User login
AGA announces its newest class of Fellows
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.
AGA Fellowship status is an honor awarded to members who demonstrate a personal commitment to the field of gastroenterology, as well as professional achievement in clinical private or academic practice and in basic or clinical research.
The most recent inductees into the AGA Fellows Program were recognized at Digestive Disease Week® (DDW) 2018 and received a digital ribbon in their AGA Community profile. The 2018 class of AGA Fellows includes 112 members, who added the designation “AGAF” in their professional activities.
Join the AGA Fellowship Recognition Panel in congratulating these distinguished members and view the 2018 class of AGA Fellows in the AGA Community forum, community.gastro.org
Learn more about joining this international community of excellence. Applications for the 2019 cohort are now being accepted. Those in clinical private or academic practice and in basic or clinical research who meet the AGAF criteria are invited to apply. Applications are due Aug. 27, 2018. Learn more at gastro.org/fellowship.
How does the Quality Payment Program affect you?
AGA asks Congress and CMS to continue to implement the Quality Payment Program (QPP) in a way that maximizes flexibility and success for you and your Medicare patients.
Most gastroenterologists participate in the Merit-Based Incentive Payment System (MIPS), which means how the QPP is implemented impacts the entire GI profession. The QPP replaced the sustainable growth rate (SGR) formula in 2015 when the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into law. The QPP is comprised of two tracks: MIPS and Advanced Alternative Payment Models (Advanced APMs).
CMS has designated 2017 and 2018 as transition years to allow providers to learn about the QPP and to gradually increase their preparedness for MIPS.
Congress also recently acted to provide CMS additional flexibility with respect to QPP and MIPS implementation, including:
• Excluding Medicare Part B drug costs from MIPS payment adjustments.
• Eliminating improvement scoring for the cost performance category for the second through fifth years of MIPS.
• Allowing CMS to weight the cost performance category at less than 30 percent, but not less than 10 percent for the second through fifth years of MIPS.
• Allowing CMS flexibility in setting the performance threshold for MIPS in years two through five to ensure a gradual and incremental transition to the performance threshold set at the mean or median for the sixth year.
QPP implementation is a top priority for AGA to ensure that the value of specialty care is recognized. Learn more on our website www.gastro.org/QPP.
AGA asks Congress and CMS to continue to implement the Quality Payment Program (QPP) in a way that maximizes flexibility and success for you and your Medicare patients.
Most gastroenterologists participate in the Merit-Based Incentive Payment System (MIPS), which means how the QPP is implemented impacts the entire GI profession. The QPP replaced the sustainable growth rate (SGR) formula in 2015 when the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into law. The QPP is comprised of two tracks: MIPS and Advanced Alternative Payment Models (Advanced APMs).
CMS has designated 2017 and 2018 as transition years to allow providers to learn about the QPP and to gradually increase their preparedness for MIPS.
Congress also recently acted to provide CMS additional flexibility with respect to QPP and MIPS implementation, including:
• Excluding Medicare Part B drug costs from MIPS payment adjustments.
• Eliminating improvement scoring for the cost performance category for the second through fifth years of MIPS.
• Allowing CMS to weight the cost performance category at less than 30 percent, but not less than 10 percent for the second through fifth years of MIPS.
• Allowing CMS flexibility in setting the performance threshold for MIPS in years two through five to ensure a gradual and incremental transition to the performance threshold set at the mean or median for the sixth year.
QPP implementation is a top priority for AGA to ensure that the value of specialty care is recognized. Learn more on our website www.gastro.org/QPP.
AGA asks Congress and CMS to continue to implement the Quality Payment Program (QPP) in a way that maximizes flexibility and success for you and your Medicare patients.
Most gastroenterologists participate in the Merit-Based Incentive Payment System (MIPS), which means how the QPP is implemented impacts the entire GI profession. The QPP replaced the sustainable growth rate (SGR) formula in 2015 when the Medicare Access and CHIP Reauthorization Act (MACRA) was signed into law. The QPP is comprised of two tracks: MIPS and Advanced Alternative Payment Models (Advanced APMs).
CMS has designated 2017 and 2018 as transition years to allow providers to learn about the QPP and to gradually increase their preparedness for MIPS.
Congress also recently acted to provide CMS additional flexibility with respect to QPP and MIPS implementation, including:
• Excluding Medicare Part B drug costs from MIPS payment adjustments.
• Eliminating improvement scoring for the cost performance category for the second through fifth years of MIPS.
• Allowing CMS to weight the cost performance category at less than 30 percent, but not less than 10 percent for the second through fifth years of MIPS.
• Allowing CMS flexibility in setting the performance threshold for MIPS in years two through five to ensure a gradual and incremental transition to the performance threshold set at the mean or median for the sixth year.
QPP implementation is a top priority for AGA to ensure that the value of specialty care is recognized. Learn more on our website www.gastro.org/QPP.
AGA opens GI Patient Center to the public
We’re proud to announce the public launch of the AGA GI Patient Center, an online hub for digestive health information developed by specialists, for patients. The GI Patient Center – previously only accessible by AGA member physicians – now directly provides patients with trusted information on a variety of GI conditions and procedures.
Browse the GI Patient Center, which includes information on more than 30 topics, available in both English and Spanish. All AGA patient education was written and reviewed by leading gastroenterologists, and developed with health literacy in mind.
You can print this information for your practice, email patients a link, include a link on your website – whatever is needed to ensure your patients are getting trusted health information about their condition, treatment, or procedure.
To get started, visit patient.gastro.org.
We’re proud to announce the public launch of the AGA GI Patient Center, an online hub for digestive health information developed by specialists, for patients. The GI Patient Center – previously only accessible by AGA member physicians – now directly provides patients with trusted information on a variety of GI conditions and procedures.
Browse the GI Patient Center, which includes information on more than 30 topics, available in both English and Spanish. All AGA patient education was written and reviewed by leading gastroenterologists, and developed with health literacy in mind.
You can print this information for your practice, email patients a link, include a link on your website – whatever is needed to ensure your patients are getting trusted health information about their condition, treatment, or procedure.
To get started, visit patient.gastro.org.
We’re proud to announce the public launch of the AGA GI Patient Center, an online hub for digestive health information developed by specialists, for patients. The GI Patient Center – previously only accessible by AGA member physicians – now directly provides patients with trusted information on a variety of GI conditions and procedures.
Browse the GI Patient Center, which includes information on more than 30 topics, available in both English and Spanish. All AGA patient education was written and reviewed by leading gastroenterologists, and developed with health literacy in mind.
You can print this information for your practice, email patients a link, include a link on your website – whatever is needed to ensure your patients are getting trusted health information about their condition, treatment, or procedure.
To get started, visit patient.gastro.org.
Phase 3 trial: Tasimelteon effective for jet lag disorder
BALTIMORE – Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase 3 trial.
“Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” Christos Polymeropoulos, MD, medical director of Vanda Pharmaceuticals, said in presenting results of the JET8 trial during the late-breaking abstracts session at the annual meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is Food and Drug Administration–approved for non-24-hour sleep-wake disorder – but not for treatment of jet lag disorder (JLD). Dr. Polymeropoulos noted there is no FDA-approved treatment for JLD.
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “JLD is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
JET8 induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary endpoint of the study was total sleep time in the first two-thirds of night measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of night versus 156.1 for those on placebo (P less than .0001), Dr. Polymeropoulos said. Full total sleep times were 315.8 minutes versus 230.3 minutes (P less than .0001), respectively.
“For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by PSG [polysomnography],” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in JLD: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four U.S. cities to London for 3 nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over 3 nights of study, the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for the placebo arm, Dr. Polymeropoulos said.
Vanda has said it plans to file a supplemental new drug application for tasimelteon for treatment of JLD in the second half of this year.
Dr. Polymeropoulos is an employee of Vanda Pharmaceuticals.
BALTIMORE – Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase 3 trial.
“Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” Christos Polymeropoulos, MD, medical director of Vanda Pharmaceuticals, said in presenting results of the JET8 trial during the late-breaking abstracts session at the annual meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is Food and Drug Administration–approved for non-24-hour sleep-wake disorder – but not for treatment of jet lag disorder (JLD). Dr. Polymeropoulos noted there is no FDA-approved treatment for JLD.
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “JLD is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
JET8 induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary endpoint of the study was total sleep time in the first two-thirds of night measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of night versus 156.1 for those on placebo (P less than .0001), Dr. Polymeropoulos said. Full total sleep times were 315.8 minutes versus 230.3 minutes (P less than .0001), respectively.
“For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by PSG [polysomnography],” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in JLD: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four U.S. cities to London for 3 nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over 3 nights of study, the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for the placebo arm, Dr. Polymeropoulos said.
Vanda has said it plans to file a supplemental new drug application for tasimelteon for treatment of JLD in the second half of this year.
Dr. Polymeropoulos is an employee of Vanda Pharmaceuticals.
BALTIMORE – Tasimelteon, a drug approved for non–24-hour sleep-wake disorder, has been shown to increase sleep times in travelers with jet lag, according to results from a phase 3 trial.
“Tasimelteon demonstrated an increase in total sleep time of 85 minutes versus placebo and also demonstrated improvement in next-day alertness versus placebo,” Christos Polymeropoulos, MD, medical director of Vanda Pharmaceuticals, said in presenting results of the JET8 trial during the late-breaking abstracts session at the annual meeting of the Associated Professional Sleep Societies.
Tasimelteon, sold under the trade name Hetlioz, is a melatonin receptor agonist that is Food and Drug Administration–approved for non-24-hour sleep-wake disorder – but not for treatment of jet lag disorder (JLD). Dr. Polymeropoulos noted there is no FDA-approved treatment for JLD.
“Jet lag disorder is a circadian disorder frequently observed in millions of travelers who cross multiple time zones,” Dr. Polymeropoulos said. “JLD is characterized by nighttime sleep disruption, decrease in daytime alertness, and impairment in social and occupational function.”
JET8 induced the circadian challenge equivalent to crossing eight time zones. The study involved 318 individuals randomized evenly to 20 mg tasimelteon or placebo 30 minutes before bedtime. The primary endpoint of the study was total sleep time in the first two-thirds of night measured by polysomnography.
Those on tasimelteon averaged 216.4 minutes of total sleep time in the first two-thirds of night versus 156.1 for those on placebo (P less than .0001), Dr. Polymeropoulos said. Full total sleep times were 315.8 minutes versus 230.3 minutes (P less than .0001), respectively.
“For total sleep time, the tasimelteon subjects gained about an hour and a half, as measured by PSG [polysomnography],” Dr. Polymeropoulos said.
Other key markers the trial measured were latency to persistent sleep and wakefulness after sleep onset. They measured 15 minutes less and 74.6 minutes less, respectively, in the tasimelteon arm.
Dr. Polymeropoulos also disclosed early results of a second trial of tasimelteon in JLD: the JET Study, a two-phase transatlantic travel study of 25 patients. The subjects flew from four U.S. cities to London for 3 nights, receiving tasimelteon or placebo each night in London. The study was terminated before reaching its enrollment goal of 90 patients because of its complexity, Vanda said in a separate press release. Over 3 nights of study, the tasimelteon arm gained a total of about 130 minutes of sleep versus 40 minutes for the placebo arm, Dr. Polymeropoulos said.
Vanda has said it plans to file a supplemental new drug application for tasimelteon for treatment of JLD in the second half of this year.
Dr. Polymeropoulos is an employee of Vanda Pharmaceuticals.
REPORTING FROM SLEEP 2018
Key clinical point: The melatonin receptor agonist tasimelteon may improve sleep in jet lag.
Major finding: Total sleep times were 315.8 minutes for tasimelteon versus 230.3 for placebo.
Study details: JET8 randomized, double-blind, placebo-controlled, multicenter trial of 318 healthy subjects with induced jet lag disorder.
Disclosures: Dr. Polymeropoulos is an employee of Vanda Pharmaceuticals.

Study questions canagliflozin amputation risk, but concerns remain
ORLANDO – but clinicians should still favor other options in patients at risk for amputations, according to investigator John Buse, MD, PhD, chief of the division of endocrinology at the University of North Carolina at Chapel Hill.
Canagliflozin is the only sodium-glucose transporter 2 (SGLT2) inhibitor that carries a black box warning of “lower limb amputations, most frequently of the toe and midfoot” but also the leg. The drug doubled the risk versus placebo in its approval trials, particularly in patients with baseline histories of prior amputations, peripheral vascular disease, neuropathy, or diabetic foot ulcers.
One trial, for instance, reported 7.5 amputations per 1,000 patient years versus 4.2 with placebo, according to labeling.
The new, observational study, which was funded by canagliflozin’s maker Johnson & Johnson and, with the exception of Dr. Buse, conducted by its employees, found no such connection. Investigators reviewed claims data from 142,800 new users of canagliflozin, 110,897 new users of the competing SGLT2 inhibitors empagliflozin (Jardiance) and dapagliflozin (Farxiga), and 460,885 new users of other diabetes drugs except for metformin, Dr. Buse said when he presented the results at the annual scientific sessions of the American Diabetes Association.
The hazard ratio for below-knee amputations with canagliflozin versus non-SGLT2 inhibitors was 0.75 (95% confidence interval, 0.40-1.41; P = 0.30). The ratio versus other SGLT2 inhibitors was 1.14 (95% CI, 0.67-1.93; P = 0.53). Overall, there were 1-5 amputations per 1,000 patient years with the drug.
However, the median follow-up was a few months, far shorter than the median follow-up of over 2 years in the randomized trials. “Therefore, the current study had limited statistical power to detect differences in the 6-12 month time period, the time at which amputation risk began to emerge” in the trials, the study report noted. Also, the investigators didn’t parse out results according to baseline amputation risk. Overall, “none of the analyses were sufficiently powered to rule out the possibility of a modest effect” on amputation rates (Diabetes Obes Metab. 2018 Jun 25. doi: 10.1111/dom.13424).
When moderator Robert H. Eckel, MD, a professor in the division of endocrinology, metabolism, and diabetes at the University of Colorado at Denver, Aurora, asked the 150 or so people who heard the presentation if they use SGLT2 inhibitors in their practices, only a small number raised their hands. Few, if any, raised their hands when he asked if the new results would make them more comfortable prescribing canagliflozin.
“I find [the study] somewhat informative,” Dr. Eckel said in an interview afterwards, “but I think the issue is that the prescribing label still demands that patients be informed of the black box warning. I think we are going to have to wait for the longer term outcomes to determine if [amputation] is a molecule effect or a class effect.”
Dr. Buse later said that “I think for the general population of patients with diabetes, they are at low risk for an amputation,” but “if you are at high risk for having an amputation, we really have to take this risk very seriously. [Canagliflozin] may increase your risk for amputation.
“If I have a patient who has had an amputation and I want to use an SGLT2 inhibitor, I wouldn’t use canagliflozin because of the label. I would use empagliflozin because [amputation] is not in the label, and there was no evidence” of it in trials, he added.
The new study, meanwhile, confirmed the cardiac benefits of SGLT2 inhibitors in type 2 patients. Canagliflozin, for instance, reduced the risk of hospitalization for heart failure by about 60%, compared with non-SGLT2 inhibitors in patients with cardiovascular disease, but it offered no statistically significant heart benefit over other members of its class.
Dr. Buse is an investigator for Johnson and Johnson.
ORLANDO – but clinicians should still favor other options in patients at risk for amputations, according to investigator John Buse, MD, PhD, chief of the division of endocrinology at the University of North Carolina at Chapel Hill.
Canagliflozin is the only sodium-glucose transporter 2 (SGLT2) inhibitor that carries a black box warning of “lower limb amputations, most frequently of the toe and midfoot” but also the leg. The drug doubled the risk versus placebo in its approval trials, particularly in patients with baseline histories of prior amputations, peripheral vascular disease, neuropathy, or diabetic foot ulcers.
One trial, for instance, reported 7.5 amputations per 1,000 patient years versus 4.2 with placebo, according to labeling.
The new, observational study, which was funded by canagliflozin’s maker Johnson & Johnson and, with the exception of Dr. Buse, conducted by its employees, found no such connection. Investigators reviewed claims data from 142,800 new users of canagliflozin, 110,897 new users of the competing SGLT2 inhibitors empagliflozin (Jardiance) and dapagliflozin (Farxiga), and 460,885 new users of other diabetes drugs except for metformin, Dr. Buse said when he presented the results at the annual scientific sessions of the American Diabetes Association.
The hazard ratio for below-knee amputations with canagliflozin versus non-SGLT2 inhibitors was 0.75 (95% confidence interval, 0.40-1.41; P = 0.30). The ratio versus other SGLT2 inhibitors was 1.14 (95% CI, 0.67-1.93; P = 0.53). Overall, there were 1-5 amputations per 1,000 patient years with the drug.
However, the median follow-up was a few months, far shorter than the median follow-up of over 2 years in the randomized trials. “Therefore, the current study had limited statistical power to detect differences in the 6-12 month time period, the time at which amputation risk began to emerge” in the trials, the study report noted. Also, the investigators didn’t parse out results according to baseline amputation risk. Overall, “none of the analyses were sufficiently powered to rule out the possibility of a modest effect” on amputation rates (Diabetes Obes Metab. 2018 Jun 25. doi: 10.1111/dom.13424).
When moderator Robert H. Eckel, MD, a professor in the division of endocrinology, metabolism, and diabetes at the University of Colorado at Denver, Aurora, asked the 150 or so people who heard the presentation if they use SGLT2 inhibitors in their practices, only a small number raised their hands. Few, if any, raised their hands when he asked if the new results would make them more comfortable prescribing canagliflozin.
“I find [the study] somewhat informative,” Dr. Eckel said in an interview afterwards, “but I think the issue is that the prescribing label still demands that patients be informed of the black box warning. I think we are going to have to wait for the longer term outcomes to determine if [amputation] is a molecule effect or a class effect.”
