User login
Fremanezumab May Be an Effective Preventive Treatment for Chronic Migraine
LOS ANGELES—Fremanezumab, a fully humanized monoclonal antibody, is a safe and effective therapy for the preventive treatment of chronic migraine, according to phase III data presented at the 70th Annual Meeting of the American Academy of Neurology. The treatment also has a flexible dosing profile.
Monthly and Quarterly Dosing Regimens
Fremanezumab selectively targets the calcitonin gene-related peptide ligand and is administered through subcutaneous injections. Stephen Silberstein, MD, Director of the Headache Center at Thomas Jefferson University Hospital in Philadelphia, and colleagues conducted a multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate two subcutaneous dose regimens of fremanezumab for the prevention of chronic migraine. Eligible patients were between ages 18 and 70. Exclusion criteria included use of onabotulinumtoxinA in the four months before screening, use of opioids or barbiturates for more than four days during the pretreatment period, and failure of two or more prior preventive medicines.
The investigators assigned 1,130 participants to one of three treatment arms. The first (monthly dosing) arm received 675 mg of fremanuzemab during the first month, followed by 225 mg of fremanezumab at months two and three. The second (quarterly dosing) arm received 675 mg of fremanezumab at month one, followed by placebo injections at months two and three. The third arm received monthly administration of matching placebo. The study’s primary efficacy end point was the mean change in the monthly average number of headache days of at least moderate severity from baseline (ie, a 28-day pretreatment period) to the 12-week double-blind treatment period. Dr. Silberstein and colleagues evaluated this end point using an analysis of covariance method or the Wilcoxon rank sum test.
During the 28-day baseline period, participants’ mean number of headache days of at least moderate severity was 13.1. During the 12-week period after the first dose, the number of monthly headache days of at least moderate severity decreased by 2.5 in the placebo arm, 4.6 in the monthly dosing arm, and 4.3 in the quarterly arm. The differences between the fremanezumab and placebo arms were statistically significant.
Secondary End Points Favored Fremanezumab
In addition, the number of monthly migraine days decreased significantly during the 12-week period after the first dose in the monthly dosing arm (by 5.0 from 16.0) and the quarterly dosing arm (by 4.9 from 16.2), compared with the placebo arm (by 3.2 from 16.3). The number of monthly migraine days also decreased significantly for both dosing regimens during the four weeks after the first dose.
Furthermore, 37.6% of patients in the quarterly dosing arm and 40.8% of patients in the monthly dosing arm had at least a 50% reduction in headache days of at least moderate severity, compared with 18.1% of the placebo arm. Similarly, 7.5% of patients in the quarterly dosing arm and 9.1% of patients in the monthly dosing arm had at least a 75% reduction in headache days of at least moderate severity, compared with 2.7% of the placebo arm.
Fremanezumab was associated with reductions in work productivity loss, compared with placebo. The change from baseline on the Work Productivity and Activity Impairment Questionnaire was −16.6 days in the quarterly dosing arm, −15.9 in the monthly dosing arm, and −9.1 in the placebo arm. In addition, mean score on the Headache Impact Test-6 decreased by 6.4 in the quarterly dosing arm, 6.8 in the monthly dosing arm, and 4.5 in the placebo arm.
The most common adverse event in the study was injection-site reaction. Discontinuation for adverse events was infrequent. Similar proportions of patients in each treatment group had at least one adverse event, and the frequency of these events was lower among controls.
“These results are consistent with [those of] the prior phase II trials in chronic migraine, with similar efficacy and similar treatment effects,” said Dr. Silberstein. Fremanezumab’s safety, tolerability, early onset of efficacy, and flexible dosing “may increase adherence and improve clinical outcomes for patients with migraine,” he concluded.
LOS ANGELES—Fremanezumab, a fully humanized monoclonal antibody, is a safe and effective therapy for the preventive treatment of chronic migraine, according to phase III data presented at the 70th Annual Meeting of the American Academy of Neurology. The treatment also has a flexible dosing profile.
Monthly and Quarterly Dosing Regimens
Fremanezumab selectively targets the calcitonin gene-related peptide ligand and is administered through subcutaneous injections. Stephen Silberstein, MD, Director of the Headache Center at Thomas Jefferson University Hospital in Philadelphia, and colleagues conducted a multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate two subcutaneous dose regimens of fremanezumab for the prevention of chronic migraine. Eligible patients were between ages 18 and 70. Exclusion criteria included use of onabotulinumtoxinA in the four months before screening, use of opioids or barbiturates for more than four days during the pretreatment period, and failure of two or more prior preventive medicines.
The investigators assigned 1,130 participants to one of three treatment arms. The first (monthly dosing) arm received 675 mg of fremanuzemab during the first month, followed by 225 mg of fremanezumab at months two and three. The second (quarterly dosing) arm received 675 mg of fremanezumab at month one, followed by placebo injections at months two and three. The third arm received monthly administration of matching placebo. The study’s primary efficacy end point was the mean change in the monthly average number of headache days of at least moderate severity from baseline (ie, a 28-day pretreatment period) to the 12-week double-blind treatment period. Dr. Silberstein and colleagues evaluated this end point using an analysis of covariance method or the Wilcoxon rank sum test.
During the 28-day baseline period, participants’ mean number of headache days of at least moderate severity was 13.1. During the 12-week period after the first dose, the number of monthly headache days of at least moderate severity decreased by 2.5 in the placebo arm, 4.6 in the monthly dosing arm, and 4.3 in the quarterly arm. The differences between the fremanezumab and placebo arms were statistically significant.
Secondary End Points Favored Fremanezumab
In addition, the number of monthly migraine days decreased significantly during the 12-week period after the first dose in the monthly dosing arm (by 5.0 from 16.0) and the quarterly dosing arm (by 4.9 from 16.2), compared with the placebo arm (by 3.2 from 16.3). The number of monthly migraine days also decreased significantly for both dosing regimens during the four weeks after the first dose.
Furthermore, 37.6% of patients in the quarterly dosing arm and 40.8% of patients in the monthly dosing arm had at least a 50% reduction in headache days of at least moderate severity, compared with 18.1% of the placebo arm. Similarly, 7.5% of patients in the quarterly dosing arm and 9.1% of patients in the monthly dosing arm had at least a 75% reduction in headache days of at least moderate severity, compared with 2.7% of the placebo arm.
Fremanezumab was associated with reductions in work productivity loss, compared with placebo. The change from baseline on the Work Productivity and Activity Impairment Questionnaire was −16.6 days in the quarterly dosing arm, −15.9 in the monthly dosing arm, and −9.1 in the placebo arm. In addition, mean score on the Headache Impact Test-6 decreased by 6.4 in the quarterly dosing arm, 6.8 in the monthly dosing arm, and 4.5 in the placebo arm.
The most common adverse event in the study was injection-site reaction. Discontinuation for adverse events was infrequent. Similar proportions of patients in each treatment group had at least one adverse event, and the frequency of these events was lower among controls.
“These results are consistent with [those of] the prior phase II trials in chronic migraine, with similar efficacy and similar treatment effects,” said Dr. Silberstein. Fremanezumab’s safety, tolerability, early onset of efficacy, and flexible dosing “may increase adherence and improve clinical outcomes for patients with migraine,” he concluded.
LOS ANGELES—Fremanezumab, a fully humanized monoclonal antibody, is a safe and effective therapy for the preventive treatment of chronic migraine, according to phase III data presented at the 70th Annual Meeting of the American Academy of Neurology. The treatment also has a flexible dosing profile.
Monthly and Quarterly Dosing Regimens
Fremanezumab selectively targets the calcitonin gene-related peptide ligand and is administered through subcutaneous injections. Stephen Silberstein, MD, Director of the Headache Center at Thomas Jefferson University Hospital in Philadelphia, and colleagues conducted a multicenter, randomized, double-blind, placebo-controlled, parallel-group study to evaluate two subcutaneous dose regimens of fremanezumab for the prevention of chronic migraine. Eligible patients were between ages 18 and 70. Exclusion criteria included use of onabotulinumtoxinA in the four months before screening, use of opioids or barbiturates for more than four days during the pretreatment period, and failure of two or more prior preventive medicines.
The investigators assigned 1,130 participants to one of three treatment arms. The first (monthly dosing) arm received 675 mg of fremanuzemab during the first month, followed by 225 mg of fremanezumab at months two and three. The second (quarterly dosing) arm received 675 mg of fremanezumab at month one, followed by placebo injections at months two and three. The third arm received monthly administration of matching placebo. The study’s primary efficacy end point was the mean change in the monthly average number of headache days of at least moderate severity from baseline (ie, a 28-day pretreatment period) to the 12-week double-blind treatment period. Dr. Silberstein and colleagues evaluated this end point using an analysis of covariance method or the Wilcoxon rank sum test.
During the 28-day baseline period, participants’ mean number of headache days of at least moderate severity was 13.1. During the 12-week period after the first dose, the number of monthly headache days of at least moderate severity decreased by 2.5 in the placebo arm, 4.6 in the monthly dosing arm, and 4.3 in the quarterly arm. The differences between the fremanezumab and placebo arms were statistically significant.
Secondary End Points Favored Fremanezumab
In addition, the number of monthly migraine days decreased significantly during the 12-week period after the first dose in the monthly dosing arm (by 5.0 from 16.0) and the quarterly dosing arm (by 4.9 from 16.2), compared with the placebo arm (by 3.2 from 16.3). The number of monthly migraine days also decreased significantly for both dosing regimens during the four weeks after the first dose.
Furthermore, 37.6% of patients in the quarterly dosing arm and 40.8% of patients in the monthly dosing arm had at least a 50% reduction in headache days of at least moderate severity, compared with 18.1% of the placebo arm. Similarly, 7.5% of patients in the quarterly dosing arm and 9.1% of patients in the monthly dosing arm had at least a 75% reduction in headache days of at least moderate severity, compared with 2.7% of the placebo arm.
Fremanezumab was associated with reductions in work productivity loss, compared with placebo. The change from baseline on the Work Productivity and Activity Impairment Questionnaire was −16.6 days in the quarterly dosing arm, −15.9 in the monthly dosing arm, and −9.1 in the placebo arm. In addition, mean score on the Headache Impact Test-6 decreased by 6.4 in the quarterly dosing arm, 6.8 in the monthly dosing arm, and 4.5 in the placebo arm.
The most common adverse event in the study was injection-site reaction. Discontinuation for adverse events was infrequent. Similar proportions of patients in each treatment group had at least one adverse event, and the frequency of these events was lower among controls.
“These results are consistent with [those of] the prior phase II trials in chronic migraine, with similar efficacy and similar treatment effects,” said Dr. Silberstein. Fremanezumab’s safety, tolerability, early onset of efficacy, and flexible dosing “may increase adherence and improve clinical outcomes for patients with migraine,” he concluded.
Is the pay-to-publish movement a good thing?
Is it me, or is anyone else worried about the online, pay-to-publish movement sweeping science?
I am being inundated with “please publish in our online journal for a fee” emails. I confess, I tried it once or twice and was pleased with the published outcome, as I communicated a concept that I thought was important to the practice of medicine. However, it was a bit disconcerting that the publishers of this online journal wanted an article within 3 weeks. Naturally, a scientific publication thrown together in 3 weeks could not be that good – unless it already had been on the drawing board for a while. Of note, the various editors of these journals often maintain that the articles are “peer reviewed.”
An article that I paid the Journal of Family Medicine and Disease Prevention to publish was one I coauthored, titled, “Prenatal vitamins deficient in recommended choline intake for pregnant women” (J Fam Med Dis Prev. 2016;2[4]1-3.)
That very straightforward article that surveyed the choline content in the top 75 prenatal vitamins showed that none of those vitamins contained the daily recommended dosage for pregnant women established by the Institute of Medicine in 1998. So, in many ways, the conclusions we drew in the article were a no-brainer and the result of simple, yet important observations that science had overlooked.
Despite the straightforward nature of that pay-to-publish article, the evidence it presented was sufficient to get the American Medical Association’s House of Delegates to pass a resolution calling for an increase in the choline content in prenatal vitamins.
So on the negative side of the ledger, I am concerned that some very “faulty science” could get published in the online, pay-to-publish journals, in light of what seems like their rush to publish. Of course, every now and then some of our prestigious journals publish information that is poorly interpreted, such as the recent article about the suicide rates among U.S. youth (JAMA Pediatr. 2018;172[7]:697-9).
Another separate, but related issue is what at least seems from a distance to be a rush by some of the tried and true medical journals (the New England Journal of Medicine, the various JAMA Network journals, The Lancet, and so on), to keep up with the trend of online journals by making their journals more accessible online.

I am concerned but not sure what to do about these new publishing trends in medicine and science. Accordingly, I will advocate that, as physicians and scientists, we learn how to read research reports critically and how to be clear when a research design is solid and leads to legitimate scientific conclusions. We must be able to discern when reports are poorly designed – and when they lead to “junk science.”
Like most things, Internet access to scientific articles is a blessing and a curse. The blessing is that more people around the world will be able to get access to scientific study and facts they can use to improve health care. The curse is that the “snake oil salespeople” may have better opportunities to convince the public that their “snake oil” works and the public should buy their “cure.”
Dr. Bell is staff psychiatrist at Jackson Park Hospital Surgical-Medical/Psychiatric Inpatient Unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; and former director of the Institute for Juvenile Research (the birthplace of child psychiatry), all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Is it me, or is anyone else worried about the online, pay-to-publish movement sweeping science?
I am being inundated with “please publish in our online journal for a fee” emails. I confess, I tried it once or twice and was pleased with the published outcome, as I communicated a concept that I thought was important to the practice of medicine. However, it was a bit disconcerting that the publishers of this online journal wanted an article within 3 weeks. Naturally, a scientific publication thrown together in 3 weeks could not be that good – unless it already had been on the drawing board for a while. Of note, the various editors of these journals often maintain that the articles are “peer reviewed.”
An article that I paid the Journal of Family Medicine and Disease Prevention to publish was one I coauthored, titled, “Prenatal vitamins deficient in recommended choline intake for pregnant women” (J Fam Med Dis Prev. 2016;2[4]1-3.)
That very straightforward article that surveyed the choline content in the top 75 prenatal vitamins showed that none of those vitamins contained the daily recommended dosage for pregnant women established by the Institute of Medicine in 1998. So, in many ways, the conclusions we drew in the article were a no-brainer and the result of simple, yet important observations that science had overlooked.
Despite the straightforward nature of that pay-to-publish article, the evidence it presented was sufficient to get the American Medical Association’s House of Delegates to pass a resolution calling for an increase in the choline content in prenatal vitamins.
So on the negative side of the ledger, I am concerned that some very “faulty science” could get published in the online, pay-to-publish journals, in light of what seems like their rush to publish. Of course, every now and then some of our prestigious journals publish information that is poorly interpreted, such as the recent article about the suicide rates among U.S. youth (JAMA Pediatr. 2018;172[7]:697-9).
Another separate, but related issue is what at least seems from a distance to be a rush by some of the tried and true medical journals (the New England Journal of Medicine, the various JAMA Network journals, The Lancet, and so on), to keep up with the trend of online journals by making their journals more accessible online.
I am concerned but not sure what to do about these new publishing trends in medicine and science. Accordingly, I will advocate that, as physicians and scientists, we learn how to read research reports critically and how to be clear when a research design is solid and leads to legitimate scientific conclusions. We must be able to discern when reports are poorly designed – and when they lead to “junk science.”
Like most things, Internet access to scientific articles is a blessing and a curse. The blessing is that more people around the world will be able to get access to scientific study and facts they can use to improve health care. The curse is that the “snake oil salespeople” may have better opportunities to convince the public that their “snake oil” works and the public should buy their “cure.”
