mg every 4 weeks for the treatment of NSCLC.
The CheckMate 384 study enrolled patients with advanced or metastatic NSCLC who had received 3 mg/kg or 240 mg of nivolumab every 2 weeks for up to 1 year. The patients had to have had relatively good performance status (Eastern Cooperative Oncology Group 0-2) and two consecutive assessments of either complete response, partial response, or stable disease.
The patients were stratified by tumor histology (squamous or nonsquamous) and response to prior nivolumab therapy at randomization, and were then randomized to receive nivolumab 240 mg every 2 weeks or 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
Dr. Garon presented an interim analysis including data on 329 of the 363 patients; the final analysis will occur after all patients have had a minimum of 12 months of follow-up. Here, he reported on 6-month progression-free survival, a coprimary endpoint with 12-month PFS.
After a median follow-up of 9.5 months in the Q4-week group and 10.2 months in the Q2-week group, the 6-month PFS rates were identical between the two dosing strategies, at 72%. The median PFS was 12.1 months and 12.2 months, respectively.
“Although the study is no longer formally powered to show noninferiority, there’s certainly nothing in these curves that makes me concerned that this 480 mg every-4-week dose would be inferior,” Dr. Garon said.
There was a slightly higher rate of treatment-related adverse events of any grade in the lower, more frequent dose group: 48% in the Q4-week versus 61% in the Q2-week arm. The respective rates of grade 3 or 4 adverse events were 8% and 12%. Rates of serious adverse events and events leading to treatment discontinuation were similar between the group; there were no treatment-related deaths.
The investigators hypothesize that the higher rate of overall events in the lower-dose group may be attributable to more frequent visits and more opportunities to report adverse events, Dr. Garon said.
“Overall, the clinical data are in agreement with the pharmacokinetic modeling and give further evidence for this 480 mg every 4 week nivolumab dosing option,” he concluded.
The study was supported by Bristol-Myers Squibb. Dr. Garon reported receiving research support from Bristol-Myers Squibb and others and consulting fees from Dracen Pharmaceuticals.
SOURCE: Garon EB et al. ASCO-SITC, Abstract 100.
SAN FRANCISCO – For patients with advanced non–small cell lung cancer (NSCLC) who previously had disease control with the checkpoint inhibitor nivolumab (Opdivo), second-line nivolumab at a higher dose every 4 weeks appeared to be comparable in efficacy and safety with standard-dose nivolumab every 2 weeks.
The key word in that last sentence is “appeared,” because the Checkmate 384 trial that was designed to show noninferiority of the every-4-weeks regimen lacked the statistical muscle to get the job done, reported Edward B. Garon, MD, from the University of California, Los Angeles.
“In many respects, extending the dosing frequency of nivolumab fulfills some of the promise of immunotherapy: The idea that we would be able to decrease the medicalization of the lives of our patients. For some people this would lead to them being able to resume a more normal work schedule, and for other people it would allow them to do things for fun, like travel on trips that would take longer than a couple of weeks,” he said at the American Society of Clinical Oncology (ASCO) – Society for Immunotherapy of Cancer (SITC): Clinical Immuno-Oncology Symposium.
However, because of difficulties in recruitment, the investigators had to stop enrollment early and settle for a sample size of 363 patients, instead of the 600 planned that would be necessary to meet a 10% noninferiority margin and one-sided 95% confidence interval. Thus, the trial analysis can only be reported as descriptive rather than definitive, Dr. Garon acknowledged.
Nivolumab is approved at a fixed dose of 240 mg every 2 weeks for the treatment of multiple tumor types in several different nations, and in the United States and Canada it is approved at a dose of 480 mg every 4 weeks for the treatment of NSCLC.
The CheckMate 384 study enrolled patients with advanced or metastatic NSCLC who had received 3 mg/kg or 240 mg of nivolumab every 2 weeks for up to 1 year. The patients had to have had relatively good performance status (Eastern Cooperative Oncology Group 0-2) and two consecutive assessments of either complete response, partial response, or stable disease.
The patients were stratified by tumor histology (squamous or nonsquamous) and response to prior nivolumab therapy at randomization, and were then randomized to receive nivolumab 240 mg every 2 weeks or 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
Dr. Garon presented an interim analysis including data on 329 of the 363 patients; the final analysis will occur after all patients have had a minimum of 12 months of follow-up. Here, he reported on 6-month progression-free survival, a coprimary endpoint with 12-month PFS.
After a median follow-up of 9.5 months in the Q4-week group and 10.2 months in the Q2-week group, the 6-month PFS rates were identical between the two dosing strategies, at 72%. The median PFS was 12.1 months and 12.2 months, respectively.
“Although the study is no longer formally powered to show noninferiority, there’s certainly nothing in these curves that makes me concerned that this 480 mg every-4-week dose would be inferior,” Dr. Garon said.
There was a slightly higher rate of treatment-related adverse events of any grade in the lower, more frequent dose group: 48% in the Q4-week versus 61% in the Q2-week arm. The respective rates of grade 3 or 4 adverse events were 8% and 12%. Rates of serious adverse events and events leading to treatment discontinuation were similar between the group; there were no treatment-related deaths.
The investigators hypothesize that the higher rate of overall events in the lower-dose group may be attributable to more frequent visits and more opportunities to report adverse events, Dr. Garon said.
“Overall, the clinical data are in agreement with the pharmacokinetic modeling and give further evidence for this 480 mg every 4 week nivolumab dosing option,” he concluded.
The study was supported by Bristol-Myers Squibb. Dr. Garon reported receiving research support from Bristol-Myers Squibb and others and consulting fees from Dracen Pharmaceuticals.
SOURCE: Garon EB et al. ASCO-SITC, Abstract 100.
REPORTING FROM ASCO-SITC