Dr. Buse later said that “I think for the general population of patients with diabetes, they are at low risk for an amputation,” but “if you are at high risk for having an amputation, we really have to take this risk very seriously. [Canagliflozin] may increase your risk for amputation.
“If I have a patient who has had an amputation and I want to use an SGLT2 inhibitor, I wouldn’t use canagliflozin because of the label. I would use empagliflozin because [amputation] is not in the label, and there was no evidence” of it in trials, he added.
The new study, meanwhile, confirmed the cardiac benefits of SGLT2 inhibitors in type 2 patients. Canagliflozin, for instance, reduced the risk of hospitalization for heart failure by about 60%, compared with non-SGLT2 inhibitors in patients with cardiovascular disease, but it offered no statistically significant heart benefit over other members of its class.
Dr. Buse is an investigator for Johnson and Johnson.
ORLANDO – but clinicians should still favor other options in patients at risk for amputations, according to investigator John Buse, MD, PhD, chief of the division of endocrinology at the University of North Carolina at Chapel Hill.
Canagliflozin is the only sodium-glucose transporter 2 (SGLT2) inhibitor that carries a black box warning of “lower limb amputations, most frequently of the toe and midfoot” but also the leg. The drug doubled the risk versus placebo in its approval trials, particularly in patients with baseline histories of prior amputations, peripheral vascular disease, neuropathy, or diabetic foot ulcers.
One trial, for instance, reported 7.5 amputations per 1,000 patient years versus 4.2 with placebo, according to labeling.
The new, observational study, which was funded by canagliflozin’s maker Johnson & Johnson and, with the exception of Dr. Buse, conducted by its employees, found no such connection. Investigators reviewed claims data from 142,800 new users of canagliflozin, 110,897 new users of the competing SGLT2 inhibitors empagliflozin (Jardiance) and dapagliflozin (Farxiga), and 460,885 new users of other diabetes drugs except for metformin, Dr. Buse said when he presented the results at the annual scientific sessions of the American Diabetes Association.
The hazard ratio for below-knee amputations with canagliflozin versus non-SGLT2 inhibitors was 0.75 (95% confidence interval, 0.40-1.41; P = 0.30). The ratio versus other SGLT2 inhibitors was 1.14 (95% CI, 0.67-1.93; P = 0.53). Overall, there were 1-5 amputations per 1,000 patient years with the drug.
However, the median follow-up was a few months, far shorter than the median follow-up of over 2 years in the randomized trials. “Therefore, the current study had limited statistical power to detect differences in the 6-12 month time period, the time at which amputation risk began to emerge” in the trials, the study report noted. Also, the investigators didn’t parse out results according to baseline amputation risk. Overall, “none of the analyses were sufficiently powered to rule out the possibility of a modest effect” on amputation rates (Diabetes Obes Metab. 2018 Jun 25. doi: 10.1111/dom.13424).
When moderator Robert H. Eckel, MD, a professor in the division of endocrinology, metabolism, and diabetes at the University of Colorado at Denver, Aurora, asked the 150 or so people who heard the presentation if they use SGLT2 inhibitors in their practices, only a small number raised their hands. Few, if any, raised their hands when he asked if the new results would make them more comfortable prescribing canagliflozin.
“I find [the study] somewhat informative,” Dr. Eckel said in an interview afterwards, “but I think the issue is that the prescribing label still demands that patients be informed of the black box warning. I think we are going to have to wait for the longer term outcomes to determine if [amputation] is a molecule effect or a class effect.”
Dr. Buse later said that “I think for the general population of patients with diabetes, they are at low risk for an amputation,” but “if you are at high risk for having an amputation, we really have to take this risk very seriously. [Canagliflozin] may increase your risk for amputation.
“If I have a patient who has had an amputation and I want to use an SGLT2 inhibitor, I wouldn’t use canagliflozin because of the label. I would use empagliflozin because [amputation] is not in the label, and there was no evidence” of it in trials, he added.
The new study, meanwhile, confirmed the cardiac benefits of SGLT2 inhibitors in type 2 patients. Canagliflozin, for instance, reduced the risk of hospitalization for heart failure by about 60%, compared with non-SGLT2 inhibitors in patients with cardiovascular disease, but it offered no statistically significant heart benefit over other members of its class.
Dr. Buse is an investigator for Johnson and Johnson.
REPORTING FROM ADA 2018
Key clinical point: A large, observational study found no increased risk of below-the-knee amputations with canagliflozin for type 2 diabetes, but clinicians should still favor other options in patients at risk for amputations.
Major finding: The hazard ratio for below-knee amputations with canagliflozin versus non-SGLT2 inhibitors was 0.75 (95% confidence interval, 0.40-1.41; P = 0.30).
Study details: An observational study of over 700,000 patients with type 2 diabetes.
Disclosures: The work was funded by canagliflozin’s maker Johnson & Johnson and, with the exception of the presenter, conducted by its employees.
FDA approves Aristada Initio for schizophrenia
The Food and Drug Administration has approved aripiprazole lauroxil (Aristada Initio) for the initiation of aripiprazole lauroxil (Aristada) for treating schizophrenia in adults, the drug’s developer, Alkermes, announced July 2 in a press release.

“,” Craig Hopkinson, MD, chief medical officer at Alkermes, said in the press release.
The standard initiation regimen for aripiprazole lauroxil previously was 21 consecutive days of oral aripiprazole starting with the first dose of Aristada. The alternative initiation regimen allows patients to achieve “relevant levels of aripiprazole within 4 days of initiation,” according to Alkermes. The result gives health care providers “an additional tool to support patients.”
One important advantage of Aristada Initio is that, in addition to monthly and 6-week dosing options, it offers a 2-month option.
Aristada and Aristada Initio both contain aripiprazole lauroxil, but the drugs are not interchangeable because they have different pharmacokinetic profiles, the company said. In addition, Aristada Initio is to be administered a single time only.
Aristada Initio has exhibited some of the same adverse events as other atypical antipsychotics, including neuroleptic malignant syndrome, tardive dyskinesia, and metabolic changes. Injection-site reactions also have been observed.
Aristada Initio is expected to become available by mid-July.
Full prescribing information and boxed warnings can be found on the Alkermes website.
The Food and Drug Administration has approved aripiprazole lauroxil (Aristada Initio) for the initiation of aripiprazole lauroxil (Aristada) for treating schizophrenia in adults, the drug’s developer, Alkermes, announced July 2 in a press release.
“,” Craig Hopkinson, MD, chief medical officer at Alkermes, said in the press release.
The standard initiation regimen for aripiprazole lauroxil previously was 21 consecutive days of oral aripiprazole starting with the first dose of Aristada. The alternative initiation regimen allows patients to achieve “relevant levels of aripiprazole within 4 days of initiation,” according to Alkermes. The result gives health care providers “an additional tool to support patients.”
One important advantage of Aristada Initio is that, in addition to monthly and 6-week dosing options, it offers a 2-month option.
Aristada and Aristada Initio both contain aripiprazole lauroxil, but the drugs are not interchangeable because they have different pharmacokinetic profiles, the company said. In addition, Aristada Initio is to be administered a single time only.
Aristada Initio has exhibited some of the same adverse events as other atypical antipsychotics, including neuroleptic malignant syndrome, tardive dyskinesia, and metabolic changes. Injection-site reactions also have been observed.
Aristada Initio is expected to become available by mid-July.
Full prescribing information and boxed warnings can be found on the Alkermes website.
The Food and Drug Administration has approved aripiprazole lauroxil (Aristada Initio) for the initiation of aripiprazole lauroxil (Aristada) for treating schizophrenia in adults, the drug’s developer, Alkermes, announced July 2 in a press release.
“,” Craig Hopkinson, MD, chief medical officer at Alkermes, said in the press release.
The standard initiation regimen for aripiprazole lauroxil previously was 21 consecutive days of oral aripiprazole starting with the first dose of Aristada. The alternative initiation regimen allows patients to achieve “relevant levels of aripiprazole within 4 days of initiation,” according to Alkermes. The result gives health care providers “an additional tool to support patients.”
One important advantage of Aristada Initio is that, in addition to monthly and 6-week dosing options, it offers a 2-month option.
Aristada and Aristada Initio both contain aripiprazole lauroxil, but the drugs are not interchangeable because they have different pharmacokinetic profiles, the company said. In addition, Aristada Initio is to be administered a single time only.
Aristada Initio has exhibited some of the same adverse events as other atypical antipsychotics, including neuroleptic malignant syndrome, tardive dyskinesia, and metabolic changes. Injection-site reactions also have been observed.
Aristada Initio is expected to become available by mid-July.
Full prescribing information and boxed warnings can be found on the Alkermes website.
Rheumatoid Arthritis vs Osteoarthritis: Comparison of Demographics and Trends of Joint Replacement Data from the Nationwide Inpatient Sample
ABSTRACT
Current literature regarding complications following total joint arthroplasty have primarily focused on patients with osteoarthritis (OA), with less emphasis on the trends and in-hospital outcomes of rheumatoid arthritis (RA) patients undergoing these procedures. The purpose of this study is to analyze the outcomes and trends of RA patients undergoing total knee arthroplasty (TKA) or total hip arthroplasty (THA) compared to OA patients.
Data from the Nationwide Inpatient Sample from 2006 to 2011 was extracted using the International Classification of Diseases, Ninth Revision codes for patients that received a TKA or THA. Outcome measures included cardiovascular complications, cerebrovascular complications, pulmonary complications, wound dehiscence, and infection. Inpatient and hospital demographics including primary diagnosis, age, gender, primary payer, hospital teaching status, Charlson Comorbidity Index score, hospital bed size, location, and median household income were analyzed.
Logistic regression analysis of OA vs RA patients with patient outcomes revealed that osteoarthritic THA candidates had lower risk for cardiovascular complications, pulmonary complications, wound dehiscence, infections, and systemic complications, compared to rheumatoid patients. There was a significantly elevated risk of cerebrovascular complication in osteoarthritic THA compared to RA THA. OA patients undergoing TKA had significantly higher risk for cardiovascular and cerebrovascular complications. There were significant decreases in mechanical wounds, infection, and systemic complications in the OA TKA patients.
RA patients are at higher risk for postoperative infection, wound dehiscence, and systemic complications after TKA and THA compared to OA patients. These findings highlight the importance of preoperative medical clearance and management to optimize RA patients and improve the postoperative outcomes.
Continue to: RA is a chronic systemic inflammatory disease...
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that causes joint deterioration, leading to pain, disability, systemic complications, short lifespan, and decline in quality of life.1-3 The deterioration primarily affects the synovial membranes of joints, causing arthritis and resulting in extra-articular sequelae such as cardiovascular disease,4 pulmonary disease,5 and increased infection rates.3,6 RA is the most prevalent inflammatory arthritis worldwide and affects up to 50 cases per 100,000 in both the US and northern Europe.2,7-9 Although the gold standard of care for these patients is medical management with immunosuppressant drugs such as disease-modifying anti-rheumatic drugs (DMARDs), total joint arthroplasty (TJA) remains an important tool in the management of joint deterioration in such patients.
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are common procedures utilized to treat disorders that cause joint pain and hindered joint mobility, including osteoarthritis (OA) and RA. Given the aging population, the amount of TKAs and THAs performed in the US has consistently increased each year, with the vast majority of this increase composed of patients with OA.10 As a result, previous studies investigated the trends and outcomes of these procedures in patients with OA, but relatively less is known about the outcomes and trends of patients with RA undergoing the same surgeries.
Given that RA is a fundamentally different condition with its own pathological characteristics, an understanding of how these differences may impact postoperative outcomes in patients with RA is important. This study aims to present a comparative analysis of the trends and postoperative outcomes between patients with RA and OA undergoing TKA and THA (Figure 1, Tables 1 and 2).
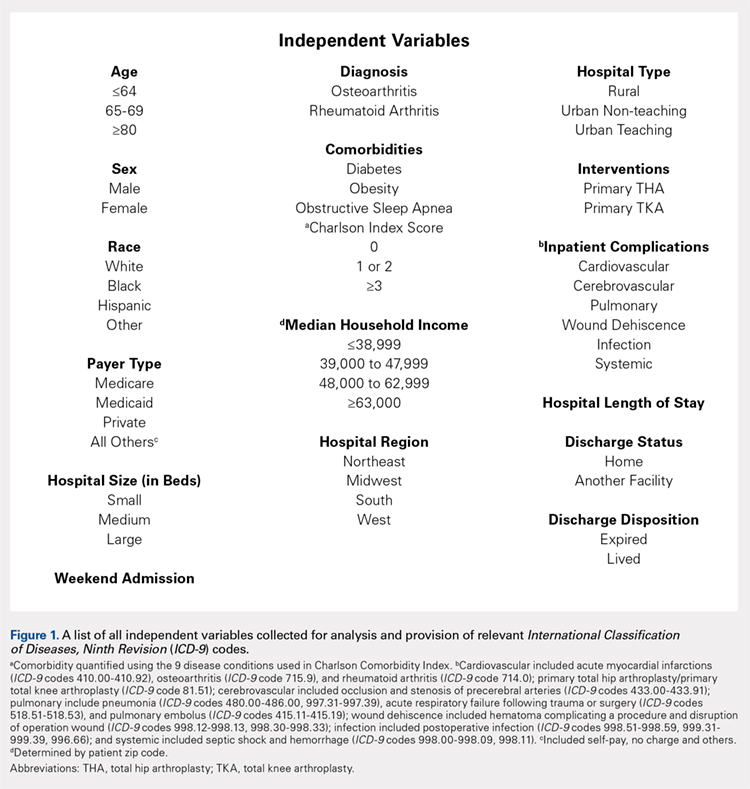
Table 1. Demographics of Total Knee Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 295,637 | 42.42 | 11,325 | 48.90 | 306,962 | 42.63 |
|
65 to 79 years | 329,034 | 47.22 | 10,055 | 43.42 | 339,089 | 47.09 |
|
≥80 years | 72,197 | 10.36 | 1780 | 7.69 | 73,977 | 10.27 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 259,192 | 37.19 | 4887 | 21.12 | 264,079 | 36.68 |
|
Female | 435,855 | 62.54 | 18,248 | 78.88 | 454,103 | 63.07 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 468,632 | 67.25 | 14,532 | 77.18 | 483,164 | 67.10 |
|
Black | 39,691 | 5.7 | 2119 | 11.25 | 41,810 | 5.81 |
|
Hispanic | 28,573 | 4.1 | 1395 | 7.41 | 29,968 | 4.16 |
|
Other | 21,306 | 3.06 | 783 | 4.16 | 22,089 | 3.07 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 112,031 | 16.08 | 3417 | 14.75 | 115,448 | 16.03 |
|
Midwest | 192,595 | 27.64 | 5975 | 25.80 | 198,570 | 27.58 |
|
South | 257,855 | 37 | 9422 | 40.68 | 267,277 | 37.12 |
|
West | 134,387 | 19.28 | 4346 | 18.77 | 138,733 | 19.27 |
|
Location/teaching status of hospital |
|
|
|
|
|
| <.0001 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban non-teaching | 333,043 | 47.79 | 10,905 | 47.46 | 343,948 | 47.77 |
|
Urban teaching | 273,326 | 39.22 | 9363 | 40.75 | 282,689 | 39.26 |
|
Hospital location |
|
|
|
|
|
| .0024 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban | 606,369 | 87.01 | 20,268 | 88.21 | 626,637 | 87.03 |
|
Hospital teaching status |
|
|
|
|
|
| <.0001 |
Teaching | 409,465 | 58.76 | 13,275 | 57.78 | 422,740 | 58.71 |
|
Non-teaching | 283,225 | 40.64 | 9702 | 42.22 | 292,927 | 40.68 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 65,342 | 9.38 | 1946 | 8.40 | 67,288 | 9.35 | <.0001 |
Diabetes | 147,292 | 21.14 | 4289 | 18.52 | 151,581 | 21.05 | <.0001 |
Obesity | 129,277 | 18.55 | 3730 | 16.11 | 133,007 | 18.47 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis.
Table 2. Demographics of Total Hip Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis or Rheumatoid Arthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 133,645 | 45.18 | 4679 | 48.02 | 138,324 | 45.27 |
|
65 to 79 years | 123,628 | 41.8 | 3992 | 40.97 | 127,620 | 41.77 |
|
≥80 years | 38,513 | 13.02 | 1073 | 11.01 | 39,586 | 12.96 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 129,708 | 43.85 | 2457 | 25.24 | 132,165 | 43.26 |
|
Female | 165,010 | 55.79 | 7278 | 74.76 | 172,288 | 56.39 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 207,005 | 69.98 | 6322 | 80.08 | 213,327 | 69.82 |
|
Black | 15,505 | 5.24 | 771 | 9.77 | 16,276 | 5.33 |
|
Hispanic | 6784 | 2.29 | 522 | 6.61 | 7306 | 2.39 |
|
Other | 7209 | 2.44 | 280 | 3.55 | 7489 | 2.45 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 58,525 | 19.79 | 1683 | 17.27 | 60,208 | 19.71 |
|
Midwest | 79,040 | 26.72 | 2446 | 25.10 | 81,486 | 26.67 |
|
South | 95,337 | 32.23 | 3716 | 38.14 | 99,053 | 32.42 |
|
West | 62,884 | 21.26 | 1899 | 19.49 | 64,783 | 21.20 |
|
Location/teaching status of hospital |
|
|
|
|
|
| .0065 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban non-teaching | 133,061 | 44.99 | 4245 | 43.87 | 137,306 | 44.94 |
|
Urban teaching | 130,150 | 44 | 4439 | 45.87 | 134,589 | 44.05 |
|
Hospital location |
|
|
|
|
|
| .4098 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban | 263,211 | 88.99 | 8684 | 89.74 | 271,895 | 88.99 |
|
Hospital teaching status |
|
|
|
|
|
| .0077 |
Teaching | 159,313 | 53.86 | 5108 | 52.78 | 164,421 | 53.82 |
|
Non-teaching | 134,852 | 45.59 | 4569 | 47.22 | 139,421 | 45.63 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 19,760 | 6.68 | 573 | 5.88 | 20,333 | 6.65 | .0028 |
Diabetes | 41,929 | 14.18 | 1325 | 13.60 | 43,254 | 14.16 | .1077 |
Obesity | 38,808 | 13.12 | 1100 | 11.29 | 39,908 | 13.06 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis
Continue to: Methods...