Dr. Bell is staff psychiatrist at Jackson Park Hospital Surgical-Medical/Psychiatric Inpatient Unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; and former director of the Institute for Juvenile Research (the birthplace of child psychiatry), all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Is it me, or is anyone else worried about the online, pay-to-publish movement sweeping science?
I am being inundated with “please publish in our online journal for a fee” emails. I confess, I tried it once or twice and was pleased with the published outcome, as I communicated a concept that I thought was important to the practice of medicine. However, it was a bit disconcerting that the publishers of this online journal wanted an article within 3 weeks. Naturally, a scientific publication thrown together in 3 weeks could not be that good – unless it already had been on the drawing board for a while. Of note, the various editors of these journals often maintain that the articles are “peer reviewed.”
An article that I paid the Journal of Family Medicine and Disease Prevention to publish was one I coauthored, titled, “Prenatal vitamins deficient in recommended choline intake for pregnant women” (J Fam Med Dis Prev. 2016;2[4]1-3.)
That very straightforward article that surveyed the choline content in the top 75 prenatal vitamins showed that none of those vitamins contained the daily recommended dosage for pregnant women established by the Institute of Medicine in 1998. So, in many ways, the conclusions we drew in the article were a no-brainer and the result of simple, yet important observations that science had overlooked.
Despite the straightforward nature of that pay-to-publish article, the evidence it presented was sufficient to get the American Medical Association’s House of Delegates to pass a resolution calling for an increase in the choline content in prenatal vitamins.
So on the negative side of the ledger, I am concerned that some very “faulty science” could get published in the online, pay-to-publish journals, in light of what seems like their rush to publish. Of course, every now and then some of our prestigious journals publish information that is poorly interpreted, such as the recent article about the suicide rates among U.S. youth (JAMA Pediatr. 2018;172[7]:697-9).
Another separate, but related issue is what at least seems from a distance to be a rush by some of the tried and true medical journals (the New England Journal of Medicine, the various JAMA Network journals, The Lancet, and so on), to keep up with the trend of online journals by making their journals more accessible online.
I am concerned but not sure what to do about these new publishing trends in medicine and science. Accordingly, I will advocate that, as physicians and scientists, we learn how to read research reports critically and how to be clear when a research design is solid and leads to legitimate scientific conclusions. We must be able to discern when reports are poorly designed – and when they lead to “junk science.”
Like most things, Internet access to scientific articles is a blessing and a curse. The blessing is that more people around the world will be able to get access to scientific study and facts they can use to improve health care. The curse is that the “snake oil salespeople” may have better opportunities to convince the public that their “snake oil” works and the public should buy their “cure.”
Dr. Bell is staff psychiatrist at Jackson Park Hospital Surgical-Medical/Psychiatric Inpatient Unit; clinical professor emeritus, department of psychiatry, University of Illinois at Chicago; and former director of the Institute for Juvenile Research (the birthplace of child psychiatry), all in Chicago. He also serves as chair of psychiatry at Windsor University, St. Kitts.
Emerging CPAP options show sustained benefits
BALTIMORE – Emerging developments for the treatment of obstructive sleep apnea have shown promise in providing options beyond continuous-positive airway pressure, investigators reported at the annual meeting of the Associated Professional Sleep Societies. These developments include a single-use nasopharyngeal airway stent, upper-airway stimulation using a pacemaker-like device, a negative-pressure device that opens the airway, and an artificial intelligence approach that can predict outcomes of oral appliance therapy.
Nasopharyngeal airway stent
Clete A. Kushida, MD, of Stanford (Calif.) University reported on recent results of a trial of the nasopharyngeal airway stent (NAS) single-use disposable insert (Seven Dreamers Laboratories, Tokyo). This device consists of a flexible semi-rigid silicone rubber tube 120-145 mm in length and coated with a hydrophilic gel. The patient inserts the distal end of the tube into the nostril, and it positions itself within the nasopharynx and retropalatal oropharynx to open the airway. A clip attaches to the exterior septum to keep the device in place. The patient removes the NAS in the morning. The device is commercially available in Japan and some European countries.
Dr. Kushida reported on two posters that were presented at Sleep 2018. The first by the Osaka University Graduate School of Dentistry in Japan investigated the predictability of NAS efficacy in patients with a velopharynx that was narrower than the hypopharynx (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.554). The study showed that 11 responders had a narrow velopharynx while 18 nonresponders had a narrow hypopharynx. Response was defined as 50% or greater reduction of apnea-hypopnea index (AHI) from baseline. “The success rate of NAS for the patients with narrowing of the velopharynx is 83.3%,” Dr. Kushida said.
He also reported on a study he led of NAS in patients with obstructive sleep apnea and healthy controls (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.555). The trial was conducted at Stanford and Tokyo sleep medical centers, with healthy controls at the Tokyo site only. AHI improved in all three obstructive sleep apnea (OSA) groups, but most significantly in those with moderate (n = 23) and severe (n = 21) OSA: 7.2 (P = .0038) and 11.7 (P = .0069), respectively. In the Stanford cohort, 2 of 32 patients originally enrolled dropped out because they found the NAS uncomfortable; none dropped out of the Tokyo cohort.
“NAS can be effective in treatment of snoring and OSA, in particular those with moderate/severe OSA, with significant improvement in mean obstructive apnea index,” Dr. Kushida said. He also noted the device is more effective in patients with narrowing of the oropharynx/velopharynx rather than the hypopharynx.
Dr. Kushida reported he had a financial relationship with the Seven Dreamers Laboratories.
Continuous negative external pressure
Jerrold A. Kram, MD, reported on a device that employs continuous negative external pressure – known as cNEP – that uses a silicone collar covering the front of the throat and a pump that applies suction to keep the airway open from the outside. He cited a small 2015 study out of Japan that found the device was effective in keeping the pharyngeal airway open in nonobese women (J Appl Physiol. 2015;118:912-20). Another small U.S. study found cNEP reduces respiratory impairment during screening colonoscopy (Endoscopy. 2016;48:584-7). Sommetrics, which has patented the technology, is developing a version of the product for obstructive sleep apnea, Dr. Kram said. The company already has a Food and Drug Administration–approved product to treat apneas that people experience when under mild to moderate sedation, such as a colonoscopy. It is approved for sale in Canada, but not in the United States.

“It gives us another tool in the box,” Dr. Kram said. “It’s very small and portable, easy to take on an airplane with you, and it reduces the chance for claustrophobia” that comes with continuous-positive airway pressure (CPAP), said Dr. Kram. There are no tubes or masks and no humidifier to deal with.
Dr. Kram conducted a small study of 15 OSA patients using cNEP last year. Among nine excellent responders, the lowest AHI was 1.5 on average, from an average baseline of 43.9; among four partial responders, the lowest observed AHI averaged 11.75 (J Clin Sleep Med. 2017;13:1009-12).
The cNEP device is also the subject of a home study of patients with OSA in Canada, Dr. Kram said. Unpublished results indicate that 46% (27/59) of patients had an initial response rate to either -25 or -30 characteristic moment waveform (cmw) of negative airway pressure. For those who completed 3 weeks of treatment, the response rate was 64% (16/25). “Seventy-six percent of subjects felt their overall experience with cNEP was better than with CPAP,” Dr. Kram said.
However, studies have noted some minor issues with cNEP, Dr. Kram said. They include mild skin irritation, choking sensation if not properly placed, limited size availability, and absence of efficacy data. Dr. Kram said a U.S. pivotal trial is scheduled to start soon.
Dr. Kram disclosed he is a paid adviser for Sommetrics.
Oral appliance therapy
Oral appliance therapy (OAT) has been very effective in some patients and has been endorsed by the American Academy of Sleep Medicine since 2006, but it has been underutilized predominantly for two reasons, noted John Remmers, MD, because fitting the device requires a trial-and-error approach that can discourage patients; and the therapeutic success rate is 50%-60%.

To predict which patients are likely to succeed with OAT, Dr. Remmers and his colleagues at Zephyr Sleep Technologies have developed an artificial intelligence (AI) platform that uses a feedback-controlled mandibular positioner, a mouthpiece-like device that opens the airway during sleep. Dr. Remmers is chief medical officer and cofounder of Zephyr Sleep Technologies, based in Calgary, Alta.
While imaging has been used in awake patients to fit OAT devices, Dr. Remmers noted a number of shortcomings with this modality. “Sleep apnea results from an anatomic problem – i.e., structural encroachment on the pharyngeal airway, which is neurally compensated when the patient is awake,” he said. “Because of this, we need to do the test when the patient is asleep.”
The AI platform with feedback-controlled mandibular positioner uses temporary dental trays to create impressions for the mouthpiece the patient uses during sleep. The mouthpiece connects to a remote-controlled device that makes real-time adjustments in the mandibular position without disturbing the patient’s sleep. “The computer identifies respiratory events all night long, adjusting the position of the mandible,” he said in explaining the AI component of the device. “Just think of it as similar to autotitration with CPAP.”
Dr. Remmers reported results of a phase 2 study of the platform presented as a poster reporting on a study of 101 patients with OSA participants. The study reported sensitivity of 86% and specificity of 92% in predicting success with the feedback-controlled mandibular positioner, he said.
“The sensitivity and overall predictive accuracy of the AI-based approach was greater than an intuitive approach using a pretreatment, temporary appliance, indicating that feedback-controlled mandibular positioning test outperformed the intuitive approach,” he said. The device has been approved by Health Canada and is awaiting clearance in the United States.
Upper airway stimulation
Upper airway stimulation (UAS) is emerging as a new class of therapy, said Patrick J. Strollo Jr., MD, of the University of Pittsburgh. The therapy involves an impulse generator (IPG) similar to a pacemaker that is implanted in the left side of the chest and connected to a stimulation lead secured to the distal hypoglossal nerve in the neck. The UAS system also incorporates a sensing lead that is implanted between the intercostal muscles and attached to the IPG allowing for phasic stimulation of the genioglossal muscle. The patient uses a remote control to turn the device on at night and off in the morning.

Dr. Strollo was lead author of the Stimulation Therapy for Apnea Reduction (STAR) trial (N Engl J Med. 2014:370;139-49), a prospective multicenter trial with a randomized therapy withdrawal arm. In 126 participants, he said, the median AHI score declined 68% in 12 months, from 29.3 at baseline to 9 (P less than .0001).
He provided updated results that showed 80% of patients continued to use the device after 5 years (Otolaryngol Head Neck Surg. 2018; doi: 10.1177/0194599818762383). Median AHI at 5 years was 6.9, Dr. Strollo said, and median Epworth Sleepiness Scale scores declined from 11.6 at baseline to 6.9 at 5 years.
Another postapproval study of UAS, the ADHERE registry, has enrolled 348 patients at 10 centers with a goal of 2,500, Dr. Strollo said (Otolaryngol Head Neck Surg. 2018: doi: 10.1177/0194599818764896). Twelve-month study results have shown reductions in AHI and Epworth Sleepiness Scale scores comparable to previous reports. ADHERE also reported that 92% of patients were satisfied with UAS.
The latest innovation for UAS is the ability to download data from the implant at office visits so the physician can review patient adherence patterns, along with energy levels and settings for sensing and stimulation, Dr. Strollo said.
“Upper airway stimulation is an additional tool in the management of properly selected, at-risk apnea patients who do not accept or adhere to positive pressure therapy,” Dr. Strollo said. “The STAR trial has provided robust evidence that upper airway stimulation is safe and effective in participants with moderate to severe OSA, and the treatment effect is maintained beyond the 12-month endpoint.”
Dr. Strollo disclosed a financial relationship with Inspire Medical Systems, manufacturer of the UAS device.
BALTIMORE – Emerging developments for the treatment of obstructive sleep apnea have shown promise in providing options beyond continuous-positive airway pressure, investigators reported at the annual meeting of the Associated Professional Sleep Societies. These developments include a single-use nasopharyngeal airway stent, upper-airway stimulation using a pacemaker-like device, a negative-pressure device that opens the airway, and an artificial intelligence approach that can predict outcomes of oral appliance therapy.
Nasopharyngeal airway stent
Clete A. Kushida, MD, of Stanford (Calif.) University reported on recent results of a trial of the nasopharyngeal airway stent (NAS) single-use disposable insert (Seven Dreamers Laboratories, Tokyo). This device consists of a flexible semi-rigid silicone rubber tube 120-145 mm in length and coated with a hydrophilic gel. The patient inserts the distal end of the tube into the nostril, and it positions itself within the nasopharynx and retropalatal oropharynx to open the airway. A clip attaches to the exterior septum to keep the device in place. The patient removes the NAS in the morning. The device is commercially available in Japan and some European countries.
Dr. Kushida reported on two posters that were presented at Sleep 2018. The first by the Osaka University Graduate School of Dentistry in Japan investigated the predictability of NAS efficacy in patients with a velopharynx that was narrower than the hypopharynx (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.554). The study showed that 11 responders had a narrow velopharynx while 18 nonresponders had a narrow hypopharynx. Response was defined as 50% or greater reduction of apnea-hypopnea index (AHI) from baseline. “The success rate of NAS for the patients with narrowing of the velopharynx is 83.3%,” Dr. Kushida said.
He also reported on a study he led of NAS in patients with obstructive sleep apnea and healthy controls (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.555). The trial was conducted at Stanford and Tokyo sleep medical centers, with healthy controls at the Tokyo site only. AHI improved in all three obstructive sleep apnea (OSA) groups, but most significantly in those with moderate (n = 23) and severe (n = 21) OSA: 7.2 (P = .0038) and 11.7 (P = .0069), respectively. In the Stanford cohort, 2 of 32 patients originally enrolled dropped out because they found the NAS uncomfortable; none dropped out of the Tokyo cohort.
“NAS can be effective in treatment of snoring and OSA, in particular those with moderate/severe OSA, with significant improvement in mean obstructive apnea index,” Dr. Kushida said. He also noted the device is more effective in patients with narrowing of the oropharynx/velopharynx rather than the hypopharynx.
Dr. Kushida reported he had a financial relationship with the Seven Dreamers Laboratories.
Continuous negative external pressure
Jerrold A. Kram, MD, reported on a device that employs continuous negative external pressure – known as cNEP – that uses a silicone collar covering the front of the throat and a pump that applies suction to keep the airway open from the outside. He cited a small 2015 study out of Japan that found the device was effective in keeping the pharyngeal airway open in nonobese women (J Appl Physiol. 2015;118:912-20). Another small U.S. study found cNEP reduces respiratory impairment during screening colonoscopy (Endoscopy. 2016;48:584-7). Sommetrics, which has patented the technology, is developing a version of the product for obstructive sleep apnea, Dr. Kram said. The company already has a Food and Drug Administration–approved product to treat apneas that people experience when under mild to moderate sedation, such as a colonoscopy. It is approved for sale in Canada, but not in the United States.
“It gives us another tool in the box,” Dr. Kram said. “It’s very small and portable, easy to take on an airplane with you, and it reduces the chance for claustrophobia” that comes with continuous-positive airway pressure (CPAP), said Dr. Kram. There are no tubes or masks and no humidifier to deal with.
Dr. Kram conducted a small study of 15 OSA patients using cNEP last year. Among nine excellent responders, the lowest AHI was 1.5 on average, from an average baseline of 43.9; among four partial responders, the lowest observed AHI averaged 11.75 (J Clin Sleep Med. 2017;13:1009-12).
The cNEP device is also the subject of a home study of patients with OSA in Canada, Dr. Kram said. Unpublished results indicate that 46% (27/59) of patients had an initial response rate to either -25 or -30 characteristic moment waveform (cmw) of negative airway pressure. For those who completed 3 weeks of treatment, the response rate was 64% (16/25). “Seventy-six percent of subjects felt their overall experience with cNEP was better than with CPAP,” Dr. Kram said.
However, studies have noted some minor issues with cNEP, Dr. Kram said. They include mild skin irritation, choking sensation if not properly placed, limited size availability, and absence of efficacy data. Dr. Kram said a U.S. pivotal trial is scheduled to start soon.
Dr. Kram disclosed he is a paid adviser for Sommetrics.
Oral appliance therapy
Oral appliance therapy (OAT) has been very effective in some patients and has been endorsed by the American Academy of Sleep Medicine since 2006, but it has been underutilized predominantly for two reasons, noted John Remmers, MD, because fitting the device requires a trial-and-error approach that can discourage patients; and the therapeutic success rate is 50%-60%.
To predict which patients are likely to succeed with OAT, Dr. Remmers and his colleagues at Zephyr Sleep Technologies have developed an artificial intelligence (AI) platform that uses a feedback-controlled mandibular positioner, a mouthpiece-like device that opens the airway during sleep. Dr. Remmers is chief medical officer and cofounder of Zephyr Sleep Technologies, based in Calgary, Alta.
While imaging has been used in awake patients to fit OAT devices, Dr. Remmers noted a number of shortcomings with this modality. “Sleep apnea results from an anatomic problem – i.e., structural encroachment on the pharyngeal airway, which is neurally compensated when the patient is awake,” he said. “Because of this, we need to do the test when the patient is asleep.”
The AI platform with feedback-controlled mandibular positioner uses temporary dental trays to create impressions for the mouthpiece the patient uses during sleep. The mouthpiece connects to a remote-controlled device that makes real-time adjustments in the mandibular position without disturbing the patient’s sleep. “The computer identifies respiratory events all night long, adjusting the position of the mandible,” he said in explaining the AI component of the device. “Just think of it as similar to autotitration with CPAP.”
Dr. Remmers reported results of a phase 2 study of the platform presented as a poster reporting on a study of 101 patients with OSA participants. The study reported sensitivity of 86% and specificity of 92% in predicting success with the feedback-controlled mandibular positioner, he said.
“The sensitivity and overall predictive accuracy of the AI-based approach was greater than an intuitive approach using a pretreatment, temporary appliance, indicating that feedback-controlled mandibular positioning test outperformed the intuitive approach,” he said. The device has been approved by Health Canada and is awaiting clearance in the United States.
Upper airway stimulation
Upper airway stimulation (UAS) is emerging as a new class of therapy, said Patrick J. Strollo Jr., MD, of the University of Pittsburgh. The therapy involves an impulse generator (IPG) similar to a pacemaker that is implanted in the left side of the chest and connected to a stimulation lead secured to the distal hypoglossal nerve in the neck. The UAS system also incorporates a sensing lead that is implanted between the intercostal muscles and attached to the IPG allowing for phasic stimulation of the genioglossal muscle. The patient uses a remote control to turn the device on at night and off in the morning.
Dr. Strollo was lead author of the Stimulation Therapy for Apnea Reduction (STAR) trial (N Engl J Med. 2014:370;139-49), a prospective multicenter trial with a randomized therapy withdrawal arm. In 126 participants, he said, the median AHI score declined 68% in 12 months, from 29.3 at baseline to 9 (P less than .0001).
He provided updated results that showed 80% of patients continued to use the device after 5 years (Otolaryngol Head Neck Surg. 2018; doi: 10.1177/0194599818762383). Median AHI at 5 years was 6.9, Dr. Strollo said, and median Epworth Sleepiness Scale scores declined from 11.6 at baseline to 6.9 at 5 years.
Another postapproval study of UAS, the ADHERE registry, has enrolled 348 patients at 10 centers with a goal of 2,500, Dr. Strollo said (Otolaryngol Head Neck Surg. 2018: doi: 10.1177/0194599818764896). Twelve-month study results have shown reductions in AHI and Epworth Sleepiness Scale scores comparable to previous reports. ADHERE also reported that 92% of patients were satisfied with UAS.
The latest innovation for UAS is the ability to download data from the implant at office visits so the physician can review patient adherence patterns, along with energy levels and settings for sensing and stimulation, Dr. Strollo said.
“Upper airway stimulation is an additional tool in the management of properly selected, at-risk apnea patients who do not accept or adhere to positive pressure therapy,” Dr. Strollo said. “The STAR trial has provided robust evidence that upper airway stimulation is safe and effective in participants with moderate to severe OSA, and the treatment effect is maintained beyond the 12-month endpoint.”
Dr. Strollo disclosed a financial relationship with Inspire Medical Systems, manufacturer of the UAS device.
BALTIMORE – Emerging developments for the treatment of obstructive sleep apnea have shown promise in providing options beyond continuous-positive airway pressure, investigators reported at the annual meeting of the Associated Professional Sleep Societies. These developments include a single-use nasopharyngeal airway stent, upper-airway stimulation using a pacemaker-like device, a negative-pressure device that opens the airway, and an artificial intelligence approach that can predict outcomes of oral appliance therapy.
Nasopharyngeal airway stent
Clete A. Kushida, MD, of Stanford (Calif.) University reported on recent results of a trial of the nasopharyngeal airway stent (NAS) single-use disposable insert (Seven Dreamers Laboratories, Tokyo). This device consists of a flexible semi-rigid silicone rubber tube 120-145 mm in length and coated with a hydrophilic gel. The patient inserts the distal end of the tube into the nostril, and it positions itself within the nasopharynx and retropalatal oropharynx to open the airway. A clip attaches to the exterior septum to keep the device in place. The patient removes the NAS in the morning. The device is commercially available in Japan and some European countries.
Dr. Kushida reported on two posters that were presented at Sleep 2018. The first by the Osaka University Graduate School of Dentistry in Japan investigated the predictability of NAS efficacy in patients with a velopharynx that was narrower than the hypopharynx (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.554). The study showed that 11 responders had a narrow velopharynx while 18 nonresponders had a narrow hypopharynx. Response was defined as 50% or greater reduction of apnea-hypopnea index (AHI) from baseline. “The success rate of NAS for the patients with narrowing of the velopharynx is 83.3%,” Dr. Kushida said.
He also reported on a study he led of NAS in patients with obstructive sleep apnea and healthy controls (Sleep. 2018;41 (suppl 1):A207: doi.org/10.1093/sleep/zsy061.555). The trial was conducted at Stanford and Tokyo sleep medical centers, with healthy controls at the Tokyo site only. AHI improved in all three obstructive sleep apnea (OSA) groups, but most significantly in those with moderate (n = 23) and severe (n = 21) OSA: 7.2 (P = .0038) and 11.7 (P = .0069), respectively. In the Stanford cohort, 2 of 32 patients originally enrolled dropped out because they found the NAS uncomfortable; none dropped out of the Tokyo cohort.
“NAS can be effective in treatment of snoring and OSA, in particular those with moderate/severe OSA, with significant improvement in mean obstructive apnea index,” Dr. Kushida said. He also noted the device is more effective in patients with narrowing of the oropharynx/velopharynx rather than the hypopharynx.
Dr. Kushida reported he had a financial relationship with the Seven Dreamers Laboratories.
Continuous negative external pressure
Jerrold A. Kram, MD, reported on a device that employs continuous negative external pressure – known as cNEP – that uses a silicone collar covering the front of the throat and a pump that applies suction to keep the airway open from the outside. He cited a small 2015 study out of Japan that found the device was effective in keeping the pharyngeal airway open in nonobese women (J Appl Physiol. 2015;118:912-20). Another small U.S. study found cNEP reduces respiratory impairment during screening colonoscopy (Endoscopy. 2016;48:584-7). Sommetrics, which has patented the technology, is developing a version of the product for obstructive sleep apnea, Dr. Kram said. The company already has a Food and Drug Administration–approved product to treat apneas that people experience when under mild to moderate sedation, such as a colonoscopy. It is approved for sale in Canada, but not in the United States.
“It gives us another tool in the box,” Dr. Kram said. “It’s very small and portable, easy to take on an airplane with you, and it reduces the chance for claustrophobia” that comes with continuous-positive airway pressure (CPAP), said Dr. Kram. There are no tubes or masks and no humidifier to deal with.
Dr. Kram conducted a small study of 15 OSA patients using cNEP last year. Among nine excellent responders, the lowest AHI was 1.5 on average, from an average baseline of 43.9; among four partial responders, the lowest observed AHI averaged 11.75 (J Clin Sleep Med. 2017;13:1009-12).
The cNEP device is also the subject of a home study of patients with OSA in Canada, Dr. Kram said. Unpublished results indicate that 46% (27/59) of patients had an initial response rate to either -25 or -30 characteristic moment waveform (cmw) of negative airway pressure. For those who completed 3 weeks of treatment, the response rate was 64% (16/25). “Seventy-six percent of subjects felt their overall experience with cNEP was better than with CPAP,” Dr. Kram said.
However, studies have noted some minor issues with cNEP, Dr. Kram said. They include mild skin irritation, choking sensation if not properly placed, limited size availability, and absence of efficacy data. Dr. Kram said a U.S. pivotal trial is scheduled to start soon.
Dr. Kram disclosed he is a paid adviser for Sommetrics.
Oral appliance therapy
Oral appliance therapy (OAT) has been very effective in some patients and has been endorsed by the American Academy of Sleep Medicine since 2006, but it has been underutilized predominantly for two reasons, noted John Remmers, MD, because fitting the device requires a trial-and-error approach that can discourage patients; and the therapeutic success rate is 50%-60%.
To predict which patients are likely to succeed with OAT, Dr. Remmers and his colleagues at Zephyr Sleep Technologies have developed an artificial intelligence (AI) platform that uses a feedback-controlled mandibular positioner, a mouthpiece-like device that opens the airway during sleep. Dr. Remmers is chief medical officer and cofounder of Zephyr Sleep Technologies, based in Calgary, Alta.
While imaging has been used in awake patients to fit OAT devices, Dr. Remmers noted a number of shortcomings with this modality. “Sleep apnea results from an anatomic problem – i.e., structural encroachment on the pharyngeal airway, which is neurally compensated when the patient is awake,” he said. “Because of this, we need to do the test when the patient is asleep.”
The AI platform with feedback-controlled mandibular positioner uses temporary dental trays to create impressions for the mouthpiece the patient uses during sleep. The mouthpiece connects to a remote-controlled device that makes real-time adjustments in the mandibular position without disturbing the patient’s sleep. “The computer identifies respiratory events all night long, adjusting the position of the mandible,” he said in explaining the AI component of the device. “Just think of it as similar to autotitration with CPAP.”
Dr. Remmers reported results of a phase 2 study of the platform presented as a poster reporting on a study of 101 patients with OSA participants. The study reported sensitivity of 86% and specificity of 92% in predicting success with the feedback-controlled mandibular positioner, he said.
“The sensitivity and overall predictive accuracy of the AI-based approach was greater than an intuitive approach using a pretreatment, temporary appliance, indicating that feedback-controlled mandibular positioning test outperformed the intuitive approach,” he said. The device has been approved by Health Canada and is awaiting clearance in the United States.
Upper airway stimulation
Upper airway stimulation (UAS) is emerging as a new class of therapy, said Patrick J. Strollo Jr., MD, of the University of Pittsburgh. The therapy involves an impulse generator (IPG) similar to a pacemaker that is implanted in the left side of the chest and connected to a stimulation lead secured to the distal hypoglossal nerve in the neck. The UAS system also incorporates a sensing lead that is implanted between the intercostal muscles and attached to the IPG allowing for phasic stimulation of the genioglossal muscle. The patient uses a remote control to turn the device on at night and off in the morning.
Dr. Strollo was lead author of the Stimulation Therapy for Apnea Reduction (STAR) trial (N Engl J Med. 2014:370;139-49), a prospective multicenter trial with a randomized therapy withdrawal arm. In 126 participants, he said, the median AHI score declined 68% in 12 months, from 29.3 at baseline to 9 (P less than .0001).
He provided updated results that showed 80% of patients continued to use the device after 5 years (Otolaryngol Head Neck Surg. 2018; doi: 10.1177/0194599818762383). Median AHI at 5 years was 6.9, Dr. Strollo said, and median Epworth Sleepiness Scale scores declined from 11.6 at baseline to 6.9 at 5 years.
Another postapproval study of UAS, the ADHERE registry, has enrolled 348 patients at 10 centers with a goal of 2,500, Dr. Strollo said (Otolaryngol Head Neck Surg. 2018: doi: 10.1177/0194599818764896). Twelve-month study results have shown reductions in AHI and Epworth Sleepiness Scale scores comparable to previous reports. ADHERE also reported that 92% of patients were satisfied with UAS.
The latest innovation for UAS is the ability to download data from the implant at office visits so the physician can review patient adherence patterns, along with energy levels and settings for sensing and stimulation, Dr. Strollo said.
“Upper airway stimulation is an additional tool in the management of properly selected, at-risk apnea patients who do not accept or adhere to positive pressure therapy,” Dr. Strollo said. “The STAR trial has provided robust evidence that upper airway stimulation is safe and effective in participants with moderate to severe OSA, and the treatment effect is maintained beyond the 12-month endpoint.”
Dr. Strollo disclosed a financial relationship with Inspire Medical Systems, manufacturer of the UAS device.
REPORTING FROM SLEEP 2018
Key clinical point: Alternative treatments have shown sustained improvement in sleep apnea symptoms.
Major finding: The negative-pressure device improved oxygen flow in OSA to 64% vs. 25% for continuous-positive airway pressure.
Data source: Multiple abstracts presented at Sleep 2018 and published studies, including ADHERE study of 326 patients and a multicenter study of 430 patients using the upper airway stimulation device; a trial of 67 patients using the nasopharyngeal airway stent; and 101 patients in the artificial intelligence study.
Disclosures: Dr. Kushida disclosed a relationship with Seven Dreamers Laboratories. Dr. Kram is a paid adviser for Sommetrics. Dr. Remmers is founder of Zephyr Sleep Technologies. Dr. Strollo is an investigator in the STAR trial, supported by Inspire Medical Systems.
Hands-on surgical training is incomparable
Hands-on surgical training is incomparable
I am not one to critique new technology or new technique. The article on use of virtual reality to not only teach technique but also to grade it caught my attention. I work in a small hospital without a million-dollar robot. Very complicated cases are sent out to larger hospitals. We have 2 new graduates who, like most new grads, have little experience with many surgical techniques. Dr. Lenihan and I were resident classmates, so I know he understands the rigors of a no-hour limit residency. Even with our residency, when we got out we relied on our partners to assist us until they knew we could do cases with a surgical assistant (SA) or a less experienced helper.
We are asking too much of our new graduates. It is up to us to provide the help and assistance with surgeries that they are not comfortable doing. While virtual reality training is great for teaching robotics and some laparoscopic techniques, it cannot teach things such as anterior and posterior repairs, tension-free vaginal tape procedures, and enterocoele repair. We can all watch YouTube tutorials, but actually doing surgery is very different. We owe it to our new graduates to provide mentoring and encouragement with their surgical cases. At our hospital, mentoring the first 10 cases performed by a new physician (new grad or otherwise) used to be required, but that requirement is gone. Our service is one of the few that still has 2 physicians at every major case. We have an SA available, but we prefer to assist each other. This makes our laparoscopic-assisted vaginal hysterectomy, bilateral salpingo-oophorectomy cases a 30- to 35-minute case. It allows us to teach anterior and posterior repair technique.
The involvement in surgical improvement is hands-on, and virtual reality training will never replace it.
Anthony J. Lemanski, MD
Kingman, Arizona
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Hands-on surgical training is incomparable
I am not one to critique new technology or new technique. The article on use of virtual reality to not only teach technique but also to grade it caught my attention. I work in a small hospital without a million-dollar robot. Very complicated cases are sent out to larger hospitals. We have 2 new graduates who, like most new grads, have little experience with many surgical techniques. Dr. Lenihan and I were resident classmates, so I know he understands the rigors of a no-hour limit residency. Even with our residency, when we got out we relied on our partners to assist us until they knew we could do cases with a surgical assistant (SA) or a less experienced helper.