METHODS
Exemptions were obtained from the Institutional Review Board. Data from the Nationwide Inpatient Sample (NIS) from 2006 to 2011 were extracted using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for patients that received primary TKA or THA, as well as their comorbid conditions. No patients or populations were excluded from the sampling process. A list of all independent variables collected for analysis and provision of relevant ICD-9 codes is included in Figure 1. The NIS is the largest all-payer stratified survey of inpatient care in the US healthcare system. As of 2011, each year provides information on approximately 8 million inpatient stays from about 1000 hospitals in 46 states. All discharges from sampled hospitals are also represented in the database. All patient information is protected, and all methods were conducted in accordance with the highest ethical standards of Human and Animal Rights Research.
STATISTICAL ANALYSIS
SAS 9.2 and PROC FREQ statistics software were used to generate P values (chi square result) and analyze the trends (Cochran-Armitage). Results were weighted utilizing standard discharge weights from the NIS to ensure accurate comparison of data from different time points. P < .05 was considered statistically significant. Multivariable logistic regression analyses were performed to generate odds ratio and 95% confidence limits to assess outcomes across different demographic variables.
RESULTS
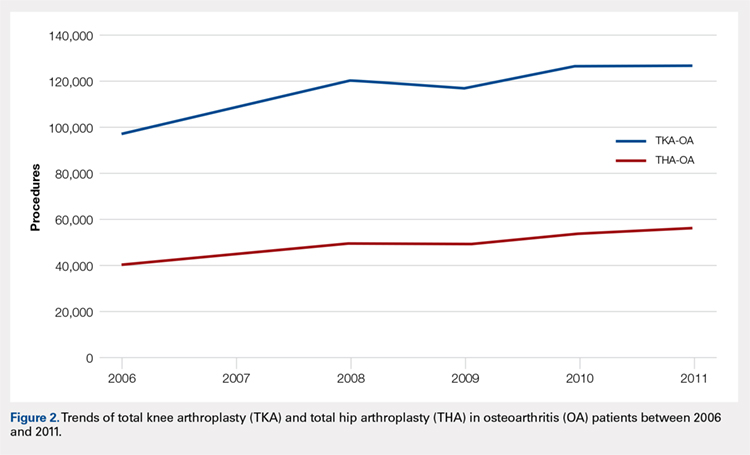
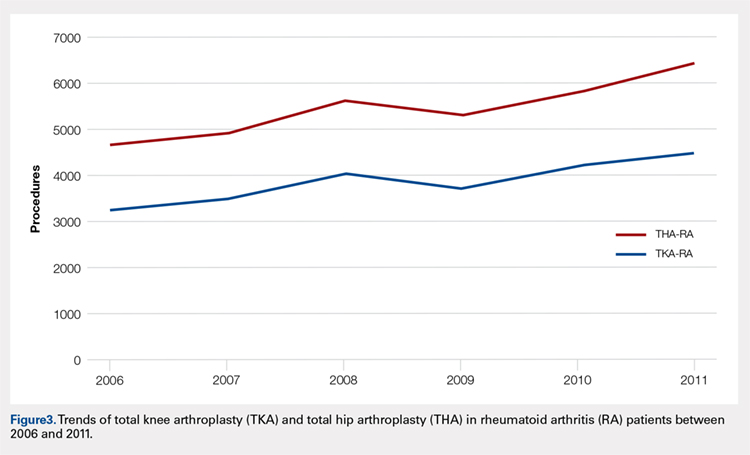
Data on 337,082 and 1,362,241 patients undergoing THA or TKA, respectively, between 2006 and 2011 were analyzed. Patients in both groups were further differentiated by a diagnosis of either OA or RA. OA was the most common diagnosis, constituting 96.8% of all arthritic THA and TKA patients. From 2006 to 2011, a 36% and 34% increase in total number of THAs and TKAs, respectively, were reported. The number of patients with OA undergoing THA and TKA steadily increased from 2006 to 2011 (Figure 2). The number of THA and TKA procedures in patients with RA followed a similar trend but at a comparatively slower rate (Figure 3). The TKA geographical trends mirrored those observed with THA. The majority of operations were performed at urban hospitals (89% THA, 87% TKA; P < .0001). Among patients with RA and OA, the majority of TKAs (47.77%; P < .0001) took place in urban non-teaching hospitals than in urban teaching hospitals (39.26%). This pattern was not the same for THA, with 44.94% being performed at urban teaching hospitals and 44.05% at urban non-teaching institutions (P < .0001). Rural hospitals accounted for a low percentage of operations for both procedures: 10.46% of THA and 12.36% of TKA (P < .0001). Large institutions (based on the number of beds) claimed the majority of cases (59% of THA and TKA).
Logistic regression analysis and odds ratios of patients with OA vs those with RA with patient outcomes adjusted for age, Charlson Comorbidity Index (CCI) score, and gender revealed that patients with OA undergoing THA had lower risk for cardiovascular (0.674; confidence interval (CI) 0.587-0.774) and pulmonary complications (0.416; CI 0.384-0.450), wound dehiscence (0.647; CI 0.561-0.747), infections (0.258; CI 0.221-0.301), and systemic complications (0.625; CI 0.562-0.695) than patients with RA. Patients with OA exhibited statistically significantly higher odds of experiencing cerebrovascular complications after THA than those with RA (1.946; CI 1.673-2.236) (Table 3). In a similar logistic regression analysis of OA vs RA in TKA, which was adjusted for age, CCI score, and gender, patients with OA had significantly higher risk for cardiovascular (1.329; CI 1.069-1.651) and cerebrovascular complications (1.635; CI 1.375-1.943) than patients with RA. Significant decreases in wound dehiscence (0.757; CI 0.639-0.896), infection (0.331; CI 0.286-0.383), and systemic complication (0.641; CI 0.565-0.729) were noted in the patients with OA and TKA (Table 4).
Table 3. Odds Ratio for In-Hospital Complications Following THA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | .674 | .587-.744 |
Cerebrovascular complication | 1.946 | 1.673-2.236 |
Pulmonary complication | .416 | .384-.450 |
Wound dehiscence | .647 | .561-.747 |
Infection | .258 | .221-.301 |
Systemic complication | .625 | .562-.695 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; THA, total hip arthroplasty.
Table 4. Odds Ratio for In-Hospital Complications Following TKA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | 1.329 | 1.069-1.651 |
Cerebrovascular complication | 1.635 | 1.375-1.943 |
Pulmonary complication | 1.03 | .995-1.223 |
Wound dehiscence | .757 | .639-.896 |
Infection | .331 | .286-.383 |
Systemic complication | .641 | .565-.729 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; TKA, total knee arthroplasty.
Continue to: Discussion...
DISCUSSION
Our results showed a continuous yearly increase from 2006 to 2011 in THA and TKA procedures at a rate of 36% and 34%, respectively; this result was consistent with existing literature.11 Despite a substantial increase in the amount of total THA and TKA procedures, the ratio of patients with RA undergoing these operations has decreased or remained nearly the same. Similar effects were found in Japan and the US when examining patients with RA undergoing TJA procedures between 2001 and 2007 and between 1992 and 2005, respectively.12-14 This observation may be explained by the advances and early initiation of pharmacologic treatment and the widespread use of DMARDs such as methotrexate (MTX), azathioprine, leflunomide, hydroxychloroquine, and biological response modifiers TNF-α and interleukin-1.15 These medications have drastically improved survival rates of patients with RA with impressive capabilities in symptom relief.15 With the increasing use of DMARDs and aggressive treatment early on in the disease process, patients with RA are showing markedly slow progression of joint deterioration, leading to a decreased need for orthopedic intervention compared with the general population.13,15
When analyzing the complication rates for patients undergoing TKA and THA, we observed that patients with RA exhibited a significant increase in the rates of infections, wound dehiscence, and systemic complications prior to discharge from the hospital compared with the OA population. The increased risk of infections was reported in previous studies assessing postoperative complication rates in TJA.16,17 A study utilizing the Norwegian Arthroplasty Registry noted an increased risk of late infection in patients with RA, leading to increased rates of revision TJA in comparison with patients with OA.16 Another study, which was based on the Canadian Institute for Health Information Discharge Abstract Database, showed that patients with RA are at an increased risk of infection only after THA and interestingly not after TKA.17 Although our study did not identify the causes of the increased infection rate, the inherent nature of the disease and the immunomodulatory drugs used to treat it may contribute to this increased infectious risk in patients with RA.6,18 Immunosuppressive DMARDs are some of the widely used medications employed to treat RA and are prime suspects of causing increased infection rates.15 The perioperative use of MTX has not been shown to cause short-term increases in infection for patients undergoing orthopedic intervention, but leflunomide and TNF-α inhibitors have been shown to cause a significant several-fold increase in risk for surgical wound infections.19,20
All patients with RA presented with significant increases for infection, wound dehiscence, and systemic complications, whereas only patients with RA undergoing THA showed increased risk of pulmonary and cardiovascular complications when compared with patients with OA. Surprisingly, in TKA, patients with RA were at a significantly decreased risk of cardiovascular complications. This observation was interesting due to cardiovascular disease being one of RA's most notable extra-articular features.4,21
Patients with RA undergoing TJA also showed significantly lower cerebrovascular complications than patients with OA. The significant reduction in risk for these complications has not been previously reported in the current literature, and it was an unexpected finding as past studies have found an increased risk in cerebrovascular disease in patients with RA. RA is an inflammatory disease exhibiting the upregulation of procoagulation factors,22 so we expected patients with RA to be at an increased risk for cerebrovascular and cardiovascular complications over patients with OA. Although we are unsure why these results were observed, we postulate that pharmaceutical interventions may confer some protection to patients with RA. For example, aspirin is commonly utilized in RA for its protective anti-platelet effect23 and may be a contributing factor to why we found low postoperative complication rates in cerebrovascular disease. However, the reason why aspirin may be protective against cerebrovascular and not cardiovascular complications remains unclear. Moreover, most guidelines suggest that aspirin be stopped prior to surgery.24 Although patients with RA were younger than those with OA, age was accounted for when analyzing the data.
A major strength of the study was the large sample size and the adjustment of potential confounding variables when examining the difference in complications between RA and OA. It is also a national US study that utilizes a validated database. Given that the patient samples in the NIS are reported in a uniform and de-identified manner, the database is considered ideal and has been extensively used for retrospective large observational cohort studies.25 However, the study also had some limitations due to the retrospective and administrative nature of the NIS database. Only data concerning patient complications during their inpatient stay at the hospital were available. Patients who may develop complications following discharge were not included in the data, providing a very small window of time for analysis. Another limitation with the database was its lack of ability to identify the severity of each patient's disease process or the medical treatment they received perioperatively. Finally, no patient-reported outcomes were determined, which would provide information on whether these complications affect the patients’ postoperational satisfaction in regard to their pain and disability.
CONCLUSION
As RA patients continue to utilize joint arthroplasty to repair deteriorated joints, understanding of how the disease process and its medical management may impact patient outcomes is important. This article reports significantly higher postoperational infection rates in RA than in patients with OA, which may be due to the medical management of the disease. Although new medications have been introduced and are being used to treat patients with RA, they have not altered the complication rate following TJA in this patient population. Thus, surgeons and other members of the management team should be familiar with the common medical conditions, co-morbidities, and medical treatments/side effects that are encountered in patients with RA. Future studies should delve into possible differences in long-term outcomes of patients with RA undergoing TKA and THA, as well as whether certain perioperative strategies and therapies (medical or physical) may decrease complications and improve outcomes.
This paper will be judged for the Resident Writer’s Award.
- Myasoedova E, Davis JM 3rd, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379-385. doi:10.1007/s11926-010-0117-y.
- Firestein GS. Evolving concepts of rheumatoid arthritis. Nature. 2003;423(6937):356-361. doi:10.1038/nature01661.
- Gullick NJ, Scott DL. Co-morbidities in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2011;25(4):469-483. doi:10.1016/j.berh.2011.10.009.
- Masuda H, Miyazaki T, Shimada K, et al. Disease duration and severity impacts on long-term cardiovascular events in Japanese patients with rheumatoid arthritis. J Cardiol. 2014;64(5):366-370. doi:10.1016/j.jjcc.2014.02.018.
- Bongartz T, Nannini C, Medina-Velasquez YF, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum.2010;62(6):1583-1591. doi:10.1002/art.27405.
- Doran MF, Crowson CS, Pond GR, O'Fallon WM, Gabriel SE. Frequency of infection in patients with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum. 2002;46(9):2287-2293. doi:10.1002/art.10524.
- Rossini M, Rossi E, Bernardi D, et al. Prevalence and incidence of rheumatoid arthritis in Italy. Rheumatol Int. 2014;34(5):659664. doi:10.1007/s00296-014-2974-6.
- Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006;36(3):182-188. doi:10.1016/j.semarthrit.2006.08.006.
- Carbonell J, Cobo T, Balsa A, Descalzo MA, Carmona L. The incidence of rheumatoid arthritis in Spain: results from a nationwide primary care registry. Rheumatology.2008;47(7):1088-1092. doi:10.1093/rheumatology/ken205.
- Skytta ET, Honkanen PB, Eskelinen A, Huhtala H, Remes V. Fewer and older patients with rheumatoid arthritis need total knee replacement. Scand J Rheumatol. 2012;41(5):345-349. doi:10.3109/03009742.2012.681061.
- Singh JA, Vessely MB, Harmsen WS, et al. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969–2008. Mayo Clin Proc. 2010;85(10):898-904. doi:10.4065/mcp.2010.0115.
- Momohara S, Inoue E, Ikari K, et al. Decrease in orthopaedic operations, including total joint replacements, in patients with rheumatoid arthritis between 2001 and 2007: data from Japanese outpatients in a single institute-based large observational cohort (IORRA). Ann Rheum Dis. 2010;69(1):312-313. doi:10.1136/ard.2009.107599.
- Jain A, Stein BE, Skolasky RL, Jones LC, Hungerford MW. Total joint arthroplasty in patients with rheumatoid arthritis: a United States experience from 1992 through 2005. J Arthroplasty. 2012;27(6):881-888. doi:10.1016/j.arth.2011.12.027.
- Mertelsmann-Voss C, Lyman S, Pan TJ, Goodman SM, Figgie MP, Mandl LA. US trends in rates of arthroplasty for inflammatory arthritis including rheumatoid arthritis, juvenile idiopathic arthritis, and spondyloarthritis. Arthritis Rheumatol 2014;66(6):1432-1439. doi:10.1002/art.38384.
- Howe CR, Gardner GC, Kadel NJ. Perioperative medication management for the patient with rheumatoid arthritis. J Am Acad Orthop Surg. 2006;14(9):544-551. doi:10.5435/00124635-200609000-00004.
- Schrama JC, Espehaug B, Hallan G, et al. Risk of revision for infection in primary total hip and knee arthroplasty in patients with rheumatoid arthritis compared with osteoarthritis: a prospective, population-based study on 108,786 hip and knee joint arthroplasties from the Norwegian Arthroplasty Register. Arthritis Care Res. 2010;62(4):473-479. doi:10.1002/acr.20036.
- Ravi B, Croxford R, Hollands S, et al. Increased risk of complications following total joint arthroplasty in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(2):254-263. doi:10.1002/art.38231.
- Au K, Reed G, Curtis JR, et al. High disease activity is associated with an increased risk of infection in patients with rheumatoid arthritis. Ann Rheum Dis. 2011;70(5):785-791. doi:10.1136/ard.2010.128637.
- Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275-2285. doi:10.1001/jama.295.19.2275.
- Scherrer CB, Mannion AF, Kyburz D, Vogt M, Kramers-de Quervain IA. Infection risk after orthopedic surgery in patients with inflammatory rheumatic diseases treated with immunosuppressive drugs. Arthritis Care Res. 2013;65(12):2032-2040. doi:10.1002/acr.22077.
- Bacani AK, Gabriel SE, Crowson CS, Heit JA, Matteson EL. Noncardiac vascular disease in rheumatoid arthritis: increase in venous thromboembolic events? Arthritis Rheum.2012;64(1):53-61. doi:10.1002/art.33322.
- Wallberg-Jonsson S, Dahlen GH, Nilsson TK, Ranby M, Rantapaa-Dahlqvist S. Tissue plasminogen activator, plasminogen activator inhibitor-1 and von Willebrand factor in rheumatoid arthritis. Clin Rheumatol. 1993;12(3):318324.
- van Heereveld HA, Laan RF, van den Hoogen FH, Malefijt MC, Novakova IR, van de Putte LB. Prevention of symptomatic thrombosis with short term (low molecular weight) heparin in patients with rheumatoid arthritis after hip or knee replacement. Ann Rheum Dis.2001;60(10):974-976. doi:10.1136/ard.60.10.974.
- Mont MA, Jacobs JJ, Boggio LN, et al. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. J Am Acad Orthop Surg.2011;19(12):768-776.
- Bozic KJ, Bashyal RK, Anthony SG, Chiu V, Shulman B, Rubash HE. Is administratively coded comorbidity and complication data in total joint arthroplasty valid? Clin Orthop Relat Res. 2013;471(1):201-205. doi:10.1007/s11999-012-2352-1.
ABSTRACT
Current literature regarding complications following total joint arthroplasty have primarily focused on patients with osteoarthritis (OA), with less emphasis on the trends and in-hospital outcomes of rheumatoid arthritis (RA) patients undergoing these procedures. The purpose of this study is to analyze the outcomes and trends of RA patients undergoing total knee arthroplasty (TKA) or total hip arthroplasty (THA) compared to OA patients.