We are asking too much of our new graduates. It is up to us to provide the help and assistance with surgeries that they are not comfortable doing. While virtual reality training is great for teaching robotics and some laparoscopic techniques, it cannot teach things such as anterior and posterior repairs, tension-free vaginal tape procedures, and enterocoele repair. We can all watch YouTube tutorials, but actually doing surgery is very different. We owe it to our new graduates to provide mentoring and encouragement with their surgical cases. At our hospital, mentoring the first 10 cases performed by a new physician (new grad or otherwise) used to be required, but that requirement is gone. Our service is one of the few that still has 2 physicians at every major case. We have an SA available, but we prefer to assist each other. This makes our laparoscopic-assisted vaginal hysterectomy, bilateral salpingo-oophorectomy cases a 30- to 35-minute case. It allows us to teach anterior and posterior repair technique.
The involvement in surgical improvement is hands-on, and virtual reality training will never replace it.
Anthony J. Lemanski, MD
Kingman, Arizona
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Hands-on surgical training is incomparable
I am not one to critique new technology or new technique. The article on use of virtual reality to not only teach technique but also to grade it caught my attention. I work in a small hospital without a million-dollar robot. Very complicated cases are sent out to larger hospitals. We have 2 new graduates who, like most new grads, have little experience with many surgical techniques. Dr. Lenihan and I were resident classmates, so I know he understands the rigors of a no-hour limit residency. Even with our residency, when we got out we relied on our partners to assist us until they knew we could do cases with a surgical assistant (SA) or a less experienced helper.
We are asking too much of our new graduates. It is up to us to provide the help and assistance with surgeries that they are not comfortable doing. While virtual reality training is great for teaching robotics and some laparoscopic techniques, it cannot teach things such as anterior and posterior repairs, tension-free vaginal tape procedures, and enterocoele repair. We can all watch YouTube tutorials, but actually doing surgery is very different. We owe it to our new graduates to provide mentoring and encouragement with their surgical cases. At our hospital, mentoring the first 10 cases performed by a new physician (new grad or otherwise) used to be required, but that requirement is gone. Our service is one of the few that still has 2 physicians at every major case. We have an SA available, but we prefer to assist each other. This makes our laparoscopic-assisted vaginal hysterectomy, bilateral salpingo-oophorectomy cases a 30- to 35-minute case. It allows us to teach anterior and posterior repair technique.
The involvement in surgical improvement is hands-on, and virtual reality training will never replace it.
Anthony J. Lemanski, MD
Kingman, Arizona
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.

Hypertensive crisis of pregnancy must be treated with all urgency
Hypertensive crisis of pregnancy must be treated with all urgency
The following happened approximately 27 years ago when I worked as an attending at a regional level 2 hospital in Puerto Rico. One afternoon I received a call from the emergency department that they had been managing a patient (G4P3) at 33 weeks of gestation for about 4 hours. The patient was consulted for hypertension when she went into a hypertensive encephalopathic coma. The patient was brought back to the birth center. Apresoline was given but did not bring the blood pressure down. Magnesium sulfate also was started at that time. I called a colleague from internal medicine and started to give nitroprusside.
Every time the patient’s blood pressure dropped from 120 mm Hg diastolic, she would become conscious and speak with us. As soon as her blood pressure went up, she would go into a coma. The patient was then transferred to a tertiary center in as stable a condition as possible. Cesarean delivery was performed, and the baby did not survive. The mother had an intracerebral hemorrhage. She was transferred to the supra-tertiary center in San Juan where she later passed away from complications of the hypertensive crisis. If the emergency physician had called me earlier, more could have been done.
This event is always fresh I my mind when I manage my patients in Ohio. Thank God for the newer medications we have available and the protocols to manage hypertensive crisis in pregnancy. I hope this experience heightens awareness of how deadly this condition can be.
David A. Rosado, MD
Celina, Ohio
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Hypertensive crisis of pregnancy must be treated with all urgency
The following happened approximately 27 years ago when I worked as an attending at a regional level 2 hospital in Puerto Rico. One afternoon I received a call from the emergency department that they had been managing a patient (G4P3) at 33 weeks of gestation for about 4 hours. The patient was consulted for hypertension when she went into a hypertensive encephalopathic coma. The patient was brought back to the birth center. Apresoline was given but did not bring the blood pressure down. Magnesium sulfate also was started at that time. I called a colleague from internal medicine and started to give nitroprusside.
Every time the patient’s blood pressure dropped from 120 mm Hg diastolic, she would become conscious and speak with us. As soon as her blood pressure went up, she would go into a coma. The patient was then transferred to a tertiary center in as stable a condition as possible. Cesarean delivery was performed, and the baby did not survive. The mother had an intracerebral hemorrhage. She was transferred to the supra-tertiary center in San Juan where she later passed away from complications of the hypertensive crisis. If the emergency physician had called me earlier, more could have been done.
This event is always fresh I my mind when I manage my patients in Ohio. Thank God for the newer medications we have available and the protocols to manage hypertensive crisis in pregnancy. I hope this experience heightens awareness of how deadly this condition can be.
David A. Rosado, MD
Celina, Ohio
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Hypertensive crisis of pregnancy must be treated with all urgency
The following happened approximately 27 years ago when I worked as an attending at a regional level 2 hospital in Puerto Rico. One afternoon I received a call from the emergency department that they had been managing a patient (G4P3) at 33 weeks of gestation for about 4 hours. The patient was consulted for hypertension when she went into a hypertensive encephalopathic coma. The patient was brought back to the birth center. Apresoline was given but did not bring the blood pressure down. Magnesium sulfate also was started at that time. I called a colleague from internal medicine and started to give nitroprusside.
Every time the patient’s blood pressure dropped from 120 mm Hg diastolic, she would become conscious and speak with us. As soon as her blood pressure went up, she would go into a coma. The patient was then transferred to a tertiary center in as stable a condition as possible. Cesarean delivery was performed, and the baby did not survive. The mother had an intracerebral hemorrhage. She was transferred to the supra-tertiary center in San Juan where she later passed away from complications of the hypertensive crisis. If the emergency physician had called me earlier, more could have been done.
This event is always fresh I my mind when I manage my patients in Ohio. Thank God for the newer medications we have available and the protocols to manage hypertensive crisis in pregnancy. I hope this experience heightens awareness of how deadly this condition can be.
David A. Rosado, MD
Celina, Ohio
Share your thoughts! Send your Letter to the Editor to [email protected]. Please include your name and the city and state in which you practice.
Tedizolid Use in Immunocompromised Patients
Immunocompromised patients are often susceptible to opportunistic infections, including those caused by multidrug-resistant organisms (MDROs). Transplant recipients are at high risk for developing infections due to lifelong immunosuppressive therapy.1,2 Additionally, patients receiving chemotherapy and those with HIV and AIDS are in an immunocompromised state.3-8
Regardless of the etiology for immunosuppression, decreased absolute neutrophil and platelet counts are seen in this condition. Although immunosuppressed individuals may be at increased risk of Gram-negative or Gram-positive infections, this review focuses on the treatment of Gram-positive bacterial infections. Of particular concern are opportunistic infections caused by Gram-positive MDROs, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus species (VRE), penicillin-resistant Streptococcus pneumoniae, and Nocardia species. Treatment of infections in the immunocompromised patient population warrants careful antimicrobial selection to ensure that a patient’s immune system is not further compromised due to adverse effects (AEs) secondary to therapy. As such, clinicians are exploring alternative antimicrobials, such as tedizolid, to treat various opportunistic infections.
Recently, requests at the William S. Middleton Memorial Veterans Hospital in Madison, Wisconsin, for off-label use of tedizolid have increased despite having other cheaper alternatives with comparable Gram-positive coverage. This review examines available literature regarding off-label use of tedizolid with a focus on use in immunocompromised patients.
Tedizolid phosphate (Sivextro) is an oxazolidinone antibiotic prodrug that joined linezolid as the second in its class in 2014. Oxazolidinones inhibit bacterial protein synthesis by binding to the 50S subunit of bacterial ribosomes in Gram-positive bacteria and are often used to treat MRSA and VRE infections.9 In vitro, oxazolidinones have shown bacteriostatic activity against Enterococcus and Staphylococcus species while exhibiting bactericidal activity against most Streptococcus species.10 Tedizolid has a US Food and Drug Administration (FDA) -approved, simplified dosing profile of 200 mg daily for 6 days compared with linezolid 400 to 600 mg twice daily for 10 to 14 days. Both medications are highly bioavailable with direct IV to oral conversion.11,12 Potential, expanded use of tedizolid against Gram-positive MDROs rests on a more favorable AE profile than does its linezolid predecessor. Tedizolid has been associated with less antibiotic-induced myelosuppression, which could prove valuable for immunocompromised patients.13
Tedizolid is approved for the sole indication of acute bacterial skin and skin structure infections (ABSSSI), whereas its predecessor has many approved indications and has been used extensively for off-label indications (Table). 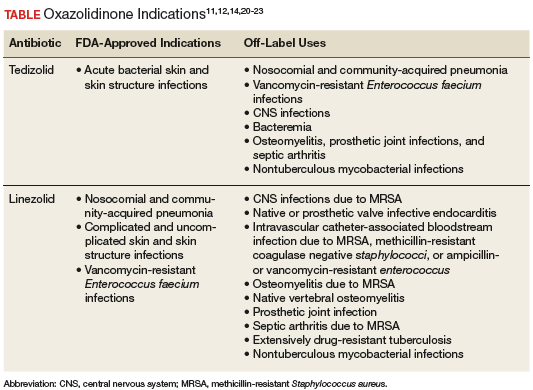
Adverse reactions, as determined by 2 phase 2 and 2 phase 3 clinical trials evaluating 1,050 patients treated with tedizolid and 662 patients treated with linezolid, were similar between the oxazolidinones. Nausea was the most common AE and was reported in 8% and 12% of patients taking tedizolid and linezolid, respectively. Other common AEs (1%-6%) reported for both agents included vomiting, diarrhea, headache, and dizziness.11 Myelosuppression, peripheral neuropathy, and optic nerve disorders were the most common severe AEs reported with oxazolidinones. Tedizolid demonstrated a significantly decreased incidence of neutropenia (3%), defined by absolute neutrophil count 9/L compared with that of linezolid (7%) (P = .024).13 Evaluation of peripheral neuropathy and optic nerve disorders within the tedizolid and linezolid groups revealed similar incidences (peripheral neuropathy 1.2% vs 0.6%; optic nerve disorders 0.3% vs 0.2%, respectively).11
There is one preclinical trial that described the use of tedizolid in a murine model. A murine model study compared the antistaphylococcal killing effect of doses of tedizolid equivalent to human exposures ranging from 200 to 3,200 mg/d in both granulocytopenic and normal mice. The mice were evaluated at 24, 48, and 72 hours after therapy initiation. The presence of granulocytes had a dramatic effect on the antimicrobial effect of tedizolid. Dose response, demonstrated by the ratio of the area under the curve over the minimum inhibitory concentration, was on average > 25-fold for nonneutropenic vs neutropenic models. Near maximal effect of the nonneutropenic group, irrespective of duration of therapy, was achieved at the lowest dose tested (an exposure of about 200-mg tedizolid phosphate per day in humans).This study suggests that immunocompromised patients may warrant higher doses of tedizolid than the currently FDA-approved dose due to a decreased number of granulocytes available for modulating bacterial infections.15
Use of tedizolid doses higher than that which is FDA-approved may negate the favorable AE profile. A phase 1 clinical study was conducted to evaluate the safety, tolerability, and pharmacokinetics of tedizolid compared with those of linezolid in 40 healthy volunteers in a 21-day multiple ascending dose study.16 Subjects were stratified into 5 treatment cohorts: 200-, 300-, or 400-mg tedizolid orally once a day, 600-mg linezolid orally twice a day, and placebo. Tedizolid given at 200 mg had a hematologic safety profile similar to that of placebo. However, mean platelet counts decreased over time in a dose-dependent manner for tedizolid, with the 400-mg tedizolid and linezolid groups reporting similar reductions in platelet counts.16
Some evidence is available examining linezolid in neutropenic patients. Rafailidis and colleagues reviewed available literature regarding linezolid in neutropenic patients with Gram-positive infections. Evaluation of linezolid administration at usual doses to 438 neutropenic patients from 2 prospective comparative studies, a prospective cohort study, 2 retrospective studies, and 8 case reports was performed. Results of the evaluation revealed a clinical cure rate between 57% and 87% in the intention-to-treat population of the prospective studies.17 Given the similarities in bacterial spectrum of activity between linezolid and tedizolid, it may be reasonable to infer that tedizolid’s decreased myelosuppression profile would make it useful in the setting of neutropenia in immunocompromised patients.
There is little evidence regarding the use of tedizolid in immunocompromised patients, as only 2 case reports were found. The first described a 60-year-old male postrenal transplant complicated with VRE bacteremia, rhabdomyolysis, and thrombocytopenia. This patient was treated with prolonged tedizolid 200 mg daily due to multiple contraindications for treatment with other antibiotics. The patient was cured with a 14-day course of tedizolid without any noted AEs.18
The second identified case report described the use of tedizolid for the treatment of central nervous system (CNS) manifestations secondary to nocardiosis. Effective treatment of CNS nocardiosis requires high concentrations and prolonged duration of antimicrobial exposure. This case report described a 68-year-old, chronically immunocompromised female patient with multiple myeloma who was hospitalized for 3 months for the treatment of a CNS nocardiosis infection. After discharge, the patient was treated with an oral regimen of 200-mg tedizolid daily in combination with sulfamethoxazole/trimethoprim (800 mg/160 mg) 3 times daily. After 6 months of combination therapy, magnetic resonance imaging revealed complete resolution of nocardiosis-related central lesions. Although the patient’s malignancy advanced during combination antibiotic therapy, the patient’s absolute neutrophil count remained stable and showed an increase in absolute CD4+ cell counts with no other documented AEs.19
Tedizolid is the latest FDA-approved oxazolidinone antibiotic for susceptible Gram-positive acute bacterial skin and skin structure infections. It has a simplified and shorter duration of treatment and imparts similar AEs at improved rates compared with that of linezolid, most notably in relation to hematologic AEs. Due to the lack of established literature and an agreed-upon dosing strategy for the use of tedizolid in immunocompromised patients, tedizolid therapy for Gram-positive infections in immunocompromised patients should be reserved for salvage therapy when more established Gram-positive antibiotic agents lack efficacy or when patient contraindications to their use exist.
1. Fishman JA, Issa NC. Infection in organ transplantation: risk factors and evolving patterns of infection. Infect Dis Clin North Am. 2010;24(2):273-283.
2. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357(25):2601-2614.
3. Nightingale SD, Byrd LT, Southern PM, Jockusch JD, Cal SX, Wynne BA. Incidence of mycobacterium avium-intracellulare complex bacteremia in human immunodeficiency virus-positive patients. J Infect Dis. 1992;165(6):1082-1085.
4. O’Brien S, Kantarjian H, Beran M, et al. Results of fludarabine and prednisone therapy in 264 patients with chronic lymphocytic leukemia with multivariate analysis-derived prognostic model for response to treatment. Blood. 1993;82(6):1695-1700.
5. Anaissie E, Kontoyiannis DP, Kantarjian H, Elting L, Robertson LE, Keating M. Listeriosis in patients with chronic lymphocytic leukemia who were treated with fludarabine and prednisone. Ann Intern Med. 1992;117(6):466-469.
6. Morrison VA, Rai KR, Peterson BL, et al. Impact of therapy with chlorambucil, fludarabine, or fludarabine plus chlorambucil on infections in patients with chronic lymphocytic leukemia: Intergroup Study Cancer and Leukemia Group B 9011. J Clin Oncol. 2001;19(16):3611-3621.
7. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211-1225.
8. Naseer M, Dailey FE, Juboori AA, Samiullah S, Tahan V. Epidemiology, determinants, and managements of AIDS cholangiopathy: a review. World J Gastroenterol. 2018;24(7):767-774.
9. Radunz S, Juntermanns B, Kaiser GM, et al. Efficacy and safety of linezolid in liver transplant patients. Transpl Infect Dis. 2011;13(4):353-358.
10. Roger C, Roberts JA, Muller L. Clinical pharmacokinetics and pharmacodynamics of oxazolidinones. Clin Pharmacokinet. 2018;57(5):559-575.
11. Sivextro [package insert]. Whitehouse Station, NJ: Merck & Co Inc; 2016.
12. Zyvox [package insert]. New York, NY: Pfizer Inc; 2018.
13. Moran GJ, Fang E, Corey GR, Das AF, De Anda C, Prokocimer P. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): a randomized, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2014;14(8):696-705.
14. Liu C, Bayer A, Cosgrove S, et al; Infectious Diseases Society of America. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55.
15. Drusano GL, Liu W, Kulawy R, Louie A. Impact of granulocytes on the antimicrobial effect of tedizolid in a mouse thigh infection model. Antimicrob Agents Chemother. 2011;55(11):5300-5305.
16. Lodise TP, Bidell MR, Flanagan SD, Zasowski EJ, Minassian SL, Prokocimer P. Characterization of the haematological profile of 21 days of tedizolid in healthy subjects. J Antimicrob Chemother. 2016;71(9):2553-2558.
17. Rafailidis PI, Kouranos VD, Christodoulou C, Falagas ME. Linezolid for patients with neutropenia: are bacteriostatic agents appropriate? Expert Rev Anti Infect Ther. 2009;7(4):415-422.
18. Sudhindra P, Lee L, Wang G, Dhand A. Tedizolid for treatment of enterococcal bacteremia. Open Forum Infect Dis. 2016;3(suppl 1):1344.
19. Matin A, Sharma S, Mathur P, Apewokin SK. Myelosuppression-sparing treatment of central nervous system nocardiosis in a multiple myeloma patient utilizing a tedizolid-based regimen: a case report. Int J Antimicrob Agents. 2017;49(4):488-492.
20. Dryden MS. Alternative clinical indications for novel antibiotics licensed for skin and soft tissue infections? Curr Opin Infect Dis. 2015;28(2):117-124.
21. Milstein M, Brzezinski A, Varaine F, Mitnick CD. (Re)moving the needle: prospects for all-oral treatment for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):18-23.
22. Winthrop KL, Ku JH, Marras TK, et al. The tolerability of linezolid in the treatment of nontuberculous mycobacterial disease. Eur Respir J. 2015;45(4):1177-1179.
23. Yuste JR, Bertó J, Del Pozo JL, Leiva J. Prolonged use of tedizolid in a pulmonary non-tuberculosis mycobacterial infection after linezlid-induced toxicity. J Antimicrob Chemother. 2017;72(2):625-628.
Immunocompromised patients are often susceptible to opportunistic infections, including those caused by multidrug-resistant organisms (MDROs). Transplant recipients are at high risk for developing infections due to lifelong immunosuppressive therapy.1,2 Additionally, patients receiving chemotherapy and those with HIV and AIDS are in an immunocompromised state.3-8
Regardless of the etiology for immunosuppression, decreased absolute neutrophil and platelet counts are seen in this condition. Although immunosuppressed individuals may be at increased risk of Gram-negative or Gram-positive infections, this review focuses on the treatment of Gram-positive bacterial infections. Of particular concern are opportunistic infections caused by Gram-positive MDROs, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus species (VRE), penicillin-resistant Streptococcus pneumoniae, and Nocardia species. Treatment of infections in the immunocompromised patient population warrants careful antimicrobial selection to ensure that a patient’s immune system is not further compromised due to adverse effects (AEs) secondary to therapy. As such, clinicians are exploring alternative antimicrobials, such as tedizolid, to treat various opportunistic infections.
Recently, requests at the William S. Middleton Memorial Veterans Hospital in Madison, Wisconsin, for off-label use of tedizolid have increased despite having other cheaper alternatives with comparable Gram-positive coverage. This review examines available literature regarding off-label use of tedizolid with a focus on use in immunocompromised patients.
Tedizolid phosphate (Sivextro) is an oxazolidinone antibiotic prodrug that joined linezolid as the second in its class in 2014. Oxazolidinones inhibit bacterial protein synthesis by binding to the 50S subunit of bacterial ribosomes in Gram-positive bacteria and are often used to treat MRSA and VRE infections.9 In vitro, oxazolidinones have shown bacteriostatic activity against Enterococcus and Staphylococcus species while exhibiting bactericidal activity against most Streptococcus species.10 Tedizolid has a US Food and Drug Administration (FDA) -approved, simplified dosing profile of 200 mg daily for 6 days compared with linezolid 400 to 600 mg twice daily for 10 to 14 days. Both medications are highly bioavailable with direct IV to oral conversion.11,12 Potential, expanded use of tedizolid against Gram-positive MDROs rests on a more favorable AE profile than does its linezolid predecessor. Tedizolid has been associated with less antibiotic-induced myelosuppression, which could prove valuable for immunocompromised patients.13
Tedizolid is approved for the sole indication of acute bacterial skin and skin structure infections (ABSSSI), whereas its predecessor has many approved indications and has been used extensively for off-label indications (Table).
Adverse reactions, as determined by 2 phase 2 and 2 phase 3 clinical trials evaluating 1,050 patients treated with tedizolid and 662 patients treated with linezolid, were similar between the oxazolidinones. Nausea was the most common AE and was reported in 8% and 12% of patients taking tedizolid and linezolid, respectively. Other common AEs (1%-6%) reported for both agents included vomiting, diarrhea, headache, and dizziness.11 Myelosuppression, peripheral neuropathy, and optic nerve disorders were the most common severe AEs reported with oxazolidinones. Tedizolid demonstrated a significantly decreased incidence of neutropenia (3%), defined by absolute neutrophil count 9/L compared with that of linezolid (7%) (P = .024).13 Evaluation of peripheral neuropathy and optic nerve disorders within the tedizolid and linezolid groups revealed similar incidences (peripheral neuropathy 1.2% vs 0.6%; optic nerve disorders 0.3% vs 0.2%, respectively).11
There is one preclinical trial that described the use of tedizolid in a murine model. A murine model study compared the antistaphylococcal killing effect of doses of tedizolid equivalent to human exposures ranging from 200 to 3,200 mg/d in both granulocytopenic and normal mice. The mice were evaluated at 24, 48, and 72 hours after therapy initiation. The presence of granulocytes had a dramatic effect on the antimicrobial effect of tedizolid. Dose response, demonstrated by the ratio of the area under the curve over the minimum inhibitory concentration, was on average > 25-fold for nonneutropenic vs neutropenic models. Near maximal effect of the nonneutropenic group, irrespective of duration of therapy, was achieved at the lowest dose tested (an exposure of about 200-mg tedizolid phosphate per day in humans).This study suggests that immunocompromised patients may warrant higher doses of tedizolid than the currently FDA-approved dose due to a decreased number of granulocytes available for modulating bacterial infections.15
Use of tedizolid doses higher than that which is FDA-approved may negate the favorable AE profile. A phase 1 clinical study was conducted to evaluate the safety, tolerability, and pharmacokinetics of tedizolid compared with those of linezolid in 40 healthy volunteers in a 21-day multiple ascending dose study.16 Subjects were stratified into 5 treatment cohorts: 200-, 300-, or 400-mg tedizolid orally once a day, 600-mg linezolid orally twice a day, and placebo. Tedizolid given at 200 mg had a hematologic safety profile similar to that of placebo. However, mean platelet counts decreased over time in a dose-dependent manner for tedizolid, with the 400-mg tedizolid and linezolid groups reporting similar reductions in platelet counts.16
Some evidence is available examining linezolid in neutropenic patients. Rafailidis and colleagues reviewed available literature regarding linezolid in neutropenic patients with Gram-positive infections. Evaluation of linezolid administration at usual doses to 438 neutropenic patients from 2 prospective comparative studies, a prospective cohort study, 2 retrospective studies, and 8 case reports was performed. Results of the evaluation revealed a clinical cure rate between 57% and 87% in the intention-to-treat population of the prospective studies.17 Given the similarities in bacterial spectrum of activity between linezolid and tedizolid, it may be reasonable to infer that tedizolid’s decreased myelosuppression profile would make it useful in the setting of neutropenia in immunocompromised patients.
There is little evidence regarding the use of tedizolid in immunocompromised patients, as only 2 case reports were found. The first described a 60-year-old male postrenal transplant complicated with VRE bacteremia, rhabdomyolysis, and thrombocytopenia. This patient was treated with prolonged tedizolid 200 mg daily due to multiple contraindications for treatment with other antibiotics. The patient was cured with a 14-day course of tedizolid without any noted AEs.18
The second identified case report described the use of tedizolid for the treatment of central nervous system (CNS) manifestations secondary to nocardiosis. Effective treatment of CNS nocardiosis requires high concentrations and prolonged duration of antimicrobial exposure. This case report described a 68-year-old, chronically immunocompromised female patient with multiple myeloma who was hospitalized for 3 months for the treatment of a CNS nocardiosis infection. After discharge, the patient was treated with an oral regimen of 200-mg tedizolid daily in combination with sulfamethoxazole/trimethoprim (800 mg/160 mg) 3 times daily. After 6 months of combination therapy, magnetic resonance imaging revealed complete resolution of nocardiosis-related central lesions. Although the patient’s malignancy advanced during combination antibiotic therapy, the patient’s absolute neutrophil count remained stable and showed an increase in absolute CD4+ cell counts with no other documented AEs.19
Tedizolid is the latest FDA-approved oxazolidinone antibiotic for susceptible Gram-positive acute bacterial skin and skin structure infections. It has a simplified and shorter duration of treatment and imparts similar AEs at improved rates compared with that of linezolid, most notably in relation to hematologic AEs. Due to the lack of established literature and an agreed-upon dosing strategy for the use of tedizolid in immunocompromised patients, tedizolid therapy for Gram-positive infections in immunocompromised patients should be reserved for salvage therapy when more established Gram-positive antibiotic agents lack efficacy or when patient contraindications to their use exist.
Immunocompromised patients are often susceptible to opportunistic infections, including those caused by multidrug-resistant organisms (MDROs). Transplant recipients are at high risk for developing infections due to lifelong immunosuppressive therapy.1,2 Additionally, patients receiving chemotherapy and those with HIV and AIDS are in an immunocompromised state.3-8
Regardless of the etiology for immunosuppression, decreased absolute neutrophil and platelet counts are seen in this condition. Although immunosuppressed individuals may be at increased risk of Gram-negative or Gram-positive infections, this review focuses on the treatment of Gram-positive bacterial infections. Of particular concern are opportunistic infections caused by Gram-positive MDROs, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus species (VRE), penicillin-resistant Streptococcus pneumoniae, and Nocardia species. Treatment of infections in the immunocompromised patient population warrants careful antimicrobial selection to ensure that a patient’s immune system is not further compromised due to adverse effects (AEs) secondary to therapy. As such, clinicians are exploring alternative antimicrobials, such as tedizolid, to treat various opportunistic infections.
Recently, requests at the William S. Middleton Memorial Veterans Hospital in Madison, Wisconsin, for off-label use of tedizolid have increased despite having other cheaper alternatives with comparable Gram-positive coverage. This review examines available literature regarding off-label use of tedizolid with a focus on use in immunocompromised patients.
Tedizolid phosphate (Sivextro) is an oxazolidinone antibiotic prodrug that joined linezolid as the second in its class in 2014. Oxazolidinones inhibit bacterial protein synthesis by binding to the 50S subunit of bacterial ribosomes in Gram-positive bacteria and are often used to treat MRSA and VRE infections.9 In vitro, oxazolidinones have shown bacteriostatic activity against Enterococcus and Staphylococcus species while exhibiting bactericidal activity against most Streptococcus species.10 Tedizolid has a US Food and Drug Administration (FDA) -approved, simplified dosing profile of 200 mg daily for 6 days compared with linezolid 400 to 600 mg twice daily for 10 to 14 days. Both medications are highly bioavailable with direct IV to oral conversion.11,12 Potential, expanded use of tedizolid against Gram-positive MDROs rests on a more favorable AE profile than does its linezolid predecessor. Tedizolid has been associated with less antibiotic-induced myelosuppression, which could prove valuable for immunocompromised patients.13
Tedizolid is approved for the sole indication of acute bacterial skin and skin structure infections (ABSSSI), whereas its predecessor has many approved indications and has been used extensively for off-label indications (Table).
Adverse reactions, as determined by 2 phase 2 and 2 phase 3 clinical trials evaluating 1,050 patients treated with tedizolid and 662 patients treated with linezolid, were similar between the oxazolidinones. Nausea was the most common AE and was reported in 8% and 12% of patients taking tedizolid and linezolid, respectively. Other common AEs (1%-6%) reported for both agents included vomiting, diarrhea, headache, and dizziness.11 Myelosuppression, peripheral neuropathy, and optic nerve disorders were the most common severe AEs reported with oxazolidinones. Tedizolid demonstrated a significantly decreased incidence of neutropenia (3%), defined by absolute neutrophil count 9/L compared with that of linezolid (7%) (P = .024).13 Evaluation of peripheral neuropathy and optic nerve disorders within the tedizolid and linezolid groups revealed similar incidences (peripheral neuropathy 1.2% vs 0.6%; optic nerve disorders 0.3% vs 0.2%, respectively).11
There is one preclinical trial that described the use of tedizolid in a murine model. A murine model study compared the antistaphylococcal killing effect of doses of tedizolid equivalent to human exposures ranging from 200 to 3,200 mg/d in both granulocytopenic and normal mice. The mice were evaluated at 24, 48, and 72 hours after therapy initiation. The presence of granulocytes had a dramatic effect on the antimicrobial effect of tedizolid. Dose response, demonstrated by the ratio of the area under the curve over the minimum inhibitory concentration, was on average > 25-fold for nonneutropenic vs neutropenic models. Near maximal effect of the nonneutropenic group, irrespective of duration of therapy, was achieved at the lowest dose tested (an exposure of about 200-mg tedizolid phosphate per day in humans).This study suggests that immunocompromised patients may warrant higher doses of tedizolid than the currently FDA-approved dose due to a decreased number of granulocytes available for modulating bacterial infections.15
Use of tedizolid doses higher than that which is FDA-approved may negate the favorable AE profile. A phase 1 clinical study was conducted to evaluate the safety, tolerability, and pharmacokinetics of tedizolid compared with those of linezolid in 40 healthy volunteers in a 21-day multiple ascending dose study.16 Subjects were stratified into 5 treatment cohorts: 200-, 300-, or 400-mg tedizolid orally once a day, 600-mg linezolid orally twice a day, and placebo. Tedizolid given at 200 mg had a hematologic safety profile similar to that of placebo. However, mean platelet counts decreased over time in a dose-dependent manner for tedizolid, with the 400-mg tedizolid and linezolid groups reporting similar reductions in platelet counts.16
Some evidence is available examining linezolid in neutropenic patients. Rafailidis and colleagues reviewed available literature regarding linezolid in neutropenic patients with Gram-positive infections. Evaluation of linezolid administration at usual doses to 438 neutropenic patients from 2 prospective comparative studies, a prospective cohort study, 2 retrospective studies, and 8 case reports was performed. Results of the evaluation revealed a clinical cure rate between 57% and 87% in the intention-to-treat population of the prospective studies.17 Given the similarities in bacterial spectrum of activity between linezolid and tedizolid, it may be reasonable to infer that tedizolid’s decreased myelosuppression profile would make it useful in the setting of neutropenia in immunocompromised patients.