Data from the Nationwide Inpatient Sample from 2006 to 2011 was extracted using the International Classification of Diseases, Ninth Revision codes for patients that received a TKA or THA. Outcome measures included cardiovascular complications, cerebrovascular complications, pulmonary complications, wound dehiscence, and infection. Inpatient and hospital demographics including primary diagnosis, age, gender, primary payer, hospital teaching status, Charlson Comorbidity Index score, hospital bed size, location, and median household income were analyzed.
Logistic regression analysis of OA vs RA patients with patient outcomes revealed that osteoarthritic THA candidates had lower risk for cardiovascular complications, pulmonary complications, wound dehiscence, infections, and systemic complications, compared to rheumatoid patients. There was a significantly elevated risk of cerebrovascular complication in osteoarthritic THA compared to RA THA. OA patients undergoing TKA had significantly higher risk for cardiovascular and cerebrovascular complications. There were significant decreases in mechanical wounds, infection, and systemic complications in the OA TKA patients.
RA patients are at higher risk for postoperative infection, wound dehiscence, and systemic complications after TKA and THA compared to OA patients. These findings highlight the importance of preoperative medical clearance and management to optimize RA patients and improve the postoperative outcomes.
Continue to: RA is a chronic systemic inflammatory disease...
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that causes joint deterioration, leading to pain, disability, systemic complications, short lifespan, and decline in quality of life.1-3 The deterioration primarily affects the synovial membranes of joints, causing arthritis and resulting in extra-articular sequelae such as cardiovascular disease,4 pulmonary disease,5 and increased infection rates.3,6 RA is the most prevalent inflammatory arthritis worldwide and affects up to 50 cases per 100,000 in both the US and northern Europe.2,7-9 Although the gold standard of care for these patients is medical management with immunosuppressant drugs such as disease-modifying anti-rheumatic drugs (DMARDs), total joint arthroplasty (TJA) remains an important tool in the management of joint deterioration in such patients.
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are common procedures utilized to treat disorders that cause joint pain and hindered joint mobility, including osteoarthritis (OA) and RA. Given the aging population, the amount of TKAs and THAs performed in the US has consistently increased each year, with the vast majority of this increase composed of patients with OA.10 As a result, previous studies investigated the trends and outcomes of these procedures in patients with OA, but relatively less is known about the outcomes and trends of patients with RA undergoing the same surgeries.
Given that RA is a fundamentally different condition with its own pathological characteristics, an understanding of how these differences may impact postoperative outcomes in patients with RA is important. This study aims to present a comparative analysis of the trends and postoperative outcomes between patients with RA and OA undergoing TKA and THA (Figure 1, Tables 1 and 2).
Table 1. Demographics of Total Knee Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 295,637 | 42.42 | 11,325 | 48.90 | 306,962 | 42.63 |
|
65 to 79 years | 329,034 | 47.22 | 10,055 | 43.42 | 339,089 | 47.09 |
|
≥80 years | 72,197 | 10.36 | 1780 | 7.69 | 73,977 | 10.27 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 259,192 | 37.19 | 4887 | 21.12 | 264,079 | 36.68 |
|
Female | 435,855 | 62.54 | 18,248 | 78.88 | 454,103 | 63.07 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 468,632 | 67.25 | 14,532 | 77.18 | 483,164 | 67.10 |
|
Black | 39,691 | 5.7 | 2119 | 11.25 | 41,810 | 5.81 |
|
Hispanic | 28,573 | 4.1 | 1395 | 7.41 | 29,968 | 4.16 |
|
Other | 21,306 | 3.06 | 783 | 4.16 | 22,089 | 3.07 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 112,031 | 16.08 | 3417 | 14.75 | 115,448 | 16.03 |
|
Midwest | 192,595 | 27.64 | 5975 | 25.80 | 198,570 | 27.58 |
|
South | 257,855 | 37 | 9422 | 40.68 | 267,277 | 37.12 |
|
West | 134,387 | 19.28 | 4346 | 18.77 | 138,733 | 19.27 |
|
Location/teaching status of hospital |
|
|
|
|
|
| <.0001 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban non-teaching | 333,043 | 47.79 | 10,905 | 47.46 | 343,948 | 47.77 |
|
Urban teaching | 273,326 | 39.22 | 9363 | 40.75 | 282,689 | 39.26 |
|
Hospital location |
|
|
|
|
|
| .0024 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban | 606,369 | 87.01 | 20,268 | 88.21 | 626,637 | 87.03 |
|
Hospital teaching status |
|
|
|
|
|
| <.0001 |
Teaching | 409,465 | 58.76 | 13,275 | 57.78 | 422,740 | 58.71 |
|
Non-teaching | 283,225 | 40.64 | 9702 | 42.22 | 292,927 | 40.68 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 65,342 | 9.38 | 1946 | 8.40 | 67,288 | 9.35 | <.0001 |
Diabetes | 147,292 | 21.14 | 4289 | 18.52 | 151,581 | 21.05 | <.0001 |
Obesity | 129,277 | 18.55 | 3730 | 16.11 | 133,007 | 18.47 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis.
Table 2. Demographics of Total Hip Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis or Rheumatoid Arthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 133,645 | 45.18 | 4679 | 48.02 | 138,324 | 45.27 |
|
65 to 79 years | 123,628 | 41.8 | 3992 | 40.97 | 127,620 | 41.77 |
|
≥80 years | 38,513 | 13.02 | 1073 | 11.01 | 39,586 | 12.96 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 129,708 | 43.85 | 2457 | 25.24 | 132,165 | 43.26 |
|
Female | 165,010 | 55.79 | 7278 | 74.76 | 172,288 | 56.39 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 207,005 | 69.98 | 6322 | 80.08 | 213,327 | 69.82 |
|
Black | 15,505 | 5.24 | 771 | 9.77 | 16,276 | 5.33 |
|
Hispanic | 6784 | 2.29 | 522 | 6.61 | 7306 | 2.39 |
|
Other | 7209 | 2.44 | 280 | 3.55 | 7489 | 2.45 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 58,525 | 19.79 | 1683 | 17.27 | 60,208 | 19.71 |
|
Midwest | 79,040 | 26.72 | 2446 | 25.10 | 81,486 | 26.67 |
|
South | 95,337 | 32.23 | 3716 | 38.14 | 99,053 | 32.42 |
|
West | 62,884 | 21.26 | 1899 | 19.49 | 64,783 | 21.20 |
|
Location/teaching status of hospital |
|
|
|
|
|
| .0065 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban non-teaching | 133,061 | 44.99 | 4245 | 43.87 | 137,306 | 44.94 |
|
Urban teaching | 130,150 | 44 | 4439 | 45.87 | 134,589 | 44.05 |
|
Hospital location |
|
|
|
|
|
| .4098 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban | 263,211 | 88.99 | 8684 | 89.74 | 271,895 | 88.99 |
|
Hospital teaching status |
|
|
|
|
|
| .0077 |
Teaching | 159,313 | 53.86 | 5108 | 52.78 | 164,421 | 53.82 |
|
Non-teaching | 134,852 | 45.59 | 4569 | 47.22 | 139,421 | 45.63 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 19,760 | 6.68 | 573 | 5.88 | 20,333 | 6.65 | .0028 |
Diabetes | 41,929 | 14.18 | 1325 | 13.60 | 43,254 | 14.16 | .1077 |
Obesity | 38,808 | 13.12 | 1100 | 11.29 | 39,908 | 13.06 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis
Continue to: Methods...
METHODS
Exemptions were obtained from the Institutional Review Board. Data from the Nationwide Inpatient Sample (NIS) from 2006 to 2011 were extracted using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for patients that received primary TKA or THA, as well as their comorbid conditions. No patients or populations were excluded from the sampling process. A list of all independent variables collected for analysis and provision of relevant ICD-9 codes is included in Figure 1. The NIS is the largest all-payer stratified survey of inpatient care in the US healthcare system. As of 2011, each year provides information on approximately 8 million inpatient stays from about 1000 hospitals in 46 states. All discharges from sampled hospitals are also represented in the database. All patient information is protected, and all methods were conducted in accordance with the highest ethical standards of Human and Animal Rights Research.
STATISTICAL ANALYSIS
SAS 9.2 and PROC FREQ statistics software were used to generate P values (chi square result) and analyze the trends (Cochran-Armitage). Results were weighted utilizing standard discharge weights from the NIS to ensure accurate comparison of data from different time points. P < .05 was considered statistically significant. Multivariable logistic regression analyses were performed to generate odds ratio and 95% confidence limits to assess outcomes across different demographic variables.
RESULTS
Data on 337,082 and 1,362,241 patients undergoing THA or TKA, respectively, between 2006 and 2011 were analyzed. Patients in both groups were further differentiated by a diagnosis of either OA or RA. OA was the most common diagnosis, constituting 96.8% of all arthritic THA and TKA patients. From 2006 to 2011, a 36% and 34% increase in total number of THAs and TKAs, respectively, were reported. The number of patients with OA undergoing THA and TKA steadily increased from 2006 to 2011 (Figure 2). The number of THA and TKA procedures in patients with RA followed a similar trend but at a comparatively slower rate (Figure 3). The TKA geographical trends mirrored those observed with THA. The majority of operations were performed at urban hospitals (89% THA, 87% TKA; P < .0001). Among patients with RA and OA, the majority of TKAs (47.77%; P < .0001) took place in urban non-teaching hospitals than in urban teaching hospitals (39.26%). This pattern was not the same for THA, with 44.94% being performed at urban teaching hospitals and 44.05% at urban non-teaching institutions (P < .0001). Rural hospitals accounted for a low percentage of operations for both procedures: 10.46% of THA and 12.36% of TKA (P < .0001). Large institutions (based on the number of beds) claimed the majority of cases (59% of THA and TKA).
Logistic regression analysis and odds ratios of patients with OA vs those with RA with patient outcomes adjusted for age, Charlson Comorbidity Index (CCI) score, and gender revealed that patients with OA undergoing THA had lower risk for cardiovascular (0.674; confidence interval (CI) 0.587-0.774) and pulmonary complications (0.416; CI 0.384-0.450), wound dehiscence (0.647; CI 0.561-0.747), infections (0.258; CI 0.221-0.301), and systemic complications (0.625; CI 0.562-0.695) than patients with RA. Patients with OA exhibited statistically significantly higher odds of experiencing cerebrovascular complications after THA than those with RA (1.946; CI 1.673-2.236) (Table 3). In a similar logistic regression analysis of OA vs RA in TKA, which was adjusted for age, CCI score, and gender, patients with OA had significantly higher risk for cardiovascular (1.329; CI 1.069-1.651) and cerebrovascular complications (1.635; CI 1.375-1.943) than patients with RA. Significant decreases in wound dehiscence (0.757; CI 0.639-0.896), infection (0.331; CI 0.286-0.383), and systemic complication (0.641; CI 0.565-0.729) were noted in the patients with OA and TKA (Table 4).
Table 3. Odds Ratio for In-Hospital Complications Following THA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | .674 | .587-.744 |
Cerebrovascular complication | 1.946 | 1.673-2.236 |
Pulmonary complication | .416 | .384-.450 |
Wound dehiscence | .647 | .561-.747 |
Infection | .258 | .221-.301 |
Systemic complication | .625 | .562-.695 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; THA, total hip arthroplasty.
Table 4. Odds Ratio for In-Hospital Complications Following TKA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | 1.329 | 1.069-1.651 |
Cerebrovascular complication | 1.635 | 1.375-1.943 |
Pulmonary complication | 1.03 | .995-1.223 |
Wound dehiscence | .757 | .639-.896 |
Infection | .331 | .286-.383 |
Systemic complication | .641 | .565-.729 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; TKA, total knee arthroplasty.
Continue to: Discussion...
DISCUSSION
Our results showed a continuous yearly increase from 2006 to 2011 in THA and TKA procedures at a rate of 36% and 34%, respectively; this result was consistent with existing literature.11 Despite a substantial increase in the amount of total THA and TKA procedures, the ratio of patients with RA undergoing these operations has decreased or remained nearly the same. Similar effects were found in Japan and the US when examining patients with RA undergoing TJA procedures between 2001 and 2007 and between 1992 and 2005, respectively.12-14 This observation may be explained by the advances and early initiation of pharmacologic treatment and the widespread use of DMARDs such as methotrexate (MTX), azathioprine, leflunomide, hydroxychloroquine, and biological response modifiers TNF-α and interleukin-1.15 These medications have drastically improved survival rates of patients with RA with impressive capabilities in symptom relief.15 With the increasing use of DMARDs and aggressive treatment early on in the disease process, patients with RA are showing markedly slow progression of joint deterioration, leading to a decreased need for orthopedic intervention compared with the general population.13,15
When analyzing the complication rates for patients undergoing TKA and THA, we observed that patients with RA exhibited a significant increase in the rates of infections, wound dehiscence, and systemic complications prior to discharge from the hospital compared with the OA population. The increased risk of infections was reported in previous studies assessing postoperative complication rates in TJA.16,17 A study utilizing the Norwegian Arthroplasty Registry noted an increased risk of late infection in patients with RA, leading to increased rates of revision TJA in comparison with patients with OA.16 Another study, which was based on the Canadian Institute for Health Information Discharge Abstract Database, showed that patients with RA are at an increased risk of infection only after THA and interestingly not after TKA.17 Although our study did not identify the causes of the increased infection rate, the inherent nature of the disease and the immunomodulatory drugs used to treat it may contribute to this increased infectious risk in patients with RA.6,18 Immunosuppressive DMARDs are some of the widely used medications employed to treat RA and are prime suspects of causing increased infection rates.15 The perioperative use of MTX has not been shown to cause short-term increases in infection for patients undergoing orthopedic intervention, but leflunomide and TNF-α inhibitors have been shown to cause a significant several-fold increase in risk for surgical wound infections.19,20
All patients with RA presented with significant increases for infection, wound dehiscence, and systemic complications, whereas only patients with RA undergoing THA showed increased risk of pulmonary and cardiovascular complications when compared with patients with OA. Surprisingly, in TKA, patients with RA were at a significantly decreased risk of cardiovascular complications. This observation was interesting due to cardiovascular disease being one of RA's most notable extra-articular features.4,21
Patients with RA undergoing TJA also showed significantly lower cerebrovascular complications than patients with OA. The significant reduction in risk for these complications has not been previously reported in the current literature, and it was an unexpected finding as past studies have found an increased risk in cerebrovascular disease in patients with RA. RA is an inflammatory disease exhibiting the upregulation of procoagulation factors,22 so we expected patients with RA to be at an increased risk for cerebrovascular and cardiovascular complications over patients with OA. Although we are unsure why these results were observed, we postulate that pharmaceutical interventions may confer some protection to patients with RA. For example, aspirin is commonly utilized in RA for its protective anti-platelet effect23 and may be a contributing factor to why we found low postoperative complication rates in cerebrovascular disease. However, the reason why aspirin may be protective against cerebrovascular and not cardiovascular complications remains unclear. Moreover, most guidelines suggest that aspirin be stopped prior to surgery.24 Although patients with RA were younger than those with OA, age was accounted for when analyzing the data.
A major strength of the study was the large sample size and the adjustment of potential confounding variables when examining the difference in complications between RA and OA. It is also a national US study that utilizes a validated database. Given that the patient samples in the NIS are reported in a uniform and de-identified manner, the database is considered ideal and has been extensively used for retrospective large observational cohort studies.25 However, the study also had some limitations due to the retrospective and administrative nature of the NIS database. Only data concerning patient complications during their inpatient stay at the hospital were available. Patients who may develop complications following discharge were not included in the data, providing a very small window of time for analysis. Another limitation with the database was its lack of ability to identify the severity of each patient's disease process or the medical treatment they received perioperatively. Finally, no patient-reported outcomes were determined, which would provide information on whether these complications affect the patients’ postoperational satisfaction in regard to their pain and disability.
CONCLUSION
As RA patients continue to utilize joint arthroplasty to repair deteriorated joints, understanding of how the disease process and its medical management may impact patient outcomes is important. This article reports significantly higher postoperational infection rates in RA than in patients with OA, which may be due to the medical management of the disease. Although new medications have been introduced and are being used to treat patients with RA, they have not altered the complication rate following TJA in this patient population. Thus, surgeons and other members of the management team should be familiar with the common medical conditions, co-morbidities, and medical treatments/side effects that are encountered in patients with RA. Future studies should delve into possible differences in long-term outcomes of patients with RA undergoing TKA and THA, as well as whether certain perioperative strategies and therapies (medical or physical) may decrease complications and improve outcomes.
This paper will be judged for the Resident Writer’s Award.
ABSTRACT
Current literature regarding complications following total joint arthroplasty have primarily focused on patients with osteoarthritis (OA), with less emphasis on the trends and in-hospital outcomes of rheumatoid arthritis (RA) patients undergoing these procedures. The purpose of this study is to analyze the outcomes and trends of RA patients undergoing total knee arthroplasty (TKA) or total hip arthroplasty (THA) compared to OA patients.
Data from the Nationwide Inpatient Sample from 2006 to 2011 was extracted using the International Classification of Diseases, Ninth Revision codes for patients that received a TKA or THA. Outcome measures included cardiovascular complications, cerebrovascular complications, pulmonary complications, wound dehiscence, and infection. Inpatient and hospital demographics including primary diagnosis, age, gender, primary payer, hospital teaching status, Charlson Comorbidity Index score, hospital bed size, location, and median household income were analyzed.
Logistic regression analysis of OA vs RA patients with patient outcomes revealed that osteoarthritic THA candidates had lower risk for cardiovascular complications, pulmonary complications, wound dehiscence, infections, and systemic complications, compared to rheumatoid patients. There was a significantly elevated risk of cerebrovascular complication in osteoarthritic THA compared to RA THA. OA patients undergoing TKA had significantly higher risk for cardiovascular and cerebrovascular complications. There were significant decreases in mechanical wounds, infection, and systemic complications in the OA TKA patients.