There is little evidence regarding the use of tedizolid in immunocompromised patients, as only 2 case reports were found. The first described a 60-year-old male postrenal transplant complicated with VRE bacteremia, rhabdomyolysis, and thrombocytopenia. This patient was treated with prolonged tedizolid 200 mg daily due to multiple contraindications for treatment with other antibiotics. The patient was cured with a 14-day course of tedizolid without any noted AEs.18
The second identified case report described the use of tedizolid for the treatment of central nervous system (CNS) manifestations secondary to nocardiosis. Effective treatment of CNS nocardiosis requires high concentrations and prolonged duration of antimicrobial exposure. This case report described a 68-year-old, chronically immunocompromised female patient with multiple myeloma who was hospitalized for 3 months for the treatment of a CNS nocardiosis infection. After discharge, the patient was treated with an oral regimen of 200-mg tedizolid daily in combination with sulfamethoxazole/trimethoprim (800 mg/160 mg) 3 times daily. After 6 months of combination therapy, magnetic resonance imaging revealed complete resolution of nocardiosis-related central lesions. Although the patient’s malignancy advanced during combination antibiotic therapy, the patient’s absolute neutrophil count remained stable and showed an increase in absolute CD4+ cell counts with no other documented AEs.19
Tedizolid is the latest FDA-approved oxazolidinone antibiotic for susceptible Gram-positive acute bacterial skin and skin structure infections. It has a simplified and shorter duration of treatment and imparts similar AEs at improved rates compared with that of linezolid, most notably in relation to hematologic AEs. Due to the lack of established literature and an agreed-upon dosing strategy for the use of tedizolid in immunocompromised patients, tedizolid therapy for Gram-positive infections in immunocompromised patients should be reserved for salvage therapy when more established Gram-positive antibiotic agents lack efficacy or when patient contraindications to their use exist.
1. Fishman JA, Issa NC. Infection in organ transplantation: risk factors and evolving patterns of infection. Infect Dis Clin North Am. 2010;24(2):273-283.
2. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357(25):2601-2614.
3. Nightingale SD, Byrd LT, Southern PM, Jockusch JD, Cal SX, Wynne BA. Incidence of mycobacterium avium-intracellulare complex bacteremia in human immunodeficiency virus-positive patients. J Infect Dis. 1992;165(6):1082-1085.
4. O’Brien S, Kantarjian H, Beran M, et al. Results of fludarabine and prednisone therapy in 264 patients with chronic lymphocytic leukemia with multivariate analysis-derived prognostic model for response to treatment. Blood. 1993;82(6):1695-1700.
5. Anaissie E, Kontoyiannis DP, Kantarjian H, Elting L, Robertson LE, Keating M. Listeriosis in patients with chronic lymphocytic leukemia who were treated with fludarabine and prednisone. Ann Intern Med. 1992;117(6):466-469.
6. Morrison VA, Rai KR, Peterson BL, et al. Impact of therapy with chlorambucil, fludarabine, or fludarabine plus chlorambucil on infections in patients with chronic lymphocytic leukemia: Intergroup Study Cancer and Leukemia Group B 9011. J Clin Oncol. 2001;19(16):3611-3621.
7. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211-1225.
8. Naseer M, Dailey FE, Juboori AA, Samiullah S, Tahan V. Epidemiology, determinants, and managements of AIDS cholangiopathy: a review. World J Gastroenterol. 2018;24(7):767-774.
9. Radunz S, Juntermanns B, Kaiser GM, et al. Efficacy and safety of linezolid in liver transplant patients. Transpl Infect Dis. 2011;13(4):353-358.
10. Roger C, Roberts JA, Muller L. Clinical pharmacokinetics and pharmacodynamics of oxazolidinones. Clin Pharmacokinet. 2018;57(5):559-575.
11. Sivextro [package insert]. Whitehouse Station, NJ: Merck & Co Inc; 2016.
12. Zyvox [package insert]. New York, NY: Pfizer Inc; 2018.
13. Moran GJ, Fang E, Corey GR, Das AF, De Anda C, Prokocimer P. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): a randomized, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2014;14(8):696-705.
14. Liu C, Bayer A, Cosgrove S, et al; Infectious Diseases Society of America. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55.
15. Drusano GL, Liu W, Kulawy R, Louie A. Impact of granulocytes on the antimicrobial effect of tedizolid in a mouse thigh infection model. Antimicrob Agents Chemother. 2011;55(11):5300-5305.
16. Lodise TP, Bidell MR, Flanagan SD, Zasowski EJ, Minassian SL, Prokocimer P. Characterization of the haematological profile of 21 days of tedizolid in healthy subjects. J Antimicrob Chemother. 2016;71(9):2553-2558.
17. Rafailidis PI, Kouranos VD, Christodoulou C, Falagas ME. Linezolid for patients with neutropenia: are bacteriostatic agents appropriate? Expert Rev Anti Infect Ther. 2009;7(4):415-422.
18. Sudhindra P, Lee L, Wang G, Dhand A. Tedizolid for treatment of enterococcal bacteremia. Open Forum Infect Dis. 2016;3(suppl 1):1344.
19. Matin A, Sharma S, Mathur P, Apewokin SK. Myelosuppression-sparing treatment of central nervous system nocardiosis in a multiple myeloma patient utilizing a tedizolid-based regimen: a case report. Int J Antimicrob Agents. 2017;49(4):488-492.
20. Dryden MS. Alternative clinical indications for novel antibiotics licensed for skin and soft tissue infections? Curr Opin Infect Dis. 2015;28(2):117-124.
21. Milstein M, Brzezinski A, Varaine F, Mitnick CD. (Re)moving the needle: prospects for all-oral treatment for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):18-23.
22. Winthrop KL, Ku JH, Marras TK, et al. The tolerability of linezolid in the treatment of nontuberculous mycobacterial disease. Eur Respir J. 2015;45(4):1177-1179.
23. Yuste JR, Bertó J, Del Pozo JL, Leiva J. Prolonged use of tedizolid in a pulmonary non-tuberculosis mycobacterial infection after linezlid-induced toxicity. J Antimicrob Chemother. 2017;72(2):625-628.
1. Fishman JA, Issa NC. Infection in organ transplantation: risk factors and evolving patterns of infection. Infect Dis Clin North Am. 2010;24(2):273-283.
2. Fishman JA. Infection in solid-organ transplant recipients. N Engl J Med. 2007;357(25):2601-2614.
3. Nightingale SD, Byrd LT, Southern PM, Jockusch JD, Cal SX, Wynne BA. Incidence of mycobacterium avium-intracellulare complex bacteremia in human immunodeficiency virus-positive patients. J Infect Dis. 1992;165(6):1082-1085.
4. O’Brien S, Kantarjian H, Beran M, et al. Results of fludarabine and prednisone therapy in 264 patients with chronic lymphocytic leukemia with multivariate analysis-derived prognostic model for response to treatment. Blood. 1993;82(6):1695-1700.
5. Anaissie E, Kontoyiannis DP, Kantarjian H, Elting L, Robertson LE, Keating M. Listeriosis in patients with chronic lymphocytic leukemia who were treated with fludarabine and prednisone. Ann Intern Med. 1992;117(6):466-469.
6. Morrison VA, Rai KR, Peterson BL, et al. Impact of therapy with chlorambucil, fludarabine, or fludarabine plus chlorambucil on infections in patients with chronic lymphocytic leukemia: Intergroup Study Cancer and Leukemia Group B 9011. J Clin Oncol. 2001;19(16):3611-3621.
7. Nucci M, Anaissie E. Infections in patients with multiple myeloma in the era of high-dose therapy and novel agents. Clin Infect Dis. 2009;49(8):1211-1225.
8. Naseer M, Dailey FE, Juboori AA, Samiullah S, Tahan V. Epidemiology, determinants, and managements of AIDS cholangiopathy: a review. World J Gastroenterol. 2018;24(7):767-774.
9. Radunz S, Juntermanns B, Kaiser GM, et al. Efficacy and safety of linezolid in liver transplant patients. Transpl Infect Dis. 2011;13(4):353-358.
10. Roger C, Roberts JA, Muller L. Clinical pharmacokinetics and pharmacodynamics of oxazolidinones. Clin Pharmacokinet. 2018;57(5):559-575.
11. Sivextro [package insert]. Whitehouse Station, NJ: Merck & Co Inc; 2016.
12. Zyvox [package insert]. New York, NY: Pfizer Inc; 2018.
13. Moran GJ, Fang E, Corey GR, Das AF, De Anda C, Prokocimer P. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): a randomized, double-blind, phase 3, non-inferiority trial. Lancet Infect Dis. 2014;14(8):696-705.
14. Liu C, Bayer A, Cosgrove S, et al; Infectious Diseases Society of America. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin Infect Dis. 2011;52(3):e18-e55.
15. Drusano GL, Liu W, Kulawy R, Louie A. Impact of granulocytes on the antimicrobial effect of tedizolid in a mouse thigh infection model. Antimicrob Agents Chemother. 2011;55(11):5300-5305.
16. Lodise TP, Bidell MR, Flanagan SD, Zasowski EJ, Minassian SL, Prokocimer P. Characterization of the haematological profile of 21 days of tedizolid in healthy subjects. J Antimicrob Chemother. 2016;71(9):2553-2558.
17. Rafailidis PI, Kouranos VD, Christodoulou C, Falagas ME. Linezolid for patients with neutropenia: are bacteriostatic agents appropriate? Expert Rev Anti Infect Ther. 2009;7(4):415-422.
18. Sudhindra P, Lee L, Wang G, Dhand A. Tedizolid for treatment of enterococcal bacteremia. Open Forum Infect Dis. 2016;3(suppl 1):1344.
19. Matin A, Sharma S, Mathur P, Apewokin SK. Myelosuppression-sparing treatment of central nervous system nocardiosis in a multiple myeloma patient utilizing a tedizolid-based regimen: a case report. Int J Antimicrob Agents. 2017;49(4):488-492.
20. Dryden MS. Alternative clinical indications for novel antibiotics licensed for skin and soft tissue infections? Curr Opin Infect Dis. 2015;28(2):117-124.
21. Milstein M, Brzezinski A, Varaine F, Mitnick CD. (Re)moving the needle: prospects for all-oral treatment for multidrug-resistant tuberculosis. Int J Tuberc Lung Dis. 2016;20(12):18-23.
22. Winthrop KL, Ku JH, Marras TK, et al. The tolerability of linezolid in the treatment of nontuberculous mycobacterial disease. Eur Respir J. 2015;45(4):1177-1179.
23. Yuste JR, Bertó J, Del Pozo JL, Leiva J. Prolonged use of tedizolid in a pulmonary non-tuberculosis mycobacterial infection after linezlid-induced toxicity. J Antimicrob Chemother. 2017;72(2):625-628.
Rare Cancer Misdiagnosed As Orchitis
A 70-year-old man underwent salvage therapy for multiple myeloma (MM). While on maintenance immunotherapy he developed a sternal plasmacytoma. After the fifth cycle of treatment, he developed swelling, erythema, and pain in his right testis.
The main differential diagnoses for those symptoms are infections and tumors; infection is more common, so his clinicians at Indiana University School of Medicine presumed orchitis and started him on IV antibiotics. The pain resolved, but the swelling persisted after the antibiotic course. The clinicians turned to biochemical marker screening for germ cell tumors, but those were negative. Serial ultrasound imaging, which they had begun during his admission, remained unchanged.
Meanwhile, the patient’s chemotherapy was being held back, and he developed another sternal mass, prompting a fluorodeoxyglucose-positron emission tomography–computed tomography (PET/CT) scan to evaluate for relapse of myeloma. The scan revealed an enlarged, diffusely hypermetabolic right testicle. Believing the symptoms were related to the myeloma and not orchitis, the clinicians advised a radical orchiectomy.
A biopsy after the surgery showed tumor cells consistent with testicular plasmacytoma.
While rare, testicular plasmacytoma is commonly associated with MM, especially in the later stages, when cancer cells are more aggressive and not relying on bone marrow for survival, the clinicians say. Unlike myeloma, which typically spreads via blood to bone sites, testicular plasmacytoma may spread via lymphatic channels to the regional lymph nodes and subsequently to distant sites, the clinicians add, similarly to lymphoma or germ cell tumor.
It is hard to diagnose, though. The clinicians say the patient’s case illustrates the challenges. Imaging studies such as ultrasound and CT scans are not specific. And although FDG-PET/CT imaging is a standard staging tool for myeloma and helpful in identifying plasmacytoma when evidenced as intramedullary or extramedullary hypermetabolic lesions, hypermetabolic lesions are not always malignant, they note. FDG-PET/CT can’t differentiate between orchitis and testicular plasmacytoma. Biopsy remains the diagnostic gold standard.
Source:
Schiavo C, Mann SA, Mer J, Suvannasankha A. BMJ Case Rep. 2018;pii:bcr-2017-222046.
doi: 10.1136/bcr-2017-222046.
A 70-year-old man underwent salvage therapy for multiple myeloma (MM). While on maintenance immunotherapy he developed a sternal plasmacytoma. After the fifth cycle of treatment, he developed swelling, erythema, and pain in his right testis.
The main differential diagnoses for those symptoms are infections and tumors; infection is more common, so his clinicians at Indiana University School of Medicine presumed orchitis and started him on IV antibiotics. The pain resolved, but the swelling persisted after the antibiotic course. The clinicians turned to biochemical marker screening for germ cell tumors, but those were negative. Serial ultrasound imaging, which they had begun during his admission, remained unchanged.
Meanwhile, the patient’s chemotherapy was being held back, and he developed another sternal mass, prompting a fluorodeoxyglucose-positron emission tomography–computed tomography (PET/CT) scan to evaluate for relapse of myeloma. The scan revealed an enlarged, diffusely hypermetabolic right testicle. Believing the symptoms were related to the myeloma and not orchitis, the clinicians advised a radical orchiectomy.
A biopsy after the surgery showed tumor cells consistent with testicular plasmacytoma.
While rare, testicular plasmacytoma is commonly associated with MM, especially in the later stages, when cancer cells are more aggressive and not relying on bone marrow for survival, the clinicians say. Unlike myeloma, which typically spreads via blood to bone sites, testicular plasmacytoma may spread via lymphatic channels to the regional lymph nodes and subsequently to distant sites, the clinicians add, similarly to lymphoma or germ cell tumor.
It is hard to diagnose, though. The clinicians say the patient’s case illustrates the challenges. Imaging studies such as ultrasound and CT scans are not specific. And although FDG-PET/CT imaging is a standard staging tool for myeloma and helpful in identifying plasmacytoma when evidenced as intramedullary or extramedullary hypermetabolic lesions, hypermetabolic lesions are not always malignant, they note. FDG-PET/CT can’t differentiate between orchitis and testicular plasmacytoma. Biopsy remains the diagnostic gold standard.
Source:
Schiavo C, Mann SA, Mer J, Suvannasankha A. BMJ Case Rep. 2018;pii:bcr-2017-222046.
doi: 10.1136/bcr-2017-222046.
A 70-year-old man underwent salvage therapy for multiple myeloma (MM). While on maintenance immunotherapy he developed a sternal plasmacytoma. After the fifth cycle of treatment, he developed swelling, erythema, and pain in his right testis.
The main differential diagnoses for those symptoms are infections and tumors; infection is more common, so his clinicians at Indiana University School of Medicine presumed orchitis and started him on IV antibiotics. The pain resolved, but the swelling persisted after the antibiotic course. The clinicians turned to biochemical marker screening for germ cell tumors, but those were negative. Serial ultrasound imaging, which they had begun during his admission, remained unchanged.
Meanwhile, the patient’s chemotherapy was being held back, and he developed another sternal mass, prompting a fluorodeoxyglucose-positron emission tomography–computed tomography (PET/CT) scan to evaluate for relapse of myeloma. The scan revealed an enlarged, diffusely hypermetabolic right testicle. Believing the symptoms were related to the myeloma and not orchitis, the clinicians advised a radical orchiectomy.
A biopsy after the surgery showed tumor cells consistent with testicular plasmacytoma.
While rare, testicular plasmacytoma is commonly associated with MM, especially in the later stages, when cancer cells are more aggressive and not relying on bone marrow for survival, the clinicians say. Unlike myeloma, which typically spreads via blood to bone sites, testicular plasmacytoma may spread via lymphatic channels to the regional lymph nodes and subsequently to distant sites, the clinicians add, similarly to lymphoma or germ cell tumor.
It is hard to diagnose, though. The clinicians say the patient’s case illustrates the challenges. Imaging studies such as ultrasound and CT scans are not specific. And although FDG-PET/CT imaging is a standard staging tool for myeloma and helpful in identifying plasmacytoma when evidenced as intramedullary or extramedullary hypermetabolic lesions, hypermetabolic lesions are not always malignant, they note. FDG-PET/CT can’t differentiate between orchitis and testicular plasmacytoma. Biopsy remains the diagnostic gold standard.
Source:
Schiavo C, Mann SA, Mer J, Suvannasankha A. BMJ Case Rep. 2018;pii:bcr-2017-222046.
doi: 10.1136/bcr-2017-222046.
‘Very encouraging’ results in BPDCN

STOCKHOLM—Tagraxofusp (SL-401) has produced “very encouraging” results in a phase 2 trial of patients with blastic plasmacytoid dendritic cell neoplasm (BPDCN), according to an investigator.
Tagraxofusp, a targeted therapy directed to CD123, produced an overall response rate (ORR) of 83% and a complete response (CR) rate of 62% in patients with previously untreated or relapsed/refractory BPDCN.
Common adverse events (AEs) related to tagraxofusp include hypoalbuminemia, transaminitis, and thrombocytopenia. There was 1 grade 5 AE—a case of capillary leak syndrome (CLS).
Study investigator Naveen Pemmaraju, MD, of The University of Texas MD Anderson Cancer Center in Houston, presented these results at the 23rd Congress of the European Hematology Association (EHA) as abstract S116.
The trial was sponsored by Stemline Therapeutics.
Dr Pemmaraju noted that there are no approved therapies for BPDCN, so patients may be treated with therapies intended for acute myeloid leukemia (AML), acute lymphoblastic leukemia, or lymphomas.
“These are usually quite intense cytotoxic chemotherapy regimens,” he said. “But even with these regimens, most groups report median overall survival times of 8 to 14 months.”
And although stem cell transplants can be effective in BPDCN, a “vast majority” of patients are not fit for transplant, according to Dr Pemmaraju.
With this in mind, he and his colleagues are conducting this trial of tagraxofusp in BPDCN.
The trial has 4 stages. In stage 1, patients received tagraxofusp at 7, 9, 12, or 16 μg/kg on days 1 to 5 of a 21-day cycle. In stages 2 and 3, patients received the drug at 12 μg/kg on days 1 to 5 of a 21-day cycle. Stage 4 is still enrolling.
Efficacy
Dr Pemmaraju presented results in 45 patients—32 with previously untreated BPDCN and 13 with relapsed/refractory BPDCN. The patients’ median age at baseline was 70 (range, 22-84), and 82% were male.
Three patients received tagraxofusp at 7 μg/kg/day, and the rest received the 12 μg/kg/day dose.
Among patients who received the 12 μg/kg/day dose, the ORR was 83% (35/42). The ORR was 90% (26/29) in previously untreated patients and 69% (9/13) in relapsed/refractory patients.
“These are very encouraging results—a 90% overall response rate in the frontline setting,” Dr Pemmaraju noted.
The composite CR rate was 62% (n=26) overall, 72% (n=21) in previously untreated patients, and 38% (n=5) in relapsed/refractory patients.
This included 13 patients with a CR (1 relapsed/refractory), 10 with a clinical CR (3 relapsed/refractory), and 3 with a CR with incomplete hematologic recovery (1 relapsed/refractory). A clinical CR was defined as absence of gross disease with minimal residual skin abnormality.
Fourteen patients went on to stem cell transplant, 1 of whom had relapsed/refractory disease at baseline.
Overall survival results were only available for the 29 previously untreated patients who received tagraxofusp at 12 μg/kg/day. In this group, the median overall survival has not been reached at a median follow-up of 13.8 months (range, 0.2 to 37.4 months).
Dr Pemmaraju said this result is important because it contrasts with the historical expectation of a median overall survival of 8 to 14 months.
Safety
Dr Pemmaraju presented safety results in 114 patients who have received tagraxofusp at 12 μg/kg/day on all trials of the drug. These data include patients with AML, myelofibrosis, and chronic myelomonocytic leukemia in addition to the 45 patients with BPDCN. However, AEs were similar regardless of disease.
Common treatment-related AEs (of any grade, occurring in at least 15% of patients) included hypoalbuminemia (49%), ALT increase (48%), AST increase (48%), thrombocytopenia (29%), nausea (27%), pyrexia (25%), chills (23%), fatigue (23%), weight increase (19%), hypotension (18%), peripheral edema (17%), and vomiting (15%).
CLS of any grade was also a common AE, occurring in 20% of patients (n=23). Most cases of CLS were grade 1 or 2, but there were grade 3 (n=5) and 4 (n=2) cases, as well as a single case of grade 5 CLS that occurred in a BPDCN patient.
Dr Pemmaraju did note that CLS has proven manageable with monitoring and pre-emptive measures. Specifically, inclusion criteria were changed so that patients must have normal cardiac function, adequate kidney function, and albumin of at least 3.2 g/dl. Investigators also began monitoring patients’ weight, albumin levels, and kidney function.
“With the combination of greater understanding of CLS, actual definitive protocol adjustments made by investigators, and monitoring, this has been a highly manageable phenomenon,” Dr Pemmaraju said.
Next steps
The investigators plan to continue enrolling patients in this study and collect additional safety and survival data, but Dr Pemmaraju and his colleagues also want to evaluate tagraxofusp in combination with other therapies.
Tagraxofusp is already under investigation in combination with azacitidine in a phase 1/2 trial of patients with high-risk myelodysplastic syndromes and AML.
Dr Pemmaraju is interested in combining hypomethylating agents with tagraxofusp for BPDCN patients as well, to build upon the encouraging results with tagraxofusp alone.
“An extraordinarily rare disease that used to not have any therapies at all now has at least one ongoing clinical trial with some encouraging activity,” he said. “I hope that gives hope to people with rare diseases, to let them know they’re not alone. There may be someone out there who’s researching their disease, no matter how rare it is.”
STOCKHOLM—Tagraxofusp (SL-401) has produced “very encouraging” results in a phase 2 trial of patients with blastic plasmacytoid dendritic cell neoplasm (BPDCN), according to an investigator.
Tagraxofusp, a targeted therapy directed to CD123, produced an overall response rate (ORR) of 83% and a complete response (CR) rate of 62% in patients with previously untreated or relapsed/refractory BPDCN.
Common adverse events (AEs) related to tagraxofusp include hypoalbuminemia, transaminitis, and thrombocytopenia. There was 1 grade 5 AE—a case of capillary leak syndrome (CLS).
Study investigator Naveen Pemmaraju, MD, of The University of Texas MD Anderson Cancer Center in Houston, presented these results at the 23rd Congress of the European Hematology Association (EHA) as abstract S116.
The trial was sponsored by Stemline Therapeutics.
Dr Pemmaraju noted that there are no approved therapies for BPDCN, so patients may be treated with therapies intended for acute myeloid leukemia (AML), acute lymphoblastic leukemia, or lymphomas.
“These are usually quite intense cytotoxic chemotherapy regimens,” he said. “But even with these regimens, most groups report median overall survival times of 8 to 14 months.”
And although stem cell transplants can be effective in BPDCN, a “vast majority” of patients are not fit for transplant, according to Dr Pemmaraju.
With this in mind, he and his colleagues are conducting this trial of tagraxofusp in BPDCN.
The trial has 4 stages. In stage 1, patients received tagraxofusp at 7, 9, 12, or 16 μg/kg on days 1 to 5 of a 21-day cycle. In stages 2 and 3, patients received the drug at 12 μg/kg on days 1 to 5 of a 21-day cycle. Stage 4 is still enrolling.
Efficacy
Dr Pemmaraju presented results in 45 patients—32 with previously untreated BPDCN and 13 with relapsed/refractory BPDCN. The patients’ median age at baseline was 70 (range, 22-84), and 82% were male.
Three patients received tagraxofusp at 7 μg/kg/day, and the rest received the 12 μg/kg/day dose.
Among patients who received the 12 μg/kg/day dose, the ORR was 83% (35/42). The ORR was 90% (26/29) in previously untreated patients and 69% (9/13) in relapsed/refractory patients.
“These are very encouraging results—a 90% overall response rate in the frontline setting,” Dr Pemmaraju noted.
The composite CR rate was 62% (n=26) overall, 72% (n=21) in previously untreated patients, and 38% (n=5) in relapsed/refractory patients.
This included 13 patients with a CR (1 relapsed/refractory), 10 with a clinical CR (3 relapsed/refractory), and 3 with a CR with incomplete hematologic recovery (1 relapsed/refractory). A clinical CR was defined as absence of gross disease with minimal residual skin abnormality.
Fourteen patients went on to stem cell transplant, 1 of whom had relapsed/refractory disease at baseline.
Overall survival results were only available for the 29 previously untreated patients who received tagraxofusp at 12 μg/kg/day. In this group, the median overall survival has not been reached at a median follow-up of 13.8 months (range, 0.2 to 37.4 months).
Dr Pemmaraju said this result is important because it contrasts with the historical expectation of a median overall survival of 8 to 14 months.
Safety
Dr Pemmaraju presented safety results in 114 patients who have received tagraxofusp at 12 μg/kg/day on all trials of the drug. These data include patients with AML, myelofibrosis, and chronic myelomonocytic leukemia in addition to the 45 patients with BPDCN. However, AEs were similar regardless of disease.
Common treatment-related AEs (of any grade, occurring in at least 15% of patients) included hypoalbuminemia (49%), ALT increase (48%), AST increase (48%), thrombocytopenia (29%), nausea (27%), pyrexia (25%), chills (23%), fatigue (23%), weight increase (19%), hypotension (18%), peripheral edema (17%), and vomiting (15%).
CLS of any grade was also a common AE, occurring in 20% of patients (n=23). Most cases of CLS were grade 1 or 2, but there were grade 3 (n=5) and 4 (n=2) cases, as well as a single case of grade 5 CLS that occurred in a BPDCN patient.
Dr Pemmaraju did note that CLS has proven manageable with monitoring and pre-emptive measures. Specifically, inclusion criteria were changed so that patients must have normal cardiac function, adequate kidney function, and albumin of at least 3.2 g/dl. Investigators also began monitoring patients’ weight, albumin levels, and kidney function.
“With the combination of greater understanding of CLS, actual definitive protocol adjustments made by investigators, and monitoring, this has been a highly manageable phenomenon,” Dr Pemmaraju said.
Next steps
The investigators plan to continue enrolling patients in this study and collect additional safety and survival data, but Dr Pemmaraju and his colleagues also want to evaluate tagraxofusp in combination with other therapies.
Tagraxofusp is already under investigation in combination with azacitidine in a phase 1/2 trial of patients with high-risk myelodysplastic syndromes and AML.
Dr Pemmaraju is interested in combining hypomethylating agents with tagraxofusp for BPDCN patients as well, to build upon the encouraging results with tagraxofusp alone.
“An extraordinarily rare disease that used to not have any therapies at all now has at least one ongoing clinical trial with some encouraging activity,” he said. “I hope that gives hope to people with rare diseases, to let them know they’re not alone. There may be someone out there who’s researching their disease, no matter how rare it is.”
STOCKHOLM—Tagraxofusp (SL-401) has produced “very encouraging” results in a phase 2 trial of patients with blastic plasmacytoid dendritic cell neoplasm (BPDCN), according to an investigator.
Tagraxofusp, a targeted therapy directed to CD123, produced an overall response rate (ORR) of 83% and a complete response (CR) rate of 62% in patients with previously untreated or relapsed/refractory BPDCN.
Common adverse events (AEs) related to tagraxofusp include hypoalbuminemia, transaminitis, and thrombocytopenia. There was 1 grade 5 AE—a case of capillary leak syndrome (CLS).
Study investigator Naveen Pemmaraju, MD, of The University of Texas MD Anderson Cancer Center in Houston, presented these results at the 23rd Congress of the European Hematology Association (EHA) as abstract S116.
The trial was sponsored by Stemline Therapeutics.
Dr Pemmaraju noted that there are no approved therapies for BPDCN, so patients may be treated with therapies intended for acute myeloid leukemia (AML), acute lymphoblastic leukemia, or lymphomas.
“These are usually quite intense cytotoxic chemotherapy regimens,” he said. “But even with these regimens, most groups report median overall survival times of 8 to 14 months.”
And although stem cell transplants can be effective in BPDCN, a “vast majority” of patients are not fit for transplant, according to Dr Pemmaraju.
With this in mind, he and his colleagues are conducting this trial of tagraxofusp in BPDCN.
The trial has 4 stages. In stage 1, patients received tagraxofusp at 7, 9, 12, or 16 μg/kg on days 1 to 5 of a 21-day cycle. In stages 2 and 3, patients received the drug at 12 μg/kg on days 1 to 5 of a 21-day cycle. Stage 4 is still enrolling.
Efficacy
Dr Pemmaraju presented results in 45 patients—32 with previously untreated BPDCN and 13 with relapsed/refractory BPDCN. The patients’ median age at baseline was 70 (range, 22-84), and 82% were male.
Three patients received tagraxofusp at 7 μg/kg/day, and the rest received the 12 μg/kg/day dose.
Among patients who received the 12 μg/kg/day dose, the ORR was 83% (35/42). The ORR was 90% (26/29) in previously untreated patients and 69% (9/13) in relapsed/refractory patients.
“These are very encouraging results—a 90% overall response rate in the frontline setting,” Dr Pemmaraju noted.
The composite CR rate was 62% (n=26) overall, 72% (n=21) in previously untreated patients, and 38% (n=5) in relapsed/refractory patients.
This included 13 patients with a CR (1 relapsed/refractory), 10 with a clinical CR (3 relapsed/refractory), and 3 with a CR with incomplete hematologic recovery (1 relapsed/refractory). A clinical CR was defined as absence of gross disease with minimal residual skin abnormality.
Fourteen patients went on to stem cell transplant, 1 of whom had relapsed/refractory disease at baseline.
Overall survival results were only available for the 29 previously untreated patients who received tagraxofusp at 12 μg/kg/day. In this group, the median overall survival has not been reached at a median follow-up of 13.8 months (range, 0.2 to 37.4 months).
Dr Pemmaraju said this result is important because it contrasts with the historical expectation of a median overall survival of 8 to 14 months.
Safety
Dr Pemmaraju presented safety results in 114 patients who have received tagraxofusp at 12 μg/kg/day on all trials of the drug. These data include patients with AML, myelofibrosis, and chronic myelomonocytic leukemia in addition to the 45 patients with BPDCN. However, AEs were similar regardless of disease.
Common treatment-related AEs (of any grade, occurring in at least 15% of patients) included hypoalbuminemia (49%), ALT increase (48%), AST increase (48%), thrombocytopenia (29%), nausea (27%), pyrexia (25%), chills (23%), fatigue (23%), weight increase (19%), hypotension (18%), peripheral edema (17%), and vomiting (15%).