RA patients are at higher risk for postoperative infection, wound dehiscence, and systemic complications after TKA and THA compared to OA patients. These findings highlight the importance of preoperative medical clearance and management to optimize RA patients and improve the postoperative outcomes.
Continue to: RA is a chronic systemic inflammatory disease...
Rheumatoid arthritis (RA) is a chronic systemic inflammatory disease that causes joint deterioration, leading to pain, disability, systemic complications, short lifespan, and decline in quality of life.1-3 The deterioration primarily affects the synovial membranes of joints, causing arthritis and resulting in extra-articular sequelae such as cardiovascular disease,4 pulmonary disease,5 and increased infection rates.3,6 RA is the most prevalent inflammatory arthritis worldwide and affects up to 50 cases per 100,000 in both the US and northern Europe.2,7-9 Although the gold standard of care for these patients is medical management with immunosuppressant drugs such as disease-modifying anti-rheumatic drugs (DMARDs), total joint arthroplasty (TJA) remains an important tool in the management of joint deterioration in such patients.
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are common procedures utilized to treat disorders that cause joint pain and hindered joint mobility, including osteoarthritis (OA) and RA. Given the aging population, the amount of TKAs and THAs performed in the US has consistently increased each year, with the vast majority of this increase composed of patients with OA.10 As a result, previous studies investigated the trends and outcomes of these procedures in patients with OA, but relatively less is known about the outcomes and trends of patients with RA undergoing the same surgeries.
Given that RA is a fundamentally different condition with its own pathological characteristics, an understanding of how these differences may impact postoperative outcomes in patients with RA is important. This study aims to present a comparative analysis of the trends and postoperative outcomes between patients with RA and OA undergoing TKA and THA (Figure 1, Tables 1 and 2).
Table 1. Demographics of Total Knee Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 295,637 | 42.42 | 11,325 | 48.90 | 306,962 | 42.63 |
|
65 to 79 years | 329,034 | 47.22 | 10,055 | 43.42 | 339,089 | 47.09 |
|
≥80 years | 72,197 | 10.36 | 1780 | 7.69 | 73,977 | 10.27 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 259,192 | 37.19 | 4887 | 21.12 | 264,079 | 36.68 |
|
Female | 435,855 | 62.54 | 18,248 | 78.88 | 454,103 | 63.07 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 468,632 | 67.25 | 14,532 | 77.18 | 483,164 | 67.10 |
|
Black | 39,691 | 5.7 | 2119 | 11.25 | 41,810 | 5.81 |
|
Hispanic | 28,573 | 4.1 | 1395 | 7.41 | 29,968 | 4.16 |
|
Other | 21,306 | 3.06 | 783 | 4.16 | 22,089 | 3.07 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 112,031 | 16.08 | 3417 | 14.75 | 115,448 | 16.03 |
|
Midwest | 192,595 | 27.64 | 5975 | 25.80 | 198,570 | 27.58 |
|
South | 257,855 | 37 | 9422 | 40.68 | 267,277 | 37.12 |
|
West | 134,387 | 19.28 | 4346 | 18.77 | 138,733 | 19.27 |
|
Location/teaching status of hospital |
|
|
|
|
|
| <.0001 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban non-teaching | 333,043 | 47.79 | 10,905 | 47.46 | 343,948 | 47.77 |
|
Urban teaching | 273,326 | 39.22 | 9363 | 40.75 | 282,689 | 39.26 |
|
Hospital location |
|
|
|
|
|
| .0024 |
Rural | 86,321 | 12.39 | 2709 | 11.79 | 89,030 | 12.36 |
|
Urban | 606,369 | 87.01 | 20,268 | 88.21 | 626,637 | 87.03 |
|
Hospital teaching status |
|
|
|
|
|
| <.0001 |
Teaching | 409,465 | 58.76 | 13,275 | 57.78 | 422,740 | 58.71 |
|
Non-teaching | 283,225 | 40.64 | 9702 | 42.22 | 292,927 | 40.68 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 65,342 | 9.38 | 1946 | 8.40 | 67,288 | 9.35 | <.0001 |
Diabetes | 147,292 | 21.14 | 4289 | 18.52 | 151,581 | 21.05 | <.0001 |
Obesity | 129,277 | 18.55 | 3730 | 16.11 | 133,007 | 18.47 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis.
Table 2. Demographics of Total Hip Arthroplasty Patients Based on Primary Diagnosis of Osteoarthritis or Rheumatoid Arthritis
| OA | RA | Total | P Value | |||
| No. | Percent | No. | Percent | No. | Percent | (RA vs OA) |
Age group |
|
|
|
|
|
| <.0001 |
<64 years | 133,645 | 45.18 | 4679 | 48.02 | 138,324 | 45.27 |
|
65 to 79 years | 123,628 | 41.8 | 3992 | 40.97 | 127,620 | 41.77 |
|
≥80 years | 38,513 | 13.02 | 1073 | 11.01 | 39,586 | 12.96 |
|
Gender |
|
|
|
|
|
| <.0001 |
Male | 129,708 | 43.85 | 2457 | 25.24 | 132,165 | 43.26 |
|
Female | 165,010 | 55.79 | 7278 | 74.76 | 172,288 | 56.39 |
|
Race |
|
|
|
|
|
| <.0001 |
White | 207,005 | 69.98 | 6322 | 80.08 | 213,327 | 69.82 |
|
Black | 15,505 | 5.24 | 771 | 9.77 | 16,276 | 5.33 |
|
Hispanic | 6784 | 2.29 | 522 | 6.61 | 7306 | 2.39 |
|
Other | 7209 | 2.44 | 280 | 3.55 | 7489 | 2.45 |
|
Region of hospital |
|
|
|
|
|
| <.0001 |
Northeast | 58,525 | 19.79 | 1683 | 17.27 | 60,208 | 19.71 |
|
Midwest | 79,040 | 26.72 | 2446 | 25.10 | 81,486 | 26.67 |
|
South | 95,337 | 32.23 | 3716 | 38.14 | 99,053 | 32.42 |
|
West | 62,884 | 21.26 | 1899 | 19.49 | 64,783 | 21.20 |
|
Location/teaching status of hospital |
|
|
|
|
|
| .0065 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban non-teaching | 133,061 | 44.99 | 4245 | 43.87 | 137,306 | 44.94 |
|
Urban teaching | 130,150 | 44 | 4439 | 45.87 | 134,589 | 44.05 |
|
Hospital location |
|
|
|
|
|
| .4098 |
Rural | 30,954 | 10.46 | 993 | 10.26 | 31,947 | 10.46 |
|
Urban | 263,211 | 88.99 | 8684 | 89.74 | 271,895 | 88.99 |
|
Hospital teaching status |
|
|
|
|
|
| .0077 |
Teaching | 159,313 | 53.86 | 5108 | 52.78 | 164,421 | 53.82 |
|
Non-teaching | 134,852 | 45.59 | 4569 | 47.22 | 139,421 | 45.63 |
|
Comorbidities |
|
|
|
|
|
|
|
Obstructive sleep apnea | 19,760 | 6.68 | 573 | 5.88 | 20,333 | 6.65 | .0028 |
Diabetes | 41,929 | 14.18 | 1325 | 13.60 | 43,254 | 14.16 | .1077 |
Obesity | 38,808 | 13.12 | 1100 | 11.29 | 39,908 | 13.06 | <.0001 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis
Continue to: Methods...
METHODS
Exemptions were obtained from the Institutional Review Board. Data from the Nationwide Inpatient Sample (NIS) from 2006 to 2011 were extracted using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes for patients that received primary TKA or THA, as well as their comorbid conditions. No patients or populations were excluded from the sampling process. A list of all independent variables collected for analysis and provision of relevant ICD-9 codes is included in Figure 1. The NIS is the largest all-payer stratified survey of inpatient care in the US healthcare system. As of 2011, each year provides information on approximately 8 million inpatient stays from about 1000 hospitals in 46 states. All discharges from sampled hospitals are also represented in the database. All patient information is protected, and all methods were conducted in accordance with the highest ethical standards of Human and Animal Rights Research.
STATISTICAL ANALYSIS
SAS 9.2 and PROC FREQ statistics software were used to generate P values (chi square result) and analyze the trends (Cochran-Armitage). Results were weighted utilizing standard discharge weights from the NIS to ensure accurate comparison of data from different time points. P < .05 was considered statistically significant. Multivariable logistic regression analyses were performed to generate odds ratio and 95% confidence limits to assess outcomes across different demographic variables.
RESULTS
Data on 337,082 and 1,362,241 patients undergoing THA or TKA, respectively, between 2006 and 2011 were analyzed. Patients in both groups were further differentiated by a diagnosis of either OA or RA. OA was the most common diagnosis, constituting 96.8% of all arthritic THA and TKA patients. From 2006 to 2011, a 36% and 34% increase in total number of THAs and TKAs, respectively, were reported. The number of patients with OA undergoing THA and TKA steadily increased from 2006 to 2011 (Figure 2). The number of THA and TKA procedures in patients with RA followed a similar trend but at a comparatively slower rate (Figure 3). The TKA geographical trends mirrored those observed with THA. The majority of operations were performed at urban hospitals (89% THA, 87% TKA; P < .0001). Among patients with RA and OA, the majority of TKAs (47.77%; P < .0001) took place in urban non-teaching hospitals than in urban teaching hospitals (39.26%). This pattern was not the same for THA, with 44.94% being performed at urban teaching hospitals and 44.05% at urban non-teaching institutions (P < .0001). Rural hospitals accounted for a low percentage of operations for both procedures: 10.46% of THA and 12.36% of TKA (P < .0001). Large institutions (based on the number of beds) claimed the majority of cases (59% of THA and TKA).
Logistic regression analysis and odds ratios of patients with OA vs those with RA with patient outcomes adjusted for age, Charlson Comorbidity Index (CCI) score, and gender revealed that patients with OA undergoing THA had lower risk for cardiovascular (0.674; confidence interval (CI) 0.587-0.774) and pulmonary complications (0.416; CI 0.384-0.450), wound dehiscence (0.647; CI 0.561-0.747), infections (0.258; CI 0.221-0.301), and systemic complications (0.625; CI 0.562-0.695) than patients with RA. Patients with OA exhibited statistically significantly higher odds of experiencing cerebrovascular complications after THA than those with RA (1.946; CI 1.673-2.236) (Table 3). In a similar logistic regression analysis of OA vs RA in TKA, which was adjusted for age, CCI score, and gender, patients with OA had significantly higher risk for cardiovascular (1.329; CI 1.069-1.651) and cerebrovascular complications (1.635; CI 1.375-1.943) than patients with RA. Significant decreases in wound dehiscence (0.757; CI 0.639-0.896), infection (0.331; CI 0.286-0.383), and systemic complication (0.641; CI 0.565-0.729) were noted in the patients with OA and TKA (Table 4).
Table 3. Odds Ratio for In-Hospital Complications Following THA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | .674 | .587-.744 |
Cerebrovascular complication | 1.946 | 1.673-2.236 |
Pulmonary complication | .416 | .384-.450 |
Wound dehiscence | .647 | .561-.747 |
Infection | .258 | .221-.301 |
Systemic complication | .625 | .562-.695 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; THA, total hip arthroplasty.
Table 4. Odds Ratio for In-Hospital Complications Following TKA for OA Patients vs RA Patients
| Odds Ratio | Confidence Limits |
Cardiovascular complication | 1.329 | 1.069-1.651 |
Cerebrovascular complication | 1.635 | 1.375-1.943 |
Pulmonary complication | 1.03 | .995-1.223 |
Wound dehiscence | .757 | .639-.896 |
Infection | .331 | .286-.383 |
Systemic complication | .641 | .565-.729 |
Abbreviations: OA, osteoarthritis; RA, rheumatoid arthritis; TKA, total knee arthroplasty.
Continue to: Discussion...
DISCUSSION
Our results showed a continuous yearly increase from 2006 to 2011 in THA and TKA procedures at a rate of 36% and 34%, respectively; this result was consistent with existing literature.11 Despite a substantial increase in the amount of total THA and TKA procedures, the ratio of patients with RA undergoing these operations has decreased or remained nearly the same. Similar effects were found in Japan and the US when examining patients with RA undergoing TJA procedures between 2001 and 2007 and between 1992 and 2005, respectively.12-14 This observation may be explained by the advances and early initiation of pharmacologic treatment and the widespread use of DMARDs such as methotrexate (MTX), azathioprine, leflunomide, hydroxychloroquine, and biological response modifiers TNF-α and interleukin-1.15 These medications have drastically improved survival rates of patients with RA with impressive capabilities in symptom relief.15 With the increasing use of DMARDs and aggressive treatment early on in the disease process, patients with RA are showing markedly slow progression of joint deterioration, leading to a decreased need for orthopedic intervention compared with the general population.13,15
When analyzing the complication rates for patients undergoing TKA and THA, we observed that patients with RA exhibited a significant increase in the rates of infections, wound dehiscence, and systemic complications prior to discharge from the hospital compared with the OA population. The increased risk of infections was reported in previous studies assessing postoperative complication rates in TJA.16,17 A study utilizing the Norwegian Arthroplasty Registry noted an increased risk of late infection in patients with RA, leading to increased rates of revision TJA in comparison with patients with OA.16 Another study, which was based on the Canadian Institute for Health Information Discharge Abstract Database, showed that patients with RA are at an increased risk of infection only after THA and interestingly not after TKA.17 Although our study did not identify the causes of the increased infection rate, the inherent nature of the disease and the immunomodulatory drugs used to treat it may contribute to this increased infectious risk in patients with RA.6,18 Immunosuppressive DMARDs are some of the widely used medications employed to treat RA and are prime suspects of causing increased infection rates.15 The perioperative use of MTX has not been shown to cause short-term increases in infection for patients undergoing orthopedic intervention, but leflunomide and TNF-α inhibitors have been shown to cause a significant several-fold increase in risk for surgical wound infections.19,20
All patients with RA presented with significant increases for infection, wound dehiscence, and systemic complications, whereas only patients with RA undergoing THA showed increased risk of pulmonary and cardiovascular complications when compared with patients with OA. Surprisingly, in TKA, patients with RA were at a significantly decreased risk of cardiovascular complications. This observation was interesting due to cardiovascular disease being one of RA's most notable extra-articular features.4,21
Patients with RA undergoing TJA also showed significantly lower cerebrovascular complications than patients with OA. The significant reduction in risk for these complications has not been previously reported in the current literature, and it was an unexpected finding as past studies have found an increased risk in cerebrovascular disease in patients with RA. RA is an inflammatory disease exhibiting the upregulation of procoagulation factors,22 so we expected patients with RA to be at an increased risk for cerebrovascular and cardiovascular complications over patients with OA. Although we are unsure why these results were observed, we postulate that pharmaceutical interventions may confer some protection to patients with RA. For example, aspirin is commonly utilized in RA for its protective anti-platelet effect23 and may be a contributing factor to why we found low postoperative complication rates in cerebrovascular disease. However, the reason why aspirin may be protective against cerebrovascular and not cardiovascular complications remains unclear. Moreover, most guidelines suggest that aspirin be stopped prior to surgery.24 Although patients with RA were younger than those with OA, age was accounted for when analyzing the data.
A major strength of the study was the large sample size and the adjustment of potential confounding variables when examining the difference in complications between RA and OA. It is also a national US study that utilizes a validated database. Given that the patient samples in the NIS are reported in a uniform and de-identified manner, the database is considered ideal and has been extensively used for retrospective large observational cohort studies.25 However, the study also had some limitations due to the retrospective and administrative nature of the NIS database. Only data concerning patient complications during their inpatient stay at the hospital were available. Patients who may develop complications following discharge were not included in the data, providing a very small window of time for analysis. Another limitation with the database was its lack of ability to identify the severity of each patient's disease process or the medical treatment they received perioperatively. Finally, no patient-reported outcomes were determined, which would provide information on whether these complications affect the patients’ postoperational satisfaction in regard to their pain and disability.
CONCLUSION
As RA patients continue to utilize joint arthroplasty to repair deteriorated joints, understanding of how the disease process and its medical management may impact patient outcomes is important. This article reports significantly higher postoperational infection rates in RA than in patients with OA, which may be due to the medical management of the disease. Although new medications have been introduced and are being used to treat patients with RA, they have not altered the complication rate following TJA in this patient population. Thus, surgeons and other members of the management team should be familiar with the common medical conditions, co-morbidities, and medical treatments/side effects that are encountered in patients with RA. Future studies should delve into possible differences in long-term outcomes of patients with RA undergoing TKA and THA, as well as whether certain perioperative strategies and therapies (medical or physical) may decrease complications and improve outcomes.
This paper will be judged for the Resident Writer’s Award.
- Myasoedova E, Davis JM 3rd, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379-385. doi:10.1007/s11926-010-0117-y.
- Firestein GS. Evolving concepts of rheumatoid arthritis. Nature. 2003;423(6937):356-361. doi:10.1038/nature01661.
- Gullick NJ, Scott DL. Co-morbidities in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2011;25(4):469-483. doi:10.1016/j.berh.2011.10.009.
- Masuda H, Miyazaki T, Shimada K, et al. Disease duration and severity impacts on long-term cardiovascular events in Japanese patients with rheumatoid arthritis. J Cardiol. 2014;64(5):366-370. doi:10.1016/j.jjcc.2014.02.018.
- Bongartz T, Nannini C, Medina-Velasquez YF, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum.2010;62(6):1583-1591. doi:10.1002/art.27405.
- Doran MF, Crowson CS, Pond GR, O'Fallon WM, Gabriel SE. Frequency of infection in patients with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum. 2002;46(9):2287-2293. doi:10.1002/art.10524.
- Rossini M, Rossi E, Bernardi D, et al. Prevalence and incidence of rheumatoid arthritis in Italy. Rheumatol Int. 2014;34(5):659664. doi:10.1007/s00296-014-2974-6.
- Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006;36(3):182-188. doi:10.1016/j.semarthrit.2006.08.006.
- Carbonell J, Cobo T, Balsa A, Descalzo MA, Carmona L. The incidence of rheumatoid arthritis in Spain: results from a nationwide primary care registry. Rheumatology.2008;47(7):1088-1092. doi:10.1093/rheumatology/ken205.
- Skytta ET, Honkanen PB, Eskelinen A, Huhtala H, Remes V. Fewer and older patients with rheumatoid arthritis need total knee replacement. Scand J Rheumatol. 2012;41(5):345-349. doi:10.3109/03009742.2012.681061.
- Singh JA, Vessely MB, Harmsen WS, et al. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969–2008. Mayo Clin Proc. 2010;85(10):898-904. doi:10.4065/mcp.2010.0115.
- Momohara S, Inoue E, Ikari K, et al. Decrease in orthopaedic operations, including total joint replacements, in patients with rheumatoid arthritis between 2001 and 2007: data from Japanese outpatients in a single institute-based large observational cohort (IORRA). Ann Rheum Dis. 2010;69(1):312-313. doi:10.1136/ard.2009.107599.
- Jain A, Stein BE, Skolasky RL, Jones LC, Hungerford MW. Total joint arthroplasty in patients with rheumatoid arthritis: a United States experience from 1992 through 2005. J Arthroplasty. 2012;27(6):881-888. doi:10.1016/j.arth.2011.12.027.
- Mertelsmann-Voss C, Lyman S, Pan TJ, Goodman SM, Figgie MP, Mandl LA. US trends in rates of arthroplasty for inflammatory arthritis including rheumatoid arthritis, juvenile idiopathic arthritis, and spondyloarthritis. Arthritis Rheumatol 2014;66(6):1432-1439. doi:10.1002/art.38384.
- Howe CR, Gardner GC, Kadel NJ. Perioperative medication management for the patient with rheumatoid arthritis. J Am Acad Orthop Surg. 2006;14(9):544-551. doi:10.5435/00124635-200609000-00004.
- Schrama JC, Espehaug B, Hallan G, et al. Risk of revision for infection in primary total hip and knee arthroplasty in patients with rheumatoid arthritis compared with osteoarthritis: a prospective, population-based study on 108,786 hip and knee joint arthroplasties from the Norwegian Arthroplasty Register. Arthritis Care Res. 2010;62(4):473-479. doi:10.1002/acr.20036.
- Ravi B, Croxford R, Hollands S, et al. Increased risk of complications following total joint arthroplasty in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(2):254-263. doi:10.1002/art.38231.
- Au K, Reed G, Curtis JR, et al. High disease activity is associated with an increased risk of infection in patients with rheumatoid arthritis. Ann Rheum Dis. 2011;70(5):785-791. doi:10.1136/ard.2010.128637.
- Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275-2285. doi:10.1001/jama.295.19.2275.
- Scherrer CB, Mannion AF, Kyburz D, Vogt M, Kramers-de Quervain IA. Infection risk after orthopedic surgery in patients with inflammatory rheumatic diseases treated with immunosuppressive drugs. Arthritis Care Res. 2013;65(12):2032-2040. doi:10.1002/acr.22077.
- Bacani AK, Gabriel SE, Crowson CS, Heit JA, Matteson EL. Noncardiac vascular disease in rheumatoid arthritis: increase in venous thromboembolic events? Arthritis Rheum.2012;64(1):53-61. doi:10.1002/art.33322.
- Wallberg-Jonsson S, Dahlen GH, Nilsson TK, Ranby M, Rantapaa-Dahlqvist S. Tissue plasminogen activator, plasminogen activator inhibitor-1 and von Willebrand factor in rheumatoid arthritis. Clin Rheumatol. 1993;12(3):318324.
- van Heereveld HA, Laan RF, van den Hoogen FH, Malefijt MC, Novakova IR, van de Putte LB. Prevention of symptomatic thrombosis with short term (low molecular weight) heparin in patients with rheumatoid arthritis after hip or knee replacement. Ann Rheum Dis.2001;60(10):974-976. doi:10.1136/ard.60.10.974.
- Mont MA, Jacobs JJ, Boggio LN, et al. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. J Am Acad Orthop Surg.2011;19(12):768-776.
- Bozic KJ, Bashyal RK, Anthony SG, Chiu V, Shulman B, Rubash HE. Is administratively coded comorbidity and complication data in total joint arthroplasty valid? Clin Orthop Relat Res. 2013;471(1):201-205. doi:10.1007/s11999-012-2352-1.
- Myasoedova E, Davis JM 3rd, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379-385. doi:10.1007/s11926-010-0117-y.
- Firestein GS. Evolving concepts of rheumatoid arthritis. Nature. 2003;423(6937):356-361. doi:10.1038/nature01661.
- Gullick NJ, Scott DL. Co-morbidities in established rheumatoid arthritis. Best Pract Res Clin Rheumatol. 2011;25(4):469-483. doi:10.1016/j.berh.2011.10.009.
- Masuda H, Miyazaki T, Shimada K, et al. Disease duration and severity impacts on long-term cardiovascular events in Japanese patients with rheumatoid arthritis. J Cardiol. 2014;64(5):366-370. doi:10.1016/j.jjcc.2014.02.018.
- Bongartz T, Nannini C, Medina-Velasquez YF, et al. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: a population-based study. Arthritis Rheum.2010;62(6):1583-1591. doi:10.1002/art.27405.
- Doran MF, Crowson CS, Pond GR, O'Fallon WM, Gabriel SE. Frequency of infection in patients with rheumatoid arthritis compared with controls: a population-based study. Arthritis Rheum. 2002;46(9):2287-2293. doi:10.1002/art.10524.
- Rossini M, Rossi E, Bernardi D, et al. Prevalence and incidence of rheumatoid arthritis in Italy. Rheumatol Int. 2014;34(5):659664. doi:10.1007/s00296-014-2974-6.
- Alamanos Y, Voulgari PV, Drosos AA. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: a systematic review. Semin Arthritis Rheum. 2006;36(3):182-188. doi:10.1016/j.semarthrit.2006.08.006.
- Carbonell J, Cobo T, Balsa A, Descalzo MA, Carmona L. The incidence of rheumatoid arthritis in Spain: results from a nationwide primary care registry. Rheumatology.2008;47(7):1088-1092. doi:10.1093/rheumatology/ken205.
- Skytta ET, Honkanen PB, Eskelinen A, Huhtala H, Remes V. Fewer and older patients with rheumatoid arthritis need total knee replacement. Scand J Rheumatol. 2012;41(5):345-349. doi:10.3109/03009742.2012.681061.
- Singh JA, Vessely MB, Harmsen WS, et al. A population-based study of trends in the use of total hip and total knee arthroplasty, 1969–2008. Mayo Clin Proc. 2010;85(10):898-904. doi:10.4065/mcp.2010.0115.
- Momohara S, Inoue E, Ikari K, et al. Decrease in orthopaedic operations, including total joint replacements, in patients with rheumatoid arthritis between 2001 and 2007: data from Japanese outpatients in a single institute-based large observational cohort (IORRA). Ann Rheum Dis. 2010;69(1):312-313. doi:10.1136/ard.2009.107599.
- Jain A, Stein BE, Skolasky RL, Jones LC, Hungerford MW. Total joint arthroplasty in patients with rheumatoid arthritis: a United States experience from 1992 through 2005. J Arthroplasty. 2012;27(6):881-888. doi:10.1016/j.arth.2011.12.027.
- Mertelsmann-Voss C, Lyman S, Pan TJ, Goodman SM, Figgie MP, Mandl LA. US trends in rates of arthroplasty for inflammatory arthritis including rheumatoid arthritis, juvenile idiopathic arthritis, and spondyloarthritis. Arthritis Rheumatol 2014;66(6):1432-1439. doi:10.1002/art.38384.
- Howe CR, Gardner GC, Kadel NJ. Perioperative medication management for the patient with rheumatoid arthritis. J Am Acad Orthop Surg. 2006;14(9):544-551. doi:10.5435/00124635-200609000-00004.
- Schrama JC, Espehaug B, Hallan G, et al. Risk of revision for infection in primary total hip and knee arthroplasty in patients with rheumatoid arthritis compared with osteoarthritis: a prospective, population-based study on 108,786 hip and knee joint arthroplasties from the Norwegian Arthroplasty Register. Arthritis Care Res. 2010;62(4):473-479. doi:10.1002/acr.20036.
- Ravi B, Croxford R, Hollands S, et al. Increased risk of complications following total joint arthroplasty in patients with rheumatoid arthritis. Arthritis Rheumatol. 2014;66(2):254-263. doi:10.1002/art.38231.
- Au K, Reed G, Curtis JR, et al. High disease activity is associated with an increased risk of infection in patients with rheumatoid arthritis. Ann Rheum Dis. 2011;70(5):785-791. doi:10.1136/ard.2010.128637.
- Bongartz T, Sutton AJ, Sweeting MJ, Buchan I, Matteson EL, Montori V. Anti-TNF antibody therapy in rheumatoid arthritis and the risk of serious infections and malignancies: systematic review and meta-analysis of rare harmful effects in randomized controlled trials. JAMA. 2006;295(19):2275-2285. doi:10.1001/jama.295.19.2275.
- Scherrer CB, Mannion AF, Kyburz D, Vogt M, Kramers-de Quervain IA. Infection risk after orthopedic surgery in patients with inflammatory rheumatic diseases treated with immunosuppressive drugs. Arthritis Care Res. 2013;65(12):2032-2040. doi:10.1002/acr.22077.
- Bacani AK, Gabriel SE, Crowson CS, Heit JA, Matteson EL. Noncardiac vascular disease in rheumatoid arthritis: increase in venous thromboembolic events? Arthritis Rheum.2012;64(1):53-61. doi:10.1002/art.33322.
- Wallberg-Jonsson S, Dahlen GH, Nilsson TK, Ranby M, Rantapaa-Dahlqvist S. Tissue plasminogen activator, plasminogen activator inhibitor-1 and von Willebrand factor in rheumatoid arthritis. Clin Rheumatol. 1993;12(3):318324.
- van Heereveld HA, Laan RF, van den Hoogen FH, Malefijt MC, Novakova IR, van de Putte LB. Prevention of symptomatic thrombosis with short term (low molecular weight) heparin in patients with rheumatoid arthritis after hip or knee replacement. Ann Rheum Dis.2001;60(10):974-976. doi:10.1136/ard.60.10.974.
- Mont MA, Jacobs JJ, Boggio LN, et al. Preventing venous thromboembolic disease in patients undergoing elective hip and knee arthroplasty. J Am Acad Orthop Surg.2011;19(12):768-776.
- Bozic KJ, Bashyal RK, Anthony SG, Chiu V, Shulman B, Rubash HE. Is administratively coded comorbidity and complication data in total joint arthroplasty valid? Clin Orthop Relat Res. 2013;471(1):201-205. doi:10.1007/s11999-012-2352-1.
TAKE-HOME POINTS
- Patients undergoing THA for OA, when compared to those with RA undergoing THA, had lower risk for postoperative cardiovascular, pulmonary, wound dehiscence, infections, and systemic complications.
- Patients with OA undergoing THA had statistically significant higher risk of cerebrovascular complication compared to RA patients undergoing the same procedure.
- In TKA, OA patients had significantly higher risk for cardiovascular and cerebrovascular complications, and a significant lower risk for mechanical wounds, infection, and systemic complications.
- RA patients are at higher risk for postoperative infection, wound dehiscence, and systemic complications after TKA and THA compared to OA patients.
- These findings highlight the importance of preoperative medical clearance and management to optimize RA patients and improve the postoperative outcomes.
New look at ATLAS suggests rivaroxaban may still have role in ACS
In a new analysis comparing only clinically similar outcomes in patients with acute coronary syndrome, the addition of rivaroxaban to standard antiplatelet therapy resulted in 115 fewer fatal or irreversible ischemic events per 10,000 patient-years than placebo, at the expense of only 10 additional fatal or seriously harmful events.
This new interpretation of the ATLAS ACS 2-TIMI 51 trial (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction-51) suggests that the factor Xa inhibitor may still carve out a place for itself in ACS therapy, despite Food and Drug Administration rejections for this indication.

Not only did the survival benefit of rivaroxaban appear early in postevent treatment, it continued to protect patients over time, C. Michael Gibson, MD, and colleagues reported in the Journal of the American College of Cardiology.
“Time-to-event analysis demonstrated that the risk of fatal or irreversible harm remained low and constant over time, whereas reduction in fatal or irreversible ischemic events expanded,” wrote Dr. Gibson, professor of medicine at Beth Israel Deaconess Medical Center, Boston, and his coinvestigators. “By 720 days, a net of 142 fatal or irreversible events would have been prevented by 2.5-mg oral doses twice per day of rivaroxaban. Additional time-to-event sensitivity analyses demonstrated similar results, even when TIMI major bleeding was included as a fatal or irreversible event.”
In conducting the new analysis, Dr. Gibson and his team argued that the original interpretation of the results of ATLAS ACS 2-TIMI 51 lumped both fatal and nonfatal events together in composite endpoints, resulting in an inaccurate real-life picture of rivaroxaban’s therapeutic potential. “All types of events [were] weighted equally; for example, reversible nonintracranial hemorrhage, nonfatal bleeds that can be managed with supportive care, are weighted equally with death and disabling stroke. Second, stroke can be either hemorrhagic or ischemic, and the relative contributions of hemorrhagic or ischemic stroke may not be appropriately assigned to risk-versus-benefit categories in many analyses.”
The net result was that, while rivaroxaban did reduce the risk of the composite endpoint (cardiovascular death, MI, or stroke), the 1.7% absolute difference in cardiovascular mortality was almost completely offset by a 1.3% increase in major bleeding. However, most of those bleeds were reversible and nonfatal, associated with a drop in hemoglobin and/or blood transfusion. The drug did not increase the risk of fatal bleeding.
Giving equal statistical weight to clinically equal events provides a clearer focus, the investigators said.
“In this form of analysis, only fatal or irreversible events were included so that benefit and seriously harmful events of similar clinical impact were compared,” they wrote. “This is particularly important when the endpoints and analyses do not include measurements of subjective clinical impact such as utility measurements or preference weights. This approach also uses risk differences rather than relative measurements such as hazard ratios, so the number of events prevented and caused are clearly distinguished.”
ATLAS comprised more than 15,000 patients with ST-segment elevation MI, non-STEMI, or unstable angina. They were randomized to either rivaroxaban 2.5 mg orally twice per day, 5 mg orally twice per day, or to placebo, in addition to standard of care, which included low-dose aspirin. Patients were stratified by the optional use of clopidogrel/ticlopidine.
Dr. Gibson and his team reanalyzed the data by comparing outcomes they judged as having a similar clinical impact: fatal and irreversible cardiovascular death, MI, and ischemic stroke. They also assessed all bleeding, TIMI life-threatening bleeding, and TIMI major bleeding.
In this analysis, the 2.5-mg dose was associated with 115 fewer fatal or irreversible ischemic deaths per 10,000 patient-years of exposure than placebo (548 vs. 663 nonbleeding cardiovascular deaths, MIs, or ischemic strokes).
However, the same dose was also associated with 10 more excessive, fatal, or irreversibly serious harmful events, compared with placebo per 10,000 patient years (33 fatal bleeds or intracranial hemorrhage vs. 23 for placebo).
“Considered together, there would be 105 fatal or irreversible events prevented per 10,000 patient-years of exposure to 2.5 mg of rivaroxaban taken orally twice a day, compared with placebo. An alternate interpretation of the data is that there would be 11 [10 of 115] fatal or irreversible ischemic events prevented for each fatal or irreversible harmful event caused,” Dr. Gibson and his colleagues wrote.
The benefit held when the outcomes were individually reckoned as well. If periprocedural MIs were excluded, rivaroxaban would still prevent 115 fatal or irreversible ischemic events. If only nonbleeding cardiovascular death or ischemic strokes were included, then 90 fatal or irreversible events would be prevented. And if only nonbleeding cardiovascular death was included, then 95 events would be prevented per 10,000 patient-years of exposure in the group taking rivaroxaban 2.5 mg twice daily.
“In all cases, the fatal or irreversible events prevented are 9-11 times the fatal or irreversible seriously harmful events caused,” the investigators said.
ATLAS ACS 2-TIMI 51 was supported by Johnson & Johnson and Bayer Healthcare. Dr. Gibson has received institutional funding, grants, and honoraria from those companies and from Portola Pharmaceuticals.
SOURCE: Gibson CM et al. J Am Coll Cardiol. 2018;72:129-36.
Balancing the risks and benefits of anticoagulation therapy after an acute coronary event leaves physicians on the horns of a dilemma. How do we choose the most effective and the least harmful antiplatelet and/or antithrombotic strategy?
To support decision making, a careful and thoughtful interpretation of the existing evidence is essential, with an explicit focus on the risk-versus-benefit assessment. Even the most well-designed trial can contain ambiguities, the study investigators noted, and ATLAS was one of these.
The reanalysis of ATLAS by Gibson et al. is an attempt to cut through some of these ambiguities. By comparing only serious or fatal outcomes, the investigators aimed to bring clinically meaningful insight into the picture. Such a way of reporting provides readers with an extra piece of information to assist in deciding whether a treatment should be used.
The analysis isn’t perfect. It doesn’t include less-serious bleeding events, which still may contribute to a poor prognosis. And the analysis didn’t take into about ischemia-driven revascularizations.
Although commonly successful, repeat revascularizations are not free from complications, which may include occurrence of large infarctions, stroke, and serious bleeding.
Nevertheless, the study enhances our understanding of how to best employ low-dose rivaroxaban therapy in addition to antiplatelet agents.