CLS of any grade was also a common AE, occurring in 20% of patients (n=23). Most cases of CLS were grade 1 or 2, but there were grade 3 (n=5) and 4 (n=2) cases, as well as a single case of grade 5 CLS that occurred in a BPDCN patient.
Dr Pemmaraju did note that CLS has proven manageable with monitoring and pre-emptive measures. Specifically, inclusion criteria were changed so that patients must have normal cardiac function, adequate kidney function, and albumin of at least 3.2 g/dl. Investigators also began monitoring patients’ weight, albumin levels, and kidney function.
“With the combination of greater understanding of CLS, actual definitive protocol adjustments made by investigators, and monitoring, this has been a highly manageable phenomenon,” Dr Pemmaraju said.
Next steps
The investigators plan to continue enrolling patients in this study and collect additional safety and survival data, but Dr Pemmaraju and his colleagues also want to evaluate tagraxofusp in combination with other therapies.
Tagraxofusp is already under investigation in combination with azacitidine in a phase 1/2 trial of patients with high-risk myelodysplastic syndromes and AML.
Dr Pemmaraju is interested in combining hypomethylating agents with tagraxofusp for BPDCN patients as well, to build upon the encouraging results with tagraxofusp alone.
“An extraordinarily rare disease that used to not have any therapies at all now has at least one ongoing clinical trial with some encouraging activity,” he said. “I hope that gives hope to people with rare diseases, to let them know they’re not alone. There may be someone out there who’s researching their disease, no matter how rare it is.”
CHMP recommends rVWF for VWD

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for vonicog alfa (Veyvondi), a recombinant von Willebrand factor (rVWF) product.
The CHMP is recommending vonicog alfa for the treatment of bleeding events and treatment/prevention of surgical bleeding in adults (age 18 and older) with von Willebrand disease (VWD) when desmopressin treatment alone is ineffective or not indicated.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion of vonicog alfa is supported by a pair of phase 3 trials.
Non-surgical setting
Results from a phase 3 trial of vonicog alfa in a non-surgical setting were published in Blood in 2015.
The study included 49 patients with VWD who received vonicog alfa with or without recombinant factor VIII (FVIII).
All participants had successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) were given an “excellent” efficacy rating (as good as or better than expected).
Most bleeds (81.8%) were resolved with a single infusion of vonicog alfa, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events (AEs) considered related to vonicog alfa, and 2 were serious. One patient experienced 2 simultaneous serious AEs—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against VWF, and no neutralizing antibodies against FVIII.
Surgical setting
Results from the phase 3 trial in a surgical setting were presented at the WFH 2018 World Congress.
The trial enrolled 15 adults with severe VWD who were undergoing elective surgical procedures (10 of them major procedures).
Patients received vonicog alfa at 40 to 60 IU per kg of body weight 12 to 24 hours before surgery. Within 3 hours of surgery, each patient’s FVIII level (FVIII:C) was assessed, with a target of 30 IU/dL for minor surgeries and 60 IU/dL for major surgeries.
Within an hour of surgery, patients received a dose of vonicog alfa, with or without recombinant factor VIII, depending on the target FVIII:C levels at the 3-hour assessment.
Ten patients received rVWF alone, 12 did not receive any preoperative FVIII, and 2 did not receive rVWF postoperatively.
The study’s primary endpoint was met. Vonicog alfa demonstrated overall hemostatic efficacy, as assessed 24 hours after the last perioperative infusion or the completion of the study visit, whichever occurred earlier.
Intra- and post-operative hemostasis was rated as “excellent” (as good as or better than expected) in 60% of patients and “good” (probably as good as expected) in 40% of patients.
One patient developed deep vein thrombosis 3 days after undergoing hip replacement surgery.
One patient tested positive for binding antibodies to VWF. None of the patients developed binding antibodies against potential impurities such as rFurin, CHO-protein, or mouse IgG.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for vonicog alfa (Veyvondi), a recombinant von Willebrand factor (rVWF) product.
The CHMP is recommending vonicog alfa for the treatment of bleeding events and treatment/prevention of surgical bleeding in adults (age 18 and older) with von Willebrand disease (VWD) when desmopressin treatment alone is ineffective or not indicated.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion of vonicog alfa is supported by a pair of phase 3 trials.
Non-surgical setting
Results from a phase 3 trial of vonicog alfa in a non-surgical setting were published in Blood in 2015.
The study included 49 patients with VWD who received vonicog alfa with or without recombinant factor VIII (FVIII).
All participants had successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) were given an “excellent” efficacy rating (as good as or better than expected).
Most bleeds (81.8%) were resolved with a single infusion of vonicog alfa, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events (AEs) considered related to vonicog alfa, and 2 were serious. One patient experienced 2 simultaneous serious AEs—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against VWF, and no neutralizing antibodies against FVIII.
Surgical setting
Results from the phase 3 trial in a surgical setting were presented at the WFH 2018 World Congress.
The trial enrolled 15 adults with severe VWD who were undergoing elective surgical procedures (10 of them major procedures).
Patients received vonicog alfa at 40 to 60 IU per kg of body weight 12 to 24 hours before surgery. Within 3 hours of surgery, each patient’s FVIII level (FVIII:C) was assessed, with a target of 30 IU/dL for minor surgeries and 60 IU/dL for major surgeries.
Within an hour of surgery, patients received a dose of vonicog alfa, with or without recombinant factor VIII, depending on the target FVIII:C levels at the 3-hour assessment.
Ten patients received rVWF alone, 12 did not receive any preoperative FVIII, and 2 did not receive rVWF postoperatively.
The study’s primary endpoint was met. Vonicog alfa demonstrated overall hemostatic efficacy, as assessed 24 hours after the last perioperative infusion or the completion of the study visit, whichever occurred earlier.
Intra- and post-operative hemostasis was rated as “excellent” (as good as or better than expected) in 60% of patients and “good” (probably as good as expected) in 40% of patients.
One patient developed deep vein thrombosis 3 days after undergoing hip replacement surgery.
One patient tested positive for binding antibodies to VWF. None of the patients developed binding antibodies against potential impurities such as rFurin, CHO-protein, or mouse IgG.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for vonicog alfa (Veyvondi), a recombinant von Willebrand factor (rVWF) product.
The CHMP is recommending vonicog alfa for the treatment of bleeding events and treatment/prevention of surgical bleeding in adults (age 18 and older) with von Willebrand disease (VWD) when desmopressin treatment alone is ineffective or not indicated.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The CHMP’s opinion of vonicog alfa is supported by a pair of phase 3 trials.
Non-surgical setting
Results from a phase 3 trial of vonicog alfa in a non-surgical setting were published in Blood in 2015.
The study included 49 patients with VWD who received vonicog alfa with or without recombinant factor VIII (FVIII).
All participants had successful treatment of bleeding episodes. Most (96.9%) treated bleeds (n=192 bleeds in 22 patients) were given an “excellent” efficacy rating (as good as or better than expected).
Most bleeds (81.8%) were resolved with a single infusion of vonicog alfa, and the treatment had a mean half-life of 21.9 hours.
There were 8 adverse events (AEs) considered related to vonicog alfa, and 2 were serious. One patient experienced 2 simultaneous serious AEs—chest discomfort and increased heart rate—but these were resolved.
There were no thrombotic events in this trial, no treatment-related binding or neutralizing antibodies against VWF, and no neutralizing antibodies against FVIII.
Surgical setting
Results from the phase 3 trial in a surgical setting were presented at the WFH 2018 World Congress.
The trial enrolled 15 adults with severe VWD who were undergoing elective surgical procedures (10 of them major procedures).
Patients received vonicog alfa at 40 to 60 IU per kg of body weight 12 to 24 hours before surgery. Within 3 hours of surgery, each patient’s FVIII level (FVIII:C) was assessed, with a target of 30 IU/dL for minor surgeries and 60 IU/dL for major surgeries.
Within an hour of surgery, patients received a dose of vonicog alfa, with or without recombinant factor VIII, depending on the target FVIII:C levels at the 3-hour assessment.
Ten patients received rVWF alone, 12 did not receive any preoperative FVIII, and 2 did not receive rVWF postoperatively.
The study’s primary endpoint was met. Vonicog alfa demonstrated overall hemostatic efficacy, as assessed 24 hours after the last perioperative infusion or the completion of the study visit, whichever occurred earlier.
Intra- and post-operative hemostasis was rated as “excellent” (as good as or better than expected) in 60% of patients and “good” (probably as good as expected) in 40% of patients.
One patient developed deep vein thrombosis 3 days after undergoing hip replacement surgery.
One patient tested positive for binding antibodies to VWF. None of the patients developed binding antibodies against potential impurities such as rFurin, CHO-protein, or mouse IgG.
CHMP supports authorization of drug for AML

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for CPX-351 (Vyxeos™), a liposomal formulation that delivers a fixed ratio (1:5) of daunorubicin and cytarabine.
The CHMP is recommending approval of CPX-351 (44 mg/100 mg) for the treatment of adults with newly diagnosed, therapy-related acute myeloid leukemia or AML with myelodysplasia-related changes.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The marketing authorization application for CPX-351 is supported by data from 5 studies, including a phase 3 study.
Data from the phase 3 study were presented at the 2016 ASCO Annual Meeting and are available in the US prescribing information for CPX-351. (The following data are taken from the prescribing information.)
This trial enrolled 309 patients, ages 60 to 75, with newly diagnosed, therapy-related AML or AML with myelodysplasia-related changes.
They received CPX-351 (n=153) or cytarabine and daunorubicin (7+3; n=156).
The complete response rate was 38% in the CPX-351 arm and 26% in the 7+3 arm (P=0.036).
The rate of hematopoietic stem cell transplant was 34% in the CPX-351 arm and 25% in the 7+3 arm.
The median overall survival was 9.6 months in the CPX-351 arm and 5.9 months in the 7+3 arm (P=0.005).
All-cause 30-day mortality was 6% in the CPX-351 arm and 11% in the 7+3 arm. Sixty-day mortality was 14% and 21%, respectively.
Six percent of patients in both arms had a fatal adverse event (AE) on treatment or within 30 days of therapy that was not in the setting of progressive disease.
The rate of AEs that led to discontinuation was 18% in the CPX-351 arm and 13% in the 7+3 arm. AEs leading to discontinuation in the CPX-351 arm included prolonged cytopenias, infection, cardiotoxicity, respiratory failure, hemorrhage, renal insufficiency, colitis, and generalized medical deterioration.
The most common AEs (incidence ≥ 25%) in the CPX-351 arm were hemorrhagic events, febrile neutropenia, rash, edema, nausea, mucositis, diarrhea, constipation, musculoskeletal pain, fatigue, abdominal pain, dyspnea, headache, cough, decreased appetite, arrhythmia, pneumonia, bacteremia, chills, sleep disorders, and vomiting.
The most common serious AEs (incidence ≥ 5%) in the CPX-351 arm were dyspnea, myocardial toxicity, sepsis, pneumonia, febrile neutropenia, bacteremia, and hemorrhage.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for CPX-351 (Vyxeos™), a liposomal formulation that delivers a fixed ratio (1:5) of daunorubicin and cytarabine.
The CHMP is recommending approval of CPX-351 (44 mg/100 mg) for the treatment of adults with newly diagnosed, therapy-related acute myeloid leukemia or AML with myelodysplasia-related changes.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The marketing authorization application for CPX-351 is supported by data from 5 studies, including a phase 3 study.
Data from the phase 3 study were presented at the 2016 ASCO Annual Meeting and are available in the US prescribing information for CPX-351. (The following data are taken from the prescribing information.)
This trial enrolled 309 patients, ages 60 to 75, with newly diagnosed, therapy-related AML or AML with myelodysplasia-related changes.
They received CPX-351 (n=153) or cytarabine and daunorubicin (7+3; n=156).
The complete response rate was 38% in the CPX-351 arm and 26% in the 7+3 arm (P=0.036).
The rate of hematopoietic stem cell transplant was 34% in the CPX-351 arm and 25% in the 7+3 arm.
The median overall survival was 9.6 months in the CPX-351 arm and 5.9 months in the 7+3 arm (P=0.005).
All-cause 30-day mortality was 6% in the CPX-351 arm and 11% in the 7+3 arm. Sixty-day mortality was 14% and 21%, respectively.
Six percent of patients in both arms had a fatal adverse event (AE) on treatment or within 30 days of therapy that was not in the setting of progressive disease.
The rate of AEs that led to discontinuation was 18% in the CPX-351 arm and 13% in the 7+3 arm. AEs leading to discontinuation in the CPX-351 arm included prolonged cytopenias, infection, cardiotoxicity, respiratory failure, hemorrhage, renal insufficiency, colitis, and generalized medical deterioration.
The most common AEs (incidence ≥ 25%) in the CPX-351 arm were hemorrhagic events, febrile neutropenia, rash, edema, nausea, mucositis, diarrhea, constipation, musculoskeletal pain, fatigue, abdominal pain, dyspnea, headache, cough, decreased appetite, arrhythmia, pneumonia, bacteremia, chills, sleep disorders, and vomiting.
The most common serious AEs (incidence ≥ 5%) in the CPX-351 arm were dyspnea, myocardial toxicity, sepsis, pneumonia, febrile neutropenia, bacteremia, and hemorrhage.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended marketing authorization for CPX-351 (Vyxeos™), a liposomal formulation that delivers a fixed ratio (1:5) of daunorubicin and cytarabine.
The CHMP is recommending approval of CPX-351 (44 mg/100 mg) for the treatment of adults with newly diagnosed, therapy-related acute myeloid leukemia or AML with myelodysplasia-related changes.
The CHMP’s recommendation will be reviewed by the European Commission, which has the authority to approve medicines for use in the European Union, Norway, Iceland, and Liechtenstein.
The European Commission usually makes a decision within 67 days of the CHMP’s recommendation.
The marketing authorization application for CPX-351 is supported by data from 5 studies, including a phase 3 study.
Data from the phase 3 study were presented at the 2016 ASCO Annual Meeting and are available in the US prescribing information for CPX-351. (The following data are taken from the prescribing information.)
This trial enrolled 309 patients, ages 60 to 75, with newly diagnosed, therapy-related AML or AML with myelodysplasia-related changes.
They received CPX-351 (n=153) or cytarabine and daunorubicin (7+3; n=156).
The complete response rate was 38% in the CPX-351 arm and 26% in the 7+3 arm (P=0.036).
The rate of hematopoietic stem cell transplant was 34% in the CPX-351 arm and 25% in the 7+3 arm.
The median overall survival was 9.6 months in the CPX-351 arm and 5.9 months in the 7+3 arm (P=0.005).
All-cause 30-day mortality was 6% in the CPX-351 arm and 11% in the 7+3 arm. Sixty-day mortality was 14% and 21%, respectively.
Six percent of patients in both arms had a fatal adverse event (AE) on treatment or within 30 days of therapy that was not in the setting of progressive disease.
The rate of AEs that led to discontinuation was 18% in the CPX-351 arm and 13% in the 7+3 arm. AEs leading to discontinuation in the CPX-351 arm included prolonged cytopenias, infection, cardiotoxicity, respiratory failure, hemorrhage, renal insufficiency, colitis, and generalized medical deterioration.
The most common AEs (incidence ≥ 25%) in the CPX-351 arm were hemorrhagic events, febrile neutropenia, rash, edema, nausea, mucositis, diarrhea, constipation, musculoskeletal pain, fatigue, abdominal pain, dyspnea, headache, cough, decreased appetite, arrhythmia, pneumonia, bacteremia, chills, sleep disorders, and vomiting.
The most common serious AEs (incidence ≥ 5%) in the CPX-351 arm were dyspnea, myocardial toxicity, sepsis, pneumonia, febrile neutropenia, bacteremia, and hemorrhage.