Although we are getting closer to therapy optimization, the final word regarding the use of low-dose rivaroxaban and other agents for secondary prevention of cardiovascular diseases has not yet been said. This is primarily because of substantial variation in the magnitude of the risks and benefits across a population. Comprehensive, individualized profiling of the patients with respect to their ischemic and bleeding risks is crucial to further improve acute coronary syndrome–related outcomes.
Eugenia Nikolsy, MD, PhD, and Freek Verheugt, MD, made these comments in an accompanying editorial (J Am Coll Cardiol. 2018;72:137-40). Dr. Nikolsy is director of clinical research in invasive cardiology at Rambam Academic Hospital, Haifa, Israel. Dr. Verheugt is a professor of cardiology at the Heart-Lung Centre at University Medical Centre, Nijmegen, the Netherlands.
Balancing the risks and benefits of anticoagulation therapy after an acute coronary event leaves physicians on the horns of a dilemma. How do we choose the most effective and the least harmful antiplatelet and/or antithrombotic strategy?
To support decision making, a careful and thoughtful interpretation of the existing evidence is essential, with an explicit focus on the risk-versus-benefit assessment. Even the most well-designed trial can contain ambiguities, the study investigators noted, and ATLAS was one of these.
The reanalysis of ATLAS by Gibson et al. is an attempt to cut through some of these ambiguities. By comparing only serious or fatal outcomes, the investigators aimed to bring clinically meaningful insight into the picture. Such a way of reporting provides readers with an extra piece of information to assist in deciding whether a treatment should be used.
The analysis isn’t perfect. It doesn’t include less-serious bleeding events, which still may contribute to a poor prognosis. And the analysis didn’t take into about ischemia-driven revascularizations.
Although commonly successful, repeat revascularizations are not free from complications, which may include occurrence of large infarctions, stroke, and serious bleeding.
Nevertheless, the study enhances our understanding of how to best employ low-dose rivaroxaban therapy in addition to antiplatelet agents.
Although we are getting closer to therapy optimization, the final word regarding the use of low-dose rivaroxaban and other agents for secondary prevention of cardiovascular diseases has not yet been said. This is primarily because of substantial variation in the magnitude of the risks and benefits across a population. Comprehensive, individualized profiling of the patients with respect to their ischemic and bleeding risks is crucial to further improve acute coronary syndrome–related outcomes.
Eugenia Nikolsy, MD, PhD, and Freek Verheugt, MD, made these comments in an accompanying editorial (J Am Coll Cardiol. 2018;72:137-40). Dr. Nikolsy is director of clinical research in invasive cardiology at Rambam Academic Hospital, Haifa, Israel. Dr. Verheugt is a professor of cardiology at the Heart-Lung Centre at University Medical Centre, Nijmegen, the Netherlands.
Balancing the risks and benefits of anticoagulation therapy after an acute coronary event leaves physicians on the horns of a dilemma. How do we choose the most effective and the least harmful antiplatelet and/or antithrombotic strategy?
To support decision making, a careful and thoughtful interpretation of the existing evidence is essential, with an explicit focus on the risk-versus-benefit assessment. Even the most well-designed trial can contain ambiguities, the study investigators noted, and ATLAS was one of these.
The reanalysis of ATLAS by Gibson et al. is an attempt to cut through some of these ambiguities. By comparing only serious or fatal outcomes, the investigators aimed to bring clinically meaningful insight into the picture. Such a way of reporting provides readers with an extra piece of information to assist in deciding whether a treatment should be used.
The analysis isn’t perfect. It doesn’t include less-serious bleeding events, which still may contribute to a poor prognosis. And the analysis didn’t take into about ischemia-driven revascularizations.
Although commonly successful, repeat revascularizations are not free from complications, which may include occurrence of large infarctions, stroke, and serious bleeding.
Nevertheless, the study enhances our understanding of how to best employ low-dose rivaroxaban therapy in addition to antiplatelet agents.
Although we are getting closer to therapy optimization, the final word regarding the use of low-dose rivaroxaban and other agents for secondary prevention of cardiovascular diseases has not yet been said. This is primarily because of substantial variation in the magnitude of the risks and benefits across a population. Comprehensive, individualized profiling of the patients with respect to their ischemic and bleeding risks is crucial to further improve acute coronary syndrome–related outcomes.
Eugenia Nikolsy, MD, PhD, and Freek Verheugt, MD, made these comments in an accompanying editorial (J Am Coll Cardiol. 2018;72:137-40). Dr. Nikolsy is director of clinical research in invasive cardiology at Rambam Academic Hospital, Haifa, Israel. Dr. Verheugt is a professor of cardiology at the Heart-Lung Centre at University Medical Centre, Nijmegen, the Netherlands.
In a new analysis comparing only clinically similar outcomes in patients with acute coronary syndrome, the addition of rivaroxaban to standard antiplatelet therapy resulted in 115 fewer fatal or irreversible ischemic events per 10,000 patient-years than placebo, at the expense of only 10 additional fatal or seriously harmful events.
This new interpretation of the ATLAS ACS 2-TIMI 51 trial (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction-51) suggests that the factor Xa inhibitor may still carve out a place for itself in ACS therapy, despite Food and Drug Administration rejections for this indication.
Not only did the survival benefit of rivaroxaban appear early in postevent treatment, it continued to protect patients over time, C. Michael Gibson, MD, and colleagues reported in the Journal of the American College of Cardiology.
“Time-to-event analysis demonstrated that the risk of fatal or irreversible harm remained low and constant over time, whereas reduction in fatal or irreversible ischemic events expanded,” wrote Dr. Gibson, professor of medicine at Beth Israel Deaconess Medical Center, Boston, and his coinvestigators. “By 720 days, a net of 142 fatal or irreversible events would have been prevented by 2.5-mg oral doses twice per day of rivaroxaban. Additional time-to-event sensitivity analyses demonstrated similar results, even when TIMI major bleeding was included as a fatal or irreversible event.”
In conducting the new analysis, Dr. Gibson and his team argued that the original interpretation of the results of ATLAS ACS 2-TIMI 51 lumped both fatal and nonfatal events together in composite endpoints, resulting in an inaccurate real-life picture of rivaroxaban’s therapeutic potential. “All types of events [were] weighted equally; for example, reversible nonintracranial hemorrhage, nonfatal bleeds that can be managed with supportive care, are weighted equally with death and disabling stroke. Second, stroke can be either hemorrhagic or ischemic, and the relative contributions of hemorrhagic or ischemic stroke may not be appropriately assigned to risk-versus-benefit categories in many analyses.”
The net result was that, while rivaroxaban did reduce the risk of the composite endpoint (cardiovascular death, MI, or stroke), the 1.7% absolute difference in cardiovascular mortality was almost completely offset by a 1.3% increase in major bleeding. However, most of those bleeds were reversible and nonfatal, associated with a drop in hemoglobin and/or blood transfusion. The drug did not increase the risk of fatal bleeding.
Giving equal statistical weight to clinically equal events provides a clearer focus, the investigators said.
“In this form of analysis, only fatal or irreversible events were included so that benefit and seriously harmful events of similar clinical impact were compared,” they wrote. “This is particularly important when the endpoints and analyses do not include measurements of subjective clinical impact such as utility measurements or preference weights. This approach also uses risk differences rather than relative measurements such as hazard ratios, so the number of events prevented and caused are clearly distinguished.”
ATLAS comprised more than 15,000 patients with ST-segment elevation MI, non-STEMI, or unstable angina. They were randomized to either rivaroxaban 2.5 mg orally twice per day, 5 mg orally twice per day, or to placebo, in addition to standard of care, which included low-dose aspirin. Patients were stratified by the optional use of clopidogrel/ticlopidine.
Dr. Gibson and his team reanalyzed the data by comparing outcomes they judged as having a similar clinical impact: fatal and irreversible cardiovascular death, MI, and ischemic stroke. They also assessed all bleeding, TIMI life-threatening bleeding, and TIMI major bleeding.
In this analysis, the 2.5-mg dose was associated with 115 fewer fatal or irreversible ischemic deaths per 10,000 patient-years of exposure than placebo (548 vs. 663 nonbleeding cardiovascular deaths, MIs, or ischemic strokes).
However, the same dose was also associated with 10 more excessive, fatal, or irreversibly serious harmful events, compared with placebo per 10,000 patient years (33 fatal bleeds or intracranial hemorrhage vs. 23 for placebo).
“Considered together, there would be 105 fatal or irreversible events prevented per 10,000 patient-years of exposure to 2.5 mg of rivaroxaban taken orally twice a day, compared with placebo. An alternate interpretation of the data is that there would be 11 [10 of 115] fatal or irreversible ischemic events prevented for each fatal or irreversible harmful event caused,” Dr. Gibson and his colleagues wrote.
The benefit held when the outcomes were individually reckoned as well. If periprocedural MIs were excluded, rivaroxaban would still prevent 115 fatal or irreversible ischemic events. If only nonbleeding cardiovascular death or ischemic strokes were included, then 90 fatal or irreversible events would be prevented. And if only nonbleeding cardiovascular death was included, then 95 events would be prevented per 10,000 patient-years of exposure in the group taking rivaroxaban 2.5 mg twice daily.
“In all cases, the fatal or irreversible events prevented are 9-11 times the fatal or irreversible seriously harmful events caused,” the investigators said.
ATLAS ACS 2-TIMI 51 was supported by Johnson & Johnson and Bayer Healthcare. Dr. Gibson has received institutional funding, grants, and honoraria from those companies and from Portola Pharmaceuticals.
SOURCE: Gibson CM et al. J Am Coll Cardiol. 2018;72:129-36.
In a new analysis comparing only clinically similar outcomes in patients with acute coronary syndrome, the addition of rivaroxaban to standard antiplatelet therapy resulted in 115 fewer fatal or irreversible ischemic events per 10,000 patient-years than placebo, at the expense of only 10 additional fatal or seriously harmful events.
This new interpretation of the ATLAS ACS 2-TIMI 51 trial (Anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction-51) suggests that the factor Xa inhibitor may still carve out a place for itself in ACS therapy, despite Food and Drug Administration rejections for this indication.
Not only did the survival benefit of rivaroxaban appear early in postevent treatment, it continued to protect patients over time, C. Michael Gibson, MD, and colleagues reported in the Journal of the American College of Cardiology.
“Time-to-event analysis demonstrated that the risk of fatal or irreversible harm remained low and constant over time, whereas reduction in fatal or irreversible ischemic events expanded,” wrote Dr. Gibson, professor of medicine at Beth Israel Deaconess Medical Center, Boston, and his coinvestigators. “By 720 days, a net of 142 fatal or irreversible events would have been prevented by 2.5-mg oral doses twice per day of rivaroxaban. Additional time-to-event sensitivity analyses demonstrated similar results, even when TIMI major bleeding was included as a fatal or irreversible event.”
In conducting the new analysis, Dr. Gibson and his team argued that the original interpretation of the results of ATLAS ACS 2-TIMI 51 lumped both fatal and nonfatal events together in composite endpoints, resulting in an inaccurate real-life picture of rivaroxaban’s therapeutic potential. “All types of events [were] weighted equally; for example, reversible nonintracranial hemorrhage, nonfatal bleeds that can be managed with supportive care, are weighted equally with death and disabling stroke. Second, stroke can be either hemorrhagic or ischemic, and the relative contributions of hemorrhagic or ischemic stroke may not be appropriately assigned to risk-versus-benefit categories in many analyses.”
The net result was that, while rivaroxaban did reduce the risk of the composite endpoint (cardiovascular death, MI, or stroke), the 1.7% absolute difference in cardiovascular mortality was almost completely offset by a 1.3% increase in major bleeding. However, most of those bleeds were reversible and nonfatal, associated with a drop in hemoglobin and/or blood transfusion. The drug did not increase the risk of fatal bleeding.
Giving equal statistical weight to clinically equal events provides a clearer focus, the investigators said.
“In this form of analysis, only fatal or irreversible events were included so that benefit and seriously harmful events of similar clinical impact were compared,” they wrote. “This is particularly important when the endpoints and analyses do not include measurements of subjective clinical impact such as utility measurements or preference weights. This approach also uses risk differences rather than relative measurements such as hazard ratios, so the number of events prevented and caused are clearly distinguished.”
ATLAS comprised more than 15,000 patients with ST-segment elevation MI, non-STEMI, or unstable angina. They were randomized to either rivaroxaban 2.5 mg orally twice per day, 5 mg orally twice per day, or to placebo, in addition to standard of care, which included low-dose aspirin. Patients were stratified by the optional use of clopidogrel/ticlopidine.
Dr. Gibson and his team reanalyzed the data by comparing outcomes they judged as having a similar clinical impact: fatal and irreversible cardiovascular death, MI, and ischemic stroke. They also assessed all bleeding, TIMI life-threatening bleeding, and TIMI major bleeding.
In this analysis, the 2.5-mg dose was associated with 115 fewer fatal or irreversible ischemic deaths per 10,000 patient-years of exposure than placebo (548 vs. 663 nonbleeding cardiovascular deaths, MIs, or ischemic strokes).
However, the same dose was also associated with 10 more excessive, fatal, or irreversibly serious harmful events, compared with placebo per 10,000 patient years (33 fatal bleeds or intracranial hemorrhage vs. 23 for placebo).
“Considered together, there would be 105 fatal or irreversible events prevented per 10,000 patient-years of exposure to 2.5 mg of rivaroxaban taken orally twice a day, compared with placebo. An alternate interpretation of the data is that there would be 11 [10 of 115] fatal or irreversible ischemic events prevented for each fatal or irreversible harmful event caused,” Dr. Gibson and his colleagues wrote.
The benefit held when the outcomes were individually reckoned as well. If periprocedural MIs were excluded, rivaroxaban would still prevent 115 fatal or irreversible ischemic events. If only nonbleeding cardiovascular death or ischemic strokes were included, then 90 fatal or irreversible events would be prevented. And if only nonbleeding cardiovascular death was included, then 95 events would be prevented per 10,000 patient-years of exposure in the group taking rivaroxaban 2.5 mg twice daily.
“In all cases, the fatal or irreversible events prevented are 9-11 times the fatal or irreversible seriously harmful events caused,” the investigators said.
ATLAS ACS 2-TIMI 51 was supported by Johnson & Johnson and Bayer Healthcare. Dr. Gibson has received institutional funding, grants, and honoraria from those companies and from Portola Pharmaceuticals.
SOURCE: Gibson CM et al. J Am Coll Cardiol. 2018;72:129-36.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Myeloproliferative neoplasms increase risk for arterial and venous thrombosis
Clinical question: What are the risks for arterial and venous thrombosis in patients with myeloproliferative neoplasms (MPNs)?
Background: Myeloproliferative neoplasms include polycythemia vera, essential thrombocythemia, and primary myelofibrosis. Prior studies have investigated the incidence of arterial and venous thrombosis in patients with myeloproliferative neoplasms, but the actual magnitude of thrombosis risk relative to the general population is unknown.
Study design: Retrospective matched-cohort study.
Setting: Sweden, using the Swedish Inpatient and Cancer Registers.

Synopsis: Using data from 1987 to 2009, 9,429 patients with MPNs were compared with 35,820 control participants to determine hazard ratios for arterial thrombosis, venous thrombosis, and any thrombosis. The highest hazard ratios were seen within 3 months of MPN diagnosis, with hazard ratios of 4.0 (95% confidence interval, 3.6-4.4) for any thrombosis, 3.0 (95% CI, 2.7-3.4) for arterial thrombosis, and 9.7 (95% CI, 7.8-12.0) for venous thrombosis. Risk decreased but remained significantly elevated through follow-up out to 20 years after diagnosis. This decrease was thought to be caused by effective thromboprophylactic and cytoreductive treatment of the MPN.
This study demonstrates significantly elevated risk for thrombosis in patients with MPNs, highest shortly after diagnosis. It suggests the importance of timely diagnosis and treatment of MPNs to decrease early thrombosis risk.
Bottom line: Patients with MPNs have increased rates of arterial and venous thrombosis, with the highest rates within 3 months of diagnosis.
Citation: Hultcrantz M et al. Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms. Ann Intern Med. 2018 Mar 6;168(5):317-25.
Dr. Komsoukaniants is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
Clinical question: What are the risks for arterial and venous thrombosis in patients with myeloproliferative neoplasms (MPNs)?
Background: Myeloproliferative neoplasms include polycythemia vera, essential thrombocythemia, and primary myelofibrosis. Prior studies have investigated the incidence of arterial and venous thrombosis in patients with myeloproliferative neoplasms, but the actual magnitude of thrombosis risk relative to the general population is unknown.
Study design: Retrospective matched-cohort study.
Setting: Sweden, using the Swedish Inpatient and Cancer Registers.
Synopsis: Using data from 1987 to 2009, 9,429 patients with MPNs were compared with 35,820 control participants to determine hazard ratios for arterial thrombosis, venous thrombosis, and any thrombosis. The highest hazard ratios were seen within 3 months of MPN diagnosis, with hazard ratios of 4.0 (95% confidence interval, 3.6-4.4) for any thrombosis, 3.0 (95% CI, 2.7-3.4) for arterial thrombosis, and 9.7 (95% CI, 7.8-12.0) for venous thrombosis. Risk decreased but remained significantly elevated through follow-up out to 20 years after diagnosis. This decrease was thought to be caused by effective thromboprophylactic and cytoreductive treatment of the MPN.
This study demonstrates significantly elevated risk for thrombosis in patients with MPNs, highest shortly after diagnosis. It suggests the importance of timely diagnosis and treatment of MPNs to decrease early thrombosis risk.
Bottom line: Patients with MPNs have increased rates of arterial and venous thrombosis, with the highest rates within 3 months of diagnosis.
Citation: Hultcrantz M et al. Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms. Ann Intern Med. 2018 Mar 6;168(5):317-25.
Dr. Komsoukaniants is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
Clinical question: What are the risks for arterial and venous thrombosis in patients with myeloproliferative neoplasms (MPNs)?
Background: Myeloproliferative neoplasms include polycythemia vera, essential thrombocythemia, and primary myelofibrosis. Prior studies have investigated the incidence of arterial and venous thrombosis in patients with myeloproliferative neoplasms, but the actual magnitude of thrombosis risk relative to the general population is unknown.
Study design: Retrospective matched-cohort study.
Setting: Sweden, using the Swedish Inpatient and Cancer Registers.
Synopsis: Using data from 1987 to 2009, 9,429 patients with MPNs were compared with 35,820 control participants to determine hazard ratios for arterial thrombosis, venous thrombosis, and any thrombosis. The highest hazard ratios were seen within 3 months of MPN diagnosis, with hazard ratios of 4.0 (95% confidence interval, 3.6-4.4) for any thrombosis, 3.0 (95% CI, 2.7-3.4) for arterial thrombosis, and 9.7 (95% CI, 7.8-12.0) for venous thrombosis. Risk decreased but remained significantly elevated through follow-up out to 20 years after diagnosis. This decrease was thought to be caused by effective thromboprophylactic and cytoreductive treatment of the MPN.
This study demonstrates significantly elevated risk for thrombosis in patients with MPNs, highest shortly after diagnosis. It suggests the importance of timely diagnosis and treatment of MPNs to decrease early thrombosis risk.
Bottom line: Patients with MPNs have increased rates of arterial and venous thrombosis, with the highest rates within 3 months of diagnosis.
Citation: Hultcrantz M et al. Risk for arterial and venous thrombosis in patients with myeloproliferative neoplasms. Ann Intern Med. 2018 Mar 6;168(5):317-25.
Dr. Komsoukaniants is a hospitalist at UC San Diego Health and an assistant clinical professor at the University of California, San Diego.
Fentanyl fears drive many opioid users, interviews suggest
SAN DIEGO – Many opioid users on the street are embracing homegrown “risk reduction” techniques to make sure they avoid the danger of fentanyl-laced heroin, while others seek out batches that have caused fatal overdoses because they figure these supplies must be extra-strong and desirable. “Anytime I hear that somebody OD’d off something,” said one user, “... I was like, ‘Oh, that stuff must be good. Where can I get it?’ ”
So say opioid users who are opening up to researchers about the deadly new American drug landscape.
There’s one common thread, said Daniel Ciccarone, MD, MPH, who presented findings from his team’s interviews at the annual meeting of the College on Problems of Drug Dependence. Attitudes about fentanyl are shifting, but not enough to turn the drug – which often is available instead of heroin – into a major crowd-pleaser.

“When we first went into the field, there was a strong negative opinion about fentanyl. It was not wanted; it was imposed,” said Dr. Ciccarone of the University of California at San Francisco. “While there is some shift now, in which some do want or like the fentanyl, it is not strong enough to have shifted the culture. i.e., .”
But fentanyl still is rampant, often making its way to users who do not want and might be actively trying to avoid it. According to the National Institute on Drug Abuse, or NIDA, fentanyl and fentanyl analogs were linked to more than 20,000 of the more than 64,000 fatal U.S. drug overdoses in 2016.
“The risks are greater with fentanyl and not just because it is more potent than heroin,” Dr. Ciccarone said. In addition, “the form (fentanyl vs. fentanyl analogs) and purity shifts on a daily basis, and it’s mixed with heroin in varying amounts. It is these vicissitudes in fentanyl/heroin types and purities that make the street blends dangerous for overdose.”
Dr. Ciccarone and his colleagues interviewed opioid users in Baltimore; Charleston, W. Va.; Lawrence and Lowell, Mass.; and Chicago. Information about some of the interviews was published previously (Intl J Drug Policy. 2017 Aug;46;146-55).
In another study whose results were released at the CPDD conference, researchers from Dartmouth College, Hanover, N.H., interviewed 76 opioid users (91% were white, average age was 34, half were female, and almost all had a history of substance abuse treatment).

Among the other findings of the studies:
- Some opioid users are shocked by the adulteration of heroin by fentanyl, and even dealers are surprised: “When we cut the dope, we don’t use fentanyl. The problem was that we were buying the dope already dirty with that, and we didn’t know it,” said a 42-year-old man from Lawrence, Mass.
- In the New Hampshire interviews, 84% of participants said fentanyl is the leading cause of overdose in the state. “Due to the fentanyl and the heroin, that’s how everyone that I know ended up passing away recently,” said one user.
- Also in New Hampshire, 84% of users interviewed said they’d used fentanyl before, accidentally in some cases. Also, study coauthor Andrea L. Meier said in an interview, “67% of users reported having a prescription for opioids in their lifetime due to some kind of illness or injury. Some were short-term prescriptions (injuries, C-sections, tooth extractions); others were prescribed long-term due to chronic pain or illness.”
Some say pursue fentanyl
In the New Hampshire interviews, 25% of the 84% who’d used fentanyl said they actively seek it out, with one expressing a preference for the “real dope” (heroin laced with fentanyl) versus the “maintenance dope” of heroin alone. Ms. Meier explained what that means: “We’ve heard that once you use fentanyl or fentanyl-laced heroin, heroin doesn’t adequately manage your withdrawal symptoms or give enough of a high. So they will use heroin to get by, but they really want fentanyl or fentanyl-laced heroin.”
She added: “We’ve learned that users are seeking fentanyl due to its potency (a stronger, better high with quicker onset than heroin), cost (cheaper than heroin, so more “bang for your buck”), and once they use fentanyl or fentanyl-laced heroin, heroin doesn’t have the same effect/high.”
As for the risk of overdose, “people want the best high they can get at the cheapest cost,” she said.” They presume it will be potent enough to produce an exceptional high but [they won’t] die from an overdose due to being sufficiently tolerant to handle it. Also, some just felt hopeless and weren’t afraid of an OD.”
Comments from users about fentanyl
- “The high is wonderful. It’s splendidly wonderful. It’s magnified heroin feeling by a great number,” said a 45-year-old man from Baltimore.
- “You spend the same amount of money or even less for it, and you’re getting 3 times as high as you did on heroin,” said one user in New Hampshire. “Who wouldn’t want that?”
Risk-reduction techniques embraced
- In Baltimore, a 39-year-old woman said: “I have a lot of associates that are letting me know, ‘Don’t go to that place because they selling fentanyl.’ ”
- Some users test their heroin. “Like when I get stuff I don’t know what it is, I do a little bit before I do something that I feel,” a Lawrence, Mass., female user in her 20s said. “Like, I want to kind of scale out how much I want to do. Because I don’t want to die. But these people are just doing a gram shot and just ... my friend just died 2 days ago.”
Dr. Ciccarone said some of the biggest proponents of harm-reduction among users were African Americans aged 60 and older who had used for many decades.
“They fear fentanyl and are using old-school harm reduction strategies for staying safer: “tooting” (snorting) and tester shots (small injections to test the quality),” he said. “These may seem like minor strategies, but if enough of the population applies them to their daily drug use, many deaths would be averted. In this crisis, we need all the wisdom we can get, so we should listen to these elders.”
Dr. Ciccarone’s research was funded by the National Institutes of Health and NIDA. Dr. Ciccarone reported no relevant disclosures. The Dartmouth College study was funded by NIDA, and those authors reported no relevant disclosures.
SAN DIEGO – Many opioid users on the street are embracing homegrown “risk reduction” techniques to make sure they avoid the danger of fentanyl-laced heroin, while others seek out batches that have caused fatal overdoses because they figure these supplies must be extra-strong and desirable. “Anytime I hear that somebody OD’d off something,” said one user, “... I was like, ‘Oh, that stuff must be good. Where can I get it?’ ”
So say opioid users who are opening up to researchers about the deadly new American drug landscape.
There’s one common thread, said Daniel Ciccarone, MD, MPH, who presented findings from his team’s interviews at the annual meeting of the College on Problems of Drug Dependence. Attitudes about fentanyl are shifting, but not enough to turn the drug – which often is available instead of heroin – into a major crowd-pleaser.
“When we first went into the field, there was a strong negative opinion about fentanyl. It was not wanted; it was imposed,” said Dr. Ciccarone of the University of California at San Francisco. “While there is some shift now, in which some do want or like the fentanyl, it is not strong enough to have shifted the culture. i.e., .”
But fentanyl still is rampant, often making its way to users who do not want and might be actively trying to avoid it. According to the National Institute on Drug Abuse, or NIDA, fentanyl and fentanyl analogs were linked to more than 20,000 of the more than 64,000 fatal U.S. drug overdoses in 2016.
“The risks are greater with fentanyl and not just because it is more potent than heroin,” Dr. Ciccarone said. In addition, “the form (fentanyl vs. fentanyl analogs) and purity shifts on a daily basis, and it’s mixed with heroin in varying amounts. It is these vicissitudes in fentanyl/heroin types and purities that make the street blends dangerous for overdose.”
Dr. Ciccarone and his colleagues interviewed opioid users in Baltimore; Charleston, W. Va.; Lawrence and Lowell, Mass.; and Chicago. Information about some of the interviews was published previously (Intl J Drug Policy. 2017 Aug;46;146-55).
In another study whose results were released at the CPDD conference, researchers from Dartmouth College, Hanover, N.H., interviewed 76 opioid users (91% were white, average age was 34, half were female, and almost all had a history of substance abuse treatment).
Among the other findings of the studies:
- Some opioid users are shocked by the adulteration of heroin by fentanyl, and even dealers are surprised: “When we cut the dope, we don’t use fentanyl. The problem was that we were buying the dope already dirty with that, and we didn’t know it,” said a 42-year-old man from Lawrence, Mass.
- In the New Hampshire interviews, 84% of participants said fentanyl is the leading cause of overdose in the state. “Due to the fentanyl and the heroin, that’s how everyone that I know ended up passing away recently,” said one user.
- Also in New Hampshire, 84% of users interviewed said they’d used fentanyl before, accidentally in some cases. Also, study coauthor Andrea L. Meier said in an interview, “67% of users reported having a prescription for opioids in their lifetime due to some kind of illness or injury. Some were short-term prescriptions (injuries, C-sections, tooth extractions); others were prescribed long-term due to chronic pain or illness.”
Some say pursue fentanyl
In the New Hampshire interviews, 25% of the 84% who’d used fentanyl said they actively seek it out, with one expressing a preference for the “real dope” (heroin laced with fentanyl) versus the “maintenance dope” of heroin alone. Ms. Meier explained what that means: “We’ve heard that once you use fentanyl or fentanyl-laced heroin, heroin doesn’t adequately manage your withdrawal symptoms or give enough of a high. So they will use heroin to get by, but they really want fentanyl or fentanyl-laced heroin.”
She added: “We’ve learned that users are seeking fentanyl due to its potency (a stronger, better high with quicker onset than heroin), cost (cheaper than heroin, so more “bang for your buck”), and once they use fentanyl or fentanyl-laced heroin, heroin doesn’t have the same effect/high.”
As for the risk of overdose, “people want the best high they can get at the cheapest cost,” she said.” They presume it will be potent enough to produce an exceptional high but [they won’t] die from an overdose due to being sufficiently tolerant to handle it. Also, some just felt hopeless and weren’t afraid of an OD.”
Comments from users about fentanyl
- “The high is wonderful. It’s splendidly wonderful. It’s magnified heroin feeling by a great number,” said a 45-year-old man from Baltimore.
- “You spend the same amount of money or even less for it, and you’re getting 3 times as high as you did on heroin,” said one user in New Hampshire. “Who wouldn’t want that?”
Risk-reduction techniques embraced
- In Baltimore, a 39-year-old woman said: “I have a lot of associates that are letting me know, ‘Don’t go to that place because they selling fentanyl.’ ”
- Some users test their heroin. “Like when I get stuff I don’t know what it is, I do a little bit before I do something that I feel,” a Lawrence, Mass., female user in her 20s said. “Like, I want to kind of scale out how much I want to do. Because I don’t want to die. But these people are just doing a gram shot and just ... my friend just died 2 days ago.”
Dr. Ciccarone said some of the biggest proponents of harm-reduction among users were African Americans aged 60 and older who had used for many decades.
“They fear fentanyl and are using old-school harm reduction strategies for staying safer: “tooting” (snorting) and tester shots (small injections to test the quality),” he said. “These may seem like minor strategies, but if enough of the population applies them to their daily drug use, many deaths would be averted. In this crisis, we need all the wisdom we can get, so we should listen to these elders.”
Dr. Ciccarone’s research was funded by the National Institutes of Health and NIDA. Dr. Ciccarone reported no relevant disclosures. The Dartmouth College study was funded by NIDA, and those authors reported no relevant disclosures.
SAN DIEGO – Many opioid users on the street are embracing homegrown “risk reduction” techniques to make sure they avoid the danger of fentanyl-laced heroin, while others seek out batches that have caused fatal overdoses because they figure these supplies must be extra-strong and desirable. “Anytime I hear that somebody OD’d off something,” said one user, “... I was like, ‘Oh, that stuff must be good. Where can I get it?’ ”
So say opioid users who are opening up to researchers about the deadly new American drug landscape.
There’s one common thread, said Daniel Ciccarone, MD, MPH, who presented findings from his team’s interviews at the annual meeting of the College on Problems of Drug Dependence. Attitudes about fentanyl are shifting, but not enough to turn the drug – which often is available instead of heroin – into a major crowd-pleaser.
“When we first went into the field, there was a strong negative opinion about fentanyl. It was not wanted; it was imposed,” said Dr. Ciccarone of the University of California at San Francisco. “While there is some shift now, in which some do want or like the fentanyl, it is not strong enough to have shifted the culture. i.e., .”
But fentanyl still is rampant, often making its way to users who do not want and might be actively trying to avoid it. According to the National Institute on Drug Abuse, or NIDA, fentanyl and fentanyl analogs were linked to more than 20,000 of the more than 64,000 fatal U.S. drug overdoses in 2016.
“The risks are greater with fentanyl and not just because it is more potent than heroin,” Dr. Ciccarone said. In addition, “the form (fentanyl vs. fentanyl analogs) and purity shifts on a daily basis, and it’s mixed with heroin in varying amounts. It is these vicissitudes in fentanyl/heroin types and purities that make the street blends dangerous for overdose.”
Dr. Ciccarone and his colleagues interviewed opioid users in Baltimore; Charleston, W. Va.; Lawrence and Lowell, Mass.; and Chicago. Information about some of the interviews was published previously (Intl J Drug Policy. 2017 Aug;46;146-55).
In another study whose results were released at the CPDD conference, researchers from Dartmouth College, Hanover, N.H., interviewed 76 opioid users (91% were white, average age was 34, half were female, and almost all had a history of substance abuse treatment).
Among the other findings of the studies:
- Some opioid users are shocked by the adulteration of heroin by fentanyl, and even dealers are surprised: “When we cut the dope, we don’t use fentanyl. The problem was that we were buying the dope already dirty with that, and we didn’t know it,” said a 42-year-old man from Lawrence, Mass.
- In the New Hampshire interviews, 84% of participants said fentanyl is the leading cause of overdose in the state. “Due to the fentanyl and the heroin, that’s how everyone that I know ended up passing away recently,” said one user.
- Also in New Hampshire, 84% of users interviewed said they’d used fentanyl before, accidentally in some cases. Also, study coauthor Andrea L. Meier said in an interview, “67% of users reported having a prescription for opioids in their lifetime due to some kind of illness or injury. Some were short-term prescriptions (injuries, C-sections, tooth extractions); others were prescribed long-term due to chronic pain or illness.”
Some say pursue fentanyl
In the New Hampshire interviews, 25% of the 84% who’d used fentanyl said they actively seek it out, with one expressing a preference for the “real dope” (heroin laced with fentanyl) versus the “maintenance dope” of heroin alone. Ms. Meier explained what that means: “We’ve heard that once you use fentanyl or fentanyl-laced heroin, heroin doesn’t adequately manage your withdrawal symptoms or give enough of a high. So they will use heroin to get by, but they really want fentanyl or fentanyl-laced heroin.”
She added: “We’ve learned that users are seeking fentanyl due to its potency (a stronger, better high with quicker onset than heroin), cost (cheaper than heroin, so more “bang for your buck”), and once they use fentanyl or fentanyl-laced heroin, heroin doesn’t have the same effect/high.”
As for the risk of overdose, “people want the best high they can get at the cheapest cost,” she said.” They presume it will be potent enough to produce an exceptional high but [they won’t] die from an overdose due to being sufficiently tolerant to handle it. Also, some just felt hopeless and weren’t afraid of an OD.”
Comments from users about fentanyl
- “The high is wonderful. It’s splendidly wonderful. It’s magnified heroin feeling by a great number,” said a 45-year-old man from Baltimore.
- “You spend the same amount of money or even less for it, and you’re getting 3 times as high as you did on heroin,” said one user in New Hampshire. “Who wouldn’t want that?”
Risk-reduction techniques embraced
- In Baltimore, a 39-year-old woman said: “I have a lot of associates that are letting me know, ‘Don’t go to that place because they selling fentanyl.’ ”
- Some users test their heroin. “Like when I get stuff I don’t know what it is, I do a little bit before I do something that I feel,” a Lawrence, Mass., female user in her 20s said. “Like, I want to kind of scale out how much I want to do. Because I don’t want to die. But these people are just doing a gram shot and just ... my friend just died 2 days ago.”
Dr. Ciccarone said some of the biggest proponents of harm-reduction among users were African Americans aged 60 and older who had used for many decades.
“They fear fentanyl and are using old-school harm reduction strategies for staying safer: “tooting” (snorting) and tester shots (small injections to test the quality),” he said. “These may seem like minor strategies, but if enough of the population applies them to their daily drug use, many deaths would be averted. In this crisis, we need all the wisdom we can get, so we should listen to these elders.”
Dr. Ciccarone’s research was funded by the National Institutes of Health and NIDA. Dr. Ciccarone reported no relevant disclosures. The Dartmouth College study was funded by NIDA, and those authors reported no relevant disclosures.
REPORTING FROM CPDD 2018